NHS Corby CCG Annual Report 2017/18
|
|
|
- Winfred Thomas
- 6 years ago
- Views:
Transcription

1 NHS Corby CCG Annual Report 2017/18 1
2 Contents Performance Report..4 PerformanceOverview...4 Clinical Chair Foreword 4 Accountable Officer's Introduction. 6 About Us.7 Our Main Providers Resetting our Priorities Key Issues Our Achievements in 2017/ Performance Summary Performance Analysis Sustainable Development Quality Report Engaging People and Communities Reducing Health Inequality Health and Wellbeing Strategy Accountability Report Corporate Governance Report Members' Report...64 Member Practices.65 Members Profiles Composition of Governing Body Committee(s), including Audit Committee Register of Interests Statement of Disclosure to Auditors Modern Slavery Act Statement of Accountable Officer s Responsibilities Governance Statement Emergency preparedness Remuneration and Staff Report
3 Remuneration Report Staff Report Parliamentary Accountability and Audit Report Other languages and formats Contact details Annual Accounts
4 PERFORMANCE REPORT Performance Overview Clinical Chair Foreword It is my pleasure to present NHS Corby Clinical Commissioning Group s (CCG) 2017/18 annual report. This document details the progress we have made in commissioning high quality health services on behalf of our local population over the past year. I have been Clinical Chair of NHS Corby CCG for the last two and a half months and continue to be passionate in my endeavours to properly serve the health needs of this population. NHS Corby CCG oversees most of the money spent on health services for the people living in and around the town. This includes the cost of hospital outpatient appointments, inpatient stays and operations, prescribed medicines, investigations, GP practice appointments and care, GP out of hours services, Corby Urgent Care Centre, community and mental health facilities, and many other services. This document also showcases how we have successfully worked closely with patients, members of the public, Corby Borough Council, Northamptonshire County Council, Kettering General Hospital NHS Foundation Trust, Northampton General Hospital, our Member Practices, CCG colleagues and health and social care professionals, to understand the needs of our community and to plan and buy healthcare services which best meet those needs. We are living though a challenging time for the NHS and I welcome the opportunity to meet these challenges and continue to deliver quality care for residents. Our priorities continue to include developing a greater emphasis on prevention for both physical and mental health, improving wellbeing and coordination of health and social care by working with partners and stakeholders and ensuring financial sustainability and cost-effective services, all while achieving and maintaining the NHS constitutional standards. We are proud of our achievements and progress made this year, due in no small part to our five-member practices and team of CCG staff, each dedicated to improving the health and wellbeing of the population we serve. I would like to express my thanks and appreciation to them all for their continued commitment as we look forward to the year ahead for NHS Corby CCG. Dr Joanne Watt, Clinical Chair NHS Corby CCG 4

5 Accountable Officer s Introduction Corby continues to be one of the fastest growing towns in England with an ever-increasingly diverse population and strong sense of community. I am pleased to report that during 2017/18 NHS Corby CCG made some notable progress on our key priorities. We have had a successful year in continuing to strive to improve health outcomes for the people of Corby and worked collaboratively with our stakeholders and patients to examine how we can best meet their health needs. To reduce avoidable emergency admissions to hospitals from care homes, we set up a proactive care home scheme which resulted in GP ward rounds every week in care homes. We also launched a successful and innovative pilot study aimed at earlier diagnosis for patients with sleep apnoea. Corby CCG measures its performance against national NHS standards. We and our providers successfully delivered many of the required standards in 2017/18 including: 6 Week Diagnostic Wait Corby CCG ensured over 99% of patients have access to a diagnostic test with 6 weeks of the referral Dementia prevalence diagnosis rate is above the required standard Not a single patient waited more than 12 hours in A&E for admission to a hospital bed 99% of patients requiring Psychological Therapies have had their treatment completed within 18 weeks (standard 95%) Significantly reduced the number of patients waiting 52 weeks or longer for elective care. However, it is still the case that access to services and recovery rates do remain challenging and we will strive towards further improvement in the coming year. The CCG has met the majority of the cancer waiting times standards but has unfortunately been challenged by the 62-day referral to treatment due to high numbers of multi-provider complex patients. We cannot avoid the financial realities of the NHS and the need to make sure we get the best health outcomes for our population, while making sure that local services are financially sustainable. This inevitably means we must demonstrate to our population we are getting the best value from all the services we commission. With this in mind we have worked closely with our colleagues at NHS Nene CCG to develop a joint operation plan which details the first two years of the over-arching five-year Sustainability and Transformation Plan (STP) for commissioners and providers in Northamptonshire. 5
6 We have worked hard to ensure that the joint operational plan for NHS Corby and NHS Nene meets all the NHS England business rules and meets our statutory responsibilities. Our STP means ever-increasing collaborative working across hospitals, GP s and community services in order to provide better care, better value and dealing with system issues for our local population. In my current dual role as Accountable Officer for Corby CCG and interim Accountable Officer for Nene CCG, I m looking forward to both CCGs continuing to build on existing close collaboration, and further focusing on integrating commissioning. This means us all working even closer together and harnessing the benefits of shared management teams. There are clearly challenging times ahead for the county s health and social care system, but this offers an opportunity for us to enhance wider collaboration with our partners to deliver services which improve the health and wellbeing of people across Northamptonshire. Together I look forward to further developing the work of the STP and the work streams which have been established. Staff may find themselves working as part of a multi-disciplinary/organisational team to ensure implementation of the STP which I hope will be welcomed in these transformational times. Carole Dehghani Accountable Officer NHS Corby CC 25 May
7 About Us NHS Corby Clinical Commissioning Group (Corby CCG) was established on 01 April 2013 under the Health and Social Care Act We are a clinically led membership organisation made up of five General Practices and are responsible for understanding the health needs of the people of Corby. The CCG was formed to improve health services for the people of Corby and to ensure that they get the best possible outcomes from services within primary care, in hospital and within the community. We achieve this through effective partnership working with national and local partners. NHS Corby CCG works closely with NHS England, NHS Nene CCG, Corby Borough Council, Northamptonshire County Council and a wide range of other local organisations and stakeholders including those in the voluntary sector to ensure services best meet the needs of the local population. As part of our NHS duty to improve quality NHS Corby CCG is committed to providing best value-for-money and the most effective, fair and sustainable use of finite resources. To aid this NHS Corby CCG and NHS Nene CCG have worked together to identify opportunities to maximise their effectiveness as commissioners. This has included aligning programmes of work, managerial and clinical leadership, governance and staffing. To oversee these new arrangements a Transition Programme was established, which will be in effect into the new financial year. Our Headquarters are based at: NHS Corby Clinical Commissioning Group Corby Enterprise Centre London Road Corby NN17 5EU Our website: Our Purpose and Activities NHS Corby Clinical Commissioning Group s mission is: To create a culture where individuals are supported to manage their own healthcare enabling people in Corby to live healthier, fuller lives. We aim to achieve this by setting out our responsibilities for commissioning healthcare for the people of Corby. The CCG Constitution describes the governing principles, rules and procedures which we have established to ensure probity and accountability in our day to day running. This ensures decisions are taken in an open and transparent way; and that the interests of patients and the public remain central to our goals. The constitution can be found on the CCG website. 7
8 Our Population Corby CCG s priorities for health and care in 2017/18 were based upon on the needs of our local population. We are responsible for commissioning most local NHS health services for the registered population of around 76,785 patients, and rapidly growing including 10,000 patients registered to our practices from outside the borough boundaries of Corby. Corby is in the county of Northamptonshire which continues to experience significant population growth, set to increase by 12% by Whilst the population has grown across all age groups, it has been particularly high for over 65-year olds and these trends are expected to continue. Corby is a town and Borough in the North East of Northamptonshire. It has a number of areas of deprivation which are in the top 20% most deprived areas in England, particularly located in and around the town centre. Socio-economic deprivation is an important health and wellbeing determinant. There are notable differences in life expectancy between the most and least deprived areas in Northamptonshire and nationally. The Borough is also expanding at a fast pace, growing by approximately 12,000 to circa 66,9007 in the past 13 years. The Office of National Statistics has reported the Borough to be in the top ten nationally for growth. Demography NHS Corby, as a small CCG, has a fast-growing population with an above-average level of social deprivation and a relatively high prevalence of smoking and obesity. Corby Borough is expanding at a fast pace, growing by approximately 12,000 in the past 13 years, to circa 66,900. The CCG s registered population has grown at a similar rate to circa 76,000. There are particular pressure points with a 44% growth in the 85+ population by 2026 and 22% growth in under 19s. The resident Corby Population is 64,000, whilst the registered practice population is 76,785. The health of people in Corby is varied compared with the England average: About 20% (2,700) of children live in low income families; Life expectancy for both men and women is lower than the England average; Life expectancy is 10.4 years lower for men in the most deprived areas of Corby than in the least deprived areas; 23.1% (167) of year 6 children are classified as obese, worse than the average for England; Levels of GCSE attainment, breastfeeding initiation and smoking at time of delivery are worse than the England average; The rate of smoking related deaths is worse than England average as are the estimated levels of adult excess weight and smoking. 8
9 Ethnicity Corby is less ethnically diverse than Northamptonshire or the East Midlands. Overall 95% of the population is estimated to be white, in particularly in the older age groups. Young people in Corby are more ethnically diverse, 88% of children prereception class were white. As the largest proportion of the population is the under 19 s and over 65 the urgent care needs will require increased children s urgent care and a focus on preventative primary care to reduce the need for reactive urgent care treatment. Population Growth NHS Corby CCG is one of the fastest growing populations in England with a considerable number of new housing developments planned across the borough. This growth in the population will need to be taken into account for the planning of health and care services in the new models of care. Key characteristics of the local population are: 0-19 year olds - the younger people population in Corby will have the biggest increase across Northamptonshire (5 year 10.9%, 10 year 21.8%); year olds - the working age population in Corby will increase again by 17% in 10 years time (5 year 8.5%, 10 year 17%); year olds - the over-65 year age group is predicted to increase by 25 % over 10 years (5 year 11%, 10 year 22%); and 85+ year olds - once people reach 85+, the increase is even more marked to nearly 45% over 10 years (5 year 22%, 10 year 44%). Growth in the Corby population is largely driven by existing ageing residents (of the 65+ age group) and the migration of younger, working people moving to the new housing developments as a commuter zone for London. The two populations have not merged, and engage with local services in line with national patterns that match their differing demographics. 9
10 Our commissioning responsibilities Our responsibilities are delegated to us from NHS England; the national body with a formal mandate to oversee the commissioning of health services in England by the Secretary of State for Health. Those known as Public Health services are now commissioned by local authorities. The accounts direction for CCGs is determined by NHS England and approved by the Department of Health (Secretary of State) and made under the following legislation: Health and Social Care Act 2012 c.7 Schedule 2 s.17. Our Allocation from NHS England for Commissioning in 2017/18 was 110m and the services we commission discharge our functions under Section 14Z15 Paragraph 2 of the National Health Service Act 2006 (as amended by the Health and Social Care Act 2012). The services we commission include: Urgent and emergency care including emergency department, ambulance and out of hours services (unplanned care) and the Urgent Care Centre in Corby Planned hospital care Community health services Mental health inpatient and community services Healthcare services for Older people Healthcare services for children and young people Healthcare services for people with learning disabilities Maternity Services Rehabilitation Services Continuing Healthcare Termination of pregnancy services Infertility Services Wheelchair Services Home Oxygen Services Treatment of infectious diseases. 10
11 Who we commission (or buy) services from The CCG has worked hard to commission high quality services making every effort to ensure that resources have been used economically, effectively and efficiently. The CCG commissions services primarily from the following providers: Kettering General Hospital NHS Foundation Trust (KGHFT) Northamptonshire Healthcare Foundation Trust (NHFT) Lakeside + Ltd (Corby Urgent Care Centre) Ramsey Healthcare (Woodlands Hospital) Northampton General Hospital (NGH) East Midlands Ambulance Services (EMAS). The CCG also has a range of other provider contracts including NHS 111, as well as other small contracts with various providers for specific services. More detail on Expenditure can be found in the Performance Report in Chapter 2. 11
12 The CCG s key strategic objectives are: 1. Prevention to prevent people becoming ill and to support people to live healthy lives. Targeting people at highest risk by working closely with our Member Practices, Public Health, Healthcare Providers and Local Authorities 2. Early Diagnosis to ensure that when people become unwell their condition is diagnosed early to ensure prompt treatment and secure better outcomes 3. Better Care to commission the right services for patients at the right time, in the right place, including end of life care 4. Commission to commission services in a way which provides seamless transition between providers, where patients need the support or intervention of primary care, community care, secondary care, social services or the voluntary sector 5. Quality to improve quality within all providers to ensure services are safe, efficient and effective 6. Engagement to engage patients, public and partner organisations to ensure that services are delivered at the right time, in the right place and to the highest quality 7. Sustainable to ensure a sustainable financial future for the CCG 8. Accountable - to be truly accountable to our population and have appropriate arrangements in place to discharge our functions effectively, efficiently and economically, and in accordance with the statutory framework and best practice principles of good governance and transparency. In September 2017 the Governing body added two overarching strategic corporate objectives, these are: Objective 1: Statutory Duties including finance, governance, cooperation. Objective 2: Health Inequalities and Access - five rights: Person, Condition, Place, Professional and Time. The CCG has developed an Operational Plan, see below, which details the activity and financial planning assumptions necessary to deliver these objectives and to achieve national performance targets and priorities. The Performance Report sets out the CCG s performance against national targets and priorities for 2016/17 and our key priorities for
13 The Northamptonshire Sustainability and Transformation Plan (STP) About the STP NHS Corby CCG is a key partner with NHS Nene CCG and the county s other leading health and care providers in the Northamptonshire Sustainability and Transformation Plan (STP). STPs have been set up across the country to find ways for organisations to work together on health and social care. The NHS is 70 this year, but health needs today are very different from when the NHS was set up, with people living longer and with more complex conditions. It has become clear that health services need to change if they are to meet those needs, now and in the future. STPs recognise that pressures on health and care cannot be addressed by organisations working in isolation but require an integrated approach. It is about transforming the ways in which we shape our services and work together so the care and support we provide can remain responsive and sustainable. The Northamptonshire STP covers the whole of the county and has been developed with doctors, other care professionals and members of the public. The organisations in the partnership include those from the health, social care and the voluntary sector. The aims of the STP Our core focus is to make practical improvements such as improving the way we share information about care, speeding up diagnosis and treatment for cancer, bringing more specialist care and treatments into local GP surgeries or offering help faster to people with mental illness. Through all our work we want to find the best ways to enable people to take more responsibility for their health and wellbeing. The STP has developed a plan setting out how services will change to improve care now and for the future. One example is our mental health crisis care concordat that has brought care providers together to shape access to local mental health crisis care. Another example is our recruitment leads who have worked together on the ground breaking Best of both worlds campaign, which pools our collective efforts and also works with private provider St Andrew s Healthcare and the University of Northampton to recruit health care workers into the county under one campaign. 13


14 Resetting our priorities Following NHS England guidance, our formal Sustainability and Transformation Plan was submitted as a working draft in June It was clear from feedback that we needed to reset our focus and think through the best ways to work together to address the priorities. In September 2017 we held an event to discuss what a local reset of our STP could focus on and how it could be shaped. The event brought together 65 stakeholders from 22 partner organisations and local stakeholder groups took part. We have clarified the most important areas for us to work together to improve outcomes for those we care for: urgent and emergency care primary, community and social care cancer mental health a unified model for acute care. Selecting these priorities doesn t mean that other areas of health and care are not important. By concentrating on these areas where we know we can make a difference, by being more efficient, coordinated and focussing on key outcomes, this will have a knock-on effect on other areas of care in our county this is the purpose of STPs and working together. Work on all these priorities will be underpinned by: a focus on prevention, health and wellbeing key support functions, such as technology, workforce, finance, estates and back office functions improved engagement and communication stakeholders working collectively to identify next steps in achieving our ambitions. 14
15 Additionally, throughout all work streams we will continue to address the three top priorities facing the NHS across the country: Health and wellbeing: By promoting healthier lifestyles, we can improve people s quality of life and reduce the pressure on our health and social care services. Care and quality: We want to ensure that needs are met by services of consistently high quality. Funding and efficiency: Efficient use of our limited resources is essential if our services are to remain effective, affordable and able to provide up-to-date treatments. Through all our work we are committed to engaging and working with the community to shape our future plans. Governance of the STP In September 2017, Angela Hillery, chief executive of Northamptonshire Healthcare NHS Foundation Trust took the STP lead role, and shortly before this the role of Programme Director was filled. In December 2017 the STP partners agreed an updated governance framework to ensure connectivity between all stakeholders. We are bringing together colleagues to support delivery of each aspect of the governance framework and the priority work streams as part of our reset and plan delivery. This governance framework represents a major change in how the organisations involved work together. Engaging all our stakeholders A core part of the structure is our collaborative stakeholder forum, which we are setting up with representatives of community organisations. It is crucial that to get we involve our staff, clinical experts, partner providers, patients, service users, carers and members of our community. Made up of key stakeholders to represent our community and quality engagement, this forum will provide engagement expertise and a crucial link between partners to ensure our community can input in the shape of our future provision. 15


16 Figure 1: Structure of Northamptonshire s STP It should be noted that as of the 1 April 2018 it known as the Northamptonshire Health and Care Partnership. Health and Wellbeing Board Health and Wellbeing Board workshops NHS Nene CCG s Chair, Dr Darin Seiger, is also a Vice Chair of the Northamptonshire Health & Wellbeing Board which is chaired by Councillor Sylvia Hughes of Northamptonshire County Council. The Health and Wellbeing Board has developed our countywide joint Health & Wellbeing strategy Supporting Northamptonshire to flourish. The Health and Wellbeing Board meets formally in public four times and has several development sessions per year. 16
17 These development sessions engage with a much wider range of organisations involved in the wider determinants of health and wellbeing in order that our local strategies and services fully meet the needs of our local population. There are 6 Health & Wellbeing Fora in the county, which are local versions of the countywide Health & Wellbeing Board. They have each agreed what their local priorities are depending on the needs of their local population and collaboratively work together to tackle these local health and wellbeing issues. The Health and Wellbeing Board is responsible for producing the Joint Strategy Needs Assessment, which identifies health and other needs in the county, and for the Health and Wellbeing Strategy. Working as a single system- The joint operational plan NHS Corby CCG and NHS Nene CCG are a part of the leadership model for the Northamptonshire Sustainability and Transformation plan (STP). Both organisations have always worked closely in the development of population-based strategy; however, they have not historically delivered integrated Operating Plans. The Operating Plan submission is the first integrated Operating Plan for the two CCGs and follows the formal issuing of Integrated Commissioning Intentions in September The plan sets out the CCGs commitment to jointly meeting the nine must do s 3 for and the processes supporting local delivery to provide assurance against key milestones and phasing plans. NHS Corby and NHS Nene CCGs are working together to answer the leadership challenge posed to us by our providers, stakeholders and populations. We aim to speak with one voice to our providers, In so doing we will reduce complexity and increase clarity for delivery. The system has commissioned a significant Organisational Development (OD) programme to support cultural change to deliver the single system approach. The CCGs are committed to drawing on national learning, best practice and targeted support programmes including the Right Care programme to drive change at pace and scale and ensure the clinical case and population case for change are co-produced. 17
18 Understanding the Local Challenges Our local challenges replicate the national challenges set out in the Five Year Forward View: Our population s health needs and personal preferences are changing, and our services do not always align with this change in demand The opportunity to use new technologies and approaches needs to be maximised further and faster Our population demographics are changing and require a different response from services to maintain and improve quality and ensure safety We have workforce shortages, key skills gaps and issues with modern working practices. These issues are driving up service cost and affecting our ability to provide the quality of service our patients require to keep them well General Practice is experiencing significant pressure and recruitment and retention has been impacted. There are a number of more specific local factors which impact on health and care outcomes: Our health and care sector includes a number of large independent providers which has an impact on the access profile of our local population There is significant population growth across all age groups in relation to new community developments Recruitment and retention is significantly influenced by the position of Northamptonshire with impact in relation to GPs, Paramedics, nurses and other key groups including social care professionals There is significant variation in the demographics across the county requiring different targeted solutions The configuration of our providers and the current commissioning landscape impact on cost and financial sustainability Some of our patients are experiencing poor access and quality of care from a range of our local providers. This is reflected in poor performance of the Accident and Emergency (A&E) 4-hour wait, Referral to Treatment Time (RTT) waiting times, (EMAS) response time and handover times and cancer waits. We are working with providers to support actions for improvement. 18
19 Local Operating Context There are a number of critical operating factors within Northamptonshire which impact on the position of health and care services within the county. This operating context supports the drive for change within the county to ensure high quality care for all and the most appropriate use of resource to ensure sustainability: Quality, safety and minimising harm The health care system has not been able to routinely maintain core constitutional standards in relation to A&E, RTT and Cancer Where organisations are in dual turnaround the impact on the organisation s financial position is significant CQC reports highlight a number of areas that require improvement Agency spend in some organisations falls into the highest agency spend band for England. Infrastructure and Estate The local model for community services has a high bed base and high overheads associated with investments to that estate and infrastructure Some local estate provides challenges in regards to its age and suitability for the provision of modern healthcare services Long term PFI contracts within the care sector are less able to move at pace to meet changing patterns of demand New contractual models that drive different outcomes from the estate are required ICT arrangements pose a challenge to delivery. Integration and models of care delivery Our Local Authority is recognised to be financially challenged which impacts on the ability to deliver change through enabling frameworks such as the Better Care Fund (BCF) The pace behind the integration of health and care continues to impact on patient flow. 19
20 GP Forward View As with the Operating Plan and the STP, NHS Corby CCG and NHS Nene CCG have chosen to work together to deliver this important plan which aims to improve and make more sustainable the delivery of Primary Care for Northamptonshire patients. For the majority of our populations, their first point of contact with health services comes with a visit to their local GP. The plan adds the context of what will need to happen in the delivery of primary care and specifically general practice to link these developments within the local STP. These themes continue with the plan which details our current intentions for primary care investment in line with operating plan guidance and in line with transformation plans. The document is not intended to replicate the narrative plan of the STP but demonstrate the alignment between the STP and the plans for implementation of the GP Forward View. NHS Corby CCG has had fully delegated responsibility for general practice contracts since April Our approach is to base our foundations of delivery in the individual practices that our populations have as a first point of contact with the health system. We have a plan of action which describes how through supporting individual practices, we will enable them to work with other practices primary care at scale to improve their offer to their own patients. Finally, the plan describes how primary care delivery will fit into the new models of care that will meet the changing needs of our population, as part of a new care model. Our new care models are beginning to integrate primary, community and other out of hospital providers with specialist support from the acute trusts to develop a robust, comprehensive out of hospital care offer. Every Practice Our vision is that there is consistent high-quality care across all Corby GP Practices, by providing consistent approaches to access and navigation so that local people understand better what their general practice can do for them and what services are available as an alternative. 20
21 Primary Care at Scale We are supporting the development of Primary Care at Scale and further detail can be found later in the Performance Report. Key Issues for 2018/19 Our priorities for 2018/19 are enshrined in our commissioning intentions; the key highlights are: As separate statutory bodies Corby and Nene CCGs are speaking with one voice to all providers This year the commissioning Intentions start with the patient pathway at their centre and focus on quality and clinical variation. This approach will demonstrate the changes required in each setting of care (prevention and self-management, primary care, enhanced primary and community care, intermediate care and acute care) to improve the overall management of health conditions. We aim to clarifying the balance between emergency care, non-elective spells and the elective options we need to offer our population. We will: Improve health outcomes and reduce variation Lead the way to safety and quality through commissioning Make best use of resources Build a health system fit for our population and maximise the opportunity to deliver across health and social care Our commissioning intentions are set within the context of unprecedented sustained and significant financial challenge across health and social care requiring new models of care, greater collaboration and joint working, a focus on prevention and self-care The move away from a traditional commissioner/provider split will reduce transactional costs and the move to an Accountable Care System (ACS) must ensure that best value opportunities are realised. This cannot reduce a focus on safety and quality across services and organisations and the necessity to drive continuous improvement across care pathway. 21
22 What does this mean in relation to primary care? For Primary Care this means working through our GP Forward View plans to secure high quality primary care services for the population of Northamptonshire from each of our practices. Continuing to utilise Personal Medical Services (PMS) reinvestment monies to: Increase the use of e-referral across the County Improve access to 24-hour blood pressure monitoring Support leg ulcer management and spirometry in general practice Commission ear syringing from general practice and Secure other services from general practice not remunerated through the core contracts Continue to encourage practices to work in partnership over populations of 30-50,000 to provide same day care at scale and develop their shared multidisciplinary team at the same time. We will continue to use the GPFV transitional OD monies to support this transformation. Continue to encourage provision of local enhanced services at scale through practices working together and secure safe and sustainable services for the whole population not by virtue of the practice people are registered with. Complete the review of near patient testing we have already started and look at services that are related to this like anticoagulation and phlebotomy to ensure adequate community capacity for these services is commissioned in accordance with the evidence base. Review the provision of ECGs in primary care to ensure adequate community capacity is used to the maximum. The priority in 2017/18 has been to create a solid platform in clustering practices to deliver same day primary care at scale and collaborative care teams. Community services have begun to pilot configuration of selected services to support primary care homes in a few areas. The development of this extended primary care family is what we mean by enhanced primary care. In 2018/19 the CCGS will support further development and reconfiguration of priority community services around primary care homes (specifically physiotherapy, community nursing and mental health support). Explore elective services within primary care homes that are either underutilised currently or need additional capacity to support primary care home needs. Continue to support practice clusters and their extended family to innovate in the use of technology to share information and process across services. Work with all providers to actively support the coming together and development of multidisciplinary extended primary care family teams in our primary care homes. Extend work done in 2017/18 on in hour s access at scale to establish a sustainable approach to provision of extended hours in primary care as part of the GP Forward View that utilises the extended primary care team. Continue engagement with the public about where the gaps are today and what their priorities might be for joined up services in primary care. 22
23 Key Achievements New patient representative group for Corby CCG Corby CCG formed a new patient representative group for people with an interest in how health services are delivered in the borough. The group were asked for their views, experiences and insight into a range of the CCG s activities and plans as it continued to review and develop health services across Corby. Members of the group are not expected to attend regular meetings but instead operate as a virtual group. The only criterion for joining is that people are registered with a Corby GP surgery. Anyone interested in finding out more can info@arch-comms.co.uk Sleep Disorder Pilot Scheme Corby CCG s launched an innovative pilot scheme for patients with a suspected sleep disorder, saving them time and inconvenience. The pilot means that local patients with suspected Obstructive Sleep Apnoea need no longer sleep overnight at clinics in Northampton or Leicester for an initial diagnosis. See news story We were the first CCG in the country to trial the technology which reduces the need for patients to undergo sleep studies by pre-filtering those patients who do not have sleep apnoea. The Trial started rolling out in October 2017 and ran until the end of March. Results show that 69 people who would previously have been referred to secondary care had the practice based test. Some 41 were subsequently onwardly referred to secondary care for further assessment and treatment, therefore 28 of those tested did not have Sleep Apnoea their disturbed sleep was down to other medical/physical issues. This cohort could commence appropriate care without the delay created by having to undergo a sleep study that would have ultimately resulted in a negative result. Harnessing the Local Media We proactively approached the local media to urge businesses in the town to join a local employer RS Components in training people in mental health first aid. Mental Health First Aid (MHFA) is an internationally recognised training course, designed to teach people how to spot the signs and symptoms of mental ill health and provide help on a first aid basis. Corby s RS Components has more than 2,000 employees on site and has trained 15 of their staff members so they can recognise the signs of anxiety, depression and many more mental health conditions. See news story 23
24 Partnership Working Stop Smoking NHS Corby CCG also teamed up with First for Wellbeing to raise awareness about the health benefits of stopping smoking NHS Corby CCG s communications team teamed up with First for Wellbeing and the Corby Telegraph to publicise how to access advice, support and information to raise awareness about the health benefits of stopping smoking. This came about when the latest Office for National Statistics figures showed that Corby again has the country s highest smoking rate % of men and 28.3% of women smoke. The story gained front-page coverage and a twopage spread in the Corby Telegraph, which also published the story online. It can be viewed here. Investors in Carers GP Accreditation standard NHS Corby CCG has worked closely with Northamptonshire Carers in 2017/18 to ensure that GPs in their five practices identify, register and refer carers to services which may be of use. The partnership also aims to ensure that GPs take needs of carers into account on home visits. In 2014 Northamptonshire Carers launched the Investors in Carers GP Standard accreditation scheme, available to all surgeries in Northamptonshire. The scheme aims to improve identification of and support available to carers, acknowledge work undertaken to support Carers by Northamptonshire GP teams and to provide an accredited framework for GP teams within which to develop services and good practice. Modelled on similar schemes operating in other parts of the UK, it is hoped that it may become part of a nationally recognised Investors in Carers Standard. There are four levels of attainment: Bronze, Silver, Gold and Gold Plus. In 2017/18 Great Oakley Medical Centre was recognised with the Silver award, Lakeside Healthcare, Corby and Woodsend Medical Centre with the Bronze award and Corby Studfall Partnership and Corby Studfall Medical Centre are continuing to work towards the accreditation. 24

25 Armed Forces Covenant In 2017 Corby and Nene CCGs were awarded the Bronze Award in the Armed Forces Covenant, Employer Recognition Scheme in recognition of our continued work with members of the Armed Forces, Cadet Forces, Reservists, Veterans and their families including: Identifying gaps across the system Working together to achieve the best outcomes Addressing any issues that have been identified locally Peer support Keeping informed of new services for Veterans in the area Ensuring Veterans are signposted quickly and efficiently to the correct support services including our voluntary sector. The armed forces covenant sets out the relationship between the nation, the government and the armed forces. It recognises that the whole nation has a moral obligation to members of the armed forces and their families, and it establishes how they should expect to be treated. National GP Patient Survey Results In NHS Corby CCG, 1,582 GP Patient Survey questionnaires were sent out, and 562 were returned completed. This represents a response rate of 36%. We are proud to announce that the CCG is rated as one of the highest CCGs nationally for 'confidence and trust in their GP,' 'confidence and trust in their nurse' and 'helpfulness of receptionists.' We recognise areas of concern which include; 'convenience of appointments,' 'experience of making appointment,' 'waiting time,' 'satisfaction of opening times' and 'satisfaction of out of hours.' These issues were reflected in the results of a survey we carried out earlier this year when we asked the people of Corby what they thought about healthcare services in the town. Variation between surgeries exists so the situation is complex, but the CCG is currently exploring ways of improving GP access and addressing these issues. Further information about individual practice results can be found on the NHS GP Patient Survey site: 25
26 Diabetes Success Lakeside Surgery in Corby was recognised for referring a high number of patients to the Healthier You: NHS Diabetes Prevention Programme. The team at Lakeside received the Practice Champion Award, presented to practices which have generated the highest referrals to the programme. The practice made 104 referrals in January. Practices in Corby CCG made 170 referrals in the same month. Members of the public were asked to complete the Diabetes UK Risk Tool and if considered to be at increased risk they were offered an HbA1c blood test. Patients who had a blood test indicating that they were at high risk of diabetes were provided with information about the Healthier You: NHS Diabetes Prevention Programme and if they consented, they were referred directly to the programme. 26
27 Performance Summary Corby CCG monitors service performance against national performance standards, including those set out in the NHS Constitution. Where standards are not met, the CCG works closely with providers and other partners to define and deliver robust actions to improve and recover performance. NHS services in Northamptonshire share similar challenges impacting NHS services nationally. In particular rising levels of non-elective demand and delayed hospital discharges, predominantly due to challenges meeting social care demand. These challenges have impacted not only impacted on urgent care performance in terms of A&E access and ambulance response times but also on elective care resulting in a large number of cancelation of routine elective activity release bed capacity and clinical time to deal with the urgent care pressures. Northamptonshire health care and social care partners continue to work collaboratively to improve the situation. The CCG has met the majority of the cancer waiting times standards in 2017/18; however, has struggled with 62-day referral to treatment due to high numbers of multi-provider complex patients. 18 week waiting time standard for planned care is an underperformance at KGH due to historic backlog. The CCG continue to work with KGH to improve the position, however this has been affected by the urgent care pressures. 27
28 Performance Analysis Corby CCG measures its performance against national NHS standards. We and our providers successfully delivered many of the required standards in 2017/18 including: 6 Week Diagnostic Wait Corby CCG have ensured over 99% of patients have access to a diagnostic test with 6 weeks of the referral Dementia prevalence diagnosis rate is above the required standard Not a single patient waited more than 12 hours in A&E for admission to a hospital bed 99% of patients requiring Psychological Therapies have had their treatment completed within 18 weeks (standard 95%) Significantly reduced the number of patients waiting 52 weeks or longer for elective care. The challenging areas that require our continued focus in 2018/19 are: A&E four-hour performance at both of Northamptonshire s acute hospitals Delivery of the new Ambulance Response Programme waiting times Continuing the improvement seen in delivery of 62-day waiting time standards at Northampton General Hospital NHS Trust Ensure Kettering General Hospital FT continue to deliver all cancer performance standards Preventing decline in the 18-week Referral to Treatment time for planned care Reducing the number of 52+ week waits for planned care to zero Improving Psychological Therapies, access and recovery rates. Corby CCG and its partners are working with all providers to ensure detailed improvement plans for each of these areas are implemented. All Key Performance Indicators (KPIs) in relation to NHS performance standards are tracked, using regular data provided by the relevant providers. Corby CCG holds a monthly operational contract meeting with each of the providers, to review their performance either directly or through national reporting systems and gain assurance where issues arise that robust action is being taken. In addition, regular meetings are held between the relevant performance leads to discuss the issues in detail. Northamptonshire also has working groups in place to ensure performance is delivered in key areas, including the Urgent Care Working Groups and the Cancer Improvement Working Group. All performance issues are escalated to the Corby CCG and Nene CCG Joint Quality Committee and the Corby CCG Governing Body. The Governing Body considers performance at every meeting. 28

29 Friends and Family Test Since December 2014 it has been requirement for all GP practices in England to undertake the NHS Friends and Family Test (FFT). The FFT is a feedback tool which supports the principle that people who use NHS services should have the opportunity to provide feedback on their experience that can be used to improve services. It is a continuous feedback loop between patients and practices. The FFT on its own does not provide results that can be used to directly compare practices - there are other robust mechanisms for that, such as national GP Patient Survey and outcomes measures - but, for each practice, it can inform current and prospective patients about the experiences of those who use the practice s services and help mark progress over time. More information can be found All practices across Corby CCG participate in FFT. During the 12 months (to date) practices are demonstrating an average of 90% of patient would recommend their practice whilst 6.7% of patients would not recommend. This is slightly higher than the all England average of 89% of patients would recommend whist 5.9% would not recommend. Figure 2: Friends and Family Test, 12 Month Average by practice 29
30 Finance Report The main areas of expenditure for the CCG during 2017/18 can be seen in Figure 3 below, the CCG had a total net spend of 108m including an administration cost allocation of 1.558m. This was our second year of holding fully delegated primary care budgets which accounted for 9.9m (9%) of the total allocation. Our core allocation (not including delegated primary care) increased by 3.16% from 16/17 moving the CCG to being only 3.8% below our fair share target allocation. Looking ahead to 2018/19 the CCG has received 3.96% growth on our nondelegated allocation which reduces the distance below target to 3.08%. Our delegated budget has increased by 5.1%. Figure 3: Main areas of expenditure for the CCG during 2017/18 4.5m,4% 2.4m,2% 9.5m, 9% 1.9m,2% 11.1m,10% 59.0m,55% 8.6m,8% 9.6m,9% Total Acute services Total Mental Health Services Total Community services Total Prescibing Services Total Primary Care Services Total Delegated Primary Care services Total Continuing Care Total Other Healthcare 30
31 Statutory Financial Duties In 2017/18 the CCG achieved its statutory duties in relation to accounting and financial standing. The achievement of these duties is detailed Figure 4 and further detail can be found in the annual accounts. Figure 4: Statutory Financial Duties Duty Target Performance Target Performance Expenditure not to exceed income 110, , Capital resource use does not exceed the amount specified in Directions Revenue resource use does not exceed the amount specified in Directions Revenue administration resource use does not exceed the amount specified in Directions n/a n/a , , , ,301 1,558 1,540 1,538 1,527 31
32 Performance against NHS Constitution and supporting measures Table 1: Urgent Care - Patients waiting four hours or less in A&E NHS Constitution measures - quarterly Std Organisation Q1 Q2 Q3 Q4 Total A&E waits Patients to be admitted, transferred or discharged within 4 hours of arrival at A&E 95% NGH 87.18% 88.54% 84.23% 82.66% 85.57% KGH 86.28% 85.66% 76.75% 68.80% 79.44% Delivering the A&E four-hour standard is a national challenge and Northamptonshire is no exception. There are a number of reasons: demand from patients with more complex care needs (for example, the frail and elderly), internal hospital operational challenges and delays in moving patients from NHS to social care services run by the local authority. The CCG continues to work with partner organisations across the whole health and social care system to improve urgent care performance and resilience. Both acute trusts Northampton General Hospital NHS and Kettering General Hospital NHS Foundation Trust - have experienced extreme pressure on their urgent care systems during the winter period, in spite of robust plans and additional funding. However, both trusts have managed to avoid any patients waiting more than 12 hours for a bed in A&E. Table 2: No waits from decision to admit to admission (trolley waits) over 12 hours NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total No waits from decision to admit to admission (trolley waits) over 12 hours 0 NGH KGH
33 Corby CCG and our partners are committed to ensuring that the system is robust, and we have developed a number of initiatives. These initiatives are broken down into three areas of focus; inflow, internal flow and outflow. Examples of the key inflow (reducing the number of patients arriving at the acute A&E) initiatives are listed below: Proactive care homes scheme Ensuring that care home are looking for the signs of illness so that patients can be seen before their condition worsens to the point of needing hospital admission Acute Psychiatric Liaison Basing acute psychiatric liaison services in the acute hospitals ensure timely assessment of patient attending A&E EMAS Frail Elderly Liaison Officer Have a paramedic dedicated to reviewing 999 calls coming from care homes to ensure the patients get referred onto the most appropriate pathway EMAS GP visiting scheme Using paramedics to supplement the GP home visiting service to ensure patients have timely access to primary care services hence reducing the number that have to use A&E as unable to access their GP Co-locating Out of Hours (OOH) GP into acute hospitals Basing the OOH service at the main hospital sites allows patients to be quickly directed from A&E to OOH or vice versa. Ensuring patients get timely effective care Emergency Care Centres in Town centres EMAS have provided static treatment centres in Northampton & Kettering on predicted busy nights in order to reduce demand on 999 and A&E. In addition to working with reduce demand for the A&E units the CCG has also worked with the acute trusts are improving internal flow (this is the process of ensuring patients move through the hospital assessment & treatment systems efficiently: Additional medical resources being placed at the front door The hospitals have placed senior specialist doctors in A&E to review patients early prior to admission. This process reduces the number of patients requiring admission Criteria-led discharge Senior medical staff create a clear set of discharge criteria for a patient, once this is met the patient can be discharged without a further consultant review. This ensures patients can leave hospital as soon as they are ready to. 33
34 Additional discharge facilitators The additional of discharge facilitators ensures improved communication between hospital, community services and the patient. This helps ensure patients can go home sooner New GP streaming area (NGH only) Walk in patients will be seen as soon as they walk in to A&E by a streaming practitioner, who can divert them to the most appropriate care in a timely fashion Moving assessment areas to be co-located (NGH only) Co-location of assessment areas allows more effective working, ensuring that patient have access to all the professionals needed to assessment / treatment in a timely fashion Hospital at home services (KGH only) Some patient requiring hospital treatment can now be discharged earlier and then treatment completed in their own home. The final area of focus is outflow; this is the process of ensuring that once acute hospital care is no longer required the patient has a place to transfer to or the support they need in their own home. Spot purchase of community beds Buying nursing or care home beds for patients that do not require hospital care but aren t able to return home. This ensures beds are available for those who do Multi Agency Discharges Events at both acute trusts These events bring in partners across the healthcare system to go to the acute hospitals to review patients to ensure that they have a plan for discharge and solve any problems Discharge to Assess Patients are discharged home with support, once at home the amount of support required is assessed, this enable patients to be discharged quicker and ensure the correct level of support. 34
35 Ambulance response times Table 3: Ambulance response times Old ambulance response measures Category A calls with emergency response arriving within 8 minutes (Red 1) Category A calls with emergency response arriving within 8 minutes (Red 2) Category A calls with ambulance arriving at the scene within 19 minutes Standard Organisation Q1 Q2 Q3 Q4 75% EMAS 72.07% N/A N/A N/A 75% EMAS 57.4% N/A N/A N/A 95% EMAS 85.57% N/A N/A N/A Table 4: New datasets from August 2017 quarter data based on Sep / Dec / Mar New NHS Constitution measures Category 1 - Mean Category 1-90th centile Standard Q1 Q2 Q3 Q4 YTD 00:07:00 n/a 00:08:16 00:09:38 00:09:46 00:09:46 00:15:00 n/a 00:14:52 00:17:11 00:17:31 00:17:31 Cat 2 - Mean 00:18:00 n/a 00:26:40 00:39:29 00:45:06 00:45:06 Cat 2-90th Percentile Cat 3-90th Percentile Cat 4-90th Percentile 00:40:00 n/a 00:56:35 01:26:08 01:40:18 01:40:18 02:00:00 n/a 03:02:38 03:59:57 04:15:55 04:15:55 03:00:00 n/a 04:16:55 04:42:22 02:58:01 02:58:01 35
36 What we are doing Nationally the ambulance service has moved this year to a new system of monitoring performance called Ambulance Response Programme. EMAS and the regional CCGs have been conducting a review to look at resourcing required to achieve the new standards. The report shows that some changes in EMAS s rota and control processes would reduce waiting times. A wider discussion is taking place across the region to ensure EMAS has the resources available to meet the new standards. Ambulance handovers All handovers between ambulance and A&E must take place within 15 minutes and crews should be ready to accept new calls within a further 15 minutes. Please note data for this measure is EMAS data and can differ to the acute trusts A&E data. Table 5: Ambulance Handover Times NHS Constitution Support Measures (Quarterly) Standard Trust Q1 Q2 Q3 Q4 Year Handovers between ambulance and A&E within 15 mins and crew ready for new calls within 15 mins (delays of over 30 mins) Handovers between ambulance and A&E within 15 mins and crew ready for new calls within 15 mins (delays of over 1 hour) 15 Mins 15 Mins NGH ,121 3,281 KGH 1, ,329 1,726 4,969 NGH KGH ,280 What we are doing The key driver in delays in ambulance handover is normally that A&E departments are beyond capacity. The actions we are taken which are detailed in the A&E sections will play a major role in resolving ambulance handover issues. In addition to those actions the Urgent Care Board continue to work with EMAS and both A&Es to improve processes on dealing with ambulance handover. The CCG has a clear escalation process for management of long delays. 36
37 Cancer Waiting Times Table 6: Cancer Waiting Times 2 week wait NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total Cancer waits 2 week wait Maximum twoweek wait for first outpatient appointment for suspected cancer Maximum twoweek wait for first outpatient appointment referred urgently with breast symptoms 93% 93% Corby CCG 95.89% 97.15% 98.40% 95.41% 96.72% NGH 89.34% 81.86% 85.64% 92.23% 87.23% KGH 96.59% 97.44% 98.43% 95.89% 97.08% Corby CCG 96.15% 97.87% 97.78% 100.0% 98.02% NGH 65.83% 39.67% 63.31% 89.51% 64.46% KGH 93.75% 98.21% 98.97% 99.07% 97.50% 37
38 Table 7: Cancer Waiting Times 31 day waits NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total Maximum one month wait from diagnosis to first definitive treatment for all cancers 96% Corby CCG 97.98% 97.98% 98.78% 98.53% 98.28% NGH 95.69% 97.20% 96.65% 97.49% 96.77% KGH 100.0% 99.39% 99.73% 98.89% 99.50% Cancer waits 31 day Maximum one month wait for subsequent surgical treatment Maximum one month wait for subsequent anti-cancer drug treatment 94% 98% Corby CCG 90.91% 100.0% 92.86% 57.14% 84.62% NGH 93.94% 92.50% 97.56% 92.11% 94.08% KGH 100.0% 100.0% 100.0% 100.0% 100.0% Corby CCG 100.0% 98.31% 97.30% 100.0% 98.89% NGH 97.10% 96.53% 98.70% 95.52% 97.03% KGH 100.0% 100.0% 100.0% 100.0% 100.0% Maximum one month wait for subsequent radiotherapy treatment 94% Corby CCG 93.55% 100.0% 93.55% 92.31% 94.87% NGH 95.80% 96.38% 96.82% 97.32% 96.90% KGH 100.0% 100.0% 100.0% No pts 100.0% 38
39 Table 8: Cancer Waiting Times 62 day waits NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 YTD Maximum two month wait from urgent GP referral to first definitive treatment 85% Corby CCG 88.64% 72.97% 78.57% 85.29% 81.53% NGH 75.61% 78.03% 83.65% 86.62% 81.07% KGH 89.06% 85.25% 85.87% 89.38% 87.34% Cancer waits 62 day Maximum two month wait from referral from an NHS screening service to first definitive treatment 90% Corby CCG 100.0% 100.0% 83.33% 100.0% 97.50% NGH 92.05% 93.18% 90.00% 92.42% 91.99% KGH 94.68% 93.10% 94.94% 96.30% 94.87% Maximum two month wait for first definitive treatment following a consultant s decision to upgrade N/A Corby CCG 80.00% 85.71% 100.0% 100.0% 89.47% NGH 85.00% 77.55% 98.00% 86.08% 86.70% KGH 70.73% 86.84% 93.22% 95.12% 87.15% Corby CCG s has seen good performance in relation to for the 31 day wait from the date of a decision to treat and 2 week wait from GP referral to specialist review. However, the CCG has struggled to consistently meet the 62-day wait from an urgent GP referral for a patient with suspected cancer to first definitive treatment; this has been due to a relatively high number of complex patients that have required transferring between providers. The CCG s largest provider, KGH, has maintained their all their cancer standards and is currently performing well. 39
40 What we are doing While there are challenges specific to each hospital, some issues are faced by services across the system. In response, the Northamptonshire Cancer Board was set up, bringing together Corby & Nene CCGs, primary care, Kettering General Hospital Foundation Trust, Northampton General Hospital, East Midlands Cancer Alliance and NHS England. All organisations individual strategies and plans have been consolidated into a high-level work plan to ensure that all services are working on the same key priority areas to improve cancer services across the county. In addition, both NGH and KGH have their improvement plans and their own internal Cancer Boards. From April 2017, Corby CCG has worked closely with the newly formed East Midlands Cancer Alliance to drive a new approach to transforming care, including prevention, diagnosis, early intervention and treatment. These groups are already seeing results. In 2017/18 we completed the following actions o o o o o o Conducted reviews of cases where patients missed 62-day waiting time, to share learning and make improvements Successfully bid for funding to test a pathway for patients who go to their GP with non-specific symptoms that might be cancer Improved communications between GPs and hospitals, for example, the development of good practice ultrasound guidelines to help select patients for whom ultrasound would be beneficial in terms of diagnosis and disease management Developed closer working links with Leicester hospitals to support timely transfer of patients referred on to a specialist treatment centre Established an Early Detection board for the county to help increase awareness of risk factors and health promotion, improve screening uptake, and increase awareness in general practice of the signs and symptoms that might be cancer. Agreed funding for a Living with and Beyond Cancer programme for the county to ensure that people who have cancer or have had treatment are leading as healthy and active a life as possible. Priorities for cancer care for 2018/19 The Cancer Pathways & Performance working group has identified key issues and pathways to drive continued improvement in 201/19, including: Improve communication between GPs and acute hospitals regarding patient choice and delays initiated by patients Implement the Faecal Immunochemical Test (FIT) to improve diagnosis of bowel cancer 40
41 Begin to implement the Nation Optimal Lung Pathway to reduce referral to diagnosis times for lung cancer patients Implement the rapid prostate pathway to streamline the referral process for prostate cancers and reduce treatment waiting times In addition, the CCG will continue to monitor all aspects of the cancer pathway to ensure that rapid action is taken to correct any emerging issues Planned care Table 9: Referral to treatment (RTT) Quarterly data based on Jun /Sep / Dec / Mar NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total Referral To Treatment (18 weeks) Patients on incomplete non-emergency pathways (yet to start treatment) 92% Corby CCG 80.62% 83.67% 81.37% 79.11% 79.11% NGH 92.02% 92.19% 91.10% 87.38% 87.38% KGH 76.03% 80.56% 79.65% 77.09% 77.09% This standard requires that at least 92% of patients waiting for consultant-led treatment have been waiting less than 18 weeks. Northampton General Hospital met this standard until December 2017, but having to cancel planned operations over the winter period due to the pressures on unplanned care saw them slip below the standard. Because of significant data quality issues, Kettering General Hospital did not submit national data for the 18-week referral to treatment standard and diagnostics between 2015 and It has a significant backlog of lengthy waits and corresponding under performance. What we are doing In order to improve performance at Kettering, Corby CCG has worked, as the lead commissioner for the hospital, closely with Nene CGG and the Trust itself to ensure a comprehensive recovery plan is in place and that robust systems are used to monitor and address the risk of harm. Kettering started reporting again in March 2017 and steadily improved performance from April until November, when winter pressures affected planned care. It has continued to reduce the number of patients waiting for 52 weeks, and is on course to have no patients waiting more than 52 weeks in the next few months. 41
42 Table 10: Quarter data based on Jun/Sep and Dec/Mar NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total No patient should wait over 52 weeks from Referral To Treatment (Incompletes) 0 Corby CCG NGH KGH *the KGH number is the total for all providers. Corby and Nene CCGs are working together to transform planned care in Northamptonshire with the aim of reducing the pressure on the acute hospitals by looking at alternative ways that patients with less complex needs can be safely treated. Diagnostics Quarterly data based on Jun /Sep / Dec / Mar This standard requires that no more than 1% of patients wait over 6 weeks for a diagnostic test. Corby has consistently met the diagnostics during 2017/18. Table 11: Diagnostic test waiting times NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total Diagnostic test waiting times Patients waiting for a diagnostic test waiting less than 6 weeks 99% Corby CCG 99.61% 99.91% 99.16% 98.89% 98.89% NGH 99.41% 99.89% 99.92% 99.87% 99.87% KGH 99.10% 99.77% 99.01% 99.11% 99.11% 42
43 Mental Health Table 12: Dementia Diagnosis Quarterly data based on Jun /Sep / Dec / Mar NHS Constitution measures Dementia prevalence diagnosis rate Std Organisation Q1 Q2 Q3 Q4 Total 66.7% Corby 85.34% 85.45% 85.78% 84.00% 85.14% What we are doing We delivered training for GPs to improve diagnosis of patients with dementia. This has helped push diagnosis recognition above the standard. We will continue to monitor this to ensure compliance is maintained. Table 13: Improved Access to Psychological Therapies (IAPT) * There is no IAPT data published yet for Quarter 4 this is not due out until end June NHS Other Support Measures Standard Org. Q1 Q2 Q3 Q4 YEAR IAPT access (Monthly) IAPT access proportion (rolling) 1.40% per month Corby CCG 3.37% 4.71% 3.59% 16.80% Corby CCG 3.37% 8.08% 11.67% No data available at time of publishing% IAPT recovery rate 50% Corby CCG 43.33% 44.00% 43.33% TBC #DIV/0! % completed 75% by TBC Corby CCG 71.33% 60.33% 74.00% treatment 6 weeks year end #DIV/0! TBC TBC % completed treatment 18 weeks 95% by year end Corby CCG 99.33% 99.00% 99.00% #DIV/0! TBC There are two performance standards for Improving Access to Psychological Therapies (IAPT); one relates to ensuring appropriate access and the other to recovery rates following IAPT. We did not meet the majority of the standards in 2017/18. What we are doing We are working closely with Northamptonshire Healthcare NHS Foundation Trust, who provide the majority of our community and mental health services, to address these issues. Since January 2017, self-referrals have been accepted, and has had resulted in an increase in the number of referrals in 2017/18 year. 43
44 The current referral and booking management systems have been overhauled. The hubs have had a positive impact on the quality of referrals and improved waiting list management. The data quality issues identified by the review of the IAPT service are being addressed by Northamptonshire Healthcare through improved processes and will be closely monitored by Corby CCG. NHS Other Measures More detail on Corby CCG s performance against the NHS Constitution and supporting measures can be found in the tables 14, 15 and 16 below: Table 14: NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total No Mixed Sex Accommodation breaches 0 Corby CCG NGH KGH NHFT Table 15: NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total No urgent operation to be cancelled for a second time 0 NGH KGH Table 16: NHS Constitution measures Std Organisation Q1 Q2 Q3 Q4 Total Operations cancelled, on or after the day of admission to be offered other binding date within 28 days. 0 NGH KGH
45 Both Operations cancelled, on or after the day of admission to be offered other binding date within 28 days and No Mixed Sex Accommodation breaches have seen a deterioration in Q3 and Q4, this is due to a government directive to focus on emergency care during December and January. The government directive also effectively suspended the Mixed Sex Accommodation target from December to March. From April 2018 these standards are expected to be achieved again. Sustainable Development NHS Corby Clinical Commissioning Group (CCG) is committed to providing high quality sustainable healthcare in the town and is committed to embedding sustainability into its operations and encouraging key partners and stakeholders to do the same. The CCG is committed to promoting environmental sustainability and to continually improve the quality of their services and environmental performance. The CCG headquarters is within the Corby Enterprise Centre and comprises one office in a serviced building which is highly energy efficient, including the following: Biomass boiler Solar thermal panels Natural ventilation Lighting Heating Natural gas installation Water saving taps Building Research Establishment Environmental Assessment Method - (BREEAM), o Corby Enterprise Centre has been designed to meet BREEAM Excellent criteria. This was considered with a selective palette of construction materials including external render, stone cladding and solar-controlled glazing panels. Maximising natural daylight and ventilation have also been factors influencing the building design which is evidenced by the use and control of areas of glazing and external window openings. o Internal lighting control has been designed to be as energy efficient as possible again in line with BREEAM requirements. External lighting is designed in accordance with Chartered Institute of Building Engineers (CIBSE) lighting Guide 6 and the BREEAM requirements. o Mechanical systems have been designed in compliance with BSD specification in line with BREEAM standard building services parameters. At a local level the CCG is committed to embedding sustainability into staff behaviour and other partners in shared premises, concentrating on the reduction of paper, increased recycling, car sharing and use of local public transport where possible. 45

46 Improve Quality Corby CCG agreed a five-year Quality Strategy in 2017, reviewed each year to reflect changing priorities. The strategy outlines the framework for ensuring that quality is at the heart of everything we do. Corby CCG has discharged its duty under Section 14R of the National Health Service Act 2006 (as amended) to improve the quality of services in a number of different ways as detailed below. What we did which went well Quality Assurance Process We have a well-developed system of quality assurance and early warning processes in place which provides information about the safety, effectiveness and patient experience of services we commission for our community. This enables us to be proactive in identifying early signs of concerns and take action where standards fall short of expectation. It also helps to inform our commissioning decisions at all stages of the commissioning cycle. Sign Up to Safety Campaign Sign Up to Safety is a NHS England three-year objective to reduce avoidable harm by 50%. In 2014/15, Corby CCG signed up to this campaign and published their pledges online. The current, three-year plan started in April Projects that have had a particular focus in 2017/18 are: Countywide joint Serious Incident investigations, and a revised GP concerns process. Implementation is monitored via the countywide patient safety forum. Corby CCG has also contributed to a countywide sign up to safety plan with partners from Kettering General Hospital NHS Foundation Trust, Northampton General Hospital NHS Trust, Northamptonshire Healthcare NHS Foundation Trust, Woodland Hospital, Three Shires Hospital and St Andrews Healthcare. The countywide patient safety plan is currently under revision following a change in leadership and the future direction of this will be developed and agreed by the countywide patient safety forum in due course. 46
47 Countywide Strategic Clinical Quality Review Meeting (CQRM) A countywide strategic CQRM has been established to: To work collaboratively to support delivery of the Sustainability and Transformation Partnership (STP) to improve the quality of care for specific cohorts of patients. To share good practice, achievement and innovation so there can be improvement for patients and carer outcomes across the county. Identify common themes from operational CQRMs, which the group can seek to resolve in a collaborative fashion Common approach to quality assurance and improvement across the county. Meeting topics to date have included CAMHS and dementia/delirium services. The format of the meeting includes sharing of patient stories to identify gaps in pathways with agreed plans on how to improve these across the system. Quality Improvement (QI) Framework The CCGs have developed a quality improvement framework to signpost those working within commissioning to a suite of quality improvement resources and methodologies that should be applied to commissioning projects across the CCGs. A tailored training programme has been developed for CCG staff with twenty staff being trained this year. Avoidable Deaths: In the last year National requirements in relation to mortality reviews have been implemented. The Learning Disabilities Mortality Review (Leeder) Programme was established following the Confidential Inquiry into the premature deaths of people with learning disabilities which found that three times more people with learning disabilities die from a cause of death amenable to good quality care. All deaths of people with learning disabilities will be notified to LeDeR and initial reviews undertaken into the deaths of people with learning disabilities aged four to 74. Reviews follow a specified format, and should the initial review highlight further investigation is required this will be undertaken. Locally a steering group has been established and training of reviewers has been undertaken. 47
48 In April 2017 the requirements of the National Guidance on Learning from Deaths came into force. All local trusts have fulfilled the requirement of publishing their policy on their public internet by the end of quarter two and from quarter three to publish data which includes: The total number of the trust s in-patient deaths (including emergency department deaths) Those deaths that the trust has subjected to case record review Estimates of how many deaths (as identified by case review) were judged more likely than not to have been due to problems in care. Infection Prevention and Control Methicillin-Resistant Staphylococcus Aureus (MRSA) Bacteraemia No cases of MRSA bacteraemia were reported across Northamptonshire in 2017/2018. Table 17: Clostridium Difficile (C. Diff) Organisati on C. Diff cases Apr 17 Mar 18 (actual) C Diff Cases year objective Corby CCG KGH NGH NHfT 3 25 All Key: Cases the number of occurrences during 2017/18 Objective the projected ceiling GP practices provide significant event audits when community cases of Clostridium Difficile are identified. Safer Staffing All hospitals are required to publish information about the number of nursing and midwifery staff working on each ward, together with the percentage of shifts meeting safe staffing guidelines. This is published on each trust website. We actively seek assurance that this guidance is followed by providers and review the information each month at ward level. Any concerns regarding nurse staffing fill rates are raised with the hospital trusts through CQRMs and when required quality visits are undertaken to gain further assurance. 48
49 Assurance on Primary Care Quality A Primary Care Quality Information and Risk Sharing Group (RSG) continues to meet; reporting to Primary Care Commissioning Committee (PCCC). Quarterly RSG meetings with NHS England, GP representation, the local medical committee (LMC), Care Quality Commission and Corby CCG where quality issues and variation in clinical practice are identified by the use of a primary care quality dashboard, discussed and actions agreed for practice improvement. All GP practices are required to be registered with the Care Quality Commission (CQC). All 5-member practices have received a comprehensive inspection. The quality team has offered support to practices both for the registration process and preparation for inspection. The new schedule of comprehensive inspections commenced in November 2017 with new key lines of enquiry that focus on impact and outcomes of systems and processes in place at the practice. This year s inspections have a particular focus on infection prevention and control. CQC Reports on Acute Trusts Both of our local trusts received inspections from the CQC this year. The report for Northampton General Hospital (NGH) rated the trust overall as good. The CQC undertook an unannounced inspection to Kettering General Hospital Foundation Trust (KGH) between June This inspection looked solely at actions taken to address the Section 29A warning notice. On 7 September 2017 the CQC published the resulting inspection report indicating that the CQC found a number of improvements had been made at the Trust since their last inspection. Given the significant improvements the CQC identified the trust had now met the requirements of the Section 29A warning notice. The CQC re-inspected the trust throughout November 2017 with the well-led review starting on 29 November The CQC inspection report was published on 27 February 2018 and rated the trust overall as Requires Improvement with Good for caring. Care home providers: Throughout the year the quality team has undertaken clinical review visits to all care homes that provide services to people with health funding. The Quality team also undertakes announced full monitoring visits. The care home provider is supplied with a RAG rated report to include recommendations where required. Providers are given 28 days to respond with an action plan. 49
50 Supplementary monitoring visits, (often unannounced) are undertaken to ensure continued development and provision of quality services. In 2017/18 there were: 142 clinical reviews (full monitoring visits) undertaken 92 supplementary visits undertaken. As part of the review people who use the services we are monitoring are spoken to. Questionnaires with regard to the services they receive are provided. The outcomes are: 93% of service users would recommend their care home to a friend or relative One care home closed last year. Domiciliary care providers: All domiciliary care providers with health funded clients undergo the same monitoring review process as the care homes. During 2017/18 the CCG quality team undertook: 44 review visits to domiciliary care providers As part of the review, services users are visited within their own homes to gain their opinions of the services they are in receipt of. 66 visits were undertaken to see people within their own home Questionnaires are also provided for completion. The outcomes of the questionnaires: 91.5% of people would recommend their care provider to a friend or relative 50
51 Safeguarding Northampton Children s Services: Northamptonshire s health and social care organisations face bigger challenges than ever before as we as a partnership strive to improve health and wellbeing, improve outcomes and make sure the most vulnerable groups in our population receive appropriate, timely, safe and effective services, in the context of a challenging financial climate across the partnership. The situation was made more difficult following the sad death of a child in our County which has highlighted issues in the management of referrals into the Multi Agency Safeguarding Hub (MASH). All partners have come together to review the MASH functions and ultimately improve the offer to children and young people. Taking forward Safeguarding priorities across Northamptonshire These areas are considered to be critical to keeping children, young people and adults at risk, safe in Northamptonshire all of which have been identified in previous Northamptonshire Serious Case Reviews (SCRs) and recent Inspection reports: Children/young people Looked after Children (LAC): We continues to see a year on year increase in the number of children coming into care in comparison to its statistically similar neighbour. However, there has been a significant improvement in all activity related to improving the health of looked after children and care leavers both accommodated within and outside the county. The outcomes for Looked after Children are poorer than children in the general population. The services that they receive in Northampton were highlighted as a particular problem. One particular area has been the application of the Early Help Assessment (EHA) across agencies and failure to engage early intervention services with families in need of additional support. Child Sexual Exploitation (CSE): This remains a national and local priority across all agencies. Adolescents and Self-Harm: Identified as a local priority due to the high incidence of self-harm. The voice of the child: Audits repeatedly identify a lack of documented evidence to demonstrate the child s views and wishes have influenced care plans. Neglect: This is a re-occurring theme from Local and national SCRs. 51
52 Adult Safeguarding Mental Capacity Act (MCA) /Deprivation of Liberty Safeguard (DoL): case reviews have identified poor and inconsistent application of the MCA and DOL safeguards. The Safeguarding have successfully delivered Mental Capacity Training to health professionals which focused on year olds. The training was extremely successful and has generated wider discussion and debate which will be followed up through themed discussions and additional training. Domestic Abuse: case reviews have identified inconsistent responses to concerns and disclosure of domestic abuse. PREVENT: The CCG have successful rolled out PREVENT training across the county. Improvements in Safeguarding within General Practice Safeguarding within GP continues to go from strength to strength with the launch of the Primary Care Safeguarding website in September 2017, supported by a robust schedule of training and forums. The Primary Care safeguarding team continue to proactively work on innovative ways to support partnership working, improve communication and develop the skills and knowledge within Primary Care. Other areas where we are working towards improvements Serious Incidents and Never Events Serious incidents in health care are defined as adverse events, where the consequences to patients, families and carers, staff or organisations are so significant or the potential for learning is so great, that a heightened level of response is justified. There were 194 serious incidents reported by NHS and independent healthcare providers in 2017/18. Seven of the serious incidents were never events. What we did about it All incidents have been subject to internal serious incident investigation scrutiny through the Corby CCG serious incident governance processes. Corby CCG always undertakes follow up quality visits to the relevant clinical area to gain assurance on the implementation of actions following never events. Learning has been shared through our countywide patient safety forum. 52
53 Urgent Care System Corby CCG recognises that both acute providers have experienced significant pressures on their A&E departments throughout the year and most specifically during the winter period. Corby CCG actively monitors the safety and experience of patients in A&E. This includes the review of any serious incidents and quality visits to both departments and is supported by a RAG rated dashboard incorporating patient safety and patient experience metrics. What we did about it The Quality team works collaboratively with the urgent care commissioning team on initiatives across the community to manage the flow of patients both into and from both acute hospitals and has developed the following: Training care homes and thereby strengthening admission avoidance from nursing home and residential care homes. This training is resulting in a reduction of conveyances to acute hospitals. Joint improvement co-ordination between CCG and NCC including the development of a memorandum of understanding regarding quality monitoring and a Care Home Standard Operating Procedure. Care Home Support via Frail Elderly Liaison Officers (FELO): The quality team are overseeing and supporting the role of the EMAS FELO to provide support for work with top twenty conveying care homes in the county with a falls focus and improving sharing of GP care plans. Introduction of Yellow Band Scheme: This scheme has been developed to enable A&E to recognise patients who have care home/domiciliary care packages in place and avoid risk aversion admission. Complaints Corby CCG is responsible for investigating all complaints or concerns raised in relation to services that we commission on behalf of our patients. Our Complaints Procedure reflects the Parliamentary Health Service Ombudsman s six principles of remedy, namely: Getting it right Being customer focused Being open and accountable Acting fairly and proportionately Putting things right Seeking continuous improvement 53
54 Corby CCG welcomes complaints as a valuable means of receiving feedback on the services they commission for the people of Northamptonshire and also on the way Corby CCG go about its business. Corby CCG aims to use information gathered from complaints as a means of improving services and the effectiveness of the organisations they commission. Corby CCG will seek to identify learning points that can be translated into positive action, and where necessary provide redress to set right any injustice that may have occurred. Between April 2017 and the end of March 2018, 10 complaints were received, and another 30 concerns were raised by members of the public or by local Members of Parliament on behalf of their constituents. Joint Quality Committee The committee is a joint committee between Corby and Nene Clinical Commissioning Groups (CCGs) and reports directly to both Governing Bodies. The Joint Committee plays a vital role in ensuring that quality remains at the heart of CCG decision-making. 54
55 Engaging People and Communities The patient voice is central to the commissioning of health care services within Corby. The CCG uses a range of engagement and communication opportunities to listen to our patients. An extensive database of community groups and other stakeholders is in place, and this is added to on an ongoing basis. NHS Corby CCG has well-structured mechanisms for engaging with patients including through Patient Participation Groups (PPGs) in each practice. Each Member Practice has a Patient Participation Group which is run by patients with support from the Practice. The groups meet regularly to represent the views of patients to staff at the Practice, including views on facilities provided and ideas to help enhance services in place. This enables patients to get involved at a very local level in discussing local health services and planned service improvements. The PPG Chairs meet regularly and input into the CCGs formal committee structure. Patient Participation Group (PPG) Chairs Engagement The CCG has a well-established PPG Chairs Group which meets regularly, with seven meetings held during 2017/18. This is a forum which brings together each of the five-member practice PPG Chairs with the CCG. The Forum provides the opportunity for patients to suggest and help to develop creative means of engagement with the local population, and for PPG Chairs to provide feedback from patients within their groups on how services operate, how accessible they are and how suitable they are for patients. The PPG Chairs Group operates as a key forum for the CCG to raise awareness of commissioning plans and for patients to provide feedback on these plans. Corby Patient Reference Group This group was formed in 2017 to provide another mechanism for engagement. Around 90 people have already been recruited to this group. We re always looking for new ways to give our patients a say about your local NHS and that s why we put together this new virtual group of people, to act as a sounding board for the CCG on a range of issues and projects. This group is open to anyone who lives in Corby, is registered with a Corby GP, and wants to have input into shaping NHS services. The Patient and Public Engagement Assurance Committee (PPEA) The Patient and Public Engagement Assurance Committee (PPEA) meets bimonthly and oversees our processes for engagement, providing productive input from local stakeholders into the CCG s engagement work and ensuring that we are engaging meaningfully with local people to meet our statutory duties set out in S14Z2 of the Health and Social Care Act More information on the work of the PPEA Committee can be found in the Governance Statement in Chapter 2. 55
56 Engaging with our Partners during 2017/18 A comprehensive programme of engagement with the people of Corby was conducted in 2017/18. The programme was designed to test public experience of primary care, awareness of the challenges facing local NHS services and acceptance of a possible case for change. The engagement was delivered in three phases. Phase 1 Gathering more than 700 responses to a public survey, supported by Patient Participation Groups, and laying on a series of workshops early in 2017 which produced valuable insights, including: Many Corby people are concerned about difficulties with access to primary care The public are over-confident about their ability to access services according to need Most accept the case for change, although there is nervousness about the detail and a significant number remain undecided People understand and support the prevention agenda People want an extended primary care offering, with access to a much wider range of co-located support and services. Phase 2 A further intensive period of engagement was undertaken between September 2017 and January This focussed in more detail on the case for change in both primary and urgent care. Activity included: A presence in public places with high footfall (supermarkets, leisure facilities, GP surgeries) Presentations to a wide range of community groups Targeted engagement with other stakeholders, including clinicians, politicians and statutory bodies (including the Overview and Scrutiny Committee and Health and Wellbeing Board) Website and social media content (including an interactive quiz to test people s ability to make the right choices about which service to access) Promotion of the issues through news coverage in all, conversations have been held with around 650 people face-to-face, and more than 20,000 were reached online. 56
57 All responses were logged and analysed to identify the following key themes: Confirmation of significant issues with primary care access in particular, getting a same day appointment. Difficulties with navigating the current system to get the right care, first time. Some patients have chosen to go to the UCC with very serious health issues when an immediate visit to A&E would have been safer and more appropriate. Strong support for: Phase 3 Extended primary care opening hours into the evenings and at weekends. The continuation of an urgent care service in Corby. The allocation of more resources to the prevention of ill health. Widespread acceptance of the need for service changes but nervousness about what that might lead to. The CCG has also involved doctors at the East Midlands Clinical Senate to secure independent clinical scrutiny. They have advised that Corby is out of step nationally. A final workshop was held in December 2017 at which Patient Reference Group members and other public representatives (including members of the group campaigning for retention of the UCC) were invited to feed directly into service options, by suggesting viable ways of addressing the clinical and financial challenges facing the local NHS. The workshop produced strong agreement around a series of key ideas/wishes for a remodelled service: Retention in Corby of an urgent service, particularly for minor injuries - Conversion of the Urgent Care Centre into a GP-led service to enhance primary care capacity, particularly for on-the-day access a Same Day Access Hub Introduction of a local integrated triage/navigation system (both by phone and at the front door) to help people get the right care, first time. The right level of training for staff doing the navigating, so that people can have confidence in their decision-making Enough phone-answering capacity to avoid barriers to making appointments, particularly at busy times of the day Longer primary care appointments for those who need them - Greater use of new technology to support people with busy lives (e.g. for GP consultations or to aid self-care) - A focus on easing the financial burden for those on the lowest incomes (e.g. a medicines bank to prescription costs). This programme of engagement was deliberately structured as an interactive process. Through it, local people have been able to explore relevant issues in increasing detail with each stage informed by what has come before. 57
58 Phase 4 The final phase ran for eight weeks between 12 February 2018 and 8 April. It was extensive and well resourced, with a dedicated operational team of three (supported by CCG officers) and strong oversight. This next period of engagement aimed to explain the context for the CCG s plans (including the pressures for change) and ask a series of questions to assess views on: The plan for extended primary care access The idea of trained navigators What will be easier when trying to make appointments a single access phone number for all of Corby, or people calling their own practice number What is a reasonable time to wait on the line and to complete an appointment booking when calling What other booking options do people want to have (online etc.) Levels of technology or human contact to improve confidence about using an appointments system for on-the-day access. All the responses gathered will be considered alongside clinical, financial and legal factors by the CCG Governing Body when making future decisions. The aim is that the evidence gathered will directly influence service access arrangements, including relevant elements of the service contract specification. Engagement activity (face-to-face, online, or both) was delivered throughout this period including in evenings and at weekends where needed. The intention was to maintain the intensity of engagement already delivered in the latter part of There was a full engagement document, with an initial print run of 3,000. Hard copies were made available through engagement activity and in public places such as GP surgeries and The Cube in the town centre. It was also accessible online, as well as by post or on request. A Freepost address (NHS Corby Responses) was procured to encourage a high return. Participants were also able to submit responses online and by . The CCG s plans have already been shaped by the extensive public and stakeholder engagement undertaken during The people of Corby have expressed strong support for the principle of retaining as much of the current urgent service facility in the town, and the CCG has listened to those views. Our intention is to preserve the core service and then to add to it, to offer a service for those whose needs are not currently being met. 58
59 Annual General Meeting NHS Corby CCG held the fourth Annual General Meeting on 07 September 2017, with more than 50 people in attendance. Members of the Governing Body talked through 2016/17 year s achievements, discussed current projects and plans for the year ahead. Examples of work included the increase in provision of mental health services in the town. Questions were taken from the audience regarding the future of The Urgent Care Centre and the challenges of the ever-increasing population. How we share news with our patients in Corby During 2017/18 the CCG continued to communicate regularly with our members, patients, public and partners; below are examples of how we did this: Corby Health News During 2017/18 we continued to publish a monthly newsletter called Corby Health News. The publication is sent to all practices where printed copies are displayed in waiting rooms. The newsletter is also published on the CCG s social media and on our website. The aim of the publication is to engage and communicate with the people of Corby and to publicise health and wellbeing events run by the CCG and in conjunction with Corby Borough Council and voluntary organisations across the town. Corby Borough Council now shares the newsletter with its staff. Large local employers such as R.S. Components and Tata Steel also distribute the newsletter to all staff. Corby CCG News We communicate with our GPs and practice staff on a monthly basis via this inhouse publication. This newsletter contains messages from the CCG, service review and feedback surveys and general information for GPs and practice staff around national NHS campaigns and resources. Knowing the Signs Campaign This campaign is aimed at raising awareness of prevalent health conditions in Corby including bowel Cancer, cervical, bowel and breast cancer screening, HIV, diabetes and stroke. This is an ongoing campaign aimed at educating patients to spot the early signs of each condition. More information can be found on our website. The campaign will continue into 2018/19. 59
60 GP in the House Corby Radio During 2017/18 Dr Joanne Watt our Clinical Chair has a regular radio slot called GP in the House, on Corby Radio 96.3FM for an hour every second Thursday at 9am. Dr Watt discusses a range of health conditions which affect the population of Corby, with a different topic covered each month. Corby radio has a potential 80,000 listeners every day. Focused on Corby Dr Joanne Watt, our Clinical Chair, has a column focusing on health care in this quarterly magazine which is delivered to 25,000 homes in Corby. 60
61 Reducing health inequality Corby is a town and Borough in the North East of Northamptonshire. The Borough is expanding at a fast pace, growing by approximately 12,000 to circa 66, 9007 in the past 13 years. The Office of National Statistics has reported the Borough as in the top ten nationally for growth. Corby has a number of areas of deprivation which are in the top 20% most deprived areas in England particularly located in and around the town centre. Socio-economic deprivation is an important health and wellbeing determinant. There are notable differences in life expectancy between the most and least deprived areas in Northamptonshire and nationally. The more recent population growth has resulted in the age demographic profile of Corby becoming younger. The CCG s commissioning strategy aims to address both the health challenges driven by Corby s historical legacy and the needs of the growing population of the borough, to meet our duties to address inequalities. This growth in the population will need to be taken into account for the planning of health and care services in the new models of care. Health deprivation has a higher occurrence than overall deprivation particularly in Corby: 1 in 3 people in Corby smoke 71.2% of the Corby population are overweight which is above the national average of 65% and the highest incidence across Northamptonshire Corby has a high incidence of mental health issues, with high levels of admission for self-harm (15 to 24 yrs.) drug and alcohol abuse as well as a poor recovery and completion rate for Improved Access to Psychological Therapies (IAPT) The estimated proportion of the Corby population meeting the recommended 5 a day in 2015 (40.7%) and average portions of fruit (2.19) and vegetable (1.97) consumed daily is significantly below the national average (52.3%, 2.51 and 2.27) The health of people in Corby is varied compared with the England average. About 20% (2,720) of children live in low income families. Life expectancy for both men and women is lower than the England average. Health and Wellbeing Strategy Corby CCG is an active partner in Northamptonshire s Health and Wellbeing Board, which brings together leaders from across the county s health and care system to work together to: improve the health and wellbeing of local people reduce health inequalities promote the integration of services 61
62 Key to this is the production and implementation of a Health and Wellbeing Strategy. Called Supporting Northamptonshire to Flourish, our five-year strategy was launched in 2016, and it sets out the partners vision to improve the health and wellbeing of all people in Northamptonshire and reduce health inequalities by enabling people to help themselves. The Board has agreed four strategic priorities: Every child gets the best start The Marmot Review tells us that what happens during the early years, starting in the womb, has lifelong effects on health and wellbeing. All the evidence shows that the health and wellbeing of Northamptonshire s children must be improved if we are to achieve sustainable improvement in health and wellbeing overall. Taking responsibility and making informed choices Men and women living in the most deprived area of the county die on average 8.9 and 6.6 years earlier, respectively, than those in the least deprived area, and that gap is widening. Healthy Lives, Healthy People, published in 2010, shows how changing adult behaviour can reduce premature death and illnesses such as circulatory disease and cancer. Promoting independence and quality of life for older adults The number of people in Northamptonshire aged is expected to increase by a fifth (21%) by Evidence suggests that by strengthening communities and integrated care systems would keep people out of hospital and ease the current pressure on our acute services. Creating an environment for all people to flourish Significant health inequalities exist in the county. Creating environments where everyone can flourish focuses our attention on the wider determinants of health and wellbeing and underpins delivery of the other three priorities. By working together we aim to create a better quality of life and improved outcomes for the people of Northamptonshire. Supporting Northamptonshire to Flourish sets out a new vision for the county and provides an unrivalled opportunity to establish for the first time a unified approach to health and wellbeing with the potential to achieve real and meaningful change for the benefit of all. 62

63 Corby Clinical Commiuionmg Group While we must deliver progress within each priority, the Board recognises the connections and interdependencies between them. Prevention, early help and early intervention are fundamental to our strategy. Successful delivery depends on integrated plans delivered by local organisations. The Sustainability and Transformation plan, which covers the same area as the Health and Wellbeing Strategy, will form the basis for frontline delivery. Carole Dehghani Accountable Officer 25 May
64
65 Further detail on Governing Body Member Profiles can be seen under the Member Profiles section of this report. During 2017/18 there have been changes to the composition of the Governing Body. Pauleen Pratt was the Registered Nurse Member on the Governing Body. Pauleen left her post in August Ms Aly Hulme took up this post in 2017/18 and is now the Governing Body Registered Nurse for both NHS Corby CCG and NHS Nene CCG. Helen Storer held the position of Independent Lay Member until 31 March At the time of submission of the Annual Report and Accounts Dr Miten Ruparelia, Clinical Vice Chair, has taken up a secondment with the STP Programme. The CCG are undertaking an appointment process for a replacement to this role, in line with the CCG s Constitution. Detail relating to the composition of the Audit and Risk Committee, can be found further on in the Corporate Governance Report. Member practices NHS Corby CCG is a membership organisation formed of the five GP practices in Corby who together have responsibility for commissioning the health services for their registered patients. Member Practices: Great Oakley Medical Centre Lakeside Healthcare Corby Studfall Partnership Corby Studfall Medical Corby Woodsend Medical Centre Further information about our member practices can be found on the CCG website 65

66 Members Profiles Carole Dehghani, Chief Executive Carole Dehghani is Chief Executive of Corby Clinical Commissioning Group and interim Accountable Officer of Nene Clinical Commissioning Group. She has more than 30 years experience working in the NHS in a variety of senior management and leadership roles including Director of Public Health. After obtaining her MSc in Health Policy and Management, Carole developed her interest in NHS policy as an Associate Director at NHS Northamptonshire. She has successfully led local implementation programmes which engaged large numbers of primary, secondary and community care clinicians together with patients and partner organisations in the scoping and identifying best models of care, creating high quality care for the population of Northamptonshire. Throughout her career Carole has taken on a number of roles which has resulted in successful pathway and service re-design for COPD, heart failure, vascular services and diabetes leading to both national and international acclaim. Carole was appointed as Chief Executive of Corby CCG in December 2013 and joined Nene CCG as interim Accountable Officer in December The new leadership arrangement across the two CCGs will enable commissioners to build on the close collaborative work already under way. Caron Williams, Director of Commissioning and Strategy Caron Williams has enjoyed a career which has spanned both the private and public sector with her progressive approach to projects earning her endeavours national recognition for her work in EoLC and a ministerial recommendation for the Transforming Community Services programme she undertook for NHS Warwickshire. She started her career with eleven years in private industry beginning her basic training in research and development, procurement for blue chips, and then new product development for GC Telecommunications - delivering new products to market. With a track record of delivering on time and to cost she was eventually promoted to the position of Senior Officer in worldwide product development. Her work then took her to the Channel Islands where she diversified into the shipping industry as a General Manager supporting operations for 4 shipping lines. After moving back to the UK, she began to work in health and social care starting at Coventry City Council where she developed markets and set up services that hitherto didn t exist - working with providers to ensure they could deliver to meet local population needs. 66

67 Her career in the NHS was launched in 2008 when she started working for Solihull Care Trust developing their end of life care services and continued life care services. Those services were regarded as the best of their kind in the UK at that time. She then moved with the NHS into Warwickshire where she transferred and transformed community services in 2010 and received ministerial recommendation. This work was also cited by The Kings Fund - an independent charity working to improve health and health care in England. More recently she moved from Warwickshire to NHS West Leicestershire CCG as a board member responsible for strategy and planning and during this time delivered the Better Care Fund. During her time there she also delivered the majority of the early shaping and development work for the five-year plan in Leicestershire and Rutland. Caron is a member of the Governing Body, Executive Directors meeting, Council of Members, Finance and Performance Committee. Dr Joanne Watt, Clinical Chair Dr Joanne Watt has been a GP at Great Oakley Medical Centre since 2005 and is now senior partner. During that time the practice has expanded from 2,500 patients to 12,300 patients and is still growing. She also works as a sexual health doctor providing confidential clinic services for non-registered patients via the department of Sexual Health. Dr Watt was her practice lead during practice-based commissioning. She then became practice delivery lead for the CCG, and in July 2012 was elected to the Governing Body as an executive GP leading on quality. In October 2015 she became interim Clinical Chair of the Governing Body and became substantive Clinical Chair in April Dr Watt has a focus on ensuring that the people of Corby receive equitable access to the high-quality care that they need, and that their requirements are considered in future Northamptonshire plans. 67


68 Dr Miten Ruparelia, Clinical Vice Chair Dr Miten Ruparelia has been a partner at Woodsend Medical Centre since 2007 and was elected as Chair of Nene CCG s Corby locality in He worked as Corby's locality lead and Nene's commissioning director until April He was Clinical Vice-Chair of NHS Corby CCG until April 2018 and he led on contracting and urgent care. Miten studied at MGM Medical College in Mumbai, qualifying in August 2001, and was the General Secretary of his university for 3 years. Dr Sanjay H Gadhia, GP Governing Body Member Dr Sanjay Gadhia qualified at the Royal Free Hospital in London in He worked in London, Stevenage and Mansfield before completing his GP vocational training scheme in Kettering. In 2006 he joined Lakeside Surgery as a partner and has been actively involved in the expansion and development of the practice. He was elected to the NHS Corby CCG board in Sanjay developed a keen interest in improving services for the community both from his work as a local GP and as a forensic medical examiner for Northamptonshire Police. He is very keen to develop services to improve healthcare services for the people of Corby. 68


69 Dr Nathan Spencer, GP Governing Body member Nathan Spencer MBChB MRCGP is a working GP at Great Oakley Medical Centre. He has special interests in mental health and sports medicine. Nathan graduated in 1999 from Leicester University and worked in a variety of hospital jobs across the country. He became a Consultant in Emergency Medicine in 2008 in the A & E Department at Kettering General Hospital. He then decided to retrain in General Practice in 2012 and completed his training last year. Nathan is delighted to be a GP member of Corby CCG and hopes to be a strong ambassador in representing the experience of patients and colleagues. Dr Sebastian Hendricks, Secondary Care Clinician Member Sebastian is an active clinical consultant in Audiovestibular Medicine and clinical lead for Paediatric Audiology & Audiovestibular Medicine for The Royal Free London NHS Foundation Trust. He is also a consultant at the Royal National Throat Nose & Ear Hospital (University College London Hospitals NHS Foundation Trust). His previous work include member of the trusts clinical governance committee in his role of chair of the children s clinical governance, trust appraiser and educational supervisor, member of the clinical excellence awards committee and lead for patient experience for children s services. In North Central London he led the local new-born hearing screening service to the unified NCL service. He was Trustee and Council Member of the British Society of Audiology (BSA) for 2 terms and chaired the Paediatric Audiology Interest Group of the BSA, representing the group also on the Audiology Advisory Group at Department of Health. He held several positions within his main professional organisation, the British Association of Audiovestibular Physicians. At present he represents the organisation at the standard developments for care records (Royal College of Physicians / Professional Record Standard Body) In the past his work for the professional organisation and at the Royal College of Physicians included the Payment for Results committee, Clinical Coding, and Expert Working Group at the NHS Health and Social Care Information Centre. Within Corby CCG, Sebastian has as a governing board member shared responsibility for all aspects of the CCG, providing a broader view on health and care issues, particularly an understanding of patient care in the secondary care setting. 69


70 Sebastian also presents an independent strategic clinical view on all aspects of CCG business as well as adding an understanding of how secondary care providers work within the health system He is member of the Joint Quality Committee with NHS Nene CCG, the council of members, the primary care commissioning committee, and the finance committee. Mike Alexander, Chief Finance Officer Mike is a qualified CIPFA accountant with over 30 years experience in NHS finance. He began his career as a regional Finance Trainee based in Romford, Essex. He held a variety of senior finance positions in North East Essex Health Authority before becoming Director of Finance at New Possibilities NHS Trust, a 2nd wave specialist Learning Disability Trust based in Colchester. In 1996 he moved to the East Midlands having been appointed Director of Finance at Grantham and District Hospital NHS Trust, where he was latterly Hospital Director. Mike was appointed Director of Finance and Deputy CE at Melton Rutland and Harborough PCT in 2001 and moved to NHS Nottinghamshire County as Director of Finance and Deputy CE in He left the NHS in April 2011 and re-joined as Chief Finance Officer of Corby CCG on a part-time basis in April Mike retired from post in April Stuart Rees, Interim Chief Finance Officer Stuart Rees was appointed as the Interim Chief Finance Officer at NHS Corby Clinical Commissioning Group on 1 April He is also the Chief Finance Officer at NHS Nene Clinical Commissioning Group. He has held a number of senior positions in the NHS. Between March and October 2015 Stuart was the Interim Accountable Officer for Nene CCG. He has also over his career held positions as Director of Finance, Contracting and Performance at Shropshire Community Health Trust and the Director of Finance and Performance at Shropshire County Primary Care Trust. Stuart has experience of working in both secondary and primary care settings and joined the NHS as part of the National Finance Management Training Scheme. Stuart s qualifications include membership of the Chartered Institute of Public Finance and Accountancy and Bachelor of Arts (Honours). 70


71 Andrew Hammond, Lay Member (Governance), Audit Chair and Deputy Lay Chair Andrew is an experienced Executive and Non-Executive Director. He spent his early career establishing a National Awareness Charity before heading to Royal Mail where he held numerous senior leadership positions from heading up advertising through to being responsible for the nation s stamps as Managing Director of Stamps & Collectibles. Notable successes include spearheading the Gold Medal Stamps and Gold Post-boxes at the 2012 London Olympics and putting the global phenomenon of Star Wars on our stamps. Andrew is currently Chief Executive of Instructus, an education charity working in the apprenticeship area, which owns companies delivering training and development programmes. He is ultimately responsible for Instructus, Instructus Skills, CQM Ltd, and the Springboard Consultancy. Andrew has a breath of experience from being ultimately responsible for organisational P&L for many years. He brings this experience to bear as Chair of Audit Committee for Corby CCG. Tansi Harper, Lay Member for Patient and Public Engagement Tansi's professional career was in education and she was Principal of two colleges as well as working in other public sector and voluntary sector positions before becoming a Regional Consultant for HEFCE for the East Midlands and Northern Ireland. She became involved on Health Boards driven by her concern that Education, Health and Social Care seemed to not work well together in the best interests of the patients, students and families and a desire to support better integration of services to meet community needs. That was 19 years ago and Tansi has been a Non- Executive Director on the Boards of a number of Health Boards since then including a Strategic Health Authority, PCTs and now Corby CCG where she represents the Patient and Public voice. She chairs a number of Committees, investing in strengthening the patient and stakeholder contribution to improving the commissioning of Health services. She has a particular interest in vulnerable groups that may need additional support to access appropriate health and wellbeing services. Until recently she chaired the County Learning Disabilities forum and actively supports Mental Health developments through her countywide networks. Since retiring Tansi has been Chair of Northamptonshire Probation Trust and subsequently Chaired a Transformation Board bringing together the Probation Trusts from Northamptonshire, Bedfordshire, Hertfordshire and Cambridgeshire in response to national policy changes in the Criminal Justice system. 71
 family of organisation's working nationally on supporting those with Mental Health and substance misuse challenges, and she is a member of")
72 She was Chair of CAN, a Northamptonshire based Substance misuse and Crisis Housing Charity, until late 2016 when she merged it with Aquarius, a larger Midlands based Charity. Both organisations are part of the Richmond Fellowship (RF) family of organisation's working nationally on supporting those with Mental Health and substance misuse challenges, and she is a member of the RF Board. Between the Summer of 2016 to Nov 2017 Tansi chaired the Northamptonshire Sustainable Transformational Plan, a countywide committee involving the CCGs, the County Council, the voluntary sector, GPs, the acute sector providers and the Mental Health trust in developing integrated health and adult social care plans based on the needs of the Northamptonshire population. She now chairs the STP Collaborative Stakeholder Forum (CSF). Helen Storer, Lay Member Helen has 26 years NHS experience and started her career as a Registered Dietitian at Leicester Royal Infirmary. She later moved to Kettering General Hospital where she ran regular community clinics in Corby. During this time, she developed an interest in public health nutrition and the prevention of diet-related problems. Helen followed this interest by becoming a Community Dietitian in Leicestershire, working with the Department of Health to set up the National School Fruit Scheme. In 2000, Helen became an Integrated Health and Social Care Manager with Nottingham CityCare Partnership. She has undertaken a variety of additional roles alongside her substantive post, including that of Professional Executive Committee Member and Board Clinician with Nottingham City PCT, Special Lecturer with Nottingham University, member of the NICE obesity guideline development group and Chair of the Nottingham School Food Group. Helen started her role as Lay Member in December 2014 and is now the Chair of the Finance Committee. Helen has resigned from her post and left the CCG on 24 April

73 Aly Hulme, Registered Nurse Member Aly has been appointed as Governing Body Registered Nurse to provide strategic nurse and clinical leadership for quality and safeguarding, ensuring that the CCG achieves the vision to improve quality, outcomes and clinical standards for all patients. Prior to joining Nene and Corby CCG, Aly was the Director for the Patient Safety Collaborative (PSC) at the North West Coast Academic Health Science Network. She was instrumental in leading and establishing the PSC with the aim of creating an effective and sustainable collaborative improvement system in patient safety. Aly has a long-standing career in the NHS as a registered nurse and midwife with over 33 years working in management roles in various organisations and has been appointed to senior nursing positions in NHS England and commissioning organisations. Aly is passionate about quality ensuring that patients are at the heart of our decision making. She has extensive expertise in patient safety and quality improvement and is a Health Foundation Quality Fellow. Aly has delivered on programmes at national level being instrumental in driving and implementing patient safety and quality improvement such as, leading on the delivery of National Patient Safety Agency (NPSA) National Learning and Reporting System and developing quality capability across the NHS. Aly has attained two master s degrees and is working towards a Doctorate in the field of Patient Safety. She is a visiting University lecture and peer reviewer. Aly also has a distinguished career in the Armed Forces with over 30 years of experience as a Reservist. She has influenced healthcare delivery at the front line through various programmes of work and is a subject matter expert for Equality and Diversity. Composition of NHS Corby CCG Governing Body Our system of governance begins with the Governing Body. The core activities of the Governing Body include: Development of strategy Approving the annual Operational Plan and Financial Plan Monitoring performance including the financial position, activity and progress against key standards including NHS Constitutional Standards Obtaining assurance that the risks are identified and that systems to manage and mitigate risk are in place Ensuring effective clinical leadership Ensuring meaningful patient and public involvement in commissioning decisions Ensuring transparent remuneration arrangements are in place for employees and others 73
74 The CCG s Constitution sets out the Governing Body s functions and the included Standing Orders details the procedures followed. Throughout 2017/18 and until the date of signing of the Annual Report and Annual Accounts, the Governing Body had 12 members, including: Clinical Chair the CCG appointed Dr Joanne Watt as the Clinical Chair who has held this role since 01 April 2016 Three GP Governing Body Members one of whom is the Clinical Vice Chair. During 2017/18 Dr Miten Ruparelia, Clinical Vice Chair, and Dr Sanjay Gadhia, GP Governing Body Member, Dr Nathan Spencer, GP Governing Body Member were in post throughout the year. Three lay members the CCG has maintained 3 Lay Members on the Governing Body during 2017/18: o Andrew Hammond, Lay Member for Governance, who also acts as the Audit Chair and the Conflict of Interests Guardian. o Tansi Harper, Lay Member for Patient and Public Engagement. o Helen Storer, Independent Lay Member, Lay Member for Finance Three Executive Directors - this includes: o Carole Dehghani, Chief Executive (Accountable Officer) o Mike Alexander, Chief Finance Officer o Caron Williams, Director of Commissioning and Strategy Secondary Care Consultant - Sebastian Hendricks has held the position of Secondary Care Consultant throughout 2017/18. Registered Nurse Member during 2017/18 Pauleen Pratt was the Registered Nurse Member on the Governing Body. Pauleen left her post in August Ms Aly Hulme took up this post in 2017/18 and is now the Governing Body Registered Nurse for both NHS Corby CCG and NHS Nene CCG. Northamptonshire Public Health supports the Governing Body, through attendance at meetings by a Consultant in Public Health. Governing Body meetings are held in public bi-monthly and during 2017/18 eight meetings took place, two of which were extraordinary. The Governing Body meetings are normally held at the CCG Headquarters and public attendance has been varied through the year, the two extraordinary meetings were held in the Corby Cube to enable more room for public attendance. Governing Body membership attendance is detailed in the table below, as per positions held up to 31 March
75 Governing Body Member Attendance Table 18: Governing Body attendance April 2017-March 2018 NAME TITLE ORGANISATION PERCENTAGE Dr Joanne Watt Clinical Chair NHS Corby CCG % Carole Dehghani Chief Executive NHS Corby CCG % Mike Alexander Chief Finance Officer NHS Corby CCG % Director of Commissioning Caron Williams & Strategy NHS Corby CCG % Pauleen Pratt Nurse Member GB NHS Corby CCG % NHS Corby CCG & Aly Hulme Nurse Member GB NHS Nene % Dr Miten Ruparelia Clinical Leader NHS Corby CCG % GP Governing Body Dr Nathan Spencer Member NHS Corby CCG % GP Governing Body Dr Sanjay Gadhia Member NHS Corby CCG % Lay Member for Andrew Hammond Governance NHS Corby CCG % Tansi Harper Lay Member for PPEA NHS Corby CCG % Helen Storer Lay Member NHS Corby CCG % Dr Sebastian Hendricks Secondary Care Consultant NHS Corby CCG % 25/04/ /06/ /07/ /08/ /08/ /10/ /12/ /01/ /02/2018 Total Sub-Committees Audit and Risk Committee The Audit and Risk Committee s work focuses on ensuring the organisation has appropriate governance and internal control in place and oversees the management of risk. The Committee provides the Governing Body with an independent and objective view of the CCG s financial systems, financial information and compliance with laws, regulations and directions governing the CCG. The Committee will seek to provide assurance to the Governing Body that an appropriate system of internal control is in place to ensure that: business is conducted in accordance with the law and proper standards and adheres to the principles of good governance public money is safeguarded and properly accounted for financial statements are prepared in a timely fashion, and give a true and fair view of the financial position of NHS Corby CCG for the period in question reasonable steps are taken to prevent and detect fraud and other irregularities 75
76 As at 31 March 2018 the Audit and Risk Committee had three members: The Chair of the Committee who was Andrew Hammond, Lay Member for Governance One other Lay member, this was undertaken by Tansi Harper, Lay Member for Patient and Public Engagement and Helen Storer, Independent Lay Member, for the purposes of quoracy One GP Governing Body Member, this was undertaken between Dr Miten Ruparelia, Clinical Vice Chair, and Dr Sanjay Gadhia and Dr Nathan Spencer, GP Governing Body Members, for the purposes of quoracy During 2017/18, the Committee met seven times. Audit and Risk Committee attendance can be seen in Figure 17 below. The meeting is considered quorate when the Chair and two members are present, one of whom must be a GP Governing Body Member. The Chief Finance Officer and External and Internal Auditors, as well as the Local Counter Fraud Specialist are regular attendees at the Committee but do not form part of the membership. The minutes of each Audit and Risk Committee are presented to the Governing Body and the Chair of the Committee draws attention to any issues that require disclosure or executive action via the Chair s highlight report. Audit and Risk Committee Member Attendance Table 19: Audit and Risk Committee attendance April 2017-March 2018 NAME TITLE ORGANISATION 25/04/ /05/ /07/ /09/ /11/ /01/ /03/2018 TOTAL PERCENTAGE Dr Miten Ruparelia Clinical Leader NHS Corby CCG % Dr Nathan Spencer GP Governing Body Member NHS Corby CCG % Dr Sanjay Gadhia GP Governing Body Member NHS Corby CCG % Andrew Hammond Lay Member for Governance NHS Corby CCG % Tansi Harper Lay Member for PPEA NHS Corby CCG % Helen Storer Lay Member NHS Corby CCG % Sebastian Hendricks Secondary Care Consultant NHS Corby CCG % * percentage is based on the number of meetings members were eligible to attend Total attendance is based on the number of meetings the Member was eligible to attend. Due to Quoracy requirements of the Audit and Risk Committee, Quoracy was achieved by the attendance of Dr Miten Ruparelia, Dr Nathan Spencer and Dr Sanjay Gadhia, as a GP Member is required to attend to ensure the Committee is quorate. Collectively 100% attendance was achieved for quoracy. For quoracy requirements the Chair of the Audit and Risk Committee must be in attendance along with one other Lay Member. Therefore, quoracy was achieved through the attendance of both Tansi Harper, Lay Member for Patient and Public Engagement and Helen Storer, Independent Lay Member. In addition to the membership above, Mike Alexander, Chief Finance Officer and the Head of Internal Audit and Head of External Audit were in attendance at each meeting of the Audit and Risk Committee. 76
77 Governance, Risk Management and Internal Control The Audit and Risk Committee Chair s report for 2017/18 highlighted the following: The Audit and Risk Committee reviewed the 2017/18 end of year draft financial accounts, Annual Report and Governance Statement at the Audit and risk Committee meeting held on 24 April The Audit committee has at previous meetings received regular reports detailing risks to delivery of financial targets and progress on recovery actions being taken following the outcome of an Expert Determination relating to a contract dispute with Lakeside Plus Limited. The outcome had a significant impact on the CCGs finances in year and required the introduction of an in year financial recovery plan. The delivery of recovery actions was overseen on behalf of the Governing Body by the Finance Committee, and progress and risks reported to the Governing Body and to Audit and Risk Committee. The CCG met its statutory breakeven duty and delivered a Surplus of 2m which included an additional 0.5% as required by NHS England. The CCG management are unaware of any material uncertainties that cast significant doubt on the CCG s ability to continue as a going concern. Head of Internal Audit presented the Head of Internal Audit Opinion to the Audit and Risk Committee, which concluded that the organisation has an adequate and effective framework for risk management, governance and internal control. At each meeting the Audit and Risk Committee has considered the risks, mitigations and assurance detailed within the Board Assurance Framework. To ensure adequate review of risks was undertaken against identified risks to the achievement of organisational objectives a series of deep dives were undertaken by the Committee. For each of these the Executive Lead for the identified risk was invited to the Committee to lead the discussion into the risks and mitigations for the strategic objectives for which they are responsible. Finance Committee The Finance Committee membership includes: One Lay Member of the Governing Body (Chair of the Committee) Chief Finance Officer (CFO)/ Deputy Chief Finance Officer (DCFO) Head of Programme Management Office (PMO) Governing Body GP Member/Nominated deputy Director of Commissioning & Strategy Contracting Team Manager. The Finance Committee makes recommendations to the Governing Body about achievement of financial and performance objectives. The Committee monitors contract activity, performance and budgets. 77
78 The Committee makes recommendations to the Governing Body on business cases for the delivery of new investments. Issues discussed and considered by the Committee during 2017/18 included: Actions planned at the main acute provider to address issues related to patient flow, impacting on A&E waits, cancelled operations and Ambulance Handover delays Resetting of Primary Care in Corby plans Performance against cancer standards Out of Hours and 111 services contract performance Performance against Referral to Treatment Times Delivery of QIPP plans IAPT (Improving Access to Psychological Therapies) Performance Refreshed Operational Planning for 2017/19 Financial Recovery plans and delivery updates. During 2017/18 the Committee met 9 times. The minutes of the Finance Committee are reported to the Governing Body meeting, with the Chair of the Committee drawing attention to any issues that require executive action via the Chair s highlight report. From October 2017 the Finance Committee moved from bi-monthly meetings to monthly meetings in response to the financial challenges the CCG faced. Finance Committee Member Attendance Table 20: Finance Committee attendance April 2017-March 2018 NAME TITLE ORGANISATION PERCENTAGE Mike Alexander Chief Finance Officer NHS Corby CCG % Dr Miten Ruparelia Clinical Leader NHS Corby CCG % Dr Nathan Spencer GP Governing Body Member NHS Corby CCG % Dr Sanjay Gadhia GP Governing Body Member NHS Corby CCG % Andrew Hammond Lay Member for Governance NHS Corby CCG % Tansi Harper Lay Member for PPEA NHS Corby CCG % Helen Storer Lay Member NHS Corby CCG % Dr Sebastian Hendricks Secondary Care Consultant NHS Corby CCG % Caron Williams Director of Commissioning & Strategy NHS Corby CCG % 18/04/ /06/ /08/ /10/ /11/ /12/ /01/ /02/ /03/2018 TOTAL Remuneration and Terms of Service Committee The Remuneration and Terms of Service Committee membership is made up of the following: 2 lay members, one of whom will act as chair. During 2017/18 Andrew Hammond Lay Member for Governance undertook the role of Chair of the Committee. Tansi Harper, Lay Member for Patient and Public Engagement and Helen Storer, Independent Lay Member, attended as required for quoracy purposes Secondary Care Consultant this is Dr Sebastian Hendricks To be quorate a minimum of 2 members must be present including the Chair. The Committee met 5 times during 2017/18. 78
79 The Remuneration Committee makes recommendations to the Governing Body regarding the remuneration, fees and other allowances for senior employees and for people who provide services to the Group. Remuneration Committee Member Attendance Table 21: Remuneration Committee attendance April 2017-March 2018 NAME TITLE ORGANISATION Percentage Lay Member Governance (Lay Vice Andrew Hammond Chair Governing Body) NHS Corby CCG % Pauline Pratt Nurse Member NHS Corby CCG % Lay Member - Patient and Public Tansi Harper Engagement NHS Corby CCG % Sebastian Hendricks Secondary Care Consultant NHS Corby CCG % Aly Hulme Nurse Member NHS Corby CCG % Helen Storer Independent Lay Member NHS Corby CCG % * This was a REMCOM held in Common with NHS Nene CCG 30/05/ /10/ /11/ /01/ /03/2018* Total Council of Members The Council of Members is a unique committee for Corby CCG, as it is a meeting which brings together representatives from all member practices. Membership of the committee includes: GP Governing Body Member (Chair) Practice Delivery Lead (practice representative) from each of our 5-member practices Chief Executive Chief Finance Officer Secondary Care Consultant (non-voting) Director of Commissioning & Strategy (non-voting). Officers of the CCG and Practice Managers are also in attendance at the Council of Members as required. The Council of Members meets bi-monthly and during 2017/18 met 6 times. The Council of Members provides assurance to the Governing Body that the organisation has delivered effective clinically-led decision making systems and processes in order to: Lead the planning, delivery and performance management of commissioning Ensure commissioning decisions meet the needs of patients, service users and wider population Formulate and deliver the CCG strategy in relation to member practices and commissioned services 79
80 During 2017/18 the Council of Members has considered the following items: Locally commissioned services (Demand Management and Leg Ulcer) Refresh of the Operating Plan Financial recovery Plan Commissioning Intentions QIPP plans Same day Access Elective demand. The minutes of the Council of Members meeting are reported to the Governing Body meeting, with the Chair of the Committee drawing attention to any issues that require Governing Body scrutiny via the Chair s highlight report. Patient and Public Engagement Assurance Committee The Patient and Public Engagement Assurance Committee (PPEA) provides assurance to the Governing Body that all decisions made by the Governing Body have been informed by the appropriate level of patients, carers and communities input in accordance with Section 14Z2 of the Health and Social Care Act The Committee upholds the core values of the NHS Constitution. The Committee membership includes: Lay Member Patient and Public Engagement (Chair) Lead GP with responsibility for Patient and Public Involvement (Deputy Chair) Commissioning Team representative A Lay Representative nominated from the GP Practice Patient Participation Chair s meeting. Other invitees include the following, although these do not form part of the formal membership of the Committee: HealthWatch Representative Member from Northamptonshire Carers Member from Voluntary Impact Northamptonshire (voluntary sector) A police representative A youth ambassador During 2017/18 the Committee met 9 times. The minutes of the Committee are reported to the Governing Body, with the Chair of the Committee drawing attention to any issues that require Governing Body scrutiny via the Chair s highlight report. The Committee went month from August 2017 in response to the financial challenges the CCG faced. 80
81 PPEA Committee Member Attendance Table 22: PPEA Committee attendance April 2017-March 2018 NAME TITLE ORGANISATION PERCENTAGE Tansi Harper Lay Member, PPEA (Chair) NHS Corby CCG % Ric Barnard Patient Participation Group Chair PPG % Dawn Cummins Deputy Chief Executive Voluntary Impact N'shire % Carole Dehghani Chief Executive NHS Corby CCG % Gwyn Roberts Deputy Chief Executive Officer Northamptonshire Carers % Joe Sim Patient Participation Group, Studfall Partnership PPG % Helen Storer Independent Lay Member NHS Corby CCG % Dr Sanjay Gadhia GP Governing Body NHS Corby CCG % Pauleen Pratt GB Registered Nurse Member NHS Corby CCG % Sonia Bray Healthwatch Officer Healthwatch N'shire % Kate Holt Healthwatch Officer Healthwatch N'shire % 18/04/ /06/ /08/ /09/ /10/ /11/ /01/ /02/ /03/2018 TO TAL Primary Care Commissioning Committee In April 2016 the CCG established the Primary Care Commissioning Committee. In accordance with its statutory powers under section 13Z of the National Health Service Act 2006 (as amended), NHS England has delegated the exercise of these functions to NHS Corby CCG. The Committee functions as a corporate decisionmaking body for the management of the delegated functions and the exercise of the delegated powers. The Committee membership includes: Chair (Lay Member) Deputy Chair (Lay Member) Chief Executive Chief Finance Officer/Deputy Chief Finance Officer Director of Commissioning & Strategy. The following organisations have a standing invitation: Two GP Governing Body Members Clinical Vice Chair Lay member for Governance CCG Quality Team representative Local Authority representative HealthWatch representative NHS England representative LMC representative External GP (external to the CCG but with the required Governing Body level experience). 81
82 During 2017/18 the Committee met 6 times on a Bi-monthly basis. The minutes of the Committee are reported to the Governing Body, with the Chair of the Committee drawing attention to any issues that require Governing Body scrutiny via the Chair s highlight report. The Primary Care Commissioning Committee meets in public and papers for the meeting can be found on the CCG website. Table 23: Primary Care Commissioning Committee attendance April March 2018 NAME TITLE ORGANISATION PERCENTAGE Mike Alexander Chief Finance Officer NHS Corby CCG % Carole Dehghani Chief Executive NHS Corby CCG % Caron Williams Director of Commissioning & Strategy NHS Corby CCG % Andrew Hammond Lay Member for Governance NHS Corby CCG % Tansi Harper Lay Member for PPEA NHS Corby CCG % Helen Storer Lay Member NHS Corby CCG % * percentage is based on the number of meetings members were eligible to attend 16/05/ /07/ /09/ /11/ /01/ /03/2018 TOTAL Joint Quality Committee The Quality Committee is a joint committee between NHS Corby CCG and NHS Nene CCG. The Committee provides assurance to the Governing Body on the quality of services commissioned and promotes a culture of continuous improvement and innovation with respect to safety of services, clinical effectiveness and patient experience to the Governing Body. Key issues debated and reviewed by the Committee during 2017/18 included: Quality overview reports received for Providers Quality Report and Quality Risk Register Complaints Annual report 2016/17 Deprivation of liberty safeguards Northamptonshire report. Safeguarding Annual Report 2016/17 Equality and inclusion updates Review of Complaints handling policy and safeguarding children and adults at risk policy Commissioning for Quality and Innovation (CQUIN) annual report 2016/17 Special Educational Needs Disability (SEND) framework Cancer long wait assurance update report Patient Stories Individual funding requests Disinvestment and De-commissioning Policy 82
83 The Committee membership is made up of: Lay representative (Deputy Chair) - NHS Nene CCG (Chair) Director of Nursing and Quality - NHS Nene and NHS Corby CCGs (Deputy Chair) Lay Member - NHS Corby CCG Clinical Executive Director for Strategy - NHS Nene CCG GP Quality Lead - NHS Corby CCG. Director of Contracting and Procurement NHS Nene CCG Secondary Care Consultant NHS Nene CCG Secondary Care Consultant NHS Corby CCG. The Committee is considered quorate when at least three voting members are present. During 2017/18 the Committee met 6 times. The minutes of the Committee are reported to the Governing Body with attention drawn to any issues that require Governing Body scrutiny via the Chair s highlight report. Joint Quality Committee Member Attendance Table 24: Joint Quality Committee attendance April 2017-March 2018 NAME TITLE ORGANISATION PERCENTAGE Christina Edwards Governing Body Lay Member NHS Corby CCG % (Chair - until ) Left Nene CCG April 2017 Dr Sebastian Hendricks (Chair - from 13/6/17) Secondary Care Consultant NHS Corby CCG % 11/04/ /06/ /08/ /10/ /12/ /02/2018 Total Mrs Sandra Bell Left Nene CCG February 2018 Vice Chair Northamptonshire Healthwatch % Mrs Pauleen Pratt (Deputy Chair until 8/8/2017) Left CCG August 17 Dr Chris Bunch (Deputy Chair from 10/10/17) Left Nene CCG February 2017 Registered Nurse Member of Governing Body NHS Corby CCG % Secondary Care Consultant NHS Nene CCG % Dr Matthew Davies Medical Director NHS Nene CCG % Mrs Carole Dehghani Mr John Wardell Left Nene CCG Dec 2017 Accountable Office (Corby) and Interim Accountable Office (Nene) Accountable Officer for Nene CCG NHS Corby CCG and NHS Nene CCG % Nene CCG % Mrs Aly Hulme Registered Nurse Member of Governing Body NHS Corby CCG and NHS Nene CCG % Mrs Alison Jamson Deputy Director of NHS Corby CCG and % Quality NHS Nene CCG Mrs Kathryn Moody Director of Contracting NHS Nene CCG % and Delivery Dr Miten Ruparelia Clinical Vice Chair NHS Corby CCG % Mrs Tina Swain Mr Peter Barker (Until 13 June 2018) Mrs Lucy Wightman (from 8/8/2017) Head of Nursing & Safeguarding Deputy Director of Public Health Director of Public Health NHS Corby CCG and NHS Nene CCG Northamptonshire County Council Northamptonshire County Council % 0 0 0% % 83
84 Register of Interests NHS Corby CCG is aware of the importance of its obligation to identify and address any potential or actual conflict of interest when transacting its business. The CCG has an embedded and robust system for: registering interests of the Governing Body, its sub-committees and staff publication of its register of interests updating the register on at least a quarterly basis taking any actual or potential conflicts into account when transacting the business of Corby CCG. The CCG s register of interests is available on the Corby CCG website. Personal Data Related Incidents All incidents reported by the CCG are investigated and reported in accordance with Department of Health guidelines. During 2017/18 there have been no serious incidents for the CCG relating to data loss or confidentiality breaches reported to the Information Commissioner. Responsibility for Information Governance rests with the Chief Finance Officer as the Senior Information Risk Owner and arrangements supporting the management of Information Governance are reviewed through the Audit and Risk Committee. Statement of Disclosure to Auditors Each individual who is a member of the CCG at the time the Members Report is approved confirms: so far as the member is aware, there is no relevant audit information of which the CCG s auditor is unaware that would be relevant for the purposes of their audit report the member has taken all the steps that they ought to have taken in order to make him or herself aware of any relevant audit information and to establish that the CCG s auditor is aware of it Modern Slavery Act Corby CCG fully supports the Government s objectives to eradicate modern slavery and human trafficking but does not meet the requirements for producing an annual Slavery and Human Trafficking Statement as set out in the Modern Slavery Act
85
86 [ljffl Corby Clmlul Commissioning Group In preparing the financial statements, the Accountable Officer is required to comply with the requirements of the Group Accounting Manual issued by the Department of Health and in particular to: Observe the Accounts Direction issued by NHS England, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis; Make judgements and estimates on a reasonable basis; State whether applicable accounting standards as set out in the Group Accounting Manual issued by the Department of Health have been followed, and disclose and explain any material departures in the financial statements; and, Prepare the financial statements on a going concern basis. To the best of my knowledge and belief, I have properly discharged the responsibilities set out under the National Health Service Act 2006 (as amended), Managing Public Money and in my Clinical Commissioning Group Accountable Officer Appointment Letter. I also confirm that: as far as I am aware, there is no relevant audit information of which the CCG's auditors are unaware, and that as Accountable Officer, I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that the CCG's auditors are aware of that information. that the annual report and accounts as a whole is fair, balanced and understandable and that I take personal responsibility for the annual report and accounts and the judgments required for determining that it is fair, balanced and understandable. Carole Dehghani Accountable Officer 25 May
87 Governance Statement Introduction and context NHS Corby CCG (the CCG) is a body corporate established by NHS England on 1 April 2013 under the National Health Service Act 2006 (as amended). The clinical commissioning group s statutory functions are set out under the National Health Service Act 2006 (as amended). The CCG s general function is arranging the provision of services for persons for the purposes of the health service in England. The CCG is, in particular, required to arrange for the provision of certain health services to such extent as it considers necessary to meet the reasonable requirements of its local population. As at 1 April 2017, the clinical commissioning group is not subject to any directions from NHS England issued under Section 14Z21 of the National Health Service Act Scope of responsibility As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the clinical commissioning group s policies, aims and objectives, whilst safeguarding the public funds and assets for which I am personally responsible, in accordance with the responsibilities assigned to me in Managing Public Money. I also acknowledge my responsibilities as set out under the National Health Service Act 2006 (as amended) and in my Clinical Commissioning Group Accountable Officer Appointment Letter. I am responsible for ensuring that the clinical commissioning group is administered prudently and economically and that resources are applied efficiently and effectively, safeguarding financial propriety and regularity. I also have responsibility for reviewing the effectiveness of the system of internal control within the clinical commissioning group as set out in this governance statement. 87
88 Governance arrangements and effectiveness The main function of the governing body is to ensure that the group has made appropriate arrangements for ensuring that it exercises its functions effectively, efficiently and economically and complies with such generally accepted principles of good governance as are relevant to it. The National Health Service Act 2006 (as amended), at paragraph 14L (2) (b) states: The main function of the governing body is to ensure that the group has made appropriate arrangements for ensuring that it complies with such generally accepted principles of good governance as are relevant to it. In accordance with this, we acknowledge within our Constitution the following principles: The highest standards of propriety involving impartiality, integrity and objectivity in relation to the stewardship of public funds, the management of the organisation and the conduct of its business by adopting: The Good Governance Standard for Public Services The standards of behaviour published by the Committee on Standards in Public Life (1995) known as the Nolan Principles The seven key principles set out in the NHS Constitution The Equality Act 2010 Standards for Members of NHS Boards and Governing Bodies in England. The roles and responsibilities of the Governing Body and sub-committees of the CCG are detailed within the CCG s Constitution including the terms of reference, and The structure can be found below in Table
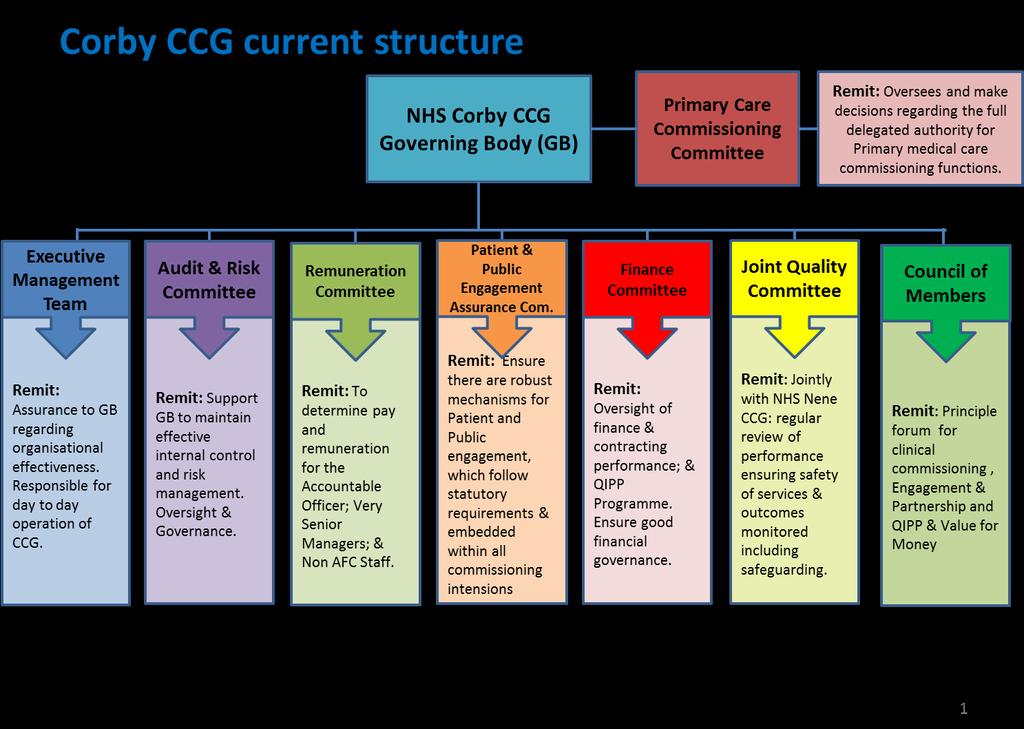
89 89
90 The CCG has established robust governance arrangements and a system of internal control. Corporate Governance is the system by which the CCG Governing Body directs and controls the organisation at the most senior level in order to achieve its objectives and meet the necessary standards of accountability and probity. The CCG s constitution sets out our organisation s commitment to good governance. It states that the Governing Body of the group will throughout each year have an ongoing role in reviewing the group s governance arrangements to ensure principles of good governance are reflected. This includes reviewing the effectiveness and the operation of Governing Body meetings and the subcommittees of this meeting. Using a risk management mechanism, the Governing Body brings together the various aspects of governance; corporate, clinical, financial and information to provide assurance on its direction and control across the whole organisation. The key features of our Constitution in relation to governance are: Discharge of functions - the arrangements made to discharge the functions of Corby CCG and the Governing Body. Our Constitution describes how we operate, the role of the Governing Body, the appointment of Committees and the specific duties of the Chair, Accountable Officer and Chief Finance Officer Primary decision-making processes - the primary decision-making processes and procedures to be followed by Corby CCG and the Governing Body including the arrangements for securing transparency in decision-making such as the provision for Governing Body meetings to be held in public Conflict of Interest management how the CCG deals with conflicts of interest, including the arrangements we have made to maintain and grant public access to registers of interest and ensure that declarations of conflicts or potential conflicts of interests are made. This is to ensure that conflicts or potential conflicts do not and do not appear to affect the integrity of the decision-making process. A copy of the CCG s register of interests is available on the CCG website Governing Body membership - details of how appointments are made to the Governing Body and how the membership of the organisation is involved in these appointments Scheme of Reservation and Delegation - sets out the decisions that are the responsibility of the Governing Body and its Committees, alongside the decisions delegated to individual members and employees. 90
91 The Constitution sets out the arrangements we have made for the discharge of the Governing Body s functions, including the following: Established sub-committees of the Governing Body Audit & Risk Committee, Remuneration Committee, Finance Committee, Council of Members, Patient and Public Engagement Assurance Committee (PPEA), Primary Care Commissioning Committee (PCCC) and Joint Quality Committee Delegated Governing Body functions for the approval of policies to the Joint Quality Committee, Audit and Risk Committee, and the Finance Committee, as committees of the Governing Body Delegated Governing Body authority to the Audit and Risk Committee to approve the Annual Report and Annual Accounts. Committee Effectiveness To ensure an accurate reflection of the work of each Committee within the CCG s governance structure each Committee Chair was asked to lead a review of the effectiveness of the work of their Committees during 2017/18. The CCG has developed the Committee Effectiveness and Meeting Checklist, which was designed to help in assessing the effectiveness of each sub-committee of the Governing Body. The first section focussed on committee/meeting and administration; the second section on how well the committee/meeting operated over a number of categories and the third section provided a free text section for each Committee Chair to provide any additional comments on the effectiveness of the Committee. Section One: Committee/Meeting Process Committee/Meeting Process Yes No Comments Does the Committee have written Terms of Reference that clearly define its role and remit? Are the Terms of Reference reviewed annually? (to take into account governance developments and the remit of other Committees within the CCG) Are the outcomes of each meeting, actions taken and Committee s view on risks, issues and mitigations reported to the Governing Body after each meeting? Does the Committee prepare an annual report on its work and performance in the preceding year for consideration? Does the Committee assess its own effectiveness periodically? Has the Committee established a plan of matters to be dealt with across the year in the form of a work programme? Has the Committee been quorate for each meeting this year? Has the Committee considered how it works with other Committees in reviewing and managing risks? 91
92 Strongly Agree Agree Disagree Strongly Disagree Unable to answer Strongly Agree Agree Disagree Strongly Disagree Unable to answer Strongly Agree Agree Disagree Strongly Disagree Unable to answer Section Two: Committee/Meeting Effectiveness Statement 2.1 Committee/Meeting Focus Comments The Committee has set itself a series of objectives it wants to achieve this year The Committee is clear on the level information it would like to receive for each of the items on the work programme Committee members contribute regularly across the range of issues discussed at the meeting The Committee is clear and fully aware of the key sources of assurance and who provides them in support of the control mitigating key risks Statement 2.2 Committee/Meeting Working Comments Committee has the right balance of experience, knowledge and skills to fulfil the role as described in its terms of reference Committee meeting has a structured agenda to cover key areas for the Committee Committee meetings have appropriate attendance from CCG officers to provide the required level of information for reports Key risks and assurances are presented to the Committee identifying any gaps in a timely fashion to avoid any gaps Committee members feel comfortable to express views, concerns and opinions in relation to key business areas Committee holds assurance providers to account for lack of assurance or missing information Committee members feel confident that where an action has been agreed, it will be implemented as agreed and in line with the agreed timescale Statement 2.3 Committee/Meeting Working Comments As Chair the quality of papers received by the Committee allows me to perform my role effectively Members provide real and genuine challenge - they do not seek clarification and/or reassurance Each agenda item has a clear conclusion so that I am clear on the action, who the action lead is and the timescale for completion and how this will be monitored The Committee agenda allows time for reflection on what has been discussed at the meeting The Committee provides a summary report to the Governing Body on a regular basis The Governing Body understands the report from the Committee There is a formal appraisal of the Committee effectiveness each year 92
93 Strongly Agree Agree Disagree Strongly Disagree Unable to answer Strongly Agree Agree Disagree Strongly Disagree Unable to answer Statement 2.4 Committee/Meeting Engagement Comments Committee actively challenges both CCG officers and other assurance providers during the year to gain a clear understanding of their findings There is clarity on the Committee s relationship with other Committees Statement 2.5 Committee/Meeting Leadership (may require discussion/review with Committee members) Comments Committee Chair has a positive impact on the performance of the Committee Committee meetings are chaired effectively and with clarity of purpose and outcome Committee Chair is visible within the organisation and is considered approachable Committee Chair allows debate to flow freely and does not assert their own views too strongly Committee Chair provides clear and concise information to the Governing Body on the activities of the Committee and the implications of identified risks and issues Section Three: Committee Effectiveness Committee Chair s Comments A text box was also used to allow further comments from the Committee Chair on the work of the Committee during the past 12 months if not covered in the comments sections above. 93
94 Performance and Effectiveness of the Governing Body The Governing Body ensures that the CCG has appropriate arrangements in place to exercise its functions effectively, efficiently and economically in accordance with the CCG s principles of good governance. The Governing Body brings together the various aspects of governance; corporate, clinical, financial and information to provide assurance on its direction and control across the whole organisation. The coordinating body for receiving assurance on these strands of governance is the Audit and Risk Committee, which oversees integrated governance and in turn provides assurance to the Governing Body. In addition, other committees oversee the risks within their specific remits, providing assurance to the Governing Body where appropriate. Governance Audit A governance audit was undertaken as part of the approved internal audit plan for 2017/18. The audit focussed on committee assurance and the controls and support mechanisms in place to ensure that the CCG's key committees are working effectively, that committee roles and responsibilities and expectations are defined and that they are reporting to the Governing Body in a timely manner. The review particularly considered the role and operation of the Primary Care Commissioning Committee (PCCC), including the views of its members. The audit confirmed that a number of improvements had been made since our previous governance audit. This included evidence of progress towards a more consistent risk management approach across the CCG s committees, and improved traceability between the committee risk registers and the Board Assurance Framework (BAF). In addition, we noted some movement away from verbal updates by the PCCC and PPEA. However, there is still work to do around the assurances that the Governing Board and Committees receive through the use of the BAF rather than through an agenda item which does ensure appropriate scrutiny and challenge is present. This is an area that the CCG will work on through 2018/19. CCG Transition Programme A paper taken to the Private Meeting in Common of the NHS Corby and NHS Nene CCG Governing Bodies in July 2017 noted that CCGs across England are coming together to work as more integrated strategic commissioning bodies in order to deliver the ambitions set out in the NHS Five Year Forward View. Additionally, the Northamptonshire STP had proposed that there should be a more integrated strategic commissioning approach for the population of Northamptonshire (the STP footprint) as a key enabler for service transformation. Corby and Nene CCGs have been working increasingly closely together over the last months in order to develop that vision and a set of aligned delivery plans. Following robust discussion, the Governing Bodies approved the following recommendations: The general approach to developing joint working arrangements between Corby and Nene CCGs 94
95 To mandate the Chief Finance Officers of Corby and Nene CCGs to develop a joint finance team that will support both CCGs. Creation of a programme of work to align the leadership (clinical and managerial) and governance arrangements of the 2 CCGs to develop a more integrated strategic commissioning approach for the population of the county, matching the STP footprint. Establishment of a Joint Transitional Programme Board, reporting to both CCG Governing Bodies to oversee the development and delivery of the joint working arrangements between the CCGs. To mandate the Audit Chairs of each CCG with a regular checkpoint scrutiny role for the purposes of assurance on the governance arrangements. Development of a communications and engagement plan with patients, members, staff and key stakeholders. To receive future reports on the progress. A Joint Transition Board was established, holding its first meeting on 14 th September 2017 to establish its terms of reference and associated work streams. Following the second meeting in November, the Programme Board continues to meet on a monthly basis chaired and attended by a lay member from each CCG, with formal reporting arrangements to the Governing Bodies Meeting in Common. An Extraordinary Governing Body meeting in Common was held in October 2017 to discuss options for an Interim Accountable Officer. A single finance team is being established, progress on this work overseen by the Transition Board; at time of writing this change is currently out to engagement with staff. The two Governing Bodies met again in January 2018 to discuss and recommend revised governance arrangements to the governing bodies of the individual organisations. A communication and engagement plan has been developed and will be presented for approval to the Transition Board in February. UK Corporate Governance Code It is worth noting that NHS Bodies are not required to comply with the UK Code of Corporate Governance, however the CCG has elected to view its governance in light of this framework as an example of best practice. Discharge of Statutory Functions In light of recommendations of the 1983 Harris Review, the clinical commissioning group has reviewed all of the statutory duties and powers conferred on it by the National Health Service Act 2006 (as amended) and other associated legislative and regulations. As a result, I can confirm that the clinical commissioning group is clear about the legislative requirements associated with each of the statutory functions for which it is responsible, including any restrictions on delegation of those functions. 95
96 Responsibility for each duty and power has been clearly allocated to a lead Director. Directorates have confirmed that their structures provide the necessary capability and capacity to undertake all of the clinical commissioning group s statutory duties. Risk management arrangements and effectiveness Leadership of the risk management process is given a high profile within Corby CCG. The CCG has a risk management policy that escalates significant risks to the Governing Body the policy was reviewed and revised in The Risk Management Strategy sets out the roles of key personnel in handling and reporting risks. Risk management is built into the strategic planning process and then managed operationally through a robust process of governance around decision making set out in the organisation s scheme of delegation. Staff receive training and support through group training and tailored one to one sessions especially with those with responsibility for maintaining risk registers. Corby encourages all employees to highlight risks and report incidents. The BAF in every Governing Body meeting. Aligned to the corporate risks of Corby CCG, it provides the Governing Body with a comprehensive method for the effective and focused management of risks that arise in meeting our strategic objectives. The Audit and Risk Committee reviews the risk register regularly and reports to the Governing Body, providing assurance that risks are being monitored and mitigated, and highlighting any exceptions. The Governing Body continues to recognise risk management as an important development area to improve internal controls and its own effectiveness during 2017/18, devoting development sessions to risk management. The Governing Body reviewed its risk appetite, and resolved to keep the existing triggers, including a lower trigger point for risks involving quality, safeguarding and safety. The BAF format has continued to be revised during the year to ensure it remains a real working document and following best practice. The Governing Body and employees receive training in Equality and Diversity, and Equality and Human Rights considerations are included in the development of all strategies, policies and business cases to ensure impacts on protected groups are understood and taken into account when making decisions. Corby CCG s Local Counter Fraud Specialist provides training and awareness as a deterrent to fraud risks arising. Capacity to Handle Risk Following on from 2017/18 Corby CCG continues to recognise risk management and the BAF as areas that need continued development. The internal audit of risk management and assurance has identified a number of improvements and work continues to embed to use of the BAF and this risk management process within the Governing body and its committees. 96
97 Risk Assessment Corby CCG s risk management policy clearly explains how to assess risk. The policy and documentation ensures every BAF and corporate risk is allocated to a committee of the Governing Body to ensure appropriate oversight and effective action. The CCG Directors and risk owners make recommendations regarding updates to the risk register which feeds through into the CCGs Committees and then finally to the BAF and Corporate Risk Register reflecting on work undertaken which would impact on the existing risks and consider any high risks identified through the risk management process. Table 26: Corby CCG major risks to governance, risk management and internal control during 2017/18 include: Risk description Mitigations and Controls Failure to achieve in year financial status for the CCG and maintain assurance status for the CCG KGH Performance against mandatory A&E targets Audit and Risk Committee monitor the BAF, reported to Governing Body. Each Committee has a risk register with escalation of risks to the Governing Body as required via the Corporate Risk Register. Quarterly assurance meetings held with NHS England, action plan from these meetings to maintain delivery. ECIP have been working with the Trust to improve areas of practice and performance in A&E and hospital flow KGH have developed an ambulatory pathway A&E Board action logs record decisions and actions taken. Monthly A&E Board action logs record decisions and actions taken. Contract monitoring and assurance meetings with providers. CCG performance managed by NHS England on National Performance Targets. CQRM monitor performance and report to the Quality Committee. Monthly review by NHSE of our performance. Regional escalation with NHSE and a new plan to address these concerns and pull them into a single space has been devised. Additional resources have been given by NHSI to KGH to support the delivery of that plan. 97
98 KGH have established an executive assurance function to support the delivery of A&E and DTOC targets. It meets fortnightly to review resolution of target achievement. Risk description KGH Performance Delayed Transfers of Care (DTOC) CQC Inspection identified areas of concern relating to patient safety and quality at Kettering General Hospital following their inspection in October 2016 resulting in a Section 29A warning notice, leading to a risk of an overarching concern regarding the Trust articulation and reporting of risk especially as winter pressures are contributing to potential risks to patient care. Mitigations and Controls This area is the key focus of regional escalation. Fortnightly review with NHSE and actions linked to BCF and winter plans. Clinical Leaders meeting work with the Deputy Medical Director to establish stranded patient work plan with the Trust. This will enable better identification. Intermediate care review will be undertaken and actioned as part of the STP Urgent Care work stream. It will develop discharge capacity, earlier support discharge for patients identified through the stranded patient work. A&E Board - outflow group have devised a Recovery Plan, and BCF resources are being reprofiled to support the delivery of the RAP. Recovery Trajectories are set. Programme alignment between BCF and UC outflow has been delivered; this has improved the clarity and accountability for individual actions. System level accountability requires some attention. All of the actions from the stabilisation plan are in place and we are due to deliver by end of February Next steps around nurse led early supported discharge are being developed. Meetings with NHS Improvement and CQC. KGH monitoring plan and position monitored at Clinical Quality Review Meeting Announced clinical quality visits undertaken bimonthly and unannounced visits undertaken as required. A&E performance managed through A&E Board. Quality Committee and Clinical Quality Review Meeting monitor and assess data submitted by KGH Clinical Quality Review Meeting, along with clinical quality visit reports, to Quality Committee. Updates through public Board papers, CCG review. Review undertaken in accordance with CCGs escalation of concerns process. Clinical Quality Review Visits. 98
99 Inspection report published in April 2017 rated the trust as inadequate Escalation of concerns via Trust Director Nursing and CQRM and Serious Incident Assurance Meeting. Quality surveillance Group provided with oversight of action taken. Quality Summit held 3 May Action notes presented at May QSG. Oversight meeting chaired by NHSI in place with representation by trust, CCG, NHSI / NHSE Trust improvement action plan approved at Trust board. Unannounced visit undertaken by CQC June Feedback letter to trust indicates areas of significant improvement. Inspection report published 7 September 2017 confirmed that improvements have been identified and the 29A warning notice has been lifted. The trust is due to be revisited by the CQC with this anticipated for October During the reporting period there were no major risks identified to Corby CCG s licence status. Risks relating to performance of providers and delivery of key performance indicators and constitutional standards are covered in the Performance section of this report. These risks are reported to the Governing Body via performance reports and updates on mitigations. Other sources of assurance Internal Control Framework A system of internal control is the set of processes and procedures in place in the clinical commissioning group to ensure it delivers its policies, aims and objectives. It is designed to identify and prioritise the risks, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control allows risk to be managed to a reasonable level rather than eliminating all risk; it can therefore only provide reasonable and not absolute assurance of effectiveness. Corby CCG and its members recognise the importance of managing conflicts of interest. Accordingly, a register of interests is maintained and updated regularly. A copy of the register of interests is available on the CCG s website. All meeting agendas of the governing body and committees include guidance and definitions of interests, and time is allocated at the start of the meeting for such declarations to be made. 99
100 The Audit and Risk Committee has oversight of the internal control mechanisms on behalf of the Governing Body. Executive directors oversee the management and delivery of internal control mechanisms. The Audit and Risk Committee bases its assessments, and therefore assurances, on the effectiveness of the CCG s controls on assurances provided by the Governing Body and Committees work programmes; Review of the Board Assurance framework which provides an oversight of the effectiveness of controls in place to manage the CCG s principle risks; Reviews of CCG policies and procedures; Provision of assurance from independent sources (e.g. internal or external audit or third-party reviews undertaken). Annual audit of conflicts of interest management The revised statutory guidance on managing conflicts of interest for CCGs (published June 2016) requires CCGs to undertake an annual internal audit of conflicts of interest management. To support CCGs to undertake this task, NHS England has published a template audit framework. The CCG undertook its annual conflict of interest Audit in November The CCG are working through the recommendations to ensure that the organisation is compliance across all Conflict of Interest Areas. Figure 5: Conflict of Interest Audit Outcomes Conflicts of Interest: this audit provided a reasonable assurance opinion and whilst a small number of medium priority weaknesses were identified an overall positive level of assurance can be taken over the controls in place for this area. Data Quality Information used by the Governing Body and its Committees enables the CCG to carry out our responsibilities and discharge its statutory functions. This information relates to operational, financial, performance, quality and patient experience. The Governing Body and its Committees are committed to improving the quality of the information received. There has been an improvement in the quality of data received and the Governing Body has taken action to continue to improve this position, including working with the Commissioning Support Unit to redesign the performance report. 100
101 Information Governance The NHS Information Governance Framework sets the processes and procedures by which the NHS handles information about patients and employees, in particular personal identifiable information. The NHS Information Governance Framework is supported by an information governance toolkit and the annual submission process provides assurances to the clinical commissioning group, other organisations and to individuals that personal information is dealt with legally, securely, efficiently and effectively. We place high importance on ensuring there are robust information governance systems and processes in place to help protect patient and corporate information. We have established an information governance management framework and have developed information governance processes and procedures in line with the information governance toolkit. We have ensured all staff undertake annual information governance training meeting the 95% staff completion rate and have implemented a staff information governance handbook to ensure staff are aware of their information governance roles and responsibilities. We have submitted a satisfactory level of compliance with the information governance toolkit assessment of 18% for 2017/18. The Information Governance Steering Group (IGSG) supports and drives the broader information governance agenda and provides the Audit and Risk Committee and ultimately the Governing Body with the assurance that effective information governance best practice mechanisms are in place within the organisation. The focus of the Information Governance audit for this year was on the preparedness for the General Data Protection Regulation (GDPR). The CCG will maintain the threshold required by NHS Digital to continue enablement of NHS digital data flows. There are processes in place for incident reporting and investigation of serious incidents. We are strengthening our information risk assessment and management procedures and a programme will be established to fully embed an information risk culture throughout the Nene and Corby CCGs against identified risks. Business Critical Models The CCG receives Service Auditor Reports on the business-critical systems operated by organisations that provide services to the CCG, which includes Shared Business Services and also the North East London Commissioning Support Unit. This enables the CCG to place reliance on quality controls established relating to business-critical systems and models delivered through the Service Level Agreement in place for 2017/18, in line with the recommendations in the 2013 Macpherson report. 101
102 Third party assurances Until 31 st July 2017 Corby and Nene CCGs relied on NHS Arden GEM CSU as a third-party provider of commissioning support services, on the 1 st August 2017 the majority of support services for Corby excluding Information Governance, Finance, HR and Health&Safety were taken on by North East London (NEL) CSU following a competitive tender exercise. On the 1 st March 2018 Finance and HR were also taken on by NEL CSU. CSUs are part of NHS England and therefore CCGs rely on NHS England-led internal and external audit of CSUs. Corby and Nene CCGs hold quarterly contract performance meetings with the NEL CSU. Control Issues No material control issues have been identified via the work undertaken by internal audit. This has been further informed by regular reporting to the Audit and Risk Committee including assurance from the External Auditors, Local Counter Fraud Specialist and Information Governance Team. These sources of assurance have not identified any areas of significant control issues. Emergency preparedness We certify that Corby Clinical Commissioning Group has incident response plans in place, which are compliant with the NHS England Emergency Preparedness Framework Corby Clinical Commissioning Group regularly reviews and makes improvements to its major incident plan and Business Continuity Plan and has a programme for regularly testing plans, the results of which are reported to the Governing Body. Providers and Commissioners of NHS funded care have a range of standards they should meet to ensure that they are prepared to meet the challenges of a business continuity incident or a major incident. A business continuity incident can be summarised as: A disruption would be any event that threatens personnel, buildings or operational capacity and requires special measures to be taken to restore normal service. Typically, business continuity disruption will consist of a denial of premises (e.g. fire or flood), a denial of staff (e.g. infectious disease, industrial action, and severe weather or transport disruption) or a loss of utilities (power, ICT or water). 102
103 And a major incident can be summarised as: Any occurrence that presents serious threat to the health of the community or causes such numbers or types of casualties, as to require special arrangements to be implemented. For the NHS this includes also an event classified as an emergency EPRR Framework Corby CCG self-certified against the NHS England Core Standards as fully compliant and this has been ratified by a panel consisting of NHS England, Public Health England and Director of Public Health, Northamptonshire County Council. Corby CCG has coordinated the NHS response to the following incidents over the previous year: Wannacry Ransomware attack coordinating the response for our providers and Primary Care in the County The rise in the National Alert Level to Critical on two occasions that necessitated appropriate communications to our providers and partners Pressures on mortuary capacity on two separate occasions Water leak into a high voltage power cable that potentially may have caused the evacuation of a community hospital Major Gas leak in Oundle affecting all properties that use gas as a fuel Severe weather and snow in December, February and March. In addition to involvement in incidents, Corby CCG has also participated in the following exercises to ensure we can provide training to Managers and Directors who perform an On-Call role and would coordinate the response to a major incident on behalf of Nene CCG, Corby CCG and the NHS in Northamptonshire. Exercise Stark 2 a winter pressures exercise to test the system preparedness with regards to escalation. Participated in Exercise Jerboa, a Local Resilience Forum led flooding exercise involving a Military Response Exercise Tartar, a mass casualty incident centred on Northampton and testing the NHS response to a terrorist fire arms attack. Corby CCG is also a part of the Local Resilience Forum, representing the NHS in Northamptonshire and is a key part of the Local Health Resilience Partnership, which consists of partners from all health and social care partners across Northamptonshire. This group is co-chaired by NHS England and the Director of Public Health, Northamptonshire County Council. This is a strategic level group and is attended by the Authorised Officer for Nene CCG, who leads on resilience for by Nene and Corby CCG s The Health Resilience Working Group is a sub-group aligned to the Local Health Resilience Partnership and is chaired by the Nene CCG and Corby CCG Head of System Resilience and EPRR. 103
104 The following plans and actions have been developed or reviewed and updated over the course of the year. Development of the Local Resilience Pandemic Influenza Plan Development the Risk and Capability Map for EPRR for Northamptonshire; Developed the Northamptonshire Health and Social Care System Surge and Escalation Plan Provided leadership for the EPRR agenda across the NHS in Northamptonshire. From the Business Continuity perspective Corby CCG has had to deal with its own response to the Wannacry Ransomware attack. In addition, the Corporate Business Continuity Plan has been fully reviewed and revised and work was commenced on combining the Business Continuity Management arrangements for Nene CCG and Corby CCG as part of our transition to closer joint working. In addition, Corby CCG had to respond to disruption caused by severe weather and snowfall in December A communications exercise was conducted to test the ability of on-call staff to access Resilience Direct from remote locations. This revealed a number of problems to be resolved. To ensure Corby CCG remains compliant with NHS England s Core Standards for EPRR and the Civil Contingencies Act 2004 the following has been identified as the priorities for the coming year: Review and update the Incident Response Plan following the introduction of the NEL Surge and Escalation Team and the changes to the on-call manager rota. Additionally the plan was exercised during Exercise Tartar Undertake the statutory exercises stated in the Civil Contingencies Act 2004 and NHS England EPRR Framework. These are: Twice yearly communications exercise Yearly table top exercise Review and update the Local Resilience Forum Pandemic Flu Plan on receipt of the updated guidance following Exercise Cygnus Develop and lead a business continuity exercise for GP Practice Managers Continuous training for on-call managers and directors Plan and Deliver, in partnership with Public Health England, an exercise to review the NHS response in Northamptonshire to incidents involving outbreaks of Meningitis, Hepatitis A and Invasive Group A Streptococcus Winter debrief and alignment of learning to plans Plan and deliver a surge and escalation exercise in late September. 104
105 Review of economy, efficiency & effectiveness of the use of resource To ensure the CCG resources are used economically, efficiently and effectively the CCG has implemented processes, which are described below: Prime and detailed financial policies, which set out the systems to be adhered to, to ensure that resources are used efficiently Developed and implemented strategic and operational plans, which include an agreed annual budget approved by the Governing Body Contracts with providers that use the national standard NHS contract and include detailed finance, activity and quality schedules. The contracts require providers to innovate to improve quality and efficiency Comprehensive programme of contract monitoring, covering all aspects of performance, quality, activity and finance against agreed plans Corporate wide process for the development and review of business cases for investment. Process includes assessment of value for money and contribution to the achievement of CCG objectives Reports on finance and quality presented on a bi-monthly basis to the Governing Body, with actions identified when performance is off track Report on identified key financial risks to Finance Committee Implemented an internal audit programme that is targeted at the strategic risks and key financial control processes Annual fraud risk assessment undertaken by an independent party, providing recommendations for key actions Comprehensive suite of Fraud and Bribery policies agreed and in place with local counter fraud specialist in place delivering an agreed work plan All staff required to undertake fraud training. Risks relating to performance of providers and delivery of key performance indicators and constitutional standards are detailed within the Performance Report under Chapter 1 of this report. The CCG has led a local assurance process with our Regulators with KGH in respect to RTT performance. To ensure delivery of assurance on that task and ensure daily business of the CCG is conducted, the CCG worked closely with system partners drawing on system resources to address the issues of patient care and experience that occur as a result of this performance challenge. The CCG and system partners understand that resources need to be used economically and efficiently to respond to the issues and review the systems in place to monitor and address the risk of harm, in line with national best practice. The CCG has continued to closely monitor this performance in 2017/18 to rectify delivery against required standards. These risks are reported to the Governing Body via the Board Assurance Framework (BAF), full papers can be found on the website. 105


106 Counter Fraud The Committee received updates on the work of the Local Counter Fraud Specialist throughout the year. The Committee received the annual Counter Fraud work plan in May It was noted that Counter Fraud did not have any outstanding concerns. The Counter Fraud Service for the CCG is provided by RSM UK, who has provided an on-going programme of prevention and detection exercises during 2017/18. The programme was developed in line with the NHS Protect Standards for Commissioners: Fraud, Bribery and Corruption, fraud planning guidance from NHS Protect and best practice. The programme is designed to ensure our staff are fully aware of the fraud risks that the organisation faces. The CCG ran a Fraud awareness process in 2017/18 for all staff, with weekly updates on fraud awareness, a training questionnaire and an banner process for raising awareness, as shown below: The Audit and Risk Committee receives regular updates on the delivery of the Counter Fraud work plan and an annual report which summarises activity through the year. The Chief Finance Officer is the responsible officer who is proactively and demonstrably responsible for tackling fraud, bribery and corruption. The Chief Finance Officer is also responsible for ensuring that appropriate action is taken in response to any NHS Protect quality assurance recommendations. During the year two partial assurance opinions have been provided to the CCG, in respect of Financial Planning and Delivery and Risk Management and Assurance. 106
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
NHS Corby CCG Public Event. 1 October 2013
 NHS Corby CCG Public Event 1 October 2013 Welcome & Introductions Tansi Harper Lay member, Patients and Public Corby CCG Governing Body Housekeeping Please turn mobile phones to silent/off No fire alarm
NHS Corby CCG Public Event 1 October 2013 Welcome & Introductions Tansi Harper Lay member, Patients and Public Corby CCG Governing Body Housekeeping Please turn mobile phones to silent/off No fire alarm
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Integrating Health & Social Care in Kirklees
 Integrating Health & Social Care in Kirklees The case for change DRAFT v3.1 June 2017 Integrated Commissioning - Building on Existing Approaches Some example Children s services Mental health Hospital
Integrating Health & Social Care in Kirklees The case for change DRAFT v3.1 June 2017 Integrated Commissioning - Building on Existing Approaches Some example Children s services Mental health Hospital
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
August Planning for better health and care in North London. A public summary of the NCL STP
 August 2017 Planning for better health and care in North London A public summary of the NCL STP Planning for better health and care in North London North London NHS organisations are working together with
August 2017 Planning for better health and care in North London A public summary of the NCL STP Planning for better health and care in North London North London NHS organisations are working together with
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
A guide to NHS Bexley Clinical Commissioning Group
 A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
Memorandum of understanding for shadow Accountable Care Systems
 Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Richmond Clinical Commissioning Group
 Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Norfolk and Waveney STP. Meeting with East Suffolk Partnership 27 September 2017
 Norfolk and Waveney STP Meeting with East Suffolk Partnership 27 September 2017 2 The Norfolk and Waveney STP Members Waveney District Council Focus of Norfolk and Waveney STP Our plan is in line with
Norfolk and Waveney STP Meeting with East Suffolk Partnership 27 September 2017 2 The Norfolk and Waveney STP Members Waveney District Council Focus of Norfolk and Waveney STP Our plan is in line with
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
South Yorkshire and Bassetlaw Accountable Care System Chief Executives
 South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Adult Social Care Assessment & care management In-house care services
 Adult Social Care Assessment & care management In-house care services Service Plan 2015/16 Date 19/03/15 Final Directorate: Education Health and Social Care 1. Introduction Policy Context The Adult Social
Adult Social Care Assessment & care management In-house care services Service Plan 2015/16 Date 19/03/15 Final Directorate: Education Health and Social Care 1. Introduction Policy Context The Adult Social
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Welcome to. Northern England and the Five Year Forward View for Mental Health. Thursday 2 February 2017 at the Radisson Blu, Durham
 Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
General Practice Commissioning Strategy Development
 General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Suffolk Health and Care Review
 Suffolk Health and Care Review Update on Health and Social Care System Redesign and Re-commissioning of GP Out of Hours, 111 and Community Healthcare services An Insight into the Health and Social Care
Suffolk Health and Care Review Update on Health and Social Care System Redesign and Re-commissioning of GP Out of Hours, 111 and Community Healthcare services An Insight into the Health and Social Care
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Item No. 9. Meeting Date Wednesday 6 th December Glasgow City Integration Joint Board Finance and Audit Committee
 Item No. 9 Meeting Date Wednesday 6 th December 2017 Glasgow City Integration Joint Board Finance and Audit Committee Report By: Contact: Sharon Wearing, Chief Officer, Finance and Resources Allison Eccles,
Item No. 9 Meeting Date Wednesday 6 th December 2017 Glasgow City Integration Joint Board Finance and Audit Committee Report By: Contact: Sharon Wearing, Chief Officer, Finance and Resources Allison Eccles,
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION
 NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
FIVE TESTS FOR THE NHS LONG-TERM PLAN
 Briefing 10 September 2018 FIVE TESTS FOR THE NHS LONG-TERM PLAN The new NHS long-term plan is a significant opportunity for the health service. It can set out a clear and achievable path for sustaining
Briefing 10 September 2018 FIVE TESTS FOR THE NHS LONG-TERM PLAN The new NHS long-term plan is a significant opportunity for the health service. It can set out a clear and achievable path for sustaining
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
Annual Report Summary 2016/17
 Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
NHS Equality Delivery System for Isle of Wight NHS Trust. Interim baseline assessment against the
 Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Local system reviews. Interim report
 Local system reviews Interim report December 2017 The Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. We make sure that health and social care services
Local system reviews Interim report December 2017 The Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. We make sure that health and social care services
NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September
 Annual General Meeting(AGM) 26th September") RIGHT CARE RIGHT TIME RIGHT PLACE NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September 2017 Introduction Matt Colledge Chair Introduction Trafford Clinical Commissioning
RIGHT CARE RIGHT TIME RIGHT PLACE NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September 2017 Introduction Matt Colledge Chair Introduction Trafford Clinical Commissioning
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Bedfordshire, Luton and Milton Keynes. Sustainability and Transformation Plan. Central Brief: February 2018
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Mental health and crisis care. Background
 briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
CCG: CO01 Access and Choice Policy
 Corporate CCG: CO01 Access and Choice Policy Version Number Date Issued Review Date V2 21 January 2016 January 2018 Prepared By: Consultation Process: NECS Commissioning Manager CCG Head of Corporate Affairs.
Corporate CCG: CO01 Access and Choice Policy Version Number Date Issued Review Date V2 21 January 2016 January 2018 Prepared By: Consultation Process: NECS Commissioning Manager CCG Head of Corporate Affairs.
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
West Wandsworth Locality Update - July 2014
 Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Manchester Health and Care Commissioning Board. A partnership between Manchester. City Council and NHS Manchester Clinical Commissioning Group
 Manchester Health and Care Commissioning Board A partnership between Manchester City Council and NHS Manchester Clinical Commissioning Group Agenda Item: Report Title: Date: Strategic Commissioning Prepared
Manchester Health and Care Commissioning Board A partnership between Manchester City Council and NHS Manchester Clinical Commissioning Group Agenda Item: Report Title: Date: Strategic Commissioning Prepared
Powys Teaching Health Board. Respiratory Delivery Plan
 Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP)
") Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP) Q. What is a Sustainability and Transformation Plan? A. The NHS and local authorities across Buckinghamshire,
Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP) Q. What is a Sustainability and Transformation Plan? A. The NHS and local authorities across Buckinghamshire,
GOVERNING BODY MEETING in Public 29 November 2017 Agenda Item 5.4
 GOVERNING BODY MEETING in Public 29 November 2017 Paper Title Paper Author Jacki Wilkes Associate Director of Commissioning Redesign of adult and older peoples specialist mental health services pre-consultation
GOVERNING BODY MEETING in Public 29 November 2017 Paper Title Paper Author Jacki Wilkes Associate Director of Commissioning Redesign of adult and older peoples specialist mental health services pre-consultation
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Enclosures Appendix 1: Annual Director of Public Health Report 2015 Rachel Wells Consultant in Public Health
 Title Health and Wellbeing Board 21 January 2016 The Five Ways to Mental Wellbeing in Barnet: The Annual Report of the Director of Public Health (2015) Report of Director of Public Health Wards All Status
Title Health and Wellbeing Board 21 January 2016 The Five Ways to Mental Wellbeing in Barnet: The Annual Report of the Director of Public Health (2015) Report of Director of Public Health Wards All Status
NHS Norwich CCG Operational Plan and
 NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Islington Practice Based Mental Health Care: Roll-out plans and progress
 Report to: Board of Directors (Public) Paper number: 3.2 Report for: Information Date: 26 th October 2017 Report author/s: Emily van de Pol, Divisional Director, Community Mental Health and Primary Care
Report to: Board of Directors (Public) Paper number: 3.2 Report for: Information Date: 26 th October 2017 Report author/s: Emily van de Pol, Divisional Director, Community Mental Health and Primary Care