Technical Note Organization of Case Management during a Cholera Outbreak June 2017
|
|
|
- Monica Crawford
- 6 years ago
- Views:
Transcription

1 Technical Note Organization of Case Management during a Cholera Outbreak June 2017 Cholera epidemics continue to be a major public health problem in many countries around the world. When epidemics strike, they can spread rapidly. The disease can also evolve quickly; patients with severe disease can die of dehydration hours after showing the first symptoms of cholera. To decrease mortality, one of the main challenges is to ensure that individuals with cholera have access to treatment as soon as possible after symptoms appear¹. This entails engagement of a network of cholera treatment structures and strategies ranging from home based or community care through to overnight stay structures with highly trained medical staff. Depending on the context, the network may be pre-existing, or may need to be established specifically during an outbreak or incorporate both established and new elements. As with childhood diarrhoea, new technological advances are not required to reduce cholera mortality². Initial access to treatment, especially in remote, rural areas is likely to be via a community health worker or a fixed oral rehydration point. Community treatment programmes for children are being developed in many countries and should be used during epidemics as much as possible. Oral therapy available in the community may not be sufficient treatment for some patients who will need to be identified quickly and referred to structures with the capacity to provide intravenous therapy. Wherever possible, transport to reduce time to access treatment should be provided to transfer patients between treatment facilities, either via a system of ambulances (car, bicycle or donkey) or by providing transport subsidies. Any vehicle providing patient transport should be cleaned and disinfected at the treatment structure and cholera prevention education provided to drivers. When setting up a treatment network, risk factors for cholera including epidemiological data from the current and previous outbreaks and access to clean water and sanitation should be taken into account, with priority given to high risk areas. In addition, cholera outbreaks frequently occur in populations with poor access to health care for geographic, economic or social reasons. Any treatment network should also take these barriers into account and be organized to maximize rapid access to treatment. Setting up a network of treatment facilities There are three levels of care, each designed to treat patients with acute watery diarrhoea and dehydration. The basic characteristics of each level are described below, but local variations will be necessary based on existing infrastructure and the skill level of those providing treatment. 1
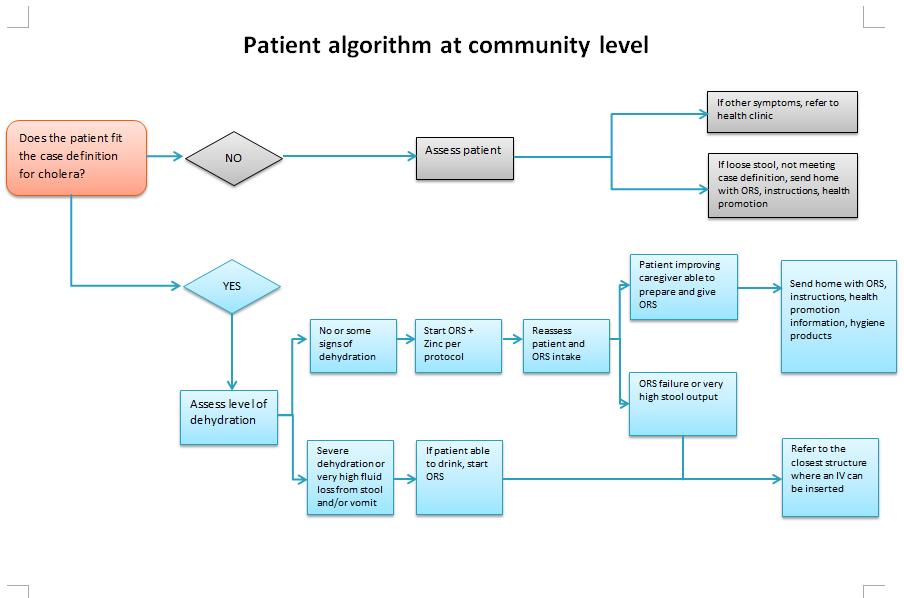
2 1.Community level oral rehydration This type of unit is frequently called an Oral Rehydration Point (ORP). This level of care provides oral treatment for patients with acute watery diarrhoea and dehydration and refers patients with severe dehydration to other parts of the treatment network (after starting ORS if possible). Health workers also provide the community with information on the prevention of cholera, including the importance of early treatment. Organisation Patients should not travel more than one hour on foot to access this type of care. In most contexts, staff providing care will not have the skills to safely insert and manage intravenous rehydration so only oral treatment with rehydration solution and zinc will be provided. Staff may already be part of a community care network (iccm, IMCI, village health workers) or may be community members who have no previous health training, but are trained specifically to provide oral rehydration therapy during a cholera outbreak. Care may be provided in a variety of modalities, either fixed or mobile, but there is no structure for overnight care for patients. As far as possible, care should be provided during all daylight hours, 7 days per week. Fixed points may include pre-existing oral rehydration points (sometimes found in refugee camps), a tent or shelter set up in communities, or in a clearly demarcated section of a health post or health centre. In the latter case, diarrhoea patients must be separated from patients with other pathologies to prevent the transmission of cholera to other patients. Mobile examples include ambulatory village health workers or Red Cross/Red Crescent volunteers. Each patient may have one caregiver (usually a family member) with them at a time. The caregiver can learn how to a help care for the patient and can also learn about cholera prevention while aiding the patient. This knowledge may help reduce cholera transmission at the home of the patient³, ⁴. In most cases, the person providing treatment will also be responsible for other community activities such as the promotion of cholera prevention (including hand washing) and distribution of materials for cholera prevention such as soap. In the event that these activities are carried out door-to-door, patients with diarrhoea can also be identified (active case finding) and ORS therapy initiated. Minimum standards Whatever their previous experience, individuals providing treatment for cholera patients must be trained on the case definitions, assessment of dehydration, appropriate treatment protocols for ORS and zinc, including monitoring of patients during treatment. Staff should also be trained to identify patients who should be transferred to receive IV rehydration. In some cases the person may have the skills to safely insert an intravenous line. In this event severely dehydrated patients may have an initial IV inserted at this level, but the patient should be transferred to a structure designed for overnight care for ongoing monitoring and to complete treatment. Whenever possible, ORS should also be started for patients given IV fluids. 2
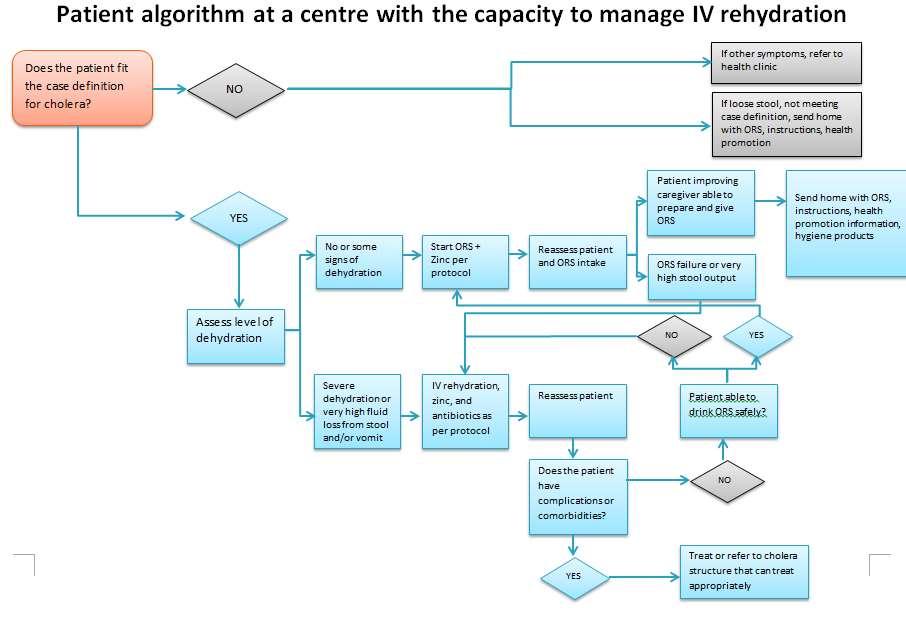
3 All staff should be trained on prevention of cholera, to protect themselves, to prevent transmission at the treatment site and to provide information on prevention of cholera for the community. Staff must have access to clean water or be provided with the means and knowledge to make safe water (disinfection tablets, filters or other sources of clean water). Staff should also be able to wash their hands. If IV treatment is to be started, appropriate waste and sharps disposal materials must also be provided. Although individual patient records may not be used at this level, basic records for epidemiological surveillance (numbers of patients, number of patients transferred, reported deaths in the community and if possible village or site of origin) and supply management should be kept. If possible referral cards should accompany patients who are transferred for higher level care. The Cholera Community, ORP Kit is designed for this type of scenario. 2. Standard oral and intravenous rehydration This type of centre has traditionally been called a Cholera Treatment Unit (CTU). This level of care provides oral and intravenous treatment. After appropriate treatment for dehydration, when possible, patients with medical complications or co-morbidities are referred to another structure in the network with more advanced facilities. Staff provides information on prevention of cholera for other staff members, patients and caregivers. The personnel also support any community level oral rehydration teams and receive transfers from these teams. Organisation Staff providing treatment have the skills to safely insert and manage intravenous rehydration, but may not have the skills to manage complications or co-morbidities. Care is provided at fixed sites which are usually open 7 days per week with infrastructure for patients to receive care 24 hours a day in either pre-existing or purpose built structures. The size usually varies from 5 to 40 beds. Both public and private structures should be considered. Patients with suspected cholera must be separated from patients with other morbidities in order to prevent transmission of cholera. In most cases, the structure will be part of a referral system receiving patients requiring intravenous therapy from sites only providing oral rehydration. Patients with complications or co-morbidities will be referred to structures with more resources. Each patient may have one caregiver (usually a family member) with them at a time. The caregiver can learn how to a help care for the patient and can also learn about cholera prevention while aiding the patient. This knowledge may help reduce cholera transmission at the home of the patient³⁴. For infection control and due to space limitations, only one caregiver at a time should be present with each patient. Minimum standards Whatever the previous experience, staff providing care for cholera patients must be trained on the case definitions, assessment of dehydration and appropriate treatment protocols for 3
4 intravenous rehydration and oral treatment with ORS and zinc, including monitoring of patients during treatment. Staff should also be trained to identify patients with complications or comorbidities who should be transferred once they no longer have cholera (e.g. malnutrition). All staff should be trained on prevention of cholera, to protect themselves, to prevent transmission at the treatment site and to provide information on prevention of cholera to patients and their care givers. Staff at this type of structure should be able to take stool samples and safely package and adequately label samples for transport to a laboratory. Significant amounts of clean water must be provided at this type of structure to prepare ORS, for infection control, laundry and general cleaning. Staff must be trained to make ORS safely and have access to clean water or provided with the means to make safe water (disinfection tablets, filters or other sources of clean water). Adequate means for infection control including hand washing, safe excreta disposal, cleaning and laundry must be available. Cholera cots should be available to enhance both patient care and infection control. As patients will be provided 24 hour care, light must be available in the structure. Food is an essential part of patient care and must be safely available for patients. Individual patient records should be kept at this level, staff should be trained to keep a register of patients, on appropriate recording of individual data and on reporting for epidemiological purposes and stock management. At this level, additional support staff such as cleaners is appropriate. The Cholera Periphery Kit is designed for this type of scenario. One Periphery Kit is enough to start a small centre, with multiple Periphery Kits necessary for larger centres. Additional kits such as the Hardware Kit may also be necessary. 3. Oral and intravenous rehydration, treatment of complications and co-morbidities This type of centre has traditionally been called a Cholera Treatment Centre (CTC). This level of care provides oral and intravenous treatment for rehydration, treatment for complications and co-morbidities and education on cholera prevention for staff, patients and caregivers. The personnel also support any community level oral rehydration teams and teams from other treatment structures and receive transfers from these teams. Organisation Staff may have a range of skills, but include members with training and competency to treat complications and co-morbidities such as hypokalemia and severe dehydration in malnourished children. Care is provided at fixed sites which are open 7 days per week with infrastructure for patients to receive care 24 hours a day in either pre-existing or purpose built structures. This type of centre will usually have anywhere from 40 to 200 beds at the peak of an outbreak. Both public and 4
5 private structures should be considered. Patients with suspected cholera must be separated from patients with other morbidities in order to prevent transmission of cholera. Each patient may have one caregiver (usually a family member) with them at a time. The caregiver can learn how to help care for the patient and can also learn about cholera prevention while aiding the patient. This knowledge may help reduce cholera transmission at the home of the patient³⁴. For infection control and due to space limitations, only one caregiver at a time should be present with each patient. In most cases, the structure will be part of a network of care receiving patients requiring intravenous therapy from sites only providing oral rehydration and/or structures that cannot adequately manage patients with complications or co-morbidities. Minimum standards Whatever the previous experience, staff providing treatment for cholera patients must be trained on the case definitions, assessment of dehydration and appropriate treatment protocols for intravenous rehydration and oral treatment with ORS and zinc, including monitoring of patients during treatment. All staff should be trained on prevention of cholera, to protect themselves, to prevent transmission at the treatment site and to provide information on prevention of cholera for the patients and their care givers. Staff at this type of structure should be able to take stool samples and safely package and adequately label samples for transport to a laboratory. Significant amounts of clean water must be provided at this type of structure to prepare ORS, for infection control, laundry and general cleaning. Cholera cots should be available to enhance both patient care and infection control. As patients will be provided 24 hour care, light must be available in the structure. Food is an essential part of patient care and must be safely available for patients. Individual patient records should be kept at this level, staff should be trained to keep a register of patients, on appropriate recording of individual data and on reporting for epidemiological purposes and stock management. At this level, additional support staff such as registrars, cleaners, laundry staff etc. will be necessary. The Central Reference Kits are designed for this type of scenario. One kit will be sufficient to start a small centre, multiple kits will be needed for larger centres. Additional kits such as the Hardware Kit may also be necessary. Note: this document recommends a general organization of a network of care for patients with suspected cholera, but is not intended to provide details of all materials required at each level of care (e.g list of materials, waste management etc). 5
6 References Page A-L, Ciglenecki I, Jasmin ER, Desvignes L, Grandesso F, Polonsky J, et al : (2015) Geogrqphic distribution qnd,ortqlity risk fqctors during the choler outbreqk in q rurql region of Hqiti, PLoS Negl Trop Dis 9(3): e : doi:10:1371/journal:pntd: World Health Organization/The United Nations Childrens Fund (UNICEF) (2013) Ending preventative child deaths from pneumonia and diarrhoea by 2025: the integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD), Geneva, Switzerland. Gartley M, Valeh P, de Lange R, DiCarlo S, Viscusi A, Lenglet A and Fesselet J. (2013) Uptake of household disinfection kits as an additonal measure in response to a cholera outbreak in urban areas of Haiti. Journal of Water and Health 11(4): George CM, Monira S, Sack DA, Rashid M, Saif-Ur-Rahman KM, Mahmud T, Rahman Z et al: (2016) Randomized controlled trial of hospital-based hygiene and water treatment intervention (CHoB17) to reduce cholera, EID, 22 (2):
7 7
8 GTFCC
Self-Assessment Tool: Are Health Facilities Capable of Managing Cholera Outbreaks?
 Self-Assessment Tool: Are Health Facilities Capable of Managing Cholera Outbreaks? Updated November, 2016 Johns Hopkins Bloomberg School of Public Health 615 N. Wolfe Street / E5537, Baltimore, MD 21205,
Self-Assessment Tool: Are Health Facilities Capable of Managing Cholera Outbreaks? Updated November, 2016 Johns Hopkins Bloomberg School of Public Health 615 N. Wolfe Street / E5537, Baltimore, MD 21205,
MULTISECTORIAL EMERGENCY RESPONSE PLAN - CHOLERA
 MULTISECTORIAL EMERGENCY RESPONSE PLAN - CHOLERA Prepared in collaboration between MISAU and Intercluster Date: 6/04/2017 Multisectorial Emergency response plan for cholera in Mozambique - 2017 1. Introduction
MULTISECTORIAL EMERGENCY RESPONSE PLAN - CHOLERA Prepared in collaboration between MISAU and Intercluster Date: 6/04/2017 Multisectorial Emergency response plan for cholera in Mozambique - 2017 1. Introduction
Objective. Note: Responsibility is ensuring the activity is done, not necessarily doing it
 Objective This document details the responsibilities of WASH Cluster, Health Cluster and Communications for AWD/Cholera response, to reduce the number of outbreaks and minimise lives lost. The WASH Cluster,
Objective This document details the responsibilities of WASH Cluster, Health Cluster and Communications for AWD/Cholera response, to reduce the number of outbreaks and minimise lives lost. The WASH Cluster,
AWD Geddo Region, South Central Somalia, 1March
 AWD Geddo Region, South Central Somalia, 1March 2008 1 WHO Somalia P.O. Box: 63565 - Nairobi, Kenya - wroffice@nbo.emro.who.int - T: +254 20 7623197/8/9 and +254 20 7622840 WHO Somalia Acute Watery Diarrhoea
AWD Geddo Region, South Central Somalia, 1March 2008 1 WHO Somalia P.O. Box: 63565 - Nairobi, Kenya - wroffice@nbo.emro.who.int - T: +254 20 7623197/8/9 and +254 20 7622840 WHO Somalia Acute Watery Diarrhoea
Cholera Overview. Recent visit to Haiti to assist with community education and prevention Mirine Richey Dye, MPH, CHES
 Cholera Overview Recent visit to Haiti to assist with community education and prevention Mirine Richey Dye, MPH, CHES Florida Keys MRC Southern point is 90 miles from Cuba 135 miles of islands connected
Cholera Overview Recent visit to Haiti to assist with community education and prevention Mirine Richey Dye, MPH, CHES Florida Keys MRC Southern point is 90 miles from Cuba 135 miles of islands connected
REPORT ON THE USE OF CERF FUNDS THE REPUBLIC OF SOUTH SUDAN RAPID RESPONSE CHOLERA 2014 RESIDENT/HUMANITARIAN COORDINATOR
 RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS THE REPUBLIC OF SOUTH SUDAN RAPID RESPONSE CHOLERA 2014 RESIDENT/HUMANITARIAN COORDINATOR Mr. Eugene Owusu REPORTING PROCESS AND CONSULTATION
RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS THE REPUBLIC OF SOUTH SUDAN RAPID RESPONSE CHOLERA 2014 RESIDENT/HUMANITARIAN COORDINATOR Mr. Eugene Owusu REPORTING PROCESS AND CONSULTATION
StC WASH, Cholera and diarrhoeal diseases
 5 th Initiative against Diarrheal and Enteric diseases in Asia (IDEA) StC WASH, Cholera and diarrhoeal diseases Humanitarian WASH, SCUK Hanoi March 2017 Overview StC and Approach to Cholera StC WASH involvement
5 th Initiative against Diarrheal and Enteric diseases in Asia (IDEA) StC WASH, Cholera and diarrhoeal diseases Humanitarian WASH, SCUK Hanoi March 2017 Overview StC and Approach to Cholera StC WASH involvement
UNICEF s response to the Cholera Outbreak in Yemen. Terms of Reference for a Real-Time Evaluation
 UNICEF s response to the Cholera Outbreak in Yemen Terms of Reference for a Real-Time Evaluation Background Two years since the escalation of violence in Yemen, a second wave of fast spreading cholera
UNICEF s response to the Cholera Outbreak in Yemen Terms of Reference for a Real-Time Evaluation Background Two years since the escalation of violence in Yemen, a second wave of fast spreading cholera
HEALTH CLUSTER BULLETIN
 HEALTH CLUSTER BULLETIN CHOLERA OUTBREAK IN HAITI FRIDAY, JANUARY 21, 2011 #15 Dear Health Cluster partners, It has been several month since we started disseminating the Health Cluster Bulletin. During
HEALTH CLUSTER BULLETIN CHOLERA OUTBREAK IN HAITI FRIDAY, JANUARY 21, 2011 #15 Dear Health Cluster partners, It has been several month since we started disseminating the Health Cluster Bulletin. During
Disaster relief emergency fund (DREF) Central African Republic: Cholera outbreak
 Central African Republic: Cholera outbreak") Disaster relief emergency fund (DREF) Central African Republic: Cholera outbreak DREF operation n MDRCF009 GLIDE n EP-2011-000153-CAF 13 October, 2011 The International Federation of Red Cross and Red
Disaster relief emergency fund (DREF) Central African Republic: Cholera outbreak DREF operation n MDRCF009 GLIDE n EP-2011-000153-CAF 13 October, 2011 The International Federation of Red Cross and Red
Disaster relief emergency fund (DREF) Republic of Congo: Epidemic
 Republic of Congo: Epidemic") Disaster relief emergency fund (DREF) Republic of Congo: Epidemic DREF operation n MDRCG014 GLIDE n EP-2013-000040-COG 12 April 2013 The International Federation of Red Cross and Red Crescent (IFRC) Disaster
Disaster relief emergency fund (DREF) Republic of Congo: Epidemic DREF operation n MDRCG014 GLIDE n EP-2013-000040-COG 12 April 2013 The International Federation of Red Cross and Red Crescent (IFRC) Disaster
Risks/Assumptions Activities planned to meet results
 Communitybased health services Specific objective : Through promotion of communitybased health care and first aid activities in line with the ARCHI 2010 principles, the general health situation in four
Communitybased health services Specific objective : Through promotion of communitybased health care and first aid activities in line with the ARCHI 2010 principles, the general health situation in four
International appeal Haiti and the Dominican Republic: Cholera prevention
 International appeal Haiti and the Dominican Republic: Cholera prevention Emergency appeal n MDR49008 5 December 2013 This International Appeal represents a distinct plan developed in close coordination
International appeal Haiti and the Dominican Republic: Cholera prevention Emergency appeal n MDR49008 5 December 2013 This International Appeal represents a distinct plan developed in close coordination
ALIMA s response to Ebola Outbreak
 ALIMA s response to Ebola Outbreak Case Situation The 2014 West Africa Ebola Virus Disease outbreak is by far the largest EVD epidemic ever recorded and potentially one of the most challenging medical
ALIMA s response to Ebola Outbreak Case Situation The 2014 West Africa Ebola Virus Disease outbreak is by far the largest EVD epidemic ever recorded and potentially one of the most challenging medical
Disaster relief emergency fund (DREF)
") Disaster relief emergency fund (DREF) Guinea: Cholera DREF operation n MDRGN005 GLIDE n EP-2012-000158-GIN 11 September 2012 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief
Disaster relief emergency fund (DREF) Guinea: Cholera DREF operation n MDRGN005 GLIDE n EP-2012-000158-GIN 11 September 2012 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief
Emergency Plan of Action (EPoA) Central Africa Republic: Cholera Epidemic Outbreak
 Central Africa Republic: Cholera Epidemic Outbreak") Emergency Plan of Action (EPoA) Central Africa Republic: Cholera Epidemic Outbreak DREF Operation Operation n MDRCF021; Glide n EP-2016-000082- CAF Date of issue:25.08.2016 Date of disaster: 07.07.2016
Emergency Plan of Action (EPoA) Central Africa Republic: Cholera Epidemic Outbreak DREF Operation Operation n MDRCF021; Glide n EP-2016-000082- CAF Date of issue:25.08.2016 Date of disaster: 07.07.2016
NEPAL EARTHQUAKE 2015 Country Update and Funding Request May 2015
 PEOPLE AFFECTED 4.2 million in urgent need of health services 2.8 million displaced 8,567 deaths 16 808 injured HEALTH SECTOR 1059 health facilities damaged (402 completely damaged) BENEFICIARIES WHO and
PEOPLE AFFECTED 4.2 million in urgent need of health services 2.8 million displaced 8,567 deaths 16 808 injured HEALTH SECTOR 1059 health facilities damaged (402 completely damaged) BENEFICIARIES WHO and
Current Situation. Haiti Cholera Response. United Nations in Haiti. December 2014
 Haiti Cholera Response United Nations in Haiti December 2014 Since the emergence of cholera in Haiti in October 2010, the Ministry of Public Health and Population (MSPP) has recorded 719,377 suspected
Haiti Cholera Response United Nations in Haiti December 2014 Since the emergence of cholera in Haiti in October 2010, the Ministry of Public Health and Population (MSPP) has recorded 719,377 suspected
Sierra Leone Cholera ERU Operation Review
 Sierra Leone Cholera ERU Operation Review Oral Rehydration Point, Mangay Loko, Bombali. Photo: Hler Gudjonsson,IFRC Peter Rees-Gildea ReesGildea Consulting January 2013 KRISTJON THORKELSSON It was with
Sierra Leone Cholera ERU Operation Review Oral Rehydration Point, Mangay Loko, Bombali. Photo: Hler Gudjonsson,IFRC Peter Rees-Gildea ReesGildea Consulting January 2013 KRISTJON THORKELSSON It was with
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. Community IMCI. Community IMCI
 Implementation in the Western Pacific Region. Community IMCI. Community IMCI") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Sudan Weekly Highlights Week 36 (4 10 September 2010)
") Emergency Preparedness and Humanitarian Action (EHA) Sudan Weekly Highlights Week 36 (4 10 September 2010) Essential and life saving drugs are regularly replenished in Kutum hospital. Regular provision
Emergency Preparedness and Humanitarian Action (EHA) Sudan Weekly Highlights Week 36 (4 10 September 2010) Essential and life saving drugs are regularly replenished in Kutum hospital. Regular provision
1) What type of personnel need to be a part of this assessment team? (2 min)
 What type of personnel need to be a part of this assessment team? (2 min)") Student Guide Module 2: Preventive Medicine in Humanitarian Emergencies Civil War Scenario Problem based learning exercise objectives Identify the key elements for the assessment of a population following
Student Guide Module 2: Preventive Medicine in Humanitarian Emergencies Civil War Scenario Problem based learning exercise objectives Identify the key elements for the assessment of a population following
PROGRAM BRIEF UGANDA. Integrated Case Management of Pneumonia, Diarrhea & Malaria through the Five & Alive Franchise Network
 PROGRAM BRIEF UGANDA Integrated Case Management of Pneumonia, Diarrhea & Malaria through the Five & Alive Franchise Network I ntegrated case management (ICM) is a strategy to reduce child morbidity and
PROGRAM BRIEF UGANDA Integrated Case Management of Pneumonia, Diarrhea & Malaria through the Five & Alive Franchise Network I ntegrated case management (ICM) is a strategy to reduce child morbidity and
Outbreak Management. Gastroenteritis Outbreak Protocol
 INFECTION PREVENTION AND CONTROL (IPAC) Outbreak Management Gastroenteritis Outbreak Protocol Infection Prevention and Control Guidelines for Acute and Residential Care R:Infection Control Manual\Outbreak
INFECTION PREVENTION AND CONTROL (IPAC) Outbreak Management Gastroenteritis Outbreak Protocol Infection Prevention and Control Guidelines for Acute and Residential Care R:Infection Control Manual\Outbreak
Self-Assessment Summary Report 2017 Accreditation
 FLA LEEND: UNMET MET ONOIN R 5.2 Team members, clients and families, and volunteers are engaged when developing the multi-faceted approach for IPC. R 1.3 The resources needed to support the IPC program
FLA LEEND: UNMET MET ONOIN R 5.2 Team members, clients and families, and volunteers are engaged when developing the multi-faceted approach for IPC. R 1.3 The resources needed to support the IPC program
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL
 DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
Dr Jean Félix ANDRIANJARANASOLO MOH MADAGASCAR
 Dr Jean Félix ANDRIANJARANASOLO MOH MADAGASCAR AREA ( km square ) : 592 000 North South : 1600 Km East West 570 Km Population : 19 000 000 Urban Population : 7 000 000 Rural Population : 12 000 000 Regions
Dr Jean Félix ANDRIANJARANASOLO MOH MADAGASCAR AREA ( km square ) : 592 000 North South : 1600 Km East West 570 Km Population : 19 000 000 Urban Population : 7 000 000 Rural Population : 12 000 000 Regions
Kenya Red Cross Cholera Response After Action Review Focused on Bomet, Homabay, Nakuru and Migori Counties February to June 2015
 Kenya Red Cross Cholera Response After Action Review Focused on Bomet, Homabay, Nakuru and Migori Counties February to June 2015 Response supported by DREF N MDRKE033, with some funding from a long term
Kenya Red Cross Cholera Response After Action Review Focused on Bomet, Homabay, Nakuru and Migori Counties February to June 2015 Response supported by DREF N MDRKE033, with some funding from a long term
Disaster relief emergency fund (DREF) Benin: Cholera outbreak
 Benin: Cholera outbreak") Disaster relief emergency fund (DREF) Benin: Cholera outbreak DREF operation n MDRBJ013 GLIDE n EP-2013-000130-BEN 10 October 2013 The International Federation of Red Cross and Red Crescent (IFRC) Disaster
Disaster relief emergency fund (DREF) Benin: Cholera outbreak DREF operation n MDRBJ013 GLIDE n EP-2013-000130-BEN 10 October 2013 The International Federation of Red Cross and Red Crescent (IFRC) Disaster
INFECTION C ONTROL CONTROL CONTROL EDUCATION PROGRAM
 INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
Clostridium difficile Infection (CDI) in children (3-16 years ) Transmission Based Precautions
 in children (3-16 years ) Transmission Based Precautions") Page 1 of 9 Standard Operating procedure (SOP) Objective To provide HCWs with details of the care required to prevent cross-infection in children s with Clostridium difficile Infection (CDI). This SOP
Page 1 of 9 Standard Operating procedure (SOP) Objective To provide HCWs with details of the care required to prevent cross-infection in children s with Clostridium difficile Infection (CDI). This SOP
Standard Operating Procedure for Community Event-Based Surveillance for Ebola Virus Disease in Sierra Leone
 Standard Operating Procedure for Community Event-Based Surveillance for Ebola Virus Disease in Sierra Leone Page 1 of 8 I. Introduction a. Background Community event-based surveillance (CEBS) is the organized
Standard Operating Procedure for Community Event-Based Surveillance for Ebola Virus Disease in Sierra Leone Page 1 of 8 I. Introduction a. Background Community event-based surveillance (CEBS) is the organized
Situation Report #26 on Cholera in South Sudan As at 23:59 Hours, 17 July 2015
 Republic of South Sudan Situation Report #6 on Cholera in South Sudan As at :9 Hours, 7 July Situation Update As of 7 July, a total of,6 cholera cases including 8 (CFR.%) have been reported in Juba and
Republic of South Sudan Situation Report #6 on Cholera in South Sudan As at :9 Hours, 7 July Situation Update As of 7 July, a total of,6 cholera cases including 8 (CFR.%) have been reported in Juba and
SOUTH AFRICA: CHOLERA
 SOUTH AFRICA: CHOLERA 29 December, 2000 appeal no. 32/00 situation report no. 2 period covered: 17 November - 19 December While the cholera operation is moving forward, particularly in the areas of health
SOUTH AFRICA: CHOLERA 29 December, 2000 appeal no. 32/00 situation report no. 2 period covered: 17 November - 19 December While the cholera operation is moving forward, particularly in the areas of health
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES. Tajikistan
 CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Guidance for contingency planning
 WHO Guidance for contingency planning World Health Organization 1 P age Everyone deserves the chance to survive. I think of this every time I see another disaster. There are probably people dying who don
WHO Guidance for contingency planning World Health Organization 1 P age Everyone deserves the chance to survive. I think of this every time I see another disaster. There are probably people dying who don
The Syrian Arab Republic
 World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
Supervision for Diarrhoea Case Management at the Oral Rehydràtion Therapy Corners and Diarrhoea Training Units in Sindh
 Supervision for Diarrhoea Case Management at the Oral Rehydràtion Therapy Corners and Diarrhoea Training Units in Sindh Pages with reference to book, From 208 To 210 Lubna A. Baig, Inayat Thaver ( Faculty
Supervision for Diarrhoea Case Management at the Oral Rehydràtion Therapy Corners and Diarrhoea Training Units in Sindh Pages with reference to book, From 208 To 210 Lubna A. Baig, Inayat Thaver ( Faculty
Clostridium difficile GDH positive (Glutamate Dehydrogenase) toxin negative
 toxin negative") Patient information Clostridium difficile GDH positive (Glutamate Dehydrogenase) toxin negative i Important information for all patients. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81
Patient information Clostridium difficile GDH positive (Glutamate Dehydrogenase) toxin negative i Important information for all patients. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81
Disaster Relief Emergency Fund (DREF) to support the national society in responding by delivering assistance.
 to support the national society in responding by delivering assistance.") Angola: Cholera Final report Emergency appeal n MDRAO001 28 May, 2008 Period covered by this Final Report: 18 May 2006 to 31 December, 2007 Appeal target (current): CHF 1,392,404 (USD 950,000 or EUR 740,000);
Angola: Cholera Final report Emergency appeal n MDRAO001 28 May, 2008 Period covered by this Final Report: 18 May 2006 to 31 December, 2007 Appeal target (current): CHF 1,392,404 (USD 950,000 or EUR 740,000);
DREF operation update Benin: Cholera outbreak
 DREF operation update Benin: Cholera outbreak DREF operation n MDRBJ013 GLIDE n EP-2013-000130-BEN Update no 1-22 November 2013 The International Federation of Red Cross and Red Crescent (IFRC) Disaster
DREF operation update Benin: Cholera outbreak DREF operation n MDRBJ013 GLIDE n EP-2013-000130-BEN Update no 1-22 November 2013 The International Federation of Red Cross and Red Crescent (IFRC) Disaster
Senegal: Cholera. DREF Operation no. MDRSN001; GLIDE no. EP SEN; 18 September, 2008
 Senegal: Cholera DREF Operation no. MDRSN001; GLIDE no. EP-2007-000187-SEN; 18 September, 2008 The International Federation s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created
Senegal: Cholera DREF Operation no. MDRSN001; GLIDE no. EP-2007-000187-SEN; 18 September, 2008 The International Federation s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created
#HealthForAll ichc2017.org
 #HealthForAll ichc2017.org Background Integrated Community Case Management (iccm) of childhood illness is an evidence-based strategy to extend the treatment of leading causes of death in children to hard-to-reach
#HealthForAll ichc2017.org Background Integrated Community Case Management (iccm) of childhood illness is an evidence-based strategy to extend the treatment of leading causes of death in children to hard-to-reach
UNICEF HUMANITARIAN ACTION UPDATE ZIMBABWE. 4 February 2009
 UNICEF HUMANITARIAN ACTION UPDATE ZIMBABWE 4 February 2009 UNICEF IS REPONDING TO THE NEEDS OF CHILDREN AND WOMEN IN THE AREAS OF HEALTH, EDUCATION, CHILD PROTECTION AND WATER, SANITATION AND HYGIENE 6
UNICEF HUMANITARIAN ACTION UPDATE ZIMBABWE 4 February 2009 UNICEF IS REPONDING TO THE NEEDS OF CHILDREN AND WOMEN IN THE AREAS OF HEALTH, EDUCATION, CHILD PROTECTION AND WATER, SANITATION AND HYGIENE 6
Floods in Pakistan Bulletin No August Pakistan Health Cluster. Highlights
 Pakistan Health Cluster Floods in Pakistan Bulletin No 12 16 August 2010 An acute diarrhoea patient is being treated in a health facility in Muzzafargarh in the province of Punjab. Photo by Syed Haider
Pakistan Health Cluster Floods in Pakistan Bulletin No 12 16 August 2010 An acute diarrhoea patient is being treated in a health facility in Muzzafargarh in the province of Punjab. Photo by Syed Haider
Clostridium difficile Infection (CDI)
") Approved by: Clostridium difficile Infection (CDI) Vice President and Chief Medical Officer Corporate Policy & Procedures Manual VI-8 Date Approved August 22, 2016 September 16, 2016 Next Review (3 years
Approved by: Clostridium difficile Infection (CDI) Vice President and Chief Medical Officer Corporate Policy & Procedures Manual VI-8 Date Approved August 22, 2016 September 16, 2016 Next Review (3 years
With more than 150,000 people reached, the operation was implemented in 3 months and was closed by end of November, 2007.
 Comoros: Cholera DREF Operation no. MDRKM001 28 March, 2008 The International Federation s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created by the Federation in 1985 to ensure
Comoros: Cholera DREF Operation no. MDRKM001 28 March, 2008 The International Federation s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created by the Federation in 1985 to ensure
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004
 UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
South Sudan Country brief and funding request February 2015
 PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
HEALTH CLUSTER BULLETIN September 2017
 HEALTH CLUSTER BULLETIN September 2017 WHO and Health Cluster partners aim to reach 10.4 million of the most vulnerable people in Yemen with health services in 2017 14.8 M IN NEED OF HEALTH ASSISTANCE
HEALTH CLUSTER BULLETIN September 2017 WHO and Health Cluster partners aim to reach 10.4 million of the most vulnerable people in Yemen with health services in 2017 14.8 M IN NEED OF HEALTH ASSISTANCE
WHEREAS, Ebola Virus Disease (EVD) is a rare and potentially deadly disease caused
 is a rare and potentially deadly disease caused") STATE OF NEW YORK : DEPARTMENT OF HEALTH --------------------------------------------------------------------------X IN THE MATTER OF THE PREVENTION AND CONTROL OF EBOLA VIRUS DISEASE ORDER FOR SUMMARY
STATE OF NEW YORK : DEPARTMENT OF HEALTH --------------------------------------------------------------------------X IN THE MATTER OF THE PREVENTION AND CONTROL OF EBOLA VIRUS DISEASE ORDER FOR SUMMARY
Learning Objectives. Successful Antibiotic Stewardship. Byron Health Center & GrandView Pharmacy
 Successful Antibiotic Stewardship Byron Health Center & GrandView Pharmacy Learning Objectives Understand the core requirements of an antibiotic stewardship program as defined by the CMS Requirements of
Successful Antibiotic Stewardship Byron Health Center & GrandView Pharmacy Learning Objectives Understand the core requirements of an antibiotic stewardship program as defined by the CMS Requirements of
NIGERIA: OUTBREAK OF CEREBRO SPINAL MENINGITIS
 NIGERIA: OUTBREAK OF CEREBRO SPINAL MENINGITIS appeal no: 04/96 4 March 1996 THIS APPEAL SEEKS CHF 2,140,000 IN CASH, KIND AND SERVICES TO ASSIST 2,000,000 BENEFICIARIES FOR 3 MONTHS Summary An epidemic
NIGERIA: OUTBREAK OF CEREBRO SPINAL MENINGITIS appeal no: 04/96 4 March 1996 THIS APPEAL SEEKS CHF 2,140,000 IN CASH, KIND AND SERVICES TO ASSIST 2,000,000 BENEFICIARIES FOR 3 MONTHS Summary An epidemic
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
ZAMBIA: CHOLERA. In Brief
 ZAMBIA: CHOLERA DREF Bulletin no. MDRZM001 6 January 2006 The Federation s mission is to improve the lives of vulnerable people by mobilizing the power of humanity. It is the world s largest humanitarian
ZAMBIA: CHOLERA DREF Bulletin no. MDRZM001 6 January 2006 The Federation s mission is to improve the lives of vulnerable people by mobilizing the power of humanity. It is the world s largest humanitarian
Safe Care Is in YOUR HANDS
 Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Disaster relief emergency fund (DREF) Togo: Cholera outbreak
 Togo: Cholera outbreak") Disaster relief emergency fund (DREF) Togo: Cholera outbreak DREF operation n MDRTG4 GLIDE n EP-213-138-TGO 4 November 213 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief
Disaster relief emergency fund (DREF) Togo: Cholera outbreak DREF operation n MDRTG4 GLIDE n EP-213-138-TGO 4 November 213 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief
Identify patients with Active Surveillance Cultures (ASC)
") MRSA CHANGE STRATEGIES The following tables include change strategies proven to be effective in healthcare settings. Implementing these changes through current or new processes may result in reducing healthcare
MRSA CHANGE STRATEGIES The following tables include change strategies proven to be effective in healthcare settings. Implementing these changes through current or new processes may result in reducing healthcare
Towards Quality Care for Patients. Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care
 Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
November, The Syrian Arab Republic. Situation highlights. Health priorities
 November, 2012 The Syrian Arab Republic Total population 20411000 5120 71/76 159/95 174 3.4 Requested 31 145 000 53 150 319 Received 7 993 078 13 648 289 25.7% 26% http://www.who.int/disasters/crises/syr
November, 2012 The Syrian Arab Republic Total population 20411000 5120 71/76 159/95 174 3.4 Requested 31 145 000 53 150 319 Received 7 993 078 13 648 289 25.7% 26% http://www.who.int/disasters/crises/syr
Prairie North Regional Health Authority: Hospital-acquired infections
 Prairie North Regional Health Authority: Hospital-acquired infections Main points... 308 Introduction... 309 Background the risk of hospital-acquired infections... 309 Audit objective, scope, criteria,
Prairie North Regional Health Authority: Hospital-acquired infections Main points... 308 Introduction... 309 Background the risk of hospital-acquired infections... 309 Audit objective, scope, criteria,
Emergency Plan of Action (EPoA) Bénin Cholera outbreak
 Bénin Cholera outbreak") Emergency Plan of Action (EPoA) Bénin Cholera outbreak DREF Operation Operation n MDRBJ15 Date of issue: 12 September 216 Date of disaster: 3 August 216 Operation manager (responsible for this EPoA): Samuel
Emergency Plan of Action (EPoA) Bénin Cholera outbreak DREF Operation Operation n MDRBJ15 Date of issue: 12 September 216 Date of disaster: 3 August 216 Operation manager (responsible for this EPoA): Samuel
Emergency Preparedness & Humanitarian Action (EHA) Week 3, January 2012
 Week 3, January 2012") Emergency Preparedness & Humanitarian Action (EHA) Week 3, 14-20 January 2012 Due to access issues, 56 health facilities out of 104 (53.8%) reported to South Kordofan s surveillance system. During the
Emergency Preparedness & Humanitarian Action (EHA) Week 3, 14-20 January 2012 Due to access issues, 56 health facilities out of 104 (53.8%) reported to South Kordofan s surveillance system. During the
Summary of UNICEF Emergency Needs for 2009*
 UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
HCAI Local implementation team action plan
 HCAI Local implementation team action plan Item Type Report Authors New Governance HCAI Group Publisher New Governance HCAI Group Download date 16/09/2018 18:12:09 Link to Item http://hdl.handle.net/10147/110814
HCAI Local implementation team action plan Item Type Report Authors New Governance HCAI Group Publisher New Governance HCAI Group Download date 16/09/2018 18:12:09 Link to Item http://hdl.handle.net/10147/110814
IASC. Mozambique Zambezi River floods and cyclone Favio crisis. Health Cluster Bulletin # March Inter-Agency Standing Committee
 IASC Inter-Agency Standing Committee Mozambique Zambezi River floods and cyclone Favio crisis #3 17 The Mozambique emergency Health Cluster Bulletin aims to give an overview of the health activities conducted
IASC Inter-Agency Standing Committee Mozambique Zambezi River floods and cyclone Favio crisis #3 17 The Mozambique emergency Health Cluster Bulletin aims to give an overview of the health activities conducted
Supportive supervision checklist on IMCI
 Supportive supervision checklist on IMCI Name of the health centre: Sub-district/municipality/Zone: District: Date of supervision:.../.../... Name of Supervisor: Designation: 1. Health services organisation
Supportive supervision checklist on IMCI Name of the health centre: Sub-district/municipality/Zone: District: Date of supervision:.../.../... Name of Supervisor: Designation: 1. Health services organisation
Guideline for the Management of Patients with Known or Suspected Diarrhoea / Viral Gastroenteritis
 Guideline for the Management of Patients with Known or Suspected Diarrhoea / Viral Gastroenteritis 1. Introduction 1.1 Patients with diarrhoea pose a risk to other patients from micro-organisms contaminating
Guideline for the Management of Patients with Known or Suspected Diarrhoea / Viral Gastroenteritis 1. Introduction 1.1 Patients with diarrhoea pose a risk to other patients from micro-organisms contaminating
COUNTRY PROFILE: LIBERIA LIBERIA COMMUNITY HEALTH PROGRAMS JANUARY 2014
 COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
JOINT PLAN OF ACTION in Response to Cyclone Nargis
 Health Cluster - Myanmar JOINT PLAN OF ACTION in Response to Cyclone Nargis Background Cyclone Nargis struck Myanmar on 2 and 3 May 2008, sweeping through the Ayeyarwady delta region and the country s
Health Cluster - Myanmar JOINT PLAN OF ACTION in Response to Cyclone Nargis Background Cyclone Nargis struck Myanmar on 2 and 3 May 2008, sweeping through the Ayeyarwady delta region and the country s
Joint statement. Scaling up the community-based health workforce for emergencies
 Joint statement Scaling up the community-based health workforce for emergencies Joint statement / Scaling-up the community-based health workforce for emergencies 2 The aim of this joint statement is to:
Joint statement Scaling up the community-based health workforce for emergencies Joint statement / Scaling-up the community-based health workforce for emergencies 2 The aim of this joint statement is to:
IMCI at the Referral Level: Hospital IMCI
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Guidelines. Camp Nursing. Guidelines for Registered Nurses
 Guidelines Camp Nursing Guidelines for Registered Nurses June 2015 CAMP NURSING: FOR REGISTERED NURSES JUNE 2015 i Approved by the College and Association of Registered Nurses of Alberta () Provincial
Guidelines Camp Nursing Guidelines for Registered Nurses June 2015 CAMP NURSING: FOR REGISTERED NURSES JUNE 2015 i Approved by the College and Association of Registered Nurses of Alberta () Provincial
Somalia Is any part of this project cash based intervention (including vouchers)? Conditionality:
? Conditionality:") Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives HEALTH POVERTY ACTION (HPA) Emergency Nutrition Interventions for IDPs in Somaliland 2018 (NutriSom) SOM-18/N/121295
Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives HEALTH POVERTY ACTION (HPA) Emergency Nutrition Interventions for IDPs in Somaliland 2018 (NutriSom) SOM-18/N/121295
Disaster relief emergency fund (DREF) Burundi: Cholera
 Burundi: Cholera") Disaster relief emergency fund (DREF) Burundi: Cholera DREF operation n MDRBI009 GLIDE n EP-2012-000187-BDI 4 December, 2012 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief
Disaster relief emergency fund (DREF) Burundi: Cholera DREF operation n MDRBI009 GLIDE n EP-2012-000187-BDI 4 December, 2012 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief
Home administration of intravenous diuretics to heart failure patients:
 Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Downloaded from:
 Mbonye, AK; Buregyeya, E; Rutebemberwa, E; Clarke, SE; Lal, S; Hansen, KS; Magnussen, P; LaRussa, P (2016) Prescription for antibiotics at drug shops and strategies to improve quality of care and patient
Mbonye, AK; Buregyeya, E; Rutebemberwa, E; Clarke, SE; Lal, S; Hansen, KS; Magnussen, P; LaRussa, P (2016) Prescription for antibiotics at drug shops and strategies to improve quality of care and patient
Outbreak Management 2015
 Outbreak Management 2015 Learning Outcomes For staff to be able to Define an outbreak To recognise an outbreak Identify the actions to be taken when an outbreak occurs Implement specific actions to be
Outbreak Management 2015 Learning Outcomes For staff to be able to Define an outbreak To recognise an outbreak Identify the actions to be taken when an outbreak occurs Implement specific actions to be
Infection Control Care Plan. Patient Demographic / label. Hospital: Ward:
 Patient Demographic / label Infection Control Care Plan for a patient with loose stools of unknown origin Statement: This care plan should be used with patients who have loose stools of unknown origin.
Patient Demographic / label Infection Control Care Plan for a patient with loose stools of unknown origin Statement: This care plan should be used with patients who have loose stools of unknown origin.
Monitoring and Evaluation of National Action Plans on AMR. Suggested approaches March 2017
 Monitoring and Evaluation of National Action Plans on AMR Suggested approaches March 2017 Role of M&E section in AMR plan Help to clarify activities and outputs expected Identify how to monitor progress
Monitoring and Evaluation of National Action Plans on AMR Suggested approaches March 2017 Role of M&E section in AMR plan Help to clarify activities and outputs expected Identify how to monitor progress
Accreditation Program: Hospital
 ccreditation Program: Hospital Infection Prevention and ontrol 2008 The Joint ommission on ccreditation of Healthcare Organizations ccreditation Program: Hospital hapter: Infection Prevention and ontrol
ccreditation Program: Hospital Infection Prevention and ontrol 2008 The Joint ommission on ccreditation of Healthcare Organizations ccreditation Program: Hospital hapter: Infection Prevention and ontrol
HEALTH CLUSTER BULLETIN
 HEALTH CLUSTER BULLETIN CHOLERA OUTBREAK IN HAITI TUESDAY, NOVEMBER 23, 2010 #4 SITUATION OVERVIEW The situation in Haiti is urgent and will only become worse over the coming weeks. One month after the
HEALTH CLUSTER BULLETIN CHOLERA OUTBREAK IN HAITI TUESDAY, NOVEMBER 23, 2010 #4 SITUATION OVERVIEW The situation in Haiti is urgent and will only become worse over the coming weeks. One month after the
Checklists for Preventing and Controlling
 Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
ANNUAL REPORT ON THE USE OF CERF GRANTS BENIN
 Country Resident/Humanitarian Coordinator ANNUAL REPORT ON THE USE OF CERF GRANTS BENIN Benin Nardos Bekele Thomas Reporting Period 15 October 2010 30 December 2010 I. Summary of Funding and Beneficiaries
Country Resident/Humanitarian Coordinator ANNUAL REPORT ON THE USE OF CERF GRANTS BENIN Benin Nardos Bekele Thomas Reporting Period 15 October 2010 30 December 2010 I. Summary of Funding and Beneficiaries
Emergency appeal (Revised) Sierra Leone: Cholera Epidemic
 Sierra Leone: Cholera Epidemic") Emergency appeal (Revised) Sierra Leone: Cholera Epidemic Revised emergency appeal n MDRSL003 GLIDE n EP-2012-000041-SLE Revised emergency appeal 29 December, 2012 This revised emergency appeal now seeks
Emergency appeal (Revised) Sierra Leone: Cholera Epidemic Revised emergency appeal n MDRSL003 GLIDE n EP-2012-000041-SLE Revised emergency appeal 29 December, 2012 This revised emergency appeal now seeks
WHO Emergency Health Programme for the Food Crisis in Niger Situation Report # 3
 Health Action in Crises WHO Emergency Health Programme for the Food Crisis in Niger Situation Report # Period: to 9 August I. Highlights The cumulative number of cholera cases from July to August is including
Health Action in Crises WHO Emergency Health Programme for the Food Crisis in Niger Situation Report # Period: to 9 August I. Highlights The cumulative number of cholera cases from July to August is including
Emergency Plan of Action operation update Kenya: Cholera Outbreak
 P a g e 1 Emergency Plan of Action operation update Kenya: Cholera Outbreak Emergency Appeal Operations update n 1 Date of Issue: 22 September, 2015. Operation n MDRKE035; Glide n EP-2015-000013-KEN Timeframe
P a g e 1 Emergency Plan of Action operation update Kenya: Cholera Outbreak Emergency Appeal Operations update n 1 Date of Issue: 22 September, 2015. Operation n MDRKE035; Glide n EP-2015-000013-KEN Timeframe
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
PLANNING HEALTH CARE FOR INTERNALLY DISPLACED PERSONS: EXPERIENCES IN UGANDA
 HEALTH POLICY AND DEVELOPMENT; 2 (2) 85-89 UMU Press 2004 THEME ONE: Coping with armed conflict PLANNING HEALTH CARE FOR INTERNALLY DISPLACED PERSONS: EXPERIENCES IN UGANDA Okware Samuel, Bwire Godfrey,
HEALTH POLICY AND DEVELOPMENT; 2 (2) 85-89 UMU Press 2004 THEME ONE: Coping with armed conflict PLANNING HEALTH CARE FOR INTERNALLY DISPLACED PERSONS: EXPERIENCES IN UGANDA Okware Samuel, Bwire Godfrey,
ANNUAL REPORT OF THE HUMANITARIAN/RESIDENT COORDINATOR ON THE USE OF CERF GRANTS. Guinea-Bissau
 ANNUAL REPORT OF THE HUMANITARIAN/RESIDENT COORDINATOR ON THE USE OF CERF GRANTS Country Humanitarian / Resident Coordinator Reporting Period Guinea-Bissau Ms. Giuseppina Mazza 01 January - 31 December
ANNUAL REPORT OF THE HUMANITARIAN/RESIDENT COORDINATOR ON THE USE OF CERF GRANTS Country Humanitarian / Resident Coordinator Reporting Period Guinea-Bissau Ms. Giuseppina Mazza 01 January - 31 December
PROVIDING GLOBAL ACCESS TO QUALITY MEDICAL CARE. Imres has the ideal medical kit solution for every international relief programme
 M E D I C A L K I T S PROVIDING GLOBAL ACCESS TO QUALITY MEDICAL CARE M E D I C A L K I T S Imres has the ideal medical kit solution for every international relief programme M E D I C A L K I T S A COMPLETE
M E D I C A L K I T S PROVIDING GLOBAL ACCESS TO QUALITY MEDICAL CARE M E D I C A L K I T S Imres has the ideal medical kit solution for every international relief programme M E D I C A L K I T S A COMPLETE
Emergency Plan of Action Operation Update 1
 Emergency Plan of Action Operation Update 1 Zambia: Cholera Outbreak Lusaka DREF n MDRZM011 For DREF; Date of issue: 18 December 2017 Project Manager (responsible for budget, compliance, implementation
Emergency Plan of Action Operation Update 1 Zambia: Cholera Outbreak Lusaka DREF n MDRZM011 For DREF; Date of issue: 18 December 2017 Project Manager (responsible for budget, compliance, implementation
Emergency Plan of Action (EPoA) Chad: Cholera outbreak
 Chad: Cholera outbreak") Page 1 Emergency Plan of Action (EPoA) Chad: Cholera outbreak DREF n MDRTD16 Glide n EP-217-129-TCD For DREF; Date of issue: October 217 Expected timeframe: 3 months Expected end date: 27 January 218 Category
Page 1 Emergency Plan of Action (EPoA) Chad: Cholera outbreak DREF n MDRTD16 Glide n EP-217-129-TCD For DREF; Date of issue: October 217 Expected timeframe: 3 months Expected end date: 27 January 218 Category
EBOLA RESPONSE: WHERE ARE WE NOW? MSF BRIEFING PAPER DECEMBER 2014
 EBOLA RESPONSE: WHERE ARE WE NOW? MSF BRIEFING PAPER DECEMBER 2014 INTRODUCTION In early September 2014, MSF urged states with biological disaster response capacity to intervene in West Africa, where an
EBOLA RESPONSE: WHERE ARE WE NOW? MSF BRIEFING PAPER DECEMBER 2014 INTRODUCTION In early September 2014, MSF urged states with biological disaster response capacity to intervene in West Africa, where an
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Vancomycin-Resistant Enterococcus (VRE)
") Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
New Diarrhea Guidelines Look Toward a Healthy Future for Vietnam s Families
 DIARRHEAL DISEASE New Diarrhea Guidelines Look Toward a Healthy Future for Vietnam s Families the problem At the National Pediatric Hospital in Hanoi, Vietnam, one in ten pediatric inpatients is admitted
DIARRHEAL DISEASE New Diarrhea Guidelines Look Toward a Healthy Future for Vietnam s Families the problem At the National Pediatric Hospital in Hanoi, Vietnam, one in ten pediatric inpatients is admitted
Benefits of improved hand hygiene
 Hand hygiene promotion reduces infections. As a result, it saves lives and reduces morbidity and costs related to health care-associated infections. Benefits of improved hand hygiene Can hand hygiene promotion
Hand hygiene promotion reduces infections. As a result, it saves lives and reduces morbidity and costs related to health care-associated infections. Benefits of improved hand hygiene Can hand hygiene promotion