LAST DAYS OF LIFE CARE PLAN
|
|
|
- Jessica Thompson
- 5 years ago
- Views:
Transcription
1 INFORMATION FOR HEALTHCARE PROFESSIONALS REGARDING THE LAST DAYS OF LIFE CARE PLAN RECOGNISE The recognition of dying is always complex. The possibility that a person may die within the next few days or hours once recognised, needs to be communicated clearly to that person, those important to them and the Multidisciplinary Team (MDT). All decisions made and actions taken are in accordance with the person s needs and wishes, and these are regularly reviewed and decisions revised accordingly. Use algorithm over page to support MDT assessment. COMMUNICATE, INVOLVE AND SUPPORT Sensitive, comprehensive, clear, communication takes place between staff and the dying person, where possible and appropriate, and those identified as important to them. Shared decisions are made about treatment and care to the extent that the dying person wants. Where there is no record to the contrary and the person does not have capacity to give consent, it is reasonable to assume that they would want their family and those important to them to be informed about their condition and prognosis. The possibility that the person may be dying in the coming days or hours is discussed with the person, and with their relative(s), whānau, friend(s) and those identified as important to them. This communication must be conducted in a way that maximises privacy, sensitivity, compassion and is culturally appropriate. The needs of the relatives, whānau and friends are actively explored, respected and met as far as possible. Staff must check and document the person s (and others who have been involved) understanding of the information that is being communicated. CREATE AN INDIVIDUALISED CARE PLAN This individualised care plan is based on the principles of Te Ara Whakapiri and includes the provision of food and drink, symptom control and physical, psychological, social and spiritual support, which is agreed, co-ordinated and delivered with dignity, care and compassion. The care plan is developed using clinical evidence and clinical judgment and discussed with the person and those important to them. Symptom Management Guidelines are provided to support the Last Days of Life Care Plan. This care plan is generic, for the use in any care setting. Each organisation using this guideline should provide its staff with further guidance as to the organisation s specific requirements, for example the use of electronic clinical records alongside this document, responsibilities for specific sections, times of routine assessments and multidisciplinary review, and contact processes with other professionals involved in the person s care. REVIEW The care plan should be dynamic, focussing on assessing the person s condition, needs and wishes and responding appropriately and reviewed at least daily. A full review of current medications is undertaken and non-essentials discontinued. The person should only be receiving medications that are beneficial at this time, with as required medication (prn) prescribed for the most common symptoms at end of life such as pain, respiratory tract secretions, restlessness and agitation, breathlessness, nausea and vomiting. See algorithm over the page for triggers for full MDT assessment. REFERENCES: International Collaborative for Best Care for the Dying Person Ellershaw J. & Wilkinson S. (2011) Care of the dying: a pathway to excellence. 2nd rev ed. Oxford: Oxford University Press. Mason S, Dowson J, Gambles M, Ellershaw J. OPCARE(optimising research for cancer patient care in the last days of life, Eur J Palliative Care 2012;19:17-9 Ellershaw J, Lakhani M. Best Care for the dying patient. BMJ 2013; 347:f4428 Ministry of Health (2015) Te Ara Whakapiri Principles and Guidelines for the Last Days of Life. Wellington: Ministry of Health.
2 ALGORITHM Decision making in recognising dying and use of the care plan to support care in the last hours or days of life. Deterioration in the person s condition suggests that the patient could be dying. ASSESSMENT Multidisciplinary Team (MDT) Assessment Is there a potentially reversible cause for the person s condition? Eg exclude opioid toxicity, renal failure, hypocalcaemia, infection. Is there an advance decision to refuse treatment, Advance Care Plan, Advanced Directive? Does the person have the capacity to make their own decisions on their own treatment at this moment in time? Is the person being cared for in the most appropriate setting or place of their choice? Is a specialist referral needed? For example Specialist Palliative Care or a second opinion. Is there an expressed wish for organ/tissue donation? The support of an advocate as appropriate. CLINICAL DECISION COMMUNICATION The person is NOT recognised as dying (in the last hours or days of life) Review the current plan of care Discussion with the person and relative or carer to explain the new or revised plan of care The person IS recognised as dying (in the last hours or days of life) The person (where appropriate) and relative or carer communication is focused on recognition and understanding that the patient is dying Discussion with the person (where appropriate) and relative or carer to explain the current plan of care MANAGEMENT The Last Days of Life Care Plan is commenced including initial, then ongoing regular assessments A full multidisciplinary team (MDT) reassessment and review of the current plan of care should be triggered when one or more of the following apply: REASSESSMENT Improved consciousness level, functional ability, oral intake, mobility, ability to perform self-care and/or Concerns expressed regarding management plan from either person, relative or carer or team member Always remember that the Specialist Palliative Care Teams are available for advice and support, especially if: Symptom control is difficult and/or if there are difficult communication issues or you need advice or support regarding your care delivery supported by the care plan. Arohanui Hospice (06) Palmerston North Hospital Palliative Care Service: (06) ext 7484
3 BARCODE AREA LAST DAYS OF LIFE CARE PLAN Section 1: Initial Assessment Recognition of Dying Recognising a person is dying is complex, irrespective of diagnosis or history. Reversible causes for the person s condition should be assessed and managed (use Health Professional s Information Sheet for guidance). Where the MDT recognises a person is in their last hours or days of life, they must ensure that the person, their relative, whānau, or friend have the opportunity to understand the possibility that death is imminent. The following should be considered: Taha Tinana - Physical Health SENIOR CLINICIAN TO COMPLETE Has an Advance Care Plan, Advanced Directive been completed?... and has this been reviewed by the clinical team?... Is this the preferred place of care for the person?... Is this the most appropriate place of care for the person?... If no, has an alternative place of care been discussed with the person, relative, whānau or friend?... If the person is to transfer to another appropriate care setting, has this been organised according to organisational policies and procedures?... To support communication, has written information been given to the relative/whanau/friend such as What to Expect When Someone is Dying?... Is the General Practice Team/ARC facility aware the person is dying?... Comments: Awareness of Person s Changing Condition First language consider need for interpreter (contact no): Taha Whānau - Family Health The person is able to take a full and active part in communication: The person is aware that they are dying: The relative, whānau spokesperson or friend* is able to take a full and active part in communication: The relative, whānau spokesperson or friend* is aware that their relative, whānau member or friend* is dying: Record outcome of the shared discussion between health professionals and with the person, relative, whānau or friend* * Included in this list is also advocate and carer. ** Senior clinician refers to most senior clinical doctor or nurse practitioner appropriate to that care setting, eg in ARC this would be general practitioner or nurse practitioner, in acute care setting it would be registrar or consultant. page 1
4 Care Plan Commenced Date care plan commenced... Time care plan commenced... Print: Name of senior clinician**/lead health practitioner (record name below) Print: Name of nurse (record name below) Signature: Signature: Name: Next of Kin/Key Spokesperson/EPOA (please circle and record name below) Name: Relative, whānau or friend* of those present for discussion (record names(s) below) Relationship: Relationship: A care plan may be discontinued after discussion with the MDT. If this care plan is discontinued please record here: Date discontinued... Time discontinued... Reasons why this care plan was discontinued by MDT Team The person is aware of changing focus of care: The relative, whānau or friend* is aware of changing focus of care: Signatures All personnel completing the care plan please sign below. You should also have read and understood the Health Care Professional Information on a separate sheet. Name (print) Full Signature Initials Professional Title Date * Included in this list is also advocate and carer. ** Senior clinician refers to most senior clinical doctor or nurse practitioner appropriate to that care setting, eg in ARC this would be general practitioner or nurse practitioner, in acute care setting it would be registrar or consultant. page 2
5 BARCODE AREA Taha Whānau - Family Health Taha Tinana - Physical Health Section 1: Initial Assessment cont... The clinical team have up to date contact information for the relative, whānau or friend* as documented below 1st contact name... Relationship to person... Tel no... Mobile no... When to contact: At any time Not at night time Staying with person overnight 2nd contact name... Relationship to person... Tel no... Mobile no... When to contact: At any time Not at night time Staying with person overnight Next of kin (this may be different from above) or Enduring Power of Attorney (EPOA) or Whānau spokesperson Name... Name... Contact details... Contact details... The relative, whānau or friend* has had a full explanation of the facilities and support available to them: and written information has been given: Base Line Information Comments: Conscious state: Conscious Semi-conscious Unconscious Alertness: Fully alert Confused Delirious In pain: Dyspnoea: Agitated: Respiratory tract secretions: Able to swallow: Nauseated: Vomiting: Continent (bladder): Continent (bowels): Catheterised: Hygiene needs assessed: Skin integrity: Mouth moist and clean: Braden score:... Other symptoms or distress (eg oedema, itch): Interventions in the Best Interest of the Person at this Moment in Time Taha Tinana - Physical Health SENIOR CLINICIAN TO COMPLETE Routine blood tests Intravenous antibiotics Blood glucose monitoring Recording of routine vital signs Oxygen therapy Currently not being taken/or given Discontinued Continued Commenced 4.1 Implantable Cardioverter Defibrillator (ICD) is deactivated: No ICD in place Contact the person s cardiologist. Refer to local/regional policy/procedure. Written information given to the person, relative, whānau or friend. page 3
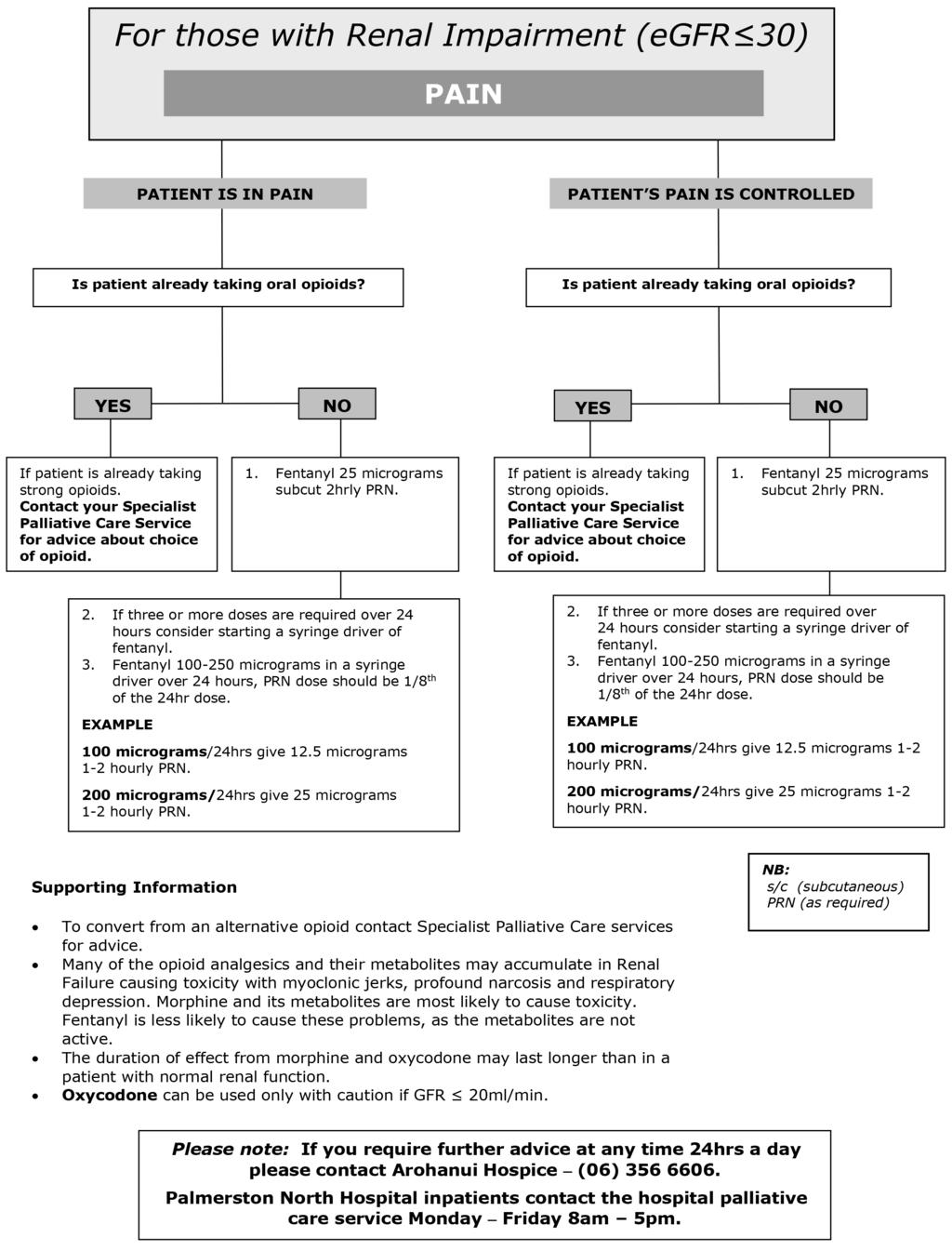
6 Medication Taha Tinana - Physical Health SENIOR CLINICIAN TO COMPLETE Current medication assessed and medications no longer essential for comfort discontinued: Medication prescribed on an as required prn basis for all of the following five symptoms which may develop in the last few days of life: Pain Agitation Respiratory tract secretions Nausea/vomiting Dyspnoea Anticipatory prescribing will ensure that there is no delay in responding to a symptom. Refer to algorithms at end of care plan. A syringe driver is available: Already in place Is available if required If a syringe driver is to be used explain the rationale to the person, relative, whānau, friend*. Not all people who are dying require a syringe driver. A four hourly checklist should be in place to monitor the use of a syringe driver. Provision of Food and Fluid A person should be supported to take fluid and foods by mouth for as long as is safe and tolerated: Taha Tinana - Physical Health SENIOR CLINICIAN TO COMPLETE Is clinically assisted (artificial) nutrition required: Not required Discontinued Continued If clinically assisted (artificial) nutrition is already in place please record the route: NG PEG/PEJ NJ TPN This review is discussed with the person where possible and appropriate and with the relative, whānau, or friend: Is clinically assisted (artificial) hydration required? Not required Discontinued Continued If clinically assisted (artificial) hydration is already in place please record the route: IV SC PEG/PEJ NG This review is discussed with the person where possible and appropriate and with the relative, whānau or friend*: Comments: Personalised Care Needs: Spiritual and Cultural Ethnicity: Which ethnic group or groups does the person identify with... It is best practice to ask the person the ethnic groups they identify with. You can gain important information at this time, for example, someone s iwi or other cultural affiliations that may be important in addressing the goals related to personalising care. Comments: Taha Wairua - Spiritual Health The person is given the opportunity to discuss what is important to them at this time, eg their wishes, feelings, faith, beliefs, values and culture. The relative, whānau spokesperson or friend* is given the opportunity to discuss what is important to them at this time, eg their wishes, feelings, beliefs, values and culture. Conversations could include identification of specific customs, traditions or cultural practices that are important to the person, relative, whānau or friend at death and after death. Religious tradition identified, please specify... Person s minister/priest/spiritual advisor/tohunga (Maori spiritual advisor) name... Phone no... Date/time... Contacted: N/A Support of the facility spiritual advisor: Name... Phone no... Date/time... Contacted: N/A The person and their family, whanau, or friends* are aware of the facility cultural support (if available), such as the Māori Health Service, Te Whare Rapuora: N/A page 4
7 BARCODE AREA Are there any specific care practices that the person, family, whānau or friend* want staff to be aware of? Including wishes regarding tissue/organ donation? Yes No After Death Care Practices Comments: Taha Wairua - Spiritual Health Checklist MDT, the person, relative, whānau or friend recognise and agree that person is dying and have been communicated with regarding plan of care: Comments: The person, relative, whānau or friend have agreed to the place of care: Yes No Initial assessment complete: Yes No The person, relative, whānau or friend have been given opportunities for further discussion about the plan of care and are aware this plan of care will be regularly reviewed in consultation with them: Yes No page 5
8 Section 2: Ongoing Assessment of the Goals of Care Date... Day... Undertake a MDT review of the current care plan. If at any time there is a change in relation to any of the following: Improved conscious level, functional ability, mobility, ability to perform self-care. Concerns expressed regarding management plan from either the person, relative, whānau or friend or MDT member. This care plan will be reviewed in its entirety daily. When each goal is assessed mark with an A if it has been achieved. If interventions are required, mark a IR and enter that change on the Interventions Required Sheet pg If using this in community enter visiting times below The person: Is pain free Is not agitated Has no respiratory tract secretions Is not breathless Is not nauseated Is not vomiting Has no urinary problems Has no bowel problems: Bowels last opened... Has no other symptoms (Record symptom here as applicable) Medication and route remain appropriate Food and fluid have been provided as appropriate (see question 6 of page 5) Has a moist and clean mouth Skin integrity is maintained Braden score... Personal hygiene needs met Receives their care in a physical environment adjusted to support their individual needs Personalised care needs met (see questions page 5) Relatives, whānau or friends* Personalised care needs met (see questions page 5) Other care needs... Signature of the registered nurse per shift: Night Morning Afternoon Night page 6 For additional pages order no:
9 BARCODE AREA What occurred? Interventions taken Interventions Required Sheet Please record intervention required on this sheet. Was intervention effective? Yes No If no, what further intervention was taken? Initials For additional pages order no: page 7
10 Interventions Required Sheet Please record intervention required on this sheet. What occurred? Interventions taken Was intervention effective? Yes No If no, what further intervention was taken? Initials page 8 For additional pages order no:
11 BARCODE AREA Date/Time Progress Notes Record significant events/conversations/medical review/significant changes to the person/visits by other specialist teams, eg palliative care/second opinion if sought/person and/or relative, whānau or friend concerns. A summary should be entered each shift. Print name and signature and role For additional pages order no: page 9
12 Date/Time Progress Notes Record significant events/conversations/medical review/significant changes to the person/visits by other specialist teams, eg palliative care/second opinion if sought/person and/or relative, whānau or friend concerns. A summary should be entered each shift. Print name and signature and role page 10 For additional pages order no:
13 BARCODE AREA Section 3: Care After Death Date of person s death... Time of person s death... Details of healthcare professional who verified death: Name... (please print) Signature... Comments... Family/whānau present at time of death... Persons present at time of death... If not present, has the relative, whānau or friend* been notified: Name of person informed... Relationship to the person... Name of Funeral Director... Telephone no... The person is treated with respect and dignity whilst care is undertaken. Universal precautions and local policy and procedures including infection risk are adhered to. Spiritual, religious cultural rituals/needs met. Organisational policy followed for the: management of ICDs storage of the person s valuables and belongings. Are valuables left on the person (if requested): The relative, whānau or friend can express an understanding of what they will need to do next and are given relevant written information. Conversation with relative, whānau or friend explaining the next steps. Written information is given such as: What to Expect When You are Grieving leaflet given: Information given regarding how and when to contact the funeral director (if appropriate) to make an appointment regarding the death certification and person s valuables and belongings where appropriate: Discuss as appropriate the following: viewing the body/ the need for a post mortem/the need for removal of cardiac devices/the need for a discussion with the coroner: Confirm wishes regarding tissue/organ donation discussed: Information given to families and whānau on child bereavement services where appropriate: A private space is available for family/whānau. Arrangements for blessing room/bed space made as appropriate: Karakia/prayer are offered in respect of cultural needs of family/whānau: The medical team and/or general practice teams/arc that supports the person in their usual place of residence are notified of the person s death: The person s death is communicated to appropriate services across the organisation: page 11
14 This page was intentionally left blank page 12

15 BARCODE AREA page 13
16 page 14

17 BARCODE AREA page 15
18 page 16
19 BARCODE AREA page 17
20 MDHB-5414 Ver This form relates to MDHB C: 1423 page 18
Liverpool Care Pathway for the Dying Patient (LCP) supporting care in the last hours or days of life
 supporting care in the last hours or days of life") Liverpool Care Pathway for the Dying Patient (LCP) supporting care in the last hours or days of life Information sheet to be given to the relative or carer following a discussion regarding the plan of
Liverpool Care Pathway for the Dying Patient (LCP) supporting care in the last hours or days of life Information sheet to be given to the relative or carer following a discussion regarding the plan of
FOR ILLUSTRATIVE PURPOSES ONLY
 - Page 1 of 15 GUIDANCE Health Professional Guidance for the Care Plan for the Dying Person - Victoria RECOGNISING DYING The possibility that a person may die within the next few days or hours is recognised
- Page 1 of 15 GUIDANCE Health Professional Guidance for the Care Plan for the Dying Person - Victoria RECOGNISING DYING The possibility that a person may die within the next few days or hours is recognised
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth
 Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
Liverpool Care Pathway for the Dying Patient (LCP) supporting care in the last hours or days of life
 supporting care in the last hours or days of life") Liverpool Care Pathway for the Dying Patient (LCP) supporting care in the last hours or days of life Please detach perforated Information sheets and give to the relative or carer following a discussion
Liverpool Care Pathway for the Dying Patient (LCP) supporting care in the last hours or days of life Please detach perforated Information sheets and give to the relative or carer following a discussion
National Care of the Dying Audit Hospitals (NCDAH) Round 3
 Round 3") National Care of the Dying Audit Hospitals (NCDAH) Round 3 This audit is being led by the Marie Curie Palliative Care Institute Liverpool in collaboration with the Royal College of Physicians, and is supported
National Care of the Dying Audit Hospitals (NCDAH) Round 3 This audit is being led by the Marie Curie Palliative Care Institute Liverpool in collaboration with the Royal College of Physicians, and is supported
Care Pathway For the last days of life
 NORTH EAST Care Pathway For the last days of life Patient Details Unit Number / NHS number August 2011 Review date: August 2013 1 Patient Details Unit Number/ NHS number CARE PATHWAY FOR THE LAST DAYS
NORTH EAST Care Pathway For the last days of life Patient Details Unit Number / NHS number August 2011 Review date: August 2013 1 Patient Details Unit Number/ NHS number CARE PATHWAY FOR THE LAST DAYS
INTEGRATED CARE PATHWAY FOR THE DYING PATIENT PATIENT S NAME.. UNIT NUMBER. DATE.. DATE OF BIRTH.. DATE OF IN PATIENT ADMISSION DIAGNOSIS: PRIMARY.
 PATIENT S NAME.. UNIT NUMBER. DATE.. DATE OF BIRTH.. DATE OF IN PATIENT ADMISSION DIAGNOSIS: PRIMARY. SECONDARY.. A Care Pathway is intended as a guide to treatment and an aid to documenting patient progress.
PATIENT S NAME.. UNIT NUMBER. DATE.. DATE OF BIRTH.. DATE OF IN PATIENT ADMISSION DIAGNOSIS: PRIMARY. SECONDARY.. A Care Pathway is intended as a guide to treatment and an aid to documenting patient progress.
Abbreviations used in Care Pathway. CNS Clinical Nurse C Chaplain / clergy / religious adviser
 Patient's Name: D.O.B: Patient GP: Named Nurse: Name: Adapted LCP Version 12 PALLIATIVE CARE PATHWAY (End Stage) PRIMARY CARE DO NOT PUT PATIENT ON THIS PATHWAY UNLESS The Multi-professional Team have
Patient's Name: D.O.B: Patient GP: Named Nurse: Name: Adapted LCP Version 12 PALLIATIVE CARE PATHWAY (End Stage) PRIMARY CARE DO NOT PUT PATIENT ON THIS PATHWAY UNLESS The Multi-professional Team have
Caring for me Advanced Care Planning
 Caring for me Advanced Care Planning Supporting guidance for Healthcare Professionals and Administrative Staff This care plan is aimed as a guide to treatment and intended to aid the documentation of patient
Caring for me Advanced Care Planning Supporting guidance for Healthcare Professionals and Administrative Staff This care plan is aimed as a guide to treatment and intended to aid the documentation of patient
Unit 301 Understand how to provide support when working in end of life care Supporting information
 Unit 301 Understand how to provide support when working in end of life care Supporting information Guidance This unit must be assessed in accordance with Skills for Care and Development s QCF Assessment
Unit 301 Understand how to provide support when working in end of life care Supporting information Guidance This unit must be assessed in accordance with Skills for Care and Development s QCF Assessment
End of Life Care Policy. Document author Assured by Review cycle. 1. Introduction Purpose Scope Definitions...
 End of Life Care Policy Board library reference Document author Assured by Review cycle P011 Lead Nurse Quality and Standards Committee 3 Years Contents 1. Introduction...3 2. Purpose...3 3. Scope...3
End of Life Care Policy Board library reference Document author Assured by Review cycle P011 Lead Nurse Quality and Standards Committee 3 Years Contents 1. Introduction...3 2. Purpose...3 3. Scope...3
End of Life Care Review Case Review Audit
 Case Review Audit : : Version: 1 NHS Wales (Intranet) / Public Health Wales (Intranet) Purpose and summary of document: This document is for use by general practices who are engaged in providing services
Case Review Audit : : Version: 1 NHS Wales (Intranet) / Public Health Wales (Intranet) Purpose and summary of document: This document is for use by general practices who are engaged in providing services
ORGANISATIONAL AUDIT
 [Type text] National Care of the Dying Audit Hospitals (NCDAH) Round 3 This audit is being led by the Marie Curie Palliative Care Institute Liverpool in collaboration with the Royal College of Physicians,
[Type text] National Care of the Dying Audit Hospitals (NCDAH) Round 3 This audit is being led by the Marie Curie Palliative Care Institute Liverpool in collaboration with the Royal College of Physicians,
Primary Care Quality (PCQ) National Priorities for General Practice
 National Priorities for General Practice") Primary Care Quality (PCQ) National Priorities for General Practice Cluster Guidance and Templates 2015/16 Authors: Primary Care Quality Team Date: November 2015 Publication/ Distribution: Version: Final
Primary Care Quality (PCQ) National Priorities for General Practice Cluster Guidance and Templates 2015/16 Authors: Primary Care Quality Team Date: November 2015 Publication/ Distribution: Version: Final
Guidance on End of Life Care-Updated July 2014
 Guidance on End of Life Care-Updated July 2014 INTRODUCTION Definition of End of Life Care: End of Life care helps all those with advanced, progressive, incurable illness to live as well as possible until
Guidance on End of Life Care-Updated July 2014 INTRODUCTION Definition of End of Life Care: End of Life care helps all those with advanced, progressive, incurable illness to live as well as possible until
Kirklees Individualised Care of the Dying Document. Guidance for clinical staff, trained carers & families/appropriate representative
 Person Name: NHS No: Hospital No: Kirklees Individualised Care of the Dying Document Guidance for clinical staff, trained carers & families/appropriate representative What is this document? This care plan
Person Name: NHS No: Hospital No: Kirklees Individualised Care of the Dying Document Guidance for clinical staff, trained carers & families/appropriate representative What is this document? This care plan
Developing individual care plans and goals for every end of life care patient
 Developing individual care plans and goals for every end of life care patient Dr. Dee Traue Consultant in Palliative Medicine We will cover How individual care plans differ from the LCP Developing and
Developing individual care plans and goals for every end of life care patient Dr. Dee Traue Consultant in Palliative Medicine We will cover How individual care plans differ from the LCP Developing and
PRIORITIES FOR CARE OF THE DYING PERSON
 PRIORITIES FOR CARE OF THE DYING PERSON Core and other useful sessions to support education and training across health and social care Fig.1 The 5 Priorities for Care of the Dying Person INTRODUCTION One
PRIORITIES FOR CARE OF THE DYING PERSON Core and other useful sessions to support education and training across health and social care Fig.1 The 5 Priorities for Care of the Dying Person INTRODUCTION One
One Chance to Get it Right:
 One Chance to Get it Right: Implementing the new priorities of Care for the Dying Person Dr Susan Salt, Medical Director Trinity Hospice, Blackpool Outline of the talk Brief look at what led to this point..
One Chance to Get it Right: Implementing the new priorities of Care for the Dying Person Dr Susan Salt, Medical Director Trinity Hospice, Blackpool Outline of the talk Brief look at what led to this point..
End of Life Care in the Acute Hospital Setting. Dr Adam Brown Consultant in Palliative Medicine
 End of Life Care in the Acute Hospital Setting Dr Adam Brown Consultant in Palliative Medicine Learning objectives Understanding a patient's priorities for end of life care How to work with the 5 priorities
End of Life Care in the Acute Hospital Setting Dr Adam Brown Consultant in Palliative Medicine Learning objectives Understanding a patient's priorities for end of life care How to work with the 5 priorities
All clinical areas of the Trust All clinical Trust staff All adults with limited prognosis Palliative care team Approved. Purpose of this document
 Trust Policy and Procedure Document Ref. No: PP(15)310 End of Life Care For use in: For use by: For use for: Document owner: Status: All clinical areas of the Trust All clinical Trust staff All adults
Trust Policy and Procedure Document Ref. No: PP(15)310 End of Life Care For use in: For use by: For use for: Document owner: Status: All clinical areas of the Trust All clinical Trust staff All adults
End of life care in Secure Psychiatric Settings
 End of life care in Secure Psychiatric Dr Nuwan Galappathie MBChB MRCPsych MMedSc LLM Consultant Forensic Psychiatrist St Andrew s Healthcare, Birmingham Visiting Researcher, Institute of Psychiatry, Kings
End of life care in Secure Psychiatric Dr Nuwan Galappathie MBChB MRCPsych MMedSc LLM Consultant Forensic Psychiatrist St Andrew s Healthcare, Birmingham Visiting Researcher, Institute of Psychiatry, Kings
ONE CHANCE TO GET IT RIGHT DERBYSHIRE
 ONE CHANCE TO GET IT RIGHT DERBYSHIRE A guide for professionals in Derbyshire who care for patients believed to be in the last year of life 1 ST edition July 2014 OCTGIRv1.29614 DERBYSHIRE ALLIANCE FOR
ONE CHANCE TO GET IT RIGHT DERBYSHIRE A guide for professionals in Derbyshire who care for patients believed to be in the last year of life 1 ST edition July 2014 OCTGIRv1.29614 DERBYSHIRE ALLIANCE FOR
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
1. Guidance notes. Social care (Adults, England) Knowledge set for end of life care. (revised edition, 2010) What are knowledge sets?
 Knowledge set for end of life care. (revised edition, 2010) What are knowledge sets?") Social care (Adults, England) Knowledge set for end of life care (revised edition, 2010) Part of the sector skills council Skills for Care and Development 1. Guidance notes What are knowledge sets? Knowledge
Social care (Adults, England) Knowledge set for end of life care (revised edition, 2010) Part of the sector skills council Skills for Care and Development 1. Guidance notes What are knowledge sets? Knowledge
End of Life Care Strategy PROUD TO MAKE A DIFFERENCE
 End of Life Care Strategy 2017-2019 PROUD TO MAKE A DIFFERENCE Background Sheffield Teaching Hospitals NHS Trust is committed to delivering high quality care to patients and those identified as important
End of Life Care Strategy 2017-2019 PROUD TO MAKE A DIFFERENCE Background Sheffield Teaching Hospitals NHS Trust is committed to delivering high quality care to patients and those identified as important
Patient details. Forename...Surname...D.O.B... Shropshire and Telford & Wrekin End of Life Care Group. End of Life Plan
 Patient details Forename...Surname...D.O.B... Shropshire and Telford & Wrekin End of Life Care Group End of Life Plan Telford and Wrekin Clinical Commissioning Group Shropshire County Clinical Commissioning
Patient details Forename...Surname...D.O.B... Shropshire and Telford & Wrekin End of Life Care Group End of Life Plan Telford and Wrekin Clinical Commissioning Group Shropshire County Clinical Commissioning
Holistic Needs Assessment (HNA) for Adult Cancer Patients Guidelines
 for Adult Cancer Patients Guidelines") Please Note: This policy is currently under review and is still fit for purpose. Holistic Needs Assessment (HNA) for Adult Cancer Patients Guidelines Handbook to accompany these guidelines is available
Please Note: This policy is currently under review and is still fit for purpose. Holistic Needs Assessment (HNA) for Adult Cancer Patients Guidelines Handbook to accompany these guidelines is available
When someone is dying Information for Relatives and Carers
 When someone is dying Information for Relatives and Carers This leaflet can be made available in other formats including large print, CD and Braille, and in languages other than English, upon request.
When someone is dying Information for Relatives and Carers This leaflet can be made available in other formats including large print, CD and Braille, and in languages other than English, upon request.
Hospice Isle of Man Education Prospectus 2018
 Hospice Isle of Man Education Prospectus 2018 Leading the Way in Palliative Care Introduction The need for palliative and end of life care is changing, with increasing demands and complexity for patients
Hospice Isle of Man Education Prospectus 2018 Leading the Way in Palliative Care Introduction The need for palliative and end of life care is changing, with increasing demands and complexity for patients
QUALIFICATION HANDBOOK
 QUALIFICATION HANDBOOK Level 2, 3 & 5 Awards and Certificates in End of Life Care (3571-02-03-04-05) May 2013 Version 5.0 Qualification at a glance Subject area City & Guilds number 3571 End of life care
QUALIFICATION HANDBOOK Level 2, 3 & 5 Awards and Certificates in End of Life Care (3571-02-03-04-05) May 2013 Version 5.0 Qualification at a glance Subject area City & Guilds number 3571 End of life care
RUH End of Life Care Annual Report April 2014 March 2015
 RUH End of Life Care Annual Report April 2014 March 2015 Chairman, Brian Stables Chief Executive, James Scott Contents 1. Introduction page 3 2. End of Life Care Working Group page 3 3. Lead Nurse Palliative
RUH End of Life Care Annual Report April 2014 March 2015 Chairman, Brian Stables Chief Executive, James Scott Contents 1. Introduction page 3 2. End of Life Care Working Group page 3 3. Lead Nurse Palliative
End Of Life Group- County Wide Clinical End of Life Care. Via training and Community Trust Communications. Document Links. Amendments History
 Title Trust Ref No 1962- Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director) Document Details Shropshire Telford and Wrekin End of
Title Trust Ref No 1962- Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director) Document Details Shropshire Telford and Wrekin End of
Serious Medical Treatment Decisions. BEST PRACTICE GUIDANCE FOR IMCAs END OF LIFE CARE
 Serious Medical Treatment Decisions BEST PRACTICE GUIDANCE FOR IMCAs END OF LIFE CARE Contents Introduction... 3 End of Life Care (EoLC)...3 Background...3 Involvement of IMCAs in End of Life Care...4
Serious Medical Treatment Decisions BEST PRACTICE GUIDANCE FOR IMCAs END OF LIFE CARE Contents Introduction... 3 End of Life Care (EoLC)...3 Background...3 Involvement of IMCAs in End of Life Care...4
Hospice Care for the Person with Cancer
 Hospice Care for the Person with Cancer Hospice is a special type of care designed to provide comfort, support and dignity to patients with a lifelimiting or terminal illness. For hospice purposes, a life-limiting
Hospice Care for the Person with Cancer Hospice is a special type of care designed to provide comfort, support and dignity to patients with a lifelimiting or terminal illness. For hospice purposes, a life-limiting
Competency Asse ssment Tool for Care of Febrile Neutropenia 2009
 Competency Asse ssment Tool for Care of Febrile Neutropenia 2009 Guidelines for use: In assessing competence, a combination of assessment methods may be utilised including clinical questioning/ interview
Competency Asse ssment Tool for Care of Febrile Neutropenia 2009 Guidelines for use: In assessing competence, a combination of assessment methods may be utilised including clinical questioning/ interview
Suffolk End of Life Care Guidelines
 In partnership with: West Suffolk NHS Foundation Trust, The Ipswich Hospital, Suffolk Community Healthcare, St Nicholas Hospice Care, St Elizabeth Hospice, Adult Community Services, NHS Ipswich and East
In partnership with: West Suffolk NHS Foundation Trust, The Ipswich Hospital, Suffolk Community Healthcare, St Nicholas Hospice Care, St Elizabeth Hospice, Adult Community Services, NHS Ipswich and East
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Learning from the National Care of the Dying 2014 Audit. Dr Bill Noble Medical Director, Marie Curie Cancer Care
 Learning from the National Care of the Dying 2014 Audit Dr Bill Noble Medical Director, Marie Curie Cancer Care MARIE CURIE Major UK end of life charity Major service provider Network of 2000 Nurses caring
Learning from the National Care of the Dying 2014 Audit Dr Bill Noble Medical Director, Marie Curie Cancer Care MARIE CURIE Major UK end of life charity Major service provider Network of 2000 Nurses caring
The School Of Nursing And Midwifery. CLINICAL SKILLS PASSPORT
 The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
What You Need To Know About Palliative Care
 www.hrh.ca Medical Program What You Need To Know About Palliative Care What s Inside: Who are your team members?... 2 Care Needs of Your Loved One: Information for the Family... 4 Options for Discharge...
www.hrh.ca Medical Program What You Need To Know About Palliative Care What s Inside: Who are your team members?... 2 Care Needs of Your Loved One: Information for the Family... 4 Options for Discharge...
Care Plan for End of Life
 Care Plan for End of Life (A hospital label may be placed here where applicable) Print Name NHS No Date of Birth Ward/Place of Care GP/Consultant Contact details District Nurse/ Clinical Nurse Specialist
Care Plan for End of Life (A hospital label may be placed here where applicable) Print Name NHS No Date of Birth Ward/Place of Care GP/Consultant Contact details District Nurse/ Clinical Nurse Specialist
NATIONAL CARE OF THE DYING AUDIT HOSPITALS (NCDAH) ROUND 3 GENERIC REPORT 2011/2012
 ROUND 3 GENERIC REPORT 2011/2012") NATIONAL CARE OF THE DYING AUDIT HOSPITALS (NCDAH) ROUND 3 GENERIC REPORT 2011/2012 Led by the Marie Curie Palliative Care Institute Liverpool (MCPCIL) in collaboration with the Royal College of Physicians
NATIONAL CARE OF THE DYING AUDIT HOSPITALS (NCDAH) ROUND 3 GENERIC REPORT 2011/2012 Led by the Marie Curie Palliative Care Institute Liverpool (MCPCIL) in collaboration with the Royal College of Physicians
It is essential that patients are aware of, and in agreement with, their referral to palliative care.
 Title: Directorate: Responsible for review: Ratified by: CHRONIC HEART FAILURE REFERRAL TO PALLIATIVE CARE SERVCES Palliative Care Consultant in Palliative Care Care and Clinical Policies Group Ref No:
Title: Directorate: Responsible for review: Ratified by: CHRONIC HEART FAILURE REFERRAL TO PALLIATIVE CARE SERVCES Palliative Care Consultant in Palliative Care Care and Clinical Policies Group Ref No:
MND Factsheet 44 Advance Directives
 MND Factsheet 44 Advance Directives Last Updated 27/10/11 Introduction Living wills, advance decisions, advance directives and advanced medical directives are all names which are, or have been, applied
MND Factsheet 44 Advance Directives Last Updated 27/10/11 Introduction Living wills, advance decisions, advance directives and advanced medical directives are all names which are, or have been, applied
What do the 5 Priorities for Care of dying people mean for the care of people with dementia?
 What do the 5 Priorities for Care of dying people mean for the care of people with dementia? Alistair Burns National Clinical Director for Dementia Bee Wee National Clinical Director for End of Life Care
What do the 5 Priorities for Care of dying people mean for the care of people with dementia? Alistair Burns National Clinical Director for Dementia Bee Wee National Clinical Director for End of Life Care
A Specialist Palliative Care Nurses Competency Framework Helen Butler Education Team Leader Mercy Hospice Auckland
 A Specialist Palliative Care Nurses Competency Framework Helen Butler Education Team Leader Mercy Hospice Auckland The aim of this session To refresh our memories about what a competency is To give a bit
A Specialist Palliative Care Nurses Competency Framework Helen Butler Education Team Leader Mercy Hospice Auckland The aim of this session To refresh our memories about what a competency is To give a bit
Document Type. Adult End of Life Care Guidelines. Document Description. Lead Author(s) Palliative Care Education Coordinator
 Palliative Care Education Coordinator") Document Title Adult End of Life Care Guidelines Document Type Service Application Version Name Kathryn Halford Sharon Yates Document Description Guide Lines Trust Wide New Lead Author(s) Job Title Director
Document Title Adult End of Life Care Guidelines Document Type Service Application Version Name Kathryn Halford Sharon Yates Document Description Guide Lines Trust Wide New Lead Author(s) Job Title Director
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
There are generally considered to be six steps in providing effective end of life care
 Page: 1 of 6 Purpose Scope Policy To provide a framework to guide best practice care and support of Service Users who have been identified as nearing the end of their life. Service Users who have been
Page: 1 of 6 Purpose Scope Policy To provide a framework to guide best practice care and support of Service Users who have been identified as nearing the end of their life. Service Users who have been
European Recommendations for End-of-Life Care for Adults in Departments of Emergency Medicine
 European Recommendations for End-of-Life Care for Adults in Departments of Emergency Medicine September 2017 European Recommendations for End-of-Life Care in Departments of Emergency Medicine * Summary
European Recommendations for End-of-Life Care for Adults in Departments of Emergency Medicine September 2017 European Recommendations for End-of-Life Care in Departments of Emergency Medicine * Summary
Prescribing for Symptom Control in End of Life Care. Dr Deborah Robertson Senior Lecturer University of Chester
 Prescribing for Symptom Control in End of Life Care Dr Deborah Robertson Senior Lecturer University of Chester #hellomynameis Dr Debs Robertson Programme leader NMP Nurse and pharmacologist Champion of
Prescribing for Symptom Control in End of Life Care Dr Deborah Robertson Senior Lecturer University of Chester #hellomynameis Dr Debs Robertson Programme leader NMP Nurse and pharmacologist Champion of
Clinical Staff Overview
 Clinical Staff Overview RESOURCES Developed by VEC Expert reference and consumer group input Last days and hours of life focus State-wide relevance acute and sub-acute care settings CARE PLAN KEY BENEFITS
Clinical Staff Overview RESOURCES Developed by VEC Expert reference and consumer group input Last days and hours of life focus State-wide relevance acute and sub-acute care settings CARE PLAN KEY BENEFITS
Submission from the National Gold Standards Framework (GSF) Centre in End of Life care on use of the Liverpool Care Pathway (LCP).
 Centre in End of Life care on use of the Liverpool Care Pathway (LCP).") Submission from the National Gold Standards Framework (GSF) Centre in End of Life care on use of the Liverpool Care Pathway (LCP). April 2013 Contents 1. Summary of submission from GSF Centre 2. About
Submission from the National Gold Standards Framework (GSF) Centre in End of Life care on use of the Liverpool Care Pathway (LCP). April 2013 Contents 1. Summary of submission from GSF Centre 2. About
Contents. Introduction 3. Required knowledge and skills 4. Section One: Knowledge and skills for all nurses and care staff 6
 Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
Policy for Anticipatory Prescribing and Just in Case Bags
 Policy for Anticipatory Prescribing and Just in Case Bags This policy was developed by Milton Keynes End of Life Care Medicine Group and has been adopted by all partner organisations (MK Clinical Commissioning
Policy for Anticipatory Prescribing and Just in Case Bags This policy was developed by Milton Keynes End of Life Care Medicine Group and has been adopted by all partner organisations (MK Clinical Commissioning
Scottish Palliative Care Guidelines Rapid Transfer Home in the Last Days of Life
 Rapid Transfer Home in the Last Days of Life Management Follow five steps below to: facilitate a peaceful death in the patient s preferred place facilitate seamless transfer from hospital or hospice to
Rapid Transfer Home in the Last Days of Life Management Follow five steps below to: facilitate a peaceful death in the patient s preferred place facilitate seamless transfer from hospital or hospice to
NSW ADVANCE CARE DIRECTIVE
 NSW ADVANCE CARE DIRECTIVE This form deals with your future health care. The time may come when you cannot speak for yourself. By completing this form, you can give directions about what medical treatment
NSW ADVANCE CARE DIRECTIVE This form deals with your future health care. The time may come when you cannot speak for yourself. By completing this form, you can give directions about what medical treatment
PALLIATIVE AND END OF LIFE CARE EDUCATION PROSPECTUS 2018/19
 #wearenhft Northamptonshire Healthcare NHS Foundation Trust PALLIATIVE AND END OF LIFE CARE EDUCATION PROSPECTUS 2018/19 DELIVERED BY: THE NORTHAMPTONSHIRE END OF LIFE CARE PRACTICE DEVELOPMENT TEAM Working
#wearenhft Northamptonshire Healthcare NHS Foundation Trust PALLIATIVE AND END OF LIFE CARE EDUCATION PROSPECTUS 2018/19 DELIVERED BY: THE NORTHAMPTONSHIRE END OF LIFE CARE PRACTICE DEVELOPMENT TEAM Working
Directive To Physicians and Family Or Surrogates (Living Will)
") Directive To Physicians and Family Or Surrogates (Living Will) INSTRUCTIONS FOR COMPLETING THIS DOCUMENT: This is an important legal document known as an Advance Directive. It is designed to help you communicate
Directive To Physicians and Family Or Surrogates (Living Will) INSTRUCTIONS FOR COMPLETING THIS DOCUMENT: This is an important legal document known as an Advance Directive. It is designed to help you communicate
Top 12 Courses for Newcross Nurses and HCAs BETTER PEOPLE BETTER TRAINED
 Top 12 Courses for Newcross Nurses and HCAs BETTER PEOPLE BETTER TRAINED Top 12 Courses for Newcross Nurses and HCAs Contents Venepuncture Syringe Drivers Catheterisation Medication Training Wound Care
Top 12 Courses for Newcross Nurses and HCAs BETTER PEOPLE BETTER TRAINED Top 12 Courses for Newcross Nurses and HCAs Contents Venepuncture Syringe Drivers Catheterisation Medication Training Wound Care
The Palliative Care Program MISSION STATEMENT
 The Palliative Care Program MISSION STATEMENT believes in providing compassionate, comprehensive, multidisciplinary care to residents living with a life threatening illness and their families to relieve
The Palliative Care Program MISSION STATEMENT believes in providing compassionate, comprehensive, multidisciplinary care to residents living with a life threatening illness and their families to relieve
Bereavement Policy. 1 Purpose of Policy 2. 2 Background 2. 3 Staff Responsibilities 3. 4 Operational Issues and Local Policies/Protocols/Guidelines 4
 Trust Policy and Procedure Bereavement Policy Document Ref. No: PP(16)252 For use in: For use by: For use for: Document owner: Status: All areas of the Trust All Trust staff The dying, their relatives
Trust Policy and Procedure Bereavement Policy Document Ref. No: PP(16)252 For use in: For use by: For use for: Document owner: Status: All areas of the Trust All Trust staff The dying, their relatives
ADVANCE DIRECTIVE PACKET Question and Answer Section
 ADVANCE DIRECTIVE PACKET Question and Answer Section Please review the following facts regarding what an Advance Directive is, as well as your right as an adult to create one. If you decide to complete
ADVANCE DIRECTIVE PACKET Question and Answer Section Please review the following facts regarding what an Advance Directive is, as well as your right as an adult to create one. If you decide to complete
National care of the dying audit for hospitals, England Executive summary May 2014
 National care of the dying audit for hospitals, England Executive summary May 2014 Foreword We only have one chance to get end of life care right and sadly sometimes we don t. There are few surprises in
National care of the dying audit for hospitals, England Executive summary May 2014 Foreword We only have one chance to get end of life care right and sadly sometimes we don t. There are few surprises in
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces.
 End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
Leadership Alliance for the Care of Dying People. Engagement with patients, families, carers and professionals.
 Leadership Alliance for the Care of Dying People Engagement with patients, families, carers and professionals. 1 Leadership Alliance for the Care of Dying People Engagement with patients, families, carers
Leadership Alliance for the Care of Dying People Engagement with patients, families, carers and professionals. 1 Leadership Alliance for the Care of Dying People Engagement with patients, families, carers
Multidisciplinary care of a patient with heart failure. patient with heart failure. Dr Claire Hookey
 Multidisciplinary care of a patient with heart failure patient with heart failure Dr Claire Hookey Mr E.S 61 year old gentleman Referred to the hospice by the heart failure specialist nurse May 2010 Heart
Multidisciplinary care of a patient with heart failure patient with heart failure Dr Claire Hookey Mr E.S 61 year old gentleman Referred to the hospice by the heart failure specialist nurse May 2010 Heart
Care and support in the last days of life
 Care and support in the last days of life Hospital Palliative Care Team 0161 206 4609 Community Palliative Care Team 0161 702 5406 Bereavement Team 0161 206 5175 All Rights Reserved 2018. Document for
Care and support in the last days of life Hospital Palliative Care Team 0161 206 4609 Community Palliative Care Team 0161 702 5406 Bereavement Team 0161 206 5175 All Rights Reserved 2018. Document for
Caring for patients in the last hours or days of life: a ten point plan
 Copyright Owner: Anne Garry, Palliative Care Team & Pharmacy Group September 2014 Version 6. Review date September 2017. Approved by York D&T Committee. Modified from Northern Cancer Network EOLC k (For
Copyright Owner: Anne Garry, Palliative Care Team & Pharmacy Group September 2014 Version 6. Review date September 2017. Approved by York D&T Committee. Modified from Northern Cancer Network EOLC k (For
End of life care. Recognise when a patient is approaching the end of life period of care
 NURSING BEST PRACTICE GUIDE End of life care This document is one of the Myeloma Academy Nursing Best Practice Guides for the Management of Myeloma series. The purpose of this Guide is to enhance knowledge
NURSING BEST PRACTICE GUIDE End of life care This document is one of the Myeloma Academy Nursing Best Practice Guides for the Management of Myeloma series. The purpose of this Guide is to enhance knowledge
Preferred Place of Care. Palliative Care Audit. Report
 Preferred Place of Care Palliative Care Audit Report Janette Barrie Jonathan Campbell Dr Catriona Ross October 2010 PPC Audit Report October 2010 1 Introduction Preferred Place of Care is a phrase which
Preferred Place of Care Palliative Care Audit Report Janette Barrie Jonathan Campbell Dr Catriona Ross October 2010 PPC Audit Report October 2010 1 Introduction Preferred Place of Care is a phrase which
Consulted With Post/Committee/Group Date Dr Dhillon Cardiology Consultant April Professionally Approved By 2. Clinical Effectiveness
 Implantable Cardioverter Defibrillator (ICD) Deactivation End of Life Type: Clinical Guidance Register No: 17007 Status: Public on ratification Developed in response to: Best Practice Contributes to CQC
Implantable Cardioverter Defibrillator (ICD) Deactivation End of Life Type: Clinical Guidance Register No: 17007 Status: Public on ratification Developed in response to: Best Practice Contributes to CQC
Planning in Advance for Your Health Care
 Planning in Advance for Your Health Care This booklet will help you to plan ahead. If you have any questions please call for assistance: NWH Patient Relations Representative 617-243-5052 NWH Pastoral Care:
Planning in Advance for Your Health Care This booklet will help you to plan ahead. If you have any questions please call for assistance: NWH Patient Relations Representative 617-243-5052 NWH Pastoral Care:
Registered Nurse Community Mental Health
 Date: Feb 2015 Job Title : Registered Nurse Department : Adult Mental Health Services Location : Waimarino, 33 Paramount Dr, Henderson Reports to : Team Manager Direct Reports : None Functional Relationships
Date: Feb 2015 Job Title : Registered Nurse Department : Adult Mental Health Services Location : Waimarino, 33 Paramount Dr, Henderson Reports to : Team Manager Direct Reports : None Functional Relationships
Standards of proficiency for nursing associates
 Standards of proficiency for nursing associates DRAFT April 2018 www.nmc.org.uk Contents Introduction 3 Standards of proficiency for nursing associates 5 Platform 1: Being an accountable professional 5
Standards of proficiency for nursing associates DRAFT April 2018 www.nmc.org.uk Contents Introduction 3 Standards of proficiency for nursing associates 5 Platform 1: Being an accountable professional 5
HEALTH CARE DIRECTIVE
 1 HEALTH CARE DIRECTIVE I,, understand this document allows me to do ONE OR BOTH of the following: PART I: Name another person (called the health care agent) to make health care decisions for me if I am
1 HEALTH CARE DIRECTIVE I,, understand this document allows me to do ONE OR BOTH of the following: PART I: Name another person (called the health care agent) to make health care decisions for me if I am
END OF LIFE CARE STRATEGY
 END OF LIFE CARE STRATEGY 2016-19 Controlled Document This document is uncontrolled when downloaded or printed. Reference number Version 12 Authors Date ratified Committee/individual responsible Issue
END OF LIFE CARE STRATEGY 2016-19 Controlled Document This document is uncontrolled when downloaded or printed. Reference number Version 12 Authors Date ratified Committee/individual responsible Issue
Deactivation of Implantable Cardioverter Defibrillators (ICD) at the end of life (Guideline)
 at the end of life (Guideline)") Bradford, Airedale, Wharfedale and Craven Joint Operational Document Deactivation of Implantable Cardioverter Defibrillators (ICD) at the end of life (Guideline) Document Reference Version: 1.0 Document
Bradford, Airedale, Wharfedale and Craven Joint Operational Document Deactivation of Implantable Cardioverter Defibrillators (ICD) at the end of life (Guideline) Document Reference Version: 1.0 Document
CLINICAL SKILLS PASSPORT
 The School Of Nursing And Midwifery. Pre-registration Postgraduate Diploma in Nursing (Adult) CLINICAL S PASSPORT NAME: COHORT: Student Details I understand that this booklet may be reviewed by my mentor,
The School Of Nursing And Midwifery. Pre-registration Postgraduate Diploma in Nursing (Adult) CLINICAL S PASSPORT NAME: COHORT: Student Details I understand that this booklet may be reviewed by my mentor,
BGS Response to LACDP System Wide Response (www.gov.uk)
") BGS BRIEFING 25 TH JUNE 2014 LEADERSHIP ALLIANCE FOR THE CARE OF DYING PEOPLE (LACDP) ANNOUNCEMENT OF PRIORITIES FOR CARE OF THE DYING PERSON BGS Response to LACDP System Wide Response (www.gov.uk) 1.
BGS BRIEFING 25 TH JUNE 2014 LEADERSHIP ALLIANCE FOR THE CARE OF DYING PEOPLE (LACDP) ANNOUNCEMENT OF PRIORITIES FOR CARE OF THE DYING PERSON BGS Response to LACDP System Wide Response (www.gov.uk) 1.
End of life care. Patient Guide
 8 End of life care Patient Guide What happens? There is a point for many in the brain tumour journey when either the disease no longer responds to treatment, or you have had all treatment that is available
8 End of life care Patient Guide What happens? There is a point for many in the brain tumour journey when either the disease no longer responds to treatment, or you have had all treatment that is available
PROCESS FOR INITIATING A SYRINGE DRIVER FOR COMMUNITY NURSE PATIENTS OUT OF HOURS
 STANDARD OPERATING PROCEDURE PROCESS FOR INITIATING A SYRINGE DRIVER FOR COMMUNITY NURSE PATIENTS OUT OF HOURS Issue History Issue Version one Purpose of Issue/Description of Change To facilitate patients
STANDARD OPERATING PROCEDURE PROCESS FOR INITIATING A SYRINGE DRIVER FOR COMMUNITY NURSE PATIENTS OUT OF HOURS Issue History Issue Version one Purpose of Issue/Description of Change To facilitate patients
We need to talk about Palliative Care. The Care Inspectorate
 We need to talk about Palliative Care The Care Inspectorate Introduction The Care Inspectorate is the official body responsible for inspecting standards of care in Scotland. That means we regulate and
We need to talk about Palliative Care The Care Inspectorate Introduction The Care Inspectorate is the official body responsible for inspecting standards of care in Scotland. That means we regulate and
Guidelines for the Management of Patients who are End of Life
 Guidelines for the Management of Patients who are End of Life This procedural document supersedes: PAT/T 65 v.1 Management of Patients who are End of Life. Did you print this document yourself? The Trust
Guidelines for the Management of Patients who are End of Life This procedural document supersedes: PAT/T 65 v.1 Management of Patients who are End of Life. Did you print this document yourself? The Trust
Section 6: Referral record headings
 Section 6: Referral record headings Referral record standards: the referral headings are primarily intended for recording the clinical information in referral communication between general practitioners
Section 6: Referral record headings Referral record standards: the referral headings are primarily intended for recording the clinical information in referral communication between general practitioners
Royal Liverpool Children s NHS Trust Alder Hey Rapid Discharge Pathway for End of Life Care
 Royal Liverpool Children s NHS Trust Alder Hey Rapid Discharge Pathway for End of Life Care Pathway for patients where a consensus decision has been made by the child s / young person s family & multi-professional
Royal Liverpool Children s NHS Trust Alder Hey Rapid Discharge Pathway for End of Life Care Pathway for patients where a consensus decision has been made by the child s / young person s family & multi-professional
Advance Directive Procedure
 Advance Directive Procedure Aim and Scope of Procedure To provide instructions on the management of Advance directives regarding care and treatment at the Phyllis Tuckwell Hospice. Adhering to the Reference
Advance Directive Procedure Aim and Scope of Procedure To provide instructions on the management of Advance directives regarding care and treatment at the Phyllis Tuckwell Hospice. Adhering to the Reference
PRACTICE ASSESSMENT DOCUMENT
 BSc (Hons) Nursing Studies / Registered Nurse Field: PRACTICE ASSESSMENT DOCUMENT Student Name: Guidance Tutor (GT): GT Tel No: Submission Dates First submission: Second submission: GT Email: GT Group
BSc (Hons) Nursing Studies / Registered Nurse Field: PRACTICE ASSESSMENT DOCUMENT Student Name: Guidance Tutor (GT): GT Tel No: Submission Dates First submission: Second submission: GT Email: GT Group
PAHT strategy for End of Life Care for adults
 PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see , Health and Safety Code) DIRECTIVE
 DIRECTIVE") DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see 166.033, Health and Safety Code) Instructions for completing this document: This is an important legal document known as an
DIRECTIVE TO PHYSICIANS AND FAMILY OR SURROGATES Advance Directives Act (see 166.033, Health and Safety Code) Instructions for completing this document: This is an important legal document known as an
MASSACHUSETTS ADVANCE DIRECTIVES
 MASSACHUSETTS ADVANCE DIRECTIVES Advance directives are legal documents that protect your right to refuse medical treatment you do not want, or to request treatment you do want, in the event you lose the
MASSACHUSETTS ADVANCE DIRECTIVES Advance directives are legal documents that protect your right to refuse medical treatment you do not want, or to request treatment you do want, in the event you lose the
The Nottinghamshire Guideline for Care in the Last Year of Life
 The Nottinghamshire Guideline for Care in the Last Year of Life A Guide for Professionals This guide was produced in partnership between Nottinghamshire Healthcare NHS Foundation Trust Nottingham CityCare
The Nottinghamshire Guideline for Care in the Last Year of Life A Guide for Professionals This guide was produced in partnership between Nottinghamshire Healthcare NHS Foundation Trust Nottingham CityCare
6: What care is available?
 6: What care is available? This section identifies and explains the types of care on offer at end of life and who is involved. The following information is an extracted section from our full guide End
6: What care is available? This section identifies and explains the types of care on offer at end of life and who is involved. The following information is an extracted section from our full guide End
When to Consider Implantable Cardioverter Defibrillator (ICD) Deactivation. A Guide for Patients and Family
 Deactivation. A Guide for Patients and Family") When to Consider Implantable Cardioverter Defibrillator (ICD) Deactivation A Guide for Patients and Family This booklet will help answer your questions about deactivating the shock function of an ICD.
When to Consider Implantable Cardioverter Defibrillator (ICD) Deactivation A Guide for Patients and Family This booklet will help answer your questions about deactivating the shock function of an ICD.
When to Consider Implantable Cardioverter Defibrillator (ICD) Deactivation. A Guide for Patients and Family
 Deactivation. A Guide for Patients and Family") When to Consider Implantable Cardioverter Defibrillator (ICD) Deactivation A Guide for Patients and Family This booklet will help answer your questions about deactivating the shock function of an ICD.
When to Consider Implantable Cardioverter Defibrillator (ICD) Deactivation A Guide for Patients and Family This booklet will help answer your questions about deactivating the shock function of an ICD.
Marie Curie Northern Ireland Patient Guide
 Marie Curie Northern Ireland Patient Guide Date of Issue: November 2014 Review date: November 2017 Contents 1. Introduction 1 2. Respect for patient s rights 3 3. What you can expect from our staff and
Marie Curie Northern Ireland Patient Guide Date of Issue: November 2014 Review date: November 2017 Contents 1. Introduction 1 2. Respect for patient s rights 3 3. What you can expect from our staff and
MENTAL HEALTH & ADDICTION SERVICES
 MENTAL HEALTH & ADDICTION SERVICES Position Description Position: Report To: Responsible For: Location: Hours Of Work: Liaise With: Registered Nurse/OT/Social worker Case Manager Team Leader/ Clinical
MENTAL HEALTH & ADDICTION SERVICES Position Description Position: Report To: Responsible For: Location: Hours Of Work: Liaise With: Registered Nurse/OT/Social worker Case Manager Team Leader/ Clinical
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing