System Quality Control and. Peter Shamamian, MD FACS Vice President and Chief Quality Officer Vice Chairman for Quality and Performance Improvement
|
|
|
- Angelina Shields
- 5 years ago
- Views:
Transcription


1 System Quality Control and Malpractice Costs Peter Shamamian, MD FACS Vice President and Chief Quality Officer Vice Chairman for Quality and Performance Improvement Disclosures 1
2 The world of healthcare is changing. The idea of the solo doctor with his or her pen doing whatever they want and getting paid whatever they charge, those days are gone. There is much more regulation much more oversight. There is much more concept of being paid for quality and meeting certain benchmarks and targets as apposed for being paid for just what you do. Dr. Michael Stewart Vice Dean of Weill Cornell Medical College and Chairman of Otolaryngology WNYC The Takeaway Job Fair: Paging Young Doctors, Monday September 8 th 2014 Consumers of Quality Measurement Data CMS Professional Societies NSQIP HIQRP NDNQI HOQRP STS VBP Others Readmission Reduction HAC Reduction Meaningful Use ESRD QIP Pioneer ACO Consumer PQRS Groups NYSPFP Hospital Report Cards CDC NHSN AHRQ Quality Indicators NHQR/NHDR Media TJC Hospital Accreditation ti Quality & Patient Safety Report Malpractice carrier Malpractice premium reduction ~900 measures/45 programs NYSDOH HAI Reporting PPR/PPC Reduction SAE Non-Payment PCI Registry Cardiac Surgery Registry Public Reporting Regulations NYPORTS MRT Commercial Insurers HEDIS P4P Contracts (Healthfirst) 2


3 WHO USES HOSPITALS WHO USES HOSPITALS PUBLICLY REPORTED QUALITY DATA? 3














4 Where Do You Find Data on Hospital Performance? 4
5 Guiding Principles of Quality Initiatives Delivery of evidence based care Elimination of patient harm Core Measures Prevention Bundles Not always evidence based Best Practices Hospital Acquired Conditions (HAC) Hospital Acquired Infections (HAI) Never Events CMS Payment Reduction Programs Value-Based Purchasing (VBP-Core Measures) Incentive program that reduces payments based on performance measures Process of care, Patient experience, Outcomes, Efficiency Hospital Acquired Condition (HAC) Reduction Program Penalty Program that Reduces Payments to Hospitals for Excess HACs Readmission (Unplanned) Reduction Program 5
6 VBP-Clinical Process or Core Measure AMI HF Pneu SCIP Aspirin prescribed at discharge Fibrinolytic agent received within 30 minutes of arrival Primary percutaneous intervention (PCI) within 90 minutes of arrival Discharge instructions Evaluation of left ventricular systolic function ACE-I or ARB for left ventricular systolic dysfunction Blood culture performed in the ED before first antibiotic Appropriate antibiotic selection for CAP Venous thromboembolism (VTE) prophylaxis within 24 hrs of surgery Prophylactic antibiotic within one hour prior to surgery Prophylactic antibiotic selection for surgical patients Prophylactic antibiotic discontinued within 24 hours (48 hrs for CTS) Cardiac surgery patients with 6 AM controlled glucose (PO day 1 & 2) Urinary catheter removed on post-op day 1 or 2 Surgery patients who received beta blockers perioperatively VBP-Patient Experience Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) HCAHPS Survey Dimensions Communication with nurses Communication with doctors Responsiveness of hospital staff Pain management Communication about medications Cleanlinessand quietness Discharge information Overall rating of hospital 6
7 CMS Value-Based Purchasing (VBP) FY 2013 Payments 10/1/12-9/30/13 Patient Experience of Care 30% Clinical Process of Care 70% SCIP HCAHPS Survey Dimensions Communication with nurses Communication with doctors Responsiveness of hospital staff Pain management Communication about medications Cleanliness and quietness Discharge information Overall rating of hospital MEASURES AMI 7a Fibrinolytic agent received w/in 30 of hospital arrival AMI 8 PCI received w/in 90 of hospital arrival HF 1 Discharge instructions PN 3b Blood culture before 1 st antibiotic i received in hospital PN 6 Initial antibiotic selection for CAP immunocompetent pt SCIP 1 Abx w/in 1 hr before incision or w/in2 hrs if Vancomycin/ Quinolone is used SCIP 2 Received prophylactic Abx consistent with recommendations SCIP 3 Prophylactic Abx discontinued w/in 24 hrs of surgery end time or 48 hrs for cardiac surgery SCIP 4 Controlled 6 AM postoperative serum glucose cardiac surgery SCIP VTE 1 Recommended VTE prophylaxis ordered during admission SCIP VTE2 Received VTE prophylaxis w/in 24 hrs prior to or after surgery SCIP Card 2 Pre admission betablocker and perioperative period beta blocker Add FY 2014 Payments 10/1/13-9/30/14 Clinical Process of Care 45% Patient Experience of Care 30% Outcome 25% SCIP 9 Postoperative Urinary Catheter Removal on Post Operative Day 1or2 HCAHPS Survey Dimensions Communication with nurses Communication with doctors Responsiveness of hospital staff Pain management Communication about medications Cleanliness and quietness Discharge information Overall rating of hospital 30 day mortality for CHF, AMI, PN Agency for Health Care Research and Quality (AHRQ) Patient Safety Indicators (PSI-90) added in 2015 PSI-3: Pressure Ulcer rate - 2.4% PSI-6: latrogenic pneumothorax rate 7.1% PSI-7: CLABSI 6.5% PSI-8: Post operative hip fracture rate 0.1% PSI-12: Perioperative PE/DVT rate 25.8% PSI-13: Post Operative sepsis rate - 7.4% PSI-14: Wound dehiscence rate - 1.7% PSI-15: Accidental puncture and laceration 49.2% 7




8 CMS Value-Based Purchasing (VBP) FY Payments 10/1/14-9/30/15 Patient Experience of Care 30% Clinical Processes of Care 20% Efficiency 20% Outcome 30% HCAHPS Survey Dimensions Communication with nurses Communication with doctors Responsiveness of hospital staff Pain management Communication about medications Cleanliness and quietness Discharge information Overall rating of hospital Central Line Associated Blood Stream Infection (CLABSI) 30 day mortality for CHF, AMI, PN PSI-90 SCIP Medicare spending per beneficiary CMS Value-Based Purchasing (VBP) FY Baseline 1/1/12-12/31/12 Performance 1/1/14-12/31/14 Payments 10/1/15-9/30/16 SCIP Measures AMI 7a Fibrinolytic agent received w/in 30 of hospital arrival PN 6 Initial antibiotic selection for CAP immunocompetent pt SCIP 2 Received prophylactic Abx consistent with recommendations SCIP 3 Prophylactic Abx discontinued w/in 24 hrs of surgery end time or 48 hrs for cardiac surgery SCIP 9 Postoperative Urinary Catheter Removal on Post Operative Day 1 or 2 SCIP-Card 2 Pre-admission beta-blocker and perioperative period beta blocker SCIP VTE2 Received VTE prophylaxis within 24 hrs prior to or after surgery New! IMM-2 Influenza Immunization Removed! AMI 8a PCI received w/in 90 of hospital arrival Removed! HF 1 Discharge instructions was removesd from FY2016 measures Removed! PN 3b Blood culture before 1 st antibiotic received in hospital Removed! SCIP 1 Abx w/in 1 hr before incision or w/in2 hrs if Vancomycin/Quinolone is used Removed! SCIP 4 Controlled 6 AM postoperative serum glucose cardiac surgery Clinical Processes of Care 10% Patient Experience of Care 25% Efficiency 25% Outcome 40% 30 day mortality CHF, AMI, PN Infection CLABSI CAUTI SSI-Colon SSI-Abdominal hysterectomy PSI-90 (6/30/14) Medicare spending per beneficiary 1/1/13-12/31/14 8

9 FY 2017 Value-Based Purchasing CLINICAL CARE - PROCESS Domain Weighting Performance Period (Payment adjustment effective for discharges from October 1, 2016 to September 30, 2017) Baseline Period January 1, 2013 December 31, 2013 January 1, 2015 December 31, 2015 Measure AMI 7a Fibrinolytic agent received w/in 30 of hospital arrival IMM-2 Influenza Immunization New! PC-01 Elective Delivery Prior to 39 Completed Weeks Gestation Removed! PN 6 Initial antibiotic selection for CAP immunocompetent pt Removed! SCIP 2 Received prophylactic Abx consistent with recommendations Removed! SCIP 3 Prophylactic Abx discontinued w/in 24 hrs of surgery end time or 48 hrs for cardiac surgery Removed! SCIP 9 Postoperative Urinary Catheter Removal on Post Operative Day 1 or 2 Removed! SCIP-Card 2 Pre-admission beta-blocker and perioperative period beta blocker Removed! SCIP VTE2 Received VTE prophylaxis within 24 hrs prior to or after surgery CMS Value-Based Purchasing (VBP) FY Payments 10/1/16-9/30/17 Patient Experience of Care 25% Process 5% Safety 20% Clinical Care 30% Outcomes 25% SCIP measures removed Efficiency 25% Baseline Period PATIENT EXPERIENCE OF CARE Performance Period January 1, 2013 December 31, 2013 January 1, 2015 December 31, 2015 SAFETY Complication/Patient Safety for Selected Indicators Baseline Period Performance Period October 1, 2010 June 30, 2012 October 1, 2013 June 30, 2015 Baseline Period Measure AHRQ PSI 90 composite Healthcare-Associated Infections Performance Period January 1, 2013 December 31, 2013 January 1, 2015 December 31, 2015 CLABSI CAUTI Measure SSI Colon SSI Abdominal Hysterectomy New! C. difficile New! MRSA CLINICAL CARE - OUTCOMES Baseline Period Performance Period October 1, 2010 June 30, 2012 October 1, 2013 June 30, 2015 Measure (Displayed as survival rate) 30-day mortality, AMI 30-day mortality, heart failure 30-day mortality, pneumonia EFFICIENCY Baseline Period Performance Period January 1, 2013 December 31, 2013 January 1, 2015 December 31, 2015 Changes in VBP Indicator Weighting: from Process to Outcome Process Outcome/Safety Pateint Experience Efficiency
10 Hospital Acquired Conditions (HAC) Defined by Deficit Reduction Act (2005): high cost (or high prevalence) result in higher DRG coding are potentially preventable The ACA mandated a 1% Medicare reimbursement penalty for hospitals in the bottom 25% ile for HACS HAC Reduction Program Framework 2016 Domain 1 (AHRQ Measure) Weighted 25% Domain 2 (CDC Measures) Weighted 75% AHRQ PSI 90 Composite This measure consists of performance period from July 1, 2012 June 30, 2014: PSI 3: pressure Ulcer rate 2.4% PSI 6: latrogenic pneumothorax rate 7.1% PSI 7: CLABSI 6.5% PSI 8: Post operative hip fracture rate 0.1% PSI 12: Perioperative PE/DVT rate 25.8% PSI 13: Post Operative sepsis rate 7.4% PSI 14: wound dehiscence rate 1.7% PSI 15: accidental puncture and laceration 49.2% 2016 (performance period CY ): CAUTI CLABSI Surgical Site Infection Colon Surgery Abdominal Hysterectomy 10

 100 98 96 94 2009 2010 92")


11 Do Physicians Adhere to Quality Standards? Improvement on National Surgical Care Improvement Project (SCIP) Measures Rates ( ) Surgical Care Composite ABX 1 hr. Correct ABX Stopping ABX Cardiac Pts before surgery Gluc Cont. Peri op Beta Blocker VTE Prophylaxis Foley Removal 11
12 Does Adherence to Process Measures Improve Outcomes? Conflicting data-depends on measure and outcome Antibiotics are necessary in reducing SSI but other factors contribute -blockers may be helpful or harmful VTE prophylaxis guidelines vary by specialty Documentation is vital to demonstrate clinical judgment and also helps with malpractice cases With the shift of emphasis on outcomes to be successful hospitals must have reliable processes Is There an Overlap Between Quality of Care Delivered and Malpractice? Quality and Safety Malpractice 12
13 Intent of Malpractice- Deterrence Assumptions Threat of malpractice deters poor care Improves adherence to standards Unintended consequences Defensive medicine Overuse of services Over testing Overtreatment More risk to patients Similar to process measures? Impact of Medical Malpractice Environment on Surgical Quality and Outcomes Though there is evidence that medical malpractice liability influences physicians clinical choices, there is little to support the theory that the threat of medical litigation improves physician adherence to quality care indicators or improves patient outcomes. JACS Vol. 218 No. 2 Feb

14 1999 IOM Report-To Err is Human 1999 IOM Report- To Err is Human 44,000 to 98,000 deaths a year from medical errors 2013 report in the Journal of Patient Safety estimated 210, ,000 deaths were associated with preventable harm Only 2% of negligent care results in law suits Surgical Morbidity and Mortality Mortality rate for inpatient surgery is 0.4 to 0.8%. Rate of major complications is 3 to 17%. At least half of all surgical complications are avoidable. 1,2 1. Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in Surgery 1999;126: Kable AK, Gibberd RW, Spigelman AD. Adverse events in surgical patients in Australia. Int J Qual Health Care 2002;14:

:629-636, 2011 Proportion of Physicians Facing a Malpractice Claim Annually by Specialty Jena AB et al.")
15 National Overview of Malpractice Data from a national liability insurer ( ) Annual cost of medical malpractice $55 billion 78% of claims did not result in payments to claimants 7.4% of physicians faced a malpractice claim each year 1.6% led to paid claim 75 to 99% of physicians will face a malpractice claim by the age of 65 Factors that drive claims are independent of the size of pay-out NEJM 365(7): , 2011 Proportion of Physicians Facing a Malpractice Claim Annually by Specialty Jena AB et al. N Engl J Med 2011;365:


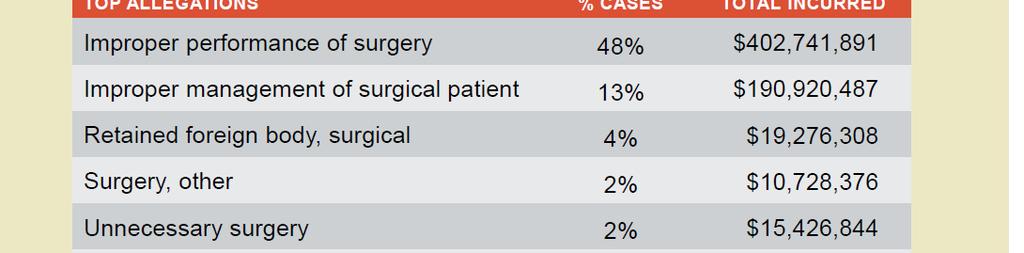
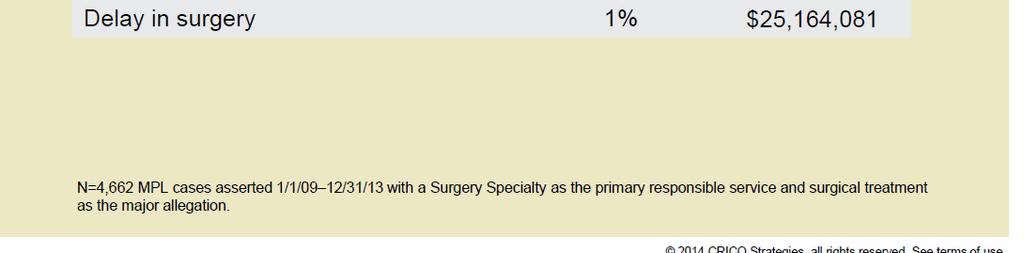
16 Amount of Malpractice Payments by Specialty. Jena AB et al. N Engl J Med 2011;365: Top 10 Claims for Surgery- Related Allegations National Practitioner Data Bank HAC/never events 16
17 Freq HAC/never events JOURNAL OF HEALTHCARE RISK MANAGEMENT VOLUME 33, NUMBER 4 Multiple opportunities were missed by all members of the team to prevent an adverse event. Nurse informs surgeon sponge count is wrong. RFID wanding was positive for a retained item. No sponge found on exploration The surgeon speculated that the sponge was beneath the patient, completed skin closure No attempt to find sponge. After months of abdominal pain X-ray shows retained sponge 17
18 Secondary Drivers of Malpractice Communication Teamwork Failure or delay in obtaining a consult Diagnostic tests Failure or delay in ordering Misinterpretation Failure to establish a differential diagnosis Treating a patient on the assumption that the prior diagnosis was correct Average Yearly Payout Between 1990 and 2011 in Inflation Adjusted 2012 Dollars JOURNAL OF HEALTHCARE RISK MANAGEMENT VOLUME 33, NUMBER 4 18
19 Impact of Malpractice on Surgeons Surgeons involved in malpractice suites Younger, worked longer hours and more night call Related to burnout, depression Less likely to recommend careers in surgery or medicine Second victims need appropriate p counseling JACS Vol. 213, No. 5, 2011 Why Do Patients File Malpractice Suits? Obvious deviation for the standard of care Financial motivations Need to find answers concern about a cover-up/poor communication Opinion outside of the care team suggested the care was substandard d Patient dissatisfaction 19
20 Patient Complaints and Malpractice (Why some may file) Physicians who have high numbers of patient complaints are: A subset linked to a disproportionate p number of complaints 9% are associated with 50% of complaints Responsible for high proportion of indemnity reserves Associate with >50% of dollars paid out and involved in high dollar cases Associated with lower patient satisfaction scores (HCAHPS) Not limited it to specific medical specialties Similar explanations or pushback for the patient complaints To Reduce Premiums Spread the cost Cut the cost Prevent the cost 20
21 Can we reduce malpractice claims with quality initiatives? Cost (Open and Closed Claims) Other 30% Surgery 34% Radiology 3% Anesthesiology 2% Gynecology 4% Emergency Medicine 6% Obstetrics 21% 21
22 Surgical Safety Initiative: Collaboration between Montefiore Medical Center Mount Sinai Health System Maimonides Medical Center Sponsored by HIC/FOJP Goals Encourage change in culture and practice Reduce adverse outcomes Increase defensibility Increase operational efficiencies i i Premium discounts 22
23 Surgical Safety Initiative OR team training- TeamSTEPPS Pre-Operative Medical Assessment Care of obese surgical patients BMI>40 Co-management/perioperative medicine Preoperative Medical Evaluation Patient is medically clear for surgery 23
24 Sample: Medical Clearance 24
25 Adequacy of Pre-operative Evaluation Question Anesthesiologist Survey ASA III & IV Patients FOJP Hospitals Were all preoperative medical problems identified when I first evaluated the patient? Were all preoperative medical problems adequately addressed when I first evaluated the patient? Response YES NO 90% 10% 85% 15% Were all relevant consults obtained? 89% 11% n=468, November 2011 Author of Pre-operative evaluation FOJP Hospitals-Survey ASA III & IV Patients Chart Review-data element % present Medical attending authored 42 Other provider authored, attending co-signature 12 Other provider authored, no attending co-signature 10 Not present in medical record 35 n=195, November,






26 What is the solution? Pre-Operative Medical Assessment Reference Pre-Operative Risk Assessment Requirements Completion of Pre-Op Risk Assessment Form (POMAF) All adult patients with significant co-morbidities (ASA III and IV) Internal Medicine Complete form Attending signature Surgeons Attending Surgeon Pre-op note that refers to POMAF Exceptions Emergent life threatening cases Must document emergent case in Attending Surgeon Pre-op note Anesthesia must classify as ASA IIIE or IVE 26
27 POMAF Compliance at Montefiore May 2013 to August % 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug POMAF Compliance Attending Note Compliance Full Compliance Target Compliance = 85% Co-management of Surgical Patients Moses Division Vascular Surgery patients Designated medical hospitalist t collaboratively l manages surgical patients, no other clinical responsibilities Daily notes by Attending Surgeon and Hospitalist Outcome data based on NSQIP measures 27
28 American College of Surgeons (ACS) National Surgical Quality Improvement Program Evaluation of Co-managed Patients Data-driven, risk-adjusted, outcomes-based surgical quality improvement program Co-managed patients data abstracted and entered into NSQIP data base Predicted outcomes determined using NSQIP calculator Observed to expected ratio calculated Risk Calculator Homepage About FAQ ACS Website ACS NSQIP Website Procedure Risk Factors Colectomy, partial; with anastomosis Age: 65-74, Male, Partially dependent functional status, ASA III, Clean/Contaminated wound, Chronic steroids, Diabetes (insulin), HTN, Previous cardiac, Dyspnea with exertion, Smoker, Overweight Change Patient Risk Factors Outcomes Serious Complication Estimated Risk 28% Chance of Outcome Above Average Any Complication 46% Pneumonia 10% Above Average Above Average Cardiac Complication Surgical Site Infection Urinary Tract Infection Venous Thromboembolism 6% 23% 6% 3% Above Average Above Average Above Average Above Average Renal Failure 6% Return to OR 12% Death 6% Above Average Above Average Above Average Discharge to Nursing or Rehab Facility 18% Above Average 0% (Better) 100% (Worse) Predicted Length of Hospital Stay: 6.0 days Surgeon Adjustment of Risks This will need to be used infrequently, but surgeons may adjust the estimated risks if they feel the calculated risks are underestimated. This should only be done if the reason for the increased risks was NOT already entered into the risk calculator. 1 - No adjustment necessary 28
29 Outcome Benefits of Co Managed Patients NSQIP analysis Outcomes Observed Rate Expected Rate O/E Ratio Trend Length of Stay NA Death Serious Complication Any Complication Pneumonia Cardiac Complication Surgical Site Infection Urinary Tract Infection Venous Thromboembolism Renal Failure Return to OR (n=167) Recommendations on Improving Quality of Care and Reducing Malpractice Risk Careful documentation Consistent effective communication Collaborative care 29
30 Questions? Redefining Professionalism Professionalism = Accountability Autonomy Authority Assertion Control Self-interest Fee for Service Collaboration Evidence Measurement Transparency Public Interest Payment for Quality 30

31 Agency for Health Care Research and Quality TeamSTEPPS program Trained a multidisciplinary team of peri-operative champions All OR personnel participated in a hospital-based training curriculum Observation program pending Teamwork poor care is inevitable when a complicated patient is cared for by myriad individuals who have not been trained to communicate effectively as a team. Gerald B. Healy, MD, FACS Presidential Address 93rd Clinical Congress American College of Surgeons October 8, 2007 Going An expert from team! a team of experts to 31


32 Care of the Obese Surgical Patient: Anesthesia/Surgery Attending Survey Change in practice for patients with BMI>40 Anesthesiology 12% 88% Other specialties 32% 68% Yes No Total 28% 72% 0% 20% 40% 60% 80% 100% 32


33 Care of the Obese Surgical Patient Goals for Compliance-Practice Standards: 1. Supplemental informed consent 2. Pre-operative medical assessment form completed 3. Nursing assessment on admission and post-op 4. Preoperative documentation plan for VTE prophylaxis 5. Documentation of two anesthesia providers at the time of induction 6. PACU dicharge note authored by an attending anesthesiologist 7. Documentation of CPAP availability 8. Difficult airway cart and/or advanced airway technology in OR 9. Appropriate size equipment for obese patients available in the OR and units 10. Perioperative nursing staff attend yearly in-service on care of obese patients 11. Pain management protocol for obese patients Supplemental Informed Consent for all patients BMI>40 33



34 Best practices for obstetrics Collaboration of 4 New York City Hospitals Including implementation ti of evidence-based d protocols, Standardized educational interventions Mandatory electronic fetal monitoring training Guidelines requiring improved documentation Each institution to develop a unique safetyrelated area of expertise that they would ultimately share and disseminate across the collaborative Improved obstetric safety through programmatic collaboration Journal of Healthcare Risk Management Volume 33, Issue 3, pages 14-22,,
 Weighted Adverse Outcome Score (WAOS) decreased from 3.")
35 Improved obstetric safety through programmatic collaboration Analysis of 19,189 deliveries January 2008 through December 2011 Adverse Outcome Index (AOI) decrease 42% (from 10.7 % to 6.2 %) Weighted Adverse Outcome Score (WAOS) decreased from 3.9 to 2.3. AOI = # deliveries affected adverse outcomes/ total number of deliveries WAOS= weighted to account for the severity of injuries Journal of Healthcare Risk Management Volume 33, Issue 3, pages 14-22,,2014 Five Stages of Grief Denial- The data is wrong Anger- It does not apply to me Bargaining- I will get the correct data Depression- There is nothing I can do about it Resolution- Acceptance and action Adapted from Elisabeth Kübler-Ross 5 stage model 35
36 It isn t reasonable to ask that we achieve perfection. What is reasonable is that we never cease to aim for it. Atul Gawande Cost (Open and Closed Claims) Other 31% Surgery 31% Anesthesiology 2% Radiology 3% Gynecology 4% Emergency Medicine 6% Obstetrics 23% 36





37 Trends in Overall Claims and Claims with an Indemnity Payment, According to Risk of Specialty. Jena AB et al. N Engl J Med 2011;365: Summary Statistics for Physician Specialties. Jena AB et al. N Engl J Med 2011;365:
38 Cumulative Career Probability of Facing a Malpractice Claim or Indemnity Payment, According to Risk of Specialty and Age of Physician. Jena AB et al. N Engl J Med 2011;365: Conclusions There is substantial variation in the likelihood of malpractice suits and the size of indemnity payments across specialties. The cumulative risk of facing a malpractice claim is high in all specialties, although most claims do not lead to payments to plaintiffs. 38
39 Risk Calculator Homepage About FAQ ACS Website ACS NSQIP Website Enter Patient and Surgical Information Procedure Colectomy, partial; with anastomosis Clear Begin by entering the procedure name or CPT code. One or more procedures will appear below the procedure box. You will need to click on the desired procedure to properly select it. You may also search using two words (or two partial words) by placing a + in between, for example: cholecystectomy+cholangiography Reset All Selections Are there other potential appropriate treatment options? Other Surgical Options Other Non-operative options None Please enter as much of the following information as you can to receive the best risk estimates. A rough estimate will still be generated if you cannot provide all of the information below. Age Group years Diabetes Insulin Sex Male Hypertension requiring medication Yes Functional status Partially Dependent Previous cardiac event Yes Emergency case No Congestive heart failure in 30 days prior to surgery No ASA class III - Severe systemic disease Wound class Clean/ Contaminated Dyspnea With Moderate exertion Steroid use for chronic condition Ascites within 30 days prior to surgery Systemic sepsis within 48 hours prior to surgery Current smoker within 1 Yes Yes year No History of severe COPD No None Dialysis No Acute Renal Failure No Ventilator dependent No BMI Calculation: Height (in) 69 Disseminated cancer No Weight (lbs) 189 Step 2 of 4 Improvement in SCIP Antibiotic Compliance does not Reduce Colon SSI Rates 39
40 SSI rates obtained from Medicare claims data SCIP rates extracted from Hospital Compare Hospitals with higher rates of SCIP compliance for antibiotic timing and selection had lower SSI rates 10% increase in compliance with timing of antibiotics led to a 5.3% decrease in SSI rates Timely discontinuing antibiotics had no effect on SSI Malpractice Risk According to Physician Specialty NEJM 365(7): ,
41 What we need to do Interdepartmental multidisciplinary efforts Clinically relevant targets of care Clinicians educated on the standards Development of workflows Feedback on performance with benchmarks Structured process designed to reduce provider variability which can be monitored J Healthc Risk Manag Sep;34(2): doi: /jhrm Analysis of patient injury based on anesthesiology closed claims data from a major malpractice insurer. Ranum D1, Ma H, Shapiro FE, Chang B, Urman RD. Reducing Risk with Clinical Decision SupportJournal:Applied Clinical InformaticsISSN: DOI: 0018Issue:Vol. 5: Issue Pages: Journal of Patient Safety: Post Author Corrections: November 13, 2014 doi: /PTS
 Hospital performance is relative to all eligible hospitals Achievement Scale Improvement Scale Two year lag from")
42 Value-Based Purchasing (VBP) Review Introduced in FY 2013 with 2 domains Clinical process- Core Measures Patient experience- Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) Expanded in FY 2014 and FY 2015 Outcomes domain Efficiency domain (FY 2015 only) Hospital performance is relative to all eligible hospitals Achievement Scale Improvement Scale Two year lag from performance and payment adjustments At risk- 1% Base DRG operating payments Increases to 2% in FY
43 CMS Reporting Requirements on Hospitals Hospital Inpatient Quality Reporting Program Authorized 100% process measures Public display of quality data begun on Hospital Compare Process measures Pti Patient texperience Affordable Care Act (ACA) Emphasis shifted from processes to outcomes Mortality Care of The Obese Surgical Patient Compliance in Obesity Cases 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Feb Mar Apr May Jun Jul Aug Moses Wakefield Weiler Target = 60% 43





44 What is in CBS? Comparative Benchmark System: a database of clinical system vulnerabilities More than 300,000 medical malpractice cases initial coding of cases provides high-level comparisons deeply coded cases provide full breadth of clinical detail for analysis 44



45 45
Objectives. Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004
 Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment
 Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment presented by Sherry Kwater, MSM,BSN,RN Chief Nursing Officer Penn State Hershey Medical Center Objectives 1. Understand
Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment presented by Sherry Kwater, MSM,BSN,RN Chief Nursing Officer Penn State Hershey Medical Center Objectives 1. Understand
National Provider Call: Hospital Value-Based Purchasing
 National Provider Call: Hospital Value-Based Purchasing Fiscal Year 2015 Overview for Beneficiaries, Providers, and Stakeholders Centers for Medicare & Medicaid Services 1 March 14, 2013 Medicare Learning
National Provider Call: Hospital Value-Based Purchasing Fiscal Year 2015 Overview for Beneficiaries, Providers, and Stakeholders Centers for Medicare & Medicaid Services 1 March 14, 2013 Medicare Learning
Value Based Purchasing
 Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
CMS in the 21 st Century
 CMS in the 21 st Century ICE 2013 ANNUAL CONFERENCE David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco November 15, 2013 The strategy is to concurrently pursue
CMS in the 21 st Century ICE 2013 ANNUAL CONFERENCE David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco November 15, 2013 The strategy is to concurrently pursue
Hospital Inpatient Quality Reporting (IQR) Program Measures (Calendar Year 2012 Discharges - Revised)
 Program Measures (Calendar Year 2012 Discharges - Revised)") The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
Value-based incentive payment percentage 3
 Report Run Date: 07/12/2013 Hospital Value-Based Purchasing Value-Based Percentage Payment Summary Report Page 1 of 5 Percentage Summary Report Data as of 1 : 07/08/2013 Total Score Facility State National
Report Run Date: 07/12/2013 Hospital Value-Based Purchasing Value-Based Percentage Payment Summary Report Page 1 of 5 Percentage Summary Report Data as of 1 : 07/08/2013 Total Score Facility State National
FY 2014 Inpatient PPS Proposed Rule Quality Provisions Webinar
 FY 2014 Inpatient PPS Proposed Rule Quality Provisions Webinar May 23, 2013 AAMC Staff: Scott Wetzel, swetzel@aamc.org Mary Wheatley, mwheatley@aamc.org Important Info on Proposed Rule In Federal Register
FY 2014 Inpatient PPS Proposed Rule Quality Provisions Webinar May 23, 2013 AAMC Staff: Scott Wetzel, swetzel@aamc.org Mary Wheatley, mwheatley@aamc.org Important Info on Proposed Rule In Federal Register
Connecting the Revenue and Reimbursement Cycles
 Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
The Wave of the Future: Value-Based Purchasing & the Impact of Quality Reporting Within the Revenue Cycle
 The Wave of the Future: Value-Based Purchasing & the Impact of Quality Reporting Within the Revenue Cycle Kim Charland, BA, RHIT, CCS Senior Vice President Clinical Innovation and Publisher VBPmonitor
The Wave of the Future: Value-Based Purchasing & the Impact of Quality Reporting Within the Revenue Cycle Kim Charland, BA, RHIT, CCS Senior Vice President Clinical Innovation and Publisher VBPmonitor
August 1, 2012 (202) CMS makes changes to improve quality of care during hospital inpatient stays
 CMS makes changes to improve quality of care during hospital inpatient stays") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
FY 2014 Inpatient Prospective Payment System Proposed Rule
 FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
Medicare Value Based Purchasing Overview
 Medicare Value Based Purchasing Overview South Carolina Hospital Association DataGen Susan McDonough Bill Shyne October 29, 2015 Today s Objectives Overview of Medicare Value Based Purchasing Program Review
Medicare Value Based Purchasing Overview South Carolina Hospital Association DataGen Susan McDonough Bill Shyne October 29, 2015 Today s Objectives Overview of Medicare Value Based Purchasing Program Review
Hospital Acquired Conditions: using ACS-NSQIP to drive performance. J Michael Henderson Jackie Matthews Nirav Vakharia
 Hospital Acquired Conditions: using ACS-NSQIP to drive performance J Michael Henderson Jackie Matthews Nirav Vakharia Your Team: Quality & Patient Safety Institute Cleveland Clinic Mike Henderson: Chief
Hospital Acquired Conditions: using ACS-NSQIP to drive performance J Michael Henderson Jackie Matthews Nirav Vakharia Your Team: Quality & Patient Safety Institute Cleveland Clinic Mike Henderson: Chief
Model VBP FY2014 Worksheet Instructions and Reference Guide
 Model VBP FY2014 Worksheet Instructions and Reference Guide This material was prepared by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under a contract with the
Model VBP FY2014 Worksheet Instructions and Reference Guide This material was prepared by Qualis Health, the Medicare Quality Improvement Organization for Idaho and Washington, under a contract with the
Improving quality of care during inpatient hospital stays
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Communications FACT SHEET FOR IMMEDIATE RELEASE Contact:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Communications FACT SHEET FOR IMMEDIATE RELEASE Contact:
Medicare Value Based Purchasing Overview
 Medicare Value Based Purchasing Overview Washington State Hospital Association Apprise Health Insights / Oregon Association of Hospitals and Health Systems DataGen Susan McDonough Lauren Davis Bill Shyne
Medicare Value Based Purchasing Overview Washington State Hospital Association Apprise Health Insights / Oregon Association of Hospitals and Health Systems DataGen Susan McDonough Lauren Davis Bill Shyne
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Care Coordination What Matters
 Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Facility State National
 Percentage Summary Report Page 1 of 5 Data As Of: 07/27/2016 Total Performance Facility State National 35.250000000000 37.325750561167 35.561361414483 Unweighted Domain Weighting Weighted Domain Clinical
Percentage Summary Report Page 1 of 5 Data As Of: 07/27/2016 Total Performance Facility State National 35.250000000000 37.325750561167 35.561361414483 Unweighted Domain Weighting Weighted Domain Clinical
Medicare Quality Based Payment Reform (QBPR) Program Reference Guide Fiscal Years
 Program Reference Guide Fiscal Years") julian.coomes@flhosp.orgjulian.coomes@flhosp.org Medicare Quality Based Payment Reform (QBPR) Program Reference Guide Fiscal Years 2018-2020 October 2017 Table of Contents Value Based Purchasing (VBP)
julian.coomes@flhosp.orgjulian.coomes@flhosp.org Medicare Quality Based Payment Reform (QBPR) Program Reference Guide Fiscal Years 2018-2020 October 2017 Table of Contents Value Based Purchasing (VBP)
Medicare Value-Based Purchasing for Hospitals: A New Era in Payment
 Medicare Value-Based Purchasing for Hospitals: A New Era in Payment Daniel J. Hettich March, 2012 I. Introduction: Evolution of Medicare as a Purchaser Cost reimbursement rewards furnishing more services
Medicare Value-Based Purchasing for Hospitals: A New Era in Payment Daniel J. Hettich March, 2012 I. Introduction: Evolution of Medicare as a Purchaser Cost reimbursement rewards furnishing more services
(202) or CMS Proposals to Improve Quality of Care during Hospital Inpatient Stays
 or CMS Proposals to Improve Quality of Care during Hospital Inpatient Stays") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE April 30, 2014 Contact: CMS Media
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE April 30, 2014 Contact: CMS Media
Medicare Payment Strategy
 Data and Analytics Medicare Payment Strategy CMS Inpatient Pay For Performance Program Update Eric Fontana, Practice Manager, Data and Analytics Group analytics@advisory.com 2011 THE ADVISORY BOARD COMPANY
Data and Analytics Medicare Payment Strategy CMS Inpatient Pay For Performance Program Update Eric Fontana, Practice Manager, Data and Analytics Group analytics@advisory.com 2011 THE ADVISORY BOARD COMPANY
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
HCAHPS. Presented by: Bill Sexton. Proudly recognized as one of the Nation s Top 100 Critical Access Hospitals - ivantage Health Analytics
 HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
CME Disclosure. HCAHPS- Hardwiring Your Hospital for Pay-for-Performance Success. Accreditation Statement. Designation of Credit.
 CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CMS Value Based Purchasing: The Wave of the Future
 CMS Value Based Purchasing: The Wave of the Future Ninth National Pay for Performance Summit David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco Betsy L. Thompson,
CMS Value Based Purchasing: The Wave of the Future Ninth National Pay for Performance Summit David Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco Betsy L. Thompson,
MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT (MBQIP)
") MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT (MBQIP) Began in September 2011 Key quality improvement activity within the Medicare Rural Hospital Flexibility grant program Goal of MBQIP: to improve
MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT (MBQIP) Began in September 2011 Key quality improvement activity within the Medicare Rural Hospital Flexibility grant program Goal of MBQIP: to improve
State of the State: Hospital Performance in Pennsylvania October 2015
 State of the State: Hospital Performance in Pennsylvania October 2015 1 Measuring Hospital Performance Progress in Pennsylvania: Process Measures 2 PA Hospital Performance: Process Measures We examined
State of the State: Hospital Performance in Pennsylvania October 2015 1 Measuring Hospital Performance Progress in Pennsylvania: Process Measures 2 PA Hospital Performance: Process Measures We examined
Accreditation, Quality, Risk & Patient Safety
 Accreditation, Quality, Risk & Patient Safety Accreditation The Joint Commission (TJC) Centers for Medicare & Medicaid Services (CMS) Wyoming Department of Health (DOH) Joint Commission: - Joint Commission
Accreditation, Quality, Risk & Patient Safety Accreditation The Joint Commission (TJC) Centers for Medicare & Medicaid Services (CMS) Wyoming Department of Health (DOH) Joint Commission: - Joint Commission
Our Hospital s Value Based Purchasing (VBP) Journey
 Journey") Our Hospital s Value Based Purchasing (VBP) Journey Linnea Huinker, MHA, Clinical Effectiveness Specialist Katie Potts, MHA, Clinical Effectiveness Specialist January 31, 2013 Presentation Outline Hospital
Our Hospital s Value Based Purchasing (VBP) Journey Linnea Huinker, MHA, Clinical Effectiveness Specialist Katie Potts, MHA, Clinical Effectiveness Specialist January 31, 2013 Presentation Outline Hospital
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD
 Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
New Mexico Hospital Association
 New Mexico Hospital Association Hospital Quality Reporting Guide Revised: November 2014 TABLE OF CONTENTS Regulatory Landscape at a Glance... 4 Key Terms and Undserstanding Timeframes... 5 Hospital Inpatient
New Mexico Hospital Association Hospital Quality Reporting Guide Revised: November 2014 TABLE OF CONTENTS Regulatory Landscape at a Glance... 4 Key Terms and Undserstanding Timeframes... 5 Hospital Inpatient
An Overview of the. Measures. Reporting Initiative. bwinkle 11/12
 An Overview of the National Hospital Quality Measures A National Voluntary Hospital Reporting Initiative bwinkle 11/12 What Are Hospital Quality Measures? The Joint Commission (TJC) and the Centers for
An Overview of the National Hospital Quality Measures A National Voluntary Hospital Reporting Initiative bwinkle 11/12 What Are Hospital Quality Measures? The Joint Commission (TJC) and the Centers for
KANSAS SURGERY & RECOVERY CENTER
 Hospital Reporting Period for Clinical Process Measures: Fourth Quarter 2012 through Third Quarter 2013 Discharges Page 2 of 13 Hospital Quality Measures Your Hospital Aggregate for All Four Quarters 10
Hospital Reporting Period for Clinical Process Measures: Fourth Quarter 2012 through Third Quarter 2013 Discharges Page 2 of 13 Hospital Quality Measures Your Hospital Aggregate for All Four Quarters 10
Mastering the Mandatory Elements of the Affordable Care Act. Melinda Hancock Walter Coleman
 Mastering the Mandatory Elements of the Affordable Care Act Melinda Hancock Walter Coleman 1 ACA Gains through 2019 Amounts in Billions Source:CBO and Joint Committee on Taxation, 2010 Projection 2 Current
Mastering the Mandatory Elements of the Affordable Care Act Melinda Hancock Walter Coleman 1 ACA Gains through 2019 Amounts in Billions Source:CBO and Joint Committee on Taxation, 2010 Projection 2 Current
SCORING METHODOLOGY APRIL 2014
 SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Brian Herdman Operations Manager, CBIZ KA Consulting Services, LLC July 30, 2015 Overview How did we get here? Summary of IPPS Quality Programs Hospital
Quality Based Impacts to Medicare Inpatient Payments Brian Herdman Operations Manager, CBIZ KA Consulting Services, LLC July 30, 2015 Overview How did we get here? Summary of IPPS Quality Programs Hospital
IMPROVING HCAHPS, PATIENT MORTALITY AND READMISSION: MAXIMIZING REIMBURSEMENTS IN THE AGE OF HEALTHCARE REFORM
 IMPROVING HCAHPS, PATIENT MORTALITY AND READMISSION: MAXIMIZING REIMBURSEMENTS IN THE AGE OF HEALTHCARE REFORM OVERVIEW Using data from 1,879 healthcare organizations across the United States, we examined
IMPROVING HCAHPS, PATIENT MORTALITY AND READMISSION: MAXIMIZING REIMBURSEMENTS IN THE AGE OF HEALTHCARE REFORM OVERVIEW Using data from 1,879 healthcare organizations across the United States, we examined
Understanding HSCRC Quality Programs and Methodology Updates
 Understanding HSCRC Quality Programs and Methodology Updates Kristen Geissler, MS, PT, CPHQ, MBA Managing Director Beth Greskovich - Director Berkeley Research Group August 19, 2016 Maryland Waiver and
Understanding HSCRC Quality Programs and Methodology Updates Kristen Geissler, MS, PT, CPHQ, MBA Managing Director Beth Greskovich - Director Berkeley Research Group August 19, 2016 Maryland Waiver and
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence
 Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
Innovative Coordinated Care Delivery
 Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
The Data Game. Vicky A. Mahn-DiNicola RN, MS, CPHQ VP Research & Market Insights
 The Data Game Vicky A. Mahn-DiNicola RN, MS, CPHQ VP Research & Market Insights My Primary Objective Today: Review Upcoming Regulatory Changes Review of Proposed IPPS Rule for FY 2016 CMS-1632-P 45 CFR
The Data Game Vicky A. Mahn-DiNicola RN, MS, CPHQ VP Research & Market Insights My Primary Objective Today: Review Upcoming Regulatory Changes Review of Proposed IPPS Rule for FY 2016 CMS-1632-P 45 CFR
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
Inpatient Quality Reporting Program
 Hospital Value-Based Purchasing Program: Overview of FY 2017 Questions & Answers Moderator: Deb Price, PhD, MEd Educational Coordinator, Inpatient Program SC, HSAG Speaker(s): Bethany Wheeler, BS HVBP
Hospital Value-Based Purchasing Program: Overview of FY 2017 Questions & Answers Moderator: Deb Price, PhD, MEd Educational Coordinator, Inpatient Program SC, HSAG Speaker(s): Bethany Wheeler, BS HVBP
Quality and Health Care Reform: How Do We Proceed?
 Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
K-HEN Acute Care/Critical Access Hospitals Measures Alignment with PfP 40/20 Goals AEA Minimum Participation Full Participation 1, 2
 Outcome Measure for Any One of the Following: Outcome Measures Meeting Either A or B: Adverse Drug Events (ADE) All measures are surveillance data Hospital Collected Anticoagulant (ADE-12) Opioid (ADE-111)
Outcome Measure for Any One of the Following: Outcome Measures Meeting Either A or B: Adverse Drug Events (ADE) All measures are surveillance data Hospital Collected Anticoagulant (ADE-12) Opioid (ADE-111)
Financial Policy & Financial Reporting. Jay Andrews VP of Financial Policy
 Financial Policy & Financial Reporting Jay Andrews VP of Financial Policy 1 Members & Groups Supported Center for Healthcare Excellence Hospital Leadership & Quality Departments Hospital Finance Departments
Financial Policy & Financial Reporting Jay Andrews VP of Financial Policy 1 Members & Groups Supported Center for Healthcare Excellence Hospital Leadership & Quality Departments Hospital Finance Departments
CCHS: Quality and Patient Safety. J Michael Henderson, MD Guido Bergomi
 CCHS: Quality and Patient Safety J Michael Henderson, MD Guido Bergomi Outline Integrated Quality & Safety structure Quality Goals and Performance Improvement Quality data sources Quality Reporting The
CCHS: Quality and Patient Safety J Michael Henderson, MD Guido Bergomi Outline Integrated Quality & Safety structure Quality Goals and Performance Improvement Quality data sources Quality Reporting The
Value Based Purchasing: Improving Healthcare Outcomes Using the Right Incentives
 Value Based Purchasing: Improving Healthcare Outcomes Using the Right Incentives One (1.0) Contact Hour Course Expires: 1/15/2015 Course Published: 12/10/2013 Reproduction and distribution of these materials
Value Based Purchasing: Improving Healthcare Outcomes Using the Right Incentives One (1.0) Contact Hour Course Expires: 1/15/2015 Course Published: 12/10/2013 Reproduction and distribution of these materials
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
Copyright 2015 Wolters Kluwer Health, Inc. All rights reserved.
 24 May 2015 Nursing Management www.nursingmanagement.com 2.5 CONTACT HOURS Value-Based Just a few years ago, we were in the infancy of the Centers for Medicare and Medicaid Services (CMS) Value-Based Purchasing
24 May 2015 Nursing Management www.nursingmanagement.com 2.5 CONTACT HOURS Value-Based Just a few years ago, we were in the infancy of the Centers for Medicare and Medicaid Services (CMS) Value-Based Purchasing
VALUE. Critical Access Hospital QUALITY REPORTING GUIDE
 better health care VALUE HEALTHIER POPULATIONS Critical Access Hospital QUALITY REPORTING GUIDE TABLE OF CONTENTS Introduction and Summary....2 Missouri Health Care-Associated Infection Reporting System
better health care VALUE HEALTHIER POPULATIONS Critical Access Hospital QUALITY REPORTING GUIDE TABLE OF CONTENTS Introduction and Summary....2 Missouri Health Care-Associated Infection Reporting System
Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA
 Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA Introduce the methods of using core measures to compare quality of health care US hospitals provide Have
Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA Introduce the methods of using core measures to compare quality of health care US hospitals provide Have
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule
 HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
Dianne Feeney, Associate Director of Quality Initiatives. Measurement
 HSCRC Quality Based Reimbursement Program Dianne Feeney, Associate Director of Quality Initiatives Sule Calikoglu, Associate Director of Performance Measurement 1 Quality Initiative Timeline Phase I: Quality
HSCRC Quality Based Reimbursement Program Dianne Feeney, Associate Director of Quality Initiatives Sule Calikoglu, Associate Director of Performance Measurement 1 Quality Initiative Timeline Phase I: Quality
Value-Based Purchasing & Payment Reform How Will It Affect You?
 Value-Based Purchasing & Payment Reform How Will It Affect You? HFAP Webinar September 21, 2012 Nell Buhlman, MBA VP, Product Strategy Click to view recording. Agenda Payment Reform Landscape Current &
Value-Based Purchasing & Payment Reform How Will It Affect You? HFAP Webinar September 21, 2012 Nell Buhlman, MBA VP, Product Strategy Click to view recording. Agenda Payment Reform Landscape Current &
Star Rating Method for Single and Composite Measures
 Star Rating Method for Single and Composite Measures CheckPoint uses three-star ratings to enable consumers to more quickly and easily interpret information about hospital quality measures. Composite ratings
Star Rating Method for Single and Composite Measures CheckPoint uses three-star ratings to enable consumers to more quickly and easily interpret information about hospital quality measures. Composite ratings
Centers for Medicare & Medicaid Services (CMS) Quality Improvement Program Measures for Acute Care Hospitals - Fiscal Year (FY) 2020 Payment Update
 Quality Improvement Program Measures for Acute Care Hospitals - Fiscal Year (FY) 2020 Payment Update") ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2020 Centers for Medicare & Medicaid Services (CMS) Improvement s for Acute
ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2020 Centers for Medicare & Medicaid Services (CMS) Improvement s for Acute
The 5 W s of the CMS Core Quality Process and Outcome Measures
 The 5 W s of the CMS Core Quality Process and Outcome Measures Understanding the process and the expectations Developed by Kathy Wonderly RN,BSPA, CPHQ Performance Improvement Coordinator Developed : September
The 5 W s of the CMS Core Quality Process and Outcome Measures Understanding the process and the expectations Developed by Kathy Wonderly RN,BSPA, CPHQ Performance Improvement Coordinator Developed : September
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Future of Quality Reporting and the CMS Quality Incentive Programs
 Future of Quality Reporting and the CMS Quality Incentive Programs Current Quality Environment Continued expansion of quality evaluation Increasing Reporting Requirements Increased Public Surveillance/Scrutiny
Future of Quality Reporting and the CMS Quality Incentive Programs Current Quality Environment Continued expansion of quality evaluation Increasing Reporting Requirements Increased Public Surveillance/Scrutiny
PASSPORT ecare NEXT AND THE AFFORDABLE CARE ACT
 REVENUE CYCLE INSIGHTS PATIENT ACCESS PASSPORT ecare NEXT AND THE AFFORDABLE CARE ACT Maximizing Reimbursements For Acute Care Hospitals Executive Summary The Affordable Care Act (ACA) authorizes several
REVENUE CYCLE INSIGHTS PATIENT ACCESS PASSPORT ecare NEXT AND THE AFFORDABLE CARE ACT Maximizing Reimbursements For Acute Care Hospitals Executive Summary The Affordable Care Act (ACA) authorizes several
Overview of the Hospital Safety Score September 24, Missy Danforth, Senior Director of Hospital Ratings, The Leapfrog Group
 Overview of the Hospital Safety Score September 24, 2013 Missy Danforth, Senior Director of Hospital Ratings, The Leapfrog Group Presentation Overview Who is getting a Hospital Safety Score? Changes to
Overview of the Hospital Safety Score September 24, 2013 Missy Danforth, Senior Director of Hospital Ratings, The Leapfrog Group Presentation Overview Who is getting a Hospital Safety Score? Changes to
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Person-Centered Care and Population Health
 Physician Leader Forum Person-Centered Care and Population Health ZIAD HAYDAR, MD, MBA Chief Medical Officer Ascension Health 2013 by the Catholic Health Association of the United States Outline Describe
Physician Leader Forum Person-Centered Care and Population Health ZIAD HAYDAR, MD, MBA Chief Medical Officer Ascension Health 2013 by the Catholic Health Association of the United States Outline Describe
The Patient Protection and Affordable Care Act of 2010
 INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
PAY FOR PERFORMANCE AND VALUE BASED PURCHASING: Leigh Humphrey, MBA, LMSW, CPHQ
 PAY FOR PERFORMANCE AND VALUE BASED PURCHASING: Leigh Humphrey, MBA, LMSW, CPHQ Objectives Define what Pay for Performance is and why CMS wants us to move in this direction Describe the process of how
PAY FOR PERFORMANCE AND VALUE BASED PURCHASING: Leigh Humphrey, MBA, LMSW, CPHQ Objectives Define what Pay for Performance is and why CMS wants us to move in this direction Describe the process of how
Scoring Methodology FALL 2017
 Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
4/10/2013. Learning Objective. Quality-Based Payment Models
 Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Quality Health Indicators: Measure List. Clinical Quality: Monthly
 Clinical Quality: Monthly Healthcare Associated Infections per 100 Inpatient Days *Core Measure* Unassisted Patient Falls per 100 Inpatient Days *Core Measure* Readmission within 30 days (All Cause) -
Clinical Quality: Monthly Healthcare Associated Infections per 100 Inpatient Days *Core Measure* Unassisted Patient Falls per 100 Inpatient Days *Core Measure* Readmission within 30 days (All Cause) -
P4P Programs 9/13/2013. Medicare P4P Programs. Medicaid P4P Programs
 P4P Programs Medicare P4P Programs Hospital Quality Reporting Programs (IQR and OQR) Hospital Value-Based Purchasing (VBP) Program Hospital Readmissions Reduction Program (HRRP) Hospital-Acquired Conditions
P4P Programs Medicare P4P Programs Hospital Quality Reporting Programs (IQR and OQR) Hospital Value-Based Purchasing (VBP) Program Hospital Readmissions Reduction Program (HRRP) Hospital-Acquired Conditions
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
Hospital-Acquired Condition Reduction Program. Hospital-Specific Report User Guide Fiscal Year 2017
 Hospital-Acquired Condition Reduction Program Hospital-Specific Report User Guide Fiscal Year 2017 Contents Overview... 4 September 2016 Error Notice... 4 Background and Resources... 6 Updates for FY 2017...
Hospital-Acquired Condition Reduction Program Hospital-Specific Report User Guide Fiscal Year 2017 Contents Overview... 4 September 2016 Error Notice... 4 Background and Resources... 6 Updates for FY 2017...
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
June 24, Dear Ms. Tavenner:
 1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 24, 2013 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 24, 2013 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
Learning Objectives. Medicare P4P Programs. How to Interpret Medicare s Hospital Pay for Performance Reports
 1 How to Interpret Medicare s Hospital Pay for Performance Reports Richard D. Pinson, MD, FACP, CCS Principal Pinson & Tang, LLC Houston, TX Learning Objectives At the completion of this educational activity,
1 How to Interpret Medicare s Hospital Pay for Performance Reports Richard D. Pinson, MD, FACP, CCS Principal Pinson & Tang, LLC Houston, TX Learning Objectives At the completion of this educational activity,
WA Flex Program Medicare Beneficiary Quality Improvement Program
 WA Flex Program Medicare Beneficiary Quality Improvement Program Medicare Rural Hospital Flexibility Grant Program Assist CAHs by providing funding to state governments to encourage quality and performance
WA Flex Program Medicare Beneficiary Quality Improvement Program Medicare Rural Hospital Flexibility Grant Program Assist CAHs by providing funding to state governments to encourage quality and performance
Overview of the Spring 2016 Hospital Safety Score March 7, Missy Danforth, Vice President of Hospital Ratings, The Leapfrog Group
 Overview of the Spring 2016 Hospital Safety Score March 7, 2016 Missy Danforth, Vice President of Hospital Ratings, The Leapfrog Group Presentation Overview Who is getting a Hospital Safety Score? Scoring
Overview of the Spring 2016 Hospital Safety Score March 7, 2016 Missy Danforth, Vice President of Hospital Ratings, The Leapfrog Group Presentation Overview Who is getting a Hospital Safety Score? Scoring
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services
 Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
VALUE. Acute Care & Critical Access Hospital QUALITY REPORTING GUIDE
 better health care VALUE HEALTHIER POPULATIONS Acute Care & Critical Access Hospital QUALITY REPORTING GUIDE TABLE OF CONTENTS Missouri Quality Transparency Measures....4 Missouri Health Care-Associated
better health care VALUE HEALTHIER POPULATIONS Acute Care & Critical Access Hospital QUALITY REPORTING GUIDE TABLE OF CONTENTS Missouri Quality Transparency Measures....4 Missouri Health Care-Associated
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Scoring Methodology SPRING 2018
 Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
June 27, Dear Ms. Tavenner:
 1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 27, 2014 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 27, 2014 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
Additional Considerations for SQRMS 2018 Measure Recommendations
 Additional Considerations for SQRMS 2018 Measure Recommendations HCAHPS The Hospital Consumer Assessments of Healthcare Providers and Systems (HCAHPS) is a requirement of MBQIP for CAHs and therefore a
Additional Considerations for SQRMS 2018 Measure Recommendations HCAHPS The Hospital Consumer Assessments of Healthcare Providers and Systems (HCAHPS) is a requirement of MBQIP for CAHs and therefore a
Hospital Quality Reporting Program Updates: An Overview of the CMS Final IPPS Rule for 2017
 Hospital Quality Reporting Program Updates: An Overview of the CMS Final IPPS Rule for 2017 Presented by Vicky Mahn-DiNicola RN, MS, CPHQ VP Clinical Analytics & Research, Midas+, A Xerox Company Accessing
Hospital Quality Reporting Program Updates: An Overview of the CMS Final IPPS Rule for 2017 Presented by Vicky Mahn-DiNicola RN, MS, CPHQ VP Clinical Analytics & Research, Midas+, A Xerox Company Accessing
Program Summary. Understanding the Fiscal Year 2019 Hospital Value-Based Purchasing Program. Page 1 of 8 July Overview
 Overview This program summary highlights the major elements of the fiscal year (FY) 2019 Hospital Value-Based Purchasing (VBP) Program administered by the Centers for Medicare & Medicaid Services (CMS).
Overview This program summary highlights the major elements of the fiscal year (FY) 2019 Hospital Value-Based Purchasing (VBP) Program administered by the Centers for Medicare & Medicaid Services (CMS).
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Table of Contents. Current and Proposed CMS Quality Measures for Reporting in 2014 through 2019 Revised 07/25/2014
 Table of Contents Current Proposed CMS Quality Measures for Reporting in through 2019 Revised 07/25/ Inpatient Measures Collected Submitted by Hospital AMI/Emergency Department/ Immunization Page 2 Heart
Table of Contents Current Proposed CMS Quality Measures for Reporting in through 2019 Revised 07/25/ Inpatient Measures Collected Submitted by Hospital AMI/Emergency Department/ Immunization Page 2 Heart
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota