NHS Wales Review of the 111 Pathfinder In Association with Janette Turner, University of Sheffield Final Report November 2017
|
|
|
- Amos Davis
- 5 years ago
- Views:
Transcription
1 NHS Wales Review of the 111 Pathfinder In Association with Janette Turner, University of Sheffield Final Report November 2017 THE POWER OF BEING UNDERSTOOD AUDIT TAX CONSULTING
2 TABLE OF CONTENTS NHS WALES REVIEW OF THE 111 PATHFINDER... 1 IN ASSOCIATION WITH JANETTE TURNER, UNIVERSITY OF SHEFFIELD... 1 FINAL REPORT SEPTEMBER GLOSSARY OF TERMS EXECUTIVE SUMMARY INTRODUCTION AND BACKGROUND STRATEGIC CONTEXT LITERATURE REVIEW CONSULTATIONS SURVEY RESULTS... 31
3 7 ACTIVITY LEVEL ANALYSIS IMPACT OF THE 111 PATHFINDER COMPARATIVE ANALYSIS CONCLUSIONS This report has been prepared on the basis set out in our Project Initiation Document ( PID ) dated April 2016 and should be read in conjunction with this. This report is for the benefit of NHS Wales ( the CLIENT ) only and has been released to the CLIENT on the basis that it shall not be copied, referred to or disclosed, in whole or in part, to any third party, knowingly or, unknowingly without our prior written consent. Other than in the limited circumstances as set out in the PID, we have not verified the reliability or accuracy of any information obtained in the course of our work. This report is not suitable to be relied upon by any party wishing to acquire rights against RSM PACEC for any purpose or in any context. Any party that obtains access to this report or a copy (under the Freedom of Information Act 2000 or otherwise) and chooses to rely on this report (or any part of it) does so at their own risk. To the fullest extent permitted by law, RSM PACEC does not assume any responsibility and will not accept any responsibility in respect of this report to any party other than the original addressee RSM UK Group LLP, all rights reserved
4 Glossary of Terms Table 0:1 Glossary of Terms Term Abandoned Call (111 Wales) Adastra A call where the caller hangs up after 60 seconds (in Wales) from being queued for a call advisor to answer. Clinical system being utilised by out-of-hours services across Wales Ambulance call Ambulance incident Auto-routed CAS Concentrator CSPT DOS ED GP OOH Minimum Data Set (MDS) MIU NHS Pathways NHS 111 Programme Board A call to the ambulance service for an emergency response originating from the emergency number, requests from other health professionals (e.g. GPs, NHS Direct) or NHS 111. All cases where an ambulance response is sent to and arrives at an incident scene. Calls routed from another service to 111 without the need for the caller to dial the number 111. Clinical Assessment Software operated by NHS Direct Wales The technical bridge linking CAS /Adastra and ensures that data flows across to the GPOOH service electronically. Call Streaming and Prioritisation Tool system within which the 111 calls are assessed and prioritised by non registrant call takers Directory of Services system that provides information on local health, Local authority and third sector services Emergency Department General practice out of hours service Routinely collected information on the efficiency and effectiveness of the different service models Minor Injury Unit Delivers a single clinical assessment tool that can provide triage over the telephone in any setting taking calls from the public (only used in England) Set up by Welsh Government to oversee the strategic development and implementation of a new telephone based service for accessing urgent care. Page 3
5 Term Primary Care Centre Ofcom A centre where patients who need to see a GP out of hours are directed to. The independent regulator and competition authority for the UK communications industries. Soft launch SPA UCC WIC Warm transfer A period of limited marketing and phased roll out across ABMU over a 3 week period with GP answerphone messages being changed to direct patients to 111 at the same time as the old GPOOH service remained operational. Single Point of Access A telephone number that manages all requests for urgent health services Urgent Care Centre (not available in Wales) Walk in Centre (not available in Wales) A call transferred to a clinical advisor at the time of the call (without the need to call back) Page 4
6 1 EXECUTIVE SUMMARY Context of the Review There have been a number of reviews and reports which have highlighted that the unscheduled care system in Wales is not resilient to unexpected and unusual surges in external demand, or demand shifted within it. This lack of resilience leads to increased attendance at ED units and increased waiting times at these units 1. In response to these issue the NHS Wales Urgent and Unscheduled Care Programme Board has developed a wider strategy to transform urgent and unscheduled care services in Wales 2. The overall aim of the strategy is to co-ordinate and manage unscheduled care demand in a different and organised way, to help meet the needs of patients within their own communities and possibly to slow the year on year increase (or, to slow the increase in demand) on hospital-based services. A key element of the strategy was the development and implementation of a free to call helpline that provides a single access point that is intended to help patients access urgent help when they need it; as well as improving access to health information and advice 3. The 3-digit number (111) that is free-to-call from both landlines and mobile telephones can offer support and advice to callers 24 hours of the day, 7 days a week. The 111 service integrated the current telephony service provided by NHS Direct Wales with the front-end call handling and triage function used by GP Out-of-Hours (GPOOH) Services in the Abertawe Bro Morgannwg University Health Board (ABMU) area to provide a single service for patients to access if they need urgent help, or access to health information and advice. Welsh Ambulance Services NHS Trust are the host organisation. A technical bridge (a concentrator) was created to enable communication between the two clinical systems in use. The service is hosted by the Welsh Ambulance Service (WAST). NHS Wales established an Implementation Board to oversee the implementation of the pilot service which is known as the 111 Pathfinder and the work is supported by a national 111 programme team who have worked closely with WAST and ABMU Health Board. The new service is being piloted in the ABMUHealth Board area and was launched in October Patients in the six other Welsh Health Boards can continue to access health advice through NHS Direct Wales and have access to urgent care through their own Health Board based GP Out-of-Hours (GPOOH) services. In May 2017, the Carmarthenshire area (which is part of the Hywel Dda University Health Board) was brought into the 111 pathfinder. However, as this was outwith the evaluation window, no data on this service has been included in this report. A comprehensive set of standards were developed for the service which provided targets and parameters for how the service should operate, for example 95% of calls should be answered within 60 seconds of the end of the telephone message, 95% of urgent (priority one) calls should receive a call back within 20 minutes and 95% of routine (priority 2/3) calls should be clinically assessed within 2 and 4 hours respectively. Terms of Reference and Methodology RSM PACEC in collaboration with the University of Sheffield (Medical Care Research Centre Unit) were appointed to undertake a review of the NHS Wales 111 / Out of Hours Pathfinder Project. Specifically the terms of reference stated, that the evaluation should include: 1 E.g. see External Factors ( Drivers ) Affecting Long-Term Trends and Recent Pressures on Unscheduled Care Use and Performance in Wales. Public Health Wales, The Way Ahead for Unscheduled Care in Wales. Unscheduled Care Improvement Board The telephony element of the 111 service is hosted by WAST under the NHSDW element of the Trust, which currently uses a CAS telephony service. GPOOH in the ABMU area which provides the triage and clinical support element of the service uses ADASTRA to handle calls and record data. Page 5
7 An analysis of the activity and performance during the first six months, with appropriate benchmarks throughout the evaluation period; An impact analysis considering the impact of 111 on other urgent care services including Emergency Departments, the Welsh Ambulance Service (WAST) and primary and community-based services; and A high-level financial evaluation. The evaluation, was also required to review the process of implementing 111 in the pilot areas and to consider what lessons can be applied if this service model was rolled out to the rest of Wales. The evaluation focused on the first full six months of operation, November 2016 to April A mixed methodology was applied to the evaluation, involving the collation and analysis of qualitative and quantitative data to demonstrate the performance and impact of the service which specifically included: User (patient) feedback through a postal questionnaire (401 responses were received); Professional feedback from staff across several services (consultations n=24; and a staff survey, n=85); Twenty-four consultations with senior policy and operational staff within the urgent and unscheduled care system. Policy staff were interviewed at the start of the evaluation to gain further insight into the policy and strategic aims of the service and operational staff were interviewed near the end of the evaluation to gain further insight into the operational impacts and any issues associated with implementation; An analysis of the activity and performance during the first six months of implementation (CAS and Adastra data), to assess if the service was meeting the standards that were set for it and a review of incidents and complaints information; An impact analysis which assessed the wider impact of 111 on other parts of the health care system, such as; Emergency Departments, the Welsh Ambulance Service (WAST) and primary care services; A high-level financial analysis which considered the cost of the service and any potential cost savings that could be identified as a result of the implementation of 111; A comparative analysis to benchmark activity levels and structures with other 111 services in the UK; A literature review of the implementation arrangements at both a national and local level and links to recognised best practice and how this may support the longer term national model. It should be noted that a number of limitations impacted on the evaluation, the most significant of these was the limited amount of data that was available. This was due to technical issues relating to the amalgamation of CAS and Adastra datasets, and the availability of data within the ABMU area. Furthermore, it is not possible to track individuals as they move through the wider health care system, for example from 111 to WAST, ED or GP in-hours services. It should be noted that the inability to track patients through the healthcare system is a systematic issue across the NHS and is not peculiar to NHS Wales or to the implementation of the 111 service. Findings from the Consultations Interviews with senior policy and operational stakeholders focused on collating feedback on the policy need for improvements to urgent care in Wales and how the 111 should contribute to this. Stakeholders provided feedback on the context in which 111 has been implemented, and the impact of the service so far. All consultees highlighted the need for reform and improvement across urgent and unscheduled care system in Wales (referring to a number of Audit Office 4 reports that highlighted a lack of resilience within the current system and pressures on ED wards) and that the implementation of the 111 Pathfinder was a key element of the strategy to deliver reform. Stakeholders highlighted several perceived benefits of the 111 Pathfinder, including improved access to 4 WAO Report Unscheduled Care Developing a Whole System Approach (2013) Page 6
8 urgent care and improved care, as well as the ability to ensure that patients get access to the right level of care for them in the appropriate setting, therefore offering improved levels of efficiency within the urgent care system. Stakeholders also noted that they expect the Pathfinder to make a positive impact on other parts of the health service, for example by reducing the level of demand for emergency care and unscheduled care (in acute hospitals), primary care teams (i.e. GP appointments) and GP Out of Hours (GPOOH) services. There was a high level of agreement amongst those who were consulted with that the standards that have been developed for the pathfinder are detailed and reflect the wide range of data that is required to adequately monitor the implementation of the service. Although it was also noted that currently it is not possible to trace patients once they leave the 111 or GPOOH system. Potential challenges highlighted by stakeholders included the limitations of the data collection, as currently patient pathways are monitored on two separate systems (CAS and Adastra). The reconciliation of data across systems has proved difficult. GPOOH services across Wales are delivered slightly differently and collect slightly different datasets. This was noted as a potential challenge for the wider rollout of the project as it could make it difficult to demonstrate the impacts of the project across all Health Board areas. All of those consulted with, highlighted the importance of ensuring that the service is sufficiently resourced both from a financial and workforce perspective. Staff shortages were highlighted as a key challenge to the service, with particular shortages of experienced nurses and GPs, (similar staff shortages across the wider healthcare system in Wales were also noted). There are known peaks in demand for unscheduled care and staffing rotas should reflect the demand profile. Furthermore, staffing levels and the technology should be able to manage any potential surges in demand, for example at weekends or bank holidays. Whilst the current technical solution was noted as a challenge, the planned all Wales NHS IT and telephony system was noted by consultees as an opportunity to improve the systems that staff are using and to maximise the opportunities for integration with other parts of the health system and to collect more detailed data in order to fully understand the impact of the service. Staff Feedback In order to collate staff views of the effectiveness of the implementation of the service and the quality of care provided, all staff engaged by WAST in the delivery of NHS Direct and 111 services were asked to complete an online survey. In total 85 staff surveys were returned (31%). The majority of respondents (65%) were either call handlers or nurse advisors. Whilst the majority of respondents (62%) believed that the service was well implemented, some areas for improvement were also highlighted. A small proportion (26%), noted that they believed that their training could be improved. Issues raised included the need for additional training on the CAS system and a reduction in time lag between completing their initial training and the implementation of the service. A small proportion of staff also believed that they would benefit from additional face-to-face, line manager support (25%). Call handlers also highlighted that the call screening prioritisation tool (CSPT) was inadequate (71%). Respondents noted that they found the system is too rigid when diagnosing illnesses and offering advice. The tool was slow and difficult to operate, particularly at times of high demand. This feedback was also mirrored by senior operational staff who were consulted noting that the algorithms used by call handlers are risk adverse, which results in too many GPOOH appointments; this in turn creates additional pressure on the wider GPOOH system. A small number of respondents (27%) to the survey stated that the hardware system was not user friendly, and that this impacts on operational performance as it takes longer than it should do to search key information to enter data. However, despite this lack of confidence in the clinical decision making tools, 75% of respondents noted that they believe patients were always or often directed to the right service. Page 7
9 Another key operational issue highlighted by staff was the rota system, 53% of respondents noted that they were satisfied with the rostering, with 27% noting that they were not satisfied. Those who were not satisfied highlighted the need for a good work-life balance, and to maintain a fair rota system. Additional concerns among staff were that the system could be abused by patients as a by-pass to the GPOOH service in order to access a GP when they were unable to get an in-hours appointment. It should be noted however that despite staff concerns, predicted demand for the service was marginally above the predicted volume (less than 5%). Feedback relating to staff morale was very mixed for example whilst only 15.4% of respondents agreed that morale was high, 62.96% of respondents were also satisfied or, quite satisfied with their current role within 111. Staff also reported high levels of satisfaction with the service they were delivering for example 55.6% of respondents noted that they believed that 111 provided a good service for patients and 67.9% of respondents reported that they believed that 111 improved access to urgent care services in AMBU. Patient Feedback Surveys were issued to patients/service users via post and 401 completed responses were received. Patients provided highly positive feedback with 92% of respondents stating that they would recommend the service. Almost all respondents (94.1%) stated that they found the health advice and information they received helpful. An analysis was also completed of the comments posted on the ABMU social media pages regarding 111. Whilst there were slightly more negative comments posted on social media than received via the survey (23%), the majority of comments were positive. Furthermore, the proportion of negative comments decreased as the service rolled out across all areas and became embedded. Whilst a small number of negative comments were receive that related to specific circumstances (such as one respondent who noted that they had received the wrong prescription via 111), the majority of negative comments related to a lack of advertising of the service. Activity Levels Activity level data was provided by ABMU and was based on amalgamated data from both the CAS and Adastra systems. This data covered the first six months of implementation (November 2016 to April 2017). In total, just under 72,000 calls were logged in the first six months of operation. This was around 3% higher than projected based on previous call volumes to GPOOH services and NHS Direct Wales. The service performed well against the standards set out in the Interim Standards and Quality Measures. In total, 98% (base=63,751) of calls were queued for less than 20 minutes (within 11). Of total calls, just 4.3% (n=538) of calls were abandoned after 60 seconds over the first six months of operation which included a busy period over the Christmas and New Year holidays. The majority of calls were made at the weekend (51%). The busiest time of the day was 6pm. The busiest day since the service was launched was on the 27th December 2016 where 1,154 calls were received over the course of 24 hours. Weekends proved busier than weekdays, and lines were busiest at 6pm and 9am. Many callers were referred onto GPOOHs (66%). Key stakeholders and senior operational staff noted that work is ongoing to better track and categorise call outcomes across the patient journey from 111 into GP out of hours services to facilitate end to end reporting and an accurate understanding of patients outcomes. This will help to add more detail on activity levels and the wider impact of the service. Impact of the Service In order to understand if the implementation of the 111 Pathfinder had impacted on other parts of the Page 8
10 health service an analysis was completed of trends in service use within the ABMU area and a comparative analysis of service use within other Health Boards. ABMU data shows that there was a decrease of 1% in ED attendance (1,343 visits) in the ABMU area (compared to the previous year) throughout the 111 pilot period. There was also a reduction in ambulance conveyances to ED, with an overall reduction of 5%. The largest reduction came from nonurgent (green) conveyances, which reduced by 29%. Although this change cannot be wholly attributed to 111 it can be surmised that the service has contributed significantly to this reduction 5. The reduction in ED attendances compares well to other Health Board areas in Wales, where four Health Board areas experienced an increase in demand. Furthermore, whilst all Health Boards have experienced a decline in non-urgent (green) ambulance conveyances over the past year the reduction is more significant in ABMU than in other Health Board areas. Economic impact of the 111 Pathfinder was also considered. The annual running cost budget of million, was off-set by cost savings to other parts of the health service. It is possible to estimate some of the savings that will have accrued because of 111 implementation. For example using financial data provided by WAST and ABMU, it is estimated that the 111 Pathfinder could have contributed notional savings in the following areas though caution should be exercised in reviewing this data as these are not actually cash releasing savings, but would in real terms be cost avoidance or efficiency gains: 60,000 through a reduction in GPOOH doctor advice calls; 218,000 through a reduction in ED attendances; 205,000 through a reduction in non-urgent (green) ambulance conveyances; 60,000 through a reduction in Minor Injury Unit (MIU) attendances. In addition to this, 111 could potentially contribut to other in-direct cost savings/efficiency gains that are more difficult to quantify, for example if it is assumed that if 10% of the proportion of patients who previously would have been conveyed to hospital via ambulance and admitted to a ward for one night then additional efficiency gains of 99,120 would also be accrued 6. Comparative Analysis The service was also compared with similar services in Scotland, Blackpool, and Great Yarmouth and Waveney. This comparative analysis highlighted that the ABMU 111 Pathfinder is structured differently to other 111 services elsewhere in the UK, for example the ABMU services are focused on clinical triage; whereas the English model is non-clinical, therefore a direct comparison is very difficult. However, elements of the services that were comparable included levels of demand and call answering times. The ABMU 111 Pathfinder compared favourably with the other more established services in the comparator areas. Demand levels were reasonably similar across all areas ranging from 0.12 calls per capita in Scotland to 0.18 per capita in Blackpool and 0.14 in ABMU. The average length of call ranged from seven minutes in Blackpool, to 18 minutes in Great Yarmouth and Waveney, average call times in ABMU were 15 minutes. Conclusions Qualitative feedback from key stakeholders, together with an analysis of the activity level data from the 5 Since the development of the 111 Pathfinder there have been a number of other initiatives undertaken across the health sector in Wales that were designed to improve both services and efficiencies, this had included work by WAST to improve response times though changes to their clinical model. It is not possible to disaggregate the impacts of the 111 Pathfinder from these other initiatives. 6 NHS Wales cost of one overnight stay in an acute hospital is stated as % = 120 days (6 months), or, months = 413x240 = Page 9
11 CAS and the Adastra system and data relating to other parts of the health care system suggest that the 111 Pathfinder has been well implemented. This is evidenced by the fact there were no increases in demand for other services such as ED or GPOOH appointments. The service also performed well against the agreed standards. For example, 94% of total calls were answered within 60 seconds and the average triage times for urgent calls was 3 minutes compared to a standard of 20 minutes. Overall there has been a positive response to the 111 Pathfinder among service users, with 95% of survey respondents reporting that they were satisfied with the service. Whilst a minority of staff (27%) suggested making some amendments to the training provided, the majority of staff (75%) reported that patients received care in the right place all or most of the time. Feedback from staff on how the new service has impacted on their role was mixed, for example whilst only 14% of respondents agreed that morale was high, 44.7% also noted that they were more satisfied with their role within 111 than their previous role. It has been difficult to disaggregate the impacts of the 111 Pathfinder from that of other ongoing health interventions in Wales. However a review of statistics and key datasets in ABMU and across Wales suggests that the 111 Pathfinder has contributed towards improvements in other parts of the healthcare system such as a reduction in ambulance conveyances and a reduction in ED attendances in ABMU, whereas other Health Board areas experienced increased attendances during the same period. Whilst it is recognised that there are limitations with the 111 IT systems which were developed by connecting two separate legacy systems (CAS and Adastra) it should also be noted that this is an interim arrangement and a new NHS Wales IT solution is being planned Future considerations The quantitative data analysis, consultations with key stakeholders and the staff and service user surveys highlighted a number of issues that should be considered for any wider roll-out of the 111 service, as summarised below: Senior operational staff noted the difficulties in recruiting experienced clinical staff such as experienced nurses and out of hours GPs. Whilst this issue is not unique to the 111 Pathfinder, it is possible that the recruitment of suitably qualified staff for out of hours services is particularly challenging (due to the required shift patterns). Feedback from key stakeholders and the staff survey suggests that the 111 service could be made a more attractive career opportunity with the potential addition of additional of professional supervision, regular staff feedback, training opportunities and more frequent on- the- job training. As the 111 Pathfinder is rolled out across Wales, NHS Wales may wish to consult with key professional bodies (such as the RCN Wales and the RCGP Wales), to further understand how working in the 111 service could be made an attractive option. Potentially low levels of staff morale were highlighted both in the staff survey and by key stakeholders. Retaining existing staff and recruiting new staff will be critical to any future expansion of the service; maintaining high levels of staff morale will be an important aspect of this. Both the staff survey and interviews with key stakeholders suggested a number of points for consideration. Firstly, rostering was highlighted (in the staf survey) as a key issue impacting on staff morale; the current rostering system should be reviewed by WAST in order to ensure that the operational needs of the service can be met whilst also maximising fairness and transparency for staff across all roles. Now that the 111 Pathfinder has been operational for more than six months and new systems and processes have become embedded, NHS Wales should consider completing a staff survey to identify key areas of staff concern and how staff morale could be improved. Almost all of those consulted with, noted the limitations of the current IT solutions. However, it was also noted that a new all Wales IT solution is due to be developed and implemented which will replace both existing systems (CAS and Adastra). This will provide the opportunity to implement a more connected service with greater potential to provide more detailed management information. Therefore, Page 10
12 the data requirements and inter-operability of the 111 service should be considered as part of the wider IT system specifications. A small number of senior clinicians involved in the operation of the service noted that the algorithms used in the triage process/clinical decision making tools should be reviewed. A structured programme of review should be considered based on the high volume/high impact so that improvements can be prioritized in line with service need. This concern was also echoed through feedback in a staff survey which highlighted a lack of confidence in the clinical decision making tools by the staff using them. Concern was expressed that current algorithms used for triage are too risk adverse resulting in too many calls being transferred to GPOOH services, which could have been dealt with by providing self care advice or in-hours GP appointments. Looking at the comparative analysis fewer callers from Wales were directed towards community and primary care settings than those within the English and Scottish regions. However, care should be taken in interpreting differences without a thorough understanding of the different tools in operation across the UK. It is also important to understand whether the there are issues around the system dispositions or whether human factors are contributing towards the overall position. The adverse impact of this is that the service may not be as efficient as it could be, and also that it makes the GPOOH service more pressurised to work in and a less attractive job role. Given that this review was completed following the first six months of delivery it was not possible to identify any trends in activity level data or, any impact on other services. NHS Wales should consider undertaking a further review of the 111 Pathfinder as it is rolled out across other Health Board areas and more longitudinal data becomes available. Page 11
13 INTRODUCTION AND BACKGROUND Introduction RSM PACEC in collaboration with the Medical Care Research Centre Unit (University of Sheffield) were appointed to undertake a review of the NHS Wales 111 / Out of Hours Pathfinder Project. This section provides an overview of the terms of reference for the review; the methodological approach and the background to the 111 Pathfinder in Wales. Terms of Reference and methodology Terms of reference The aim and objective of the review was to identify whether the introduction of the NHS Wales 111/ Out of Hours Pathfinder (hereafter 111 Pathfinder) within the Abertawe Bro Morgannwg University Health Board (ABMU), provides an effective service for patients who needed to access urgent care, in line with Prudent Healthcare principles 7. The evaluation was also required to review the process of implementing 111 in the pilot areas and to consider what lessons can be applied if this service model is rolled out to the rest of Wales. The terms of reference (2016) note that the evaluation is specifically required to include: User (patient) feedback; Professional feedback from staff across a number of services; An analysis of the activity and performance during the first six months, with appropriate benchmarks throughout the evaluation period; An impact analysis considering the impact of 111 on other urgent care services including Emergency Departments, the Welsh Ambulance Service (WAST) and primary and community-based services. It is recognised that some of this will be difficult to evaluate formally (in terms of establishing direct, causal relationships), however the evaluator will be expected to review existing datasets and advise accordingly A high-level financial evaluation to supplement existing modelling work which identifies the cost of the service on a per patient basis with appropriate benchmarks; and A documentary review of the implementation arrangements at both a national and local level and links to recognised best practice and how this may support the longer term national model. 7 The four Prudent Healthcare Principles are: 1. Achieve health and wellbeing with the public, patients and professionals as equal partners through co-production; 2. Care for those with the greatest health need first, making the most effective use of all skills and resources; 3. Do only what is needed, no more, no less; and do no harm. 4. Reduce inappropriate variation using evidence based practices consistently and transparently. Page 12
14 Methodology As summarised in the following table the methodology involved nine stages of work. Table 0:1 Summary of Review Methodology Stages Stage 1: Project Initiation Stage 2: Desk Research Stage 3: Stakeholder Consultations Stage 4: Evaluation Framework & Logic Model Stage 5: Patient Feedback Stage 6: Staff and Stakeholder consultations Stage 7: Analysis & Benchmarking Stage 8: Case Studies Stage 9: Reporting & Dissemination Activities Agree and refine methodology with the 111 Programme Team Baseline Assessment Policy Review Literature Review Interviews with key stakeholders involved in the development and operation of the Pathfinder Development of Evaluation framework Design & agree patient survey Pilot survey Fieldwork Design & delivery staff survey Interviews with key operational stakeholders Analysis of Performance, Impact & Economic data Case studies for each pilot area Interim Report Draft Report Final Report Source: RSM PACEC Programme Initiation Document Overview of the 111 Pathfinder The 111 service is part of a wider strategy to transform urgent and unscheduled care services in Wales 8. As set out in the following section, the overall aim of the strategy is to co-ordinate and manage unscheduled care demand in a different and organised way, to help meet the needs of patients within their own communities and possibly to slow the year on year increase (or, to slow the increase in demand) on hospitalbased services. The key components of the service are summarised below, however, not all the functionality listed below will be available from the outset: A simple telephone number which is available 24 hours a day, every day, and is free to the public from a landline or mobile phone; Well-trained call handlers using agreed protocols, including a safe and reliable decision support tool; Additional capacity for management of calls and triage, removing double-handling (instances where patients must repeat their details more than once) as far as possible; Ability to request a 999 ambulance quickly where necessary; Assessment by experienced clinicians, co-located with the trained call handlers; 8 The Way Ahead for Unscheduled Care in Wales. Unscheduled Care Improvement Board Page 13
15 An up-to-date all-wales directory of service that provides information on local services (phase 1) and ideally integrates with local authority single points of access (phase 2); A common clinical Out of Hours (OOH) 9 database with appropriate access to the Individual Health Record and care plans for high-risk and special-needs patients; Providing an appropriate, booked face-to-face assessment when required; and Providing guidance to the public on treatment in the European Union. The service model for 111 Wales differs from that in operation elsewhere in the UK. In Wales, the model is based on an integrated approach to the delivery of call taking, clinical assessment by the 111 service, and clinical assessment services provided by the ABMU GP Out of Hours Service (GPOOH). The 111 service integrated the current telephony service provided by NHS Direct Wales with the front-end call handling and triage function used by GP Out-of-Hours (GPOOH) Services to provide a single service for patients to access if they need urgent help, or access to health information and advice 10. Welsh Ambulance Services NHS Trust are the host organisation. A technical bridge (a concentrator) was created to join the two clinical assessment systems, as summarised in the following diagram. 9 In ABMU Out of Hours clinical services are those operating from 6pm to 8am. 10 The telephony element of the 111 service is hosted by WAST under the NHSDW element of the Trust, which currently uses a CAS telephony service. GPOOH in the ABMU area which provides the triage and clinical support element of the service uses ADASTRA to handle calls and record data. Page 14

16 Figure 0:1 111 Pathfinder Call Flow Source: ABMU This approach, combined with the complexities of operating two separate clinical systems that have a technical bridge between them, makes analysis of activity levels and performance challenging. It is recognised that these issues have made it difficult locally, to be able to assess end to end performance since the service was introduced, but also acknowledged that it makes the evaluation piece complex. A further factor is that the 111 service operates on a 24/7 basis, whilst the GPOOH service operates from 6.30pm until 8am on weeknights, and from 6.30pm on a Friday through to 8am Monday (excluding bank holidays). Calls within the 111 service are assessed through the Call Streaming Prioritisation Tool (CSPT). This tool is predominantly used by trained call takers (though it is also used by clinical staff during busy periods when the service is focussing on maintaining access levels). CSPT has 60+ protocols which the call takers use to assess and prioritise calls to reach the appropriate patient outcome. This system is based on a previous model designed by NHS Direct England which uses evidence based clinical protocols to direct callers to an appropriate level or place of care, within an appropriate time frame. Having said this, a number of CSPT protocols were prioritised for clinical review (e.g. infants under 18 months, children aged 18 months to 5 years) to the desired call flow model for 111 whilst maintaining the 0845 service. The purpose of the Pathfinder was to field test the clinical model to fully test and evaluate the benefits of the service within ABMU, towards ensuring a smooth transition across the rest of Wales. The 111 Pathfinder became operational in the ABMU area in mid October It is intended that once the service has been fully tested it will then be rolled out nationally after due consideration of the evaluation. A fulltime programme board was created to oversee the full development of the service and the implementation of the Pathfinder in The following diagram summarises the overall service model and patient pathways and processes that have been established with the implementation of the new 111 service. Page 15
 Page")
17 Figure 0:2 Overview of 111 Pathways Source: 111 Project Board (2015) Page 16
18 The 111 Strategic Outline Business Case (December, 2015) notes that the critical success factors for the project are: Patients will: Be appropriately assessed (either by phone or face-to-face) by the right service, at the right time; Be able to receive treatment in their own home (or as close to their home as possible) in a community setting on a consistent basis, where appropriate, and avoid unnecessary transportation by ambulance to the ED; Have access to information to enable them to care for themselves, if appropriate, by having timely access to information, direct advice from a clinician if necessary, and signposting to the right service; Be able to have access to health information, advice and clinical assessment through a variety of channels (e.g. website, mobile devices); Have a better understanding of what services to access; and Be able to have information on their individual care needs shared with relevant clinicians (with consent) to facilitate the delivery of high quality care and avoid unnecessary duplication. The expectations for 111 are: Demand for inappropriate 999 ambulance responses will reduce; Demand for face-to-face assessment by GPOOHs will reduce; Overall demand impact on the Emergency Department (ED) services will be marginal, however 111 will not place additional demands on acute services; There will be reductions in inappropriate attendances to ED & GPOOHs; There will be an increase in utilisation of clinical pathways and alternatives to hospital admission (via the Directory of Service) as part of Local Health Boards (LHBs) primary care and community strategies; and The 111 service has been designed to support prudent healthcare principles by supporting effective navigation through the unscheduled care system, promoting self-care, providing high quality information for patients to access as they need, and using technology within a new all-wales service to support effective workforce deployment and development. Page 17
19 Need for 111 There have been a number of reviews and reports which have highlighted that the unscheduled care system in Wales is not resilient to unexpected and unusual surges in external demand, or demand shifted within it. This lack of resilience leads to increased attendance at ED units and increased waiting times at these units 11. A series of Welsh Audit Office reports 12 have also noted a range of problems within the unscheduled care system in Wales resulting in the system of unscheduled care operating in a disjointed way for people who need help. The reports note many factors which have placed considerable pressure on unscheduled care services, including rising demand, financial constraints, workforce challenges and problems with patient flow through hospitals. The first report 13 concluded that radically new ways of delivering unscheduled care should be introduced in order to improve unscheduled care. This included a number of recommendations, for example, that Health Boards should seek to provide points of access to unscheduled care that better reflect the nature of demand, including; a single point of access should be contactable by phone at all times of the day. The 111 Pathfinder Strategic Outline Business 14 case highlights the strategic, economic, commercial and management need for the development of an Urgent Care Advice and Treatment Service, accessible via the 111 telephone number across Wales. This Business Case notes that the unscheduled care system in Wales is complex and difficult to navigate for patients, carers and for health professionals alike. In addition to NHS Wales Direct (that is provided nationally) each individual LHB has its own, unconnected GPOOH service. The current, fragmented service delivery model has led to disjointed provision and duplication of a number of functions. Outside the hours of Monday to Friday (8am to 6.30pm), urgent primary care services are provided or commissioned by Local Health Boards and each has different service models and operating systems in place. The GPOOH services in each of the seven Local Health Boards operate independently of each other but all provide telephone assessment with signposting to other clinical services and/or face to face appointments or home visits when required. NHSDW provides a 24-hour service offering health information /advice and signposting services, alongside a range of other services as required. All OOH and NHSDW services provide call handling and clinical assessment services in addition to the local face to face services, even at times when there is a low level of demand (e.g. after midnight). Therefore, services could be provided more efficiently if organised on a national basis, or supported by a national access infrastructure. In addition to different service delivery models and operating systems across the 7 LHBs, the GPOOH services and NHSDW also have different service and quality standards, including the prioritisation categories for clinical assessment and appointment. Neither NHSDW nor GPOOH standards reflect those of in-hours primary care services or are properly aligned in a strategic manner with other parts of the unscheduled care system. The Business Case also notes that all elements of the Unscheduled Care system across Wales, (i.e. 999 ambulances (WAST, ED, and GPOOHs) remain under significant pressure which is often compounded by attendances whose needs could be more effectively met by other services or by direct advice or signposting. Service demand, particularly in GPOOH is high and increasing, with significant peaks in activity for all services at key times. The patterns of service demand for OOH services are broadly consistent across all LHB areas. The differences in the service delivery models used across each LHB means that it is not possible to manage this as effectively as a single, nationwide service would do. 11 E.g. see External Factors ( Drivers ) Affecting Long-Term Term Trends and Recent Pressures on Unscheduled Care Use and Performance in Wales. Public Health Wales, Unscheduled Care. An update in Performance. Welsh Audit Office, Unscheduled Care: Developing a whole system approach. WAO e%20for%20easc%2026%20jan%2016.pdf Page 18
20 Unlike hospital or many community services, the clinical service model currently operating within NHSDW is provided entirely by nurses, meaning that staff do not have the opportunity to refer to other professionals within the service for additional guidance or support. This has led, in part, to the development of a risk averse culture, with more complex or acute patients being signposted to external service provision rather than supported to self-care. This situation has been compounded in recent years by the lack of investment to update the clinical decision software; the algorithms of which have not been altered to reflect changes to clinical practice (e.g. issue of NICE guidelines) or service developments. As a result, staff operate a dual system, referring to paper/electronic based guidelines, supported by education, where changes to clinical practice were needed until much needed development to the clinical system (CAS) was undertaken in 2016 as a pre-cursor to 111 Pathfinder roll out in ABMU. The Business Case also notes significant and ongoing difficulties in the recruitment of experienced clinical staff, particularly GPs within OOH services across Wales and also Nurse Advisor posts within NHSDW, which has led to service capacity gaps with a resultant impact on timely service delivery. It is anticipated that the new 111 service will provide opportunities to redesign roles and challenge current set patterns of working, which in turn will lead to the redesign of roles, create new ways of working, increase job satisfaction and provide opportunities for career development. These could then help tackle recruitment difficulties. The historic IT infrastructure (pre 111 pathfinder) for the GPOOH service and NHSDW services did not support the transfer or sharing of data, leading to duplication and delays in callers accessing the right service for their needs. Furthermore, within GPOOH services, there are separate contractual arrangements in place with commercial providers and the LHBs all use different versions of a single IT system (Adastra), meaning that NHS Wales has not been able to take advantage of combined purchasing power to deliver a more cost-effective IT system. In addition to this the NHSDW IT infrastructure is now obsolete and must be replaced by Therefore, in summary the Business Case noted that there was a need to provide a more integrated, efficient and effective urgent care system in Wales that is easy for patients and clinicians to navigate and can flexibly manage demand on a national basis. Page 19
21 STRATEGIC CONTEXT Introduction This section provides a high-level overview of the policy context in which the 111 Pathfinder was developed. Table 0:1 Summary of key relevant policies Policy / Strategy The Way Ahead for Unscheduled Care in Wales (2014) Our Plan for a Primary Care Service for Wales up to March 2018 (2015) Quality and Delivery Framework for Emergency Ambulance Services (2015) Informed Health and Care: A Digital Health and Social Care Strategy for Wales (2015) Prudent Healthcare Principles (2014) Relevance / Impact of the 111 Service In February 2014, the Unscheduled Care Improvements Programme produced its vision for how unplanned care needs should be met. Included in this report were key objectives for NHS Wales such as the need to provide rapid, reliable advice when it is needed; to support for self-care; to provide easy access to urgent care across Wales; and enhanced information systems and care networks that cross organisations. A key component in The Way Ahead was for the unscheduled care systems in Wales to implement a free, 24 hour telephony service to meet out-of-hours, urgent, primary care needs. The Welsh Government s February 2015 document Our Plan for Primary Care Service Delivery for Wales up to March 2018 iterates the commitment of the Welsh Government to deliver 111 in Wales. Specifically it states that 111 should provide access to a wide range of reliable health and wellbeing information, advice and assistance and coordinating access to urgent care for people. This document emphasised the specific role the 111 service was to have in supporting carers, including those in care homes, to feel supported and well informed to meet the needs of those they are caring for and to help avoid inappropriate hospital admissions. This report presents a 5 Step Ambulance Pathway that provided a framework against which emergency ambulance services in Wales should be commissioned. It also had direct links to the development of 111. Specifically, steps 1 and 2 of the Framework (helping to choose and Answering my call) refers to the development of the 111 service, which will build on the success of NHSDW and its website. It notes that WAST will work with LHBs and other elements of the health and social care system to ensure that callers access the right health care for them in the most appropriate place. This includes referrals to other sources of advice such as NHSDW and a 111. The report emphasised the significant role that technology could play in enabling more effective service delivery through information sharing at a personal level to help service users make informed decisions and choices to support their wellbeing and amongst professionals to reduce duplication and enhance informed decision making. The creation of 111 supports further development and provides a platform to support access to trusted information and advice by service users. In January 2014, the Welsh Government NHS Confederation Conference sought to embed a set of Prudent Healthcare Principles across the NHS in Wales. The principles are as follows: Page 20
22 Policy / Strategy WAO Report Unscheduled Care Developing a Whole System Approach (2013) Welsh Government Manifesto (2011) Ten High Impact Steps to Transform Unscheduled Care (2011) Setting the Direction. Relevance / Impact of the 111 Service Do no harm; Carry out minimum appropriate intervention; Organise the workforce most appropriately; Promote equity between professionals and patients; and Co-create health with the public, patients and partners. The 111 service has been designed to support in particular the second, third and fourth principles by supporting effective navigation through the unscheduled care system, promoting self-care, providing high quality information for patients to access as they need, and using technology within a new all-wales service to support effective workforce deployment and development. This report detailed a number of recommendations in relation to strategic planning to improve unscheduled care. In particular one of the recommendations related to the development of the 111 service and the construction of a proposed service model that would include: A single point of access that should be contactable by phone at any time of day; The establishment of a hub for all referrals to unscheduled care and transfers between parts of the unscheduled care service; That different services could use and agree, common triage and clinical governance systems; and The maintenance of a regularly updated directory of services. The Welsh Government s Manifesto Commitments (2011) were very clear that introducing a 111 system should: Build on the success of the NHS Direct service and offer a single; number for accessing OOH health care in Wales, linked into the local OOH services; and Ensure all out-of-hours services are provided by the local NHS. The introduction of the 111 service builds on these key policy commitments and emphasises the need to move towards a model of care that is based on the development of strong primary and community services. The Unscheduled Care Programme Board 15 published Ten High Impact Steps to Transform Unscheduled Care in August This document highlights the key steps that were required to transform the unscheduled care pathway in Wales at Local and National level. The 111 service was recognised as a fundamental requirement in delivering a number of steps and as a key enabler for the wider service transformation. This document sets out a framework to assist LHBs to develop and deliver improved primary care and community based services for their local 15 The Unscheduled Care Programme Board consists of 24 Senior Health and Social Care Professional, including representatives from LHBs and Unscheduled Care specialists from across Wales. Page 21
23 Policy / Strategy Primary & Community Services Strategic Delivery Programme. (Welsh Assembly Government, 2010) Relevance / Impact of the 111 Service populations. It notes the need to effectively manage the interface between in hours and out-of-hours services so that governance and accountability for care is clearly defined and understood. It also highlights that the current system of out of hours services and its relationship within mainstream primary care services is disjointed and lacks cohesion and co-ordination; NHS Direct appears to have had little impact in deflecting demand from primary care services. Furthermore, too many people are in the wrong place in the care system and there is an over reliance on hospital care and ED Departments. As one of a number of issues to be considered to address deficiencies in the system this reports suggests that a single number access point for all unscheduled care is developed. Page 22
24 LITERATURE REVIEW Introduction The following paragraphs provide a summary of the key findings of rapid review of the literature relating to urgent care and telephone triage conducted by Sheffield University, School of Health and Related Research (ScHARR). Background Demand for urgent care (including emergency care) has increased year on year over the last 40 years. The reasons for this are only partly understood but comprise a complex mix of changing demographic, health and social factors. Over the last 15 years there have been a number of reviews of urgent care, policy recommendations for service changes and service level innovations, all of which were aimed at improving access to and delivery of urgent care. Despite this, the emergency and urgent care system remains under greater pressure than ever. It is increasingly recognised that provision of urgent care is a complex system of interrelated services and that this whole-system approach will be key to improvement and development in the future. Data sources used for this review were MEDLINE, EMBASE, The Cochrane Library, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) and the Web of Science Methods A rapid, framework-based, evidence synthesis approach to ensure the efficient identification and synthesis of the most relevant evidence, was used. A range of search methods was used. First, Sheffield University performed a broad general search on MEDLINE. This was then supplemented by targeted database searches for each of the five themes mentioned below. Searches were conducted for the years To increase efficiency existing search strategies from related research that the School of Health and Related Research (ScHARR) and from existing related systematic reviews were utilised. Additional references were identified by scrutinising reference lists of included systematic reviews, utilising Sheffield s extensive archive of related research and new research provided by internal and external topic experts. A single reviewer sifted searches and a second reviewer checked a 10% random sample. Only empirical evidence was included. Data extraction from individual studies was only carried out for papers that met the inclusion criteria and had not been included in a systematic review. Data were extracted directly into summary tables. Formal quality assessments were not undertaken but provided a narrative summary of study quality based on the limitations reported by study authors. The evidence for each theme is summarised common issues that overlap between themes have been identified. Results Five separate rapid evidence reviews were conducted on themes related to the delivery of emergency and urgent care in the NHS. These themes were (1) trends in and characteristics of demand; (2) telephone triage and advice; (3) management of patients in the community by ambulance clinicians; (4) models of service delivery in the ED; and (5) emergency and urgent care networks. The outcomes of which are summarised below Demand for emergency and urgent care Four systematic reviews and 39 primary studies were included. This highlighted that there is remarkably little empirical evidence that can fully explain the increases in demand for urgent care. The key evidence gaps and challenges identified from the existing evidence relate to a need to examine demand from a whole-system perspective and to gain better understanding of the relative proportions of demand for different parts of the system and the characteristics of patients within each sector. This could be addressed by developing research studies that build on the existing knowledge about factors that may be influencing demand and the contribution each one makes, and mapping these onto a coherent system model. This would then support the development of service design and planning to meet current and future needs of local populations. Page 23
25 Telephone triage and advice A total of 10 systematic reviews and 44 primary studies were included. There is an existing, substantial evidence base regarding the operational and clinical effectiveness of telephone-based triage and advice services for management of requests for urgent health care. Overall, these services provide appropriate and safe decision-making and patient satisfaction is generally high, as is the likelihood that patients will accept advice, although this varies depending on the clinician providing it. There is little evidence, though, on the efficiency of these services from a whole-system perspective. Evidence gaps and aspects of service delivery that warrant further study are centred around the need for (1) further assessment of the whole-system impact of telephone access services for emergency and urgent care, including the associated costs, to establish how it contributes to improving system efficiency; (2) more focused research on the broad area of the optimum requirements for different skill levels needed in the NHS 111 service; and (3) more detailed evaluation of the accuracy and appropriateness of call assessment decisions would help answer some of the questions about the appropriateness of referrals made by the NHS 111 service Management of patients with urgent care needs by the ambulance service in community settings Seven systematic reviews and 12 primary studies were included. Extended paramedic roles have been implemented in various health systems and settings; these appear to be successful at reducing transports to hospital, making safe decisions about the need for transport and delivering acceptable care out of hospital, and are potentially cost-effective. The key evidence gaps and areas for further research include (1) further work on ways to support paramedic decision-making and development of integrated care pathways for a range of conditions that mediate safe management in the community setting; (2) more detailed study on the necessary skill mix of paramedics, and paramedics with advanced and specialist skills needed to provide a safe and high-quality, community-based service for patients; and (3) more accurate estimations of the likely proportion of patients who could be safely managed outside hospital to support ambulance resource and paramedic workforce planning Models of service delivery in the emergency department Attempting to assess the evidence on different models of delivering ED services was challenging. Sheffield University conducted two reviews. One updated an existing systematic review on co-location of primary care in the ED and identified potential for this initiative. Two systematic reviews and seven primary studies were included in this review. Sheffield University have only been able to conduct a review of reviews (22 systematic reviews) about the wider ED service and, given the complexity of the subject area, it was not possible to identify clear evidence gaps. The review highlighted some areas worth further consideration. Additional focused reviews utilised the existing search library with, where necessary, targeted focused additional searches. One of these could be management of the frail elderly in EDs, as this is a key area for development, but there is little evidence on interventions to improve care. There is scope to identify more recent primary studies from our existing search library. One clear evidence gap is the lack of studies conducted at scale. The emphasis on developing co-located primary care services within EDs is one area in which there is an opportunity to undertake a broader study Emergency and urgent care networks No evidence was identified on how to best organise and operate an emergency and urgent care network, nor any empirical evidence on the effectiveness of this type of network model. Research activities which could support emergency and urgent care network development include (1) a more detailed and targeted rapid review to further explore the related theoretical literature and identify evidence concerning design and strategies for successful network development; (2) some rapid scoping research to identify and map current emergency and urgent care network development nationally; and (3) a programme of research to evaluate emergency and urgent care networks and measure effectiveness. Some common themes were identified across subject areas. These included (1) the relationship between better understanding of the drivers of demand and the planning of health services by networks; (2) the need to develop integrated care and referral pathways to improve effectiveness for telephone services and Page 24
26 support patient management in the community; and (3) the need to measure whole-service and system impact, and associated costs, when evaluating interventions and initiatives. A substantial number of included studies for most themes were from the UK, but this was not the case for the trends in demand theme Limitations This was a large-scope rapid review; therefore, it was not possible to conduct a detailed analysis of the quality of the evidence base. Some of the key themes identified are summarised below: Overall, the evidence base on the clinical effectiveness of different models of care for delivering emergency and urgent care is weak, with small numbers of randomised controlled trial designs and a reliance on uncontrolled before-and-after studies. There is an emphasis on process measurement, such as times and attendance rates, rather than patient outcomes other than satisfaction. Little attention has been paid to the costs and cost-effectiveness associated with interventions. A quality assessment of the 22 systematic reviews on delivery of ED care found that, overall, the quality of these reviews was good, with 20 out of 22 conducting adequate searching, 13 out of 22 assessing risk of bias and 17 out of 22 using appropriate methods of synthesis; in 14 out of 22 the evidence presented was judged to support author conclusions. The limitations of the rapid review method used are as follows: (1) it was not possible to exhaustively search for and synthesise all the relevant literature; (2) existing systematic reviews were drawn extensively; and (3) because of the potential scope and scale, there are related themes that have been excluded from this review. The most obvious gaps are separate reviews of models of urgent care within primary care and specific attention to workforce issues, such as skills, education and retention. It was also not possible to include patient and public involvement input to this review, but this will be of benefit when prioritising which evidence gaps should be addressed to assess importance to patients. Conclusions There is a paucity of evidence to explain the complex reasons that have driven the increases in demand for emergency and urgent care and to support the development of emergency and urgent care networks. There exists a considerable evidence base on the clinical effectiveness and cost-effectiveness of some interventions to improve service delivery, but the evidence base is weak overall and based in small singlesite studies with no assessment of impact at scale or on the wider emergency and urgent care system. The evidence gaps that appear to be in most immediate need of addressing are: Research to characterise and map demand at a population level and link this to service need so that emergency and urgent care systems can be designed that can effectively, efficiently and safely respond to patient needs; An assessment of the current state of play in the development of emergency and urgent care networks, and longer-term evaluation of the clinical effectiveness and cost-effectiveness of different network models to identify how best networks can deliver NHS Wales objectives; and Expanding the current evidence base on existing interventions that are viewed as central to delivery of the NHS Wales plan by assessing the implications of increasing interventions at scale and measuring costs and system impact. Although not an evidence gap, a clear theme that emerged across the reviews was the need for robust, high-quality and linked patient data to support these tasks. Finally, given the large number of related programmes already at work in the NHS, it would be prudent to develop a national picture of existing pilot projects or interventions in development to support decisions about research commissioning. Page 25
27 CONSULTATIONS Introduction This section summarises the main findings emerging from consultations with key stakeholders associated with the 111 Pathfinder Project. A suite of consultations were completed prior to the implementation of the service which focused on the design phase of the project, with further consultation completed with senior operational staff surrounding the six months of service delivery. Consultations where conducted with members of the following groups: Abertawe Bro Morgannwg Community Health Council; Abertawe & Bro Morgannwg University Health Board; Aneurin Bevan University Health Board; Cwm Taf University Health Board; Royal College of Nursing; Wales Ambulance Service NHS Trust (WAST) who provide NHS Direct Wales; Welsh Government; All Wales GP Out of Hours Forum; and The 111 National Programme Team. A full list of those interviewed is set out in Appendix A. Policy Context and Need for the Service All of those consulted highlighted that the 111 Pathfinder is highly consistent with and contributes towards several key government policies, relating to unscheduled care and Out of Hours Care. Consultees stated that the strategy and policy supporting the concept of a 111 service has been in development for a number of years. Specifically, consultees indicated that 111 Pathfinder also contributes to and is consistent with the aims and objectives set out in the Ministerial Review of GPOOH Care and the Unscheduled Care Policy paper (The Way Ahead, 2014). Both note the need for an accessible telephone service for those who require urgent health advice and clinical assessment. In addition to the policy direction, the majority of those consulted with stated that there is a need to provide the public with increased access to clinical advice and information by appropriately trained clinicians, in order to reduce the pressure on other parts of the health system. These consultees highlighted that there are high and increasing levels of demand on all types of unscheduled care, including GP OOH, ED units and 999 ambulance service 16. Many of those consulted with noted that they believed that the high levels of demand on ED units can often led to unnecessary hospital attendances and admissions. There are a number of reports referring to this, for example, Unscheduled Care: An Update on Progress Report (Welsh Audit Office, 2013). Those who were consulted with prior to the launch also highlighted that the Welsh Government was keen to ensure that any new system being developed was appropriate for Wales, that opportunities should be taken to learn from elsewhere, and that members of the Programme Board undertook research and completed study visits (in England and Scotland) as part of the development of 111. A number of key staff including clinicians who were consulted with after the launch of the service highlighted that the Welsh model was unique and that the clinical triage and clinical hub were important elements of the service. Data from Welsh Ambulance Service, Adastra and Emergency Department Data Set (EDDS) shows a steady increase in ambulance service call volumes, A&E attendances and call to GPOOH services across Wales (see section 7) Page 26
28 Implementation Those consulted after the implementation of the 111 service in ABMU were asked their views on how well the service was introduced. The general feedback from staff who were working in unscheduled care was that the launch of the 111 Pathfinder was very well organised. There was a general perception amongst those consulted that an important aspect to the successful launch of the service was the dedicated programme team. There was a general agreement that having a team of experienced and dedicated staff would also be crucial to any further roll-out of the service in other Health Board areas. Key staff within WAST, GPOOHs and ABMU felt the implementation went well and demand for the service was there among the public. Consultees felt they were kept informed at each stage of the Pathfinder s development. The decision did not have significant amounts of publicity about the service and to stagger the implementation across the three main areas with the ABMU Health Board was considered by most consultees to be particularly helpful and should be considered if the service is to be rolled-out to other parts of Wales. A small number of consultees felt that there was insufficient communication about the service and that more could have been done to inform staff to minimise the potential for any confusion when the service went live. Another factor that was identified as being key to the successful launch of the service was the clinical support and leadership that the service received in its development and implementation from a small number of senior clinicians and unscheduled care experts. Around half of those who were interviewed following the launch of the service highlighted that the support and involvement of senior clinical staff was also important to not only ensuring that the service was clinically safe and effective. These consultees also noted that if the service is to be rolled-out elsewhere it is crucial to have buy-in and support from local clinicians to ensure that the service is complementary to existing models of care. Impacts All of those consulted with prior to the start of the service expected the 111 Pathfinder to have a positive impact in three key areas: callers experience of the service; the health and well-being of patients; and the effectiveness and efficiency of the health service in Wales. Specifically, these consultees expected the 111 service to reduce the number of unnecessary or inappropriate ambulance call outs and unnecessary attendances in ED, which in turn should have a positive impact on waiting times and patient flow in unscheduled care. These consultees also believed that by offering access to clinical advice and support the 111 Pathfinder should also reduce the level of demand for GPOOH services. A small number of consultees were also concerned that the service could potentially increase demand at ED and MIUs, as was the case when some of the 111 services were launched in England. Those who were consulted with after the launch believed that a number of positive impacts that were achieved for both patients and staff and the overall health economy. Senior operational staff believed that 111 will be beneficial for a wide range of clinical staff, for example paramedics can call clinicians at the clinical hub directly which potentially could result in a reduction in ambulance conveyances. Clinical staff from nursing homes could also potentially use the 111 service, which in the long-term could reduce the number of GPOOH call-outs and ED attendances. Senior clinical staff noted that they have received positive informal feedback from GPs noting a reduction in OOH appointments although the impact on inhours GP appointments is more difficult to gauge as there is no data either before or after to measure the impact against. It must be stressed however that the information in this section is anecdotal and not based on evidence, rather opinion. Conversely, other senior clinicians involved in out of hours care, also noted concern regarding the volume of triaged calls that are being referred to GPOOH noting that these appeared high. These clinicians noted that whilst the models of care were developed for the 111 service, NHS Wales is reasonable risk adverse, which could lead to more GPOOH referrals than 111 services in other regions. However, more staff training and a review of the algorithms should be conducted to minimise inappropriate referrals and unnecessary GPOOH burden. However, it is important to note that during the period between November and April, there were frequent periods of escalation when calls were being managed directly by the GPOOH to support the wider 111 service when workforce challenges within 111 prevented the planned call flow model from operating consistently. Page 27
29 Challenges IT solutions The development of the 111 service, required connecting two existing IT systems. Almost all of those consulted with noted that whilst this was the only technical solution that was available at the point of development, it was not ideal and created limitations with data flows and limited the amount of data that can be extracted from the system. For example, some clinicians and senior stakeholders responsible for planning and delivering services noted that they would like more information about how the service is operating at each key stage, for example, the number of callers who do not get through, the length of the queue (i.e. the number of calls waiting to be answered) and times across each stage of the process and more information about the full patient pathway. It was also noted that the implementation of an all Wales IT infrastructure will be important to an all Wales roll-out of 111, as it has the potential to provide inter-operability for the system and should be designed to enable service managers to access live information on the service Data requirements and data outputs Consultees were asked what information they believe is required to demonstrate the effectiveness of the 111 Pathfinder. All consultees noted that there were a number of key areas that the data should focus on, mainly, the processes (e.g. call handling data), patient experience/satisfaction and that the care provided is effective. All of those interviewed agreed that the clinical standards 17 that have been developed to monitor the implementation of the service are comprehensive and if reported on accurately and on a timely basis they will provide a useful overview of how the project is performing against key service criteria. Whilst most of these are operational standards such as call volumes and onward referrals they also include standards for patient/caller experience, which is an important aspect of the overall assessment of the service. Consultees highlighted how important it is to ensure that the clinical standards that have been established for the pathfinder are an accurate reflection of the effectiveness of the service. This is because the service will be assessed against these standards which therefore will influence the wider rollout of the service nationally. It was also generally agreed that there will be the opportunity to refine the standards further (should it required) once the project becomes operational. As the 111 project is expected to impact upon the whole health service, most consultees emphasised that robust baseline information from across the health service is essential to understanding the impact of the Pathfinder. This includes, Primary Care (e.g. GPOOHs), Acute Hospitals (especially attendances at ED Departments) and the Ambulance Service (call out rates and potentially response times). Consultees expected to see an impact on all aspects of unscheduled care. However, there may also be an increase in scheduled care, for example an increase in GP in-hours appointments from patients who have been triaged through 111 and advised to contact their GP. Around half of those who were interviewed after the service had been implemented noted the limitations in the data that is currently available particularly on patient outcomes. It was recognised that this is partly due to the fact that the current service is required to operate from two distinct IT systems that have been joined through the use of a connector. Therefore, at this point in time it is not possible to get information on individual patients on their pathway through the system. These consultees also highlighted that NHS Wales are in the process of developing specification for a new all Wales ICT system and hoped that issues associated with extracting data from the system would be eased with the new systems. Page 28
30 Staffing Almost all of those who were consulted with after the implementation noted the need more staff at all levels. Consultees believed that greater efficiencies could be achieved if it was possible to recruit more experienced nurses and call handlers. However, this point was noted within the wider context of staff recruitment difficulties across NHS Wales 18. Consultees also highlighted the shortage of experienced nurses and GPs and the difficulties of recruiting staff into out-of- hours services. Consultees also noted that in order to maximise the efficiency of the service, it is important get the balance or, skills mix of staff right across the 111 service. Consultees believed that more call takers should be recruited and that the 111 Programme team should consider how to make the job more attractive; bearing in mind that shifts and rotas need to be weighted to out of hours service provision (i.e. 6.30pm to 8am). A small number of consultees highlighted that if more nurses or, other advanced practitioners are employed fewer GPs would be required. As the service is rolled out across Wales other staff roles could also be considered, such as pharmacists, paediatricians and palliative care specialists. Mainstreaming Consultees noted that greater efficiencies or, economies of scale could be achieved if the service is rolled out across Wales at both a regional and national level. This could potentially release some staff from other OOHs roles to work within the 111 service and the scale of the service could also indicate a need for a more range of health care support such as g. palliative care, pharmacists and mental health practitioners. Furthermore, when a single IT solution for all of NHS Wales is developed it should take into consideration the data monitoring and reporting needs of the 111 service. The development of a new IT system provides the opportunity to have a more responsive service that can provide live data and information on the endto-end patient pathway. A small number of consultees also noted that the governance of any system that is rolled out across Wales should also be considered in great detail. In order to ensure a safe, efficient and effective service it is important to understand who has managerial, monitoring and clinical responsibilities for each stage of the service. This is also an important consideration for funding and resourcing any future service. Most consultees also highlighted the need for more staff if the service was to be rolled out further and that this would also provide an opportune time to provide further or refresher training to existing staff, whilst ensuring that the team are structured so that staff feel supported in their role. Other Issues All of those who were interviewed post implementation highlighted the significant technical challenges in delivering the new service and the restrictions Almost all of these who were consulted with post implementation highlighted the importance of getting the balance of staff to deliver the service. Experienced and trained nurses are required to undertake clinical triage and trained call handlers are also required to answer calls. It was noted that during a period of exceptionally high levels of demand (Christmas 2016), nurses were required to answer calls, which is not an efficient use of nurses time. Furthermore, like other parts of NHS Wales it was noted that the 111 Pathfinder experienced difficulties in recruiting nurses. 18 There is a wide range of reports highlighting the staff shortages and recruitment challenges across NHS Wales, for example, see Page 29
31 Summary The main points arising from the discussions with key stakeholders are: The 111 Pathfinder has created the opportunity to create a better patient experience, by providing patients with easy access to trained clinicians who can triage calls and ensure that calls get access to the right level of care for them in the appropriate setting. In addition to improved patient experience all of those consulted with noted that the Pathfinder should have a positive impact on other parts of the health service by reducing the level of demand for, emergency care (in acute hospitals), primary care teams (i.e. GP appointments) and GPOOH services. There was a high level of agreement that the standards that have been developed for the pathfinder are detailed and reflect the wide range of data that is required to adequately monitor the implementation of the service. It was generally agreed that this data will help to inform decisions regarding the wider rollout of the project. The difference in approaches to data collection and GPOOH services across Wales was also noted as a potential challenge for the wider rollout of the project as it could make it difficult to demonstrate the impacts of the project across all Health Board areas. All of those consulted with, highlighted the importance of ensuring that the service is sufficiently resourced. There are known peak demand times for unscheduled care in and staffing rotas should reflect these peak times. Furthermore, staffing levels and the technology should be able to manage and potential surges in demand, for example at weekends or bank holidays. Page 30
32 SURVEY RESULTS Introduction A key part of the evaluation was to gather qualitative feedback from both the 111 Pathfinder operational staff and service users to understand their experiences of the service. This section provides a brief outline of the key findings from both the service user and staff surveys. The questionnaires used are set out in Appendix B and C and a detailed analysis of each question is set out in C and D. Service user feedback has also been augmented with an analysis of comments and tags on the ABMU Facebook page relating to the 111 Pathfinder. Service User Survey In December 2016 and February ,600 hard copy surveys were posted to a random selection of 111 service users, (with pre-paid return envelopes) 19, 401 completed surveys were returned. The following paragraphs summarise the key findings from this survey Respondent demographics This sections NHS 111 service user demographics. This will include a breakdown of age of service user, gender, as well as ethnic origins, and area of residence. Figure 0:1 Gender Breakdown of Service Users Source: RSM PACEC Service User Survey 2016/17 The above graph highlights that the majority (70.2%) of respondents were female and 29.8% were male. This is consistent with the profile of service users, there was a higher percentage of female respondents. 19 In order to adhere to data protection the surveys were issued by ABMU staff. Page 31
33 Figure 0:2 Service user age breakdown Source: RSM PACEC Service User Survey 2016/17 The most common age group (17.97%) of respondents was The same number of users were aged between 45 and 54, 55 and 64, and 75 and over (15.44%). A further 13.67% are aged between 35 and 44, and 13.42% are aged between 45 and 54. Fewer young people are likely to use the service. Just 5.57% of users were between 18 and 24, 1.52% between 12 and 17, or under 12. In reality, a larger proportion of younger people used the service, with 22.94% of calls being made on behalf of children between 0-4. This suggests there could be potential limitations within the survey. Figure 0:3 Percentage of respondents with a long term illness Source: RSM PACEC Service User Survey 2016/17 Most respondents (59.14%) do not have a long-term illness. This is compared to 38.83% who reported that they have a long-term illness. The remaining 2.03% were unable to answer the question. Page 32
34 Figure 0:4 Area in which the survey respondent lives Source: RSM PACEC Service User Survey 2016/17 The majority (51.13%) of survey respondents live within the Swansea area. The second most common area of residence is Bridgend (24.06%), followed by Neath Port Talbot (21.30%). The remaining 3.75% of respondents reported that they lived in different areas. These areas include: Carmarthenshire (0.75%); Powys (0.5%); Rhondda Cynon Taff (0.75%); Winchester (0.25%); Oldham (0.25%); Cwm Rar (0.25%); RCI (0.25%) and Cwm Taff (0.25%). Page 33
35 Accessing the Service Service users were asked how they heard about the 111 service; how they first accessed the support, as well as overall attempts to access support, and length of time spent on the call. Figure 0:5 How respondents first heard about the 111 Service Source: RSM PACEC Service User Survey 2016/17 Almost a third (32.32%) heard about 111 through their healthcare provider. A further 19.59% heard about the service through friends and family. Just over 12% (12.72%) heard about 111 through their health service telephone messages (redirected from NHS Direct, GP voic etc.); 9.67% of respondents heard about the service through the media (TV, newspaper, radio etc.); 8.91% of respondents heard about the service through the internet; and 5.85% of respondents heard about the service through disseminated leaflets. Less than 1% of respondents heard about the service through either social services, family working within healthcare, through the hospital, or out of hours. In total 9.16% of respondents were unaware of how they first heard about the service. Page 34
36 Figure 0:6 How the respondents accessed the 111 service Source: RSM PACEC Service User Survey 2016/17 Most 111 callers (55.84%) knew about the service and called 111 directly. Over a third (34.03%) were redirected to 111 from another service. A further 3.64% of respondents were redirected by their GP, or doctors and nurses at medical centres (minor injury, out of hours, pharmacy); 1.82% accessed the service after finding the number online; 0.26% accessed the service through someone else, or were told by a friend. The remaining respondents (4.16%) do not recall how they accessed the service. Page 35
37 Figure 0:7 How many times respondent called 111 before reaching a call handler Source: RSM PACEC Service User Survey 2016/17 The majority of respondents (92.46%) only had to call the service once. A further 4.11% got through to the service on their second call. The remaining 3.41% phoned the service three or more times. Page 36
38 Figure 0:8 Length of time before respondents heard back from service provider Source: RSM PACEC Service User Survey 2016/17 Most service users heard back within the first hour (79.69%); with 43.36% of the overall sample heard back within the 20 minutes. Under six percent (5.47%) of respondents heard back within the first and second hour. Just over five percent (5.86%) heard back between the second hour and the forth hour, whereas just 0.78% received a call back after the fourth hour. The remaining respondents (8.20%) were unable to recall the length of time between the initial call and call back. Page 37
39 Figure 0:9 Number of people spoken to while on 111 line Source: RSM PACEC Service User Survey 2016/17 The majority of respondents spoke with two people (62.78%). The second largest proportion of respondents (27.84%) reported speaking to just one person. The remaining 9.38% of respondents spoke to three or more people, or could not recall Satisfaction with Service This section outlines respondent satisfaction with the 111 pathfinder. This includes satisfaction with how they were treated, as well as whether they would recommend the service to their friends and relatives, and their general health five days after using the service. Page 38
40 Figure 0:10 Overall Helpfulness of Advice Given Source: RSM PACEC Service User Survey 2016/17 The majority of respondents (72.53%) found that the service was very helpful. A further 21.60% found that the support was quite helpful. Only 5.86% of respondents found the service the unhelpful, 2.93% stating it was not very helpful, and 2.93% stating it was not helpful at all. Page 39

41 Qualitative comments relating to how helpful the service was include: Very useful. I can never get any response with my out of hours GP at my surgery. 111 was effective, helpful, will use again. - Made an appointment at A&E and my daughter was seen straight away very happy that the 111 service helped me avoid long wait at A&E connecting me to the appropriate service Figure 0:11 Percentage of respondents reporting that 111 made it easier to access urgent care Source: RSM PACEC Service User Survey 2016/17 Most respondents (97.63%) stated that they found it easy to access urgent care through the 111 service. Just 2.37% reported that the service did not make it easier to access to urgent care. The people are always knowledgeable and helpful. It is reassuring to have a service where you can obtain advice when you are unable to contact a doctor or do not want to sit in A&E for hours on end Figure 0:12 Percentage of respondents reporting improved access to urgent care because of the 111 service Source: RSM PACEC Service User Survey 2016/17 The majority of respondents (74.80%) report that the service has increased access to urgent care. Just 7.43% report that it does not. The remaining 17.77% of respondents were unsure. Brilliant, so easy to access, good advice given, simple instructions, caring people Page 40
42 Figure 0:13 Percentage of Respondents who believe they were treated kindly and with respect Source: RSM PACEC Service User Survey 2016/17 Over ninety-eight percent (98.70%) of respondents reported that they believe they were treated politely and with respect. Just 1.30% believed that they were not. Dealt with my problem efficiently and professionally Lovely call handler, and I was given an appointment to avoid hanging around waiting Figure 0:14 Percentage of Respondents who believe they were treated with kindness and compassion Source: RSM PACEC Service User Survey 2016/17 The majority of respondents (96.11%) believed they were treated kindly and with compassion. Two percent felt they were not treated with the appropriate kindness or compassion. The remaining 1.55% were not sure. Reasons for this include: Ultimately because my problem was not addressed, despite speaking to two nurses In similar situation with another child, NHS direct sent ambulance. 111 told me to drive to A&E myself with a child with shortness of breath. (5 weeks old baby) Due to the number of inappropriate questions it was difficult to feel this. Page 41
43 Figure 0:15 Overall Satisfaction with 111 Service Source: RSM PACEC Service User Survey 2016/17 In total, 76.96% responded were very satisfied with the 111 service. An additional 14.14% stated they were satisfied. Four percent of respondents reported they were neither satisfied nor dissatisfied, whereas the remaining 4.72% reported that they were dissatisfied, or very dissatisfied. Positive comments included: Helpful for my problem, arranging a prescription without having to see a doctor I feel like it is a valuable asset to the NHS Page 42
44 The majority of all comments on the 111 service were positive, however the very small number of negative comments include: I see this as another tier, a) call 111, b) put through to out of hours, c) seen by a GP, d) transferred to A&E, e) spend 7 hours there. Person on phone was polite and competent but I would not use the service again. No help at the time and I was crying with pain and couldn't eat or sleep. The process prolonged my agony. Figure 0:16 Percentage of Respondents who would recommend the service to someone else Source: RSM PACEC Service User Survey 2016/17 The response to this question was largely positive with 92.19% or respondents reporting that they would recommend the service to someone else. Just 3.39% of the respondents would not recommend the service. The remaining 4.43% were unsure. Figure 0:17 Percentage of Respondents who would use the service again if faced with a similar issue Source: RSM PACEC Service User Survey 2016/17 Ninety-one percent of respondents stated that they would use the service again if faced with a similar health problem. A further 4.70% stated that they would not. The remaining 3.92% were not sure as to whether they would use the service again. Reasons respondents would not use the service again include: That the GPOOH service was sufficient in dealing with issues; That they would not use the service as they did not believe that adequate care is available through the service; and That the correct prescription was not provided and this caused the respondent s health to deteriorate. Page 43
45 The respondents that were not sure as to whether they would use the service again stated: That they were alone, in pain, and the length of time between calls caused concern; That they would use the service only if they had to; and That they considered the service just as another tier in the many tiers of NHS support. The respondents that stated they would use the service again gave a variety of reasons: That it provides 24-hour support which is crucial to some people; That it is easy to access, that good advice is given, and that the people are caring and responsive; and It is nice to have a central access point to avoid confusion over who to call. Overall feedback suggests that the 111 service is working effectively within the pilot area. Page 44
46 Feedback provided via Social Media The ABMU Health Board s presence on Facebook is very active, with the administrator often posting several times per day. With over 15,000 people following the Board s Facebook page, it is a very large platform to disseminate information about the new 111 service. Since October 2016, five of these posts have been in relation to the launch of the new 111 service, with other Facebook users posting a variety of comments under each update. The feedback given by these users provides an informal context to gauge the public s response to the new service. Data collected from the Facebook page reveals that some of the posts relating to the 111 service reached upwards of 71,000 Facebook users. The number of these users commenting on the posts can vary anywhere between 5 and 39. Response rates on these comments is excellent, with the page s administrator generally responding within 1 to 3 working hours to address any comments made by users. 79 comments were posted by other Facebook users on the posts relating to the 111 service. This is thematically analysed below: Table 0:1 Feedback on the 111 Pathfinder Facebook posts Positive Feedback Negative Feedback Tagging Friends Queries Poor Advertising Total Post 1 15% 5% 40% 30% 10% 100% Post 2 28% 26% 31% 5% 10% 100% Post 3 20% 80% 0% 0% 0% 100% Post 4 30% 30% 30% 10% 0% 100% Post 5 100% 0% 0% 0% 0% 100% Aggregate 29% 23% 29% 11% 8% 100% Source: Facebook.com As summarised above, 29% of all comments (23/79) were users tagging other users in these posts. This high percentage of the total number of comments indicates that people were keen to share this information with their Facebook friends, possibly inferring that they were excited about the arrival of the new service and wanted to let others know about it. Dennhardt et al. (2013) 20 find that engagement with a Facebook page has positive effects on consumers' brand awareness as well as word of mouth activities, demonstrating that these tags help increase public awareness of the 111 service. Prior to these comments, there were users who believed that the service had been poorly advertised. Examples of these comments include: They haven't advertised this very well, I for one had no idea! Not even staff in NPT Minor Injuries Department knew. They were still giving out Prime Care telephone number out to patients. Don t you think ABMU Management staff in Unscheduled Care should have been informed of change in service to relay to nursing staff? It made them look uninformed. These negative comments reflect the Health Board s chosen approach for a soft launch of the service, i.e. one with very little marketing. This is the reason why table 6.18 separates these comments from other negative feedback. While 10% of comments on the initial two posts were in relation to the service s poor advertising, the following three posts had no comments relating to this issue. Therefore, the public s awareness of the service appears to have improved over this six month period Page 45
47 Overall, positive comments exceeded the number of negative comments. It is in the nature of social media that people are likely to use it as a medium to express their dissatisfaction, which possibly explains why the proportion of negative responses on Facebook exceeds the amount of negative feedback received from RSM s survey (which was less than 1%). As Clarke (2013) 21 notes, social media is largely used by Millennials for venting their anger against organisations. Within the positive and negative feedback, several key themes were identified. The following table breaks down these themes and includes examples for each one. Table 0:2 Positive and Negative comments received via Facebook Positive Excellent call handlers Efficient service Have used the service the past two weekends. Found the service excellent each time. Very friendly staff who didn't sound like robots even though they had set questions to ask on both calls. Very efficient in determining my child needed to be seen by GP for further assessment. Fast follow up call from out of hours and seen within a few hours of call. Very grateful to have a service available when my doctors is closed. Used them about two weeks ago on a Sunday for my wife, details taken, doctor phoned back, faxed a prescription to the local chemist, all sorted in less than two hours, very impressed. Negative Poor service Poor advice Problems with coverage Sceptical comments I used the service last night and was patronised until I hung up Your 111 service gave a prescription over the phone today which would have seriously endangered my son!!!! Luckily Boots in Neath noticed. I'm disgusted with the service I received today. Medical negligence! And I live in Port Talbot with the dangerous pilot scheme! My little girl had croup the other night, we live in Bridgend, phoned 111 like I was told by doctor s number and I was told to phone NHS direct as the service wasn't running in my area. Lucky, it wasn't more urgent! Just a re-launch of NHS Direct. Waste of money. Help!!! It doesn't seem to have worked very well elsewhere! Another category to address is the number of queries people had in relation to each post (which made up 11% of all comments). Social media, and especially Facebook, provides another format for the Health Board to informally respond to any questions people have. The questions people asked broadly fell under three categories: Job opportunities provided by the service; How deaf people may access the service; and Areas covered by the service Page 46
48 While addressing these questions is beneficial to users, it also offers insights into ways the service may improve. The most notable of these was in relation to access for deaf people. While deaf people may access 111 using TypeTalk, the problem was raised that this feature is not widely used. Instead, users expressed that they believed an SMS version would make a massive difference to the deaf community. The high level of user interaction with the Board s Facebook page demonstrates that people are keen to engage with the service over social media, as it provides a quick and easy means of interaction and access to information Service User Summary The majority of respondents (70.21%) were female, and do not suffer from long-term health conditions (59.14%); The majority of respondents were from the Swansea area (51.13%); The most common way people heard about the 111 service was through their healthcare provider (GP, dentist, etc.), and most respondents phoned the service directly (55.84%); Most callers phoned the service once (92.47%) and received a call back within the first hour (79.69%); Most people spoke to two members of staff (62.78%) and found the advice helpful (94.13%); Most people would recommend the service (92.19%) and would call the number back again (91.38%); and Positive feedback on social media increased over time and the number of complaints referring to poor advertisement fell from 10% in the first post to zero in the fifth. Page 47
49 Staff Survey Results All operational staff from the 111 Pathfinder were ed a link to an online survey with a covering explaining the purpose of the survey and assuring confidentiality. In total 85 surveys were completed from the 270 members of staff, represents response rate of 31%. The following paragraphs provide a brief outline of the staff feedback Respondent Demographics The following section provides an overview of where respondents gender, age and job role. Figure 0:18 Staff Gender Source: RSM PACEC Staff Survey 2016/17 The majority (82.72%) of staff respondents who provided their gender were female. A further 17.28% were male. Actual split in the workforce is 92% female staff to 8% male. Figure 0:19 Location of Workplace Source: RSM PACEC Staff Survey 2016/17 Most respondents (73.49%) work in Thanet House in Swansea. A further 14.46% work in Vantage Point House, Cwmbran, and the remaining respondents that provided an answer work within Snowdon House in Bangor. Figure 0:20 Number of Staff Recruited to 111 Team Source: RSM PACEC Staff Survey 2016/17 Most staff (85.54%) previously worked within the wider NHSDW service before joining the 111 team. Less than one fifth (14.46%) of staff were recruited to be part of the 111 team. Prior to their involvement as part of the 111 team job roles include: clerical worker, dental practice manager, NHSDW call handler, nurse in primary care, nurse in an acute hospital, registered dental nurse, and pharmacy dispenser. Page 48
50 Figure 0:21 Current Job Role Source: RSM PACEC Staff Survey 2016/17 Over half of respondents were either call takers (32.84%), or nurse advisors (31.34%). The other roles among respondents include: Managers, (site, clinical and team); Dental Nurse Advisor; Health Information Advisor and Practice Coach. Page 49

51 Training and 111 Implementation The following paragraphs summarise staff views on the training received and the manner in which the 111 pilot was implemented. Figure 0:22 Introductory Training Source: RSM PACEC Staff Survey 2016/17 The majority (74.07%) of respondents believed that the training they received was appropriate and equipped them for their job role. A quarter of respondents (25.93%) believed that it did not. Reasons given for this include: Not enough training / practice sessions between training & Go Live date; No training team support on the floor when we did Go Live - very poor/inadequate launch to service; Ad hoc training was not as in-depth as normal training; Training was too short and should be longer to cover all aspects safely; Not enough training was provided prior to going live- learnt a lot from listening into call and from being in the position; Initial questions were met with We don t know but this has improved; In the beginning things were changing daily and were very confusing; Training was provided prior to the system being uploaded so staff were not able to access the training database. Staff had to train themselves on the job meaning for long assessments due to the unfamiliarity with the tools; Too long a period between training and the go live date; and It would be beneficial if further training could be given with regards clinical practice and referring patients to other services. Respondents felt that initial training was insufficient or not detailed enough, and that there was a lot of uncertainty among trainers initially, and that the system would often change during the initial training causing confusion. The feedback however does also suggest that once systems were in place training improved. Figure 0:23 Additional Training Needs Source: RSM PACEC Staff Survey 2016/17 Just over a quarter (27.16%) believed that they would benefit from additional training. Suggested areas of training include: Additional training using the Adastra System as staff often have to answer to GP/ nurses who request information from Adastra that staff cannot access/ do not know how to access; Regular practice coaching and updating on changes; Additional training on end of life and special notes; Page 50
52 Negligible training for the clinical desk; Additional training for specific illnesses to enable more efficient and effective call handling; More training on the clinical hub; and Constant training on the updated systems. A key theme that developed from respondents is that constant training or on the job coaching ought to be given. This is reflective of the comments provided regarding training. Figure 0:24 Line Manager Support Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (75.31%) believed that they did receive enough support from their line manager. Reasons for this include that the line manager was involved at a high level in all implementation work; and that regular daily briefings were held. Of the 24.69% that responded no, reasons for this include: As they were not operational staff they were unable to help once the system went live; The line manager only provided limited information, but this was due to limited information being provided to them; As the line manager was not accessing the system, the majority of assistance was gathered from nurses who had experience using it; and There were no face-to-face conversations, only s. Page 51
53 Satisfaction with Service Figure 0:25 Quality of the Telephony System Source: RSM PACEC Staff Survey 2016/17 Most respondents stated that the system is good or very good (61.73%). A quarter rated it as fair. Only 8.64% believed the system was poor or very poor. Figure 0:26 Greeting Process Source: RSM PACEC Staff Survey 2016/17 Over half or respondents (59.26%) believe that the greeting process is working well. Just 2.47% stated that it did not. The remaining 38.27% did not know, or did not provide an answer. Page 52
54 Figure 0:27 CAS/ Call Screening Prioritisation Tool (CSPT) Source: RSM PACEC Staff Survey 2016/17 Just 13.75% of participants believed that the clinical decision making tool was adequate. Over two thirds (71.25%) believed that it was not. The remaining 15% did not know. Reasons why staff consider the system to be inadequate include: Not enough protocol actions for individual situations; The system is not user friendly; Have to go roundabout ways to reach outcome e.g. call handlers do not have details of the nurse CSPT has and has to go down the head injury route for facial injuries; The system is unstable; The system is repetitive; Too long and complex which impacts on operational performance; Children CSPT is long winded and includes inappropriate questions; Symptom categories too restrictive; Computer system should be more holistic; CAS should not have been implemented at the same time as 111 too much to take on board; Questions can be too long or inappropriate; Advice derived from the system often not what the patient needs; The system does not account for co-morbid illnesses; and CSPT is too clinical a system for non-clinical staff to operate. The key finding from this question is that the system is too rigid when diagnosing illnesses and offering advice. It is also difficult to operate for staff and too slow to deal with the high demand and pressure situation patients are in. Figure 0:28 System Hardware Source: RSM PACEC Staff Survey 2016/17 Whilst the majority of respondents (65.43%) believed that the system hardware was user friendly, over a quarter (27.16%) believed it was not. The remaining 7.41% did not know. Possible improvements to the service as indicated by respondents include: Improve navigation- currently have to go in and out of pages to view different aspects of information; It is difficult to identify GPs- add in a recent search or search by area function to improve this; Improve formatting (print size etc.); Reduce the number of CAS questions; Page 53
.")
55 The cancel button on the system is too close to the save button; Bring back the tabbing function from the old system; Too many errors with regard to dispositions; Interim care advice too hard to identify- should be highlighted; and Include a basic rationale in instances where the caller has to exit early, e.g. exit here for remote TP adults/ or proceed for remote TP children (to log their details in CAS). Figure 0:29 Signposting Service Source: RSM PACEC Staff Survey 2016/17 Despite a lack of confidence in the clinical decision making tools, most respondents (72.50%) believe that calls are signposted to the appropriate services often (62.50%) or always (10%). Over one fifth (23.75%) believe that patients are signposted to the correct service some of the time, and just 3.75% believe that patients are rarely, or never signposted to the correct service. Page 54
 were neither satisfied nor dissatisfied. Just over a quarter of respondents were dissatisfied (28.75%). Reasons for this include: Shifts not being the same as those requested; Rostering")
56 Figure 0:30 Satisfaction with Rosters Source: RSM PACEC Staff Survey 2016/17 Just over half of respondents (52.50%) were satisfied with the rosters. Just under one fifth (18.75%) were neither satisfied nor dissatisfied. Just over a quarter of respondents were dissatisfied (28.75%). Reasons for this include: Shifts not being the same as those requested; Rostering impacting upon work-life balance; Having to work multiple weekends in a row, or multiple unsociable hours (50% of working hours at night); Given the upheaval of the current system there is a lot of uncertainty, and people are worried with regard to work-life balance; Call numbers are low around 9am (peak MIU time) and between 3pm and 4pm, meaning nurses are often required to take calls; and Inequality among the workforce- some staff get better time off than others (i.e. around bank holidays). Page 55
57 Figure0:31 Satisfaction with Workload Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (66.67%) are satisfied with their workload. Just under a fifth (19.75%) are neither satisfied nor dissatisfied % of respondents reported being dissatisfied. Reasons provided include: It is difficult to meet demands of the role in addition to those of 111; There are not enough staff members available, especially during out of hours shift. It is incredibly stressful and staff often have to go from wrap up calls to live calls; As registered nurses the fact that some shifts are spent call handling can be frustrating, and is not a good use of skill; and Too much demand to take calls, meaning previous calls cannot be researched and resolved- not good for the patient. Figure 0:32 Level of Contentment Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (65.82%) report feeling the same as before. 7.59% report feeling more content. The remaining respondents (26.58%) that did respond report feeling less content than before. Reasons given for the decreased level of contentment include: The constant changes caused anxiety and stress for many staff members; Having to use both the Adastra system and the CAS is time consuming and repetitive- doctors should use one system; There are not enough staff to deal with the increased workload; Nurses appear to require more training in the system and there are more Datix errors during the weekend period; A GP should be present at consultation during 111 hours to improve communication; Less support is available for operational staff now despite higher pressures and demand; and Nurses are de-valued and often during OOH time periods triage nurses are underutilized and calls sent straight to the GP. Page 56
 were neither satisfied nor dissatisfied. Only 11.11% reported being dissatisfied. Figure 0:34 Proud to work for WAST Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (74.")
58 Figure 0:33 Satisfaction with Current Role Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (62.96%) reported being satisfied or very satisfied in their current role. A quarter (25.93%) were neither satisfied nor dissatisfied. Only 11.11% reported being dissatisfied. Figure 0:34 Proud to work for WAST Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (74.07%) are proud to work for WAST. Just under a fifth (23.46%) neither agree nor disagree with the statement. Only 2.47% are not proud to work for WAST. Page 57
59 Figure 0:35 Colleagues are Helpful and Supportive Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (90%) agree that their colleagues are helpful and supportive. Seven percent (7.5%) neither agree nor disagree and only 2.5% believe their colleagues are unhelpful and unsupportive. Almost half of respondents (52.50%) feel well informed about the changes that affect them within the service. Over a fifth (21.25%) of respondents neither agree nor disagree. Over a quarter (26.25%) of all respondents disagree however and feel they have not received enough information. Page 58

60 Figure0:36 Clear of Expectations Source: RSM PACEC Staff Survey 2016/17 Almost four fifths (79.48%) of respondents are clear of what is expected of them % are neither clear nor unclear and just 7.69% of respondents are unclear of what is expected of them. Figure 0:37 Opportunity to Develop Skills Source: RSM PACEC Staff Survey 2016/17 Page 59
 neither agree nor disagree and over a third (35%) disagree, stating they do not get the opportunity to develop their skills within the service.")
61 Just over a third of respondents (38.75%) agree that they have an opportunity to develop their skills. Over a quarter (26.25%) neither agree nor disagree and over a third (35%) disagree, stating they do not get the opportunity to develop their skills within the service. Staff were also asked to what extent do they agree that morale is high, responses are summarised in the following chart. Figure 0:38 Morale is high Source: RSM PACEC Staff Survey 2016/17 Only 15.39% of staff members report having a high morale. Just over a third (34.62%) neither agree nor disagree that morale is high. However, half of respondents (50%) disagreed or strongly disagrred with this stafement. Almost one quarter of responses (23.53%) to this question were from Call Takers or Nurse Advisors who disagreed or strongly disagreed with the statement. Whilst no Nurse Adviors agreed or, strongly agreed that morale is high, 5.9% of all responses were from Call Takers, who agreed or strongly agreed. The following chart sets out the proportion of respondents within each role who disagreed that staff morale is high. Page 60

62 Figure 6.39: Proportion of staff in each role disagreeing that morale was high Therefore, as set out above there was a reasonable spread of respondents disagreeing that staff morale was high across all roles. On average 54% of respondents in each role, disagreed that morale was high. Staff were also asked if their role within the 111 team was less stressful than their previous role, as summarised in the following chart. Page 61
 report no difference. The remaining 35.80% percent believed that their role is now more stressful. Staff were also asked their views on the service they were delivering, as summarised below.")
63 Figure 0:40 Less Stress than previous role Source: RSM PACEC Staff Survey 2016/17 Just over a fifth (22.22%) of respondents feel less stress than in their previous role. Over forty percent (41.98%) report no difference. The remaining 35.80% percent believed that their role is now more stressful. Staff were also asked their views on the service they were delivering, as summarised below. Page 62
 feel that their job makes a difference to service users. Only 8.75% neither agree nor disagree. Just 7.")
64 Figure 0:41 Role makes a difference to patients/ service users Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (83.75%) feel that their job makes a difference to service users. Only 8.75% neither agree nor disagree. Just 7.50% believe that job makes little difference to patients or service users. Page 63
 believe that the telephony service provides a good service to patients.")
65 Figure 0:42 Do you think that 111 telephony service provides a good service to patients? Source: RSM PACEC Staff Survey 2016/17 Most respondents (55.56%) believe that the telephony service provides a good service to patients. Reasons given include: It provides easier access to OOH services; It is more streamlined and appropriate for users needs; It is free; Callback is within targets and usually includes a GP; Call handlers are experienced and well-trained; and It provides a one stop shop for assessments. The remaining 44.44% of respondents believe the service does not provide good support to patients (17.28%), or else they are unsure (27.16%). Reasons given for this include: Not having enough staff; CSPT being too long for the system to cope with; There are too many assessments/ calls before the patient can get a face to face appointment. Nurses should have the authority to book appointments; Patients are transferred to OOH where nurses can provide accurate self-care information; There is a lack of consistency between patients (e.g. dependent on postcode they are directly transferred to OOH); and Staff are not provided with access to patient pathway. Page 64
66 Figure 0:43 Do you think that the introduction of the 111 number has improved access to urgent care for patients in the ABMU area? Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (67.90%) believe 111 has improved access to urgent care within the ABMU. Just 4.94% believe it does not improve access to emergency care. Over a quarter of respondents (27.16%) are unsure whether 111 improves access to emergency care. Reasons provided by those who believe it improves access include: It provides more appropriate access; It is a more streamlined service; Use of one number makes it easier; Protocol allows for 20-minute callback in urgent cases; Calls are answered promptly; and Calls are free. Those who stated that 111 has not improved access provide reasons such as: Patients often end up having to speak to more people (call handler, nurse, GP); System is often abused by patients who want to use the service to access OOH in non-urgent cases; and Some patients have complained about having to wait. Figure 0:44 Does NHSDW/111 help service users to access health care and advice in the place that is most appropriate for them? Source: RSM PACEC Staff Survey 2016/17 The majority of respondents (74.07%) believe that the 111 service has helped service-users access appropriate health care. The remaining 25.92% who provided a response were either unsure (17.28%), or did not believe the service helped access the most appropriate response (8.64%). Reasons why staff believe the service has improved access include: All the information provided in the directory of service can signpost public to services; It is an effective signposting tool; It is more streamlined; The nurse and health team are well-informed and call handlers work their hardest to help; Page 65
67 Service is good for offering general advice; Use of an effective software system by call handling staff and assessment by experienced nurse clinicians; Staff who are unsure, or do not think the service provides better access claim that this is due to: Patients not having a full idea of what the service should be used for; The service provides an easier and cheaper access route, but it is uncertain whether patients follow guidelines, or just go to the ED; Nurses are without the ability to signpost or act in serious cases of illness; and In most cases calls are redirected directly to OOHs, which makes the service somewhat ineffective. Figure 0:45 Do you think that the overall quality of service for patients has improved since the introduction of the 111 pathfinder into ABMU? Source: RSM PACEC Staff Survey 2016/17 Over half of respondents (51.25%) were unsure when asked if they believed the quality of service for patients has improved since the introduction of the 111 pathfinder. Over two fifths (41.25%) believed the overall quality of service for patients had improved with the introduction of 111. Only 7.50% percent reported that the quality of service had not improved. Reasons provided as to why people were unsure of whether the service had improved quality of service include: Patients still have to wait a long time and numerous patients phone back chasing calls; Patients report conflicting information; Although the service is streamlined at times demand can be high and feedback slow; Quality does not seem to be as important as the quantity of calls answered. Page 66
 reported that 111 has helped create a centralised service (i.e. allowed for the collaboration across health care areas, as well as providing a single point of contact for patients).")
68 Figure 0:46 Key Outcomes from the 111 Pathfinder as Identified by Staff Source: RSM PACEC Staff Survey 2016/17 The above graph provides an aggregate overview of key outcomes reported by staff. Over a third (44.88%) reported that 111 has helped create a centralised service (i.e. allowed for the collaboration across health care areas, as well as providing a single point of contact for patients). In total 22.05% of respondents stated that the service has created better access routes for patients; 3.15% of respondents also suggest that 111 has allowed for standardised care- where patient information can be easily transferred from one health professional to another. A further 15.75% of staff believe that it is important that the service is free; 12.6% percent also report the benefits of staffing within 111. This has led to the introduction of more experienced and diverse teams. It is also reported however that staff are under more pressure due to 111. The remaining.079% of respondents list reduced patient time, and relief to other services as outcomes of the 111 service. Page 67
69 Figure 0:47 Things that could Improve 111 Source: RSM PACEC Staff Survey 2016/17 A fifth (20.39%) of all respondents claimed that further work could be done to standardise the call process. An improved methodogy to standardise the process may reduce the administrative tasks and witing times. Just under a fifth (18.47%) report the demand within the service for more staff. A further 1.91% highlight the need for experienced staff, and an additional 8.28% highlight the need for better staff support. Nearly eleven percent (10.19%) of staff highlight the need for improved communication both internally and across health teams. Just over a tenth of respondents (10.83%) highlight the need to develop a better IT system. A further 8.28% highlight that CSPT is too lengthy and issues relating to it ought to be resolved; 4.46% suggest that nurses should be given more autonomy in decision making with regard to patient health and 4.46% suggest that more should be done to improve public knowledge of 111 and the support it provides. When asked what potential changes they would make to the 111-triage service staff provided a range of answers such as: Greater communication with senior operational staff; Gradual introduction of services into the workspace; More staff; Better algorithms to aid decision making; Improved IT systems (e.g. Cisco system similar to 999 make CSPT more robust and Electronic records which link with the other parts of the health service to ensure continuity/reduce repetition/simplify the healthcare process for the public.); Streamline service to improve service functionality for staff and service users; Increase training opportunities in the workforce; Allow nurses to access Adastra system; Have coaches on the floor when new workers start and ensure the ratio of call handlers to supervisors is safe; Ensure only appropriate calls are directed to OOH; Allow nurses to schedule appointments; Page 68
70 Improve questions relating to children- currently too long winded; Reduce the amount of scripted dialogue and allow for a rapport between handler and patient; Open hub even when the GP is unavailable; Return focus to giving advice during calls, instead of catching every call; Improve staff morale- which is at an all-time low; and Allow staff to see how busy the service is as well as appointment availability. When asked if they had any additional comments staff stated: Better communication to develop the role of the nurse to expand the service; Emergency provisions should be available during stressful periods such as the weekend; Steps need to be taking to improve training opportunities and boost morale- this was previously good; and Staff work-life balance needs to be taken into account Staff Survey Summary The following subsection summarises the key points from the staff survey: The majority of respondents were female (82.72%) and worked in the Swansea area (73.49%) and were already an existing member of staff prior to 111 (85.54%); Nearly a third of respondents were call handlers (32.84%), or a nurse advisor (31.34%); Whilst the majority of respondents (74%) reported that they were satisfied with the introductory training, around one quarter (26%) of respondents believe the introductory training was not satisfactory. Reasons for this included: there was too long between training and the go live date; staff were unable to access the system during training; and initially management staff were not skilled to answer queries; Just over one quarter of respondents (27%) report that they would like additional training. The type of training requested included; updates to changes within the system; additional training with the Adastra system; illness specific training; and additional training surrounding the clinical hub; Staff also indicated that they would benefit from additional face-to-face line manager support, and that they there was an issue with receiving information from upper levels of staff; The majority of staff (71.25%) stated that the CSPT system was inadequate. Reasons for this include: the system is not user friendly and is repetitive impacting upon operational performance, protocol is too general and sometimes inappropriate, the process for dealing with children is too long, and the final outcome is often not relevant to the patient; Over a quarter of staff (28.75%) were dissatisfied with rostering. Reasons included: shifts were not those requested, staff often have to work multiple weekends in a row, it impacts work-life balance, nurses are often made to answer calls during peak times, and there are instances were some staff get better shifts than others; Feedback relating to staff morale was mixed for example whilst only 15.4% of respondents agreed that morale was high, 62.96% of respondents also reported that they were satisfied or, quite satisfied with their current role within 111. Staff have expressed concerns over the number of staff, that the CSPT system is too long-winding, and the service could potentially be abused by patients who want to use it to access OOH in non-urgent cases; and Some staff expressed concern that the service may not increase quality of care, stating that they are unaware if patients follow advice, and that nurse staff do not have the appropriate authority to signpost staff onwards. Page 69
71 ACTIVITY LEVEL ANALYSIS Introduction The following section provides a detailed analysis of the call levels received by the 111 Pathfinder from November 2016 to the end of April 2017, i.e. the first full six months of operation. During the OOH period calls are managed according to patient complexity: Calls that are assessed as requiring a 20-minute response, are streamed directly by call takers into the GPOOH service for assessment (priority one) this was designed as part of the model to ensure that the sickest patients were assessed by the most experienced clinician Calls that are assessed as more routine will be assessed by nursing staff within the 111 service, and only if they need to receive either a further telephony clinical assessment or a face to face appointment, will be passed onto the GPOOH service (priority two and three) Calls that are more complex in nature (for example, calls from paramedics, or from care homes) will be managed by the clinical support hub during operational hours (and outside of these hours by the GPOOH service). During the launch period (which coincided with winter), the 111 Programme, WAST and ABMU were keen to ensure that the service had an opportunity to bed down properly. A key focus was on ensuring that the wider unscheduled care system was not destabilised during implementation. An escalation plan was agreed between all parties prior to launch, which set out the circumstances that calls would be escalated through to the GPOOH period. Workforce and other challenges meant that during the first six months of the service, there were a considerable number of occasions when all calls that required clinical assessment during the OOH period were therefore handled by the GPOOH service. The extended period of escalation impacted on the outcomes from service delivery until the early part of April 2017, when the normal call flow (as depicted above) was managed routinely. Although the workforce calculations had assumed that demand would increase because of the introduction of a free-to-call service, demand over the initial period exceeded expectations by an estimate of 5%. There were also some challenges in rostering sufficient staff to meet the peak demand periods. This resulted in further recruitment to provide more flexibility. The 111 service in Wales uses a combination of both CAS (this is a clinical system in use within WAST to support both NHSDW and 111 activity) and Adastra (which is a system used by the GPOOH services to manage workflow) data. There is a technical bridge (called a concentrator ) between CAS & Adastra which ensures that data flows across to the GPOOH service electronically. The concentrator is technically operational 24/7 but it is set up to only transmit information during GPOOH opening times. This has caused several technical issues. For example, during the OOH period some calls will transfer across as a no action call (for example, dental calls). Furthermore, unlike Adastra, the CAS system is able to identify duplicate calls (i.e. when a caller who has phoned initially follows up their call with another after a short period), and groups them to create one record. This is an issue as once this data passes the concentrator onto the Adastra system the record will split leading the system to log two separate calls. This means that on the Adastra system call volume may be slightly inflated with multiple callers. It is important to note at this stage that the current system is not ideal for monitoring 111 calls. Although staff have merged the two systems to an extent there are still several issues which would be expected at this pilot stage. The process through which this data is logged is illustrated on the following page: Page 70
.")
72 Figure 0:1 111 Call Flow Diagram Source: ABMU Health Board (2017) The following section provides a summary of the volume of calls to 111 as captured through the CAS and Adastra systems and collated by WAST. The data was used to determine call profile (abandoned, answered, in-hour, out-of-hour). The data provided by WAST ranges from the start of November 2016 to the end of April 2017, covering the first full six months of 111 operation in ABMU. This activity level data was also used to determine the 111 pilot s performance against the interim standards and quality measures 22. Key metrics are outlined below, and a summary of additional standards and performance is detailed in Appendix H. 22 Defined in the Interim Standards and Quality Measures for the 111 Pathfinder in Wales Page 71

73 Figure 0:2 Standard and Quality Measures Source: ABMU Health Board (2017) It is important to note that the approach to introducing the 111 service was by way of a soft launch. This means that marketing was limited to leaflets, posters, press releases and use of social media to avoid confusing patients who did not live in the ABMU Health Board area. ABMU residents still have access to the service via the number but there has been a gradual shift away from 0845 to use of the 111 number. However, this is still not complete and further marketing is now ongoing. The average monthly call volume of residents from ABMU using the 0845 service has dropped from 5,000 per month (September 16) to around 2,000 (April 2017). These calls to 0845 are excluded from the analysis. Also excluded are calls from Health Care Professionals working in community settings (e.g. paramedics, district nurses etc.) as ABMU decided that these calls should be routed directly into the Clinical Support Hub through the GPOOH service in order to provide a timely and appropriate response. These cases are therefore only captured on the Adastra system unless the health care professional has mistakenly called 111 and not used the alternative number. Separate analysis of call volumes from health care professionals and the impact of the introduction of the service is shown in section 8. Page 72
74 Activity Level Data Yearly Call Projection The table below presents the projected call volume of the 111 service, alongside current actual calls, and previous call volume for the original 0845 and GPOOH numbers. Figure 0:3 Projected call volume Original volume (2014) call Actual call volume 111 /0845 (November to April 6 months) Projected Call Volume Annual *calls answered *calls presented to queue GPOOH Service (including 20% uplift) 115,868 71, , call volume 52,529 (on average, circa 2,500 contacts per month from ABMU patients to 0845 since 111 launched) 30,000 (estimate full year impact) Total 168, ,706 Source: WAST The above table suggests that call volume was 3% higher than planned. Having said this, the original figure is based on calls answered, whereas the projected annual call volume is based on actual demand (total calls answered and abandoned) so a direct comparison is misleading. An additional point that should be considered is that the projected annual call volume will be disproportional, as it contains both data from the Christmas and Easter seasons. Page 73
75 Call Volume As indicated, 71,853 calls were made to 111 in the November to April period. The figure below provides an overview of call volume per day throughout the six-month period, firstly together, and split for weekday and weekend. Figure 0:4 Telephony Call Volume Source: WAST (2017) The busiest day over the six months of data was 27 th December, where a total of 1,154 calls were logged. The least busy days were 3 rd and 4 th of November where 164 calls were logged on each day. Consistently across the six month period the weekend period was busier than the weekdays. On average 404 calls were logged per day on weekends. Average call volume during weekdays was 280 per day. Weekend calls ranged from 345 (9 th April) to 904 (24 th December). Average calls per day totalled 712. Page 74
 to 458 (Christmas Day). Average call volume during bank holidays is 802 per day. Total calls during the bank holiday period equates to 4,010.")
76 Figure 0:5Bank Holiday Call Volume Source: WAST (2017) The above graph provides an overview of 111 call volume during the bank holiday period. Call volume ranged from 1,038 (Boxing Day) to 458 (Christmas Day). Average call volume during bank holidays is 802 per day. Total calls during the bank holiday period equates to 4,010. Callers receive a 60 second automated message before being put through to a call handler. Some callers hang up before being put through to the queue for answer, therefore the total number of calls answered is less than the calls offered. Calls where the caller has exited the system after the message and therefore presenting to a queue for answer (hung-up) are classified as abandoned. Those who exit before or during the message are terminated as they have not presented through to a queue for answer. Page 75
77 Answered Calls Figure 0:6Total Answered Calls Source: WAST (2017) The above table illustrates the total calls received by the service (calls offered) alongside calls that are presented to the queue for answer, as well as the total number of answered calls for the 111 service. Of the 71,853 calls made to 111, 67,466 were answered by a call handler. The largest disparity in total calls to answered calls occurred on the 27 th December the day with the highest overall demand. In total, 151 calls (13% of total calls, n=1,154) went unanswered, compared to 1 unanswered call on 2 nd November, (the quietest day of the first six months of operation). On 2 nd November, the call was abandoned at 2am. The standards set out in the Interim Standards and Quality Measures document detail that 95% of calls should be answered within 60 seconds of the end of the pre-recorded message. A third of total calls (47,855) were answered within 60 seconds. During the weekend period 58% (n=21,149) of total calls were answered in under 60 seconds. During the week, this was higher with four fifths (75%, n=26,706) calls answered in under 60 seconds. Further work is required to identify how workforce patterns need to be realigned to ensure that patient experience is not comprised. Mean time to answer since the service launched is 85 seconds. Page 76
78 Calls In and Out of Hours Figure 0:7 Total Calls in and Out of Hours Source: WAST (2017) The above graph compares answered calls to total calls both in-hours and out-of-hours. In total, 11,153 calls were carried out in-hours (15.5% of calls). The remaining 84.5% (56,313) were conducted out-ofhours. This analysis has important implications for the development of service model and workforce requirements going forward as the pattern of use of 111 services presents a significant shift away from the traditional model for NHSDW. Page 77
79 Abandoned Calls Figure 0:8 Abandoned Calls against Total Calls Source: WAST (2017) The table above illustrates total calls against abandoned calls. The graph illustrates that as call volume increased so did the total volume of abandoned calls. The key performance metric in respect of access to the service, and abandonment is that no more than 5% of calls are abandoned (measured 60 seconds after the end of the messaging). In total, just 4.3% (3,094) of calls were abandoned after the 60 second message. No more than five percent of calls were abandoned after the initial message during the weekend period (5%, n= 1941), or the weekday (3%, n=1153). Where call volume was at its lowest, abandoned calls equate for just 1% of total calls. Where call volume was at its highest, abandonment rate increased to 13%. There was no significant change in number of calls abandoned, or received in the 6-month period. In total 1210 calls (1.7%) were abandoned within the first minute. There are multiple reasons why people may terminate the call including decided to try to access the service at an alternative time; following directions set out within the messaging (e.g. accessing website information) or telephoning another service. Page 78
80 Time of Call This data was also examined at on an hour-by-hour basis of calls both during the week and at the weekend: Figure 0:9 Call Volume Telephony Source: WAST (2017) More calls were logged at 6pm than at any other time of day. The fewest calls were logged at 4am. Over the course of the day (00:00-23:59) calls increase significantly (indicated by the red trend lines in the figure above) (p=0.002). Between 4am and 9am calls increase consecutively hour on hour before decreasing hour on hour until 3pm where calls then begin to increase once more to 6pm. After 6pm call volume decreases. During the weekend period across the six months there were 36,311 calls made. This accounted for 51% of calls. The remaining 49% were made during the week. The busiest hour during the week was 6pm, where 4,532 calls were made. This accounted for 13% of daily calls. The busiest hour during the weekend was 9am, where 3,483 calls were made, which accounted for 10% of calls. As the day progressed there was a statistical increase in calls during the week (p<0.05), but not at the weekend. The busiest time of the weekend was 9am, when 9.5% of all weekend calls were answered. The quietest time of day was 4am. Page 79
. Across the six months 4,304 calls were abandoned (5.9%).")
81 Call Disposition Figure 0:10 Call Disposition Source: WAST (2017) In total 67,466 calls were handled out of 71,853 (93.8%). The day with the highest number of calls handled was 27 th December, 2016 (n=1003). Across the six months 4,304 calls were abandoned (5.9%). The day which saw the highest number of abandoned calls (n=135) was also the day with the most calls. In total 83 callers were de-queued to speak to a clinical specialist, 72 of which were de-queued during the out of hour s period. Across the 6-month period there was no significant statistical change for number of handled calls, or number of abandoned calls. There is however a statistical significance change for number of calls dequeued (p=0.02). Page 80
82 User Demographic This section provides a breakdown of gender, and specific details such as age, and outcome of call. This dataset provides information on 63,751 NHS Wales 111 users. Figure 0:11 Gender of Caller Source: WAST (2017) In total, 58.45% of calls related to females and 41.55% to males. Figure 0:12 Age of Caller Source WAST (2017) Over a fifth of calls (22.94%) were on behalf of someone aged between 0 and 4. The second most common age group was 20 to 24 (7.91%), followed by 25 to 29 (7.46%). Just 18.33% of calls were made by those aged 65 or over. It is important to consider the age of caller for future planning or mainstreaming purposes, as this should be considering when assessing potential future call volumes. As noted above, the largest proportion of calls were made on behalf of someone under 5 years old (23%). Page 81
83 CSPT Outcome Figure 0:13 CSPT Outcome from CAS Source: WAST (2017) As mentioned in section 2.3, the 111 service uses a Call Streaming and Prioritisation Tool (CSPT). A number of CSPT protocols were reviewed and tailored to the desired call flow model for 111 (and also are in use across the remainder of Wales supporting call flow via 0845). Reviewing outcomes has proved to be the most challenging aspect of service delivery and agreement on aligning informational outcome reporting across CAS and Adastra is still being taken forward. At this stage therefore, it is only possible to review the outcomes separately until full end to end reporting is available (expected in September 2017). Page 82
84 The above table provides an overview of CSPT outcomes. The most common outcome was other (19%), followed by A&E (15.21%) and Dental (14.86%) Reason for Call Figure 0:14 Reason for Call Source: ABMU Health Board (2017) The above figure provides a summary of reasons for calls to the 111 service. The figure highlights that 21.86% of all calls are triaged to a nurse advisor. The remaining 78.14% of problems are dealt with by call handlers and GPOOHs. The most common issues dealt with by call handlers include intake* (10.65%) (see definition below), a child related problem (8.1%), or an infant related problem (7.5%). This accounts for 26.25% of all calls to the 111 service. The largest proportion of nurse advisor calls are related to dental problems (4.36%). Additional calls involving nurse advisors relate to various issues of muscular, and bone pain or swelling (2.01%), toddler related issues (1.25%), issues relating to 5-16 year olds (1.08%), head injury (0.46%), and chest pain (0.88%). * Intake refers to cases where no specific protocol is run by the call taker. This could include cases whereby the caller is seeking simple information that doesn t result in a CAS record being created such as, where is my nearest pharmacy. The 111 Pathfinder team noted that further work is ongoing to verify intake reporting following changes made to the background tables by the system supplier in This work has now been completed and the majority of intake calls refer to remote third party callers and follow up calls. A full breakdown of the other (misc.) category is outlined in appendix F. Page 83
85 Triage Figure 0:15 Call Priority Category Volume by Hour of the Day Source: WAST (2017) The above graph provides an overview of caller priority through the day. In each of the priorities there is a significant increase on an hour by hour basis (p<0.05). In both the P1 and P2 categories 6pm was the busiest hour of the day. For priority three calls the busiest time of day was 9am. The quietest time of day across each of the categories was 4am. In total 32,240 callers received a priority category. Of these calls 36% were priority one calls, 40% were priority 2 calls, and 24% were priority 3. One of the 111 Pathfinder identified standards is that 95% of all priority one calls receive a call back within 20 minutes. An examination of the data for 111 only (full data review across 111 and GPOOH not possible due to data limitations) shows that 98% of priority 1 calls were answered within 20mins. Of these calls 2,509 (21%) were queued. In total, 286 priority one calls were queued for more than 20 minutes, accounting for just 2% of all priority one calls. The average time to triage for priority one calls was 3 minutes, well under the proposed standard for 20 minutes. The remaining 64% (n=20,522) of priority calls were classed as priority two or three. Of these calls 917 were queued for over two hours, accounting for just 4% of total priority two and three queues. The average time to triage for priority two calls was 26 minutes, below the proposed 2-hour standard. Average time to triage for priority three calls was also below the standard, with average time of 45 minutes. Page 84
86 Figure 0:16 Final Patient Outcome Source: WAST (2017) The above graph outlines caller outcome. The data used is a combination of both call handler assessment (n=49,912) and nurse assessment (n=13,732). Most calls (66.08%) resulted in referral to GP Out of Hours (GPOOH). The second largest outcome was referral to ED (7.45%). Following this, the most common outcomes were other (5.39%), 999 (4.23%), dental (4.17%), and self-care (2.77%) Appointment Details The following sub-section refers to Adastra data only. Figure 0:17 Appointment Date Weekday and Weekend Comparison Source: WAST (2017) The above graph illustrates total number of triage appointments over the six-month period. In total 21,880 appointments were made, 63% of which were on weekends. The remaining 8,030 appointments (37%) Page 85
87 were made during the week. The average number of appointments per day was 62 during the week, and 266 at the weekend Appointment Length Figure 0:18 Average Appointment Length (Minutes) Weekday and Weekend Comparison Source: WAST (2017) The above table provides an insight into the average appointment length on a day to day basis. In total 360,709 minutes of appointments were organised through 111/GPOOH. This was across 22,986 appointments, averaging minutes per appointment. Appointment length ranged from minutes (2 nd February, 2017) and 9.93 minutes (11 th April, 2017). Both days were weekdays (a Thursday and a Tuesday). The average length of a weekday appointment was minutes. Compared to this, the weekend period had a lower range in appointment length, minutes (24 th December) to minutes (22 nd April, 2017). Average length of appointment was also below the weekly average (15.43 minutes). Page 86
88 Caller Priority Figure 0:19 Caller Priority at Reception Source: WAST (2017) The above graph indicates the priority assigned to callers. In total, 50,575 callers were assigned a priority. Of these attendees: 27.37% (n=8,145) of callers were to be called back within 20 minutes (urgent) (priority 1); 64.69% were to be called back within 2 hours (less urgent) (priority 2); and 7.94% were to be called back within 4 hours (priority 3). A review of face to face appointments shows that 67% of priority 1 calls were within their targets (1 hour to face to face). Given the small number of instances, and the variability in user experience it is difficult to assess the performance. 77% of priority 2 calls were within their target (2 hours), and 90% of priority three calls were within target (6 hours). It should be noted that at the time of this analysis, it was recognised that the there were a number of failed contacts within the dataset. A failed contact is where a clinician has been unable to contact the patient to undertake an assessment following their initial call to the service. A policy is in place to manage these contacts, and a review of the dataset identified that a small number of cases where case had been left open whilst the clinician attempted to contact the patient but the timestamp was taken from the time that the case was closed (which may have been several hours later or longer over the weekend period). A small number of cases therefore had excessive consultation lengths and this will have skewed the data. A fix is being applied to allow these cases to be excluded from further analysis Appointment Timeliness Figure 0:20 Appointment Late Bookings or Arrivals. Source: WAST (2017) The majority of appointments (98.5%) were booked within the standards set for the service. The remaining 1.5% were booked late. Most patients also arrived on time (99.73%). Page 87
89 Service Complaints The following sub-section provides an overview of complaints submitted to WAST surrounding the 111 service. Of total complaints 49 (94%) were insignificant and the remaining 6% caused minor, or short-term harm to callers. The table below provides a breakdown of complaints between October 2016 and April Figure 0:21 Complaints to 111 Service (WAST) Incidents by Category Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017 Mar 2017 Apr 2017 Total Access, admission, transfer and discharge Clinical assessment / diagnosis / tests Advanced Medical Priority Dispatch System (AMPDS) Issues Implementation of care and ongoing monitoring / review Consent, communications confidentiality interpersonal and CAS related issues NHSDW - Call Handling Issues IT, Radio & Telecommunications Total Source: WAST Most complaints (63%, n=33) related to call handlers. Nearly half of these complaints (15) were made during the month of March. March was also the busiest month (29%, n=15) for complaints. This is despite being the second least busy month in terms of call volume (16%, n=11,270). The second largest proportion of complaints related to consent, interpersonal communication, and confidentiality (10%, n=5), followed by clinical assessment, diagnosis, and tests (8%, n=4) Page 88
90 Summary of 111 Pathfinder data Key points relating to the activity that has taken place from November 2016 to April 2017 are: Almost 72,000 calls were received by the service, over the six months of operation. 67,466 (94%) of calls were answered by a call handler. The service performed well against the majority of standards that were set for it. For example, the average triage time for priority 1 calls was 3 minutes against a standard of 20 minutes; 98% of priority 1 calls were queued for less than 20 minutes against a service standard of 95% within 111; In total, just 4.3% (3,094) of calls were abandoned after the 60 second message. No more than five percent of calls were abandoned after the initial message during the weekend period (5%, n= 1941), or the weekday (3%, n=1153). The key performance metric in respect of access to the service, and abandonment is that no more than 5% of calls are abandoned (measured 60 seconds after the end of the messaging). The busiest day so far was 27 th December 2016, when 1,154 calls were received in one 24 hour period; 9.00am and 6.00pm are the busiest times of the day and Saturdays and Sundays are the busiest days; 42,053 (66%) of calls were referred to GPOOHs; and Total calls recorded are currently just 3% higher than the original demand assumptions. This suggests that the same assumptions used to estimate ABMU volume would largely apply to Wales and that the decision to include a 20% uplift factor for GPOOH call volumes at the launch of 111 was correct. Page 89
91 IMPACT OF THE 111 PATHFINDER A key element of the evaluation was to consider the impact of the 111 Pathfinder on the wider urgent care system. The following paragraphs provide an overview of the level of demand for unscheduled care in the ABMU area before and after the introduction of 111. Where possible a comparative analysis of unscheduled care in other Health Boards across Wales has also been included. This section also considers the economic consequences of changes in the use of unscheduled care. Data is provided for the first six months of 111 operation, and for the corresponding period in the previous year, for the volume of use. The following paragraphs highlight the key areas of interest, with further analysis set out in Appendix G. It should be noted that there are limitations in the extent to which changes to other parts of the health care system can be directly attributed to the 111 Pathfinder. The changes noted within this section have been made in a context of increasing demand for NHS services, and the delivery of other initiatives designed to provide efficiencies within the wider health and social care system; for example, the new Clinical Response Model for ambulance services introduced by WAST. To attribute observed changes to the 111 service, it would be necessary to have data from several years, to establish trends. It would also be necessary to have data from another comparable Health Board which did not introduce a service like 111, for example Aneurin Bevan or Cwm Taf, to act as a baseline to benchmark ABMU against 23. Call Volume Calls to 111, NHSDW, and GPOOH As noted in section 6, since it s launched in October 2016 to May 2017 the 111 Pathfinder service received over 71,000 calls. During this period, callers to GPOOH services and NHSDW from the ABMU area received an automated message directing them to 111. The table below compares the number of calls made to 111 in 2016/17, and GPOOH and NHSDW during the same period of 2015/16. Table 0:1 Call Volumes for NHSDW, GPOOH and NHSDW GPOOH GPOOH/ NHSDW Total Nov 4,241 8,320 12,561 10,635 Dec 4,779 9,737 14,516 14,149 Jan 4,956 10,261 15,217 12,867 Feb 4,289 8,767 13,056 10,887 Mar 5,198 11,773 16,971 11,270 Apr 4,343 8,463 12,806 12,045 6 months 27,806 57,321 85,127 71,853 Source: ABMU, ABMU calls volume NHSDW/GPOOH; 111 data The above table indicates that there just over 13,000 less calls within the 111 system compared to the NHSDW and GPOOH during the same period of the previous year. This would suggest that there is less demand for the 111 service. Having said this, there are several reasons why demand may be lower. Potential reasons include that during the 2015/16 period, calls may have been signposted to NHSDW from GPOOH and vice versa, resulting in some queries being double counted and an inaccurate increased demand in the 2015/16 period. Furthermore, in the current year the NHSDW service ( ) is still 23 See Turner, J., et al., 2012, Evaluation of NHS 111 Pilot Sites, Final Report, for evaluation design using control sites. Page 90
92 open within the ABMU area, meaning that not all calls that are redirected to 111 are accounted for as set out in figure Calls to 999 taken through Medical Priority Dispatch System (MPDS) The 111 service was intended to field non-urgent calls which may have otherwise gone to 999. The number of 999 calls that are taken through Medical Priority Dispatch System (MPDS) 24 and resulted in ambulance attendance at the scene are recorded through the WAST Ambulance Quality Indicators (AQI) by Local Health Board. The totals for the equivalent periods where data are available are virtually identical between 2015/16 and 2016/17. This is outlined below: Table 0:2 ABMU calls to 999 taken through MPDS Change Change (%) Nov 6,001 6, % Dec 6,638 7, % Jan 6,644 6, % Feb 6,380 5, % Mar 6,958 6, % Apr 5,928 6, % Six months 38,549 38, % Source: AQI Indicators, WAST 24 Medical Priority Dispatch System the algorithm-based software designed to prioritise emergency ambulance calls in terms of the speed of response required (lights and sirens or not) and whether advanced or basic life support is needed. Page 91
93 Conveyances WAST and Paramedic Referrals to 111/GPOOH Comparison ED Conveyance By WAST In addition to the number of calls that were made to 999 it was also important to consider the number of calls that result in a conveyance to hospital. WAST categorise calls as red (immediately life-threatening calls), amber (patients with conditions which may need treatment and care at the scene and fast transport to a healthcare facility), or green (non-serious calls, which can often be managed by other health services, including healthcare advice or through self-care) conveyances 25. Green conveyances are the least urgent of conveyances. Figure 0:1 ED Conveyance by Severity of Case Source: WAST The above graph details ED conveyances between October 2015 and May These are conveyances directly to the emergency department. In this measurement period, there was a significant change in green conveyances (p<0.001). It should also be noted that since 111 commencement there has not been a net increase in ED conveyances, which was a concern when planning the pathfinder. In terms of total conveyances, in ABMU the number of conveyances decreased following 111 implementation. Overall there has been a 5% decrease in total conveyances to ED between October 2015 and May This is detailed by conveyance type below: 25 Page 92
94 Table 0:3 ED Conveyance by WAST Comparison Time Period Red Conveyances Amber Conveyances Green Conveyances Total Conveyance November May ,606 19,071 4,389 25,066 November 2016-May 2017 (111 implemented) 1,679 19,062 3,098 23,839 Percentage Change +5% 0% -29% -5% Source: WAST Comparing ED conveyances for November 2015 to May 2016 and November 2016 to May 2017 there has been a decrease in overall conveyance by 5%. Green conveyances saw the largest decrease (29%). There was a minimal decrease in amber conveyances. The number of red conveyances increased by 5% in this period. It should be noted that 111 was not intended to have an impact on emergency and urgent care, therefore an impact on red ambulance conveyances was not expected. Page 93
95 Green conveyances to ABMU ED Units As highlighted above, non-emergency ambulance (green) conveyances to ED fell by almost 30% from the pre-111 level. The fall was sharpest in December and January, when the number of conveyances was almost halved from the previous year; this coincided with a sharp rise in referrals to GPOOH services, and may have been a reaction to the queueing of ambulances and long waits for admission over the winter. Since January there have been more conveyances and fewer referrals. Table 0:4 WAST Green calls: conveyances to ABMU ED Units Change Change (%) Nov % Dec % Jan % Feb % Mar % Apr % May % 6 months 4,389 3,098-1,291-29% Source: WAST (Ambulance conveyances and paramedic referrals) The AQIs include a breakdown by LHB of the number of GREEN category incidents resulting in a response : the eventual conveyances are a subset of this number but the data does give an indication of whether the change in conveyances might be specific to ABMU or a national phenomenon. The overall number of GREEN incidents fell for Wales as a whole, and in all LHB areas except Cwm Taf, over the time period for which comparable data is available (April 2016 July 2017). However, the number of incidents in ABMU was falling more rapidly than any other LHB, and around double the rate of Wales as a whole, as the graph below shows. The indexed data must be interpreted with care, however, if ABMU had had a particularly high number of incidents at the beginning of the time period (April 2016), this would be responsible for the relative drop which followed. Trends for each of Wales s Health Boards is details below. Figure 0:2 WAST Green category incidents resulting in a response, by LHB, Apr 2016 Jul Apr-16 Jul-16 Oct-16 Jan-17 Apr-17 Jul-17 All ABM AB BCU C&V CT HD P Source: WAST AQI Page 94
96 Lost hours and queues There has been ongoing concern about ambulances queuing at hospitals, unable to unload patients because hospitals have insufficient capacity to receive them. This has been a problem across Wales. The delays have been highly seasonal, and tending to increase year on year 26, but peaked in Figure 0:3 WAST Lost hours due to admission delays Source: WAST AQI ABMU AB BCU C&V CT HD P As shown above the number of ambulance service hours that have been lost due to delayed admissions has decreased since The changes in ABMU have closely tracked the pan-wales trends, and so are probably not attributable to the local pilot. Figure 0:4 WAST Lost hours due to admission delays, indexed All ABMU Source: WAST AQI. Indexed; Jan 2016 = PACEC and Turner, 2017, NHS Wales Ambulance Service & Emergency Ambulance Services Committee, Clinical Model Pilot Evaluation, Final Report, section 4.9. Page 95
97 GPOOH services The total demand for GPOOH services has risen over the past two years. This total includes services which were not counted as GPOOH in Clinical Support Hub (CSH) and NHS Direct Nurse Advice (NHSDNA) and pharmacy (pharm). The graph below details service usage for new, and existing services. Figure 0:5 GPOOH Existing and New Services Source: WAST The above graph provides an overview of total contacts to GPOOH divided into total contacts through existing routes (Doctor Advice (DA), Home Visits (HV), Prescription Pick Up (PPU), and the Primary Care Centre (PCC)), and through new services (NHS Direct Nurse Advice (NHSDNA), the Clinical Support Hubs (CSH), and the Pharmacy (Pharm)). In four of the seven contact routes, there has been a significant change in total contacts made (Primary Care Centre, Prescription Pick Up, Clinical Support Hub, and NHS Direct Nurse Advice; p<0.05). During the 111 pilot period, there was a significant increase in number of contacts made through NHS Direct Nurse Advice (p=0.004). This measure relates to the number of contacts that have been assessed and closed by nurses working within 111/NHS Direct Wales. This started to increase in September (just as the 111 pilot was beginning) as the technical configuration of the system allowed calls undertaken through the 0845/111 service to be counted within the GPOOH dataset. Overall there has been a significant increase in people using new services (p< ). Existing services have continued to operate as normal. A side by side comparison of GPOOH usage rates (2015/16 and 2016/17) are detailed below. Page 96
98 Table 0:5 GPOOH Services Change Change (%) Nov 8,308 9,746 1,438 17% Dec 10,135 12,647 2,512 25% Jan 9,723 11,848 2,125 22% Feb 8,695 9,792 1,097 13% Mar 11,982 9,829-2,153-18% Apr 8,586 11,894 3,308 39% 6 months 57,429 65,756 8,327 14% Source: WAST (Contacts referrals) The above table indicates that usage of GPOOH services has increased 14% between the 2015/16 and the 2016/17 period. However, when comparing the demand for GPOOH service on a like-for-like basis (i.e. excluding CSH and NHSDNA), demand fell by 5%. This is summarised below. Table 0:6 GPOOH services, like for like Change Change (%) Nov 8,308 8, % Dec 10,135 10, % Jan 9,723 10, % Feb 8,695 7, % Mar 11,982 7,897-4,085-34% Apr 8,586 9, % 6 months 57,429 54,299-3,130-5% Source: WAST (Contacts referrals) The above tables suggest that the GPOOH usage is higher than the previous year, but the additional services have directed demand from existing services. Increased use of GPOOH services is consistent with the feedback provided by senior operational staff who believed that that the algorithms used by call handlers was too risk adverse and directs too many service users to GPOOH services, thus putting additional pressure on GPOOH staff. However as noted earlier, during the initial implementation period it is recognized that the GPOOH service were also managing lower priority calls (P2 and P3) during periods of escalation when workforce gaps were impacting on service delivery. The above table will therefore not offer a true reflection of the desired call flow model which will be skewed by these periods of escalation (which occurred at busy times and especially at weekends). The potential benefit of the 111 service therefore in reducing the number of calls being managed by the GPOOH services is not able to be assessed from the initial 6 month period of evaluation. Page 97
99 Referrals to GPOOH Services The following subsection details referrals to GPOOH services through WAST, the ambulance service, the emergency department, nursing homes, and the district nurse. The GPOOH service operates from 6.30pm to 8am on weekdays and all day weekends and bank holidays 27. Currently the GPOOH number is still in operation, but this will be replaced by 111. Services provided by GPOOH include: call handling, triage and advice by nurse or doctor, face to face consultations in treatment centre by GP or Nurse Practitioner, and home visits by healthcare professional WAST Referrals to GPOOH The graph below outlines WAST referrals to GPOOHs. Figure 0:6 WAST Referrals to GPOOH The above chart shows that referrals from WAST to 111/GPOOH increased when the 111 service went live in November 2016, (i.e. an increase of 118 referrals per month, October 2016 (n=243) and December 2016 (n=361); this however was not significant (p=0.06). WAST referrals to GPOOH significantly decreased from December 2016 consecutively to February 2017 (p=0.03). Compared to the previous year, however, there was a 77% increase in activity during the pilot months of 111. This is detailed overleaf: 27 Page 98
100 Table 0:7 WAST referrals to GPOOH services Change Change (%) Nov % Dec % Jan % Feb % Mar % Apr % 6 months 1,017 1, % Source: WAST (Ambulance conveyances and paramedic referrals) It should be noted that this increase may not be entirely attributable to 111. Other services which may impact upon this is the WAST New Clinical Response Model. The new model measures quality of care, as opposed to the old model, which measured timeliness of response Page 99
101 Ambulance Referrals to GPOOH Figure 0:7 Ambulance Referrals to GPOOH Source: WAST The above graph illustrates total ambulance referrals to 111/GPOOH across the four categories: DA, HV, PCC, and PPU. Across three of the four categories there has been a significant increase in referrals from ambulance to GPOOH from April 2015 onwards. The categories are: DA (p<0.0001), PCC (p<0.001), and PPU (p<0.0001). However, the 111 service has not been operational for long enough to determine any specific trends in the data. It should be noted that for Doctor s Advice, the Primary Care Centre, and Prescription Pick Up there was an increase following the pre-pathfinder clinical support hub commencement date. In the months leading up to 111 commencement these routes continued to increase, following slight decreases postcommencement from January onwards. This suggests a decrease in demand post-111, but it is too soon to tell whether this is significant or not Page 100
102 Emergency Department Referral to GPOOH Figure 0:8 ED Referrals Source: WAST The above chart indicates total ED referrals to GPOOH from April 2015 to May Across this period there has been a small insignificant decrease (p=0.17) in total ED referrals to GPOOH. Since the 111 pilot commenced, total ED referrals equalled to 2,270. This is a decrease of 11% from 2,541 in the same period of the previous year (November-May). The practice of GPOOH accepting referrals from ED hasn t changed since the launch of 111, and therefore the decrease is unlikely to be related to the introduction of the 111 service. The trend lines in the graph above are indicative of the months surrounding the pre-pathfinder clinical support hub, and 111. Page 101
103 Nursing Home Referrals to GPOOH Figure 0:9 Nursing Home Referral GPOOH Source: WAST The above chart details nursing home referrals to 111/GPOOH across five areas of DA, HV, PCC, PPU, and Pharmacy. Across four outcomes (DA, HV, Pharmacy, and PCC, p<0.05) there has been a significant increase in nursing home referrals over the measurement period (April May 2017). This suggests that 111 is having a wider impact on services and has impacted nursing home referrals to GPOOH. The increase in referrals in visibly greater post 111, and highlights greater success than following the commencement of the pre-pathfinder clinical support hub. Overall, referrals to GPOOH from nursing homes have increased significantly following 111. This change was more pronounced than during the implementation of the pre-pathfinder clinical support hub. Page 102
104 District Nurse Referrals to GPOOH Figure 0:10 District Nurse Referrals Source: WAST The above graph illustrates district nurse referrals to GPOOH. The largest proportion of referrals were through DA (54%), HV (21%), PCC (13%), followed by PPU (12%). In the measurement period referrals resulting in home visits saw a significant increase (p=0.002). There was no significant change in other referral outcomes as a result of the 111 pilot period. ED Attendance The impact of 111 on ED attendance was also considered. The following section sets out ED attendance rates across all seven Health Boards before and after the implementation of 111. Page 103
105 All Wales ED Attendance Comparison Figure 0:11Total ED Attendance Source: StatsWales.gov.wales As shown above from October 2015 to June 2017 ABMU had the second highest number of ED attendees (309,401), after Betsi Cawadalr (392,061). In total, ABMU made up 17.6% of ED attendances. The graph indicates a trend for increasing ED attendances across Wales. As detailed overleaf, four of the seven Health Boards experienced increased attendances in ED compared to the same six months previous. Table 0:8 ED Attendance Change Region November to June 2015/16 November to June 2016/17 % change Abertawe Bro Morgannwg University Health Board 122, , % Aneurin Bevan University Health Board 108, , % Betsi Cadwaladr University Health Board 146, , % Cardiff and Vale University Health Board 91,557 92, % Cwm Taf 85,680 86, % Hywel Dda University Health Board 94,405 94, % Powys Teaching Health Board 11,962 12, % All Wales 660, , % Source: StatsWales.gov.wales This may not be in direct response to the 111 service, but it does suggest that the service has neither a negative or positive impact, and may have potentially attributed to the reduction in ED attendances of 0.6% Page 104
106 (762 attendances). This slight decrease in ED attendances since the introduction of 111 is also important as ED attendances in England increased after the introduction of Unlike ABMU, neighbouring Health Boards (Cwm Taf, Hywel Dda, and Cardiff and Vale) saw an increase in attendance. This may suggest that 111 as part of an overall changing healthcare system has had a positive impact on ED attendances All Wales Performance against the 4-hour waiting time target As changes in ED attendance rates can also impact on waiting times performance against 4-hour waiting time targets was also considered. NHS Wales aim to have 95 per cent of patients spending less than 4 hours in all emergency care facilities from arrival until admission, transfer or discharge. Figure 0:12ED Attendances within 4 Hour Target Source: StatsWales.gov.wales ED attendances within the 4-hour waiting time target per month ranged from 74% to 83% within ABMU. 29 Since the commencement of the 111 pilot, the Health Board has met ED waiting time targets (both minor and major injuries collectively) in at least 76% of cases each month. Overall since 111 commencement (November 2016 June 2017) there has been no significant change in ED attendances meeting the 4-hour waiting time target. Compared with the same period of the previous year however on average there has been a 2.4% increase in total cases per month within the target. In both measurement periods targets met fell during the winter months before increasing consecutively from March. This is detailed overleaf. 29 Target: 95 per cent of patients should spend less than 4 hours in all emergency care facilities from arrival until admission, transfer or discharge NHS Wales Emergency Department Dataset Page 105
107 Table 0:9 ED Cases with 4-hour target year by year comparison Health Board Average 2015/16 Average 2016/17 Percentage Change Abertawe Bro Morgannwg University Health Board 76.60% 79% 2.4% Aneurin Bevan University Health Board 81.30% 80.60% -0.7% Betsi Cadwaladr University Health Board 77.80% 77.90% 0.1% Cardiff and Vale University Health Board 80.30% 83.60% 3.3% Cwm Taf 81.10% 84.40% 3.3% Hywel Dda University Health Board 83.80% 85.80% 2.0% Powys Teaching Health Board 99.80% 99.90% 0.1% All Wales 83% 84.4% 1.4% Source: StatsWales.gov.wales In total, across Wales s seven LHBs six areas saw an improvement against the 4-hour target between these two periods. The average increase in targets met when comparing both periods was 1.4%. Aneurin Bevan was the only Health Board to experience a decrease, which was marginal. This indicates that compared to the national average, ABMU is performing well. Feedback from key stakeholders have indicated that that it was also positive that the introduction of a new service and new process did not negatively impact upon waiting times at ED. Page 106
108 ABMU ED Attendance by Transport Type The following subsection details Emergency Department (ED) attendance in ABMU by transportation, alongside hospital, and ED conveyance by severity of case. Figure 0:13 ED Attendance by Transport Type Source: WAST The above graph illustrates ED attendance. Looking at the 111 pilot period there was no significant change in number of ambulance arrivals (ambulance and air ambulance), or private arrivals (private motor, bicycle, and public transport). There was however a significant decrease in other conveyances (police, other, and non-applicable). As noted previously (see table 8.8) overall ED attendance has decreased slightly since November Page 107
109 Minor Injury Units Attendance rates at minor injury units (MIUs) were also considered, as summarised below across each of Wales s Health Boards. Figure 0:14 Minor Injury Unit Attendance Source: Statswales Minor Injury Units (MIUs) are self-referral walk-in centres which treat minor injuries. There has been a very small fall in use. For example, from November 2016 June 2017 there were 92,073 MIU attendances in ABMU compared with 93,001 during the same period in the previous year. Similar changes were also noted in other Health Boards which have not introduced the 111 service, and so are probably not attributable to 111. Page 108
110 Summary of impacts Overall, the changes in service demand are shown in the table below. Table 0:10 Service demand change, to Change Change (%) 111 calls 71,583 71,583 NHSDW calls 27,806-27,806 _ 999 calls 38,549 38, % GPOOH calls 57,321-57,321 _ GPOOH services 57,429 65,756 8,327 14% GPOOH services (like for like) 57,429 54,299-3,130-5% A&E attendances 74,046 72, % Red conveyances 1,606 1, % Amber conveyances 19,071 19, % Green conveyances 4,389 3,098-1,291-29% Total conveyances 25,066 23,839-1,277-5% Minor Injury Unit attendances 93,001 92, % Performance against the 4- hour waiting time 76.6% 79% 2.4% 2.4% Note: Six month totals. Source: RSM PACEC Regards 111 calls, no data was available for the 2015/16 period as the service was not in operation. For both NHSDW and GPOOH calls no data was available for the 2016/17 period. Because of this, these factors could not be compared. Overall when comparing time periods an increase was seen in: the use of GPOOH services, red ambulance conveyances, and performance against the four-hour waiting time standard. A decrease was seen in like for like GPOOH services, overall ED attendance, green ED conveyances, total ED attendance, and MIU attendance. It is possible that 111 has impacted upon overall volume of use. Page 109
111 Economic Impact Changes to the use of other health services since the launch of the 111 Pathfinder (as noted in the preceding paragraphs) form the basis for this cost-consequence analysis. The intent behind the 111 service is that it should improve signposting, replace the NHS Direct Wales and GPOOH numbers, provide assistance using the Clinical Hub, and divert non-emergency users away from emergency services and towards services such as GPOOH. Qualitative feedback from key stakeholders such as senior operational staff (see section 5) suggests that this has been achieved, and this, to an extent is visible in the usage statistics. However, it is not possible to attribute all changes in demand over this time period to the 111 service. The 2016/17 running cost budget of the 111 pathfinder was 1.673m (including 212,000 for telephony and IT costs). The call volume in the first six months of the service was 71,853. The call volume in the second half of the year is likely to rise, since not all NHSDW calls were being routed through 111 until April Furthermore, the Pathfinder has now also been extended to cover the Carmarthenshire area of Hywel Dda. An analysis of the data suggests that there has been changes in the demand for urgent care since the introduction of the 111 service, especially non-urgent ambulance conveyances (Green, -29%) and from like-for-like GPOOH services (-5%). Using cost per incident estimates, it is possible to make ballpark estimates of the financial implications of these changes. However, this is purely a before-and-after comparison; it has not been possible to establish direct attribution to the 111 service. The major components of cost change are as follows: Cost of GPOOH Doctor Advice: - 60k (accountable for by use of 111 Clinical Hub advice or transfer to new GPOOH services); Cost of A&E attendances: - 218k (potentially attributable to use of 111 advice); Cost of ambulance conveyances (coded Green): - 205k (whilst it is unlikely that the reduction in green ambulance conveyance is wholly attributable to the 111 Pathfinder, due to the new clinical model implemented by WAST six months previously, it should be noted that green conveyances reduced more steeply in ABMU than in other Health Board areas therefore it is reasonable to assume that 111 has had a positive impact, but it is not possible to apportion the cost savings associated with this); and Cost of MIU attendances: - 60k (probably not attributable to use of 111 advice). In addition to the direct cost avoidance noted above the 111 with Pathfinder will also have contributed towards indirect cost savings that are more difficult to accurately quantify. For example a proportion of those who would have previously been conveyed to hospital would also have been admitted for an overnight stay in an acute hospital. As noted above the majority of savings relate to Green conveyances. Currently data is not available on the proportion of green conveyances that result in a hospital admission, whilst this is likely to be much lower proportion than that of amber or red conveyances, relatively small reductions in hospital admissions can still accrue significant cost savings. For example, if a conservative estimation that 10% of Green conveyances result in one overnight stay in an acute hospital is applied then the 111 Pathfinder would have contributed to a reduction in 120 days of acute hospital time. This equates to cost savings in the region of 49,560 [1] for the first six months of the 111 service or 99,120 per annum. [1] NHS Wales cost of one overnight stay in an acute hospital is stated as Page 110
112 COMPARATIVE ANALYSIS Introduction To understand the progress made in the implementation of 111 in ABMU, and to set the impacts of the service in context, ideally a comparison would be made between ABMU and similar regions within the UK. To do this, we compared 111 services in other regions of the UK. However, on examination of staff structure, volume, and patient pathways it became apparent that each of these services is structured very differently to 111 in ABMU, and a direct comparison therefore would not be meaningful. Therefore, the following section provides a summary of available data on how the other services are structured, and the activity levels associated with them. Detailed information is provided in Appendix I. There are limitations on the extent to which data from each region can be compared. For example, in addition to differences in the way in which each service is structured, data on each service is gathered and collated slightly differently. Therefore, caution should be applied when making direct comparison across services. The NHS National Minimum dataset was examined for key statistics relating to the 111 service in potentially comparable areas of England. Scottish data was obtained through NHS 24 s information services. There is an issue when comparing the different systems as they record information differently. Primarily, the ABMU 111 service is clinical, as opposed to the non-clinical English equivalent, with specialist clinicians working within the service to deal with caller issues. Over 75% of ABMU calls did not fit into the 111 Minimum dataset outcome groupings. The largest proportion of these calls were referred on to GPOOH (66% of total calls), or to other services such as 999 (4%), dental services (4%), or advised to administer self-care (3%) Comparator Regions As set out in the table below two English regions were selected as comparator regions based on demographic data, alongside Scotland. Table 0:1 Comparator Region Demographic Overview ABMU Scotland Blackpool Great Yarmouth and Waveney Total population 525,466 5,404, , ,560 Size in proportion to ABMU % over 65 years 19.7% 7.2% 20.5% 12.82% % under 4yrs 5% 5.3% 6.1% 11.16% Life expectancy - males Life expectancy female Average deprivation rank score Top 25% least deprived Top 25% most deprived (rank: 1 st ) Top 25% most deprived (rank: 20 th ) Page 111
113 Comparator 1 NHS 24 Scotland Key Available Data As each area operates differently, the available data varies from region to region. The following section provides an overview of the available Scottish data. This includes data on staffing, call volume, and call outcome Overview of Staff In total, NHS 24 has 839 clinical and call handling staff. This is summarised below: Table 0:2 NHS 24 Staff Overview Staff Staff as at 31/03/2016 (WTE) Clinical Staff Clinical Service Managers 16 Lead Nurse Dental 1 Team Leaders Nurses Advisory Staff (pharmacy and physio) Dental Nurses Total Clinical Front Line Total Non-Clinical Front Line (incl call handlers) Total Staff Page 112
114 Activity Levels This section outlines call activity in Scotland. All data is sourced through the Urgent Care Datamart and is provided at the financial year level (March 2015-March 2016). In Scotland System Watch is used to monitor and predict emergency. Table 0:3 NHS24 Yearly Call Volume Year Number of Calls Percentage Change from Previous Year 2011/12 1,330, /13 1,407,268 +5% 2013/14 1,318,971-8% 2015/16 1,442,848 +9% Increase ,820 8% The above table shows that call volume is fairly consistent across the four-year period for which data is provided. In total, between 2011/12 and 2015/16 number of calls have increased 8%. Within the Welsh 111 data calls have also remained consistent, with no significant increase over the 6 months of data availability (p=0.7). The table below illustrates total call volume for both Wales and Scotland between the months of November and March. The most recent year of available data has been used in both instances. Table 0:4 NHS 24 and ABMU 111 call volumes Month NHS 24 (November March 2016) % of total calls ABMU 111 (November March 2017) % of total calls November 106,544 17% 10,635 18% December 129,892 21% 14,149 24% January 142,401 23% 12,867 22% February 113,644 18% 10,887 18% March 134,066 21% 11,270 19% Total Calls 626,547 59,808 Population of Area 5,295, ,466 Number of Calls per Capita Whilst the call volume of NHS24 calls is significantly greater to that of ABMU, the number of calls per capita is broadly similar. This is something to consider if planning to expand 111 to cover all of Wales. The Scottish service covers a much larger population and received 9.5 times as many calls as the ABMU Pathfinder. However, similar trends appear in both areas. Therefore, as expected, and in line with ABMU call trends, December and January are the busiest times of the year. Page 113
115 With regards age, for the financial year of in Scotland, the largest proportion of calls were made on behalf of those aged 0-4 (15%). Within Wales during November April 2017 this age group also made up the largest proportion of calls (23%, n=14,502). Within Scotland the second largest age group was (9%, n=119,606). Within Wales the second largest group was 15-19, making up 8% of overall callers (n=3,255). In both instances the 90+ age group used the number the least, with just 3% in Scotland (n=37,058), and 2% in Wales (n=1,494). Within Scotland 42% of calls were made by men and 58% women. The Welsh 111 service had a similar breakdown of male to female callers, with 58.45% of callers being female, and 41.55% male. Time of Call Both NHS 24 and ABMU s 111 pathfinder provided data on time of call. This is detailed in the graph below: Figure 0:1Percentage of Calls per Hour The above graph provides an overview of call proportion in both the Scottish NHS 24 and the ABMU 111 Pathfinder services. In both scenarios, the largest proportion of calls are at 6pm, 10% (n=143,961) in Scotland, and 9% (n=6,391) in Wales. In both scenarios, the least busy hour was between 4am and 5am. This illustrates that despite difference in call volume, both regions have a similar pattern of usage. Unlike ABMU, Scotland redirects callers to their GP practice during working hours. ABMU s model is centred on 24-hour delivery. Caller outcome More detailed information on call outcome is set out in appendix I. The most noticeable difference between the two services are the proportion of calls resulting in a GPOOH appointment. A larger proportion of Welsh callers were directed to GPOOH (66%), when compared to Scotland (36%). Page 114
116 Comparator 2 Blackpool NHS Overview of the Service NHS 111 in Blackpool is staffed through two organisations, North West Ambulance Service (NWAS) and Fylde Coast Medical Services (FCMS, a non-profit healthcare provider). It was established in In total, there are 211 staff. There are 119 NWAS directly employed call handlers and clinicians, and 82 FCMS call handlers and clinicians. Supporting their work are 35 front line staff split across three management roles: Shift Supervisors, Team Supervisors, and Clinical Duty Managers. All staff are supported by the Senior Management Team who are linked with NWAS s Executive team. A Clinical Duty Manager is also on duty 24/7 to ensure clinical safety in the service NWAS state that they provide a team of fully-trained call handlers supported by experienced senior clinical advisors, who assess the symptoms and then signpost the caller directly to the most appropriate place of care Activity Levels The information below sets out the most recently available data for the months November to April in Blackpool ( ), and in ABMU ( ) Call Volume Call volume for NHS 111 Blackpool and ABMU regions are detailed below: Table 0:5 Call Volume Blackpool CCG and ABMU Variable Blackpool % total calls ABMU % total calls Population 468, ,466 Number of Calls 84, % 71, % Per Capita Dealt call 31 84,890 63,751 Number of answered calls 82, % 67, % Answered within 60 seconds 76, % 47, % Number of Abandoned Calls 2, % 4, % Transferred to clinical advisor 17, % 32,488 51% Handling time worked by clinical staff (mins) 175,291 1,727,267 Average Call Length 7 minutes 15 minutes Source: NHS England Minimum Dataset/ NHS Wales This refers to calls within ABMU area which went through the patient pathway (i.e. was not abandoned/ resolved early) Page 115
117 Whilst there are broadly similar levels of calls in the Blackpool and ABMU areas there are significant differences in the amount of time spent on calls by clinical staff. This reflects the clinical model applied by ABMU. Fifty-one percent of ABMU calls were triaged. Each triaged call in ABMU was handled by a clinical call handler. Compared to this just 20.21% of Blackpool 111 callers spoke to a clinical advisor Call Outcome The section below provides an overview of the outcome of calls for both the Blackpool and ABMU region: Table 0:6 Call Outcome Comparison Blackpool (November 2014 April 2015) % total disposition ABMU (November 2016 April 2017) % total disposition Total Population 468, ,466 Recommended to attend A&E 6, % 4, % Number per Capita Recommended to attend primary and community care Recommended to attend other service Not recommended to attend other service Given Health Information Not recommended to attend other service Recommended home care Not recommended to attend other service Other nonclinical 50, % 4, % % 3, % 13, % 2, % 4, % 1, % 8, % - - Other n/a n/a 47, % Total Disposition 76, % 63, % Number per Capita Source: NHS England Minimum Dataset/ NHS Wales As summarised above a similar proportion of calls in each area were referred to A&E (Blackpool, 8.14%; ABMU 7.43%). A larger percentage of callers from the Blackpool region were recommended to attend primary or community care (65.87%) when compared to ABMU (6.35%). As highlighted, it is not clear from the NHSE 111 Minimum Dataset what proportion of callers are referred to GPOOH. Page 116
118 Comparator 3 Great Yarmouth and Waveney NHS Overview of the Service The GY and W service was established in No information was available on the number, or structure of staff for the service. The service is provided by social enterprise IC Activity Levels This subsection sets out the levels of activity of the NHS 111 service in Great Yarmouth and Waveney (GY and W). All NHS 111 English data is sourced from the NHS Minimum Data Set. The information below details data from corresponding months for both GY and W and ABMU Call Volume The table below details call volume in both Great Yarmouth and Waveney, and ABMU for the most recent year between November and April. Table 0:7 Call Volume for NHS 111 in GY and W and ABMU Variable Great Yarmouth and Waveney % total calls ABMU % total calls Population 215, ,466 Number of Calls % 71, % Per Capita Dealt call % 63,751 Number of answered calls Answered within 60 seconds Number of Abandoned Calls Transferred to clinical advisor Handling time worked by clinical staff (mins) % 67, % % 47, % % 4, % % 32,488 51% ,727, Average Call Length 18 minutes 15 minutes Source: NHS Minimum Data Set/ NHS Wales Telephony Data The above table shows that per capita there are slightly more calls in the Great Yarmouth and Waveney area (0.16) than ABMU (0.14). GY and W also had a larger proportion of calls answered (98.1%) when compared with ABMU (83.89%). A higher percentage of ABMU calls however were transferred to a clinical advisor (51%), when compared with Great Yarmouth and Waveney (25%). Per capita Great Yarmouth and Waveney provided 0.31 minutes Page 117
119 of clinical time, compared to ABMU which was over ten times this (3.3 minutes). As with Blackpool, this highlights the clinical model applied to the Welsh 111 service Call Outcome The table below sets out caller outcome data relating to 111 service dispositions for the NHS 111 GY and W and ABMU regions. The most recent year s data for GY&W was used to compare with ABMU. Table 0:8 Call Disposition GY and W (November 15- April 16) ABMU (November 2016-April 2017) Total Population 215, ,466 Recommended to attend A&E 1, % 4, % Number per Capita Recommended to attend primary and community care Recommended to attend other service Not recommended to attend other service Given Health Information Not recommended to attend other service Recommended home care 18, % 4, % 1, % 3, % % 2, % 1, % 1, % Not recommended to attend other service Recommended other non-clinical Source: NHS England Minimum Dataset/ NHS Wales 2, % - - The above table summarises comparable call disposition data. A similar percentage of ABMU and Great Yarmouth calls results in attendance at A and E (0.009 per capita), or were recommended to attend other services (6.57% GY&W; 5.73% ABMU). A greater percentage of ABMU calls result in health information (3.2%) when compared with GY&W (1.4%). In total, just under 10% of GY&W calls had a non-clinical outcome. Page 118
120 User Experience It was also possible to provide some limited information on the extent to which users were satisfied with 111 services across the four regions. The table below provides a summary of caller experience. As with previous sections the data for the English services used was that of the MDS. Welsh data was taken from RSM PACEC s patient survey (as detailed in section 6.2). Data on Scottish satisfaction was taken from McAteer et al. s questionnaire (2016). 32 Table 0:9Patient Experience Summary Measure ABMU Scotland Great Yarmouth and Waveney 33 Blackpool 34 Average % respondents satisfied with service % respondents complied with advice % respondents improved health 94% (n=382) 83% (n=556) 87% (n=252) 99% (n=100) 91% 98% (380) n/a 88% (n=252) 98% (n=100) 95% 72% (n=380) n/a 74% (n=252) 96% (n=85) 81% The table above indicates that levels of patient satisfaction within ABMU s 111 service compares well to other more established 111 services. However, as different questionnaires, approaches, and sample sizes were used in each area this data is indicative rather than directly comparable. Due to the nature of the questionnaire this data should not be taken as a definitive image of quality of care and of the 111 service. Reasons for this include the differing sample sizes, and the wording of the questionnaire, e.g. in the Welsh survey, improved health was recorded for five days after the call, whereas in England this distinction was not made April-September April-September 2015 Page 119
121 Comparator Summary The following section provides a summary of 111, and equivalent, call services in each comparator region. Table 0:10 Comparator Summary ABMU Scotland Blackpool GY and W Population 525,466 5,295, , ,560 Calls 71, ,547 84,890 35,196 Per capita Total Staff 270 1, n/a Callers referred to ED (%) Patients satisfied with service (%) 7% 7% 8% 6% 94% 83% 99% 87% Peak call time 6pm 6pm Whilst the level of directly comparable data is limited, the outlined data does suggest that the 111 pathfinder in ABMU compares favorably to other more established 111 services elsewhere. For example, the ABMU service is handling similar levels of calls per capita as the other regions and has similar levels of patient satisfaction. The comparable data can also be used to inform on the potential rollout across Wales. Data such as peak call time and caller demographics could be used to inform staffing structures and rotas. Page 120
122 CONCLUSIONS Summary of key findings This section summarises the findings from the evaluation of the first full six months of operation for the 111 Pathfinder and sets out considerations for the future development of the service. The key findings are: The 111 Pathfinder was successfully implemented in October 2016 and received over 71,000 calls in the first six months of operation, 94% of which were answered by call takers; The 111 Pathfinder generally met the standards that were set for it (under the Interim Standards and Quality Measures) for example the average triage times for priority ones calls was 3 minutes compared to a standard of 20 minutes. Also, only 2% of priority one calls were queued for more than 20 minutes against a quality standard that notes 95% of priority calls should be answered within 20 minutes. There was a high level of service user satisfaction with 95% of survey respondents stating that they were satisfied or very satisfied with the whole 111 process. Furthermore, the service has received a very small percentage of formal complaints, all of which were minor (0.07% of all calls). There has been a very small reduction (1%) in the number of ED attendances during the first six months of operation compared to the same six months in the previous year. However, other Health Boards across Wales experienced a slight increase in ED attendances during the same period. Therefore, whilst this is not a statistically significant reduction it is an important one. The number of non-urgent (green) ambulance conveyances has decreased since the introduction of the service (29%) compared to the same time the previous year. Key stakeholders involved in the development and the operation of the service are enthusiastic about the Pathfinder and believe that greater benefits and efficiencies could be achieved with careful roll-out across Wales. Whilst it is difficult to disaggregate the impact of the 111 Pathfinder from other ongoing initiatives within urgent and emergency care services in the ABMU region, it is possible that the 111 Pathfinder contributed towards efficiencies particularly in ED and MIU attendances and Ambulance conveyances. For example, ED attendances in ABMU decreased slightly compared to increases in other LHBs. It must be stressed however that this cannot be directly attributed to the 111 service, and that these findings are based on the limited available data. Feedback from operational staff and senior stakeholders suggests that the service requires more clinical staff and experience call handles to facilitate any further expansion Key Operational Concerns: Based on the information provided by both staff the key operational concerns are summarised below: The majority of staff (who responded to the survey) reported that the introductory training was appropriate and equipped them for their job role (74%), one quarter of respondents (26%) were not satisfied with the traioing they received.. Reasons for this included: it was too long between training and the go live date; staff were unable to access the system during training; and initially management staff were not skilled to answer queries;potential areas of additional training include information on: updates to changes within the system; additional training with the Adastra system; illness specific training; and training surrounding the clinical hub; Additional face-to-face line manager support would be helpful; There are issues with the operational utility of the CSPT system; There are issues with current staffing structure and rostering; and Page 121
123 Some staff expressed concern that the service may not increase quality of care, stating that they are unaware if patients follow advice, and that nurse staff do not have the appropriate authority to signpost patients onwards although the decision support software is there to support their decisions and should be alongside their professional judgement. Strengths and Limitations Whilst the methodology selected for the evaluation has many strengths such as the mixed approach that was applied to collating qualitative and quantitative data, there have been a number of limitations that have restricted the analysis that can be completed and the conclusions that can be drawn. Firstly, as the Pathfinder is essentially a pilot service that was only introduced within the ABMU area it was difficult to collect data. Furthermore, the 111 Pathfinder was developed and introduced using existing telecommunications services, (NHSDW (which is still operational across the other six Welsh Health Board areas)) and GPOOH services in ABMU). Since additional resources and additional staff have been utilised it has not been possible to undertake detailed financial analysis of the full implementation costs and cost per call. Furthermore, the IT solution that was developed to enable the Pathfinder to operate was an interconnector to join the two separate operating systems together (CAS and Adastra). Whilst this connector worked in that it allowed calls to flow from one service to another (111 to GPOOH ), it limited the amount of data that could be generated. For example, a small number of clinicians noted that it is not possible to see the total size of the queue of calls waiting to be answered across systems and that it is not possible to trace service users across the wider health care system. Whilst it is recognised that Welsh Government required information urgently on the impact and effectiveness of the 111 Pathfinder in order to make funding and policy decisions, in an ideal world the evaluation of the service would be based on a full operational year in order to realise the full benefits of the service. Evaluations on the development of other 111 service in England 35 noted that it can take time for problems in new services to be identified and rectified and for the service to become established with users. It should also be noted that the service was implemented within the environment of wider change across the health service in Wales. For example, WAST recently implemented a new model of care to reprioritise 999 calls which could also have impacted upon ambulance conveyances and ED attendances therefore not all changes to urgent care will be directly attributable to the 111 service. Future considerations The quantitative data analysis, consultations with key stakeholders and the staff and service user surveys highlighted a number of issues that should be considered for any wider roll-out of the 111 service, as summarised below: The Pathfinder Directors and operational staff noted the difficulties in recruiting experienced clinical staff. Whilst this issue is not unique to the 111 Pathfinder, it is possible that the recruitment of suitably qualified staff for out of hours services is particularly challenging. Feedback from key stakeholders and the staff survey suggests that the 111 service could be made a more attractive career opportunity with the potential addition of additional of professional supervision, regular staff feedback and training opportunities and more frequent on- the- job training. Now that the 111 Pathfinder has been operational for more than six months and new systems and processes have become embedded, NHS Wales should 35 Turner, J., et al (2012) Evaluation of NHS 111 Pilot Sites. University of Sheffield Page 122
124 consider completing a staff survey to identify key areas of staff concern and how staff morale could be improved. Potentially low levels of staff morale were highlighted both in the staff survey and by key stakeholders. Retaining existing staff and recruiting new staff will be critical to any future expansion of the service; maintaining high levels of staff morale will be an important aspect of this. Both the staff survey and interviews with key stakeholders suggested a number of points for consideration. Firstly, rostering was highlighted (in the staff survey) as a key issue impacting on staff morale; the current rostering system should be reviewed by WAST in order to ensure that the operational needs of the service can be met whilst also maximising fairness and transparency for staff across all roles. Now that the 111 Pathfinder has been operational for more than six months and new systems and processes have become embedded, NHS Wales should consider completing a staff survey to identify key areas of staff concern and how staff morale could be improved. Almost all of those consulted with noted the limitations of the current IT and telephony solution. However, it was also noted that a new all Wales IT solution is due to be developed and implemented that will replace all existing systems across the NHS Wales. This will provide the opportunity to implement a more connected service with greater potential to provide more detailed management information. Therefore, the data requirements and inter-operability of a 111 service should be considered as part of the wider IT system specifications. A small number of senior clinicians involved in the operation of the service noted that the algorithms used in the triage process/clinical decision making tools should be reviewed. A structured programme of review should be considered based on the high volume/high impact so that improvements can be prioritized in line with service need. This concern was also echoed through feedback in a staff survey which highlighted a lack of confidence in the clinical decision making tools by the staff using them. Concern was expressed that current algorithms used for triage are too risk adverse resulting in too many calls being transferred to GPOOH services, which could have been dealt with by providing self care advice or in-hours GP appointments. Looking at the comparative analysis fewer callers from Wales were directed towards community and primary care settings than those within the English and Scottish regions. However, care should be taken in interpreting differences without a thorough understanding of the different tools in operation across the UK. It is also important to understand whether the there are issues around the system dispositions or whether human factors are contributing towards the overall position. The adverse impact of this is that the service may not be as efficient as it could be, and also that it makes the GPOOH service more pressurised to work in and a less attractive job role. Given that this review was completed following the first six months of delivery it was not possible to identify any trends in activity level data or, impacts on other services. NHS Wales should consider undertaking a further review of the 111 Pathfinder as it is rolled out across other Health Board areas and more longitudinal data becomes available. Page 123
125 APPENDIX A: CONSULTEE LIST Name Sarah Paul Clare Jenkins Sue Evans Kevin Duff Dr Steven Basset Hillary Dover Helen Thomas Susan Bailey Alex Howells Judith Paget Chris Powell Dr Peter Thomas Dr Chris Jones Nicola Davis-Job Aled Williams James Moore Richard Lee Hannah Evans Helen Rees Stephanie Kneath Roger Perks Sharon Rosser Organisation Abertawe Bro Morgannwg Community Health Council Abertawe Bro Morgannwg Community Health Council Abertawe Bro Morgannwg Community Health Council ABMU Health Board ABMU Health Board ABMU Health Board ABMU Health Board ABMU Health Board ABMU Health Board ABU Health Board and SRO 111 Programme WAST 111 Programme Cwm Taf University Health Board Royal College of Nurses WAST WAST WAST WAST WAST/ NHS Direct Wales WAST/ NHS Direct Wales Welsh Government Welsh Government Appendices
126 APPENDIX B: SERVICE USER QUESTIONNAIRE Patient profile information Q1. Are you? Male Female Q2. What age group is the patient? Under 12 years old years old years old years old years old years old years old years old 75+ Q3. Which local authority do you live in? (Tick one) Swansea Neath Port Talbot Bridgend Other (please specify) Q4. What is your ethnic group? (Tick one) White Asian or Asian British Mixed Appendices
127 Black or Black British Chinese Don t know Other (please specify) Q5. Which of the following, if any, best describes the status of your main occupation? (Tick one) Company director Self-employed Employed full time Employed part time Unemployed / seeking employment Student Retired Looking after home / family Permanently sick / disabled Other economically inactive (i.e. not working or seeking work) None of the above Don t know Q6. Do you have any long-term health problems or disabilities which limit your daily activities or the work you can do? (including problems which are due to old age) (Tick one) Yes No Don t know Q7. How did you first hear about the 111 telephone service? (Tick one) Media (TV, newspaper, radio etc.) Leaflet Appendices
128 Friends / relatives Healthcare provider (GP, dentist etc.) Social services Health service telephone message Online / internet Don t know Other (please specify) Accessing the 111 service Q8. How did you access the 111 telephone service? (Tick one) I knew about the 111 service and I called 111 first I called another service and a message told me to call 111 If redirected from another service, please state which one: I don t recall Other (please specify) Q9. How quickly did you get through to a 111 call handler? (Tick one) The call was answered immediately (within 60 seconds) I was held in a queue for more than 60 seconds I hung up before talking to someone I don t recall Q10. How many times did you try before getting through to a 111 call handler? (Please enter a number) Appendices
129 Q11. When you first got through to the 111 call handler, what happened? (Tick one) I was assessed only by the person who answered the telephone I was told that a nurse advisor will call me back (if ticked, please go to Q13) I was told that a GP or pharmacist would contact me back (if ticked please go to Q13) I was transferred immediately to a nurse advisor for further assessment I don t recall Q12. How long did you have to wait for someone to call you back? (Tick one) Less than 20 minutes Less than 1 hour Between 1 hour and 2 hours Between 2 hours and 3 hours Between 3 hours and 4 hours Over 4 hours I don t recall Q13. Did the call back time meet your expectations? (Tick one) Yes No Not sure If not sure why not? Q14. How many people did you speak to before receiving final advice? (Please enter a number) Q15. Did you feel you were treated politely and with respect during your call? (Tick one) Appendices
130 If not sure why not? Yes No Not sure Q16. Did you feel you were treated with kindness and compassion during your call? (Tick one) Yes No Not sure If not sure why not? About the advice you were given Q17. At the end of the call what did the 111 advisor tell you? (Tick one) Your call would be transferred to the 999 service The 111 service arranged an appointment for you with an out of hours health professional You must go to an A&E department / Minor Injury Unit centre by yourself Contact your GP or a doctor at your usual practice Contact another health professional yourself (e.g. dentist, optician etc.) Visit a pharmacy You were informed about how to look after the problem yourself I don t recall Other (Please specify) Appendices
131 If the 111 service arranged an appointment for you with an out of hours health professional, answer Q18 otherwise, please skip to Q19 Q18. If the 111 service arranged an appointment with an out of hours health professional, how long after the call were you contacted by this person? Less than 20 minutes Less than 1 hour Between 1 hour and 2 hours Between 2 hours and 4 hours Between 4 hours and 6 hours Over 6 hours I don t recall Q19. How helpful was the advice given by the 111 service? (Tick one) Very helpful Quite helpful Not very helpful Not helpful at all Don t know (please explain below) Q20. Did you follow the advice that you were given by the 111 service? (Tick one) Yes If you did not follow the advice, please say why? (Tick one) No I did not understand the advice I tried to follow the advice but it did not work I was unable to follow the advice Other (Please specify) Appendices
132 After the 111 call Q21. During the five days after you made the call to the NHS Wales 111 service, did you have contact with any health services for the same problem? (Tick one) Yes Go to Q22 No Go to Q23 Q22. What was your main reason to contact the health service? (Tick one) The 111 service did it on my behalf I was told to do it by the 111 service I wanted a second opinion My health problem worsened My health problem improved Other (Please specify below) Other (Please specify) Q23. How was your health problem five days after you made the 111 call? (Tick one) Completely solved Improved The same Worse If worse please provide details Appendices
133 Access to Urgent Care via 111 Q24. Did you find it easy to access urgent care via the 111 service? (Tick one) Yes No Not sure If no, why not? Q25. Do you feel that the 111 service has improved access to the urgent care system? (Tick one)? Yes No Not sure If no, why not? Q26. If the 111 service had not been available, would you have contacted another urgent care service (i.e. A&E, Minor Injury Unit, GP Out of Hours)? (Tick one) Definitely Probably Possibly Probably not Definitely not If Definitely or Probably, which of the following would you have been most likely to contact? (Tick one) A&E Department Minor Injury Unit GP Out of Hours Service Appendices
134 Overall satisfaction with the service Q27. From your experience of the 111 service, please rate the extent to which you agree or disagree with the statements. (Tick one per row) Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Don t know The 111 call handler was knowledgeable The 111 staff were helpful The 111 service dealt with my problem quickly The advice I received worked well in practice The 111 service helped me to make contact with the right service The 111 service is efficient I was happy with 111 service I trust the 111 service Using the 111 service reassured me The 111 service is a valuable addition to the NHS in Wales Q28. Overall, how satisfied or dissatisfied were you with the way the 111 service handled the whole process? (Tick one) Very satisfied Somewhat satisfied Neither satisfied of dissatisfied Somewhat dissatisfied Very dissatisfied Please describe anything about the 111 service that you were particularly satisfied or dissatisfied with. Appendices
135 Q29. Would you recommend the 111 service to your friends and family? (Tick one) Yes No Not sure Q30. If you faced a similar health problem in the future would you use the 111 service? (Tick one) Yes No Not sure Q31. Do you have any further comments about your experience of the NHS Wales 111 service? Appendices
136 APPENDIX C: STAFF QUESTIONNAIRE Q1 Are you: Male Female Q2 What is your age group? year-old year-old year-old year-old year-old 65+ Q3 Where do you work? Swansea, Thanet House Cwmbran, Vantage Point House Bangor, Snowdon House Q4 Have you been recently recruited to the 111 team or were you an existing member of staff? Part of the 111 recruitment (go to Q5) Existing member of staff (go to Q6) Q5 What was your role prior to commencing in the Welsh Ambulance Service (WAST)? (Tick one) Nurse (Acute Hospital) Nurse (primary care including GPOOH) Nurse Other Setting Call Taker/Admin & Clerical (non NHS) Call Taker/Admin & Clerical NHS Appendices
137 NHSDW call handler NHSDW Nurse Adviser NHSDW Health Information Adviser NHSDW Dental Health Adviser Other (please specify): Specify Q6 What is your current position? (Tick one) Call Taker Nurse Advisor Dental Nurse Advisor Team manager (CHC/HIC) Team Manager (SNA) Practice Coach/Training team Reception staff Health Information Adviser Other (please specify): Specify Can you give a brief description of your role within WAST? Q7 Yes No Did you feel that the introductory training you received was appropriate & equipped you for the role? (Please tick one) If no, why not? Q8 Do you feel that you need more training? (Please tick one) Yes No If yes, please specify what training you require? Appendices
138 Q9 Yes No Do you feel that you received enough support regarding the implementation of the ABMU 111 pathfinder from your line manager, e.g. Briefings, feedback, advice etc.? (Please tick one) Explain your answer Q10 How would you rate the quality of the telephony system? (Please tick one) Very Good Good Fair Poor Very Poor Don t know Q11 Is the greetings process working well? (Please tick one) Yes No Don t know Explain your answer Q12 Yes No Is the clinical decision making Tool (CAS/CSPT) adequate? (Please tick one) Don t know If you think that the CAS/CSPT is inadequate, please provide details of how it could be improved: Q13 Is the computer system/hardware user friendly? (Please tick one) Yes Appendices
139 No Don t know If you think that the computer hardware could be more user friendly please, explain which areas require improvement: Q14 How often do you think that calls are signposted to the right service? Always Often Sometimes Rarely Never Q15 How satisfied or dissatisfied are you with the rosters? (Please tick one) Very Satisfied Quite Satisfied Neither Satisfied or Dissatisfied Quite Dissatisfied Very Dissatisfied If dissatisfied, please say why. Q16 How satisfied or dissatisfied are you with your workload? (Please tick one) Very Satisfied Quite Satisfied Neither Satisfied or Dissatisfied Quite Dissatisfied Very Dissatisfied If dissatisfied, please say why. Q17 Do you feel content at work now since the introduction of the 111 Pathfinder? (Please tick one) More content than before Appendices
140 Same as before Less content If less content than before, please say why. Q18 In general, how satisfied or dissatisfied are you with your current role (Please tick one) Very Satisfied Quite Satisfied Neither Satisfied or Dissatisfied Quite Dissatisfied Very Dissatisfied Q19 Please rate the extent to which you agree or disagree with each of the following statements. (Tick one per row) Strongly Agree Agree Neither Agree nor Disagree Disagree Strongly Disagree I am proud to work for WAST. My WAST colleagues are helpful and supportive. I feel well informed about the changes that affect me in the service I am clear what is expected of me. I am given a real opportunity to develop my skills in the service. The training provided meets my needs for my current job. I am more empowered to make effective decisions now than I was before. I am encouraged to work to the best of my ability. I feel I have a positive attitude towards change. Morale is high. I am more satisfied in my current role than I was in my previous one. Appendices
141 I feel that my role makes a difference to patients / service users. I feel less stress now than I did in my previous role. I feel less time pressure now than I did before the introduction of 111. Q20 Yes No Do you think that 111 telephony service provides a good service to patients? (Please tick one) Not sure Please explain your answer Q21 Yes No Do you think that the introduction of the 111 number has improved access to urgent care for patients in the ABMU area? (Please tick one) Not sure Please explain your answer Q22 Yes No In your opinion, does NHSDW/111 help service users to access health care and advice in the place that is most appropriate for them? (Please tick one) Not sure Please explain your answer Q23 In your opinion what are the main 3 things that works well with the introduction of the 111 service? Appendices
142 Q24 Yes No Do you think that the overall quality of service for patients has improved since the introduction of the 111 pathfinder into ABMU? (Please tick one) Not sure Please explain your answer Q25 In your opinion what are the main 3 things that could be improved with the introduction of the 111 service? Q26 If you had the opportunity to make any changes to NHSDW/111 telephone triage service, what would they be? Q26 Do you have any further comments about working for WAST and delivering the NHSDW/111 services? Appendices
143 APPENDIX D: SERVICE USER SURVEY RESPONSES Appendices
144 Appendices
145 Appendices
146 Accessing the Service Appendices
147 Appendices
148 Appendices
149 Appendices
150 Appendices
151 Satisfaction with Service Appendices

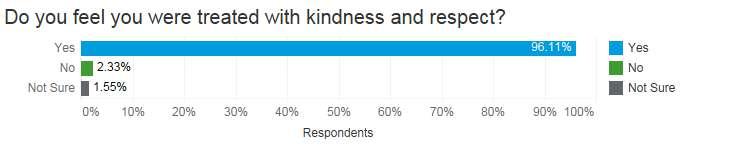
152 Appendices
153 Appendices
154 Staff Responses (Appendix E) User Demographic Appendices
155 Appendices
156 Training and Implementation Appendices

157 Satisfaction with Service Appendices

158 Appendices
159 Appendices

160 Appendices
161 Appendices
162 Appendices
163 Appendices
164 Appendices
165 Appendices
166 Appendices
167 Appendices
168 Appendices
169 Appendices
170 Appendices
171 Appendices
172 Appendices

173 Appendices

174 Appendices
175 Appendices
176 Appendices
177 APPENDIX F: ACTIVITY LEVEL ANALYSIS Demographics Appendices
178 Call Outcome Appendices
179 Reason for Call Table 11 Reason for Call Protocol Title Protocol User % of Calls Number of Calls Intake Call Handler 10.65% 6,791 Child 18 months to 5 years Call Handler 8.10% 5,163 Infant Under 18 months Call Handler 7.50% 4,782 Chest Pain or Upper Back Pain Call Handler 4.85% 3,094 Dental Problems Nurse Advisor 4.38% 2,791 Urinary Problems Call Handler 3.43% 2,184 Abdominal Pain 12 years and over Call Handler 3.14% 2,001 Throat Problems Call Handler 3.01% 1,922 Health Information Call Handler 3.01% 1,919 Safety Questions Over 2 Years Call Handler 2.97% 1,891 Breathing Difficulties or Wheezing Call Handler 2.95% 1,878 Rash or Skin Problems Call Handler 2.36% 1,502 Earache Call Handler 1.90% 1,211 Leg Pain or Calf Pain Call Handler 1.62% 1,033 Headache Call Handler 1.42% 907 Abdominal Pain Adult Nurse Advisor 1.38% 877 Appendices
180 Wounds Call Handler 1.35% 862 Low Back Pain Call Handler 1.32% 842 Cough 12 Years and Over Call Handler 1.28% 815 Eye Problems Call Handler 1.04% 664 Collapse Call Handler 0.94% 599 Vomiting 12 Years and Over Call Handler 0.93% 595 Chest Pain Nurse Advisor 0.88% 561 Generally Unwell 12 Years and Over Call Handler 0.88% 559 Flank Pain Call Handler 0.86% 548 Pregnancy Problems Call Handler 0.82% 522 Head Injury Call Handler 0.82% 521 Dizziness or Light-Headedness Call Handler 0.81% 516 Limb Injury Call Handler 0.78% 499 Miscellaneous Algorithm Nurse Advisor 0.77% 494 Sore Throat Adult Nurse Advisor 0.76% 487 Ear Problem Nurse Advisor 0.76% 483 Toothache and or Swelling Call Handler 0.70% 448 Suicide or Self Harm Call Handler 0.64% 408 Vaginal Bleeding Call Handler 0.63% 404 Rectal Bleeding Call Handler 0.57% 366 Toxic Substance Call Handler 0.54% 343 Confusion or Behaviour Change Call Handler 0.51% 327 Abdominal Pain 0-11 years Call Handler 0.51% 326 Ingestion Toxic Substance Nurse Advisor 0.51% 324 Generally Unwell Under 12 Years Call Handler 0.46% 294 Appendices
181 Head Injury Nurse Advisor 0.46% 292 Cough Adult Nurse Advisor 0.45% 289 Safety Questions Remote Over 2 Years Call Handler 0.42% 270 Colds and Flu Symptoms Call Handler 0.42% 265 Breathing Problems Adult Nurse Advisor 0.39% 250 All Other Injuries Call Handler 0.39% 249 Back Pain Nurse Advisor 0.39% 246 Headache Adult Nurse Advisor 0.37% 238 Rash Adult Nurse Advisor 0.36% 228 End of Life Care Call Handler 0.35% 224 Falls Nurse Advisor 0.34% 218 Eye Problem Nurse Advisor 0.34% 216 Diarrhoea 12 Years and Over Call Handler 0.33% 213 All Other Symptoms Call Handler 0.32% 202 Diabetes Concern Call Handler 0.31% 196 Vomiting Adult Nurse Advisor 0.30% 191 Rash Toddler - Age 1-4 years Nurse Advisor 0.29% 188 Cough Under 12 Years Call Handler 0.29% 187 Diarrhoea Adult Nurse Advisor 0.28% 179 Fever Toddler - Age 1-4 years Nurse Advisor 0.27% 175 Diarrhoea and Vomiting 12 Years and Over Call Handler 0.25% 159 Abdominal Pain Child - Age 1-16 years Nurse Advisor 0.24% 152 Dizziness or Vertigo Nurse Advisor 0.24% 151 Sore Throat Child - Age 5-16 years Nurse Advisor 0.24% 151 Rash Child - Age 5-16 years Nurse Advisor 0.23% 149 Appendices
182 Bites and Stings Call Handler 0.22% 139 Rectal Problems Nurse Advisor 0.22% 138 Unwell or Irritable Infant - Age 0-1 year Nurse Advisor 0.21% 135 Lumps Nurse Advisor 0.20% 130 Vomiting Under 12 Years Call Handler 0.20% 130 Vaginal Bleeding Nurse Advisor 0.19% 122 Neck Pain Call Handler 0.18% 116 Leg Pain Nurse Advisor 0.18% 113 Catheter Problems Call Handler 0.17% 107 Wound Infection Nurse Advisor 0.17% 107 Unwell or Irritable Newborn - Age 0-3 months Nurse Advisor 0.16% 99 Suicide Ideation Nurse Advisor 0.15% 96 Fever Adult Nurse Advisor 0.15% 95 Symptomatic Protocol Selection Call Handler 0.15% 95 Back Injury Call Handler 0.15% 94 Breathing Problems Toddler - Age 1-4 years Nurse Advisor 0.15% 94 Anxiety Nurse Advisor 0.14% 91 Nosebleed Call Handler 0.14% 89 Burns or Electric Shock Call Handler 0.13% 84 Lacerations Nurse Advisor 0.13% 82 Cough Toddler - Age 1-4 years Nurse Advisor 0.13% 81 Fever Child - Age 5-16 years Nurse Advisor 0.13% 80 Neck Pain or Swelling Nurse Advisor 0.12% 77 Nosebleeds Nurse Advisor 0.12% 75 Appendices
183 Depression Nurse Advisor 0.12% 74 Knee Pain Nurse Advisor 0.11% 71 Shoulder Pain or Swelling Nurse Advisor 0.11% 71 Rash Infant - Age 0-1 year Nurse Advisor 0.11% 69 Flank Pain Nurse Advisor 0.11% 68 Foot Pain or Swelling Nurse Advisor 0.11% 67 Palpitations Nurse Advisor 0.10% 65 Allergic Reactions Nurse Advisor 0.10% 63 Fever Infant - Age 0-1 year Nurse Advisor 0.10% 63 Vomiting Toddler - Age 1-4 years Nurse Advisor 0.09% 59 Colds and Flu Adult Nurse Advisor 0.09% 58 Back Injury Nurse Advisor 0.09% 57 Facial Pain or Swelling Nurse Advisor 0.09% 56 Cough Child - Age 5-16 years Nurse Advisor 0.08% 54 Arm Pain Nurse Advisor 0.08% 53 Dysuria Female Adult Nurse Advisor 0.08% 53 Confusion Nurse Advisor 0.08% 52 Constipation Adult and Child Nurse Advisor 0.08% 51 Hip Pain or Buttock Pain Nurse Advisor 0.08% 51 Facial Injury Nurse Advisor 0.08% 48 Mouth Problems Nurse Advisor 0.08% 48 Headache Child - Age 5-16 years Nurse Advisor 0.07% 47 Fatigue Nurse Advisor 0.07% 45 Muscle Problems Nurse Advisor 0.07% 44 Fainting or Syncope Nurse Advisor 0.07% 43 Appendices
184 Haemoptysis Nurse Advisor 0.07% 42 Burns Nurse Advisor 0.06% 40 Diarrhoea and Vomiting Under 12 Years Call Handler 0.06% 38 Groin Pain or Swelling Nurse Advisor 0.06% 38 Testicular Pain or Swelling Nurse Advisor 0.06% 38 Vaginal Discharge Nurse Advisor 0.06% 37 Haematuria Nurse Advisor 0.06% 36 Cough Infant - Age 0-1 year Nurse Advisor 0.05% 35 Sinus Pain Nurse Advisor 0.05% 35 Toe Pain or Problems Nurse Advisor 0.05% 35 Breast Problems Female Nurse Advisor 0.05% 34 Facial Injury Call Handler 0.05% 34 Other Dental Problems Call Handler 0.05% 34 Sore Throat Toddler - Age 1-4 years Nurse Advisor 0.05% 34 Vomiting Child - Age 5-16 years Nurse Advisor 0.05% 34 Breathing Problems Child - Age 5-16 years Nurse Advisor 0.05% 33 Leg Injury Nurse Advisor 0.05% 33 Diarrhoea Toddler - Age 1-4 years Nurse Advisor 0.05% 32 Urinary Frequency Nurse Advisor 0.05% 32 Breathing Problems Infant - Age 0-1 year Nurse Advisor 0.05% 30 Ingestion Foreign Body Nurse Advisor 0.05% 30 Foreign Body Call Handler 0.05% 29 Infant under 1 year Call Handler 0.05% 29 Vomiting Infant - Age 0-1 year Nurse Advisor 0.05% 29 Calf Pain Nurse Advisor 0.04% 28 Appendices
185 Chest Injury Call Handler 0.04% 27 Hand Pain or Swelling Nurse Advisor 0.04% 25 Behaviour Change Nurse Advisor 0.04% 24 Finger Pain or Swelling Nurse Advisor 0.04% 23 Pregnancy Vaginal Bleeding Nurse Advisor 0.04% 23 Ankle Pain or Swelling Nurse Advisor 0.03% 22 Arm Injury Nurse Advisor 0.03% 22 Chest Injury Nurse Advisor 0.03% 22 Pregnancy Nausea or Vomiting Nurse Advisor 0.03% 22 Finger Injury Nurse Advisor 0.03% 21 Jaw Pain or Temporomandibular Joint Pain Nurse Advisor 0.03% 21 Penile Problems Nurse Advisor 0.03% 21 Seizures Nurse Advisor 0.03% 21 Diarrhoea Child - Age 5-16 years Nurse Advisor 0.03% 20 Dysuria Male Adult Nurse Advisor 0.03% 20 Numbness Leg Nurse Advisor 0.03% 20 Puncture Wounds Nurse Advisor 0.03% 20 Urinary Retention Nurse Advisor 0.03% 20 Haematemesis Nurse Advisor 0.03% 19 Knee Injury Nurse Advisor 0.03% 19 Numbness Arm Nurse Advisor 0.03% 19 Foot Injury Nurse Advisor 0.03% 18 Itching Nurse Advisor 0.03% 18 Diarrhoea Under 12 Years Call Handler 0.03% 17 Appendices
186 Urogenital Problems Male Toddler - Age 1-4 years Nurse Advisor 0.03% 17 Ankle Injury Nurse Advisor 0.03% 16 Blisters Nurse Advisor 0.03% 16 Diarrhoea Infant - Age 0-1 year Nurse Advisor 0.03% 16 Neck Injury Nurse Advisor 0.03% 16 Purpura Nurse Advisor 0.03% 16 Wrist Pain or Swelling Nurse Advisor 0.03% 16 Dental Impact Injury Call Handler 0.02% 15 Elbow Pain or Swelling Nurse Advisor 0.02% 15 Bites or Scratches Cat Nurse Advisor 0.02% 14 Nail Problems Nurse Advisor 0.02% 14 Safety Questions Remote Under 2 Years Call Handler 0.02% 14 Sleep Problems Nurse Advisor 0.02% 14 Toe Injury Nurse Advisor 0.02% 14 Geriatric Dizziness or Vertigo Nurse Advisor 0.02% 13 Wrist Injury Nurse Advisor 0.02% 13 Bites Dog Nurse Advisor 0.02% 12 Bites Insect Nurse Advisor 0.02% 12 Heartburn Nurse Advisor 0.02% 11 Pregnancy Back Pain Nurse Advisor 0.02% 11 Urogenital Problems Female Child - Age 5-16 years Urogenital Problems Female Toddler - Age 1-4 years Nurse Advisor 0.02% 11 Nurse Advisor 0.02% 11 Inhalation Injury Nurse Advisor 0.02% 10 Numbness Generalised Nurse Advisor 0.02% 10 Appendices
187 Dental Bleeding Call Handler 0.01% 8 Hearing Loss Nurse Advisor 0.01% 8 Urogenital Problems Male Child - Age 5-16 years Nurse Advisor 0.01% 8 Inhalation Injury Call Handler 0.01% 7 Nasal Congestion Adult Nurse Advisor 0.01% 7 Abdominal Injury Nurse Advisor 0.01% 6 Bites Wild Animal Nurse Advisor 0.01% 6 Breast Problems Male Nurse Advisor 0.01% 6 Constipation Infant - Age 0-1 year Nurse Advisor 0.01% 6 Dental Protocol Selection Call Handler 0.01% 6 Amenorrhoea Nurse Advisor 0.01% 5 Constipation Toddler - Age 1-4 years Nurse Advisor 0.01% 5 Elbow Injury Nurse Advisor 0.01% 5 Hand Injury Nurse Advisor 0.01% 5 Hiccups Nurse Advisor 0.01% 5 Pregnancy Vaginal Discharge Nurse Advisor 0.01% 5 Crisis Call (Abuse or Violence) Call Handler 0.01% 4 Dysmenorrhoea Nurse Advisor 0.01% 4 Excessive Sweating Nurse Advisor 0.01% 4 Mole Change Nurse Advisor 0.01% 4 Nasal Congestion Infant - Age 0-1 year Nurse Advisor 0.00% 3 Stings Nurse Advisor 0.00% 3 Belching Nurse Advisor 0.00% 2 Bites Human Nurse Advisor 0.00% 2 Contraceptive Enquiries Nurse Advisor 0.00% 2 Appendices
188 Hoarseness Nurse Advisor 0.00% 2 Smell Disturbance Nurse Advisor 0.00% 2 Tinnitus Nurse Advisor 0.00% 2 Colds and Flu Child - Age 1-16 years Nurse Advisor 0.00% 1 Crisis Call Assault or Violence Nurse Advisor 0.00% 1 Geriatric Itching Nurse Advisor 0.00% 1 Grazes Nurse Advisor 0.00% 1 Major Trauma Nurse Advisor 0.00% 1 Nasal Congestion Child - Age 5-16 years Nurse Advisor 0.00% 1 Nasal Congestion Toddler - Age 1-4 years Nurse Advisor 0.00% 1 Sun or Heat Exposure Nurse Advisor 0.00% 1 Urinary Incontinence Nurse Advisor 0.00% 1 Appendices
189 Call Priority Time to Triage Appendices
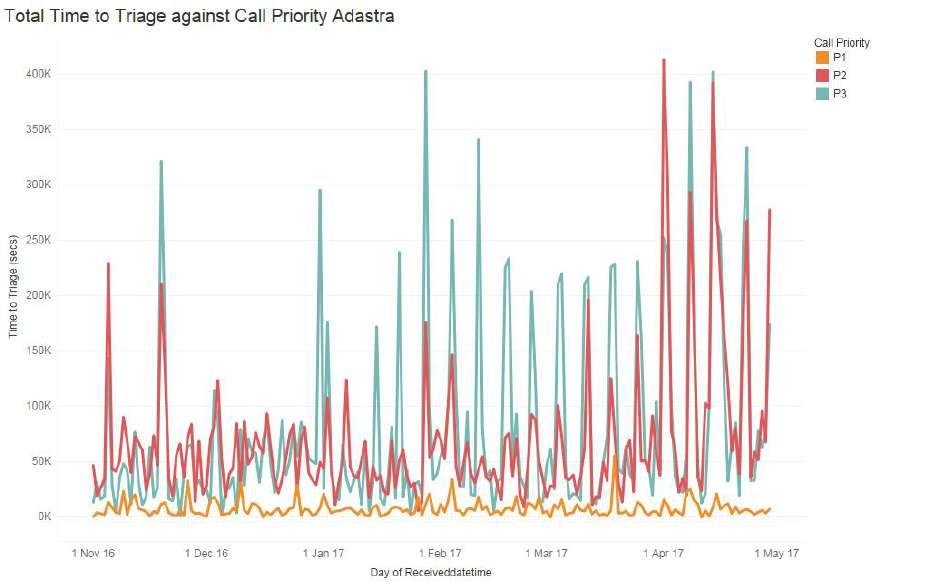
190 Appendices
191 Appendices
192 Appendices
193 Appointment Details Appendices
194 Appendices

195 Length of Assessments Appendices
196 Appendices
197 Appendices
198 Appendices
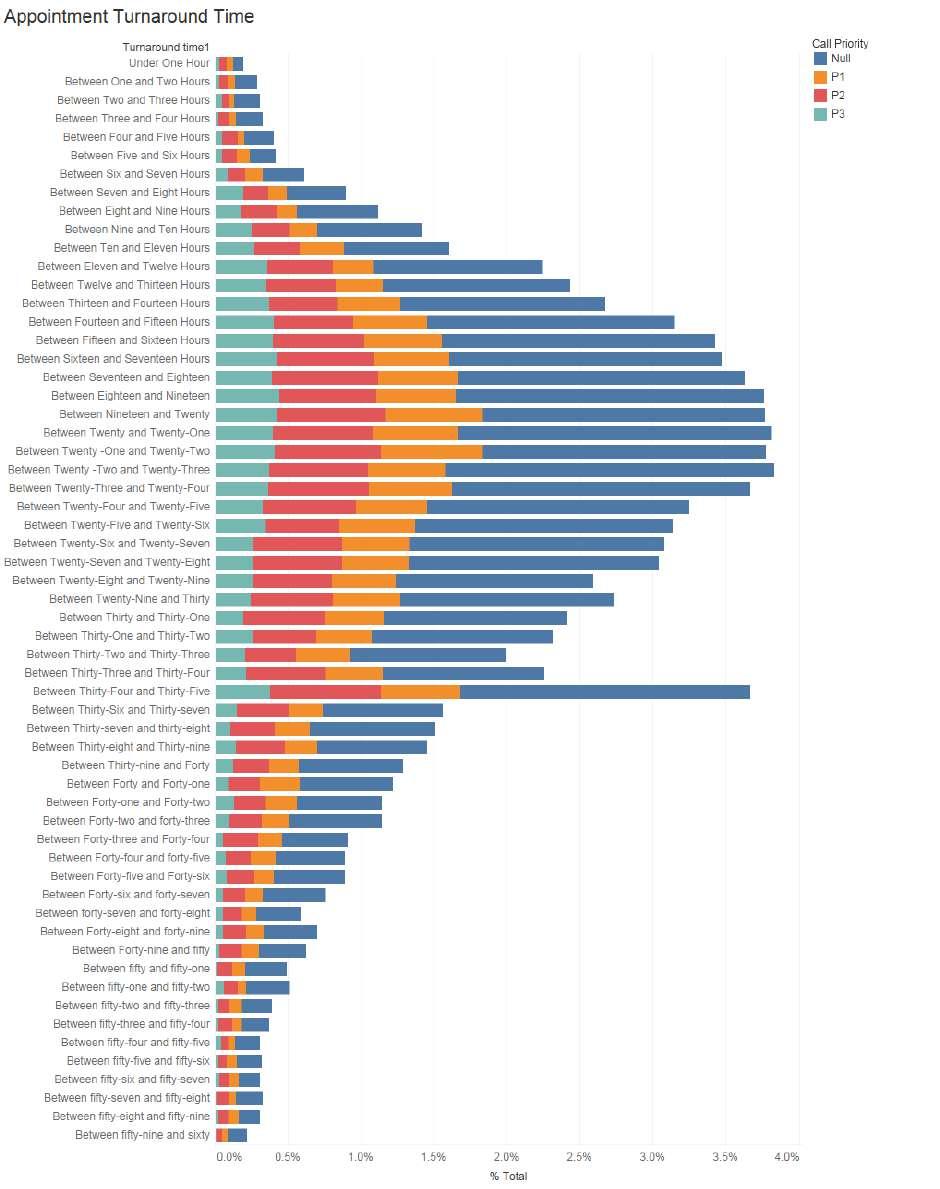
199 Appendices
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
111 Wales: Frequently Asked Questions
 111 Wales: Frequently Asked Questions What is 111 and why are you introducing it now? The 111 service will join up two services that are currently provided by different parts of the NHS in Wales namely
111 Wales: Frequently Asked Questions What is 111 and why are you introducing it now? The 111 service will join up two services that are currently provided by different parts of the NHS in Wales namely
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
IMPROVING UNSCHEDULED CARE IN WALES - UPDATE
 AGENDA ITEM No. 10 MEETING : TRUST BOARD DATE : 22 APRIL 2009 REPORT OF : CLINICAL DIRECTORATE Contact : Grayham McLean, Unscheduled Care Lead Officer Tel: 01792 562900 Email: grayham.mclean@ambulance.wales.nhs.uk
AGENDA ITEM No. 10 MEETING : TRUST BOARD DATE : 22 APRIL 2009 REPORT OF : CLINICAL DIRECTORATE Contact : Grayham McLean, Unscheduled Care Lead Officer Tel: 01792 562900 Email: grayham.mclean@ambulance.wales.nhs.uk
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
NHS 111 Service Specification
 NHS 111 Service Specification NHS 111 Programme Version 2.8 November 2011 Document control Audience Document Title Document Status NHS 111 programme and stakeholders NHS 111 Service Specification Approved
NHS 111 Service Specification NHS 111 Programme Version 2.8 November 2011 Document control Audience Document Title Document Status NHS 111 programme and stakeholders NHS 111 Service Specification Approved
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
NHS 111 specification
 NHS 111 specification Contents NHS 111 Specification introduction 2 Vision/aims of NHS 111 3 NHS 111: The basics 3 Who is NHS 111 for? 3 What patients can expect the new service to do: 3 Basic service
NHS 111 specification Contents NHS 111 Specification introduction 2 Vision/aims of NHS 111 3 NHS 111: The basics 3 Who is NHS 111 for? 3 What patients can expect the new service to do: 3 Basic service
Committee of Public Accounts
 Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Greater Manchester Health and Social Care Strategic Partnership Board
 Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
NHS 111 urgent care service
 NHS 111 urgent care service Frequently Asked Questions (FAQs) Contents Background 2 Operational 3 NHS Direct 5 999 5 101 6 Training 7 Service Impact 7 Telephony 8 Marketing 8 1 Background Why are you introducing
NHS 111 urgent care service Frequently Asked Questions (FAQs) Contents Background 2 Operational 3 NHS Direct 5 999 5 101 6 Training 7 Service Impact 7 Telephony 8 Marketing 8 1 Background Why are you introducing
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Transforming Welsh Ambulance Service: scrapping times, supporting patients!
 Transforming Welsh Ambulance Service: scrapping times, supporting patients! Dr Brendan Lloyd Medical Director Welsh Ambulance Services Trust Founding Senior Fellow FMLM Dr John Kotter: Leading Change 8-stage
Transforming Welsh Ambulance Service: scrapping times, supporting patients! Dr Brendan Lloyd Medical Director Welsh Ambulance Services Trust Founding Senior Fellow FMLM Dr John Kotter: Leading Change 8-stage
NHS 111. Introduction. Background
 NHS 111 Introduction The NHS 111 service is being introduced to make it easier for the public to access healthcare services when they need medical help fast, but it s not a lifethreatening situation. The
NHS 111 Introduction The NHS 111 service is being introduced to make it easier for the public to access healthcare services when they need medical help fast, but it s not a lifethreatening situation. The
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
The costs and benefits of managing some low-priority 999 ambulance calls by NHS Direct nurse advisers
 The costs and benefits of managing some low-priority 999 ambulance calls by NHS Direct nurse advisers Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO)
The costs and benefits of managing some low-priority 999 ambulance calls by NHS Direct nurse advisers Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO)
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
Charlotte Banks Staff Involvement Lead. Stage 1 only (no negative impacts identified) Stage 2 recommended (negative impacts identified)
 Stage 2 recommended (negative impacts identified)") Paper Recommendation DECISION NOTE Reporting to: Trust Board are asked to note the contents of the Trusts NHS Staff Survey 2017/18 Results and support. Trust Board Date 29 March 2018 Paper Title NHS Staff
Paper Recommendation DECISION NOTE Reporting to: Trust Board are asked to note the contents of the Trusts NHS Staff Survey 2017/18 Results and support. Trust Board Date 29 March 2018 Paper Title NHS Staff
Surge Management. Prepared by NEAS Resilience,
 Surge Management Prepared by NEAS Resilience, 13.09.2017 Plans for Winter 2017/18 Overview of system within locality The Strategic principles of the NEAS Surge Management Plan are to ensure: Response standards
Surge Management Prepared by NEAS Resilience, 13.09.2017 Plans for Winter 2017/18 Overview of system within locality The Strategic principles of the NEAS Surge Management Plan are to ensure: Response standards
Medical and Clinical Services Directorate Clinical Strategy
 www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Sunderland Urgent Care: Frequently asked questions
 Sunderland Urgent Care: Frequently asked questions What is Urgent care? We ve tried to make it as simple as possible for people to understand what it means and our definition is that urgent care is a sudden
Sunderland Urgent Care: Frequently asked questions What is Urgent care? We ve tried to make it as simple as possible for people to understand what it means and our definition is that urgent care is a sudden
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
OFFICIAL. Integrated Urgent Care Key Performance Indicators and Quality Standards Page 1 of 20
 Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Efficiency Review of The Welsh Ambulance Services NHS Trust
 Efficiency Review of The Welsh Ambulance Services NHS Trust Undertaken by Lightfoot Solutions in association with Lis Nixon Associates And Baker Tilly on behalf of Health Commission Wales and The Welsh
Efficiency Review of The Welsh Ambulance Services NHS Trust Undertaken by Lightfoot Solutions in association with Lis Nixon Associates And Baker Tilly on behalf of Health Commission Wales and The Welsh
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
NHS Pathways and Directory of Services
 NHS Pathways and Directory of Services Core Narrative Purpose The NHS Pathways and the Directory of Services core narrative has been designed to support NHS communications leads and/or project managers
NHS Pathways and Directory of Services Core Narrative Purpose The NHS Pathways and the Directory of Services core narrative has been designed to support NHS communications leads and/or project managers
OFFICIAL. Integrated Urgent Care Key Performance Indicators 2016/17. Integrated Urgent Care Key Performance Indicators Nov 16 Page 1 of 33
 Integrated Urgent Care Key Performance Indicators 2016/17 Integrated Urgent Care Key Performance Indicators Nov 16 Page 1 of 33 NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Integrated Urgent Care Key Performance Indicators 2016/17 Integrated Urgent Care Key Performance Indicators Nov 16 Page 1 of 33 NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Transforming Mental Health Services Formal Consultation Process
 Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement
 Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement NHS Hull Clinical Commissioning Group Governing Body Meeting 23 rd March 2018 1. Purpose Integrated Urgent Care (IUC) is
Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement NHS Hull Clinical Commissioning Group Governing Body Meeting 23 rd March 2018 1. Purpose Integrated Urgent Care (IUC) is
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Patient Pathway Guidelines:
 Welsh Ambulance Services NHS Trust: Patient Pathway Guidelines: For Fallers, Resolved Hypoglycaemia and Resolved Epileptic Seizures aged 18 years and over Version 1.7 DOCUMENT CONTROL SHEET Document Version
Welsh Ambulance Services NHS Trust: Patient Pathway Guidelines: For Fallers, Resolved Hypoglycaemia and Resolved Epileptic Seizures aged 18 years and over Version 1.7 DOCUMENT CONTROL SHEET Document Version
Economic Evaluation of the Implementation of an Electronic Palliative Care Coordination System (EPaCCS) in Lincolnshire using My RightCare
 in Lincolnshire using My RightCare") Economic Evaluation of the Implementation of an Electronic Palliative Care Coordination System (EPaCCS) in Lincolnshire using My RightCare This paper will provide an economic assessment of utilising the
Economic Evaluation of the Implementation of an Electronic Palliative Care Coordination System (EPaCCS) in Lincolnshire using My RightCare This paper will provide an economic assessment of utilising the
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Integrated Urgent Care Minimum Data Set Specification Version 1.0
 Integrated Urgent Care Minimum Data Set Specification Version 1.0 1. Document control Audience Document Title Document Status Integrated Urgent Care and NHS 111 service providers and commissioners Integrated
Integrated Urgent Care Minimum Data Set Specification Version 1.0 1. Document control Audience Document Title Document Status Integrated Urgent Care and NHS 111 service providers and commissioners Integrated
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Executive Summary Independent Evaluation of the Marie Curie Cancer Care Delivering Choice Programme in Somerset and North Somerset October 2012
 Executive Summary Independent Evaluation of the Marie Curie Cancer Care Delivering Choice Programme in Somerset and North Somerset October 2012 University of Bristol Evaluation Project Team Lesley Wye
Executive Summary Independent Evaluation of the Marie Curie Cancer Care Delivering Choice Programme in Somerset and North Somerset October 2012 University of Bristol Evaluation Project Team Lesley Wye
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health and Social Care Directorate Quality standards Process guide
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
HEALTH AND CARE (STAFFING) (SCOTLAND) BILL
 (SCOTLAND) BILL") HEALTH AND CARE (STAFFING) (SCOTLAND) BILL POLICY MEMORANDUM INTRODUCTION 1. As required under Rule 9.3.3 of the Parliament s Standing Orders, this Policy Memorandum is published to accompany the Health
HEALTH AND CARE (STAFFING) (SCOTLAND) BILL POLICY MEMORANDUM INTRODUCTION 1. As required under Rule 9.3.3 of the Parliament s Standing Orders, this Policy Memorandum is published to accompany the Health
Evaluation of the Links Worker Programme in Deep End general practices in Glasgow
 Evaluation of the Links Worker Programme in Deep End general practices in Glasgow Interim report May 2016 We are happy to consider requests for other languages or formats. Please contact 0131 314 5300
Evaluation of the Links Worker Programme in Deep End general practices in Glasgow Interim report May 2016 We are happy to consider requests for other languages or formats. Please contact 0131 314 5300
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Organisational factors that influence waiting times in emergency departments
 ACCESS TO HEALTH CARE NOVEMBER 2007 ResearchSummary Organisational factors that influence waiting times in emergency departments Waiting times in emergency departments are important to patients and also
ACCESS TO HEALTH CARE NOVEMBER 2007 ResearchSummary Organisational factors that influence waiting times in emergency departments Waiting times in emergency departments are important to patients and also
Mental Health (Wales) Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities
 Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities") Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Performance Evaluation Report Pembrokeshire County Council Social Services
 Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Briefing on Shaping Our Future urgent care work stream progress
 Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
Investment Committee: Extended Hours Business Case (Revised)
") PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
The Duty to Review Final Report Post-Legislative Assessment of the Mental Health (Wales) Measure 2010
 Measure 2010") The Duty to Review Final Report Post-Legislative Assessment of the Mental Health (Wales) Measure 2010 Crown copyright 2015 WG27249 Digital ISBN 978 1 4734 5289 3 Acknowledgements We would like to thank
The Duty to Review Final Report Post-Legislative Assessment of the Mental Health (Wales) Measure 2010 Crown copyright 2015 WG27249 Digital ISBN 978 1 4734 5289 3 Acknowledgements We would like to thank
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE
 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE") NHS Board Meeting Tuesday 16 October 2012 Chief Operating Officer (Acute Services Division) Board Paper No. 12/45 PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE Recommendation:
NHS Board Meeting Tuesday 16 October 2012 Chief Operating Officer (Acute Services Division) Board Paper No. 12/45 PATIENT RIGHTS ACT (SCOTLAND) 2011 ACCESS POLICY FOR TREATMENT TIME GUARANTEE Recommendation:
5. Integrated Care Research and Learning
 5. Integrated Care Research and Learning 5.1 Introduction In outlining the overall policy underpinning the reform programme, Future Health emphasises important research and learning from the international
5. Integrated Care Research and Learning 5.1 Introduction In outlining the overall policy underpinning the reform programme, Future Health emphasises important research and learning from the international
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales.
 Welsh Affairs Committee. Purpose: The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales. Contact: Nesta Lloyd Jones, Policy and Public Affairs
Welsh Affairs Committee. Purpose: The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales. Contact: Nesta Lloyd Jones, Policy and Public Affairs
Papers for the. West Kent Primary Care Commissioning Committee (Improving Access) Tuesday 21 st August at 4 4:30 pm
 Tuesday 21 st August at 4 4:30 pm") Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
OFFICIAL. Commissioning a Functionally Integrated Urgent Care Access, Treatment and Clinical Advice Service
 Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
OUTLINE PROPOSAL BUSINESS CASE
 OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
NATIONAL LOTTERY CHARITIES BOARD England. Mapping grants to deprived communities
 NATIONAL LOTTERY CHARITIES BOARD England Mapping grants to deprived communities JANUARY 2000 Mapping grants to deprived communities 2 Introduction This paper summarises the findings from a research project
NATIONAL LOTTERY CHARITIES BOARD England Mapping grants to deprived communities JANUARY 2000 Mapping grants to deprived communities 2 Introduction This paper summarises the findings from a research project
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire
 Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
NHS CONFEDERATION RESPONSE TO THE EMERGENCY ADMISSIONS MARGINAL RATE REVIEW (JUNE 2013)
") NHS CONFEDERATION RESPONSE TO THE EMERGENCY ADMISSIONS MARGINAL RATE REVIEW (JUNE 2013) 1. ABOUT THE NHS CONFEDERATION 1.1 The NHS Confederation is the only body to bring together the full range of organisations
NHS CONFEDERATION RESPONSE TO THE EMERGENCY ADMISSIONS MARGINAL RATE REVIEW (JUNE 2013) 1. ABOUT THE NHS CONFEDERATION 1.1 The NHS Confederation is the only body to bring together the full range of organisations
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
Torfaen North Neighbourhood Care Network Action Plan
 Torfaen North Neighbourhood Care Network Action Plan 2015-16 1 Torfaen North Draft Action Plan 2015-16 Strategic Aim 1: To understand the needs of the population served by the Network No Objective Agreed
Torfaen North Neighbourhood Care Network Action Plan 2015-16 1 Torfaen North Draft Action Plan 2015-16 Strategic Aim 1: To understand the needs of the population served by the Network No Objective Agreed
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Implementation of Quality Framework Update
 Joint Committee Meeting 26 January 2016 Title of the Committee Paper Framework Update Executive Lead: Director of Nursing & Quality Assurance Author: Director of Nursing & Quality Assurance Contact Details
Joint Committee Meeting 26 January 2016 Title of the Committee Paper Framework Update Executive Lead: Director of Nursing & Quality Assurance Author: Director of Nursing & Quality Assurance Contact Details
Mandating patient-level costing in the ambulance sector: an impact assessment
 Mandating patient-level costing in the ambulance sector: an impact assessment August 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that are
Mandating patient-level costing in the ambulance sector: an impact assessment August 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that are
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Developing an outcomes-based approach in mental health. The policy context
 briefing December 2011 Issue 231 Developing an outcomes-based approach in mental health Key points A new Mental Health Network report explores the issue of outcome measurement in mental health. The report
briefing December 2011 Issue 231 Developing an outcomes-based approach in mental health Key points A new Mental Health Network report explores the issue of outcome measurement in mental health. The report
Transforming NHS ambulance services
 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1086 SESSION 2010 2012 10 JUNE 2011 Department of Health Transforming NHS ambulance services 4 Summary Transforming NHS ambulance services Summary 1 In
REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1086 SESSION 2010 2012 10 JUNE 2011 Department of Health Transforming NHS ambulance services 4 Summary Transforming NHS ambulance services Summary 1 In
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Redesigning the Acute Coronary Syndrome (NSTE- ACS) pathway at Morriston Cardiac Centre - The case for change
 pathway at Morriston Cardiac Centre - The case for change") Redesigning the Acute Coronary Syndrome (NSTE- ACS) pathway at Morriston Cardiac Centre - The case for change 4 th July 2012 Dr D Smith & Dr S Dorman Introduction... 2 NSTE-ACS Where are we now?... 2 NSTE-ACS
Redesigning the Acute Coronary Syndrome (NSTE- ACS) pathway at Morriston Cardiac Centre - The case for change 4 th July 2012 Dr D Smith & Dr S Dorman Introduction... 2 NSTE-ACS Where are we now?... 2 NSTE-ACS
Delivering the Five Year Forward View. through Business Intelligence
 Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
RESPONSE TO RECOMMENDATIONS FROM THE HEALTH & SOCIAL CARE COMMITTEE: INQUIRY INTO ACCESS TO MEDICAL TECHNOLOGIES IN WALES
 Recommendations 1, 2, 3 1. That the Minister for Health and Social Services should, as a matter of priority, identify means by which a more strategic, coordinated and streamlined approach to medical technology
Recommendations 1, 2, 3 1. That the Minister for Health and Social Services should, as a matter of priority, identify means by which a more strategic, coordinated and streamlined approach to medical technology
Consultant Radiographers Education and CPD 2013
 Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
The Dementia Challenge:- Every Nurse s business providing care and support to everybody affected by dementia and their carers.
 The Dementia Challenge:- Every Nurse s business providing care and support to everybody affected by dementia and their carers. Dementia Self-Assessment Framework for all in patient settings Dementia Self-Assessment
The Dementia Challenge:- Every Nurse s business providing care and support to everybody affected by dementia and their carers. Dementia Self-Assessment Framework for all in patient settings Dementia Self-Assessment
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Wales Psychological Therapies Plan for the delivery of Matrics Cymru The National Plan 2018
 Wales Psychological Therapies Plan for the delivery of Matrics Cymru The National Plan 2018 Written by the National Psychological Therapies Management Committee, supported by 1000 Lives Improvement, Public
Wales Psychological Therapies Plan for the delivery of Matrics Cymru The National Plan 2018 Written by the National Psychological Therapies Management Committee, supported by 1000 Lives Improvement, Public
Agenda Item 3.3 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE
 FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health