NHS London. QIPP milestone Tracker Reform Milestone Tracker
|
|
|
- Robert Fletcher
- 5 years ago
- Views:
Transcription
1 NHS London QIPP milestone Tracker Reform Milestone Tracker
2 ENCLOSURE: H Agenda Item: 78/12 Date: 26 April 2012 BEXLEY CLINICAL COMMISSIONING GROUP FORMAL MEETING 26th April 2012 SOUTH EAST LONDON JOINT OPERATING PLAN AND JOINT CSP Action Required Note the South East London Joint Operating Plan and Joint CSP. Executive Summary Earlier versions of these documents have been to several cabinet meetings since November These documents now form the final documents that were approved by the SEL Joint Boards on the 29 th March The following points were noted at the Joint Boards SEL Joint Operating Plan Amendments to the final document may be required to accommodate possible changes to the contracts as they are still being finalised; and further information is required on innovation themes (ICCGs). SEL Joint CSP Appendix D item 5.3 contains a stakeholder map. This is an example and is not the actual stakeholder map for South East London. This is being compiled by the SEL communications team and will be included at a later date. Next steps The CCG has been closely involved in submitting information to be included in the joint documents. A final version of the local plans is being drafted. The letter to stakeholders, agreed at the last formal cabinet, outlining our outcomes and achievements from 2011/12 and highlighting our proposed priorities for 2012/13 has been sent out to key stakeholders. This information, along with information from our internal objective setting process will inform the final details in the Operating Plan and CSP.
3 Organisational implications Financial Plans demonstrate how resources will be broadly committed Equality and Diversity Forms part of plans Risk (governance and/or clinical) Patient impact NHS constitution Which objective does this paper support? Improve choice and access to integrated health services for Bexley patients Reduce the level of health inequalities across Bexley Improve care for patients with long term conditions & increase the range of services offered within the community Improving the health & wellbeing for people in Bexley Maximizing the opportunities of joint working (A Picture of Health, Joint Strategy Needs Assessment, Wellness agenda etc) Using our resources in the most efficient & effective manner (organisational & financial) Consideration by Other Committees/Groups Insert Tick ) Author Beth Hill Executive Sponsor Chair and MDs Date 17 th April 2012 A partnership of Primary Care Trusts in Bromley, Greenwich, Lambeth, Lewisham, Southwark and Bexley Care Trust Chair: Caroline Hewitt Chief Executive: Andrew Kenworthy
4 3rd DRAFT (TO BE FINALISED FOR SUBMISSION MAR 9 th ) NHS South East London Cluster Better for You Commissioning Strategy Plan 2012/ /15
5 ii
6 Dear Colleagues, We are all very pleased to introduce to you Better for You, our health Commissioning Strategy Plan for 2012/13 to 2014/15 for the people of South East London. As chairs of each of the six Clinical Commissioning Pathfinders in South East London, we are positive and excited about the future for our local health services and about the role that we and other clinical leaders can take to enable more local people to stay healthy and experience joinedup care that meets their individual health needs in the most effective way. We will continue to work with our local partners, for example across health and social care, to make sure that our plans are fully integrated and reflect the health and well-being needs of local people. We believe in involving patients in their healthcare arrangements. We already work closely with our Local Involvement Networks (LINks) and look forward to working with our local Healthwatch organisations as they emerge in order to gain independent perspectives on patients experiences of their health services. We will use this feedback to monitor current and improve future services. There are differing needs within our respective populations and some common ones. In every case our ambition is to meet the same strategic goals which will put patients and carers at the centre of decision making. As Pathfinders, we are collaborating with one another with the aim of maximising health benefits from collective approaches and achieving a sustainable health economy for South East London. Over the last year we have been supported to take a local leadership role in developing our long term plans and we are confident that we have the right mechanisms in place to ensure delivery of those plans. We are continuing to work with the NHS in South East London to develop our future commissioning capability. Our plan for a full year of shadow working from April 2012 will enable us to take full delegation and gain confidence prior to the authorisation process for the establishment of Clinical Commissioning Groups commencing in summer We would welcome any comments or feedback on our first South East London Commissioning Strategy Plan. Dr Adrian McLachlan, Chair, Lambeth Collaborative Clinical Commissioning Board Dr Andrew Parson, Chair, Bromley Collaborative Clinical Commissioning Board Dr Howard Stoate, Chair, Bexley Collaborative Clinical Commissioning Board Dr Helen Tattersfield, Chair, Lewisham Collaborative Clinical Commissioning Board Dr Hany Wahba, Chair, Greenwich Collaborative Clinical Commissioning Board Dr Amr Zeineldine, Chair, Southwark Collaborative Clinical Commissioning Board iii
7 Contents 1. Introduction Context Approach Engagement with the public and patients Partnership working Working with providers Joint Commissioning Engagement on pan-london initiatives Governance and leadership at cluster and across boroughs Vision Better for You Our vision for Our strategic goals Case for Change The People of South East London Local context Local population needs Financial case for change Quality and performance Achievements on the 2011/12 Plan Summary case for change Priorities and Opportunities Our strategic programmes and the key role of primary care Opportunities delivered through four strategic programmes Enablers Clinical engagement and leadership The Commissioning Support Organisation (CSO) Workforce Integrated health informatics Estates Managing our finances Impact on the System Impact on patients and public Summary Income and Expenditure Plan iv
8 8.3 Impact of savings initiatives across care settings Provider Impact Sustainable Commissioning Implementation How will we implement the strategic programmes How we will measure success of the strategic programmes Delivering our strategy Risks and mitigations Foundation Trust pipeline Appendices See separate document Appendix A: CSP Summaries by Borough Appendix B: Cluster Measurement Framework Appendix C: Financial Case for Change and Delivery of Financial Balance Appendix D: South East London Communications and Engagement Plan v
9 1. Introduction NHS South East London (NHS SEL) is a partnership of Bromley, Greenwich, Lambeth, Lewisham and Southwark Primary Care Trusts (PCT) and Bexley Care Trust. Better for You, our Commissioning Strategy Plan (CSP) for 2012/13 to 2014/5 is our vision for improving health and healthcare for the communities that we serve over the next three years. "We each have to find our own solutions, and I realise that the health service can't provide all of those, but it could still have a role in helping us find what we need" Patient interview, Lambeth & Southwark, 2010 Our population is rising and demands on health services are rising at a faster pace than our income, meaning that we need to be more efficient to meet the health needs of the people of South East London. In this strategy we show how we will meet this challenge. There is a history of collaboration between the six PCTs, and the integrated care initiatives described in this strategy show how, through the emerging health system for South East London, we are pursuing opportunities to work together to deliver solutions that are tailored to meet the needs of local and, where appropriate, larger populations. At the same time, we are in a period of very significant organisational change in the NHS. The Government proposes to replace Primary Care Trusts, the current NHS commissioners, with Clinical Commissioning Groups (CCGs) from April By establishing and developing Commissioning Pathfinders in our boroughs, we are already making the arrangements for this transfer of responsibility to happen effectively. The development of this CSP represents an important step in the development of our Pathfinders towards authorisation as CCGs, planned for April Bringing these aspects of our work together, we show in this strategy how we will lever reform the increasing accountability of clinicians as commissioners and clinical leaders, the development of viable and innovative providers and the introduction of integrated care solutions to achieve our commissioning goals as we transition to a new health system. This CSP is a high-level document which articulates our challenge as commissioners for South East London and describes how we propose to meet this challenge. It is laid out in the following sections: Context: The population of South East London, its health needs and associated trends and the landscape of providers currently delivering healthcare services to local patients Approach: The steps we have taken to seek input from patients, the public and our providers, leverage pan-london initiatives and formed effective clinically-led governance to oversee the development of a CSP which meets local needs and achieves scale to deliver within available resources. Vision and strategic goals: Our ambition for the health and quality of healthcare to be provided for our population and the future performance of our health system 1
10 Case for Change: The current performance of our health system in terms of finance, quality and productivity, and the scale of improvement now required to deliver our vision and strategic goals Priorities and Opportunities: A description of our four priorities integrated care, London-wide programmes, productive care and staying healthy and respective change programmes, together with their associated sets of opportunities (initiatives), which will deliver our vision and strategic goals Enablers: Our underpinning plans for clinical engagement and leadership; a South London commissioning support organisation; workforce; integrated health informatics; estates; and management of our finances Impact on the System: The projected outcomes of our strategy in terms of patients and the public, activity and finance; potential implications for key providers Sustainability: How we are working to deliver our commitments to sustainable commissioning Implementation: Our overall implementation plan; approach to the governance and monitoring of delivery; risks identified and planned mitigations. 2
11 2. Context This section describes the population of South East London, its health needs and associated trends and the landscape of providers currently delivering healthcare services to SEL patients South East London has a population of million people 1. The population size in each borough ranges from 220,300 in Bexley, to 306,400 in Bromley (estimate for 2011). The total population is projected to grow to 1.73 million by Greenwich is predicted to see the largest increase in population, with a growth over the next five years of 13%; Southwark will have the second highest at 8%. The biggest increase in births is projected for Greenwich with an 11% increase in the period 2011 to South East London contains the extremes of deprivation and wealth with a large percentage of the population being amongst the most deprived fifth in the country while other parts of the sector contain those who are in the most affluent fifth of the population in England. South East London is served by four acute trusts; two Foundation Trusts and two NHS Trusts in the process of FT application: Guy s and St. Thomas NHS Foundation Trust (GST) primarily serves the population of Lambeth, Lewisham and Southwark but activity does flow across the whole of South East London and it provides specialist services for patients from much further afield. It is also the integrated community health provider for Lambeth and Southwark. King s College Hospital NHS Foundation Trust (KCH) is one of London s largest teaching hospitals, providing a full range of general hospital services for over 700,000 people in the boroughs of Lambeth, Lewisham and Southwark and providing specialised services that are available to patients across a wider area. Lewisham Healthcare NHS Trust, located in the centre of Lewisham, offers medical, surgical and emergency services for the local community and specialised services for South East London and beyond. It is also the provider for community health services for Lewisham. It is in the process of applying for Foundation Trust status. South London Healthcare Trust (SLHT) provides a wide range of healthcare to the people of South East London, in particular to the communities living in Bexley, Bromley and Greenwich. SLHT is in the process of applying for Foundation Trust status. Mental health services are provided by two mental health foundation trusts: 1 Source for all population data: GLA 2010 Round Demographic Projections and GLA 2010 Round Ethnic Group Population Projection (EGPP) figures, Greater London Authority, Figures are rounded to nearest 100 per GLA requirements 3

12 South London and Maudsley Foundation Trust (SLaM) provides the most extensive portfolio of mental health and substance misuse services in the UK. The trust serves a local population of 1.1 million in south London and offers specialist expertise nationally resulting in an annual turnover of approximately 350 million. Oxleas NHS Foundation Trust provides a wide range of health and social care services and specialises in caring for people with mental health problems and learning disabilities. It is the main provider of specialist mental health and adult learning disabilities services for Bexley, Bromley and Greenwichand is is also the provider of community health services to Bexley and Greenwich. Bromley Healthcare, a newly created social enterprise, provides a range of community healthcare services for the people of Bromley. Across South East London there are over 200 General Practices made up of Personal Medical Services (over 140), General Medical Services (over 50) and Alternative Provider Medical Services (over six) contracts. We have one of only five Academic Health Sciences Centres (AHSC) in England. King s Health Partners (KHP) is a partnership between King s College London, Guy s and St. Thomas Foundation Trust, King s College Hospital Foundation Trust and South London and Maudsley NHS Foundation Trust. The KHP partners are considering organisational merger. NHS Lambeth and NHS Southwark Health Promotion Training 4
13 3. Approach How the development of this CSP has been governed and what engagement has taken place with representatives of the patients, public, providers and other stakeholders NHS South East London s role is to enable our clinical leaders to balance the importance of meeting the needs of local populations in our six boroughs with the need to be effective commissioners of services from the major providers of acute and mental health care in our area. As part of the London health economy, we actively participate in, and extract value from initiatives delivering for the whole of the capital. Our starting point for the development of this CSP is that it should serve as: a coherent commissioning plan for South East London an umbrella for the CSPs developed for each of our six boroughs and under the leadership of Pathfinder clinicians, and a vehicle to articulate and deliver the impact of pan-london initiatives for our communities. Our approach, described below, has therefore been to: Engage systematically with the public, our patients and clinicians across our six boroughs to gain qualitative insight into local needs, building on public health assessments Maintain on-going dialogue with stakeholders, such as Local Government, Local Involvement Networks (LINks), NHS Trusts, independent and third sector organisations, in a variety of forums, ensuring that CSP plans and their potential impact are anticipated Engage with the London Specialist Commissioning Group (LSCG) and owners of other pan-london initiatives to ensure alignment of plans Ensure strong governance and leadership at cluster level and across our Pathfinders to pull together coherent and ambitious plans which meet local needs within available resources. 3.1 Engagement with the public and patients "Thank you for a good meeting and we must have more! It s all to do with communicating concerns, strategy and policy for patients of the wonderful NHS." Peckham and Camberwell workshop for community organisations, October 2010 We believe that engagement is vital in helping us to deliver local services that are right for local people and we have a record of effective engagement in South East London. We have robust arrangements that involve the public and patients, staff, clinicians and stakeholder organisations, such as Local Authorities, NHS Trusts and the voluntary sector. Over recent years major programmes such as Healthcare for London, A Picture of Health and local PCT strategies have benefited from the views of the public and patients and 5
14 produced the Peoples Principles governing our approach to change. The role of clinical leaders has been instrumental in designing and delivering our service improvements. We have a tailored approach to involving the public at borough and pan borough levels, including deliberative events, borough-wide public conversations and targeted engagement activities, with active LINks networks and an effective stakeholder reference group. We actively seek to engaged traditionally hard to reach and hard to hear groups and expand our ways of communicating to reach a wider audiences. In 2009 we won the Department of Health award for best communications leadership. We have developed our approach to engagement at cluster level, with three stakeholder reference groups. These groups bring together local councillors, Links, council officers and partners from the voluntary sector to ensure that public engagement and patient choice are included in all service change proposals. The NHS South East London Stakeholder Reference Group provides the overarching framework for pan-south East London clinical service change programmes. The Bexley, Bromley and Greenwich Stakeholder Reference Group and the Lambeth, Southwark and Lewisham Stakeholder Reference Group operate alongside this group to offer guidance on change to services that cuts across more than one borough. The establishment of shadow Health and Well-being Boards within each borough is progressing well. Each Pathfinder has engaged with council representatives of the HWB with regards to the development of their CSP and QIPP plans. Working in conjunction with local social care organisations, Pathfinders are developing local methodologies for engaging patients. Some are built up from patient participation groups, and in Bexley a patient council. These structured forms of engagement are a central part of how Pathfinders ensure the patient voice is at the centre of what they do. 3.2 Partnership working Aspirant CCGs in South East London work in partnership to ensure that services are coherent for local people and that plans across organisations are aligned. In this way larger more timely changes can be made. There are different dimensions to partnership working: Joint programmes across CCGs Joint programmes with local authorities Joint programmes where providers are encouraged and incentivised to work together to improve outcomes for service users In South East London models of each of these have been developed and renewed as CCGs increasingly lead commissioning. In outer South East London there is a Bexley, Bromley and Greenwich Commissioning Group chaired by Dr. Andrew Parson (Clinical Chair in Bromley) that has identified significant workstreams that are being progressed across all three boroughs. In Lambeth and Southwark an integrated care pilot is driving a significant change programme for the benefit of older adults living with long term conditions. Lewisham s focus is integration across the care pathway; maximising the benefit of the vertically integrated community and acute hospital services available from Lewisham Healthcare NHS Trust. There is a South East London Clinical Strategy Group that brings together clinicians 6
15 from CCGs with the cancer and cardiac and stroke networks and has set a priority to develop a clinical strategy for urgent and unplanned care in 2012/ Working with providers Across South East London we have engaged with our providers to discuss and develop a number initiatives: In Lambeth and Southwark, we participate with King s College Hospital and Guy s and St. Thomas Foundation Trusts in joint steering groups for planned care and an urgent care network, and we are working jointly with King s Health Partners on an integrated care pilot, delivery of which is a priority within our CSP. In Lewisham, we have ensured that Lewisham Healthcare Trust s application for foundation trust status contains activity and finance assumptions which are aligned with commissioning plans. Bexley, Bromley and Greenwich commissioners have been working jointly and with South London Healthcare Trust in a cross-borough urgent care network and on estates initiatives at Queen Mary s Sidcup, Orpington and Elmstead. 3.4 Joint Commissioning South East London CCGs recognise the importance of building on the strong joint commissioning arrangements with local authorities that already exist in South East London. Our pathfinders and their relevant borough authorities understand the need for innovative solutions and joint working and individual CCG CSPs set out specific priorities for partnership working based on local JSNAs. For example: In Southwark joint commissioning priorities have been set in relation to the provision of effective urgent care responses across health and social care; the prevention of ill health and disability; tackling health inequalities; and safeguarding. Bexley Care Trust maintains a Joint Commissioning Unit (a shared mechanism between the GP consortium and Bexley Council) to ensure that health and local authority funding is used collaboratively and effectively to deliver a coordinated and cohesive system of support for residents and patients with long-term conditions. Detailed discussion of joint commissioning and partnership arrangements for each borough is beyond the scope of this document but can be found in individual CCG CSPs. 3.5 Engagement on pan-london initiatives To ensure that our patients have access to high quality specialised care, such as neonatal intensive care, complex arterial surgery and rare cancers, when they need it, we work 7
16 closely with the London Specialised Commissioning Group, clinical networks such as the cancer and the cardiac and stroke networks, other London PCT clusters and London Health Programmes. Our clinical leaders are involved in developing cases for change, setting priorities and in ensuring that the interface between local services and specialised services is designed and operates effectively. They are active members of London s Clinical Senate and also the London-wide Clinical Council. A separate commissioning strategy for London is published by the London Specialised Commissioning Group on behalf of all London PCTs. 3.6 Governance and leadership at cluster and across boroughs NHS SEL s strategy has been developed through our GP Pathfinder leaders within each of the six boroughs, working both as local leaders and as members of the SEL Clinical Strategy Group. This will ensure that our plans are clinically led, patient focussed and owned by the clinical commissioners who will assume responsibility for its delivery. At cluster level, the joint Board of the five PCTs and Bexley Care Trust and its committees have overall responsibility for the development and delivery of this strategy. This Board includes the Clinical Chairs of Pathfinders. At borough level our local Clinical Commissioning Committees operate with significant delegated responsibilities, including delivery of borough based Quality, Innovation, Productivity and Prevention (QIPP) initiatives. The committees build on existing Clinical Commissioning structures and are the place where local commissioning issues are considered with GP colleagues and key stakeholders. The committees also support the development of consortia and lead on relations with each Borough s Health and Well-Being Boards. 8
17 4. Vision Our ambition for the health and quality of healthcare provided for our population, within available financial resources, as informed by our engagement 4.1 Better for You Our vision for 2015 More people in South East London will stay healthy, and every patient will experience joined-up healthcare which meets their needs in the most effective way. 4.2 Our strategic goals "Now I see my consultant regularly at my GP surgery - he does an outpatient clinic there which is much more convenient. I'd rather not visit hospital unless I need to even though I don't live far away... It would be good to have a more responsive service as sometimes I have appointments in the summer when I feel well and don't really need to see anyone, while in the winter my health can deteriorate pretty quickly. Luckily my GP is excellent and has been great referring me to whatever specialist advice I've needed. I get a great service there" Patient Interview, 2011 In South East London we commission physical and mental healthcare across home, primary, community and acute settings from a variety of NHS, voluntary and independent sector providers. In every case, our ambition is to meet the same strategic goals, that: 1. In every contact with the NHS and local public service partners, people are encouraged and enabled to positively manage their own health, in partnership with health professionals and their carers. 2. Patients experience the NHS as a joined-up personalised service, rather than a disconnected set of services they are required to navigate. 3. Patients are treated fairly with dignity and the respect due to them at all times. 4. Clinical decision-making and healthcare delivery is in line with evidence-based best practice and takes account of value for money. 5. The logistics of healthcare delivery, within and across different care settings, are designed to meet patients clinical needs, whether long-term or acute, in the most effective way. In setting these goals we have taken account of both the views of local stakeholders (see Section 3) and of lessons learnt more widely across the NHS, such as the quality issues at Mid Staffordshire and recent Care Quality Commission audits of care of older people. More effective clinical decision-making and healthcare delivery logistics will drive a significant increase in productivity and enable the health and social care system in South East London to manage increasing levels of demand without an equivalent increase in resources. We have set an ambitious target for our health economy of productivity improvement to the value of 117 million over four years. Through monitoring execution of this plan and the achievement of our strategic goals, we will be able to ensure and demonstrate to our population that we have been able to make savings without compromising our ambition, or patients expectations, for care quality. 9
18 South East London is home to a highly diverse population living in many local communities, each with their own needs, priorities and expectations of the NHS. Ourstrategic goals are informed by the work of our Pathfinders to develop their local strategic health goals and QIPP plans as part of borough based commissioning plans. These build on local joint strategic needs assessments and local stakeholder engagement. Proposed measures for each strategic goals have been developed and work is underway to agree trajectories for these. These sit alongside SMART measures for strategic priorities, set out in Section 9, to form the overall measurement framework for the CSP. Appendix B sets out the measurement framework in full including baselines and proposed trajectory assumptions. Table 1: SMART Measures for Cluster Strategic Goals 1. Cluster Strategic Goal 2. Proposed Measure I. In every contact with the NHS and local public service partners, people are encouraged and enabled to positively manage their own health, in partnership with health professionals and their carers II. Patients experience the NHS as a joined-up personalised service, rather than a disconnected set of services they are required to navigate III. Patients are treated with dignity and the respect due to them at all times IV. Clinical decision-making and healthcare delivery is in line with evidence-based best practice and takes account of value for money Structured Patient Feedback Smoking Quitters NHS Healthchecks Patient experience survey MSA breaches 3. Detail of Measures 4. Other Goals Where Measure Applies? Number of 4-week smoking quitters that have attended NHS Stop Smoking Services Number of eligible people who have received an NHS Healthcheck Outliers identified using NHS Performance Framework approach and narrative and results of local surveys Numbers of unjustified breaches See also additional measures under other goals, below (column 4) Length of stay (Acute) Performance in Prescribing incentive schemes Average spell duration for nonsame day acute discharges % of generic Losartan/Candesartan items as % of total Angiotensin Receptor Blocker (ARB) items Appropriate prescribing of specials Compliance with All providers to give assurance NICE guidance that systems are in place to comply with NICE guidance, with monitoring mechanisms in place Bowel screening Extension of bowel screening program to men and women aged 70 up to 75 birthday See also additional measures under other goals, below (column 4) 10
19 1. Cluster Strategic Goal 2. Proposed Measure V. The logistics of healthcare delivery, within and across different care settings, are designed to meet patient needs, whether long-term or acute, in the most effective way. A&E Quality Indicators - Unplanned reattendance 3. Detail of Measures 4. Other Goals Where Measure Applies? Unplanned re-attendance at A&E Goal IV within 7 days of original attendance (including if referred back by another health professional) Emergency readmissions within Goal IV 30 days % of people with LTCs who said Goal I they had had enough support from local services/orgs Emergency Readmissions People with Long Term Conditions feeling independent and in control of their condition % deaths at home No. registered deaths at home/no. registered deaths Goal I 11
20 5. Case for Change The performance of our current health system in terms of quality and productivity, progress made to-date and the scale of improvement still required to meet our ambition 5.1. The People of South East London Local context Population Size and Growth South East London has a population of 1.635, million people2. The population size in each borough ranges from 220,300 in Bexley to 306,400 in Bromley (estimate for 2011). The total population is projected to grow to 1.73 million by Greenwich is predicted to see the largest increase in population, with a growth over the next five years of 13%; Southwark will have the second highest at 8%. The biggest increase in births is projected for Greenwich with an 11% increase in the period 2011 to Table 2. Population size and age for South East London by borough in 2011 Total population size Percentage Borough All ages South East London Population Pyramid Bexley 40, ,900 35, ,300 18% 66% 16% GLA Projections for 2001 and 2016 Bromley 54, ,200 49, ,400 18% 66% 16% 90+ Greenwich 51, ,900 29, ,400 21% 67% 12% Lambeth 54, ,600 24, ,400 18% 74% 8% Lewisham 52, ,900 24, ,900 19% 72% 9% Southwark , ,500 25, ,800 19% 73% 9% SE London ,100 1,140, ,000 1,635,200 19% 70% 11% Bromley (16%) and Bexley (16%) have relatively high proportions of older people compared Age band with Lambeth (8%) and Lewisham and Southwark (9%). In contrast Southwark and Lambeth have relatively high proportions of people of working age (73% and 74% compared with Bexley and Bromley South with 30 - East 34 66%). London The main Population expected Pyramid population growth is in those of working GLA 25-29Projections for and age and in the under fifteen year s olds rather than amongst the older population Age band Male Female Male Female 2001 Figure 1. South-East London Population Pyramid for 2011 and Source for all population data: GLA 2010 Round Demographic Projections and GLA 2010 Round Ethnic Group Population Projection (EGPP) figures, Greater London Authority, Figures are rounded to nearest 100 per GLA s requirements 12

21 Diversity Ethnicity 71% of the population is White, and 29% from Black and Ethnic Minority groups (BME). Black Africans, Black Caribbeans and Black other groups form the largest combined ethnic minority in South East London, accounting for 67% of the total minority population in Black Africans form the largest single group amongst the ethnic minorities (33% in 2011). Southwark has the largest population of Black African, while Lewisham has the largest Black Caribbean population. Black Caribbean and Black African population are more prone to problems such as hypertension and diabetes. People from Asian communities are high risk of diabetes and heart disease. Patterns of risk factors such as diet and exercise and beliefs about disease may differ between different communities. BME Populations 2011 Figure 2: Ethnic populations Boroughs for in South East East London London sector (GLA by 2010 borough, projections) 2011 (Source: Based on data from GLA 2010 Round Ethnic Group Projections) persons Black African Black Caribbean Black Other Other Subcontinental Bexley Bromley Greenwich Lambeth Lewisham Southwark Diversity Deprivation and Wealth South East London contains the breadth and extremes of deprivation and wealth with a large percentage of the population being amongst the most deprived fifth in the country while other parts of the sector contain those who are in the most affluent fifth of the population in England. There is a well established link betweeren deprivation and ill health with increased incidence and prevalence of disease amongst most deprived population groups with increased risk of early death and shortened life expectancy. Figure 3. Index of Multiple deprivation by super output area, South East London (Source: Index of Multiple Deprivation 2010)3 3 Contains Ordnance Survey data (c) Crown copyright and database rights
 is improving for both men and women, with particular improvements noted for LE in women and men in Southwark.")

22 Life Expectancy The overall indicators of health for SEL show a positive trend. The trend for life expectancy (LE) is improving for both men and women, with particular improvements noted for LE in women and men in Southwark. However there remains the challenge for Lambeth, Lewisham and Greenwich in narrowing the gap with the national average. Figure 4.South East London Male and Female Life Expectancy by Borough Index of Inequality The improvement can hide some internal difference in local boroughs with a widening of the gap in the slope index of inequality especially for Southwark men. Figure 5.South East London Inequality (Slope) Index by Borough Premature mortality An important place to start is to focus on premature deaths i.e. deaths under the age of 75 years, where there is potential for action that will prolong life especially through better management of long term conditions (LTCs). While there is a trend for improvement there remains more to be achieved for both men and women in four of the clinical commissioning areas- Lambeth, Southwark, Lewisham and Greenwich. 14


23 Figure 6.South East London Premature Mortality by Borough 5.2 Local population needs Based on local assessment of needs and building on the JSNAs for the individual local boroughs,the five key health challenges for South East London have been agreed. These are the key health problems that are common to all areas. The tables below summarises the most significant local health challenges across SEL with illustration of specific local needs. While there are common themes across areas there are differences in the profiles of diseases between the diffent areas driven by the specific demographic features in each community. For instance diseases that more commonly occur earlier in Black communities increase prevalence in those boroughs with a greateer concentration of people from black communities e.g. diabetes and hypertension. Likewise those living in deprived comunities are more risk of becoming ill, having more severe disease,complications early death. Challenge Detail Example of local needs Table 3: Key Health Challenges across SEL Related Priority See Section 6 Cancer A major cause or premature mortality with variations in the outcomes for different people Breast: higher incidence in Bexley and Bromley related to more affluent population, but mortality higher in Lambeth. Lung: incidence and mortality rates are high with all age mortality higher than England average in Greenwich, Lambeth, Lewisham and Southwark Prostate: higher incidence in more deprived areas linked to deprivation and ethnicity. Causes of high mortality in Bexley not clear London-wide Cardiovascular Diseases (CVD) Major cause of premature death and some rates higher than the national average CHD: Lambeth, Southwark, Lewisham and Greenwich have higher mortality rates than London and National average linked to deprivation London-wide and Integrated Care 15
24 Challenge Detail Example of local needs Related Priority See Section 6 Long Term Conditions (including Diabetes, COPD and HIV) High rates of diabetes across SEL Many COPD deaths are preventable and can lead to excess demand on hospital beds if not managed well. COPD: standardised mortality rates are significantly higher than the national average in all areas except Bexley and Bromley associated with longterm smoking patterns and appporaches to management Diabetes: Black African, Black Caribbean and South Asian ethnic groups are at higher risk of developing diabetes, so a considerable percentage of SEL population at high risk. Lambeth and Southwark have the highest prevalences of HIV in England Integrated Care and Productive Care Mental Health A significant cause of disability and distress Reported mental illness prevalence in higher than average in most areas (highest in Lambeth and Lewisham linked to ethnicity and poverty) Demand on mental health services by children in South East London is more than double the national average and higher than the London average linked to complex local communities and deprivation. Integrated Care Healthy Living Many of the factors driving ill health are due to how people eat, drink and take exercise Smoking: identified as a leading risk factor for the top causes of early death in South East London. Obesity: high rates of obesity for young people at Reception and Year 6 Preventable infections: immunisation rates do not reach the necessary target levels to protect children from the spread of disease. Healthy Living Learning from local differences in health outcomes As part of the overarching approach to QIPP in South East London, a Staying Healthy plan has been implemented over the last couple of years to support cluster-wide shared approaches and monitoring of improvements in key areas of public health importance. The areas the plan concentrates on, linked to borough and cluster-wide JSNA priorities, are as follows: Tuberculosis Childhood Immunisations Cancer Screening Smoking Cessation NHS Health Checks Programme Implementation Obesity Sexual Health Through the Directors of Public Health regular meetings in South East London, the plan is monitored and action to bring about improvements in performance considered. The group 16
25 reviews a set of KPIs linked to performance in all of these areas which are updated on a quarterly basis. A DPH is identified as the lead for each of the areas listed above; their role is to review performance across the cluster, support boroughs to share good practice and make recommendations about improvement actions to be considered. This process has resulted, for example, in the establishment of a cluster Tobacco Control working group, convened by the Bromley DPH, to consider the variation in 4-week quitters performance across the cluster as part of the drive to make improvements and achieve targets. Where there are concerns about performance against these key priorities and targets are not on track to be delivered, action plans are escalated to the full Cluster Board meeting to provide assurance that arrangements are in place to make the necessary improvements. At the meeting of the cluster Board in January 2012, the Board received actions plans for specific under-performing boroughs in relation to smoking, health checks, bowel screening and immunisations. For many areas within the Staying Healthy Plan, good progress is being made by a number of the boroughs, but there are generally some that are not on track to hit targets. The monitoring process that is in place through the DPH meeting provides a regular opportunity for performance to be reviewed, improvement actions to be considered, and escalation to the board to be provided where needed. The GP suggested a referral to the STAR clinic who sent me onto the Pulmonary Rehab team at St Thomas. It was a set no. of appointments, 16 I think, and it was absolutely marvellous. They taught me an awful lot about my condition, how and when to use the inhaler, we had specialist talks from consultants and experts in their field. There's a gym there and the nurses and physios give so much encouragement, they explain how your lungs are muscles that need to be exercised and how you can safely push yourself to improve. To start with I could only do the easiest machines but they don't let you just do the bare minimum; they push you so you're working harder. At first it feels quite tough, but once you see how quickly you can build up it's amazing for your confidence. Some of the people that were there are incredible. People in their 80s with oxygen tanks and tubes attached, and all doing the most they can. I met a woman, she was 82 and could barely shuffle around on portable oxygen, but by the end of the course she told me she'd been out dancing. It was the lease of life I needed, as to be honest I'd started to give up on myself." Patient interview, Lambeth & Southwark,

26 Figure 7: Summary Local Healthmap
27 5.3 Financial case for change South East London faces continuing growth in demand and cost of acute services, driven by: Population growth Demographic changes The expansion of available health technologies Increased expectations The rate of increase of funding for the NHS is now below inflation. The underlying rate of deficit will increase if no action is taken and there is an unprecedented level of financial challenge facing the NHS over the next few years. A step change will be required in the approach to development and delivery of QIPP plans. Redesign of the system, the ownership of the plans by local CCGs and change led by primary care clinicians working in conjunction with acute clinical colleagues to improve care pathways and patient experience, eliminate duplication and improve productivity are required. South East London commissioners must secure significant efficiency and productivity savings over the next three years to provide the financial resource to support delivery of their vision and the supporting strategies. If no action is taken then the underlying financial positions will deteriorate, resulting in a deficit in 2014/15 across South East London PCTs of 89.4 million. In order to achieve the required 1% surplus in 2014/15, QIPP savings totalling million will be needed over the three-year period. In order to achieve the 1% surplus in each year, the required QIPP savings will need to be front loaded, with 59.4 million of the savings requirement being in 2012/13 as set out below. Table 4: The Financial Case for Change Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Forecast Surplus/ (Deficit) 2011/12 QIPP savings requirement 2012/13 QIPP savings requirement 2013/14 QIPP savings requirement 2014/15 Total QIPP savings requirement Do-Nothing Forecast Surplus/ (Deficit) 2014/15 0 5,992 4,612 6,605 5,375 5,857 28,441 (10,778) (4,710) (12,419) (11,974) (8,469) (11,043) (59,393) (5,145) (3,140) (7,817) (7,562) (5,278) (6,636) (35,578) (3,161) (2,426) (3,911) (4,635) (3,909) (4,789) (22,830) (19,084) (10,276) (24,147) (24,171) (17,656) (22,468) (117,801) (19,084) (4,284) (19,535) (17,566) (12,281) (16,611) (89,360) 19
28 The financial challenge in 2012/13 is therefore the most challenging and delivery of QIPP savings and the overall delivery of planned surpluses in 2012/13 are key to the delivery of financial balance over the medium term and also in ensuring a sound and sustainable financial legacy to CCGs. It is important to note that the delivery of the required QIPP savings are not only across the acute/primary care interface but across all areas of commissioning spend including mental health, community and primary care contracts. As commissioning responsibilities are transferred across the new commissioning authorities, QIPP savings requirements will also need to be transferred. 5.4 Quality and performance We aim to continue to maintain and improve quality and performance across all areas. Across South East London we are performing well on a number of areas including Methicillin-Resistant Staphylococcus Aureus (MRSA) indicators and stroke, proportion of people who have had a stroke who spend at least 90% of their time in hospital on a stroke unit. However, we recognise that there are some quality and performance gaps present in the provision of acute care across SEL: Indicator Setting Detail Table 5: Quality and Performance Gaps Healthcare Acquired Infections (HCAIs) Referral to Treat (RTT) Cancer waiting times Mixed Sex Accommodation (MSA) Ambulance handover Pan - Cluster SLHT / GST GST SLHT Pan- Cluster The DH continues to set challenging targets for both MRSA and Clostridium difficile reduction for 2011/12. It is expected that SEL Boroughs will achieve targets for reported cases of MRSA. Targets for reported cases of C. Difficile will not expected to be achieved in any of the boroughs Two Trusts within SEL, SLHT and GST have failed to meet referral to treatment (RTT) standards on a continued basis in the current year. Particular areas of concern have been orthopaedics (both trusts), bariatric and gynaecology (SLHT) and plastic surgery and oral surgery (GST). Both trusts are subject to detailed action plans with Cluster review and ongoing monitoring by the DH. GST has consistently performed below the 85% standard for the 62- day target for time from urgent GP referral. A significant proportion of the breaches are due to late referrals from cancer units, including SLHT and outside London. Reduction in the number of MSA breaches with step change in July and August, however September has shown an increased number of breaches Performance against the KPIs is variable, and the issue of most concern is the number of 60 minute patient handover breaches. The Cluster is meeting with each trust to review their action plans, trajectories, and numbers of 60 minute breaches 20
29 We aim to continue to maintain and improve quality and performance across other areas. The following quality and performance gaps are present in the provision of community care and health promotion services across SEL. Indicator Setting Detail Immunisation Lewisham Table 6: Quality Gaps - Health Promotion Lewisham Borough has the lowest immunisation rate across all indicators, especially for children at 5 years of age where the rate is significantly below the target as well as the London and sector average. Breast-feeding Lambeth In Lambeth data coverage and hence reported continuation of breastfeeding have been below trajectory for some years. Smoking quitters Southwark Data quality and data capture is a known issue due to a reduction in resources and lack of clarity around processes Improving the standards and reducing variation in performance across primary care is a continuous priority across South East London. 5.5 Achievements on the 2011/12 Plan Achievements against our 2011/12 plan have included: Reforming urgent care. Delivery of an Urgent Care Centre (UCC) in Southwark at the front end of King s A&E department. At the same time plans are underway in Lambeth to replace the minor injuries unit (MIU) with a UCC at St. Thomas Hospital and in Lewisham a UCC has been opened at the front end of Lewisham Hospital s A&E department. Walk in centres (WIC) are in place at the Lister Centre in Peckham, the Waldron Health Centre in New Cross and Thames Reach Health Centre, Thamesmead, all of which provide care 365 days per year between the hours of 8am and 8pm. In Greenwich a new UCC service has been procured to replace the successful pilot at the Queen Elizabeth Hospital Woolwich site. New models of care for integrated intermediate care services have been implemented in Bromley and Greenwich, for example through Intermediate Care Services and Joint Emergency Teams. A new directory of urgent care services (DoS) has been populated for South East London in preparation for the procurement of an NHS 111 implementation pilot during early 2012 with a target go-live date of January The Transforming Community Services (TCS) programmes have completed. 21
30 Planned care. Milestones include implementation of referral management systems across SEL. Outpatient referrals now go through locally agreed referral management systems for specific conditions/clinical specialities. Pathway redesign. A community scheme for cardiology and consultant-led rapid access chest pain clinics has been implemented in Bexley. The diabetes pathway has been redesigned across South East London, and primary eye assessment and referral service (PEARS) initiatives have been implemented in Bexley and Greenwich and are in progress in Bromley. Mental Heath. Improving access to psychological therapies (IAPT) services have been extended across SEL. Additionally the Living Well Collaborative is now in place in Lambeth 5.6 Summary case for change Demands are increasing on the healthcare system in South East London due to a combination of our changing and growing population, worsening health risk factors and increased identified need. We know that too many of our patients are dissatisfied with their healthcare experience, and there are many examples where performance of our NHS providers and the health outcomes that we are achieving fall short of our expectations. Economically, the demand for, and costs of healthcare are both rising at a rate higher than our income, creating a position where doing the same things as before is not an option. We therefore need to achieve step changes in the way in which healthcare is delivered, the outcomes that we achieve and create the circumstances to ensure that our healthcare system is effective and clinically financially sustainable. 22

31 6. Priorities and Opportunities The case for change in Section 5 above demonstrates that a significant step change in performance of the SEL health system will be required to realise the vision and strategic goals of the cluster, our clinical leaders and borough partners, as described in Section 4. This section describes how, working together, we intend to make that step change to achieve our vision and strategic goals. As illustrated in Figure 8, our plan is to deliver our vision and strategic goals through the pursuit of four strategic change programmes, each representing a strategic priority for the Cluster, and addressing one or more of the Health Needs identified in the Clinical Case for Change. i. Integrated care ii. Productive care iii. Staying Healthy iv. London-wide programmes Figure 8: Mapping priorities and strategic programmes to vision and Cluster health needs 23
32 A strategic change programme has been established for each priority, and each strategic change programme contains a set of initiatives, or opportunities, enacted at borough, crossborough, cluster or pan-london level. Together with a set of enablers, described in section 7, this constitutes our delivery agenda. In the following we pages we present a consolidated view for each priority of: Rationale why we have selected the area as a priority Principles the principles we see informing the approach to improving performance and, where relevant, the design of new care models across the South East London health economy Opportunities the opportunities, or initiatives, which are being, or will be, pursued to improve performance, delivering new care models as appropriate; showing progress to-date and planned investment/disinvestment and expected benefits 6.1 Our strategic programmes and the key role of primary care Our approach to implementation and delivery monitoring is described in Section 8. In doing so we are conscious that high quality primary care underpins the successful delivery of all of our plans for out of hospital care and primary and community services transformation, being the foundation of each care pathway (e.g. safe care, right care, end of life care, urgent and emergency care, long term conditions) and our vision for integrated care networks. Our ambition is to achieve continuous improvements in quality, productivity, patient experience and health outcomes of primary care and produce a legacy for our CCGs to build upon. To drive efficiency and productivity improvements we have completed reviews of PMS contracts in four boroughs and have commenced PMS reviews in Lambeth and Southwark with the aim of commissioning services to match the identified health needs of the population through a core offering to be delivered by each practice. APMS contracts will be reviewed across the Cluster to ensure value for money. There is a strong need for greater transparency of performance information. Using the London-wide List Maintenance policy, we will ensure that all practices have accurate and validated registered lists. This will enable monitoring of practices actual performance regarding, for example, immunisation levels, screening coverage and prevalence levels of long term conditions. This information will feed into the pan-london dashboard for quality outcomes and contract compliance that we will utilise to support improved performance in 2012/13. We will continuously monitor contract performance and quality of services delivered. The performance framework reviews infection control, health and safety, business continuity, child protection, employment checks and clinical governance domains. 24
33 As regards infection control, we have agreed a process whereby an initial 25% of practices will be visited by a PCT infection control adviser and assessed using an audit proforma which will be used to trigger conversations with the practice about how they might best and reasonably reduce their risk. These visits are designed to be developmental in nature and, except in the most serious and obvious cases of unacceptable practice, we expect that sensible and pragmatic solutions will be found to any problems identified. The programme will continue to all practices throughout 2012/13 and 2013/14. We have a track record of, and will continue to, proactively managing instances of poor performance in South East London, including the issue of breach and remedial notices as required. Opportunities are being taken on retirement of practitioners to review the current provision and to agree new arrangements such as list dispersal. PCTs are entitled to inspect premises and ensure that they are suitable for the delivery of those services and sufficient to meet the reasonable needs of patients. For 2011/12, the Cluster is undertaking premises inspections for statutory and contractual compliance and where agreed CQC requirements. All practices are required to make their premises available for inspection, subject to reasonable notice. These surveys will inform our premises strategy. Many of our practices struggle to deliver services from premises that are less than ideal and therefore, we are in the process of bidding for Improvement Grant monies in the order of 5 million during 2012/13 and 2013/14. Unplanned care in SEL London is provided through a complex network of services, including primary and secondary care services. We have an opportunity to build upon existing services and developments to ensure quality and value for money. Through our priorities (see section 6) we aim to: Understand the current issues regarding the delivery of unplanned care both in and out of hours Understand what is driving demand Review how services are commissioned and develop best practice consistent approaches to support future contractual arrangements, where appropriate Understand future changes and their impact, including but not exclusive to the implementation of 111 Map potential duplication in provision of unscheduled care services within and across boroughs and make recommendations for cost effective commissioning of services to future CCGs and the NHS National Commissioning Board. 25
34 6.2 Opportunities delivered through four strategic programmes Integrated Care Rationale There is a clear and national direction of travel towards integrated care Integrated care enables improved individualised care to people with long term conditions and to frequent users of services by addressing their specific care needs using a case managed approach By undertaking population risk stratification to predict need we can respond to provide evidence-based care on a proactive and planned basis for the individual. We will develop greater integration between primary, community, acute hospital and social care in order to improve clinical outcomes, care planning and patient satisfaction through seamless patient and care pathways We see integrated care systems as key to unlocking significant improvements in patient experience and satisfaction. The quality of care will rise. Patients will experience better healthcare as close as possible to their home and be better equipped to self-manage their conditions. Integrated care, in areas such as diabetes and the care of the elderly, offer significant improvements to clinical outcomes and efficiency. Principles We see the core components of integrated care systems across South East London as: Maintaining robust patient registers Patient risk stratification to focus on patients at risk of developing illness Common clinical protocols applied along patient pathways by all providers Defined care packages, tailored to the needs of each individual Care that is proactively planned, co-ordinated and delivered A multi-disciplinary team approach across health and social care Case conferences for patients with complex needs Continuous review of performance of and by multi-disciplinary teams with peer support. Integrated care systems will reduce hospital based care and increase care in home and closer to home settings. This will require A different and mobile workforce. New and better payment mechanisms to ensure that money flows to care providers appropriately. With our partners, we will build the right incentives to ensure that happens to close hospital capacity where necessary. Improved community health facilities. We are developing a number of new purpose-built buildings in Greenwich and Lambeth to deliver integrated care in community settings. We are also progressing strategic solutions for services at Orpington Hospital and for future services on the Queen Mary s Hospital site 26
35 High quality primary care underpins our plans for Integrated Care systems. We believe that integrated care will deliver better care closer to home. We recognise that there is not a one size fits all solution and we are therefore developing and testing different models of models of integrated care for different populations and geographies: Lambeth and Southwark: The Integrated Care Programme is designed to deliver sustainable integrated health and social care services. It is being delivered through a partnership between NHS Lambeth, NHS Southwark, London Boroughs of Lambeth and Southwark, King s Health Partners Academic Health Sciences Centre and GP practices. This will redesign the health and social care system and its services and will redefine the way professionals engage with each other around the assessed needs of individuals. It will fundamentally change the way in which people are supported in taking charge of their own care and conditions. The programme s initial focus is on caring for older people and its scope will be systematically broadened over the next three years ( ). From its third year onwards the changes made to the systems and to services for older people will become self financing and the transformation seen will mean that every year in Lambeth and Southwark: 15,900 unnecessary bed days currently spent in hospital are avoided for older people (a reduction of 14%) 118 older people are supported in a way that means they do not have to go into care homes (18% fewer care home packages) Savings of 13.9m per annum are released across the system. We will drive up the quality of care and drive down costs, improving the value of care we provide to people in Lambeth and Southwark by: 27
36 Joining up care around people, across providers Identifying and managing people s care needs better and intervening earlier Ensuring care is provided in the most appropriate setting, particularly at times of acute crisis Ensuring the right incentives exist for providers to work in integrated ways The system will by led by a Federation of health and social care providers with an overarching Integrated Board Structure, working in partnership with clinical commissioners and responsible for the shared delivery of care along agreed pathways. The process of service change will be evolutionary during 2011/12 we have established programme structures and plans and commissioned new admissions avoidance schemes such as the Virtual Ward, community based Rapid Response and enhanced re-ablement services. During 2012/13 we will develop patient based risk registers and reporting in GP practices, holistic health assessment (including mental health) and case management for older people through GP practices and urgent access hot geriatric outpatient clinics for rapid diagnosis of older people. Bexley, Bromley and Greenwich: a whole system strategic approach for outer South East London is being taken, building on existing integrated care models in each borough and supported by client or pathway specific joint working groups. Key principles underpinning this approach are: To provide and deliver sustainable, fully integrated, high quality health and social care for patients, and their carers; To gain better knowledge about these client groups and increase the potential to be able to act upon that knowledge in a proactive way to maintain standards of health; To ensure better clinical outcomes for these patients; To describe a clinical case for change which is illustrated with real cases; To facilitate, as far as possible, an environment where patients can self-manage their own condition and feel confident enough to do so A new model of care for elderly patients with long term conditions is currently being developed. The core aims and values of this model are to ensure at risk patients are identified and proactively managed to maintain independence using the skills of the primary health and social care teams. A patient risk stratification tool is being used with the aim of commissioning responsive and timely care to avoid inappropriate hospital admissions. There are aspirations to align community health and social care services and an elderly care assessment service to aid senior decision making to ensure individual patient care is planned effectively. Lewisham: Lewisham is continuing the development of an integrated commissioning model to deliver joined up care for patients with long term conditions and the elderly, especially 28
37 working with Lewisham Healthcare as a Trust combining public health, community services and acute care in innovative ways. We have already developed a Joint Management Board for the Urgent Care Centre and worked together on a Clinical Assessment Service to reduce admissions or length of stay for those admitted. The further developments in 2012/13 will concentrate on integrated clinical teams, case management and risk profiling approaches with full engagement of general practice and pathway providers including third sector. Patient involvement in redesign decisions and underpinning contractual arrangements will be overseen by Joint Management Pathway Boards and a joint Service Redesign Group. Work includes developing pathway budgets arrangements in conjunction with the DH Long Term Conditions Programme support. The first two priority pathways are COPD and diabetes. Phase 2 pathways are under consideration and may include heart failure and stroke care. Offender Health: HMP Brixton, HMP Belmarsh and HMP and YOI Isis are located in South East London. A fourth prison is due to open in We aim, to give prisoners access to the same quality and range of Healthcare services as the general public receives from the National Health Service. Prisoners disproportionately come from disadvantaged socio-economic groups, with more physical and more mental and social health problems than the general population, and more frequently high risk behaviours. We are modelling our prison health services along an integrated approach involving joined up primary and secondary care, within the prison establishment where possible. Opportunities Opportunity Impact Integrated care case management LTC Case Management and Admissions Avoidance SEL-wide End of life care Greenwich, Lambeth, Southwark Pathway redesign SEL-wide Referral management SEL-wide Primary Eyecare Acute Referral Service (PEARS) Bexley, Bromley, Greenwich Including COPD, MSK, Dermatology, Diabetes Reduction in admissions and high cost attendances (pre HRG4) Improved quality of care for patients Work with local Hospices and Marie Curie to implement the integrated EOLC model of care, incl. evaluation of the model, tendering, and implementation of best practice pathways. Redesign of pathways including: Cardiology, Anticoagulation, Palliative Care, Minor oral surgery, Oxygen Management, Neuro Rehab, Gynaecology Changes to reduce the number of inappropriate GP initiated referrals to OP, shifting activity from acute setting to community. Reduce variation in GP referrals Skills of optometrists used to prioritise and manage patients presenting with the majority of minor eye conditions. This enables as many patients as possible to be seen quickly and in a local primary care setting, avoiding secondary referrals 29
38 Opportunity Intermediate care Bromley, Greenwich, Lambeth, Southwark Elderly care Bexley, Greenwich, Lambeth, Southwark Develop Primary Care and expand Mental Health IAPT SEL-wide Redesign child and adolescant mental health services (CAMHs) Greenwich, Southwark Impact Redesigning the intermediate care model to rebalance bed provision and community rehabilitation. Redesigned care pathway for older people: Integrated primary and secondary care Risk Stratification Modeling (part of ProMISE - management of frail & elderly patients) Redesign of the QMS campus Integration with Mental Health services Implement SEL Mental Health case for change focusing on Support for those with LTC and MH Primary care services IAPT Crisis services Working in partnership with Local Authority colleagues redesign of CAMHS services Integrated care urgent care Integrated provision of urgent care and OOH Expand UCCs Retendering of existing multiple providers Achieve seamless provision at lower cost Whole system model, redesign undertaken collaboratively with neighbouring CCGs. Redesign front end of A&E to reduce unnecessary admissions Enabling Integration of Community, Primary, Mental Health and Acute Care Eltham Community Hospital Greenwich QMS campus Bexley Orpington Bromley Dulwich Southwark Heart of East Greenwich Centre Greenwich Kidbrooke Greenwich Offers opportunity to integrate Primary, Community and Acute services networked with local GP surgeries Design a health campus focus on elderly care, integrated primary and secondary services Strategic opportunity to integrate Primary, Community and Acute services. Plans under development therefore no delivery milestone as yet Strategic opportunity to integrate Primary, Community and Acute services. Plans under development therefore no delivery milestone as yet Strategic opportunity to integrate Primary, Community and Acute services. Plans under development therefore no delivery milestone as yet Strategic opportunity to integrate Primary, Community and Acute services for the Urban village development replacing the Ferrier estate. Plans under development therefore no delivery milestone as yet 30
39 Productive Care Rationale We believe that patients should be treated in hospital where necessary and at home or closer to home where possible. The majority of patients are best cared for in the community, providing better access to care closer to home and avoiding unnecessary visits to hospitals for routine care. Patients with long term conditions such as COPD and diabetes particularly benefit from a more localised model for routine healthcare. A more localised model of care closer to home also enables patients and carers to take greater control over their care and selfmanagement of their conditions. Currently, South East London has a high level of emergency hospital admissions which could be managed in primary and community care, particularly for patients with diabetes and respiratory illnesses. Primary care services need to achieve greater economies of scale to ensure better access for patients, for example improving access to urgent care services through GP-led networks, particularly out of hours. Primary care services can also support moving care out of hospital to more cost effective settings closer to home, for example day-case surgery, diagnostics and outpatient services. Localising routine medical services with primary care would enable patients to access a wider range of services closer to home, under one roof and would enable providers to offer more convenient services such as better out of hours access. Principles We will drive the health system to be more productive across primary and hospital and community based secondary care settings. Our approach includes: Clinically led re/designed clinical pathways Using integrated care models to unlock innovation across care settings Common protocols with acute providers where possible Care closer to home where possible; hospital where necessary Right care, right place, right time philosophy Improving access to services Transforming primary care services Use of contractual levers to drive productivity Review of Personal Medical Service contracts Use of systematic patient and user feedback Evidence based practice Developing new workforce Making good quality referrals Expanding diagnostics for primary care Avoiding unnecessary treatments and appointments 31
40 Co-ordinating patient journeys Creating the right incentives for providers Driving up standards in primary care and reducing variation in performance Opportunities Opportunity Impact Productive care Primary & Community Improve access to primary care Improved access Open 12 hours a day 7 days a week service Developing the scope and capacity of primary care to manage care more SEL wide effectively in the community. PMS Reviews Improved efficiency and productivity of Primary Care services through review Lambeth & Southwark of the PMS contract Prescribing in Primary Care Deliver cost effective prescribing within budget, reduce variation between SEL wide practices in prescribing spend, improve quality of prescribing. Alternative care pathways and delivery protocols SEL wide Community Services integration Lambeth, Lewisham Extension of alternative care pathways and redesign delivery protocols so that A&E is not default destination. Improved efficiency and productivity of community services to ensure more people can be managed in the community. Productive care Acute Treatment Access Policy SEL wide OP follow up appointments SEL wide Medicines management initiatives SEL wide Emergency admissions SEL wide Acute KPIs and thresholds SEL wide Contract challenge SEL wide Demand management and decommissioning of POLCE. Ensure adherence to South East London Treatment Access Policy for SEL patients by GPs and trusts Change in thresholds for outpatient follow up activity, in contracts negotiated by cluster acute contracting team Prescribing enteral feeds, Patient Drug Waste and Direct Supply Dressing Shared formulary with SLHT, GST, KCH and LHNT for high cost drugs/high risk conditions, new anti-coagulation drugs, challenging PbR excluded drugs, management of the RAG list of drugs Improved cost effectiveness of care and movement of people into planned steams of care. Lambeth and Southwark: review Virtual Ward pilot and commission extension if evidence of impact; work with KHP to improve admitted emergency pathways and further alternatives to admission based on integrated care pilot All: develop single point of access for community based service via 111; re-commission EoL care Opportunities to generate savings and improve quality by encouraging acute providers to achieve benchmarks and KPIs Clinical and technical contract challenge Awaiting further detail 32
41 Staying Healthy Rationale The main causes of premature death are common across South East London. We believe that by creating opportunities for people to choose and maintain healthy lifestyles we will make major contributions to increasing life expectancy, reducing health inequalities, reducing hospital admissions and preventing and delaying the development of long term conditions. Smoking is a leading risk factor for the top causes of premature death for our population (CVD, some cancers, respiratory diseases). Smoking contributes to other conditions such as osteoporosis, cataracts, childhood infections and digestive disorders Physical inactivity is a leading risk factor for the main causes of premature death for our population (CVD, cancers, and respiratory diseases. Childhood obesity rates are high in South East London Babies who are not breastfed are much more likely to develop illnesses such as gastroenteritis and respiratory infections requiring hospitalisation as children. In later life they are more likely to develop high blood pressure and cholesterol levels and associated illness. Mothers who do not breastfeed have increased risk of breast and ovarian cancers and may find it difficult to return to pregnancy weight Too many people die of alcohol related problems in South East London. Alcohol-related problems place a major burden on health services in primary care, A&E, acute and specialist services and also across wider societal areas of crime, accidents, domestic violence and unemployment. Principles We will: Employ strategies aimed at the whole population as well as focusing on specific local patient groups Tailor solutions to local populations while at the same time applying national and London polices at a local level. Work together across the cluster where this is the most appropriate approach to achieve better outcomes Seek to achieve maximum benefit in health for our populations, to reducing inequalities in health 33
42 Opportunities Opportunity Tackling Obesity, Diet and Physical Activity Smoking NHS Health Checks Implement fall prevention programme Tuberculosis Cancer Immunisations Sexual Health Impact Reduce the level of obesity in adults and children reducing the impact on heart, diabetes etc. Increase the numbers of people quitting smoking with NHS stop smoking services in SEL, reduce the prevalence of smoking amongst our population and reduce smoking attributable acute activity and premature mortality Fully implement the new NHS Health Checks programme in SEL, reducing the major risk factors for vascular disease and reducing the prevalence of heart disease, strokes and diabetes within our population over time` In conjunction with London-wide TB programme, improve the early detection and effective treatment of TB in SEL and reduce the burden of disease within the population In conjunction with London-wide Cancer programme, improve coverage of cancer screening programmes across SEL, increasing early detection of treatable breast, cervical and bowel cancers within and improving survival rates Reduce the level of obesity in adults and children reducing the impact on heart, diabetes etc. To improve the coverage of childhood immunisation across SEL and reduce the incidence of outbreaks and cases To improve sexual health within our population by reducing late diagnosis of HIV, reducing teenage conceptions, improving the early detection and treatment of chlamydia and improving access to sexual health and contraceptive services 34
43 London-wide Priorities Rationale Our strategy reflects that we need to adopt different strategies for different populations and some services better tackled at populations larger than South East London, due to for example the rarity of condition, specialism and complexity of care or the scalability of solutions to common issues. Evidence suggests that centralising the most specialist services so that specialist teams treat higher numbers of patients and develop their skills would improve clinical outcomes and reduce lengths of stay in hospital. For example, complex arterial surgery, e.g. abdominal aortic aneurysm (AAA) repair, has also been shown to produce better outcomes when performed by specialist vascular surgeons Healthcare practice and technologies change rapidly. Increasingly care can and is being provided at home and closer to home settings, which reduce hospital income. Strategic solutions are required to ensure that hospital services remain viable or are replaced by high quality alternatives. NHS South East London, together with other London PCTs, is driving a series of patient care pathway service redesign programmes to improve the quality, efficiency and productivity of commissioned services. Principles We will work in partnership with the London Specialised Commissioning Group, clinical networks, other PCT clusters and other stakeholders to build and deliver strategic solutions to London wide issues and to develop more effective clinical interfaces between tertiary, secondary and primary care services. The programmes set out below will impact on 2012/13 contracts: Better hospitals: We aim to improve hospital productivity, develop a programme approach to raising quality and safety standards; develop strategic approaches to service reconfigurations where required and to inform a potential London model for future health campuses. Stronger specialist care: We will implement agreed best practice pathways for: cancer, stroke, trauma & cardio-vascular services. We will implement agreed models of care for cancer and tertiary paediatrics. The move to commissioning cancer on the basis of patient pathways and contracting through the Integrated Cancer Systems (ICS) and not individual organisations requires commissioners to work together to commission the ICS, for common pathway specifications and common metrics. We will build best practice expectations into our contracts with providers of specialised services along whole patient pathways: Prevention, Awareness, Screening, Genetic risk, Access and Presentation, Diagnostics, Treatment, Follow up, Living with illness, End of life care. 35
44 Opportunities (All being implemented SEL-wide) Opportunity Cancer Stroke and Cardiovascular Tertiary paediatrics Adult emergency services Building better hospitals and hospital services Modernising Pathology Services Tuberculosis Maternity Services Implementation of 111 Impact Implementation of agreed model of care and best practice pathways Implementation of NHS Institute for Innovation: transforming inpatient cancer care programme Implementation of cardiovascular model of care and agreed pathways for stroke and cardiovascular services Implementation of agreed model of care for tertiary paediatric services & complex paediatric surgery: Implementation of agreed best practice pathways Decommissioning from some sites and ending of services in networks that are clinically determined as being unsafe or severely isolated Commissioning standards for AES applied to local providers' acute medicine and emergency general surgery services Service reconfigurations where needed and development of London model for health campuses, to deliver improved hospital productivity and quality and safety, and deliver strategic solutions for financially challenged NHS providers Shift towards commissioning direct access services based on a London wide acceptable price range and currency Procurement of services from Providers which meet the Modernising Pathology Services in London approved turnaround times for both direct access and acute services. Pan-London protocols agreed for the use of directly observed therapy and cohort review All Providers expected to adhere to these protocols and use risk assessment tool available through London TB Register, to identify patients at risk of non-compliance with treatment TB prevention opportunities included under Staying Healthy programme Continued local improvement programmes to: Improve the quality and safety of maternity services minimum clinical standards Use key indicators from the maternity dashboard to improve clinical standards, particularly on reducing PP haemorrhage, 3rd degree tear and mortality rates. Deliver direct access/self referral for patients Ensure transparent capacity planning to enable choice for caesarian section. Reduce caesarian section rates and implement NICE guidance on choice Meet 12+6 week booking standards Develop new care pathways, based on comprehensive needs assessments, for patients with low to high social and medical risks. Increase the workforce by 17% Expand physical capacity for births Single point of access for all non urgent unscheduled care services including GP in and out of hours, community health, walk in centres, Urgent Care Centres, A&E Departments, pharmacy 36
45 7. Enablers Our work around clinical engagement and leadership, commissioning support, workforce, integrated health informatics, incentives and contractual levers, better use of estate, financial management and CSP delivery monitoring, which will support delivery. 7.1 Clinical engagement and leadership Clinical engagement is excellent throughout the cluster, with every Pathfinder having their own local mechanisms in place to engage with practices to support the delivery of the local QIPP strategy. Within each Borough, elections have been held to appoint a Pathfinder Chair and a number of clinical executives, these leaders will be key to the achievement of authorisation as CCGs in the coming year and beyond. Each Pathfinder has their own learning and organisational development programme which is supported by external consortia of specialist providers who are providing a tailored programme to meet their individual local needs in their journey to becoming authorised by April All Pathfinders play a key role in leading the local development of their local strategies and in consultation with their Health and Well-Being Boards and local LINks. Clinical leadership is key to the success of driving forward this plan over the next three years. The clinical leaders are together developing health economy ways of working with providers to ensure coordination in designing and implementing integrated ways of working. NHS SEL fully supports the proposals for co-production and testing of Local Professional Networks to strengthen clinical input for primary care commissioning across the NHS National Commissioning Board built around each profession (pharmacy, dental and ophthalmic). 7.2 The Commissioning Support Organisation (CSO) NHS South East London has been working with Pathfinders to develop a CSO for south London which will enable future CCGs to retain local skills and functions for them to operate within the 25 per head running cost allowance by purchasing a selection of services at scale. The South London CSO will be a fundamentally different organisation to the current PCT clusters and will require an organisational development programme to move to a customer-orientated organisation, with improved quality and responsiveness. A commercial outlook will also be key to its success with a decision made in 2012 on the future CSO organisational shape to take effect by 2015/16. The core service offering being developed must further strengthen the enablers described in this section. 37
46 7.3 Workforce It is not strategies, hospitals or surgeries that deliver healthcare to patients, it is people doctors, nurses and the myriad of other staff groups, and workforce accounts for about 65% of healthcare costs. For South East London s vision that more people In South East London will stay healthy, and every patient will experience joined-up healthcare which meets their needs in the most effective way to be realised, a reshaping of the workforce will be fundamental. The challenge will be to develop the right skills and capacity in the workforce to undertake an extended range of services across different mix of care settings, working in a more integrated way and continuing to maintain safety and quality standards. To achieve this, our workforce agenda is threefold: 1. Establish workforce indicators and assurance for clinical quality and safety In the current climate whilst productivity is important, ensuring patient safety and care quality must be paramount. Research has shown that reviewing a number of workforce indicators gives an organization a health check, and a direct link to clinical quality and safety. Research also shows the better engaged and motivated the workforce, the better productivity and discretionary effort will be offered. Workforce assurance indicators will therefore be incorporated as part of each organisation s performance metrics across South East London, ensuring balances are achieved between control and freedom to act, staff engagement and productivity, and patient safety. Details are shown at Appendix C. 2. Facilitate a strategic shift in skills and capacity NHS SEL s role will be to oversee and influence the overall shape of the future workforce as a whole system, with particular focus on general practice, integrated care, and specialist services. We will do this by: raising awareness of the impact, implications and opportunities workforce can have on commissioner service intentions co-ordinating workforce plans across the cluster promoting collaboration across organisations identifying and trialling innovative solutions to workforce challenges and share learning. Transformation will focus on different styles of working and skill-mix to achieve integration and better end to end care. In particular, our plan is to move many aspects of care such as management of long term conditions, increased prevention and screening, and some mental health management to general practice. 38
47 It is important the primary care workforce has the capacity and capability to take on extended roles, to teach patients to become self-carers, and to deliver care the local population the needs, in a safe and qualitative manner. This will be done through projects such as a practice staff skills audit (leading to a better understanding of education and development requirements), practice nurse leadership courses, and Making the Move (an initiative supporting secondary care nurses to move into general practice); these are already being developed and implemented. This improved profile for the primary care workforce will be an important legacy for NHS SEL. 3. Develop leadership talent both clinical and managerial As delivery of healthcare evolves, so health leadership must evolve and reflect it. Future leaders will focus on leading whole health systems, partnerships and collaboration, and need development accordingly, supported by the National Leadership Academy. NHS South East London is participating in a London-wide scheme which uses a transparent, systematic approach to recognising top talent. Senior managers identified through this as having leadership potential will be eligible to join regional and national talent programmes. SEL recognises the need for the leadership of clinical networks and the contribution they bring to the local and regional levels. 7.4 Integrated health informatics We know that our clinical commissioners will need high quality integrated health informatics to support and track delivery of our CSP. Our objective is to revolutionise the informatics available to commissioners and the health system. As a first step, the cluster will undertake an evaluation of informatics needs and current provision, with the aspiration to use the South London CSO as the vehicle for future service provision if this can meet requirements. Based on current knowledge, we envisage the establishment of a commercial-standard business intelligence function, with the ability to collect and analyse data from different care settings and to delivery standard and bespoke reports to a variety of commissioners at different levels, thereby enabling effective monitoring and decision-making. This would involve the creation of a single customer-focused informatics team and the development of a pan-south London data warehouse, containing data from primary, community, social and secondary care for physical and mental health. The data warehouse will adhere to agreed service levels in terms of performance, availability, resilience, business continuity, disaster recovery and security. While commissioning support is our primary focus, there are further aspects of informatics we need to support and influence: Delivery of a GP practice information system. We will roll out EMIS Web to 138 practices across Lambeth, Southwark, Lewisham and Greenwich which will allow the delivery of the 39
48 electronic transfer of patient records between GP practices, the uploading of the summary care record and the next iteration of the electronic prescription service (EPS2). EPS2 will allow patients to nominate their pharmacy for prescription pickup and assist practices in reducing repeat prescription workload. Proactive management of individual patients healthcare. A number of boroughs in South East London are implementing a population health management and patient risk stratification solution, which will enable GP practices to identify patients at risk of hospital admission and ensure they are taking steps to prevent it. The information available will help GPs to take accountability for their patients whole experience of NHS care. NHS SEL will facilitate active learning and sharing between the early borough adopters and those which have not yet progressed a population health management informatics solution. Enabling of joined-up care, through electronic scheduling and shared patient records Whilst ownership of clinical and booking systems rests with providers, the availability of the right informatics is, from NHS SEL s perspective, crucial to the implementation of its vision of joined up care and its priorities around integrated care. By maintaining delivery focus on outcomes, the cluster will ensure local solutions are pragmatic and business-led. 7.5 Estates Buildings are key enablers to the delivery of high quality health services, and in particular for us to deliver our ambition for expanding integrated care and care out of hospital services. We have a portfolio of 138 properties; 72 leasehold and 66 freehold. Whilst there are some high quality buildings in the portfolio, many older properties need significant new investment or replacement. Backlog maintenance has been estimated at 8-10m and a capital programme of 7.244m is anticipated in 2011/12 of which 2.625m comprises grant to assist the transfer of properties used by Learning Disability services. We also have scope for disinvestment in some properties. With careful planning, up to 10% of the older stock could be released, creating more scope for future investment in the remaining properties. Key new developments include plans in Lambeth for Ackerman Road and Norwood Hall, in Greenwich for Eltham Community Hospital and the Heart of East Greenwich Health Centre, in Southwark the strategy for the Dulwich Hospital site and in Bromley the disposal of Bassetts House We are not only interested in estates that we own or operate. In Bromley we are working with partners to transform services currently provided from the Orpington Hospital site. We want to revitalise health services for Orpington patients and end the uncertainty about the future of the hospital site. In Bexley, we are at the early stages of planning a community healthcare campus model to support elderly and integrated care. We are exploring options that involve Queen Mary s Hospital. Both of these developments are being clinically led to meet identified needs and the estate solutions will be designed to meet the care models. We are conscious that the sites are owned by a significantly financially challenged NHS Trust, South London Healthcare 40
49 Trust, that will be seeking value for money solutions to match its estate with the future capacity required to meet the needs of patients. Our strategy to expand integrated approaches to healthcare in community settings will reduce the requirement for hospital capacity (e.g. beds). In line with Department of Health guidelines, we will develop plans to offer to transfer approximately 30% of our health centres to a small number of NHS community service providers, where they are the majority occupier. This will require disaggregation of the contracts and leases transfers. Other premises will remain under the management of NHS SEL pending further guidance from the Department of Health. The General Practice estate is important, in particular as we aim to deliver more services in community settings. In South East London there are 268 practices. A challenge over the coming year will be to understand the investment required in that estate to ensure that it is both fit for purpose and can comply with the new requirements anticipated with the Care Quality Commission registration in April Our estate includes 11 administrative buildings of varying sizes and quality, located across the six South East London boroughs. We have indentified scope to reduce and rationalise our administrative buildings. We anticipate that there will be a number of disposals in 2012/13 that will result in more efficient use of office premises to support our emerging CCGs. An early priority will be to secure a strategic solution to ensure that any retained administrative premises are fit for purpose, provide value for money and enable commissioning support staff to be accessible to and readily support the new CCGs or the National Commissioning Board. 7.6 Managing our finances Financial balance is a statutory requirement for our six PCTs. Delivery of the PCTs planned financial positions is a core priority. The Cluster and Pathfinders play a vital leadership role in this. The financial position is reviewed regularly by local Pathfinders, the Cluster Joint Board and the Board s Performance, Finance and QIPP Committee. Quarterly Joint Cluster and BSU QIPP stocktake meetings provide executive assurance of financial and service performance including QIPP delivery and review progress against the achievement of full authorisation. Internal and external audit review the PCTs financial management, reporting and controls. The achievement of in-year and underlying financial balance is supported by the delivery of Recovery Plans. These plans are kept under Board review as part of the agreed overall financial reporting arrangements. Savings proposals are developed through a process of budget challenge across all areas of activity, which includes an approach of targeting a stretch 150% of savings required in order ensure delivery of 100% of targeted savings. Organisational change and the associated period of transition bring significant changes in the responsibilities of individual staff members, different reporting lines and changes in key personnel and represents an organisational risk. The Cluster and BSU finance teams is working 41
50 with senior staff to ensure changes to the budgetary framework are quickly embedded, including: Revised budgetary framework Refreshed budgetary delegation to budget holders Refreshed authorised signatory lists Enhanced reporting arrangements Budget holder guidance and training We actively pursue debtor management to ensure all income due to the PCTs is recovered. Our processes ensure that creditors are paid efficiently and on time within the Better Payment Practice Code. Outstanding creditor balances are, wherever possible, minimised. 42
51 8. Impact on the System The projected outcomes of our strategy in terms of activity and finance, together with its potential implications on key providers of NHS SEL, the associated risks and planned mitigations 8.1 Impact on patients and public The Equality Delivery System (EDS) is a new tool with a new nine-step approach to equality and human rights has been developed for the NHS. The aim is to improve transparency, engagement and performance on equality and human rights across all aspects of NHS activity. The intention is that as far as possible the equality responsibilities of an organisation should be part of routine business, whether strategic development, business planning, commissioning or service provision, (i.e. all). In the SEL Cluster, we have been working with the equality leads from the six BSUs and from the local Provider Trusts in conjunction with the Cluster Corporate Equalities Group, to ensure that our EDS implementation plan meets its objectives. On 14 November 2011, the SEL Cluster held an Equality Delivery System launch event to explain the system, roles and expectations to stakeholders. Local interested parties who attended included LINks, staff, GP Pathfinders, clincial leads, local authorities, voluntary organisations and union representatives. Work on reviewing the QIPP programme in the light of equalities is being pursued and we are in discussions with NHS London and the Department of Health regarding the potential of jointly working to implement the EDS framework in detail to two areas, unscheduled care and introduction of the 111 number. Our strategy will transform primary and community services and provide care and support in home and community settings. Fewer patients will need to attend hospital services. Our integrated approach will be built around the needs of patients. Better joined up and personalised care will result in better patient experiences, fewer duplicated diagnostic tests and better co-ordination of contacts with health and social care professionals. We aim to develop a more structured approach to gaining feedback and experiences of patients and ensuring that our service plans are improved by building upon patient feedback. 8.2 Summary Income and Expenditure Plan Financial Plans have been updated for each borough and for each the three years based on NHS London s CSP planning guidance and locally developed investment and QIPP savings plans. Changes to income and expenditure, by PCT, is set out in the Appendices and also summarised in total for South East London below: 43

52 Figure 9: Change in Income and Expenditure 2012/ /15 It should be noted that annual plans for 2012/13 have been refined to take account of Operating Framework guidance and further work to set detailed budgets and contracts, which will be reflected in 2012/13 Operating Plans. There has in particular been a review of Bexley s financial plans and further details are set at Appendix C. 8.3 Impact of savings initiatives across care settings Existing detailed QIPP savings plans have been reviewed by CCGs with support from Cluster teams. New QIPP schemes have been initiated and included in financial plans. In total QIPP savings schemes across 2012/ /15 total 173.5m, however schemes have been RAG rated to deliver savings of 117.8m and it is this total that is assumed to be delivered within financial plans. 44
53 A summary of QIPP initiatives and their impact by expenditure area over 2012/13 to 2014/15 is set out below: Table 7: QIPP Savings by Expenditure Area 2012/ /15 Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Planned QIPP Savings Before Risk Rating Acute 24,170 14,173 25,146 18,441 20,682 16, ,174 Client Groups 1, ,062 11,417 3,300 3,961 26,631 Primary Care 1,250 3,612 3,037 4,207 1,650 4,869 18,624 Corporate 0 0 1, ,343 4,716 Other Budgets and Reserves 3, ,373 Total 30,952 18,417 35,436 34,846 26,132 27, ,518 Planned QIPP Savings After Risk Rating Acute 12,802 8,100 16,345 13,249 13,668 13,353 77,517 Client Groups 1,244 (23) 4,148 7,371 2,475 3,761 18,977 Primary Care 1,250 1,836 2,462 3,160 1,238 3,350 13,295 Corporate 0 0 1, ,003 3,786 Other Budgets and Reserves 3, ,227 Total 19,084 10,276 24,147 24,171 17,656 22, ,801 It should be noted in Table 7 the Bexley QIPP programme includes unidentified savings of 3.488m in 2012/13, which will be required for the Care Trust to deliver a 1% surplus in 2012/13 (see Appendix C paragraph 9). 8.4 Provider Impact An initial impact assessment of plans on local providers income from SEL is set out below with further detail by year in the Financial Appendix. This assessment will continue to be refined based on discussions and negotiations with providers, further detailed working up of QIPP implementation plans and taking into account detailed guidance for 2012/13 and beyond. 45

54 Figure 10: Change in Local Trust Income 2012/ /15 Discussion of QIPP and commissioning intentions with providers Engagement has taken place with providers on the impact of QIPP plans and commissioning intentions and contractual negotiations for 2012/13 are well advanced. For Acute providers. The SEL Acute Contracting team has shared QIPP intentiions with acute providers (SLHT, GST and King s) in November and December 2011, leading to a timetable of contracting and negotiations through to year end, with clinical commissioners, supported by the Acute Contracting Team, engaging with hospital clinicians at borough level. With SLHT there is a specific concordat/proposed strategic framework that looks to the next 3-5 year planning cycle and a BBG clinical contract group to negotiate the detail. For out of major out of area providers. BSUs and CCGs have also engaged in the commissioning planning process for providers outside SEL. For example Bexley have engaged with NHS Kent and Medway and Dartford, Gravesham and Swanley CCG in relation to priorities and financial projections for Dartford & Gravesham Trust. For Community and Mental Health Providers. Individual BSUs have shared QIPP intentions with community providers: Oxleas, Bromley Healthcare, Lewisham Healthcare, GST Community Services and King s. Where appropriate boroughs have worked jointly for example for GST community services QIPP was flagged as part of the bilateral transfer agreement signed at the end of March 2011 between Lambeth and Southwark and GST, with current QIPP positions confirmed as part of contract negotiations during early
55 9. Sustainable Commissioning NHS SEL is committed to the NHS Carbon Reduction Strategy. We recognise the imperative of driving the sustainability vision through greater resource efficiency, reducing emissions and environmental impact, and delivering positive impact on the local economy. Some examples of the schemes which are helping to deliver a more sustainable local health system include: Further rollout of telehealth schemes such as GP telephone consultation scheme in Bromley, reducing the need for patients to travel to their GP practice Development of Bromley Healthcare; delivering community services to the borough of Bromley through a social enterprise model Urgent Care redesign across all our boroughs including the rollout and/or expansion of existing Urgent Care Centres across all boroughs, enabling more efficient and effective use of resources to treat urgent care needs Rollout of schemes that promote care at home and in the community, for example the virtual ward pilot and further rollout in Southwark, and the piloting of the Marie Curie choice model for end of life care in Greenwich Various capital developments ensuring sustainable and energy efficient designs in development of future healthcare premises. We recognise the opportunity to go further than this with a consistent joined up vision and approach across all of our boroughs, and will seek to continue to improve sustainability plans and arrangements, building these principles into all that we do. 10. Implementation How opportunities that make up our four strategic programmes will be delivered and monitored and how we will address the risks associated with the Commissioning Strategy 10.1 How will we implement the strategic programmes The following figures set out implementation plans for each strategic priority programme across SEL. Each shows the delivery trajectory for our most critical opportunities (current and new). In each case we have worked with BSUs to outline the key strategic milestones within each borough over the next three years. More detailed twelve-month plans are being developed and will be included in the 2012/13 Operating Plan. 47
")
56 (i) Integrated Care Programme Key schemes in each borough (1 of 3) 48
")
57 Integrated Care Programme Key schemes in each borough (2 of 3) 49
")
58 Integrated Care Programme Key schemes in each borough (3 of 3) 50

59 (ii) Productive Care Programme Key schemes in each borough 51

60 (iii) Staying Healthy Programme Key schemes in each borough 52

61 (iv) London-wide Programme 10.2 How we will measure success of the strategic programmes A set of SMART measures has been selected encompassing the strategic priorities for South East London. This is intended to sit alongside the measures set out in Section 4 for SEL strategic goals, to give an overall outcome framework for the CSP, with a number of measures shared across both. A national consultation is currently taking place on the Commissioning Outcomes Framework that will result in new measures coming into effect from 2013/14, and at the same time SEL pathfinders and Health and Wellbeing Boards are currently selecting local outcome measures associated with their own borough-level commissioning strategies. The proposed metrics have therefore been selected pragmatically, building where possible on measures that are currently being tracked and monitored, to give a simple monitoring framework common to all boroughs within South East London. Each borough will track and report progress against these common measures, in addition to any locally-specific measures for that borough. Detailed baseline and trajectory assumptions are included at Appendix B. Table 7: SMART Measures for Cluster Strategic Priorities 1. Strategic Priority (Programme) 2. Proposed Measure 3. Detail of Measure 4. Other Priorities & Goals Where Measure Applies? 1. Integrated care (physical, mental) People with Long Term Conditions feeling independent and in control of their condition Receiving psychological therapies % of people with LTCs who said they had had enough support from local services/orgs The proportion of people who have depression and/or anxiety disorders who are moving to recovery Priority 2, Goal II 53
62 1. Strategic Priority (Programme) 2. Proposed Measure 3. Detail of Measure 4. Other Priorities & Goals Where Measure Applies? 2. Productive care % deaths at home Registered deaths at home/registered deaths See also additional measures under other priorities, below (see column 6) Priority 2 A&E Quality Indicators Time to treatment in department Goal IV GP Practice Performance Number of measures on GP Performance Dashboard within 2 standard deviations tolerance Performance in prescribing metrics % of generic Losartan/Candesartan items as % of total Angiotensin Receptor Blocker (ARB) items Goal IV 3. Staying Healthy Appropriate prescribing of specials Emergency Readmissions Emergency readmissions within 30 days See also additional measures under other priorities, below (column 4) Childhood Obesity(year 6) Percentage of children in Year 6 with height and weight recorded who are obese. Smoking Quitters Number of 4-week smoking quitters that have attended NHS Stop Smoking Services NHS Healthchecks Number of eligible people who have received an NHS Healthcheck Goal V Goal I Priority 4, Goal I 4. Londonwide Priorities All-age All-cause Mortality (males) All-age All-cause Mortality (females) Mortality rate per 100,000 (directly age standardised) population, males, from all causes at all ages Mortality rate per 100,000 (directly age standardised) population, females, from all causes at all ages Childhood Immunisation Immunisation (MMR at age 2, 2 doses) See also additional measures under other priorities, below (column 4) Cancer 2 week wait from urgent GP referral Cancer 62 days from urgent GP referral to treatment 2 week wait - % seen in 2 weeks of urgent GP referral 62 day wait - % treated in 62 days from urgent GP referral Maternity Percentage of first appointments within 12week +6 day booking target See also additional measures under other priorities, above (column 4) Priorities 1, 2, 4 Priorities 1, 2, 4 Priority 2 54
63 10.3 Delivering our strategy Through our strategy, we will enable more people In South East London to stay healthy and mean that every patient will experience joined-up healthcare which meets their needs in the most effective way. It is also a crucial element of CCG authorisation and an effective transition to a reformed health system. Our monitoring will be effective, issues will be promptly resolved, risks identified and managed and impediments to delivery will be removed at the earliest opportunity. Our approach will be: Governance: 2012/13 will be the shadow year for Clinical Commissioning and the final year of transition prior to the abolition of Primary Care Trusts in April From April 2013 a revised governance model will enable Local Clinical Commissioning Committees (LCCCs) to exercise delegated approaches to quality, performance and finance as part of preparation for full statutory establishment, following authorisation. Core components are: CCGs to take full shadow responsibility reflected in LCCC business and reporting to the joint boards A joint integrated governance committee (incorporating Quality and Safety and Finance, Performance and QIPP) Three tier focus on o Lambeth, Southwark and Lewisham o Bexley, Bromley and Greenwich o South East London wide Monthly performance reporting and committee arrangements Improvements to the Board Assurance Framework Information: build CSP delivery monitoring information needs into the requirements for commissioning support arrangements from April 2012; designed to give early warning of issues to be addressed. Of particular importance will be the development, with borough and provider partners, LINks/Health Watch and patient participation group, of an integrated approach to the collection and review of patient feedback necessary to measure the achievement of our strategic goals Support and intervention: resources at cluster level will be organised to provide targeted support for the resolution of issues arising, whether with borough or cross-borough initiatives and performance or with wider threats to the delivery of the South East London strategic goals. The figure below sets out our thinking on governance and information at this stage. Further work is planned to specify and put in place fully-functional arrangements by April

64 Figure 11: Governance Framework 10.4 Risks and mitigations This section provides a high-level summary of the risks identified to the successful delivery of the CSP, together with mitigating actions. Table 8: Strategic Risks and Mitigation # Risk Mitigation There is a risk that attention on CSP delivery causes a loss of focus on operational performance and the quality and safety of services There is a risk that there will be insufficient clinical leadership to drive the strategy and sustain it to 2015 and beyond There is a risk that the delivery of QIPP savings will slip, resulting in failure to meet CSP strategic goals around effectiveness and a lack of funding to invest in the change required for CSP delivery SEL Cluster continues to manage the SEL All Risk Register. See Clinical Leadership section QIPP planning has identified 150% of the requirement Refreshed governance to track QIPP delivery 56

65 # Risk Mitigation There is a risk that the projected impact of CSP delivery, combined with their current position, will mean that NHS hospital trusts in SEL fail to achieve a viable position and are unable meet the requirements of Foundation Trust status There is a risk that the skillset and capacity of SEL workforce will not support the new models of care envisaged in the CSP as necessary to deliver our strategic goals See detailed mitigation actions below in respect of South London Healthcare Trust and Lewisham Healthcare Trust See Workforce section 6. There is a risk that, on top of recent changes, further reorganisation and restructuring will diminish our organisation s ability to deliver: staff focus on delivery may suffer, skilled individuals may leave and organisational memory may be lost Use delivery of this strategy as a rallying point. Continue to build ownership and develop capability and capacity at borough level Organise cluster resources to provide responsive and targeted support to cluster and borough level initiatives 7. There is a risk that insufficient business intelligence will be available to enable cluster and borough leadership to monitor CSP delivery and make early interventions to remove barriers to the realisation of benefits See Delivery Monitoring and Integrated Health Informatics sections 10.5 Foundation Trust pipeline South East London contains a number of established Foundation Trusts in the form of acute providers, GST and King s, and mental health providers, SLaM and Oxleas. Additionally NHS South East London is heavily involved in supporting the Foundation Trust pipeline process for NHS Trusts; SLHT and Lewisham Healthcare. South London Healthcare Trust In considering the provider landscape South East London commissioners are live to the fact that South London Healthcare Trust is a highly financially challenged provider. It provides most of the general acute services for Bexley, Bromley and Greenwich patients and receives the majority of its patient income from South East London commissioners. There is consequently a high degree of interdependency 57
66 between the Trust s financial position and the financial health of the PCTs and future CCGs. The historical context is seen to be important here. South East London commissioners have already led and successfully implemented a major reconfiguration of the acute services platform in outer South East London through the A Picture of Health (APOH) programme saw the closure of an Accident and Emergency (A&E) department and maternity services on the Queen Mary s site in Bexley and consolidation of these services on the Queen Elizabeth site in Greenwich and the Princess Royal site in Bromley. Whilst many of the clinical benefits of this programme have been secured, including the mission critical improvement required in patient safety in A&E and in maternity services, the benefits have not resolved the financial problems of the Trust. We will need to take this into account in our strategic planning in order to secure the continuance of the core and essential services SLHT provides to our patients. Our approach will include commissioner support for the work streams and milestones outlined in the Tripartite Framework agreement which sets out the journey that the Trust has committed to in respect of achieving Foundation Trust status and financial viability. A significant element of that work is internal productivity work to be undertaken within the Trust and the Challenged Trust Board has already supported a significant programme of work exploring the opportunities for such gains. Commissioners will therefore be working alongside other signatories to that agreement to understand the firm time line for delivery of improved cost control and productivity. In addition SE London Commissioners will be driving a clinically led process to design services that meet the identified needs of patients across primary, community and secondary care. Our overall strategy reduces the need for hospital capacity and increasingly delivers integrated care in community nad home settings. Our clinical commissioners will explore and agree the service model to be delivered for Bexley and work with the Trust to find solutions to the QMS campus proposals and for the future of the Orpington site. As part of this work we will participate in the planned simulation programme around the future of the Trust in the context of service disposition across a broader acute platform. We acknowledge that these are potential areas of cost reduction for the Trust as part of a required capacity reduction programme and as such the business cases for both of these areas and the services required within them must be sound, robust and affordable from both a commissioning perspective and a provider perspective. This is complex work and it is recognised that the business case development requires particular attention and priority. The commissioner view is that focus needs to promptly turn from income generation to capacity and associated cost reduction based on a needs led strategy in favour of a supply led strategy. The combination of financial and organisational issues for SLHT pose considerable risk to the delivery of the South East London commissioning strategy and the financial viability of Bexley, Bromley and Greenwich PCTs and the future CCGs. 58


67 Lewisham Healthcare Lewisham Healthcare is a combined acute and community NHS Trust with a strong track record of close partnership working with local commissioners. Our approach to supporting its ambition to become a Foundation Trust is set within the context of the Tripartite Framework agreement which sets out the journey that the Trust has committed to in respect of achieving Foundation Trust status and associated financial viability. Commissioners are continuing with the significant raft of service redesign work streams already in train in Lewisham and which seek to maximise the benefits of an integrated Trust, such as Lewisham Healthcare. As part of the supporting programme, clinical commissioners have successfully worked with Trust partners to bring forward the agreement of the 2012/13 contract. This means that there is a clear robust baseline for moving forward and a shared set of priorities for change between the Trust and commissioners. 59
68 3 rd DRAFT (TO BE FINALISED FOR SUBMISSION MAR 9 th ) NHS South East London Cluster Better for You Commissioning Strategy Plan 2012/ /15 DETAILED APPENDICES 1
69 Contents Appendix A: Commissioning Strategy Plan Summaries by Borough... 3 Appendix B: Cluster Measurement Framework Appendix C: Financial Case for Change and Delivery of Financial Balance Appendix D: South East London Communications and Engagement Plan
70 Appendix A: Commissioning Strategy Plan Summaries by Borough Bexley Vision Our vision is one of Excellent Healthcare, Locally Delivered. Bexley Care Trust works in partnership to improve the health and well-being of the local population. Three-Year Goals Full SMART measures being developed as part of 12/13 Operational Plan and ongoing work. Improving Health Improve the health and wellbeing of the local population. Long-term conditions Improve care for patients with long-term conditions, with a focus on integration. Sexual Health Empower the population of Bexley to make informed choices about their sexual health. Mental Health Greater focus on mental health and wellbeing. Child Health Improve the life chances of local children. 3

71 Implementation Roadmap Bexley Key strategic milestones over the next three years are set out below. 4
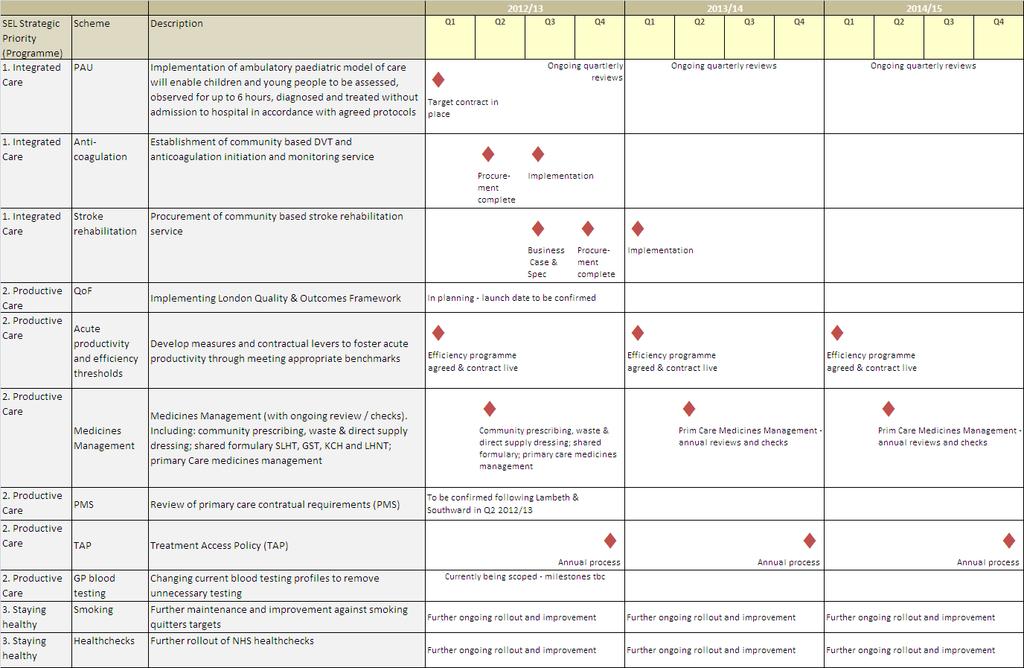
72 5
73 Bromley Vision Our vision is to help the people of Bromley live longer, healthier, happier lives and to provide the best possible services to support them. Arising from our focus upon services and clinical relationships we will continue to pursue the reform and integration of the services we provide. Three-Year Goals Full SMART measures being developed as part of 12/13 Operational Plan and ongoing work ACCESS/CHOICE. To improve access to and extend choice of services to all patients, services users and their carers, ensuring that clinical pathways are fit for purpose and that the services we commission meet the highest possible quality standards, whilst increasing the pace on delivery of the quality, innovation productivity and prevention (QIPP) challenge. PREVENTION. Empower those people in Bromley with long term conditions, particularly older people, to exercise control over their own lives and prevent problems arising or worsening and enabling them to independently manage their own health and wellbeing, thus improving their health outcomes and preventing them dying prematurely. To strengthen and fully integrate the infrastructure supporting this cohort of people ensuring that their health needs are met 24/7 in a planned and structured way. ENGAGEMENT/EDUCATION. To ensure that patients, service users and their carers are at the centre of all decisions we take around their healthcare, and have a positive experience of care. Reduce health inequalities by keeping them better informed around adopting a healthier lifestyle through a programme of education and targeted interventions known to work to increase the control they have over their own health and wellbeing. To undertake a process of education and reform to ensure our workforce have the necessary skills to deliver new and changing pathways of care. REFORM. To support the process of reforms within the NHS by ensuring that Bromley Clinical Commissioning works transparently and has full engagement and integration across the health and social care sector; maintains financial balance; is fully accountable for its performance and, through a process of development, is ready to take on statutory responsibilities by 2013/14. 6

74 Implementation Roadmap Bromley Key strategic milestones over the next three years are set out below. 7
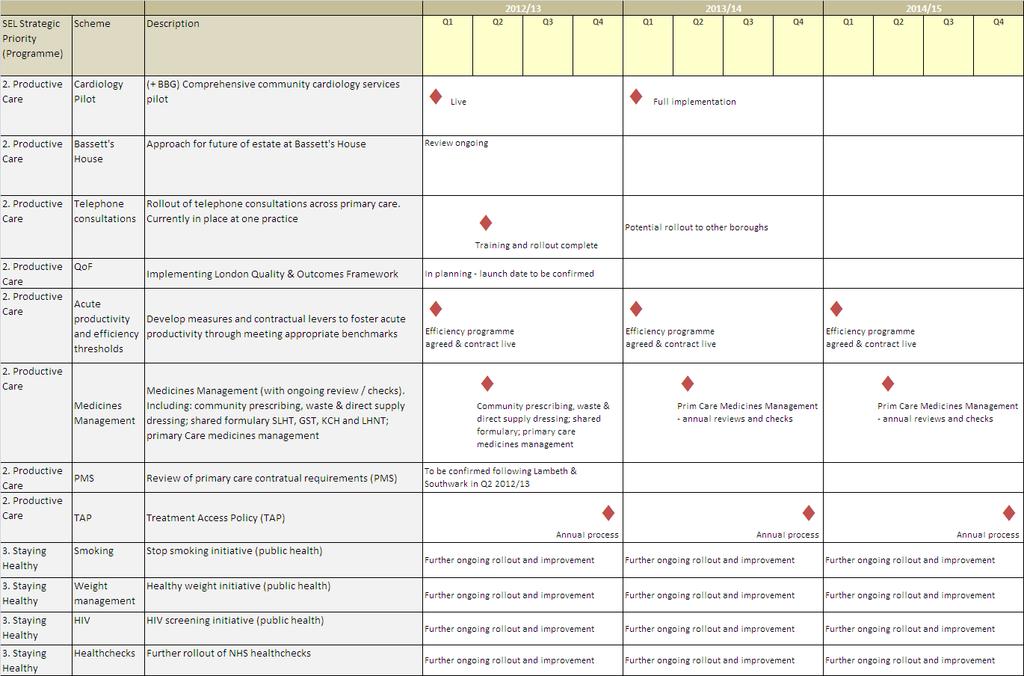
75 8
76 Greenwich Vision We are ambitious to deliver our vision for health to the population we serve. To secure the best possible health and care services: Developed in consultation with patients and the public, and in collaboration with health and social care professionals and partner organizations In primary care and community settings where possible, and in hospital where necessary to reduce health inequalities and improve health outcomes. Three-Year Goals Full SMART measures being developed as part of 12/13 Operational Plan and ongoing work Improve long-term conditions care for all ages, through: Prevention and self-management support/support to carers Targeting interventions according to need & extending the range of services available Better coordination between providers & integration between health, social and other care Increase capacity in high quality cost effective alternatives to hospital based planned care, linking these to hospital services in ways that avoid fragmentation and duplication Co-ordinate the provision of urgent and out of hours care, reducing duplication Improve mental health care, by focusing on: The interface between primary and secondary care Increase service users choice (children and young people, adults of working age and older adults) Access to services that maximise recovery, prevent relapse and admissions to acute care Children and Young People s Services: A whole system approach, focusing on prevention and developing integrated care pathways and services. Enhance the quality of end of life care, through: Better coordination between service providers, implementing an integrated model Enabling people to die in the place of their choice Implementing best practice pathways and frameworks Improve the health of our population through the Staying Healthy programme 9

77 Implementation Roadmap Greenwich Key strategic milestones over the next three years are set out below. 10
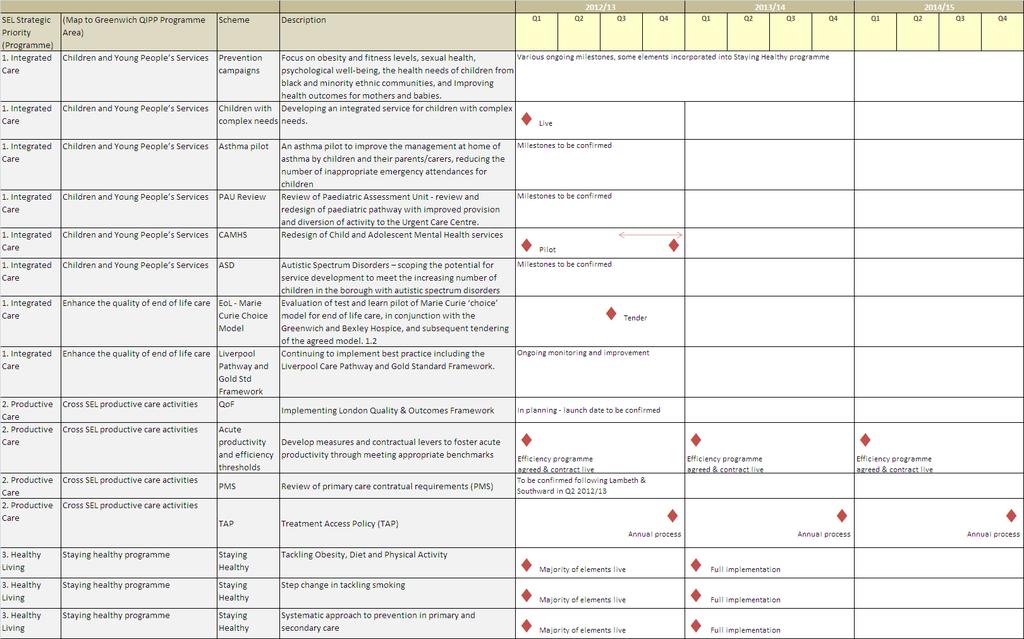
78 11
79 Lambeth Mission Our mission is to improve the health and reduce the health inequalities of Lambeth people and to commission the highest quality health services on their behalf. Vision 1. Health improvement is at the heart of all we do. We will increase life expectancy for all and reduce the difference in life expectancy between the most and least deprived in our diverse communities. 2. We will maintain a thriving, financially viable, health economy delivering safe and effective high quality care. 3. We will commission comprehensive integrated care that meets the needs of local people. We will value diversity amongst providers, but will expect excellent outcomes. 4. In delivering this Vision we recognise the need: for a rigorous, population needs based approach to commissioning, supported by public health expertise. to work with Lambeth people and their representatives to commission services that best meet their needs. to work in partnership with colleagues, across geographic, organisational and professional boundaries. This will include primary care practitioners, the London Borough of Lambeth, King's Health Partners and neighbouring health commissioners. to support innovation in workforce development and in the local application of teaching, training and research. to look first to local colleagues for management support Three-Year Health Goals Enable 1000 people with serious mental illness to move on from secondary care by accessing a new asset/recovery based service offer. Measure: 98% users in CPA with HONOS Improve hypertension control of 1000 more people in Lambeth. Measure: 76% of people with hypertension with BP <= 150/90 Help 5000 more people with diabetes bring their blood sugar under control. Measure: 74.5% for HbA1c <8 Halve the proportion of Lambeth residents diagnosed very late with HIV (<200 CD4 cells/mm3). Measure: 26% (2009) to 13% (by 2015) Help over 12,500 more people in Lambeth quit smoking. Measure: 1062 smoking quitters per 100,000 Help 900 more children overcome or avoid obesity; and help over children maintain a healthy weight. Measure: 22.3% Year 6 obesity prevalence in children Increase the number of frontline staff who have received training in screening and brief intervention for alcohol misuse. Measure: 90% of the identified frontline staff have received training in screening and brief intervention for alcohol misuse (to be confirmed) 12

80 Implementation Roadmap Lambeth Key strategic milestones over the next three years are set out below. 13
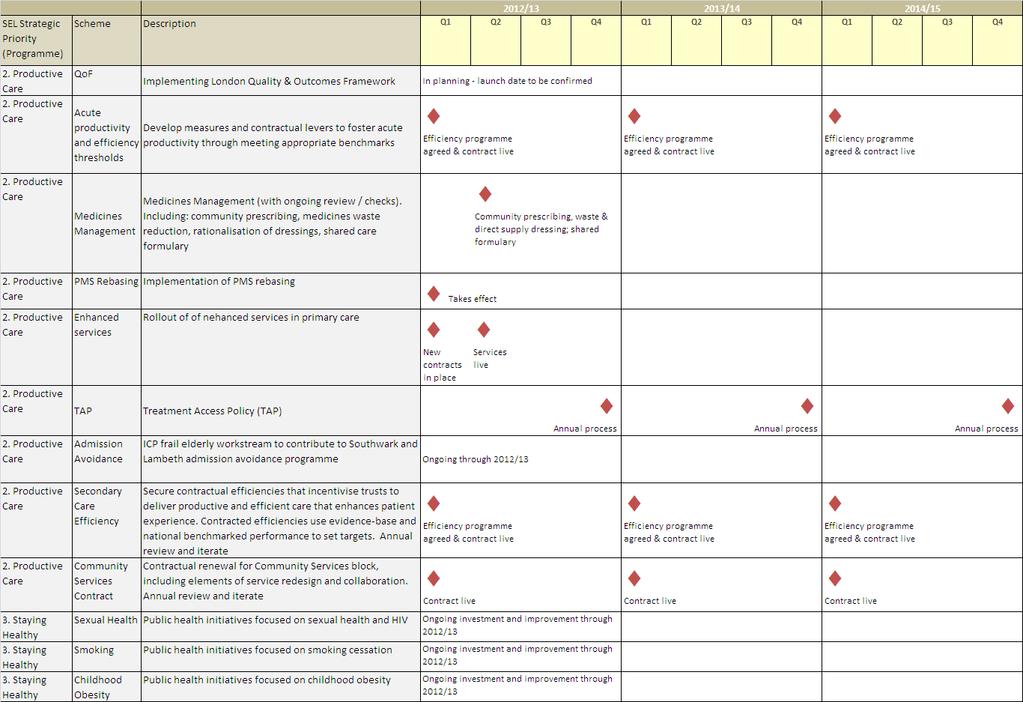
81 14
82 Lewisham Vision 1. Our vision is to improve the health of the people living in the borough and where possible to reduce health inequalities. 2. We will achieve this by working co-operatively between practices, community and primary care and also with secondary care colleagues, partners in the borough and the voluntary sector. 3. We also welcome the active involvement of our established patient participation groups, expert patients and the wider public. Three-Year Goals Full SMART measures being developed as part of 12/13 Operational Plan and ongoing work. Improve quality of care for people with long term conditions, thereby reducing their needs for emergency services Improve quality and productivity of services for people with urgent or unplanned needs Continue to integrate services between Lewisham Healthcare, social care and primary care services in order to improve productivity across the system and improve outcomes for patients Develop locally accessible services for Lewisham residents, especially at the Lewisham Hospital site Continue to focus on acute productivity to meet benchmarked levels. This will focus on all acute services, including Kings College Foundation Trust and Guys and St Thomas Foundation Trust Develop prevention services in primary care building on efforts in 2011/12 to improve immunisation rates Improve quality and productivity in mental health services Continue with focus on GP outpatient referrals and prescribing along with tackling corporate overheads. 15

83 Implementation Roadmap Lewisham Key strategic milestones over the next three years are set out below. 16
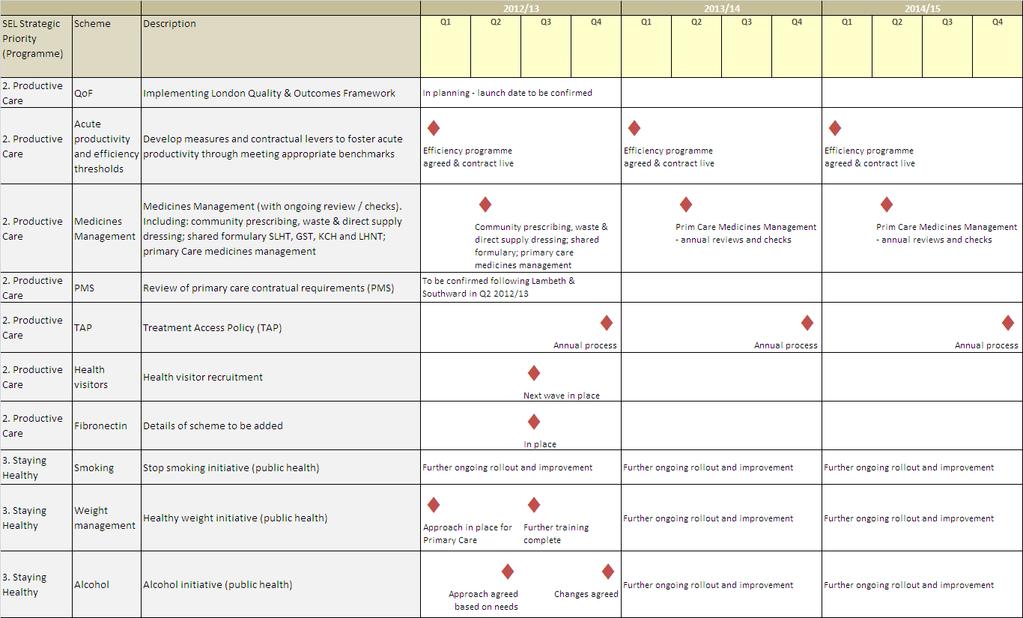
84 17
85 Southwark Vision As the Southwark Clinical Commissioning Committee our vision is to improve the health outcomes of our population. We will commission services that continually enhance the quality of care provided to patients as we believe quality services are efficient services. We want to change local health provision so that services are structured around safe, high quality and efficient pathways of care that are expertly coordinated and managed so they work well for patients. As Clinical Commissioners we want: 1. Better, more productive and safer provision and to improve patient experience of these services 2. Better care closer to home with more delivered in community settings that are efficiently integrated with specialist care in hospitals 3. Stronger specialist care in hospitals and in mental health services 4. To make sure NHS resources are utilised to continually improve performance across the health economy 5. To directly engage local people in shaping their services. Three-Year Goals Full SMART measures being developed as part of 12/13 Operational Plan and ongoing work. The following Strategic Goals are aligned to the Southwark Joint Strategic Needs Assessment (JSNA) and reflect identified priorities. The over-arching strategic goal of clinically-led commissioning is to improve the health and wellbeing of Southwark s population and to achieve a reduction in health inequalities. We will give particular emphasis to cardiovascular and respiratory disease, diabetes, mental health, and other long term conditions. Commission and manage effective integrated care pathways. The goal of developing integrated care is to reduce duplication, improve coordination across care settings and to structure services so they are increasingly patient-focused. Achieving this goal will improve the quality of commissioned services and support cost effective care. Lead the local NHS as part of a broader network of partner organisations through the Southwark Health & Wellbeing Board so that we can achieve excellence in commissioning and improve outcomes for our residents Bring patients and the public into the centre of decision-making locally by involving more people in decision making and, ensuring local views drive commissioning decisions Maintain a robust system of financial control with clinical leads overseeing the effective management of resources including the delivery of a QIPP programme 150% the size of our identified do nothing gap. 18

86 Implementation Roadmap Southwark Key strategic milestones over the next three years are set out below. 19
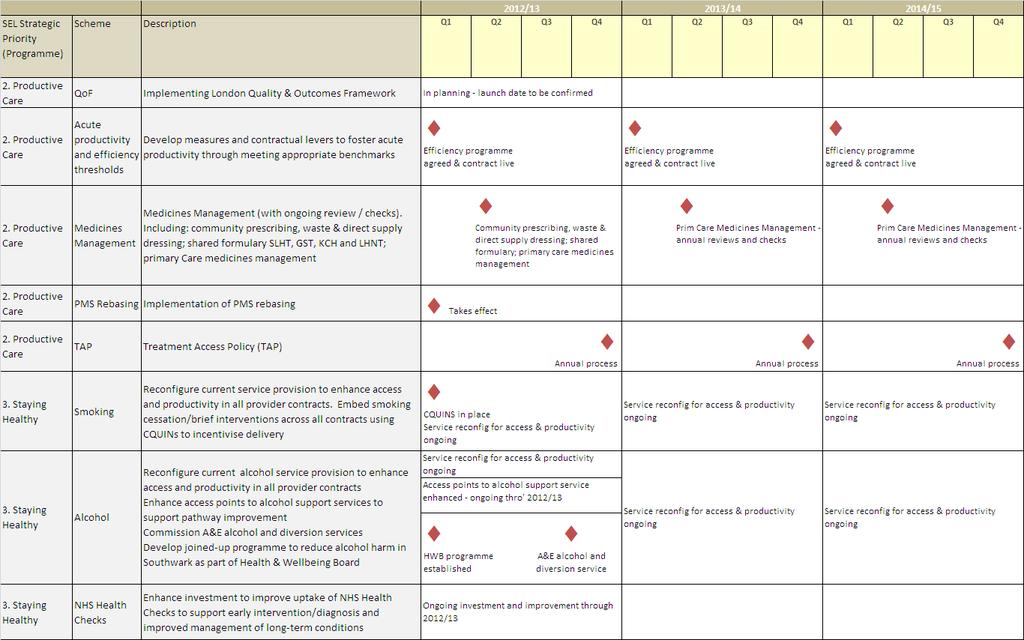
87 20
88 Appendix B: Cluster Measurement Framework (i) Measures to support Strategic Goals 21
89 (ii) Measures to support Strategic Priorities (Programmes) (1 of 2) 22
90 (ii) Measures to support Strategic Priorities (Programmes) (2 of 2) 23
91 Appendix C: Financial Case for Change and Delivery of Financial Balance 1. Introduction 1.1. This section sets out information in support of the NHS South East London Commissioning Strategy plan, including: Background on the PCTs financial positions in NHS and how financial plans have been updated Aims of the financial plans The Financial Case for Change Summary income and expenditure plans for all 6 boroughs and associated assumptions An initial assessment of the impact of commissioner plans on local NHS Trust and Foundation Trust providers How we will ensure financial delivery 2. Current Financial Position 2.1. The South East London Cluster includes four Foundation Trusts (FTs), a Trust in the process of applying for FT status and a significantly financially challenged Trust SEL PCTs have a strong track record of financial delivery. In 2011/12, all six PCTs in South East London are projecting that they will meet surpluses in line with 2011/12 plans. There are significant financial risks associated with these positions which will require close co-ordination and management for the remainder of the financial year. The financial challenge in 2011/12 is particularly great for Bexley Care Trust and the Cluster is working closely with the CCG to address this in 2011/12. This will have an impact on financial plans going forward. 3. South East London Process in Updating Financial Plans 3.1. Finance teams across the SEL Cluster central teams and in CCGs have worked closely together jointly to own and manage financial and QIPP plans and as part of larger multi-disciplinary teams. This has ensured both local clinical ownership of plans and an improved consistency in approach across SEL boroughs. 24
92 3.2. Updates to financial plans have been developed in line with NHS London CSP guidance in respect of assumptions around PCT uplifts, tariff, efficiency and other inflationary cost changes, required contingencies and surpluses. Plans are supported by a locally developed financial model shared across cluster and CCG teams and also a detailed activity model, providing a high level of granularity when developing activity projections, including the impact of QIPP initiatives Financial plans within the CSP are based on CSP guidance and assumptions. They are strategic in nature. While they are reconciled to more detailed and specific Operating Plan and budget setting work (see Annex H), they are not equal to the annual plans for 2012/13. The latter have been refined to take account of Operating Framework guidance and further work to set detailed budgets and contracts.a great deal of detailed work has been undertaken with regard to Bexley s financial plans and further details are set out at section Aims of the 3 Year Financial Plans 4.1. The aim of the Cluster s financial plans are to: Ensure financial balance and stability through the effective management of available resources and financial risks to ensure statutory duties are met each year. Support Operating Plans, Commissioning Strategy Plans and individual service strategies through the effective use of available resources on a one-off (invest to save) and recurrent basis and to support innovation in service redesign and health improvement. Secure value for money and efficiency through enhanced Quality, Innovation, Productivity and Prevention (QIPP) in our commissioning responsibilities. Ensuring a sound and sustainable financial legacy to CCGs. 5. The Financial case for Change 5.1. All of the commissioning organisations in South East London face continuing growth in demand and cost of acute services, driven by population growth, demographic changes and expansion of available health technologies. There is also an increased expectation of the quality and extent of health service delivery. At the same time the rate of increase of funding for the NHS has considerably slowed down to just above inflation. This means that the underlying rate of deficit will increase 25
93 if no action is taken It is clear that the level of financial challenge facing the NHS over the next few years is unprecedented, especially when compared to the significant levels of financial growth enjoyed by the NHS over the last decade. Furthermore, it is clear that in order to address the level of financial deficit in the do - nothing scenario, a step change will be required in how we approach the development and delivery of QIPP plans. We therefore need to continue to ensure that the redesign of the system and the ownership of the plans are with local CCGs and led by primary care clinicians working in conjunction with acute clinical colleagues to improve care pathways and patient experience, eliminate duplication and improve productivity The financial challenge facing SEL is therefore to secure significant efficiency and productivity savings from all commissioning and provider organisations over the course of the next three years to provide the financial resource to support delivery of our vision and the supporting strategies. If no action is taken then the underlying financial positions will deteriorate, year on year resulting in a worsening in the current cumulative position from 2012/13 to 2014/15 and a deficit in 2014/15 across South East London PCTs of 89.4m. In order to achieve the required 1% surplus in 2014/15, QIPP savings totalling 117.8m will need to be delivered over the three year period In order to achieve the 1% surplus in every year the required QIPP savings will need to be front loaded, with 59.4m of the savings requirement being in 2012/13 as set out below: Table 1: The Financial Case for Change 26
94 Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Forecast Surplus/ (Deficit) 2011/12 0 5,992 4,612 6,605 5,375 5,857 28,441 QIPP savings requirement 2012/13 (10,778) (4,710) (12,419) (11,974) (8,469) (11,043) (59,393) QIPP savings requirement 2013/14 (5,145) (3,140) (7,817) (7,562) (5,278) (6,636) (35,578) QIPP savings requirement 2014/15 (3,161) (2,426) (3,911) (4,635) (3,909) (4,789) (22,830) Total QIPP savings requirement (19,084) (10,276) (24,147) (24,171) (17,656) (22,468) (117,801) "No Change" Forecast Surplus/ (Deficit) 2014/15 (19,084) (4,284) (19,535) (17,566) (12,281) (16,611) (89,360) 5.5. The financial challenge in 2012/13 is therefore the most challenging and delivery of QIPP savings and the overall delivery of planned surpluses in 2012/13 are key to the delivery of financial balance over the medium term and also in ensuring a sound and sustainable financial legacy to CCGs It is important to note that the delivery of the required QIPP savings are not only across the acute/ primary care interface but across all areas of commissioning spend including mental health, community and primary care contracts. As commissioning responsibilities are transferred across the new commissioning authorities, QIPP savings requirements will also need to be transferred. 6. Summary Income and Expenditure Plan 6.1. Financial Plans have been updated for each borough and for each the three years based on NHS London planning guidance and locally developed investment and QIPP savings plans. Changes to income and expenditure, by PCT, is set out at Annexes A to C and also summarised in total for South East London below: Chart 1: Change in Income and Expenditure 2012/ /15 27

95 300 SEL Cluster - Movement from 2011/12 surplus to planned Surplus in 2014/ Income/ Saving 200 Expenditure 150 Surplus/ (Deficit) 'million (50) (100) (150) Forecast Surplus 2011/12 Recurrent Uplift Full year effect of Tariff and generic Efficiency within prior year outturn uplifts Tariffs demographic growth Non-demographic Investment growth Proposals and cost pressures QIPP Savings Initiatives Planned Surplus 2014/ Assumptions are set out further below. Recurrent Uplifts, Tariff and Generic Uplifts, Demographic & Non-Demographic Growth and Primary Care Prescribing Uplifts A summary of uplift assumptions, on average across South East London are set out below. Details by expenditure area and by borough are at Annex D. Table 2: Uplift Assumptions 28
96 2012/ / /15 Recurrent uplift 2.25% 2.48% 2.70% demographic Growth 0.83% 0.82% 0.87% Non-demographic growth 1.05% 1.04% 1.02% Prescribing growth 5.20% 5.21% 5.21% Tariff/ Inflation Uplift 2.22% 2.21% 2.20% Tariff efficiency assumption/ Price Efficiency applied (3.12%) (3.09%) (3.05%) Further details on uplift assumptions are provided below: Recurrent Uplifts PCT Revenue Resource Limit (RRL) uplifts are in line with NHS London guidance. This set uplifts at a national average allocated growth of 2.38% in 2012/13, 2.62% in 2013/14 and 2.84% in 2014/15. As Southwark and Bexley were allocated 2.20% growth in 2011/12, in line with the national average, we have also used the percentage above for future years. All other Cluster PCT are currently over their weighted capitation targets so were funded 0.2% less uplift than average in 2011/12, so 0.2% less than average uplifts have been assumed for these PCTs going forward. It should be noted that actual RRL uplifts for 2012/13 and beyond are not yet confirmed. Tariff and Generic Uplifts Tariff uplifts have been assumed at a net -1.5%, including a built in 4.0% efficiency assumption. This has been applied to acute, mental health and community spend. Demographic & Non-Demographic Growth Detailed work has been undertaken to review planning assumptions related to demographic and non demographic acute growth for the CSP. The objective has been to ensure robust and realistic borough based planning assumptions related to population and incidence factors, which take account of demographic growth estimates and historic acute demand trends. To do so the following process has been undertaken : A review of population growth assumptions by borough (including GLA and ONS figures) for acute services. 29
97 A review of historic demand trends by borough for acute services, with supporting trend analysis completed for the following key areas of acute activity outpatients, elective, A&E attendances, and emergency admissions, maternity and other. The development of proposed demographic and non demographic growth assumptions by CCG by admission method, applied on a consistent basis across the six SEL boroughs. The testing of assumptions with SEL clinical commissioners, CCGs and CSP leads, to confirm proposed planning assumptions. This process has resulted in a consensus agreement, supported by robust analytics, on the demographic and non demographic assumptions to be utilised for the CSP. Brought Forward Surpluses Forecast surpluses for 2011/12 have been assumed to be carried forward into 2012/13. This assumption has also been made for future years. Full Year effect of 2011/12 outturn The full year recurrent impact of 2011/12 forecast outturn expenditure has been included within 2012/13 expenditure plans, including the costs of reinstating PCT contingencies at 0.5% of recurrent resource limits. Investment Proposals and Cost Pressures Borough investments and cost pressures have been included in financial plans for all years. While detailed expenditure plans are in place for 2012/13, these remain draft pending the release of all detailed planning guidance for 2012/13 and also while detailed implementation plans are put in place for the delivery of QIPP savings initiatives. QIPP Savings Initiatives Existing detailed QIPP savings plans have been reviewed by CCGs with support from Cluster teams. New QIPP schemes have been initiated and included in financial plans. In total QIPP savings schemes across 2012/ /15 total 173.5m, however schemes have been RAG rated to deliver savings of 117.8m and it is this total that is assumed to be delivered within financial plans. A summary of QIPP initiatives and their impact by expenditure area over 2012/13 to 2014/15 is set out below: 30
98 Table 3: QIPP Savings by Expenditure Area 2012/ /15 Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Planned QIPP Savings Before Risk Rating Acute 24,170 14,173 25,146 18,441 20,682 16, ,174 Client Groups 1, ,062 11,417 3,300 3,961 26,631 Primary Care 1,250 3,612 3,037 4,207 1,650 4,869 18,624 Corporate 0 0 1, ,343 4,716 Other Budgets and Reserves 3, ,373 Total 30,952 18,417 35,436 34,846 26,132 27, ,518 Planned QIPP Savings After Risk Rating Acute 12,802 8,100 16,345 13,249 13,668 13,353 77,517 Client Groups 1,244 (23) 4,148 7,371 2,475 3,761 18,977 Primary Care 1,250 1,836 2,462 3,160 1,238 3,350 13,295 Corporate 0 0 1, ,003 3,786 Other Budgets and Reserves 3, ,227 Total 19,084 10,276 24,147 24,171 17,656 22, ,801 It should be noted in Table 3 the Bexley QIPP programme includes unidentified savings of 3.488m in 2012/13, which will be required for the Care Trust to deliver a 1% surplus in 2012/13 (see paragraph 9 below). 2% Non-Recurrent Funds Plans for all SEL PCTs assume and include use of the 2% funds in full as an enabler for QIPP delivery and to effectively manage the transition to the new commissioning environment. 7. Provider Impact 7.1. An initial impact assessment of plans on local providers income from SEL is set out below with further detail by year at Annex E. This assessment will continue to be refined based on discussions and negotiations with providers, further detailed working 31
99 up of QIPP implementation plans and taking into account detailed guidance for 2012/13 and beyond. Chart 2: Change in Local Trust Income 2012/ /15 Change in SEL Cluster Expenditure - Local Contracts / /15 increase in Trust Income reduction in Trust Income 110% 105% 100% 95% 90% TAR TAR EFF DEM NON- DEM QIPP TAR TAR EFF DEM NON- DEM QIPP TAR TAR EFF DEM NON- DEM QIPP TAR TAR EFF DEM NON- DEM QIPP TAR TAR EFF DEM NON- DEM QIPP TAR TAR EFF DEM NON- DEM QIPP TAR = Tariff/ Generic Uplift; TAR EFF = Tariff efficiency deflator; DEM= Demographic Growth; NON-DEM= Non-Demographic Growth; QIPP = QIPP Savings 8. Ensuring Financial Delivery 32
100 8.1. Financial balance and the delivery of the PCTs planned financial positions is a core priority and a statutory requirement for NHS SE London. The Cluster and Clinical Commissioning Groups (CCGs) play a vital leadership role in this The financial position is reviewed regularly by local CCGs, the Cluster Joint Board and the Cluster Performance, Finance & QIPP Committee. Quarterly Joint Cluster and BSU QIPP Stocktake meetings provide executive assurance of financial and service performance including QIPP delivery and review progress against the achievement of full authorisation. Internal and external audit review the PCTs financial management, reporting and controls. Further external assurance is also put in place where this is needed The achievement of in-year and underlying financial balance is supported by the delivery of Recovery Plans. These plans are kept under Board review as part of the agreed overall financial reporting arrangements. Savings proposals are developed through a process of budget challenge across all areas of activity CCGs are implementing development plans that take account of the NHS London Roadmap recognised by the Department of Health as a means of achieving full authorisation. The Roadmap s eight domains include finance and governance and development programmes will strengthen CCGs skills in these areas Organisational change and the associated period of transition bring significant changes in the responsibilities of individual staff members, different reporting lines and changes in key personnel and represents an organisational risk. The Cluster and BSU finance teams is working with senior staff to ensure changes to the budgetary framework are quickly embedded, including: Revised budgetary framework Refreshed budgetary delegation to budget holders Refreshed authorised signatory lists Enhanced reporting arrangements Budget holder guidance and training 8.6. The Cluster is actively pursuing debtor management to ensure all income due to the PCTs is recovered. Processes are in place to ensure that creditors are paid efficiently and on time so that the Better Payment Practice Code (BPPC) can be met 33
101 and outstanding creditor balances are, wherever possible, minimised. This involves regular reporting of outstanding invoices supported by staff training in the use of electronic workflow systems. 9. Moving onto 2012/13 Operating Plans 9.1. While financial plans within the CSP are based on CSP guidance and assumptions, annual plans for 2012/13 have been refined to take account of Operating Framework guidance and further work to set detailed budgets and contracts, which will be reflected in 2012/13 Operating Plans. There has, in particula,r been a review of Bexley s financial plans and further details are set out below: Operating Framework and Operating Plan guidance for 2012/13 Operating Framework guidance for 2012/13 was released on 24 th November This includes some further clarity on finance and business rules for 2012/13, particularly in relation to PCT uplifts and changes to national tariffs. While most of the guidance is consistent with planning guidelines used to inform South East London s CSP there are some additional flexibilities from confirmed PCT uplifts and tariff deflators but also additional financial pressures relating to the announcement that CQUIN will be increased by 1% to 2.5%. Detailed financial plans for 2012/13 have been updated within Operating Plans as finance rules have been confirmed and negotiations with providers progress. In response to this guidance, the SEL Cluster and CCGs have reviewed cost pressures, investments and the delivery of QIPP savings plans to address the level of financial challenge ans this has been reflected in 2012/13 Operating Plans. A summmary of the changes in financial assumptions for 2012/13 from the CSP to 2012/13 Operating Plans is set out at Annex H. Bexley Operating Plan Review The initial Bexley QIPP programme within the CSP included an unidentified QIPP of 3.488m in 2012/13, which would be required for the Care Trust to deliver a 1% surplus in 2012/13. In moving to 2012/13 Operating Plans Bexley BSU has reviewed its financial plans, as summarised below: 34
102 An increase in the 2012/13 recurrent growth uplift Increase in brought forward surplus from 2011/12 Increase in tariff deflator to 1.8% Review of 2012/13 investment proposals Removal of unidentified QIPP savings assumptions Mutual financial support across SEL in 2012/13 Bexley s plans have been revised to include identified recovery initiatives required for future financial sustainability. To deliver the required 1% surplus over the medium term, specifically to deliver a 1% surplus in each of 2012/13, 2013/14 and 2014/15, requires financial support in 2012/13 to smooth the transition from deficit to surplus. Bexley s plan includes an assumption that sustained financial stability will be reached in 2013/14 and that it will generate a surplus that is greater than support received in 2012/13, in addition to the required 1% surplus. The SEL Cluster will facilitate the agreement of mutual financial support in 2012/13 to support Bexley s delivery plan. 10. Conclusion This paper sets out financial information in support of the Cluster Commissioning Strategy Plan. Separate plans will continue be updated over the remainder of the financial year in line with Operating Plan, contract negotiation and budget setting requirements. 35
103 Summary Income and Expenditure 2012/ /15 Annex A Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Income Recurrent Uplift 27,411 36,430 33,342 45,497 38,464 41, ,755 Prior Year Surplus brought forward 0 5,992 4,612 6,605 5,375 5,857 28,441 Total Income Changes 27,411 42,422 37,954 52,102 43,839 47, ,196 Expenditure Full year effect of 2011/12 outturn 9,957 3,546 12,128 12,489 7,798 3,816 49,734 Net Generic Uplifts Tariff and generic uplifts 22,912 33,883 28,789 43,457 36,045 36, ,109 Efficiency with Tariff (31,213) (46,842) (40,464) (61,987) (49,886) (50,464) (280,857) Net Tariff/ Generic Uplift (8,302) (12,959) (11,675) (18,530) (13,841) (14,440) (79,747) Demographic & Non-Demographic Growth demographic Growth 4,128 5,774 19,182 9,596 11,467 25,620 75,767 Non-demographic growth 12,859 17,786 13,375 20,781 11,314 17,498 93,613 Total Demographic & Non-Demographic Growth 16,988 23,559 32,558 30,378 22,780 43, ,380 Investment Proposals and cost pressures 24,171 33,275 24,260 44,936 38,997 31, ,225 QIPP Savings Initiatives (19,084) (10,276) (24,147) (24,171) (17,656) (22,468) (117,801) Change in Recurrent Expenditure 23,730 37,144 33,123 45,102 38,079 41, ,789 Surplus/ (Deficit) 3,682 5,278 4,830 7,000 5,760 5,857 32,407 Surplus as % of Recurrent RRL 1.0% 1.0% 1.0% 1.1% 1.0% 1.0% 1.0% 36
104 Summary Income and Expenditure 2012/ /15 By Year Annex B Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL 2012/ / / / / / / / / / / / / / / / / / / / /15 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 '000 Income Recurrent Uplift 8,108 9,138 10,165 10,709 12,148 13,573 9,802 11,118 12,422 13,375 15,171 16,951 11,626 12,675 14,162 12,308 13,872 15,431 65,929 74,122 82,704 Prior Year Surplus brought forward 0 3,488 3,579 5,992 5,020 5,141 4,612 4,710 4,830 6,605 7,000 7,000 5,375 5,492 5,618 5,857 5,857 5,857 28,441 31,568 32,027 Total Income Changes 8,108 12,627 13,744 16,701 17,168 18,714 14,414 15,828 17,252 19,980 22,171 23,951 17,001 18,167 19,781 18,165 19,729 21,288 94, , ,731 Expenditure Full year effect of 2011/12 outturn 9, , , , , , , Net Generic Uplifts Tariff and generic uplifts 7,490 7,739 7,683 10,980 11,307 11,596 9,619 9,580 9,590 14,179 14,476 14,802 11,747 12,014 12,284 11,773 11,975 12,276 65,789 67,091 68,230 Efficiency with Tariff (10,549) (10,414) (10,250) (15,284) (15,630) (15,928) (13,565) (13,467) (13,432) (20,262) (20,671) (21,054) (16,382) (16,633) (16,872) (16,552) (16,777) (17,135) (92,594) (93,592) (94,671) Net Tariff/ Generic Uplift (3,059) (2,675) (2,568) (4,304) (4,324) (4,332) (3,945) (3,887) (3,843) (6,083) (6,196) (6,252) (4,635) (4,618) (4,588) (4,779) (4,801) (4,860) (26,805) (26,501) (26,441) Demographic & Non-Demographic Growth demographic Growth 1,384 1,376 1,369 1,891 1,928 1,955 5,703 5,701 7,779 3,156 3,195 3,246 3,800 3,818 3,849 8,421 8,518 8,681 24,354 24,534 26,878 Non-demographic growth 4,330 4,287 4,242 5,800 5,945 6,041 4,492 4,445 4,438 6,815 6,910 7,057 3,776 3,763 3,775 5,762 5,821 5,914 30,975 31,171 31,467 Total Demographic & Non-Demographic Growth 5,714 5,663 5,611 7,690 7,873 7,996 10,195 10,145 12,217 9,970 10,105 10,303 7,576 7,581 7,623 14,184 14,339 14,595 55,329 55,706 58,345 Investment Proposals and cost pressures 2,786 11,204 10,181 9,459 11,617 12,199 3,745 12,556 7,958 8,577 18,824 17,535 9,239 14,864 14,894 10,131 10,970 10,484 43,939 80,037 73,250 QIPP Savings Initiatives (10,778) (5,145) (3,161) (4,710) (3,140) (2,426) (12,419) (7,817) (3,911) (11,974) (7,562) (4,635) (8,469) (5,278) (3,909) (11,043) (6,636) (4,789) (59,393) (35,578) (22,830) Change in Recurrent Expenditure 4,620 9,047 10,063 11,681 12,026 13,437 9,703 10,998 12,422 12,980 15,171 16,951 11,509 12,549 14,021 12,308 13,872 15,431 62,801 73,663 82,324 Surplus/ (Deficit) 3,488 3,579 3,681 5,020 5,142 5,277 4,710 4,830 4,830 7,000 7,000 7,000 5,492 5,618 5,760 5,857 5,857 5,857 31,568 32,027 32,406 Surplus as % of Recurrent RRL 1.0% 1.0% 1.0% 1.0% 1.0% 1.0% 1.0% 1.0% 1.0% 1.1% 1.1% 1.1% 1.0% 1.0% 1.0% 1.1% 1.1% 1.0% 1.1% 1.0% 1.0% 37
105 Income and Expenditure 2012/ /15 Waterfall Diagrams Annex C/1 30 Bexley - Movement from 2011/12 surplus to planned Surplus in 2014/15 60 Bromley - Movement from 2011/12 surplus to planned Surplus in 2014/15 25 Income/ Saving Expenditure 50 Income/ Saving 20 Expenditure Surplus/ (Deficit) 'million 5 Surplus/ (Deficit) 'million 0 20 (5) 10 (10) (15) 0 (20) Forecast Surplus Recurrent Uplift Full year effect of Tariff and generic Efficiency within 2011/12 prior year outturn uplifts Tariffs demographic Non-demographic Investment QIPP Savings growth growth Proposals and cost Initiatives pressures Planned Surplus 2014/15 (10) Forecast Surplus Recurrent Uplift Full year effect of Tariff and generic Efficiency within 2011/12 prior year outturn uplifts Tariffs demographic Non-demographic Investment QIPP Savings growth growth Proposals and cost Initiatives pressures Planned Surplus 2014/15 50 Greenwich - Movement from 2011/12 surplus to planned Surplus in 2014/15 70 Lambeth - Movement from 2011/12 surplus to planned Surplus in 2014/15 40 Income/ Saving 60 Income/ Saving Expenditure 50 Expenditure Surplus/ (Deficit) 'million 10 Surplus/ (Deficit) 'million (10) (10) (20) (20) (30) Forecast Surplus Recurrent Uplift Full year effect of Tariff and generic Efficiency within 2011/12 prior year outturn uplifts Tariffs demographic Non-demographic Investment QIPP Savings growth growth Proposals and cost Initiatives pressures Planned Surplus 2014/15 (30) Forecast Surplus Recurrent Uplift Full year effect of Tariff and generic Efficiency within 2011/12 prior year outturn uplifts Tariffs demographic Non-demographic Investment QIPP Savings growth growth Proposals and cost Initiatives pressures Planned Surplus 2014/15 38
106 Summary Income and Expenditure 2012/ /15 Waterfall Diagrams Annex C/2 60 Lewisham - Movement from 2011/12 surplus to planned Surplus in 2014/15 70 Southwark - Movement from 2011/12 surplus to planned Surplus in 2014/15 50 Income/ Saving 60 Income/ Saving Expenditure 50 Expenditure Surplus/ (Deficit) 'million 20 Surplus/ (Deficit) 'million (10) (10) (20) (20) (30) Forecast Surplus Recurrent Uplift Full year effect of Tariff and generic Efficiency within 2011/12 prior year outturn uplifts Tariffs demographic Non-demographic Investment QIPP Savings growth growth Proposals and cost Initiatives pressures Planned Surplus 2014/15 Forecast Surplus Recurrent Uplift Full year effect of Tariff and generic Efficiency within 2011/12 prior year outturn uplifts Tariffs demographic Non-demographic Investment QIPP Savings growth growth Proposals and cost Initiatives pressures Planned Surplus 2014/15 39
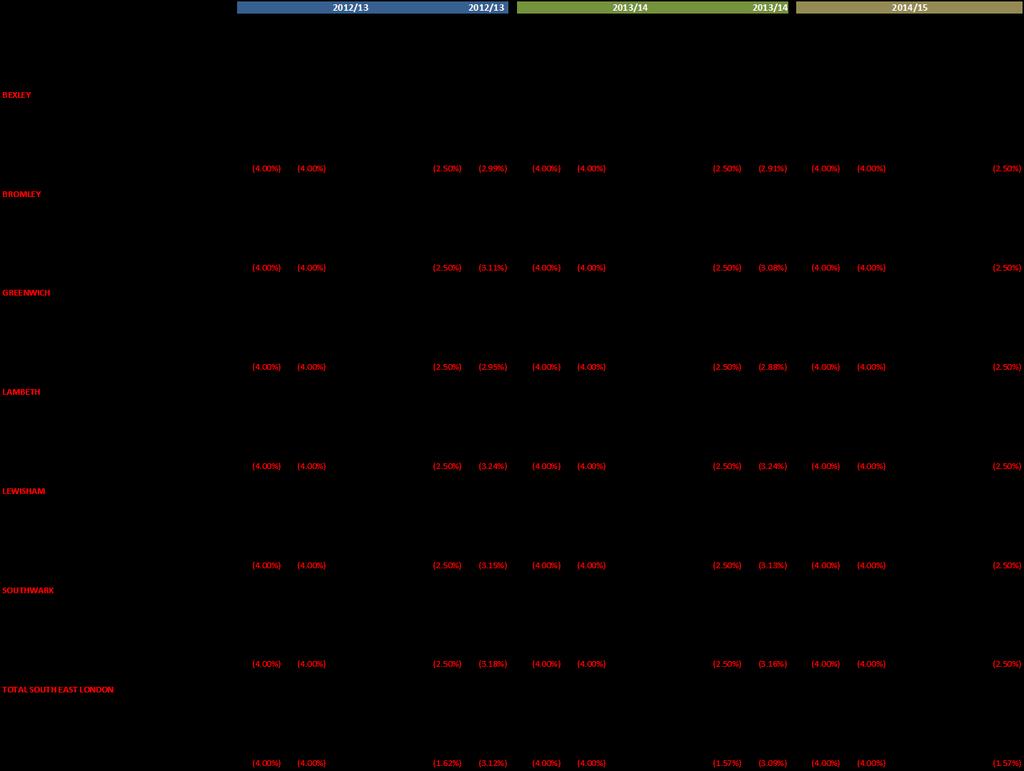
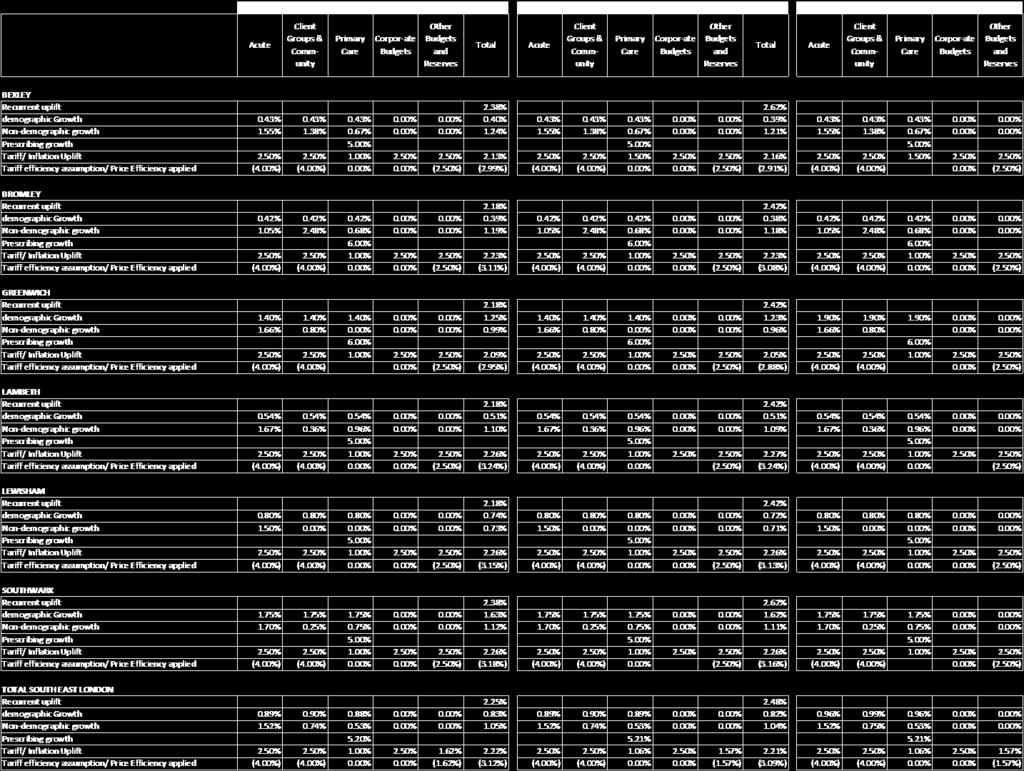
107 Uplift Assumptions Annex D 40
108 Change in SEL Cluster expenditure at local Trusts 2012/ /15 Annex E/1 41
109 Change in SEL Cluster expenditure at local Trusts 2012/ /15 Annex E/2 42
110 Change in SEL Cluster expenditure at local Trusts 2012/ /15 Annex E/3 43
111 Change in SEL Cluster expenditure at local Trusts 2012/ /15 Annex E/4 Annex E/5 44
112 Change in SEL Cluster expenditure at local Trusts 2012/ /15 Change in SEL Cluster expenditure at local Trusts 2012/ /15 Annex E/6 45
113 46
114 Annex F SEL Cluster - CSP 2012/ /15 QIPP Savings by SEL Strategic Programme Values '000 - SAVINGS 2012/13 Plan Pre RAG Activity 2013/14 Plan Pre RAG Activity ACTIVITY: (note: Positive = reduction in activity) 2014/15 Plan Pre RAG Activity 2012/13 Plan post RAG activity 2013/14 Plan post RAG activity PCT CSP Strategic Programme 2012/13 Plan Pre RAG 2013/14 Plan Pre RAG 2014/15 Plan Pre RAG 2012/13 Plan post RAG 2013/14 Plan Post RAG 2014/15 Plan post RAG BEXLEY Integrated Care 1,872 2,384 1,384 1,622 1, , , London-wide Priorities , , Other Savings/ Investments 4, , , Productive Care 8,856 7,406 4,937 5,153 3,703 2,469 21,012 21,012 18,006 10,506 10,506 9,003 BEXLEY Total 14,841 9,790 6,321 10,778 5,145 3,161 97,525 21,740 18,734 87,881 10,870 9,367 BROMLEY Integrated Care 3,196 3,091 2,341 2,289 1,670 1,170 12,736 1,388 1,388 8, London-wide Priorities Other Savings/ Investments Productive Care 3,055 2,939 2,511 1,658 1,469 1,256 16,394 16,374 10,916 8,207 8,187 5,458 Staying Healthy BROMLEY Total 7,535 6,029 4,852 4,710 3,140 2,426 29,364 17,762 12,304 17,268 8,881 6,152 GREENWICH Integrated Care 6,640 3,031 1,579 4,490 1, ,289 1, , Other Savings/ Investments Productive Care 10,940 7,787 3,922 7,333 5,693 2,526 20,545 18,185 11,997 10,727 9,481 6,193 Staying Healthy GREENWICH Total 18,176 11,231 6,028 12,419 7,817 3,911 56,042 19,368 12,797 35,172 10,219 6,625 LAMBETH Integrated Care 4,494 3,994 2,501 2,900 2,511 1,322 16,831 8,933 8,911 12,334 6,597 6,581 Other Savings/ Investments Productive Care 12,309 6,572 4,195 8,684 5,051 3,314 27,007 20,819 20,819 20,230 15,614 15,614 LAMBETH Total 17,584 10,566 6,696 11,974 7,562 4,635 43,837 29,752 29,730 32,564 22,211 22,195 LEWISHAM Integrated Care 3,113 3,538 3,051 1,860 2,116 1,873 4,617 11,645 11,651 3,463 8,305 8,309 Other Savings/ Investments Productive Care 9,000 4,216 2,714 6,334 3,162 2,036 23,505 15,314 15,289 17,629 11,485 11,466 LEWISHAM Total 12,613 7,754 5,765 8,469 5,278 3,908 28,122 26,959 26,940 21,092 19,790 19,776 SOUTHWARK Integrated Care 1,741 2,141 1, , ,188 8,104 2,690 11,008 5,710 1,650 Other Savings/ Investments 1, , Productive Care 10,718 5,057 4,056 8,696 4,924 3,923 33,202 22,159 22,142 33,085 22,089 22,072 SOUTHWARK Total 14,302 7,698 5,735 11,043 6,636 4,788 48,390 30,264 24,832 44,093 27,800 23,722 Grand Total 85,052 53,067 35,396 59,393 35,577 22, , , , ,070 99,771 87, /15 Plan post RAG activity 47

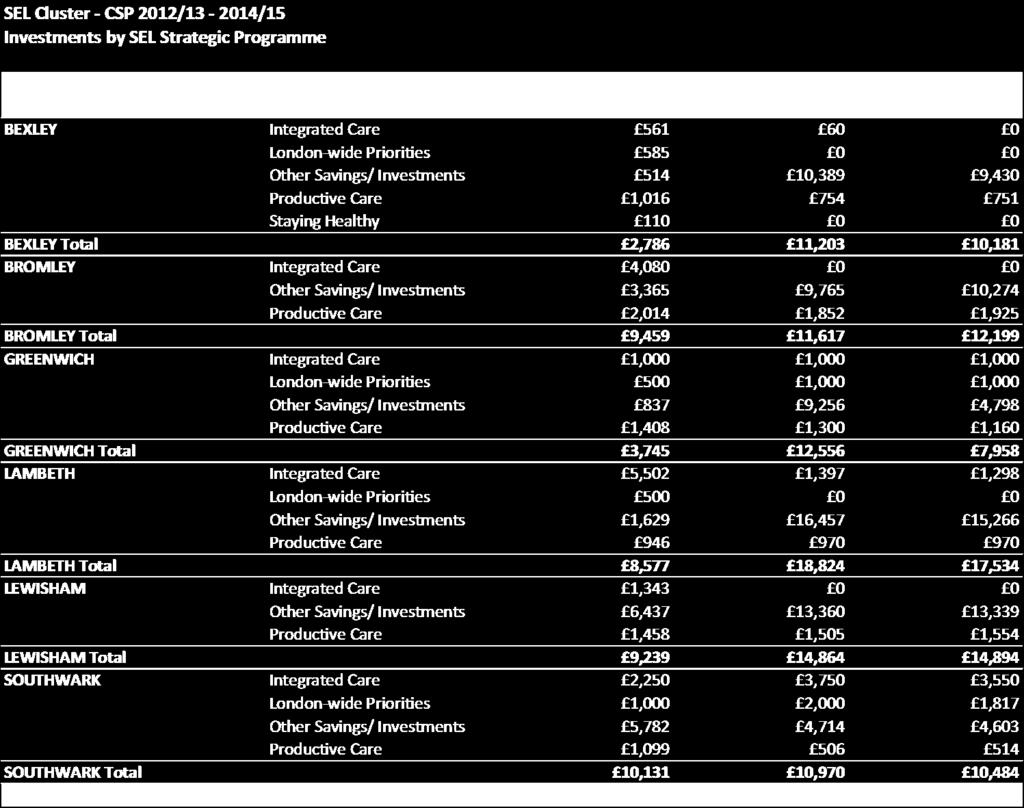
115 Annex G 48
116 Change in Financial Assumptions CSP to 2012/13 Operating Plans to reflect Operating Framework Guidance Annex H Bexley Bromley Greenwich Lambeth Southwark Lewisham SEL Total '000 '000 '000 '000 '000 '000 '000 CSP Planned Surplus 3,488 5,020 4,710 7,000 5,857 5,492 31,568 Changes - CSP to Operating Plan: Income Changes - Increase/ (decrease) Recurrent Uplift 2,032 3,913 3,581 4,887 3,085 3,618 21,116 Prior Year Surplus brought forward 2, ,245 Total Income Changes 4,277 3,913 3,581 4,887 3,085 3,618 23,361 Expenditure - Increase/ (decrease) Full year effect of 2011/12 outturn (239) (612) (2,227) 4,576 1,566 3,118 6,182 Net Generic Uplifts Tariff and generic uplifts (886) (1,119) (961) (1,398) (1,165) (1,118) (6,648) Efficiency with Tariff 125 (47) (64) (9) (83) (110) (189) Net Tariff/ Generic Uplift (762) (1,166) (1,025) (1,407) (1,248) (1,228) (6,837) Population & Incidence Growth demographic Growth (14) 9 (5) (6) (2) 15 (3) Non-demographic growth (53) Total Population & Incidence Growth (67) /13 Investment Proposals and cost pressures 863 5,657 4,298 4,979 2,765 2,340 20,902 QIPP Savings Initiatives 4, ,527 (3,282) 0 (681) 3,027 Total Expenditure 4,257 3,913 3,581 4,887 3,085 3,591 23,315 Operating Plan Surplus 3,508 5,020 4,710 7,000 5,857 5,519 31,613 Planned Surplus 3,508 5,020 4,710 7,000 5,857 5,518 31,614 Remaining Financial Gap
117 Appendix D: South East London Communications and Engagement Plan COMMISSIONING STRATEGY PLAN Communications and Engagement 2012/2014 Strategy Paradoxically, the most important first task in creating a successful quality and cost improvement strategy is not to identify the size of the challenge or to work out which areas of service delivery offer the greatest opportunity for change The framing for QIPP should not just be about cost and quality improvement. We should be thinking deeply about the meaning of what we are asking people to do in an era of QIPP. Fundamentally, it should be about the higher purpose of the NHS and the calling that each of us has to serve that purpose. NHS Institute for Innovation and Improvement This plan sets out the communications and engagement activity required to support the delivery of the south east London Quality Innovation and Improvement Plan (QIPP). 1. Quality and improvement in south east London 1.1. The case for change nationally was set out in the Government s white paper, Equity and Excellence, Liberating the NHS (2010). The challenges presented in the white paper for the NHS are set firmly in the need to provide continuous improvement within the context of achieving savings and at the same time finding new ways to meet the healthcare needs of local people In south east London demand for services are increasing. All of the PCTs and Care Trusts in South East London face continuing growth in demand for services, driven by population growth, demographic changes and expansion of available health technologies that assist with health problems There are major inequalities in health and in health services in south east London and within individual boroughs. We have some of the best health provision in the country and some of the greatest levels of challenge. Whilst there are some very active patient representative groups in the cluster, engagement activities do not always reflect all sections of the community Shadow GP clinical commissioning groups differ too in how well their arrangements for communication and engagement work locally and indeed in their own level of development as commissioners. While GP-led commissioning has been accepted as being the way forward, is still being negotiated in some parts of the Cluster and during this period of transition, it is important to provide clarity both on the expectations for communication and engagement and output. Page 50
118 1.5. The expectation of Government is that quality is best delivered by focusing on outcomes giving real power to patients, and devolving power and accountability to the frontline. However the degree of change fatigue for many staff, patients and the public mean that there is a difficult barrier to cross when we ask people to think differently and urge them to try out new ideas. However, there are many people across the cluster who recognise that in an uncertain future the best chance of a more secure future which goes far beyond survival, is to deliver a better patient experience. 2. Communication and engagement challenges 2.1. The direction and purpose of the NHS is a subject of almost continuous public and political debate. At the heart of the healthcare system are the patient and the public whose healthcare needs drive the commissioning intentions of the CCGs. Change is no longer cyclical but continuous, a situation that means not more communication and engagement but better, more targeted, timely communication and more purposeful and meaningful engagement The extent of collaboration required to create a sustainable health economy for local people in south east London presents a challenge that is being met in many of joint plans and initiatives described in the commissioning strategy plan The on-going service changes required to keep the focus on individual patient needs and seek the most cost-efficient options for services, are seen by many as mutually exclusive. Yet, this is the balance that commissioners wish to strike, and it is a core message for this strategy. This strategy acknowledges the extent of this challenge and specifically: 51 Public and patient perception that the changes to the NHS are driven solely by the need to achieve savings as a result innovation is simply a way to disguise reductions in services. This view may also be shared among those working in healthcare. Regular, often negative, coverage of the NHS in the national media could make it difficult to encourage constructive debate about the services that do work really well in south east London. In supporting the CCGs in their aspiration to enable more local people to stay healthy and experience joined-up care that meets their individual health needs in the most effective way, it is important to acknowledge the particular challenge this poses with regard to communication and engagement. There are significant differences in population and in expectations. Engagement listening and responding to people is an important way of uncovering, and often addressing, individual needs. However, engagement must be framed within the context of available resources and need. South east London has a number of vocal and active locally-based groups working to oppose the health reform bill. While it is unlikely that any centrally or locally
119 delivered strategy will substantially alter the views of those fundamentally opposed to the changes, this strategy acknowledges their views as valid, and proposes a commitment to offer full explanations of why particular decisions have been made or are being proposed. There is support for proactive engagement and communications from the central public affairs team, which can provide strategic advice and guidance to individual boroughs. Delivering the activities outlined in the action plan (Appendix 2.) will depend upon: the level of available resources; a co-ordinated, responsive approach; and the full commitment of commissioners and staff across the cluster to clear, open and timely communication. 3. Overarching communication and engagement objectives 3.1. This strategy aims: To support clinical commissioners in ensuring that stakeholders are actively involved in making and executing decisions that affect how services are designed and delivered; and advise on how to communicate their decisions to the patients and public. Ensure there is sufficient planned and monitored communications and engagement activity to support delivery of the south east London CSP. To communicate clearly to all identified stakeholders, a robust case for change. To communicate the outcomes of the QIPP Plan to staff, providers and the public. To ensure that communication to all stakeholders is timely, accessible and clear. To ensure there is on-going communication and consultation where appropriate with stakeholders. To demonstrate that the QIPP will be delivered in a fair and transparent manner. To ensure that the cluster is prepared for any media attention/patient response to the QIPP. Ensure that communications and engagement activities mirror the commitment of commissioners to equality and diversity in commissioning and delivering services. To work across the sector with commissioners, partners, patients and the public These objectives will be achieved by: Effectively co-ordinating communication activities; carrying out on-going medium and long-term horizon-scanning of issues that may affect the patient experience; working closely with local community and voluntary groups to ensure that the views and experiences of patients and the public are sought and accurately reflected in subsequent communications; By asking commissioners what they want from their communications and engagement support and staying focused on providing value for money solutions that meet those needs. 52
120 4. Key messages 4.1. Some of the messages in this plan may need to be modified over time to reflect progress and any changes to the plans. QIPP and NHS reform: national messages Delivering innovative, cost-effective services Using existing resources wisely The government believes GPs are best placed to make decisions about how money should be spent locally Tough choices must be made savings will be re-invested in patient care by supporting front line staff, funding innovative treatments and giving patients more choice. QIPP: local messages are underpinned by a focus upon quality and outcomes The NHS has to make financial savings in order to respond to the increasing demands for services, new technologies and advances in treatment. There is no additional funding available for the NHS investments have to be made within the current resources. The QIPP programme is about ensuring that NHS funds are used to the very best possible effect to bring maximum benefit to the patient. We have engaged with GPs, patients and other stakeholders to develop plans which set out how savings will be made taking into account borough and cluster populations. It is important that we continue to work closely with GPs and clinicians as they will be key to the successful implementation of this plan. Over the next four to five years, the local NHS has to save in order to invest and those savings made will only be reinvested in those areas identified in our goals i.e. COPD (Chronic obstructive pulmonary disease), cancer, long-term care, areas covered in the clinical pathway redesigns etc. 5. Stakeholders 5.1. Our stakeholders are important to the successful delivery of the QIPP. A number of them will not only receive information about the plan and take part in engagement activities, they will also be the communicators, delivering the messages outlined above, and leading engagement work to inform and involve local people and interested parties. To do this well, they will need accurate information; the confidence to take and answer questions; and mechanisms to feedback responses promptly to stakeholders Identifying the role of each stakeholder and where they are in terms of their understanding and commitment to the QIPP is crucial if we are to ensure that the limited resources available are used to best effect. Stakeholder mapping allows us to see firstly if we have correctly identified all the people we need to talk with and listen to, 53
121 and ensure that we have appropriate methods/opportunities to engage with them. It will also help us to be clear about what we are saying and why Who are the key stakeholders? An indicative list of key stakeholders is listed below, however, a stakeholder mapping exercise will be carried out with cluster engagement leads (Appendix 2.) to produce a more detailed map. Patients, carers and public Clinical commissioners/clinicians delivering services in Lewisham (hospital, primary care, community, mental health etc). Staff LINks/HealthWatch/Third sector Local Authority/Health Overview Scrutiny panels Partners/Alliance/Sector NHS London Media Stakeholder mapping Meet their needs (try to increase level of interest and engage on interest areas) GPs Clinicians delivering services (i.e. hospital, primary care, community, mental health etc). Local Authorities/Director s of Public Health Councillors/Lead Members/OSC s LINks/HealthWatch Community and voluntary sector providers Key Player able to communicate/engage other groups (focus efforts on this group, involve them in decision making groups and engage and consult regularly) Clinical commissioners LMC s Trust Board members NHS London Least important (inform via general communication newsletters, website etc) Local media Show consideration (involve in low risk areas and keep informed and consult on interest area. Potential supporter/ambassador) Patients, carers and public Cluster & BSU staff Patient support groups & networks Community and voluntary sector organisations Interest 6. Resources 54
122 6.1. Appropriate resources will need to be identified to deliver this strategy. Wherever possible opportunities to share resources will be investigated particularly with regard to consultation and events. 7. Tools and systems 7.1. Different audience groups present their own communication challenges. There will need to be a number of tools and systems in place to enable effective communication and engagement with the range of audience groups The following is a list of the communication and engagement tools available. Additional ones can be created depending on budget and the services in question. We will consult with stakeholders to decide upon the most appropriate methods of informing and engaging them. information/deliberative Events organisational newsletters and bulletins including briefing systems etc in PCT and other NHS organisations and partners and bespoke electronic bulletins and updates existing stakeholder meetings partner and cluster websites meetings and face to face briefings with staff, patients and stakeholders newspaper/council publications features/advertising direct mail news releases and media briefings road shows and exhibitions Contact people on the established PPI Database LINks contacts and newsletter Community Development Workers 8. Action Plan 8.1. Attached at Appendix 1 is the communications and engagement implementation plan for the QIPP. This maps out the activity required linked to timescales, resources and risks. 9. Evaluation 9.1. Detailed evaluation measures will be identified with cluster engagement leads and progress monitored against them, and will include patient surveys and analysis of feedback forms. We expect that the cluster stakeholder reference group will wish to receive regular updates on the progress of the agreed actions. Such scrutiny is welcomed and will be actively supported. 10. Equality Impact Assessment Review actions against the EIA and ensure this plan reflects the key deliverables in the EIA. This will be tracked once the EIA is completed. 55
123 Appendix 1 Communications and Engagement Implementation Plan for the implementation of the SEL QIPP Plan 1. Ensure there is planned and monitored C&E activity to support delivery of the QIPP. 2. Ensure there are specific C&E action plans for each QIPP initiative in south east London with leads identified. 3. To ensure clinical commissioners are actively involved and engaged in decision making around the savings that need to be made and that the case for change is robust and will stand up to scrutiny. 4. To ensure that all identified savings are assessed against the service variation criteria and appropriate involvement/consultation is undertaken where appropriate. 5. To ensure all relevant stakeholders in the cluster are involved where appropriate and informed about the Case for Change and the savings that need to be made. 6. To communicate the outcomes of the QIPP Plan to staff, providers and the public. 7. To ensure that communication to all stakeholders is timely, accessible and clear. 8. To ensure there is on-going communication and consultation where appropriate with stakeholders. 9. To demonstrate that the QIPP will be delivered in a fair and transparent manner. 10. To ensure that the cluster is prepared for any media attention/patient response to the QIPP. 56
124 Action Plan 2011/2012 Activity required Half-day workshop for Cluster engagement leads: stakeholder mapping evaluation Timescale/ Milestone Quarter /13 Lead/ Resource required Stakeholder Engagement leads Cluster-wide online communications and engagement stakeholder survey Quarter /13 Stakeholder engagement cluster lead Update of stakeholder database Quarter /13 Stakeholder engagement cluster lead Presentation to public sector communication, marketing and engagement leads to discuss agreement of protocols covering joint-working Quarter /13 Director of Corporate Affairs Draft action plan for 2012/13 agreed with BSUs Quarter /13 Director of Corporate Affairs/ Stakeholder engagement cluster lead 57

125 Cluster Name: South East London Operating Plan 2012/13
126 Cluster name: South East London DRAFT Cluster Operating Plan Version: SEL Master Key Cluster Contacts: Name Title Telephone Executive Lead for operating planning: Finance: Penny Emerit Director of Delivery Richard Chapman Acting Director of Finance Workforce: Ana Selby Director of Workforce Performance: Penny Emerit Director of Delivery Sean Morgan Director of Knowledge Management & Performance Improvement Informatics: Commissioning Development: Leroy Adamson-Parks Head of ICT Gill Galliano Executive Director of Development Engagement/ Sign off: Supporting statement outlining process of consultation and engagement with stakeholders in development of Operating Plan for NHS South East London (SEL) is a partnership of Bromley, Greenwich, Lambeth, Lewisham and Southwark Primary Care Trusts and Bexley Care Trust. The Operating Plan for 2012/13 builds on the work undertaken in the development of Better for You the NHS SEL Cluster Commissioning Strategy Plan for 2012/ /15 which was developed through: Engaging systematically with the public, our patients and clinicians across six boroughs to gain insight into local needs, building on public health assessments Maintaining ongoing dialogue with stakeholders, such as Local Government, Local Involvement Networks (LINks), NHS Trusts, independent and third sector organisations, ensuring that plans and their potential impact are anticipated Engaging with the London Specialist Commissioning Group (LSCG) and owners of other pan- London initiatives to ensure alignment of plans Ensuring strong governance and leadership at cluster level and across our pathfinders to pull together coherent and ambitious plans which meet local needs within available resources. Clinical Commissioning Groups were involved in the process of developing commissioning intentions for 12/13and more recently, as BSUs and CCGs have matured, CCGs have developed a focus on local programmes of work, each with clinical leadership. BSUs and CCGs have an established process of engagement with other stakeholders such as Links and the local authority. Patients and the public are represented on local programme boards and shared plans are developed through Health & Well Being 1
127 Boards. There is ongoing engagement with service users and the public on a number of specific issues to gain views and input into service redesign such as Orpington Hospital in Bromley and long term conditions and unplanned care in Lewisham. Clinical Commissioners have also worked together on a number of initiatives to support the planning process. Each BSU has constructive relationships with their providers and there are effective commissioning and contractual processes that underpin these relationships. Provider organisations are represented on local programme boards which have responsibility for developing both the CSP and Operating Plans and specific sessions have been run to share the QIPP plans with providers. The draft NHS South East London Operating Plan has been presented to each CCG in February or March alongside initial drafts of local Operating Plans which develop the borough specific priorities for 12/13, aligned to the cluster operating plan. CCGs will be held accountable for delivery of the local plan under full delegation in 12/13. Final versions of both the NHS South East London plan and borough specific plans will be considered by the CCGs in public. Cluster Medical Director Cluster Director of Nursing Cluster CEO Emerging CCG Leads Enter signature here Enter signature here Andrew Kenworthy Bexley Bromley Greenwich Lambeth Lewisham Southwark Section One: Strategic Overview Reproduce from your strategic plans for 2012/15 the key strategic priorities and the main initiatives you have planned for 2012/13 to deliver these. Please indicate whether and how these will impact on performance against the National Performance Measures as outlined in the Operating Framework 2012/13 and other performance priorities: Better for You Our vision for 2015 More people In South East London will stay healthy, and every patient will experience joined-up healthcare which meets their needs in the most effective way. Our strategic goals In South East London we commission physical and mental healthcare across home, primary, community and acute settings from a variety of NHS, voluntary and independent sector providers. In every case, our ambition is to meet the same strategic goals, that: 1. In every contact with the NHS and local public service partners, people are encouraged and enabled to positively manage their own health, in partnership with health professionals and their carers. 2. Patients experience the NHS as a joined-up personalised service, rather than a disconnected set of services they are required to navigate. 3. Patients are treated with dignity and the respect due to them at all times. 4. Clinical decision-making and healthcare delivery is in line with evidence-based best practice and takes account of value for money. 5. The logistics of healthcare delivery, within and across different care settings, are designed to meet patient needs, whether long-term or acute, in the most effective way. More effective clinical decision-making and healthcare delivery logistics will drive a significant increase in productivity and enable the health and social care system in South East London to manage increasing 2
128 levels of demand without an equivalent increase in resources. We have set an ambitious target for our health economy of productivity improvement to the value of 117m over four years. Through monitoring execution of plan and the achievement of our strategic goals, we will be able to ensure and demonstrate to our population that we have been able to make savings without compromising our ambition, or patients expectations, for care quality. Overview of case for change Demands are increasing on the healthcare system in South East London due to a combination of our changing and growing population, worsening health risk factors and increased identified need. We know that too many of our patients are dissatisfied with their healthcare experience, and there are many examples where performance of our NHS providers and the health outcomes that we are achieving fall short of our expectations. Economically, the demand for, and costs of healthcare are both rising at a rate than our income, creating a position where doing the same things as before is not an option. We therefore need to achieve step changes in the way in which healthcare is delivered, the outcomes that we achieve and create the circumstances to ensure that our healthcare system is effective and clinically financially sustainable. Our strategic approach has been to: Engage systematically with the public, our patients and clinicians across our six boroughs to gain qualitative insight into local needs, building on local Joint Strategic Needs Assessments Maintain on-going dialogue with stakeholders, such as Local Government, Local Involvement Networks (LINks), NHS Trusts, independent and third sector organisations, in a variety of fora, ensuring that CSP plans and their potential impact are anticipated Engage with the London Specialist Commissioning Group (LSCG) and leaders of other pan-london initiatives to ensure alignment of plans Ensure strong governance and leadership at cluster level and across pathfinders to pull together coherent and ambitious plans which meet local needs within available resources. Priorities and Opportunities The case for change above demonstrates that a significant step change in performance of the SEL health system will be required to realise the vision and strategic goals of the cluster, our clinical leaders and borough partners. Our plan is to deliver our vision and strategic goals through the pursuit of four priorities: i. Integrated care ii. Productive care iii. Staying Healthy iv. London-wide programmes Primary Care High quality primary care underpins the successful delivery of all of our plans for out of hospital care and primary and community services transformation, being the foundation of each care pathway (e.g. safe care, right care, end of life care, urgent and emergency care, long term conditions) and our vision for integrated care networks. Our ambition is to achieve continuous improvements in quality, productivity, patient experience and health outcomes of primary care and produce a legacy for our Pathfinders to build upon. The Cluster is fully engaged and supportive of the NHSL Primary Care Transformation Programme. To drive efficiency and productivity improvements we have completed reviews of PMS contracts in four boroughs and have commenced PMS reviews in Lambeth and Southwark with the aim of commissioning services to match the identified health needs of the population through a core offering to be delivered by each practice. There is a strong need for greater transparency of performance information. Using the London-wide List Maintenance policy, we will ensure that all practices have accurate and validated registered lists. This will enable monitoring of practices actual performance regarding, for example, immunisation levels, screening coverage and prevalence levels of long term conditions. This information will feed into the pan- London dashboard for quality outcomes and contract compliance that we will utilise to support improved 3
129 performance in 2012/13. We will continuously monitor contract performance and quality of services delivered. The performance framework reviews on infection control, health and safety, business continuity, child protection, employment checks and clinical governance domains. We have a track record of, and will continue to, proactively managing instances of poor performance in south east London, including the issue of breach and remedial notices as required. Opportunities are being taken on retirement of practitioners to review the current provision and to agree new arrangements such as list dispersal. We will roll out EMIS Web (a GP practice information system) to 138 practices across Lambeth, Southwark, Lewisham and Greenwich which will allow the delivery of the electronic transfer of patient records between GP practices, the uploading of the summary care record (SCR) and the next iteration of the electronic prescription service (EPS2). EPS2 will allow patients to nominate their pharmacy for prescription pickup and assist practices in reducing repeat prescription workload. Bexley practices have already completed their deployments of SCR and EPS2 enabling their patients to benefit from having their summary care records uploaded to the spine as well as having their repeat prescriptions sent electronically to their chosen pharmacists. Unplanned care in SEL London is provided through a complex network of services, including primary and secondary care services. We have an opportunity to build upon existing services and developments to ensure quality and value for money. Through our priorities (see section 6) We aim to: Understand the current issues regarding the delivery of unplanned care both in and out of hours Understand what is driving demand Review how services are commissioned and develop best practice consistent approaches to support future contractual arrangements, where appropriate Understand future changes and their impact, including but not exclusive to the implementation of 111 Map potential duplication in provision of unscheduled care services within and across boroughs and make recommendations for cost effective commissioning of services to future CCGs and the NHS National Commissioning Board. Integrated Care Integrated care enables improved individualised care to people with long term conditions and to frequent users of services by addressing their specific care needs using a case managed approach. By undertaking population risk stratification to predict need we can respond to provide evidence-based care on a proactive and planned basis for the individual. We will develop greater integration between primary, community, acute hospital and social care in order to improve clinical outcomes, care planning and patient satisfaction through seamless patient and care pathways. We see integrated care systems as key to unlocking significant improvements in patient experience and satisfaction. The quality of care will rise. Patients will experience better healthcare as close as possible to their home and be better equipped to self-manage their conditions. Integrated care, in areas such as diabetes and the care of the elderly, offer significant improvements to clinical outcomes and efficiency. The core components of integrated care systems across south east London are: Maintaining robust patient registers Patient risk stratification to focus on patients at risk of developing illness Common clinical protocols applied along patient pathways by all providers Defined care packages, tailored to the needs of each individual Care that is proactively planned, co-ordinated and delivered A multi-disciplinary team approach across health and social care Case conferences for patients with complex needs Continuous review of performance of and by multi-disciplinary teams with peer support. High quality primary care underpins our plans for Integrated Care systems. We believe that integrated care will deliver better care closer to home. We recognise that there is not a one size fits all solution and we are therefore developing and testing different models of models of integrated care across different populations and geographies: 4
130 Lambeth ad Southwark Lewisham Bexley, Bromley and Greenwich. Productive Care We believe that patients should be treated in hospital where necessary and at home or closer to home where possible. The majority of patients are best cared for in the community, providing better access to care closer to home and avoiding unnecessary visits to hospitals for routine care. Patients with long term conditions such as COPD and diabetes particularly benefit from a more localised model for routine healthcare. A more localised model of care closer to home also enables patients and carers to take greater control over their care and self-management of their conditions. Currently, south east London has a high level of emergency hospital admissions which could be managed in primary and community care, particularly for patients with diabetes and respiratory illnesses. Primary care services need to achieve greater economies of scale to ensure better access for patients, for example improving access to urgent care services through GP-led networks, particularly out of hours. Primary care services can also support moving care out of hospital to more cost effective settings closer to home, for example day-case surgery, diagnostics and outpatient services. Localising routine medical services with primary care would enable patients to access a wider range of services closer to home, under one roof and would enable providers to offer more convenient services such as better out of hours access. Staying Healthy The main causes of premature death are common across south east London. By creating opportunities for people to choose and maintain healthy lifestyles we will make major contributions to increasing life expectancy, reducing health inequalities, reducing hospital admissions and preventing and delaying the development of long term conditions. Smoking is a leading risk factor for the top causes of premature death for our population (CVD, some cancers, respiratory diseases). Smoking contributes to other conditions such as osteoporosis, cataracts, childhood infections and digestive disorders. Physical inactivity is a leading risk factor for the main causes of premature death for our population (CVD, cancers, and respiratory diseases. Childhood obesity rates are high in south east London. Babies who are not breastfed are much more likely to develop illnesses such as gastroenteritis and respiratory infections requiring hospitalisation as children. In later life they are more likely to develop high blood pressure and cholesterol levels and associated illness. Mothers who do not breastfeed have increased risk of breast and ovarian cancers and may find it difficult to return to pregnancy weight. Too many people die of alcohol related problems in south east London. Alcohol-related problems place a major burden on health services in primary care, A&E, acute and specialist services and also across wider societal areas of crime, accidents, domestic violence and unemployment. London-wide Priorities We recognize the need to adopt different strategies for different populations. Some service changes are better tackled at populations larger than south east London, due to for example the rarity of condition, specialism and complexity of care or the scalability of solutions to common issues. Evidence suggests that centralising the most specialist services so that specialist teams treat higher numbers of patients and develop their skills would improve clinical outcomes and reduce lengths of stay in hospital. For example, complex arterial surgery, e.g. abdominal aortic aneurysm (AAA) repair, has also been shown to produce better outcomes when performed by specialist vascular surgeons. Healthcare practice and technologies change rapidly. Increasingly care can and is being provided at home and closer to home settings, which reduce hospital income. Strategic solutions are required to ensure that hospital services remain viable or are replaced by high quality alternatives. NHS South East London, together with other London PCTs, is driving a series of patient care pathway service redesign programmes to improve the quality, efficiency and productivity of commissioned services. Commissioner Support to Foundation Trust status South East London contains a number of established Foundation Trusts in the form of acute providers, GST and King s, and mental health providers, SLaM and Oxleas. Additionally NHS South East London is 5
131 heavily involved in supporting the Foundation Trust pipeline process for NHS Trusts; SLHT and Lewisham Healthcare. In considering the provider landscape south east London commissioners are live to the fact that South London Healthcare Trust is a highly financially challenged provider. It provides most of the general acute services for Bexley, Bromley and Greenwich patients and receives the majority of its patient income from south east London commissioners. There is consequently a high degree of interdependency between the Trust s financial position and the financial health of the PCTs and future CCGs. Our approach will include commissioner support for the work streams and milestones outlined in the Tripartite Framework agreement which sets out the journey that the Trust has committed to in respect of achieving Foundation Trust status and financial viability. A significant element of that work is internal productivity work to be undertaken within the Trust and the Challenged Trust Board has already supported a significant programme of work exploring the opportunities for such gains. Commissioners will therefore be working alongside other signatories to that agreement to understand the firm time line for delivery of improved cost control and productivity. In addition SE London Commissioners will be driving a clinically led process to design services that meet the identified needs of patients across primary, community and secondary care. Our overall strategy reduces the need for hospital capacity and increasingly delivers integrated care in community and home settings. Our clinical commissioners will explore and agree the service model to be delivered for Bexley and work with the Trust to find solutions to the QMS campus proposals and for the future of the Orpington site. As part of this work we will participate in the planned simulation programme around the future of the Trust in the context of service disposition across a broader Acute Platform. We acknowledge that these are potential areas of cost reduction for the Trust as part of a required capacity reduction programme and as such the business cases for both of these areas and the services required within them must be sound, robust and affordable from both a commissioning perspective and a provider perspective. This is complex work and it is recognised that the business case development requires particular attention and priority. The commissioner view is that focus needs to promptly turn from income generation to capacity and associated cost reduction based on a needs led strategy in favour of a supply led strategy. The combination of financial and organisational issues for SLHT pose considerable risk to the delivery of the south east London commissioning strategy and the financial viability of Bexley, Bromley and Greenwich PCTs and the future CCGs. Lewisham Healthcare is a combined acute and community NHS Trust with a strong track record of close partnership working with local commissioners. Our approach to supporting its ambition to become a Foundation Trust is set within the context of the Tripartite Framework agreement which sets out the journey that the Trust has committed to in respect of achieving Foundation Trust status and associated financial viability. Commissioners are continuing with the significant raft of service redesign work streams already in train in Lewisham and which seek to maximise the benefits of an integrated Trust, such as Lewisham Healthcare. As part of the supporting programme clinical commissioners have successfully worked with Trust partners to bring forward the agreement of the 2012/13 contract. This means that there is a clear robust baseline for moving this work forward and a shared set of priorities for change between the Trust and commissioners. Milestones / Key Actions 1. Integrated Care Case Management LTC Case Management and Admission Avoidance including COPD, MSK, Dermatology, Diabetes 1. Reduction in admissions and high cost attendances (pre HRG4) 2. Improved quality of care for patients 2. Integrated Care Case Management End of Life Care work with local Hospices and Marie Curie to implement the integrated EOLC model of care, including evaluation of the model, tendering, and implementation of best practice pathways. Achievement Date March 2013 Ongoing 6
132 3. Integrated Care Shifting Care Closer to Home March 2013 Pathway Re-design Re-design of pathways including: Cardiology, Anticoagulation, Palliative Care, Minor Oral Surgery, Oxygen Management, Neuro Rehab, Gynaecology 4. Integrated Care Shifting Care Closer to Home Referral Management changes to reduce the number of inappropriate GP initiated referrals to OP, shifting activity from acute setting to community. Reduce variation in GP referrals. April 2012 for first outpatient appointments 5. Integrated Care Shifting Care Closer to Home Intermediate Care re-designing the intermediate care model to rebalance bed provision and community rehabilitation. October Productive Care Primary & Community October 2012 Improve Access to Primary Care Services improved access: working with individual providers and their patient groups to determine appropriate access times matching the population requirements. Developing the scope and capacity of primary care to manage care more effectively in the community. 7. Productive Care Primary & Community PMS Reviews improved efficiency and productivity of Primary Care services through review of the PMS contract. 8. Productive Care Primary & Community Prescribing in Primary Care deliver cost effective prescribing within budget, reduce variation between practices in prescribing spend, improve quality of prescribing. 9. Productive Care Primary & Community Alternative Care Pathways and Delivery Protocols extension of alternative care pathways and re-design delivery protocols so that A&E is not default destination. 10. Productive Care Primary & Community Community Services Integration improved efficiency and productivity of community services to ensure more people can be managed in the community. 11. Productive Care Acute Treatment Access Policy demand management and decommissioning of POLCE. Ensure adherence to South East London Treatment Access Policy for SEL patients by GPs and Trusts. Commenced in December 2011Complete by April 2012 September 2012 Quarter /13 Ongoing Ongoing 12. Productive Care Acute April 2012 OP Follow-up Appointments change in thresholds for outpatient follow-up activity, in contracts negotiated by cluster acute contracting team. 13. Productive Care Acute Medicines Management Initiatives: prescribing enteral feeds, Patient Drug Waste and Direct Supply Dressing. Shared formulary with SLHT, GST, KCH and LHNT for high cost drugs/high risk conditions, new anti-coagulation drugs, challenging PbR excluded drugs, management of the RAG list of drugs. 14. Productive Care Acute Emergency Admissions improve cost effectiveness of care and movement of people into planned streams of care: Lambeth and Southwark: review Virtual Ward pilot and commissioning extension if evidence of impact; work with KHP to improve admitted September 2012 December 2012 Evaluation 1 September
133 emergency pathways and further alternatives to admission based on integrated care pilot All: develop single point of access for community based services via 111; re-commission EoL care 15. Productive Care Acute Acute KPIs and Thresholds: Opportunities to generate productivity and quality improvement. Evaluation 2 December 2012 Mainstream March 2013 December 2012 By April
134 Section Two: London Health Programmes 2.1 Summarise the key outstanding actions that need to be taken in 2012/13 in your cluster to ensure completion of the cardiovascular, stroke and trauma programmes (NB a core set of metrics on these 3 London programmes will be agreed with the clinical networks in advance of 2012/13). The cardiovascular programmes have been focused on improving patient access and management to ensure equal access to specialist services. In the case of cardiac surgery vascular surgery NSTEACS and complex arrhythmia this has involved improvements in local networks, changes to patient pathways and consolidation of services and specialist care on to a single site within the network. The Stroke programme has been focussed on the acute aspect of the pathway for all stroke and TIA patients and is nearing completion. For stroke patients the area of focus is now shifting to improving discharge and rehabilitation services. Cardiovascular and Stroke Milestones specific to South East London are to be developed and included in later versions of the Operating Plan. The major trauma system for London is now fully operational with four Trauma Networks, each consisting of a Major Trauma Centre and a number of Trauma Units. The Major Trauma Centre for SEL is King s College Hospital. Activity is monitored by completion and submission of reports to TARN, (Trauma Audit & Research Network) which is a contractual requirement for all Major Trauma Centres and Trauma Units. The London Trauma Office hosted by the London Specialised Commissioning Group is responsible for developing, implementing and monitoring a performance framework supported by in-year onsite assessments. The performance framework will be managed through the London SCG specialised services contract with the Major Trauma Centre (King s College Hospital). Payment of the quality premium (c 2.5M per Major Trauma Centre to support the additional costs of meeting the higher service and quality standards) is linked to evidencing compliance/achievement with the performance framework and Major Trauma Centre service specification, with payment managed through the London SCG contract. In the priority areas for inclusion in the performance framework will be o Completion of a rehabilitation prescription for each patient o Completion and submission of the TARN data set to TARN for each eligible patient o Specific areas of clinical care as described in the framework The Trauma Office is developing a Performance Framework and from this will be developed milestones specific to South East London. These will be available in a later version of the Operating Plan. Milestones / Key Actions Achievement Date 1. Cardiovascular: All NSTEACS centres will be delivering all A2 quality standards September Cardiovascular: Direct LAS transfers of emergency arrhythmia to centrally commissioned units, that meet the quality care standards for management of emergency on 24/7 basis 3. Cardiovascular: All devices and EP/ablations procedures are being delivered at units that meet the devices and EP/ablations quality standards 4. Cardiovascular: Non-emergency mitral valve operations will only be undertaken cardiac surgeons with a specialist interest and training in mitral valve surgery. All units and surgeons will provide audit data to demonstrate they meet the quality standards for care delivery 5. Cardiovascular: Complex arterial vascular surgery centralised on to designated site that meets all commissioning standards for 2011/12 6. Cardiovascular: Improvements have been made to the cardiac surgery, vascular surgery, NSTEACS and complex arrhythmia local networks, changes to patient pathways and consolidation of services and specialist care on to a single site within the network 7. Stroke: Systematic assessment process against all the standards set out in London Stroke Tariff completed November 2012 April 2012 through to March 2013 March 2013 June 2012 April 2012 April
135 8. Stroke: Annual assessment process for stroke introduced with regular April 2012 monitoring of standards via SINAP/SSNAP and visits, where necessary. Completion of SLHT HASU assessment (April 2013) and SU assessments (November 2012) 9. All stroke rehabilitation providers will have met the 5 recommendations set out April 2013 in the Commissioning Support for London Stroke Rehabilitation Guide 10. Stroke: Life after stroke: commissioning guide - progress in implementing recommendations in the Life after stroke: commissioning guide April 2013 Section Three: Performance and Quality 3.1 Summarise performance in 2011/12 against the Headline and Supporting Measures, identifying areas of weak performance which will need to be addressed in 2012/13 During 2011/12 (based on April to October) the Cluster performed well against a number of the acute performance measures, notably: The Cluster is on track to meet the overall Cluster MRSA target CAT A performance in SEL has been consistently at or above the target Every month from April October the Cluster has met the overall cancer targets for: o 2 weeks urgent referrals o 31 day referral to treatment o 31 day subsequent chemotherapy o 62 day referral from screening In addition significant progress has been made in Eliminating Mixed Sex Accommodation in 3 of the 4 acute trusts, and on RTT performance at Lewisham Healthcare Trust During 2011/12 (based on April to October) the Cluster performed well against a number of the non acute performance measures, notably: The Cluster is on track to meet the overall Health Visitor trajectory for 2011/12. Every month from April October the Cluster has met the overall Mental Health targets for: o o The number of new cases of psychosis served by early intervention teams IAPT - Proportion of people with depression referred for (and receiving) psychological therapy. In 2011/12 there have also been some acute areas which have performed below the expected levels: Referral to treatment at South London Healthcare Trust and Guy s & St Thomas FT for admitted patients Diagnostic waits at KCH, SLHT and GST Emergency access including A & E DTA and ambulance handover C Difficile cases at both PCT and acute trust level 62 day urgent referral to treatment at Guy s & St Thomas FT Mixed Sex Accommodation at SLHT VTE at SLHT In 2011/12 there have also been some non acute areas which have performed below the expected levels: Immunisation Breast Feeding Smoking Quitters Cervical Screening Test Results Below is a summary of the key performance challenges faced by the South East London Business Support Units. The key performance challenges have been identified through the quarterly stocktake process between Cluster Directors and all six Clinical Commissioning groups. Joint agenda s focus discussion across all performance areas. Areas of acute performance issues such as RTT, CDIF and A&E waits have been discussed with actions agreed by the Clinical Commissioning Groups which have informed the provider recovery process. The Managing Directors of the Lewisham, Lambeth and Bromley Business Support Units also chair the three Urgent Care Networks (Lewisham, Lambeth and Southwark, Bexley, Bromley and Greenwich). 10
136 Referral to Treatment During 2012/13 both GST and SLHT had waiting list backlogs in a number of specialties, predominately in admitted care. Both Trusts continue to receive support with waiting list management from the Intensive Support Team. For SLHT, the backlog was reduced in year in some specialties, leaving Gynaecology, Bariatric Surgery and Orthopaedics for admitted and Ophthalmology for non admitted as outstanding issues at year end. Through access bids monies additional capacity has been secured, with the intention to reduce the backlog in these specialties through a combination of additional in-house capacity and outsourcing to independent providers. A residual backlog will however remain in 2012/13. For GST, the specialties of Plastics, Orthopaedics, Bariatric Surgery, Oral Surgery and Paediatric Surgical specialties (ENT, orthopaedic, urology) are outstanding issues at year end. The Cluster has worked with the trust to seek alternative providers however this has not yet delivered benefit, and there is insufficient capacity at the trust to clear backlog in these specialties in 2011/12. Late in 2011/12 a backlog issue was identified at Kings College Hospital. The Cluster is working through the implications for performance in 2011/12 and 2012/13 with the trust, including timescales for recovering the position. Diagnostics Waits for endoscopy has been an issue across a number of trusts in 2011/12. Trusts have used a combination of additional in house capacity, mobile units, and outsourcing to independent providers to redress the imbalance between capacity and demand. At GST, there are additionally waiting time issues for urodynamics and sleep studies. The ability to deliver the agreed trajectories have been compromised by emergency pressures in the later months of 2012/13. There will therefore be an outstanding issue in these service areas in 2012/13. Diagnostic waits at SLHT have mostly been resolved. Emergency access Performance against the 4 hour target has varied across acute trusts this financial year. With all trusts except SLHT performing well against this target up until summer. Since that time, however performance has deteriorated at a number of trusts. Access monies have been used to bolster capacity and out of hospital provision in the final quarter of 2011/12. Performance at Queen Elizabeth Hospital has noticeably improved in February Ambulance Handover has been a pressure point at all trusts with the exception of GST most of this financial year. Trusts have developed action plans in conjunction with the LAS to improve electronic capture of handover times using HAS and improve performance against the key performance targets relating to handover. C Difficile KCH, GST and SLHT have all taken part in external independent assessment of their respective infection control policies and procedures, as part of improvement plans to bring performance in line with CDI targets. It should be noted that the CDI objective for GST did not take account of a change in testing regime which was introduced part way through the previous year. 62 Day Cancer Access Target As a tertiary provider, GST has experienced delays with patients being referred from both within and outside the Cancer network. This is one of the key drivers for the performance on this target at GST, however there is still a requirement for the trust to reduce waits for internal referrals. This will improve the overall performance for this target but on its own will not bring performance up to the required standard. The Cancer Network continues to work with referring hospitals within the SEL, to reduce delays. Mixed Sex Accommodation At SLHT there has been a residual number of mixed sex accommodation breaches throughout the year. The issues on the PRUH site experienced earlier in the year have mostly been eliminating with the issues now mostly relating to the Day Surgery unit on the QEH site. The trust has implemented weekend closure on this site, and will continue to operate this measure, emergency pressures permitting. VTE SLHT has implemented a new system for capturing real time information. The trust were previously reporting performance based on one off audits. Initial figures show a coverage rate of approximately 60% in January. The trust will be providing information to Unify on time for the next deadline. Further work is required to agree a recovery trajectory with the cluster to bring performance up to the required standard but the Trust has indicated that it expects levels of 70% in February and 80% in March. 11
137 In 2011/12 there have also been some non acute areas across the borough which have performed below the expected levels: Immunisation Breast Feeding Smoking Quitters Cervical Screening Test Results Immunisation, Breast Feeding, Smoking Quitters and Cervical Screening have all been identified as performance priorities in 2012/13. Actions against objectives, milestones and dates have been detailed in section 3.2 for the relevant BSU s that provide assurance of the Clusters focus in 2012/13, so the information has not been repeated in this section. RTT, A&E and Healthcare Acquired Infections have been an issue for all six BSUs across all provider Trusts across South East London. The issues and challenges relating to these are summarised above, and the ongoing issues and 2012/13 challenges together with accompanying actions and milestones for RTT, A&E and HCAI s have been detailed in section 3.2 and so do not appear in this section. Bexley: The key performance challenges in 11/12 have been RTT, CDIF, A&E waits, Stroke TIA, Smoking quitters and the Learning Disability self assessment framework. For IAPT, there has been a low number of those referred receiving treatment due to the recent establishment of the service and there is ongoing work to address backlog issues. Smoking quitters has seen performance dip to Red in 11/12 and this is due to the particularly strong performance in 10/11 inflating the trajectory. There continues to be a focus in this area and performance is still above the cluster average. Bexley scored poorly in the LD self assessment framework and subsequently was required to provide an action plan for improvement in LD and autism. The autism plan has been sent to NHSL and the strategy is to be signed off in April. Work on the LD improvement plan has started in February and will be submitted by the end of April Bromley: The key performance challenges in 11/12 have been RTT, CDIF, A&E waits, Diagnostic waits, Mixed Sex Accommodation, Smoking quitters, Health Checks and IAPT. IAPT has been an issue in year although this is a small service that has been ramped up and is now one of the most improved PCTs in country. Health Check performance has been addressed through a GP incentive scheme and filling health check nurse vacancies. Greenwich: The key performance challenges in 11/12 have been RTT, CDIF, A&E waits, Mixed Sex Accommodation, Cancer Waits, Stroke TIA, Maternity Access, Mixed Sex Accommodation, the Learning Disability self assessment framework and IAPT. IAPT has been a similar issue to Bexley in that it is a new service and there needs to be work done to understand the backlog issues. The IAPT trajectory has not been met and the CPA standard has not been achieved either. The Learning Disability improvement plan was submitted to NHS London and improvement against these milestones will be monitored for progress on a weekly basis. Lambeth: The key performance challenges in 11/12 have been RTT, CDIF, Diagnostic Waits and Breastfeeding at 6-8 weeks. There has been significant improvement in the second half of this year in Breastfeeding and actions to continue improvements are included in section 3.2. Lewisham: The key performance challenges in 11/12 have been CDIF, Immunisations, and IAPT. A recovery plan for IAPT was submitted to NHS London and actions such as people moving off sick pay and benefits have been realised. There has also been work between commissioner and provider to improve waiting list management. Although performance is falling short of the trajectory set by NHS London there is a clear understanding of the issues and a robust approach to develop the services in line with the requirements of the Operating Framework. Although Immunisations has been an issue Performance has improved across all indicators in both Quarters 2 and 3 apart from DTaP/IPV/Hib at age 1 although this continues to be the strongest area of performance. Improved communications, work with stakeholders, implementation of a new MMR pathway and engagement with primary schools have all improved performance. Southwark: The key performance challenges in 11/12 have been RTT, CDIF, MRSA, Diagnostic Waits, Smoking quitters, Immunisation and health checks. Southwark is currently bottom of the London league table for 4 week quitters although data quality and capture has improved and performance is expected to 12
138 meet the required targets going forward through the actions addressed in section Summarise the Cluster's performance priorities and challenges for 2012/13: From April 2012, all acute areas will be delegated to the emerging CCGs within South East London. The Cluster has undertaken a risk assessment of the 2012/13 Operating Framework measures attached as an appendix. The risk assessment was based on the latest performance data and the degree of stretch required to achieve the 2012/13 standards, both at individual PCT and Cluster level. The highest risk measures for the Cluster as a whole are: MRSA CDI RTT (admitted and incomplete) Proportion of GP referrals booked using Choose and Book The next highest risk measures are: 62-day Cancer waits Patient experience survey Diagnostic waits A&E waits VTE risk assessment Smoking quitters There are a number of Operating Framework measures which are very high risk for individual organisations but not for the aggregate performance of the Cluster: Proportion of unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) per 100,000 population (2 PCTs) Emergency admissions for acute conditions that should not usually require hospital admission (1 PCT) Mixed sex accommodation (1 acute Trust and 1 PCT) Coverage of NHS Health Checks (1 PCT) % of Patients with access to their medical records (2 PCTs) Bookings to services where named consultant led team was available (1 Trust and 1 other Trust which uses a non-standard field to show named consultants in Choose and Book) The Cluster s priorities and challenges for 2012/13 acute areas in some cases lead on from 2011/12 issues: Referral to Treatment SLHT will have a residual backlog in April The focus will be on reducing this backlog while maximising performance levels in 2012/13. GSTFT s current recovery plan is to eliminate the admitted backlog by quarter 2, 2012/3. As with SLHT, the focus will be on sustaining specialty level monthly performance. Both trusts have made significant improvements in reducing the number of patients on incomplete pathways and will continue to reduce these in 2012/13. Diagnostic waits The 3 local Trusts (SLHT, King s and GST) have made significant inroads in addressing diagnostics backlogs. SLHT latest performance is within the new 1% tolerance and King s expects to achieve this by March. GST has made significant progress in dealing with the endoscopy waits over 6 weeks, and has put in place additional capacity for both paediatric urodynamics and sleep studies although this recently been constrained by emergency pressures over spilling into these beds. The Cluster is working with trusts to establish a suitable level of capacity to manage the increased in workload expected from the Bowel Cancer Awareness Campaign and screening age extension. Emergency Access- SLHT is working closely with the wider health care community to improve appropriate use of emergency services, and maximise the use of community and out of hospital provision. The successful re-tendering of the UCC on the QEH in December 2011, has already resulted in an increase in throughput of the UCC on that site, releasing capacity in the main ED. 13
139 Further work will be needed in 2012/13 to improve urgent care pathways on the QEH site which will assist in reducing the number of Mixed Sex Accommodation breaches at QEH, improve ambulance handover times and reduce 60 minute handover breaches. Similarly on the PRUH site, work is underway to improve throughput at the beginning of the pathway, which in turn would improve the DTA performance and ambulance handover times. The focus in 2012/13 will be to maintain improvement in QEH and deliver step change on the PRUH site. Reducing avoidable emergency admissions is a priority within our commissioning strategy and QIPP plans, underpinned by a commitment to high quality primary care. In addition to improvements in A&E and UCC services our approach is to expand predictive modelling to identify patients at higher risk of requiring urgent care together with disease specific case management. We are also expanding existing services, through diffusion, that have proved successful such as community falls prevention and COPD services, home based care and supporting self care. MRSA and C difficile the 2012/13 objectives are challenging both at acute trust and PCT level (some organisations have an annual trajectory of 1 MRSA bacteraemia). Acute trusts have participated in external independent reviews of policies and procedures to aid implementation of best practice examples from elsewhere. Trajectories for delivering both MRSA and CDI objectives are in place with all BSUs. 62 day urgent referrals to treatment GST has made improvements in the urology pathway earlier in the year and more recently in the pathway for Lower GI, particularly access to colonoscopies through the use of the additional endoscopy capacity on the St Thomas site. Early indications are that this has resulted in improved performance (Oct-Dec 2011). If this level of performance is maintained then this performance threshold should not present an issue in 2012/13. CAT A - key events that could impact upon performance in 2012/13 are as follows: o Olympics separate funding has been agreed with the DH in order to maintain business as usual and includes funding for a expected general rise in activity. o Other large events Queen s Jubilee, Public Demonstrations o Implementation of 111 ambulance activity could potentially rise while new providers bed in. o Further Industrial Action Plans are already underway to mitigate against the risks identified above. In July 2011 the South East London Cluster delegated the responsibility for non acute targets to Bexley and Lambeth Clinical Commissioning. From April 2012, all non acute areas will be delegated to the other Clinical Commissioning Groups within South East London. Smoking Quitters In line with the 2012/13 Operating Framework Smoking Quitters performance measure, this area will be a Cluster priority. All PCT s have struggled with performance to date in 2011/12 and performance will continue to be an issue in 2012/13. Data Quality has been an issue in particular obtaining timely data from providers caused in part by a reduction in resource to chase returns. Moving into 2012/13 there is commitment to train smoking advisors to use data capture system to assist provision of data and performance. There will also be local based marketing campaigns in the local communities. Southwark reduced investment for smoking quitters midway through 2010/11. Although resource has since been increased the proposed trajectory will still be challenging. Bexley and Lambeth have historically performed well and although the trajectories submitted do not meet the sign-off criteria of an increase in performance on 2010/11 they are still above the Cluster average, in terms of the rate of quitters per 100,000 population. A request for approval of the trajectories has been made to NHS London. Health Checks - In line with the 2012/13 Operating Framework this area will be a priority for the Cluster. Southwark is currently behind the rest of the cluster on establishing the NHS Health Checks programme and is currently implementing an action plan to extend the programme across the whole borough during the remainder of the year, building on the learning from the pilot phase and also lessons on what has worked elsewhere. All Boroughs will be achieving the required performance from quarter /13 apart from Southwark which will ramp up performance from quarter 3 sufficiently to hit the 20% trajectory by the end of the year. 14
140 Immunisation The Clusters priority in 2012/13 will be to improve performance in immunising children under the age of 5 years. In particular, Lewisham PCT has the lowest immunisation rate across all indicators, especially for children at 5 years of age where the rate is significantly below the target as well as the London and sector average. Several actions are underway and will be progressed in 2012/13. The Immunisations Strategy Group has been re-organised with amended Terms of Reference and is reviewing a proposal for a catch-up programme for older children through Health Visitors. Communication will improve with the publication of a new e- newsletter and the distribution of immunisation schedules to parents of all children under 5. There will be engagement with primary schools and early years providers to implement standardised collection of information on the immunisation status of new entrants, exploring options for offering vaccinations to under-vaccinated children, and identify opportunities to promote immunisation. Furthermore, to improve local coverage, Bexley is taking part in a birthday card scheme project led by Barking and Dagenham as a host borough for the Olympics. The name of the project is Celebrate and Protect and its purpose is to support practices in the area of call and recall to increase the uptake of the pre-school vaccinations including MMR2. Breast Feeding Although performance has improved there is still some way to go in 2012/13. There will be commissioning of a development of a breastfeeding and weaning policy for Lambeth and the BSU has identified capacity within the service improvement team to provide project support to the work. There will be a Focus on improving and making consistent the way practices capture information and forward for entry onto RiO as well as work to improve data flow between GP practices and community services to ensure accurate population of the RiO system. An action plan to take into account learning from partners in Southwark where results for prevalence at 6-8- weeks are considerably higher than Lambeth will be developed and utilised in 2012/13. Cervical Screening Test Results Performance will be challenging across 3 out of the 4 providers in South East London in 2012/13. Performance has been an issue at South London Hospital Trust, Guy s & St Thomas Trust and King s Hospital. Actions have already been taken with SLHT moving letters sent out second class to first class to hit the 14 day turnaround target. Improvements are being made to the lab and a concerted effort to improve the Lab Information technology systems is planned. Guy s & St Thomas Trust has acknowledged that it has been understaffed in the laboratories and has provided a commitment to staff up to sufficient levels to improve performance above the target. King s Hospital believe that they do not have a performance issue and believe that validation of the numbers will reflect good performance so the initial work with the trust will be to establish an accurate performance position. Bowel Screening - The bowel cancer national awareness which started on the 28th January poses a risk to performance in 2012/13 across the cluster as projected demand increases. Planning with the Acute Trusts to increase capacity has commenced and performance leads will continue to work with the Cancer Screening Lead for South East London and the South East London Cancer Network who are concentrating on the age awareness and national campaign in Bowel Screening. Work streams have been identified and are currently being worked through and the recently formed South East London Cancer Screening Board will be reviewing performance and progress. Please note that the following acute milestones are subject to final contract negotiation. Milestones / Key Actions Achievement Date 1. HCAI CDI and MRSA Objectives to be delivered by all BSUs and trusts Mar RTT Delivery of performance targets for: - specialty level admitted at GST - specialty level non- admitted at GST - incompletes at GST - specialty level admitted at KCH - specialty level non- admitted at KCH - incompletes at KCH - specialty level admitted at SLHT - specialty level non- admitted at SLHT - incompletes at SLHT Sep-12 Apr-12 Sep-12 TBC TBC TBC Jun-12 Jun-12 Jun-12 15
141 - All RTT at LHT Apr Delivery of diagnostic performance requirements at all trusts Jun Emergency access - 4 hour DTA target delivery - Reduction in ambulance handover breaches Jun-12 Apr Day Cancer access at GST Jun Declaration for Eliminating Mixed Sex Accommodation Compliance at SLHT Apr Delivery of VTE target at SLHT Jun Health Checks Required performance to be delivered by Bexley, Bromley, Greenwich, Lambeth and Lewisham. Quarter 1 9. Health Checks Required performance to be delivered by Southwark. Quarter Smoking Quitters Required performance to be delivered by Bromley, Greenwich and Lewisham. 11. Smoking Quitters Required Annual performance to be delivered by Southwark. Quarter 1 Quarter 4 16
142 Section Four: Priority areas Priority areas To be inserted by NHSL once Op Framework is out Health visitors/family Nurse Partnerships DH Requirement Clusters to work towards delivering provider-based No 2012/13 trajectories due to be issued by NHSL w/c 5 th December. This is in line with the Government commitment of an additional 4200 by April Maintain existing delivery and continue expansion of the Family Nurse Partnership programme in line with the Government commitment to double capacity to 13,000 places by April (Section 2.13 of Operating Framework) Delegation to CCGs (yes/no)? Actions required to maintain or achieve requirement. Please include key risks and mitigations. All cluster have service specification in place for health visiting 2012/13 and this includes health child programme. Work is on-going to improve the HV service and numbers by 2015 and align these programmes with provider plans All Trusts are on line with trajectory to increase health visitors to 2012/13 number and investment requirements. The required FTE staff are funded and in contracts for 2012 /13. Achievement Date Olympic- Paralympic Games-time delivery Deliver business as usual performance levels, whilst meeting any increase in demand associated with the Games ( Games Effect ) at Games-time. Meet the bid commitments by providing LOCOG with the necessary ambulance and paramedic resources at all LOCOG Events and through the Designated Hospitals (Non-designated hospitals if clinically appropriate) providing free healthcare for the accredited members of the Games Family. Provide appropriate contingency for health resilience at Games Time in compliance with DH guidance as part of the contribution to the Olympic Security and Safety Programme. A comprehensive NHS Games Planning toolkit and reference pack has been produced by NHS London, this can be accessed at: games. Games time is between the 9 th of July 2012 and the 12 th September No A pan Cluster Olympics and Paralympics coordinating group, chaired by the deputy CEO, was established in Summer This reports to the Senior Management Team and to the Cluster Board. The approach is to focus on borough working with pan-sel co-ordination. This group recognises that it is the Cluster s role to co-ordinate a system response to Games time planning across SE London and it is working to the requirements and timescales of the of the London wide games time delivery group and overseeing the delivery of a comprehensive project plan with six priority work streams :- Emergency planning and response Human resources and staffing Communications and engagement Readiness of Acute Hospital services Readiness of Primary, community and non acute hospital services Delivering the Health Legacy 17
143 The key risks identified that we are working to mitigate are :- Transportation: Ensuring Staff in Cluster and NHS providers can get to work/manage their work remotely etc Workforce: Ensuring staff leave properly planned, that staff are prepared to minimise disruption and that all guidance on volunteering followed Emergency response: Ensuring 101% robust and fit for purpose with clarity of communications between NHS bodies Greenwich: Ensuring we can manage the pinch point in Greenwich where many significant Olympics events are being held Transformation: Ensuring we can handle an event of this scale whilst also undergoing very significant multi dimensional organisational change with potential for key staff to move on before and during event. It is important to note that, as we aim to be 'games ready' by April 2012, these workstreams will be complete and risks mitigated prior to the commencement of this operating plan period [progress in 2011/12 is being reported to the London wide Olympics delivery group and presented to SE London Cluster Public Board in January 2012 and presented to the SE London Health Council in March 2012] Key forward milestones for 2012/13:- April 27th 2012 : To undertake a assurance process across the Cluster in respect of the 'games readiness' across Acute Trusts, Mental Health Trusts, Primary care Providers and other Providers of NHS services in SE London. The domains identified in the NHS London assurance template will all be comprehensively and 18
144 evidenced. May 2012 : To finalise arrangements for games time reporting [once confirmation received from DH and NHS L of their requirements] and to train all Cluster 'On call' Directors so that they can enact this process. May 2012 :- To finalise arrangements for Pan Cluster communications and reporting during this period e.g. daily teleconferences [once confirmation received from DH and NHS L of their requirements]and to hold meeting with on call and operational leads in all major organisations to confirm common understanding of processes to be adopted has been achieved. May-June 2012 : To have addressed any areas where gaps in assurance were identified, either from the Cluster led games time assurance undertaken in April and the NHS L led Emergency Planning audit undertaken in February and to have finalized plans for areas where further information has been received since the assurance process. July-August-September 2012: Mobilisation of plans with particular focus on Torch relay through SE London in w/c July 20th, and games periods 27 July - 12th August and 29th August -11th September. Innovation Evidence the PCT Cluster is preparing to implement the Innovation Review. Please outline the key milestones that will ensure implementation of the review with particular reference to compliance with list of high impact innovations and accelerating adoption and diffusion of innovative best practice. End September: Stand down and review learning. A baseline review will be undertaken on the high impact innovations. The expectation is that this will have been completed by March 2012 and that this will inform the Business Plans for 2012/13 of the Pathfinder CCGs and the Cluster as a whole. 19
145 Informatics digitalassets/documents/digitalasset/dh_ pdf Include evidence of consideration of informatics capability and capacity necessary to support the transition. Include a credible proposal for giving patients online access to their medical records, starting with their GP records. Provide an achievable trajectory for providing Summary Care Records by March 2013 to all residents who have been written to. (Section 3.26 of Operating Framework) There are three ICT teams within the South East London Cluster - one covering Bexley, one covering Bromley, and one covering Greenwich, Lambeth, Lewisham and Southwark. A Primary care ICT team within the LSLG ICT service is responsible for overseeing the full rollout of SCR, ensuring that the rollout is undertaking alongside the EMIS Web rollout for EMIS practices. The Cluster will continue to work with EMIS to ensure that its plan to deploy SCR takes into account the proposed accreditation of CSR within EMIS Web. The Cluster is reviewing its informatics capability (including information management, technology and governance) to ensure that it remains fit for purpose for current and emerging organisations. The Cluster Management Board is responsible for considering informatics capacity and capability, and considering proposals for strengthening this key service area. The South London Commissioning Support Service programme will oversee the specific development of a capable informatics service to support emerging Clinical Commissioning Groups. This programme will also oversee the provision of ICT services to a range of other third parties, such as the South East London health Protection Unit, to assure service provision through 2012/13 and beyond. The ICT service will dovetail with Estates services to ensure collaboration and the development of complementary strategies. For Bexley, the capacity and capability to support the transition is identified in both the IT strategy and also within the CSO and proposed BSU structures going forward. The Primary Care Directorate are working with primary care contractors, emerging Clinical 20
146 Commissioning Groups and the LMC to ensure that giving access for patients to their GP records, and moving forwards to their full medical record, is considered a key priority. In Bexley this is being addressed using Health Space. The ICT function is and will continue to engage with clinical system providers to ensure that a) the technical capability is in place across all GP practices within South East London, and b) that a deployment plan will be created in partnership with GPs and patients to ensure that access is granted in line with national, regional and locally agreed timetables. Progress in delivering this capability will be overseen by the Cluster s ICT Steering Group, supported by a Primary Care ICT Programme Board. As the first completed London Trust on SCR, Bexley already has a significant proportion of live records uploaded to the SCR. Bexley completed its SCR deployment ahead of schedule with all Bexley practices uploading their SCR to the spine. The next stage would be the promotion of an advanced Health Space account for patients who wish to view their GP records online. The resources and rollout of this programme will need to be scoped and approved by the BSU CCG. Once we have this, we can move forwards with the implementation of this programme and the relevant timelines can then be more accurate. There are 267 practices of which 114 practices have uploaded SCR covering 768,000 patients (41%). SEL has a Primary Care IT Programme Board responsible for overseeing the implementation of SCR, EMIS Web and EPS, which meets monthly to review progress against plans. This Board is responsible for monitoring and responding to key risks as such as the current lack of accreditation of SCR with EMIS 21
147 Web. A Business Case identifying the benefits of the programme, as well as necessary deployment resources has been approved, including project managers, clinical transformation leads, technical leads, and RA. SEL has a Communications Strategy that sets out the Comms plan with the key stakeholders. There remains a further 153 deployments to be completed by 31st March 2013 with 19 being deployed by 31st March Bexley & Bromley manage their deployment within current resources. SCR completed for all practices within Bexley except the Albion Practice who is forecast to be complete by March Public Sector Equality Duty (PSED) Include assurance that due regard is given to the Public Sector Equality Duty (PSED), both specific and general, and that equality objectives are integrated into the plan considering using the Equality Delivery System as the framework. (Section 2.4 of Operating Framework) The majority of organisations, i.e. 93% (13), have Governance and Leadership structures in place to ensure the implementation of the EDS. 64% (9) have attained Board Sign-Up from their Boards. 100% (6) of CCCs have signed up to the EDS as well as signing up to the EDS as part of the Pathfinder Delegation application process. 86% (12) of the organisations have identified resources for EDS implementation and the remainder are working towards this. Most organisations, i.e. 79% (11) have started to engage/involve with local interests and identified those who will take part in the grading/objective setting process. One organisation has successfully carried out the engagement process. Ensuring good quality engagement with local interests was identified as being the main risk by 64% of the organisations. The major challenge for some of the smaller organisations is to do this with limited resources. How to carry out meaningful engagement with all the protected groups is identified as another challenge. Larger and smaller organisations state the key 22
148 Safeguarding Children Safeguarding Adults Ensure a sustained focus on robust safeguarding arrangements (to include how the Board assures itself). To work in partnership through Local Safeguarding Children Boards (LSCBs) and ensure ongoing access to the expertise of designated professionals. Work with developing CCGs to ensure they are prepared for their safeguarding responsibilities. (Section 2.43 of Operating Framework) Ensure a sustained focus on robust safeguarding arrangements. challenges at this stage are ensuring that the self-assessment and subsequent engagement with the local interest groups is managed within the expected timescale and that relevant equality objectives are agreed, both by the stakeholders and the organisation s E&D Committee. However, it is felt that partnership working across the SEL cluster and working SMART with stakeholders, public health and the local government will help mitigate to some extent. Organisations are also concerned about lack of capacity, competing priorities, organisational change. Specifically, lack of staff and resources as a result of workforce transformation and lack of expertise in service plans. Most organisations will be undergoing workforce transformations over the coming year (some of them large-scale) and this could potentially add further pressure to an already unpredictable working environment. CP safeguard lead appointed for cluster. Policies and procedures in place for all provider units. All staff remains in place in line with working together. In contracts with primary care/ BSU s and Trusts to ensure compliance with Working Together. Escalation procedures in place with designated professionals to ensure that executive and board members are aware of safeguarding issues throughout cluster. Multi-agency work continues with appropriate health representation Training numbers and serious case review recommendations and implementation monitored by Quality and safety subgroup of the board. Quarterly meeting with clinical commissioners with safeguarding responsibilities set up GP s to ensure transfer of CP knowledge and governance. The subgroup reports to the joint clinical board. Safeguarding lead meets with borough safeguarding lead. Areas of focus for the cluster are to ensure annual reviews of all vulnerable adults out of area by 23
149 Military and veterans health Work with developing CCGs to ensure they are prepared for their safeguarding responsibilities. (Section 2.43 of Operating Framework) Work with the London Armed Forces Network to ensure the principles of the Armed Forces Network Covenant are met for the armed forces, their families and veterans. Ensure that the Ministry of Defence/NHS Transition Protocol for those who have been seriously injured in the course of their duty is implemented in any commissioned service. PCT Clusters, and organisations they commission from, should be supportive towards those staff who volunteer for reserve duties. (Section 2.12 of Operating Framework) Sept Work with nursing homes to improve pressure area care reducing grade 3 s and 4 s by 50% by acute providers targeting homes by Nov The Adult safeguarding lead at cluster in post. Safeguarding leads in BSU s relating to borough safeguarding boards. Adult safeguarding processes and procedures in place in all Trusts and primary care. Adult safeguarding meetings in place to prepare Clinical commissioners identified as adult safeguarding leads for safeguarding responsibilities. Greenwich has historically had strong ties with the military. Woolwich barracks is home to two battalions and living quarters for current service personnel. Currently a small station command team is based at Woolwich barracks while the Princess of Wales troop are overseas approx. 500 soldiers. Their families and about children are at home in Woolwich. The King's troop (Ceremonial), a small unit with only about 36 horses - arrive on Feb 6 th We support the London Armed Forces Network with our Local Authority to ensure that we understand any impact of having a military barracks in the Borough and the needs of current and ex-service personnel that may need support form statutory services outside of the MoD. Greenwich BSU has formed links with military health leads within the Borough and began to map out how we can support them with their delivery of healthcare for physical and mental health. We intend to meet further Ministry of Defence representatives that oversee healthcare delivery across South East London in April This will assist us in undertaking a health needs assessment to ensure that we better acknowledge and respond to the needs of the military and 24
150 veterans of Greenwich as we are conscious that this has not been explicitly covered in previous health needs assessments. This will help us understand what the MoD deliver, what pressures/gaps they have and what use of secondary/specialist services they require etc.. It will additionally enable us to assess the numbers of service personnel that retire on health grounds within the Borough, the needs of the families of service personnel and veterans and ensure that we link more appropriately with our Local Authority colleagues across housing, education, adult and children s services. We have developed IAPT in Greenwich with local veterans being a priority target group. We will review activity to ensure appropriate take up of services. PTSD treatment is available from our local secondary care provider and additional services are purchased from other specialist providers if local services are not appropriate. We commission quick access to prosthesis for current and ex-service personnel and work with sector leads to ensure access to individual and exceptional treatments. Existing services provided within Greenwich will link with future Pan London and National strategies. We are currently reviewing care services available to service personnel and their families and working with our local GP practices within Woolwich to support existing health services provided by the MoD and to ensure appropriate access to services for ex veterans within Greenwich and South East London. 25
151 Mental health Continue to meet expectations within No Health Without Mental Health and NHS Outcomes Framework. IAPT to meet 15% prevalence with recovery rate of at least 50%. Focus needed on minority groups, older people, people with serious mental illness and long term conditions. Reduction of mortality from physical illness in those with mental illness. Focus on joint working with National Offender Management Service. Focus on mental health prevention in looked after children and other young people at risk. QIPP achievement monitored against MH Performance Framework covering new cases of psychosis served by EIT, gatekeeping of acute admissions by crisis teams, 7-day post discharge follow up for those on CPA. Elimination of mixed sex accommodation (Section 2.23 of Operating Framework) Mental health services are provided by two mental health foundation trusts; South London & Maudsley, (SLaM) serving a population of 1.1million in South London and Oxleas, the main provider of specialist mental health and learning disabilities service for Bexley, Bromley and Greenwich. Representatives from across BBG collaborate to commission services from Oxleas to promote improvement of services and better ways of working. The early intervention in psychosis service delivered by Oxleas is an example of the commissioners working together to raise concerns and shape the service delivered by the provider. NHS SEL is committed to continuing to meet expectations within the mental health outcomes strategy; No Health Without Mental Health. All boroughs are taking action locally to ensure this target is met by 2012 and based on current performance we are on track to do so. There are initiatives underway across all boroughs to ensure increased access to black and minority ethnic groups and older people, and increased availability of psychological therapies for people with severe mental illness and long term health problems. The focus on the physical healthcare of those with mental health illness to reduce their excess mortality continues to be an area of priority. The development of CQUINs over the last two years has increased awareness within mental health services of physical health needs as demonstrated in the achievement of the CQUIN indicators and this will continue to be a priority in 2012/2013. We support the need to focus on improving offender health and working in partnership with 26
152 the National Offender Management Service. Responsible commissioner guidance supports the provision of services for offenders in the community and their access to local acute and community mental health services including substance misuse services. A range of Tier 2 and Tier 3 community services are in place for 2012/2013 and each borough has local arrangements in place to ensure a greater focus in this area. We continue to monitor QIPP achievement against MH Performance Framework covering new cases of psychosis served by EIT, gatekeeping of acute admissions by crisis teams and 7 day post discharge follow up for those on CPA through monthly and quarterly monitoring meetings with our providers. The requirement for eliminating mixed sex accommodation is fully complete across all our providers. Borough based focus and assurances are detailed below. Bexley The BSU is currently working towards the IAPT target of 15% prevalence with recovery rate of at least 50%. The option to take on further trainees, expanding the IAPT resource to ensure we meet this target by 2014 is being explored. Recovery rates for quarter 2 were reported at 64% and therefore we are confident we are on track to meet 2014 target. The BSU has identified a need to focus on minority groups, older people, people with serious mental illness and long term conditions. This requirement will be met following the re-tender of the Bexley IAPT and counselling service using a 27
153 service specification amended to specifically include these groups. The standard IAPT data set reports that currently 3.5% of service users are over 65 years and 6.4% of services are BME. The BSU anticipates that the new mental health minimum data set will include people with serious mental illness and long term conditions in order for us to report figures in the future. The BSU has identified a need to focus on working with the National Offender Management Service and to establish if the provider has carried out any work to date on this requirement with the forensic provider Oxleas Foundation Trust. There is also the possibility that the Specialist Commissioning Group will take on responsibility of the commissioning of forensic services in the South East, pending appropriate discussions and process and procedure assurance to commissioners. Reduction of mortality from physical illness in those with mental illness. We had a CQUIN for 10/11 to encourage physical health checks by our main mental health provider and this has now been integrated into main services. In addition Mind in Bexley provides a physical health trainer via a public health contract, which mental health clients can access. Furthermore GP s have/had a QOF target for them to provide physical health checks for patients Bromley Bromley has an operational IAPT service Bromley Working for Well-being, which is compliant with the national model. Bromley is a wave 3 site, with the service starting in October The service is being delivered in partnership between Bromley Healthcare (Community Interest 28
154 Company) and Bromley Mind (3rd Sector Provider). The current service has only been commissioned to meet approximately 5% of local prevalence (~2000 new cases per year), and local plans have been developed to incrementally increase the service capacity over the next two years to meet 15% prevalence (~5100 new cases) by 2014/2015. Increasing service capacity is subject to agreement to commission an expanded service. The current service is achieving a recovery rate of over 50%. In the first two quarters of being fully operational (Q1, 2011/2012 and Q2, 2011/2012) the service achieved recovery rates of 58% and 57% respectively. In line with the no health without mental health framework, significant focus has been given to the improvement of physical health of people with a mental illness in collaboration with the local mental health provider and primary care. This has been demonstrated through the development and monitoring of CQUIN indicators being included within the mental health contract over the past two years. There is significantly increased awareness within mental health services of the physical health needs of individuals that is demonstrated by provider achievement of the local CQUIN indicators. This will continue to be a local priority, and is also highlighted in the providers Quality Accounts in 2010/2011. Greenwich Over the next year we are seeking to develop our Health and Wellbeing programme to ensure that care and support will be delivered which will offer choice, in the least restrictive environment and that is accessible and available to service users 29
155 and carers across the lifespan. We will be continuing to support our providers to deliver a programme that promotes Recovery and Wellbeing and challenges health inequalities particularly amongst difficult to reach groups such as older adults, people with a learning Disability, ethnic minority groups in the community and patients who have a Dual Diagnosis. IAPT in Greenwich is provided by Oxleas Foundation Trust at the Greenwich Time to Talk service and we are in the third year of the contract. The service was launched in October 2008 and since this time 8670 people have been referred to the service. This year we have also supported the permanent appointment of an Employment Coordinator based within our IAPT service at Greenwich Time to Talk. In the past the emphasis for the service has been to maintain people in employment rather than assist with finding employment. The appointment of the Employment Coordinator means that in the coming year, as part of the assessment process, all clinical staff will be expected to focus on employment as a goal in therapy and refer on to the Coordinator to access support to return to the workplace. Targeted projects are in place as well for people with Long Term Conditions, recurrent depression and chronic physical health conditions such as chronic fatigue. To achieve this the BSU will be supporting the interim appointment of a worker to start networking and set up collaborations with GP s, Long Term Condition Primary Teams and acute hospital physical health Teams. In the longer term we are developing a Business Case with Oxleas to appropriately fund interventions and a programme for these groups. In terms of a focus on minority groups, older 30
156 people, people with serious mental illness and long term conditions, LTC is addressed through the IAPT agenda. For the other groups, Greenwich are developing a borough wide mental health service user group which aims to: Develop a group to represent all mental health service users in the borough. It does not represent one interest group or organisation but will focus on groups who are historically difficult to reach and have problems accessing services. Provide service user training Promote peer support, peer mentoring and mystery shopping. The group will feed into the decision making structures for mental health such as the Joint Commissioning Group. Ideally in the future service users can give views on service design, commissioning decisions and changes in the boroughs mental health services. Greenwich Council and NHS Greenwich are joint funding the service user group. The BSU is currently working towards the IAPT target of 15% prevalence with recovery rate of at least 50%. In the last year the Greenwich Time to Talk service has achieved a recovery rate of 48% and feedback from Service Users and GP s continues to be positive. We are confident that there will be an improvement in Recovery Rates over the coming year through targeted projects in respect of Long Term Conditions and the provision of Mindfulness Training to staff which specifically supports people with recurrent depression and chronic physical health conditions such as chronic fatigue. THE BSU support the need to focus on improving offender health and working in partnership with 31
157 the National Offender Management Service. Responsible commissioner guidance supports the provision of services for offenders in the services including substance misuse services. The Court Diversion Scheme has done much to ensure the detection of mental illness earlier within the forensic pathway and has seen a corresponding increase in the number of offenders detained under civil sections and referred to low and medium secure accommodation at the Bracton and Memorial sites. The BSU has supported the Business Case to increase the provision of low secure Forensic hostel accommodation at the Goldie Lee site and a corresponding decrease in the number of Forensic beds commissioned from Oxleas. This development will come on line in 2012/2013. Local CQUINs are in the process of being discussed and agreed at a meeting scheduled with Oxleas NHS Foundation trust on the 15th March. The local CQUINs being considered are: Safeguarding: 1. Improving and standardising reporting of safeguarding issues: number of alerts, outcomes, completion of investigations, escalation to other agencies. 2. Ensuring that the needs of adult service user s children are met. this will require an audit and it may be possible to combine the audit with a survey to consider - 3. Domestic Violence combine an audit with 2 4. Pregnancy - this would include some identification of Service users who are known to be expectant fathers having the needs of the 32
158 unborn child/ impact of parental mental illness included within their assessment and care plan. Vulnerable adults - following on from the results from the last LD SAF several CQUIN Indicators have been developed in respect of Autism and LD. These include ensuring that Pathways of care are reasonably adjusted to meet the health needs of people with learning disabilities and autism and that the trust has protocols in place to provide suitable support for family carers who support patients with learning disabilities including the provision of information regarding learning disabilities, relevant legislation and carers' rights PbR this is being developed and Oxleas are leading on constructing a draft a proposal. Lambeth Minority groups Lambeth s various initiatives are addressing needs of minority groups as outlined here Mortality CQUIN physical health targets are being met by SLaM ; the improved primary care and secondary care interface through the primary care mental health support service will further sustain improvements in this key target area. Offender health - NHS Lambeth works with NOMS and other criminal justice agencies in a number of ways. The re-role of HMP Brixton is being undertaken in a planned, collaborative way with the Prison, the providers, NHS Wandsworth (in relation to HMP Wandsworth transfers) and NOMS to 33
159 ensure a smooth transition for patient health care. NHS Lambeth is involved in development and operation of the Integrated Offender Management (IOM) programme in Lambeth. The Lambeth MHIP Criminal Justice Pathway project (as above) involves the entire criminal justice pathway, per the Bradley Report, including prisons and Probation. Looked After Children (LAC) - range of Tier 2 and Tier 3 community services in place for 2012/2013, including a LAC CAMH Service (CLAMHS), YOS CAMH Service and an integrated Early Intervention Service. Implementation of CAMHS IAPT service in Lambeth is in process, which will be integrated with existing parenting programmes. QIPP Key performance targets - CPA, HONOS, EI and HTT are being met together with MH QIPP savings target SLaM continue to comply with the Mixed sex accommodation policy with no breaches during Lewisham The BSU have an IAPT action plan in place to reduce the large waiting list. The current activity levels are 11% prevalence and 48% recovery so the service is in a good position to meet the national targets by 2014/15. The plan for 2012/13 is to stabilise the service at this level due to the focus on financial recovery in Lewisham and to focus on recovery and cementing the good performance on moving people off sick pay and benefits. Physical health continues to be at the forefront of developments in mental health services. Local CQUINs are specifically targeting physical health 34
160 whilst further projects are being developed to ensure appropriate GP input to mental health inpatient services in the community. During 11/12 a further assessment and liaison service has been developed with SLAM to ensure that people leaving prison are placed appropriately and, if in medium secure, this period is managed appropriately and length of stay reduced. QIPP targets are monitored through monthly pooled budget meetings between SLaM, the PCT and the Local Authority. Specific targets around EIS, 7 day follow ups and gatekeeping those in crisis are monitored through the SLaM Core Contract meeting and monthly quality reports. In 2011/12 these areas are where SLaM is performing very well and this drive for quality is expected to continue into 2012/13. Southwark Southwark is currently achieving its IAPT targets and the MH Programme has a project devoted to increasing the access to psychological therapies. Working with all providers, Southwark are on track to meet the 15% IAPT target. The BSU have a project devoted to increasing the access to psychological therapies. A review of current joint working will be undertaken to assess how Southwark can work better to support the National Offender Management Service. The Substance Misuse Project Group is taking this forward and is currently supported by SLaM through the high support team. Southwark also has strong operational links with the Courts where a liaison officer is employed to support offenders who may 35
161 require mental health interventions. Strong partnership working with the Local Authority will support the joint working National Offender Service. Carers Publication by 30 September 2012 of Local Authority and PCT Cluster joint needs assessment with agreed plans policies and identified budgets with Local Authorities and voluntary groups to support carers. To include identification of total budget to support carers breaks and indicative number of breaks available within the budget. (Section 2.11 of Operating Framework) The PCare & LTC MH (Crisis / Psychosis) is focusing on improving physical health and well being by supporting primary, community and secondary care to identify and address the physical needs of those who present with MH and other LTCs. The local CQUIN with SLaM for physical health and recovery supports reduction in mortality. Development of Carers strategies are being led locally by BSUs with each of the Local Authorities and voluntary groups. Engagement with Local authorities is at different stages across the Cluster but has commenced in all boroughs and the implications being worked through. The carers strategies across the Cluster also vary in maturity. Lambeth, Bexley and Southwark have all recently undergone the process of updating or refreshing their carers strategy whereas Bromley, Greenwich and Lewisham are undertaking the process now with the strategies due to be completed in September. Funding for carers breaks have been identified where available across the Cluster although this has not been possible for every borough. Where this has not been practical at present plans to make this possible have been addressed. Carers allocations are being aligned to with the 2012/13 operating framework with details of provision being established by joint commissioning groups and governance structures being adjusted to reflect working across BSU s, Local Authorities and voluntary groups. A summary for each borough is below: 36
162 Bexley: Bexley completed a carers' needs assessment at the end of The CCG and London Borough of Bexley have agreed to develop a Joint Carers Strategy. This will support the out of hospital agenda and elderly care pathway redesign. The aim being to pool resource as part of joint commissioning arrangements overseen by the Shadow Health and Well Being Board. As part of this we are jointly reviewing all Voluntary sector grants to align funding to reduce duplication in carers support services. A draft carers' strategy will be completed by Jan 31 st 12. A final strategy and total budget will be published by the end of March The carers sub group will continue to work with health and the local authority to monitor progress and implementation of the strategy. Bexley has about 21,000 carers, 4,000 of these providing more than 50 hours of care each week. We recognise that we need to work together with partners across the public, private and voluntary sectors to meet the challenge of delivering the changes required to improve the living of carers. A final strategy and total budget will be published by the end of Mar-12. The strategy will also look to address the key priorities in the national strategy as well as local priories identified through the needs assessment to include; (September 2012 key actions) Carers and cares organisations are partners in the planning, delivery and development of approaches and services which are flexible and better targeted to their needs There is earlier identification, awareness 37
163 and understanding by service providers, of the role and importance of the carer; carers have access to emergency care and support systems when they need it, that reduce and prevent ill health and improve the quality of life for carers; carers are identified from all sections of the community; all carers in Bexley have access to improved information and advice. (March 2013) Bexley has a contract with the Alzheimer s Society to provide Day Support and Dementia Support Service for Dementia sufferers and their carers. The value of the contract is currently 50,000. The Memory Service provides support to carers as part of the service specification (for newly diagnosed, then signposted to Alzheimer s Society service) in line with NICE guidance. The BSU also have a contract with Re-Instate Ltd This model is for service users offering Social Inclusion and Employment Service. However, whilst the clients are at Re-Instate it does offer their carers a break too. Bexley have two different respite schemes provided by Crossroads with a joint budget of approximately 30,000. These include the Ethnicity project and the respite project, which both provide respite care. Another project with the voluntary sector called Carers Support has a total budget for carers of 60,000. Over a third of this is spent on respite care; the rest of this is spent on information, support and advice for carers. Individual care packages for patients receiving continuing health care also includes elements of respite where required. 38
164 All of the contracts from carers will be reviewed in the next financial year to bring the service models more in line with the carer s assessment undertaken this financial year. The budget allocation for 2012/13 has been provisionally set at 200,000. Bromley: Bromley has a joint Carers Strategy between the Local Authority and PCT since The strategy is currently being refreshed focusing on the 4 key priority areas of enabling, supporting, personalising and for carers to remain mentally and physically well as set out in the government's National Carers Strategy (2011). The re-fresh process is governed by the local Carers Strategy Group, chaired by the CEO of Carers Bromley and members includes local authority and Bromley CCG colleagues alongside multiple representation from voluntary sectors, other health and social care provision partners and some service users. A survey was sent out to 2771 carers in 2011 with a 12% response rate. The information is key in developing the refreshed strategy. The refreshed strategy which would be completed by spring 2012 will include agreed action plans and policies and spend (budget) from both organisations to support carers. Both Bromley Local Authority and CCG spent approximately 1.5m in total so far in 2011/12 in providing carers breaks. There are provided in private care homes, voluntary sector care homes, service users own homes, specialist care homes and relatives homes. There is an assumption that the provision of carers breaks will remain a priority for both organisations in the refreshed strategy. The plan for 2012/13 is to work with London 39
165 Borough of Bromley and jointly spot purchase more specialist placements as there are currently many patients with complex neurological long term conditions who are currently being cared for at home. These placements are costly and by working with the local authority, we will be able to expand on choice and obtain best value for money. It also saves resources for both organizations when it comes to contract and quality monitoring. Greenwich: The Current Carers Strategy (2011/2012) will be reviewed and a revised version published by September The Local Authority will lead on this process, with full engagement of NHS partners, the voluntary sector, user groups and other stakeholders. A listening event with carers held in the summer informed the joint dementia strategy which was published in The developing Joint Commissioning Plans all address the identification and needs of carers. Carers can benefit both directly and indirectly by the services provided to the cared for person. Therefore, the current support package in place for the cared for person will be considered to ensure the carer s needs have been properly reflected in the service users Personal Budget. If the Carer s Assessment confirms eligibility, the outcome can be either: provision of services to the cared for person or the payment of a one-off personal budget to the carer. In some cases, both outcomes will apply. Carer s will not be financially assessed and are not expected to make a contribution to services. Funding for carers was earmarked in 2011/12 in line with the 2011/12 operating framework. Year to date, the uptake against this allocation equates 40
166 to approximately 50%. We currently fund: Bedded respite services for people with learning disabilities and mental health Additional hours of home care support to relieve carers of people with continuing health care needs Specialist respite services for people with complex and severe health needs Top up of placements within care homes for short breaks There are also a number of council managed schemes. For 2012/13, the carers allocation will be expanded in line with the 2012/13 operating framework, with the detail of provision to be drawn up within the relevant joint commissioning groups. An Older Adults Joint Commissioning Plan and revised governance structures are also being reviewed and will be in place by April/May 2012.Greenwich funds: Greenwich Carers Centre: provides information advice, advocacy and building social capital for carers. Adults and Older People Services provides 148k funding and Children's Services funds 74k; Crossroads provides a Carers Dementia Cafe - 19,500 from Adults and Older People Services Volcare provides a Sitting Service - 37,000 from Adults and Older People Services The tables below shows the total numbers of people who have received respite breaks (01/04/2011 to 31/12/2011), and the spend on these. 41
167 Nursing Respite Care Residential Respite Care Adult Placement Scheme Respite Number of clients receiving respite breaks Number of respite weeks provided (approxi mate figure) Gross cost (this figure does not include pct reclaim) , , , Greenwich BSU have a four year allocation towards developing and supporting services for carers of 547, 755 covering the following areas: Bedded respite services for people with learning disabilities and mental health Additional hours of home care support to relieve carers of people with continuing health care needs Specialist respite services for people with complex and severe health needs Top up of placements within care homes for short breaks 3,492 per annum is directly pooled with the local authority and the remainder supports health and social care clients packages of carer as well as carers events. The arrangements outlined in the updated narrative constitute a new plan which we do not expect to change in the near future as we are near the start of a three year spending plan cycle 42
168 for LAs, but may be subject to review. The Greenwich JSNA 2011/12 update has been completed and presented in public at the Greenwich Clinical Commissioning Committee. Lambeth: Following the publication of the Refreshed National Carers Strategy, the Lambeth Carers Strategy was refreshed in The Refreshed Lambeth Carers Strategy which took into consideration the needs of carers outlined agreed plans and identified budgets to support carers till the end of the financial year 2012/2013 including the number of available breaks. The Carers Strategy is a joint LB Lambeth/NHS Lambeth document. A major piece of work is currently being carried out to review all forms of respite provision for carers in Lambeth. The intended outcome is to develop policy proposals leading to new models of care, direct payment for carers and ensuring investment equity for carers of all types. Lewisham: A Carer Strategic Development Officer has been recruited and will be leading on the development of a new Carer's Commissioning Strategy for Health and Social Care. NHS Lewisham is leading work on identifying carers in healthcare settings in both Lewisham Healthcare and GP Services so that better referrals can take place with social care. Joint Commissioners between the Local Authority and Lewisham Clinical Commissioners will develop and publish the plans and policies for carers by September The Group will involve Public Health colleagues to assist with needs analysis, 43
169 although this will need to be further refined when Census level detail becomes available later in the year. The development will involve Carers in the plan development including a Lewisham Carers event. In 12/13 PCT budgets will include: 100k which will fund: Yew Tree project to provide carer support at the End of Life Carer support workers to provide support to Lewisham Healthcare and GP staff to deliver for carers 122k which funds the core costs of Carers Lewisham via London Borough of Lewisham via Section 256 arrangements. Southwark: Southwark BSU have agreed a Carers Strategy (Vision and Direction of Travel) with Southwark Social Services, this is published on the website. Southwark PCT and Southwark Council are committed to working together to develop services to meet the diverse needs of carers, including child carers of adults. This document sets out the strategic direction of travel in respect of our planned approach for Plans are in place to ensure personal health budgets are implemented by We are submitting an expression of interest to become a pilot site for PHB in Continuing health Care in in January The pilot site will include a focus on supporting clients and carers to have more control and choice over packages of care in order to support their individual needs. 44
170 The BSU Assistant Director for Adults, Older People and Dementia is the lead for carers within the BSU and will be working jointly for the BSU Chief Finance Officer during the budget setting process in March 2012 to identify the total budget to support carers and the indicative number of breaks available within this budget. Development of Carers strategies is being led in Southwark by the CCG and BSU in collaboration with the Local Authority and voluntary groups. The allocation of personal budgets to carers for breaks is managed through Southwark Carers, which is commissioned by the local authority. To date since the Carers Hub went live in August 2011 there have been 383 PB's allocated. Planning for carer's breaks next year will use this data as a baseline and aim to build on these within the 400k investment allocation Dementia and care of older people Ensure providers are compliant with NICE quality standards and information published in provider quality accounts. Work with GPs to ensure improvements in general practice and community services including improvement of diagnostic rates. Ensure participation in and publication of national clinical audits. Outline initiatives to reduce inappropriate antipsychotic prescribing. Southwark has identified a 400k investment to fund support for carers and will deploy these resources in collaboration with the Local Authority. This agreement has been confirmed by both organisations with funds to be transferred for 12/13. Resources will be invested in services for carers of people with dementia; in the development of a Southwark Carers Hub; and to fund further respite packages for carers in the borough. Ensure providers are compliant with NICE quality standards and information published in provider quality accounts Providers are required to comply with NICE quality standards and to publish as part of Quality Accounts as part of our contractual requirements We will continue to monitor this through a well established process of quality outcome review meetings and challenging providers to improve quality and improve efficiency. 45
171 Continued drive to eliminate Mixed Sex Accommodation. Reporting of inappropriate admission rates. Non payment for emergency readmissions within 30 days of discharge from elective admission. (Section 2.08 of Operating Framework) Bexley BSU will continue to monitor this through a well established process of quality outcome review meetings and challenging providers to improve quality and improve efficiency to evidence compliance with NICE guidance. In developing new specifications for care of older peoples services evidencing quality outcomes for patients will be a core part of any service specification. The timeframe for this will be ongoing. Bexley, Bromley and Greenwich have been working jointly with Oxleas. BBG have worked together on the establishment of Quality Meetings with Oxleas and ensuring that there is on-going review of the progress being made in respect of the delivery of services benchmarked against NICE quality frameworks and indicators. This has been agreed in the Quality and Safety Improvement Plan and CQUIN goals. Over the next year BBG will continue to monitor progress against the CQUIN indicators and the three quality domains Patient Experience, Patient Safety and Clinical Effectiveness and work with service users and carers to insure information is shared and appropriate training is available for health care professional. From a joint commissioning perspective, Social Care providers are required to comply with the CQC Essential Standards of Quality and Safety measures and council contract officers monitor provider s compliance status as part of a comprehensive monitoring programme which includes visits to services. In Southwark Contract negotiations are underway these will ensure all providers are compliant with NICE quality standards and that this information is published in provider quality accounts. 46
172 In Lambeth Providers are required to comply with NICE quality standards and to publish as part of Quality Accounts as part of our contractual requirements. In Lewisham all providers of Lewisham s dementia support services, including SLaM and Mindcare voluntary sector support, are aware of and remain compliant with NICE guidance and quality standards, which are outlined in all provider service specifications. Lewisham was asked by NHS London to present their local Dementia model as a good practice example on in January Work with GPs to ensure improvements in general practice and community services including improvement of diagnostic rates. There is an established regular liaison meeting between local GP leads and clinical leads in the local provider. This is providing a framework for the improvement of local services In Southwark the GP Meeting in January focussed on Mental Health. This meeting discussed the programme plan and each project. In Lambeth and Southwark work is underway with GPs to ensure improvements in general practice and community services including improvement of diagnostic rates. The Lambeth and Southwark Mental Health for Older Adults Group and the workplan for this group, that is currently in development will include a workstream to establish innovative ways of working with GPs to improve earlier diagnosis and increase diagnostic rates. Ensure participation in and publication of national clinical audits. We are seeking to improve participation in 47
173 national audit and would hope to confirm a programme of participation in national audits over the coming year. We propose that participation in national clinical audit should form part of contractual requirements for 2012/13. It is part of the national Quality Accounts template. The Lambeth & Southwark Dementia workplan will ensure Lambeth and Southwark participate in and publish results of national clinical audits. Southwark is seeking to improve participation in national audit and would hope to confirm a programme of participation in national audits over the coming year. We propose that participation in national clinical audit should form part of contractual requirements for 2012/13. It is part of the national Quality Accounts template. The Lambeth & Southwark Dementia workplan will ensure Lambeth and Southwark participate in and publish results of national clinical audits. Outline initiatives to reduce inappropriate prescribing of anti-psychotic medication Following the POMH-UP audit, GP reviews in respect of prescribing has commenced in partnership with Oxleas. Following completion of the reviews, if necessary, an Action Plan will be constructed to support the need for regular monitoring and review. Bexley, Bromley and Greenwich have been working jointly with Oxleas. Oxleas is rolling out an education and support programme to local care homes to help them improve the management of dementia and resulting challenging behaviours, and subsequent prescribing of anti-psychotics. This programme has demonstrated a reduction in attendance at A&E, as well as referrals and admissions to MHOA inpatient services. The following actions are 48
174 being taken by BBG commissioners: Oxleas report admission rates within the monthly contract monitoring meetings where commissioners are given an opportunity to consider admission trends and identify admissions through the Home treatment team and under provision of the Mental Health Act. We are working with Oxleas to support the review of all patients inappropriately prescribing of anti-psychotic medication and the drive to consider alternatives. We are also supporting the work underway by Oxleas to support the development of Shared prescribing and the addressing of any obstacles that exist between primary and secondary care. We will continue to monitor this through a well-established process of quality outcome review meetings which are held on a quarterly basis. Oxleas report on their clinical audits on a rolling basis as the audits are completed. We have received specific assurance that Oxleas will be participating in and publishing national clinical audits for 12/13. This will be documented in the audit schedule for 12/13 which is also shared with commissioners In Lewisham a Pharmacy post has been commissioned to review those on anti-psychotics and reducing prescribing as clinically appropriate. In Southwark Medicine Management are currently auditing the use of antipsychotic prescribing in Southwark. Our prescribing rates are low anyway as the National Lead works from Southwark, but this audit is expected to confirm these findings. 49
175 Continued Drive to eliminate Mixed Sex Accommodation. Reporting of inappropriate admission rates Local mental health services are compliant with privacy and dignity requirements and elimination of mixed sex accommodation. Any breach in same sex accommodation requirements is received in the reporting data from providers and monitored through the course of our contract monitoring arrangements. In Southwark there is ontinued Drive to eliminate Mixed Sex Accommodation and eporting of inappropriate admission rates. Local mental health services are compliant with privacy and dignity requirements and elimination of mixed sex accommodation. Any breach in same sex accommodation requirements is received in the reporting data from providers and monitored through the course of our contract monitoring arrangements. Non payment for emergency readmissions within 30 days of discharge from elective admission. We have agreed proposals in 2011/12 contracts for non payment for emergency readmissions within 30 days of discharge from elective admissions and propose a similar agreement for 2012/13 with commensurate re-investment in schemes to prevent inappropriate readmission. In Lewisham 30 day readmissions are identified and not paid for. This along with reablement funding provides a fund for agreed system wide schemes. This is agreed and monitored by the Whole Systems Group (Lewisham s Urgent Care Network) that has representation by commissioners, Lewisham Healthcare NHS Trust and London Borough of Lewisham social care 50
176 commissioners and providers. In Southwark, there is a plan in place to withhold payment for these readmissions. Additionally there is a Programme for Admission Avoidance, which is funded by re-investing these monies into several projects that provide alternatives to admission implement the Virtual Ward model and implement several improvements around Enhanced Rapid Response to aid swift discharge and manage people for longer in their own home. The Lambeth & Southwark programme for Admission Avoidance (Virtual Ward project) will evaluate all admissions in the pilot sites to monitor inappropriate admissions. This project will roll out in all localities early 2012.There is a plan in place to withhold payment for these readmissions with contracts to secure withholding of payment where these are shown to have breached the 30 day rule. Trust progress is managed in monthly contract reporting and monitoring meetings, which are led by Southwark clinical leads and BSU officers. For Lambeth and Southwark implementation is overseen by the Lambeth & Southwark Mental Health of Older Adults Group, with a clear work plan agreed and underway. The membership of this group includes representatives from BSUs, LAs and SLaM. In addition, Southwark BSU has identified 55k new investment in the further development of local memory services. The Action plan for bexley, Bromley & Greenwich with milestones is included below: 1. (BBG) 12/13 contract negotiations ensure any new and or relevant NICE guidance is included as much is possible in the reporting process. This year 12/13 the NICE 15 quality domains for user 51
177 experience have been included as part of the QSIP (reviewed quarterly). 2012/13-Q1,2,3 &4 2. (BBG) Quarterly quality meetings are held with our mental health service provider throughout the year which provide assurance against the 3 quality domains and agreed QSIP (national targets mandated). Commissioners can seek further assurance where there is any lack of evidence; through the quarterly meetings 2012/13-Q1,2,3 &4 3. Local CQUAG Quarterly meetings are held for the above content to be presented, further scrutinised and discussed at an organisational level ensuring further assurance checks are carried out 2012/13-Q1,2,3 &4 4. SEL Joint Quality meetings are held quarterly for the above content to be shared and discussed at SEL Cluster 2012/13-Q1,2,3 &4 5. Clinical Governance and Quality Lead provides alerts to new NICE guidance throughout the financial year and requests and monitors agreed action plan against the guidance for organisational NICE policy On-going 6. Provider quality accounts are shared and feedback is requested from the 52
178 commissioner in Q1 for the previous financial year April Dementia outcomes framework to be agreed and in place July Key objectives of Dementia outcomes framework to be monitored and reported to HWBB 2012/13 Q3 & Q4 9. Identify any priority areas and or gaps in progress (Via Dementia Steering Group) 2012/13 Bi-monthly and quarterly 10. Carry out a Dementia Needs Assessment across Health and Social Care to review pathways and Integration opportunities (Last assessment 2009) 2012/13 Q4 11. Review and update local dementia strategy to reflect areas of need 2012/13 Q4 & 2013/14 Q1 12. Commissioners will ensure 12/13 audit schedule is shared at Q1 Quality Monitoring Meeting 2012/13 Q1 13. Commissioners will cross reference audit schedule and ensure this is in line with 53
179 national audit participation requirements 2012/13 Q1 14. Commissioners will ensure recommendations and or findings following the audits have a clear action plan that can be monitored by commissioners. 2012/13 Q1 15. Commissioners will request and ensure they are notified by Oxleas when audit publications are due 2012/13 Q4 & or 2013/14 Q1 16. Commissioners/Oxleas to agree schedule for reviewing audit recommendations/findings and monitoring progress 2012/13 Q4 & or 2013/14 Q1 The Action plan for Lewisham with milestones is included below: In operation and ongoing: Lewisham Dementia pathway has been recommissioned in line with the National Strategy to meet all 17 objectives and has been launched in 2011/12 and will continue into 2012/13. Clinical Commissioners are very supportive of the approach. The project objectives are to: - encourage help-seeking and help-offering by changing public and professional 54
180 attitudes - make early diagnosis and treatment the rule rather than the exception - enable people with dementia and their carers to life well with dementia Single Point Of Access service is in place for all Dementia referral in the borough. All providers of Lewisham s dementia support services, including SLaM and Mindcare voluntary sector support, are aware of and remain compliant with NICE guidance and quality standards, which are outlined in all provider service specifications. Between 1 April December 2011 a total of 334 people were referred to Lewisham s new Memory Service. This is a significant increase in the number of referrals Since April 2011 the number of people diagnosed with dementia has steadily increased; 80 out of 220 people referred to the Memory Service in recent months were diagnosed with dementia. Since April 2011 Lewisham has delivered an assistive technology service for all people diagnosed with dementia whether they are Fair Access to Care Services (FACS) or Care Programme Approach (CPA) eligible. This has seen a steady increase in the number of people accessing AT services. A programme of dementia training and coaching will be systematically rolled out to staff and managers of residential and nursing homes from early The programme will be extended to Extra Care Housing providers and domiciliary care providers in Dementia awareness training will be rolled 55
181 out to nursing, A&E staff, community staff including district nurses and members of the social care team based at University Hospital Lewisham in The training will capture staff groups not included in an earlier round of dementia training in early The quality of the training support was highlighted as an area of best practice in a recent HIEC review of dementia services. Mixed Sex Accommodation Lewisham Healthcare has reported minimal Mixed Sex Accommodation breaches. Any Qualified Provider Extend patient choice of community and mental health services to AQP in 3 service lines per Cluster between April and September Outcome-based service specifications should be developed with input from CCGs and patients. The nationally developed provider qualification questionnaire should be used to qualify providers. Include further service lines as per Government announcement (expected in December). (Section 3.21 of Operating Framework) No CCGs have selected three service lines for implementation across the south east London Cluster (Continence, adult Hearing and Wheelchairs for children). CCGs have established working groups for the implementation of the service lines with LINkS representation. These groups will enhance the national service specification to meet local needs and ensure an outcome focus. The CCG working groups have developed high level milestones for the programme (see below). Each service line will have its own detailed implementation plan, in line with the advertising windows provided by the Quality Centres of Excellence. London Clusters are collaborating to achieve consistency enabling London windows to be agreed with the Quality Centres of Excellence. Hearing and Continence - September 2012 Wheelchairs December 2012 * * The Department of Health extended national deadline in this service area in order to ensure that local commissioners are able to engage with key stakeholders and achieve the level of service 56
182 improvement and innovation indicated by the national implementation pack for wheelchairs. Service Line: General Date: November 2011 Committee/Lead: South East London Clinical Strategy Group Milestone: Clinical Strategy Group to provide final decision on service line selection Date: January 2012 Committee/Lead: Working Groups Milestone: Evaluation of current service provision (contract, activity and finance) and identification of issues Date: February to March 2012 Committee/Lead: Responsible Director Milestone: Provision of variation notices to providers Service Line: Hearing Date: March- April 2012 Committee/Lead: Working Group Milestone: Local amendments to national specification to ensure local reflection including LINKs and clinical input Date: March- April 2012 Committee/Lead: London Network Milestone: Agreement with London groups on principles of tariff and currency definition, enhancing National Specification Date: March April 2012 Committee/Lead: Working Group Milestone: Define evaluation criteria for qualification based on national guide Date: April 2012 Committee/Lead: Steering Group 57
183 Milestone: Sign off of specification and evaluation criteria Date: May 2012 Committee/Lead: Steering Group Milestone: Provide specification to QCE Date: June 2012 Committee/Lead: QCE Milestone: Advert on Supply2Health (QCE Window) Date: August 2012 Committee/Lead: QCE/CCG Boards Milestone: Recommendations to CCG Boards to approve providers Date: September 2012 Committee/Lead: Commissioners Milestone: Provision of contracts and go live of services Service Line: Continence Date: March- April 2012 Committee/Lead: Working Group Milestone: Local amendments to national specification to ensure local reflection including LINKs and clinical input Date: March- April 2012 Committee/Lead: London Network Milestone: Agreement with London groups on principles of tariff and currency definition, enhancing National Specification Date: March April 2012 Committee/Lead: Working Group Milestone: Define evaluation criteria for qualification based on national guide Date: April May 2012 Committee/Lead: Steering Group 58
184 Milestone: Sign off of specification and evaluation criteria Date: June 2012 Committee/Lead: Steering Group Milestone: Provide specification to QCE Date: July 2012 Committee/Lead: QCE Milestone: Advert on Supply2Health (QCE Window) Date: August September 2012 Committee/Lead: QCE/CCG Boards Milestone: Recommendations to CCG Boards to approve providers Date: End September October 2012 Committee/Lead: Commissioners Milestone: Provision of contracts and go live of services Service Line: Wheelchairs Date: March- April 2012 Committee/Lead: Working Group Milestone: Finalise information (activity, finance and contractual) and identify issues Date: April- May 2012 Committee/Lead: Working Group Milestone: Local amendments to national specification to ensure local reflection including LINKs and clinical input Date: May - June 2012 Committee/Lead: London Network Milestone: Agreement with London groups on principles of tariff and currency definition, enhancing National Specification Date: June 2012 Committee/Lead: Working Group Milestone: Define evaluation criteria for qualification based on national guide Date: July
185 Committee/Lead: Steering Group Milestone: Sign off of specification and evaluation criteria Date: July 2012 Committee/Lead: Steering Group Milestone: Provide specification to QCE Date: September 2012 Committee/Lead: QCE Milestone: Advert on Supply2Health (QCE Window) Date: September October 2012 Committee/Lead: QCE/CCG Boards Milestone: Recommendations to CCG Boards to approve providers Integrated Care Systems Clusters are asked to describe how they plan to: Identify the geographies and population segments the ICS will cover Establish a coalition of leadership at the most senior levels Develop a business case, which defines clinical scope and financial model, approved by all parties (commissioners and providers) Develop a detailed operational plan, setting out day-to-day working arrangements e.g. the operating model of the MDGs, information sharing protocols Invite all parties to sign up to all elements of the operational arrangements, including information governance arrangements Prepare for operational launch, including establishment of the integrated management board with its independent chair. Develop local measures of integrated care that will support improved delivery such as patient reported experience of co-ordinated care. Profile the expected point at which clinical Yes Date: November to December 2012 Committee/Lead: Commissioners Milestone: Provision of contracts and go live of services The core components of integrated care systems across south east London are: Maintaining robust patient registers Patient risk stratification to focus on patients at risk of developing illness Common clinical protocols applied along patient pathways by all providers Defined care packages, tailored to the needs of each individual Care that is proactively planned, coordinated and delivered A multi-disciplinary team approach across health and social care Case conferences for patients with complex needs Continuous review of performance of and by multi-disciplinary teams with peer support. High quality primary care underpins our plans for Integrated Care systems. We believe that integrated care will deliver better care closer to 60


186 benefits and cost-savings will begin home. We recognise that there is not a one size fits all solution and we are therefore developing and testing different models of models of integrated care across different populations and geographies: Lambeth ad Southwark Lewisham Bexley, Bromley and Greenwich. The systems will by led by a Federation of health and social care providers with an overarching Integrated Board Structure, working in partnership with clinical commissioners and responsible for the shared delivery of care along agreed pathways. Lambeth and Southwark: The Integrated Care Programme is designed to deliver sustainable integrated health and social care services. It is being delivered through a partnership between NHS Lambeth, NHS Southwark, London Boroughs 61
187 of Lambeth and Southwark, King s Health Partners Academic Health Sciences Centre and GP practices. A coalition of leaders is in place, led by the CCG clinical chairs. This will redesign the health and social care system and its services and will redefine the way professionals engage with each other around the assessed needs of individuals. It will fundamentally change the way in which people are supported in taking charge of their own care and conditions. The programme s initial focus is on caring for older people and its scope will be systematically broadened over the next three years ( ). From its third year onwards the changes made to the systems and to services for older people will become self financing and the transformation seen will mean that every year in Lambeth and Southwark: 15,900 unnecessary bed days currently spent in hospital are avoided for older people (a reduction of 14%) 118 older people are supported in a way that means they do not have to go into care homes (18% fewer care home packages) Savings of 13.9m per annum are released across the system. We will drive up the quality of care and drive down costs, improving the value of care we provide to people in Lambeth & Southwark by: Joining up care around people, across providers Identifying and managing people s care needs better and intervening earlier Ensuring care is provided in the most appropriate setting, particularly at times of 62
188 acute crisis Ensuring the right incentives exist for providers to work in integrated ways The process of service change will be evolutionary during 2011/12 we have established programme structures and plans and commissioned new admissions avoidance schemes such as the Virtual Ward, community based Rapid Response and enhanced re-ablement services. During 2012/13 we will develop patient based risk registers and reporting in GP practices, holistic health assessment (including mental health) and case management for older people through GP practices and urgent access hot geriatric outpatient clinics for rapid diagnosis of older people. We have submitted a bid to Guy s & St. Thomas Charity to pump prime the programme, but are also working together on use of emergency admissions and readmissions funding, community care and mental health contract resources and primary care. In particular we are seeking the charity s support to deliver information technology that would allow a sophisticated single view of real time information related to the care of individuals and take the findings of the department of Health s whole systems demonstrator pilots of telehealth and telecare and deliver them at scale. Bexley, Bromley and Greenwich: a whole system strategic approach for outer south east London is being taken, building on existing integrated care models in each borough and supported by client or pathway specific joint working groups. Key principles underpinning this approach are: To provide and deliver sustainable, fully integrated, high quality health and social 63
189 care for patients and their carers; To gain better knowledge about these client groups and increase the potential to be able to act upon that knowledge in a proactive way to maintain standards of health; To ensure better clinical outcomes for these patients; To describe a clinical case for change which is illustrated with real cases; To facilitate, as far as possible, an environment where patients can selfmanage their own condition and feel confident enough to do so Lewisham: Lewisham is continuing the development of an integrated commissioning model to deliver joined up care for patients with long term conditions and the elderly, especially working with Lewisham Healthcare as a Trust combining public health, community services and acute care in innovative ways. We have already developed a Joint Management Board for the Urgent Care Centre and worked together on a Clinical Assessment Service to reduce admissions or length of stay for those admitted. The further developments in 2012/13 will concentrate on integrated clinical teams, case management and risk profiling approaches with full engagement of general practice and pathway providers including third sector. Patient involvement in redesign decisions and underpinning contractual arrangements will be overseen by Joint Management Pathway Boards and a joint Service Redesign Group. Work includes developing pathway budgets arrangements in conjunction with the DH Long Term Conditions Programme support. The first two priority pathways are COPD and diabetes. Phase 2 pathways are under consideration and may include heart failure and stroke care. 64
190 Primary care Clusters are asked to describe how they plan to: No Implement the full NHS Operating Plan requirements relating to Primary Care (list cleansing / practice boundary changes / practice choice pilots) Enable CCGs to develop primary care improvement intentions / transformation approaches for authorisation and to support integrated care / out of hospital strategy Transition to using the GPOS and Once for London principles in 12/13 Gear up for the Olympic games Complete confirmed transition actions contract stock take, premises stock take, LPN piloting Working within the principles of the Once for London List Maintenance policy, the Cluster has established a working group with the LMC to add pace to the London policy. Using 2011/12 non recurrent resources, first letters establishing current address and GP registration will be sent to patients not subject to similar exercises in the last 12 months by the 31 st March Engagement with practices on non-responders to this first letter will occur in the 1 st Quarter 2012/13 and second letters sent in the 2 nd quarter of 2012/13 where registration cannot be established. FP69 flags will be set by 1 st October 2012 with training being provided to practices on FP69 processes and the required level of evidence to remocve the FP69 flag. De-registration of patients where contract has not been established will occur on or before the 1 st April AS part of the programme of contract assignment, existing contract documentation is being reviewed including practice boundaries. Mapping software has been purchased to improve the quality and accuracy of existing catchment areas. In the first quarter of 2012/13, engagement will occur with practices to establish inner and outer boundaries. The Cluster will work with INEL on the practice choice pilots and establish common policies and pricing for taking this initiative forward. The Joint Board has received a development plan for primary care and the Primary Care Directorate has engaged with individual CCGs to take this work forward. Existing dashboards have been reviewed and a common approach agreed across the Cluster building on the GPOS work. A common data extraction tool, used in three of the PCTs will be expanded to all six to provide a common tool across the Cluster. 65
191 The PMS reviews, following the principles of the Once for London framework are identifying from Public Health Reports areas of improvement in the needs of the population and these are forming the basis of the common basket of services and delivery is incorporated as a contractual requirement. The Cluster is chairing the Once for London premises programme. The Primary Care Directorate has recently appointed a Project Manager until September 2012 to co-ordinate the response in primary care to the challenges of the Olympics. Engagement events have been organised and those contractors either affected by their location or transport routes will be subject to planning visits to ensure business as usual. An assurance agreement is being sought from each contractor. The first stage, the stocktake, of the contract transition process has been completed by a dedicated team. Circa 2,500 risks have been identified and these are now being resolved. The biggest risk identified has been the novation to a successor body not being a PCT and this has been raised with the NHSL team overseeing this work. Existing information is being shared with contractors and new documentation being issued where required. A standard contract file requirement has been developed and existing paper and electronic files are being updated to meet this requirement. This work is ongoing. Leases for those contractors in PCT owned properties are being reviewed and work has commenced with the LMC to ensure resolution within 2012/13. There is full engagement with both NHSL and 66
192 representative bodies to complete the stabilisation phase by October Clusters are asked to describe how they plan to: Develop NHS 111 service go-live plans that meet London and national 111 service specifications developed with and endorsed by local CCGs meeting the April 2013 DH deadline. Develop a business case and 111 local service specification approved by CCGs. Build contingency for service commencement slippage built into the rollout plan. Put in place robust project management and governance arrangements to ensure delivery. Secure local clinical leadership, clinical governance and clinical engagement of DoS and pilot implementation plans. Further develop and refine the Directory of Services with the inclusion of mental health crisis and specialist palliative care services, by linking with social care, local government and the third sector (to support veterans). Put in place contractual arrangements (agreed with providers) to ensure resilience and sustainability of the DoS. Monitor the performance of NHS 111 pilots post go-live including patient experience & professional feedback and whole system impact against agreed KPIs. Develop a single electronic end of life register for London Coordinate my Care Agree electronic bookable appointment systems between NHS111 service and DoS providers. Y/N Existing networks are being utilised to develop the LPNs within South East London. SEL is included in Batch 4 of the London procurement of 111 implementation plans. Procurement documentation includes national, London and SEL specification. SEL 111 business case developed SEL CCG sign off of SEL 111 specification Rollout plan to include slippage contingency 111 Programme Board established 111 Implementation group to be established Clinical governance arrangements in place Three Clinical Champions across SEL Engagement strategy in place Mental health crisis services listed on DoS To be validated. Risk involvement of MH providers. Mitigation targeted comms and engagement work. Specialist palliative care listed on DoS and validated Links to social care, LA and third sector. Risk involvement of MH providers. Mitigation targeted comms and engagement work. Maintenance of DoS included in provider contracts Apr-12 Monitoring system to be established Dec-12 Patient experience and professional feedback KPIs In place included in SEL spec and contract Bexley Update (05-Mar-12) May Mar-12 Jun to Dec-12 In place Jun-12 Jun-12 In place In place In place Aug-12 Aug-12 Aug-12 67
193 Primary care contracting team to negotiate with willing NHS 111 services ability to include bookable appointments. Oct-12 NHS SEL 111 will deliver a universal free service available 24 hours a day, 7 days a week, 365 days a year to respond to people s health care needs acting as a Single Point of Access to SEL unscheduled care services including GP Out of Hours (OOH), community services, OOH dental services, end of life care services and some mental health services, providing a signposting service to pharmacy, optometry, and GUM and providing an appointment booking service with GPs (where appropriate). The service will also include provision of general and specialist health care advice and the ability to warm transfer a call to a GP for further clinical assessment where appropriate.[1][1] SEL Core 111 will be available 24 hours a day, 7 days a week, 365 days a year to respond to people s healthcare needs when: it s not a 999 emergency; the caller thinks they need to go to A&E or another NHS urgent care service; they don t think it can wait for an appointment with their GP; they don t know who to call for medical help; or the caller requires reassurance about what to do next. SEL 111 answers the call, asks questions to assess callers needs and determines the most appropriate course of action, including: for callers facing an emergency, an ambulance will be despatched without 68
194 delay; where a face to face consultation is required, an appointment will be booked or the caller will be referred to the service that has the appropriate skills and resources to meet their needs in the required timeframe, or warm transferred to a GP for further clinical assessment; for callers who do not require a face-toface consultation, information, advice and reassurance will be provided; and where the call is outside the scope of NHS 111, the caller will be signposted to an alternative service. SEL 111 provides management information to commissioners regarding the demand, usage and performance of services in order to enable the commissioning of more effective and productive services that are designed to meet people s needs. 69
195 Section Five: Commissioning Development PCT Clusters have an important role in the development of commissioning structures and processes in their area during 2012/13. This includes: o successful establishment of the new commissioning architecture to ensure effective clinical commissioning and handover by April 2013, comprising; commissioning support organisations, or the transfer of commissioning responsibilities to the NHS Commissioning Board, and nurturing clinical leadership through emerging CCGs, o and delivering full authorisation of as many CCGs as possible by April 2013 wherever emerging CCGs are ready and willing to achieve this. The following areas are subject to change depending on the passage of the Health and Social Care Bill and the drafting of the commissioning development section of the NHS Operating Framework 2012/ Summarise the PCT Cluster s commissioning development priorities for 2012/13 and how these will be implemented: The sections below outline how South East London will take forward taking CCGs to full authorisation, the development of the South London Commissioning Support Organisation, establishment of local health and well being boards. We plan to work with and support the emerging NHS Commissioning Board to ensure an effective transition of functions, along with local authorities for public health and the CCGs We are still at a point where there is still clarity needed on the policy detail and our plans will continue to be adapted as further detail on the policy implementation is known. Each system change area (including closedown) has its own plan which is reported to NHSL on a monthly basis highlighting progress planned and made, highlighted risks and mitigations, and areas for escalation. The cluster has its own System Transition group (chaired by the CE) to oversee the plans for each area and provide each lead Director an opportunity to discuss common issues and actions, and allow coordination across the change areas. The group also acts as a filter for the CE who is member of the NHSL System Transition Board. Lead Directors are: CCG authorisation Deputy CE and CCGs CSO CSO MD Public Health Cluster DPH NHSCB Director of Primary Care Closedown Deputy CE Other changes (e.g. Prop co) Deputy CE Objectives are for each work stream Director to deliver the policy changes within an agreed (and evolving) timetable for implementation by ,whilst at the same time ensuring that all other areas of the operating plan are delivered A. Summarise how the PCT Cluster will oversee and ensure the delivery of commissioning responsibilities that have been delegated, during 2012/13, including; setting out the approach to delegation including eligible commissioning budgets allocating non pay running costs and staff: - How delegated responsibilities will operate during 2012/13 - How the experience of delegated responsibilities will be captured to support emerging CCGs in developing a track record for Authorisation, and - Summarising plans for the transition of all commissioning responsibilities to 70
196 CCGs and others by the end of March During 2011/12 we worked closely with our developing Clinical Commissioning Groups (CCGs) in south east London in order to enable each to take on delegated responsibilities for commissioning at their own pace, and in accordance with our local governance arrangements. From April 2012 it is planned that each of the six CCGs in SE London will assume full responsibility for delegated budgets. Additionally, the planning round for 2012/13 has been jointly delivered by clinical commissioners, and a programme plan towards full authorisation by April 2013 has commenced within each of the emerging CCGs, with support from the cluster team. It is proposed that a full shadow year of running takes place from April 2012, with the central cluster team continuing to support each CCG as required. The commissioning support offer to CCGs for south London has been designed in order to be delivered, in shadow form, from April Current arrangements for performance management of delegation are through the borough Stocktake meetings, and the emphasis and remit of these will change from April 2012 as each emerging CCG has full responsibility for delegated budgets. The Stocktake meetings are used to review performance, and any escalation/intervention necessary will happen between these meetings using existing management structures. Following agreement of first elements of delegation by the PCT Board(s), the remaining elements are delegated based on recommendation from the Finance & QIPP Committee to the Board following the Borough stocktake meeting with each Pathfinder/CCG In SE London all 6 CCGs are borough based and all 6 CCG areas have been overseen by a borough based Local Commissioning Committee which is established as a formal committee of the Board. The CCG chairs of the committee are also full members of the PCT Board, Managing Directors of the business support units underpinning our CCGs delivery programme are also full members of both the relevant Board and the Local Clinical Commissioning Committee and a minimum of two Non Executives sit on each of the 6 Committees. These formally established committees, which have been running successfully since the inception of the Cluster and which are an embedded part of our ongoing governance processes, are a strong platform for the governance of local borough based activity including that activity now delegated to the CCG. Each committee formally reports back to the Cluster Board at every Public Cluster Board meeting. In addition, and to enable a more detailed and in depth scrutiny of progress and risk by wider members of the relevant PCT Board, the Cluster Board has recently established two additional integrated governance committees, one for the Lambeth, Southwark and Lewisham geography and one for Bromley, Bexley and Greenwich geography. These will drill down in more depth than is possible at the Public Cluster Board in respect of the local CCG positions in respect of finance, performance, QIPP delivery and quality. These committees will be directly informed by the outcome of quarterly stock take process which is described above and which form the key plank of the executive aspects of the management of delegated responsibilities. These formally established subcommittees, which have been running successfully since the inception of the Cluster and which are an embedded part of our ongoing governance processes, are a strong platform for the governance of local borough based activity including that activity now delegated to the CCG. B. Summarise, including key milestones, how the PCT Cluster will support and develop its pathfinders/emerging CCGs to prepare for and navigate the authorisation process. This includes developing the track record in preparation for authorisation. (e.g. on QIPP, primary care, tackling health inequalities, relationships with local partners including participation in emerging health and wellbeing boards, patient engagement and public involvement). It is expected that the majority of CCGs in south east London will wish to apply for authorisation sooner rather than later. There is considerable enthusiasm and energy amongst the CCG leaders locally, and we will be supporting them from the PCT cluster in order ensure their applications are successful. There is s joint organisational development group in place to coordinate activities for authorisation and to enable 71
197 CCGs to learn from each other and agree areas where they may wish to do joint work. Milestones / Key Actions 1. Have delegated authority for 100% of commissioning budgets.(cluster) Achievement Date 2. Have an updated Development Plan in place and agreed.(all) 3. April Finalise conflict of interest policy.(all) 4. March Ensure development plans describe how intend to source and manage the external commissioning support service. CCGs 5. Confirm relationship between CCG and its constituent practices including arrangements for membership and voting.(ccgs) 6. Have discussed and agreed with PCT cluster the transition plan for staff and infrastructure support. (CCGs) 7. Identify and agree a CCG corporate lead for CSS, and identify any need to access specialist procurement advice where alternative or additional commissioning support is required to be secured. 8. Be leading the local health system including finance, performance, quality and activity for commissioned services.(ccgs) 1. November April 2012 (differing timelines for each CCG) 5. March March March March April Prepare authorisation application.-ccgs 10. April - July Implement the Development Plan.-CCGs 11. May Have staff formally allocated to manage and support the development of the emerging CCG. 12. Agree collaborative commissioning arrangements and formalise (likely LSL and BBG arrangements). 13. Confirm the identification of senior leaders either through a local or national process.(all) 14. Work with NHS CSS to ensure the local and national offers reflect needs of CCGs. (all) 15. Have determined and agreed CSS option, and working to agree SLA(s) associated with this.(cluster) 16. Clarify involvement of patients, carers and local communities in CCG executive decision making process. (all) 12. May May June June June July Agree and adopt Equality and Diversity Scheme. (all) 18. July Agree new CCG Constitution.(CCGs) 19. July Finalise authorisation application-ccgs 20. July - September 2012 (majority of our CCGs likely to be in the earlier "waves") 20. Work with SHA and PCT cluster to shape and refine further the NHS CSS offer, ahead of final business review checkpoint.(all) 21. CCGs Signal intention for commissioning support for 2013/14 to enable completion of business plans by NHS CSS. 22. Agree risk sharing arrangements between practices/localities in CCG. 21. August August September CCGs complete formal CCG authorisation process. 24. December 2012 (at latest) 24. CCGs Have SLA in place with hosted NHS CSS ahead of taking on full responsibilities from 1 April CCGs Be operating and preparing to take on full statutory responsibilities January March 2013 (at latest) - but intention is that this would be earlier for our CCGs Summarise, including key milestones, the PCT Cluster s plan for the development of a Commissioning Support Organisation to provide the required commissioning support for the local market. This includes identifying local need, mapping the scope and scale of services to be provided and developing cost models to ensure that the overarching strategic approach to 72
198 commissioning support will be affordable. Work has been undertaken with functional leads, CCGs and other stakeholders to map out how commissioning support services will best be provided within SEL. Following discussions with colleagues in South West London who also have strong NHS Borough based teams, it has been agreed that a three point solution to commissioning support services should be developed with: Effective local clinical commissioning teams; Strong local teams in collaboration with Local Authorities/CCGs; A strong South London Commissioning Support Service (SLCSS). A draft SLCSS prospectus was developed in December based on five functional pillars: Provider contacting and monitoring; Information, Communication and Technology; Strategy and business planning; Specialist advice and clinical expertise; Corporate support. Work continues with the CCGs to identify the most efficient and effective use of the 25 per head running costs. It is clear that in order to achieve this, some commissioning support services will best be provided at scale but delivered locally. In developing the OBP for the SL CSS, NHS South East London has acknowledged the importance of responding to clinical leadership and delivering commissioning support as locally as possible within the CCGs. External support for the development of the Outline Business Plan for South London CSS (due 31 March 2012) has been procured and we are now in the final stages of describing, in detail: The business and pricing model A transition and development plan, covering all aspects of the transition from Clusters to a Commissioning Support Service and the development of the Commissioning Support Services over the next months Organisational structure options with recommendations and preferred structure An interim Managing Director has been appointed for the organisation and has recruited an interim senior leadership team, The interim Managing Director has started the recruitment processes for the substantive Directors. Further recruitment will commence once the business model is finalised for the Outline Business Case and the overall transition HR plan agreed. Engagement with CCGs is ongoing and it is anticipated that the South London CSS will agree a memorandum of understanding with each CCG effective from April. Engagement will continue with the CCGs to develop more detailed products and services to be reflected in detailed Service Level Agreements. Commissioning support including the development of a South London Commissioning Support Service is an integral part of the overall South East London Transition Programme. Dependencies with the development of CCGs and with the wider programme, including public health transition and the HR processes are managed as part of the programme governance. NHS SE and SW London have worked closely with emerging CCGs and with LAs to produce an overarching plan for the development of a South London CSS. By transforming current working practice it is believed that a SL CSS will be able to provide significant benefits to CCGs, the NHS CB and other potential customers in delivering both improved health outcomes and value for money. It will also support CCGs in their application for authorisation as they demonstrate access to robust and cost effective commissioning support arrangements. Although complex and challenging to deliver, a South London solution provides stability and opportunities for the development of commissioning support services and staff during the transition and beyond, thus retaining NHS expertise. 73

199 Development work has been lead by the directors of transition from SE and SW London supported by a programme director and a development group of 10 service heads drawn from both clusters. Building on this, and following the appointment of an interim managing director in December 2011, an interim core project team has now been appointed. Recruitment for a substantive managing director and head of acute contracting has started. Once the remaining structure and operating model has been finalised, recruitment to other key posts will commence. The service offering of the SL CSS reflects the current requirements of local CCGs. This has been achieved by CCGs and NHS SE and SW London through their commitment to the joint development of this organisation through a varied engagement strategy. Through this engagement, the PCT cluster has mapped the scope and scale of all the services to be offered by the CSS. The CCGs have clearly articulated they wish to see an offering which provides a core level of support, and flexibility around other that service offerings. This is reflected below. Ongoing engagement with CCGs has indicated that there is a broad consensus about the services CCGs would like CSS to offer, and those they prefer to maintain in-house Based on this feedback, we have structured our offer in a package structure to ensure that our Core offering is as affordable as possible, having regard to the needs of CCGs and a desire to achieve scale and provide value for money The Core package therefore represents the consensus view of those services which the CCGs wish to procure from the CSS We have clearly identified those capabilities which CCGs wish to maintain in-house, and we have excluded these from the Core We have devised alternative packages to meet the needs of CCGs who wish to leverage the expertise of the CSS for a more extensive service offering The rationale for this structure is to ensure that our offer is affordable within the financial envelope available to CCGs for spending on external commissioning support. A detailed pricing package for the three bundled packages of support has been developed in more detail within the OBC The pricing package, also recognises the costs of business development, both to secure 74
200 new business and to protect existing income streams. The operating model for the SL CSS has been designed to reflect the expectations of CCGs. Each seeks a strong local focus and close working relationship so that the needs of their local population remain the priority whilst maintaining access to high levels of technical expertise. Services will also be delivered with the help of a number of partner organisations as the benefits will allow SL CSS : Ability to quickly build expertise / gain capabilities; Scale for transactional elements of service delivery; Flexibility to obtain right resources quickly for services with cyclical or unpredictable demand. Work is underway to explore partnerships with other suppliers including the independent sector, voluntarily organisations, LAs. Developing and commissioning new models of integrated care will be a priority for all CCGs across South London. The SL CSS service offer will support existing and proposed joint commissioning arrangements through its locally focused teams and integrated performance framework and contract support. Discussions are currently underway with LAs including PH to consider how a collaborative structure with improved partnership working can develop. This will be further reflected in Outline Business Case. Key to the success of the SL CSS will be the development of effective partnerships between Primary, Secondary and the tertiary sector. The detailed financial modelling is included in the OBP due for submission at the end of March. However it is helpful to confirm here that the core package is expected to be priced at between 7-8. At the time of writing, 11 of the 12 South London CCGs are committed to buying into this as well as buying some services from the other additional packages.due to the current lack of certainty around these other services, the OBP will reflect various scenarios but emphasising the fundamental premise, that given the population size and the volume of the agreed core offering, the SLCSS will be financially viable. In preparation for the submission of the Outline Business Case, significant progress has been made in the following areas: Greater consensus on the level of support CCGs require from SL CSS; Further challenge and scrutiny of SL CSS costs to achieve margin and lower unit costs; Development of business strategy for SL CSS and consequential financing requirements; Mapping and transition from current state to future state. As a result of the very detailed work which has been undertaken and led by the CCGs and supported by the cluster, there is now a much clearer picture emerging of the overall affordability of the CCG and CSS structures within the 25 per head target. This is a particular issue for South West London as there are four CCGs with a population of less than 200,000. This work includes Further iteration on the balance between running costs of services provided CCG in-house versus outsourced to SL CSS; Further testing of the ability of all services to deliver the required quality and capacity and an understanding of how CSS core services integrate with CCG services; The development of proposals for collaborative or joint commissioning with other CCGs and LAs; Clarification of the ability of CCGs to invest in new services that are not part of the current system (e.g. Integration of primary care data to data warehouse, risk stratification of patients); More detailed modelling of the transition to end state. The service offering will continue to evolve over the next few months as discussions further shape the detail of the CSS strategy and offer which in turn will be reflected in the FBP to be submitted in August. Developing the SL CSS will be achieved through the already established SL CSS transformational programme. The priorities for this programme build on feedback from all pathfinders and local authorities 75
201 and include a focus on: Delivering a large scale cultural change: Setting a pace for the transition which will involve trade-offs e.g. long-term structure by 2012 vs. 2013; Improving the quality of services providing the architecture, tools, products and services to deliver the new clinical model of commissioning; Access to new skills and capabilities (obtained either by building internally or sourcing from outside) to secure the customer base thus ensuring the organisation remains commercially viable. Alongside this programme of work the SL CSS will, over the next 15 months, drive forward its business planning with the support of a number of enabling strategies including: Marketing & Business Development strategies; An OD plan; A Communications and Engagement strategy; A HR strategy; IT and Estates strategies. Key Risks in the development of Commissioning Support are detailed below: Risk 1. Leadership Engagement Lack of visible and committed leadership to fulfil obligations. 2. Continuing to provide commissioning support using the existing model within South London leads to economic unviability of the organisation in Risk of alienating key stakeholders throughout the transformation process, in particular LAs. 4. Inability to Deliver OBP to schedule will lose confidence of NHS London and customers 5. Poor quality submission can be extremely damaging to this newly emerging organisations reputation 6. Programme Decisions Requiring Sign off - good governance 7. Potential Distraction from PCT Cluster Activities Mitigation MD recruited. CSS Interim Leadership and CSS Development Team recruited. Development of CSS Executive programme meeting for South London, Discussion now under way re developing workstream leads with interim leadership team Leverage economic modelling to understand viability of any future operating model. Identify key areas to gain scale within commissioning support, either through partnership or JVs, e.g. Information. Current modelling suggests financial viability based on 9 out of 12 CCGs buying in Active engagement of LA as partners in the transformation process. Ensure communication channels are continually open. MD in post, strike up good relationship with NHS London as an organisation to be taken seriously. Ensure Delivery with quality. Additional support of NHS London Anthony Perry from NHS London as Advisor. Delay submission through negotiation as necessary to ensure appropriate quality Pathway for Board sign-off defined. Executive engagement through Executive Programme Group Programme to support staff through Process. MD and Team recruited 8. Initial delay to the process means a lot to do to achieve deadlines when compared to other London PCT clusters Balance planning and delivery of CSO with need to protect critical teams from distraction in crucial January to March period 76
202 Greater programme focus, keeping = to schedule and spreading the workload across the clusters 9. Lack of delivery in 2011/12 that undermines CCG belief in CSS as a partner 10. Decisions to be made with all the information not just based in silos 11. Risk of alienating customers throughout the transformation process. As part of OBC, build in service improvement into 2012/13 delivery efforts to create CCG confidence in CSS ability Facilitate integrated work across the work groups e.g. estates, IT, finance to provide information to make the right decisions. Engagement of right people with expertise to make the decisions Key events with CCGs conducted. Making the case for CCG and ensuring the business message is sold to CCGs competitively Active engagement of CCGs throughout the development process on the future of the organisation. Creation of a CCG advisory group to ensure full alignment with the ongoing transformation. 12. Staff Attrition lack of engagement 13. Period of transition April- October will require on-going programme dedicated support requirements. 14. Securing people with the right skills to support transformation 15. Failure to deliver business as usual 16. Lack of ability to compete with incoming private providers post Loss in flexibility for deciding end state of the organisation HR key member of transition team. Require on-going engagement strategy Adequate plans in place. Continual resource assessment. Marketing / tendering / buying in additional expertise / developing staff within the organisation with potential Tight central and internal performance management: workstream leads need to report business capabilities in interim leadership meetings Leverage advantage of current monopoly position to drive development of high value service for CCGs. Identify any outstanding skill gaps and address them through partnering or recruiting. Price competitive by leveraging scale and standardisation where possible. Working closely with the DH and SHA to understand the shape of other centralised services Milestones / Key Actions 1. Have identified experienced transitional leaders focussed specifically on the development of NHS CCS. 2. Build on the work done for checkpoint one of the business review process in the development of an outline business plan for checkpoint two. 3. Ensure that governance arrangements are in place which support the development of the SL CSS in an arm s length type arrangement clearly distinguishable from the SEL Joint Boards. 4. Ensure that shadow SLA arrangements or MoUs are developed and ready to be put in place between emerging CCGs and their choice of NHS commissioning support service. 5. Meet all requirements of BDU checkpoint three of the business review process. Deliverables 1. By end March By end March By April From April August
203 6. Develop and implement people transition plan for CSS in line with overall plan. 6. From April Finalise OBP. 7. March 2012 Outline Business Case, transition plan including organisation structure submitted 8. Expectations of each CCG clarified. 8. March 2012 MoUs with each CCG signed 9. Ensure clear leadership. 9. June 2012 Substantive Leadership appointed 10. CSS operating at arms length. 10. Sub-committee established 11. Governance arrangements in place to support. 11. April Organisation culture of CSS defined and developed. 12. September 2012 OD programme commissioned and in place May Develop full Business Case. 13. April 2012 to August 2012 Full Business Case and staged implementation, subject to HR framework 14. SL CSS fully operational October Summarise, including key milestones, the PCT Cluster s provision of development support and leadership development for pathfinders, which will be delivered during 2012/13. Work has taken place in 11/12 with CCGs to support their work with providers and through the cluster OD group share and learn together. This has enabled each CCG to have their own individualised plans which were devised with their providers to put them in a strong position for authorisation. (details of the milestones are monitored by cluster and NHSL) This will continue during 12/13, (confirmation is outstanding on 12/13 development monies) to ensure authorisation by April Milestones / Key Actions 1. Update and implement development plan in place (cluster) 1. April Ongoing monitoring of plans (cluster) and actions taken where needed Milestones / Key Actions 2. April OD terms of reference reviewed (all) 3. April Review and update development plans to all new policy guidance(all) June 2012 Summarise, including key milestones, the PCT Cluster s role in the development of the single operating model for the direct commissioning responsibilities the NHS Commissioning Board will have (including primary care, dental services, armed forces etc.), and plans for handover to ensure a safe and proper transfer of responsibilities in 2013 through an agreed process of convergence. Over the last nine months, the cluster has proactively supported the Once For London Pan-London Operating Principles and chaired the development of the PMS Review Principles within this work. The Cluster has developed through its Joint Standing Liaison Committee with the LMC, cluster wide policies for: Primary Care Performers List Management GP Locum Reimbursement GP Premises Cost Reimbursements & Rent Reviews- Application and Review Process 2011/12 QOF Process GP Performance Management (incorporating Pan London GPOC) 78
204 Infection Control and Prevention Programme GP Site Surveys Cluster wide policies developed for other contractor groups include: Primary Care Performers List Management Policy agreed with the LDC, LPC and LOC. Optometry Contract Compliance Arrangements Optometry PVV arrangements Pharmacy Contract Performance Management Arrangements Pharmacy Application Process Dental Performance Management Arrangements Initial discussions have been held with NHS South West Primary Care colleagues on joint programmes of work and sharing best practice to the advantage of both clusters. Directorate representation at DH/SHA events has assisted the development of policy. The above activity is assisting in creating a single operating model within NHS South East London which will assist in the transfer to the NCB model. The Cluster has commenced the stocktake stage of the contracts transition PCT Implementation Plan and will complete the sign off of the transition controls data capture tool and risk assessment for primary care contracting by the 16th January This has been achieved with the recruitment of interim support and it is intended to continue with this support through to the end of March Circa 1,200 contracts have been identified during this stocktake stage and a risk assessment is being completed to inform a development programme to provide a comprehensive and consistent contract portfolio for transfer to the NCB. This will address the regularisation of contract documentation and financial sign off of contract values by commissioner/provider. The Cluster will undertake a GP premises survey to ensure statutory compliance and to assist practices to prepare for CQC registration from April An application for improvement grant funds forms part of the 2012/13 capital bids to address highlighted issues. The issue of leases for those practices occupying PCT premises will be addressed and appropriate charging mechanisms put in place. The cluster has approved capital monies to rollout EMIS web with SCR and EPS2 capability to 138 practices in LSLG with a similar programme in Bromley. In Bexley there are 2 sites wishing to go over to EMIS web/vision. Early discussions have been had with local representative groups and cluster clinical advisors to form pilot LPNs and to work through this grouping to develop fully functioning LPNs to assist in commissioning decisions for the planning round 2013/14. The cluster is developing plans based on the Once for London List maintenance policy to undertake a review with practices of their registered lists. This work is aimed to set FP69 flags by the 1st October 2012 to regularise lists for the 1st April Milestones / Key Actions Milestones / Key Actions 1. Completion of Stocktake /01/ Risk Assessment and development of Action Plan /01/ Stabilisation of contract documentation and financial signoff within resource envelope. 4. Development of Local Professional Networks Pilots to fit for purpose vehicles /03/ /09/ Regularisation of Premises Issues /09/ List Maintenance Exercise /09/ EMIS Web Rollout with SCR and EPS2 capability /03/
205 Summarise, including key milestones, how the PCT Cluster will develop with emerging CCGs and local authorities the Joint Strategic Needs Assessment, Joint Health and Well Being Strategy, and joint/integrated commissioning arrangements during 2012/13. How will the PCT Cluster ensure successful handover to CCGs, NHS CB, and local authorities for these responsibilities? Each CCG is working very closely with their respective Public Health departments and with Local Authority colleagues on the JSNA and Health and Well Being Strategies. In all boroughs, local GP commissioners, the managing director, the DPH and NEDs sit on the Health and Well Being Board alongside local authority colleagues, councillors and patient and public representatives, to shape and develop health and social care strategies and policy. For each SE London borough, the Health and Well Being Strategy has arisen out of the JSNA, and has informed the CCG plan. Local strategies and QIPP plans have been presented to H&WB Boards to ensure good stakeholder engagement. In each borough, it is intended that the H&WB Board will be responsible for the regular refresh of the JSNA and relevant strategies, ensuring that there is appropriate engagement. Production of the JSNA is led by the borough DPH, who also supports the CCG by undertaking a range of tasks such as the production of specific needs assessments. Local CCG commissioning strategy plans have been collated by Cluster colleagues into a single CSP for SE London. This has been overseen and shaped by the SE London Clinical Strategy Group. All six CCGs will continue to work together through the Clinical Strategy Group, CSS arrangements and other coordinating systems (such as the joint office of the MDs, the SE London DPH group and the clinical networks) to ensure that there are robust and co-ordinated SE London strategies and plans in place. A single cluster JSNA has been produced out of which several public health priorities have been identified. These include immunisation. screening, TB, sexual health and vascular checks. All borough health and social care economies, led by local PH departments are linking into these cluster priorities. The DPH group monitors progress against the relevant targets, feeding into cluster wide performance management systems. In addition to the Cluster wide arrangements, South East London CCGs also work in specific groupings (eg BBG) to develop plans that respond to the needs of local populations and also provide a coherent platform for commissioning with key providers. Each CCG works within its borough to support and develop existing joint commissioning arrangements, and all are committed to further joint working underpinned by joint teams, pooled budgets, section 75 agreements, etc In preparation for the separation of functions, CCGs are already working very closely with Cluster colleagues to ensure a robust handover of arrangements to new organisations such as the NHS Commissioning Board and Public Health England. A systematic approach is being taken to ensuring as smooth a transition as possible, for example: - CCGs and Cluster colleagues have agreed funding for Commissioning Support Services and are about to commence on jointly shaping the new organisation - a transition board for public health has been set up with a specific workstream on transition of non local public health functions (to Public Health England) - all contracts, including those with independent contractors, have been identified and categorised in readiness for transfer to appropriate bodies Milestones / Key Actions 1. Shadow Health and Well Being Boards in operation in all 6 boroughs. Milestones / Key Actions 1. May Refreshed JSNA. 2. Late Health and Wellbeing strategies agreed in all 6 boroughs 3. March
206 4. Full Health and Well Being Boards operational 4. By March Summarise, including key milestones, the PCT Cluster s plan for the development of a Public Health transition plan to ensure successful handover of responsibilities to local authorities and Public Health England NHS SE London cluster has developed a detailed Project Initiation document (PID) incorporating a template for a local transition plan. These have been consulted on with all six local authorities and BSUs/PCTs. The PID formed the focus for structured reviews of progress taking place to develop robust local public health transition plans with each of the six boroughs across the SE London Cluster. Invited to these meetings which took place in February and early March 2012 were Borough lead officers and their colleagues in different functions including HR, Finance and Information as well as CCG Chairs or representatives, each DPH and local BSU representatives including Managing Directors as well as Finance, HR and Information. These meetings were well attended by a range of participants. The output of these local meetings has been to; Prompt progress in all areas of the transition process and ensure the development of robust transition plans at a local level. Ensure local ownership of the PID and transition plan template with local authority and health colleagues. Clarify where there is better value in having single SE London Cluster wide work streams. These have been agreed as HR, Information, Communications and Non local service delivery in Public Health transition. The HR work stream is already underway and has met several times. Draft terms of reference and participants for these other named work streams have been identified and dates for the first meeting of these work streams are planned. NHS Finance leads and their local authority finance colleagues will meet at the end of March 2012 to focus on improving understanding of the allocations and queries relating to the transfer of functions. Offer an opportunity to highlight areas where there are particular local challenges. Confirm all local boroughs are proceeding to design and develop local transition plans including local work streams on their future operating models, communications and engagement, HR, Finance and Information. The table in Appendix 1 shows responses from all local boroughs/dsph to the four questions identified by the NHSL Public Health Transition Director. The draft Memo of Understanding between health and local authorities and put forward by NHSL was reviewed at the SE London Public Health Transition Board in February It was agreed that a revised statement of intent based on the MOU would be shared with all Boroughs to develop and adapt to local circumstances for use with local health colleagues. It is expected these are all likely to be signed by the end of March The exception may be Bexley due to the continuing discussion about the level of financial allocation. Building on the work undertaken by the DsPH in Lambeth, Southwark, Lewisham and Greenwich looking at the potential for sharing public health services in the Autumn 2011, further work is being taken forward to explore this option based on the expressed interest of the four local authority Chief Executives. A first meeting of the design group is planned for the 20th of March 2012 and it is proposed that this work will continue up to the end of May It is agreed work will proceed in parallel to develop public health transition for each local authority in order that progress in the shadow year does not lose pace while considering the four Borough model in the first part of 2012/13. The cluster Public Health Transition Board is meeting monthly to coordinate all aspects of transition of 81
207 Public Health functions to local authorities, Public Health England and NHS Commissioning Board. Dates have been proposed for the shadow year 2012/13 and the group will continue to meet and oversee all aspects of transition throughout the transition period. The group will work to support 6 local transition plans in accordance with annex 6 of national guidance on transition. The Board is Chaired by the Director of Development, SE London Cluster. There are two recognised areas of risk to the timetable for creation and implementation of transition plans: 1. Bexley s allocation was the lowest in London and so they are to explore why this is the case and have started a process of comparison with neighbouring and comparable authorities. Bexley local authority has indicated they may not be able to proceed with Public Health transition without the allocation being reviewed. Work is underway to identify the impact of the relatively low allocation and the specific functions where there is currently low investment. This work is informing discussion about how to increase the allocation to Bexley. In the meantime, work on a transition plan is well established including co-location of staff with the local authority Bexley has not had a Director of Public Health for some time. The Borough have indicated they wish to build on the initial contract already in place to obtain public health advice through Kings Health Partners, Department of Public Health and Primary Care. Prof Peter Littlejohns has been appointed to the role of adviser on Public Health on a part time basis. 2. The design process of a possible four borough shared Public Health service is expected to have an initial report in May 2012 and a final proposal ready by September It is unclear at present what the likely outcome of that design process will be. This means that the timetable for transition will be challenged. As a result each local PH/BSU/council partnership is also working to plan a one on one local transfer of public health functions in order to ensure a fall back position in readiness for 1 st April Milestones / Key Actions 1. NHS SEL Public Health Transition Group established 1. Underway Milestones / Key Actions 2. Design processes for each borough underway 2. Underway 3. Assessment of implications of Shadow budgets 3. February Borough based plans for Transition of the Public Health functions 4. March Implementation of Transition Plans 5. Throughout 2012/13 6. Transfer of functions, staff and responsibilities 6. By end March Summarise, including key milestones, how the PCT Cluster will develop plans for the transition of specific responsibilities to local authorities, for example in addition to Public Health above, the known areas of, Complaints and advocacy, information and signposting, and Independent Mental Health Advocates (IMHA). This section should describe any planning to date and activities the PCT Cluster will undertake to agree and plan jointly with Local Authorities to ensure a safe and proper transfer of responsibilities during 2012/13. Enter text here outlining risks and mitigations where necessary. 82
208 Milestones / Key Actions 1. Enter text here NB. ensure actions listed are not business as usual activity NHSL will pre-populate milestones and dates where possible. Milestones / Key Actions 1. Enter text here NB. ensure actions listed are not business as usual activity NHSL will pre-populate milestones and dates where possible Section Six: QIPP Summarise the Cluster's key QIPP priorities and challenges for 2012/13: Our case for change outlines: increasing demand on the healthcare system in South East London, examples where patient experience needs to improve, the main determinants of ill health and mortality examples where performance of our NHS providers and the health outcomes that we are achieving fall short of our expectations and the economic imperative to achieve this within the context that the demand for, and costs of healthcare are both rising at a faster rate than our income. Doing the same things as before is not an option. Our Quality, Innovation, Productivity and Prevention (QIPP) programme, therefore, is designed to achieve step changes in the way in which healthcare is delivered, the outcomes that we achieve and to create the circumstances to ensure that our healthcare system is effective and clinically financially sustainable. This requires us to deliver the QIPP agenda at scale and pace. Productivity requirement In total QIPP savings schemes deliver productivity gains/savings of m in 2012/13. Although this represents a decrease of 17.54m from last year s target of m, 2012/13 presents a major challenge and is the most challenging year within the 3 year strategic planning cycle. Existing detailed QIPP savings plans have been reviewed by CCGs with support from Cluster teams. New QIPP schemes have been initiated and included in financial plans. We acknowledge that there are inherent risks to the delivery of QIPP plans and associated savings Performance against the 2011/12 QIPP target is projected to deliver savings at m (over 76% of target), a shortfall of m against plan. Despite the shortfall, this represents an unprecedented level of savings in any year and the following learning has been taken forward into the 2012/13 plan: It took longer than planned to implement a range of pathway redesign initiatives due to the wide ranging clinical and stakeholder engagement and procurement processes. Our 12/13 plans are more realistic in identifying lead times and ensuring enabling actions are completed early 11/12 initiatives that started later than planned provide a full year effect benefit within our 12/13 plans We have made significant progress already in agreeing 12/13 contracts with our main NHS providers, for example Lewisham contract was signed on 29 February We have risk assessed our 12/13 plans and scoped m savings in order to achieve the target of m (which is the value that our risk adjusted plans will save) 83
209 The impact of shortfalls against the 11/12 plans have been incorporated into the 12/13 plan We recognise the risks associated with increasing demand and implementation of QIPP plans and have identified reserves of m. QIPP savings and investments are phased appropriately throughout the year, linked to milestones QIPP savings targets for 2013/14 and 2014/15 are as follows (see also QIPP tracker) Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 QIPP savings requirement 2013/14 (5,145) (3,140) (7,817) (7,562) (5,278) (6,636) (35,578) QIPP savings requirement 2014/15 (3,161) (2,426) (3,911) (4,635) (3,909) (4,789) (22,830) The QIPP programme supports the 4 strategic priorities; Integrated care, Productive care, Staying Healthy and London-wide programmes Aspirant CCGs in South East London work in partnership to ensure that services are coherent for local people and that QIPP plans across commissioners are aligned. In this way larger more timely changes can be made through pursuing joint programmes across CCGs, with local authorities or across providers. In South East London models of each of these have been developed and renewed as CCGs increasingly lead commissioning. In outer South East London there is a Bexley, Bromley and Greenwich Commissioning Group chaired by Dr. Andrew Parson (Clinical Chair in Bromley) that has identified significant workstreams that are being progressed across all three boroughs. In Lambeth and Southwark an integrated care pilot is driving a significant change programme for the benefit of older adults living with long term conditions. Lewisham s focus is integration across the care pathway; maximising the benefit of the vertically integrated community and acute hospital services available from Lewisham Healthcare NHS Trust. There is a South East London Clinical Strategy Group that brings together clinicians from CCGs with the cancer and cardiac and stroke networks and has set a priority to develop a clinical strategy for urgent and unplanned care in 2012/13. This also facilitates the diffusion and sharing of innovative and good practice across south east London. The following table shows the 2012/13 QIPP plans by PCT by strategic priority Bexley Bromley Greenwich Lambeth Lewisham Southwark Total '000 '000 '000 '000 '000 '000 '000 Integrated Care 525 2,539 3,447 2,030 2, ,221 Productive Care 5,016 1,807 5,849 12,326 5,890 9,082 39,969 Staying Healthy Londonwide Other ,503 4,940 Total 6,316 4,710 9,892 15,256 9,150 11,043 56,366 Elements of the QIPP programme have been designed across more than one borough in order that the impacts are consistent on local providers that provide services to those boroughs for example: Lambeth and Southwark Lewisham Bexley, Bromley and Greenwich Kings and Guy s and St. Thomas NHS FTs Lewisham Healthcare South London Healthcare Trust The impact of the QIPP programme has been shared with all main providers with a view to agreeing whole health system changes and cost efficiencies and assisting provider organisation planning. Reducing avoidable emergency admissions is a priority within our commissioning strategy and QIPP 84
210 CCGs are the future local leaders of the NHS and, through delegation, are responsible for delivery QIPP. Our approach has been led by local clinicians at borough level, designing three year QIPP plans that address local issues where necessary and that also take opportunities where appropriate to address larger scale issues and achieve larger scale benefits across bigger populations. QIPP plans are therefore a rich blend of local, pan borough and cluster wide initiatives to improve quality and productivity, create opportunities for people to live healthier lives and to foster environments where innovation can flourish. Underpinned by a commitment to high quality primary care, our plans will improve A&E and UCC services. Our approach is to prioritise the creation of new large scale integrated care systems, including expanding predictive modelling to identify patients at higher risk of requiring urgent care together with disease specific case management. We are also expanding existing services, through diffusion, that have proved successful such as community falls prevention and COPD services, home based care and supporting self care. 2011/12 is year one of our three year strategic planning horizon. The following table shows the 2012/13 QIPP plans by PCT by QIPP level 2 category Bexley Bromley Greenwich Lambeth Lewisham Southwark Total '000 '000 '000 '000 '000 '000 '000 Activity Shifts 450 1,739 1, ,775 Acute Sector 3,620 1, ,000 3,759 4,459 18,434 Back Office Community Support services ,699 1, ,924 Decommissioning Ineffective Procedures End of Life Care Estates ,253 4,490 Long Term Conditions ,668 Mental health ,354 2,820 1,350 1,561 7,659 Planned Care Prescribing ,057 1, ,503 Prevention Primary care productivity 0 0 1,000 3, ,613 7,500 Referral management ,055 Staffing Staying Healthy Urgent care ,718 Total 6,316 4,710 9,892 15,256 9,150 11,043 56,366 85
211 Impact on Main Providers The following table shows the income impact on main providers excluding potential new income from activity shifts Bexley Bromley Greenwich Lambeth Lewisham Southwark Total '000 '000 '000 '000 '000 '000 '000 GST ,922 1,337 2,411 7,043 Kings , ,628 6,101 Lewisham , ,572 Oxleas SLAM ,120 1,350 1,561 6,156 SLHT 3,502 3,040 6, ,372 St Georges Darent Valley Other Total 4,545 3,328 7,765 8,370 6,956 6,730 37,694 Governance Responsibility for the delivery of the QIPP programme rests with designated Directors on behalf of the chairs of the 6 aspirant CCGs and the Chief Executive. For the final year of transition (2012/13 being the shadow year ) we have revised our governance model to enable Local Clinical Commissioning Committees (LCCCs) to exercise delegated approaches to quality, performance and finance as part of preparation for full statutory establishment, following authorisation, from April This is underpinned by new integrated governance and reporting framework. This approach formalises our aspiration that every pathfinder will have full commissioning delegation covering Acute, Community and Mental Health from April The Chief Executive remains the formal Accountable Officer until April Our monitoring will be effective, issues will be promptly resolved, risks identified and managed and impediments to delivery will be removed at the earliest opportunity. Our approach will be: 2012/13 will be the shadow year for Clinical Commissioning and the final year of transition prior to the abolition of Primary Care Trusts in April From April 2013 a revised governance model will enable Local Clinical Commissioning Committees (LCCCs) to exercise delegated approaches to quality, performance and finance as part of preparation for full statutory establishment, following authorisation. Core components are: CCGs to take full shadow responsibility reflected in LCCC business and reporting to the joint boards A joint integrated governance committee (incorporating Quality and Safety and Finance, Performance and QIPP) Three tier focus on o o o Lambeth, Southwark and Lewisham Bexley, Bromley and Greenwich South east London wide Monthly performance reporting and committee arrangements Improvements to the Board Assurance Framework The operating plan and CSP delivery monitoring information needs are built into the requirements for commissioning support arrangements from April 2012; designed to give early warning of issues to be addressed. Our cluster level resources will be organised to provide targeted support for the resolution of issues arising, whether with borough or cross-borough initiatives and performance or with wider 86
212 threats to the delivery of the South East London QIPP plans. Provider Engagement and Agreement QIPP plans, and their impacts and opportunities, have been discussed with all main providers as part of our usual business cycle, alongside our commissioning intentions. Contractual negotiations for 2012/13 are well advanced and agremeent has been reached with Lewisham Healthcare Trust. For Acute providers. The SEL Acute Contracting team has shared QIPP intentiions with acute providers (SLHT, GST and King s) in November and December 2011, leading to a timetable of contracting and negotiations through to year end, with clinical commissioners, supported by the Acute Contracting Team, engaging with hospital clinicians at borough level. With SLHT there is a specific concordat/proposed strategic framework that looks to the next 3-5 year planning cycle and a BBG clinical contract group to negotiate the detail. For out of major out of area providers. BSUs and CCGs have engaged in the commissioning planning process for providers outside SEL. For example Bexley have engaged with NHS Kent & Medway and Dartford, Gravesham & Swanley CCG in relation to priorities and financial projections for Dartford & Gravesham Trust. For Community and Mental Health Providers. Individual BSUs have shared QIPP intentions with community providers: Oxleas, Bromley Healthcare, Lewisham Healthcare, GST Community Services and King s. Where appropriate boroughs have worked jointly for example for GST Community services QIPP was flagged as part of the bilateral transfer agreement signed at the end of March 2011 between Lambeth & Southwark and GST, with current QIPP positions confirmed as part of contract negotiations during early QIPP Tracker The QIPP tracker is appended to this Operating Plan. It shows key milestones to be achieved in the delivery of our QIPP plans and will be used for monitoring performance throughout 2012/13. Borough Based QIPP plans The following sections provide an overview of QIPP priorities by borough/aspirant CCG Bexley Acute: The approach to driving up the quality and productivity within the acute care system is based on a balance of incentives and penalties to create change in the system. Through the contracting round with the local acute providers, agreements are being made that seek to support the drive to care for more patients in the community setting, integrate care and reduce the unnecessary admissions into hospital. 50% of the projected efficiency gains next year will come from; Reductions in the consultant to consultant referrals, Reduction in the number of operational first to follow up appointments Reduction in the number of short stay emergency admissions from A&E Reduction in the length of stay for some speciality areas including general surgery and elderly care Reduction in the variance of GP referrals to bring practices to median quartile or above for both outpatient and inpatient elective referrals Client Groups: Quality and productivity savings have been identified through specific client groups and service areas. Priorities include: Mental Health Out of Borough placements Crisis and outreach teams ADHD pathway redesign SLAM referral management 87
213 Community services Community Nursing services Step up/ step down beds Primary care: Prescribing in primary care Referral management Productive General Practice scheme A key local priority is to improve the co- Many of these programmes are focused on Long-term condition pathways and integrated care: ordination of care across providers for individual patients. patients with long-term conditions including; Diabetes COPD / oxygen management Long Term Neurological Rehabilitation MSK Cardiology Anticoagulation Transformational programme longer term programmes In order to manage the rising incidences of long term conditions and increasing elderly dependency, a longer term and transformational programme of work is also being developed which takes a whole system approach, linking improvements in integrated care, primary care performance and elective care. Some of the strands of work that are being explored include: Development of the QMS campus Development of an integrated care model across primary, secondary and social care for older people and patients with long term conditions Development of a locality delivery network in primacy care to provide extended weekday and weekend out of hours from a hub practice, supported from other local practices and extended range of services including community services, outpatient appointments, minor procedures, urgent care services, diagnostics. This could include; o Increase in GP appointment capacity and redesign skill mix to absorb outpatient appointments o Expand use of GP telephone consultations o Implement productive primary care o Review risk stratification process, care planning and extend multi-disciplinary team working for all major pathways to improve the co-ordination of care and a registry of all patients to be held by the MDT o Develop clinical protocols ad care packages (pathways of care) o Improve peer review and encourage learning between practices, which includes the use of comparisons tables between GP practices and monthly tracking. o Robust monitoring and review of non GP referrals (e.g. consultant to consultant referrals) o Streamline out of hours access, integrated with the new 111 service. Bromley Access and Choice: To improve access to and extend choice of services to all patients, services users and their carers, ensuring that clinical pathways are fit for purpose and that the services we commission meet the highest possible quality standards, whilst increasing the pace on delivery of the quality, innovation productivity and prevention (QIPP) challenge. Schemes include the rollout of telephone across primary care and providing care closer to home on specific care pathways such as dermatology and gynaecology. Prevention: Empowering those people in Bromley with long term conditions, particularly older people, to exercise control over their own lives and prevent problems arising or worsening and enabling them to independently manage their own health and wellbeing; thus improving their health outcomes and preventing them dying prematurely. 88
214 Strengthening and fully integrating the infrastructure supporting this cohort of people ensuring that their health needs are met 24/7 in a planned and structured way. Schemes contributing towards this include the development of the Proactive Management of Integrated Services for the Elderly (ProMISE) and improvements to intermediate care. Engagement/Education: Ensuring that patients, service users and their carers are at the centre of all decisions we take around their healthcare, and have a positive experience of care. This aims to reduce health inequalities by keeping patients, service users and their carers better informed around adopting a healthier lifestyle through a programme of education and targeted interventions known to work to increase the control they have over their own health and wellbeing. Staying Healthy schemes contribute to this, such as improving the rate of smoking cessation and proactive weight management. Greenwich: Improve long-term conditions care for all ages, through: Prevention and self-management support/support to carers Targeting interventions according to need & extending the range of services available Better coordination between providers & integration between health, social and other care Schemes include integrating primary care incorporating the development of intermediate care at home and building up consultant led sub-acute capacity in existing beds and case finding of vulnerable patients Increase capacity in high quality cost effective alternatives to hospital based planned care, linking these to hospital services in ways that avoid fragmentation and duplication. Schemes include the development of a comprehensive community cardiology services pilot Co-ordinate the provision of urgent and out of hours care, reducing duplication including the development of a whole systems model for an integrated urgent care system enabling the development of a specification to tender for the whole system. Improving mental health care, by focusing on: The interface between primary and secondary care Increase service users choice (children and young people, adults of working age and older adults) Access to services that maximise recovery, prevent relapse and admissions to acute care Children and Young People s Services: A whole system approach, focusing on prevention and developing integrated care pathways and services. Enhance the quality of end of life care, through: Better coordination between service providers, implementing an integrated model Enabling people to die in the place of their choice Implementing best practice pathways and frameworks Staying Healthy initiatives targeting obesity, diet and Physical Activity and smoking cessation Lewisham Improving long term conditions care thereby reducing emergency admissions and improving outcomes for patients. Schemes include agreeing and implementing new pathways for diabetes and COPD and proactive management through improved assistance in taking prescribed medicines and telehealth pilot. It is for a limited number of patients and an exit route may be needed if the scheme does not prove successful. Improving Urgent Care through the development and provision of medical assessment and a simplified route to social care assessment. Provision of integrated care through aligning community, acute and prevention services. Promotion of staying healthy initiatives, such as smoking cessation and weight management. 89
215 Lambeth Lambeth faces continuing growth in demand and cost of secondary care services, driven by population growth, demographic changes and the expansion of available health technologies. People are living longer in Lambeth in the past 10 years average life expectancy for men has increased by 4 years and women by 2 years. There is also an increased expectation of the quality and extent of health service delivery as a consequence of advances in medicine. At the same time the rate of increase of funding for the NHS has considerably slowed down to just above inflation. This means that the underlying rate of deficit will increase if no action is taken. It is clear that the level of financial challenge facing the NHS over the next few years is unprecedented, especially when compared to the significant levels of financial growth enjoyed by the NHS over the last decade. A step change in how we approach the development and delivery of QIPP plans is therefore required to address the level of financial deficit in the do - nothing scenario. The financial challenge facing NHS Lambeth is therefore to secure significant QIPP delivery over the course of the next three years to provide the financial resource to support delivery of our vision, health goals and supporting strategies. If no action is taken then the underlying financial positions will deteriorate, year on year resulting in a worsening in the current cumulative position. The plans to achieve this are set out in Section 7. Governance Lambeth has developed a programme approach to the delivery of QIPP supported by formal contract management arrangements. The programme structure is set out overleaf. Staying Healthy: Improving health inequalities and the preventions of ill health. Schemes include smoking cessation and alcohol work in A&E to reduce harm and target younger people. Improving Long Term conditions: Focusing on next stages of pathway redesign for diabetes, cardiovascular disease and respiratory services, including the Increase in access to patient education. Multi-disciplinary community based services with a remit to support and develop skills in general practice will be commissioned to support patients. Patients will be identified at an earlier stage of disease and get them into to treatment Mental Health: Supporting and developing self management through personalisation and peer support. Implementing the next stage of the Living Well Collaborative co-production approach and new service offers to people with long term mental illness in partnership with SLaM, social care, primary care and the third sector. Review of residential provision for people with dementia. Unplanned care: Developing a single point of access for community based services and reviewing the implementation of the pilot of the virtual ward (with Southwark) which uses patient registers and risk stratification to identify patients. Urgent Care: Commissioning Urgent Care Centres in conjunction with Southwark at Guys and St Thomas, which will redirect patients from A&E through an alternative pathway. Southwark Working with Lambeth BSU we have agreed a major programme of investment in community admission avoidance services, funded from reinvested 30 day readmission penalties. Services will include: Enhanced Rapid Response services, accessible both directly from GPs, community and via A&E/acute hospital referral Virtual Ward - Risk stratification and early intervention - a multi-disciplinary team model, led by community matrons using risk stratification tools and providing timely interventions Specialist respiratory nursing support to provide a hospital at home approach and support the management of COPD linking to community respiratory team 90
216 Enhanced social care assessments, rehabilitation interventions and availability of community equipment on a rapid delivery basis Night Owl Service with generic workers to respond to basic health, social or domestic needs Link to re-ablement strategy to support earlier discharge and prevent re-admission Improved management of LTC focussing on diabetes, respiratory and heart failure Mental Health: Southwark BSU and SLaM jointly manage a two-year programme of change to efficiencies across Mental Health services. The programme of change focuses on delivering quality interventions as part of improved and costeffective patient pathways, achieved by service redesign, synergy of provision, reduction of activity by enhancing the provision of effective recovery services, delivering care out of hospital and specialist settings and de-commissioning clinically unnecessary activity - more specifically: 1. Redesigning Community Mental Health Team (CMHT) 2. Redesigning Crisis intervention and management by reconfiguration of Assertive outreach and Home support teams, including the liaison teams that support crisis management. 3. Reducing Length of Stay (LoS) with a programme to deliver a greater proportion of care in primary care and decommission the work from SLaM. 4. Rationalising and redesigning Counselling 5. Reduce out-of-area provision for CAMHS placements 6. Redesign Psychosis management, to enable earlier intervention, maximise maintenance and minimise crisis intervention Urgent Care: Procurement of Urgent Care centres at front end of A&E to manage minor activity. Re-commission GP-led Walk in centre, with an emphasis on redirection from A&E and A&E avoidance Improved LTC management in primary care, supported by community services for diabetes, respiratory and heart failure should reduce A&E admissions Improving walk in access to primary care including extended hours High level Risk Summary Risk Impact Mitigation Planned activity shift to out of hospital settings is not Shortfall against QIPP savings plan Robust implementation planning fully effective Budget overspend Risk assessed plans Scoped 86m savings in order to achieve the target of m Financial reserves QIPP savings and investments are phased appropriately throughout the year, linked to milestones Robust PMO arrangements Robust monitoring of activity and finance performance Planned admissions avoidance is not fully Shortfall against QIPP savings plan Robust implementation planning effective Budget overspend Risk assessed plans Scoped 86m savings in order to achieve the target of m 91
217 Referrals are higher than planned Providers do not close capacity Providers do not agree with QIPP schemes QIPP plans reduce provider income faster than providers can reduce cost Shortfall against QIPP savings plan Budget overspend Unplanned expenditure on supply led unplanned activity Budget overspend Provider overspend if activity does not flow Provider does not close capacity Unplanned expenditure on supply led unplanned activity Budget overspend Provider overspend if activity does not flow Whole system instability Provider financial position worsens FT application adversely affected Whole system instability Provider financial position worsens FT application adversely affected Financial reserves QIPP savings and investments are phased appropriately throughout the year, linked to milestones Robust PMO arrangements Robust monitoring of activity and finance performance Robust implementation planning Risk assessed plans Scoped 86m savings in order to achieve the target of m Financial reserves QIPP savings and investments are phased appropriately throughout the year, linked to milestones Robust PMO arrangements Robust monitoring of activity and finance performance Early agreement of contracts Borough QIPP plans are consistent in objective and timing for common local providers Clinical agreement on evidence based pathways Decommissioning plans Robust monitoring of activity and finance performance Early agreement of contracts Borough QIPP plans are consistent in objective and timing for common local providers Clinical agreement on evidence based pathways Decommissioning plans Early agreement of contracts Borough QIPP plans are consistent in objective and timing for common local providers 92
218 Insufficient clinical leadership to lead the QIPP agenda Shortfall in numbers and/or skills of workforce in out of hospital settings System reform reduces focus on QIPP Slippage in QIPP delivery Lack of agreement with provider clinicians Clinical agreement on evidence based pathways Decommissioning plans Full delegation to clinical commissioning committees from April 2012 Early authorisation of CCGs Full compliment of clinicians on clinical commissioning committees Development of clinical champions GP leader development programmes Cluster workforce plan Shortfall in capacity in out of hospital services Patients will flow to hospitals if capacity has not been closed Quality may reduce if workforce lacks skills Workforce uncertainty Early CCG authorisation Robust CSO plans 93
219 Section Seven: Finance Planning Please complete the financial planning spreadsheets attached as Annex A Overview of financial position Delivery in 2012/13, including FCOT, risks, opportunities, non-recurrent matters, etc. Pan-Cluster overview for 2012/13: All CCGs within South East London have developed plans to deliver surpluses in line with the 1% surplus requirement, although it should be noted that this is dependent on the return of 2011/12 surpluses. The underpinning plans that enable the delivery of 2012/13 surplus requirements have been developed utilising robust processes, modelling and methodologies for assessing underlying demand and service pressures, price pressures and issues, QIPP initiatives and delivery plans. In doing so we have reviewed historic performance and trends and also ensured lessons from 2011/12 processes and delivery have been learnt. In addition to robust underpinning processes we have focussed specifically on risks and opportunities in finalising our plans for 2011/13, including ensuring that we have taken proactive steps to mitigate risks where feasible at this stage of the planning process. The key risk risks and opportunities are summarised below: Over performance against 2012/13 start plans Our modelling of underlying demand has been more sophisticated for 2012/13, utilising an approach that moves away from a straight line outturn projection to one that models on the basis of seasonality and working days. We consider that this approach provides a more realistic baseline for our contracts. In addition we have worked with providers to assess the further activity impact of meeting key targets for 2012/13, particularly RTT, to enable these to be quantified up front for start contracts. Finally we have set aside population and incidence reserves to fund further expected increases in demand over 2012/13. Pace and scale of change associated with the delivery of QIPP savings Key mitigations have been: learning lessons form 2011/12 QIPP delivery in terms of allowing within our plans for the phased delivery of savings over the year, the development of plans in excess of the bottom line savings requirements to mitigate against under delivery, collaborative work with providers over 2011/12 on 2011/12 plans and a contractual approach that makes explicit the responsible owner and risk holder for each QIPP initiatives. The impact of PbR tariff in 2012/13, including for mental health providers We have been prudent in our assumptions and have established reserves to cover prices pressures such as Best Practice Tariffs and to mitigate against areas of the contract where national average assumptions are not delivered due to case mix. In addition we have worked with providers to complete as much work as possible on expected and known tariff issues, across both PbR and local prices, to ensure prior agreements have been reached at an early stage, thus enabling accurate assumptions to be reflected in our 2012/13 plans. Return of 2012/12 surpluses, thus providing the flexibility to ensure delivery of 2012/13 surplus requirements. Successful negotiation of 2012/13 contractual agreements Our intention is to sign contracts in a timely manner, thus providing financial certainty in relation to contractual agreements and commitments for the start of the year. To facilitate this we have been working with providers since the summer to enable early agreement on approaches to key issues. Agreed contract terms represent an opportunity in terms of enabling effective risk mitigation, particularly in relation to QIPP, as above. Access to 2% non-recurrent funds 2 % non-recurrent funds will provide opportunities for delivery and risks if funds are not forthcoming to facilitate the delivery of QIPP initiatives. As this stage CCGs have been prudent in committing 2% non-recurrent funds while we await confirmation of the proposed NHS London 94
220 approach in 2012/13. However at this stage some assumptions have been made and these are listed in section Key assumptions in 2012/13 Including but not limited to: - Service developments - Tariff impact / changes - Workforce - Commissioning intentions - N/R items - Cluster access to 2% N/R funds - Readmissions and reablement funds - Cluster risk pooling fund (CTB) - sources and applications CCGs across the Cluster have work closely together and with Cluster colleagues in developing robust and consistent budgetary assumptions for 2012/13 in line with Operating Framework guidance, building on and updating previous plans and sharing intelligence across boroughs as well as learning the lessons from 2011/12. Service developments A range of service developments are planned for 2012/13 focussed specifically on supporting the delivery of SEL CCG Commissioning Intentions and agreed service redesign initiatives to support QIPP delivery. Over and above these locally initiated service developments the SEL Cluster will be implementing though contracts London Commissioning Intentions, new NICE guidance and new cancer drugs. The key focus of our agreed service developments is agreement and implementation of developments that further our strategic intention of shifting work from acute to community based settings and delivering care pathway redesign to do so. Tariff impact/changes Looking back on 2011/12, it is clear PCTs assumptions around the level of underlying growth, particularly in the acute sector, were in line with expected population and incidence growth but that price pressures had limited the ability of PCTs to ensure adequate investment in volumes to meet underlying demand. In developing 2012/13 budgets and in preparing for the negotiation of 2012/13 contracts, contracting teams have agreed up front a number of assumptions relating to price changes in 2012/13 and these assumptions are included in CSPs and Operating Plans. In terms of the impact of the 2012/13 PbR tariff, while a national -1.8% tariff deflator was expected and this is built into budgets, past experience would suggest that such as assumption is risky and CCGs have therefore assumed a further 0.5% cost pressure relating to the acute tariff. In addition, QIPP savings plans have not been delivered in full in 2011/12, which has contributed to financial pressures faced by PCTs. The Cluster is mitigating against this by the development of additional QIPPs in 2012/13, allowing the establishment of QIPP risk reserves as a contingency should the pace of delivery be slower than planned. Workforce Agreement of contracts and triangulation of plans across London should ensure that provider workforce plans are informed. The impact of structural reform on commissioner workforce plans continues to be understood and refined in line with ongoing CCG and CSO developments. Commissioning Intentions Each CCG has developed its own local commissioning intentions as part of the SEL Cluster CSP and in addition the CSP includes a number of Cluster wide priorities and commissioning intentions. For the 2012/13 operating Plan we will be implementing year 1 deliverables, focussing specifically on implementing agreed service and care pathway redesign to support QIPP and on supporting the delivery in SEL of London and national commissioning priorities. From a financial perspective where commissioning intentions require investment or pump priming these have been accounted for within our plans for 2011/12 and where it is anticipated that they will deliver savings these have been reflected in our plans, but with mitigation with respect to QIPP particularly also built in to our plans. 95
221 Recurrent Uplifts, Tariff and Generic Uplifts, Demographic & Non-Demographic Growth and Primary Care Prescribing Uplifts A summary of uplift assumptions, on average across South East London are set out below. Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL Recurrent uplift 2.80% 2.80% 2.80% 2.80% 2.80% 2.80% 2.80% Reablement 0.18% 0.18% 0.18% 0.18% 0.18% 0.18% 0.18% Total Uplift 2.98% 2.98% 2.98% 2.98% 2.97% 2.98% 2.98% demographic Growth 0.40% 0.39% 1.25% 0.51% 0.74% 1.63% 0.83% Non-demographic growth 1.24% 1.20% 0.99% 1.10% 0.73% 1.12% 1.05% Total population & incidence growth 1.64% 1.59% 2.24% 1.60% 1.47% 2.75% 1.88% Prescribing growth 5.00% 6.00% 5.00% 5.00% 5.00% 5.00% 5.21% Tariff/ Inflation Uplift 1.90% 2.01% 1.88% 2.03% 2.03% 2.03% 1.99% Tariff efficiency assumption/ Price Efficiency applied (2.99%) (3.12%) (2.97%) (3.21%) (3.15%) (3.19%) (3.12%) Net Tariff/ Inflation Uplift (1.09%) (1.11%) (1.08%) (1.19%) (1.12%) (1.16%) (1.13%) Further details on uplift assumptions are provided below: Recurrent Uplifts PCT Revenue Resource Limit (RRL) uplifts are as per confirmed allocation uplifts of 2.8% plus a further 0.18% in respect of reablement. Tariff and Generic Uplifts Tariff uplifts have been assumed at a net -1.8%, including a built in 4.0% efficiency assumption. This has been applied to acute, mental health and community spend. Funds have also been earmarked to fund the expected impact of the ending of the MFF payment cap, applied to Guy s & St Thomas in 2011/12. Demographic & Non-Demographic Growth Detailed work has been undertaken to review planning assumptions related to demographic and non demographic acute growth for the CSP. The objective has been to ensure robust and realistic borough based planning assumptions related to population and incidence factors, which take account of demographic growth estimates and historic acute demand trends. To do so the following process has been undertaken: A review of population growth assumptions by borough (including GLA and ONS figures) for acute services. A review of historic demand trends by borough for acute services, with supporting trend analysis completed for the following key areas of acute activity outpatients, elective, A&E attendances, and emergency admissions, maternity and other. The development of proposed demographic and non demographic growth assumptions by CCG by admission method, applied on a consistent basis across the six SEL boroughs. The testing of assumptions with SEL clinical commissioners, CCGs and CSP leads, to confirm proposed planning assumptions. This process has resulted in a consensus agreement, supported by robust analytics, on the demographic and non demographic assumptions to be utilised for the CSP. Brought Forward Surpluses Forecast surpluses for 2011/12 have been assumed to be carried forward into 2012/13. Full Year effect of 2011/12 outturn The full year recurrent impact of 2011/12 forecast outturn expenditure has been included within 96
222 2012/13 expenditure plans, including the costs of reinstating PCT contingencies at 0.5% of recurrent resource limits. Investment Proposals and Cost Pressures Borough investments and cost pressures as developed by CCGs have been included in financial plans for 2012/13. Cluster teams have facilitated the sharing of information and guidance across CCGs to ensure plans are robust. QIPP Savings Initiatives Existing detailed QIPP savings plans have been reviewed by CCGs with support from Cluster teams. New QIPP schemes have been initiated and included in financial plans. In total QIPP savings schemes across in 2012/13 total m. However schemes have been RAG rated to deliver savings of m and it is this total that is assumed to be delivered within financial plans. A summary of QIPP initiatives and their impact by expenditure area over 2012/13 are set out below: Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Planned QIPP Savings Before Risk Rating Acute 7,998 6,058 8,430 7,134 8,663 6,629 44,912 Client Groups 1,028 (103) 2,558 6,542 1,800 1,130 12,955 Primary Care 750 1,095 1,692 7,407 1,650 4,700 17,294 Corporate , ,843 3,685 Other Budgets and Reserves , ,068 Total 10,551 7,535 13,122 22,883 13,521 14,302 81,914 Planned QIPP Savings After Risk Rating Acute 4,245 3,917 7,189 5,251 5,606 5,429 31,636 Client Groups 733 (148) 1,144 3,998 1, ,976 Primary Care ,117 5,107 1,238 3,213 11,814 Corporate ,503 2,645 Other Budgets and Reserves ,295 Total 6,316 4,710 9,892 15,256 9,150 11,043 56,366 2% Non-Recurrent Funds Plans assume that 2% funds will be made available in full as an enabler for QIPP delivery and to effectively manage the transition to the new commissioning environment. However, at this stage CCGs have been prudent in committing 2% non-recurrent funds while we await confirmation of the proposed NHS London approach in 2012/13. Emergency, Readmissions and reablement funds No assumptions have been made relating to the reinvestment of 70% emergency over-performance funds transferred to NHS London, noting that these funds are minimal across South East London, due to the high 2008/09 emergency baseline and the fact that emergency admissions have reduced since 2008/09 in most areas. New reablement funds allocated to PCTs in 2012/13 have been earmarked for investment in agreed whole system initiatives. National guidance for emergency readmissions has recently been confirmed. We will be reflecting the guidance in our contracts with SEL providers for 2012/13 with an agreed clinically led audit over Q1 to agree appropriate non-funding agreements and targets with providers. However a number of local commitments have already been made in relation to investment in admissions avoidance schemes and where this is the case all parties have agreed that existing commitments will be honoured. 97
223 Risk Pooling CCGs in South East London agreed a policy of mutual financial assistance in 2011/12 so the importance of ensuring financial balance and legacy across the local commissioners as CCGs move towards full authority by 1 st April 2013 is supported and understood. The Operating Plan for Bexley includes an assumption that 4.8m of financial support made available to the CCG in 2012/13 and that this is repayable in 2014/15. The SEL Cluster is facilitating the agreement of this support, initially on a voluntary basis and then by using 2% non-recurrent funds across all CCGs. Running Costs QIPP plans assume the delivery of running costs reductions in 2012/13. The Cluster is in the process of assessing the redundancy provisions requirement to include in 2011/12 PCT accounts Key bridging movements from 2011/12 FCOT to 2012/13 plan Including changes by revenue type, cost type, QIPP, overall surplus/deficit and underlying surplus/deficit. Key bridging movements for each CCG and for the cluster as a whole are set out below: Income and Expenditure changes 2012/13 Bexley Bromley Greenwich Lambeth Lewisham Southwark Total SEL cluster '000 '000 '000 '000 '000 '000 '000 Income Recurrent Uplift 10,140 14,622 13,383 18,262 15,244 15,393 87,044 Prior Year Surplus brought forward 2,245 5,992 4,612 6,605 5,375 5,857 30,686 Total Income Changes 12,385 20,614 17,995 24,867 20,619 21, ,730 Expenditure Full year effect of 2011/12 outturn 9,718 2,934 9,901 17,065 10,916 5,382 55,916 Net Generic Uplifts Tariff and generic uplifts 6,629 9,861 8,658 12,781 10,618 10,616 59,163 Efficiency with Tariff (10,425) (15,331) (13,629) (20,271) (16,480) (16,671) (92,807) Net Tariff/ Generic Uplift (3,795) (5,470) (4,971) (7,490) (5,863) (6,054) (33,644) Demographic & Non-Demographic Growth demographic Growth 1,370 1,900 5,698 3,150 3,815 8,422 24,354 Non-demographic growth 4,277 5,824 4,506 6,841 3,803 5,763 31,016 Total Demographic & Non-Demographic Growth 5,647 7,724 10,204 9,991 7,618 14,185 55,370 Investment Proposals and cost pressures 3,623 15,116 8,043 13,556 11,579 12,923 64,840 QIPP Savings Initiatives (6,316) (4,710) (9,892) (15,256) (9,150) (11,043) (56,366) Change in Recurrent Expenditure 8,877 15,594 13,285 17,867 15,100 15,393 86,116 Surplus/ (Deficit) 3,508 5,020 4,710 7,000 5,519 5,857 31,615 Surplus as % of Recurrent RRL 1.0% 1.0% 1.0% 1.1% 1.0% 1.1% 1.0% 98
224 7.4. Delegation of budgets to pathfinders / CCGs Including commentary on: - 2/head GP development - Budgets delegated to pathfinders / CCGs at 1st April Timeline for delegation of budgets (if not fully delegated at 1st April 2012) The Cluster and CCGs are working towards completing the process of full delegation of budgets to CCGs by 1st April The active involvement of Clinical Commissioners in the 2012/13 acute contracting round is part of the process of embedding full responsibility for these budgets. All CCGs are planning on 2/ head GP development funds being available in full in 2012/13. These funds are included within the 2012/13 Operating Plan and will be used to support the development of CCGs. This includes meeting the cost of supporting organisational development and systems of governance, developing a strong local clinical network and taking forward practice level information analysis. Planned outcomes for delegated commissioning activities are incorporated within Operating Plan and Business Plans. Outcome measures cover: Delivery of Financial balance and our QIPP plans Quality assurance of ongoing safety of services Patient reported outcomes and improved patient experience of services Enhanced effectiveness of services and care pathways Shift of care to out of hospital settings and from treatment to prevention Delivery of performance standards. It should be noted Operating Plan budgets include specialist commissioning and public health budgets in full. Specialist commissioning budgets have been set in line with agreed LSCG budgets and therefore the impact on other CCG held budgets has been built into assumptions Activity 99
225 Overall activity levels, split by providers where significant, specifically: - Summarise your overarching objectives around activity across the Cluster in relation to particular providers and settings - Include intentions in relation to outpatient, elective and emergency growth / reductions in comparison with forecast 2011/12 outturn - Cover how this links to commissioning intentions and the QIPP priorities outlined in section 6 and your Milestone Tracker - Cover how planned activity provides the capacity to deliver RTT - Outline those productivity metrics to be met/achieved at key providers - Include value of 70% emergency admissions threshold monies to the SHA Overarching objectives Our activity plans support our strategic goals, as described in Section 1 above. The overall productivity improvement target is 117m over four years. We believe that patients should be treated in hospital where necessary and at home or closer to home where possible. The majority of patients are best cared for in the community, providing better access to care closer to home and avoiding unnecessary visits to hospitals for routine care. A more localised model of care closer to home also enables patients and carers to take greater control over their care and self-management of their conditions. Currently, south east London has a high level of emergency hospital admissions which could be managed in primary and community care, particularly for patients with diabetes and respiratory illnesses. These objectives are shared across the Cluster and are equally applicable to all providers. Intentions for Outpatients, Elective and Emergency Admissions Activity modelling for this Operating Plan builds on the assumptions in the CSP. The methodology takes the forecast outturn for 2011/12 (which incorporates a seasonal adjustment for emergency admissions) and builds in the demographic growth forecasts for each borough and adds an assumed level of acute activity growth (based on historical trends) to reach a forecast baseline. Some adjustments are then made for known non-recurrent activity changes occurring in-year, e.g. service developments. The borough-specific QIPP initiatives are then factored in to give a planning figure for each activity category for each borough. This modelling is applied across all acute providers to give a projected activity plan to inform the contract negotiations. The following is a summary of the amalgamation of the six CCG plans, there are naturally differences at local level reflecting local CCG priorities and local circumstances. The CCG plans aim to reduce GP referrals by 5% in 2012/13 (compared with this year s projected outturn). These plans comprise re-design of a number of pathways to provide alternatives to traditional hospital-based outpatient services and the implementation and expansion of referral management services to ensure that the new pathways are being consistently adhered to. These plans are ambitious (given the 2% increase in GP referrals seen this year) but reflect the CCG commissioning intentions and the anticipated boost to delivery through full delegation from April The approach to reducing consultant-to-consultant referrals will build on this year s plan delivery with ratios (compared with GP referrals) built into contracts and the risk against delivery of these KPIs lying with the providers. The aim remains that all providers should implement best practice and that KPIs should be based on upper quartile performance. The plans for elective activity take account of the demographic growth, forecast outturn, planned reduction in first referrals through QIPP and also the requirement to deliver and sustain the RTT standards (including the new standard on incomplete pathways). The overall growth is 0.4% above the 2011/12 forecast outturn. Planning for emergency admissions is based on the strategic direction described above, with the aim of strengthening the range of out-of-hospital services to provide much more care closer to home and reduce the number of avoidable admissions. This builds on the current plans, and in the year to date (to November) there has been a 1.9% reduction in emergency admissions compared with the same period last year. The overall Cluster plan is a further reduction of 1.1% in emergency admissions in 2012/13 100
226 compared with this year s forecast outturn. Productivity Metrics 2012/13 contracts with providers will include a range of contracted Key Performance Indicators (KPIs), which will set a stretch performance target for each indicator plus a payment threshold to be applied in the event that agreed targets are not met. SE London is working closely with Associate Commissioners to ensure that the overall approach and the degree of performance improvement being sought for 2012/13 from providers is consistent with and an equivalent stretch to that being applied in other London Clusters. In agreeing contractual KPIs we will expect to distinguish between tertiary and non tertiary workload. The KPIs that we intend to agree as part of the contractual KPIs include : outpatient follow up ratios, internal consultant to consultant referral rates, A&E conversion ratios, day case to outpatient procedures rates, planned procedures not carried out, preoperative bed days, length of stay and excess bed days. Value of 70% emergency admissions threshold to the SHA The value of the 70% emergency threshold for 2012/13 is assessed as being 1,651million across South East London. This figure will be confirmed as negotiations with providers around the emergency quantum are finalised, as some emergency baseline changes may be required to take account of agreed service changes between providers for 2012/ Triangulation Describe the triangulation activity that has taken place to ensure robustness in respect of: - Activity - SLA values - Workforce Enter text here [this should include a specific link between the QIPP schemes, activity and SLAs] outlining risks and mitigations where necessary. Activity and QIPP schemes are covered in detail in Section 7.5: Activity. SLAs for have not been finalised as yet and this information will be included in later a later version of the Operating Plan Key capital schemes Include scheme name, values, purpose, funding source, etc. Bassetts Campus Disposal - Bromley The Bassetts Campus in Bromley has been identified for disposal, and subject to business case approval is anticipated to be sold late in 2012/13. Plans are being developed to relocate existing services to more appropriate sites. Eltham Community Hospital Greenwich Subject to approval this 13.5m, 4300m2 LIFT development will reach financial and commercial close in 2012/13. The new community hospital is key to delivering service change and improvement in Greenwich, and it is intended that it will open in 2014/15. Services will include general practice, community health services, minor surgery and intermediate and stroke inpatient care. Heart of East Greenwich Greenwich This scheme forms and forms part of a wider Homes and Communities led initiative with Greenwich Council to regenerate a part of East Greenwich, on the former Greenwich District Hospital site, and will include general practice and community health services. The development is subject to business case approval and will require a capital injection from the PCT of circa 5m, much of which will be funded from the disposal for 3m of the nearby Vanbrugh Health Centre. Akerman Road Lambeth This 13.1m, 5200m2 LIFT funded development is under construction and will be completed in July 2012 and provides a local neighbourhood resource centre hub for 3 general practice, community health 101
227 services, dental services and a base for adult social care services. This is a key development in a highly deprived part of Lambeth. Norwood Lambeth Subject to approval this 14.2m, 5402m2 LIFT development will reach financial and commercial close in This development is being carried out jointly with Lambeth Council, who will take the head lease, and will provide a customer service centre, swimming pool and other sports facilities as well as health services covering 2460m2 of space including general practice, community health services and a specialist dental school. Norwood is scheduled to open in 2014/15. Guy s Urgent Care Centre - Southwark An Urgent Care Centre will be developed at Guy s Hospital in the current Minor Injuries Service and is scheduled to open in 2012/13. Circa 900k capital works will be funded from PCT capital programme. The services will include primary care minor illness provision as well as minor injuries Liquidity / cash flow / loan requirements All the PCTs in the SEL Cluster are on target to achieve their 2011/12 cash target by drawing down their cash limits in full with minimal cash balances at 31 March It is, therefore, assumed that the availability of cash resources in 2012/13 will not be impacted by adjustments relating to 2011/12. The Cluster PCTs cash assumptions in 2012/13 are based on the availability of cash resources in line with both recurrent and non-recurrent revenue and capital resources, with the exception of carry forward surpluses from 2011/12. Cash in 2012/13 will be managed through the movement in working balances. It is, therefore, anticipated that the Cluster PCTs will not require additional cash support from NHS London Key financial risks and opportunities in 2012/13 All NHS organisations are facing ongoing financial pressures, after many years of unprecedented growth in available funds. The main risks and mitigating actions and reserves are set out in summary below and explained further below. It is important to note that the risk assessment will be updated following the finalisation of contract negotiations with providers within which the balance between upfront investment and savings and in year financial risk will change. Bexley Bromle Greenwic Lambet Lewisha Southwar SEL y h h m k Total '000 '000 '000 '000 '000 '000 '000 Risks In year activity growth: Acute services 3,799 3,932 6,519 6,972 5,837 9,866 36,926 Client Groups 1,159 2,826 2,671 1,490 1,101 2,255 11,503 Primary Care ,014 1, ,064 6,941 QIPP delivery 4,236 2,825 3,230 7,628 4,371 3,259 25,548 Running Costs RTT pressures 975 1,377 1,078 1,613 1,303 1,475 7,822 Return of 2011/12 Surpluses 2,245 5,992 4,612 6,605 5,375 5,857 30,686 Access to 2% Non- Recurrent Funds 7,016 10,118 9,260 12,636 10,548 10,651 60,229 Acute price pressures 984 1,360 1,066 1,344 1,692 1,340 7,785 Downside Risks 21, , ,628 39,945 31,102 36, ,
228 Bexley Bromle Greenwic Lambet Lewisha Southwar SEL y h h m k Total '000 '000 '000 '000 '000 '000 '000 Mitigation QIPP risk reserves 4,236 2,825 3,230 7,628 4,371 3,259 25, % contingency 1,754 2,593 2,275 3,300 2,772 2,663 15,357 Population & Incidence reserves 5,647 7,724 10,204 9,991 7,618 14,185 55,370 2% non-recurrent funds reserves 7,016 10,118 9,260 12,636 10,548 10,651 60,229 Planned 2012/13 surplus reserves 3,508 5,020 4,710 7,000 5,519 5,857 31,615 Acute price pressures earmarked reserves 984 1,360 1,344 1,692 1,340 6,719 Mitigation 23, , ,679 41,899 32,520 37, , /12 Outturn Outturn assumptions have been updated since submission of the CSP and in the Operating Plan we have funded 2011/12 outturn based on the latest forecasts, taking into account the use of nonrecurrent savings or sources of funds and the impact of this in 2012/13, as well as seasonality, working days and RTT requirements. The extent to which actual outturn deviates from this may provide some financial risks, which will present itself as over-performance against contracted levels of activity in 2012/13, which would need to be funded from contingency reserves. Acute over performance The risk of over performance against planned levels of activity and expenditure in the acute sector has historically been the most significant financial risk facing commissioners. We have however utilised a more sophisticated demand and capacity modelling for start contract agreements - start baselines are therefore considered to be realistic particularly in relation to activity required to sustain RTT targets over 2012/13. In addition population and incidence reserves have been established to provide a funding source for increased demand over 2012/13 define by population and incidence factor. Start contract agreements in relation to QIPP implementation, supported by contractual commitments to deliver to commissioners guaranteed savings for Trust led initiatives and robust implementation and contingency plans for CCG led initiatives. The Cluster and CCGs will continue to deliver robust, timely contract monitoring and management to ensure action is taken to contain demand in year as appropriate. RTT pressures Risk remains that the delivery of RTT waiting times targets on a sustained basis over 2012/13 results in demand and activity pressures in excess of planned levels. This is mitigated by the utilisation of more sophisticated demand and capacity modelling for start contract agreements - start baselines are therefore considered to be realistic in relation to activity required to sustain RTT targets over 2012/13. In addition QIPP initiatives are being implemented to reduce a number of RTT related areas of demand in relation to outpatient care pathways, including referral management, improved productivity and efficiency related to outpatient follow up performance, shift from day case to outpatient procedures and care pathway redesign to reduce steps in the care pathway. Continued robust, timely contract monitoring and management will continue, to ensure action is taken to contain demand in year as appropriate. QIPP All QIPP initiatives have been risk-assessed to give increased confidence that the savings that will be achieved in 2012/13. GP Leads and Project managers are clear that their objective is to aim for the stretch QIPP plans in 2012/13 and implementation plans have been developed and signed-off by individual CCGs. For those initiatives that are owned by the provider we expect out contract 103
229 terms to mitigate the risk of non-delivery from the PCT/CCG perspective and Trusts are equally committed to ensuring full delivery of agreed targets. Each local health economy has in place processes to ensure the effective monitoring and management of QIPP delivery in year. A risk rated approach has been applied to start plans, so plans are being implemented to deliver on a full year effect basis more than 100% of 2012/13 requirements, thus mitigating against pace of change issues in year and QIPP reserves have been established to cover potential pace of change or part year effect shortfalls in delivery. Robust, real time motoring of QIPP delivery during 2012/13 will enable contingency plans to be implemented as appropriate early in the contract year. 2% Non-Recurrent Funds Plans assume and include use of the 2% funds in full as an enabler for QIPP delivery and to effectively manage the transition to the new commissioning environment. This represents both a risk and opportunity in 2012/13 and the Cluster and CCGs will ensure robust plans are in place at an earlier stage to ensure access to funds at an earlier stage in the financial year. The 2% Non Recurrent Investment Fund is recognised as being important to deliver QIPP targets and ensure the achievement of underlying financial balance over 2012/13 and the strategic period. However at this stage, limited assumptions made for 2012/13 start plans in relation to the utilisation of 2% non recurrent funds and where access to the 2% has been assumed this has been limited to non recurrent issues, thus minimising any on going risk or liability and recurrent commissioning reserves have been set at levels as high as possible to cover potential in year pressures and issues. Return of 2011/12 Surpluses The remains uncertainty on the return of our planned 2011/12 surpluses in This is current Treasury policy but there is the risk that this may be used to manage overall NHS cost pressures. The Operating Plan assumes that this surplus is returned in full. If this was not the case our QIPP plans would need to increase accordingly and/ or planned surpluses in 2012/13 are reduced. The impact of PbR tariffs in 2012/13, including for mental health providers. We are currently assessing the impact of the final acute PbR tariff the impact of the new tariffs will differ by provider and for each CCG and any deviation from the assumed -1.8% could present financial risks. However our financial plans have assumed under delivery of the -1.8% and we consider therefore that in aggregate terms the impact of 2012/13 acute PbR tariffs will be manageable within our existing plans. The impact and timing of the introduction of Mental Health Payment by Results (PbR) remains unclear. Commissioners have agreed principles for rebasing contract baselines in negotiation with SLAM associated with the introduction of PbR full implementation of responsible commissioner guidance, to minimise risk across both commissioners and provider. Work is jointly being undertaken during 2011/12 and in 2012/13, the introductory year to ensure that activity and financial information is robust and forms a strong base for the implementation of PbR. Successful negotiation of 2012/13 contractual agreements. For acute providers we have now received costed proposals for the majority of our key providers and negotiations are progressing well. We expect to have achieved early signing of the contract with LHNT (end February 2012), and also to reach a timely agreement with GST and KCH. A successful negotiation in terms of securing early agreement and financial certainty in relation to SLHT however remains a risk we are working with SLHT, with senior level Chief Executive involvement, to try to mitigate against SLHT related risks. Good progress is being made with nonacute provider negotiations for 2012/13 and we expect to be able to reach timely agreement within the parameters set out in our 2012/13 plans. Emergency readmissions 104
230 The implementation of 2012/13 final PbR guidance may reduce level of unfunded emergency readmissions and mean there is a shortfall against CCG admission avoidance investment plans. In SEL however agreement has been reached with providers to fund prior commitments related to admissions avoidance schemes for an agreed period and a whole system process has been agreed for reviewing existing commitments and re-profiling commitments to match available funds from unfunded emergency readmissions as required. Running Costs Transitional arrangements will continue in 2012/13 as CCGs move towards full authorisation and associated CSOs are developed. Risks relating to double running costs and also costs associated with additional management remain but supported by GP Development Funds (funded in 2011/12) and potentially 2% non-recurrent funds. Ensuring Financial Delivery Financial balance and the delivery of the PCTs planned financial positions is a core priority and a statutory requirement for NHS SE London. The Cluster and Clinical Commissioning Groups (CCGs) play a vital leadership role in this. The financial position is reviewed regularly by local CCGs, the Cluster Joint Board and the Cluster Performance, Finance & QIPP Committee. Quarterly Joint Cluster and BSU QIPP Stocktake meetings provide executive assurance of financial and service performance including QIPP delivery and review progress against the achievement of full authorisation. Internal and external audit review the PCTs financial management, reporting and controls. Further external assurance is also put in place where this is needed. The achievement of in-year and underlying financial balance is supported by the delivery of Recovery Plans. These plans are kept under Board review as part of the agreed overall financial reporting arrangements. Savings proposals are developed through a process of budget challenge across all areas of activity. CCGs are implementing development plans that take account of the NHS London Roadmap recognised by the Department of Health as a means of achieving full authorisation. The Roadmap s eight domains include finance and governance and development programmes will strengthen CCGs skills in these areas. Organisational change and the associated period of transition bring significant changes in the responsibilities of individual staff members, different reporting lines and changes in key personnel and represents an organisational risk. The Cluster and BSU finance teams are working with senior staff to ensure changes to the budgetary framework are quickly embedded, including: o o o o o Revised budgetary framework Refreshed budgetary delegation to budget holders Refreshed authorised signatory lists Enhanced reporting arrangements Budget holder guidance and training The Cluster is actively pursuing debtor management to ensure all income due to the PCTs is recovered. Processes are in place to ensure that creditors are paid efficiently and on time so that the Better Payment Practice Code (BPPC) can be met and outstanding creditor balances are, wherever possible, minimised. This involves regular reporting of outstanding invoices supported by staff training in the use of electronic workflow systems. The Cluster has implemented a new Sollis information system across all boroughs and is continuing to develop opportunities to improve data validation, claims management and forecasting Overall contingency / reserves 105
231 All CCGs within the SEL Cluster have set aside the following reserves and contingencies in 2012/13 initial budgets and plans: Contingency reserves of 0.5%, in line with NHS London guidance. Funds to deliver surpluses equivalent to 1.0% of recurrent resource limits. This will however be dependent on the carry forward of surpluses from 2011/12. Earmarked sums for population & incidence growth. These vary across CCGs, as set out in section 7.2 above. These will be released to fund activity above 2011/12 forecast outturn, as agreed with providers. These may also need to be used, in part, to fund any unanticipated cost pressures in 2012/13, including the impact of final PbR tariffs. Reserves relating to the difference between 150% QIPP savings and the 100% required. These reserves will be released to fund reductions in agreed QIPP savings, closer to the 100%, should savings be guaranteed to CCGs. 106
232 Section Eight: Workforce 8.1. Workforce impact of strategic goals Will your service vision for the cluster have a workforce impact for your providers? Please provide a description of the anticipated impact for workforce within local provider Trusts and Community providers as a result of the cluster s strategic initiatives e.g. describing anticipated increases / decreases for your main providers and services that may see significant change. NHS SEL expect all SEL providers bar Oxleas to see a reduction in income by the end of the CSP period (2014/15), with the biggest impact being felt in 2012/13. The reductions are as a result of changes to tariff, the tariff efficiency deflator, demographic/non-demographic growth, and QIPP savings. As workforce accounts for such a large proportion of cost, this will inevitably impact on size and shape, however no major reconfiguration of either organisations or workforce is envisaged. The CSP service vision for SEL has four main priorities: Integrated Care, Productive Care, Staying Healthy and implementing London-wide strategies. The focus is for specialised centres only where necessary, local delivery where possible, with repatriation of work from central London to local providers. All of these priorities will impact the workforce however the general vision or services to be delivered more efficiently and in more local settings, means the workforce will see a slight downturn in numbers resulting from efficiencies and some moves in location, but overall will be stable. Sensible reviews to release productivity savings will also occur; examples of this would be community midwife follow-up visits where historic organisational mergers mean some workers travel a long distance from their base, whilst the patient actually lives close to another Trust, or extending the use of community pharmacists for repeat prescribing, community optometrists for minor eye conditions. Integrated care and productive care both require a flexible, multi-disciplinary approach, putting the varying need of individual patients at the centre of the pathway. The workforce must be able to work effectively in different settings, often independently, and respond to each patient s unique needs, within the framework of an overall pathway. It also means team working and good communication skills are important to provide a seamless, efficient service. Lewisham, GSTT and Oxleas all took over community staff/services as part of TCS. Each have set their delivery models up differently; we will monitor and assess the success of each during 2012/13 and recommend alternative workforce interventions where appropriate. All are on track to achieve their Health Visitor numbers in 2012/13. Regarding productive care, we will work closely with providers regarding workforce productivity during 2012/13 and plan to establish a pan-cluster group to focus on this during Q1. Staying healthy requires a holistic preventative approach, often with primary care staff taking on new, extended responsibilities. In 2011/12 we prioritised the development of practice staff with this in mind, and will continue to support them through 2012/13. Workforce plans are discussed with clinical and operational colleagues to assess potential risks. We will continue our dialogue with SEL provider workforce leads, and with BSU/CCG and cluster contract leads, about workforce impact Effective communication with providers Does your organisation have a process in place by which it can assure the Yes:; no comment workforce strategies of its provider organisations are fully integrated with service and financial plans; have clinical ownership and aligned with the cluster s vision as highlighted in its commissioning intentions communicated to its providers? NHS SEL is still an emerging organisation, forged from elements of the 6 former PCTs, and with a limited life due to on-going NHS changes. This means corporate memory, any precedents or long standing 107
233 relationships are weakened though it does have a culture of flexibility and adapting to emerging priorities. Consequently the cluster does not have an established process in place by which it will assure provider workforce strategies, but the work will be done. Discussions have already begun with SEL cluster contract leads and with providers about it, though in reality it cannot be completed until the service/finance plan is more robust. As the development of Local Education and Training Boards (LETBs) progresses through 2012/13, a framework for the regular involvement of clinicians and of providers in reviewing service and workforce plans will be more clearly visible. To underpin this in SEL we have already established two forums (one for Bexley, Bromley and Greenwich, another for Lambeth, Southwark and Lewisham) which will feed in primary and community views. Discussion will take place to ensure triangulation has occurred between workforce, service and finance, that clinicians have been involved and approve the plan, meaning the plans are likely to be achievable, and will be safe for patients. As mentioned above, we will work closely with providers regarding workforce productivity during 2012/13 and plan to establish a pan-cluster group to focus on this during Q1. We see building co-operative relationships with providers as more effective than performance management routes, and will continue to focus on this during 2012/ Quality of service / education considerations Has the cluster made clear to their provider organisations that their education and training funding should be used to transform their workforce to support the delivery of the cluster s service vision, and does the cluster have mechanisms in place to assess whether provider organisations have appropriate plans to support this objective? SEL will ensure the workforce implications of the commissioning strategy plan on provider education and training needs are reviewed, once the CSP is settled. Through a development, rather than performance management lens we keep the strategy and performance teams informed of CPPD money available to contribute to implementing successful service vision. An example of this recently was a successful CPPD bid written by the SEL strategy team to support training for community opticians to take on management of minor eye conditions. Part of SEL s workforce transformation brief is promoting collaboration, and building local relationships in advance of greater provider involvement in LETBs. The standard commissioning contract includes a clause whereby providers are required to cooperate with relevant bodies to understand and plan local healthcare workforce requirements. Although the contract clause exists as a backstop, we prefer to manage through developing effective working relationships and will do so to support LETBs. As the development of Local Education and Training Boards (LETBs) progresses through 2012/13, a structure for SEL will be created to review the investment of education and training funding and will enable it to be better directed towards delivery of the cluster s service vision Does the cluster have processes in place to ensure that provider organisations carry out appropriate workforce risk assessments and address capability or capacity issues ahead of the changes that the Cluster s local service vision will require? Yes: no comment The standard commissioning contract has been revamped for 2012/13, moving it from four separate contracts into one. The requirement for workforce capability and capacity to deliver the service continues to be part of the contract (now section E), and provides a lever for performance discussions should they be required. In SEL we have agreed that workforce will become a standing item on the cluster s Quality and Safety Committee, which includes senior commissioner and clinician representatives. Going forward into 2012/13 indicators from the national workforce tool will also form part of regular discussions between the cluster and its providers, with the Q&S committee providing an escalation route if required. 108
234 Additionally, as sector developments such as Eltham Community Hospital, QMS campus, Orpington, Dulwich and Heart of East Greenwich Centre come on stream we will ensure workforce is part of the early design planning, to make sure capability and capacity are properly addressed Statutory workforce obligations Does the organisation have a process in place by which it can assure statutory workforce obligations (e.g. EWTD, mandatory training, % appraisal rates, quality of appraisals, medical revalidation) are delivered within its provider organisations? Yes: no comment The revamped standard commissioning contract continues to include performing statutory workforce checks, and provides a lever for performance discussions should it be required. We ask providers to guarantee their compliance with this, during regular visits and discussions, and again, see the national workforce tool and Quality and Safety committee as the SEL vehicles to discuss these Monitoring and performance management Does the cluster include workforce metrics, benchmarking, trends and plans within its contract performance process with its providers? Are these metrics incorporated with related quality metrics and intelligence, and used to identify and raise concerns about future trends and performance? Where the workforce indicators of a provider raises concern, please describe the process that the cluster will take to resolve the risk identified? How will the cluster ensure that CQC and Monitor have been involved as appropriate? Whilst recognizing that commissioning is for outcomes, not inputs or processes, SEL does take note of the workforce required to deliver the contract in its discussions with providers. Monthly contract meetings occur with each provider to discuss quality and service delivery. In preparation for that meeting the provider sends in KPIs covering a range of areas, including workforce indicators (sickness, turnover, bank and agency use, fte, etc); information in the KPIs directs the meeting to areas which need more scrutiny, including workforce as an integral metric. A discussion regarding the cluster s strategic plans has been had with all providers. These have highlighted poor internal discussions within some providers, especially about reduced commissioning intentions and the impact on future income. This message will continue to be delivered as changing income will impact the workforce and the provider needs to reduce accordingly, whilst maintaining quality. Going forward into 2012/13 workforce metrics will be part of a new monthly integrated performance dashboard being created for the Board Managing of workforce risk Where workforce changes have been identified, please describe the risks that these changes may have to patient care standards during the transition and the process by which the Cluster will mitigate these risks with the providers? As outlined above, workforce changes to delivery vision are minor, not major. Consequently any risks to delivery of the vision which would impact patient safety relate more to moving services to new settings (community) rather than new services, per se. All change plans are reviewed by clinicians and operational managers thus ensuring the patient safety element is paramount. 109
235 Appendices Appendix A: The 2012/13 QIPP Milestone Tracker Return Appendix B: The Risk Assessment for Performance Framework Appendix C: The Progress Towards Public Health Transition - SE London Cluster 110
236 PROGRESS TOWARDS PUBLIC HEALTH TRANSITION, SE LONDON CLUSTER. FRIDAY 9 TH MARCH How much of the desired content of the planning documents (memorandum and transition plan) are in place already Bexley Bexley BSU and LBB already have a memorandum of understanding in place which includes the transition process in general terms. Bexley BSU and LBB are currently working to finalise a transition plan for the integration of Public Health Services which will include any transfers for Public Health England and the National Commissioning Board. This is being undertaken in conjunction with SEL Cluster plans. Bromley Bromley have completed an MoU which has been signed by the LA Chief Executive and the Cluster Chief Executive on behalf of the PCT. The transition plan is being completed by LA identified leads and will be submitted as a cluster return to NHSL by 30 March Greenwich About 20% Lambeth Lewisham We are confident that all of the desired content of the NHS planning documents are in place in Lambeth. These are not yet in final form but a draft transition plan has been prepared which identifies and confirms the individual work strands and the related activity required to ensure a smooth transition. Leaders and team members who will work on each strand have also been identified and they will review the draft plan and refine as necessary. Southwark With the other boroughs in South East London we have created a statement of joint working for the transition process for Public Health between the NHS and local authority. This statement is currently being refined locally. The development of the Transition Plan is underway, based on the template proposed by NHS South East London. The lead names for each of the transition workstreams have been identified from both the council and the PCT, including representation from the NHS Southwark Business Support Unit and Public Health team. Discussions are taking place about how a plan for transition will be set out for each domain or workstream. In some instances where there is a cluster wide workstream e.g. HR, the leads will liaise with that programme of work and complete the local plan based on the cluster wide work. 1
237 PROGRESS TOWARDS PUBLIC HEALTH TRANSITION, SE LONDON CLUSTER. FRIDAY 9 TH MARCH Confirmation that a governance statement (memorandum or some other form) will be in place by 1 st April 2012, if not already? Bexley As previously stated, there is a broad statement of intent MOU in place. Bromley Greenwich Lambeth Bromley has a section 75 agreement in place. A draft statement is attached and is due to be signed off in the next few days. We can confirm our statement on joint working will be signed in advance of the 1 st April. A copy is attached and this has been signed by the CE SE London Cluster and is in the process of being signed off by the local authority. This is expected in the next few days Lewisham We anticipate that a statement setting out the governance arrangements for the transition will be in place by April Southwark The statement of joint working is going through its final editing process and it is likely that it will be signed off before 1 st April The current proposed sign-offs for Southwark include the Council, the NHS cluster, the Clinical Commissioning Group and the Director of Public Health. 2
238 PROGRESS TOWARDS PUBLIC HEALTH TRANSITION, SE LONDON CLUSTER. FRIDAY 9 TH MARCH Confirmation that each PCT/borough partnership has in place, an agreed process for finalisation of its transition plan, and the agreed date for completion (including sign-off at appropriate levels in cluster and council) Bexley Bexley BSU and LBB are working to finalise the transition plan by 31 st March 2012 per the original deadline. Currently, there is a comprehensive draft in place which is being reviewed by the project leads for each area to ensure that there are no significant gaps in the process. In terms of sign off, the BSU plan to include this in their Clinical Cabinet meeting at the end of March 2012, where it is expected to be agreed. It is understood that the CEO of the Bexley Council may agree to sign off the document subject to a number of caveats including the recognition that the funding advised to date is to be challenged. Bromley Greenwich Lambeth Lewisham Bromley s Chief Executive will sign off the completed transition plan which will then be sent to the Cluster Chief Executive for sign off. The cluster level sign off will take place by 27/3 in order to be submitted to NHSL by 30/3/12. Yes, we can confirm that there is a comprehensive PID for Public Health transition that identifies the timelines We can confirm we are in the final stages of agreeing a transition plan and have an agreed process for its finalisation by 31 March The transition plan will be completed and signed off initially by the programme board. Discussion is currently taking place on where further sign off is required. This will include at relevant points the LCCG, the Shadow Health and Wellbeing Board and ultimately Mayor and Cabinet Southwark A process has been agreed locally in which the Southwark BSU Managing Director (NHS Cluster), the Director of Public Health (Public Health) and Director of Corporate Strategy (Southwark Council) sign-off the transition plans. It is expected this will be submitted to NHS South East London Cluster by the 23 March The Cabinet Member for Health and Adult Social Care and other key directors in the Council will be briefed on the plans. 3
239 PROGRESS TOWARDS PUBLIC HEALTH TRANSITION, SE LONDON CLUSTER. FRIDAY 9 TH MARCH Any issues that may cause local planning to be unduly delayed or may impede implementation. Bexley The following issues have been identified as potential items which may cause a delay in implementation; Bromley Greenwich Lambeth Challenge to the level of funding advised to date Sign off of the transition plan by all parties Approval of bill through parliamentary process Resources to undertake levels of work required Delays in setting up Public Health England/National Commissioning Board and their structures and functions being agreed Any delays in further guidance being released by DH Resolution of staff pension issues when TUPE applies Dis-aggregation of block contracts for a number of community services to various parties e.g Oxleas, SLHT Any local Public Health incident which would require staff to mobilise emergency planning arrangements None foreseen The Royal Borough of Greenwich is currently exploring with Lewisham, Southwark and Lambeth, the possibility of some functions being delivered across 4 Boroughs, including the Director of Public Health, and will seek to minimise the impact of this parallel discussion on implementation. No other statutory or senior officer function functions are shared across LSLG. In Greenwich 1, it is anticipated that the DPH will report to the DASS following transfer. The reporting status of the DPH might vary across the boroughs even if the post is shared. 1 The reporting line of the DPH within the Royal Borough of Greenwich has not yet been formally agreed through any of our constitutional decision making processes. Whilst we are confident that we have strong local processes in place to ensure an effective transition we have identified a number of external factors which have the potential to cause our local planning to be unduly delayed and/or to impede local implementation: Financial Uncertainty: There is an increasingly urgent need for clarity on future funding allocations. We are clear that our future public health functions must be designed to be affordable. For detailed design work to take place there must therefore be clarity on the funding that will be available. We understand that the baseline is now likely to be reassessed. We are also aware that work is underway on a future funding formula, including a transition from baseline to formula allocations, however no details of this have yet been made public. This continued uncertainty presents a substantial risk to our ability to advance the design of our future public health functions. Health Protection: There continues to be a high degree of uncertainty as to the specific roles of different agencies in the new health protection system, including the specific levers the DPH will have to exert local leadership. This continued uncertainty presents a rising and substantial risk to the resilience of our post April 2013 health protection systems. To ensure new 4

240 PROGRESS TOWARDS PUBLIC HEALTH TRANSITION, SE LONDON CLUSTER. FRIDAY 9 TH MARCH Any issues that may cause local planning to be unduly delayed or may impede implementation. arrangements are in place, tested and proven to be robust by April 2013 it will be essential that there is clarity on these issues Lewisham Southwark within the next two to three months. Engagement with National Bodies: At present we do not have mechanisms to engage with the NHS Commissioning Board or Public Health England on the transition of those functions for which they will in future be accountable. We have not therefore been able to engage then in our local transition planning process. It will be essential that there are clear and effective mechanisms for engagement with both agencies within the next two to three months. HR transition: We now have strong Lambeth and SE London mechanisms to oversee HR transfer. However despite the significant quantities of guidance issued on the HR transition there continues to be substantial uncertainty on three key issues: 1) the transfer of pension rights and liabilities; 2) the possible/desirable timing of any necessary reorganisations (pre or post transfer); 3) the availability of funding to cover any resulting redundancy costs prior to transfer, at the point of transfer and thereafter. These are issues that require an urgent national resolution. Infection Control: At present infection control within NHS Lambeth is led by our public health team. However future accountabilities remain unclear, including the responsibilities of CCGs, PHE and NHSCB as well as those of local authority public health teams (if any). In order to ensure effective transition urgent clarification of future accountabilities is now required. Implementation of the transition plan is dependent on the provision of accurate and confirmed information including that relating to budgets, contracts and HR. There is a project underway to consider how the four councils of Lambeth, Southwark, Lewisham and Greenwich might create a shared public health service. This project will produce a preliminary report in May which will provide a steer on the functions and staff for shared development. There will be a final report in September This work will need to be coordinated with the design of how the public health function will operate in the local authority to ensure an integrated and coherent delivery of all the new local authority responsibilities. The current timetable for transition is extremely challenging due to the timeline set by the Department of Health for the announcement of a funding formula and grant for public health (December 2012), and the finalised set of outcomes framework indicators (autumn 2012). A consultation on the public health workforce is also expected imminently but has not at this time been published. There are risks that local implementation may be delayed due to a lack of certainty at a national level. These issues may not allow enough time for statutory and appropriate consultation with affected staff. It may also be a consideration regarding notice periods on any affected contracts. However within these limitations Southwark is moving forward with its plan and preparing for the transition, implementing a series of workstreams as far as possible within the constraints of existing national guidance. 5
DRAFT NHS South East London Cluster Better for You
 DRAFT NHS South East London Cluster Better for You Commissioning Strategy Plan 2012/13 2014/15 Page 2 of 51 Dear colleagues, We are all very pleased to introduce to you Better for You, our health Commissioning
DRAFT NHS South East London Cluster Better for You Commissioning Strategy Plan 2012/13 2014/15 Page 2 of 51 Dear colleagues, We are all very pleased to introduce to you Better for You, our health Commissioning
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
NHS LEWISHAM CLINICAL COMMISSIONING GROUP. COMMISSIONING INTENTIONS 2014/15 and 2015/16
 NHS LEWISHAM CLINICAL COMMISSIONING GROUP COMMISSIONING INTENTIONS 2014/15 and 2015/16 1 CONTENTS Introduction 1. Who We Are p5-6 1.1 CCG s Responsibilities p5 1.2 Partnership Working p6 2. CCG s Strategic
NHS LEWISHAM CLINICAL COMMISSIONING GROUP COMMISSIONING INTENTIONS 2014/15 and 2015/16 1 CONTENTS Introduction 1. Who We Are p5-6 1.1 CCG s Responsibilities p5 1.2 Partnership Working p6 2. CCG s Strategic
Southwark s Primary and Community Care Strategy
 Southwark s Primary and Community Care Strategy 2013/2014 2017/2018 Southwark Primary and Community Care Strategy 2013/2014 2017/2018 Table of Contents Section Page Number Executive Summary 3 1. Introduction,
Southwark s Primary and Community Care Strategy 2013/2014 2017/2018 Southwark Primary and Community Care Strategy 2013/2014 2017/2018 Table of Contents Section Page Number Executive Summary 3 1. Introduction,
A guide to NHS Bexley Clinical Commissioning Group
 A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Greenwich Clinical Commissioning Group. Patient and Public Engagement Strategy ( )
") Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
A review of 2017/18 and a summary of the Greenwich Commissioning Strategy. Transforming our health and social care system 2018 to 2022
 A review of 2017/18 and a summary of the Greenwich Commissioning Strategy Transforming our health and social care system 2018 to 2022 Welcome... 4 Who we are and what we do... 6 Our achievements... 8 Our
A review of 2017/18 and a summary of the Greenwich Commissioning Strategy Transforming our health and social care system 2018 to 2022 Welcome... 4 Who we are and what we do... 6 Our achievements... 8 Our
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
DARLINGTON CLINICAL COMMISSIONING GROUP
 DARLINGTON CLINICAL COMMISSIONING GROUP CLEAR AND CREDIBLE PLAN 2012 2017 Working together to improve the health and well-being of Darlington May 2012 Darlington Clinical Commissioning Group Clear and
DARLINGTON CLINICAL COMMISSIONING GROUP CLEAR AND CREDIBLE PLAN 2012 2017 Working together to improve the health and well-being of Darlington May 2012 Darlington Clinical Commissioning Group Clear and
South East London: Sustainability and Transformation Plan
 South East London: Sustainability and Transformation Plan 21 October 2016 Key information details Name of footprint and no: South east London; no. 30 Region: South east London (Bexley; Bromley; Greenwich;
South East London: Sustainability and Transformation Plan 21 October 2016 Key information details Name of footprint and no: South east London; no. 30 Region: South east London (Bexley; Bromley; Greenwich;
Summary annual report 2014/15
 1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
GOVERNING BODY PAPER
 Enclosure: E Agenda item: 7 GOVERNING BODY PAPER Title of paper: To approve South London Commissioning Strategy Programme Case for change Date of meeting: Wednesday 26 th March 2014 Presented by: Dr Hany
Enclosure: E Agenda item: 7 GOVERNING BODY PAPER Title of paper: To approve South London Commissioning Strategy Programme Case for change Date of meeting: Wednesday 26 th March 2014 Presented by: Dr Hany
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
NHS West Cheshire Clinical Commissioning Group
 NHS West Cheshire Clinical Commissioning Group Five Year Strategy: 2014/15-2018/19 1 Our Planning Footprint In developing our system vision for 2018/2019 NHS West Cheshire Clinical Commissioning Group
NHS West Cheshire Clinical Commissioning Group Five Year Strategy: 2014/15-2018/19 1 Our Planning Footprint In developing our system vision for 2018/2019 NHS West Cheshire Clinical Commissioning Group
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
South East London Commissioning Strategy Programme. Case for Change
 South East London Commissioning Strategy Programme Office South East London Commissioning Strategy Programme Case for Change (DRAFT) 28 February 2014 DOCUMENT CONTROL Version Date Author Comments V0.14
South East London Commissioning Strategy Programme Office South East London Commissioning Strategy Programme Case for Change (DRAFT) 28 February 2014 DOCUMENT CONTROL Version Date Author Comments V0.14
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Our Healthier South East London Consolidated Strategy. Draft v1.0 June 2015
 Our Healthier South East London Consolidated Strategy Draft v1.0 June 2015 Section Page No. Executive Summary 3 Purpose of the document 35 Introduction to south east London 38 Introduction to the Our Healthier
Our Healthier South East London Consolidated Strategy Draft v1.0 June 2015 Section Page No. Executive Summary 3 Purpose of the document 35 Introduction to south east London 38 Introduction to the Our Healthier
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS. September 2014
 OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby
 STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
BROMLEY CLINICAL COMMISSIONING GROUP - GOVERNING BODY MEETING THURSDAY 20 NOVEMBER 2014
 BROMLEY CLINICAL COMMISSIONING GROUP - GOVERNING BODY MEETING THURSDAY 20 NOVEMBER 2014 PUBLIC QUESTIONS AND ANSWERS QUESTIONS RAISED FOR THE PUBLIC FORUM PRIOR TO THE MEETING ON 20 NOVEMBER 2014 WRITTEN
BROMLEY CLINICAL COMMISSIONING GROUP - GOVERNING BODY MEETING THURSDAY 20 NOVEMBER 2014 PUBLIC QUESTIONS AND ANSWERS QUESTIONS RAISED FOR THE PUBLIC FORUM PRIOR TO THE MEETING ON 20 NOVEMBER 2014 WRITTEN
GOVERNING BODY. Purpose of the report: To ensure the Governing Body has knowledge of and approve the annual report ahead of submission to NHS England.
 Enclosure: L Agenda item: 15 GOVERNING BODY Title of paper: NHS Greenwich CCG Annual Report 2015/16 Date of meeting: 25 May 2016 Presented by: Diane Jones Prepared by: Diane Jones Title: Director of Integrated
Enclosure: L Agenda item: 15 GOVERNING BODY Title of paper: NHS Greenwich CCG Annual Report 2015/16 Date of meeting: 25 May 2016 Presented by: Diane Jones Prepared by: Diane Jones Title: Director of Integrated
NHS Leeds West CCG Clinical Commissioning Strategy. 2013/14 to 2015/16
 NHS Leeds West CCG Clinical Commissioning Strategy 2013/14 to 2015/16 Working together locally to achieve the best health and care in all our communities 1 Contents Section 1: Summary Page 3 Section 2:
NHS Leeds West CCG Clinical Commissioning Strategy 2013/14 to 2015/16 Working together locally to achieve the best health and care in all our communities 1 Contents Section 1: Summary Page 3 Section 2:
South Yorkshire and Bassetlaw Accountable Care System Chief Executives
 South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
General Practice Commissioning Strategy Development
 General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
Summary Annual Report 2017/18
 Summary Annual Report 2017/18 Reporting back Guy s and St Thomas has, once again, performed well both operationally and financially, despite a challenging year which has seen unprecedented demand on our
Summary Annual Report 2017/18 Reporting back Guy s and St Thomas has, once again, performed well both operationally and financially, despite a challenging year which has seen unprecedented demand on our
Sustainability and transformation plan (STP)
") Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Source Question Summary response Action Proposal to set up a review of community services:
 NHS Lambeth CCG Public forum 1 st March 2017 tes Source Question Summary response Action Proposal to set up a review of community services: In light of the Primary Care Trusts transfer to CCGs in 2013
NHS Lambeth CCG Public forum 1 st March 2017 tes Source Question Summary response Action Proposal to set up a review of community services: In light of the Primary Care Trusts transfer to CCGs in 2013
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.
 MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.") CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP)
") Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP) Q. What is a Sustainability and Transformation Plan? A. The NHS and local authorities across Buckinghamshire,
Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP) Q. What is a Sustainability and Transformation Plan? A. The NHS and local authorities across Buckinghamshire,
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
Southend-on-Sea Health System Strategic Plan
 Southend-on-Sea Health System Strategic Plan 2014-19 Contents Introduction... Plan on a page.. 4 Executive summary The Southend-on-Sea health system 7 Our vision.. 14 Planning for outcomes. 19 Involving
Southend-on-Sea Health System Strategic Plan 2014-19 Contents Introduction... Plan on a page.. 4 Executive summary The Southend-on-Sea health system 7 Our vision.. 14 Planning for outcomes. 19 Involving
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
Integrated Performance Report
 ENC Bi Integrated Performance Report M1 2014/15 26 June 2014 Contents 1. Structure of the Document... 3 2. Southwark CCG and Providers Performance Summary Dashboard... 4 3. Southwark CCG Dashboard... 5
ENC Bi Integrated Performance Report M1 2014/15 26 June 2014 Contents 1. Structure of the Document... 3 2. Southwark CCG and Providers Performance Summary Dashboard... 4 3. Southwark CCG Dashboard... 5
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
NHS Southwark Clinical Commissioning Group (CCG) General Practice (GP) Services. Locality PPGs March 2017
 General Practice (GP) Services. Locality PPGs March 2017") NHS Southwark Clinical Commissioning Group (CCG) General Practice (GP) Services Locality PPGs March 2017 Our strategy is to maximize the value of health and care for Southwark people, ensuring our services
NHS Southwark Clinical Commissioning Group (CCG) General Practice (GP) Services Locality PPGs March 2017 Our strategy is to maximize the value of health and care for Southwark people, ensuring our services
Direct Commissioning Assurance Framework. England
 Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Central Lancashire Local Delivery Plan 2016/ /21
 Central Lancashire Local Delivery Plan 2016/17 2020/21 1 Contents 1. Introduction and context 2. Our priorities 3. The health and wellbeing gap 4. The care and quality gap 5. Financial challenges, gap
Central Lancashire Local Delivery Plan 2016/17 2020/21 1 Contents 1. Introduction and context 2. Our priorities 3. The health and wellbeing gap 4. The care and quality gap 5. Financial challenges, gap
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
NHS Southwark CCG Operating Plan 2016/17. Council of Members 30 March 2016
 NHS Southwark CCG Operating Plan 2016/17 Council of Members 30 March 2016 Operating Plan 2016-17: contents Section Page Introduction and context 3 Delivering the CCG s Forward View into Action 2016-17:
NHS Southwark CCG Operating Plan 2016/17 Council of Members 30 March 2016 Operating Plan 2016-17: contents Section Page Introduction and context 3 Delivering the CCG s Forward View into Action 2016-17:
South East London Commissioning Strategy Programme
 South East ondon Commissioning Strategy Programme Office South East ondon Commissioning Strategy Programme Commissioning Strategy 2014-19 Appendices A, B and C 20 June 2014 Version 1.0 SUBISSION TO NS
South East ondon Commissioning Strategy Programme Office South East ondon Commissioning Strategy Programme Commissioning Strategy 2014-19 Appendices A, B and C 20 June 2014 Version 1.0 SUBISSION TO NS
NHS North West London
 NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Integrating Health & Social Care in Kirklees
 Integrating Health & Social Care in Kirklees The case for change DRAFT v3.1 June 2017 Integrated Commissioning - Building on Existing Approaches Some example Children s services Mental health Hospital
Integrating Health & Social Care in Kirklees The case for change DRAFT v3.1 June 2017 Integrated Commissioning - Building on Existing Approaches Some example Children s services Mental health Hospital
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
Worcestershire Public Health Directorate. Business plan 2011/12
 Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Commissioning Plan. NHS Gateshead Clinical Commissioning Group
 Commissioning Plan NHS Gateshead Clinical Commissioning Group 2012-2017 (Incorporating the 2012-13 Integrated Plan and Draft Commissioning Intentions 2013-14) Contents Foreword... 4 1. Overview... 5 2.
Commissioning Plan NHS Gateshead Clinical Commissioning Group 2012-2017 (Incorporating the 2012-13 Integrated Plan and Draft Commissioning Intentions 2013-14) Contents Foreword... 4 1. Overview... 5 2.
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
West Wandsworth Locality Update - July 2014
 Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Richmond Clinical Commissioning Group
 Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Committee of Public Accounts
 Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
REPORT TO CROYDON CLINICAL COMMISSIONING GROUP GOVERNING BODY Meeting in Public. 30 October 2012
 REPORT TO CROYDON CLINICAL COMMISSIONING GROUP GOVERNING BODY Meeting in Public 30 October 2012 Title: CROYDON CCG AND CROYDON PUBLIC HEALTH MEMORANDUM OF UNDERSTANDING Lead Director Report Author Contact
REPORT TO CROYDON CLINICAL COMMISSIONING GROUP GOVERNING BODY Meeting in Public 30 October 2012 Title: CROYDON CCG AND CROYDON PUBLIC HEALTH MEMORANDUM OF UNDERSTANDING Lead Director Report Author Contact
Operational Plan
 1 Introduction This two year operating plan is written to provide NHS England with assurance that Sandwell and West Birmingham CCG has plans in place aligned to the Black Country Sustainability and Transformation
1 Introduction This two year operating plan is written to provide NHS England with assurance that Sandwell and West Birmingham CCG has plans in place aligned to the Black Country Sustainability and Transformation
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Westminster Health and Wellbeing Board
 Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
A consultation on the Government's mandate to NHS England to 2020
 A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
NHS Norwich CCG Operational Plan and
 NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare