Adult BH Home & Community Based Services (HCBS) In Person Trainings JULY, 2016
|
|
|
- Delilah Doyle
- 5 years ago
- Views:
Transcription
1 Adult BH Home & Community Based Services (HCBS) In Person Trainings JULY, 2016 July 8, 2016
2 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will be reviewed and incorporated into future trainings and presentations, added to Q&A resources when possible. Reminder: Information and timelines are current as of the date of the presentation
3 Schedule 9:30-10:30: HCBS Foundations 10:30-11:15: Hab/Rehab/CPST 11:15-11:30: BREAK 11:30-12:15: Hab/Rehab/CPST Cont. 12:15-1: LUNCH 1-2:30: Peer Support & Family Support 2:30-2:45: BREAK 2:45-4: Education & Employment 4-5: Crisis Respite/Tools/Future Offerings
4 Adult BH HCBS Value/Core Principles
5 Value/Core Principles The development of Health and Recovery Plans (HARPs) is intended to promote significant improvements in the Behavioral Health System as we move into a recovery- based Managed Care delivery model. A recovery model of care emphasizes and supports a person's potential for recovery by optimizing quality of life and reducing symptoms of mental illness and substance use disorders through empowerment, choice, treatment, educational, employment, housing, and health and well-being goals. The Behavioral Health Home and Community Based Services (BH HCBS) provide opportunities for adult Medicaid beneficiaries with mental illness and/or substance use disorders to receive services in their own home or community. Implementation of BH HCBS will help to create an environment where managed care plans, service providers, plan members, families, and government partner to help members prevent and manage chronic health conditions and recover from serious mental illness and substance use disorders. The partnership will be based on these core principles:
6 Value/Core Principles Cont. Person-Centered Care: Services should reflect an individual s goals and emphasize shared decisionmaking approaches that empower members, provide choice, and minimize stigma. Services should be designed to optimally treat illness and emphasize wellness and attention to the persons overall well- being and full community inclusion. Recovery-Oriented: Services should be provided based on the principle that all individuals have the capacity to recover from mental illness and/or substance use disorders. Specifically, services should support the acquisition of living, employment, and social skills and be offered in home and community-based settings that promote hope and encourage each person to establish an individual path towards recovery.
7 Value/Core Principles Cont. Integrated: Services should address both physical and behavioral health needs of individuals. Care coordination activities should be the foundation for care plans, along with efforts to foster individual responsibility for health awareness. Data-Driven: Providers should use data to define outcomes, monitor performance, and promote health and well-being. Performance metrics should reflect a broad range of health and recovery indicators beyond those related to acute care. Evidence-Based: Services should utilize evidence-based practices where appropriate and provide or enable continuing education activities to promote uptake of these practices. Trauma-Informed: Trauma-informed services are based on an understanding of the vulnerabilities or triggers experienced by trauma survivors that may be exacerbated through traditional service delivery approaches so that these services and programs can be more supportive and avoid re-traumatization. All programs should engage all individuals with the assumption that trauma has occurred within their lives. (SAMHSA, 2014)
8 Value/Core Principles Cont. Peer-Supported: Peers will play an integral role in the delivery of services and the promotion of recovery principles. Culturally Competent: Culturally competent services that contain a wide range of expertise in treating and assisting people with Serious Mental Illness (SMI) and Substance Use Disorder (SUD) in a manner responsive to cultural diversity. Flexible and Mobile: Services should adapt to the specific and changing needs of each individual, using off-site community service delivery approaches along with therapeutic methods and recovery approaches which best suit each individual s needs. BH HCBS, where indicated, may be provided in home or off-site, including appropriate community settings such as where an individual works, attends school or socializes. Inclusive of Social Network: The individual, and when appropriate, family members and other key members of the individual s social network are always invited to initial meetings, or any necessary meetings thereafter to mobilize support. Coordination and Collaboration: These characteristics should guide all aspects of treatment and rehabilitation to support effective partnerships among the individual, family and other key natural supports and service providers.
9 Adult BH HCBS Eligibility
10 Adult BH Medicaid Managed Care MEDICAID MANAGED CARE BH MEDICAID MANAGED CARE MAINSTREAM HEALTH & RECOVERY PLAN (HARP) Adults 21 + HIV SNPs HCBS Eligibility Assessment HCBS Eligible Tier 1 or 2 Not Eligible
11 Adult BH HCBS Eligibility State Identified HARP enrolled Medicaid beneficiaries age 21 and older Individuals enrolled in HIV SNPs determined by the State to be HARP-eligible Meets eligibility criteria on the HCBS Eligibility Assessment Tier 1 -- Services include employment, education and peer supports services Tier 2 -- Includes the full array of Adult BH HCBS H Codes indicate HCBS eligibility - available on EPACES
12 HCBS Eligibility Assessment & Referral Role of the Health Home HH Workflow conducts eligibility assessment (for HARP enrolled) develops person-centered Plan of Care Refers to HCBS designated provider of choice (after MCO approves Level of Service Determination) in a conflict-free manner Completes full CMHA (best practice 30 days, up to 90 days) 7/8/2016
13 New York State Process for Conflict Free Adult BH HCBS Referral HARP enrollees shall be provided with a choice of HCBS designated providers from the MCO s network of a particular service. With respect to conflict-free care management requirements for Health Homes: To promote and ensure integrated care for the best interest of the client, it is possible that an individual may receive care management and direct care services from the same entity, however, in these instances the care management and direct service components will be under different administrative/supervisory structures.
14 Adult BH HCBS Service Specific Intake/Evaluation (Assessment) BH HCBS provider receives referral and POC from HH and completes the following within 3 visits/14 days (of first visit) conducts an service specific intake/evaluation (assessment) develops an Individualized Service Plan submits Authorization Form to MCO with frequency, intensity, and duration It is recommended that providers talk to the Managed Care Organization to determine their specific health plan s process as it relates to LOS and Authorization for the 3 visits.
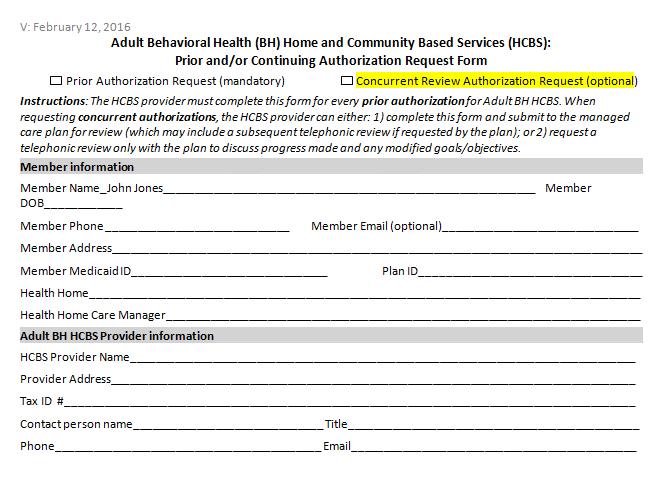
15 Adult BH HCBS Prior and/or Continuing Authorization Process
16 BH HCBS Authorization Adult BH HCBS Providers must complete the prior authorization form for every Adult BH HCBS. When requesting concurrent authorizations, the HCBS provider can choose to either: 1) complete this form and submit it to the managed care plan for review (which may include a subsequent telephonic review if requested by the plan); or 2) request a telephonic review only with the plan to discuss progress made and any modified goals/objectives.
17 BH HCBS Authorization Cont. Plans may not require providers to complete and submit the form for concurrent reviews if the provider does not wish to. Submission of authorization form does not preclude telephonic review, which may be required by MCO/BHO. NYS encourages providers to reach out to the MCO/BHO regarding authorization protocol to ensure timely delivery of services for members. Request telephonic reviews at any point in the review process Plans may request case documentation as needed to ensure appropriate access to services and desired outcomes.
18 Adult BH HCBS Prior and/or Continuing Authorization Request Form Form Review The Managed Care Technical Assistance Center of New York
19
20
21
22
23
24
25
26 Billing Guidelines
27 Billing Guidelines/Requirements Co-Mingling Not Allowed Space Use OASAS & OMH There is nothing prohibiting an OMH or OASAS outpatient licensed provider from allowing an HCBS service to be provided out of their licensed space, so long as such services do not take away from the resources that the licensed program is licensed/funded by OASAS or OMH to provide Staff Sharing Allowed. Staff time must be allocated and meet all regulatory requirements Group Services Not Allowed except for PSR & Family Support Services cannot be provided telephonically
28 HCBS Utilization Thresholds HCBS services will be subject to utilization caps at the recipient level that apply on a calendar year basis. These limits will fall into three categories: 1. Tier 1 HCBS services will be limited to $8,000 as a group. There will also be a 25% corridor on this threshold that will allow plans to go up to $10,000 without a disallowance. 2. There will also be an overall cap of $16,000 on HCBS services (Tier 1 and Tier 2 combined). There will also be a 25% corridor on this threshold that will allow plans to go up to $20,000 without a disallowance. 3. Both cap 1 and cap 2 are exclusive of crisis respite. The two crisis respite services are limited within their own individual caps (7 days per episode, 21 days per year). If a Plan anticipates they will exceed any limit for clinical reasons they should contact the HARP medical director from either OMH or OASAS and get approval for a specific dollar increase above the $10,000 effective limit.
29 HCBS/State Plan Services Allowable Billing Combinations of State Plan and HCBS Clinic/OTP ACT PROS IPRT/CDT Partial Hospital* PSR YES YES CPST YES/NO YES Habilitation YES YES YES YES Family Support and Training YES YES YES Education Support Services YES YES YES YES Peer Support Services YES YES YES YES Employment Services YES YES YES *If a participant is admitted into a Partial Hospital program, their HCBS payments will be suspended so that their services will not be terminated. ** All HARP Members are eligible for Crisis Respite Services
30 Allowable Billing Combinations of HCBS and HCBS HCBS Combinations PSR CPST Habilitation Family Support and Training Education Support Services Peer Support Services Employment Services PSR* YES YES YES YES YES YES CPST YES YES YES YES YES YES Habilitation* YES YES YES YES YES YES Family Support and Training YES YES YES YES YES YES Education Support Services YES YES YES YES YES YES Peer Support Services YES YES YES YES YES YES Employment Services YES YES YES YES YES YES * PSR and Habilitation may only be provided at the same time by the same agency. ** All HARP Members are eligible for Crisis Respite Services
31 Documentation Requirements & Quality Assurance/Improvement
32 Documentation Requirements Adult BH HCBS Service Specific Intake/Evaluation (Assessment) Encounter Note Individual Service Plan Discharge Plan It is recommended that HCBS providers have a copy of the Plan of Care and NYS Community Mental Health Assessment
33 Documentation Requirements Cont. BH HCBS Documentation requirements for individual service encounters: Name of consumer Type of service provided Date of service provided Location of service Duration of service, including start and end times Description of interventions to meet Plan of Care goals Outcome (s) or progress made toward goal achievement Follow up/ next steps Your name, qualifications, signature and date
34 Quality Assurance Reviews Quality Assurance reviews and claims audits will be conducted by NYS or its designee, including Local Government Units, to ensure providers comply with the rules, regulations, and standards of the program, and may be conducted without prior notice. The Quality Assurance reviews will focus on program aspects, but may include technical requirements such as billing, claims, and other Medicaid program requirements. Managed care plans may also be developing protocols to oversee the provision of these services in their provider networks.
35 CMS Settings Rule Summary of CMS Final Rule Regarding Settings The CMS final rule requires that all Home and Community Based settings meet certain qualifications. These include that the setting: Is integrated in and supports full access to the greater community; Is selected by the individual from among setting options; Ensures individual rights of privacy, dignity, and respect, and freedom from coercion and restraint; Optimizes autonomy and independence in making life choices; and Facilitates choice regarding services and who provides them
36 CMS Settings Rule Cont. Under the final CMS rule, in a provider-owned or controlled residential setting, the following conditions must be met: 1) The unit can be owned, rented or occupied under an agreement by the individual receiving services, and the individual has, at a minimum, the same responsibilities and protections from eviction that tenants have under landlord tenant law. 2) Each individual has privacy in their sleeping or living unit: Units have entrance doors lockable by the individual, with only appropriate staff having keys to doors as needed. 3) Individuals sharing units have a choice of roommates in that setting. 4) Individuals have the freedom to furnish and decorate their sleeping or living units within the lease or other agreement. 5) Individuals have the freedom and support to control their own schedules and activities, and have access to food at any time. 6) Individuals are able to have visitors of their choosing at any time. 7) The setting is physically accessible to the individual.
37 Adult BH HCBS Residential Settings Adult BH HCBS Approved Settings Still Under Review Adult Residential Not Meeting CMS Standard for Community Setting OMH Supported Housing Independent Community Housing OMH Apartment Treatment Programs OMH CR-SRO OMH SP-SRO OMH 100% special needs SP-SRO OMH SP-SRO Mixed Use OASAS Supportive Living OASAS Residential Reintegration/Scatter Site Setting Shelters OMH Community Residence OMH Adult Home OMH Housing located adjacent to and on State Hospital Grounds (not for profit and state run) OASAS Intensive Residential OASAS Community Residence OASAS Inpatient Rehab OASAS Residential Rehabilitation OASAS Residential Reintegration/Congregate Setting
38 Adult BH Home & Community Based Services Overview
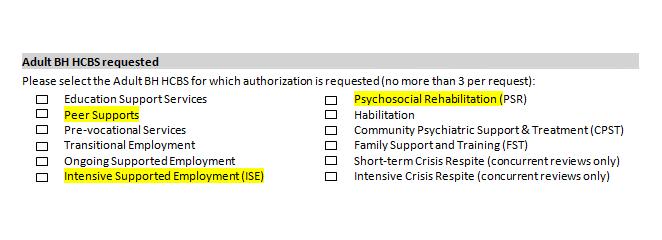
39 Adult BH HCBS Services Rehabilitation Psychosocial Rehabilitation Community Psychiatric Support and Treatment (CPST) Habilitation Crisis Respite Short-Term Crisis Respite Intensive Crisis Respite Educational Support Services Individual Employment Support Services Pre-vocational Transitional Employment Support Intensive Employment Support On-going Supported Employment Empowerment Services -- Peer Supports Family Support and Training
40 Rehabilitation and Habilitation PSR/CPST/Habilitation Services
41 Psychosocial Rehabilitation (PSR) PSR services are designed to assist the individual with compensating for or eliminating functional deficits and interpersonal and/or environmental barriers associated with their behavioral health condition (i.e., SUD and/or mental health). The intent of PSR is to restore the individual s functional level to the fullest possible (i.e., enhancing SUD resilience factors) and as necessary for integration of the individual as an active and productive member of his or her family, community, and/or culture with the least amount of ongoing professional intervention.
42 PSR Components Independent Living: A close working relationship between staff and participant to develop and strengthen the individual s independent community living skills and support community integration Social: Establishing and sustaining friendships and a supportive recovery social network, developing conversation skills and a positive sense of self; Community: Support the identification and pursuit of personal interests (e.g. creative arts, reading, exercise, faith-based pursuits, cultural exploration); Personal autonomy: Learning to manage stress, unexpected daily events and disruptions, mental health symptoms, relapse triggers and cravings with confidence; Health: Developing constructive and comfortable interactions with health-care professionals, Relapse Prevention Planning; Social Skills: Engaging with people respectfully, appropriate eye contact, conversation skills, listening skills and advocacy skills Wellness: meal planning, healthy shopping and meal preparation, nutrition awareness, exercise options Personal Care: grooming, sustaining living environment, managing finances and other independent living skills
43 Habilitation Habilitation services are designed to assist individuals with a behavioral health diagnosis in acquiring, retaining and improving skills such as communication, self-help, domestic, self-care, socialization, fine and gross motor skills, mobility, personal adjustment, relationship development, use of community resources and adaptive skills necessary to reside successfully in home and community-based settings. These services assist individuals with developing skills necessary for community living and, if applicable, to continue the process of recovery from an SUD disorder.
44 Habilitation Components Instruction in accessing and using community resources such as transportation, translation, and communication assistance Instruction in developing or sustaining financial stability and security (e.g., understanding budgets, managing money, and the right to manage their own money). Skill training and hands-on assistance of instrumental activities of daily living, including assistance with shopping, cooking, cleaning, and other necessary activities of community and civic living (voting, civic engagement via community activities, volunteerism) Habilitation provide onsite modeling, training, and/or supervision to assist the participant in developing maximum independent functioning in community living activities. Facilitation of family reunification through coordination of family services as applicable and self-advocacy instruction. Housing preservation and advocacy training, including assistance with developing positive landlord-tenant relationships, and accessing appropriate legal aid services if needed including skills to successfully live with roommates
45 Habilitation Components Cont. Assistance with developing strategies and supportive interventions for avoiding the need for more intensive services Assistance with increasing social opportunities and developing social support skills that ameliorate life stressors Instruction in developing strategies to manage trauma induced behaviors and/or PTSD as per a Trauma Informed Assessment Instruction in self-advocacy skills
46 Community Psychiatric Support and Treatment (CPST) CPST is designed to help individuals with serious mental illness to achieve stability and functional improvement in the following areas: daily living, finances, housing, education, employment, personal recovery and/or resilience, family and interpersonal relationships and community integration. CPST is designed to provide mobile treatment and rehabilitation services to individuals who have difficulty engaging in sitebased programs who can benefit from off-site rehabilitation or who have not been previously engaged in services, including those who had only partially benefited from traditional treatment or might benefit from more active involvement of their family of choice in their treatment.
47 CPST Components Assist the individual and family members or other collaterals1 to identify strategies or treatment options associated with the individual s behavioral health disorder Provide individual and their family supportive counseling, solution-focused interventions, emotional and behavioral management, Facilitate participation in and utilization of strengths based planning and treatments which include assisting the individual and family members or other collaterals with identifying strengths and needs, resources, natural supports, and developing goals and objectives to utilize personal strengths, resources, and natural supports to address functional deficits Assist the individual with effectively responding to or avoiding identified precursors or triggers that would risk their remaining in a natural community location, Provide ongoing rehabilitation support for individuals pursuing employment, housing, or education goals. Assist the individual with independent living skills to promote recovery and growth specific to managing their own home including managing their money, medications, and using community resources and other self-care requirements Implement interventions using evidence-based and best practice techniques, drawn from cognitive-behavioral therapy and other evidence-based psychotherapeutic interventions that ameliorate targeted symptoms and/or recover the person s capacity to cope with or prevent symptom interference with daily activities.
48 PSR CPST Habilitation Rehabilitation/Habilitation Settings/Limitations/Exclusions and Staffing Setting Limitations/Exclusions Staffing Services must be offered in the setting best suited for desired outcomes, including home, or other community-based setting in compliance with Medicaid regulations and the Home and Community Based Settings Final Rule (see appendix). The setting may include programs that are peer driven/operated or peer informed and that provide opportunities for drop-in. Services may be provided individually or in a group setting and should utilize (with documentation) evidence-based practices in rehabilitation and recovery. All individual and group interventions should be driven by the goal and objectives identified in the Plan of Care. On or off site. Services must be offered in the setting best suited for desired outcomes, including home or other community-based setting. Off site Habilitation may be delivered (on-site), or in the community (off-site). This service can be provided by the individual s provider of housing services. The total combined hours for Psychosocial Rehabilitation, Community Psychiatric Support and Treatment, and Habilitation are limited to no more than a total of 500 hours in a calendar year. Providers of service may include unlicensed behavioral health staff (see appendix). Workers who provide PSR services should periodically report to a supervising professional staff on participants progress toward the recovery and re-acquisition of skills. Staff to Member Ratio: 1:20. The intent of this service is to eventually transfer the care to a place based clinical setting. Professional staff (see appendix) must provide this service. The total combined hours for CPST, Psychosocial Rehabilitation Decisions about how to balance caseloads will be left to the (PSR) and Habilitation are limited to no more than a total of 500 provider agencies as they see appropriate to ensuring quality of hours in a calendar year. care and maintaining acceptable performance outcomes. Services must be offered in the setting best suited for desired outcomes, including home or other community-based setting. Setting must be Off site The total combined hours for Psychosocial Rehabilitation, Community Psychiatric Support and Treatment and Habilitation are limited to no more than a total of 500 hours in a calendar year. Providers of service may include unlicensed behavioral health staff (see appendix). Workers who provide this service should periodically report to a supervising by a professional staff on participants progress toward the recovery and re-acquisition of skills. Staff ratio of 1:20 or less Supervisory ratio: 1:5 (1 supervisor to 5 Direct Care Staff).
49 Empowerment Peer and Family Support Services
50 Empowerment Peer Services Peer Support services are peer-delivered services with a rehabilitation and recovery focus. They are designed to promote skills for coping with and managing behavioral health symptoms while facilitating the utilization of natural resources and the enhancement of recovery-oriented principles (e.g. hope and self-efficacy, and community living skills). Peer support uses trauma-informed, non-clinical assistance to achieve long-term recovery from a behavioral health disorder. Activities included must be intended to achieve the identified goals or objectives as set forth in the individuals individualized service plan, which delineates specific goals that are flexibly tailored to the participant and attempt to utilize community and natural supports. The intent of these activities is to assist individuals in initiating recovery, maintaining recovery, and enhancing the quality of personal and family life in long-term recovery. The structured, scheduled activities provided by this service emphasize the opportunity for peers to support each other in the restoration and expansion of the skills and strategies necessary to move forward in recovery. Individuals providing these services will do so through the paradigm of the shared personal experience of recovery.
51 Advocacy Peer Services Components Outreach and Engagement Self Help Tools Recovery Supports Transitional Supports Pre-Crisis and Crisis Supports
52 Peer Services Business/Billing Rules Peer supports may be provided in a variety of setting including, outpatient settings and in the community, and respite programs. The majority of the contacts with the individual should be offsite in the community. Meeting at community locations such as may include: an individual s home, homeless shelters and soup kitchens for the purpose of opening up a dialogue. Note: Peer Support must be the individual s recovery plan. Peer support services are limited to no more than a total of 500 hours in a calendar year. Individuals receiving SUD outpatient treatment may not receive Peer Supports, if they are receiving an OASAS state plan peer service. Note: peer services while an individual is incarcerated or institutionalized are not Medicaid reimbursable. Time spent on the phone with individuals is not Medicaid reimbursable. The cost of admission to an event (i.e., sports event or concert) is not Medicaid reimbursable. Advocacy for community improvement (not specific to the Medicaid eligible individual) is not Medicaid reimbursable. Certification/Provider Qualifications Peer support providers must have a certification as of the following: OMH established Certified Peer Specialist OASAS Certified Peer Advocate Staffing: 1 FTE to 20 Consumers
53 Family Support Services Training and support necessary to facilitate engagement and active participation of the family in the treatment planning process and with the ongoing instruction and reinforcement of skills learned throughout the recovery process. This service is provided only at the request of the individual. A person-centered or person-directed, recovery oriented, trauma-informed approach to partnering with families and other supporters to provide emotional and information support, and to enhance their skills so that they can support the recovery of a family member with a substance use disorder/mental illness. The individual, his or her treatment team and family are all primary members of the recovery team. For purposes of this service, family is defined as the persons who live with or provide care to a person served on the waiver and may include a parent, spouse, significant other, children, relatives, foster family, or in-laws. Family does not include individuals who are employed to care for the participant. Training includes instruction about treatment regimens, elements, recovery support options, recovery concepts, and medication education specified in the Individual Service Plan and shall include updates, as necessary, to safely sustain the participant at home and in the community. All family support and training must be included in the individual s service plan and for the benefit of the Medicaid covered participant.
54 Family Support Services Components Training on treatment regimens Assisting the family to provide a safe and supportive environment in the home and community for the individual Facilitate family and friends support groups under the direction of a certified peer Provide family mediation and conflict resolution services Development and enhancement of the family s specific problem-solving skills, coping mechanisms, and strategies for the individual s symptom/behavior management and prevention of relapse. Collaboration with the family and caregivers in order to develop positive interventions to address specific presenting issues and to develop and sustain healthy, stable relationships among all caregivers, including family members Assisting the family in the acquisition of knowledge and skills necessary to understand and address the specific needs of the Medicaid eligible individual in relation to their substance use disorder/mental illness and treatment Provide family with training/workshops Assisting the family in understanding various requirements of the waiver process Training on community integration and self-advocacy Training on behavioral intervention strategies Training on mental health conditions, services and supports including providing benefits and entitlements counseling and providing skills and knowledge to parents with mental illness and
55 Family Support Services Business/Billing Rules This is a face-to-face service which may be provided 1:1 or in groups consisting of family members. This service can be provided onsite and where an individual lives and community locations such as where an individual works or socializes. The total combined hours for Family Support and Training are limited to no more than a total of 40 hours in a calendar year. Unlicensed staff (see appendix) may provide this service. Staffing Ratio/Case Limits 1:15 for staff to individual ratio, 1:16 for groups with family members.
56 Individual Education & Employment Support Services (IESS)
57 Individual Education Support Service: OVERALL COMPONENTS Education Support Services are provided to assist individuals with a behavioral health disorders who want to start or return to school or formal training with a goal to achieve skills necessary to obtain employment. Identify financial aid resources and assist with applications. Assist with transitions and/or withdrawals from programs such as those resulting from mental health or substance abuse challenges, issues and medical conditions and other cooccurring disorders. Orient individual to school settings, navigating the school system and student services particularly disability services. Provide/referral to cognitive remediation services to improve executive functioning abilities such as attention, organizing, planning and working memory Provide instruction on self-advocacy skills in relation to independent functioning in the educational environment.
58 Individual Education Support Service SETTINGS & STAFF QUALIFICATIONS The actual educational setting site is ideal, but this service may be provided on education site or off site. Education Specialists should possess a BA, and two years of experience supporting individuals in pursuing education goals. An Education Supervisor may be unlicensed (see appendix) and requires a minimum of a BA (preferably a Masters in Rehabilitation or a relevant field), a minimum of three years of relevant work experience preferably as an education specialist. All staff should have minimum of two years working in the behavioral health. Staffing Ratio/Case Limits: Maximum caseload for a full-time education specialist is 20 individuals and proportional number for part-time staff.
59 INDIVIDUAL EMPLOYMENT SUPPORT SERVICES PRE-VOCATIONAL SERVICES TRANSITIONAL SERVICES INTENSIVE SUPPORTED EMPLOYMENT ONGOING EMPLOYMENT SUPPORT
60 Individual Employment Support Services: OVERALL COMPONENTS Assists individuals to establish positive workplace relationships, including interactions with supervisors, and co-workers Helps individuals to build and sustain skills in the workplace Provides reminders of effective workplace practices and reinforcement of skills gained during the period of intensive supported employment services: Assist individuals to manage symptoms that may impact their ability to sustain employment The basic tenet is that all individuals are capable of working in competitive employment in the community even without prior training and all individuals interested in employment should be given the opportunity.
61 Individual Employment Support Service SETTINGS: Setting This service is generally provided at the program site, but also includes support at a work location where the individual may acquire workrelated experience such as volunteering and internships in the community. Admission/Eligibility Criteria -- Individual must have a clear desire to work in competitive employment.
62 Individual Employment Support Services: STAFF QUALIFICATIONS -- Employment Specialists may be non-licensed and possess an education and experience equivalent to an undergraduate degree in employment services, disabilities services, business personnel management, or behavioral health counseling. An Employment Program Manager requires a minimum of a BA (preferably a Masters Degree in Rehabilitation or Behavioral Health Counseling) and a minimum of three years relevant work experience preferably as an Employment Specialist with a minimum of 18 months of management experience in a Behavioral Health setting. OASAS Certified Clinics and in community based programs. Staffing ratios/case limits -- 1:20 for staff to individual ratio The recommended program manager to staff ratio is 1:10
63 PREVOCATIONAL SERVICE COMPONENTS To teach employment concepts such as: Work compliance Attendance Task completion Problem solving and safety How to identify obstacles to employment How to obtain paperwork necessary for employment applications How to interact with others in the work setting Provide scheduled activities outside the individual s home that support acquisition, retention, and/or improvement in job-related skills Gain work-related experience considered crucial for job placement Services do not include development of job specific skills.
64 TRANSITIONAL EMPLOYMENT SUPPORT SERVICES Providing on the job supports, including: On-site job training Assisting the participant to develop natural supports in the workplace Adopt an identity as a worker Accept responsibility for decisions Examine past work experiences for failure and successes. Consider potential for transferability of skills Coordinate with employers and coworkers
65 Intensive Supportive Employment Assist the participant to locate a job or develop a job that includes Rapid job search Acquisition of hard and soft skills to retain employment Training and systematic instruction Provide support for the job application process Support the individual to establish or maintain selfemployment, including home-based self- employment Provide ongoing job related discovery and assessment
66 ONGOING SUPPORTED EMPLOYMENT Provide support in a variety of settings, particularly work sites Assists individuals to identify reasonable accommodations necessary to manage symptoms that may emerge at work Provides activities needed to retain paid work Assessment of issues and linkage/referral to other community resources as appropriate Provide activities needed to sustain paid work by participants, including supervision and training: Provides supports to individuals who are currently employed in settings that are competitive and integrated
67 Crisis Respite Short Term Crisis Respite & Intensive Crisis Respite
68 Crisis Respite Based on Residential Settings Respite staff should coordinate with HH care coordinators and MCOs to assist with the housing process (brokering enrollment in Health Homes, identifying housing readiness skills, etc.) and should focus care and discharge planning on moving the housing process along as they are able, but will not be expected or required to find housing or to hold recipients in Respite until housing is available. If someone enters a Respite program from a shelter, it is appropriate to discharge them back to a shelter If someone enters a Respite program from the street, it is strongly recommended that client be discharged to a shelter Providers should develop policies and procedures and recipient consent and orientation processes to address these points
69 Short Term Crisis Respite Short-term Crisis Respite is a short-term care and intervention strategy for individuals who have a mental health or co-occurring diagnosis and are experiencing challenges in daily life that create risk for an escalation of symptoms that cannot be managed in the individual s home and community environment without onsite supports including: A mental health or co-occurring diagnosis and are experiencing challenges in daily life that create imminent risk for an escalation of symptoms and/or a loss of adult role functioning but who do not pose an imminent risk to the safety of themselves or others A challenging emotional crisis occurs which the individual is unable to manage without intensive assistance and support When there is an indication that an individual s symptoms are beginning to escalate Referrals to Crisis Respite may come from the emergency room, the community, self-referrals, a treatment team, or as part of a step-down plan from an inpatient setting. Crisis respite is provided in site-based residential settings. Crisis Respite is not intended as a substitute for permanent housing arrangements.
70 Short Term Crisis Respite Components Onsite peer support during the respite stay Working with existing treatment providers Health and wellness coaching Relaxation techniques to help reduce stress, anxiety, emerging panic or feelings of losing control Coordinating with primary care, Health Home or other BH providers (on-site or through referrals) Relapse Prevention planning
71 Short Term Crisis Respite Components Continue Wellness activities Family support Conflict resolution Ongoing communication between the individual, crisis respite staff, natural supports, and the individuals established mental health providers to assure collaboration and continuity in managing the crisis situation and identifying subsequent support and service systems Collaboration with the individual, BH providers, Health Home Care manager and natural supports to make recommendations for modifications to the recipients plan of care and treatment.
72 Intensive Crisis Respite Intensive Crisis Respite (ICR) is a short-term, residential care and clinical intervention strategy for individuals who are facing a behavioral health crisis, including individuals who are suicidal, express homicidal ideation, or have a mental health or cooccurring diagnosis and are experiencing acute escalation of mental health symptoms. In addition, the person must be able to contract for safety. Individuals in need of ICR are at imminent risk for loss of functional abilities, and may raise safety concerns for themselves and others without this level of care. The immediate goal of ICR is to provide supports to help the individual stabilize and return to previous level of functioning or as a step-down from inpatient hospitalization.
73 Intensive Crisis Respite Components Comprehensive assessment including screening for physical health conditions Comprehensive risk assessment medication management Individual and group counseling Training in de-escalation strategies Relaxation techniques to help reduce stress, anxiety, panic or feelings of losing control Monitoring for high risk behavior Psychiatric evaluation for competency
74 Intensive Crisis Respite Components Continue Linkage to resources and referrals to community-based mental health and substance abuse treatment Peer support Relapse prevention planning Wellness activities Family support Engagement of Natural Supports Conflict resolution Ongoing communication between individuals receiving ICR, crisis respite staff, and the individuals established mental health providers is necessary to assure collaboration and continuity in managing the crisis, as well as to identify effective subsequent support and service resources. At the conclusion of an Intensive Crisis Respite period, clinical staff, together with the individual, will make recommendations for modifications to the individual s Plan of Care.
75 Short Term Crisis Short Term Crisis Respite Settings/Limitations/Exclusions and Staffing Setting Limitations/Exclusions Staffing Site-based residential settings will offer a supportive home-like environment with a maximum preferred capacity of 8-10 individuals (fewer in rural areas), preferably in single rooms. The setting must be code compliant. Staffed and open 24 hours a day, seven days a week when a resident is present. Residents should be allowed to leave and return as needed, maintaining employment and other daily activities to the extent possible. To the greatest extent possible, guests will be encouraged to maintain contact with significant others, including family members, friends, and spouses. To facilitate this contact, guests may have visitors at any time that is convenient and practical for the guest as well as the operations of the crisis respite center. No longer than 1 week per episode, not to exceed a maximum of 21 days per year. Individual stays of greater than 72 hours require prior authorization. Individuals requiring crisis respite for longer periods may be evaluated on an individual basis and approved for greater length of stay based on medical necessity. Crisis Respite services may be delivered by peers or unlicensed staff (see appendix): Peer Respite staff will have experience as a recipient of mental health services with a willingness to share personal, practical experience, knowledge, and first-hand insight to benefit program enrollees Crisis Respite should have a Program Director (1 FTE) who will have 3-5 years of management experience working in a social service or related setting and will supervise Crisis Respite staff and coordinate the day-to-day activities associated with managing the Crisis Respite Peer Respite staff will possess the competency to meet requirements outlined in the job description, and will complete any relevant trainings within 90 days of employment. All Peer staff must be OMH or OASAS certified There shall be a minimum of one staff person on-site for every four guests from 7 am to 8 pm. Between the hours of 8 pm and 7 am, there shall be a minimum of two staff on-site. The director or a designee shall be available at all times by cell phone.
76 Intensive Crisis Respite Settings/Limitations/Exclusions and Staffing Intensive Crisis Setting Limitations/Exclusions Staffing Individuals are encouraged to receive respite in the most integrated and cost-effective settings appropriate to meet their respite needs, preferably in a residential, community-based setting. Please refer to the appendix for BH HCBS settings requirements. Intensive Crisis Respite services include a limit of 21 days per year. Individuals requiring Intensive Crisis Respite for longer periods than those specified may be evaluated on an individual basis and approved for greater length of stay based on medical necessity. 7 days maximum Have an acute medical condition requiring higher level of care. Agency must possess a current license to provide crisis and/or treatment services (i.e. clinic, Comprehensive Psychiatric Emergency Programs (CPEP), Partial Hospital, PROS, Psychiatric Inpatient or have licensed professionals who have a minimum of 1 year of experience in delivering off-site crisis services including conducting psychiatric evaluations and providing treatment. Agency must demonstrate capacity for mobile crisis visits to be conducted by a minimum of 2 staff persons one of whom must be a licensed clinician. This service will be provided by a multidisciplinary team of licensed, unlicensed and certified peer staff. Every ICR shall have at least one psychiatrist as primary medical coverage. Back-up coverage may be a physician who will consult with the psychiatrist. The psychiatrist or physician shall be on call 24-hours-a-day and will make daily rounds. Counties of less than 50,000 population may utilize a licensed physician for on-call activities and daily rounds as long as the physician has postgraduate training and experience in diagnosis and treatment of SMI and SUD At least one registered nurse shall be on duty 24-hours-a-day, 7- days-a-week when there is an individual in care. Staffing ratio: 1-10 Beds Requires 1 RN and 1 Mental Health Treatment Staff Beds Requires 1 RN and 2 Mental Health Treatment Staff
77 Adult BH HCBS Designation Changes and Manual Providers who are interested in becoming a new designated Adult BH HCBS provider or changing their existing designation status by: Adding New Adult BH HCBS Removing Adult BH HCBS Inactive Status Should notify the state by ing at omh.sm.co.hcbs-application@omh.ny.gov Providers should also inform Managed Care Organizations of any changes to their HCBS designation. Updated Adult BH HCBS Provider Manual Link:
78 Frequently Asked Questions (FAQ) The Managed Care Technical Assistance Center of New York
79 Frequently Asked Questions Are Home and Community Based Services (HCBS) only made available for HARP eligible clients? Yes, HCBS services are only available to clients that are enrolled in a HARP or an HIV SNP after they've undergone a brief and full assessment using the New York State Community Mental Health Assessment and the assessment has indicated that they are eligible and for which services. For more information consult a recent workflow presentation. Will Managed Care Organizations know who the designated Home and Community Based Services (HCBS) providers are? How will CM know who the HCBS providers are and which ones are in each plan's network? Yes, Plans are provided this information and the list of the designated providers is also publicly available on the OMH website, and can be accessed here. CM should have a list of designated providers and should also have a list of HCBS providers in each plan's network. Can homeless clients use the Crisis Respite Home and Community Based Service? If an individual is HARP eligible, yes, but note that Crisis Respite has usage caps outlined in the HCBS manual and MCTAC trainings. How do agencies identify if a client is HARP/HCBS eligible? HARP/HCBS eligibility information is available using epaces. Are HARPs required to have case managers? How are clients assigned to Home Health Care Managers? Yes, HARPs are required to have case managers. The expectation is that most face to face care management will be done through the Health Homes. Each Health Home has its own assignment process.
80 Tools and Resources The Managed Care Technical Assistance Center of New York
81
82
83
84 Future Training Opportunities MCTAC, CPI, and NYAPRS are currently with NYS DOH, OMH, and OASAS partners on developing a more comprehensive longterm training approach for Adult BH HCBS providers. Stay tuned to MCTAC s website and list for more information in late fall/winter Small Business Initiative: Adult BH HCBS providers who have minimal experience billing for Medicaid BH Services are encouraged to take advantage of this training opportunity coordinated by NYAPRS, ASAP, and the Coalition for Behavioral Health agencies. Please visit the MCTAC website for more training opportunities and an existing HCBS related training resources.

85 Visit to view past trainings, sign-up for updates and event announcements, and access
Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016
 Foundations Webinar JUNE 29, 2016") Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016 June 30, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016 June 30, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Adult BH Home & Community Based Services (HCBS) In Person Trainings JULY, 2016
 In Person Trainings JULY, 2016") Adult BH Home & Community Based Services (HCBS) In Person Trainings JULY, 2016 July 26, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Adult BH Home & Community Based Services (HCBS) In Person Trainings JULY, 2016 July 26, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Rehabilitation (PSR/CPST) & Habilitation. November 13 th & 16 th The Managed Care Technical Assistance Center of New York
 & Habilitation. November 13 th & 16 th The Managed Care Technical Assistance Center of New York") Rehabilitation (PSR/CPST) & Habilitation November 13 th & 16 th 2015 The Managed Care Technical Assistance Center of New York Welcome MCTAC Overview Business/Billing Rules Services Definition Service Components
Rehabilitation (PSR/CPST) & Habilitation November 13 th & 16 th 2015 The Managed Care Technical Assistance Center of New York Welcome MCTAC Overview Business/Billing Rules Services Definition Service Components
Practical Facts about Adult Behavioral Health Home and Community Based Services. (Adult BH HCBS)
") Section I: Introduction: Practical Facts about Adult Behavioral Health Home and Community Based Services (Adult BH HCBS) The development of Health and Recovery Plans (HARPs) is intended to promote significant
Section I: Introduction: Practical Facts about Adult Behavioral Health Home and Community Based Services (Adult BH HCBS) The development of Health and Recovery Plans (HARPs) is intended to promote significant
New York State: Health and Recovery Plan (HARP) Adult Behavioral Health Home and Community Based Services (BH HCBS) Provider Manual
 Adult Behavioral Health Home and Community Based Services (BH HCBS) Provider Manual") New York State: Health and Recovery Plan (HARP) Adult Behavioral Health Home and Community Based Services (BH HCBS) Provider Manual New York State is pleased to release the Adult Behavioral Health Home
New York State: Health and Recovery Plan (HARP) Adult Behavioral Health Home and Community Based Services (BH HCBS) Provider Manual New York State is pleased to release the Adult Behavioral Health Home
The Managed Care Technical Assistance Center of New York
 The Managed Care Technical Assistance Center of New York The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that
The Managed Care Technical Assistance Center of New York The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that
Understanding and Using the Adult BH HCBS Billing Rates and Codes. February 22, The Managed Care Technical Assistance Center of New York
 Understanding and Using the Adult BH HCBS Billing Rates and Codes February 22, 2016 The Managed Care Technical Assistance Center of New York Housekeeping Slides are posted at MCTAC.org Questions not addressed
Understanding and Using the Adult BH HCBS Billing Rates and Codes February 22, 2016 The Managed Care Technical Assistance Center of New York Housekeeping Slides are posted at MCTAC.org Questions not addressed
Home and Community Based Services (HCBS) Presented by: Meredith L. Ray-LaBatt, MA, MSW Douglas P. Ruderman, LSCW-R
 Presented by: Meredith L. Ray-LaBatt, MA, MSW Douglas P. Ruderman, LSCW-R") Home and Community Based Services (HCBS) Presented by: Meredith L. Ray-LaBatt, MA, MSW Douglas P. Ruderman, LSCW-R 2 Meredith Ray-LaBatt CHILDREN S HCBS SERVICES Children s Transition Timelines 3 Children
Home and Community Based Services (HCBS) Presented by: Meredith L. Ray-LaBatt, MA, MSW Douglas P. Ruderman, LSCW-R 2 Meredith Ray-LaBatt CHILDREN S HCBS SERVICES Children s Transition Timelines 3 Children
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Home & Community Based Services (HCBS) for Adults. Non-Medical Transportation July 24, 2015
 for Adults. Non-Medical Transportation July 24, 2015") Home & Community Based Services (HCBS) for Adults Non-Medical Transportation July 24, 2015 1 Presented by: Kate Federici & Jordana Vanderselt, MCTAC/CASAColumbia Alyssa Slezak, New York State Department
Home & Community Based Services (HCBS) for Adults Non-Medical Transportation July 24, 2015 1 Presented by: Kate Federici & Jordana Vanderselt, MCTAC/CASAColumbia Alyssa Slezak, New York State Department
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York Conference of Local Mental Hygiene Directors November 19, 2013 Agenda Goals Timeline BH Benefit Design Overview
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York Conference of Local Mental Hygiene Directors November 19, 2013 Agenda Goals Timeline BH Benefit Design Overview
Welcome to the Webinar!
 Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Clinical Services. clean NYS Driver s License, fingerprinting, criminal record check, and approval from NYS Office of Mental Health.
 Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
Critical Time Intervention (CTI) (State-Funded)
 (State-Funded)") Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
LOUISIANA MEDICAID PROGRAM ISSUED: 08/24/17 REPLACED: 07/06/17 CHAPTER 2: BEHAVIORAL HEALTH SERVICES APPENDIX B GLOSSARY/ACRONYMS PAGE(S) 5 GLOSSARY
 5 GLOSSARY") GLOSSARY The following is a list of abbreviations, acronyms and definitions used in the Behavioral Health Services manual chapter. Ambulatory Withdrawal Management with Extended On-Site Monitoring (ASAM
GLOSSARY The following is a list of abbreviations, acronyms and definitions used in the Behavioral Health Services manual chapter. Ambulatory Withdrawal Management with Extended On-Site Monitoring (ASAM
PART 512 Personalized Recovery Oriented Services
 PART 512 Personalized Recovery Oriented Services (Statutory authority: Mental Hygiene Law 7.09[b], 31.04[a], 41.05, 43.02[a]-[c]; and Social Services Law, 364[3], 364-a[1]) Sec. 512.1 Background and intent.
PART 512 Personalized Recovery Oriented Services (Statutory authority: Mental Hygiene Law 7.09[b], 31.04[a], 41.05, 43.02[a]-[c]; and Social Services Law, 364[3], 364-a[1]) Sec. 512.1 Background and intent.
Overview of Key Policies and CMS Statements of Intent Regarding the Medicaid State Plan HCBS Benefits and HCBS Waiver Final Rule
 January 16, 2014 Overview of Key Policies and CMS Statements of Intent Regarding the Medicaid State Plan HCBS Benefits and HCBS Waiver Final Rule On January 10, 2014, the Centers for Medicare and Medicaid
January 16, 2014 Overview of Key Policies and CMS Statements of Intent Regarding the Medicaid State Plan HCBS Benefits and HCBS Waiver Final Rule On January 10, 2014, the Centers for Medicare and Medicaid
Access to Adult BH HCBS for Non-Health Home Enrollees: The State Designated Entity. February 22, 2018
 Access to Adult BH HCBS for Non-Health Home Enrollees: The State Designated Entity February 22, 2018 February 22, 2018 Agenda Overview of HARP and Adult BH HCBS What is a State Designated Entity? Becoming
Access to Adult BH HCBS for Non-Health Home Enrollees: The State Designated Entity February 22, 2018 February 22, 2018 Agenda Overview of HARP and Adult BH HCBS What is a State Designated Entity? Becoming
Adult BH HCBS Town Hall ROS Designated Providers. June 13, 2017
 Adult BH HCBS Town Hall ROS Designated Providers June 13, 2017 June 28, 2017 2 Why Behavioral Health Transformation is Needed June 28, 2017 3 Why Behavioral Health Transformation is Needed In NYS, members
Adult BH HCBS Town Hall ROS Designated Providers June 13, 2017 June 28, 2017 2 Why Behavioral Health Transformation is Needed June 28, 2017 3 Why Behavioral Health Transformation is Needed In NYS, members
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS
 UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
June 2017 NYS Department of Health NYS Office of Mental Health NYS Office of Alcoholism and Substance Abuse Services
 Guidance for Behavioral Health Home and Community Based (BH HCB) Non-Medical Transportation Services for Adults in HARPs and HARP Eligibles in SNPs June 2017 NYS Department of Health NYS Office of Mental
Guidance for Behavioral Health Home and Community Based (BH HCB) Non-Medical Transportation Services for Adults in HARPs and HARP Eligibles in SNPs June 2017 NYS Department of Health NYS Office of Mental
Rule 132 Training. for Community Mental Health Providers
 Rule 132 Training for Community Mental Health Providers October 2013 Goals for training Understand purpose and vision of Rule 132 Understand Rule 132 requirements Understand the appropriate application
Rule 132 Training for Community Mental Health Providers October 2013 Goals for training Understand purpose and vision of Rule 132 Understand Rule 132 requirements Understand the appropriate application
Medicaid Managed Care Utilization Management and Integrated Billing Overview
 Medicaid Managed Care Utilization Management and Integrated Billing Overview March, 23 2016 The Managed Care Technical Assistance Center of New York 1 st webinar in series about UM and Billing. In- person
Medicaid Managed Care Utilization Management and Integrated Billing Overview March, 23 2016 The Managed Care Technical Assistance Center of New York 1 st webinar in series about UM and Billing. In- person
Children s Medicaid System Transformation: HCBS Rates & SPA Rate Code Review. December 21, 2017
 Children s Medicaid System Transformation: HCBS Rates & SPA Rate Code Review December 21, 2017 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Children s Medicaid System Transformation: HCBS Rates & SPA Rate Code Review December 21, 2017 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Transition Management Services (TMS) (Previously known as Tenancy Support Team) Revised 6/3/16
 (Previously known as Tenancy Support Team) Revised 6/3/16") Transition Management Services (TMS) (Previously known as Tenancy Support Team) Revised 6/3/16 Service Definition and Required Components Transition Management Services (TMS) is a service provided to individuals
Transition Management Services (TMS) (Previously known as Tenancy Support Team) Revised 6/3/16 Service Definition and Required Components Transition Management Services (TMS) is a service provided to individuals
Iowa Medicaid Habilitation Services Criteria Utilization Management Guidelines
 https://providers.amerigroup.com Iowa Medicaid Habilitation Services Criteria Utilization Management Guidelines Description State plan home- and community- based habilitation services are intended to meet
https://providers.amerigroup.com Iowa Medicaid Habilitation Services Criteria Utilization Management Guidelines Description State plan home- and community- based habilitation services are intended to meet
October 5 th & 6th, The Managed Care Technical Assistance Center of New York
 October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
Clinical Services. clean NYS Driver s License, fingerprinting, criminal record check, and approval from NYS Office of Mental Health.
 Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
Clinical Services Clinical Social Worker- Fee for Service Location: Wyandanch- Clinic Job Function: Provide direct clinical care to clients as needed as a member of a multi-disciplinary treatment. Qualifications:
NEW YORK STATE CHILDREN S HEALTH AND BEHAVIORAL HEALTH (BH) SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL
 SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL") NEW YORK STATE CHILDREN S HEALTH AND BEHAVIORAL HEALTH (BH) SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL 1 Table of Contents General... 5 Purpose of this Manual... 5 New
NEW YORK STATE CHILDREN S HEALTH AND BEHAVIORAL HEALTH (BH) SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL 1 Table of Contents General... 5 Purpose of this Manual... 5 New
Medicaid Funded Services Plan
 Clinical Communication Bulletin 007 To: From: All Enrollees, Stakeholders, and Providers Cham Trowell, UM Director Date: May 10, 2016 Subject: Medicaid Funded Services Plan benefit changes, State Funded
Clinical Communication Bulletin 007 To: From: All Enrollees, Stakeholders, and Providers Cham Trowell, UM Director Date: May 10, 2016 Subject: Medicaid Funded Services Plan benefit changes, State Funded
1915(k) Community First Choice Overview
 Community First Choice Overview") 1915(k) Community First Choice Overview 1 Today s Objectives 1. Brief overview of Community First Choice (CFC) Program & Key Features Other materials available: http://www.medicaid.gov/medicaid-chip-program-information/by-topics/longterm-services-and-supports/home-and-community-based-services/communityfirst-choice-1915-k.html\
1915(k) Community First Choice Overview 1 Today s Objectives 1. Brief overview of Community First Choice (CFC) Program & Key Features Other materials available: http://www.medicaid.gov/medicaid-chip-program-information/by-topics/longterm-services-and-supports/home-and-community-based-services/communityfirst-choice-1915-k.html\
HCBS: Getting Started with Implementation
 HCBS: Getting Started with Implementation Presentation to ACL members by Cindy Freidmutter, CLF Consulting August 4 & 5, 2016 HCBS Presentation Agenda HCBS Framework How HCBS Works HCBS Start-up Challenges
HCBS: Getting Started with Implementation Presentation to ACL members by Cindy Freidmutter, CLF Consulting August 4 & 5, 2016 HCBS Presentation Agenda HCBS Framework How HCBS Works HCBS Start-up Challenges
INTEGRATED CASE MANAGEMENT ANNEX A
 INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
Children's System MCO Contracting Fair. November 6, 2017
 Children's System MCO Contracting Fair November 6, 2017 2 Guiding Principles Behind Children s Health and Behavioral Health MC Transition Key components of the managed care transition is to: Early identification
Children's System MCO Contracting Fair November 6, 2017 2 Guiding Principles Behind Children s Health and Behavioral Health MC Transition Key components of the managed care transition is to: Early identification
NORTH CAROLINA DEPARTMENT OF HEALTH & HUMAN SERVICES
 NORTH CAROLINA DEPARTMENT OF HEALTH & HUMAN SERVICES Division of Mental Health, Developmental Disabilities and Substance Abuse Services State-Funded MH/DD/SA SERVICE DEFINITIONS Revision Date: September
NORTH CAROLINA DEPARTMENT OF HEALTH & HUMAN SERVICES Division of Mental Health, Developmental Disabilities and Substance Abuse Services State-Funded MH/DD/SA SERVICE DEFINITIONS Revision Date: September
Covered Service Codes and Definitions
 Covered Service Codes and Definitions [01] Assessment Assessment services include the systematic collection and integrated review of individualspecific data, such as examinations and evaluations. This
Covered Service Codes and Definitions [01] Assessment Assessment services include the systematic collection and integrated review of individualspecific data, such as examinations and evaluations. This
New Federal Regulations for Home and Community-Based Services Program: Offers Greater Autonomy, Choice, and Independence
 New Federal Regulations for Home and Community-Based Services Program: Offers Greater Autonomy, Choice, and Independence The Centers for Medicare and Medicaid Services (CMS) has published a Final Rule
New Federal Regulations for Home and Community-Based Services Program: Offers Greater Autonomy, Choice, and Independence The Centers for Medicare and Medicaid Services (CMS) has published a Final Rule
MHANYS Behavioral Health Managed Care Update
 MHANYS Behavioral Health Managed Care Update Mental Health Association in New York State, Inc. October 28, 2016 September 22, 2016 2 Presentation Overview What are the Goals for the Medicaid Changes? Changes
MHANYS Behavioral Health Managed Care Update Mental Health Association in New York State, Inc. October 28, 2016 September 22, 2016 2 Presentation Overview What are the Goals for the Medicaid Changes? Changes
All Providers Frequently Asked Questions (FAQs)
") All Providers Frequently Asked Questions (FAQs) The new Independent Assessment / Community-Based Care Management process for access to Medicaid Adult Home and Community Based Services available through
All Providers Frequently Asked Questions (FAQs) The new Independent Assessment / Community-Based Care Management process for access to Medicaid Adult Home and Community Based Services available through
Starting January 1, 2016, new behavioral health Home and Community Based Services (HCBS) became available for adults enrolled in HARPS.
 became available for adults enrolled in HARPS.") Starting January 1, 2016, new behavioral health Home and Community Based Services (HCBS) became available for adults enrolled in HARPS. These consist of rehabilitation and recovery services such as psychosocial
Starting January 1, 2016, new behavioral health Home and Community Based Services (HCBS) became available for adults enrolled in HARPS. These consist of rehabilitation and recovery services such as psychosocial
I. General Instructions
 Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
Health Home Care Management & Behavioral Health HCBS
 Health Home Care Management & Behavioral Health HCBS Person-Centered Planning, Completing the BH HCBS Plan of Care, & the Expedited Workflow Developed by the OMH Bureau of Rehabilitation Services & Care
Health Home Care Management & Behavioral Health HCBS Person-Centered Planning, Completing the BH HCBS Plan of Care, & the Expedited Workflow Developed by the OMH Bureau of Rehabilitation Services & Care
Children and Family Treatment and Support Services. In-Depth Training w/ Review of New Implementation Timeline
 Children and Family Treatment and Support Services In-Depth Training w/ Review of New Implementation Timeline Introduction & Housekeeping Slides will be posted at MCTAC.org following the last training
Children and Family Treatment and Support Services In-Depth Training w/ Review of New Implementation Timeline Introduction & Housekeeping Slides will be posted at MCTAC.org following the last training
Medicaid Managed Care Readiness For Agency Staff --
 Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Draft Children s Managed Care Transition MCO Requirements
 Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Division of Mental Health, Developmental Disabilities & Substance Abuse Services NC Mental Health and Substance Use Service Array Survey
 Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
Table 1 Service Name Include any subcategories of service on a separate line In Table 2, please add service description and key terms Outpatient Treatment Behavioral Health Urgent Care (a type of outpatient)
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
Bulletin. DHS Provides Policy for Certified Community Behavioral Health Clinics TOPIC PURPOSE CONTACT SIGNED TERMINOLOGY NOTICE NUMBER DATE
 Bulletin NUMBER 17-51-01 DATE February 27, 2017 OF INTEREST TO County Directors Social Services Supervisors and Staff Case Managers and Care Coordinators Managed Care Organizations Mental Health Providers
Bulletin NUMBER 17-51-01 DATE February 27, 2017 OF INTEREST TO County Directors Social Services Supervisors and Staff Case Managers and Care Coordinators Managed Care Organizations Mental Health Providers
Overview of Medicaid. and the 1115 Medicaid Transformation Waiver. Opportunities for Supportive Housing Providers and Tenants August 2, 2016
 Overview of Medicaid and the 1115 Medicaid Transformation Waiver Opportunities for Supportive Housing Providers and Tenants August 2, 2016 Speaker Carol Wilkins, MPP Consultant carol.wilkins.ca@gmail.com
Overview of Medicaid and the 1115 Medicaid Transformation Waiver Opportunities for Supportive Housing Providers and Tenants August 2, 2016 Speaker Carol Wilkins, MPP Consultant carol.wilkins.ca@gmail.com
Intensive In-Home Services Training
 Intensive In-Home Services Training Intensive In Home Services Definition Intensive In Home Services is an intensive, time-limited mental health service for youth and their families, provided in the home,
Intensive In-Home Services Training Intensive In Home Services Definition Intensive In Home Services is an intensive, time-limited mental health service for youth and their families, provided in the home,
Office of Long-Term Living Waiver Programs - Service Descriptions
 Adult Daily Living Office of Long-Term Living Waiver Programs - Descriptions *The service descriptions below do not represent the comprehensive Definition as listed in each of the Waivers. Please refer
Adult Daily Living Office of Long-Term Living Waiver Programs - Descriptions *The service descriptions below do not represent the comprehensive Definition as listed in each of the Waivers. Please refer
Macomb County Community Mental Health Level of Care Training Manual
 1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
HCBS Settings Residential Program Assessment. June 27 th and June 28 th 2016
 HCBS Settings Residential Program Assessment June 27 th and June 28 th 2016 Introductions and Overview 2 Raná Meehan & Amber Vanderwarker NYS Office of Mental Health Bureau of Housing Development and Support
HCBS Settings Residential Program Assessment June 27 th and June 28 th 2016 Introductions and Overview 2 Raná Meehan & Amber Vanderwarker NYS Office of Mental Health Bureau of Housing Development and Support
LAKESHORE REGIONAL ENTITY Clubhouse Psychosocial Rehabilitation Programs
 Attachment A LAKESHORE REGIONAL ENTITY This service must be provided consistent with requirements outlined in the MDHHS Medicaid Provider Manual as updated. The manual is available at: http://www.mdch.state.mi.us/dch-medicaid/manuals/medicaidprovidermanual.pdf
Attachment A LAKESHORE REGIONAL ENTITY This service must be provided consistent with requirements outlined in the MDHHS Medicaid Provider Manual as updated. The manual is available at: http://www.mdch.state.mi.us/dch-medicaid/manuals/medicaidprovidermanual.pdf
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES NOTICE OF PROPOSED POLICY
 MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES NOTICE OF PROPOSED POLICY Public Act 280 of 1939, as amended, and consultation guidelines for Medicaid policy provide an opportunity to review proposed
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES NOTICE OF PROPOSED POLICY Public Act 280 of 1939, as amended, and consultation guidelines for Medicaid policy provide an opportunity to review proposed
Service Array: Mental Health Medicaid Specialty Supports and Services Descriptions Note:
 Service Array: Mental Health Medicaid Specialty Supports and Services Descriptions Note: If you are a Medicaid beneficiary and have a serious mental illness, or serious emotional disturbance, or developmental
Service Array: Mental Health Medicaid Specialty Supports and Services Descriptions Note: If you are a Medicaid beneficiary and have a serious mental illness, or serious emotional disturbance, or developmental
New HCBS Regulations: Transition Plan Requirements. Background Final HCBS Regulations
 New HCBS Regulations: Transition Plan Requirements Presentation by: Background Final HCBS Regulations Regulations published in the Federal Register on January 16, 2014 The Final Rule combined responses
New HCBS Regulations: Transition Plan Requirements Presentation by: Background Final HCBS Regulations Regulations published in the Federal Register on January 16, 2014 The Final Rule combined responses
4.401 Substance Use Partial Hospitalization Program (Adults and Adolescents)
") 4.40 STRUCTURED DAY TREATMENT SERVICES 4.401 Substance Use Partial Hospitalization Program (Adults and Adolescents) Description of Services: Substance use partial hospitalization is a nonresidential treatment
4.40 STRUCTURED DAY TREATMENT SERVICES 4.401 Substance Use Partial Hospitalization Program (Adults and Adolescents) Description of Services: Substance use partial hospitalization is a nonresidential treatment
PROS Clarification. Structured Skill Development and Support
 PROS Clarification Guidance 1: Guidance 2: Guidance 3: Guidance 4: Guidance 5: Guidance 6: Guidance 7: Guidance 8: Guidance 9: IRP Development and Timeframes The PROS Assessment and Timeframes Progress
PROS Clarification Guidance 1: Guidance 2: Guidance 3: Guidance 4: Guidance 5: Guidance 6: Guidance 7: Guidance 8: Guidance 9: IRP Development and Timeframes The PROS Assessment and Timeframes Progress
GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS
 GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS Table of Contents Introduction... 2 Purpose... 2 Serving Senior Medicare-Medicaid Enrollees... 2 How to Use This Tool... 2
GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS Table of Contents Introduction... 2 Purpose... 2 Serving Senior Medicare-Medicaid Enrollees... 2 How to Use This Tool... 2
Transitioning to Community Services: HARPS, Health Homes and SPOA
 Transitioning to Community Services: HARPS, Health Homes and SPOA P R E S E N T E R : G L E N N L I E B M A N, C EO Mental Health Association in New York State, Inc. Brief History of Health and Recovery
Transitioning to Community Services: HARPS, Health Homes and SPOA P R E S E N T E R : G L E N N L I E B M A N, C EO Mental Health Association in New York State, Inc. Brief History of Health and Recovery
HCBS Settings Rule and Minnesota s Transition Plan
 HCBS Settings Rule and Minnesota s Transition Plan Aimee Rumpza, Program Administrator, Aging and Adult Services Division, DHS 5/1/2017 2017 Assisted Living and Home Care Conference August 2 nd, 2017 10:45-11:45
HCBS Settings Rule and Minnesota s Transition Plan Aimee Rumpza, Program Administrator, Aging and Adult Services Division, DHS 5/1/2017 2017 Assisted Living and Home Care Conference August 2 nd, 2017 10:45-11:45
907 KAR 10:014. Outpatient hospital service coverage provisions and requirements.
 907 KAR 10:014. Outpatient hospital service coverage provisions and requirements. RELATES TO: KRS 205.520, 42 C.F.R. 447.53 STATUTORY AUTHORITY: KRS 194A.030(2), 194A.050(1), 205.520(3), 205.560, 205.6310,
907 KAR 10:014. Outpatient hospital service coverage provisions and requirements. RELATES TO: KRS 205.520, 42 C.F.R. 447.53 STATUTORY AUTHORITY: KRS 194A.030(2), 194A.050(1), 205.520(3), 205.560, 205.6310,
NEW YORK STATE MEDICAID PROGRAM OFFICE OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES HOME AND COMMUNITY BASED SERVICES WAIVER MANUAL
 NEW YORK STATE MEDICAID PROGRAM OFFICE OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES HOME AND COMMUNITY BASED SERVICES WAIVER MANUAL POLICY GUIDELINES Table of Contents SECTION I - DESCRIPTION OF
NEW YORK STATE MEDICAID PROGRAM OFFICE OF MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIES HOME AND COMMUNITY BASED SERVICES WAIVER MANUAL POLICY GUIDELINES Table of Contents SECTION I - DESCRIPTION OF
Individual and Family Guide
 0 0 C A R D I N A L I N N O V A T I O N S H E A L T H C A R E Individual and Family Guide Version 9 revised November 1, 2016 2016 Cardinal Innovations Healthcare 4855 Milestone Avenue Kannapolis, NC 28081
0 0 C A R D I N A L I N N O V A T I O N S H E A L T H C A R E Individual and Family Guide Version 9 revised November 1, 2016 2016 Cardinal Innovations Healthcare 4855 Milestone Avenue Kannapolis, NC 28081
Balance of State Continuum of Care Program Standards for Permanent Supportive Housing Programs
 1 Balance of State Continuum of Care Program Standards for Permanent Supportive Housing Programs The Balance of State Continuum of Care developed the following Permanent Supportive Housing Program standards
1 Balance of State Continuum of Care Program Standards for Permanent Supportive Housing Programs The Balance of State Continuum of Care developed the following Permanent Supportive Housing Program standards
Alternative or in Lieu of Service Description Alliance Behavioral Healthcare
 Alternative or in Lieu of Service Description Alliance Behavioral Healthcare 1. Service Name and Description: Rapid Response Crisis Services for Children and Youth Service Name: Rapid Response Procedure
Alternative or in Lieu of Service Description Alliance Behavioral Healthcare 1. Service Name and Description: Rapid Response Crisis Services for Children and Youth Service Name: Rapid Response Procedure
Contemporary Psychiatric-Mental Health Nursing. Deinstitutionalization. Deinstitutionalization - continued
 Contemporary Psychiatric-Mental Health Nursing Chapter 12 Creating Hospital and Community-Based Therapeutic Environments Deinstitutionalization Began in the post World War II period Large public mental
Contemporary Psychiatric-Mental Health Nursing Chapter 12 Creating Hospital and Community-Based Therapeutic Environments Deinstitutionalization Began in the post World War II period Large public mental
OUTPATIENT SERVICES. Components of Service
 OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
1915(i) State Plan Home and Community-Based Services Overview
 State Plan Home and Community-Based Services Overview") GOVERNMENT OF THE DISTRICT OF COLUMBIA Department of Health Care Finance 1915(i) State Plan Home and Community-Based Services Overview Purpose: The Adult Day Health Program- 1915(i) is a new service under
GOVERNMENT OF THE DISTRICT OF COLUMBIA Department of Health Care Finance 1915(i) State Plan Home and Community-Based Services Overview Purpose: The Adult Day Health Program- 1915(i) is a new service under
October 5 th & 6th, The Managed Care Technical Assistance Center of New York
 October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
Prior Authorization and Continued Stay Criteria for Adult Serious Mentally Ill (SMI) Behavioral Health Residential Facility
 Behavioral Health Residential Facility") Prior Authorization and Continued Stay Criteria for Adult Serious Mentally Ill (SMI) Behavioral Health Residential Facility AUTHORIZATION CRITERIA FOR BEHAVIORAL HEALTH RESIDENTIAL FACILITY, ADULT Title
Prior Authorization and Continued Stay Criteria for Adult Serious Mentally Ill (SMI) Behavioral Health Residential Facility AUTHORIZATION CRITERIA FOR BEHAVIORAL HEALTH RESIDENTIAL FACILITY, ADULT Title
DEPARTMENT OF HUMAN SERVICES DIVISION OF MENTAL HEALTH & ADDICTION SERVICES
 DEPARTMENT OF HUMAN SERVICES DIVISION OF MENTAL HEALTH & ADDICTION SERVICES ADDENDUM to Attachment 3.1-A Page 13(d).10 Service Description Community Support Services consist of mental health rehabilitation
DEPARTMENT OF HUMAN SERVICES DIVISION OF MENTAL HEALTH & ADDICTION SERVICES ADDENDUM to Attachment 3.1-A Page 13(d).10 Service Description Community Support Services consist of mental health rehabilitation
1. SMHS Section of CCR Title 9 (Division 1, Chapter 11): this is the regulation created by the California Department of Health Care Services (DHCS).
: this is the regulation created by the California Department of Health Care Services (DHCS).") Clinical Documentation Tool This tool compares the definitions of outpatient Specialty Mental Health s (SMHS) that appear in two different sources: 1. SMHS Section of CCR Title 9 (Division 1, Chapter 11):
Clinical Documentation Tool This tool compares the definitions of outpatient Specialty Mental Health s (SMHS) that appear in two different sources: 1. SMHS Section of CCR Title 9 (Division 1, Chapter 11):
DEVELOPING A MEDICAID SUPPORTIVE HOUSING SERVICES BENEFIT
 DEVELOPING A MEDICAID SUPPORTIVE HOUSING SERVICES BENEFIT CONSIDERATIONS AND DECISION POINTS EXECUTIVE SUMMARY This tool is designed to assist States in the development of a Medicaid benefit to pay for
DEVELOPING A MEDICAID SUPPORTIVE HOUSING SERVICES BENEFIT CONSIDERATIONS AND DECISION POINTS EXECUTIVE SUMMARY This tool is designed to assist States in the development of a Medicaid benefit to pay for
Adult Autism Waiver HCBS Transition Plan
 Section 1: Identification The Bureau of Autism Services (BAS) will use its Adult Autism Waiver (AAW) transition plan as a way to determine its compliance with CMS rule on home and community-based services
Section 1: Identification The Bureau of Autism Services (BAS) will use its Adult Autism Waiver (AAW) transition plan as a way to determine its compliance with CMS rule on home and community-based services
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Non- PAPH Outpatient Mental Health
 Fee-for-Service Provider Manual Non- PAPH Outpatient Mental Health Updated 05.2014 PART II Introduction Section 7000 7010 8100 8200 8300 8400 8410 Appendix BILLING INSTRUCTIONS Non-PAHP Outpatient Mental
Fee-for-Service Provider Manual Non- PAPH Outpatient Mental Health Updated 05.2014 PART II Introduction Section 7000 7010 8100 8200 8300 8400 8410 Appendix BILLING INSTRUCTIONS Non-PAHP Outpatient Mental
Approved Curriculum and Equivalency Standards. Parent Support and Training/Youth Support and Training
 Approved Curriculum and Parent Support and Training/Youth Support and Training Introduction to Wraparound This initial training introduces new parent support and training and youth support and training
Approved Curriculum and Parent Support and Training/Youth Support and Training Introduction to Wraparound This initial training introduces new parent support and training and youth support and training
(c) A small client to staff caseload, typically 10:1, to consistently provide necessary staffing diversity and coverage;
 A small client to staff caseload, typically 10:1, to consistently provide necessary staffing diversity and coverage;") 309-019-0225 Assertive Community Treatment (ACT) Overview (1) The Substance Abuse and Mental Health Services Administration (SAMHSA) characterizes ACT as an evidence-based practice for individuals with
309-019-0225 Assertive Community Treatment (ACT) Overview (1) The Substance Abuse and Mental Health Services Administration (SAMHSA) characterizes ACT as an evidence-based practice for individuals with
Clinical Utilization Management Guideline
 Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
BEHAVIOR HEALTH LEVEL OF CARE GUIDELINES for Centennial Care
 BEHAVIOR HEALTH LEVEL OF CARE GUIDELINES for Centennial Care Acute Inpatient Hospitalization I. DEFINITION OF SERVICE: Acute Inpatient Psychiatric Hospitalization is a 24-hour secure and protected, medically
BEHAVIOR HEALTH LEVEL OF CARE GUIDELINES for Centennial Care Acute Inpatient Hospitalization I. DEFINITION OF SERVICE: Acute Inpatient Psychiatric Hospitalization is a 24-hour secure and protected, medically
Mental Health and Substance Abuse Services Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE. Effective Date:
 Mental Health and Substance Abuse Services Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE Date of Issue: July 30, 1993 Effective Date: April 1, 1993 Number: OMH-93-09 Subject By Resource
Mental Health and Substance Abuse Services Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE Date of Issue: July 30, 1993 Effective Date: April 1, 1993 Number: OMH-93-09 Subject By Resource
Prepaid Inpatient Health Plans (PIHP), Community Mental Health Services Programs (CMHSP)
, Community Mental Health Services Programs (CMHSP)") Bulletin Michigan Department of Health and Human Services Bulletin Number: MSA 15-42 Distribution: Prepaid Inpatient Health Plans (PIHP), Community Mental Health Services Programs (CMHSP) Issued: October
Bulletin Michigan Department of Health and Human Services Bulletin Number: MSA 15-42 Distribution: Prepaid Inpatient Health Plans (PIHP), Community Mental Health Services Programs (CMHSP) Issued: October
Navigating New York State s Transition to Managed Care
 Navigating New York State s Transition to Managed Care December 3, 2014 Mary McKernan McKay, Ph.D Andrew F. Cleek, Psy.D. Meaghan E. Baier, LMSW Agenda Introduction of the Managed Care Technical Assistance
Navigating New York State s Transition to Managed Care December 3, 2014 Mary McKernan McKay, Ph.D Andrew F. Cleek, Psy.D. Meaghan E. Baier, LMSW Agenda Introduction of the Managed Care Technical Assistance
New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session. Comments of Christy Parque, MSW.
 New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session Comments of Christy Parque, MSW President and CEO November 29, 2017 The Coalition for Behavioral Health, Inc. (The Coalition)
New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session Comments of Christy Parque, MSW President and CEO November 29, 2017 The Coalition for Behavioral Health, Inc. (The Coalition)
Provider Frequently Asked Questions
 Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services.
 907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
256B.0943 CHILDREN'S THERAPEUTIC SERVICES AND SUPPORTS.
 1 MINNESOTA STATUTES 2016 256B.0943 256B.0943 CHILDREN'S THERAPEUTIC SERVICES AND SUPPORTS. Subdivision 1. Definitions. For purposes of this section, the following terms have the meanings given them. (a)
1 MINNESOTA STATUTES 2016 256B.0943 256B.0943 CHILDREN'S THERAPEUTIC SERVICES AND SUPPORTS. Subdivision 1. Definitions. For purposes of this section, the following terms have the meanings given them. (a)
empowering people to build better lives their efforts to meet economic, social and emotional challenges and enhance their well-being
 Community Care Alliance empowering people to build better lives Adult Mental Health Services Basic Needs Assistance Child & Family Services Education Employment & Training Housing Stabilization & Residential
Community Care Alliance empowering people to build better lives Adult Mental Health Services Basic Needs Assistance Child & Family Services Education Employment & Training Housing Stabilization & Residential
From HARPs to DSRIP to VBP: What Do They Mean To You?
 From HARPs to DSRIP to VBP: What Do They Mean To You? North Country NYAPRS 2016 Winter Forum Harvey Rosenthal Executive director 1 New York Association of Psychiatric Rehabilitation Services (NYAPRS) A
From HARPs to DSRIP to VBP: What Do They Mean To You? North Country NYAPRS 2016 Winter Forum Harvey Rosenthal Executive director 1 New York Association of Psychiatric Rehabilitation Services (NYAPRS) A
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
UnitedHealthcare Guideline
 UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
Update on the Home and Community- Based Services Rule. Presentation Outline. Home and Community Based Services
 Michigan Department of Health & Human Services Update on the Home and Community- Based Services Rule Heather Hill and Phil Kurdunowicz LeadingAge Training Day October 22 nd, 2015 Putting people first,
Michigan Department of Health & Human Services Update on the Home and Community- Based Services Rule Heather Hill and Phil Kurdunowicz LeadingAge Training Day October 22 nd, 2015 Putting people first,
CHILDREN S INITIATIVES
 CHILDREN S INITIATIVES Supports and Specialty Services for Children, Youth and Families October 8, 2013 Calgie, MSW Intern, Eastern Michigan University Carlynn Nichols, LMSW, Detroit Wayne Mental Health
CHILDREN S INITIATIVES Supports and Specialty Services for Children, Youth and Families October 8, 2013 Calgie, MSW Intern, Eastern Michigan University Carlynn Nichols, LMSW, Detroit Wayne Mental Health
Housing as Health Care Webinar. Wrapping Tenancy Supports into Your Housing Strategy
 Housing as Health Care Webinar Wrapping Tenancy Supports into Your Housing Strategy National Governors Association Friday, October 28th, 2016 12-1pm EST Dial-in: 888-858-6021; Passcode 2026245354 1 Agenda
Housing as Health Care Webinar Wrapping Tenancy Supports into Your Housing Strategy National Governors Association Friday, October 28th, 2016 12-1pm EST Dial-in: 888-858-6021; Passcode 2026245354 1 Agenda
David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health
 David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation,
David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation,
HOME AND COMMUNITY-BASED SETTINGS & TRANSITION PLANNING. August 2014
 HOME AND COMMUNITY-BASED SETTINGS & TRANSITION PLANNING August 2014 Presentation Overview Brief overview of the CMS Final Rule. Person-Centered Planning Requirements. Transition planning to come into compliance
HOME AND COMMUNITY-BASED SETTINGS & TRANSITION PLANNING August 2014 Presentation Overview Brief overview of the CMS Final Rule. Person-Centered Planning Requirements. Transition planning to come into compliance