Staffordshire, Shropshire & Black Country Newborn and Maternity Network. Neonatal Care Pathways 2015
|
|
|
- Chrystal Sullivan
- 5 years ago
- Views:
Transcription

1 Staffordshire, Shropshire & Black Country Newborn and Maternity Network Neonatal Care Pathways
2 Introduction This is a revision to the original Staffordshire, Shropshire and Black Country Newborn Network Care Pathway document (August 2011), which reflected the principles within the Toolkit for High Quality Neonatal Services 1 and the NICE quality standards 2. The aim of the Staffordshire, Shropshire & Black Country Newborn and Maternity Network (SSBCNMN) neonatal pathways is to put collaborative clinical decision making at the centre of care for babies and parents utilising the clear clinical thresholds within the NHS England neonatal critical care service specification 3 to reduce inappropriate transfers whilst maintaining high quality care. The pathways maintain the principle that care for extremely premature and complex neonates should be in Network Lead Neonatal Intensive Care Centres. Process The revision of the SSBCNMN neonatal clinical pathways has been through consultation with Neonatal and Maternity services representatives from all provider trusts in SSBCNMN, NHS England Specialist Commissioners, parent representatives and local commissioners. The original SSBC Newborn Network Clinical Care Pathways document was circulated with the NHS England neonatal critical care service specification in January 2015 to the neonatal and maternity service leads in each provider trust in SSBCNMN for review in order to identify any changes required to the network neonatal care pathways. Following this, each unit was visited in February 2015 by the Network Manager/Lead Nurse and the Neonatal & Obstetric Clinical Leads to discuss the individual unit pathways. Neonatal, Maternity and managerial representation at the meetings was provided as deemed appropriate by each Trust. The individual pathways were refined as necessary following the visits with the units. Agreement of the principles of this approach to neonatal care in SSBCNMN was obtained at the SSBCNMN board meeting held in September The pathways are fully supported by the West Midlands Specialised Commissioners. The Staffordshire, Shropshire & Black Country Newborn and Maternity Network, with the Specialised Commissioners will continue to monitor the care received by infants in the SSBC Newborn and Maternity Network and suggest changes as appropriate in agreement with the provider Trusts and Specialised Commissioners. General principles Collaborative Clinical decision making Discussion and collaboration on clinical aspects of individual care between the Network Lead NICU Centres and referring neonatal units has been formalised at key points of care and reflects unit designation, resource availability of the neonatal unit and the unit s status of escalation at the time care is required in the Staffordshire, Shropshire & Black Country Newborn and Maternity Network. Transfer for specialist neonatal medical care Each unit has an agreed set of clinical indicators that are key points of decision making for the continuance of care for that baby at that unit. Where a babies clinical indicators fall below that unit s trigger points then transfer to the Lead NICU Centre or other neonatal unit able to provide care at that 2
3 threshold and appropriate to the unit s care pathway is expected. Babies at thresholds of care may possibly stay within the referring unit if it is expected that the baby s condition will significantly and timely improve against an agreed plan of care with the referring clinician and Lead Centre clinician, and that the referring unit within local resources and designation can safely deliver this plan. Similarly the thresholds for transferring a baby out from an individual unit will alter to reflect the escalation status at the time care is required. Both the referring unit and Lead NICU Centre must ensure appropriate and accurate record keeping of any discussion leading to agreement for the continuation of care at a referring unit outside of that units care pathway and clinical threshold. See Appendix A- Exception Report Templates Individual Baby Exception Report Repatriation for continuance of care Within the care pathways, neonatal units within the network must ensure timely repatriation of babies to referring units when that baby s care falls within the referring unit s thresholds and is stable for transfer. This will ensure the most effective use of neonatal cot capacity within the network units whilst ensuring that babies receive care as close to home as possible The Lead NICU Centre must ensure appropriate and accurate record keeping of any local decisions or discussions with referring units that delay repatriation appropriate to referring units care thresholds. Neonatal Units should keep a record of all occasions when the repatriation of a baby to the referring unit is delayed beyond 48 hours of the initial request for repatriation. Exception monitoring and compliance to pathways In order to monitor the effectiveness of the pathways the Staffordshire, Shropshire & Black Country Newborn and Maternity Network require each neonatal unit to provide a collated record of the exceptions for babies whose continuation of care falls outside of a referring units pathway and care thresholds either for transfer or repatriation. Each maternity service provides the network with a collated record of the in utero transfers that are exceptions to the neonatal care pathways The Network will provide a quarterly report of neonatal pathway exceptions to the Network Board and to the Specialised Commissioners. In order to ensure that all exception reports are provided, the Network will monitor neonatal unit activity and cross-reference this through the following; Admission activity The Clevermed neonatal data system in all neonatal units in the Staffordshire, Shropshire & Black Country Newborn and Maternity Network will be monitored to identify any baby admitted to a neonatal unit that is an exception to the SSBCNMN care pathways. Pathway exception monitoring The Network has developed agreed collated exception report templates, both ex utero and in utero, for return to the Network by quarterly, see appendix A. Where an exception to the pathway is identified by the Network from the Clevermed neonatal data system which is not reflected in the submitted collated exception report, the Network will write to the neonatal unit involved to request further information about the exception. 3
4 Care pathways for the Staffordshire, Shropshire & Black Country Newborn and Maternity Network Neonatal Units Introduction These Care Pathways reflect the clinical thresholds within the NHS England neonatal critical care service specification as appropriate to the neonatal unit designations in SSBCNMN. They support the NHS England s strategy for Neonatal Services in the West Midlands by providing details of how infants should be cared for across the Staffordshire, Shropshire & Black Country Newborn and Maternity Network. The underlying aim of the care pathways are to provide a neonatal service that ensures that mothers and babies are able to access the best and most appropriate level of care at the right place and at the right time, as close to home as possible. This is underpinned by a focus on clinical discussions, agreement and monitoring. The care pathways will be supported in operation by the SSBCNMN Daily Communication Policy, see appendix B, and Repatriation Policy, see appendix C, and by using an agreed escalation procedure in each unit. The escalation procedure will reflect unit staffing, activity and dependency level of each neonate, maximising the safe delivery of care in the appropriate level of neonatal services where possible within network. The organisation of neonatal care within the Staffordshire, Shropshire & Black Country Newborn and Maternity Network is explained to pregnant women in an Information Leaflet, see appendix D 4
5 PRINCESS ROYAL HOSPITAL UNIT SPECIFICATION The neonatal service at Princess Royal Hospital is designated as a local neonatal unit (LNU) which will provide; 1. Neonatal services commensurate with national guidelines and professional standards where; singleton births are anticipated after 26+6 weeks gestational age and multiple births are anticipated after 27+6 weeks gestational age providing the anticipated birth weight is above 800g. 2. Babies with an antenatal diagnosis of congenital anomaly will deliver in Princess Royal Hospital if an agreed postnatal management plan is in place. 3. Following input from a Paediatric Cardiologist (BCH), it will also be appropriate to deliver the majority of antenatally detected cardiac problems at Princess Royal Hospital if an agreed post natal management plan is in place. 4. Fetuses identified with Diaphragmatic hernia, will normally be delivered in a neonatal surgery unit (Liverpool Women s with close proximity to Alderhey Children s Hospital or Birmingham Women s Hospital unit with close proximity to neonatal surgery at Birmingham Children s Hospital). 5. Where ever possible, women will be transferred in-utero to the Network NICU at Royal Stoke Hospital or Royal Wolverhampton Hospital, when gestational age less than 27 weeks, birth weight less than 800gms or need for complex or prolonged intensive care is anticipated including antenatally detected fetal hydrops, this list is not exhaustive. 6. Short term intensive care Short periods of intubated ventilator support will be provided, however the clinical condition of any baby requiring this care must be discussed with a consultant in the Network NICU at Royal Stoke Hospital by 48 hours and at agreed periods thereafter if intubated ventilator support continues. An agreed management plan including decisions regarding transfer criteria and review periods whilst intubated ventilator support continues will be documented 7. The stabilisation of babies prior to transfer to the Network NICU who require complex High dependency care and special care for their local population. 8. Referrals from other network neonatal units who are unable to undertake high dependency and special care work, due to capacity reasons and/or network guidelines. 9. Women in preterm labour at or above 27 weeks gestation may be accepted in for delivery in consultation with the maternity unit lead. 10. On-going high dependency and special care for babies who have undergone specialist surgery following repatriation from the surgical NICU. 11. High dependency and special care for local babies repatriated from elsewhere in the network who no longer require positive pressure ventilation. 12. In order to facilitate early repatriation of babies to their referral unit and to ensure integrity of capacity for SSBCNMN babies Princess Royal LNU will not accept out of network referrals without prior discussion with the Lead NICU at Royal Stoke Hospital. 13. Babies less than 27 weeks gestation, less than 800gms, and/or requiring complex (see 3. on next page) or prolonged intensive care (> 48 hours) in the LNU at Princess Royal Hospital will be referred to the Consultant on call of the Network Lead NICU centre at Royal Stoke Hospital to discuss and an agreed management plan will be recorded and put in place. Referrals to the Consultant on call of the Network Lead NICU centre at Royal Stoke Hospital will usually have been made within 6 hours from admission to the neonatal unit, however resuscitation and stabilisation of the baby will take priority before referral to the NICU unless the Consultant in Telford requires advice in order to stabilise the baby. 5
6 14. If there is doubt about necessity for transfer (e.g. baby is in good condition and not likely to need intensive care for more than 48 hours or baby is dying), there will be consultant to consultant discussion with the Neonatologist on call for Royal Stoke Hospital, the Network Lead Centre for the Princess Royal Hospital and an agreed management plan will be recorded and put in place. 15. Therapeutic Hypothermia (Cooling): Newly born infants who require cooling for treatment of perinatal asphyxia will be transferred to Royal Stoke Hospital or Royal Wolverhampton Hospital or the next appropriate Neonatal Intensive Care Unit. 16. Surgery including NEC: Babies who require surgery or a surgical opinion (including for NEC) will be transferred out to Alderhey Children s neonatal surgical centre, sometimes this may include a transfer to the surgical cots on the neonatal unit at Liverpool Women s Hospital. Babies who require surgery or a surgical opinion can also be transferred to Birmingham Children s Hospital dependent on cot availability and sometimes this may include transfer to the surgical cots on the neonatal unit at Birmingham Women s Hospital. 17. Any baby where it is anticipated specialist treatment with high frequency oscillatory ventilation (HFOV) and/or nitric oxide (NO) may be necessary should be discussed early prior to initiating either treatment with the Consultant on call of the Network Lead NICU centre at Royal Stoke Hospital and an agreed management plan recorded and put in place. The Local Neonatal unit at Princess Royal Hospital will not ordinarily be commissioned to provide the following: 1. On-going intensive care beyond initial stabilisation and intensive care to babies less than 27+0 weeks of gestation 2. On-going intensive care beyond initial stabilisation to babies with a birth weight below 800g 3. Complex intensive care including babies requiring respiratory support with symptoms of additional organ failure (e.g. hypotension, disseminated intravascular coagulation (DIC), renal failure, metabolic acidosis) or babies requiring the following treatment and support: Support of more than one organ, for example ventilation via a tracheal tube plus any one of the following: Inotrope infusion, insulin infusion, presence of a chest drain, exchange transfusion and prostaglandin infusion. Nitric Oxide (NO) High frequency oscillatory ventilation (HFOV) Therapeutic hypothermia beyond initial stabilisation. Prolonged Intensive care (intubated ventilatory support) for greater than 48 hours NB. There may be cases which are exceptions to the above and a baby may remain at the Princess Royal Hospital where the case has been discussed with the Neonatologist on call for Royal Stoke Hospital, the Network Lead Centre for the Princess Royal Hospital and an agreed management plan has been recorded and put in place. ESCALATION The above care pathways will be managed within unit designation as a local neonatal unit (Toolkit for high- quality neonatal services pg ). Any babies who cannot be offered care due to unit escalation procedure being activated will move where possible within network to the appropriate level neonatal unit. DISCHARGE CRITERIA Discharge to Transitional Care/ Post Natal Ward Criteria weeks gestation On full oral feeds Individual basis following review by Nursing and Medical staff Discharge Home Criteria Baby well Established feeds and gaining weight Maintaining temperature in a cot 6
7 Parent(s) agree Babies can be discharged home on oxygen and /or receiving tube feeds, these are decided on an individual basis Transition into Primary Care The liaison Health Visitor attends the neonatal unit daily and she alerts the relevant health visitor about the babies on the neonatal unit. On the day of discharge either the community midwife and/or the health visitor (as appropriate) are telephoned to inform them of the discharge of the baby from the neonatal unit. Babies meeting the following criteria are referred for follow up by the community neonatal outreach team: Less than 30 weeks gestation at birth Less than 1.8kgs on discharge O 2 Dependent NAS on prescribed medication Feeding problems/poor weight gain Screening follow up PKU Shared care with Paediatric community team (up to 6 months) Other babies at the discretion of NNU Nursing and Medical staff Follow Up Babies discharged from the neonatal unit meeting the following criteria undergo regular follow up. Birth weight 1500 g Gestation <32 weeks Requiring IPPV or CPAP for more than a few hours Significant cranial ultrasound abnormality o cystic PVL or IVH with significant ventricular dilation defined by consultant following final scan on NICU Acute neonatal encephalopathy grade 2 or 3 Seizures of whatever cause Neonatal meningitis Exchange transfusion for any reason Major congenital anomalies Other babies may be followed up at the discretion of the Consultant. Long Term Neurodevelopmental Follow Up Network Programme All babies born at less than 31 weeks gestation and/or those with a very low birth weight of less than 1250g have a Bayley III developmental assessment at a corrected age of 2 years 2 years 3 months 7
8 ROYAL STOKE HOSPITAL (NETWORK LEAD NICU CENTRE FOR NEONATAL UNITS IN STAFFORDSHIRE & SHROPSHIRE) UNIT SPECIFICATION The service will provide in addition to services provided by SCUs and LNUs: 1. Neonatal services commensurate with national guidelines and professional standards where births are anticipated after 22+6 weeks gestation (BAPM & Nuffield Council on Bioethics). 2. Intensive care for all the babies born within the network according to ODN approved care pathways including those less 27+0 / 27+6 weeks gestation, or with a birth weight < 800g and any baby requiring complex or prolonged intensive care. ODNs and the Trusts responsible for these units should monitor adherence to the care pathways 3. Babies with an antenatal diagnosis of cardiac or other congenital anomaly will deliver in Royal Stoke Hospital if an agreed postnatal management plan is in place. Fetuses with some identified surgical conditions will normally be delivered at Royal Stoke Hospital. Following input from a Paediatric Cardiologist, it is appropriate to deliver antenatally detected cardiac problems in Royal Stoke Hospital. Perinatal Meeting Care Plan Made Antenatal Counselling clinic letter to parents Delivery following care plan 4. Fetuses with some identified surgical conditions including Diaphragmatic hernia, will normally be delivered in a neonatal surgery unit (Liverpool Women s with close proximity to Alderhey Children s Hospital or Birmingham Women s Hospital unit with close proximity to neonatal surgery at Birmingham Children s Hospital). 5. Neonatal intensive care service for other local neonatal networks or out of area neonatal units when they cannot access a cot in their network NICU because of lack of capacity at that unit 6. Leadership within neonatology for the neonatal ODN units and 24 hour acute clinical telephone consultations as required by the network hospitals and, if required neonatal transport services. The NICU at Royal Stoke Hospital shall provide 24 hour acute clinical telephone consultations for the LNU at Princess Royal Hospital 7. Care for local network babies repatriated from elsewhere requiring on-going care from a NICU. 8. Therapeutic Hypothermia (Cooling): Newly born infants in SSBCNMN who require cooling for treatment of perinatal asphyxia will be managed at Royal Stoke Hospital or Royal Wolverhampton Hospital 9. Surgery (including NEC): Babies who require surgery or a surgical opinion (including for NEC) will be transferred out to Alderhey Children s neonatal surgical centre, sometimes this may include a transfer to the surgical cots on the neonatal unit at Liverpool Women s Hospital. ANTENATAL TRANSFERS INTO ROYAL STOKE HOSPITAL (NETWORK LEAD NICU CENTRE) Except in the presence of known severe antenatally detected surgical problems (where delivery in a supra-specialist centre is recommended), all women below 28 weeks gestation may be considered for delivery at Royal Stoke Hospital. Women at 28 weeks gestation and above should not routinely be considered for delivery at Royal Stoke Hospital unless the woman is very sick or there are indications that the baby will require complex or long term intensive care or the request to transfer the woman has been declined by the three network local neonatal units at Telford, Walsall and Dudley. NETWORK LEAD NICU CENTRE NEONATOLOGIST ROLE As the network lead NICU centre in Staffordshire & Shropshire, Neonatologists on the neonatal unit at Royal Stoke Hospital will be actively involved in the decisions required in the exception reports completed for individual babies born in the network LNUs who fall outside of the usual criteria for that unit but for 8
9 whom it is deemed appropriate for them to remain in their local unit rather than transfer out to a neonatal intensive care unit or local neonatal unit. REPATRIATION OF BABIES TO REFERRING UNIT Discussion regarding repatriation must commence between Royal Stoke Hospital and the babies referring unit as soon after admission as possible and before the baby meets the clinical pathway threshold for the referring unit, see SSBCNMN Daily Communication Policy. Arrangements for repatriation should be commenced as soon as the baby is stable for transfer see SSBCNMN Repatriation Policy. ESCALATION The above care pathways will be managed within unit designation as a neonatal intensive care unit (Toolkit for high- quality neonatal services pg ). Any babies who cannot be offered care due to unit escalation procedure being activated will move where possible within network to the appropriate level neonatal unit. DISCHARGE CRITERIA Discharge from the neonatal unit to: Postnatal Ward Mother is an in patient Baby well, establishing feeding, maintaining temperature in a cot and not needing continuous specialist neonatal care/monitoring E.g. Completing 48 hour course of IV antibiotics Home Baby well On full feeds and gaining weight Maintaining temperature in a cot Parent(s) agree Babies can be discharged home on oxygen and /or receiving tube feeds, these are decided on an individual basis Transition into Primary Care Babies discharged home with long term medical problems are referred to the appropriate paediatric community team for follow up at home All babies born below 34 week gestation are referred to the Hospital at Home Team. Babies 34 weeks and above are referred to the Health Visitor. All babies below 28 days of life are automatically referred to the Community Midwife. Helping hands parent support group meet monthly at the Hope Children s Centre in Hanley. All babies discharged from NICU and their siblings are invited to attend. Follow Up Babies are followed up in the neonatal clinic as per the SSBCNN Neonatal Guideline Babies discharged from the neonatal unit meeting the following criteria undergo regular follow up. Birth weight 1500 g Gestation <32 weeks Requiring IPPV or CPAP for more than a few hours Significant cranial ultrasound abnormality o cystic PVL or IVH with significant ventricular dilation defined by consultant following final scan on NICU Acute neonatal encephalopathy grade 2 or 3 Seizures of whatever cause Neonatal meningitis Exchange transfusion for any reason Major congenital anomalies Other babies may be followed up at the discretion of the Consultant. Long Term Neurodevelopmental Follow Up Network Programme All babies born at less than 31 weeks gestation and/or those with a very low birth weight of less than 1250g have a Bayley III developmental assessment at a corrected age of 2 years 2 years 3 months. 9
10 WALSALL MANOR HOSPITAL UNIT SPECIFICATION The neonatal service at Walsall Manor Hospital is designated as a local neonatal unit which will provide; 1. Neonatal services commensurate with national guidelines and professional standards where; singleton and multiple births are anticipated after 27+6 weeks gestational age providing the anticipated birth weight is above 800g. 2. Babies with an antenatal diagnosis of congenital anomaly will deliver in Walsall Manor Hospital if an agreed postnatal management plan is in place. 3. Following input from a Paediatric Cardiologist (BCH), it will also be appropriate to deliver the majority of antenatally detected cardiac problems at Walsall Manor Hospital if an agreed post natal management plan is in place. 4. Fetuses identified with Diaphragmatic hernia, will normally be delivered in Birmingham Women s Hospital unit with close proximity to neonatal surgery at Birmingham Children s Hospital 5. Wherever possible, babies with gastroschisis will be delivered at Birmingham Women s Hospital. (short term until 24/7 ANNP cover secured at WMH) 6. Where ever possible, women will be transferred in-utero to the Network NICU at Royal Wolverhampton Hospital or Royal Stoke Hospital, when gestational age less than 28 weeks, birth weight less than 800gms or need for complex or prolonged intensive care is anticipated including antenatally detected fetal hydrops, this list is not exhaustive. 7. Short term intensive care Short periods of intubated ventilator support will be provided, however the clinical condition of any baby requiring this care must be discussed with a consultant in the Network NICU at Royal Wolverhampton Hospital by 48 hours and at agreed intervals thereafter if intubated ventilator support continues. An agreed management plan including decisions regarding transfer criteria and review periods will be documented 8. The stabilisation of babies prior to transfer to the Network NICU who require complex High dependency care and special care for their local population. 9. Referrals from other network neonatal units who are unable to undertake high dependency and special care work, due to capacity reasons and/or network guidelines. 10. Women in preterm labour at or above 28 weeks gestation may be accepted in for delivery in consultation with the maternity unit lead. 11. On-going high dependency and special care for babies who have undergone specialist surgery following repatriation from the surgical NICU. 12. High dependency and special care for local babies repatriated from elsewhere in the network who no longer require positive pressure ventilation. 13. In order to facilitate early repatriation of babies to their referral unit and to ensure integrity of capacity for SSBCNMN babies Walsall Manor Hospital LNU will not accept out of network referrals without prior discussion with the Lead NICU at Royal Wolverhampton Hospital. 14. Babies less than 28 weeks gestation, less than 800gms, and/or requiring complex (see 3. On next page) or prolonged intensive care (> 48 hours) in the LNU at Walsall Manor Hospital will be referred to the Consultant on call of the Network Lead NICU centre at Royal Wolverhampton Hospital to discuss and an agreed management plan will be recorded and put in place. Referrals to the Consultant on call of the Network Lead NICU centre at Royal Wolverhampton Hospital will usually have been made within 6 hours from admission to the neonatal unit, however resuscitation and stabilisation of the baby will take priority before referral to the NICU unless the Consultant in Walsall requires advice in order to stabilise the baby. 10
11 15. If there is doubt about necessity for transfer (e.g. baby is in good condition and not likely to need intensive care for more than 48 hours or baby is dying), there will be consultant to consultant discussion with the Neonatologist on call for Royal Wolverhampton Hospital, the Network Lead Centre for the Walsall Manor Hospital and an agreed management plan will be recorded and put in place. 16. Therapeutic Hypothermia (Cooling): Newly born infants who require cooling for treatment of perinatal asphyxia will be transferred to Royal Wolverhampton Hospital or Royal Stoke Hospital or the next appropriate Neonatal Intensive Care Unit. 17. Surgery (including NEC): Babies who require surgery or a surgical opinion (including for NEC) will be transferred out to Birmingham Children s neonatal surgical centre, sometimes this may include a transfer to the surgical cots on the neonatal unit at Birmingham Women s Hospital. 18. Any baby where it is anticipated specialist treatment with high frequency oscillatory ventilation (HFOV) and/or nitric oxide (NO) may be necessary should be discussed early prior to initiating either treatment with the Consultant on call of the Network Lead NICU centre at Royal Wolverhampton Hospital and an agreed management plan recorded and put in place The Local Neonatal unit at Walsall Manor Hospital will not ordinarily be commissioned to provide the following: 1. On-going intensive care beyond initial stabilisation and intensive care to babies less than 28+0 weeks of gestation 2. On-going intensive care beyond initial stabilisation to babies with a birth weight below 800g 3. Complex intensive care including babies requiring respiratory support with symptoms of additional organ failure (e.g. hypotension, disseminated intravascular coagulation (DIC), renal failure, metabolic acidosis) or babies requiring the following treatment and support: Support of more than one organ, for example ventilation via a tracheal tube plus any one of the following: Inotrope infusion, insulin infusion, presence of a chest drain, exchange transfusion and prostaglandin infusion. Nitric oxide High frequency oscillatory ventilation (HFOV) Therapeutic hypothermia beyond initial stabilisation. Prolonged Intensive care (intubated ventilatory support) for greater than 48 hours NB. There may be cases which are exceptions to the above and a baby may remain at Walsall Manor Hospital where the case has been discussed with the Neonatologist on call for Royal Wolverhampton Hospital, the Network Lead Centre for Walsall Manor Hospital and an agreed management plan has been recorded and put in place. ESCALATION The above care pathways will be managed within unit designation as a local neonatal unit (Toolkit for high- quality neonatal services pg ). Any babies who cannot be offered care due to unit escalation procedure being activated will move where possible within network to the appropriate level neonatal unit. DISCHARGE Discharge to Post Natal Ward Criteria Mother is an in patient Baby well, establishing feeding, maintains temperature in a cot, not needing continuous specialist neonatal care/monitoring. E.g. Completing 48 hour course of IV antibiotics Discharge Home Criteria feeding well 3 hourly gaining weight appropriately clinically well corrected to 35 weeks gestation or more Transition into Primary Care Follow up based on birth weight and gestation 11
12 >2.3kg AND > 34/40 Follow up with community midwife / Health visitor contacted prior to discharge <2.3kg OR < 34/40 Short term weekly follow up with community neonatal nurse alongside Health visitor then care transferred to Health visitor Babies going home on oxygen Follow up by community neonatal nurse initially then care transferred to community children s nurses Discharge planning meetings take place prior to discharge for any of the following reasons: Going home on oxygen Social issues Complex needs 12
13 RUSSELL S HALL HOSPITAL UNIT SPECIFICATION The neonatal service at Russell s Hall Hospital is designated as a local neonatal unit (LNU) which will provide; 1. Neonatal services commensurate with national guidelines and professional standards where; singleton births are anticipated after 26+6 weeks gestational age and multiple births are anticipated after 27+6 weeks gestational age providing the anticipated birth weight is above 800g. 2. Babies with an antenatal diagnosis of congenital anomaly will deliver in Russell s Hall Hospital if an agreed postnatal management plan is in place. Antenatal Detected Problem Condition decision of care Obstetrician and Specialist at BCH/BWH Antenatal care and deliver at BWH BCH Antenatal care and deliver at RHH BCH/BWH 3. Following input from a Paediatric Cardiologist (BCH), it will also be appropriate to deliver the majority of antenatally detected cardiac problems at Russell s Hall Hospital if an agreed post natal management plan is in place. 4. Fetuses identified with Diaphragmatic hernia, will normally be delivered in Birmingham Women s Hospital unit with close proximity to neonatal surgery at Birmingham Children s Hospital. 5. Where ever possible, women will be transferred in-utero to the Network NICU at Royal Wolverhampton Hospital or Royal Stoke Hospital, when gestational age less than 27 weeks, anticipated birth weight less than 800gms or need for complex or prolonged intensive care is anticipated including antenatally detected fetal hydrops, this list is not exhaustive. 6. Limited intensive care Short periods of intubated ventilator support will be provided, however the clinical condition of any baby requiring this care must be discussed with a consultant in the Network NICU at Royal Wolverhampton Hospital by 48 hours and at agreed intervals thereafter if intubated ventilator support continues. An agreed management plan including decisions regarding transfer criteria and review periods will be documented 7. The stabilisation of babies prior to transfer to the Network NICU who require complex High dependency care and special care for their local population. 8. Referrals from other network neonatal units who are unable to undertake high dependency and special care work, due to capacity reasons and/or network guidelines. 9. Women in preterm labour at or above 27 weeks gestation may be accepted in for delivery in consultation with the maternity unit lead. 10. On-going high dependency and special care for babies who have undergone specialist surgery following repatriation from the surgical NICU. 11. High dependency and special care for local babies repatriated from elsewhere in the network who no longer require positive pressure ventilation. 13
14 12.. In order to facilitate early repatriation of babies to their referral unit and to ensure integrity of capacity for SSBCNMN babies Russells Hall Hospital LNU will not accept out of network referrals without prior discussion with the Lead NICU at Royal Wolverhampton Hospital. 13. Babies less than 27 weeks gestation, less than 800gms, and/or requiring complex (see 3. Below) or prolonged intensive care (> 48 hours) in the LNU at Russell s Hall Hospital will be referred to the Consultant on call of the Network Lead NICU centre at Royal Wolverhampton Hospital to discuss and an agreed management plan will be recorded and put in place. Referrals to the Consultant on call of the Network Lead NICU centre at Royal Wolverhampton Hospital will usually have been made within 6 hours from admission to the neonatal unit, however resuscitation and stabilisation of the baby will take priority before referral to the NICU unless the Consultant in Dudley requires advice in order to stabilise the baby. 14. If there is doubt about necessity for transfer (e.g. baby is in good condition and not likely to need intensive care for more than 48 hours or baby is dying), there will be consultant to consultant discussion with the Neonatologist on call for Royal Wolverhampton Hospital, the Network Lead Centre for the LNU at Russell s Hall Hospital and an agreed management plan will be recorded and put in place. 15. Therapeutic Hypothermia (Cooling): Newly born infants who require cooling for treatment of perinatal asphyxia will be transferred to Royal Wolverhampton Hospital or Royal Stoke Hospital or the next appropriate Neonatal Intensive Care Unit. 16. Surgery including NEC: Babies who require surgery or a surgical opinion (including for NEC) will be transferred out to Birmingham Children s neonatal surgical centre, sometimes this may include a transfer to the surgical cots on the neonatal unit at Birmingham Women s Hospital. 17. Any baby where it is anticipated specialist treatment with high frequency oscillatory ventilation (HFOV) and/or nitric oxide (NO) may be necessary should be discussed early prior to initiating either treatment with the Consultant on call of the Network Lead NICU centre at Royal Wolverhampton Hospital and an agreed management plan recorded and put in place The Local Neonatal unit at Russell s Hall Hospital will not ordinarily be commissioned to provide the following: 1. On-going intensive care beyond initial stabilisation and intensive care to babies less than 27+0 weeks of gestation 2. On-going intensive care beyond initial stabilisation to babies with a birth weight below 800g 3. Complex intensive care including babies requiring respiratory support with symptoms of additional organ failure (e.g. hypotension, disseminated intravascular coagulation (DIC), renal failure, metabolic acidosis) or babies requiring the following treatment and support: Support of more than one organ, for example ventilation via a tracheal tube plus any one of the following: Inotrope infusion, insulin infusion, presence of a chest drain, exchange transfusion and prostaglandin infusion. Nitric oxide High frequency oscillatory ventilation (HFOV) Therapeutic hypothermia beyond initial stabilisation. Prolonged Intensive care (intubated ventilatory support) for greater than 48 hours NB. There may be cases which are exceptions to the above and a baby may remain at Russell s Hall Hospital where the case has been discussed with the Neonatologist on call for Royal Wolverhampton Hospital, the Network Lead Centre for Russell s Hall Hospital and an agreed management plan has been recorded and put in place. ESCALATION The above care pathway will be managed within unit designation as a local neonatal unit (Toolkit for highquality neonatal services pg ). Any babies who cannot be offered care due to unit escalation procedure being activated will move where possible within network to the appropriate level neonatal unit. 14
15 Each neonatal unit will require to develop a locally owned Unit Escalation Procedure that reflects both staffing and activity to ensure safe delivery of care. DISCHARGE CRITERIA Each baby is individually assessed by a Consultant/Registrar or ANNP to ensure they are well enough to be discharged home. Although there are no set criteria for discharge, the following points are adhered to: A sustained pattern of weight gain rather than a specific achieved weight Physiologic stability defined as the ability to suckle feed and maintain normal body temperature in an open environment. An active programme of parental involvement and preparation for post hospital care, which incorporates the optimisation of their parenting skills and enhancing their confidence to care for their baby independently. This is accomplished by offering all parents the use of the self-contained flat on the neonatal unit before discharge. Frequent outpatient follow-up to assure adequate weight gain for the smallest infants commencing four to six weeks immediately after discharge. Referral to the Children s Ward via completion of a Paediatric Alert Form to ensure timely treatment is delivered if admission to hospital is necessary Transition into Primary Care An active programme of parental support after discharge of the baby in the home setting is ensured by the community neonatal team. Babies who require extra support after discharge e.g. oxygen dependent babies, will need the community team to organise a pre-discharge meeting with other multidisciplinary community team members On discharge, all parents will be provided with a Discharge letter. The Discharge letter (a copy of which is retained in the notes and also faxed to the GP and Health Visitor), will be sealed and addressed to the GP A monthly parent support group for babies discharged from the neonatal unit in Dudley is held at Woodside Childrens Centre, Dudley Follow Up Babies discharged from the neonatal unit meeting the following criteria undergo regular follow up. Birth weight 1500 g Gestation <32 weeks Requiring IPPV or CPAP for more than a few hours Significant cranial ultrasound abnormality o cystic PVL or IVH with significant ventricular dilation defined by consultant following final scan on NICU Acute neonatal encephalopathy grade 2 or 3 Seizures of whatever cause Neonatal meningitis Exchange transfusion for any reason Major congenital anomalies Other babies may be followed up at the discretion of the Consultant. Long Term Neurodevelopmental Follow Up Network Programme All babies born at less than 31 weeks gestation and/or those with a very low birth weight of less than 1250g have a Bayley III developmental assessment at a corrected age of 2 years 2 years 3 months 15
16 ROYAL WOLVERHAMPTON HOSPITAL (NETWORK LEAD NICU CENTRE FOR NEONATAL UNITS IN THE BLACK COUNTRY) UNIT SPECIFICATION The service will provide in addition to services provided by SCUs and LNUs: 1. Neonatal services commensurate with national guidelines and professional standards where births are anticipated after 22+6 weeks gestation (BAPM & Nuffield Council on Bioethics). 2. Intensive care for all the babies born within the network according to ODN approved care pathways including those less 27+6 weeks gestation, or with a birth weight < 800g and any baby requiring complex or prolonged intensive care. ODNs and the Trusts responsible for these units should monitor adherence to the care pathways 3. Babies with an antenatal diagnosis of cardiac or other congenital anomaly will deliver in Royal Wolverhampton Hospital if an agreed postnatal management plan is in place. Fetuses with some identified surgical conditions will normally be delivered at Royal Wolverhampton Hospital. Following input from a Paediatric Cardiologist, it is appropriate to deliver antenatally detected cardiac problems in Royal Wolverhampton Hospital. 4. Fetuses with some identified surgical conditions including Diaphragmatic hernia, will normally be delivered in Birmingham Women s Hospital unit with close proximity to neonatal surgery at Birmingham Children s Hospital. 5. Neonatal intensive care service for other local neonatal networks or out of area neonatal units when they cannot access a cot in their network NICU because of lack of capacity at that unit 6. Leadership within neonatology for the neonatal ODN units and 24 hour acute clinical telephone consultations as required by the network hospitals and, if required neonatal transport services. The NICU at Royal Wolverhampton Hospital shall provide 24 hour acute clinical telephone consultations for the LNUs at Walsall Manor and Russell s Hall Hospitals 7. Care for local network babies repatriated from elsewhere requiring on-going care from a NICU. 8. Therapeutic Hypothermia (Cooling): Newly born infants in SSBCNMN who require cooling for treatment of perinatal asphyxia will be managed at Royal Wolverhampton Hospital or Royal Stoke Hospital 9. Surgery (including NEC): Babies who require surgery or a surgical opinion (including for NEC) will be transferred out to Birmingham Children s neonatal surgical centre, sometimes this may include a transfer to the surgical cots on the neonatal unit at Birmingham Women s Hospital. ANTENATAL TRANSFERS INTO ROYAL WOLVERHAMPTON HOSPITAL (NETWORK LEAD NICU CENTRE) Except in the presence of known severe antenatally detected surgical problems (where delivery in a supra-specialist centre is recommended), all women below 28 weeks gestation may be considered for delivery at ROYAL WOLVERHAMPTON HOSPITAL. Women at 28 weeks gestation and above should not routinely be considered for delivery at Royal Wolverhampton Hospital unless the woman is very sick or there are indications that the baby will require complex or long term intensive care or the request to transfer the woman has been declined by the three network local neonatal units at Telford, Walsall and Dudley. NETWORK LEAD NICU CENTRE NEONATOLOGIST ROLE As the network lead centre in the Black Country, Neonatologists on the neonatal unit at ROYAL WOLVERHAMPTON Hospital will be actively involved in the decisions required in the exception reports completed for individual babies born in the network LNUs who fall outside of the usual criteria for that unit but for whom it is deemed appropriate for them to remain in their local unit rather than transfer out to a neonatal intensive care unit or local neonatal unit. 16
17 ESCALATION The above care pathways will be managed within unit designation as a neonatal intensive care unit (Toolkit for high- quality neonatal services pg ). Any babies who cannot be offered care due to unit escalation procedure being activated will move where possible within network to the appropriate level neonatal unit. REPATRIATION OF BABIES TO REFERRING UNIT Discussion regarding repatriation must commence between ROYAL WOLVERHAMPTON HOSPITAL and the babies referring unit as soon after admission as possible and before the baby meets the clinical pathway threshold for the referring unit, see SSBCNMN Daily Communication Policy. Arrangements for repatriation should be commenced as soon as the baby is stable for transfer, see SSBCNMN Repatriation Policy. DISCHARGE TO TRANSITIONAL CARE Transitional Care Admission Guideline Admission criteria from Delivery Suite Gestation weeks. Lower weight limit 1.7 kg Upper weight limit kg dependent on gestation All babies below 36 weeks and / or < 2.45kg must be admitted to Transitional Care Babies who are borderline and not treated as T/C should be observed to ensure there are no feeding issues. Babies can be transferred into Transitional Care if any problems develop. Substance misuse Admission criteria from NNU Gestation weeks. Weight below 2.5kg Babies of 33 weeks gestation who have been stable on NNU for 24 hours are suitable for transfer to Transitional Care DISCHARGE HOME Referral criteria to Neonatal Community Liaison Team (NCLT) A gestation of 34 weeks and below Less than 2kgs A baby that has been on the neonatal unit for more than 10 days A request from neonatal consultants Oxygen at home The baby must be established on full feeds, managing their temperature in a cot and all observations stable. The NCLT attend the morning ward rounds three times a week and work closely with the consultants in planning all discharges from the neonatal unit. Prior to discharge all babies and families will meet a member of NCLT to discuss support they will receive at home. A discharge pack is given to parents prior to discharge. The team offer a 7 day a week service and the option to take babies home on short term tube feeding if appropriate. Babies and families can be discharged from the NCLT once there have been 4 good weight gains and the family feels supported enough for discharge to happen. Once discharge has been agreed the red book is completed with current weight and a brief entry of care during this period. A referral is made to the health visitor so they are aware that the baby has been discharged from the NCLT. If the baby requires on going medical care then appropriate referrals are made. A monthly parent support group Helping Hands is held at the GEM Centre in Wolverhampton for all discharged babies born within the Wolverhampton area at 31 weeks or earlier, or below a birth weight of 1,250 grams (2lb 12oz) or other babies referred by a healthcare professional. 17
18 FOLLOW UP All babies less than 32 weeks gestation discharged from the neonatal unit have developmental follow up at 6 weeks, 6 months and 1 year corrected and are generally discharged at 2 years corrected. In addition any ventilated baby, babies who have received therapeutic cooling or who are identified as having complex needs will also be followed up as above. Any baby with specific medical needs e.g. renal pelvic dilatation, O 2 dependent, cardiac problem etc would have follow up in the neonatal clinic in children s OPA and would be jointly managed with BCH or other specialists as appropriate. Long Term Neurodevelopmental Follow Up Network Programme All babies born at less than 31 weeks gestation and/or those with a very low birth weight of less than 1250g have a Bayley III developmental assessment at a corrected age of 2 years 2 years 3 months 18
19 19
20 Appendix A- Exception Report Templates Individual Baby Exception Report Care Pathway Exception Report Referring Unit: Baby: Name: DOB: Hospital Number/NHS Number: Staffordshire, Shropshire & Black Country Newborn and Maternity Network (Complete patient details or Affix Patient Identification label on copy for patient notes) Name of Consultant at Referring Hospital: Date: Time: Brief Details of the exception(s) to care pathway: Network Lead Centre: (Tick box as appropriate) Royal Stoke Royal Wolverhampton Name of Consultant at Network Lead Centre: Outcome of Consultant to Consultant discussion: (Tick box as appropriate) Baby to be transferred to: Baby to remain at referring unit with the following agreed management plan: Agreed Date for review with Network Lead Centre: Additional Comments: 20
21 Staffordshire, Shropshire & Black Country Newborn and Maternity Network Guidance for completing Exception reports Guidance for completing SSBCNMN Exception reports 1. An individual exception report should be completed for any baby admitted to a neonatal unit in the SSBCNMN that falls outside of that unit s criteria for care or normal care pathway E.g. babies admitted below the gestation and/or weight threshold babies requiring longer than 48 hours ventilation babies admitted who were booked in another network any baby that is not repatriated to its referring unit once the baby s care falls within the criteria of care for that unit. 2. Copies of the exception report template can be downloaded from the network website. For babies admitted to a unit that fall outside of that unit s criteria for care 3. The referring unit (where the baby has been admitted) should download an exception report template and complete sections 1, 2, 3 & 6 before telephoning the appropriate network lead NICU centre. Princess Royal Hospital = Royal Stoke Hospital. Walsall Manor and Russell s Hall Hospital s = Royal Wolverhampton Hospital 4. Sections 5, 7 9 should be completed by the referring unit consultant during/immediately following the telephone call with the network lead NICU centre consultant on take/call. Examples for exception from pathway;- agreed with Lead Centre as clinically appropriate & why transport availability neonatal capacity within network maternity capacity within network (IUT) unit escalation status Other (state) 5. Section 10 can be used for additional information such as any difficulties with locating a cot and/or arranging the transfer 6. A copy of the exception report should be printed off and a copy of this should be faxed to the network lead centre unit for their records before filing the original in the baby s notes. Royal Stoke Hospital NNU Fax No Royal Wolverhampton Hospital NNU Fax No: If a review date with the network lead centre unit is set as part of the management plan then a second exception report form should be completed on the date of the review and the above steps followed again To report delays in repatriating babies closer to home 8. An exception report should be commenced by the referring unit if the repatriation of a baby to a unit closer to home is delayed for 48 hours after the initial request for repatriation has been made. 9. The exception report should be completed with the final outcome, I.E. the date the baby was eventually repatriated or the date the baby went home or was discharged to another destination. 10. A copy of the final form should be sent to the receiving unit and the original filed in the baby s Notes Reporting Neonatal Exceptions to the Network 11. The network will a template form to each NNU quarterly to collect information regarding neonatal exceptions that have occurred as described above. This should be completed and returned to the network office via To report IUT exceptions to the care pathways 12. A template form is ed quarterly to collect information regarding IUT s that are exceptions to care pathways which is completed and returned by to the network office 21
22 Exception Report Templates Neonatal Ex-Utero Exceptions Collated Report Ex Utero Neonatal Care Pathway Exceptions Quarterly Collation Report Template Hospital Trust: Quarter: Name of Person Completing the Form: Please return to: Sarah Carnwell, Network Administrator 1. Babies who require care above the clinical threshold for unit designation (Including: Gestation, Birthweight, Ventilation > 48 hours) *Reported in quarter exception occurs on NNU Date of Birth Exception Reason (Gestation/ Weight/ Ventilation / Other) Discussed with Network NICU Consultant (Name) Staffordshire, Shropshire & Black Country Newborn & Maternity Network Outcome Transfer destination or Agreed Management plan Comments 2. Delayed Repatriations > 48 hours after initial request for transfer * Reported in quarter baby discharged from NNU Place of booking Number of Comments days delayed Date of discharge Destination (Name of Hospital or Discharged home) 3. Admissions from outside the SSBCNMN (Home postcode external to SSBCNMN, do not include SSBCNMN babies born outside of network and repatriated) * Reported in quarter baby discharge from NNU Date of Birth Date of admission Place of Booking Date of Discharge Destination (Name of Hospital or Discharged home) Comments 22
23 Exception Report Templates In Utero Exceptions Collated Report Staffordshire, Shropshire & Black Country Newborn& Maternity Network Hospital Trust: Quarter: Name of person Completing the Form: Please return to: Ruth Moore, Network Manager In Utero Transfer Neonatal Care Pathway Exception Report Template Date &Time Gestation Reason(s) for IUT Below gestational threshold for NNU NNU Full No NNU Capacity in Network No Labour Ward Capacity in Network Other (please state) Transfer Destination Previous IUT in this Pregnancy Y / N Outcome (If Known) Delivered Y / N Comments 23
24 Appendix B Staffordshire, Shropshire & Black Country Newborn and Maternity Network NICU / LNU Daily Communication Policy 1. The SSBCNMN Repatriation Policy Algorithm (see appendix) identifies a need for a daily conversation between the respective NICU and LNU to review the progress of any LNU babies currently being cared for on the NICU to keep both the LNU staff and the baby s parents up to date with progress and an anticipated timeframe for repatriation to the LNU. 2. This NICU / LNU Daily Communication policy aims to strengthen communication between the NICUs and the LNUs through the introduction of a daily telephone call between the Consultants of the Week and neonatal unit shift co-ordinators of the respective units. This will provide a mechanism to enable regular review of babies within neonatal services in the SSBCNMN to ensure timely repatriation and effective use of neonatal capacity within the network. 3. Following completion of the daily ward round in the NICU the NICU Consultant of the week and the neonatal unit shift co-ordinator will telephone the LNUs that they are responsible for in terms of the network care pathway, see table below, to speak with the Consultant of the Week and the shift coordinator on the LNU. NICU University Hospital of North Midlands NHS Trust Royal Wolverhampton Hospital NHS Trust LNU Shrewsbury and Telford Hospital NHS Trust Walsall Healthcare NHS Trust Dudley Group NHS Foundation Trust 4. The daily communication between the two neonatal units has two objectives; Provide an opportunity for the NICU to update the LNU of any babies on the NICU that may be suitable for repatriation (babies booked at LNU) or continuing care (other babies not booked at LNU to create capacity in the NICU) and the anticipated time frame for being ready for transfer Provide the LNU an opportunity to identify and discuss with the NICU any existing or potential babies that require care outside of the LNUs care pathway in order that a plan of care can be agreed and an exception report completed. 5. The timing of the routine daily telephone call should be agreed between the two respective units. It is acknowledged that there will be days when the activity within either or both neonatal units may prevent this routine daily communication from occurring. 6. It may not always be possible for the neonatal shift co-ordinator to join in the daily telephone call, when this is the case the Consultant of the week will update their shift co-ordinator of the key points discussed and any planned or anticipated transfers between units. 7. There will be times when babies booked at an LNU may be being cared for at a different NICU than the NICU with responsibility for that LNU, in these cases it is good practice for each NICU to have a daily communication with the LNU where the baby was booked in order to update them on the baby s progress and identify the anticipated time frame for a timely repatriation. The neonatal transfer service should be informed of any planned transfers at the earliest opportunity. 24
25 25
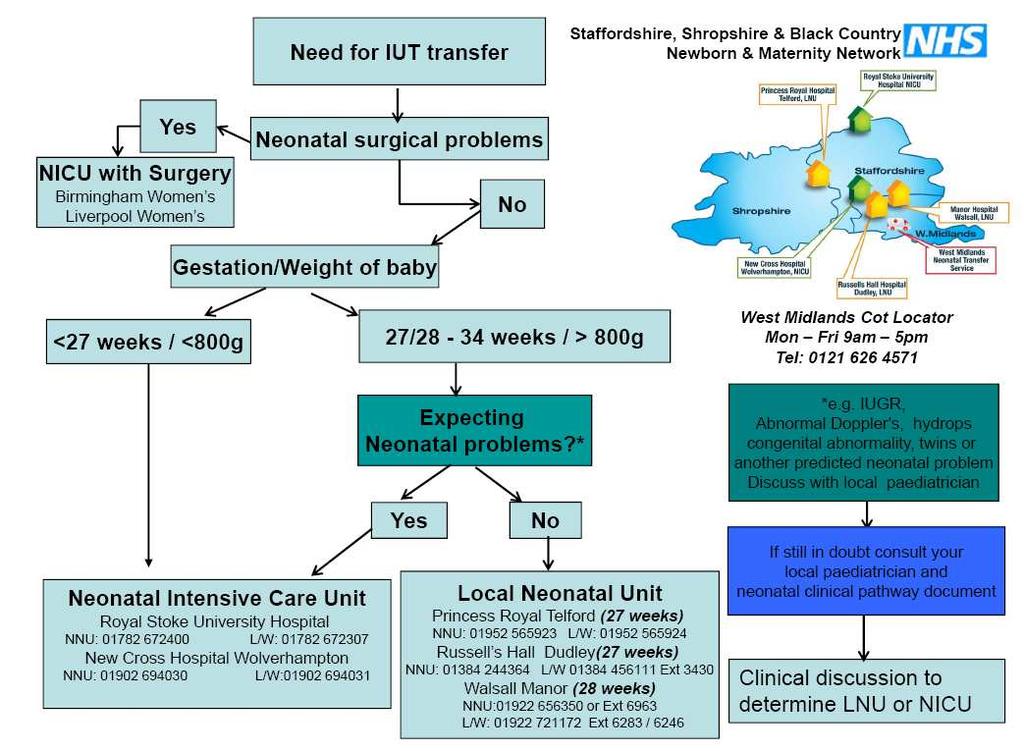
26 Appendix C Staffordshire, Shropshire & Black Country Newborn and Maternity Network Repatriation Policy 1. The Staffordshire, Shropshire & Black Country Newborn and Maternity Network (SBCNMN) was established to facilitate the neonatal service providers in the network to work collectively to provide the right level of care for the right baby in the right hospital at the right time. The ultimate aim is to keep babies within the network as close to home as clinically appropriate. 2. There are three types of neonatal unit with the following designations; a. Neonatal Intensive Care Units (NICU) b. Local Neonatal Units (LNU) c. Special Care Units (SCU) 3. The neonatal units in SSBCNMN have the following designation: a. Royal Stoke University Hospital, University Hospital of North Midlands NHS Trust NICU (All gestations) b. Royal Wolverhampton Hospital NHS Trust NICU (All gestations) c. Shrewsbury and Telford Hospitals NHS Trust LNU (27 weeks and above) d. Dudley Group of Hospitals NHS Foundation Trust LNU (27 weeks and above) e. Walsall Healthcare NHS Trust LNU (28 weeks and above) 4. Babies who require a higher level of care than is available at their place of delivery (SCU/LNU) are routinely transferred to the Local Neonatal Unit (LNU) or Neonatal Intensive Care Unit (NICU) in order to receive either High Dependency (HD) or Intensive care (IC) as appropriate to their level of care needs. However, once they are well enough they should be repatriated to their place of booking (SCU/LNU) for ongoing management and preparation for discharge. 5. One of the challenges in running a network of units providing different levels of care for babies is the refusal by parents to repatriate their baby(s) to their place of booking once they no longer require the IC/HD level of care. As a result of this, the cot capacities in the NICU and LNU are compromised by babies occupying IC/HD cots when they no longer require this level of care. 6. Given the constraints with the resources, the network needs to ensure that the cot capacity is maintained for the most vulnerable and sick babies in the NICUs and LNUs. Babies need to be repatriated to their LNU/SCBU as soon as they are well enough to do so. There is no parental choice in this matter. 7. In order to work effectively as a network and ensure there is the capacity to accommodate network babies the proposed algorithm and escalation pathway shown in Figure 1 will be followed. 8. Parents will be informed about the pathway of care in the antenatal period and again on admission to the neonatal unit. 9. An Information Leaflet is available to inform pregnant women about how neonatal services are organised within SSBCNMN. 10. Routine isolation practice should be reviewed by each unit to ensure this is not an obstacle to repatriation of babies with no known colonisation of organisms. 11. West Midlands Neonatal Transfer Service has developed the Repatriation Without Parental Assent Policy to facilitate repatriations within SSBCNMN. See Appendix 1. 26
27 Figure 1. Algorithm for the repatriation of babies to their LNU/SCBU following in-utero or ex-utero transfer Antenatal Period All women are to be given network information about how neonatal services are organised and the care pathways in the network. Where possible all ELBW (<800gms) referrals into NICUs should be in utero. Where transfer is ex utero there must be case review at network level (BAPM 2014). The LNU/SCU where the ELBW baby was born should include this in the unit s monthly collated exception report to the network. In Utero Transfers When the baby is delivered, the admitting unit will notify and update their local unit on the status of the baby. On Admission to the NNU All Parents to be given the leaflet on the network pathway and repatriation policy to ensure cot capacity for vulnerable and sick babies. This should be documented and signed in the Parent Passport. Daily review of the baby to ensure baby is repatriated to their LNU/SCBU as soon as it is safe to do so. Parents made aware of this. NICU/LNU updates the LNU/SCBU daily on the baby s progress and anticipated timeframe for repatriation. Parents made aware of this. Receiving LNU/SCBU should have these babies in their workbook and make all efforts to repatriate them as soon as clinically appropriate. If the baby has not been repatriated within 48hrs after the initial request, this should be escalated to both unit managers and included in the unit s monthly exception report to the network. If babies are not repatriated within 5 days from the initial request the network should be informed via telephone call and confirmed in an with the reason for this delay. Escalation to both unit managers and the network should be via a telephone call and confirmed with an . Network Office Tel: (Answerphone available out of office hours) Network Manager ruth.moore2@nhs.net Reference: BAPM, 2014, Optimal Arrangements for Neonatal Intensive Care Unit in the UK including guidance on their Medical Staffing: A Framework for Practice 27
28 Appendix 1 West Midlands Neonatal Transfer Service - Repatriation Without Parental Assent Policy INSERT LINK TO POLICY HERE 28

29 Appendix D 29

30 30
2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) E8a SSNDS 23
 E8a SSNDS 23") E8a 2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No. Service
E8a 2012/13 NHS STANDARD CONTRACT FOR ACUTE, AMBULANCE, COMMUNITY AND MENTAL HEALTH AND LEARNING DISABILITY SERVICES (MULTILATERAL) SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No. Service
SCHEDULE 2 THE SERVICES. A. Service Specifications
 Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E08/S/a Neonatal Critical Care (Intensive Care, HDU
Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E08/S/a Neonatal Critical Care (Intensive Care, HDU
CYMRU INTER HOSPITAL ACUTE NEONATAL TRANSFER SERVICE - NORTH WALES
 CYMRU INTER HOSPITAL ACUTE NEONATAL TRANSFER SERVICE - NORTH WALES STANDARD OPERATING PROCEDURES Ysbyty Glan Clwyd Telephone No: 01745 534686 Fax No: 01745 534681 Date: June 2015 Authors: Neonatal Transport
CYMRU INTER HOSPITAL ACUTE NEONATAL TRANSFER SERVICE - NORTH WALES STANDARD OPERATING PROCEDURES Ysbyty Glan Clwyd Telephone No: 01745 534686 Fax No: 01745 534681 Date: June 2015 Authors: Neonatal Transport
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Carol Jackson Cheshire and Merseyside Neonatal Network Nurse Consultant for Neonatal Transport
 Carol Jackson Cheshire and Merseyside Neonatal Network Nurse Consultant for Neonatal Transport Transport Service Facilities 1. Access to 24/7 Cheshire and Merseyside Perinatal Cot Bureau and Data Management
Carol Jackson Cheshire and Merseyside Neonatal Network Nurse Consultant for Neonatal Transport Transport Service Facilities 1. Access to 24/7 Cheshire and Merseyside Perinatal Cot Bureau and Data Management
North West London Perinatal Network (NWLPODN) Induction Package. NWLPODN March
 Induction Package. NWLPODN March") North West London Perinatal Network (NWLPODN) Induction Package NWLPODN March 2015 1 Introduction This package is for staff working within the 7 NWLPODN hospitals: To explain how the NWLPODN functions
North West London Perinatal Network (NWLPODN) Induction Package NWLPODN March 2015 1 Introduction This package is for staff working within the 7 NWLPODN hospitals: To explain how the NWLPODN functions
Discharge Care Pathway for Infants from Neonatal Unit, CAH
 Title: Author: Designation: Speciality / Division: CLINICAL GUIDELINES ID TAG Discharge care pathway for infants from the neonatal unit, Craigavon Area Hospital Una Toland Lead Nurse for Neonatal Services,
Title: Author: Designation: Speciality / Division: CLINICAL GUIDELINES ID TAG Discharge care pathway for infants from the neonatal unit, Craigavon Area Hospital Una Toland Lead Nurse for Neonatal Services,
Managing Emergency Pressures Within The Neonatal Unit. Escalation Policy. V3
 Managing Emergency Pressures Within The Neonatal Unit. Escalation Policy. V3 Lead Person(s) : Ian MacLennan, Nurse Manager. Centre : Women and Children s First developed : March 2012 Last updated : March
Managing Emergency Pressures Within The Neonatal Unit. Escalation Policy. V3 Lead Person(s) : Ian MacLennan, Nurse Manager. Centre : Women and Children s First developed : March 2012 Last updated : March
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
MIDWIFE AND HEALTH VISITOR COMMUNICATION PROCEDURE
 Appendix 2a of the Health Visiting Overarching Policy MIDWIFE AND HEALTH VISITOR COMMUNICATION PROCEDURE 1. Introduction 1.1. This procedure sets out standards of best practice regarding communication
Appendix 2a of the Health Visiting Overarching Policy MIDWIFE AND HEALTH VISITOR COMMUNICATION PROCEDURE 1. Introduction 1.1. This procedure sets out standards of best practice regarding communication
^Çãáëëáçå=íç=íÜÉ=kÉçå~í~ä=råáí==
 tljbkûpeb^iqe j^qbokfqvrkfq ^ÇãáëëáçåíçíÜÉkÉçå~í~äråáí ^ãéåçãéåíë Date Page(s) Comments Approved by July 2012 Whole Document Document Reviewed Women s Health Guidelines Group Jan 2013 Admission to SCU
tljbkûpeb^iqe j^qbokfqvrkfq ^ÇãáëëáçåíçíÜÉkÉçå~í~äråáí ^ãéåçãéåíë Date Page(s) Comments Approved by July 2012 Whole Document Document Reviewed Women s Health Guidelines Group Jan 2013 Admission to SCU
West Midlands Maternity and Children s Strategic Clinical Network. Maternity Bereavement Services Audit
 West Midlands Maternity and Children s Strategic Clinical Network Maternity Bereavement Services Audit Alison Davies, Quality Improvement Lead March 2015 Contents Page Background 3 Aim 3 Approach 3 Audit
West Midlands Maternity and Children s Strategic Clinical Network Maternity Bereavement Services Audit Alison Davies, Quality Improvement Lead March 2015 Contents Page Background 3 Aim 3 Approach 3 Audit
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
Criteria for Registration in Paediatric Neonatology
 Criteria for Registration in Paediatric Neonatology Any doctor can request to be registered in Paediatric Neonatology if he/she fulfils ALL the following requirements: 1. A recognised basic medical degree
Criteria for Registration in Paediatric Neonatology Any doctor can request to be registered in Paediatric Neonatology if he/she fulfils ALL the following requirements: 1. A recognised basic medical degree
Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014
 Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014") + Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014 Northern Michigan Perinatal Summit July 23, 2014 Tulika Bhattacharya, CON Michigan
+ Certificate of Need (CON) Review Standards for NICU Beds & Special Newborn Nursery Services Effective March 3, 2014 Northern Michigan Perinatal Summit July 23, 2014 Tulika Bhattacharya, CON Michigan
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Clinical Director for Women s and Children s Directorate
 FEEDING PRETERM AND SMALL FOR GESTATIONAL AGE INFANTS ON THE POSTNATAL WARD CLINICAL GUIDELINES Register No: 08094 Status: Public Developed in response to: Contributes to CQC Regulation 9,11 Intrapartum
FEEDING PRETERM AND SMALL FOR GESTATIONAL AGE INFANTS ON THE POSTNATAL WARD CLINICAL GUIDELINES Register No: 08094 Status: Public Developed in response to: Contributes to CQC Regulation 9,11 Intrapartum
Congenital Heart Disease Services
 Congenital Heart Disease Services We are changing the way care is delivered across the North West of England, North Wales and Isle of Man for people living with congenital heart disease. Please read below
Congenital Heart Disease Services We are changing the way care is delivered across the North West of England, North Wales and Isle of Man for people living with congenital heart disease. Please read below
Consulted With Post/Committee/Group Date Dr Agrawal
 DRUG AND ALCOHOL MISUSE IN PREGNANCY CLINICAL GUIDELINES Register No: 06056 Status: Public Developed in response to: Contributes to CQC Outcome 4 Intrapartum NICE Guidelines RCOG guideline Consulted With
DRUG AND ALCOHOL MISUSE IN PREGNANCY CLINICAL GUIDELINES Register No: 06056 Status: Public Developed in response to: Contributes to CQC Outcome 4 Intrapartum NICE Guidelines RCOG guideline Consulted With
Acutely ill patients in hospital
 Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Karen King (Link) Kathleen Hamblin Carole McBurnie Frances Wright Joyce Linton Catriona Thomson
 Kathleen Hamblin Carole McBurnie Frances Wright Joyce Linton Catriona Thomson") Name of Local Supervising Authority: Dumfries and Galloway Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising
Name of Local Supervising Authority: Dumfries and Galloway Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising
PIPER. Defined transfer (Time Critical Newborn)
") PIPER Paediatric Infant Perinatal Emergency Retrieval Defined transfer (Time Critical Newborn) Review date: June 2018 1 P a g e Defined transfer (Time Critical Newborn) Retrieval System Paediatric Infant
PIPER Paediatric Infant Perinatal Emergency Retrieval Defined transfer (Time Critical Newborn) Review date: June 2018 1 P a g e Defined transfer (Time Critical Newborn) Retrieval System Paediatric Infant
KIDS INTENSIVE CARE & DECISION SUPPORT (KIDS) & NEONATAL TRANSFER SERVICE (NTS)
 & NEONATAL TRANSFER SERVICE (NTS)") KIDS INTENSIVE CARE & DECISION SUPPORT (KIDS) & NEONATAL TRANSFER SERVICE (NTS) KIDS-NTS SERVICE DESCRIPTION & OPERATIONAL OVERVIEW Alex Philpott Sanjay Revanna V1 November 2017 Next Review November 2018
KIDS INTENSIVE CARE & DECISION SUPPORT (KIDS) & NEONATAL TRANSFER SERVICE (NTS) KIDS-NTS SERVICE DESCRIPTION & OPERATIONAL OVERVIEW Alex Philpott Sanjay Revanna V1 November 2017 Next Review November 2018
PROTOCOL FOR UNIVERSAL ANTENATAL CONTACT (FOR USE BY HEALTH VISITING TEAMS)
") Scope - CP12 PROTOCOL FOR UNIVERSAL ANTENATAL CONTACT (FOR USE BY HEALTH VISITING TEAMS) RATIONALE The Healthy Child Programme Pregnancy and the first five years of life (DH, 2009) states that health professionals,
Scope - CP12 PROTOCOL FOR UNIVERSAL ANTENATAL CONTACT (FOR USE BY HEALTH VISITING TEAMS) RATIONALE The Healthy Child Programme Pregnancy and the first five years of life (DH, 2009) states that health professionals,
The New NCCMDS, Neonatal HRGs 2016 and Reference Costs. A Guide for Clinicians
 The New NCCMDS, Neonatal HRGs 2016 and Reference Costs A Guide for Clinicians Aim To help clinicians involved in neonatal care to understand the changes that have taken place to the NCCMDS dataset the
The New NCCMDS, Neonatal HRGs 2016 and Reference Costs A Guide for Clinicians Aim To help clinicians involved in neonatal care to understand the changes that have taken place to the NCCMDS dataset the
An improvement resource for neonatal care
 National Quality Board Edition 1, June 2018 Safe, sustainable and productive staffing An improvement resource for neonatal care This document was developed by NHS Improvement on behalf of the National
National Quality Board Edition 1, June 2018 Safe, sustainable and productive staffing An improvement resource for neonatal care This document was developed by NHS Improvement on behalf of the National
Specialised Services Service Specification. Adult Congenital Heart Disease
 Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
STUDENTS WELCOME TO YOUR PLACEMENT. On the. Neonatal Unit, RHCH
 STUDENTS WELCOME TO YOUR PLACEMENT On the Neonatal Unit, RHCH Dear Student Welcome to Hampshire Hospitals NHS Foundation Trust. We hope you find your placement at HHFT rewarding and enjoyable and your
STUDENTS WELCOME TO YOUR PLACEMENT On the Neonatal Unit, RHCH Dear Student Welcome to Hampshire Hospitals NHS Foundation Trust. We hope you find your placement at HHFT rewarding and enjoyable and your
CTG Interpretation Training: High Level Audit
 CTG Interpretation Training: High Level Audit West Midlands Maternity & Children s Strategic Clinical Network Alison Davies, Quality Improvement Lead March 2015 Background The West Midlands Strategic Clinical
CTG Interpretation Training: High Level Audit West Midlands Maternity & Children s Strategic Clinical Network Alison Davies, Quality Improvement Lead March 2015 Background The West Midlands Strategic Clinical
Critical Care in Obstetrics Guideline
 This is an official Northern Trust policy and should not be edited in any way Critical Care in Obstetrics Guideline Reference Number: NHSCT/12/515 Target audience: This guideline is directed to all obstetricians,
This is an official Northern Trust policy and should not be edited in any way Critical Care in Obstetrics Guideline Reference Number: NHSCT/12/515 Target audience: This guideline is directed to all obstetricians,
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines. Version 1.0
 South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines Version 1.0 Ratified: 28 th August 2018 Date for Review: 28 th August 2019 Suzanne.sweeney@uclpartners.com South London
South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines Version 1.0 Ratified: 28 th August 2018 Date for Review: 28 th August 2019 Suzanne.sweeney@uclpartners.com South London
Nenatal Simulation Programme & WONEP Network Study Days Princess Anne Hospital 2017
 Nenatal Simulation Programme & WONEP Network Study Days Princess Anne Hospital 2017 MPROvE NEONATAL SIMULATION PROGRAMME Dear Trainees, We would like to welcome you to the NNU at Princess Anne Hospital.
Nenatal Simulation Programme & WONEP Network Study Days Princess Anne Hospital 2017 MPROvE NEONATAL SIMULATION PROGRAMME Dear Trainees, We would like to welcome you to the NNU at Princess Anne Hospital.
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005
 Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Specialised Services Service Specification: Inherited Bleeding Disorders
 Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
South Central Neonatal Network
 South Central Neonatal Network Education and training strategy: Continuing education and professional development Authored by Sue Turrill, School of Healthcare, University of Leeds, February 2012 Final
South Central Neonatal Network Education and training strategy: Continuing education and professional development Authored by Sue Turrill, School of Healthcare, University of Leeds, February 2012 Final
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Indicator. unit. raw # rank. HP2010 Goal
 Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
Neonatal Intensive Care Unit (NICU) Level of Care Authorization and Reimbursement Policy
 Level of Care Authorization and Reimbursement Policy") In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
Mapping maternity services in Australia: location, classification and services
 Accessory publication Mapping maternity services in Australia: location, classification and services Caroline S. E. Homer 1,4 RM, MMedSci(ClinEpi), PhD, Professor of Midwifery Janice Biggs 2 BA(Hons),
Accessory publication Mapping maternity services in Australia: location, classification and services Caroline S. E. Homer 1,4 RM, MMedSci(ClinEpi), PhD, Professor of Midwifery Janice Biggs 2 BA(Hons),
Medical Training Initiative Post Neonatal Fellow with specialist interest in Neonatal Retrieval. Job Description Lead Clinician Dr Joanna Behrsin
 Leicester Royal Infirmary, University Hospitals of Leicester NHS Trust Medical Training Initiative Post Neonatal Fellow with specialist interest in Neonatal Retrieval. Job Description Lead Clinician Dr
Leicester Royal Infirmary, University Hospitals of Leicester NHS Trust Medical Training Initiative Post Neonatal Fellow with specialist interest in Neonatal Retrieval. Job Description Lead Clinician Dr
Catherine Hughson Kathryn Kearney Number of supervisors relinquishing role since last report:
 Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Preparing and Registering S.T.A.B.L.E. Support Instructors
 Preparing and Registering S.T.A.B.L.E. Support Instructors If a person is unable to attend an official National or Private Instructor course, but they wish to co-teach a S.T.A.B.L.E. Learner course with
Preparing and Registering S.T.A.B.L.E. Support Instructors If a person is unable to attend an official National or Private Instructor course, but they wish to co-teach a S.T.A.B.L.E. Learner course with
Advanced Training Skills Module - Labour Ward Lead August Labour Ward Lead
 Labour Ward Lead The labour ward is an area of complexity within any hospital. At any time there may be women experiencing normal childbirth, as well as others, fortunately fewer in number, who may be
Labour Ward Lead The labour ward is an area of complexity within any hospital. At any time there may be women experiencing normal childbirth, as well as others, fortunately fewer in number, who may be
PROTOCOL FOR DISCHARGING A BABY
 PROTOCOL FOR DISCHARGING A BABY Parents of babies who stay on the neonatal unit are fully supported during their baby s admission and the unit promotes a philosophy of family-centred care. Families often
PROTOCOL FOR DISCHARGING A BABY Parents of babies who stay on the neonatal unit are fully supported during their baby s admission and the unit promotes a philosophy of family-centred care. Families often
Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience.
 Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience. Jo Maitland Perinatal Mental Health Training & Service Development Lead 5 Year Forward View Community
Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience. Jo Maitland Perinatal Mental Health Training & Service Development Lead 5 Year Forward View Community
Pregnancy Information Sharing Pathway for Safeguarding Children (Midwifery, Health Visiting and Primary Care)
") Pregnancy Information Sharing Pathway for Safeguarding Children (Midwifery, Health Visiting and Primary Care) July 2010 Originator: Women and Child Health /Primary Care/Safeguarding Team Submitted by:
Pregnancy Information Sharing Pathway for Safeguarding Children (Midwifery, Health Visiting and Primary Care) July 2010 Originator: Women and Child Health /Primary Care/Safeguarding Team Submitted by:
Perinatal Designation Matrix 3/21/07
 Codes: N = Neonatal Criteria M= Maternal Criteria P= Perinatal Criteria (both N & P) Perinatal Designation Matrix 3/21/07 Service/ 1. (N) Minimum NICU bed capacity Minimum of 10 NICU beds. Minimum of 15
Codes: N = Neonatal Criteria M= Maternal Criteria P= Perinatal Criteria (both N & P) Perinatal Designation Matrix 3/21/07 Service/ 1. (N) Minimum NICU bed capacity Minimum of 10 NICU beds. Minimum of 15
Burton Hospitals NHS Foundation Trust. On: 24 October Review Date: October Corporate / Directorate. Clinical / Non Clinical
 POLICY DOCUMENT Burton Hospitals NHS Foundation Trust DISCHARGE POLICY Approved by: Trust Executive Committee On: 24 October 2017 Review Date: October 2020 Corporate / Directorate Clinical / Non Clinical
POLICY DOCUMENT Burton Hospitals NHS Foundation Trust DISCHARGE POLICY Approved by: Trust Executive Committee On: 24 October 2017 Review Date: October 2020 Corporate / Directorate Clinical / Non Clinical
SBAR Report phase 1 Maternity, Gynaecology & Neonatal services
 North Wales Maternity, Gynaecology, Neonatal and Paediatric service review SBAR Report phase 1 Maternity, Gynaecology & Neonatal services Situation The Minister for Health and Social Services has established
North Wales Maternity, Gynaecology, Neonatal and Paediatric service review SBAR Report phase 1 Maternity, Gynaecology & Neonatal services Situation The Minister for Health and Social Services has established
Examination of the Newborn by Registered Midwives Protocol (CG484)
") Examination of the Newborn by Registered Midwives Protocol (CG484) Approval and Authorisation Approved by Maternity Clinical Governance Committee Job Title or Chair of Committee Chair, Maternity Clinical
Examination of the Newborn by Registered Midwives Protocol (CG484) Approval and Authorisation Approved by Maternity Clinical Governance Committee Job Title or Chair of Committee Chair, Maternity Clinical
Trust Guideline for the Management of Postnatal Care: Planning, Information and Discharge Guideline
 Trust Guideline for the Management of Postnatal Care: Planning, A Clinical Guideline recommended for use In: Women s health - Obstetrics By: For: Key words: Written by: Obstetricians, Midwives, Paediatricians
Trust Guideline for the Management of Postnatal Care: Planning, A Clinical Guideline recommended for use In: Women s health - Obstetrics By: For: Key words: Written by: Obstetricians, Midwives, Paediatricians
SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Staffordshire, Shropshire & Black Country Newborn Network
 SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Staffordshire, Shropshire & Black Country Newborn Network TRANSPORT USER GROUP Minutes of meeting held on Friday
SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Staffordshire, Shropshire & Black Country Newborn Network TRANSPORT USER GROUP Minutes of meeting held on Friday
Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and
 Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and Wales NHS England INFORMATION READER BOX Directorate
Management of surge and escalation in critical care services: standard operating procedure for Adult and Paediatric Burn Care Services in England and Wales NHS England INFORMATION READER BOX Directorate
Services for People with Stroke (Acute Phase) & TIA
 & TIA") West Midlands Partnership of Cardiac and Stroke Networks Services for People with Stroke (Acute Phase) & TIA West Midlands Overview Report Report Date: March 2011 Visit Dates: May to November 2010 Images
West Midlands Partnership of Cardiac and Stroke Networks Services for People with Stroke (Acute Phase) & TIA West Midlands Overview Report Report Date: March 2011 Visit Dates: May to November 2010 Images
SuRNICC Full Business Case. Benefits Realisation Strategy and Framework
 SuRNICC Full Business Case Benefits Realisation Strategy and Framework Purpose The purpose of this document is to set out the arrangements for the identification of potential benefits, their planning,
SuRNICC Full Business Case Benefits Realisation Strategy and Framework Purpose The purpose of this document is to set out the arrangements for the identification of potential benefits, their planning,
The specification includes conditions which are diagnosed antenatally for which surgical intervention is required.
 E02/S/c 2013/14 NHS STANDARD CONTRACT FOR PAEDIATRIC SURGERY: NEONATES SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review
E02/S/c 2013/14 NHS STANDARD CONTRACT FOR PAEDIATRIC SURGERY: NEONATES SECTION B PART 1 - SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review
JOB DESCRIPTION Safe, compassionate, effective care provided to our communities with a transparent, open approach.
 JOB DESCRIPTION Safe, compassionate, effective care provided to our communities with a transparent, open approach. JOB TITLE: GRADE: BASE: MANAGED BY: Advanced Neonatal Nurse Practitioner Band 8a Homerton
JOB DESCRIPTION Safe, compassionate, effective care provided to our communities with a transparent, open approach. JOB TITLE: GRADE: BASE: MANAGED BY: Advanced Neonatal Nurse Practitioner Band 8a Homerton
M: Maternal/ Newborn Care
 M: Maternal/ Newborn Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 113 Competency: M-1 Maternal/Newborn Nursing M-1-1 M-1-2 M-1-3 Demonstrate knowledge
M: Maternal/ Newborn Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 113 Competency: M-1 Maternal/Newborn Nursing M-1-1 M-1-2 M-1-3 Demonstrate knowledge
TRUST POLICY FOR THE MANAGEMENT OF CHILDREN, YOUNG PEOPLE AND NEONATES WHO ARE NOT BROUGHT FOR THEIR APPOINTMENTS. Status. Final
 TRUST POLICY FOR THE MANAGEMENT OF CHILDREN, YOUNG PEOPLE AND NEONATES WHO ARE NOT BROUGHT FOR THEIR APPOINTMENTS Reference Number Version: Status Author: POL-CL/ 1887/2011 V2 Final Jane O Daly- CLCHPROT/2011/036
TRUST POLICY FOR THE MANAGEMENT OF CHILDREN, YOUNG PEOPLE AND NEONATES WHO ARE NOT BROUGHT FOR THEIR APPOINTMENTS Reference Number Version: Status Author: POL-CL/ 1887/2011 V2 Final Jane O Daly- CLCHPROT/2011/036
Palliative care (supportive and end of life care) A framework for clinical practice in Perinatal medicine
 A framework for clinical practice in Perinatal medicine") British Association of Perinatal Medicine Working group report Palliative care (supportive and end of life care) A framework for clinical practice in Perinatal medicine Palliative care for [fetus, neonate
British Association of Perinatal Medicine Working group report Palliative care (supportive and end of life care) A framework for clinical practice in Perinatal medicine Palliative care for [fetus, neonate
Wiltshire Safeguarding Children Board Multi agency Pre-birth Protocol to Safeguard Unborn Babies. December 2015
 Wiltshire Safeguarding Children Board Multi agency Pre-birth Protocol to Safeguard Unborn Babies December 2015 1 List of Contents Introduction 3 Risk Factors 4 Early Intervention and Common Assessment
Wiltshire Safeguarding Children Board Multi agency Pre-birth Protocol to Safeguard Unborn Babies December 2015 1 List of Contents Introduction 3 Risk Factors 4 Early Intervention and Common Assessment
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50
 Acutely ill adults in hospital: recognising and responding to deterioration Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50 NICE 2018. All rights reserved. Subject to Notice of rights
Acutely ill adults in hospital: recognising and responding to deterioration Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50 NICE 2018. All rights reserved. Subject to Notice of rights
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Outline. Case 1. Progress 4/23/2013. From hospital to hospice or home How the neonatal team can enable palliative care
 Outline From hospital to hospice or home How the neonatal team can enable palliative care Dr Sharon English Lead Clinician Neonatal Services Leeds Teaching Hospitals NHS Trust Case stories Background Practicalities
Outline From hospital to hospice or home How the neonatal team can enable palliative care Dr Sharon English Lead Clinician Neonatal Services Leeds Teaching Hospitals NHS Trust Case stories Background Practicalities
Obstetric, Maternity and Gynaecology Services
 Action Plan Arising from RCPCH Evaluation Recommendation Obstetric, Maternity and Gynaecology Services Strategy and Patient safety 1 Expedite the Phase Two business case and commence development to provide
Action Plan Arising from RCPCH Evaluation Recommendation Obstetric, Maternity and Gynaecology Services Strategy and Patient safety 1 Expedite the Phase Two business case and commence development to provide
Neonatal Complex and Palliative Care
 1 Neonatal Complex and Palliative Care Alex Mancini Pan London Lead Nurse for Neonatal Palliative 2018 Training Workshops Alexandra.mancini@chelwest.nhs.uk www.londonneonatalnetwork.org.uk 2 Growing challenge
1 Neonatal Complex and Palliative Care Alex Mancini Pan London Lead Nurse for Neonatal Palliative 2018 Training Workshops Alexandra.mancini@chelwest.nhs.uk www.londonneonatalnetwork.org.uk 2 Growing challenge
Review of Stroke (Acute Phase) & TIA Services
 & TIA Services") West Midlands Partnership of Cardiac and Stroke Networks Review of Stroke (Acute Phase) & TIA Services Report Date: June 2011 Visit Dates: May to November 2010 Images courtesy of The Stroke Association,
West Midlands Partnership of Cardiac and Stroke Networks Review of Stroke (Acute Phase) & TIA Services Report Date: June 2011 Visit Dates: May to November 2010 Images courtesy of The Stroke Association,
SHREWSBURY AND TELFORD HOSPITAL NHS TRUST Training guideline (Includes the Training Needs Analysis as an Appendix)
") SHREWSBURY AND TELFORD HOSPITAL NHS TRUST Training guideline (Includes the Training Needs Analysis as an Appendix) Lead Person : Angela Hughes Lead Midwife for Clinical Education Division : 2 Implemented
SHREWSBURY AND TELFORD HOSPITAL NHS TRUST Training guideline (Includes the Training Needs Analysis as an Appendix) Lead Person : Angela Hughes Lead Midwife for Clinical Education Division : 2 Implemented
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification. 12 months
 E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
April 23, 2014 Ohio Department of Health Regulations and Noncompliance Findings
 April 23, 2014 Ohio Department of Health Regulations and Noncompliance Findings Shannon Richey, R.N. Assistant Bureau Chief Bureau of Community Health Care Facilities and Services Ohio Department of Health
April 23, 2014 Ohio Department of Health Regulations and Noncompliance Findings Shannon Richey, R.N. Assistant Bureau Chief Bureau of Community Health Care Facilities and Services Ohio Department of Health
The Makings of a Small Baby Unit. Objectives. What s the big deal? 9/28/16
 The Makings of a Small Baby Unit Anamika B. Mukherjee, MD, MS Assistant Professor of Pediatrics Loma Linda Children s Hospital Division of Neonatology September 28, 2016 Objectives What is a Small Baby
The Makings of a Small Baby Unit Anamika B. Mukherjee, MD, MS Assistant Professor of Pediatrics Loma Linda Children s Hospital Division of Neonatology September 28, 2016 Objectives What is a Small Baby
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
British Association of Perinatal Medicine. A Framework for Neonatal Transitional Care. October 2017
 British Association of Perinatal Medicine A Framework for Neonatal Transitional Care October 2017 Executive Summary Keeping mothers and babies together should be the cornerstone of newborn care. Neonatal
British Association of Perinatal Medicine A Framework for Neonatal Transitional Care October 2017 Executive Summary Keeping mothers and babies together should be the cornerstone of newborn care. Neonatal
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Visiting Professional Programme: Neonatal ICU
 Visiting Professional Programme: Neonatal ICU 1 Introduction The Guy s and St Thomas NHS Foundation Trust Neonatal ICU Visiting Professional Programme (VPP) is designed to provide international visiting
Visiting Professional Programme: Neonatal ICU 1 Introduction The Guy s and St Thomas NHS Foundation Trust Neonatal ICU Visiting Professional Programme (VPP) is designed to provide international visiting
Access to Public Information Response
 Access to Public Information Response December 24 th 2016 REQUEST UNDER THE CODE OF PRACTICE FOR ACCESS TO PUBLIC INFORMATION Request sent on December 24 th 2016: I am making a request under the Code of
Access to Public Information Response December 24 th 2016 REQUEST UNDER THE CODE OF PRACTICE FOR ACCESS TO PUBLIC INFORMATION Request sent on December 24 th 2016: I am making a request under the Code of
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
BASIC STANDARDS FOR SUBSPECIALTY FELLOWSHIP TRAINING IN NEONATAL MEDICINE
 BASIC STANDARDS FOR SUBSPECIALTY FELLOWSHIP TRAINING IN NEONATAL MEDICINE American Osteopathic Association and American College of Osteopathic Pediatricians TABLE OF CONTENTS 1 Article I. Introduction...
BASIC STANDARDS FOR SUBSPECIALTY FELLOWSHIP TRAINING IN NEONATAL MEDICINE American Osteopathic Association and American College of Osteopathic Pediatricians TABLE OF CONTENTS 1 Article I. Introduction...
Wolverhampton s 0-19 Healthy Child Programme
 Wolverhampton s 0-19 Healthy Child Programme Consultation document for a proposed new service model Public Health and Well-being August 2016 Wolverhampton s Healthy Child Programme Consultation Document
Wolverhampton s 0-19 Healthy Child Programme Consultation document for a proposed new service model Public Health and Well-being August 2016 Wolverhampton s Healthy Child Programme Consultation Document
NCEPOD On the Right Trach?
 NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
Key findings from the Healthwatch network
 BRIEF ING Maternity Services Key findings from the Healthwatch network Local Healthwatch are independent organisations working across all 152 local authorities in England and give communities a stronger
BRIEF ING Maternity Services Key findings from the Healthwatch network Local Healthwatch are independent organisations working across all 152 local authorities in England and give communities a stronger
Register No: Status: Public
 ADMINISTRATION OF VITAMIN K FOR NEONATES CLINICAL GUIDELINES Register No: 08095 Status: Public Developed in response to: Contributes to CQC Outcome 11,12 Intrapartum NICE Guidelines CNST Requirement Consulted
ADMINISTRATION OF VITAMIN K FOR NEONATES CLINICAL GUIDELINES Register No: 08095 Status: Public Developed in response to: Contributes to CQC Outcome 11,12 Intrapartum NICE Guidelines CNST Requirement Consulted
Neonatal Implementation. TRANSPORT PATHWAYS (Logistics)
") Neonatal Implementation TRANSPORT PATHWAYS (Logistics) The plan is to transfer the longer term and complex neonatal intensive care to the Neonatal Intensive Care Unit (NICU) in Arrowe Park from January
Neonatal Implementation TRANSPORT PATHWAYS (Logistics) The plan is to transfer the longer term and complex neonatal intensive care to the Neonatal Intensive Care Unit (NICU) in Arrowe Park from January
CERTIFICATE OF NEED Department Staff Project Summary, Analysis & Recommendations Maternal and Child Health Services
 CERTIFICATE OF NEED Department Staff Project Summary, Analysis & Recommendations Maternal and Child Health Services Name of Facility: Our Lady of Lourdes Medical CN# FR 140701-04-01 Center Name of Applicant:
CERTIFICATE OF NEED Department Staff Project Summary, Analysis & Recommendations Maternal and Child Health Services Name of Facility: Our Lady of Lourdes Medical CN# FR 140701-04-01 Center Name of Applicant:
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Local Maternity System Board Plan
 Local Maternity System Board Plan Fay Baillie on behalf of the Herefordshire & Worcestershire LMS Board September 2017 1 Executive Summary The birth of a child should be a wonderful, life changing time
Local Maternity System Board Plan Fay Baillie on behalf of the Herefordshire & Worcestershire LMS Board September 2017 1 Executive Summary The birth of a child should be a wonderful, life changing time
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Advance Care Plan for a Child or Young Person
 Advance Care Plan for a Child or Young Person West Midlands Paediatric Palliative Care Network NHS Number: Advance Care Plan for a Child or Young Person This document is a tool for discussing and communicating
Advance Care Plan for a Child or Young Person West Midlands Paediatric Palliative Care Network NHS Number: Advance Care Plan for a Child or Young Person This document is a tool for discussing and communicating
SOUTH CENTRAL NEONATAL NETWORK
 SOUTH CENTRAL NEONATAL NETWORK Audit of the current provision of education and training within the Neonatal South Central Network 1.0 Background The driving principles for the reform of the NHS education
SOUTH CENTRAL NEONATAL NETWORK Audit of the current provision of education and training within the Neonatal South Central Network 1.0 Background The driving principles for the reform of the NHS education
SCHEDULE 2 THE SERVICES. A. Service Specifications. E07/S/c Paediatric Long Term Ventilation
 Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Annie Hunter Head of Midwifery Isle of Wight NHS
 Annie Hunter Head of Midwifery Isle of Wight NHS The Isle of Wight has a population of 140,500, this doubles in the holiday season with the Island receiving approximately 2.8 million visitors each year.
Annie Hunter Head of Midwifery Isle of Wight NHS The Isle of Wight has a population of 140,500, this doubles in the holiday season with the Island receiving approximately 2.8 million visitors each year.
SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS
 SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS About The Chartis Group The Chartis Group is an advisory services firm that provides management consulting and applied research to
SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS About The Chartis Group The Chartis Group is an advisory services firm that provides management consulting and applied research to
1. CRITICAL CARE. Preamble. Adult and Pediatric Critical Care
 1. CRITICAL CARE Complete understanding of the following paragraphs is essential to appropriate billing of the critical care fees. Members of the team billing the Critical Care Payment Schedule can not
1. CRITICAL CARE Complete understanding of the following paragraphs is essential to appropriate billing of the critical care fees. Members of the team billing the Critical Care Payment Schedule can not
TFN Impact Report. MAITS (Multi-Agency International Training and Support)
") Name of your Organisation: Name of the project TFN funded: Date Funded by TFN: 6 July 2017 Were you able to undertake your project as planned? Can you describe and/or demonstrate the specific impact that
Name of your Organisation: Name of the project TFN funded: Date Funded by TFN: 6 July 2017 Were you able to undertake your project as planned? Can you describe and/or demonstrate the specific impact that
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,