ADULT NASOGASTRIC FEEDING TUBE INSERTION AND MANAGEMENT. Type: Clinical Guideline Register No: Status: Public
|
|
|
- Julian Davidson
- 5 years ago
- Views:
Transcription
1 ADULT NASOGASTRIC FEEDING TUBE INSERTION AND MANAGEMENT Type: Clinical Guideline Register No: Status: Public Developed in response to: Best practice: NHSI Patient Safety Alert (NHS/PSA/RE/2016/006) CQC Fundamental Standard: 11, 12, 14, 17 Consulted With: Post/Committee/Group: Date: Dr S Webster Nutrition Lead, Consultant Gastroenterologist Dr A Lwin Consultant, ITU Marie Hellon Nutrition CNS Suzanne Slaughter Advanced Specialist Dietitian Andrea Francis Clinical Lead for Radiology Dan Spooner Chair of Nutrition Steering Group Professionally Approved By: Dr Ellie Makings Medical Director Version Number 4.0 Issuing Directorate Medicine Ratified by: Document Ratification Group Ratified on: 22 nd November 2017 Trust Executive Sign Off Date December 2017/ January 2018 Implementation Date 6 th December 2017 Next Review Date October 2020 Author/Contact for Information Marie Hellon, Nutrition CNS Policy to be followed by (target All clinical staff staff) Distribution Method Intranet, Website Related Trust Policies (to be read in conjunction with) Incident Policy Consent to examination or treatment Clinical record keeping Mental Capacity Act (2005) Policy for standard infection control procedures Guideline for Passing a Naso/oro-gastric tube and intermittent tube feeding for Children (10 days-16 years) Dementia Policy Nasal Retention Devices Adult Clinical Guidelines Restrictive Interventions Document Review History: Version No: Reviewed by: Active Date: 1.1 Angela Wade, Rachael Frost, Cathy Powis 26 September Dr L Westcott, Dr R Dobson 28th April Sibo Maponga (Nutrition CNS) November Sibo Maponga (Nutrition CNS) 15 April Marie Hellon (nutrition CNS) 6 th December
2 Contents 1.0 Purpose 2.0 Scope 3.0 Definitions 3.1 Nasogastric feeding tube (NGT) 3.2 Wide bore tubes or gastric drainage tubes (Ryles) 3.3 CE marked ph paper 4.0 Roles and responsibilities 5.0 Pre-procedure 5.1 Decision making 5.2 Indications for NGT feeding 5.3 Contraindications for NGT feeding 5.4 Consent 5.5 Equipment 6.0 Insertion procedure 7.0 Post procedure 7.1 Initial confirmation of NGT position following insertion 7.2 First line testing: ph testing of NGT aspirate 7.3 Second line testing: Chest Radiography 7.4 Methods that must not be used 8.0 On-going management of NGT in situ 8.1 Regular tube position checks 8.2 Positioning of the patient 8.3 Flushing 8.4 Managing a blocked NGT 8.5 Inadvertent NGT removal 8.6 Transfer of care to the community setting 9.0 Education and training 2
3 10.0 Audit and monitoring 11.0 Communication and implementation 12.0 References 13.0 Appendices Appendix 1 Decision tree for nasogastric tube placement checks in ADULTS Appendix 2 Recommended procedure for checking the position of NG feeding tubes Appendix 3 Additional guidelines of nasogastric tube placement Appendix 4 Competency for nasogastric tube (NG) insertion and management Appendix 5 NG tube insertion and management form Appendix 6 NG tube position check record Appendix 7 BAPEN nasogastric tube insertion decision tree 3
4 1.0 Purpose 1.1 This guideline has been developed to support clinical staff in the correct insertion of nasogastric feeding tubes (NGT) and in the confirmation of tube placement to reduce risk to patients in line with current best practice, clinical governance standards, and National Patient Safety Agency (NPSA) Patient Safety Alerts (NHS/PSA/RE/2016/006). It aims to promote a clear, consistent and evidenced based approach to the safe insertion, care and management of an NGT in adult patients. 2.0 Scope 2.1 This guideline applies to the insertion and management of an NGT in adult patients admitted to the Trust. 2.2 Patients in a critical care setting, e.g. general Intensive care, Burns Centre, may have additional needs beyond the scope of this guideline. 2.3 It is the responsibility of the Critical care unit to ensure that all care and equipment for the continuity of patient care is compliant to practice, Trust policies and equipment available on general adult care wards at time of patient transfer. 2.4 This guideline does not apply to paediatric patients (under age of 16 years old). 3.0 Definitions 3.1 Nasogastric feeding tube (NGT) An NGT is a flexible tube that can be inserted trans-nasally into the stomach. It is commonly used for delivery of feed, fluids, medication, or drainage of gastric contents For a NGT to be fit for the purpose of feeding, the NGT is required to be NPSA compliant, i.e.: Fully radio-opaque throughout its length; Externally visible length markings. Other features will include: EnFit compliant; Can remain in situ for up to days (dependant on manufactures instructions); Made of Polyurethane; Will often have a guidewire throughout its length to aid insertion; Size 6-12fg (recommended size for feeding 8fg). 3.2 Wide bore tubes or gastric drainage tubes (Ryles) Wide bore gastric drainage tubes (Ryle s tubes) are usually made of polyvinylchloride (PVC) and may be used for a maximum of 7-10 days (as per 4
5 manufacturers instructions) size of tubes start at 12fg. These tubes are not NPSA compliant, therefore must not be used for the purpose of feeding (NPSA 002, 2011) These tubes may also be associated with the following complications: Rhinitis; Pharyngitis; Oesophageal ulceration; Gastric erosion; Increased tendency for reflux; Patient discomfort; Difficulty swallowing PVC material has the risk of leaching plasticizers within the tube causing it to become brittle and increasing the risk of gastric erosions and ulceration. 3.3 CE marked ph paper ph indicator paper must be CE marked and intended by the manufacturer to test human gastric aspirate. 4.0 Roles and responsibilities 4.1 Chief Executive The Chief Executive is responsible for ensuring that systems are in place to ensure the safe and effective placement and management of an NGT. This responsibility is delegated to the Medical Director. 4.2 Medical Director The Medical Director is responsible for ensuring compliance with systems in place to ensure the safe and effective placement and management of an NGT. 4.3 Nutrition Lead The Nutrition Lead is responsible for approving the document and monitoring clinical effectiveness. 4.4 Consultants Consultants are responsible for the everyday clinical care of their patients including decisions about NGT insertion and use They are also responsible for the dissemination of this policy within their area of responsibility. 5
6 4.5 Nutrition Clinical Nurse Specialist The Nutrition CNS will provide training in the insertion of NGT, ensure that all policies and procedures for the placement and management of enteral feed equipment are up to date and evidence based, and facilitate decisions regarding artificial nutrition in complex individual cases. 4.6 Dietitians Dietitians are responsible for the assessment, guidance and prescription of the most clinically appropriate feeding regimen for the patient and on-going dietetic assessment and review of the patient. 4.7 All other Clinical Staff All healthcare professionals must adhere to the principles described in this policy A decision to insert an NGT for the purpose of feeding and/or administration of medications must be made and documented by a senior member of the medical team responsible for the patients care Only staff with the relevant skills and expertise should insert and confirm the placement of an NGT. 4.8 Ward Sister / Charge Nurse Senior ward nurses should identify which members of staff are trained and competent to undertake insertion and management of an NGT They should monitor standards of practice in their environment in relation to an NGT. An up to date record is to be kept in the clinical area to evidence that training and competencies have been completed. 4.9 Radiographer When an NGT Chest X-ray is requested, radiographers should ensure they are able to justify the examination and provide an image to clearly demonstrate the presence and position of the NGT. 5.0 Pre-procedure 5.1 Decision making A decision to insert an NGT for the purpose of feeding and/or administration of medications should be made by a senior doctor responsible for the patient s care and in the case of complex, vulnerable patients should involve the multidisciplinary team. This decision should only be made following careful assessment of the risks and benefits, with the patient s best interests at the centre of this process. Consideration should be given to the patient s previously expressed wishes, an Advanced Care Plan, family involvement or an independent advocate. 6
7 5.1.2 Once a decision has been made to insert an NGT an entry must be made in the medical notes, it must be signed, dated and timed, clearly documenting the purpose of the NGT, e.g. administration of medication only, for nutrition, hydration & medication. In complex cases where a timed trial is appropriate for nutrition, a review date must be set at the start of the trial Prior to insertion the rationale for insertion of an NGT must be considered and responses to the following documented on the NGT Insertion & Management form (Appendix 5): Is NGT feeding the right decision for this patient? Is this the right time to place the NGT and is appropriate equipment available? Is there sufficient expertise available at this time to test for safe placement? An NGT should only be placed when there is experienced support available for insertion and confirmation of the NGT position. If there is not sufficient, experienced support available (for example at night) then, unless clinically urgent, placement should be delayed until that support is available. Rationale for any decisions made should be recorded in the patients medical notes Where longer term enteral feeding is required (> 4 6 Weeks) consideration should be given to gastrostomy placement Ventilated patients may have the NGT inserted under direct laryngoscopy. All critical care/ventilated patients have X-ray to confirm initial NGT placement. 5.2 Indications for NGT feeding NGT feeding is the most common method of providing short-term artificial nutrition support in the acute setting. A decision to feed via an NGT should be a multidisciplinary one NGT feeding should be considered for patients who have a functioning gastrointestinal (GI) tract and require short-term tube feeding (up to 4-6 weeks) The insertion of an NGT facilitates access to the GI tract, enabling nutrition and medicines to be administered whilst other assessments or therapies are being considered or carried out. 5.3 Contraindications for NGT feeding This list is not definitive. Some patients may require referral to specialist teams, e.g. ENT, Gastroenterology or Interventional Radiology for further assessment/advice/assistance with the procedure. An NGT may be contraindicated in the following conditions: Non-functioning GI tract e.g. ileus; Maxillo-facial disorders/surgery/trauma; Laryngectomy; Trachoesophageal fistula; Oesophageal/Pharyngeal pouch; 7
8 Oesophageal Stricture or other Oesophageal abnormalities; Oesophageal tumours or Oesophageal surgery; Actively bleeding Oesophageal or gastric varices; Gastric outflow obstruction; Basal skull fracture; Nasal CPAP (Continuous Positive Airway Pressure) can be considered for enteral feeding with close observation due to the increased risk of reflux aspiration - NJ feeding should be considered as a safer option; Unstable Cervical Spinal Injuries; Choana atresia. 5.4 Consent Informed verbal consent must be sought prior to the insertion of the NGT. A clear explanation of the procedure should be given and verbal consent gained. If the patient is unable to respond verbally, other means of communication should be sought If the patient lacks mental capacity, staff should refer to the Trust s Consent to examination or treatment Policy and Mental Capacity Act (2005) Policy. A Mental Capacity Assessment (MCA) should be completed in full and a copy submitted to the adult safeguarding team. 5.5 Equipment Plastic apron and gloves; Radio-opaque NGT with externally visible length markings; CE marked for human gastric aspirate ph indicator strips/paper with a range of 0 to 6 and 0.5 gradations; Water based lubricating jelly; Freshly drawn water to flush the tube once NGT position has been confirmed; Purple Enteral EnFit Syringe; Receiver/kidney bowl; Glass of water and a straw (only if the patient has a safe swallow reflex); 1 st line securement - cheek dressing to secure tube (Grip Lok dressing); 2 nd line securement - consider Nasal Retention Device (refer to Guideline No ); NG Tube Insertion and Management form (Appendix 5) 8
9 6.0 Insertion procedure Action Refer to medical notes to ensure a clear purpose for the NGT has been documented. Prior to insertion of the NGT refer to notes to check for any potential complications e.g. previous nasal trauma, disease, surgery or congenital abnormalities and any required investigations e.g. blood clotting tests. Prior to insertion, check the NG tube is patent with a 50 ml sterile bladder syringe filled with air. Explain the procedure and associated risks to the patient. Where the patient demonstrates lack of capacity - a best interest decision must be documented in the medical notes and a mental capacity assessment completed. Arrange a signal so that the patient can communicate with the nurse during the procedure e.g. raise a hand. Wash hands and put on non-sterile gloves and an apron. Assist the patient in a semi-upright position. Support the head in a slightly forward position. Check that the nostrils are patent by completing The Sniff Test, asking the patient to cover on nostril and sniff through the alternative nostril. Repeat with the other side. Ask the patient to clean nose by blowing prior to placement/if patient unable to do this - please assist as required. Alternate nostrils if replacing a tube. Check packing prior to opening. Noting the description of the device, size expiry date, Lot Number. Unpack the tube, observe full length of NGT observing for any damage and that the NGT is not kinked. Gently manipulate the guidewire to ensure it can move freely ensure the guidewire is secured back into place before insertion. Rationale To ensure the appropriate tube is inserted to meet the patient s needs and clinical condition. To insert the NGT safely and minimise complications. To ensure the NG tube is patent and fit for purpose. To ensure that the patient understands and is able to give consent and co-operate with the procedure. To demonstrate compliance with current legislation, evidence of wider consultation for the best interest decision. Helps to alleviate fear as the patient has some control over the procedure. Where possible also have a second health care professional present for patient support. Adherence to local Infection Prevention policy. Assists swallowing and helps prevent tracheal placement if the swallow is compromised. Patient comfort. Helps identify potential obstruction. Prevents nasal irritation and potential ulceration. Ensuring the NGT is not damaged, that the appropriate NGT is to be inserted for purpose. Traceability of the device. The size of a NGT for enteral feeding should be between 6-12fg. Facilitates smooth insertion of NGT. 9
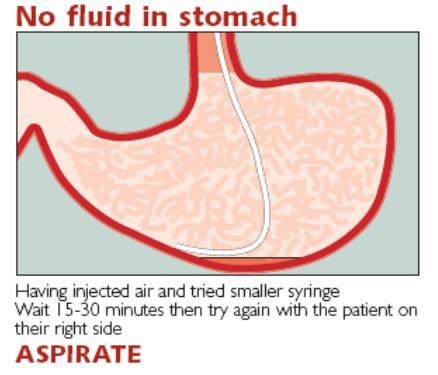
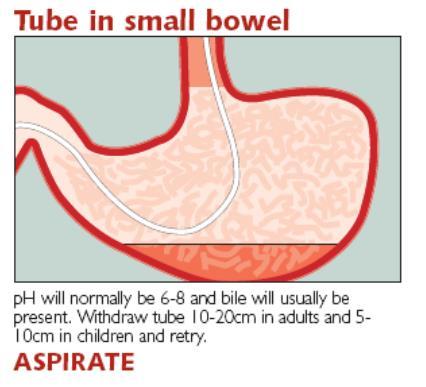
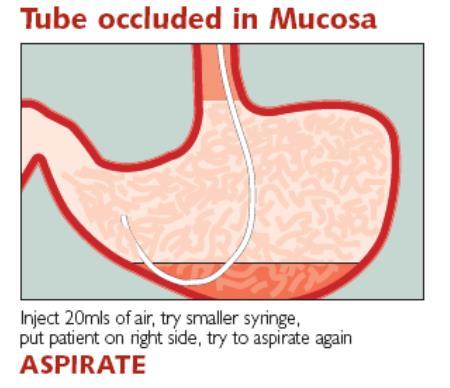
10 Estimate length of tube using NEX measurement - Nose, Earlobe & Xiphisternum: Place tube tip to the tip of the nose, extend to ear lobe & down to the Xiphisternum; Note the measurement at the point of the Xiphisternum. Lubricate the tube. Use a thin coating of water based jelly (please refer to manufactures guidelines). Insert the tip of the tube into the chosen nostril, advancing it horizontally and gently along the floor of the nostril; parallel to the nasal septum, to the nasopharynx and then oropharynx. At this point ask the patient to swallow fluid if it is safe and they have capacity to follow instruction. In the absence of a safe swallow ask to them to try a dry swallow. A chin tuck may also assist. Continue advancement to NEX measurement. If resistance is felt, stop the procedure pull back slightly before attempting to re-insert (check the patients mouth in case the tube has coiled). If the patient sneezes or coughs pull back slightly on the NGT wait until the patient is settled. If the patient becomes distressed it is advised to stop NGT insertion and seek specialist advice. A maximum of 3 attempts should be made at one time to insert the NGT - PLEASE SEEK SENIOR/SPECIALIST ADVICE. Once the NGT has been inserted: Leave the guide wire in place (do not remove); Attach a 60ml Enteral EnFit syringe to the NGT end; Flush NGT with 10ml of air to clear the tip of any debris; Then pull back on the syringe to withdraw a gastric aspirate. To gain an estimated measurement- to ensure that the NGT tip will reach the patient s stomach. Please note that the NEX measurement is only an estimation, to gain a gastric aspirate you may need to adjust the position by 10% by further advancing or pulling back of the NGT. Facilitates easy passage of the tube. To achieve insertion of tube into the stomach. To minimise any risk of trauma or distress to the patient. To assist intubation into the oesophagus and reduce the risk of tracheal intubation. To minimise any risk of trauma or distress to the patient. To confirm position of NGT in the stomach and that it is safe to feed/administer medication 10
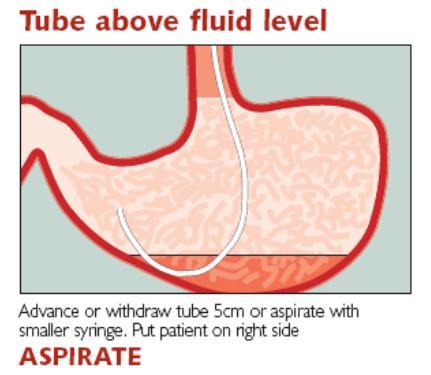
11 Confirm the position of the NGT by testing the aspirate, using ph strips that are CE marked for human gastric aspirate. The ph reading must be 5.5 or below to confirm the position of NGT. When an aspirate of 5.5 or below is obtained tube position is confirmed and it is safe to remove the guidewire and administer medication/feed. If difficulty is found in obtaining a gastric aspirate follow manufactures advice. To gain an aspirate (check for a aspirate after each technique is attempted): Check mouth for coiling of NGT; Position patient on their side; Re-flush the tube with air to dislodge debris from insertion; If patient has a safe swallow offer a drink then wait minutes and re-check aspirate; Advance or withdraw NGT by cm. Refer to Appendix 1 (NPAS decision tree for NGT placement checks in adults). If an aspirate cannot be obtained then request an X-ray to confirm position of NGT. State clearly on the request that attempts have been made to gain an aspirate or that the ph is more than 5.5 NB: do not remove the guidewire until the position of the NGT has been confirmed. Fix the NGT to the patient s cheek using 1 st line securement - Grip Lok dressing. 2 nd line securement - Nasal retention devices may be suitable for certain patients. Refer to local guideline No.16026, full patient assessment is required with the lead clinician and MDT agreement for the use of this securement device. Document in the NG Tube Insertion & Management form (Appendix 5): Type of tube, size and lot number; Name of person inserting the tube; Date and time of insertion; The cm measurement on the tube at the exit point from the nostril; To confirm position of NGT in the stomach and that it is safe to feed/administer medication. To confirm position of NGT in the stomach and that it is safe to administer medication/feed. An X-ray is the final option to confirm the position of the NGT. To reduce the risk of tube misplacement. Securing the NGT to the cheek rather than the nose will reduce the risk of nasal erosion/ulceration. To reduce the risk of repeated NGT displacement. Repeated NGT displacement may prevent the patient receiving adequate nutrition, hydration and medications and cause increased risk of distress & discomfort from repeated attempts to insert another NGT. Tracking and traceability; For audit and training requirements; Allows the user to assess whether the tube has changed position; 11
12 The ph value (if gastric aspirate obtained); Which nostril used; Ease of insertion; The Doctor reviewing the X-ray should record the result on the NG tube Insertion and Management form and in the patient s Medical notes (entry should be signed, dated and timed). Allows staff to compare with previous readings; Prevents trauma caused by using the same nostril repeatedly; Useful information for other healthcare professionals inserting subsequent tubes; To identify whether the tube is safe for use and for tracking and accountability. 7.0 Post procedure 7.1 Initial confirmation of NGT position following insertion The ideal position for the NGT is in the stomach below the diaphragm. The position of the NGT must be checked to confirm it is in the stomach. The procedure is summarised in the flow charts and guidance on ph testing in Appendices 1 and 2. Further information is available in the NPSA Supporting information document An NGT must not be flushed or liquid/feed introduced through the tube following initial placement, until the tube tip is confirmed to be in the stomach by ph testing or X-ray. 7.2 First line testing: ph testing of NGT aspirate Aspirate 2ml of stomach content using a sterile syringe and test using CE marked for human gastric aspirate ph paper. A ph of 5.5 or below can be considered gastric in origin Only if a ph of 5.5 or below has been obtained and documented or the correct placement confirmed and documented by a competent person through X-ray can an NGT be used Initial and on-going ph checks must be documented on the NG Tube Insertion & Management form and the NG Tube Position Check Record (Appendices 5 & 6) which should be kept at the patient s bedside ph readings should be 5.5 or below for feeding to commence safely. However, the NPSA has identified the potential difficulty in differentiating ph readings using between ph 5 and 6. Therefore, any readings between ph 5 and 6 should have a second check undertaken by a registered nurse, who has completed their competency assessment Consideration should be given to the impact of medication such as antacids, H2 antagonists like Ranitidine or Proton pump inhibitors like Lansopazole & Omeprazole and the frequency of feeds on stomach ph Refer to Appendices 1, 2 & 3 for further advice on attempting to gain aspirate 12
13 7.2.7 Any staff still having difficulty obtaining an aspirate must request help from a more experienced member of staff. 7.3 Second line testing: Chest Radiography If staff are unable to obtain aspirate or ph indicator paper fails to confirm the location of the NGT in the stomach, then a request for an X-ray of the chest should be made. The request form must clearly state that the purpose of the X-ray is to establish the position of the NGT and which type of NGT tube was inserted. The request should also state the result of gastric aspiration whether aspirate could be obtained and if so what ph it was. This helps radiology staff to determine if radiation exposure is justified. If a fine bore tube is used, the guide wire must be left in place until after imaging and interpretation of the resultant image X-rays must only be interpreted and NGT position confirmed by a doctor assessed as competent to do so. The doctor must document in the patient s medical notes that the NGT position has been confirmed as safe to use. This entry should be signed, dated and timed. In addition the NG Tube Insertion & Management form will require updating and signing If there is any difficulty in interpretation of the X-ray, the advice of a radiologist should be sought. The radiologist must document the position of the NGT and tip and whether it is safe to use the NGT If the NGT is not in the correct position, it must be repositioned and further checks carried out or removed and a new NGT inserted If there is any relevant past medical history such as Hiatus Hernia or previous gastric surgery, staff should consider using X-ray after discussion with the senior medical team. 7.4 Methods that must not be used: Auscultation of air insufflated through the tube ( whoosh test ); Testing aspirate with Blue Litmus paper; Presence / absence of respiratory distress; Monitoring bubbling at the end of the tube; Observing the appearance of the aspirate. 8.0 On-going management of NGT in situ 8.1 Regular tube position checks Prior to use of an NGT the healthcare professional must re-assess the risk to the patient and ensure the tube is still correctly positioned. NGT position should be checked: At least once daily during continuous (pump) feeds; at the end of the rest period before starting the next feed; 13
14 Before all administration of medication or flushes when the patient is not currently receiving continuous feed; Before administering each bolus feed; Following episodes of vomiting/retching/coughing or suction (the absence of coughing does not rule out misplacement or migration); If the patient complains of a change in level of discomfort; If the patient develops difficulty in breathing during administration of feeds, medicines or flushes; In the presence of any new or unexplained respiratory symptoms or reduction in oxygen saturation; Following any evidence or suggestion of tube displacement (e.g. loose tape or portion of visible tube appears longer) Where feed/medication has already passed through the tube wait a minimum of an hour (without any further feeding) prior to testing of gastric aspirate using ph paper In some situations, such as when patients are fed continuously, when they are treated with acid-reducing medication and when medications are given frequently via the NGT, it may not be possible to obtain aspirate with a ph of 5.5 or below, and daily X-rays are not practical or safe. In circumstances where the initial placement was appropriately confirmed, and there is no reason to suspect displacement (i.e. no vomiting, retching, suction or coughing spasms and no unexplained respiratory symptoms) the only practical method of determining if the NGT remains correctly placed is through external observation. This should include: confirmation that the length of the external tube remains identical to that recorded initially in the patient s notes; confirmation that fixation tapes or plasters have not moved or worked loose; This confirmation should be clearly documented on the NG Tube Position Check Record (Appendix 6) Tube length should be recorded on a daily basis and prior to administration of any liquid via the NGT on the bedside chart (Appendix 6). If there is any indication that the length has changed, appropriate action should be taken to assess tube tip position prior to using the NGT If there is evidence that the tube has become displaced, for whatever reason, then only checking the position at the nose would be inappropriate as it could be coiled in the back of the mouth, so in this circumstance second line testing through X-ray, or removal of the tube if seen to be coiled in the mouth, is appropriate When requesting an X-ray to confirm the position of an existing NGT, the clinician must clearly document that the guidewire is not in situ. This will enable the Radiographer to determine whether or not a portrait image is required to enable the NGT tip to be demonstrated. 14
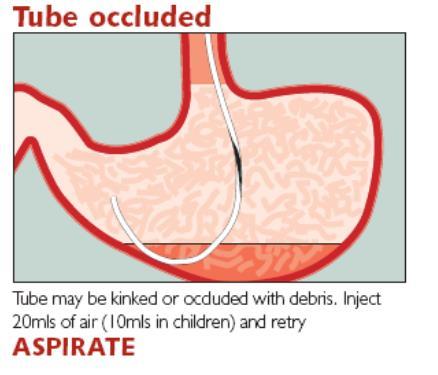
15 8.2 Positioning of the patient The risk of oesophageal reflux and aspiration during enteral feeding can be minimised by: Elevating the head of the bed at a minimum of 30 degrees during feeding and for at least an hour after feeding; Sitting the patient in a chair whilst feed is running. 8.3 Flushing Tubes should be flushed with 50ml water before and after the administration of medication. If more than one medicine is to be administered, flush between each one with at least 10ml of water to ensure that the drug is cleared from the tube. Liaise with Pharmacy as to the most suitable form of medications to administer via an NGT. If the patient is on a fluid restriction, consult the dietitian and pharmacist about the quantity of water to be given before and after medication. Tubes should be flushed with at least 50ml water at the start and finish of the administration of each feed. All fluid given as a flush must be clearly documented on the patient s fluid balance chart. 8.4 Managing a blocked NGT Possible causes of a blocked NGT are: Possible causes Not flushing or inadequate flushing after feed and medication. Unsuitable medicine preparations for giving via an NGT, e.g. large particles, viscous liquids. Multiple medications being given together without a flush in between each drug. Kinked NGT Intervention Flush with 50ml water before and after feed or medication. Review medication and consider alternative medication. All medication given via NG tube should be in either liquid or dissolvable form if possible. Liaise with pharmacist. All medications should be given separately, flushing about 10ml of water in between each medication. NGT may be kinked in the stomach, pull back slightly (1-2cm) and confirm NGT position. The new measurement confirming NGT Position including ph of gastric aspirate should be recorded and actions documented Flushing with water can shift most blockages. Check length marking to confirm NGT position has not changed before flushing with any fluid to unblock the tube. Use a 60ml enteral EnFit syringe; 15
16 Prime with 20-30mls warm water, carbonated (sparkling) water or soda water (do not use Coca-Cola/Lucozade/Pineapple juice or anything other than warm water, carbonated water or soda water); Flush using a pumping action; Squeeze along the tube, and then retry flushing; Once cleared, flush thoroughly; If the NGT remains blocked remove it and insert a new one. 8.5 Inadvertent NGT removal In the case of repeated NGT displacement consider use of mittens or a nasal retention device. Please refer to the following guidlines: Mittens/DOLS Restrictive Interventions policy No.15005, Nasal Retention Device Adult Guidelines No Transfer of care to the community setting Mid Essex CCG do not currently support the care of patients with an NGT in the Community, alternative means of nutrition should be sought prior to discharge. 9.0 Education and Training 9.1 Only registered Nurses, doctors or allied health care professionals e.g. Dietitians trained and assessed as competent (Appendix 4) to insert or check the position of an NGT should attempt these procedures. 9.2 Health Care Assistants (HCAs) or Health Care Practioners cannot attempt to insert or check the position of an NGT. 9.3 Bank and Agency staff must have completed the appropriate MEHT training and competencies prior to attempting to insert or check the position of an NGT. 9.4 Doctors may only insert an NGT if they have been trained to do so or are supervised by a competent member of staff. Doctors who have completed the mandatory training for checking Chest X-rays for NGT placement can confirm correct tube position and document in the patients notes and supporting documents that the tube can be used. All entries should be signed, dated and timed Audit and Monitoring 10.1 A clinical incident (Datix) risk event form should be completed to report any incident related to NGT care and management, inclusive of near misses or never events An annual audit of compliance with this policy will be undertaken with the support of Clinical Audit Findings, the audit will be reviewed by the Nutrition Steering Group and where deficiencies are identified; actions will be developed, implemented and monitored by this group. 16
17 11.0 Communication & Implementation 11.1 The policy will be available to staff and the public on the Trust s intranet site and website The policy will be sent to all Clinical Directors and Corporate Nursing for information and dissemination amongst their teams by the author References British Association of Parental and Enteral Nutrition (BAPEN) /NNNG NasoGastric (NG) Tube Insertion- Decision Tree NHS/PSA/RE/2016/006, Patient Safety Alert: Nasogastric tube misplacement: continuing risk of death and severe harm. July 2016 Good practice guideline- safe insertion of Nasogastric (NG) Feeding Tubes in Adults NNNG National Nurses Nutrition Group April NPSA/2012/RRR001, Rapid Response Report: Harm from flushing of nasogastric tubes before confirmation of placement. March 2012 NPSA / 2011 / PSA 002. Patient safety alert: Reducing the harm caused by misplaced Nasogastric feeding tubes in adults, children and infants. March 2011 Royal Marsden Online procedures NPSA How to confirm the correct position of nasogastric feeding tubes in infants, children and adults, February 2005 Rajaraman D 2009 Nasogastric tubes 1: Insertion technique and confirming the correct position. Nursing Times Vol. 105, Iss. 16,
18 Appendix1 18
19 Appendix 2 Recommended Procedure for Checking NGT Position Action Check whether the patient is on medication that may increase the ph level of gastric contents. Check for signs of tube displacement. Sufficient aspirate (0.5 to 1ml) obtained. Aspirate is ph 5.5 or below. Aspirate is ph 6 or above. Wait up to one hour before re-aspirating to check ph level. Problems obtaining aspirate? Turn patient onto their side. Inject air 10-20ml using a 20ml or 50ml syringe. Wait for minutes and try again This is NOT a testing procedure: DO NOT carry out auscultation of air ( whoosh test) to test tube position. Advance the tube by 10-20cm Consider X-ray All radiographs should be read by appropriately trained staff. Rationale Medications that could elevate the ph level of gastric contents are; antacids, H2 antagonists and proton pump inhibitors. For those patients who are regularly on antacids, the initial risk assessment needs to identify actions that staff should take in this scenario, and document them in the care plan. The initial ph of the aspirate should also be documented in the case notes. Documenting the external length of the tube initially and checking external markings prior to feeding will help to determine if the tube has moved. The documentation will also assist radiographers if an X-ray is needed. 0.5 to 1ml of aspirate will cover an adequate area on the single, double or triple reagent panels of ph testing strips/paper. Allow ten seconds for any colour change to occur. Commence feed. There are no known reports of pulmonary aspirates at or below this figure. The range of ph 0 to 5.5 balances the risk between increasing the potential problems for clinical staff e.g. removing tubes that are actually in the stomach, increased use of X-ray, with the as yet, unreported possibility of feeding at ph 5.5 when the tube is in the respiratory tract. DO NOT FEED. Possible bronchial secretion; leave up to one hour and try again. The initial risk assessment should identify actions for staff to take in this scenario for each patient. The actions should be documented in the care plan and/or in local policies. If there is ANY doubt about the position and/or the clarity of the colour change on the ph indicator strip/paper, particularly between the ranges ph 5 and 6, then feeding should NOT commence seek advice. The most likely reason for failure to obtain gastric aspirate below ph of 5.5 is the dilution of gastric acid by enteral feed. Waiting for up to an hour will allow time for the stomach to empty and the ph to fall. The time interval will depend on the clinical need of the patient and whether or not they are on continuous or bolus feeds. This will allow the tip of the NG tube to enter the gastric fluid pool. Injecting air through the tube will dispel any residual fluid (feed, water or medicine) and may also dislodge the exit-port of the NG feeding tube from the gastric mucosa. Using a large EnFit enteral syringe allows gentle pressure and suction; smaller syringes may produce too much pressure and split the tube (check manufacturers guidelines). Polyurethane syringes are preferable to other syringes. It is safe practice to use NG tubes and enteral syringes that have non leur connectors (Building a Safer NHS for Patients: Improving Medication Safety published 22/01/2004 available at Advancing the tube may allow it to pass into the stomach if it is in the oesophagus. X-ray should not be used routinely. The radiographer will need to know that this advice has been followed, what the problem has been and the reason for the request. The radiographer should document this. Fully radio-opaque tubes with markings to enable measurement, identification and documentation of their external length should be used. 19

20 Appendix 3 Additional Guidelines for Nasogastric Tube Placement 20
21 Appendix 4 Name Competency for Nasogastric Tube (NG) Insertion and Management (Competency training should include theoretical and practical learning (NPSA/2011/PSA002) Ward This competency document is designed to be used in conjunction with the generic core competency document. Initial Self/mentor Assessment Level Nasogastric tube insertion and management Date of initial self/mentor assessment Date of Review Date Final Level achieved Final Level Achieved Comments/Action Plan Signature of preceptor/ Mentor Understands the indications for nasogastric tube ( NGT) placement self mentor mentor Understands the contraindications for NGT placement Understands the differences and indications for fine bore feeding tubes or wide bore (Ryles) e.g. for drainage/aspirate Understands and implements the NPSA NHS/PSA/RE/2016/006 directives and Trust Policy for the insertion and management of NG feeding tubes Able to undertake NGT placement including all aspects of health & safety. Maintains patient comfort/dignity and safety throughout Able to check position of NGT immediately following insertion using 1 st line ph testing (aspirate is 5.5 or below). Understands when 2 nd line testing (x-ray) is appropriate i.e. If no
22 aspirate is obtained or if aspirate is above 5.5 Understands when and how often NG tube should be checked for correct position post insertion Understands what action to take if: Unable to obtain aspirate ph is 5.5 or above affected by patient receiving PPI Can provide care for a patient with a NG tube including changing NG tapes, checking skin, providing mouth care Documents insertion, care of, tube details (For traceability), difficulties during insertion, tube measurements and position checks of NG tubes, nostril of Placement Able to administer enteral feeding and medication according to prescription and feeding regime agreed by MDT prior to insertion of NG tube Has an understanding of re-feeding syndrome. Is aware of re-feeding syndrome guidelines and out of hours NG feeding regime and how to access on the trust intranet Nutrition CNS # or Ext:
23 Appendix 5 NG Tube Insertion & Management To be filed in patient s medical record Please affix patient demographics label or complete the following details Surname: DOB: NHS Number: First Name Ward: Hospital Number: Reason for NG Tube insertion: Identify the senior doctor responsible for the patient s care who has agreed to the NG tube insertion: Is Nasogastric tube feeding the right decision for this patient? Yes / No Is this the right time to place the NG tube and is appropriate equipment available? Yes / No Is there sufficient expertise available at this time to confirm correct placement of NGT? Yes / No Has verbal consent been given by the patient? Yes / No / NA If NO/ NA, please complete MCA2 as per trust policy for consent & Mental capacity Act NG Tube Type: Size: Length: Date: / / Time: : Inserted by: Signature: Designation: Please note nostril of placement: Placement check: First line test method Aspirate checked using ph indicator paper that is CE marked Yes / No Was aspirate obtained: Yes / No Date: / / Time: : Initial ph test result: Safe range for feeding ph of 5.5 or below Is it confirmed as safe to administer feed / medication Yes / No Checked by: Signature: Designation: If ph between 5 and 6, signature & designation of second competent person checking result: Please confirm that the tube was not flushed prior to the placement check by ticking this box Second line check X-ray authorised by: Interpretation of x-ray: Position of tube confirmed on: / / Time: : Name: Signature: Designation: Plan: Was the x-ray reviewed the most current available? Yes / No If tube placed in lung was the NG tube removed immediately? Yes / No
24 Appendix 6 NG Tube Position MUST be confirmed Prior to every episode of use including medication, water flushes or feeding Patient Surname: First Name ph of NG Aspirate ph 5.5 or below proceed to feed or administer medication ph greater than 5.5 additional checks or action required as per policy NHS / Hospital Number Initial tube length on insertion Date / time Name of person checking NGT (print) Signature Tapes intact Y/N Tube length (daily / prior to feed) Aspirate obtained Y/N ph before feed / drugs Name of 2 nd checker (competent RN) if ph between (Print name) Signature Agreed ph Outcome e.g. proceed to feed; record additional checks carried out; escalate to medical team (record name and grade of Dr) 24


25 Appendix 7 BAPEN Naso Gastric Tube insertion Decision Tree 25


26 Appendix 7 BAPEN Naso Gastric Tube insertion Decision Tree (contd) 26
Trust Standard for Assessment and Management of Physical Health Practice Guidance Note Insertion and Management of NG Feeding Tubes V01
 Trust Standard for Assessment and Management of Physical Health Practice Guidance Note Insertion and Management of NG Feeding Tubes V01 Date Issued Planned Review PGN No: Issue 1 Aug 16 Aug 19 AMPH-PGN-02.2
Trust Standard for Assessment and Management of Physical Health Practice Guidance Note Insertion and Management of NG Feeding Tubes V01 Date Issued Planned Review PGN No: Issue 1 Aug 16 Aug 19 AMPH-PGN-02.2
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: RM82 Version: 1.0 Name of Policy: Paediatric Nasogastric Tube Policy Effective From: 25/07/2018 Date Ratified 07/06/2018 Ratified Paediatric SafeCare Review Date 01/06/2020 Sponsor Kathryn Brown
Policy No: RM82 Version: 1.0 Name of Policy: Paediatric Nasogastric Tube Policy Effective From: 25/07/2018 Date Ratified 07/06/2018 Ratified Paediatric SafeCare Review Date 01/06/2020 Sponsor Kathryn Brown
Good Practice Guideline. Safe Insertion of Nasogastric (NG) Feeding Tubes in Adults
 Feeding Tubes in Adults") Good Practice Guideline Safe Insertion of Nasogastric (NG) Feeding Tubes in Adults (Not ongoing care) March 2012 Review date: March 2015 Description: A nasogastric tube is inserted through the nose, into
Good Practice Guideline Safe Insertion of Nasogastric (NG) Feeding Tubes in Adults (Not ongoing care) March 2012 Review date: March 2015 Description: A nasogastric tube is inserted through the nose, into
Reducing the Harm Caused by Misplaced Nasogastric & Orogastric Feeding Tubes Policy April 2017
 Reducing the Harm Caused by Misplaced Nasogastric & Orogastric Feeding Tubes Policy April 2017 Page 1 of 12 Title Author(s) Reducing the Harm Caused by Misplaced Nasogastric & Orogastric Feeding Tubes
Reducing the Harm Caused by Misplaced Nasogastric & Orogastric Feeding Tubes Policy April 2017 Page 1 of 12 Title Author(s) Reducing the Harm Caused by Misplaced Nasogastric & Orogastric Feeding Tubes
Nasogastric Tube Management and Care
 Nasogastric Tube Management and Care This procedural document supersedes: PAT/T 17 v.4 - Nasogastric Tube Management and Care Did you print this document yourself? The Trust discourages the retention of
Nasogastric Tube Management and Care This procedural document supersedes: PAT/T 17 v.4 - Nasogastric Tube Management and Care Did you print this document yourself? The Trust discourages the retention of
INSERTION OF A NASOGASTRIC TUBE, CONFIRMATION OF CORRECT POSITION AND ONGOING CARE IN ADULTS, CHILDREN AND INFANTS (NOT NEONATES) PROCEDURE
 PROCEDURE") INSERTION OF A NASOGASTRIC TUBE, CONFIRMATION OF CORRECT POSITION AND ONGOING CARE IN ADULTS, CHILDREN AND INFANTS (NOT NEONATES) PROCEDURE Reference No: UHB 114 Version No: 1 Previous Trust / LHB Ref
INSERTION OF A NASOGASTRIC TUBE, CONFIRMATION OF CORRECT POSITION AND ONGOING CARE IN ADULTS, CHILDREN AND INFANTS (NOT NEONATES) PROCEDURE Reference No: UHB 114 Version No: 1 Previous Trust / LHB Ref
Reference Number: UHB 114 Version Number: 5. Date of Next Review: 09 Mar 2021 Previous Trust/LHB Reference Number:
 Reference Number: UHB 114 Version Number: 5 Date of Next Review: 09 Mar 2021 Previous Trust/LHB Reference Number: Insertion of a nasogastric feeding tube, confirmation of correct position and ongoing care
Reference Number: UHB 114 Version Number: 5 Date of Next Review: 09 Mar 2021 Previous Trust/LHB Reference Number: Insertion of a nasogastric feeding tube, confirmation of correct position and ongoing care
Nasogastric tube feeding
 What is nasogastric tube feeding? Nasogastric (NG) feeding is where a narrow feeding tube is placed through your nose down into your stomach. The tube can be used to give you fluids, medications and liquid
What is nasogastric tube feeding? Nasogastric (NG) feeding is where a narrow feeding tube is placed through your nose down into your stomach. The tube can be used to give you fluids, medications and liquid
Best Practice Guidelines BPG 2 Enteral Feeding
 Best Practice Guidelines BPG 2 Enteral Feeding Wolverhampton Clinical Commissioning Group Best Practice Guideline BPG 2 - Enteral Feeding 1 DOCUMENT STATUS: Approved DATE ISSUED: 10 th November 2015 DATE
Best Practice Guidelines BPG 2 Enteral Feeding Wolverhampton Clinical Commissioning Group Best Practice Guideline BPG 2 - Enteral Feeding 1 DOCUMENT STATUS: Approved DATE ISSUED: 10 th November 2015 DATE
Information for Patients
 Having a Radiologically Inserted Gastrostomy (RIG) Information for Patients In this leaflet: Introduction.. 2 What is a RIG feeding tube?. 2 Why do I need a RIG?. 2 Are there any risks?.2 Are there any
Having a Radiologically Inserted Gastrostomy (RIG) Information for Patients In this leaflet: Introduction.. 2 What is a RIG feeding tube?. 2 Why do I need a RIG?. 2 Are there any risks?.2 Are there any
NASOGASTRIC TUBE INSERTION AND MANAGEMENT POLICY AND PROCEDURES FOR ADULTS
 NASOGASTRIC TUBE INSERTION AND MANAGEMENT POLICY AND PROCEDURES FOR ADULTS Policy Title: Executive Summary: Nasogastric tube Insertion and Management for Adults To optimise the nutritional care of adult
NASOGASTRIC TUBE INSERTION AND MANAGEMENT POLICY AND PROCEDURES FOR ADULTS Policy Title: Executive Summary: Nasogastric tube Insertion and Management for Adults To optimise the nutritional care of adult
Insertion and Confirmation of Position of Nasogastric Tubes for Adults and Children
 This is an official Northern Trust policy and should not be edited in any way Insertion and Confirmation of Position of Nasogastric Tubes for Adults and Children Reference Number: NHSCT/10/296 Target audience:
This is an official Northern Trust policy and should not be edited in any way Insertion and Confirmation of Position of Nasogastric Tubes for Adults and Children Reference Number: NHSCT/10/296 Target audience:
Policies & Procedures
 Policies & Procedures Title: ENTERAL FEEDING TUBE WITH A STYLET: ASSISTING WITH INSERTION OF: CARE OF, REMOVAL OF Authorization [X] SHR Nursing Practice Committee ID Number: 1109 Source: Nursing Date Reaffirmed:
Policies & Procedures Title: ENTERAL FEEDING TUBE WITH A STYLET: ASSISTING WITH INSERTION OF: CARE OF, REMOVAL OF Authorization [X] SHR Nursing Practice Committee ID Number: 1109 Source: Nursing Date Reaffirmed:
Radiology Standard Operating Procedure
 Title Purpose Scope and responsibilities Owner(s) Authors Confirmation of site of Naso-Gastric Tube using Chest X-ray This SOP details the operating procedure for clinical staff when confirming by Chest
Title Purpose Scope and responsibilities Owner(s) Authors Confirmation of site of Naso-Gastric Tube using Chest X-ray This SOP details the operating procedure for clinical staff when confirming by Chest
Nasal Bridle Policy. PAT/T 69 v.1. This is a new procedural document, please read in full.
 Nasal Bridle Policy This is a new procedural document, please read in full. Did you print this document yourself? The Trust discourages the retention of hard copies of policies and can only guarantee that
Nasal Bridle Policy This is a new procedural document, please read in full. Did you print this document yourself? The Trust discourages the retention of hard copies of policies and can only guarantee that
Trust Standard for the Assessment and Management of Physical Health Practice Guidance Note Enteral Tube Feeding Overview V01
 Trust Standard for the Assessment and Management of Physical Health Practice Guidance Note Enteral Tube Feeding Overview V01 Date Issued Planned Review PGN No: Issue 1 Aug 16 Issue 2 Nov 16 Aug 19 AMPH-PGN-02
Trust Standard for the Assessment and Management of Physical Health Practice Guidance Note Enteral Tube Feeding Overview V01 Date Issued Planned Review PGN No: Issue 1 Aug 16 Issue 2 Nov 16 Aug 19 AMPH-PGN-02
After your child s NasoGastric (NG) Tube Discharge Information
 Tube Discharge Information") After your child s NasoGastric (NG) Tube Discharge Information Children s services This leaflet provides information and advice following the insertion of your child s nasogastric (NG) tube. It is important
After your child s NasoGastric (NG) Tube Discharge Information Children s services This leaflet provides information and advice following the insertion of your child s nasogastric (NG) tube. It is important
Purpose: This document states the procedure for giving medicines via nasogastric tube, gastrostomy and jejunostomy to children in the community
 The Redway School Procedure for Administration of Medicines via External Feeding Tubes Purpose: This document states the procedure for giving medicines via nasogastric tube, gastrostomy and jejunostomy
The Redway School Procedure for Administration of Medicines via External Feeding Tubes Purpose: This document states the procedure for giving medicines via nasogastric tube, gastrostomy and jejunostomy
TUBE FEEDING WITH NUTRICIA CHOICE
 TUBE FEEDING WITH NUTRICIA CHOICE NURSE SUPPORT FLEXIBLE DELIVERIES OUT OF HOURS SUPPORT ENTERAL FEEDING PUMP SUPPORTING ALL YOUR TUBE FEEDING NEEDS EASY TO ORDER & PAY COMPREHENSIVE TUBE FEED PACKAGE
TUBE FEEDING WITH NUTRICIA CHOICE NURSE SUPPORT FLEXIBLE DELIVERIES OUT OF HOURS SUPPORT ENTERAL FEEDING PUMP SUPPORTING ALL YOUR TUBE FEEDING NEEDS EASY TO ORDER & PAY COMPREHENSIVE TUBE FEED PACKAGE
Replacement Of Balloon Retained Gastrostomy (BRG) Procedure Introduction and Aim
 Procedure Introduction and Aim") Reference Number: UHB 189 Version Number: 2 Date of Next Review: 10 th Dec 2018 Previous Trust/LHB Reference Number: Replacement Of Balloon Retained Gastrostomy (BRG) Procedure Introduction and Aim The
Reference Number: UHB 189 Version Number: 2 Date of Next Review: 10 th Dec 2018 Previous Trust/LHB Reference Number: Replacement Of Balloon Retained Gastrostomy (BRG) Procedure Introduction and Aim The
Document control information (Published as separate document) Document Control 37 Policy Implementation Plan 37. Nasogastric Feeding Policy
 Document Control 37 Policy Implementation Plan 37. Nasogastric Feeding Policy") Classification: Policy Lead Author: Brenda Blackett, Nutrition Nurse Specialist (on behalf of the Nutrition Steering Group) Additional author(s): N/A Authors Division: Surgery Unique ID: TWCG20(11) Issue
Classification: Policy Lead Author: Brenda Blackett, Nutrition Nurse Specialist (on behalf of the Nutrition Steering Group) Additional author(s): N/A Authors Division: Surgery Unique ID: TWCG20(11) Issue
Nasojejunal feeding tube
 Nasojejunal feeding tube This leaflet provides information about having a nasojejunal feeding tube and how to take care of your tube at home. If you have any further questions, please speak to the team
Nasojejunal feeding tube This leaflet provides information about having a nasojejunal feeding tube and how to take care of your tube at home. If you have any further questions, please speak to the team
Enteral Feeding - Children, Young People and Families
 Standard Operating Procedure 3 (SOP 3) Enteral Feeding - Children, Young People and Families Why we have a procedure? Children who are unable to meet their nutritional requirements orally but have a functioning
Standard Operating Procedure 3 (SOP 3) Enteral Feeding - Children, Young People and Families Why we have a procedure? Children who are unable to meet their nutritional requirements orally but have a functioning
Nasogastric Intubation and Check Image Interpretation. Robert Law DCR, MRCR (Hon). Consultant GI Radiographer - Frenchay Hospital, Bristol
. Consultant GI Radiographer - Frenchay Hospital, Bristol") Nasogastric Intubation and Check Image Interpretation. Robert Law DCR, MRCR (Hon). Consultant GI Radiographer - Frenchay Hospital, Bristol National Patient Safety Agency (NPSA) NPSA suggests 171,000 fine
Nasogastric Intubation and Check Image Interpretation. Robert Law DCR, MRCR (Hon). Consultant GI Radiographer - Frenchay Hospital, Bristol National Patient Safety Agency (NPSA) NPSA suggests 171,000 fine
Home enteral tube feeding a guide for patients and carers
 University Teaching Trust Home enteral tube feeding a guide for patients and carers Ladywell Building Nutrition and Dietetics 0161 206 4255 All Rights Reserved 2017. Document for issue as handout. Contents
University Teaching Trust Home enteral tube feeding a guide for patients and carers Ladywell Building Nutrition and Dietetics 0161 206 4255 All Rights Reserved 2017. Document for issue as handout. Contents
Subacute Care. 1. Define important words in the chapter. 2. Discuss the types of residents who are in a subacute setting
 175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
You and your gastrostomy feeding tube
 The Clatterbridge Cancer Centre NHS Foundation Trust You and your gastrostomy feeding tube Rehabilitation and Support A guide for patients and carers Contents Skin care...1 Daily tube care...2 Feeding
The Clatterbridge Cancer Centre NHS Foundation Trust You and your gastrostomy feeding tube Rehabilitation and Support A guide for patients and carers Contents Skin care...1 Daily tube care...2 Feeding
Tube Feeding Status Critical Element Pathway
 Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Use this pathway for a resident who has a feeding tube. Review the Following in Advance to Guide Observations and Interviews: Most current comprehensive and most recent quarterly (if the comprehensive
Care of your Radiologically Inserted Gastrostomy (RIG) Tube
 Tube") Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Care of your Radiologically Inserted Gastrostomy (RIG) Tube Nursing and Clinical Governance The purpose of this leaflet is
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Care of your Radiologically Inserted Gastrostomy (RIG) Tube Nursing and Clinical Governance The purpose of this leaflet is
Title Nasopharyngeal Suction Standard Operating Procedure
 Document Control Title Nasopharyngeal Suction Standard Operating Procedure Author s job title Community Respiratory Physiotherapist Directorate Health and Social Care Community Services Date Version Status
Document Control Title Nasopharyngeal Suction Standard Operating Procedure Author s job title Community Respiratory Physiotherapist Directorate Health and Social Care Community Services Date Version Status
Intravenous Medication Administration via a Central Venous Line
 Standard Operating Procedure 11 (SOP 11) Intravenous Medication Administration via a Central Venous Line Why we have a procedure? This procedure is to assist/ inform healthcare professionals on how to
Standard Operating Procedure 11 (SOP 11) Intravenous Medication Administration via a Central Venous Line Why we have a procedure? This procedure is to assist/ inform healthcare professionals on how to
Care of a Freka Percutaneous Endoscopic Gastrostomy (PEG)
") Care of a Freka Percutaneous Endoscopic Gastrostomy (PEG) Information for patients and carers Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets
Care of a Freka Percutaneous Endoscopic Gastrostomy (PEG) Information for patients and carers Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets
MANAGEMENT OF DYSPHAGIA POLICY
 MANAGEMENT OF DYSPHAGIA POLICY Latest Revision September 2015 Next Revision September 2016 Reviewer: Head of Governance and Clinical Services; Clinical team Compliance Associated Policies Contents 1. Introduction
MANAGEMENT OF DYSPHAGIA POLICY Latest Revision September 2015 Next Revision September 2016 Reviewer: Head of Governance and Clinical Services; Clinical team Compliance Associated Policies Contents 1. Introduction
Tube Feeding at Home A Guidebook for Patients and Caregivers
 Tube Feeding at Home A Guidebook for Patients and Caregivers This manual provides information on the following: What is Tube Feeding? How to Flush Your Feeding Tube Problems That May Occur With Tube Feeds
Tube Feeding at Home A Guidebook for Patients and Caregivers This manual provides information on the following: What is Tube Feeding? How to Flush Your Feeding Tube Problems That May Occur With Tube Feeds
Enteral Feeding Policy For Adults with Operational Guidelines
 Enteral Feeding Policy For Adults with Operational Guidelines Policy Number: 331 Supersedes: Enteral feeding guidelines Standards For Healthcare Services No/s 7,8,11,13,14,15,16, 18, 19 Version Date Of
Enteral Feeding Policy For Adults with Operational Guidelines Policy Number: 331 Supersedes: Enteral feeding guidelines Standards For Healthcare Services No/s 7,8,11,13,14,15,16, 18, 19 Version Date Of
10 Appendix 7 1 Competence for insertion of nasal bridle 7 2 Nasal bridle care plan 10 3 Discharge care sheet 11
 Classification: Policy Lead Author: Brenda Blackett, Nutrition Nurse, on behalf of the Nutrition Steering Group Authors ivision:surgery Unique I: TWCG8(11) Issue number: 4 Expiry ate: February 2021 Contents
Classification: Policy Lead Author: Brenda Blackett, Nutrition Nurse, on behalf of the Nutrition Steering Group Authors ivision:surgery Unique I: TWCG8(11) Issue number: 4 Expiry ate: February 2021 Contents
Percutaneous Endoscopic Gastrostomy (PEG)
") Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Percutaneous Endoscopic Gastrostomy (PEG) Nursing and Clinical Governance Why do I need a feeding tube? You may be due to have
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Percutaneous Endoscopic Gastrostomy (PEG) Nursing and Clinical Governance Why do I need a feeding tube? You may be due to have
Caring for Patients at Risk for Aspiration
 Nursing Assistants Sample Peak Development Resources, LLC P.O. Box 13267 Richmond, VA 23225 Phone: (804) 233-3707 Fax: (804) 233-3705 After reading the newsletter, the nursing assistant should be able
Nursing Assistants Sample Peak Development Resources, LLC P.O. Box 13267 Richmond, VA 23225 Phone: (804) 233-3707 Fax: (804) 233-3705 After reading the newsletter, the nursing assistant should be able
After your child s Jejunostomy Discharge Information
 After your child s Jejunostomy Discharge Information Children s Services This leaflet provides information and advice following the insertion of your child s jejunostomy tube. It is important that you
After your child s Jejunostomy Discharge Information Children s Services This leaflet provides information and advice following the insertion of your child s jejunostomy tube. It is important that you
PROCEDURE FOR CHECKING THE WATER IN BALLOON RETAINED GASTROSTOMY TUBE / LOW PROFILE DEVICES FOR BOTH ADULTS AND CHILDREN
 PROCEDURE FOR CHECKING THE WATER IN BALLOON RETAINED GASTROSTOMY TUBE / LOW PROFILE DEVICES FOR BOTH ADULTS AND CHILDREN First Issued Issue Version Purpose of Issue/Description of Change Planned Review
PROCEDURE FOR CHECKING THE WATER IN BALLOON RETAINED GASTROSTOMY TUBE / LOW PROFILE DEVICES FOR BOTH ADULTS AND CHILDREN First Issued Issue Version Purpose of Issue/Description of Change Planned Review
Having an Oesophageal Dilatation
 Having an Oesophageal Dilatation Information for Patients In this leaflet: Introduction 2 What is an Oesophageal Dilatation?...2 What are the benefits of an Oeosphageal Dilatation? 2 Are there any risks?.2
Having an Oesophageal Dilatation Information for Patients In this leaflet: Introduction 2 What is an Oesophageal Dilatation?...2 What are the benefits of an Oeosphageal Dilatation? 2 Are there any risks?.2
Placement and Care of Your Gastrojejunostomy Tube (GJ Tube) Interventional Radiology
 Interventional Radiology") Placement and Care of Your Gastrojejunostomy Tube (GJ Tube) Interventional Radiology Your healthcare team recommended that you undergo gastrojejunostomy tube (GJ tube) placement. This procedure will be
Placement and Care of Your Gastrojejunostomy Tube (GJ Tube) Interventional Radiology Your healthcare team recommended that you undergo gastrojejunostomy tube (GJ tube) placement. This procedure will be
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth
 Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
Title Oropharyngeal & Oral Yankauer Suction Standard Operating Procedure
 Document Control Title Oropharyngeal & Oral Yankauer Suction Standard Operating Procedure Author s job title Community Respiratory Physiotherapist Directorate Health & Social Care Community Services Date
Document Control Title Oropharyngeal & Oral Yankauer Suction Standard Operating Procedure Author s job title Community Respiratory Physiotherapist Directorate Health & Social Care Community Services Date
TRAINEE BOOKLET. Selection, insertion and ongoing safe use of nasogastric (NG) tubes in adults with the CORTRAK Enteral Access System (EAS)
 tubes in adults with the CORTRAK Enteral Access System (EAS)") TRAINEE BOOKLET Selection, insertion and ongoing safe use of nasogastric (NG) tubes in adults with the CORTRAK Enteral Access System (EAS) This programme has been accredited by the RCN Centre for Professional
TRAINEE BOOKLET Selection, insertion and ongoing safe use of nasogastric (NG) tubes in adults with the CORTRAK Enteral Access System (EAS) This programme has been accredited by the RCN Centre for Professional
Pleural procedures and thoracic ultrasound British Thoracic Society Pleural Disease Guideline 2010
 Pleural procedures and thoracic ultrasound British Thoracic Society Pleural Disease Guideline 2010 Tom Havelock, Richard Teoh, Diane Laws, Fergus Gleeson On behalf of the BTS Pleural Disease Guideline
Pleural procedures and thoracic ultrasound British Thoracic Society Pleural Disease Guideline 2010 Tom Havelock, Richard Teoh, Diane Laws, Fergus Gleeson On behalf of the BTS Pleural Disease Guideline
Good Practice Guideline Changing of a Balloon Gastrostomy Tube (BGT) into the Stomach for Adults and Children. October 2016 Review date: October 2019
 into the Stomach for Adults and Children. October 2016 Review date: October 2019") Good Practice Guideline Changing of a Balloon Gastrostomy Tube (BGT) into the Stomach for Adults and Children October 2016 Review date: October 2019 Description A balloon gastrostomy (BGT) is a feeding
Good Practice Guideline Changing of a Balloon Gastrostomy Tube (BGT) into the Stomach for Adults and Children October 2016 Review date: October 2019 Description A balloon gastrostomy (BGT) is a feeding
Percutaneous Endoscopic Gastrostomy (PEG) Tube Insertion
 Tube Insertion") Percutaneous Endoscopic Gastrostomy (PEG) Tube Insertion Patient Information Ninewells Hospital Endoscopy Unit Telephone: 01382 660111, extension: 40078 or bleep 4470 Perth Royal Infirmary Endoscopy Unit
Percutaneous Endoscopic Gastrostomy (PEG) Tube Insertion Patient Information Ninewells Hospital Endoscopy Unit Telephone: 01382 660111, extension: 40078 or bleep 4470 Perth Royal Infirmary Endoscopy Unit
About your PICC line. Information for patients Weston Park Hospital
 About your PICC line Information for patients Weston Park Hospital This booklet explains what a PICC line is, how it is inserted and some general advice on its use and care. What is a PICC line? A Peripherally
About your PICC line Information for patients Weston Park Hospital This booklet explains what a PICC line is, how it is inserted and some general advice on its use and care. What is a PICC line? A Peripherally
Policy Review Sheet. Review Date: 14/10/16 Policy Last Amended: 19/10/17. Next planned review in 12 months, or sooner as required.
 Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
PICU tracheostomy protocol
 PICU tracheostomy protocol This protocol is based on the joint Royal Brompton & Harefield NHS Trust and Great Ormond Street Hospital for Children NHS Trust, Great Ormond Street Hospital Manual of Children
PICU tracheostomy protocol This protocol is based on the joint Royal Brompton & Harefield NHS Trust and Great Ormond Street Hospital for Children NHS Trust, Great Ormond Street Hospital Manual of Children
Peripherally inserted central catheter (PICC line) Information to accompany consent
 Information to accompany consent") Peripherally inserted central catheter (PICC line) Information to accompany consent Exceptional healthcare, personally delivered What is a PICC line? PICC stands for peripherally inserted central venous
Peripherally inserted central catheter (PICC line) Information to accompany consent Exceptional healthcare, personally delivered What is a PICC line? PICC stands for peripherally inserted central venous
Effective: Revised: April 15, 2016 SUCTIONING, MODIFIED STERILE TRACHEAL
 SUCTIONING, MODIFIED STERILE TRACHEAL Purpose: Tracheal suctioning is performed to remove secretions and maintain a patent airway. Additional Authority: Nevada Revised Statute, Nevada Nurse Practice Act,
SUCTIONING, MODIFIED STERILE TRACHEAL Purpose: Tracheal suctioning is performed to remove secretions and maintain a patent airway. Additional Authority: Nevada Revised Statute, Nevada Nurse Practice Act,
Formative DOPS: Percutaneous endoscopic gastrostomy (PEG)
") Date of procedure Trainee name Trainer name Formative DOPS: Membership no. (eg. GMC/NMC) Membership no. (eg. GMC/NMC) Outline of case Difficulty of case Easy Moderate Complicated Please tick appropriate
Date of procedure Trainee name Trainer name Formative DOPS: Membership no. (eg. GMC/NMC) Membership no. (eg. GMC/NMC) Outline of case Difficulty of case Easy Moderate Complicated Please tick appropriate
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Injectable Medicines Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Injectable Medicines Policy Version No.: 4.3 Effective From: 24 March 2017 Expiry Date: 21 January 2019 Date Ratified: 11 January 2017 Ratified By:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Injectable Medicines Policy Version No.: 4.3 Effective From: 24 March 2017 Expiry Date: 21 January 2019 Date Ratified: 11 January 2017 Ratified By:
Care Instructions AMT G-JET
 Care Instructions AMT G-JET Patient name Date of Insertion Conversion Primary Placement The device size is: FR G CM J CM Balloon Fill Volume: ml Safe to gastric feed Y N Useful numbers Professional Name
Care Instructions AMT G-JET Patient name Date of Insertion Conversion Primary Placement The device size is: FR G CM J CM Balloon Fill Volume: ml Safe to gastric feed Y N Useful numbers Professional Name
URINARY CATHETER MANAGEMENT CARE PLAN
 URINARY CATHETER MANAGEMENT CARE PLAN Care planning: Clear set of actions that enable a patient/ client and nurse to achieve a goal in relation to a specific problem or need. Focus for care Continuity
URINARY CATHETER MANAGEMENT CARE PLAN Care planning: Clear set of actions that enable a patient/ client and nurse to achieve a goal in relation to a specific problem or need. Focus for care Continuity
NCEPOD On the Right Trach?
 NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
Standard operating procedure for gastrostomy tube care
 Document level: West Locality Code: CC47 Issue number: 1 Standard operating procedure for gastrostomy tube care Lead executive Authors details Type of document Target audience Document purpose General
Document level: West Locality Code: CC47 Issue number: 1 Standard operating procedure for gastrostomy tube care Lead executive Authors details Type of document Target audience Document purpose General
Undergoing a Percutaneous Endoscopic Gastrostomy (PEG) Tube procedure
 Tube procedure") Page 1 of 7 Undergoing a Percutaneous Endoscopic Gastrostomy (PEG) Tube procedure Introduction This leaflet only contains information regarding a PEG tube and includes important information about the procedure.
Page 1 of 7 Undergoing a Percutaneous Endoscopic Gastrostomy (PEG) Tube procedure Introduction This leaflet only contains information regarding a PEG tube and includes important information about the procedure.
Adult Enteral Feeding guidelines
 Adult Enteral Feeding guidelines Full Title of Guideline: Adult Enteral Feeding guidelines Section 10.0 Procedure for discharging patients on Home Enteral feeding Author (include email and role): Anne
Adult Enteral Feeding guidelines Full Title of Guideline: Adult Enteral Feeding guidelines Section 10.0 Procedure for discharging patients on Home Enteral feeding Author (include email and role): Anne
Vascular Access Department Insertion of a tunnelled Central Venous Catheter Information for patients
 Vascular Access Department Insertion of a tunnelled Central Venous Catheter Information for patients What is a tunnelled central venous catheter (CVC)? A CVC is a long, narrow tube (catheter) that is put
Vascular Access Department Insertion of a tunnelled Central Venous Catheter Information for patients What is a tunnelled central venous catheter (CVC)? A CVC is a long, narrow tube (catheter) that is put
All About Your Peripherally Inserted Central Catheter (PICC)
") All About Your Peripherally Inserted Central Catheter (PICC) General Information Intravenous (IV) therapy is the delivery of fluid directly into a vein. An intravenous catheter is a hollow tube that is
All About Your Peripherally Inserted Central Catheter (PICC) General Information Intravenous (IV) therapy is the delivery of fluid directly into a vein. An intravenous catheter is a hollow tube that is
TRAINEE BOOKLET. Selection, insertion and ongoing safe use of nasogastric (NG) tubes in adults with the CORTRAK TM 2 Enteral Access System (EAS TM )
 tubes in adults with the CORTRAK TM 2 Enteral Access System (EAS TM )") TRAINEE BOOKLET Selection, insertion and ongoing safe use of nasogastric (NG) tubes in adults with the CORTRAK TM 2 Enteral Access System (EAS TM ) This programme has been accredited by the RCN Centre
TRAINEE BOOKLET Selection, insertion and ongoing safe use of nasogastric (NG) tubes in adults with the CORTRAK TM 2 Enteral Access System (EAS TM ) This programme has been accredited by the RCN Centre
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY
 DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
CLINICAL GUIDELINE FOR THE EMERGENCY DEFILL OF AN ADJUSTABLE GASTRIC BAND
 CLINICAL GUIDELINE FOR THE EMERGENCY DEFILL OF AN ADJUSTABLE GASTRIC BAND 1. Aim/Purpose of this Guideline The aim of this guideline to enable the effective care of patients needing emergency defill of
CLINICAL GUIDELINE FOR THE EMERGENCY DEFILL OF AN ADJUSTABLE GASTRIC BAND 1. Aim/Purpose of this Guideline The aim of this guideline to enable the effective care of patients needing emergency defill of
THE USE OF MITTS (HAND CONTROL MITTENS) IN ADULT PATIENTS POLICY
 IN ADULT PATIENTS POLICY") THE USE OF MITTS (HAND CONTROL MITTENS) IN ADULT PATIENTS POLICY Policy Number: 171 Supercedes: Standards For Healthcare Services No/s 7, 10, 11, 14 and 16 Version No: Date Of Review: Reviewer Name: Completed
THE USE OF MITTS (HAND CONTROL MITTENS) IN ADULT PATIENTS POLICY Policy Number: 171 Supercedes: Standards For Healthcare Services No/s 7, 10, 11, 14 and 16 Version No: Date Of Review: Reviewer Name: Completed
NASAL ENDOSCOPY IN THE OUTPATIENTS DEPARTMENT (OPD)
") NASAL ENDOSCOPY IN THE OUTPATIENTS DEPARTMENT (OPD) Version Number V2 Date of Issue January 2017 Reference Number Review Interval Approved By Name: Fionnuala O Neill Title: Nurse Practice Coordinator Authorised
NASAL ENDOSCOPY IN THE OUTPATIENTS DEPARTMENT (OPD) Version Number V2 Date of Issue January 2017 Reference Number Review Interval Approved By Name: Fionnuala O Neill Title: Nurse Practice Coordinator Authorised
SELF - ADMINISTRATION OF MEDICINES AND ADMINISTRATION OF MEDICINES SUPPORTED BY FAMILY/INFORMAL CARERS OF PATIENTS IN COMMUNITY NURSING
 CLINICAL PROTOCOL SELF - ADMINISTRATION OF MEDICINES AND ADMINISTRATION OF MEDICINES SUPPORTED BY FAMILY/INFORMAL CARERS OF PATIENTS IN COMMUNITY NURSING RATIONALE Medication errors can cause unnecessary
CLINICAL PROTOCOL SELF - ADMINISTRATION OF MEDICINES AND ADMINISTRATION OF MEDICINES SUPPORTED BY FAMILY/INFORMAL CARERS OF PATIENTS IN COMMUNITY NURSING RATIONALE Medication errors can cause unnecessary
Comprehensive Aspiration Risk Management Plan (CARMP) Individual s Name: Case Manager: Date of CARMP: DOB:
 Individual s Name: Case Manager: Date of CARMP: DOB:") Individual s Name: Case Manager: Date of CARMP: DOB: Case Management Agency: NOTE: Individuals at moderate risk for aspiration due to Risky Eating Behaviors (REB) identified as the only Aspiration Risk
Individual s Name: Case Manager: Date of CARMP: DOB: Case Management Agency: NOTE: Individuals at moderate risk for aspiration due to Risky Eating Behaviors (REB) identified as the only Aspiration Risk
Table of Contents. Nursing Skills. Page 2 of 8. Nursing School Made Simple Guaranteed 2014 SimpleNursing.com All Rights Reserved.
 Table of Contents 1 Universal Competencies... 3 1.1 Universal Elements... 3 2 Critical Thinking Question... 4 3 Documentation... 4 4 Handwashing... 4 5 Moving a patient up in bed... 4 6 Applying restraints...
Table of Contents 1 Universal Competencies... 3 1.1 Universal Elements... 3 2 Critical Thinking Question... 4 3 Documentation... 4 4 Handwashing... 4 5 Moving a patient up in bed... 4 6 Applying restraints...
Surgical Treatment for Cancer of the Oesophagus
 Oxford Oesophagogastric Centre Surgical Treatment for Cancer of the Oesophagus Information for patients This leaflet gives you information about your planned operation, possible risks and complications,
Oxford Oesophagogastric Centre Surgical Treatment for Cancer of the Oesophagus Information for patients This leaflet gives you information about your planned operation, possible risks and complications,
Enteral Feeding Infection Control Policy (Interim)
") This is an official Northern Trust policy and should not be edited in any way Enteral Feeding Infection Control Policy (Interim) Reference Number: NHSCT/12/494 Target audience: This policy is aimed at
This is an official Northern Trust policy and should not be edited in any way Enteral Feeding Infection Control Policy (Interim) Reference Number: NHSCT/12/494 Target audience: This policy is aimed at
Bowel Surgery Hartmann s Procedure Your operation explained
 Bowel Surgery Hartmann s Procedure Your operation explained Introduction This information is for people considering having a Hartmann s Procedure operation. It explains what is involved and some possible
Bowel Surgery Hartmann s Procedure Your operation explained Introduction This information is for people considering having a Hartmann s Procedure operation. It explains what is involved and some possible
Competency Based Training for Enteral Tube Feeding. Record of Achieving Competency for Staff
 West of Scotland Gastroenterology, Hepatology and Nutrition Competency Based Training for Enteral Tube Feeding Record of Achieving Competency for Staff Purpose This document will provide a record of the
West of Scotland Gastroenterology, Hepatology and Nutrition Competency Based Training for Enteral Tube Feeding Record of Achieving Competency for Staff Purpose This document will provide a record of the
Going home with a redivac drain after surgery
 Going home with a redivac drain after surgery This leaflet explains about going home with a redivac drain following your surgery. If you have any further questions, please speak to the nurse or doctor
Going home with a redivac drain after surgery This leaflet explains about going home with a redivac drain following your surgery. If you have any further questions, please speak to the nurse or doctor
CLINICAL GUIDELINE FOR THE USE OF RECTUS SHEATH CATHETERS IN CHILDREN. 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR THE USE OF RECTUS SHEATH CATHETERS IN CHILDREN. 1. Aim/Purpose of this Guideline 1.1. Guidelines for the use of rectus sheath catheters for the management of pain following laparotomy
CLINICAL GUIDELINE FOR THE USE OF RECTUS SHEATH CATHETERS IN CHILDREN. 1. Aim/Purpose of this Guideline 1.1. Guidelines for the use of rectus sheath catheters for the management of pain following laparotomy
TRUST POLICY & PROCEDURES FOR ENTERAL FEEDING Reference Number POL-CL/1194/11
 TRUST POLICY & PROCEDURES FOR ENTERAL FEEDING Reference Number POL-CL/1194/11 Version / Amendment History Version: V1.3.1 Status Final Version Date Author Reason V1.2 Sept 2011 V1.3 Nov 2014 V1.3 May 2017
TRUST POLICY & PROCEDURES FOR ENTERAL FEEDING Reference Number POL-CL/1194/11 Version / Amendment History Version: V1.3.1 Status Final Version Date Author Reason V1.2 Sept 2011 V1.3 Nov 2014 V1.3 May 2017
Policy for use of the Royal Marsden Manual of Clinical Nursing Procedures (9th Edition)
") Policy for use of the Royal Marsden Manual of Clinical Nursing Procedures (9th Edition) Document Summary This Policy defines the clinical procedures for all Clinical staff (including temporary staff, contracted
Policy for use of the Royal Marsden Manual of Clinical Nursing Procedures (9th Edition) Document Summary This Policy defines the clinical procedures for all Clinical staff (including temporary staff, contracted
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Hickman line insertion and caring for your line
 Hickman line insertion and caring for your line Information for patients This booklet explains how a Hickman line is put in, the benefits, the risks and the alternatives, as well as how to care for your
Hickman line insertion and caring for your line Information for patients This booklet explains how a Hickman line is put in, the benefits, the risks and the alternatives, as well as how to care for your
Skin Tunnelled Catheter (STC), also known as Central line
, also known as Central line") Skin Tunnelled Catheter (STC), also known as Central line Intravenous Therapy Department Patient information leaflet What is a skin tunnelled catheter? A skin tunnelled catheter (STC) is a long flexible
Skin Tunnelled Catheter (STC), also known as Central line Intravenous Therapy Department Patient information leaflet What is a skin tunnelled catheter? A skin tunnelled catheter (STC) is a long flexible
Curriculum For The LMA Supreme
 Curriculum For The LMA Supreme Course Description This course is designed to provide instruction in a procedure for the use of the LMA Supreme by the EMT-Intermediate `99 and Paramedic. Prerequisites 1.
Curriculum For The LMA Supreme Course Description This course is designed to provide instruction in a procedure for the use of the LMA Supreme by the EMT-Intermediate `99 and Paramedic. Prerequisites 1.
Endoscopy Unit Having an Oesophageal Stent insertion
 Endoscopy Unit Having an Oesophageal Stent insertion Information for patients Your doctor has recommended that you have an Oesophageal Stent Insertion. This leaflet will explain the procedure and what
Endoscopy Unit Having an Oesophageal Stent insertion Information for patients Your doctor has recommended that you have an Oesophageal Stent Insertion. This leaflet will explain the procedure and what
Gastrostomy tube care
 All of our publications are available in different languages, larger print, braille (English only), audio tape or another format of your choice. Tha gach sgrìobhainn againn rim faotainn ann an diofar chànanan,
All of our publications are available in different languages, larger print, braille (English only), audio tape or another format of your choice. Tha gach sgrìobhainn againn rim faotainn ann an diofar chànanan,
Register No: Status: Public on ratification
 Private Patient Policy Type: Policy Register No: 12024 Status: Public on ratification Developed in response to: Service Development Contributes to CQC Outcome number: 4 Consulted With Post/Committee/Group
Private Patient Policy Type: Policy Register No: 12024 Status: Public on ratification Developed in response to: Service Development Contributes to CQC Outcome number: 4 Consulted With Post/Committee/Group
Nutrition by Artificial Means Guide. Know your rights and have your say about your mental health care and treatment.
 Nutrition by Artificial Means Guide Know your rights and have your say about your mental health care and treatment. What is nutrition by artificial means? Sometimes, as a result of an eating disorder or
Nutrition by Artificial Means Guide Know your rights and have your say about your mental health care and treatment. What is nutrition by artificial means? Sometimes, as a result of an eating disorder or
ADVANCE DIRECTIVE FOR HEALTH CARE
 ADVANCE DIRECTIVE FOR HEALTH CARE This document includes a list of definitions and the two types of Advance Directives (together called a Combined Directive). Some people choose to fill out only one portion.
ADVANCE DIRECTIVE FOR HEALTH CARE This document includes a list of definitions and the two types of Advance Directives (together called a Combined Directive). Some people choose to fill out only one portion.
SOP Venesection Registered Nurses
 HAEM / ONC WARD & DAY UNIT STANDARD OPERATING PROCEDURE SOP Venesection Registered Nurses Document Code Version Number 1 Issue Number 1 Date of Issue 07/03/2014 Review Interval 2 years Author (original
HAEM / ONC WARD & DAY UNIT STANDARD OPERATING PROCEDURE SOP Venesection Registered Nurses Document Code Version Number 1 Issue Number 1 Date of Issue 07/03/2014 Review Interval 2 years Author (original
Administration of IV Medication in the Community by the Children s Community Nursing Team Standard Operating Procedure
 Administration of IV Medication in the Community by the Children s Community Nursing Team Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Quality and Standards Group Date
Administration of IV Medication in the Community by the Children s Community Nursing Team Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Quality and Standards Group Date
patients by referral to x-ray by cardiac nurses, within clearly defined parameters. Contributes to CQC Core Outcome: Outcome 4
 Referral of Patients for Chest X-Rays Post Pacemaker Insertion by Cardiac Nurses/ Cardiac Radiographers Type: Register No: 06026 Status: Public Clinical Guidelines Developed in response to: To reduce treatment
Referral of Patients for Chest X-Rays Post Pacemaker Insertion by Cardiac Nurses/ Cardiac Radiographers Type: Register No: 06026 Status: Public Clinical Guidelines Developed in response to: To reduce treatment
Caring for children and young people in the community receiving enteral tube feeding
 Best Practice Statement ~ September 2007 Caring for children and young people in the community receiving enteral tube feeding NHS Quality Improvement Scotland is committed to equality and diversity. We
Best Practice Statement ~ September 2007 Caring for children and young people in the community receiving enteral tube feeding NHS Quality Improvement Scotland is committed to equality and diversity. We
Diagnostic Upper Gastrointestinal Endoscopy
 Diagnostic Upper Gastrointestinal Endoscopy Endoscopy Department Patient information leaflet This leaflet explains more about having a gastroscopy, including the benefits, risks and any alternatives and
Diagnostic Upper Gastrointestinal Endoscopy Endoscopy Department Patient information leaflet This leaflet explains more about having a gastroscopy, including the benefits, risks and any alternatives and
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee
 TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
Eating, drinking and speech following surgery for cancer of the mouth
 Eating, drinking and speech following surgery for cancer of the mouth Speech and Language Therapy Information for Patients i Leaflet number: 504 Version: 3 Produced: July 2018 Review: July 2021 Introduction
Eating, drinking and speech following surgery for cancer of the mouth Speech and Language Therapy Information for Patients i Leaflet number: 504 Version: 3 Produced: July 2018 Review: July 2021 Introduction
Endoscopy Department Patient Information Gastroscopy with Oesophageal Dilation
 Endoscopy Department Patient Information Gastroscopy with Oesophageal Dilation This leaflet provides information about the Endoscopy and Dilation procedure. It aims to answer any questions you may have
Endoscopy Department Patient Information Gastroscopy with Oesophageal Dilation This leaflet provides information about the Endoscopy and Dilation procedure. It aims to answer any questions you may have
Subject: Skilled Nursing Facilities (Page 1 of 6)
") Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Based on the comprehensive assessment of a resident, the facility must ensure that:
 7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * )
 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * )") County of Los Angeles INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * ) * Staff who work in patient care areas 1 ANNUAL CORE
County of Los Angeles INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * ) * Staff who work in patient care areas 1 ANNUAL CORE