Hitting the mark... sometimes. Improve the accuracy of CPT code distribution. MGMA Connexion, Vol. 5, Issue 1, January 2005
|
|
|
- Lindsay Gilmore
- 5 years ago
- Views:
Transcription

1 MGMA Connexion, Vol. 5, Issue 1, January 2005 Hitting the mark... sometimes Improve the accuracy of CPT code distribution By Margie C. Andreae, MD, associate director for clinical services, Division of General Pediatrics, Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor, Gary L. Freed, MD, MPH, director, Division of General Pediatrics, Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor and Max Fawley, consultant, Finanical Office, Faculty Group Practice, University of Michigan Health System, Ann Arbor Scrutiny of physician billing and coding practices has increased steadily over the past several years. The federal government has led this initiative to reduce improper payments for Medicare-related services. 1 Private insurance carriers soon followed, with heightened investigation of health care billing and coding practices at the state and local levels. Health care providers worry about the implications of this increased oversight. Changes in billing regulations in the past decade have simplified monitoring and comparison of medical claims. 2 In 1992, in response to the need for standardized medical terminology and procedures, all payers began requiring current procedural terminology (CPT) billing codes for payment of reported services. 3 That same year, the American Medical Association and the Centers for Medicare &Medicaid Services (CMS) jointly developed CPT guidelines for coding evaluation and management (E&M) services. CMS intended these guidelines to standardize claims for different levels of E&M service. The agency revised the guidelines in and again in 1997; both versions are currently in use. 4
2 Despite revisions, many health care providers believe that the CPT E&M coding guidelines are clinically irrelevant and overly complex. 5 Physicians tend to have little understanding of the coding guidelines, and many find it difficult to apply them to clinical practice. 6 This lack of understanding results in a high rate of coding inaccuracy. 7 Physicians risk much by improper coding. Penalties may include loss of revenue, financial sanctions, disciplinary action and exclusion from participation in government programs. 8 To avoid these penalties, practices must invest significant resources in compliance management: 9 employing professional staff to monitor billing practices, buying software to enhance accuracy and training physicians to understand the guidelines for assigning the appropriate visit code. Physicians learn that proper code selection is critical to avoid coding patterns that may violate compliance regulations. 10 Even if applied properly, use of more lower-level codes (undercoding) or higher-level codes (overcoding) than the accepted norm for a particular specialty may trigger an audit. Based on a review of Medicare claims, a bell-curve distribution of CPT E&M codes has long been regarded as the norm for primary care specialties, including pediatrics. 11,12 Although modeling a bell-curve distribution in clinical practice may provide a sense of security against audits, the dogma of the bell curve has never been tested for coding accuracy. We examined the CPT E&M code distribution for a sample pediatric practice before and after applying corrections for the inaccuracy of code assignment to actual CPT E&M claims. Methods We collected data from a university health system practice with 28 general pediatricians. The practice has eight primary care health centers located in suburban and rural communities in the Midwest. The clinicians see their own patients four days a week and supervise residents and medical students one day a week in their clinic. The physicians are compensated under a productivity-based program using the relative value unit as the measure of clinical productivity. 13 Compensation is independent of collection rate or payer mix. To analyze the annual frequency distribution of CPT E&M code use for the practice as a whole, we collected claims data for all E&M established patient visits (CPT codes ) for the
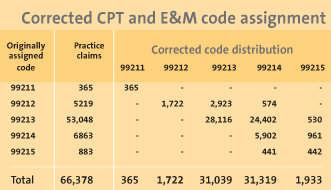
3 practice from Jan. 1-Dec. 31, We excluded resident encounters. The institution s Professional Fee Audit and Education Division of the Compliance Office conducted its own review of the accuracy of CPT E&M code assignment for a subsample of practice claims over a five-month period (January-May) in The division did this as part of its annual compliance review of each clinical department. The coding analysts two registered nurses with experience in medical records review and coding reviewed the documentation of four to five E&M established patient visit claims for every general pediatrician and determined the number of claims that had been originally assigned the correct CPT E&M code, as well as the appropriate code for claims initially assigned incorrect codes. Using the information from the compliance review, we calculated the proportion of claims in each CPT E&M category that were under- or overcoded, and the degree of coding error (e.g., undercoded by one level, two levels). We calculated these proportions for each originally assigned CPT E&M code, indicating the fraction that would have been more appropriate to code as 99211, 99212, 99213, and 99215, respectively. By applying these proportions to the larger number of claims originally assigned to each CPT E&M level in our general pediatric practice sample, we estimated the corrected number of claims for each of the five CPT E&M established patient visit codes. Results We collected 72,857 E&M established patient visit claims for the practice, which represented 95 percent of the total E&M visits; the other 5 percent were new patient visits. We excluded 6,479 of these visit claims from the data set because a resident had seen the patient. The coding analysts reviewed 125 E&M established patient visit claims for the practice (0.5 percent of all E&M established patient visits during that period). The ratio of claims for each CPT E&M code reviewed by the coding analysts (i.e., the number of vs. the number of 99212) was similar to the actual ratio of the pediatric practice claims, with representing the highest proportion in both data sets. Using the 1994/95 CPT E&M guidelines, the analysts found that 56 (45 percent) of the E&M established patient visits were improperly coded. Of these, 55 (44 percent)
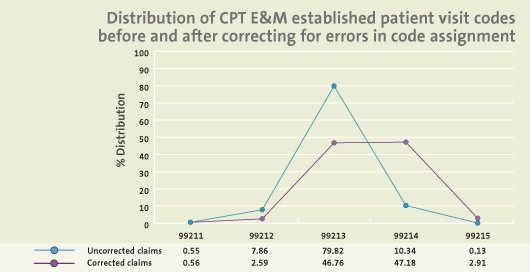
4 were undercoded by one or more levels and one (1 percent) was overcoded. The (table) shows the proportion of claims for each CPT E&M code that were under-, over- or accurately coded based on the information available from the independent review. This subsample analysis demonstrated, for example, that a large proportion of the claims (56 percent) should have been coded as and a smaller proportion should have been coded as (11 percent). After applying these proportions for each CPT E&M code to the claims in the general pediatric practice sample, we developed a corrected number of claims for each code. The uncorrected CPT E&M code distribution for the practice demonstrated a bell curve, with the predominance of claims at the mid-level (99213) for established patient visits. Application of the proportion of error based on the subsample analysis to the practice claims resulted in a shift in the configuration of the CPT E&M code distribution (see graph). The bell-shaped curve with its peak at the midline in the uncorrected sample was replaced with one that demonstrated a more equal distribution of mid- (99213) and upper-level (99214) codes. Commentary We found that the CPT E&M code distribution differed dramatically after the practice claims were corrected for coding errors identified by analysts. The corrected distribution may more accurately represent the level of complexity of services provided in general pediatric practices. Though the pediatric literature contains no data on coding accuracy, the rate of coding error in the independent compliance review in this study resembles that in the family medicine literature on larger sample sizes of both academic and private practices. In one study from the Department of Family Medicine at Northwestern University Medical School, Chicago, surveys went to 600 family physicians in both private and academic practice asking them to assign a CPT code for six different clinical scenarios. 7 Physician responses agreed with expert CPT E&M code assignment for 52 percent of the established patient visits. Undercoding was the most common error, identified in 33 percent of cases. In another study, research nurses reviewed 4,000 claims from 138 family physicians. 14 Fifty-five percent of the CPT codes generated by medical record review corresponded with the codes
5 assigned by physicians. Undercoding overcoding occurred at frequencies of 21 percent and 24 percent, respectively. Both studies attributed the high level of coding inaccuracy to the complexity of the CPT guidelines. A poor understanding of the complex and inconsistent coding guidelines may explain the difference in the distribution of CPT E&M code use for the uncorrected and corrected claims in our study. The difference may also reflect the regulatory pressure on physicians under the current system. The limited variation in code use with a sharp peak at the level for the uncorrected practice data suggests that general pediatricians consider this a comfort area, safe from increased scrutiny and costly audits. Even with better understanding of the coding guidelines, physicians will probably not change their coding patterns until payers and regulatory agencies accept a higher coding distribution as an accurate reflection of physician effort and intensity of service delivery. Regulatory authorities may perceive any increase in use of higher-level codes as upcoding rather than a correction in coding behavior. Some practices may choose to err on the side of undercoding rather than deviate from the accepted notion of the bell-curve distribution and risk being audited. The practice in our study had a reimbursement rate for a visit from $14 to $35 more than a visit, depending on the carrier. Looking only at the frequency of undercoding of the visits, the estimated annual loss in potential revenue ranged from $12,000 to $30,500 per physician. Limitations We did not assess inter-rater reliability of the coding analysts. The number of claims reviewed by the Compliance Office limited the size of our subsample analysis of accuracy of CPT E&M code assignment. The study was limited to one multisite practice and may not represent practices in other settings. However, since the CPT E&M coding guidelines are universal for the entire country and the regulatory pressure to adhere to accepted coding norms is the same across regions, our findings may apply to other general pediatric practices.
6 Correcting for coding errors may dramatically alter the CPT E&M code distribution for a general pediatric practice. Larger studies should be conducted in conjunction with an assessment of the accuracy of code assignment to determine the correct CPT E&M code distribution norm for general pediatrics and other specialties. notes 1. U.S. Department of Health and Human Services. Audit shows sustained drop in improper Medicare payments. HHS News. March 6, Available at: Accessed Feb. 6, Sgammato J. HCFA answers questions about its new documentation guidelines. Fam Pract Manag. 1995;2(1): American Medical Association. CPT Process. Chicago: American Medical Association; Moss MM, Schexnayder SM. Coding and billing in the pediatric intensive care unit. Pediatr Clin North Am. 2001;48(3): Lasker RD, Marquis MS. The intensity of physicians work in patient visits implications for the coding of patient evaluation and management services. N Engl J Med ;341(5): Martin S. Indefinite delay on E&M. American Medical News. May 11, 1998:1,7. 7. King MS, Sharp L, Lipsky MS. Accuracy of CPT evaluation and management coding by family physicians. J Am Board Fam Pract. 2001;14(3): Adams DL, Norman H, Burroughs VJ. Addressing medical coding and billing part II: A strategy for achieving compliance. A risk management approach for reducing coding and billing errors. J Natl Med Assoc. 2002;94(6): Hospital Billings on Behalf of Physicians (Resolution 820,1-97). Council on Medical Service [committee report]. December. Available at: Accessed Nov. 26, Statz KL. Protecting your practice against coding inaccuracies. SVA Consulting, Inc. [newsletter article]. Available at: Accessed Nov. 26, Navsaria D. Coding and documentation: a brief guide. Medscape Med Students.
:44-50, 52, 54. 14.")
7 2001;3(2):1-7. Available at Accessed Sept. 25, E&M Curve Data Book: 2000 Edition. Rockville: Part B News; Andreae MC, Freed GL. A new paradigm in academic health centers: Productivity-based physician compensation. Med Group Manage J. 2001;48(3):44-50, 52, Chao J, Gillanders WG, Flocke SA, Goodwin MA, Kikano GE, Stange KC. Billing for physician services: a comparison of actual billing with CPT codes assigned by direct observation. J Fam Pract. 1998;47(1):28-32.
8
ORIGINAL INVESTIGATION. Expert Agreement in Current Procedural Terminology Evaluation and Management Coding
 ORIGINAL INVESTIGATION Expert Agreement in Current Procedural Terminology Evaluation and Management Coding Mitchell S. King, MD; Martin S. Lipsky, MD; Lisa Sharp, PhD Background: Available data suggest
ORIGINAL INVESTIGATION Expert Agreement in Current Procedural Terminology Evaluation and Management Coding Mitchell S. King, MD; Martin S. Lipsky, MD; Lisa Sharp, PhD Background: Available data suggest
HA, A, CFE, E, CHC,, CPC P,, CPC P -H
 Using a Page from the Government s Play Book: Using Data to Monitor Physician Practices Andrei M. Costantino, MHA, CFE, CHC, CPC, CPC-H Director, Organizational integrity & Audit Services Compliance Institute
Using a Page from the Government s Play Book: Using Data to Monitor Physician Practices Andrei M. Costantino, MHA, CFE, CHC, CPC, CPC-H Director, Organizational integrity & Audit Services Compliance Institute
NP or PA as Billing Provider
 NP or PA as Billing Provider Claire Agnew, CPA MBA CHC Vice President of Financial Operations Phoenix Children s Medical Group Phoenix Children s Hospital Arizona s only children s hospital recognized
NP or PA as Billing Provider Claire Agnew, CPA MBA CHC Vice President of Financial Operations Phoenix Children s Medical Group Phoenix Children s Hospital Arizona s only children s hospital recognized
Compliance Program Updated August 2017
 Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
A Day in the Life of a Compliance Officer
 A Day in the Life of a Compliance Officer (for small physician practices) Mina Sellami, MBA, PMP, JD MedProv, LLC Julia Konovalov Medical Business Partners September 29, 2016 Agenda Government Regulations
A Day in the Life of a Compliance Officer (for small physician practices) Mina Sellami, MBA, PMP, JD MedProv, LLC Julia Konovalov Medical Business Partners September 29, 2016 Agenda Government Regulations
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
UNIVERSITY OF ROCHESTER MEDICAL CENTER BILLING COMPLIANCE PLAN
 UNIVERSITY OF ROCHESTER MEDICAL CENTER BILLING COMPLIANCE PLAN Revised December 31, 1998 INTRODUCTION This plan is an integral part of the University s ongoing efforts to achieve compliance with federal
UNIVERSITY OF ROCHESTER MEDICAL CENTER BILLING COMPLIANCE PLAN Revised December 31, 1998 INTRODUCTION This plan is an integral part of the University s ongoing efforts to achieve compliance with federal
3M Health Information Systems Should physicians assign their own codes?
 3M Health Information Systems Should physicians assign their own codes? The practical guide to striking a coding balance It started with the EHR boom The adoption of electronic health records (EHR) significantly
3M Health Information Systems Should physicians assign their own codes? The practical guide to striking a coding balance It started with the EHR boom The adoption of electronic health records (EHR) significantly
Evaluation and Management Documentation and Coding Technology Adoption
 Evaluation and Management Documentation and Coding Technology Adoption by Susan H. Fenton, PhD, MBA, RHIA; and Larry D. Gamm, PhD Introduction The adoption of information technology in healthcare is anticipated
Evaluation and Management Documentation and Coding Technology Adoption by Susan H. Fenton, PhD, MBA, RHIA; and Larry D. Gamm, PhD Introduction The adoption of information technology in healthcare is anticipated
Common Errors on the T3010 related to fundraising costs. Know how to avoid them
 Common Errors on the T3010 related to fundraising costs Know how to avoid them 1 Focus of presentation Many errors that charities make in the reporting of their fundraising expenses on the T3010 occur
Common Errors on the T3010 related to fundraising costs Know how to avoid them 1 Focus of presentation Many errors that charities make in the reporting of their fundraising expenses on the T3010 occur
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM
 The Harvard Pilgrim Independence Plan SM") Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Getting Started with OIG Compliance
 Getting Started with OIG Compliance Kathy Mills Chang, MCS-P CCPC Do You Feel Like This? Or This? Does Your Business Deserve the Same Focus Your Patients Do? How This Training Will Protect You! Stay within
Getting Started with OIG Compliance Kathy Mills Chang, MCS-P CCPC Do You Feel Like This? Or This? Does Your Business Deserve the Same Focus Your Patients Do? How This Training Will Protect You! Stay within
2011 Electronic Prescribing Incentive Program
 2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Medicare Regulations and Rules Update What Should You Know?
 Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Medicare Regulations and Rules Update What Should You Know? Presenters: Gary Massey, CPA & Emily Wetsel, CPA Investment advisory services are offered through CliftonLarsonAllen Wealth Advisors, LLC, an
Decrease in Hospital Uncompensated Care in Michigan, 2015
 Decrease in Hospital Uncompensated Care in Michigan, 2015 July 2017 Introduction The Affordable Care Act (ACA) expanded access to health insurance coverage for Michigan residents in 2014 through the creation
Decrease in Hospital Uncompensated Care in Michigan, 2015 July 2017 Introduction The Affordable Care Act (ACA) expanded access to health insurance coverage for Michigan residents in 2014 through the creation
Table of Contents. Overview. Demographics Section One
 Table of Contents Overview Introduction Purpose... x Description... x What s New?... x Data Collection... x Response Rate... x How to Use This Report Report Organization... xi Appendices... xi Additional
Table of Contents Overview Introduction Purpose... x Description... x What s New?... x Data Collection... x Response Rate... x How to Use This Report Report Organization... xi Appendices... xi Additional
Doris V. Branker, CPC, CPC-I, CEMC
 Doris V. Branker, CPC, CPC-I, CEMC 1 Identify the common sources for missed reimbursement in the specialty practice Identify the common sources for reduced reimbursement in the specialty practice Identify
Doris V. Branker, CPC, CPC-I, CEMC 1 Identify the common sources for missed reimbursement in the specialty practice Identify the common sources for reduced reimbursement in the specialty practice Identify
A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans. Optimizing revenue from a compliance perspective
 A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
Agenda. National Landscape. Background. Optimizing revenue from a compliance perspective. Mitigate the risk: Data mining and coding audits
 A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
A Physician Led Comprehensive Coding Compliance Program: Datamining to Disciplinary Action Plans Keith Ponitz, M.D. October 16,2012 Agenda Background Optimizing revenue from a compliance perspective Mitigate
Shared and Incident To Billing of E/M Services in Radiation Oncology Updated November 2017
 ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
CRCE Exam Study Manual Update for 2017
 CRCE Exam Study Manual Update for 2017 This document reflects updates made to the instructional content from the Certified Revenue Cycle Executive (CRCE-I, CRCE-P) Exam Study Manual - 2016 to the 2017
CRCE Exam Study Manual Update for 2017 This document reflects updates made to the instructional content from the Certified Revenue Cycle Executive (CRCE-I, CRCE-P) Exam Study Manual - 2016 to the 2017
The Impact of Physician Quality Measures on the Coding Process
 The Impact of Physician Quality Measures on the Coding Process The Impact of Physician Quality Measures on the Coding Process by Mark Morsch, MS; Ronald Sheffer, Jr., MA; Susan Glass, RHIT, CCS-P; Carol
The Impact of Physician Quality Measures on the Coding Process The Impact of Physician Quality Measures on the Coding Process by Mark Morsch, MS; Ronald Sheffer, Jr., MA; Susan Glass, RHIT, CCS-P; Carol
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
Clinical Policy: Automated Ambulatory Blood Pressure Monitoring Reference Number: CP.MP. 262
 Clinical Policy: Reference Number: CP.MP. 262 Effective Date: 4/06 Last Review Date: 01/17 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Clinical Policy: Reference Number: CP.MP. 262 Effective Date: 4/06 Last Review Date: 01/17 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Few non-clinical issues have created as
 from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
from October 2001 How to Get All the 99214s You Deserve It s easier than you might think to get what s coming to you. Emily Hill, PA-C Few non-clinical issues have created as much controversy as the CPT
March 6, Dear Administrator Verma,
 March 6, 2018 Seema Verma Administrator Centers for Medicare and Medicaid Services U.S. Department of Health and Human Services Room 445 G, Hubert H. Humphrey Building 200 Independence Avenue SW Washington,
March 6, 2018 Seema Verma Administrator Centers for Medicare and Medicaid Services U.S. Department of Health and Human Services Room 445 G, Hubert H. Humphrey Building 200 Independence Avenue SW Washington,
The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare
 The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare AT&T, Healthcare, and You Overview The American Recovery and Reinvestment Act of 2009 (ARRA) allocated more than $180
The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare AT&T, Healthcare, and You Overview The American Recovery and Reinvestment Act of 2009 (ARRA) allocated more than $180
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Using Data for Risk Assessment, Benchmarking, and Creating Physician Scorecards
 Using Data for Risk Assessment, Benchmarking, and Creating Physician Scorecards Presented by: Marsha Martin, RHIT, CCS-P Margaret Nusbaum, CPC Andrei Costantino, MHA, CHC, CPC, CPC-H Sunday April 13, 2008
Using Data for Risk Assessment, Benchmarking, and Creating Physician Scorecards Presented by: Marsha Martin, RHIT, CCS-P Margaret Nusbaum, CPC Andrei Costantino, MHA, CHC, CPC, CPC-H Sunday April 13, 2008
Medicare Advantage PPO participation Termination - Practice Name (Tax ID #: <TaxID>)
") July xx, 2013 INDIVDUAL PRACTICE VERSION RE: Medicare Advantage PPO participation Termination - Practice Name (Tax ID #: ) Dear :
July xx, 2013 INDIVDUAL PRACTICE VERSION RE: Medicare Advantage PPO participation Termination - Practice Name (Tax ID #: ) Dear :
3M Health Information Systems. A case study in coding compliance: Achieving accuracy and consistency
 3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
Best Practices Contracting for Health IT Supporting Pay-for-Performance (P4P) Early Findings
 Early Findings") Best Practices Contracting for Health IT Supporting Pay-for-Performance (P4P) Early Findings Researchers: Martin, Thomas R. PhD, Assistant Professor St. Joseph s University Department of Health Services;
Best Practices Contracting for Health IT Supporting Pay-for-Performance (P4P) Early Findings Researchers: Martin, Thomas R. PhD, Assistant Professor St. Joseph s University Department of Health Services;
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
The E/M Essentials Pocket Guide
 The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
Observation Care Evaluation and Management Codes Policy
 Policy Number Observation Care Evaluation and Management Codes Policy 2017R0115A Annual Approval Date 3/8/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible
Policy Number Observation Care Evaluation and Management Codes Policy 2017R0115A Annual Approval Date 3/8/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible
Certified Ophthalmic Executive (COE) Review Day
 Review Day") Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
9/25/2012 AGENDA. Set the Stage Monitoring versus Audit Identifying Risk Strategies related to an audit plan Corrective Action Plans Examples
 The Art and Science of Designing a Physician Practice Audit : Unique Techniques Lori Laubach, Partner MOSS ADAMS LLP 1 AGENDA Set the Stage Monitoring versus Audit Identifying Risk Strategies related to
The Art and Science of Designing a Physician Practice Audit : Unique Techniques Lori Laubach, Partner MOSS ADAMS LLP 1 AGENDA Set the Stage Monitoring versus Audit Identifying Risk Strategies related to
Avoiding the Cap Trap What Every Hospice Needs to Know. Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc.
 Avoiding the Cap Trap What Every Hospice Needs to Know Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc. Overview 11% of hospices exceeded the cap in 2012 with an average overage
Avoiding the Cap Trap What Every Hospice Needs to Know Matthew Gordon, CPA Principal Consultant / Founder Cap Doctor Associates, Inc. Overview 11% of hospices exceeded the cap in 2012 with an average overage
The Transition to Version 5010 and ICD-10
 The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
THIRD WAVE. Over the last 20 years, we have observed two GETTING READY FOR THE OF PHYSICIAN-HOSPITAL INTEGRATION
 4 GETTING READY FOR THE THIRD WAVE OF PHYSICIAN-HOSPITAL INTEGRATION Over the last 20 years, we have observed two major waves of physician-hospital integration. Now, partly in response to the recently
4 GETTING READY FOR THE THIRD WAVE OF PHYSICIAN-HOSPITAL INTEGRATION Over the last 20 years, we have observed two major waves of physician-hospital integration. Now, partly in response to the recently
Should PCMH accreditation be the next step in your quest for high-quality care delivery?
 This Web version may be reproduced for individual use. Should PCMH accreditation be the next step in your quest for high-quality care delivery? Lessons learned from one organization that achieved PCMH
This Web version may be reproduced for individual use. Should PCMH accreditation be the next step in your quest for high-quality care delivery? Lessons learned from one organization that achieved PCMH
Compliance Workplan for Physician Practices
 Compliance Workplan for Physician Practices Ronda Tews, CPC, CHC, CCP-P St. John s Health System Springfield, MO www.hcca-info.org 888-580-8373 Put together a practical plan for your physician s practice
Compliance Workplan for Physician Practices Ronda Tews, CPC, CHC, CCP-P St. John s Health System Springfield, MO www.hcca-info.org 888-580-8373 Put together a practical plan for your physician s practice
COMPARATIVE STUDY OF HOSPITAL ADMINISTRATIVE DATA USING CONTROL CHARTS
 International Jour. of Manage.Studies.,Statistics & App.Economics (IJMSAE), ISSN 2250-0367, Vol. 7, No. I (June 2017), pp. 1-12 COMPARATIVE STUDY OF HOSPITAL ADMINISTRATIVE DATA USING CONTROL CHARTS SUCHETA
International Jour. of Manage.Studies.,Statistics & App.Economics (IJMSAE), ISSN 2250-0367, Vol. 7, No. I (June 2017), pp. 1-12 COMPARATIVE STUDY OF HOSPITAL ADMINISTRATIVE DATA USING CONTROL CHARTS SUCHETA
POLICY BRIEF. Identifying Adverse Drug Events in Rural Hospitals: An Eight-State Study. May rhrc.umn.edu. Background.
 POLICY BRIEF Identifying Adverse Drug Events in Rural Hospitals: An Eight-State Study Michelle Casey, MS Peiyin Hung, MSPH Emma Distel, MPH Shailendra Prasad, MBBS, MPH Key Findings In 2013, Critical Access
POLICY BRIEF Identifying Adverse Drug Events in Rural Hospitals: An Eight-State Study Michelle Casey, MS Peiyin Hung, MSPH Emma Distel, MPH Shailendra Prasad, MBBS, MPH Key Findings In 2013, Critical Access
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
GUIDELINES FOR CRITERIA AND CERTIFICATION RULES ANNEX - JAWDA Data Certification for Healthcare Providers - Methodology 2017.
 GUIDELINES FOR CRITERIA AND CERTIFICATION RULES ANNEX - JAWDA Data Certification for Healthcare Providers - Methodology 2017 December 2016 Page 1 of 14 1. Contents 1. Contents 2 2. General 3 3. Certification
GUIDELINES FOR CRITERIA AND CERTIFICATION RULES ANNEX - JAWDA Data Certification for Healthcare Providers - Methodology 2017 December 2016 Page 1 of 14 1. Contents 1. Contents 2 2. General 3 3. Certification
SCRIBES, SMAS AND INCIDENT T0
 SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
Presentation Objectives
 Managed Care Negotiation Strategies Using Transparency and Case Data to demonstrate to Payers How ASCs Save Money I. Naya Kehayes, M.P.H., Managing Principal & CEO R. Matthew Kilton, M.B.A., M.H.A., Principal
Managed Care Negotiation Strategies Using Transparency and Case Data to demonstrate to Payers How ASCs Save Money I. Naya Kehayes, M.P.H., Managing Principal & CEO R. Matthew Kilton, M.B.A., M.H.A., Principal
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters. Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014
 Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014 Agenda Medicare cost report myths Common cost reporting
Medicare Cost Reporting and PPS FFY 2015 Proposed Rule Why it Still Matters Glenn Grigsby, CPA OACHC 2014 Annual Spring Conference March 11, 2014 Agenda Medicare cost report myths Common cost reporting
Impact of Financial and Operational Interventions Funded by the Flex Program
 Impact of Financial and Operational Interventions Funded by the Flex Program KEY FINDINGS Flex Monitoring Team Policy Brief #41 Rebecca Garr Whitaker, MSPH; George H. Pink, PhD; G. Mark Holmes, PhD University
Impact of Financial and Operational Interventions Funded by the Flex Program KEY FINDINGS Flex Monitoring Team Policy Brief #41 Rebecca Garr Whitaker, MSPH; George H. Pink, PhD; G. Mark Holmes, PhD University
time to replace adjusted discharges
 REPRINT May 2014 William O. Cleverley healthcare financial management association hfma.org time to replace adjusted discharges A new metric for measuring total hospital volume correlates significantly
REPRINT May 2014 William O. Cleverley healthcare financial management association hfma.org time to replace adjusted discharges A new metric for measuring total hospital volume correlates significantly
Are There Hospice Patients Living in Your Home Health Agency?
 Are There Hospice Patients Living in Your Home Health Agency? July 10, 2012 Presented by: Cindy Campbell, RN, BSN Associate Director, Operational Consulting Fazzi Associates 243 King Street, Suite 246
Are There Hospice Patients Living in Your Home Health Agency? July 10, 2012 Presented by: Cindy Campbell, RN, BSN Associate Director, Operational Consulting Fazzi Associates 243 King Street, Suite 246
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
About the AHA Central Office and Coding Clinic
 About the AHA Central Office and Coding Clinic AHA Central Office Clearinghouse service established by 1963 Memorandum of Understanding with HHS to provide free assistance with ICD-9-CM advice Switched
About the AHA Central Office and Coding Clinic AHA Central Office Clearinghouse service established by 1963 Memorandum of Understanding with HHS to provide free assistance with ICD-9-CM advice Switched
Medical Billing Audits for Local Health Departments
 Medical Billing Audits for Local Health Departments Submitted to: Illinois Public Health Association Submitted by: NCG Medical, Inc. January 13, 2017 1 Executive Summary Local health departments (LHDs)
Medical Billing Audits for Local Health Departments Submitted to: Illinois Public Health Association Submitted by: NCG Medical, Inc. January 13, 2017 1 Executive Summary Local health departments (LHDs)
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
Procedural andpr Diagnostic Coding. Copyright 2012 Delmar, Cengage Learning. All rights reserved.
 Procedural andpr Diagnostic Coding What is Coding? Converting descriptions of disease, injury, procedures, and services into numeric or alphanumeric descriptors Accurate coding maximizes reimbursement
Procedural andpr Diagnostic Coding What is Coding? Converting descriptions of disease, injury, procedures, and services into numeric or alphanumeric descriptors Accurate coding maximizes reimbursement
August 25, Dear Ms. Verma:
 Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
Seema Verma Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, S.W. Room 445-G Washington, DC 20201 CMS 1686 ANPRM, Medicare Program; Prospective
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
Alabama Primary Health Care Association October 4, Separating Clinical Documentation, Professional Coding, and Billing: A Workflow Analysis
 Alabama Primary Health Care Association October 4, 2017 Separating Clinical Documentation, Professional Coding, and Billing: A Workflow Analysis Presented by: Gary Lucas, M.Sc., CPC, CPC-I, AHIMA ICD-10
Alabama Primary Health Care Association October 4, 2017 Separating Clinical Documentation, Professional Coding, and Billing: A Workflow Analysis Presented by: Gary Lucas, M.Sc., CPC, CPC-I, AHIMA ICD-10
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY
 OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 232.10 T0 Effective Date: March 1, 2017 Table of Contents Page INSTRUCTIONS
OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 232.10 T0 Effective Date: March 1, 2017 Table of Contents Page INSTRUCTIONS
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
Caring for the Whole Patient Predictive Analytics Technology, Socio-demographic Insights, and Improved Patient Outcomes Randy K.
 WHITE PAPER Caring for the Whole Patient Randy K. Hawkins, MD Caring for the Whole Patient Socio-demographic data, not normally present in the electronic health record, and not routinely found in the hands
WHITE PAPER Caring for the Whole Patient Randy K. Hawkins, MD Caring for the Whole Patient Socio-demographic data, not normally present in the electronic health record, and not routinely found in the hands
EXECUTIVE SUMMARY. Introduction. Methods
 EXECUTIVE SUMMARY Introduction University of Michigan (UM) General Pediatrics offers health services to patients through nine outpatient clinics located throughout South Eastern Michigan. These clinics
EXECUTIVE SUMMARY Introduction University of Michigan (UM) General Pediatrics offers health services to patients through nine outpatient clinics located throughout South Eastern Michigan. These clinics
Washington Update. Agenda
 Washington Update Agenda Trending topics Quality Payment Program: Mid-Year Status Report Proposed 2018 Medicare regulations Healthcare Reform Update Q&A 1 Non Discrimination Standards Where did it come
Washington Update Agenda Trending topics Quality Payment Program: Mid-Year Status Report Proposed 2018 Medicare regulations Healthcare Reform Update Q&A 1 Non Discrimination Standards Where did it come
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Clinical Episode-Based Payment (CEBP) Measures Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach
Clinical Episode-Based Payment (CEBP) Measures Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach
HCA. Coding, Billing, and Documentation Regarding Inpatient, Outpatient, Ambulatory Surgery, and Physician Patient Accounts 3/17/2015
 Coding, Billing, and Documentation Regarding Inpatient, Outpatient, Ambulatory Surgery, and Physician Patient Accounts Mark J. Eddy, CPA Vice President HCA Internal Audit 1 HCA Headquarters: Nashville,
Coding, Billing, and Documentation Regarding Inpatient, Outpatient, Ambulatory Surgery, and Physician Patient Accounts Mark J. Eddy, CPA Vice President HCA Internal Audit 1 HCA Headquarters: Nashville,
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals
 NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
Cloning and Other Compliance Risks in Electronic Medical Records
 Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
CIO Legislative Brief
 CIO Legislative Brief Comparison of Health IT Provisions in the Committee Print of the 21 st Century Cures Act (dated November 25, 2016), H.R. 6 (21 st Century Cures Act) and S. 2511 (Improving Health
CIO Legislative Brief Comparison of Health IT Provisions in the Committee Print of the 21 st Century Cures Act (dated November 25, 2016), H.R. 6 (21 st Century Cures Act) and S. 2511 (Improving Health
Are physicians ready for macra/qpp?
 Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
REGULATION, ACCREDITATION, AND PAYMENT PRACTICE GROUP (June, July, August 2004)
") REGULATION, ACCREDITATION, AND PAYMENT PRACTICE GROUP (June, July, August 2004) Lester J. Perling Broad and Cassel Fort Lauderdale, Florida I. Case Summaries CMNs Document Medical Necessity In Maximum
REGULATION, ACCREDITATION, AND PAYMENT PRACTICE GROUP (June, July, August 2004) Lester J. Perling Broad and Cassel Fort Lauderdale, Florida I. Case Summaries CMNs Document Medical Necessity In Maximum
POLICIES AND PROCEDURE MANUAL
 POLICIES AND PROCEDURE MANUAL Policy: MP017 Section: Medical Benefit Policy Subject: Ambulance Transport Service I. Policy: Ambulance Transport Service II. Purpose/Objective: To provide a policy of coverage
POLICIES AND PROCEDURE MANUAL Policy: MP017 Section: Medical Benefit Policy Subject: Ambulance Transport Service I. Policy: Ambulance Transport Service II. Purpose/Objective: To provide a policy of coverage
Medical Fee Schedule (MFS) Frequently Asked Questions (FAQs) General FAQs
 Frequently Asked Questions (FAQs) General FAQs") Medical Fee Schedule (MFS) Frequently Asked Questions (FAQs) General FAQs 1. What is the Medical Fee Schedule (MFS)? The MFS is the schedule of maximum fees payable for scheduled medical services rendered
Medical Fee Schedule (MFS) Frequently Asked Questions (FAQs) General FAQs 1. What is the Medical Fee Schedule (MFS)? The MFS is the schedule of maximum fees payable for scheduled medical services rendered
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
Updates in Coding & Billing Strategies.
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
The Law and EHRs in Medical Education: The ARRA World. Overview
 The Law and EHRs in Medical Education: The ARRA World David Donnersberger MD, JD Clinical Assistant Professor of Medicine MS3 Site Director University of Chicago Pritzker School of Medicine Overview American
The Law and EHRs in Medical Education: The ARRA World David Donnersberger MD, JD Clinical Assistant Professor of Medicine MS3 Site Director University of Chicago Pritzker School of Medicine Overview American
Population and Sampling Specifications
 Mat erial inside brac ket s ( [ and ] ) is new to t his Specific ati ons Manual versi on. Introduction Population Population and Sampling Specifications Defining the population is the first step to estimate
Mat erial inside brac ket s ( [ and ] ) is new to t his Specific ati ons Manual versi on. Introduction Population Population and Sampling Specifications Defining the population is the first step to estimate
MACRA MACRA MACRA 9/30/2015. From the Congress: A New Medicare Payment System. The Future of Medicare: A Move Toward Value Driven Healthcare W20.
 W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Reimbursement Update MAPA Tricia Marriott, PA-C, MPAS, DFAAPA AAPA Director of Reimbursement on Twitter
 Reimbursement Update MAPA 2012 Tricia Marriott, PA-C, MPAS, DFAAPA AAPA Director of Reimbursement Advocacy tmarriott@aapa.org @TriciaPAC on Twitter Disclaimer This presentation was current at the time
Reimbursement Update MAPA 2012 Tricia Marriott, PA-C, MPAS, DFAAPA AAPA Director of Reimbursement Advocacy tmarriott@aapa.org @TriciaPAC on Twitter Disclaimer This presentation was current at the time
The Home Health Groupings Model (HHGM)
") The Home Health Groupings Model (HHGM) September 5, 017 PRESENTED BY: Al Dobson, Ph.D. PREPARED BY: Al Dobson, Ph.D., Alex Hartzman, M.P.A, M.P.H., Kimberly Rhodes, M.A., Sarmistha Pal, Ph.D., Sung Kim,
The Home Health Groupings Model (HHGM) September 5, 017 PRESENTED BY: Al Dobson, Ph.D. PREPARED BY: Al Dobson, Ph.D., Alex Hartzman, M.P.A, M.P.H., Kimberly Rhodes, M.A., Sarmistha Pal, Ph.D., Sung Kim,
REPORT OF THE BOARD OF TRUSTEES
 REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
Facility Survey of Providers of ESRD Therapy. Number of Dialysis and Transplant Units 1989 and Number of Units ,660 2,421 1,669
 Annual Data Report Facility Survey of Providers of ESRD Therapy Chapter X Annual Facility Survey of Providers of ESRD Therapy T he Annual Facility Survey conducted, by HCFA, is the source of all the results
Annual Data Report Facility Survey of Providers of ESRD Therapy Chapter X Annual Facility Survey of Providers of ESRD Therapy T he Annual Facility Survey conducted, by HCFA, is the source of all the results
CMS Meaningful Use Incentives NPRM
 CMS Meaningful Use Incentives NPRM Margret Amatayakul MBA, RHIA, CHPS, CPHIT, CPEHR, CPHIE, FHIMSS President, Margret\A Consulting, LLC Faculty and Board of Examiners, Health IT Certification, LLC Notice
CMS Meaningful Use Incentives NPRM Margret Amatayakul MBA, RHIA, CHPS, CPHIT, CPEHR, CPHIE, FHIMSS President, Margret\A Consulting, LLC Faculty and Board of Examiners, Health IT Certification, LLC Notice
Tools and Resources: Staying Up-To-Date with the Medicare Physician Fee Schedule
 April 2015 Tools and Resources: Staying Up-To-Date with the Medicare Physician Fee Schedule The Medicare Physician Fee Schedule is complex and has a lot of moving parts as evidenced by correction notices
April 2015 Tools and Resources: Staying Up-To-Date with the Medicare Physician Fee Schedule The Medicare Physician Fee Schedule is complex and has a lot of moving parts as evidenced by correction notices
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #374: Closing the Referral Loop: Receipt of Specialist Report National Quality Strategy Domain: Effective Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
Quality ID #374: Closing the Referral Loop: Receipt of Specialist Report National Quality Strategy Domain: Effective Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
TITLE 37. HEALTH -- SAFETY -- MORALS CHAPTER HOSPITALS HOSPITAL MEASURES ADVISORY COUNCIL. Go to the Ohio Code Archive Directory
 Page 1 ß 3727.31. Hospital measures advisory council created HOSPITAL MEASURES ADVISORY COUNCIL ORC Ann. 3727.31 (2012) There is hereby created the hospital measures advisory council. The council shall
Page 1 ß 3727.31. Hospital measures advisory council created HOSPITAL MEASURES ADVISORY COUNCIL ORC Ann. 3727.31 (2012) There is hereby created the hospital measures advisory council. The council shall
The Impact of Medicaid Primary Care Payment Increases in Washington State
 EXECUTIVE SUMMARY BACKGROUND Enhanced payments for primary care services provided to Medicaid patients in 2013 and 2014, authorized by the federal Patient Protection and Affordable Care Act (ACA) of 2010,
EXECUTIVE SUMMARY BACKGROUND Enhanced payments for primary care services provided to Medicaid patients in 2013 and 2014, authorized by the federal Patient Protection and Affordable Care Act (ACA) of 2010,
Responding to Today s Health Care Regulatory Environment
 Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
The Trauma System. Prevention Pre-hospital care and transport Acute hospital care Rehab Research
 An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
September 8, 2015 EXECUTIVE SUMMARY
 AMERICAN ASSOCIATION OF NEUROLOGICAL SURGEONS THOMAS A. MARSHALL, Executive Director 5550 Meadowbrook Drive Rolling Meadows, IL 60008 Phone: 888-566-AANS Fax: 847-378-0600 info@aans.org President H. HUNT
AMERICAN ASSOCIATION OF NEUROLOGICAL SURGEONS THOMAS A. MARSHALL, Executive Director 5550 Meadowbrook Drive Rolling Meadows, IL 60008 Phone: 888-566-AANS Fax: 847-378-0600 info@aans.org President H. HUNT
2017 Freestanding Ambulatory Surgery Center Survey
 2017 Freestanding Ambulatory Surgery Center Survey Part A : General Information 1. Identification UID: Facility Name: County: Street Address: City: Zip: Mailing Address: Mailing City: Mailing Zip: 2. Report
2017 Freestanding Ambulatory Surgery Center Survey Part A : General Information 1. Identification UID: Facility Name: County: Street Address: City: Zip: Mailing Address: Mailing City: Mailing Zip: 2. Report
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice