Regional Complex Continuing Care Review: Final Report and Recommendations
|
|
|
- Allyson Adams
- 5 years ago
- Views:
Transcription
1 Regional Complex Continuing Care Review: Final Report and Recommendations Submitted to: North Simcoe Muskoka LHIN Leadership Council January 2010 Submitted by Sara Lankshear, RN PhD (c) Relevé Consulting Services Judith Skelton Green, RN PhD Transitions-HOD Consultants Inc.
2 Table of Contents Executive Summary 2 Background 6 Project Scope and Objectives 7 Guiding Principles and Assumptions 7 Project Timelines 8 Complex Continuing Care Client Profile 9 Utilization Patterns 10 Stakeholder Engagement 12 Care Delivery and Staffing Models 15 Funding 17 Recommendations and Timelines 18 Conclusions and Next Steps 24 Appendix 25
3 Executive Summary Project Scope and Objectives Purpose: To review current Regional Complex Continuing Care (CCC) Service design and recommend future design or modifications that would assist the North Simcoe Muskoka (NSM) Complex Continuing Care Steering Committee in moving to design a CCC Centre of Excellence model for healthcare improvements across the continuum of care. Objectives: 1. Standardize the CCC patient definition for the regional service including a description of patient population to be served (e.g., palliative, slow stream rehabilitation (SSR), and medically complex); 2. Evaluate the current CCC program model highlighting key lessons learned and barriers to implementation; 3. Review current practices and variances, standardized care practices / policies (e.g., admission and discharge criteria, repatriation agreements, communication and referral processes, etc.) for the CCC Regional Service; 4. Recommend a leadership model to support a Regional CCC Centre of Excellence model within the LHIN environment including accountabilities and roles of the partners involved to ensure an accountable and sustainable service; 5. Recommend a cost-effective staffing model inclusive of frontline staff (nurse practitioners, physicians, etc.) and ensure medical coverage is provided across the continuum of CCC care; 6. Recommend a funding model to support this regional service that is within the scope of the regional service and the defined patient population; and 7. Based on cost efficiencies, current patterns of patient flow, patient needs, the health of the population and the future projected needs, review the appropriate sizing of CCC beds for North Simcoe Muskoka to recommend an appropriate number of CCC regional beds. Regional Complex Continuing Care Review Final Report January 2010 Page 2 of 35
4 Summary of Recommendations Area 1. CCC Regional Vision Statement 2. CCC Client Definitions Recommnedation / Description Adoption of CCC Vision statement All residents of North Simcoe-Muskoka will receive quality* complex continuing care appropriate to their needs. Vision statement for CCC program will provide a short, succinct sound bite that can be consistently used when speaking to Board members, physicians, community partners, staff, patients/family and also act as a criterion/filter for decision making (e.g. will proposed activities enable or hinder achievement of the vision). *Quality as defined by the Ontario Health Quality Council and the Institute for Health Improvement Effective, Efficient, Equitable, Accessible, Safe, Patient- Centred, Focus on Population Health, Integrated, Appropriately Resourced. Revise CCC client defintions to adopt a rehabilitation / goal orientation to client descriptions. Definitions to be goal focused and to include specific indicators and exclusion criteria for each of the CCC client subcategories. See Appendix A for CCC definitions and indicators 3. CCC Sizing Total number of CCC beds reduced from 118 to 102 Regional beds: Georgian Bay General = 32 beds (including 6 Palliative Care beds) Muskoka Algonquin Healthcare / Huntsville = 10 beds Muskoka Algonquin Healthcare / Bracebridge = 16 beds Orillia Soldiers Memorial Hospital = 44 beds (including addition of 11 Extensive Care beds) Key messages regarding number of CCC beds: 1. Consistent with Integration Order 2. Reflective of current utilization trends 3. Facilitates care based on a critical mass of similar clients / care needs 4. Recognizes co-siting (or not) of CCC beds with acute care services 5. Enables a goal orientation to the care of CCC clients 6. Consistent with LHIN Strategic Priority to create an integrated health system in North Simcoe Muskoka 4. Role Review and Redesign To ensure optimal functioning and role clarity, conduct a role review to determine degree of involvement of staff in CCC admission, patient flow, team leadership, and discharge processes; identification of current practices within Regional Complex Continuing Care Review Final Report January 2010 Page 3 of 35
5 Area Recommnedation / Description and across programs, areas of overlap, role ambiguity and opportunities for role redesign. Role review to include the following roles: a. Service Manager b. Unit Clerk c. Nurse Practitioner d. Team Leader e. Social Work / Discharge Planner f. CCAC Client Care Coordinator g. Registered Nurse 5. Staffing Model: Nursing 6. Staffing Model: Rehab Disciplines Implementation of a Nursing Dyad Model of care delivery: no more than two categories of care providers to enhance role clarity, accountability and continuity of care. (e.g., RN/PSW model or RN/RPN model) Nursing Leadership from CCC program partners to come together to determine most appropriate Nursing Dyad Model. Principles to guide Nursing Dyad Model development will be based on: 1. Client population needs 2. Principles of care delivery, include a focus on Total Patient Care 3. Evidence re: staffing and impact on staff and patient outcomes 4. Optimized scope of practice 5. Financial sustainability 6. Physical layout: number of location of client rooms 7. Educational/regulation qualifications of dyad parties (specifically RNs and RPNs licenced through the College of Nurses of Ontario; PSWs graduates of Georgian College or equivalent program) 8. Human resource implications 9. Consistent approach across CCC program; with possible exception of Extensive Care Services and increased complexity of client needs. Enhanced rehabilitation staffing for all CCC programs with designated time for CCC program. Incorporation of Rehab Dyads : Physiotherapist / Occupational Therapists and Rehab Assistant to optimize use of available rehab staffing resources and expertise. See Appendix C for Recommended Health Disciplines staffing based on current and projected CCC client needs and comparator consultations. Regional Complex Continuing Care Review Final Report January 2010 Page 4 of 35
6 Area 7. Leadership and Governance Model Recommnedation / Description Leadership Dyad Model: a. Regional Program Director Role (1 Full Time) b. Physician Leadership Role (Stipend) 8. Quality Monitoring Development of Scorecard specific to CCC program using the CCC program scorecard to be in sync with LHIN Balanced Scorecard. Scorecard to include indicators that can be applied to both program and regional aspects of CCC care delivery. 9. Process Improvements Recognition that all processes are dynamic in nature. Development of timeframes for review and refinement ( e.g. short-term, interim and ongoing). Clarification of eligible versus suitable based on match between criteria, client needs and availability of required resources (e.g. physician availability, nurse practitioner (NP) workload, adequate staffing, necessary equipment and/or competencies required). Determine system for prioritization of clients (e.g., weighting based on established criteria) Within North Simcoe Muskoka LHIN Inpatient referrals Direct from community / Day Hospital Outside of LHIN boundaries 10. Funding Reinvestment of funding from bed reductions into Staffing Models (e.g., Nursing and Health Disciplines) and newly identified roles (e.g., CCC Program Educator, Regional CCC Program Director, Regional Physician Leader). Determine OSMH s ability to access Post Construction Operational Plan (PCOP) funding to support addition of 11 Extensive Care Service beds. Regional Complex Continuing Care Review Final Report January 2010 Page 5 of 35
7 Background In the spring of 2007, at the request of the Ministry of Health and Long-Term Care (MOHLTC) and Royal Victoria Hospital, the North Simcoe Muskoka Local Health Integration Network (NSM LHIN) established a group to explore current utilization of Complex Continuing Care services, to project future need and to make recommendations regarding the most appropriate utilization, configuration and distribution of CCC resources within the LHIN. In March 2008, the North Simcoe Muskoka LHIN Board of Directors issued an integration decision pursuant to subsection 25(2) (a) of the Local Health System Integration Act, 2006 (LHSIA), that the NSM CCAC, RVH, MAHC-SMMH site, MAHC-HDMH site, NSHA-PGH, NSHA-HDH and OSMH are hereby required to implement by end of May 2008 a centralized access to CCC beds, coordinated through the NSM CCAC, and including: Standardized eligibility determination (eligibility criteria and assessment tools) Central management of the waiting list(s) Standardized discharge criteria. In January 2009, letters were received from North Simcoe Hospital Alliance and Orillia Soldiers Memorial Hospital indicating they were unable to meet the terms of the integration due to lack of physician resources and full implementation compliance by all partners. In July 2009, the Steering Committee, supported by the North Simcoe Muskoka LHIN, identified the need to review the current status of the Regional CCC program and determine future directions. Definition of Organizational Acronyms: Muskoka Algonquin Healthcare (MAHC) o South Muskoka Memorial Hospital (SMMH) Bracebridge o Huntsville District Memorial Hospital (HDMH) Huntsville North Simcoe Hospital Alliance (NSHA) o Penetanguishene General Hospital (PGH) o Huronia District Hospital (HDH) o NOTE: As of December 2009, name changed to Georgian Bay General Hospital (GBGH) North Simcoe Muskoka Community Care Access Centre (NSM CCAC) Orillia Soldiers Memorial Hospital (OSMH) Royal Victoria Hospital (RVH) Regional Complex Continuing Care Review Final Report January 2010 Page 6 of 35
8 Project Scope and Objectives Purpose: To review current Regional CCC Service design and recommend future design or modifications that would assist the North Simcoe Muskoka Complex Continuing Care Steering Committee in moving to design a CCC Centre of Excellence model for healthcare improvements across the continuum of care. Objectives: 1. Standardize the CCC patient definition for the regional service including a description of patient population to be served (e.g., palliative, slow stream rehabilitation (SSR), and medically complex); 2. Evaluate the current CCC program model highlighting key lessons learned and barriers to implementation; 3. Review current practices and variances, standardized care practices / policies (e.g., admission and discharge criteria, repatriation agreements, communication and referral processes, etc.) for the CCC Regional Service; 4. Recommend a leadership model to support a Regional CCC Centre of Excellence model within the LHIN environment including accountabilities and roles of the partners involved to ensure an accountable and sustainable service; 5. Recommend a cost-effective staffing model inclusive of frontline staff (nurse practitioners, physicians, etc.) and ensure medical coverage is provided across the continuum of CCC care; 6. Recommend a funding model to support this regional service that is within the scope of the regional service and the defined patient population; and 7. Based on cost efficiencies, current patterns of patient flow, patient needs, the health of the population and the future projected needs, review the appropriate sizing of CCC beds for North Simcoe Muskoka to recommend an appropriate number of CCC regional beds. Guiding Principles and Underlying Assumptions The following were used to guide the review and development of recommendations: 1. The objective of the Regional CCC program is to meet the needs of the North Simcoe Muskoka Local Health Integration Network s population by effectively utilizing resources to achieve the appropriate level of Complex Continuing Care services in the right place at the right time. 2. Build upon experiences to date and lesson learned from both internal and external stakeholders and content experts. 3. Recommendations will be focused on a five year time frame: This will enable implementation of recommendations, formal evaluation of impacts and consideration for future siting and sizing needs based on population needs. 4. Recommendations to be implemented within existing funding. 5. Consensus model to be used to enhance open and supportive communication and decision making. Regional Complex Continuing Care Review Final Report January 2010 Page 7 of 35
9 Strategies to Conduct the Review The following strategies were used to guide the review and development of recommendations: 1. Review of relevant background information and relevant literature regarding complex continuing care models, integrated care delivery, staffing models, and published reports. 2. Consultation with stakeholders directly involved with Regional Complex Continuing Care program, including hospitals with designated CCC beds and hospitals within North Simcoe Muskoka who refer to CCC clients to CCC program, and CCAC partners. 3. Consultation with comparator CCC programs within Ontario. Comparators were chosen based on similar program characteristics (e.g., CCC program within community hospitals), CCC programs with demonstrated quality outcomes (e.g. as per 2007 Hospital Report Complex Continuing Care) and those also providing Regional service. 4. Presentation of recommendations to both the CCC Program Steering Committee and Operations Committee for input and consultation. Project Timelines The Regional CCC Program Review project began in August 2009 and was completed in February Data collection and consultations (internal and external) occurred from September to December Initial recommendations were presented to the joint CCC Steering / Operations Committee on December 9, 2009, with a follow-up meeting held on January 13, 2010 were consensus was reached on the recommendations contained in this report. The final report and recommendations will be presented to the North Simcoe Muskoka LHIN Leadership Council for review and direction. NSM Regional CCC Program Review Project Timelines March 2008 Integration Order issued Feb Recommendations Presented to LHIN Leadership Council January 2009 Notification by GBG and OSMH re: unable to fully implement Integration Orders August 2009 Review of Regional CCC program initiated; consultants contracted Sept Initial meeting with members of CCC Operation and Steering Committees. Sept Dec Data collection, stakeholder consultations Dec ; Jan Presentation of Recommendations Regional Complex Continuing Care Review Final Report January 2010 Page 8 of 35
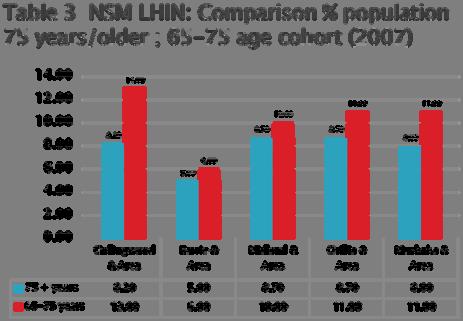
10 CCC Client Profile North Simcoe Muskoka LHIN population statistics for 2001, 2006 and 2007 were reviewed with specific attention to age categories relevant to CCC client population reveals the following: 1. Of the five geographic areas within the North Simcoe Muskoka LHIN, Barrie and Area has the greatest overall number of residents who are 75 years or age / older. (See Appendix B: Table 1) 2. Although Barrie and Area has the greatest overall number of residents who are 75 years and older, each of the four other geographic areas (Collingwood / Wasaga and Area, Orillia and Area, Midland / Penetanguishene and Area, and Muskoka) have a higher percentage of residents 75 years and older when compared to the overall population. (See Appendix B: Table 2) 3. When compared to the other geographic areas, Wasaga / Collingwood and Area has the highest percentage of residents who are years. This age cohort has significance as they will become the future clients for the CCC program, and therefore may have an impact on the number and location of CCC beds in the future. (See Appendix B: Table 3). CCAC Admission assessment data provided a snapshot of CCC client health status and care needs for all clients admitted to CCC program from April September A review of the most commonly identified Client Assessment Protocols (CAPs) reveals client care needs that would be associated with CCC population. The types of care needs documented were consistent across all CCC program sites. Examples of CCC care needs included: a) Assisted Daily Living (ADL) rehab potential b) Pain c) Urine (incontinence) d) Pressure Ulcers e) Cognition f) Falls g) Communication Disorders h) Psychotropic Drug Additional assessment data such as Case Mix Index (CMI) values revealed a wide range in CMI scores (care requirements) within and across the CCC program sites. This may be due to presence of Alternate Level of Care (ALC) patients within designated CCC beds. The table below depicts the mean CMI scores for each of the CCC programs and the range. CMI Mean score (Range) GBGH / PGH MAHC / Huntsville MAHC/ Bracebridge OSMH ( ) ( ) ( ) ( ) Regional Complex Continuing Care Review Final Report January 2010 Page 9 of 35
11 Utilization Patterns Data was collected from each of the CCC programs (sending and receiving hospitals) and CCAC for all clients referred to the CCC program for the six month time frame of April September The following information has been derived from the data received. It is therefore important to note that the information presented here is based on a snapshot of a six month period of time and therefore may not be reflective of current status or overall trends throughout the year. Admission Patterns The admission patterns for each of the CCC programs were reviewed. The table below depicts the Top 3 sources of referrals / admissions for each of the CCC program sites. # 1 # 2 # 3 GBGH /PGH GBGH RVH CGMH MAHC/ Huntsville MAHC/ Bracebridge MAHC MAHC OSMH OSMH RVH Referrals, Eligibility and Placements The table below depicts the number of referrals made to each of the CCC program sites (April September 2009), degree of eligibility and overall percent of admission of CCC clients. The percent of clients referred, who were then deemed eligible ranges from 69% to 100%; thus indicating an opportunity to re-visit CCC admission eligibility criteria to ensure clarity and optimal utilization of resources. # of Referrals % Eligible (#) % Admission (#) Location GBGH/PGH 39 90% (35) 69% (25) 24 admitted to GBGH 1 admitted to MAHC/H MAHC/Huntsville 27 89% (24) 79% (19) All MAHC/H MAHC/Bracebridge % (17) 59% (10) All MAHC/B OSMH 64 69% (44) 56% (24) All to OSMH RVH 54 78% (42) 90% (38) 22 admitted to OSMH 16 admitted to GBGH CGMH 14 86% (12) 100% (12) All to GBGH Regional Complex Continuing Care Review Final Report January 2010 Page 10 of 35
12 Discharge destinations Each of the CCC programs was asked to rank order the most common discharge destinations for CCC clients. The results were fairly consistent across the CCC program sites. The most common discharge destination for CCC clients is long-term care (LTC), followed by Other (i.e. death), community and lastly, acute care. CCC Bed Utilization Data provided by the CCC program partners was used to determine overall CCC bed occupancy, and impacts of ALC pressures on the overall CCC bed utilization within the region. The results from the weekly ALC reports generated by the North Simcoe Muskoka LHIN were also used to review ALC impacts. The table below depicts overall CCC bed utilization. The percent of ALC clients in CCC beds ranges from 9-53%. Based on the CCC occupancy reported a revised number of actual CCC beds used is generated. The calculation is based on the total number of CCC beds X highest CCC utilization / occupancy rate. # CCC Beds budget # Beds Operational Occupancy % CCC clients % ALC clients # beds used for CCC clients* % Referrals from other communities ( e.g. regions) GBGH /PGH % 81-93% 7-19% 34 50% MAHC/H % 50-70% 30-50% 7 0% MAHC/B % 5-19% 29-52% 5 0% OSMH % 46-91% 9-53% 34 50% Total Please Note: In December 2009, MAHC/ Bracebridge site verbally reported a significant increase in CCC bed utilization due to increased support from ALC Flow Coordinator, increased team collaboration, physician engagement and enhanced understanding of CCC admission criteria. Increased utilization as high as 75% reported. Based on the review of data provided, the status of Regional CCC Program bed utilization can be described as follows: a. Number of Beds on paper (as per Integration Order) = at OSMH; 36 at PGH and 34 at MAHC b. Actual number of beds in operation = 107 c. Actual number of beds used for CCC clients (as per utilization rates) = 80 d. Actual number of Regional beds in operation = 73 (GBGH and OSMH participating in Regional CCC Program) Regional Complex Continuing Care Review Final Report January 2010 Page 11 of 35
13 Stakeholder Engagement The following internal and external stakeholders were engaged in the review of the North Simcoe Muskoka Regional CCC program. Stakeholders represented CCC program leadership roles, direct care providers, CCAC, and North Simcoe Muskoka LHIN hospitals that refer clients to the Regional CCC program. In addition to those directly involved in the CCC program, a list of CCC comparator programs across Ontario was generated for additional consultation regarding program delivery and staffing models. Stakeholder Group Organizations Participants Method CCC Program Providers Georgian Bay General Hospital Orillia Soldiers Memorial Hospital Muskoka Algonquin Healthcare ( Huntsville and Bracebridge sites) CCC Program Leadership; Discharge planners, direct care providers (nursing and rehab professions); Decision Support; Physicians, Nurse Practitioners Focus Groups CCC Program Partners Royal Victoria Hospital Collingwood General and Marine Hospital NSM CCAC CCAC Client Care Coordinators; Patient Flow, Decision Support, Medical program; Discharge Coordinators, Utilization Focus Groups Total Number of Participants involved in consultations listed above = 56 Stakeholder Group Organizations Participants Method Comparator CCC Programs Others Headwaters Health Care Centre (Orangeville) West Park Healthcare Centre (Toronto) Bridgepoint Health * (Toronto) Almonte General Hospital (Almonte) St. Joseph s Care Group ( Thunder Bay) St. Mary s / Providence CCC (Kingston) North Simcoe Muskoka Palliative Care Network CCC Program Managers / Directors *Professional Practice Leadership Executive Director Telephone consultation Site Visit* Telephone consultation Regional Complex Continuing Care Review Final Report January 2010 Page 12 of 35
14 Results from Stakeholder Consultations Participants were asked to provide their perspectives regarding the CCC program in terms of: a. What s working well? b. What is not working well? c. Suggestions for improvement? The findings reported here represent the information obtained from the consultation processes. Unless otherwise indicated, the themes presented here present the views commonly expressed by the participant groups. The themes are listed according to the frequency in which they were mentioned. As with all consultations involving stakeholder engagement and feedback, findings should be reviewed with the awareness that for every opinion expressed during the consultations (and hence presented here) there may be an alternate view held by others who were not involved in the consultation process. Question # 1: What is working well Theme Description Team / Teamwork Staffing / Resources Physician Involvement Client Identification Provision of Client Care Client Outcomes Utilization Despite examples of growing pains, overall team work between various partners viewed as being effective. Specific examples of teams mentioned include: interprofessional teams, MD/NP relationship, CCAC/CCC programs, and the effectiveness of the Q2 weekly conference calls to review CCC wait lists and projected bed availability. Two main areas identified: the benefits of access to rehab professionals and the importance of the RN team leader role as a knowledgeable resource to the team. Increased continuity of client care associated with increased physician involvement. Improved identification and assessment of eligible clients for CCC program Improved goal orientation to client care planning, introduction of case conferences and interprofessional rounds / team meetings; as well as the benefits of client groupings (e.g., SSR and Active Rehab clients; CCC and Interim LTC clients). Demonstrated benefits to the clients in terms of functional mobility and social impacts; having the extra time to recover and improve before moving to final placement / next destination; anecdotal evidence re: decreased readmissions. Need for program demonstrated by the number of referrals and bed utilization; increased acute care bed utilization; equal regional access (2/3 sites participating). Regional Complex Continuing Care Review Final Report January 2010 Page 13 of 35
15 Question # 2: What is not working well? Theme Patient Care Processes Physician Involvement Lack of Rehab Philosophy Space / Equipment Staffing Utilization Patient Status Description Lack of consistent goal setting and specific care delivery model; Mixing ALC with CCC client inhibits effective care delivery and goal setting for CCC clients. Lack of physician involvement impacting the number of CCC clients that can be admitted to program; Physician reluctance to admit to CCC program due to lack of knowledge re: program goals; and funding inadequate as it s based on chronic care model vs. complexity of patients seen. Lack of structure and processes to support/reinforce a rehabilitation approach to CCC client care; Nursing philosophy mainly based on chronic care model rather than rehabilitation focused; lack of educational roles/resources to support learning needs. Limited space and equipment to provide rehabilitation services and interventions. Lack of adequate staffing for rehabilitation professionals; lack of dedicated time allocated to CCC program therefore acute care needs take precedence; limited amount of physicians involved impacting future sustainability of CCC program (Physician reimbursement / billing model cited as main barrier to physician engagement), lack of consistent team leader for all CCC units; recruitment challenges (e.g., NP role for MAHC) and implications for care delivery and program effectiveness. Perceptions of delays in referral process, increased admissions impacting workload for all professionals; not all beds are open / or available for regional referrals; ALC pressures impacting CCC utilization. Differing perceptions regarding eligible patients and what defines complex ; CCC patient status changes frequently therefore increased need for re-assessment. Regional Complex Continuing Care Review Final Report January 2010 Page 14 of 35
16 Question # 3: Suggestions for improvement Theme Staffing Education Clear Expectations Space / Equipment Goal Orientation Consistency in Practices Description Increased dedicated time for rehabilitation professions to CCC program; Team leader for all CCC units; increased physician involvement; all roles functioning to full scope of practice / elimination of organizational policies limiting scope of practice; Educator role for CCC program to support clinical and professional development needs of staff. Investment in education to reinforce rehabilitation philosophy of care for all members of the interprofessional team; increased education for staff, physicians, and clients/families re: the objectives of CCC program (e.g., this is not substandard care or LTC). Review policies and guidelines re: admission and discharge criteria; who makes decisions re: admission and who can override decisions. Increased space and resources to support adequate rehabilitation interventions and programming. Incorporation of clearly stated goals and outcomes for all CCC clients; reinforcement of approach to CCC not as a final destination, but rather an interim destination to enhance functional mobility and health status. Consistent application of CCC policies (e.g., co-payment) currently there is inconsistency among sites in terms of application of co-payment policy. This has negative impacts on client/family satisfaction as well as fiscal impacts. Care Delivery and Staffing Models A review of the literature reveals an extensive amount of information regarding the various factors that can impact patient, staff and organizational outcomes. A full review of the literature was beyond the scope of this review, yet the following provide some examples of the evidence regarding the relationship between staffing and patient outcomes. Registered Nurse (RN) staffing and patient outcomes Increased RN staffing associated with decreased 30-day mortality, increased satisfaction, decreased falls, decreased nosocomial infections, and decreased length of stay (Kane et al, 2007; Aiken, 2008; Dall et al, 2009). External factors impacting staffing Key factors to consider when determining staffing levels should include the following: availability of specialized equipment and technology, availability of support services, the model of care delivery in place, administrative practices, and proximity of patients, patient acuity and patient turnover (DeVandry & Cooper, 2009, Thomas & Herrin, 2009). Regional Complex Continuing Care Review Final Report January 2010 Page 15 of 35
17 Team communication Less hierarchy within teams is associated with better patient outcomes (Institute of Medicine, 2004). Effectiveness of interpersonal communication between nurses and other team members has a positive impact on patient outcomes such as self-care activities (e.g., bathing), ambulation and transfers (Doran et al, 2001). Characteristics of the work environment A study conducted by Tourangeau et al (2008) revealed high levels of staff burnout, low ratings of workplace empowerment, low job satisfaction and high turnover rates especially with health disciplines categories of CCC staff. When considering the evidence, there is no one single care delivery model identified as providing the best outcomes (e.g., Primary Nursing, Total Patient Care, Team Nursing, Modular Nursing,). Rather, it is the combined effects of key elements of care delivery that should be considered when implementing a nursing and/or interprofessional care delivery model (See Appendix C). These essentials elements include: 1. Continuity of care provider 2. Continuity of care 3. Effective communication 4. Care assignments based on patient care needs 5. Clear accountability Based on the existing literature, these are the essential elements to be considered in the design, implementation and evaluation of care delivery model for CCC. Nursing Staffing Model Nurse staffing patterns for each of the four CCC program sites was obtained revealing a significant variability in the staff mix and staffing patterns within the CCC Regional program. Recent changes to the staff mix included the introduction of the Personal Support Worker role (PSW) at all sites to the existing RN and RPN skill mix. At present, only two of the six CCC units have an all nursing skill mix model (MAHC/ Huntsville site and OSMH/SSR). The nurse staffing patterns of the comparator CCC programs was also reviewed (See Appendix D: Nursing Staffing). Of particular interest was the Nursing Care Delivery Model currently being implemented at Bridgepoint Health. The principles of the model are drawn from the Ottawa Nursing Care Delivery Model which highlights the benefit of having no more than two categories of care providers, working as a dyad team, when determining nursing skill mix model. Verbal reports regarding the evaluation results from the Ottawa experience reveals increases in role clarity, accountability, continuity of care provider and team communication. Health Disciplines Staffing Model Health disciplines staffing patterns for each of the four CCC program sites was obtained revealing a significant variability in the staff mix and staffing patterns within the CCC Regional program (See Appendix E: Table 1 for current health disciplines staffing). Verbal feedback from staff obtained through the focus Regional Complex Continuing Care Review Final Report January 2010 Page 16 of 35
18 groups revealed that staff time is often split between in-patient and CCC program; there is no specific dedicated time allocated to CCC program. This creates delays in assessment and development of treatment plans for CCC patients. The health discipline staffing patterns of the comparator CCC programs was also reviewed (See Appendix E: Table 2). As a result of the internal and external review, a Rehab Dyad Model is also proposed with increased allocation of rehabilitation professions within the CCC program. This will support the principle that CCC is not a final destination, but rather an interim placement to enhance health status and optimal functioning. (See Appendix E: Table 3). Funding Throughout the review and consultation process, the following funding gaps were identified as having an actual and or potential impact on the success of the Regional CCC program: 1. Physician reimbursement model a. Current OMA funding reimbursement for CCC clients remains as Chronic Care; detriment to the recruitment and retention of physicians willing to assume care for CCC clients. 2. Need for enhanced Rehab services a. Lack of dedicated rehab staffing for CCC program impacting ability to provide rehab care and programming. 3. Funding support for Roles a. Lack of ongoing funding for NP and Most Responsible Physician (MRP) roles (has been provided as one-time dollars from the LHIN) b. Regional Program Director Role new role c. Regional Physician Leader new role (stipend) d. CCC Program Educator / Professional Practice role new role 4. CCC Program Needs a. Equipment (e.g., Rehab equipment, bariatric equipment) b. Pharmacy costs related to multi-system co-morbidities associated with CCC client population 5. Potential Human Resource implications associated with changes to staffing models a. Recruitment b. Severance dependent on changes to staffing models and skill mix. 6. OSMH ability to access PCOP funding to support expansion of 11 beds/ Extensive Care Service. i. $285.00/bed/day X 11 beds = $1,144,275/year See Appendix F for a listing of Funding knowns, assumptions and unknowns that have a direct impact of the Regional CCC program and ability to meet the needs of the NSM CCC client population. Regional Complex Continuing Care Review Final Report January 2010 Page 17 of 35
19 Recommendations Recommendation Description Potential Risks Proposed Timeline for Implementation CCC Vision Statement CCC Definitions CCC Bed Sizing Adoption of CCC Vision statement All residents of North Simcoe-Muskoka will receive quality complex continuing care appropriate to their needs. Vision statement for CCC program will provide a short, succinct sound bite that can be consistently used when speaking to Board members, physicians, community partners, staff, patients/family and also act as a criterion/filter for decision making (e.g. will proposed activities enable or hinder achievement of the vision. *Quality as defined by the Ontario Health Quality Council and the Institute for Health Improvement Effective, Efficient, Equitable, Accessible, Safe, Patient- Centred, Focus on Population Health, Integrated, Appropriately Resourced. Revise CCC client defintions to adopt a rehabilitation / goal orientation to client descriptions. Definitions to be goal focused and include specific indicators and exclusion criteria for each of the CCC client subcategories. See Appendix A for CCC definitions and indicators Total number of CCC beds reduced from 118 to 102 Regional beds: Georgian Bay General Hospital = 32 beds (including 6 Palliative Care beds) Muskoka Algonquin Healthcare / Huntsville = 10 beds Muskoka Algonquin Healthcare / Bracebridge = 16 beds Orillia Soldiers Memorial Hospital = 44 beds (including addition of 11 Extensive Care beds) None March 2010 None March 2010 Initiate April 2010 phased approach over 2 years. Regional Complex Continuing Care Review Final Report January 2010 Page 18 of 35
20 Recommendation Description Potential Risks Proposed Timeline for Implementation Foci for CCC program sites: 1. All of the CCC program sites will provide care for CCC clients within the following categories: clinically complex and slow stream rehabilitation clients. 2. GBGH/PGH will be identified as the designated site for CCC clients requiring Palliative Care. Please note: Although GBGH/PGH has 6 regional palliative care beds; this does not preclude other sites from providing palliative care or end of life services to clients. 3. OSMH will be identified as the designated site for CCC clients requiring Extensive Care services as this will enable timely access to acute care services such as diagnostic and laboratory services. Key messages regarding sizing of CCC beds: 1. Consistent with Integration Order 2. Reflective of current utilization trends 3. Facilitates care based on a critical mass of similar clients / care needs 4. Recognizes co-siting (or not) of CCC beds with acute care services 5. Enables a goal orientation to the care of CCC clients 6. Consistent with LHIN Strategic Priority to create an Integrated Health System in North Simcoe Muskoka Role Review and Redesign To ensure optimal functioning and role clarity, conduct role review to determine degree of staff involvement in CCC admission, patient flow, team leadership, and discharge processes; identification of current practices within and across programs; areas of overlap, role ambiguity and opportunities for role redesign. Role review to include the following roles: None Initiate June 2010 Regional Complex Continuing Care Review Final Report January 2010 Page 19 of 35
21 Recommendation Description Potential Risks Proposed Timeline for Implementation a) Service Manager b) Unit Clerk c) Nurse Practitioner d) Team Leader e) Social Work / Discharge Planner f) CCAC Client Care Coordinator g) Registered Nurse Nursing Staffing Model Implementation of a Nursing Dyad Model* of care delivery: no more than two categories of care providers (e.g. RN/PSW model or RN/RPN model) to enhance role clarity, accountability, communication and continuity of care (*Honours Ottawa Nursing Care Delivery Model recommendation of no more than two categories of caregivers to enhance accountability and role clarity). Proposed Nurse Staffing Model (Proposed for a 24 bed unit) Team Leader / RN Care Coordinator (M-F; days) Unit Clerk (M-F; days) RN PSW Dyads* assigned to groups of patients Human Resource implications: recruitment and retention of required care provider roles. Collective agreement implications related to changes in skill mix s and/or FTE allocation Financially sustainable Initiate March dyads; 8 patients per dyad (days); 2 dyads; 12 patients per dyad (evenings; nights) 1 dyad; 24 patients (nights) Role Focus RN: Most Responsible Nurse - assessment, teaching, care planning, discharge preparation, direct client care Regional Complex Continuing Care Review Final Report January 2010 Page 20 of 35
22 Recommendation Description Potential Risks Proposed Timeline for Implementation PSW: ADL, aspects of care as assigned by RN Both: rehabilitation and promotion of self-care and / or optimal functioning Action: Nursing Leadership from CCC program partners to come together to determine most appropriate Nursing Dyad Model. Principles to guide Nursing Dyad Model development will be based on: 1. Client population needs 2. Principles of care delivery including a focus on Total Patient Care 3. Evidence re: staffing and impact on staff and patient outcomes 4. Optimized scope of practice 5. Financial sustainability 6. Physical layout: number of location of client rooms 7. Educational / regulation qualifications of dyad parties (specifically RNs and RPNs licenced through the College of Nurses of Ontario; PSWs graduates of Georgian College or equivalent program) 8. Human resource implications 9. Consistent approach across CCC program; with possible exception of Extensive Care Services and increased complexity of client needs. Health Disciplines Staffing Model Enhanced rehabilitation staffing for all CCC programs with designated time for CCC program. Incorporation of Rehab Dyads: Physiotherapist / Occupational Therapists and Rehab Assistant to optimize use of available rehab staffing resources and expertise. Human Resource implications: recruitment and retention of required care provider roles. Collective agreement implications related to changes in skill mix s Initiate March 2010 Regional Complex Continuing Care Review Final Report January 2010 Page 21 of 35
23 Recommendation Description Potential Risks Proposed Timeline for Implementation See Appendix C for the following Comparison of current Rehab staffing within CCC; projected staffing requirements (based on CCC utilization and client need) Health discipline staffing from comparator CCC programs Recommended Health Disciplines staffing based on current and projected CCC client needs and comparator consultations. and/or FTE allocation. Financially sustainable CCC Program Leadership and Governance A Leadership Dyad Model to be implemented in order to support the Regional CCC Program through the next phase of development. Leadership Dyad to consist of the following roles: a) Regional Program Director Role (1 Full Time) b) Physician Leadership Role (Stipend 1-2 days/month) The primary focus of the roles is to provide strategic leadership to the Regional CCC program, systems integration, development of quality monitoring indicators and processes, clarifying expectations and to act as liaison for Regional CCC program with internal and external partners. This will enable a focused approach to the implementation and monitoring of the Regional CCC program. Regional CCC Program Steering Committee to remain in place until Regional Program role is established and the Regional Governance structure has been developed. Financially sustainable Recruitment of appropriate candidates Initiate April 2010 Quality Monitoring Development of CCC Program Balanced Scorecard. Scorecard to include indicators that can be used to monitor and review program specific and regional aspects of CCC care delivery, while keeping in sync with the foci of the LHIN Balanced Scorecard. None Initiate March 2010 Regional Complex Continuing Care Review Final Report January 2010 Page 22 of 35
24 Recommendation Description Potential Risks Proposed Timeline for Implementation Process Improvements Recognition that all processes are dynamic in nature; Development of timeframes for review and refinement (e.g. short-term, interim and ongoing) Clarification of eligible versus suitable based on match between criteria*, client needs and availability of required resources (e.g. MD availability, NP workload, adequate staffing, necessary equipment and/or competencies...) Determine system for prioritization of clients (e.g. weighting based on established criteria) Within LHIN Inpatient referrals Direct from community / Day Hospital Outside of LHIN boundaries None Initiate April 2010 Funding Reinvestment of funding from bed reductions into Staffing Models (e.g. Nursing and Health Disciplines) and newly identified roles (e.g. CCC Program Educator, Regional CCC Program Director, Regional Physician Leader) Determine OSMH ability to access PCOP funding to support addition of 11 Extensive Care Service beds. Continuing fiscal pressures impacting ability to meet CCC program care delivery needs. Initiate March 2010 Regional Complex Continuing Care Review Final Report January 2010 Page 23 of 35
25 Conclusions 1. Based on current utilization trends and population demographics, there is a demonstrated need for a Regional Complex Continuing Care program for the North Simcoe Muskoka LHIN. 2. Effective partnerships have been established between health care partners within the LHIN, with an opportunity for continued growth and development of relationships. 3. Demonstrated commitment to the Regional Complex Continuing Care program by all partners and service providers. 4. The act of integrating this program regionally is forefront and aligns with the North Simcoe Muskoka LHIN s strategic priority to create an integrated health system. Next Steps 1. Presentation of report and recommendations to the North Simcoe Muskoka LHIN Leadership Council (February 10, 2010) 2. Direction required regarding the following areas: a. Agreement with recommendations and proposed next steps b. Funding: Reinvestment of funding from bed deductions into staffing model for both Nursing and Health Disciplines; and other key / new roles c. Availability of PCOP funding to support opening of Extensive Care service beds within OSMH d. Strategies to address any remaining funding gaps e. Expectations regarding timelines for implementation: Revision to bring Integration Order up to date. 3. Upon agreement and support of recommendations, the North Simcoe Muskoka LHIN Board of Directors will be informed of the recommendations and next steps associated with this facilitated integration. Regional Complex Continuing Care Review Final Report January 2010 Page 24 of 35
26 Appendix A: CCC Client Definitions and Indicators CCC Category Criteria Admission criteria Exclusion Criteria Indicators Clinically Complex Clients are medically complex with stabilized disease processes and predictable outcomes. Clients are able to participate in a minimum of 45 minutes/week of therapy provided by members of the interdisciplinary team. Clients are medically complex with stabilized disease processes and predictable outcomes. Clients are able to participate in a minimum of 45 minutes/week of therapy provided by members of the interdisciplinary team. Clients with unstable conditions requiring acute care services including frequent diagnostic services CMI (target) ADL (target) CHESS score (target) The goal is to improve overall health status and level of functioning to the point where care needs can be met at home / community or long term care. Slow Stream Rehab / Reactivation Clients present with varying diagnoses, medically stable, no longer needing an acute care setting. Clients are cognitively able to participate and follow instructions, and have the desire and motivation to participate in rehabilitation. Clients present with varying diagnoses, medically stable, no longer needing an acute care setting. Clients are cognitively able to participate and follow instructions, and have the desire and motivation to participate in rehabilitation. Client independent with ADL Cognitive deficits sufficient to prevent rehabilitation interventions CMI (target) ADL (target) CHESS score (target) The goal is to provide time-limited interdisciplinary rehabilitative care. Regional Complex Continuing Care Review Final Report January 2010 Page 25 of 35
27 CCC Category Criteria Admission criteria Exclusion Criteria Indicators Palliative Clients present with complex palliative supportive care needs. The goal is to regain control of pain/symptom management or to facilitate end of life care. Clients present with complex palliative supportive care needs. Clients with unstable conditions requiring acute care services including frequent diagnostic services CMI (target) ADL (target) CHESS score (target) Extensive Care Clients present with an exacerbation of a chronic disease process and/or multiple comorbidities and complex extensive service needs. Client outcomes are less predictable and require extensive nursing intervention. Clients present with an exacerbation of a chronic disease process and/or multiple comorbidities and complex extensive service needs. Client outcomes are less predictable and require extensive nursing intervention. Clients with unstable conditions requiring acute care. CMI (target) LOS (unit average) The goal is to improve overall health status and/or maintain current level of functioning. Adapted from: St. Joseph s Care Group (Thunder Bay) Regional Complex Continuing Care Review Final Report January 2010 Page 26 of 35











28 Appendix B: NSM LHIN CCC Population Demographics Data Source: Pop Est Summary PHU County Municip LHIN Tables. Ontario Ministry of Health and Long-Term Care: IntelliHealth ONTARIO. Oct. 9, Last refreshed [May/2009]. Data Source: Pop Est Summary PHU County Municip LHIN Tables. Ontario Ministry of Health and Long-Term Care: IntelliHealth ONTARIO. Oct. 9, Last refreshed [May/2009]. Regional Complex Continuing Care Review Final Report January 2010 Page 27 of 35



29 Appendix C: Care Delivery Model Essential Elements Regional Complex Continuing Care Review Final Report January 2010 Page 28 of 35
30 Appendix D: Nursing Staffing Models Current CCC program staffing and Comparators RN RPN PSW GBGH/PGH Level1 (CCC) x x x GBGH/PGH Level 2 (SSR / Palliative) x x x OSMH / C4 (CCC) x x x OSMH / C5 (SSR) x x MAHC / H (CCC / Interim LTC beds) x x MAHC / B (CCC) x x x Bridgepoint Health Care x x Phasing out; April 2010 St. Joseph`s Care Group x x St. Mary`s Providence x x Not currently in place, in future West Park Healthcentre x X Almonte General Hospital x x Not currently in place, in future Headwaters Health x x Introducing Regional Complex Continuing Care Review Final Report January 2010 Page 29 of 35
31 Appendix E: Health Disciplines Staffing Table 1: Current CCC Program Staffing (FTEs) GBGH / PGH Actual > Projected* OSMH** Actual > Projected* MAHC / H Actual > Projected* MAHC / B Actual > Projected* Current # of beds Physiotherapy 0.8 > > > > 1.0 Occupational Therapy 0.6 > > > > 0.5 Rehab Assistant.053 > > 1.5 Pharmacist 0.05 > > 0.2 Dietitian 0.2 > > > > 0.1 Speech Language 0.0 > > > > 0.2 Pathologist Social Work 0.6 > > > > 0.4 Recreation Therapist 1.0 > > > > 1.0 * Projected need based on the assumption of decrease in % of ALC patients in CCC beds, resulting in an increased need for rehab services to meet needs of growing CCC population. ** Not inclusive of Extensive care services beds proposed for OSMH. Regional Complex Continuing Care Review Final Report January 2010 Page 30 of 35
32 Appendix E: Health Disciplines Staffing Table 2: Comparator CCC programs: Health Disciplines Staffing (FTEs) Current # of beds Bridgepoint 6W 52 SSR Bridgepoint 7E 50 Clin Complex West Park Almonte General Hospital Headwaters Healthcare St. Joseph s Care Group Reactivation St. Joseph s Care Group 40 Clin. Complex PT am/week OT am/week Rehab Assistant Pharmacist Consult Unable to Consult 0 obtain information Dietitian Consult SLP Social Work Consult Recreation Therapist Consult Regional Complex Continuing Care Review Final Report January 2010 Page 31 of 35
33 Appendix E: Health Disciplines Staffing Table 3: Proposed Health Disciplines Staffing for NSM Regional CCC Program Health Discipline FTE Based on 24 bed unit Physiotherapy 1.0 Occupational Therapy Rehab Assistant 1.0 Pharmacist 0.2 Dietitian 0.2 Speech Language Pathologist 0.2 Social Work / Discharge Planning* 1.0 Recreation Therapist / Activation 1.0 Regional Complex Continuing Care Review Final Report January 2010 Page 32 of 35
34 Appendix F: Funding. the knowns, assumptions, and unknowns Knowns Assumptions Unknowns Demonstrated need for CCC program within NSM LHIN No additional operating funds available Ability to recruit and retain NP and MDs for CCC program? Demonstrated commitment to CCC regional program by partners Urgent Priority Funding extended to Current funding model sustainable for MDs Continued support from LHIN to continue the program Current OMA/ MD funding model not adequate One time funding for NPs and Hospitalists ends March 2010 Without the NPs and Hospitalists there is no regional program Although regional in principle, CCC program not truly regional CCAC Funding to support Regional CCC program one time only (2007/08) Utilization of existing resources - dedicated time allocated to CCC program Existing funds can be moved from one category of staff to another within a hospital Existing funds can be moved from one department / program /service to another within an organization Existing funds can be moved from one organization to another within the LHIN Status of Urgent Priority Funding; ongoing funding after 2011? Ability of OSMH to access Post Capital Operating Plan funding to support 11 beds / Extensive care services? Optimal Funding model: Centralized or decentralized? Regional Complex Continuing Care Review Final Report January 2010 Page 33 of 35


35 Contact information regarding this report: Sara Lankshear, RN PhD (c) Relevé Consulting Services 280 Silver Birch Drive Penetanguishene, Ontario L9M 2H7 Phone: Fax: Judith Skelton Green RN, PhD Transitions-HOD Consultants Inc. Unit 10 8 Beck Street Penetanguishene, Ontario L9M 1C3 Phone: judith.skelton-green@transitions-hod.ca
Waterloo Wellington Community Care Access Centre. Community Needs Assessment
 Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Waterloo Wellington Community Care Access Centre Community Needs Assessment Table of Contents 1. Geography & Demographics 2. Socio-Economic Status & Population Health Community Needs Assessment 3. Community
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Stroke Interprofessional Collaboration : Working Together for Better Patient Care
 Stroke Interprofessional Collaboration : Working Together for Better Patient Care Dean Lising, Collaborative Practice Lead, Strategy Lead, IPE Curriculum Centre for Interprofessional Education, University
Stroke Interprofessional Collaboration : Working Together for Better Patient Care Dean Lising, Collaborative Practice Lead, Strategy Lead, IPE Curriculum Centre for Interprofessional Education, University
Health System Performance and Accountability Division MOHLTC. Transitional Care Program Framework
 Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Nurse Managers Role in Promoting Quality Nursing Practice
 Nurse Managers Role in Promoting Quality Nursing Practice Mission Critical: Nurse Manager Summit Fredericton, New Brunswick April 30, 2015 Jeanne Besner, C.M., PhD, RN 1 Outline of Presentation Background
Nurse Managers Role in Promoting Quality Nursing Practice Mission Critical: Nurse Manager Summit Fredericton, New Brunswick April 30, 2015 Jeanne Besner, C.M., PhD, RN 1 Outline of Presentation Background
UNDERSTANDING DETERMINANTS OF OUTCOMES IN COMPLEX CONTINUING CARE
 UNDERSTANDING DETERMINANTS OF OUTCOMES IN COMPLEX CONTINUING CARE FINAL REPORT DECEMBER 2008 CO PRINCIPAL INVESTIGATORS 1, 5, 6 Ann E. Tourangeau RN PhD Katherine McGilton RN PhD 2, 6 CO INVESTIGATORS
UNDERSTANDING DETERMINANTS OF OUTCOMES IN COMPLEX CONTINUING CARE FINAL REPORT DECEMBER 2008 CO PRINCIPAL INVESTIGATORS 1, 5, 6 Ann E. Tourangeau RN PhD Katherine McGilton RN PhD 2, 6 CO INVESTIGATORS
Hospital Care for Future Generations
 Hospital Care for Future Generations May 26 Huntsville; May 27 Bracebridge; May 28 - Gravenhurst Outstanding Care ~ People Focused Purpose & Desired Outcomes Provide an overview of the required planning
Hospital Care for Future Generations May 26 Huntsville; May 27 Bracebridge; May 28 - Gravenhurst Outstanding Care ~ People Focused Purpose & Desired Outcomes Provide an overview of the required planning
Toronto Central LHIN 2016/2017 QIP Snapshot Report. Health Quality Ontario The provincial advisor on the quality of health care in Ontario
 Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Transitions in Care. Discharge Planning Pathway & Dashboard
 Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
2006 Strategy Evaluation
 Continuing Care 2006 Strategy Evaluation Executive Summary June 2015 Introduction In May 2006, the Department of Health and Wellness (DHW) released the Continuing Care Strategy entitled Shaping the Future
Continuing Care 2006 Strategy Evaluation Executive Summary June 2015 Introduction In May 2006, the Department of Health and Wellness (DHW) released the Continuing Care Strategy entitled Shaping the Future
Reference materials are provided with the criteria and should be used to assist in the correct interpretation of the criteria.
 InterQual Level of Care Criteria Rehabilitation Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Rehabilitation Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
MUSKOKA AND AREA HEALTH SYSTEM TRANSFORMATION COUNCIL TERMS OF REFERENCE
 MUSKOKA AND AREA HEALTH SYSTEM TRANSFORMATION COUNCIL TERMS OF REFERENCE Table of Contents Background... 1 Vision for our Future... 1 Purpose of Health System Transformation Council... 2 Accountability...
MUSKOKA AND AREA HEALTH SYSTEM TRANSFORMATION COUNCIL TERMS OF REFERENCE Table of Contents Background... 1 Vision for our Future... 1 Purpose of Health System Transformation Council... 2 Accountability...
Rapid Recovery Therapy Program. GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen
 Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Sub-Acute Care Capacity Plan
 Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
INTERQUAL REHABILITATION CRITERIA REVIEW PROCESS
 REVIEW RP-1 RP-2 INTERQUAL CRITERIA REVIEW REVIEW The InterQual Criteria provide support for determining the appropriateness of admission, continued stay and discharge destination. The Acute Rehabilitation
REVIEW RP-1 RP-2 INTERQUAL CRITERIA REVIEW REVIEW The InterQual Criteria provide support for determining the appropriateness of admission, continued stay and discharge destination. The Acute Rehabilitation
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
North Simcoe Muskoka Local Health Integration Network. Working Together to Achieve Better Health, Better Care, Better Value.
 North Simcoe Muskoka Local Health Integration Network Working Together to Achieve Better Health, Better Care, Better Value. Annual Business Plan 2010-2011 Table of Contents Annual Business Plan Context
North Simcoe Muskoka Local Health Integration Network Working Together to Achieve Better Health, Better Care, Better Value. Annual Business Plan 2010-2011 Table of Contents Annual Business Plan Context
AH3600 Repatriation Policy
 1.0 PURPOSE AH3600 Repatriation Policy This policy outlines the standard operating procedure and performance expectations for Patient Repatriation activities originating at Interior Health (IH) acute care
1.0 PURPOSE AH3600 Repatriation Policy This policy outlines the standard operating procedure and performance expectations for Patient Repatriation activities originating at Interior Health (IH) acute care
MODULE 01 INTRO TO RN & RPN PRACTICE: THE CLIENT, THE NURSE AND THE ENVIRONMENT
 RN & RPN PRACTICE: THE CLIENT, THE NURSE AND THE ENVIRONMENT College of Nurses of Ontario (2014) MODULE 01 INTRO TO RN & RPN PRACTICE: THE CLIENT, THE NURSE AND THE ENVIRONMENT Prepared by: Donna Rothwell,
RN & RPN PRACTICE: THE CLIENT, THE NURSE AND THE ENVIRONMENT College of Nurses of Ontario (2014) MODULE 01 INTRO TO RN & RPN PRACTICE: THE CLIENT, THE NURSE AND THE ENVIRONMENT Prepared by: Donna Rothwell,
An Integrated Program for Complex Care in the Hamilton Niagara Haldimand Brant Local Health Integration Network
 An Integrated Program for Complex Care in the Hamilton Niagara Haldimand Brant Local Health Integration Network Final Report from the Task Group on Coordinated Strategy for Complex Care to the Hamilton
An Integrated Program for Complex Care in the Hamilton Niagara Haldimand Brant Local Health Integration Network Final Report from the Task Group on Coordinated Strategy for Complex Care to the Hamilton
Introduction. 1 Health Professions Regulatory Advisory Council. (2015) Registered Nurse Prescribing Referral, A Preliminary Literature
 Registered Nurse Prescribing Referral, A Preliminary Literature") RN Prescribing Home Care Ontario & Ontario Community Support Association Submission to the Health Professions Regulatory Advisory Committee February 2016 Introduction The Ontario government has confirmed
RN Prescribing Home Care Ontario & Ontario Community Support Association Submission to the Health Professions Regulatory Advisory Committee February 2016 Introduction The Ontario government has confirmed
Expression of Interest for Wound Care Project
 Expression of Interest for Wound Care Project November 11, 2016 Telewound Care EOI Page 1 of 12 Contents 1 Introduction... 3 2 Telewound Care Project Background... 4 2.1 Background... 4 2.2 Purpose...
Expression of Interest for Wound Care Project November 11, 2016 Telewound Care EOI Page 1 of 12 Contents 1 Introduction... 3 2 Telewound Care Project Background... 4 2.1 Background... 4 2.2 Purpose...
RECOMMENDATION STATUS OVERVIEW
 Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Review Process. Introduction. InterQual Level of Care Criteria Subacute & SNF Criteria. Reference materials. Informational notes
 InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
Review Process. Introduction. InterQual Level of Care Criteria Long-Term Acute Care Criteria
 InterQual Level of Care Criteria Long-Term Acute Care Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of Long-Term Acute Care (LTAC) admission,
InterQual Level of Care Criteria Long-Term Acute Care Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of Long-Term Acute Care (LTAC) admission,
Environmental Scan of Ontario s Behavioural Support Transition Units (BSTUs)
") Environmental Scan of Ontario s Behavioural Support Transition Units (BSTUs) Report Created by the Behavioural Support Transition Unit (BSTU) Collaborative Part of Ontario s Best Practice Exchange June
Environmental Scan of Ontario s Behavioural Support Transition Units (BSTUs) Report Created by the Behavioural Support Transition Unit (BSTU) Collaborative Part of Ontario s Best Practice Exchange June
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ
 Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
ONTARIO COMMUNITY REHABILITATION: A PROFILE OF DEMAND AND PROVISION
 ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network ONTARIO COMMUNITY REHABILITATION: A PROFILE OF DEMAND AND PROVISION March 2007 Prepared by: Laura Passalent Emily Borsy
ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network ONTARIO COMMUNITY REHABILITATION: A PROFILE OF DEMAND AND PROVISION March 2007 Prepared by: Laura Passalent Emily Borsy
Assisted Living Services for High Risk Seniors Policy, 2011 An updated supportive housing program for frail or cognitively impaired seniors
 Assisted Living Services for High Risk Seniors Policy, 2011 An updated supportive housing program for frail or cognitively impaired seniors January 2011 (as updated September 2012) Ministry of Health and
Assisted Living Services for High Risk Seniors Policy, 2011 An updated supportive housing program for frail or cognitively impaired seniors January 2011 (as updated September 2012) Ministry of Health and
Exploring the Hip Fracture and Joint Replacement Landscape in a Changing Context: Implications and Recommendations GTA REHAB NETWORK
 Exploring the Hip Fracture and Joint Replacement Landscape in a Changing Context: Implications and Recommendations GTA REHAB NETWORK MARCH 2006 TABLE OF CONTENTS EXECUTIVE SUMMARY 7 1.0 BACKGROUND AND
Exploring the Hip Fracture and Joint Replacement Landscape in a Changing Context: Implications and Recommendations GTA REHAB NETWORK MARCH 2006 TABLE OF CONTENTS EXECUTIVE SUMMARY 7 1.0 BACKGROUND AND
EXECUTIVE COMPENSATION PROGRAM
 EXECUTIVE COMPENSATION PROGRAM 2 Background In 2010, the Province legislated a two-year compensation freeze for all non-unionized employees in the Broader Public Sector (BPS) which prohibited increases
EXECUTIVE COMPENSATION PROGRAM 2 Background In 2010, the Province legislated a two-year compensation freeze for all non-unionized employees in the Broader Public Sector (BPS) which prohibited increases
Developmental /Category III Explanatory/Category II Not Defined Explanatory/Category II Defined Proposed Priority
 The Rehabilitative Care System supports high quality patient experiences through the utilization of best practices to enhance outcomes for individuals with functional goals. This evaluationframework has
The Rehabilitative Care System supports high quality patient experiences through the utilization of best practices to enhance outcomes for individuals with functional goals. This evaluationframework has
Care in Your Home. North West CCAC
 Care in Your Home Care in Your Home Home and community support services can help you manage your health care while living in your own home. At the Community Care Access Centre (CCAC), we provide information
Care in Your Home Care in Your Home Home and community support services can help you manage your health care while living in your own home. At the Community Care Access Centre (CCAC), we provide information
Quality Improvement Plans (QIP): Progress Report for QIP
: Progress Report for QIP") Excellent Care for All Act Quality Improvement Plans (QIP): Progress Report for 2013-14 QIP This document uses the standard Health Quality Ontario (HQO) template for reporting on the progress as of April
Excellent Care for All Act Quality Improvement Plans (QIP): Progress Report for 2013-14 QIP This document uses the standard Health Quality Ontario (HQO) template for reporting on the progress as of April
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/24/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/24/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Supporting Best Practice for COPD Care Across the System
 Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
Enhancing Patient Care through Effective and Efficient Nursing Documentation
 Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Interim Results: Rapid Cycle Evaluation. Anna Greenberg, Director, Transformation Secretariat, MOHLTC
 Interim Results: Rapid Cycle Evaluation Anna Greenberg, Director, Transformation Secretariat, MOHLTC Current Evaluation Activities Rapid Cycle Evaluation Baseline conditions Early implementation results
Interim Results: Rapid Cycle Evaluation Anna Greenberg, Director, Transformation Secretariat, MOHLTC Current Evaluation Activities Rapid Cycle Evaluation Baseline conditions Early implementation results
Proudly Serving our Communities - Delivering Best Patient Outcomes with High Standards & Compassion. MASTER PROGRAM Revised 2016 FEBRUARY
 Proudly Serving our Communities - Delivering Best Patient Outcomes with High Standards & Compassion MASTER PROGRAM Revised 2016 FEBRUARY Resource Planning Group Inc. 502-703 Evans Ave. Toronto ON M9C 5E9
Proudly Serving our Communities - Delivering Best Patient Outcomes with High Standards & Compassion MASTER PROGRAM Revised 2016 FEBRUARY Resource Planning Group Inc. 502-703 Evans Ave. Toronto ON M9C 5E9
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard /10 Q3
 MLAA Performance Assessment Dashboard /10 Q3") MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
The South West Regional Wound Care Program: A Collaborative Approach to Wound Care
 The South West Regional Wound Care Program: A Collaborative Approach to Wound Care 2016 OACCAC Conference June 6, 2016 #OACON16 I @OACCAC I @SWRWCP Objectives By the end of this presentation, participants
The South West Regional Wound Care Program: A Collaborative Approach to Wound Care 2016 OACCAC Conference June 6, 2016 #OACON16 I @OACCAC I @SWRWCP Objectives By the end of this presentation, participants
Long-Term Care Homes Protocol
 Long-Term Care Homes Protocol Ministry of Health and Long-Term Care October 9, 2009 Table of Contents Page # Context...................................... 3 Roles and Responsibilities of Individual Ministry
Long-Term Care Homes Protocol Ministry of Health and Long-Term Care October 9, 2009 Table of Contents Page # Context...................................... 3 Roles and Responsibilities of Individual Ministry
Sub-Acute Care Capacity Plan
 Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Executive Compensation Policy and Framework BLUEWATER HEALTH
 Executive Compensation Policy and Framework BLUEWATER HEALTH 1. Background The Province of Ontario introduced The Broader Public Sector Accountability Act in 2010 (BPSAA), which introduced controls on
Executive Compensation Policy and Framework BLUEWATER HEALTH 1. Background The Province of Ontario introduced The Broader Public Sector Accountability Act in 2010 (BPSAA), which introduced controls on
Nursing and Personal Care: Funding Increase Survey
 Nursing and Personal Care: Funding Increase Survey Prepared for: Ministry of Health and Long-Term Care Long Term Care Facilities Branch 5 th Floor, Hepburn Block 80 Grosvenor Street Toronto, Ontario Prepared
Nursing and Personal Care: Funding Increase Survey Prepared for: Ministry of Health and Long-Term Care Long Term Care Facilities Branch 5 th Floor, Hepburn Block 80 Grosvenor Street Toronto, Ontario Prepared
Rehab V Vita Square Operational Guideline
 Southern Adelaide Local Health Network Rehab V Vita Square Operational Guideline Consultation Paper Version 2.2 January 2018 Purpose The purpose of this document is to provide an overview of operational
Southern Adelaide Local Health Network Rehab V Vita Square Operational Guideline Consultation Paper Version 2.2 January 2018 Purpose The purpose of this document is to provide an overview of operational
Hard Decisions / Hard News:
 Hard Decisions / Hard News: The Ethical (& Human) Dilemmas of Allocating Home Care Resources When Supply Demand Champlain Ethics Symposium Catherine Butler VP, Clinical Care Champlain CCAC September 29,
Hard Decisions / Hard News: The Ethical (& Human) Dilemmas of Allocating Home Care Resources When Supply Demand Champlain Ethics Symposium Catherine Butler VP, Clinical Care Champlain CCAC September 29,
Grey Bruce Health Services (GBHS) Executive Compensation Framework. February Final Copy
 Executive Compensation Framework. February Final Copy") Grey Bruce Health Services (GBHS) Executive Compensation Framework February 2018 Final Copy Grey Bruce Health Service has established an Executive Compensation Framework, a new requirement of the provincial
Grey Bruce Health Services (GBHS) Executive Compensation Framework February 2018 Final Copy Grey Bruce Health Service has established an Executive Compensation Framework, a new requirement of the provincial
PANEL DISCUSSION SEPTEMBER 22, 2017
 Comparing and contrasting 3 models of Nurse Practitioner MRP in Ontario public hospitals PANEL DISCUSSION SEPTEMBER 22, 2017 Hôpital Montfort, Ottawa Vanessa Helleur NP (Adult), BScN, MN St-Joseph s Health
Comparing and contrasting 3 models of Nurse Practitioner MRP in Ontario public hospitals PANEL DISCUSSION SEPTEMBER 22, 2017 Hôpital Montfort, Ottawa Vanessa Helleur NP (Adult), BScN, MN St-Joseph s Health
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Quality Improvement Plans (QIP): Progress Report for 2013/14 QIP
: Progress Report for 2013/14 QIP") Excellent Care for All Quality Improvement Plans (QIP): Report for 201/14 QIP The following template has been provided to assist with completion of reporting on the progress of your organization s QIP.
Excellent Care for All Quality Improvement Plans (QIP): Report for 201/14 QIP The following template has been provided to assist with completion of reporting on the progress of your organization s QIP.
Long-Term Care Homes Financial Policy
 Ministry of Health and Long-Term Care Long-Term Care Homes Financial Policy Policy: LTCH Level-of-Care Per Diem Funding Policy Date: April 1, 2011 1.1 Introduction The policy outlines the funding approach
Ministry of Health and Long-Term Care Long-Term Care Homes Financial Policy Policy: LTCH Level-of-Care Per Diem Funding Policy Date: April 1, 2011 1.1 Introduction The policy outlines the funding approach
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Beacon Award for Excellence Audit Tool
 Beacon Award for Excellence Audit Tool The Beacon Award for Excellence audit tool and application are best completed collaboratively between the unit leadership and staff. The audit tool provides you with
Beacon Award for Excellence Audit Tool The Beacon Award for Excellence audit tool and application are best completed collaboratively between the unit leadership and staff. The audit tool provides you with
Provincial Dialysis Capacity Assessment Executive Summary. April 2012
 Provincial Dialysis Capacity Assessment 2011-2020 Executive Summary April 2012 Table of Contents Introduction... 2 Planning Process... 2 Methodology... 3 Dialysis Planning Support Model... 3 Data... 3
Provincial Dialysis Capacity Assessment 2011-2020 Executive Summary April 2012 Table of Contents Introduction... 2 Planning Process... 2 Methodology... 3 Dialysis Planning Support Model... 3 Data... 3
OVERVIEW. 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: Toll Free: Fax:
 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
SW LHIN Complex Continuing Care Eligibility Guidelines
 SW LHIN Complex Continuing Care Eligibility Guidelines Name: Referring site: HIN: Date: Definition: OHA defines Complex Continuing Care as a specialized program of care providing programs for medically
SW LHIN Complex Continuing Care Eligibility Guidelines Name: Referring site: HIN: Date: Definition: OHA defines Complex Continuing Care as a specialized program of care providing programs for medically
Determining the Appropriate Inpatient Rehabilitation Candidate
 Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Beacon Award for Excellence Audit Tool
 Beacon Award for Excellence Audit Tool The Beacon Award for Excellence audit tool and application is best completed collaboratively between the unit leadership and staff. The audit tool provides you with
Beacon Award for Excellence Audit Tool The Beacon Award for Excellence audit tool and application is best completed collaboratively between the unit leadership and staff. The audit tool provides you with
LONG TERM CARE LONG TERM CARE 2005 SERVICE STRATEGY BUSINESS PLAN
 TABLE OF CONTENTS A. Background A.1 Preparing the Service Strategy Business Plan... 1 A.2 Key Contacts... 1 A.3 Additional Information... 1 B. Description of Current Services B.1 Program Location Map...
TABLE OF CONTENTS A. Background A.1 Preparing the Service Strategy Business Plan... 1 A.2 Key Contacts... 1 A.3 Additional Information... 1 B. Description of Current Services B.1 Program Location Map...
Grey Bruce Health Services. Executive Compensation Framework. January 2018
 Grey Bruce Health Services Executive Compensation Framework January 2018 2 Grey Bruce Health Service (GBHS) is in the process of establishing an Executive Compensation Framework, a new requirement of the
Grey Bruce Health Services Executive Compensation Framework January 2018 2 Grey Bruce Health Service (GBHS) is in the process of establishing an Executive Compensation Framework, a new requirement of the
OVERVIEW SCOPE & DEMONSTRATION OF IMPACT
 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
Family and Community Support Services (FCSS) Program Review
 Program Review") Family and Community Support Services (FCSS) Program Review Judy Smith, Director Community Investment Community Services Department City of Edmonton 1100, CN Tower, 10004 104 Avenue Edmonton, Alberta,
Family and Community Support Services (FCSS) Program Review Judy Smith, Director Community Investment Community Services Department City of Edmonton 1100, CN Tower, 10004 104 Avenue Edmonton, Alberta,
Hospital Improvement Plan Niagara Health System Staff Report December 16, Hamilton Niagara Haldimand Brant Local Health Integration Network
 Hospital Improvement Plan Niagara Health System Staff Report December 16, 2008 Hamilton Niagara Haldimand Brant Local Health Integration Network Question: Emergency Medical Services (EMS) The EMS stated
Hospital Improvement Plan Niagara Health System Staff Report December 16, 2008 Hamilton Niagara Haldimand Brant Local Health Integration Network Question: Emergency Medical Services (EMS) The EMS stated
Background: As described below, 70 years of RN effectiveness makes it clear that RNs are central to a high-performing health system.
 Background: Nurses are the largest group of regulated health professionals in Canada, accounting for about half the health-care workforce. This includes more than 115,000 Ontario registered nurses (RN)
Background: Nurses are the largest group of regulated health professionals in Canada, accounting for about half the health-care workforce. This includes more than 115,000 Ontario registered nurses (RN)
The Re-ACT Program. Remote Access to Care Technology
 w w w.w E C A R E. C A The Re-ACT Program Remote Access to Care Technology January 2011 Introduction Almost 80% of Canadian adults over the age of 65 have some form of chronic disease. Treating and caring
w w w.w E C A R E. C A The Re-ACT Program Remote Access to Care Technology January 2011 Introduction Almost 80% of Canadian adults over the age of 65 have some form of chronic disease. Treating and caring
Assignment Of Client Care: Guidelines for Registered Nurses
 Assignment Of Client Care: Guidelines for Registered Nurses May 2014 Approved by the College and Association of Registered Nurses of Alberta (CARNA) Permission to reproduce this document is granted; please
Assignment Of Client Care: Guidelines for Registered Nurses May 2014 Approved by the College and Association of Registered Nurses of Alberta (CARNA) Permission to reproduce this document is granted; please
 AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2010 B E T W E E N: NORTH SIMCOE MUSKOKA LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) - and - MUSKOKA ALGONQUIN
AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2010 B E T W E E N: NORTH SIMCOE MUSKOKA LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) - and - MUSKOKA ALGONQUIN
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Northeastern Ontario Clinical Services Review
 Northeastern Ontario Clinical Services Review FINAL PROJECT REPORT Hay Group Health Care Consulting March, 2014 2014 Hay Group Limited. All rights reserved Contents 1.0 EXECUTIVE SUMMARY... 1 1.1 BACKGROUND
Northeastern Ontario Clinical Services Review FINAL PROJECT REPORT Hay Group Health Care Consulting March, 2014 2014 Hay Group Limited. All rights reserved Contents 1.0 EXECUTIVE SUMMARY... 1 1.1 BACKGROUND
A PROFILE OF COMMUNITY REHABILITATION WATERLOO WELLINGTON LOCAL HEALTH INTEGRATION NETWORK ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU)
") ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network A PROFILE OF COMMUNITY REHABILITATION WATERLOO WELLINGTON LOCAL HEALTH INTEGRATION NETWORK March 2007 Prepared by: Laura
ARTHRITIS COMMUNITY RESEARCH & EVALUATION UNIT (ACREU) University Health Network A PROFILE OF COMMUNITY REHABILITATION WATERLOO WELLINGTON LOCAL HEALTH INTEGRATION NETWORK March 2007 Prepared by: Laura
Renfrew Victoria Hospital
 Renfrew Victoria Hospital Implementation of a Functional Abilities Measurement Tool TEAM MEMBER NAMES: Randy Penney, Executive Sponsor Charlene Hanniman, Team Lead Stefanie Coughlin, Team Member Chris
Renfrew Victoria Hospital Implementation of a Functional Abilities Measurement Tool TEAM MEMBER NAMES: Randy Penney, Executive Sponsor Charlene Hanniman, Team Lead Stefanie Coughlin, Team Member Chris
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
MEASURING THE JOB STICKINESS OF COMMUNITY NURSES IN ONTARIO ( ): Implications for Policy & Practice
: Implications for Policy & Practice") MEASURING THE JOB STICKINESS OF COMMUNITY NURSES IN ONTARIO (2004 2010): Implications for Policy & Practice Alameddine, M., Baumann, A., Laporte, A. & Deber, R. Background Over the past two decades, many
MEASURING THE JOB STICKINESS OF COMMUNITY NURSES IN ONTARIO (2004 2010): Implications for Policy & Practice Alameddine, M., Baumann, A., Laporte, A. & Deber, R. Background Over the past two decades, many
SELKIRK MENTAL HEALTH CENTRE ACQUIRED BRAIN INJURY PROGRAM MODEL OCTOBER Striving for Excellence in Rehabilitation, Recovery, and Reintegration.
 SELKIRK MENTAL HEALTH CENTRE ACQUIRED BRAIN INJURY PROGRAM MODEL OCTOBER 2008 Striving for Excellence in Rehabilitation, Recovery, and Reintegration. SELKIRK MENTAL HEALTH CENTRE ACQUIRED BRAIN INJURY
SELKIRK MENTAL HEALTH CENTRE ACQUIRED BRAIN INJURY PROGRAM MODEL OCTOBER 2008 Striving for Excellence in Rehabilitation, Recovery, and Reintegration. SELKIRK MENTAL HEALTH CENTRE ACQUIRED BRAIN INJURY
Appendix B: Restorative Care Training Presentation. Audience: All Staff Release date: December
 Appendix B: Restorative Care Training Presentation Audience: All Staff Release date: December 17 2010 Objectives At the completion of this session, participants will be able to: Understand the principles
Appendix B: Restorative Care Training Presentation Audience: All Staff Release date: December 17 2010 Objectives At the completion of this session, participants will be able to: Understand the principles
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Better at Home. 3 Ways to Improve Home and Community Care in Ontario. Recommendations to meet the changing needs of clients
 Better at Home 3 Ways to Improve Home and Community Care in Ontario Recommendations to meet the changing needs of clients Ontario Community Support Association 2018 Contents Introduction 01 Impacting clients,
Better at Home 3 Ways to Improve Home and Community Care in Ontario Recommendations to meet the changing needs of clients Ontario Community Support Association 2018 Contents Introduction 01 Impacting clients,
Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network
 Healthcare Quarterly ONLINE CASE STUDY Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network Jessica Meleskie and Katrina Wilson 1 Abstract The Grey Bruce Health
Healthcare Quarterly ONLINE CASE STUDY Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network Jessica Meleskie and Katrina Wilson 1 Abstract The Grey Bruce Health
Evaluation Framework to Determine the Impact of Nursing Staff Mix Decisions
 Evaluation Framework to Determine the Impact of Nursing Staff Mix Decisions CANADIAN PRACTICAL NURSES ASSOCIATION A. Introduction In 2004, representatives from the Canadian Nurses Association (CNA), the
Evaluation Framework to Determine the Impact of Nursing Staff Mix Decisions CANADIAN PRACTICAL NURSES ASSOCIATION A. Introduction In 2004, representatives from the Canadian Nurses Association (CNA), the
Excellent Care for All Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP
: Progress Report for 2016/17 QIP") Excellent Care for All Quality Improvement Plans (QIP): Progress Report for QIP The Progress Report is a tool that will help organizations make linkages between change ide and improvement, and gain insight
Excellent Care for All Quality Improvement Plans (QIP): Progress Report for QIP The Progress Report is a tool that will help organizations make linkages between change ide and improvement, and gain insight
Recommendations for Adoption: Diabetic Foot Ulcer. Recommendations to enable widespread adoption of this quality standard
 Recommendations for Adoption: Diabetic Foot Ulcer Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
Recommendations for Adoption: Diabetic Foot Ulcer Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
MUST SUBMIT STATE APPLICATION PD 107
 NORTHAMPTON COUNTY HEALTH DEPARTMENT NOTIFICATION OF VACANCY Department: Northampton County Health Department Position Title: Public Health Nurse II (RN) Community Care Program (CCP) Position Grade: 72
NORTHAMPTON COUNTY HEALTH DEPARTMENT NOTIFICATION OF VACANCY Department: Northampton County Health Department Position Title: Public Health Nurse II (RN) Community Care Program (CCP) Position Grade: 72
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016
 Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016 Introduction The Ministry of Health and Long Term Care s (MOHLTC) Patients First: Action Plan for Health Care exemplifies
Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016 Introduction The Ministry of Health and Long Term Care s (MOHLTC) Patients First: Action Plan for Health Care exemplifies
Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost
 Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost Narendra Shah COO MH LHIN September 29, 2010 1 Implications of Alternate Level of Care
Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost Narendra Shah COO MH LHIN September 29, 2010 1 Implications of Alternate Level of Care
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
UNIT DESCRIPTIONS. 2 North Musculoskeletal Rehabilitative Care
 UNIT DESCRIPTIONS 2 North Musculoskeletal Rehabilitative Care Musculoskeletal Rehabilitation The Musculoskeletal Service provides rehabilitation following multiple trauma, or orthopaedic surgery (primarily
UNIT DESCRIPTIONS 2 North Musculoskeletal Rehabilitative Care Musculoskeletal Rehabilitation The Musculoskeletal Service provides rehabilitation following multiple trauma, or orthopaedic surgery (primarily
Quality Standards. Process and Methods Guide. October Quality Standards: Process and Methods Guide 0
 Quality Standards Process and Methods Guide October 2016 Quality Standards: Process and Methods Guide 0 About This Guide This guide describes the principles, process, methods, and roles involved in selecting,
Quality Standards Process and Methods Guide October 2016 Quality Standards: Process and Methods Guide 0 About This Guide This guide describes the principles, process, methods, and roles involved in selecting,
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
North East Behavioural Supports Ontario Sustainability Plan
 North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
Long-term Ventilation Service Inventory Program. Final Summary Report July 31, 2008
 Long-term Ventilation Service Inventory Program Final Summary Report July 31, 2008 Table of Contents EXECUTIVE SUMMARY... I 1.0 INTRODUCTION...1 1.1 BACKGROUND...1 1.2 LTV ACTION PLAN...2 1.3 LTV INFORMATION
Long-term Ventilation Service Inventory Program Final Summary Report July 31, 2008 Table of Contents EXECUTIVE SUMMARY... I 1.0 INTRODUCTION...1 1.1 BACKGROUND...1 1.2 LTV ACTION PLAN...2 1.3 LTV INFORMATION
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
MINISTRY OF HEALTH AND LONG-TERM CARE. Summary of Transfer Payments for the Operation of Public Hospitals. Type of Funding
 MINISTRY OF HEALTH AND LONG-TERM CARE 3.09 Institutional Health Program Transfer Payments to Public Hospitals The Public Hospitals Act provides the legislative authority to regulate and fund the operations
MINISTRY OF HEALTH AND LONG-TERM CARE 3.09 Institutional Health Program Transfer Payments to Public Hospitals The Public Hospitals Act provides the legislative authority to regulate and fund the operations
INTERQUAL LONG-TERM ACUTE CARE CRITERIA REVIEW PROCESS
 REVIEW RP-1 RP-2 INTERQUAL CRITERIA REVIEW REVIEW The InterQual Criteria provide support for determining the appropriateness of admission, continued stay and appropriate discharge destinations. Supporting
REVIEW RP-1 RP-2 INTERQUAL CRITERIA REVIEW REVIEW The InterQual Criteria provide support for determining the appropriateness of admission, continued stay and appropriate discharge destinations. Supporting
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans
 Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders