BENIN Work Plan FY 2018 Project Year 7
|
|
|
- Vivian Alexander
- 6 years ago
- Views:
Transcription


1 BENIN Work Plan FY 2018 Project Year 7 October 2017 September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation, Helen Keller International, IMA World Health, Light for the World, Sightsavers, and World Vision. ENVISION is funded by the US Agency for International Development under cooperative agreement No. AID-OAA-A The period of performance for ENVISION is September 30, 2011, through September 30, The author s views expressed in this publication do not necessarily reflect the views of the US Agency for International Development or the United States Government.
2 ENVISION Project Overview The US Agency for International Development (USAID) s ENVISION project ( ) is designed to support the vision of the World Health Organization (WHO) and its member states by targeting the control and elimination of seven neglected tropical diseases (NTDs), including lymphatic filariasis (LF), onchocerciasis (OV), schistosomiasis (SCH), three soil-transmitted helminths (STH; roundworm, whipworm, and hookworm), and trachoma. ENVISION s goal is to strengthen NTD programming at global and country levels and support ministries of health (MOHs) to achieve their NTD control and elimination goals. At the global level, ENVISION in close coordination and collaboration with WHO, USAID, and other stakeholders contributes to several technical areas in support of global NTD control and elimination goals, including the following: Drug and diagnostics procurement, where global donation programs are unavailable Capacity strengthening Management and implementation of ENVISION s Technical Assistance Facility (TAF) Disease mapping NTD policy and technical guideline development NTD monitoring and evaluation (M&E). At the country level, ENVISION provides support to national NTD programs by providing strategic technical and financial assistance for a comprehensive package of NTD interventions, including the following: Strategic annual and multi-year planning Advocacy Social mobilization and health education Capacity strengthening Baseline disease mapping Preventive chemotherapy (PC) or mass drug administration (MDA) Drug and commodity supply management and procurement Program supervision M&E, including disease-specific assessments (DSAs) and surveillance. In Benin, ENVISION project activities are implemented by RTI International. ii
3 TABLE OF CONTENTS ENVISION Project Overview... ii TABLE OF TABLES... iv TABLE OF FIGURES... iv ACRONYMS LIST... v COUNTRY OVERVIEW ) General Country Background... 8 a) Administrative Structure... 8 b) Overview of ENVISION support ) National NTD Program Overview a) Lymphatic Filariasis b) Trachoma c) Onchocerciasis d) Schistosomiasis e) Soil-Transmitted Helminths ) Snapshot of PC NTD Status in Benin PLANNED ACTIVITIES ) NTD Program Capacity Strengthening a) Strategic Capacity Strengthening Approach b) Capacity Strengthening Objectives and Interventions c) Monitoring Capacity Strengthening ) Project Assistance a) Strategic Planning b) NTD Secretariat c) Building Advocacy for a Sustainable National NTD Program d) MDA Coverage e) Social Mobilization to Enable NTD Program Activities f) Training g) Drug and Commodity Supply Management and Procurement h) Supervision for MDA i) M&E j) Supervision for M&E and DSAs k) Dossier Development ) Maps iii
4 APPENDIX 1: Work Plan Timeline APPENDIX 2. Table of USAID-supported Regions and Districts in FY TABLE OF TABLES Table 1: Snapshot of the expected status of PC NTDs in Benin as of September 30, Table 2: Project assistance for capacity strengthening Table 3: Districts targeted for MDA with USAID support in FY Table 4: Social mobilization/communication activities and materials checklist for NTD work planning Table 5: Planned DSAs for FY18 by disease TABLE OF FIGURES Figure 1: Organization of the cascade training for the various MDA campaigns iv
5 ACRONYMS LIST AE AFRO ALB APOC ATP AZT CAME CDD CDTI CES Co-RUP CP CRP DDS D-FEAT DFID DNSP DPS DQA DSA DSME ESPEN EU FOG FTS FY GOB GTMP HAT HQ HZ ICT IEC IITA INSAE ITI IVM JRSM KCCO LF LOE M&E MDA Adverse Event Regional Office for Africa (WHO) Albendazole African Program for Onchocerciasis Control Annual Transmission Potential Azithromycin Centrale d Achat des Médicaments Essentiels Community Drug Distributor Community-Directed Treatment with Ivermectin Coverage Evaluation Survey Co-Responsable d Unité Pédagogique (Pedagogical Unit Deputy Chief) Conseiller Pédagogique (Pedagogical Advisor) Chef de Région Pédagogique (Head of School District) Direction Départementale de la Santé (Departmental Health Directorate) District Filariases Elimination Action Tool UK Department for International Development Direction Nationale de la Santé Publique (National Public Health Directorate) (MOH) Direction de la Promotion de la Scolarisation (Schooling Promotion Directorate) Data Quality Assessment Disease-Specific Assessment Direction de la Santé de la Mère et de l Enfant (Mother and Child Health Directorate) (MOH) Expanded Special Project for Elimination of Neglected Tropical Diseases (WHO AFRO) Evaluation Unit Fixed Obligation Grant Filariasis Test Strip Fiscal Year Government of Benin Global Trachoma Mapping Project Human African Trypanosomiasis Headquarters Hôpital de Zone (Health Zone Hospital) Immunochromatographic Test Information, Education, and Communication International Institute for Tropical Agriculture Institut National de la statistique et de l analyse économique (National Institute of Statistics and Economic Analysis) International Trachoma Initiative Ivermectin Joint Request for Selected PC Medicines (WHO) Kilimanjaro Center for Community Ophthalmology Lymphatic Filariasis Level of Effort Monitoring and Evaluation Mass Drug Administration v
6 MDSC MEMP Mf MMDP MOH NGO NTD OCP OV PC PCR PNLLUB PNLMT PZQ RPRG RUP SAC SAE SAFE SCH SNIGS SOP STH STTA SWOT TAF TAP TAS TEO TF TFGH TIPAC TIS TS TSO TT TV USAID WASH WHO ZTH Multi-Disease Surveillance Center (Burkina Faso) Ministère de l Enseignement Maternelle et Primaire (Ministry of Kindergarten and Primary Education) Microfilaraemia Morbidity Management and Disability Prevention Ministry of Health Nongovernmental Organization Neglected Tropical Disease Onchocerciasis Control Program Onchocerciasis Preventive Chemotherapy Polymerase Chain Reaction Programme National de Lutte contre la Lèpre et l Ulcère de Buruli (National Leprosy and Buruli Ulcer Control Program) Programme National de Lutte contre les Maladies Transmissibles (National Program for Control of Communicable Diseases) Praziquantel Regional Programme Review Group Responsable d Unité Pédagogique (Pedagogical Unit Chief) School-Age Children Severe Adverse Event Surgery Antibiotics Facial Cleanliness Environmental Improvement Schistosomiasis Système National d Information et de Gestion Sanitaire (National Health Information and Management System) Standard Operating Procedure Soil-Transmitted Helminths Short-Term Technical Assistance Strengths, Weaknesses, Threats and Opportunities Technical Assistance Facility Trachoma Action Plan Transmission Assessment Survey Tetracycline Eye Ointment Trachomatous Inflammation Follicular Task Force for Global Health Tool for Integrated Planning and Costing Trachoma Impact Survey Trachomatous Scarring Technicien supérieur en ophtalmologie (Senior Ophthalmological Officer) Trachomatous Trichiasis Television United States Agency for International Development Water, Sanitation, and Hygiene World Health Organization Zithromax vi
7 Health Facility Terms, Translations, and Acronyms English French Acronym Hubert Koutoukou Maga National University Hospital National Hospital of Respiratory Medicine Lagune Mother and Children s Hospital Centre National Hospitalier et Universitaire Hubert Koutoukou Maga Centre National Hospitalier de Pneumo- Phtisiologie Hôpital de la Mère et de l Enfant la Lagune Departmental hospital Centre Hospitalier Départemental CHD Center for detection and treatment of Buruli ulcer Centre de dépistage et de traitement de l ulcère de Buruli CNHU-HKM HOMEL CDTUB Leprosy treatment center Centre de traitement anti lèpre CTAL Village health unit Unité villageoise de santé UVS Sub-district health center Centre de santé de l arrondissement CSA District health center Centre de santé de la commune CSC Health zone referral hospital Hôpital de zone HZ Full health center Standalone clinic Standalone maternity ward Denominational health center Centre de santé complet Dispensaire isolé Maternité isolée Centre de santé confessionnel vii
8 COUNTRY OVERVIEW 1) General Country Background a) Administrative Structure Benin s administrative and financial capital is Cotonou. In 1999, the country s six political and administrative départements (departments) were reorganized into a total of 12 departments (Alibori, Atacora, Atlantique, Borgou, Collines, Couffo, Donga, Littoral, Mono, Ouémé, Plateau, and Zou). These departments are further subdivided into a total of 77 communes (hereafter referred to as districts), which are composed of a total of 546 arrondissements (boroughs, hereafter referred to as sub-districts) and 5,295 1 villages. The Ministry of Health (MOH) is responsible for initiation, planning, implementation, coordination, and monitoring and evaluation (M&E) of the country s health programs, with plans laid out in its National Health Development Plan, the current version of which covers the period Facilities at the central level include Hubert Koutoukou Maga National University Hospital, National Hospital of Respiratory Medicine, National Psychiatric Center, Gerontology Center, Lagune Mother and Children s Hospital, and the National Medical Laboratory, all located in Cotonou. At the intermediate level, the country s reorganization into 12 departments became effective in February 2017 with the nomination of a Director of Health for each department. Across the departments, there are five departmental hospitals, four centers for detection and treatment of Buruli ulcer, eight leprosy treatment centers, and a center for respiratory medicine. The Hospital Saint Jean de Dieu, in Tanguiéta, serves as a sentinel site for monitoring Human African Trypanosomiasis (HAT). The peripheral levels consist of health zones (34 in the country), each made up of one or more districts. One department has between two and four health zones. Each health zone is supervised by a medical doctor (health zone coordinator), and is intended to consist of a network of first-line health facilities (village health units, stand-alone maternity wards and clinics, sub-district health centers, district health centers), and private health facilities, all of which are supported by a health zone referral hospital (Hôpital de Zone [HZ]), serving a population ranging from 100,000 to 200,000. Across the entire country, there are 27 public or private HZs one per health zone with an additional 7 HZs still to be established, 571 full health centers, 118 stand-alone clinics, 113 stand-alone maternity wards, and 59 denominational health centers. Many private health facilities are involved in collecting data for the National Health Information and Management System (Système National d Information et de Gestion Sanitaire [SNIGS]). The MOH s National Public Health Directorate (Direction Nationale de la Santé Publique [DNSP]) oversees the National Communicable Disease Control Program (Programme National de Lutte contre les Maladies Transmissibles [PNLMT]) and the National Leprosy and Buruli Ulcer Control Program (Programme National de Lutte contre la Lèpre et l Ulcère de Buruli [PNLLUB]). The PNLMT is responsible for lymphatic filariasis (LF), onchocerciasis (OV), schistosomiasis (SCH), soil-transmitted helminths (STH), and trachoma, as well as hepatitis, HAT, Guinea worm (dracunculiasis), and loiasis; and the PNLLUB is responsible for Buruli ulcer, leprosy, and yaws. 1 Law N o (May 27, 2013). 8
9 The structure of the Ministry of Kindergarten and Primary Education (Ministère de l Enseignement Maternelle et Primaire [MEMP]) is similar to that of the MOH, including a technical department called the Schooling Promotion Directorate (DPS). The MEMP is present in all 12 departments, and has had an office in each department since These offices oversee a total of 85 school districts, which are further subdivided into teaching units, jointly managed by the Pedagogical Unit Chiefs (Responsable d Unité Pédagogique [RUP]) and Pedagogical Unit Deputy Chiefs (Co-Responsable d Unité Pédagogique [Co-RUP]). The MEMP is responsible for all 10,015 private and public schools in the country. The MEMP s DPS collaborates closely with the PNLMT in the context of school-based mass drug administration (MDA) for PC NTDs. b) Overview of ENVISION support RTI, through the ENVISION project, has supported the PNLMT in its efforts to control and eliminate PC NTDs in the country, since fiscal year 2013 (FY13). This has included technical and financial support for disease mapping and surveys, MDA for all the PC NTDs, social mobilization, technical training, advocacy, and M&E. ENVISION also procures necessary drugs (including tetracycline eye ointment [TEO]) that are not provided by the drug donation programs) and diagnostic tools (filariasis test strips [FTS] and Kato- Katz kits, among others) for surveys. ENVISION s support includes technical assistance, via expert local and/or international consultants, to enable quality completion of PC NTD-related PNLMT activities and to build the PNLMT s capacity to lead these activities on its own. 9
10 2) National NTD Program Overview The MOH strategy for NTD control and elimination is laid out in its National Master Plan for NTD Control , which was approved by MOH leadership in February 2017 and launched at a ceremony held on September 28, 2017 in Cotonou. This document succeeds the prior Master Plan, which covered the period The current document addresses LF, OV, SCH, STH, and trachoma, along with Buruli ulcer, Guinea worm, HAT, leprosy, and loiasis; it also mentions yaws, while specifying that loiasis and yaws have not been shown to be endemic and that both are simply under surveillance. The plan proposes intensified scaling up of interventions and consideration of cross-cutting determinants of health (health education, access to potable water, hygiene, and sanitation). Disease-specific updates include the findings of SCH, STH, and trachoma baseline mapping completed since the previous plan; a more defined strategy for trachoma elimination, based on the trachoma action plan (TAP) developed in 2015; and an updated strategy for OV, reflecting WHO s 2016 OV elimination guidelines. The plan aims for elimination of LF, OV, and trachoma, as well as HAT and leprosy, by 2020; control of SCH, STH, and Buruli ulcer; and maintenance of the certification of eradication of Guinea worm (certified since 2010). Control and elimination of PC NTDs is the responsibility of the PNLMT, as noted above. Baseline mapping is complete for all five PC NTDs. The PNLMT uses two strategies to reach targeted populations with PC: (1) MDA or community-directed treatment, involving community drug distributors (CDDs) in communities; and (2) school-based MDA for SAC (5 14 years), involving teachers as distributors. Typically, the first approach is used for OV and LF (which includes STH, as appropriate), as well as for trachoma; and the second approach is used for SCH and STH. In 2017, the PNLMT experimented with using the first approach for SCH/STH MDA in selected districts. In districts where two or more NTDs are co-endemic, and based on disease prevalence and the treatment cycle, the PNLMT has conducted integrated MDA in the following combinations: OV+LF, OV+LF+STH, LF+STH, and STH+SCH. In line with the standard practice in most countries of the region, trachoma MDA is conducted separately from MDA for the other diseases. The F and E elements of the SAFE strategy (Surgery Antibiotics Face cleanliness Environmental improvement) are being addressed on a small-scale, ongoing basis by NGOs, the MEMP, and one division of the MOH (under the DNSP) in selected areas: the E component in Kalalé District and the F and E components (community hygiene, including hand washing and sanitation) in Nikki, Pèrèrè, Tchaourou, Toukountouna, Banikoara, and Natitingou districts. The PNLMT includes six units: (1) M&E, managed by the data manager; (2) MDA, led by the nurseepidemiologist; (3) Biological and Entomological Activities, managed by the biologist-entomologist; (4) Prevention and Social Mobilization, managed by the senior social work specialist; (5) Financial Management, under the responsibility of the financial controller; and (6) Equipment and Logistics, under the responsibility of the logistician. The PNLMT has designated health professionals outside its structure as national focal points for certain of the PC NTDs; these focal points are involved in PNLMT disease-related meetings, as well as in programmatic decisions and in training whenever their expertise is needed. a) Lymphatic Filariasis The PNLMT s goal is to eliminate LF in the country by Specific objectives are to reduce LF s prevalence rate to <1% in endemic districts, to identify cases of LF-related morbidity in endemic districts, and to provide case management of LF-related morbidity. Strategies are MDA, vector control, surgery, personal hygiene and home self-care, and epidemiological surveillance. Channels for service 10
11 delivery include the community, long-lasting insecticide-treated nets, health facilities, home care, and local radio stations. LF baseline mapping was conducted in 2000, following the standard WHO protocol and using immunochromatographic tests (ICTs), and taking the district as the implementation unit. This mapping showed 50 districts (including Cotonou and Porto-Novo, the country s largest cities) to be endemic for the disease ( 1%), with village-level prevalence ranging from 0% to 12.5%. Remapping of Cotonou and Porto Novo in 2016, with epidemiological and entomological components, confirmed that neither district requires MDA, reducing the number of endemic districts to 48. Based on the findings of baseline mapping, 36 districts progressively initiated LF MDA (IVM+ALB) over the period (12 in 2002, 11 in 2004, 1 in 2005, 5 in 2006, and 7 in 2011). Twelve other districts launched MDA in As of June 2017, 25 districts 2 are on a treatment schedule for LF; this does not include 23 districts that passed a transmission assessment survey (TAS) and met the criteria to stop MDA (see below). The PNLMT conducted pre-tas in four districts in 2007, and in a further five districts in 2009, with neither showing any positive cases. The surveys followed WHO guidelines on site selection (a stable population of at least 500 people, with known high transmission of LF) and use of nocturnal microfilaraemia (Mf) as the diagnostic tool. The 2007 surveys took place in Aplahoué, Djakotomé (both in Couffo Department), Bopa, and Grand-Popo (both in Mono Department); the 2009 surveys took place in Boukoumbé, Malanville (both in Atacora Department), Tchaourou (Borgou Department), Savalou (Collines Department), and Zogbodomey (Zou Department). In 2012, the PNLMT implemented TAS1 in 23 districts (grouped into six evaluation units [EUs]) that had regularly had at least five rounds of MDA with more than 65% epidemiologic coverage. TAS1 was carried out in these districts with TFGH support. The survey found only one positive case among the 9,629 children surveyed. As a result, MDA was stopped. The PNLMT conducted TAS2 in the same 23 districts in 2014, using ICT cards and with support from ENVISION, showing no positive cases. The TAS2 was conducted in schools in the 21 districts where school enrollment was 75% and in the community in the two other districts (Karimama and Malanville, both in Alibori Department) where school enrollment was below 75%. The PNLMT conducted school-based TAS3 in the 21 districts with high school enrollment (mentioned above) grouped into five EUs during April May 2017, using FTS and with support from ENVISION. Final results showed no positive cases. In 14 of these districts, the TAS3 survey was paired with an STH assessment (see Soil-Transmitted Helminths section below). The PNLMT anticipates conducting community-based TAS3 in the two remaining districts (in Alibori Department, and constituting an additional EU), also with support from ENVISION, in FY18. Of the 25 districts still on a treatment cycle for LF, 13 have conducted pre-tas, all using nocturnal mf and led by the PNLMT with ENVISION support. Pre-TAS in five districts of Zou Department (Agbangnizoun, Ouinhi, Zagnanado, Za-Kpota, and Zogbodomey) in 2013 showed prevalences exceeding 1% in two of the districts (1.17% in Agbangnizoun and 1.98% in Za-Kpota); MDA therefore continued in all of these districts. Pre-TAS in 2016 included the two districts that failed pre-tas in 2013, along with eight others (Allada, Kpomassè, Ouidah, Torri-Bossito [in Atlantique Department], Parakou [Borgou Department], Bonou [Ouémé Department], Adja-Ouèrè [Plateau Department], and Covè [Zou Department]); all showed prevalence below 1%. 2 Includes the 13 that started MDA between 2005 and 2011 and the 12 that started MDA in
12 Pending a definitive and complete reply from the RPRG on the PNLMT s October 2017 request for TAS1 in the 13 districts, ENVISION plans to support the TAS1 in those districts. Should the eventual reply from the RPRG expected for November or December 2017 indicate that certain of the proposed districts are not approved (and should continue to conduct LF MDA), ENVISION will update plans accordingly. The MOH established a Technical Committee of Experts for Elimination of OV and LF, which is tasked with developing a national guide and roadmap for elimination of both diseases; this committee will meet for the first time in late FY17, with ENVISION support. The PNLMT lacks an estimate of the LF morbidity burden, but LF MDA treatment registers designed in FY16 are helping to estimate the number of people living with LF-related disability. The 25 districts currently on a treatment cycle for LF are all co-endemic for STH (including 13 districts that had baseline STH prevalence rates of 20%, the WHO-indicated threshold for MDA). Nine of these districts are also endemic for OV. b) Trachoma The PNLMT s goal is to eliminate trachoma in the country by Specific objectives are to reduce prevalence of trachomatous inflammation-follicular (TF) to <5%, to reduce TT to <0.1% in the total population, and to provide case management for trachoma-related complications. The PNLMT subscribes to the SAFE strategy. Channels for service delivery include the community, health facilities, and local radio stations. The PNLMT conducted baseline mapping in , following GTMP protocol and with support from ENVISION and Sightsavers (the latter with GTMP funding from DFID). The activity was carried out by 11 two-person teams (consisting of one GTMP-certified grader and one recorder each). The surveys were carried out in the 26 districts that were suspected to be endemic for the disease; these were grouped into 11 EUs each consisting of between one and four districts. Results across the 11 EUs showed TF prevalence among children ages 1 9 years ranging from 2% to 24%, and trichiasis prevalence among people ages 15 years ranging from 0.1% to 1.9%. 3 A total of four EUs, comprising eight districts, were found to be endemic, which is defined as having TF prevalence of 5%. Among these, Banikoara (Alibori Department), Boukoumbé, Natitingou, and Toukountouna (Atacora Department) registered TF prevalence in children of 10% and <30%, requiring three rounds of MDA; and Kalalé, Nikki, Pèrèrè, and Tchaourou (Borgou Department) registered TF prevalence in children of 5% and <10%, for which a single round of MDA is indicated. 4 Overall, nine EUs, comprising 19 districts, registered trichiasis prevalence in adults of 0.2%, constituting a public health problem in those districts. 5 The other 51 districts were not included in the mapping surveys, as they were not suspected to be endemic. Following 3 Prevalence was calculated for trichiasis, which can be due to multiple causes, rather than for TT because the presence or absence of trachomatous scarring was not recorded in eyes with trichiasis. Consensus for recording trachomatous scarring was established after these surveys were completed. WHO Alliance for the Global Elimination of Blinding Trachoma by (2016). Second Global Scientific Meeting on Trachomatous Trichiasis. Cape Town, November 4 6, Geneva. 4 ITI. (2017, June). Diagram on Decision Making for the Antibiotic Treatment of Trachoma, version 10. In version 9 of the diagram, from 2014, MDA in such districts was at the discretion of the MOH. 5 Banikoara, Gogonou, Karimana, Kandi, Malanville, and Segbana (Alibori Department); Boukoumbé, Kérou, Kouandé, Natitingou, Pehunco, and Toukountouna (Atacora Department); and Bembékéré, Kalalé, N dali, Nikki, Pèrèrè, Sinendé, and Tchaourou (Borgou Department). See WHO, Report of the 2 nd Global Scientific Meeting on Trachoma, Geneva, August, 2003 (Geneva, 2003) and WHO, Report of the 3 rd Global Scientific Meeting on Trachoma, Johns Hopkins University, Baltimore, MD, July 2010 (Geneva, 2010). 12
13 these findings, the PNLMT held a workshop in 2015 to develop a TAP, with support from ENVISION and involving the Kilimanjaro Center for Community Ophthalmology (KCCO) and ITI. The PNLMT initiated MDA for trachoma in As of June 2017, two rounds (FY16 and FY17) have been completed in the four districts with TF prevalence of 10% and <30%, and one round (FY17) in the four districts with TF prevalence of 5% and <10%, all supported by ENVISION. All four districts targeted in FY16 reported sufficient program coverage; in FY17, all eight targeted districts reached sufficient program coverage. The PNLMT is slated to conduct its third (and final) round of MDA in 2018, in the four districts with baseline TF prevalence of 10% and <30%. MDA is community-based, with door-to-door distribution by CDDs of TEO (1%) for children ages 0 6 months (for twice-daily application over six weeks), Zithromax (ZTH) suspension for children ages 6 59 months, and ZTH tablets for people ages 5 years and up. The population denominator is established through CDD registration of the population in target areas (whole districts, apart from Natitingou, where only rural areas are treated). According to the PNLMT 2015 TAP, 75% of the country s TT cases (5,998 cases) must be operated on by 2020 to reach the elimination threshold. The PNLMT plans to initially focus on the priority districts of Banikoara (2,113 surgeries required), Malanville (900), Boukoumbé (740), Natitingou (696), and Tchaourou (1,769). As noted above, the Trachoma Focal Point and one other ophthalmologist will be trained on trichiasis surgery in July 2017; in FY18, these trainers are expected to train three TSOs, who will then provide surgical services in the five priority districts, with funding from the USAID-funded Morbidity Management and Disability Prevention (MMDP) project and WHO AFRO. The country has one Tropical Data-certified trachoma clinical grader and two Tropical Data-certified trachoma data recorders; the aforementioned grader served as a master trainer, and the recorders as trainees, at the regional trachoma-focused Tropical Data training in Senegal in July Loupes that were provided by GTMP for the mapping activity are still in country and available. c) Onchocerciasis The PNLMT s goal is to eliminate OV in the country by The specific objective is to reduce prevalence of OV to <0.1% (as measured by Ov16) in endemic districts. Presently, the strategy to reach this goal is MDA for people ages 5 years (until 2002, under the Onchocerciasis Control Program in West Africa [OCP], larviciding of black fly breeding sites was also part of the country s strategy), with monitoring via entomological and epidemiological assessments (with skin snip microscopy to be replaced by Ov16 rapid diagnostic tests starting in FY17). Channels for service delivery include the community, health facilities, and local radio stations. Baseline assessments conducted in the 1970s showed 51 districts to be hyper- or meso-endemic for OV. The total number of hypo-endemic districts is not known because the other 26 districts were considered either hypo- or non-endemic. A total of 5,978 sentinel sites were selected across the country and assessed. Before 1974, when OCP launched control operations for the disease, OV Mf prevalence ranged from 25% to 98% (as measured by the skin snip method); OV-related blindness 6 ranged between 1% and 3% in hyper-endemic areas and 1% in meso-endemic areas; and annual transmission potential (ATP) registered at several capture points exceeded 800 infective larvae per individual per year. 7 Follow-up epidemiological and entomological assessments conducted from 2000 to 2002 showed that control activities had an effect: most surveyed villages registered Mf prevalence below 5%, and ATP was below 100 at most capture points. 6 Assessed via clinical diagnosis by health personnel. 7 Well over the ATP of 20 that is (as of 2017) thought to be necessary for sustainable transmission within a focus. 13
14 OCP conducted larviciding of black fly breeding sites, using a rotation of insecticides (Temephos, Phoxim, Pyraclofos, Carbosulfan, Permethrin, Etofenprox, and Bacillus thuringiensis var israeliensis), in some of the aforementioned 51 districts from 1977 until OCP s close in Larviciding continued in special intervention zones in upper Ouémé under the lead of the African Programme for Onchocerciasis Control (APOC). The special intervention zones include Natitingou, Boukoumbé, Kouandé, Toukountouna, Bassila, Copargo, Djougou, Ouaké, Parakou, N Dali, and Tchaourou districts from 2003 to 2007, following survey results. Treatment with IVM started in 1988, distributed by mobile teams from OCP headquarters (HQ) in Burkina Faso. In 1997, this was replaced by community-directed treatment with IVM (CDTI), led by the MOH. Until 2002, the 51 districts conducted twice-yearly CDTI alongside the vector-control activities. In the upper Ouémé river basin special intervention zone, twice-yearly CDTI continued until 2007, while the other endemic districts continued to conduct a single round of treatment per year. Since 2008, all districts have conducted MDA once per year. Since 2013, with support from ENVISION, the PNLMT has conducted annual community-based MDA, integrated with LF and/or STH as appropriate by district. In 2015, the PNLMT conducted epidemiological surveys using skin-snip microscopy in 48 villages that had never been assessed or where at least three years had passed since the previous epidemiological assessment. All villages were targeted through the OV MDA campaign. The villages are in 12 districts (Banikoara, Kérou, Natitingou, Boukoumbé, Bassila, Bantè, Sinendé, Nikki, Ouèssè, Savè, Kétou, and Zagnanado) along 10 river basins (Ouémé, Zou, Sota, Couffo, Mekrou, Okpara, Alibori, Keran, Terou, and Pendjari). Standardized Mf prevalence varied from 0% to 4.7%. The PNLMT plans to rotate assessments through all known endemic districts over a several-year period. In 2016, the PNLMT conducted an entomological assessment (impact survey) in four sites identified as productive by OCP: Manta in Boukoumbé (Atacora Department); Vossa in Ouèssè District; Zoundji in Savalou District; and Kaboua in Savè District all in Collines Department. A total of 34,802 black flies were collected and sent to MDSC for PCR analysis, showing infectivity rates below 0.5/ In 2017, the PNLMT conducted epidemiological and entomological assessments (impact surveys) in 65 villages of 6 endemic districts to help identify districts where transmission is still occurring. Black fly breeding sites were mapped a decade ago with the support of APOC. The PNLMT plans to remap the breeding sites with technical support from WHO AFRO s Expanded Special Project for Elimination of Neglected Tropical Diseases (ESPEN). As noted in the Lymphatic Filariasis section above, the MOH established a Technical Committee of Experts for Elimination of OV and LF, which is tasked with developing a national guide and roadmap for elimination of both diseases; this committee met for the first time in August The meeting report included the following recommendations: updating the map of breeding sites, sentinel villages, and transmission zones; conducting nationwide epidemiological and entomological surveys; developing a national OV elimination plan; increasing intra- and intersectoral collaboration within the country and with neighboring countries; requesting missing data from WHO, and developing written operating procedures. 8 This was the entomological threshold used under APOC s Conceptual and Operational Framework of Onchocerciasis Elimination with Ivermectin Treatment (Ouagadougou, 2010) for Phase 1b. evaluations to [c]onfirm that breakpoint has been reached and treatment can be stopped. The threshold used under WHO s Guidelines for stopping mass drug administration and verifying elimination of human onchocerciasis: criteria and procedures (Geneva, 2016) is a different one. 14
15 d) Schistosomiasis The PNLMT s goal is to control SCH in the country by The specific objective is to reduce prevalence of SCH to <10% among 75% of SAC by Strategies are MDA in schools and in the community; and behavior change communication. Channels for service delivery include schools, the community, health facilities, local radio stations, television (TV), and organized groups. From , the PNLMT remapped all districts for both SCH and STH, all with support from ENVISION and using Kato-Katz and urine filtration as the diagnostic tools. Those results are considered the baseline. Eight districts were remapped in 2013; 30 districts in 2014; and the remaining 39 districts in SCH results ranged from 0% to 65.6%, with only Kpomassè District (Atlantique Department) registering 0%. A total of 31 districts were classified as low-risk (>0 and <10%); 37 as moderate-risk ( 10% and <50%); and 8 as high-risk ( 50%). The PNLMT s control strategy for SCH is MDA with PZQ for all in- and out-of-school SAC (ages 5 14 years); the entire district is treated. The PNLMT decided in 2017 that beginning in FY18, it will only target districts with 10% prevalence, either at baseline or following a prevalence evaluation survey. In districts with baseline prevalence of 10%, the PNLMT follows WHO guidance for treatment based on prevalence: once every two years in moderate-risk communities (10% to <50% by parasitological methods), and once a year in high-risk communities ( 50% by parasitological methods). 9 The PNLMT has conducted SCH MDA with PZQ, with support from ENVISION, beginning in 2013, and since 2016 reaching all endemic districts requiring MDA (in 2017, all districts with baseline prevalence of 10% are on a treatment cycle). SCH MDA over the past 5 years is as follows: 2013: School-based integrated SCH/STH MDA, with PZQ and ALB, in the eight districts mapped that year 2014: School-based integrated MDA in districts out of the 38 districts mapped in : School-based SCH MDA (PZQ only) in 4 districts, and school-based integrated SCH/STH MDA in 12 districts 2016: School-based SCH-only MDA in 16 districts and school-based integrated SCH/STH MDA in 18 districts 2017: School-based SCH/STH MDA in 19 districts, school-based SCH-only MDA in 10 districts, community-based SCH/STH MDA in 2 districts (pilot activity), and community-based SCH-only MDA in 1 district (pilot activity) the first time that 6 of these districts were treated for SCH. In FY18, 33 districts are targeted for SCH MDA, including 13 districts through school-based SCH-only MDA, 3 districts through community-based SCH-only MDA, 12 districts through school-based integrated SCH/STH MDA, and 5 districts through community-based integrated SCH/STH MDA. The choice to use a community-based approach in selected districts is based on the successful experience of the pilot of community-based MDA for SCH and/or STH in FY17; in FY18, this approach will be used in districts with recurrent low coverage and/or where lack of collaboration from the MEMP s peripheral-level personnel (teachers and head teachers) has been reported for school-based MDA. As noted, beginning in FY18 the PNLMT will not conduct SCH MDA in districts with SCH prevalence <10%. Accordingly, the 12 districts with prevalence rates <10% where MDA has been initiated between 2014 and 2016 will no longer be treated, along with 19 other districts that have never been targeted. 9 WHO, Schistosomiasis: Progress Report and Strategic Plan (Geneva, 2013), Table Includes the 8 districts targeted in FY13, so 13 newly targeted districts. 15
16 In FY18, the PNLMT is planning a meeting to discuss and develop strategies for continued SCH/STH control, particularly once support for existing complementary MDA platforms (namely LF MDA, which will be stopped in many districts if TASs indicate that transmission was interrupted) stops. Please see Strategic Planning, Activity 5: Meeting to develop a strategy for sustained control of SCH and STH, below, for more detail on this meeting. e) Soil-Transmitted Helminths The PNLMT s goal is to control STH in the country by The specific objective is to reduce the prevalence of STH to <20% among 75% of SAC by Preschool-age children (pre-sac) are treated by the MOH s Mother and Child Health Directorate (Direction de la Santé de la Mère et de l Enfant [DSME]). Strategies are MDA in schools and in the community, and promotion of hygiene and environmental sanitation. Channels for service delivery include schools, the community, the framework for intersectoral dialogue on NTDs, and local radio stations. From 2013 to 2015, the PNLMT remapped all districts for both STH and SCH (as noted above), all with support from ENVISION and using Kato-Katz as the diagnostic for STH. This was considered the baseline mapping. A total of 8 districts were remapped in 2013, 30 districts in 2014, and the remaining 39 districts in The surveys showed that either Ancylostoma duodenale (hookworm) or Ascaris lumbricoides (roundworm), or both species, were present in all districts. Trichuris trichiura (whipworm) was observed in some districts. The three types of STH were observed with intra-specific and interspecific variation in the prevalence and intensity of infection. Overall, 2 districts were shown to be highrisk ( 50%); 43 districts moderate-risk ( 20 and <50%); and 32 districts low-risk (<20%) for STH. Fourteen of the districts that require STH MDA passed TAS1 and stopped MDA for LF in The PNLMT s control strategy for STH is MDA with ALB for all in- and out-of-school SAC (ages 5 14 years); the entire district is treated. The PNLMT decided in 2017 that beginning in FY18, it will only target districts with 20% prevalence, either at baseline or following a prevalence evaluation survey. The PNLMT conducts STH MDA once per year in both moderate-risk districts (baseline prevalence of 20% and <50%) and high-risk districts (baseline prevalence 50%).. The PNLMT has conducted STH MDA with ALB, with support from ENVISION, beginning in 2013 and reached full national scale for annual MDA with ALB in all moderate- and high-risk districts (i.e., all districts with prevalence rates of 20%) in STH MDA for the past 5 years is as follows: 2013: School-based integrated SCH/STH MDA with PZQ and ALB in the eight districts mapped that year 2014: School-based integrated SCH/STH MDA in 21 districts 2015: School-based STH-only MDA in 12 districts, school-based integrated SCH/STH MDA in 12 districts, and community-based integrated LF/STH MDA with IVM and ALB in 25 districts. 2016: School-based STH-only MDA in 14 districts, school-based integrated SCH/STH MDA in 18 districts, and community-based integrated LF/STH MDA in 25 districts. 2017: School-based STH-only MDA in 5 districts, school-based integrated SCH/STH MDA in 12 districts, community-based integrated LF/STH MDA in 4 districts, community-based STH-only MDA in 2 districts (pilot activity), and community-based integrated SCH/STH MDA in 5 districts (pilot activity). In FY18, 28 districts are targeted for STH treatment, including 5 districts through school-based STH-only MDA (one of which, Comé, will be supported by DeWorm3 in the framework of research on STH elimination); 12 districts through school-based integrated SCH/STH MDA; and 4 districts through 16
17 community-based integrated LF/STH MDA. 11 The other seven districts, which have either recurrent low coverage or where the MEMP s collaboration with the MOH is not optimal, will conduct communitybased STH MDA following the successful example of the pilot of community-based SCH and/or STH MDA conducted in FY17. This includes two districts that will conduct STH-only MDA and five districts that will conduct integrated SCH/STH MDA. Fourteen districts with baseline STH prevalence <20% have been conducting STH MDA via integrated MDA, with either LF or SCH. This includes 12 districts that conducted integrated LF/STH MDA (among which 4 districts will conduct TAS1 in FY18, potentially stopping MDA for LF), and 2 districts that conducted integrated SCH/STH MDA. As noted above, starting in FY18, the PNLMT will no longer treat the districts with STH prevalence <20% (using results of initial mapping or STH assessment during TAS3). As noted above (see Lymphatic Filariasis section), the PNLMT conducted an STH assessment, using Kato- Katz kits and with support from ENVISION, in 14 districts April May 2017 as part of the TAS3 conducted in a wider group of 21 districts. The STH assessment was limited to those districts that registered 20% in baseline mapping in Preliminary results show a significant reduction in STH prevalence in 13 of the 14 surveyed districts. As noted above, in FY18, the PNLMT is planning a meeting to discuss and develop strategies for continued SCH/STH control, particularly after support for existing complementary MDA platforms ends (namely LF MDA, which will no longer be conducted in many districts because those districts have data showing that transmission has been stopped). It is expected that the meeting will explore alternative platforms, such as other public health and/or maternal and child health interventions. 11 Those districts will not conduct MDA if they pass TAS1. STH MDA can easily be integrated with OV MDA because most of the districts will continue to conduct the latter. 17
18 3) Snapshot of PC NTD Status in Benin Table 1: Snapshot of the expected status of PC NTDs in Benin as of September 30, 2017 Columns C+D+E=B for each Columns F+G+H=C for each disease disease MDA MAPPING GAP DETERMINATION MDA GAP DETERMINATION DSA NEEDS ACHIEVEMENT A B C D E F G H I Disease Total no. of districts in Benin No. of districts classified as initially endemic No. of districts classified as initially nonendemic No. of districts in need of initial mapping No. of districts receiving MDA as of 09/30/17 USAIDfunded Others No. of districts expected to be in need of MDA at any level: MDA not yet started or prematurely stopped as of 09/30/17 Expected no. of districts where criteria for stopping districtlevel MDA have been met as of 09/30/17 No. of districts requiring DSA as of 09/30/17 LF g TAS1: Pre-TAS: 12 TAS3: 2 13 OV SCH STH Trachoma TIS: 4 12 Pending approval of the WHO AFRO RPRG, which met in October Includes four districts with TF 5% 9.9% at baseline. 14 As of FY18, per the MOH decision, only districts with SCH prevalence 10% are considered by the MOH to require MDA. This is different from previous years, where all districts with prevalence >0% were considered endemic and requiring MDA. 31 districts are considered by the MOH to be endemic, but without need of MDA, with SCH prevalence of >0% and <10%. 15 The PNLMT considers these districts non-endemic (and not in need of SCH MDA) because SCH prevalence is <10%; this includes 31 districts with prevalence >0% and <10%, and 1 district with prevalence of 0%. However, 12 of the districts conducted SCH MDA at least once in the past four years. 16 These districts, all with SCH prevalence 10%, are on an SCH treatment cycle (i.e., those with 50% prevalence treat annually, and those with 10% to <50% prevalence treat once every two years). 17 Districts with STH prevalence 20%. 18 The 45 districts endemic above the STH treatment threshold ( 20%) conducted STH MDA with USAID support in FY17. In addition, 19 districts with prevalence <20% have also been treated in conjunction with either the LF/OV or the SCH MDA, based on a national policy to treat all districts with ALB when and where possible (because there is no additional cost for the distribution, apart from the WHO-donated medicines). Beginning in FY18, only districts with STH prevalence 20% among SAC (whether from baseline mapping or from an STH prevalence evaluation survey) will be targeted. 19 Includes four districts with TF 5% 9.9% at baseline. 18
19 PLANNED ACTIVITIES 1) NTD Program Capacity Strengthening a) Strategic Capacity Strengthening Approach Capacity Goals 1. Increased capacity of district-level MOH personnel to plan, implement, and evaluate PC NTDrelated activities: The PNLMT s primary goal, as indicated in its National Master Plan for NTD Control , is to strengthen its NTD-related results-based planning, resource mobilization, and financial sustainability. The central PNLMT team has demonstrated that it can plan, implement, and monitor PC NTD-related activities. It is also essential that the district-level health personnel in charge of NTD activities (district head doctors and NTD focal points) have the capacity to analyze challenges, identify needs, plan, implement, and evaluate PC NTDrelated activities. 2. Financial autonomy and greater diversity of partners for the PNLMT: The PNLMT requires financial autonomy, with a greater number of partners, to sustain its PC NTD-related activities. 3. The country s LF and trachoma data compiled and held in one place by the central-level PNLMT: Having these data on hand will enable preparation of the elimination dossier for each disease at a later stage (process anticipated to start in FY19). It is anticipated that the MOH s Integrated NTD Database will be used in this process. Capacity Strengthening Strategy 1. Training, with support from ENVISION, to strengthen capacity of central- and health zone-level MOH personnel, focusing on PC NTD-related tools and activities (e.g., use of the Integrated NTD Database at central level, use of the Integrated NTD Database s Excel import forms at health zone level, and PC NTD-related data analysis and use at both levels). 2. Support from ENVISION to develop a resource mobilization strategy to expand and sustain PNLMT PC NTD activities. The PNLMT will continue to advocate for financial and in-kind support from health zones and municipalities. The PNLMT will also continue to seek new partners. 3. Assistance with compilation of LF and trachoma data, for eventual use in elimination dossiers. 20 It is anticipated that the MOH s Integrated NTD Database will be used in this process. b) Capacity Strengthening Objectives and Interventions Objective 1: Develop a resource mobilization strategy and implement its recommendations Activity 1: Assist the PNLMT in developing a resource mobilization strategy for PC NTDs: ENVISION will provide a qualified local consultant to assist the PNLMT in developing a resource mobilization strategy document aimed at identifying prospective partners and establishing a strategy to mobilize resources from those partners, in support of the MOH s activities to control and/or eliminate PC-NTDs. The proposed strategy will focus on enabling the MOH to maintain or expand MDA and other control activities for SCH and STH, after the MOH reaches the WHO-defined elimination targets for LF, OV, 20 Work on the LF and trachoma elimination dossier templates should begin in FY19. 19
20 and/or trachoma and stops its MDA for those diseases. The strategy document will identify potential partners, the types of support those partners could provide, and ways to secure that support. The PNLMT will then hold a meeting with the MOH technical directorates (e.g., DNSP director, MOH General Secretary, etc.) for official validation of the strategy. Activity 2: Meeting to advocate with partners for funding of PC NTD-related activities: ENVISION will financially support the PNLMT in organizing an advocacy meeting bringing together potential partners identified in the resource mobilization strategy document. The PNLMT will present its PC NTD-related needs via PowerPoint presentations to enable those potential partners to assess how and where they might assist technically and/or financially. The PNLMT will follow up with partners that show interest and/or make commitments to provide support. Objective 2: Strengthen the capacities of central- and health zone-level staff for data management and use in decision-making Activity 3: Train health zone-level NTD focal points how to fill out the Excel import forms for the Integrated NTD Database, and how to better analyze and use their PC NTD data: To enable better access to district- and sub-district-level PC NTD data at the central level (for inclusion in the PNLMT s Integrated NTD Database), and to enable health zone-level NTD focal points (and, by extension, the district-level personnel whom they support/oversee) to more effectively analyze and use the data generated by each district, ENVISION will technically and financially support the PNLMT in organizing a training in Parakou (Borgou Department) for health zone-level NTD focal points (from the four northern departments Alibori, Atacora, Borgou, and Donga) to enable the focal points to (1) fill out the Excel import forms with sub-district-level data, for sharing with the PNLMT, and (2) analyze and use those data to identify performance and trends in MDA coverage and to tailor strategies for those areas when microplanning for MDA, and to review the findings of surveys and assessments and draw programmatic conclusions in coordination with the PNLMT. Three central-level personnel will serve as trainers. This training will foster compilation of data that can be used in the process laid out in ENVISION s NTD Data for Action Guide (March 2016), which was adapted for use by and rolled out at health zone and district levels in FY17. Activity 4: Train central- and district-level PNLMT staff on how to perform a TIS: Four districts with TF prevalence rates of 5% and <10% (Nikki, Kalalé, Pèrèrè, and Tchaourou) completed the required single round of trachoma MDA in FY17 and will conduct a TIS in FY18 with ENVISION support. These will be the country s first TISs. Surveyors (graders and recorders) and supervisors will be trained in Parakou (Borgou Department). Objective 3: Compile data on LF and trachoma, for eventual use in elimination dossiers Activity 5: Compile data on LF and trachoma: RTI staff will assist the PNLMT in compiling the country s LF and trachoma data for storing by the PNLMT at the central level, incorporating them into and/or drawing from the MOH s Integrated NTD Database where possible. Data to be compiled include baseline prevalence, sentinel sites, MDA coverage, and DSA results. Having these data on hand will enable the PNLMT to begin filling out the dossier templates in later years (process anticipated to start in FY19). c) Monitoring Capacity Strengthening PNLMT and RTI staff will jointly assess progress in reaching the MOH s capacity strengthening goals and objectives, via their existing weekly meetings. Four times during the year the following indicators will be evaluated: 20
21 Objective 1: Implement the recommendations of the advocacy and resource mobilization strategy Indicators: (1) Proportion of recommendations effectively implemented by the PNLMT, (2) Number of contacts made with new partners by the PNLMT, and (3) Facilitation of communications with new partners by the PNLMT Objective 2: Strengthen the capacities of PNLMT and district-level MOH personnel for ownership of PC NTD-related activities and better management of data Indicators: Activity 1: (1) Number of health zone-level and/or district-level NTD focal points trained and (2) Proportion of health zone-level and/or district-level NTD focal points trained who fill out the Integrated NTD Database s Excel import forms with sub-district-level data, for sharing with the PNLMT Activity 2: (1) Number of Tropical Data trachoma graders and recorders trained for TIS Objective 3: Compile data on LF and trachoma, for eventual use in elimination dossiers Indicators: (1) LF data are compiled and stored at central level in the Integrated NTD Database and other files as appropriate (e.g., for qualitative data) and (2) Trachoma data are compiled and stored at central level in the Integrated NTD Database and other files as appropriate (e.g., for qualitative and F&E data) Table 2: Project assistance for capacity strengthening Project assistance area Building advocacy for a sustainable national NTD program M&E Dossier development Capacity strengthening interventions/activities Assist in developing a resource mobilization strategy for PC NTDs Conduct advocacy meeting with potential partners Train health zone/district-level NTD focal points on filling out Integrated NTD Database s Excel import forms with subdistrict-level data, for sharing with the PNLMT Train health zone/district-level NTD focal points to analyze and use those data to tailor strategies and to draw programmatic conclusions Train additional trachoma graders and recorders Compile and store data for development of LF and trachoma elimination dossiers How these activities will support the PNLMT s PC NTD program Establish a roadmap for further fundraising efforts Identify additional resources to help sustain and/or expand the PNLMT s PC NTD-related activities after stopping MDA for LF and trachoma Ensure sub-district-level data related to PC NTD activity data are available at the health zone level Better data-based decision making as MDA activity results are available at health zone/district level Country able to implement a TIS without assistance of an external consultant Data to be included in the LF and trachoma elimination dossiers are stored in one place for each disease. 21
22 2) Project Assistance a) Strategic Planning Activity 1: Annual PC NTD review meeting (for FY17 activities) and MOH PC NTD annual planning meeting (for FY18 activities): Each year toward the end of the calendar-year, the PNLMT organizes backto-back meetings for review of the previous (USAID fiscal) year s PC NTD activities and for planning of the coming (USAID fiscal) year s PC NTD activities. Over the course of the two meetings, the PNLMT and its partners review the preceding year s successes and challenges related to MDA, surveys, and M&E; develop strategies to improve MDA coverage as needed; coordinate health district-level activities; and plan activities for the coming year (including those planned as part of the ENVISION work plan for that same period). Participants have included MOH representatives from the central, departmental, health zone, and district levels; MEMP representatives from the central and departmental levels; village chiefs; and CDDs. ENVISION will fund and provide logistical support for this activity, and assist the PNLMT in preparing data for the meetings. In FY18, these two types of meetings will take place in the form of three smaller paired meetings (review and planning), held successively in different parts of the country, given that Benin is getting closer to reaching its elimination goals for LF and for trachoma and it will be more productive to work in smaller groups that share common challenges. The sets of paired meetings will be held at three different locations: representatives of the four northern departments (Alibori, Atacora, Borgou, and Donga) will meet in Parakou (Borgou Department); representatives of the four central departments (Collines, Couffo, Mono, and Zou) will meet in Lokossa (Mono Department); and representatives of three southern departments (Atlantique, Ouémé, Plateau) will meet in Kétou (Plateau Department). PNLMT personnel and RTI staff will collectively attend all three meetings, and Cabinet personnel and MEMP personnel who will each attend one of the three meetings. PNLMT, RTI, health zone and/or district-level staff will each give presentations on MDA coverage rates reported by districts, on districts with recurrent low coverage, on the various causes of low coverage identified, and on the results of DSAs conducted in FY17 and their implications. Presentations will aim to help participants think about solutions to improve coverage rates, especially in districts where causes of low coverage have not been clearly identified. Activity 2: PC NTD Steering Committee meetings: ENVISION will fund the quarterly meetings of the MOH s NTD Steering Committee in Cotonou. The Steering Committee is responsible for coordinating integration of PC NTD activities, assessing progress, and addressing challenges for PC NTD control in Benin; it oversees implementation of the PNLMT s PC NTD program, including community-based and school-based MDA. Activity 3: Cross-border OV meeting with Togo: With ENVISION support, the PNLMT is continuing its collaboration with the neighboring country of Togo to develop common strategies for PC NTD (mainly OV for now) control and elimination along their shared border areas. In FY18, ENVISION will financially support a meeting in Lokossa (Mono Department), bringing together the same number and types of participants as in previous years: Benin s side will include members of the MOH NTD team (district head doctors from districts that border Togo, heads of departmental public health services, and central-level PNLMT staff) and RTI staff members. From Togo s side, it is expected that the NTD program coordination staff and collaborators will attend the meeting, with their own funding. 22
23 Activity 4: Meetings of the Technical Committee of Experts for Elimination of OV and LF: ENVISION will technically and financially support the PNLMT in organizing two meetings of the committee in FY18, the first with domestic participants only and the second adding international participants (apart from the RTI personnel, the international partners would cover their own travel to attend the meeting). The meetings will assess progress of the OV elimination strategy and activities (it is expected that in FY17 and FY18, the committee will focus on OV only; it will expand its focus to include LF starting in FY19). The first meeting, for three days in Bohicon (Zou Department), will review progress made by the PNLMT toward fulfillment of recommendations from the late-fy17 meeting. The second meeting will be in Cotonou. The PNLMT will present a summary of what has been achieved so far (based on recommendations from previous meeting), and the committee will assist the PNLMT in figuring out the next steps to achieve elimination. Activity 5: Meeting to develop a strategy for sustained control of SCH and STH: ENVISION will give the PNLMT financial support to organize a meeting in Bohicon (Zou Department) to develop a clear strategy to sustain SCH/STH control activities. The meeting will bring together SCH/STH experts from the University of Abomey-Calavi, members of research institutions, members of the MEMP, and PNLMT staff. Activity 6: FY19 ENVISION work plan workshop: ENVISION will financially support the PNLMT and RTI in organizing a workshop in Bohicon (Zou Department) to develop the Benin ENVISION FY19 work plan. PNLMT and RTI will review the FY18 work plan activities and identify new activities that are needed to help achieve elimination of NTDs by b) NTD Secretariat Activity 1: Support for PNLMT operational costs (office equipment, communication costs, and supplies): ENVISION will provide minor financial support for operational costs and supplies related to PNLMT PC NTD activities (including paper, copies, office maintenance, and communications). Activity 2: Vehicle maintenance and related supplies: In FY18, ENVISION will provide financial support for vehicle maintenance and purchase of routine vehicle-related supplies. c) Building Advocacy for a Sustainable National NTD Program Activity 1: Assist the PNLMT in developing a resource mobilization strategy for PC NTDs: ENVISION will provide a qualified local consultant to assist the PNLMT in developing a resource mobilization strategy document aimed at identifying prospective partners and in developing a strategy to mobilize resources from those partners, in support of the MOH s activities to control and/or eliminate PC-NTDs. The proposed strategy will focus on enabling the MOH to maintain or expand MDA and other control activities for SCH and STH, after the MOH reaches the WHO-defined elimination targets for LF, OV, and/or trachoma and stops its MDA for those diseases. Activity 2: Meeting to advocate with partners for funding of PC NTD-related activities: ENVISION will financially support the PNLMT in organizing a meeting, in Cotonou, to advocate with existing and prospective partners for funding for PC NTDs. PNLMT and RTI staff will attend this meeting along with potential partners. It is expected that the PNLMT will then follow up with partners that express interest. d) MDA Coverage 23
24 Following the success of the community-based SCH/STH MDA in FY17, the PNLMT has decided to use this strategy in districts that have often reported low coverage rates or where collaboration between the MOH and the MEMP is not optimal. In FY18, the SCH/STH MDA campaign will be conducted in the community (rather than in schools) in 10 of the districts targeted for STH separately from LF MDA: 3 are targeted for SCH treatment alone, 2 for STH alone, and 5 for both SCH and STH. Table 3: Districts targeted for MDA with USAID support in FY18 LF OV SCH STH NTD Age groups targeted Entire population 5 years Entire population 5 years Number of rounds of distribution annually SAC ages 5 14 years 1 SAC ages 5 14 years 1 Entire population 5 years SAC only 1 SAC only 1 Trachoma Entire population Distribution platform(s) Communitybased MDA Communitybased MDA Communitybased MDA School-based MDA Communitybased MDA 23 Communitybased MDA School-based MDA Communitybased MDA Number of districts to be treated in FY SCH + 5 SCH/STH 13 SCH + 12 SCH/STH 4 2 STH + 5 SCH/STH 4 STH + 12 SCH/STH 4 Activity 1: MDA supplies (registers for CDDs involved in community SCH/STH MDA, dose poles for CDDs involved in community SCH/STH MDA, reporting forms, and vests for CDDs: ENVISION will financially support printing registers for registration and treatment data collection. ENVISION will financially support manufacturing of dose poles for districts that will conduct communitybased SCH MDA, for districts that previously conducted school-based SCH MDA for which dose poles were not needed. ENVISION will financially support printing reporting forms for school-based integrated SCH/STH MDA. Those forms will be used for MDA data collection by teachers and head teachers. ENVISION will procure vests for those CDDs who did not receive one during previous distribution. The CDDs will wear the vests during the MDA, promoting the campaign, increasing the visibility of the MDA, and valorizing their work. After the MDA campaign, supplies that were used during the campaign are kept at sub-district level; any extra supplies are returned to the districts for storage. 21 Comé is excluded here because it will be supported by the DeWorm3 project. 22 MDA targets depend on RPRG approval of TAS1; if RPRG does not approve proposed TAS1 plans, the districts will instead be treated with USAID support in FY MDA targets depend on RPRG approval of TAS1; if RPRG does not approve proposed TAS1 plans, the districts will instead be treated with USAID support in FY18. 24
25 Activity 2: School-based MDA for SCH and/or STH in 29 districts: School-based SCH/STH MDA campaigns distributing ALB (400 mg) and PZQ generally last one week. Prior to the MDA, the PNLMT and the Steering Committee, in collaboration with the MEMP (for school-based MDA), meet to agree on the planning and implementation of treatment in all schools of the targeted districts. The MDA schedule is then transmitted through the MEMP hierarchy to the teachers, who serve as drug distributors in schools. For FY18, the treatment in schools will target 13 districts for SCH alone, 4 districts 24 for STH alone, and 12 districts for the combined treatment of STH/SCH. Catch-up campaigns involving teachers, assisted by the CDDs, will be organized in districts where the targets are missed. A total of 2,950 schools will receive treatment; in each school, one CDD will assist in the treatment of SAC who do not attend school and who are invited to come to school to receive their treatment during the MDA day. A week before the treatment day, community radio stations inform the community about the treatment day and encourage all parents (with an emphasis on parents whose children are school age but do not attend school) to take their children to the nearest school on the treatment day to receive the drugs. Religious and traditional leaders will be briefed by nurses to communicate the same information in their communities. The same message is relayed by town criers, CDDs, and cars equipped with megaphones circulating in the villages two days before the treatment day. The MDA is carried out on a single day at each school under the supervision of the head teachers, district head doctors, NTD focal points, and heads of the sub-district health center (nurses). Each child receives treatment in his/her classroom, and the data is immediately collected by the teacher (often assisted by a teacher s assistant). On the treatment day, SAC who do not attend school receive drugs from the head teachers or from CDDs. All teachers and head teachers are considered volunteers. Activity 3: Community-based SCH/STH MDA in 10 districts: ENVISION will support the PNLMT in conducting community-based STH-only MDA in two districts, community-based integrated SCH/STH MDA in five districts, and community-based SCH-only MDA in three districts. This community-based MDA will be conducted in the same period as the school-based MDA. Switching to a community-based platform in these districts will reduce the challenges of cooperation with the MEMP and teachers, help CDDs successfully incorporate additional drugs packages, and is expected to address the low-coverage problems in those districts. To verify the accuracy of the denominators used for the campaign, the registration will be performed using a register. In villages where there is more than one CDD, they will be organized in groups of two and go door-todoor to distribute drugs. While one CDD measures the height (PZQ treatment only) and fills out the register, the second CDD offers the treatment. The CDDs make sure the pills are swallowed and the data are recorded according to gender. Activity 4: Community-based MDA for LF and/or OV in 62 districts: The drugs are distributed by CDDs under the supervision of sub-district nurses and district head doctors. In villages where there is more than one CDD, they are organized in groups of two and go door-to-door to distribute drugs. While one CDD measures height and fills out the register, the second CDD offers treatment. The CDDs make sure the pills are instantly swallowed (directly observed treatment) and the data are recorded according to gender. The same information on CDD allowances as is applied for the SCH/STH MDA is applicable here. 24 Excluding Comé, which will be treated with the support of DeWorm3. 25
26 Activity 5: Trachoma MDA in four districts: MDA in four districts (Banikoara, Boukoumbé, Toukountouna, and Natitingou) with TF prevalence of 10% 29.9% for three consecutive years with funding from ENVISION started in 2016 and will be completed in FY18. CDDs will go house to house to provide treatment. ITI will provide the ZTH, and ENVISION will provide the TEO 1% for children 0 6 months old. As in FY17, the treatment will be distributed over 15 days for two reasons: (1) figures reported by the villages on the tenth day of FY17 MDA supervision indicated a coverage rate inferior to 70%, and (2) the time needed for ZTH treatment administration is greater than for IVM/ALB because the entire population is targeted. ENVISION will provide financial support for payment of MDA per diems to CDDs, as well as provide technical assistance for drug distribution, MDA supervision, and data collection and reporting. e) Social Mobilization to Enable NTD Program Activities Activity 1: Printing of posters and banners: ENVISION will support the printing and distribution of posters in targeted districts for all ENVISION-supported MDA in FY18. The posters and banners are distributed a few days before the MDA. Posters are displayed in classrooms and around schools for STH and SCH school-based campaigns; the teachers refer to these when discussing the campaign with their students, the students view the illustrations and report back to their families, and any other visitors to the school (whether literate or not) understand the posters message thanks to the pictures that are included. LF, OV, and trachoma posters are displayed in public places such as the town halls, health centers, and markets. They are also used by CDDs, who carry them when visiting households for drug administration. Posters will be used before and during SCH and STH, LF/OV, and trachoma MDA. In non-educational settings, one of the following three types of posters will be displayed in the communities for OV, LF, and trachoma MDA, according to the disease being treated in the targeted districts. One poster focuses on LF prevention and annual treatment, the second provides information on OV treatment, and the third focuses on describing trachoma and its prevention and treatment. These three posters inform the community about the importance of not missing the annual IVM (OV), IVM and ALB (LF), and TEO/ZTH (trachoma) treatments. Posters will be displayed by the CDDs and volunteers in public places in communities and villages a week before the MDA. The LF, OV, and trachoma posters will target the whole community. For SCH/STH MDA, three types of posters will be used to inform and educate children and parents about the risks of STH/SCH infections and the basic rules of prevention a poster on STH control, a poster on SCH control, and a poster on the risk factors and prevention of both STH and SCH. The last of these will also highlight the importance of using toilets. These posters will also be used as reinforcement to remind viewers of the previously broadcast messages. All districts targeted for STH and SCH MDA will be provided with an appropriate number of posters necessary to cover their area. Posters will be displayed in classrooms and/or at strategic locations, such as toilet front doors and on notice boards, allowing not only the students but also their families and other visitors to the school to see them. The head teachers will assist the teachers in ensuring that these posters are properly displayed at their respective schools. Banners will be used to announce the beginning of STH/SCH as well as LF/OV and trachoma MDA campaigns. For SCH/STH MDA campaigns, banners will be displayed at the entrance of the DDS offices, the MEMP Departmental Directors offices, the school district, and in public places. For LF/OV and trachoma MDA, banners will be displayed at the entrance of the city and around the markets. The 26
27 banners will remind the community of the MDA date and the treatment strategy (i.e., whether it is a community-based or school-based MDA). Activity 2: Broadcasting of TV and radio commercials and announcements: ENVISION will financially support the PNLMT in broadcasting radio and TV commercials and announcements in all targeted districts. To promote the FY18 STH/SCH, LF/OV, and trachoma MDA campaigns, ENVISION will provide financial support for these advertisements to be broadcast at the peak listening or viewing time blocks on major TV channels and community radio stations in targeted districts. For trachoma, a message will be broadcast on local and community radio stations in four targeted districts (Banikoara, Boukoumbé, Natitingou, and Toukountouna). Activity 3: Message broadcast by mobile sound system: ENVISION will financially support broadcasting of MDA messages via mobile sound systems (rental of cars or motorbikes equipped with loudspeakers) in 39 districts 25 for STH/SCH for one day, 67 districts for two days of messages for LF/OV, and 4 districts for three days of trachoma messages before the respective MDA. The trachoma MDA lasts longer than the LF/OV MDA (15 versus 10 days), hence the need for more days of broadcasting for the former. The mobile sound system is used to reinforce the above-stated messages in the communities particularly to inform all parents (of districts targeted through the school-based platform) with nonenrolled SAC that they should go to the nearest school in their community to receive treatment and the exact dates of distribution in each community. Activity 4: Village-to-village awareness-raising by Red Cross volunteers or town criers: ENVISION will support the PNLMT in using the services of Red Cross volunteers in districts where there are enough people to conduct effective social mobilization; in those districts without volunteers, ENVISION will continue to fund the work of town criers. The volunteers (or town criers) will be briefed by district head doctors, assisted by NTD focal points, on each disease before the MDA campaign and given posters for their social mobilization activities. The volunteers/town criers will inform the public of MDA dates and hold awareness-raising sessions with the aim of increasing the communities participation in the MDA campaigns. ENVISION will financially support the Red Cross volunteers to travel from village to village by motorcycle, bicycle, or on foot, using the megaphones purchased in previous years to broadcast information. 25 Comé is not included as it will conduct MDA with support from DeWorm3. 27
28 Table 4: Social mobilization/communication activities and materials checklist for NTD work planning Category MDA announce ment Disease prevention Key messages MDA will take place in schools on a specific date (SCH/STH) or in the community during a specific timeframe (SCH/STH, LF/OV, and trachoma). Category of person targeted by each MDA The drugs provided are free and safe Target population Community members Community members IEC activity (e.g., materials, medium, training groups) Banners, radio and TV announcem ents Radio and TV commercials Posters Where/when will they be distributed Banners: hung at the entrance of the Departmental Directorate for Education, DDS, and school district for school-based MDA and at the entrance of the city and around the markets for communitybased MDA, one two weeks before MDA Radio and TV announcements : broadcast on national TV and local radio channels one two weeks before the MDA National TV stations (4) and local radio stations (number depends on the district targeted) a few days before OV/LF MDA campaign Posters: Hung in classrooms and around schools for SCH/STH MDA; in public places (town hall, health centers, and markets) for LF/OV and trachoma one Frequency Radio announce ment: frequency according to district coverage TV announce ment: at least one time a day (frequency depends on popularity of TV channel) Banners: Before each MDA campaign Radio commercia ls: three times per day TV commercia ls: at least one per day (frequency depends on popularity of TV channel) Posters: Before each MDA campaign 28
29 Category Key messages Target population IEC activity (e.g., materials, medium, training groups) Where/when will they be distributed week before MDA Frequency Disease Prevention Some AEs are normal and they will pass. Drugs distributed at school are safe and keep you healthy. Prevent SCH, STH, LF, OV, and trachoma Drug distributors Schoolaged children Community members CDD training module Social mobilization activities (town criers, mobile sound systems, CDD information session before treatment, TV/radio commercials Posters Radio and TV commercials District-level CDD refresher training TV/radio commercials: national TV stations (4) and local radio stations (number depends on the district targeted) a few days before OV/LF MDA campaign. Town criers, mobile sound systems: Two days before MDA campaign and during MDA information sessions Posters: Hung in the classrooms and around schools for SCH/STH MDA; Training modules will be distributed once annually in newly targeted districts. Radio commercia ls: three times per day TV commercia ls: at least one time a day (frequency depends on popularity of TV channel) Town criers: at least two times by village (before and during MDA) Mobile sound systems: one round by village CDD informatio n: before drug administrat ion Posters: Before each MDA campaign 29
30 Category Other Key messages Avoid complicati ons of LF, OV, and trachoma Promoting visibility of NTD Program Target population IEC activity (e.g., materials, medium, training groups) Where/when will they be distributed in public places (town hall, shops, health centers, and markets) for LF/OV and trachoma one week before MDA. Radio and TV commercials: Broadcast on national and radio channels during a specific period (a few days before and during campaign) CDDs Vests Distribution of vests to CDDs before FY18 MDA campaign Frequency Radio commercia ls: three times per day TV commercia ls: at least one time a day (frequency depends on popularity of TV channel) One time 30
31 f) Training Activity 1: MDA training of departmental trainers: ENVISION will financially and technically support the MOH s team of national trainers in training trainers for each of the six areas targeted for MDA in the departments of Atacora/Donga, Mono/Couffo, Borgou/Alibori, Ouémé/Plateau, Atlantique/Littoral, and Zou/Collines; trainees will include DDS directors, heads of departmental public health services, and heads of the Division of Epidemiology and Sanitary Surveillance. For the departmental training, DDS directors, heads of departmental public health services, heads of the Division of Epidemiology and Health Surveillance, health zone coordinators, district head doctors, and NTD focal points will participate in Atacora/Donga and Borgou/Alibori, and in the other grouped departments. They will be trained on the PC NTDs targeted in Benin (with less focus on trachoma in districts not requiring treatment for that disease). The training workshop aims to remind former participants and teach new participants about the different types of MDA campaigns in terms of preparation, implementation, social mobilization, and supervision of MDA. Activity 2: MDA training of nurses and CDDs for OV/LF MDA in 62 districts: ENVISION will support the PNLMT in providing refresher training to nurses for OV and LF MDA. The nurses will travel and meet at their respective district health centers to receive training from the supervising medical doctor. On their return, these nurses will conduct refresher training sessions for CDDs involved in OV and LF MDA. The central level MOH dispatches its staff to different locations across the country to supervise the training. Departmental (DDS) and district-level (doctors and NTD focal points) also supervise this activity. Activity 3: Training CRPs, CPs, RUPs, Co-RUPs, trainers, and supervisors of teachers, and training of teachers: To ensure continuity of school-based MDA, the GOB included the school-based MDA cost and training in the teaching staff work plan and budget. Consequently, ENVISION will no longer support per diems for head-teachers and teachers for this activity. ENVISION will support the per diems of participants (RUPs, Co-RUPs, CRPs, and CPs) for refresher training. The CRPs and the CPs are the hierarchical superiors of the heads of the educational units, so they will be the RUP and Co-RUP supervisors during the teachers training. These RUPs and Co-RUPs will train the head teachers and teachers, who will be paid by the local government. The training module will then be included in the training package for the teaching staff in each education unit. This package also encourages teachers to educate children on the impact of NTDs on their society and the different ways to prevent and control NTDs, especially SCH and STH, in school. (The RUPs have numerous other opportunities to train teachers and head teachers, without funding from ENVISION.) In addition to the RUPs and Co-RUPs, the CRPs and the CPs will receive training. The CRPs and CPs are in charge of planning and the choice of themes to be developed in the educational units. 31



32 Figure 1: Organization of the cascade training for the various MDA campaigns Regional NTD focal persons (medical doctors) Medical doctors from targeted districts Medical doctors from targeted districts Cascade-like training for school-based MDA RUP and Co-RUP Nurses Cascade-like training for community-based MDA School directors Teachers CDDs Activity 4: Training of nurses and CDDs for community-based SCH/STH MDA in 10 districts: ENVISION will support district head doctors in providing refresher training for nurses on SCH/STH MDA preparation, implementation, and supervision for community-based SCH/STH MDA in 10 districts. ENVISION will then support the nurses in providing training for CDDs, enabling them to properly perform registration and treat targeted persons. Activity 5: Training of health workers and CDDs for trachoma MDA in four districts: ENVISION will financially and technically support refresher training in Natitingou for heads of departmental public health services, health zone coordinators, district head doctors, the national Trachoma Focal Point, nurses, heads of the Division of Epidemiology and Sanitary Surveillance, and the NTD focal points involved in trachoma MDA in the four targeted districts. ENVISION will then support nurses in conducting training for CDDs in their respective districts, under the supervision of the district head doctors. Participants will be taught about trachoma and the SAFE strategy, the trachoma situation in the country and respective districts, the pharmacology of ZTH (with emphasis on uses, doses, and possible AEs), ZTH dosing and use of the dose pole, writing patient details, and how to write the daily summary reports. The different duties of the health zone coordinators, supervisors, nurses, and CDDs will be clearly explained to each respective group. Activity 6: Integrated NTD Database refresher training for central-level PNLMT and RTI personnel: ENVISION will technically and financially support the PNLMT in holding a refresher training for PNLMT and RTI staff in Cotonou. Activity 7: Training on filling out Excel import forms and data use for health zone-level NTD focal points from four departments: To enable better access to district-level PC NTD data at the central level (for inclusion in the PNLMT s Integrated NTD Database), and to enable health zone-level NTD focal points (and, by extension, the district-level personnel whom they support/oversee) to more effectively analyze and use the data generated by each district, ENVISION will technically and financially support the PNLMT in organizing a training in Parakou (Borgou Department) for health zone-level NTD focal points (from the four northern departments Alibori, Atacora, Borgou, and Donga) to enable the focal 32
33 points to (1) fill out the Excel import forms with sub-district-level data, for sharing with the PNLMT, and (2) analyze and use those data to identify performance and trends in MDA coverage and to tailor strategies for those areas, and to review the findings of surveys and assessments and draw programmatic conclusions in coordination with the PNLMT. Three central-level personnel will serve as trainers. A coaching approach will be used, with RTI encouraging the PNLMT to contact the trainees at defined moments in the months following the training, to check on their progress. Activity 8: Printing of training modules and guides for CDDs and training modules for nurses for community-based SCH/STH MDA in 10 districts: ENVISION will financially support printing of training modules and guides for the CDDs. Activity 9: Training on Coverage Evaluation Surveys in two districts: ENVISION will train surveyors and PNLMT staff on the updated WHO method for coverage evaluation surveys (CES), to ensure high quality implementation of the survey in two districts. The training will cover electronic survey data capture. g) Drug and Commodity Supply Management and Procurement Activity 1: NTD drug quantification: The PNLMT uses the Tool for Integrated Planning and Costing (TIPAC) to estimate the quantity of ALB, IVM, and PZQ needed, and to generate applications for those drugs. RTI will participate in the work session to finalize the MOH s Joint Request for Selected PC Medicines (JRSM) for 2019, with the PNLMT s permission. For TEO and ZTH, application forms are provided by RTI and ITI respectively and are filled out by the PNLMT; RTI staff will assist. Activity 2: Transport and store PC NTD MDA drugs and diagnostics within country: Donated drugs are sent to the country through WHO, which assists the PNLMT to obtain customs clearance. Diagnostics are delivered directly to the PNLMT office. After ALB, PZQ, ZTH, TEO, and IVM clear customs, the drugs are delivered to the central medical store (Centrale d Achat des Médicaments Essentiels [CAME]). ENVISION will financially support the PNLMT in storing and transporting drugs for school-based and community-based SCH/STH MDA, and for community-based trachoma and OV/LF MDA. This financial support will cover vehicle rental and fuel to transport the drugs from the port to the CAME via two trucks, from Cotonou to the departments, and then to districts targeted for MDA and/or DSAs. 26 Activity 3: Annual monitoring of supplies of PC NTD MDA drugs and diagnostics: At the end of all MDA campaigns (SCH/STH, trachoma, and OV/LF), the remaining drugs in each district are counted. ENVISION will fund the reverse supply chain of drug and diagnostic stocks. Two teams will carry out the inventory in all targeted districts for each of the MDA campaigns. The inventory for OV/LF and trachoma drugs will be combined. Teams travel and visit all health zones, including districts, after each MDA. They are in charge of counting the remaining drug supply at the health zone level (number of bottles converted into number of pills). When needed, districts are also visited to count the remaining supply. This ensures that the remaining drugs are returned to the health zones for proper storage until the next campaign. ENVISION ensures that all medicines distributed via ENVISION-supported MDA are valid and not expired. The PNLMT s MDA Officer checks drugs before they are shipped from the central level; MOH personnel 26 The GOB will provide the PNLMT with equipment to transfer the drugs from the districts to target villages prior to the distribution and repackaging of the drugs. The transportation and storage of drugs for OV/LF community-based MDA are provided by the MOH. The costs of the various activities involved in the supply chain are fully supported by the PNLMT as a cost-share for NTD control and elimination. Transport of drugs from the central level to the district level for OV/LF MDA is paid for by the PNLMT. Diagnostics are not included in these shipments. 33
34 at health zone, district, and sub-district levels do the same. They are trained on how to avoid wasting drugs by using the remaining, unexpired supplies from previous campaigns before using newer supplies. h) Supervision for MDA Activity 1: Supervision of MDA cascade training: Supervisory visits at all levels of training include assessment of knowledge about WHO guidelines, use of IEC materials, treatment strategies, management of SAEs, management of drugs, and data collection and reporting. ENVISION will provide per diem support to enable the PNLMT s pool of supervisors tasked with overseeing the proper implementation of training; the MOH provides the PNLMT with staff, vehicles, and fuel. Activity 2: Supervision of OV/LF MDA: For the OV/LF community-based MDA in 62 districts, staff members from the central level, from the departmental level, district head doctors, nurses, and NTD focal points in targeted health zones will supervise the treatment. In urban districts reporting low coverage on a recurrent basis, the new strategy (using maps and social mobilization in churches and mosques before MDA) will be implemented to ensure sufficient coverage is reached in the coming years of MDA. Activity 3: Supervision of SCH/STH MDA: For the 39 districts 27 targeted for SCH/STH MDA (through school- and community-based MDA), staff members from the central level, from the departmental level, from the MEMP, district head doctors, CRPs and their assistants, CPs, representatives of teachers union, and NTD focal points from the health zones targeted will supervise the treatment, including supervision of 120 nurses for the 10 districts targeted through community-based MDA. Activity 4: Supervision of trachoma MDA: For the trachoma MDA, staff members from the central level, at the department level, district head doctors, nurses, and NTD focal points in the targeted health zones will supervise the treatment. i) M&E Activity 1: LF TAS1 in 13 districts: The PNLMT presently anticipates conducting TAS1 in 13 districts (Agbangnizoun, Za-Kpota, Ouinhi, Zagnanado, Zogbodomey, Allada, Ouidah, Kpomassè, Torri-Bossito, Bonou, Adja-Ouèrè, Parakou, and Covè). Of these 13 districts, 3 passed pre-tas in 2013, and the other 10 in As of early August 2017, RPRG approval has not yet been formally granted for TAS1 in all of these districts. ENVISION will support the TAS1 in those districts where it is approved, and will continue to support MDA in those districts (if any) where the survey is not approved. The survey will be school-based as all districts have primary-school enrollment of 75%. FTS will be used as the diagnostic test. ENVISION will financially support a training in Bohicon (Zou Department) just before the start of the survey, and per diem for field work. Activity 2: LF TAS3 in two districts: ENVISION will support the PNLMT in conducting a TAS3 in two districts (1 EU) that did not complete the planned TAS3 assessment in FY17 due to the late arrival of FTS. 27 Comé is not included as the MDA in this district will be financially supported by the DeWorm3 project. 34
35 The surveys will be conducted in the community as the proportion of children enrolled in school is <75%, and FTS will be used as the diagnostic. In FY17, the nurses recruited CDDs to record the population in households within the clusters selected, based on a map established by INSAE; this same information will be used in FY18. ENVISION will fund a refresher training in Parakou (Borgou Department), and per diem for the duration of the field-work. Activity 3: LF pre-tas in 12 districts: The PNLMT will conduct pre-tas in 12 districts (Adjarra, Adjohoun, Aguégués, Akpro-Missérété, Avrankou, Dangbo, Sèmè-Kpodji, Ifangni, Pobè, Sakété, Abomey, and Bohicon) that have completed five rounds of MDA (FY13 FY17), all with 65% epidemiological coverage, using CDD registration for the denominator. FTS will be used as the diagnostic test. ENVISION will provide financial support for a training for supervisors and surveyor teams in Bohicon (Zou Department), the day before the beginning of the activity, and for field work. Activity 4: TIS in four districts: ENVISION will support the PNLMT in conducting TIS in four districts that have completed the required single round of MDA with sufficient program coverage (Nikki, Kalalé, Pèrèrè, and Tchaourou). Each district will be considered as an EU. TF, TT, and Trachomatous Scarring (TS) will be graded, following the WHO/Tropical Data protocol. Surveyors (graders and recorders) and supervisors will be trained during four days in Parakou (Borgou Department). ENVISION will provide financial support for a training and for the activity itself. Activity 5: Coverage Evaluation Surveys in two districts: ENVISION will support the PNLMT in conducting coverage evaluation surveys in two districts, following ENVISION-supported LF/OV MDA. The immediate purpose will be to validate reported coverage in those two districts, which will be purposively selected. Until additional surveys are performed in FY19, the results from these FY18 surveys will apply (for validation of reported coverage) to these two districts alone. ENVISION will purchase smartphones for use in electronic data collection for these surveys. These devices will be used for all ENVISION-supported surveys that involve electronic data capture. Table 5: Planned DSAs for FY18 by disease Disease No. of endemic districts (as of July 2017) No. of districts planned for DSA No. of EUs planned for DSA (if known) Type of assessment Diagnostic method 2 1 TAS3 FTS LF TAS1 FTS 12 N/A Pre-TAS FTS Trachoma TIS Clinical grading j) Supervision for M&E and DSAs Activity 1: Supervision of LF TAS1 in 13 districts: ENVISION will financially support supervision by MOH or affiliated staff during the period allocated to data collection. The supervisors will ensure that the 35
36 teams follow the recommended operating procedures and that they have adequate supplies to carry out the surveys. The supervisors will also help facilitate the field work for the teams. Activity 2: Supervision of LF TAS3 in two districts: ENVISION will financially support supervision by MOH or affiliated staff during the period of the survey. The supervisors will ensure that the teams follow the SOPs for TAS3 and that they have the adequate supplies to carry out the survey. Activity 3: Supervision of LF Pre-TAS in 12 districts: ENVISION will financially support supervision by supervisors (PNLMT central-level staff) for the entire duration of the survey. They will ensure that the teams follow the SOPs recommended by WHO for this activity and solve any issues that can hinder the success of the activity. Activity 4: Supervision of TIS in four districts: ENVISION will financially support supervision by supervisors (MOH or affiliated staff) for the period of the survey. They will ensure that the teams follow the SOPs recommended by WHO for this activity and solve any issues that can hinder the success of the activity. Activity 5: Supervision of Coverage Evaluation Survey in two districts: ENVISION will provide financial support for supervisors to oversee data collection of the CES. These supervisors will ensure surveyors are adhering to the protocol and the updated WHO methodology on CES. A supervisor will visit all of their assigned team(s) at least once per day during data collection. k) Dossier Development Activity 1: Assistance in compiling LF and trachoma data: ENVISION will assist the PNLMT in compiling available data on LF and trachoma, incorporating them into and/or drawing from the MOH s Integrated NTD Database where possible, to be stored by the PNLMT at the central level. After these data are on hand, they can be used to begin to fill out the template for the elimination dossier for each disease (activity anticipated for FY19). 36

37 3) Maps 37
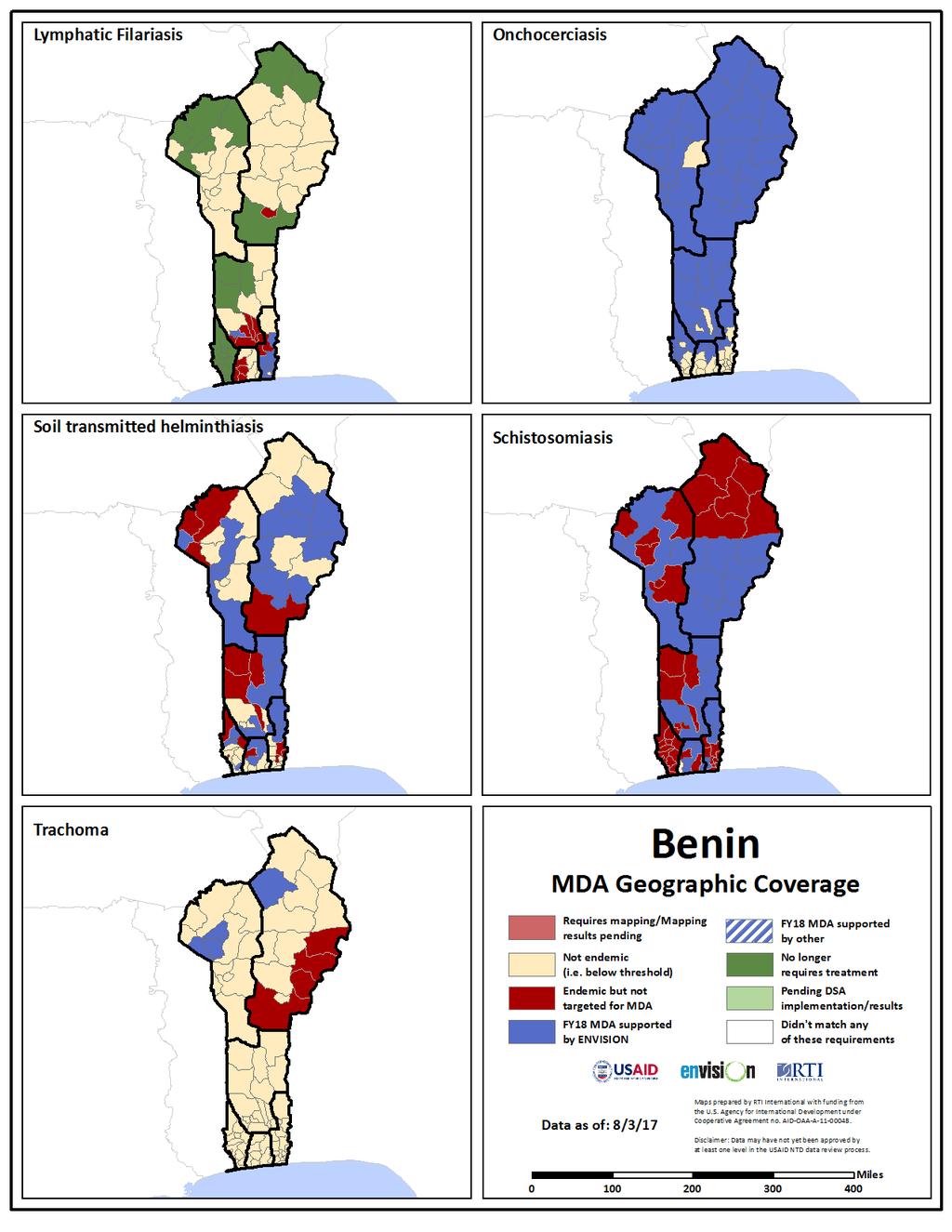
38 38
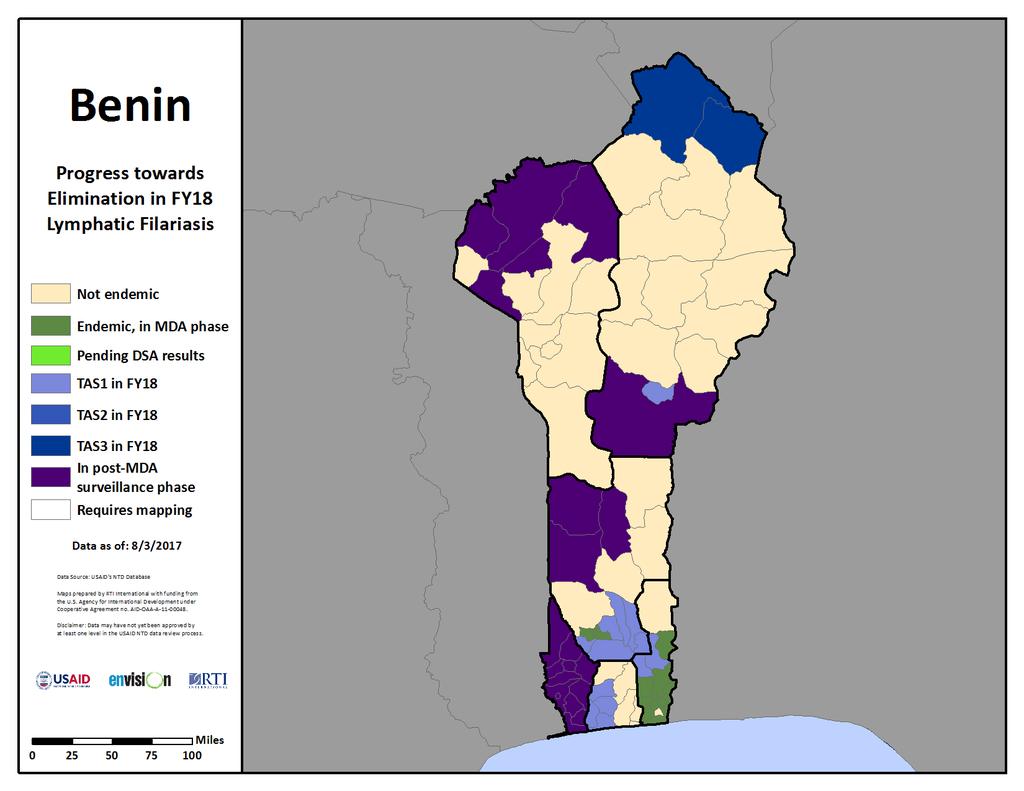
39 39
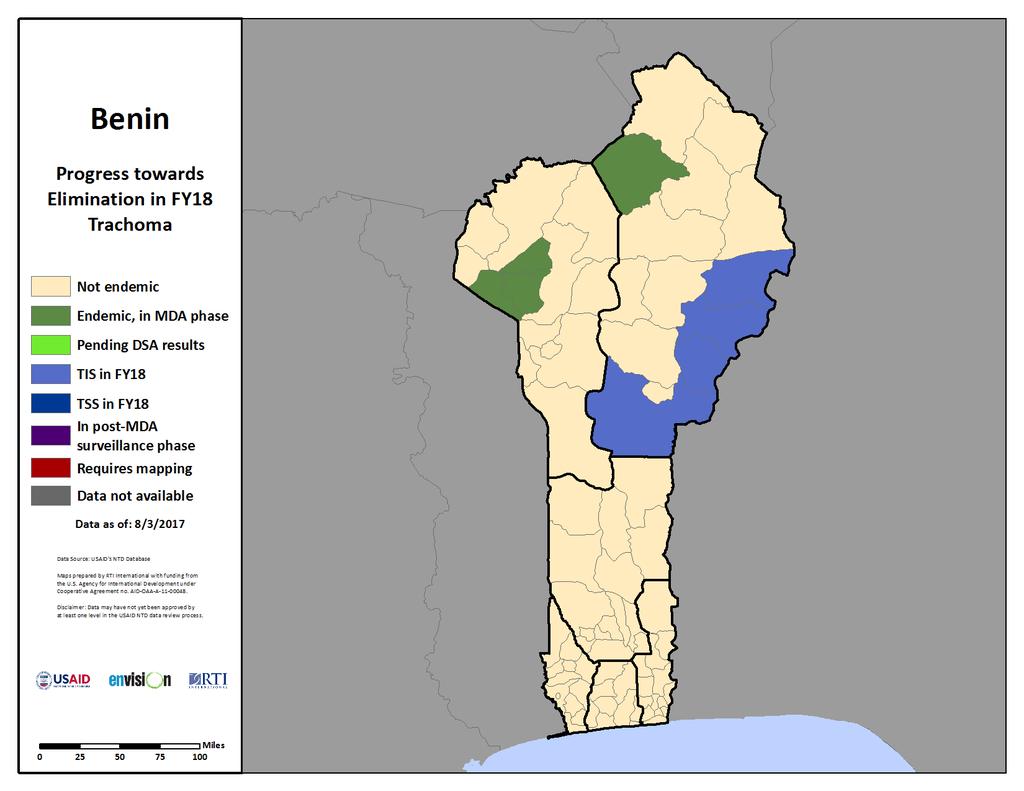
40 40
MOZAMBIQUE Work Plan FY 2018 Project Year 7
 MOZAMBIQUE Work Plan FY 2018 Project Year 7 October 2017 September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation,
MOZAMBIQUE Work Plan FY 2018 Project Year 7 October 2017 September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation,
THE PHILIPPINES Work Plan FY 2017 Project Year 6
 THE PHILIPPINES Work Plan FY 2017 Project Year 6 October 2016 September 2017 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows
THE PHILIPPINES Work Plan FY 2017 Project Year 6 October 2016 September 2017 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows
Ghana FY2015. A n n u a l W o r k P lan October 2014 to September Date: 30 th July 2014
 Ghana FY2015 C o n trol of Neglected Tropical Diseases A n n u a l W o r k P lan October 2014 to September 2015 Date: 30 th July 2014 Submitted to: Bolivar Pou Project Director End in Africa Project FHI
Ghana FY2015 C o n trol of Neglected Tropical Diseases A n n u a l W o r k P lan October 2014 to September 2015 Date: 30 th July 2014 Submitted to: Bolivar Pou Project Director End in Africa Project FHI
GUINEA Work Plan FY 2018 Project Year 7
 GUINEA Work Plan FY 2018 Project Year 7 October 2017-September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation,
GUINEA Work Plan FY 2018 Project Year 7 October 2017-September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation,
FY2017. End Neglected Tropical Diseases in Africa (End in Africa) Annual Work Plan October 1, 2016 September 30, 2017
 Annual Work Plan October 1, 2016 September 30, 2017") FY2017 End Neglected Tropical Diseases in Africa (End in Africa) Annual Work Plan October 1, 2016 September 30, 2017 Submitted to: United States Agency for International Development (USAID) Submitted by:
FY2017 End Neglected Tropical Diseases in Africa (End in Africa) Annual Work Plan October 1, 2016 September 30, 2017 Submitted to: United States Agency for International Development (USAID) Submitted by:
CAMEROON Work Plan FY 2018 Project Year 7
 CAMEROON Work Plan FY 2018 Project Year 7 October 2017 September 2018 ADD PARTNER LOGO(S) HERE ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center,
CAMEROON Work Plan FY 2018 Project Year 7 October 2017 September 2018 ADD PARTNER LOGO(S) HERE ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center,
Tanzania Work Plan FY 2018 Project Year 7
 Tanzania Work Plan FY 2018 Project Year 7 October 2017 September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation,
Tanzania Work Plan FY 2018 Project Year 7 October 2017 September 2018 ENVISION is a global project led by RTI International in partnership with CBM International, The Carter Center, Fred Hollows Foundation,
BURKINA FASO F Y C ontrol of N e glec t e d T r o p ic al Diseases. A n n u a l Work Pl a n October 1, 2017 August 31, Date: July
 BURKINA FASO F Y 2018 C ontrol of N e glec t e d T r o p ic al Diseases A n n u a l Work Pl a n October 1, 2017 August 31, 2018 Date: July 17 2017 Submitted to: Mr. Bolivar Pou Project Director END in
BURKINA FASO F Y 2018 C ontrol of N e glec t e d T r o p ic al Diseases A n n u a l Work Pl a n October 1, 2017 August 31, 2018 Date: July 17 2017 Submitted to: Mr. Bolivar Pou Project Director END in
OPERATIONAL PLAN 2013 FOR NEGLECTED TROPICAL DISEASES CONTROL IN BURKINA FASO
 OPERATIONAL PLAN 2013 FOR NEGLECTED TROPICAL DISEASES CONTROL IN BURKINA FASO Annual Work Plan Period Covered: October 2012 September 2013 Date: December 2012 Submitted to: FHI 360 Submitted by: Helen
OPERATIONAL PLAN 2013 FOR NEGLECTED TROPICAL DISEASES CONTROL IN BURKINA FASO Annual Work Plan Period Covered: October 2012 September 2013 Date: December 2012 Submitted to: FHI 360 Submitted by: Helen
Neglected Tropical Disease
 Neglected Tropical Disease Control Program Final Report November 212 The NTD Control Program, led by RTI International, was made possible by the generous support of the American People and USAID under
Neglected Tropical Disease Control Program Final Report November 212 The NTD Control Program, led by RTI International, was made possible by the generous support of the American People and USAID under
Validation of elimination of lymphatic filariasis as a public health problem ISBN
 Validation of elimination of lymphatic filariasis as a public health problem ISBN 978-92-4-151195-7 World Health Organization 2017 Some rights reserved. This work is available under the Creative Commons
Validation of elimination of lymphatic filariasis as a public health problem ISBN 978-92-4-151195-7 World Health Organization 2017 Some rights reserved. This work is available under the Creative Commons
An African Region free of Neglected Tropical Diseases
 An African Region free of Neglected Tropical Diseases Regional Programme Review Group 2 nd Meeting PREVENTIVE CHEMOTHERAPY 17-20 February 2015 Brazzaville, Congo NTD PROGRAMME PREVENTIVE CHEMOTHERAPY 1
An African Region free of Neglected Tropical Diseases Regional Programme Review Group 2 nd Meeting PREVENTIVE CHEMOTHERAPY 17-20 February 2015 Brazzaville, Congo NTD PROGRAMME PREVENTIVE CHEMOTHERAPY 1
Focusing on 2020: 4 Years Remaining
 Summary Proceedings Eighteenth Annual Trachoma Program Review Focusing on 2020: 4 Years Remaining Atlanta, Georgia March 22-24, 2017 Focusing on 2020: 4 Years Remaining The Eighteenth Annual Trachoma Control
Summary Proceedings Eighteenth Annual Trachoma Program Review Focusing on 2020: 4 Years Remaining Atlanta, Georgia March 22-24, 2017 Focusing on 2020: 4 Years Remaining The Eighteenth Annual Trachoma Control
Report on Trachoma mapping in Malawi July 2015
 Report on Trachoma mapping in Malawi July 2015 Background of trachoma in the country The Trachoma Control Programme was launched in Malawi 2011 to implement the SAFE strategy through the Government and
Report on Trachoma mapping in Malawi July 2015 Background of trachoma in the country The Trachoma Control Programme was launched in Malawi 2011 to implement the SAFE strategy through the Government and
The Expanded Special Project for Elimination of Neglected Tropical Diseases espen 2017 ANNUAL REPORT
 The Expanded Special Project for Elimination of Neglected Tropical Diseases espen 2017 ANNUAL REPORT TABLE OF CONTENTS Foreword 4 2017 In A Snapshot 5 Challenges and Lessons Learned 6 About ESPEN 6 Guiding
The Expanded Special Project for Elimination of Neglected Tropical Diseases espen 2017 ANNUAL REPORT TABLE OF CONTENTS Foreword 4 2017 In A Snapshot 5 Challenges and Lessons Learned 6 About ESPEN 6 Guiding
DOSSIER DOCUMENTING ELIMINATION OF TRACHOMA AS A PUBLIC HEALTH PROBLEM. Ghana. Date of Submission: January 2018
 DOSSIER DOCUMENTING ELIMINATION OF TRACHOMA AS A PUBLIC HEALTH PROBLEM Ghana Date of Submission: January 2018 Date of Review: February 2018 1 TABLE OF CONTENTS DOSSIER DOCUMENTING ELIMINATION OF TRACHOMA
DOSSIER DOCUMENTING ELIMINATION OF TRACHOMA AS A PUBLIC HEALTH PROBLEM Ghana Date of Submission: January 2018 Date of Review: February 2018 1 TABLE OF CONTENTS DOSSIER DOCUMENTING ELIMINATION OF TRACHOMA
Fourteenth meeting of the Regional Programme Review Group on lymphatic filariasis elimination and other preventive chemotherapy programmes
 Report on the Fourteenth meeting of the Regional Programme Review Group on lymphatic filariasis elimination and other preventive chemotherapy programmes Cairo, Egypt 12 14 October 2015 Report on the Fourteenth
Report on the Fourteenth meeting of the Regional Programme Review Group on lymphatic filariasis elimination and other preventive chemotherapy programmes Cairo, Egypt 12 14 October 2015 Report on the Fourteenth
2017 Progress Report. Breaking Barriers to NTD Care
 2017 Progress Report Breaking Barriers to NTD Care The vision of AIM is to see people thrive in a world free from the burden of NTDs. Every step of the process mapping, planning and implementing is driven
2017 Progress Report Breaking Barriers to NTD Care The vision of AIM is to see people thrive in a world free from the burden of NTDs. Every step of the process mapping, planning and implementing is driven
Looking Back, Moving Forward
 Summary Proceedings Sixteenth Annual Trachoma Program Review Looking Back, Moving Forward Atlanta, Georgia March 2-4, 2015 Supported by: Looking Back, Moving Forward The Sixteenth Annual Trachoma Control
Summary Proceedings Sixteenth Annual Trachoma Program Review Looking Back, Moving Forward Atlanta, Georgia March 2-4, 2015 Supported by: Looking Back, Moving Forward The Sixteenth Annual Trachoma Control
Report on the Meeting on postendemic Surveillance for Blinding Trachoma. World Health Organization, Geneva, 4 to 5 November 2008.
 Report on the Meeting on postendemic Surveillance for Blinding Trachoma World Health Organization, Geneva, 4 to 5 November 2008. 1 1. INTRODUCTION The Meeting on post-endemic Surveillance for Blinding
Report on the Meeting on postendemic Surveillance for Blinding Trachoma World Health Organization, Geneva, 4 to 5 November 2008. 1 1. INTRODUCTION The Meeting on post-endemic Surveillance for Blinding
The Regional Strategic Plan for Elimination of Lymphatic Filariasis Regional Office for South-East Asia
 The Regional Strategic Plan for Elimination of Lymphatic Filariasis 2010-2015 Regional Office for South-East Asia SEA-CD-203 Distribution: Limited The Regional Strategic Plan for Elimination of Lymphatic
The Regional Strategic Plan for Elimination of Lymphatic Filariasis 2010-2015 Regional Office for South-East Asia SEA-CD-203 Distribution: Limited The Regional Strategic Plan for Elimination of Lymphatic
REPUBLIC OF MALAWI MINISTRY OF HEALTH
 REPUBLIC OF MALAWI MINISTRY OF HEALTH REPORT FOR TRACHOMA SITUATION ANALYSIS IN MALAWI JANUARY 2014 This report was compiled by: Associate Prof Khumbo Kalua, University of Malawi, BICO and MOH Dr Bagrey
REPUBLIC OF MALAWI MINISTRY OF HEALTH REPORT FOR TRACHOMA SITUATION ANALYSIS IN MALAWI JANUARY 2014 This report was compiled by: Associate Prof Khumbo Kalua, University of Malawi, BICO and MOH Dr Bagrey
Report from the Kenyan Healthcare Outreach Programme
 Report from the Kenyan Healthcare Outreach Programme Background Kenya has a population of 43 million people, of which half live in rural communities. In rural Kenya, around 70% of people are living below
Report from the Kenyan Healthcare Outreach Programme Background Kenya has a population of 43 million people, of which half live in rural communities. In rural Kenya, around 70% of people are living below
INTRODUCTION I CONTEXTUAL OVERVIEW
 INTRODUCTION This document lays out the MPHP s (Ministry of Public Health and Population) strategic plan for the neglected tropical disease (NTD) program. It is a description of the planned activities
INTRODUCTION This document lays out the MPHP s (Ministry of Public Health and Population) strategic plan for the neglected tropical disease (NTD) program. It is a description of the planned activities
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
Mozambique Country Profile
 Lepr Rev (2015) 86, 89 95 SHORT PAPER Mozambique Country Profile ARIE DE KRUIJFF* *Country leader for the Leprosy Mission Mozambique Accepted for publication 11 February 2015 Introduction Mozambique is
Lepr Rev (2015) 86, 89 95 SHORT PAPER Mozambique Country Profile ARIE DE KRUIJFF* *Country leader for the Leprosy Mission Mozambique Accepted for publication 11 February 2015 Introduction Mozambique is
UNICEF WCARO October 2012
 UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
Report of the 18th meeting. the Global Elimination of. Trachoma by Addis Ababa, April 2014
 Report of the 18th meeting of the WHO Alliance for the Global Elimination of Trachoma by 2020 Addis Ababa, 28 29 April 2014 Report of the 18th meeting of the WHO Alliance for the Global Elimination of
Report of the 18th meeting of the WHO Alliance for the Global Elimination of Trachoma by 2020 Addis Ababa, 28 29 April 2014 Report of the 18th meeting of the WHO Alliance for the Global Elimination of
Feasibility of Scaling-up Interventions: The Role of Intervention Design
 Disease Control Priorities Project Personal Health Services Workshop London, 23 July 2003 Feasibility of Scaling-up Interventions: The Role of Intervention Design Christian Gericke 1,2, Christoph Kurowski
Disease Control Priorities Project Personal Health Services Workshop London, 23 July 2003 Feasibility of Scaling-up Interventions: The Role of Intervention Design Christian Gericke 1,2, Christoph Kurowski
EDCTP2 - Opportunities for clinical research on poverty-related diseases in sub-saharan Africa.
 EDCTP2 - Opportunities for clinical research on poverty-related diseases in sub-saharan Africa. Info Day, Horizon 2020 Societal Challenge 1: Health, demographic change and wellbeing 8 July 2016, Brussels
EDCTP2 - Opportunities for clinical research on poverty-related diseases in sub-saharan Africa. Info Day, Horizon 2020 Societal Challenge 1: Health, demographic change and wellbeing 8 July 2016, Brussels
TURKANA EYE PROJECT. Annual report
 2013 TURKANA EYE PROJECT Annual report After 10 years working in Turkana, 2013 has led to a crucial qualitative change: for the first time, three organizations have brought together our efforts to fight
2013 TURKANA EYE PROJECT Annual report After 10 years working in Turkana, 2013 has led to a crucial qualitative change: for the first time, three organizations have brought together our efforts to fight
Senior Fellowships Call for Proposals 2017
 Senior Fellowships Call for Proposals 2017 Type of action TMA Call budget 3M Funding level Up to 100% of eligible costs Expected number of grants 6-8 Opening date 3 November 2017, 17:00 CET Closing date
Senior Fellowships Call for Proposals 2017 Type of action TMA Call budget 3M Funding level Up to 100% of eligible costs Expected number of grants 6-8 Opening date 3 November 2017, 17:00 CET Closing date
Report of the Ninth Meeting of the WHO Alliance for the Global Elimination of Blinding Trachoma
 WHO/PBD/GET/05.1 Prevention of Blindness and Deafness Report of the Ninth Meeting of the WHO Alliance for the Global Elimination of Blinding Trachoma Geneva 21 23 March, 2005 GLOBAL ELIMINATION OF BLINDING
WHO/PBD/GET/05.1 Prevention of Blindness and Deafness Report of the Ninth Meeting of the WHO Alliance for the Global Elimination of Blinding Trachoma Geneva 21 23 March, 2005 GLOBAL ELIMINATION OF BLINDING
Introduction SightFirst Program Goals
 LIONS CLUBS INTERNATIONAL FOUNDATION SIGHTFIRST GRANT APPLICATION Introduction The mission of the Lions Clubs International Foundation s SightFirst program is to build eye care systems to fight blindness
LIONS CLUBS INTERNATIONAL FOUNDATION SIGHTFIRST GRANT APPLICATION Introduction The mission of the Lions Clubs International Foundation s SightFirst program is to build eye care systems to fight blindness
REPORT OF THE 19TH MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF TRACHOMA BY 2020 HAMMAMET, TUNISIA, APRIL 2015
 REPORT OF THE 19TH MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF TRACHOMA BY 2020 HAMMAMET, TUNISIA, 27 29 APRIL 2015 REPORT OF THE 19TH MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION
REPORT OF THE 19TH MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF TRACHOMA BY 2020 HAMMAMET, TUNISIA, 27 29 APRIL 2015 REPORT OF THE 19TH MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION
Call for Proposals. EDCTP Regional Networks. Expected number of grants: 4 Open date: 5 November :00 18 February :00 (CET); 16:00 (GMT)
; 16:00 (GMT)") Call for Proposals EDCTP Regional Networks Type of Action: Coordination & Support actions (CSA) Call budget: 12,000,000 Funding threshold: 3,000,000 per network Funding Level: 100% of eligible costs Expected
Call for Proposals EDCTP Regional Networks Type of Action: Coordination & Support actions (CSA) Call budget: 12,000,000 Funding threshold: 3,000,000 per network Funding Level: 100% of eligible costs Expected
ANNUAL REPORT ON THE USE OF CERF GRANTS BENIN
 Country Resident/Humanitarian Coordinator ANNUAL REPORT ON THE USE OF CERF GRANTS BENIN Benin Nardos Bekele Thomas Reporting Period 15 October 2010 30 December 2010 I. Summary of Funding and Beneficiaries
Country Resident/Humanitarian Coordinator ANNUAL REPORT ON THE USE OF CERF GRANTS BENIN Benin Nardos Bekele Thomas Reporting Period 15 October 2010 30 December 2010 I. Summary of Funding and Beneficiaries
How to Apply for an LCIF SightFirst Grant SIGHTFIRST GRANT APPLICATION GUIDE AND CRITERIA
 How to Apply for an LCIF SightFirst Grant SIGHTFIRST GRANT APPLICATION GUIDE AND CRITERIA Mission Statement: The Lions Clubs International Foundation SightFirst program funds the efforts of Lions, nongovernmental
How to Apply for an LCIF SightFirst Grant SIGHTFIRST GRANT APPLICATION GUIDE AND CRITERIA Mission Statement: The Lions Clubs International Foundation SightFirst program funds the efforts of Lions, nongovernmental
Case study: Joint action on water, sanitation and hygiene (WASH) and Neglected Tropical Diseases (NTDs)
 and Neglected Tropical Diseases (NTDs)") Case study: Joint action on water, sanitation and hygiene (WASH) and Neglected Tropical Diseases (NTDs) The Testing Integrated WASH Implementation Models for Neglected Tropical Disease (NTD) Prevention
Case study: Joint action on water, sanitation and hygiene (WASH) and Neglected Tropical Diseases (NTDs) The Testing Integrated WASH Implementation Models for Neglected Tropical Disease (NTD) Prevention
The theme of the eleventh annual
 Eye e of the Eagle Volume 3, Number 1 THE CARTER CENTER January y 2002 OEPA: President Carter Att ttends the Eleventh enth IACO in Mexico City; ; Increased Mectizan Cover erage Repor eported ed The theme
Eye e of the Eagle Volume 3, Number 1 THE CARTER CENTER January y 2002 OEPA: President Carter Att ttends the Eleventh enth IACO in Mexico City; ; Increased Mectizan Cover erage Repor eported ed The theme
The WHO African Programme for Onchocerciasis Control Final Evaluation Report
 JAF21.6 AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL The WHO African Programme for Onchocerciasis Control Final Evaluation Report October 2015 www.who.int/apoc Copyright African Programme for Onchocerciasis
JAF21.6 AFRICAN PROGRAMME FOR ONCHOCERCIASIS CONTROL The WHO African Programme for Onchocerciasis Control Final Evaluation Report October 2015 www.who.int/apoc Copyright African Programme for Onchocerciasis
Optimization of chemotherapy for control and elimination of onchocerciasis and lymphatic filariasis-ghana sites
 Optimization of chemotherapy for control and elimination of onchocerciasis and lymphatic filariasis-ghana sites Objective 2 Group: Bonn/Germany Kumasi/Ghana Prof. Achim Hoerauf Dr. Sabine Mand Dr. Alex
Optimization of chemotherapy for control and elimination of onchocerciasis and lymphatic filariasis-ghana sites Objective 2 Group: Bonn/Germany Kumasi/Ghana Prof. Achim Hoerauf Dr. Sabine Mand Dr. Alex
Readiness Checklist for Plague V Country: Date:
 Readiness Checklist for Plague V3 05.10.17 Country: Date: This checklist aims to help countries to assess and test their level of readiness for a plague response, and be used as a tool for identifying
Readiness Checklist for Plague V3 05.10.17 Country: Date: This checklist aims to help countries to assess and test their level of readiness for a plague response, and be used as a tool for identifying
Final Evaluation Report 11 th October 2016
 Summative Evaluation of a project to eliminate trachoma, implemented by Orbis Ethiopia, in Gamo Gofa, Derashe, Konso and Alle in Southern Nations, Nationalities, and Peoples' Region Ethiopia from 2006-2016
Summative Evaluation of a project to eliminate trachoma, implemented by Orbis Ethiopia, in Gamo Gofa, Derashe, Konso and Alle in Southern Nations, Nationalities, and Peoples' Region Ethiopia from 2006-2016
Report of the Eighth Meeting of the. WHO Alliance for the. Global Elimination of Blinding Trachoma
 WORLD HEALTH ORGANIZATION Prevention of Blindness and Deafness WHO/PBD/GET/04.2 Report of the Eighth Meeting of the WHO Alliance for the Global Elimination of Blinding Trachoma Geneva 29 30 March, 2004
WORLD HEALTH ORGANIZATION Prevention of Blindness and Deafness WHO/PBD/GET/04.2 Report of the Eighth Meeting of the WHO Alliance for the Global Elimination of Blinding Trachoma Geneva 29 30 March, 2004
Standard Operating Procedure for Community Event-Based Surveillance for Ebola Virus Disease in Sierra Leone
 Standard Operating Procedure for Community Event-Based Surveillance for Ebola Virus Disease in Sierra Leone Page 1 of 8 I. Introduction a. Background Community event-based surveillance (CEBS) is the organized
Standard Operating Procedure for Community Event-Based Surveillance for Ebola Virus Disease in Sierra Leone Page 1 of 8 I. Introduction a. Background Community event-based surveillance (CEBS) is the organized
SPECIAL PROGRAMME FOR RESEARCH AND TRAINING IN TROPICAL DISEASES: MEMBERSHIP OF THE JOINT COORDINATING BOARD
 WORLD HEALTH ORGANIZATION ORGANISATION MONDIALE DE LA SANTE REGIONAL OFFICE FOR THE WESTERN PACIFIC BUREAU REGIONAL DU PACIFIQUE OCCIDENTAL REGIONAL COMMITTEE Forty-fifth session Kuala Lumpur 19-23 September
WORLD HEALTH ORGANIZATION ORGANISATION MONDIALE DE LA SANTE REGIONAL OFFICE FOR THE WESTERN PACIFIC BUREAU REGIONAL DU PACIFIQUE OCCIDENTAL REGIONAL COMMITTEE Forty-fifth session Kuala Lumpur 19-23 September
Senegal Humanitarian Situation Report
 Senegal Humanitarian Situation Report Highlights 4,015 children have been admitted to treatment in January and February, or 11% of the annual target. The national Infant and Young Child Feeding policy
Senegal Humanitarian Situation Report Highlights 4,015 children have been admitted to treatment in January and February, or 11% of the annual target. The national Infant and Young Child Feeding policy
HOW TO MONITOR LEPROSY ELIMINATION IN YOUR WORKING AREA. World Health Organization
 HOW TO MONITOR LEPROSY ELIMINATION IN YOUR WORKING AREA World Health Organization HOW TO MONITOR LEPROSY ELIMINATION IN YOUR WORKING AREA contents The Final Push to Eliminate Leprosy 2 Why do we monitor?
HOW TO MONITOR LEPROSY ELIMINATION IN YOUR WORKING AREA World Health Organization HOW TO MONITOR LEPROSY ELIMINATION IN YOUR WORKING AREA contents The Final Push to Eliminate Leprosy 2 Why do we monitor?
Study to Identify and Analyse National Experiences that foster the Nutritional Wellbeing in Latin America and the Caribbean
 Executive Summary Study to Identify and Analyse National Experiences that foster the Nutritional Wellbeing in Latin America and the Caribbean Community of Latin American and Caribbean States (CELAC) Food
Executive Summary Study to Identify and Analyse National Experiences that foster the Nutritional Wellbeing in Latin America and the Caribbean Community of Latin American and Caribbean States (CELAC) Food
PROGRAMME BUDGET PERFORMANCE ASSESSMENT REPORT
 PBPA06-07 PROGRAMME BUDGET 2006-2007 PERFORMANCE ASSESSMENT REPORT PROGRAMME BUDGET 2006-2007 The designations employed and the presentation of the material in this document do not imply the expression
PBPA06-07 PROGRAMME BUDGET 2006-2007 PERFORMANCE ASSESSMENT REPORT PROGRAMME BUDGET 2006-2007 The designations employed and the presentation of the material in this document do not imply the expression
Ebola Preparedness and Response in Ghana
 Ebola Preparedness and Response in Ghana Final report to the Japan Government World Health Organization Ghana Country Office November 2016 0 TABLE OF CONTENTS SUMMARY... 2 I. SITUATION UPDATE... 3 II.
Ebola Preparedness and Response in Ghana Final report to the Japan Government World Health Organization Ghana Country Office November 2016 0 TABLE OF CONTENTS SUMMARY... 2 I. SITUATION UPDATE... 3 II.
Rapid Assessment of the Health System in Benin, April Grace Adeya Alphonse Bigirimana Karen Cavanaugh Lynne Miller Franco
 Grace Adeya Alphonse Bigirimana Karen Cavanaugh Lynne Miller Franco Printed: February 2007 This report was made possible through support provided by the U.S. Agency for International Development. The opinions
Grace Adeya Alphonse Bigirimana Karen Cavanaugh Lynne Miller Franco Printed: February 2007 This report was made possible through support provided by the U.S. Agency for International Development. The opinions
Building Pharmaceutical Management Capacity in South Sudan
 Building Pharmaceutical Management Capacity in South Sudan January 2017 BACKGROUND South Sudan s health system is struggling to overcome a myriad of challenges, including poor pharmaceutical supply management
Building Pharmaceutical Management Capacity in South Sudan January 2017 BACKGROUND South Sudan s health system is struggling to overcome a myriad of challenges, including poor pharmaceutical supply management
MONITORING AND EVALUATION PLAN
 GHANA HEALTH SERVICE MONITORING AND EVALUATION PLAN National tb control programme Monitoring and evaluation plan for NTP INTRODUCTION The Health System Structure in Ghana The Health Service is organized
GHANA HEALTH SERVICE MONITORING AND EVALUATION PLAN National tb control programme Monitoring and evaluation plan for NTP INTRODUCTION The Health System Structure in Ghana The Health Service is organized
Democratic Republic of Congo
 World Health Organization Project Proposal Democratic Republic of Congo OVERVIEW Target country: Democratic Republic of Congo Beneficiary population: 8 million (population affected by the humanitarian
World Health Organization Project Proposal Democratic Republic of Congo OVERVIEW Target country: Democratic Republic of Congo Beneficiary population: 8 million (population affected by the humanitarian
FEDERAL MINISTRY OF HEALTH NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME TERMS OF REFERENCE FOR ZONAL CONSULTANTS MARCH, 2017
 FEDERAL MINISTRY OF HEALTH NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME EPIDEMIOLOGICAL ANALYSIS OF TUBERCULOSIS BURDEN AT NATIONAL AND SUB NATIONAL LEVEL (EPI ANALYSIS SURVEY) TERMS OF REFERENCE
FEDERAL MINISTRY OF HEALTH NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME EPIDEMIOLOGICAL ANALYSIS OF TUBERCULOSIS BURDEN AT NATIONAL AND SUB NATIONAL LEVEL (EPI ANALYSIS SURVEY) TERMS OF REFERENCE
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
Malaria surveillance, monitoring and evaluation manual
 Malaria surveillance, monitoring and evaluation manual Abdisalan M Noor, Team Leader, Surveillance Malaria Policy Advisory Committee (MPAC) meeting 22-24 March 2017, Geneva, Switzerland Global Technical
Malaria surveillance, monitoring and evaluation manual Abdisalan M Noor, Team Leader, Surveillance Malaria Policy Advisory Committee (MPAC) meeting 22-24 March 2017, Geneva, Switzerland Global Technical
ASSOCIATION FRANCAISE RAOUL FOLLEREAU
 ASSOCIATION FRANCAISE RAOUL FOLLEREAU Support from the Association Française aise Raoul Follereau for Buruli ulcer control 2005-2006 2006 Jehan-Michel RONDOT Director, Support and Programmes AFRF 1995-2006
ASSOCIATION FRANCAISE RAOUL FOLLEREAU Support from the Association Française aise Raoul Follereau for Buruli ulcer control 2005-2006 2006 Jehan-Michel RONDOT Director, Support and Programmes AFRF 1995-2006
Period of June 2008 June 2011 Partner Country s Implementing Organization: Federal Cooperation
 Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
EVALUATION OF THE IMPACT OF GLOBAL FUND CONTRIBUTIONS ON BENIN S NATIONAL TUBERCULOSIS PROGRAM
 EVALUATION OF THE IMPACT OF GLOBAL FUND CONTRIBUTIONS ON BENIN S NATIONAL TUBERCULOSIS PROGRAM EVALUATION REPORT DEVELOPED BY Evaluation Team URC-CHS Support Team Dr Frantz SIMEON, Team Leader Dr Jean
EVALUATION OF THE IMPACT OF GLOBAL FUND CONTRIBUTIONS ON BENIN S NATIONAL TUBERCULOSIS PROGRAM EVALUATION REPORT DEVELOPED BY Evaluation Team URC-CHS Support Team Dr Frantz SIMEON, Team Leader Dr Jean
South Sudan National Master Plan ( ) For Neglected Tropical Diseases
 For Neglected Tropical Diseases") GET South Sudan National Master Plan (2016 2020) For Neglected Tropical Diseases NTDs South Sudan (2015-2016) Contents PART 1: SITUATION ANALYSIS.8 1.1 Country profile... 8 11 1.1.2 Geographical Characteristics...
GET South Sudan National Master Plan (2016 2020) For Neglected Tropical Diseases NTDs South Sudan (2015-2016) Contents PART 1: SITUATION ANALYSIS.8 1.1 Country profile... 8 11 1.1.2 Geographical Characteristics...
Human Resources for Eye Health. Regional Advocacy Strategy
 Human Resources for Eye Health Regional Advocacy Strategy 2014-2018 Narrative In Africa there are an estimated 5.9 million people who are blind and 26.3 million who are visually impaired. This is not a
Human Resources for Eye Health Regional Advocacy Strategy 2014-2018 Narrative In Africa there are an estimated 5.9 million people who are blind and 26.3 million who are visually impaired. This is not a
Performance-based financing (PBF) has been used
 has been used") January 2017 PERFORMANCE-BASED FINANCING IMPROVES QUANTITY AND QUALITY OF HEALTH SERVICES IN HAITI Photo by Colin Gilmartin Performance-based financing (PBF) has been used increasingly to improve the quantity
January 2017 PERFORMANCE-BASED FINANCING IMPROVES QUANTITY AND QUALITY OF HEALTH SERVICES IN HAITI Photo by Colin Gilmartin Performance-based financing (PBF) has been used increasingly to improve the quantity
REQUEST FOR PROPOSAL. Issue date: 28 March RFP closing date: 20 April 2018 RFP closing time: 18:00 Central European Time
 REQUEST FOR PROPOSAL Development and implementation of a country-specific strategy for demand creation and advocacy activities on HCV diagnostics and diagnosis in Cameroon, Georgia, India, Malaysia, Myanmar
REQUEST FOR PROPOSAL Development and implementation of a country-specific strategy for demand creation and advocacy activities on HCV diagnostics and diagnosis in Cameroon, Georgia, India, Malaysia, Myanmar
Emergency Plan of Action (EPoA) Bénin Cholera outbreak
 Bénin Cholera outbreak") Emergency Plan of Action (EPoA) Bénin Cholera outbreak DREF Operation Operation n MDRBJ15 Date of issue: 12 September 216 Date of disaster: 3 August 216 Operation manager (responsible for this EPoA): Samuel
Emergency Plan of Action (EPoA) Bénin Cholera outbreak DREF Operation Operation n MDRBJ15 Date of issue: 12 September 216 Date of disaster: 3 August 216 Operation manager (responsible for this EPoA): Samuel
#HealthForAll ichc2017.org
 #HealthForAll ichc2017.org 1 Positioning CHW s within HRH Strategies: Key Issues and Opportunities Liberia Case Study Ochiawunma Ibe, MD, MPH, Msc (MCH), FWACP Background Outline Demographic profile and
#HealthForAll ichc2017.org 1 Positioning CHW s within HRH Strategies: Key Issues and Opportunities Liberia Case Study Ochiawunma Ibe, MD, MPH, Msc (MCH), FWACP Background Outline Demographic profile and
Emergency Preparedness & Humanitarian Action (EHA) Week 3, January 2012
 Week 3, January 2012") Emergency Preparedness & Humanitarian Action (EHA) Week 3, 14-20 January 2012 Due to access issues, 56 health facilities out of 104 (53.8%) reported to South Kordofan s surveillance system. During the
Emergency Preparedness & Humanitarian Action (EHA) Week 3, 14-20 January 2012 Due to access issues, 56 health facilities out of 104 (53.8%) reported to South Kordofan s surveillance system. During the
STRATEGIC OBJECTIVES & ACTION PLAN. Research, Advocacy, Health Promotion & Surveillance
 STRATEGIC OBJECTIVES & ACTION PLAN Research, Advocacy, Health Promotion & Surveillance February 2012 INTRODUCTION Addressing the rising trends of Non-Communicable Diseases in low and middle income countries
STRATEGIC OBJECTIVES & ACTION PLAN Research, Advocacy, Health Promotion & Surveillance February 2012 INTRODUCTION Addressing the rising trends of Non-Communicable Diseases in low and middle income countries
BENIN PRIVATE HEALTH SECTOR CENSUS
 BENIN PRIVATE HEALTH SECTOR CENSUS December 2014 This document was produced for review by the United States Agency for International Development. It was prepared by Andrew Carmona, Sean Callahan, and Kathryn
BENIN PRIVATE HEALTH SECTOR CENSUS December 2014 This document was produced for review by the United States Agency for International Development. It was prepared by Andrew Carmona, Sean Callahan, and Kathryn
DRAFT VERSION October 26, 2016
 WHO Health Emergencies Programme Results Framework Introduction/vision The work of WHE over the coming years will need to address an unprecedented number of health emergencies. Climate change, increasing
WHO Health Emergencies Programme Results Framework Introduction/vision The work of WHE over the coming years will need to address an unprecedented number of health emergencies. Climate change, increasing
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 TONGA Tonga is a lower-middle-income country in the Pacific Ocean with an estimated population of 102 371 (2005), of which 68% live on the main island Tongatapu and 32% are distributed on outer islands.
TONGA Tonga is a lower-middle-income country in the Pacific Ocean with an estimated population of 102 371 (2005), of which 68% live on the main island Tongatapu and 32% are distributed on outer islands.
Incremental Cost of Conducting Population-Based Prevalence Surveys for a Neglected Tropical Disease: The Example of Trachoma in 8 National Programs
 Incremental Cost of Conducting Population-Based Prevalence Surveys for a Neglected Tropical Disease: The Example of Trachoma in 8 National Programs Chaoqun Chen 1, Elizabeth A. Cromwell 2, Jonathan D.
Incremental Cost of Conducting Population-Based Prevalence Surveys for a Neglected Tropical Disease: The Example of Trachoma in 8 National Programs Chaoqun Chen 1, Elizabeth A. Cromwell 2, Jonathan D.
Call for grant applications
 Call for grant applications Research on the impact of insecticide resistance mechanisms on malaria control failure in Africa Deadline for submissions: 2 December 2013, 17:00 hours CET Research teams from
Call for grant applications Research on the impact of insecticide resistance mechanisms on malaria control failure in Africa Deadline for submissions: 2 December 2013, 17:00 hours CET Research teams from
Terms of Reference For Cholera Prevention and Control: Lessons Learnt and Roadmap 1. Summary
 Terms of Reference For Cholera Prevention and Control: Lessons Learnt 2014 2015 and Roadmap 1. Summary Title Cholera Prevention and Control: lessons learnt and roadmap Purpose To provide country specific
Terms of Reference For Cholera Prevention and Control: Lessons Learnt 2014 2015 and Roadmap 1. Summary Title Cholera Prevention and Control: lessons learnt and roadmap Purpose To provide country specific
Mauritania Red Crescent Programme Support Plan
 Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
AREAS OF FOCUS POLICY STATEMENTS
 ENGLISH (EN) AREAS OF FOCUS POLICY STATEMENTS With respect to the areas of focus policy statements, The Rotary Foundation notes that 1. The goals of the Foundation are to increase efficiency in grant processing
ENGLISH (EN) AREAS OF FOCUS POLICY STATEMENTS With respect to the areas of focus policy statements, The Rotary Foundation notes that 1. The goals of the Foundation are to increase efficiency in grant processing
ERN Assessment Manual for Applicants
 Share. Care. Cure. ERN Assessment Manual for Applicants 3.- Operational Criteria for the Assessment of Networks An initiative of the Version 1.1 April 2016 History of changes Version Date Change Page 1.0
Share. Care. Cure. ERN Assessment Manual for Applicants 3.- Operational Criteria for the Assessment of Networks An initiative of the Version 1.1 April 2016 History of changes Version Date Change Page 1.0
Monitoring and Evaluation of National Action Plans on AMR. Suggested approaches March 2017
 Monitoring and Evaluation of National Action Plans on AMR Suggested approaches March 2017 Role of M&E section in AMR plan Help to clarify activities and outputs expected Identify how to monitor progress
Monitoring and Evaluation of National Action Plans on AMR Suggested approaches March 2017 Role of M&E section in AMR plan Help to clarify activities and outputs expected Identify how to monitor progress
MALARIA. Continuous LLIN Distribution Senegal s Push and Pull Combination Strategy. Lessons in Brief No. 10 BACKGROUND HOW IT WORKS.
 MALARIA Continuous LLIN Distribution Senegal s Push and Pull Combination Strategy In 2013, Senegal piloted an innovative combination model, where multiple channels for continuous distribution of long-lasting
MALARIA Continuous LLIN Distribution Senegal s Push and Pull Combination Strategy In 2013, Senegal piloted an innovative combination model, where multiple channels for continuous distribution of long-lasting
COMMISSION IMPLEMENTING DECISION. of
 EUROPEAN COMMISSION Brussels, 16.10.2014 C(2014) 7489 final COMMISSION IMPLEMENTING DECISION of 16.10.2014 laying down rules for the implementation of Decision No 1313/2013/EU of the European Parliament
EUROPEAN COMMISSION Brussels, 16.10.2014 C(2014) 7489 final COMMISSION IMPLEMENTING DECISION of 16.10.2014 laying down rules for the implementation of Decision No 1313/2013/EU of the European Parliament
Original Article. Full list of authors affiliations is available at the end of the article.
 http://ijhpm.com Int J Health Policy Manag 2017, 6(10), 587 600 doi 10.15171/ijhpm.2017.17 Original Article Ineffective Healthcare Technology Management in Benin s Public Health Sector: The Perceptions
http://ijhpm.com Int J Health Policy Manag 2017, 6(10), 587 600 doi 10.15171/ijhpm.2017.17 Original Article Ineffective Healthcare Technology Management in Benin s Public Health Sector: The Perceptions
Federal Ministry of Health Department of Public Health
 Neglected Tropical Diseases REPORT ON PILOT ROLL-OUT MALARIA-NTD-WASH CO-IMPLEMENTATION Report submitted to Federal Ministry of Health Department of Public Health National Malaria Elimination Programme,
Neglected Tropical Diseases REPORT ON PILOT ROLL-OUT MALARIA-NTD-WASH CO-IMPLEMENTATION Report submitted to Federal Ministry of Health Department of Public Health National Malaria Elimination Programme,
Country accountability roadmap Niger
 Country accountability roadmap 2012 2015 In support of implementing the recommendations of the Commission on Information and Accountability for Women's and Children's Health Niger Draft version* 21 Novembre
Country accountability roadmap 2012 2015 In support of implementing the recommendations of the Commission on Information and Accountability for Women's and Children's Health Niger Draft version* 21 Novembre
Improved Maternal, Newborn and Women s Health through Increased Access to Evidence-based Interventions. Source:DHS 2003
 KENYA Improved Maternal, Newborn and Women s Health through Increased Access to Evidence-based Interventions INTRODUCTION Although Kenya is seen as an example among African countries of rapid progress
KENYA Improved Maternal, Newborn and Women s Health through Increased Access to Evidence-based Interventions INTRODUCTION Although Kenya is seen as an example among African countries of rapid progress
ERN board of Member States
 ERN board of Member States Statement adopted by the Board of Member States on the definition and minimum recommended criteria for Associated National Centres and Coordination Hubs designated by Member
ERN board of Member States Statement adopted by the Board of Member States on the definition and minimum recommended criteria for Associated National Centres and Coordination Hubs designated by Member
Strategy of TB laboratories for TB Control Program in Developing Countries
 Strategy of TB laboratories for TB Control Program in Developing Countries Borann SAR, MD, PhD, Institut Pasteur du Cambodge Phnom Penh, Cambodia TB Control Program Structure of TB Control Establish the
Strategy of TB laboratories for TB Control Program in Developing Countries Borann SAR, MD, PhD, Institut Pasteur du Cambodge Phnom Penh, Cambodia TB Control Program Structure of TB Control Establish the
Executive summary. 1. Background and organization of the meeting
 Regional consultation meeting to support country implementation of the top ten indicators to monitor the End TB Strategy, collaborative TB/HIV activities and programmatic management of latent TB infection
Regional consultation meeting to support country implementation of the top ten indicators to monitor the End TB Strategy, collaborative TB/HIV activities and programmatic management of latent TB infection
Translating recommendations into practice for surgical site infection prevention. Claire Kilpatrick IPC Global Unit SDS, HIS, WHO HQ
 Translating recommendations into practice for surgical site infection prevention Claire Kilpatrick IPC Global Unit SDS, HIS, WHO HQ XXVIII e Congrès National de la Société Française d Hygiène Hospitalière
Translating recommendations into practice for surgical site infection prevention Claire Kilpatrick IPC Global Unit SDS, HIS, WHO HQ XXVIII e Congrès National de la Société Française d Hygiène Hospitalière
Health: UNDAP Plan. Report Summary Responsible Agency # Key Actions Action Budget UNFPA 8 15,900,000 UNICEF 15 39,110,000 WFP 2 23,250, ,085,000
 Health: UNDAP Plan Report Summary Responsible Agency # Key Actions Action Budget 8 5,900,000 5 9,0,000 WFP,50,000 6 5 50,85,000 9,085,000 Relevant MDAs and LGAs develop, implement and monitor policies,
Health: UNDAP Plan Report Summary Responsible Agency # Key Actions Action Budget 8 5,900,000 5 9,0,000 WFP,50,000 6 5 50,85,000 9,085,000 Relevant MDAs and LGAs develop, implement and monitor policies,
REPORT OF THE FIRST MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF TRACHOMA. Geneva, Switzerland 30 June - 1 July 1997
 WORLD HEALTH ORGANIZATION WHO/PBL/GET/97.1 Distr.: General Original: English REPORT OF THE FIRST MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF TRACHOMA Geneva, Switzerland 30 June - 1 July
WORLD HEALTH ORGANIZATION WHO/PBL/GET/97.1 Distr.: General Original: English REPORT OF THE FIRST MEETING OF THE WHO ALLIANCE FOR THE GLOBAL ELIMINATION OF TRACHOMA Geneva, Switzerland 30 June - 1 July
Grant Aid Projects/Standard Indicator Reference (Health)
") Examples of Setting Indicators for Each Development Strategic Objective Grant Aid Projects/Standard Indicator Reference (Health) Sector Development strategic objectives (*) Mid-term objectives Sub-targets
Examples of Setting Indicators for Each Development Strategic Objective Grant Aid Projects/Standard Indicator Reference (Health) Sector Development strategic objectives (*) Mid-term objectives Sub-targets
GLOBAL PROGRAM. Strengthening Health Systems. Collaborative Partnerships with Health Ministries
 GLOBAL PROGRAM Strengthening Health Systems Collaborative Partnerships with Health Ministries WHO WE ARE WHAT WE DO The National Alliance of State and Territorial AIDS Directors (NASTAD) represents U.S.
GLOBAL PROGRAM Strengthening Health Systems Collaborative Partnerships with Health Ministries WHO WE ARE WHAT WE DO The National Alliance of State and Territorial AIDS Directors (NASTAD) represents U.S.
Health and Life Sciences Committee. Advancing the ASEAN Post-2015 Health Development Agenda
 Health and Life Sciences Committee Advancing the ASEAN Post-2015 Health Development Agenda Introduction The US-ASEAN Business Council s Health and Life Sciences (HLS) Committee is comprised of multinational
Health and Life Sciences Committee Advancing the ASEAN Post-2015 Health Development Agenda Introduction The US-ASEAN Business Council s Health and Life Sciences (HLS) Committee is comprised of multinational
Meeting Report MEETING FOR STRENGTHENING SURVEILLANCE OF MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC REGION
 Meeting Report MEETING FOR STRENGTHENING SURVEILLANCE OF MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC REGION 21 23 June 2017 Manila, Philippines WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR
Meeting Report MEETING FOR STRENGTHENING SURVEILLANCE OF MALARIA CONTROL AND ELIMINATION IN THE WESTERN PACIFIC REGION 21 23 June 2017 Manila, Philippines WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR
GOVERNMENT OF THE REPUBLIC OF SIERRA LEONE MINISTRY OF HEALTH AND SANITATION. National Infection Prevention and Control Policy
 GOVERNMENT OF THE REPUBLIC OF SIERRA LEONE MINISTRY OF HEALTH AND SANITATION National Infection Prevention and Control Policy Page 1 of 24 Contents 1 Introduction... 8 1.1 Background... 8 1.2 Healthcare-Associated
GOVERNMENT OF THE REPUBLIC OF SIERRA LEONE MINISTRY OF HEALTH AND SANITATION National Infection Prevention and Control Policy Page 1 of 24 Contents 1 Introduction... 8 1.1 Background... 8 1.2 Healthcare-Associated
GOARN Request for Assistance: Ebola Virus Disease in West Africa
 GOARN Request for Assistance: Ebola Virus Disease in West Africa Date: 19 June 2015 Country: Guinea, Sierra Leone and Liberia WHO Region: Africa (AFR) Classification: Restricted not to be disseminated
GOARN Request for Assistance: Ebola Virus Disease in West Africa Date: 19 June 2015 Country: Guinea, Sierra Leone and Liberia WHO Region: Africa (AFR) Classification: Restricted not to be disseminated
In , WHO technical cooperation with the Government is expected to focus on the same WHO strategic objectives.
 PAPUA NEW GUINEA Papua New Guinea, one of the most diverse countries in the world and the largest developing country in the Pacific, is classified as a low-income country. PNG s current population is estimated
PAPUA NEW GUINEA Papua New Guinea, one of the most diverse countries in the world and the largest developing country in the Pacific, is classified as a low-income country. PNG s current population is estimated
INTEGRATED DISEASE SURVEILLANCE PROGRAMME (IDSP)
") Introduction:- INTEGRATED DISEASE SURVEILLANCE PROGRAMME (IDSP) The Integrated Disease Surveillance Programme (IDSP) was launched in the year 2004 by Ministry of Health & family welfare GOI. In Jammu &
Introduction:- INTEGRATED DISEASE SURVEILLANCE PROGRAMME (IDSP) The Integrated Disease Surveillance Programme (IDSP) was launched in the year 2004 by Ministry of Health & family welfare GOI. In Jammu &