How often do you brush your teeth? How often do you floss? Yes No. Yes No
|
|
|
- Samantha Shields
- 5 years ago
- Views:
Transcription
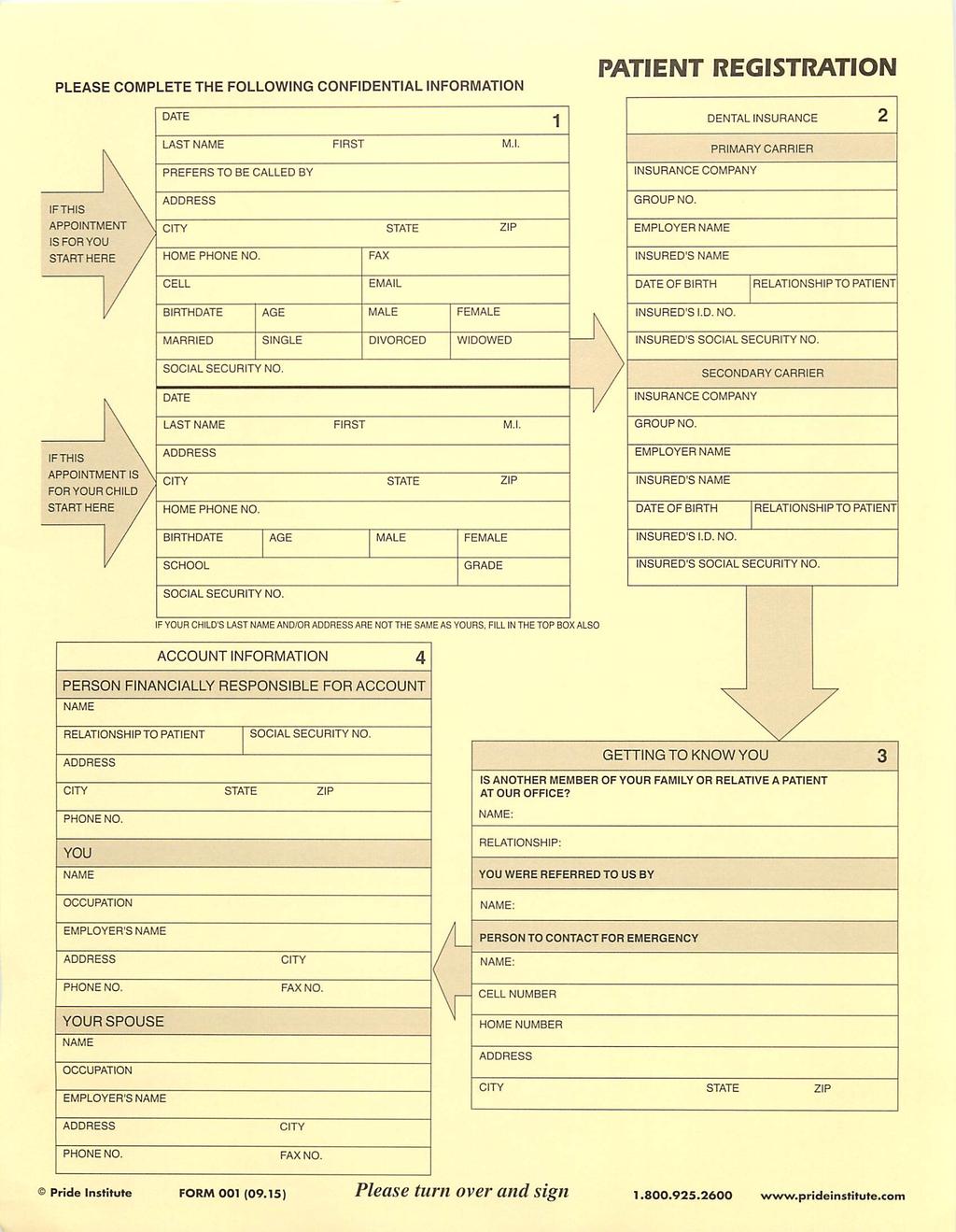
1
2
3 Patient Name Medical Alert DENTAL HISTORY Welcome! So that we may provide you with the best possible care please complete both sides of this medical / dental history form. All information is completely confidential. What is the reason for your visit today? Date of last dental visit Last dental cleaning Last full mouth X-rays What was done at your last dental visit? Previous Dentist s name Address Telephone How often do you have dental examinations? How often do you brush your teeth? How often do you floss? Have you ever used or are currently using topical fluoride? Yes What other dental aids do you use? (Interplak, toothpick, etc.) Do you have any dental problems now? Yes If yes, please describe: Are any of your teeth sensitive to: Hot or cold?... Sweets?... Biting or chewing?... Have you noticed any odors or bad tastes?... Do you frequently get cold sores, blisters, or any oral lesions?... Do your gums bleed or hurt?... Have your parents experienced gum disease or tooth loss?... Have you noticed any loose teeth or change in your bite?... Does food tend to become caught between your teeth?... If yes, where? Have you ever had: Orthodontic treatment?... Oral surgery?... Periodontal treatment?... Your teeth ground or bite adjusted?... A bite plate or mouth guard?... A serious injury to the mouth or head?... If so, please describe, including cause Have you experienced: Clicking or popping of the jaw?... Yes Pain? (Joint, ear, side of face)... Yes Difficulty in opening or closing the mouth?... Yes Difficulty in chewing on either side of the mouth?... Yes Headaches, neckaches or shoulder aches?... Yes Sore muscles (neck, shoulder)?... Yes Do you: Are you satisfied with your teeths appearance? Clench or grind your teeth while awake or asleep? Would you like to keep your teeth all your life? Bite your lips or cheeks regularly?... Hold foreign objects with your teeth?... Do you feel nervous about having dental treatment? (Pencils, pipe, pins, nails, fingernails) If so, what is your biggest concern? Mouth breathe while awake or asleep?... Have tired jaws, especially in the mornings?... Have you ever had an upsetting dental experience? Snore or have any other sleeping disorders?... If yes, please describe Smoke/chew tobacco or use other tobacco products?... Have you ever been told to take pre-medication prior to dental treatment? Is there anything else about having dental treatment that you would like us to know? If yes, please describe
4 Patient Name: MEDICAL HISTORY Medical Alert: 1. Physician s Name #1 Phone ( ) Physician s Name # 2 Phone ( ) 2. Have you had any medical care within the past two years?... Date of last heath care exam or physical: What was this exam for? 3. Are you currently being treated for any medical conditions?... Please list 4. Are you currently taking any medication, drugs, pills or herbal remedies, including regular dosages of asprin?... Drug Medical Condition Being Treated Dosage For How Long 5. Have you ever taken bone loss prevention drugs such as Fosamax, Actonel, Boniva or other similar drugs? Have you been a patient in the hospital during the past five years? Do you get headaches? How often? 8. Does anything trigger your headaches? 9. To what degree would you say your headaches affect your life? 10. On a scale of one to ten, what is the range of your headaches? 11. Have you been treated or evaluated for your headaches? 12. Indicate which of the following you have had, or have at present. Circle yes or no to each item. Heart (Surgery, Disease, Attack)... Chest Pain or Angina... Congenital Heart Disease... Heart Murmur... High/Low Blood Pressure... Endocarditis... Artificial Heart Valve/Transplant.. Snoring or Sleep Apnea... Arthritis/Rheumatism... Cortisone Medicine... Pacemaker... Stroke... Slow Healing Mouth Sores... Alcohol / Drug Use... Kidney Disease... Heart Stent?... Artificial Joints (hip, knee)... Ulcers... Diabetes... Thyroid Problems... Glaucoma... Contact lenses... Emphysema/Lung Illness... Chronic Cough... Tuberculosis... Asthma... Hay Fever/Allergy/Hives... Latex Sensitivity... Sinus Trouble... Radiation Therapy... Chemotherapy... Cancer or Tumors... Hepatitis A B C (Circle)... Take Blood Thinners... A.I.D.S/H.I.V. Positive... Cold Sores/Fever Blisters... Anemia or Blood Disorder... Hemophilia... Sickle Cell Disease... Bruise Easily... Liver Disease/Yellow Jaundice... Neurological Disorders... Epilepsy or Seizures... Fainting or Dizzy Spells... Nervous/Anxious... Psychiatric/Psychological Care Are you aware of having an allergic (or adverse) reaction to any substance or medication?... If yes, please list 14. Have you lost or gained more than 10 pounds in the last year? Do you have or have you had any disease, condition or problem not listed?... If yes, please list: 16. Women: Are you pregnant or think you could be pregnant? Yes Months Nursing? Do you use birth control prescriptions Do you use tobacco? In what form? How much per day? For how long? I understand the above information is necessary to provide me with dental care in a safe and efficient manner. I have answered all questions to the best of my knowlegde. Should further information be needed, you have my permission to ask the respective health care provider or agency, who may release such information to you. I will notify the doctor of any change in my health or medication. Patient/Guardian Signature When placed? When placed? Date

5 HIPAA PRIVACY FORM 1 tice of Privacy Practices Purpose: This form, tice of Privacy Practices, presents the information that federal law requires us to give our patients regarding our privacy practices. { te: this form may need to be changed to reflect the dental practice's particular privacy policies and/or stricter state laws.} We must provide this tice to each patient beginning no later than the date of our first service delivery to the patient, including service delivered electronically, after April 14, We must make a good-faith attempt to obtain written acknowledgement of receipt of the tice from the patient. We must also have the tice available at the office for patients to request to take with them. We must post the tice in our office in a clear and prominent location where it is reasonable to expect any patients seeking service from us to be able to read the tice. Whenever the tice is revised, we must make the tice available upon request on or after the effective date of the revision in a manner consistent with the above instructions. Thereafter, we must distribute the tice to each new patient at the time of service delivery and to any person requesting a tice. We must also post the revised tice in our office as discussed above American OE11tal Assoc1at1on All Rlg,ts Reserved Reproduction and use of this foon bydenhsts and thetr staff 1s pern111led Any 01her use. dupilcauon or d1stnbution a this fam by any other pany requires the pnor wn\len approval a the Ameru:an Dental Assoc1ahon This Form 1s educa11onal only. does not constitute legal advice. and covers only federal. not state. law (August 14, 2002) H I PAA PRIV ACY FOR M S 61

6 { NAME OF PRACllCE} NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. THE PRIVACY OF YOUR HEALTH INFORMATION IS IMPORTANT TO US. OUR LE~L DUTY We are required by applicable federal and state law to maintain the privacy of your health information. We are also required to give you this tice about our privacy practices, our legal duties, and your rights concerning your health information. We must follow the privacy practices that are described in this tice while it is in effect. This tice takes effect 01 / 01 / 15, and will remain in effect until we replace it. We reserve the right to change our privacy practices and the terms of this tice at any time, provided such changes are permitted by applicable law. We reserve the right to make the changes in our privacy practices and the new terms of our tice effective for all health information that we maintain, including health information we created or received before we made the changes. Before we make a significant change in our privacy practices, we will change this tice and make the new tice available upon request. 'tbu may request a copy of our tice at any time. For more information about our privacy practices, or for additional copies of this tice, please contact us using the information listed at the end of this tice. USES AND DISCLOSURES OF HEALTH INFORMATION We use and disclose health information about you for treatment, payment, and healthcare operations. For example: Treatment: We may use or disclose your health information to a physician or other healthcare provider providing treatment to you. Payment: We may use and disclose your health information to obtain payment for services we provide to you. Healthcare Operations: We may use and disclose your health information in connection with our healthcare operations. Healthcare operations include quality assessment and improvement activities, reviewing the competence or qualifications of healthcare professionals, evaluating practitioner and provider performance, conducting training programs, accreditation, certification, licensing or credentialing activities. Your Authorization: In addition to our use of your health information for treatment, payment or healthcare operations, you may give us written authorization to use your health information or to disclose it to anyone for any purpose. If you give us an authorization, you may revoke it in writing at any time. 'tbur revocation will not affect any use or disclosures permitted by your authorization while it was in effect. Unless you give us a written authorization, we cannot use or disclose your health information for any reason except those described in this tice. To Your Family and Friends: We must disclose your health information to you, as described in the Patient Rights section of this tice. We may disclose your health information to a family member, friend or other person to the extent necessary to help with your healthcare or with payment for your healthcare, but only if you agree that we may do so. Persons Involved In Care: We may use or disclose health information to notify, or assist in the notification of (including identifying or locating) a family member, your personal representative or another person responsible for your care, of your location, your general condition, or death. If you are present, then prior to use or disclosure of your health information, we will provide you with an opportunity to object to such uses or disclosures. In the event of your incapacity or emergency circumstances, we will disclose health information based on a determination using our professional judgment disclosing only health information that is directly relevant to the person's involvement in your healthcare. We will also use our professional judgment and our experience with common practice to make reasonable inferences of your best interest in allowing a person to pick up filled prescriptions, medical supplies, x-rays, or other similar forms of health information. Marketing Health-Related Services: We will not use your health information for marketing communications without your written authorization. Required by Law: We may use or disclose your health information when we are required to do so by law. Abuse or Neglect: We may disclose your health information to appropriate authorities if we reasonably believe that you are a possible victim of abuse, neglect, or domestic violence or the possible victim of other crimes. We may disclose your health information to the extent necessary to avert a serious threat to your health or safety or the health or safety of others.

7 National Security: We may disclose to military authorities the health information of Armed Forces personnel under certain circumstances. We may disclose to authorized federal officials health information required for lawful intelligence, counterintelligence, and other national security activities. We may disclose to correctional institution or law enforcement official having lawful custody of protected health information of inmate or patient under certain circumstances. Appointment Reminders: We may use or disclose your health information to provide you with appointment reminders (such as voic messages, postcards, or letters). PATIENT RIGHTS Access: You have the right to look at or get copies of your health information, with limited exceptions. 'tbu may request that we provide copies in a format other than photocopies. We will use the format you request unless we cannot practicably do so. ('tbu must make a request in writing to obtain access to your health information. 'tbu may obtain a form to request access by using the contact information listed at the end of this tice. We will charge you a reasonable cost-based fee for expenses such as copies and staff time. You may also request access by sending us a letter to the address at the end of this tice. If you request copies, we will charge you $0. 25c for each page, $15.00 per hour for staff time to copy your health information, and postage if you want the copies mailed to you. If you request an alternative format, we will charge a cost-based fee for providing your health information in that format. If you prefer, we will prepare a summary or an explanation of your health information for a fee. Contact us using the information listed at the end of this tice for a full explanation of our fee structure.) Disclosure Accounting: You have the right to receive a list of instances in which we or our business associates disclosed your health information for purposes, other than treatment, payment, healthcare operations and certain other activities, for the last 6 years, but not before April 14, If you request this accounting more than once in a 12-month period, we may charge you a reasonable, cost-based fee for responding to these additional requests. Restriction: You have the right to request that we place additional restrictions on our use or disclosure of your health information. We are not required to agree to these additional restrictions, but if we do, we will abide by our agreement (except in an emergency). Alternative Communication: )bu have the right to request that we communicate with you about your health information by alternative means or to alternative locations. ('1bu must make your request in writing.) )bur request must specify the alternative means or location, and provide satisfactory explanation how payments will be handled under the alternative means or location you request. Amendment: You have the right to request that we amend your health information. ('1bur request must be in writing, and it must explain why the information should be amended.) We may deny your request under certain circumstances. Electronic tice: If you receive this tice on our Web site or by electronic mail ( ), you are entitled to receive this tice in written form. QUESTIONS AND COMPLAINTS If you want more information about our privacy practices or have questions or concerns, please contact us. If you are concerned that we may have violated your privacy rights, or you disagree with a decision we made about access to your health information or in response to a request you made to amend or restrict the use or disclosure of your health information or to have us communicate with you by alternative means or at alternative locations, you may complain to us using the contact information listed at the end of this tice. '1bu also may submit a written complaint to the U.S. Department of Health and Human Services. We will provide you with the address to file your complaint with the U.S. Department of Health and Human Services upon request. We support your right to the privacy of your health information. We will not retaliate in any way if you choose to file a complaint with us or with the U.S. Department of Health and Human Services. Contact Officer: Mark W. Langberg Telephone: Fax: drlangber@rlangberg.com Address: W. 12 Mile Rd. Ste 303. Southfield M C American Dental Association. All rights reserved. Reproduction and use of this form by dentists and their staff for non-eommercial use is permitted. Any other use, duplication or distribution of this form by any other party requires the prior written approval of the American Dental Association. This Form is educational only, does not constitute legal advice, and covers only federal, not state, law (August ).
8 MARK W LANGBERG DDS, MAGD, PC W. 12 MILE RD, STE 303 SOUTHFIELD, MI (248) We are grateful you have chosen us. Please help us learn more about our web presence. How did you hear about us? If you found us on the internet, how did you search? Google Yahoo Bing 0 Angie's List. Other What specific search words did you use? What about our website attracted you? Acknowledgement of Receipt of this Practices Privacy tice I acknowledge that I have been given the choice of reviewing the tice of Privacy Practices of this office. I am aware that I may receive a paper copy of this notice if I request it. In addition, I acknowledge that the tice of Privacy Practice is kept in each treatment room of the office where I can review it if desired. Patient or Patient Representative or Parent (If patient representative signs above, please include relationship to patient) Date The patient presented for treatment on this date and was provided with the Practice Privacy tice. A good faith effort was made to obtain written acknowledgement of receipt. A written acknowledgement was not obtained because: Patient refused to sign, with the reason Patient is unable to sign due to. There was a medical emergency preventing timely signature, and an attempt will be made to obtain acknowledgement later. Other Employee Signature Date
Welcome and thank you for choosing Jerman Family Dentistry
 Welcome and thank you for choosing Jerman Family Dentistry We provide dental services for the entire family. The following is helpful information to serve you better as a patient. If there are questions
Welcome and thank you for choosing Jerman Family Dentistry We provide dental services for the entire family. The following is helpful information to serve you better as a patient. If there are questions
City. Whom may we thank for referring you to us?
 CAMBRIDGE DENTAL CENTER - PATIENT REGISTRATION Date Patient's Last Name First :Kame MI Age Soc. Sec. No.: Home Work Phone: Home rujul
CAMBRIDGE DENTAL CENTER - PATIENT REGISTRATION Date Patient's Last Name First :Kame MI Age Soc. Sec. No.: Home Work Phone: Home rujul
Ivis M. Getz, D.M.D. Caring For Kids Pediatric Dentistry, P.C. 140 Lockwood Avenue, Suite 315, New Rochelle, NY 10801
 How did you hear of our office? New Patient Registration SECTION 1: PATIENT INFORMATION Patient Name: M / F Date of Birth: Address: City: State: Zip Code: SECTION 2: PARENT / GUARDIAN / INSURANCE Name:
How did you hear of our office? New Patient Registration SECTION 1: PATIENT INFORMATION Patient Name: M / F Date of Birth: Address: City: State: Zip Code: SECTION 2: PARENT / GUARDIAN / INSURANCE Name:
PATIENT INFORMATION. Patient name: Date of birth: Sex: Age: Home address: City: State: Zip: Billing address (if different): City: State: Zip:
: City: State: Zip:") PATIENT INFORMATION Welcome to our office. We appreciate the confidence you place with us to provide dental services. To assist us in serving you, please complete the following form. The information provided
PATIENT INFORMATION Welcome to our office. We appreciate the confidence you place with us to provide dental services. To assist us in serving you, please complete the following form. The information provided
Broomall Patients ONLY may send forms via to:
 Thank you for choosing Children s Dentistry! To expedite your check in, please complete the forms in this packet and bring with you to your appointment. You may also FAX these forms to the office where
Thank you for choosing Children s Dentistry! To expedite your check in, please complete the forms in this packet and bring with you to your appointment. You may also FAX these forms to the office where
Thank you for choosing Smileology for your implant, cosmetic and family dentistry needs!
 Thank you for choosing Smileology for your implant, cosmetic and family dentistry needs! Please complete the attached health record prior to your arrival. By choosing us, you have selected a practice whose
Thank you for choosing Smileology for your implant, cosmetic and family dentistry needs! Please complete the attached health record prior to your arrival. By choosing us, you have selected a practice whose
Lost/broken filing(s) Teeth grinding/clenching Ringing in ears Broken/chipped tooth Gum disease Stained Teeth Bad Breath Swelling/lumps in mouth
 Teeth grinding/clenching Ringing in ears Broken/chipped tooth Gum disease Stained Teeth Bad Breath Swelling/lumps in mouth") 3148 N Swan Rd PATIENT INFORMATION Page 1 Title: Mr. Ms. Mrs. Dr. Name *: Nickname: First MI Last Gender: Male Female Birth Date: Age: Email *: Street *: Apt.: City *: State *: Zip *: Home Phone: Cell
3148 N Swan Rd PATIENT INFORMATION Page 1 Title: Mr. Ms. Mrs. Dr. Name *: Nickname: First MI Last Gender: Male Female Birth Date: Age: Email *: Street *: Apt.: City *: State *: Zip *: Home Phone: Cell
Acknowledgement of Receipt of Notice of Privacy Practices
 HIPAA PRIVACY FORM 2 Acknowledgement of Receipt of Notice of Privacy Practices Purpose: This form is used to obtain acknowledgement of receipt of our Notice of Privacy Practices or to document our good
HIPAA PRIVACY FORM 2 Acknowledgement of Receipt of Notice of Privacy Practices Purpose: This form is used to obtain acknowledgement of receipt of our Notice of Privacy Practices or to document our good
Kim E. Stiegler, D.M.D.
 Kim E. Stiegler, D.M.D. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Kim E. Stiegler, D.M.D. NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Patient Registration and Dental History
 Patient Registration and Dental History PATIENT INFORMATION DENTAL INSURANCE Date SS/HIC/Patient ID # Patient Name Last Name First Name Middle Name Address Email City State Zip Sex M F Birthdate Married
Patient Registration and Dental History PATIENT INFORMATION DENTAL INSURANCE Date SS/HIC/Patient ID # Patient Name Last Name First Name Middle Name Address Email City State Zip Sex M F Birthdate Married
 !W"]FamiIY First Dentistry, 1611 Sands Place SE, Suite 100, Marietta, GA30067 PH: 770.226.0008 FX:770.226.0700 We welcome you as part of our family. Please provide information to assist us with assisting
!W"]FamiIY First Dentistry, 1611 Sands Place SE, Suite 100, Marietta, GA30067 PH: 770.226.0008 FX:770.226.0700 We welcome you as part of our family. Please provide information to assist us with assisting
BETHESDA DENTAL GROUP
 PLEASE COMPLETE ALLINFORMATION THAT APPLIES TO YOU - THANK YOU PATIENT LAST NAME: FIRST: INITIAL How did you hear about us? Whom may we thank for your referral? Date of Birth: Single: Married: Divorced:
PLEASE COMPLETE ALLINFORMATION THAT APPLIES TO YOU - THANK YOU PATIENT LAST NAME: FIRST: INITIAL How did you hear about us? Whom may we thank for your referral? Date of Birth: Single: Married: Divorced:
Spouse's Work ( ) Best time and place to reach you _ IN CASE OF EMERGENCY, CONTACT (Specify someone who does not live in your household.
 Best time and place to reach you _ IN CASE OF EMERGENCY, CONTACT (Specify someone who does not live in your household.") PATIENT Date INF\ORMATION W E L ( 0 M DENTAL I NSVRAN(E E Who is responsible for this account? SS/HIC/Patient 10 # Patient ~ Relationship to Patient -----=,,------------- Insurance Co. -------- Address
PATIENT Date INF\ORMATION W E L ( 0 M DENTAL I NSVRAN(E E Who is responsible for this account? SS/HIC/Patient 10 # Patient ~ Relationship to Patient -----=,,------------- Insurance Co. -------- Address
Pediatric Dental Specialists
 Pediatric Dental Specialists Notice of Privacy Practices This Notice describes how your health information may be used and disclosed and how you can get access to this information. Please review it carefully.
Pediatric Dental Specialists Notice of Privacy Practices This Notice describes how your health information may be used and disclosed and how you can get access to this information. Please review it carefully.
Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION. Cell Phone ( ) Employer s Name
 Employer s Name") Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION Name Last First M.I. Social Security. Home Address Street City State Zip Mailing Address
Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION Name Last First M.I. Social Security. Home Address Street City State Zip Mailing Address
Sample Notice of Privacy Practices 2 of 6 cda.org/practicesupport
 Sample Notice of Privacy Practices 2 of 6 cda.org/practicesupport RUSSELL L. CURETON D.D.S. Notice of Privacy Practices This Notice describes how your health information may be used and disclosed and how
Sample Notice of Privacy Practices 2 of 6 cda.org/practicesupport RUSSELL L. CURETON D.D.S. Notice of Privacy Practices This Notice describes how your health information may be used and disclosed and how
Welcome. We are very happy to welcome you as a new patient.
 100 Saratoga Village Blvd Suite 31 B Malta NY Phone: 518-899-6068 Fax: 518-899-6069 Email: office@salvatoredental.com Welcome Our mission is to deliver exceptional comprehensive dental care to all of our
100 Saratoga Village Blvd Suite 31 B Malta NY Phone: 518-899-6068 Fax: 518-899-6069 Email: office@salvatoredental.com Welcome Our mission is to deliver exceptional comprehensive dental care to all of our
Patient Registration Form
 Patient Registration Form Please Complete the Following Information-Thank You Patient Information: Name: Last First MI Address: City: State: Zip: Home Telephone: Work Telephone: Best to Reach? Home? Work?
Patient Registration Form Please Complete the Following Information-Thank You Patient Information: Name: Last First MI Address: City: State: Zip: Home Telephone: Work Telephone: Best to Reach? Home? Work?
Associated Pediatric Dentistry Belleville, Edwardsville, O Fallon, IL
 Associated Pediatric Dentistry Belleville, Edwardsville, O Fallon, IL Patient Name: DOB: ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES AND CONSENT **You May Refuse to Sign This Consent Acknowledgement**
Associated Pediatric Dentistry Belleville, Edwardsville, O Fallon, IL Patient Name: DOB: ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES AND CONSENT **You May Refuse to Sign This Consent Acknowledgement**
Medical History. Patient Information. Dental History. Your current physical health is: Good Fair Poor
 Medical History Your current physical health is: Good Fair Poor Cruse Dental Center complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin,
Medical History Your current physical health is: Good Fair Poor Cruse Dental Center complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin,
TRINITY DENTAL CLINIC Medical History Form Date:
 Page 1of 4 TRINITY DENTAL CLINIC Medical History Form Date: NAME DATE OF BIRTH ADDRESS CITY STATE ZIP PHONE NUMBERS PHYSICIAN DO WE HAVE PERMISSION TO LEAVE A MESSAGE AT THE PHONE NUMBERS LISTED ABOVE?
Page 1of 4 TRINITY DENTAL CLINIC Medical History Form Date: NAME DATE OF BIRTH ADDRESS CITY STATE ZIP PHONE NUMBERS PHYSICIAN DO WE HAVE PERMISSION TO LEAVE A MESSAGE AT THE PHONE NUMBERS LISTED ABOVE?
DIRECTIONS TO OUR OFFICE:
 8008 Frost St. Suite 300, San Diego, Ca 92123 Office Number: (858)292-5050 DIRECTIONS TO OUR OFFICE: PermaDontics is located at 8008 Frost Street in San Diego off the 163 freeway by Sharp Memorial and
8008 Frost St. Suite 300, San Diego, Ca 92123 Office Number: (858)292-5050 DIRECTIONS TO OUR OFFICE: PermaDontics is located at 8008 Frost Street in San Diego off the 163 freeway by Sharp Memorial and
J. MATOVICH, DMD HOW DID YOU HEAR ABOUT OUR OFFICE? SECONDARY INSURANCE COMPANY NAME PHONE
 MARTI J. MATOVICH, DMD PATIET IFORMATIO AME DETAL ISURACE PRIMAR ISURACE COMPA last first m.i. ADDRESS AME OF ISURED CIT STATE ZIP RELATIOSHIP TO PATIET self spouse child other HOME PHOE CELL PHOE GROUP
MARTI J. MATOVICH, DMD PATIET IFORMATIO AME DETAL ISURACE PRIMAR ISURACE COMPA last first m.i. ADDRESS AME OF ISURED CIT STATE ZIP RELATIOSHIP TO PATIET self spouse child other HOME PHOE CELL PHOE GROUP
Patient Name Today s Date: Mailing Address Home Phone: City State Zip: Work Phone: Cell Phone: Birth Date: / / Age: SSN: Sex: Male Female
 Patient Registration Patient Name Today s Date: Mailing Address Home Phone: City State Zip: Work Phone: Email: Cell Phone: Birth Date: / / Age: SSN: Sex: Male Female Marital Status: Single Married Widowed
Patient Registration Patient Name Today s Date: Mailing Address Home Phone: City State Zip: Work Phone: Email: Cell Phone: Birth Date: / / Age: SSN: Sex: Male Female Marital Status: Single Married Widowed
351 Osborne Road, Loudonville, New York ARWynnykiwDDS. Welcome!
 351 Osborne Road, Loudonville, New York 12211 518.432.3991 518.432.3987 smile@albanydds.com ARWynnykiwDDS www.albanydds.com Welcome! When it comes to dentists, I know that you have many options. My goal
351 Osborne Road, Loudonville, New York 12211 518.432.3991 518.432.3987 smile@albanydds.com ARWynnykiwDDS www.albanydds.com Welcome! When it comes to dentists, I know that you have many options. My goal
PATIENT REGISTRATION
 PATIENT REGISTRATION Patient Information Last Name: First Name: Middle Initial: Address: Address2: City: FL: Zipcode: Home Phone: Work Phone: Cellular: Sex: Male Female Marital Status: Married Single Divorced
PATIENT REGISTRATION Patient Information Last Name: First Name: Middle Initial: Address: Address2: City: FL: Zipcode: Home Phone: Work Phone: Cellular: Sex: Male Female Marital Status: Married Single Divorced
Welcome to St. Mary s Family Dentistry
 Welcome to St. Mary s Family Dentistry We would like to thank you for choosing St. Mary s Family Dentistry as your dental care provider. We are pleased to meet any dental needs you or your family have.
Welcome to St. Mary s Family Dentistry We would like to thank you for choosing St. Mary s Family Dentistry as your dental care provider. We are pleased to meet any dental needs you or your family have.
EMERALD ISLE SMILES DENTAL STUDIO WELCOMES YOU
 EMERALD ISLE SMILES DENTAL STUDIO WELCOMES YOU ~We Are Honored by Your Call for an Appointment~ A warm welcome from Emerald Isle Smiles Dental Studio! Thank you for choosing us to contribute to your dental
EMERALD ISLE SMILES DENTAL STUDIO WELCOMES YOU ~We Are Honored by Your Call for an Appointment~ A warm welcome from Emerald Isle Smiles Dental Studio! Thank you for choosing us to contribute to your dental
THE COUNSELING PLACE ADULT INTAKE FORM Yearly Family Income:
 Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Louis R. Vita, D.D.S., F.A.G.D. 991 Van Houten Avenue Clifton, NJ Phone:
 Louis R. Vita, D.D.S., F.A.G.D. 991 Van Houten Avenue Clifton, NJ 07013 Phone: 973-777-1933 Fax: 973-777-4727 Email: Vitaoffice991@gmail.com Website: DrLouisVita.com We are pleased to welcome you to our
Louis R. Vita, D.D.S., F.A.G.D. 991 Van Houten Avenue Clifton, NJ 07013 Phone: 973-777-1933 Fax: 973-777-4727 Email: Vitaoffice991@gmail.com Website: DrLouisVita.com We are pleased to welcome you to our
Welcome to our office! Please fill out this form as completely as possible and return it to the desk.
 Welcome to our office! Please fill out this form as completely as possible and return it to the desk. Name of Doctor you wish to see: Today's Date Name Email Address Address Home Male Female Cell City
Welcome to our office! Please fill out this form as completely as possible and return it to the desk. Name of Doctor you wish to see: Today's Date Name Email Address Address Home Male Female Cell City
PATIENT INFORMATION RECORD
 Laurence D. Popowich, D.D.S. Robert Laski, D.M.D. Jaime M. Cernansky, D.M.D., M.D. Niral Parikh, D.D.S., B.D.S. Mark H. Grim, D.M.D., Emeritus Diplomates American Board of Oral and Maxillofacial Surgery
Laurence D. Popowich, D.D.S. Robert Laski, D.M.D. Jaime M. Cernansky, D.M.D., M.D. Niral Parikh, D.D.S., B.D.S. Mark H. Grim, D.M.D., Emeritus Diplomates American Board of Oral and Maxillofacial Surgery
WELCOME TO OUR OFFICE!
 WELCOME TO OUR OFFICE! Name Date: / / Address City State Zip Home Phone Cell Phone E-Mail Birthdate Age SS# Race: Marital Status: M W D S Employer Work Phone Occupation Name & Birthdate of Primary Insured
WELCOME TO OUR OFFICE! Name Date: / / Address City State Zip Home Phone Cell Phone E-Mail Birthdate Age SS# Race: Marital Status: M W D S Employer Work Phone Occupation Name & Birthdate of Primary Insured
Person to Contact in Case of Emergency. THE COUNSELING PLACE YOUTH INTAKE FORM Yearly Family Income:
 Person to Contact in Case of Emergency Name Relationship Best Contact Number Alt. Number Office Use Only Intake Date Reason for referral Counselor Who Can Pick Up Client (if Minor) THE COUNSELING PLACE
Person to Contact in Case of Emergency Name Relationship Best Contact Number Alt. Number Office Use Only Intake Date Reason for referral Counselor Who Can Pick Up Client (if Minor) THE COUNSELING PLACE
Patient Information Form
 Patient Information Form Full Name: Date of Birth: / / Gender: M or F SS#: Marital Status: Single Married Widowed Divorced Employment Status: Employed Unemployed Retired Disabled Address: City: State:
Patient Information Form Full Name: Date of Birth: / / Gender: M or F SS#: Marital Status: Single Married Widowed Divorced Employment Status: Employed Unemployed Retired Disabled Address: City: State:
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient s Legal Name: Preferred Name: First Middle Last
 Douglas County Dental Clinic Patient Registration Revised August 2016 We REQUIRE A Parent, Guardian, Or Other Legally Responsible Party To Complete & Sign all forms. Please provide a photo ID, Proof of
Douglas County Dental Clinic Patient Registration Revised August 2016 We REQUIRE A Parent, Guardian, Or Other Legally Responsible Party To Complete & Sign all forms. Please provide a photo ID, Proof of
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Surgery Handbook. ! a GUIDE to PREPARING for your OPERATION Lincoln Circle SE Orange City, IA ochealthsystem.org
 Surgery Handbook! a GUIDE to PREPARING for your OPERATION Hospital 712.737.4984 Patient Information 712.737.5238 Toll free: 800.808.6264 Fax: 712.737.5252 1000 Lincoln Circle SE Orange City, IA 51041 ochealthsystem.org
Surgery Handbook! a GUIDE to PREPARING for your OPERATION Hospital 712.737.4984 Patient Information 712.737.5238 Toll free: 800.808.6264 Fax: 712.737.5252 1000 Lincoln Circle SE Orange City, IA 51041 ochealthsystem.org
POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX
 Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
PATIENT NUMBER. Address. Telephone. Relationship to patient. Name of Insurance Co. Address
 Patient s Name Date of Birth Male Female Age Last First Initial Date If Child: Parent s Name How do you wish to be addressed Single Married Separated Divorced Widowed Minor Residence - Street City State
Patient s Name Date of Birth Male Female Age Last First Initial Date If Child: Parent s Name How do you wish to be addressed Single Married Separated Divorced Widowed Minor Residence - Street City State
Practice Limited to Infants, Children, & Adolescents
 Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL
 Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Julie Gussenhoven, OD 3416 Bechelli Lane Redding, CA 96002
 Julie Gussenhoven, OD OCULAR AND MEDICAL HISTORY QUESTIONNAIRE Name: M F Date: Date of Birth: Home Phone: Social Security #: Cell Phone: Address: Work Phone: City: Zip: Email: Please complete all personal
Julie Gussenhoven, OD OCULAR AND MEDICAL HISTORY QUESTIONNAIRE Name: M F Date: Date of Birth: Home Phone: Social Security #: Cell Phone: Address: Work Phone: City: Zip: Email: Please complete all personal
PATIENT NOTICE OF PRIVACY PRACTICES Effective Date: June 1, 2012 Updated: May 9, 2017
 PREMIER PSYCHIATRY Psychiatric and Behavioral Health Services PATIENT NOTICE OF PRIVACY PRACTICES Effective Date: June 1, 2012 Updated: May 9, 2017 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU
PREMIER PSYCHIATRY Psychiatric and Behavioral Health Services PATIENT NOTICE OF PRIVACY PRACTICES Effective Date: June 1, 2012 Updated: May 9, 2017 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
Community Outreach Services, Inc Greenbelt Road Suite 206 College Park, MD (301) Fax: (301)
 Fax: (301)") Community Outreach Services, Inc. 6215 Greenbelt Road Suite 206 College Park, MD 20740 (301)345-1459 Fax: (301) 345-1305 Office Policies Form *Office Hours *Times are subject to change. Please contact
Community Outreach Services, Inc. 6215 Greenbelt Road Suite 206 College Park, MD 20740 (301)345-1459 Fax: (301) 345-1305 Office Policies Form *Office Hours *Times are subject to change. Please contact
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group
 DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center
 Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Welcome to Pinnacle Chiropractic Spine and Sports Center Name: Social Security Number: : Address: City: State: Zip: _ Telephone Home: Work: Mobile: _ Age: of Birth: Height: Weight: Gender: M / F Employer:
Dr. Ian C. MacIntyre
 coburg dentistryinc.bsc, DDS Patient Information Dr. Ian C. MacIntyre Name: DOB: (dd/mm/yyyy) / / Telephone: home cell work email: preferred contact method: Address: Street city province postal code Healthcard:
coburg dentistryinc.bsc, DDS Patient Information Dr. Ian C. MacIntyre Name: DOB: (dd/mm/yyyy) / / Telephone: home cell work email: preferred contact method: Address: Street city province postal code Healthcard:
Over. 1. What is the primary reason that you are here? 2. What three aesthetic changes would you like to effect?
 New Patient Questionnaire Please help us help you by filling out the following information. It is our intention to make your consultation and surgical experience with us productive, enjoyable and goal
New Patient Questionnaire Please help us help you by filling out the following information. It is our intention to make your consultation and surgical experience with us productive, enjoyable and goal
Karen Lopez - Bartlett, FNP-C 2400 Augusta Suite 210 Houston, Texas Phone: Fax:
 Karen Lopez - Bartlett, FNP-C 2400 Augusta Suite 210 Houston, Texas 77057 Phone: 832.970.0228 Fax: 713.278-7885 Welcome! We are honored that you have chosen us to help in your search for optimum health.
Karen Lopez - Bartlett, FNP-C 2400 Augusta Suite 210 Houston, Texas 77057 Phone: 832.970.0228 Fax: 713.278-7885 Welcome! We are honored that you have chosen us to help in your search for optimum health.
DAHIYA FACIAL PLASTIC SURGERY AND LASER CENTER CONSULTATION AND MEDICAL HISTORY. Name Date of Birth Today s Date Address: Street City State Zip
 DAHIYA FACIAL PLASTIC SURGERY AND LASER CENTER CONSULTATION AND MEDICAL HISTORY Name Date of Birth Today s Date Address: Street City State Zip Home phone: May we contact you on your home phone? YES NO
DAHIYA FACIAL PLASTIC SURGERY AND LASER CENTER CONSULTATION AND MEDICAL HISTORY Name Date of Birth Today s Date Address: Street City State Zip Home phone: May we contact you on your home phone? YES NO
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES Effective Date: 2013 Wisconsin Dental Association (800) 243-4675 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
NOTICE OF PRIVACY PRACTICES Effective Date: 2013 Wisconsin Dental Association (800) 243-4675 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS
CAPITAL SURGEONS GROUP, PLLC
 CAPITAL SURGEONS GROUP, PLLC NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
CAPITAL SURGEONS GROUP, PLLC NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
MEDICAL HISTORY QUESTIONNAIRE Last name First Name MI DOB. Please answer the following questions about your current eye problems and medical history:
 MEDICAL HISTORY QUESTIONNAIRE Last name First Name MI DOB Please answer the following questions about your current eye problems and medical history: 1. What problems are you CURRENTLY having with your
MEDICAL HISTORY QUESTIONNAIRE Last name First Name MI DOB Please answer the following questions about your current eye problems and medical history: 1. What problems are you CURRENTLY having with your
Patients Name. Insurance policy holders name and Social security number. Address. Home Phone number. Work Phone Number
 Patient Registration Form Print out this form and also the Health History Form. Bring both fully completed forms and your insurance card with you and give them to our staff as you check in for your appointment.
Patient Registration Form Print out this form and also the Health History Form. Bring both fully completed forms and your insurance card with you and give them to our staff as you check in for your appointment.
Dodge. County. Schools
 Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
NOTICE OF PRIVACY PRACTICE UNIVERSITY OF CALIFORNIA SAN FRANCISCO DENTAL CENTER
 Effective Date: February 1, 2018 NOTICE OF PRIVACY PRACTICE UNIVERSITY OF CALIFORNIA SAN FRANCISCO DENTAL CENTER THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW
Effective Date: February 1, 2018 NOTICE OF PRIVACY PRACTICE UNIVERSITY OF CALIFORNIA SAN FRANCISCO DENTAL CENTER THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW
R. B. KO L A C H A L A M M. D. GENERAL SURGERY
 GENERAL SURGERY Patient Information (Please Print and Circle or check the appropriate response) Patient s Name: DOB: _ Address: City: _ Zip: Home Phone: Cell: Work:_ Email Address: Patient s SSN: Male
GENERAL SURGERY Patient Information (Please Print and Circle or check the appropriate response) Patient s Name: DOB: _ Address: City: _ Zip: Home Phone: Cell: Work:_ Email Address: Patient s SSN: Male
NOTICE OF PRIVACY PRACTICES UNIVERSITY OF CALIFORNIA RIVERSIDE CAMPUS HEALTH CENTER
 NOTICE OF PRIVACY PRACTICES UNIVERSITY OF CALIFORNIA RIVERSIDE CAMPUS HEALTH CENTER Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
NOTICE OF PRIVACY PRACTICES UNIVERSITY OF CALIFORNIA RIVERSIDE CAMPUS HEALTH CENTER Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
MAIN STREET RADIOLOGY
 MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
NOTICE OF PRIVACY PRACTICES
 EFFECTIVE DATE: APRIL 14, 2003 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
EFFECTIVE DATE: APRIL 14, 2003 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
School Based Oral Health Services
 Seal a Smile Oral Health Program A project of Whitney M. Young Jr. Health Services and the Healthy Capital District Initiative School Based Oral Health Services Oral health classroom education Dental screenings
Seal a Smile Oral Health Program A project of Whitney M. Young Jr. Health Services and the Healthy Capital District Initiative School Based Oral Health Services Oral health classroom education Dental screenings
Patient Demographic Sheet
 Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Patient Demographic Form Please PRINT Patient Demographic Sheet Last name First Name Middle Initial Date of Birth Social Security Number Gender Male Female Marital Status Married Single Divorced Life Partner
Advanced Oral & Maxillofacial Surgery, Ltd. NOTICE OF PRIVACY PRACTICES
 Advanced Oral & Maxillofacial Surgery, Ltd. NOTICE OF PRIVACY PRACTICES This notice describes how health information about you may be used and disclosed and how you can get access to this information.
Advanced Oral & Maxillofacial Surgery, Ltd. NOTICE OF PRIVACY PRACTICES This notice describes how health information about you may be used and disclosed and how you can get access to this information.
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Orthopedic Specialty Clinic, Ltd. Updated 05/2014
 Orthopedic Specialty Clinic, Ltd. Updated 05/2014 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Orthopedic Specialty Clinic, Ltd. Updated 05/2014 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Johns Hopkins Notice of Privacy Practices for Health Care Providers
 Johns Hopkins Notice of Privacy Practices for Health Care Providers This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please
Johns Hopkins Notice of Privacy Practices for Health Care Providers This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please
*Family Chiropractic Care* New Patient Information Worksheet*
 *Family Chiropractic Care* New Patient Information Worksheet* Name: SSN: Age: Address: City: State: Zip: Phone Hm: Wk: Date of Birth: E-Mail Employer: Insurance: Policy/I.D. # : Spouses Name: Marital Status:
*Family Chiropractic Care* New Patient Information Worksheet* Name: SSN: Age: Address: City: State: Zip: Phone Hm: Wk: Date of Birth: E-Mail Employer: Insurance: Policy/I.D. # : Spouses Name: Marital Status:
Last Name: First Name: Sex: Male Female. Birth Date: / / Age: Home Address: Home Phone #: Cell Phone #: Work Phone #:
 Today s Date: / / Last Name: First Name: Sex: Male Female Birth Date: / / Age: Email: Home Address: City: State: Zip Code: Home Phone #: Cell Phone #: Work Phone #: Which is the best number to reach you?
Today s Date: / / Last Name: First Name: Sex: Male Female Birth Date: / / Age: Email: Home Address: City: State: Zip Code: Home Phone #: Cell Phone #: Work Phone #: Which is the best number to reach you?
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
physicians, nurses, and technicians and other Facility personnel for review and learning purposes. We may also combine the medical information we
 WESTMINSTER CANTERBURY - RICHMOND NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
WESTMINSTER CANTERBURY - RICHMOND NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
This notice describes Florida Hospital DeLand s practices and that of: All departments and units of Florida Hospital DeLand.
 MRN: FIN: FLORIDA HOSPITAL DELAND HIPAA NOTICE OF PRIVACY PRACTICES Effective Date: September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
MRN: FIN: FLORIDA HOSPITAL DELAND HIPAA NOTICE OF PRIVACY PRACTICES Effective Date: September 23, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
ALFRED ALINGU, MD INTERNAL MEDICINE
 Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
SUMMARY OF NOTICE OF PRIVACY PRACTICES
 LAKE REGIONAL MEDICAL GROUP 54 HOSPITAL DRIVE OSAGE BEACH, MO 65065 SUMMARY OF NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU
LAKE REGIONAL MEDICAL GROUP 54 HOSPITAL DRIVE OSAGE BEACH, MO 65065 SUMMARY OF NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU
PATIENT'REGISTRATION'FORM'FOR'KURT'R'WHARTON S'OFFICE' ' Last%Name:% %%%%%%%%%%%First%Name:% %%%%%%%%%%%%%%Middle:% %% % Responsible%Party:%
 PATIENT'REGISTRATION'FORM'FOR'KURT'R'WHARTON S'OFFICE' ' LastName: FirstName: Middle: ResponsibleParty: Relationship: Address: Zip: City: State: PreferredPhone: Email: MaritalStatus: S M D W LegallySeparated
PATIENT'REGISTRATION'FORM'FOR'KURT'R'WHARTON S'OFFICE' ' LastName: FirstName: Middle: ResponsibleParty: Relationship: Address: Zip: City: State: PreferredPhone: Email: MaritalStatus: S M D W LegallySeparated
Middle Initial: Street Address: City: Date of Birth: Age: Marital Status: Occupation: Employer: Name of Spouse: Emergency Contact:
 SALT LAKE EYE ASSOCIATES, LLC (801) 281-2020 1025 E 3300 S, SLC, Utah * Patient Information Sheet First Name: Last Name: Middle Initial: Referred By Family Doctor EMAIL Street Address: City: State: Zip:
SALT LAKE EYE ASSOCIATES, LLC (801) 281-2020 1025 E 3300 S, SLC, Utah * Patient Information Sheet First Name: Last Name: Middle Initial: Referred By Family Doctor EMAIL Street Address: City: State: Zip:
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003
 NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION CONSENT TO USE OR DISCLOSE MEDICAL INFORMATION
 Patient Name (PLEASE PRINT): Date of Birth: ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION The & Center of Southern Oregon, PC s Notice of Privacy Practices contains information about the uses and disclosures
Patient Name (PLEASE PRINT): Date of Birth: ACKNOWLEDGEMENT OF HIPAA PRIVACY INFORMATION The & Center of Southern Oregon, PC s Notice of Privacy Practices contains information about the uses and disclosures
Choptank Community Health System Caroline County School Based Health Centers Healthy Children Are Better Learners MEDICAL
 Choptank Community Health System Caroline County School Based Health Centers Healthy Children Are Better Learners MEDICAL Dear Parent/Guardian: As a student in the Caroline County Public School system,
Choptank Community Health System Caroline County School Based Health Centers Healthy Children Are Better Learners MEDICAL Dear Parent/Guardian: As a student in the Caroline County Public School system,
J.C. Blair Memorial Hospital Huntingdon, PA
 J.C. Blair Memorial Hospital Huntingdon, PA Notice of Privacy Practices Effective Date: 4/14/03 Revised Date: 1/21/14 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
J.C. Blair Memorial Hospital Huntingdon, PA Notice of Privacy Practices Effective Date: 4/14/03 Revised Date: 1/21/14 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
RECEIPT OF NOTICE OF PRIVACY PRACTICES WRITTEN ACKNOWLEDGEMENT FORM. I,, have received a copy of Dr. Andy Hand s Notice of Privacy Practice.
 Central Texas Institute Of Plastic Surgery, PA Dr. Andy Hand, M.D. Plastic and Reconstructive Surgery Cosmetic Plastic Surgery RECEIPT OF NOTICE OF PRIVACY PRACTICES WRITTEN ACKNOWLEDGEMENT FORM I,, have
Central Texas Institute Of Plastic Surgery, PA Dr. Andy Hand, M.D. Plastic and Reconstructive Surgery Cosmetic Plastic Surgery RECEIPT OF NOTICE OF PRIVACY PRACTICES WRITTEN ACKNOWLEDGEMENT FORM I,, have
ERIE COUNTY MEDICAL CENTER CORPORATION NOTICE OF PRIVACY PRACTICES. Effective Date : April 14, 2003 Revised: August 22, 2016
 ERIE COUNTY MEDICAL CENTER CORPORATION NOTICE OF PRIVACY PRACTICES Effective Date : April 14, 2003 Revised: August 22, 2016 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
ERIE COUNTY MEDICAL CENTER CORPORATION NOTICE OF PRIVACY PRACTICES Effective Date : April 14, 2003 Revised: August 22, 2016 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED
Name DOB / / SS# / / Street Address City/State/Zip. Home ( ) - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -
 - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -") Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
Privacy Practices Home Visit Doctor, LLC July 2017
 Privacy Practices Home Visit Doctor, LLC July 2017 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Privacy Practices Home Visit Doctor, LLC July 2017 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
College of Sequoias Physical Therapist Assistant Program Student Health Release Form
 Part A: College of Sequoias Physical Therapist Assistant Program Student Health Release Form To be completed by the Student Name: Telephone: Cell Number: Address: City: ZIP Code: Birth Date: Family Health
Part A: College of Sequoias Physical Therapist Assistant Program Student Health Release Form To be completed by the Student Name: Telephone: Cell Number: Address: City: ZIP Code: Birth Date: Family Health
TOS Health Questionnaire
 Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
NORTH COUNTY PHYSICAL THERAPY, INC. DBA MISSION PHYSICAL THERAPY GROUP
 NORTH COUNTY PHYSICAL THERAPY, INC. DBA MISSION PHYSICAL THERAPY GROUP Last Name First Name MI Mailing Address City State Zip Date of Birth Age SSN: - - Gender: M or F Home Phone Cell Phone Email: Patient
NORTH COUNTY PHYSICAL THERAPY, INC. DBA MISSION PHYSICAL THERAPY GROUP Last Name First Name MI Mailing Address City State Zip Date of Birth Age SSN: - - Gender: M or F Home Phone Cell Phone Email: Patient
School Based Health Services Consent Form
 MRN: PCP: Teacher: Grade: School Based Health Services Consent Form Before your child sees a provider, we are asking you to authorize medical and/ or dental treatment. We will work with you to improve
MRN: PCP: Teacher: Grade: School Based Health Services Consent Form Before your child sees a provider, we are asking you to authorize medical and/ or dental treatment. We will work with you to improve
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE Phone: Fax:
 School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
HIPAA PRIVACY NOTICE
 HIPAA PRIVACY NOTICE PLEASE REVIEW THIS NOTICE CAREFULLY. IT DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU MAY GAIN ACCESS TO THAT INFORMATION. POLICY STATEMENT This Practice
HIPAA PRIVACY NOTICE PLEASE REVIEW THIS NOTICE CAREFULLY. IT DESCRIBES HOW YOUR MEDICAL INFORMATION MAY BE USED AND DISCLOSED AND HOW YOU MAY GAIN ACCESS TO THAT INFORMATION. POLICY STATEMENT This Practice
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES Ihosvani Miguel, MD, PA DBA: Endo Care of South Florida 1400 S Andrews Avenue Fort Lauderdale, FL 33316 Effective Date: April 2, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION
NOTICE OF PRIVACY PRACTICES Ihosvani Miguel, MD, PA DBA: Endo Care of South Florida 1400 S Andrews Avenue Fort Lauderdale, FL 33316 Effective Date: April 2, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION
JOINT NOTICE OF PRIVACY PRACTICES
 JOINT NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. Who Will Follow This Notice PLEASE REVIEW
JOINT NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. Who Will Follow This Notice PLEASE REVIEW
James M. Wilson, M.D. - Medical Information to (fax to ) PATIENT INFORMATION Last name: First: D.O.
 PATIENT INFORMATION Last name: First: D.O.") James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
James M. Wilson, M.D. - Medical Information Email to wilson@houstonmds.org (fax to 713-790-1605) PATIENT INFORMATION Last name: First: D.O.B: SSN: Age: Gender: M F Home Phone #: Cell Phone #: Work Phone
PEDIATRIC HEALTH ASSOCIATES HIPAA NOTICE OF PRIVACY PRACTICES
 Policy effective date: 4-14-2003 Revised January 2014 PEDIATRIC HEALTH ASSOCIATES HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
Policy effective date: 4-14-2003 Revised January 2014 PEDIATRIC HEALTH ASSOCIATES HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND