Mortality Report. 1. Introduction / Background
|
|
|
- Georgia Singleton
- 5 years ago
- Views:
Transcription
1
2
3 Mortality Report 1. Introduction / Background 1.1 The Board is reminded of the findings from the CQC review in December 2016, 'Learning, candour and accountability: a review of the way trusts review and investigate the deaths of patients in England'. The review found that some providers were not giving learning from deaths sufficient priority and so were missing valuable opportunities to identify and make improvements in quality of care. In March 2017, the National Quality Board (NQB) introduced new guidance for NHS providers on how they should learn from the deaths of people in their care. NHS Improvement are now leading this agenda and supporting trusts to meet the requirements of the new guidance. The purpose of the report is to present the current positon of mortality rates to the Board and the Trust s progress in implementing the National Guidance on Learning from Deaths (2017). 2. Review of RCHT Mortality Data 2.1 RCHT mortality data is submitted to an online benchmarking solution for healthcare called Healthcare Evaluation Data (HED). HED was developed by United Hospitals Birmingham NHS Foundation Trust. RCHT uses the following mortality indices when comparing its mortality data with other similar trusts: 2.2 The Hospital Standardised Mortality Ratio (HSMR) The HSMR is calculated each month for each hospital in England. It includes deaths in the most common conditions in hospital which account for around 80% of deaths in hospital. HSMR is the ratio of observed to expected deaths, multiplied by 100, from 56 baskets of the 80% most common diagnoses. If the HSMR is above 100 then there are more observed deaths than expected deaths. Upper and lower Confidence Intervals are applied to the HSMR. HSMRs with values between the confidence intervals are consistent with random or chance variation. To have a red flag means that that the HSMR is above 100 and the lower Confidence Interval Value is also above 100 which signifies that the variation is unlikely to be due to random or chance variation and that other issue may be causing this variation. These are the HSMRs that the trust refers to as Red Flags. RCHT is alerted to Red Flags using the dashboards and tools provided HED 2.3 Summary Hospital-level Mortality Indicator (SHMI) The SHMI score includes all deaths in hospital and within 30 days of discharge from hospital. 1
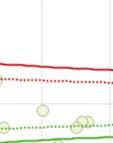
4 2.4 HSMR data (Rolling 12 month period Sept 16 to Aug 17) The RCHT mortality position has continued on its improved trajectory with a 12 month rolling HMSR of sitting well below the national benchmark of 100. In addition to improved overall mortality, we have seen a progressive narrowing of the differential between the HMSR for patients admitted at the weekend and for patients admitted during the week (the so called weekend effect). For the rolling 12 month period the weekend and non-weekend HMSR s were weekend 96.81, non-weekend Rolling 12 month HSMR Sep 16 Oct 16 Nov 16 Dec 16 Jan 17 Feb 17 Mar 17 Apr 17 May 17 Non weekend Weekend Grand Total Jun 17 Jul 17 Aug 17 2













5 SHMI data The SHIMII data for Aug 2016 July 2017 was well below the national benchmark of
6 2.5.2 Despite the overall positive picture however, the Trust has two diagnostic group red flags alerting on HSMR. The first refers to acute cerebrovascular disease (stroke). We have been aware of this flag for some time and made improvements in the stroke pathway in November 2016 by creating a dedicated stroke unit, two hyper-acute stroke beds and a 24/7 stroke nurse outreach provision to the Emergency Department to increase the number of patients admitted with stroke getting to the stroke unit within four hours. This criterion is one of the key determinants of good stroke outcomes. We have also recently flagged nationally (on 6/10/2017) on the Sentinel Stroke National Audit Programme (SSNAP). We had already commissioned the Stroke Team to perform a deep dive review of stroke mortality. This included an analysis of the Local Stroke Database and coding, and an in-depth case review on a series of 50 stroke deaths The case review was performed using structured judgement review (SJR) methodology as recommended by the National Guidance on Learning from Deaths. The results were very reassuring with the overall care judged as excellent or good in 44 cases. In no case was the care scored as poor. The coding and data recording review identified a number of issues that contribute to the reported increased mortality. The first was the inclusion in the Local Stroke Database of a number of patients who did not have a primary diagnosis of stroke: including patients with traumatic sub-arachnoid haemorrhage and those with a secondary diagnosis of stroke with an alternative primary diagnosis. Secondly, a number of cases with a primary diagnosis of stroke who survived were not captured on the Local Stroke Database. Finally RCHT currently treats a number of patients with minor stroke through the outpatient TIA Service rather than through inpatient pathways. All three of these factors may therefore have potentially have worsened the reported Stroke Mortality Rate The findings from the in depth case review process and the data quality analysis have been sent to Professor Tony Rudd at SSNAP for further comment. We are reviewing performance of the stroke team on a monthly basis through the stroke operational group meeting. Our current priorities are developing a responsive TIA clinic that is co-located with the stroke unit allowing assessment and treatment of all patients referred with a TIA within 24 hours. It further includes a business case for 7- day therapy cover and expanding the consultant workforce allowing review of stroke patients by a consultant trained in stroke medicine with 14 hours of arrival The stroke team are keen to improve the performance of the stroke team and pathway. Members of the team partook in the Stroke Improvement Program in Senior members of the RCHT stroke service visited the Bournemouth stroke team in 2011 and have emulated their CT scanning pathway. We were visited by the British Associated of Stroke Physicians (BASP) and Royal College of Physician Stroke Peer Review team in 2012 who gave us good advice, and also by Professor Tony Rudd in On his advice we went to visit the Beacon stroke unit at St George s hospital to emulate some of their practices. A further BASP / RCP visit has been planned (no date fixed as yet) with the national stroke team to review our stroke care pathway and we continue to review performance at the monthly stroke operational group meeting There is a high rate of atrial fibrillation (AF) related strokes and the percentage of patients who are not on anticoagulation in the community is high (58% as per recent SSNAP audit). The stroke service is working with the commissioners and healthcare colleagues in the community to address this, ie endeavour to identify and treat atrial fibrillation earlier in patients in the community. 4
7 2.5.7 Stroke has not flagged in the most recent HED data set (Sept 16 to Aug 17) The second red flag is for other perinatal conditions. This refers to stillbirth. Although it is a recent red flag, the issue of data collection in stillbirth has been an historical concern for RCHT. This is reflected in national reporting to MBRRACE-UK, where the reported increased rate of stillbirth was felt to reflect under reporting of the total number of births in Cornwall. The Mortality Review and Oversight Committee (November 2017) has requested a deep dive into stillbirth. 2.6 Mortality review at RCHT The National Guidance for Learning from death guidance 2017 requires each trust to publish the following: Trust data on the total number of deaths from the previous quarter Those deaths that have been subject to case review Estimates of those judged more likely than not to be due to problems in care The learning points 2.7 Current situation (Quarter 2) The review of deaths for July September is displayed in the local RCHT dashboard see Appendix Current process: RCHT aims to review 100% of its deaths using a short screening form and then in-depth review where a concern has been raised. Some specialities, most notably critical care, review all of their deaths on an in-depth form There is a 1-5 grading scheme on the screening form. Any screened death graded as a 4 there were areas of concern which may have contributed to the patient's death is subject to an in depth review on the local Trust form Any death graded as a 5 there were areas of concern which significantly contributed to the death of this patient, who would otherwise have been expected to survive is reported on the Trust s incident reporting system, Datix, and considered for classification as a serious incident (SI) that is externally reportable, with a full investigation using root cause analysis techniques Although most specialities are able to review the majority of their deaths on a screening form, specialities which experience a large volume of patient deaths such as care of the elderly and respiratory medicine have struggled to do so, because of the number of case reviews required and on-going senior medical staff shortages For Q2 the existing Trust mortality processes were employed to review deaths. During Q2, there were 411 deaths of which 186 (45%) were reviewed. Of these, five concerns deaths were identified; 3 deaths were graded as 4 and 2 as 5 on the system described above. One of the deaths graded as 5 has been declared an SI and the other is currently going through the grading process. Of the 3 grade 4 deaths which were subject to in-depth mortality reviews, the following issues were highlighted: poor junior doctor handover, failure to recognise and escalate the deteriorating patient (two cases), failure to comment on and repeat abnormal blood test results, untreated sepsis, and delay in recognition of a complication of surgery., In total 6 SIs were declared in this period. Of these, one was identified through the mortality review process and five were declared through the Datix incident reporting 5
8 system, and are all investigations are currently in process. One of these was a paediatric death which occurred after transfer of the child to a regional centre For Q2, there were also three completed SI reports on three different patients, whose deaths occurred prior to this period, where death was judged to be avoidable. Review of these highlighted the following: Tumour lysis syndrome o In patients at high risk of tumour lysis syndrome as a result of chemotherapy, this should be clearly identified with an appropriate management plan and the renal physicians made aware. Such patients should receive their chemotherapy early in the day to facilitate appropriate monitoring. Medical and nursing staff should be educated on any new drugs uploaded onto the Aria system. Failure to monitor and supply oxygen therapy for transportation on discharge o Care rounding and observations need to be recorded for patients in the discharge lounge. Staff need to be aware of the importance of booking oxygen for patient and the expected length of transportation time. Staff need to be competent in the delivery of supplemental oxygen. Failure to detect the deteriorating patient The importance of correct selection procedures and induction/training of overseas staff. Now, new overseas nurses attend a patient observations and NEWS study day. This is a full day s training and covers recognising the deteriorating patient, sepsis, normal parameters for patient observations, how to complete the NEWS and how to carry out patient observations following the Royal Marsden's current guidelines. They undertake practical assessment in the clinical skills area in the knowledge Spa and are then enrolled as part of RCH preceptee programme In addition to our existing processes, we have included three of the priority groups identified in the National Guidance 2.8 Learning Disabilities These are patient deaths in cases where learning disabilities were identified. For Q2, there were two such cases. In these cases, the deaths were reviewed by both the Trust Mortality lead and the Learning Disabilities team, using SJR methodology recommended by the National Guidance on Learning from Deaths Neither death was judged to be potentially avoidable. No concerns were identified in the first case. In the second case, which was a subject of post mortem examination, death was judged not to be avoidable but there were some concerns identified around venous thrombosis (VTE) management, lack of a treatment escalation plan (TEP) and lack of death certificate data or evidence of discussion with the Coroner. 2.9 Perinatal/Stillbirths awaiting report from Karen Stoyles All neonatal deaths (NNDs) and stillbirths (SB) are reviewed in the weekly Multidisciplinary Patient Safety Meeting which is led by a consultant obstetrician and attended by other obstetricians, midwives and anaesthetists. In addition they are 6
9 presented and discussed in the monthly Perinatal Mortality Meeting involving midwives, obstetricians and neonatologists. Any cases where substandard care is identified which was likely to have changed the outcome would normally be subjected to an SI investigation In Q2 there 3 stillbirths, 3 NND s (>24 weeks) and 2 NND s (<24 weeks therefore pre-viable). Of the stillbirths there was no cases in which the care was inadequate to the extent that the death would have been avoided. There was one case in which there was a delay in investigating a report of decreased fetal movements however when the patient came to the Day Assessment Unit the fetal movements appeared to be normal and the CTG s appeared to show both babies had normal heart rate traces Of the 3 cases of NND >24 weeks the babies had either known chromosomal or other lethal conditions incompatible with life. The other 2 deaths were of pre-viable foetuses who showed signs of life at delivery but died of prematurity There was one potentially avoidable death, the learning from which focused around the need to ensure that in twin pregnancies, the foetuses are monitored independently on cardiotocography 2.10 Paediatric/Child deaths There was 1 paediatric death that was unavoidable Complaints about the care of a patient who has died There were complaints surrounding the deaths of 2 patients in Q2. One of these is closed and one remains open. In the complaint that is closed, the death was not regarded as avoidable but there were issues identified regarding death certification and discussion of safe-guarding concerns related to out of hospital care with the coroner. This resulted in a delay in the funeral and caused obvious distress to the relatives of the deceased.as a result of this complaint, there have been several changes in Trust policy namely; all juniors have been instructed to discuss the cause of death with their consultant or his/her deputy before completion of death certificates. The coroner s office has been asked to consult the responsible consultant in the first instance, rather than a junior doctor, where there are queries about a death. The Trust legal team have been asked to involve a junior doctor s consultant in any case where a junior has been asked to provide any additional information to the coroner. The bereavement office has been made aware of the above Learning from deaths Learning identified from adult deaths for Q2 will be included in the December 2017 Mortality Newsletter Learning from paediatric deaths is shared via the following methods: urgent learning identified is shared via message of the week - read out at multidisciplinary handover. Mortality reviews are presented at the paediatric business/governance meeting. Important learning is shared through the risk management newsletter. The child death mortality meeting reviews in-hospital deaths and the deaths of local children who have died in regional hospitals. Child Death Overview Panel (CDOP) panels (responsibility of the Local Safeguarding Children s Board) review all deaths. Cornwall and the Isles of Scilly have a joint CDOP with Plymouth SCP and Devon 7
10 and Torbay SCP. The overall aim of CDOP is to understand how and why children die; and when necessary to put in place interventions that will help to safeguard children in the future Learning from perinatal/stillbirth Learning is shared through the risk management newsletter, staff safety briefings and communication from the matron for antenatal and day assessment unit areas with staff. 3. Recommendations of the National Guidance on Learning from Deaths The priority groups for case record review are as follows: i. all deaths where bereaved families and carers, or staff, have raised a significant concern about the quality of care provision; ii. all in-patient, out-patient and community patient deaths of those with learning disabilities (either through the LeDeR review in those regions where the programme is available or by using Structured Judgement Review (SJR) or another robust and evidence-based methodology, or severe mental illness. Note the LeDeR programme is not yet available in Cornwall; iii. all deaths in a service specialty, particular diagnosis or treatment group where an alarm has been raised with the provider through whatever means (for example via a Summary Hospital-level Mortality Indicator or other elevated mortality alert, concerns raised by audit work, concerns raised by the CQC or another regulator); iv. all deaths in areas where people are not expected to die, for example in relevant elective procedures; v. deaths where learning will inform the provider s existing or planned improvement work, vi. a further sample of other deaths that do not fit the identified categories so that providers can take an overview of where learning and improvement is needed most overall. 3.2 The above minimum requirements are additional to existing requirements for providers to undertake specific routes of reporting, review or investigations for specific groups of patient deaths, such as deaths of patients detained under the Mental Health Act Providers should review a case record review following any linked inquest and issue of a Regulation 28 Report on Action to Prevent Future Deaths 3.4 Providers should apply rigorous judgement to the need for deaths to be subject to a Serious Incident reporting and investigation. For example, there may be instances where deaths clearly meet Serious Incident criteria and should be reported as such (whether or not a case record review has already been undertaken). Equally, problems identified in case record review may lead to the need for investigation whether this is an investigation under the Serious Incident Framework or other framework/procedure 3.5 Progress against the above recommendations An updated mortality review policy was submitted to Trust Board (Sept 2017) and approved incorporating processes to align RCHT mortality review to National Guidance on Learning from Deaths (2017). 8
11 3.5.2 The Trust Mortality Lead and the Learning Disabilities team have reviewed the Q2 learning disabilities deaths pending rollout of the national LeDeR programme. The medical review has been completed using the SJR methodology. Deaths from stroke, which has alerted on the HED dataset have been reviewed using SJR methodology The Clinical Effectiveness team is working with the trust coding team to establish means to identify other priority groups such as patients with severe mental health problems and deaths in patient undergoing elective procedures The paediatric and obstetric teams are modifying their mortality review processes to align with quarterly Board reporting The Bereavement Team will continue to support bereaved families and relay any concerns to the Mortality Review Oversight Committee The terms of reference of the MROC are being adapted to ensure the committee is fit for purpose to deliver the National Guidance The Trust Mortality Lead and the Interim Medical Director have been trained in the SJR methodology. 4. Next steps (by Q3) A team of reviewers will be trained in the SJR process allowing in-depth case reviews to be performed in the priority areas using SJR methodology (2018 training days 03 Jan, 23 rd Jan, 02 Feb. 30% of the deaths identified as priority for review will be reviewed 5. Recommendation 5.1 The Board is asked to Note the report in light of the requirements for Trust Boards following publication of the 2017 Learning from Deaths national guidance. Confirm their support for the on-going work that is currently taking place. Appendix FINAL - Learning From Deaths Dashboa 9
12 NHS ROYAL CORNWALL HOSPITAL: Learning from Deaths Dashboard - July-September 2017 Summary of total number of deaths and total number of cases reviewed Total Number of Deaths in Q2 July August September July August September Total Number of Reviews Completed in Q2 Total this Quarter (QTD) 186 % this quarter (QTD) 45% Summary of total number of learning disabilities deaths and total number of cases reviewed July August September Total Number of Deaths Total Number of Reviews Completed Total Number of Learning Disabilities Deaths Total Number of Reviews Completed by Learning disabilities team Total Number of Reviews Completed by Specialites team Grade of Mortality Review July August September July August September July August September Total this Quarter (QTD) % this quarter (QTD) Total this Quarter (QTD) % this quarter (QTD) Total Potentially Avoidable deaths % 2 100% 0 Summary of total number of concern deaths and total number of cases reviewed Total Number of "Concern" Deaths in Q2 (Grade 4 and 5) Total Number of Reviews Completed by Screening/Web Form Total Number of Reviews Completed by In-Depth Form Grade of Mortality Review - final grade following both screening/in-depth July August September July August September July August September Total Potentially Avoidable deaths 5
13 Summary of total number of Perinatal/Stillbirth deaths and total number of cases reviewed Total Number of Perinatal/Stillbirth deaths July August September Not Avoidable Avoidability in this quarter (QTD) Potentially Avoidable Data provided by the Bereavement Midwives which is not included on the data tab as pt identifiable relates to mother not baby Summary of total number of Paediatric/Child deaths and total number of cases reviewed Total Number of Paediatric/Child deaths Avoidability in this quarter (QTD) July August September Not Avoidable Potentially Avoidable Data provided by Paediatrics Team Total Number of complaints relating to a death Summary of total number of complaints relating to a death and total number of cases reviewed Total Number of Reviews Completed by Screening/Web Form Total Number of Reviews Completed by In-Depth Form Grade of Mortality Review - final grade following both screening/in-depth July August September July August September July August September Total this Quarter (QTD) % this quarter (QTD) Total Potentially Avoidable deaths % 0 Summary of SI's Number of SI's by date of death in Q2 Number of SI's completed and sent to KCCG July August September July August September Notes: Date of death - SI status could be at any stage and not reported and closed within the same quarter Date sent to KCCG - may relate to a patient with a DoD outside this quarter
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Learning from the Deaths of Patients in our Care Policy
 Learning from the Deaths of Patients in our Care Policy Approved By: Date of Original Approval: UHL Mortality Review Committee UHL Policies & Guidelines Committee September 2017 Trust Reference: B31/2017
Learning from the Deaths of Patients in our Care Policy Approved By: Date of Original Approval: UHL Mortality Review Committee UHL Policies & Guidelines Committee September 2017 Trust Reference: B31/2017
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Policy
 Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Learning from Deaths; Mortality Review Policy
 Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Authors: Head of Outcomes & Effectiveness, Quality Project Manager and Deputy MD, Sponsor: Medical Director
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
TRUST CORPORATE POLICY RESPONDING TO DEATHS
 SCOPE OF APPLICATION AND EXEMPTIONS CONSULT ATION COR/POL/224/2017-001 TRUST CORPORATE POLICY RESPONDING TO DEATHS APPROVING COMMITTEE(S) EFFECTIVE FROM DISTRIBUTION RELATED DOCUMENTS STANDARDS OWNER AUTHOR/FURTHER
SCOPE OF APPLICATION AND EXEMPTIONS CONSULT ATION COR/POL/224/2017-001 TRUST CORPORATE POLICY RESPONDING TO DEATHS APPROVING COMMITTEE(S) EFFECTIVE FROM DISTRIBUTION RELATED DOCUMENTS STANDARDS OWNER AUTHOR/FURTHER
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
h. HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST LEARNING FROM DEATHS POLICY. Broad Recommendations / Summary
 201 2017.473h. HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST LEARNING FROM DEATHS POLICY Broad Recommendations / Summary In-hospital death occurs. Patient 18 years of age or above. Yes Child Death Review
201 2017.473h. HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST LEARNING FROM DEATHS POLICY Broad Recommendations / Summary In-hospital death occurs. Patient 18 years of age or above. Yes Child Death Review
Mortality Policy - Learning from Deaths (CG627)
") Mortality Policy - Learning from Deaths (CG627) Approval Approval Group Job Title, Chair of Committee Date Policy Approval Group Chair, Policy Approval Group September 2017 Change History Version Date
Mortality Policy - Learning from Deaths (CG627) Approval Approval Group Job Title, Chair of Committee Date Policy Approval Group Chair, Policy Approval Group September 2017 Change History Version Date
Learning from Deaths Policy
 Policy Author: Owner: Publisher: Version: 1 Peter Wanklyn, Helen Noble Medical Director Medical Governance Date of version issue: September 2017 Approved by: Executive Board Date approved: September 2017
Policy Author: Owner: Publisher: Version: 1 Peter Wanklyn, Helen Noble Medical Director Medical Governance Date of version issue: September 2017 Approved by: Executive Board Date approved: September 2017
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Mortality Policy. Learning from Deaths
 Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
SWH Mortality Review Policy
 Corporate Governance SWH 01785 The Trust s Intranet holds the current approved guidance documents. Notice to staff using a paper copy of this document. Staff must ensure that they are using the most up-to-date
Corporate Governance SWH 01785 The Trust s Intranet holds the current approved guidance documents. Notice to staff using a paper copy of this document. Staff must ensure that they are using the most up-to-date
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
RM57 HOSPITAL MORTALITY REVIEW POLICY
 RM57 HOSPITAL MORTALITY REVIEW POLICY Version: 1 Name of ratifying committee: Clinical Quality Assurance Committee Date ratified: 20 th September 2017 Name of originator/author: Julie Grice, Chair of Hospital
RM57 HOSPITAL MORTALITY REVIEW POLICY Version: 1 Name of ratifying committee: Clinical Quality Assurance Committee Date ratified: 20 th September 2017 Name of originator/author: Julie Grice, Chair of Hospital
Unique Identifier: Review Date: November Issue Status: Approved Version No: 1.4 Issue Date: November 2017
 Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Policy Authors Name & Title: Dr Mark Jackson, Director of Research & Informatics Dr Raphael Perry, Medical Director Scope: Trust Wide Classification: Non Clinical Replaces: version 1.3 To be read in conjunction
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
A summary of: Five years of cerebral palsy claims
 A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Learning from Deaths - Mortality Report
 Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
LEARNING FROM DEATHS (Mortality Policy)
") LEARNING FROM DEATHS () Version: 1.0 Date issued: October 2017 Review date: September 2020 Applies to: All Clinical Staff Groups This document is available in other formats, including easy read summary
LEARNING FROM DEATHS () Version: 1.0 Date issued: October 2017 Review date: September 2020 Applies to: All Clinical Staff Groups This document is available in other formats, including easy read summary
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Active date: 25 th Sept Exclusions: None
 Trust Policy Title: Mortality review Author(s): James Coulston - Mortality Lead, Stuart Walker - Medical Director, Lincoln Andrews - Compliance and Audit Manager, Charlie Davis - Palliative Care Lead Document
Trust Policy Title: Mortality review Author(s): James Coulston - Mortality Lead, Stuart Walker - Medical Director, Lincoln Andrews - Compliance and Audit Manager, Charlie Davis - Palliative Care Lead Document
Indicator 5c Mortality Survey
 Indicator 5c Mortality Survey Undertaken by NCEPOD on behalf of NHS England Dr Neil Smith - Clinical Researcher and Deputy CEO Dr Hannah Shotton - Clinical Researcher Dr Marisa Mason - Chief Executive
Indicator 5c Mortality Survey Undertaken by NCEPOD on behalf of NHS England Dr Neil Smith - Clinical Researcher and Deputy CEO Dr Hannah Shotton - Clinical Researcher Dr Marisa Mason - Chief Executive
Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September 2009
 Summary Report Q2 July September 2009") Agenda 24/1 Public Board Meeting, 28 JAN 21 Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September Presented by: Colin Johnston, Medical Director 1. Purpose The following CLIP
Agenda 24/1 Public Board Meeting, 28 JAN 21 Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September Presented by: Colin Johnston, Medical Director 1. Purpose The following CLIP
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
Mortality Monitoring Policy
 Mortality Monitoring Policy Document Information Version: 3.0 Date: 25/07/2016 Ratified by: King s Executive Date ratified: 31 July 2017 Author(s): Responsible Director: Responsible committee: Date when
Mortality Monitoring Policy Document Information Version: 3.0 Date: 25/07/2016 Ratified by: King s Executive Date ratified: 31 July 2017 Author(s): Responsible Director: Responsible committee: Date when
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
Evidence Search Completed by..joanne Phizacklea.Date
 Document Type: Procedure Unique Identifier: CORP/PROC/073 Document Title: Mortality Review Process Scope: Consultants, Nursing Staff, Clinical Coding Staff, Clinical Audit & Effectiveness Staff, Quality
Document Type: Procedure Unique Identifier: CORP/PROC/073 Document Title: Mortality Review Process Scope: Consultants, Nursing Staff, Clinical Coding Staff, Clinical Audit & Effectiveness Staff, Quality
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Policy on Learning from Deaths
 Policy on Learning from Deaths Version number: 1 Consultation: Governance Committee Board Committee Director of Quality Assistant Director of Governance & Compliance Patient Safety Manager Ratified by:
Policy on Learning from Deaths Version number: 1 Consultation: Governance Committee Board Committee Director of Quality Assistant Director of Governance & Compliance Patient Safety Manager Ratified by:
Learning from Deaths Trust Board in public
 Learning from Deaths Trust Board in public Date: 30 th August 2018 Agenda item: 2.4 Executive sponsor Professor Des Holden Medical Director Dr Richard Brown Director of Outcomes Report author(s) Jonathan
Learning from Deaths Trust Board in public Date: 30 th August 2018 Agenda item: 2.4 Executive sponsor Professor Des Holden Medical Director Dr Richard Brown Director of Outcomes Report author(s) Jonathan
Tele Stroke ( Telemedicine in Practice)
") Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Document Title Investigating Deaths (Mortality Review) Policy
 Policy") Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Document Title Investigating Deaths (Mortality Review) Policy Document Description Document Type Policy Service Application DWMH Trust wide Version 1.0 Policy Reference no. POL 351 Lead Author(s) Name
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
LEARNING FROM DEATHS POLICY
 Summary LEARNING FROM DEATHS POLICY Learning from a review of the care provided to patients who die is integral to a provider s clinical governance and quality improvement work. To fulfil the standards
Summary LEARNING FROM DEATHS POLICY Learning from a review of the care provided to patients who die is integral to a provider s clinical governance and quality improvement work. To fulfil the standards
Integrated Quality Report
 Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
MORTALITY REVIEW & LEARNING FROM DEATHS POLICY
 MORTALITY REVIEW & LEARNING FROM DEATHS POLICY Document Reference Document status Target Audience MD25.MRLD.V1.1 Final All clinical staff involved in mortality case record reviews and investigations and
MORTALITY REVIEW & LEARNING FROM DEATHS POLICY Document Reference Document status Target Audience MD25.MRLD.V1.1 Final All clinical staff involved in mortality case record reviews and investigations and
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Worcestershire Acute Hospitals NHS Trust
 Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Paper 8 DECISION NOTE. Recommendation
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Our Achievements. CQC Inspection 2016
 Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
SSNAP data: What are the benefits? Tony Rudd
 SSNAP data: What are the benefits? Tony Rudd Without the audit data services would not have improved 2001 2005 2007 2010 2013 What does SSNAP measure? Organisation of care (measures structure) Clinical
SSNAP data: What are the benefits? Tony Rudd Without the audit data services would not have improved 2001 2005 2007 2010 2013 What does SSNAP measure? Organisation of care (measures structure) Clinical
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Visiting Professional Programme: Obstetric Medicine
 Visiting Professional Programme: Obstetric Medicine Visiting Professional Programme Obstetric Medicine 1 Introduction The Guy s and St Thomas NHS Foundation Trust Obstetric Medicine Visiting Professional
Visiting Professional Programme: Obstetric Medicine Visiting Professional Programme Obstetric Medicine 1 Introduction The Guy s and St Thomas NHS Foundation Trust Obstetric Medicine Visiting Professional
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
LEARNING FROM DEATHS POLICY SEPTEMBER 2017
 LEARNING FROM DEATHS POLICY SEPTEMBER 2017 Learning From Deaths Policy_RM09_V1 Policy title Learning from Deaths Policy Policy RM09 reference Policy category Corporate Relevant to Clinical Staff Date published
LEARNING FROM DEATHS POLICY SEPTEMBER 2017 Learning From Deaths Policy_RM09_V1 Policy title Learning from Deaths Policy Policy RM09 reference Policy category Corporate Relevant to Clinical Staff Date published
Learning From Deaths Policy
 Learning From Deaths Policy The purpose of this policy is to provide a systematic approach to ensure that the Trust has robust governance arrangements in place to review, report and learn from patient
Learning From Deaths Policy The purpose of this policy is to provide a systematic approach to ensure that the Trust has robust governance arrangements in place to review, report and learn from patient
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
Diagnostic Testing Procedures in Urodynamics V3.0
 V3.0 09 01 18 Table of Contents Summary.... 1. Introduction... 3 1.1. Diagnostic testing information... 3 2. Purpose of this Policy/Procedure... 3 2.1. Approved Document Process... 3 3. Scope... 3 3.1.
V3.0 09 01 18 Table of Contents Summary.... 1. Introduction... 3 1.1. Diagnostic testing information... 3 2. Purpose of this Policy/Procedure... 3 2.1. Approved Document Process... 3 3. Scope... 3 3.1.
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Statement 2: Patients/carers are offered verbal and written information on VTE prevention as part of the admission process.
 THROMBOSIS GROUP Venous thromboembolism (VTE) is a collective term referring to deep vein thrombosis (DVT) and pulmonary embolism (PE). VTE is defined by the following ICD-10 codes: I80.0-I80.3, I80.8-I80.9,
THROMBOSIS GROUP Venous thromboembolism (VTE) is a collective term referring to deep vein thrombosis (DVT) and pulmonary embolism (PE). VTE is defined by the following ICD-10 codes: I80.0-I80.3, I80.8-I80.9,
Working in partnership to improve the identification and treatment of sepsis
 Identifying and Tackling Sepsis in Healthcare Tuesday 25 th April 2017 Working in partnership to improve the identification and treatment of sepsis Tracy Broom Associate Director Wessex Patient Safety
Identifying and Tackling Sepsis in Healthcare Tuesday 25 th April 2017 Working in partnership to improve the identification and treatment of sepsis Tracy Broom Associate Director Wessex Patient Safety
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Learning from Deaths Policy
 Learning from Deaths Policy Document Reference No. CLIN041v4 Version No. 4 Issue Date 16/11/2017 Review Date 1 st September 2020 Document Author Document Owner Accountable Executive Approved by Deputy
Learning from Deaths Policy Document Reference No. CLIN041v4 Version No. 4 Issue Date 16/11/2017 Review Date 1 st September 2020 Document Author Document Owner Accountable Executive Approved by Deputy
Status: Information Discussion Assurance Approval
 Report to: Trust Board Agenda item: Date of Meeting: July 2017 Report Title: Safe Nurse Staffing 6 Monthly Assurance Report Status: Information Discussion Assurance Approval X x Prepared by: Sarah Dodds,
Report to: Trust Board Agenda item: Date of Meeting: July 2017 Report Title: Safe Nurse Staffing 6 Monthly Assurance Report Status: Information Discussion Assurance Approval X x Prepared by: Sarah Dodds,
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
Handover of Care (Maternity) Guidelines Author s job title Lead Clinical Midwife Department Ladywell Unit. Comment / Changes / Approval
 Guidelines Author s job title Lead Clinical Midwife Department Ladywell Unit. Comment / Changes / Approval") Document Control Title Author Directorate Surgery Date Version Issued 0.1 Oct 2009 0.2 Nov 2009 1.0 Nov 2009 1.1 Feb 2010 2.0 Feb 2010 2.1 Aug 2011 2.2 Oct 2011 Handover of Care (Maternity) Guidelines
Document Control Title Author Directorate Surgery Date Version Issued 0.1 Oct 2009 0.2 Nov 2009 1.0 Nov 2009 1.1 Feb 2010 2.0 Feb 2010 2.1 Aug 2011 2.2 Oct 2011 Handover of Care (Maternity) Guidelines
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Specialised Services Service Specification: Inherited Bleeding Disorders
 Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone Fax
 Agenda Item Meeting of Lanarkshire NHS Board 25 February 2009 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.co.uk WAITING TIMES 1.
Agenda Item Meeting of Lanarkshire NHS Board 25 February 2009 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.co.uk WAITING TIMES 1.
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
Section 1 - Key Performance Indicators
 Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD