E M E R G E N C Y O P E R A T I O N A L (DI S A S T E R )PLAN ( E O P )
|
|
|
- Laurence Esmond Oliver
- 5 years ago
- Views:
Transcription
 PLAN (EOP) Reviewed by: Date: Revision Date MAY 2005 Effective Date MAY 2010 Due for Revision on:")
1 E M E R G E N C Y O P E R A T I O N A L (DI S A S T E R )PLAN ( E O P ) Title: KING SAUD UNIVERSITY HOSPITALS (King Khalid University Hospital and King Abdul Aziz University Hospital ) Committee: EMERGENCY MANAGEMENT Issue Date: MAY 2002 Prepared/Revised by: Date: EMERGENCY OPERATIONAL (DISASTER) PLAN (EOP) Reviewed by: Date: Revision Date MAY 2005 Effective Date MAY 2010 Due for Revision on: Authorized by: Date: Dr. Zohair Ahmed Al Aseri Chairman, Department of Emergency Medicine Co-Chairman Emergency Management Committee Authorized by: Date: Dr. Farheen Shaikh Policy and Procedure Review Committee Authorized by: Date: Dr. Badr Al Jabri KKUH-Medical Director Authorized by: Date: Dr. Abdul Rahman Al Muammar KAUH Medical Director Approved by: Date: Dr. Ayman Abdo Vice Dean for Quality Dr. Abdulaziz Al Saif Vice Dean for Hospitals Chairman of Emergency Management Committee Prof. Mussaad Al Salman Dean College of Medicine and Supervisor for University Hospitals 1
2 E M E R G E N C Y O P E R A T I O N A L (D I S A S T E R ) P L A N ( E O P ) Table of Content Content Page Purpose 3 Introduction 4 Activation Of Response 5 Command Authority 7 Communication 11 Level Of Activation 14 Emergency Codes 16 External Emergency Plan 17 Utility Failure Code Gray 19 Fire Code Red 22 Alert 4- Evacuation 24 Cardio Pulmonary Resuscitation-Code Blue 28 Disruptive Behavior-Code White 29 Bomb Threat-Code Orange 32 The Emergency Operation Plan Of Safety And Security Department 37 Dem Disaster Response 39 Disaster Plan- Blood Bank 43 Incident Respond Guides (IRG) 44 Bomb Threat 45 Alert 4 Evacuation, Complete Or Partial Facility 49 Fire 53 Hazardous Material Spill (Code Brown) 58 Code Green (DEM Overcrowding) 61 Hostage / Barricade 65 Infant / Child Abduction (Code Pink) 68 Internal Flooding 71 Loss of Heating / Ventilation/ Air Conditioning (HVAC) 75 Loss of Power 79 Loss of Water 83 Severe Weather 87 Appendix 1 Command Center 91 Appendix 2 Emergency Codes 92 Appendix 3 Triage Algorithms 93 Appendix 4 Mettag 95 Appendix 5 Call List 100 Appendix 6 Job Action Sheet (JAS) 111 2
3 Emergency (Disaster) Operations Plan (EOP): Purpose Hospitals confront a myriad of operational and fiscal challenges on a daily basis. To effectively manage emergencies, whether external (e.g., fires, sever weather) or internal (e.g., child abductions, utility failure), KKUH must invest the time and necessary funds to ensure adequate preparations are in place. Hospital Emergency Incident Command System (HEICS) and Emergency (Disaster) Operations Plan (EOP) serve as an important emergency management foundation for this institute. We recognized the value and importance of using an incident management system, not only in emergency situations but also in daily operations, preplanned events, and nonemergent situations. We believe this Emergency (Disaster) Operations Plan (EOP) and the accompanying materials can play a major role in advancing KKUH preparedness while providing needed local, state, and national standardization of hospital emergency response and recovery. We believe the new Hospital Incident Command System has built upon the benefits and successes of the original Disaster Plan and provides our hospital with tools needed to advance their emergency preparedness and response capability both individually and as a member of the broader response community. This Emergency (Disaster) Operations Plan (EOP) is intended to explain in a clear and concise manner the critical components of the Hospital Incident Command System (HICS) as well as the suggested manner for using the accompanying materials. The primary beneficiaries of HICS will be physicians, nurses, hospital administrators, department chairman, and other personnel in hospitals who will assume command roles during an incident. Students preparing for a career in medicine, nursing, and hospital administration, whose education should include understanding hospital emergency preparedness principles and practices, will also find the material useful. The reader should find the short-paragraph and bulleted-information format helpful in quickly understanding and applying vitally important tenets of response planning, incident command, and effective response. A copy of the KKUH Emergency Plan shall be available within each unit/department for all staff to read. It is the responsibility of Chairmen/units heads to ensure that all staff being oriented and assure continuous training for all staff toward emergency preparedness plan. Since all staff employed by KKUH involved with patient care should be trained in techniques for the safe evacuation of patients from their area. A list of code red associate (wardens) and emergency floor plans should be centered prominently in all work areas. Evacuation blanket/sheet should be available in all clinical areas. 3
4 INTRODUCTION There are two types of emergencies that may impact on this hospital Internal and External Emergencies. Internal Emergencies involve only the hospital and its capabilities that may be reduced. External Emergencies will usually be sited outside the hospital and the hospital s capabilities may remain intact. INTERNAL EMERGENCIES Internal emergencies are any incidents which threaten the safety of the physical structure of the hospital, staff, patients and visitors and which may also reduce the capacity of the hospital to function normally. In most cases, staff in departments and units will be responsible for their own initial response. EXTERNAL EMERGENCIES KKUH will resume Incident Command for all emergencies within King Saud University. KKUH will participate with other facility in order to provide emergency medical care during emergencies outside the University Medical City. External emergencies are managed as a part of an overall plan. HOSPITAL EMERGENCY STATUS Whenever the internal or external emergency plan is activated, the hospital will be considered to be in EMERGENCY STATUS with specific command responsibilities to facilitate resource allocation. 4
5 ACTIVATION OF RESPONSE KSUHS response to an incident begins with recognition that an untoward incident could happen (advance warning) or has happened (post-incident warning) that may disrupt normal business operations. Advance warning information may come from several sources. The Chairman of DEM or the Consultant on duty must be contacted during the initial emergency notification call. If possible, the call reporting the emergency should be transferred through to the Consultant in DEM, so he/she is able to obtain a full appreciation of the situation. If the call cannot be transferred through, the Telecommunications Operator must ascertain all related details regarding the emergency, and those details should be relayed to the Chairman of DEM or the Consultant on duty. Chairman of DEM or the Consultant on duty shall advise the Telecommunications Operator of one of the four principle responses: Alert 0 - NO RESPONSE Do nothing further at this time. Alert 1 -STANDBY STATUS A warning notice, and the incident command group should be contacted and advised of the emergency, and a brief report of the situation provided; or Alert 2 - EMERGENCY STATUS Activate The Partial call-in list contacted, according to Incident Commander. all parties advised of the emergency, given a brief report of the situation and directed to initiate their response immediately. Alert 3- EMERGENCY STATUS Activate The full call-in list contacted, all parties advised of the emergency, given a brief report of the situation and directed to initiate their response immediately. Alert 4- EVACUATION Activate the total evacuation process. Important information to obtain as soon as possible should include but not be limited to: Type of incident, including specific hazard/agent, if known Location of incident Number and types of injuries Special actions being taken (e.g., decontamination, transporting persons on buses) Estimated time of arrival of first-arriving red crescent units 5
6 Initiation of Disaster Notification All key personnel on the Initial Disaster Notification (Appedinx1) will be notified accordingly during initial disaster notification, those personnel and the disaster code number-8888-should notify the appropriate personnel under their command of the alert status for the response (appendix 5). All subsequent staff will be called in by using a cascade system, where the primary contacts call in other personnel as required. Telecommunication Operators shall obtain from the Incident Command Centre: Instructions for dealing with inquiries from: o Emergency response services o Other Hospitals o Relatives, etc., inquiring about persons involved in the emergency incident Offers from volunteers Name of PIO from the Dean Office to whom all media enquiries should be directed. The primary communications will be through the switchboard. The Emergency number will be according to Emergency Codes System (appendix2) REMEMBER Communication capacity will be severely taxed during the emergency, so restrict calls to critical matters do not phone for an update. SWITCHBOARD Emergency hot line is 953 The Telecommunications Operator will be crucial in assisting with the appropriate response to any emergency. Notification of the emergency, and its status, may be received first by either the Department of Emergency Medicine (DEM) or the Telecommunications Operator. 6
7 Command Authority GENERAL DEM (Team Leader) and/or the ADON-DEM (after working hours the Nursing Supervisor) will have the authority to activate the disaster plan and initiate the disaster notification. They will immediately consult with the DEM Chairman/designee. The Incident Commander will have the authority to move to any alert phases according to the level of emergency. In a sudden rush of casualties to DEM before the arrival of the Incident commander, the Emergency Team Leader will have the authority to activate the disaster response. During Disaster announcement every member of the KKUH staff shall follow the job action Sheet (JAS) assigned to his/her. (Appendix 6) If an emergency requires a response from Civil Defense, Police, Fire or other professional response agencies, they will assume command to the service the render and will liaise with the Hospital Command Centre to forward information and the use of hospital resources when required. COMMAND CENTREE LOCATION: 0 LEVEL, Conference Room DEM For major emergencies, the Command Centre will be established in the College Board Room, this room contains: o Telephone services on dedicated outside lines to facilitate communication in the event of hospital communications failure or overload. o Internal telephones o A complete set of Emergency Plans and associated documentations o Site Maps and Whiteboard o A Fax Machine o A rotated stock of torches, stationery and materials appropriate to the need o An AM/FM band radio battery operated The COMMAND CENTREE will operate upon the announcement of alert 1,2 or 3. by Command Member In the event the Incident Command Centre in DEM conference room, level 0 cannot be utilized the Incident Command Centre will be established in the College Board Room. PERSONNEL COMMAND CENTREE For the purpose of all Emergency Plans in this document, the following defines the Hospital Emergency Incident Command System (Appendix 1) that will decide on the management of the emergency and the activation of resources. The Incident Commander will be in charge of the total response and the other members of the team will coordinate with him. For each designated role in the plan, the responsible officer will be the most senior officer from each group on site and available at the time. INCIDENT COMMAND TEAM Incident Commander (Chairman-DEM) Members Liaison Officer (Medical Director) PIO Dean Office IT Branch Director Medical/Technical Specialist(s) Safety & Security Director Exec. Director of Services Medical Director Director of Nursing Exec. Dir. Of Patient Affairs 7
8 DUTIES COMMAND TEAM When informed of an incident by the Incident Commander/ DEM Consultant/ Telecommunications Operator, find out the: Nature of incident Time and place By whom reported Move to the Command Centre and initiate action to control initial minor problems. Liaise with the Director, Safety and Security Services Department, and Manager, Security Services in the area (using Safety and Security Services radio if necessary) to establish if the incident is under control or if additional staff is required. Ensure the appropriate response for the type of incident that is being followed: Establish communications with the Civil Defense, KSU Fire Services and/or Police as required Obtain additional staff resources as required and oversee any evacuation deemed necessary. Determine if the incident will be brought under control quickly or is likely to escalate to a larger incident. If the incident is being effectively managed and likely to be brought to a prompt conclusion, ensure all patients are safely accommodated, evaluate the final impact of the incident and advise respective senior staff of the events. Where the incident is escalating or is likely to be protracted, the Command Team should ensure that all designated personnel are on site. INCIDENT COMMAND TEAM Incident Commander (Chairman-DEM) Members Liaison Officer (Medical Director) PIO Dean Office IT Branch Director Medical/Technical Specialist(s) Safety & Security Director Exec. Director of Services Medical Director Director of Nursing Exec. Dir. Of Patient Affairs 8
9 DUTIES OF INCIDENT COMMANDER (Chairman, DEM) 1. Initiate the activation phase 2. Supervision of the whole plan 3. Modification of the plan steps as necessary 4. Notify and mobilize additional support as necessary 5. Call more senior staff and officials as necessary 6. Communication with the disaster site 7. Formation and direction of medical teams to go to the scene 8. Coordination of disaster plan with outside agencies as appropriate a. Police b. Red Crescent c. Civil Defense d. Other Hospitals 9. Communication and coordination with all clinical and non-clinical departments 10. Make announcements as necessary 11. Terminate the disaster DUTIES OF THE MEDICAL DIRECTOR 1. Supervise the clinical care in all areas of the hospital including Department of Emergency Medicine 2. Make sure the plan is being carried out in the right manner 3. Call up the necessary medical specialists as needed 4. Assist in the areas where help is required 5. Monitor the number of patients admitted and their distribution in the surgical/ medical/ pediatric wards. These details are available from the disaster patient tracking form. 6. Allocate a clinician to reassess all patients for possible discharge to improve patient bed availability. 9
10 DUTIES OF THE EXECUTIVE DIRECTOR of SERVICES 1. Initiate the call in of his Associate directors and their teams 2. Liaise with the Associate Director, Support Services to ensure disaster plan and job action sheets are being carried out. DUTIES OF THE EXECUTIVE DIRECTOR of PATIENT AFFAIRES 1. Initiate the call in of his Associate directors and their teams 2. Liaise with the Associate Director, Patient Relations to ensure disaster plan and job action sheets are being carried out 3. Liaise with the Executive Director for Support Services to ensure disaster plan and job action sheets are being carried out 4. Allocate the Public Relations Officers to the DEM AOD 5. Allocate Patient Relations Officers to arrange together with security supervisor to keep property of injured patients safe DUTIES OF DIRECTOR OF NURSING 1. Initiate the call in of the relevant nursing departments 2. Direct Associate Directors of Nursing to commence their job action sheets 3. Allocate a Nursing Supervisor to the Physiotherapy department to control and delegate call in nursing staff. (nursing staff pool) 4. Initiate the commencement of the patient discharge area 5. Monitor that the disaster plan is being carried out in the right manner 7. Enhance nurse s assistance in discharging patient that clinically discharged to improve patient bed availability. 11
11 COMMUNICATION COMMAND CENTREE RADIO PROCEDURES Call 953. The relevant code name of the disaster response must be used at all times (e.g. Code Orange) DIRECT TELEPHONE NUMBER 1) ) ) ) Fax COMMUNICATIONS ALTERNATIVE In the event that a malfunction of the switchboard occurs as a result of the emergency, a number of available alternative systems such as direct external telephones in Executive Offices, mobile telephones and two-way radio systems are available. CANCELLATION OF CODE After consultation with appropriate emergency services, the Incident Commander shall indicate ALL CLEAR and advise of subsequent action. It is important to observe that ALL CLEAR is given and followed by the emergency code corresponding to the emergency to which it relates. For example, where emergency color codes are used, in a fire Code Red. If the fire is extinguished prior to completion of evacuation then ALL CLEAR Code Red is given. DEBRIEF At the conclusion of the activity, a formal debrief and counseling sessions should be made available for all staff. The Head of Psychiatric Services will coordinate this after the emergency is over. WORKPLACE HEALTH AND SAFETY REQUIREMENTS If during the course of an Internal or External Emergency, either of the following occurs: o o SERIOUS BODILY INJURY: an injury that causes death or impairs a person to such an extent that as a consequence of the injury, the person becomes an overnight or longer stay patient in a hospital. DANGEROUS EVENT: an event at a workplace involving imminent risk of explosion, fire or serious bodily injury. The Safety and Security Services Department is to be immediately notified by pager through the switchboard. Before an area is re-entered, following an evacuation due to smoke or a fire, the Safety and Security Services Department is to be notified by pager through the switchboard to enable atmospheric monitoring to be conducted. 11
12 COMMUNICATION Role of the Department of Emergency Medicine 1. The Deputy Chairman of Emergency Medicine is to assume control of the Department of Emergency Medicine (DEM) if the chairman is not available ROLE: Direct the clearing of patients in the department Prepare for the reception of casualties into the department i. Communicate with Incident Command Centre ii. Organize site medical teams, equipment as required. Safety and Security Services staff will control access to the Department of Emergency Medicine. 2. Patients will be directed to an appropriate area on arrival by the Triage Officer (Emergency Department Team Leader). All patients will be identified, recorded and issued a disaster chart number. A Mettag (Appendix 4) will be attached to the patient if not already present. The number on the Mettag should be recorded with the disaster chart number on the patient tracking form. 3. The distribution of casualties within the emergency department will be according to their triage acuity (Appendix 3). All adult, ambulatory patients with minor injuries will be directed to Urgent Care Unit. All pediatric, ambulatory patients with minor injuries will be directed to the Pediatric Emergency Unit. 4. Following initial assessment and treatment, patients are transferred to appropriate areas of the hospital Wards. 5. For critically ill patients requiring intensive care: Surgical Intensive Care Unit (SICU) Medical Intensive Care Unit (MICU) Pediatric Intensive Care Unit (PICU) Coronary Care Unit (CCU) High dependency unit (HDU) beds to be converted to Intensive Care Unit (ICU) beds Ward 21B 4 beds Ward 25A 3 beds These beds will accommodate chronic patients in the related intensive care units so that the patients from the emergency department will be transferred to the appropriate ICU. The beds in ICU will be vacated by transferring patients to the HDU beds. If there are any patients in the HDU, they will be transferred to their corresponding ward. The HDU will serve as backup for any patients from ICU requiring minimal care. All ICU s should have designated chronically ill patients requiring minimal care who can be transferred to HDU as required. Heads of clinical areas should arrange to discharge patients from the wards. The discharged patients will be directed to Ward 35A. In this area, the discharge medications, clinic appointments and patient transport will be dealt with. A Patient Relations Officer will be placed here to assist with contacting patient s relatives if necessary. Discharged patients will use the elevator near ward 35A as their exit out of the hospital. 6. Evacuation of casualties by helicopter 12
13 The number of casualties to be evacuated by air from a major incident/ disaster should be established as soon as possible. Arrangements should be made to send KKUH ambulances to the university helipad. A staging point with medical/nursing support to be established adjacent to the heliport when resources permit. NOTE: If casualties are being transported in large numbers by helicopter, consideration should be given to request the assistance of the Red Crescent to transport casualties to KKUH Department of Emergency Medicine. 13
14 LEVEL OF ACTIVATION STANDY Alert1 When the decision is made to move to Standby Status pending possible activation of the External Medical Emergency Plan, the Emergency Department Consultant/Team Leader, will ensure that the following senior personnel are notified. Emergency Department Standby Hospital Standby Chairman Department of Emergency Medicine Emergency Department Consultant On-call Associate Director of Nursing, DEM Head Nurse, Emergency (Adult& Pediatric) ACTIVATION Alert 2, 3 1. When the decision to activate the external emergency plan has been made, the above senior personnel must be asked to come immediately to the Incident Command, Department of Emergency Medicine for briefing and to collect their job action sheets. They then have the responsibility of notifying and mobilizing the other key response personnel. 2. The Consultants on-call of Surgery, Medicine, Anesthesia and Orthopedics should report initially to the Chairman of Emergency Medicine or his designee for a briefing on the disaster. 3. The Trauma Team should initially report to the doctor s room in DEM for an initial briefing before entering the clinical area. 4. Security officers are responsible for immediately securing the entrances and perimeters of the emergency department (map 1) and for organizing the flow of ambulances to the emergency department triage area. 5. In the emergency department, patients waiting for admission or who are likely to require admission are to be sent directly to an allocated ward. Those patients who can be discharged should be discharged from the emergency department. Those patients with minor complaints should be asked to go to another hospital 6. Patients from KKUH wards will be transferred to KAUH, as a back-up in case more beds are needed than can be made available at KKUH. Patients with minor injuries may also be referred to KAUH if the need arises. The Deputy Director of Nursing (KKUH) can be contacted on /1621, bleep 0059 or 1798 and the Director of Nursing (KAUH) on , bleep 0879 for this arrangement to be initiated (agreement Plan in process with king Fahad Medical City) in order to reduce patient travel distance. 7. When necessary back up ambulances from KAUH can be utilized throe the Head Paramedic/designee. KKUH ambulance will be the person responsible for contacting KAUH on if the need arises. 8. All personnel who are called in to report for duty must have their hospital ID visible to be given entry to the hospital by the security officers. All staff should enter thorough the main entrance at the front of the hospital. 9. All DEM staff who are called in are to assemble in the Ortho Clinic to await further instructions and allocation of their duties. 10. All medical and nursing staff from other areas who have been called in should report to the Ortho Clinic to await further allocation of their duties. 14
15 11. Staff called in for other departments of the hospital should report to their designated areas 12. An information center staffed by Public Relations Officers will be established in the orthopedic female waiting room. Media representatives e.g. reporters, TV crews will not be permitted into any area on O Level. Security officers should direct all such representatives to the Dean Office, College of Medicine on the first floor. 13. Security should direct any people who come to volunteer either medical students or those wishing to give blood to the student cafeteria area. A Patient Relations Officer should be stationed there to assist as needed. NO STAFF OTHER THAN THOSE ISSUED WITH DISASTER PASSES ARE PERMITTED ACCESS TO THE DEPARTMENT EMERGENCY MEDICICNE. The underlying principle is early mobilization of key personnel in control of departments who will play a pivotal role in the hospital response. These key personnel are then responsible for contacting and mobilizing staff required for their own internal response as decided by each department. Each department has the responsibility to ensure that all their employees are familiar with the Hospital as well as the department disaster plan 15
16 EMERGENCY CODES Identification: To facilitate identification of and communication about the various types of emergency, particularly when using open communication such as a public address system and two-way radios, the following color codes have been developed. The Color Codes are based on a Standard for an Emergency Response for Health Care Facilities: Blue Yellow Brown Orange White Green Black Pink Gray Medical Emergency Missing Patient Toxic or Radiological Leak Bomb Threat Disruptive Behavior ED Overcrowding External Disaster Infant/Child Abduction Utility Failure 16
17 EXTERNAL EMERGENCY PLAN EXTERNAL DISASTER - CODE BLACK DEFINITION: An incident occurring outside the hospital, which causes casualties in such numbers and severity that would overwhelm the capabilities of existing clinical services. At KKUH, ten (10) or more injured casualties with potentially serious injuries constitute a DISASTER. A MAJOR INCIDENT will be activated if there are five (5) or more seriously injured casualties. CATEGORIES OF CASUALTY SEVERITY Explanation: The aim of the KKUH external emergency plan (Code Black) is to coordinate the hospital services to receive and optimally manage any influx of patients of such numbers that would otherwise overwhelm the capabilities of existing services. The external emergency plan for KKUH is activated in response to incidents, which temporarily increases the demands on the hospital emergency patient handling capacity above the normal level, and/or requires on-site clinical teams to undertake assessments and assign priorities to the treatment and evacuation of the victims. This plan seeks to ready the hospital to receive patients within 30 minutes of notification of an external disaster. PRINCIPLES The following principles are based on three (3) phases: Acts to dispatch teams to the pre-hospital site Acts to sort the Emergency Department resources Acts to sort the hospital resources The principles underlying this plan are: Immediate assessment of likely demands on current services and activation when a potentially overwhelming demand is confirmed. Central command and coordination of the hospital response, with best possible communication to the incident site, other emergency response agencies, and other responding health care facilities Managing the response within normal operational protocols wherever possible, and only implementing special procedures where the demand is excessive. Activation of key hospital personnel, who will use their professional skill and expertise to provide an appropriate response guided by Job Action sheets which provide prompts/reminders for necessary activities that differ from normal daily practice. Progressive build up of response (Key staff activate additional staff as required) to match the demand arising from the incident. Careful management of the response to ensure that the operation of the hospital addresses the continuing demands of existing patients as well as incident victims, both in the short and long term. Accurate documentation of treatment as well as casualty movements. 17
18 Progressive integration of incident victims into the mainstream of hospital routine, although in the first few days there may be a need to allocate an appropriately staffed separate ward to cope with the numbers involved. Addressing not only the physical but also the psychological and emotional needs of victims and their families, as well as those of KKUH staff participating in the response. Detailed debriefing and assessment after the event to review the effectiveness of the response and to identify where improvement is required to better future responses. Ongoing training and periodic drills for key hospital staff to ensure an effective and appropriate response when the plan is activated. NOTIFICATION Notification is most likely to come from Red Crescent, Civil Defense or Police via a call to the Department of Emergency Medicine. The person receiving the call notifying an external disaster should record the following information: Time of notification Who is calling and their contact telephone number Description of disaster Location of disaster Number and type of persons injured and severity of injuries Any other information available The person taking the call must immediately notify the Consultant on duty in the Emergency Department, who will then notify those who have authority to activate the External Medical Emergency Plan (Code Black). AUTHORITY TO ACTIVATE The decision to move to Standby Status and/or activate the External Emergency Plan will be made by the Incident Commander. 18
19 UTILITY FAILURE CODE GRAY Dial 953, state Code Gray, the location and the nature of the emergency If necessary, move people to a safe area Follow the instructions of the Senior Safety & Security Officer or authorized person in charge Prepare to evacuate if instructed by the Senior Safety & Security Officer or authorized person in charge. EXPLANATION Internal Emergencies are any incidents that threaten the safety of the physical structure of the hospital, staff, patients, and visitors and which may also reduce the capacity of the hospital to function normally. Such incidents include: Explosion Natural Disaster (Earthquakes) Engineering failures (burst water mains, loss of electricity, gas leak, etc.) Impacts on buildings or grounds (aircraft, etc.) Incidents in the immediate surrounds of the hospital (Chemical spills with noxious vapors affecting people) The Internal Emergencies that are most likely to occur in the hospital will be of short duration and low intensity. Staff in the affected area, will manage such emergencies with provision for coordination by the most senior medical, nursing, and security staff actually on site at the time of the incident. These staff will constitute the Command Group. However, some emergencies will increase to a serious nature, and others will have a long time frame. In these situations, an Incident Command, staffed by senior hospital personnel, will be established to manage the hospital activities and liaise with external Emergency Services. These incidents will require the systematic evacuation of patients and others from all or part of the hospital. To address these needs, the plan has specific instructions for each incident category and the systematic evacuation of the building. When any of these incidents happen, the hospital is in EMERGENCY STATUS, and this affects allocation of personnel, command responsibilities, etc. PRINCIPLES OF EMERGENCY RESPONSE The basic principles of managing the response to an internal emergency are: Removal of people from danger as quickly as possible. Prevent other people unknowingly coming into a danger area Minimize the damage to the physical structure of the hospital Maintain the hospital function and re-establish services There are specific sections of this plan addressing major emergency categories. All staff must be familiar with the appropriate initial action for each emergency. It is important that there are effective management processes that can be implemented rapidly and that personnel and facility risks/danger are minimized. STAFF OBLIGATIONS INTERNAL EMERGENCY During the initial phase of an emergency, all staff will be under the direction of the Director, Safety and Security Services and the Senior Staff Member on duty in the affected area. If necessary, the Command Team will be formed and assume responsibility for managing the response. In major incidents an Incident Command Team will be established and these personnel assume control. In the event of a major internal emergency, where there has been significant damage to hospital property and casualties among patients and staff, there will be a reverse flow of patients. This means the casualties (staff, patients) will be taken 19
20 from wards to the Department of Emergency Medicine for treatment and transferred to another health facility for care. The underlying principle of the plan is that as far as possible staff will be doing their normal job. However, all staff may be required to assist in activities not normally part of their duties. While the EMERGENCY STATUS exists for the hospital, staff will be expected to undertake any allocated tasks for which they are physically capable position descriptions and duty statements are suspended for the duration of the emergency. Staff off-duty should not come to the hospital until the starting time of their normal shift and they should not telephone the hospital as this places a higher demand on the telephone services. In situations where off duty staff are called to assist in making the hospital safe or to evacuate patients, all staff are expected to return promptly to duty if called. It is the responsibility of managers/supervisors to ensure: That up-to-date call in lists are maintained That the Switchboard is informed of changes as necessary It is the responsibility of employees to: Be aware that their names are on the call in lists Be aware of their obligations if called Regularly exercise their roles in such emergencies Know where to report to in evacuation. There is an obligation for all off duty staff to return to duty when requested in an emergency and to assist as required by the Incident Command Team. Staff returning to duty must ensure them WEAR THEIR HOSPITAL STAFF ID BADGE, so they will have their usual freedom of movement around the hospital. COMMUNICATION In the normal course of events the hospital telephone system will be used, but there are back-up systems in the form of Safety and Security two-way radios and hand carried messages TRAFFIC CONTROL / PARKING Pedestrian Non-Evacuation Traffic Safety and Security Services staff shall ensure that all non-essential people do not enter the hospital grounds. If the emergency is major, Police should assist in the control of people traffic. Vehicular Traffic While the hospital is in Emergency Status, only emergency response vehicles will gain access to KKUH. Media vehicles will not gain access. All vehicles on site and not involved in the emergency but which may interfere with the management of the emergency, must be removed by their owners. If this cannot be managed, then, on the authority of the Command Team, a towing contractor can be called to remove the vehicles. Illegal Occupancy KKUH may become a target for illegal intruders. In the event of the above incident occurring the Senior Safety and Security Officer on duty will: Notify the Police and request assistance Ensure appropriate Emergency Services have been alerted. Notify the Director, Safety & Security Services Department. 21
21 Initiate action to restrict: a. Entrance to the building b. Illegal occupants gaining entry, and c. Contact between the illegal occupants and the hospital occupants. For the duration of the incident, the Senior Security Officer will utilize all available officers to assist with the control of pedestrians / traffic and to liaise with the relevant Emergency Services. 21
22 ACTION ON DISCOVERY OF FIRE FIRE - CODE RED DO NOT PANIC as panic may cause more serious injuries than that caused by the fire. Alert staff near to the fire to remove patients from the immediate area. REMOVE or RESCUE people from the immediate area. ALERT others of the presence of the fire by: o Verbally telling others in the immediate area o Activating the nearest break glass alarm (manual call point) o Contacting the emergency operator on extension 953 on any internal telephone. State your name and the exact location and the nature of the fire. CONFINE by closing doors and windows. This will provide occupants with additional time to evacuate EXTINGUISH the fire if: o It is safe to do so o You have someone with you o You have previously used a Fire Extinguisher TURN OFF ALL SERVICES Any decision to withdraw patient life support systems for the duration of the evacuation rests with the Medical Director. The decision to turn off the main oxygen supply to a building would be made by the Chief Fire Officer in conjunction with the Chief of Staff / Vice Dean. Lifts are not to be used in a fire emergency unless authorized by a Fire Officer. Save records (without personal risk) The procedures and equipment discussed below relate to the initial response to the fire emergency. Standard procedures will normally have a Safety and Security Officer at the site of a fire alarm in 2 minutes. The Civil Defense can be expected on site within 15 minutes. REPORTING A FIRE Remove all people from immediate danger Investigate any trace of smoke or burning smell Contact Safety and Security Services when the source of the smoke or smell cannot be identified. Dial 953 Tell your name and classification (e.g. Staff Nurse) Location of the fire, what is burning and if patients are being evacuated Activate any manual alarms in the vicinity use a hard object to break glass alarms. Do not shout or panic, this may cause confusion Where possible isolate any oxygen outlets by closing the shut off valve Remove oxygen cylinders from the area COMMAND RESPONSIBILITY For the initial response to a fire emergency, the senior staff member present is in command. If your position takes you to a number of wards and units each day, you do not have to know each area s fire plan, but you should understand the basic principles and be prepared to work under the direction of a fire marshal or the senior nursing staff member present at the time of the initial response. You may be asked to guide ambulant (walking) patients from the ward, allowing nursing staff to deal with non-ambulant (bedridden) patients. FIRE FIGHTING EQUIPMENT 22
23 Know the location and use of the fire fighting equipment in your area. All areas of the hospital have fire hoses and portable fire extinguishers. The location of the fire fighting equipment is shown on the evacuation plan displayed in your area. Use of the wrong fire extinguishers can make the situation worse. Water based equipment used on fires involving energized electrical equipment can result in electrocution. Furthermore, water from a hose or extinguisher applied to burning flammable liquids will spread the fire. FIRE EXTINGUISHERS Fire extinguishers are mounted on brackets either on the wall or in fire hose cupboards depending upon the hospital location. Make certain that you are familiar with the action required. Know how to activate the fire extinguishers in your area. Free the fire extinguisher from the bracket Balance the weight of the fire extinguisher Release the safety pin Squeeze the trigger or lever. Hold and direct the hose if necessary FIRE HOSES Located throughout the building are hose reels, which are similar to large garden hoses. DO NOT USE fire hoses if: Live electrical circuits are in area of the fire Flammable liquids are the source of the fire Procedure for using Fire Hoses Turn on the hose at the valve attached directly to the hose reel (in some cases this also releases the hose from a clamp). The hose is still turned off at the nozzle. Drag the hose to the scene of the fire Turn the nozzle in the direction as indicated on the nozzle. Play the stream of water on the fire. If hose nozzles are fitted with an upright lever, pull or push the lever to activate the hose. Following the completion of the fire emergency, the message CODE RED, ALL CLEAR will be given by the incident commander. Evacuation If evacuation from the area or building is required see CODE ALERT 4 23
24 Alert 4 - EVACUATION Do not panic or shout as this may cause panic in others. An orderly response will save more people. Under no circumstances should lifts be used in a fire related evacuation unless directed by the Fire authorities. Remove people from the immediate danger area e.g. a room containing the fire or alleged to contain a bomb. Evacuate people in the following order: o Ambulant (walking) o Semi-Ambulant (support when walking\0 o Non-Ambulant (bedridden) Move people adjacent (sideways) to a safe area if possible, or go down using fire stairs to another level below. The best choice is to move adjacent (sideways) through smoke doors on the same level. PROGRESSIVE EVACUATION OF THE BUILDING When evacuation requires movement outside the building, personnel will move via their directed route to the designated assembly area (via fire stairs) GENERAL Evacuation involves the movement of patients, staff and other people within or from the hospital in a rapid and as safe a manner as possible. ASSESSING THE SITUATION Before the decision to evacuate is made, a senior staff member present in the area should assess the situation at the time, in relation to the: Seriousness of the fire threat to human safety Proximity of hazards which may be relevant to the situation; and The nature and type of patients in the area AUTHORITY TO EVACUATE The authority to order evacuation of an area shall be with the Fire Marshal or senior staff member present in the area at the time. Responsibility for the evacuation should be given to the incident commander who would act on his/her own initiative. Staff such as medical officers, nursing staff, or engineers if present may provide advice. The decision for which patients are for immediate evacuation should be made by the nurse-in-charge or medical officer (or both). The Fire Services will assume control on their arrival. STAGES IN EVACUATION Evacuation should be conducted in three distinct stages according to the severity of the emergency. STAGE 1 REMOVAL OF PEOPLE FROM THE IMMEDIATE DANGER AREA. Patients and other people in the immediate area, and if necessary on the whole floor will need to be assembled a safe distance from the cause of the emergency. In the case of fire and smoke, once the area has been evacuated, doors should be closed to localize the fire and smoke. 24
25 STAGE 2 - STAGE 3- REMOVAL TO A SAFE AREA Should the seriousness of the situation warrant further evacuation, patients should be moved through the fire and/or smoke doors/exits to safe areas. This may be to an adjoining ward protected by fire and smoke doors on the same floor level or to another floor level. When evacuating a complete floor, patients should generally be moved to a floor on a lower level of the occupied building. COMPLETE EVACUATION OF A BUILDING Evacuation of the entire building will require all available staff to assist in the movement of the patients to a safe place. STAGES IN EVACUATION 1. Away from immediate danger 2. To safe area beyond fire or smoke doors 3. Complete evacuation of the building An evacuation plan should be displayed in your area. Evacuation should be by using exit routes as indicated on that plan. It is important that all staff are familiar with evacuation plans for their own work area. EXIT ROUTES The presence of fire or smoke (or both) in an emergency situation may govern the choice of evacuation routes and prohibit the use of nearby exits, in which case the nearest accessible exit should be used. For this purpose, prior knowledge of the building layout by staff is very important. Fire Marshals play a vital role in the education of staff and in controlling any necessary evacuations. LIFTS Lifts shall not be used in a fire emergency unless authorized by the fire service officers. Electric power may fail or be switched off causing people to be trapped in a lift. The lift shaft could act as a chimney and thus contribute to the spread of fire, heat and smoke to other parts of the building. Fire isolated stairs; fire escapes and other safe routes should be used. EVACUATION OF STAFF AND PATIENTS For the purpose of evacuation it is desirable to sub-divide patients into three groups taking into account the type of patients present: GROUP 1 - Ambulatory patients who require only a staff member to guide or direct them to a place of safety. GROUP 2 - Semi-ambulant patients, requiring minimal assistance GROUP 3 - Non-ambulant patients who have to be physically moved or carried. Once people have been removed from immediate danger it is generally recommended that Group 1 be moved first, then Group 2, and finally Group 3. ASSEMBLY AREAS In the event of a major fire/emergency, patients, visitors and staff will be advised of the required assembly area within the hospital grounds. It is desirable to wrap a blanket around each patient. A blanket provides protection from radiated heat if required. NOTE: It must be stressed that the first responsibility of the staff in proximity to the fire/ emergency is to remove patients from the immediate danger area. Staff must be familiar with all exits and exit routes to facilitate the quickest movement of patients. 25
26 ROOM CHECK / RECORD COLLECTION When all patients have been removed from the danger area, a staff member should check that the area is clear. Provided no risk is involved, staff lists and patients records should be collected at this time. FIRE EXIT MONITORS A staff member should be positioned to prevent other people entering the danger area by alternative entrances, provided no risk is involved and the person nominated can be spared. A head count should also be conducted once the evacuation is complete. Staff and patients must be instructed to stay in the evacuation area, until advised they can leave, to enable an accurate head count to be made. The senior staff member or designee should report to the Fire Service Officer or Senior Safety and Security Services Officer present to indicate if anyone is missing after having conducted a staff and patient check. FACTORS FOR CONSIDERATION Factors that must be considered in the emergency handling of patients include: The nature of the emergency The weight and condition of the patient The strength, skill and training of the rescuer(s) The height of the bed The availability of resources both human and material Correct lifting techniques should be observed at all times. When using a blanket to drag a patient, it should be grasped and pulled from the end near the patient s feet. The beds of intensive care patients may be wheeled to safety if the situation permits. Do not obstruct corridors, doorways, and stair entrances with beds or bedding. AMBULATORY PATIENTS Ambulatory patients should be taken in a group to a safe area. A responsible person must be given control to minimize panic and ensure that all are accounted for. Ambulatory patients and visitors can be used to assist in the orderly removal of other ambulatory patients. WHEELCHAIR PATIENTS If the need for wheelchairs is acute, patients who have reached a safe area should vacate their chairs so that other patients may be evacuated. Do not obstruct corridors, doorways and stairs with wheelchairs NON-AMBULATORY PATIENTS Non-ambulatory patients may be carried on stretchers, blankets or specially designed equipment, e.g. evacuation sheets. They may also be moved by emergency removal techniques such as: Blanket drag Swing carry Fore and aft carry Other improvised techniques to suit the situation. PATIENT CARE FOLLOWING EVACUATION After patients and staff are evacuated the all clear may be given. Patient care will probably require an extraordinary effort by staff until such time as the patients can be returned to their ward, found alternative accommodation within the hospital or transported to another hospital. 26
27 SISTER WARDS An evacuation that has patients being placed outside of a building will, in addition to subjecting the patient to the weather conditions at the time, effectively reduce the following: Medical air and gas Suction Communication Medical support It is therefore strongly recommended that all patient care areas develop a sister ward protocol with at least two other wards/clinics that would be able to look after patients in the event of an evacuation. Each ward would be required to provide as much as possible, similar medical functions that the patients were receiving prior to the evacuation. This process would be reciprocal and should be confirmed on a regular basis. 27
28 CARDIO PULMONARY RESUSCITATION CODE BLUE 1. Commence basic life support and call for assistance 2. Dial , state the Code Blue and the location 3. Continue resuscitation with CPR, use of bag-valve mask and AED (if available) until the arrival of the Cardiac Arrest Team MEDICAL EMERGENCY NON CARDIAC ARREST This process applies to situations where the patient is not experiencing a cardiac arrest but where clinical staff believes that the patient requires medical attention urgently (i.e. within minutes). Guidelines for following this process include: Airway threatened Breathing unexpected change in respiratory rate. Under 5 or over 36. Circulation unexpected change in pulse rate. Under 40 or over 140 Drop in Systolic BP under 90 Unexpected significant bleeding Nervous System sudden loss of consciousness. Aggression. Prolonged or repeated seizure activity. Other any patient whom you are seriously concerned about. Procedure: Dial 6. Notify switchboard as to which is the primary treating team for the patient and ask to have them paged urgently or the be paged urgently by the ward staff. 28
29 DISRUPTIVE BEHAVIOR CODE WHITE Definition: Armed or unarmed persons threatening to injure others or cause injury to themselves. This procedure is the initial response to a personal threat that may arise from an armed or unarmed person confronting staff or others in a violent or threatening manner or where a person threatens to commit suicide. Once Safety and Security Services, Police or other professional response groups arrive, they will assume command. WARNING! UNDER NO CIRCUMSTANCES SHOULD STAFF, PATIENTS OR VISITORS PLACE THEMSELVES IN FURTHER DANGER. Whenever there are unlawful demands for hospital property (Money, drugs, equipment, etc.) with threats of violence, the property should be handed over without question. ARMED CONFRONTATION Obey the offender s instructions, Keep calm and be observant. Do only what you are told and nothing more Do not volunteer any information Stay out of danger if not directly involved Leave the building if it is safe to do so Raise the alarm Dial 953 with details of the: o Location o Nature of incident o Person reporting The switchboard operator should announce CODE WHITE then notify Safety and Security. Safety and Security Services on arrival at the scene will inform the switchboard operator of the situation to be relayed to the Police. Carefully observe any vehicle used by the offender(s) taking particular note of its registration number, type and color and number of occupants and their descriptions. Observe the offender(s) as much as possible. In particular, note the speech, mannerisms, clothing, scars or any other distinguishing features. Record these observations as quickly as possible after the event, as the police will want individual descriptions of what happened, not influenced by others. Keep other people out of the area and Centre Safety and Security Services staff at entrances to stop people from entering into the area. Do not move or take anything from the area until the police have checked for fingerprints and other clues. Ask all witnesses to remain until the police arrive. Explain to the witnesses that their view of what happened, however brief, could provide vital information when put together with other evidence. All members of the media must be excluded from the Hospital and all media contact will be made through the Public Relations Office. Should injuries occur, only attempt to assist where there is no risk to yourself and the offender consents? Do not place more people in danger. Explanation In the hospital environment, personal threats can take many forms, and therefore a specific response cannot be detailed. However, the basic principles that should always be addressed are: o Remove as many people from the danger and prevent other people from getting into danger o Always carry out the demands of the offender exactly nothing more, nothing less. 29
30 o o If hospital property is demanded, it should always be handed over. Do not try to be a hero Aims of the Plan Saving of life Minimum disruption to the patients, staff, visitors and the running of the hospital Where possible, protection of assets. RAISING THE ALARM In most cases involving personal threat, the person directly involved with the offender will not be in a position to raise the alarm. In such cases, the staff member must try to draw the attention of other persons to the situation, without placing any person at risk. Each work area should develop a code that indicates that an individual is under threat. The alarm should be raised by dialing 953 and advising the switchboard of the nature of the incident, the number of people involved, the location of the incident and who is reporting the incident. The operator will immediately notify Safety and Security Services and the Police. Medical Team The Department of Emergency Medicine will be informed by the switchboard operator and placed on Alert 1 -STANDBY STATUS in the event of injuries. Minimizing People Involved Every effort should be made to minimize the number of people involved or potentially involved in a personal threat situation. All people who are not directly under threat should leave the area if safe to do so. Outside the threat area, security should be Centered to ensure that other people do not become involved in the incident. The unexpected arrival of other people may panic the offender into rash action, or increase the number of people at risk. ARMED HOLD UP Armed hold up is the most likely personal threat, and this could be for cash, drugs or some other item. In all cases, the persons in contact with the offender should be as agreeable as possible, while trying to signal to other staff to raise the alarm. DRUGS HOLD UP The pharmacies and every clinical area are potential sites for unlawful demands for drugs. Where possible, you should tell the offender that the demanded drugs are not held in the area or that the key to the storage cupboard is unavailable. If the threats become more menacing, then every effort should be made to meet the offender s demands. If there are genuine reasons to be unable to meet the demands, such as not having the key to drug cupboards, then explain the procedure used to access the drugs and why you are unable to access them. For any type of hold up, try to keep a mental note of the property taken, and as soon as the threat is removed, write down the list of stolen property. It is also important that nothing is touched and only essential people enter the area until the Police are on the site, so that fingerprints and other evidence is maintained intact HOSTAGE The hostage may be a patient, staff member or a visitor. The reasons for taking such a hostage can be several, but could include: demands for money or drugs; demands for action or inaction regarding the treatment of an individual (this may or may not be the offender); some political motivation, retribution for some real or perceived wrong; a domestic matter. The major concerns should be to minimize the number of hostages and to minimize the risk to each. 31
31 People who can, should immediately leave the threat area. The offender s instructions should be carried out as closely as possible. Because of the likely lengthy nature of this category of personnel threat, a Command Centre would be established to manage liaison between the Police, Hospital staff, and the threat area. The locations will depend upon the site of the threat, and all communication should be relayed through the switchboard. Twoway radio communication should be used only out of earshot of the hostage taker(s). It is important that there is a clear understanding of the nature of the demands including the reasons for the event and the expectations of the offender. This information must be relayed to the Command Centre by Senior Safety and Security Services Officer. Once Police and other professional response groups are on site, they will assume control. This response may be armed so staff will need to be aware of the risks not only from the offender, but also Police, and should immediately obey any instructions. If you are in a location that is low risk, stay there until the situation is resolved. When the situation is resolved, there will be an announcement CODE WHITE ALL CLEAR. At that time, it is safe to resume normal activities. IRRATIONAL PERSON When an irrational person undertakes a campaign of damage against staff and/or the environment of the hospital, there is essentially an unmanageable situation. The first concern should be to move as many people away from the expected path of the offender and the violence. If these people cannot escape from the area, they should minimize their exposure by moving behind furniture, etc., which will isolate them from the offender. The alarm should be raised by dialing 953. The switchboard operator will contact Safety and Security Services and the Police. All personnel who are able should leave the threatened area as quickly as possible. If possible, staff should exit one by one, not in groups to minimize target opportunities. Once Police and other professional response groups are at the hospital, they will assume control. 31
32 BOMB THREAT CODE ORANGE This procedure is this hospital s response to a bomb threat. Once Police, Civil Defense and other professional response groups arrive, they will work with staff of the hospital to assess the level and nature of the threat. A bomb threat will usually be received by phone or in the mail. Do not panic but treat the threat as genuine. Phone Threat Record all available information given by the person on the telephone. DO NOT HANG UP AFTER CALL UNTIL INSTRUCTIONS ARE GIVEN. Mail Threat Suspicious Parcel Do not touch. Remove all people from the area. Written Threat Envelope and correspondence should be kept, do not handle further. Place in a plastic bag if possible to assist in fingerprinting, Centre marks, etc. Dial 953; state CODE ORANGE and location (use another internal phone if threat is by phone). Follow instructions of the Senior Safety and Security Services Officer or Police. Prepare to evacuate in accordance with the Evacuation Plan ALERT 4. Assist by visual search of your work area look for unusual parcels, objects, etc. NOT normally in your work area. If object found: Do not touch Report find by dialing 953 on internal telephone Keep clear BOMB / ARSON THREAT CHECKLIST Any indication that a bomb or improvised explosive device has been planted must be regarded as genuine and the bomb/arson protocol implemented. If such threats are genuine and the device is activated resulting in an explosion and/or fire, then the Fire Plan Code Red, Code Gray and Alert 4 will be implemented. Bomb threats may be specific or non-specific as follows: SPECIFIC THREAT The caller provides more detailed information which could include statements describing the device, why it was placed, its location, the time of activation and other details. Although less common, the specific threat is more credible. NON-SPECIFIC THREAT The caller may make a simple statement to the effect that a device has been placed. Generally, very little, if any additional detail is said before the caller ends the conversation. The non-specific threat is more common but neither type of threat should be immediately discredited without investigation. Every threat should be treated as genuine until proven otherwise. INITIAL RESPONSE The staff member receiving the threat must gain as much information as possible and document it immediately. Details that should be gained include: The location of the bomb or other device and in what it is contained. When the device is set to be activated The reason for the threat Any identifying characteristics of the caller which might be available, including: Location 32
33 Identity Age Sex Accent or speech impediment Background sounds e.g. aircraft, etc. Immediately after the phone call, or during the phone call, another staff member must try to contact the switchboard on 953 and advise them of the threat and they will initiate the appropriate protocol for CODE ORANGE. It is best if you can raise the alarm while keeping the caller on the phone as long as possible to enable a phone trace and action the CODE ORANGE protocol earlier than the caller would anticipate. NOTIFICATION The staff member receiving the call must immediately contact the switchboard operator on 953. The switch immediately contacts the Director, Safety and Security Services Department IN HOURS OR AFTER HOURS. The Duty Senior Safety and Security Services Officer will immediately contact the staff member who received the call or information. The Director, Safety and Security Services or the Senior Safety and Security Services Officer will contact the Police. The Police will contact other emergency services as necessary. The Security Officer will then delegate the Safety and Security Officers to inform staff within close proximity to the Code Orange Area. EVALUATION Following an analysis of the information received, the Director or Senior Safety and Security Services Officer shall make the decision whether to institute one of the three possible actions, as follows: Search without evacuation Evacuate and search Evacuate (without search) SWITCHBOARD / SAFETY & SECURITY SERVICES Ensure that radio transmitters including two-way radios and mobile telephones are not used within 30 meters of the suspect bomb location. (This action reduces the risk of setting off the detonators, etc. by radio emission). SEARCH The aim of the search is to identify any object which is not normally found in an area or location, or for which an owner is not readily identifiable or becomes suspect for any other reason e.g. suspiciously labeled (similar to that described in the threat), unusual size, shape, sound and presence of pieces of tape, wire, string or explosive wrappings. If any suspect object is found, the Safety and Security Officers shall ensure that it is not touched or moved, and that the area is kept clear. The Safety and Security Officer shall notify the Incident Commander immediately. NOTE: More than one suspect object may have been planted. The search may be made without evacuation or made after evacuation. 33
34 SEARCH WITHOUT EVACUATION If the decision is made to search without evacuation, Incident Commander shall execute the following: Alert all Security Officers and the Police of the situation, identifying the location, if known. If the location is unknown, state that it is unknown Delegate Security Officers to supervise and assist in the search for any objects. All Safety and Security Officers and members of staff within the area will search their immediate areas. A sticker should be placed on each sector of an area after a search has been completed to indicate that each area has been searched. This negates double searching and identifies area, which have been missed. If any suspect object is found, the Staff member will notify the Security Supervisor IMMEDIATELY. The Security supervisor will ensure that it is not touched or moved and that the area is kept clear. The Security Supervisor will notify the Police and switchboard operator IMMEDIATELY that a suspect object has been located. The Incident Commander will then notify the following officers: Dean Vice Dean for hospital affairs Medical Director Executive Director of Services Executive Director of Patients Affairs EVACUATION Implement ANNOUNCEMENT OF Alert 4- EVACUATION. Ensure all personal items are removed As soon as all persons are at the evacuation assembly point, all persons shall move to a secondary assembly area at least 100 meters distance from the building where the bomb is placed. Doors and windows should be opened as the building is evacuated to allow any explosive device to vent. Once evacuation has been completed no person should re-enter the building without the authority of the Police or Safety and Security Services Officer. PATIENT CARE AREAS: EVACUATION OPTION The following options need to be assessed by Senior Medical and Nursing Staff in consultation with the Director or Senior Safety & Security Services Officer: Total Evacuation Partial Evacuation TOTAL EVACUATION Immediate and total evacuation would seem to be the most appropriate response to any bomb threat. However, there are significant safeties factors associated with a bomb threat that may weigh against immediate evacuation. These are as follows: RISK INJURY As a general rule, the easiest area in which to plant an object is the shrubbery sometimes found outside a building, an adjoining car park, or in an area to which the public has the easiest access. Immediate evacuation through these areas may increase the injury risk. Car parks should not normally be used as assembly areas. The Security Supervisor should ensure that exit routes and assembly areas are searched for suspicious objects prior to any evacuation. 34
35 RESPONSE IMPAIRMENT Total evacuation will remove personnel who may be required to make a search. Panic. A sudden bomb threat evacuation may cause panic and unpredictable behavior, leading to unnecessary risk of injury. Patient Dependency. At least some of the patients in any area under bomb threat may be dependent upon life support equipment. Reduction in patient care. Although evacuation of patients to any assembly area may ensure their safety, repeated threats and evacuation could compromise patient care. The above factors may make total evacuation an undesirable response to the bomb threat. NOTE: Total and immediate evacuation, although risky, is the easy decision. After taking the easy way, the hard decision of when to return still has to be made. PARTIAL EVACUATION One alternative to total evacuation is partial evacuation. This response is particularly effective when the threat includes the specific or general location of the object or in those instances where a suspicious object has been located without prior warning. Partial evacuation can reduce risk of injury by evacuating ambulant patients, visitors and non-essential personnel. Staff essential to a search can remain, critical services can be continued and in cases of repeated threat, risk of injury is minimized. SEARCH AFTER EVACUATION If the decision is made to evacuate and search, the Security Supervisor should try to see that personal belongings are removed. Experts should check unidentified and unattended suspicious objects e.g. Police, and no attempt to remove such objects should be made. The following areas shall be searched in the order stated below: 1. Outside areas including evacuation assembly area 2. Building entrances and exits, and in particular evacuation routes. 3. Public areas within buildings 4. After external and public areas have been cleared, a search should be conducted beginning at the lowest levels and continuing upwards until every floor including the roof has been searched. 5. After a floor or room has been searched, it should be distinctively marked to avoid duplication of effort. If a device has been located, Police will establish a Command Centre. The following staff will be required at the Command Centre location: During Working Hours: Hospital Incident Commander Vice Dean Medical Director Deputy Director of Nursing Executive Directors Director, Safety & Security Department After Hours: The following officers will report to the Command Centre until replaced by more senior members of staff. Officers identified in During Working Hours will be notified of the incident by switchboard: Senior Safety & Security Officer DEM Team Leader Nursing Supervisor 35
36 At the conclusion of this stage, Police will advise when Code Orange is cancelled. Code Orange All Clear Telecommunications Operator will then advise all sections Stand down Safety and Security Services and Switchboard 36
37 THE EMERGENCY OPERATION PLAN OF SAFETY AND SECURITY DEPARTMENT OBJECTIVE To secure the site by scrutinizing everything entering to it and by making sure that alarm system and fire fighting means are available and in place; evacuation points, routes utilized, temporary collection and evacuation places are known; the readiness of site to receive ordinary and emergency cases is kept and maintained. THE MISSION The mission of Safety and Security Unit at College of Medicine and King Khalid University Hospital is presented in the following: 1) to prepare the site for receiving emergency cases at any time. 2) To make sure that all internal and external traffic areas leading to emergency exits and doors are clear. 3) To continuously make sure that all corridors are not blocked and free from any obstacles that may hinder or hamper evacuation. 4) To provide vigilance to all service sites, energy sources, and vital sites and prevent unauthorized personnel from entrance. 5) To spread awareness among staff, patients and watchers in respect of what they should know about: a. Siren tones b. Safety places that they can go to during an internal disaster c. Receiving instructions during emergency occurrence and not acting alone. d. Not approaching any suspicious items and reporting its presence. 6) To make sure that contact devices are properly working and urgent contact can be made with the Civil Defense Dept. 7) To make sure that the service tunnel is secure and periodic patrols are routed in and around it. 8) To schedule the working hours pro-rota to be every six hours in the field area. 9) To keep record of places from which necessary needed vehicles or machinery can be brought over in time of crisis such as fire break -out or building collapse. 10) When a disaster occurs, the most important acts of safety and security will be: a) To initiate immediate intervention with the purpose of accommodating the situation and lessening the disaster s effects. b) To request help from the parties concerned. c) To extinguish fires and prevent spreading of fires. d) To participate in the evacuation process. e) To carry out evacuation plan in the site and nearby sites that could be exposed to danger as result of the situation. 37
38 f) To prepare evacuation sites for affected people. g) To mobilize all potentials for confronting the situation. Mobilization to include mobilizing human resources, equipment and machinery. h) To safeguard and maintain discipline in the area (affected site, medical evacuation, support site, accommodation places). i) To account for losses and harms, and to conduct an investigation for establishing the cause of the internal disaster. j) To restore the situation to its normal status. THE PLAN OF RECEIVING CASES IN EMERGENCY 1. The casualties who are brought in by ambulances will enter through the southern entrance of the hospital. A security man at the entrance will direct the injured to the Emergency Triage Area at the main door (Ambulance Bay). 2. Security Officers will be allocated to all points of entry on 0 level from the Emergency Department to Primary Care Clinics (PCC). No persons other than those wearing disaster passes will be permitted entry to the Emergency Department and surrounding areas on 0 level. 3. An iron rail separating the E/entrance and the visit entrance (20) will be put in place so that the injured are separated from the discharged patients who leave their wards. A security man will guide the patients and their watchers to the exit. 4. A security man will be stationed in the covered parking lot in order to prevent private cars from parking in Ambulance Parking Area. 5. Additional security man will be stationed at the circle in order to guide the injured to the right place and to prevent at random parking, and to facilitate the entrance of the ambulances. 6. The exit route for inpatients from their wards will be through the southern entrance of the hospital and the emergency exits of the wards. A security man will be stationed and he will guide the inpatients and the watchers to the exit place. 38
39 DEM DISASTER RESPONSE ROLE OF THE DEPARTMENT of EMERGENCY MEDICINE The Chairman of the DEM is a Incident Commander and is responsible for initiating the appropriate response to the disaster that has been notified. The Chairman should follow his/her action sheet for the directions to be commenced. If the number of victims is 10 or less, the DEM doctors with the help of medical staff on-call (trauma team) will deal with the incident. The nurse-in-charge will ask for more nurses if required. If the number of victims is more than 10, the team leader of DEM will advise the in charge nurse to initiate the Code Black and commence an activated response. On arrival, the Chairman of DEM will assume control of the department. He/she is responsible to Direct the clearing of patients from the department. Patients waiting for admission/likely to need admission should be sent to the ward. Patients requiring an emergency intervention should be triaged as normal. Patients waiting in the waiting room should be directed to another hospital. If afterhours, the nursing supervisor should provide nursing staff until on-call staff arrives. For critically ill patients requiring intensive care SICU PICU CCU MICU NICU High dependency beds Ward 21B 4 beds Ward 25A 3 beds These beds will accommodate chronic patients in the related intensive care units so that the patients from the emergency department will be transferred to the appropriate ICU s. The beds in the ICU will be vacated by transferring patients to the HDU beds. If there are any patients in the HDU, they will be transferred to their corresponding ward. The HDU will serve as back up for any patients from ICU requiring minimal care. All ICU s should have designated chronically ill patients requiring minimal care who can be transferred to the HDU as required. Organize the department for the reception of patients. ORGANISATION OF THE DEPARTMENT During a disaster, the emergency department staff will continue to manage patients as normal in the appropriate assessment areas, the difference being the number of patients will be increased and not all investigations and treatment will be completed before the patient leaves the assessment area. This is to ensure a continuous flow of patients through the department during the disaster response. A senior doctor will be responsible for prioritization of investigations such as X-ray, CT scan. TRIAGE Triage area will be set up outside the main door in the Ambulance bay. All available stretchers and wheelchairs should be brought to this area. This area will be staffed by: An emergency physician A pediatric doctor 2 staff nurses 2 receptionists All available paramedics/emt s 39
40 Role of the doctors and nurses This staff will be responsible for allocating a triage category to the patient and disposal to an appropriate assessment area. They should check the Mettag that is attached to the patient for relevant information. If no Mettag is attached to the patient, then triage staff is responsible for attaching a tag. If a patient not involved in the disaster, but requiring emergency care arrives, they should be treated the same as a disaster patient and a Mettag should be attached to their person. The triage staff are also responsible for directing the patient to the appropriate assessment area (see diagram). Each team should consist of: 1 doctor 1 staff nurse 1 receptionist Role of the receptionists The receptionists are responsible for the documentation of all patients who arrive to the emergency department. The form that is used is the disaster patient tracking form. They should not remove the Mettag from the patient. They are responsible for keeping an accurate list of all patients who arrive either alive or dead. They must record the number of the Mettag with the number of the disaster chart that is allocated to the patient. They must also record the assessment area that the patient is sent to. This list should be kept by the reception staff and not given to anyone. The people who may require access to the list are either a patient relation officer or a public relations officer. Under no circumstances are they to remove the list from the department. Role of the paramedics The paramedics/emt who are available should assist in transferring the patients to the assessment areas. They must ensure that staff in the area know that a patient has arrived. They should return to the triage area as soon as possible. When the casualties are no longer being transported to the department, the paramedics/emt should be allocated throughout the department to assist with patient care/ transfer. Resuscitation Unit Function of the area: To resuscitate the critically ill/injured patients with life-threatening conditions that may require airway management/assisted ventilation This area should be staffed by 3 anesthetists 3 doctors 16 nurses (1 nurse per patient, 2 nurses as runners) Comprehensive care should be given to these patients until a decision is made about their transfer to ICU or operating room. Acute Care Unit Function of the area: To resuscitate the critically ill/injured patients with life-threatening conditions that do not need airway support. This area should be staffed by 1 emergency consultant 5 doctors 9 nurses (1 nurse per patient, 2 nurses as runners) Stabilizing care should be given to these patients until a decision is made about their transfer to the ward or operating room. 41
41 Stabilizing care should be given to these patients until a decision is made about their transfer to the ward or operating room. Some of these patients may be admitted to the ward prior to having investigations completed e.g. X-ray Fast track Room Function of the area: To treat the seriously ill/injured patients e.g. long bone fractures with hypotension, <15% burns. This area should be staffed by: 2 doctors 4 nurses 1 emergency consultant should move between Acute Care 1 and Consultation room. Stabilizing care should be given to these patients until a decision is made about their transfer to the ward or operating room. Some of these patients may be admitted to the ward prior to having investigations completed e.g. X-ray Urgent Care Unit Function of the area: To treat patients with minor injuries who are non-ambulatory e.g. multiple lacerations, fractures This area should be staffed by: 1 doctor 3 nurses All adult ambulatory patients with minor injuries should be directed to the Primary Care Clinics. PEDIATRIC PATIENTS Pediatric Emergency Consultant/Team Leader should direct the clearing of patients in the department. Patients waiting for admission/likely to need admission should be sent to the ward. Patients waiting in the waiting room should be re-triaged and those able to leave should be directed to another hospital. All pediatric patients from the disaster will be seen at the Triage area (ambulance bay). The triage staff will be responsible for applying a triage category to the patient and allocation to an assessment area. They should check the Mettag that is attached to the patient for relevant information. If no Mettag is attached to the patient, then the triage staff is responsible for attaching a tag to the patient. If a patient not involved in the disaster but requiring emergency care arrives, they should be treated the same as a disaster patient and a Mettag should be attached to their person. They are also responsible for directing the patient to the appropriate assessment area (see diagram). Observation area Function of the area: To resuscitate the critically ill/injured patients with life-threatening conditions that do not need airway support. This area should be staffed by 2 doctors 4 nurses (1 nurse as a runner) 41
42 Stabilizing care should be given to these patients until a decision is made about their transfer to the ward or operating room. POPD All pediatric ambulatory patients with minor injuries will be directed to the Pediatric Outpatient Clinic area. This area should be staffed by: 6 doctors 12 nurses DOCUMENTATION ALL CLINICAL AREAS It is critically important that accurate and timely documentation is kept during the period of the disaster response. All patients must have two identifying numbers one taken from the Mettag and the other from the disaster chart. These two numbers should be written on any and all documentation relating to the patient even when transferred from the emergency department. The correct identity of the patient will be matched with these numbers when the disaster response has been stood down and time can be taken to establish correct information. All ambulatory patients should have correct identification information taken before they are permitted to leave the hospital. 42
43 DISASTER PLAN BLOOD BANK 1. MAIN OBJECTIVES o To ensure that the necessary stock of blood and blood products is maintained throughout the emergency. o To ensure the policy of issuing blood in a major disaster is maintained. 2. MAINTENANCE OF THE NECESSARY STOCK OF BLOOD AND BLOOD PRODUCTS Suspending blood issue for non-emergency transfusions. Increasing stock to the desired level by: o Delivery from other hospitals o Emergency donor bleeding Policy for blood issue in a major disaster (same as of emergency transfusion but will be dictated by the color code of the patient: Red, Yellow, or Green). o Compatibility done wherever possible. o Attempt to determine ABO and Rh groups to allow issue of group specific blood. o Issue group O Rh+ve to boys and men, O Rh-ve to women (except if O-ve is not available). o FFP & PC: usually available in good stocks (PC reserved for those who receive massive transfusion. PPF reserved for burns), o The Disaster & Mettag No. should be used in the: Identification of casualties Labeling samples of blood, reports of X-matched blood units 3. EMERGENCY DONORS ROOMS o Provision of bigger space and personnel to man the extended donor area. o Blood bank 4 rooms plus Student Cafeteria area. o This area should be clearly sign posted; hospital security and Public Relations, KKUH Telephone Operator and local radio or TV station should know of it in advance. o The King Saud University student rooms (the Health Center 5th floor) may be used in extremes of need. o Specially labeled bags and tubes should be ready to allow collection of blood from about 100 donors. o The currently used Blood Transfusion Requisition Form will be employed. It will carry the Disaster No. & Mettag No. which is to be issued by DEM. o Extra personnel to man the emergency donor rooms will be recruited from: o Hematology personnel (both medical and technical) o Hospital Phlebotomy personnel (both males and females) o Other laboratory personnel, if needed. o Porters (at least 2) should be allocated to Blood Bank Copies of this document will be circulated to all departments concerned to make their staff aware of the proposed commitments to this disaster plan. P.S.: 43
44 INCIDENT RESPONSE GUIDES ( IRG) To assist the incident command staff to optimally react to the situation they are confronting, Incident Response Guides have been devised for external and internal scenarios. Each IRG lists fundamental decision considerations specific to managing that situation by timeframe. The IRGs are intended to complement the hospital EOP and provide a primer that will provide some directional assistance and a means of initially documenting the actions undertaken. 44
45 BOMB THREAT INCIDENT RESPONSE GUIDE Mission: To safely manage staff, patients, and visitors during a bomb threat or suspicious package situation. Directions Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives Document all bomb threat information Immediate respond to the bomb threat when received or suspicious object is found Maintain security of the facility, consider lockdown and/or evacuation Control and inspect packages and materials entering critical areas for suspicious objects Maintain patient care services Ensure safety of the staff, patients, and visitors Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate Command staff and Section Chiefs as appropriate Consider the possibility of a dirty bomb and evaluate/prepare for secondary radiation, chemical, and/or biological contamination (Liaison Officer): Notify appropriate authorities of bomb threat and coordinate internal and external response agencies (e.g., law enforcement, bomb squad) Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. COMMAND (Safety Officer): Consider immediate evacuation of areas if threat is identified. Monitor response activities to ensure safety of staff, patients, and responders. (Public Information Officer): Establish a media staging/briefing area and secure the media area to ensure media remain in designated areas. Conduct media briefings and situation updates. OPERATIONS Implement the bomb threat procedure. Secure the facility and stop visitors and others from entering the facility. Evacuate non-essential personnel out of the facility to a safe area. 45
46 Initiate and coordinate search activities to identify suspicious objects or suspicious activity. Liaison with responding and investigating law enforcement agencies Consider evacuation or relocation of patients. PLANNING Establish operational periods, incident objectives and Incident Action Plan, in collaboration with Incident Commander. Prepare to track patients and personnel. LOGISTICS If necessary, establish an external evacuation safe area. Prepare to implement patient tracking protocols. Prepare for possible transportation for evacuated patients. Account for all personnel currently in the facility. Provide staff information and mental health services, as appropriate. Intermediate (Operational Period 2-12 Hours) COMMAND (Incident Commander): Meet with Command Staff and Section Chiefs to evaluate the overall impact of incident on the facility. (PIO): Continue monitoring media reporting Develop briefings and updates for staff, patients and visitors (Safety Officer): Conduct ongoing analysis of existing response practices for health and safety issues related to staff, patients, and facility, and implement corrective actions to address. OPERATIONS Continue securing the hospital and grounds and restricting non-essential personnel from entering the building. Continue facility search procedures. Evacuate patients and staff, as indicated. Continue to liaison with law enforcement LOGISTICS Continue to support facility response by providing appropriate personnel or equipment. FINANCE/ADMINISTRATION Track expenses and lost revenues. Extended (Operational Period Beyond 12 Hours) COMMAND (Incident Commander): Implement patient, staff and visitor evacuation of the facility. Update and revise the Incident Action Plan. (PIO): Continue media briefings and situation updates. (Liaison Officer): 46
47 Continue updating local emergency management, fire and EMS of situation status and need to evacuate facility. (Safety Officer): Continue monitoring safety practices and oversee safe evacuation of the facility OPERATIONS Continue patient management activities and evacuation of the facility Oversee evacuation of the facility and transfer of patients to other hospitals Continue hospital and grounds security, deny entry to non-essential personnel PLANNING Implement patient and staff tracking during the evacuation Update and revise the Incident Action Plan LOGISTICS Continue to provide mental health support to staff and patients as needed FINANCE Continue to track response expenses Demobilization/System Recovery COMMAND (Incident Commander): Ensure local law enforcement/bomb squad issue an all clear for the facility. Oversee restoration of normal hospital operations (PIO): Conduct final media briefing providing situation status, appropriate patient information and termination of the incident. (Liaison Officer): Notify local emergency management, fire and EMS of termination of the incident. (Safety Officer): Oversee the safe return to normal operations and repatriation of patients OPERATIONS Restore patient care and management activities. Repatriate evacuated patients Re-establish visitation and non-essential services PLANNING Finalize the Incident Action Plan and demobilization plan. Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation. Write after-action report and corrective action plan to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions Recommendations for correction actions 47
48 LOGISTICS Provide debriefing and mental health support services for staff and patients. FINANCE/ADMINISTRATION Compile final response and recovery cost and expenditure summary and submit to the Incident Commander for approval. Documents and Tools Hospital Emergency Operations Plan Hospital Evacuation Plan Hospital Bomb Threat Procedure (telephone vs. suspicious object threat) Facility and Departmental Business Continuity Plans 48
49 (ALERT4) EVACUATION, COMPLETE OR PARTIAL FACILITY INCIDENT RESPONSE GUIDE Mission: To safely perform a complete or partial facility evacuation. Directions: Read this entire response guide and review incident management team chart. Use this response guide as a checklist to ensure all tasks are addressed and completed. Objectives: Maintain safety of patients, staff, visitors Maintain life support functions Conduct safe and rapid evacuation of the facility Plan for patient repatriation and restoration of services Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the facility emergency operations plan and the Incident Command structure. Appoint Command Staff and Section Chiefs. Determine type of evacuation needed: Immediate vs. delayed Vertical, horizontal, complete Order the organized and timely evacuation of the facility (PIO): Conduct regular media briefings on situation status and appropriate patient information. Oversee patient family notifications of evacuation/transfer/early discharge (Liaison Officer): Notify and regularly communicate with local emergency management agency, Fire, EMS and law enforcement about facility status and evacuation order. (Safety Officer): Oversee the immediate stabilization of the facility and basement flooding Recommend areas for immediate evacuation to protect life Ensure the safe evacuation of patients, staff and visitors OPERATIONS: Implement emergency life support procedures to sustain critical services (i.e., power, water, communications) until evacuation can be accomplished. Determine type of evacuation needed, in conjunction with the Incident Commander: Immediate vs. delayed Vertical, horizontal, complete Implement planning for immediate evacuation of the facility. Prioritize patients/areas of the facility to be evacuated Prepare patient records, medications and valuables for transfer 49
50 Confirm the transfer and timeline with accepting hospitals, providing patient information as appropriate Discharge patients as appropriate Establish a safe area for holding patients until transferred. Ensure patient records, medications and belongings are transferred with the patient Secure the facility and restrict visitors and entry of non-essential personnel Activate business continuity plans and procedures Relocate hazardous materials from flooded areas to prevent area/facility contamination Coordinate ambulances, aero medical services, and other transportation Implement the evacuation plan and move patients and staff PLANNING: Track patients and personnel including evacuation location and receiving facility Establish operational periods, incident objectives and develop the Incident Action Plan in collaboration with the Incident Commander Ensure documentation of all actions and activities Intermediate (Operational Period 2-12 Hours) COMMAND: (Incident Commander): Notify hospital Board, Dean and other internal authorities of situation status and evacuation. (Liaison): Integration with external agencies, including healthcare facilities (PIO): Continue staff, patient, visitor and media briefings (Safety Officer): Conduct ongoing analysis of existing response practices for health and safety issues related to staff, patients, and facility, and implement corrective actions to address OPERATIONS: Ensure appropriate patient care and management during evacuation Continue facility security, traffic and crowd control Ensure family notification of patient transfer Continue facilitating discharges Continue to communicate patient information and status to receiving facilities PLANNING: Continue patient and personnel tracking and documentation Update and revise the Incident Action Plan Ensure complete documentation of activities, decisions and actions LOGISTICS: Supply supplemental staffing to key areas to facilitate evacuation Provide for staff food and water and rest periods Monitor facility damage and initiate repairs, as appropriate, as long as it does not hinder evacuation of the facility Initiate salvage operations of damaged areas and relocate equipment from evacuated areas to secure areas or to other facilities. FINANCE/ADMINISTRATION: Track costs and expenditures of response and evacuation 51
51 Track estimates of lost revenue due to evacuation of the facility Extended (Operational Period Beyond 12 Hours) COMMAND (Incident Commander): Meet with Command Staff and Section Chiefs to update evacuation progress and situation status. (Liaison Officer): Continue to update local emergency management, Fire, EMS and law enforcement officials on situation status and evacuation progress (Safety Officer): Continue ongoing evaluation of evacuation practices for health and safety issues related to staff, patients, and facility, and implement corrective actions. OPERATIONS: Ensure patient care and management for patients waiting evacuation Secure all evacuated areas, equipment, supplies and medications Continue business continuity and recovery actions PLANNING: Continue to track patients and staff locations Track materiel and equipment transferred to other hospitals Prepare a demobilization plan and deactivate HCC positions and staff when they are no longer necessary Discuss staff utilization and salary practices during evacuation and closure of the facility with Human Resources; provide information to employees when determined Continue to ensure documentation of actions, decisions and activities Update and revise the Incident Action Plan LOGISTICS: Maintain information technology security Support evacuation of supplies (medical, food, water, other equipment) Assess and secure utility systems FINANCE/ADMINISTRATION: Continue to track and report response costs and expenditures and lost revenue Demobilization/System Recovery COMMAND: (Incident Commander): Assess if criteria for partial or complete reopening of the facility is met, and order reopening and repatriation of patients Oversee restoration of normal hospital operations (PIO): Conduct final media briefing providing situation status, appropriate patient information and termination of the incident (Liaison Officer): Notify local emergency management, fire and EMS of termination of the incident and reopening of the facility (Safety Officer): Oversee the safe return to normal operations and repatriation of patients OPERATIONS Restore patient care and management activities 51
52 Repatriate evacuated patients Re-establish visitation and non-essential services PLANNING: Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Write after-action report and corrective action plan to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions LOGISTICS: Implement and confirm facility cleaning and restoration, including: Structure Medical equipment certification Provide debriefing and mental health support services for staff and patients Inventory supplies, equipment, food, and water, and return to normal levels FINANCE/ADMINISTRATION: Compile final response and recovery cost and expenditure and estimated lost revenues summary and submit to the Incident Commander for approval Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate Documents and Tools: Hospital Emergency Operations Plan Patient Evacuation Plan Utility Failure Plans Facility and Departmental Business Continuity Plans 52
53 FIRE INCIDENT RESPONSE GUIDE Mission: To reduce the loss of life and property during an internal fire incident. Directions: Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives: Confine the fire/reduce the spread of the fire Rescue and protect patients and staff Implement internal emergency management plan fire Implement partial/full evacuation Communicate situation to staff, patients, and the public Investigate and document incident details Immediate Actions (Operational Period 0-2 Hours): COMMAND: (Incident Commander): Activate the facility emergency operations plan and the Incident Command structure Appoint Command Staff and Section Chiefs Consider the formation of a unified command with hospital and fire officials Determine need for and type of evacuation (PIO): Establish a media staging area Conduct regular media briefings to update situation status and provide appropriate patient and employee information Oversee patient family notifications of incident and evacuation/relocation, if ordered COMMAND (Liaison Officer): Notify and regularly communicate with local emergency management agency, Fire, EMS and law enforcement about facility status Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. (Safety Officer): Oversee the immediate stabilization of the facility Recommend areas for immediate evacuation or temporary relocation to protect staff and patients Monitor the condition of the facility during the event and immediately notify the Incident Commander of any situations that are an immediate threat to life or health OPERATIONS: Implement fire response plan and conduct extinguishment/rescue operations, if needed and/or if possible Evaluate need for evacuation or temporary relocation of nearby areas damaged from smoke or fire Evaluate safety of involved structure after obtaining damage assessment from emergency response agency (fire department) 53
54 Secure the facility and deny entry to non-essential and unauthorized personnel Establish alternate laboratory testing sites through other locations or contracted services Follow up on injured employees and patients and document condition PLANNING: Conduct an immediate count of hospital patients and their locations Initiate patient tracking procedures Account for on-duty staff by name and location Establish operational periods, incident objectives and develop Incident Action Plan, in collaboration with the Incident Commander LOGISTICS: Assist with facility damage assessment Perform salvage operations in damaged laboratory areas, if possible Ensure communications systems and IT/IS is functioning Initiate follow up and documentation on injured employees, and assist with notification of family members Call back additional staff to assist with operations and possible evacuation, as needed Intermediate (Operational Period 2-12 Hours) COMMAND (Incident Commander): Meet regularly with Command Staff and Section Chiefs to review overall impact of the fire on the facility and reevaluate the need for evacuation or temporary relocation of patient care area and services (Liaison): Continue to communicate with area hospitals and local emergency management to update on situation status and request assistance Establish the patient information center, in collaboration with the PIO (PIO): Continue briefings for staff, patients and the media Establish the patient information center, in collaboration with the Liaison Officer (Safety Officer): Conduct ongoing analysis of existing response practices for health and safety issues related to staff, patients, and facility, and implement corrective actions to address OPERATIONS: Continue patient care and management activities Relocate or evacuate patients from damaged/impacted areas, as appropriate Ensure notification of patient s families of incident and patient condition Continue to re-establish laboratory services Ensure critical infrastructure services to essential area Initiate facility clean up procedures Initiate facility repairs Continue facility security and secure all unsafe areas Ensure business continuity operations were not damaged and are fully functional PLANNING: Continue patient and personnel tracking Update and revise the Incident Action Plan Ensure documentation of actions, decisions and activities LOGISTICS: Continue salvage operations, as appropriate Provide mental health support for staff Provide for staff food, water and rest periods Continue to monitor condition of injured employees and report to Incident Commander 54
55 Order supplies and equipment as needed to facilitate patient care and recovery operations Arrange transportation for relocated or evacuated patients Assist with re-establishment of laboratory services through relocation or contracted services Continue to provide supplemental staffing, as needed FINANCE/ADMINISTRATION: Track response and recovery costs and expenditures, including estimates of lost revenue Initiate documentation and claims for injured employees and patients, if any Facilitate procurement of supplies, equipment, medications, contracted services and staff needed for effective response and recovery Extended (Operational Period Beyond 12 Hours) COMMAND: (Incident Commander): Meet with Command Staff and Section Chiefs to update situation status and patient relocation/evacuation progress (PIO): Continue to brief staff, patients, families and the media on the situation status and appropriate patient information Continue patient information center, as needed (Liaison Officer): Continue to update local emergency management, Fire, EMS and law enforcement officials on situation status and evacuation progress (Safety Officer): Continue ongoing evaluation of evacuation practices for health and safety issues related to staff, patients, and facility, and implement corrective actions OPERATIONS: Continue patient care and management activities Ensure safe patient relocation/evacuation, if necessary If patients are evacuated to other facilities, ensure patient records, medications and belongings are transferred with the patient Continue to assess facility damage and services Provide for food and water for patients, families and visitors Continue security of the facility and unsafe areas within the facility PLANNING: Plan for demobilization of incident and system recovery Update and revise the Incident Action Plan Ensure documentation of actions, decisions and activities Continue patient and personnel tracking LOGISTICS: Provide mental health support and debriefings to staff Continue to provide food, water and rest periods for staff Continue to monitor the condition of injured employees and report to the Incident Commander Replace or reorder damaged supplies and equipment to provide laboratory services as soon as possible Provide additional staffing as needed FINANCE/ADMINISTRATION: Continue to track and report response costs and expenditures and lost revenue Complete claims/risk management reports on injured employees or patients Demobilization/System Recovery: 55
56 COMMAND: (Incident Commander): Assess if criteria for partial or complete reopening of areas within the facility is met, and order reopening and repatriation of patients Oversee restoration of normal hospital operations Provide appreciation and recognition to solicited and non-solicited volunteers, staff, state and federal personnel that helped during the incident (PIO): Conduct final media briefing providing situation status, appropriate patient information and termination of the incident (Liaison Officer): Notify local emergency management, fire and EMS of termination of the incident and reopening of the facility (Safety Officer): Oversee the safe return to normal operations and repatriation of patients OPERATIONS: Restore patient care and management activities Repatriate evacuated patients Re-establish visitation and non-essential services Provide mental health support and information about community services to patients and families, as needed PLANNING: Finalize the Incident Action Plan and demobilization plan Prepare a summary of the status and location of patients. Disseminate to Command Staff and Section Chiefs and to other requesting agencies, as appropriate Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Write after-action report and improvement plan to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Future response actions Corrective actions LOGISTICS: Provide mental health support and conduct stress management debriefings, as needed Monitor health status of staff Restock and resupply equipment, medications, food and water and supplies to normal levels Itemize all damaged equipment and supplies and submit to Finance/Administration Section Return borrowed equipment after proper cleaning/disinfection Restore normal non-essential services (i.e., gift shop, etc.) FINANCE/ADMINISTRATION: Compile final response and recovery cost and expenditure and estimated lost revenues summary and submit to the Incident Commander for approval Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate Documents and Tools: Hospital Emergency Operations Plan 56
57 Fire Emergency Response Plan Hospital Patient Evacuation Plan Patient Tracking Form Hospital Damage Assessment Procedures Forms Job Action Sheets Hospital Organization Chart Facility and Departmental Business Continuity Plans Television/radio/internet to monitor news Telephone/cell phone/satellite phone/internet for communication 57
58 HAZARDOUS MATERIAL SPILL (CODE BROWN) INCIDENT RESPONSE GUIDE Mission: To effectively and efficiently manage a spill or leak involving hazardous material within the hospital. Directions: Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives: Isolate the contaminated area Identify the hazardous material Patient triage and medical management Protection of patients, staff and visitors Immediate (Operational Period 0-2 Hours) & Intermediate (Operational Period 2-12 Hours) COMMAND: (Incident Commander): Establish Incident Command and activate PIO, Safety Officer, Liaison Officer and Operations and Logistics Section Chiefs Alert/notification of internal staff via overhead page (e.g., Code Orange: Internal) Activate and implement the hospital s Spill Response Team Establish Hospital Command Center (HCC) and assemble incident management team Activate the Medical/Technical Specialist Chemical to assess the incident Activate Medical Care, Infrastructure, HazMat, and Security Branch Director Establish operational periods and operational objectives (e.g., protecting life safety of existing personnel and patients, limit further spread/damage, provide decontamination, and account for all personnel and patients) (PIO): Establish a patient information center; coordinate with the Liaison Officer and local Emergency Management/Public Health/EMS COMMAND (Liaison): Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. (Safety Officer): Conduct ongoing analysis of existing response practices for health and safety issues related to staff, patients, and facility, and implement corrective actions to address OPERATIONS: Ensure proper triage of symptomatic and non-symptomatic patients, staff, volunteers and others with possible exposure Initiate and maintain patient care and management activities Coordinate with the Security Officer, as necessary, to isolate the spill area Communicate with local emergency management to identify toxic chemicals Isolate the contaminated area Identify the hazardous material Provide situation report to IC including 58
59 Substance description and damage inflicted Response / clean-up plan including potential notification and activation of contracted Hazardous Materials spill response provider PLANNING: Establish operational periods and develop Incident Action Plan: Engage other hospital departments Share Incident Action Plan through Incident Commander with these areas Provide instructions on needed documentation including completion detail and deadlines Prepare and implement patient tracking protocols LOGISTICS: Monitor the health status staff who participated in decontamination activities and actively provide rehabilitation as necessary Anticipate an increased need for medical/surgical supplies, personal protective equipment, transporters, and personnel Extended (Operational Period Beyond 12 Hours) COMMAND (PIO): Continue patient information center, as necessary (Liaison): Obtain a summary of the status and location of all incident patients from the Patient Tracking Officer. Disseminate to public health/ems, local EOC, local Fire/HazMat Teams, or others as appropriate OPERATIONS: Continue spill clean up and decontamination of the laboratory Continue patient management activities Monitor environmental conditions/fumes and continue to control HVAC operations to limit or prevent spread LOGISTICS: Continue to monitor the health status of staff who were exposed to the fumes or who participated in decontamination activities Monitor, in collaboration with the Medical Care Branch Director, all patients who were exposed or may have been exposed to the fumes/chemical Ensure restoration or relocation of laboratory services FINANCE/ADMINISTRATION: Monitor and track all personnel time and response costs Track costs for outside resources assisting in response Prepare summary reports for the Incident Commander every 8 hours and as requested Demobilization/System Recovery COMMAND: (Incident Commander): Once notified of complete clean up and decontamination of the affected area(s), declare the emergency terminated and demobilize the HCC (PIO): Notify the media of the termination of the event, outcomes and other pertinent information (Safety Officer): Ensure safety of impacted area(s) and notify the IC of status 59
60 (Liaison): Notify local officials, Fire/HazMat teams and other hospitals of all clear status OPERATIONS: Complete clean up operations and assess decontamination Implement local hazmat protocols to follow up with the local/state/federal agencies as appropriate (e.g., EPA) PLANNING: Conduct after-action review with the following: Command personnel and Section Chiefs Laboratory Staff Spill Team Response Members Staff, patients and volunteers Write after-action report and corrective action plan to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions Recommendations for correction actions LOGISTICS: Monitor the health status staff who participated in decontamination activities for an extended period Conduct stress management and after-action debriefings and meetings as necessary Inventory all HCC and hospital supplies and replenish as necessary and appropriate FINANCE/ADMINISTRATION: Compile expense reports and submit to Incident Commander and proper authorities for reimbursement Documents and Tools Hospital Emergency Operations Plan Hospital Spill Response Plan Hospital Decontamination Protocol Hospital Mass Casualty Incident Protocol Patient Tracking Form 61
61 CODE GREEN (DEM OVERCROWDING) HOSPITAL OVERLOAD INCIDENT RESPONSE GUIDE Mission: To safely manage periods of limited bed capacity, facilitate the timely admission of patients, and minimize holding time in the department of emergency medicine (DEM). Directions: Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives: Maintain current census of ED and inpatients, number waiting to be seen, waiting for admission and pending discharges Activate alternate care sites Provide safe and appropriate patient care Communicate situation status regularly to patients, families, staff, other hospitals and local officials Evaluate diversion criteria and outpatient/urgent care clinic resources Immediate Actions (From Decision to Activate EOP to 2 Hours) COMMAND (Incident Commander): Activate Hospital Command Center, Command Staff and Section Chiefs, as appropriate Activate the Medical/Technical Specialists Hospital Administration, Clinic Administration, Medical Staff and Pediatric Care Establish the operational period, incident objectives and initial Incident Action Plan (PIO): Provide information to visitors and families regarding situation status and hospital measures to meet the demand Activate the media staging area and provide regular briefings and updates COMMAND: (Liaison Officer): Establish communications with the local Emergency Operations Center to report the activation of the Emergency Operations Plan/HCC, situation status and critical issues/needs Contact licensing authorities for potential need to alter staff/patient ratio s, as necessary Communicate with local EOC and Regional Hospital Coordination Center for local, regional and state bed availability Communicate with other healthcare facilities to determine: Situation status Surge capacity and capability Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. (Safety Officer): Ensure safety practices are being used Ensure that non-traditional areas used for patient care and other services are safe and hazard free OPERATIONS: Activate Branch Directors and Unit Leaders and brief on the current situation Activate the hospital s surge capacity plan Activate alternate care sites, as appropriate 61
62 Review all surgeries and outpatient appointments and procedures for cancellation and/or rescheduling Identify inpatients for early discharge or transfer to other facilities and direct staff to expedited discharges Establish a discharge area to free beds until patient can be transported Assess current staffing and project staffing needs/shortages for the next operational period and out Ensure the rapid cleaning and turn-over of patient care beds and areas to expedite discharge and admission Ensure the use of appropriate personal protective equipment by staff and volunteers Consider extending outpatient hours to accommodate additional patient visits PLANNING: Establish operational periods, incident objectives and develop Incident Action Plan, in collaboration with the Incident Commander Institute patient, bed, personnel and materiel tracking and project needs for the next hours LOGISTICS: Anticipate an increased need for supplies, equipment, medications and personnel and obtain resources as appropriate Ensure the operations of communication systems and IT/IS Assist the Operations Section with the establishment of alternate care sites Manage solicited and unsolicited volunteers Intermediate and Extended (Operational Period 2- greater than 12 Hours) COMMAND (Incident Commander): Communicate current hospital status to CEO, Board of Directors and other appropriate internal and external officials Regularly update and revise initial Incident Action Plan, in collaboration with Planning Section Consider deploying a Liaison Officer to the local EOC (PIO): Continue to provide information to visitors and families regarding situation status and hospital measures to meet the demand Provide regular staff situation status updates and information Continue to provide regular briefings and updates to the media Establish the patient information center, if appropriate, in conjunction with the Liaison Officer (Liaison Officer): Continue regular communications with the local Emergency Operations Center to report the hospital s situation status and critical issues/needs Continue to communicate with local EOC and Regional Hospital Coordination Center for local, regional and state bed availability Continue to communicate with and update other healthcare facilities regarding: Situation status Surge capacity and capability Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. (Safety Officer): Conduct ongoing analysis of existing response practices for health and safety issues related to staff, patients, and facility, and implement corrective actions to address 62
63 OPERATIONS: Continue patient care and management activities Assist with transportation of discharged/transferred patients to residences, skilled nursing facilities, alternate care sites, etc. Expedite discharge medication processing and dispensing Regularly reassess and reevaluate patients waiting for admission Continue to review scheduled/elective procedures and surgeries for cancellation or rescheduling Ensure the re-triage and observation of all patients waiting to be seen Continue or implement alternate care sites Consider need for and provision of alternate standards of care (austere care) and prioritization of resources PLANNING: Update and revise the Incident Action Plan and distribute to Command Staff and Section Chiefs Continue patient, bed, personnel and materiel tracking and reporting Ensure complete documentation of actions, decisions and activities Begin planning for demobilization and system recovery LOGISTICS: Continue to call in additional staff to supplement operations Continue to coordinate solicited and unsolicited volunteers Obtain needed supplies, equipment and medications to support patient care activities for a 72 hour period Provide for food, water and rest periods for staff Establish a dependent care area, as appropriate Ensure the rapid investigation and documentation of injuries or employees exposed to illness and provide appropriate follow up FINANCE/ADMINISTRATION: Facilitate procurement of needed supplies, equipment, medications and contractors to meet patient care and facility needs Track all costs and expenditures of the response and estimate lost revenues due to cancelled procedures/surgeries and other services Ensure the rapid investigation and documentation of injuries or employees exposed to illness and provide appropriate follow up Demobilization/System Recovery COMMAND (Incident Commander): Establish priorities for restoring normal operations using the hospital s continuity of operations and business plans Approve the demobilization plan and finalize the Incident Action Plan Provide appreciation and recognition to solicited and non-solicited volunteers, staff, state, and federal personnel that helped during the incident (Public Information Officer): Conduct final briefings for media, in cooperation with the JIC Close the patient information center, if activated (Liaison Officer): Communicate hospital status and final patient condition and location information to appropriate authorities (i.e., local and state public health, local EOC) (Safety Officer): Oversee the safe and effective restoration of normal services OPERATIONS: 63
64 Restore normal facility operations and visitation Provide mental health and information about community services for patients and families PLANNING: Compile all documentation and forms for archiving Write after-action report and improvement plan, including the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions Recommendations for correction actions LOGISTICS: Conduct stress management and after-action debriefings and meetings for staff Monitor health status of staff exposed to infectious patients and provide appropriate medical and mental health follow up, as needed Restock all supplies and medications Restore/repair/replace broken equipment Return borrowed equipment after proper cleaning/disinfection Restore normal non-essential services (i.e., gift shop, etc.) FINANCE: Compile final response expense reports, submit to IC for approval and to appropriate authorities for reimbursement Documents and Tools: Emergency Operations Plan, including: Infectious Patient Surge Plan and Alternate Care Site Plan Mass Prophylaxis Plan Risk Communication Plan Hospital Security Plan Patient/staff/equipment tracking procedures Behavioral health support for staff/patients procedures Mass Fatalities Plan Infection Control Plan Employee Health Monitoring/Treatment Plan All other relevant protocols/guidelines relating to biological/infectious disease/mass casualty incidents Hospital Organization Chart Television/radio/internet to monitor news 64
65 HOSTAGE / BARRICADE INCIDENT RESPONSE GUIDE Mission: To safely manage a hostage or barricade situation. Directions: Read this entire response guide and review incident management team chart. Use this response guide as a checklist to ensure all tasks are addressed and completed. Objectives: Protect safety of staff, patients, and visitors Manage the media Coordinate with law enforcement and other external response agencies Provide for mental health support and stress debriefing/management services to patients, staff and families Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Notify law enforcement agencies of incident and provide details, as able Establish a unified command with law enforcement, upon arrival Safely evacuate the immediate area surrounding the unit, if possible or provide security to the nearby areas Determine need to activate Medical/Technical Specialist Risk Management, as appropriate (Public Information Officer): Establish a media staging area in a safe and secluded location Provide regular media briefings and situation status updates (Liaison Officer): Establish communication with area hospitals to notify of the incident and potential need for evacuation of patients (Safety Officer): Ensure the safety of patients, families, visitors and staff in non-impacted areas of the hospital Collaborate with law enforcement and hospital security staff on safe evacuation of nearby areas OPERATIONS: Suspend non-essential services Secure the facility and do not allow entrance or exit of people except essential personnel Evacuate the immediate area around the critical care unit, if safe to do so Consider and prepare for additional gunman or perpetrators Liaison with law enforcement and provide facility and utility drawings/schematics upon arrival Provide space and communications systems near the unit for law enforcement operations including negotiations Be prepared to maintain or shut off selective utility or HVAC systems upon the request of law enforcement Ensure continuation of patient care management activities in the hospital Institute ambulance diversion status; notify local EMS and ambulance providers Notify family members of hostages of the situation, including staff, families and visitors Prepare to render care to injured hostages and/or the perpetrator PLANNING: 65
66 Establish operational periods, incident objectives and develop Incident Action Plan, in collaboration with the Incident Commander and law enforcement Implement patient tracking LOGISTICS: Prepare for mental health support needs of hostages Provide mental health support for on-duty staff, patients and visitors, patients, family and staff Intermediate and Extended (Operational Period 2 to Greater than 12 Hours) COMMAND (Incident Commander): Assess the impact of the situation and response on the hospital; Update and revise the Incident Action Plan in conjunction with law enforcement and Planning Section Chief Establish a procedure, in conjunction with local law enforcement, to provide care for hostages, when released COMMAND (PIO): Continue to conduct regular media briefings as the incident evolves Establish a patient information center, if needed, in collaboration with Liaison Officer Continue to provide staff, patients and visitors with situation status updates and information (Liaison Officer): Continue to communicate with local officials to provide situation updates and hospital critical issues/needs (Safety Officer): Conduct ongoing analysis of existing response practices for health and safety issues related to staff, patients, and facility, and implement corrective actions to address OPERATIONS: Reassess evacuations and need for further evacuation Continue hospital/facility security and restriction of entry and exit except for essential personnel Continue to liaison with law enforcement and provide requested supplies and services Continue patient care and management operations Ensure documentation of actions, decisions and activities Provide ongoing victim family support PLANNING: Update and revise the Incident Action Plan Continue patient tracking, if needed Plan for demobilization and system recovery LOGISTICS: Continue to supply hostage support needs (water, medications, etc.) as directed by law enforcement Assess impact of ongoing incident on services FINANCE: Track costs and expenditures of response, including lost revenues Demobilization/System Recovery 66
67 COMMAND (Incident Commander): Ensure local law enforcement issues an all clear for the facility Oversee restoration of normal hospital operations Conduct immediate debriefing with law enforcement (PIO): Conduct final media briefing providing situation status, appropriate patient information and termination of the incident (Liaison Officer): Notify local emergency management, fire and EMS of termination of the incident (Safety Officer): Oversee the safe return to normal operations and repatriation/relocation of patients OPERATIONS Restore normal patient care operations Restore normal visitation and non-essential services Facilitate clean up and repair of the critical care unit and reopening Provide mental health support services to patients and patient s families Restore utilities to the unit, if needed Reunite hostages with family Immediately debrief staff hostages, as directed by law enforcement PLANNING Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Write after-action report and corrective action plan to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions Recommendations for correction actions LOGISTICS Provide staff debriefing, mental health support and stress management services Continue providing support to hostages, as needed FINANCE/ADMINISTRATION Compile final response and recovery cost and expenditure summary and submit to the Incident Commander for approval Complete documentation and follow up of personnel injury and/or line of duty death as appropriate Documents and Tools Hospital Emergency Operations Plan Hospital Evacuation Pan Hospital Building and Utilities Plans Fatality Management Plan 67
68 INFANT/CHILD ABDUCTION (CODE PINK) INCIDENT RESPONSE GUIDE Mission: To manage and collaborate in the process of locating and recovering a lost or abducted infant or child. Directions Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives: Confirm that an abduction has taken place Secure mother and staff involved with infant or child s care Activate the Infant/Child Abduction Response Plan Collaborate with law enforcement to recover the infant or child Provide mental health support services to the patient and staff Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the Infant/Child Abduction Plan Notify law enforcement agencies of incident and provide details, as able Establish a unified command with law enforcement, upon arrival Activate appropriate Command Staff and Section Chiefs (Public Information Officer): Establish a media staging area Provide regular media briefings and situation status updates, releasing only information that has been approved by the hospital Incident Commander and law enforcement Provide informational bulletin for current patients to notify them of the incident and the measures initiated, as appropriate COMMAND (Liaison Officer): Notify and liaison with local government officials, as needed Call local law enforcement to initiate an Amber Alert Call the National Center for Missing and Exploited Children, 800-THE-LOST, for assistance in handling the ongoing investigation and crisis (Safety Officer): Ensure the safety of patients, families, visitors and staff during hospital search procedures OPERATIONS Secure the facility and deny access or exit. Search any persons exiting the facility, as appropriate Assign staff to conduct a floor-by-floor, door-by-door search of the facility Assign a liaison to coordinate with law enforcement/fbi Conduct staff and mother/family interviews to gather information and evidence, in conjunction with law enforcement Provide law enforcement with photos, footprints of child, etc., if available Provide additional information to staff and security about the abductor as information is available to facilitate internal search Provide mental health support to the patient and other family members 68
69 PLANNING Establish operational periods, incident objectives and develop the Incident Action Plan, in collaboration with the Incident Commander Intermediate and Extended (Operational Period 2- Greater than 12 Hours) COMMAND (Incident Commander): Update and revise the Incident Action Plan Ensure the continuation of normal hospital operations Activate Medical/Technical Specialist Risk Management to assist with response and documentation of incident Continue to brief key senior management on the situation Appropriately report incident to state, JCAHO and other regulatory agencies as a sentinel event (PIO): Continue regular media briefings and updates, in conjunction with law enforcement Provide situation status updates to hospital staff and patients (Liaison Officer): Update local officials and other agencies, as appropriate OPERATIONS If it is determined that abductor has left facility, consider releasing staff posted at doors to normal duties Continue to provide mental health support and physical care to the mother and family members Provide assurance and support to other new mothers or parents of children in the facility, regarding the safety of their infant/child Consider maintaining a visible security presence in the impacted department Re-register the mother under a fictitious name and move her room location to maintain privacy Ensure the continuation of normal patient care services and hospital operations Continue communications and collaboration with law enforcement Provide appropriate medical exam of infant/child, and unification with parents PLANNING Revise and/or complete Incident Action Plan LOGISTICS Provide mental health support and stress management services to department staff FINANCE/ADMINISTRATION Track costs and expenditures of response Demobilization/System Recovery COMMAND (Incident Commander): Oversee the hospital s return to normal operations Ensure continued liaison and communication with law enforcement (PIO): Conduct final media briefing providing situation status, appropriate patient information and termination of the incident (Liaison Officer): 69
70 Notify appropriate local officials of the termination of the incident OPERATIONS Restore normal operations and patient care services Restore normal visitation and non-essential services PLANNING Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Write after-action report and corrective action plan to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions Recommendations for correction actions LOGISTICS Provide ongoing mental health support and stress management services for involved employees, as needed FINANCE/ADMINISTRATION Compile final response and recovery cost and expenditure summary and submit to the Incident Commander for approval Documents and Tools Emergency Operations Plan Hospital s Infant/Child Abduction Response Plan Secure surveillance media (tapes or other video) 71
71 INTERNAL FLOODING INCIDENT RESPONSE GUIDE Mission: To safely manage an internal flooding incident within a hospital. Directions: Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives Prevent facility flooding Protect patients, staff and facility Ensure safe patient care and medical management Evacuate the facility (partial or complete) as needed Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the facility Emergency Operations Plan Activate Command Staff and Section Chiefs, as appropriate (Liaison Officer): Notify local emergency management of situation and immediate actions Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. (Public Information Officer): Inform staff, patients and families of situation and actions underway to prevent/limit flooding Prepare media staging area in a safe locations Conduct regular media briefings, in collaboration with the local EOC/Joint Information Center (Safety Officer): Conduct safety assessment of low lying flooded areas and assess risks and impacts to patients, staff and facility OPERATIONS Activate the hospital s Internal Flooding Plan Ensure continuation of patient care and essential services Consider partial or complete evacuation of the facility, or relocation of patients and services into safe areas of the facility Ensure the operations of alternate power supplies (i.e., back up generators) Maintain communications systems, activate alternate communications systems, as needed Evaluate the flooded area(s) and identifying safety issues Institute measures to prevent flooding and protect facility resources, as appropriate Secure the facility and limit access and egress Implement business continuity planning and protection of patient records PLANNING Establish operational periods, incident objectives and develop the Incident Action Plan, in collaboration with the Incident Commander Implement patient and staff tracking, as appropriate 71
72 LOGISTICS Assess facility damage and project impacts of rising flood waters on the facility Maintain utilities and activate alternate systems as needed Intermediate (Operational Period 2-12 Hours) COMMAND (PIO): Establish a patient information center in coordination with the Liaison Officer to notify patient families of situation and patient locations (Liaison Officer): Notify local emergency management and EOC of situation status, critical needs and plans for evacuation, if appropriate OPERATIONS Continue essential patient care management and services Initiate clean up operations, as appropriate Reassess need for or prepare for evacuation Continue to maintain utilities Provide mental health support to patients and families, as needed Continue to secure the facility, including unsafe areas Activate business continuity plans, including protection of records and possible relocation of business functions PLANNING Continue patient and personnel tracking, as needed Update and revise the Incident Action Plan and distribute to Command Staff and Section Chiefs LOGISTICS Continue to evaluate facility integrity and safety of flooded areas Initiate clean up as appropriate FINANCE/ADMINISTRATION Track costs and expenditures and estimate cost of facility damage and lost revenue Initiate documentation of any injuries or facility damage Facilitate the procurement of supplies, equipment and medications and contracting for facility clean up or repair Extended (Operations/EOC Activation Beyond 12 Hours) COMMAND (Incident Commander): Update and revise the Incident Action Plan and prepare for demobilization Continue to update internal leaders on the situation status (PIO): Continue with briefings and situation updates with staff, patients and families Continue patient information center operations, in collaboration with Liaison Officer (Liaison Officer): Continue to notify local EOC of situation status Continue patient information center operations, in collaboration with PIO. (Safety): Continue to evaluate flooded areas and facility integrity for safety and take immediate corrective actions OPERATIONS 72
73 Continue essential patient care management and services Continue repair and clean up operations, as appropriate Continue evacuation of the facility, if implemented Ensure the transfer of patient s belongings, medications and records, when evacuated Continue to maintain utilities Continue to secure the facility, including unsafe areas Continue business continuity activities and relocation of business services, if appropriate Prepare for demobilization and system recovery PLANNING Revise and update the incident action plan Initiate demobilization plan and plan for system recovery LOGISTICS Provide supplemental staffing as needed Continue to evaluate facility damage and integrity and initiate clean up and repair activities FINANCE/ADMINISTRATION Continue to track costs and expenditures Continue to facilitate contracting for facility repair and clean up Demobilization/System Recovery COMMAND (Incident Commander): Determine hospital status and declare termination of the incident (Liaison Officer): Communicate final hospital status and termination of the incident to local EOC, area hospital and officials Assist with the repatriation of patients transferred (PIO): Conduct final media briefing and assist with updating staff, patients, families and others of the termination of the event (Safety Officer): Ensure facility safety and restoration of normal operations Ensure facility repairs are completed, in conjunction with the Operations and Logistics Sections OPERATIONS Restore normal patient care operations Ensure restoration of utilities and communications Complete a facility damage report, progress of repairs and estimated timelines for restoration of facility to pre-event condition PLANNING Complete a summary of operations, status, and current census Conduct after-action reviews and debriefings Develop the after-action report and improvement plan for approval by the Incident Commander LOGISTICS Restock supplies, equipment, medications, food and water Ensure communication and IT/IS operations return to normal Provide stress management and mental health support to staff 73
74 FINANCE/ADMINISTRATION Compile a final report of response and facility repair costs for approval by the Incident Commander Work with local, state, and federal emergency management to begin reimbursement procedures for cost expenditures related to the event Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate reimbursement and claims procedures Documents and Tools Hospital Emergency Operations Plan Hospital Evacuation Plan Flood Response Plan Utility Failure Plans Facility and Departmental Business Continuity Plans 74
75 LOSS OF HEATING/VENTILATION/AIR CONDITIONING (HVAC) INCIDENT RESPONSE GUIDE Mission: To safely manage the loss of HVAC within the hospital. Directions Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives Identify the extent and duration of the loss of HVAC Protect patient, family, staff and facility Minimize the impact of the loss of HVAC on patients and staff and consider evacuations Communicate situation status and updates to staff, patients, visitors and facility Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the facility Emergency Operations Plan Activate Command Staff and Section Chiefs, as appropriate (Liaison Officer): Notify local emergency management of situation and immediate actions Notify local EMS and ambulance providers about the situation and possible need to evacuate Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. Contact the Regional Hospital Coordination Center, if exists, to notify about the situation and request assistance with patient evacuation destinations COMMAND (Public Information Officer): Inform staff, patients and families of situation and actions underway to cool the facility and protect life Prepare media staging area in a safe locations Conduct regular media briefings, in collaboration local emergency management, as appropriate (Safety Officer): Evaluate safety of patients, family, staff and facility and recommend protective and corrective actions to minimize hazards and risks OPERATIONS Assess patients for risk and prioritize care as appropriate Implement alternate cooling measures for the patients, perishable supplies and the facility Secure the facility and implement limited visitation policy Assess the HVAC system and prepare a plan and timeline for repair and restoration of service Ensure continuation of patient care and essential services Consider partial or complete evacuation of the facility, or relocation of patients and services within the facility Maintain communications systems and other utilities 75
76 PLANNING Establish operational periods, incident objectives and develop the Incident Action Plan, in collaboration with the Incident Commander Implement patient and personnel tracking, as appropriate LOGISTICS Assess HVAC system damage and project impacts of heat on the facility, equipment and perishables Maintain other utilities and activate alternate systems as needed Investigate and provide recommendations for rental of portable HVAC units Investigate and provide recommendations for rental of portable filtration such as HEPA units and temporary isolation capability Identify needed replacement air filters (e.g. HEPA) for HVAC system Provide for water, food and rest periods for staff Monitor staff for heat related injuries and provide appropriate follow up Obtain supplemental staffing, as needed Prepare for transportation of evacuated patients Intermediate and Extended (Operational Period 2 to Greater than 12 Hours) COMMAND (Incident Commander): Update and revise the Incident Action Plan and prepare for demobilization Continue to update internal officials on the situation status Monitor evacuation, if activated (PIO): Continue with briefings and situation updates with staff, patients and families Continue patient information center operations, in collaboration with Liaison Officer (Liaison Officer): Continue to notify local EOC of situation status, critical issues and request assistance, asneeded Continue patient information center operations, in collaboration with PIO Continue communications with area hospitals and facilitate patient transfers (Safety): Continue to evaluate facility operations for safety and hazards and take immediate corrective actions OPERATIONS Continue evaluation of patient and visitors for heat impacts and maintain cooling measures Cancel elective surgeries and procedures Prepare the staging area for patient transfer/evacuation Initiate ambulance diversion procedures Continue or implement patient evacuation Ensure the transfer of patient s belongings, medications and records upon evacuation Continue evaluation and provision of temporary HVAC systems and portable filtration units Ensure facility security and restricted visitation Ensure provision of water and food to patients, visitors and families Continue to maintain other utilities Monitor patients for adverse affects of heath and psychological stress Institute HVAC repairs and services Prepare demobilization and system recovery plan PLANNING Continue patient, bed and personnel tracking Update and revise the Incident Action Plan Plan for repatriation of patients 76
77 Prepare demobilization and system recovery plan Ensure documentation of actions, decisions and activities LOGISTICS Continue provision of portable HVAC units and filtration systems Continue to provide staff for patient care and evacuation Monitor staff for adverse affects of heath and psychological stress Monitor, report, follow up on and document staff or patient injuries Continue to provide transportation services for internal operations and patient evacuation FINANCE/ADMINISTRATION Continue to track costs and expenditures and lost revenue Continue to facilitate contracting for facility repair and clean up Demobilization/System Recovery: COMMAND (Incident Commander): Determine hospital status and declare restoration of HVAC services and termination of the incident (Liaison Officer): Communicate final hospital status and termination of the incident to local EOC, area hospital and officials Assist with the repatriation of patients transferred (PIO): Conduct final media briefing and assist with updating staff, patients, families and others of the termination of the event (Safety Officer): Ensure facility safety and restoration of normal operations Ensure facility repairs are completed, in conjunction with the Operations and Logistics Sections OPERATIONS Restore normal patient care operations Ensure restoration of HVAC services and negative pressure isolation rooms Repatriate evacuated patients Discontinue ambulance diversion and visitor limitations PLANNING Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Conduct after-action reviews and debriefing Write after-action report and corrective action plan for approval by the Incident Commander to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement LOGISTICS Restock supplies, equipment, medications, food and water Ensure communication and IT/IS operations return to normal Replace all damaged or soiled air handling filters (e.g. HEPA) Provide stress management and mental health support to staff 77
78 FINANCE/ADMINISTRATION Compile a final report of response and facility repair costs for approval by the Incident Commander Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate reimbursement and claims procedures Documents and Tools Hospital Internal Utility Failure Plan Emergency Operations Plan Facility Evacuation Plan (as needed) 78
79 LOSS OF POWER INCIDENT RESPONSE GUIDE Mission: To safely manage the operations of the facility during a power outage and minimize time to restore service. Directions Read this entire response guide and review incident management team chart Use this response guide as a checklist to ensure all tasks are addressed and completed Objectives Maintain emergency power systems Maintain patient care management and safety Minimize impact on hospital operations and clinical services Evacuate patients to other facilities, if appropriate Communicate situation to staff, patients, the media and community officials Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the facility Emergency Operations Plan Activate Command Staff and Section Chiefs, as appropriate (Liaison Officer): Notify local emergency management/eoc of hospital situation status and obtain incident information and estimated timelines for restoration of power Notify local EMS and ambulance providers about the situation and possible need to evacuate Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. Contact the Regional Hospital Coordination Center, if exists, to notify about the situation and request assistance with patient evacuation destinations COMMAND (Public Information Officer): Inform staff, patients and families of situation and measures to provide power and protect life Prepare media staging area Conduct regular media briefings, in collaboration local emergency management, as appropriate (Safety Officer): Evaluate safety of patients, family, staff and facility and recommend protective and corrective actions to minimize hazards and risks OPERATIONS Evaluate the emergency power supply and appropriate usage within the facility Initiate power conservation measures Assess patients for risk and prioritize care and resources, as appropriate Secure the facility and implement limited visitation policy Ensure continuation of patient care and essential services Consider partial or complete evacuation of the facility, or relocation of patients and services within the facility 79
80 Maintain communications systems and other utilities and activate redundant (back up) systems, as appropriate Implement business continuity plans and protection of records PLANNING Establish operational periods, incident objectives and develop the Incident Action Plan, in collaboration with the Incident Commander Prepare for patient and personnel tracking in the event of evacuations Monitor weather conditions LOGISTICS Maintain other utilities and activate alternate systems as needed Investigate and provide recommendations for auxiliary power (i.e., battery powered lights,etc) Provide for water, food and rest periods for staff Obtain supplies to maintain functioning of emergency generators (i.e., fuel, parts, etc.) Obtain supplemental staffing, as needed Prepare for transportation of evacuated patients Validate and/or activate the backup communications systems Intermediate and Extended (Operational Period 2 to Greater than 12 Hours) COMMAND (Incident Commander): Update and revise the Incident Action Plan and prepare for demobilization Continue to update internal officials on the situation status Monitor evacuation, if activated (PIO): Continue with briefings and situation updates with staff, patients and families Continue patient information center operations, in collaboration with Liaison Officer (Liaison Officer): Continue to notify local EOC of situation status, critical issues and request assistance, as needed Continue to communicate with local utilities incident details and duration estimates Continue patient information center operations, in collaboration with PIO Continue communications with area hospitals and facilitate patient transfers : (Safety): Continue to evaluate facility operations for safety and hazards and take immediate corrective actions OPERATIONS Continue evaluation of patients and patient care Determine if any equipment can be taken off emergency power to minimize load on generators Cancel elective surgeries and procedures Prepare the staging area for patient transfer/evacuation Initiate ambulance diversion procedures Continue or implement patient evacuation Ensure the transfer of patient s belongings, medications and records upon evacuation Continue evaluation and provision of emergency power Ensure facility security and restricted visitation Ensure provision of water and food to patients, visitors and families Continue to maintain other utilities Monitor patients for adverse affects of heath and psychological stress Prepare demobilization and system recovery plan 81
81 PLANNING Continue patient, bed and personnel tracking Update and revise the Incident Action Plan Prepare the demobilization and system recovery plans Plan for repatriation of patients Ensure documentation of actions, decisions and activities LOGISTICS Contact vendors to schedule regular deliveries of fuel to maintain emergency power Contact vendors on availability of supplies and fresh food Continue provision of emergency power to critical areas Continue to provide staff for patient care and evacuation Monitor staff for adverse affects of heath and psychological stress Monitor, report, follow up on and document staff or patient injuries Continue to provide transportation services for internal operations and patient evacuation FINANCE/ADMINISTRATION Continue to track costs and expenditures and lost revenue Continue to facilitate contracting for emergency power and other services Demobilization/System Recovery COMMAND (Incident Commander): Determine hospital status and declare restoration of normal power and termination of the incident Notify state licensing, accreditation or regulatory agency of sentinel event (Liaison Officer): Communicate final hospital status and termination of the incident to local EOC, area hospitals and officials Assist with the repatriation of patients transferred (PIO): Conduct final media briefing and assist with updating staff, patients, families and others of the termination of the event (Safety Officer): Ensure facility safety and restoration of normal operations OPERATIONS Restore normal patient care operations Ensure restoration of power and services Repatriate evacuated patients Discontinue ambulance diversion and visitor limitations Ensure business continuity of operations and return to normal services PLANNING Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Conduct after-action reviews and debriefing Write after-action report and corrective action plan for approval by the Incident Commander to include the following: Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions LOGISTICS 81
82 Perform evaluation and preventative maintenance on emergency generators and ensure their readiness Restock supplies, equipment, medications, food and water Ensure communications and IT/IS operations return to normal FINANCE/ADMINISTRATION Compile a final report of response costs and expenditures and lost revenue for approval by the Incident Commander Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate reimbursement and claims procedures Documents and Tools Hospital Emergency Operations Plan Hospital Evacuation Plan Emergency Power Plans Emergency Communications Plans Facility and Departmental Business Continuity Plans 82
83 LOSS OF WATER INCIDENT RESPONSE GUIDE Mission: To effectively and efficiently manage the effects of a loss of water in the facility. Directions Read this entire response guide and review incident management team chart. Use this response guide as a checklist to ensure all tasks are addressed and completed. Objectives Conserve water and restore water supply Identify and obtain alternate sources of potable water Maintain patient care management Monitor heating and cooling systems Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the facility Emergency Operations Plan Activate Command Staff and Section Chiefs, as appropriate Establish incident objectives and operational period (Liaison Officer): Notify local emergency management of hospital situation status, critical issues and timeline for water service repairs and restoration Notify the water utility and outside agencies of water loss and estimated time for water main repair and restoration of service Notify local EMS and ambulance providers about the situation and possible need to evacuate Communicate with other healthcare facilities to determine:. Situation status. Surge capacity. Patient transfer/bed availability. Ability to loan needed equipment, supplies, medications, personnel, etc.. Contact the Regional Hospital Coordination Center, if exists, to notify about the situation and request assistance with patient evacuation destinations COMMAND (Public Information Officer): Inform staff, patients and families of situation and measures to conserve water and protect life Prepare media staging area Conduct regular media briefings, in collaboration local emergency management, as appropriate (Safety Officer): Evaluate safety of patients, family, staff and facility and recommend protective and corrective actions to minimize hazards and risks OPERATIONS Determine loss of water impact on systems and patients Estimate potable and non-potable water usage and needs and collaborate with Logistics Section and Liaison Officer to obtain back up supplies 83
84 Access alternate sources of water to provide for fire suppression, HVAC system and other critical systems, as able Institute rationing of water, as appropriate Initiate water conservation measures Assess patients for risk and prioritize care and resources, as appropriate Monitor infection control practices Provide alternate toilet and hand washing facilities Secure the facility and implement limited visitation policy Ensure continuation of patient care and essential services Consider partial or complete evacuation of the facility, or relocation of patients and services within the facility Activate facility and impacted departmental business continuity plans PLANNING Establish operational periods, incident objective and develop the Incident Action Plan, in collaboration with the Incident Commander Prepare for patient and personnel tracking in the event of evacuations LOGISTICS Maintain other utilities and activate alternate systems as needed Investigate and provide recommendations for alternate water supplies, including potable water Assist with rationing water, as appropriate Obtain supplemental staffing, as needed Prepare for transportation of evacuated patients, if activated Oversee and conduct water main repairs and restoration of services Intermediate and Extended (Operational Period 2 hours to Greater than 12 Hours) COMMAND (Incident Commander): Update and revise the Incident Action Plan and prepare for demobilization Continue to update internal officials on the situation status Monitor evacuation (PIO): Continue with briefings and situation updates with staff, patients and families Continue patient information center operations, in collaboration with Liaison Officer Assist with notification of patient s families about situation and evacuation, if activated (Liaison Officer): Continue to notify local EOC of situation status, critical issues and request assistance, as needed Continue to communicate with local utilities incident details and duration estimates Continue patient information center operations, in collaboration with PIO Continue communications with area hospitals and facilitate patient transfers (Safety Officer): Continue to evaluate facility operations for safety and hazards and take immediate corrective actions OPERATIONS Continue evaluation of patients and patient care Cancel elective surgeries and procedures Prepare the staging area for patient transfer/evacuation Initiate ambulance diversion procedures Continue or implement patient evacuation Ensure the transfer of patient s belongings, medications and records upon evacuation Continue to ration water, especially potable water, as appropriate Maintain facility security and restricted visitation Continue to maintain other utilities 84
85 Monitor patients for adverse affects of heath and psychological stress Prepare demobilization and system recovery plan PLANNING Continue patient, bed and personnel tracking Update and revise the Incident Action Plan Prepare the demobilization and system recovery plans Plan for repatriation of patients Ensure documentation of actions, decisions and activities LOGISTICS Continue with nutritional, sanitation, and HVAC support and operations Contact vendors to provide emergency potable and non-potable water supplies and portable toilets Monitor the impact of the loss of water on critical areas Continue to provide staff for patient care and evacuation Monitor staff for adverse affects of heath and psychological stress Monitor, report, follow up on and document staff or patient injuries Continue to provide transportation services for internal operations and patient evacuation FINANCE/ADMINISTRATION Continue to track costs and expenditures and lost revenue Continue to facilitate contracting for emergency repairs and other services Demobilization/System Recovery COMMAND (Incident Commander): Determine hospital status and declare restoration of normal water services and termination of the incident Notify state licensing, accreditation or regulatory agency of sentinel event Provide appreciation and recognition to solicited and non-solicited volunteers and to state and federal personnel sent to help (Liaison Officer): Communicate final hospital status and termination of the incident to local EOC, area hospital and officials Assist with the repatriation of patients transferred (PIO): Conduct final media briefing and assist with updating staff, patients, families and others of the termination of the event (Safety Officer): Ensure facility safety and restoration of normal operations OPERATIONS Confirm water restoration plan with local water authority and complete bacteriological testing and final potable water safety verification Restore normal patient care operations Ensure restoration of water and other infrastructure (i.e., HVAC) Repatriate evacuated patients Discontinue ambulance diversion and visitor limitations PLANNING Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Conduct after-action reviews and debriefing Write after-action report and corrective action plan for approval by the Incident Commander to include the following: 85
86 Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions LOGISTICS Perform evaluation and preventative maintenance on emergency generators and ensure their readiness Restock supplies, equipment, medications, food and water Ensure communications and IT/IS operations return to normal Conduct stress management and after-action debriefings and meetings, as necessary FINANCE/ADMINISTRATION Compile a final report of response costs and expenditures and lost revenue for approval by the Incident Commander Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate reimbursement and claims procedures Documents and Tools Hospital Emergency Operations Plan Hospital Loss of Water Plan Hospital Loss of Sewer Plan Hospital Loss of HVAC Plan Facility and Departmental Business Continuity Plans 86
87 SEVERE WEATHER INCIDENT RESPONSE GUIDE Mission: To provide for the safety of patients, visitors, and staff during a severe weather emergency such as rain, flooding, etc. Directions: Read this entire response guide and review incident management team chart. Use this response guide as a checklist to ensure all tasks are addressed and completed. Objectives Implement Emergency Operations Plan and Severe Weather Emergency Response Plan Initiate facility hardening Protect patients, visitors, staff and facility Maintain patient care and medical management Restore normal operations as soon as feasible Immediate (Operational Period 0-2 Hours) COMMAND (Incident Commander): Activate the facility Emergency Operations Plan Activate Command Staff and Section Chiefs, as appropriate Establish incident objectives and operational period (Liaison Officer): Notify local emergency management of hospital situation status, critical issues and resource requests Notify local EMS and ambulance providers about the situation and possible need to evacuate or relocate patients Communicate with other healthcare facilities to determine: Situation status Surge capacity Patient transfer/bed availability Ability to loan needed equipment, supplies, medications, personnel, etc. Monitor weather conditions, structural integrity, and facility security COMMAND (Public Information Officer): Inform staff, patients and families of situation status and provide regular updates Prepare media staging area Conduct regular media briefings, in collaboration local emergency management, as appropriate (Safety Officer): Evaluate safety of patients, family, staff and facility and recommend protective and corrective actions to minimize hazards and risks OPERATIONS Assess patients for risk and prioritize care and resources, as appropriate Secure the facility and implement limited visitation policy Ensure continuation of patient care and essential services Prepare to implement emergency plans and procedures as needed (i.e., loss of power, water, HVAC, communications, etc.) Consider partial or complete evacuation of the facility, or relocation of patients and services within the facility Develop storm staffing plan and triggers for activation 87
88 Initiate facility hardening activities Designate an area(s) to accommodate community boarders including those who may be electrically dependent or have medical needs Distribute appropriate equipment throughout the facility (i.e. portable lights), as needed Determine timeline and criteria for discontinuation of non-essential services and procedures PLANNING Establish operational periods, incident objective and develop the Incident Action Plan, in collaboration with the Incident Commander Conduct a hospital census and identify potential discharges, in coordination with Operations Section Initiate tracking system for patients and arriving community boarders and visitors that will remain in the facility during the storm LOGISTICS Maintain utilities and communications and activate alternate systems as needed Obtain supplies, equipment, medications, food and water to sustain operations Obtain supplemental staffing, as needed Prepare for transportation of evacuated patients, if activated Intermediate and Extended (Operational Period 2 hours to Greater than 12 Hours) COMMAND (Incident Commander): Update and revise the Incident Action Plan and prepare for demobilization Continue to update internal officials on the situation status Monitor evacuation, if activated (PIO): Continue to monitor weather reports and conditions Continue with briefings and situation updates with staff, patients and families Continue patient information center operations, in collaboration with Liaison Officer Assist with notification of patient s families about situation and evacuation, if activated (Liaison Officer): Continue to notify local EOC of situation status, critical issues and request assistance, as needed Continue patient information center operations, in collaboration with PIO Continue communications with area hospitals and facilitate patient transfers, if activated (Safety Officer): Continue to evaluate facility operations for safety and hazards and take immediate corrective actions OPERATIONS Continue evaluation of patients and maintain patient care Cancel elective surgeries and procedures Prepare the staging area for patient transfer/evacuation Regularly perform facility damage assessments and initiate appropriate repairs Ensure the functioning of emergency generators and alternative power/light resources, if needed Initiate ambulance diversion procedures, if possible Continue or implement patient evacuation Ensure the transfer of patient s belongings, medications and records upon evacuation Maintain facility security and restricted visitation Continue to maintain utilities and communications 88
89 Monitor patients for adverse affects of heath and psychological stress Prepare for demobilization and system recovery PLANNING Continue patient, bed and personnel tracking Update and revise the Incident Action Plan Prepare the demobilization and system recovery plans Plan for repatriation of patients Ensure documentation of actions, decisions and activities LOGISTICS Continue evaluation of facility for damage and initiate repairs Continue to obtain needed supplies, equipment, medications, food and water Continue to provide staff for patient care and evacuation Monitor staff for adverse affects of heath and psychological stress Monitor, report, follow up on and document staff or patient injuries Continue to provide transportation services for internal operations and patient evacuation FINANCE/ADMINISTRATION Continue to track costs and expenditures and lost revenue Continue to facilitate contracting for emergency repairs and other services Demobilization/System Recovery COMMAND (Incident Commander): Determine hospital status and declare restoration of normal water services and termination of the incident Provide appreciation and recognition to solicited and non-solicited volunteers and to state and federal personnel sent to help (Liaison Officer): Communicate final hospital status and termination of the incident to local EOC, area hospital and officials Assist with the repatriation of patients transferred (PIO): Conduct final media briefing and assist with updating staff, patients, families and others of the termination of the event (Safety Officer): Ensure facility safety and restoration of normal operations OPERATIONS Restore normal patient care operations Ensure integrity of and/or restoration of utilities and communications Repatriate evacuated patients Discontinue ambulance diversion and visitor limitations PLANNING Finalize the Incident Action Plan and demobilization plan Compile a final report of the incident and hospital response and recovery operations Ensure appropriate archiving of incident documentation Conduct after-action reviews and debriefing Write after-action report and corrective action plan for approval by the Incident Commander to include the following: 89
90 Summary of actions taken Summary of the incident Actions that went well Area for improvement Recommendations for future response actions LOGISTICS Ensure facility repairs and restoration of utilities Restock supplies, equipment, medications, food and water Ensure communications and IT/IS operations return to normal Conduct stress management and after-action debriefings and meetings, as necessary FINANCE/ADMINISTRATION Compile a final report of response costs and expenditures and lost revenue for approval by the Incident Commander Contact insurance carriers to assist in documentation of structural and infrastructure damage and initiate reimbursement and claims procedures Documents and Tools Hospital Emergency Operations Plan Hospital Severe Weather Emergency Procedure Facility and Departmental Business Continuity Plans Television/radio to monitor weather Hospital Emergency Operations Plan Hospital Severe Weather Emergency Procedure Telephone/cell phone/radio/satellite phone/intranet for communication 91

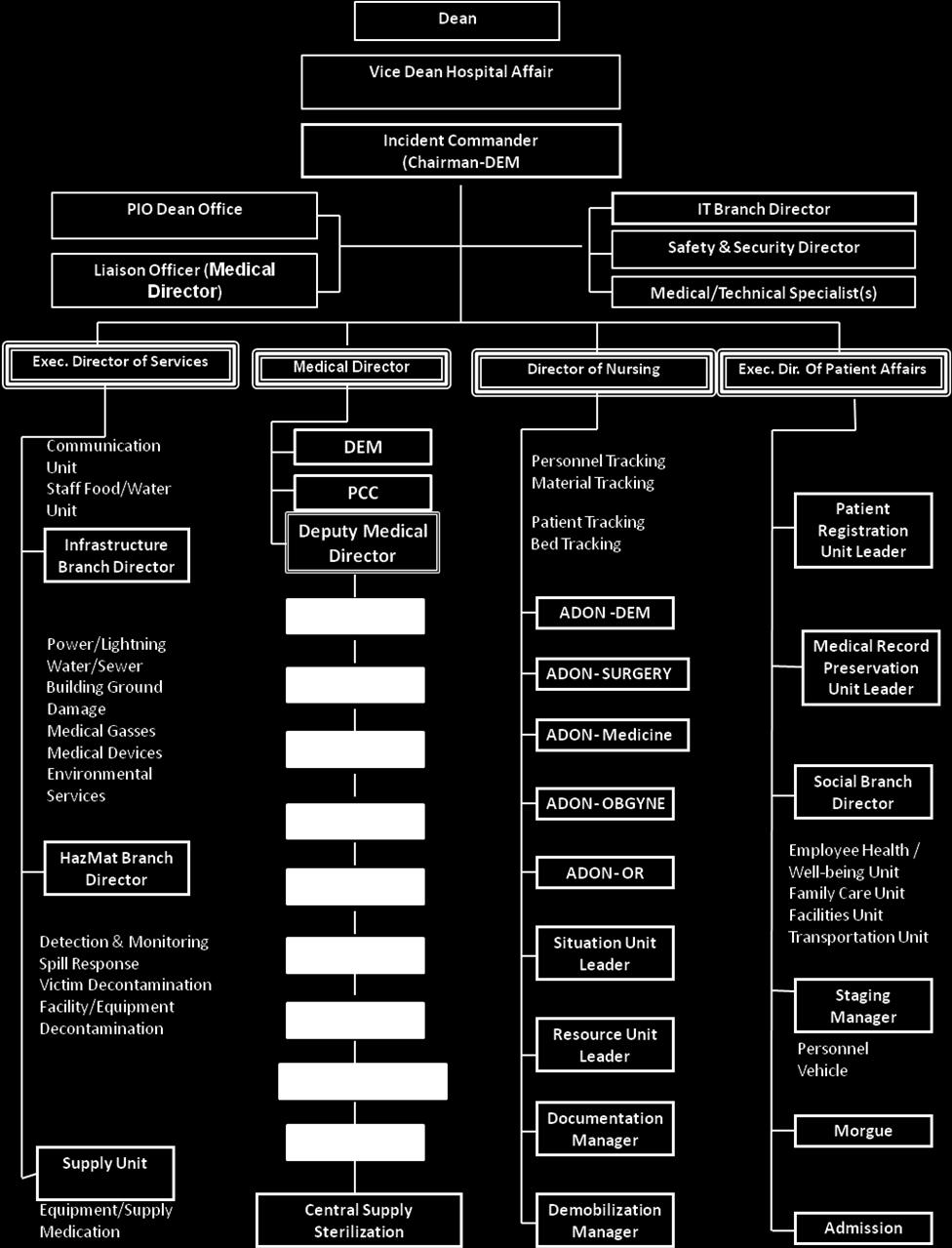
91 Appendix1 (Command Team) 91

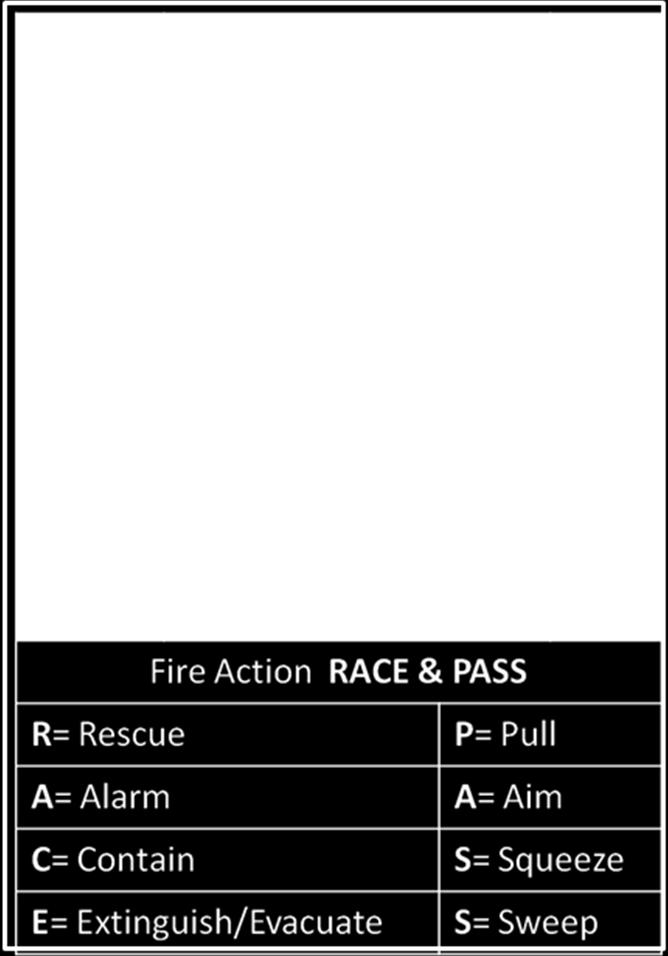
92 Appendix 2 (Emergency Codes) 92
93 Appendix 3 START Adult Triage Algorithm 93
94 Appendix 3 Jump START Pediatric Triage Algorithm 94
95 Appendix 4 Mettag 95
96 Appendix 5 Call List LIST OF INCEDENT COMMAND GROUP Name Position Bleep Office Fax Cell phone Prof. Mussad mohammed Alsalman Dr. Abdulaziz Abdullah Al-Saif Dr. Zohair Ahmed Al- Aseri Dr. Bader Bin Abdulrahman Al Jabri Mr. Mansour Saeed AlSuwaidan Mr. Hamdan Daham Alenezi Mr. Nasser Salash AL Thbaib Dr. Bader Bin Abdulrahman Al Jabri Mr. Mohammed Mofleh Dean Vice Dean for Hospital Affairs Incident Command (DEM Chairman) PIO Dean Office Liaison Officer (Medical Director) IT&C Branch Director Safety & Security Director Medical/Technical Specialist(s) Exec. Director of Services Medical Director Director of Nursing Mr. Motlaq Abdullah Alrasheed Exec. Dir. Of Patient Affairs Engr. Sayed Abdul Infrastructure Hafiz Hassanein Branch Director Pro.Taj aldin Omar HazMat Branch Mlinbary Director Mr. Ahmed Ali Security Branch Albashiri Director Dr.Talal Daian AL Otaibi Supply Unit Dr. Zohair Bin Ahmad Al Aseri DEM Mr. Sultan Al Rashid PCC Dr. Mohammed Deputy Medical Ibrahim Almajid Director Prof. Hana Ahmad Habib LABORATORY Dr. Abdulmoneam Al Othman BLOOD BANK Dr. Ayed Mohammed Al Shamrani PHARMACY
97 Dr. Abdullah Dohayan Al Dohyan SURGERY Prof. Ahmad Abdulrahim Turkstani ANESTHESIA Dr. Fawaz Fahad Al Jasir ORTHOPEDIC Dr. Nizar Naqshbandi RADIOLOGY Dr. Abdulaziz Hamad Al Zeer CRITICAL CARE Prof. Mohammed Abdulaziz Al Sahger PSYCHIATRY Mrs. Sara Al Banyan Central Supply Sterilization Mr. Haytam Mosleh ADON -DEM Ms. Rosely Varghese ADON- SURGERY Ms. Mhardiya Al Fad ADON- Medicine Ms. Maggie Taiwo ADON- OBGYNE Ms. Neda Salcedo ADON- OR Physician's Name Dr. Abdulla Mohammed Ahmed Al-Sakka Dr. Abdulmoniem Mohammed Al- Mubarak Dr. Ahad Alhassan Saud Abdulaziz LIST OF ADULT EMERGENCY PHYSICIANS ADULT ER STAFF Computer Number Bleep Number Home Phone Mobile Dr. Ahmad Fathy Al-maghrabi Dr. Ahmed Abdullah Bin Obaid Dr. Abdulaziz Sulaiman Al- Mehlisi Dr. Ala'a Eldeen Al-Jundi Dr. Ala'a Mostafa Sultan Dr. Asa'ad Sulaiman Mohammed Hamza Al Shuja'a Dr. Ammar Abdulkader El Sammra Dr. Adel Abdullah Obaid Al- Tamimi
98 Dr. Adel Mohammed El Hardallo Dr. Bandar Youssef Al-Eissa Dr. Fahad Ibrahim Abuguyan Dr. Fawaz Abdulrahman Al- Tuwaijri Dr. Hossam Aldin Hassan Abdulrazik Dr. Hani Ali Al Ibrahim Dr. Jalal El-Noor Yousif Dr. Khalid Abdelkarim Gabralla Hamed Dr. Majed Alawe Al Otaibi Dr. Mohammed Moustafa Izzideen Dr. Mohammed Owais Suriya Dr. Mohammed Shoukry Ibrahim Ahmed Dr. Mohammed Ahmed El Zubair Dr. Mohammed Mahamoud Mohammed Abdulrahim Dr. Mohammed Khalid Al-Ageel Dr. Mohammed Shami Al-Zahri Dr. Mushtaq Moh'd Ghulam Jilani Dr. Neda'a Mohammed Romaili Dr. Abdulaziz Dawas Al-Dawas Dr. Abdulmajeed bin Mubarad Dr. Bayan Abdullah Hassan Abdulbaqi Dr. Bashayer Al-Mahdi Al-Bogami Dr. Fatimah Saif Alibrahim Dr. Hanan Saad Al Zeer Dr. Mohammad Mosleh Al Gehani
99 Dr. Mohannad Fahad Al Eeban Dr. Rakan Saleh Al Rasheed Dr. Yasser Abdulkarim Alaska Dr. Tariq Abdulrahman Jaber Al Thobaiti Physician's Name Dr. Abdulrahim Mahmoud Aljaraddah PEDIATRIC STAFF Computer Number Bleep Number Home Phone Mobile Dr. Abdulshaheed Khan Dr. Adel Hassan M. Suleiman N/A Dr. Hashim Mohammed Bin Salleeh Dr. Lina Abdulaziz Al Bakry Dr. Mahmoud Mahmed Al Hag Ibrahim Dr. Manal Eltoum Hassan Abou Dr. Mohammed Abdulaziz Al Othman Dr. Mohammed Masirul Haque Dr. Mohey Eldin Mahmoud Ismail Dowidar Dr. Moutaz Mohammed Kudaimi Dr. Mudasir Mushtaq Ahmad Dr. Nazik Abdulaziz Al Bawardi Dr. Saleh Abdullah Al Tamimi Dr. Sayed Ahmed Ammer Dr. Tahani Awad Al Ahmadi Dr. Uzma Yasmeen Majed Kashif Dr. Varky Ashok Dr. Yasmeen Ahmed Sayed
100 IT Staff Staff Name Tel. Bleep Mansour Saad M. Al-Swaidan (IT Director) NA Khawla Al Harbi (IT Deputy Director) Fairzia A. Lim( Administration) Suha Ayoub( Administration) Help Desk Khalil Ibrahim Joudah (Supervisor) NA Imran Abdulrahman Mohammed Sujath Ali Raheemuddin Mohd. Saleem Sari alsayed Mohd. Mofleh Yahya Zakaria Sultan Nelson Raul Patacsil Salman Khalid Baksh Majid Jazi Al Mutairi Mohammed Shafeeq ur Rahman Kamran Ahmed Khan Abdulrazzak Pannam Kutil NA Mohammed Feroz Kamaruddin NA Mohammed Yakub Ali NA Warda Mohammed Bawazeer NA Najwa Abdulhaq Merriki NA Meshael Mubtil Al Otaibi NA Wasim Khalil Ali Ramy Mohammed Mustafa NA Mohd. Mahmoud Mohd. Farghali NA Mohd. Mamdouh Abdulaziz NA 111
101 Ghada Nasser AlBakr NA Amro Mohammed Fekry Ibrahem Ahmed Al Bajjaly NA Mustafa Majed Yamak NA Mohammed Aamir AbdulQayyum Syed Afzal Ali Mohammed Abdulnaim Aqter Al Ameen Mohammed Khair NA Mohammed Abdullah Ali NA Khalid Abdullah Al Enizi NA Surgery Department GASTRO-INTESTINAL SURGERY GENERAL SURGERY LAST NAME M. NAME FIRST NAME Degree/Position FRCSC, Associate Professor & 1 Al-Naami Yahya Mohammed 2 Al- Dohayan Dohayan Abdullah Al- Bin 3 Tameem Mubarak COLORECTAL SURGERY Mohsin 1 Al-Obaid Abdulaziz Omar 2 Zubaidi Mohammed Ahmad 3 Al-Khayal Abdulmalik Khayal 4 El-Faroug Yousif Omer COMP. # PAGER OFFICE MOBILE HOME TEL Consultant FRCSGlas, Professor & Consultant, Chairman D/S Professor & Consultant General surgeon FRCSC, Asst. Prof.Cons Colorectal & Min. Inv Sur FRCSC, Asstistant Prof. & HEAD of G.S FRCSC, FRCSC (Colorectal) A/Cons Colorectal Surgeon FRCS, Asst. Prof & Consultant ENDOCRINE/BREAST & ENDOCRINE SURGERY 1 Al-Shehri Yahya Mohammed 2 Al-Saif Abdullah Abdulaziz 3 Abdulkareem Abdullatif Amal 4 Gamal Aldin Ahmed Khairy Professor & Consultant General surgeon FRCS, FRACS, Asst. Prof. & Cons. Breast/ Endocrine Surg American Board, Asst. Professor & Consultant FRCS, Assoc. Prof & Consultant
102 VASCULAR SURGERY HEPATO-BILIARY SURGERY 1 Al-Saif Abdullah Faisal Al- 2 Qahtani Hadi Hamad HEPATO-BILIARY SURGERY 1 Safdar Mufti Mohammed 2 Anjum Nawaz Muhammad Bokhari Abdullah Areej El- 4 Sayed Saad Magdy 5 Al-Enazi Abdullah Naif 6 Al-Alawi Salamah Khalil FRCSC, Asst. Prof. Cons Hep.- Pancreato Bil & Transplant Surgery General & Hepato biliary surgery FCPS, Senior Registrar FCPS, Senior Registrar Saudi Board of General Surgery, Senior Registrar FRCSI, Senior Registrar General Surgery, Senior Registrar General Surgery, Senior Registrar PLASTIC SURGERY LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE MD, FRCSC, Associate Professor, 1 Al-Jabri A'rahman Badr Head & Consultant Al- FRCSC, FACS, Professor of Surgery & 2 Salman Mohammed Mussaad Consultant Al- MD, MSc, FRCSC, Assoc. Professor & Omran A'rahman Mohammed Consultant Iqbal Shikh Kaisor FRCS, Consultant Vascular Surgeon Al-Nasr Mahmoud Tawfiq FRCS, Sr. Registrar Al- Tuwaijri A'rahman Talal MB;BS, Sr. Registrar Batheeb Abo Bakr Nabil FRCSI, Sr. Registrar MB; Bch, SB of Gen. Surg. Fellow, 8 Zoghby Ahmed Kamal Vascular Surgery AlToijry Hamad Abdulmajeed MBBS, Demonstrator Al- Sheikh Omar Sultan MBBS, Demonstrator Home Tel
103 Home Tel. NGH LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE FRCSC, Professor, Head & 1 Al-Qattan Manaa Mohammed Consultant FRCSGlas, Assist. Professor & 2 Hassanain Mahjoub Jamaleldin Consultant Al- Jordanian Board, Acting Consultant Shanawani Nawras Bisher Surgeon Al-Zahrani Jaman Khalid Saudi Board of Plastic Surgery MRCS & Arab Board in GS, Sr. 5 Keyyali Essam Mohammed Registrar Zeidan Ibrahim Mohammed FRCS, Sr. Registrar A'Hamid Mahmoud Mokhtar MRCSEng, Registrar Al-Arfaj A'Hamid Nawarah MB;BS, Registrar, Plastic Surgery Al-Humsi Riyadh Taghreed MB;BS, Resident, Plastic Surgery Al-Ghamdi Gormulla Hisham MB;BS, Demonstrator, Plastic Surgery Adult UROLOGY LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE FRCSC, FACS, Assoc. Professor, 1 Rabah Manthar Danny Head & Consultant FRCSEd, Professor of Urology & 2 Talic Fouad Riyadh Andrology FRCSEng, Associate Professor & 3 El-Faqih Rashid Salah Consultant FRCSC, Asst. Professor & 4 Alomar Abdulaziz Mohammad Consultant Arahman 5 Bin Saleh Abd. Saleh FRCSC, Asst. Prof. & Consultant Al-Turaifi El-Gaili Abdulmonem FRCS, Consultant Urologist Home Tel Pediatric LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE FRCSI, Assoc. Professor & Cons. 1 Fouda Neel Ali Khalid Pediatric Urologist Al-Hazmi Hammad Ayed Hamdan Asst. Professor & Cons. Pediatric Urologist Home Tel REGISTRARS & SENIOR REGISTRARS/RESIDENT LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE Home Tel. 1 Sallem Abdallah Mahmoud FRCS, Senior Registrar, Pedia Urology Gomha Bahaaeddin Abdulmoneim Masters in Urology, Senior Registrar, Pedia Urology Mohamad Mohamad Ahmad MBSc, Masters Degree in Urology, Sr. Registrar, Pedia Urol Seida Atia, Atwa Mohammed FRCS, Registrar Urodynamics Abou Mustafa Abdullah Nebal Arab Board, Registrar, Adult Urol Ahmed Siddique Tauheed M.S. Registrar Adwan Ahmad Ayman Registrar AlThunayan Mohammed Abdulaziz MB;BS Resident
104 THORACIC SURGERY 1 LAST NAME M. NAME FIRST NAME Al- Nassar Abdulaziz Sami 2 Hajjar Mohammed Waseem 3 Kim Joon Dae DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE MD, FRCSC, Asst Prof. & Head Consultant Thoracic surgeon FRCS, Asst. Professor & Consultant Gen Thoracic MD, Asst. Professor & Consultant Gen Thoracic Home Tel Rahhal Mahmoud Salah FRCS,.Registrar, General Thoracic El- 5 Akeed Nageeb Ahmad MD, Registrar, General Thoracic Ahmed Chaudary Iftikhar FCPS, Registrar, General Thoracic NEUROSURGERY LAST NAME M. NAME FIRST NAME 1 Al-Habib Fayez Amro 2 Jamjoom Alabedeen Zain 3 El-Watidy Mohammed Sherif 4 El-Gamal Eldin Ali Essam DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE FRCSC, Asst. Prof. & Consultant Neurosurgeon FACHARZT, Professor, Head & Consultant Neurosurgeon FRCS, Professor & Consultant Neurosurgeon FRCS, Asst. Professor & Consultant Neurosurgeon Malik Hussain Safdar FCPS, Senior Registrar Abdel 6 Ahmed Raouf Aly MS, Registrar Zakaria Mohammed Amr MS., Registrar Zaidi Ghalib Syed FCPS Neurosurgery, Registrar Home Tel
105 PEDIATRIC SURGERY LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE Home Tel. 1 Al-Jazaeri Hassan Ayman FRCSC, Asst. Professor & Consultant Al-Bassam Ahmed Abdulrahman FRCSEd, Professor & Head & Consultant Al-Qahtani Robiaan Aayed FRCSC, Assoc. Professor & Consultant Al-Zahem Mohammed A'rahman FRCSC, Asst. Professor & Consultant Mallick Mohammad Saquib FRCS, Assoc. Professor & Consultant Gado Mohammed Abdulmonem FRCS, Senior Registrar Al-Sayed Hamdy Osama MD, FRCSEd, Senior Registrar Aziz Asher Muhammad MRCSI, Senior Registrar Al-Shehri Fadl Abdullah MB BS; Demonstrator Fallatah Mohd Amein Amnah MB;BS; Gen. Surgery Specialist, Fellow GENERAL SURGERY - RMC LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE 1 Alam Kurshid Mohammed FRCS, Professor of Surgery Bin FRCS, Assoc. Professor of 2 Al-Salamah Mohamed Saleh Surgery FRCS, Assoc. Professor of 3 Al-Aqeely Bin Hamed Mohammed Surgery FRCS, Consultant General 4 Bismar A'Rahman Hayan Surgeon / Gul Home Tel Malik Mushtaq Rahman FRCS, Senior Registrar / Ibrar Hussein Mohammed FRCS, Senior Registrar / Anzari Uddin Fraz FRCS, Senior Registrar / Abdullah Yaqoob Muhammad FCPS, FRCS, Senior Registrar / DEMONSTRATORS LAST NAME M. NAME FIRST NAME DEGREE/POSITION COMP. # BLEEP OFFICE MOBILE MBBS, Demonstrator, Vascular 1 AlToijry Hamad Abdulmajeed Surgery Al-Buraikan Adnan Ahmed MB;BS, Demonstrator - G.S Al-Subaie Saud Hamad MB;BS, Demonstrator - G.S Bin Drees Khalid Hind MB;BS, Demonstrator - G.S Al-Qahtanij Mansour Saad MB;BS, Demonstrator - G.S Al-Turaiki Abdullah Thamer MB;BS, Demonstrator - G.S MB BS; Demonstrator, Pediatric 7 Al-Shehri Fadl Abdullah Surgery MB;BS, Demonstrator - 8 Al-Mutairi Sallem Fawaz Neurosurgery MB;BS, Demonstrator, Plastic 9 Al-Ghamdi Gormulla Hisham Surgery Home Tel
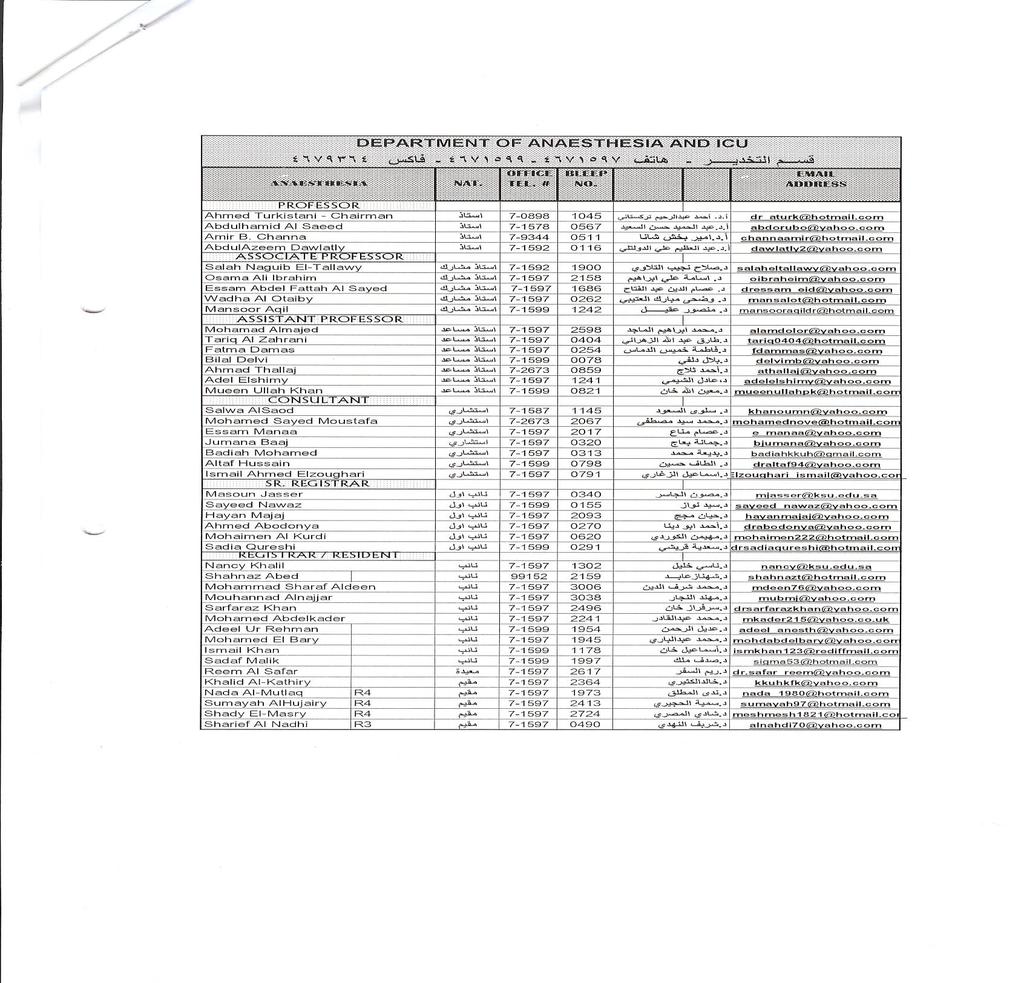
106 116
KENTUCKY HOSPITAL ASSOCIATION OVERHEAD EMERGENCY CODES FREQUENTLY ASKED QUESTIONS
 KENTUCKY HOSPITAL ASSOCIATION OVERHEAD EMERGENCY CODES FREQUENTLY ASKED QUESTIONS Question - Why have standard overhead emergency codes? Answer Lessons learned from recent disasters shows that the resources
KENTUCKY HOSPITAL ASSOCIATION OVERHEAD EMERGENCY CODES FREQUENTLY ASKED QUESTIONS Question - Why have standard overhead emergency codes? Answer Lessons learned from recent disasters shows that the resources
Emergency Codes. ~( Code Triage
 Emergency Codes ~( Code Red ~( Code Green ~( Code Blue/Code Broselow ~( Code Gray ~( Code Pink ~( Code Brown ~( Code White ~( Code Yellow ~( Code Black ~( Code Triage Code Red (Code Green- Drill} Code
Emergency Codes ~( Code Red ~( Code Green ~( Code Blue/Code Broselow ~( Code Gray ~( Code Pink ~( Code Brown ~( Code White ~( Code Yellow ~( Code Black ~( Code Triage Code Red (Code Green- Drill} Code
Objective: Emergency Access Number Always use the code words, not the actual emergency!
 Emergency Codes Objective: At the end of this self-study module, participants will be able to demonstrate knowledge of all emergency codes and their responsibilities during each code. All codes are initiated
Emergency Codes Objective: At the end of this self-study module, participants will be able to demonstrate knowledge of all emergency codes and their responsibilities during each code. All codes are initiated
A Unit nurse acts as recorder until the arrival of an Advanced Life Support (ALS) qualified nurse, who will then take over recording.
 qualified nurse, who will then take over recording.") Title: Code Blue Team and Resuscitation Services Reviewed by: King Khalid University Hospital King Abdulaziz University Hospital Department: Unit: Policy Number: HWCPP-035 Issue JULY 2010 Prepared/Revised
Title: Code Blue Team and Resuscitation Services Reviewed by: King Khalid University Hospital King Abdulaziz University Hospital Department: Unit: Policy Number: HWCPP-035 Issue JULY 2010 Prepared/Revised
IVROP JOB SHADOW PROGRAM ORIENTATION
 IVROP JOB SHADOW PROGRAM ORIENTATION Hospital Incident Command System (HICS) Emergency Codes Hospital Emergency Incident Command System Emergency Codes HEICS Emergency Codes These codes are part of the
IVROP JOB SHADOW PROGRAM ORIENTATION Hospital Incident Command System (HICS) Emergency Codes Hospital Emergency Incident Command System Emergency Codes HEICS Emergency Codes These codes are part of the
Emergency Codes - Ouellette Campus
 The Emergency Codes # is: 555 CODE RED - FIRE 555 CODE PURPLE - HOSTAGE SITUATION OR PERSON WITH WEAPON CODE BLUE - CARDIAC ARREST CODE GREEN - EVACUATION CODE YELLOW - MISSING PATIENT CODE BLACK - CODE
The Emergency Codes # is: 555 CODE RED - FIRE 555 CODE PURPLE - HOSTAGE SITUATION OR PERSON WITH WEAPON CODE BLUE - CARDIAC ARREST CODE GREEN - EVACUATION CODE YELLOW - MISSING PATIENT CODE BLACK - CODE
By then end of this course the participant will be able to: 0 Identify the emergency codes and what extension to use to activate the system.
 Agenda: By then end of this course the participant will be able to: 0 Identify the emergency codes and what extension to use to activate the system. 0 Explain the staff role in keeping RCHSD a safe place
Agenda: By then end of this course the participant will be able to: 0 Identify the emergency codes and what extension to use to activate the system. 0 Explain the staff role in keeping RCHSD a safe place
Life Safety for Students
 Life Safety for Students DISASTER RESPONSE Tift Regional Health System s Disaster Response includes an emergency code system and general actions each employee should take in the specified emergency situation.
Life Safety for Students DISASTER RESPONSE Tift Regional Health System s Disaster Response includes an emergency code system and general actions each employee should take in the specified emergency situation.
GREY NUNS COMMUNITY HOSPITAL ACTIVE ASSAILANT EMERGENCY RESPONSE PLAN
 GREY NUNS COMMUNITY HOSPITAL ACTIVE ASSAILANT EMERGENCY RESPONSE PLAN ACTIVE ASSAILANT EMERGENCY RESPONSE PLAN ALGORITHM Staff Member Discovering the incident Staff in close proximity to the incident Recognizes
GREY NUNS COMMUNITY HOSPITAL ACTIVE ASSAILANT EMERGENCY RESPONSE PLAN ACTIVE ASSAILANT EMERGENCY RESPONSE PLAN ALGORITHM Staff Member Discovering the incident Staff in close proximity to the incident Recognizes
Corporate Safety. Contents
 Corporate Safety This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Target Audience: All Employees Contents Instructions...2
Corporate Safety This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Target Audience: All Employees Contents Instructions...2
Emergency Management Plan and Emergency Operations Plan
 Carolinas HealthCare System Blue Ridge Emergency Management Introduction Carolinas Healthcare System Blue Ridge uses a uniform system of Codes and Conferences to alert staff to emergencies in their facility.
Carolinas HealthCare System Blue Ridge Emergency Management Introduction Carolinas Healthcare System Blue Ridge uses a uniform system of Codes and Conferences to alert staff to emergencies in their facility.
Orientation. Revised May
 Orientation Revised May 2017 1 Volunteers are not expected to take a lead role in dealing with emergency situations. This is the role and responsibility of staff. However, volunteers should follow staff
Orientation Revised May 2017 1 Volunteers are not expected to take a lead role in dealing with emergency situations. This is the role and responsibility of staff. However, volunteers should follow staff
EMERGENCY PREPAREDNESS 2017 Additional information for staff of Children s Hospital of Pittsburgh
 EMERGENCY PREPAREDNESS 2017 Additional information for staff of Children s Hospital of Pittsburgh CHP Emergency Preparedness Program (EPP) Children s Hospital of Pittsburgh of UPMC Emergency Preparedness
EMERGENCY PREPAREDNESS 2017 Additional information for staff of Children s Hospital of Pittsburgh CHP Emergency Preparedness Program (EPP) Children s Hospital of Pittsburgh of UPMC Emergency Preparedness
Nursing Student Orientation. Emergency Codes
 Nursing Student Orientation Emergency Codes EMERGENCY CODES CODE RED - FIRE CODE PURPLE HOSTAGE OR PERSON WITH A WEAPON CODE BLUE CARDIAC ARREST CODE GREEN - EVACUATION CODE YELLOW MISSING PATIENT CODE
Nursing Student Orientation Emergency Codes EMERGENCY CODES CODE RED - FIRE CODE PURPLE HOSTAGE OR PERSON WITH A WEAPON CODE BLUE CARDIAC ARREST CODE GREEN - EVACUATION CODE YELLOW MISSING PATIENT CODE
UNIVERSITY POLICE/PUBLIC SAFETY EMERGENCY PREPAREDNESS MANAGEMENT PLAN
 UNIVERSITY POLICE/PUBLIC SAFETY EMERGENCY PREPAREDNESS MANAGEMENT PLAN Introduction This procedure provides a brief overview of the types of disasters posing a potential threat to Downstate Medical Center.
UNIVERSITY POLICE/PUBLIC SAFETY EMERGENCY PREPAREDNESS MANAGEMENT PLAN Introduction This procedure provides a brief overview of the types of disasters posing a potential threat to Downstate Medical Center.
University of Virginia Health System TABLE OF CONTENTS
 TABLE OF CONTENTS ACTIVE SHOOTER (RED ALERT)... Tab 1 BIOLOGICAL SPILL... Tab 2 BOMB THREAT... Tab 3 CHEMICAL SPILL... Tab 4 COMPUTER SYSTEMS... Tab 5 EARTHQUAKE... Tab 6 EVACUATION... Tab 7 FIRE... Tab
TABLE OF CONTENTS ACTIVE SHOOTER (RED ALERT)... Tab 1 BIOLOGICAL SPILL... Tab 2 BOMB THREAT... Tab 3 CHEMICAL SPILL... Tab 4 COMPUTER SYSTEMS... Tab 5 EARTHQUAKE... Tab 6 EVACUATION... Tab 7 FIRE... Tab
Emergency Codes ilearn Module Text Version
 Emergency Codes ilearn Module Text Version Introduction LHSC is committed to providing a safe environment. But unforeseen emergencies can and do happen, both within and outside of our facilities. These
Emergency Codes ilearn Module Text Version Introduction LHSC is committed to providing a safe environment. But unforeseen emergencies can and do happen, both within and outside of our facilities. These
Western New Mexico University Crisis Intervention Plan
 Western New Mexico University Crisis Intervention Plan Table of Contents Purpose... 3 Definition... 3 Policy... 3 Crisis Response Plan... 4 I. Response Priorities... 4 II. Crisis Intervention Response
Western New Mexico University Crisis Intervention Plan Table of Contents Purpose... 3 Definition... 3 Policy... 3 Crisis Response Plan... 4 I. Response Priorities... 4 II. Crisis Intervention Response
EMERGENCY PREPAREDNESS POLICY
 MANUAL OF POLICIES, PROCEDURES AND BY-LAWS EMERGENCY PREPAREDNESS POLICY Code: Policy 6.7 Date of Coming into Force: September 15, 2014 Number of Pages: 13 Origin: Equipment Services Operator and Storage
MANUAL OF POLICIES, PROCEDURES AND BY-LAWS EMERGENCY PREPAREDNESS POLICY Code: Policy 6.7 Date of Coming into Force: September 15, 2014 Number of Pages: 13 Origin: Equipment Services Operator and Storage
POLCIE, AMBULANCE, FIRE DEPARTMENT DIAL FIRE, DISASTER, EVACUATE 3 BELLS
 FANNINDEL ISD EMERGENCY PROCEDURES MANUAL POLCIE, AMBULANCE, FIRE DEPARTMENT 911 DIAL FIRE, DISASTER, EVACUATE 3 BELLS FANNIN COUNTY SHERIFF 903-583-2143 DELTA COUNTY SHERIFF 903-395-2146 FANNINDEL ISD
FANNINDEL ISD EMERGENCY PROCEDURES MANUAL POLCIE, AMBULANCE, FIRE DEPARTMENT 911 DIAL FIRE, DISASTER, EVACUATE 3 BELLS FANNIN COUNTY SHERIFF 903-583-2143 DELTA COUNTY SHERIFF 903-395-2146 FANNINDEL ISD
WRHA OCCUPATIONAL HEALTH AND SAFETY OPERATIONAL PROCEDURES
 WRHA OCCUPATIONAL HEALTH AND SAFETY OPERATIONAL PROCEDURES Subject: First Responder Program Effective Date: November 1, 2007 Review Date: 3 years or legislation changes 1.0 GUIDING PRINCIPLES: The following
WRHA OCCUPATIONAL HEALTH AND SAFETY OPERATIONAL PROCEDURES Subject: First Responder Program Effective Date: November 1, 2007 Review Date: 3 years or legislation changes 1.0 GUIDING PRINCIPLES: The following
UNIVERSITY OF TOLEDO
 UNIVERSITY OF TOLEDO SUBJECT: CODE GREEN - INTERNAL EVACUATION PROCEDURE Procedure No: EP-08-005 PROCEDURE STATEMENT Specific procedures will be followed in handling the shelter in place/evacuation of
UNIVERSITY OF TOLEDO SUBJECT: CODE GREEN - INTERNAL EVACUATION PROCEDURE Procedure No: EP-08-005 PROCEDURE STATEMENT Specific procedures will be followed in handling the shelter in place/evacuation of
WHAT IS AN EMERGENCY? WHY IT IS IMPORTANT TO PREPARE COMMUNICATIONS
 OVERVIEW The purpose of this plan is to provide for the carrying out of emergency functions to save lives; establish responsibilities necessary to performing these functions; prevent, minimize, and repair
OVERVIEW The purpose of this plan is to provide for the carrying out of emergency functions to save lives; establish responsibilities necessary to performing these functions; prevent, minimize, and repair
Incident Command System Awareness Participant Guide May 2016
 Incident Command System Awareness Participant Guide May 2016 Copyright 2016 Midwest Consortium for Hazardous Waste Worker Training Acknowledgments The Midwest Consortium developed this course for Hazardous
Incident Command System Awareness Participant Guide May 2016 Copyright 2016 Midwest Consortium for Hazardous Waste Worker Training Acknowledgments The Midwest Consortium developed this course for Hazardous
Effective Date: 7/2004
 MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
ORIENTATION HANDBOOK FOR AGENCY STAFF
 ORIENTATION HANDBOOK FOR AGENCY STAFF January 2018 1 A message from Carmel To begin with, I would like to welcome you to the Blackrock Clinic. It is our intention that you are as familiar as is possible
ORIENTATION HANDBOOK FOR AGENCY STAFF January 2018 1 A message from Carmel To begin with, I would like to welcome you to the Blackrock Clinic. It is our intention that you are as familiar as is possible
Model Policy. Active Shooter. Updated: April 2018 PURPOSE
 Model Policy Active Shooter Updated: April 2018 I. PURPOSE Hot Zone: A geographic area, consisting of the immediate incident location, with a direct and immediate threat to personal safety or health. All
Model Policy Active Shooter Updated: April 2018 I. PURPOSE Hot Zone: A geographic area, consisting of the immediate incident location, with a direct and immediate threat to personal safety or health. All
Commack School District District-Wide. Emergency Response Plan
 Commack School District District-Wide Emergency Response Plan 2016-2017 Date of Acceptance/Revision: Introduction 1.1 Purpose The purpose of this plan is to provide emergency preparedness and response
Commack School District District-Wide Emergency Response Plan 2016-2017 Date of Acceptance/Revision: Introduction 1.1 Purpose The purpose of this plan is to provide emergency preparedness and response
EMERGENCY CONDITIONS & BASIC STAFF RESPONSE
 EMERGENCY CONDITIONS & BASIC STAFF PROBLEM CODE NAME DESCRIPTION INITIAL Admitted Adult Patient Missing Code Brown or has left where patient s leaving may be life-threatening to patient. Code Brown Procedure
EMERGENCY CONDITIONS & BASIC STAFF PROBLEM CODE NAME DESCRIPTION INITIAL Admitted Adult Patient Missing Code Brown or has left where patient s leaving may be life-threatening to patient. Code Brown Procedure
* Indicates lot is available for associate parking from 5pm on Friday to 7:30am on Monday.
 L I I A Physician / CTC / Handicapped Only / VIP B Patient / Visitor / Tenant Visitor * C Tenant Staff * D Patient / Visitor / Tenant Visitor/ Vendors/ Contractors * E Tenant Staff * E East Associate Parking
L I I A Physician / CTC / Handicapped Only / VIP B Patient / Visitor / Tenant Visitor * C Tenant Staff * D Patient / Visitor / Tenant Visitor/ Vendors/ Contractors * E Tenant Staff * E East Associate Parking
1. Purpose. In any emergency, Bellarmine University s overriding concerns are as follows:
 Active Aggressor Preparedness Plan Bellarmine University 2017 1. Purpose The basic procedures outlined in this plan are intended to enhance the protection of the Bellarmine University campus and facilities
Active Aggressor Preparedness Plan Bellarmine University 2017 1. Purpose The basic procedures outlined in this plan are intended to enhance the protection of the Bellarmine University campus and facilities
Mission. Directions. Objectives
 Incident Response Guide: Tornado Mission To provide a safe environment for patients, staff, and visitors within the hospital before and after a tornado impacts the campus, structural integrity of the buildings
Incident Response Guide: Tornado Mission To provide a safe environment for patients, staff, and visitors within the hospital before and after a tornado impacts the campus, structural integrity of the buildings
FAMILY DISASTER PLAN. Name: Date: 4 STEPS OF SAFETY LOCAL OFFICE:
 FAMILY DISASTER PLAN Name: Date: It is recommended that every employee of the judicial branch have a personalized Family Disaster Plan. Families can - and do - cope with disaster by preparing in advance
FAMILY DISASTER PLAN Name: Date: It is recommended that every employee of the judicial branch have a personalized Family Disaster Plan. Families can - and do - cope with disaster by preparing in advance
ACTIVE SHOOTER HOW TO RESPOND
 ACTIVE SHOOTER HOW TO RESPOND October 2008 Emergency Numbers EMERGENCY SERVICES: 9-1 -1 LOCAL EMERGENCY INFORMATION LINE: LOCAL POLICE DEPARTMENT: LOCAL FIRE DEPARTMENT: LOCAL HOSPITAL: LOCAL FBI FIELD
ACTIVE SHOOTER HOW TO RESPOND October 2008 Emergency Numbers EMERGENCY SERVICES: 9-1 -1 LOCAL EMERGENCY INFORMATION LINE: LOCAL POLICE DEPARTMENT: LOCAL FIRE DEPARTMENT: LOCAL HOSPITAL: LOCAL FBI FIELD
The 2018 edition is under review and will be available in the near future. G.M. Janowski Associate Provost 21-Mar-18
 The 2010 University of Alabama at Birmingham Emergency Operations Plan is not current but is maintained as part of the Compliance Certification for historical purposes. The 2018 edition is under review
The 2010 University of Alabama at Birmingham Emergency Operations Plan is not current but is maintained as part of the Compliance Certification for historical purposes. The 2018 edition is under review
ABUDHABI INDIAN SCHOOL DISASTER MANAGEMENT POLICY-STANDARD OPERATING PROCEDURES FOR EVICTION
 ABUDHABI INDIAN SCHOOL DISASTER MANAGEMENT POLICY-STANDARD OPERATING PROCEDURES FOR EVICTION DISASTER MANAGEMENT POLICY Name of Policy : Disaster Management Policy- Standard Operating procedures for Eviction
ABUDHABI INDIAN SCHOOL DISASTER MANAGEMENT POLICY-STANDARD OPERATING PROCEDURES FOR EVICTION DISASTER MANAGEMENT POLICY Name of Policy : Disaster Management Policy- Standard Operating procedures for Eviction
ACTIVE SHOOTER HOW TO RESPOND. U.S. Department of Homeland Security. Washington, DC
 U.S. Department of Homeland Security Washington, DC 20528 cfsteam@hq.dhs.gov www.dhs.gov ACTIVE SHOOTER HOW TO RESPOND October 2008 MANAGING THE CONSEQUENCES OF AN ACTIVE SHOOTER SITUATION LESSONS LEARNED
U.S. Department of Homeland Security Washington, DC 20528 cfsteam@hq.dhs.gov www.dhs.gov ACTIVE SHOOTER HOW TO RESPOND October 2008 MANAGING THE CONSEQUENCES OF AN ACTIVE SHOOTER SITUATION LESSONS LEARNED
CIVIL AND NATURAL DISASTER POLICY AND PROCEDURES
 CIVIL AND NATURAL DISASTER POLICY AND PROCEDURES Revised 2016 This document and the Crusader Defense Plan serve as the Emergency Procedures for Ascension of our Lord School. No policy can cover every emergency
CIVIL AND NATURAL DISASTER POLICY AND PROCEDURES Revised 2016 This document and the Crusader Defense Plan serve as the Emergency Procedures for Ascension of our Lord School. No policy can cover every emergency
Emergency Plan Guidelines For Child Care Providers
 South Carolina Division of Early Care and Education Health. Safety. Supervision. Emergency Plan Guidelines For Child Care Providers Visit us on the Web at: www.scchildcare.org Phone Numbers Region 1 (Upstate):
South Carolina Division of Early Care and Education Health. Safety. Supervision. Emergency Plan Guidelines For Child Care Providers Visit us on the Web at: www.scchildcare.org Phone Numbers Region 1 (Upstate):
Emergency Preparedness
 In the interest of maintaining a safe environment for all visitors at Stanford University, it is important for your program s staff and participants to know the following procedures in the unlikely event
In the interest of maintaining a safe environment for all visitors at Stanford University, it is important for your program s staff and participants to know the following procedures in the unlikely event
Coldspring Excelsior Fire and Rescue Standard Operating Policies 6565 County Road 612 NE Kalkaska, MI Section 4.13 INCIDENT COMMAND MANAGEMENT
 Coldspring Excelsior Fire and Rescue Standard Operating Policies 6565 County Road 612 NE Kalkaska, MI 49646 Section 4.13 INCIDENT COMMAND MANAGEMENT The purpose of an Incident Command Management System
Coldspring Excelsior Fire and Rescue Standard Operating Policies 6565 County Road 612 NE Kalkaska, MI 49646 Section 4.13 INCIDENT COMMAND MANAGEMENT The purpose of an Incident Command Management System
St. Vincent's Birmingham Patient Care & Service Area Locations
 St. Vincent's Birmingham Patient Care & Service Area Locations STUDENT NURSE GUIDE West Wing Main Wing East Wing South Tower Women's Center North Tower Ortho Sports Ground Floor Central Sterile Pre Admission
St. Vincent's Birmingham Patient Care & Service Area Locations STUDENT NURSE GUIDE West Wing Main Wing East Wing South Tower Women's Center North Tower Ortho Sports Ground Floor Central Sterile Pre Admission
4.1.2 The admitting physician will complete an initial physical, psychological social, nutritional and pain assessment.
 Title: PATIENT ASSESSMENT AND RE-ASSESSMENT Reviewed by: King Khalid University Hospital King Abdulaziz University Hospital Department: Unit: Policy Number: HWCPP - 004 Issue DEC 2009 Prepared/Revised
Title: PATIENT ASSESSMENT AND RE-ASSESSMENT Reviewed by: King Khalid University Hospital King Abdulaziz University Hospital Department: Unit: Policy Number: HWCPP - 004 Issue DEC 2009 Prepared/Revised
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency Acute Care
 Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
Banff Mineral Springs Hospital EMERGENCY RESPONSE CODE BLUE Cardiac Arrest / Medical Emergency EMERGENCY RESPONSE CODE BLUE ALGORITHM First Person On-Scene First Person On-Scene Call for HELP Push code
This policy applies to any hospital staff, within KKUH/KAUH, who has privileges to enter data into medical records.
 King Khalid K University Hospital King Abdulaziz University Hospital Title: CLINICAL DOCUMENTATION Reviewed by: Date: Department: Unit: Policy Number: HWCPP - 005 Issue Date: DEC 2009 Prepared/Revised
King Khalid K University Hospital King Abdulaziz University Hospital Title: CLINICAL DOCUMENTATION Reviewed by: Date: Department: Unit: Policy Number: HWCPP - 005 Issue Date: DEC 2009 Prepared/Revised
Tidewater Community College Crisis and Emergency Management Plan Appendix F Emergency Operations Plan. Annex 8 Active Threat Response
 Tidewater Community College Crisis and Emergency Management Plan Appendix F Emergency Operations Plan A. Purpose Annex 8 Active Threat Response This Annex has been developed to direct actions in response
Tidewater Community College Crisis and Emergency Management Plan Appendix F Emergency Operations Plan A. Purpose Annex 8 Active Threat Response This Annex has been developed to direct actions in response
Chelan & Douglas County Mass Casualty Incident Management Plan
 Chelan & Douglas County Mass Casualty Incident Management Plan Updated 6/2016 1.0 Purpose 2.0 Scope 3.0 Definitions 4.0 MCI Management Principles 4.1 MCI Emergency Response Standards 4.2 MCI START System
Chelan & Douglas County Mass Casualty Incident Management Plan Updated 6/2016 1.0 Purpose 2.0 Scope 3.0 Definitions 4.0 MCI Management Principles 4.1 MCI Emergency Response Standards 4.2 MCI START System
MASS CASUALTY INCIDENT S.O.P January 15, 2006 Page 1 of 13
 January 15, 2006 Page 1 of 13 INTRODUCTION This plan establishes a standard structure and guidelines for the management of fire and E.M.S. Operations in a multi-casualty emergency medical situation. This
January 15, 2006 Page 1 of 13 INTRODUCTION This plan establishes a standard structure and guidelines for the management of fire and E.M.S. Operations in a multi-casualty emergency medical situation. This
St. Vincent s Health System Page 1 of 11. TITLE: Mass Casualty Plan Code Yellow 12/11/07 12/11/07
 St. Vincent s Health System Page 1 of 11 TITLE: Mass Casualty Plan Code Yellow FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Safety HOSPITAL SHARED POLICY? Yes No DOCUMENT NUMBER: 802 ORIGINATION
St. Vincent s Health System Page 1 of 11 TITLE: Mass Casualty Plan Code Yellow FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Safety HOSPITAL SHARED POLICY? Yes No DOCUMENT NUMBER: 802 ORIGINATION
OVERVIEW OF EMERGENCY PROCEDURES
 OVERVIEW OF EMERGENCY PROCEDURES TYPE: Bolded items have procedures listed below Active Threat/Active Shooter (incl. Hostage, Assault, Murder, Kidnapping) ALICE Bomb Threat Weather (Ice & snow, Flooding,
OVERVIEW OF EMERGENCY PROCEDURES TYPE: Bolded items have procedures listed below Active Threat/Active Shooter (incl. Hostage, Assault, Murder, Kidnapping) ALICE Bomb Threat Weather (Ice & snow, Flooding,
ACTIVE SHOOTER GUIDEBOOK
 ACTIVE SHOOTER GUIDEBOOK HOW TO RESPOND WHAT IS AN ACTIVE SHOOTER? An Active Shooter is an individual actively engaged in killing or attempting to kill people in a confined and populated area; in most
ACTIVE SHOOTER GUIDEBOOK HOW TO RESPOND WHAT IS AN ACTIVE SHOOTER? An Active Shooter is an individual actively engaged in killing or attempting to kill people in a confined and populated area; in most
Hospital Codes. North York General Hospital Student Orientation revised Sept 2013
 Hospital Codes North York General Hospital Student Orientation revised Sept 2013 Attention Attention Code Now what?? Refer to the Code Manual or Intranet Code RED Code WHITE Code PURPLE Code BLACK Code
Hospital Codes North York General Hospital Student Orientation revised Sept 2013 Attention Attention Code Now what?? Refer to the Code Manual or Intranet Code RED Code WHITE Code PURPLE Code BLACK Code
Administrative Procedure
 Administrative Procedure Number: 408 Effective: Interim Supersedes: 07/28/1998 Page: 1 of 7 Subject: EMERGENCY ACTION PLAN 1.0. PURPOSE: To establish procedures for the evacuation of University buildings
Administrative Procedure Number: 408 Effective: Interim Supersedes: 07/28/1998 Page: 1 of 7 Subject: EMERGENCY ACTION PLAN 1.0. PURPOSE: To establish procedures for the evacuation of University buildings
Health, Safety and Environment Management System
 Health, Safety and Environment Management System HSE-PRO-019 Management Procedure Page 1 of 12 Table of Contents 1 Intent... 3 2 Scope... 3 3 Definitions... 3 4 Management Planning... 4 5 Preparedness:
Health, Safety and Environment Management System HSE-PRO-019 Management Procedure Page 1 of 12 Table of Contents 1 Intent... 3 2 Scope... 3 3 Definitions... 3 4 Management Planning... 4 5 Preparedness:
AUSTIN/MOWER COUNTY-WIDE
 PART A - RADIOLOGICAL PROTECTION The purpose of this standard operating guideline is to outline the actions and responsibilities of personnel designated to protect the citizens of Mower County from the
PART A - RADIOLOGICAL PROTECTION The purpose of this standard operating guideline is to outline the actions and responsibilities of personnel designated to protect the citizens of Mower County from the
Programmatic Policy and Procedure
 Page 11 of 7 Programmatic Policy and Procedure Section Sub-section Policy Psychiatric Health Facility (PHF) Crisis and Emergency Response Emergency Facility Evacuation Effective: 11/29/2017 Version: 1.0
Page 11 of 7 Programmatic Policy and Procedure Section Sub-section Policy Psychiatric Health Facility (PHF) Crisis and Emergency Response Emergency Facility Evacuation Effective: 11/29/2017 Version: 1.0
Base Hospital Advanced Life Support Program for Durham Region
 Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
UCL MAJOR INCIDENT TEAM MAJOR INCIDENT PLAN. Managing and Recovering from Major Incidents
 UCL MAJOR INCIDENT TEAM MAJOR INCIDENT PLAN Managing and Recovering from Major Incidents June 2017 MAJOR INCIDENT PLAN - June 2017 Title Primary author (name and title) UCL Major Incident Plan (public
UCL MAJOR INCIDENT TEAM MAJOR INCIDENT PLAN Managing and Recovering from Major Incidents June 2017 MAJOR INCIDENT PLAN - June 2017 Title Primary author (name and title) UCL Major Incident Plan (public
Integrated Safe School Plan. Emergency Team Duties and Supply Lists. Incident Command System
 Emergency Team Duties and Supply Lists Incident Command System The Incident Command System (ICS) is used by first responder and government agencies to manage emergencies, crises, and disasters nationwide.
Emergency Team Duties and Supply Lists Incident Command System The Incident Command System (ICS) is used by first responder and government agencies to manage emergencies, crises, and disasters nationwide.
Emergency Management
 Slide 1 Emergency Management Annual Training Module Welcome to the Emergency Management Learning Module. Emergency Management, Safety and Security are critical areas of operation within Lehigh Valley Health
Slide 1 Emergency Management Annual Training Module Welcome to the Emergency Management Learning Module. Emergency Management, Safety and Security are critical areas of operation within Lehigh Valley Health
Topic 3 Contribute to safe work practices in the workplace 43
 Contents Before you begin vii Topic 1 Follow safe work practices 1 1A Follow workplace policies and procedures for safe work practices 2 1B Identify existing and potential hazards, and report and record
Contents Before you begin vii Topic 1 Follow safe work practices 1 1A Follow workplace policies and procedures for safe work practices 2 1B Identify existing and potential hazards, and report and record
July 1, 2017 EMERGENCY PROCEDURES FOR DEPARTMENT OF ALLIED HEALTH SCIENCES IN BONDURANT HALL
 EMERGENCY PROCEDURES FOR DEPARTMENT OF ALLIED HEALTH SCIENCES IN BONDURANT HALL These procedures set forth the steps to be followed in the event of an emergency. It is important that all employees thoroughly
EMERGENCY PROCEDURES FOR DEPARTMENT OF ALLIED HEALTH SCIENCES IN BONDURANT HALL These procedures set forth the steps to be followed in the event of an emergency. It is important that all employees thoroughly
Critical Incident Policy (Business Continuity Plan)
") Critical Incident Policy (Business Continuity Plan) Lead Reviewed by Staff Reviewed by Students Business Manager N/A N/A Approved by Directors July 2016 Interim Review Full Review TBC TBC Page 1 of 11
Critical Incident Policy (Business Continuity Plan) Lead Reviewed by Staff Reviewed by Students Business Manager N/A N/A Approved by Directors July 2016 Interim Review Full Review TBC TBC Page 1 of 11
Benton Franklin Counties MCI PLAN MASS CASUALTY INCIDENT PLAN
 Benton Franklin Counties MCI PLAN MASS CASUALTY INCIDENT PLAN Adopted January 2000 Revised February 2008 TABLE OF CONTENTS 1.0 Purpose 2.0 Policy 3.0 Definitions 4.0 Organizations Affected 5.0 Standard
Benton Franklin Counties MCI PLAN MASS CASUALTY INCIDENT PLAN Adopted January 2000 Revised February 2008 TABLE OF CONTENTS 1.0 Purpose 2.0 Policy 3.0 Definitions 4.0 Organizations Affected 5.0 Standard
Crisis Response Planning
 Crisis Response Planning Table of Contents Crisis Response Planning... 1 Building your Crisis Response Team (CRT)... 2 Potential Threats... 4 Identifying Potential Partners & Resources... 5 Developing
Crisis Response Planning Table of Contents Crisis Response Planning... 1 Building your Crisis Response Team (CRT)... 2 Potential Threats... 4 Identifying Potential Partners & Resources... 5 Developing
Macfeat Early Childhood Lab School Emergency Plan Withers Building Room 41 Rock Hill, SC (803)
") Emergency Plan Macfeat Early Childhood Lab School Emergency Plan Withers Building Room 41 Rock Hill, SC 29733 (803) 323-2219 The director may be contacted for further information or explanation of this
Emergency Plan Macfeat Early Childhood Lab School Emergency Plan Withers Building Room 41 Rock Hill, SC 29733 (803) 323-2219 The director may be contacted for further information or explanation of this
Inverclyde Royal Hospital Major Incident Plan. May 2016 Version 1.1
 Inverclyde Royal Hospital Major Incident Plan May 2016 Version 1.1 1 One Page Overview - Initial Actions.4 Legal Requirement to Plan...5 Hospital Major Incident Medical Management...5 Governance of the
Inverclyde Royal Hospital Major Incident Plan May 2016 Version 1.1 1 One Page Overview - Initial Actions.4 Legal Requirement to Plan...5 Hospital Major Incident Medical Management...5 Governance of the
NEW EMPLOYEE ORIENTATION SAFTEY QUIZ EMPLOYEE ID#: DEPARTMENT: DATE:
 NEW EMPLOYEE ORIENTATION SAFTEY QUIZ NAME: EMPLOYEE ID#: DEPARTMENT: DATE: Directions: Please read Annual Safety Training and complete Safety Quiz. Sign the acknowledgement form regarding Steward s Privacy
NEW EMPLOYEE ORIENTATION SAFTEY QUIZ NAME: EMPLOYEE ID#: DEPARTMENT: DATE: Directions: Please read Annual Safety Training and complete Safety Quiz. Sign the acknowledgement form regarding Steward s Privacy
TILLAMOOK COUNTY, OREGON EMERGENCY OPERATIONS PLAN ANNEX R EARTHQUAKE & TSUNAMI
 TILLAMOOK COUNTY, OREGON EMERGENCY OPERATIONS PLAN ANNEX R EARTHQUAKE & TSUNAMI I. PURPOSE A. Tillamook coastal communities are at risk to both earthquakes and tsunamis. Tsunamis are sea waves produced
TILLAMOOK COUNTY, OREGON EMERGENCY OPERATIONS PLAN ANNEX R EARTHQUAKE & TSUNAMI I. PURPOSE A. Tillamook coastal communities are at risk to both earthquakes and tsunamis. Tsunamis are sea waves produced
Town of Brookfield, Connecticut Mass Casualty Incident Plan
 Town of Brookfield, Connecticut Mass Casualty Incident Plan 1.0 Definition Of Mass Casualty Incident: A Mass Casualty Incident is an incident having multiple patients that would exceed the amount Brookfield
Town of Brookfield, Connecticut Mass Casualty Incident Plan 1.0 Definition Of Mass Casualty Incident: A Mass Casualty Incident is an incident having multiple patients that would exceed the amount Brookfield
Active Shooter Guideline
 1. Purpose: This procedure establishes guidelines for Monterey County Public Safety Personnel who respond to Active Shooter Incidents (ASI). The goal is to provide effective rescue and treatment procedures,
1. Purpose: This procedure establishes guidelines for Monterey County Public Safety Personnel who respond to Active Shooter Incidents (ASI). The goal is to provide effective rescue and treatment procedures,
TITLE: LOCKDOWN (INTERNAL ACTIVE THREAT) Page 1 of 5 ST. CLOUD HOSPITAL/RIVER CAMPUS
 Page 1 of 5 ST. CLOUD HOSPITAL/RIVER CAMPUS") TITLE: LOCKDOWN (INTERNAL ACTIVE THREAT) Page 1 of 5 CentraCare Health (CCH) adopts the following policy/procedure for: St. Cloud Hospital River Campus Original: 3/12 Minor Revisions: 10/13, 6/15 Full
TITLE: LOCKDOWN (INTERNAL ACTIVE THREAT) Page 1 of 5 CentraCare Health (CCH) adopts the following policy/procedure for: St. Cloud Hospital River Campus Original: 3/12 Minor Revisions: 10/13, 6/15 Full
Canadian Mental Health Association Durham Emergency Preparedness & Business Continuity Plan. June 2015 Revised June 2016
 Canadian Mental Health Association Durham Emergency Preparedness & Business Continuity Plan June 2015 Revised June 2016 0 Contents 1.0 Introduction... 2 2.0 Purpose of Emergency Preparedness and Business
Canadian Mental Health Association Durham Emergency Preparedness & Business Continuity Plan June 2015 Revised June 2016 0 Contents 1.0 Introduction... 2 2.0 Purpose of Emergency Preparedness and Business
LAKE VALLEY FIRE PROTECTION DISTRICT JOB DESCRIPTION Apprentice Firefighter/Paramedic
 LAKE VALLEY FIRE PROTECTION DISTRICT JOB DESCRIPTION Apprentice Firefighter/Paramedic Nature of Agency The is a local government agency created and operated pursuant to California State Law; by the Fire
LAKE VALLEY FIRE PROTECTION DISTRICT JOB DESCRIPTION Apprentice Firefighter/Paramedic Nature of Agency The is a local government agency created and operated pursuant to California State Law; by the Fire
Emergency Management Plan
 Emergency Management Plan Purpose: To develop procedures to follow and lines of responsibility in the event of an emergency situation. To provide information to emergency services so they are aware of
Emergency Management Plan Purpose: To develop procedures to follow and lines of responsibility in the event of an emergency situation. To provide information to emergency services so they are aware of
DISASTER MANAGEMENT PLAN
 DISASTER MANAGEMENT PLAN Purpose This Allen University Disaster Management Plan (AUDMP) will be the basis to establish policies and procedures, which will assure maximum and efficient utilization of all
DISASTER MANAGEMENT PLAN Purpose This Allen University Disaster Management Plan (AUDMP) will be the basis to establish policies and procedures, which will assure maximum and efficient utilization of all
Emergency Preparedness and Response Plan
 2014-2015 Emergency Preparedness and Response Plan Charlton Heston Academy (CHA) 1350 N. St. Helen Rd. St. Helen, Michigan 48656 989-632-3390 CHA Emergency Response Team David Patterson, Superintendent-313-622-9173
2014-2015 Emergency Preparedness and Response Plan Charlton Heston Academy (CHA) 1350 N. St. Helen Rd. St. Helen, Michigan 48656 989-632-3390 CHA Emergency Response Team David Patterson, Superintendent-313-622-9173
(Name of Organization) Model Hospital Mutual Aid Memorandum of Understanding 1
 Model Hospital Mutual Aid Memorandum of Understanding 1") (Name of Organization) Model Hospital Mutual Aid Memorandum of Understanding 1 I. Introduction and Background (month, day, year) As in other parts of the nation, (name of city, county, and or state served
(Name of Organization) Model Hospital Mutual Aid Memorandum of Understanding 1 I. Introduction and Background (month, day, year) As in other parts of the nation, (name of city, county, and or state served
Mission. Directions. Objectives
 Incident Response Guide: Severe Weather with Warning Mission To provide for the safety of patients, visitors, and staff during a severe weather emergency such as ice storms, snowstorms, rain, flooding,
Incident Response Guide: Severe Weather with Warning Mission To provide for the safety of patients, visitors, and staff during a severe weather emergency such as ice storms, snowstorms, rain, flooding,
Active Threat Procedure - Facility
 Active Threat Procedure - Facility Containment Activated in response to an external active threat In the event that an external active threat is identified by staff, patients and/or visitors, call 911.
Active Threat Procedure - Facility Containment Activated in response to an external active threat In the event that an external active threat is identified by staff, patients and/or visitors, call 911.
Emergency Management Resource Guide. Kentucky Center for School Safety. School Plan
 Emergency Management Resource Guide Kentucky Center for School Safety 51 Checklist for ning Under the direction of the principal, each school is to complete the following according to its unique needs
Emergency Management Resource Guide Kentucky Center for School Safety 51 Checklist for ning Under the direction of the principal, each school is to complete the following according to its unique needs
Nature Alliance Family Day Care Service
 Nature Alliance Family Day Care Service Serious Incidents, Emergencies & Evacuation Policy POLICY IN THIS SECTION AS REQUIRED BY Education and Care Services National Law (WA) Act 2012: Section 169(5);
Nature Alliance Family Day Care Service Serious Incidents, Emergencies & Evacuation Policy POLICY IN THIS SECTION AS REQUIRED BY Education and Care Services National Law (WA) Act 2012: Section 169(5);
Required Contingency Plans for CMHCM Providers
 Required Contingency Plans for CMHCM Providers 1. Medical Emergency 2. Missing Consumer 3. Power Outage 4. Water Shortage 5. Fire 6. Bad Weather 7. Chemical/Shelter in Place 8. Choking 9. Death of Consumer
Required Contingency Plans for CMHCM Providers 1. Medical Emergency 2. Missing Consumer 3. Power Outage 4. Water Shortage 5. Fire 6. Bad Weather 7. Chemical/Shelter in Place 8. Choking 9. Death of Consumer
Emergency Management Policy and Procedures
 Emergency Management Policy and Procedures Name of Child Care Centre: Immanuel Child Care Centre Date Policy and Procedures Established: July 1, 2017 Date Policy and Procedures Updated: July 14, 2017 Purpose
Emergency Management Policy and Procedures Name of Child Care Centre: Immanuel Child Care Centre Date Policy and Procedures Established: July 1, 2017 Date Policy and Procedures Updated: July 14, 2017 Purpose
Dealing with Emergencies & Evacuation
 1 Dealing with Emergencies & Evacuation Purpose The Education and Care Services National Regulations require John Street to have a policy on Emergency Evacuation. To provide a policy through which appropriate
1 Dealing with Emergencies & Evacuation Purpose The Education and Care Services National Regulations require John Street to have a policy on Emergency Evacuation. To provide a policy through which appropriate
UNIVERSITY OF TOLEDO
 UNIVERSITY OF TOLEDO SUBJECT: CODE VIOLET VIOLENT SITUATION Procedure No: EP-08-015 PROCEDURE STATEMENT Code Violet will be initiated for serious situations involving any individual(s) exhibiting or threatening
UNIVERSITY OF TOLEDO SUBJECT: CODE VIOLET VIOLENT SITUATION Procedure No: EP-08-015 PROCEDURE STATEMENT Code Violet will be initiated for serious situations involving any individual(s) exhibiting or threatening
Emergency and Evacuation Procedures CO 500.4:
 Emergency and Evacuation Procedures CO 500.4: Purpose The Morehouse College Emergency Action Plan provides an organizational structure capable of responding to on-campus emergencies ranging in complexity.
Emergency and Evacuation Procedures CO 500.4: Purpose The Morehouse College Emergency Action Plan provides an organizational structure capable of responding to on-campus emergencies ranging in complexity.
CITY OF SAULT STE. MARIE EMERGENCY RESPONSE PLAN
 CITY OF SAULT STE. MARIE EMERGENCY RESPONSE PLAN 12/13/2017 Fire Service, Emergency Management Division Schedule A to By-law 2017-236 Page 1 CONTENTS 1. INTRODUCTION... 3 2. PURPOSE... 3 3. SCOPE... 3
CITY OF SAULT STE. MARIE EMERGENCY RESPONSE PLAN 12/13/2017 Fire Service, Emergency Management Division Schedule A to By-law 2017-236 Page 1 CONTENTS 1. INTRODUCTION... 3 2. PURPOSE... 3 3. SCOPE... 3
CHILD CARE FACILITIES INTRODUCTION TO THE DISASTER PLAN
 CHILD CARE FACILITIES INTRODUCTION TO THE DISASTER PLAN Disaster Plan Information Procedures Protocols To allow your facility to respond to an emergency or disaster in an effective, coordinated & integrated
CHILD CARE FACILITIES INTRODUCTION TO THE DISASTER PLAN Disaster Plan Information Procedures Protocols To allow your facility to respond to an emergency or disaster in an effective, coordinated & integrated
Centre for Education Clinical Experience at Western Health Sunbury Day Hospital
 Centre for Education Clinical Experience at Western Health Information for Students and Clinical Facilitators Contents Welcome to Western Health... 2 Aims of Clinical Experience at Western Health... 3
Centre for Education Clinical Experience at Western Health Information for Students and Clinical Facilitators Contents Welcome to Western Health... 2 Aims of Clinical Experience at Western Health... 3
EMERGENCY MANAGEMENT
 EMERGENCY MANAGEMENT The purpose of this policy is to provide clear direction for staff and licensees to follow in dealing with emergency situations. The procedures set out steps for staff to follow to
EMERGENCY MANAGEMENT The purpose of this policy is to provide clear direction for staff and licensees to follow in dealing with emergency situations. The procedures set out steps for staff to follow to
DANGEROUS/THREATENING PERSON PROCEDURES Code Blue
 DANGEROUS/THREATENING PERSON PROCEDURES Code Blue We have established the following procedure to be followed by employees and visitors in the event a dangerous/threatening person enters the facility. The
DANGEROUS/THREATENING PERSON PROCEDURES Code Blue We have established the following procedure to be followed by employees and visitors in the event a dangerous/threatening person enters the facility. The
University Crisis Management. July 2014
 University Crisis Management July 2014 The Crisis Management document can be used as a reference for integrating internal plans into the University s strategic operational plans, it does not replace departments
University Crisis Management July 2014 The Crisis Management document can be used as a reference for integrating internal plans into the University s strategic operational plans, it does not replace departments
Emergency & Critical Incident Policy
 Emergency & Critical Incident Policy 1. Preamble Emergency and Critical Incident Management is the management of emergencies and critical incidents from a human, hazard identification, and risk assessment
Emergency & Critical Incident Policy 1. Preamble Emergency and Critical Incident Management is the management of emergencies and critical incidents from a human, hazard identification, and risk assessment
Emergency Management Policy and Procedures
 Purpose YMCA of OAKVILLE Emergency Management Policy and Procedures The purpose of this policy is to provide clear direction for staff and licensees to follow and deal with emergency situations. The procedures
Purpose YMCA of OAKVILLE Emergency Management Policy and Procedures The purpose of this policy is to provide clear direction for staff and licensees to follow and deal with emergency situations. The procedures
Kings Crisis and Critical Incident Management Policy
 Kings Crisis and Critical Incident Management Policy All Kings policies will be ratified by the Board of Directors and signed by the Chairperson. Each policy will be co-signed by the principal of each
Kings Crisis and Critical Incident Management Policy All Kings policies will be ratified by the Board of Directors and signed by the Chairperson. Each policy will be co-signed by the principal of each
INCIDENT COMMANDER. Date: Start: End: Position Assigned to: Signature: Initial: Hospital Command Center (HCC) Location: Telephone:
 Location: Telephone:") COMMAND INCIDENT COMMANDER Mission: Organize and direct the Hospital Command Center (HCC). Give overall strategic direction for hospital incident management and support activities, including emergency
COMMAND INCIDENT COMMANDER Mission: Organize and direct the Hospital Command Center (HCC). Give overall strategic direction for hospital incident management and support activities, including emergency
EMERGENCY RESPONSE FOR SCHOOLS Checklists
 EMERGENCY RESPONSE FOR SCHOOLS Checklists For: Lafayette Parish School System Date: July 24, 2009 According to the Federal Emergency Management Agency (FEMA), there are a number of phases included in the
EMERGENCY RESPONSE FOR SCHOOLS Checklists For: Lafayette Parish School System Date: July 24, 2009 According to the Federal Emergency Management Agency (FEMA), there are a number of phases included in the
2017 Annual Mandatory Education. Sarasota Memorial Health Care System
 2017 Annual Mandatory Education Sarasota Memorial Health Care System Self-Study Module Questionnaire The goals of Annual Mandatory Education are to provide employees with information pertinent to their
2017 Annual Mandatory Education Sarasota Memorial Health Care System Self-Study Module Questionnaire The goals of Annual Mandatory Education are to provide employees with information pertinent to their
CODE ORANGE. MASS CASUALTY INCIDENT (MCI) RESPONSE PLAN Covenant Health Edmonton Acute Care Hospitals
 RESPONSE PLAN Covenant Health Edmonton Acute Care Hospitals") Code Orange 1 CODE ORANGE MASS CASUALTY INCIDENT (MCI) RESPONSE PLAN Covenant Health Edmonton Acute Care Hospitals This document contains information specific to Grey Nuns Hospital (page 14) and information
Code Orange 1 CODE ORANGE MASS CASUALTY INCIDENT (MCI) RESPONSE PLAN Covenant Health Edmonton Acute Care Hospitals This document contains information specific to Grey Nuns Hospital (page 14) and information