2012 ICD-10-CM. Session I: Introduction to ICD-10-CM. Your Presenters Today
|
|
|
- Sabina Barker
- 5 years ago
- Views:
Transcription
1 2012 ICD-10-CM Session I: Introduction to ICD-10-CM August 24, 2012 Your Presenters Today Barbara Flynn, RHIA, CCS AHIMA Approved ICD-10-CM/PCS Trainer & Ambassador Vice President/Health Information and Denial Management Services Florida Hospital Association Management Corporation 307 Park Lake Circle, Orlando, FL p and Linda Renn, RHIT, CCS, CPC, CPC-H, HITPRO TR AHIMA Approved ICD-10-CM/PCS Trainer & Ambassador Vice President, Education & Communications STAT Solutions, Inc. P.O. Box 0397 New Port Richey FL info@statsolutionsinc.com 1



 Review Your Understanding")
2 Preparation is Your Key to Success Course Objectives: Review Your Understanding of: The Format, Code Structure and Coding Conventions of ICD 10 CM The Requirements of the Uniform Hospital Discharge Data Set The Requirements of the 2012 Version 5010 and HIPAA Requirements Identify Ethical Coding and Reporting Standards The Official Coding Guidelines for the ICD 10 CM and the Assignment of POA Indicators The ICD-10-CM General Equivalence Mappings (GEMs) Review Your Understanding the History of ICD 10 CM 2
3 What are ICD-10-CM and ICD-10-PCS? The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) and the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) were developed as a replacement for ICD-9-CM. ICD-10-CM consists of diagnosis codes: Clinical modification of the World Health Organization s (WHO) ICD-10. ICD-10-PCS consists of procedure codes: Classification of operations and procedures developed for use in the United States; not a part of the WHO classification. Review Your Understanding of the Rationale for Change fromicd-9-cm to ICD-10-CM 3
4 Rationale for Change ICD-9-CM has been in use in the United States since Many improvements in medical practice and technology have taken place since ICD-9-CM was first implemented. ICD-9-CM is limited in its ability to expand enumeration because of physical numbering constraints. t Some categories have vague and imprecise codes. Rationale for Change cont. Lack of specificity creates problems, such as: Inability to collect accurate data on new technology. Increased requirements for submission of documentation to support claims. Lack of quality data to support health outcomes. Less accurate reimbursement. Many of the ICD-9-CM categories have become full, making it difficult to create new codes. Once a category is full, several types of similar diagnoses or procedures are combined under one code, or a place is found in another section of the classification for a new code. 4
5 Rationale for Change cont. Due to a lack of space in the classification, several distinct procedures performed in different parts of the body with widely different resource utilization may be grouped together under the same procedure code. The structural integrity of the ICD-9-CM procedure classification has already been compromised: New code numbers have been assigned to chapter 00 and chapter 17 when new numbers were not available within the appropriate body system chapter. ICD-10-CM Improvements and Major Modifications Significant improvements in coding primary care encounters, external causes of injury, mental disorders, neoplasms, and preventive health Advances in medicine and medical technology that have occurred since the last revision Codes with more detail on socioeconomic conditions, family relationships, ambulatory care conditions, problems related to lifestyle, and the results of screening tests More space to accommodate future expansions (alphanumeric structure) New categories for post-procedural disorders 5
6 ICD-10-CM Improvements and Major Modifications The addition of laterality specifying which organ or part of the body is involved when the location could be on the right, the left, or bilateral Expanded distinctions for ambulatory and managed care encounters Expansion of diabetes and injury codes Creation of combination diagnosis/symptom codes to reduce the number of codes needed to fully describe a condition Greater specificity in code assignment Inclusion of trimester information in pregnancy codes Review Your Understanding of the g ICD-10-CM Compliance Date 6
7 Compliance Date HHS adopting ICD-10-CM and ICD-10-PCS as medical data code sets under HIPAA: Replacing volumes 1 and 2 for reporting diagnoses. Replacing volume 3 for reporting procedures. Replacing the official coding guidelines. ICD-10-PCS codes are not used in outpatient transactions, or by physicians: ICD-10-PCS codes are used only by hospitals for inpatient procedures. Full compliance was initially required for claims received for encounters and discharges on or after October 1, 2013 (FY 2014). Compliance Date (cont.) Compliance date is based on the date of discharge for inpatient claims, and the date of service for outpatient claims. Consistent with the practice for inpatient facilities to use the version of ICD codes in effect at the date of discharge. ICD-10-CM/PCS codes may not be reported before the compliance date. 7
 ICD-10 Implementation Schedule Pending Final Rule Previously HHS had mandated October 1, 2013 as the single compliance date where all covered entities must begin using the ICD- 10 code set.")
8 Compliance Date (cont.) ICD-10 Implementation Schedule Pending Final Rule Previously HHS had mandated October 1, 2013 as the single compliance date where all covered entities must begin using the ICD- 10 code set. On April 17, 2012, HHS published a rule proposing postponement of the ICD-10-CM/PCS for one year to take place then October 1, (provisional date) Compliance Date (cont.) On May 17, 2012, the comment period for interested parties to express and detail their particular position for or against the delay ended. We are now in limbo for what the final rule will be, and although there is no set standard for the timeline in the rule-making process, the final decision currently was scheduled to be announced on June 30, The announcement is still pending as of this date. 8
 Proposed a one year delay in ICD-10-CM is to the")



9 Compliance Date (cont.) Proposed a one year delay in ICD-10-CM is to the implementation date and not to the code set. The HIM community to move forward, to: Take a leadership role in educating colleagues about the benefits of ICD-10, Use any time gained from a deadline extension to ensure a smooth transition and fine tune your preparations Keep moving forward lead the way Watch on AHIMA s YouTube channel, AHIMA on Demand. Compliance Date (cont.) 9
10 Review Your Understanding of the ICD-10-CM CM Coding and Reporting Guidelines Coders Must Understand and Follow The basic principles behind the classification system in order to use ICD-10-CM and ICD-10-PCS appropriately and effectively. This knowledge is also the basis for understanding and applying the official coding advice provided through the AHA Coding Clinic, published by the Central Office of the American Hospital Association Note: There are plans to publish ICD-10 coding advice in Coding Clinic for ICD-9-CM starting with Fourth Quarter 2012, and Coding Clinic for ICD- 10-CM and ICD-10-PCS in
11 Coders Must Understand and Follow Official Guidelines for Coding and Reporting Developed through the editorial board for the Coding Clinic and approved by the four cooperating parties: American Hospital Association, American Health Information Management Association, Centers for Medicare & Medicaid Services (CMS), and National Center for Health Statistics (NCHS). ICD-10-CM Official Guidelines for Coding and Reporting The term encounter is used for all settings, including hospital admissions. In the context of these guidelines, the term provider is used throughout the guidelines to mean physician or any qualified health care practitioner who is legally accountable for establishing the patient s diagnosis. Only this set of guidelines, approved by the Cooperating Parties, is official. 11
12 ICD-10-CM Official Guidelines for Coding and Reporting cont. The guidelines are organized into sections. Section I includes the structure and conventions of the classification and general guidelines that apply to the entire classification, and chapter-specific guidelines that correspond to the chapters as they are arranged in the classification. ICD-10-CM Official Guidelines for Coding and Reporting cont. The guidelines are organized into sections. Section II includes guidelines for selection of principal diagnosis for non-outpatient settings. Section III includes guidelines for reporting additional diagnoses in non-outpatient settings. 12

13 ICD-10-CM Official Guidelines for Coding and Reporting cont. Section IV is for outpatient coding and reporting. It is necessary to review all sections of the guidelines to fully understand all of the rules and instructions needed to code properly. Review Your Understanding of Section I. Conventions, general coding guidelines and chapter specific guidelines 13
14 ICD-9-CM Vol. 1 & 2 & ICD-10-CM Comparison ICD 9 CM Diagnosis Codes ICD 10 CM Diagnosis Codes 3 5 characters in length 3 7 characters in length Approximately 13,000 codes First digit may be alpha (E or V) or numeric; Digits 2 5 are numeric Approximately 68,000 available codes First digit is alpha; Digits 2 3 are numeric; Digits 4 7 are alpha or numeric Limited space for adding new codes Lacks detail Lacks laterality Flexible for adding new codes Very specific Has laterality Example: Venous embolism and thrombosis of deep vessels of proximal lower extremity Example: I Embolism and thrombosis of right femoral vein Differences in the ICD-10-CM Code Structure All ICD-10-CM codes have an alphanumeric structure with all codes starting with an alphabetic character except the letter U. The basic code structure consists of three characters. A decimal point is used to separate the basic three-character category code from its subcategory and subclassifications. For example, L




15 Differences in the ICD-10-CM Code Structure Most ICD-10-CM codes contain a maximum of six characters, with a few categories having a seventh-character code extension. Each chapter in the main classification is structured to provide the following subdivisions: Sections (groups of three-character categories), e.g., Infections of the skin and subcutaneous tissue (L00-L08) Official Guidelines for Coding and Reporting 15



16 ICD-10-CM Section I. Conventions, general coding guidelines and chapter specific guidelines The conventions, general guidelines and chapter-specific guidelines are applicable to all health care settings unless otherwise indicated. The conventions and instructions of the classification take precedence over guidelines. Current ICD-10-CM Guidelines 16
17 ICD-10-CM Section I.A. A. Conventions for the ICD-10-CM The conventions for the ICD-10-CM are the general rules for use of the classification independent of the guidelines. These conventions are incorporated within the Alphabetic Index and Tabular List of the ICD-10-CM as instructional notes. ICD-10-CM Section I.A The Alphabetic Index and Tabular List The ICD-10-CM is divided into the Alphabetic Index, an alphabetical list of terms and their corresponding code, and the Tabular List, a chronological list of codes divided into chapters based on body system or condition. Continued 17
18 ICD-10-CM Section I.A The Alphabetic Index and Tabular List Continued The Alphabetic Index consists of the following parts: the Index of Diseases and Injury, the Index of External Causes of Injury, the Table of Neoplasms and the Table of Drugs and Chemicals. See Section I.C2. General guidelines See Section I.C.19. Adverse effects, poisoning, underdosing and toxic effects ICD-10-CM Section I.A Format and Structure: The ICD-10-CM CM Tabular List contains categories, subcategories and codes. Characters for categories, subcategories and codes may be either a letter or a number. All categories are 3 characters. A three-character category that has no further subdivision is equivalent to a code. Continued 18
19 ICD-10-CM Section I.A Format and Structure: Continued Subcategories are either 4 or 5 characters. Codes may be 3, 4, 5, 6 or 7 characters. That is, each level of subdivision after a category is a subcategory. The final level of subdivision is a code. Codes that have applicable 7th characters are still referred to as codes, not subcategories. A code that has an applicable 7th character is considered invalid without the 7th character. The ICD-10-CM uses an indented format for ease in reference. Review Your Understanding of ICD-10-CM Code Structure For example: K29 Gastritis and duodenitis (category) K29.0 Acute gastritis (subcategory) K29.00 Acute gastritis without bleeding (code) R10 Abdominal and pelvic pain (category) R10.8 Other abdominal pain (subcategory) R10.81 Abdominal tenderness (subcategory) R Right upper quadrant (code) abdominal tenderness 19
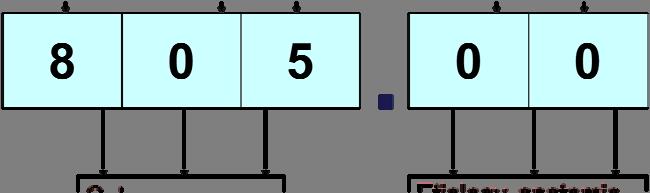
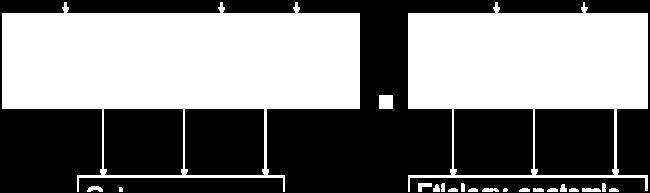


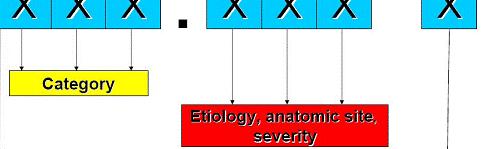
20 Changes Classifications ICD-9-CM Structured Format ICD-10-CM Format 20

 e.g.")




21 Review Your Understanding of ICD-10-CM Code Structure Subdivisions continued: Categories (three-character code numbers) e.g., L02, Cutaneous abscess, furuncle and carbuncle Subcategories (four-character code numbers), e.g., L02.2, Cutaneous abscess, furuncle and carbuncle of trunk Fifth-, sixth-, or seventh-character subclassifications (five-, six-, or sevencharacter code numbers), e.g., L02.211, Cutaneous abscess of abdominal wall Changes Classifications ICD-10-CM Structured Format 21
22 ICD-10-CM Section I.A Use of codes for reporting purposes For reporting purposes only codes are permissible, not categories or subcategories, and any applicable 7th character is required. ICD-10-CM Section I.A Placeholder character The ICD-10-CM utilizes a placeholder character X. The X is used as a placeholder at certain codes to allow for future expansion. An example of this is at the poisoning, adverse effect and underdosing codes, categories T36- T50. Where a placeholder exists, the X must be used in order for the code to be considered a valid code. 22
23 ICD-10-CM Section I.A Placeholder character Continued For Example, the use of the placeholder character x and the seventh-character extension is shown: T16 Foreign body in ear Includes: foreign body in auditory canal The following seventh-character extensions are to be added to each code from category T16: A initial encounter D subsequent encounter S sequela T16.1 Foreign body in right ear T16.2 Foreign body in left ear T16.9 Foreign body in ear, unspecified ear ICD-10-CM Section I.A th Characters Certain ICD-10-CM categories have applicable 7th characters. The applicable 7th character is required for all codes within the category, or as the notes in the Tabular List instruct. The 7th character must always be the 7th character in the data field. If a code that requires a 7th character is not 6 characters, a placeholder X must be used to fill in the empty characters. 23

 Chapter 15 represents fetus in multiple gestation affected by condition")
24 Coding and Use of 7 th Character Obstetrics Injury External cause Injury and External Cause - Identifies Injury Either alpha or numeric Placeholder X Meanings vary Initial Receiving active treatmentt t Coding and Use of 7 th Character Aftercare Z codes are not used for aftercare for injuries Combination codes for poisonings and external cause (accidental, intentional self-harm, assault, undetermined) Chapter 15 represents fetus in multiple gestation affected by condition being coded 24
25 ICD-10-CM Section I.A.6.a. 6. Abbreviations a. Alphabetic Index abbreviations NEC Not elsewhere classifiable This abbreviation in the Alphabetic Index represents other specified. When a specific code is not available for a condition, the Alphabetic Index directs the coder to the other specified code in the Tabular List. NOS Not otherwise specified This abbreviation is the equivalent of unspecified. Continued ICD-10-CM Section I.A.6.b. 6. Abbreviations Continued b. Tabular List abbreviations NEC Not elsewhere classifiable This abbreviation in the Tabular List represents other specified. When a specific code is not available for a condition the Tabular List includes an NEC entry under a code to identify the code as the other specified code. NOS Not otherwise specified This abbreviation is the equivalent of unspecified. 25
26 ICD-10-CM Section I.A Punctuation [ ] Brackets are used in the Tabular List to enclose synonyms, y alternative wording or explanatory phrases. Brackets are used in the Alphabetic Index to identify manifestation codes. ( ) Parentheses are used in both the Alphabetic Index and Tabular List to enclose supplementary words that may be present or absent in the statement of a disease or procedure without affecting the code number to which it is assigned. The terms within the parentheses are referred to as nonessential modifiers. Continued ICD-10-CM Section I.A Punctuation Continued : Colons are used in the Tabular List after an incomplete term which needs one or more of the modifiers following the colon to make it assignable to a given category. 26
27 ICD-10-CM Section I.A Use of and When the term and is used in a narrative statement it represents and/or. ICD-10-CM Section I.A.9.a 9. Other and Unspecified codes a. Other codes Codes titled other or other specified are for use when the information in the medical record provides detail for which a specific code does not exist. Alphabetic Index entries with NEC in the line designate other codes in the Tabular List. These Alphabetic Index entries represent specific disease entities for which no specific code exists so the term is included within an other code. 27
28 ICD-10-CM Section I.A.9.b. 9. Other and Unspecified codes b. Unspecified codes Codes titled unspecified are for use when the information in the medical record is insufficient to assign a more specific code. For those categories for which an unspecified code is not provided, the other specified code may represent both other and unspecified. ICD-10-CM Section I.A Includes Notes This note appears immediately under a three character code title to further define, or give examples of, the content of the category. 28
29 ICD-10-CM Section I.A Inclusion terms List of terms is included under some codes. These terms are the conditions for which that code is to be used. The terms may be synonyms of the code title, or, in the case of other specified codes, the terms are a list of the various conditions assigned to that code. The inclusion i terms are not necessarily exhaustive. Additional terms found only in the Alphabetic Index may also be assigned to a code. ICD-10-CM Section I.A Excludes Notes The ICD-10-CM has two types of excludes notes. Each type of note has a different definition for use but they are all similar in that they indicate that codes excluded from each other are independent of each other. 29
30 ICD-10-CM Section I.A.12.a. 12. Excludes Notes a. Excludes1 A type 1 Excludes note is a pure excludes note. It means NOT CODED HERE! An Excludes1 note indicates that the code excluded should never be used at the same time as the code above the Excludes1 note. An Excludes1 is used when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition. ICD-10-CM Section I.A.12.b. 12. Excludes Notes b. Excludes2 A type 2 excludes note represents Not included here. An excludes2 note indicates that the condition excluded is not part of the condition represented by the code, but a patient may have both conditions at the same time. When an Excludes2 note appears under a code, it is acceptable to use both the code and the excluded code together, when appropriate. 30



31 Exclusion 1 Exclusion 2 NEVER USE Together MAY USE Together Pure Exclude Note NEVER USE CANNOT occur together Is NOT INCLUDED Is NOT PART OF CONDITION May have SIMULTANEOUS conditions ICD-10-CM Section I.A Etiology/manifestation convention ( code first, use additional code and in diseases classified elsewhere notes) Certain conditions have both an underlying etiology and multiple body system manifestations due to the underlying etiology. For such conditions, the ICD-10-CM has a coding convention that requires the underlying condition be sequenced first followed by the manifestation. Wherever such a combination exists, there is a use additional code note at the etiology code, and a code first note at the manifestation code. These instructional notes indicate the proper sequencing order of the codes, etiology followed by manifestation. Continued 31
32 ICD-10-CM Section I.A Etiology/manifestation convention ( code first, use additional code and in diseases classified elsewhere notes). Continued In most cases the manifestation codes will have in the code title, in diseases classified elsewhere. Codes with this title are a component of the etiology/ manifestation convention. The code title indicates that it is a manifestation code. In diseases classified elsewhere codes are never permitted to be used as first-listed or principal diagnosis codes. They must be used in conjunction with an underlying condition code and they must be listed following the underlying condition. See category F02, Dementia in other diseases classified elsewhere, for an example of this convention. Continued ICD-10-CM Section I.A Etiology/manifestation convention ( code first, use additional code and in diseases classified elsewhere notes) ). Continued There are manifestation codes that do not have in diseases classified elsewhere in the title. For such codes a use additional code note will still be present and the rules for sequencing apply. In addition to the notes in the Tabular List, these conditions also have a specific Alphabetic Index entry structure. In the Alphabetic Index both conditions are listed together with the etiology code first followed by the manifestation codes in brackets. The code in brackets is always to be sequenced second. Continued 32
33 ICD-10-CM Section I.A Etiology/manifestation convention ( code first, use additional code and in diseases classified elsewhere notes) ). Continued An example of the etiology/manifestation convention is dementia in Parkinson s disease. In the Alphabetic Index, code G20 is listed first, followed by code F02.80 or F02.81 in brackets. Code G20 represents the underlying etiology, Parkinson s disease, and must be sequenced first, whereas codes F02.80 and F02.81 represent the manifestation of dementia in diseases classified elsewhere, with or without behavioral disturbance. Continued ICD-10-CM Section I.A Etiology/manifestation convention ( code first, use additional code and in diseases classified elsewhere notes) ). Continued Code first and Use additional code notes are also used as sequencing rules in the classification for certain codes that are not part of an etiology/ manifestation combination. See Section I.B.7. Multiple coding for a single condition. 33
34 ICD-10-CM Section I.A And The word and should be interpreted to mean either and or or when it appears in a title. ICD-10-CM Section I.A With The word with should be interpreted to mean associated with or due to when it appears in a code title, the Alphabetic Index, or an instructional note in the Tabular List. The word with in the Alphabetic Index is sequenced immediately following the main term, not in alphabetical order. 34
35 ICD-10-CM Section I.A See and See Also The see instruction following a main term in the Alphabetic Index indicates that another term should be referenced. It is necessary to go to the main term referenced with the see note to locate the correct code. Continued ICD-10-CM Section I.A See and See Also Continued A see also instruction following a main term in the Alphabetic Index instructs that there is another main term that may also be referenced that may provide additional Alphabetic Index entries that may be useful. It is not necessary to follow the see also note when the original main term provides the necessary code. 35
36 ICD-10-CM Section I.A Code also note A code also note instructs that two codes may be required to fully describe a condition, but this note does not provide sequencing direction. ICD-10-CM Section I.A Default codes A code listed next to a main term in the ICD- 10-CM Alphabetic Index is referred to as a default code. The default code represents that condition that is most commonly associated with the main term, or is the unspecified code for the condition. If a condition is documented in a medical record (for example, appendicitis) without any additional information, such as acute or chronic, the default code should be assigned. 36
37 Review Your Understanding of I.B. General Coding Guidelines for ICD-10-CM Section I.B.1. General Coding Guidelines 1. Locating a code in the ICD-10-CM: There are basic principles that all coders must follow. It is important to use both the Alphabetic Index and the Tabular List during the coding process. Follow all instructional notes Even if common codes have been memorized, refer to the Alphabetic Index and Tabular List 37
38 Section I.B.2. General Coding Guidelines 2. Level of Detail in Coding: Always assign codes to the highest level of detail. All characters must be used None can be omitted or added NEC and NOS codes should be assigned only when appropriate. Combination codes should be used if they are available. Assign multiple codes as needed to fully describe a condition. Avoid coding irrelevant information. Section I.B.3. General Coding Guidelines 3. Code or codes from A00.0 through T88.9, Z The appropriate code or codes from A00.0 through T88.9, Z00-Z99.8 must be used to identify diagnoses, symptoms, conditions, problems, complaints or other reason(s) for the encounter/visit. 38
39 Section I.B.4. General Coding Guidelines 4. Signs and symptoms Codes that describe symptoms and signs, as opposed to diagnoses, are acceptable for reporting purposes when a related definitive diagnosis has not been established (confirmed) by the provider. Chapter 18 of ICD-10-CM, Symptoms, Signs, and Abnormal Clinical i l and Laboratory Findings, Not Elsewhere Classified (codes R R99) contains many, but not all codes for symptoms. Section I.B.5. General Coding Guidelines 5. Conditions that are an integral part of a disease process Signs and symptoms that are associated routinely with a disease process should not be assigned as additional codes, unless otherwise instructed by the classification. 39
40 Section I.B.6. General Coding Guidelines 6. Conditions that are not an integral part of a disease process Additional signs and symptoms that may not be associated routinely with a disease process should be coded when present. Section I.B.7. General Coding Guidelines 7. Multiple coding for a single condition In addition to the etiology/ manifestation convention that requires two codes to fully describe a single condition that affects multiple body systems, there are other single conditions that also require more than one code. Use additional code notes are found in the Tabular List at codes that are not part of an etiology/manifestation pair where a secondary code is useful to fully describe a condition. The sequencing rule is the same as the etiology/manifestation pair, use additional code indicates that a secondary code should be added. 40
41 Section I.B.8. General Coding Guidelines 8. Acute and Chronic Conditions If the same condition is described as both acute (subacute) and chronic, and separate subentries exist in the Alphabetic Index at the same indentation level, code both and sequence the acute (subacute) code first. Section I.B.9. General Coding Guidelines 9. Combination Code A combination code is a single code used to classify: Two diagnoses, or A diagnosis with an associated secondary process (manifestation) Adi diagnosis i with an associated complication 41
42 Section I.B.10. General Coding Guidelines 10. Sequela (Late Effects) A sequela is the residual effect (condition produced) after the acute phase of an illness or injury has terminated. There is no time limit on when a sequela code can be used. The residual may be apparent early, such as in cerebral infarction, or it may occur months or years later, such as that due to a previous injury. Coding of sequela generally requires two codes sequenced in the following order: The condition or nature of the sequela is sequenced first. The sequela code is sequenced second. Section I.B.11. General Coding Guidelines 11. Impending or Threatened Condition Code any condition described at the time of discharge as impending or threatened as follows: If it did occur, code as confirmed diagnosis. If it did not occur, reference the Alphabetic Index to determine if the condition has a subentry term for impending or threatened and also reference main term entries for Impending and for Threatened. If the subterms are listed, assign the given code. If the subterms are not listed, code the existing underlying condition(s) and not the condition described as impending or threatened. 42
43 Section I.B.12. General Coding Guidelines 12. Reporting Same Diagnosis Code More than Once Each unique ICD-10-CM diagnosis code may be reported only once for an encounter. This applies to bilateral conditions when there are no distinct codes identifying laterality or two different conditions classified to the same ICD-10-CM diagnosis code. Section I.B.13. General Coding Guidelines 13. Laterality For bilateral sites, the final character of the codes in the ICD-10-CM indicates laterality. An unspecified side code is also provided should the side not be identified in the medical record. If no bilateral l code is provided d and the condition is bilateral, assign separate codes for both the left and right side. 43
44 Section I.B.14. General Coding Guidelines 14. Documentation for BMI and Pressure Ulcer Stages For the Body Mass Index (BMI) and pressure ulcer stage codes, code assignment may be based on medical record documentation from clinicians who are not the patient s provider (i.e., physician or other qualified healthcare practitioner legally accountable for establishing the patient s diagnosis), since this information is typically documented by other clinicians involved in the care of the patient (e.g., a dietitian often documents the BMI and nurses often documents the pressure ulcer stages). Section I.B.15. General Coding Guidelines 15. Syndromes Follow the Alphabetic Index guidance when coding syndromes. In the absence of Alphabetic Index guidance, assign codes for the documented manifestations of the syndrome. 44




45 Section I.B.16. General Coding Guidelines 16. Documentation of Complications of Care Code assignment is based on the provider s documentation of the relationship between the condition and the care or procedure. The guideline extends to any complications of care, regardless of the chapter the code is located in. It is important to note that not all conditions that occur during or following medical care or surgery are classified as complications. There must be a cause-and-effect and effect relationship between the care provided and the condition, and an indication in the documentation that it is a complication. Query the provider for clarification, if the complication is not clearly documented. Review Your Understanding of I.C. Chapter Specific Coding Guidelines for ICD-10-CM 45
46 Chapter-Specific Coding Guidelines Chapter-Specific Coding Guidelines In addition to general coding guidelines, there are guidelines for specific diagnoses and/or conditions in the classification. These will be reviewed and discussed later in the FHA ICD-10-CM CM series. Please consult your FHA schedule. Review your Understanding of Section Review your Understanding of Section II. Selection of Principal Diagnosis 46
47 Section II. Selection of Principal Diagnosis The circumstances of inpatient admission always govern the selection of principal i diagnosis. The principal diagnosis is defined in the Uniform Hospital Discharge Data Set (UHDDS) as that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care. Continued Section II. Selection of Principal Diagnosis cont. The UHDDS definitions are used by hospitals to report inpatient t data elements in a standardized manner. Since that time the application of the UHDDS definitions has been expanded to include all non-outpatient settings (acute care, short term, long term care and psychiatric hospitals; home health agencies; rehab facilities; nursing homes, etc.). Continued 47
48 Section II. Selection of Principal Diagnosis cont. In determining principal diagnosis, coding conventions in the ICD-10-CM, the Tabular List and Alphabetic Index take precedence over these official coding guidelines. (See Section I.A., Conventions for the ICD-10-CM) The importance of consistent, complete documentation in the medical record cannot be overemphasized. Without such documentation the application of all coding guidelines is a difficult, if not impossible, task. Section II.A. Selection of Principal Diagnosis cont. A. Codes for symptoms, signs, and illdefined conditions Codes for symptoms, signs, and ill-defined conditions from Chapter 18 are not to be used as principal diagnosis when a related definitive diagnosis has been established. 48
49 Section II.B. Selection of Principal Diagnosis cont. B. Two or more interrelated conditions, each potentially meeting the definition for principal diagnosis. When there are two or more interrelated conditions (such as diseases in the same ICD- 10-CM chapter or manifestations characteristically associated with a certain disease) potentially meeting the definition of principal diagnosis, either condition may be sequenced first, unless the circumstances of the admission, the therapy provided, the Tabular List, or the Alphabetic Index indicate otherwise. Section II.C. Selection of Principal Diagnosis cont. C. Two or more diagnoses that equally meet the definition for principal diagnosis In the unusual instance when two or more diagnoses equally meet the criteria for principal diagnosis as determined by the circumstances of admission, diagnostic workup and/or therapy provided, and the Alphabetic Index, Tabular List, or another coding guidelines does not provide sequencing direction, any one of the diagnoses may be sequenced first. 49
50 Section II. Selection of Principal Diagnosis cont. D. Two or more comparative or contrasting conditions. In those rare instances when two or more contrasting or comparative diagnoses are documented as either/or (or similar terminology), they are coded as if the diagnoses were confirmed and the diagnoses are sequenced according to the circumstances of the admission. If no further determination can be made as to which diagnosis should be principal, either diagnosis may be sequenced first. Section II.E & II.F Selection of Principal Diagnosis cont. E. A symptom(s) followed by contrasting/comparative diagnoses When a symptom(s) is followed by contrasting/comparative diagnoses, the symptom code is sequenced first. All the contrasting/comparative diagnoses should be coded as additional diagnoses. F. Original treatment plan not carried out Sequence as the principal diagnosis the condition, which after study occasioned the admission to the hospital, even though treatment may not have been carried out due to unforeseen circumstances. 50
51 Section II.G Selection of Principal Diagnosis cont. G. Complications of surgery and other medical care When the admission is for treatment of a complication resulting from surgery or other medical care, the complication code is sequenced as the principal diagnosis. If the complication is classified to the T80-T88 series and the code lacks the necessary specificity in describing the complication, an additional code for the specific complication should be assigned. Section II.H Selection of Principal Diagnosis cont. H. Uncertain Diagnosis If the diagnosis documented at the time of discharge is qualified as probable, suspected, likely, questionable, possible, or still to be ruled out, or other similar terms indicating uncertainty, code the condition as if it existed or was established. The bases for these guidelines are the diagnostic workup, arrangements for further workup or observation, and initial therapeutic approach that correspond most closely with the established diagnosis. Note: This guideline is applicable only to inpatient admissions to short-term, acute, long-term care and psychiatric hospitals. 51
52 Section II.I.1. Selection of Principal Diagnosis cont. I.1. Admission Following Medical Observation When a patient is admitted to an observation unit for a medical condition, which either worsens or does not improve, and is subsequently admitted as an inpatient of the same hospital for this same medical condition, the principal diagnosis would be the medical condition which led to the hospital admission. Section II.I.2. Selection of Principal Diagnosis cont. I.2. Admission Following Post- Operative Observation When a patient is admitted to an observation unit to monitor a condition (or complication) that develops following outpatient surgery, and then is subsequently admitted as an inpatient of the same hospital, hospitals should apply the Uniform Hospital Discharge Data Set (UHDDS) definition of principal diagnosis as "that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care." 52
53 Section II.J Selection of Principal Diagnosis cont. J. Admission from Outpatient Surgery When a patient receives surgery in the hospital's outpatient surgery department and is subsequently admitted for continuing inpatient care at the same hospital, the following guidelines should be followed in selecting the principal diagnosis for the inpatient admission: Continued Section II.J Selection of Principal Diagnosis cont. J. Admission from Outpatient Surgery continued If the reason for the inpatient admission is a complication, assign the complication as the principal diagnosis. If no complication, or other condition, is documented as the reason for the inpatient admission, assign the reason for the outpatient surgery as the principal diagnosis. If the reason for the inpatient admission is another condition unrelated to the surgery, assign the unrelated condition as the principal diagnosis. 53
54 Review your Understanding of Section III. Reporting Additional Diagnoses Section III. Reporting Additional Diagnoses General Rules for Other (Additional) Diagnoses For reporting purposes the definition iti for other diagnoses is interpreted as additional conditions that affect patient care in terms of requiring: clinical evaluation; or therapeutic treatment; or diagnostic procedures; or extended length of hospital stay; or increased nursing care and/or monitoring. Continued 54
55 Section III. Reporting Additional Diagnoses cont. General Rules for Other (Additional) Diagnoses The UHDDS item #11-b defines Other Diagnoses as all conditions that coexist at the time of admission, that develop subsequently, or that affect the treatment received and/or the length of stay. Diagnoses that relate to an earlier episode which have no bearing on the current hospital stay are to be excluded. UHDDS definitions apply to inpatients in acute care, short-term, long term care and psychiatric hospital setting. The UHDDS definitions are used by acute care short-term hospitals to report inpatient data elements in a standardized manner. Section III. Reporting Additional Diagnoses cont. General Rules for Other (Additional) Diagnoses Since that time the application of the UHDDS definitions has been expanded to include all non-outpatient settings (acute care, short term, long term care and psychiatric hospitals; home health agencies; rehab facilities; nursing homes, etc.). The following guidelines are to be applied in designating other diagnoses when neither the Alphabetic Index nor the Tabular List in ICD-10-CM CM provide direction. The listing of the diagnoses in the patient record is the responsibility of the attending provider. 55
56 Section III. Reporting Additional Diagnoses cont. A. Previous conditions If the provider has included a diagnosis in the final diagnostic statement, such as the discharge summary or the face sheet, it should ordinarily be coded. Some providers include in the diagnostic statement resolved conditions or diagnoses and status-post procedures from previous admission that have no bearing on the current stay. Such conditions are not to be reported and are coded only if required by hospital policy. However, history codes (categories Z80-Z87) may be used as secondary codes if the historical condition or family history has an impact on current care or influences treatment. Section III. Reporting Additional Diagnoses cont. B. Abnormal findings Abnormal findings (laboratory, x-ray, pathologic, and other diagnostic results) are not coded and reported unless the provider indicates their clinical significance. If the findings are outside the normal range and the attending provider has ordered other tests to evaluate the condition or prescribed treatment, it is appropriate p to ask the provider whether the abnormal finding should be added. Please note: This differs from the coding practices in the outpatient setting for coding encounters for diagnostic tests that have been interpreted by a provider. 56


57 Section III. Reporting Additional Diagnoses cont. C. Uncertain Diagnosis If the diagnosis documented at the time of discharge is qualified as probable, suspected, likely, questionable, possible, or still to be ruled out or other similar terms indicating uncertainty, code the condition as if it existed or was established. The bases for these guidelines are the diagnostic workup, arrangements for further workup or observation, and initial therapeutic approach that correspond most closely with the established diagnosis. Note: This guideline is applicable only to inpatient admissions to short-term, acute, long-term care and psychiatric hospitals. Review your Understanding of Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient Services 57
58 Diagnostic Coding and Reporting Guidelines for Outpatient Services Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient Services These coding guidelines for outpatient diagnoses have been approved for use by hospitals/ providers in coding and reporting hospital-based outpatient services and provider-based office visits. Continued Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient ti t Services Continued Information about the use of certain abbreviations, punctuation, symbols, and other conventions used in the ICD-10-CM Tabular List (code numbers and titles), can be found in Section IA of these guidelines, under Conventions Used in the Tabular List. Information about the correct sequence to use in finding a code is also described in Section I. Continued 58
59 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient ti t Services Continued The terms encounter and visit are often used interchangeably in describing outpatient service contacts and, therefore, appear together in these guidelines without distinguishing one from the other. Continued Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient ti t Services Continued Though the conventions and general guidelines apply to all settings, coding guidelines for outpatient and provider reporting of diagnoses will vary in a number of instances from those for inpatient t diagnoses, recognizing i that: t The Uniform Hospital Discharge Data Set (UHDDS) definition of principal diagnosis applies only to inpatients in acute, short-term, long-term care and psychiatric hospitals. Coding guidelines for inconclusive diagnoses (probable, suspected, rule out, etc.) were developed for inpatient reporting and do not apply to outpatients. 59
60 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. A. Selection of first-listed condition In the outpatient setting, the term firstlisted diagnosis is used in lieu of principal diagnosis. In determining the first-listed diagnosis the coding conventions of ICD-10-CM, as well as the general and disease specific guidelines take precedence over the outpatient guidelines. Cont. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. A. Selection of first-listed condition Diagnoses often are not established at the time of the initial encounter/visit. It may take two or more visits before the diagnosis is confirmed. The most critical rule involves beginning the search for the correct code assignment through the Alphabetic Index. Never begin searching initially in the Tabular List as this will lead to coding errors. 60
61 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. A1. Outpatient Surgery When a patient presents for outpatient surgery (same day surgery), code the reason for the surgery as the first-listed diagnosis (reason for the encounter), even if the surgery is not performed due to a contraindication. ti Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. A.2. Observation Stay When a patient is admitted for observation for a medical condition, assign a code for the medical condition as the first-listed diagnosis. When a patient presents for outpatient surgery and develops complications requiring admission to observation, code the reason for the surgery as the first reported diagnosis (reason for the encounter), followed by codes for the complications as secondary diagnoses. 61
62 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. B. Codes from A00.0 through T88.9, Z00- Z99 The appropriate code(s) from A00.0 through T88.9, Z00-Z99 must be used to identify diagnoses, symptoms, conditions, problems, complaints, or other reason(s) for the encounter/visit. C. Accurate reporting of ICD-10-CM diagnosis codes For accurate reporting of ICD-10-CM diagnosis codes, the documentation should describe the patient s condition, using terminology which includes specific diagnoses as well as symptoms, problems, or reasons for the encounter. There are ICD-10-CM codes to describe all of these. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. D. Codes that describe symptoms and signs Codes that describe symptoms and signs, as opposed to diagnoses, are acceptable for reporting purposes when a diagnosis has not been established (confirmed) by the provider. Chapter 18 of ICD-10-CM, Symptoms, Signs, and Abnormal Clinical and Laboratory Findings Not Elsewhere Classified (codes R00-R99) contain many, but not all codes for symptoms. 62
63 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. E. Encounters for circumstances other than a disease or injury ICD-10-CM provides codes to deal with encounters for circumstances other than a disease or injury. The Factors Influencing Health Status and Contact with Health Services codes (Z00-Z99) are provided to deal with occasions when circumstances other than a disease or injury are recorded as diagnosis or problems. See Section I.C.21. Factors influencing health status and contact with health services. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. F. Level of Detail in Coding 1. ICD-10-CM codes with 3, 4, 5, 6 or 7 characters ICD-10-CM is composed of codes with 3, 4, 5, 6 or 7 characters. Codes with three characters are included in ICD-10-CM as the heading of a category of codes that may be further subdivided by the use of fourth, fifth, sixth or seventh characters to provide greater specificity. 63
64 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. F. Level of Detail in Coding 2. Use of full number of characters required for a code A three-character code is to be used only if it is not further subdivided. A code is invalid if it has not been coded to the full number of characters required for that code, including the 7th character, if applicable. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. G. ICD-10-CM code for the diagnosis, condition, problem, or other reason for encounter/visit List first the ICD-10-CM code for the diagnosis, condition, problem, or other reason for encounter/visit shown in the medical record to be chiefly responsible for the services provided. List additional codes that describe any coexisting conditions. In some cases the first-listed diagnosis may be a symptom when a diagnosis has not been established (confirmed) by the physician. 64
65 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. H. Uncertain diagnosis Do not code diagnoses documented as probable, suspected, questionable, rule out, or working diagnosis or other similar terms indicating uncertainty. Rather, code the condition(s) to the highest degree of certainty for that encounter/visit, such as symptoms, signs, abnormal test results, or other reason for the visit. Please note: This differs from the coding practices used by short-term, acute care, longterm care and psychiatric hospitals. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. I. Chronic diseases Chronic diseases treated on an ongoing basis may be coded and reported as many times as the patient receives treatment and care for the condition(s) 65
66 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. J. Code all documented conditions that coexist Code all documented conditions that coexist at the time of the encounter/visit, and require or affect patient care treatment or management. Do not code conditions that were previously treated and no longer exist. However, history codes (categories Z80-Z87) may be used as secondary codes if the historical condition or family history has an impact on current care or influences treatment. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. K. Patients receiving diagnostic services only For patients receiving diagnostic services only during an encounter/visit, sequence first the diagnosis, condition, problem, or other reason for encounter/visit shown in the medical record to be chiefly responsible for the outpatient services provided d during the encounter/visit. it Codes for other diagnoses (e.g., chronic conditions) may be sequenced as additional diagnoses. 66
67 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. K. Patients receiving diagnostic services only Continued For encounters for routine laboratory/radiology testing in the absence of any signs, symptoms, or associated diagnosis, assign Z01.89, Encounter for other specified special examinations. If routine testing is performed during the same encounter as a test t to evaluate a sign, symptom, or diagnosis, it is appropriate to assign both the Z code and the code describing the reason for the non-routine test. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. K. Patients receiving diagnostic services only Continued For outpatient encounters for diagnostic tests that have been interpreted by a physician, and the final report is available at the time of coding, code any confirmed or definitive diagnosis(es) documented in the interpretation. Do not code related signs and symptoms as additional diagnoses. Please note: This differs from the coding practice in the hospital inpatient setting regarding abnormal findings on test results. 67
68 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. L. Patients receiving therapeutic services only For patients receiving therapeutic services only during an encounter/visit, sequence first the diagnosis, condition, problem, or other reason for encounter/visit shown in the medical record to be chiefly responsible for the outpatient services provided during the encounter/visit. Codes for other diagnoses (e.g., chronic conditions) may be sequenced as additional diagnoses. The only exception to this rule is that when the primary reason for the admission/encounter is chemotherapy or radiation therapy, the appropriate Z code for the service is listed first, and the diagnosis or problem for which the service is being performed listed second. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. M. Patients receiving preoperative evaluations only For patients receiving preoperative evaluations only, sequence first a code from subcategory Z01.81, Encounter for preprocedural examinations, to describe the preop consultations. Assign a code for the condition to describe the reason for the surgery as an additional diagnosis. Code also any findings related to the pre-op evaluation. 68
69 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. N. Ambulatory surgery For ambulatory surgery, code the diagnosis for which the surgery was performed. If the postoperative diagnosis is known to be different from the preoperative diagnosis at the time the diagnosis i is confirmed, select the postoperative diagnosis for coding, since it is the most definitive. Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. O. Routine outpatient prenatal visits See Section I.C.15. Routine outpatient prenatal visits. P. Encounters for general medical examinations with abnormal findings The subcategories for encounters for general medical examinations, Z00.0-, provide codes for with and without abnormal findings. Should a general medical examination result in an abnormal finding, the code for general medical examination with abnormal finding should be assigned as the first-listed diagnosis. A secondary code for the abnormal finding should also be coded. 69





70 Diagnostic Coding and Reporting Guidelines for Outpatient Services cont. Q. Encounters for routine health screenings See Section I.C.21. Factors influencing health status and contact with health services, Screening Identify Ethical Coding and Reporting Review Standards Your Understanding of Ethical Coding and Reporting Standards 70
71 Ethical Coding and Reporting Medicare reimbursement depends on: The correct designation of the principal diagnosis, The presence or absence of additional codes that represent complications, comorbidities, or major complications or comorbidities as defined by the MSDRG system, and Procedures performed. Other third-party payers may follow slightly different reimbursement methods, but the accuracy of ICD-9-CM coding is always vital. Ethical Coding and Reporting cont. Accurate and ethical ICD-9-CM coding Depends on correctly following all instructions in the coding manuals, official guidelines, and Coding Clinic for ICD-9-CM. Requires the correct selection of conditions that meet the criteria set by the UHDDS and the official guidelines. Over-coding and over-reporting is unethical and may be considered fraudulent. Failure to include all diagnoses or procedures that meet reporting criteria may result in financial loss for the health care provider. Coders should abide by the AHIMA Standards of Ethical Coding. 71




72 Ethical Coding and Reporting cont. Medicare identifies certain codes as unacceptable as the principal diagnosis. Third-party payers may question or deny payment. It is important to code correctly, and then make whatever adjustment is required for reporting. Otherwise, the coder runs the risk of developing incorrect coding practices that will distort data used for other purposes. A facility may collect nonreportable diagnoses or procedures for internal use if the information is maintained outside the external reporting system. Review Your Understanding of the 2012 Version 5010 and HIPAA Requirements The Version 5010 enforcement discretion period ended on June 30,
73 Overview All health plans, providers, and clearinghouses that conduct business electronically are preparing p to convert to the next Health Insurance Portability and Accountability Act (HIPAA) standard for electronic transactions Version HIPAA will require entities conducting electronic claim submissions, claim status requests and responses, referral/authorization requests and responses, eligibility/benefit requests and responses, and claim remittances to use Version Version 5010 and HIPAA Requirements Version 5010 is Critical The Version 5010 enforcement discretion period ended on June 30, Make sure to submit claims in Version 5010 to ensure that your claims are not rejected. Software upgrades to Version 5010 are required for your systems to accommodate ICD-10 codes. As of January 1, 2012, everyone covered by HIPAA should have completed the upgrade to Version


74 ICD-10-CM Resources and References ICD-10-CM Resources & References ICD-10-CM Draft Official Guidelines for Coding and Reporting Release of ICD-10-CM Code Guidelines, Addenda, List of Codes, GEMS HHS Announces Intent to Delay ICD-10-CM/PCS Compliance Date Search for the February 16, 2012 press release 74

75 ICD-10-CM Resources & References 2012 ICD-10-CM is available at or hhs 2012 ICD-10-CM Index to Diseases and Injuries 2012 ICD-10-CM Tabular List of Diseases and Injuries Instructional Notations 2012 Official Guidelines for Coding and Reporting 2012 Table of Drugs and Chemicals 2012 Neoplasm Table 2012 Index to External Causes 2012 Mapping ICD-9-CM to ICD-10-CM and ICD-10-CM to ICD-9-CM ICD-10-CM Resources & References General ICD-10 Information General Equivalence Mappings and User s Guides 0_ICD10PCS.asp _ICD_10_CM.asp 75
76 ICD-10-CM Resources & References ICD-10-CM: The Complete Official Draft Code Set 2012 (by OptumInsight, formerly Ingenix) Introduction ICD-10-CM Draft Conventions ICD-10-CM Official Guidelines for Coding and Reporting (Draft 2012) ICD-10-CM Index to Diseases and Injuries ICD-10-CM Neoplasm Table Table of Drugs and Chemicals ICD-10-CM Index to External Causes ICD-10-CM Tabular List of Diseases and Injuries ICD-10-CM Resources & References 2013 Release of ICD-10-CM The National Center for Health Statistics has posted some of the 2013 ICD-10-CM files, including the ICD-10-CM Addenda and the 2013 version of ICD- 10-CM in PDF and XML format. Watch for further updates as additional 2013 ICD- 10-CM files are posted, including mapping files and the updated ICD-10-CM CM coding guidelines. Click here to access the 2013 ICD-10-CM files: 76



77 Audience Questions August 24,
THE ART OF DIAGNOSTIC CODING PART 1
 THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
a. General E Code Coding Guidelines
 19. Supplemental Classification of External Causes of Injury and Poisoning (E-codes, E800-E999) Introduction: These guidelines are provided for those who are currently collecting E codes in order that
19. Supplemental Classification of External Causes of Injury and Poisoning (E-codes, E800-E999) Introduction: These guidelines are provided for those who are currently collecting E codes in order that
Institute on Medicare and Medicaid Payment Issues March 28 30, 2012 Robert A. Pelaia, JD, CPC
 I. Introduction Institute on Medicare and Medicaid Payment Issues March 28 30, 2012 Robert A. Pelaia, JD, CPC Senior University Counsel for Health Affairs - Jacksonville 904-244-3146 robert.pelaia@jax.ufl.edu
I. Introduction Institute on Medicare and Medicaid Payment Issues March 28 30, 2012 Robert A. Pelaia, JD, CPC Senior University Counsel for Health Affairs - Jacksonville 904-244-3146 robert.pelaia@jax.ufl.edu
FY2013-FY2014 CHANGES TO ICD-9-CM CODING HANDBOOK WITH ANSWERS
 FY2013-FY2014 CHANGES TO ICD-9-CM CODING HANDBOOK WITH ANSWERS Narrative changes appear in bold italicized text; deletions show as strike-through text. Revised 4/10/14 Page FY2012 Text Number 39 Because
FY2013-FY2014 CHANGES TO ICD-9-CM CODING HANDBOOK WITH ANSWERS Narrative changes appear in bold italicized text; deletions show as strike-through text. Revised 4/10/14 Page FY2012 Text Number 39 Because
Presented by: Gary Lucas, CPC, CPC-I, AHIMA Approved ICD-10-CM & PCS Trainer and Ambassador
 Presented by: Gary Lucas, CPC, CPC-I, AHIMA Approved ICD-10-CM & PCS Trainer and Ambassador President, Discover Compliance Resources, Inc. Atlanta/Decatur, GA June 5, 2013 Alabama-Georgia Rural Health
Presented by: Gary Lucas, CPC, CPC-I, AHIMA Approved ICD-10-CM & PCS Trainer and Ambassador President, Discover Compliance Resources, Inc. Atlanta/Decatur, GA June 5, 2013 Alabama-Georgia Rural Health
PPS Coding in the Rehabilitation Setting. Copyright (c) 2015 by American Hospital Association. All rights reserved.
 2015 by American Hospital Association. All rights reserved.") PPS Coding in the Rehabilitation Setting 1 Gretchen Young-Charles, RHIA Senior Coding Consultant 2 Disclaimer This presentation is designed to provide accurate and authoritative information in regard to
PPS Coding in the Rehabilitation Setting 1 Gretchen Young-Charles, RHIA Senior Coding Consultant 2 Disclaimer This presentation is designed to provide accurate and authoritative information in regard to
ICD-10-CM/PCS Building Expert Trainers in Diagnostic and Procedure Coding. Information Provided by: AHIMA Academy for ICD-10-CM/PCS Trainers
 ICD-10-CM/PCS 2011 Building Expert Trainers in Diagnostic and Procedure Coding Information Provided by: AHIMA Academy for ICD-10-CM/PCS Trainers www.ahima.org/icd10 About Version HIPAA 5010 To process
ICD-10-CM/PCS 2011 Building Expert Trainers in Diagnostic and Procedure Coding Information Provided by: AHIMA Academy for ICD-10-CM/PCS Trainers www.ahima.org/icd10 About Version HIPAA 5010 To process
Inappropriate Primary Diagnosis Codes Policy
 Policy Number 2017R0122H Inappropriate Primary Diagnosis Codes Policy Annual Approval Date 11/8/2017 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission
Policy Number 2017R0122H Inappropriate Primary Diagnosis Codes Policy Annual Approval Date 11/8/2017 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission
ICD-10 is Here! What Now? Process, Pitfalls and Proactive Solutions
 ICD-10 is Here! What Now? Process, Pitfalls and Proactive Solutions Maureen McCarthy, RN, BS, RAC-MT President & CEO Celtic Consulting, LLC www.celticconsulting.org Define ICD-10 Discuss the impact of
ICD-10 is Here! What Now? Process, Pitfalls and Proactive Solutions Maureen McCarthy, RN, BS, RAC-MT President & CEO Celtic Consulting, LLC www.celticconsulting.org Define ICD-10 Discuss the impact of
HomeTown Health HCCS. Hospital Consortium Project: Track 1 Nuts and Bolts of: CDI Proficiencies
 HomeTown Health HCCS Hospital Consortium Project: Track 1 Nuts and Bolts of: CDI Proficiencies Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD 10 CM/PCS Trainer Director of Coding Healthcare Coding
HomeTown Health HCCS Hospital Consortium Project: Track 1 Nuts and Bolts of: CDI Proficiencies Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD 10 CM/PCS Trainer Director of Coding Healthcare Coding
Questions. 2. What is printed in bold in Volume 2? a. Subterms b. Anatomical sites c. Latin words d. Main terms e. Procedures
 2009 Home Health ICD-9 Basics Competencies Examination Outline These questions represent the variety of subjects that are involved in the ICD-9 Basics exam. All of the questions on this competency exam
2009 Home Health ICD-9 Basics Competencies Examination Outline These questions represent the variety of subjects that are involved in the ICD-9 Basics exam. All of the questions on this competency exam
Ten Tips for ICD-10. September 17, Theresa Marshall, Sr. Director Compliance Data Experian Health
 Ten Tips for ICD-10 September 17, 2015 Theresa Marshall, Sr. Director Compliance Data Experian Health Experian and the marks used herein are service marks or registered trademarks of Experian Information
Ten Tips for ICD-10 September 17, 2015 Theresa Marshall, Sr. Director Compliance Data Experian Health Experian and the marks used herein are service marks or registered trademarks of Experian Information
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #38 Transitioning from ICD-9 to ICD-10 Wednesday, August 7 10:30 to 11:30 a.m. Atlantic 3 Upon completion
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #38 Transitioning from ICD-9 to ICD-10 Wednesday, August 7 10:30 to 11:30 a.m. Atlantic 3 Upon completion
Presented by: Sparkle Sparks, PT MPT HCS-D COS-C AHIMA Approved ICD-10 Coding Instructor OASIS Answers, Inc. Senior Associate Consultant
 Presented by: Sparkle Sparks, PT MPT HCS-D COS-C AHIMA Approved ICD-10 Coding Instructor OASIS Answers, Inc. Senior Associate Consultant This educational presentation is provided by The preferred partner
Presented by: Sparkle Sparks, PT MPT HCS-D COS-C AHIMA Approved ICD-10 Coding Instructor OASIS Answers, Inc. Senior Associate Consultant This educational presentation is provided by The preferred partner
Jurisdiction 1 Part B Updated ICD-10 Implementation Information. 1 of 7 10/1/12 8:44 AM
 ^ Back to Top Palmetto GBA CorporatePalmetto GBA Medicare Palmetto GBA Home / Jurisdiction 1 Part B / Browse by Topic / ICD-10 / Updated ICD-10 Implementation... Jurisdiction 1 Part B Updated ICD-10 Implementation
^ Back to Top Palmetto GBA CorporatePalmetto GBA Medicare Palmetto GBA Home / Jurisdiction 1 Part B / Browse by Topic / ICD-10 / Updated ICD-10 Implementation... Jurisdiction 1 Part B Updated ICD-10 Implementation
Transitioning to ICD-10-CM
 Transitioning to ICD-10-CM August 6, 2015 1488_0115 Today s Presenters Arlene Dunphy, CPC Provider Outreach and Education Consultant Alicia Forbes, CPC Provider Outreach and Education Consultant 2 Disclaimer
Transitioning to ICD-10-CM August 6, 2015 1488_0115 Today s Presenters Arlene Dunphy, CPC Provider Outreach and Education Consultant Alicia Forbes, CPC Provider Outreach and Education Consultant 2 Disclaimer
ICD-9 (Diagnosis) Coding
 Coding") 1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
Overview and Checklist
 How to Prepare for ICD-10 in Medical Practices:????? Overview and Checklist? By Betsy Nicoletti, M.S., CPC? $? A Resource Provided by Medical-Billing.com Table of Contents About the Author 3 How to Prepare
How to Prepare for ICD-10 in Medical Practices:????? Overview and Checklist? By Betsy Nicoletti, M.S., CPC? $? A Resource Provided by Medical-Billing.com Table of Contents About the Author 3 How to Prepare
ICD-10: Preparation and Implementation Strategies Leah Killian-Smith
 Transitioning from ICD 9 to 10, LNHA, RHIA Director of Corporate Accounts OBJECTIVES Know what ICD-10 is & why coding is changing Know differences between ICD-9 and ICD-10 Identify regulatory requirements
Transitioning from ICD 9 to 10, LNHA, RHIA Director of Corporate Accounts OBJECTIVES Know what ICD-10 is & why coding is changing Know differences between ICD-9 and ICD-10 Identify regulatory requirements
Pathway Health, Inc. 1
 OBJECTIVES Transitioning from ICD 9 to 10 Leah Killian-Smith, LNHA, RHIA Director of Corporate Accounts Know what ICD-10 is & why coding is changing Know differences between ICD-9 and ICD-10 Identify regulatory
OBJECTIVES Transitioning from ICD 9 to 10 Leah Killian-Smith, LNHA, RHIA Director of Corporate Accounts Know what ICD-10 is & why coding is changing Know differences between ICD-9 and ICD-10 Identify regulatory
L6615. Coding CPCS. what Every. Professional Should Know 90.1
 CPT S8092 D6212 ICD-9-CM L6615 Coding and You CPCS 86567 what Every 0 90.1 Healthcare Professional Should Know 423 172.2 D6212 092 L6615 Coding and You what Every healthcare Professional Should Know is
CPT S8092 D6212 ICD-9-CM L6615 Coding and You CPCS 86567 what Every 0 90.1 Healthcare Professional Should Know 423 172.2 D6212 092 L6615 Coding and You what Every healthcare Professional Should Know is
ICD-10 Readiness. Adriana Villagrana
 ICD-10 Readiness Adriana Villagrana Where Does ICD-10 Fit In? Common reliance on complete and accurate data and clinical documentation Meaningful Use Quality reporting Value-based purchasing Hospital-acquired
ICD-10 Readiness Adriana Villagrana Where Does ICD-10 Fit In? Common reliance on complete and accurate data and clinical documentation Meaningful Use Quality reporting Value-based purchasing Hospital-acquired
FAQ for Coding Encounters in ICD 10 CM
 FAQ for Coding Encounters in ICD 10 CM Topics: Encounter for Routine Health Exams Encounter for Vaccines Follow Up Encounters Coding for Injuries Encounter for Suture Removal External Cause Codes Tobacco
FAQ for Coding Encounters in ICD 10 CM Topics: Encounter for Routine Health Exams Encounter for Vaccines Follow Up Encounters Coding for Injuries Encounter for Suture Removal External Cause Codes Tobacco
Diagnosis Code Requirements - Invalid As Primary
 Manual: Policy Title: Reimbursement Policy Diagnosis Code Requirements - Invalid As Primary Section: Administrative Subsection: Diagnosis Codes Date of Origin: 1/1/2000 Policy Number: RPM054 Last Updated:
Manual: Policy Title: Reimbursement Policy Diagnosis Code Requirements - Invalid As Primary Section: Administrative Subsection: Diagnosis Codes Date of Origin: 1/1/2000 Policy Number: RPM054 Last Updated:
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Addressing and clarifying 2017 Guideline recommendations
 Addressing and clarifying 2017 Guideline recommendations WHITE PAPER z FEATURES Supportive documentation..2 Tipping the scales... 3 Reminders... 3 Additional changes... 4 PCS concerns... 5 Sepsis... 7
Addressing and clarifying 2017 Guideline recommendations WHITE PAPER z FEATURES Supportive documentation..2 Tipping the scales... 3 Reminders... 3 Additional changes... 4 PCS concerns... 5 Sepsis... 7
PROFESSIONAL MEDICAL CODING AND BILLING WITH APPLIED PCS LEARNING OBJECTIVES
 The Professional Medical Coding and Billing with Applied PCS classes have been designed by experts with decades of experience working in and teaching medical coding. This experience has led us to a 3-
The Professional Medical Coding and Billing with Applied PCS classes have been designed by experts with decades of experience working in and teaching medical coding. This experience has led us to a 3-
ICD-CM Coding The Structural Considerations
 The Challenge ICD-CM Coding The Structural Considerations Hospices are being called upon to 1. Start using ICD-9 CM coding on its claims 2. Be prepared to transition to ICD-10-CM by 10/1/2014 Complicating
The Challenge ICD-CM Coding The Structural Considerations Hospices are being called upon to 1. Start using ICD-9 CM coding on its claims 2. Be prepared to transition to ICD-10-CM by 10/1/2014 Complicating
HEALTH DEPARTMENT BILLING GUIDELINES
 HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
HEALTH DEPARTMENT BILLING GUIDELINES Acknowledgement: Current Procedural Terminology (CPT ) is copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative
Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims
 March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
Anatomy and Physiology: A Critical First Step
 LET THE COUNT DOWN BEGIN Anatomy and Physiology: A Critical First Step Getting Medical Coders Ready for ICD-10-CM/PCS Authored by Clare Carvel, M.Ed., RHIA, CCS Education Consultant Barry Libman, Inc.
LET THE COUNT DOWN BEGIN Anatomy and Physiology: A Critical First Step Getting Medical Coders Ready for ICD-10-CM/PCS Authored by Clare Carvel, M.Ed., RHIA, CCS Education Consultant Barry Libman, Inc.
COMPREHENSIVE BILLING SERIES - PART 8 DIAGNOSIS CODING. for clients of: Content developed and presented by:
 COMPREHENSIVE BILLING SERIES - PART 8 DIAGNOSIS CODING for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: Polaris Group 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607
COMPREHENSIVE BILLING SERIES - PART 8 DIAGNOSIS CODING for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: Polaris Group 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607
ICD-10 and Gastroenterology
 ICD-10 and Gastroenterology Steven M. Verno, CMBSI, CEMCS, CMSCS, CPM-MCS Page 1 of 31 ICD-10 and Gastroenterology Steven M. Verno, CMBSI, CEMCS, CMSCS, CPM-MCS Note: ICD-9-CM and ICD-10 are owned and
ICD-10 and Gastroenterology Steven M. Verno, CMBSI, CEMCS, CMSCS, CPM-MCS Page 1 of 31 ICD-10 and Gastroenterology Steven M. Verno, CMBSI, CEMCS, CMSCS, CPM-MCS Note: ICD-9-CM and ICD-10 are owned and
Procedural andpr Diagnostic Coding. Copyright 2012 Delmar, Cengage Learning. All rights reserved.
 Procedural andpr Diagnostic Coding What is Coding? Converting descriptions of disease, injury, procedures, and services into numeric or alphanumeric descriptors Accurate coding maximizes reimbursement
Procedural andpr Diagnostic Coding What is Coding? Converting descriptions of disease, injury, procedures, and services into numeric or alphanumeric descriptors Accurate coding maximizes reimbursement
June 12, Dear Dr. McClellan:
 June 12, 2006 Mark McClellan, MD, PhD Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1488-P PO Box 8011 Baltimore, Maryland 21244-1850 Dear
June 12, 2006 Mark McClellan, MD, PhD Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1488-P PO Box 8011 Baltimore, Maryland 21244-1850 Dear
ICD 10 Preparation for NSMM
 This document explains regulation changes coming in 2014 that will impact how we collect and document clinical appropriateness using diagnosis codes (ICD-9 conversion to ICD-10). Please familiarize yourself
This document explains regulation changes coming in 2014 that will impact how we collect and document clinical appropriateness using diagnosis codes (ICD-9 conversion to ICD-10). Please familiarize yourself
ICD-10: The History, the Impact, and the Keys to Success. White Paper
 ICD-10: The History, the Impact, and the Keys to Success White Paper Contents: Executive Summary ICD-10 History ICD-9-CM Limitations ICD-10 Specifics Benefits of ICD-10 Impact of ICD-10 Successful ICD-10
ICD-10: The History, the Impact, and the Keys to Success White Paper Contents: Executive Summary ICD-10 History ICD-9-CM Limitations ICD-10 Specifics Benefits of ICD-10 Impact of ICD-10 Successful ICD-10
Diagnostic Coding. Psychomotor Domain. Affective Domain
 UNIT THREE MANAGING THE FINANCES IN THE PRACTICE CHAPTER 11 Diagnostic Coding Learning Outcomes Cognitive Domain 1. Spell and define the key terms 2. Describe the relationship between coding and reimbursement
UNIT THREE MANAGING THE FINANCES IN THE PRACTICE CHAPTER 11 Diagnostic Coding Learning Outcomes Cognitive Domain 1. Spell and define the key terms 2. Describe the relationship between coding and reimbursement
ICD-10 Frequently Asked Questions for Providers Q Updates
 ICD-10 Frequently Asked Questions for Providers Q4 2012 Updates What is ICD-10? International Classification of Diseases, 10th Revision (ICD-10) is a diagnostic and procedure coding system endorsed by
ICD-10 Frequently Asked Questions for Providers Q4 2012 Updates What is ICD-10? International Classification of Diseases, 10th Revision (ICD-10) is a diagnostic and procedure coding system endorsed by
2017 CDI Pocket Guide is published by HCPro, a division of BLR. Copyright 2016 Pinson&Tang LLC. Printed in the United States of America.
 2017 CDI Pocket Guide is published by HCPro, a division of BLR. Copyright 2016 Pinson&Tang LLC. Printed in the United States of America. ISBN: 978-0-98276-646-0 No part of this publication may be reproduced,
2017 CDI Pocket Guide is published by HCPro, a division of BLR. Copyright 2016 Pinson&Tang LLC. Printed in the United States of America. ISBN: 978-0-98276-646-0 No part of this publication may be reproduced,
ICD-10 Transition Provider Roadshow. October 2012
 ICD-10 Transition Provider Roadshow October 2012 About ICD-10 ICD-10 CM for diagnosis coding For use in all US healthcare settings Uses 3 to 7 digits instead of the 3 to 5 digits ICD-10-PCS for inpatient
ICD-10 Transition Provider Roadshow October 2012 About ICD-10 ICD-10 CM for diagnosis coding For use in all US healthcare settings Uses 3 to 7 digits instead of the 3 to 5 digits ICD-10-PCS for inpatient
HCS-D Exam Update. Tricia A. Twombly BSN RN HCS-D HCS-O COS-C CHCE AHIMA Approved ICD-10 CM Trainer Senior Director, DecisionHealth CEO, BMSC
 HCS-D Exam Update Lisa Selman-Holman JD, BSN, RN, HCS-D, HCS-O, COS-C AHIMA Approved ICD-10 CMPCS Trainer Owner, Selman-Holman and Associates Chair, BMSC Tricia A. Twombly BSN RN HCS-D HCS-O COS-C CHCE
HCS-D Exam Update Lisa Selman-Holman JD, BSN, RN, HCS-D, HCS-O, COS-C AHIMA Approved ICD-10 CMPCS Trainer Owner, Selman-Holman and Associates Chair, BMSC Tricia A. Twombly BSN RN HCS-D HCS-O COS-C CHCE
Transition to ICD 10 CM/PCS Preparing for October 1, 2015
 Transition to ICD 10 CM/PCS Preparing for October 1, 2015 July 17, 2014 10 am - Noon Irene Mueller, EdD, RHIA AHIMA Approved ICD-10-CM/PCS Trainer 2014 by Irene L. E. Mueller By attending this workshop,
Transition to ICD 10 CM/PCS Preparing for October 1, 2015 July 17, 2014 10 am - Noon Irene Mueller, EdD, RHIA AHIMA Approved ICD-10-CM/PCS Trainer 2014 by Irene L. E. Mueller By attending this workshop,
ICD Codes health health health
 1-10-2017 Encounter for screening for malignant neoplasm of cervix. 2016 2017 2018 Billable/Specific Code Female Dx POA Exempt. Z12.4 is a billable/specific ICD-10. ICD-10 is the 10th revision of the International
1-10-2017 Encounter for screening for malignant neoplasm of cervix. 2016 2017 2018 Billable/Specific Code Female Dx POA Exempt. Z12.4 is a billable/specific ICD-10. ICD-10 is the 10th revision of the International
Choosing the Principal Diagnosis Symptoms, Signs and Ill Defined Conditions. Related Definitive Diagnosis
 Choosing the Principal Diagnosis Symptoms, Signs and Ill Defined Conditions Department of Health and Human Services, "ICD-9-CM Official Guidelines for Coding and Reporting." UCenters for Disease Control
Choosing the Principal Diagnosis Symptoms, Signs and Ill Defined Conditions Department of Health and Human Services, "ICD-9-CM Official Guidelines for Coding and Reporting." UCenters for Disease Control
Guide to Documentation and Medical Coding 2017
 Guide to Documentation and Medical Coding 2017 Office of Compliance 933 Bradbury SE, Suite 3053 Albuquerque, NM 87106 Phone: 505-925-6053 Fax: 505-925-0934 i ii Table of Contents INTRODUCTION... V CHAPTER
Guide to Documentation and Medical Coding 2017 Office of Compliance 933 Bradbury SE, Suite 3053 Albuquerque, NM 87106 Phone: 505-925-6053 Fax: 505-925-0934 i ii Table of Contents INTRODUCTION... V CHAPTER
Disclosure of Proprietary Interest
 HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
ICD-10/APR-DRG. HP Provider Relations/September 2015
 ICD-10/APR-DRG HP Provider Relations/September 2015 Agenda ICD-10 ICD-10 General Overview Who is affected Preparation Testing Prior Authorization APR-DRG Inpatient hospital rates Crosswalks Questions 2
ICD-10/APR-DRG HP Provider Relations/September 2015 Agenda ICD-10 ICD-10 General Overview Who is affected Preparation Testing Prior Authorization APR-DRG Inpatient hospital rates Crosswalks Questions 2
Preparing for ICD-10: Education and Clinical Documentation
 Preparing for ICD-10: Education and Clinical Documentation Agenda Background Road to Readiness Education Clinical Documentation Quick Start Today s presentation and recording will be sent to all attendees
Preparing for ICD-10: Education and Clinical Documentation Agenda Background Road to Readiness Education Clinical Documentation Quick Start Today s presentation and recording will be sent to all attendees
Learning Objectives. Denver Health Medical Center. Complex Coding Scenarios and Resolution
 Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Sample page. Podiatry. A comprehensive illustrated guide to coding and reimbursement CODING COMPANION
 CODING COMPANION 2018 Podiatry A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com. Contents
CODING COMPANION 2018 Podiatry A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com. Contents
CARING & CODING FOR MALNUTRITION
 CARING & CODING FOR MAL Sandy Routhier RHIA, CCS, CDIP, AHIMA Approved ICD-10CM/PCS Trainer CloudMed Solutions Michelle Mathura, RDN, LRD, CDE Director, Nutrition Division DM&A Our Presenters Sandra Routhier,
CARING & CODING FOR MAL Sandy Routhier RHIA, CCS, CDIP, AHIMA Approved ICD-10CM/PCS Trainer CloudMed Solutions Michelle Mathura, RDN, LRD, CDE Director, Nutrition Division DM&A Our Presenters Sandra Routhier,
ICD 10 CM State of Transition
 ICD 10 CM State of Transition Tricia A. Twombly, RN, BSN, HCS D, HCS C, COS C, CHCE, AHIMA ICD 10 Trainer, ICE Certified Credentialing Specialist, CEO Board of Medical Coding and Compliance, Senior Director
ICD 10 CM State of Transition Tricia A. Twombly, RN, BSN, HCS D, HCS C, COS C, CHCE, AHIMA ICD 10 Trainer, ICE Certified Credentialing Specialist, CEO Board of Medical Coding and Compliance, Senior Director
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System
 Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Diagnostic Coding. 1. Spell and define the key terms
 CHAPTER 14 Diagnostic Coding Learning Outcomes Cognitive Domain 1. Spell and define the key terms 2. Describe the relationship between coding and reimbursement 3. Name and describe the coding system used
CHAPTER 14 Diagnostic Coding Learning Outcomes Cognitive Domain 1. Spell and define the key terms 2. Describe the relationship between coding and reimbursement 3. Name and describe the coding system used
11/24/2014. External Causes Morbidity (V00-Y99) Toxic Effects
 Toxic Effects") Toxic Effects Harmful substance is ingested or comes in contact with a person Associated intent: Accidental Intentional self-harm Assault Undetermined 223 Chapter 19 Take Away Point With all the extensive
Toxic Effects Harmful substance is ingested or comes in contact with a person Associated intent: Accidental Intentional self-harm Assault Undetermined 223 Chapter 19 Take Away Point With all the extensive
Truly Understanding Clinical Documentation Improvement for ICD-10
 Truly Understanding Clinical Documentation Improvement for ICD-10 John Hailes ASC-E/M, CCS, CCS-P, CPC, CPC-H, CIRCC, CPMA, CPC-I, CEMC, CFPC, ICD-10-CM/PCS Trainer 1 Objectives Identify areas in ICD-10-CM
Truly Understanding Clinical Documentation Improvement for ICD-10 John Hailes ASC-E/M, CCS, CCS-P, CPC, CPC-H, CIRCC, CPMA, CPC-I, CEMC, CFPC, ICD-10-CM/PCS Trainer 1 Objectives Identify areas in ICD-10-CM
Implementation Issues of the Physician Practice. for ICD-10-CM
 Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Coding and Payment Guide for Chiropractic Services. A comprehensive coding, billing, and reimbursement resource for chiropractic services
 Coding and Payment Guide for Chiropractic Services A comprehensive coding, billing, and reimbursement resource for chiropractic services 2014 Contents Introduction...1 Coding Systems... 1 Claim Forms...
Coding and Payment Guide for Chiropractic Services A comprehensive coding, billing, and reimbursement resource for chiropractic services 2014 Contents Introduction...1 Coding Systems... 1 Claim Forms...
Icd 10 code health maintenance
 Icd 10 code health maintenance The Borg System is 100 % Icd 10 code health maintenance Codes. Z13 Encounter for screening for other diseases and disorders. Z13.0 Encounter for screening for diseases of
Icd 10 code health maintenance The Borg System is 100 % Icd 10 code health maintenance Codes. Z13 Encounter for screening for other diseases and disorders. Z13.0 Encounter for screening for diseases of
HHGM is Alive and Kicking: How Can You Prepare for What s Next?
 HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
HHGM is Alive and Kicking: How Can You Prepare for What s Next? New England Home Care & Hospice Conference and Trade Show April 26, 2018 Presented by: Chris Attaya VP of Product Strategy, SHP Sue Payne
ICD-10 is Coming What s A Provider to do?
 ICD-10 is Coming What s A Provider to do? Texas Osteopathic Medical Association Friday, January 31, 2014 Yolanda Doss, MJ, RHIA, CHPS Director, Compliance and Payment Advocacy Presentation developed for
ICD-10 is Coming What s A Provider to do? Texas Osteopathic Medical Association Friday, January 31, 2014 Yolanda Doss, MJ, RHIA, CHPS Director, Compliance and Payment Advocacy Presentation developed for
HC 1930 HC 1930 ICD-9-CM III/CPT Coding II
 South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
a. 95 guidelines are based on body systems 97 systems based on bullet points.
 Interview questions for freshers Medical Coding Interview Questions 1) What is the basic difference between 95 and 97 guidelines? a. 95 guidelines are based on body systems 97 systems based on bullet points.
Interview questions for freshers Medical Coding Interview Questions 1) What is the basic difference between 95 and 97 guidelines? a. 95 guidelines are based on body systems 97 systems based on bullet points.
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Chapter 2 Nursing Process
 Chapter 2 Nursing Process Definition of the Nursing Process Organized sequence of problem-solving steps Used to identify and manage the health problems of clients Accepted standard for clinical practice:
Chapter 2 Nursing Process Definition of the Nursing Process Organized sequence of problem-solving steps Used to identify and manage the health problems of clients Accepted standard for clinical practice:
Standards for ethical conduct in clinical coding
 Standards for ethical conduct in clinical coding ICD-10-AM/ACHI/ACS Tenth Edition 2017 Education program Background: The code of ethics has been in the Appendices of the Australian Coding Standards since
Standards for ethical conduct in clinical coding ICD-10-AM/ACHI/ACS Tenth Edition 2017 Education program Background: The code of ethics has been in the Appendices of the Australian Coding Standards since
5/30/2012. ICD 10 Implementation HCCA. Agenda. Understanding ICD 10. June 8, ICD 10 Overview Planning Communication Education Physician Training
 ICD 10 Implementation HCCA June 8, 2012 1 Agenda ICD 10 Overview Planning Communication Education Physician Training 2 Understanding ICD 10 The key to accepting any change is understanding Why is this
ICD 10 Implementation HCCA June 8, 2012 1 Agenda ICD 10 Overview Planning Communication Education Physician Training 2 Understanding ICD 10 The key to accepting any change is understanding Why is this
HIPE Coding Process. Extraction of information from medical record to summary of the discharge in HIPE record
 HIPE Coding Process Extraction of information from medical record to summary of the discharge in HIPE record HIPE Record Summary of admitted episode of care Demography information (from PAS) Administrative
HIPE Coding Process Extraction of information from medical record to summary of the discharge in HIPE record HIPE Record Summary of admitted episode of care Demography information (from PAS) Administrative
What s Up Wednesday. Together Let s Get ICD-10 Ready. Date: February 18, 2015 Time: 2 3 p.m. Phone Number: Pass code:
 What s Up Wednesday Together Let s Get ICD-10 Ready Date: February 18, 2015 Time: 2 3 p.m. Phone Number: 800-882-3610 Pass code: 5411307 Presented by the Pennsylvania Blues Plans 2 What s Up Wednesday
What s Up Wednesday Together Let s Get ICD-10 Ready Date: February 18, 2015 Time: 2 3 p.m. Phone Number: 800-882-3610 Pass code: 5411307 Presented by the Pennsylvania Blues Plans 2 What s Up Wednesday
Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition
 Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition") 2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
American Health Information Management Association 2008 House of Delegates
 2008 House of Delegates ACTION ITEM TITLE: Standards of Ethical Coding MOTION: I move to approve the Standards of Ethical Coding. The motion is proposed by: Laurinda Harman, PhD, RHIA Virginia Mullen,
2008 House of Delegates ACTION ITEM TITLE: Standards of Ethical Coding MOTION: I move to approve the Standards of Ethical Coding. The motion is proposed by: Laurinda Harman, PhD, RHIA Virginia Mullen,
Health Informatics. Health Informatics professionals treat technology as a tool that helps patients and healthcare professionals.
 Health Informatics Health Informatics professionals treat technology as a tool that helps patients and healthcare professionals. 3.02 Understand health informatics 2 Health Informatics A career area that
Health Informatics Health Informatics professionals treat technology as a tool that helps patients and healthcare professionals. 3.02 Understand health informatics 2 Health Informatics A career area that
AAPC Richardson, TX Chapter. Monthly Meeting. 6pm. Location:
 AAPC Richardson, TX Chapter Monthly Meeting 4/17/2017 @ 6pm Location: Methodist Richardson/Renner Medical Center-Physician Pavilion I 2821 E President George-Physician Services Building, 2nd floor Conference
AAPC Richardson, TX Chapter Monthly Meeting 4/17/2017 @ 6pm Location: Methodist Richardson/Renner Medical Center-Physician Pavilion I 2821 E President George-Physician Services Building, 2nd floor Conference
ICD-10-CM. Objectives
 ICD-10-CM What is it? Why? Now What? Debbie Johnson, RHIT, CHP American Health Care Association Webinar September 12, 2013 Objectives Learn what ICD-10-CM is what the main differences in ICD-9 and ICD-10
ICD-10-CM What is it? Why? Now What? Debbie Johnson, RHIT, CHP American Health Care Association Webinar September 12, 2013 Objectives Learn what ICD-10-CM is what the main differences in ICD-9 and ICD-10
ICD-10 Frequently Asked Questions - SurgiSource
 ICD-10 Frequently Asked Questions - SurgiSource What Version of SurgiSource is ICD-10 Compliant? Version 6.0 Where can I find ICD-10 Training Materials for SurgiSource? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - SurgiSource What Version of SurgiSource is ICD-10 Compliant? Version 6.0 Where can I find ICD-10 Training Materials for SurgiSource? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - AdvantX
 ICD-10 Frequently Asked Questions - AdvantX What Version of AdvantX is ICD-10 Compliant? Version 5.0.01 Where can I find ICD-10 Training Materials for AdvantX? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - AdvantX What Version of AdvantX is ICD-10 Compliant? Version 5.0.01 Where can I find ICD-10 Training Materials for AdvantX? 1. Visit our Client Portal (portal.sourcemed.net)
Essentials for Clinical Documentation Integrity 2017
 Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
General Background of CDI
 Clinical Documentation Improvement The Physician Champion ILHIMA 04/30/16 1 General Background of CDI 2 1 CMS Federal Register August 2008 Final Rule (CMS-1533-FC page 208) We do not believe there is anything
Clinical Documentation Improvement The Physician Champion ILHIMA 04/30/16 1 General Background of CDI 2 1 CMS Federal Register August 2008 Final Rule (CMS-1533-FC page 208) We do not believe there is anything
ICD-10 Frequently Asked Questions
 ICD-10 Frequently Asked Questions September 2015 pulseinc.com + 1.800.444.0882 We care for your practice, as if it were our own. Acknowledgments Document Number: 01 Date: September 7, 2015 Pulse Systems
ICD-10 Frequently Asked Questions September 2015 pulseinc.com + 1.800.444.0882 We care for your practice, as if it were our own. Acknowledgments Document Number: 01 Date: September 7, 2015 Pulse Systems
Subject: Updated UB-04 Paper Claim Form Requirements
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
Countdown to ICD-10-CM: Three Months to Go. Presented by: Rhonda Granja, BS, CMA, CMC, CPC, CMIS, CMOM
 Countdown to ICD-10-CM: Three Months to Go Presented by: Rhonda Granja, BS, CMA, CMC, CPC, CMIS, CMOM Overview Setting the Stage ICD-10-CM Coding System Overview Planning Your ICD-10 Transition Assessing
Countdown to ICD-10-CM: Three Months to Go Presented by: Rhonda Granja, BS, CMA, CMC, CPC, CMIS, CMOM Overview Setting the Stage ICD-10-CM Coding System Overview Planning Your ICD-10 Transition Assessing
The new semester for this Certificate will begin Fall 2018
 Great Basin College Professional Medical Coding and Billing Program Certificate of Achievement The new semester for this Certificate will begin Fall 2018 For more information, Contact: Gaye Terras 775-753-2241
Great Basin College Professional Medical Coding and Billing Program Certificate of Achievement The new semester for this Certificate will begin Fall 2018 For more information, Contact: Gaye Terras 775-753-2241
ICD-10 Awareness Training International Classification of Diseases Tenth Revision
 ICD-10 Awareness Training International Classification of Diseases Tenth Revision Course Objective This course will provide basic awareness training on ICD-10, BMS planning and implementation phases, and
ICD-10 Awareness Training International Classification of Diseases Tenth Revision Course Objective This course will provide basic awareness training on ICD-10, BMS planning and implementation phases, and
Ensuring a Successful Transition to ICD-10-CM and ICD-10-PCS for Post Acute Care Settings
 Ensuring a Successful Transition to ICD-10-CM and ICD-10-PCS for Post Acute Care Settings August 9, 2012 Nelly Leon-Chisen, RHIA Director Coding and Classification American Hospital Association Recent
Ensuring a Successful Transition to ICD-10-CM and ICD-10-PCS for Post Acute Care Settings August 9, 2012 Nelly Leon-Chisen, RHIA Director Coding and Classification American Hospital Association Recent
network news Exciting updates to kp.org coming soon! FOR NETWORK PROVIDERS OF KAISER PERMANENTE
 network Produced by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc., with the Mid-Atlantic Permanente Medical Group, P.C. Web site: www.providers.kp.org/mas news MARCH 2011 FOR NETWORK PROVIDERS
network Produced by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc., with the Mid-Atlantic Permanente Medical Group, P.C. Web site: www.providers.kp.org/mas news MARCH 2011 FOR NETWORK PROVIDERS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
PASRR IN SKILLED NURSING Regulatory Overview
 PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
3rd Quarter Vol.5 Issue 3. Coding Signs, Symptoms & Abnormal Findings in ICD-10-CM By Connie Calvert RHIA, CCS, CCDS
 3rd Quarter 2015 Vol.5 Issue 3 I N S I D E T H I S I S S U E : PCS: An ICD-10 Refresher Tricky Codes: An ICD-10 Refresher CMS Flexibility Policy for Part B Claims ICD-10 Sample Documentation Contact Us
3rd Quarter 2015 Vol.5 Issue 3 I N S I D E T H I S I S S U E : PCS: An ICD-10 Refresher Tricky Codes: An ICD-10 Refresher CMS Flexibility Policy for Part B Claims ICD-10 Sample Documentation Contact Us
A McKesson Perspective: ICD-10-CM/PCS
 A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
American Health Information Management Association Standards of Ethical Coding
 American Health Information Management Association Standards of Ethical Coding Introduction The Standards of Ethical Coding are based on the American Health Information Management Association's (AHIMA's)
American Health Information Management Association Standards of Ethical Coding Introduction The Standards of Ethical Coding are based on the American Health Information Management Association's (AHIMA's)
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services
 Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
ICD-10: Capturing the Complexities of Health Care
 ICD-10: Capturing the Complexities of Health Care This project is a collaborative effort by 3M Health Information Systems and the Healthcare Financial Management Association Coding is the language of health
ICD-10: Capturing the Complexities of Health Care This project is a collaborative effort by 3M Health Information Systems and the Healthcare Financial Management Association Coding is the language of health
Sample page. Orthopaedics: Hips & Below. A comprehensive illustrated guide to coding and reimbursement CODING COMPANION
 CODING COMPANION 2018 Orthopaedics: Hips & Below A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
CODING COMPANION 2018 Orthopaedics: Hips & Below A comprehensive illustrated guide to coding and reimbursement POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
# December 29, 2000
 #00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
#00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
ICD-10: The History, the Impact, and the Keys to Success. White Paper
 ICD-10: The History, the Impact, and the Keys to Success White Paper Contents: Executive Summary ICD-10 History ICD-9-CM Limitations ICD-10 Specifics Benefits of ICD-10 Impact of ICD-10 Successful ICD-10
ICD-10: The History, the Impact, and the Keys to Success White Paper Contents: Executive Summary ICD-10 History ICD-9-CM Limitations ICD-10 Specifics Benefits of ICD-10 Impact of ICD-10 Successful ICD-10