Authors: Head of Outcomes & Effectiveness, Quality Project Manager and Deputy MD, Sponsor: Medical Director
|
|
|
- Nicholas Randall
- 5 years ago
- Views:
Transcription
1 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER 2017 Author: [insert] Sponsor: [insert] Date: [MM/YY] MORTALITY REPORT Trust Board paper G PAGE 1 OF 3 Authors: Head of Outcomes & Effectiveness, Quality Project Manager and Deputy MD, Sponsor: Medical Director Executive Summary Background and Context UHL s crude and risk-adjusted mortality rates, and the work-streams being undertaken to review and improve review these, are overseen by the Trust s Mortality Review Committee (MRC), chaired by the Medical Director. MRC also oversee UHL s Mortality and Morbidity process which has recently been revised in line with national requirements i, ii, iii which focus on Learning from Deaths in hospitals in order to improve the care of all patients. One of the Learning from Deaths requirements is for Trusts to submit nationally and publish mortality data on a quarterly basis, from December 2017, including the number of deaths reviewed and/or investigated, and the number of those found to be more than likely due to problems in care. In addition to the work being undertaken in response to national guidance, the locally commissioned health economy-wide audit looking at the care provided to patients who died either in LPT or UHL or within 30 days of discharge from UHL - has started. Questions 1. What are the data telling us around UHL s mortality rates and what actions are being taken to improve these? 2. What has been the Learning from Deaths in Quarters 1 and 2 and are we on track to meet the national mortality reporting requirements? 3. What progress has been made with the LLR Clinical Quality Audit? 1. UHL s Mortality Rates and Actions A summary of UHL s mortality rates, both risk adjusted and crude, are set out in the slide deck (Appendix 1). UHL s published Summary Hospital-level Mortality Indicator (SHMI) is 101 (for the time period April 16 to March 17) and our Hospital Standardised Mortality Ratio (HSMR) is 102 and are both within the expected range. Analysis of our SHMI and HSMR, using the HED clinical benchmarking tool, shows that our HSMR is 97 for the 12 months August 16 to July 17 and our unpublished SHMI is expected to reduce further for the 12 months July 16 to June 17.
2 UNIVERSITY HOSPITALS OF LEICESTER MORTALITY REPORT TO TRUST BOARD PAGE 2 OF 3 There have been a number of actions undertaken to reduce mortality as part of our Quality Commitment over the past 3 years. The work on recognition and appropriate management of the deteriorating patient continues with a particular focus on sepsis and acute kidney injury. A current area of focus is cardiac patients both those presenting medically and for surgical intervention. Our HSMR has been above expected for 2 diagnosis and 1 procedure group related to cardiac disease and detailed reviews have not shown any significant concerns with the service. 2. UHL s Learning from Deaths Process and Publication of Data UHL s Learning from the Deaths of Patients in our Care Framework is underpinned by the: Medical Examiner Process, in collaboration with Bereavement Services Specialty Mortality & Morbidity Meetings and Structured Judgement Review Process Bereavement Support Service Serious Incident Reporting and Investigation Process In Quarters 1 & 2, MEs screened 1378 (97% of all adult deaths, to include community and ED). Part of this screening process involves contacting the next of kin. Where MEs identify potential for learning or the bereaved raise a concern about clinical care, the case is referred to the Specialty M&M for full Structured Judgement Review (SJR) using the national mortality review template. To date, 249 deaths have been referred or met the national requirement for SJR in Quarters 1 and 2. This includes 9 deaths of patients with Learning Disability and 49 deaths of children/neonates. 112 SJRs have been completed and death classifications confirmed. Our internally set target is that 75% of SJRs should be completed within 4 months of death and 100% within 6 months. Therefore all April s deaths should have had SJRs completed at the end of October and 75% of May and June s deaths should have had completed SJRs. However, not all SJR details have been collated due to resource constraints within the Corporate M&M Admin team and capacity within the Specialty M&M teams. There was one patient where problems in care were thought more likely than contributed to the death and this has been investigated as a Patient Safety Incident and confirmed as being a Serious Incident with Major Harm as the outcome The investigation into this case identified multiple contributory factors with specific learning for both ED and the Difficult Asthma Clinic. Completion of actions and learning points will be tracked through the Adverse Events Committee with escalation to the CMG Assurance Performance Review meetings as required by exception. In addition to our Medical Examiners speaking to the bereaved relatives/carers to ask if they have any concerns about the care provided to the deceased, follow up by the Bereavement Support Nurse (BSN) is offered to all families/carers of patients who have died in our care.
3 UNIVERSITY HOSPITALS OF LEICESTER MORTALITY REPORT TO TRUST BOARD PAGE 3 OF 3 Most concerns raised by the bereaved relate to the last few days of life or the death and often because of communication difficulties. Where concerns can t be resolved over the phone, or the bereaved would like a better understanding about clinical management plans or decisions made about end of life care, the BSN will arrange a meeting with the clinical team. Further details about the number of deaths, how many have been through the SJR process and Death Classification agreed plus emerging themes are given in the slide deck (Appendix 1). The final slide in Appendix 1 provides an overarching summary of UHL s Learning from Deaths framework (meeting the requirements to publish a Learning from Deaths Dashboard). 3. LLR Clinical Quality Audit Following on from the Learning Lessons to Improve Care (LLTIC) review published in 2014, a follow up LLR system-wide review has been commissioned. The audit has commenced, is being undertaken by Mazars and is expected to report to the LLTIC task force in February Input Sought Members of the Trust Board are requested to receive this report and appendix and to: Be advised that UHL s mortality rates are closely monitored and that any patient groups with a higher HSMR or SHMI are being reviewed and learning and action taken where applicable. Note the good progress made with screening of adult deaths by the Medical Examiners and completion of Structured Judgment Reviews by Specialty M&Ms. Be advised that resource issues are affecting tracking of progress with the Learning from Deaths programme and also analysis of data. Be assured that where deaths have been considered to be more than likely due to problems in care these have been investigated by the Patient Safety Team as a Serious Incident. Note that the LLR Clinical Quality Audit is underway. i Learning, candour and accountability - A review of the way NHS trusts review and investigate the deaths of patients in England, Care Quality Commission, December ii National Guidance on Learning from Deaths - A Framework for NHS Trusts and NHS Foundation Trusts on Identifying, Reporting, Investigating and Learning from Deaths in Care, National Quality Board, March iii Implementing the Learning from Deaths framework: key requirements for trust boards, NHS Improvement, July Implementing_LfD_- _information_for_boards_jh_amend_3.pdf
4 Appendix 1 UHL Trust Board Mortality Report Slide-deck 2017/18 - Quarter 1 & 2 Report from UHL Medical Director 1
5 What are UHL s current overall crude and risk adjusted mortality rates? 2
6 Crude mortality: i.e. number deaths and proportion of discharges where death is the outcome 3
7 How many people died in the Trust during the first 6 months of this financial year and what is the Trust s crude mortality rate? What actions are being taken What is the data telling us? There were 1,368 in-patient deaths during Q1-Q2 with August and September having the lowest number of deaths since August 15. The monthly mortality rate has been between % during the first 6 months of this financial year. However, it should be noted that these are typically the months with fewer deaths. Please note: Figures for the latest months discharges may change due to late data recording on the system 4
8 HSMR: Hospital Standardised Mortality Ratio HSMR is risk adjusted mortality where patients die in hospital (either in UHL or if transferred directly to another NHS hospital trust) over a 12 month period within 56 diagnostic groups (which contribute to 80% of in-hospital deaths). The HSMR methodology was developed by the Dr Foster Unit at Imperial College (DFI) and is used as by the CQC as part of their assessment process, however the rolling 12 month data presented in the next chart is taken from the Hospital Evaluation Dataset (HED) as their HSMR has been more recently rebased against all other trusts. NOTE: Following upload of new national data, both HED and DFI rebase their HSMR dataset and therefore Trusts may see a change in their previously reported HSMR. 5
 Apr15- Mar16 Apr16- Mar17 What is the data telling us?")

9 What is the Trust s current Hospital Standardised Mortality Ratio (HSMR)? UHL s Rolling 12 month HSMR (as reported by HED) Apr15- Mar16 Apr16- Mar17 What is the data telling us? UHL s HSMR was above 100 for the financial year 2016/17 (as reported by HED) but was still within the expected range compared to all trusts. The latest rolling 12 month HSMR (Aug 16 to Jul 17) is 97 and our monthly HSMR has been below 100 for the past 5 months in both the HED and DFI tools. 6
10 How does UHL s latest HSMR* compare with other trusts? (Aug 16 Jul 17) *Data taken from HED UHL 97 What is the data telling us? UHL s HSMR is within the funnel plot (i.e. within expected) and whilst it was above 100 for the financial year Apr 16 to Mar 17 our latest 12 month HSMR is now at 97. 7
11 SHMI: Summary Hospital Mortality Index ie risk adjusted mortality where patients die either in UHL or within 30 days of discharge (incl those transferred to a community trust) The SHMI is published on a Quarterly basis by NHS Digital (previously the HSCIC). UHL subscribes to the University Hospitals of Birmingham s Hospital Evaluation Dataset Clinical Benchmarking tool (HED) which uses HSCIC methodology to replicate SHMI. This then allows us to review our SHMI pre publication. NOTE: Although HED rebase their SHMI database following uploading of new data, the unpublished SHMI value is usually 1 or 2 below the final NHS Digital published SHMI Due to the SHMI involving out of hospital deaths the reporting timeframe is a month behind that for the HSMR. 8
 Jun 15")
12 What is the Trust s current Summary Hospital Mortality Index (SHMI)? UHL s Published SHMI and latest 12 months HED unpublished SHMI Apr11- Mar12 Apr12- Mar13 Apr13- Mar14 unpublished Apr14- Mar15 Apr15- Mar16 Apr16- Mar17 UHL s monthly SHMI (as reported by HED) Jun 15 Jun 17 What is the data telling us? UHL s published SHMI was above 100 for the first 3 financial years of reporting and was then below 100 for the next 2. Our latest published SHMI is 101 for the financial year 16/17. UHL s unpublished SHMI - as reported by HED - has come down to 98 for Jul16-Jun 17 which is the next reporting period for the Published SHMI due end of December 17. It is therefore anticipated that, following national rebasing, our next published SHMI will be
13 How does UHL s SHMI as reported by HED - compared against all Trusts (Jul 16 to Jun 17) UHL 98 What is the data telling us? UHL is one of the England top 5 trusts for activity and also for the number of deaths. Our SHMI is s unpublished SHMI for the period Jul 16 to Jun 17 is 98 which is slightly below the expected of 100 and is in line with other trusts with similar numbers of deaths. 10

14 Which are the diagnosis groups most contributing to our SHMI? Diagnosis Groups with a SHMI above 100 (Jul 16 to Jun 17) What is the data telling us? The above chart presents those diagnosis groups with a SHMI above 100. The size of the box indicates the number of deaths and the colour indicates the SHMI i.e. The larger the box, the greater the number of deaths; and the darker the colour, the higher the SHMI Open wounds of head; neck; and trunk, Other Perinatal Conditions, and Intrauterine hypoxia and birth asphyxia are the top 3 diagnosis groups with the highest SHMIs. For these groups, the numbers of deaths are small (18, 11 and 6 respectively) but only 8, 5 and 2 deaths were expected, hence the high SHMI. Of all the diagnosis groups with a SHMI above 100, Acute cerebrovascular disease has the most deaths (225 against an expected 198). 11
15 Actions being taken to improve UHL s SHMI and HSMR Case note reviews have been undertaken for those diagnosis groups with a higher SHMI or HSMR and whilst none have found deaths more than likely due to problems in care, we have identified areas for improvement (see below). Whilst we have identified learning to improve patient pathways, a common theme from the reviews has also been the need to improve the accuracy of the primary reason for hospital admission as this affects the adjusted mortality risk prediction. Diagnosis Group Acute Myocardial Infarction / Coronary Atherosclerosis and Other Heart Disease Stroke Other Perinatal Conditions, Small for Gestation, Intrauterine Hypoxia Cardiac Arrest Open Wounds of Head, Neck & Trunk Review Findings / Improvement Work Stream Ongoing case note review of patients admitted to LRI with AMI as primary diagnosis to confirm appropriateness of admission and cardiology involvement. Acute Coronary Syndrome Clinical Decision Tool developed and launched in Aug 17 aim to support more accurate diagnosis and earlier referral. Cardiology Consultant presence in ED Review of pathway for patients referred urgently from other centres for cardiac surgery. Correlation of data with the national Stroke Audit (SSNAP) Mortality reporting this shows UHL s mortality rate is in line with the national average. Liaison with Clinical Coders to improve depth of coding of type of stroke Continued focus on improving time to thrombolysis and time to stroke unit. Comparison of UHL s perinatal mortality data as reported to MBRRACE (the Maternal, Newborn and Infant Clinical Outcome Review Programme). For 2015 significantly more of the stillbirths and neonatal deaths at UHL were due to congenital anomaly compared to the UK average. The GROW protocol has been implemented in maternity to support earlier recognition of foetal growth retardation. Reflects increased number of patients having an out of hospital cardiac arrest being admitted directly to the Coronary Care Unit at Glenfield. OoHCA patients in other trusts will usually be taken to the Emergency Dept and therefore fewer deaths included in the HSMR/SHMI. Review identified that although the patients had a wound on admission, they had an underlying significant condition (cancer, dementia) which had necessitated hospital stay and had been the primary cause of death. 12
16 Learning From the Deaths of Patients in our Care 13
17 What s involved? In December last year, the Care Quality Commission published its review Learning, candour and accountability: A review of the way NHS Trusts review and investigate deaths of patients in England. In response to the review recommendations, the National Guidance on Learning from Deaths has been published which includes a requirement for Acute Trusts to publish on a quarterly basis: total numbers of in-hospital deaths from 1 st April 2017 numbers of deaths fully reviewed as part of the relevant Specialty M&M process (using the Structured Judgement Review tool (SJR) which is part of the National Mortality Case Record Review programme) number of deaths assessed as having been more likely than not to have been caused by problems in care evidence of learning and action that is happening as a consequence of this information There are certain categories of deaths where a full review is automatically expected (ie patients with Learning Disabilities, Severe Mental Illness, following an elective procedure). Full reviews should also be undertaken where family, carers or staff have raised a concern about the quality of care provision; there is the potential for learning and improvement There is a CUSUM alert for a diagnosis group 14
18 Learning from Deaths Terminology Review vs Investigation Case record review can identify problems with the quality of care so that common themes and trends can be seen, which can help focus organisations quality improvement work. Review also identifies good practice that can be spread. Investigation starts either after case record review or straight after an incident, where problems in care that need significant analysis are likely to exist. Investigation is more indepth than case record review as it gathers information from many additional sources. The investigation process provides a structure for considering how and why problems in care occurred so that actions can be developed that target the causes and prevent similar incidents from happening again. Data generated from case record review and investigation, for example estimates of the number of deaths thought more likely than not to be due to problems in care, are subjective and so not useful for making external judgements about the safety of trusts. Death due to a problem in care: A death that has been clinically assessed using a recognised method of case record review, where the reviewers feel the death is more likely than not to have resulted from problems in care delivery/service provision. Note, this is not a legal term and is not the same thing as cause of death. The term avoidable mortality should not be used as this has a specific meaning in public health that is distinct from death due to problems in care.
19 UHL s Learning from Deaths Framework Medical Examiners (MEs) screen all adult cases, speak to relatives Specialty Mortality & Morbidity Programme (M&M) Mortality Reviews (SJRs), Learning Lessons and taking forward Actions Bereavement Support Nurse (BSN) follow up contact for bereaved families of adult patients Patient Safety Team (PST) Investigation where death considered to be due to problems in care All part of the Trust s Quality Commitment 16
20 UHL s LFD Framework Medical Examiners In order to meet the NHS England requirement of high level assessment of all deaths UHL implemented the Medical Examiner Process (from July 16) which is now in place across all 3 sites Currently we have 11 Senior Consultants providing 10.5 Medical Examiner sessions a week Medical Examiners: Are involved in the death certification and screening of adult in-patient and ED deaths Provide advice to certifying doctor cause of death for the death certificate and which Deaths should be referred to the Coroner (where not nationally mandated) Complete Part 2 of the Cremation Form (LRI only) Speak to the bereaved to confirm they understand the cause of death and also if they have any concerns about care provided Undertake mortality screening of the clinical record (paper and electronic) to see if any potential problems in care Cross reference with the Trust s Patient Safety Incident reporting data as part of the mortality screening process Refer cases to the relevant Specialty M&M for further review or formal structured judgement review as applicable. 17
21 How are deaths in UHL selected for Structured Judgment Review? National requirements for Structured Judgement Review (Case Record Review) Infant and Child Deaths and Maternal Deaths Deaths where the patient had a Learning Disability or Severe Mental Illness Deaths following an elective procedure Deaths where primary diagnosis on admission is part of a SHMI/HSMR alert UHL Medical Examiner Criteria for SJR referral - identified either via case note screening or bereaved relatives feedback or from speaking to the Certifying Doctor All cases identified as having potential problems in care relating to Assessment, Investigation, Diagnosis Medication, IV fluids / Electrolytes / Oxygen Treatment and Management Plan Infection control Operation/Invasive Procedure Clinical Monitoring Resuscitation following cardiac or respiratory arrest Other Criteria for SJR referral Members of the clinical team consider potential learning Bereaved Relatives feedback to Bereavement Support Nurse Death occurred in diagnosis/patient group that is part of a quality improvement work-stream
22 How is the Case Record Review process carried out? Using the Royal College of Physician s Structured Judgement Review method: Involves a detailed review of patient s case notes by a Consultant / Senior Trainee in the relevant Specialty, but not involved in the care of the patient, to assess the quality of care for each phase of admission as shown below: On admission (first 36 hours) - Ongoing Procedural and Post Operative - End of Life/Discharge Each phase given a score of 1 to 5 with a score also being given to the overall care: 1 = very poor care 2 = poor care 3 = adequate care 4 = good care 5 = Excellent care An explicit statement then needs to be given to support the score given for each phase of care / overall, for example: Very good care rapid triage and identification of diabetic ketoacidosis with appropriate treatment. (On admission care = 5) Good documentation of clinical findings, investigation results, management plan and discussion with other teams (Ongoing care = 4) Overall, a fundamental failure to recognise the severity of this patient s respiratory failure (Overall care = 2). The Reviewer is also asked to confirm whether there were problems in care, what type of problems and in which phase of care these occurred. Where problems identified, these are then assessed as to whether caused harm or not 19
23 What are UHL s Death Classification Criteria and Next Steps? Following review of phases of care and confirmation as to whether any problems in care led to harm, deaths are classified in line with the criteria below and action taken accordingly: Category Rationale Next Steps 1* 2* 3* Death is more likely than not to have resulted from a problem in care Problems in care which may have contributed to death but not very likely Problems in care but very unlikely that these contributed to death 4** No problems in care 5** Good or Excellent Care. Upon initial classification of DC = 1 (i.e. by Reviewer, M&M Lead or at MDT M&M): Confirm Category as applicable. Check if reported as Patient Safety Incident (PSI). If not already on Datix as Moderate, Major or Death graded incident, M&M Lead to ensure reported as PSI with Major Harm on Datix. Reporter to advise PSI identified thru SJR Review/M&M. MDT M&M to Escalate to MRC for further review via Mortality Mailbox and Confirm learning and actions. Upon initial classification of DC = 2 (i.e. by Reviewer, M&M Lead or at MDT M&M): Confirm Category as applicable. Check if reported as PSI If not consider if requires reporting as PSI. SJR findings to be reported to MRC via Mortality Mailbox. Update SJR proforma. Confirm learning and actions. Discuss at M&M meeting. Confirm learning and actions and Patient Safety Implications. Update SJR proforma with M&M discussion and send to Mortality Mailbox Confirm if any learning and disseminate accordingly. Update SJR proforma if discussed at M&M meeting and send to Mortality Mailbox Confirm if any learning /sharing of best practice and disseminate accordingly. Update SJR proforma if discussed at M&M meeting and send to Mortality Mailbox * MUST be discussed at Specialty M&M ** Death Classification can be signed off by M&M Lead
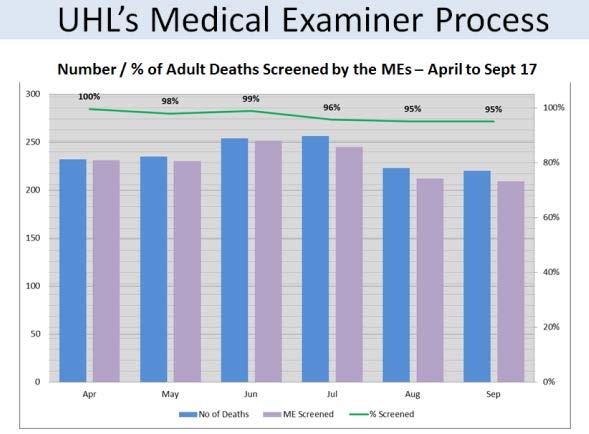
24 UHL s Learning from Death process April to September 17 PLACE OF DEATH ADULT / CHILD / NEONATE NUMBER OF DEATHS ED 88 Adult 85 Child 3 Inpatient 1358 Adult 1308 Child 13 Neonate 37 TOTAL 1446 What is the data telling us? UHL is one of the England top 5 trusts for activity and also for the number of deaths. The table above shows the number of patients who died either in the Emergency Department or as an in-patient. Neonates are babies who are born in UHL or in another hospital and transferred to our Neonatal Unit. 21

25 UHL s Medical Examiner Process Number / % of Adult Deaths Screened by the MEs April to Sept 17 What. is the data telling us? UHL target is 95% of all Adult Deaths to be screened Of the Jul to Sept cases not yet screened, most were referred to the Coroner and cause of death details required to inform ME Screening 22
26 Structured Judgement Review Criteria What is the data telling us? ME referral for SJR makes up over half the cases with paediatric/neonatal deaths being the next largest group. 23
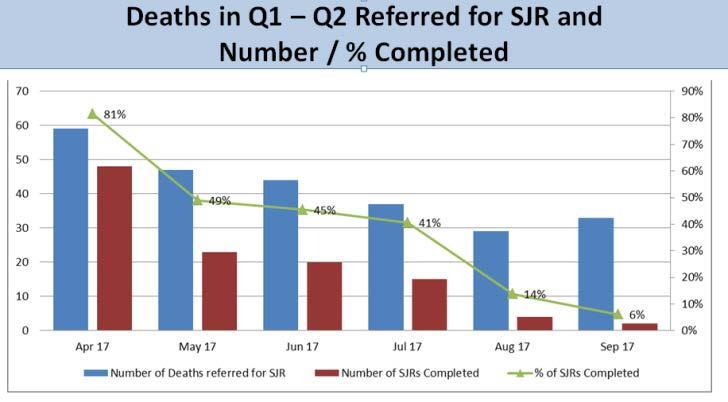
 Following discussion with the Specialty M&M Leads, an internally set target for completion of SJRs was")
27 Deaths in Q1 Q2 Referred for SJR and Number / % Completed What is the data telling us? 112 of the 249 cases referred for SJR between April to September 17 have been completed (45%) Following discussion with the Specialty M&M Leads, an internally set target for completion of SJRs was agreed as: 75% within 4 months of death and 100% within 6 months. Therefore all April s deaths should have had SJRs completed at the end of October and 75% of May and June s deaths should have had completed SJRs. However, not all SJR details have been collated due to capacity constraints within the Corporate M&M Admin team and capacity within the Specialty 24 M&M teams.
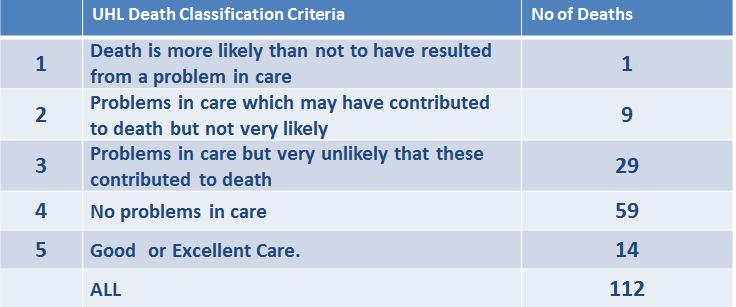
28 Death Classifications where SJR Completed UHL Death Classification Criteria Death is more likely than not to have resulted from a problem in care Problems in care which may have contributed to death but not very likely Problems in care but very unlikely that these contributed to death No of Deaths 4 No problems in care 59 5 Good or Excellent Care. 14 ALL What is the data telling us? The number of deaths where there was a problem in care that contributed to the patient s death is small. In a significant number of cases, no problems were found or good or excellent care was identified. The death in Category 1 has been investigated as a Serious Incident and identified multiple contributory factors with specific learning for both ED and the Difficult Asthma Clinic at Glenfield. 25
29 Learning from Deaths Quarters 1 & 2 Wide range of learning identified but most fall into the following categories: Escalation of the deteriorating patient / sepsis treatment / acting on results Communication where bloods or investigations not carried out Senior review / Setting of Ceilings of Care Recognition of patients at the end of life Actions being taken For most cases, the actions were around raising awareness and disseminating the clinical teams lessons learnt specifically: risk of paralytic ileus for patients receiving chemotherapy risk of sudden deterioration of patients with endocarditis risks for patients on long term steroids importance of referral to Anticoagulation clinic 26
30 How is UHL engaging with bereaved families and carers 27
31 Bereavement Support Service Follow up contact by the Bereavement Support Service is offered to the bereaved relative/carer for all UHL deaths. Contact is made by the Bereavement Support Nurse (BSN) 6-8 weeks after the death 60% of bereaved requested follow up in Quarter 1 and 60% of those were spoken to by phone (letter sent to all where the Bereavement Support Nurse was unable to make telephone contact) Further information was requested by 38 families as part of the follow up contact Meetings with the clinical team were facilitated for 15 families Signposting to bereavement services eg CRUSE, LOROS, Sharma Women s Centre, Child Bereavement UK was given to 60 bereaved relatives/carers 28
32 Deaths being investigated under the Serious Incident framework Deaths for investigation have been identified by: ME mortality screening SJR Patient Safety Incident reporting 4 deaths have been investigated in Q1 and Q2 1 investigation has been completed and confirmed as a serious incident (relates to case given a Death Classification of 1 in slide 25) Remaining 3 investigation ongoing 29




33 December 2017 Learning from the Deaths of Patients in our Care Q1&2 Summary
Learning from the Deaths of Patients in our Care Policy
 Learning from the Deaths of Patients in our Care Policy Approved By: Date of Original Approval: UHL Mortality Review Committee UHL Policies & Guidelines Committee September 2017 Trust Reference: B31/2017
Learning from the Deaths of Patients in our Care Policy Approved By: Date of Original Approval: UHL Mortality Review Committee UHL Policies & Guidelines Committee September 2017 Trust Reference: B31/2017
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Mortality Policy - Learning from Deaths (CG627)
") Mortality Policy - Learning from Deaths (CG627) Approval Approval Group Job Title, Chair of Committee Date Policy Approval Group Chair, Policy Approval Group September 2017 Change History Version Date
Mortality Policy - Learning from Deaths (CG627) Approval Approval Group Job Title, Chair of Committee Date Policy Approval Group Chair, Policy Approval Group September 2017 Change History Version Date
TRUST CORPORATE POLICY RESPONDING TO DEATHS
 SCOPE OF APPLICATION AND EXEMPTIONS CONSULT ATION COR/POL/224/2017-001 TRUST CORPORATE POLICY RESPONDING TO DEATHS APPROVING COMMITTEE(S) EFFECTIVE FROM DISTRIBUTION RELATED DOCUMENTS STANDARDS OWNER AUTHOR/FURTHER
SCOPE OF APPLICATION AND EXEMPTIONS CONSULT ATION COR/POL/224/2017-001 TRUST CORPORATE POLICY RESPONDING TO DEATHS APPROVING COMMITTEE(S) EFFECTIVE FROM DISTRIBUTION RELATED DOCUMENTS STANDARDS OWNER AUTHOR/FURTHER
h. HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST LEARNING FROM DEATHS POLICY. Broad Recommendations / Summary
 201 2017.473h. HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST LEARNING FROM DEATHS POLICY Broad Recommendations / Summary In-hospital death occurs. Patient 18 years of age or above. Yes Child Death Review
201 2017.473h. HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST LEARNING FROM DEATHS POLICY Broad Recommendations / Summary In-hospital death occurs. Patient 18 years of age or above. Yes Child Death Review
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Mortality Policy. Learning from Deaths
 Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Learning from Deaths Policy
 Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Learning from Deaths Policy
 Policy Author: Owner: Publisher: Version: 1 Peter Wanklyn, Helen Noble Medical Director Medical Governance Date of version issue: September 2017 Approved by: Executive Board Date approved: September 2017
Policy Author: Owner: Publisher: Version: 1 Peter Wanklyn, Helen Noble Medical Director Medical Governance Date of version issue: September 2017 Approved by: Executive Board Date approved: September 2017
Learning from Deaths; Mortality Review Policy
 Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Mortality Report. 1. Introduction / Background
 Mortality Report 1. Introduction / Background 1.1 The Board is reminded of the findings from the CQC review in December 2016, 'Learning, candour and accountability: a review of the way trusts review and
Mortality Report 1. Introduction / Background 1.1 The Board is reminded of the findings from the CQC review in December 2016, 'Learning, candour and accountability: a review of the way trusts review and
MORTALITY REVIEW & LEARNING FROM DEATHS POLICY
 MORTALITY REVIEW & LEARNING FROM DEATHS POLICY Document Reference Document status Target Audience MD25.MRLD.V1.1 Final All clinical staff involved in mortality case record reviews and investigations and
MORTALITY REVIEW & LEARNING FROM DEATHS POLICY Document Reference Document status Target Audience MD25.MRLD.V1.1 Final All clinical staff involved in mortality case record reviews and investigations and
RM57 HOSPITAL MORTALITY REVIEW POLICY
 RM57 HOSPITAL MORTALITY REVIEW POLICY Version: 1 Name of ratifying committee: Clinical Quality Assurance Committee Date ratified: 20 th September 2017 Name of originator/author: Julie Grice, Chair of Hospital
RM57 HOSPITAL MORTALITY REVIEW POLICY Version: 1 Name of ratifying committee: Clinical Quality Assurance Committee Date ratified: 20 th September 2017 Name of originator/author: Julie Grice, Chair of Hospital
SWH Mortality Review Policy
 Corporate Governance SWH 01785 The Trust s Intranet holds the current approved guidance documents. Notice to staff using a paper copy of this document. Staff must ensure that they are using the most up-to-date
Corporate Governance SWH 01785 The Trust s Intranet holds the current approved guidance documents. Notice to staff using a paper copy of this document. Staff must ensure that they are using the most up-to-date
LEARNING FROM DEATHS (Mortality Policy)
") LEARNING FROM DEATHS () Version: 1.0 Date issued: October 2017 Review date: September 2020 Applies to: All Clinical Staff Groups This document is available in other formats, including easy read summary
LEARNING FROM DEATHS () Version: 1.0 Date issued: October 2017 Review date: September 2020 Applies to: All Clinical Staff Groups This document is available in other formats, including easy read summary
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Mortality Monitoring Policy
 Mortality Monitoring Policy Document Information Version: 3.0 Date: 25/07/2016 Ratified by: King s Executive Date ratified: 31 July 2017 Author(s): Responsible Director: Responsible committee: Date when
Mortality Monitoring Policy Document Information Version: 3.0 Date: 25/07/2016 Ratified by: King s Executive Date ratified: 31 July 2017 Author(s): Responsible Director: Responsible committee: Date when
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
Active date: 25 th Sept Exclusions: None
 Trust Policy Title: Mortality review Author(s): James Coulston - Mortality Lead, Stuart Walker - Medical Director, Lincoln Andrews - Compliance and Audit Manager, Charlie Davis - Palliative Care Lead Document
Trust Policy Title: Mortality review Author(s): James Coulston - Mortality Lead, Stuart Walker - Medical Director, Lincoln Andrews - Compliance and Audit Manager, Charlie Davis - Palliative Care Lead Document
Learning from Deaths Policy
 Learning from Deaths Policy Document Reference No. CLIN041v4 Version No. 4 Issue Date 16/11/2017 Review Date 1 st September 2020 Document Author Document Owner Accountable Executive Approved by Deputy
Learning from Deaths Policy Document Reference No. CLIN041v4 Version No. 4 Issue Date 16/11/2017 Review Date 1 st September 2020 Document Author Document Owner Accountable Executive Approved by Deputy
Using the structured judgement review method
 National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
Indicator 5c Mortality Survey
 Indicator 5c Mortality Survey Undertaken by NCEPOD on behalf of NHS England Dr Neil Smith - Clinical Researcher and Deputy CEO Dr Hannah Shotton - Clinical Researcher Dr Marisa Mason - Chief Executive
Indicator 5c Mortality Survey Undertaken by NCEPOD on behalf of NHS England Dr Neil Smith - Clinical Researcher and Deputy CEO Dr Hannah Shotton - Clinical Researcher Dr Marisa Mason - Chief Executive
National Mortality Case Record Review Programme. Using the structured judgement review method A guide for reviewers (England)
") National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
Surrey & Sussex Healthcare NHS Trust. Learning from Deaths (Mortality Review) Policy
 Policy") Surrey & Sussex Healthcare NHS Trust Learning from Deaths (Mortality Review) Policy Status (Draft/ Ratified): Ratified Date ratified: 14/09/2017 Version: 1 Ratifying Board: Effectiveness Committee Approved
Surrey & Sussex Healthcare NHS Trust Learning from Deaths (Mortality Review) Policy Status (Draft/ Ratified): Ratified Date ratified: 14/09/2017 Version: 1 Ratifying Board: Effectiveness Committee Approved
CRM012 - Identifying, Reporting, Investigating And Learning From Deaths In Care
 CRM012 - Identifying, Reporting, Investigating And Learning From Deaths In Care 1 Table of Contents Why we need this Policy 3 What the Policy is trying to do..3 Which stakeholders have been involved in
CRM012 - Identifying, Reporting, Investigating And Learning From Deaths In Care 1 Table of Contents Why we need this Policy 3 What the Policy is trying to do..3 Which stakeholders have been involved in
Unique Identifier: Review Date: November Issue Status: Approved Version No: 1.4 Issue Date: November 2017
 Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
LEARNING FROM DEATHS POLICY
 Issue number: 1st Edition LEARNING FROM DEATHS POLICY Author with contact details Dr Neil Mercer, Associate Medical Director for Clinical Governance Neil.mercer@aintree.nhs.uk tel. 529-5152 Original Issue
Issue number: 1st Edition LEARNING FROM DEATHS POLICY Author with contact details Dr Neil Mercer, Associate Medical Director for Clinical Governance Neil.mercer@aintree.nhs.uk tel. 529-5152 Original Issue
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Learning from Deaths - Mortality Report
 Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Evidence Search Completed by..joanne Phizacklea.Date
 Document Type: Procedure Unique Identifier: CORP/PROC/073 Document Title: Mortality Review Process Scope: Consultants, Nursing Staff, Clinical Coding Staff, Clinical Audit & Effectiveness Staff, Quality
Document Type: Procedure Unique Identifier: CORP/PROC/073 Document Title: Mortality Review Process Scope: Consultants, Nursing Staff, Clinical Coding Staff, Clinical Audit & Effectiveness Staff, Quality
Quality Improvement Strategy
 / Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
/ Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
CO119, Learning from Deaths policy
 CO119, Learning from Deaths policy Consultation Draft v.1* September 2017 *Awaiting standardised Structured Judgement Review for Mental Health Trusts & wider consultation with workforce and stakeholder
CO119, Learning from Deaths policy Consultation Draft v.1* September 2017 *Awaiting standardised Structured Judgement Review for Mental Health Trusts & wider consultation with workforce and stakeholder
Learning from Deaths Policy
 Learning from Deaths Policy September 2017 To be reviewed by April 2018 Contents Page 1 Introduction 3 2 Scope 4 3 Purpose 4 4 SHMI/HSMR data 5 5 Roles and responsibilities 6 6 Definitions 11 7 Deaths
Learning from Deaths Policy September 2017 To be reviewed by April 2018 Contents Page 1 Introduction 3 2 Scope 4 3 Purpose 4 4 SHMI/HSMR data 5 5 Roles and responsibilities 6 6 Definitions 11 7 Deaths
Document Title Investigating Deaths (Mortality Review) Policy
 Policy") Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Assessing Quality of Hospital Services - the importance of national clinical audits
 Assessing Quality of Hospital Services - the importance of national clinical audits Professor Sir Mike Richards Chief Inspector of Hospitals November 2015 1 Overview CQC s role and purpose Our approach
Assessing Quality of Hospital Services - the importance of national clinical audits Professor Sir Mike Richards Chief Inspector of Hospitals November 2015 1 Overview CQC s role and purpose Our approach
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
National Clinical Audit & Patient Outcome Programme: An update
 National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
National Clinical Audit & Patient Outcome Programme: An update Jenny Mooney Director of Operations www.hqip.org.uk Healthcare Quality Improvement Partnership Our structure and funding The National Clinical
SUBJECT: CLINICAL GOVERNANCE
 Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Learning from Deaths Trust Board in public
 Learning from Deaths Trust Board in public Date: 30 th August 2018 Agenda item: 2.4 Executive sponsor Professor Des Holden Medical Director Dr Richard Brown Director of Outcomes Report author(s) Jonathan
Learning from Deaths Trust Board in public Date: 30 th August 2018 Agenda item: 2.4 Executive sponsor Professor Des Holden Medical Director Dr Richard Brown Director of Outcomes Report author(s) Jonathan
Bereavement Policy. 1 Purpose of Policy 2. 2 Background 2. 3 Staff Responsibilities 3. 4 Operational Issues and Local Policies/Protocols/Guidelines 4
 Trust Policy and Procedure Bereavement Policy Document Ref. No: PP(16)252 For use in: For use by: For use for: Document owner: Status: All areas of the Trust All Trust staff The dying, their relatives
Trust Policy and Procedure Bereavement Policy Document Ref. No: PP(16)252 For use in: For use by: For use for: Document owner: Status: All areas of the Trust All Trust staff The dying, their relatives
Learning from Deaths, Mortality Review Policy
 Learning from Deaths, Mortality Review Policy Policy Number: 981 Version: 1.0 Category Authorisation Committee/Group Clinical Patient Safety Committee Date of Authorisation: 29 th August 2017 Ratification
Learning from Deaths, Mortality Review Policy Policy Number: 981 Version: 1.0 Category Authorisation Committee/Group Clinical Patient Safety Committee Date of Authorisation: 29 th August 2017 Ratification
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Paper 8 DECISION NOTE. Recommendation
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Warrington and Halton Hospitals NHS Foundation Trust Quality Report
 Warrington and Halton Hospitals NHS Foundation Trust Quality Report 2016-2017 Contents Part 1 Statement of Quality from the Chief Executive 7 Part 2 Improvement Priorities & Statement of Assurance from
Warrington and Halton Hospitals NHS Foundation Trust Quality Report 2016-2017 Contents Part 1 Statement of Quality from the Chief Executive 7 Part 2 Improvement Priorities & Statement of Assurance from
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Northumbria Healthcare NHS Foundation Trust. Clinical Governance Policies and Procedures
 Clin Gov 108 Northumbria Healthcare NHS Foundation Trust Clinical Governance Policies and Procedures Learning from Deaths Policy Version 1 Sub Committee & approval date Mortality and Outcomes Data Group
Clin Gov 108 Northumbria Healthcare NHS Foundation Trust Clinical Governance Policies and Procedures Learning from Deaths Policy Version 1 Sub Committee & approval date Mortality and Outcomes Data Group
Integrated Quality Report
 Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Percent Unadjusted Inpatient Mortality (NHSL Acute Hospitals) Numerator: Total number of in-hospital deaths
 Numerator: Total number of in-hospital deaths") Page 1 of 23 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable harm, a sustainable infrastructure for patient
Page 1 of 23 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable harm, a sustainable infrastructure for patient
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Policy on Learning from Deaths
 Policy on Learning from Deaths Version number: 1 Consultation: Governance Committee Board Committee Director of Quality Assistant Director of Governance & Compliance Patient Safety Manager Ratified by:
Policy on Learning from Deaths Version number: 1 Consultation: Governance Committee Board Committee Director of Quality Assistant Director of Governance & Compliance Patient Safety Manager Ratified by:
Pressure ulcers: revised definition and measurement. Summary and recommendations
 Pressure ulcers: revised definition and measurement Summary and recommendations June 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that are
Pressure ulcers: revised definition and measurement Summary and recommendations June 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that are
Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - October 2015
 Page 1 of 22 Print :15/1/215 Page 2 of 22 Print :15/1/215 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable
Page 1 of 22 Print :15/1/215 Page 2 of 22 Print :15/1/215 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust
 Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
TRUST BOARD/DIRECTORS GROUP 2016 Key Performance Indicators
 TRUST BOARD/DIRECTORS GROUP 2016 Key Performance Indicators Introduction This paper provides an update on our progress towards our vision to be England s best acute teaching trust in 2016 and beyond. The
TRUST BOARD/DIRECTORS GROUP 2016 Key Performance Indicators Introduction This paper provides an update on our progress towards our vision to be England s best acute teaching trust in 2016 and beyond. The
Learning From Deaths Policy
 Learning From Deaths Policy The purpose of this policy is to provide a systematic approach to ensure that the Trust has robust governance arrangements in place to review, report and learn from patient
Learning From Deaths Policy The purpose of this policy is to provide a systematic approach to ensure that the Trust has robust governance arrangements in place to review, report and learn from patient
LEARNING FROM DEATHS POLICY
 Summary LEARNING FROM DEATHS POLICY Learning from a review of the care provided to patients who die is integral to a provider s clinical governance and quality improvement work. To fulfil the standards
Summary LEARNING FROM DEATHS POLICY Learning from a review of the care provided to patients who die is integral to a provider s clinical governance and quality improvement work. To fulfil the standards
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Sepsis Collaborative May 2015 Report
 Report Table of Contents Background... 3 Collaborative set up... 3 Impact... 4 Process measures... 4 Outcome measures... 4 1. Coding... 4 2. Mortality in patients undergoing a blood culture... 5 Sustainability...
Report Table of Contents Background... 3 Collaborative set up... 3 Impact... 4 Process measures... 4 Outcome measures... 4 1. Coding... 4 2. Mortality in patients undergoing a blood culture... 5 Sustainability...
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Using mortality data to improve the quality and safety of patient care December 2015
 Using mortality data to improve the quality and safety of patient care December 2015 Version Date Published Notes 12.0 18/12/2015 12 th publication 11.0 18/09/2015 11 th publication 10.0 19/06//2015 10
Using mortality data to improve the quality and safety of patient care December 2015 Version Date Published Notes 12.0 18/12/2015 12 th publication 11.0 18/09/2015 11 th publication 10.0 19/06//2015 10
Reducing In-hospital Mortality
 Advancing Quality Alliance Reducing In-hospital Mortality Observations arising from AQuA s work May 2013 Contents Introduction and background Understanding mortality rates Mortality rates SMR methodologies
Advancing Quality Alliance Reducing In-hospital Mortality Observations arising from AQuA s work May 2013 Contents Introduction and background Understanding mortality rates Mortality rates SMR methodologies
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme
 The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
A summary of: Five years of cerebral palsy claims
 A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
Hospital Standardised Mortality Ratios
 Hospital Standardised Mortality Ratios Quarterly Release Publication date 15 May 2018 A National Statistics publication for Scotland This is a National Statistics Publication National Statistics status
Hospital Standardised Mortality Ratios Quarterly Release Publication date 15 May 2018 A National Statistics publication for Scotland This is a National Statistics Publication National Statistics status
Quality Strategy: Liverpool Women s NHS Foundation Trust
 Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
NLG (15) 401. DATE 29 September Trust Board of Directors Public REPORT FOR. Mr Lawrence Roberts, Medical Director REPORT FROM
 401. DATE 29 September Trust Board of Directors Public REPORT FOR. Mr Lawrence Roberts, Medical Director REPORT FROM") NLG (15) 401 DATE 29 September 2015 REPORT FOR Trust Board of Directors Public REPORT FROM Mr Lawrence Roberts, Medical Director CONTACT OFFICER Jeremy Daws, Head of Quality Assurance SUBJECT Monthly Mortality
NLG (15) 401 DATE 29 September 2015 REPORT FOR Trust Board of Directors Public REPORT FROM Mr Lawrence Roberts, Medical Director CONTACT OFFICER Jeremy Daws, Head of Quality Assurance SUBJECT Monthly Mortality
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP. Corporate Parenting Board. Date of Meeting: 23 rd Feb Agenda item: ( 7 )
") WOLVERHAMPTON CLINICAL COMMISSIONING GROUP Corporate Parenting Board Agenda Item No. 7 Health Services for Looked After Children Annual Report September 2014 -August 2015 Date of Meeting: 23 rd Feb 2016.
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP Corporate Parenting Board Agenda Item No. 7 Health Services for Looked After Children Annual Report September 2014 -August 2015 Date of Meeting: 23 rd Feb 2016.
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement