Governing Body Meeting (in public) Agenda
|
|
|
- Noel Mills
- 6 years ago
- Views:
Transcription
1 Governing Body Meeting (in public) Agenda Thursday 10 October am-12.30pm Diamond Meeting Room, The Gateway, Gatehouse Road, Aylesbury, Bucks Clinical Chair: Dr Graham Jackson No Agenda Item Desired Outcome(s) Contributor Papers Welcome & Apologies Declarations of Interest Minutes of the meeting held on 12 September 2013 Action points update Questions from the public Dr Graham Jackson Dr Graham Jackson For approval Dr Graham Jackson GB Dr Graham Jackson Corporate and Governance Chief Officer s Report: To inform the Governing Body of local and national developments in the context of NHS Aylesbury Vale CCG For information & discussion Louise Patten, Chief Officer GB Board Assurance Framework: To update the Governing Body on the key risks to the CCG For approval Robert Majilton, Chief Finance Officer GB a GB b Accountability Forum update For information Louise Patten, Chief Officer Verbal update Clinical Commissioning Commissioning Intentions & update on progress with locality development For discussion Colin Thompson, Director of Operations and Performance GB a GB b
2 Quality & Performance Quality Report including Keogh update For information Jane McVea, Director of Quality GB A Promise to Learn a commitment to act, improving the safety of patients in England For discussion Jane McVea, Director of Quality GB QIPP: Update on progress against Quality Innovation Productivity and Prevention (QIPP) plans For information Colin Thompson, Director of Operations and Performance GB a GB b Performance Report & Dashboard: Update on progress against National Operating and Outcome framework For information Colin Thompson, Director of Operations and Performance GB a GB b Finance Chief Finance Officer s Report: To update the Governing Body on the financial status of the CCG For Information Robert Majilton, Chief Finance Officer GB a GB b For Information Executive Team Minutes of the meeting held on 22 August 2013 For information Commissioning for Quality For information Minutes of the July 2013 meeting Audit Committee For information Minutes of the July 2013 meeting Meeting agendas will be published on the Anyone may ask questions relating to the agenda in advance either by post, telephone or , or on the day in the question time slot at the start of the meeting. Questions about topics not included in the agenda are welcome by post, telephone or and they will be answered, depending on the number, either in or outside of the meeting. All questions and answers will be published on the website. By post: Aylesbury Vale Clinical Commissioning Group, First Floor, The Gateway, Gatehouse Road, Aylesbury, Bucks HP19 8FF Tel: avccg.feedback@nhs.net Website: If you would like to attend a meeting and need extra help to do so, for example because of a disability, please contact us as early as possible so that we can try to put in place the right support. For further information about these meetings please contact: Administration team on or avccg.feedback@nhs.net.

3 Meeting of the Governing Body- Main Points on a Page Thursday 12 September am 12.30pm Ground Floor Meeting Room, The Gateway, Gatehouse Road, Aylesbury, Bucks Item no. Agenda Item Summary Key Decisions 3 Questions from the public Question sent in by the public were asked and responded 4 Chief Officer Report Report containing key messages from the CCG For Information 5 Engaging our Public Plans for Public & Patient Engagement 6 Board Assurance Framework Report updating them on the principal risks identified. For Information 7 Quality report including Keogh update Report updating on the issues that have arisen during the preceding month For Information 8 QIPP Quality, Innovation Report providing a Month 4 position for QIPP Noted 9 Performance Report & Dashboard Report of the CCG s performance against the NHS England CCG Assurance 10 Chief Finance Officers Report Report on the Financial Position to the end of July 2013 Page 1 of 13
4 Governing Body Meeting Minutes Thursday 16 January am 12.30pm Diamond Meeting Room, The Gateway, Gatehouse Road, Aylesbury, Bucks Governing Body Present: Dr. Jonathan Fielden, Secondary Care Consultant Specialist (JF) Dr. Graham Jackson, - Chair (GJ) David Lunn, Interim Lay Member & Audit Committee Lead Vice Chair (DL) Robert Majilton, Chief Finance Officer (RM) Louise Patten, Chief Officer (LP) Graham Smith, Lay Member Patient & Public Engagement (GS) Crystal Oldman - Registered Nurse Specialist (CO) Other Attendees: Colin Thompson Director of operations and Performance (CT) Jane McVea Director of Quality (JMcV) Apologies: Dr Karen West (KW) Dr. Kevin Suddes, Clinical Lead (KS) Minute taker: Angela Harvey, Executive Assistant Page 2 of 13
5 1 Welcome & Apologies GJ welcomed all to the meeting and the Governing Body members introduced themselves to those present. 2 Minutes of the meeting held on 22 August 2013 (Document reference: GB ) Minutes agreed as a true record Questions from the public Question: In light of the Keogh report on Buckinghamshire Healthcare NHS Trust, what will the CCG do differently, compared to the Primary care Trust, when monitoring the quality of care provided by the NHS for Buckinghamshire residents? Response: Jane McVea (JMcV) - Covered in Agenda item 7 of today s meeting. Question: One of the ways that providers and commissioners of services can identify services that need improvement is to collect information from patients on their experiences and their concerns. However it appears that many people do not wish to raise these concerns directly with the authorities. Can we find out why this is so and identify ways in which we can give patients, their relatives and carers the confidence to raise concerns without fear? Response: Lou Patten (LP) This will be covered in today s meeting, particularly in the presentation which will be given under agenda item Question: How do the CCG board plan to involve the public in determining this year s commissioning plans? Page 3 of 13 Response: Colin Thompson (CT) This year s commissioning intentions have been informed in a number of ways; Health & Wellbeing Board Strategy we use this and the strategy has been consulted on Patient and public involvement has been sought in determining the projects planned for the forthcoming year. For example, there is a Long Term Conditions workshop later today and a
6 commissioning workshop took place recently and these involved patients, public and providers. We do, however, recognise that more work needs to be done to provide more information as to how people can get involved. 3.4 Question: In light of the decision by central Government to raid the NHS budget to pay for social care services how much of the CCG budget for health services has been transferred to the county council to pay for social care? Response: As part of the Governments Comprehensive Spending Review (CSR), money has been transferred to Social Care for health outcomes. This will form part of our joint commissioning intentions and funds such initiatives as Prevention Matters. It has also funded the dementia care initiative which has taken place in our North locality which has helped with the diagnosis of dementia in the population Chief Officer Report (Document reference: GB ) Organisational Development: CCG Assurance Framework Over the summer Louise Patten (LP) and Graham Jackson (GJ) the Clinical Chair, attended one of five national events focussing on CCG feedback to the proposed CCG development and assurance process. The key messages from CCGs regarding Development were: 1. CCG training needs are diverse and offers of support should be made specific to each situation; 2. Help with sorting the variety and quantity of support that s on offer would be appreciated; 3. CCGs are keen to see the national team support a variety of development approaches including: networks for learning; a comprehensive, online and searchable directory of development support from both the public and private sector; support for their Organisational Development planning and delivery; differential personal and team development for all CCG members; Page 4 of 13
7 a desire for shared development with Area Teams and our Health & Wellbeing Board. The key messages from CCGs regarding Assurance were: 1. The key principle of assurance should be one of no surprises ; engendering positive local relationships between CCGs and area teams that provide mutual support and development; 2. The assurance model needs to take into consideration local pressures, including those which CCGs have less ability to influence because of the complexity of co-commissioning relationships. An assurance summit took place on 24 July where the detail underpinning the annual assurance framework was developed further, the output of this event will be shared with stakeholders again on 3 September to further fine tune; before being drawn up into a final assurance framework to be presented to NHS England Board for approval on 8 November, with publication shortly thereafter. Further work is on-going nationally regarding aspirational development of CCGs beyond assurance; Dr Jackson is deputy chair of this CCG Development Group. 4.2 Call to Action - National Context The NHS Belongs to the People A Call to Action is a programme of engagement that will allow everyone to contribute to the debate about the future of health and care provision in England. The programme aims to be the broadest, deepest and most meaningful public discussion that the NHS has ever undertaken. The NHS constitution states that patients and public must be involved in this debate and we are currently working to map local groups and communities and ways in which we can engage more fully with them. The CCG will be performance managed on its success in this area. The aim is to engage our populations through our local events, as well as using alternative communication channels such as online and digital resources to enable us to produce meaningful views, data and information that the CCG can use to develop 5 year commissioning plans. Currently, there are three locality groups, North, South and Central, who meet regularly and hold frequent public meetings. The GP surgeries within these localities have Patient Engagement Representative groups and patients are able to join these groups. We are also currently recruiting to the Governing Body Lay Member role for public and patient Page 5 of 13
8 involvement. Interviews are planned and candidates will be asked to present to a group of patients from each of our member practice Patient Representative Groups, as part of the selection process. We are pleased to report that Alex Hannaford, Chief Executive of Healthwatch has agreed to sit on the interview panel and we hope to provide news of appointment shortly. Our future Public and Patient Engagement plans will include as many opportunities as possible for local feedback on this national engagement strategy as well as for our own more localised services feedback. 4.3 Local Context: Keogh Enquiry and maintaining high quality services We continue to work closely with Buckinghamshire Hospitals Trust (BHT) to ensure that actions arising from the Keogh Review into the quality of care & treatment are completed within the timescales agreed at the Risk Summit held on the 11th July A weekly task and finish action group has been established to achieve this and AVCCG has active membership on this group. Further details are in our Quality Report and will be in our Commissioning for Quality sub- committee minutes. We are pleased with the progress made to date. 5 Engaging our Public: presentation by Lou Patten, Chief Officer (Document reference: GB ) Lou Patten (LP) gave a presentation detailing our plans for Public and Patient Engagement over the coming months. These include: A listening exercise which will actively seek patient views and how they can be involved. A Schools competition Page 6 of 13
9 6 Board Assurance Framework (Document reference: GB ) A paper was presented to the Governing Body by Robert Majilton (RM) to update them on the principal risks identified for 2013/14. The Governing Body Assurance Framework (GBAF) sets out the principal risks to the 5 Strategic Objectives identified in the Operating Plan. There are currently 15 risks identified on the GBAF: 3 Extreme Risks No. 8, 10, High Risks No. 2, 3, 4, 5, 6, 7, 9, 12, 14, 15 2 Moderate / Low Risks No. 1, 13 Out of a potential risk score of 375 the current risk score is 46% against a target of 26%. (43% as at July). The 3 extreme risks are: 8 - Economic environment, demand / cost pressures and in-year changes to CCG allocations create increased requirement for QIPP or reductions in spending plans 10 - Operational plans (including QIPP) are not delivered, leading to contract over-performance and the need for in-year additional financial measures and service changes 11 Commissioning Support organisations are not fully delivering commissioned services 4 Risk scores have increased since July and these reflect: Continued problems getting systematic, good quality information to support commissioning decisions and reviews of quality of services (Risk 5) Increasing financial pressures within the CCG and across key providers (Risks 8 and 9) Concerns on the performance of Central Southern CSU which have led to the CCG issuing a Corrective Action Plan notice (Risk 11) The Governing Body are asked to note the updated GBAF, especially the mitigation around the extreme risks. Page 7 of 13
10 7 Quality Report including Keogh update (Document reference: GB ) A paper was presented to the Governing Body by Jane McVea (JMcV) to update them on issues that have arisen during the preceding month. Provider updates Buckinghamshire Healthcare Trust The steering group for the Keogh action plan is meeting weekly with CCG representation. Heatherwood and Wexham Park Foundation Trust The Risk Summit to review the quality of care at HW&WP was held on 30 July. Action plans are in place against all the standards with which the Trust was found to be non-compliant. A second summit will be held on 30 September Cancer peer review Both HW&WP and BHT have had their urology cancer pathways peer reviewed. In common with all other Trusts in Thames Valley neither are compliant with Improving Outcomes Guidance (IOG) which are the national standards for cancer. As there is no single commissioner for cancer pathways anymore the Thames Valley Area Team Medical Director has met with the peer review team and also spoken with Sean Duffy, National Clinical Director for Cancer Services on the issue. There is a meeting of the urology TSSG on 27 August which Bernadette Lavery will attend as Clinical Director of the Southern Cancer Network. The agreed outcome we wish to see from this meeting is the outline of an agreed workable solution that moves us to IOG compliance in a reasonable time frame. The peer review team realise that it could take 1-2 years to achieve full IOG compliance given the capacity issues. The team confirmed that there were no quality concerns and that the surgeons were performing sufficient numbers of procedures, just not in the single centre that the IOG stipulates. NHS 111 Service With the public announcement of the withdrawal of NHS Direct from its 111 contracts we have had discussions with the provider on how the CCGs can be assured that quality is maintained during the transition. We have agreed a method for making both announced and unannounced visits to the Milton Keynes service. This methodology will be replicated across other out of hours services. Page 8 of 13 The Quarter one patient experience survey for the 111 service shows 25% of callers took part in the survey and of those 79% reported they were satisfied with the service. 88% reported they had received
11 clear advice about what to do next and 83% found that advice helpful. 7.5 A promise to learn a commitment to act Following on from the Francis report professor Don Berwick President Emeritus and Senior Fellow of the Institute of Health Improvement was asked to distil for the Government and the NHS the lessons learnt and to specify the changes that are needed. The report is now published and makes ten recommendations: To reduce patient harm by embracing an ethic of learning. All leaders should place quality and, in particular, safety at the head of their agenda. Patients and carers should be present, powerful and involved at all levels of healthcare organisations. Government, Health Education England and NHS England should make sure sufficient staff are available now and in the future. Healthcare organisations should ensure staff are present in appropriate numbers to provide safe care and are well supported. Mastery of quality and patient safety science and practices should be part of initial preparation and lifelong education of all health care professionals including managers and executives. NHS should become a learning organisation. Transparency should be complete and unequivocal. All organisations should seek out the patient voice as an essential asset in monitoring quality and safety. Supervisory and regulatory systems should be simple and clear. We support responsive regulation of organisations. A paper will be circulated to the Governing Body shortly which describes the journey from the Francis Report, through the Keogh investigations to the Berwick report Inspection and regulation The Care Quality Commission consultation on its inspection processes closed on the 12 August This consultation focuses on hospital care with a further consultation on adult social care and general practice going out later this year. The new regime will be in place by October Executive Team Reporting August was the first month that the detailed Quality Report had been completed by the CSU for the Executive Team. This report will provide the executive with a better understanding of the key quality risks in the system and what actions are being taken to mitigate them. Page 9 of 13
12 8 QIPP Quality, Innovation, (Document reference: GB ) The corporate reporting framework should be the spine of the organisation providing sufficient information for the Governing Body and Executive Team to be assured of the organisations progress towards delivering the corporate objectives. The QIPP report summarises the reports received from the QIPP Programme Leads to provide information regarding the progress, delays and risks associated with delivery of individual QIPP programmes. A report was presented to the Governing Body, providing a Month 4 position for QIPP delivery for Aylesbury Vale CCG. 9 Performance Report & Dashboard 10 A report was presented to the Governing Body informing them as to the CCGs performance against the NHS England CCG Assurance Framework. Chief Finance Officer s Report (Document reference: GB /7a) A report was presented to the Governing Body giving an update as to the Financial Position to the end of July 2013 and the forecast position to the 12 months ending in March The report highlights the areas of variance to the plan and key risks to the forecast position Financial Position Highlights are: Plan The current financial plan is based on a resource allocation of 201.6m ( 196.7m for Programme Costs and 4.9m for Running Costs). The budget has been reduced by 3.9m for additional transfers to NHS England for Specialist Commissioning, however these are held as potential adjustments as further work to validate the baseline is required before formal agreement is made. No gain or loss on this transfer has been factored into the current or forecast position. To the end of July, 60% of the Headroom has been committed in Contracts (50% [ 2m] to BHT and 10% [ 0.5m] to cover pressures in baseline funding issues). The remaining headroom has been factored into the financial mitigation plan developed in response to the emerging pressures within the overall plan. Page 10 of 13
13 10.2 Year to Date The CCG has developed a plan that delivers the 1% surplus planning requirement of 1,996k, resulting in a year to date actual surplus of 665k. Pressures on budgets ( 1.6m / 3.6%) within Planned and Unscheduled care reflecting contract overspends mainly on Acute and Ambulance contracts. In the majority of cases the report reflects the contract position as at the end of June with estimations for July. This overspend has been reduced by underspends within Joint and Continuing Care where the level of Adult Continuing Care activity is not high as expected. To the end of July 1.1m of reserves (21% of the total available) have been factored into the position in order to maintain the surplus position Programme Budgets Planned Care budgets have a 503k over spend against plan at the end of the 4 months to July Of the Planned Care overspend, 191k relates to BMI activity, with anticipated pressure from the OUH Contract when the Plan is aligned to the funding available. Unscheduled Care budgets have a 935k deficit against plan at the end of the 4 months to July Of this overspend, 395k relates to MKHFT with emerging pressures across other Acute contracts. The Ambulance contract is still showing over performance based on the Month 3 report, although this adverse variance has reduced form previous months. The underspend of 371k in Joint and Continuing Care mainly reflects the reduction in Adult Continuing Care. Care activity Prescribing is balanced year to date against plan pending a review of total spend when the month 3 actual spend data becomes available for all categories of the prescribing budget. GP Prescribing over the 12 months to May 2013 averaged 7.3% below the budget set for 2013/ Page 11 of 13 QIPP Delivery of 807k against a plan of 1.5m (55% achievement). The adverse year to date position is partly mitigated by the use of headroom in the BHT contract and other underspends on budgets not covered by QIPP. The forecast position is a year-end under delivery of the plan as in order to deliver this target, savings will need to be generated at a rate of 16% above the original plan for the remainder of the year.
14 Further details on the individual schemes are available from the separate QIPP report Forecast The Executive Team reviewed the financial mitigation plan at its meeting on the 22 August which identified a gross risk of 8.2m, less 6.8m of in-year mitigations, leaving a c 1.4m of additional unmitigated in-year financial pressure. Factored into the Mitigation plan is the worsening of the BHT month 4 SLAM position to a year to date pressure of 1.5m. Work on the mitigation plan continues but should this gap not be able to be closed the forecast position would worsen by up to that amount. This assumes that the most likely pressures included in the plan do not worsen. The Governing Body should note that the majority of the 6.8m of in-year mitigations is non-recurrent, leaving c 8m of recurrent pressure going into the 2014/15 financial year. The Governing Body were asked to note the reported financial position, forecast and development of a financial mitigation plan to support delivery of the planned surplus, and to be aware of the further risks to the reported position and potential impact on the ability of the CCG to deliver its original financial plan. Next meeting: Thursday 10 October, am to 12.30pm Venue Diamond Room, Aylesbury Vale District Council offices, The Gateway, Gatehouse Road, Aylesbury Page 12 of 13
15 GOVERNING BODY MEETING October 2013 CHIEF OFFICER REPORT Agenda item: GB Purpose of Paper To inform the Governing Body of local and national developments in the context of NHS Aylesbury Vale CCG Actions Required For information Objectives supported by this Paper (Please Tick) Support delivery of in-year performance and the financial plan Support transition to clinically led commissioning Support development of the CCG to take on the commissioning role Development of the working relationship between the Commissioning Support Services (CSS) and AVCCG Supports Quality Agenda X X X X
16 Chief Officer Report to the Governing Body, October Organisational Development: Primary Care Strategy Our commissioning strategy, developing through our three localities, remains committed to shifting activity from hospitals to the community and through significant integration of health, social and voluntary care. This will ensure that people do not spend any longer in hospital than necessary and will prevent the need for hospital admission wherever possible. Our commissioning intentions reflect this strategic direction. However, our strategy must be aligned with the development of Primary Care. If we are to shift significant resource to the community, our local Primary Care providers need to be ready to take on this challenge. As the first point of contact for over 90% of patients in accessing health care, General Practitioners (GPs) and their wider teams are at the forefront of developing improvements in chronic disease management, early interventions & diagnostics, end of life care and support for selfmanagement. Our plans over the next 5-8 months is to work with member practices and their commissioners (the NHS England Area Team) in order to establish how primary care will develop over the next few years to meet the challenge of shifting significant healthcare activity nearer to home for patients and their carers. 2. Workforce Development: Appointment to the Governing Body I am pleased to report that we have appointed Graham Smith as our second Lay Member, with responsibility for Public and Patient engagement. Graham is a barrister, with practical experience of advocating in the county courts. He is a resident in Aylesbury Vale and is very keen to take up the responsibility of overseeing our public engagement strategy. 3. Integrating Health and Social Care Lesley Perkin has been appointed to the Director of Integration post, a role that reports directly to the Healthy Bucks Leaders group. This is a one year appointment that aims to significantly develop the integration agenda through early implementation in one or more localities across the county. Lesley will be presenting to the Executive Committee in the near future. Chief Officer Report NOT PROTECTIVELY MARKED 2
17 4. Local Context: Keogh Enquiry I attended the Health and Social Care Select Committee (HASC) last week, where Buckinghamshire Hospitals Trust (BHT) alongside CCGs were presenting an update on progress with Keogh. The meeting was very thorough and the HASC were satisfied that BHT were making good progress. The webcast can be seen on the County Council website at: We continue to attend the weekly operational meetings and the monthly review meetings with BHT and the Trust Development Agency, (the Regulator). We remain pleased that good progress is being made against milestones. Louise Patten Chief Officer Chief Officer Report NOT PROTECTIVELY MARKED 3
18 Agenda item: GB a GOVERNING BODY MEETING OCTOBER 2013 GOVERNING BODY ASSURANCE FRAMEWORK Purpose of Paper To update the Governing Body on the principal risks identified for 2013/14 Executive Summary The Governing Body Assurance Framework (GBAF) sets out the principal risk to the 5 Strategic Objectives identified in the Operating Plan. There are currently 15 risks identified on the GBAF: 3 Extreme Risks No. 8, 10, High Risks No. 2, 3, 4, 5, 6, 7, 9, 12, 14, 15 2 Moderate / Low Risks No. 1, 13 Out of a potential risk score of 375 the current risk score is 46% against a target of 26%. (46% as at July) The 3 extreme risks are: 8 - Economic environment, demand / cost pressures and in-year changes to CCG allocations create increased requirement for QIPP or reductions in spending plans 10 - Operational plans (including QIPP) are not delivered, leading to contract overperformance and the need for in-year additional financial measures and service changes 11 Commissioning Support organisations are not fully delivering commissioned services No risk scores have changed since September Actions Required Review updated GBAF, especially the mitigation around the extreme risks
19 Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG X X ROBERT MAJILTON CHIEF FINANCE OFFICER 2
20 Glossary A&E Accident and Emergency BHT Buckinghamshire Healthcare NHS Trust CCG 1 Clinical Commissioning group CHC 2 Continuing Healthcare CO Chief Officer CFO Chief Finance Officer CQR Clinical Quality Review CQuIN Commissioning for Quality and Innovation CSU 3 Commissioning Support Unit C4Q 4 Commissioning for Quality Committee DO Director of Operations and Performance ECIST Emergency and Urgent Care Intensive Support Team IT Information Technology JSNA Joint Strategic Needs Assessment KPI Key Performance Indicator LTC Long Term Condition MK Milton Keynes PbR Payment by Results PCT 5 Primary Care Trust QIPP Quality, Innovation, Productivity & Prevention SLAM 6 Service Level Agreement Monitoring TDA Trust Development Authority TV 7 Thames Valley TVAEO Thames Valley Accountable Emergency Officer 1 Refers mainly to NHS Aylesbury Vale CCG ( 2 Refer to NHS Choices for background on Continuing Healthcare ( 3 Refers to Central Southern Commissioning Support Unit ( 4 This is a joint sub-committee of NHS Aylesbury Vale CCG and NHS Chiltern CCG 5 Refers mainly to NHS Buckinghamshire PCT 6 General term for Contract Monitoring Information for NHS contracts 7 Reflects Thames Valley Area team of NHS England and the CCGs within that area (Oxfordshire, Berkshire & Buckinghamshire) 3
21 Aylesbury Vale Clinical Commissioning Group Board Assurance Framework October 2013 Strategic Objective Principal Risk Initial Current Acceptable Change Improve people's health and reduce inequalities The CCG does not fully assess or understand the impact of its plans on health 1 inequalities That tensions may exist between a locality approach and whole system delivery 2 which makes priorities more difficult to deliver Enhance quality, safety and experience of patient services Quality handover from the PCT has identified issues with the CCGs main acute provider which may, until resolved, negatively impact on the quality, safety and 3 experience of the CCGs population and will take operational resource to resolve The ability to positively influence patient services is impacted by the size of the CCG 4 and the relative responsibility of commissioning organisations The availability of quality information and resources taken on acute providers means 5 the CCG cannot properly assure itself on other non-acute services Ensure local people have greater influence and management of The CCG fails to engage productively with stakeholders, patients and the public so they are not able to take advantage of the opportunities to positively influence their own care 6 own care Legacy financial issues create pressures in-year which are not fully mitigated within 7 the CCGs financial plan Deliver financial sustainability with headroom to invest Economic environment, demand / cost pressures and in-year changes to CCG 8 allocations create increased requirement for QIPP or reductions in spending plans Financial pressures within services commissioned creates financial fragility within 9 providers Operational plans (including QIPP) are not delivered, leading to contract overperformance and the need for in-year additional financial measures and service 10 changes Perform well as a CCG 11 Commissioning Support organisations are not fully delivering commissioned services Performance issues across the system creating risks to patients treatment times, 12 and delivery of patient services Service continuity is disrupted in key areas Organisational delivery is disrupted by unexpected adverse events or capacity to 14 deliver CCG does not manage its external reputation and loses credibility with stakeholders 15 and the public Page 1 of 18
22 Initial May Jul Sept Nov Jan Mar Objective: Improve people's health and reduce inequalities Clinical Lead Karen West Managerial Lead Lou Patten Risk: The CCG fails to align its priorities and plans with the emergent whole systems approach to reduction of health inequalities Date last reviewed 2 Oct 2013 Risk Rating 10 Rationale for current score: Likelihood Consequence 5 The emerging nature of relationships with Health and Wellbeing board and Initial Acceptable Public Health makes it more difficult to achieve whole system alignment of 0 Current Current priorities in terms of health outcomes and inequalities Acceptable Controls (What are we currently doing about the risk?) 1) Joint Strategic Needs Assessment reported & reviewed by Governing Body to understand our health inequalities, updated JSNA reported to Executive 2) CCG engaged in setting Health & Wellbeing Board Strategic Objectives & action plan 3) Public Health engaged to support the CCG in understanding the impact of our plans Mitigating actions (What have we done/what more should we do?) 1) Work with Health & Wellbeing Board to develop measurable performance indicators 2) Ensure all Executive and Locality plans address the 5 priorities set out in the Health & Wellbeing Action plan 3) Developing 2014/15 Commissioning Intentions in line with H&WB Strategy Assurances (How do we know if the things we are doing are having an impact?) Quarterly review of progress against the performance indicators set out within the Health & Wellbeing Action plan Gaps in assurance (What additional measures should we seek?) Current performance (with these actions taken, how serious is the problem?) Additional comments Page 2 of 18

23 Initial May Jul Sept Nov Jan Mar Objective: Improve people's health and reduce inequalities Clinical Lead Locality Leads Managerial Lead Colin Thompson Risk: That tensions may exist between a locality approach and whole system delivery which makes priorities more difficult to deliver Date last reviewed 2 Oct 2013 Risk Rating 20 Rationale for current score: Likelihood Consequence 10 Clear alignment on variation of use of resources across the system but lack of Initial Acceptable monitoring information available for practices. 0 Current Current Acceptable Controls (What are we currently doing about the risk?) a) Clear locality QIPP descriptions (activity & costs) b) Locality leads workplans, aligned to the delivery plan - improving as data becomes more available c) Locality version of the delivery plan d) Referral point and Price on Ice implemented Mitigating actions (What have we done/what more should we do?) a) CFO/CO/DO visiting each of the members 21 practices to listen to concerns and opportunities for improvement in system delivery. b) Systemwide fortnightly Director of Ops meeting being established to review system delivery. Assurances (How do we know if the things we are doing are having an impact?) a) Impact assessments being undertaken, for each system change b) Monthly QIPP and Performance report c) Further alignment will be achieved across the system with individual practices as the new directly enhanced services come on-line, both of these link directly to system wide plans, for example risk stratification and digital first. d) Referral information being routinely sent to practices and localities Current performance (with these actions taken, how serious is the problem?) These actions will reduce the risk, the challenge will be if the system reaches a point of nondelivery and how then mitigation can be quickly agreed across the system. Gaps in assurance (What additional measures should we seek?) a) Clear performance on Choose & book take up, prescribing performance and diagnostic utilisation is not yet routine b) Locality budgets not yet issued due to data issues Additional comments Page 3 of 18
24 Initial May Jul Sept Nov Jan Mar Objective: Enhance quality, safety and experience of patient services Clinical Lead Karen West Managerial Lead Jane McVea Risk: Quality handover from the PCT has identified issues with the CCGs main acute providers which may, until resolved, negatively impact on the quality, safety and experience of the CCGs population and will take operational resource to resolve Date last reviewed 2 Oct 2013 Risk Rating 40 Rationale for current score: Likelihood Consequence 20 The Keogh review confirmed the issues identified in the quality handover. BHT Initial Acceptable has been placed on special measures and an action plan agreed with the TDA. 0 Current Current Monitoring of progress is through the TDA oversight meeting of which the CCG Acceptable is a member. Controls (What are we currently doing about the risk?) a) An individual risk assessment has been carried out for each risk identified. b) Individual management plans are in place for all known risks, co-ordinated through the TDA action plan. c) Safeguarding action plan in place monitored through the Safeguarding Boards d) Patient safety - incident reporting will be monitored through CQR meetings with provider Mitigating actions (What have we done/what more should we do?) a) Risk summit confirmed and formalised the actions agreed at the Quality Strategy meeting. b) Action plan and monitoring processes in place. Assurances (How do we know if the things we are doing are having an impact?) a) Agreed Quality Schedule in 2013/14 Contract. b) Agreed CQuIN plans in 2013/14 Contract. Q1 report received and achieved c) Forward plan in place for Commissioning for Quality Committee (C4Q), minutes of C4Q sent to Governing Body. Gaps in assurance (What additional measures should we seek?) a) Have received partial information from BHT on Quarter 1. CSU is discussing provision of the rest of the data. There has been some progress in receiving the data but there are still gaps in assurance. These have been filled using intelligence from other sources. Current performance (with these actions taken, how serious is the problem?) There are clear actions in place to deliver the the priorities. Keogh review gave assurance that the priorities which the CCG had identified were correct. Additional comments Page 4 of 18
25 Initial May Jul Sept Nov Jan Mar Objective: Risk: Risk Rating Enhance quality, safety and experience of patient services Lead Lou Patten The ability to positively influence patient experience is impacted by the size of the CCG and the relative responsibility of commissioning organisations Date last reviewed 2 Oct Rationale for current score: Likelihood Consequence 10 The CCG should act as a role model for involving patients, families and carers in Acceptable assessing need and understanding what is important to patients. Such as 0 Current communication pathways Initial Current Acceptable Controls (What are we currently doing about the risk?) 1) Establishing comprehensive patient feedback systems through localities to ensure decisions are informed by knowledge of patient experience 2) Working with our providers to develop shared patient experience goals as part of developing good working relationships 3) Schools Competition approved by Executive 4) Lay member for Patient & Public Engagement appointed Assurances (How do we know if the things we are doing are having an impact?) 1) Providers' patient feedback surveys report improved feedback 2) Locality feedback reports improvements to patient experience Mitigating actions (What have we done/what more should we do?) 1) Further alignment of incentive systems to recognise and reward innovative patient experience measurement and improvement in local provider organisations 2) Look at Patient Experience across pathways of care 3) The CCG should act as a role model for involving patients, families and carers in assessing need and understanding what is important to patients 4) Obtaining additional capacity short term on Comms & Engagement Gaps in assurance (What additional measures should we seek?) Methods of collecting and reporting patients' feedback should be linked to clinical services so that clinicians identify with the results. Current performance (with these actions taken, how serious is the problem?) Additional comments Page 5 of 18
26 Initial May Jul Sept Nov Jan Mar Objective: Risk: Risk Rating Enhance quality, safety and experience of patient services Lead Robert Majilton The availability of good quality information and resources taken on acute providers means the CCG cannot properly assure itself on other non-acute services Date last reviewed 2 Oct Rationale for current score: Likelihood Consequence Acceptable 10 While CSU provider performance function gets fully established this remains a probable risk, the impact is expected to be mitigated as information improves 0 and targeted action can be taken on areas of non-acute services where quality Current or performance is less than desired. Initial Current Acceptable Controls (What are we currently doing about the risk?) a) Quarterly quality reporting on a wider range of services b) Performance report b) Continue to work with partner agencies e.g. BCC on Care Homes c) Quality KPIs are included in non-acute contracts and reported on by CSU Mitigating actions (What have we done/what more should we do?) a) Continued to develop performance report with CSU paricularly provider performance to ensure a more systematic way of identifying key themes and quality issues Assurances (How do we know if the things we are doing are having an impact?) a) Regular reporting of quality information from contracts b) Review of narrative quality reports on regular basis by Commissioning for Quality Committee c) Safeguarding will be reviewed by Safeguarding Boards d) Patient safety - incident reporting will be monitored through CQR meetings with provider Gaps in assurance (What additional measures should we seek?) a) Other lead commissioners negotiating quality schedules - need to improve local CCG involvement Current performance (with these actions taken, how serious is the problem?) a) Current quality report identifies some areas where further work on quality is being undertaken Additional comments Page 6 of 18
27 Initial May Jul Sept Nov Jan Mar Objective: Ensure local people have greater influence and management of own care Clinical Lead Stuart Logan Managerial Lead Lou Patten Risk: The CCG fails to engage productively with stakeholders, patients and the public so they are not able to take advantage of the opportunities to positively influence their own care Date last reviewed 2 Oct 2013 Risk Rating 40 Rationale for current score: Likelihood Consequence 20 Increasing self care will happen when patients and carers are equipped with the Initial Acceptable necessary knowledge, skills and confidence to manage their own conditions. 0 Current Current CCG capacity and the large patient groups who require this proactive Acceptable engagement means this is one of the greatest challenges for the CCG Controls (What are we currently doing about the risk?) 1) Communication and engagement strategy developed with action plan 2) Linking to County Council for use of their communications networks 3) Using social marketing analysis to understand why some groups are higher users of services 4) To actively equip patients and carers with the necessary knowledge skills and confidence to manage their own care Assurances (How do we know if the things we are doing are having an impact?) Patients and carers report it is easy to find out information about their conditions Mitigating actions (What have we done/what more should we do?) 1) Long Term Conditions strategy to be widely published 2) To further 'reach out' to less accessible populations and make them part of the engagement and involvement process. 3)To align the necessary knowledge and support for patients and carers across health and social care providers 4) Additional Communications resource dedicated to public engagement in place Gaps in assurance (What additional measures should we seek?) Providers reporting comprehensive arrangements to offer information to patients and carers Current performance (with these actions taken, how serious is the problem?) Additional comments Page 7 of 18
28 Initial May Jul Sept Nov Jan Mar Objective: Risk: Risk Rating Deliver financial sustainability with headroom to invest Lead Robert Majilton Legacy financial issues create pressures in-year which are not fully mitigated within the CCGs financial plan Date last reviewed 2 Oct Rationale for current score: Likelihood Consequence 10 Main areas of relevant provisions are around Continuing Health Care where Acceptable there remains a material contingent liability. Provision for 15% has been made 0 Current (subject to audit) in 2012/13 accounts Initial Current Acceptable Controls (What are we currently doing about the risk?) a) Provision carried-forward from 2012/13 b) Process to dissagregate PCT balances c) Review through the Continuing Healthcare Project Board Mitigating actions (What have we done/what more should we do?) a) Review of final audited PCT balance sheet to ensure provisions are correctly allocated through to CCG b) Regular review of progress on clearing CHC retrospectives Assurances (How do we know if the things we are doing are having an impact?) a) Audit of PCT 2012/13 Accounts b) Continued clearance of CHC retrospective claims Gaps in assurance (What additional measures should we seek?) a) Dissagregation of PCT Balance sheet not likley to be completed until end of Quarter 2 b) Over 70% of original retrospective claims are still to reach conclusion Current performance (with these actions taken, how serious is the problem?) Additional comments Page 8 of 18
29 Objective: Risk: Risk Rating Deliver financial sustainability with headroom to invest Lead Robert Majilton Economic environment, demand / cost pressures and in-year changes to CCG allocations create increased requirement for QIPP or reductions in spending plans Date last reviewed 2 Oct 2013 Rationale for current score: Likelihood Consequence 20 Current uncertaintly around impact of further baseline adjustments particuarly Acceptable specialist. 5% Pressure on BHT SLAM as at July 2013 ( 1.5m) Initial Current Acceptable Current Controls (What are we currently doing about the risk?) a) Work with Area Team and CSU to ensure impact of allocation adjustments are understood and cost neutral b) Agreed financial plan and regular monitoring to identify variances and mitigating actions c) Contingency and 40% Headroom remain to mitigate financial risks d) Mitigation plan reviewed by Executive team August and weekly meetings in place to oversee and further develop mitigations Assurances (How do we know if the things we are doing are having an impact?) a) Work continues to ratify the expected specialist adjustment, the additional work gives more assurance that the adjustment can be linked to contract / cost adjustments b) Report on Mitigations to August Exec and regular meetings in place to further oversee and develop this work Mitigating actions (What have we done/what more should we do?) a) Idenitfy in-year financial mitigations b) Agree allocation adjustment with Area Team for Specialist c) Review of legacy balances Gaps in assurance (What additional measures should we seek?) a) Number of significant contracts not yet signed or financial value aligned b) Number of allocation adjustments proposed by Area Team or not yet finalised e.g. Specialist c) Month 4 SLAM from BHT shows 5% over spend against contract ( 1.5m) Current performance (with these actions taken, how serious is the problem?) a) Specialist adjustment not agreed but work continuing b) Work on SLAM validation and challenge continues with the CSU c) Forecast still at planned surplus (1%/ 2m as at Month 4) but additional financial risks Additional comments Page 9 of 18
30 Initial May Jul Sept Nov Jan Mar Objective: Deliver financial sustainability with headroom to invest Lead Robert Majilton Risk: Financial pressures within services commissioned creates financial fragility within providers Date last reviewed 2 Oct 2013 Risk Rating 20 Rationale for current score: Likelihood Consequence 10 Need for continued efficiencies and tight economic environment may cause Initial Acceptable unstainable financial pressures across providers 0 Current Current Acceptable Controls (What are we currently doing about the risk?) a) Where appropriate contracts include financial schedules setting out expected income levels for providers to plan b) CCG involvement in reviewing Long Term Financial Model for BHT FT application Mitigating actions (What have we done/what more should we do?) a) Develop better understanding of system wide financial outlook, working with partners b) Continue to explain CCG financial outlook to stakeholders Assurances (How do we know if the things we are doing are having an impact?) a) Signed Contracts b) Review of main provider CIPs for quality impact Gaps in assurance (What additional measures should we seek?) a) Financial stability, linked to performance on contracts in other areas, of NHS Direct 111 Contracts has led NHS Direct to announch their withdrawl from NHS 111 and means the CCG has to obtain a step-in provider Current performance (with these actions taken, how serious is the problem?) Additional comments Page 10 of 18
31 Initial May Jul Sept Nov Jan Mar Objective: Perform well as a CCG Lead Colin Thompson Risk: Operational plans (including QIPP) are not delivered, leading to contract over-performance and the need for in-year additional financial measures and service changes Date last reviewed 2 Oct 2013 Risk Rating 25 Rationale for current score: Likelihood Consequence Localities are receiving referral information regularly but are not receiving Initial Acceptable information on diagnostics. Current Current Acceptable Controls (What are we currently doing about the risk?) The team have reviewed the first 100 days of the CCGs being live against the operational framework developed by PWC to support a focus on delivery. Several schemes of mitigation are also being developed and assessed through the CCG weekly operational meetings. Mitigating actions (What have we done/what more should we do?) The team is monitoring the weekly BHT referral information and the increase experience in April/May for the last two years is not being seen to the same degree this year. However a range of mitigation schemes are being developed. Assurances (How do we know if the things we are doing are having an impact?) Increased monitoring against individual workplans, linked to activity trajectories. Gaps in assurance (What additional measures should we seek?) Lack of Business Intelligence information to support locality reporting Current performance (with these actions taken, how serious is the problem?) Referrals are 17% above allocation (1,628) for April July at the top 5 providers BUT 4.9% (580) BELOW the same point last year Additional comments Strength in delivery in Planned care and Prescribing, issue of pace on implementation of LTC QIPP and delivery issues on emergency care. Page 11 of 18
32 Initial May Jul Sept Nov Jan Mar Objective: Perform well as a CCG Lead Robert Majilton Risk: Commissioning Support organisations are not fully delivering commissioned services Date last reviewed 2 Oct 2013 Risk Rating 20 Rationale for current score: Likelihood Consequence 10 Current gaps in capacity and bedding down of new ways of working make it Initial Acceptable likely that currently the CSU will not deliver fully against the service 0 Current Current specification. The impact of this is mitigated by active dialogue and escalation of Acceptable issues. Controls (What are we currently doing about the risk?) a) Monthly contract meetings - reporting across KPIs b) Embedding key CSU staff in CCG office (e.g. Communications) to improve understanding of CCG c) Regular meetings with account manager and CFO Mitigating actions (What have we done/what more should we do?) a) Corrective Action Plan response reviewed - further information on specific milestones around key service improvements requested b) CCG to produce Commissioning Intentions for Commissioning Support as part of planning Assurances (How do we know if the things we are doing are having an impact?) a) More KPIs being reported on and undertanding improved - now incorporated into organisational development section of the CCG performance report. Gaps in assurance (What additional measures should we seek?) a) Concerns on some areas of KPIs and Service Planning & redesign yet to report b) Drop in performance on complaints response times to 33% in June but returned to 100% in July Current performance (with these actions taken, how serious is the problem?) Additional comments NHS England proposing to allow extension of contracts to April 2016 ( Page 12 of 18
33 Initial May Jul Sept Nov Jan Mar Objective: Risk: Risk Rating Perform well as a CCG Lead Colin Thompson Performance issues across the system creating risks to patients treatment times, and delivery of patient services Date last reviewed 2 Oct Rationale for current score: Likelihood Consequence 10 Three main areas of concern A&E now seeing sustained green rating A&E delivery above Acceptable 95% for over 7 weeks, 18 weeks still holding although pressure on black-log 0 Current increasing. Ambulance response times still not delivering at CCG level. Delayed transfers of care still low, issues emerging on C-Diff levels Initial Current Acceptable Controls (What are we currently doing about the risk?) a) System resilience plans in place, ECIST report on A&E now available b) Heads of Terms agreed with South Central Ambulance Trust Mitigating actions (What have we done/what more should we do?) PbR contract in place to support 18 weeks Ambulance contract documentation to be signed Assurances (How do we know if the things we are doing are having an impact?) Weekly and monthly performance monitoring to the operational team and clinical executive Gaps in assurance (What additional measures should we seek?) Full implementation at pace of ECIST report Current performance (with these actions taken, how serious is the problem?) Additional comments A&E performance has improved although was under 95% for Week Commencing the 12th & 19th August Page 13 of 18
34 Initial May Jul Sept Nov Jan Mar Objective: Perform well as a CCG Lead Jane McVea Risk: Service continuity is disrupted in key areas Date last reviewed 2 Oct 2013 Risk Rating 20 Rationale for current score: Likelihood Consequence 10 The major providers all have Business Continuity Plans and Major Incident in Initial Acceptable place which are tested regularly. Currently area of greatest risk would be a 0 Current Current single care home failure, however the Local Authority have plans in place to Acceptable mitigate against this. Controls (What are we currently doing about the risk?) a) Whole system teleconference with action plans takes place daily to manage capacity and reduce risk in the system. b) Health Resilience Partnership provides forum to monitor incidents across Thames Valley and learn lessons. c) Bucks Quality Surveillance group set up Mitigating actions (What have we done/what more should we do?) a) Emergency planning standards in each contract. b) Urgent Care action plans from ECIST report will improve functioning of urgent care pathway. c) MK has joined the AEOs meeting giving greater visibility of the issues d) Support for the Clincial Commisioner is being sought. Assurances (How do we know if the things we are doing are having an impact?) a) Whole system teleconference reporting. b) Monitoring of A&E targets. c) TV Escalation framework approved d) Fire at BHT provided a live test of processes which were resilient e) Winter planning exercise has taken place across system f) MK has joined the TVAEO meeting Current performance (with these actions taken, how serious is the problem?) Daily resilence has amber/red during Septemeber indicating pressure in the system Gaps in assurance (What additional measures should we seek?) a) Lack of clarity on who is responsible for maintaining resilience in primary care. b) action plan being developed from winter planning exercise c) Winter Plan in development Additional comments Page 14 of 18
35 Initial May Jul Sept Nov Jan Mar Objective: Perform well as a CCG Lead Jane McVea Risk: Organisational delivery is disrupted by unexpected adverse events or capacity to deliver Date last reviewed 2 Oct 2013 Risk Rating 20 Rationale for current score: Likelihood Consequence 10 The CCG has in place processes which will support remote working and therefore is Initial Acceptable not relient on the functioning of either a single building or transport links. As a small 0 Current Current organisation we currently have some areas reliant on individuals (single points of Acceptable failure). Controls (What are we currently doing about the risk?) a) All staff have ability to remote work. b) Video conferencing implemented. c) CCG needs to formalise a Business Continuity Plan Mitigating actions (What have we done/what more should we do?) a) Need to work with other CCGs and CSU to reduce risk of single points of failure. b) Introduction of more formal structure to shared IT drive improving remote acccess c) Business continuity support is in place across the CCG but this needs to be formally captured in a plan focussed on remote working. Assurances (How do we know if the things we are doing are having an impact?) Whole system test of plans has taken place. Gaps in assurance (What additional measures should we seek?) a) Some areas reliant on individuals b) Co-ordinated Business Continuity Plan Current performance (with these actions taken, how serious is the problem?) Additional comments Page 15 of 18
36 Initial May Jul Sept Nov Jan Mar Objective: Perform well as a CCG Lead Lou Patten Risk: CCG does not manage its external reputation and loses credibility with stakeholders and the public Date last reviewed 2 Oct 2013 Risk Rating Rationale for current score: 20 Likelihood Consequence 10 Recent public renewed questioning of the Better Healthcare in Bucks Initial Acceptable consultation and the Keogh review of our main secondary care provider (we are 0 Current Current the Contract Lead) has increased our need to manage our external reputation Acceptable Controls (What are we currently doing about the risk?) 1) Active engagement with stakeholders through groups already set up and functioning 2) Communication and engagement strategy developed with action plan 3) Training for staff in stakeholder communications 4) Active engagement by the Governing Body members with key stakeholder groups 5) A whole system approach to developing open and honest answers to queries raised about local services Assurances (How do we know if the things we are doing are having an impact?) CCG has positive reporting in local media and with patient and stakeholder groups CCG engagement groups report positive feedback Patient & Public Lay role appointed Mitigating actions (What have we done/what more should we do?) 1) Further development of whole system alignment across Buckinghamshire 2) Continue to develop culture of openness and transparency throughout the organisation, our population and our stakeholders Gaps in assurance (What additional measures should we seek?) a) Withdrawl of NHS Direct from 111 service, requiring Buckinghamshire to recommission step-in provider may adversly affect external reputation Current performance (with these actions taken, how serious is the problem?) Additional comments Healthwatch attended July Executive to be part of discussion around Keogh review Page 16 of 18

37 Page 17 of 18
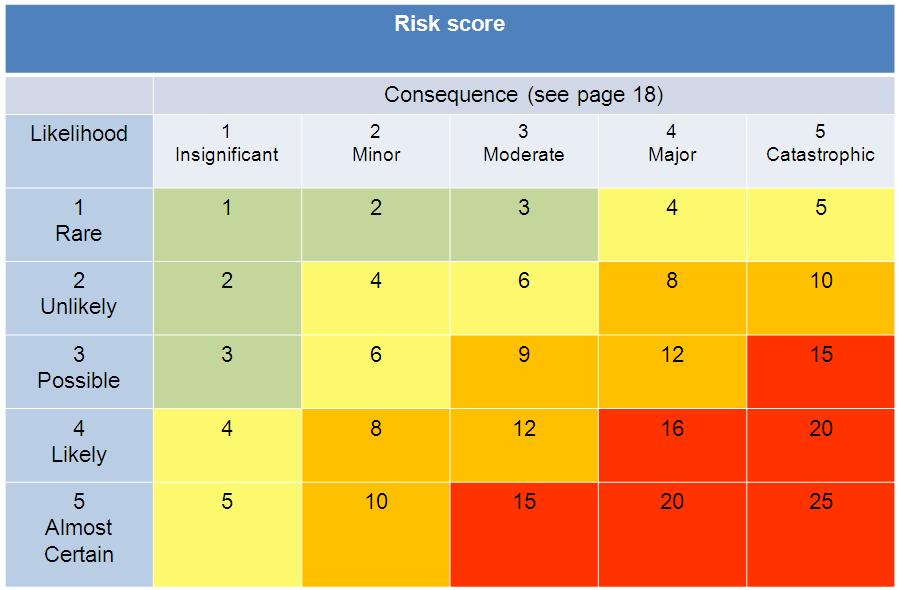
38 Consequence (Severity) Descriptor Insignificant Minor Moderate Major Catastrophic Objectives / Projects Insignificant cost increase / schedule slippage. Barely noticeable reduction in scope or quality < 5% over budget / schedule slippage or minor reduction in quality / scope 5-10% over budget / schedule slippage or reduction in scope or quality % over budget / schedule slippage or failure to meet secondary objectives > 25% over budget / schedule slippage or doesn't meet primary objectives Injury (Physical / Psychological) Minor injury not requiring first aid or no apparent injury Minor injury or illness, first aid treatment needed RIDDOR / Agency reportable Major injuries, or long term incapacity / disability (loss of limb) Death or major permanent incapacity Patient Experience / Outcome Unsatisfactory patient experience not directly related to patient care Unsatisfactory patient experience - readily resolvable Mismanagement of patient care, short term effects (less than a week) Serious mismanagement of patient care, long term effects (more than a week) Totally unsatisfactory patient outcome or experience Complaints / Claims Locally resolved complaint Justified complaint peripheral to clinical care Below excess claim. Justified complaint involving lack of appropriate care Claim above excess level. Multiple justified complaints Multiple claims or single major claim Service / Business Interruption Loss / interruption > 1 hour Loss / interruption > 8 hours Loss / interruption > 1 day Loss / interruption > 1 week Permanent loss of service or facility HR / Organisational Development Staffing and Competence Financial Inspection / Audit Adverse Publicity / Reputation Short term low staffing level temporarily reduces service quality (< 1 day) Small loss (under 50k) Minor recommendations Minor noncompliance with standards Rumours Ongoing low staffing level reduces service quality Loss > 0.1% of allocation ( 50k - 250k) Recommendatio ns given. Noncompliance with standards Local Media - short term. Minor effect on staff morale. Page 18 of 18 Late delivery of key objective / service due to lack of staff. Minor error due to ineffective training. Ongoing unsafe staffing level Loss > 0.25% of allocation ( 250k - 500k) Reduced rating. Challenging recommendations. Non-compliance with core standards Local Media - long term. Significant effect on staff morale. Uncertain delivery of key objective / service due to lack of staff. Serious error due to ineffective training Loss > 0.5% of allocation ( 500k - 2m) Enforcement Action. Low rating. Critical report. Major noncompliance with core standards National Media < 3 Days Non delivery of key objective / service due to lack of staff. Loss of key staff. Critical error due to insufficient training Loss > 1% of allocation (Over 2m Prosecution. Zero Rating. Severely critical report National Media > 3 Days. MP Concern (Questions in House)
39 Agenda item: GB a GOVERNING BODY MEETING OCTOBER 2013 COMMISSIONING INTENTIONS Purpose of Paper To provide the Governing body with an update to the 2014/2015 contracting round, through an overview of the commissioning intentions section. Executive Summary It is our aim to continue to work with patients, carers and users to review the services we provide and look to establish meaningful outcomes for those services. This paper introduces a new framework approach to contracting which aims to achieve this through supporting the population as a whole. Actions requested / recommendation To support progress to date Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG X X x x X Equality Analysis completed (please tick ) Author of paper Colin Thompson Yes No Not applicable Lead Director(s) responsible for this area of work Operations Delivery and Performance
40 Working paper Review and Development of our (AVCCG) Commissioning Intentions The Setting The Buckinghamshire Health & Well Being strategy is a three year partnership between County and District Counsellors, GPs and other partners. The strategy supports the system to focus on addressing the big issues that will improve the health and wellbeing of individuals. The top line objectives of the strategy are: Every child has the best start in life Everyone takes greater responsibility for their own health and wellbeing and the health and wellbeing of others Everyone has the best opportunity to fulfil their potential Adding years to life and life to years The Need The Executive team received a detailed health needs presentation from Public Health at the July meeting. The Rationale and practical recommendations for commissioning were also discussed directly with each clinical lead. The Challenge Six months into the contracting year the system is already experiencing significant pressures. In the 2013/14 intentions our ambition was to see a shift in the care setting and use of resources. We have made a start through the locality investment fund, but are currently in dispute with BHT over costs of activity being experienced there. Equally we had an ambition to ensure that patients admitted for urgent care received high quality care in the correct speciality and remain in hospital for as short a time as possible. At present BHT is still in special measures. Public and Stakeholder engagement Re-launch of our strategy presented earlier in the meeting. activities include: Other recent engagement 200 of BHT members list contribution comments to the system work on reducing follow ups 43 individuals from across providers and 3 rd sector involved in a commissioning intention workshop in August 31 patients and voluntary sector representatives involved in the September LTC workshop Involved of all practices during September/October in the ACHT review 1
41 Developments by localities in 2013/14 Some examples of new projects developed and now starting implementation, led by localities in the last six months include: MK discharge co-ordinator for North locality Care Home matron for South locality Paediatric education urgent care for Central locality Leg ulcer management for all localities The learning from these developments has been valuable in understanding both the capacity and capability required to make this level of progress. A framework under development (IPOC) The outcomes of any system depend on how that system is built. Therefore as a clinical commissioner we want to start and test new models of commissioning and new payment arrangements which encourage organisations to work collaboratively to improve the patient s health and delivery of integrated care and support. The framework we want to develop is IPOC or Integrated Population based Outcome Contracts. The main drive will be to improve outcomes for our population. Proposed clinical focus for 2014/15 Planned care To work closely with secondary care to ensure that referrals have the best possible health outcomes for the patient by: Review of current Anti-coagulation services, with the aim of supporting individuals receiving care in a primary care setting. Evaluation of current services available to patients for Obesity treatment, including overlap to current activity referral schemes. Understanding of demand and capacity within direct access radiology and pathology services Continue to progress further the appropriate digitalisation of outpatient consultations. Carry out initial stage of reviewing end to end MSK services Chronic disease management & Meds Management To ensure a patient-centred approach to managing long term conditions with a focus on inequality and cost effective care by: Continue living well project, integrating psychological therapies with LTC management in general practice. Support Self Care, a new resource programme to empower patients in Aylesbury Vale to maximise self-management. Primary Care Development, new approaches to address multiple co-morbidities. Medicines management will continue to focus on Diabetes, anticoagulation and nutrition, but will add a further focus on waste and ideally a review of stoma care. 2
42 Unscheduled care To integrate urgent care and reduce A&E attendances and emergency admissions by: Care homes commission appropriate medical support to care homes. Quantify the demand for same day care home placements. Shared plans & information aim to improve planning and shared EOL & management plans agreed between patients, relatives and GPs and shared with urgent care services. Discharge to access maximise discharge to access through effective utilisation of reablement and other services including ACHTs. Maximise existing services and access ensuring previous service changes and investments are fully utilised. Establish ambulatory emergency care to reduce LOS and avoid emergency admission. ACHT review implement recommendations from the review. Re-contract bundle of urgent care services work on re-contracting 111, MIIU and OOH within a framework to improve alignment of outcomes. Early years (Achieving a healthy baby and a healthy mother) To ensure that every child has the best start in life by early intervention and prevention and reduction of inequalities by: Decreasing percentage of mothers who smoke at delivery. Improving emotional health and mental health. Reducing the level of crisis admissions. Partnership and Joint Commissioning To work in partnership and deliver shared priorities, with joint planning to ensure people in the community live a s healthy a life as possible for as long as possible by: Maximise the co-ordination between GP, Carer and Individual. Purchasing against revised outcomes in Mental Health based on the individual s needs. Achieving increased quality in the new Learning Disability contract. Quality Intention Patient safety Reduce harm VTE Pressure ulcers Falls Catheter related UTIs Reduce avoidable deaths in all our providers by improving the quality of the urgent care pathway, reducing suicide Outcome measure Reduction in harm as measured by Safety Thermometer Reduction in HSMR in BHT Reduction in community suicides of people in receipt of MH care 3
43 Patient Experience Supporting providers in developing their safety culture by ensuring that all Sis have appropriate action plans to stop recurrence. Reducing the admissions to Intensive Therapy Units by ensuring providers have implemented NEWS Increase knowledge of mental capacity act and improved confidence in the use of Deprivation of Liberty safeguards to ensure least restrictive option is used. Support the development of the Multi Agency Safeguarding Hub Supporting the identification of children exposed to sexual exploitation and gang activity and ensure multiagency pathways are in place to support them. Increase the proportion of patients who would recommend the services we commission including A&E, maternity, out of hours. Work with providers to improve the staff experience as measured by the national staff survey as this is closely related to patient experience and quality. Work closely with Healthwatch to expand the feedback we receive on patient experience from direct observation and feedback from patients, clinicians and the public including those from hard to reach communities. Work with providers to ensure that appropriate levels of available clinical expertise and safe working practices in all services Encourage all staff and patients to act as quality inspectors Increase in low risk incidents reported to NRLS with a decrease in serious incidents by all our providers Increase in DoLs applications from all providers Measure at Safeguarding Board level Measure at Safeguarding Board level Increasing net promoter scores in providers Increase in Patients and the public describe the CCG as a listening organisation. 4
44 Clinical Effectiveness Improve the information given to patients? Work with partner organisations through healthy Bucks leaders to agree a single quality improvement model for Buckinghamshire and develop the capacity and capability across the system. Next Steps This is a working paper. Considerable detail sits behind the proposed areas for review. The draft discussion paper will continue to be refined and the following actions completed. 1. Complete draft consulted with practices, localities and the community 2. Presentation to H&WB in October 3. Alignment with CCCG 4. Alignment to Providers also updates on PbR changes 5. Economic appraisal of proposals against the investment schedule 5
45 Agenda Item: GB GOVERNING BODY MEETING OCTOBER 2013 Director of Quality Report Purpose of Paper To provide assurance to the Governing Body that quality is adequately monitored across the commissioned services and that appropriate action is taken where that quality falls below standard. Executive Summary The paper reviews the quality of care at Buckinghamshire Healthcare Trust including the progress against the Mortality action plan. A follow up risk summit has been held to review the progress Heatherwood and Wexham Park have made following the initial Summit in July. Assurance processes have been put in place to ensure that the quality of service provided by 111 is maintained during the transition phase to the step in provider. The Commissioning for Quality Committee has reviewed the assurance we receive on the quality of care provided for learning Disability clients with Southern Health and made some suggestions to make this more robust. The Insight Dashboard has been published which draws together a variety of information on the patient experience at all NHS Trusts across England. Actions requested / recommendation For note
46 Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG X X X Equality Analysis completed (please tick ) Author of paper Jane McVea Yes No Not applicable Lead Director(s) responsible for this area of work Director of Quality 2
47 1. Introduction This paper reviews the current quality issues in the services commissioned by Aylesbury Vale and Chiltern CCGs and provides assurance that these issues are being managed. 2. Acute Care 2.1 Buckinghamshire Healthcare Trust The Trust now has processes in place to report against the quality schedule each month. The October Clinical Quality review meeting will review the current reports to ensure that the indicators clearly understood Community acquired pneumonia pathway This was one of the pathways that the Keogh Review identified could be improved. The Trust has put in place a care bundle approach which ensures that all patients get all elements of the correct treatment in the recommended time window. This will be regularly audited along with the number of patients who are not placed within the speciality Mortality The mortality reviews which have been in place for some years have been further developed. The divisions have set up systems to review all deaths and to identify any learning The deteriorating patient The Early Warning Scoring system has been relaunched to identify deteriorating patients and ensure that prompt actions are taken. The Scores are audited to ensure they are correctly implemented. In addition all patients that are admitted to ITU are reviewed by a consultant and, if any learning relating to early identification is identified theses are shared with the ward based team. This will ensure that not only is the system of identifying patients in place but systematic quality improvement cycles are also present to ensure continuous learning Safety culture The Board has carried out the Manchester Safety Assessment Framework which is a self-assessment of the safety culture in the organisation. This is being cascaded through the divisions to ward level. The Trust is working with commissioners to identify an expert who could help the Trust embed the lessons learnt Staff awards Commissioners attended the Buckinghamshire Health Care Trust award ceremony which celebrated a wide range of quality improvements across the organisation. 2.2 Heatherwood and Wexham Park A follow up risk summit was held on 30 September. The lead commissioners provided assurance that they were closely monitoring the action plans. There was challenging discussion to seek assurance from the Trust on the progress made against the action plans. 3
48 3. Out of hours The step in 111 provider has been identified as South Central Ambulance Trust. A transition plan is in place. The quality of the service is monitored through the Key Performance Indicators and a robust Clinical Governance system. In addition the commissioners carried out an unannounced visit on 2 October. The visit was targeted at assuring commissioners that the system remained robust during transition. The service was fully staffed with both call handlers and clinicians. Those staff interviewed were able to articulate how the escalation system worked and confirm that they were well supported. 4. Southern Health The Commissioning in Quality Committee has reviewed the quality of care in the Learning Disability Service in Buckinghamshire. One of the issues noted was a lack of information specific to the LD service in Buckinghamshire as most information was recorded Trust wide. A recent Safeguarding investigation had made a number of recommendations however the commissioners had not at the time of writing received confirmation that these had been implemented. The joint commissioner is seeking confirmation through the contract process. 5. Insight Dashboard Overview NHS England made the Insight dashboard to be accessible to the public on 30 August What s in the dashboard? A summary of data sets currently included in the dashboard, appear below. Many of the data sets used have been available for some years and national data sets. Other data flows are new and in some cases have been put in place to support the dashboard: Experiences of NHS services and care (Viewable for England or NHS Trust) Friends and family test monthly scores; Comments that patients are making about the NHS (from NHS Choices, which includes comments patients make through other routes, such as Patient Opinion); What patients are complaining about (from the annual complaints return); How satisfied patients are with NHS services (from the inpatient survey); and Whether staff would recommend services to friends and family (from the annual staff survey and monthly from monthly data collected by YouGov); 4
49 Views/conversations about the NHS (Viewable for England only) Trending topics in healthcare; Top healthcare tweets; Key themes the public engaged with about the NHS on social media; How satisfied citizens are with NHS services; and Public perceptions of the NHS brand (covering a range of themes including recommendation, corporate reputation, quality and value for money) The dashboard can be found here Why is the dashboard important? The Insight Dashboard provides a never before seen view of experiences and views about the NHS from patients, the public and NHS staff. These data sets have historically either been difficult to find, poorly presented or not available at all. 5.3 Next steps for the Insight Dashboard NHS England will be undertaking a range of engagement activities and are encouraging structured feedback on the following areas. 1. Potential audiences for the dashboard; 2. How different audiences would use the dashboard; 3. Functionality that it would be useful to incorporate; 4. Data sets/functionality that is missing; 5. Additional data sets that could be incorporated that we are unaware of; 6. Suggested changes to current format and structure Options with regards to the longer term future of the dashboard will be informed by the feedback provided. Initial feedback suggested that incorporation into the Integrated Customer Service Platform would be a preferred option. This needs to be explored further. Jane McVea Director of Quality October
50 Agenda Item: GB GOVERNING BODY MEETING OCTOBER 2013 A PROMISE TO LEARN A COMMITMENT TO ACT. IMPROVING THE SAFETY OF PATIENTS IN ENGLAND Purpose of Paper To inform the Governing Body of the recommendations made in A promise to learn and to describe the actions the CCG will take in response to these. Executive Summary In August A promise to learn a commitment to act. Improving the Safety of patients in England was published as a result of a review of the recommendations from the Mid Staffordshire investigation, the Francis report, the Winterbourne report by Professor Don Berwick, President Emeritus and senior fellow for the Institute of Healthcare Improvement. The aim of this report is to collate the lessons learnt and specify the changes needed. ck_report.pdf Professor Berwick emphasises that culture will trump rules, standards and control strategies every time and achieving a vastly safer NHS will depend far more on cultural change than on a new regulatory regime. The paper outlines the actions the CCG proposes to take in response to the recommendations and describes how success will be measured. Actions requested / recommendation The Governing Body is asked to note the recommendations and approve the proposed actions. 1
51 Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG X X X X Equality Analysis completed (please tick ) Yes No Not applicable Author of paper Jane McVea Lead Director(s) responsible for this area of work Director of Quality
52 1. Introduction The year September 2012 to September 2013 has been a transition period for the NHS with the new Clinical Commissioning Groups taking over the majority of local commissioning from the Primary Care Trusts and NHS England taking over the oversight role from the old Strategic Health Authorities. At the same time a number of key documents have been published which have developed the thinking on quality and quality improvement within the NHS. In August A promise to learn a commitment to act. Improving the Safety of patients in England was published as a result of a review of the recommendations from the Mid Staffordshire investigation, the Francis report, the Winterbourne report by Professor Don Berwick, President Emeritus and senior fellow for the Institute of Healthcare Improvement. The aim of this report is to collate the lessons learnt and specify the changes needed. In the report three different types of unnecessary risk of harm are identified: risk of harm due to neglect or wilful misconduct; risk of harm due to failures in the system; risk of harm from error. They are not the same. Most errors are made by wellintentioned people or arise from failures in systems. The critical task for leaders in healthcare systems is to improve the reliability and safety of healthcare systems. It is only by developing a reporting culture where both patients and staff feel confident in reporting mistakes that continuous improvement will take place. 3/Berwick_Report.pdf 2. Problems identified Professor Berwick identified the following problems recurred across all the findings he reviewed 3. Changes required Patient safety problems exist throughout all healthcare services including the NHS. In the vast majority of cases these are due to the systems, procedures, conditions, environment and constraints rather than being due to individual staff. Incorrect priorities do damage. The central focus must always be on patients. Clear warning signals are sometimes not heeded, especially the voices of patients and carers. When responsibility is diffused, it is not clearly owned: no-one is in charge. Improvement needs to be resourced and supported by an agenda of capability building. Fear is toxic to both safety and improvement. The problems listed above are not unique to the NHS. They occur in all large healthcare systems. Recognising them is the first step. Below are the principles that guided the choice of recommendations. Recognise with clarity and courage the need for wide systemic change
53 Abandon blame as a tool and trust the goodwill and intentions of the staff. Reassert the primacy of working with patients and carers to achieve health care goals. Use quantitative targets with caution and never allow them to displace the primary goal of better care. Recognise that transparency is essential and expect and insist on it. Ensure that responsibility for functions related to safety and improvement are assigned clearly and simply. Support career long learning of quality improvement methods. Make sure pride and joy in work, not fear, infuse the NHS. The pursuit of improving safety should permeate every action and level in the NHS. Professor Berwick emphasises that culture will trump rules, standards and control strategies every time and achieving a vastly safer NHS will depend far more on cultural change than on a new regulatory regime. 4. Lessons for Boards 1. Listen to and involve patients and carers in every organisational process and at every step in their care. 2. Monitor the quality and safety of care constantly, including variation within the system. 3. Respond directly, openly, faithfully and rapidly to safety alerts, early warning systems and complaints from patients and staff. Welcome all of these. 4. Embrace complete transparency. 5. Train and support all staff all the time to improve the processes of care. 6. Join multi-organisational collaboratives networks in which teams can learn from and teach each other. 7. Use evidence based tools to ensure adequate staffing levels. 5. Local Response In May we presented a set of promises which had been developed in response to the Francis Report to the public (appendix 1). The majority of the actions fall under Promises 1 and 2 or our constitution and Organisation Development plan. The Table 1 outlines the actions Aylesbury Vale CCG will take in response to A promise to learn and a description of how we will know we have succeeded. Professor Berwick emphasises that the single, most important action is to develop an NHS which focusses on continual learning and improvement of patient care. Aylesbury Vale CCG is committed to delivering its part in that change. 6. Summary As a universal healthcare system, free at the point of access, with common goals, structures and systems, the NHS is unique and can do what no other system can. It has the potential to be the safest healthcare system in the world. In Buckinghamshire we need to build on the strengths of the local healthcare system with the opportunities for integrated care but also to be clear on the areas where we need to improve and deliver targeted improvements e.g. the urgent care pathway particularly for the frail elderly. Jane McVea Director of Quality Sept 2013
54 Table 1 Local response The report said Action which we will take How we will know we are achieving 1. The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning. Promise 1 In Buckinghamshire there will be a continual reduction in harm measured by a reduction in serious incidents; a reduction in repeat incidents and an increase in minor incidents and near misses. 2. All leaders concerned with NHS healthcare should place quality of care, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement and support. Promise 2 3. Patients and carers should be present, powerful and involved at all levels of healthcare organisations. Promise 1 4. Healthcare organisations should ensure that staff are present in appropriate numbers to provide safe care at all times and are well supported. Promise 2 Work with Clinical Commissioners during the 2014/15 contract round to develop quality schedules to support each clinical portfolio. Provide training on implementing the Human Factors in healthcare for all Clinical Commissioners. From September to December 2013 we will deliver a programme of engagement at all levels of the organisation to ensure patients and the public and members are fully involved in planning and decision making at all levels. Develop systems to provide assurance that staffing levels are actively monitored and shared with patients and the public in provider organisations. Ensure all staff in the CCG act as a quality inspector, never knowingly passing on an error, risk or defect to a colleague or patient Clinical Commissioner s reports on their portfolios will describe the quality of the services they commission as well as the activity and finance. Patients, carers and the public will describe the CCG as a listening organisation. Patients and the public will report that they were treated with dignity and respect by staff who had time to include them in the making decisions about their care. 5
55 The report said Action which we will take How we will know we are achieving 5. All staff should have training in quality and patient safety sciences 6. Leaders in the NHS must create and support the capability for learning and change at scale. Organisational development plan Work with partner organisations through Healthy Bucks Leaders to agree a single quality improvement model for Buckinghamshire and develop the capacity and capability across the system. All members of staff within the CCG will be able to describe their role in quality improvement and demonstrate the skills required to deliver it. 7. Transparency should be complete, timely and unequivocal. Data on quality should be shared in an accessible form with patients and the public. CCG constitution 8. All organisations should seek out the patient voice as an essential asset in monitoring the quality and safety of care Promise 1 9. Supervisory and regulatory systems should be simple and clear 10. Commissioners should practice responsive regulation Quality dashboards will be developed to cover the full range of commissioned services and will be shared with the public along with the actions we are taking to improve quality. Gathering feedback from patients will be embedded in all routine quality monitoring, service redesign, strategy development. We will be developing a strategic alliance with Healthwatch to ensure we are hearing people and communities which are hard to reach. We are working with our partner organisations to create clear supervisory and regulatory systems based on a Quality Surveillance Group for Buckinghamshire Patients and the public will report that where quality standards are not met they had access to the information and what the improvement plan is.
56 Appendix 1 P Promise 1 Develop systems to collate the views of local people, both clinicians and the public and to feed back the actions we have taken in response to these views. Ro Pro Prom Promise 2 We will work with our partners to monitor the quality of care provided to our patients. We will wor k wit h our partners to of care provided to our patients with regard to compassion Promise Promise 3 We will develop a visiting schedule covering the range of services we commission to understand the patient pathway. Promise 4 We will monitor the mortality rates in our providers and where these are above the expected work with providers to reduce them. Promise 6 We will publish a quality framework which describes the accountability for quality assurance and for quality improvement. We will ensure that the public and our member practices are informed of the actions taken wit 1romise 1 By xxx 2013 we will have in place systems to collate the views of local people, both clinicians and the public and to feed back the actions we have taken in response to these views. By xxx 2013 we will have in place systems to collate the views of local people, both clinicians and the public and to feed back the actions we have taken in response to these vie 7
57 Agenda Item: GB a GOVERNING BODY MEETING OCTOBER 2013 QIPP REPORT Purpose of Paper The corporate reporting framework should be the spine of the organisation providing sufficient information for the Governing Body and Executive Team to be assured of the organisations progress towards delivering the corporate objectives. The QIPP report summarises the reports received from the QIPP Programme Leads to provide information regarding the progress, delays and risks associated with delivery of individual QIPP programmes. Executive Summary This report provides a Month 5 position for QIPP delivery for Aylesbury Vale CCG. The reports are provided directly from programme managers and should have the authorisation of the Clinical Executive Leads, via Joint Executive Team (JET) meetings prior to inclusion within this report. Each Clinical Executive is responsible for the information provided in this report. Actions requested / recommendation The Governing Body is asked to review the report and provide feedback on the quality and style of the report to support further development. The Governing Body is asked to note the report and issues identified with delivery to Month 5. Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG Equality Analysis completed (please tick ) Yes No Not applicable 1
58 Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children s) Planned Care (Right Care) Localities Joint care This report highlights the key issues and risks in the 2013/4 QIPP Plan during Month 5 (August), although much of the supporting data analysis relates to month 4. The table to the left provides a high level assessment of current and forecast delivery of the QIPP challenge in 2013/14 for each of the constituent programmes. Assessment of QIPP programme delivery is made on achievement of the required activity reduction aligned to delivery of the QIPP projects (activity and finance) and the assessment of delivery from the highlight reports (milestones). The body of the report provides a summary highlight report for each programme including the high level Key Performance Indicators (KPIs) for each programme where these have been agreed. Where they have not, work continues with programme managers to identify KPIs and these should all be in place by October (some services do not start until later in the year). More detailed highlight reports are available from the programmes.
59 2. Summary of QIPP Delivery - QIPP Finance Annual Budget Year to Date Budget Year to Date Actual Year to Date Variance Achieved Year to Date % Impact Rating Forecast Actual Forecast Variance Forecast Achievem ent % - INPACT 1, (60) 73% Amber 829 (260) 76% Red - Chronic Disease 1, (434) 42% Red 769 (1,068) 42% Red - Early Years (20) 0% Amber 0 (109) 0% Amber - Planned Care 1, (126) 67% Amber 1,031 (330) 76% Red - Localities (100) 60% Amber 525 (75) 88% Amber - Joint Care % Green % Green Total Gross Savings 5,594 1,874 1,134 (740) 61% Red 3,752 (1,842) 67% Red Mitigtion - BHT - Use of Headroom Blue Blue Total Net QIPP Programm 5,594 1,874 1,417 (457) 76% Blue 4,430 (1,164) 79% Blue Key: High Impact/Risk of not achieving plan (variance 25%/ 250k or over Medium Impact/Risk of not achieving plan (variance against plan belo On target or marginally positive Positive variances against plan Red Amber Green Blue Risk Rating Table One (left) provides a summary of Month 5 QIPP achievement by programme and a forecast position for year end in financial terms. Actual reported position was 1,134k savings against a plan of 1,874k (61% achievement). This is partly off-set by 283k mitigation from underspend on budgets not covered by QIPP schemes The mitigated QIPP position is an under achievement of 457k (24%) The forecast position is a year-end delivery of 79% of the plan. It should be noted that it is assumed that delivery has been achieved on budgets that are currently showing as being on Plan in Prescribing and Joint Care, and for those elements that will be delivered under the risk sharing rules established within the BHT contract.
 shows that the InPACT programme is estimated")

60 3. QIPP Programmes 3.1 InPACT CLINICAL LEAD: DR KEVIN SUDDES RAG rating Activity Finance Milestones Table 2: Delivery of savings against plan by project InPACT Table 2 (left) shows that the InPACT programme is estimated to be delivering 163K of its expected 223k (73% achievement). Summary For AVCCG, admissions at all providers are lower than last year but above plan at BHT. However, these figures exclude admissions to CDU, SAU and the cardiac and stroke unit. CDU admissions are well above plan and leading to a significant rise in overall cost of urgent care at BHT. To identify the cause of this higher CDU activity than expected an audit has been undertaken. Results of this will inform a planned review of the CDU tariff. Pathway changes at SMH are having benefits to patents as the Trust has achieved it s A&E 4 hour standard consistently since April and there are fewer delays in ambulance handovers than at other local trusts. Key Performance Indicators (KPIs): Activity trends for emergency admissions, A&E attendances Further communications are planned to increase public awareness of alternatives to A&E for urgent care including a video for use in GP waiting rooms. Ambulance demand: Calls to SCAS have increased by 6% (569 extra calls) in AVCCG in April Aug compared to the same period last year. Analysis that SCAS has produced shows that Red 1 (life threatening) calls from 999 have remained fairly constant in Chiltern but risen in AVCCG. In addition, red (urgent and life threatening) calls from NHS 111 have added to the demand. SCAS are not allowed to re-triage these calls so this has significantly added to their workload. Patient level clinical analysis is being undertaken as part of NHS 111 work to determine whether these NHS 111 red calls, clinically required an ambulance response. This will identify whether the NHS 111 national triage pathway would benefit from modification, or whether NHS 111 is identifying new patients who warrant an ambulance but who would not have called 999.



61 Winter pressure funding has not been awarded to Buckinghamshire. The InPACT Board and UC JET are identifying mitigating actions to support delivery of resilient A&E services during the winter period and support change in the urgent care system. These include making maximum use of services such as MIIU and MuDAS, and new services such as the expanded local authority re-ablement service. Winter plans are being collated and submitted to the NHS England TV Area Team, to demonstrate how Buckinghamshire will manage the expected demand within existing resources. Key achievements last month: Shared Patient Notes: Completion of pilot and commenced review to decide whether system requires any modification before being rolled out across Bucks for EoL and other patients. NHS 111, Directory of Services: Review the ranking strategy for border OOHs Comms: MIIU posters have been sent out to practices. Not achieved Brokerage for self funding DTOC: Identify pilot ward and meet with hospital/ward staff. Escalated issue via InPACT Operating Board to BHT Key next steps for next month: Shared Patient Notes deployment decision depending on JET approval by end of September NHS111, finalise on report process for repeat callers for OOH s MAG s: continue presentations to 35 practices through September and October. MAGs: Roll out plan being developed in line with practices signing up to the DES. Also recruit Care Coordinator Officers x 5 working with BCC Corporate Comms: Winter messaging develop specific activities in line with funding available and create materials. Centaur: Continue to engage with GP practices in order to increase referral rates Falls & bone health: develop outline business case with an options appraisal

62 Children s Urgent Care: Roll out of Bronchiolitis, D&V and Head Injury including printing and disseminating of electronic copies needs to be undertaken in Sept Transforming discharge: Start of pilot of home tomorrow 3.2 Planned Care (Right Care Steering Group) CLINICAL LEAD: DR CHRISTINE CAMPLING RAG rating Activity Finance Milestones Table 3: Delivery of savings against plan by project: Planned Care Project Title & Brief Description (categorised by w orkstream type) Net Savings YTD Planned Net Saving YTD Actual Saving YTD Variance From Plan Planned Forecast Outturn Revised Forecast Outturn Variance Forecast Outturn '000 '000 '000 '000 '000 '000 '000 New approach to follow ups 1, , Total 1, ,361 1, Key Performance Indicators: Follow-ups and elective admissions Two thirds of the QIPP savings expected from the reduction in followups are being generated (Table 3). The programme is delivering the agreed milestones. However there is a forecast over performance (at BHT) against key areas in planned care leading to the development of a mitigation plan for Planned Care The programme has developed a draft action plan which was discussed at the RCSG 19th September. This plan will not mitigate against the total forecast overspend and there is a need to work in collaboration with other programmes for example, locality working and referral management. This Plan has been produced as a joint effort by BHT, CCGs and the CSU. The key areas that require acceleration of work are T & O complete review of pathway, management of back log, understand waiting list profile and reduce follow up appointments General Surgery - complete review of pathway including pre and post-operative management and adherence to LPP &TDP and reduce follow up appointments Dermatology escalate pace of and capacity for community clinics, widen access to teledermataology (photo links) to all GPs Ophthalmology escalate pace of discharge of glaucoma


 CLINICAL LEAD: DR STUART LOGAN RAG rating Activity Finance Milestones Table 4: Delivery of savings against plan by project: Chronic Diseases Long term")
63 patients to the practice, review pathway including referral of and procedures for cataracts Pathology full roll out of ICE format for ordering and education, practice information of monthly activity and trends Direct Access Radiology review pathways to and between BHT and Care UK continue exploration of possible causes - check all coding and themes. Followed by revamp of protocols and education. Reduction in Consultant Led Follow Ups at BHT by 1.5m in year during 13/14 This project is on target against all milestones. Most of the reductions in follow appointments will be realised in quarters 3 and 4. So far the biggest reductions are being seen in Paediatrics and Gynaecology. A business case for audio visual software programme to support non face to follow up is being discussed at the right care steering group (RCSG) on 19 th September. 3.3 Chronic Diseases (Long Term Conditions LTCs) CLINICAL LEAD: DR STUART LOGAN RAG rating Activity Finance Milestones Table 4: Delivery of savings against plan by project: Chronic Diseases Long term conditions The Primary Care Long Term Conditions Programme covers the Psychological Therapies 'Live Well', AIM, and diabetes and respiratory skills projects. Planned QIPP savings for these schemes are not yet being met as work to date has mostly been preparatory, or in too early stages of implementation. The Live Well clinics are receiving patients for assessment and treatment, but will take time to realise benefits to the system. Similarly, the AIM telehealth project, whilst achieving very good take up across the CCG is still completing training for practices. Key Performance Indicators: to be confirmed for LTCs and to be finalised for A risk has emerged with the Live Well project in that the required data for risk stratification cannot be captured in one practice because a mass Read code conversion is required to allow patients to be included. A solution has been identified and will be implemented. Medicines management
64 medicines management but will be in the areas of dexa scan and pathology test rates by practice. The updated national forecasting model is now available and indicates an improved forecast under spend on M3 prescribing. The interim review of the Diabetes specialist nurse post and dietician post is complete and continued funding is being sought. Anticoagulation service specification first draft complete for wider consultation. We are actively inputting into the insulin management of T2DM LES 3.4 Early Years (including Children s Urgent Care) CLINICAL LEAD: DR JULIET SUTTON RAG rating Activity Finance Milestones Table 5: Delivery of savings against plan by project: Early Years Project Title & Brief Description (categorised by w orkstream type) Net Savings YTD Planned Net Saving YTD Actual Saving YTD Variance From Plan Planned Forecast Outturn Revised Forecast Outturn Variance Forecast Outturn '000 '000 '000 '000 '000 '000 '000 Paediatric urgent care Paediatric urgent care KPIs: Emergency admissions for under 5s and fever pathway (from September) plus other pathways as they come on stream. Table 5 (left) shows that the Early years programme is not delivering it s expected 17k of savings to date. Children s urgent care Following receipt of governance approval the D&V, Bronchiolitis and Head Injury pathways have been approved. D&V is now with the Quality Committee whilst Bronchiolitis and Head Injury are going through the Trust (BHT) Governance process and then will go the Quality Committee. D&V will be published on 1st October subject to Quality Committee approval and Bronchiolitis and Head injury shortly thereafter. The ChildhealthBucks website for making information regarding the local services available for children s health support and providing simple health advice is in the final stages of development and is expected to be delivered in October. A communications plan for publicising this website and health advice is being developed and will run concurrently with the publicity for the pathways, the website and the overarching social marketing campaign for urgent care in October/November. This plan will link with the central locality paediatric urgent care initiative.
65 3.5 Joint Care: CLINICAL LEAD: DR KAREN WEST RAG rating Activity Finance Milestones Table 6: Delivery of savings against plan by project: Joint Care Project Title & Brief Description (categorised by workstream type) Gross Savings Investment Net Savings YTD Planned Net Saving YTD Actual Saving YTD Variance From Plan Planned Forecast Outturn Revised Forecast Outturn Variance Forecast Outturn '000 '000 '000 '000 '000 '000 '000 '000 '000 Reduce Grow th The following key performance indicators have now been agreed and will be monitored from the date specified. KPIs Referrals to memory clinics (from October); Number of people with a learning disability receiving a health check (from September (ie September data)); Number of practices signing up for Remote monitoring DES (from August) The QIPP savings generated through the joint care programme are related to reducing and containing growth Projects covered by programme are: Autism; Dementia; Neuro-rehab services review; Stroke support. Key achievements this month were: Autism: Review of actions from the 2012/13 action plan. Governance changes achieved so that the work sits under Integrated Care Pathways National self assessment has gone to Adult JET for discussion final comments due on 20/09/13 Self assessment has been forwarded to Autism Strategy Board for comment Meeting held with Cheryl Gillian MP, NAS and local carers to discuss developments locally. Dementia: Dementia friendly community coordinator post has gone out to advert. PTL on Dementia and Frail Elderly for AVCCG
66 MRI Scans initial discussion has taken place before meeting is arranged to agree change to the protocol for Dementia patients. Four new memory clinics are under development in addition to the current three in Aylesbury, Amersham and High Wycombe. The seven clinics will give geographical coverage for the county. Neuro-rehab services review: Completion of high level mapping for inpatient, outpatient and day case pathways (covering Inpatient, community neuro-rehab & community head injury services). Comparative data gained from site visits to Nottingham Neuro Rehab Unit & Oxford Centre for Enablement (OCE) Stroke support: Further revisions to the stroke action plan ToR reviewed and direction for the Stroke Network Group agreed with CSU and Public Health leads Revised stroke patient portfolio complete and rolled out Mental Health Pathway Redesign IAPT : Funds secured for proposed 7k increase in Couples Counselling for Depression (Relate). Contract finalised and with provider Richmond Fellowship contract finalised and with provider Expanding COPD/IAPT Pathfinder geographically - project group secured agreement from SCN for evaluation funding, to include economic analysis IAPT PbR pilot in Buckinghamshire proposed - awaiting national response Education and training group established with GP clinical leadership GP clinical lead identified for Maternal & Infant MH scoping project Specialist community review: OHFT are on target with the review of CMHTs, assertive outreach, crisis/home treatment services. Pathway design is shaping up for two locality teams - covering the two CCG areas, with sub-team structures. New hospital: On track for completion within agreed timescale. Commissioner visit has taken place. Personality Disorder (complex needs) review: OHFT have carried out early discussions with the staff at the therapeutic community. OHFT contract/pbr Performance meetings are being led by the CSU. Cluster specifications are in place. Psychiatric In-Reach and Liaison Service (PIRLS Provider/
 of which 225k per annum is new investment LD Pathway and Integration: Review workshop regarding the forensic pathway with Southern")
67 commissioner meetings have happened to discuss specification. Specification is agreed within a 400k per annum limit (2 years) of which 225k per annum is new investment LD Pathway and Integration: Review workshop regarding the forensic pathway with Southern Health was held on 16/9/13 in Oxford Literature review re. LD integrated services models started Challenging Behaviour: Project Initiation Document (PID) under development. Literature review of Challenging Behaviour Strategies 3.6 Localities: CLINICAL LEADS: DR CHARLES TODD & DR MALCOLM JONES RAG rating Activity Finance Milestones Table 7: Delivery of savings against plan by project: localities First out-patient attendances are above plan year to date and referral activity is above allocation But has shown a reduction compared to 2012/13 of approximately 4% across all localities. Practices in localities are being encouraged to review specialties with high referral patterns as part of the QOF QP process in 2013/14 to support the CCG to reduce utilisation of acute care. The locality meetings in October and November will be used to undertake peer review to support practices to challenge each other as to proposals to improve referral management. Central locality in particular has engaged with the use of QP to support mitigating the CCGs activity position and has made innovative suggestions regarding how practices can buddy together to improve practice, we are negotiating with the Area Team to ensure this work by practices is recognised as part of the QP process. Key Performance Indicators: First out-patient attendances and first outpatient attendances which are GP referred; diagnostic activity exact KPI to be agreed. Leg Ulcers A preferred provider for the proposed pilot scheme has been agreed and it is intended to complete the contract by early October to start as soon as possible. This is an AVCCG-wide project support is required to encourage take-up across all our practices. In the long run this should lead to

68 improved patient outcomes and reduced use of nurse time. Strengthened Parental Care for Sick Children This project is now being supported by the Communications Lead; engagement events for mothers and children are being planned for October/November and further work is being put in place to target areas of high activity. Milton Keynes Discharge Coordinator Discharge coordinator has been in post for two months, work is on-going to strengthen communication between acute, social care and primary care to support improved patient care and quality of discharge. This includes ensuring appropriate access to information and patient records. Electronic Discharge notes are now being shared between the trust and primary care at the start of admission. The Coordinator has identified a cohort of patients who are regular users of services across the healthcare system and is working with partners to understand drivers for usage patterns and solutions to support both the patients and the services. Primary Care colleagues have welcomed the support from the discharge coordinator. Care Home Matron A launch event for the care homes matron project was held on 19 th September with South Locality practices to introduce the service. The project is now moving forward to provide support on the ground to care homes and practices.
69 Agenda Item: GB a Purpose of Paper GOVERNING BODY MEETING OCTOBER 2013 CORPORATE PERFORMANCE REPORT To inform the Executive Team of CCG performance against national performance indicators and seek guidance to address areas of concern. Executive Summary This report provides assurance of performance against the NHS England CCG Assurance Framework. Actions requested / recommendation The Governing Body is asked to note the report. Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG Equality Analysis completed (please tick ) Author of paper Sian Barry, AV CCG Katherine Woolley, CSU Yes No Not applicable Lead Director(s) responsible for this area of work Colin Thompson, Director of Operations & Performance 1
70 Organisational Performance Report, Month 5 September 2013 Introduction The corporate reporting framework is intended to be the spine of the organisation providing sufficient information for the Governing Body and Executive Team to be assured of the organisations progress towards delivering the corporate objectives. The following reports are the core set of monthly reports to provide assurance to the Executive Team and the Governing Body. Organisational Performance Report Finance Report QIPP Report Quality Report Board Assurance Framework This report, the Organisational Performance Report provides a high level summary across all areas covered by the Corporate Reporting Framework for more detail please follow the hyperlinks to the relevant supporting reports. The Balanced Scorecard This report provides a summary of Aylesbury Vale CCG performance against national and local indicators during Month 5 (August 2013), presented using a balanced scorecard developed by the Area Team. It provides a summary of quality and performance indicators that describe how services that the CCG is responsible for commissioning are delivering care. The indicators within the report are presented as a balanced scorecard. A balanced scorecard allows the CCG as an organisation to review all aspects of its business to make an assessment in the round, identifying areas of good progress or concern. It allows the Executive Team to review all information when making decisions. The five areas of the balanced scorecard are: Assuring Quality of Care (Are local people getting good quality care?) Achieving Patient Standards (Are patient s rights under the NHS Constitution being promoted?) Improving Health Outcomes (Are health outcomes improving for local people?) Finance (Is the CCG commissioning services within its financial allocation?) Organisational Development The areas of the balanced scorecard amalgamate a number of indicators under each heading. The RAG (Red, Amber, Green) assessment is made by allocating a score for each indicator, amalgamating these scores and assessing the result against the agreed framework. Where an area is assessed as Amber or Red a short summary of issues generating these concerns is provided with assurance of the actions being taken to improve delivery. The full set of indicators included in each area of the scorecard is included for reference in the appendices to this report. 1
71 CCG Balanced Scorecard : Are local people getting good quality care? Provider indicators R CCG assurance indicators A Quality Dashboard A (not part of LAT scorecard, included for Additional local measures) Are patient's rights under the NHS constitution being promoted? NHS Constitution A Supporting measures G CCG Local Priorities A Are health outcomes improving for local people? Preventing people from dying prematurely (domain 1) G Enhancing quality of life for people with an LTC (domain 2) A Helping people to recover from episodes of ill health (domain 3) G Patients Experience (domain 4) G Patient safety (domain 5) A Finance: Is the CCG commissioning services within its financial allocation? Financial Performance G Financial Management A QIPP - year to date delivery (finance) A Activity trends - year to date A Activity trends - full year forecast A QIPP - full year forecast (finance) A (amber after mitigation) Organisational Development Domain 1: Clinical involvement G Domain 2: Engagement and communication G Domain 3: Planning and performance G Domain 4: Governance G Domain 5: Collaborative working G Domain 6: Leadership G CSU Key Indicators 2
72 High Level Summary Are local people getting good quality care? Has a local provider been subject to enforcement action by the CQC? Following an inspection held in February 2013, Stoke Mandeville Hospital location within Buckinghamshire Healthcare Trust (BHT) was subject to an enforcement action by way of a warning notice to be met by 31 May 2013 in relation to Regulation 23 Supporting workers. A further standard was subject to a compliance action. BHT submitted an action plan to the CQC which is monitored by the CQC. Note: Report published in September In July 2013 a follow up inspection to check whether improvements had been made was carried out. This resulted in the enforcement action being removed and replaced by a compliance action. Note: Report published in September In July 2013 a follow up inspection of Amersham Hospital, where there had been compliance actions was carried out. This resulted in an enforcement action by way of a warning notice to be met by 30 September 2013 in relation to Regulation 22 Staffing Has a local provider been identified as a negative outlier on SHMI or HSMR (mortality)? BHT are reporting that the HSMR has improved and this will be confirmed when rebasing is complete. However, the action plan to reduce mortality is on-going with implementation monitored by the Putting Patients First steering group Does the feedback from the Friends and Family Test (FFT) indicate areas of concern? BHT did not meet the required baseline of 15% response rate for Quarter /14. An action plan is in place and there has been some improvement. The combined response rate for July was 9.5% (published). Provisional data for August indicates an improvement to a combined response rate of 18.9%. Has the provider experienced any Never Events in the last quarter? One Never Event was reported in August at HWPHFT. This related to wrong site surgery. A superficial incision was made to a hand before the wrong site was recognised. An investigation and root cause analysis is underway and commissioners expect an action plan to prevent recurrence to be developed. 3
73 Other Concerns The review of the safeguarding arrangements at BHT has concluded and the action plan agreed by Buckinghamshire Safeguarding Boards has been updated. There are still concerns re data quality and gaps in data submitted by BHT. Commissioners and the Central Southern Commissioning Support Unit (CSCSU) are working with BHT to improve data submission. Are patient s rights under the NHS constitution being promoted The CCG is monitored against pledges given in the NHS Constitution. The report below covers indicators which are currently performing at red or amber. Ambulance Response Times These indicators monitor the time it takes for an ambulance to respond to a 999 call. Category A calls are the most serious, and are monitored as Category A8 and A19, these calls are those that resulted in an emergency response arriving at the scene of the incident within 8 minutes and within 19 minutes. Category A8 is further split into two parts, Red 1 and Red 2. Red 1 calls are the most time critical and cover cardiac arrest patients who are not breathing and do not have a pulse, and other severe conditions such as airway obstruction. Red 2 calls are serious but less immediately time critical and cover conditions such as stroke and fits. Red 1 patients account for less than 5% of all ambulance calls. SCAS are currently commissioned, and the CCGs monitored, on performance at a Thames Valley level and not at CCG level. On that basis SCAS performance hit all targets, both for the month of August and on a year to date (YTD) basis. However, on a local level not all targets were met: Aylesbury CCG August breakdown Ambulance Clinical Quality - Category A 8 Minute Response Time - Red 1, the 75% target was met, with performance at 87.9% Ambulance Clinical Quality - Category A 8 Minute Response Time - Red 2, the 75% target was not met but the monthly performance improved to 72.9% against a Year to Date average of 71.2% Ambulance Clinical Quality- Category A 19 Minute Transportation Time, the 95% target was not met, with an achievement of 92.9%, which brings the YTD slightly under target at 94.5% Calls to SCAS have increased by 6% (569 extra calls) in April August compared to the same period last year. Analysis that SCAS has produced shows that Red 1 (life threatening) have risen in AVCCG, and increased activity has been experienced in urgent and life threatening calls directed to the ambulance service from NHS 111. The Ambulance Service is required to send an emergency response to these calls. 4
74 Actions taken to recover performance Patient level clinical analysis is being undertaken to determine whether these NHS 111 red calls, clinically required an ambulance response. This will identify whether the NHS 111 national triage pathway would benefit from modification, or whether NHS 111 is identifying new patients who warrant an ambulance but who would not have called 999. A&E Four Hour Wait This indicator is a measure of the time that patients wait within an A&E department (or Minor Illness/Injuries Unit) before either being admitted, treated & discharged or transferred to another hospital and is measured by provider to ensure patients are seen within nationally set time limits. For AV CCG the main hospitals residents attend are Buckinghamshire Healthcare Trust (BHT), Oxford University Hospitals (OUH) and Milton Keynes NHS Foundation trust (MKFT)). In August BHT & MKFT achieved the 95% standard required for this indicator with OUH underachieving at 92.88%. Year to date OUH remains below the required standard (93.59%). OUH has been awarded additional funding to manage winter pressures and will use this funding to improve patient flows in A&E and ambulatory capacity. Diagnostics > 6 week wait for diagnostic tests This indicator is a measure of the number of people waiting longer than 6 weeks for a diagnostic test, the indicator measures all Aylesbury Vale patients waiting at any hospital trust. The over 6 week 1% target was met in the month of July, with 0.8% being seen outside the 6 weeks target. However, YTD percentage of patients seen over 6 weeks is 2.1%. This is due to OUH missing their diagnostic target. While OUH have improved over the previous few months, they did not meet the Diagnostic target in July. The Trust has assured Commissioners that the standard will be met in August. Cancer All cancer targets were met, with the exception of the All Cancer 62 days from Urgent Referral from a cancer screening service to Treatment. The 90% target was not achieved in July with 88.89% (8 out of 9 patients) being seen within the timescale, this brings the Year to Date percentage to just under target at 89.7%. The breech patient was at Milton Keynes Hospital and the patient was treated two days later. 18 weeks incomplete pathways This indicator measures the number of patients across all hospital trusts that have waited longer than 18 weeks for either first definitive outpatient or inpatient treatment. The standard of 92% of patients with an incomplete pathway within 18 weeks was missed in the month of July. There is a known backlog issue of patients waiting more than 18 weeks for Trauma & Orthopaedics (T&O) at Buckinghamshire Health Care Trust (BHT). The Trust has put in place actions to ensure that these patients are treated; this includes securing additional capacity at a private hospital provider to treat those patients who are able or willing to transfer their care. 5
75 The number of Patients with Referral to Treatment (RTT) pathways greater than 52 weeks There was one Incomplete Pathway at Oxford University Hospital in Trauma and Orthopaedics reported as being over 52 weeks in July. This case is being investigated with the Trust. Local priority People Feeling Supported to Manage their own condition Since July 2011, the GP Patient Survey takes place twice a year. Questionnaires are sent to a selection of around 2.7 million adults who are registered with a GP in England over the course of the year. The latest results show Aylesbury Vales CCG to be just below target on this measure. The last GP survey data published related to the period July 2012-March It showed that the score for people feeling supported to manage their own condition for AV CCG was 50.1 which is 3.1 under the local target of This score is calculated from the proportion of people answering YES or YES TO SOME EXTENT to the question In the last 6 months, have you had enough support from local services or organisations to help you manage your long-term condition(s)? In AV CCG district there were 1,545 responses, 600 answered yes, and a further 348 answered yes to some extent. The GP survey results are issued bi-annually, and the first GP survey of 2013/14 will be issued in Autumn 2013 which will enable a first indication of whether people s perceptions have changes since the CCG was established. Are health outcomes improving for local people The CCG is monitored for delivery of improvements against a range of health outcomes for local people as described within the NHS Outcomes Framework. Many of these indicators are only reported annually and should be assessed over the long-term to understand progress. This report includes only those indicators within the framework which are updated monthly or quarterly; an annual report assessing all indicators will be produced each year. The report below covers indicators which are currently performing at red or amber. Infection control: CDIFF Summary of Concerns CCGs are assessed on all cases of C-DIFF for their population including community cases. AVCCG has a limit of 46 C. difficile cases for 2013/14. To achieve this limit a 27% reduction is needed from the 63 cases that occurred in 2012/13. During 2012/13 75% of AVCCG cases were community cases. The cumulative number of cases at the end of August was 22. This is 3 cases above the cumulative limit. However, for the month of 6
76 August, the number of cases reduced to 3 cases, which is 1 case below the monthly limit of 4 cases. One community case occurred in a patient in their own home and two acute cases occurred at BHT. For BHT as a Trust there was an increase in cases in August: After having only a single case in July there have been 6 cases which is 3 cases above their monthly limit. This means that BHT is currently 4 cases over their cumulative limit of 15 cases to the end of August. BHT are typing all cases and this has shown that the cases are not linked and therefore cross infection has not occurred. Actions taken to recover performance All cases are being reviewed in order to identify the source of infection. A countywide C. difficile reduction action plan is in place. This action plan incorporates actions to reduce cases in both acute and community settings. Monthly performance meetings are being held with BHT s Director for Infection Prevention and Control and Lead Nurse for Infection Prevention and Control. Community antibiotic prescribing is being monitored and performance is being reported to practices via the monthly prescribing dashboard. A report on the learning from community C. difficile cases for quarter one 2013/14 has been compiled and will be disseminated to primary care with information on how to reduce and manage C. difficile cases. BHT actions include; Restricting use of high risk antibiotics on Medicine for Older People wards and in patients on other wards over 65 years of age. Key infection control messages have been disseminated to Nursing and Domestic staff, stressing the need to ensure that high standards of cleaning are maintained. The inspection of commodes has been added to weekly Matrons Rounds. BHT have been asked to compile a report covering the learning identified in the root cause analysis of cases of C. difficile that occurred in quarter one 2013/14. Infection control: MRSA Summary of Concerns The DH has set a limit of zero cases of MRSA bacteraemia for all CCGs and Acute Trusts. An MRSA bacteraemia has occurred in an AVCCG patient during August. This patient was in the community and the infection is associated with the patients urinary catheter. 7
77 Actions taken to recover performance A post infection review has been carried out, with learning identified. Finance: Is the CCG commissioning services within its financial allocation Financial Performance The CCG has delivered its year to date planned surplus of 831k, and whilst it is on target to deliver its 1% planned surplus for the year of 1,996k, there are significant risks within Acute portfolio and a mitigation plan has been developed. Financial Management The CCG is within its cash limit plan, however cash balances held at the end of the month are in excess of the DH tolerance level of 5%. The BPCC percentage of 82.4% is below the target of 95% but shows a continuing improvement over previous months. Further details are available in the Finance Report QIPP Delivery Finance The actual reported position on achievement of QIPP savings was 1,134k against a plan of 1,874k (61% achievement).at month 4. This is partly off-set by 283k mitigation from underspend on budgets not covered by QIPP schemes The mitigated QIPP position is an under achievement of 457k (24%) The forecast position is a year-end delivery of 79% of the plan. Activity In line with the financial position, acute activity is over performing across all areas except for A&E attendances: All first out-patient attendances are 6.1% above plan with the largest over-performance at OUH Elective admissions are 3.7% above plan Non-elective admissions are the key area of concern as they are 19.6% above plan. A&E attendances (excluding MIIU attendances at Wycombe) are on plan. This represents the position against the activity plan however, it is not consistent with the financial plan which was over adjusted down to take account of BHiB. 8
78 Organisational Development Aylesbury Vale CCG was authorised as a statutory body in March 2013 following assessment by NHS England against 119 criteria and the current indicators reflect those criteria. A first draft Organisational Development (OD) plan has been developed and shared with the management team for discussion and feedback. The current indicators will be replaced by appropriate measures from the new plan once these have been finalised. Central Southern Commissioning Support Unit - Key Performance Indicators AVCCG has identified a set of KPIs by which it will hold the Central Southern Commissioning Support Unit to account. These are shown in Appendix 3 with the current RAG rating where this is available. Following concerns raised by the CCG, corrective action plans are in place to improve performance. 9
79 APPENDICES Table 1 Are People Getting Good Quality Care Providers BHT Ox Health OUH Milton Keynes SCAS Has local provider been subject to enforcement action by the CQC? Y Enforcement Action N N Y-Action Plan in place N Has local provider been flagged as as a 'quality compliance risk' by Monitor and/or are requirements in place around breaches of provider licence conditions? N/A N N/A Y-Action Plan in place N Has local provider been been subject to enforcement action by the NHS TDA based on 'quality' in place N N N/A N Does feedback from the Friends and Family test (or any other patient feedback) indicate any causes for concern? Y-Action Plan in place N N Y-Action Plan in place N Has the provider been identified as a 'negative outlier' on SHMI or HSMR? Y-Action Plan in place N N N N Do provider level indicators from the National Quality Dashboard show that: MRSA cases are above zero N N Y-Action Plan in place N N the provider has reported more C difficile cases than trajectory Y-Action Plan in place N N N N MSA breaches are above zero N N N N N Y-Action Plan in place Does the provider currently have any unclosed Serious Untoward Incidents (SUIs)? Y-Action Plan in place Y-Action Plan in place Y-Action Plan in place Y-Action Plan Has the provider experienced any 'Never Events' during the last quarter? in place N N N N Is provider meeting the 15% response rates of FFT N Y Y N Y Y-Action Plan in place CCG Assurance Framework Clinical Governance Does the CCG have any outstanding conditions of authorisation in place on clinical governance? Has the CCG self-assessed and identified any risks associated with the following Concerns around quality issues being discussed regulary by the CCG governing body Concerns around the arrangements in place to proactively identify early warnings of a failing service Concerns around the arrangements in place to deal with and learn from serious untoward incidents and never events Concerns around being an active participant in its Quality Surveillance Group EPRR If there was an emergency event in the last quarter, has the CCG self-assessed and identified any areas of concern on the arrangements in place for dealing with such an event? Winterbourne View Has the CCG self-assessed and identifed any risk to progess against its Winterbourne View action plan N Y - Action plan in place N N N N N 10
80 Table 2: Are patients rights under the NHS constitution being promoted Ref Measure Frequency Latest Data Target Actual Y-T-D Percent from target Movement Baseline Data NHS Constitution CB_B1 % of admitted pathways within 18 weeks for admitted patients whose clocks stopped during the period on an adjusted basis Monthly Jul-13 90% 91.7% 1.9% 93.20% CB_B2 % of non-admitted pathways within 18 weeks for non-admitted patients whose clocks stopped during the period Monthly Jul-13 95% 97.5% 2.6% 98.60% CB_B3 % of incomplete pathways within 18 weeks for patients on incomplete pathways at the end of the period Monthly Jul-13 92% 91.6% -0.5% 95.10% CB_B4 The percentage of patients waiting 6 weeks or more for a diagnostic test Monthly Jul-13 1% 2.1% 105.0% 1.4% CB_B5 A&E waiting time - total time in the A&E Department, % less than 4 hours (BHT) Monthly Aug-13 95% 96.5% 1.6% 92.40% CB_B5 A&E waiting time - total time in the A&E Department, % less than 4 hours (OUH) Monthly Aug-13 95% 93.6% -1.5% CB_B5 A&E waiting time - total time in the A&E Department, % less than 4 hours (MK) Monthly Aug-13 95% 95.6% 0.6% CB_B6 All cancer two week wait Monthly Jul-13 93% 96.2% 3.4% 98.70% CB_B7 Two week Wait for Breast Symptoms (where cancer not initially suspected) Monthly Jul-13 93% 98.0% 5.4% 97.60% CB_B8 Percentage of patients receiving first definitive treatment within one month of a cancer diagnosis (measured from date of decision to treat ) Monthly Jul-13 96% 98.3% 2.4% 98.60% CB_B9 31-Day Standard for Subsequent Cancer Treatments-Surgery Monthly Jul-13 94% 100% 6.4% 99.10% CB_B10 31-Day Standard for Subsequent Cancer Treatments-Anti Cancer Drug Regimens Monthly Jul-13 98% 100% 2.0% 100% CB_B11 31-Day Standard for Subsequent Cancer Treatments-Radiotherapy Monthly Jul-13 94% 98.2% 4.5% 97.20% CB_B12 All Cancer Two Month Urgent Referral to Treatment Wait Monthly Jul-13 85% 87.6% 3.0% 89% 62-Day Wait for First Treatment Following Referral from an NHS CB_B13 Cancer Screening Service Monthly Jul-13 90% 89.7% -0.4% 96.90% 62-Day Wait for First Treatment For Cancer Following a Consultants CB_B14 Decision to Upgrade The Patient s Priority Monthly Jul-13 85% 100.0% 17.6% 100% Ambulance Clinical Quality- Category A 8 Minute Response Time - CB_B15_01 Red 1 Monthly Aug-13 75% 83.5% 11.3% 72.50% Ambulance Clinical Quality- Category A 8 Minute Response Time - CB_B15_02 Red 2 Monthly Aug-13 75% 71.2% -5.1% 68.90% Ambulance Clinical Quality- Category A 19 Minute Transportation CB_B16 Time Monthly Aug-13 95% 94.5% -0.5% 94.60% C_B19 Care Programme Approach (CPA) Quartery Q1 13/14 95% 98.6% N/A Percentage of patients who have operations cancelled, on or after Quarterly Q1 13/ % N/A BHT CB_B18 the day of admission (including the day of surgery), for non-clinical Quarterly Q1 13/ % N/A OUH reasons who are offered another binding date within 28 days, or the Quarterly Q1 13/ % N/A MK *SCAS are commissioned for performance targets at Thames Valley contract level but are providing data at CCG level for information. The CCG level data is shown in these reports, however, currently year to date the contract is meeting all the required targets at Thames Valley level. 11
81 Ref Measure Frequency Latest Data Target Actual Performance Percent from target Movement Baseline Data Supporting Measures CB_S6 i The number of Referral to Treatment (RTT) pathways greater than 52 weeks for completed admitted pathways (un-adjusted), Monthly* Jul The number of Referral to Treatment (RTT) pathways greater than CB_S6 ii 52 weeks for completed non-admitted pathways Monthly* Jul The number of Referral to Treatment (RTT) pathways greater than CB_S6 iii 52 weeks for incomplete pathways. Monthly* Jul CB_S7 i Ambulance handover delays of over 30 minutes (SMH) Aug Ambulance handover delays of over 30 minutes (High Wyc) Aug Ambulance handover delays of over 30 minutes (OUH) Aug Ambulance handover delays of over 30 minutes (MK) Aug Monthly* CB_S7 ii Ambulance handover delays of over 1 hour (SMH) Aug Ambulance handover delays of over 1 hour (High Wyc) Aug Ambulance handover delays of over 1 hour (OUH) Aug Ambulance handover delays of over 1 hour (MK) Aug CB_S8 i Crew clear delays of over 30 minutes (SMH) Monthly* Aug CB_S8 i Crew clear delays of over 30 minutes (High Wyc) Monthly* Aug-13 3 CB_S8 i Crew clear delays of over 30 minutes (OUH) Monthly* Aug CB_S8 i Crew clear delays of over 30 minutes (MK) Monthly* Aug CB_S8 ii Crew clear delays of over 1 hour (SMH) Monthly* Aug-13 1 CB_S8 ii Crew clear delays of over 1 hour (High Wyc) Monthly* Aug-13 0 CB_S8 ii Crew clear delays of over 1 hour (OUH) Monthly* Aug-13 7 CB_S8 ii Crew clear delays of over 1 hour (MK) Monthly* Aug-13 3 CB_S9 Trolley waits in A&E Monthly N/A N/A CB_S10 Urgent operations cancelled for a second time (BHT) Jul CB_S10 Urgent operations cancelled for a second time (OUH) Monthly Jul CB_S10 Urgent operations cancelled for a second time (MK) Jul Local Priorities L1 People feeling supported to manage their own condition Bi-Annual 7/12 to 3/ % 50.10% -5.8% L2 Patient Experience of Out of Hours Service Bi-Annual 7/12 to 3/ % 72.70% 3.9% L3 Emergency admissions age 0-5 (excluding lower respiratory tract infection, Monthly asthma, diabetes and epilepsy) YTD Jul % * Actual data for this indicator is based on the most recent period, rather than a cumulative or annual-average ie the monthly actual 12
82 Table 3 Are health outcomes improving for local people Ref Measure Frequency Latest Data Target Actual Percent from target Movement Baseline Data 1. Preventing people from dying prematurely C1.13 Antenatal assessments <13 weeks 1 Quarterly Q4 12/13 by PCT 90% 91.7% 1.9% N/A 91.70% C1.14 Maternal smoking at delivery 1 Quarterly Q4 12/13 by PCT 7.8% N/A 7.9% C1.15 Breast feeding prevalence at 6-8 weeks 1 Quarterly Q4 12/13 by PCT 56.30% 58.5% 3.9% N/A 58.50% CB_B19 Mental Health Measure - Care Programme Approach Quarterly Q1 13/14 95% 98.6% 3.8% N/A 97.75% 2. Enhancing quality of life for people with long term conditions CB-A (per Unplanned hospitalisation for chronic ambulatory care sensitive C2.6* Monthly Jul % 100,00 conditions (adults) pop) CB-A6-02 C2.7* Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s Monthly Jul % CB-A7 People with long-term conditions feeling independent and in C2.2 control of their condition Bi-Annual 7/12 to 3/ % 50.10% -5.8% 51.2% CB-A8 Health-related quality of life for people with long-term C2.1 conditions Bi-Annual N/A N/A Helping people to recover from episodes of ill health or following injury CB-A (per Emergency admissions for acute conditions that should not C3.1* Monthly Jul % 100,00 usually require hospital admission pop) CB-A6-04 C3.4* Emergency admissions for children with lower respiratory tract infections Monthly Jul % CB-A10 Emergency re-admissions within 30 days of discharge from C3.2 hospital Quarterly Q4 2012/13 4.2% N/A 10.1% CB-A11- Patient reported outcome measures for elective procedures: 01 C3.3 hip replacement 2 Quarterly Q3 2012/ N/A 0.39 CB-A11- Patient reported outcome measures for elective procedures: 02 C3.3 knee replacement 2 Quarterly Q3 2012/ N/A 0.32 CB-A11- Patient reported outcome measures for elective procedures: 03 C3.3 groin hernia 2 Quarterly Q3 2012/ N/A 0.12 CB-A11- Patient reported outcome measures for elective procedures: 04 C3.3 varicose veins 2 Quarterly Q3 2012/13 0 N/A 4. Patient Experience - Ensuring that people have a positive experience of care CB-A12-02Patient experience of GP out-of-hours services Bi-Annual 7/12 to 3/13 70% 72.70% 3.9% N/A 68% 5.Patient Safety - Treating and caring for people in a safe environment and protecting them from avoidable harm C5.2 Risk Assessment of venous thromboembolism (VTE) (BHT) Jun-13 90% 93.56% 4.0% C5.2 Risk Assessment of venous thromboembolism (VTE) (OUH) Monthly* Jun-13 90% 96.03% 6.7% C5.2 Risk Assessment of venous thromboembolism (VTE) (MK) Jun-13 90% 96.87% 7.6% CB_A15 HCAI measure (MRSA) C5.3* Monthly Aug CB_A16 HCAI measure (Clostridium difficile infections) C5.4* Monthly Aug % CB_B17 MSA Breaches Monthly* Aug (per 100,00 pop) 376 (per 100,00 pop) 1 Data for these indicators is collected bi-annually 2 The questionnaires returned for this organisation, had a count of less than 30. No adjusted results have been calculated as the underlying statistical methods break down when counts are low and aggregate calculations based on small denominators may return unrepresentative results for the raw figures * Actual data for this indicator is based on the most recent period, rather than a cumulative or annual-average ie the monthly actual 13
83 Tables 4A & B Finance and QIPP Activity Trends Table 4A finance Financial Performance Number Indicator Underlying recurrent surplus Surplus - year to date performance Surplus - full year forecast Management of 2% NR funds within agreed processes Running Costs Clear identification of risks against financial delivery and mitigations CCG position RAG movement Financial Management Number Indicator This covers Internal and external audit opinions, and an assessment of the timeliness and quality of returns. Balance sheet indicators including cash management and BPCC CCG position movement Programme YTD budget YTD Actual Percent from target CCG position Month 4 " 000 " INPACT % - Chronic Disease % - Early Years % - Planned Care % - Localities % - Joint Care % Total Gross Savings 1,874 1,134 39% Mitigation 283 Total following mitigation 1,874 1,417 24% RAG 14
84 Programme FY budget FY forecast Percent from target " 000 " INPACT 1, % - Chronic Disease 1, % - Early Years % - Planned Care 1,361 1,031 24% - Localities % - Joint Care % Total Gross Savings 5,594 3,752 33% Mitigation 678 Total following mitigation 5,594 4,430 21% CCG position Table 4b Activity Trends Ref Measure Latest Data Target Actual Percent from target Activity trends - year to date GP referred First out-patients (made)(g&a) Jul % CB_S2 All first outpatient attendances all providers Jul % CB_S3 Elective Admissions (spells) all providers Jul % CB_S1 Non-elective admissions (spells) all providers Jul % AE Attendances Aylesbury Vale CCG proportion * Aug % Mental Health measure IAPT - the proportion of people that enter treatment against the level of need in the general population (the level of prevalence addressed or captured by Q4 2012/ % 11% (2012/13 target was 10%) CB_S5 referral routes) Mental Health measure IAPT - the proportion of people who complete treatment who are Q4 2012/13 45% 48% CB_S5 moving to recovery * This is the proportion of attendances from those hospitals allocated to AVCCG by the DoH against which they monitor the CCG. The proportions are 38% of BHT total; 6% of Milton Keynes total and 2% of OUH total. 15

85 Appendix 2 Quality Dashboard 16

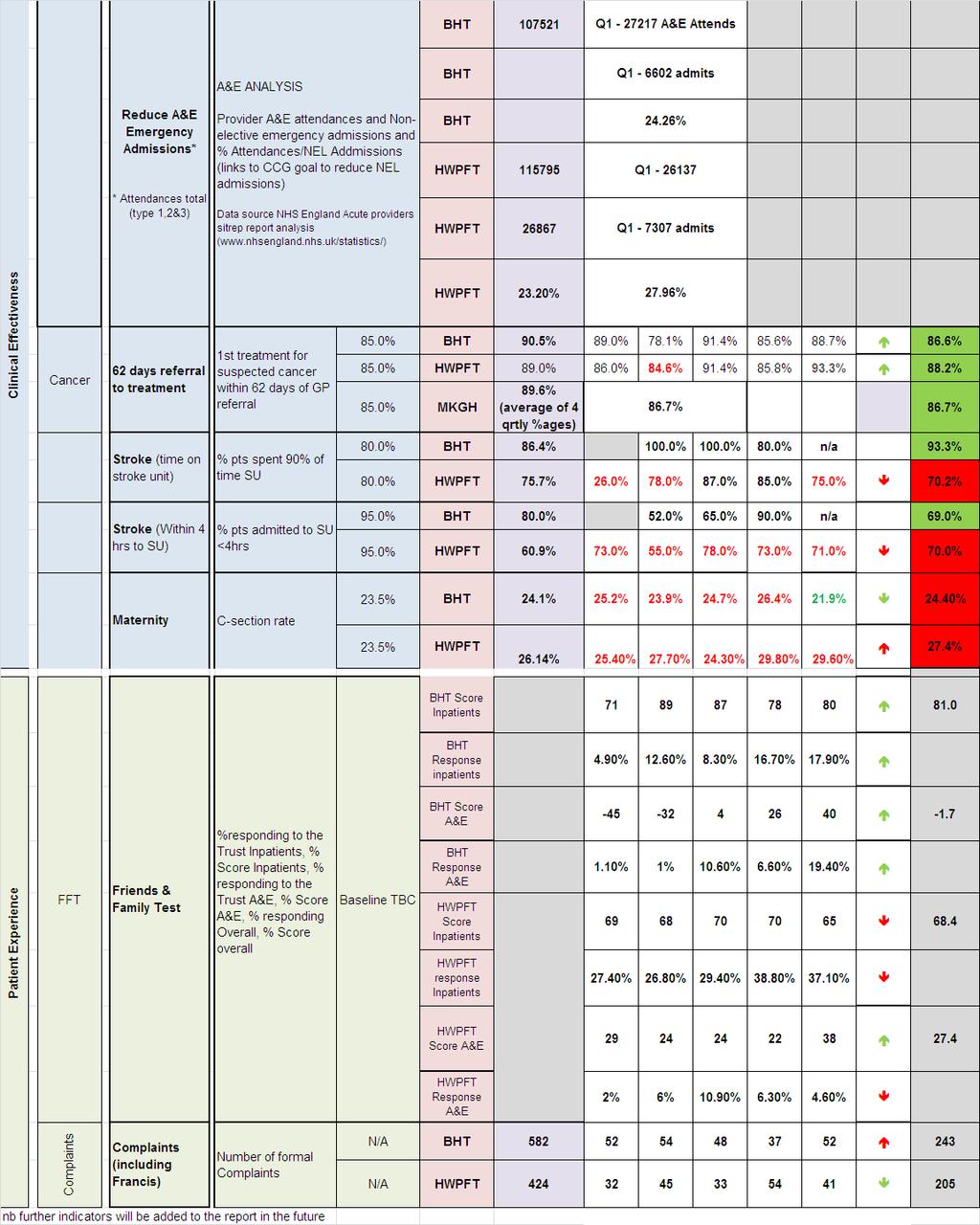
86 17

87 APPENDIX 3 KEY CSU PERFORMANCE INDICATORS 18
88 19
89 Glossary NHS England has developed a set of national standards and requirements by which it holds NHS organisations to account. These indicators are set out in a number of key documents: NHS constitution The national requirements, in terms of operational standards expected are set out in the NHS Constitution, which sets out patients rights for treatment within set timescales and quality standards indicators included in this document is included in table 2. In addition to the specific measures set out in the Constitution there are a number of indicators called supporting measures which are seen as good indicators for measuring progress towards a target which is otherwise difficult to measure. CCG Outcomes Indicator Set which are a group of outcome measures which CCGs are expected to meet. These are grouped into 5 categories or domains which are aligned to national objectives. They are: C1 Preventing people from dying prematurely C2 Enhancing quality of life for people with long-term conditions C3 Helping people to recover from episodes of ill health or following injury C4 Ensuring that people have a positive experience of care C5 Treating and caring for people in a safe environment and protecting them from avoidable harm These are the indicators shown in Table 3. Local Priorities NHS England expects CCGs to develop their own local priorities through their input into the Joint Health and Wellbeing Strategy and it asks each CCG to identify three local priorities against which it will make progress during the year. These priorities will be taken into account when determining if the CCG should be rewarded through the Quality Premium. For AVCCG these are L1 people being supported to manage their own condition L2 Patient experience of out of hours service L3 emergency admissions age 0-5 (excluding lower respiratory tract infection, asthma, diabetes and epilepsy) Quality Premium The quality premium is intended to reward clinical commissioning groups (CCGs) for improvements in the quality of the services that they commission and for associated improvements in health outcomes and reducing inequalities. It is paid based on achievement of four national measures and the three local priority measures (see above). The four national measures, all of which are based on measures in the NHS Outcomes Framework, are: reducing potential years of lives lost through amenable mortality (12.5 per cent of quality premium): the overarching objective for Domain 1 of the NHS Outcomes Framework; reducing avoidable emergency admissions (25 per cent of quality premium): a composite measure drawn from four measures in Domains 2 and 3 of the NHS Outcomes Framework; ensuring roll-out of the Friends and Family Test and improving patient experience of hospital services (12.5 per cent of quality premium), based on one of the overarching objectives for Domain 4 of the NHS Outcomes Framework; preventing healthcare associated infections (12.5 per cent of quality premium), based on one of the objectives for Domain 5 of the NHS Outcomes Framework. These indicators have been marked with an * in the above tables. CCG Assurance Framework 20
90 These indicators, together with financial performance, provider quality measures and organisational development are the criteria by which NHS England is assured that the CCG is performing to the required standard. This has been developed into a balsnaced scorecard as presented here. Further information can be found in the following link: Everyone Counts: Planning for Patients 2013/14 Additional definitions: Six week waits for diagnostic tests The following tests are included: MRI; CT; NON_OBSTETRIC_ULTRASOUND; BARIUM_ENEMA; DEXA_SCAN; AUDIOLOGY_ASSESSMENTS; ECHOCARDIOGRAPHY; ELECTROPHYSIOLOGY; PERIPHERAL_NEUROPHYS; SLEEP_STUDIES; URODYNAMICS; COLONOSCOPY; FLEXI_SIGMOIDOSCOPY; CYSTOSCOPY; GASTROSCOPY Patient s reported Outcome Measures (PROMS): These indicators are designed to measure the perceived improvement in health status following an elective procedure. The procedures currently covered are groin hernia, hip replacement, knee replacement and varicose veins. PROMs are calculated from the patient s responses to a pair of questionnaires which are completed, one before and one after the surgery. A gap of at least 3 months is required following surgery before completing the second questionnaire (Six months for hip replacement). A comparison of responses shows whether and to what extent the procedure has improved the health status of the patient. The higher the number reported in the indicator the better. 21
91 Agenda item: GB a GOVERNING BODY MEETING OCTOBER 2013 FINANCE REPORT Purpose of Paper The attached report provides an update from the Chief Finance Officer on the Financial Position to the end of August 2013 and the forecast position to the 12 months ending March The report highlights the areas of variance to the plan and key risks to the forecast position. Executive Summary Position to the end of August A surplus of 831,000, in line with delivering the 2m planned surplus by the end of March Pressures on budgets ( 2.6m / 4.8%) within Planned and Unscheduled care reflecting contract overspends mainly on Acute and Ambulance contracts. In the majority of cases the report reflects the contract position as at the end of July with estimations for August. This overspend has been reduced by underspends within Joint and Continuing Care where the level of Adult Continuing Care activity is not high as expected. To the end of August 1.5m of reserves (33% of the total available) have been factored into the position in order to maintain the surplus position. Forecast Position The forecast position remains at 2m surplus and the report highlights the major risks to the forecast position. Mitigation Work is on-going to progress areas to mitigate the financial risks highlighted at the last governing body meeting and the CCG has taken part in a review of its Run-Rate (reviewing expenditure to date against forecast to highlight any areas which may impact on the forecast) with the Thames Valley Area team which did not highlight any significant concerns on the reporting on our financial position. Legacy NHS England has recent published the approach to transferring remaining legacy balances to receiving organisations and we have received initial information from the Thames Valley Area Team which is currently being reviewed.
92 Actions requested / recommendation Note the reported financial position, forecast and development of a financial mitigation plan to support delivery of the planned surplus. Be aware of the further risks to the reported position and potential impact on the ability of the CCG to deliver its original financial plan Strategic Objectives supported by this Paper (Please Tick) Improve people's health and reduce inequalities Enhance quality, safety and experience of patient services Ensure local people have greater influence and management of own care Deliver financial sustainability with headroom to invest Perform well as a CCG X X Equality Analysis completed (please tick ) Author of paper Robert Majilton, Chief Finance Officer Yes No Not applicable X Lead Director(s) responsible for this area of work Robert Majilton, Chief Finance Officer 2
93 FINANCIAL PERFORMANCE TO AUGUST 2013 Section A At a glance MONTH /14 Actual Spend Year to Date Running Costs L Red K Amber J Green Significant Increasing Over Performance on Non- Elective Admissions at BHT, and elective admissions at BMI Pressures emerging across Planned Care with regard to waiting list catch up On Plan to Deliver Target Surplus Ambulance Prescribing Joint & Continuing Care Other Acute Planned Care Unscheduled Care YTD Surplus / (Deficit) Area '000 Planned Care (979) Unscheduled Care (1,371) Other Acute (122) Ambulance (161) Prescribing 525 Joint & Continuing Care 408 Running Costs 204 Other 2,326 Total 830 Annual Budget Year to Date Budget Year to Date Actual Year to Date Variance Financial Performance to August 2013 (Month /14) Page 1 of 18 Achieved Year to Date % Impact Rating Forecast Actual Forecast Variance Forecast Achieve ment % - INPACT 1, (60) 73% Amber 829 (260) 76% Red - Chronic Disease 1, (434) 42% Red 769 (1,068) 42% Red - Early Years (20) 0% Amber 0 (109) 0% Amber - Planned Care 1, (126) 67% Amber 1,031 (330) 76% Red - Localities (100) 60% Amber 525 (75) 88% Amber Risk Rating - Joint Care % Green % Green Total Gross Savings 5,594 1,874 1,134 (740) 61% Red 3,752 (1,842) 67% Red Mitigtion - BHT - Use of Headroom Blue Blue Total Net QIPP Programme 5,594 1,874 1,417 (457) 76% Blue 4,430 (1,164) 79% Blue
94 Section B - Contents Performance Against Plan This Month Last Month Year to date 831k Surplus v Plan Spend 84m 665k Surplus v Plan Spend 67m 3 In month 166k Surplus v Plan Spend 17m 166k Surplus v Plan Spend 17.6m 3 Forecast 2.0m Surplus (Range - 9m to + 9m) 2.0m Surplus (Range - 1.9m to + 6.2m) 5 Risks to forecast Unmitigated risk of c 1.5m 5 QIPP In month 327k + 57k of mitigation v Plan 414k 272k + 57k of mitigation v Plan 401k 4 Year-to-date 1.1m + 283k of mitigation v Plan 1.9m 0.8m + 226k of mitigation v Plan 1.5m 4 Forecast Under delivery of 1,842k less 678k mitigation Under delivery of 1,772k less 678k mitigation 4 Commissioning Planned Care 979k Adverse Variance v Plan Spend 25.3m 503k Adverse Variance v Plan Spend 19.7m 6 Unscheduled Care 1.4m Adverse Variance v Plan Spend 14.8m 935k Adverse Variance v Plan Spend 11.8m 6 Ambulance 161k Adverse Variance v Plan Spend 2.4m 131k Adverse Variance v Plan Spend 1.9m 6 Prescribing 525k favourable variance v Plan Spend 10.6m Balanced v Plan Spend 8.5m 7 Joint & Continuing Care 408k Favourable Variance v Plan Spend 15.2m 371k Favourable Variance v Plan Spend 11.9m 8 Reserves 1.5m released from 4.5m Total Reserves available 1.1m released from 5.2m Total Reserves available 5 Running Costs Running Costs 205k Favourable Variance v Plan Spend 1.9m 122k Favourable Variance v Plan Spend 1.4m 9 Locality Budgets Month 4 Due 18 September 2013 Other Changes to Plan Internal Transfers 758k, Release from Reserves Internal Only 10 1m supported by additional funding of 323k Contract Monitoring Summary of Main Contracts Summary of Main Contracts 11 Treasury Management Underperformance against Cash Plan by 8.8m Underperformance against Cash Plan by 3.9m 15 Glossary Table of Abbreviations Table of Abbreviations 17 Page Ref Financial Performance to August 2013 (Month /14) Page 2 of 18
95 m Section C Financial Performance Previous August 13 month Annual Plan YTD Plan YTD Actual Variance to plan Variance to plan To Date '000 '000 '000 '000 % '000 Commissioning Planned and Unscheduled Car 128,734 54,336 56,969 (2,633) (4.8%) (1,580) Prescribing 25,392 10,580 10, % 0 Joint & Continuing Care 36,459 15,191 14, % 371 Reserves 4,480 1,495-1, % 1,086 Commissioning sub-total 195,065 81,602 81,807 (205) (0.3%) (122) Running Costs 4,890 1,867 1, % 122 Surplus 1, % 665 Total CCG 201,951 84,300 83, % , , ,000 Resource Limit Compared to Planned Spend & Actual (Cumulative) Key Points The CCG has developed a plan that delivers the 1% surplus planning requirement of 1,996k, resulting in a year to date actual surplus of 831k. Actual spend within Planned and Unscheduled Care is based on the available month 4 Contract Reports and estimated for month 5. The over spend of 2.6m mainly relates to urgent care pressures within the main Acute Contracts and the Ambulance Trust, together with Planned Care pressures from BMI activity and the shortfall in funding available for the OUH contract. The underspend of 408k in Joint and Continuing Care mainly reflects Adult Continuing Care activity based on month 4 data with an estimate for month 5. QIPP The reported under-delivery is mainly arising from overspends reported against Contract Plans and expected slippage on delivery, which has been partly mitigated within the BHT Contract through use of the CCG headroom reserve. Development of the mitigation plan continues and there remains c 1.5m unsecured at the moment. 50,000 - Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Resource Limit 16,802 33,037 49,392 66,970 84, , , , , , , ,951 Planned Spend 16,636 32,705 48,893 66,304 83, , , , , , , ,955 Actual Spend 16,636 32,466 48,893 66,304 83,469 Financial Performance to August 2013 (Month /14) Page 3 of 18
96 '000 Section D QIPP Annual Budget Year to Date Budget Year to Date Actual Year to Date Variance Achieved Year to Date % Impact Rating Forecast Actual Forecast Variance Forecast Achieve ment % Risk Rating - INPACT 1, (60) 73% Amber 829 (260) 76% Red - Chronic Disease 1, (434) 42% Red 769 (1,068) 42% Red - Early Years (20) 0% Amber 0 (109) 0% Amber - Planned Care 1, (126) 67% Amber 1,031 (330) 76% Red - Localities (100) 60% Amber 525 (75) 88% Amber - Joint Care % Green % Green Total Gross Savings 5,594 1,874 1,134 (740) 61% Red 3,752 (1,842) 67% Red Mitigtion - BHT - Use of Headroom Blue Blue Total Net QIPP Programme 5,594 1,874 1,417 (457) 76% Blue 4,430 (1,164) 79% Blue Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Total QIPP Plan Total QIPP Actual Key Points QIPP Planned Savings vs Actual savings '000 The majority of QIPP will be reported through the specific QIPP & Performance report. The table above shows the QIPP plan and delivery to August Actual reported was 1.1m against a plan of 1.9m (61% achievement). The under delivery to date is partially mitigated in-year through the use of non-recurrent headroom reserves within the BHT contract. The table to the left shows how the QIPP plan is phased over the year. The forecast position is a year-end under delivery of the plan as in order to deliver this target, savings will need to be generated at a rate of 20% above the original plan for the remainder of the year. Financial Performance to August 2013 (Month /14) Page 4 of 18
 to a 9m deficit (the worst case ). After reviewing the month 5 position the current forecast is to deliver the 1% planned surplus ( 2.0m).")
97 Section E Forecast, Risks and Mitigation E1 Risk Assessed Forecast Key Points The first table shows the potential range of risks for the 12 months to March The current range is from a 9.3m surplus (the best case ) to a 9m deficit (the worst case ). After reviewing the month 5 position the current forecast is to deliver the 1% planned surplus ( 2.0m). Further review of the forecast and mitigation plan is planned before the half year (Month 6) report to firm up on both the range and areas of further mitigation. Major risks to the forecast include: o Continuing pressures from growth in Acute Care that cannot be contained by planned reductions in activity under QIPP schemes, from the delivery of the in-year mitigation or from CCG reserves o Uncertainty over the impact of additional Resource Allocation adjustments, particularly relating to the changes around commissioning for Specialised Services o Present activity in Adult Continuing Care indicates a flattening out of activity in most care categories, the overall financial position cannot be confirmed until the previous year s provisions have been analysed particularly in relation to the Retrospective Reviews, in that the legacy provision is being passed to CCG s. Financial Performance to August 2013 (Month /14) Page 5 of 18
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE
 PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE Page 1 DOCUMENT CONTROL SHEET Name of Document: Patient Safety and Quality Committee Terms of Reference Version: 5 File Location / Document Name:
PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE Page 1 DOCUMENT CONTROL SHEET Name of Document: Patient Safety and Quality Committee Terms of Reference Version: 5 File Location / Document Name:
Direct Commissioning Assurance Framework. England
 Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September 2013
 Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Joint framework: Commissioning and regulating together
 With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July C Hickson, Head of Management Accounts
 NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July 2013 9.4 Date of the meeting 18/09/2013 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July 2013 9.4 Date of the meeting 18/09/2013 Author Sponsoring GB member Purpose of report Recommendation Resource
TERMS OF REFERENCE. Transformation and Sustainability Committee. One per month (Second Thursday) GP Board Member (Quality) Director of Commissioning
 GP Board Member (Quality) Director of Commissioning") TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7
 Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7") Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7 Title Sponsoring Director (name and job title) Sponsoring
Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7 Title Sponsoring Director (name and job title) Sponsoring
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
PEC meeting Patient and Public. Quality and Governance meeting Quarterly from August PEC meeting
 Appendix 3 PPI strategy Bristol CCG Patient and Public Involvement (PPI) Action Plan 2014/15 To be read in conjunction with the CCG Equality and Diversity Action Plan, and Communications Action Plan Strategic
Appendix 3 PPI strategy Bristol CCG Patient and Public Involvement (PPI) Action Plan 2014/15 To be read in conjunction with the CCG Equality and Diversity Action Plan, and Communications Action Plan Strategic
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS Portsmouth CCG 2013/14 Contract Agreements Summary. Michelle Spandley Deputy Chief Finance Officer May Improving health services
 NHS Portsmouth CCG 2013/14 Contract Agreements Summary Michelle Spandley Deputy Chief Finance Officer May 2013 Contents Contracts Summary Portsmouth Hospitals NHS Trust Solent NHS Trust South Central Ambulance
NHS Portsmouth CCG 2013/14 Contract Agreements Summary Michelle Spandley Deputy Chief Finance Officer May 2013 Contents Contracts Summary Portsmouth Hospitals NHS Trust Solent NHS Trust South Central Ambulance
Bury Health and Wellbeing Board. Annual Report for 2016/17
 Bury Health and Wellbeing Board Annual Report for 2016/17 Bury Health and Wellbeing Board Annual Report for 2016-17 Contents 1. Introduction... 3 2. Background to the Health and Wellbeing Board... 5 3.
Bury Health and Wellbeing Board Annual Report for 2016/17 Bury Health and Wellbeing Board Annual Report for 2016-17 Contents 1. Introduction... 3 2. Background to the Health and Wellbeing Board... 5 3.
Draft Minutes. Agenda Item: 16
 Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
Quality Strategy
 Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, October 2013
 Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, October 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, October 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016
 Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Kingston Clinical Commissioning Group Report Summary
 Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 9 th January 2018 Report Title Minutes of the 34 th Meeting held on 7 th November 2017 Agenda Item 3 Attachment
Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 9 th January 2018 Report Title Minutes of the 34 th Meeting held on 7 th November 2017 Agenda Item 3 Attachment
Facilitating shared ownership on Health and Wellbeing Boards
 Facilitating shared ownership on Health and Wellbeing Boards 11 February 2014 Hallam Conference Centre, London Follow the conversation on Twitter #hwblearn Welcome & introduction Dr Graham Jackson, Clinical
Facilitating shared ownership on Health and Wellbeing Boards 11 February 2014 Hallam Conference Centre, London Follow the conversation on Twitter #hwblearn Welcome & introduction Dr Graham Jackson, Clinical
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
Alison Jamson, Head of Quality & Clinical Standards NHSMK&N Commissioning Support Hub
 Enc 11/10f Subject: Meeting: NHSMK CQUIN Schemes MK Commissioning Board Date of Meeting: 13 December 2011 Report of: Alison Jamson, Head of Quality & Clinical Standards NHSMK&N Commissioning Support Hub
Enc 11/10f Subject: Meeting: NHSMK CQUIN Schemes MK Commissioning Board Date of Meeting: 13 December 2011 Report of: Alison Jamson, Head of Quality & Clinical Standards NHSMK&N Commissioning Support Hub
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
CCG authorisation: the role of medicines management
 May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015
 NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015 Title Locality Committee Reports Q2 2015/16 Agenda Item: 13 Purpose (tick one only) Responsible Director(s) and Job Title
NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015 Title Locality Committee Reports Q2 2015/16 Agenda Item: 13 Purpose (tick one only) Responsible Director(s) and Job Title
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
General Practice Commissioning Strategy Development
 General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
BOARD PAPER - NHS ENGLAND
 Paper NHSE130904 BOARD PAPER - NHS ENGLAND Title: Implementing the Recommendations of the Government s Response to the Francis Report and its Winterbourne Review Report Clearance: Bill McCarthy, National
Paper NHSE130904 BOARD PAPER - NHS ENGLAND Title: Implementing the Recommendations of the Government s Response to the Francis Report and its Winterbourne Review Report Clearance: Bill McCarthy, National
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Better Healthcare in Bucks Reconfiguring acute services
 service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
MINUTES. Name of meeting. Quality and Clinical Governance Committee. Date and time Tuesday 2 May :30-17:00. Venue. Board Room, Dominion House
 MINUTES Name of meeting Quality and Clinical Governance Committee Date and time Tuesday 2 May 2017 14:30-17:00 Venue Board Room, Dominion House Name Title Chair Dr Sue Tresman (ST) Lay Vice Chair (Lay
MINUTES Name of meeting Quality and Clinical Governance Committee Date and time Tuesday 2 May 2017 14:30-17:00 Venue Board Room, Dominion House Name Title Chair Dr Sue Tresman (ST) Lay Vice Chair (Lay
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Partnership Agreement between NHS Trust Development Authority and Care Quality Commission
 Partnership Agreement between NHS Trust Development Authority and Care Quality Commission June 2013 Joint Statement Through this partnership agreement we commit the Care Quality Commission (CQC) and the
Partnership Agreement between NHS Trust Development Authority and Care Quality Commission June 2013 Joint Statement Through this partnership agreement we commit the Care Quality Commission (CQC) and the
NHS Equality Delivery System for Isle of Wight NHS Trust. Interim baseline assessment against the
 Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Regional Medicines Optimisation Committees
 Regional Medicines Optimisation Committees Operating Model First Edition, April 2017 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans.
Regional Medicines Optimisation Committees Operating Model First Edition, April 2017 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans.
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Strategy for Delivery of Clinical Quality and Patient Safety. North Norfolk Clinical Commissioning Group
 Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
West Mid Beds Locality Development Plan
 West Mid Beds Locality Development Plan 2013-14 Contents Introduction..3 1. Key Progress 2012/13.. 4 2. Locality Objectives 2013/14.5 2.1 Commissioning.5 2.2 Performance & Finance.. 9 2.3 Engagement 11
West Mid Beds Locality Development Plan 2013-14 Contents Introduction..3 1. Key Progress 2012/13.. 4 2. Locality Objectives 2013/14.5 2.1 Commissioning.5 2.2 Performance & Finance.. 9 2.3 Engagement 11
PATIENT AND SERVICE USER EXPERIENCE STRATEGY
 PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting. Meeting Date: 25 October Executive Lead: Rajesh Nadkarni
 Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Delegated Commissioning in NW London: Frequently Asked Questions
 Delegated Commissioning in NW London: Frequently Asked Questions 16 November 2016 Contents General questions 3 Benefits and risks of delegated commissioning 4 2017 V 2018 6 Conflict of interest 9 Contracting
Delegated Commissioning in NW London: Frequently Asked Questions 16 November 2016 Contents General questions 3 Benefits and risks of delegated commissioning 4 2017 V 2018 6 Conflict of interest 9 Contracting
CLINICAL COMMISSIONING GROUP RESPONSIBILITIES TO ENSURE ROBUST SAFEGUARDING AND LOOKED AFTER CHILDREN ARRANGEMENTS
 MEETING DATE: 14 March 2013 AGENDA ITEM NUMBER: Item 8.6 AUTHOR: JOB TITLE: DEPARTMENT: Sarah Glossop Designated Nurse Safeguarding Children NHS North Lincolnshire Clinical Commissioning Group REPORT TO
MEETING DATE: 14 March 2013 AGENDA ITEM NUMBER: Item 8.6 AUTHOR: JOB TITLE: DEPARTMENT: Sarah Glossop Designated Nurse Safeguarding Children NHS North Lincolnshire Clinical Commissioning Group REPORT TO
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
OFFICIAL. Integrated Urgent Care Key Performance Indicators and Quality Standards Page 1 of 20
 Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Bedfordshire, Luton and Milton Keynes. Sustainability and Transformation Plan. Central Brief: February 2018
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Any Qualified Provider: your questions answered
 Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Buckinghamshire Health & Social Care. Operational Resilience & Capacity Plan
 Operational Resilience & Capacity Plan 1 DOCUMENT CONTROL Title Operational Resilience and Capacity Plan Author Bernadette Devine Urgent Care Commissioning Lead Owner Approval Routes Robert Majilton Buckinghamshire
Operational Resilience & Capacity Plan 1 DOCUMENT CONTROL Title Operational Resilience and Capacity Plan Author Bernadette Devine Urgent Care Commissioning Lead Owner Approval Routes Robert Majilton Buckinghamshire
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
South Yorkshire and Bassetlaw Accountable Care System Chief Executives
 South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement
 Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement NHS Hull Clinical Commissioning Group Governing Body Meeting 23 rd March 2018 1. Purpose Integrated Urgent Care (IUC) is
Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement NHS Hull Clinical Commissioning Group Governing Body Meeting 23 rd March 2018 1. Purpose Integrated Urgent Care (IUC) is
The Sustainability and Transformation Plan (STP) for Buckinghamshire, Oxfordshire and Berkshire West (BOB). A short summary.
 for Buckinghamshire, Oxfordshire and Berkshire West (BOB). A short summary.") The Sustainability and Transformation Plan (STP) for Buckinghamshire, Oxfordshire and Berkshire West (BOB). A short summary. The problem which the STP was set up to solve is a financial one, to balance
The Sustainability and Transformation Plan (STP) for Buckinghamshire, Oxfordshire and Berkshire West (BOB). A short summary. The problem which the STP was set up to solve is a financial one, to balance
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
The Chair Dr Raj Bajwa (RB) welcomed the Governing Body members and members of the public
 welcomed the Governing Body members and members of the public") CHILTERN AND AYLESBURY VALE CLINICAL COMMISSIONING GROUPS GOVERNING BODY (in Public) 8 th December 2016 Jubilee Room, The Gateway, Gatehouse Road, Aylesbury, HP19 8FF Governing Body Members Present Chair
CHILTERN AND AYLESBURY VALE CLINICAL COMMISSIONING GROUPS GOVERNING BODY (in Public) 8 th December 2016 Jubilee Room, The Gateway, Gatehouse Road, Aylesbury, HP19 8FF Governing Body Members Present Chair
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT
 KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating