,[*J. Caprock Cardiovascular Center, LLP CAPROCK
|
|
|
- Sabrina Holland
- 5 years ago
- Views:
Transcription


1




2

3
4 Caprock Cardiovascular Center, LLP ' 41 Street Lubbock, TX Phone: (806) Fax: (806)?0_! _57,[*J CAPROCK ;_AJllll!r '.tr. CLILAR: CLNT,;;"' "Iii CONSENT TO TREATEMENT: I (the patient/parent/guardian/legal representative of the patient acting on the patient's behalf) give permission for medical treatment, including radiology and laboratory procedures, to be performed by the physicians and staff of Caprock Cardiovascular Center, LLP. (Center). This consent is valid from this date forward. FINANCIAL AGREEMENT: The person signing below agrees, whether he/she signs as patient or representative of the patient, that in consideration of the services rendered to the patient, he/she hereby individually obligates himself/herself to pay the account of the Center at the Regular rates and terms of the Center. Should the account be referred to an attorney or collection agency for collection, the person signing below shall pay reasonable attorney's fees and collection expenses. "I assign payment for the unpaid charges for certain medical treatment furnished by the physicians and staff of Caprock Cardiovascular Center, LLP and by attending physicians for whom the Center is authorized to bill. I understand that 1 am responsible for any health insurance deductible and coinsurance at the time services are rendered." AGREEMENT AS TO GOVERNING LAW AND FORUM: The patient or patient's representative and health care provider, including employees and agents of the healthcare provider, rendering or providing medical care, health care, or safety, professional or administrative services directly related to the health care of the patient agree: (1) that all health care rendered shall be governed exclusively and only by Texas Law and in no event shall the law of any other state apply to any health care rendered to patient; and (2) in the event of a dispute, any lawsuit, action, or cause of which in any way relates to health care provided to the patient shah only be brought in a Texas Court in the county/district where all or substantially all of the health care was provided or rendered and in no event will any lawsuit, action or cause of action ever be brought in any other state. The choice of law and forum selection provisions of this paragraph are mandatory and are not permissive. ASSIGNMENT OF BENEFITS: In consideration of services rendered, I hereby assign to Caprock Cardiovascular Center, LLP, and/or any physician who has treated me, all rights, title and interest in any payment due me for services described herein as provfded in the policy or policies of insurance. I agree to pay the charges of the Center and/or attending physician which is greater than the amount paid by the insurance company or companies. ADVANCE DIRECTIVE/LIVING WILL: Do you have an Advance Directive/Living Will? Yes No If you answered No, would you like more information on Advance Directives? Yes No Patient Name: Patient Signature: Date:



5




6
7


8

9



10

11

12

13 CAPROCK ASSESSMENT SUMMARY SHEET Jason T. Bradley, MD, FACC Juan Kurdi, MD Date of visit: PCP; Name: Referring Physician: Date of Birth: Age: Sex: Marital Status: D M D S D W D D Chief Complaint: History (please do not write in this area): 1. Cardiovascular Review of Systems (Please mark yes or no to all questions) Place of Treatment 1. Myocardial Infarction (heart attack) 2. Heart Catherization 3. Coronary Angioplasty 4. Coronary Artery Bypass 5. Stress Test 6. Echocardiogram 7. Holter Monitor 8.EBT 9. Carotid Doppler 10. Lower Extremity Doppler 11. Bypass/ Angioplasty/S ent 1n Other Locations
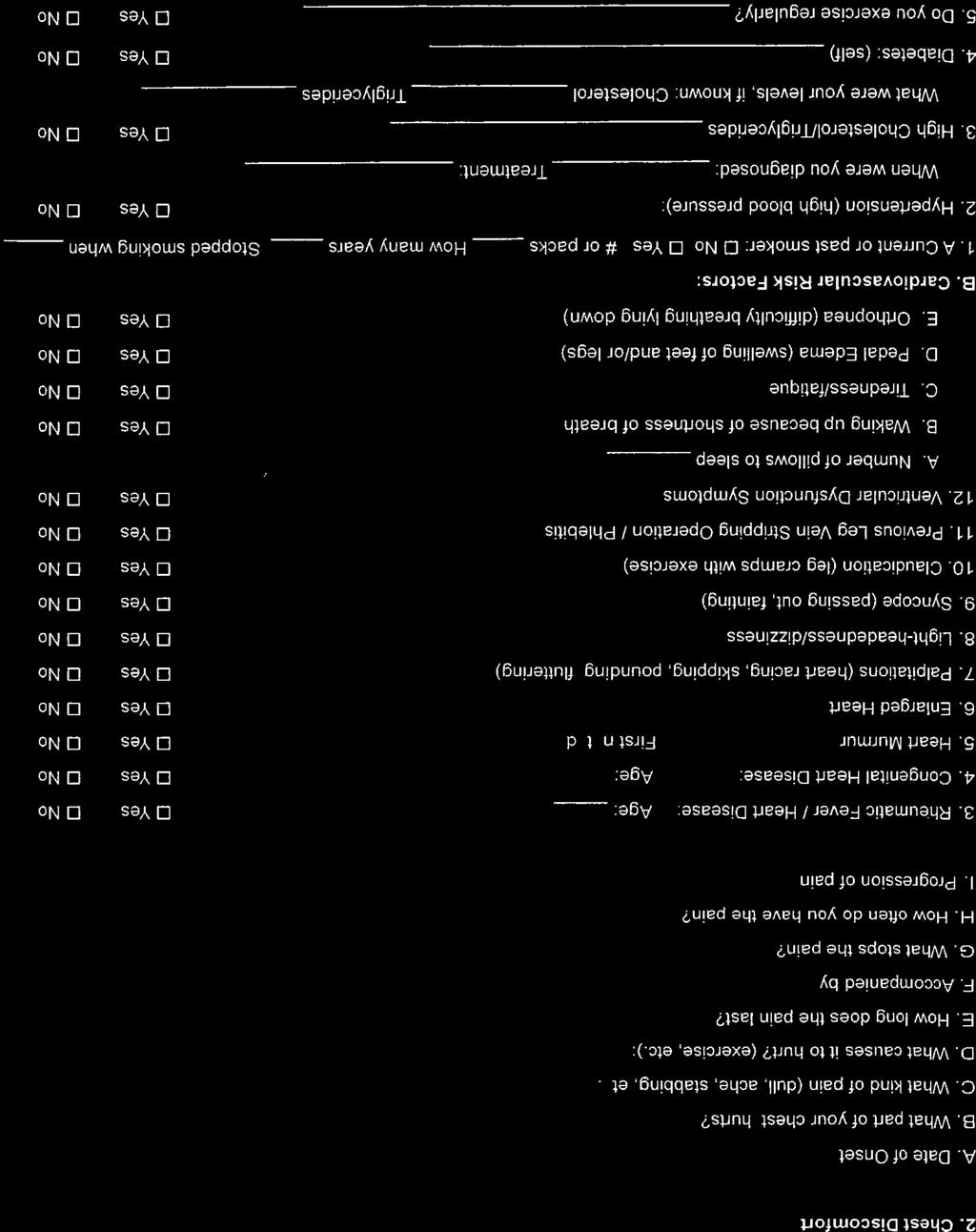
14 2. Chest Discomfort A. Date of Onset B. What part of your chest hurts? C. What kind of pain (dull, ache, stabbing, etc.): D. What causes it to hurt? (exercise, etc.): E. How long does the pain last? F. Accompanied by G. What stops the pain? H. How often do you have the pain? I. Progression of pain 3. Rheumatic Fever/ Heart Disease: Age: DYes D No 4. Congenital Heart Disease: Age: 5. Heart Murmur First noted: 6. Enlarged Heart 7. Palpitations (heart racing, skipping, pounding, fluttering) 8. Light-headedness/dizziness 9. Syncope (passing out, fainting) 10. Claudication (leg cramps with exercise) 11. Previous Leg Vein Stripping Operation I Phlebitis 12. Ventricular Dysfunction Symptoms A. Number of pillows to sleep B. Waking up because of shortness of breath C. Tiredness/fatique D. Pedal Edema (swelling of feet and/or legs) E. Orthopnea (difficulty breathing lying down) B. Cardiovascular Risk Factors: OYes D No OYes 0 No DYes D No DYes D No DYes D No DYes D No DYes 0 No DYes 0 No DYes 0 No DYes D No DYes D No DYes D No DYes D No 1. A Current or past smoker: D No D Yes # or packs How many years Stopped smoking when 2. Hypertension (high blood pressure): DYes D No When were you diagnosed: Treatment: 3. High Cholesterol/Triglycerides DYes D No What were your levels, if known: Cholesterol Triglycerides 4. Diabetes: (self) DYes ONo 5. Do you exercise regularly? DYes DNo
15 C. Present Medications: (Name of medication, dosage, how often you take medication) D. Allergies: Drugs: Foods: E, Past Medical/Surgical History: Reason for hospitalization Name of Hospital Dates of Hospitalizations Other Medical Problems: F. Social/Personal History: Place of Birth: Place of Residence ( city/state ) : Occupation: Do you drink caffeine: How much/ how often: Do you drink alcohol: Do you use recreational drugs: How much I how often: What kind/how much/how often: Do you have any religious restrictions: Have you had any recent stresses:

16


17
18 Caprock Cardiovascular Center, L.L.P. Consent For Use And Disclosure Of Protected Health Information For Treatment, Payment, Or Healthcare Operations I understand that as part of my healthcare, the Physician originates and maintains medical records describing my health history, symptoms, examination and test results, diagnosis, treatment, financial and demographic information, and any plans for future care or treatment. The Physician also originates and maintains billing records. I understand and consent to this infonnation being used or disclosed for the following purposes: Planning my care and treatment; Communications between my Physician and healthcare professionals that act under the direction of my Physician and participating in my diagnosis, evaluation, or treatment; Collection of fees for medical services; Detennining liabi1ity for payment and obtaining reimbursement; Conducting healthcare operations, including the evaluation of healthcare services, appropriateness and quality of healthcare treatment, and the qualifications of healthcare practitioners. I have been provided with a copy of the Physician's Notice of Privacy Practices that provides information about how the Physician uses and discloses Protected Health Infonnation about me. I understand that I have the following rights and privileges: The right to review the notice prior to signing this consent; and The right to request restrictions as to how my health information may be used or disclosed to carry out treatment, payment, or healthcare operations. The Physician is not required to agree to the requested restrictions. but is bound to any restrictions agreed to. I understand that as provided in the Notice of Privacy Practices, the terms of the Notice may change. If they do, I may obtain a revised copy from the privacy officer by calling (806) I understand that I may revoke this consent in writing, except to the extent that the Physician has already taken action in reliance thereon. I also understand that by refusing to sign or revoking this consent, the Physician may refuse to treat me. I wish to restrict the use or disclosure of my health information as follows: I understand that my confidential information may be released to the following individuals: Signature of Patient or Representative Date Patient Name Patient Identification Number (SSN) Name of Representative (if applicable) Relationship
19 Caprock Cardiovascular Center, LLP "' Street Lubbock, TX Phone: (806) Fax: (806) 701-S799 l+j CAPROCK -, i.:iji YA 1:':1'L..._ 4iii,t:;""1Tlrft, t..'-. MEDICARE AND/OR MEDICAID CERTIFICATION: The person signing below certifies that he/she has read this document and is the patient, or is duly authorized by the patient as the patient's representative, to execute the above and accept its terms. "I certify that the information given by me in applying for payment under Title XVII and/or Title XIX of the Social Security Administration is correct. I authorize any holder of medical or other information about me to release to the Social Security Administration or its intermediaries / carriers any information for this or related Medicare claim. I request that payment of authorized benefits be made on my behalf." Patient Name: Patient Signature: Date:
NAME SS# ADDRESS CITY STATE ZIP. TELEPHONE (home) (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE
 (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE") REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
CURE CARDIOVASCULAR CONSULTANTS
 NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Statement of Financial Responsibility
 Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
Statement of Financial Responsibility Patient Name: Date: Acct : BIR JV, LLP including; Out-Patient, In-Patient and, Home Health Rehab appreciates the confidence you have shown in choosing us to provide
DRUG / MEDICATION ALLERGIES: (include: Type/Reaction)
") NASSAU CHEST PHYSICIANS PC MEDICAL QUESTIONNAIRE 1 DATE: PATIENT NAME: DOB: DRUG / MEDICATION ALLERGIES: (include: Type/Reaction) 9/1/2014 PHARMACY NAME PHARMACY PHONE PHARMACY Street Address City State
NASSAU CHEST PHYSICIANS PC MEDICAL QUESTIONNAIRE 1 DATE: PATIENT NAME: DOB: DRUG / MEDICATION ALLERGIES: (include: Type/Reaction) 9/1/2014 PHARMACY NAME PHARMACY PHONE PHARMACY Street Address City State
POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX
 Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
James M. Wilson, M.D. - Medical Information to (fax to ) PATIENT INFORMATION Last name: First: D.O.
 PATIENT INFORMATION Last name: First: D.O.") James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
James B. Duke, MD PA Orthopedic Surgery 2300 SE 17 th Street, Suite 500 Ocala, FL
 James B. Duke, MD PA Orthopedic Surgery 2300 SE 17 th Street, Suite 500 Ocala, FL 34471 352-867-0444 Dear Patients: Welcome to our orthopaedic office. We appreciate your confidence and will take great
James B. Duke, MD PA Orthopedic Surgery 2300 SE 17 th Street, Suite 500 Ocala, FL 34471 352-867-0444 Dear Patients: Welcome to our orthopaedic office. We appreciate your confidence and will take great
New Patient Paperwork
 Your Vision Is Our Focus New Patient Paperwork Dear Patient, Please fill out all of the following pages, and bring them with you to your scheduled appointment time. If you have questions regarding your
Your Vision Is Our Focus New Patient Paperwork Dear Patient, Please fill out all of the following pages, and bring them with you to your scheduled appointment time. If you have questions regarding your
Patient: Gender: Male Female. Mailing Address: Ethnicity: Not Hispanic or Latin Hispanic/Latin Home Phone #:
 5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Medical History Form
 Medical History Form Patient Name of Birth Medical History Do you have or have you had any of the following? Condition Yes No Condition Yes No Condition Yes No ADHD Stroke Menopausal Syndrome Allergies
Medical History Form Patient Name of Birth Medical History Do you have or have you had any of the following? Condition Yes No Condition Yes No Condition Yes No ADHD Stroke Menopausal Syndrome Allergies
Patient Registration. City, State & Zip Code Date of Birth Age. Occupation: Family Physician: Married Single Other Spouse's Name
 *SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
*SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group
 DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
We welcome you as a patient
 St. Augustine Cardiology Associates, P.A. Ferris E. George, M.D. Robert N. Signor, M.D. Billie J. Russell, PhD, ARNP-BC Susan W. Morrow, ARNP 201 Health Park Blvd., Suite 105 St Augustine, FL. 32086 904-824-1776
St. Augustine Cardiology Associates, P.A. Ferris E. George, M.D. Robert N. Signor, M.D. Billie J. Russell, PhD, ARNP-BC Susan W. Morrow, ARNP 201 Health Park Blvd., Suite 105 St Augustine, FL. 32086 904-824-1776
- Cardiac Catherization - Cardiac Angioplasty - Cardiac Bypass - MUGA - CT Scan
 Thank you for making an appointment with our office. We look forward to meeting you. Please help us to prepare for your appointment by gathering the information we will need to make the most of your time
Thank you for making an appointment with our office. We look forward to meeting you. Please help us to prepare for your appointment by gathering the information we will need to make the most of your time
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD
 Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD PATIENT LAST NAME: FIRST NAME: MI: MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE: WORK PHONE: CELL PHONE: MARITAL STATUS: DATE OF BIRTH:
Retina Center of Oklahoma Demographic Information Sam S. Dahr,MD PATIENT LAST NAME: FIRST NAME: MI: MAILING ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE: WORK PHONE: CELL PHONE: MARITAL STATUS: DATE OF BIRTH:
LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W
 CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W") PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
Patient Demographic Sheet
 Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with?
 Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
Filling out this form will help us provide the best possible care for you. What are the main questions or problems you would like help with? 1. 2. 3. IMPORTANT PLEASE BRING A COMPUTER DISK WITH ANY BRAIN
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
New Patient Intake Questionnaire
 New Patient Intake Questionnaire NAME: DATE: / / BIRTHDATE: / / REFERRED BY: AGE: REASON FOR VISIT: LOCATION OF PAIN: BACK HIP BUTTOCK LEG FOOT RIGHT LEFT NECK ARM SHOULDER HAND RIGHT LEFT OTHER (DESCRIBE)
New Patient Intake Questionnaire NAME: DATE: / / BIRTHDATE: / / REFERRED BY: AGE: REASON FOR VISIT: LOCATION OF PAIN: BACK HIP BUTTOCK LEG FOOT RIGHT LEFT NECK ARM SHOULDER HAND RIGHT LEFT OTHER (DESCRIBE)
St. Mary s Industrial Medicine 4017 Atlanta Hwy, Ste B Bogart, GA Phone: (706) Fax: (706)
 Fax: (706)") Please Fill Out Completely: St. Mary s Industrial Medicine Patient s Last Name First Name MI Social Security Number Date of Birth Age Gender Race Marital Status Ethnicity (Circle one): Language Latino
Please Fill Out Completely: St. Mary s Industrial Medicine Patient s Last Name First Name MI Social Security Number Date of Birth Age Gender Race Marital Status Ethnicity (Circle one): Language Latino
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
APPOINTMENT INFORMATION SHEET
 APPOINTMENT INFORMATION SHEET All appointments for new patients will require a one-time, refundable deposit of $50.00 to secure your appointment. You may use cash, check or credit card. The check or credit
APPOINTMENT INFORMATION SHEET All appointments for new patients will require a one-time, refundable deposit of $50.00 to secure your appointment. You may use cash, check or credit card. The check or credit
Sage Medical Center New Patient Forms
 Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
PATIENT INFORMATION Please Print
 PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
New Patient Information
 New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
Amarillo Endoscopy Center Srinivas Pathapati, MD., PA 6833 Plum Creek Drive Amarillo, TX (806)
") Today s Date: / / PATIENT INFORMATION Patient s Last Name First Middle Mr. Miss Mrs. Ms. Marital Status (Circle one) Single / Mar / Div / Sep / Widow Legal Name (If applicable) Maiden Name Birth Date Age
Today s Date: / / PATIENT INFORMATION Patient s Last Name First Middle Mr. Miss Mrs. Ms. Marital Status (Circle one) Single / Mar / Div / Sep / Widow Legal Name (If applicable) Maiden Name Birth Date Age
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
TOS Health Questionnaire
 Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
May Family Chiropractic Health Information and Health History Patient Name: Gender: Male Female
 1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
PETER BOWER, M.D Rolkin Court, Suite 301. Charlottesville VA (434) F(434) Today's date. Name:
 F(434) Today's date. Name:") PETER BOWER, M.D. A N D A S S O C I A T E S 1415 Rolkin Court, Suite 301 Charlottesville VA 22911 (434)964-0159 F(434)978-1667 Today's date Name: Date of Birth: Male Female Social Security # Mailing Address:
PETER BOWER, M.D. A N D A S S O C I A T E S 1415 Rolkin Court, Suite 301 Charlottesville VA 22911 (434)964-0159 F(434)978-1667 Today's date Name: Date of Birth: Male Female Social Security # Mailing Address:
Neck & Spine Patient Demographic
 Neck & Spine Patient Demographic o New Patient o Return Patient o Update Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg.
Neck & Spine Patient Demographic o New Patient o Return Patient o Update Account #: Physician: Last Name First Name MI: Address City State Zip Home Phone o OK to Leave Msg. Work Phone o OK to Leave Msg.
Women s Specialty Care, P.C 682 Hemlock Street Suite 300 Macon GA WELCOME
 Women s Specialty Care, P.C 682 Hemlock Street Suite 3 Macon GA 3121 478-744-9683 WELCOME Thank you for choosing Women s Specialty Care, P.C. for your OB/GYN needs. We ask that you complete all of the
Women s Specialty Care, P.C 682 Hemlock Street Suite 3 Macon GA 3121 478-744-9683 WELCOME Thank you for choosing Women s Specialty Care, P.C. for your OB/GYN needs. We ask that you complete all of the
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c
 W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
PATIENT REGISTRATION FORM (ecw)
") PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
SPOUSE/GUARDIAN (If patient is married, give spouse information. If patient is a child, give parent information.)
") Please Fill Out Completely: St. Mary s Women s Center 1000 Cowles Clinic Way, Suite D-300 Greensboro, GA 30642 762-243-3860 phone 762-243-3879 fax Patient s Last Name First Name MI Social Security Number
Please Fill Out Completely: St. Mary s Women s Center 1000 Cowles Clinic Way, Suite D-300 Greensboro, GA 30642 762-243-3860 phone 762-243-3879 fax Patient s Last Name First Name MI Social Security Number
Name DOB / / SS# / / Street Address City/State/Zip. Home ( ) - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -
 - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -") Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
PATIENT REGISTRATION
 of Appointment: Referring Physician: Denton Watumull, M.D. Derek Rapp, M.D. Joshua Lemmon, M.D. Chase Derrick, M.D. Submit completed form to your patient coordinator s email, print out or email to: Bruce
of Appointment: Referring Physician: Denton Watumull, M.D. Derek Rapp, M.D. Joshua Lemmon, M.D. Chase Derrick, M.D. Submit completed form to your patient coordinator s email, print out or email to: Bruce
PATIENT INFORMATION Indiana Plastic Surgery Center, PC
 PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
INSURANCE INFORMATION
 2014 575 Hill Country Dr. Ste 202 Kerrville, TX 78028 (830)258-6237 Office (830)315-1366 Fax Patient Name (last, first, MI) of Birth Social Security Number Mailing Address Home Telephone Work Telephone
2014 575 Hill Country Dr. Ste 202 Kerrville, TX 78028 (830)258-6237 Office (830)315-1366 Fax Patient Name (last, first, MI) of Birth Social Security Number Mailing Address Home Telephone Work Telephone
Welcome to Rebound Sports & Physical Therapy!
 Welcome to Rebound Sports & Physical Therapy! We are happy you chose us to assist with your care. We strive towards providing an excellent experience for all our patients as we assist you in regaining
Welcome to Rebound Sports & Physical Therapy! We are happy you chose us to assist with your care. We strive towards providing an excellent experience for all our patients as we assist you in regaining
Louis R. Vita, D.D.S., F.A.G.D. 991 Van Houten Avenue Clifton, NJ Phone:
 Louis R. Vita, D.D.S., F.A.G.D. 991 Van Houten Avenue Clifton, NJ 07013 Phone: 973-777-1933 Fax: 973-777-4727 Email: Vitaoffice991@gmail.com Website: DrLouisVita.com We are pleased to welcome you to our
Louis R. Vita, D.D.S., F.A.G.D. 991 Van Houten Avenue Clifton, NJ 07013 Phone: 973-777-1933 Fax: 973-777-4727 Email: Vitaoffice991@gmail.com Website: DrLouisVita.com We are pleased to welcome you to our
We must have ALL paperwork least 72 hrs prior to your appointment, Thanks.
 Thomas A. Lombardo, MD T. Randolph Lombardo, MD Jorge A. Hernandez, MD Alfred B. Brady, MD Mark Fasulo, MD Allen D. McGrew, DO, FACC Sheila DeVaugh, APRN, BC Greg Gilbreath, APRN, BC Amanda J. Reneau,
Thomas A. Lombardo, MD T. Randolph Lombardo, MD Jorge A. Hernandez, MD Alfred B. Brady, MD Mark Fasulo, MD Allen D. McGrew, DO, FACC Sheila DeVaugh, APRN, BC Greg Gilbreath, APRN, BC Amanda J. Reneau,
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
MAIN STREET MEDICAL NEW PATIENT QUESTIONNAIRE
 NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
Department of Internal Medicine Division of Cardiology
 Department of Internal Medicine Division of Cardiology APPOINTMENTS: (813) 259-0600 TOLL FREE: (888) USF-DOCS WEB: www.usfdocs.com Provider: Appt. Date: Appt. Time: We1come to the University of South Florida
Department of Internal Medicine Division of Cardiology APPOINTMENTS: (813) 259-0600 TOLL FREE: (888) USF-DOCS WEB: www.usfdocs.com Provider: Appt. Date: Appt. Time: We1come to the University of South Florida
 ADVANCED DIRECTIVES ACKNOWLEDGEMENT FORM Patient Name: Date: I do have an Advanced Directive / Living Will / Durable Power of Attorney for medical or health care decisions. I do not have an Advanced Directive
ADVANCED DIRECTIVES ACKNOWLEDGEMENT FORM Patient Name: Date: I do have an Advanced Directive / Living Will / Durable Power of Attorney for medical or health care decisions. I do not have an Advanced Directive
Bay area Advanced Gastroenterology Care
 Authorization to Release Medical Information Date: Patient s Name: Patient s Address: Date of Birth: I hereby authorize you to transfer or make available all medical records or reports relating to my care
Authorization to Release Medical Information Date: Patient s Name: Patient s Address: Date of Birth: I hereby authorize you to transfer or make available all medical records or reports relating to my care
WELCOME TO THE UPMC LIVER CANCER CENTER PLEASE FILL OUT AND BRING WITH YOU TO YOUR APPOINTMENT
 WELCOME TO THE UPMC LIVER CANCER CENTER PLEASE FILL OUT AND BRING WITH YOU TO YOUR APPOINTMENT You are scheduled to have an appointment at the UPMC Liver Cancer Center which is located in the UPMC Montefiore
WELCOME TO THE UPMC LIVER CANCER CENTER PLEASE FILL OUT AND BRING WITH YOU TO YOUR APPOINTMENT You are scheduled to have an appointment at the UPMC Liver Cancer Center which is located in the UPMC Montefiore
Last Name First Middle. Mailing Address. City State Zip Phone. Date of Birth Age Soc. Sec# Cell. Employer Work Phone
 Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
Last Name First Middle Mailing Address City State Zip Phone Date of Birth Age Soc. Sec# Cell Employer Work Phone Email Address Emergency contact Phone # Relation: Name of Primary Insurance Policy # -----
Patient Information: Last Name First Name MI. Address Apt/Room # City Zip. Community name (if not at home) Martial Status: S M W D
 Martial Status: S M W D") HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
PATIENT INFORMATION & CONDITION FORM
 PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
PATIENT INFORMATION & CONDITION FORM Patient Name: Today's Date: / / Social Security Number Birth Date: / / Age: Gender: F M Email Height : Weight: Specify Right or Left Handed Have you ever been in our
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
Patient Information. Insurance Information. Emergency Contact
 Page 1 of 2 Name: Patient Information RVC-A1 Social Security Number: Gender:!Male!Female of birth: Mailing Address: City: State: Zip: Home phone: ( ) Work phone: ( ) Insurance Information Name of policyholder:
Page 1 of 2 Name: Patient Information RVC-A1 Social Security Number: Gender:!Male!Female of birth: Mailing Address: City: State: Zip: Home phone: ( ) Work phone: ( ) Insurance Information Name of policyholder:
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
HEALTH. CENTER Main St NE, Suite 101 PO Box 507 Duvall, WA ph fax Dr. Jeffrey P. Metcalf
 Welcome To Our Office Name I prefer to be called First MI Last Home Address: Street City Zip Mailing Address: Street City Zip Phone: ( ) ( ) ( ) Home Cell Work E-mail: Birth : / / Age: Male / Female Marital
Welcome To Our Office Name I prefer to be called First MI Last Home Address: Street City Zip Mailing Address: Street City Zip Phone: ( ) ( ) ( ) Home Cell Work E-mail: Birth : / / Age: Male / Female Marital
CATARACT AND LASER CENTER, LLC
 CATARACT AND LASER CENTER, LLC Patient Information Date: Patient Name: M F Address: Street City State Zip Home Phone: Work Phone: Cell Phone: E-Mail : Referred by: Medical Doctor: Who is your regular eye
CATARACT AND LASER CENTER, LLC Patient Information Date: Patient Name: M F Address: Street City State Zip Home Phone: Work Phone: Cell Phone: E-Mail : Referred by: Medical Doctor: Who is your regular eye
Patient Name Age Date of Birth. Patient Address. City State Zip Code. Home Phone Cell Phone Work Phone
 Patient Registration Date Patient Information Patient Name Age Date of Birth Patient Address City State Zip Code Home Phone Cell Phone Work Phone Last 4 Digits of Your Social Security Number Email Marital
Patient Registration Date Patient Information Patient Name Age Date of Birth Patient Address City State Zip Code Home Phone Cell Phone Work Phone Last 4 Digits of Your Social Security Number Email Marital
Dear New Patient: Sincerely, The Scheduling Staff
 Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Pediatric Patient History
 Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Fax: Do not mail the forms!
 Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
NEW PATIENT PACKET. Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone. Address: Driver s License #:
 Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Psychological Services Agreement
 John A. Watterson, Ph.D. 4101 Parkstone Heights Drive, Suite 260 Austin, Texas 78746 Phone: 512-306-0663 Fax: 512-306-8086 Website: www.johnwatterson.com Psychological Services Agreement Welcome to my
John A. Watterson, Ph.D. 4101 Parkstone Heights Drive, Suite 260 Austin, Texas 78746 Phone: 512-306-0663 Fax: 512-306-8086 Website: www.johnwatterson.com Psychological Services Agreement Welcome to my
Family Care Health Centers
 Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
ALFRED ALINGU, MD INTERNAL MEDICINE
 Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Welcome to Hawaii Women s Healthcare
 Cheryl Lynn T. Rudy, M.D. Cheryl L. Leialoha, M.D. Erin C. Gertz, M.D. Laura A. Spector, D.O. Andrea Wieland, APRN Welcome to Hawaii Women s Healthcare Hawaii Women s Healthcare strives to provide you
Cheryl Lynn T. Rudy, M.D. Cheryl L. Leialoha, M.D. Erin C. Gertz, M.D. Laura A. Spector, D.O. Andrea Wieland, APRN Welcome to Hawaii Women s Healthcare Hawaii Women s Healthcare strives to provide you
Independent Wellness Center 1000 W. Apache Trail, Suite #108, Apache Junction, AZ Phone# Fax #
 PATIENT INTAKE Welcome t o Independent Wellness Center. In order to provide you with the best health care and assist you with other details of our clinic, we have provided the following information. We
PATIENT INTAKE Welcome t o Independent Wellness Center. In order to provide you with the best health care and assist you with other details of our clinic, we have provided the following information. We
PATIENT INFORMATION RESPONSIBLE PARTY INFORMATION NAME: DOB: SEX: M / F SOCIAL SECURITY # RELATIONSHIP TO PATIENT: PHONE #: CELL#: EMPLOYER:
 PATIENT INFORMATION NAME: DOB: SEX: MALE / FEMALE SOCIAL SECURITY #: MARITAL STATUS: ADDRESS: CITY: STATE: ZIP CODE: PHONE #: CELL#: E-MAIL: PATIENT'S EMPLOYER: OCCUPATION: WORK PHONE: WHERE IS THE BEST
PATIENT INFORMATION NAME: DOB: SEX: MALE / FEMALE SOCIAL SECURITY #: MARITAL STATUS: ADDRESS: CITY: STATE: ZIP CODE: PHONE #: CELL#: E-MAIL: PATIENT'S EMPLOYER: OCCUPATION: WORK PHONE: WHERE IS THE BEST
ANNUAL FOLLOW-UP FORM
 Public reporting burden for this collection of information is estimated to average 6-15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and
Public reporting burden for this collection of information is estimated to average 6-15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and
THE COUNSELING PLACE ADULT INTAKE FORM Yearly Family Income:
 Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Burton M. Sundin, M.D. / Reps B. Sundin, M.D. Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: address:
: Address: Zip, City, State: Home#: Work#: Cell#: address:") Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
Patient Registration Form
 Patient Registration Form Please Complete the Following Information-Thank You Patient Information: Name: Last First MI Address: City: State: Zip: Home Telephone: Work Telephone: Best to Reach? Home? Work?
Patient Registration Form Please Complete the Following Information-Thank You Patient Information: Name: Last First MI Address: City: State: Zip: Home Telephone: Work Telephone: Best to Reach? Home? Work?
Worker s Compensation Forms
 Patient Name: DOB: Employer Name: Address: Claim Number: Date of Injury/DOI: Description of Accident: Adjuster s Information Adjuster s Name: Adjuster s Phone Number: Fax Number: Workers Compensation Insurance
Patient Name: DOB: Employer Name: Address: Claim Number: Date of Injury/DOI: Description of Accident: Adjuster s Information Adjuster s Name: Adjuster s Phone Number: Fax Number: Workers Compensation Insurance
Please allow us hours to refill the medication; approval from your medical provider is required on all refills.
 Thank you for choosing Rex Primary Care of Holly Springs for your primary care needs. To keep our patients better informed we have created a list of our office policies to make your visit and continuation
Thank you for choosing Rex Primary Care of Holly Springs for your primary care needs. To keep our patients better informed we have created a list of our office policies to make your visit and continuation
MR #: Patient Name: Page: 1 of 4 PROGRESSIVE PHYSICAL THERAPY PATIENT DATA SHEET. May we send you text messages relating to your care with us?
 MR #: Patient Name: Page: 1 of 4 PROGRESSIVE PHYSICAL THERAPY PATIENT DATA SHEET First: MI: Last: of Birth: Age: Gender: Male Female Mailing Address: Physical Address: May we send you text messages relating
MR #: Patient Name: Page: 1 of 4 PROGRESSIVE PHYSICAL THERAPY PATIENT DATA SHEET First: MI: Last: of Birth: Age: Gender: Male Female Mailing Address: Physical Address: May we send you text messages relating
Patient Name: Last First Middle
 Wilmington Ear Nose & Throat Associates, PA Patient Information Form Patient Name: Last First Middle Mailing Address: Street Address (if different from above): City: State: Zip Code: Social Security #:
Wilmington Ear Nose & Throat Associates, PA Patient Information Form Patient Name: Last First Middle Mailing Address: Street Address (if different from above): City: State: Zip Code: Social Security #:
Flossmoor: (708) Harvey: (708) Tinley Park: (708) ICOR: (708) Crestwood: (708) Patient Signature:
 Harvey: (708) Tinley Park: (708) ICOR: (708) Crestwood: (708) Patient Signature:") Patient Information Guidelines Department of Outpatient Therapy Services Physical, Speech and Occupational Therapy The staff at Ingalls Outpatient Therapy Services Department is dedicated to providing
Patient Information Guidelines Department of Outpatient Therapy Services Physical, Speech and Occupational Therapy The staff at Ingalls Outpatient Therapy Services Department is dedicated to providing
Emergency Contact Name: Relationship: Home #: ( ) Cell #: ( ) Alternate #: ( ) Pharmacy Information Pharmacy Name: Phone #: ( ) Location:
 Cell #: ( ) Alternate #: ( ) Pharmacy Information Pharmacy Name: Phone #: ( ) Location:") New Patient Office Information Last Name: First Name: Initial Date of Birth: SSN # Marital Status: Single Married Divorced Widowed Address: City: State: Zip: Gender: M Parent/ Legal Guardian if Patient
New Patient Office Information Last Name: First Name: Initial Date of Birth: SSN # Marital Status: Single Married Divorced Widowed Address: City: State: Zip: Gender: M Parent/ Legal Guardian if Patient
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD
 Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
Patient History. Name: Date: / / 20. Street Address: City: State: ZIP:
 Patient History Name: Date: / / 20 Street Address: City: State: ZIP: Social Security Number: / / Date of Birth: / / Age: Marital Status: Single Married Divorced Widow/er Employer: Occupation: Spouse's
Patient History Name: Date: / / 20 Street Address: City: State: ZIP: Social Security Number: / / Date of Birth: / / Age: Marital Status: Single Married Divorced Widow/er Employer: Occupation: Spouse's
Body Basics Physical Therapy Medical History
 Body Basics Physical Therapy Medical History Name Date Age Height Weight Hand Dominance: Right/Left Primary Language Do you require an interpreter? Yes/No How did you hear about us? Doctor s First and
Body Basics Physical Therapy Medical History Name Date Age Height Weight Hand Dominance: Right/Left Primary Language Do you require an interpreter? Yes/No How did you hear about us? Doctor s First and
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL
 Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Lives (circle one): in assisted living with a relative alone
: in assisted living with a relative alone") Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip
 PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
NEW PATIENT INFORMATION: ADULT
 NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
Patient Information. Address: City: State: Zip: Spouse/Guardian s Last 4 Digits S.S. #: Phone: ( ) Cell Phone: ( ) Emergency Contact Information
 Cell Phone: ( ) Emergency Contact Information") Patient Information Patient Name: D.O.B: Marital Status: Age: Address: Gender: Male Female City: State: Zip: Last 4 Digits S.S #: Home: ( ) Cell Phone: ( ) E-mail Address: Patient Occupation: Phone: (
Patient Information Patient Name: D.O.B: Marital Status: Age: Address: Gender: Male Female City: State: Zip: Last 4 Digits S.S #: Home: ( ) Cell Phone: ( ) E-mail Address: Patient Occupation: Phone: (
Authorization, Fees, and Office Policy
 a Authorization, Fees, and Office Policy Authorization for Treatment I hereby authorize the staff of Compassionate Care Clinics of Pinellas to render medical services as deemed necessary. I also certify
a Authorization, Fees, and Office Policy Authorization for Treatment I hereby authorize the staff of Compassionate Care Clinics of Pinellas to render medical services as deemed necessary. I also certify
PATIENT INSTRUCTIONS FOR PAPERWORK
 330 Mallory Sta-on Rd., Suite B3 Franklin, TN 37067 Ph. 615-944-3530 Fax. 615-550.2641 PATIENT INSTRUCTIONS FOR PAPERWORK Thank you so much for trus0ng your care to Integra0ve Family Medicine. A
330 Mallory Sta-on Rd., Suite B3 Franklin, TN 37067 Ph. 615-944-3530 Fax. 615-550.2641 PATIENT INSTRUCTIONS FOR PAPERWORK Thank you so much for trus0ng your care to Integra0ve Family Medicine. A
Bellevue Neurology PATIENT DEMOGRAPHIC FORM
 PATIENT DEMOGRAPHIC FORM Name Today s date / / Last First M.I. Mailing Address Age Number, Street, Apartment Number City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Date of Birth / / SS # Marital
PATIENT DEMOGRAPHIC FORM Name Today s date / / Last First M.I. Mailing Address Age Number, Street, Apartment Number City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Date of Birth / / SS # Marital