Mansfield and Ashfield NHS Clinical Commissioning Group. Strategic Plan
|
|
|
- Marilyn Cooper
- 5 years ago
- Views:
Transcription

1 Mansfield and Ashfield NHS Clinical Commissioning Group Strategic Plan April 2012, following consultation Page 1 of 75
2 Contents Page 1. Foreword and statement of Governing Body Approval 3 2. Working together to Improve the Health and Wellbeing of people in Mansfield and Ashfield 6 3. Our priorities for action: Our financial plan Commissioning with our partners How will we know we are making an impact? 19 List of Appendices 1 Links to further sources of information 2 Diagram showing leadership and decision-making arrangements 3 Map showing alignment between practices and resident and registered populations 4 Federated Commissioning Group (FCG) organisation and support 5 How we have consulted on the development of our priorities. 6 Glossary/Abbreviations Page 2 of 75
3 1. Foreword 1.1. In order to achieve authorisation as a Clinical Commissioning Group Mansfield and Ashfield NHS Clinical Commissioning Group (MACCG) must demonstrate that, as an organisation we achieve key competencies in the following areas: Clinical focus and added value Capacity and capability (including governance) Engagement with patients and communities Leadership capacity and capability Collaborative arrangements Governance And that we have a: o Clear and credible plan to meet its duties to serve the population of Ashfield and Mansfield and its objectives as a Clinical commissioning group. We want to be known as an organisation that contributes to making a real difference to improving the health and wellbeing of people in Mansfield and Ashfield This document is our first strategic plan as an organisation that has the ambition to become authorised as a Statutory Clinical Commissioning Group by 1 April Our starting point for developing the plan has been to look closely at the health needs of the people who live in Mansfield and Ashfield. We are working closely with the Health and Wellbeing Board to inform the Health and Wellbeing Strategy for Nottinghamshire as a whole. In the meantime, we have used the County Health Needs Assessment and the District Health Profiles which set out these health needs (please refer to Appendix 1) Our second consideration has been our financial position. As a CCG we need to establish our organisation and deliver better health, whilst at the same time making productivity and efficiency gains of approximately 4% in each of the next 3 years. This is necessary to address rising demand for healthcare at a time when financial resources that we will receive from the Department of Health will not increase in line with that increase in demand. This will be delivered through ensuring that the services we commission deliver high Quality, exploit Innovation, maximise Productivity, and take a strong approach to Prevention of ill health. This is known as the QIPP challenge. This is a significant challenge indeed, and to succeed we intend to work in partnership with patients, members of the public, clinicians, managers, local authorities and voluntary organisations across our area. Page 3 of 75
4 1.5. It is with this in mind that our Governing Body has approved the following values as PARTNERS in healthcare: P atient Our focus will always be on our service to patients A ccountable We will be accountable for, and honest and open about, the decisions we make R esponsive We will listen and respond to what people tell us about the services we commission T rue partners We will work collaboratively with all of our partners who can help to Improve the Health and Wellbeing of People in Mansfield and Ashfield N ear to home Services Near to home, so long as they are Safe, Clinically Effective and Cost Effective E quitable We will recognise the diverse needs of our population and ensure services are available on a fair and equitable basis R espect We will be mindful of how we work and of the impact our actions might have on others S eamless We will work hard with others to provide integrated services to improve the patient experience (These values support the principles set out in the NHS constitution) 1.6 Mansfield and Ashfield CCG has been established as a sub-committee of the PCT (NHS Nottinghamshire County) since July 2011 and is accountable to NHS Nottinghamshire County for performance, quality and finance. The PCT Cluster remains accountable for all functions delegated to its CCGs, until the CCGs become statutory bodies in their own right. Therefore the PCT Cluster Chief Executive remains the Accountable Officer during the transition period. Mansfield and Ashfield CCG s Governing Body minutes and financial reports are reported to the PCT Cluster Board during the transition. CCGs have also adopted and adapted the PCT s policies and standing financial instructions. 1.7 We have made great progress in the past six months. We have: Broadened and deepened clinical involvement and engagement Established a cohort of clinical leaders across the Mansfield and Ashfield areas Overhauled organisational governance arrangements in line with what is expected from the Health and Social Care Bill Extended Governing Body membership and have appointed secondary care doctor and board nurse member posts Put in place innovative arrangements for patient and public involvement at every level of our organisation. In addition, we plan to: Re-develop our inter-practice agreement so that it better reflects the requirements of practices as clinical commissioners. Appoint a lay person/non-executive with responsibility for Audit, once the requirements of such a post have been clarified. We aim to continue on this trajectory of success and need your help in making this happen so that we can make the most of this opportunity to target effort and services to make a difference in Mansfield and Ashfield. A shortened version of this plan is available on request from Julie Andrews (julie.andrews@nottspct.nhs.uk ). We can also arrange for it to be made available in alternative formats. Page 4 of 75
5
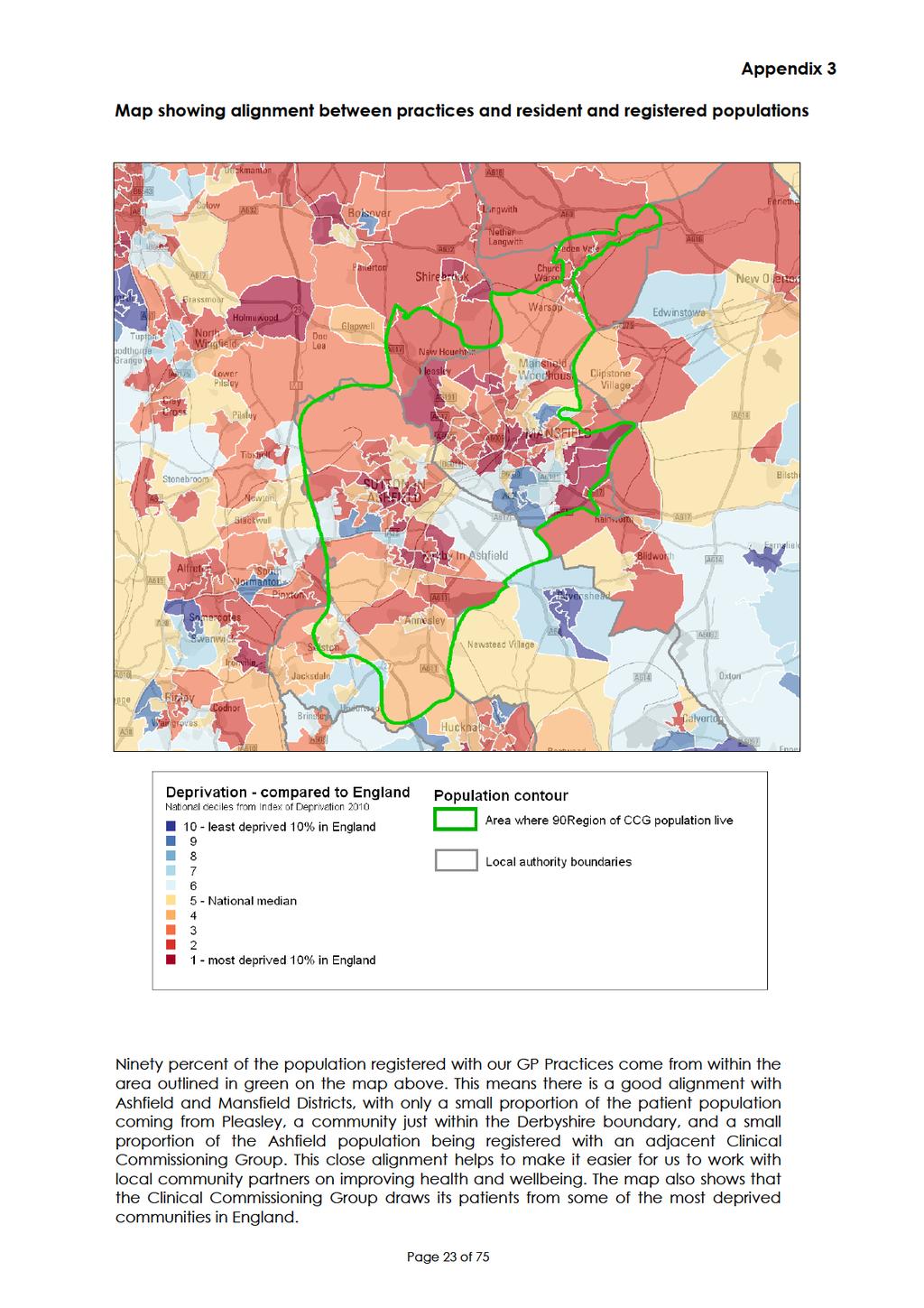
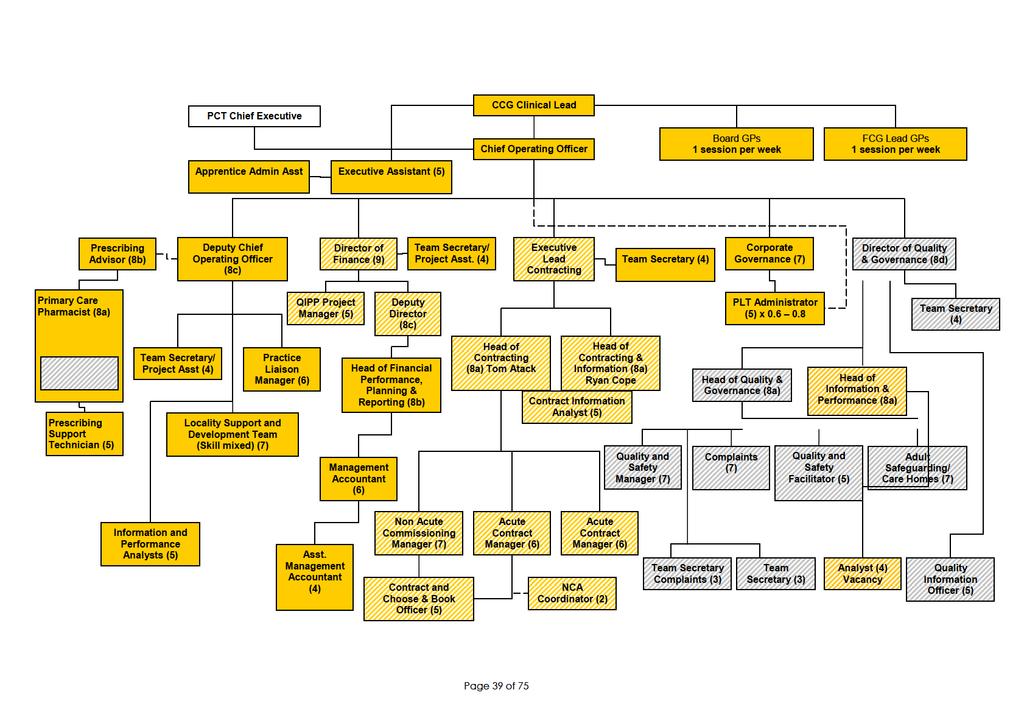
6 2. Working together to Improve the Health and Wellbeing of People in Mansfield and Ashfield 2.1 About Mansfield and Ashfield CCG Clinical Commissioning Group Our geography Mansfield and Ashfield CCG is one of 6 Clinical Commissioning Groups in the Nottinghamshire cluster. We formed in April 2011 from the 31 GP practices which made up the former Mansfield and Ashfield Practice Based Commissioning Group (formerly known as High Point Health ). We cover all of the Mansfield and Ashfield areas with the exception of Hucknall. GP practices in Mansfield and Ashfield first came together to work as commissioners when Ashfield and Mansfield PCTs were created in Throughout a series of changes to the NHS we have retained continuity as like-minded practices who are committed to working together for the best interests of patients in our area. We see this as a strength going forward Leadership and accountability We anticipate that Mansfield and Ashfield CCG will start the authorisation process in October From April 2013, we will take on the responsibilities of a statutory organisation (such as being responsible for negotiating contracts) and will have full budgetary accountability. Until that time, we will continue to lead contract negotiations and be responsible for financial balance of the CCG in shadow form. We are currently operating with delegated responsibility through a Memorandum of Understanding with NHS Nottinghamshire County. Therefore, our governing body acts as a subcommittee of the NHS Nottinghamshire County Board. Our authority and decision-making powers are delegated to us from the PCT s Board, and we are accountable to the PCT Cluster Chief Executive and PCT Board. Detailed arrangements about how this works in practice can be found in the Transfer of Commissioning Functions Memorandum of Understanding, and details of how to access this are in Appendix 1. Mansfield and Ashfield CCG has an elected Clinical lead and elected Governing Body GPs. These posts are supported by a management team led by a Chief Operating Officer (COO) and appointed lay Chair and secondary care doctor and board nurse members. Public Health advice to the Governing Body is through a named Public Health Consultant. A diagram showing our leadership and decision-making arrangements is to be found at Appendix 2. We have put in place a programme of organisation and leadership development to take us through the transition period to ensure we have the right structures, staff and skills needed to perform our statutory duties as a CCG. Mansfield and Ashfield CCG is responsible for a budget of 236million and for purchasing healthcare for a population totalling 183,000 people. It is important that the CCG commissions effectively for our registered and resident populations. The map at Appendix 3 illustrates the good alignment between our practices and registered population. ( Registered population refers to the people who are registered as a patient with one of our 31 practices. Resident population refers to those people who live in our geographical area, but who are registered as a patient elsewhere). Page 6 of 75
7 Partnership working Health and Wellbeing Board The Nottinghamshire Health and Wellbeing Strategy will guide our vision and direction. The CCG will have the opportunity to help develop the strategy and, once approved, the Health and Wellbeing Strategy will provide the framework for our future plans. Partnership working will be embedded through joint commissioning with the County Council, where this is relevant. Newark and Sherwood Clinical Commissioning Group Mansfield and Ashfield Clinical Commissioning Group is one of six CCGs in the Nottinghamshire cluster. Amongst these, Newark and Sherwood is our key partner for commissioning. Between Mansfield and Ashfield and Newark and Sherwood CCGs, we account for approximately 85% of the income of Sherwood Forest Hospitals NHS Foundation Trust, (SFHFT). It is important, therefore, that we have a shared approach to agreeing commissioning intentions for this trust. Clinical leaders from Mansfield and Ashfield and Newark and Sherwood CCGs meet with clinical leaders from SFHFT as a Clinical Executive group to discuss, debate and agree key clinical issues and consider proposals for pathway changes. In order to commission services effectively, we have a number of managers who are responsible to both CCG Governing Bodies (Mansfield and Ashfield and Newark and Sherwood). In this way, and through sharing management costs, both CCGs are able to benefit from the expertise of a range of high calibre managers who lead the contracting process on behalf of both organisations. (Please see Appendix 1 for additional information). Other Nottinghamshire CCGs In addition, for the other larger NHS provider contracts, each of the Nottinghamshire CCGs has taken a role as first amongst equals as leaders of the contracting process. We are currently developing a Memorandum, of Understanding between the CCGs to describe how these arrangements will work in practice. Mansfield and Ashfield CCG has taken this leadership role in respect of: Sherwood Forest Hospitals NHS Foundation Trust East Midlands Ambulance Service NHS Trust (linking in to Derbyshire CCGs) Central Nottinghamshire Clinical Services (our out of hours primary care provider) Patients and the Public Mansfield and Ashfield CCG currently has a lay Chair, lay Vice Chair, and one further lay member as full voting members of our governing body. Our governing body has recently agreed the principles for developing a Citizen s Reference Panel (CRP) that will be made up of a range of key individuals such as : Representatives from practices Patients Reference Groups Interest Groups and Voluntary Groups working in our area Page 7 of 75
8 Interested members of the public District councillors We will consult with the CRP in relation to proposed service changes and will ask them to be our sounding board to ensure we know what we need to change and how we might need to commission differently. The Citizens Reference Panel will elect 2 of it members to be the lay members of the governing body in future in this way we will ensure that the voice of the patients and public in our own locality is heard and is listened to. This should help us to enshrine the ward to board principles of good governance. A further lay member/non-executive will be appointed to have oversight of our audit committee, once the requirements of this Governing body member are better understood and in time for us being a statutory organisation. Details of how to access our Patient and Public Engagement Strategy are set out in Appendix 1. Practices All but one of our practices will have Patient Reference Groups (PRG) by the end of 2011/12 (some are developing more quickly than others), and these are the foundation of our Engagement Strategy. Discussions are ongoing with the remaining practice who does not yet have a PRG in place to see how we can facilitate this development. We have established 5 Federated Commissioning Groups (FCGs) consisting of between 5 and 7 practices that have agreed to work in partnership as commissioners. All of our 31 practices are members of an FCG. (Please refer to Appendix 4 for full details). We are revising our Inter-Practice Agreement to which all practices are signatories. We are enlisting the help of the NHS Alliance with this work. In addition, all practices are expected to sign up to their formal participation as members of the CCG through a national constitution. This will be completed in line with the authorisation process and requirements. 2.2 About health in Mansfield and Ashfield Increasingly, we are shaping our thinking about improvements in health services in line with the NHS Outcomes Framework. We are using the Outcomes Framework in each of our health priority workstreams. The vast majority of people registered with our Clinical Commissioning Group live within the boundaries of either Mansfield or Ashfield District. Since the CCG is responsible for the resident as well as the registered population, this is an advantage to the CCG in the way it plans services. Life expectancy is a quick and easy way of indicating health in the population. For both Mansfield and Ashfield, life expectancy overall is significantly worse than the England average. So whilst health has been improving here, it has not been enough to close the health inequalities gap. Health status is shaped by many factors outside the control of the NHS, and these are often described as the wider determinants of health. The level of multiple deprivations in the community is a good proxy for describing this, so it is perhaps unsurprising that both Districts have scores higher than the national average. At District level these figures mask more inequalities, for instance in Page 8 of 75
9 Mansfield 40% of residents live in the worst 20% of deprivation nationally. (Please refer to Appendix 5 to see our Health Profiles). This helps to define the health needs of our population and, in turn, impacts on the delivery of primary care services and the commissioning of health services in the area. For instance, we know that in our populations we have higher than average levels of unhealthy behaviours e.g. smoking and obesity. These, in turn, mean that we have higher than average levels of chronic and lifethreatening diseases such as Cancer, Diabetes and Chronic Respiratory Diseases. We therefore recognise the importance of working with the Health and Wellbeing Board to ensure that we take a joined-up approach to developing the Health and Wellbeing Strategy and tackling the causes of ill health. At the same time we are driving up the quality of clinical care (including chronic disease management) provided in our practices, so that we can reduce unplanned admissions to hospital, and optimise health for our populations, in line with the NHS Outcomes Framework. We also need to plan for, and develop services to address, the changing profile of our populations. We know that the incidence of dementia is growing all the time and, with more people living longer, the incidence of that disease will increase yet further. The 2011 health profiles recently published for Mansfield and Ashfield (Appendix 1) tell us that the topmost priorities for both localities are smoking, obesity and alcohol all of which have impact on the prevalence of the longterm conditions referenced above. Our Diverse population We confirm our commitment to ensure our priorities meet the needs of our diverse populations in Mansfield and Ashfield. The Equality Act 2010 requires public services to ensure that all people have a good access to, and experience of, those services. This includes people specifically listed with the protected characteristics relating to: Age Disability Gender reassignment Marriage and civil partnership Pregnancy and maternity Race Religion or belief Sex Sexual orientation For Mansfield and Ashfield, the level of disability appears to be of greatest significance and this is recognised within our health priorities and our workstreams. In addition, the most significant factor affecting health in Mansfield and Ashfield, although not addressed specifically be the protected characteristics is deprivation. Our populations are significantly overrepresented in the most deprived groups. Approximately a third of our registered population live within the 20% most deprived areas of England. We will ensure that we comply with our duties under the Equality Act as an employer and as a commissioner of health services. Page 9 of 75
10
11
12 Rationale Mansfield and Ashfield CCG Workstreams Workstream objectives Working in partnership (Link to Health needs and/or financial position/qipp in MACCG) Increase access to consultants in health care of the elderly, particularly in the community. Implement MACCG Care Homes co-ordinator pilot across Mansfield and Ashfield. 1. Care of the elderly in the community Bring about a reduction in the number of falls, which lead to fractures. Ensure referrals to the community falls team have a multi-factorial falls assessment in primary care, and that the recommendations of the falls team are actioned. Tackle preventable ill health and disability, and help people live independently Engage with all care homes to ensure EMAS protocols are up to date and the good practice guidance is followed. Improve the early diagnosis of dementia. Implement a MACCG community dermatology service, to include primary care education. Decommission anticoagulation services from SFHT and provide community based alternative 2. Planned care Implement an increased range of direct access diagnostic services. Optimise the use of Advice and Guidance on Choose and Book in the pilot specialties (Cardiology and ENT) and expand the range of specialties for which Advice and Guidance is available. Audit reasons for Ophthalmology referral and referral outcome. Develop and use a Minimum Data Set (MDS) for referrals to ensure better triage. Ensure reduction in unwarranted clinical variation when referring for procedures of limited clinical value and where referral thresholds can be applied. Prevent unnecessary hospital visits Revise and implement Limited Clinical Value Policy and adopt and implement evidencebased thresholds for referral. Prevent unnecessary hospital admissions Prevent unnecessary hospital visits Adopt uro-gynae stress and urge incontinence pathways Systematically apply the evidence-based pathway for heavy menstrual bleeding. Implement the alcohol pathway, to include primary care training. Reduce the impact of harmful drinking Page 12 of 75
13 Mansfield and Ashfield CCG Workstreams Workstream objectives Working in partnership Rationale (Link to Health needs and/or financial position/qipp in MACCG) 3. Mental Health and substance misuse Undertake PBR data validation for high volume service users (and put bespoke action plans in place for high volume service users) such as individual case management. Improve access to dementia services and improve services for younger people with dementia, and their carers. Reduce use of atypical anti-psychotics for people with dementia through review of patients in nursing and residential homes, initially. Increase the availability of talking therapies, review demand for specialist mental health services. Reduce the number of alcohol-related admissions to hospital Prevent unnecessary hospital visits Prevent unnecessary hospital admissions Tackle preventable disability and help people live independently Demonstrate utilisation of high quality and cost effective prescribing Prevent unnecessary demand on specialist mental health services 4. Prescribing 5. End of Life Ensure adherence to agreed formulary and achievement of incentive scheme objectives. Develop and implement local prescribing formulary. Agree prescribing improvement plans, e.g. waste reduction. Ensure comprehensive implementation of the end of life (EOL) pathway. Provide anticipatory prescribing for patients who are terminally ill. Demonstrate utilisation of high quality and cost effective prescribing Support more people to die at home if that is their choice Demonstrate utilisation of high quality and cost effective prescribing Prevent unnecessary hospital admissions 6. Cardiovascular disease and prevention Review and progress the Heart Failure integrated care pathway. Implement vascular checks to provide earlier intervention and reduce cardiac disease. Reduce the number of people that die and who have life-limiting disability after suffering a stroke, by improving primary prevention. Increase number of smoking quitters Prevent unnecessary hospital admissions Tackle preventable disability and help people live independently 7. Access and urgent care Reduce inappropriate urgent care activity through introduction of integrated primary care front door to Emergency Department (ED). Targeted use of emergency care practitioners for community pathways such as intravenous antibiotics. Improve access to primary care as a means of reducing use of secondary care. Prevent unnecessary hospital admissions Prevent unnecessary hospital visits Reduce the number of patients who do not attend their GP appointments. Page 13 of 75
14 Mansfield and Ashfield CCG Workstreams Workstream objectives Working in partnership Rationale (Link to Health needs and/or financial position/qipp in MACCG) 8. COPD (Chronic Obstructive Pulmonary Disease) Review and strengthen the primary care element of the COPD pathway Implement the MACCG plan for increased community oxygen assessment, through practice review of oxygen registered patients GP review within 6 weeks of a hospital discharge, patient personalised management plan, medication review, seasonal vaccination. Increase number of smoking quitters Prevent unnecessary hospital admissions Prevent unnecessary hospital visits Tackle preventable disability and help people live independently Demonstrate utilisation of high quality and cost effective prescribing Reduce the rate of teenage conception. 9. Children s health Improve mental health and well-being of children Reduce childhood obesity e.g. by improving rates of breastfeeding. Implement Multi-Disciplinary Teams (MDTs) in primary care. Addressing the identified health needs of our population. Taking a positive approach to promoting good health and preventing ill health. 10. Cancer Improve early diagnosis and prevention. Reduce the rate of smoking. Addressing the identified health needs of our population. 3.3 A strategy for primary care To date, we have not yet completed work on a primary care strategy. To achieve success, each of the 10 health priorities listed above, require significant effort and input from primary care clinicians reflecting the commitment of local practices to manage patients in primary care, where possible, to provide care to patients in the most appropriate setting. However, more work remains to be done on an over-arching primary care strategy, which will: Demonstrate the overall service strategy, including the ways in which we intend to improve the quality of, and access to, primary care in Mansfield and Ashfield. Indicate how we will use the Estate to support the primary care service strategy Address workforce development and education issues Indicate how, through management of local resources, we could incentivise more services to be carried out in primary care settings to achieve best value for money. Work will continue on this emergent primary care strategy and this will be taken to the CCG governing body in May for approval. Page 14 of 75
15 4. Our Financial Plan 4.1 Financial context At its meeting in March 2011, the PCT considered the key planning assumptions that reflected the latest Operating Framework and SHA guidance. These assumptions fed into the 4-year financial plan (2011 to 2015), developed in support of the overarching PCT strategy, Strategic Operational Plan (SOP) and CCG financial positions. The revised financial plan for 2011/12 onwards was developed using the following base case inflation planning assumptions: BASE CASE 11/12 12/13 Growth 2.20% 0.00% Uplift Assumptions (net of efficiency) Service Level Agreements (SLAs) - Tariff Inflation -1.50% -1.50% SLAs - CQUIN (09/10 0.5%, uplifted to 1.5% in 10/11) 0.00% 0.00% Primary Care (net) 1.00% 1.00% Dental (net) 0.20% 0.20% Prescribing (gross) 5.00% 5.00% (The planning assumptions for 13/14 onwards are to be found at high level in the PCT Integrated plan, to which we have contributed.) 4.2 Financial position compared to likely growth in activity As the majority of spend relates to provider activity, activity models are developed. These activity models include growth assumptions for the next four years, derived from activity trends across the Health Community and are specific to the differing healthcare points of delivery. We have checked and validated these growth assumptions to ensure they are in line with PCT expectations. These are represented below. BASE CASE 11/12 12/13 NHS East Midlands Growth Assumptions A&E Attendances Growth 3.60% 3.60% Out-Patients Growth 1.50% 1.50% Non-Elective Growth 2.80% 2.80% Elective Growth 3.40% 3.40% Other Growth 0.70% 0.70% (The planning assumptions for 13/14 onwards are to be found at high level in the PCT Integrated plan, to which we have contributed.) Combining the nil funding growth from 2012/13 onwards with the anticipated continued growth in activity, which will also impact on other areas of spend, means that the financial outlook is challenging. There will be insufficient resources available to meet the investment requirements to allow the CCG to focus on prevention and quality and continue to meet increasing demands. Delivery of recurrent QIPP savings, therefore, is essential for the ongoing financial balance of the CCG (and PCT Cluster) and for delivery Page 15 of 75
16 of the organisation s strategic objectives. The required level of savings to be delivered in total through cost improvements and improving Quality, Innovation, Prevention and Productivity (QIPP) has been identified. The table below shows the QIPP target over the life of the Plan, based on current planning assumptions. 4.3 Financial allocation going forwards Considerable work is being undertaken at a national level to determine the financial allocations at CCG level. Until this work is concluded, (which was expected to be by December 2011) we have made an assumption that the CCG will be no better off, nor no worse off, than if we inherit our current budget share of the PCT allocation. This means that in 2012/13 the value of our QIPP requirement is 9.5m, which represents 4.1% of our total resource. This reduces to 3.7% and 3.2% in subsequent years, however, this is a significant challenge. Year At PCT level At CCG level 4.4 QIPP alignment PCT Resource Limit QIPP Requirement % of total Resources QIPP Requirement % of total Resources 1,068m 1,057m 1,048m 1,047m 46.4m 36.7m 33.1m 28.0m 4.34% 3.47% 3.2% 2.7% 12.0m 9.5m 8.6m 7.3m 5.1% 4.1% 3.7% 3.2% Work has already been undertaken in the current planning year (2011/12) to align the CCG QIPP requirement with the health priorities for action. Financial values are as set out in the table below Alignment of QIPP requirement with health priorities for action 2011/12 Mansfield & Ashfield Clinically led schemes 2011/ Care of the elderly in the Community Planned care 1,515 3 Mental health and substance misuse Prescribing 1,314 5 End of Life Cardiovascular disease and prevention 47 7 Access and urgent care 4,151 8 Chronic obstructive pulmonary disease (COPD) Children s health (*) 10 Cancer (*) Subtotal 8, Data validation Other QIPP Schemes 1,260 TOTAL 9,492 (*)QIPP requirement not yet agreed Page 16 of 75
17 QIPP schemes led by other CCGs/PCT Cluster 2011/ Management & Admin 1,453 Estates 852 Continuing Care 1,094 Long Term Conditions and Specialised Commissioning 108 Primary Care 43 NUH 1247 Mental health 655 Community 1,401 TOTAL 7,320 TOTAL MANSFIELD & ASHFIELD SCHEMES 16,775 In line with best practice, the CCG has identified potential QIPP schemes higher than its QIPP target. (138% identified). This is to ensure that in the event that schemes do not deliver the full savings, the target is still met Alignment of QIPP requirement with health priorities for action 2012/13 The alignment of QIPP requirement with health priorities is underway for 2012/13. We expect this to be broadly in line with 2011/12. Mansfield & Ashfield clinically led schemes aligned to CCG health priorities 2012/ Sherwood Forest Hospitals 3,801 Prescribing 821 Other 443 TOTAL 5,065 QIPP schemes led by other CCGs/PCT Cluster 2012/ Management & Admin 48 Estates 15 Continuing Care 1,090 Nottingham University Hospitals 688 Mental health 702 Community 677 TOTAL 3,220 TOTAL MANSFIELD & ASHFIELD SCHEMES 8,285 Two exceptions to this are mental health and prescribing expenditure because benchmarking information indicates a low level of savings opportunity. It will be necessary to review the 2012/13 alignment of QIPP with the health priorities at the end of March 2012 because we will need to: Review QIPP delivery by health priority areas for 2011/12 Review any available benchmarking information Page 17 of 75
18 4.5 Clinical leadership Each of the priorities for action will be sponsored by one of the GPs on the Executive Team or governing body and supported managerially. Progress will be monitored at the Executive Team and reported periodically to the governing body. 5. Commissioning with our partners Our success as a Clinical Commissioning Group will rely upon successful working and collaboration with others. 5.1 Current arrangements We have a range of arrangements in place already. The clinical lead is a member of the Health and Wellbeing Board. As previously detailed, we work closely with Newark and Sherwood CCG to commission the services of SFHT. There is close clinical dialogue between SFHT and the CCGs through the Clinical Executive group. We work closely with the other Nottinghamshire CCGs on a first among equals basis to enable each of the CCGs to take responsibility for leading contracting processes on our behalf. A Memorandum of Understanding will be developed to describe these arrangements. In order to deliver QIPP across organisations, we participate in Productive Nottinghamshire to assist in the delivery of system-wide reform and transformation. The clinical lead is a member of the Mansfield Area Strategic Partnership to ensure that our thinking is aligned with the Mansfield District stakeholders. Similarly, we are seeking to develop strategic links with Ashfield District Council to ensure that our thinking is aligned with the Ashfield District stakeholders. We are developing a service level agreement to describe the support we commission from our Commissioning Support Unit, Nottinghamshire Commissioning Support Hub. This provides a range of services (technical contract and procurement support, legal services, Estates support and advice, Human Resources support). We intend to put in place joint commissioning arrangements with the County Council where this is relevant to improving services currently offered. 5.2 Future Plans We already have some plans in place for financial risk sharing within Nottinghamshire. Since we are smaller organisations, variation in activity can have a more dramatic impact on our separate financial positions. In order to mitigate the impact of the risk of variation, we are working with the other CCGs to develop a managed financial risk-sharing approach. We are seeking advice from an external organisation to develop the terms of the risk sharing arrangements. 5.3 Benefits of collaboration We see the benefits of collaboration as: Enabling us to increase our knowledge base and provide greater management and clinical capacity and capability, whilst remaining within our running costs allowance. Affording us the opportunities for integrating commissioning and provision in the medium term. Page 18 of 75
19 Sharing best practice and the opportunity to implement good ideas more quickly. Enabling us to scale our size and commissioning influence appropriately. (using the opportunity for CCGs to influence what only CCGs can influence and, at the same time, commissioning as a group of CCGs where a larger scale is more appropriate). 6. How will we know we are making an impact? 6.1 Ensuring a good process Planning and performance as part of our structure As the CCG has developed in recent months a number of changes to our structure and processes have strengthened planning and performance management. For example: Workgroups have been revised and aligned with our health priorities for action. Although not included in this document, detailed plans for each of the workstreams have been developed (or are currently being developed in consultation with practices). These include the outcomes that are to be achieved through the work along with timescale for delivery. Federated Commissioning Groups (FCGs) of Mansfield and Ashfield CCG practices were introduced in April, and are working actively. They are accountable to our Executive, which reports to the CCG governing body, which is in turn accountable to the PCT Cluster. Clinical leadership in Mansfield and Ashfield CCG is now fully embedded at FCG, Executive and governing body level, and has been further boosted by the appointment of a secondary care doctor and board nurse. Mansfield and Ashfield CCG took over the management of Protected Learning Time (professional training for GPs and practice clinical and administrative staff) with effect from September This enables us to tailor the local education agenda to meet our own local needs and health priorities, and ensure that training and service developments run hand-in-hand. The PCT Cluster has set up a robust Performance Management Office (PMO) at which our financial and activity plans are objectively challenged and our performance and outcomes are regularly monitored. Mansfield and Ashfield CCG has established a mechanism for independently considering and approving cases for change that are generated by our practices. A panel of officers considers innovative ideas, or business cases, from practices and/or FCGs. This group is called the business case panel and, through its membership, removes any potential conflict of interest for individual clinicians and/or practices and this also improves the likelihood of rapid spread of good practice). Each of the workstreams has a clinical lead who will report progress on a quarterly basis to the Executive Team. In this way, clinical leads and workstream groups will be held accountable for progress and delivery of plans. Page 19 of 75
20
21 Appendix 1 Links to further sources of information (These are available on the CCG website) Additional information 1. Transfer of Commissioning Functions Memorandum of Understanding 2. Joint management structure showing shared posts 3. Mansfield and Ashfield CCG Patient Engagement Strategy 4. Delivery plan and clinical lead arrangements for 10 workstreams 5. List of the names of key officers, Governing Body and Executive team members, work stream leads and appointees. HPB.11.27b final MOU as amended by S:\Mansfield & Ashfield CCG\HR_Adm S:\Mansfield & Ashfield CCG\Strateg S:\Mansfield & Ashfield CCG\Strateg Contact List.doc Location 6. Equality Impact assessment 7. Single Equality and Diversity Strategy Mansfield and Ashfield CCG Public Health Practice Profile S:\Mansfield & Ashfield CCG\Strateg Single Equality and Diversity Strategy inc App 1 - Mansfield Ashfield 2011 final.do Page 21 of 75

22
23
24 Appendix 4 Federated Commissioning Group (FCG) organisation and support Background to Federated Commissioning Group working within Mansfield & Ashfield Constituent practices of Mansfield & Ashfield Clinical Commissioning Group (CCG) made a collective decision early during its organisational development to adopt the concept of groups of practices working together as Federated Commissioning Groups (FCG). 1. Rationale The model was proposed for a number of reasons: To develop a way for practices to work together effectively in order for the CCG to be successful Enable all practices within Mansfield & Ashfield to be involved in Clinical Commissioning Improve opportunity for clinical engagement across 31 practices simultaneously Facilitate variation in level of engagement for clinicians, from local level through to wider leadership roles 2. How have the groupings been derived? Largely a geographical allocation to groups Groups of no more than 6-7 practices Approximately same sized population in each grouping Each group containing at least one member of the former PBC Implementation Team for continuity Where possible, groupings took account of individual practice preferences 3. The Federated Commissioning Groups are not intended to: Coerce practices to merge or to share provider functions Take away a practice s individual accountability for its allocated share of the consortium commissioning budget 4. The Federated Commissioning Groups will: Meet regularly Tackle performance and clinical or practice variation in the group Review referral data Generate ideas for service redesign and innovation Be supported by a strengthened consortia management team Include a clinical lead for the group to represent the group at the CCG Executive Team, and provide two way feedback between practices and strategic groups Have agreed terms of reference within which to work 5. The benefits of federated working: Improved communication and accountability across the consortium Supports smaller practices, and those practices previously less engaged with PBC Good practice can be shared Page 24 of 75
25 Group 1 Group 2 Group 3 Group 4 Group 5 Name of Group Name of Group Name of Group Name of Group Name of Group Vantage Point Practices: JAKS Practices: Hardwick Practices: ROSEWOOD Practices: Kirkwood Practices: Oakwood Surgery Oaktree Lane Surgery Meden Vale Medical Centre Bull Farm Primary Care Centre Riverbank Medical Services Pleasley Surgery Ashfield House Selston Surgery Jacksdale Medical Centre Kirkby Surgery Kirkby Health Centre Kirkby Community Primary Care Centre Kirkby Family Medical Centre Healdswood Surgery Ashfield Medical Centre Dr R Sharma (St John Street) The Pantiles Medical Centre Orchard Medical Practice Sandy Lane Surgery Drs Law and Mountcastle Rosemary St Health Centre Millview Surgery Drs Ward, Pearce & Simm Roundwood Surgery Acorn Medical Practice Woodside Surgery Huthwaite Health Centre Willowbrook Medical Practice Woodlands Medical Practice Harwood Close Kirkby Healthcare complex Chair: Chair: Chair: Chair: Chair: Dr Khalid Butt CCG governing body GP(s) Locality SDM Support: Dr Julian Law CCG governing body GP(s) Dr Julian Law Dr Peter Macdougall Locality SDM Support: Dr James Mills CCG governing body GP(s) Dr Dean Temple Locality SDM Support: Dr Milind Tadpatrikar CCG governing body GP(s) Locality SDM Support: Dr Paul Temple CCG governing body GP(s) Dr Piyush Oza Dr Hilary Lovelock Locality SDM Support: Jacqui Kemp Finance Support: Ruth Willis Finance Support: Jo Riddell Finance Support: Jane Thornley Finance Support: Kirsty Ball Finance Support: TBC TBC TBC TBC TBC Information Support: Information Support: Information Support: Information Support: Information Support: Michael Seagrave TBC Julie Shortland Julie Shortland TBC Page 25 of 75
26 Appendix 5 How we have consulted on the development of our priorities Consultation on the Strategic Plan has been undertaken with clinicians, patients, carers and members of the communities of Mansfield and Ashfield. The purpose of the engagement has been to: Raise awareness of the Strategic Plan and to offer the opportunity for involvement with key stakeholders. Provide appropriate and proportionate mechanisms for patients, carers, the public and other stakeholders to contribute to the setting of health priorities and underpinning objective to address health needs and reduce health inequalities in Mansfield and Ashfield. This has been delivered through: o o o o o Discussion of the outline plan by the governing body followed by further detailed discussion at a subsequent governing body Development session. Both sessions included input from Lay Advisors. Discussion with clinicians and practice staff facilitated through Federated Commissioning Groups Federated Commissioning Groups engaging with their constituent Patient Reference Groups Seeking patient, carer and public views through a dedicated engagement event that included presentations and facilitated group discussions with clinical input provided by GPs Utilisation of existing meetings to obtain views The focus of discussion has been on reviewing the ten commissioning health priorities and the underpinning objectives for each priority. Following the engagement process all comments have been reviewed and the Strategic Plan has been amended and refined to reflect those comments. Participants involved in the consultation will be informed of the impact of their deliberations on the Strategic Plan. Wider consultation of stakeholders will be undertaken on the Strategic Plan following formal sign off by the governing body on 10 November Page 26 of 75
27 Appendix 6 Glossary/Abbreviations A&E Accident and emergency departments assess and treat people with serious injuries and those in need of emergency treatment. They are sometimes referred to as casualty departments or emergency departments. Anticipatory prescribing Anticipatory prescribing describes the prescribing of a defined list of medicines for patients who are identified as being in the last stages of life, to ensure they have all medicines needed to manage their symptoms, e.g. pain, sickness. Atypical anti-psychotics Atypical antipsychotic drugs are a group of medicines used to manage symptoms such as agitation, anxiety, mania and aggression in people with conditions such as schizophrenia or dementia. Evidence shows that the use of these drugs for elderly patients with dementia increase their risk of suffering cerebro-vascular events including stroke and this outweighs the likely benefits in the treatment of behavioural symptoms of dementia. Guidance suggests they should not be prescribed and GPs are reviewing those patients who have been prescribed atypical anti-psychotics to decide whether it is still appropriate. Authorisation Authorisation is a process that will determine Clinical Commissioning Groups (CCGs) readiness to be established as a statutory organisation. CCGs will be judged on a number of areas, e.g. governance arrangements, clinical and professional focus and leadership. Care Homes Co-Ordinator Pilot The Care Homes Co-Ordinator Pilot is a time limited jointly funded project through health and social care to support care homes and their residents in the prevention of inappropriate admissions to hospital. Care pathway A care pathway defines a patient's journey through care for a specific health condition. The pathway identifies what care and treatment is required along the pathway and the expected outcomes of that care and treatment. Choose and Book This is a system whereby patients referred mainly to hospital usually by their GP are offered a choice of hospital and a choice of time and date for their booked appointment. Clinical Commissioning Group Clinical Commissioning Group is the term given to a form of commissioning that is clinically led by a group of GPs and other staff working together within a defined area, e.g. geographical. They are currently operating in shadow form and, subject to authorisation, will become statutory organisations from 2012/13 (subject to passage of legislation). Clinical Executive Group The Clinical Executive Group comprises GPs and management team reporting to the Mansfield and Ashfield NHS CCG governing body, which meets on a monthly basis to take forward the strategic direction of the Clinical Commissioning Group. Page 27 of 75
28 CQUIN Commissioning for Quality and Innovation (CQUIN) is a framework that enables commissioners of care to financially reward providers where they can demonstrate they are delivering high quality care to agreed standards. Commissioning Commissioning relates to the purchasing and contracting of health care services. It involves identifying health needs, service planning and design and purchasing services from appropriate providers and subsequently managing the contracts put in place. ED An emergency department (ED), also known as accident & emergency (A&E), or casualty department, assesses and treats people with serious injuries and those in need of emergency treatment without prior appointment, who arrive there either by their own means or by ambulance. The emergency department is usually found in a hospital. Elective Care Elective care is pre-arranged, non-emergency care that includes planned operations. It is usually provided by consultants in a hospital setting. Patients are usually referred from a primary care professional such as a GP. Federated Commissioning Groups Federated Commissioning Groups are a local initiative that brings together groups of 6-7 practices, usually in a geographical area, to work together to share good practice and generate ideas for service redesign and innovation. Health Needs Assessment Health needs assessment is a method for reviewing the health issues facing a population, leading to agreed priorities and allocation of resources that will improve health and reduce inequalities Health and Wellbeing Board Local authorities will have a responsibility to establish a Health and Wellbeing Board that will lead on improving the strategic co-ordination of commissioning across NHS, social care and related children s and public health services. Clinical Commissioning Groups will be represented on the Health and Wellbeing Board. Health and Social Care Bill Proposals for a Health Bill were included in the Queen s Speech for the first Parliamentary session of the coalition Government. The Health and Social Care Bill will bring forward the legislative changes required for the implementation of the proposals in the White Paper: Equity and Excellence, Liberating the NHS which includes the establishment of Clinical Commissioning Groups. Inter-practice agreement A locally developed agreement between Mansfield and Ashfield GP practices which defines the governance arrangements and underpinning principles of working together as a group. Mansfield Area Strategic Partnership (MASP) MASP is the Local Strategic Partnership (LSP) for the Mansfield District. LSP s bring together a wide range of people and organisations in a single co-ordination framework. It sets the strategic aims for the area and ensures they are delivered with all partners contributing, e.g. health, crime and disorder. Page 28 of 75
29 Memorandum of Understanding A Memorandum of Understanding is a written agreement put in place to establish a clear understanding of how an arrangement will practically function and each party's role and responsibilities. Such an agreement is in place between the Primary Care Trust and Clinical Commissioning Groups. MDS Minimum Data Set describes key information that is required to ensure that the next stage of care in a patient care pathway is high quality, timely, safe, and appropriate, e.g. referral to secondary care. Multi-factorial falls assessment The multi-factorial falls assessment is a process followed to assess the likelihood of a patient experiencing a fall. It is usually undertaken with older people who have fallen or who are at risk of falling. NHS Alliance The NHS Alliance is an organisation that champions, supports and represents NHS primary care and all those working within it.. NHS East Midlands NHS East Midlands forms part of the NHS Midlands and East Strategic Health Authority (SHA) cluster. Its role is to ensure that services for patients are developed, financial control is maintained and to lead the implementation of the Government s reforms of the NHS including the provision of support to emerging Clinical Commissioning Groups. Non-elective Non-elective refers to a patient who is admitted to hospital but not in a planned way from a waiting list, for example the patient would be admitted as an emergency. Non-Executive Director Non-executive directors bring expertise and experience, and often particular, knowledge as a member of the local community, to the work of the Board or governing body. Their focus is at a strategic level and is impartial, providing an independent view that is removed from the day-to-day running of the organisation NHS Operating Framework The NHS Operating Framework is a document issued by the Department of Health annually in December giving the planning and priorities for the year ahead. This enables NHS organisations to plan for the financial year starting in April. Patient Reference Groups Patient Reference Groups, or Patient Participation Groups as they are sometimes known, bring together a group of registered patients of a GP practice with the aim of involving them in decisions about the range and quality of services provided, and, over time, commissioned by their practice through the Clinical Commissioning Group. Primary Care Trust Primary Care Trusts are currently responsible for the planning and paying for health care services in its area. The responsibility for this is due to transfer to Clinical Commissioning Groups by April 2013 when Primary Care Trusts will cease to exist. PCT Cluster A Primary Care Trust (PCT) Cluster is a partnership of PCTs working together with a joint management team. Within Nottinghamshire, NHS Nottingham City and NHS Page 29 of 75
30 Nottinghamshire County have joined together to form a cluster. Each organisation continues to have a separate Board. Prescribing formulary A prescribing formulary is a list of medicines recommended for prescribing based on latest evidence for medicines including efficacy, safety, outcomes and cost. Primary Care Services Primary Care Services are services provided by GP practices, dental practices, community pharmacies and high street optometrists. Procedures of limited clinical value A list of procedures of limited clinical value has been drawn up that will only be paid for by the local NHS in certain restricted circumstances, and also a number of treatments which don t work well enough to justify any use within the local NHS. A similar list has been drawn up for medications, to ensure that the local NHS gets the greatest possible value for the local population. Productive Nottinghamshire In recognition of the need across the Nottinghamshire health community to improve efficiency and productivity whilst delivering quality and innovation, all NHS organisations in Nottinghamshire have joined together to form an alliance known as Productive Nottinghamshire. This will ensure that the Nottinghamshire Health community makes best use of limited resources to deliver the QIPP agenda. Quality, Innovation, Prevention and Productivity (QIPP) QIPP is a programme that supports the NHS to deliver Quality, Innovation, Productivity and Prevention programmes. QIPP programmes are necessary because the funding the NHS is set to receive is lower than funding estimated to be required to meet increasing demand on health services (due to the aging population, increase in long terms conditions, more expensive drugs and technologies). The QIPP gap is a term sometimes used to describe the extent of the funding gap between what is available and what is estimated to be needed. By adopting QIPP programmes, we will deliver more for our money to be able to meet the health need of our patients. Registered population Registered population refers to persons registered with a GP practice in a particular area. Resident population Resident population refers to persons usually resident in a particular area. Secondary care Secondary care is defined as a service provided by medical specialists who generally do not have first contact with patients. Secondary care is usually delivered in hospitals or clinics and patients have usually been referred to secondary care by their primary care provider (usually their GP). Triage Triage is a process used to assess symptoms and severity of illness or injury to determine when, where and by whom the patient should be seen as the next part of the care pathway. It is often used in emergency departments and may be used in primary care to assess referrals made to specialist services. Unnecessary hospital visits Page 30 of 75
31 In some circumstances, additional care provided in the community can prevent the need for people to receive their care in hospital. An example might include the provision of community-based dermatology or ENT services. When a patient s medical condition deteriorates, they may need to access hospitalbased services. In some cases, more comprehensive care outside of hospital (in primary care or in community-based services) can prevent or delay this deterioration. An example might include the provision of comprehensive, community-based diagnosis and treatment of long term conditions. Where prevention or treatment services are in place, they can be said to prevent unnecessary hospital visits. Page 31 of 75
32 Nottinghamshire County Transfer of Commissioning Functions Memorandum of Understanding PURPOSE: In response to the Health and Social Care Bill 2011, NHS Nottinghamshire County has put in place arrangements to transfer commissioning services to Clinical Commissioning Groups (CCGs). Five CCGs have been established within Nottinghamshire: High Point Health Newark and Sherwood Nottingham West Nottingham North and East Principia Partners in Health. This Memorandum of Understanding describes the relationship between the CCGs and the PCT Cluster and NHS Nottinghamshire County Board (the PCT Board) during the transition period until the CCGs become statutory bodies and the role of the PCT ceases. This Memorandum of Understanding applies only while the CCG Shadow Boards operate as sub committees of the PCT Board and will not apply once the CCGs are separate statutory bodies. The arrangements set out in this document will take effect from 1 August The PCT Board has established five sub committees of the Board, one for each of the CCGs. The sub committees have the role of shadow boards of the CCGs during the transition period. CONTEXT: In line with national guidance the PCT has formed a PCT Cluster with NHS Nottingham City. A Cluster Chief Executive to cover both PCTs was appointed in October A Cluster Executive Team to provide the management function for the PCT Cluster has also been established. The PCT Cluster is not a statutory body or separate legal entity. NHS Nottinghamshire County and NHS Nottingham City remain separate legal entities and retain statutory responsibility for functions. Both PCTs are legally required to retain a PCT Board. A Nottinghamshire Clinical Commissioning Hub (the hub) has been established to support the CCGs during the transition period. Employees within the hub are employed by the PCT. Oversight of the performance and direction of the hub lies with the CCGs. STATEMENT OF ACCOUNTABILITY: The PCT Cluster remains accountable for all functions delegated to CCGs, until such time as the CCGs become statutory bodies. The PCT Cluster Chief Executive remains the Accountable Officer during the transition period. GOVERNANCE ARRANGEMENTS: General arrangements: The PCT Board has delegated authority to CCGs, through the CCG Shadow Boards and Chief Operating Officers, to manage commissioning functions on behalf of the PCT Cluster until the it ceases to exist. Page 32 of 75
33 As sub committees of the PCT Board, the CCG Shadow Boards are accountable to the PCT Board. Any changes to terms of reference of the CCG Shadow Board must be approved by the PCT Board. Authority to manage functions and delegated decision-making powers are set out in the PCT s Scheme of Delegation. The CCG Shadow Boards report to each meeting of the PCT Board through the presentation of its Board minutes, the standard reports set out in the assurance section below and any other documentation as may be agreed between the PCT Cluster or PCT Board and individual CCGs. Chief Operating Officers or other CCG representatives will attend PCT Board meetings as requested by the Board, to provide specialist input where needed or to give clarification on specific issues. Representatives of the PCT Cluster may attend CCG Shadow Board meetings as observers by prior arrangement with the relevant Chief Operating Officer. CCGs are responsible for ensuring they have robust governance arrangements in place and provide the necessary support required for the Chief Executive to produce an annual Statement on Internal Control. The sub committee structure hosted by the CCGs provides assurance to the CCG Shadow Boards and the PCT Board. The CCGs will initially adopt NHS Nottinghamshire County policies and procedures but in areas where they have delegated authority they may wish to amend those policies and procedures without approval by the PCT Cluster. A central database of policies and procedures will be retained by the PCT Cluster. CCGs should therefore inform the Cluster Executive Lead for Governance if policies and procedures are revised so that the database may be updated. Risk Management: The CCGs will establish appropriate risk management arrangements and will maintain and monitor its own Assurance Framework which links to the Cluster Board Assurance Framework. The Chief Operating Officer will provide a regular update to the Executive Lead for Governance to assist with the regular review of the Board Assurance Framework. CCG Shadow Boards will provide a written report in the agreed format to each meeting of the PCT Board highlighting risk issues which could impact on the achievement of the PCT s strategic objectives. The Quality and Risk Sub Committee has oversight of risk management arrangements in the CCGs. This committee is hosted by Newark and Sherwood in the north and Nottingham North and East in the south. CCGs will inform the relevant PCT Cluster lead of all significant issues or risks as soon as they arise. This includes issues relating to quality, patient safety and safeguarding and matters of major reputational risk which could attract media attention or be of concern to the Department of Health or regulators. Health and Safety: All CCGs are responsible for ensuring that statutory Health and Safety responsibilities (including fire safety) within the CCGs are met. Support will be provided if required by the Estates team within the hub. The element of the Quality and Risk Sub Committee hosted by Nottingham North and East has oversight of Health and Safety compliance. The committee will provide a written report of all Health and Safety incidents to the PCT Board. The Cluster Chief Executive retains ultimate responsibility for Health and Safety across the PCT, including the CCGs until they are established as statutory bodies. Internal Audit and Counter Fraud and Security Management Services (CFSMS): Page 33 of 75
34 The contracting arrangements for Internal Audit and CFSMS continue to be controlled and monitored by the PCT Cluster. Resource to support audits within CCGs will be provided as agreed between the Cluster Director of Finance and the Chief Operating Officer at the beginning of each year. CCGs will participate in discussions with the PCT Cluster and its Internal Audit service to ensure its audit requirements are included within the annual plan. Serious Incidents: CCGs are responsible for reporting and monitoring Serious Incidents. All Serious Incidents must be reported through the STEIS system. CCGs will inform the Cluster Chief Executive or his/her representative of all high profile Serious Incidents and those where there has been extensive harm within 24 hours of the incident being highlighted to the CCG. CCGs have responsibility for ensuring that learning arising from the investigation of all incidents, is introduced into working practice and monitored for effectiveness. Emergency Planning and Business Continuity: Responsibility for statutory emergency planning duties remain with the PCT Cluster. CCGs are expected to make staff available to support emergency planning duties as required and to provide any information required to enable the PCT Cluster to maintain up to date emergency plans. The CCG is responsible for ensuring it has adequate business continuity arrangements in place to ensure the services provided by the CCG are maintained. These arrangements must be agreed with the PCT Cluster. The PCT Cluster will maintain a senior manager on-call rota to enable a co-ordinated response to all incidents requiring the input of senior management. Senior mangers in the CCGs, Cluster and the hub will take part in the rota. Chief Operating Officers must ensure that members of CCG staff are available to undertake on-call duties. External Visits / Inspections: In the event of a CCG being notified of an assessment or visit by an external or regulatory body, the Chief Operating Officer will notify the Cluster Chief Executive as soon as possible taking full account of the immediacy of the visit / inspection. A joint decision will be taken about how the visit will be managed. Information Governance: CCGs are responsible for complying with statutory and Department of Health information governance requirements, including complying with the Information Governance Toolkit, responding to Freedom of Information requests, Subject Access Requests and complying with the Data Protection Act. Information Governance support is available from the hub as required. The Information Governance team within the hub will have a co-ordination role in dealing with any Freedom of Information requests relating to more than one CCG or where the PCT Cluster is involved. The Information Governance team based in the hub will complete the annual assessment of the Information Governance Toolkit on behalf of the PCT Cluster. CCGs are required to provide the necessary evidence to support the assessment. The Information Governance and Information Management Sub Committee oversees information governance arrangements. The committee is hosted by Nottingham North and East. Page 34 of 75
35 The roles of Caldicott Guardian and Senior Information Risk Owner sit within the PCT Cluster, although CCGs will need to establish their own arrangements for these roles when they become statutory bodies. Complaints: CCGs have responsibility for responding to all complaints relating to their area. This will be undertaken by separate complaints teams in the north and the south which will co-ordinate and oversee complaints investigations and responses. CCGs will comply with the NHS Nottinghamshire County complaints policy. CCGs will provide written reports regarding complaints management to the PCT Board quarterly. Infection Prevention and Control: The Quality and Risk Sub Committee has oversight of infection prevention and control arrangements. This committee is hosted by Newark and Sherwood in the north and Nottingham North and East in the south. Safeguarding CCGs are responsible for ensuring compliance with statutory and Department of Health requirements in relation to Safeguarding. The Safeguarding Sub Committee has oversight of Safeguarding arrangements. This committee is hosted by Newark and Sherwood. The Designated Nurse post is shared across all five CCGs. Equality, Diversity and Human Rights CCGs are responsible for ensuring statutory and Department of Health requirements relating to equality, diversity and human rights are met. Support is available from the Executive Lead for Equality and Diversity within the PCT Cluster. The Quality and Risk Sub Committee hosted by Newark and Sherwood CCG has oversight of equality, diversity and human rights arrangements. Human Resources and Organisational Development: NHS Nottinghamshire County continues to be the employing body of all staff within CCGs, although day-to-day line management is undertaken by CCGs. The Chief Operating Officers for each CCG have delegated authority as Appointing Officer and to undertake the role of Chief Executive when enacting any Human Resources Policies and Procedures when applied to staff working within the CCGs. Public Health CCGs are responsible for ensuring that Public Health matters are taken into account in making commissioning decisions. The Public Health team will remain within the PCT Cluster pending a national decision on the future of the function. A separate Memorandum of Understanding setting out the service required by CCGs from the Public Health team will be agreed. CORPORATE GOVERNANCE: Provision of legal advice Legal advice should be sourced via the Executive Lead for Governance in the PCT Cluster during the transition period expect in the case of employment law advice which can be sourced by the Human Resources team based in the hub. Page 35 of 75
36 Contract and Other Legal Documentation During the transition period any legal documents must be entered into in the name of the PCT as the legal entity. Responsibility for the sealing of documents remains with the Cluster Chief Executive and is undertaken on his behalf by the Executive Lead for Governance (Company Secretary). The requirements for signing and sealing documents as set out in the PCT Standing Orders and Standing Financial Instructions should be followed by CCGs. Claims management Liaison with the NHS Litigation Authority in relation to the management of claims is dealt with by the PCT Cluster. Investigation of claims relating to the functions of CCGs is delegated to CCGs. FINANCIAL ARRANGEMENTS: The Cluster Director of Finance remains accountable for the financial performance of NHS Nottinghamshire County including the CCGs until they are established as statutory bodies. NHS Nottinghamshire County s annual accounts will include the financial results of the CCGs. Each CCG has a designated financial management function. CCGs are responsible for ensuring they operate within the financial resources allocated for the financial year and for providing any information requested by the Cluster Director of Finance or his representative. Scheme of Delegation: Details of expenditure authority levels are set out in the PCT s Scheme of Delegation. The sub delegation of authority to approve expenditure and other decision-making below this can be agreed by the CCG. In which case the CCG should produce its own Scheme of Delegation to supplement that of the PCT. Standing Financial Instructions (SFI) / Standing Orders (SO): CCGs must adhere to and abide by, as applicable, the SFI / SO regulatory controls of the PCT Cluster, to ensure that they are acting within delegated powers. Individual CCGs may wish to produce financial procedures to provide staff with more detailed guidance in applying the SFI and SO. Reporting Requirements: CCGs will provide timely and accurate information on their financial position to each meeting of the PCT Board in a format required by the Cluster Director of Finance and on an ad hoc basis as requested by the Cluster Director of Finance. This includes providing information requested of the PCT Cluster by the Strategic Health Authority or the NHS Commissioning Board. Annual Reporting Requirements NHS Nottinghamshire County has a statutory responsibility to produce annual accounts for the Department of Health, following a detailed, prescribed format and timetable. The annual accounts are subject to external audit by the Audit Commission. CCGs will provide such supporting working papers as are required for audit purposes, to the appropriate standard, and in line with the prescribed timetable. CCGs will participate in the production of NHS Nottinghamshire County s consolidated annual accounts as required. Page 36 of 75
37 Audit Committee The Audit and Governance Committee, a committee of the PCT Board has responsibility for audit functions across NHS Nottinghamshire County and the CCGs. The CCGs may be required to provide information requested by the Audit and Governance Committee and to ensure a representative is available to attend meetings where the committee wishes to review a particular issue relevant to the CCG. CCGs have responsibility for monitoring all audit action plans relating to its activities and reporting progress to the Cluster Director of Finance to enable timely reporting to the Audit and Governance Committee. CCGs will also need to develop their own arrangements for oversight of audit responsibilities during the transition period, including having a lay member of the board to oversee audit. ESTATES: Responsibilty for the Estates Strategy and approval of all expenditure on Estates remains with the PCT Cluster. The Estates team within the hub will provide support to the Cluster on Estates matters. PARTNERSHIP WORKING: Responsibility has been allocated to individual CCGs to co-ordinate arrangements for specific functions. The responsibility for contract management and negotiation with providers is as follows: Sherwood Forests Hospitals NHS Foundation Trust - High Point Health East Midlands Ambulance Service NHS Trust High Point Health Nottinghamshire Healthcare NHS Foundation Trust Newark and Sherwood County Health Partnerships and other community services Nottingham North and East Nottingham University Hospitals NHS Trust Nottingham West. Principia Partners in Health is responsible for oversight of the hub and out-sourcing arrangements. CCGs are expected to work in partnership with each other and NHS Nottingham City s CCG to ensure effective commissioning across the county and robust monitoring of provider contracts. CCGs are committed to collaborating wherever possible to achieve this aim. SERVICE LEVEL AGREEMENTS: The hub provides the following support functions as required by individual CCGs: Human Resources Organisational Development Communications Technical Finance Supplies Information Governance Estates Medicines Management Continuing Care. Service Level Agreements will be agreed between the hub and CCGs for all services provided. All services purchased by CCGs will be paid for from the annual budgets allocated to CCGs at rates agreed through the Service Level Agreement. Page 37 of 75
38 Principia Partners in Health has responsibility for overseeing the management of the hub to ensure it provides the services required by the CCGs. There may be some support which the CCGs will provide to the PCT Cluster where staff with the necessary skills and experience are based in the CCG. These services will also be carried out under the terms of a service level agreement. ASSURANCE CCGs will provide the following assurance to each meeting of the PCT Board: Minutes from each CCG Shadow Board meeting A timely financial performance report for each meeting of the PCT Board in a format agreed with the Cluster Director of Finance A timely performance and quality report for each meeting of the PCT Board in accordance with the format agreed at the PCT s Governance Committee on 27 June 2011 A Risk and Assurance report highlighting significant issues of concern, serious incidents and matters of corporate significance or risks which could impact on the achievement of the PCT s strategic objectives. This should also detail the CCG s strategic risks at the time the report is produced and should be in the same format as the Risk and Assurance Report received by the PCT s Governance Committee on 27 June Page 38 of 75
39

40 Page 40 of 75
41 1. Background Embedding Engagement in High Point Health NHS Clinical Commissioning Group (CCG) 1.1 Statutory requirement for engagement The National Health Service Act 2006 (section 242 (1B), 243 and 244) states that NHS organisations must make arrangements, in respect of health services for which they are responsible, which ensure that users of those services, whether directly or through representatives, are involved in: a) The planning of the provision of those services. b) The development and consideration of proposals for changes in the way those services are provided. c) Decisions to be made by that body affecting the operation of those services. In addition, to responsibilities described above, CCGs will be required by law (subject to parliamentary approval) to: consult on annual commissioning plans report on involvement through an Annual Report have two lay members on their governing body have due regard to the findings from local HealthWatch make clear how the voice of patients and the public will be heard and acted upon in the CCGs constitution 1.2 Towards Authorisation for High Point Health One of the six domains against which High Point Health will need to have evidence of competency to achieve authorisation is Engagement with patients, carers and their communities. The domain description states that: CCGs will need to be able to show how they will ensure inclusion of patients, public, communities of interest and geography, health and wellbeing boards and local authorities in everything they do especially their commissioning decisions. They should include mechanisms for gaining a broad range of views then analysing and acting on these. It should be evident how the views of individual patients from the consulting room are translated into commissioning decisions and how the voice of each practice population will be sought and acted upon To evidence achievement of the competencies relating to this authorisation domain High Point Health will need to demonstrate that engagement is undertaken throughout the commissioning cycle and across a continuum from individual through to collective engagement, and that the information gathered is acted upon. Therefore High Point Health will need robust reporting mechanisms to be in place to evidence how engagement has influenced it s decision making at every stage. Page 41 of 75
42 2. Guiding Principles for Engagement Lay members across Nottinghamshire have developed a set of guiding principles which have been applied in the development of High Point Health s engagement model: Local needs people in local communities are able to make their views known about the services they want from a CCG; Decisions early people are having a say right at the start of a decision making process PPI access at the care interface people are engaged at the closest point to where they access care or whenever/wherever they use their NHS; Integrated people are embedded into the decision making processes Wider Community engagement people from the wider local community are engaged in giving their views about services; Consistency of care high quality services, monitored across the community, and which are delivered to the same standards wherever individuals live; Patient expectations patient expectations are realistic, and informed by education and information, thereby better informing their choice of services; Flexibility services which are flexible in meeting individual needs as well as those of the local community; Public input into commissioning decisions Lay Advisers, Patients and Public directly involved in CCG commissioning decisions; Countywide health services - people having a say in which clinical (or CCG support services) should be delivered by the CCG, and which should be delivered centrally; Asset management people involved in making decisions about the best use of CCG resources; Networks of engagement - people are engaged in a variety of ways, at different levels in the community, and from different interest groups, including hard to reach groups; Cross-section of engagement - there is representation on CCG PPE structures e.g. PPG groups, from across different community interests; Monitoring information - there is a process in place to capture, and improve the patient experience, which enables the CCG to prevent illness and encourage self care; Countywide infrastructure for health and social care - people having a say in the impact of organisations such as HealthWatch, Care Quality Commission, Local Authorities, on the provision of local services. 3. Model for engagement in High Point Health A model of engagement has been developed that incorporates the guiding principles developed locally, and which will enable High Point Health to meet the competencies required for authorisation as a statutory body. Diagram 1, shows how High Point Health will ensure the inclusion of patients, public, and communities will be gathered in the membership of the proposed Citizen s Reference Panel. It also demonstrates how patient and public engagement links to High Point Health s planning (task and finish groups) and decision making bodies (Executive and Board). Page 42 of 75
43
44
45 3.1 Patient Participation Groups (PPGs) PPGs are the backbone of the proposed structures, and PPG members will be encouraged and supported to be involved in the Citizen s Reference Panel. All Practices that are members of High Point Health Clinical Commissioning Group will have a PPG. 3.2 High Point Health s Citizen s Reference Panel (CRP) The Citizen s Reference Panel will be a sub-committee of the High Point Health Board. Membership of the CRP would comprise two lay members from PPGs within each of the five Federated Commissioning Groups. Community and voluntary sector representatives, local politicians and members of networks such as the Take a Healthy Interest scheme will also have members on the CRP. The CRP would act as an important point of reference for the High Point Health Board in ensuring that engagement in High Point meets the aspirations of the guiding principles and the engagement domain for authorisation. 3.3 Big Health Forum The Big Health Forum is an open meeting that will be advertised widely and to which any member of the local public may come. The aim of the forum is to engage with the patients and the public across all of Mansfield and Ashfield on health issues, and it will also provide a mechanism for engaging the wider public on High Point Health as a commissioning organisation. The forum will have a flexible agenda and format to meet the needs of participants and the CCG alike. The first Big Health Forum for High Point Health will be held on 6 September The objectives of this forum meeting will be to provide information about the NHS Reforms, and specifically what this means for High Point Health, including the development of patient and public engagement. It is planned to hold Big Health Forum meetings once or twice a year, as issues arise. 3.4 Countywide Strategic Panel (CSP) The County-wide strategic panel (CSP) will be a forum which the Citizens reference panel chair (and their equivalent from other Nottinghamshire CCGs) meet regularly. It will be a means of sharing best practice and co-ordinating patient and public engagement where a countywide approach is needed. A good example being the most recent consultations conducted on the Review of the Walk-In Centre. It is proposed that the CSP meets quarterly. The CSP will also provide a means for the public to link into the development of both HealthWatch and the Health and Wellbeing Board. 4. Review It will be necessary to evaluate and review these proposals to ensure this engagement model works simply and efficiently and delivers on its objectives, for both the members of public who commit to become involved in it, and for High Point Health CCG. It is proposed that an evaluation be carried out within 6 months of implementation. 5. Recommendation to Board The Board of High Point Health is asked to endorse the model suggested in this paper and agree that it will: Ensure inclusion of patients, public, communities of interest and geography Be a mechanism for gaining a broad range of views Be a means of hearing the views of individual patients and the voice of each practice population. Page 45 of 75
46 Strategic Plan, Work Stream Areas Work Stream Lead Clinician Clinical Support Management Support Public Health Contract Lead Care of the elderly in James Mills Raian Sheikh Kirsty Ball Mary Corcoran Tom Atack the community Planned care Julian Law Ruth Willis Jonathan Gribbin Richard Moles Mental health, learning disabilities and substance misuse Hilary Lovelock Jacqui Kemp Barbara Brady Karon Glynn / Marie Crowley Prescribing Khalid Butt James Mills Jane Creedon Piyush Oza Alison Hale End of life Milind Tadpatrikar Jacqui Kemp John Tomlinson Linda Clarke Cardio-vascular disease and prevention Peter MacDougall Jo Riddell John Tomlinson Tom Atack Access and urgent care Dean Temple Jane Thornley Ruth Willis (ECN) Tom Atack COPD Khalid Butt Kirsty Ball John Tomlinson Tom Atack Children s health Julian Law Jane Thornley Kate Allen Linda Clarke Cancer Milind Tadpatrikar Jacqui Kemp Mary Corcoran Richard Moles Diabetes and Obesity Dr Piyush Oza Page 46 of Jo 75 Riddell John Tomlinson
47 Key Contacts Board Members Mr David Pearson Ms Deborah Jaines Dr Raian Sheikh Mr Peter Green Mr Peter Robinson Professor Rachel Munton Dr Ben Pearson Dr Julian Law Dr Hilary Lovelock Dr Peter MacDougall Dr Piyush Oza Dr Dean Temple Ms Helen Pledger Chairman Chief Operating Officer Clinical Lead Lay Vice Chair Lay Member Board Nurse Secondary Care Clinician Board GP Board GP Board GP Board GP Board GP Director of Finance Executive Team Members Ms Deborah Jaines Dr Raian Sheikh (Chair) Ms Barbara Brady Ms Lesley Carman Mr Ian Ellis Ms Helen Pledger Dr Hilary Lovelock Dr Peter MacDougall Dr Dean Temple Dr Khalid Butt Dr Paul Temple Dr Julian Law Dr James Mills Dr Milind Tadpatrikar Chief Operating Officer Clinical Lead Public Health Consultant Deputy Chief Operating Officer Assistant Director of Acute Contracts, Productivity and Performance Director of Finance Board GP Board GP Board GP FCG Chair Vantage Point FCG Chair Kirkwood FCG Chair - JAKS FCG Chair Hardwick FCG Chair - Rosewood Page 47 of 75
48 EQUALITY ANALYSIS (E.A) Completing this document is a Statutory Duty under Equality Legislation Name and address of organisation Clinical Commissioning Group Name and full description of service, policy, development Name and title of person completing the Equality Analysis Date Signature of person completing the Equality Analysis (EIA) Declaration we confirm that we have made all the necessary enquiries in relation to this service and in good faith believe that relevant steps and plans are in place to mitigate any potential discrimination in the service we provide. We understand that progress will be monitored through your contract reviews. Equality Impact Assessment Overview This section should be completed once you have answered questions 1 5 overleaf. Please identify the protected characteristics where action is required Age Yes No Disability Yes No Gender identity (transgender) Yes No Marriage and civil partnership Yes No Pregnancy and maternity Yes No Race Yes No Religion and belief Yes No Sex (Gender) Yes No Sexual orientation Yes No Social Exclusion & Economic Deprivation Yes No Page 48 of 75
49 Equality Analysis Completion guidance: Please ensure that all the questions within this EIA are completed and that written evidence is provided. Should you have any problems when filling out this EIA please refer to: The Guide to completing an Equality Assessment (EA) Equality Group full explanation is within the guidance documentation 1. Would the service be aimed at any particular equality group? Please tick all that apply 1. If yes, please provide a brief explanation why particular group (s) would be targeted Age Yes No Disability Yes No Gender identity (transgender) Yes No Marriage and civil partnership Yes No Pregnancy and Maternity Yes No Race Yes No Religion and belief Yes No Sex (gender) Yes No Page 49 of 75
50
51 Religion and belief Yes No Sex (gender) Yes No Sexual orientation Yes No Social Exclusion & Economic Deprivation Yes No Protected characteristics 3. Are there any known barriers which could obstruct access to the benefits of the service? 3. Barriers could be physical, geographical, or communication. If yes, explain what you intend to do to remove these barriers. Age Yes No Disability Yes No Gender identity (transgender) Yes No Marriage and civil partnership Yes No Page 51 of 75
52 Pregnancy and Maternity Yes No Race Yes No Religion and belief Yes No Sex (gender) Yes No Sexual orientation Yes No Social Exclusion & Economic Deprivation Yes No Protected characteristics 4. Please confirm you will collect personal data to ensure your service is targetted at the right people. 4. This is a yes/no response to using the CCG s personal data monitoring form (forms are supplied) which should be collected from each service user. (if there is a NO response using the PCT CCGs personal data form, please tell us the reason why) Age Yes No Disability Page 52 of 75
53 Gender identity (transgender) Marriage and civil partnership Pregnancy and Maternity Race Religion and belief Sex (gender) Sexual orientation Social Exclusion & Economic Deprivation Page 53 of 75
54 5. What evidence has been used to assist you to make your judgements in questions 1-3? 5. Please provide any other evidence that you feel may be appropriate or details of how you will gather evidence in the future Demographic data and other statistics including census findings Result of research findings including studies of deprivation Results of recent consultations and surveys Results of ethnic monitoring data and any equalities data from the local authority/joint services Information from groups and agencies within Nottinghamshire Comparisons between similar functions/policies Analysis of Patient and Public Involvement Analysis of audit reports and review Community Engagement and consultation events Page 54 of 75
55
56 MANSFIELD AND ASHFIELD CCG PUBLIC HEALTH PRACTICE PROFILE OCT 2011 Page 56 of 75
57 CONTENTS 1. Introduction Key Messages Demographics Life Expectancy Deprivation Child Poverty Healthy Lifestyle Behaviours Smoking Binge Drinking Obesity Levels Fruit & Vegetable Consumption Key Admissions Statistics Mental Health Admissions Hip Fractures in people over 65 years old Elective and Non-elective Admissions Selected Long Term Conditions COPD Heart Failure Diabetes Page 57 of 75
58 1. Introduction Wider Determinants of Health are various demographic, socio-economic and behavioural characteristics of a population that have been widely tied to health outcomes, as well as to health inequalities which may exist between and among populations. In order to have a full picture of the health needs for any population therefore, these wider determinants should be considered. Considering Wider Determinants of Health at the level of GP registered practice presents certain complications in regards to data collection for this population. These issues generally fall into one of the following two categories: Data is collected based on geographical residence and not on a registered population. Data is collected at a geographical area larger than can be reasonably extrapolated to a GP population (e.g., collected only at Nottinghamshire County level). For purposes of this report, information has been translated from resident population data into registered population using a weighting methodology. The geographic areas for which the data was available (e.g., Middle-Super-Output-Area (MSOA) or Ward area) were compared against the registered population of each GP practice. Each registered person s area of residence was noted and a percent allocated for each area, thereby building a picture of where the registered population for each GP practice lives. From here, a weighting was applied to the health indicator in question, thereby providing a weighted figure per GP practice. In the cases where information was not available at areas lower than a County (or previously, a PCT) level, it was not included at a GP level within this report. Within this report, data is provided in most cases as an estimated and weighted percent of population. Where results are reported as directly standardised rates (DSRs) they have been standardised for age. National practice profiles The Association of Public Health Observatories (APHO) have produced practice profiles based upon nationally available data. The Public Health Information and Intelligence Team (PHIIT) have defined clusters for these profiles which can only be accessed by selecting the link below. RPROFILE&clstr=4140 Help regarding interpretation and use of the tool can be found by selecting supporting documents at the weblink above. A note regarding naming of practices. The information contained within this report is derived from a variety of sources. The same practice may be given a different (nationally recognised) name depending on the source of the data. In subsequent reports practices will be referred to consistently using their preferred name. Page 58 of 75
59 2. Key Messages Approximately a third of Mansfield and Ashfield CCG s registered population live within the 20% most deprived areas in England, and the overall life expectancy for Mansfield and Ashfield CCG populations is below the England average (78.3) for all practices except one. There is approximately a two year gap in life expectancy between the highest and lowest GP practice. The proportion of children living in income deprived households varies among practices in Mansfield and Ashfield between 16% and 35%. Mansfield and Ashfield residents are estimated to have higher levels of smoking and binge drinking than the Nottinghamshire average. Estimated levels of obesity were also higher than the East Midlands average, and the level of consumption of fruit and vegetables is lower than average. Admission rates (DSRs) for mental health diagnoses within the CCG were significantly higher than Nottinghamshire. Practices within the CCG show variation in admission rates, with some practices showing significantly higher rates compared with the CCG average. Admissions for hip fractures showed no significant variation across Nottinghamshire s CCGs Patterns of access to secondary care showed variations with age and deprivation. Across Nottinghamshire the ratio of emergency to elective admissions was highest in children and young people where there is also a clear relationship with deprivation: practices with populations from the most deprived areas were more likely to access secondary care as an emergency compared with practices from less deprived areas. The rate of emergency admissions (DSR) was highest amongst older people (65+) within Nottinghamshire where the rate was approximately three times that of younger age groups. This pattern is reflected across all the CCGs. Mansfield and Ashfield CCG had emergency admission rates significantly higher than the average for Nottinghamshire across all age groups. Practices within the CCG showed a 2 fold variation in emergency admission rates, with some practices showing significantly higher rates compared with the CCG average. For the majority of practices in Mansfield and Ashfield Health, observed numbers of patients on the COPD, Heart Failure and Diabetes registers were lower than expected estimates, this suggests there may be some undiagnosed need within Mansfield and Ashfield Health CCG. Page 59 of 75
60 3. Demographics Mansfield and Ashfield CCG consists of 31 GP practices, these vary in size from Oakwood Surgery which makes up around 8% of the whole population of the CCG to Pantiles Medical Centre and Dr Kahn s Practice which make up only 1.4% respectively. The population pyramid shows the age and sex breakdown of Mansfield and Ashfield s registered population is slightly older than that of Nottinghamshire County as a whole, with slightly higher proportions of older age groups and a lower proportion of year olds. Table 1: Mansfield and Ashfield CCG GP Practices and Registered Populations Source: Data Warehouse registered population July 2010 Page 60 of 75

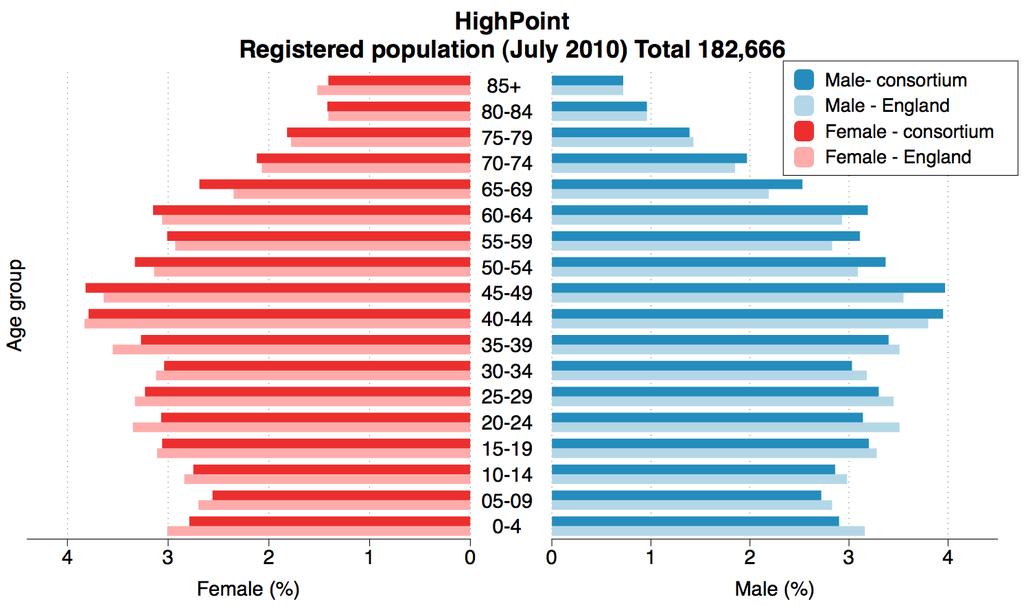
61 Page 61 of 75
 for all practices except Oaktree Lane Surgery (78.6).")
62 Map showing Nottinghamshire s Districts and contour showing where 90% of the CCG registered population live (green). Areas of higher deprivation are marked with darker shades of purple. 4. Life Expectancy The overall life expectancy for Mansfield and Ashfield residents is below the England average (78.3) for all practices except Oaktree Lane Surgery (78.6). There is an estimated 2 year difference in overall life expectancy between Oaktree Lane Surgery Page 62 of 75

 also had a life expectancy greater than the England average (80.6).")
63 (78.6) and Colwick Vale Surgery (76.1) the practice with the lowest life expectancy in the CCG. The pattern in life expectancy was similar for males with only Oaktree Lane Surgery having an expected life expectancy greater than the England average, however in females Huthwaite Medical Practice (80.8) also had a life expectancy greater than the England average (80.6). Page 63 of 75
64 Page 64 of 75


65 5. Deprivation Approximately a third of Mansfield and Ashfield s registered population live within the 20% most deprived areas in England. This represents almost 62,000 people within the CCG s registered population. There is substantial variation in deprivation at practice level with Selston Surgery having only 1% of its registered population in the most deprived quintile and to Dr Khan s Practice having over 60% of their population living in the most deprived quintile. Table 2: Mansfield and Ashfield Medical Registered Population Estimated patients living within each deprivation quintile Source: Data warehouse, July 2007 Registered Population and IMD2007 Scores, national Page 65 of 75
 (defined as either households receiving Income Based Job Seekers Allowance / Income Support /Pension Credit or those not in receipt")
66 6. Child Poverty Overall in England around 23.5% of children aged 0-15 live in income deprived households (IDACI) (defined as either households receiving Income Based Job Seekers Allowance / Income Support /Pension Credit or those not in receipt of these benefits but in receipt of Working Tax Credits / Child Tax Credits with an equivalised income below 60 per cent of the national median before housing costs). Again substantial variation is observed between practices from 16% of children living in income deprived households in Jacksdale Medical Centre to 35% in Pleasley Surgery. There were no figures available for 3 practices (Kirkby Community Primary Care Centre, Churchside Medical Centre and Churchside Surgery). Page 66 of 75


67 7. Healthy Lifestyle Behaviours 7.1 Smoking Approximately 30% of Mansfield and Ashfield s registered population is estimated to smoke cigarettes, this is higher than the Nottinghamshire average of 25%. All practices within Mansfield and Ashfield CCG are estimated to have a higher smoking prevalence than the Nottinghamshire average. Using these estimates, approximately 17,000 people in Mansfield and Ashfield smoke. 7.2 Binge Drinking Approximately 19% of Mansfield and Ashfield s registered population are estimated to binge drink, this is slightly higher than the East Midlands average of 18%. Only Meden Medical Services are estimated to have a lower binge drinking prevalence (17%) than the Nottinghamshire average. Using these estimates, over 10,000 people within the Mansfield and Ashfield engage in binge drinking. Page 67 of 75


68 7.3 Obesity Levels Around 29% of the registered population of Mansfield and Ashfield are estimated to be obese, this is higher than the Nottinghamshire average of 26%. All practices in Mansfield and Ashfield are estimated to have obesity levels above the Nottinghamshire average with 12 practices estimated to have more than 30% of residents being obese. Using these estimates, approximately 16,500 people in Mansfield and Ashfield CCG would be considered obese. 7.4 Fruit & Vegetable Consumption Approximately 22% of the population of Mansfield and Ashfield are estimated to consume the recommended amount of fruit and vegetables, this is lower than the Nottinghamshire estimate of 27%, and all practices are estimated to have a lower prevalence of fruit and vegetable intake than the Nottinghamshire average. Using these estimates, there are approximately 44,000 people in Mansfield and Ashfield who do not achieve the recommended level of fruit and vegetable consumption. 8. Key Admissions Statistics Page 68 of 75
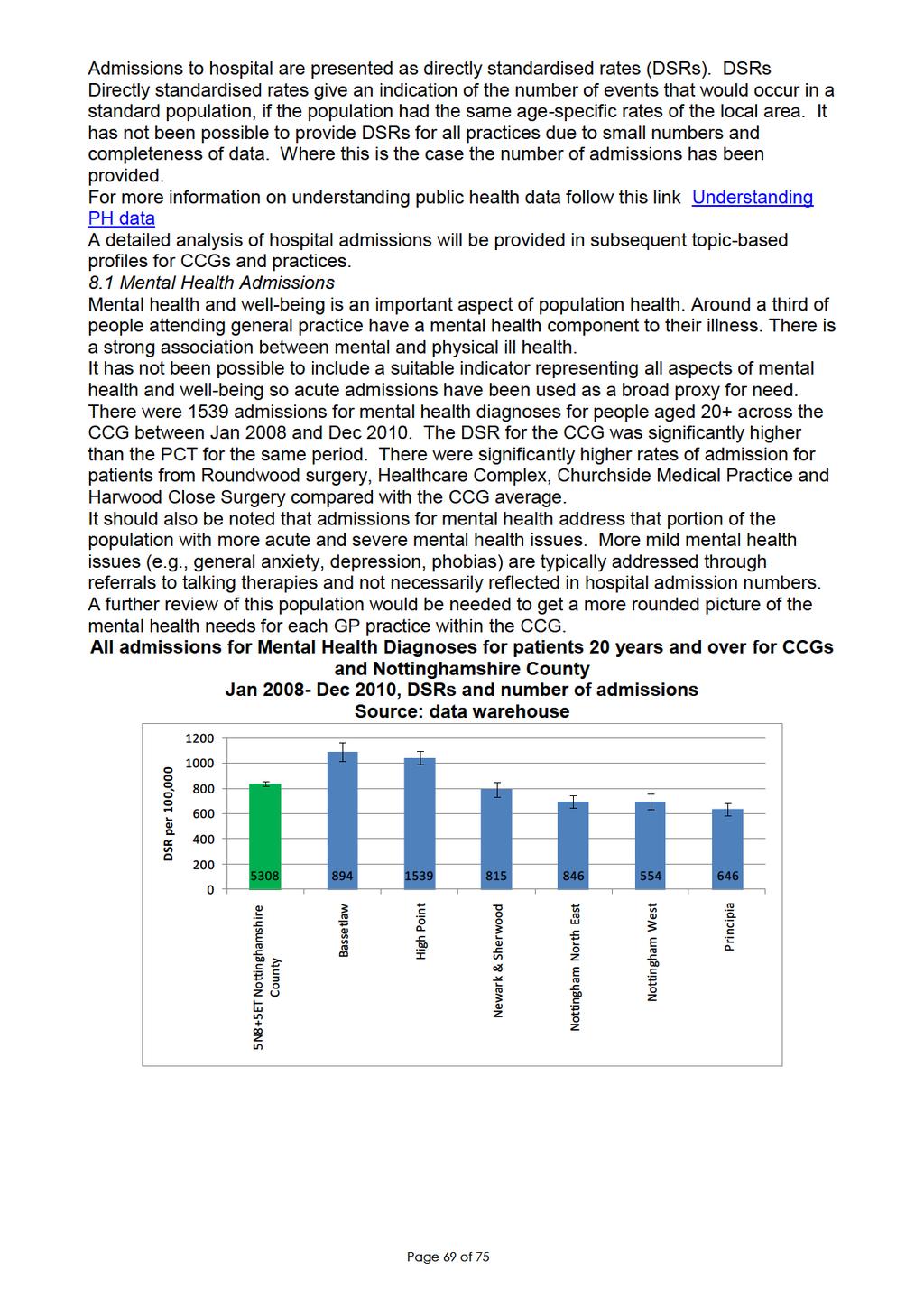
69
70
71 All admissions for fractured neck of femur in patients 65 years and over by CCG Jan Dec 2010, DSRs and number of admissions Source: data warehouse 2500 DSR per 100, Principia Newark & Sherwood Nottingham West High Point 5N8+5ET Nottinghamshire County Nottingham North East Bassetlaw 8.3 Elective and Non-elective Admissions Admissions patterns are potentially informative regarding populations and health behaviour. Comparisons of elective to non-elective admissions point to patterns of planned versus emergency care, and can shed light on areas where further analysis might be required. Across Nottinghamshire, the ratio of emergency to elective admissions varies with broad age group. Children and young people aged under 20 years are more likely to be admitted as an emergency, rather than for planned care. There is an apparent relationship between ratio of emergency and elective admission rate and deprivation. This is clearest in children and young people where those practices with the most deprived populations are almost twice as likely to access secondary care as an emergency compared with those practices with the least deprived populations where they are equally likely to be admitted as an emergency or for planned care. Page 71 of 75
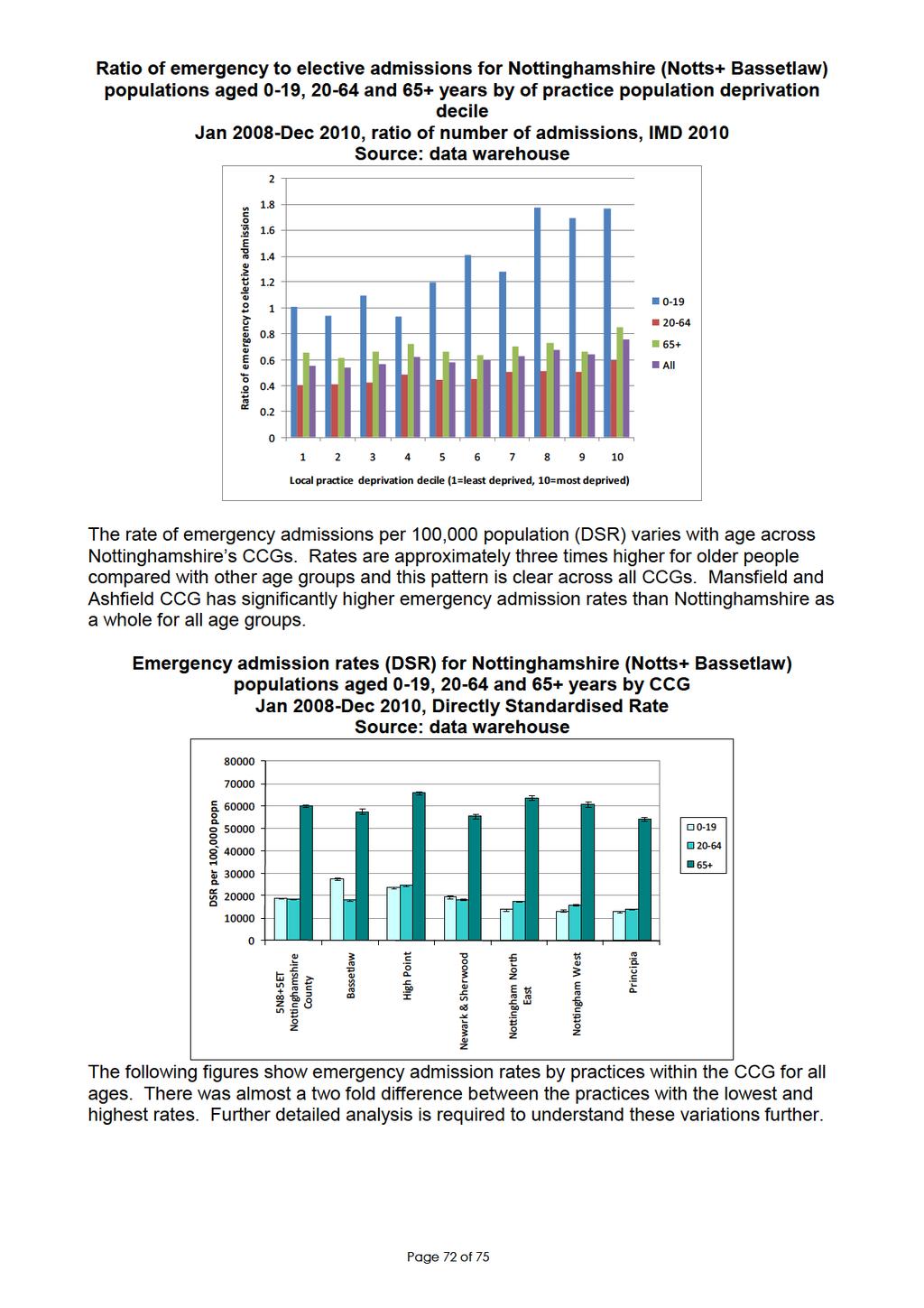
72
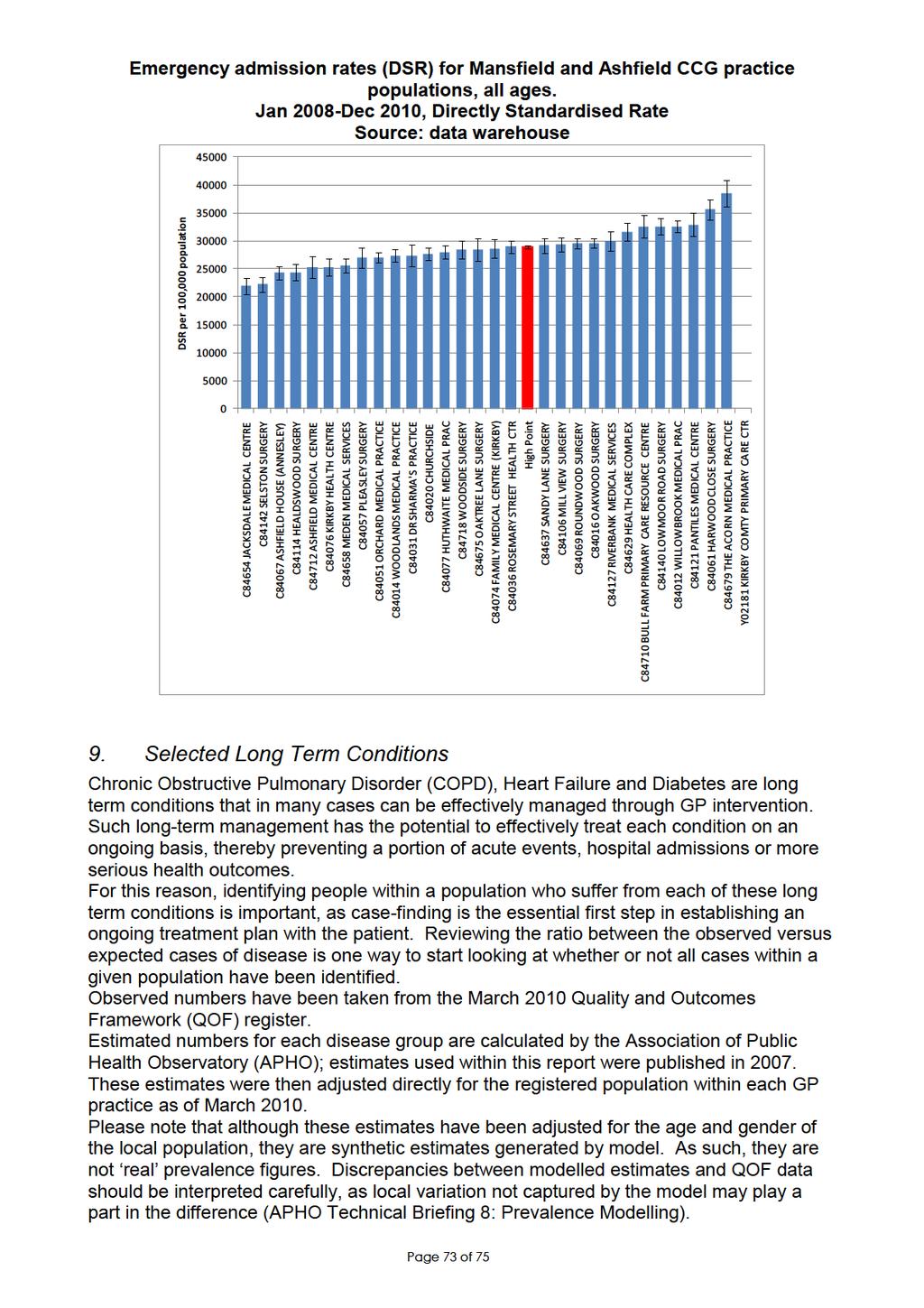
73

74 9.1 COPD Within Mansfield and Ashfield, practices varied in terms of the number of COPD cases that were observed compared to the number that was expected using the model. They varied from only a third of the expected number in Pantiles Medical Centre to 115% in Health Care Complex. In Health Care Complex, Meden Medical Services, Family Medical Centre (Kirkby) and Oakwood Surgery there are more patients registered with COPD than the model would expect. However in some of the other practices including Pantiles the model may suggest that not all people who have COPD have been identified. Information was not available for Kirkby Community Primary Care Centre or Churchside Medical Centre. 9.2 Heart Failure There is substantial variation between practices in terms of the observed versus expected number of Heart Failure patients. They varied from Mill View Surgery which only had 23% of the expected number of heart failure patients to Dr Khan s practice which had 83% of the expected number. This suggests that potentially not all people who have Heart Failure in Mansfield and Ashfield have been identified. Information was not available for Kirkby Community Primary Care Centre or Churchside Medical Centre. Page 74 of 75


75 9.3 Diabetes There was substantial variation between practices with 11 practices having more cases than the model would expect, however other practices including Churchside Surgery and Pantiles Medical Centre only had 64% of the expected number of diabetes cases. This suggests that not all people registered who have Diabetes have been identified within Mansfield and Ashfield CCG. Page 75 of 75
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
DARLINGTON CLINICAL COMMISSIONING GROUP
 DARLINGTON CLINICAL COMMISSIONING GROUP CLEAR AND CREDIBLE PLAN 2012 2017 Working together to improve the health and well-being of Darlington May 2012 Darlington Clinical Commissioning Group Clear and
DARLINGTON CLINICAL COMMISSIONING GROUP CLEAR AND CREDIBLE PLAN 2012 2017 Working together to improve the health and well-being of Darlington May 2012 Darlington Clinical Commissioning Group Clear and
Agreeing the methodology used to calculate weighted rates for CCG GP practice reporting
 Agreeing the methodology used to calculate weighted rates for CCG GP practice reporting Introduction The mid-nottinghamshire analytics team are currently reviewing the reporting methodology used to support
Agreeing the methodology used to calculate weighted rates for CCG GP practice reporting Introduction The mid-nottinghamshire analytics team are currently reviewing the reporting methodology used to support
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Version Number Date Issued Review Date V1: 28/02/ /08/2014
 Corporate CCG CO01 Access and Choice Policy Version Number Date Issued Review Date V1: 28/02/2013 31/08/2014 Prepared By: Consultation Process: Governance Lead, NHS South of Tyne and Wear Information Governance
Corporate CCG CO01 Access and Choice Policy Version Number Date Issued Review Date V1: 28/02/2013 31/08/2014 Prepared By: Consultation Process: Governance Lead, NHS South of Tyne and Wear Information Governance
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Telford and Wrekin Clinical Commissioning Group. Prospectus 2013/2014
 Telford and Wrekin Clinical Commissioning Group Prospectus 2013/2014 Who we are Telford and Wrekin Clinical Commissioning Group (CCG) is responsible for healthcare in the Telford and Wrekin area. We Plan
Telford and Wrekin Clinical Commissioning Group Prospectus 2013/2014 Who we are Telford and Wrekin Clinical Commissioning Group (CCG) is responsible for healthcare in the Telford and Wrekin area. We Plan
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
CCG authorisation: the role of medicines management
 May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Committee of Public Accounts
 Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
4 Year Patient and Public Involvement Strategy
 4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Any Qualified Provider: your questions answered
 Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY
 PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
South Yorkshire and Bassetlaw Accountable Care System Chief Executives
 South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Worcestershire Public Health Directorate. Business plan 2011/12
 Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Collaborative Agreement for CCGs and NHS England
 RCCG/GB/15/164 Collaborative Agreement for CCGs and NHS England East Midlands Collaborative Commissioning Oversight Group (EMCCOG) 1. Particulars 1.1. This Agreement records the particulars of the agreement
RCCG/GB/15/164 Collaborative Agreement for CCGs and NHS England East Midlands Collaborative Commissioning Oversight Group (EMCCOG) 1. Particulars 1.1. This Agreement records the particulars of the agreement
West Wandsworth Locality Update - July 2014
 Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
CCG: CO01 Access and Choice Policy
 Corporate CCG: CO01 Access and Choice Policy Version Number Date Issued Review Date V2 21 January 2016 January 2018 Prepared By: Consultation Process: NECS Commissioning Manager CCG Head of Corporate Affairs.
Corporate CCG: CO01 Access and Choice Policy Version Number Date Issued Review Date V2 21 January 2016 January 2018 Prepared By: Consultation Process: NECS Commissioning Manager CCG Head of Corporate Affairs.
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Memorandum of understanding for shadow Accountable Care Systems
 Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION
 NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
5. Does this paper provide evidence of assurance against the Governing Body Assurance Framework?
 Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting. Meeting Date: 25 October Executive Lead: Rajesh Nadkarni
 Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Transforming Clinical Services. Our developing clinical strategy
 Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS
 MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
A guide to NHS Bexley Clinical Commissioning Group
 A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby
 STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Staff Health, Safety and Wellbeing Strategy
 Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
CCG Involvement Strategy and 2016/19 action plan
 CCG Involvement Strategy and 2016/19 action plan 1 Contents 1. Introduction and purpose of document 5 2. Our commitment to effective involvement 5 3. Legislation our statutory obligations 7 4. Aims of
CCG Involvement Strategy and 2016/19 action plan 1 Contents 1. Introduction and purpose of document 5 2. Our commitment to effective involvement 5 3. Legislation our statutory obligations 7 4. Aims of
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Living With Long Term Conditions A Policy Framework
 April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS. September 2014
 OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
Central Lancashire Local Delivery Plan 2016/ /21
 Central Lancashire Local Delivery Plan 2016/17 2020/21 1 Contents 1. Introduction and context 2. Our priorities 3. The health and wellbeing gap 4. The care and quality gap 5. Financial challenges, gap
Central Lancashire Local Delivery Plan 2016/17 2020/21 1 Contents 1. Introduction and context 2. Our priorities 3. The health and wellbeing gap 4. The care and quality gap 5. Financial challenges, gap
The Suffolk Marie Curie Delivering Choice Programme
 The Suffolk Marie Curie Delivering Choice Programme Phase III A report on progress and achievements Date: April 2012 Author: Sandy Barron Project Lead Manager Design and Development - MCDCP 1 Table of
The Suffolk Marie Curie Delivering Choice Programme Phase III A report on progress and achievements Date: April 2012 Author: Sandy Barron Project Lead Manager Design and Development - MCDCP 1 Table of
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
General Practice Commissioning Strategy Development
 General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
NHS Right Care expanding the approach in the context of delivering the Five Year Forward View
 NHS Right Care expanding the approach in the context of delivering the Five Year Forward View Background 1. NHS Right Care originated as part of the QIPP programme within the Department of Health in 2009.
NHS Right Care expanding the approach in the context of delivering the Five Year Forward View Background 1. NHS Right Care originated as part of the QIPP programme within the Department of Health in 2009.
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Five year strategy for Leeds A view from the Leeds Unit of Planning June submission.
 Five year strategy for Leeds A view from the Leeds Unit of Planning June submission. Background - Leeds Leeds has an ambition to be internationally renowned for its excellent health and social care economy
Five year strategy for Leeds A view from the Leeds Unit of Planning June submission. Background - Leeds Leeds has an ambition to be internationally renowned for its excellent health and social care economy
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Cabinet Member for Education, Children and Families
 Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
NHS BORDERS CLINICAL STRATEGY. 'A plan for person-centred, innovative healthcare to help the Borders flourish'
 NHS BORDERS CLINICAL STRATEGY 'A plan for person-centred, innovative healthcare to help the Borders flourish' CONTENTS NHS BORDERS CLINICAL STRATEGY FOREWORD 3 EXECUTIVE SUMMARY 4 THE CASE FOR CHANGE 5
NHS BORDERS CLINICAL STRATEGY 'A plan for person-centred, innovative healthcare to help the Borders flourish' CONTENTS NHS BORDERS CLINICAL STRATEGY FOREWORD 3 EXECUTIVE SUMMARY 4 THE CASE FOR CHANGE 5
Delivering the QIPP programme: making existing services improve patient outcomes
 Delivering the QIPP programme: making existing services improve patient outcomes Produced by Glyn Davies MP, Chair All-Party Parliamentary Group on AF in association with the Atrial Fibrillation Association
Delivering the QIPP programme: making existing services improve patient outcomes Produced by Glyn Davies MP, Chair All-Party Parliamentary Group on AF in association with the Atrial Fibrillation Association
Update on NHS Central London CCG QIPP schemes
 Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
NHS Norwich CCG Operational Plan and
 NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
5. Integrated Care Research and Learning
 5. Integrated Care Research and Learning 5.1 Introduction In outlining the overall policy underpinning the reform programme, Future Health emphasises important research and learning from the international
5. Integrated Care Research and Learning 5.1 Introduction In outlining the overall policy underpinning the reform programme, Future Health emphasises important research and learning from the international
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Health and care in South Yorkshire and Bassetlaw. Sustainability and Transformation Plan a summary
 Health and care in South Yorkshire and Bassetlaw Sustainability and Transformation Plan a summary Introduction This is the summary version of the South Yorkshire and Bassetlaw Sustainability and Transformation
Health and care in South Yorkshire and Bassetlaw Sustainability and Transformation Plan a summary Introduction This is the summary version of the South Yorkshire and Bassetlaw Sustainability and Transformation
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Greenwich Clinical Commissioning Group. Patient and Public Engagement Strategy ( )
") Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local