Session 15 Accountable Care Organizations Richard Lopez, MD August 12, 2015
|
|
|
- Randolf Morrison
- 5 years ago
- Views:
Transcription

1 Practicing Medicine in the Era of Health Reform Session 15 Accountable Care Organizations Richard Lopez, MD August 12, 2015 Tufts Health Care Institute 1
2 Accountable Care Organizations Richard Lopez, MD Chief Medical Officer Atrius Health August 12,
3 Today s Discussion Introductions Health Care Crisis Reactions to Rising Cost of Healthcare ACO Concept as a Provider Solution Global Payments in support of ACO s ACO Model: BCBSMA AQC ACO Model: Pioneer ACO ACO Results 3

4 Atrius Health The Northeast s largest nonprofit independent multi-specialty medical group. A national leader in delivering high-quality, patient-centered coordinated care. Dedham Medical Associates Granite Medical Group Harvard Vanguard Medical Associates VNA Care Network Providing care for ~ 675,000 adult and pediatric patients with 750 physicians across more than 35 specialties. 4
5 Atrius Health Core Competencies Corporate Data Warehouse integrates single platform, electronic health record data with multi-payer claims data Widespread Extensive Population Health Management including disease-based and risk-based rosters, population managers Long history with and majority of revenue under Global Payment across commercial and public payers Sophisticated development and reporting of Quality and Performance Measures leading to high achievement Patient-Centered Medical Home foundation, achieving level 3 NCQA across all primary care practices Atrius Health, Inc. All rights reserved. Not for distribution.
6 US Health Care Costs as Compared to Gross National Product 6
7 National Healthcare Perspective: Spending vs Life Expectancy The U.S. is off the charts when it comes to health expenditures per capita, but this extensive spending is not performance-based and is not correlated to longer life expectancy. CT MA

8 Workers Are Paying a Greater Share of Health Care Premiums as Employers Strive to Reduce Their Costs 8

 15% 38% 33% 23% 13% 50% 11% Health Care Coverage (State Employees/GIC; Medicaid/Health Reform) Public Health Mental Health Education Infrastructure/")
9 State Healthcare Perspective: Burden of Healthcare Expenditures Growing healthcare expenditures are putting enormous pressure on state budgets throughout the country, forcing budget cuts in most other areas to make room for the growing healthcare component. Massachusetts State Budget ($ Billions), FY 2001 FY2001 FY2011 vs $5.1 B (+59%) -$4.0 B (-20%) 15% 38% 33% 23% 13% 50% 11% Health Care Coverage (State Employees/GIC; Medicaid/Health Reform) Public Health Mental Health Education Infrastructure/ Housing Human Services Local Aid Public Safety SOURCE: Massachusetts Budget and Policy Center 2013 Atrius Health, Inc. All rights reserved.
10 10
11 Response of Commercial Payers and Employers Consumer Driven Products (cost sharing) High deductables Higher copays Defined contribution Tiered physician and hospital networks GIC Tufts Navigator HPHC Independence Limited networks Increased pre-authorization programs Imaging High cost drugs Sleep studies Increased risk sharing with providers (ACO) Employers: Employee Wellness Programs 11
12 Response of Government Part One Federal Accountable Care Organizations Shared Savings Program (CMS) Pioneer ACO Program (CMMI) NexGen ACO (CMMI) Payment Decreases for hospitals and physicians Penalties for hospitals for re-admissions and never events Bundled Payments Bundle Payment for Care Improvement Initiative 12
13 Response of Government Part Two State Chapter 224 passed in August 2012 Limits rate of increase in health care costs to the State s Gross Product Requires payers and providers to provide performance improvement plans if rates exceed SGP Regulates ACO s Requires transparency in pricing by both payers and providers Municipalities Conversion from traditional high cost BCBSMA plans to lower cost Group Insurance Commission (GIC) plans with higher copays and deductibles 13
14 Marketplace Response: Disruptive innovation? Limited service and retail clinics CVS MinuteClinics and Walgreens Take Care Clinics Doctors Express (franchise) CareWell (in partnership with UMASS and Lahey) MedSpring (in partnership with Partners Health Care Best Doctors expert opinion program Video visits, e.g. American Well, Find a doctor when needed: ZocDoc Potential use of out-of-state MDs for telemedicine Employee wellness companies 14
15 Response from Providers (Hospitals, Health Systems, Physician Groups) Heavy pressures on reimbursement rates are resulting in shifts towards accountable care and risk based contracting models Tighter network management of leakage across the spectrum hospital, SNF, outpatient, specialty Stronger care management models- PCMH, High Risk Management Healthcare delivery systems are integrating across the spectrum to optimize care management Hospitals acquiring physicians Physician groups acquiring hospitals Systems acquiring insurance companies Insurance companies acquiring delivery systems Consolidation of health systems, with scale providing significant advantages Access to capital Efficiencies of scale both clinical and administrative Opportunity for white label insurance products Opportunity for direct-to-employer contracting 15
16 The concept of an Accountable Care Organization is not new The existing deficiencies in health care cannot be corrected simply by supplying more personnel, more facilities and more money. These problems can only be solved by organizing the personnel, facilities and financing into a conceptual framework and operating system that will provide optimally for the health needs of the population. Dr. Robert Ebert, Founder, Harvard Community Health Plan, Atrius Health, Inc. All rights reserved
17 Definitions of Accountable Care Organization Academic: Devers & Berenson in RWJ Brief: The ability to provide, and manage with patients, the continuum of care across different institutional settings, including at least ambulatory and inpatient hospital care and possibly post acute care; The capability of prospectively planning budgets and resource needs; and Sufficient size to support comprehensive, valid, and reliable performance measurement. Federal Law: PPACA: an organization of health care providers that agrees to be accountable for the quality, cost, and overall care of Medicare beneficiaries who are enrolled in the traditional fee-forservice program who are assigned to it. Certification: NCQA: provider-based organizations that take responsibility for meeting the health care needs of a defined population with the goal of simultaneously improving health, improving patient experience and reducing per capita costs. MA State Law: Health Policy Commission will define ACO through its certification process and Model ACO certification


18 Migration Towards Accountable Care This means a radical transformation from the perspective of providers, who will need to develop the capabilities to manage a population s health, as well as payors, who will need to transition to risk-based contracting models. Commercial Payors Providers Regulators The act of providers assuming responsibility and financial risk for the quality and total cost of care of a defined population 18


19 Implications for Providers Managing a population s health, and remaining financially viable in a riskbased contracting environment, requires healthcare delivery systems to be truly integrated across the spectrum of care. From Fragmented Care Systems Towards Integrated Care and Population Health Management
20 Massachusetts is a Leader in Medicare ACOs Pioneer ACOs: Atrius Health BIDPO MACIPA Partners Steward Of total 22 nationally Medicare Shared Savings: Accountable Care Clinical Services Accountable Care Org of NE BMC Integrated Care Services Cape Cod Health Network Circle Health Alliance, LLC Collaborative Health ACO Emerald Physicians Harbor Medical Associates, PC Lahey clinical Performance ACO LLC NEQCA Accountable Care Physicians Accountable Care Pioneer Valley Accountable Care Southcoast ACO UMASS Memorial ACO Winchester Community ACO Of total 404 nationally 20
21 Impact of ACO s: Consolidation The Massachusetts market is rapidly moving towards consolidation It is widely predicted that in 3-5 years, a large percentage of healthcare in the Commonwealth will be provided by 5-6 large health care systems: Partners Stewart BIDCO Atrius Health UMass??? 21
22 First Year Results of Medicare Shared Savings ACO Program the numbers Number ACO s Participating: 114 Number of ACO s that saved money: 54 Number of ACO s that saved enough money to collect a bonus: 29 Amount saved: $126M 22
23 Accountable Care is driving fundamental change in health delivery Increase in population management registries, outreach Increased use of data to manage cost and quality Use of nurses to coordinate care for high-risk patients Use of community health workers Creation of preferred post-acute provider network (SNF and VNA) Connecting with local community elder service agencies to provide community-based supports Systematic ways to honor, across the care continuum, patients wishes around end of life care Delivery of a proven post-discharge bundle of services to prevent readmission Increase in disease management programs Patient engagement in shared decision making 23

24 Global Payments provide financing model for an Accountable Care Organization Infrastructure can be Planned and maintained without dependence on patient activity Provided even if not funded in under Fee-for-Service payment Provides stimulus for more efficient use of physician and office time with more convenience to the patient. Funds innovations such as e-portals, text messaging, phone calls and new roles necessary to be with the patient where life is actually being lived by the patient. Fosters use of diverse medical teams working at top of license
25 BCBSMA Alternative Quality Contract was Early Model for ACO Accountability for quality and resource use across full care continuum Long-term (5-years) Annual inflation tied to Consumer Price Index Improved quality, safety & outcomes as compared with traditional Pay-for-Performance Robust performance measure set (60+ measures) creates accountability for quality, safety & outcomes across continuum and over time Substantial financial incentives for high performance
26 Experience with AQC helped us step up our game Early adopter based on prior managed care experience Investments made to retool factory include Lean, Leadership Academy, Patient Centered Medical Home Quality framework provided focus and common language across Atrius Health groups Established strong precedent for joining Medicare Pioneer ACO Program Other Mass payers have followed suit


27 Lean is an important Foundation for our work 27

28 Why Participate in Pioneer ACO? Reason for Action High quality, high value care for all Medicare eligible patients across the care continuum with spillover for commercial risk Unique opportunity to be accountable for quality and costs for a PPO population Further Atrius Health position as a market leader in payment reform, moving towards 100% global payment Achieving Triple Aim Goals Ạtrius 28
29 Key Features of Pioneer & Performance Measures Three year contract effective January 2012 with two additional year options; accountable for all Medicare A and B benefits Partnership with Center for Medicare and Medicaid Innovation (CMMI) Medicare FFS beneficiaries aligned with ACO based on their historical claims data Global budget: performance measured against national benchmark Incentives rewards to achieve high quality performance measurements Upside & downside risk sharing with CMS Accountable to Pioneer ACO Obligations 29
30 Financial Measures: Shared saving/loss Atrius Health Goal: To beat the Benchmark Benchmark Think Global Budget Baseline Based on Actual Claim for ACO population Based on Growth Rate from National Matched Cohort 30
31 Quality Measures: Key Features Patient/caregiver experience, measured by CG-CAHPS 33 Quality Measures: many new, or with new features Care coordination/patient safety using claims data (eg. Readmission rates) At Risk Population, using EHR measures Diabetes IVD CAD Heart Failure Hypertension Preventive Health


32 Pioneer ACO Strategies Address Gaps Hospital Strategy Dual Population Medicare/Medicaid Strategy Geriatric Care Model Care Management Strategy Post-Acute Strategy PATIENT CENTERED MEDICAL HOME Costs: Beat the Trend Quality:100% Reporting th Percentile 2013 Quality & Safety Electronic Health Records & Health Information Exchange Data Analytics & Reporting Regulatory Internal Communication & Structure
33 ACO = Medicare Population Health Strategy Approximately 52,000 Medicare Beneficiaries in Outcomes-Based Contracts with Triple-Aim Accountability 1000 Pioneer Aligned 21,000 30,000 Medicare Advantage Duals HMOs 33
34 Accountable Care = Population Management What is the target population? How is the cohort defined? How is accountability defined? What population outcomes do we want & how are they measured? What conceptual framework links potential care processes to target outcomes? What are the overall key indicators? What are interim process/operational indicators? How do we support the key processes required to achieve outcomes? Which of these processes are most effective, efficient, and patient centered? What infrastructure is required to ensure reliable frontline process execution?. 34
35 Medicare Population Health Approach Close medical management at end of life Tight coordination of 5% highest risk Medical Management of chronic conditions Preventative Care for well patients Advanced Illness Management - Top 2% Other High Risk/Acute - Another 3% Chronic Care Management - Next 15% Population Management - Remaining 80%» Local Implementation Practices at different starting points.» Central support to reach goals, manage CMS relationship and obligations. Atrius Health All rights 35 reserved
36 Focus One: High Risk Patients, High Cost Events Advanced Illness Management - Top 2% Other High Risk/Acute - Another 3% Chronic Care Management - Next 15% Population Management - Remaining 80% Advance Care Planning High Risk Roster Review Care Transitions Post Acute Episode Mgmt CKD Community Support for Dual Eligibles 36


37 Focus Two: Health Risk Prevention Advanced Illness Management - Top 2% Other High Risk/Acute - Another 3% Chronic Care Management - Next 15% Population Management - Remaining 80% Falls Risk/Fractures Depression Screening Med Reconciliation 37
38 Keep Working the Medicare Population Pyramid Advanced Illness Management - Top 2% Other High Risk/Acute - Another 3% Chronic Care Management - Next 15% Population Management - Remaining 80% 2015 Focus: Custodial Nursing Home program Palliative Care/Hospice Care Transitions COPD Expanded home telemonitoring New ACO Quality Measures 38
39 The Triple Aim Population Health Per Capita Cost Experience Of Care The root of the problem in health care is that the business models of almost all US health care organizations depend on keeping these aims separate. Society on the other hand needs these three aims optimized (given appropriate weightings on the components) simultaneously. Tom Nolan, PhD. Source: IHI.org 39

40 Outputs: Population Health Initiatives Identify Gaps Design Program Develop Tools Implement Track & Measures Continuous Improvement Triple Aim Inputs: Quality Measurement and Improvement, Data Analytics, Medical Management, Clinical Champions, Internal Best Practices, External Peer Accomplishments 40
41 Key ACO Initiatives: Our Investments Geriatric Care Model Patient Risk Stratification Multidisciplinary Roster Reviews Advance Care Planning Chronic Kidney Disease Care Management ( Post Acute Home ) VNACNH Integration Local Elder Services Agencies Programs for Dual-Eligibles Shared standards and best practices Data Analytics & Reporting Ongoing Support for Workgroup Initiatives Trackers to monitor performance against goals Electronic Health Record and Health Information Exchange Tools to Support ACO Quality Metrics & Workflow Acute/Post Acute Preferred Providers Strategies Preferred SNF Network with service standards/facility expectations SNF Provider Expectations Preferred Hospital strategy Preferred ambulance strategy Quality & Safety ACO Quality Metric Reporting Performance Improvement/Best Practices 41

42 Medicare High Risk Model: Patient Risk Stratification Tool Using both claims and Electronic Health Records databases, the tool allows to identify members at risk of hospitalization, poor health outcomes, high costs Factor The model consists of five key factors: Likelihood of Hospitalization Hospital admissions or ED visits Behavioral Health diagnosis CHF or COPD >= 15 medications Pts DxCG Likelihood of Hospitalization Score 3 (Model 71) Hospital Admissions or ED Visits 3 Behavioral Health (Psychiatric, Substance 2 Abuse, Dementia) CHF or COPD or CKD 1 Poly-pharmacy (Excludes Topical & 1 Supplies) Maximum Score 10 Proportions of High Cost (Atrius Health ACO) Patients & attributable to them Costs (Aug 2012) 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 20% of patients Patients 60% of costs ACO TME % DECEASED % ALIVE H/VH Risk % OTHERS 42
43 High Risk Patient Roster Review Confirm diagnoses Review medications Address quality measures Social assessment Care needs assessment PCP-Led Team Advance directives Palliative care discussion Care plan documentation & orders. 43

44 High Risk Roster Participants Each site may choose to have any number or combination of participants so long as the goals of high risk roster reviews are being met. Typical participants include: PCP Primary Nurse or Medical Assistant Population Manager Care Manager Geriatric Champion or Palliative Care Specialist Social Worker VNA representative Clinical Pharmacist Atrius Health All rights reserved 44
45 Geriatric Care Model: Multidisciplinary Roster Reviews Review and confirm accuracy of diagnosis Adopted common standards for High Risk Patient Roster Reviews Review appropriateness of medications Perform a care needs assessment Create a clinical summary of the patient Perform a social assessment Review applicable diseases related quality measures Confirm existence and need for advance directives Update the patient s care plan and document next steps Early adopters of HRRR saw greater reductions in TME 45
46 Advance Care Planning Initiatives Description: Developed advance care planning (ACP) curriculum with CME/CEU credits. Established site based ACP champions to train and provide ongoing ACP support locally Developed new tools in Epic to track and document advance care planning Expected Outcomes: Improve PCP knowledge and comfort with ACP Increase end of life conversations and collection of patient s care wishes, advance directives and proxy information Minimize use of aggressive curative care when not aligned with patient s care wishes 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% ACP and 2014 MOLST Trainings ACP 82% MOLST 86%
47 Advance Care Planning: Results Implemented EMR checklist 47
48 Geriatric Care Model: Chronic Kidney Disease Description Clinical guidelines Provider education & training Patient education and engagement Keeping services in house when appropriate Expectations for outside nephrologists Epic tools Risk score modification Results In first 5 months, 66% of patients with lab defined criteria were diagnosed with CKD triggering clinical interventions. Expected Outcomes Improve diagnosis Slow progression of CKD 48
49 CKD: Clinical Guidelines Atrius Health CKD Guidelines for Primary Care Stage (egfr) Albuminuria? ( 30mg/g) Serum egfr and Urine Microalbumin Hgb, 25-OH Vit D, Phos, PTH, Lipids, Ca Electrolytes Initial Renal Ultrasound Nephrology Consult Stage 3a (45-59) No Annually* Annually* Consider Stage 3a; (45-59) Yes Q6 Month* Annually* Consider Recommend Stage 3b; (30-44) No Q6 Month* Annually* Consider Recommend Stage 3b; (30-44) Yes Q4-6 Month* Annually* Consider Recommend Stage 4; (15-29) N/A Q3 Month* Annually* Consider Recommend * Might require more frequent monitoring if abnormal and/or if undergoing changing treatment strategies Kidney International, Jan 2013; Supplement 3 KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: Approved by the Atrius Health Accountable Care Organization s Geriatric Care Model CKD Workgroup, which includes the Harvard Vanguard Chief of Nephrology; February
 - Clinical Outcomes (BP, LDL, HgA1c) - Referral to Nephrologist Specialist - Visit to")
50 CKD Dashboard/Roster Primary Care Dashboard: Merge of EPIC and Claims Data - Lab Result Based Total CKD Population - Laboratory Screening (Ca, Phos, CBC, UA, Vit D, PTH) - Clinical Outcomes (BP, LDL, HgA1c) - Referral to Nephrologist Specialist - Visit to Nephrologist 50
51 CKD: Impact 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Patients w/egfr<60 CKD Dx No CKD Dx. 51
52 Post-Acute Home Workgroup: Stronger Collaboration with VNACN Developed Standard Work for referrals to and communication with VNACNH during episode of care. Care plan transmitted to EPIC within 48 hours of admission, including: Advance care planning forms Follow up appointment with PCP within 7 days of hospital discharge Collection of ACO quality metrics * Fall risk assessment * Medication review * Depression screen (PHQ) 2 We see a decrease in VNA $pmpm and a decrease in readmits during VNA episode Atrius Health, Inc. All rights reserved.
53 PAH Tracker: By Medical Group Post Acute Home (by Medical Group) YTD Jan 2014 thru October 2014 YTD (Claims paid through December 2014) VNACNF Episodes as % total HHA Episodes PION VNACNF Episodes as % total HHA Episodes TMP ED visit/k during VNACNF Episode PION Readmit Rate during VNACNF Episode PION % Patients with VNACNF Episode with ACP in Epic PION % Duals Enrolled DMA 53% 72% 84 17% 86% 15% GRN 40% 64% 92 20% 67% 15% HVMA 32% 65% % 67% 20% RMG 42% 68% % not available 50% SMG 35% 61% % 75% 22%
54 Tracking VNA Performance PAH 2015 Q1 Utilization A. ED Visit per 1000 during NON VNACNF episode/admission B. ED Visit per 1000 during VNACNF episode/admission C. Readmit rate during NON VNACNF episode/admission D. Readmit rate during VNACNF episode/admission E. VNACNF episodes/admissions as % of all home health episodes/admissions Quality % of patients admitted to VNACNF who have Falls Risk Assessment (FRA) scanned in EPIC within the episode/admission % of patients admitted to VNACNF who have Depression Screening scanned in EPIC within the episode/admission % of patients admitted to VNACNF who have ACP form (MOLST, Adv Dir, or HCP) in EPIC VNACNF Pre op Joint visits completed (all payers) % of total joint replacement discharges going home with VNA 2015 PION Goal Atrius YTD thru TMP PION NA VNACNF lower than NON VNACNF NA 22% 11% VNACNF lower than NON VNACNF 17% 11% 37% 68% 37% 94% 95% 88% 94% 93% 87% watch until Q4 79% 75% watch 65 Q1 watch 20% 37% PION YTD RPM Program (began May 2015 all payers) a. # of referrals Q2 & Q3 watch b. accepted to program Q2 & Q3 watch Acute hospital admissions during an RPM Q2 & Q3 watch episode VNACNF Patient Experience A. % of referrals with timely initiation of care 95% 94% B. AH complaints % of investigations initiated within 48 hours C. AH complaints % resolved within 30 days 92% 92% 2015 YTD thru 100% (12/12) 75% (9/12) May 5 3 0

55 Post-Acute Home Workgroup: Integrate Local Elder Services (ASAPs) 55
56 Variation in 2010 Medicare Average Length of Stay for Skilled Nursing Facilities Difference Between Top & Bottom Quartile 10 Days = $4, Quartile 1 Quartile 2 Quartile 3 Quartile 4 ALOS Source: Adapted from Office of HHS Inspector General December Adapted from Slides presented by Robert Mechanic, Brandeis University, with permission
57 Variation in 2009 Risk Adjusted Readmission Rates from Skilled Nursing Facilities 30.0% 25.0% 20.0% 15.0% 10.0% 5.0% 14.4% 18.1% 22.0% 0.0% 25th Percentile Median 75th Percentile Readmissions Source: MedPAC Report to Congress, March Adapted from Slides presented by Robert Mechanic, Brandeis University, with permission 57


58 Development of Preferred SNFs Network Meet service standards SNF willingness to collaborate Good metrics* Created preferred SNF network to enhance the delivery and coordination of care Atrius Health team on site History of positive relationship Geographic needs *Good Metrics: Medicare Compare; State survey; Readmission during SNF stay; LOS 58






59 Managing SNF Events Developed expectations and tools to manage length of stay Facility level expectations Provider level expectations Discharge workflow EHR documentation Monitoring & reporting Use of preferred discharge providers 2.0 LOS = $2M 2% Readmit Rate = $.5M 59


60 Still Lots of Opportunity Preferred Non-Preferred 60
61 EHR tools to support ACO: Standard Checklist and Shared Workflows Tools were developed to facilitate: Advanced Care Planning Fall Risk Assessment Depression screening Medication Reconciliation Patient Care Checklist Advance Care Planning documents are not on file A Falls Risk Assessment has not been completed in the current calendar year A PHQ-2 or PHQ-9 has not been completed in the current calendar year Tobacco use has not been reviewed in the current calendar year BMI has not been updated within the past 6 months CHARTING Patient Checklist Visit Info Allergies Vitals Patient Care Checklist Advance Care Planning documents on file A Falls Risk Assessment has been completed in the current calendar year A PHQ-2 or PHQ-9 has been completed in the current calendar year Tobacco use has been reviewed in the current calendar year BMI has been updated within the past 6 months 61
62 Depression Screen & Fall Risk Assessment Reset FRA, PHQ Checklist Implemented EMR checklist 62




63 Data Analytics and Reporting provides Ongoing Support for Workgroup Initiatives

64 #1 ACO in New England; #2 Pioneer Nationally 64
 control < 8 BP = % of hypertensive patient population with blood pressure control")
65 First Year Pioneer Results: 2012 ACO Quality Metrics Atrius Health compared to Pioneer ACO Range A1c = % of diabetic patient population with blood sugar (hgba1c) control < 8 BP = % of hypertensive patient population with blood pressure control <140/90 Tobacco = % of diabetic patient population who do not currently smoke Aspirin = % of diabetics with ischemic vascular disease (IVD) who are currently taking aspirin ACE/ARB = % of patients with coronary artery disease (CAD) who are also diabetics OR have left ventricular systolic dysfunction (LVSD) and are on an angiotensin converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) 65
:2152-2161. doi:10.1001/jama.2015.4930.")
66 Independent Near Market Evaluation, May 2015 Association of Pioneer Accountable Care Organizations vs Traditional Medicare Fee for Service With Spending, Utilization, and Patient Experience JAMA. 2015;313(21): doi: /jama Pioneer ACOs saved $384M over two years Atrius Health saved $36M compared to near market Ten of 32 Original Pioneers had statistically significant savings in both years Atrius Health was one of the ten Atrius Health noted as one of three Pioneers accounting for 70% of savings in
67 Pioneer Financial Performance Year over Year Improvement 2012 (PY1) = 1% loss, in the noise Atrius Health expenditure $10,700 vs. Massachusetts Pioneer Expenditure $12, (PY2) = 1% savings, in the noise * $3M saved for Medicare 2014 (PY3) = Projecting 1.4% savings, would be: * $4.5M saved for Medicare * $2.8M share to Atrius Health 67
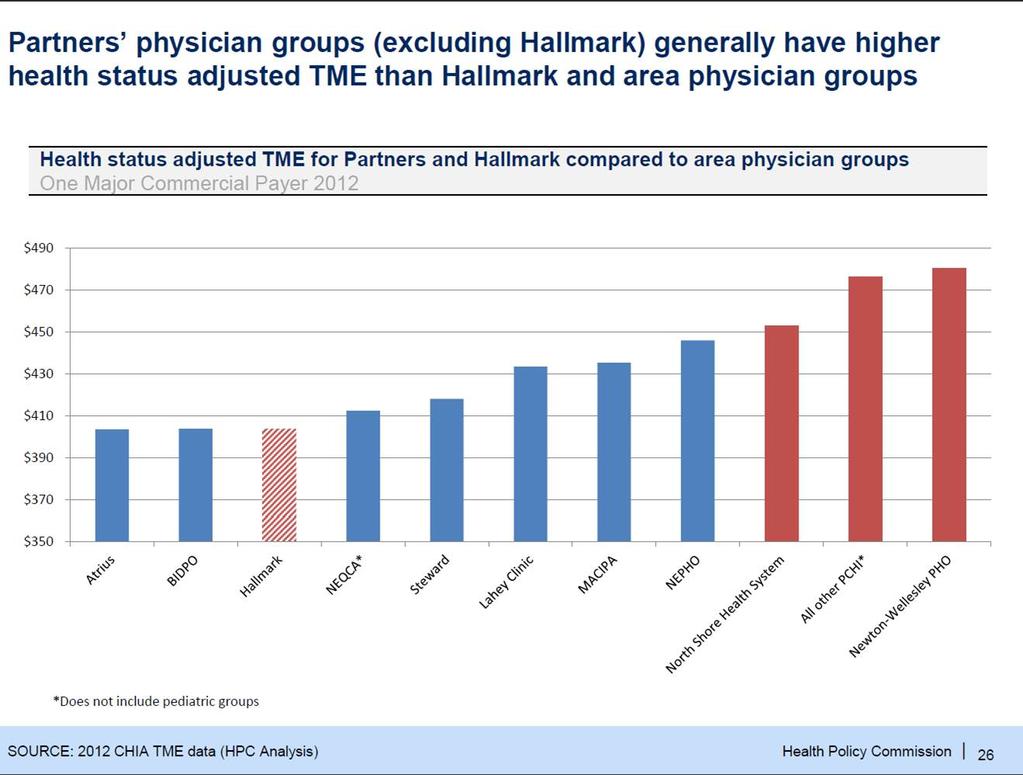
68 From the JAMA Article BIDCO MACIPA Steward Atrius Health Partners 68
69 Side by Side Settlement: Beat the Trend. 69
70
71 71
72 Keys to Success Leadership and Facilitation Create the data-based hypothesis Identify evidence-based best practice Develop standards & tools to close gaps Measure and track Outcomes Fidelity to Process Core Competencies Small team with operational credibility Diverse clinical expertise Share resources clustered together (no silos) Home for shared values Exploratory mindset Laser focus on triple aim 72

73 Lessons Learned Internal MD engagement key to driving change Wide adoption of Lean problem solving methodology created strong foundation for change One Model, One Contract provided burning platform Making long-lasting change takes time Our ability to partner effectively is key CMS More unknowns = more risk It s bigger than CMS - many federal agencies have a stake Engagement of other Pioneers big opportunity, but differing priorities CMS is moving up the learning curve too
74 This image cannot currently be displayed. This image cannot currently be displayed. We will challenge Simple rules I am accountable We are accountable From Accountable Care Organizations, Marc Bard and Mike Nugent,
75 Two Kinds of Change Technical Problem is well-defined Solution is known, can be found Implementation is clear From Jack Silversin, Amicus Adaptive Challenge is complex To solve requires transforming longstanding habits and deeply held assumptions and values Involves feelings of loss, sacrifice (sometimes betrayal to values) Solutions requires learning and a new way of thinking, new relationships 75
76 Reflections We shall not cease from exploration. And the end of all our exploring will be to arrive where we started and know that place for the first time. T.S. Eliot 76
77 Reflections The future we predict today is not inevitable. We can influence it, if we know what we want it to be We can and should be in charge of our own destinies in a time of change. Charles Handy The Age of Unreason 77
How ACO s Are Thinking of Home Care: the Atrius Health Experience
 How ACO s Are Thinking of Home Care: the Atrius Health Experience Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org May 29, 2014 Contents Overview of Atrius Health Overview of Pioneer
How ACO s Are Thinking of Home Care: the Atrius Health Experience Richard Lopez, MD Chief Medical Officer Richard_Lopez@AtriusHealth.org May 29, 2014 Contents Overview of Atrius Health Overview of Pioneer
Medical Management in the Era of Value Based Payments. Rick Lopez, MD
 Medical Management in the Era of Value Based Payments Rick Lopez, MD 1 Brief Overview of Today s Discussion Value Based Payment: The Changing Environment of Alternative Payments Ideal Organizational Attributes
Medical Management in the Era of Value Based Payments Rick Lopez, MD 1 Brief Overview of Today s Discussion Value Based Payment: The Changing Environment of Alternative Payments Ideal Organizational Attributes
Medical Home as a Platform for Population Health
 Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
3/29/2013. Effective ACO Compliance. Objectives THE HEALTH CARE DILEMMA: ARE ACOS THE ANSWER? HCCA Compliance Institute April 21, 2013
 Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
National ACO Summit. Third Annual. June 6 8, Follow us on Twitter and use #ACOsummit.
 Third Annual National ACO Summit June 6 8, 2012 Follow us on Twitter at @ACO_LN and use #ACOsummit. The Engelberg Center for Health Care Reform at Brookings The Dartmouth Institute Infrastructure for Quality
Third Annual National ACO Summit June 6 8, 2012 Follow us on Twitter at @ACO_LN and use #ACOsummit. The Engelberg Center for Health Care Reform at Brookings The Dartmouth Institute Infrastructure for Quality
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Long term commitment to a new vision. Medical Director February 9, 2011
 ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Practice Implications for Accountable Care Organizations
 Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Quality Measurement, Population Health and Payment Reform
 Quality Measurement, Population Health and Payment Reform The Move from Volume to Value Dale W. Bratzler, DO, MPH, FACOI, FIDSA Professor, Colleges of Medicine and Public Health Associate Dean, College
Quality Measurement, Population Health and Payment Reform The Move from Volume to Value Dale W. Bratzler, DO, MPH, FACOI, FIDSA Professor, Colleges of Medicine and Public Health Associate Dean, College
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
ACO Information Required to be Published on ACO Website per CMS Regulations
 ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Slide 1. Slide 2 Rural Princeton. Slide 3 Agenda Rural ACO RURAL ACOS CAN WORK AND LEAD THE WAY
 Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Holding the Line: How Massachusetts Physicians Are Containing Costs
 Holding the Line: How Massachusetts Physicians Are Containing Costs 2017 Massachusetts Medical Society. All rights reserved. INTRODUCTION Massachusetts is a high-cost state for health care, and costs continue
Holding the Line: How Massachusetts Physicians Are Containing Costs 2017 Massachusetts Medical Society. All rights reserved. INTRODUCTION Massachusetts is a high-cost state for health care, and costs continue
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together
 Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
PCMH to ACO: Carilion Clinic s Journey
 PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
Intro to Global Budgeting
 Intro to Global Budgeting Jim Hester House Health Care Committee & Senate Health & Welfare Committee 1/21/10 Agenda Goal of global budgeting Global budget models and examples Global payment model and examples
Intro to Global Budgeting Jim Hester House Health Care Committee & Senate Health & Welfare Committee 1/21/10 Agenda Goal of global budgeting Global budget models and examples Global payment model and examples
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
The Accountable Care Organization Specific Objectives
 Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS
 UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Health System Transformation. Discussion
 Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Future of Patient Safety and Healthcare Quality
 Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011
 Accountable Care: Health System View CHC Best Practices Forum Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011 Who we are Southeastern New Jersey s largest health system
Accountable Care: Health System View CHC Best Practices Forum Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011 Who we are Southeastern New Jersey s largest health system
Beyond the Horizon: What s Next? Session PH6, March 5, 2018 Don Calcagno, President, Advocate Physician Partners
 Beyond the Horizon: What s Next? Session PH6, March 5, 2018 Don Calcagno, President, Advocate Physician Partners 1 Conflict of Interest Don Calcagno Has no real or apparent conflicts of interest to report.
Beyond the Horizon: What s Next? Session PH6, March 5, 2018 Don Calcagno, President, Advocate Physician Partners 1 Conflict of Interest Don Calcagno Has no real or apparent conflicts of interest to report.
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
1.01 Government Programs: CMS and Pay for Performance: Current Issues. CMS Regional Administrator March 2009
 1.01 Government Programs: CMS and Pay for Performance: Current Issues David Saÿen CMS Regional Administrator March 2009 Overview Why value-based purchasing? What demonstrations are underway? Hospital demonstrations
1.01 Government Programs: CMS and Pay for Performance: Current Issues David Saÿen CMS Regional Administrator March 2009 Overview Why value-based purchasing? What demonstrations are underway? Hospital demonstrations
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance
 Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Oregon s Health System Transformation: The Coordinated Care Model. March 2014 Jeanene Smith MD, MPH Chief Medical Officer- Oregon Health Authority
 Oregon s Health System Transformation: The Coordinated Care Model March 2014 Jeanene Smith MD, MPH Chief Medical Officer- Oregon Health Authority The Challenges Oregon Faced Rising healthcare costs outpacing
Oregon s Health System Transformation: The Coordinated Care Model March 2014 Jeanene Smith MD, MPH Chief Medical Officer- Oregon Health Authority The Challenges Oregon Faced Rising healthcare costs outpacing
Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations
 Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations Executive Summary Rural networks across the nation have been working with rural providers to assist
Proposed CMMI Rural Shared Savings Demonstration Project: Frontier/Rural Community Care Organizations Executive Summary Rural networks across the nation have been working with rural providers to assist
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
The Center for Medicare & Medicaid Innovations: Programs & Initiatives
 The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
A strategy for building a value-based care program
 3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
AGENDA. QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, /21/2014
 QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
HOME DIALYSIS REIMBURSEMENT AND POLICY. Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation
 HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Actionable Data and Physician Engagement Drive ACO Success
 Actionable Data and Physician Engagement Drive ACO Success Session #100, February 21, 2017 Christy Cawthon, University of Texas Southwestern Medical Center Sam Stearns, Verscend Technologies 1 Speaker
Actionable Data and Physician Engagement Drive ACO Success Session #100, February 21, 2017 Christy Cawthon, University of Texas Southwestern Medical Center Sam Stearns, Verscend Technologies 1 Speaker
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Payment Reform Strategies. Ann Thomas Burnett BlueCross BlueShield of South Carolina
 Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015
 Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Keeping Your Diabetes Education Program Stable In the Era Of Health Care Reform and Accountable Care Organizations
 Keeping Your Diabetes Education Program Stable In the Era Of Health Care Reform and Accountable Care Organizations Nicole Downey, MBA, RD, CDE Program Director Diabetes Services The Polyclinic Seattle,
Keeping Your Diabetes Education Program Stable In the Era Of Health Care Reform and Accountable Care Organizations Nicole Downey, MBA, RD, CDE Program Director Diabetes Services The Polyclinic Seattle,
Shared Savings Program ACO Public Report
 ACO ame and Location Shared Savings Program ACO Public Report University of Health Alliance Accountable Care Organization, LLC 1227 E. Rusholme Street Davenport, 52803 ACO Primary Contact Primary Contact
ACO ame and Location Shared Savings Program ACO Public Report University of Health Alliance Accountable Care Organization, LLC 1227 E. Rusholme Street Davenport, 52803 ACO Primary Contact Primary Contact
Creating a Population Health Strategy that Scales
 Creating a Population Health Strategy that Scales Session #72, March 6, 2018 Renee Broadbent, AVP, Population Health IT & Strategy, UMass Memorial Health Care 1 Conflict of Interest Renee Broadbent, MBA
Creating a Population Health Strategy that Scales Session #72, March 6, 2018 Renee Broadbent, AVP, Population Health IT & Strategy, UMass Memorial Health Care 1 Conflict of Interest Renee Broadbent, MBA
Improving Clinical Outcomes
 Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth