ED OVERCROWDING: Evidence Based review
|
|
|
- Alfred Lang
- 5 years ago
- Views:
Transcription



1 ED OVERCROWDING: Evidence Based review Prof Drew Richardson BMedSc MBBS(Hons) FACEM GradCertHE MD NRMA-ACT Road Safety Trust Chair of Road Trauma and Emergency Medicine Australian National University Medical School
2 Declaration This research was carried out whilst an employee of the Australian National University Medical School and was not separately funded Views expressed are those of the author and do not necessarily reflect those of any of his employers Overcrowding is my major research interest The Unit has received research funding Author has received travel/other expenses to speak Author owns no related shares
3 Objectives Outline the history of research into ED overcrowding Describe the major landmark studies in the field Identify generally accepted research about the causes, effects, and possible solutions Review research developments over the last three years in detail Since this is a rather dry topic, intersperse with anecdote, data and analogy which may help explain the issues
4 ACEP Crowding (rev Feb 2013) Crowding occurs when the identified need for emergency services exceeds available resources for patient care in the emergency department (ED), hospital, or both. The causes of crowding are multifactorial and span the entire health care delivery system. Research has shown a continued increase in ED visits, which has outpaced population growth. Current trends show increasing patient acuity as well, requiring more complex evaluation and treatment plans that increase care delivery times, as well as ED and inpatient lengths of stay. The resultant strain on hospital inpatient bed capacity creates downstream pressure to board admitted patients* in the ED. These factors exacerbate crowding by utilizing limited ED resources, including beds and nursing care. Evidence has shown an increase in morbidity and mortality because of boarding. *A boarded patient is defined as a patient who remains in the ED after being admitted to the facility but has not been transferred to an inpatient unit. Results of crowding include the following: treatment of patients in areas not designated for treatment, such as hallways treatment of boarded inpatients by outpatient (ED) nurses increased morbidity and mortality for both boarded and other ED patients increased disability in older patients who are discharged to facilities rather than admitted increased inpatient length of stay decreased patient satisfaction significant delay in evaluation and treatment of emergency patients patients leaving before completion of medical treatment increased ambulance diversion time increased costs It is the responsibility of hospital leadership to address well identified recurrent causes of crowding (such as unavailability of inpatient beds) to prevent poor outcomes related to crowding. It is imperative that local and national health care systems be active in addressing the more global and systemic causes of crowding, including hospital funding. Emergency medicine leadership should be actively involved in helping to identify successful solutions to crowding at both the local and national levels.

5 Overcrowding Concept of overcrowding is almost as old as the concept of crowds Wherever herd animals gather, the useful maximum number is sometimes exceeded unless there are external controls




6 Overcrowding Earliest descriptions of overcrowding in a healing setting date to biblical times Hospital Overcrowding and adverse effects described since at least the mid nineteenth century

: 20-5 Can Med Assoc J 1974 May")
7 Overcrowding Studies reporting increased ED workload pre-date recognition of ED as a specialty Multiple proposed solutions started 40 years ago Emerged as a significant subject for research NEJM 1958 Jan 2; 258(1): 20-5 Can Med Assoc J 1974 May 4; 110(9):

8 1148 papers in international literature to Feb 2016 Read all these abstracts so you don t have to
9 History Overcrowding became a major issue in USA in late 1980s Traditionally started in New York Others lay claim Scientific descriptions started in 1990s General Medical Literature Health Services Literature Emergency Medicine Literature Clear recognition that cause and solutions lay outside ED Gallagher EJ, Lynn SG. The etiology of medical gridlock: causes of emergency department overcrowding in New York City. J Emerg Med Nov-Dec;8(6): Schneider S, Zwemer F, Doniger A, Dick R, Czapranski T, Davis E. Rochester, New York: a decade of emergency department overcrowding. Acad Emerg Med Nov; 8(11): Bindman AB, Grumbach K, Keane D, Rauch L, Luce JL. Consequences of Queuing for Care at a Public Hospital Emergency Department. JAMA Aug 28;266(8): Baker DW, Stevens CD, Brook RH. Patients who leave a public hospital emergency department without being seen by a physician. Causes and consequences. JAMA Aug 28;66(8): Kellermann AL, Hackman BB. Patient 'dumping' post-cobra. Am J Public Health Jul;80(7):864-7 Grumbach K, Keane D, Bindman A. Primary Care and Public Emergency Deaprtment Overcrowding. Am J Public Health Mar;83:372-8 Andrulis DP, Kellermann A, Hintz EA, Hackman BB, Weslowski VB. Emergency departments and crowding in United States teaching hospitals. Ann Emerg Med Richards JR, Navarro ML, Derlet RW. Survey of directors of emergency departments in California on overcrowding. West J Med Jun;172(6):385-8
10 History Despite a lack of supporting evidence, unambiguously stated that overcrowding was a threat to patient safety Early publications tended to start from this assumption then describe ways to fix it Triage Short stay Units Multimodal interventions G Dickinson. Emergency department overcrowding. CMAJ Feb 1;140(3): Shah CP, Carr LM. Triage: a working solution to over crowding in the emergency department. Can Med Assoc J May 4;110(9): Neville L, Rowand RS. Short stay unit solves emergency overcrowding. Dimens Health Serv Feb;60(2): 26-7 Feferman I, Cornell C. How we solved the overcrowding problem in our emergency department. CMAJ Feb 1;140(3): Lynn SG, Kellermann AL. Critical decision making: managing the emergency department in an overcrowded hospital. Ann Emerg Med Mar;20(3): Cooke J, Finneran K. A clearing in the crowd: innovations in emergency services. Pap Ser United Hosp Fund N Y Jan: 1-43
11 History First systematic research showed association with increased costs Krochmal P, Riley TA. Increased health care costs associated with ED overcrowding. Am J Emerg Med May;12(3):265-6 Actually spending midnight in ED not associated with less ward LOS First outcome study showed increased mortality in Spain Miró O, Antonio MT, Jiménez S, De Dios A, Sánchez M, Borrás A, Millá J. Decreased health care quality associated with emergency department overcrowding. Eur J Emerg Med Jun;6(2):105-7 Weak methodology, weekly presentations, no correction for seasonal factors First Review article listed 8 adverse effects but provided a reference for only one of them (ambulance diversion) Derlet RW, Richards JR. Overcrowding in the nation's emergency departments: complex causes and disturbing effects. Ann Emerg Med Jan;35(1):63-8
12 Systematic studies New generation of researchers entered the field in 2000s Systematically examined Definitions (still needs work) Causes Effects Process Quality Patient Outcome including mortality Solutions Fair to say that even with good data it has proven difficult to persuade our inpatient and administrative colleagues Even if our children think we research the bleeding obvious
13 Colleges needed no persuasion Crowding occurs when the identified need for emergency services exceeds available resources for patient care in the emergency department (ED), hospital, or both Overcrowding is the situation where Emergency Department function is impeded primarily because the number of patients waiting to be seen, undergoing assessment and treatment, or waiting for departure exceeds either the physical or the staffing capacity of the Emergency Department Access Block is the situation where patients in the ED requiring inpatient care are unable to gain access to appropriate hospital beds within a reasonable time frame. It is expressed as the proportion of patients requiring formal admission to hospital who have a total ED time greater than 8 hours American College of Emergency Physicians. Crowding. Ann Emerg Med Jun;47(6):585 Australasian College for Emergency Medicine. Policy document standard terminology. Emerg Med (Aust) 2002; 14: Australasian College for Emergency Medicine. Policy document standard terminology. Emerg Med (Aust) 2002; 14:
 Australia: 37% over decade 2000-01 to 2009-10 1.")
14 Causes of Overcrowding - 1 Increasing demand at the front door noted since 1950s Build it and they will come USA: 102.8M in 1999 to 136.1M in 2009 (32%) 37.8/100 to 45.1/100 persons (19%) Australia: 37% over decade to % annual increase after population growth Development of EM as a specialty has contributed to a positive attitude towards ER Development of medical care in general increases demand Population aging is important Shortliffe EC, Hamilton TS, Noroian EH. The emergency room and the changing pattern of medical care. N Engl J Med Jan 2;258(1):20-5

15 Causes of Overcrowding - 2 Accepted by professional bodies that access to inpatient beds ( access block ) and resultant boarders causative This research base started in 2003 Clear statistical link between hospital occupancy and ED LOS Subsequently confirmed in multiple studies around world Mostly retrospective Ever increasing sophistication Forster AJ, Stiell I, Wells G, Lee AJ, van Walraven C. The effect of hospital occupancy on emergency department length of stay and patient disposition. Acad Emerg Med Feb;10(2): Dunn R. Reduced access block causes shorter emergency department waiting times: an historical control observational study. Emerg Med Australas Jun;15(3):232-8 Fatovich DM, Nagree Y, Sprivulis P. Access block causes emergency department overcrowding and ambulance diversion in Perth, Western Australia. Emerg Med J May;22(5):351-4 Fatovich DM, Hirsch RL. Entry overload, emergency department overcrowding, and ambulance bypass. Emerg Med J Sep;20(5):406-9
16 Causes of Overcrowding - 3 Politicians and funders tended to blame nonurgent patients, GP-type patients, uninsured Language and reasoning varied but everywhere Nagree Y, Ercleve TN, Sprivulis PC. After-hours general practice clinics are unlikely to reduce low acuity patient attendances to metropolitan Perth emergency departments. Aust Health Rev Dec 13;28(3): Dent AW, Phillips GA, Chenhall AJ, McGregor LR. The heaviest repeat users of an inner city emergency department are not general practice patients. Emerg Med (Fremantle) Aug;15(4):322-9 Sprivulis P. Estimation of the general practice workload of a metropolitan teaching hospital emergency department. Emerg Med (Fremantle). 2003;15:32-37 Sprivulis P, Grainger S, Nagree Y. Ambulance diversion is not associated with low acuity patients attending Perth metropolitan emergency departments. Emerg Med Australas Feb;17(1):11-5 Research response also Health Services Research Foundation. Myth: Emergency room happened around the world Canadian overcrowding is caused by non-urgent cases. J Health Serv Res Policy Jul;15(3):188-9 Retrospective studies of load Schull MJ, Kiss A, Szalai JP. The effect of low-complexity patients on Some prospective studies of emergency department waiting times. Ann Emerg Med. 2007;49: MF, Keirns CC, Cunningham R, et al. Uninsured adults telephone advice lines, low- Newton presenting to US emergency departments: assumptions vs data. JAMA. 2008;300: acuity services Rimsza ME, Butler RJ, Johnson WG. Impact of Medicaid on health care use and cost. Pediatrics. 2007;119: Low acuity patients do not disenrollment e block ambulances from Munro J, Nicholl J, O'Cathain A, Knowles E. Impact of NHS Direct on demand for immediate care : observational study. BMJ. 2000;321: unloading Dunt D, Wilson R, Day SE, et al. Impact of telephone triage on emergency after hours GP Medicare usage: a time-series analysis. Aust New Zealand Health Policy. 2007;4:21
17 Causes of Overcrowding - Recent More prospective studies on the effects of closing inpatient beds Crilly J, Keijzers G, Krahn D, Steele M, Green D, Freeman J. The impact of a temporary medical ward closure on emergency department and hospital service delivery outcomes. Qual Manag Health Care Oct-Dec;20(4): Not good for ED Ever more complex models used in analysis Admission practice in off-peak times does impact results at peaks Distinct Choke points found in large hospitals around discharge timing from the wards Hospital Occupancy and complexity as measured by admissions important Same patterns across broad groups of hospitals Luo W, Cao J, Gallagher M, Wiles J. Estimating the intensity of ward admission and its effect on emergency department access block. Stat Med Nov 21. doi: /sim.5684 Khanna S, Boyle J, Good N, Lind J. Unravelling relationships: Hospital occupancy levels, discharge timing and emergency department access block. Emerg Med Australas Oct;24(5):510-7 Rathlev NK, Obendorfer D, White LF, Rebholz C, Magauran B, Baker W, Ulrich A, Fisher L, Olshaker J. Time series analysis of emergency department length of stay per 8-hour shift. West J Emerg Med May;13(2):163-8 Wiler JL, Handel DA, Ginde AA, Aronsky D, Genes NG, Hackman JL, Hilton JA, Hwang U, Kamali M, Pines JM, Powell E, Sattarian M, Fu R. Predictors of patient length of stay in 9 emergency departments. Am J Emerg Med Nov;30(9):

 Occupancy up 3.")
18 Causes of Overcrowding - Recent Sep and Dec 2012 Annals of EM 424 hospitals: Throughput performance measures highly dependent on exogenous variables Seeking a way to adjust measures for hospital and outside factors Concluded no simple way exists Volume, casemix, age, teaching etc 8 years of National Ambulatory Medical Care Surveys Visits up 1.9% per annum (15%) Occupancy up 3.1% per annum (27%) Increase driven by practice intensity Doing more for each patient


19 Causes of Overcrowding - Recent Boarding still contributes to crowding, but is no longer getting worse the way it was a decade ago In this US series growth is in practice intensity Older and sicker? Substituting admissions? Doing too much? Most growth in imaging Most contribution simple tests and treatment Much more research to be done Pitts SR, Pines JM, Handrigan MT, Kellermann AL. National trends in emergency department occupancy, 2001 to 2008: effect of inpatient admissions versus emergency department practice intensity. Ann Emerg Med Dec;60(6):
20 Consequences of Overcrowding As noted, in 2000 it was accepted as a given that ED overcrowding was bad, but no evidence base The next generation of researchers set about seeking any relationship between overcrowding and undesirable outcomes Broadly this came to 3 different approaches: Is a crowded ED a functional place? Process Is a crowded ED a safe place? Quality What happens to patients in a crowded ED? Outcome Subdivided by: What happens to those who board / have access block? What happens to those who come to a crowded ED?

21 Process Perhaps surprising that little immediate followup to the 1994 study linking overcrowding with costs First published report statistically linking access block with ED function (mean wait) Nov 2000 Followed by a series of confirmatory studies Richardson DB. Quantifying the effects of access block. Annual Scientific Meeting of the Australasian College for Emergency Medicine, Canberra, November Emerg Med Australas Mar; 13(1): A10
22 Process Statistical Links Demonstrated Access Block EMS Bypass Divert Status Ambulance delay for chest pain NEDOCS LWBS Access Block Waiting Times Subjective overcrowding Waiting Time Boarding Hours Multiple flow measures Boarder Burden Median LOS discharged ED 8am boarders >6h LOS daily Largely retrospective studies Fatovich DM, Nagree Y, Sprivulis P. Access block causes emergency department overcrowding and ambulance diversion in Perth, Western Australia. Emerg Med J May;22(5): Schull MJ, Morrison LJ, Vermeulen M, Redelmeier DA. Emergency department overcrowding and ambulance transport delays for patients with chest pain. CMAJ 2003; 168: Weiss SJ, Ernst AA, Derlet R, King R, Bair A, Nick TG. Relationship between the National ED Overcrowding Scale and the number of patients who leave without being seen in an academic ED. Am J Emerg Med May;23(3): Dunn R. Reduced access block causes shorter emergency department waiting times: An historical control observational study. Emerg Med (Aust) Jun;15(3): Vieth TL, Rhodes KV. The effect of crowding on access and quality in an academic ED. Am J Emerg Med Nov;24(7): Timm NL, Ho ML, Luria JW. Pediatric emergency department overcrowding and impact on patient flow outcomes. Acad Emerg Med Sep;15(9): White BA, Biddinger PD, Chang Y, Grabowski B, Carignan S, Brown DF. Boarding inpatients in the emergency department increases discharged patient length of stay. J Emerg Med Jan;44(1):230-5 Fogarty E, Saunders J, Cummins F. The effect of boarders on emergency department process flow. J Emerg Med May;46(5):706-10
23 Individual Quality Large studies linked delay in reaching an inpatient bed with: Defined adverse events in various groups (all, ICU, >65) Delay to provision of home medications Worse adherence to AMI guidelines Pneumonia in intubated patients Chalfin DB, Trzeciak S, Likourezos A, et al; DELAY-ED study group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med Jun; 35(6): Liu SW, Thomas SH, Gordon JA, Hamedani AG, Weissman JS. A pilot study examining undesirable events among emergency department-boarded patients awaiting inpatient beds. Ann Emerg Med Sep; 54(3): Liu SW, Chang Y, Weissman JS, Griffey, RT, Thomas J, Nergui S, Hamedani AG, Camargo, CA, Singer S. An Empirical Assessment of Boarding and Quality of Care: Delays in Care Among Chest Pain, Pneumonia, and Cellulitis Patients. Acad Emerg Med doi: /j x Ackroyd-Stolarz S, Read Guernsey J, Mackinnon NJ, Kovacs G. The association between a prolonged stay in the emergency department and adverse events in older patients admitted to hospital: a retrospective cohort study. BMJ Qual Saf Jul; 20(7): Diercks DB, Roe MT, Chen AY, Peacock WF, Kirk JD, Pollack CV Jr, Gibler WB, Smith SC Jr, Ohman M, Peterson ED. Prolonged emergency department stays of non-stsegmentelevation myocardial infarction patients are associated with worse adherence to the American College of Cardiology/American Heart Association Guidelines for management and increased adverse events. Ann Emerg Med Nov; 50(5): Carr BG, Kaye AJ, Wiebe DJ, et al. Emergency department length of stay: a major risk factor for pneumonia in intubated blunt trauma patients. J Trauma 2007 Jul; 63(1): 9-12
24 Overall Quality Worse pain care in Hip fracture Severe pain Back pain Sickle Cell Crisis Children with long bone fractures Hwang U, Richardson LD, Sonuyi TO, Morrison RS. The effect of emergency department crowding on the management of pain in older adults with hip fracture. J Am Geriatr Soc Feb;54(2):270-5 Pines JM, Hollander JE. Emergency department crowding is associated with poor care for patients with severe pain. Ann Emerg Med Jan;51(1):1-5 Hwang U, Richardson L, Livote E, et al. Emergency department crowding and decreased quality of pain care. Acad Emerg Med Dec;15(12): Pines JM, Shofer FS, Isserman JA, Abbuhl SB, Mills AM. The effect of emergency department crowding on analgesia in patients with back pain in two hospitals. Acad Emerg Med Mar;17(3): Shenoi R, Ma L, Syblik D, Yusuf S. Emergency department crowding and analgesic delay in pediatric sickle cell pain crises. Pediatr Emerg Care Oct;27(10):911-7 Lesser patient satisfaction in admitted and discharged patients Sills MR, Fairclough DL, Ranade D, Mitchell MS, Kahn MG. Emergency department crowding is associated with decreased quality of analgesia delivery for children with pain related to acute, isolated, long-bone fractures. Acad Emerg Med Dec;18(12): Pines JM, Iyer S, Disbot M, et al. The effect of emergency department crowding on patient satisfaction for admitted patients. Acad Emerg Med Sep;15(9): Tekwani KL, Kerem Y, Mistry CD, Sayger BM, Kulstad EB. Emergency Department Crowding is Associated with Reduced Satisfaction Scores in Patients Discharged from the Emergency Department. West J Emerg Med Feb;14(1):11-5
25 Overall Quality Greater risk of Missed AMI Delay to thrombolysis in AMI Delay to antibiotics in CA pneumonia Schull MJ, Vermeulen MJ, Stukel TA. The risk of missed diagnosis of acute myocardial infarction associated with emergency department volume. Ann Emerg Med Dec;48(6): Schull MJ, Vermeulen MJ, Slaughter G, et al. Emergency department crowding and thrombolysis delays in acute myocardial infarction. Ann Emerg Med Dec;44(6): Pines JM, Hollander JE, Localio AR, Metlay JP. The association between emergency department crowding and hospital performance on antibiotic timing for pneumonia and percutaneous intervention for myocardial infarction. Acad Emerg Med Aug;13(8):873-8 Fee C, Weber EJ, Maak CA, Bacchetti P. Effect of emergency department crowding on time to antibiotics in patients admitted with community acquired pneumonia. Ann Emerg Med Nov;50(5):501-9, 509.e1 Pines JM, Localio AR, Hollander JE, et al. The impact of emergency department crowding measures on time to antibiotics for patients with community-acquired pneumonia. Ann Emerg Med Nov;50(5):510-6
26 Overall Quality Adverse events in AMI Delay to surgery in #NOF Fishman PE, Shofer FS, Robey JL, Zogby KE, Reilly PM, Branas CC, Pines JM, Hollander JE. The impact of trauma activations on the care of emergency department patients with potential acute coronary syndromes. Ann Emerg Med Oct;48(4):34753 Richardson DB, McMahon K. Emergency Department Access Block Occupancy Predicts Delay to Surgery in Patients with Fractured Neck of Femur. Emerg Med Australas Aug; 21(4): Compliance with Sepsis Bundle Delay to Steroids in pediatric asthma Delay to resuscitation Shin TG, Jo IJ, Choi DJ, Kang MJ, Jeon K, Suh GY, Sim MS, Lim SY, Song KJ, Jeong YK. The adverse effect of emergency department crowding on compliance with the resuscitation bundle in the management of severe sepsis and septic shock. Crit Care Oct 6;17(5):R224 Bekmezian A, Fee C, Bekmezian S, Maselli JH, Weber E. Emergency department crowding and younger age are associated with delayed corticosteroid administration to children with acute asthma. Pediatr Emerg Care Oct;29(10): Hong KJ, Shin SD, Song KJ, Cha WC, Cho JS. Association between ED crowding and delay in resuscitation effort. Am J Emerg Med Nov 15
27 Overall Quality Violence towards ED staff Defined complications in boarders Contamination of Blood cultures Time to antibiotics in febrile neonates Quality and timeliness (but not equity) in paediatric asthma Preventable Medical Errors (National ED Safety Study) Blood culture contamination Medley DB, Morris JE, Stone CK, Song J, Delmas T, Thakrar K. An association between occupancy rates in the emergency department and rates of violence toward staff. J Emerg Med Oct;43(4): Zhou JC, Pan KH, Zhou DY, Zheng SW, Zhu JQ, Xu QP, Wang CL. High hospital occupancy is associated with increased risk for patients boarding in the emergency department. Am J Med Apr;125(4):416.e1-7 Lee CC, Lee NY, Chuang MC, Chen PL, Chang CM, Ko WC. The impact of overcrowding on the bacterial contamination of blood cultures in the ED. Am J Emerg Med Jul;30(6): Kennebeck SS, Timm NL, Kurowski EM, Byczkowski TL, Reeves SD. The association of emergency department crowding and time to antibiotics in febrile neonates. Acad Emerg Med Dec;18(12): Sills MR, Fairclough D, Ranade D, Kahn MG. Emergency department crowding is associated with decreased quality of care for children with acute asthma. Ann Emerg Med Mar; 57(3): e1-7 Epstein SK, Huckins DS, Liu SW, Pallin DJ, Sullivan AF, Lipton RI, Camargo CA Jr. Emergency department crowding and risk of preventable medical errors. Intern Emerg Med Apr; 7(2): Halverson S1, Malani PN, Newton DW, Habicht A, Vander Have K, Younger JG. Impact of hourly emergency department patient volume on blood culture contamination and diagnostic yield. J Clin Microbiol Jun;51(6):1721-6


28 Overall Quality - Recent Literature So many to choose from Acting on IOM research priorities Quality defined by timeliness of therapy in asthma, fracture 9 overcrowding measures Large statistical adjustment Best overcrowding measures Total patient care hours Arrivals last 6 hours Retrospective, limited input variables (no boarding) Simple measures often best Sills MR, Fairclough D, Ranade D, Kahn MG. Emergency department crowding is associated with decreased quality of care for children. Pediatr Emerg Care Sep; 27(9):


29 2006: Institute of Medicine Report Marked the widespread acceptance outside the EM community that there is a problem Multiple recommendations Improved efficiency and flow Coordination and accountability Increased resources Pay attention to Children Research agenda
30 Correlation or Causation? Demonstrating causality is generally agreed to require the Bradford-Hill criteria: Strength of association Consistency Specificity Temporality A dose response relationship Biological plausibility Coherence Reversibility Consideration of alternative explanations Hill AB. The environment and disease: association or causation? Proc R Soc Med 1965; 58:
31 Patient Outcomes Self evident to EPs that after the presenting emergency condition has been identified and managed, prolonged care in the ED is not in the best interests of the patient Boarding or Access Block represents restricted access to timely urgent care, which delays definitive therapy, prolongs hospital stay and increases complications ED staff equipped to provide acute care are not the most appropriate providers to inpatients An ED working at 200% of its capacity is likely to provide a lesser standard of care than a ward never exceeding 100% Less self-evident to outsiders

 hospital LOS Dose-response")
32 Patient Outcome beyond the ED 2002: First study to show effect of prolonged ED LOS on subsequent (not total) hospital LOS Dose-response curve
33 Patient Outcome beyond the ED Same result when correcting for age, time of day, casemix Same result in other countries Same result in ICU patients Adverse events in over 65 Adverse events in AMI Pneumonia in trauma patients Defined adverse events in boarders Again mostly retrospective but confounders addressed with multivariate techniques Liew D, Liew D, Kennedy MP. Emergency department length of stay independently predicts excess inpatient length of stay. Med J Aust Nov 17; 179(10): Nippak PM, Isaac WW, Ikeda-Douglas CJ, et al. Is there a relation between emergency department and inpatient lengths of stay? Can J Rural Med Winter;19(1):12-20 Chalfin DB, Trzeciak S, Likourezos A, et al; DELAY-ED study group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med Jun; 35(6): Ackroyd-Stolarz S, Read Guernsey J, Mackinnon NJ, Kovacs G. The association between a prolonged stay in the ED and adverse events in older patients admitted to hospital: a retrospective cohort study. BMJ Qual Saf. 2011Jul; 20(7): Diercks DB, Roe MT, Chen AY, Peacock WF, Kirk JD, et al. Prolonged emergency department stays of non-st segmentelevation myocardial infarction patients are associated with worse adherence to the American College of Cardiology/AHA Guidelines for management and increased adverse events. Ann Emerg Med Nov; 50(5): Carr BG, Kaye AJ, Wiebe DJ, et al. Emergency department length of stay: a major risk factor for pneumonia in intubated blunt trauma patients. J Trauma 2007 Jul; 63(1) :9-12 Zhou JC, Pan KH, Zhou DY, Zheng SW, et al. High hospital occupancy is associated with increased risk for patients boarding in the ED. Am J Med Apr; 125(4): 416.e1-7 Fishman PE, Shofer FS, Robey JL, Zogby KE, Reilly PM, Branas CC, Pines JM, Hollander JE. The impact of trauma activations on the care of emergency department patients with potential acute coronary syndromes. Ann Emerg Med Oct; 48(4):
34 Overall Outcome beyond the ED Medical care strives to produce best patient outcomes rather than simply best measures of process or documented quality Mortality is the unequivocal outcome for which research seeking any link with ED overcrowding is critical Death after ED presentation is multifactorial and rare so large series are required First published study from Spain was poorly controlled but found an excess of deaths Second published study from Houston was underpowered but found a trend towards excess trauma mortality Third & fourth studies were well designed from Australia Miró O, Antonio MT, Jiménez S, De Dios A, Sánchez M, Borrás A, Millá J. Decreased health care quality associated with emergency department overcrowding. Eur J Emerg Med Jun;6(2):105-7 Begley CE, Chang Y, Wood RC, Weltge A. Emergency Department Diversion and Trauma Mortality: Evidence from Houston, Texas. J Trauma Dec;57(6):1260-5


35 2006: Overcrowding and Mortality Two studies from different places with totally different methodological approaches One retrospective matched cohort in a single ED over 3 years One multivariate 3-hospital study of admissions through ED Both found around 30% increase in short term mortality from presenting to a crowded ED or crowded hospital
36 Overcrowding and Mortality Multiple major studies have reported an increased mortality Intensive care patients Sepsis and pneumonia patients All patients discharged from ED All presentations In places with ambulance diversion during overcrowding Hospital mortality lower as ambulances are turned away Citywide AMI mortality higher Two neutral findings Suggested these are settings where overcrowding so severe that no adequate control periods Chalfin DB, Trzeciak S, Likourezos A, et al; DELAY-ED study group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med Jun;35(6): Hong YC, Chou MH, Liu EH, et al. The effect of prolonged ED stay on outcome in patients with necrotising fasciitis. Am J Emerg Med May;27(4): Jo S, Kim K, Lee JH, Rhee JE, Kim YJ, Suh GJ, Jin YH. Emergency department crowding is associated with 28-day mortality in community-acquired pneumonia patients. J Infect Mar;64(3): Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. BMJ Jun 1; 342:d2983 Jo S, Jin YH, Lee JB, Jeong T, Yoon J, Park B. Emergency department occupancy ratio is associated with increased early mortality. J Emerg Med Feb;46(2):241-9 Shenoi RP, Ma L, Jones J, Frost M, Seo M, Begley CE. Ambulance diversion as a proxy for emergency department crowding: the effect on pediatric mortality in a metropolitan area. Acad Emerg Med Feb;16(2): Fatovich D. M. Effect of ambulance diversion on patient mortality: How access block can save your life. Med J Aust Dec 5-19;183(11/12): Yankovic N, Glied S, Green LV, Grams M. The impact of ambulance diversion on heart attack deaths. Inquiry. 2010;47(1):81-91

37 Recent Work yr of admissions in academic ED Stratified by boarding interval Adjusted for measures of severity and comorbidity Hospital with an overcapacity protocol: low-risk boarders could be moved to ward hallways patients Singer AJ, Thode HC Jr, Viccellio P, et al. The association between length of emergency department boarding and mortality. Acad Emerg Med. 2011; 18:

38 Recent Work - 2 Highly significant dose-response relationship between boarding duration and ICU admission, mortality and inpatient LOS Overcapacity protocol is a theoretical weakness but the data is compelling

39 Recent Work - 2 Case-crossover study of Medicare patients with AMI from 4 Californian counties All Medicare claims All ambulance diversion logs 6 years ( ) No AMI specific transport policies Each case linked to closest ED by mailing address EDs acted as their own controls Adjustments for demographics, comorbidities, hospitals AMIs, 149 EDs Shen Y, Hsia RY. Association Between Ambulance Diversion and Survival Among Patients With Acute Myocardial Infarction. JAMA. 2011; 305(23):

40 Recent Work - 2 When hospital on diversion >12h per day, less AMI patients admitted to hospitals with a catheter lab (78% vs 87%) Diversion >12hr associated with 3% increase in mortality at 30 days, persisting for at least 1 year Unable to separate ambulance, ED and hospital effects, but ambulance diversion is bad for patients

41 Recent Work admissions through ED to 187 hospitals California, 2007 Crowding defined as days of top quartile of ambulance diversion for that hospital Model included demographics, day of week, time of year, comorbidities Effect of Emergency Department Crowding on Outcomes of Admitted Patients. Sun BC, Hsia RY, Weiss RE, Zingmond D, Liang LJ, Han W, McCreath H, Asch SM. Ann Emerg Med Dec 5. doi:pii: S (12)01699-X

42 Recent Work - 3 Results highly significant 5% greater chance of inpatient death [300 deaths] 0.8% longer hospital stay [6200 bed-days] 1.1% increased costs [$17M]

43 Recent Work - 4 Used existing dataset from large ED in Korea over 2 years Overcrowding measured by simultaneous occupancy ratio 1846 with BP<90 In-hospital outcome Mortality higher No dose-response Mostly trauma, ID Fits with experience Jo S, Jeong T, Jin YH, Lee JB, Yoon J, Park B. ED crowding is associated with inpatient mortality among critically ill patients admitted via the ED: post hoc analysis from a retrospective study. Am J Emerg Med Dec;33(12): doi: /j.ajem
44 The Debate is well and truly over Finally now accepted that ED and hospital crowding do cause harm to patients Strength of association Consistency Specificity Temporality A dose response relationship Biological plausibility Coherence Reversibility Consideration of alternative explanations Hill AB. The environment and disease: association or causation? Proc R Soc Med 1965; 58:
45 Two mortality reversibility studies A randomised controlled trial of overcrowding unlikely Two reports of reversibility of the mortality effect so far Requires a well documented system which improves its overcrowding status in a short period State of Western Australia done that PA Hospital in Brisbane has done that WA: Access block from 40% to 10% in 3 tertiary hospitals Mortality reduced from 1.12% to 0.98% in same period WA is best regarded as an encouraging first report Too many variables and changes in hospitals practice to be certain it is causative Documentation is ongoing a more definitive result is expected Geelhoed GC, de Klerk NH. Emergency department overcrowding, mortality and the 4-hour rule in Western Australia. Med J Aust Feb 6;196:122-6


46 Two mortality reversibility studies PA Hospital: Well described hospital-wide intervention Studied Jan-Mar over 3 years Overall NEAT 32% to 62% to 72% HS Mortality Rate 93 to 72 to 55 Sullivan CM, Staib A, Flores J, Aggarwal L, Scanlon A, Martin JH, Scott IA. Aiming to be NEAT: safely improving and sustaining access to emergency care in a tertiary referral hospital. Australian Health Review, 2014, 38,



47 Two mortality reversibility studies Also reported Absolute drop in in-hospital death Strong negative association between NEAT and HSMR Fits with the theory and understanding of overcrowding Definitely an encouraging second report Time series and close to 1 life saved every second day Likely some other changes at work Further analysis undertaken
48 Cures for Overcrowding? Three basic approaches Mitigating the bad effects and decreasing ED LOS (ED internal) Cutting occupancy with particular groups (ED collaborative) Whole of hospital change There is sufficient before-after jurisdiction-wide evidence that it can be changed longer term Reversibility of flow issues demonstrated, as noted awaiting good studies on outcome Not specific interventions, but indication that financial incentives and extra resources work Weber EJ, Mason S, Carter A, Hew RL. Emptying the corridors of shame: organizational lessons from England's 4-hour emergency throughput target. Ann Emerg Med Feb; 57(2): e1 Ben-Tovim DI, Dougherty ML, O Connell TJ, McGrath KM. Patient journeys: the process of clinical redesign. Med. J. Aust. 2008; 188 (6 Suppl): S14 17 Richardson DB, Kelly A-M, Kerr D. Prevalence of Access Block in Australia Emerg Med Australas Dec; 21(6): Geelhoed GC, de Klerk NH. Emergency department overcrowding, mortality and the 4-hour rule in Western Australia. Med J Aust Feb 6;196:122-6
49 Multiple successful approaches Small, mostly before-after studies with publication bias We report what works Local process changes, staff Streaming Fast-track and Mid-track Early Senior input Joint with radiology/pathology Overcapacity protocols Top-down incentives Shetty A, Gunja N, Byth K, Vukasovic M. Senior Streaming Assessment Further Evaluation after Triage zone: a novel model of care encompassing various emergency department throughput measures. Emerg Med Australas Aug; 24(4): Huang EP, Liu SS, Fang CC, Chou HC, Wang CH, Yen ZS, Chen SC. The impact of adding clinical assistants on patient waiting time in a crowded ED. Emerg Med J Nov 22 Sterner SE, Coco T, Monroe KW, King WD, Losek JD. A new after-hours clinic model provides cost-saving, faster care compared with a pediatric emergency department. Pediatr Emerg Care Nov;28(11): Soremekun OA, Shofer FS, Grasso D, Mills AM, Moore J, Datner EM. The Effect of an Emergency Department Dedicated Midtrack Area on Patient Flow. Acad Emerg Med Apr;21(4): Grouse AI, Bishop RO, Gerlach L, de Villecourt TL, Mallows JL. A stream for complex, ambulant patients reduces crowding in an emergency department. Emerg Med Australas Apr;26(2):164-9 Jang JY, Shin SD, Lee EJ, Park CB, Song KJ, Singer AJ. Use of a Comprehensive Metabolic Panel Point-of-Care Test to Reduce Length of Stay in the Emergency Department: A Randomized Controlled Trial. Ann Emerg Med Aug 15 Khanna S, Boyle J, Good N, Lind J. Early discharge and its effect on ED length of stay and access block. Stud Health Technol Inform. 2012;178:92-8 Birkhahn RH, Wen W, Datillo PA, Briggs WM, Parekh A, Arkun A, Byrd B, Gaeta TJ. Improving patient flow in acute coronary syndromes in the face of hospital crowding. J Emerg Med Aug;43(2):356-65
50 Multiple successful approaches Journey Coordinators Logistic Management Senior Assessment and Streaming Only intervention consistently reported as not working is telephone advice lines Sharieff GQ, Burnell L, Cantonis M, Norton V, Tovar J, Roberts K, VanWyk C, Saucier J, Russe J. Improving emergency department time to provider, left-without-treatment rates, and average length of stay. J Emerg Med Sep;45(3): Rogg JG, White BA, Biddinger PD, Chang Y, Brown DF. A longterm analysis of physician triage screening in the emergency department. Acad Emerg Med Apr;20(4): Asha SE, Ajami A. Improvement in emergency department length of stay using a nurse-led 'emergency journey coordinator': A before/after study. Emerg Med Australas Apr;26(2): Asha SE, Ajami A. Improvement in emergency department length of stay using an early senior medical assessment and streaming model of care: A cohort study. Emerg Med Australas Oct;25(5): Healy-Rodriguez MA, Freer C, Pontiggia L, Wilson R, Metraux S, Lord L. Impact of a logistics management program on admitted patient boarders within an emergency department. J Emerg Nurs Mar;40(2): Graber DJ, Ardagh MW, O Donovan P, St George I. A telephone advice line does not decrease the number of presentations to Christchurch Emergency Department, but does decrease the number of phone callers seeking advice Jul 11;116(1177):U495



51 Telephone Advice Lines Politically popular Still trying to spin them as effective The data really does not support One from 2015 Cat 4-5 patients went UP May help to decrease loweracuity patient visits So Wrong Howell T. ED Utilization by Uninsured and Medicaid Patients after Availability of Telephone Triage. doi: /j.jen

52 Learning from Others Overcrowding is not unique to Medicine As noted at the start, any herd animal likely to experience dysfunctionally large herds at times Common to say that Medicine should learn from hospitality and airlines for flow, air traffic control and nuclear power for safety
 EM cannot simply queue or deny without triage Flights with Oversales If at departure time more")
53 Learning from Others There are many lessons we can take from other services Some really good things in hospitality for elective surgery, invasive tests These services have better demand management strategies available Emergency Medicine cannot say no large groups after 5pm (surgeons do every day) EM cannot simply queue or deny without triage Flights with Oversales If at departure time more customers with confirmed reservations are present than there are seats available, gate agents will first ask for volunteers who are willing to give up their seats in exchange for compensation and a confirmed seat on a later flight. On extremely rare occasions, a customer may be denied boarding on an involuntary basis, if a sufficient number of volunteers are not obtained. In such events, we will usually deny boarding based upon check-in time, but we may also consider factors such as severe hardships, fare paid, and status within the AAdvantage program. With few exceptions, persons denied boarding involuntarily are entitled to compensation under federal law.
54 Learning from Others Doctors are highly regulated and highly rewarded Food Services are safety regulated but poorly rewarded Medical skills are in short supply, food preparation skills not The snake oil era of the 19th Century provides an illustration of unregulated medicine In economic theory terms the disparity in information between the vendor and the consumer is too great for market forces alone to work Little need for restaurants to publicise their results Most customers eat out 2-3 times per week (or more) Little desire for hospitals to publish (or even examine) theirs Most customers use their elective services twice a decade and their emergency services a little more, never get to compare Better information makes a better market (internal/external)

55 Learning from Others This talk is not really about quality or reproducibility beyond the effect of overcrowding EM lacks the option of providing quality of care to the first arrivals and closing the door to latecomers In food service 5% get meals worse than the 5th centile mostly indistinguishable If you see 200 patients/day, 10 will get care less than 5th centile you know it when you see it and sometimes they do Difficult to establish benchmarks for assessment and management simultaneously but we need to standardise


56 New Literature There is more to be learnt about streaming Recent poster at SAEM described changes to model of care when 8 new patient spaces added to an overcrowded ED Reorganised ED from a large Acute stream with 23% Fasttrack and 3% Psych to balanced A-stream and B-stream 50% and 41%, still 3% Psych Staff rotate to both sides


57 Productivity gain without new Doctors Nationally recognised Performance Indicators improved significantly accounting for workload Median waiting time to be seen fell from 0:44 to 0:42, 90th centile from 3:25 to 3:08 Mean number tracked to a waiting area rather than a clinical space fell by 36% (P<10E-6) Interesting that no effect on time spent in ED A lot more remains to be learnt Largest sub-acute stream in Australasian Literature


58 New Literature Ambulance Diversion does not make a difference At least in Massachusetts where it was banned 1/1/2009 Before and after study, 9 hospitals comparing two years After adjustments, volume increased, admitted LOS decreased, ambulance turnaround time decreased Burke LG, Joyce N, Baker WE, Biddinger PD, Dyer KS, Friedman FD, Imperato J, King A, Maciejko TM, Pearlmutter MD, Sayah A, Zane RD, Epstein SK. The effect of an ambulance diversion ban on emergency department length of stay and ambulance turnaround time. Ann Emerg Med Mar;61(3):

59 New Literature A cluster randomised trial Setting of financial incentives Intervention was an additional nurse and doctor working in Triage area Intervention effective for nonconsulted discharged patients Wait decreased 25min High Acuity LOS decreased 24min Low Acuity LOS by 56min if seen LWBS 1.5% vs 2.2% (p=0.06) Not a surprising result Cheng I, Lee J, Mittmann N, Tyberg J, Ramagnano S, Kiss A, Schull M, Kerr F, Zwarenstein M. Implementing wait-time reductions under Ontario government benchmarks (Pay-forResults): a Cluster Randomized Trial of the Effect of a Physician-Nurse Supplementary Triage Assistance team (MDRNSTAT) on emergency department patient wait times. BMC Emerg Med Nov 11;13:17

60 New Literature - Alberta Accepted 2016 by AEM Large and Well controlled Main intervention was improving General Internal Medicine (GIM) Reduced IP LOS 1.4 days No adverse effects like readmission ED LOS for GIM patients fell by 2.8 hours 1 in 30, so only 15 min ED overall Statistically significant but obviously needs to involve more inpatient units McAlister FA, Bakal JA, Rosychuk RJ, Rowe BH. Does reducing inpatient length of stay have upstream effects on the emergency room: exploring the impact of the general Internal Medicine care Transformation initiative. Acad Emerg Med Feb 6. doi: /acem [Epub ahead of print]
61 Newer Literature - Systematic Reviews Now so much work that we have seen the rise of the systematic review Mostly fairly critical of the methodologies used Appear to work Triage Liaison Physician Triage nurse ordering Rapid Assessment/Fasttrack Rowe BH, Guo X, Villa-Roel C, Schull M, Holroyd B, Bullard M, Vandermeer B, Ospina M, Innes G. The role of triage liaison physicians on mitigating overcrowding in emergency departments: a systematic review. Acad Emerg Med Feb;18(2): Rowe BH, Villa-Roel C, Guo X, Bullard MJ, Ospina M, Vandermeer B, Innes G, Schull MJ, Holroyd BR. The role of triage nurse ordering on mitigating overcrowding in emergency departments: a systematic review. Acad Emerg Med Dec;18(12): Oredsson S, Jonsson H, Rognes J, Lind L, Göransson KE, Ehrenberg A, Asplund K, Castrén M, Farrohknia N. A systematic review of triage-related interventions to improve patient flow in emergency departments. Scand J Trauma Resusc Emerg Med Jul 19;19:43 Bullard MJ, Villa-Roel C, Guo X, Holroyd BR, Innes G, Schull MJ, Vandermeer B, Ospina M, Rowe BH. The role of a rapid assessment zone/pod on reducing overcrowding in emergency departments: a systematic review. Emerg Med J May;29(5):372-8 Elder E, Johnston AN, Crilly J. Review article: systematic review of three key strategies designed to improve patient flow through the emergency department. Emerg Med Australas Oct;27(5): Chan SS, Cheung NK, Graham CA, Rainer TH. Strategies and solutions to alleviate access block and overcrowding in emergency departments. Hong Kong Med J Aug;21(4):34552
62 Newer Literature - Systematic Reviews Appear not to work Primary care professionals in ED Insufficient evidence Overcapacity protocols Crawford K, Morphet J, Jones T, Innes K, Griffiths D, Williams A. Initiatives to reduce overcrowding and access block in Australian emergency departments: a literature review. Collegian. 2014;21(4): Mason S, Mountain G, Turner J, Arain M, Revue E, Weber EJ. Innovations to reduce demand and crowding in emergency care; a review study. Scand J Trauma Resusc Emerg Med Sep 11;22:55 Khangura JK, Flodgren G, Perera R, Rowe BH, Shepperd S. Primary care professionals providing non-urgent care in hospital emergency departments. Cochrane Database Syst Rev Nov 14;11:CD Villa-Roel C, Guo X, Holroyd BR, Innes G, Wong L, Ospina M, Schull M, Vandermeer B, Bullard MJ, Rowe BH. The role of full capacity protocols on mitigating overcrowding in EDs. Am J Emerg Med Mar;30(3):412-20
63 This is likely to change The biggest news in the field of overcrowding cures came in 2012 with the series of abstracts from Alberta Canadian Emergency Medicine meeting, International conference on Emergency Medicine, Society for Academic Emergency Medicine (prize winning) Cannot really call it equivalent to peer-reviewed study until it is published, but this is the most exciting work

64
65 Access Block in Alberta Many flow projects and capacity expansions: A multi-million dollar system-wide acute access program (GRIDLOCC 2007 / 2008) failed to improve hospital access or reduce ED boarding times For > a decade, ED and hospital access block increasing Dec 2010: Implementation of the Alberta Overcapacity Plan 14 Teaching Hospitals across Alberta simultaneously >650,000 patients /year Results mean that the evidence based reviws are likely to change their views shortly
66

67
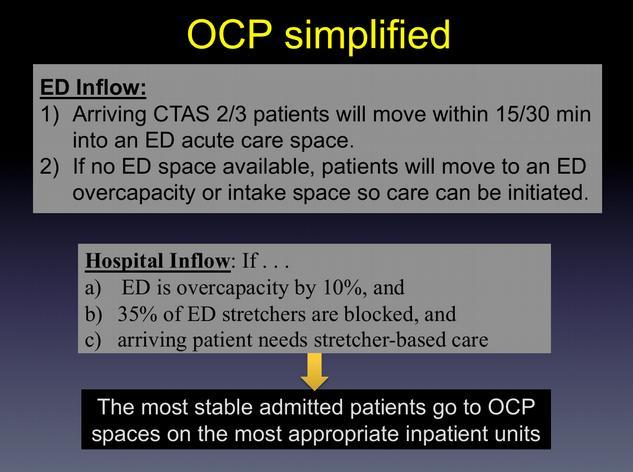
68 5 Philosophical tenets of a successful OCP The same care standards apply throughout the hospital, from patient arrival to discharge Overcrowding (access block) is addressed by the entire system Best outcomes and efficiencies occur when patients are matched to the right unit and team ASAP All units have important care missions and require reasonable access to their resources in order to provide acceptable care and meet performance targets Hallways are undesirable locations for patient care
October 14, Dear Ms. Leslie:
 October 14, 2015 Ruth W. Leslie, Director e mail: ruth.leslie@health.ny.gov Division of Hospitals and Diagnostic & Treatment Centers New York State Department of Health Empire State Plaza, Corning Tower
October 14, 2015 Ruth W. Leslie, Director e mail: ruth.leslie@health.ny.gov Division of Hospitals and Diagnostic & Treatment Centers New York State Department of Health Empire State Plaza, Corning Tower
Specifications Manual for National Hospital Inpatient Quality Measures Discharges (1Q17) through (4Q17)
 through (4Q17)") Last Updated: Version 5.2a EMERGENCY DEPARTMENT (ED) NATIONAL HOSPITAL INPATIENT QUALITY MEASURES ED Measure Set Table Set Measure ID # ED-1a ED-1b ED-1c ED-2a ED-2b ED-2c Measure Short Name Median Time
Last Updated: Version 5.2a EMERGENCY DEPARTMENT (ED) NATIONAL HOSPITAL INPATIENT QUALITY MEASURES ED Measure Set Table Set Measure ID # ED-1a ED-1b ED-1c ED-2a ED-2b ED-2c Measure Short Name Median Time
Emergency department overcrowding, mortality and the 4-hour rule in Western Australia. Abstract. Methods
 Research Gary C Geelhoed FRACP, FACEM, MD, Director, 1 and Professor, 2 Nicholas H de Klerk BSc, MSc, PhD, Head of Biostatistics and Bioinformatics 3,4 1 Emergency Department, Princess Margaret Hospital
Research Gary C Geelhoed FRACP, FACEM, MD, Director, 1 and Professor, 2 Nicholas H de Klerk BSc, MSc, PhD, Head of Biostatistics and Bioinformatics 3,4 1 Emergency Department, Princess Margaret Hospital
Measure Information Form. Admit Decision Time to ED Departure Time for Admitted Patients Overall Rate
 Last Updated: Version 4.4 Measure Set: Emergency Department Set Measure ID #: ED-2 Measure Information Form Set Measure ID# ED-2a ED-2b ED-2c Performance Measure Name Admit Decision Time to ED Departure
Last Updated: Version 4.4 Measure Set: Emergency Department Set Measure ID #: ED-2 Measure Information Form Set Measure ID# ED-2a ED-2b ED-2c Performance Measure Name Admit Decision Time to ED Departure
OP ED-THROUGHPUT GENERAL DATA ELEMENT LIST. All Records
 Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
When Overcrowded Means Unsafe: A Research Review Of Patient Outcomes In Over-Capacity Emergency Departments
 When Overcrowded Means Unsafe: A Research Review Of Patient Outcomes In Over-Capacity Emergency Departments An overcrowded hospital should now be regarded as an unsafe hospital. Introduction A growing
When Overcrowded Means Unsafe: A Research Review Of Patient Outcomes In Over-Capacity Emergency Departments An overcrowded hospital should now be regarded as an unsafe hospital. Introduction A growing
OP ED-THROUGHPUT GENERAL DATA ELEMENT LIST. All Records
 Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Material inside brackets ( [ and ] ) is new to this Specifications Manual version. HOSPITAL OUTPATIENT QUALITY MEASURES ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
LWOT Problem Tool. Quotes Surge Scenarios LWOT. Jeffery K. Cochran, PhD James R. Broyles, BSE
 LWOT Problem Tool Quotes Surge Scenarios LWOT 1 Jeffery K. Cochran, PhD James R. Broyles, BSE Analysis Goals With this tool, the user will be able to answer the question: In our Emergency Department (ED),
LWOT Problem Tool Quotes Surge Scenarios LWOT 1 Jeffery K. Cochran, PhD James R. Broyles, BSE Analysis Goals With this tool, the user will be able to answer the question: In our Emergency Department (ED),
OP ED-Throughput General Data Element List. All Records All Records. All Records All Records All Records. All Records. All Records.
 Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Material inside brackets ([and]) is new to this Specifications Manual version. Hospital Outpatient Quality Measures ED-Throughput Set Measure ID # OP-18 OP-20 OP-22 Measure Short Name Median Time from
Improving patient satisfaction by adding a physician in triage
 ORIGINAL ARTICLE Improving patient satisfaction by adding a physician in triage Jason Imperato 1, Darren S. Morris 2, Leon D. Sanchez 2, Gary Setnik 1 1. Department of Emergency Medicine, Mount Auburn
ORIGINAL ARTICLE Improving patient satisfaction by adding a physician in triage Jason Imperato 1, Darren S. Morris 2, Leon D. Sanchez 2, Gary Setnik 1 1. Department of Emergency Medicine, Mount Auburn
Median Time from Emergency Department (ED) Arrival to ED Departure for Admitted ED Patients ED-1 (CMS55v4)
 Arrival to ED Departure for Admitted ED Patients ED-1 (CMS55v4)") PIONEERS IN QUALITY: EXPERT TO EXPERT: Median Time from Emergency Department (ED) Arrival to ED Departure for Admitted ED Patients ED-1 (CMS55v4) Median Admit Decision Time to ED Departure Time for Admitted
PIONEERS IN QUALITY: EXPERT TO EXPERT: Median Time from Emergency Department (ED) Arrival to ED Departure for Admitted ED Patients ED-1 (CMS55v4) Median Admit Decision Time to ED Departure Time for Admitted
1. Introduction. Keywords Emergency department, Inpatient, Overcrowding, Boarding, Patients preference, Cardiovascular mortality
 Clinical Practice 2018, 7(1): 1-5 DOI: 10.5923/j.cp.20180701.01 Patient Preference for the Boarding at Emergency Department of Aseer Central Hospital when Emergency is Working with Its Maximum Capacity
Clinical Practice 2018, 7(1): 1-5 DOI: 10.5923/j.cp.20180701.01 Patient Preference for the Boarding at Emergency Department of Aseer Central Hospital when Emergency is Working with Its Maximum Capacity
January 1, 20XX through December 31, 20XX. LOINC(R) is a registered trademark of the Regenstrief Institute.
 is a registered trademark of the Regenstrief Institute.") e Title Median Time from ED Arrival to ED Departure for Admitted ED Patients e Identifier ( Authoring Tool) 55 e Version number 5.1.000 NQF Number 0495 GUID 9a033274-3d9b- 11e1-8634- 00237d5bf174 ment
e Title Median Time from ED Arrival to ED Departure for Admitted ED Patients e Identifier ( Authoring Tool) 55 e Version number 5.1.000 NQF Number 0495 GUID 9a033274-3d9b- 11e1-8634- 00237d5bf174 ment
January 1, 20XX through December 31, 20XX. LOINC(R) is a registered trademark of the Regenstrief Institute.
 is a registered trademark of the Regenstrief Institute.") e Title Median Admit Decision Time to ED Departure Time for Admitted Patients e Identifier ( Authoring Tool) 111 e Version number 5.1.000 NQF Number 0497 GUID 979f21bd-3f93-4cdd- 8273-b23dfe9c0513 ment
e Title Median Admit Decision Time to ED Departure Time for Admitted Patients e Identifier ( Authoring Tool) 111 e Version number 5.1.000 NQF Number 0497 GUID 979f21bd-3f93-4cdd- 8273-b23dfe9c0513 ment
The effect of a zero-diversion policy on emergency department performance measures
 ORIGINAL ARTICLE The effect of a zero-diversion policy on emergency department performance measures Eman Spaulding 1, Laurie Byrne 1, Eric Armbrecht 2, Collin Jackson 1, Preeti Dalawari 1 1. Division of
ORIGINAL ARTICLE The effect of a zero-diversion policy on emergency department performance measures Eman Spaulding 1, Laurie Byrne 1, Eric Armbrecht 2, Collin Jackson 1, Preeti Dalawari 1 1. Division of
Thank you for joining us today!
 Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Racial disparities in ED triage assessments and wait times
 Racial disparities in ED triage assessments and wait times Jordan Bleth, James Beal PhD, Abe Sahmoun PhD June 2, 2017 Outline Background Purpose Methods Results Discussion Limitations Future areas of study
Racial disparities in ED triage assessments and wait times Jordan Bleth, James Beal PhD, Abe Sahmoun PhD June 2, 2017 Outline Background Purpose Methods Results Discussion Limitations Future areas of study
Accepted Manuscript. Discharge before noon: an urban legend. Dan Shine. S (14) DOI: /j.amjmed Reference: AJM 12824
 DOI: /j.amjmed Reference: AJM 12824") Accepted Manuscript Discharge before noon: an urban legend Dan Shine PII: S0002-9343(14)01230-3 DOI: 10.1016/j.amjmed.2014.12.011 Reference: AJM 12824 To appear in: The American Journal of Medicine Received
Accepted Manuscript Discharge before noon: an urban legend Dan Shine PII: S0002-9343(14)01230-3 DOI: 10.1016/j.amjmed.2014.12.011 Reference: AJM 12824 To appear in: The American Journal of Medicine Received
A Conceptual Model of Emergency Department Crowding
 HEALTH POLICY/CONCEPTS A Conceptual Model of Emergency Department Crowding Brent R. Asplin, MD, MPH David J. Magid, MD, MPH Karin V. Rhodes, MD Leif I. Solberg, MD Nicole Lurie, MD, MSPH Carlos A. Camargo,
HEALTH POLICY/CONCEPTS A Conceptual Model of Emergency Department Crowding Brent R. Asplin, MD, MPH David J. Magid, MD, MPH Karin V. Rhodes, MD Leif I. Solberg, MD Nicole Lurie, MD, MSPH Carlos A. Camargo,
Overcrowding in the Emergency Department Does Volume of Emergency Room Patients Affect Ordering of CT Scans?
 ISPUB.COM The Internet Journal of Emergency Medicine Volume 6 Number 1 Overcrowding in the Emergency Department Does Volume of Emergency Room Patients Affect Ordering of CT Scans? F Moser, M Maya, S Young,
ISPUB.COM The Internet Journal of Emergency Medicine Volume 6 Number 1 Overcrowding in the Emergency Department Does Volume of Emergency Room Patients Affect Ordering of CT Scans? F Moser, M Maya, S Young,
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals
 A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
ED crowding: Causes, Consequences, Solutions
 ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
Emergency care workload units: A novel tool to compare emergency department activity
 Bond University epublications@bond Faculty of Health Sciences & Medicine Publications Faculty of Health Sciences & Medicine 10-1-2010 Emergency care workload units: A novel tool to compare emergency department
Bond University epublications@bond Faculty of Health Sciences & Medicine Publications Faculty of Health Sciences & Medicine 10-1-2010 Emergency care workload units: A novel tool to compare emergency department
Improving emergency department patient flow
 Clin Exp Emerg Med 2016;3(2):63-68 http://dx.doi.org/10.15441/ceem.16.127 Improving emergency department patient flow Paul Richard Edwin Jarvis Emergency Department, Calderdale & Huddersfield NHS Foundation
Clin Exp Emerg Med 2016;3(2):63-68 http://dx.doi.org/10.15441/ceem.16.127 Improving emergency department patient flow Paul Richard Edwin Jarvis Emergency Department, Calderdale & Huddersfield NHS Foundation
Research Article The Impact of Psychiatric Patient Boarding in Emergency Departments
 Emergency Medicine International Volume 2012, Article ID 360308, 5 pages doi:10.1155/2012/360308 Research Article The Impact of Psychiatric Patient Boarding in Emergency Departments B. A. Nicks and D.
Emergency Medicine International Volume 2012, Article ID 360308, 5 pages doi:10.1155/2012/360308 Research Article The Impact of Psychiatric Patient Boarding in Emergency Departments B. A. Nicks and D.
Emergency department visit volume variability
 Clin Exp Emerg Med 215;2(3):15-154 http://dx.doi.org/1.15441/ceem.14.44 Emergency department visit volume variability Seung Woo Kang, Hyun Soo Park eissn: 2383-4625 Original Article Department of Emergency
Clin Exp Emerg Med 215;2(3):15-154 http://dx.doi.org/1.15441/ceem.14.44 Emergency department visit volume variability Seung Woo Kang, Hyun Soo Park eissn: 2383-4625 Original Article Department of Emergency
Research Article Factors Associated with Overcrowded Emergency Rooms in Thailand: A Medical School Setting
 Emergency Medicine International, Article ID 576259, 4 pages http://dx.doi.org/10.1155/2014/576259 Research Article Factors Associated with Overcrowded Emergency Rooms in Thailand: A Medical School Setting
Emergency Medicine International, Article ID 576259, 4 pages http://dx.doi.org/10.1155/2014/576259 Research Article Factors Associated with Overcrowded Emergency Rooms in Thailand: A Medical School Setting
Rapid assessment and treatment (RAT) of triage category 2 patients in the emergency department
 of triage category 2 patients in the emergency department") Trauma and Emergency Care Research Article Rapid assessment and treatment (RAT) of triage category 2 patients in the emergency department S. Hassan Rahmatullah 1, Ranim A Chamseddin 1, Aya N Farfour 1,
Trauma and Emergency Care Research Article Rapid assessment and treatment (RAT) of triage category 2 patients in the emergency department S. Hassan Rahmatullah 1, Ranim A Chamseddin 1, Aya N Farfour 1,
The Effect of Emergency Department Crowding on Paramedic Ambulance Availability
 EMERGENCY MEDICAL SERVICES/ORIGINAL RESEARCH The Effect of Emergency Department Crowding on Paramedic Ambulance Availability Marc Eckstein, MD Linda S. Chan, PhD From the Department of Emergency Medicine
EMERGENCY MEDICAL SERVICES/ORIGINAL RESEARCH The Effect of Emergency Department Crowding on Paramedic Ambulance Availability Marc Eckstein, MD Linda S. Chan, PhD From the Department of Emergency Medicine
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Hospital Performance Report for Emergency Department Measures
 QUALIS HEALTH Hospital Outpatient Quality Reporting Hospital Performance Report for Emergency Department Measures Community: Washington State Includes Data Through: Q2 2015 - Q1 2016 Report Created: April
QUALIS HEALTH Hospital Outpatient Quality Reporting Hospital Performance Report for Emergency Department Measures Community: Washington State Includes Data Through: Q2 2015 - Q1 2016 Report Created: April
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
CDU. Clinical Decision Unit Ward for
 CDU Clinical Decision Unit Ward for Can t Observational Decide Medicine Unit What are observation medicine units? Observation medicine delivers intensive shortterm assessment, observation or therapy to
CDU Clinical Decision Unit Ward for Can t Observational Decide Medicine Unit What are observation medicine units? Observation medicine delivers intensive shortterm assessment, observation or therapy to
A Model for Psychiatric Emergency Services
 A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
What good looks like in the emergency pathway
 What good looks like in the emergency pathway @ECISTNetwork @PeteGordon68 I m going to cover Safer Faster Better The evidence Myths What we ve found over 150 engagements Why we need simple rules We recommend
What good looks like in the emergency pathway @ECISTNetwork @PeteGordon68 I m going to cover Safer Faster Better The evidence Myths What we ve found over 150 engagements Why we need simple rules We recommend
The number of patients admitted to acute care hospitals
 Hospitalist Organizational Structures in the Baltimore-Washington Area and Outcomes: A Descriptive Study Christine Soong, MD, James A. Welker, DO, and Scott M. Wright, MD Abstract Background: Hospitalist
Hospitalist Organizational Structures in the Baltimore-Washington Area and Outcomes: A Descriptive Study Christine Soong, MD, James A. Welker, DO, and Scott M. Wright, MD Abstract Background: Hospitalist
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC
 Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
AMBULANCE diversion policies are created
 36 AMBULANCE DIVERSION Scheulen et al. IMPACT OF AMBULANCE DIVERSION POLICIES Impact of Ambulance Diversion Policies in Urban, Suburban, and Rural Areas of Central Maryland JAMES J. SCHEULEN, PA-C, MBA,
36 AMBULANCE DIVERSION Scheulen et al. IMPACT OF AMBULANCE DIVERSION POLICIES Impact of Ambulance Diversion Policies in Urban, Suburban, and Rural Areas of Central Maryland JAMES J. SCHEULEN, PA-C, MBA,
Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed.
 Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed. ANALYZING THE PATIENT LOAD ON THE HOSPITALS IN A METROPOLITAN AREA Barb Tawney Systems and Information Engineering
Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed. ANALYZING THE PATIENT LOAD ON THE HOSPITALS IN A METROPOLITAN AREA Barb Tawney Systems and Information Engineering
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
Healthcare Informatics: Supporting Collaborative Sensemaking in the Emergency Department
 Healthcare Informatics: Supporting Collaborative Sensemaking in the Emergency Department It is a busy day in the emergency room with the monitors beeping, the alarms blaring intermittently, the phones
Healthcare Informatics: Supporting Collaborative Sensemaking in the Emergency Department It is a busy day in the emergency room with the monitors beeping, the alarms blaring intermittently, the phones
Capital Zone Emergency Services Council CZESC
 Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2016) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2016) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Analysing completion times in an academic emergency department: coordination of care is the weakest link
 S P E C I A L A R T I C L E Analysing completion times in an academic emergency department: coordination of care is the weakest link I.L. Vegting 1,2, P.W.B. Nanayakkara 1,2*, A.E. van Dongen 1, E. Vandewalle
S P E C I A L A R T I C L E Analysing completion times in an academic emergency department: coordination of care is the weakest link I.L. Vegting 1,2, P.W.B. Nanayakkara 1,2*, A.E. van Dongen 1, E. Vandewalle
Overcrowding and Its Association With Patient Outcomes in a Median-Low Volume Emergency Department
 Original Article J Clin Med Res. 2017;9(11):911-916 Overcrowding and Its Association With Patient Outcomes in a Median-Low Volume Emergency Department J. Laureano Phillips a, Bradford E. Jackson b, c,
Original Article J Clin Med Res. 2017;9(11):911-916 Overcrowding and Its Association With Patient Outcomes in a Median-Low Volume Emergency Department J. Laureano Phillips a, Bradford E. Jackson b, c,
Cause of death in intensive care patients within 2 years of discharge from hospital
 Cause of death in intensive care patients within 2 years of discharge from hospital Peter R Hicks and Diane M Mackle Understanding of intensive care outcomes has moved from focusing on intensive care unit
Cause of death in intensive care patients within 2 years of discharge from hospital Peter R Hicks and Diane M Mackle Understanding of intensive care outcomes has moved from focusing on intensive care unit
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
The Waiting Time at Emergency Departments at Khartoum State-2005
 Original Article The Waiting Time at Emergency Departments at Khartoum State-2005 Sara AM Abd Elaal MD 1, Yousif A. Ibrahim MD 2, 1 General Specialist, 2 Professor of Community Medicine, Head Department
Original Article The Waiting Time at Emergency Departments at Khartoum State-2005 Sara AM Abd Elaal MD 1, Yousif A. Ibrahim MD 2, 1 General Specialist, 2 Professor of Community Medicine, Head Department
Version 2 15/12/2013
 The METHOD study 1 15/12/2013 The Medical Emergency Team: Hospital Outcomes after a Day (METHOD) study Version 2 15/12/2013 The METHOD Study Investigators: Principal Investigator Christian P Subbe, Consultant
The METHOD study 1 15/12/2013 The Medical Emergency Team: Hospital Outcomes after a Day (METHOD) study Version 2 15/12/2013 The METHOD Study Investigators: Principal Investigator Christian P Subbe, Consultant
Capital Zone Emergency Services Council CZESC
 Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2015) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2015) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Boarding Impact on patients, hospitals and healthcare systems
 Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
The CAHPS Ambulatory Care Improvement Guide
 The CAHPS Ambulatory Care Improvement Guide Practical Strategies for Improving Patient Experience To download the Guide s other sections, including descriptions of improvement strategies, go to https://cahps.ahrq.gov/quality-improvement/improvementguide/improvement-guide.html.
The CAHPS Ambulatory Care Improvement Guide Practical Strategies for Improving Patient Experience To download the Guide s other sections, including descriptions of improvement strategies, go to https://cahps.ahrq.gov/quality-improvement/improvementguide/improvement-guide.html.
Cost Effectiveness of Physician Anesthesia J.P. Abenstein, M.S.E.E., M.D. Mayo Clinic Rochester, MN
 Mayo Clinic Rochester, MN Introduction The question of whether anesthesiologists are cost-effective providers of anesthesia services remains an open question in the minds of some of our medical colleagues,
Mayo Clinic Rochester, MN Introduction The question of whether anesthesiologists are cost-effective providers of anesthesia services remains an open question in the minds of some of our medical colleagues,
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Racial and Ethnic Differences and Disparities in Chronic Wounds ASP Workshop on Wound Repair and Healing in Older Adults
 Racial and Ethnic Differences and Disparities in Chronic Wounds ASP Workshop on Wound Repair and Healing in Older Adults Caroline E. Fife, MD Executive Director, U.S. Wound Registry Racial and Ethnic Disparities
Racial and Ethnic Differences and Disparities in Chronic Wounds ASP Workshop on Wound Repair and Healing in Older Adults Caroline E. Fife, MD Executive Director, U.S. Wound Registry Racial and Ethnic Disparities
available at journal homepage:
 Australasian Emergency Nursing Journal (2009) 12, 16 20 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/aenj RESEARCH PAPER The SAPhTE Study: The comparison of the SAPhTE (Safe-T)
Australasian Emergency Nursing Journal (2009) 12, 16 20 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/aenj RESEARCH PAPER The SAPhTE Study: The comparison of the SAPhTE (Safe-T)
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Cost-effective critical care: What does it look like?
 Cost-effective critical care: What does it look like? Scott D. Halpern, M.D., Ph.D. Associate Professor of Medicine, Epidemiology, and Medical Ethics & Health Policy Director, Fostering Improvement in
Cost-effective critical care: What does it look like? Scott D. Halpern, M.D., Ph.D. Associate Professor of Medicine, Epidemiology, and Medical Ethics & Health Policy Director, Fostering Improvement in
A QUEUING-BASE STATISTICAL APPROXIMATION OF HOSPITAL EMERGENCY DEPARTMENT BOARDING
 A QUEUING-ASE STATISTICAL APPROXIMATION OF HOSPITAL EMERGENCY DEPARTMENT OARDING James R. royles a Jeffery K. Cochran b a RAND Corporation, Santa Monica, CA 90401, james_broyles@rand.org b Department of
A QUEUING-ASE STATISTICAL APPROXIMATION OF HOSPITAL EMERGENCY DEPARTMENT OARDING James R. royles a Jeffery K. Cochran b a RAND Corporation, Santa Monica, CA 90401, james_broyles@rand.org b Department of
Technology Overview. Issue 13 August A Clinical and Economic Review of Telephone Triage Services and Survey of Canadian Call Centre Programs
 Technology Overview Issue 13 August 2004 A Clinical and Economic Review of Telephone Triage Services and Survey of Canadian Call Centre Programs Publications can be requested from: CCOHTA 600-865 Carling
Technology Overview Issue 13 August 2004 A Clinical and Economic Review of Telephone Triage Services and Survey of Canadian Call Centre Programs Publications can be requested from: CCOHTA 600-865 Carling
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT)
") Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Is Emergency Department Quality Related to Other Hospital Quality Domains?
 ORIGINAL CONTRIBUTION Is Emergency Department Quality Related to Other Hospital Quality Domains? Megan McHugh, PhD, Jennifer Neimeyer, PhD, Emilie Powell, MD, MS, Rahul K. Khare, MD, MS, and James G. Adams,
ORIGINAL CONTRIBUTION Is Emergency Department Quality Related to Other Hospital Quality Domains? Megan McHugh, PhD, Jennifer Neimeyer, PhD, Emilie Powell, MD, MS, Rahul K. Khare, MD, MS, and James G. Adams,
Psychiatric Patient Boarding Problems in the Emergency Department
 Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
The Impact of Input and Output Factors on Emergency Department Throughput
 The Impact of Input and Output Factors on Emergency Department Throughput Phillip V. Asaro, MD, Lawrence M. Lewis, MD, Stuart B. Boxerman, DSc Abstract Objectives: To quantify the impact of input and output
The Impact of Input and Output Factors on Emergency Department Throughput Phillip V. Asaro, MD, Lawrence M. Lewis, MD, Stuart B. Boxerman, DSc Abstract Objectives: To quantify the impact of input and output
TRIAGE SYSTEMS FOR TRAUMA CARE
 Indep Rev July-Aug 2014;16(7-9) IR-333 TRIAGE SYSTEMS FOR TRAUMA CARE Awais Shuja FRCS (Ed), FCPS Assistant Professor of Surgery Independent Medical College, Faisalabad. Correspondence Address: Awais Shuja
Indep Rev July-Aug 2014;16(7-9) IR-333 TRIAGE SYSTEMS FOR TRAUMA CARE Awais Shuja FRCS (Ed), FCPS Assistant Professor of Surgery Independent Medical College, Faisalabad. Correspondence Address: Awais Shuja
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
Analyzing Readmissions Patterns: Assessment of the LACE Tool Impact
 Health Informatics Meets ehealth G. Schreier et al. (Eds.) 2016 The authors and IOS Press. This article is published online with Open Access by IOS Press and distributed under the terms of the Creative
Health Informatics Meets ehealth G. Schreier et al. (Eds.) 2016 The authors and IOS Press. This article is published online with Open Access by IOS Press and distributed under the terms of the Creative
Ambulance Diversion and Lost Hospital Revenues
 HEALTH POLICY AND CLINICAL PRACTICE/ORIGINAL RESEARCH Ambulance Diversion and Lost Hospital Revenues K. John McConnell, PhD Christopher F. Richards, MD Mohamud Daya, MD, MS Cody C. Weathers, BS Robert
HEALTH POLICY AND CLINICAL PRACTICE/ORIGINAL RESEARCH Ambulance Diversion and Lost Hospital Revenues K. John McConnell, PhD Christopher F. Richards, MD Mohamud Daya, MD, MS Cody C. Weathers, BS Robert
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Chapter 39 Bed occupancy
 National Institute for Health and Care Excellence Final Chapter 39 Bed occupancy Emergency and acute medical care in over 16s: service delivery and organisation NICE guideline 94 March 218 Developed by
National Institute for Health and Care Excellence Final Chapter 39 Bed occupancy Emergency and acute medical care in over 16s: service delivery and organisation NICE guideline 94 March 218 Developed by
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Health care process improvement teams often
 Original Article Causal Analysis of Emergency Department Delays Raya E. Kheirbek, MD; Shervin Beygi, PhD; Manaf Zargoush, PhD; Farrokh Alemi, PhD; Alyshia W. Smith, DNP, RN; Ross D. Fletcher, MD; Philip
Original Article Causal Analysis of Emergency Department Delays Raya E. Kheirbek, MD; Shervin Beygi, PhD; Manaf Zargoush, PhD; Farrokh Alemi, PhD; Alyshia W. Smith, DNP, RN; Ross D. Fletcher, MD; Philip
Dashboard Review First Quarter of FY-2017 Joe Selby, MD, MPH
 Dashboard Review First Quarter of FY-217 Joe Selby, MD, MPH Executive Director 1 Board of Governors Dashboard First Quarter FY-217 (As of 12/31/216) Our Goals: Increase Information, Speed Implementation,
Dashboard Review First Quarter of FY-217 Joe Selby, MD, MPH Executive Director 1 Board of Governors Dashboard First Quarter FY-217 (As of 12/31/216) Our Goals: Increase Information, Speed Implementation,
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Nursing skill mix and staffing levels for safe patient care
 EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
The Current State of CMS Payfor-Performance. HFMA FL Annual Spring Conference May 22, 2017
 The Current State of CMS Payfor-Performance Programs HFMA FL Annual Spring Conference May 22, 2017 1 AGENDA CMS Hospital P4P Programs Hospital Acquired Conditions (HAC) Hospital Readmissions Reduction
The Current State of CMS Payfor-Performance Programs HFMA FL Annual Spring Conference May 22, 2017 1 AGENDA CMS Hospital P4P Programs Hospital Acquired Conditions (HAC) Hospital Readmissions Reduction
Implementation of crowding solutions from the American College of Emergency Physicians Task Force Report on Boarding
 Int J Emerg Med (2010) 3:279 286 DOI 10.1007/s12245-010-0216-6 ORIGINAL RESEARCH ARTICLE Implementation of crowding solutions from the American College of Emergency Physicians Task Force Report on Boarding
Int J Emerg Med (2010) 3:279 286 DOI 10.1007/s12245-010-0216-6 ORIGINAL RESEARCH ARTICLE Implementation of crowding solutions from the American College of Emergency Physicians Task Force Report on Boarding
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS
 APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
Reduction of Admit Wait Times: The Effect of a Leadership-based Program
 ORIGINAL CONTRIBUTION Reduction of Admit Wait Times: The Effect of a Leadership-based Program Pankaj B. Patel, MD, Mary A. Combs, and David R. Vinson, MD Abstract Objectives: Prolonged admit wait times
ORIGINAL CONTRIBUTION Reduction of Admit Wait Times: The Effect of a Leadership-based Program Pankaj B. Patel, MD, Mary A. Combs, and David R. Vinson, MD Abstract Objectives: Prolonged admit wait times
MBQIP Measures Fact Sheets December 2017
 December 2017 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U1RRH29052, Rural Quality
December 2017 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U1RRH29052, Rural Quality
Capital District Emergency Services Council CDESC
 Capital District Emergency Services Council CDESC Quarterly Report Quarter 4 With focus on the Emergency Departments of Cobequid Community Health Centre and Hants Community Hospital 1 Introduction Emergency
Capital District Emergency Services Council CDESC Quarterly Report Quarter 4 With focus on the Emergency Departments of Cobequid Community Health Centre and Hants Community Hospital 1 Introduction Emergency
Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds.
 Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds. IDENTIFYING THE OPTIMAL CONFIGURATION OF AN EXPRESS CARE AREA
Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds. IDENTIFYING THE OPTIMAL CONFIGURATION OF AN EXPRESS CARE AREA
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Placing Physician Orders at Triage: The Effect on Length of Stay
 HEALTH POLICY AND CLINICAL PRACTICE/ORIGINAL RESEARCH Placing Physician Orders at Triage: The Effect on Length of Stay Stephan Russ, MD, MPH, Ian Jones, MD, Dominik Aronsky, MD, PhD, Robert S. Dittus,
HEALTH POLICY AND CLINICAL PRACTICE/ORIGINAL RESEARCH Placing Physician Orders at Triage: The Effect on Length of Stay Stephan Russ, MD, MPH, Ian Jones, MD, Dominik Aronsky, MD, PhD, Robert S. Dittus,
At-Risk Populations and the Critically Ill Rely Disproportionately on Ambulance Transport to Emergency Departments
 EMERGENCY MEDICAL SERVICES/ORIGINAL RESEARCH At-Risk Populations and the Critically Ill Rely Disproportionately on Ambulance Transport to Emergency Departments Benjamin T. Squire, MD, Aracely Tamayo, MSW,
EMERGENCY MEDICAL SERVICES/ORIGINAL RESEARCH At-Risk Populations and the Critically Ill Rely Disproportionately on Ambulance Transport to Emergency Departments Benjamin T. Squire, MD, Aracely Tamayo, MSW,
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
VJ Periyakoil Productions presents
 VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER
 SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER 1 WHY IS SAN FRANCISCO GENERAL HOSPITAL IMPORTANT? and Trauma Center (SFGH) is a licensed general acute care hospital which is owned and operated by the
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER 1 WHY IS SAN FRANCISCO GENERAL HOSPITAL IMPORTANT? and Trauma Center (SFGH) is a licensed general acute care hospital which is owned and operated by the
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
IN EFFORTS to control costs, many. Pediatric Length of Stay Guidelines and Routine Practice. The Case of Milliman and Robertson ARTICLE
 Pediatric Length of Stay Guidelines and Routine Practice The Case of Milliman and Robertson Jeffrey S. Harman, PhD; Kelly J. Kelleher, MD, MPH ARTICLE Background: Guidelines for inpatient length of stay
Pediatric Length of Stay Guidelines and Routine Practice The Case of Milliman and Robertson Jeffrey S. Harman, PhD; Kelly J. Kelleher, MD, MPH ARTICLE Background: Guidelines for inpatient length of stay
The characteristics of children who visit pediatric
 Research Recherche Patients who leave the pediatric emergency department without being seen: a case control study Ran D. Goldman, Alison Macpherson, Suzanne Schuh, Crystal Mulligan, Jonathan Pirie DOI:10.1503/cmaj.1031817
Research Recherche Patients who leave the pediatric emergency department without being seen: a case control study Ran D. Goldman, Alison Macpherson, Suzanne Schuh, Crystal Mulligan, Jonathan Pirie DOI:10.1503/cmaj.1031817
Low Acuity Emergency Department Visits. Joanna Cohen, MD June 2018
 Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact