WHO ANNUAL REPORT 2017 YEMEN
|
|
|
- Adam Thornton
- 5 years ago
- Views:
Transcription


1 WHO ANNUAL REPORT 2017 YEMEN
2 2 ANNUAL REPORT 2017 World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. [Title]. Cairo: WHO Regional Office for the Eastern Mediterranean; Licence: CC BYNC-SA 3.0 IGO. Sales, rights and licensing. To purchase WHO publications, see To submit requests for commercial use and queries on rights and licensing, see Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-partyowned component in the work rests solely with the user. General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.

3 WHO Annual Report 2017 YEMEN

4 4 ANNUAL REPORT 2017 Table of Contents Foreword Executive Summary Key figures on health in Yemen Part I. The Health Cluster Leading the response to rising health needs in Yemen Vulnerability rate increases in Yemen Strengthening WHO s Presence and support accross Yemen Building local capacity while supporting hospitals Ensuring access to priority health services Providing the essentials to keep health facilities running Part II. The Minimum Service Package (MSP): Lifeline for a rapidly collapsing health system Meeting a country s health needs through solid partnership Laying the foundation for tailored health service delivery Managing the medical side of malnutrition Maternal, newborn, child and adolescent health Combating communicable diseases Part III. Outbreak alert and response operations: Cholera and Diphtheria and other communicable diseases Cholera: The largest cholera outbreak in the world Diphtheria: Responding to a long forgotten disease Vector-borne diseases Neglected tropical diseases Emergency Operations Centres Rapid detection: Risk assessment and response Part IV. Managing the treatment of endemic and noncommunicable diseases Cancer: Care Crisis in Yemen The silent impact of war in Yemen Scaling up access to treatment for noncommunicable diseases Supporting trauma care and referral services Part V. Priority needs and gaps Financial overview

5 Credit: Sadeq Al-Wesabi 5


6 6 ANNUAL REPORT 2017 Foreword Dr Nevio Zagaria WHO Representative in Yemen As the war rages on in Yemen, it is the people of Yemen who suffer. The scale of this crisis is unimaginable. Almost three years of conflict have led to the world s largest food crisis, the world s worst cholera epidemic and the near collapse of the nation s health and social systems. The humanitarian situation is catastrophic and continues to deteriorate. This report presents the work done by WHO to support the delivery of preventive and curative health services in Yemen during 2017, in partnership with the Health Cluster and other partners. At the beginning of the year, WHO generated a vulnerability matrix at district levels to identify areas with the highest priority needs. The vulnerability matrix presented in detail in this report, was updated October 2017, following the revised Clusters indicators. The matrix was used to generate the health section of the Humanitarian Needs Overview (HNO). The trend analysis showed a serious deterioration of the situation between the beginning and the end of 2017, with an increase of districts categorized with very high and high vulnerabilities. A deteriorating situation, an innovative approach The situation on the ground has deteriorated across 2017 in terms of accessibility, commercial and humanitarian blockades in accessing the country, bureaucratic impediments in the importation of medical supplies, and in the logistics of their distribution across the country, difficult dialogue with the health authorities and other authorities at national and sub-national levels. In summary, it has been a very difficult year resulting in an increased number of Yemenis suffering, increased morbidity, disabilities, and mortality, particularly among the most vulnerable. Displaced people in Ibb governorate. Credit: Christine Cool

7 7 Dr Zagaria, visits a WHOsupported diarrhoea treatment centre in Sana a, Yemen Credit: Sadeq Al-Wesabi As WHO, during 2017, we did everything possible to address the health needs of the affected population, coordinating the Health Cluster partners in the scaling up of the health sector response. While continuing the preventive health interventions and the support to the tertiary hospitals at governorate levels, WHO developed, in consultation with health authorities and Health Cluster partners, a Minimum Service Package (MSP) to prioritize and standardize the health services on which to focus the scale up of the coverage at both primary (i.e. health centres and health units), and secondary (i.e. district hospitals) levels of care. We increased two and a half times over the funds utilized in 2017 as compared to 2016, and we have formulated the plan for a further substantial expansion in 2018, in order to match the increased health needs of the people of Yemen. All this has been possible thanks to the generous support provided by many donors and partners. Valuable health partnerships In this context, the innovative partnership signed with the World Bank by WHO and UNICEF in February 2017, and the following additional financial agreements focused on malnutrition and cholera responses, as well as the important financial resources made available for a three year period ( ), catalyzed a new way of working. Medium-term planning in a protracted humanitarian context, has made it possible to bridge the delivery of life saving interventions, with the delivery of basic health needs. In addition to this, noncommunicable diseases, which continue to plague Yemen, cannot remain neglected in a protracted crisis, in a country with a collapsing health system. Traditional humanitarian response operations alone will not be enough to alleviate the suffering and neither will the classic developmental approach. What started in 2017, is an embryonic new way of delivering health services in a protracted humanitarian crisis, that aligns the different funding streams based on one comprehensive strategic framework. At the center of this are humanitarian lifesaving interventions, and the basic health services needed as part of the population s right to health. As the WHO Representative in Yemen, I would like to continue to work during 2018 to further increase the support of the delivery of health services across Yemen, hoping the peace process can move forward. Only peace will bring a halt to the enormous suffering that the people of Yemen are experiencing. We will do all we can to relieve the suffering in this country and work towards peace.
8 8 ANNUAL REPORT 2017 Executive summary The World Health Organization (WHO) is leading the health response, ensuring access to life-saving health services. This report covers the WHO and health partners response to this humanitarian crisis from January to December 2017, and spans five crucial parts: the Health Cluster, the Minimum Service Package (MSP), the cholera and diphtheria outbreaks, managing the treatment of endemic and noncommunicable diseases and financial priority needs and gaps. Part 1: WHO supports health authorities and the Health Cluster Nearly 16.4 million people lack access to basic healthcare. To respond to this massive need, WHO, Health Cluster partners and other health sector actors are delivering health services to the people of Yemen despite the critical security situation, logistical difficulties and the collapsing health system. WHO and Health Cluster partners have scaled-up their presence to meet rising health needs, reaching 9.5 million beneficiaries in 2017 with preventive and curative interventions in health facilities and with 239 emergency medical mobile teams (EMMTs) out of a target set in the 2017 Humanitarian Response Plan of 10.4 million people. Part 2: The Minimum Service Package (MSP): Lifeline for a rapidly collapsing health system Far from the spotlight, thousands of people are dying as infectious and noncommunicable diseases continue to spread. More women are dying in childbirth. Those injured cannot receive appropriate surgical care due to lack of skilled surgeons in district hospitals. People with chronic diseases cannot access the treatment they need to stay alive. The Minimum Service Package (MSP), ensures access to basic health services, and covers priority services across the 8 health care components: general services and trauma care, reproductive/maternal and newborn health, child care, mental health and psychosocial support, nutrition, noncommunicable diseases, communicable diseases and environmental health in health facilities. Part 3: Outbreak alert and response: Cholera and Diphtheria and other communicable diseases WHO and partners scaled up the overall operational response to infectious disease outbreaks. This section illustrates the immediate upsurge in outbreak response activities. At the peak of the cholera outbreak, there were 229 Diarrhoea Treatment Centres (DTCs) with in-patient capacities, and Oral Rehydration Corners (ORCs) for early detection, treatment and referral of severe cholera cases. WHO supported the technical and operational work of the response, to contain outbreaks and build local capacity at governorate and district level health facilities and community levels. In particular, during this cholera outbreak response the establishment of rapid response teams (RRTs) across all 333 districts in Yemen took place, in order to be able to detect, assess, alert and respond to cholera and all other potential infectious disease outbreaks. For vector-borne diseases, WHO distributed of basic and supplementary malaria kits that can test patients for malaria and treat an estimated cases. 1.5 million bed nets were delivered to 76 districts in Yemen. In the area of neglected tropical diseases (NTDs), a treatment plan for onchocerciasis was devised for approximately more than half a million people eliminate the disease in affected areas and identify populations requiring treatment. For Leishmaniasis, WHO provided national health authorities with vials of stibogluconate (leishmaniasis drug) and leishmaniasis laboratory tests (i.e. rapid diagnostic tests). While for the treatment of Rabies, rabies vaccines were procured. Part 4: Managing the treatment of endemic and noncommunicable diseases There are new expected cancer patients per year out of which patients received some form of cancer treatment in The percentage of full treatment out of WHO s work in numbers 1500 tonnes of medicines and supplies delivered million litres of clean water provided to more than 100 health facilities million litres of fuel provided for health facility generators and ambulances 49 Health Cluster partners coordinated as part of emergency response

9 9 these patients, increased from 30% to 60% of full treatments, thanks to the donation of cancer treatment drugs from WHO in 2017 as compared to Part 5: Financial overview, priority needs and gaps The full list of our valued partners are located in the financial overview of this annual report. All of our generous donors have provided much of the financial resources needed by WHO to carry out health response activities in Acknowledging the magnitude and scale of this emergency as well as its associated vulnerabilities, the Humanitarian Country Team (HCT) launched the 2018 Yemen Humanitarian Response Plan (YHRP) to prioritize life-saving and protection response across the country, which include a targeted set of humanitarian-plus activities to ensure the delivery of essential services and livelihoods in the most affected areas in-country. The 2018 YHRP aims to assist 13.1 million people across the country and is seeking US$2.96 billion, a considerable increase from the US$2.2 billion sought after in 2017, which is a key indicator that the needs are still monumental even after In spite of serious challenges such as access restrictions by all parties to the conflict, including bureaucratic impediments, partners provided assistance that saved or improved the lives of more than 10 million people in With the continued support from our donors, the response to the crisis in 2017 will be even more robust in New ways of working and humanitarian access In light of the current economic crisis in Yemen, the commitment and support needed to find innovative and sustainable solutions for the payment of health workers and other civil servants is desperately needed. Without these real-life heroes, timely health service delivery would be impossible. The attacks on health facilities, patients and personnel must also be stopped. WHO has made a commitment to support the strengthening of Yemen s health system as part of rehabilitation and recovery efforts, for years to come. Credit: Sadeq Al-Wesabi emergency mobile medical teams in 3 governorates fixed health teams in 13 governorates surgical teams in 14 conflict-affected governorates therapeutic feeding centres in 10 priority governorates




10 10 ANNUAL REPORT 2017 Key facts on health in Yemen million people lack access to health services people have been injured or killed in the conflict health facilities have been partially damaged or destroyed








11 11 50% 50% of mortality is caused by communicable diseases, maternal, and poor nutritional conditions of health facilities are closed or only partially functioning 39% of mortality caused by noncommunicable diseases 350 out of every expected mothers die in childbirth
12 12 ANNUAL REPORT 2017 Part I: The Health Cluster
13

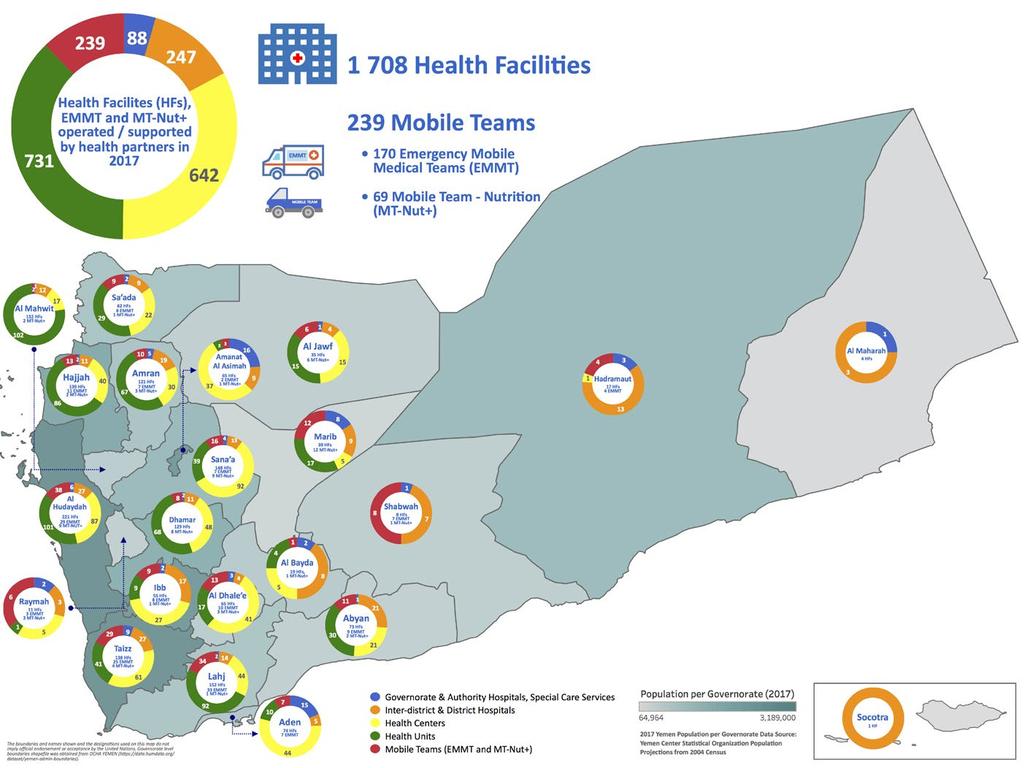
14 14 ANNUAL REPORT 2017 Leading the response to rising health needs in Yemen In emergencies, coordination is paramount. No one organization can respond to a health crisis alone. This is why the Health Cluster approach was used in Yemen to ensure effective emergency coordination since the very beginning of the crisis. The World Health Organization (WHO) is the Cluster Lead Agency supporting health authorities at central and at hub, and governorate levels by coordinating the efforts of all health response partners, which include international organizations (INGOs), national nongovernmental organizations (NNGOs), affected communities, specialized agencies, academic and training institutes, and UN agencies. The Health Cluster exists to relieve suffering and save lives in humanitarian emergencies, while advancing the well-being and dignity of affected populations. In Yemen, the health authorities, supported by the Cluster, coordinated the efforts of 20 International Non-Governmental (INGOs), 34 National Non- Governmental (NNGOs) and 7 UN agencies, who have been involved in the implementation of the health activities outlined in 2017 according to the health section of Yemen Humanitarian Response Plan (YHRP). Health Cluster partners were represented in 237 districts within all 22 governorates across Yemen. To ensure close and effective coordination of health activities across Yemen, subnational cluster coordination systems were established in five hubs: Aden, Hudaydah, Ibb, Sa ada and San a, with dedicated subnational cluster coordinators. By the end of December 2017, Health Cluster partners had successfully delivered health services benefitting 9.5 million people. In cooperation with health authorities, WHO reprioritized the response in the beginning of 2017, focusing on ensuring access to lifesaving health services in the most vulnerable districts, and scaling up the adoption of the Minimum Service Package (MSP), including the prevention and treatment of noncommunicable diseases. In 2017, the number of health facilities operated/ supported by Health Cluster partners across all 22 governorates was This included 88 governorate and authority hospitals as well as specialized hospitals, 247 district hospitals, 642 health centres and 731 health units, comprising a large volume of healthcare
 were also supported by partners.")
15 15 In 2017, Health Cluster partners delivered health services benefiting 9.5 million people Credit: Sadeq Al-Wesabi provision given that year. At least 239 mobile teams (170 Emergency Mobile Medical Teams and 69 Mobile Team Nutrition) were also supported by partners. More help needed to reach those in need To support Health Cluster partners in prioritizing their interventions, WHO carried out an in-depth analysis to determine, down to the district level, where needs were the greatest, generating a vulnerability matrix presented in the dedicated chapter of this report. In 2017, the Health Cluster aimed to reach 10.4 million people with life-saving health services. WHO is supporting its health partners in this endeavor, providing them with technical guidance, epidemiological data and medical supplies. However, many of the Organization s partners were constrained by a lack of funding. The Health Cluster received only 35.6% of total funds requested under the Yemen Humanitarian Response Plan for More resources are desperately needed to sustain the response to this ongoing crisis moving forward.

16 16 ANNUAL REPORT 2017 WHO s work in numbers consultations provided by WHO and partners disease alerts detected and investigated surgical interventions conducted by surgical teams million people reached by the Health Cluster Yemen's most vulnerable Disaster risk refers to the complex interaction between a hazard and the characteristics that make people and places vulnerable and exposed; and is affected by risk drivers such as poverty and inequality, urban and regional development, climate change and environmental degradation (UNISDR, 2015). An important aspect of understanding disaster risk is by acknowledging that a disaster is also an indicator of development failures (UNISDR, 2015). In the beginning of 2017, the World Health Organization (WHO) Country Office in Yemen generated the vulnerability matrix using the available data at district level from the following: hazards, the impact of these hazards on the exposed populations, health system capacities, morbidity of selected communicable diseases and other conditions, WASH, nutrition, and food security key clusters indicators, as well as social determinants and health outcomes. The vulnerability matrix has been used to identify districts with higher vulnerabilities and the main drivers of such local vulnerabilities, in order to prioritize both geographical areas, and health and non-health interventions. The table on the following page illustrates the differences in terms of the number of districts in the four categories of vulnerability, between the beginning and the end of Clearly the number of districts with higher vulnerabilities increased, as well the exposed populations, challenging the humanitarian response to cover larger geographical areas and higher number of beneficiaries. The vulnerability matrix also highlights the need of a multi-sectoral approach in delivering humanitarian interventions. *UNISDR (United Nations International Strategy for Disaster Reduction), Global Assessment Report on Disaster Risk Reduction million people live in 39 extremely and 86 highly vulnerable districts million live in 158 moderately vulnerable districts million people live in 50 districts that are deemed stable. (6 and 4,5 on the vulnerability scale). (2,3 on the vulnerability scale). (0,1 on the vulnerability scale).


17 million 99.7% million children vaccinated against polio severely malnourished children received treatment at WHO supported therapeutic feeding centres people treated for suspected cholera of people with suspected cholera who are able to access treatment are surviving This table illustrates the trends of the vulnerability matrix in terms of number of districts and their population across the 4 levels of vulnerability. Between February and November 2017, Yemen faced an important deterioration of the situation highlighted by the 21.3% increase of number of population leaving in the 125 districts with very high or high vulnerabilities. Vulnerability level Very high (6) # Districts # Population 2017 # Districts # Population High (5,4) Moderate (3,2) Low (1,0) Total February 2017 November

18 18 ANNUAL REPORT 2017 Strengthening WHO s presence and support across Yemen The Health Cluster response, though robust, is not enough for a crisis of this magnitude. As complement WHO strengthened its presence in Yemen in Surge capacity--no regrets Compared to 64 staff at the end of 2016, the Organization had 204 staff, comprised of consultants, international experts and national staff dedicated to the Yemen response across various locations (i.e. one sub-office, three hubs and two regional hubs in Amman and Djibouti) by the end of 2017, as part of a no-regrets policy under the WHO s Emergency Response Framework. In addition, staff from WHO s Eastern Mediterranean Regional Office and Headquarters Office also deployed on surge missions to support the country office, providing much needed capacity in response to cholera and malnutrition. Four sub-national hubs: Aden, Ibb, Hudaydah and Sa ada were established, and a logistics hub was set-up to manage incoming medicines and supplies for the response, with warehouses in key areas: Aden, Sana a and Hudaydah. The expansion of the
.")
19 19 WHO Yemen team, especially the scale-up of the Organization s presence at the sub-national level, is in line with continued reforms taking place since the establishment of the WHO Health Emergencies Programme (WHE). This expansion allows WHO to be closer to communities, faster in detecting and responding to needs on the ground, better able to manage the distribution of life saving supplies through a decentralized model/ approach and support partners and counterparts delivering on the ground, including those present in the sub-offices of other UN agencies, for greater technical and institutional dialogue. Creating an efficient response network The situation in Yemen is unfolding amidst the backdrop of a civil war. WHO established the Aden office to support Yemen health authorities in the southern part of the country and setting-up three hubs scattered across key areas in Yemen to ensure the implementation of critical health activities. Establishing a sub-office and sub-national hubs creates an operational response network that makes emergency coordination, in a country as large as Yemen, possible-- ensuring closer coordination of health activities at governorate and district levels. The potential risks to the staff safety and security is always a primary consideration when setting up a field office. Nonetheless, the health needs in the country were so great, that WHO needed to ensure that both the northern and southern parts of Yemen were covered. Strengthening WHO sub-offices and hubs is not just a matter of hiring additional people. Rather, considerable improvements had to be made to each of these locations, to enhance security, including the creation of safe areas and the installation of CCTV and secure access control in some instances.

, providing them with incentives, medicines/supplies and capacity building through regular trainings for health care workers.")
20 20 ANNUAL REPORT 2017 Building local capacity while supporting health facilities WHO supports emergency mobile medical teams, providing them with financial incentives, medicines and capacity building through regular trainings for health care workers Credit: WHO The Aden sub-office and established hubs were responsible for carrying out key health interventions in areas in need of critical humanitarian support. WHO supported mobile and fixed teams in seven district trainings where armed clashes were heaviest (i.e. Majz, Sahar, Haydan, Rezah, Baqim, Shada, Dhahar), providing them with incentives, medicines/supplies and capacity building through regular trainings for health care workers. In the context of noncommunicable diseases, WHO hubs also facilitated the importation of dialysis supplies for an entire year for local hospitals, such as Al Jumori hospital. Cancer centers were also provided with supportive drugs for cancer patients and supplies to implement 500 renal dialysis sessions. In Al Hudaydah alone, which had over 12,000 confirmed malaria cases, 135 malaria kits were distributed to governorate health offices (GHOs) sufficient to treat 52,650 patients. Mental health and psychosocial support activities were also supported in this hospital through an already established psychiatric unit.

21 21 Yemeni doctors continue saving lives amidst a suffocating crisis Dr. Abdul-Kareem Qasem, a pediatric surgeon in Al Sabeen Hospital in Sana a, vividly remembers the moment when his head was bleeding following a blast that damaged the hospital where he was working. Since 2003, Dr. Qasem has worked with sick and injured children at the Al Sabeen Hospital, but he never expected he would be injured while working at the hospital. At that moment, I realized what it meant to be injured, he recalled. I felt as if it was an earthquake when a bomb hit a house just near the hospital 2 years ago. Glass from the building flew to my head and my face was covered with blood. For 14 years, Dr. Qasem worked under difficult circumstances, but the current situation is becoming unbearable. We were already under suffocating crisis but this one is totally different. We are not only working under a shortage of medicines and lack of regular salaries, but the security problems have also added a heavy burden on us, he explained. and serve the country during these exceptional conditions, then when will we?. Over the last two and a half years, Dr. Qasem has noticed the gradual deterioration of the financial situation of patients. Some ask to be exempted from even the very low, almost token, fees for the health services provided. Our living conditions as doctors are also worsening. We ve not received our salaries for one year and I cannot even pay for the rent of my apartment, he says. Al Sabeen Hospital in Sana a is just one of over 350 health facilities that have been partially or fully damaged by the conflict. Unfortunately, the health facilities and medical personnel in Yemen have fallen victims to this war. My message to the national and international warring parties is to respect medical workers and health facilities. They must know that we provide health services to all people regardless of political and geographical considerations. Since March 2015, the security situation has further deteriorated in Yemen. Several doctors, could not leave the country to find work elsewhere. For his part, Dr Qasem says I will not leave my country under any circumstances. I studied medicine for 15 years outside Yemen to return to my country and dedicate my expertise to save my people. I will not allow any wound to prevent me from doing my job and serving them. In addition to his main work in the hospital, Dr. Qasem responds to distress calls made by public hospitals during mass casualty incidents. We cannot see the injured in need while we stand silent. If we don t help our people Around 40,000 health workers have not received their salaries in over a year Credit: Sadeq Al-Wesabi

22 22 ANNUAL REPORT 2017 Ensuring access to priority health services country's health system is crumbling under the weight of almost three years of intense conflict Credit: WHO Cholera and diphtheria are not the only health issues facing Yemen. According to the Health Cluster s analysis, the main causes of avoidable deaths in Yemen are communicable diseases, maternal, perinatal and poor nutritional conditions, accounting for 50% of mortality and noncommunicable diseases (NCDs), accounting for 39% of mortality, while remaining mortality percentages are from casualties of war. The country's health system is crumbling under the weight of almost three years of intense conflict. Only 50% of health facilities in Yemen are fully functioning. To further assess the functionality and health service availability, the Health Resources and Services Availability Monitoring System (HeRAMS) is currently being implemented. A HeRAMS workshop was conducted for district health officers and data managers of Sana'a Governorate in December The workshop will be conducted for other governorates in WHO is working with partners, including United Nation Children's Fund (UNICEF) and the World Bank, through the Emergency Health and Nutrition Project (EHNP) to meet emergency health needs related to the current humanitarian crisis, while at the same time strengthening the national health system for the future. Negotiating access to populations in need WHO is committed to reaching all people-in-need of health care across Yemen, regardless of their geographical location, ethnic background, religion, political affiliation or any other consideration. This is a direct reflection of the Organization s core principles and mandate. In practice, this requires that the Organization negotiates access to affected populations, with the support of the United Nations Office for the Coordination of Humanitarian Affairs (OCHA). In March, for example, WHO negotiated the safe passage of a truck carrying more than eight tonnes of essential medicines and medical supplies to the Taiz enclave, where more than people were in need of health services. This was the first delivery of essential medicines and medical supplies to cross conflict lines since the beginning of the conflict. WHO continues to call on parties to the conflict to allow for the free movement of health workers, medical supplies and other humanitarian assistance to reach those in need.


23 23 Providing the essentials to keep health facilities running In 2017, WHO delivered 40 fullyequipped ambulances to main hospitals in Yemen with the support of the UAE Red Crescent Credit: WHO In major emergencies, people who die due to lack of health care can far outnumber those reported as immediate casualties. The conflict in Yemen has taken a severe toll on the health system. An estimated 278 health facilities were partially damaged and 72 health facilities fully damaged, with many more forced to close due to a lack of operational costs, medicines and staff. Similarly, 13 emergency mobile medical teams provided consultations to communities living in Al Hudaydah, Hajjah, and Sa ada. These teams provided reproductive health, routine immunization and nutrition services. In addition, 43 fixed health facility-based teams in 13 governorates provided primary health care consultations during WHO is working to keep priority health facilities running across Yemen. This includes the provision of more than 1500 tonnes of medicines and supplies, 76 million litres of clean water to more than 100 health facilities and 4.4 million litres of fuel to 147 hospitals and clinics to run generators. When necessary, the Organization is also providing direct financial support, travel costs and overtime for health personnel. At the same time, WHO is working with UNICEF and partners to conduct integrated outreach activities in remote areas of the country. Five rounds of outreach activities have taken place in 2017, during which children under the age of one were immunized with routine vaccines. Vulnerable communities were also provided with reproductive health and nutrition services, as well as treatment for common conditions such as high blood pressure. More than 1500 tonnes of medicines and medical supplies were delivered by WHO in 2017 Credit: Sadeq Al-Wesabi
: Lifeline for a rapidly collapsing health")
24 24 ANNUAL REPORT 2017 Part II: The Minimum Service Package (MSP): Lifeline for a rapidly collapsing health system

25 25 WHO and the World Bank have partnered to equip 72 hospitals with a suite of essential life-saving health services, better know as the Minimum Service Package (MSP) Credit: Sadeq Al-Wesabi Meeting a country s health needs through solid partnership Currently, 16.4 million Yemenis desperately require assistance to access essential healthcare. Over the course of almost three years of conflict, WHO has moved proactively to save lives through multiple emergency interventions. As the situation continues to evolve, the crisis has shifted from an acute emergency to a complex and protracted humanitarian crisis. This means that a traditional humanitarian approach alone cannot meet the health needs of the affected population. Without access to health care, many more Yemenis are dying from conditions that would be easily treatable within the context an effective and functioning health system. Solid health systems tailored to specific needs is, therefore, a must for saving lives. WHO and the World Bank have partnered to equip 72 hospitals with a suite of essential life-saving health services, better known as the Minimum Service Package (MSP). The two organizations are also working with UNICEF to strengthen the referral system from the primary to the tertiary level. The Emergency Health and Nutrition Project (EHNP), is the cross-cutting response framework designed specifically to meet all acute health needs and support the national health system in the middle of this ongoing conflict. The MSP is the delivery mechanism for the EHNP, and aims to deliver health services even in situations of extreme stress, addressing major health threats. These priority health interventions fall within 8 major areas and are to be implemented within the country s District Health System to ensure maximum impact. This enormous but essential undertaking requires partnerships with health facilities in local districts, as well as with national and international health partners. This is the lifeline needed by the people of Yemen to ensure accessible and targeted health service delivery amidst the volatile backdrop of civil war.






26 26 ANNUAL REPORT 2017 The crucial components of WHO health interventions are: General services and trauma care Reproductive, Maternal and Newborn Health Childcare at all levels Mental health and psychosocial support Nutrition Noncommunicable diseases Communicable diseases Environmental health About 50% of deaths caused by communicable diseases, maternal, perinatal and nutritional conditions could have been avoided more than health workers have not received their salaries regularly in almost a year


27 27 Credit: Sadeq Al-Wesabi Laying the foundation for innovative and tailored health service delivery In 2017, this work focused on providing health facilities with essential drugs, supplies and equipment including clean water, generators and fuel. During the final quarter of the year, transitional work had begun, linking the major disease outbreak response to district level health service delivery, strengthening readiness and resilience to future outbreaks. Intensive district level health planning ensured that scarce resources went towards the most urgent needs, beginning with the Al Thawra Hospital in Al Hudaydah. This is where a pilot programme for results-based approaches to supporting tertiary hospitals serving the most vulnerable were conducted. This lay the groundwork for a roll-out of MSP over the course of These partnerships allow for the adaptation and expansion of the tertiary hospitals support to secondary and primary levels and the support to inter-district hospitals. With sufficient resources, this work will then be expanded over 2019, with the goal of stabilizing the national health system. Only 50% of health facilities are fully functioning At least 278 health facilities have been partially damaged in the violence, while 72 health facilities were fully damaged
 are food insecure and require")
28 28 ANNUAL REPORT 2017 Over 4018 children under the age of five suffering from severe acute malnutrition with medical complications received treatment at WHOsupported therapeutic feeding centres in 2017 Credit: Abdullah Al-Halabi Managing severe acute malnutrition with medical complications An estimated 17 million people (almost 60% of the total Yemeni population) are food insecure and require urgent humanitarian assistance. WHO plays a special role in responding to malnutrition, by providing live-saving treatment for severely acute malnourished (SAM) children with medical complications. Children with SAM are nine times at higher risk of death compared with normal or moderately malnourished children, and WHO supports specialized care for these children, the majority of whom would die without it. This is a complementary role to those played by partners such as WFP and UNICEF. In 2017, WHO trained 164 health workers at Stabilization Centres (SCs) in 10 priority governorates in Yemen on the medical management of SAM with complications. Given the sheer scale of the need for nutrition services in Yemen, WHO has stepped in as the provider of last resort. The Organization has established 26 SCs across the country, which admitted around 5000 SAM cases. There are plans to establish a further 25 centres in This entails the physical rehabilitation of existing health facility structures to make them suitable SCs, and the provision of furniture, equipment and kits containing supplies for the medical management SAM. WHO has procured 120 SAM kits to distribute to all therapeutic feeding centres (TFCs) in the country, whether established by WHO or another partners. From January to December 2017, more than 4430 children under the age of five suffering from severe acute malnutrition with medical complications received treatment at WHO-supported stabilization centres. Treatment in the centres is free-of-charge, including provision of therapeutic feeding and medicines, meals to the caregivers, as well as health education for parents and relatives attending the facility. To help ensure quality of care, WHO conducts regular supervision and on-the-job training, using its strengths as a technical agency to provide guidance on how best to treat malnutrition with medical complications, updating related guidelines, and tailoring them to the local context. In addition, the Organization is working with local health authorities and partners to pilot a nutrition surveillance system. In April alone, 55 sentinel sites in 6 governorates were opened out of 100 planned in pilot districts in 10 priority governorates. Training was provided to 220 health workers on surveillance and data collection. Nutrition surveillance reporting in these governorates commenced in May 2017.

29 Zahraa s story 29 Three-month-old Zahraa was admitted to a WHO-supported therapeutic feeding centre at Al-Thawra Hospital in Hudaydah governorate suffering from severe acute malnutrition After receiving intensive treatment, Zahraa fully recovered and was discharged. Since the beginning of the year, the centre has treated more than 450 children. WHO/ Sadeq Al-Wesabi

30 30 ANNUAL REPORT 2017 Maternal, newborn, child and adolescent health When health systems collapse in protracted emergencies, the consequences for mothers and infants are dire. Reductions in the maternal mortality ratio, achieved by Yemen prior to the escalation of the conflict, have been reversed as expectant mothers face increasing difficulties 148 in accessing life-saving emergency obstetric care Maternal mortality rate per 100,000 live births Ranging from 350 to 400 WHO, together with the World Bank and UNICEF, under the Health and Population Project (HPP) prepared a major scale-up of support to emergency obstetric care capacities across the country. This was done through in-kind contributions of supplies and fuel, capacity building through training and direct support to health workers, resulting in the support of 73 health facilities in 6 governorates. WHO has worked with the local health authorities and other UN agencies, UNICEF and UNFPA, to update the National Reproductive Health Strategy for Maternal Health, Newborn, Advocacy and BCC for The strategy is in line with both the Sustainable Development Goals (SDGs) and global guidelines, but is designed to address these within the context of the current protracted crisis and ongoing humanitarian response needs. This strategy was implemented, starting with building the capacity of 52 general practitioners from 12 governorates on Emergency Maternal, Newborn Obstetric Care (EmONC), in order for them to pass on their knowledge to colleagues. Sixteen general practitioners from 12 governorates, 13 anaesthesia technicians, and 160 midwives across 6 governorates were also trained on EmONC. WHO Yemen worked closely with UNICEF to update the national community based maternal and newborn health care guidelines for community midwives. Similarly, national guidelines for the integrated management of childhood illnesses (IMCI) have been updated, and 479 health workers have received training on IMCI. WHO/ Sadeq Al-Wesabi
31 31 Combating communicable diseases: Detection, prevention and control in Yemen WHO remains vigilant in the detection, prevention and control communicable diseases Surveillance Rapid detection is key to bringing outbreaks to a halt. Through the support of the WHO, an estimated 1982 sentinel sites are now reporting regularly resulting in more than disease alerts that have been detected and investigated in WHO continues to support the strengthening of Yemen s disease surveillance system capacities with 1655 health workers from all 23 governorates already trained on rapid response, disease surveillance and data collection this year Sentinel sites supported Disease alerts detected and investigated health workers trained on rapid response Vaccination WHO and UNICEF are stepping up their long-term support to keep Yemen poliofree, ensuring that all children receive essential vaccinations. As a result, vaccination coverage remains high (above 80%). Despite the ongoing conflict, WHO, UNICEF and national health authorities successfully implemented two house-to-house polio vaccination campaigns in February and October 2017, reaching almost 4.87 million children under the age of 5. Measles and rubella mop-up campaigns successfully reached children in Amran and Sa ada. above 80% vaccination coverage 4.78 million children vaccinated against polio To protect the effectiveness of vaccines stored in a context where the electricity supply is often interrupted, solar power refrigerators were provided following a cold chain assessment conducted in 22 governorates. To help counter increasing reluctance to vaccinate in some areas of the country, a strategic plan for Information, Education and Communication (IEC) for the Expanded Programme on Immunization (EPI) has been developed for governorates provided solar-powered refrigerators 370 thousand children vaccinated against measles and rubella
 is a complement to UNICEF s Community Engagement and Awareness for Development Programme (C4D).")
32 32 ANNUAL REPORT 2017 In Yemen, the strengthening of laboratory functions has been a priority especially with the ongoing outbreaks of cholera and diphtheria Credit: Sadeq Al-Wesabi Emergency risk communication Here in Yemen, emergency risk communication (ERC) is a complement to UNICEF s Community Engagement and Awareness for Development Programme (C4D). For both cholera and diphtheria, as well as other disease outbreaks, ERC is a public health intervention that is instrumental in informing communities on how to protect themselves from disease, as well as training healthcare workers on how to effectively disseminate public health messages that carefully consider a community s knowledge, attitudes and practices (KAP). In every disease outbreak, WHO and UNICEF work hand-in-hand to ensure public health messages reach affected communities, since an effective emergency risk communications (ERC) system is part of the process of combating communicable diseases. For cholera alone, a nationwide awareness campaign conducted by WHO and UNICEF in August supported national health authorities, ensuring that cholera key messages reached an estimated 14 million people across all 22 governorates in Yemen. Laboratory diagnostics Due to the collapsing health system in Yemen, laboratory strengthening is a critical priority, since lab diagnostics is an essential component of communicable disease surveillance, for routine confirmation of infections and the rapid identification of outbreaks and epidemics. In Yemen, the strengthening of laboratory functions has been a priority especially with the ongoing outbreaks of cholera and diphtheria. WHO has been actively involved in building laboratory capacity in-country through training, supplying reagents, culture and transport media to enable the diagnosis and confirmation of probable cases of diphtheria. Under the International Health Regulations (IHR 2005), countries like Yemen, ideally, should have the capacity to provide support in response to a public health emergency of international concern (PHEIC) through specialized staff, laboratory analysis of samples (domestically or through collaborating centres) and logistical assistance (e.g. equipment, supplies and transport).
33 33 Part III: Outbreak alert and response operations: Cholera and Diphtheria and other communicable diseases
 more than 1 million suspected cases of cholera were reported, including over 2200 deaths.")
34 34 ANNUAL REPORT 2017 Cholera Responding to an unprecedented outbreak One of the world s largest cholera outbreaks Yemen is currently facing one of the world s largest cholera outbreaks. Between 27 April and 31 December 2017 (the period covered by this report) more than 1 million suspected cases of cholera were reported, including over 2200 deaths. WHO and health partners are working to ensure access to clean water and sanitation, setting up treatment centres, training health workers, reinforcing surveillance, and working with communities on prevention. Their efforts have already had an impact. The over 1 million suspected cases that have been reported are all people who have received treatment. The case fatality ratio (CFR) of 0.22% implies that almost 99% of people who become sick with suspected cholera and who are able to access health services are surviving. Life-saving oral rehydration corners (ORCs) and diarrhoea treatment centres (DTCs) must be provided for as many people as possible. Yemen s cholera outbreak is far from over. There is a continued need to scale up the response, especially during 2018 when a potential third wave of cholera is expected during Yemen s rainy season.
 of the most-affected districts in all 22 governorates.")
35 35 Guiding the WHO and partners outbreak response activities WHO and its health partners have responded quickly to the explosive situation, rapidly scaling up their support to local health authorities to tackle cholera in 305 (out of 333) of the most-affected districts in all 22 governorates. As of the end of 31 December 2017, Health Cluster partners were operating 3211 Diarrhoea Treatment Centre (DTCs) beds in 208 DTCs in addition to 906 Oral Rehydration Points (ORPs) in 20 Governorates and 232 affected districts in Yemen. They also engaged in health systems strengthening and preparedness with the initial integration of cholera treatment facilities into Yemen s health system. WHO implemented district and governorate level rapid response teams (RRTs) to tackle the epidemic. The aim of these RRTs is to detect, alert and respond to potential outbreaks of cholera. Ongoing support to strengthen laboratory sampling and diagnostics in-country (i.e. collection of stool samples for lab testing, transporting samples to lab and provision of operational costs), and availability of supplies and reagents have occurred, as well the use of rapid diagnostic tests (RDTs), 740 RDTs were conducted in the last week of December 2017, with 136 positive RDTs, 1094 have been confirmed by culture. Empowering communities through sound public health messaging An estimated people were reached by partners with cholera key messages through household visits, and community and school events in 122 districts in 15 governorates. WHO and UNICEF worked side by side to support local health authorities in rolling out a nationwide house-to-house awareness campaign, reaching more than 14 million people in all 22 governorates. The campaign deployed over volunteers working through mobile teams, 2650 fixed teams and supported by 4795 supervisors. WHO has continued to advocate with local authorities for an oral cholera vaccination (OCV) campaign and worked with academics, health authorities and UNICEF to lessen the severity and spread of of the expected third wave of this disease. WHO is also supporting the coordination of day-to-day operations of the intersectoral response of health, WASH and risk communication partners hosted at Emergency Operations Centres (EOC). There is a continued need to scale up the response, especially during 2018 when a potential third wave of cholera is expected during Yemen s rainy season. Credit: Sadeq Al-Wesabi Another key contribution WHO is making to the cholera response is the provision of timely data to guide partners response activities. Epidemiological bulletins provide a weekly in-depth analysis of the progression of the outbreak, and epidemiological updates provide brief, daily overviews of the current situation. The underlying data is available through an online platform for partners who wish to conduct their own analysis. A recently developed web-based dashboard includes data on both the status of the outbreak and the latest data on the response activities of health and WASH partners.

36 36 ANNUAL REPORT 2017 Diphtheria Responding to a long forgotten disease Diphtheria is a real concern, since the overall prevention, treatment and control of the disease is more complex than that of cholera, requiring more resources. On 29 October 2017, the WHO team in Sana a, Yemen received reports of suspected cases of diphtheria from Ibb governorate. From 13 August through 21 December 2017, a total of 333 probable cases including 35 deaths were reported from 20 out of 23 governorates. In the absence of laboratory-confirmation, the event was treated as an outbreak of probable diphtheria based on clinical diagnosis. The last major diphtheria outbreak in Yemen was in Therefore, most clinicians had to be re-introduced on how to manage this deadly disease, affecting mainly adolescents and young children, over 60% of whom were not vaccinated. In early November and December almost 350,000 children under 7 years of age were vaccinated in the areas most affected by diphtheria. On the 20th December, UNICEF brought in 2.5 million doses of Pentavalent vaccine, which protects against diphtheria, tetanus, whooping cough, pertusis, hepatitis B and haemophilus influenza type b. An estimated 3 million doses of Td vaccine, which protects against tetanus and diphtheria, were also brought in, with an additiional 6 million doses of Td and 2.5 million of Penta in pipeline. WHO response efforts focused on the following key outbreak surveillance, prevention and control activities: Surveillance and detection: WHO worked hard to strengthen surveillance and confirmation of cases through refinement of the standard case definition and complementary training activities to ensure this was implemented properly. Laboratory: WHO brought in lab reagents for the culture test to be conducted in-country. Capacity building: Healthcare workers (HCWs) were trained on the clinical case management of probable diphtheria cases; rapid response teams (RRT) in all 23 governorates and 333 districts level are fully activated Despite a global supply shortage of diphtheria anti-toxin (DAT) in 2017, WHO managed to bring in 1000 doses of DAT for the lifesaving treatment of severe cases of diphtheria Credit: Sadeq Al-Wesabi

37 37 Yaseen, 4, has been discharged from Al Sabeen Hospital in Sana a, where he was receiving treatment for diphtheria. Credit: Sadeq Al-Wesabi and the ones in affected districts have been trained and received antibiotics to contact tracing and preventable antibiotics, in line with WHO guidelines. Diphtheria antitoxin (DAT): Despite a global supply shortage of DAT in 2017, as of December the supply of DAT worldwide was 5000 doses, WHO managed to bring in 1000 doses of DAT for the lifesaving treatment of severe cases of diphtheria. Diphtheria specific treatment antibiotics: Targeting a population of have been procured and distributed; antibiotics included: Erythromycin packs of tablets and bottles of syrup; Azithromycin packs of tablets and 8280 bottles of syrup; and Penicillin vials. Emergency risk communication (ERC): Social mobilization for prevention and containment of the outbreak. UNICEF and WHO have developed key messages for communities about cases early symptoms, prevention, access to care and about vaccination. Training of the 9000 Yemeni Health Promotion/ Social mobilisation volunteers were completed by UNICEF. Communities are being engaged through these mobilisers, religious leaders and community volunteers to actively participate in early case identification, referral, contact tracing and treatment to contain and halt the outbreak and creating community resilience. The fight against the disease is far from over, the commitment of health authorities, vaccination, targeted outbreak control measures and community empowerment remain primary prevention and mitigation measures that can rapidly contain the spread of this deadly disease. About diphtheria Diphtheria is an infectious respiratory disease caused by a potent toxin produced by certain strains of the bacterium Corynebacterium diphtheriae. It spreads through air droplets by coughing or sneezing. Vaccination against diphtheria is safe and effective for prevention of the disease.
 at least 40% people are displaced and located in close proximity to")



38 38 ANNUAL REPORT 2017 Vector-borne diseases The triangle of war, poverty and disasters have led to further deterioration of the malaria situation. The current conflict has led to the displacement of 3 million people (2 million still in displacement and 1 million returned) at least 40% people are displaced and located in close proximity to malaria endemic areas. Limited access to clean water and sanitation has significantly increased the risk of vector-borne diseases. While malaria and dengue fever, for example, are endemic in parts of Yemen, a sudden upsurge in cases of both diseases was reported in 2015 and To maintain malaria control and prevention and avoid any deterioration, WHO increased its response to the needs of malaria control and prevention in Yemen to ensure the continuation of life-saving interventions such as case management, vector control and malaria surveillance. The support provided by the World Bank has enabled WHO to expand and improve its response to malaria and other vector-borne diseases in Yemen such as dengue and chikungunya. In 2017, however, malaria and dengue fever have been kept largely in check, although WHO remains vigilant given the imminent start to the malaria season. WHO distributed 1137 of basic and supplementary malaria kits which enables health facilities to test to patients for malaria detection by rapid diagnostic tests and treat cases. It facilitated the transportation of 1.5 million bednets to 76 districts in Yemen. This activity contributed to the increase in coverage by bednets to 3 million people in 8 governorates. WHO supported the implementation of an indoor residual spraying campaign which provides protection to 1.3 million people against malaria. The planned vector control campaigns in 2018 will target 2 million people in Tehama region and Southern governorates. Almost 300 medical doctors and health workers were trained on the clinical management of malaria in 2017, and the national surveillance system known as edews increased the number of sentinel surveillance sites from 442 to 1982, increasing the capacity to detect the disease early on. Credit: WHO Yemen
")
39 39 Neglected tropical diseases (NTDs) are commonplace in IDP camps. More attention and funding are required to eliminate NTDs Credit: Sadeq Al-Wesabi Neglected tropical diseases The conflict has also increased the spread of neglected tropical diseases (NTDs) including rabies and leishmaniasis, and has brought serious new challenges in implementing control measures. New strategies for control are needed in this context. In early August, WHO in coordination with national health authorities, succeeded in bringing together 30 experts from across the entire country and drafted the National Neglected Tropical Diseases Master Plan (NTDs MP) within the context of the current crisis. This is a continuation of work over the past ten years to tackle the top neglected tropical diseases affecting the people of Yemen. Notably, implementation of mass treatment has reduced the prevalence of schistosomiasis from 19.4% in 2010 to 6.9% in 2017 where two treatment campaigns were conducted targeting 1.3 million and 0.8 million adults and children, respectively. Leprosy elimination efforts are still conducted with full support from the WHO, focusing on areas where the disease is endemic, despite security threats and challenges in these areas, healthcare workers are still implementing active examination in the form of rapid skin surveys and contacts, adapting the situation and targeting more the contacts, hotspots, IDPs, capacity building, monitoring and supervision. Deworming has reached 85% of the targeted areas and leprosy is on the verge of being eliminated. WHO regularly provides supplies for the treatment of NTDs. The Organization provided doses of rabies vaccine and more than 7 million tablets (5 million praziquantel and 2.1 million albendazole tablets) for the treatment of schistosomiasis and other soil-transmitted parasitic diseases in For the treatment of onchocerciasis a plan has been devised for approximately more than half a million people in western Yemen to eliminate onchocerciasisaffected areas and identify populations requiring treatment. For Leishmaniasis, WHO provided national health authorities with vials of stibogluconate (leishmaniasis drug) and 9600 leishmaniasis laboratory tests (i.e. rapid diagnostic tests). While for the treatment of Rabies, WHO provided the country with 11,000 rabies vaccines and 5000 anti-sera. Procured doses of rabies vaccine million tablets for the treatment of schistosomiasis and other parasitic disease

40 40 ANNUAL REPORT 2017 Emergency operations centres have been established in Yemen to ensure faster, more efficient and effective response to outbreaks and other health emergencies. Credit: Sadeq Al-Wesabi Emergency Operations Centres: Responding to health emergencies A faster, more efficient and effective response to outbreaks and other health emergencies this is the purpose of a network of Emergency Operation Centres (EOCs) established across Yemen by national health authorities, with the support of partners including WHO, UNICEF, UN OCHA, the World Bank, WFP and others. Central EOCs in Aden and Sana a will support governorate-level EOCs established in the governorates most affected by the cholera outbreak. Health, water, sanitation and risk communication partners, including UN agencies and partner NGOs, are not only collaborating, but working physically in the same place. This facilitates greater information-sharing and allows the group to benefit from each agency s strengths. For example, WFP is taking on logistics for the partnership, while WHO continues to work with the local health authorities to analyse epidemiological data, and UNICEF coordinates efforts to expand access to safe water and sanitation facilities. While the network is being strengthened to facilitate the response to the cholera outbreak, the EOCs will also provide the technological infrastructure for an incident command system for future health emergencies. At the central EOC in Sana a, for example, an existing ambulance dispatch centre has been incorporated into the structure, and an emergency response telephone number has been reactivated.

41 41 WHO conducts on-the job training on cholera case management, infection and prevention control according to WHO guidelines and protocols. Credit: Sadeq Al-Wesabi Rapid detection: Risk assessment and response WHO is providing technical and operational support to strengthen the national surveillance system to help meet the additional demands of the cholera outbreak. Thirty-six disease surveillance and data entry personnel from 21 governorates have been trained on cholera data entry and analysis. Alongside other agencies, WHO has contributed to the provision of computers and other communications technology to strengthen the timely reporting of suspected cases of cholera. Increasing numbers of rapid response teams are being trained and deployed, with 98 teams comprised of 5 people per team trained in 2017, to ensure the timely and thorough investigation of potential cholera cases and to chlorinate wells and water sources. Each team is comprised of a district surveillance coordinator, an epidemiologist, health education officer, water and sanitation officer and the director of the district health office. At the end of 2017, WHO was on track to have rapid response teams present in all of the country s 333 districts ready and available to detect and respond rapidly to cholera and other future outbreaks.

42 42 ANNUAL REPORT 2017 Mohannad: One of the 99% of patients who have survived suspected cholera Credit: Sadeq Al-Wesabi Eight-year-old Mohannad overcame cholera following three days of treatment in the diarrhoea treatment centre at Al Sabeen Hospital in Sana'a. Mohannad lost his mother and sister when a bomb went off near their home in Hajjah. He and his father have since fled to Sana a. Mohannad is all I have in this life after my wife and daughter died. When he was infected with cholera I was very anxious that he would have the same fate as his mother and sister, said Mohannad s father.

43 43 Delivering medicines and supplies to support the joint cholera response Since the 27th April, WHO has procured and distributed more than two million items for the cholera response, including 1.04 million bags of intravenous fluids, 1450 beds with cleaning supplies and 158 kits containing supplies for the treatment of cholera and diarrhoeal diseases. While the majority of these items have been delivered to health facilities and to district health offices, 10 NGOs have also been provided with WHO-procured cholera supplies. WHO has established a partnership with the World Food Programme (WFP) and the Logistics Cluster to scale up logistics support for the cholera response. In addition to providing vessels and aircraft for the transportation of medical supplies, WFP is playing a prominent role in the establishment of treatment centres and emergency operations centres (EOCs). Credit: Sadeq Al-Wesabi

44 44 ANNUAL REPORT 2017 A workshop was conducted in Sana'a to review and asses the epidemiological situation of NTDs in Yemen, discuss challenges, identify the key public-health interventions required to control and eliminate NTDs Credit: OCHA Communicating risk and engaging communities in the response to cholera Every Yemeni has an important role to play in keeping themselves and their families safe from cholera. A key pillar of the cholera response is community engagement, which depends on easily understood and technically sound messaging on how to reduce risks and seek care. WHO and UNICEF supported local health authorities to conduct a nationwide house-to-house awareness campaign from August, reaching more than 14 million people in all 23 governorates. Throughout the campaign, individuals and communities were provided with life-saving information on proper handwashing, preparation of oral rehydration solution (ORS), and proper home care of the people with cholera, including referral to health facilities. The campaign deployed over volunteers working through mobile teams and 2650 fixed teams, supported by 4795 supervisors. WHO is now working with UNICEF to analyse the effectiveness of the risk communications campaign. This information will be used to identify gaps and needs raised by communities and will help inform future activities. WHO will also link epidemiological and social data to refine messaging and strategies focusing on high risk districts. Beyond the campaign, WHO continues to provide technical advice on the messages delivered by partners and has disseminated brochures to NGOs, UN partners and health centres to ensure communities know how to keep themselves safe from cholera.
45 Part IV: Managing the treatment of endemic and noncommunicable diseases 45

46 46 ANNUAL REPORT 2017 The cancer care crisis in Yemen In Yemen, more than cancer patients (12% of whom are children) have received treatment at the National Oncology Centre in Sana a since But the Centre, which treats patients from across the country, had its annual budget come to a grinding halt. Before the crisis, the Government used to provide the centre with around USD 12 million a year, but the Centre has not received any funding for nearly two years, leaving it dependent on limited external support. Almost 6000 patients received cancer treatment at the Centre in 2017, however, challenges in cancer care still remain. An estimated cancer patients are in need of active treatment (i.e. chemotherapy, radiation therapy, hormonal treatment or palliative treatment). Keeping this lifeline alive The Centre has been on the verge of closing several times, which would deprive thousands of patients from receiving life-saving chemotherapy and radiation therapy. The challenges facing the centre are not only confined to shortages of medicines and lack of operational costs. Professional oncologists and other medical staff are leaving the country due to the ongoing conflict, unpaid health care worker salaries and the deteriorating economic situation. We try to do our best to keep functioning, but we don t have enough medicines, and we have no choice but to watch our patients die due to lack of treatment. Poor patients simply leave us and die at home because they cannot afford treatment, said Dr Ali Al-Ashwal, Director of the National Oncology Centre. Life-saving support from donors

47 47 Akram, 8, and Ashjan, 7, a brother and sister, lie on one bed suffering from lymphoma and a brain tumour, respectively. Their father has brought them from Wesab District in Dhamar Governorate to receive treatment. Credit: Sadeq Al-Wesabi With support from the World Bank and Germany, WHO is in the process of providing the centre with USD 2.5 million worth of anti-cancer medicines and chemotherapy medications, sufficient for almost patients. The anti-cancer drugs and chemotherapy medication have been procured and will be shipped to the country by early To fill the gap until the arrival of this precious cargo, WHO provided the National Oncology Centre in Sana a with various cancer drugs and chemotherapy medications sufficient to treat 5000 patients for one month. In 2017 alone, more than cancer patients were registered but only 40% of them received appropriate and complete treatment. This is a clear indication of the critical conditions these patients are in. The families of cancer patients in Yemen are suffering from the agony of watching their children endure the pain of this disease, or die due to lack of full treatment. It is a tragedy that treatment for noncommunicable diseases such as cancer, diabetes and hypertension is available in only 20% of health facilities across Yemen. As a result, these chronic conditions are now killing more people than bullets or bombs, accounting for 39% of all reported deaths in 2017.

48 48 ANNUAL REPORT 2017 The silent impact of war in Yemen Thirteen year-old Mohannad was playing with his friend and brother in Taiz City when a mortar shell landed nearby. Suddenly his carefree days were turned into days of pain. Previously cheerful and sociable Mohannad became an introvert, a shadow of his former self. Mohannad lost his brother in this attack. His friend was blinded and lost his leg. Mohannad suffered extensive burns and was transferred to Sana a for surgery. To support his recovery Mohannad was referred to the mental health and psychosocial care unit at Al Jumhouri hospital in Sana a. These rehabilitation sessions are designed to help Mohannad cope with what happened. The 9 months of treatment was conducted by a WHO trained team. The care started with psychological first aid two weeks after this traumatizing event. The psychological rehabilitation then moved to narrative exposure therapy, where Mohannad was able to tell his story and even to draw the events. Mohannad s story represents one of a thousand others, who live with disturbing, psychological reminders of this ongoing war. Dr Mohammed Al-Kholaidi, a mental health specialist, based in Sana'a, notes the increasing numbers of patients coming to him for mental health care. He reports seeing a population suffering from anxiety, depression, insomnia, and obsessive compulsive disorder. All of these are symptoms of post-traumatic stress disorder (PTSD). For 12-year-old Dhia Khaled, the sound of massive explosions in the Faj Attan district of Sa'ana have left him inconsolable and suicidal. Yehia Al-Fatemi from Dhamar governorate was diagnosed with severe depression after The ongoing conflict has left men, women and children traumatised and in need of mental health and psychosocial support in order to cope with this dire situation. Credit: WHO returning to his house to find the charred bodies of his wife, son and two daughters, killed by an airstrike. The people and their horrific stories are endless. Mental health and psychosocial support is a crucial component of health service delivery, especially during a conflict that shows no signs of abating. WHO is leading the integration of mental health and psychosocial support into the Yemen primary health care system. WHO in cooperation with the Ministry of Public Health has conducted several workshop courses on providing psychosocial support for crisis victims. These workshops

49 49 trained around 200 psychologists and primary healthcare workers from conflict-affected governorates. We plan to build up professional human resource capacity by providing them with knowledge and practical management protocols to deal with the rising rate of people suffering from psychological stress," said Dr Nevio Zagaria, WHO Representative in Yemen. There are undoubtedly huge needs for psychological support, a huge challenge being that Yemen has only forty psychiatrists, therefore alternative strategies are needed. "Mental health is usually ignored in terms of prioritizing health in a poor country. People with pre-existing mental problems become more vulnerable due to displacement, abandonment and lack of access to mental health services," said Dr Zagaria. "WHO will keep utilizing the available community resources to become more active and reach a significant percent of population who are in need of psychosocial support."

50 50 ANNUAL REPORT 2017 Seham: Seeking dialysis in the midst of crisis It is not only the kidney pain and gradual loss of vision that make 10-year-old Seham s life challenging. Because of this disease, I had to stop going to school, said Seham. All I want is to be free from this disease and to go back to my studies. Accessing dialysis has always been an issue in Yemen, the poorest country in the Middle East. But the conflict has created additional challenges, with health facilities facing a shortage of dialysis supplies and travel complicated by checkpoints and insecurity. WHO is working to ensure that people in need of dialysis, like Seham, can access the treatment they need. In late August, the Organization helped to transport 100 tonnes of supplies provided through a private-public partnership to the dialysis centre she regularly attends at Al Jumhoori Hospital in Sa ada. WHO s involvement helped to facilitate the shipment s swift and unhindered entry into the country and on to Sa ada. Health data indicates that more than 6000 chronic kidney disease patients are registered country-wide, and need regular haemodialysis sessions, in addition to 2500 kidney-transplant patients in continuous need of immunosuppressant drugs. WHO/ Sadeq Al-Wesabi
51 51 Scaling up access to treatment for noncommunicable diseases As the health system crumbles, noncommunicable diseases a category which includes highly treatable illnesses such as kidney disease, diabetes, high blood pressure, and many forms of cancer are being left undetected and unmanaged. Basic treatment for noncommunicable diseases is available in an estimated 20% of health facilities. These chronic conditions already accounted for 39% of all mortality before the conflict, but now they are all the more deadly, killing far more people than bullets, bombs or cholera. The noncommunicable diseases medical supply pipelines dried out due to logistical constraints and a dramatic decline of both Ministry of Health budget and the purchasing power of Yemeni citizens. Chronic disease patients are less able to cope without access to adequate health service, medicines and nutrition due to financial hardship and serious shortage of essential medicines. WHO is bolstering the availability of treatment for noncommunicable diseases in USD USD USD USD urgent anti-cancer drugs and lab reagents of materials for dialysis sessions of life-saving drugs for kidney transplant patients of insulin for diabetic patients Supporting trauma care and referral services for those caught in the crossfire The conduct of hostilities in Yemen has been brutal. More than 8500 deaths and injuries were registered between March 2015 and August But these figures are only based on health-facility reporting and are likely to be an underestimate of the actual casualties resulting from the conflict. Many more people are estimated to have died before reaching one of the still functioning health facilities. Conflict related-casualties 19 March December 2017 Female Children Male Total Deaths Injuries Total

52 52 ANNUAL REPORT 2017 Supporting trauma care and referral services With the intensification of the conflict in several areas of Yemen, the need for emergency trauma care has increased. At the same time, the departure and displacement of specialized medical staff and a critical shortage of essential medicines and supplies is impeding the provision of life-saving care. A substantial portion of trauma-related mortality occurs outside of the health system, when people die at or near the scene of their injuries. The second wave of mortality occurs after entry into the health system. This second wave is avoidable, and is the main target of WHO support. WHO is currently supporting 41 surgical teams in 14 governorates to provide emergency trauma care (Abyan, Al Hudaydah, Al Jawf, Al Mahweet, Amran, Hajjah, Marib, Sa ada, Sana a, Shabwa, Aden, Taiz, Ibb and Hadramout). In 2017, these teams provided more than life-saving surgical interventions to people in conflict-affected areas. In comparison, 10 surgical teams delivered interventions throughout the whole of WHO has also supported major hospitals across the country with 55 emergency trauma kits, including medicines, surgical supplies, and dressings to meet the needs of 5500 patients requiring surgical care. To increase access to pre-hospital care and referral services, WHO has procured and delivered 40 fully equipped ambulances through the support of Emirates Red Crescent: 20 delivered through the port in Al Hudaydah and 20 delivered through Aden. WHO also supports the central emergency control room with communications equipment and staff incentives. This control room monitors the hospitalbased trauma surveillance system, identifies any needs and gaps in times of mass casualty incidents, manages pre-hospital care, and coordinates interhospital transfers. Safe blood transfusion is a critical, life-saving intervention directly linked to mass casualty management and trauma care. WHO continues to support safe blood transfusion services and has provided 9000 triple blood bags, single blood bags, testing kits and other supplies for blood collection, testing, processing and storage to the central blood bank. The blood cold chain is also being supported through the provision of fuel for generators. In parallel, WHO is supporting training on the safe administration of blood and blood products, and sharing standard operating procedures for bedside transfusion.

53 53 Conflict in Yemen 19 March December 2017 Deaths 9245 Injuries Total Credit: Sadeq Al-Wesabi

54 54 ANNUAL REPORT 2017
 and from new actors such as the World Bank, allowed WHO to have a two-pronged approach to deal with the challenges of the health sector in a")
55 55 Part V: Priority needs and gaps Increased financial support, increased response activities Credit: Abdullah Al-Halabi Increased financial support during 2017 from traditional humanitarian donors in response to the Humanitarian Response Plan (HRP) and from new actors such as the World Bank, allowed WHO to have a two-pronged approach to deal with the challenges of the health sector in a protracted humanitarian crisis. Activities such as, engaging in medium term planning and linking life-saving health interventions with the delivery of basic health services to cover communicable and noncommunicable diseases, and provide effective, quality preventive and curative interventions are top priorities. This also includes: Expanding and enhancing key public health functions, such as epidemiological surveillance and outbreak rapid response teams (RRTs) across all 333 districts of the country, Increasing immunization activities in fixed posts in health facilities as well as outreach services for remote populations with no access to health care Undertaking communicable disease public health control activities, including the response to the massive cholera outbreak, in strong collaboration with UNICEF and Health Cluster partners; and Scaling-up and improving the provision of key inputs for the reactivation and sustaining of the health facility network in terms of fuel, water, oxygen, essential drugs and medical supplies and equipment, with priority to district hospitals to bridge the primary and tertiary levels of care.
56 56 ANNUAL REPORT 2017 Moving forward In 2018, WHO will focus on scaling up the implementation of the Minimum Service Package (MSP) at primary and secondary levels of care, while continuing to support the tertiary governorate hospitals. However, in order to do this, WHO and the Health Cluster partners will continue the dialogue with the health authorities at central levels, and augment the technical and operational support to the Governorate Health Offices (GHOs) with fully functioning Emergency Operation Centres (EOCs) in all the 23 GHOs. They will also work to strengthen the capacities of the District Health Offices (DHOs) starting from the most vulnerable districts, with technical and operational support, to identify gaps in service delivery and plan the use of available resources to target priority areas for national and Financial overview The overall revised request of the Health Cluster was million USD, including the final cholera response plan of million USD for HRP In 2017, WHO and Health Cluster partners were in a relatively good position financially, thanks to the generosity of the contributors, however, the overall health sector humanitarian response remained underfunded. international NGOs interventions that are in line with the MSP guidelines. New health financing mechanisms are needed to reduce out-of-pocket health expenditures, as well as the consistent and regular payment of incentives to health workers in the public health system. An overall transitional solution for public social services should be identified and implemented, to accommodate the protracted nature of the crisis and the high attrition rate of civil servants, most of them without salaries for more than a year. WHO continues to advocate for this, while discussing options with local health authorities and piloting mechanisms to provide health staff with forms of compensation that allow them to work, to be expanded in the very near future. The Health Cluster had a financial gap of 37% to carry out planned activities under the Yemen Humanitarian Response Plan (YHRP) 2017, as highlighted in the figure below, while WHO had a financial gap of 38%. In 2017 WHO utilized 49.1 million USD for the health sector HRP 2017 activities response funded by the traditional humanitarian donors. Health Cluster funding received in 2017 under HRP WHO funding received in 2017 under HRP Received Funding gap Received Funding gap USD million requested by Health Cluster partners, without WHO, under the Yemen Humanitarian Response Plan (HRP) 2017 USD million received in 2017, according to the Financial Tracking System 37% funding gap USD 190 million requested for WHO under the revised Yemen Humanitarian Response Plan (HRP) 2017, including USD 64 million for cholera USD million received 38% funding gap In October 2016, WHO became a member of the International Aid Transparency Initiative (IATI). Funds allocated for the WHO Yemen response can therefore be traced back by programme area on the WHO website:
57 57 Strong partnerships WHO signed in February 2017 the Emergency Health and Nutrition Project (EHNP) for a total of 76 million USD and two additional financing arrangements to respond to the acute malnutrition and cholera for an additional 91 million USD. The timeframe for the implementation of the World Bank interventions is February 2017 to June Out of this funding 52.6 million USD was utilized during WHO has been in the position to respond and scale up both humanitarian and non-humanitarian interventions considering the important financial contribution of the World Bank, and adopting a medium term planning cycle, as illustrated in previous sections of this report, particularly in the response to the cholera outbreak. WHO has also implemented activities under the developmental umbrella for a total of 11.5 million USD during 2017, for earmarked specific activities, such as the ones targeting Neglected Tropical Diseases (NTDs), malaria, and dengue. WHO started in 2017 to develop one strategic agenda to tackle the health challenges in responding to the needs of a large-scale, protracted humanitarian crisis. The convergence of different funding streams in supporting of one strategic approach in responding to the Yemen crisis started during For 2018 the overall needs to be addressed are going to be larger, while further efforts will be needed in enhancing complementarity and having a common strategic vision, prioritizing life saving interventions, and at the same time responding to basic health needs of the affected population in terms of preventive and curative care. Humanitarian donor contribution to WHO received in 2017 (for the period of ) Donor Amount received Percentage USAID Saudi Arabia United Arab Emirates ECHO OCHA Oman Germany Japan CERF Kuwait China Norway Republic of Korea Canada - DFATD Algeria Total "WHO would like to extend its sincerest thanks to all donors and partners for their generous support to this humanitarian response. Without your contributions we would not be able to help this country and its beautiful people. Our deepest thanks go out to all of you and we look forward to your continued and valued support."

58 58 ANNUAL REPORT 2017 How the international community can help? In addition to ensuring that the health response to the humanitarian crisis in Yemen is fully funded, the international community can help the people of Yemen by advocating for the following: A peaceful, political resolution to the conflict A solution for the payment of health workers and other civil servants of the social sectors An end to attacks on health care in Yemen The unimpeded delivery of life-saving supplies to all affected areas Long-term investments in Yemen s health system
59 59 Contact details: Dr Nevio Zagaria, WHO Representative in Yemen Christine Tiffany Cool, Emergency Communication Lead Sadeq Al-Wesabi, Communication Officer Front cover: A child from an IDP camp in Ibb, Yemen Credit: Christine Tiffany Cool

60 60 ANNUAL REPORT 2017 /WHOYemen WHOYemen
HEALTH CLUSTER BULLETIN APRIL 2018
 Photo Credit: INTERSOS HEALTH CLUSTER BULLETIN APRIL 2018 16.4 M IN NEED OF HEALTH ASSISTANCE 12.3 M TARGETED WITH HEATLH INTERVENTIONS 3 M INTERNALLY DISPLACED & RETURNEES HIGHLIGHTS HEALTH CLUSTER Health
Photo Credit: INTERSOS HEALTH CLUSTER BULLETIN APRIL 2018 16.4 M IN NEED OF HEALTH ASSISTANCE 12.3 M TARGETED WITH HEATLH INTERVENTIONS 3 M INTERNALLY DISPLACED & RETURNEES HIGHLIGHTS HEALTH CLUSTER Health
The Syrian Arab Republic
 World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
South Sudan Country brief and funding request February 2015
 PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
HEALTH CLUSTER BULLETIN September 2017
 HEALTH CLUSTER BULLETIN September 2017 WHO and Health Cluster partners aim to reach 10.4 million of the most vulnerable people in Yemen with health services in 2017 14.8 M IN NEED OF HEALTH ASSISTANCE
HEALTH CLUSTER BULLETIN September 2017 WHO and Health Cluster partners aim to reach 10.4 million of the most vulnerable people in Yemen with health services in 2017 14.8 M IN NEED OF HEALTH ASSISTANCE
Planning meeting to set up a diploma in mental health, human rights and law at the International Islamic University, Islamabad, Pakistan
 Summary report on the Planning meeting to set up a diploma in mental health, human rights and law at the International Islamic University, Islamabad, Pakistan WHO-EM/MNH/208/E Cairo, Egypt 24 26 September
Summary report on the Planning meeting to set up a diploma in mental health, human rights and law at the International Islamic University, Islamabad, Pakistan WHO-EM/MNH/208/E Cairo, Egypt 24 26 September
ERM HUMANITARIAN HEALTH RESPONSE IN YEMEN KAREN HOBDAY, WHO. Photos: Acknowledgements to Dr Ahmed Zouiten
 HUMANITARIAN HEALTH RESPONSE IN YEMEN KAREN HOBDAY, WHO Photos: Acknowledgements to Dr Ahmed Zouiten ERM Demographic indicators Total population (2014) 26,052,966 Population under the age of 15 40.2% Gross
HUMANITARIAN HEALTH RESPONSE IN YEMEN KAREN HOBDAY, WHO Photos: Acknowledgements to Dr Ahmed Zouiten ERM Demographic indicators Total population (2014) 26,052,966 Population under the age of 15 40.2% Gross
NEPAL EARTHQUAKE 2015 Country Update and Funding Request May 2015
 PEOPLE AFFECTED 4.2 million in urgent need of health services 2.8 million displaced 8,567 deaths 16 808 injured HEALTH SECTOR 1059 health facilities damaged (402 completely damaged) BENEFICIARIES WHO and
PEOPLE AFFECTED 4.2 million in urgent need of health services 2.8 million displaced 8,567 deaths 16 808 injured HEALTH SECTOR 1059 health facilities damaged (402 completely damaged) BENEFICIARIES WHO and
Regional consultation on the availability and safety of blood transfusion during humanitarian emergencies
 Summary report on the Regional consultation on the availability and safety of blood transfusion during humanitarian emergencies WHO-EM/LAB/387/E Tunis, Tunisia 15 16 May 2016 Summary report on the Regional
Summary report on the Regional consultation on the availability and safety of blood transfusion during humanitarian emergencies WHO-EM/LAB/387/E Tunis, Tunisia 15 16 May 2016 Summary report on the Regional
Northeast Nigeria Health Sector Response Strategy-2017/18
 Northeast Nigeria Health Sector Response Strategy-2017/18 1. Introduction This document is intended to guide readers through planned Health Sector interventions in North East Nigeria over an 18-month period
Northeast Nigeria Health Sector Response Strategy-2017/18 1. Introduction This document is intended to guide readers through planned Health Sector interventions in North East Nigeria over an 18-month period
JOINT PLAN OF ACTION in Response to Cyclone Nargis
 Health Cluster - Myanmar JOINT PLAN OF ACTION in Response to Cyclone Nargis Background Cyclone Nargis struck Myanmar on 2 and 3 May 2008, sweeping through the Ayeyarwady delta region and the country s
Health Cluster - Myanmar JOINT PLAN OF ACTION in Response to Cyclone Nargis Background Cyclone Nargis struck Myanmar on 2 and 3 May 2008, sweeping through the Ayeyarwady delta region and the country s
UNICEF s response to the Cholera Outbreak in Yemen. Terms of Reference for a Real-Time Evaluation
 UNICEF s response to the Cholera Outbreak in Yemen Terms of Reference for a Real-Time Evaluation Background Two years since the escalation of violence in Yemen, a second wave of fast spreading cholera
UNICEF s response to the Cholera Outbreak in Yemen Terms of Reference for a Real-Time Evaluation Background Two years since the escalation of violence in Yemen, a second wave of fast spreading cholera
WORLD HEALTH ORGANIZATION
 WORLD HEALTH ORGANIZATION EXECUTIVE BOARD EB115/6 115th Session 25 November 2004 Provisional agenda item 4.3 Responding to health aspects of crises Report by the Secretariat 1. Health aspects of crises
WORLD HEALTH ORGANIZATION EXECUTIVE BOARD EB115/6 115th Session 25 November 2004 Provisional agenda item 4.3 Responding to health aspects of crises Report by the Secretariat 1. Health aspects of crises
Joint external evaluation of IHR Core Capacities of the Republic of Uganda. Executive summary June 26-30, 2017
 Joint external evaluation of IHR Core Capacities of the Republic of Uganda Executive summary June 26-30, 2017 WHO/WHE/CPI/SUM/2017.39 World Health Organization 2017 Some rights reserved. This work is available
Joint external evaluation of IHR Core Capacities of the Republic of Uganda Executive summary June 26-30, 2017 WHO/WHE/CPI/SUM/2017.39 World Health Organization 2017 Some rights reserved. This work is available
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Health Cluster Coordination Meeting. Friday December 4, 2015, Kiev
 Health Cluster Coordination Meeting Friday December 4, 2015, Kiev Agenda Polio vaccination update Humanitarian Response Plan 2016 Partners updates MHPSS update TB/HIV/AIDs and OST AOB BACKGROUND On 28
Health Cluster Coordination Meeting Friday December 4, 2015, Kiev Agenda Polio vaccination update Humanitarian Response Plan 2016 Partners updates MHPSS update TB/HIV/AIDs and OST AOB BACKGROUND On 28
DRAFT VERSION October 26, 2016
 WHO Health Emergencies Programme Results Framework Introduction/vision The work of WHE over the coming years will need to address an unprecedented number of health emergencies. Climate change, increasing
WHO Health Emergencies Programme Results Framework Introduction/vision The work of WHE over the coming years will need to address an unprecedented number of health emergencies. Climate change, increasing
Summary of UNICEF Emergency Needs for 2009*
 UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES. Tajikistan
 CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
November, The Syrian Arab Republic. Situation highlights. Health priorities
 November, 2012 The Syrian Arab Republic Total population 20411000 5120 71/76 159/95 174 3.4 Requested 31 145 000 53 150 319 Received 7 993 078 13 648 289 25.7% 26% http://www.who.int/disasters/crises/syr
November, 2012 The Syrian Arab Republic Total population 20411000 5120 71/76 159/95 174 3.4 Requested 31 145 000 53 150 319 Received 7 993 078 13 648 289 25.7% 26% http://www.who.int/disasters/crises/syr
Background Paper & Guiding Questions. Doctors in War Zones: International Policy and Healthcare during Armed Conflict
 Background Paper & Guiding Questions Doctors in War Zones: International Policy and Healthcare during Armed Conflict JUNE 2018 This discussion note was drafted by Alice Debarre, Policy Analyst on Humanitarian
Background Paper & Guiding Questions Doctors in War Zones: International Policy and Healthcare during Armed Conflict JUNE 2018 This discussion note was drafted by Alice Debarre, Policy Analyst on Humanitarian
Informal note on the draft outline of the report of WHO on progress achieved in realizing the commitments made in the UN Political Declaration on NCDs
 Informal note on the draft outline of the report of WHO on progress achieved in realizing the commitments made in the UN Political Declaration on NCDs (NOT AN OFFICIAL DOCUMENT OR FORMAL RECORD 1 ) Geneva,
Informal note on the draft outline of the report of WHO on progress achieved in realizing the commitments made in the UN Political Declaration on NCDs (NOT AN OFFICIAL DOCUMENT OR FORMAL RECORD 1 ) Geneva,
ACHIEVING QUALITY UNIVERSAL HEALTH COVERAGE THROUGH BETTER WATER, SANITATION AND HYGIENE SERVICES IN HEALTH CARE FACILITIES
 ACHIEVING QUALITY UNIVERSAL HEALTH COVERAGE THROUGH BETTER WATER, SANITATION AND HYGIENE SERVICES IN HEALTH CARE FACILITIES A focus on Cambodia and Ethiopia ACHIEVING QUALITY UNIVERSAL HEALTH COVERAGE
ACHIEVING QUALITY UNIVERSAL HEALTH COVERAGE THROUGH BETTER WATER, SANITATION AND HYGIENE SERVICES IN HEALTH CARE FACILITIES A focus on Cambodia and Ethiopia ACHIEVING QUALITY UNIVERSAL HEALTH COVERAGE
Syrian Arab Republic unrest Regional situation report # 1 Date: 9 August 2012
 unrest Regional situation report # 1 Date: 9 August 2012 According to the Syrian Ministry of Health, 38 out of 88 hospitals have been damaged Photo: WHO Highlights The health system in the is only partially
unrest Regional situation report # 1 Date: 9 August 2012 According to the Syrian Ministry of Health, 38 out of 88 hospitals have been damaged Photo: WHO Highlights The health system in the is only partially
COMMONWEALTH OF THE NORTHERN MARIANA ISLANDS WHO Country Cooperation Strategy
 COMMONWEALTH OF THE NORTHERN MARIA ISLANDS WHO Country Cooperation Strategy 2018 2022 OVERVIEW The Commonwealth of the Northern Mariana Islands is one of five inhabited United States island territories.
COMMONWEALTH OF THE NORTHERN MARIA ISLANDS WHO Country Cooperation Strategy 2018 2022 OVERVIEW The Commonwealth of the Northern Mariana Islands is one of five inhabited United States island territories.
MARSHALL ISLANDS WHO Country Cooperation Strategy
 MARSHALL ISLANDS WHO Country Cooperation Strategy 2018 2022 OVERVIEW The Marshall Islands covers 181 square kilometres in the Pacific Ocean and comprises 29 atolls and five major islands. The population
MARSHALL ISLANDS WHO Country Cooperation Strategy 2018 2022 OVERVIEW The Marshall Islands covers 181 square kilometres in the Pacific Ocean and comprises 29 atolls and five major islands. The population
TONGA WHO Country Cooperation Strategy
 TONGA WHO Country Cooperation Strategy 2018 2022 OVERVIEW The Kingdom of Tonga comprises 36 inhabited islands across 740 square kilometres in the South Pacific Ocean. The population was about 103 000 in
TONGA WHO Country Cooperation Strategy 2018 2022 OVERVIEW The Kingdom of Tonga comprises 36 inhabited islands across 740 square kilometres in the South Pacific Ocean. The population was about 103 000 in
Sudan High priority 2b - The principal purpose of the project is to advance gender equality Gemta Birhanu,
 Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
WHO s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies
 SIXTY-FIFTH WORLD HEALTH ASSEMBLY A65/25 Provisional agenda item 13.15 16 March 2012 WHO s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies
SIXTY-FIFTH WORLD HEALTH ASSEMBLY A65/25 Provisional agenda item 13.15 16 March 2012 WHO s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies
MULTISECTORIAL EMERGENCY RESPONSE PLAN - CHOLERA
 MULTISECTORIAL EMERGENCY RESPONSE PLAN - CHOLERA Prepared in collaboration between MISAU and Intercluster Date: 6/04/2017 Multisectorial Emergency response plan for cholera in Mozambique - 2017 1. Introduction
MULTISECTORIAL EMERGENCY RESPONSE PLAN - CHOLERA Prepared in collaboration between MISAU and Intercluster Date: 6/04/2017 Multisectorial Emergency response plan for cholera in Mozambique - 2017 1. Introduction
Biennial Collaborative Agreement
 Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Managing possible serious bacterial infection in young infants 0 59 days old when referral is not feasible
 WHO/UNICEF Joint Statement Managing possible serious bacterial infection in young infants 0 59 days old when referral is not feasible Key points in this Joint Statement n Infections are currently responsible
WHO/UNICEF Joint Statement Managing possible serious bacterial infection in young infants 0 59 days old when referral is not feasible Key points in this Joint Statement n Infections are currently responsible
Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E
 Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E WHO-EM/RDO/002/E Shaping the future of health in the WHO Eastern Mediterranean Region:
Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E WHO-EM/RDO/002/E Shaping the future of health in the WHO Eastern Mediterranean Region:
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION
 COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION") UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
Water, Sanitation and Hygiene Cluster. Afghanistan
 Water, Sanitation and Hygiene Cluster Afghanistan Strategy Paper 2011 Kabul - December 2010 Afghanistan WASH Cluster 1 OVERARCHING STRATEGY The WASH cluster agencies in Afghanistan recognize the chronic
Water, Sanitation and Hygiene Cluster Afghanistan Strategy Paper 2011 Kabul - December 2010 Afghanistan WASH Cluster 1 OVERARCHING STRATEGY The WASH cluster agencies in Afghanistan recognize the chronic
Special session on Ebola. Agenda item 3 25 January The Executive Board,
 Special session on Ebola EBSS3.R1 Agenda item 3 25 January 2015 Ebola: ending the current outbreak, strengthening global preparedness and ensuring WHO s capacity to prepare for and respond to future large-scale
Special session on Ebola EBSS3.R1 Agenda item 3 25 January 2015 Ebola: ending the current outbreak, strengthening global preparedness and ensuring WHO s capacity to prepare for and respond to future large-scale
Mauritania Red Crescent Programme Support Plan
 Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Guidance for contingency planning
 WHO Guidance for contingency planning World Health Organization 1 P age Everyone deserves the chance to survive. I think of this every time I see another disaster. There are probably people dying who don
WHO Guidance for contingency planning World Health Organization 1 P age Everyone deserves the chance to survive. I think of this every time I see another disaster. There are probably people dying who don
Democratic Republic of Congo
 World Health Organization Project Proposal Democratic Republic of Congo OVERVIEW Target country: Democratic Republic of Congo Beneficiary population: 8 million (population affected by the humanitarian
World Health Organization Project Proposal Democratic Republic of Congo OVERVIEW Target country: Democratic Republic of Congo Beneficiary population: 8 million (population affected by the humanitarian
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder
 Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
2.5 m (People in Need)
") HEALTH Jan - December 2016 Dashboard The quarterly dashboard summarizes the progress made by partners involved in the Lebanon Crisis Response and highlights trends affecting people in need. The Health
HEALTH Jan - December 2016 Dashboard The quarterly dashboard summarizes the progress made by partners involved in the Lebanon Crisis Response and highlights trends affecting people in need. The Health
AMERICAN SAMOA WHO Country Cooperation Strategy
 AMERICAN SAMOA WHO Country Cooperation Strategy 2018 2022 OVERVIEW American Samoa comprises five volcanic islands and two atolls covering 199 square kilometres in the South Pacific Ocean. American Samoa
AMERICAN SAMOA WHO Country Cooperation Strategy 2018 2022 OVERVIEW American Samoa comprises five volcanic islands and two atolls covering 199 square kilometres in the South Pacific Ocean. American Samoa
YEMEN SITUATION REPORT
 YEMEN SITUATION REPORT May UNICEF Yemen/ Highlights By the end of May, over 65,000 suspected cases of cholera and at least 532 deaths have been reported, the number of cases increases by the minute*. The
YEMEN SITUATION REPORT May UNICEF Yemen/ Highlights By the end of May, over 65,000 suspected cases of cholera and at least 532 deaths have been reported, the number of cases increases by the minute*. The
Papua New Guinea Earthquake 34, 100. Situation Report No. 2 HIGHLIGHTS HEALTH CONCERNS 65% OF HEALTH FACILITIES IN AFFECTED AREAS ARE DAMAGED
 Papua New Guinea Earthquake Situation Report No. 2 28 MARCH 2018 544 000 PEOPLE AFFECTED 270 000 NEED IMMEDIATE ASSISTANCE WHO team with displaced villagers in the Southern Highlands of Papua New Guinea
Papua New Guinea Earthquake Situation Report No. 2 28 MARCH 2018 544 000 PEOPLE AFFECTED 270 000 NEED IMMEDIATE ASSISTANCE WHO team with displaced villagers in the Southern Highlands of Papua New Guinea
National Health Strategy
 State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
Humanitarian Bulletin Libya: The crisis that should not be. Escalating crisis amidst depleting resources. Total Requested US$165.
 Humanitarian Bulletin Libya: The crisis that should not be Issue 01 16 02-2016 Escalating crisis amidst depleting resources P.1 Health system attacked and weakened P.2 The Humanitarian Response Plan (HRP)
Humanitarian Bulletin Libya: The crisis that should not be Issue 01 16 02-2016 Escalating crisis amidst depleting resources P.1 Health system attacked and weakened P.2 The Humanitarian Response Plan (HRP)
2016 YEMEN EMERGENCY RESPONSE
 2016 YEMEN EMERGENCY RESPONSE YEMEN CRISIS I KEY FACTS & FIGURES 14.8 MILLION PEOPLE WHO NEED BASIC HEALTHCARE 14.5 MILLION PEOPLE IN NEED OF WATER AND SANITATION 18.8 MILLION PEOPLE ARE IN NEED OF HUMANITARIAN
2016 YEMEN EMERGENCY RESPONSE YEMEN CRISIS I KEY FACTS & FIGURES 14.8 MILLION PEOPLE WHO NEED BASIC HEALTHCARE 14.5 MILLION PEOPLE IN NEED OF WATER AND SANITATION 18.8 MILLION PEOPLE ARE IN NEED OF HUMANITARIAN
IASC. Mozambique Zambezi River floods and cyclone Favio crisis. Health Cluster Bulletin # March Inter-Agency Standing Committee
 IASC Inter-Agency Standing Committee Mozambique Zambezi River floods and cyclone Favio crisis #3 17 The Mozambique emergency Health Cluster Bulletin aims to give an overview of the health activities conducted
IASC Inter-Agency Standing Committee Mozambique Zambezi River floods and cyclone Favio crisis #3 17 The Mozambique emergency Health Cluster Bulletin aims to give an overview of the health activities conducted
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 TONGA Tonga is a lower-middle-income country in the Pacific Ocean with an estimated population of 102 371 (2005), of which 68% live on the main island Tongatapu and 32% are distributed on outer islands.
TONGA Tonga is a lower-middle-income country in the Pacific Ocean with an estimated population of 102 371 (2005), of which 68% live on the main island Tongatapu and 32% are distributed on outer islands.
DEMOCRATIC PEOPLE S REPUBLIC OF KOREA
 DEMOCRATIC PEOPLE S REPUBLIC OF KOREA Assessment of Capacities using SEA Region Benchmarks for Emergency Preparedness and Response SEA-EHA-22-DEMOCRATIC PEOPLE S REPUBLIC OF KOREA Assessment of Capacities
DEMOCRATIC PEOPLE S REPUBLIC OF KOREA Assessment of Capacities using SEA Region Benchmarks for Emergency Preparedness and Response SEA-EHA-22-DEMOCRATIC PEOPLE S REPUBLIC OF KOREA Assessment of Capacities
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL
 DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
Talia Frenkel/American Red Cross. Emergency. Towards safe and healthy living. Saving lives, changing minds.
 Talia Frenkel/American Red Cross Emergency health Towards safe and healthy living www.ifrc.org Saving lives, changing minds. Emergency health Saving lives, strengthening recovery and resilience ISSUE 2
Talia Frenkel/American Red Cross Emergency health Towards safe and healthy living www.ifrc.org Saving lives, changing minds. Emergency health Saving lives, strengthening recovery and resilience ISSUE 2
UNICEF YEMEN CRISIS SITUATION REPORT 7-12 May, 2015
 /2015/Mohamed Yasin Yemen Humanitarian Situation Report 7-12 May, 2015 SITUATION IN NUMBERS Highlights People in need of urgent humanitarian assistance: Despite the challenging operating conditions, UNICEF
/2015/Mohamed Yasin Yemen Humanitarian Situation Report 7-12 May, 2015 SITUATION IN NUMBERS Highlights People in need of urgent humanitarian assistance: Despite the challenging operating conditions, UNICEF
HEALTH EMERGENCY MANAGEMENT CAPACITY
 Module 3 HEALTH EMERGENCY MANAGEMENT CAPACITY INTER-REGIONAL TRAINING COURSE ON PUBLIC HEALTH AND EMERGENCY MANAGEMENT IN ASIA AND THE PACIFIC Learning Objectives By the end of this module, the participant
Module 3 HEALTH EMERGENCY MANAGEMENT CAPACITY INTER-REGIONAL TRAINING COURSE ON PUBLIC HEALTH AND EMERGENCY MANAGEMENT IN ASIA AND THE PACIFIC Learning Objectives By the end of this module, the participant
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
Disaster Management Structures in the Caribbean Mônica Zaccarelli Davoli 3
 Disaster Management Structures in the Caribbean Mônica Zaccarelli Davoli 3 Introduction This chapter provides a brief overview of the structures and mechanisms in place for disaster management, risk reduction
Disaster Management Structures in the Caribbean Mônica Zaccarelli Davoli 3 Introduction This chapter provides a brief overview of the structures and mechanisms in place for disaster management, risk reduction
Health workforce coordination in emergencies with health consequences
 SEVENTIETH WORLD HEALTH ASSEMBLY A70/11 Provisional agenda item 12.1 13 April 2017 Health workforce coordination in emergencies with health consequences Report by the Secretariat 1. This report describes
SEVENTIETH WORLD HEALTH ASSEMBLY A70/11 Provisional agenda item 12.1 13 April 2017 Health workforce coordination in emergencies with health consequences Report by the Secretariat 1. This report describes
Laboratory Assessment Tool
 WHO/HSE/GCR/LYO/2012.2 Laboratory Assessment Tool Annex 1: Laboratory Assessment Tool / System Questionnaire April 2012 World Health Organization 2012 All rights reserved. The designations employed and
WHO/HSE/GCR/LYO/2012.2 Laboratory Assessment Tool Annex 1: Laboratory Assessment Tool / System Questionnaire April 2012 World Health Organization 2012 All rights reserved. The designations employed and
In , WHO technical cooperation with the Government is expected to focus on the same WHO strategic objectives.
 PAPUA NEW GUINEA Papua New Guinea, one of the most diverse countries in the world and the largest developing country in the Pacific, is classified as a low-income country. PNG s current population is estimated
PAPUA NEW GUINEA Papua New Guinea, one of the most diverse countries in the world and the largest developing country in the Pacific, is classified as a low-income country. PNG s current population is estimated
UNICEF HUMANITARIAN ACTION UPDATE ZIMBABWE. 4 February 2009
 UNICEF HUMANITARIAN ACTION UPDATE ZIMBABWE 4 February 2009 UNICEF IS REPONDING TO THE NEEDS OF CHILDREN AND WOMEN IN THE AREAS OF HEALTH, EDUCATION, CHILD PROTECTION AND WATER, SANITATION AND HYGIENE 6
UNICEF HUMANITARIAN ACTION UPDATE ZIMBABWE 4 February 2009 UNICEF IS REPONDING TO THE NEEDS OF CHILDREN AND WOMEN IN THE AREAS OF HEALTH, EDUCATION, CHILD PROTECTION AND WATER, SANITATION AND HYGIENE 6
UNICEF Evaluation Management Response
 UNICEF Evaluation Management Response Evaluation title: Evaluation of UNICEF s Response to the Ebola Outbreak in West Africa, 2014 2015 Region: Global Office: New York headquarters Evaluation year: 2016
UNICEF Evaluation Management Response Evaluation title: Evaluation of UNICEF s Response to the Ebola Outbreak in West Africa, 2014 2015 Region: Global Office: New York headquarters Evaluation year: 2016
YEMEN SITUATION REPORT
 YEMEN SITUATION REPORT June 2017 UNICEF Yemen/2017 Highlights Yemen is today one of the world s largest humanitarian crises. It was estimated in the April 2017 Periodic Monitoring Report that 20.7 million
YEMEN SITUATION REPORT June 2017 UNICEF Yemen/2017 Highlights Yemen is today one of the world s largest humanitarian crises. It was estimated in the April 2017 Periodic Monitoring Report that 20.7 million
Disaster relief emergency fund (DREF) Palestine (Gaza): Complex emergency
 Palestine (Gaza): Complex emergency") Disaster relief emergency fund (DREF) Palestine (Gaza): Complex emergency DREF operation n MDRPS006 GLIDE n CE-2012-000194-PSE 17 November 2012 The International Federation of Red Cross and Red Crescent
Disaster relief emergency fund (DREF) Palestine (Gaza): Complex emergency DREF operation n MDRPS006 GLIDE n CE-2012-000194-PSE 17 November 2012 The International Federation of Red Cross and Red Crescent
Regional meeting of directors of national blood transfusion services
 Summary report on the Regional meeting of directors of national blood transfusion services WHO-EM/LAB/386/E Tunis, Tunisia 17 19 May 2016 Summary report on the Regional meeting of directors of national
Summary report on the Regional meeting of directors of national blood transfusion services WHO-EM/LAB/386/E Tunis, Tunisia 17 19 May 2016 Summary report on the Regional meeting of directors of national
Senegal Humanitarian Situation Report
 Senegal Humanitarian Situation Report Highlights 4,015 children have been admitted to treatment in January and February, or 11% of the annual target. The national Infant and Young Child Feeding policy
Senegal Humanitarian Situation Report Highlights 4,015 children have been admitted to treatment in January and February, or 11% of the annual target. The national Infant and Young Child Feeding policy
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004
 UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
Highlights HEALTH SECTOR 59 WHO STAFF 70 HEALTH CLUSTER PARTNERS FUNDING REQUIREMENTS FOR 2018 $ 5 M WHO
 WHO Special WHO Situation Special Report Situation Report occupied Palestinian Mosul Crisis, territory, Iraq Gaza December to Issue January No 12: 2018 26 March to 01 April 2017 2 MILLION PEOPLE AFFECTED
WHO Special WHO Situation Special Report Situation Report occupied Palestinian Mosul Crisis, territory, Iraq Gaza December to Issue January No 12: 2018 26 March to 01 April 2017 2 MILLION PEOPLE AFFECTED
Women (Million) Boys (Million) Men (Million) Yemen: Humanitarian Response Plan 2017 Revision (August 2017). https://goo.
 Boys (Million) Men (Million) Yemen: Humanitarian Response Plan 2017 Revision (August 2017). https://goo.") UNICEF Yemen/2017/A.Rasheed Yemen Humanitarian Situation Report SITUATION IN NUMBERS Highlights The world s worst Acute Watery Diarrhea (AWD)/cholera outbreak continues spreading in Yemen. Between late-april
UNICEF Yemen/2017/A.Rasheed Yemen Humanitarian Situation Report SITUATION IN NUMBERS Highlights The world s worst Acute Watery Diarrhea (AWD)/cholera outbreak continues spreading in Yemen. Between late-april
Provisional agenda (annotated)
") EXECUTIVE BOARD EB140/1 (annotated) 140th session 21 November 2016 Geneva, 23 January 1 February 2017 Provisional agenda (annotated) 1. Opening of the session 2. Adoption of the agenda 3. Report by the
EXECUTIVE BOARD EB140/1 (annotated) 140th session 21 November 2016 Geneva, 23 January 1 February 2017 Provisional agenda (annotated) 1. Opening of the session 2. Adoption of the agenda 3. Report by the
Minister. Secretaries of State. Department of Planning and Health Information. Department of Human Resources Development
 KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
Guidelines for Preventive and Social Medicine/Community Medicine/Community Health Curriculum in the Undergraduate Medical Education
 SEA-HSD-325 Distribution: General Guidelines for Preventive and Social Medicine/Community Medicine/Community Health Curriculum in the Undergraduate Medical Education World Health Organization 2010 All
SEA-HSD-325 Distribution: General Guidelines for Preventive and Social Medicine/Community Medicine/Community Health Curriculum in the Undergraduate Medical Education World Health Organization 2010 All
ANNEX V - HEALTH A. INTRODUCTION
 ANNEX V - HEALTH A. INTRODUCTION 1. Health care services in Sri Lanka are mainly provided through a well organized curative and preventive health network in the country. The damage to the health sector
ANNEX V - HEALTH A. INTRODUCTION 1. Health care services in Sri Lanka are mainly provided through a well organized curative and preventive health network in the country. The damage to the health sector
AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE. CHF 7,993,000 2,240,000 beneficiaries. Programme no 01.29/99. The Context
 AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE CHF 7,993,000 2,240,000 beneficiaries Programme no 01.29/99 The Context Twenty years of conflict in Afghanistan have brought a constant deterioration
AFGHANISTAN HEALTH, DISASTER PREPAREDNESS AND RESPONSE CHF 7,993,000 2,240,000 beneficiaries Programme no 01.29/99 The Context Twenty years of conflict in Afghanistan have brought a constant deterioration
What happened? WHO Early Recovery in Ebola affected countries: What did we learn? 13/10/2015
 WHO Early Recovery in Ebola affected countries: What did we learn? What happened? Shams Syed MD, MPH, DPH(Cantab), FACPM Department of Service Delivery & Safety WHO Headquarters ISQua 2015 October 5, 2015
WHO Early Recovery in Ebola affected countries: What did we learn? What happened? Shams Syed MD, MPH, DPH(Cantab), FACPM Department of Service Delivery & Safety WHO Headquarters ISQua 2015 October 5, 2015
Emergency appeal operation update Ukraine: Civil unrest
 Emergency appeal operation update Ukraine: Civil unrest Emergency appeal n MDRUA007 Operation update n 1 Emergency operation start date: 13 December 2013 Appeal budget: Appeal coverage: CHF 1,375,100 23%
Emergency appeal operation update Ukraine: Civil unrest Emergency appeal n MDRUA007 Operation update n 1 Emergency operation start date: 13 December 2013 Appeal budget: Appeal coverage: CHF 1,375,100 23%
Assistance. FOR people affected by armed conflict and other situations of violence
 Assistance FOR people affected by armed conflict and other situations of violence second edition April 2012 Assistance FOR people affected by armed conflict and other situations of violence ASSISTANCE
Assistance FOR people affected by armed conflict and other situations of violence second edition April 2012 Assistance FOR people affected by armed conflict and other situations of violence ASSISTANCE
WHO s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies
 130th session EB130.R14 Agenda item 6.15 21 January 2012 WHO s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies The Executive Board, Having
130th session EB130.R14 Agenda item 6.15 21 January 2012 WHO s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies The Executive Board, Having
Lesotho Humanitarian Situation Report June 2016
 Humanitarian Situation Report June 2016 UNICEF//2015 Highlights UNICEF provided support for the completed Vulnerability Assessment Committee (LVAC), which revised the number of people requiring humanitarian
Humanitarian Situation Report June 2016 UNICEF//2015 Highlights UNICEF provided support for the completed Vulnerability Assessment Committee (LVAC), which revised the number of people requiring humanitarian
Emergency Response Fund Yemen Fund Annual Report Yemen. Photo: UNOCHA. Annual Report Office for the Coordination of Humanitarian Affairs
 Emergency Response Fund Yemen Fund Annual Report 2013 Yemen Photo: UNOCHA Annual Report 2013 Office for the Coordination of Humanitarian Affairs Table of Contents NOTE FROM THE HUMANITARIAN COORDINATOR...1
Emergency Response Fund Yemen Fund Annual Report 2013 Yemen Photo: UNOCHA Annual Report 2013 Office for the Coordination of Humanitarian Affairs Table of Contents NOTE FROM THE HUMANITARIAN COORDINATOR...1
Dr. AM Abdullah Inspector General, MOH THE HEALTH SITUATION IN IRAQ 2009
 Dr. AM Abdullah Inspector General, MOH THE HEALTH SITUATION IN IRAQ 2009 AIMS AND OBJECTIVES The principle objective of the health system is to ensure that the healthcare needs of all Iraqi citizens are
Dr. AM Abdullah Inspector General, MOH THE HEALTH SITUATION IN IRAQ 2009 AIMS AND OBJECTIVES The principle objective of the health system is to ensure that the healthcare needs of all Iraqi citizens are
Somalia Is any part of this project cash based intervention (including vouchers)? Conditionality:
? Conditionality:") Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives HEALTH POVERTY ACTION (HPA) Emergency Nutrition Interventions for IDPs in Somaliland 2018 (NutriSom) SOM-18/N/121295
Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives HEALTH POVERTY ACTION (HPA) Emergency Nutrition Interventions for IDPs in Somaliland 2018 (NutriSom) SOM-18/N/121295
WHO Special Situation Report occupied Palestinian territory, Gaza February 2018
 WHO Special Situation Report occupied Palestinian territory, Gaza February 2018 OCCUPIED PALESTINIAN TERRITORY 2 MILLION PEOPLE AFFECTED 31 HOSPITALS IMPACTED 23 CLINICS DISRUPTED 42% DRUGS TOTALLY DEPLETED
WHO Special Situation Report occupied Palestinian territory, Gaza February 2018 OCCUPIED PALESTINIAN TERRITORY 2 MILLION PEOPLE AFFECTED 31 HOSPITALS IMPACTED 23 CLINICS DISRUPTED 42% DRUGS TOTALLY DEPLETED
Dr. Carissa F. Etienne acceptance speech Jan 2018 WHO EB
 Dr. Carissa F. Etienne acceptance speech Jan 2018 WHO EB Good morning! Chair of the Executive Board, EB Members, Member State Representatives, Director General of WHO Tedros, fellow Regional Directors,
Dr. Carissa F. Etienne acceptance speech Jan 2018 WHO EB Good morning! Chair of the Executive Board, EB Members, Member State Representatives, Director General of WHO Tedros, fellow Regional Directors,
Improving Patient Safety: First Steps
 The African Partnerships for Patient Safety Framework Improving Patient Safety: First Steps This resource outlines an approach to improving patient safety using a partnership model, structured around 12
The African Partnerships for Patient Safety Framework Improving Patient Safety: First Steps This resource outlines an approach to improving patient safety using a partnership model, structured around 12
Burkina Faso: Meningitis
 Burkina Faso: Meningitis DREF operation n MDRBF009 GLIDE n FL-2010-000039-BFA 3 March 2010 The International Federation s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created
Burkina Faso: Meningitis DREF operation n MDRBF009 GLIDE n FL-2010-000039-BFA 3 March 2010 The International Federation s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created
Strengthening nursing and midwifery in the Eastern Mediterranean Region
 WHO-EM/NUR/429/E Strengthening nursing and midwifery in the Eastern Mediterranean Region A framework for action 2016-2025 Strengthening nursing and midwifery in the Eastern Mediterranean Region A framework
WHO-EM/NUR/429/E Strengthening nursing and midwifery in the Eastern Mediterranean Region A framework for action 2016-2025 Strengthening nursing and midwifery in the Eastern Mediterranean Region A framework
Saving Every Woman, Every Newborn and Every Child
 Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Risks/Assumptions Activities planned to meet results
 Communitybased health services Specific objective : Through promotion of communitybased health care and first aid activities in line with the ARCHI 2010 principles, the general health situation in four
Communitybased health services Specific objective : Through promotion of communitybased health care and first aid activities in line with the ARCHI 2010 principles, the general health situation in four
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Conclusion: what works?
 Chapter 7 Conclusion: what works? Fishermen (Abdel Inoua) 7. Conclusion: what works? It is a convenient untruth that there has been no progress in health in the Region. This report has used a wide range
Chapter 7 Conclusion: what works? Fishermen (Abdel Inoua) 7. Conclusion: what works? It is a convenient untruth that there has been no progress in health in the Region. This report has used a wide range
Emergency Plan of Action (EPoA) Cameroon: Ebola virus disease preparedness
 Cameroon: Ebola virus disease preparedness") Emergency Plan of Action (EPoA) Cameroon: Ebola virus disease preparedness DREF Operation Operation n MDRCM019 Date of issue: 25 August 2014 Date of disaster: N/A Operation manager : Viviane Nzeusseu Point
Emergency Plan of Action (EPoA) Cameroon: Ebola virus disease preparedness DREF Operation Operation n MDRCM019 Date of issue: 25 August 2014 Date of disaster: N/A Operation manager : Viviane Nzeusseu Point
Ebola Preparedness and Response in Ghana
 Ebola Preparedness and Response in Ghana Final report to the Japan Government World Health Organization Ghana Country Office November 2016 0 TABLE OF CONTENTS SUMMARY... 2 I. SITUATION UPDATE... 3 II.
Ebola Preparedness and Response in Ghana Final report to the Japan Government World Health Organization Ghana Country Office November 2016 0 TABLE OF CONTENTS SUMMARY... 2 I. SITUATION UPDATE... 3 II.
Swaziland Humanitarian Mid-Year Situation Report January - June 2017
 Swaziland Humanitarian Mid-Year Situation Report January - June 2017 Day of the African Child commemorations, 2017 Highlights In response to the state of emergency due to the El Niño drought, the Government
Swaziland Humanitarian Mid-Year Situation Report January - June 2017 Day of the African Child commemorations, 2017 Highlights In response to the state of emergency due to the El Niño drought, the Government
Solomon Islands experience Final 5 June 2004
 Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
MALAWI Humanitarian Situation Report
 MALAWI Humanitarian Situation Report HIGHLIGHTS SITUATION IN NUMBERS The Education cluster administered a situation analysis of the most affected schools over a period of 4 days via the Real Time Monitoring
MALAWI Humanitarian Situation Report HIGHLIGHTS SITUATION IN NUMBERS The Education cluster administered a situation analysis of the most affected schools over a period of 4 days via the Real Time Monitoring
Nepal Humanitarian Situation and ACF response update n 3, May 28, 2015
 Nepal Humanitarian Situation and ACF response update n 3, May 28, 2015 Context and humanitarian situation ACF visiting affected neighborhood of Balaju in Kathmandu. 2015 Daniel Burgui Iguzkiza / ACF One
Nepal Humanitarian Situation and ACF response update n 3, May 28, 2015 Context and humanitarian situation ACF visiting affected neighborhood of Balaju in Kathmandu. 2015 Daniel Burgui Iguzkiza / ACF One
RE-ENGINEERING PRIMARY HEALTH CARE FOR SOUTH AFRICA Focus on Ward Based Primary Health Care Outreach Teams. 7June 2012
 RE-ENGINEERING PRIMARY HEALTH CARE FOR SOUTH AFRICA Focus on Ward Based Primary Health Care Outreach Teams 7June 2012 CONTEXT PHC RE-ENGINEERING Negotiated Service Delivery Agreement (NSDA) Strategic Outputs
RE-ENGINEERING PRIMARY HEALTH CARE FOR SOUTH AFRICA Focus on Ward Based Primary Health Care Outreach Teams 7June 2012 CONTEXT PHC RE-ENGINEERING Negotiated Service Delivery Agreement (NSDA) Strategic Outputs
7 Attacks on health facilities since 24 June
 Syria crisis SOUTHERN SYRIA UPDATE WHOLE OF SYRIA Issue 2 29 June-1 July 2018 Supplies from the 27.5-ton shipment delivered last week have been distributed to Dar a National Hospital, SARC, Izr a Hospital,
Syria crisis SOUTHERN SYRIA UPDATE WHOLE OF SYRIA Issue 2 29 June-1 July 2018 Supplies from the 27.5-ton shipment delivered last week have been distributed to Dar a National Hospital, SARC, Izr a Hospital,
TERMS OF REFERENCE: SECURITY FRAMEWORK ADAPTATION -LIBYA MISSION-
 TERMS OF REFERENCE: SECURITY FRAMEWORK ADAPTATION -LIBYA MISSION- Zone/Country Libya Start Date March 2017 Duration Proposition of a 3 phases consultancy - First phase : 7 days - Second phase : 2 weeks
TERMS OF REFERENCE: SECURITY FRAMEWORK ADAPTATION -LIBYA MISSION- Zone/Country Libya Start Date March 2017 Duration Proposition of a 3 phases consultancy - First phase : 7 days - Second phase : 2 weeks
1) What type of personnel need to be a part of this assessment team? (2 min)
 What type of personnel need to be a part of this assessment team? (2 min)") Student Guide Module 2: Preventive Medicine in Humanitarian Emergencies Civil War Scenario Problem based learning exercise objectives Identify the key elements for the assessment of a population following
Student Guide Module 2: Preventive Medicine in Humanitarian Emergencies Civil War Scenario Problem based learning exercise objectives Identify the key elements for the assessment of a population following
JOB PROFILE. Grade: 3 Child Protection Level: Line Management Responsibility: 3 Yes
 JOB PROFILE Job Title: Reports to: Grade: 3 Child Protection Level: Line Management Responsibility: East and Southern Africa Regional Humanitarian Nutrition Adviser Senior Humanitarian Nutrition Adviser
JOB PROFILE Job Title: Reports to: Grade: 3 Child Protection Level: Line Management Responsibility: East and Southern Africa Regional Humanitarian Nutrition Adviser Senior Humanitarian Nutrition Adviser