CRE and XDRO for Long Term Care Facilities. May 28, 2014
|
|
|
- Bernadette Estella Williams
- 6 years ago
- Views:
Transcription


1 CRE and XDRO for Long Term Care Facilities May 28, 2014



2 Featured Presenters Deb Burdsall, MSN, RN-BC, CIC Infection Preventionist Lutheran Home/Lutheran Life Communities William Trick, M.D. Director, Collaborative Research Unit Cook County Health & Hospitals System Michael Lin, M.D., MPH Assistant Professor, Infectious Diseases Rush University The opinions, viewpoints, and content presented in this webinar may not represent the position of the Illinois Department of Public Health
3 CRE Detect and Protect webinar for long-term care staff Deb Patterson Burdsall MSN, RN-BC, CIC Infection Preventionist: Lutheran Home/Lutheran Life Communities
4 Questions: Inquiring minds want to know how do we prevent or contain CRE? how do we implement prevention programs in a long term facility? how do we educate frontline staff on identification and prevention what cleaning products are effective
5 What to Do? Define Collaborate Prepare Watch Identify and Report Respond and Control

6 Definitions CRE Enterobacteriaceae - A family of bacteria. These types of bacteria have developed ways to become very resistant to commonly used antibiotics. The resistance makes the bacteria very difficult to kill and infections very hard to treat. There are 2 main types. E-coli (a common intestinal bacteria), and Klebsiella pneumoniae PCR (Polymerase Chain Reaction) A test that makes copies of DNA (or RNA) in order to identify specific organisms Modified Hodge Test Lab test that can identify organisms that produce carbapenemase

7 Illinois Detect and Protect Campaign
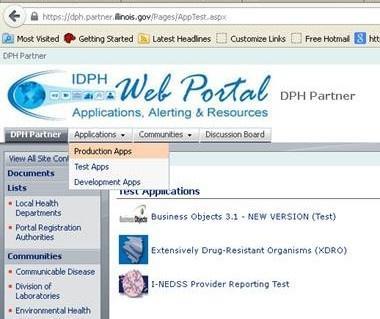
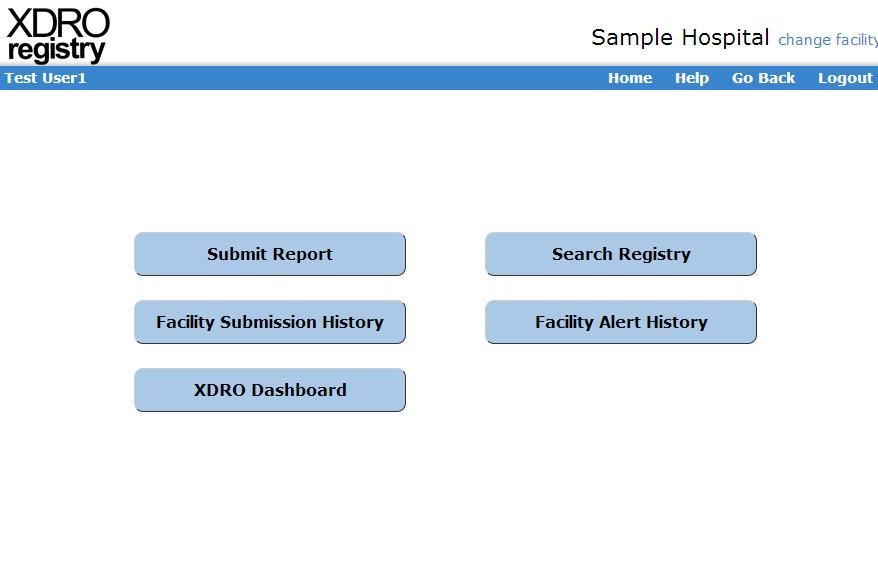
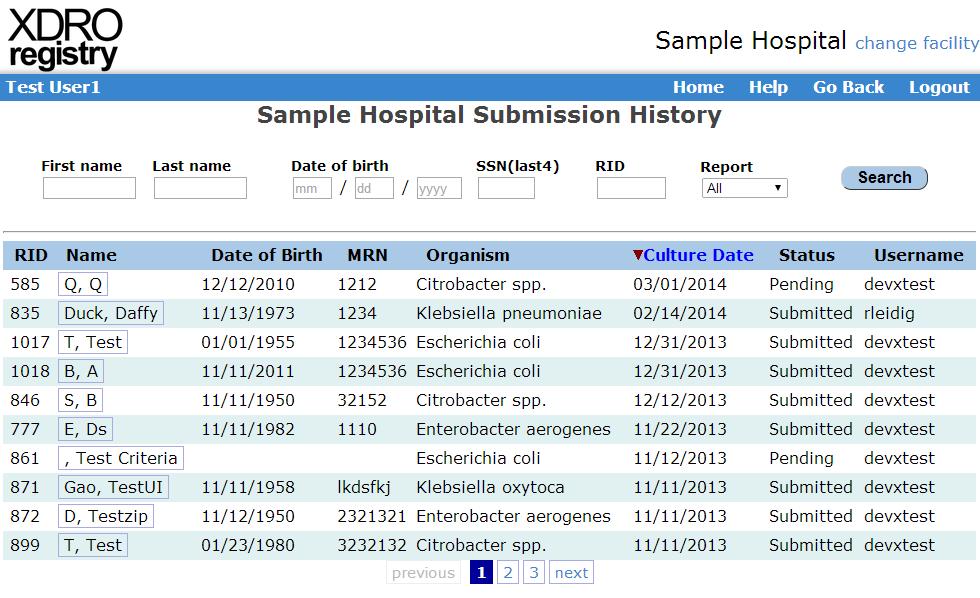
8 The XDRO Registry Purpose #1 Report CRE-carrying patients to the XDRO Purpose #2 Query the XDRO registry to determine whether or a person has a history of CRE LTC in Illinois is required to report Need access to the XDRO registry through the IDPH portal Get access BEFORE you need it Lessons Learned. Access to SIREN does not mean you have access to the XDRO registry..
9 Talk to your Micro Lab Ask what kind of CRE detecting capability is available? How will they let you know if they detect a CRE/KPC? Will they report to the XDRO registry?

10 Burdsall High C s of Infection Prevention and Control Clean Hands Clean Clothes Clean Equipment and Environment Contained Drainage Covered Wounds Careful Assessment Careful Use of Antimicrobials Collaborative Approach Communication

11 The care we provide is undertaken as a Human issue, and we need to approach care in a biopsychosocial and spiritual framework The person does not become the bacteria


12 SUPPORT OLDER ADULTS WITH KNOWLEDGE/EVIDENCE BASED INTERVENTIONS AND RESPONSES THIS IS THE IDEAL Environment
13 Readiness Build on systems that consider biological, psychological, social, and spiritual needs Put systems in place to respond to colonization and infection Focus on risk factors that can be addressed to prevent colonization and infection Avoid using limitations as an excuse not to provide care OR admit residents and patients However, understanding limits of each level of LTC is very important
 http://www.cdc.gov/hai/organisms/cre/cre-toolkit/index.")
14 2012 CRE Toolkit - Guidance for Control of Carbapenem-resistant Enterobacteriaceae (CRE)
15 CRE Toolkit Guidance: Core Measures for All Acute and Long-term Care Facilities Minimize use of invasive devices Get them out! Promote antimicrobial stewardship Avoid antibiotic pressure Avoid pressuring the prescribers for antibiotics
16 CRE Toolkit Guidance: Core Measures for All Acute and Long-term Care Facilities Hand Hygiene Promote hand hygiene Monitor hand hygiene adherence and provide feedback Ensure access to hand hygiene stations

17 Proper Glove Use is a PhD Level Skill Gloves are useful when used correctly Gloves can be a nightmare when used in the wrong way Do not wear 1 pair of gloves for more than 1 job!! Photo: Medline.com
.")
18 Hand Hygiene is one of the most important interventions to stop the spread of disease causing organisms! Reported worldwide hand hygiene participation rates ranging from 5% to 89% overall average reported to be 38.7% Pittet, D., Allegranzi, B., & Boyce, J. (2009). The World Health Organization guidelines on hand hygiene in health care and their consensus recommendations Infection Control and Hospital Epidemiology, 30(7),
19 F-441 Based Hand Hygiene Hand Sanitizer OR Soap and Water Wash or sanitize hands When coming to work and before going home When going room to room Before and after each resident contact After handling soiled equipment Before using gloves and after removing gloves F Soap and Water Are visibly soiled (dirty) If they have come in contact with blood or other body fluids Before and after eating Before and after handling food Before and after assisting a resident with toileting after contact with a resident with infectious diarrhea After performing your own personal hygiene or personal use of the toilet


20 Hand Hygiene Observations iscrub Fries J. #69. Presented at: SHEA 2011 Annual Scientific Meeting; April 1-4, 2011; Dallas. 20


21 Edited locations and notes 21

22 Examples of iscrub lite Feedback opportunities HCW opportunity Hand Hygiene Nurse Before Touching a Patient No Nurse After Touching Patient Surroundings Rub Nurse Before Touching a Patient No Nurse After Touching a Patient No Nurse Before Touching a Patient Wash Nurse After Touching a Patient Rub Nurse Before Touching a Patient Rub Nurse Med Pass After Touching a Patient Rub Nurse Med Pass Before Touching a Patient Rub Nurse Med Pass After Touching a Patient Rub Nurse Med Pass After Touching Patient Surroundings Rub Nurse Med Pass Before Touching a Patient Rub Nurse Med Pass After Touching a Patient No Nurse Med Pass After Touching a Patient Wash 22

23 CLEAN ENVIRONMENT The more I think about it, the more I realize cleanliness is the key with multi-drug resistant organisms Pat Rosenbaum RN, CIC
24 Ideal Cleaner Disinfectant Single step (clean and disinfect in one step) Stable Low toxicity/danger for humans and pets EPA approved Rapid kill of wide range of microorganisms with minimal contact time Does not damage surfaces
25 Some Common LTC Sanitizing and Disinfecting Products Isopropyl or Ethyl Alcohol Chlorine products Hydrogen Peroxide [Advanced hydrogen peroxide products (AHP)] Quaternary Ammonium Compounds
26



27 Clean and Disinfect Cleaning is everyone s responsibility Concentrate general cleaning/disinfecting on high touch/high use areas Equipment must be cleaned/disinfected between each resident/client use Cleaning/disinfecting supplies must be available at the point of care
28 Diffusion of Responsibility for Cleaning Equipment and Environment Not Cleaned
 Patients/residents at lower risk for transmission use Standard Precautions for most")
29 CRE Toolkit Guidance: Core Measures for All Acute and Long-term Care Facilities Contact Precautions Long-term care: CRE colonized or infected residents Patients/residents at high-risk for transmission on CP (as described in text) Patients/residents at lower risk for transmission use Standard Precautions for most situations




30 Standard Precautions does not mean no precautions Standard Precautions require that PPE is Always Available PPE Closets, Housekeeping carts Stock with gloves, gowns, goggles, masks
31 Dr Stone: CDC Standard Precautions: When should PPE be used? Gloves: Before any possible contact with blood or body fluids, mucous membranes (eyes, nose, mouth) or potentially infectious materials such as contaminated medical equipment or waste Face masks or shields To protect eyes during situations where blood or body fluids may spray or splatter Gowns To protect skin and clothing during situations where blood or body fluids may spray or splatter or care of resident could result in contamination of skin/clothing
32 Contact Precautions Dr Stone: CDC Hand Hygiene Before / after PPE use During resident care as appropriate (e.g., if gloves changed) Use of gown and gloves for direct resident care Don prior to room entry Remove prior to room exit Dedicating non-essential items for resident care May help decrease transmission due to contamination Blood pressure cuffs; Stethoscopes; IV poles and pumps Private rooms or cohorting residents if possible





33 Individual with active infection on Contact Precautions Social Interaction or Minimal Contact Personal Care Dressing Changes Hand Hygiene Gown, Glove, possibly Mask and Eye Protection, Hand Hygiene
34 Dr Stone: CDC Challenges with Contact Precautions in LTC Lack of private rooms / limited ability to move residents Moving people is disrupting to residents and staff Ability to identify carriers to cohort is limited (no active surveillance in most facilities) Determining duration of contact precautions Unable to restrict resident mobility and participation in social events/therapy for prolonged periods Unlikely to document clearance of carriage Large population of residents with unrecognized MDRO carriage Underestimating the sources of potential transmission
35 Dr Stone: CDC Strategic placement of residents based on risk factors New roommate assignments on resident characteristics and history of MDRO carriage Try to avoid placing two high risk residents together May be safer to cohort low-risk and high-risk residents Don t necessarily change stable room assignments just because of a new culture result unless it now poses new risk Roommates who ve been together for a long time have already had opportunity to share organisms in the past (even if you only learned about it recently)
36 CRE Toolkit Guidance: Core Measures for All Acute and Long-term Care Facilities Patient and staff cohorting When available cohort CRE colonized or infected patients and the staff that care for them even if patients are housed in single rooms If the number of single patient rooms is limited, reserve these rooms for patients with highest risk for transmission (e.g., incontinence)
37 CRE Toolkit Guidance: Core Measures for All Acute and Long-term Care Facilities Supplemental Measures for Healthcare Facilities with CRE Transmission Active Surveillance and screening Preemptive Contact Precautions Chlorhexidine bathing Bathe patients with 2% chlorhexidine
38 Case Study Mr. Jones, an 86 year old white male, is a planned admission. He has some sort of resistant bacterial colonization (he flagged in the hospital system), but the hospital staff nurse giving report did not have the history on hand. He is not being treated with an antibiotic at this time.
39 Situation What is the situation, and what information do you need to care for Mr. Jones? What do you need to tell the Physician or the Infection Preventionist?
40 Background What background information is needed to get a good picture of the individual and the situation?
41 Exam Temperature is 98 F tympanic (normal range is 97.8 to 98.2 F) Blood pressure is 122/78 (normal range is 116/70 to 130/82) Pulse is 76 and regular (normal range is 68-80) His respiratory rate is 16. His lungs are clear. He has no open wounds or rashes- skin is clear and in good condition He has a urinary catheter inserted in the hospital, but there is no documentation about why he needs the catheter.
42 With Lab Result A
43 Lab Result A Source: URINE 01/13/13 clean catch FINAL REPORT 01FEB14 100,000 COLONIES/ML KLEBSIELLA PNEUMONIAE SUSCEPTIBILITY TESTING KLEPNE MIC MIC AMPICILL/SULBAC 8 S CEFAZOLIN <=4 S CIPROFLOXACIN <=0.25 S ESBL NEGATIVE GENTAMICIN <=1 S MEROPENEM <=0.25 S NITROFURANTOIN 64 I TIGECYCLINE 1 S TOBRAMYCIN <=1 S TRIMETH/SULFA <=20 S ZOSYN <=4 S
44 With Lab Result B
45 Lab Result B 13 January, ,000 COLONIES/ML PROTEUS MIRABILIS EXTENDED SPECTRUM BETA LACTAMASE PRODUCER RENDERING CEPHALOSPORINS, PENICILLINS, AND AZTREONAM CLINICALLY RESISTANT TO THERAPY. INSTITUTE CONTACT ISOLATION PRECAUTIONS AS PER INFECTION CONTROL POLICY. PROMIR MIC MIC INTERP AMPICILLIN R CEFAZOLIN R CEFEPIME R CEFOTAXIME R CIPROFLOXACIN >2 R ESBL POSITIVE GENTAMICIN >8 R LEVOFLOXACIN >4 R MEROPENEM <=1 S TOBRAMYCIN >8 R TRIMETH/SULFA >2 R ZOSYN R
46 With Lab Result C
47 SUSCEPTIBILITY PHONED TO: RN 0900 ON 01/13/13 100,000 COLONIES/ML KLEBSIELLA PNEUMONIAE MULTIPLE DRUG RESISTANT STRAIN. INSTITUTE CONTACT ISOLATION PRECAUTIONS AS PER INFECTION CONTROL POLICY. CONFIRMED CARBAPENEMASE PRODUCER (CONFIRMATORY TESTING PERFORMED BY OUTSIDE LABORATORY Lab Result C SUSCEPTIBILITY TESTING KLEPNE MIC MIC AMPICILL/SULBAC >=32 R CEFAZOLIN >=64 R CEFEPIME R CEFTRIAXONE R CIPROFLOXACIN >=4 R ESBL NEGATIVE GENTAMICIN <=1 S IMIPENEM R NITROFURANTOIN 256 R TOBRAMYCIN >=16 R TRIMETH/SULFA >=320 R
48 Recommendation Recommendation based upon scope of practice. How should the problem be corrected? Source: The SBAR Communication Technique, Thomas et al.,
49 Assessment What is your assessment of this patient s immediate needs?
50 Summary for Long term Care Register for the XDRO registry Educate direct care staff about CRE/KPC Involve the residents/patients and their families Hand Hygiene Cleaner/disinfectants at point of care Empower direct care staff re: Contact Precautions Minimize Antimicrobial Use Get tubes and lines out Rapid identification of symptoms Prompt isolation of infections (immune imbalance: host/microbe) Accurate and ongoing assessment

51 Realize we are part of a larger healthcare community and must work together in a spirit of cooperation.
52 XDRO Registry for long term care facilities: 6 month update May 2014 Michael Lin, MD MPH William Trick, MD Chicago CDC Prevention Epicenter
53 Objectives 1. CRE overview and recent trends 2. CRE definition / laboratory considerations 3. XDRO registry sign-up and website update 4. Querying and automated alerts 5. Question and answer
 with few antibiotic options, high mortality rate cdc.")
54 CRE: nightmare bacteria Carbapenem-resistant Enterobacteriaceae (CRE) are extensively drug resistant organisms (XDROs) with few antibiotic options, high mortality rate cdc.gov
55 Enterobacteriaceae Family of bacteria that include: Escherichia coli Klebsiella species Enterobacter species Citrobacter species Cause healthcare and community-associated infections Example: urinary tract infections
 Resistance iceberg")
56 CRE Normally found in GI tract, sometimes skin. Most CRE patients are asymptomatic carriers ( colonized ) Resistance iceberg Some patients develop CRE infections
57 CRE: 2 dominant types Stands for: Bacterial species KPC Klebsiella pneumoniae carbapenemase Usually Klebsiella, sometimes E. coli NDM New Delhi metallo-β-lactamase Often E. coli (in U.S.) but variable Prevalence Most common CRE Rare but emerging Treatment Nearly impossible Nearly impossible Concerning? Yes! Yes!! Because it is still rare in U.S. and spreads aggressively. If your lab suspects it, report right away to IDPH
58 CRE in Chicagoland Chicago area facilities (REALM project), Facility type CRE colonization prevalence Short stay acute care hospitals (adult ICUs) 3% Long term acute care hospitals (LTACHs) 30% Lin MY et al. CID, 2013 CRE are relatively common in some Chicago healthcare facilities, particularly LTACHs Data unclear for nursing homes, but data suggest that skilled nursing facilities with ventilated patients have CRE rates similar to LTACHs Lin et al. CID, (9): Prabaker et al. ICHE (12):
59 CRE definition and laboratory considerations
60 CRE definition: Enterobacteriaceae with one of the following test results: 1. Molecular test (e.g., PCR) specific for carbapenemase OR 2. Phenotypic test (e.g., Modified Hodge) specific for carbapenemase production OR 3. For E. coli and Klebsiella species only: non-susceptible to ONE of the carbapenems (doripenem, meropenem, or imipenem) AND resistant to ALL third generation cephalosporins tested (ceftriaxone, cefotaxime, and ceftazidime). Report 1 st CRE event per patient per encounter
61 CRE reporting: points of confusion What are Enterobacteriaceae? Common Less common E. coli, Klebsiella spp. Enterobacter, Proteus, Citrobacter, Serratia, Morganella, or Providentia species Never Pseudomonas, Acinetobacter Ignore ertapenem susceptibility ESBL (extended spectrum β-lactamase) does not qualify as CRE
62 Laboratory considerations Criterion Lab test Common? 1: Molecular PCR Some 2: Phenotypic Modified Hodge Some 3: Susceptibility Automated system All labs Ask your lab about testing capability Currently, many facilities will only use criterion 3 Molecular testing (PCR) tests for the presence of CRE genes, and is currently the only way to confirm the carbapenemase type (KPC vs NDM)
 Ceftriaxone was only 3 rd gen cephalosporin reported Non-susceptible to at least")
63 Laboratory example This laboratory performed confirmation testing and thus was able to determine carbapenemase presence. (but I had to ask the lab that the test was PCR and that it confirmed KPC) Ceftriaxone was only 3 rd gen cephalosporin reported Non-susceptible to at least 1 carbapenem Ignore ertapenem results
64 Questions to ask your lab 1) What kind of testing do you perform for CRE? a. Modified Hodge testing? b. PCR testing? c. Metallo-β-lactamase E-test [MBL E-test]? 2) Are you (the lab) reporting CRE results to IDPH on our behalf? (if yes, LTCF needs to let IDPH know)
65
66 (Facility data is fictitious, but state data is real)
67 Illinois CRE trend (unique pts) Mandatory reporting 618 total patients reported; 471 pts since Nov (average 2 to 3 patients reported per day)
68 Resistance mechanisms reported to XDRO registry 100% 86% 80% 60% 40% 20% 9% 5% 0% KPC NDM Other n=338 n=34 n=19 Data through May 5, 2014; from pts with reported mechanism data, 63% of total
69 Organism distribution KPC (N=338) NDM (N=34) 100% 93% 100% 94% 80% 80% 60% 60% 40% 40% 20% 0% 2% 4% Klebsiella E. coli Other 20% 0% 6% Klebsiella E. coli Data through May 5, 2014; from pts with reported mechanism data, 63% of total
70 Specimen sources of reported CRE % Urine 49 Wound 14 Sputum 13 Rectal (screening) 12 Blood 7 Body fluid, tissue, other 5
71 XDRO registry website: orientation and updates

72
73

74 Registration Page: New Users

75 User Sign-In
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94 Querying the XDRO registry
95 Querying the registry Currently, querying requires typing patient information into the webpage Reasonable if few admissions per day (e.g., long term care facilities) Large facilities may want to query only high-risk patients (e.g., transfers)
96 Automated CRE alerts All Illinois facilities Your facility 1. Send patient info (encrypted) 2. Receive CRE alert if match XDRO registry Automated alerts will be piloted at limited hospitals in 2014; anticipate wider availability in 2015
97 Take home points 1. You are required to report CRE to the XDRO registry. Discuss with your lab about CRE testing and reporting. 2. Even if your lab reports CRE for you, we advise every facility to designate an infection preventionist to sign up for the XDRO registry - Query the registry to see if new patients have been reported as CRE-colonized
98 Question and answer forum
99 Upcoming Webinars Target Webinar Audience recordings Topics and slides will be available at Date Laboratorians CRE testing guidelines, June 6 Reporting to XDRO Long Term Care staff Antibiotic Use in Nursing Homes June 26 Webinar recordings and slides will be available at


100 Survey and Continuing Education Units Fill out webinar evaluation on SurveyMonkey at: Instructions on applying for CEUs will appear at the end of the SurveyMonkey Surveys and CEU applications must be completed by Monday, June 9! Contact: or
State of the State Address on HAI Prevention Activities
 State of the State Address on HAI Prevention Activities Disclaimer/Conflict of Interest I have no disclaimers or conflicts of interest to report Objectives Identify priority action areas and components
State of the State Address on HAI Prevention Activities Disclaimer/Conflict of Interest I have no disclaimers or conflicts of interest to report Objectives Identify priority action areas and components
Enterobacteriaceae. Preventing the Spread of Carbapenemresistant. in LTCFs. Nimalie D. Sto ne, MD, MS CDC Division of Healthcare Quality Promotion
 Preventing the Spread of Carbapenemresistant Enterobacteriaceae in LTCFs Nimalie D. Sto ne, MD, MS CDC Division of Healthcare Quality Promotion March 29, 2016 Preventing the Spread of Carbapenemresistant
Preventing the Spread of Carbapenemresistant Enterobacteriaceae in LTCFs Nimalie D. Sto ne, MD, MS CDC Division of Healthcare Quality Promotion March 29, 2016 Preventing the Spread of Carbapenemresistant
Guidance for Control of Carbapenem-resistant Enterobacteriaceae (CRE) 2012 CRE Toolkit
 2012 CRE Toolkit") Guidance for Control of Carbapenem-resistant Enterobacteriaceae (CRE) 2012 CRE Toolkit National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion Guidance for
Guidance for Control of Carbapenem-resistant Enterobacteriaceae (CRE) 2012 CRE Toolkit National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion Guidance for
Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas
 Prevention and Management Toolkit for Inpatient Areas") Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas This toolkit includes examples advice leaflets and forms which may be helpful for use by teams or
Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas This toolkit includes examples advice leaflets and forms which may be helpful for use by teams or
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent
 Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
The Growing Threat of Antibiotic Resistance in Post-Acute Care
 The Growing Threat of Antibiotic Resistance in Post-Acute Care Jennifer Han, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Associate Healthcare Epidemiologist
The Growing Threat of Antibiotic Resistance in Post-Acute Care Jennifer Han, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Associate Healthcare Epidemiologist
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Prevention and Control of Carbapenem Resistant Enterobacteriaceae Infections
 01.41 - Prevention and Control of Carbapenem Resistant Purpose To prevent healthcare-associated infections in patients caused by carbapenem-resistant Enterobacteriaceae (CRE). Audience All healthcare workers
01.41 - Prevention and Control of Carbapenem Resistant Purpose To prevent healthcare-associated infections in patients caused by carbapenem-resistant Enterobacteriaceae (CRE). Audience All healthcare workers
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Prevention, Control & Immunizations
 Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
TRUST POLICY AND PROCEDURES FOR CARBAPENEM RESISTANT ENTEROBACTERIACEAE (CRE) AND CARBAPENEM RESISTANT ORGANISMS (CRO)
 AND CARBAPENEM RESISTANT ORGANISMS (CRO)") TRUST POLICY AND PROCEDURES FOR CARBAPENEM RESISTANT ENTEROBACTERIACEAE (CRE) AND CARBAPENEM RESISTANT ORGANISMS (CRO) Reference Number POL- IC/1082/14 Version 1.2.0 Status Final Author: Helen Forrest
TRUST POLICY AND PROCEDURES FOR CARBAPENEM RESISTANT ENTEROBACTERIACEAE (CRE) AND CARBAPENEM RESISTANT ORGANISMS (CRO) Reference Number POL- IC/1082/14 Version 1.2.0 Status Final Author: Helen Forrest
STANDARD PRECAUTIONS POLICY Page 1 of 8 Reviewed: May 2017
 Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
Vancomycin-Resistant Enterococcus (VRE)
") Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
8. Droplet/Contact Precautions. 8.1 Introduction
 8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Objectives. IPC Open calls - bi-weekly series. Introduction to Infection Prevention & Control (IPC) Open Call Series
 Open Call Series") Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
How to Add an Annual Facility Survey
 Add an Annual Facility Survey https://nhsn.cdc.gov/nhsndemo/help/patient_safety_component/how_to/add_an_annual... Page 1 of 1 10/9/2017 Show Patient Safety Component > How To > Facility > Add an Annual
Add an Annual Facility Survey https://nhsn.cdc.gov/nhsndemo/help/patient_safety_component/how_to/add_an_annual... Page 1 of 1 10/9/2017 Show Patient Safety Component > How To > Facility > Add an Annual
Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home
 Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
1/28/2014. Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home. Thank you to AANAC
 Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Objectives. Industry Landscape. Infection Prevention and Control Changes, Updates and Quality Results!
 Infection Prevention and Control Changes, Updates and Quality Results! Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health 1 Objectives 1.Describe the recent industry
Infection Prevention and Control Changes, Updates and Quality Results! Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health 1 Objectives 1.Describe the recent industry
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 CONTACT PRECAUTIONS... 4 DROPLET PRECAUTIONS... 6 ISOLATION PROCEDURES... 7
 ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
Approval Signature: Date of Approval: December 6, 2007 Review Date:
 Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
LPN 8 Hour Didactic IV Education
 LPN 8 Hour Didactic IV Education Infection Prevention and Control By Pamela Truscott, MSN, Nurse Educator, RN Infection Prevention and Control Background Healthcare-acquired infections are increasing 1
LPN 8 Hour Didactic IV Education Infection Prevention and Control By Pamela Truscott, MSN, Nurse Educator, RN Infection Prevention and Control Background Healthcare-acquired infections are increasing 1
Safe Care Is in YOUR HANDS
 Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
2014 Annual Continuing Education Module. Contents
 This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
New Programs and Required Reporting for Long Term Care (LTC)
") New Programs and Required Reporting for Long Term Care (LTC) New Centers for Medicare and Medicaid Services (CMS) Requirements Slide: D. Burdsall 1 The mission of the U.S. Centers for Medicare & Medicaid
New Programs and Required Reporting for Long Term Care (LTC) New Centers for Medicare and Medicaid Services (CMS) Requirements Slide: D. Burdsall 1 The mission of the U.S. Centers for Medicare & Medicaid
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards. Infection Prevention and Control: Personal Protective Equipment
 PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care
 Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care Melissa Schaefer, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care Melissa Schaefer, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Carbapenamase Producing Enterobacteriaceae: A Draining Concern
 Carbapenamase Producing Enterobacteriaceae: A Draining Concern Heather Candon, B.Sc., M.Sc., MHM, CIC Lorraine Maze dit Mieusement, RN, MN, CIC Natasha Salt, B.Sc., B.A.Sc., CPHI (C), CIC Introduction
Carbapenamase Producing Enterobacteriaceae: A Draining Concern Heather Candon, B.Sc., M.Sc., MHM, CIC Lorraine Maze dit Mieusement, RN, MN, CIC Natasha Salt, B.Sc., B.A.Sc., CPHI (C), CIC Introduction
Routine Practices. Infection Prevention and Control
 Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases
 Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Alert Organisms Multi-Resistant Gram Negative Bacteria (MR-GNB) excluding MRSA
 excluding MRSA") Infection Prevention and Control Assurance - Standard Operating Procedure 22 (IPC SOP 22) Alert Organisms Multi-Resistant Gram Negative Bacteria (MR-GNB) excluding MRSA Why we have a procedure? To ensure
Infection Prevention and Control Assurance - Standard Operating Procedure 22 (IPC SOP 22) Alert Organisms Multi-Resistant Gram Negative Bacteria (MR-GNB) excluding MRSA Why we have a procedure? To ensure
Personal Hygiene & Protective Equipment. NEO111 M. Jorgenson, RN BSN
 Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
BEHAVIORAL HEALTH & LTC. Mary Ann Kellar, RN, MA, CHES, IC March 2011
 BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION
 NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
11/3/2017. Infection Control Assessment and Response (ICAR) Tools. Infection Control Assessment and Response (ICAR) Tools
 Tools. Infection Control Assessment and Response (ICAR) Tools") Infection Control Assessment and Response (ICAR) Tools Fresh Eyes Collaborative Approach Infection Control Assessment and Response (ICAR) Tools Comprehensive documents/questionnaires identify elements
Infection Control Assessment and Response (ICAR) Tools Fresh Eyes Collaborative Approach Infection Control Assessment and Response (ICAR) Tools Comprehensive documents/questionnaires identify elements
Infection Control Assessment and Response (ICAR) Tools. Fresh Eyes Collaborative Approach
 Tools. Fresh Eyes Collaborative Approach") Infection Control Assessment and Response (ICAR) Tools Fresh Eyes Collaborative Approach Infection Control Assessment and Response (ICAR) Tools Comprehensive documents/questionnaires identify elements
Infection Control Assessment and Response (ICAR) Tools Fresh Eyes Collaborative Approach Infection Control Assessment and Response (ICAR) Tools Comprehensive documents/questionnaires identify elements
TRANSMISSION-BASED PRECAUTIONS
 TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
2017 State of the State Address on Prevention of Health Care Associated Infections and Antimicrobial Resistance
 2017 State of the State Address on Prevention of Health Care Associated Infections and Antimicrobial Resistance Erica Runningdeer, MSN, MPH, RN HAI Prevention Coordinator Division of Patient Safety & Quality
2017 State of the State Address on Prevention of Health Care Associated Infections and Antimicrobial Resistance Erica Runningdeer, MSN, MPH, RN HAI Prevention Coordinator Division of Patient Safety & Quality
Infection Prevention and Control
 Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
Oregon Health & Science University Department of Surgery Standard Precautions Policy
 Standard Precautions Policy 1. Policy Standard Precautions are to be followed by all employees for all patients within and entering the OHSU system. Standard Precautions are designed to reduce the risk
Standard Precautions Policy 1. Policy Standard Precautions are to be followed by all employees for all patients within and entering the OHSU system. Standard Precautions are designed to reduce the risk
The Role of Isolation and Contact Precautions in the Elimination of Transmission of MRSA
 The Role of Isolation and Contact Precautions in the Elimination of Transmission of MRSA Marcia Patrick, RN, MSN, CIC Infection Control Director MultiCare Health System Tacoma, WA APIC/BD MRSA Presentation
The Role of Isolation and Contact Precautions in the Elimination of Transmission of MRSA Marcia Patrick, RN, MSN, CIC Infection Control Director MultiCare Health System Tacoma, WA APIC/BD MRSA Presentation
Assessing Evidence of Transmission and End of Transmission of Carbapenemase Producing Enterobacterales 1 (CPE)
") Assessing Evidence of Transmission and End of Transmission of Carbapenemase Producing Enterobacterales 1 (CPE) CPE Expert Group National Guidance Document, Version 1.0 Scope of this Guidance This guidance
Assessing Evidence of Transmission and End of Transmission of Carbapenemase Producing Enterobacterales 1 (CPE) CPE Expert Group National Guidance Document, Version 1.0 Scope of this Guidance This guidance
Infection Prevention Isolation Precautions Toolkit
 Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Clinical Research in Antibiotic Resistance
 Clinical Research in Antibiotic Resistance Mary-Claire Roghmann, MD, MS Professor of Epidemiology and Public Health and Medicine Assocaite Hospital Epidemiologist, Staff Physician and Research Health Scientist
Clinical Research in Antibiotic Resistance Mary-Claire Roghmann, MD, MS Professor of Epidemiology and Public Health and Medicine Assocaite Hospital Epidemiologist, Staff Physician and Research Health Scientist
Preventing Further Spread of CPE
 Provisional Guidance relating to CPE for General Practice. May 26 2017. Issued by the HSE Health Care Associated Infection and Antimicrobial Resistance Response Team. What is CPE (Carbapenemase Producing
Provisional Guidance relating to CPE for General Practice. May 26 2017. Issued by the HSE Health Care Associated Infection and Antimicrobial Resistance Response Team. What is CPE (Carbapenemase Producing
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Department of Infection Control and Hospital Epidemiology. New Employee Orientation
 Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL
 NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
Principles of Infection Prevention and Control
 Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
INFECTION CONTROL POLICY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT
 Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
01/09/2014. Infection Prevention and Control A Foundation Course WHO Provides a Consensus on Hand Hygiene. WHO - My 5 Moments Approach
 Infection Prevention and Control A Foundation Course 2014 WHO Provides a Consensus on Hand Hygiene WHO - My 5 Moments Approach Recommendations given on 1. Indications for Hand Hygiene 2. Hand Hygiene Technique
Infection Prevention and Control A Foundation Course 2014 WHO Provides a Consensus on Hand Hygiene WHO - My 5 Moments Approach Recommendations given on 1. Indications for Hand Hygiene 2. Hand Hygiene Technique
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings
 in Healthcare Settings") Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Prioritization in isolation a reality in Infection Control. WH Seto Chief Infection Control Officer Hong Kong, China
 Prioritization in isolation a reality in Infection Control WH Seto Chief Infection Control Officer Hong Kong, China 1935 2004 Daniel Seto Guideline for Isolation Precautions: Preventing Transmission of
Prioritization in isolation a reality in Infection Control WH Seto Chief Infection Control Officer Hong Kong, China 1935 2004 Daniel Seto Guideline for Isolation Precautions: Preventing Transmission of
INFECTION C ONTROL CONTROL CONTROL EDUCATION PROGRAM
 INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
Healthcare Antibiotic Resistance Prevalence DC (HARP-DC)
") Healthcare Antibiotic Resistance Prevalence DC (HARP-DC) Jacqueline Reuben, MHS Center for Policy, Planning and Evaluation District of Columbia Department of Health October 29, 2016 Nothing to Disclose
Healthcare Antibiotic Resistance Prevalence DC (HARP-DC) Jacqueline Reuben, MHS Center for Policy, Planning and Evaluation District of Columbia Department of Health October 29, 2016 Nothing to Disclose
HEALTHCARE ASSOCIATED INFECTIONS RISK ASSESSMENT PROCEDURE
 HEALTHCARE ASSOCIATED INFECTIONS RISK ASSESSMENT PROCEDURE Author: Jenny Boyce, Lead Infection Prevention & Control Nurse Approved by and date: March 2016 Any other linked ICP 000 - Infection Prevention
HEALTHCARE ASSOCIATED INFECTIONS RISK ASSESSMENT PROCEDURE Author: Jenny Boyce, Lead Infection Prevention & Control Nurse Approved by and date: March 2016 Any other linked ICP 000 - Infection Prevention
Part II Quality improvement in long-term care: Partnership of infection prevention and environmental services
 Part II Quality improvement in long-term care: Partnership of infection prevention and environmental services Using the Centers for Medicare and Medicaid Services (CMS) Quality Assurance Performance Improvement
Part II Quality improvement in long-term care: Partnership of infection prevention and environmental services Using the Centers for Medicare and Medicaid Services (CMS) Quality Assurance Performance Improvement
Prevention and Control of Infection in Care Homes. Infection Prevention and Control Team Public Health Norfolk County Council January 2015
 Prevention and Control of Infection in Care Homes Infection Prevention and Control Team Public Health Norfolk County Council January 2015 Content for today Importance of IPAC -refresher IPAC audits in
Prevention and Control of Infection in Care Homes Infection Prevention and Control Team Public Health Norfolk County Council January 2015 Content for today Importance of IPAC -refresher IPAC audits in
Patient and Visitor Involvement: The Hand Hygiene Missing Link?
 Patient and Visitor Involvement: The Hand Hygiene Missing Link? Jim Gauthier, MLT, CIC CHICA-Canada Past President Providence Care, Kingston, ON CPSI April 2013 1 Objectives Review some of our issues with
Patient and Visitor Involvement: The Hand Hygiene Missing Link? Jim Gauthier, MLT, CIC CHICA-Canada Past President Providence Care, Kingston, ON CPSI April 2013 1 Objectives Review some of our issues with
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Reducing the risk of healthcare associated infection
 i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Infection Prevention and Control and Isolation Authored by: Infection Prevention and Control Department
 Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention & Control (IPAC):
:") Windsor Regional Hospital believes that Infection Prevention and Control is vital to patient safety. ALL persons working in the hospital have a RESPONSIBILITY to practice good infection prevention and
Windsor Regional Hospital believes that Infection Prevention and Control is vital to patient safety. ALL persons working in the hospital have a RESPONSIBILITY to practice good infection prevention and
SECTION 11.4 VANCOMYCIN RESISTANT ENTERCOCCUS (VRE)
") SECTION 11.4 VANCOMYCIN RESISTANT ENTERCOCCUS () Introduction Definitions Associated with Risk Groups Signs and Symptoms Source Mode of Transmission Diagnosis Treatment Screening Transport Communication
SECTION 11.4 VANCOMYCIN RESISTANT ENTERCOCCUS () Introduction Definitions Associated with Risk Groups Signs and Symptoms Source Mode of Transmission Diagnosis Treatment Screening Transport Communication
Self-Instructional Packet (SIP)
") Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
& ADDITIONAL PRECAUTIONS:
 INFECTION CONTROL GUIDELINES: STANDARD PRECAUTIONS & ADDITIONAL PRECAUTIONS: LESSON PLAN Lesson overview Time: One hour This lesson covers the guidelines developed by the U.S. Centers for Disease Control
INFECTION CONTROL GUIDELINES: STANDARD PRECAUTIONS & ADDITIONAL PRECAUTIONS: LESSON PLAN Lesson overview Time: One hour This lesson covers the guidelines developed by the U.S. Centers for Disease Control
Cystic Fibrosis Foundation Recommendations
 Hospital Epidemiology and Infection Control Department Presenters: Sandra Kistler, RN, PHN, MSN, ICP Cystic Fibrosis Foundation Recommendations Contact Precautions for ALL patients with Cystic Fibrosis
Hospital Epidemiology and Infection Control Department Presenters: Sandra Kistler, RN, PHN, MSN, ICP Cystic Fibrosis Foundation Recommendations Contact Precautions for ALL patients with Cystic Fibrosis
Emergency Department Isolation Precautions
 Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
Nosocomial Infection in a Teaching Hospital in Thailand
 Nosocomial Infection in a Teaching Hospital in Thailand Somsak Lolekha, M.D., Ph.D.,* Banchong Ratanaubol R.N.** and Pranom Manu R.N.** (*Department of Pediatrics; **Department of Nursing, Faculty of Medicine
Nosocomial Infection in a Teaching Hospital in Thailand Somsak Lolekha, M.D., Ph.D.,* Banchong Ratanaubol R.N.** and Pranom Manu R.N.** (*Department of Pediatrics; **Department of Nursing, Faculty of Medicine
a. Goggles b. Gowns c. Gloves d. Masks
 Scrub In A patient is isolated because of an undetermined respiratory condition. Which PPEs will healthcare professionals need before caring for the patient? a. Goggles b. Gowns c. Gloves d. Masks A patient
Scrub In A patient is isolated because of an undetermined respiratory condition. Which PPEs will healthcare professionals need before caring for the patient? a. Goggles b. Gowns c. Gloves d. Masks A patient
Single room with negative pressure ventilation in relation to surrounding areas
 7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
Hand Hygiene: Train the Trainer. National Hand Hygiene Training Programme for Healthcare Workers in Community and Primary Care
 Hand Hygiene: Train the Trainer National Hand Hygiene Training Programme for Healthcare Workers in Community and Primary Care HCAI AMR Clinical Programme 2017 Who can become a trainer? The trainer will
Hand Hygiene: Train the Trainer National Hand Hygiene Training Programme for Healthcare Workers in Community and Primary Care HCAI AMR Clinical Programme 2017 Who can become a trainer? The trainer will
Reducing the risk of healthcare associated infection
 i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
i Reducing the risk of healthcare associated infection Healthcare associated infection Introduction The Royal Marsden takes the safety of our patients very seriously. That means doing everything we can
Antibiotic Use and Resistance in Nursing Homes
 Antibiotic Use and Resistance in Nursing Homes GHINWA DUMYATI, MD PROFESSOR OF MEDICINE CENTER FOR COMMUNITY HEALTH UNIVERSITY OF ROCHESTER MEDICAL CENTER FEBRUARY 8, 2017 Nicolle LE, et al. Antimicrobial
Antibiotic Use and Resistance in Nursing Homes GHINWA DUMYATI, MD PROFESSOR OF MEDICINE CENTER FOR COMMUNITY HEALTH UNIVERSITY OF ROCHESTER MEDICAL CENTER FEBRUARY 8, 2017 Nicolle LE, et al. Antimicrobial
Standard Precautions
 Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Clostridium difficile Infection (CDI)
") Approved by: Clostridium difficile Infection (CDI) Vice President and Chief Medical Officer Corporate Policy & Procedures Manual VI-8 Date Approved August 22, 2016 September 16, 2016 Next Review (3 years
Approved by: Clostridium difficile Infection (CDI) Vice President and Chief Medical Officer Corporate Policy & Procedures Manual VI-8 Date Approved August 22, 2016 September 16, 2016 Next Review (3 years
Surveillance Protocol for Carbapenemase- Producing Organisms (CPO) in British Columbia
 in British Columbia") Surveillance Protocol for Carbapenemase- Producing Organisms (CPO) in British Columbia December 2017 Contacts: Dr. Linda Hoang Program Head, Public Health Advanced Bacteriology & Mycology BCCDC Public
Surveillance Protocol for Carbapenemase- Producing Organisms (CPO) in British Columbia December 2017 Contacts: Dr. Linda Hoang Program Head, Public Health Advanced Bacteriology & Mycology BCCDC Public
ACG GI Practice Toolbox. Developing an Infection Control Plan for Your Office
 ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
Recommendation II. Recommendation I. Who s on Your Team? Recommendation III
 Infection Prevention In the Surgical Suite Janie Kinsey, RN, CASC Administrator, St. Luke s South Surgery Center President, Kansas Association of Ambulatory Surgery Centers Objectives Recommendation I
Infection Prevention In the Surgical Suite Janie Kinsey, RN, CASC Administrator, St. Luke s South Surgery Center President, Kansas Association of Ambulatory Surgery Centers Objectives Recommendation I
ISOLATION PRECAUTIONS INTRODUCTION. Standard Precautions are used for all patient care situations, but they
 ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
Infection Prevention and Control
 Infection Prevention and Control Infection Control in the Healthcare Setting Chain of Infection Hand Hygiene Hospital Acquired Infections Isolation Exposures Tuberculosis Chain of Infection Most Common
Infection Prevention and Control Infection Control in the Healthcare Setting Chain of Infection Hand Hygiene Hospital Acquired Infections Isolation Exposures Tuberculosis Chain of Infection Most Common
THE INFECTION CONTROL STAFF
 INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
Erlanger Infection Control Program. Resident Resident Orientation and. and
 Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance
 Open Call Series #1 Surveillance") Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Early detection, management and control of carbapenemase-producing Enterobacteriaceae Policy V3.0
 Early detection, management and control of carbapenemase-producing Enterobacteriaceae Policy V3.0 01.05.2018 Summary - Patient admission flow chart for the infection prevention and control of carbapenemase-producing
Early detection, management and control of carbapenemase-producing Enterobacteriaceae Policy V3.0 01.05.2018 Summary - Patient admission flow chart for the infection prevention and control of carbapenemase-producing
Overview of Revised LTC Surveillance Definitions
 Surveillance in Long-Term Care Facilities: Urinary Tract Infections (UTI) and Multidrug-Resistant Organisms (MDRO) Wisconsin Division of Public Health May-June 2014 Overview of Revised LTC Surveillance
Surveillance in Long-Term Care Facilities: Urinary Tract Infections (UTI) and Multidrug-Resistant Organisms (MDRO) Wisconsin Division of Public Health May-June 2014 Overview of Revised LTC Surveillance
PRECAUTIONS IN INFECTION CONTROL
 PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
01/09/2014. The very first requirement in a hospital is that it should do the sick no harm!!!!
 Infection Prevention and Control A Foundation Course Update on recent Guidelines and Recommendations Ros Cashman Cork University Maternity Hospital, Cork 2014 The very first requirement in a hospital is
Infection Prevention and Control A Foundation Course Update on recent Guidelines and Recommendations Ros Cashman Cork University Maternity Hospital, Cork 2014 The very first requirement in a hospital is
Training Your Caregiver: Hand Hygiene
 Infections are a serious threat to fragile patients. They are often spread by healthcare workers and family members who are providing frontline care. In fact, one of the major contributors to infections
Infections are a serious threat to fragile patients. They are often spread by healthcare workers and family members who are providing frontline care. In fact, one of the major contributors to infections
Chapter 10. medical and Surgical Asepsis. safe, effective Care environment. Practices that Promote Medical Asepsis
 chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
How we Got Here: Implementing Stewardship in Rochester Nursing Homes
 How we Got Here: Implementing Stewardship in Rochester Nursing Homes Ghinwa Dumyati, MD Professor of Medicine Center for Community Health University of Rochester Medical Center Ghinwa_dumyati@urmc.rochester.edu
How we Got Here: Implementing Stewardship in Rochester Nursing Homes Ghinwa Dumyati, MD Professor of Medicine Center for Community Health University of Rochester Medical Center Ghinwa_dumyati@urmc.rochester.edu
Infection Prevention and Control Guidelines for Cystic Fibrosis Patients
 AU Medical Center Policy Library Infection Prevention and Control Guidelines for Cystic Fibrosis Patients Policy Owner: Epidemiology POLICY STATEMENT Based upon best practices for the care of cystic fibrosis
AU Medical Center Policy Library Infection Prevention and Control Guidelines for Cystic Fibrosis Patients Policy Owner: Epidemiology POLICY STATEMENT Based upon best practices for the care of cystic fibrosis
Infection Control in General Practice
 Infection Control in General Practice August 2017 Magali De Castro Clinical Director, HotDoc Infection Control in General Practice This session will cover: Key infection control considerations for general
Infection Control in General Practice August 2017 Magali De Castro Clinical Director, HotDoc Infection Control in General Practice This session will cover: Key infection control considerations for general
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE)
") DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others