Physiological Observations Policy
|
|
|
- Shavonne Blake
- 5 years ago
- Views:
Transcription


1 Physiological Observations Policy Reference No: P_CS_16 Version: 3.0 Ratified by: LCHS Trust Board Date ratified: 14 th November 2017 Name of originator / author: Name of responsible committee / individual: Jill Anderson/Tim Balderstone Safeguarding & Patient Safety Date Approved by committee: 18 th October 2017 Date issued: November 2017 Review date: October 2019 Target audience: Distributed via: All Staff Website Chair: Elaine Baylis, QPM Chief Executive: Andrew Morgan
2 Version Control Sheet Physiological Observations Policy Version Section/Para/ Appendix Version/Description of Amendments Date Author/Amended by 1 New Policy November 2012 Jill Anderson 2 Minor wording changes, updates to policy references, external references and links to external sites. November 2014 Tim Balderstone 2.1 Extension agreed January 2017 Corporate Assurance Team 2.2 Extension agreed September 2017 Corporate Assurance Team 3 Full review. Incorporation of paediatric POPS process. Revised NEWS processes and Adjusted Parameter Trigger process October 2017 Tim Balderstone Copyright 2017 Lincolnshire Community Health Services NHS Trust, All Rights Reserved. Not to be reproduced in whole or in part without the permission of the copyright owner. 2
3 Physiological Observations Policy Contents Page No. Policy Statement... 5 Background... 5 Statement... 5 Responsibilities... 5 Training... 5 Dissemination... 5 Resource implication... 5 Abbreviations / Definitions... 6 Introduction and Summary... 7 Aims and Objectives... 8 Scope... 8 Inclusion Criteria... 8 NEWS System... 8 POPS System... 8 Review... 9 Evidence Base... 9 Risk Management... 9 Duties within the organisation... 9 Recording Vital Signs - Adults Patient Observations Urgent Care Services Routine Observations In-patient Areas NEWS Clinical Response to NEWS Alteration of Routine Monitoring Frequency for In-Patient Areas Exclusion from Routine Monitoring Altered Escalation Triggers Patient consent Documentation National Early Warning Score (NEWS) Suspected Sepsis NEWS Scoring Parameters Respiratory rate Heart Rate Temperature Blood Pressure Oxygen saturation Neurological Assessment (AVPU) Assessing the patient with significant deterioration
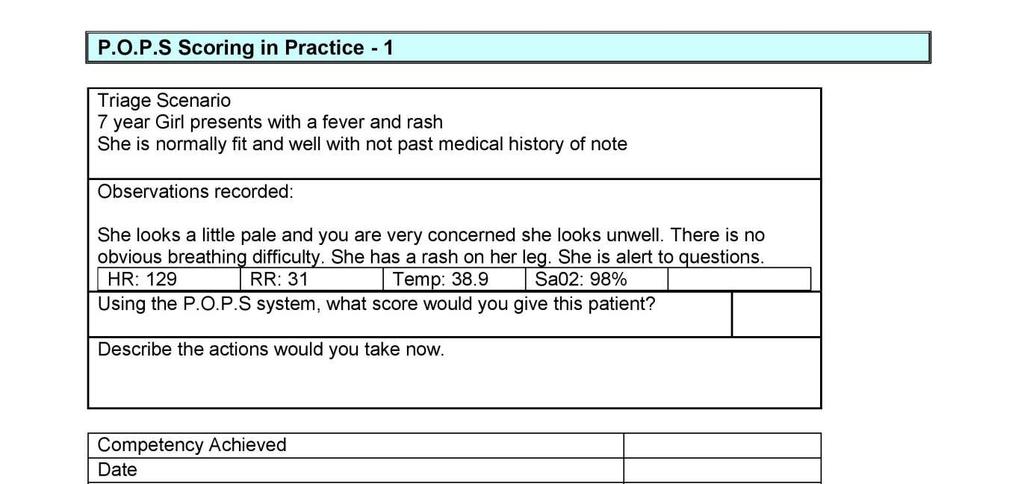
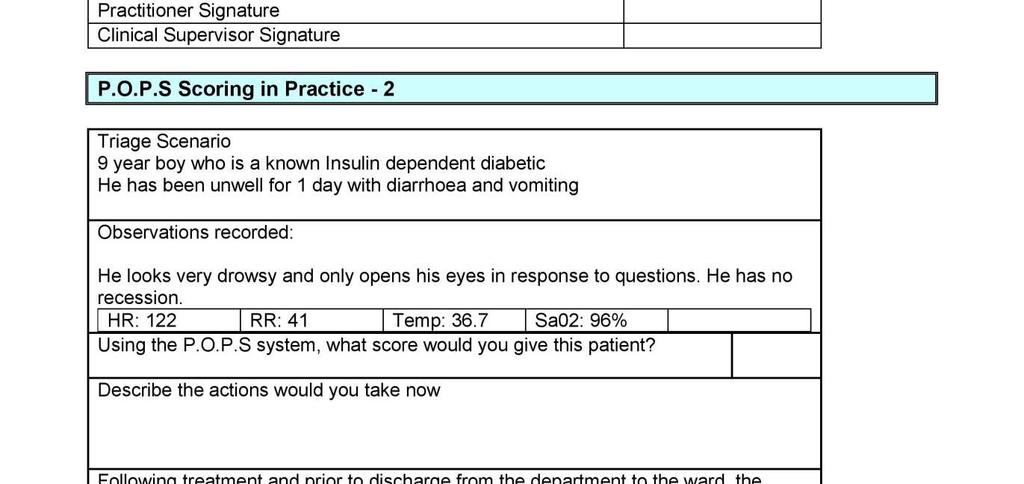
4 Seeking Help Recording Vital Signs Children POPS Vital Signs Additional POPS Chart Components POPS Scoring Matrix Escalation Handover Communication SBAR Printable Documents References Monitoring Template Equality Analysis Appendix 1 NEWS Observation Chart Appendix 2 NEWS Parameters Appendix 3 NEWS Clinical Response Appendix 4 Adjusted Escalation Triggers Form Appendix 5 POPS Form Appendix 6 POPS Learning Package
5 Policy Statement Physiological Observations Policy Background Physiological observations are fundamental to ensuring that patients in hospital are safe and that healthcare professionals are aware of the health status of patients. Patients within all hospital settings are at risk of physiological deterioration and not all patient deterioration can be predicted, so all patients (with the exception of some patients at the end of their life) require observation which includes the taking and recording of vital signs. Statement This policy outlines how LCHST will meet the duties set out in the NHSLA Risk Management Standard (4.8), which requires that all organisations have an approved documented process for managing the risks associated with the deteriorating patient. It is intended that the NEWS and POPS systems be utilised by all members of clinical staff who perform clinical observations as a part of patient management. Responsibilities Compliance with the guideline will be the responsibility of all Lincolnshire Community Health Services NHS Trust staff. Training National Early Warning Score e-learning Clinical Observation Teaching and Assessment Pack Face to Face teaching clinical observations LCHS POPS Teaching Package Dissemination Website/Intranet Resource implication Staff will require an understanding of process and time to complete training pack. 5
6 Abbreviations / Definitions Acronym AVPU ECG EWS GCS GLUC IV LCHS NEWS NICE NPSA RCP SP0² WBC POPS SBAR MDT Term / Definition Alert, Pain, Verbal, Unresponsive Electro cardiogram Early Warning Score Glasgow Coma Score Glucose Intra-venous Lincolnshire Community Health Services NHS Trust National Early Warning Score National Institute for Clinical Excellence National Patient Safety Agency Royal College of Physicians Oxygen Saturation White Blood Count Paediatric Observation Priority Score Situation, Background, Assessment, Response Multi-Disciplinary Team 6
7 Introduction and Summary Physiological observations are fundamental to ensuring that patients in hospital are safe and that healthcare professionals are aware of the health status of patients (NICE 20071a.1,2 NPSA 20071,2. 3,4 ). This form of clinical monitoring may be regarded as being a task and as having a low status / a task based activity by clinical professionals (NPSA, ), rather than the gathering of clinical information. This poses a real danger for patients, without effective leadership from nurses in senior roles, there is potential for patient observations not to be seen as a serious responsibility Patients within all healthcare and community settings are at risk of physiological deterioration and not all patient deterioration can be predicted so all patients (with the exception of some patients at the end of their life) require observation which includes the taking and recording of vital signs. It is well documented that patients who deteriorate, have abnormalities that are detectable by physiological observations well in advance. There is also evidence that there is poor recognition of physiological deterioration and although deterioration can be recognised through vital signs, these are not always regularly recorded by the healthcare community despite being the primary indicator of altered physiology. Early detection, timeliness and competency of clinical response are a triad of determinants of clinical outcome in people with acute illness (RCP ), numerous national reports have advocated the use of early warning scores (EWS) to efficiently identify and respond to patients who present with or develop acute illness and the use of Track and Trigger was established within the Trust. Work by a Royal College of Physicians task force led to the development of the National Early Warning Score, providing a standardised track and trigger system for acute illness in people presenting to, or within hospital and this was adopted by LCHS The NEWS system is used as a surveillance system for all patients in hospitals, tracking their clinical condition, alerting the clinical team to any deterioration and triggering a timely clinical response. Patients within community hospital settings although not acutely ill, often have complex medical conditions, co-morbidities, and multiple pharmacopeia predisposing them to the risk of further episodes of acute illness and are therefore equally requiring of continued physiological monitoring. It is therefore important that all adult patients in hospitals settings, should have regular physiological observations as a minimum standard. These observations should always lead to the calculation and recording of an NEWS and if abnormal should be acted upon according to protocol (see NEWS Clinical Response - Appendix 2), which describes a graded response. To facilitate this the healthcare team should be competent to undertake, document, interpret and act upon these observations and should have access to appropriate monitoring and measurement equipment (MHRA , NICE 2007¹; NPSA ,4, ). 7
8 Aims and Objectives The purpose of this policy is to ensure a standardised Trust wide approach to the recording of physiological monitoring and the actions which should be triggered in the case of abnormality. To articulate the standards expected of those working as clinical staff within the Trust. Improve the quality of patient monitoring and observation Define the expectation for physiological observations within the Urgent Care services Define the physiological observations that should be undertaken on all adult inpatients. The frequency of observations and when they should be stepped up or down How observations should be recorded and assessed Using the NEWS or POPS process to guide clinical decision making The process of referral when a patient is found to be deteriorating The initial actions that can be taken to prevent deterioration or promote a dignified death. Scope This policy outlines the minimum standard expected from clinical professionals for what is defined and referred to throughout the document as routine monitoring. This applies to all patient settings across Lincolnshire Community Health Services NHS Trust (LCHS). To discuss all possible clinical circumstances is beyond the scope of this policy and therefore the reader is also referred to local policies and protocols, which describe monitoring and observations specific to certain conditions. The policy is concerned with the prevention of deterioration and should be read in conjunction with the Resuscitation Policy (P_CS_ 08 ) and DNACPR Policy (P_CS_07). Inclusion Criteria NEWS System It is anticipated that all adult patients requiring vital signs observations will have NEWS applied to the results. Whilst the NEWS system is not yet fully validated for use within pre-hospital or Emergency Department areas an increasing evidence base suggests its use here has significant merit 26 and acts as the trigger for other clinical tools such as sepsis screening. Its use in all areas of LCHS undertaking patient observations is therefore required. POPS System Use of the POPS system is mandated on presentation of a child with the following situations and conditions;- o all infants < 1 year o all infants/children with apparent or reported breathing difficulty o all infants/children with apparent or reported altered level of alertness o all infants/children presenting with or a recent history of D&V 8
9 o repeat attenders (>2 contacts in last 72 hours) o pre-existing morbidity (e.g. known asthma, heart disease) o any infant or child where parental/carer concern is high. In all other situations it is appreciated that individual clinicians may consider through clinical judgement a complete POPS assessment is not required. In this situation records must reflect the clinicians rationale for proceeding without exclusion of abnormal physiology. It is anticipated that a full examination of a child is undertaken and that this process will normally capture the majority of POPS scoring elements and significant observational indicators of the child s wellbeing. Review This policy will be reviewed tri-annually by the group fulfilling the function of Safeguarding & Patient Safety Group. Evidence Base See References Risk Management The NHSLA Risk Management Standards (NHS Litigation Authority Section 4.8, states that all organisations must have an appropriate documented process for managing the risks associated with the deteriorating patient and outlines the requirement for: A documented plan for vital signs monitoring, that identifies which variables need to be measured, including the frequency of measurement. Use of an early warning system within the organisation to recognise patients at risk of deterioration. Actions to be taken to minimise or prevent further deterioration. This policy provides for a record of both the initiation of observation screening and treatment interventions using NEWS and POPS systems applicable to all LCHS responsible healthcare settings. NICE Quality Standard 64 Fever in Under 5 s 8 requires organisations to evidence Infants and children under 5 years who are seen in person by a healthcare professional have their temperature, heart rate, respiratory rate and capillary refill time measured and recorded if fever is suspected. Full completion of the POPS process will provide such evidence. Duties within the organisation The Chief Executive: has overall responsibility for the strategic and operational management of Lincolnshire Community Health Services NHS Trust, including ensuring that the organisation s policies comply with all legal, statutory and good practice requirements. 9
10 Heads of Clinical Service: Responsible for identifying and implementing policies relevant to their area of responsibility. They are also responsible for ensuring that all staff have access to and are made aware of, policies that apply to them. All staff Responsible for the implementation of LCHS policies as part of their core duties. Practitioners measuring and recording the observations It is the responsibility of these individuals to ensure that they are competent to undertake, record and report abnormalities in physiological observations in accordance with the screening tools outlined in this policy. Practitioners interpreting observations It is the responsibility of these individuals to ensure that they are competent to interpret observations and make judgements about them taking into account normal parameters, baseline parameters for the individual patient and acceptable or target parameters according to the plan of care. Interpretation should lead to appropriate action where there is abnormality (NEWS/POPS) and use of the relevant sepsis screening tool if appropriate. This action should consider necessary action by the interpreting individual or other clinical professional. If there is any doubt about abnormal observations and the potential for sepsis these should always be reported to a more senior and experienced professional (Senior Nurse, Advanced Nurse Practitioner, Paramedic Specialist Practitioner,Doctor). Practitioners responding to abnormal observations It is the responsibility of the practitioner responding to abnormal observations and undertaking the screening process to ensure that they are competent to intervene should treatment be indicated and recognise the limits of their competence. All clinical professionals Who are involved in monitoring, recording, interpreting and acting to treat changes in physiological observations should be aware of this policy and its principles. Documentation and communication are pivotal to minimising risks for patients and all actions must be documented contemporaneously or as soon as possible after the event in accordance with the organisational policy. Senior help and advice should be sought by all professionals who are concerned about patients regardless of their observations. All should be aware of the screening systems (NEWS/POPS) and what actions are necessitated by the range of scores generated. Any individual recording observations should be able to interpret these in the light of the NEWS/POPS protocols and should ensure that escalation is occurring in accordance with the NEWS. This includes Registered (e.g. Nurses, Physiotherapists, Doctors) and nonregistered (e.g. Healthcare Assistants/Support Workers) staff. Failures to comply with this policy and adverse clinical incidents occurring in relation to physiological monitoring should be reported in accordance with Trust policy. The senior clinician in charge of the clinical area 10
11 It is the responsibility of the senior clinicain working in conjunction with Clinical Practice Educators to ensure that all staff are competent to undertake their role in relation to physiological observations to facilitate correct use of the NEWS/POPS tools. The senior clinician should identify any additional training that may be required for appropriate staff. This responsibility extends to ensuring that staff have access to appropriate monitoring equipment (NPSA 2007a 1 ; 2007b 2 ) and documentation for the recording of observations. All documents where patient s observations are recorded should be located together and in close proximity to the patient (NPSA, 2007b 2 ). The senior clinicain, in collaboration with the matron and other relevant professionals such as the Resuscitation Lead, should investigate all adverse clinical incidents in relation to physiological monitoring and develop action plans to prevent their future occurrence. Monitoring Compliance The senior clinicain (usually ward manager in the case of in-patient areas ans team/locality lead for urgent care) in charge of each clinical area is responsible for ensuring that the standard of physiological monitoring in their clinical area is audited for compliance with this document at least annually. In addition for ward areas monthly sel-audit of compliance with National Early Warning Scoring should be undertaken using the Trust NEWS Audit tool and reported to the Resuscitation Lead. Competence for Practice Physiological observations should be recorded and acted upon by staff who have been trained to undertake these procedures and understand their clinical relevance. (NICE, 2007a 1 ). An online training resource can be found via All healthcare staff recording data for, or responding to, the NEWS should be trained in its use and should understand the significance of the scores with regard to local policies for responding to the NEWS triggers and the clinical response required. Training can be accessed via A clear understanding of the escalation protocols applicable to each service area MUST form an element of the local induction process for staff. This understanding should be checked regularly and the clinican in charge should ensure all staff are aware of any changes. All healthcare staff recording data for, or responding to, the POPS tool should be trained in its use.(lchs POPS Teaching Package Appendix 6) It is the responsibility of all individuals to ensure that they are competent to undertake their role and responsibilities in relation to physiological monitoring. This competence should be assessed and documented only by professionals who are themselves competent at this area of practice, who are able to assess competence in others and who are registered 11
12 professionals (e.g. Registered Nurse/ Clinical Educator/ Education & Workforce Development Team). Recording Vital Signs - Adults Patient Observations Urgent Care Services Physiological observations remain the mainstay investigations for assessment of patients physiology. Patients presenting at Urgent Care Services are by their very nature therefore requiring a full and thorough assessment, including physiological observations, and the results should therefore be subject to the NEWS process. Patients attending Urgent Care Services who have physiological observations taken should therefore all have the NEWS recorded. Any parameter not assessed and not used for NEWS, through patient nonconcordance for example, should have an explanatory record detailing the reason or rationale for omission. Whilst prolonged periods of physiological monitoring are not allpicable to Urgent Care settings the baseline the measurements provide can be of significant benefit to secondary care and so these records should move with the patient whenever possible. Routine Observations In-patient Areas All patients should have heart rate*, respiratory rate, blood pressure, level of consciousness (AVPU), oxygen saturation (SP02), blood glucose and temperature recorded on admission together with a pain score if appropriate. Other assessments e.g. MUST and falls should be assessed as per local policy. (*Important clinical information such as pulse volume, rate and rhythm, are all lost if automatic equipment is used alone.) All patients should have a NEWS score attributed to every set of observations.(rcp ) All in-patients should have their weight recorded on admission All in-patient s observations should be recorded on the Trust observation chart. Patients should retain the same observation chart, when moving between departments and reference made to previous charts when transferred from other hospitals, in order that physiological trends can be identified. All patients should have a clear written monitoring plan that specifies which physiological observations should be recorded and how often (NICE CG50 1 ). The plan should take account of the patient s diagnosis, presence of co-morbidities and agreed treatment plan. It 12
13 is acceptable to state in this plan that patients should have routine monitoring and in this case the minimum parameters and frequencies described below will apply Physiological observations should be recorded at least every 12 hours (Routine Monitoring), (NICE CG50 1, Royal College of Physicians 5.) unless a decision has been made at MDT to alter the frequency of observation. A full and detailed rationale to support this MDT decision must be recorded in the patient s notes. Some patient, may have pre-existing conditions and the scoring may need to be interpreted accordingly, e.g. hypercapnoeic failure due to COPD and scoring is outlined within the guidance (e.g. target saturations of 88-92% should be used (British Thoracic Society 9 ), scoring if the saturations drop below 92% and when supplementary oxygen is used. However, should the scoring escalation protocol may be re-set by a competent clinical decision maker to allow for long term physiological changes in one or more parameter the rationale must be recorded in the patient record by completion of an Adjusted Parameter form. Any adjustment to escalation protocols MUST NOT result in a lowering of basic observation frequency below the minimum 12 hourly unless the patient is on a defined end of life plan and DNACPR is in place or until an MDT decision and rationale is recorded. Patients with abnormal physiology are at greater risk of deterioration and reducing observation frequency could result in increased potential for un-noticed deterioration. The frequency of monitoring should increase when abnormal physiology is detected or the patient is at risk of deterioration e.g. exacerbation of condition, infection. NEWS The NEW Score should be used to inform the frequency of clinical monitoring within the impatient areas. In urgent care services it is accepted the majpority of patients may be subjected to just a single set of recordings, although the resulting score will again inform of the requirement for increased scrutiny. 0 the minimum frequency of monitoring should be 12 hourly 1-4 monitoring increased to 4 6 hourly unless more or less frequent monitoring is considered appropriate by a competent clinical decision-maker (senior nurse or ward doctor) This may include patients undergoing rehabilitation or in a stable condition, daily monitoring may be considered if supported by a documented rationale for the decision. 5 6 The frequency of monitoring should be increased to a minimum of hourly or a RED score (ie a score of 3 in any single parameter) until the patient is reviewed and a plan of care documented. 7 Continuous care, monitoring and recording of vital signs for those with a NEWS aggregate score of 7 or more. 13
14 Clinical Response to NEWS Depending on the NEW score there are recommendations for the frequency of clinical monitoring, the urgency of clinical review, the competency requirements of the clinical team required to undertake the review and the most appropriate environment for on-going care (NEWS Clinical Response - Appendix 3). Clinical response to the NEWS should be recorded on the chart. This will provide a continuous record of actions taken in response to variations in the NEWS and act as a prompt for escalating care if necessary. Concern about a patient s clinical condition should always override the NEWS if the attending healthcare professional considers it necessary to escalate care. Within Urgent Care settings the escalation process used will depend on the environment and clinical expertise available, to cover all settings within this policy is not possible. Staff MUST be aware of the processes and escalation options available within their clinical setting. Alteration of Routine Monitoring Frequency for In-Patient Areas For all patients within in-patient areas NICE (CG50 1 ) expectations are that patients physiological observations should be recorded at least every 12 hours, any alteration from that minimum standard, such as reduction to daily observation recording, requires an MDT decision and the rationale to be supported by detailed clinical notes by a senior clinician. Until such time as the MDT has taken place observations must continue at the minimum threshold of 12 hourly. Exclusion from Routine Monitoring This policy does not apply to patients who have been commenced on an End of Life care plan and are subject to a DNACPR order. It is not considered appropriate to continue to undertake routine all physiological observations in instances where deterioration changes will not result in active treatment. However it is important to understand that some palliative treatments will still require some vital signs to be monitored and recorded. In these circumstances a documented note detailing what parameters should be monitored to facilitate safe treatment and the range of acceptable results is required along with any escalation actions required if results are outside of these ranges. Altered Escalation Triggers 14
15 Exceptions to standard monitoring protocols may be appropriate for patients with physiological abnormalities due to long term conditions that permanently derange the score in certain parameters. The desired effect of the Altered Escalation Triggers Form is to alter escalation trigger levels in response to elevated results in specified isolated NEWS scoring parameters by discounting the score for the particular deranged observation. E.g. A 72 year old patient with stable copd has a normal oxygen saturation of 91% and a respiratory rate of 22 even at rest. It therefore be appropriate to consider the NEW Score of 3 for the SpO 2 element and 2 for the respiratory element to be discounted from the total when considering escalation actions for this patient. However, the rationale for the decision must be documented in the patients notes and an Altered Escalation Triggers Form completed to confirm the revised plan. This form alone cannot be used to effect the reduction of observation frequency below the 12 hourly threshold, this requires a MDT decision and full rationale documented. It is important that the acknowledgement of altered physiology, and resultant NEW score component results, should NOT change the basis for the calculation of the total score and it is simply the trigger actions arising from increased scores in specified parameters that are altered. There has to be understanding by the entire care team that the NEWS escalation actions are only reduced where increased scores are present in the clinical parameters specified in the Adjusted Escalation Triggers paperwork. Increased scores in any other parameters should result in the specified escalation actions being followed. Clinical notes should reflect revised escalation actions for the specified abnormal parameters and also define any circumstances in which the reduced actions do not apply. Patient consent Informed verbal consent should always be obtained from the patient to undertake observations. In most instances this will be a simple process of informing the patient what needs to be done, why and what they are likely to experience. In circumstances where observations are indicated and a patient refuses consent it is important to give a clear explanation of the need to perform observations and to explore the reason for refusal. All explanations, refusal of consent by the patient and actions by clinical staff should be dated, timed and signed as entries in the clinical or nursing notes. Senior nursing staff/ doctor should always be informed when patients refuse consent for observations and an entry made in the clinical record to reflect this reporting process. Clinical staff, both nursing and medical, should constantly review the risk and implications of not undertaking observations and should consider whether the patient has the mental 15
16 capacity to consent. Mental Capacity must be formally assessed in circumstances where there is any doubt. Should any staff member have concerns regarding the refused consent for observations and potential safeguarding implications the line manager should be involved and consider whether specialist safeguarding advice is required. Documentation To facilitate standardisation and a national unified approach, a colour coded NEWS chart has been developed to record routine clinical data and track a patient s clinical condition. Routine monitoring, as described above, should be clearly and legibly recorded, contemporaneously on the NEWS chart. The NEWS chart is colour-coded (Red, Amber, Green RAG coded) to provide both visual and numeric prompts to aid identification of abnormal clinical parameters. Other key parameters not incorporated in the score, including urine output and pain scores, should be recorded separately in the sections included at the bottom of the chart or on additional specific charts if required. This chart must be completed in Black Ink. It should be noted that whilst the use of colour (e.g.red ink) may appear to enhance visibility on the original document this will not necessarily be transferred to photocopies which may be used in the supply of documents to other parties outside the Trust, for example in the case of litigation. This chart must always be maintained even if another chart with similar information (for example, the Neurological monitoring chart or Glasgow Coma Score) is also used. The recorded entries for temperature, pulse and pain should be joined by a single straight line to produce a graph against time. National Early Warning Score (NEWS) The NEWS is based on a simple scoring system in which a score is allocated to physiological measurements. Six physiological parameters form the basis of the scoring system: i. Respiratory rate ii. Oxygen saturation iii. Temperature iv. Systolic Blood pressure v. Pulse rate vi. Level of Consciousness The NEWS scoring system The NEW score should be determined from seven parameters (six physiological plus one weighting score for supplemental oxygen): 16
17 Six physiological parameters routinely recorded: i) respiratory rate, ii) oxygen saturations, iii) temperature, iv) systolic blood pressure, v) pulse rate and vi) level of consciousness. In addition, a weighting score of 2 should be added for any patient requiring supplemental oxygen (oxygen delivery by mask or nasal cannula). Each of the six NEWS physiological parameters is allocated a score reflecting the magnitude of disturbance to each of the physiological parameters. The individual parameter scores should then be combined with a score for use of supplemental oxygen to derive the aggregate NEWS score for the patient. Three trigger levels are recommended for a clinical alert requiring clinician assessment based on the NEWS: A low score: an aggregate NEW score of 1 4 A medium score: a NEWS aggregate score of 5 or more, or a RED score, i.e. an extreme variation in an individual physiological parameter (a score of 3 in any one parameter which is colour coded RED on the observation chart). A high score: an aggregate NEWS score of 7 or more. The triggers should determine the urgency of the clinical response and the clinical competency of the responder/s (** physiological abnormalities due to long term conditions should be considered at admission**) A low score (NEW score 1 4) should prompt assessment by a competent registered clinician who should decide if a change to frequency of clinical monitoring or an escalation of clinical care is required. A medium score (i.e. NEW score of 5 6 or a RED score) should prompt an urgent (within 1 hour) review by a clinician skilled with competencies in the assessment of acute illness which will be either the Senior Clinician with appropriate skills, GP responsible for the ward, Urgent Care Doctor, Nurse Practitioner or Specialist Paramedic Practitioner with relevant experience, who should consider whether escalation of care to an acute hospital is required. To ensure clinical cover 24/7, this role will be undertaken by an Out of Hours doctor, nurse or emergency care practitioner A high score (NEW score of 7 or more) should prompt emergency assessment (immediate) and/ or usually transfer of the patient to an acute care setting. An urgent transfer (999) will be arranged by the senior clinician within the clinical area (where appropriate) using their clinical judgement and this should not be delayed to await a more senior assessment. 17
18 Supplemental oxygen Remember for oxygen therapy the prescription should be to achieve a specified minimum SpO 2 rather than the concentration or flow of gas. The method of delivery, device and flow rate therefore need to be recorded within the patient record and the resulting SpO 2 reading obtained marked on the NEWS chart. Pain Pain is not recorded as part of NEWS, but is incorporated within the NEWS observation chart. Pain and/or its cause will usually but not always generate physiological disturbances that should be captured by the scoring system so should always be considered. Urine Output It is recognised that monitoring urine output is essential for some patients as dictated by their clinical condition and this has therefore been included on the NEWS observation chart. The optimum urine output is 1ml / kg / hr. In a 70kg adult this is equal to 70 mls/hr. The minimum desired urine output is 0.5mls / kg / hr, which is equal to 35 mls/hr. Urine output is generally assessed over a two hour period. In the majority of patients urine output does not need to be routinely measured, but should be considered in the following instances: o Patients with other abnormal signs such as high fever. o Patients with other abnormal fluid losses such as vomiting, drains, stomas or diarrhoea. o Patients with primary urological or renal problems Fluid Balance Charts The balance of fluids within the body is vitally important, many conditions and situations impact the bodies ability to manage fluids and in such circumstances measurement of input and output may be required. (NICE CG ) When a fluid balance chart is in use all measures of both input and output fluid quantities and times should be recorded. All patients receiving IV fluid require a fluid chart All patients required to be nil by mouth for any period exceeding four hours require a fluid chart Daily and cumulative balances should be entered onto the fluid chart. Insensible losses are not normally recorded, but should be considered and accounted for in patients with fluid balance problems. Normal insensible loss is approximately 1L in 24 hours but can greatly increase when a patient has a high temperatures or rapid respiratory rate. Head Injury In patient falls where a head injury cannot be excluded e.g. un-witnessed falls, the patient should be considered at risk of deterioration and observed closely until clinically significant 18
19 head injury has been excluded. (See also Patient Falls and Injuries Prevention Guidelines PAT/PS 11 and NPSA Rapid Response Report 2011/RRR ). After initial assessment Routine monitoring plus pupil size and reaction and Glasgow Coma Scale should be commenced immediately (NICE, 2007b 1 ). Suspected Sepsis In ALL cases of known or strongly suspected infection full assessments MUST be undertaken with the view to EXCLUDE THE POSSIBILITY of sepsis. Sepsis screening using the Trust tools should be performed and even where no current signs or symptoms are presently evident clear advice should be given regarding any signs of deterioration. This safety netting process should be fully recorded detailing the information given to the patient if deterioration occurs or concern increases. BE SUSPICIOUS, a significant number of patients with early stages of sepsis may look well, not all will show classic sepsis symptoms and can present with high or low temperatures. NEWS Scoring Parameters Respiratory rate Respiratory rate is the most sensitive indicator of deteriorating physiology and MUST be recorded in all patients Respiratory rate should be recorded for 60 seconds to account for variations in respiratory rate and pattern. A respiratory rate of <9 or >20 is significant and will generate an alert, this will be form part of the aggregated score and trigger a clinical response. Depth, symmetry and pattern of respiration should also be note and recorded if abnormal together with any associate sounds e.g. wheeze, cough and should form part of any assessment. Heart Rate A manual pulse MUST be taken with every set of observations to assess the pulse properties. If the pulse is irregular or the patient is known to be in atrial fibrillation, then the apex beat should be used to assess the patient s heart rate. The normal resting pulse varies in different client groups, a pulse rate of >90 and < 51 will generate an alert within the NEWS. The rate and regularity should be recorded. Sepsis should be considered when the heart rate is >90 b/min. 19
20 A 12 lead ECG should be performed on any patient who has a new irregular pulse noted, or any other concerns with their pulse. Patients receiving a rate limiting medication i.e. beta blocker will not be able to increase their heart rate to compensate for hypoperfusion conditions and therefore other abnormal signs (high respiratory rate and low urine output) will have extra significance. Temperature Low temperature is as significant as high temperature. The Surviving Sepsis campaign defines one of the parameters for sepsis, as having a core temperature of >38.3 C or 36 C (patients who are immune compromised who develop a temperature > 38 C should be treated as high risk. Hypothermia is defined as a core temperature <35 C, which can become fatal at < 32 C. These patients should be warmed slowly and require transfer to acute care. Tympanic thermometers are known to become less reliable below 34 C and alternative systems should be used. Patients with a temperature < 35 are defined as hypothermic and require acute hospital care, with core temperature (rectal / oesophageal) monitoring. Blood Pressure The gold standard for assessing a patients blood pressure is to use a manual device. There is a role for using an electronic device for frequent recordings in suitable uncomplicated patients, however there should be a high index of suspicion and reversion to a manual device if patients have abnormal recordings e.g. very low BP. Electronic devices are known to become less reliable below 80 mmhg systolic, therefore all patients with blood pressures below this level MUST have a manual recording undertaken Manual sphygmomanometers MUST be available to all areas and staff should be competent to use them as it is accepted that for patients with cardiac arrhythmias automated blood pressure devices may give unreliable results (MHRA ) Although BP is important to monitor, it can be a late sign of clinical deterioration, sick patients can physiologically compensate and may only fail to maintain their BP, when they are very sick. Systolic blood pressure (SBP) less than 100 mmhg will initiate an alert on the NEWS A SBP 90mmHg may be a sign of severe sepsis and requires further assessment of the patient (Surviving Sepsis Campaign ) The SBP should be greater than the heart rate. If the heart rate increases above the SBP it should initiate an alert. 20
21 If the pulse is irregular, the accuracy of electronic BP measuring devices may not be accurate. If the patient s pulse is irregular, manual recording of blood pressure must be undertaken. Oxygen saturation Oxygen saturation is the fifth vital sign. This is a very useful tool, however it maybe limited by many variables: - Nail Varnish and artificial nails - Bright or fluorescent room lighting - Conditions such as jaundice, anaemia, atrial fibrillation or hypothermia, carbon monoxide exposure, oedema and vasoconstriction - Poorly positioned probe - Movement e.g. shivers, rigors - Certain vascular diseases Oxygen saturation (SpO2) and the amount of oxygen at the time of the recording i.e. air or % of oxygen should be recorded on all patients on admission. For most patients a target oxygen saturation should be 94% or above. The exceptions are patients at risk of hypercapnic respiratory failure (usually patients with moderate or severe chronic obstructive pulmonary disease, severe chest wall or spinal disease, neuromuscular disease or severe obesity) for this group the target oxygen saturation is usually set at 88 to 92% (until arterial blood gases have been checked). Unless normal for that patient, a saturation 90%, with or without supplemental oxygen needs to be addressed urgently. The concentration of supplemental oxygen should be recorded and the oxygen delivery device documented. If the patient has an oxygen saturation reading 90%, the device, flow rate, cylinder or wall outlet should all be checked to ensure optimum oxygenation. Oxygen saturation does not measure carbon dioxide levels and therefore arterial blood gases should be considered in all patients with abnormal SpO2, breathing difficulties or unexplained low levels of consciousness, despite supplementary oxygen (urgent transfer to acute care will be required). Oxygen saturations will not be accurate in patients with hypoperfusion conditions i.e. those with irregular heart rhythms. A capillary refill time (CRT) test and mottled knee sign can give further information on the patients perfusion and may initiate an alert. It must be remembered that Oxygen is a drug and for all but emergency life saving administration requires a written prescription and rationale for use recorded in the patient record. 21
22 Neurological Assessment (AVPU) Neurological condition is an important marker of deterioration in clinical condition. Changes in neurological status are highly significant A neurological assessment conscious level should be initially assessed on all patients using the AVPU scale, unless they have a primary neurological problem when the Glasgow Coma Score (GCS) should be used by a competent practitioner. The AVPU scale score is adequate for normal purposes. A = Alert (Awake) V = Responds to voice (Lethargy) P = Responds to pain (Stupor) U = Unresponsive (Coma) Deteriorations in conscious level can be caused by many factors, and a more comprehensive physical assessment should be undertaken by a competent practitioner. New confusion is a significant indicator of deteriorating physiology and should be recorded on the NEW score. A response only to pain or unresponsive, correlates to a GCS of 8 and should be treated as a medical emergency. Any deterioration in conscious level should be followed by a more in depth assessment of GCS. Patients having seizures are at significant risk and all should have a medical review. Assessing the patient with significant deterioration Vital signs and the NEW score will give an indication of the patients condition. If the patient is deteriorating, a more comprehensive assessment is warranted to fully understand any life threatening presentations. The ABCDE model of assessment is recommended as it gives a rapid, initial assessment of the patients condition. (RC[UK] Resuscitation Guidelines 2015). Using ABCDE assessment it may be apparent here may be simple interventions that are appropriate to treat potentially life threatening problems however, help must be sought as soon as possible if any practitioner feels unable to adequately deal with the situation, or feels that the patient could deteriorate further. Seeking Help Any concerns about the patient must be relayed to the senior clinician on the ward and discussed with the medical staff, this should be recorded in the patients records. Other experts may be required to deal with the patient and there should be no delay 22
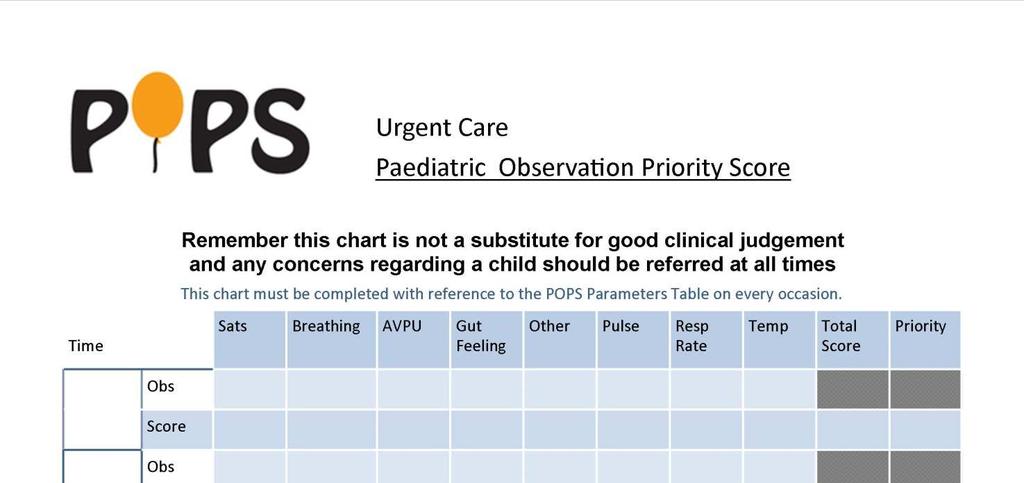
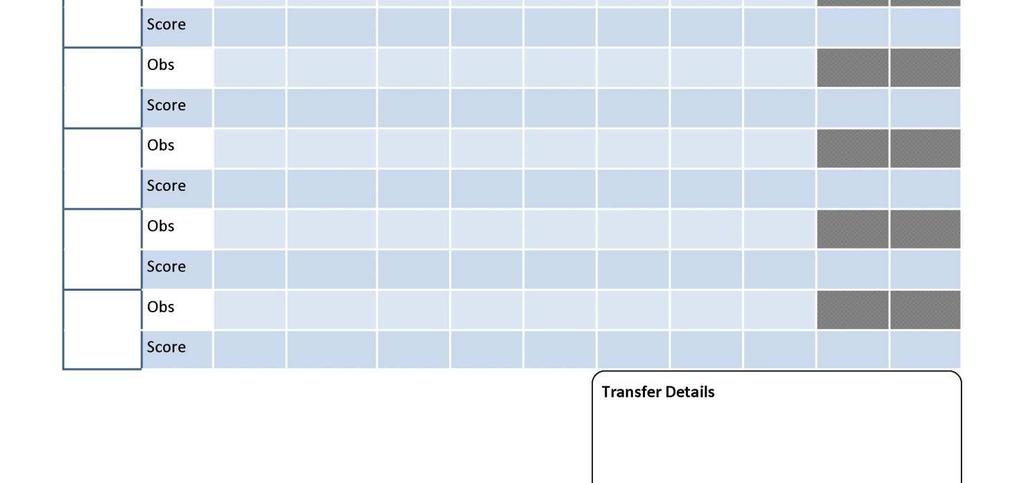
23 In referring the patient to an acute care setting in an emergency situation a 999 call should be made, to effect immediate transfer. Transfer should not be delayed if the ward doctor is unavailable or delayed (nurse led units). Recording Vital Signs Children POPS Vital Signs Using the Paediatric Observation Priority Score (POPS 13 ) system requires the ability to undertake specific observations within all age s groups of children and considers observatory assessments as well as measurements to complete the assessment. If using the paper POPS Form (Appendix 5) additional non-scoring observations can be added to the overall assessment to provide a wider clinical picture. Oxygen saturation Oxygen saturation measurement requires equipment appropriate to the patients age and size to provide accurate readings Oxygen saturation should be recorded at the point of assessment for all patients. For most patients a target oxygen saturation should be 94% or above. For emergency life saving a prescription for oxygen is not required but administration is limited to high flow/high concentration devices. Administration of oxygen for therapeutic purposes requires a written prescription and rationale for use recorded in the patient record. Respiratory Rate & Breathing Appropriate respiratory rates for children vary widely by age and whilst normal parameters are quoted in a number of sources and categorised by age for the system it also considers an examination of breathing effort, work, and quality. POPS Respirations should be counted for one minute. Neurological Assessment (AVPU) Neurological condition is an important marker of deterioration in clinical condition. Changes in neurological status are highly significant The AVPU scale score is adequate for normal purposes. A = Alert (Awake) V = Responds to voice (Lethargy) 23
24 P = Responds to pain (Stupor) U = Unresponsive (Coma) Gut Feeling Many studies show the importance of acknowledging parents or carers subjective assessments of children and how the addition of these improves the usefulness of physiological scoring systems. Professionals clinical intuition has long been recognised as a significant factor in determining patients general state but gut feeling is equally important and this section allows concern from all parties to be recognised. Other Children presenting with pre-existing health issues are known to have increased risk factors. Four categories automatically gain an identified POPS risk score;- Oncology patients Diabetic or long term steroid users Ex-prem or any syndromic condition patients Congenital Heart Condition Patients Heart Rate A pulse should be taken manually wherever possible. Pulse oximetry devices can provide data but should be cross-checked by auscultation or palpation of the heart/pulse rate. Stethoscope auscultation of the apex heart rate is required in children less than two years of age. Heart/pulse rates should be counted for one minute. Temperature A temperature should be recorded on all children who attend with an acute presentation of illness with the device applicable for age. In infants under the age of four weeks, temperature should be measured with an electronic thermometer in the axilla (NICE, CG ). For infants and children aged from four weeks to five years an electronic/chemical dot thermometer in the axilla or an infrared tympanic thermometer should be used. Whenever a child feels warm to the touch the temperature should immediately be measured even if it was normal a short time before (Hockenberry, ). 24
25 POPS Chart supplementary investigations Blood Pressure Blood Pressure is not part of the POPS scoring system but should be taken in any child who there is concern about their cardiovascular status whether this be a primary cardiac problem or secondary shock, dehydration or concern with renal problems. Blood Sugar A normal blood glucose level is between approximately 4-7mmol/L (Gilbert , Hanas ). Although not an element of the POPS score blood glucose levels outside this range in children not known to be diabetic will prompt further examination and will inform decision making. Blood sugar measurement is mandated for ALL patients with a POPS score of 3 or more. Capillary Refill Time (CRT) Poor capillary refill and differential pulse volumes are neither sensitive nor specific indicators of shock in infants/children, but are useful clinical indicators when used in conjunction with other signs, also note that the presence of a temperature does not affect the sensitivity of a delayed capillary refill in children with hypovolaemia, but a low ambient temperature will reduce its specificity. It should not be used solely as an indication of deterioration of clinical status (APLS ). CRT is however a required element of the minimum observation dataset in any child under 5 who presents with suspected fever. (NICE CG ) Although not part of the POPS scoring system CRT should be recorded on the form to help aid decision making. Pupil Reactions It is important to consider any existing or administered medication that may alter pupil responses. Assess pupil reactions and sizes, recording size in an ambient light and reactions using a bright narrow torch beam. Reactions should be recorded thus;- brisk reaction = + no reaction = - sluggish reaction = SL Check visual acuity if child of an appropriate age. If the child is too young to check visual acuity, ascertain whether the child can fix and follow - for toddlers try a toy, for infants try a toy or a light. 25
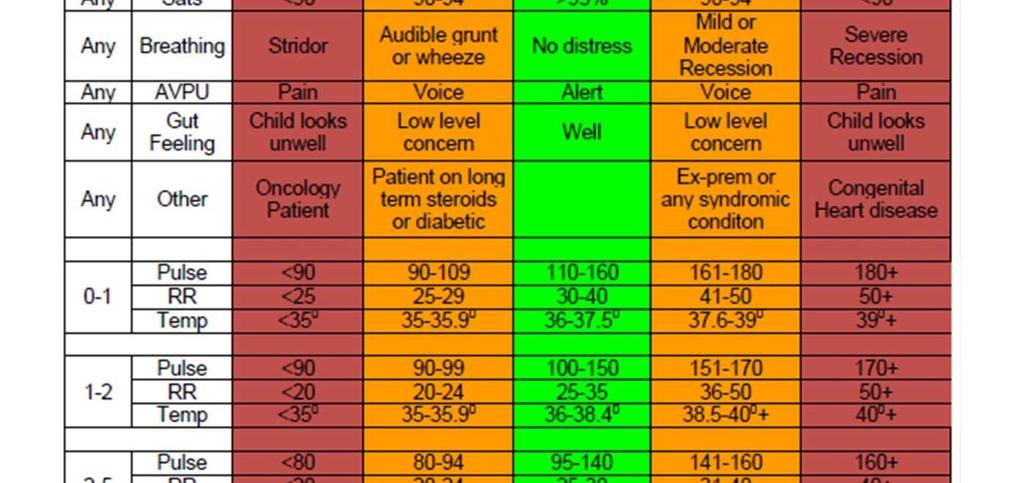
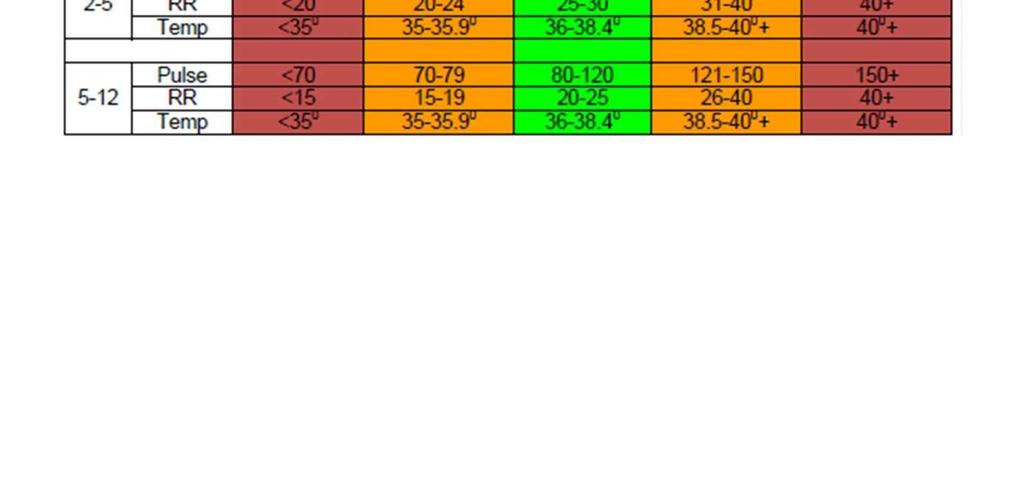
26 Additional POPS Chart Components Pain Assessment Many differing systems for assessing pain in children are in use. POPS uses a 10 point scale that equates to scoring systems from both the FLACC BEHAVIOURAL SCALE (Merkel et al, ) and the Wong Baker FACES Pain Scale Analgesia given prior to presentation needs to be established and if analgesia administered re-assessment at time of anticipated peak effect planned and recorded. Communication Good interactions and communications are essential to provide the best possible care post referral or discharge. This component should be fully completed to provide evidence of best practice and as prompts to inform or involve other services and systems. Planned interventions Record A visual indicator showing the need for each test or intervention and the timed history of application or completion gives a timeline of treatment processes. In conjunction with the monitoring score grid this gives a treatment history and allows ongoing assessment of progress. POPS Scoring Matrix The POPS matrix was developed to provide an age related score for each parameter. (Appendix 3) Aggregate scoring provides a total used to discriminate potential treatment or referral outcome, with higher values indicating a greater degree of potential illness. The setting of response actions for each matrix band score are based upon local service situations and availability of clinical services and expertise. Escalation of care requiring greater resources is mapped and priority indicated. The matrix boundaries, actions and priority ranking for LCHS are;- POPS Score & Priority Ranking 0 1 Consider treatment options A 2 3 Consider ED transfer B 4 7 Urgent ED/Paeds referral C Emergency Transfer D The Priority Ranking action statements are based upon the ability of LCHS to offer treatment options and therefore POPS acts as a discriminatory triage tool. 26
27 Practitioners must however not be limited in their ability to make referrals if concerned about a child s condition even if the POPS score suggests referral thresholds have not been reached. Children presenting with a POPS score beyond Level A show an obvious and significant increase in admission rates. Commencing with Level B escalation to Emergency Department treatment is indicated and at Level C a referral discussion is indicated. With scores of 8 or more the Level D response, 999 transfer, a pre-alert for ED is required to enable suitable paediatric attention on Arrival. Escalation Handover The POPS system is designed to assist all members of the healthcare team interacting with children in an urgent care environment to provide an improved quality of care for patients. The POPS tool includes a section on elements of communication specific to care of a child and includes safeguarding considerations and use of the LCHS Safeguarding Discharge Guidance. The POPS tool is not used universally amongst healthcare providers so communication with other organisations needs to follow a structure that ensures all relevant observation information is transferred and the priority of care is explained. Use SBAR, not just a POPS score! Communication It is well known that communication at transitions of care, handover, is frequently found to be poor especially in high acuity environments.(who ) In a 2013 review of studies addressing communication errors during handover, the greatest problem reported was the omission of detailed patient information. The use of scores for handover was found to be potentially misleading, the communication of individual vital signs had the highest confidence amongst clinicians. (Flemming et al ) It has also been recognised structured handover systems, such as SBAR, show significant improvements both in the level of information transferred and the ability of clinicians to make appropriate treatment decisions in a timely manner. (Pope et al ) SBAR is the system recommended by the Royal College of Physicians clinical toolkits (RCP 2013, ) and this should be used to provide a comprehensive handover dataset including not just an overall warning score but the individual parameter results. 27
28 SBAR The use of SBAR, (Situation, Background, Assessment, Recommendation) is now widely used within UK healthcare. The system offers a sensible effective, timely communications tool that improves information transfer between individuals from differing clinical backgrounds and hierarchies. This system should be used to convey information when making any referral or providing a pre-alert: Situation I am (name) from (location) I am calling about a patient (x) I am calling because I am concerned that (BP is low/ high, pulse is low or high etc) and wish advice on further actions/transfer Background Patient has presented with (for example a chest infection) Vital signs obs are.. Assessment I think the problem is (x) and I have given (oxygen/ analgesia etc) OR I don t know but I am really worried, the patient s condition now is. Recommendation Please advise on actions from now and transfer options? SBAR hand-over is the LCHS system of choice and included within the Trust NEWS record form. Printable Documents High printable versions of documents within this policy may be found in the Deteriorating Patient & Resuscitation pages of the Trust intranet site. Deteriorating Patient & Resuscitation : Printable Documents 28
29 References 1.National Institute for Health and Clinical Excellence (2007¹) Acutely ill patients in hospital.recognition of and response to acute illness in adults in hospital. Clinical Guideline 50. (CG50) National Institute for Health and Clinical Excellence, London. 2. National Institute for Health and Clinical Excellence (2007²) Head injury: Triage, assessment, investigation and early management of head injury in infants, children and adults. Clinical Guideline 56. (CG56) NICE, London. 3.National Patient Safety Agency (2007) The fifth report from the Patient Safety Observatory: Safer Care for the acutely ill patient: learning from serious incidents. PSO/05.The National Patient Safety Agency, London. 4.National Patient Safety Agency (2007²) Recognising and responding appropriately to early signs of deterioration in hospitalised patients. The National Patient Safety Agency, London. 5. Royal College of Physicians (2012), National Early Warning Score (NEWS), standardising the assessment of acute illness severity in the NHS. RCP, London 6. Medicines & Healthcare products Regulatory Agency (2013) Blood Pressure Measurement Devices. MHRA, London NICE (2014) Fever in Under 5 s. Quality Standard (QS64) 9. British Thoracic Society (2008) (BTS) Guideline for emergency Oxygen use in adult patients.british Thoracic Society, London. 10. NICE (2016) Intravenous fluid therapy in adults in hospital. Clinical Guideline 174 (CG174) 11. National Patient Safety Agency (2011) Essential care after an inpatient fall. Rapid Response Report. NPSA/2011/RRR Roland, D., Lewis, G., Fielding, P., Hakim, C., Watts, A. and Davies, F. (2016) The Paediatric Observation Priority Score: A System to Aid Detection of Serious Illness and Assist in Safe Discharge. Open Journal of Emergency Medicine, 4, NICE (2013) Fever in under 5s: assessment and initial management Clinical Guideline [CG160] 15. Hockenberry & Wilson (2003), Wong s Nursing Care of Infants & Children 16. Gilbert C (2009) Investigation and management of congenital hyperinsulinism. British Journal of Nursing 18 (20:
30 17. Hanas R (2004) Type 1 diabetes in children, adolescents and young adults. Class Publishing, London. Edition 2nd edition. 18. Advanced Life Support Group (2106) Advanced Paediatric Life Support (APLS): A Practical Approach to Emergencies, 6th Edition 19. Merkel et al, (1997) FLACC Behavioural Pain Assessment Scale 20. Wong & Baker (1988) FACES Pain Scale, Pain in Children: Comparison of Assessment Scales. 21. World Health Organisation. Communication during patient hand-overs. Patient safety solutions Flemming, Daniel; Hübner, Ursula (2013). "How to improve change of shift handovers and collaborative grounding and what role does the electronic patient record system play? Results of a systematic literature review". International Journal of Medical Informatics. 82 (7): Pope, BB; Rodzen, L; Spross, G (March 2008). "Raising the SBAR: how better communication improves patient outcomes.". Nursing. 38 (3): Royal College of Physicians Acute Care Toolkits 1, 6. (2013, 2015) 25. Resuscitation Council (UK) Resuscitation Guidelines Daniel J.Silcock et al (2015) - Validation of the National Early Warning Score in the prehospital setting. Resuscitation April West of England Academic Health Science Network Safer care for the deteriorating patient NEWS implememntation & use in six NHS Trusts (Apr 2017) 30
31 Monitoring Template Minimum requirement to be monitored Process monitoring audit for e.g. Responsible individuals/ group/ committee Frequency of monitoring/a udit Responsible individuals/ group/ committee (multidisciplina ry) for review of results Responsible individuals/ group/ committee for development of action plan Responsible individuals/ group/ committee monitoring action plan for of POPS Patient Observation records Audit completed by each clinical area and reported to Resuscitation Lead Safeguarding & Patient Safety Group Quarterly / spot audits Safeguarding & Patient Safety Group Safeguarding & Patient Safety Group Safeguarding & Patient Safety Group NEWS Patient Observation Records Audit completed by each in-patient clinical area and reported to Resuscitation Lead Safeguarding & Patient Safety Group Monthly / spot audits Safeguarding & Patient Safety Group Safeguarding & Patient Safety Group Safeguarding & Patient Safety Group 31
32 Equality Analysis Name of Policy/Procedure/Function* Phsyiologoical Observations Policy Equality Analysis Carried out by: Tim Balderstone Date: 3 rd October 2017 Equality & Human rights Lead: Rachel Higgins Director\General Manager: Lisa Green *In this template the term policy\service is used as shorthand for what needs to be analysed. Policy\Service needs to be understood broadly to embrace the full range of policies, practices, activities and decisions: essentially everything we do, whether it is formally written down or whether it is informal custom and practice. This includes existing policies and any new policies under development. 32
33 Section 1 to be completed for all policies A. B. C. D. Briefly give an outline of the key objectives of the policy; what it s intended outcome is and who the intended beneficiaries are expected to be Does the policy have an impact on patients, carers or staff, or the wider community that we have links with? Please give details Is there is any evidence that the policy\service relates to an area with known inequalities? Please give details Will/Does the implementation of the policy\service result in different impacts for protected characteristics? To ensure that patients presenting to LCHS services are assessed in a uniform and structured manner to inform trigger actions which should be undertaken in the case of abnormality. Impacts on patients and staff No Disability Sexual Orientation Sex Gender Reassignment Race Marriage/Civil Partnership Maternity/Pregnancy Age Religion or Belief Carers Yes If you have answered Yes to any of the questions then you are required to carry out a full Equality Analysis which should be approved by the Equality and Human Rights Lead please go to section 2 The above named policy has been considered and does not require a full equality analysis Equality Analysis Carried out by: Tim Balderstone Date: 3 rd October 2017 No x x x x x x x x x x 33
34 Section 2 Equality analysis Title: Relevant line in: What are the intended outcomes of this work? Include outline of objectives and function aims Who will be affected? e.g. staff, patients, service users etc Evidence The Government s commitment to transparency requires public bodies to be open about the information on which they base their decisions and the results. You must understand your responsibilities under the transparency agenda before completing this section of the assessment. What evidence have you considered? List the main sources of data, research and other sources of evidence (including full references) reviewed to determine impact on each equality group (protected characteristic). This can include national research, surveys, reports, research interviews, focus groups, pilot activity evaluations etc. If there are gaps in evidence, state what you will do to close them in the Action Plan on the last page of this template. Disability Consider and detail (including the source of any evidence) on attitudinal, physical and social barriers. Sex Consider and detail (including the source of any evidence) on men and women (potential to link to carers below). Race Consider and detail (including the source of any evidence) on difference ethnic groups, nationalities, Roma gypsies, Irish travellers, language barriers. Age Consider and detail (including the source of any evidence) across age ranges on old and younger people. This can include safeguarding, consent and child welfare. Gender reassignment (including transgender) Consider and detail (including the source of any evidence) on transgender and transsexual people. This can include issues such as privacy of data and harassment. Sexual orientation Consider and detail (including the source of any evidence) on heterosexual people as well as lesbian, gay and bi-sexual people. Religion or belief Consider and detail (including the source of any evidence) on people with different religions, beliefs or no belief. Pregnancy and maternity Consider and detail (including the source of any evidence) on working arrangements, part-time working, infant caring responsibilities. 34
35 Carers Consider and detail (including the source of any evidence) on part-time working, shift-patterns, general caring responsibilities. Other identified groups Consider and detail and include the source of any evidence on different socioeconomic groups, area inequality, income, resident status (migrants) and other groups experiencing disadvantage and barriers to access. Engagement and involvement Was this work subject to the requirements of the Equality Act and the NHS Act 2006 (Duty to involve)? (Y/N) How have you engaged stakeholders in gathering evidence or testing the evidence available? How have you engaged stakeholders in testing the policy or programme proposals? For each engagement activity, please state who was involved, how and when they were engaged, and the key outputs: Summary of Analysis Considering the evidence and engagement activity you listed above, please summarise the impact of your work. Consider whether the evidence shows potential for differential impact, if so state whether adverse or positive and for which groups. How you will mitigate any negative impacts. How you will include certain protected groups in services or expand their participation in public life. Now consider and detail below how the proposals impact on elimination of discrimination, harassment and victimisation, advance the equality of opportunity and promote good relations between groups. Eliminate discrimination, harassment and victimisation Where there is evidence, address each protected characteristic (age, disability, gender, gender reassignment, pregnancy and maternity, race, religion or belief, sexual orientation). Advance equality of opportunity Where there is evidence, address each protected characteristic (age, disability, gender, gender reassignment, pregnancy and maternity, race, religion or belief, sexual orientation). Promote good relations between groups Where there is evidence, address each protected characteristic (age, disability, gender, gender reassignment, pregnancy and maternity, race, religion or belief, sexual orientation). What is the overall impact? Consider whether there are different levels of access experienced, needs or experiences, whether there are barriers to engagement, are there regional variations and what is the combined impact? 35
36 Addressing the impact on equalities Please give an outline of what broad action you or any other bodies are taking to address any inequalities identified through the evidence. Action planning for improvement Please give an outline of the key actions based on any gaps, challenges and opportunities you have identified. Actions to improve the policy/programmes need to be summarised (An action plan template is appended for specific action planning). Include here any general action to address specific equality issues and data gaps that need to be addressed through consultation or further research. Please give an outline of your next steps based on the challenges and opportunities you have identified. Include here any or all of the following, based on your assessment For the record Name of person who carried out this assessment: Date assessment completed: Name of responsible Director/ General Manager: Date assessment was signed: 36

37 Appendix 1 NEWS Observation Chart 37

38 Appendix 2 NEWS Parameters 38

39 Appendix 3 NEWS Clinical Response A medium score (i.e., NEW score of 5 6 or a RED score) should prompt an urgent review (<1 hour) by a clinician skilled with competencies in the assessment of acute illness. The Senior Nurse with appropriate skills, GP responsible for the ward, Urgent Care Doctor or a Nurse/EC Practitioner with relevant experience, should consider whether escalation of care to the acute hospital is required. This role will be undertaken by an Out of Hours doctor or Nurse/EC practitioner to ensure clinical cover 24 hours a day, 7 days a week. A high score (NEW score of 7 or more) should prompt emergency assessment (immediate) and/ or usually transfer of the patient to an acute care setting. An urgent transfer (999) will be arranged by the senior clinician within the clinical area (where appropriate) using their clinical judgement and this should not be delayed to await a more senior assessment. 39

40 Appendix 4 Adjusted Escalation Triggers Form Chair: Elaine Baylis, QPM Chief Executive: Andrew Morgan


41 Appendix 5 POPS Form Chair: Elaine Baylis, QPM Chief Executive: Andrew Morgan
42 42
43 43

44 Appendix 6 POPS Learning Package 44
45 45
46 46
47 47
48 48
49 49
50 50
51 51
52 52
53 53
54 54
55 55
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting
 NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50
 DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50 Applies to: Committee for Approval Date of Approval September 2012 Date Ratified: September 2012 Review Date: September 2015 Name of Lead Manager Version:
DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50 Applies to: Committee for Approval Date of Approval September 2012 Date Ratified: September 2012 Review Date: September 2015 Name of Lead Manager Version:
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in
 These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
The ROHNHSFT Experience: Implementing BWCH PEWS
 The ROHNHSFT Experience: Implementing BWCH PEWS Alison Warren Clinical Matron for Children and Young Peoples Services The Royal Orthopaedic Hospital NHS Foundation Trust RGN, RSCN, ENB 415 & 998 PG Cert
The ROHNHSFT Experience: Implementing BWCH PEWS Alison Warren Clinical Matron for Children and Young Peoples Services The Royal Orthopaedic Hospital NHS Foundation Trust RGN, RSCN, ENB 415 & 998 PG Cert
PHYSIOLOGICAL OBSERVATIONS OF ADULT PATIENTS IN THE COMMUNITY SETTING POLICY
 PHYSIOLOGICAL OBSERVATIONS OF ADULT PATIENTS IN THE COMMUNITY SETTING POLICY To be read in conjunction with Physiological Observations Policy for Inpatients and Minor Injury Units (including Wessex House)
PHYSIOLOGICAL OBSERVATIONS OF ADULT PATIENTS IN THE COMMUNITY SETTING POLICY To be read in conjunction with Physiological Observations Policy for Inpatients and Minor Injury Units (including Wessex House)
Acutely ill patients in hospital
 Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: RM64 Version: 5.0 Name of Policy: Use of the National Early Warning Score System in Adult Patients Policy Effective From: 21/07/2016 Date Ratified 22/06/2016 Ratified Resuscitation and Deterioration
Policy No: RM64 Version: 5.0 Name of Policy: Use of the National Early Warning Score System in Adult Patients Policy Effective From: 21/07/2016 Date Ratified 22/06/2016 Ratified Resuscitation and Deterioration
Irish Paediatric Early Warning System (PEWS)
") Irish Paediatric Early Warning System (PEWS) Learning Outcomes By the end of the session, you will be able to: Discuss the importance of clinical judgement and individualised assessment Discuss the use
Irish Paediatric Early Warning System (PEWS) Learning Outcomes By the end of the session, you will be able to: Discuss the importance of clinical judgement and individualised assessment Discuss the use
Early Warning Score Procedure
 Procedure Contents Purpose... 2 Scope/Audience... 2 Associated documents... 3 Definitions... 4 Adult patients... 4 Maternity patients... 4 Paediatric patients... 4 Equipment... 5 Education and training
Procedure Contents Purpose... 2 Scope/Audience... 2 Associated documents... 3 Definitions... 4 Adult patients... 4 Maternity patients... 4 Paediatric patients... 4 Equipment... 5 Education and training
Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50
 Acutely ill adults in hospital: recognising and responding to deterioration Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50 NICE 2018. All rights reserved. Subject to Notice of rights
Acutely ill adults in hospital: recognising and responding to deterioration Clinical guideline Published: 25 July 2007 nice.org.uk/guidance/cg50 NICE 2018. All rights reserved. Subject to Notice of rights
Standard Operating Procedure for Patients Referred for Blood Transfusion to Louth Clinical Decision Unit by General Practitioners.
 Standard Operating Procedure for Patients Referred for Blood Transfusion to Louth Clinical Decision Unit by General Practitioners. Reference number: G_CS_87 Version: 1 Ratified by: LCHS Trust Board Date
Standard Operating Procedure for Patients Referred for Blood Transfusion to Louth Clinical Decision Unit by General Practitioners. Reference number: G_CS_87 Version: 1 Ratified by: LCHS Trust Board Date
Assessment and Reassessment of Patients
 Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
CHILDREN S OBSERVATIONS & SEVERITY TOOL (COAST FORMELY PEWS) & PAEDIATRIC OBSERVATION CHART POLICY
 & PAEDIATRIC OBSERVATION CHART POLICY") CHILDREN S OBSERVATIONS & SEVERITY TOOL (COAST FORMELY PEWS) & PAEDIATRIC OBSERVATION CHART POLICY Document Author Written By: Paediatric Sister Authorised Authorised By: Chief Executive Date: July 2017
CHILDREN S OBSERVATIONS & SEVERITY TOOL (COAST FORMELY PEWS) & PAEDIATRIC OBSERVATION CHART POLICY Document Author Written By: Paediatric Sister Authorised Authorised By: Chief Executive Date: July 2017
RECOGNISING AND RESPONDING TO EARLY DETERIORATION OF ACUTELY ILL PATIENTS ON THE WARDS. Presented by Primary Health Care Team
 RECOGNISING AND RESPONDING TO EARLY DETERIORATION OF ACUTELY ILL PATIENTS ON THE WARDS Presented by Primary Health Care Team 2013/2014 Aims of Session Any patient in hospital may become acutely ill, however,
RECOGNISING AND RESPONDING TO EARLY DETERIORATION OF ACUTELY ILL PATIENTS ON THE WARDS Presented by Primary Health Care Team 2013/2014 Aims of Session Any patient in hospital may become acutely ill, however,
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services
 Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Paediatrics. PEWS & Deteriorating Patients Linda Clerihew
 Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Deteriorating Patient Policy
 Deteriorating Patient Policy (Applicable for all Patients Admitted into Acute Inpatient and Emergency Settings at RGH, NHH, YYF and Mental Health Patients at YYF and to all Health Board Staff Who Care
Deteriorating Patient Policy (Applicable for all Patients Admitted into Acute Inpatient and Emergency Settings at RGH, NHH, YYF and Mental Health Patients at YYF and to all Health Board Staff Who Care
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Title Protocol for the Management of Chest Wall Injuries (over 12 years of age) in MIU s and WIC s.
 in MIU s and WIC s.") Document Control Title Protocol for the Management of Chest Wall Injuries (over 12 years of age) in MIU s and WIC s. Author Author s job title Professional Lead, Minor Injuries Unit Directorate Department
Document Control Title Protocol for the Management of Chest Wall Injuries (over 12 years of age) in MIU s and WIC s. Author Author s job title Professional Lead, Minor Injuries Unit Directorate Department
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Adult Observation Chart Policy (Incorporating National Early Warning Score NEWS)
") Adult Observation Chart Policy (Incorporating National Early Warning Score NEWS) Document Author Written By: Sister Critical Care Outreach Service Authorised Authorised By: Chief Executive Date: 1 st April
Adult Observation Chart Policy (Incorporating National Early Warning Score NEWS) Document Author Written By: Sister Critical Care Outreach Service Authorised Authorised By: Chief Executive Date: 1 st April
1. Storyboard Title Use of the proposed National Early Warning System (NEWS) scoring matrix in a community hospital setting
 scoring matrix in a community hospital setting") Powys teaching Health Board Storyboard submission: Improving Patient Safety 1. Storyboard Title Use of the proposed National Early Warning System (NEWS) scoring matrix in a community hospital setting 2.
Powys teaching Health Board Storyboard submission: Improving Patient Safety 1. Storyboard Title Use of the proposed National Early Warning System (NEWS) scoring matrix in a community hospital setting 2.
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Standard Operating Procedure Safe To Wait in Urgent Care Services
 Standard Operating Procedure Safe To Wait in Urgent Care Services Reference No: G_CS_91 Version 2 Ratified by: LCHS Trust Board Date ratified: 5 th April 2018 Name of originator / author: Teresa McNally
Standard Operating Procedure Safe To Wait in Urgent Care Services Reference No: G_CS_91 Version 2 Ratified by: LCHS Trust Board Date ratified: 5 th April 2018 Name of originator / author: Teresa McNally
AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN RECOMMENDATIONS ON MONITORING DURING ANAESTHESIA
 Review PS18 (2008) AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS ON MONITORING DURING ANAESTHESIA The terms Anaesthetist, medical practitioner and practitioner
Review PS18 (2008) AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS ON MONITORING DURING ANAESTHESIA The terms Anaesthetist, medical practitioner and practitioner
National Quality Improvement Project 2018/2019 Vital Signs in Adult Information Pack
 National Quality Improvement Project 2018/2019 Vital Signs in Adult Information Pack Introduction... 3 Methodology... 4 Inclusion criteria... 4 Exclusion criteria... 4 Flow of data searches to identify
National Quality Improvement Project 2018/2019 Vital Signs in Adult Information Pack Introduction... 3 Methodology... 4 Inclusion criteria... 4 Exclusion criteria... 4 Flow of data searches to identify
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
Core competencies for the care of acutely ill and injured children and young people. May 2006
 Core competencies for the care of acutely ill and injured children and young people May 2006 Contents Introduction 3 How the competencies can be used 6 Core competencies : Assessment domain 7 Core competencies
Core competencies for the care of acutely ill and injured children and young people May 2006 Contents Introduction 3 How the competencies can be used 6 Core competencies : Assessment domain 7 Core competencies
Do Not Attempt Resuscitation Policy
 Do Not Attempt Resuscitation Policy PROV 27 March 2009 1 Document Management Title of document Do Not Attempt Resuscitation Policy Type of document Policy PROV 27 Description To ensure that do not resuscitate
Do Not Attempt Resuscitation Policy PROV 27 March 2009 1 Document Management Title of document Do Not Attempt Resuscitation Policy Type of document Policy PROV 27 Description To ensure that do not resuscitate
Stage 2 GP longitudinal placement learning outcomes
 Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
Policy Review Sheet. Review Date: 14/10/16 Policy Last Amended: 19/10/17. Next planned review in 12 months, or sooner as required.
 Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Brief Summary. Educational Rationale. Learning Objectives: Nurse. Learning Objectives: Doctor
 Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE
 PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE This Practice Guideline sets out a method for implementing triage in the Emergency Centre. Excluding the cover page, this Practice
PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE This Practice Guideline sets out a method for implementing triage in the Emergency Centre. Excluding the cover page, this Practice
Aneurin Bevan University Health Board Clinical Record Keeping Policy
 N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
Wessex Regional All Cause Deterioration (including Sepsis) Guidance
 Guidance") Wessex Regional All Cause Deterioration (including Sepsis) Guidance For Adult ( 16 non-pregnant) patients WACDG v1 11 th May 2018 Guidance includes models for the following healthcare settings Hospital
Wessex Regional All Cause Deterioration (including Sepsis) Guidance For Adult ( 16 non-pregnant) patients WACDG v1 11 th May 2018 Guidance includes models for the following healthcare settings Hospital
Choice on Discharge Policy
 Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: Fluid Balance Policy for adult in-patient areas Version: 2 Reference Number: Supersedes Minor Amendment Author Ratification Supersedes: Version 1 Changes: See Minor Amendments
DOCUMENT CONTROL PAGE Title Title: Fluid Balance Policy for adult in-patient areas Version: 2 Reference Number: Supersedes Minor Amendment Author Ratification Supersedes: Version 1 Changes: See Minor Amendments
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK
 PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK 0 CONTENTS Course Description Period of Learning in Practice Summary of Competencies Guide to Assessing Competencies Page 2 3 10 14 Course
PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK 0 CONTENTS Course Description Period of Learning in Practice Summary of Competencies Guide to Assessing Competencies Page 2 3 10 14 Course
Minimum Standards of Physical Health Assessment Policy. Choice, Responsiveness, Integration & Shared Care
 Minimum Standards of Physical Health Assessment Policy Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document
Minimum Standards of Physical Health Assessment Policy Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document
Wales Critical Care & Trauma Network (North)
") Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Wales Critical Care & Trauma Network (North) CRITICAL CARE ADMISSION & DISCHARGE GUIDELINES Revised 2016 1 CONTENTS: 1.0 Introduction 1.1 Scope of the Guideline 1.2 Levels of Care 2.0 Admission Guidance
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease
 Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Document Ratification Group Chairman s Action
 Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
#NeuroDis
 Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY
 DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
SITE APPLICABILITY This practice applies to all pediatric patient care areas that have been designated by your health authority.
 GUIDELINE PURPOSE To provide guidance and direction for the use of the Pediatric Early Warning System (PEWS). The PEWS system supports the recognition, mitigation, notification, and response to the pediatric
GUIDELINE PURPOSE To provide guidance and direction for the use of the Pediatric Early Warning System (PEWS). The PEWS system supports the recognition, mitigation, notification, and response to the pediatric
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Type: Policy. Cathy Geddes Chief Nurse June 2016 Professionally Approved By Dr Ronan Fenton
 Trigger Response Team Operational Policy (Adults) Type: Policy Register No: 12042 Status: Public Developed in response to: Patient Safety Contributes to CQC Outcome number: 9,12 Consulted With Post/Committee/Group
Trigger Response Team Operational Policy (Adults) Type: Policy Register No: 12042 Status: Public Developed in response to: Patient Safety Contributes to CQC Outcome number: 9,12 Consulted With Post/Committee/Group
1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure
 ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
EMERGENCY CARE DISCHARGE SUMMARY
 EMERGENCY CARE DISCHARGE SUMMARY IMPLEMENTATION GUIDANCE JUNE 2017 Guidance for implementation This section sets out issues identified during the project which relate to implementation of the headings.
EMERGENCY CARE DISCHARGE SUMMARY IMPLEMENTATION GUIDANCE JUNE 2017 Guidance for implementation This section sets out issues identified during the project which relate to implementation of the headings.
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
A guide to the Home Oxygen Order Form
 A guide to the Home Oxygen Order Form Part A front cover Air Products Clinicians Helpline Telephone: 01270 218050 8.00am-5.00pm, Monday to Friday (open 24 hours for urgent calls only) Introduction During
A guide to the Home Oxygen Order Form Part A front cover Air Products Clinicians Helpline Telephone: 01270 218050 8.00am-5.00pm, Monday to Friday (open 24 hours for urgent calls only) Introduction During
London s Urgent and Emergency Care Collaborative
 London s Urgent and Emergency Care Collaborative Katy Millard London Community Services Director Claire Eves Operational Head of Hillingdon Health Care Partnership Thomas Dowle Clinical & Operational Lead,
London s Urgent and Emergency Care Collaborative Katy Millard London Community Services Director Claire Eves Operational Head of Hillingdon Health Care Partnership Thomas Dowle Clinical & Operational Lead,
Title Audit of Compliance with the Irish Paediatric Early Warning System National Clinical Guideline No. 12.
 1 QUALITY ASSURANCE AND VERIFICATION DIVISION HEALTHCARE AUDIT SUMMARY REPORT Title Audit of Compliance with the Irish Paediatric Early Warning System National Clinical Guideline No. 12. Number QAV008/2016
1 QUALITY ASSURANCE AND VERIFICATION DIVISION HEALTHCARE AUDIT SUMMARY REPORT Title Audit of Compliance with the Irish Paediatric Early Warning System National Clinical Guideline No. 12. Number QAV008/2016
VERIFICATION OF LIFE EXTINCT POLICY DECEMBER Verification of Life Extinct Policy December 2009 Page 1 of 18
 VERIFICATION OF LIFE EXTINCT POLICY DECEMBER 2009 Page 1 of 18 POLICY TITLE: Verification of Life Extinct Policy POLICY REFERENCE NUMBER: Med01/009 IMPLEMENTATION DATE: December 2009 REVIEW DATE: December
VERIFICATION OF LIFE EXTINCT POLICY DECEMBER 2009 Page 1 of 18 POLICY TITLE: Verification of Life Extinct Policy POLICY REFERENCE NUMBER: Med01/009 IMPLEMENTATION DATE: December 2009 REVIEW DATE: December
MANAGEMENT OF DYSPHAGIA POLICY
 MANAGEMENT OF DYSPHAGIA POLICY Latest Revision September 2015 Next Revision September 2016 Reviewer: Head of Governance and Clinical Services; Clinical team Compliance Associated Policies Contents 1. Introduction
MANAGEMENT OF DYSPHAGIA POLICY Latest Revision September 2015 Next Revision September 2016 Reviewer: Head of Governance and Clinical Services; Clinical team Compliance Associated Policies Contents 1. Introduction
Unit CHS19 Undertake physiological measurements (Level 3)
") About this workforce competence This workforce competence covers taking and recording physiological measurements as part of the individuals care plan. Measurements include: blood pressure both by manual
About this workforce competence This workforce competence covers taking and recording physiological measurements as part of the individuals care plan. Measurements include: blood pressure both by manual
Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation
 Health Informatics Unit Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation April 2011 Funded by: Acknowledgements This project was funded by the Academy of
Health Informatics Unit Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation April 2011 Funded by: Acknowledgements This project was funded by the Academy of
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
National Early Warning Scoring System
 National Early Warning Scoring System A common language for health care The deteriorating patient Professor Derek Bell January 2013 Adult National Early Warning Score Background Overview of NEWS Next Steps
National Early Warning Scoring System A common language for health care The deteriorating patient Professor Derek Bell January 2013 Adult National Early Warning Score Background Overview of NEWS Next Steps
Anaphylactic Reaction Emergency Treatment Reference Number:
 This is an official Northern Trust policy and should not be edited in any way Anaphylactic Reaction Emergency Treatment Reference Number: NHSCT/12/551 Target audience: Nursing Staff Groups included are:
This is an official Northern Trust policy and should not be edited in any way Anaphylactic Reaction Emergency Treatment Reference Number: NHSCT/12/551 Target audience: Nursing Staff Groups included are:
Policy & Procedure for assessing and measuring vital signs on Paediatric Patients and using the Paediatric Early warning score
 Policy & Procedure for assessing and measuring vital signs on Paediatric Patients and using the Paediatric Early warning score 1 Procedure Title: Executive Summary: Supersedes: Description Amendment(s):
Policy & Procedure for assessing and measuring vital signs on Paediatric Patients and using the Paediatric Early warning score 1 Procedure Title: Executive Summary: Supersedes: Description Amendment(s):
Clinical Skills Passport for Relief and Temporary Staff in Neonatal Units
 Clinical Skills Passport for Relief and Temporary Staff in Neonatal Units This work is drawn from the Scottish Neonatal Nurses Group document The Competency Framework and Core Clinical Skills for Neonatal
Clinical Skills Passport for Relief and Temporary Staff in Neonatal Units This work is drawn from the Scottish Neonatal Nurses Group document The Competency Framework and Core Clinical Skills for Neonatal
Lincolnshire CCGs. Non-Emergency Patient Transport. Eligibility Criteria Policy
 Lincolnshire CCGs Non-Emergency Patient Transport Eligibility Criteria Policy Reference No: Version: 1.0 Ratified by: ClG058 Date ratified: May 2018 Name of originator/author: Name of responsible committee/individual:
Lincolnshire CCGs Non-Emergency Patient Transport Eligibility Criteria Policy Reference No: Version: 1.0 Ratified by: ClG058 Date ratified: May 2018 Name of originator/author: Name of responsible committee/individual:
Chan Man Yi, NC (Neonatal Care) Dept. of Paed. & A.M., PMH 16 May 2017
 Dept. of Paed. & A.M., PMH 16 May 2017") The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
Community Nurse Prescribing (V100) Portfolio of Evidence
 Portfolio of Evidence") ` School of Health and Human Sciences Community Nurse Prescribing (V100) Portfolio of Evidence Start date: September 2016 Student Name: Student Number:. Practice Mentor:.. Personal Tutor:... Submission
` School of Health and Human Sciences Community Nurse Prescribing (V100) Portfolio of Evidence Start date: September 2016 Student Name: Student Number:. Practice Mentor:.. Personal Tutor:... Submission
General Practice Triage: An update for Reception & Clinical Staff
 General Practice Triage: An update for Reception & Clinical Staff October 2017 Magali De Castro Clinical Director, HotDoc This update will cover Essential components of a robust triage system Accreditation
General Practice Triage: An update for Reception & Clinical Staff October 2017 Magali De Castro Clinical Director, HotDoc This update will cover Essential components of a robust triage system Accreditation
Hospital Discharge and Transfer Guidance. Choice, Responsiveness, Integration & Shared Care
 Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
National Early Warning Score (ViEWS) System. Recommendations for Audit. February 2012
 System. Recommendations for Audit. February 2012") National Early Warning Score (ViEWS) System Recommendations for Audit February 2012 Version 3 Acknowledgement: The National Early Warning Score and associated Education Programme Audit and Evaluation sub-group
National Early Warning Score (ViEWS) System Recommendations for Audit February 2012 Version 3 Acknowledgement: The National Early Warning Score and associated Education Programme Audit and Evaluation sub-group
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: Early Warning Score Policy Version: 6 (May 2010) Amended version Reference Number: Supersedes Originator or modifier Approval Supersedes: EWS Policy v5 2009 August 2009
DOCUMENT CONTROL PAGE Title Title: Early Warning Score Policy Version: 6 (May 2010) Amended version Reference Number: Supersedes Originator or modifier Approval Supersedes: EWS Policy v5 2009 August 2009
Course Outline and Assignments
 Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Critical Care in Obstetrics Guideline
 This is an official Northern Trust policy and should not be edited in any way Critical Care in Obstetrics Guideline Reference Number: NHSCT/12/515 Target audience: This guideline is directed to all obstetricians,
This is an official Northern Trust policy and should not be edited in any way Critical Care in Obstetrics Guideline Reference Number: NHSCT/12/515 Target audience: This guideline is directed to all obstetricians,
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
CERTIFICATE OF COMPLETION OF PAEDIATRIC LEVEL 1 COMPETENCY V1.0
 Applicants applying for ST4 posts in paediatrics may use this certificate to successful, satisfactory completion of Level 1 paediatric competences, as defined in the RCPCH Level 1 Paediatrics and Child
Applicants applying for ST4 posts in paediatrics may use this certificate to successful, satisfactory completion of Level 1 paediatric competences, as defined in the RCPCH Level 1 Paediatrics and Child
Guidelines for the appointment of. General Practitioners with Special Interests in the Delivery of Clinical Services. Respiratory Medicine
 Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
The School Of Nursing And Midwifery. CLINICAL SKILLS PASSPORT
 The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
PATIENT ASSESSMENT POLICY Page 1 of 7
 Page 1 of 7 Policy applies to: All staff and allied health professionals involved in patient care delivery at Mercy Hospital including Manaaki. Related Standards: Health & Disability Services (core) Standards
Page 1 of 7 Policy applies to: All staff and allied health professionals involved in patient care delivery at Mercy Hospital including Manaaki. Related Standards: Health & Disability Services (core) Standards
Handover of Care (Maternity) Guidelines Author s job title Lead Clinical Midwife Department Ladywell Unit. Comment / Changes / Approval
 Guidelines Author s job title Lead Clinical Midwife Department Ladywell Unit. Comment / Changes / Approval") Document Control Title Author Directorate Surgery Date Version Issued 0.1 Oct 2009 0.2 Nov 2009 1.0 Nov 2009 1.1 Feb 2010 2.0 Feb 2010 2.1 Aug 2011 2.2 Oct 2011 Handover of Care (Maternity) Guidelines
Document Control Title Author Directorate Surgery Date Version Issued 0.1 Oct 2009 0.2 Nov 2009 1.0 Nov 2009 1.1 Feb 2010 2.0 Feb 2010 2.1 Aug 2011 2.2 Oct 2011 Handover of Care (Maternity) Guidelines
PATIENT IDENTIFICATION POLICY
 PATIENT IDENTIFICATION POLICY DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Effectiveness Committee Date ratified: 12 th January 2012 Name of originator/author: Clinical Policy Advisor Name of responsible
PATIENT IDENTIFICATION POLICY DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Effectiveness Committee Date ratified: 12 th January 2012 Name of originator/author: Clinical Policy Advisor Name of responsible
Framework for Cancer CNS Development (Band 7)
") Framework for Cancer CNS Development (Band 7) Opening Statement This framework provides a common understanding of the CNS role across the London Cancer Alliance and will be used to support the development
Framework for Cancer CNS Development (Band 7) Opening Statement This framework provides a common understanding of the CNS role across the London Cancer Alliance and will be used to support the development
Title: MIU Meningococcal Disease and Bacterial Meningitis, management of. Services/Nurse Consultant Emergency Care
 Title: MIU Ref No: 1961 Version 2 Document Author: Ratified by: Senior Manager MIU Services/Nurse Consultant Emergency Care Care & Clinical Policies Group Meeting Clinical Director of Pharmacy Date 18
Title: MIU Ref No: 1961 Version 2 Document Author: Ratified by: Senior Manager MIU Services/Nurse Consultant Emergency Care Care & Clinical Policies Group Meeting Clinical Director of Pharmacy Date 18
INDEPENDENT NON-MEDICAL PRESCRIBING (NMPs) POLICY. Suffolk GP Federation Board
 POLICY. Suffolk GP Federation Board") INDEPENDENT NON-MEDICAL PRESCRIBING (NMPs) POLICY Version: 1.0 Policy owner: Ratified by: Clinical Governance Lead Chief Executive Date approved: 28 th November 2014 Approved by: Suffolk GP Federation
INDEPENDENT NON-MEDICAL PRESCRIBING (NMPs) POLICY Version: 1.0 Policy owner: Ratified by: Clinical Governance Lead Chief Executive Date approved: 28 th November 2014 Approved by: Suffolk GP Federation
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
SCHEDULE 2 THE SERVICES. A. Service Specifications. E07/S/c Paediatric Long Term Ventilation
 Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Standard Operating Procedure Hospital Pre-alert & Patient Handover
 Standard Operating Procedure Hospital Pre-alert & Patient Handover No of Pages: 6 Unique reference No: Implementation date: 17 th May 2010 Version: Final Version 2.0 Next review date: May 2013 Title of
Standard Operating Procedure Hospital Pre-alert & Patient Handover No of Pages: 6 Unique reference No: Implementation date: 17 th May 2010 Version: Final Version 2.0 Next review date: May 2013 Title of
SOP for the Receiving and Actioning of Laboratory Results into the Out of Hours Service
 SOP for the Receiving and Actioning of Laboratory Results into the Out of Hours Service Reference No: G_CS_38 Version 2 Ratified by: LCHS Trust Board Date ratified: 14 August 2018 Name of originator /
SOP for the Receiving and Actioning of Laboratory Results into the Out of Hours Service Reference No: G_CS_38 Version 2 Ratified by: LCHS Trust Board Date ratified: 14 August 2018 Name of originator /
South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines. Version 1.0
 South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines Version 1.0 Ratified: 28 th August 2018 Date for Review: 28 th August 2019 Suzanne.sweeney@uclpartners.com South London
South London Neonatal Network Hypoxic Ischemic Encephalopathy Transfer Guidelines Version 1.0 Ratified: 28 th August 2018 Date for Review: 28 th August 2019 Suzanne.sweeney@uclpartners.com South London
Patient Identification
 Patient Identification Reference No: Version: 5 Ratified by: P_CS_24 LCHS Trust Board Date ratified: 10 th April 2018 Name of originator/author: Name of approving committee/responsible individual: Date
Patient Identification Reference No: Version: 5 Ratified by: P_CS_24 LCHS Trust Board Date ratified: 10 th April 2018 Name of originator/author: Name of approving committee/responsible individual: Date
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol