Panel II: Real Time Critical Issues
|
|
|
- Harvey Bryant
- 6 years ago
- Views:
Transcription
1 Panel II: Real Time Critical Issues
2 Dr. Gabrielle Goldberg, M.D.

3 Palliative Care 2012 November 16, 2012 Gabrielle Goldberg, MD Assistant Professor Brookdale Department of Geriatrics and Palliative Medicine Samuel Bronfman Department of Medicine, Division of Hematology and Medical Oncology Medical Director, Wiener Family Palliative Care Unit HERTZBERG PALLIATIVE CARE INSTITUTE
4 Objectives Define Palliative Care Summarize the impact of palliative care on patients, families, clinicians and hospitals Review the growth of Palliative Care

5 Mr. W 91 year old WWII veteran with a history of mild HTN, BPH, Afib with TIAs on coumadin, CHF s/p AICD/PM placement for episodes of NSVT documented during a hospitalization for a TIA in Prior to that hospitalization, Mr. W, a widower, was living in Queens independently performing all of his ADLs and IADLs
6 Post-discharge Mr. W had a prolonged delirium. Over the ensuing 2 years he became increasingly dependent for all his ADLs and required 24 hour companionship His daughters were distressed about his deteriorating QOL and asked the cardiologist about shutting off his AICD. He was referred to a hospice agency in January 2010 who deemed him not appropriate for hospice care.


7 Conceptual Shift OLD Life Prolonging Care Hospice Benefit NEW Dx Life Prolonging Care Life Prolonging Care Palliative Care Hospice Benefit Death
8 Advanced Illness in the Hospital > 80% of people who die in US have a long, progressive illness Everybody with serious illness spends at least some time in a hospital... 98% of Medicare decedents spend at least some time in a hospital in the year before death % of decedents had at least one stay in an ICU in the 6 months before death. 80% patients say they want to avoid hospitalization and intensive care when they are dying Dartmouth Atlas of Health Care 1999 & 2006

9
10 Disease Trajectory 100 Cancer Heart Failure Dec-04 Feb-05 Apr-05 Jun-05 Aug-05 Oct-05 Dec-05 Feb-06 Apr-06 Jun-06 Aug-06 Oct-06 Dec-06 Feb-07 Apr-07 Jun-07 Aug-07 Oct-07 Dec-07 Feb-08 Apr-08 Jun-08 Aug-08 At what point in the trajectory will a patient die?
11 Palliative Care Definition: Palliative care is specialized care for patients and families facing serious illnesses. Care is focused on providing patients with relief from the symptoms, pain, and stress of a serious illness whatever the diagnosis.
12 How Does Palliative Care Differ From Hospice? Non-hospice palliative care is appropriate at any point in a serious illness. It is provided at the same time as life-prolonging treatment. No prognostic requirement, no need to choose between treatment approaches. Hospice is a form of palliative care that provides care for those in the last weeks/few months of life. Patients must have a 2 MD-certified prognosis of <6 months + give up insurance coverage for curative/life prolonging treatment in order to be eligible.
13 Palliative Care Benefits Patients Symptom management Quality of li Navigate complex medical system Understand pros & cons of tx options Allows simultaneous treatment of symptoms along with curative care Practical and emotional support for the exhausted family caregivers
14 Early Palliative Care for Patients with Metastatic Non Small-Cell Lung Cancer Non-blinded, randomized, controlled trial of early PC with standard oncologic care vs. standard oncologic care alone in patients with newly diagnosed metastatic NSCL PC group Improved quality of life Less depressive symptoms (16% vs. 38%) Less use of aggressive end-of-life care (33% vs 54%) Lived longer (11.6 months vs. 8.9 months) Temel J, et al.n Engl J Med 2010; 363:
15 Palliative Care Benefits Clinicians Save time by helping to handle repeated, intensive patient-family communications, coordination of care across settings, comprehensive discharge planning Bedside management of pain and distress of highly symptomatic and complex cases, supports the treatment plan of the primary physician Promote patient and family satisfaction with the clinician s quality of care
16 Palliative Care Benefits Hospitals Effectively treat outliers with complex advanced illness Provide service excellence, patient-centered care Increase patient and family satisfaction Improve staff satisfaction and retention Meet TJC quality standards Rationalize the use of hospital resources Increase bed/icu capacity and throughput, reduce cost per day

17 The Growth of Palliative Care 65.7% of hospitals An increase of 148 % between 2000 and 2010

18 Back to Mr. W In March 2010, Mr. W was again referred and accepted for hospice care His daughter was greatly relieved that calls from his caregiver about changes in his medical condition could now be referred to hospice. In April 2010, Mr. W had the opportunity to meet his 5 th great-grandchild
19 The hospice MD assisted in shutting off his AICD The hospice HHA assisted his 24 hour caregiver with day to day care The hospice RN notified his daughter in May 2010 that his prognosis was hours to days 4 out of his 5 grandchildren had the opportunity to visit with him the night before he died peacefully in his sleep in his own home
20 Take Home Points Palliative Care is specialized care for patients and families facing a serious illness and is appropriate at any stage of illness. Palliative Care is beneficial to patients, families, clinicians and hospitals Palliative Care continues to grow as a specialty Efforts to increase availability of high quality palliative care to all patients continue
21 For more information: For the Media For Clinicians For Policymakers For Family Caregivers
22 The new england journal of medicine clinical practice Palliative Care R. Sean Morrison, M.D., and Diane E. Meier, M.D. From the Hertzberg Palliative Care Institute, Brookdale Department of Geriatrics and Adult Development, Mount Sinai School of Medicine, New York. Address reprint requests to Dr. Morrison at the Department of Geriatrics, Box 1070, Mount Sinai School of Medicine, One Gustave L. Levy Place, New York, NY 10029, or at mssm.edu. N Engl J Med 2004;350: Copyright 2004 Massachusetts Medical Society. An 85-year-old man with New York Heart Association class IV heart failure, hypertension, and moderate Alzheimer s disease is admitted to the hospital after a hip fracture. His postoperative course is complicated by pneumonia, delirium, and pressure ulcers on his heels and sacrum. He is losing weight and is unable to participate in rehabilitation because of his confusion. This is his fourth hospitalization in the past year. His 84-year-old wife, who has been caring for him at home, feels overwhelmed by his medical and personal care needs. The patient s physician is increasingly frustrated by his frequent readmissions. What might she do to address his needs, alleviate his suffering, and facilitate his discharge from the hospital and subsequent care at home? the clinical problem By 2030, 20 percent of the U.S. population will be over the age of 65 years. 1 For most people, the years after the age of 65 are a time of good health, independence, and integration of a life s work and experience. Eventually, most adults will have one or more chronic illnesses with which they will live for years before they die. These years are often characterized by physical and psychological distress, progressive functional dependence and frailty, and increased needs for family and external support. 1 Studies suggest that medical care for patients with serious and advanced illnesses is characterized by the undertreatment of symptoms, conflict about who should make decisions about the patient s care, impairments in caregivers physical and psychological health, and depletion of family resources. 2-5 strategies and evidence the role of palliative care There are many reasons why patients who have advanced illnesses receive inadequate care, but most of those reasons are rooted in a medical philosophy that is focused almost exclusively on curing illness and prolonging life, rather than on improving the quality of life and relieving suffering. Traditionally, medical care has been articulated as having two mutually exclusive goals: either to cure disease and prolong life or to provide comfort care. 1 Given this dichotomy, the decision to focus on reducing suffering is made only after life-prolonging treatment has been ineffectual and death is imminent. 6 In the United States, this forced choice is driven largely by the reimbursement system that is, regular Medicare covers curative therapies and the Medicare hospice benefit covers comfort care. That division of services results both in the provision of burdensome and costly life-prolonging treatments when they are no longer beneficial and in preventable suffering during all stages of advanced illness. 7 In contrast, patients would benefit most from care that included a combination of life-prolonging treatment (when possible and appropriate), palliation of symptoms, rehabilitation, and support for caregivers. Meeting the needs of patients will require that physicians employ skills that are 2582 n engl j med 350;25 june 17, 2004 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
23 clinical practice not traditionally taught in medical schools. 8 Palliative care aims to relieve suffering and improve the quality of life for patients with advanced illnesses and their families through specific knowledge and skills, including communication with patients and family members; management of pain and other symptoms; psychosocial, spiritual, and bereavement support; and coordination of an array of medical and social services. 1 Palliative care should be offered simultaneously with all other medical treatment. physician patient communication Communicating with patients is a core skill of palliative medicine. 9 Studies suggest that in a typical clinical encounter, clinicians elicit fewer than half of patients concerns and consistently fail to discuss patients values, goals of care, and preferences with regard to treatment. 10 Empirical evidence supports the effectiveness of clinicians use of specific communication skills in enhancing disclosure of the issues of concern to a patient, decreasing anxiety, assessing depression, and improving a patient s well-being and the level of the patient s and the family s satisfaction with the treatment. 10 Those communication skills include making eye contact with patients, asking open-ended questions, responding to a patient s affect, and demonstrating empathy. When a physician is informing a patient about a poor prognosis, conducting an open, patient-centered interview (in which the emphasis is on empathy, openness, and reassurance), rather than the traditional closed, physiciancentered interview (in which the physician is focused on the task), has been associated with an improved level of satisfaction on the part of patients and their families. 11 Guidelines have been developed for establishing goals of medical care, communicating bad news, and withholding or withdrawing medical treatments (Fig. 1). 12,13 Whether the use of these protocols actually helps patients and their families has not been empirically determined, but we and others have found these guidelines to be useful in clinical practice. One randomized trial in the United Kingdom showed that a postgraduate course in communication skills that had cognitive, behavioral, and affective components led to improved communication skills among the physicians. 17 Similar courses are offered annually in the United States. 18,19 Palliative care begins with establishing the goals Establishing Goals of Medical Care Communicating Bad News Figure 1. Protocols for Communicating with Patients about Major Topics in Palliative Care. Adapted from the Education on Palliative and End-of-life Care Project. 12 of care. Outlining realistic and attainable goals assumes an increased importance in the setting of advanced disease, in which treatments intended to cure the disease and prolong life may be more burdensome than beneficial. Whereas the goal for Withdrawing Treatment Create the right setting: plan what to say, allow adequate time, and determine who else should be present at the meeting Establish what the patient knows: clarify the situation and context in which the discussion about goals is occurring Explore what the patient is hoping to accomplish: help distinguish between realistic and unrealistic goals Suggest realistic goals: explore how goals can be achieved and work through unrealistic expectations Establish what the patient knows: clarify what the patient can comprehend; reschedule the talk if necessary Establish how much the patient wants to know: recognize and support preferences; people handle information in different ways Share the information: avoid jargon, pause frequently, check for understanding, use silence; do not minimize the information Establish and review the goals of care Establish the context of the current discussion: discuss what has changed to precipitate the discussion Discuss specific treatment in the context of the goals of care: talk about whether the treatment will meet the goals of care Discuss alternatives to the proposed treatment: talk about what will happen if the patient decides not to have the treatment Respond empathetically to feelings: be prepared for strong emotions and allow time for response, listen, encourage description of feelings, allow silence Make a plan and follow through: discuss which treatments will be undertaken to meet the goals, establish a concrete plan for follow-up, review and revise the plan periodically as needed Follow up: plan for next steps, discuss potential sources of support, share contact information, assess the patient s safety and support, repeat news at future visits Plan for the end of treatment: document a plan for withdrawal of treatment and give it to the patient, the patient s family, and members of the health care team n engl j med 350;25 june 17, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
24 The new england journal of medicine some patients may be to prolong life at any cost, studies suggest that what most seriously ill patients want is to have their pain and other symptoms relieved, improve their quality of life, avoid being a burden to their family, have a closer relationship with loved ones, and maintain a sense of control. 9,20 Establishing clear goals can facilitate decision making regarding treatment. For example, in the case of a patient with end-stage dementia who has dysphagia, placement of a percutaneous endoscopic gastrostomy (PEG) tube may be considered. If the primary goal is to reduce suffering and enhance the quality of life, then placing a PEG tube is unlikely to meet these goals, since it requires a painful, invasive procedure; eliminates the pleasurable oral sensations of eating and drinking; is associated with an increased use of restraints; can cause cellulitis, vomiting, diarrhea, and fluid imbalances; and is unlikely to reduce the risk of aspiration. 21 Even in cases in which a primary goal is to prolong life, the role of a PEG tube remains questionable; no survival benefits have been shown in observational studies in which patients with dementia who received feeding tubes were compared with similar patients who did not receive feeding tubes. 21 Expert opinion suggests that clinicians can assist patients and their families in establishing their own goals by means of open-ended and probing questions. Some examples of the types of questions include What makes life worth living for you? Given the severity of your illness, what are the most important things for you to achieve? What are your most important hopes? What are your biggest fears? and What would you consider to be a fate worse than death? 16 The goals that patients establish may overlap, be contradictory, rise and fall in importance, and shift with the progression of the disease. 12,16 Warning signs of poorly established or conflicting goals can include frequent and lengthy hospitalizations; feelings of frustration, anger, or powerlessness on the part of the physician; and feelings of being burdened on the part of caregivers. 15 Once goals are established, they can be used to construct advance directives about the types of care that patients want. Most studies, 22 although not all, 23,24 have shown that few patients have advance directives and that the documents they do have are relatively ineffectual in enhancing physician patient communication, facilitating decision making about resuscitation, 25 or influencing terminal care in hospitals. 22 It is possible that the gradual rise in the prevalence of advance directives over the past decade will improve their effectiveness, as physicians and patients become more familiar with them and physicians become more comfortable using them for assistance in guiding the care of cognitively impaired adults. A recent report suggested that the focus of advance care planning should shift from discussing specific treatments to defining an acceptable quality of life and setting goals for care under various likely clinical scenarios. 26,27 Whether this goal-centered approach to advance care planning will affect clinical outcomes is unknown. assessment and treatment of symptoms A fundamental goal of palliative care is the relief of pain and other symptoms. 9,20 Successful approaches to the assessment and management of pain and some physical and psychological symptoms have been established in controlled trials. 12,28-30 Despite these advances, undertreatment of symptoms persists in the majority of patients and settings. 2,31 Relief of suffering begins with routine and standardized symptom assessment with use of validated instruments. Routine assessment has been shown to identify overlooked and unreported symptoms, facilitate treatment, and enhance patient and family satisfaction. 32,33 Clinically useful assessment instruments can be found on the Web sites of the Center to Advance Palliative Care ( and of Brown University s Center for Gerontology and Health Care Research, which features a tool kit of instruments to measure end-of-life care (www. chcr.brown.edu/pcoc/toolkit.htm). Improved treatment of symptoms has been associated with the enhancement of patient and family satisfaction, functional status, quality of life, and other clinical outcomes. 32,34 Although a comprehensive review of strategies for assessment and therapy of symptoms is beyond the scope of this review, Table 1 summarizes approaches to commonly encountered symptoms in advanced illnesses. psychosocial, spiritual, and bereavement support Providing psychosocial, spiritual, and bereavement support to patients and caregivers is a key component of palliative care. Patients who experience spiritual and psychological distress are more likely to express a desire for death than are other patients, 42 and their family members are more likely to have an extended or complicated grief and bereavement process (defined as grief that lasts for 2584 n engl j med 350;25 june 17, 2004 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
25 clinical practice Table 1. Approaches to the Management of Pain and Other Common Symptoms.* Symptom Assessment Treatment Anorexia and cachexia Anxiety Constipation Depression Delirium Is a disease process causing the symptom, or is it secondary to other symptoms (e.g., nausea and constipation) that can be treated? Is the patient troubled by the symptom? Does the patient exhibit restlessness, agitation, insomnia, hyperventilation, tachycardia, or excessive worry? Is the patient taking opioids? Does the patient have a fecal impaction? How does the patient respond to the question Are you depressed? Does the patient express or exhibit any of the following feelings: helplessness, hopelessness, anhedonia, loss of self-esteem, worthlessness, persistent dysphoria, and suicidal ideation? (Somatic symptoms are not reliable indicators of depression in this population.) Was the onset of confusion acute? Is the patient disoriented or experiencing changes in the level of consciousness or minute-to-minute fluctuations? Is the condition reversible? Consider megestrol acetate or dexamethasone. Recommend supportive counseling and consider prescribing benzodiazepines (in the elderly, avoid benzodiazepines with long half-lives). Prescribe a stool softener (ineffective alone) plus escalating doses of a stimulant; if escalation of the dose is ineffectual, agents from other classes (e.g., osmotic laxatives and enemas) should be added. Recommend supportive psychotherapy, cognitive approaches, behavioral techniques, pharmacologic therapies, or a combination of these interventions; prescribe psychostimulants for rapid treatment of symptoms (within days) or selective serotoninreuptake inhibitors, which may require three to four weeks to take effect; tricyclic antidepressants are relatively contraindicated because of their side effects. Identify underlying causes and manage symptoms; recommend behavioral therapies, including avoidance of excess stimulation, frequent reorientation, and reassurance; ensure presence of family caregivers; prescribe haloperidol, risperidone, or olanzapine. (Chlorpromazine can be used for agitated or terminal delirium, but benzodiazepines have been found to exacerbate delirium and should be avoided.) Dyspnea Does the symptom have reversible causes? Prescribe oxygen to treat hypoxia-induced dyspnea or to provide symptomatic relief, when hypoxia is absent, through stimulation of the V2 branch of the trigeminal nerve. Opioids relieve breathlessness without measurable reductions in respiratory rate or oxygen saturation; effective doses are often lower than those used to treat pain. Consider anxiolytics (e.g., low-dose benzodiazepines) and use reassurance, relaxation, distraction, and massage therapy. Nausea Pain Which mechanism is causing the symptom (e.g., stimulation of the chemoreceptor trigger zone, gastric stimulation, delayed gastric emptying or squashed stomach syndrome, bowel obstruction, intracranial processes, or vestibular vertigo)? How severe is the symptom (as assessed with the use of validated instruments)? Prescribe an agent directed at the underlying cause. Multiple agents directed at various receptors or mechanisms may be required. Prescribe medications to be administered on a standing or regular basis; as-needed or rescue doses should be available for breakthrough pain or pain not controlled by the standing regimen; start a regimen to prevent constipation for all patients receiving opioids. For mild pain: use acetaminophen or a nonsteroidal antiinflammatory agent (consider opioids in older adults). For moderate pain: titrate short-acting opioids. For severe pain: rapidly titrate shortacting opioids until pain is relieved or intolerable side effects develop; start long-acting opioids (e.g., sustained-release morphine or oxycodone and transdermal fentanyl) once pain is well controlled; use methadone only if experienced in its use. Rescue doses: prescribe immediate-release opioids consisting of 10% of the 24-hour total opioid dose to be given every hour (orally) or every 30 minutes (parenterally) as needed. Concomitant analgesics (e.g., corticosteroids, anticonvulsants, tricyclic antidepressants, and bisphosphonates) should be used when applicable. * For details of recommendations and more information about the management of symptoms, see Foley, 35 American Geriatrics Society Panel on Persistent Pain in Older Persons, 36 Luce and Luce, 37 Casarett and Inouye, 38 Strasser and Bruera, 39 Block, 40 and Regnard and Comiskey. 41 n engl j med 350;25 june 17, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
26 The new england journal of medicine at least 14 months after the death and results in a failure of the survivor to return to his or her normal activities) and are at higher risk for illness and death. 43 Studies suggest that patients welcome inquiries about their spiritual well-being from their physicians, 44 although interventions to address spiritual distress have not been well developed or well evaluated. Support groups have been found to reduce stress and depression experienced by caregivers. 45,46 Although many formal interventions to address complicated grief and bereavement have been described, data are lacking on their effects on outcomes. 47 Two recent studies reported lower morbidity and mortality 48 and better emotional support 49 among surviving family members of hospice patients than among family members of patients who did not receive hospice services, although it is uncertain whether this difference reflects the nature of families who elect hospice care rather than the effects of the intervention. 48 coordination of care Several studies demonstrate that the personal and practical care needs of patients who are seriously ill and their families are not adequately addressed by routine office visits or hospital and nursing home stays and that this failure results in substantial burdens medical, psychological, and financial on patients and their caregivers. 3-5,49,50 In the context of chronic progressive disease, the ability of physicians to coordinate an array of social and medical services on behalf of patients and families assumes increased importance. Various comprehensive care programs are available to help physicians manage the care of their patients who have serious and complex illnesses. Palliative care programs within home care organizations, hospitals, and nursing homes are increasingly prevalent in the United States and provide comprehensive interdisciplinary care for patients and families in collaboration and consultation with primary care physicians. 51 Hospice services, under the Medicare benefit, are available in most U.S. communities and provide palliative care, primarily at home, for patients with a life expectancy of six months or less who are willing to forgo insurance coverage for life-prolonging treatments. Studies suggest that referral to palliative care programs and hospice results in beneficial effects on patients symptoms, reduced hospital costs, a greater likelihood of death at home, and a higher level of patient and family satisfaction than does conventional care. 49,50,52,53 Other programs that coordinate care for patients who have complex illnesses are available in most communities. Programs that coordinate home care services for patients with chronic conditions (e.g., depression, heart failure, or the acquired immunodeficiency syndrome) have been associated with increased patient and family satisfaction and reductions in mortality, use of hospital services, visits to physicians offices, and admission to nursing homes Case management is usually provided by managed-care organizations, Medicare managed-care services, commercial insurers, some home health care agencies, and privately hired case managers. The quality, cost, and extent of the services provided are highly variable. Comprehensive multidisciplinary home care programs that serve frail older adults have been evaluated under Medicare and the Veterans Health Administration (VHA). The Program of All-Inclusive Care for the Elderly (PACE) is a capitated Medicare and Medicaid benefit for frail older adults that offers comprehensive medical and social services at 25 adult day health centers, in homes, and at inpatient facilities. (More information about the program is available online at Patients who use the services provided by PACE have higher rates of completing advance directives for their care 57 and lower rates of admission to nursing homes, 58 hospitalization, 59 and death in the hospital 59 than do patients who do not use the services. Similar programs of team-coordinated home-based care exist within the VHA. 60 Until comprehensive palliative care programs become widely available, the responsibility for coordination of care falls to the primary care physician, since patients and their families frequently have problems negotiating the current health care system. Table 2 details the range of palliative care services that should be considered at various stages of a serious illness; Table 3 lists services that are covered by Medicare. areas of uncertainty Physicians have few data to guide them in improving their communication with patients and in their management of pain and other symptoms. The communication guidelines presented in Figure 1, although widely taught and used by palliative care experts, have not been shown to be associated with 2586 n engl j med 350;25 june 17, 2004 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
27 clinical practice Table 2. Coordination of Care for Early, Middle, and Late Stages of Serious Chronic Illnesses.* Palliative Care Services Early Stage Middle Stage Late Stage Goals of care Programmatic support Discuss diagnosis, prognosis, likely course of the illness, and disease-modifying therapies; talk about patientcentered goals, hopes, and expectations for medical treatments. Advise patient to sign up for visiting nurse and home care services and casemanagement services (if available). Financial planning Advise patient to seek help in planning for financial, longterm care, and insurance needs and to begin transfer of assets if patient is considering a future Medicaid application; refer patient to a lawyer who is experienced in health issues. Family support Inform patient and family about support groups; ask about practical support needs (e.g., transportation, prescription-drug coverage, respite care, and personal care); listen to concerns. Review patient s understanding of prognosis; review efficacy and benefit-to-burden ratio for disease-modifying treatments; reassess goals of care and expectations; prepare patient and patient s family for a shift in goals; encourage paying attention to important tasks, relationships, and financial affairs. Advise patient to sign up for visiting nurse and home care services; consider palliative care program in hospital or at home, hospice, subacute rehabilitation, casemanagement services, and PACE. Advise patient to reassess adequacy of planning for financial, medical, home care, prescription, long-term care, and family-support needs; consider hospice referral and Medicaid eligibility. Encourage support or counseling for family caregivers; ensure that caregivers have information about practical resources, stress, depression, and adequacy of medical care; identify respite and practical support resources; recommend help from family and friends; raise the possibility of hospice and discuss its benefits; listen to concerns. Assess patient s understanding of diagnosis, disease course, and prognosis; review appropriateness of disease-modifying treatments; review goals of care and recommend appropriate shifts; help patient explicitly plan for a peaceful death; encourage completion of important tasks and increased attention to relationships and financial affairs. Advise patient to sign up for a palliative care program in hospital or at home, case-management services, hospice, or PACE; consider nursing home placement with hospice or palliative care if patient s home caregivers are overwhelmed. Advise patient to review all financial resources and needs; inform patient and family about financial options for personal and long-term care (e.g., hospice and Medicaid) if resources are inadequate to meet needs; explicitly recommend hospice and review its advantages; consider Medicaid eligibility. Encourage out-of-town family to visit; refer caregivers to disease-specific support groups or counseling; inquire routinely about health, wellbeing, and practical needs of caregivers; offer resources for respite care; after death, send bereavement card and call after one to two weeks; screen for complicated bereavement; maintain occasional contact after patient s death; listen to concerns. * Early stage refers to the stage of disease at the time of diagnosis, middle stage to progressive disease and increasing functional decline, and late stage to the stage when death is imminent. PACE denotes Program of All-Inclusive Care for the Elderly. improved outcomes. Similarly, although data are available to guide the treatment of pain due to cancer, data are lacking regarding the treatment of other pain syndromes, symptoms other than pain (such as dyspnea, fatigue, delirium, and anxiety), spiritual distress, and complicated grief and bereavement. guidelines The National Comprehensive Cancer Network 61 has developed guidelines for patients who have advanced incurable cancer, and the National Consensus Project for Quality Palliative Care, 62 a collaborative effort of five national palliative care organizations, has similar guidelines for patients who have advanced chronic illnesses. These guidelines encompass many of the recommendations detailed in this article, and the National Consensus Project guidelines also include recommendations regarding the spiritual, religious, and existential aspects of care; cultural aspects of care; and care of patients whose death is imminent. 62 Although the guidelines of the National Comprehensive Cancer Network are targeted to patients with terminal cancer, many patients who have early stages of the disease or uncertain prognoses or who are undergoing active curative or life-prolonging therapies can benefit from the organization s recommendations. The application of those recommendations should not be restricted to patients with a limited life expectancy. n engl j med 350;25 june 17, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
28 The new england journal of medicine Table 3. Summary of Medicare Coverage for Common Services Required by Patients with Serious and Chronic Illnesses. Medicare Part A* Service Coverage Out-of-Pocket Cost Ambulance Transportation only to a hospital or skilled nursing facility and only if 20% of Medicare-approved amounts transportation in any other type of vehicle endangers health Custodial care No coverage for custodial care if this is the only care needed 100% Home health care Skilled nursing care in the home for treatment of an acute illness if at least one of the following is needed: intermittent skilled nursing care, physical or speech therapy, or continuing occupational therapy and if the patient is unable to leave the house except with major effort None; if the patient has only Part B coverage, services are covered by Part B Hospice Hospital inpatient care Skilled nursing facility or rehabilitation Eligibility: life expectancy of 6 mo or less if disease follows its usual course and willingness to relinquish Medicare-reimbursed services focused on prolongation of life or cure; coverage includes physician and nursing services, durable medical equipment and supplies, medications for pain or symptom control, home health aide and homemaker services (4 hr/day on average), physical and occupational therapy, short-stay hospitalizations and respite care, social work services, and bereavement services; regular Medicare covers services not related to hospice diagnosis; room and board are covered only for respite care and short hospital stays, not for nursing home or residential hospice stays None for regular hospice services; copayment of up to $5 for outpatient prescription drugs; 5% of Medicare-approved amount for inpatient respite care General hospital services with semiprivate room For each benefit period, deductible of $812 for days 1 60, $203/day for days 61 90, and $406/day for days ; benefit period begins on hospital day 1 and ends when hospital or skilled nursing care has not been received for 60 consecutive days If patient has Part A benefit days remaining after hospitalization; qualified hospital stay (inpatient stay of 3 consecutive days and entry into a skilled nursing facility within 30 days of discharge); need for a skilled service to treat a medical condition that was treated in the hospital or started while getting Medicare-covered skilled nursing care; no coverage for nursing home custodial care Medicare Part B For each benefit period, none for days 1 20, $101.50/day for days , and 100%/day for day 101 Service Coverage Out-of-Pocket Cost Custodial care No coverage for custodial care if this is the only care needed 100% Durable medical Air-fluidized beds, canes, commode chairs, crutches, home oxygen Variable after $100 deductible equipment and equipment (with qualifications), hospital beds, nebulizers, patient lifts, suction pumps, walkers, and wheelchairs Office visits to doctors No coverage for routine physical and gynecologic examinations 20% of Medicare-approved rates Outpatient mental health services Nonphysician health care services Prescription drugs Transportation Office visits to physicians, clinical social workers, psychologists, nurse specialists, and physician assistants Office visits to clinical social workers, psychologists, physician assistants, and nurse practitioners (for medically necessary services) Limited coverage for erythropoietin only in end-stage renal disease, injectable drugs, limited oral cancer medications, limited oral antiemetics (if a Medicare-covered cancer drug), some infusion therapies (if considered reasonable and necessary). A Medicare discount card is currently available for other prescription drugs and a $600 credit is available for qualifying low-income individuals. In 2005, a Medicare prescription-drug plan will become available. No coverage for transportation to physicians offices, laboratory tests, outpatient physical therapy, or ambulette (van) services 50% of Medicare-approved rates 20% of Medicare-approved rates In 2004, 75 to 90 percent for most prescriptions. In 2005, a $35 monthly premium and a $250 deductible; 25 percent of pharmacy costs between $250 and $2,250 in drug spending, 100 percent of costs between $2,250 and $3,600, and 5 percent of costs over $3, % * Under Part A, the patient pays no premium if the patient or the patient s spouse has paid Medicare taxes while working for 40 or more quarters. Under Part B, the patient pays for optional coverage with a premium of $58.70 per month n engl j med 350;25 june 17, 2004 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
29 clinical practice conclusions and recommendations The aim of palliative care is to relieve suffering and improve the quality of life for patients with advanced illnesses and their families. It is based on an interdisciplinary approach that is offered simultaneously with other appropriate medical treatments and involves close attention to the emotional, spiritual, and practical needs and goals of patients and of the people who are close to them. The patient who is described in the vignette, who has multiple chronic and serious medical conditions but is not actively dying, is ideally suited to receive high-quality palliative care. Specifically, we suggest the following approach. The patient s symptoms should be assessed and treated, as discussed in Table 1. If available, consultation with a palliative care team should be strongly considered to help with evaluating and managing his symptoms. Once the patient is comfortable, a discussion about realistic goals should be held, with particular attention given to clarifying the patient s opinion about an acceptable quality of life, identifying conditions under which the patient would consider life not worth living, establishing attainable short- and long-term goals, and designating a health care proxy. We recommend that this discussion be summarized in a treatment directive and that a health-care-proxy form be completed. Once goals are clarified, appropriate treatment and discharge planning can begin. In the case described in the vignette, for example, the treatment goal might be to focus on the patient s comfort and on caring for him at home, and the appropriate treatments might be spoon-feeding rather than placement of a PEG tube, diuretics and bisphosphonates, avoidance of hospitalization, and a trial of physical and occupational therapy with the aim of regaining function. The patient s discharge services will depend on the goals, the patient s insurance coverage and financial resources, and available home care services. Since a hospice program will support these goals, a referral to hospice should be considered. If hospice is not an option (e.g., because of limited home care hours or uncertainty about the prognosis), the patient should be referred to a case-management program, PACE, or a certified home care agency. The family s ability to afford medications should be evaluated, and alternative sources (such as mail-order drug plans or state-sponsored prescription plans for low-income elderly people) or less costly medications should be considered. Before discharge, a home-safety and home-needs evaluation should be performed either by an occupational therapist or through a structured interview with the patient s caregiver. An assessment of support requirements for the caregiver should be conducted to ensure that the personal care needs of the patient and the patient s family are met. Referral to a social worker can help identify community alternatives and determine Medicaid eligibility. Finally, a regular system of communication should be established between the treating physician and the home care team. Dr. Morrison is a Paul Beeson Faculty Scholar in Aging Research, an Open Society Institute Project on Death in America Faculty Scholar, and the recipient of a Mid-Career Investigator Award in Patient- Oriented Research (K24AG022345) from the National Institute on Aging. Dr. Meier is an Open Society Institute Project on Death in America Faculty Scholar, the recipient of an Academic Career Leadership Award (K07AG00903) from the National Institute on Aging, and the director of the Center to Advance Palliative Care, a program office of the Robert Wood Johnson Foundation. references 1. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life. Washington, D.C.: National Academy Press, The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients: the Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995;274: [Erratum, JAMA 1996;275:1232.] 3. Emanuel EJ, Fairclough DL, Slutsman J, Emanuel LL. Understanding economic and other burdens of terminal illness: the experience of patients and their caregivers. Ann Intern Med 2000;132: Emanuel EJ, Fairclough DL, Slutsman J, Alpert H, Baldwin D, Emanuel LL. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. N Engl J Med 1999;341: Covinsky KE, Goldman L, Cook EF, et al. The impact of serious illness on patients families. JAMA 1994;272: Christakis NA, Escarce JJ. Survival of Medicare patients after enrollment in hospice programs. N Engl J Med 1996;335: Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. 2. Health outcomes and satisfaction with care. Ann Intern Med 2003;138: Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-oflife care: a national report. J Gen Intern Med 2003;18: Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000;284: Tulsky JA. Doctor-patient communication. In: Morrison RS, Meier DE, eds. Geriatric palliative care. New York: Oxford University Press, 2003: Dowsett SM, Saul JL, Butow PN, et al. Communication styles in the cancer consultation: preferences for a patient-centered approach. Psychooncology 2000;9: The EPEC Project: Education on Palliative and End-of-life Care. (Accessed April 21, 2004, at n engl j med 350;25 june 17, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
30 clinical practice 13. Buckman R. How to break bad news: a guide for health care professionals. Baltimore: Johns Hopkins University Press, Goold SD, Williams B, Arnold RM. Conflicts regarding decisions to limit treatment: a differential diagnosis. JAMA 2000;283: Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA 2001;286: Quill TE. Perspectives on care at the close of life: initiating end-of-life discussions with seriously ill patients: addressing the elephant in the room. JAMA 2000; 284: Fallowfield L, Jenkins V, Farewell V, Saul J, Duffy A, Eves R. Efficacy of a Cancer Research UK communication skills training model for oncologists: a randomised controlled trial. Lancet 2002;359: Harvard Medical School Center for Palliative Care. Practical aspects in palliative medicine: integrating palliative care into clinical practice. (Accessed April 21, 2004, at American Academy on Physician and Patient. Upcoming courses and meetings. (Accessed April 21, 2004, at physicianpatient.org/default.htm.) 20. Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients perspectives. JAMA 1999;281: Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA 1999;282: Miles SH, Koepp R, Weber EP. Advance end-of-life treatment planning: a research review. Arch Intern Med 1996;156: Hammes BJ, Rooney BL. Death and endof-life planning in one midwestern community. Arch Intern Med 1998;158: Morrison RS, Meier DE. High rates of advance care planning in New York City s elderly. Arch Intern Med (in press). 25. Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the Patient Self- Determination Act and the SUPPORT intervention. J Am Geriatr Soc 1997;45: Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med 2002;346: Meier DE, Morrison RS. Autonomy reconsidered. N Engl J Med 2002;346: Doyle D, Hanks GW, Cherny NI, Calman K. Oxford textbook of palliative medicine. 3rd ed. Oxford, England: Oxford University Press, TIME: Toolkit of Instruments to Measure End of life care. (Accessed April 21, 2004, at toolkit.htm.) 30. Morrison RS, Meier DE. Geriatric palliative care. New York: Oxford University Press, Bernabei R, Gambassi G, Lapane K, et al. Management of pain in elderly patients with cancer. JAMA 1998;279: [Erratum, JAMA 1999;281:136.] 32. Bookbinder M, Coyle N, Kiss M, et al. Implementing national standards for cancer pain management: program model and evaluation. J Pain Symptom Manage 1996; 12: Manfredi PL, Morrison RS, Morris J, Goldhirsch SL, Carter JM, Meier DE. Palliative care consultations: how do they impact the care of hospitalized patients? J Pain Symptom Manage 2000;20: Morrison RS, Magaziner J, McLaughlin MA, et al. The impact of post-operative pain on outcomes following hip fracture. Pain 2003;103: Foley KM. Advances in cancer pain. Arch Neurol 1999;56: AGS Panel on Persistent Pain in Older Persons. The management of persistent pain in older persons. J Am Geriatr Soc 2002;50:Suppl:S205-S Luce JM, Luce JA. Perspectives on care at the close of life: management of dyspnea in patients with far-advanced lung disease: once I lose it, it s kind of hard to catch it.... JAMA 2001;285: Casarett DJ, Inouye SK. Diagnosis and management of delirium near the end of life. Ann Intern Med 2001;135: Strasser F, Bruera ED. Update on anorexia and cachexia. Hematol Oncol Clin North Am 2002;16: Block SD. Assessing and managing depression in the terminally ill patient. Ann Intern Med 2000;132: Regnard C, Comiskey M. Nausea and vomiting in advanced cancer a flow diagram. Palliat Med 1992;6: McClain CS, Rosenfeld B, Breitbart W. Effect of spiritual well-being on end-of-life despair in terminally-ill cancer patients. Lancet 2003;361: Stroebe MS, Stroebe W. The mortality of bereavement: a review. In: Stroebe MS, Stroebe W, Hansson RO, eds. Handbook of bereavement: theory, research, and intervention. Cambridge, England: Cambridge University Press, 1993: Ehman JW, Ott BB, Short TH, Ciampa RC, Hansen-Flaschen J. Do patients want physicians to inquire about their spiritual or religious beliefs if they become gravely ill? Arch Intern Med 1999;159: Mittelman MS, Ferris SH, Shulman E, Steinberg G, Levin B. A family intervention to delay nursing home placement of patients with Alzheimer disease: a randomized controlled trial. JAMA 1996;276: Mittelman MS, Ferris SH, Shulman E, et al. A comprehensive support program: effect on depression in spouse-caregivers of AD patients. Gerontologist 1995;35: Stroebe MS, Stroebe W, Hansson RO. Handbook of bereavement: theory, research, and intervention. Cambridge, England: Cambridge University Press, Christakis NA, Iwashyna TJ. The health impact of health care on families: a matched cohort study of hospice use by decedents and mortality outcomes in surviving, widowed spouses. Soc Sci Med 2003;57: Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place of care. JAMA 2004;291: Miller SC, Mor V, Teno J. Hospice enrollment and pain assessment and management in nursing homes. J Pain Symptom Manage 2003;26: Center to Advance Palliative Care home page. (Accessed April 21, 2004, at Finlay IG, Higginson IJ, Goodwin DM, et al. Palliative care in hospital, hospice, at home: results from a systematic review. Ann Oncol 2002;13:Suppl 4: Smith TJ, Coyne P, Cassel B, Penberthy L, Hopson A, Hager MA. A high-volume specialist palliative care unit and team may reduce in-hospital end-of-life care costs. J Palliat Med 2003;6: West JA, Miller NH, Parker KM, et al. A comprehensive management system for heart failure improves clinical outcomes and reduces medical resource utilization. Am J Cardiol 1997;79: Wasson J, Gaudette C, Whaley F, Sauvigne A, Baribeau P, Welch HG. Telephone care as a substitute for routine clinic followup. JAMA 1992;267: Elkan R, Kendrick D, Dewey M, et al. Effectiveness of home based support for older people: systematic review and meta-analysis. BMJ 2001;323: Mukamel DB, Bajorska A, Temkin- Greener H. Health care services utilization at the end of life in a managed care program integrating acute and long-term care. Med Care 2002;40: Eng C, Pedulla J, Eleazer GP, McCann R, Fox N. Program of All-Inclusive Care for the Elderly (PACE): an innovative model of integrated geriatric care and financing. J Am Geriatr Soc 1997;45: Wieland D, Lamb VL, Sutton SR, et al. Hospitalization in the Program of All-Inclusive Care for the Elderly (PACE): rates, concomitants, and predictors. J Am Geriatr Soc 2000;48: [Erratum, J Am Geriatr Soc 2001;49:835.] 60. Hughes SL, Weaver FM, Giobbie-Hurder A, et al. Effectiveness of team-managed home-based primary care: a randomized multicenter trial. JAMA 2000;284: The National Comprehensive Cancer Network. Guidelines for supportive care. (Accessed April 21, 2004, at nccn.org/physician_gls/f_guidelines.html.) 62. The National Consensus Project for Quality Palliative Care (NCP) home page. (Accessed April 21, 2004, at nationalconsensusproject.org.) Copyright 2004 Massachusetts Medical Society n engl j med 350;25 june 17, 2004 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2004 Massachusetts Medical Society. All rights reserved.
31 The new england journal of medicine original article Early Palliative Care for Patients with Metastatic Non Small-Cell Lung Cancer Jennifer S. Temel, M.D., Joseph A. Greer, Ph.D., Alona Muzikansky, M.A., Emily R. Gallagher, R.N., Sonal Admane, M.B., B.S., M.P.H., Vicki A. Jackson, M.D., M.P.H., Constance M. Dahlin, A.P.N., Craig D. Blinderman, M.D., Juliet Jacobsen, M.D., William F. Pirl, M.D., M.P.H., J. Andrew Billings, M.D., and Thomas J. Lynch, M.D. Abstract Background Patients with metastatic non small-cell lung cancer have a substantial symptom burden and may receive aggressive care at the end of life. We examined the effect of introducing palliative care early after diagnosis on patient-reported outcomes and end-of-life care among ambulatory patients with newly diagnosed disease. Methods We randomly assigned patients with newly diagnosed metastatic non small-cell lung cancer to receive either early palliative care integrated with standard oncologic care or standard oncologic care alone. Quality of life and mood were assessed at baseline and at 12 weeks with the use of the Functional Assessment of Cancer Therapy Lung (FACT-L) scale and the Hospital Anxiety and Depression Scale, respectively. The primary outcome was the change in the quality of life at 12 weeks. Data on end-of-life care were collected from electronic medical records. From Massachusetts General Hospital, Boston (J.S.T., J.A.G., A.M., E.R.G., V.A.J., C.M.D., J.J., W.F.P., J.A.B.); the State University of New York, Buffalo (S.A.); Adult Palliative Medicine, Department of Anesthesiology, Columbia University Medical Center, New York (C.D.B.); and Yale University, New Haven, CT (T.J.L.). Address reprint requests to Dr. Temel at Massachusetts General Hospital, 55 Fruit St., Yawkey 7B, Boston, MA 02114, or at jtemel@partners.org. N Engl J Med 2010;363: Copyright 2010 Massachusetts Medical Society. Results Of the 151 patients who underwent randomization, 27 died by 12 weeks and 107 (86% of the remaining patients) completed assessments. Patients assigned to early palliative care had a better quality of life than did patients assigned to standard care (mean score on the FACT-L scale [in which scores range from 0 to 136, with higher scores indicating better quality of life], 98.0 vs. 91.5; P = 0.03). In addition, fewer patients in the palliative care group than in the standard care group had depressive symptoms (16% vs. 38%, P = 0.01). Despite the fact that fewer patients in the early palliative care group than in the standard care group received aggressive end-of-life care (33% vs. 54%, P = 0.05), median survival was longer among patients receiving early palliative care (11.6 months vs. 8.9 months, P = 0.02). Conclusions Among patients with metastatic non small-cell lung cancer, early palliative care led to significant improvements in both quality of life and mood. As compared with patients receiving standard care, patients receiving early palliative care had less aggressive care at the end of life but longer survival. (Funded by an American Society of Clinical Oncology Career Development Award and philanthropic gifts; ClinicalTrials.gov number, NCT ) n engl j med 363;8 nejm.org august 19, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
32 The new england journal of medicine The quality of care and the use of medical services for seriously ill patients are key elements in the ongoing debate over reform of the U.S. health care system. 1 Oncologic care is central to this debate, largely because anticancer treatments are often intensive and costly. 2 Comprehensive oncologic services for patients with metastatic disease would ideally improve the patients quality of life and facilitate the efficient allocation of medical resources. Palliative care, with its focus on management of symptoms, psychosocial support, and assistance with decision making, has the potential to improve the quality of care and reduce the use of medical services. 3,4 However, palliative care has traditionally been delivered late in the course of disease to patients who are hospitalized in specialized inpatient units or as a consultative service for patients with uncontrolled symptoms. 5,6 Previous studies have suggested that late referrals to palliative care are inadequate to alter the quality and delivery of care provided to patients with cancer. 7,8 To have a meaningful effect on patients quality of life and end-of-life care, palliative care services must be provided earlier in the course of the disease. Metastatic non small-cell lung cancer, the leading cause of death from cancer worldwide, 9 is a debilitating disease that results in a high burden of symptoms and poor quality of life; the estimated prognosis after the diagnosis has been established is less than 1 year We previously found that introducing palliative care shortly after diagnosis was feasible and acceptable among outpatients with metastatic non small-cell lung cancer. 13 The goal of the current study was to examine the effect of early palliative care integrated with standard oncologic care on patientreported outcomes, the use of health services, and the quality of end-of-life care among patients with metastatic non small-cell lung cancer. We hypothesized that patients who received early palliative care in the ambulatory care setting, as compared with patients who received standard oncologic care, would have a better quality of life, lower rates of depressive symptoms, and less aggressive end-of-life care. Methods Study Design From June 7, 2006, to July 15, 2009, we enrolled ambulatory patients with newly diagnosed metastatic non small-cell lung cancer in a nonblinded, randomized, controlled trial of early palliative care integrated with standard oncologic care, as compared with standard oncologic care alone. The study was performed at Massachusetts General Hospital in Boston. Eligible patients were enrolled within 8 weeks after diagnosis and were randomly assigned to one of the two groups in a 1:1 ratio without stratification. Patients who were assigned to early palliative care met with a member of the palliative care team, which consisted of board-certified palliative care physicians and advanced-practice nurses, within 3 weeks after enrollment and at least monthly thereafter in the outpatient setting until death. Additional visits with the palliative care service were scheduled at the discretion of the patient, oncologist, or palliative care provider. General guidelines for the palliative care visits in the ambulatory setting were adapted from the National Consensus Project for Quality Palliative Care and were included in the study protocol. 14 Using a template in the electronic medical record, palliative care clinicians documented the care they provided according to these guidelines (see Table 1 in the Supplementary Appendix, available with the full text of this article at NEJM.org). Specific attention was paid to assessing physical and psychosocial symptoms, establishing goals of care, assisting with decision making regarding treatment, and coordinating care on the basis of the individual needs of the patient. 14,15 Patients who were randomly assigned to standard care were not scheduled to meet with the palliative care service unless a meeting was requested by the patient, the family, or the oncologist; those who were referred to the service did not cross over to the palliative care group or follow the specified palliative care protocol. All the participants continued to receive routine oncologic care throughout the study period. Before enrollment in the study was initiated, the protocol was approved by the Dana Farber/Partners CancerCare institutional review board. All participants provided written informed consent. The protocol, including the statistical analysis plan, is available at NEJM.org. All the authors attest that the study was performed in accordance with the protocol and the statistical analysis plan. Patients Patients who presented to the outpatient thoracic oncology clinic were invited by their medical on- 734 n engl j med 363;8 nejm.org august 19, 2010 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
33 Early Palliative Care for Metastatic Cancer cologists to enroll in the study; all the medical oncologists in the clinic agreed to approach, recruit, and obtain consent from their patients. Physicians were encouraged, but not required, to offer participation to all eligible patients; no additional screening or recruitment measures were used. Patients were eligible to participate if they had pathologically confirmed metastatic non small-cell lung cancer diagnosed within the previous 8 weeks and an Eastern Cooperative Oncology Group (ECOG) performance status of 0, 1, or 2 (with 0 indicating that the patient is asymptomatic, 1 that the patient is symptomatic but fully ambulatory, and 2 that the patient is symptomatic and in bed <50% of the day) 16 and were able to read and respond to questions in English. Patients who were already receiving care from the palliative care service were not eligible for participation in the study. Patient-Reported Measures Health-related quality of life was measured with the use of the Functional Assessment of Cancer Therapy Lung (FACT-L) scale, which assesses multiple dimensions of the quality of life (physical, functional, emotional, and social well-being) during the previous week. 17 In addition, the lungcancer subscale (LCS) of the FACT-L scale evaluates seven symptoms specific to lung cancer. The primary outcome of the study was the change from baseline to 12 weeks in the score on the Trial Outcome Index (TOI), which is the sum of the scores on the LCS and the physical well-being and functional well-being subscales of the FACT-L scale. Mood was assessed with the use of both the Hospital Anxiety and Depression Scale (HADS) and the Patient Health Questionnaire 9 (PHQ- 9). 18,19 The 14-item HADS, which consists of two subscales, screens for symptoms of anxiety and depression in the previous week. Subscale scores range from 0, indicating no distress, to 21, indicating maximum distress; a score higher than 7 on either HADS subscale is considered to be clinically significant. The PHQ-9 is a nine-item measure that evaluates symptoms of major depressive disorder according to the criteria of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). A major depressive syndrome was diagnosed if a patient reported at least five of the nine symptoms of depression on the PHQ-9, with one of the five symptoms being either anhedonia or depressed mood. Symptoms had to be present for more than half the time, except for the symptom of suicidal thoughts, which was included in the diagnosis if it was present at any time. Measures of Health Care Use Data were collected from the electronic medical record on the use of health services and end-oflife care, including anticancer therapy, medication prescriptions, referral to hospice, hospital admissions, emergency department visits, and the date and location of death. Patients were classified as having received aggressive care if they met any of the following three criteria: chemotherapy within 14 days before death, no hospice care, or admission to hospice 3 days or less before death Finally, we assessed whether patients resuscitation preferences were documented in the outpatient electronic medical record. 23 Data Collection Participants completed baseline questionnaires before randomization. Follow-up assessments of quality of life and mood were performed at 12 weeks (or at an outpatient clinic visit within 3 weeks before or after that time point). Participants who had no scheduled clinic visits within this period received the questionnaires by mail. When responses on questionnaires were incomplete, research staff documented the reasons for which the participant did not give a full response. Statistical Analysis Data obtained through December 1, 2009, were included in the analyses. The primary outcome was the change in the score on the TOI from baseline to 12 weeks. We estimated that with 120 patients, the study would have 80% power to detect a significant between-group difference in the change in the TOI score from baseline to 12 weeks, with a medium effect size of 0.5 SD. 24 The protocol was amended in August 2008 to allow for the enrollment of an additional 30 participants in order to compensate for the loss of any patients to follow-up. Statistical analyses were performed with the use of SPSS software, version 16.0 (SPSS). Descriptive statistics were used to estimate the frequencies, means, and standard deviations of the study variables. Differences between study groups in baseline characteristics and clinical outcomes were assessed with the use of two-sided Fisher s exact tests and chi-square tests for categorical n engl j med 363;8 nejm.org august 19, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
34 The new england journal of medicine variables and independent-samples Student s t-tests for continuous variables. Multivariate linear regression analyses, adjusted for baseline scores, were used to examine the effect of early palliative care on quality-of-life outcomes. For intentionto-treat analyses, we used the conservative method of carrying baseline values forward to account for all missing patient-reported outcome data, including data that were missing owing to death. Survival time was calculated from the date of enrollment to the date of death with the use of the Kaplan Meier method. Data from patients who were alive at the last follow-up (December 1, 2009) were censored on that date. A Cox proportional-hazards model was used to assess the effect of early palliative care on survival, with adjustment for demographic characteristics and baseline ECOG performance status. Results Baseline Characteristics of the Patients A total of 151 patients were enrolled in the study (see the figure in the Supplementary Appendix). The percentage of patients enrolled was similar for each of the thoracic oncologists in the clinic. Table 1. Baseline Characteristics of the Study Participants.* Variable Standard Care (N = 74) Early Palliative Care (N = 77) P Value Age yr 64.87± ± Female sex no. (%) 36 (49) 42 (55) 0.52 Race no. (%) 0.06 White 70 (95) 77 (100) Black 3 (4) 0 Asian 1 (1) 0 Hispanic or Latino ethnic group 1 (1) 1 (1) 1.00 Marital status no. (%) 1.00 Married 45 (61) 48 (62) Single 9 (12) 9 (12) Divorced or separated 12 (16) 12 (16) Widowed 8 (11) 8 (10) ECOG performance status no. (%) (41) 26 (34) 1 35 (47) 46 (60) 2 9 (12) 5 (6) Presence of brain metastases no. (%) 19 (26) 24 (31) 0.48 Initial anticancer therapy no. (%) Platinum-based combination chemotherapy 35 (47) 35 (45) Single agent 3 (4) 9 (12) Oral EGFR tyrosine kinase inhibitor 6 (8) 6 (8) Radiotherapy 26 (35) 27 (35) Chemoradiotherapy 3 (4) 0 No chemotherapy 1 (1) 0 Receipt of initial chemotherapy as part of a clinical trial no. (%) Never smoked or smoked 10 packs/yr no./ total no. (%) Assessment of mood symptoms no./total no. (%) HADS** (27) 16 (21) /73 (22) 18/76 (24) 0.85 Anxiety subscale 24/72 (33) 28/77 (36) 0.73 Depression subscale 18/72 (25) 17/77 (22) 0.70 PHQ-9 major depressive syndrome 12/72 (17) 9/76 (12) n engl j med 363;8 nejm.org august 19, 2010 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
35 Early Palliative Care for Metastatic Cancer Table 1. (Continued.) Variable Scores on quality-of-life measures Standard Care (N = 74) Early Palliative Care (N = 77) P Value FACT-L scale 91.7± ± Lung-cancer subscale 18.7± ±4.4 Trial Outcome Index 55.3± ±13.4 * Plus minus values are means ±SD. Percentages may not total 100 because of rounding. ECOG denotes Eastern Cooperative Oncology Group, EFGR epidermal growth factor receptor, FACT-L Functional Assessment of Cancer Therapy Lung, HADS Hospital Anxiety and Depression Scale, and PHQ-9 Patient Health Questionnaire 9. P values were calculated with the use of two-sided chi-square and Fisher s exact tests for categorical variables and the independent-samples Student s t-tests for continuous variables. Race or ethnic group was self-reported. The P value is for the between-group comparison of the proportions of patients who were white and those who were members of a minority group (black and Asian), calculated with the use of Fisher s exact test. An ECOG performance status of 0 indicates that the patient is asymptomatic, 1 that the patient is symptomatic but fully ambulatory, and 2 that the patient is symptomatic and in bed less than 50% of the day. The P value is for the between-group comparison of the proportion of patients receiving platinum-based combination chemotherapy and the proportion receiving other treatments, calculated with the use of Fisher s exact test. ** The HADS consists of two subscales, one for symptoms of anxiety and one for symptoms of depression. Subscale scores range from 0, indicating no distress, to 21, indicating maximum distress; a score higher than 7 indicates clinically meaningful anxiety or depression. The PHQ-9 is a nine-item measure that evaluates symptoms of major depressive disorder according to the criteria of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). A major depressive syndrome was diagnosed if a patient reported at least five of the nine symptoms of depression on the PHQ-9, with one of the five symptoms being either anhedonia or depressed mood. Symptoms had to be present for more than half the time, except for the symptom of suicidal thoughts, which was included in the diagnosis if it was present at any time. The quality of life was assessed with the use of three measures: the FACT-L scale, on which scores range from 0 to 136, with higher scores indicating a better quality of life; the lung-cancer subscale of the FACT-L scale, on which scores range from 0 to 28, with higher scores indicating fewer symptoms; and the Trial Outcome Index, which is the sum of the scores on the lung-cancer, physical well-being, and functional well-being subscales of the FACT-L scale (scores range from 0 to 84, with higher scores indicating a better quality of life). No significant differences in demographic characteristics or overall survival were seen between the study participants and eligible patients who were not enrolled in the study. The baseline characteristics were well matched between the two study groups (Table 1). Known prognostic factors, including age, sex, ECOG performance status, presence or absence of brain metastases, smoking status, and initial anticancer therapy, were also balanced between the study groups. Although genetic testing was not routinely performed, the proportions of patients with mutations in the epidermal growth factor gene (EGFR) were similar between the study groups among the patients who underwent testing (9% in the palliative care group and 12% in the standard-treatment group, P = 0.76). No significant between-group differences were seen in baseline quality of life or mood symptoms. Palliative-Care Visits All the patients assigned to early palliative care, except for one patient who died within 2 weeks after enrollment, had at least one visit with the palliative care service by the 12th week. The average number of visits in the palliative care group was 4 (range, 0 to 8). Ten patients who received standard care (14%) had a palliative care consultation in the first 12 weeks of the study, primarily to address the management of symptoms, with seven patients having one visit and three having two visits. Quality-of-Life and Mood Outcomes A comparison of measures of quality of life at 12 weeks showed that the patients assigned to early palliative care had significantly higher scores than did those assigned to standard care, for the total FACT-L scale, the LCS, and the TOI, with effect sizes in the medium range (Table 2). Patients in the palliative care group had a 2.3-point increase in mean TOI score from baseline to 12 weeks, as compared with a 2.3-point decrease in the standard care group (P = 0.04) (Fig. 1). With the use of linear regression to control for baseline quality-of-life values, the group assignment significantly predicted scores at 12 weeks on the total FACT-L scale (adjusted difference in mean n engl j med 363;8 nejm.org august 19, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
36 The new england journal of medicine Table 2. Bivariate Analyses of Quality-of-Life Outcomes at 12 Weeks.* Variable Standard Care (N = 47) Early Palliative Care (N = 60) Difference between Early Care and Standard Care (95% CI) P Value Effect Size FACT-L score 91.5± ± ( ) LCS score 19.3± ± ( ) TOI score 53.0± ± ( ) * Plus minus values are means ±SD. Quality of life was assessed with the use of three scales: the Functional Assessment of Cancer Therapy Lung (FACT-L) scale, on which scores range from 0 to 136, with higher scores indicating better quality of life; the lung-cancer subscale (LCS) of the FACT-L scale, on which scores range from 0 to 28, with higher scores indicating fewer symptoms; and the Trial Outcome Index (TOI), which is the sum of the scores on the LCS and the physical well-being and functional well-being subscales of the FACT-L scale (scores range from 0 to 84, with higher scores indicating better quality of life). The P value was calculated with the use of two-sided Student s t-tests for independent samples. The effect size was determined with the use of Cohen s d statistic, which is a measure of the difference between two means (in this case, the mean in the group assigned to early palliative care group minus the mean in the group assigned to standard care) divided by a standard deviation for the pooled data. According to the conventional classification, an effect size of 0.20 is small, 0.50 moderate, and 0.80 large. [±SE] scores, 5.4±2.4; 95% confidence interval [CI], 0.7 to 10.0; P = 0.03) and the TOI (adjusted difference in mean scores, 5.2±1.8; 95% CI, 1.6 to 8.9; P = 0.005), but not on the LCS (adjusted difference in mean scores, 1.0±0.6; 95% CI, 0.2 to 2.3; P = 0.12). In addition, the percentage of patients with depression at 12 weeks, as measured by the HADS and PHQ-9, was significantly lower in the palliative care group than in the standard care group, although the proportions of patients receiving new prescriptions for antidepressant drugs were similar in the two groups (approximately 18% in both groups, P = 1.00) (Fig. 2). The percentage of patients with elevated scores for symptoms of anxiety did not differ significantly between the groups. The figure in the Supplementary Appendix includes an explanation of missing data according to study group. There was no significant association between missing data on patient-reported outcomes at 12 weeks and any baseline characteristic (although there was a trend toward a significant association between missing data and assigned treatment [P = 0.07]). When we carried the baseline scores of the participants forward for the missing data on patient-reported outcomes, all primary treatment effects were replicated with respect to quality of life (P = 0.04 for the 12-week FACT-L score, P = 0.01 for the 12-week LCS score, P = 0.04 for the 12-week TOI score, and P = 0.04 for the mean change from baseline to 12 weeks in the TOI score) and mood (P = 0.04 for the comparison of patients with elevated scores on the HADS depression subscale, and P = 0.02 for the comparison of patients with symptoms of major depression on the PHQ-9). End-of-Life Care At the time of the analysis of end-of-life care, 105 participants (70%) had died; the median duration of follow-up among participants who died was 5.7 months. Within this subsample, a greater percentage of patients in the group assigned to standard care than in the group assigned to early palliative care received aggressive end-of-life care (54% [30 of 56 patients] vs. 33% [16 of 49 patients], P = 0.05). In addition, fewer patients in the standard care group than in the palliative care group had resuscitation preferences documented in the outpatient electronic medical record (28% [11 of 39 patients who had preferences documented during the course of the study] vs. 53% [18 of 34 patients], P = 0.05). The study did not have adequate power to examine specific indicators of aggressive care at the end of life. However, analyses of various measures of utilization, such as rates of hospitalization and emergency department visits (Table 2 in the Supplementary Appendix), as well as the duration of hospice care (median duration, 11 days in the palliative care group vs. 4 days in the standard care group; P = 0.09 with the use of the Wilcoxon rank-sum test), suggested an improvement in the quality of care with early palliative care. Despite receiving less aggressive end-of-life care, patients in the palliative care group had significantly longer survival than those in the standard care group (median survival, 11.6 vs. 8.9 months; P = 0.02) (Fig. 3). 738 n engl j med 363;8 nejm.org august 19, 2010 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
37 Early Palliative Care for Metastatic Cancer Figure 1. Mean Change in Quality-of-Life Scores from Baseline to 12 Weeks in the Two Study Groups. Quality of life was assessed with the use of the Functional Assessment of Cancer Therapy Lung (FACT-L) scale, on which scores range from 0 to 136, with higher scores indicating a better quality of life; the lung-cancer subscale (LCS) of the FACT-L scale, on which scores range from 0 to 28, with higher scores indicating fewer symptoms; and the Trial Outcome Index (TOI), which is the sum of the scores on the LCS and the physical well-being and functional well-being subscales of the FACT-L scale (scores range from 0 to 84, with higher scores indicating a better quality of life). With study group as the independent variable, two-sided independent-samples Student s t-tests showed a trend toward a significant between-group difference in the mean (±SD) change in scores from baseline to week 12 on the FACT-L scale ( 0.4±13.8 in the standard care group vs. 4.2±13.8 in the palliative care group; difference between groups, 4.6; 95% confidence interval [CI], 0.8 to 9.9; P = 0.09) (Panel A), no significant betweengroup difference in the mean change in scores on the LCS (0.3±4.0 and 0.8±3.6 in the two groups, respectively; difference between groups, 0.5; 95% CI, 1.0 to 2.0; P = 0.50) (Panel B), and a significant between-group difference in the mean change in scores on the TOI ( 2.3±11.4 vs. 2.3±11.2; difference between groups, 4.6; 95% CI, 0.2 to 8.9; P = 0.04) (Panel C). Data are from the 47 patients in the standard care group and the 60 patients in the palliative care group who completed the 12-week assessments. I bars indicate 95% confidence intervals. A FACT-L Mean Change B LCS Mean Change C TOI Standard Care Standard Care Early Palliative Care Early Palliative Care Discussion 5.0 Mean Change Standard Care Early Palliative Care This study shows the effect of palliative care when it is provided throughout the continuum of care for advanced lung cancer. Early integration of palliative care with standard oncologic care in patients with metastatic non small-cell lung cancer resulted in survival that was prolonged by approximately 2 months and clinically meaningful improvements in quality of life and mood. Moreover, this care model resulted in greater documentation of resuscitation preferences in the outpatient electronic medical record, as well as less aggressive care at the end of life. Less aggressive end-of-life care did not adversely affect survival. Rather, patients receiving early palliative care, as compared with those receiving standard care alone, had improved survival. Previous data have shown that a lower quality of life and depressed mood are associated with shorter survival among patients with metastatic non smallcell lung cancer We hypothesize that improvements in both of these outcomes among patients assigned to early palliative care may account for the observed survival benefit. In addition, the integration of palliative care with standard oncologic care may facilitate the optimal and appropriate administration of anticancer therapy, especially during the final months of life. With earlier referral to a hospice program, patients may receive care that results in better management of symptoms, leading to stabilization of their condition and prolonged survival. These hypotheses require further study. Improving quality of life and mood in patients n engl j med 363;8 nejm.org august 19, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
38 The new england journal of medicine Patients with Mood Symptoms (%) Standard care Early palliative care HADS-D HADS-A PHQ-9 Figure 2. Twelve-Week Outcomes of Assessments of Mood. Depressive symptoms were assessed with the use of the Hospital Anxiety and Depression Scale (HADS), which consists of two subscales, one for symptoms of anxiety (HADS-A) and one for symptoms of depression (HADS-D) (subscale scores range from 0, indicating no distress, to 21, indicating maximum distress; a score higher than 7 on either HADS subscale is considered to be clinically significant) and with the use of the Patient Health Questionnaire 9 (PHQ-9). The PHQ-9 is a nine-item measure that evaluates symptoms of major depressive disorder according to the criteria of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). A major depressive syndrome was diagnosed if a patient reported at least five of the nine symptoms of depression on the PHQ-9, with one of the five symptoms being either anhedonia or depressed mood. Symptoms had to be present for more than half the time, except for the symptom of suicidal thoughts, which was included in the diagnosis if it was present at any time. The percentages of patients with mood symptoms, assessed on the basis of each of these measures, in the group assigned to standard treatment and the group assigned to early palliative care, respectively, are as follows: HADS-D, 38% (18 of 47 patients) versus 16% (9 of 57), P = 0.01; HADS-A, 30% (14 of 47 patients) and 25% (14 of 57), respectively; P = 0.66; and PHQ-9, 17% (8 of 47 patients) versus 4% (2 of 57); P = The analyses were performed with the use of a two-sided Fisher s exact test. with metastatic non small-cell lung cancer is a formidable challenge, given the progressive nature of the illness. 28 The improvement we observed in the quality of life among patients assigned to early palliative care, as indicated by a mean change in the TOI score by 12 weeks that was approximately 5 points higher in the palliative care group than in the standard care group, is similar to the improvement in the quality of life that has been observed among patients who have a response to cisplatin-based chemotherapy. 29 Most studies show that there is a deterioration in the quality of life over time, which is consistent with the results in the standard care group in our study Despite similar cancer therapies in our two study groups, the patients assigned to early palliative care had an improved quality of life, as compared with those receiving standard care. Rates of depression also differed significantly between the groups, with approximately half as many patients in the palliative care group as in the standard care group reporting clinically significant depressive symptoms on the HADS, and this effect was not due to a betweengroup difference in the use of antidepressant agents. To date, evidence supporting a benefit of palliative care is sparse, with most studies having notable methodologic weaknesses, especially with respect to quality-of-life outcomes. 8 One study with sufficient power to examine quality-of-life outcomes showed that among patients receiving radiation therapy, a multidisciplinary intervention focused on education, behavioral modification, and coping style resulted in improvements in the quality of life. 33 A recent study showed that Project ENABLE (Educate, Nurture, Advise, Before Life Ends), a telephone-based, psychoeducational program for patients with advanced cancer, significantly improved both quality of life and mood. 34 However, the percentage of patients who completed the study assessments was somewhat low, and the study did not use a traditional palliative care model. Our study also showed that early outpatient palliative care for patients with advanced cancer can alter the use of health care services, including care at the end of life. Other studies of outpatient palliative care have failed either to investigate these outcomes or to show an effect on the use of resources. 5,34,35 In our trial, significantly more patients in the group assigned to early palliative care than in the standard care group had resuscitation preferences documented in the outpatient electronic medical record, an essential step in clarifying and ensuring respect for patients wishes about their care at the end of life. 36 Early introduction of palliative care also led to less aggressive end-of-life care, including reduced chemotherapy and longer hospice care. Given the trends toward aggressive and costly care near the end of life among patients with cancer, timely introduction of palliative care may serve to mitigate unnecessary and burdensome personal and societal costs. 20, n engl j med 363;8 nejm.org august 19, 2010 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
39 Early Palliative Care for Metastatic Cancer Our study has several advantages over previous studies, in which investigators have often relied on referrals to palliative care instead of using a recruitment approach designed to obtain a representative sample. 5,35 Because all patients with a new diagnosis of metastatic non small-cell lung cancer were eligible for enrollment in our study, we extended the generalizability of our findings. Another strength of our trial was the low rate of loss to follow-up and the high percentage of participants who completed the study assessments. In addition, the dropout rate by week 12 was less than 1%, further supporting the feasibility and acceptability of early palliative care. Finally, the trial was adequately powered to detect changes in both quality of life and mood, and we prospectively collected data on end-oflife care. Several limitations of the study deserve mention. It was performed at a single, tertiary care site with a specialized group of thoracic oncology providers and palliative care clinicians, thereby limiting generalization of the results to other care settings or patients with other types of cancer. In addition, because the sample lacked diversity with respect to race and ethnic group, we were unable to assess the effect of these important factors on study outcomes. Although we used a randomized, controlled design, both the patients and the clinicians were aware of the study assignments. To account for possible influences of care that are not specific to the palliative care provided, follow-up investigations should include a control group that receives a similar amount of attention. In addition, we did not deny palliative care consultations to participants receiving standard care, and a small minority of patients in the standard care group was seen by the palliative care team. The data from these patients were analyzed with the data from their assigned study group (standard care), a factor that may have diluted our findings. Finally, carrying the last observation forward for all missing data in the intention-to-treat analyses is a conservative approach; therefore, the actual treatment effect of early palliative care may be greater than we report. Early integration of palliative care for patients with metastatic non small-cell lung cancer is a clinically meaningful and feasible care model that has effects on survival and quality of life that are similar to the effects of first-line chemotherapy in such patients. 28,38,39 As compared with Patients Surviving (%) Months Standard care Early palliative care Figure 3. Kaplan Meier Estimates of Survival According to Study Group. Survival was calculated from the time of enrollment to the time of death, if it occurred during the study period, or to the time of censoring of data on December 1, Median estimates of survival were as follows: 9.8 months (95% confidence interval [CI], 7.9 to 11.7) in the entire sample (151 patients), 11.6 months (95% CI, 6.4 to 16.9) in the group assigned to early palliative care (77 patients), and 8.9 months (95% CI, 6.3 to 11.4) in the standard care group (74 patients) (P = 0.02 with the use of the log-rank test). After adjustment for age, sex, and baseline Eastern Cooperative Oncology Group performance status, the group assignment remained a significant predictor of survival (hazard ratio for death in the standard care group, 1.70; 95% CI, 1.14 to 2.54; P = 0.01). Tick marks indicate censoring of data. the study participants who received standard care, those who were assigned to early palliative care had improved mood, more frequent documentation of resuscitation preferences, and less aggressive end-of-life care. Although our findings must be replicated in a variety of care settings and cancer populations, the results nonetheless offer great promise for alleviating distress in patients with metastatic disease and addressing critical concerns regarding the use of health care services at the end of life. Supported by an American Society of Clinical Oncology Career Development Award and philanthropic gifts from the Joanne Hill Monahan Cancer Fund and Golf Fights Cancer. Dr. Temel reports receiving payment for developing continuing medical education (CME) programs from InforMEDical; and Dr. Lynch, serving on the board of Infinity Pharmaceuticals, receiving consulting fees from Roche, Boehringer Ingelheim, Merck, AstraZeneca, Bristol-Myers Squibb, and Sanofi-Aventis, royalties from Partners HealthCare, and payment for developing CME programs from InforMEDical. No other potential conflict of interest relevant to this article was reported. Disclosure forms provided by the authors are available with the full text of this article at NEJM.org. n engl j med 363;8 nejm.org august 19, The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
40 Early Palliative Care for Metastatic Cancer References 1. Mongan JJ, Ferris TG, Lee TH. Options for slowing the growth of health care costs. N Engl J Med 2008;358: Weinstein MC, Skinner JA. Comparative effectiveness and health care spending implications for reform. N Engl J Med 2010;362: Ferris FD, Bruera E, Cherny N, et al. Palliative cancer care a decade later: accomplishments, the need, next steps from the American Society of Clinical Oncology. J Clin Oncol 2009;27: Levy MH, Back A, Benedetti C, et al. NCCN clinical practice guidelines in oncology: palliative care. J Natl Compr Canc Netw 2009;7: Follwell M, Burman D, Le LW, et al. Phase II study of an outpatient palliative care intervention in patients with metastatic cancer. J Clin Oncol 2009;27: Jordhøy MS, Fayers P, Loge JH, Ahlner- Elmqvist M, Kaasa S. Quality of life in palliative cancer care: results from a cluster randomized trial. J Clin Oncol 2001; 19: Morita T, Akechi T, Ikenaga M, et al. Late referrals to specialized palliative care service in Japan. J Clin Oncol 2005;23: Zimmermann C, Riechelmann R, Krzyzanowska M, Rodin G, Tannock I. Effectiveness of specialized palliative care: a systematic review. JAMA 2008;299: Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, CA Cancer J Clin 2009;59: Hopwood P, Stephens RJ. Depression in patients with lung cancer: prevalence and risk factors derived from quality-oflife data. J Clin Oncol 2000;18: Hopwood P, Stephens RJ. Symptoms at presentation for treatment in patients with lung cancer: implications for the evaluation of palliative treatment. Br J Cancer 1995;71: Lutz S, Norrell R, Bertucio C, et al. Symptom frequency and severity in patients with metastatic or locally recurrent lung cancer: a prospective study using the Lung Cancer Symptom Scale in a community hospital. J Palliat Med 2001;4: Temel JS, Jackson VA, Billings JA, et al. Phase II study: integrated palliative care in newly diagnosed advanced non-smallcell lung cancer patients. J Clin Oncol 2007;25: Clinical practice guidelines for quality palliative care. 2nd ed. Pittsburgh: National Consensus Project, (Accessed July 23, 2010, at Jackson VA, Jacobsen JC, Greer J, et al. Components of early intervention outpatient palliative care consultation in patients with incurable NSCLC. J Clin Oncol 2009;27:Suppl: abstract. 16. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5: Cella DF, Bonomi AE, Lloyd SR, Tulsky DS, Kaplan E, Bonomi P. Reliability and validity of the Functional Assessment of Cancer Therapy-Lung (FACT-L) quality of life instrument. Lung Cancer 1995;12: Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983;67: Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001; 16: Earle CC, Landrum MB, Souza JM, Neville BA, Weeks JC, Ayanian JZ. Aggressiveness of cancer care near the end of life: is it a quality-of-care issue? J Clin Oncol 2008;26: American Society of Clinical Oncology Quality Oncology Practice Initiative. ASCO QOPI summary of measures. Fall (Accessed July 23, 2010, at qopi.asco.org/documents/qopifall2009 MeasuresSummary pdf.) 22. Tang ST, Wu SC, Hung YN, Chen JS, Huang EW, Liu TW. Determinants of aggressive end-of-life care for Taiwanese cancer decedents, 2001 to J Clin Oncol 2009;27: Temel JS, Greer JA, Admane S, et al. Code status documentation in the outpatient electronic medical records of patients with metastatic cancer. J Gen Intern Med 2010;25: Cella D. The Functional Assessment of Cancer Therapy Lung and Lung Cancer Subscale assess quality of life and meaningful symptom improvement in lung cancer. Semin Oncol 2004;31:Suppl 9: Maione P, Perrone F, Gallo C, et al. Pretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: a prognostic analysis of the Multicenter Italian Lung Cancer in the Elderly Study. J Clin Oncol 2005;23: Movsas B, Moughan J, Sarna L, et al. Quality of life supersedes the classic prognosticators for long-term survival in locally advanced non-small-cell lung cancer: an analysis of RTOG J Clin Oncol 2009;27: Pirl WF, Temel JS, Billings A, et al. Depression after diagnosis of advanced non-small cell lung cancer and survival: a pilot study. Psychosomatics 2008;49: Brown J, Thorpe H, Napp V, et al. Assessment of quality of life in the supportive care setting of the Big Lung Trial in non-small-cell lung cancer. J Clin Oncol 2005;23: Cella D, Eton DT, Fairclough DL, et al. What is a clinically meaningful change on the Functional Assessment of Cancer Therapy-Lung (FACT-L) Questionnaire? Results from Eastern Cooperative Oncology Group (ECOG) Study J Clin Epidemiol 2002;55: Bonomi P, Kim K, Fairclough D, et al. Comparison of survival and quality of life in advanced non-small-cell lung cancer patients treated with two dose levels of paclitaxel combined with cisplatin versus etoposide with cisplatin: results of an Eastern Cooperative Oncology Group trial. J Clin Oncol 2000;18: Langer CJ, Manola J, Bernardo P, et al. Cisplatin-based therapy for elderly patients with advanced non-small-cell lung cancer: implications of Eastern Cooperative Oncology Group 5592, a randomized trial. J Natl Cancer Inst 2002;94: Sandler AB, Nemunaitis J, Denham C, et al. Phase III trial of gemcitabine plus cisplatin versus cisplatin alone in patients with locally advanced or metastatic nonsmall-cell lung cancer. J Clin Oncol 2000; 18: Rummans TA, Clark MM, Sloan JA, et al. Impacting quality of life for patients with advanced cancer with a structured multidisciplinary intervention: a randomized controlled trial. J Clin Oncol 2006; 24: Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial. JAMA 2009;302: Rabow MW, Dibble SL, Pantilat SZ, McPhee SJ. The comprehensive care team: a controlled trial of outpatient palliative medicine consultation. Arch Intern Med 2004;164: Walling A, Lorenz KA, Dy SM, et al. Evidence-based recommendations for information and care planning in cancer care. J Clin Oncol 2008;26: Emanuel EJ, Ash A, Yu W, et al. Managed care, hospice use, site of death, and medical expenditures in the last year of life. Arch Intern Med 2002;162: Non-Small Cell Lung Cancer Collaborative Group. Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. BMJ 1995; 311: Spiro SG, Rudd RM, Souhami RL, et al. Chemotherapy versus supportive care in advanced non-small cell lung cancer: improved survival without detriment to quality of life. Thorax 2004;59: Copyright 2010 Massachusetts Medical Society. 742 n engl j med 363;8 nejm.org august 19, 2010 The New England Journal of Medicine Downloaded from nejm.org at MOUNT SINAI SCHOOL OF MEDICINE on November 14, For personal use only. No other uses without permission. Copyright 2010 Massachusetts Medical Society. All rights reserved.
41 Paul Menzel & Bonnie Steinbock


42 ADVANCE DIRECTIVES, DEMENTIA, AND PHYSICIAN-ASSISTED DEATH Bonnie Steinbock, PhD, U of Albany/SUNY Paul Menzel, PhD, Pacific Lutheran University Freedom of Choice at the End of Life: Patients Rights in a Shifting Legal and Political Landscape New York Law School, Nov. 16, 2012
43 Physician-Assisted Death (PAD) and Contemporary Competence Almost all jurisdictions where PAD is legal require contemporary competence Intended to ensure that PAD limited to: people who really want to die have cognitive capacity to make such momentous decision not suffering from depression or any disorder that impairs judgment
44 Physician-Assisted Death and Contemporary Competence (continued) Along with terminal illness, contemporary competence is regarded as an essential safeguard against mistake and abuse
45 Implications of Contemporary Competence Requirement Rules out PAD for all patients with dementia, even if terminally ill and suffering terrible and unrelievable pain Rules out PAD for individuals with strong, long-held and unwavering desires not to end their lives in dementia Many are more afraid of living in severe dementia for years than a few months of suffering at the end of life
46 Global Context From 2000 to 2040, number of people in the world over 85 will nearly quadruple Almost half of those over 85 have some form of dementia Issue must be faced: Do competent individuals have a right to be assisted in dying when they become severely demented?

47 PAD in The Netherlands Both physician-assisted suicide and euthanasia legal by statute since 2002 Two doctors must certify that: Patient s decision is voluntary and informed Desire to die stems from hopeless and unbearable suffering
48 PAD in The Netherlands (cont d) 2011 Dutch woman in severe dementia received euthanasia frequently crying, with longstanding request not to be in nursing home New guidelines issued: Voluntariness requirement can be satisfied by evidence that patient wanted euthanasia, even if now no longer competent
49 Advance Directives (ADs) ADs created by competent individuals to control medical decisions when they become incompetent Can thereby refuse medical treatment, including the most critical and life-saving treatment Includes medically administered nutrition and hydration, withholding/withdrawing of which ensures death
 Technically advance directives for physician-assisted dying (ADPAD) A way to satisfy")
50 Advance Directives (cont d) Where aid-in-dying is legal (OR, WA), should the right to die be expanded to avoid living in dementia? Could be expressed in advance euthanasia directives (AEDs) Technically advance directives for physician-assisted dying (ADPAD) A way to satisfy voluntariness requirement
51 Arguments for Expansion (1) Same as basic moral arguments in favor of PAD 1. Respect for autonomy Provides basis for the right to refuse even life-sustaining treatment Inconsistent to allow people to die by refusing treatment or refusing food and water, but not let them have their doctors help them with quick, painless death
52 Arguments for Expansion (2) Same as basic moral arguments in favor of PAD (continued ) 2. Avoidance of suffering Not limited to competent individuals; those in dementia may suffer as much, or more
53 Arguments Against Expansion Disability critique Problem of precedent autonomy the then-self/now-self problem The possibility of a change of mind
54 The Disability Critique People often think prospectively that living with a particular disability would be unbearable, when it turns out not to be adaptation Some positive aspects to dementia Ignorance about and prejudice toward disability
55 The Disability Critique (cont d) Sub-standard conditions in nursing homes Fix it, rather than help people to die Desire to die need not be based on ignorance, prejudice, failure to appreciate adaptation, or fear of poor care Can be based on convictions about the meaning of one s life

56 The Then-self/Now-self Problem Person who wrote the AD (then-self) has radically changed in dementia No longer has the same interests Doesn t remember writing the AD Doesn t care about autonomy Doesn t find her very diminished life unbearable Scrap autonomy, focus on best interests of the patient as she is now (now-self)
57 Autonomy and Previously Competent Choosers To focus only on interests of the nowself treats the person as if she had never been competent Ignores most of the elements in her life that made her the person she is The competent individual is the one to decide what s in her own best interest when she is no longer competent to make decisions
58 Changing One s Mind Someone in dementia may come to value new activities, find life worth living Why should we hold her to an AD she no longer believes in? But at some point in dementia, no longer possible to change one s mind Not enough of a mind to change
59 Importance of Narrative Identity Our conception of ourselves values, character, commitments For many (not all), one s stake in continued existence is connected with narrative identity What makes survival into severe dementia horrifying is the loss of self How people end their lives is crucial part of the meaning of their lives
60 Always Respect AEDs? Depends on the details of the cases Strongest case: where there s a clear, knowledgeable AED and contemporary suffering 2011 Dutch case Somewhat less strong: no suffering, but no interest or enjoyment in living Case for respecting AED weakens as contemporary interests in living strengthen
61 A Sliding Scale Approach An AED written by informed, competent person gains in authority as the person s abilities to enjoy life decrease An AED loses authority where the person is engaged in activities and gives every evidence of valuing her life Helping her to die not in her best interest Conflicts with social, professional values The argument for AEDs does not require that they be carried out in every case
62 From PAD to AEDs Strong basis of PAD is respect for autonomy People more concerned re loss of autonomy, dignity, meaningful activity than about pain control all apply in dementia Primary basis of ADs is respect for autonomy one does not lose one s rights with incompetence Combine PAD and ADs: the logical result is AEDs w/ strong safeguards

63 Conclusion Strong case for ADs for dementia To give people control over the way they die, in both refusing treatment and requesting aid-in-dying Countervailing considerations How informed the AD is Possibility of a change of mind Stake of the person in continued life A sliding scale allows us to differentiate between cases
64 DRAFT DRAFT DRAFT (November 2012) NOT FOR TO BE DISTRIBUTED OR QUOTED UNLESS PERMITTED BY AUTHORS Advance Directives, Dementia, and Physician-Assisted Death Paul T. Menzel and Bonnie Steinbock I. Introduction Almost all jurisdictions where physician-assisted death (PAD) 1 is legal require that the requesting individual be competent to make medical decisions at time of assistance. 2 The requirement of contemporary competence is intended to ensure that PAD is limited to people who really want to die and have the cognitive ability to make a final choice of such enormous import. Along with terminal illness, defined as prognosis of death within six months, contemporary competence is regarded as an important safeguard against mistake and abuse, arguably the strongest objections to legalizing PAD. The insistence on contemporary competence is problematic. It means that someone who has dementia is ruled out as a candidate for PAD, even if she is terminally ill and suffering terrible and unrelievable pain. It also rules out individuals with strong and unwavering desires not to end their life in dementia. Many people are more afraid of living in a severely demented state for years than they fear a few months of suffering at the end of life. 3 They think that they have just as much right to choose death to avoid living long in dementia as they do to choose death when terminally ill. This issue will become particularly pressing as the world s population ages. By 2040, the number of people over 85 will nearly quadruple from what it was in Studies have shown that almost half of people over 85 have some form of dementia. 5 About 5.4 million Americans have Alzheimer s disease, the most common form. The numbers will rise progressively over the next several decades. Thus, the issue must be squarely faced: Do competent individuals have a right to decide to be assisted in dying when they become severely demented? The question has sparked a great deal of discussion in The Netherlands, where PAD both assisted suicide and voluntary euthanasia has been legal by statute since Two doctors must certify that the patient s decision is voluntary and informed, and that the desire to die stems from hopeless and unbearable suffering. In 2011 an important Dutch case, to which we return below,
65 Advance Directives, Dementia, and Physician-Assisted Death raised specifically the question of whether the voluntariness requirement requires contemporaneous competence. One way in which the voluntariness requirement might be satisfied would be with advance directives. They would be written by competent individuals, expressing their desire to be helped to die when they are demented, and no longer capable of making medical decisions. Such directives, written in jurisdictions where euthanasia is permitted such as The Netherlands, are known as advance euthanasia directives (AEDs). Obviously, where euthanasia is illegal, there cannot be operative advance euthanasia directives. However, in jurisdictions that allow for aid-in-dying, but not euthanasia, individuals might be allowed, while they are competent, to write advance directives asking for assisted dying in severe dementia. In this paper, we argue that such directives should be permitted and, in many cases, followed. The insistence on contemporaneous competence is not warranted. When carefully written, advance directives for assisted death can satisfy the voluntariness requirement, which is the rationale for the requirement of contemporary competence. Technically, such directives, if created in states where PAS is legal but euthanasia is illegal, would be advance directives for physician assisted suicide (ADPAS). Instead of using this awkward neologism, we use the shorter term AED. Though we will argue that AEDs can be morally justified, the issue is complex and multifaceted. One complexity has to do with the range of cognitive abilities and quality of life in dementia. We recognize that in some cases, the demented person may change her mind about preferring death to living with dementia. In that case respect for autonomy requires us not to hold the person to her AED. In some other cases, moreover, even where there has been no change of mind, due consideration of the demented person s best interests, as well as societal considerations, point toward not implementing an AED. Thus the question of whether people should be able to create AEDs to avoid prolonged life in dementia does not have a simple yes-or-no answer, but depends on the details of cases. In the remainder of this introduction we first set the stage by briefly reviewing the main arguments in favor of PAD. It turns out that they apply not only to terminal illness but also to avoiding prolonged life in dementia. Next we describe the highly relevant developing situation in The Netherlands. Section II then lays out some basic information about dementia. Section III considers the disability critique of attitudes toward living in dementia. Sections IV and V take up the important challenges to advance directives from Rebecca Dresser and John Robertson. In sections VI and VII we elaborate the debate between Ronald Dworkin and Agnieszka Jaworska on 2
66 Advance Directives, Dementia, and Physician-Assisted Death respecting autonomy and argue that neither has got the issue exactly right. In the Jaworska section we begin to delineate our own view, which we flesh out in detail in sections VIII-X. Basic Moral Arguments in Favor of PAD The two basic moral arguments in favor of physician-assisted death focus on suffering and on autonomy. The former maintains that it is cruel to force a terminally ill patient to continue to suffer terrible pain at the end of life, when such pain cannot be eradicated or adequately controlled and has no purpose, such as restoring the patient to health. Clearly, the argument from suffering is not limited to competent individuals; those in dementia may suffer as much, or more, as those with greater cognitive capacity. The argument from autonomy focuses on the right of people to make crucial decisions about how their lives will go for themselves, without interference from the state. The right to refuse medical treatment, including life-sustaining medical treatment, is well-established in the United States by common law and landmark court decisions, including Quinlan, 7 Cruzan, 8 and Bouvia. 9 Many have argued that the same value of autonomy that underlies the right to refuse life-sustaining treatment is also implicated in a right to choose death. They regard as irrational the fact that the law allows people to die certain and expedited deaths by refusing to eat and drink 10 or by refusing lifesupportive treatment but does not allow them to choose to have their doctors provide them with a quick and painless death. 11 Opposition to PAD may be based on sanctity of life, views about the appropriate role of physicians, or concerns about the risks of mistake and abuse. 12 We do not discuss these objections and put to one side the general debate about the legitimacy of PAD. Instead, we focus on the question of whether PAD could justifiably be expanded, first, by dropping the requirement of contemporaneous competence and allowing AEDs, and second, to allow for application of those AEDs to situations of dementia, relaxing the requirement of a prognosis of death within six months. We turn now to Dutch law, where PAD has been expanded on both counts. Dutch Law In The Netherlands, a vigorous dementia debate about the eligibility of patients with severe dementia for euthanasia has taken place for over two decades. 13 The requirement that the person requesting euthanasia make a voluntary and carefully considered request has traditionally been interpreted by Dutch doctors to rule out euthanasia on patients with dementia. Then, in March 2011 it was reported that a Dutch woman in severe dementia received euthanasia. 3
67 Advance Directives, Dementia, and Physician-Assisted Death The woman was not named, but we will refer to her as Lotte. She was 64 years old and a long-time supporter of the Dutch euthanasia law. While fully competent, she had written an advance directive in which she expressed her desire to die rather than go into a nursing home. Lotte repeated this desire over time to her family physician and was supported in her request by husband and children. As dementia grew more severe, she could remember only bits of her directive. Nevertheless, in every conversation with her doctor, she said she would rather die than go into a nursing home. Also, she appeared to be suffering; she was angry, confused, and cried a lot. Thus, the doctors involved considered the legal requirements of voluntariness and unbearable suffering to be met. Because the case was so sensitive it was looked at by all five relevant regional committees; all concluded that her doctor had acted within the criteria of due care. 14 The significance of the Lotte decision is magnified by the fact that shortly thereafter, in June 2011, the Royal Dutch Medical Association (KNMG) issued a major position paper including new guidelines for interpreting the 2002 Euthanasia Act. An obvious concern about the expansion of euthanasia to patients in early or late-stage dementia or with chronic psychiatric illness is abuse. The KNMG addressed this issue, calling such cases especially difficult. Any assessment of the considerations prompting such a request and of whether the suffering is indeed unbearable and lasting is generally much more complicated in this category of patients than among those who are suffering due to somatic problems and ailments. Physicians [need to] act with extreme caution and restraint. 15 In addition to unbearable suffering, patient volition is critical in Dutch law. The new guidelines indicate that the voluntariness requirement can be satisfied by evidence that euthanasia is what the patient wanted, even if the patient is no longer competent. One of the clearest kinds of evidence of one s desires is a carefully considered advance directive, written when one is still competent, that speaks to the current situation and has been reiterated over time, especially in early dementia when one presumably has a clearer idea of what life in dementia means. 16 When we ask whether competent individuals have a right to create AEDs, we are thinking of directives that meet these criteria, including reiteration in early dementia. II. Stages and Types of Dementia Any responsible discussion of expanding PAD to advance directives for dementia needs to be well informed about dementia itself. 4
68 Advance Directives, Dementia, and Physician-Assisted Death Dementia refers to a wide range of cognitive impairments and memory loss sufficiently severe to interfere with the normal functions of daily life. The range of dementia from mild to severe/advanced is conveyed in the array of various deficits clinically used in assessment tests (e.g., the Functional Assessment Staging Test 17 ). In mild dementia the deficits affect daily functions such as bill paying, cooking, housecleaning, and traveling. A person in moderate dementia requires help in slightly more basic daily activities, such as selecting one s clothes. In moderately severe dementia the person has difficulty putting on clothes, bathing, and toileting, and with urinary or fecal incontinence. In severe dementia one is unable to speak daily more than 5-6 words at all or more than two words clearly, and one lacks either the ability to walk, to sit up, to hold up one s head, or to smile. For a specific individual at a particular point in time, deficits that would normally indicate only mild or moderate dementia may combine with some from severe dementia, making the assignment of a stage from mild to severe at any particular point in time ambiguous. Some scales define a more advanced very severe stage. In the longstanding (since 1982) seven-stage Global Deterioration Scale s stage 7, all verbal abilities are lost. These patients require assistance in toileting and eating. They lose psychomotor skills as though the brain is no longer able to tell the body what to do. 18 Other authors, labeling this stage advanced, add the clarification of inability to recognize familiar faces or to walk, and incontinence of urine and stool. 19 The extent to which the impairments of dementia interfere with quality of life varies a great deal. The cognitive level of mental life has changed, of course, but the effect of this on affective temperament can range from highly negative to positive. Some persons with dementia are continually frightened or at moments extremely scared, or anxious and irritable, and even violent. Others are evidently happy, sometimes eagerly participating in the activities of which they are still capable. Judgments about the degree of personality change with dementia are complicated by the fact that capacities lost most of the time may briefly re-emerge in moments of temporary lucidity. At such times it may be possible to determine whether the individual still holds the beliefs or values previously expressed in an advance directive or in actions throughout their lives. The patient may show flashes of her old self, providing evidence of a continuous personality even into severe dementia. 5
69 Advance Directives, Dementia, and Physician-Assisted Death The variety and unpredictability within dementia, even within a given type such as Alzheimer s, must be taken into account if an advance directive for a future state of dementia is to be reasonably well informed. No one can know in advance whether she will be among the happy demented or the terribly frightened and anxious. Such limitations may affect how informed an AD is, and therefore how much moral weight it can carry. III. The Disability Critique Difficulties in writing an informed AED for application in case of dementia stem not only from unpredictable variation in dementia s stages and effects. Members of the disability community have forcefully addressed a related problem: people often think prospectively that they would find a particular disabling condition unbearable or worse than death, only to find when they actually experience it that it is not nearly as bad as they thought it would be. In part this may be due to a failure of imagination about what life will be like. One might focus only on the abilities and pleasurable experiences one will lose, without recognizing that there could be positive aspects to living in an eternal present. For example, Robert Leleux writes about his grandmother, JoAnn, who had been estranged from her daughter. In Alzheimer s, as she lost memory and sense of time, grudges and old hurt feelings disappeared. She simply forgot what made her angry and was able to be reunited with daughter. 20 A related aspect is the phenomenon of adaptation, confirmed many times in the psychological literature. 21 While people experience a drop in subjective well-being upon becoming disabled, within a relatively short period of time they often regain the level of happiness they had previously. Moreover, adaptation can be fostered. An AED written in ignorance of adaptation may be inadequately informed, and for that reason have less moral force. Another aspect of the disability critique concerns attitudes toward disability that stem from ignorance and prejudice. Enlightened people no longer call infants born with severe disabilities monsters. Parents are no longer routinely advised to place their children with Down syndrome in institutions, or told that the children will never talk or learn or recognize their parents. Some of the recoiling from dementia, especially such aspects as incontinence, drooling, loss of mobility, and in general the dependence dementia entails, may spring from equally unenlightened attitudes. 22 An additional fact is that undoubtedly, some people view living in dementia as a fate worse than death because of the lamentable, sub-standard conditions that characterize some nursing homes. It goes without saying that such conditions are unacceptable and that steps to improve the 6
70 Advance Directives, Dementia, and Physician-Assisted Death lives of people with dementia need to be taken. Nevertheless, the desire to die to avoid dementia need not stem only from ignorance and prejudice, lack of imagination, failure to appreciate adaptation, and fear of poor nursing home care. As will become clear later, it can be based on profound convictions about the meaning and narrative of one s life, and when it is, it is deserving of respect. Moreover, dementia has profound effects on selfhood, making dementia arguably different from other disabling conditions. This contrast is brought out by the way Asch explains how many people with profound disabilities can be helped to live full, meaningful lives: [With] personal assistants, they live in their own homes by themselves or with family and friends. They are in the community, not in institutions. They hold jobs, engage in volunteer activities, visit friends and generally participate in ordinary family, civic, and social life. Wheelchairs do not confine; they liberate. Using the services and skills of a personal assistant who helps them get into and out of bed or travel to their next appointment is no more shameful or embarrassing than it is for a nondisabled person to value the expertise of a mechanic. 23 Little of this applies to people in severe dementia. They do not hold jobs, engage in volunteer activities, or socialize with family and friends. Moreover, the interest in determining how one s life should go, including how it ends, is one shared equally by the temporarily-abled and disabled alike. IV. Advance Directives: the Dresser/Robertson Challenge The deeper and more general objection to ADs is that the very condition that effectuates them, the inability to participate in medical decision making, often so dramatically changes the person s interests as to undercut the authority of the directive. Rebecca Dresser and John Robertson make this criticism of what they call the orthodox approach of American courts to the withdrawing or withholding of medical treatment from previously competent patients. 24 In the orthodox approach, competent patients have the right to refuse medical treatment, including treatment necessary to save their lives, and they retain this right if they become incompetent. Courts then assume that respect for incompetent patients requires according such patients the same right to refuse treatment accorded competent patients. 25 Refusal is based on the patient s own wishes, either stated in an advance directive or as determined by the patient s appointed proxy or family and close friends. Allegedly, this both respects the autonomy of the nowincompetent person and avoids over-treatment treatment the patient does not want. 7
71 Advance Directives, Dementia, and Physician-Assisted Death Dresser and Robertson argue that this approach is based on a fiction. The now-incompetent person is not an autonomous chooser; the autonomous chooser, who made the advance directive, no longer exists. Moreover, the incompetent individual now before us likely has quite different interests than she did previously. She may no longer have the same interests in preserving control or autonomy or in not being dependent on or a burden to caregivers. An existence that seems demeaning and unacceptable to the competent person may still be of value to the incompetent patient, whose abilities, desires, and interests have so greatly narrowed. 26 In part, the Dresser-Robertson critique of the orthodox approach rests on epistemic considerations: It is difficult, if not impossible, for competent individuals to predict their interests in future treatment situations when they are incompetent because their needs and interests will have so radically changed. 27 They also suggest that philosophical theories of identity which emphasize psychological continuity might be used to bolster their view. Derek Parfit, 28 for example, has suggested that a person s life can consist in a series of successive selves, with a new self emerging as the individual undergoes significant changes in beliefs, desires, memories, and intentions. If the successive selves are not identical, the authority of a prior self over a later self would be questionable. V. Is Identity the Issue? Is the person who wrote the directive sufficiently the same person as the later person with dementia, for the directive to have authority in the new situation? DeGrazia perspicuously labels this the someone else problem. 29 If psychological continuity is the basis for numerical identity what makes a person the same person over time then radical changes in a person s beliefs, desires, and concerns can affect identity itself. And if the later individual is not the same person as the earlier person who wrote the AD, why should the wishes of the earlier person control what happens to the later person? The psychological account thus threatens advance directives generally. The event that triggers the use of an advance directive, after all, is incompetence, and especially in dementia, that may involve changes radical enough to affect identity. The phenomenon of a very different self in dementia is well illustrated by the case of Margo, brought to prominence in the literature by Ronald Dworkin. 30 Andrew Firlik, a medical student, repeatedly visits Margo, a patient with Alzheimer s. With each arrival Margo behaves as if she knows him, though without ever using his name. She says she reads mysteries, but Firlik notices 8
72 Advance Directives, Dementia, and Physician-Assisted Death that her place in the book jumps randomly from day to day. She feels good just sitting and humming to herself, nodding off liberally, occasionally turning to a fresh page. In attending an art class for dementia patients, she paints virtually the same picture each time. She takes abundant pleasure in simple acts like eating peanut-butter-and-jelly sandwiches. Firlik writes that despite her illness, or maybe somehow because of it, Margo is undeniably one of the happiest people I have ever known. 31 We know little about Margo s past life and concerns, but they were undoubtedly different than the concerns and life she has now. Does such difference, considerable as it is, now make her a different person? The basic intuition behind the very notion of advance directives is that they represent a claim to control by persons over their later lives; the unspoken assumption is that the incompetent individual is the same person as the prior competent one. Departing from this common assumption would create all kinds of difficulties, especially in the law, something even Dresser and Robertson acknowledge. 32 Pragmatically, bodily identity has huge advantages as a criterion of same-individual identity compared to any psychological continuity standard, with its line-drawing and intersubjective discernment difficulties. 33 Interpersonally, people just do use bodily identity when they uphold contracts, blame people or praise them, discern criminal and civil liability, etc. 34 People also, of course, speak of becoming a different person, but their usual reference then is to personality changes, not to the going out of existence of one person and the coming in of another. As a realistic framework for discussing the authority of ADs, therefore, we will assume that Margo (for example) is numerically the same person as she was before her change into dementia. That, however, does not settle the question of the moral authority of her AD, given the enormous changes in her personality caused by her dementia. Following DeGrazia 35 and Schechtman, 36 we shall regard these personality-related dimensions as part of the notion of narrative identity. Full selfhood involves such identity, not just continuation as numerically the same individual. The inquiry Who are you? calls for a different response than the bodily focus typically used for numerical identity: something of the history, experiences, beliefs, values, and other psychological features that make you the person you are. In the narrative aspect of their identity people think as persisting subjects of memory and anticipation and form an autobiographical narrative ( story ) of their lives. This need not be sophisticated or philosophically reflective. Even individuals with diminished mental capacity often have a firstperson perspective on their lives that involves memory and anticipation. 9
73 Advance Directives, Dementia, and Physician-Assisted Death Though Margo has changed significantly and become less a self as she loses much of her narrative identity, not replaced with other narrative elements, Margo (now with dementia) is still Margo, the individual who previously wrote the advance directive. Even if the Parfitian, psychological continuity view of identity is thus rejected and Margo is still Margo, however, Dresser and Robertson s critical challenge remains: have Margo s interests changed so radically in dementia that her earlier advance directive is no longer relevant and should be disregarded? VI. Dworkin s View: Autonomy and Best Interests Ronald Dworkin 37 acknowledges that some of a person s interests can change radically in dementia. He maintains, however, that this does not undercut the moral authority of advance directives, including ones for euthanasia. In this section we explain Dworkin s distinction between experiential and critical interests, and the role it plays in his defense of AEDs. Autonomy and Critical Interests Autonomy refers both to the ability of normal adults to make important decisions in their lives, and the right to make such decisions for themselves. Because infants and young children lack the mental capacity to weigh different and often conflicting factors and make their own decisions, it makes no sense to ascribe to them a right to do so. It is also absurd to invoke respect for autonomy in the case of never-competent adults, severely impaired from birth. In such cases the relevant basis for decision-making is best interests. The situation is different for incompetent adults who were previously competent. The beliefs, desires, and values they have while autonomous choosers form what Dworkin calls critical interests. These are second-order interests, which involve a certain level of thought and reflection. They include, for example, convictions about what helps to make a life good on the whole. 38 These and other values have as their object states of affairs that can obtain when people are no longer competent or even alive. While experiential interests continue to exist only as long as someone is experiencing, critical interests are not confined to conscious experiences. They exist, to be satisfied or not satisfied, even after one no longer experiences them. Thus, while the dead and those in PVS no longer have experiential interests, they continue to have critical interests. If someone cares about what happens to his property, his family, or his reputation after he dies, he has a critical interest in these things. To dispose of property contrary to his will, to violate the provisions of an advance directive, to unfairly tarnish his reputation after his 10
74 Advance Directives, Dementia, and Physician-Assisted Death death all are ways of harming and wronging people. That we make judgments of this kind is evidence of the existence of non-experiential, critical interests. While dead and permanently unconscious individuals can have only critical interests, people with dementia have both experiential and critical interests, and these may conflict. 39 Suppose that Margo wrote a strong advance directive stipulating PAD in any level of dementia equal to or worse than what she now has, but she is now experiencing her days as a happy and rather energetic person. How should this conflict between her current experiential interest in living and her critical interest in not living in dementia be resolved? According to Dworkin, respect for autonomy requires us to respect the AD because it represents a judgment about the overall shape of the kind of life he wants to have led. 40 To ignore the AD, sacrificing a person s critical interests to satisfy his experiential interests, would be a violation of his autonomy. In particular, making someone die in a way that others approve, but he believes a horrifying contradiction of his life, is a devastating, odious form of tyranny. 41 Best Interests For Dworkin, however, sacrificing a person s critical interests to satisfy her experiential interests is not only a violation of autonomy. It also misconstrues what is in her best interest. Suppose that Margo has the advance directive previously described, written when she was fully competent. If we consider only her experiential interests, we should not follow it. Margo is now happy and enjoys her life, and presumably does not even remember writing an AD. According to Dworkin, however, what is best for Margo is not determined by her experiential interests, but by her critical interests, which are formed when she is competent. If I decide, when I am competent, that it would be best for me not to remain alive in a seriously and permanently demented state, then a fiduciary could contradict me only by exercising an unacceptable form of moral paternalism. Once we rule out that form of paternalism once we accept that we must judge Margo s critical interests as she did when competent to do so then the conflict between autonomy and beneficence seems to disappear. 42 Critical interests not only reflect the focus of autonomy on integrity and reflective, second-order desires; they outweigh they trump experiential interests in construing what is in a person s best interest. Reinforced at the second-order level, they are people s most important interests, interests about what ultimately matters to them. Thus Dworkin concludes that Margo s best interest as well as her autonomy support following her AD. 11
75 Advance Directives, Dementia, and Physician-Assisted Death VII. Jaworska s Critique: New Critical Interests explains: Jaworska grants Dworkin this claim about the dominant weight of critical interests. As she In the case of an ordinary competent person, when his critical interests (his judgments and values) come into conflict with his experiential interests (what would lead to the optimal state of mind for him), we do not hesitate to give precedence to his well-considered values and judgments, and we concede that this is, overall, best for him. The case of our demented person turns out to be no different: in his conflict between ongoing experiential and critical interests, it is also best to privilege the latter. 43 Where Jaworska disagrees with Dworkin is about the ability of demented individuals to generate new critical interests, including ones about the value of life. The conflict is therefore not merely between experiential and critical interests (in which case critical interests win out); it is between older and newer critical interests. To show that people in dementia can generate new critical interests, Jaworska appeals to the distinction between values and desires. Desiring is the more basic, first-order notion. By contrast, valuing involves reflection. We do not always value what we desire think of trying to break a habit. To value something is not merely to want it, but to think that it is good, a kind of secondorder appraisal. For Dworkin, to form critical interests one must be capable of having convictions about what makes life one s own life good as a whole, but this is just what Jaworska denies. Critical interests, on her view, issue from convictions about what is good to have, which do not require the ability to grasp or review one's whole life. 44 Jaworska provides the example of Mrs. D., diagnosed with probable Alzheimer s, now moderately to severely impaired. Mrs. D. volunteers for medical research and explains her decision: I could have said, 'no,' but believe me, if I can help me and my [fellow] man, I would do it." This suggests that Mrs. D. had considered her decision and thought it would be wrong to refuse, a clear second-order activity. Mrs. D. does not have mere desires and experiential interests; she has values. Jaworska writes, In the context of dementia,so long as [the person] still holds values, he is capable of self-governance and can form new critical interests. 45 Jaworska s key point is that what often happens to persons in dementia is a change in their values. Given their diminishing capabilities, people in dementia: are naturally inclined to savor and appreciate simpler pleasures. Thus, after developing Alzheimer's, even former highbrow intellectuals come to value, or value 12
76 Advance Directives, Dementia, and Physician-Assisted Death more highly, the pleasures of listening to music, gardening, yoga, simple art-making, telling fanciful stories to their grandchildren. 46 Such changes, Jaworska argues, are crucial in assessing the validity of an advance directive. It is one thing for someone to write an AD directing their treatment in case of permanent unconsciousness; the AD has full authority because later there is no current active agent. It is quite different to write an AD to apply in case of dementia, when there will still be a valuer, though one with different interests. The person executing an advance directive for dementia is more akin to someone who anticipates that his values will change for the worse in the future and attempts to hold his future self to his current values by making others promise that they will, at a future time, enforce his current values against his will. 47 What, Jaworska asks, would justify privileging the earlier values? Few of us would want to be held to the values we espoused in our teens or twenties. Roger Daltrey sang, Hope I die before I get old, 48 when he was 21; it s unlikely he would want to be held to that today at age 68. Then why should the demented person be held to values she no longer holds or remembers? In Jaworska s view, Dworkin fails to appreciate the ability of people with dementia to generate new critical interests. In giving such different accounts of critical interests, however, Dworkin and Jaworska are largely talking past each other. For Jaworska, anyone capable of secondorder desires is a valuer, and for that reason capable of generating new critical interests. For Dworkin, critical interests are not just any values or second-order desires; they intrinsically involve notions like character, life-long convictions, and views of what makes life good as a whole. Thus, Jaworska has not shown that Dworkin is factually mistaken about the ability of patients in dementia to have new critical interests. Rather, she has offered a different conception of critical interests, one that does not address the kinds of reasons Dworkin offers for their importance their roots in character, convictions, and the value one sees in one s life as a whole. Jaworska is right, however, to note that a person s values and self-concept can change, and change radically, certainly over a lifetime and perhaps in dementia, at least in the early stages when people come to appreciate activities that were of little interest to them before. This is the force of Jaworska s highly intellectual grandmother, whom we will call Helen. Her new appreciation of yoga, gardening, simple art-making, and telling stories indicates not only new values, but perhaps a change of mind about what makes living worthwhile, even if she no longer has sufficient memory to consider her life as a whole. 13
77 Advance Directives, Dementia, and Physician-Assisted Death We say perhaps because the mere fact that Helen has new values of some kind, and a new appreciation of certain activities, is not conclusive evidence that she has changed her mind about the value of her life in dementia. (We discuss this further in Section IX.) Moreover, even if Helen, as described, has changed her mind, at some point persons in dementia cannot change their minds in the relevant sense. As Ron Berghmans poignantly puts it, with dementia, at the time you would most likely change your mind [about your directive], you don t have enough mind left to change. 49 At that point demented persons only critical interests are the ones generated previously. If Jaworska s claim 50 that Margo falls into the category of someone capable of generating new critical interests is plausible, it is because Margo is not severely demented. At best, then, the Jaworska critique applies only to those in mild or possibly moderate dementia. The analysis is very different for someone in severe dementia who is no longer capable of valuing of any kind, and certainly not generating new critical interests. This is the case of a person we will call Ruth, who is in severe dementia. Ruth does not reflect on her desires, or deem them good or bad; she simply has them, like an infant or very young child. Ruth does not actively engage in a range of activities, like Margo, but neither is she suffering, like Lotte (the Dutch woman described in Section I). Indeed, Ruth gives every indication of being happy, or at least contented. She eats with pleasure, she often smiles and utters sounds of apparent pleasure when she is stroked and talked to, and she enjoys cuddling her stuffed animals. Suppose Ruth has an AED, reiterated over time, asking that if she becomes severely and permanently demented, all life-sustaining aid should be withdrawn so she can die, and if that is not possible because she is needs no such life-support, that she should be helped to die. Should we follow her directive? Dresser and Robertson would say no, focusing on Ruth s present interests. Dworkin presumably would say yes on grounds of respecting her autonomy and best interests, because a person s best interests are ultimately determined by her critical interests. It is not entirely clear what Jaworska would say, as she does not consider this sort of case. Given that she agrees with Dworkin that critical interests trump merely experiential ones in determining best interest, though, it seems that she should agree with Dworkin here and see Ruth as a case where the AED should be followed. However happy Ruth is, she does not value her satisfactions and therefore, even for Jaworska, she 14
78 Advance Directives, Dementia, and Physician-Assisted Death does not generate new critical interests that might conflict with the ones she still has, expressed in her AED. At this point we can see that in addition to their disagreement over the nature of critical interests, the debate between Dworkin and Jaworska turns on the very different picture each gives of dementia. Jaworska tends to focus on those in the early and moderate stages. Early stage is represented in her example of Julian, who has Alzheimer s. For a dinner where he was going to be honored for his accomplishments in science, Julian wanted to make a thank-you speech. When he tried to write it he was able to produce only unconnected phrases. By patiently interviewing him, however, his wife was able to write the speech he wanted to make about why he cared passionately about science but was now ending his work. He needed his colleagues to know why he had left. He wanted them to know, too, that people with Alzheimer's are still 'regular folks.'" 51 This example, as moving as it is, surely does not provide a counter-example to Dworkin s view. Julian s problem is not that he cannot reflect on his life-long values, or that his character has radically changed. His only problem is an inability to find the words to express the thoughts and values he has. So although Julian needs help with many aspects of living, he is autonomous in a full sense, as Dworkin would surely acknowledge. We do not know what Julian s attitudes toward dementia were in his earlier life. However, even if he once thought that becoming demented would be intolerable and make his life no longer worth living, his remark about wanting to let people know that people with Alzheimer s are still regular folks suggests that he might have changed his mind. Someone like Julian can change his mind about when life is worth living. Unlike Ruth, he still has a mind to change. In marked contrast to Julian, Helen, or Margo is Dworkin s characterization of someone in late-stage Alzheimer s disease: Patients in the late stages have lost substantially all memory of their earlier lives and cannot, except periodically and in only a fragmented way, recognize or respond to other people, even those to whom they were formerly close. They may be incapable of saying more than a word or two. They are often incontinent, fall frequently, or are unable to walk at all. They are incapable of sustaining plans or projects or desires of even a very simple structure. A specialist describes the degeneration as occurring gradually and inexorably, usually leading to death in a severely debilitated, immobile state between four and twelve years after onset. 52 Clearly, persons in late-stage dementia no longer have the capacity for any degree of selfgovernance or autonomy. 15
79 Advance Directives, Dementia, and Physician-Assisted Death But does that matter should it matter in terms of their value and moral standing? Surely such persons still have worth, must be treated with dignity, and are entitled to respect. The notion of dignity applicable to dementia, though, has to do with more than present capacities. We respect the person now in part because of what she was an autonomous, self-constituting, self-conscious narrative self and because of the narrative identity she still has. But we respect the person also because of the remaining consciousness present in late-stage dementia, and because of her continuing role in a network of relations. The patient with dementia is still someone s husband or wife, someone s mother or father, grandmother or grandfather. Dementia does not banish someone from the human family. Beyond the issue between Dworkin and Jaworska of who has new critical interests and can change their mind in the relevant sense, the question thus remains: How do we best demonstrate respect for the patient in dementia who has an AED by following or by disregarding it? In the remaining sections we argue that because of numerous complicating factors, there is no yes-or-no answer to this question. VIII. The Value of Life in Dementia Two factors, psychological continuity and narrative identity, fundamentally affect the value of life in dementia. In severe dementia, experiential interests remain, but there is very little if any anticipation or memory. Without them, psychological continuity within the person s subjective life is weak. This has notable implications for the stake someone has in continuing to exist. 53 The person lives in a kind of eternal present, without the ability to envisage her future existence or have desires about it. In such a state the value of survival to the person at the time is greatly diminished. Consider Ruth, who derives enjoyment from various kinds of experiences. She wants to have these experiences, and in that sense wants to go on living, since being alive is a condition of her having these experiences. Yet she cannot be said to value her survival, or to have a stake in her continued existence, since her cognitive deficits prevent her from even anticipating it. As her future existence, it cannot matter to her now. And when she actually gets to the future moment that she cannot anticipate, she cannot see it as her survival, since she has no memory of her earlier existence. In this respect, she is comparable to an infant. The infant, however, is rapidly developing into a being who will have strong psychological connections to his or her own future. By contrast, Ruth s psychological continuity will get progressively weaker, and as it does her stake in her own 16
80 Advance Directives, Dementia, and Physician-Assisted Death continued existence diminishes. This is also true for someone like Margo, although Margo s experiential interests her enjoyment of a range of activities, her energy for living are considerably stronger than Ruth s. The conflict between Margo s experiential interests in continuing to live and her critical interest in not living in dementia, as expressed in her AED, is thus much stronger than this conflict is in the case of Ruth. A different kind of situation arises with a person, let us call him Walter, who is as severely demented as Lotte and Ruth, but who is neither suffering (as Lotte appears to be) nor one of the happily demented (as is Ruth). Walter s affect is flat. He appears to derive no enjoyment from activities and experiences, a situation not uncommon in end-stage dementia. Like Ruth, he lives in an eternal present, but unlike her, he seems to derive no pleasure from the experiences he has. Walter s current experiential interests thus do not conflict with his critical interest in not surviving in severe dementia (suppose that he, too, has a clear AED for this). They provide no reason to disregard his directive. In addition to the role psychological continuity plays in the strength of someone s interest in survival, narrative identity also affects the value of life in dementia. The subjective personal value of a life is not simply a matter of continuing to exist as a particular biological organism. If it were, we would have a strong stake in continuing to live in PVS, without any subjective experience or awareness at all. For most people, however, the value of surviving in a state of diagnosed PVS is (at best) nil. Apart from the remote chance of recovery to consciousness, continuing to live in PVS has no value to the individual at all. For most people it is not one s existence simply as a biological organism that matters, but rather one s existence as a conscious being. Moreover, our stake in continuing to exist is largely as the individuals we conceive ourselves to be that is, with our narrative identity. The further a future departs from our conception of ourselves and the story of our lives our characters, commitments, values the weaker the stake we have in it. What makes survival into severe dementia to many so valueless, and to some even horrifying, is the thought that they will have lost this identity: they will no longer be themselves. Biological death for them is thus preferable to the loss of narrative self. In summary, where previously expressed critical interests do not conflict with experiential interests, as in the case of someone who is experiencing severe and unrelievable suffering, the case for respecting an AED is clear. The hard cases are those in which there is a genuine conflict between experiential and critical interests. In such cases, do we best show respect for the patient in 17
81 Advance Directives, Dementia, and Physician-Assisted Death dementia who has an AED by following it, or by disregarding it? In the next section, we outline the factors that must be considered and offer a sliding scale approach to weighing them. IX. Our View: The Rationale for Implementing AEDs in Severe Dementia How people end life is an important part of the meaning of their lives. Respect for persons includes giving them control over that end. Advance directives enable them to do this and should in general be followed. On this point we agree with Dworkin and Rhoden. Not all advance directives, however, have the same moral force. Carefully considered AEDs that are based on realistic assessment of the facts and reflect the person s enduring values have greater moral force than AEDs that do not. People who wish to avoid severe dementia through an advance directive must inform themselves about the various stages of dementia and what life may be like in those stages. This includes the fact that it is likely impossible to know whether one will be one of the happy demented, or one of the frightened, anxious, and confused. Reiteration of a directive in the relatively early stages of dementia when a person can still understand a directive adds to its moral weight. All this places a burden on people who want to make advance directives for PAD, but not an unreasonable burden. An AED, after all, puts a grave burden on others: it calls on them to end one s life! Carefully considered AEDs should also not be the result of mere prejudice or unthinking assumption that life in dementia is unmitigated horror. Carefully considered AEDs should not express other kinds of blatantly unreasonable preferences, either. To Ludwig Minelli, the founder of Dignitas, a Swiss organization that caters to foreigners coming to Switzerland for euthanasia, it does not matter why the person wants to die; the only value is self-determination. 54 We think it does matter. As Rhoden put it, When they start saying, If I can't do higher mathematics, kill me, we will have to worry in earnest about the limits of precedent autonomy. 55 Even when a directive is written with adequate knowledge of and without prejudice against dementia, the substantive question of employing PAD to avoid living in dementia does not admit of a simple yes or no answer. One complicating factor, discussed in Section VII, is the possibility that the writer of the AED, who preferred death to living in dementia, might change her mind. If there is a genuine change of mind, then it is wrong to bind the person to her previous values. Helen is arguably such a person
82 Advance Directives, Dementia, and Physician-Assisted Death Jaworska sees Margo also as an example of a person who has changed her mind. Yet from the fact that Margo plainly enjoys her life, does it follow that she has changed her mind about the value of her life in dementia? One might think that Margo s enjoyment of various activities is evidence that her life now has value to her, a value she did not anticipate when she wrote her AED. On this interpretation, Margo has changed her mind about whether death is preferable to living in dementia. If so, it is plainly wrong to hold her to her prior values. One could also argue, however, that while Margo retains a capacity for enjoyment, she no longer has the cognitive capacity to consider or reflect on what makes her life as a whole worth living, and therefore she is not capable of revising or rejecting her previous values, or changing her mind about them. It may well just not be clear whether Margo has changed her mind about the value of her life. Note, however, that her AED could be written to clarify this matter. Suppose Margo specifically addressed the possibility that in dementia she might have a period in which she would be enjoying her life. Suppose she said that nevertheless she wants to die then because, given her deepest values and character, she regards death as preferable to being sustained in pleasant dementia. Once she becomes demented, she may no longer remember the AED she wrote, but it is the AED that expresses Margo s reflective preferences and relevant critical interests. Respect for Margo s autonomy supports following her AED. Autonomy, though, is not the only consideration. Margo also has experiential interests in continued life. The happier she is, the stronger are her experiential interests in living, and the harder it is to justify ending her life. Another consideration is whether following the AED of a happily demented person is socially tolerable. Aid-in-dying implicates many more people than just the recipient. It involves the individual physician who participates, and the medical community as a whole insofar as it provides the guidelines and safeguards for responsible use. Also involved, as part of the web of relationships of the person with dementia, are friends, family members, and other care givers. The decision to allow people to receive aid-in-dying is a social one, and therefore it is entirely appropriate that the values of the community have some role in deciding whether and under what conditions assistance in dying should be allowed. To put the point starkly, do we really want to be the sort of society where people who are living happy lives, lives they enjoy and which they apparently want now to continue, are put to death? Dworkin himself acknowledges that there might be valid reasons for refusing to follow the AD of a happily demented person, namey, that we might reject living in a community where officials carried out such ADs. 57 Dworkin only insists that if the refusal to carry out the AD is thus 19
83 Advance Directives, Dementia, and Physician-Assisted Death justifiable, we cannot claim to be acting for her [the demented person s] sake. 58 As noted in Section VI, Dworkin thinks that when we consider the critical interests of the happily demented person, we realize that carrying out the AD is in her best interest, all things considered. We agree with Dworkin that carrying out Margo s AED would respect her autonomy, but we are doubtful it would be in her best interest. Dworkin thinks it would be because in his view, critical interests invariably trump experiential interests. But what is the argument for thinking that this is invariably the case? 59 Why cannot experiential interests of sufficient number and strength outweigh fewer or weaker critical interests? Even if we acknowledge an autonomy-based right to choose not to live as a happily demented person, it strains credibility to insist that the happily demented person who still has a real zest for life would be better off dead. The case for following an AED is strongest where the individual experiences severe and irremediable suffering, as was found to be the case with Lotte. But while we accept unbearable suffering as a sufficient condition for voluntary euthanasia, it is not a necessary condition. That is, we reject the Dutch view that voluntary euthanasia is permissible only in the presence of unbearable suffering. Imagine that Walter, who is neither happy nor miserable, left a clear and carefully considered AED. Even if we grant that someone like Margo is capable of changing her mind something we left unresolved certainly someone in Walter s condition is not. In the late stages of dementia such as his there isn t enough of a mind to change, so the only values to be considered are those of the previously competent person. Suppose that Walter, when autonomous and reflective on his life as a whole, found death preferable to the prospect of living in complete dependence, without any compensating pleasures, and unable to recognize, much less converse with, family and loved ones, and using up all the final resources he badly wanted to leave for particular persons and causes. And suppose that he reiterated that choice in the last part of his life, including when he was mildly demented. Then his choice should be respected both out of respect for his autonomy and in recognition that his stake in continuing to live is vanishingly small. To maintain that Walter is now experiencing unbearable suffering would only be a pretense to justify carrying out his AED. The justification for carrying it out is not that he is currently suffering. It is that he never wanted to end his life this way, and his current experiential interests in continuing to live are not strong enough to justify ignoring his previous wishes. These various considerations can be brought together by viewing the moral situation as a sliding scale where both autonomy and the capacity for enjoyment are considered. 60 An advance directive for PAD, written by an informed and competent person, gains in authority as the 20
84 Advance Directives, Dementia, and Physician-Assisted Death capacities of a person to generate new critical interests and to enjoy life decrease. This is so even in the absence of suffering, such as Walter. By contrast, an AED has less authority where the person still retains the ability to value and generate new critical interests and gives every indication of enjoying her life. This is exemplified by Helen and perhaps by Margo. In such cases, not following the AED would appear to be in the patient s best interest. Moreover, the social reasons against carrying out the AED here are decisive. It is difficult to imagine a compassionate physician being willing to participate in killing patients still actively engaged in activities and relationships, and who neither want to die nor remember having asked to be killed. In applying this sliding scale, a case for AED implementation can be made for Ruth. Ruth is not as happy as Margo; still less does she have the zest for life exemplified by Helen. But her life is not empty of pleasure and enjoyment, as is Walter s. Should Ruth s AED be followed? It depends on the strength of the relevant critical and experiential interests. If Ruth had very strong views about not living in dementia like Lotte did, say her AED should be followed, for her experiential interests in continued life are relatively weak. In this respect, Ruth is significantly different from Margo or Helen. Ruth s situation also differs in another important way. Because she is significantly more demented than are Helen and Margo, she has less stake in her own survival. Thus, if Ruth had a strong desire not to survive in severe dementia because this would be contrary to own conception of what her life was about a conviction that she can now in no sense change respect for her autonomy should prevail, and her AED should be respected. Something else should be noticed about Ruth. To allow AEDs for dementia to be implemented only in cases like Walter but not Ruth would say something striking and unacceptable about the balance between autonomy and best interest. The autonomy and convictions about the whole of one s life at issue in Ruth s directive are clear, and they are not diminished or modified by any new values about life she now has or expresses. To say that they are then still outweighed by even what is to her the greatly decreased value of survival would be saying that autonomy and deep convictions about the whole of one s life count for very, very little so little, in fact, that in effect we would be treating the incompetent but previously competent person as if she had never been competent. Thus, the path from Walter, whose AED we would implement, back to Ruth is clear: Ruth s AED, too, should be implemented. Now, though, comparison in the other direction demands attention: the path from Margo to Ruth. We have doubted that Margo s AED should be implemented. She perhaps has new critical interests, though arguably slim, which run against the grain of the critical interests represented by 21
85 Advance Directives, Dementia, and Physician-Assisted Death her AED. As a valuer she still has a modicum of autonomy and self-governance. Most importantly, her survival is valuable to her in more than just the recurring present she very much looks forward, for instance, to her next art class, at least in moments right before or after it. Even survival in the present is more valuable to her than it is to Ruth; at times she is truly engaged in life, not merely contented. We should be able to recognize that in real life, a graduated spectrum runs between Margo and Ruth, and that the hardest case of all, harder than either of them, lies somewhere in between. There is no sharp line at which the things we have said about Ruth suddenly apply and those about Margo no longer do. Moreover, persons with severe dementia who are well along the road to Ruth s status may have moments of temporary lucidity; depending on what is expressed in them, they can either complicate or clarify judgments about the critical interests that reflect a person s whole-life convictions and autonomy. None of this gradation damages the validity of a sliding scale as the appropriate moral lens for applying AEDs in severe dementia. Rather, the gradation confirms the need to see the situation in terms of a sliding scale. In real time there may be few if any bright lines of distinction along the path of deepening dementia. This fact of life must be recognized, but it should not mislead us into failing to discern the moral difference in implementing AEDs that does accumulate as one moves all the way from Margo to Ruth. At this point, it may be objected that the sliding scale gives insufficient guidance. How are we to know how strong Ruth s previously expressed desire not to live in dementia is? Who is supposed to make this determination? Finally, what is the use of an advance directive if it can be disregarded on the basis of other people s assessments? We acknowledge the problems but note that health care professionals always have to interpret ADs, to determine what the person had in mind and how best to carry out her wishes. In the attempt to understand what an AD means, health care professionals will often talk with the family, who are usually in the best position to know the person s choices and decisions over a lifetime. They will be able to provide some guidance about the strength of the person s values, and how to balance them against her contemporaneous interests. The interpretation of AEDs is not appreciably different from other ADs. 61 The last question, about what value ADs have if they can be disregarded, is harder to answer. The whole point of making an AD, a document which has legal force, is to have a means of ensuring that one s wishes will be respected. To suggest that an AED ought not to be followed seems inconsistent with the rationale for having ADs in the first place. Our response is two-fold. 22
86 Advance Directives, Dementia, and Physician-Assisted Death First, we acknowledge the possibility of a change of mind. If someone who thought all her life that death would be preferable to dementia now appears to think that living in dementia is not as bad as she feared, there is no reason to hold her to her earlier values. Jaworska is right about this. Second, even in cases where there isn t a clear change of mind, we maintain that strong experiential interests in continuing to live can trump weak critical interests in dying. The argument for allowing people to create AEDs is not an argument for requiring that they be carried out in every case. X. Conclusion There is a strong prima facie case for following advance directives in dementia, both for the withdrawal of life-sustaining treatment and for aid-in-dying. Advance directives enable people to have some measure of control over the way they die, and the way they die is an important reflection of how they have lived. We cannot say it better than Rhoden: Something is wrong when we treat formerly competent patients as if they were never competent. Someone who makes a prior directive sees herself as the unified subject of a human life. She sees her concern for her body, her goals, or her family as transcending her incapacity. One component of treating persons with respect [is] that we view them as they view themselves. If we are to do this, we must not ignore their prior choices and values. 62 At the same time, there are countervailing factors to consider. We have laid these out throughout this paper. In conclusion we wish to emphasize three points. 1. The more informed, thoughtful, and based in fact an advance directive is, the more moral authority it has. This points to the need for solid provider-patient relationships that include serious discussions of patients values and commitments. 2. The case for following an AED is strongest in the presence of severe and unrelievable suffering. This is exemplified by the case of Lotte, the woman in advanced dementia who received euthanasia in The Netherlands in March For other cases a sliding scale that considers both autonomy and the capacity for enjoyment provides the justification for determining when an AED should be followed. An AED written by an informed and competent person gains in authority as that person s capacities to generate new critical interests and to enjoy life now decrease. This sliding scale can be used to generate conclusions in the six cases besides Lotte featured in our discussion. The two easiest, on opposite ends of the spectrum of dementia, are Julian and Walter. Julian is still perfectly capable of deep convictions and valuing his life as a whole. He can 23
87 Advance Directives, Dementia, and Physician-Assisted Death generate new critical interests about the value of his survival; he can change his mind about whether he wants to be allowed or helped to die. For this reason, any advance directive he may have created would be superseded by his current wishes, which can be determined by patient conversation with him. A strong and reiterated AED by Walter, on the other hand, should be implemented. He has no capacity to generate new critical interests, and he takes little if any enjoyment in life. Mrs. D. and Helen are cases on the not yet end of our moral conclusions. Their AEDs should not be followed at this time. Although both Mrs. D. and Helen have significant dementia, making them incapable of changing their minds about their critical interests, they not only enjoy but clearly value the lives they are living. They may even still be capable of some reflection on their lives as a whole, and Helen, especially, has adapted to her dementia with new interests and real zest for life. Thus, their strong experiential interests in living outweigh their critical interest in not living in dementia. Dementia at this time has turned out not to be as dreadful as they predicted, although this may change as the dementia inexorably worsens. This is the stage that Ruth is in. Admittedly, she is contented and perhaps can even be characterized as modestly happy. Thus, unlike Lotte and Walter, she has some experiential interests in continued survival. But because she has no capacity to generate any new critical interests, and because the value of her life to herself is greatly diminished by her inability either to remember or to anticipate, a substantive moral decision becomes clear: her AED, assuming it was a clear indication of her character and deepest values of her life, should be implemented. The hardest case among the six is Margo. She can likely still value particular experiences, and many she certainly enjoys. It is not clear, however, whether she can observe or reflect on life enough to value it, and she appears not to have the capacity to reflect on her life as a whole. If she has a strong and reiterated AED aimed at the moderately severe level of her current dementia, she exemplifies a sharp clash between autonomy and critical interests, on the one hand, and current experiential interests on the other. Margo has enough capacity for memory and anticipation to generate great enjoyment of life. In light of that enjoyment, we believe that on balance, society should say firmly in her case, not yet. We conclude, finally, with two observations about the larger legal context for AEDs. First, the emergence of AEDs as morally acceptable has more than one logical legal home. One, evidenced by the real case of Lotte, is The Netherlands, where euthanasia is legal. There, voluntariness, not just unbearable suffering, is a required condition for permissible euthanasia, and a strong and reiterated AED can then be interpreted as making euthanasia voluntary. An equally 24
88 Advance Directives, Dementia, and Physician-Assisted Death logical home for AEDs, however, is the legalized PAS of Oregon, Washington, British Columbia, and Switzerland. There, too, the emphasis on voluntariness can be plausibly extended to include AEDs. Their laws, of course, would have to be rewritten, but the current requirements of terminal prognosis within six months and current competency 63 are at odds with PAS s fundamental emphasis on voluntariness. The legal and moral framework of these jurisdictions, too, could readily incorporate carefully implemented AEDs. Second, most of our analysis of implementing advance directives for dementia applies as much to the refusal of life supporting treatment as it does to physician assisted dying. The same dilemmas about interpreting change of mind and weighing critical and experiential interests arise. All the specific persons with dementia we have analyzed and come to conclusions on regarding implemention of an AED could also have ADs for refusal of life support. Presumably, anyone whose aim in an AED was not to live long in severe dementia would want to include in their directive not just PAD, but withholding and withdrawal of feeding tubes, for example, and refusal of hospitalization from nursing homes. Such regular ADs for treatment refusal pair logically with AEDs, and where AEDs are not now legally permitted, clear ADs that speak to refusing life support in dementia typically are. This has great practical importance. A high percentage of patients with advanced dementia in nursing homes develop infectious episodes and eating problems, and many are hospitalized for acute crises multiple times a year. 64 And in so far as ADs to refuse life support are already being implemented for patients like Ruth and Walter, for example, and to the extent that we are confident that implementation of such ADs is justified, they provide important precedent for the eventual acceptance of AEDs. NOTES 1. Physician-assisted death (PAD) covers both physician-assisted suicide (PAS) and euthanasia. In PAS the patient takes lethal drugs made available through a physician s prescription; in euthanasia, the physician delivers the drugs, usually by injection. The term physician-assisted suicide has fallen out of favor in Oregon; proponents, wishing to distinguish it from suicide in general, often prefer aid-in-dying. We continue to use PAS. 2. Physician-assisted suicide (PAS) is legal in the United States in Oregon and Washington by statute: Oregon Death With Dignity Act, Or. Rev. Stat (1997); Washington Death with Dignity Act, Wash. Rev. Code (2009). It is legal by a decision of the state supreme court in Montana: Baxter v. Montana No. DA (2009). In British Columbia it is conditionally legal as of June 2012 by order of the Supreme Court of British Columbia: Carter v. Canada (Attorney General) 2012 BCSC 886 (15 June 2012), available at < (last visited September 14, 2012). In Switzerland, PAS and assisted suicide more generally are legal by statute, without restriction to terminal illness; voluntary self-administration is still required (that is, only assisted suicide, not 25
89 Advance Directives, Dementia, and Physician-Assisted Death euthanasia, is allowed): S. A. Hurst and A. Mauron, Assisted Suicide and Euthanasia in Switzerland: Allowing a Role for Non-Physicians, British Medical Journal 326: 7383 (1 Feb 2003): Even in Oregon and Washington, the three most frequently mentioned reasons for requesting aid-in-dying are loss of autonomy, decreasing ability to engage in activities that make life enjoyable, and loss of dignity. Inadequate pain control is cited much less often. See Oregon Public Health Division Report, at Act/Documents/year14.pdf, p. 2 (last visited September 14, 2012; Washington State Department of Health 2011 Death with Dignity Act Report, at < p. 1 (last visited September 14, 2012). 4. Retirement Policy.org, at < (last visited September 14, 2012). 5. National Institute of Neurological Disorders and Stroke, at < (last visited September 14, 2012). 6. Termination of Life on Request and Assisted Suicide (Review Procedures) Act (2002), at < Ley 2002.pdf> (last visited September 14, 2012). The procedures codified in the law reflect Dutch medical practice since 1973, when doctors began openly providing euthanasia on request. 7. In In re Quinlan, 70 N.J. 10, 355 A.2d 647 (NJ 1976), the New Jersey Supreme Court held that incompetent patients do not lose their right to privacy, including the right to refuse lifesustaining treatment, and that this right could be exercised on their behalf by a guardian. 8. In Cruzan v. Director, Missouri Department of Health, 497 U.S. 261 (1990), the United States Supreme Court upheld the right of guardians to discontinue life-sustaining treatment, both respirators and feeding tubes, from patients in permanent vegetative states, while also upholding states rights to require clear and convincing evidence of the patient s prior wishes. 9. In Bouvia v. Superior Court, 225 Cal. Rptr. 297 (Ct. App. 1986), the California Court of Appeals held that a competent patient has the right to refuse tube feeding and may not be force-fed against her will. 10. For an extensive defense of this path to death, see S. A. Terman (with R. B. Miller and M. S. Evans), The Best Way to Say Goodbye: A Legal Peaceful Choice at the End of Life (Carlsbad, CA: Life Transitions Publications, 2007). 11. R. Dworkin, Life s Dominion: An Argument About Abortion, Euthanasia and Individual Freedom (New York: Alfred A. Knopf, 1993), at 184, and D. W. Brock, Voluntary Active Euthanasia, Hastings Center Report 22 (1992): 2: For an opposing view, see H. Hendin and K. Foley, Physician-Assisted Suicide in Oregon: A Medical Perspective, Issues in Law and Medicine 24 (2008): 2: M.P. Cees, M. Hertogh, M. E. de Boer, R. Droees, and J. A. Eefsting, Would We Rather Lose Our Life than Lose Our Self? Lessons from the Dutch Debate on Euthanasia for Patients with Dementia, American Journal of Bioethics 7 (2007): 4:
90 Advance Directives, Dementia, and Physician-Assisted Death 14. Michael Cook, Informed Consent in Netherlands: Euthanasia, BioEdge, Nov. 12, 2011, at < (last visited September 14, 2012). 15. Koninklijke Nederlandsche Maatschappij tot bevordering der Geneeskunst (KNMG, Royal Dutch Medical Association), Position Paper: The Role of the Physician in the Voluntary Termination of Life (June 2011), p. 7, at < (last visited September 14, 2012). 16. In Legal Euthanasia: Ethical Issues in an Era of Legalized Aid in Dying, Journal of Medicine and Philosophy 18 (1993): 3: , Leslie P. Francis argues that if any advance directives for euthanasia are to be granted authority, they should have been made repeatedly in advance, with the patient now confirming that the time has come. 17. Medical Care Corporation, Functional Assessment Staging Test, 2010, at < (last visited September 14, 2012). 18. B. Reisberg, S. H. Ferris, M. J. De Leon, and T. Crook, The Global Deterioration Scale for Assessment of Primary Degenerative Disease, American Journal of Psychiatry 139 (1982): 9: , at S. L. Mitchell, B. S. Black, M. Ersek, L. C. Hanson, S. C. Miller, G. A. Sachs, J. M. Teno, and R. S. Morrison, Advanced Dementia: State of the Art and Priorities for the Next Decade, Annals of Internal Medicine 156 (2012): 45-51, at R. Leleux, The Living End: A Memoir of Forgetting and Forgiving (New York: St. Martin s Press, 2012). 21. S. Frederick and G. Loewenstein, Hedonic Adaptation, in D. Kahneman, E. Diener, and N. Schwarz (eds), Well-being: The Foundations of Hedonic Psychology (New York, NY: Russell Sage Foundation, 1999), pp ; P. T. Menzel, P. Dolan, J. Richardson, and J. A. Olsen, The Role of Adaptation to Disability and Disease in Health State Valuation: A Preliminary Analysis, Social Science and Medicine 55 (2002): ; and D. Arnold, A. Girling, A. Stevens, and R. Litford, Comparison of Direct and Indirect Methods of Estimating Health State Utilities for Resource Allocation: Review and Empirical Analysis, British Medical Journal 339: b2688 (22 July 2009), doi: /bmj.b A. Asch, Recognizing Death While Affirming Life: Can End of Life Reform Uphold a Disabled Person s Interest in Continued Life? Hastings Center Report 35: 6 (Nov-Dec 2005): S31-S Asch (2005), id., at S32-S R. Dresser and J. S. Robertson, Quality of Life and Non-Treatment Decisions for Incompetent Patients, Law, Medicine & Health Care 17 (1989): 3: For an insightful and comprehensive treatment of this challenge that deals with Dresser s numerous other writings, see L. W. Sumner, Assisted Death (Oxford: Oxford University Press, 2011), pp Sumner also gives a detailed treatment of Dworkin s position, including the Margo case that features centrally in Dworkin s discussion. 25. Dresser and Robertson (1989), id., at Dresser and Robertson (1989), id., at Dresser and Robertson (1989), id., at
91 Advance Directives, Dementia, and Physician-Assisted Death 28. D. Parfit, Reasons and Persons (Oxford, UK: Oxford University Press, 1985), pp D. DeGrazia, Advance Directives, Dementia, and the Someone Else Problem, Bioethics 13 (1999): 5: , and Human Identity and Bioethics (New York: Cambridge University Press, 2005), pp Dworkin (1993), supra note 10, at A. D. Firlik, Margo s Logo, JAMA 265 (1991): 2: Dresser and Robertson (1989), supra note 23, at H. Klepper and M. Rorty, Personal Identity, Advance Directives, and Genetic Testing for Alzheimer Disease, Genetic Testing 3 (1999): 1: , and N. Rhoden, The Limits of Legal Objectivity, North Carolina Law Review 68 (1990): Even someone who espouses a psychological theory of identity and denies that identity is based essentially on bodily continuity could maintain that the now-demented person is the same individual as before. For example, on Jeff McMahan s mind essentialism, the criteria for numerical identity are satisfied so long as the individual has the capacity for consciousness. Since persons with dementia are conscious, their numerical identity remains the same. See McMahan, The Ethics of Killing: Problems at the Margins of Life (New York: Oxford University Press. 2002), at DeGrazia (2005), supra note M. Schechtman, The Constitution of Selves (Ithaca, NY: Cornell University Press, 1996). 37. Dworkin (1993), supra note Dworkin (1993), id., at Dworkin (1993), id., at Dworkin (1993), id, at Dworkin (1993), id., at Dworkin (1993), id., at A. Jaworska, Respecting the Margins of Agency: Alzheimer's Patients and the Capacity to Value, Philosophy & Public Affairs 28 (1999): 2: , at Jaworska (1999), id., at Jaworska (1999), id., at Jaworska (1999), id., at Jaworska (1999), id., at The Who, My Generation (song), The citation of Daltrey is ours, not Jaworska s. 49. R. Berghmans, Advance Directives and Dementia, Annals of the New York Academy of Sciences 913 (2000): , at Jaworska (1999), supra note 42, at Jaworska (1999), supra note 42, at Dworkin (1993), supra note 10, at
92 Advance Directives, Dementia, and Physician-Assisted Death 53. McMahan (2002), supra note 33, at 503. In that larger work McMahan develops a Time- Relative Interest Account (TRIA) of the harm of death: the harm is not determined solely by how much good life (in terms of quantity and quality) one loses, but also by the extent to which one is psychologically connected with one s future. For a concise statement and defense of the TRIA, see D. DeGrazia, Creation Ethics: Reproduction, Genetics, and Quality of Life (New York: Oxford University Press, 2012), at A. Gentleman, Inside the Dignitas House, The Guardian, November 18, 2009, available at < (last visited September 14, 2012). 55. Rhoden (1990), supra note 32, at Unlike Mrs. D. and Julian, who are based on actual people, Helen is a fictitious example. How realistic is Helen? We should point out that when one of us presented this paper, a physician in the audience said that he had never met a demented person like Helen. 57. R. Dworkin makes this point in his response to Seana Shiffrin in Ronald Dworkin Replies, in J. Burley, ed., Dworkin and His Critics (Oxford: Blackwell Publishing Company, 2004), at Dworkin (1993), supra note 10, at Similar reservations about the dominance of critical interests are expressed by Sumner (2011), supra note 23, at The notion of a sliding scale is used by A. Buchanan and D. W. Brock, Deciding for Others: Competency, Milbank Quarterly 64 (1986): 2: Some of the factors we include in our sliding scale are used by L. P. Francis, Decisionmaking at the End of Life: Patients with Alzheimer s or Other Dementia, Georgia Law Review 35 (2001): , at 588 and An alternative approach would be to stipulate that AEDs be implemented only in the later stages of dementia. This would have the advantage of not requiring clinicians to make subjective decisions about the strength of desires; they would base their decisions to uphold AEDs on clear medical diagnoses. Moreover, this approach would reach the same results we have recommended, upholding the AEDs of Ruth, Walter, and Lotte, but not Margo or Helen. From a philosophical perspective, however, our sliding scale approach explains why some AEDs should be implemented and others not. 62. Rhoden (1990), supra note 32 at In Switzerland, only current competency. 64. In as study of 323 nursing home residents with advanced dementia, 45 percent lived longer than 18 months, 86 percent developed an eating problem, and the average number of transfers to a hospital in the last 90 days of life was 1.6. See Mitchell et al. (2012), supra note 18, at 45-46, and S. L. Mitchell, J. M. Teno, D. K. Kiely, M. L. Shaffer, R. N. Jones, H. G. Prigerson, L. Volicer, J. L. Givens, and M. B. Hamel, The Clinical Course of Advanced Dementia, N. Engl. J. Med. 361 (2009): 16:
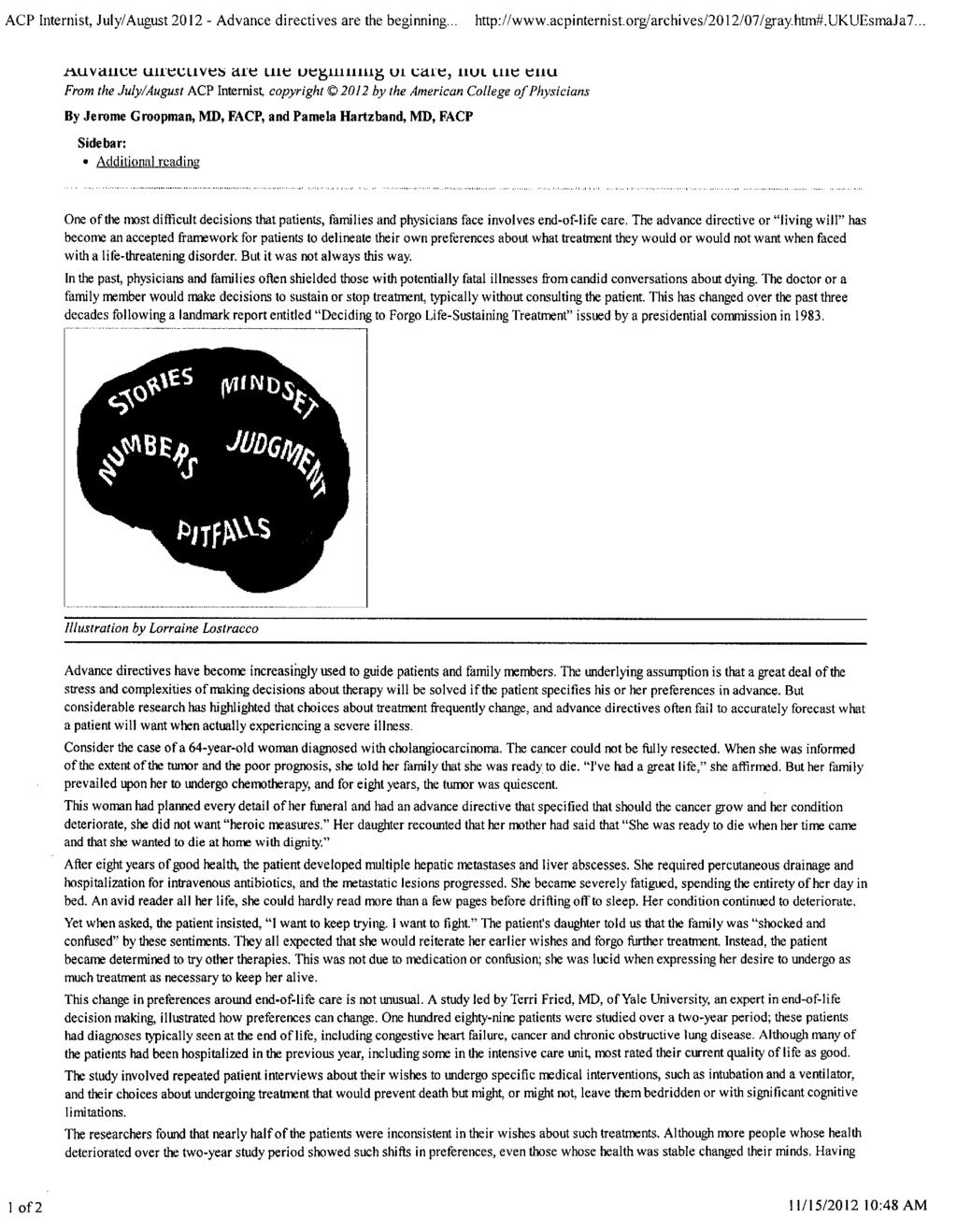
93
94
95 Thaddeus M. Pope
96 Legal Mechanisms for Resolving Medical Futility Disputes Thaddeus Mason Pope, J.D., Ph.D. New York Law School November 16,
97 What is a futility dispute? 2
98 Clinician Surrogate CMO LSMT
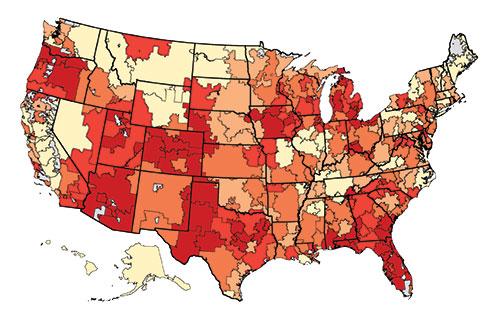
99 4
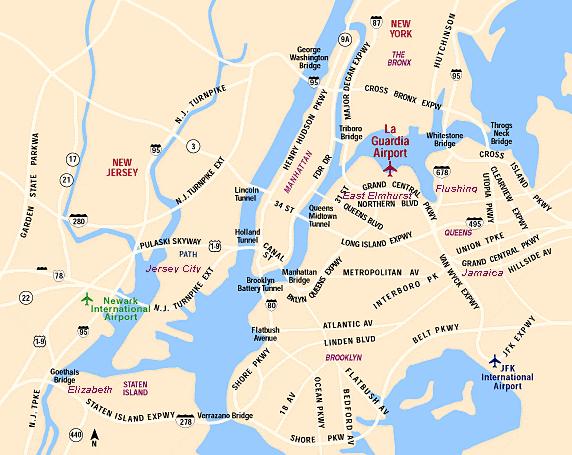
100 5

101 Betancourt v. Trinitas Hospital
102 73yo male PVS COPD End-stage renal disease Hypertensive cardiovascular disease Stage 4 decubitus ulcers Osteomyeletitus Diabetes Parchmentlike skin
103 The only organ that s functioning really is his heart. It all seems to be ineffective. not getting us anywhere. It s We re allowing the man to lay in bed and really deteriorate.
104 Clinician Surrogate CMO LSMT
105 1. Prevention 2. Consensus 3. Transfer 4. Surrogate selection 5. Unilateral action
106 1. Prevention 11
107 12
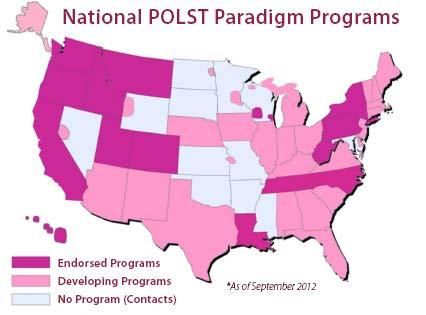
108
109 14
110 Palliative Care Information Act N.Y. Pub. Health L. 2997c (eff. Feb 2011) 15
111 A8176 S7329 Clinical Education in Palliative Care 16
112 2. Consensus 17
113 18
114 3. Transfer 19
115 Rare, but possible 20
116 4. Surrogate Selection 21
117 Substituted judgment Best interests 22
118 Agent PHL 2952 Surrogate PHL 2994-D(4)(A)(I)

119 PHL
120 66% accurate 50% = pure chance
121 Moorman & Carr 62% 2010 Barrio-Catelejo et al. 63% 2009 Shalowitz et al. 58% 2006
122

123 28
124 Helga Wanglie (Minn. 1991)

125 Albert Barnes 30

126 31

127 32

128 Baby M 33

129 34

130 35

131 Dorothy Livadas

132
133 38
134 In re Rochester Gen. Hosp., 601 N.Y.S.2d 375 (1993).

135 Gary Harvey

136 41
137 Consent and Capacity Board 42
138 Limits 43

139 Hassan Rasouli 44

140 45
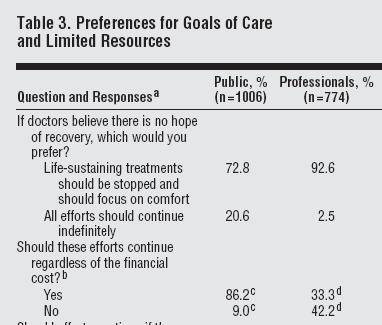
141
142 20%: More important to prolong life. National Journal (Mar. 2011) Archives Surgery (Aug. 2008)
143


144
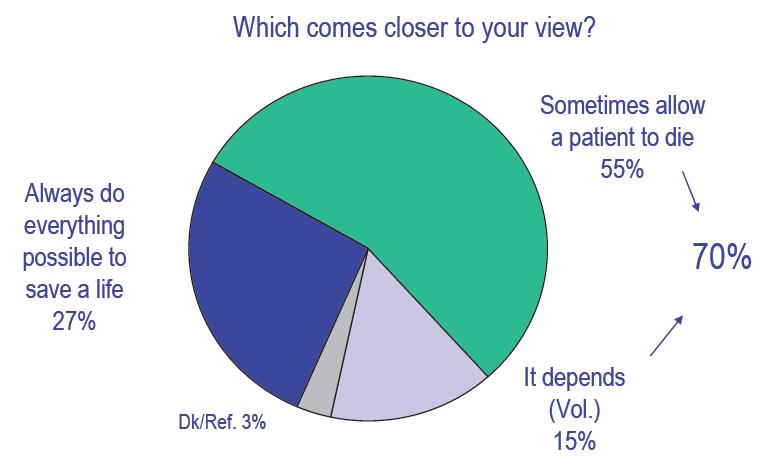
145

146 If cannot replace surrogate, then provide the treatment Truog
147 5. Unilateral action 52

148 53

149

150 55
151 56

152
153 You may stop LSMT for any reason - with immunity - if your HEC agrees Tex. H&S
154

155 60

156 61
157 Why they follow... SDMs instead of doing what they feel is appropriate... lack of legal support.
158 Typical response to bad law claims Safe harbor immunity

159 64


160 65
161 66

162 67
163 Treat til transfer 68

164 Miss. Code
 (died in")
165 Okla. H.B (2012) (died in committee) 70
166 71
167 generally accepted health care standards

168

169 74

170
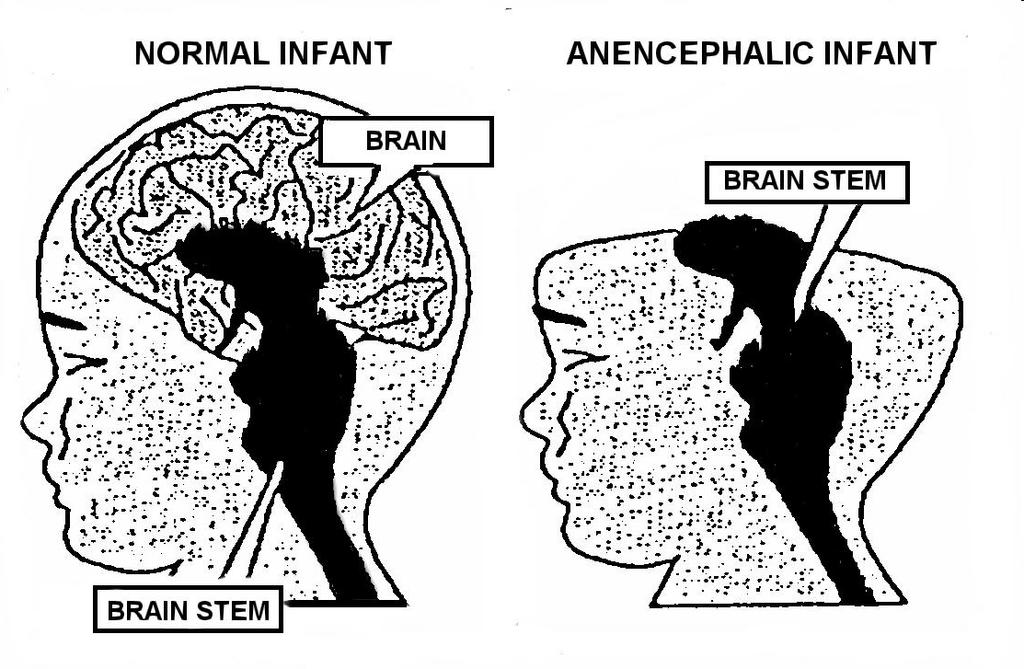
171

172
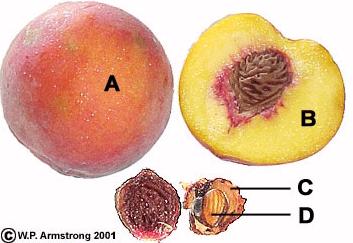
173
174 Risk > 0
175 Liability averse Litigation averse too
176 Even prevailing parties pay transaction costs

177 82
178 =
179 84

180 85
181 Surrogate 2994f(3) Agent
182 If surrogate directs [LST]... provider that does not wish to provide... shall nonetheless comply
183 Idaho Discrimination in Denial of Life Preserving Treatment Act (2012) 88
184 Health care... may not be... denied if... directed by... surrogate 89
185 Futile care exception 90
186 death is imminent within hours... OR denial... will not result... death. 91

187 S.B (2012) Passed Senate, died House 92
 CPR only,")
188 SB 172, HB 309 (2012) CPR only, died 93
189 94
190 FRCP 65 95
191 Conclusion 96
192 97
193 98

194 99

195 100
196 Thaddeus Mason Pope Associate Professor of Law Hamline University School of Law 1536 Hewitt Avenue Saint Paul, Minnesota T F E tpope01@hamline.edu W B medicalfutility.blogspot.com 101
197 References White DB & Pope TM, The Courts, Futility, and the Ends of Medicine, 307(2) JAMA (2012). Pope TM, Physicians and Safe Harbor Legal Immunity, 21(2) ANNALS HEALTH L (2012). Pope TM, Medical Futility, in GUIDANCE FOR HEALTHCARE ETHICS COMMITTEES ch.13 (MD Hester & T Schonfeld eds., Cambridge University Press 2012). 102
198 Pope TM, Review of LJ Schneiderman & NS Jecker, Wrong Medicine: Doctors, Patients, and Futile Treatment, 12(1) AM. J. BIOETHICS (2012). Pope TM, Responding to Requests for Non- Beneficial Treatment, 5(1) MD-ADVISOR: A J FOR THE NJ MED COMMUNITY (Winter 2012) at Pope TM, Legal Fundamentals of Surrogate Decision Making, 141(4) CHEST (2012). 103
199 Pope TM, Legal Briefing: Medically Futile and Non-Beneficial Treatment, 22(3) J. CLINICAL ETHICS (Fall 2011). Pope TM, Surrogate Selection: An Increasingly Viable, but Limited, Solution to Intractable Futility Disputes, 3 ST. LOUIS U. J. HEALTH L. & POL Y (2010). Pope TM, Legal Briefing: Conscience Clauses and Conscientious Refusal, 21(2) J. CLINICAL ETHICS (2010). 104
200 Pope TM, The Case of Samuel Golubchuk: The Dangers of Judicial Deference and Medical Self- Regulation, 10(3) AM. J. BIOETHICS (Mar. 2010). Pope TM, Restricting CPR to Patients Who Provide Informed Consent Will Not Permit Physicians to Unilaterally Refuse Requested CPR, 10(1) AM. J. BIOETHICS (Jan. 2010). Pope TM, Legal Briefing: Medical Futility and Assisted Suicide, 20(3) J. CLINICAL ETHICS (2009). 105
201 Pope TM, Involuntary Passive Euthanasia in U.S. Courts: Reassessing the Judicial Treatment of Medical Futility Cases, 9 MARQUETTE ELDER S ADVISOR (2008). Pope TM, Medical Futility Statutes: No Safe Harbor to Unilaterally Stop Life-Sustaining Treatment, 75 TENN. L. REV (2007). Pope TM, Mediation at the End-of-Life: Getting Beyond the Limits of the Talking Cure, 23 OHIO ST. J. ON DISP. RESOL (2007). 106
202

203 C AMBRIDGE UNIVERSITY PRESS Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, Siio Paulo, Delhi, Mexico City Cambridge University Press The Edinburgh Building, Cambridge CB2 8RU, UK Published in the United States of America by Cambridge University Press, New York Information on this title: Cambridge University Press 2012 This publication is in copyright. Subject to statutory exception and to the provisions of relevant collective licensing agreements, no reproduction of any part may take place without the written permission ofcambridge University Press. First published 2012 Printed in the United Kingdom at the University Press, Cambridge A catalog record for this publication is available from the British Library Library ofcongress Cataloging in Publication da ta Guidance for healthcare ethics committees I edited by D. Micah Hester, Toby Schonfeld. p.; cm. Includes bibliographical references and index. ISBN (pbk.) I. Hester, D. Micah. II. Schonfeld, Toby. [DNLM: 1. Ethics Committees, Clinical. 2. Delivery of Health Care ethics. 3. Ethics, Clinical. 4. Hospital Administration - ethics. 5. Practice Guidelines as Topic. WX 150.1J dc ISBN Paperback Cambridge University Press has no responsibility for the persistence or accuracy ofurls for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate. Every effort has been made in preparing this book to provide accurate and up-to-date information which is in accord with accepted standards and practice at the time of publication. Although case histories are drawn from actual cases, every effort has been made to disguise the identities of the individuals involved. Nevertheless, the authors, editors and publishers can make no warranties that the information contained herein is totally free from error, not least because clinical standards are constantly changing through research and regulation. The authors, editors and publishers therefore disclaim all liability for direct or consequential damages resulting from the use of material contained in this book. Readers are strongly advised to pay careful attention to information provided by the manufacturer ofany drugs or equipment that they plan to use.

204 Contents List ofcontributors Preface xi page ix Section 1 - The Context of Healthcare Ethics Committee Work Introduction to healthcare ethics committees 1 D. Micah Hester and Toby Schonfeld 2 Brief introduction to ethics and ethical theory 9 D. Micah Hester and Toby Schonfeld 3 Healthcare ethics committees and the law 17 Stephen Latham 4 Cultural and religious issues in healthcare 25 Alissa Hurwitz Swota Section 2 - Consultation 5 Mission, vision, goals: defining the parameters of ethics consultation 32 Martin L. Smith 6 Ethics consultation process Jeffrey Spike 41 7 Informed consent, shared decision-making, and the ethics committee 48 Randall Horton and Howard Brody 8 Decision-making capacity 55 Arthur R. Derse 9 Family dynamics and surrogate decision-making 63 Lisa Soleymani Lehmann 10 Confidentiality Toby Schonfeld 11 Advance care planning and end-of-life decision-making Nancy M. P. King and John C. Moskop 12 Medical futility 88 Thaddeus Mason Pope 13 Ethical issues in reproduction Anne Drapkin Lyerly 14 Ethical issues in neonatology John D. Lantos 15 Ethical issues in pediatrics D. Micah Hester Section 3 - Policy Development and Organizational Issues 16 Ethics committees and distributive justice 122 Nancy s. Jecker 17 Developing effective ethics policy 130 Anne Lederman Flamm 18 Implementing policy to the wider community 139 Mary Faith Marshall and Joan Liaschenko vii

205 viii Contents 19 Ethics in and for the 21 Education as prevention 164 organization 147 Kayhan Parsi Mary V Rorty Section 4 - Educating Others 20 The healthcare ethics committee as educator 155 Kathy Kinlaw 22 Understanding ethics pedagogy 172 Felicia Cohn Index 180 (on1 Howarc Institut( Univers Galvest( Felicia ( Kasier F CA, US, Arthur I Medical WI, US, Anne LE Departr Clevelar D.Mica Univers Sciencei Childrel USA Randall Institute Universi Galvestc Nancy 5 Departn Universi Medicin Nancy ~ Departn Policy, v Winstor: Kathy K Center f Atlanta,
206 ;4 Contributors Howard Brody Institute for the Medical Humanities, University of Texas Medical Branch, Galveston, TX, USA Felicia Cohn Kasier Permanente Orange County, Irvine, CA,USA Arthur R. Derse Medical College of Wisconsin, Milwaukee, WI, USA Anne Lederman Flamm Department of Bioethics, Cleveland Clinic, Cleveland, OH, USA D. Micah Hester University of Arkansas for Medical Sciences, and Clinical Ethicist, Arkansas Children's Hospital, Little Rock, AR, USA Randall Horton Institute for the Medical Humanities, University of Texas Medical Branch, Galveston, TX, USA Nancy S. Jecker Department of Bioethics and Humanities, University of Washington School of Medicine, Seattle, WA, USA Nancy M. P. King Department of Social Sciences and Health Policy, Wake Forest School of Medicine, Winston-Salem, NC, USA Kathy Kinlaw Center for Ethics, Emory University, Atlanta, GA, USA John D. Lantos Bioethics Center, Children's Mercy Hospital, Kansas City, MO, USA Stephen Latham Interdisciplinary Center for Bioethics, Yale University, New Haven, CT, USA Lisa Soleymani Lehmann Center for Bioethics, Brigham and Women's Hospital, Boston, MA, USA Joan Liaschenko Center for Bioethics, University of Minnesota, Minneapolis, MN, USA Anne Drapkin Lyerly University of North Carolina, Chapel Hill, NC, USA Mary Faith Marshall Center for Bioethics, University of Minnesota, Minneapolis, MN, USA John C. Moskop Department of Internal Medicine, Wake Forest School of Medicine, Winston -Salem, NC, USA Kayhan Parsi Neiswanger Institute for Bioethics and Health Policy, Loyola University, Maywood, IL, USA Thaddeus Mason Pope Health Law Institute, Hamline University, St Paul, MN, USA Mary V. Rorty Stanford University, Stanford, CA, USA ix

207 Consultation Objectives Medical futility Thaddeus Mason Pope l. Describe the three main definitions of "medical futility." 2. Identify the key factors at the heart of disagreements between surrogates and providers concerning whether a treatment is beneficial. 3. Distinguish six strategies that ethics committees can use to prevent and to resolve medical futility disputes. Case One year ago, 73-year-old Mr. B came to your hospital for surgery on a thymus gland tumor. While the surgery was successful, during his post-operative recovery, Mr. B's endotracheal tube became dislodged. This resulted in severe, irreversible brain damage. Mr. B was subsequently discharged to other facilities. But, 6 months ago, he was readmitted to your hospital with a diagnosis of renal failure. He has remained there ever since, in a persistent vegetative state, dependent for survival on mechanical ventilation, hemodialysis, and tube feedings. Mr. B has developed increasingly severe decubitus ulcers and recurrent infections. He remains a full code. In light of his deteriorating status, Mr. B's physicians have determined that he is beyond medical rescue. They think that it is medically inappropriate and outside the standard of care to continue his life-sustaining treatment. Indeed, they think it is ethically inappropriate and inhumane to sustain Mr. B artificially while his body is decomposing. The treatment team wants to discontinue dialysis and issue a DNAR order. They have carefully explained their proposed treatment plan to Mr. B's surrogate, his daughter. But, even after many conferences, she will not consent. Mr. 8's family is very close. Discussion with his wife and sons confirms that the surrogate is acting in accordance with Mr. B's consistent, considered, and deliberated preferences. The hospital tried to transfer Mr. B to another facility willing to provide the disputed treatment, but none could be found. Mr. B's attending physician has sought guidance from the ethics committee. Introduction: Medical futility Like Mr. B, hospitalized patients at the end of life frequently lack decision-making capacity. So, decisions regarding their treatment are usually made by surrogate decision-makers Guidance for Healthcare Ethics Committees, ed. D. M. Hester and T. Schonfeld. Published by Cambridge University Press. Cambridge University Press (Chapter; wants to, but the hi withdraw surrogate without c Medi( committe It first p tions of ' disputes. After how mee a treatm( question! ing medi Defini1 For deca seemingl ments. Ir term as, rationale To a, "medical replacin! offer orr ing that I an argun tative fu1 Physiol The nan logical fi ate beca' a multit! forming chemott Witt assessm, no norn I While surrog the tre Third,

208 Chapter 12: Medical futility 89 :n surrogates and Jrevent and to resolve n a thymus gland tumor. Mr. B's endotracheal tube :. Mr. B was subsequently d to your hospital with a?rsistent vegetative state, j tube feedings. Mr. B has Ins. He remains a full code. ed that he is beyond medle standard of care to conppropriate and inhumane AR order. They have care s daughter. But, even after scussion with his wife and onsistent, considered, and ~rfacilitywilling to provide )hysician has sought guid :k decision-making capacsurrogate decision-makers IOfeld. 5s2012. (Chapters 8, 9). A futility dispute is typically described as a situation in which a surrogate wants to continue the patient's non-palliative treatment (usually life-sustaining treatment) but the healthcare provider wants to stop. Providers normally need consent to withh old or withdraw treatment. Therefore, to resolve futility disputes, providers must: (1) accede to the surrogate, (2) obtain consent, or (3) find a legitimate basis to withhold or withdraw treatment without consent. l Medical futility is one of the most common reasons for ethics consultation and ethics committee review. This chapter serves as a basic primer to medical futility disputes. It first provides some essential context and background, including the leading definitions of "medical futility." Then it reviews the primary factors that cause medical futility disputes. After providing this conceptual and SOCiological background, this chapter then addresses how medical futility disputes can be avoided and resolved. Included in this discussion is a treatment of preventative ethics, leading mechanisms for resolving futility con flicts, and questions for further discussion to motivate HEC members' thinking on the issues surrounding medical futility. Definitions of "medical futility" For decades, bioethicists have warned that there is a temptation and tendency to use the seemingly objective and scientific term "medical futility" to mask heavily value-laden judgments. Indeed, many healthcare providers, and even ethics committee members, employ the term as an excuse to stop treatment without devoting sufficient attention to the underlying rationale for refusing or wanting to refuse treatment. To avoid this danger, some have suggested that, rather than describing treatm ent as "medically futile," it should instead be described as "non-beneficial" or "inappropriate." But replacing the adjective does not solve the problem. The proposition that clinicians need not offer or provide inappropriate treatment seems uncontroversial. But it is also vacuous. Applying that proposition to any particular situation requires more than affixing a label. It requires an argument. There are three fundamental types of arguments: physiological futility, quantitative futility, and qualitative futility. Physiological futility The narrowest and most clearly defined type of "medically futility" is referred to as "physiological futility" (Pope, 2007). Physiologically futile interventions are considered inappropriate because they have a zero percent chance of being effective. Commentators have offered a multitude of colorful examples, including: prescribing antibiotics for a viral illness, performing CPR in the presence of cardiac rupture or severe outflow obstruction, and offering chemotherapy for an ulcer. With physiological futility, the ethics committee member does not make any evaluative assessment that the treatment's effect is too unlikely, too small, or not worthwhile. There is no normative disagreement. Instead, healthcare providers can readily ascertain physiological While medical futility disputes are paradigmatically between the responsible physician and the surrogate, there are three other types. First, there is intra-professional conflict, between members of the treatment team. Second, there is intra-familial conflict, among members of the patient's family. Third, there are questions regarding patients without proxies.

209 90 Section 2: Consultation futility based solely upon their clinical knowledge. The basis for refusing treatment is an to make t empirical one: the treatment simply will not work. committe, However, this objectivity comes at a steep price. Physiological futility has a very lim would. Fa ited applicability. Decisions about withholding and withdrawing treatment are usually based tions and on probabilities as opposed to certainties. Providers can rarely be certain that there is a treatment 100 percent probability that a given intervention will have zero effect. In the case ofmr. B, for Never1 example, neither ventilation nor dialysis are physiologically futile. They have been working itatively f successfully for months. (2) perm, have refer Quantitative futility nently un. tion, awar While few disputed interventions are physiologically futile, many more are probably inefnot comn fective. Accordingly, some commentators have proposed a quantitative standard for detersimply ex mining when life-sustaining treatment is inappropriate. Proponents of quantitative futility note that clinical studies and scoring systems can provide enough information to provide an empirical basis for establishing percentage thresholds. Perhaps the most common quantita Summal tive futility standard holds that a treatment should be regarded as medically futile if it has Consensu not worked in the last 100 cases (Schneiderman & Jecker, 2011). which ph~ At first blush, quantitative futility seems ethically defensible. The ethics committee memminewhe ber only determines whether the requested intervention can reasonably achieve the patient's futility" a goals. The member does not necessarily challenge the patient's goals themselves. However, quantitative futility suffers from two serious problems. First, it is unclear where the threshold percentage should be set. Should it be 2 percent, 1 percent, or even 0.1 percent? Causes Setting the threshold of probability is a value judgment about which there is considerable Medical f variability. Second, even if healthcare providers and society could settle upon a threshold donotwa percentage, available measures from population-level studies are very imprecise. It is diffisurrogate cult for physicians to ascertain whether a given threshold standard applies to any particular that surrc patient. main rea5 Qualitative futility With a quantitative standard, the ethics committee member starts with the patient's own goals and determines whether those goals are sufficiently achievable. However, when applying a qualitative futility standard, the member questions whether the patient's goals themselves are worthwhile. Qualitative futility has two primary forms. The first form ofqualitative futility asserts that treatment is medically inappropriate when its prospective benefits are outweighed by its associated burdens to the patient. For example, providing long-term dialysis to a patient with severe dementia arguably prolongs agony with no likelihood ofa good outcome. Similarly, performing CPR on a patient with metastatic cancer is arguably disproportionately burdensome. It cannot restore the patient but, by causing multiple rib fractures, would serve to increase the patient's suffering. The second form ofqualitative futility asserts that treatment is inappropriate when it simply cannot provide the patient a minimum quality oflife worth living. The expected outcome is oflittle or no value in light of the patient's extremely poor condition or prognosis. Providing the disputed treatment might not cause the patient to suffer. But neither does it offer the patient any reasonable benefit. Qualitative futility is heavily criticized. While an individual may make a personal choice to forgo treatment, it is a very different matter for an ethics committee or healthcare provider Reason~ Repeated believe th that surf( (1) distru gion, and Distrust SurrogatE in the pa physician more con Distn stantial e' prolongar to withdr to growit!

210 l Chapter 12: Medical futility 91 for refusing treatment is an gical futility has a very limstreatment are usually based iy be certain that there is a :ffect. In the case ofmr. B, for :ile. They have been working any more are probably inefmtitative standard for deter 'nents of quantitative futility sh information to provide an the most common quantitad as medically futile if it has I.. The ethics committee mem Lsonably achieve the patient's goals themselves. ems. First, it is unclear where percent, or even 0.1 percent? which there is considerable :mld settle upon a threshold Lre very imprecise. It is diffilard applies to any particular ts with the patient's own goals ~. However, when applying a 1e patient's goals themselves nedically inappropriate when s to the patient. For example, Lrguably prolongs agony with a patient with metastatic can re the patient but, by causing ering. is inappropriate when it sim living. The expected outcome ldition or prognosis. Provid.. But neither does it offer the may make a personal choice mittee or health care provider to make that decision on the patient's behalf. Most problematic is the risk that an ethics committee or provider may judge the patient's quality of life to be far less than the patient would. For example, people with physical and cognitive disabilities obtain many satisfactions and rewards in their lives. But others may not recognize those possible benefits of treatment. Nevertheless, there is growing consensus that continued life-sustaining treatment is qualitatively futile in two situations: (1) when a patient is permanently unconscious and/or (2) permanently totally dependent on intensive medical care. Some Canadian authorities have referred the former as the "minimum goal" oflife-sustaining treatment. When permanently unconscious, patients have no thoughts, sensation, purposeful action, social interaction, awareness ofself, or awareness oftheir environment. Therefore, the minimum goal does not comment on the quality ofthe patient's experience; rather it states that the patient must simply experience his/her own existence. Summary Consensus on a definition of "medical futility" remains elusive. Except in the rare case in which physiological futility applies, the ethics committee member has no algorithm to determine when requested treatment is inappropriate. Nevertheless, the concepts of "quantitative futility" and "qualitative futility" provide a useful framework to guide thinking and analysis. Causes of futility disputes Medical futility disputes typically result from surrogates requesting treatment that clinicians do not want to provide. To understand the causes ofthese disputes, it is useful to examine why surrogates insist and why clinicians resist. First, this section summarizes the main reasons that surrogates demand non-recommended treatment. Second, this section summarizes the main reasons why clinicians are unwilling to provide the desired treatment. Reasons for surrogate requests Repeated surveys demonstrate that the public is far more likely than health care providers to believe that patients have a right to demand care that doctors think will not help. The reasons that surrogates request non-recommended treatment can be grouped into four categories: (1) distrust; (2) cognitive issues; (3) psychological and emotional issues; and (4) values, religion, and miracles. Distrust Surrogates are aware of the limits of prognostication, sometimes because of a prior error in the patient's treatment. Accordingly, they may doubt that things are actually as bad as physicians represent. Moreover, with greater access to medical information, surrogates are more confident in opposing health care providers. Distrust is especially prevalent among African-Americans and Hispanics. There is substantial evidence that these patients and surrogates are more likely to request unconditional prolongation oflife-sustaining treatment and are less likely to agree with a recommendation to withdraw or withhold. Furthermore, even non-minorities are increasingly distrustful, due to growing attention on providers' economic incentives.

211 92 Section 2: Consultation Cognitive issues Unfortunately, surrogates frequently do not understand the clinical status of the patients whom they represent. Some studies have shown that less than halfofsurrogates, regardless of educational level, had adequate knowledge ofwhat was going on and what would happen to the patient. Sometimes, the surrogate lacks capacity to make the relevant decisions. But even when the surrogate has capacity, there are three key iatrogenic causes ofsurrogate misunderstanding. First, providers often fail to explain clearly the patient's condition and prognosis with clear, jargon-free language. Second, providers may place undue pressure on the surrogate and fail to allow sufficient time to process information. Third, different specialists often supply the surrogate with uncoordinated, even conflicting, information. Psychological and emotional issues In addition to cognitive issues, many surrogates have clinically diagnosable conditions such as stress, depression, and anxiety. These psychological problems may impair the surrogate's decision-making capacity. But, even if the surrogate has capacity, she may find it difficult to carry out her fiduciary duties, because of loyalty, guilt, or uncertainty about the patient's wishes, or because of other family dynamics. Furthermore, some surrogates may have "dubious motives" in that they are looking out for their own interests rather than the patient's interests. Values, religion, and miracles While some requests for inappropriate treatment can be explained by the surrogate's distrust or by cognitive or psychological impairment, the most intractable futility disputes tend to be those in which the surrogate's decision is based on a value difference over "odds and ends," over what is a worthwhile chance or what is a worthwhile outcome. Religion is at the bottom of the most intractable futility disputes (Zier et ai., 2009). For example, in the widely discussed Samuel Golubchuk case, physicians determined that their patient had minimal brain function and that his chances for recovery were slim. Mr. Golubchuk's insurmountable problem with wound infections required providers repeatedly to hack away surgically at his skin ulcers. Several physicians resigned because they thought this was tantamount to "torture." Still, Mr. Golubchuk's adult children argued that taking their father offlife support would be a sin under their Orthodox Jewish faith. Even apart from religion, many surrogates request treatment with very low odds ofsuccess, because they think that any chance is worth taking when the stakes are life and death. Indeed, a majority of the American public believes in miracles. They believe that, even if doctors said futility had been reached, divine intervention by God could save their family member. Reasons for provider resistance Since the surrogate speaks for the patient, respect for autonomy means that providers should generally follow surrogate decisions. But medical futility concerns the limits of autonomy. There are five main reasons why providers resist surrogate treatment requests. 2 They want These are professional reasons for wanting to refuse a surrogate's request for life-sustaining treatment. Increasingly, healthcare providers are also asserting personal, conscience-based objections to patient treatment requests (Chapter 18). to: (1) avoid medical pro Avoid patien Perhaps the avoid being surrogate-if another cast not Auschw Of coun fort (e.g., d outweighed plicit in cau suffering." Respect pati Providers '\I the surroga Indeed, Sigl treatment ( that most p Protect the Physicians beholden t "indenture sion is a sel Avoid mora Medical fu thing to d course ofa It can also other patif Promote 91 Finally, pn they balan must be b subject of at the bed "hard" res Summal Identifyin successful

212 Chapter 12: Medical futility 93 :linical status of the patients alf ofsurrogates, regardless of m and what would happen to e relevant decisions. But even :auses ofsurrogate misunder ~ nt's condition and prognosis undue pressure on the surrotird, different specialists often Jrmation. T diagnosable conditions such ns may impair the surrogate's lcity, she may find it difficult ncertainty about the patient's o.e surrogates may have "dubi ~e s ts rather than the patient's ned by the surrogate's distrust.ble futility disputes tend to be ference over "odds and ends," :ome. isputes (Zier et al., 2009). For fsicians determined that their recovery were slim. Mr. Gol [uired providers repeatedly to.ned because they thought this ldren argued that taking their Nish faith. ~nt with very low odds of suc 1 the stakes are life and death. les. They believe that, even if y God could save their family ly means that providers should tcerns the limits of autonomy. eatment requests. 2 They want ~quest for life-sustaining sanal, conscience-based to: (1) avoid patient suffering, (2) respect patient autonomy, (3) protect the integrity of the medical profession, (4) avoid moral distress, and (5) promote good stewardship. Avoid patient suffering Perhaps the most significant reason that providers resist surrogate requests is the desire to avoid being engaged in causing suffering. In the Golubchuk case, one physician described the surrogate-requested treatment as "abomination," "immoral," and "tantamount to torture." In another case from Boston, a staff member said: "This is the Massachusetts General Hospital, not Auschwitz." Of course, healthcare providers are willing to inflict things that cause pain and discomfort (e.g., chemotherapy). But they are willing to do this only because such side effects are outweighed by some benefit. In other words, providers are not really opposed to being complidt in causing patient suffering per se. They are opposed to participating in "unwarranted suffering. " Respect patient autonomy Providers want to do what they think the patient would have wanted. They often doubt that the surrogate's decision accurately reflects the patient's wishes, preferences, or best interest. Indeed, significant empirical evidence shows that surrogates frequently do not make the same treatment decision that the patient would have made for herself. Significant evidence shows that most patients prefer less aggressive medicine at the end of life. Protect the integrity of the medical profession Physicians want to defend the integrity of the medical profession. They do not want to be beholden to provide whatever treatment patients or surrogates want. Physicians are not "indentured servants," "reflexive automatons," or "vending machines." The medical profession is a self-governing one with its own standards of professional practice. Avoid moral distress Medical futility is the leading cause of moral distress among nurses. Nurses "know the right thing to do," but institutional constraints make it nearly impossible to pursue that right course of action. Moral distress can drive people from the profession and thus reduce access. It can also reduce staffing levels and make people operate less well, thus adversely impacting other patients' quality of care. Promote good stewardship Finally, providers want to be good stewards of healthcare resources. In most futility disputes they balance autonomy against beneficence or non-maleficence. But sometimes, autonomy must be balanced against justice (Chapter 16). While end-of-life costs have been a major subject of health policy debates, they have not played, and generally should not play, a role at the bedside. On the other hand, physicians do want to be careful with the allocation of "hard" resources like ICU beds, particularly in true triage situations. Summary Identifying and understanding the causes ofmedical futility disputes are important for their successful collaborative resolution. In particular, with a better understanding of surrogates'

213 94 Section 2: Consultation motivations and rationales for resisting provider recommendations to discontinue life support, the ethics committee can better develop empirically derived interventions. The committee can incorporate targeted interventions into its dispute resolution mechanisms and deploy them according to the precise basis for surrogate dissent. For example, if the basis for disagreement is prognostic distrust, it might be effective to offer an independent second opinion or a time-limited trial of the disputed therapy. Preventative ethics If possible, it is preferable to prevent medical futility disputes from arising in the first place, rather than to attempt resolution after they have arisen. There are three main mechanisms by which an ethics committee can engage in preventative ethics: (1) surrogate training, (2) staff education, and (3) mandatory consults. Surrogate training Surrogates find themselves performing a new role, for the first time, under difficult circumstances. Therefore, healthcare providers should advise the surrogate of the duties of a good substitute decision-maker and provide statistical information on patient preferences. The ethics committee can help by making resources available like the American Bar Association's booklet, Making Medical Decisions for Someone Else: A How- To Guide. Staff education and good communication Most conflict over end-of-life treatment is due to communication failures. The ethics committee can pre-emptively address these deficiencies by arranging for staff education and training. Importantly, providers must establish goals of care early and evaluate them routinely. They must foster realistic expectations. And they must reassure surrogates that the patient will never be abandoned. Palliative care is always appropriate. The patient's comfort and dignity must always be maintained. Mandatory consults Most of the medical futility literature focuses on surrogate demands for therapy that the provider thinks is non-beneficial. But surrogates are not always the problem. Many healthcare providers recommend or insist on overly aggressive treatment at the end of life. There are many causes for this, including: (1) the physician's anti-death attitude, (2) the physician's desire to maintain hope, (3) the physician's need to avoid failure and shame, (4) the physician's religion, (5) the physician's reimbursement incentives, and (6) the physician's sense of the goals and ends of medicine. These situations rarely mature into conflict. Sometimes the physician accedes to the surrogate's demands to avoid the potential time and stress of litigation. Usually there is no conflict because the surrogate is unaware of the treatment's low chances, side effects, or alternatives. In response, some states, like New York and California, have enacted "right to know" laws that require providers to tell terminally ill patients their end-of-life options, including palliative care and hospice. There are at least two ways that an ethics committee can check physician-driven overtreatment. First, it can permit not only physicians but also nurses, consultants, and family members to refer cases to the ethics committee. Second, the committee can institute mandatory ethics or pa facilities au Dispute While gooe inate them resolve con ond, the co modation. J recommen( refusal of tr Institutio In 1996, the futility poli and impler sometimes Having providers ij for clarifyii transparem The AIY Since there committee decision, w Goal clari Most futili! ers, chaplai are quite e putes prov 7 steps in mediation. Accomm Even when accon1mo( bye, and tc hours or d Surrogat Only rarel: priate. As
 surrogate training, (2) staff ethics or palliative care consultation for")
214 Chapter 12: Medical futility 95 ltions to discontinue life supived interventions. The com ~ resolution mechanisms and ent. For example, if the basis I offer an independent second from arising in the first place, Ire three main mechanisms by 1) surrogate training, (2) staff ethics or palliative care consultation for certain populations of patients. For example, some facilities automatically trigger a consult for all ICU patients after a defined number of days. Dispute resolution While good preventative ethics can reduce the number of futility disputes, it will not eliminate them altogether. Procedurally, there are six things that an ethics committee can do to resolve conflict. First, the committee can draft and implement an institutional policy. Second, the committee can serve as a mediator. Third, the committee can recommend accommodation. Fourth, the committee can facilitate surrogate selection. Fifth, the committee can recommend the patient's transfer. Sixth, the committee can support or authorize unilateral refusal of treatment. : time, under difficult circum Togate of the duties of a good 1 on patient preferences. The le American Bar Association's oguide. ltion failures. The ethics comg for staff education and trainand evaluate them routinely. Ire surrogates that the patient The patient's comfort and dig ::!emands for therapy that the ys the problem. Many healthtment at the end of life. There lth attitude, (2) the physician's ure and shame, (4) the physind (6) the physician's sense of e physician accedes to the suration. Usually there is no conlances, side effects, or altern a have enacted "right to know" end-of-life options, including ck physician-driven overtreatconsultants, and family memnittee can institute mandatory Institutional policy In 1996, the American Medical Association recommended that all hospitals adopt a medical futility policy (AMA et al., 1999). Over the past 15 years, more hospitals have been drafting and implementing medical futility policies. Sometimes, these are stand-alone policies and sometimes they are amendments to a DNAR or other policy. Having an institutional policy can provide significant benefits (Chapter 18). It can assist providers in decision-making about inappropriate interventions. It can provide mechanisms for clarifying values and goals. And a futility policy can offer guidelines that ensure a fair and transparent process for resolving conflict (Joseph, 2011). The AMA recommends that policies on medical futility follow a "due process" approach. Since there are no accepted substantive criteria or formulas for medical futility, the ethics committee member must resort to procedural criteria. If we cannot identify what is a right decision, we can at least address how to reach it. Goal clarification and mediation Most futility disputes are resolved informally and internally. Ethics consultants, social workers, chaplains, ethics committees, legal counsel, ombudspersons, and other hospital resources are quite effective at achieving consensus. Only around 5 percent of medical futility disputes prove intractable. Given this kind of data, it is wholly appropriate that the first 4 of 7 steps in the AMA model futility policy are aimed at communication, negotiation, and mediation. Accommodation Even when treatment is deemed non-beneficial, it may be appropriate to make a short-term accommodation. This provides the family with time: to resolve personal matters, to say goodbye, and to grieve. Even brain-dead patients are often maintained on life support for several hours or days as a matter of sensitivity to religious, cultural, or moral values. Surrogate selection Only rarely do disputes remain intractable. In such cases, surrogate selection may be appropriate. A surrogate is the patient's agent and, as such, must act according to the patient's

215 96 Section 2: Consultation L instructions, known preferences, and best interests. When a surrogate exceeds the scope of her authority, she can and should be replaced (Pope, 2010). While an effective mechanism for many disputes, surrogate selection cannot resolve some categories of conflict. In some cases it will be difficult to demonstrate surrogate deviation. Since too few individuals engage in adequate advance care planning, applicable instructions and other evidence regarding patient preferences are rarely available. Other times, the available evidence shows that the surrogate is acting faithfully and making decisions consistent with the patient's instructions, preferences, and values. Transfer When surrogate selection is not available and efforts at reaching consensus have failed, the ethics committee may transition from a mediation role to an adjudication role. The AMA model policy provides that, if the committee supports the surrogate's position and the physician remains unpersuaded, transfer of care to another physician within the institution may be arranged. If the committee supports the physician's position and the surrogate remains unpersuaded, the patient's transfer to another institution may be sought. The disputed treatment should continue pending transfer. Referer American Medic theca JAml1 Joseph R I futility anden Acad ~ Luce JM ( over el the Un PopeTM safe ha life-su: LawR, PopeTM and as: 274-8( Unilateral refusal The final step of the AMA's due process approach provides that, if transfer is not possible, then the intervention need not be offered. This should not happen without giving the surrogate reasonable notice and time to seek judicial intervention. But the AMA also noted that "the legal ramifications of this course of action are uncertain" (AMA, 1999). Indeed, only in Texas does the decision of the ethics committee clearly confer legal immunity on healthcare providers who withhold or withdraw life-sustaining treatment without consent. Other states have purported legal safe harbors, but these are usually materially limited in two ways. First, they are often linked to compliance with the standard of care. Because there is significant variability and no clear standard of care, the scope of protection is uncertain, making these safe harbors ineffective. Second, these safe harbors often require treatment until transfer. Since the transfer of patients who are the subjects of futility disputes is typically impossible, this condition is rarely satisfied. Nevertheless, the ethics committee can still serve a useful role even in states where the ethics committee has no special authority. 'The process itself usually helps all stakeholders reach consensus. Discussion questions 1. Conceptual: Is it a goal ofmedical care not only to relieve physical and emotional pain and suffering and to enhance the quality and functionality of life, but also to extend the length oflife? 2. Pragmatic: Does your institution have a medical futility policy? Has your community developed model standards and guidelines? 3. Strategic: What elements are essential to fair processes for resolving intractable conflict? Formulate a guideline document that highlights these essential features.
 (1999).")
216 J ~ LI C_h_a e_r_'_2:_m_e_d_ic_a_l_fu_t_ili_ty ~ 97 pt surrogate exceeds the scope of e selection cannot resolve some monstrate surrogate deviation. anning, applicable instructions vailable. Other times, the availld making decisions consistent References American Medical Association (AMA) (1999). Medical futility in end-of-life care: report of the Council on Ethical and Judicial Affairs. JAm Med Assoc; 281: Joseph R (2011). Hospital policy on medical futility - does it help in conflict resolution and ensuring good end-of-iife care? Ann Acad Med Singapore; 40: Luce JM (2010). A history of resolving conflicts over end-of-life care in intensive care units in the United States. Crit Care Med; 38: Pope TM (2007). Medical futility statutes: no safe harbor to unilaterally refuse life-sustaining medical treatment. Tennessee Law Review; 71: Pope TM (2009). Legal briefing: medical futility and assisted suicide. J Clin Ethics; 20: Pope TM (2010). Surrogate selection: an increasingly viable, but limited, solution to intractable futility disputes. St. Louis Univ J HIth Law & Policy; 3: Pope TM (2011). Legal briefing: medically futile and non-beneficial treatment. J Clin Ethics; 22: Schneiderman LJ, Jecker NS (2011). Wrong Medicine: Doctors, Patients, and Futile Treatment, 2nd edn. Baltimore, MD: The Johns Hopkins University Press. Truog R, Brett AS, Frader J (1992). The problem with futility. N EngI J Med; 326: Wilkinson DJ, Savulescu J(2011). Knowing when to stop: futility in the ICU. CurT Opin Anaesth; 24: Zier LS, Burack JH, Micco G, et al. (2009). Surrogate decision makers' responses to physicians' predictions of medical futility. Chest; 136: hing consensus have failed, the ell adjudication role. The AMA 'rogate's position and the physician within the institution may tion and the surrogate remains ybe sought. The disputed treates that, if transfer is not poslid not happen without giving Itervention. But the AMA also 1 are uncertain" (AMA, 1999). ittee clearly confer legal immue-sustaining treatment without are usually materially limited in standard of care. Because there cope of protection is uncertain, ors often require treatment until ; of futility disputes is typically Ul role even in states where the If usually helps all stakeholders ~ physical and emotional pain ty of life, but also to extend the policy? Has your community )r resolving intractable conflict? sential features.
217 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 277 Thaddeus Mason Pope, Legal Briefing: Futile or Non-Beneficial Treatment, The Journal of Clinical Ethics 22, no. 3 (Fall 2011): Law Legal Briefing: Futile or Non-Beneficial Treatment Thaddeus Mason Pope Readers who learn of cases, statutes, or regulations that they would like to have reported in this column are encouraged to Thaddeus Pope at tmpope@ widener.edu. ABSTRACT This issue s Legal Briefing column covers recent legal developments involving futile or non-beneficial medical treatment. 1 This topic has been the subject of recent articles in JCE. 2 Indeed, it was the subject of a Legal Briefing in fall Accordingly, this column focuses on legal developments from the past two years. These developments are usefully grouped into the following 11 categories: 1. Texas Advance Directives Act 2. Ontario Consent and Capacity Board 3. Surrogate selection 4. Ex post cases for damages 5. Ex ante cases for injunctions 6. Coercion and duress 7. Assent and transparency 8. Brain-death cases 9. Criminal and administrative sanctions 10. Conscientious objection 11. Penalties for providing futile treatment Thaddeus Mason Pope, JD, PhD, is an Associate Professor with the Health Law Institute at Widener University School of Law, Wilmington, Deleware, tmpope@widener.edu by The Journal of Clinical Ethics. All rights reserved. INTRODUCTION Medical treatment at the end of life is the subject of significant conflict. One type of conflict, medical futility dispute, arises when a healthcare provider wants to refuse treatment (usually life-sustaining treatment) that the patient or surrogate wants. Fortunately, most futility disputes are resolved consensually and informally. Only rarely do they become intractable. And even more rarely do surrogates or careproviders bring futility disputes to court or to another adjudicative tribunal. 4 But the relative absence of futility disputes from courts does not mean they are not contentious. Cases are often tried in the mass media. 5 Newspapers and television broadcasts frequently report cases in which a patient miraculously defies the odds. For example, in March 2010, Brianna Manns gave birth to conjoined twins at the University of Illinois Medical Center at Chicago. The twins share a liver and a malformed heart and can never be surgically separated, and will eventually outgrow the ability of their single heart to support their bodies. Manns refused to authorize a recommended donot-resuscitate (DNR) order. 6 Nevertheless, the twins were stable more than a year later. 7 The Manns s case is hardly unique. In December 2010, New Zealand teenager Kimberly McNeill was in a serious car crash; 15 days later
218 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 278 The Journal of Clinical Ethics Fall 2011 careproviders at Auckland City Hospital turned off her life support. McNeill survived and is now enrolling in university classes. 8 In March 2011, Gloria Cruz had a stroke in her sleep and was rushed to Royal Darwin Hospital in Australia, where she was later diagnosed as being brain dead. After her husband begged careproviders not to switch off the ventilator, Cruz woke up. 9 In addition to miracle cases, the media frequently cover cases involving neonates. 10 In September 2009, Sarah Capewell gave birth to a baby boy, 21 weeks and five days into her pregnancy. Physicians at Britain s James Paget Hospital refused to provide medical support, citing national guidelines that babies born before 22 weeks should not be given medical treatment. 11 Similarly, in March 2010, careproviders at Britain s Southend Hospital refused to resuscitate Tracy Godwin s son born at 22 weeks, because its policy was not to resuscitate babies born earlier than 24 weeks into pregnancy. 12 Not all media coverage materially impacts the resolution of futility cases. Neither do all court cases. But media coverage has caused hospitals to change their positions. Further, the threat of such coverage has chilled hospitals from pursuing such cases in the first place. It is important to remember that the effect of pressure from negative public relations can be just as effective as pressure from pending or threatened litigation. TEXAS ADVANCE DIRECTIVES ACT The Texas Advance Directive Act (TADA) permits physicians to refuse life-sustaining treatment without consent, for any reason, and with legal immunity, so long as an institutional committee agrees. 13 A hospital must give a surrogate 48 hours notice before the institutional committee meeting occurs. If a committee agrees with the attending physician that life-sustaining treatment is inappropriate, the hospital must give the surrogate 10 days after the meeting to find a facility that will provide the treatment desired. TADA proved very controversial and was the subject of significant legislative activity during the 2007 and 2009 sessions of the Texas Legislature. Bills, particularly one requiring treatment of a patient until transfer to another facility, were again proposed and debated in the 2011 session, 14 but, as in prior sessions, none were enacted into law. 15 Particularly regrettable was a failure to enact an amendment that would require the Texas Health and Human Services Commission to promulgate regulations requiring hospitals to report detailed statistical and demographic information concerning use of the act s futility provision. 16 Apparently, the original absence of a reporting mechanism was inadvertent. The 2011 proposal died because it was attached to a bill on another issue that was not voted out before the end of the session. While cases concerning TADA were widely discussed in the mass media during the mid- 2000s, far fewer cases have been reported more recently. One of those was at Texas Children s Hospital in June Physicians explained to the parents of 14-year-old Jordan Allen that there was nothing more they could do for the boy, who had inoperable glioblastoma (a brain tumor). When his parents would not consent to stopping life support, the hospital utilized the TADA process. In most cases this does not result in the unilateral removal of life support. Some surrogates consent after a committee s decision, and some patients die during the TADA process. In this case, Allen s parents were able to transfer him, five days into the 10-day waiting period, to Atrium Medical Center, a nearby long-term acute-care facility. Several weeks later, he was weaned from the ventilator and discharged home. 17 TADA as a Model Physicians in most U.S. jurisdictions are afraid to refuse surrogate-requested treatment that they deem inappropriate or even cruel. In contrast, TADA has proven effective at allowing physicians to avoid providing such treatment. Accordingly, other jurisdictions have been looking to TADA as a model. Major conferences were held in Connecticut 18 and Maryland 19 in late Medical and bar association resolutions were introduced in California, 20 New Jersey, 21 New York, 22 and Washington. 23 But no new legislation has been enacted.
219 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 279 TADA as Cautionary Lesson While some states are looking at giving careproviders more discretion, others are working to constrain the ability of careproviders to refuse life-sustaining treatment that is desired by a surrogate. For example, New York s 2010 Family Healthcare Decisions Act imposes a requirement for treatment until transfer. It provides, if a surrogate directs the provision of lifesustaining treatment, the denial of which in reasonable medical judgment would be likely to result in the death of the patient, a hospital or individual health care provider that does not wish to provide such treatment shall nonetheless comply with the surrogate s decision pending either transfer of the patient to a willing hospital or individual health care provider, or judicial review. 24 Such patient transfers are usually not found. A New Jersey bill would also impose a requirement for treatment until transfer. The bill would require, if a surrogate directs the provision of lifesustaining treatment for a patient, the denial of which in reasonable medical judgment would be likely to result in the patient s death, a health care facility or health care professional that does not wish to provide that treatment shall comply with the surrogate s decision pending: transfer of the patient to a health care facility or health care professional willing to receive the patient; or a review of the matter by a court of competent jurisdiction. 25 For decades, Virginia has had a futility provision similar to, although not quite as strong as, the one in TADA. 26 It provides that a physician is not required to prescribe or render medical treatment to a patient that the physician determines to be medically or ethically inappropriate. A bill introduced in 2011 proposed to clarify the legitimate bases on which treatment could be deemed inappropriate. The bill, which died in the legislature, would have prohibited medical treatment from being deemed medically or ethically inappropriate on the basis of a view (i) that values extending the life of a younger, nondisabled individual who is not terminally ill more than extending the life of an elderly, disabled, or terminally ill individual or (ii) different from that of the patient, or the individual authorized to act on the patient s be half, on the tradeoff between extending the length of the patient s life and the risk of disability. 27 ONTARIO CONSENT AND CAPACITY BOARD Apart from TADA, the other leading adjudicative mechanism for the resolution of medical futility disputes is Ontario s Consent and Capacity Board (CCB). 28 There are three important distinctions between TADA and CCB. First, unlike TADA committees that are part of a hospital, the CCB is an independent, quasi-judicial tribunal, a neutral, expert board. Second, unlike a TADA committee s decision that is unreviewable, even a legal and binding CCB decision can be reversed on appeal through the courts. 29 Third, while TADA committees can deem treatment inappropriate on any ground, CCB is limited to replacing surrogates who fail to act in a patient s best interests. 30 Nevertheless, both TADA committees and the CCB also handle reverse futility cases, in which the surrogate wants to stop and the careprovider wants to continue treatment. The CCB has repeatedly directed surrogates to either (1) accede to careproviders recommendations to limit treatment or (2) be replaced. 31 Perhaps the most high-profile recent case involved one-year-old Joseph Maraachli, who was suffering from a severe and progressively deteriorating neurological state. Doctors concluded that the child had no prospect of recovery and would only continue to deteriorate. Accordingly, they decided to remove his breathing tube. His parents opposed that decision; they wanted doctors to perform a tracheotomy so they could take the boy home. In January 2011, the CCB ordered the parents to comply with the doctors recommendation. 32 The parents appealed that decision to the Ontario Superior Court, which affirmed the CCB in February.
220 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 280 The Journal of Clinical Ethics Fall 2011 While considering whether to file a further appeal to the Court of Appeal for Ontario, the parents arranged a transfer to Cardinal Glennon Children s Medical Center in St. Louis. 33 In a more recent case, a patient known as B.S. was in a persistent vegetative state and developed a number of complications. His physicians proposed a palliative care plan of treatment, but his surrogate refused to consent. There was no evidence of B.S. s wishes, values, or beliefs. Applying a pure, objective best interest standard, the CCB determined that B.S. had a poor quality of life and that his condition would not improve. He was being subjected to daily indignities through invasive medical procedures that would not improve the likelihood he would recover. Accordingly, the CCB ruled that B.S. s surrogate had not complied with the principles for substitute decision making. Accordingly, the CCB directed the surrogate to consent to the proposed treatment plan. 34 Limitations of the CCB While the CCB works effectively across a range of futility disputes, it is less useful when a surrogate has reliable evidence that a patient really wanted a non-recommended treatment. 35 For example, in In re S.S., the patient was admitted to an intensive care unit (ICU) in October 2010 with catastrophic brain injuries from a multivascular stroke involving the neurocortex, and an ischemic brain lesion. S.S. had a history of diabetes, severe neuropathy, renal failure, hypertension, glaucoma, and was wheelchair bound. She had a tracheotomy and had been on life support for months. The medical team was of the opinion that S.S. would not recover from her medical difficulties and that acute interventions such as ventilation, resuscitation, life support sustaining measures and future admission to an ICU are futile and therefore not medically indicated. 36 Because S.S. s daughter, her substitute decision maker, refused to follow the medical team s advice, the team applied to the CCB. In January 2011, the CCB found that S.S. s surrogate proved that S.S. was of the Muslim faith and would want life to be sustained at all costs, even if there is pain.... Since a surrogate can be replaced only if she or he violates Section 21 of the Ontario Health Care Consent Act (HCCA), the CCB dismissed the physicians application. The surrogate complied with Section 21, because she made her treatment decision in accordance with S.S. s values and beliefs. Similarly, a physician for Desmond Watson determined that continued treatment was inappropriate. Watson had been an inpatient for almost 14 continuous months. He had severe dementia and was bedridden and non-communicative. He suffered from, and would continue to suffer from, opportunistic infections and suffered discomfort and pain from intrusive interventions such as airway suctioning, wound dressing, feeding, incontinence, repositioning, and daily care. The patient had no hope of a meaningful recovery. But his surrogate, his wife of 69 years, would not consent to withdrawing ventilatory support. She testified that Watson was a religious Catholic who would have wanted continued aggressive treatment. She and her daughter testified that Watson would choose discomfort and prefer to suffer because withdrawing life support would be a sin. In March 2011, the CCB stated that on a pure objective best interest standard, it would have ruled for the physician. But because the CCB found that the wife s and daughter s testimony about the patient s religious preferences was sincere, the CCB determined it must rule for them. 37 Recognizing the limits of the CCB in cases such as S.S. and Watson, careproviders have attempted to circumvent the CCB. For example, Mann Kee Li, a 46-year-old Toronto accountant, created an extraordinarily detailed record documenting that he wanted doctors to use all medical measures possible to save him in the event of a life-threatening emergency. But when Li was later a cancer inpatient at Sunnybrook Health Sciences Centre, his physician imposed a DNR order without Li s consultation or consent. In October 2010, the Ontario Superior Court issued an order that suspended this order and directed that the CCB conduct a hearing. 38 The court made clear that it was not compelling providers to actually resuscitate Li in case of emergency, leaving the matter to their own judgment.
221 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 281 The case soon became moot when Li s condition deteriorated. Li s family no longer felt that his previous request to receive CPR was still applicable. The exclusivity of the CCB was more directly challenged in Rasouli v. Sunnybrook Health Sciences Center. In October 2010, careproviders determined that Hassan Rasouli was in a permanent vegetative state and had no realistic hope of medical recovery. They thought it was in Rasouli s best interest to take him off life support and provide him with palliative care until he died. Rasouli s wife, Parichehr Salasel, would not consent. The careproviders and Salasel applied to court, seeking a declaration on whether her consent was required for the proposed treatment plan. In March 2011, the Ontario Court of Justice held that the Health Care Consent Act (HCCA) always requires consent to treatment. If a careprovider cannot obtain consent from a surrogate, then the careprovider must obtain consent from the CCB. In other words, healthcare providers must bring intractable surrogate-physician disputes regarding the appropriateness of continuing life-sustaining treatment to the CCB. 39 In June 2011, the Court of Appeal of Ontario affirmed. 40 However, the appellate court narrowed its own ruling in three ways. First, it clarified that only disputes over continuing life-sustaining treatment must go to the CCB. Only withdrawing not withholding treatment requires consent. If a certain intervention was never offered to a patient/surrogate in the first place, then no consent is needed. Second, the court held that interventions that offer a patient no therapeutic value do not constitute treatment. Therefore, consent would not be required to disconnect such interventions. Third, the court held that the HCCA requires consent for withdrawing futile medical interventions only when such withdrawal causes immediate death. For example, consent is not required to stop medically worthless chemotherapy. Nevertheless, the court held that consent to stop life-sustaining treatments, like those at issue in Rasouli, was still required, because the withdrawal was inextricably intertwined with the provision of palliative care. Since palliative care is treatment (requiring consent), consent is required for the associated withdrawal. Dissatisfied with this ruling, in August 2011 the providers in Rasouli filed an Application for Leave to Appeal to the Supreme Court of Canada. The court has not yet ruled on whether or nor it will accept the appeal. If it does, this could be the most significant court case to address medical futility. The core issues are rarely so clearly framed. And they have never been adjudicated by a nation s highest court. The CCB as a Model Just as TADA is seen as a model, so is the CCB. As I explained elsewhere, 41 Queensland, Australia, has a mechanism similar to the CCB. It was used to replace a surrogate in April Careproviders at Gold Coast Hospital urged Ziv Magen to consent to stopping life support for his wife, who was dying of lymphoma cancer. But Magen was not ready to let her go until he was sure that everything possible had been done to save her. Unable to obtain consent from Magen, the hospital called and was about to obtain consent from the adult guardian, when Magen s wife died while still on life support. 42 In Manitoba, Canada, a working group recommended the legislation of a CCB-like tribunal with authority to adjudicate futility disputes. 43 This was part of the broader development of end-of-life guidelines for hospitals undertaken by the Winnipeg Regional Health Authority after the high-profile medical futility case of Samuel Golubchuk in In 2011, the Manitoba Ministry of Health rejected the proposal and decided to focus exclusively on preventing intractable futility disputes through better education and communication, rather than on resolving them once they arise. 44 SURROGATE SELECTION While the U.S. lacks a special dedicated tribunal such as the CCB, careproviders are frequently able to resolve futility disputes by the selection of surrogates using regular courts. 45 Indeed, careproviders probably have an obliga-
222 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 282 The Journal of Clinical Ethics Fall 2011 tion to replace a surrogate when they lack a good-faith belief that the surrogate is faithfully making decisions on behalf of the patient. 46 For example, the DuPage County (Illinois) Public Guardian executed a DNR order for Mary Rauschenberger, despite her relatives objections. The family had been living off Rauschenberger s trust, paying their own bills, staying in her condo, and going on vacations to Disney World and Las Vegas. 47 Perhaps the most notable recent example of surrogate selection is the case of Albert Barnes. Barnes was a patient at Park Nicollet Methodist Hospital in Minneapolis. Healthcare providers determined that continued treatment for Barnes was inappropriate, but his wife insisted that all interventions continue. Unable to resolve the dispute internally, the hospital asked the Hennepin County Probate Court to transfer decision-making authority from Barnes s wife to Alternate Decision Makers, Inc., a professional guardian. Once the proceedings began, it became clear that Barnes s wife had altered her husband s advance care planning documents that confirmed he would not have wanted the treatment she was asking for. The court found her deceiving and took medical decisionmaking authority from her. 48 In some cases, a hospital selects a new surrogate without going to court. For example, in February 2010, 40-year-old Rebecca Bennett went into a coma due to complications from diabetes. After a few weeks, the ethics committee at Ruby Memorial Hospital in Morgantown, West Virginia, decided that it would stop Bennett s dialysis, despite the objections of her daughter and default surrogate, Sierra Kisner. The hospital apparently had significant evidence from other family members and co-workers that she would refuse dialysis under the circumstances. 49 The parties settled the case, whereby the hospital agreed to continue dialysis for about 10 days to allow Kisner an opportunity to transfer Bennett to another facility. 50 Child Abuse Sadly, one type of case in which surrogates are regularly replaced is homicide child abuse. In such cases, an abusive parent has a clear conflict of interest, as prolonging the child s life helps the abuser avoid more serious homicide charges. 51 For example, the Worcester, Massachusetts Juvenile Court authorized careproviders to remove seven-year-old Nathaniel Turner from life support over the objections of his father, who had been charged with assault and battery on a child. 52 In Ohio, John Jones was convicted of shaking his infant girl, Jada Ruiz-Jones, so hard that bones in her legs were fractured, and bleeding was caused in her brain. The infant was in pediatric intensive care at Akron Children s Hospital on a breathing machine in a persistent vegetative state. While her mother consented to the withdrawal of life-sustaining medical treatment, her father objected. 53 The Summit County, Ohio Probate Court ruled that the mother could remove her baby from life support over the father s objections. 54 In Wisconsin, Michael Below beat his infant daughter into a catastrophic but non-vegetative state. Life support was withdrawn, even though Wisconsin law permits the withdrawal of life support from a child only when the child is in a persistent vegetative state. Below was convicted of first-degree reckless homicide and physical abuse of a child. On appeal, he argued that the wrongful withdrawal of life support broke the chain of causation causing the child s death, and that his conviction must be reversed because the jury should have been, but was not, so instructed. In April 2011, the Wisconsin Court of Appeals rejected Below s argument. 55 Limitations of Surrogate Selection Just as there are limits to the CCB, there are limits to surrogate selection in the U.S. Sometimes a surrogate is not replaceable because she is faithful to the patient. Take, for example, the 2010 Ruben Betancourt case in New Jersey. In addition to arguing that it did not need consent to stop dialysis or to write a DNR order, Trinitas Hospital argued surrogate selection. It contended that Betancourt s surrogate, his daughter Jacqueline, suffered from a conflict of interest, because a potential medical malpractice action would be more valuable if her father were still alive. 56 (I assisted the daughter in her ef-
223 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 283 forts, as described more fully below, in the section The Rare Permanent Injunction. ) But while a financial conflict of interest could be a basis for replacing a surrogate, family members will almost always be personally impacted by a patient s death. Since there is usually a conflict of interest, this alone cannot be sufficient to disqualify a surrogate. Instead, a careprovider must establish a material conflict of interest: the issue is not the existence of a conflict of interest, but its pervasiveness and its effect. 57 There was no such evidence in the Betancourt case. In fact, the testimony of three family members indicated that Betancourt would have wanted to continue treatment. His wife testified that he would want to continue living until God wished. 58 In the New York case S.I. v R.S., the patient S.S. had designated his wife, R.S., as healthcare proxy. R.S. directed the removal of life-sustaining treatment, but that decision, as well as the appointment of R.S., was challenged by the patient s brother and sister, F.H. and S.I. The court found that the patient s siblings failed to establish any ground upon which R.S. s treatment should be removed. They did not establish that R.S. was acting in bad faith. 59 Sometimes, after being replaced by a courtappointed guardian, family members turn around and challenge the appropriateness of the guardian s decisions, just as the hospital had earlier challenged the appropriateness of the family s decisions. For example, in February 2011, Georgetown University Medical Center removed Rachel Nyirahabiyambere s feeding tube with the consent of her court-appointed guardian. In November 2010, Georgetown had sought a guardian because careproviders determined that Nyirahabiyambere s family was not making medical decisions in her best interest. 60 In March 2011, the family challenged and obtained a temporary injunction against the court-appointed guardian who seemed to be making decisions on the basis of her personal moral and political views. 61 Similarly, in the case of Gary Harvey, the court replaced Harvey s wife as surrogate, and his wife has been challenging the new substitute decision maker. In January 2006, Harvey fell down his basement stairs, leaving him in a persistent vegetative state. Careproviders soon determined that he was suffering and had little to no chance of recovery. While his wife was initially appointed guardian, she showed a pattern of dangerous behavior. So, in February 2007, a court transferred the wife s decisionmaking authority to Chemung County (New York) because she failed to use good judgment and follow medical advice. 62 Harvey s wife has been litigating for nearly five years in the New York courts to regain custody. 63 She claims that the county is not an appropriate guardian and is not taking care of her husband properly. 64 CASES FOR DAMAGES In several comprehensive studies of reported court cases, commentators have concluded that healthcare providers are overwhelmingly successful in lawsuits brought against them for stopping life-sustaining treatment without consent. 65 A study of unreported cases is finding the same thing. 66 Over the past two years, this trend has continued. For example, in Wheelock v. Doers, careproviders allegedly wrote a DNR order and then later refused to perform cardiopulmonary resuscitation (CPR) for Gene Wheelock, notwithstanding his advance directive and the specific and vocal instructions of his appointed agent and other family members. 67 The family filed a medical malpractice action in In September 2010, the Tennessee Court of Appeals affirmed summary judgment in favor of the careprovider-defendants. 68 With respect to the physician-defendant, the trial court explained: We have had a great deal of discussion here about medical services and the request of medical care providers as to whether there can be a cause of action for not providing medical services that a health care provider finds are not within those services required to be given under the standard of care, but at this point I don t believe the law of this state allows a patient or others to bring an action against a health care provider for not providing services that, within the standard of care, would not have been provided. [69]
224 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 284 The Journal of Clinical Ethics Fall 2011 The court continued: Just because a patient says I want it, does that mean you have to give it and continue giving it to when? But those are the reasons why it is left to the standard of care With respect to the hospital-defendant, the trial court explained that there was no proof that continuing CPR or giving CPR would have changed the end result. 71 In 2003, Tara Bottoms-Hawkins, a pregnant college freshman, was knocked down by an acquaintance. The fall injured her neck, and she lapsed into a coma. Bottoms-Hawkins had been in a coma for almost four months when she spontaneously delivered a son in her hospital bed. Two days later, doctors removed Bottoms- Hawkins from the ventilator against the wishes of her mother. In 2006, the mother filed a lawsuit alleging tortuous termination of life support, claiming that DeKalb Medical Center discontinued life support without consent. In 2007, the Georgia Court of Appeals ruled that lawsuit could proceed. 72 In August 2010, the jury returned a verdict for the defendants. 73 In 2009, Mel Marin brought his mother to the Cleveland Clinic for medical tests pursuant to his power of attorney. Once there, careproviders refused to comply with Marin s demands that they administer a certain medication to his mother. He subsequently sued the clinic. The court dismissed his lawsuit, holding, in part, that Ohio law allows a doctor or health care facility to refuse to comply with the instructions of an attorney-in-fact for any basis. 74 Futility Cases Still in Litigation Several other lawsuits are ongoing. In Miami, careproviders recommended that Nelson Francois authorize the removal of a ventilator for his wife, who had suffered a catastrophic brain bleed. Francois refused. A University of Miami transplant coordinator allegedly proceeded to disconnect Francois s wife s life support. Francois filed a lawsuit in While the trial court granted summary judgment in favor of the University of Miami, it later reversed that ruling. The trial court s order vacating its earlier judgment is now on appeal. 76 In California, Van Pena, MD, an employee of the Sonoma Developmental Center (SDC), was fired for writing a unilateral DNR order. Pena argued that since CPR would have been medically ineffective and non-beneficial, the DNR order was appropriate. Therefore, contended Pena, SDC s ground for dismissal was clearly pretextual. The actual basis for dismissal, Pena contends, was retaliation in violation of his civil rights for reporting substandard care. In November 2009, a jury disagreed; in May 2011, the U.S. Court of Appeals for the Ninth Circuit remanded the case for retrial. 77 While damages lawsuits (usually on claims for medical malpractice) are typically unsuccessful, families have been comparatively more successful on claims for intentional infliction of emotional distress. Here, a claim is based not on the unilateral refusal itself, but on its outrageous manner. 78 Wawrzyniak v. Livingstone is an example: in August 2010 in Toronto, Joy Wawrzyniak filed a $1 million lawsuit against Sunnybrook Health Sciences Centre and two of its physicians. The lawsuit claims that while Wawrzyniak and her father had repeatedly requested he receive life-saving treatment in case of a medical emergency, doctors unilaterally overruled those wishes, not only without consent, not only without consultation, but in an especially deceptive and insensitive manner. 79 CASES FOR INJUNCTIONS Surrogates and families not only bring ex post cases for damages after life-sustaining treatment is stopped, but they also bring ex ante actions to prevent careproviders from removing treatment in the first place. In contrast to damages action, surrogates are often successful in obtaining injunctive relief. For example, in November 2009, Catherine Palmer, with the assistance of the Alliance Defense Fund, sought a temporary restraining order and injunction against East Tennessee Children s Hospital (ETCH) on the basis of an alleged violation of the Tennessee Health Care Decisions Act. 80 The hospital had planned to withdraw treatment from her nine-month-old infant son upon the formal approval of its ethics committee. Palmer dropped the lawsuit after reaching an agreement that her son would remain a patient at ETCH.
225 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 285 On 24 October 2009, in Edmonton, Alberta, Isaiah May was born with severe oxygen deprivation and was dependent on life support. In January 2010, careproviders at the Stollery Children s Hospital determined that all medical procedures had been exhausted and there was no hope for May s recovery. Unable to obtain consent from his parents to remove the ventilator, physicians told the family they were going to remove life support. The family secured an order from the Alberta Court of Queen s Bench ordering the hospital not to remove the ventilator until a court hearing could be held on the baby s medical condition. The injunction lasted nearly two months, until 11 March By then the family had obtained independent medical assessments that substantially agreed with those of the treating team. Thus, there was little point in proceeding with the litigation, and the parents consented to the treatment team s recommendation. The baby was taken off life support and died in his parents arms. 81 The case of Baby RB in the United Kingdom (U.K.) followed a similar path. In November 2009, a British hospital asked the High Court for permission to remove one-year-old Baby RB s ventilator, over his father s objections. Baby RB s mother, who was separated from his father, supported the hospital s application. Baby RB, hospitalized since birth, was born with congenital myasthenic syndrome, a muscle condition that severely limits both the ability to breathe independently and limb movement. After several days of court hearings, Baby RB s father changed his mind. Substantial medical evidence suggested it would be in the best interests of Baby RB if medical support were withdrawn. The court issued Words of Endorsement, declaring that the conclusion reached by the parents and clinicians was the only tenable outcome for RB. 82 Courts Do Not Always Issue Temporary Injunctions In Alberta, Canada, Samir Sweiss had significant health problems, including ischemic cardiomyopathy, hypertension, type II diabetes, and chronic obstructive pulmonary disease. By late 2009, he had nearly 100 hospital admissions before suffering a 40-minute cardiac arrest that left him in an even worse state. A neurologist determined that Sweiss had a 0 percent chance of recovery. His careproviders entered a DNR order and informed his family that they were going to discontinue ventilation support. The family disagreed with this treatment plan and obtained a temporary injunction to get an independent assessment. In court, they established that Sweiss wished that all Islamic law be followed. The Court of Queen s Bench of Alberta determined that a patient s wishes and beliefs would not always trump other best interest factors. The court ruled that a temporary injunction (from 25 to 30 September 2009) was justified, given Sweiss s wishes and beliefs, but the judge refused to grant the family s request to lift the DNR order, crediting the physician s testimony that CPR would provide the patient no benefit. 83 In Victoria, Australia, Ljupco Slaveski petitioned the court to enjoin careproviders at Austin Hospital from removing life support from his father who had suffered a catastrophic stroke. Aiming to take the course that carried lower risk of injustice if it should turn out to have been wrong, the Supreme Court granted a temporary injunction, from 14 to 22 October This permitted the court to obtain a better understanding of the circumstances. It also allowed the family to obtain an independent assessment of the patient. By then, all the medical evidence indicated that ongoing and active intervention was futile and not in the patient s best interests. Accordingly, the court refused to continue intervening by injunctive relief. It refused to further restrain the Austin Hospital and the doctors who work there in the way that they have and will discharge their duties and obligations in the patient s treatment and management. 85 Courts Typically Refuse Permanent Injunctions While courts regularly grant temporary injunctions as temporary stopgap measures in exigent circumstances, they usually deny permanent injunctions. For example, in Britain the brother of AVS, a patient dying of sporadic Jakob-Creutzfeldt disease, sought to compel the
226 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 286 The Journal of Clinical Ethics Fall 2011 administration of an experimental (but probably beneficial) therapy. In November 2010, the Court of Protection denied the application. The court refused to make a declaration that administration of the therapy was in the best interest of the patient. It ruled that such a declaration would be wholly academic and purely hypothetical, as no physician was willing to offer that treatment. The court also refused to force the hospital to provide treatment against its clinician s judgment. In January 2011, the High Court of Justice affirmed. 86 In New South Wales, Australia, the prison health system sought a judicial declaration that it could lawfully discontinue all life-sustaining treatment and medical support measures for an incapacitated inmate with end-stage lung cancer. In March 2011, the Supreme Court entered that order. The Court observed that it had not even been necessary for the medical practitioners to resort to the Court for such a declaration. It explained: medical practitioners are not the mere instruments of their patients, at their patient s behest, but are also expected to bring to their tasks professional medical judgment. No patient has a right to insist on being given any particular treatment. The patient s right is that the medical practitioner use reasonable professional care in the interests of the patient s health and well-being. A patient is not entitled to insist on being prescribed particular drugs or receiving particular treatment but to that treatment, which the medical practitioner, using reasonable care, judges is best for the patient in the circumstances. The Court concluded that it would be a rare case in which the Court would require a medical practitioner to render to a patient a particular form of medical treatment, which the practitioner genuinely and reasonably thought was not warranted or appropriate in the circumstances. 87 The Rare Permanent Injunction The injunctions that courts issue in medical futility cases are almost always temporary. But Betancourt v. Trinitas Hospital, discussed above, is an important exception. In January 2008, 73-year-old Ruben Betancourt suffered severe, irreversible brain damage when his endotracheal tube became dislodged after surgery at Trinitas Hospital in Elizabeth, New Jersey. He was discharged, but was readmitted to Trinitas in July He remained there until May 2009, in a persistent vegetative state, dependent for survival on mechanical ventilation, hemodialysis, and tube feedings. He developed severe decubitus ulcers and recurrent infections. His physicians eventually determined that it was medically inappropriate and outside the standard of care to continue life-sustaining treatment for a dying patient whose body was decomposing. Since Betancourt lacked decision making capacity, the Trinitas careproviders explained their proposed treatment plan to the his surrogate, his daughter. But, even after many conferences, the daughter would not consent. Trinitas tried to transfer Betancourt to another facility that was willing to provide treatment, but none could be found. Ultimately, in January 2009, notwithstanding the daughter s objections, Trinitas careproviders wrote a DNR order and discontinued dialysis. At this time, the daughter was already talking to attorneys about a potential malpractice action concerning the dislodging of her father s breathing tube. With their help, she filed an action with the Chancery Division of the Union County Superior Court to enjoin Trinitas from stopping treatment. The court temporarily enjoined the hospital until it could hold an evidentiary hearing. Given the irreparable harm at stake, courts almost always enter these temporary restraining orders, and, given the fragile state of patients in medical futility disputes, these orders, while only intended to be only stopgap measures, often end up being practically dispositive. Pending resolution of the dispute, patients typically die while still on the disputed life support. But the temporary restraining order was not the final order for Betancourt. While dialysis may have been inappropriate and non-beneficial, it was not ineffective or physiologically
227 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 287 futile, as it worked to sustain his life. In February 2009, the Chancery Division heard testimony from witnesses on behalf of both the hospital and the Betancourt family. The hospital s witnesses testified that, while medically inappropriate, if treatment were continued at the present level, the patient could go on for quite a while. In March 2009, the court did what few courts have done in litigated medical futility disputes: it issued its final ruling on the merits. Specifically, the court granted a permanent injunction ordering Trinitas Hospital not to discontinue or suspend Betancourt s treatment without his daughter s consent. This was a case of first impression. No New Jersey case had ever addressed the right of physicians to refuse life-sustaining treatment over a surrogate s objections. Accordingly, Trinitas Hospital appealed the trial court s order to seek clarity and guidance. 88 But Betancourt died in May 2009, just as the appellate process began. Although the appellate case was still fully briefed and argued in August 2010, the Appellate Division declined to rule and dismissed the case as moot. Courts typically adjudicate only active and ongoing cases and controversies affecting the parties. Here, Trinitas s appeal questioned the correctness of the Chancery Division s injunction ordering careproviders to continue life support, but the patient was no longer receiving life support because of his death. No decision from the Appellate Division could have any practical effect on that controversy. When Betancourt died, the dispute died too. The Appellate Division did not enter its dismissal lightly. It recognized that New Jersey courts have decided appeals notwithstanding mootness where the underlying issue is one of substantial importance, likely to reoccur but capable of evading review. But the court determined that the particular circumstances of the Betancourt case were not likely to reoccur. The hospital s ethical and medical motivations were clouded by allegations of medical negligence and substantial unpaid hospital bills. The Appellate Division concluded that those unique facts did not provide an appropriate platform for consideration of the broader issues presented. 89 COERCION AND DURESS It is wholly appropriate that careproviders work to educate and even to persuade surrogates that a particular treatment plan is appropriate. Patients want guidance from physicians. Physicians can and should share, and even defend, their opinion as to the best course of action, offering evidence and reasons. But when argumentation and persuasion rise to manipulation or coercion, surrogates have sued. 90 For example, in 2009, Disability Rights Wisconsin (DRW) sued the University of Wisconsin Hospitals and Clinics (UWHC), alleging it broke the law by withholding treatment from two developmentally disabled patients with apparent cases of pneumonia. 91 With respect to one patient, J.L., DRW alleged the attending physician strongly encouraged J.L. s family to discontinue antibiotics and accept hospice services, even though J.L. was recovering from her acute illness. Among other claims, DRW alleged, UWHC policies and practices [provide] insufficient protections to people with developmental disabilities from UWHC pressuring guardians and families to discontinue life sustaining medical treatment under circumstances that are not permitted by law. 92 In July 2010, the Dane County (Wisconsin) Circuit Court denied the defendants motion to dismiss DRW s disability discrimination claims. In Yarick v. PacifiCare of California, 93 the family of Joseph Yarick brought a lawsuit alleging that doctors at Bakersfield Family Medical Group first counseled, and later pressured, them to terminate efforts at curing Yarick and to substitute, instead, comfort or end-of-life care. Yarick had been diagnosed with multiple conditions, including pneumonia and congestive heart failure. The complaint further alleges that this coercion and pressure were due to financial incentives; specifically, that the physicians insurance contracts offered insufficient payment to permit them to make decisions and to provide care based on patients reasonable medical needs, requiring the careproviders to substitute a standard of financial expediency. In Ireland, Simon Fitzmaurice claims that careproviders pressured him to refuse a ventila-
228 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 288 The Journal of Clinical Ethics Fall 2011 tor. 94 Shortly after being admitted, a doctor informed him it was rare and expensive for patients with his condition (amyotrophic lateral sclerosis ALS) to have a ventilator at home. The doctor said, This is it now for you. It is time for you to make the hard choice. In West Virginia, Terrie Lincoln described how careproviders pressured her parents to withdraw life support after she severed her spine and broke her neck in an automobile accident. 95 ASSENT AND TRANSPARENCY Sometimes conflict centers not on whether providers may unilaterally refuse treatment, but on the manner of the refusal. Families often complain about a lack of transparency and the failure of providers to involve them with, or even apprise them of, decisions to stop treatment. Take, for example, the case of Barbara Evans, who was being treated at St. James s Hospital in Leeds in 2006, when her daughter noticed a DNR order in her chart. The National Health Service (NHS) Trust explained that CPR decisions are discussed with patients and/or their relatives when physicians think it could be successful, but when physicians think it will not be successful, there is no real decision for the patient or relatives to make. Information about interventions that would not be clinically successful would be unnecessarily burdensome and of little or no value. 96 In 2010, the U.K. General Medical Council, which registers doctors to practice medicine, issued new guidance requiring that if a surrogate asks for treatment that a physician determines is not clinically appropriate, the physician should explain the basis for this view and explore the reasons for the request. The guidance further advises that physicians should explain the options of seeking a second opinion and applying to the appropriate statutory body or court for an independent ruling. 97 In March 2011, following Janet Tracey s admission to Addenbrooke s Hospital in Cambridge, providers placed a DNR order on her chart without her consent, even though she had capacity. On Tracey s request, the order was canceled. But just a few days later, providers entered another DNR order on her chart. Tracey died in March But in late August 2011, the Tracey family filed a lawsuit against the NHS Trust responsible for Addenbrooke s Hospital and against the Secretary of State for Health seeking declarations from the court that the NHS Trust s policy on the use of DNR is unlawful, and for the Secretary of State for Health to issue national guidance for patients and their families to know their rights concerning the use of DNR orders. 98 In 2010, a New Zealand hospital placed a DNR order on the chart of Juanita Wallace without consulting either her or her surrogate. While the DNR order may have been appropriate, the lack of transparency was not. Professor Grant Gillett explained: It is a misconception among medical staff, that because it is permissible for them to make the decision, that they don t need to bother discussing it. 99 While Swedish law permits physicians to refuse life-support care to patients to whom it offers no medical benefit, a refusal should be carried out in consultation with the patient and family as far as possible. Unfortunately, a number of studies report decisions are commonly made without the patient s knowledge. 100 In response, the Swedish National Board of Health and Welfare issued new life-support regulations that came into force in August In Singapore, hospitals can cease treatment they deem futile even when it is opposed by the patient s family. 102 In July 2011, the family of the late Lee Ah Cheo opposed a move by doctors from Khoo Teck Puat Hospital to stop her assisted ventilation. The family acknowledged that Cheo was ill, but had hoped she would continue to fight. The family also felt that the hospital did not give them enough time to gather relatives. The family s disruptive behavior led to the hospital calling the police for the protection of other nearby patients and staff. 103 BRAIN DEATH CASES One category of futility dispute that is comparatively far more legally settled is brain death. Once a patient has been determined to be brain dead, careproviders rarely have any legal obli-
229 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 289 gation to continue life-sustaining treatment, although they may do so as a short-term accommodation. 104 Nevertheless, there are a handful of conflicts each year. In August 2009, 22-year-old Christian Lanciano overdosed on heroin. Subsequently, doctors at Martinsburg (West Virginia) City Hospital determined he was brain dead. But his mother, Angela Lanciano Moreno, did some research on her own and thought that he would recover. The Berkeley County Circuit Court granted Moreno a temporary restraining order, giving her 10 days to find another facility to take over care for her son or to come up with another plan. 105 But after just a few days Moreno was satisfied that all of the appropriate medical tests had been done to determine her son s true physical condition. The order was dissolved, and life support was discontinued. 106 In March 2011, 19-year-old Florida resident Arthur Johnson, III, was shot in the head. He was declared brain dead and Charlotte Regional Medical Center prepared to harvest his organs, consistent with his prior consent. But his parents protested. They wanted a second opinion on whether he was actually brain-dead or if he could have recovered. The parents were unable to obtain a second opinion and, a few days later, consented to stopping life support. 107 In March 2010, the military s Joint Theater Trauma System issued recommendations that brain-dead troops be transported to advanced military hospitals to permit family members an opportunity for a final reunion with their loved ones before life support is removed. Traditionally, doctors in combat operations have not needed permission to remove a brain-dead patient from life support. 108 CRIMINAL AND ADMINISTRATIVE SANCTIONS While most legal actions concerning medical futility are private ones taken by surrogates or careproviders, sometimes government officials impose administrative or even criminal sanctions. For example, at the John Radcliffe Hospital in Oxford, England, careproviders turned off Mr. C s life support machine after a do not attempt resuscitation note was made in his medical records. The DNR note was entered despite his daughter s stating expressly that the life support was not to be switched off. The case was investigated and was the subject of a report by the Parliamentary and Health Service Ombudsman. The hospital was ordered to pay 1,000 to the family. 109 In the U.S., one significant area of medical regulatory compliance is the Emergency Medical Treatment and Labor Act (EMTALA), the 1986 federal law requiring emergency departments to screen all individuals who arrive at a hospital and stabilize any discovered emergency medical conditions. Notwithstanding the infamous Baby K case, EMTALA is generally irrelevant to medical futility disputes, as almost all such disputes concern inpatients. For decades, most federal courts, as well as the Centers for Medicare and Medicaid Services (CMS), have held that EMTALA does not apply to inpatients. However, this consensus was recently eroded. First, the U.S. Court of Appeals for the Sixth Circuit (comprising Michigan, Ohio, Kentucky, and Tennessee) held there is no inpatient exception. 110 Second, in 2011, CMS issued an advance notice of proposed rulemaking, announcing its intention to solicit comments on the need to publish a proposed rule to address the applicability of EMTALA to hospital inpatients. 111 In 2009, the Queensland [Australia] Coroner released its Findings of Inquest in the death of June Woo. 112 Woo was an 82-year-old Cantonese woman with acute respiratory failure and other co-morbidities. On her final admission to the emergency department (ED), an emergency physician entered a DNR in her chart. Since the physician believed CPR would be ineffective and inappropriate, he did not consider the decision one the relatives could consent or object to. The coroner, however, observed that, had Woo arrested in the ED, significant legal consequences may have followed. In fact, Woo did not arrest. Instead, she was admitted as an inpatient. While the family s consent to a DNR order was contested, several careproviders testified that they discussed the treatment plan with the family. The providers testified that since they had not documented
230 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 290 The Journal of Clinical Ethics Fall 2011 any disagreement, the family must have tacitly accepted. The coroner concluded that in the absence of any rejection of their proposals, the careproviders were entitled to consider they had the family s consent to the order. 113 Criminal prosecution is not uncommon when a provider is accused of deliberately hastening a patient s death through administration of pain medication and other drugs. 114 It is very rare in the medical futility context that a provider is accused of withholding or withdrawing life-sustaining treatment without consent. 115 One such ongoing case is proceeding in Dubai, in which the patient, a quadriplegic, was in a critical condition and needed continuous monitoring because of chronic heart complications. Prosecutors say that two days before the patient died, an emergency room doctor issued orders that the patient was not be resuscitated if he suffered a heart attack. The doctor also allegedly removed an oxygen monitor and other life-support apparatus, and ordered an increase in the dosage of morphine and a decrease in the quantity of oxygen below the necessary limit for the ICU patient. Euthanasia is illegal under federal law in the United Arab Emirates, and doctors are required to revive patients regardless of the patients wishes. 116 CONSCIENTIOUS OBJECTION While it has not been tested in the futility context, a healthcare provider s right to conscientious objection (CO) has been the subject of significant legal action in state legislatures and courts across the U.S. 117 While CO rights are typically invoked with respect to interventions pertaining to reproduction, CO can also be used to justify the denial of life-sustaining treatment. 118 Nevertheless, careproviders CO rights are materially limited in most states, because they are conditioned on continuing the disputed treatment until the patient is transferred to a new careprovider. PENALTIES FOR FUTILE TREATMENT The focus of legislative and judicial developments, as well as the focus of the literature on medical futility, is on the permissibility of healthcare providers refusing desired treatment. But, increasingly, policy makers have been exploring when it is mandatory for careproviders to refuse treatment. Careproviders usually must stop treatment when stopping treatment is what the patient or the surrogate wants. 119 But sometimes careproviders have a duty to stop treatment even when a patient or a surrogate wants it to continue. In 2010, the Parliament of the Spanish state of Andalusia enacted the Bill of Rights and Guarantees of the Dignity of Terminally Ill Persons. 120 Article 21 of the statute requires the responsible physician to limit the therapeutic effort, when the clinical situation warrants, avoiding therapeutic obstinacy. The statute separately defined therapeutic obstinacy in Article 5 as the initiation or continuation of life support or other interventions that lack clinical utility, which only prolong biological life, or have little chance of improvement or recovery for a person in a terminal condition or in agony from a serious and irreversible disease. 121 Some breaches of the act are classified as minor or serious ; a breach of Article 21 is defined as a very serious offense 122 and carries a fine from C15,000 = to C600,000. = 123 The legislation has recently been copied both by other provinces and is being considered by the Spanish federal government. 124 Like Andalusia, France has also encouraged its medical professionals to withhold and withdraw futile treatment at the end of life. Its 2005 Code of Medical Ethics provides that the physician must avoid any unreasonable obstinacy in diagnosis or treatment, and cannot pursue or continue treatments that appear unnecessary, disproportionate, or which have no object other than the artificial maintenance of life. 125 Applying this law, in June 2009, the Administrative Court of Nîmes (Vaucluse, France) ordered the public hospital in the city of Orange to pay damages for providing futile treatment. 126 An apparently stillborn infant who suffered from intrauterine hypoxia for 30 minutes was resuscitated after a further 25 minutes of effort. The court held that the hospital was guilty of unreasonable obstinacy in saving the life of
231 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 291 this child because the medical team could not have been unaware of the highly predictable serious neurological consequences of a long intrauterine hypoxia and because of the excessive duration of the resuscitation efforts. 127 The child is now 11 years old and suffers from severe physical and mental disabilities. Increasingly, U.S. jurisdictions are also imposing sanctions for providing overly aggressive end-of-life treatment. New York recently joined California by enacting a right to know act. These statutes typically require that, for those patients diagnosed with a terminal illness or condition, the patient s attending healthcare practitioner must offer to provide the patient with information and counseling regarding palliative care and end-of-life options appropriate to the patient, including: (1) the range of options appropriate to the patient; (2) the prognosis, risks, and benefits of the various options; and (3) the patient s legal rights to comprehensive pain and symptom management at the end of life. 128 A violation of California s disclosure law is now being litigated. 129 While not an end-of-life case, the recent case of Michael Kamrava, MD, is instructive. In June 2008, the California fertility doctor implanted a dozen embryos in Nadya Suleman ( Octomom ), which resulted in the birth of eight babies. 130 Suleman demanded all 12 embryos that were available for the procedure and would not accept anything less. 131 Kamrava did not think he could refuse to transfer less embryos than those to which N.S. would agree because he believed at the time that the ultimate decision should be largely driven by the patient s wishes. 132 He said that he felt bound to honor her wishes. 133 But the California Medical Board revoked his license. It found gross negligence. 134 The board held that while it is appropriate to consider a patient s wishes, a physician cannot be oblivious to standards of care. It concluded that Kamrava failed to exercise sound judgment. 135 Finally, an American Bar Association resolution, considered at the ABA s annual meeting in August 2011, called on the Centers for Medicare and Medicaid Services (CMS) to take preventive and corrective action in response to evidence that some institutional and individual healthcare careproviders are violating their obligations under the Medicare and Medicaid Conditions of Participation (CoPs), thwarting the treatment wishes expressed by terminally ill patients, and seeking reimbursement for these practices. The ABA Resolution calls on CMS to inform providers that their legal obligations to provide the standard of care and to honor the expressed wishes of patients may [not] be ignored without jeopardizing federal reimbursement for services that have been provided contrary to the patient s wishes. 136 CONCLUSION With better advance care planning, the rate of futility conflict may decrease. But it will not disappear. Hopefully, policy makers can learn from experience with TADA and the CCB to develop additional and better dispute resolution mechanisms. Increasingly, the message from legislative and adjudicative tribunals is that, in certain end-of-life circumstances, not only may patients autonomy be limited, but it must be limited. NOTES 1. This article focuses on medical futility. It does not cover related legal developments pertaining to involuntary active euthanasia. This article also excludes coverage of negligent (as opposed to deliberate) refusals of treatment. 2. J. Hardwig, Families and Futility: Forestalling Demands for Futile Treatment, The Journal of Clinical Ethics 16, no. 4 (Winter 2005): T.M. Pope, Legal Briefing: Medical Futility and Assisted Suicide, The Journal of Clinical Ethics 20, no. 3 (Fall 2009): A few later developments were discussed in T.M. Pope, Legal Update, The Journal of Clinical Ethics 21, no. 1 (Spring 2010): T.M. Pope and E.A. Waldman, Mediation at the End-of-Life: Getting Beyond the Limits of the Talking Cure, Ohio State Journal on Dispute Resolution 23, no. 1 (2007): ; T.M. Pope, Medical Futility, in Guidance for Healthcare Ethics Committees, ed. M.D. Hester and T. Schonfeld (Cambridge, U.K.: Cambridge University Press, forthcoming, 2012).
232 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 292 The Journal of Clinical Ethics Fall L. Ballinger, Did Hospital Turn Off Mother s Life Support Machine to Save Cash? Daily Mail, 2 February 2010 (reporting case of Lai-Mai Pang- Cheung). 6. D.L. Shelton, Mom: They Are My Babies Conjoined Twins Locked in Battle for Life, Chicago Tribune, 8 June A Medical Miracle: Conjoined Twins Kameron and Kaydon Celebrate their First Birthday, Daily Mail, 4 April E.A. Roy, Parents Refused to Let Daughter Die, Stuff, 3 July N. Adlam, Stroke Victim s Miracle Survival, NT News, 11 May While careproviders at IWK Health Centre in Halifax resuscitated Krista Cook s premature son Bryson, the mother and medical team fought about how long to sustain the severely brain-injured infant. N.S. Mother Fights for Comatose Son, CBC News, 28 February Similarly, while physicians in Sweden could unilaterally refuse treatment for catastrophically brain-injured Baby Malin, they sought consultations because they wanted the discontinuation to be consensual. De har Rätt att Avbryta Meningslös Behandling, Expressen, 5 February V. Allen and A. Levy, Doctors Told Me it was against the Rules to Save My Premature Baby, Daily Mail, 9 September T. Cohen, They Left My Baby to Die in My Arms, Daily Mail, 20 April The hospital did apologize to Godwin for failing to communicate properly and tell her what would happen. My Baby Lived for 46 minutes, but Doctors Didn t Help Him, Southend Standard, 17 March The Southend coroner s office has ordered an inquest. 13. Tex. Health & Safety Code Tex. H.B. 3520, 82nd Legislature (2011) (Hughes). 15. C. Lindell, Sensitive Topic of Futile Medical Care Faces Long Road in Legislature, Austin- American Statesman, 8 May 2011; E. Ramshaw, Texas End-of-Life Bills Appear Dead, Texas Tribune, 23 May 2011; J. Tone, How Long Should Texas Docs Treat Untreatable Patients? The Debate That Won t Go Away, Dallas Observer, 8 July Tex. S.B. 8, 82nd Legislature (First Called Session) (2011) (Nelson), House Committee Amendment 10 (Hughes). A proposed amendment for an interim study also failed. Tex. S.B. 8, 82nd Legislature (First Called Session) (2011) (Nelson), House Committee Amendment 11 (Truitt). 17. T. Ackerman, Teen s Move Sidesteps Futile-Care Controversy, Houston Chronicle, 1 July 2011; L. Frillici, Family Fights to Keep Teen Alive as Hospital Decides to End Life Support, KHOU 11 News, 30 June 2011; T. Ackerman, Brain Cancer Patient Going Home after Texas Children s Hospital Had Invoked Futile Care Law, Houston Chronicle, 23 August Hartford Hospital Ethics Committee, A Summit Medical Futility: Medicine, Law and Ethics, 21 October 2010, accessed 3 September T.M. Pope, Medical Futility and Maryland Law, Mid-Atlantic Ethics Committee Newsletter, Winter 2011, 1-3. Earlier, similar proposals have been considered in Idaho, North Carolina, and Wisconsin. 20. California Medical Association, 2009 House of Delegates, Resolution : End-of-Life Care and Futile Treatment, HODCommERes.pdf, accessed 3 September Betancourt v. Trinitas Hospital, No. A T2 (N.J. Sup. Ct. A.D. 7 August 2009) (Brief of New Jersey Hospital Association, Catholic Healthcare Partnership of New Jersey, and Medical Society of New Jersey), _small_.pdf, accessed 3 September New York State Bar Association Health Law Section, Summary Report on Healthcare Costs: Legal Issues, Barriers and Solutions (September 2009). 23. Washington State Medical Association, 2010 House of Delegates, Resolution A-2: WSMA Opinion on Medical Futility in End-of-Life Care, Official_Actions_2010.pdf, accessed 12 August N.Y. Pub. Health L f(3). 25. N.J. A.B (2011) (Conaway). 26. Va. Code Va. H.B (2011) (Bell) index.asp, accessed 12 August The Yukon has a similar tribunal called the Capability and Consent Board, board.ca, accessed 12 August M. Handelman and B. Parke, The Beneficial Role of a Judicial Process When Everything Is Too Much, Healthcare Quarterly 11, no. 4 (Winter 2008): 46, In re L.F., 2010 CanLII (ON C.C.B.); In re B.T., 2011 CanLII (ON C.C.B.). 31. See Pope, note 3 above. The CCB can also appoint substitute decision makers for friendless
233 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 293 patients. For example, in August 2010, the CCB appointed a public guardian for Kulendran Mayandy. That guardian consented to withdrawing life-sustaining treatment over the objections of some close to the patient. P. Criscione, Pastor Centre of Pro- Life Battle, Brampton Guardian, 26 August In re J.M., 2011 CanLII 7955 (ON C.C.B.). 33. R. D Aliesso, Ontario Infant at Centre of Ethics Debate Has Surgery in U.S., Globe and Mail, 21 March 2011; B. Bernhard, Cardinal Glennon Chief Answers Plea for Help, St. Louis Post-Dispatch, 27 April The appeal served to stay an application to the Provincial Guardian and Trustee, which likely would have taken custody of the infant. 34. In re B.S., 2011 CanLII (ON C.C.B.). 35. T.M. Pope, Surrogate Selection: An Increasingly Viable, but Limited, Solution to Intractable Futility Disputes, St. Louis University Journal of Health Law and Policy 3, no. 2 (2010): In re S.S., 2011 CanLII 5000 (ON C.C.B.). 37 In re DW, 2011 CanLII (ON C.C.B.). 38. Li v. Sunnybrook Health Sciences Centre (22 October 2010) (Conway, J.). 39. Rasouli v. Sunnybrook Health Sciences Centre, 2011 ONSC Rasouli v. Sunnybrook Health Sciences Centre, 2011 ONCA See Pope, note 35 above. 42. G. Stolz, Final Hours Lost in Battle over Wife s Right to Life at Gold Coast Hospital, Courier-Mail, 6 April Radio interviews with the patient s husband and with the adult guardian are available at and files/ziv-on-mornings-2.mp3, accessed 12 August Report of the WRHA Working Group on Withholding and Withdrawing Life-Sustaining Treatment (22 March 2011), healthinfo/reports/files/endoflife-report.pdf, accessed 12 August 2011; Withholding/Withdrawing Life-Sustaining Treatment: WRHA Board Working Group Report, December 2010, mb.ca/healthinfo/reports/files/endoflife- BoardReport.pdf, accessed 12 August WRHA, Access to End-of-Life Supports and Resources to Increase for Patients, Families and Professionals, 25 March 2011, media/releases/2011/ php, accessed 12 August Surrogate selection is also used in other situations. For example, in November 2010, Northwestern Memorial Hospital near Chicago asked a public guardian to be appointed for its patient Dolores Bedin, because her daughter refused to consent to her discharge home. D.L. Shelton, Hospital Says Elderly Woman Ready for Discharge; Daughter Says No, Chicago Tribune, 8 November Cardoza v. U.S.C. University Hospital, No. B195092, 2008 WL (Cal. App. 13 August 2008) (reversing demurrers granted to careproviders because: [1] they were bound to comply with the patient s directive, [2] the patient s agent was not authorized to depart from the directive, and [3] compliance with an agent s decision that is at odds with the patient s directive does not qualify as in good faith ). 47. J. Sturges, Public Guardian Often Can Help the Helpless, Naperville Sun, 26 July In re Emergency Guardianship of Albert N. Barnes, No. 27-GC-PR (Hennepin Cty. Dist. Ct., Probate Div., Minn., 11 February 2011) (Order). 49. Kisner v. West Virginia University Hospitals, No. 10-C-190 (Monongalia Cty. Circuit Court, W. Va., 25 March 2010) (Verified Complaint). 50. B. Brubaker, Woman in Coma out of Ruby: Bennett Still Needs Tracheal, Dialysis Treatment Facility, Dominion Post, 14 April In one case, the infant patient s father admitted that his motivation for seeking to prevent the hospital from removing life support was to avoid charges of murder/homicide by continuing to artificially ventilate the infant s body for a year and a day. Hernandez v. Abel., No (4th Cir. 7 July 2010) (Brief of Appellee). 52. S.H. Foskett Jr., A Family Decision Judge Says Ventilator Removal Not Up to Court, Worcester Telegram, 25 June 2009; B.B. Kush, 7-year-Old Removed from Life-Support, Pronounced Dead, Worcester Telegram, 27 June P. Trexler, Father Accused of Beating Girl Resists Removing Life Support, Akron Beacon-Journal, 9 April Judge Rules in Favor of Removing Life Support from Baby Jada, Akron Beacon-Journal, 16 July State v. Below, 2011 WI APP 64 (2011). 56. See NJHA-CHPNJ-MSNJ Brief, note 21 above. 57. A. Meisel and K.L. Cerminara, The Right to Die: the Law of End-of-Life Decisionmaking (New York: Aspen, 2010) 3.24[C]. 58. Betancourt v. Trinitas Hospital, No. UNN-C (Union Cty. Sup. Ct., N.J.) (Trial Transcript), to_show_cause_hearings_ ,_ _ pdf, accessed 12 August S.I. v. R.S., 877 N.Y.S.2d 860 (2009).
234 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 294 The Journal of Clinical Ethics Fall D. Sontag, Immigrant s Health Crisis Leaves Her Family on Sideline, New York Times, 3 March D. Sontag, Virginia: Judge Orders Nutrition for Immigrant in Nursing Home, New York Times, 11 March J. Zick, Man s Life in Court s Hands, Corning Leader, 22 June 2009; R. Finger, Wife Accused of Abuse Wants Guardianship of Husband, Star Gazette, 18 September 2009, 6A; S. Cook and T. Fioraliso, Gary Harvey s Daughter Speaks Out, WENY News, 16 December Court Allows Suit against Chemung, Star Gazette, 8 July S. Smink, Fighting for Her Husband s Custody, WETM News, 18 March See Pope, notes 3 and 35 above; D.E. Hoffmann and J. Schwartz, Who Decides Whether a Patient Lives or Dies? Trial (October 2006): J.M. Luce, A History of Resolving Conflicts over End-of-Life Treatment in Intensive Care Units in the United States, Critical Care Medicine 38, no. 8 (2010): ; C. Huff, Agreeing on Ending: Hospitalists Struggle with End-of-Life Disputes, ACP Hospitalist, November There was a factual dispute over whether the patient had revoked his advance directive, but that dispute was irrelevant to the summary judgment motion. The judge ruled on the motion assuming the patient had not revoked his advance directive. 68. Wheelock v. Doers, No. E COA- R3-CV, 2010 WL (Tenn. Ct. App. 14 September 2010). 69. Wheelock v. Doers, Technical Record 5-6 (hearing on summary judgment before the Knox County Circuit Court, Tenn., 24 July 2009). 70. Wheelock v. Doers, Technical Record Wheelock v. Doers, Technical Record DeKalb Medical Center v. Hawkins, No. A07A1405, 2007 Ga. App. LEXIS 1269 (29 November 2007). 73. K.H. Tucker, Malpractice Verdict Favors Doctors, Daily Report, 1 September The case is now on appeal. Oral argument was heard in May Marin v. Cleveland Clinic, No. 1:09CV2090, 2010 WL (N.D. Ohio 29 January 2010) (citing Ohio Rev. Code ). 75. Francois v. University of Miami, No CA-31 (11th Judicial Circuit Court, Fla. 19 May 2008) (Amended Complaint); C.M. Miller, Lawsuit asks: Was Woman Breathing when Plug Was Pulled? Miami Herald, 1 March The docket at the Miami-Dade County Clerk of Court shows that a notice of appeal was filed on 6 December Book 27512, Page Pena v. Meeker, No , 2011 WL (9th Cir. 27 May 2011). 78. See Pope, notes 3 and 35 above. 79. Wawrzyniak v. Livingstone, No. CV (Ontario Superior Court of Justice 30 August 2010) (Statement of Claim); R. Cribb, Lawsuit Could Set Precedent about End-of-Life Decisions, Toronto Star, 4 September Palmer v. Tennessee Children s Hospital, No (Knox Cty. Chancery Court, Tenn., 23 November 2009) (Complaint). 81. May v. Alberta Health Services, 2010 ABQB 213 (30 March 2010). 82. In re RB (a Child), [2009] EWHC 3269 (Fam). 83. Sweiss v. Alberta Health Services, 2009 ABQB Slaveski and Ors. v. Austin Health [2010] VSC 493 (22 October 2010). 85. The court observed: I am in no doubt that the Court has no place on the case management committee which oversees the management of Mr. Slaveski senior nor do I consider there is any serious question that it should take up such a place. 86. AVS v. A NHS Foundation Trust, [2011] EWCA Civ Application of Justice Health; re a Patient [2011] NSWSC The hospital was supported by four amici curiae: the Medical Society of New Jersey, the New Jersey Hospital Association, the Catholic Healthcare Partnership of New Jersey, and the Greater New York Hospital Association. The patient s daughter was supported by a coalition of disability groups, a coalition of Jewish groups, and me. 89. This characterization of the case was adapted from T.M. Pope, Responding to Requests for Non- Beneficial Treatment, MD-Advisor: A Journal for the New Jersey Medical Community (forthcoming 2012). 90. Jacobs v. CORE, No. 1:09-CV (W.D. Pa. filed 4 March 2009); Ussery v. Children s Healthcare of Atlanta, Inc., 656 S.E.2d 882 (Ga. Ct. App. 2008). 91. J. Stein, Group Sues UW Hospital over Policy on Withholding Treatment from Disabled Patients, Wisconsin State Journal, 14 May Disability Rights Wisconsin v. University of Wisconsin Hospital and Clinics, No 09-CV-2340 (Dane County Circuit Court, Wisc., 14 May 2009) (Complaint). 93. Yarick v. Pacificare of California, No. F (Cal. App. 1 December 2009). 94. A. Kelly, Doctors Pressured Irish Man to
235 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. Volume 22, Number 3 The Journal of Clinical Ethics 295 Refuse Ventilator and Face Death, Irish Central, 16 April T. Lincoln, Never Take No for an Answer, accessed 12 August M. Waites, Anger after Doctors Put Do Not Resuscitate Note on Records, Yorkshire Post, 1 June A similar case in which the family complained about a non-consensual DNR order is that of Margaret Cummins. E. Andrews, We ll Do Cancer Scan on Monday... If She s Still Alive : Agony of Family of Dying Grandmother Who Devoted Her Life to NHS, Daily Mail, 20 August General Medical Council, Treatment and Care towards the End of Life: Good Practice in Decision Making (20 May 2010), 16(i). 98. Leigh Day Serve Judicial Review and Human Rights Challenge to Use of Do Not Resuscitate Orders, 30 August 2011, co.uk/news/2011/august-2011/leigh-day-serve-judicial-review-and-human-rights-c, accessed 3 September 2011; S. Greenhill and J. Geoghegan, Husband s Battle to Re-draw Do Not Resuscitate Rules after Wife Dies in Hospital Blunder, Daily Mail, 31 August J. Rankin, Hospital Accused of Acting Like God, Manawatu Standard, 29 October 2010; J. Rankin, Doctors Must Consult about Resuscitation Orders, Manawatu Standard, 30 October D. Jonasson, Doctors Violate Life-Support Rules, Stockholm News, 28 June 2011; A. Bäsén, Så Bestämmer Läkarna om ditt liv är Värt att Räddas, Expressen, 27 June SOSFS 2011:7 Socialstyrelsens Föreskrifter och Allmänna råd om Livsuppehållande Behandling, accessed 12 August Hospitals Can Cease Treatment if They Think It Is Futile, New Paper, 1 August N.C. Chin, More Patients, Families Engage Doctors in Treatment Discussions, Today, 12 July In California, New Jersey, and New York, providers may be legally required to accommodate certain treatment requests for brain-dead patients J. Vincent, Judge Grants Request for Restraining Order, Martinsburg Journal, 1 September J. Vincent, Family Opts to End Care, Martinsburg Journal, 5 September J. Davis, Brain-Dead Teen Taken off Life Support and Dies, Herald Tribune, 29 March 2011; J. Davis, Family Considers Taking Brain-Dead Son off Life Support, Herald Tribune, 28 March Joint Theater Trauma System, Clinical Practice Guideline: Management of Patients with Catastrophic, Non-Survivable Head Injury, 1 March 2010, Catastrophic_Care_16_Feb_10.pdf, accessed 12 August 2011; G. Zoroya, Military Offers Closure in Brain Deaths, USA Today, 22 March Parliamentary and Health Service Ombudsman, Care and Compassion? Report of the Health Service Ombudsman on Ten Investigations into NHS Care of Older People, February 2011, home, accessed 12 August Moses v. Providence Hospital, 561 F.3d 573 (6th Cir. 2009), cert. denied, 130 S. Ct (2010) U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, Medicare Program; Emergency Medical Treatment and Labor Act: Applicability to Hospital and Critical Access Hospital Inpatients and Hospitals with Specialized Capabilities, 75 Fed. Reg. 80,762 (23 December 2010) Inquest into the Death of June Woo, No. COR 2713/02 (Queensland Coroner s Court, 1 June 2009) The coroner also concluded that the family s consent was valid because: (1) there was no prior opposition by the patient, (2) it was in the patient s best interest, (3) it was the least intrusive course of action, (4) it best preserved the patient s dignity, and (5) it constituted good medical practice E.g. T. Plohetski, Former Austin Nurse on Trial in 3 Deaths, Austin-American Statesman, 18 November State v. Naramore, 965 P.2d 211 (Kan. App. 1998) M. Nammour, Doctors Stand Trial for Killing Patient, Khaleej Times, 18 July T.M. Pope, Legal Briefing: Conscience Clauses and Conscientious Refusal, The Journal of Clinical Ethics 21, no. 2 (Summer 2010): ; T.M. Pope, Conscientious Objection, Lahey Clinic Medical Ethics Journal 18, no. 1 (Winter 2011): B.J. Balch, Some Conscience Laws Authorize Involuntary Euthanasia, National Right to Life News (April/May 2011): T.M. Pope, Legal Briefing: Compliance with Advance Directives, The Journal of Clinical Ethics 23, no. 4 (Winter 2012), forthcoming Ley de Derechos y Garantías de la Dignidad de la Persona ante el Proceso de la Muerte, noticias.juridicas.com/base_datos/ccaa/an-l html, accessed 12 August The statute also requires: (1) that the justification for the limitation appear in the medical
236 Articles from The Journal of Clinical Ethics are copyrighted, and may not be reproduced, sold, or exploited for any commercial purpose without the express written consent of The Journal of Clinical Ethics. 296 The Journal of Clinical Ethics Fall 2011 record, (2) that the limitation be concurred in by another physician, (3) that the identity of these professionals and their views be recorded in the medical record, and (4) that these professionals provide health interventions necessary to ensure proper care and comfort Article 31(1)(b) Article 32 provides, Offences under this Act shall be subject to administrative sanctions provided for in Article 36 of Law 14/1986 of April 25, General Health. That law specifies a fine from 2,500,001 to 100,000,000 pesetas. I converted that amount into Euros at An earlier version of the legislation proposed sanctioning physicians up to = C1 million for maintaining the life of a terminally ill patient without the prospect of recovery. R. Rincón, Salud Multará Hasta con un Millón el Ensañamiento Terapéutico, El Pais, 3 September In 2011, the northern Spanish states Navarro and Aragon enacted end-of-life statutes similar to the one earlier enacted in Andalusia. In May 2011, the federal government approved plans for nearly identical national legislation. The legislation was sent to consultative bodies of the Interterritorial Health Council, so that its introduction can be standardized across all regions. The draft legislation will then be submitted for debate in Spanish Parliament. E. de Benito, La Ley de Muerte Digna Consagra el Derecho a Morir en una Habitación Individual, El Pais, 13 May Code de Deontologie Medicale, Code de la Sante Publique, Article R G. Mollaret, Un hôpital condamné pour acharnement thérapeutique, Le Figaro, 10 November I. Plu et al., Condamnation d un Hopital pour Obstination Deraisonable sur un Noveau-ne: Reflexion Medico-Legal et Ethique, La Revue de Médecine Légale 2, no. 2 (2011): T.M. Pope, Legal Briefing: Informed Consent, The Journal of Clinical Ethics 21, no. 1 (Spring 2010): 72-82; Ariz. S.B. 1447, 50th Legisl (2011) (Lopez); Cal. Health & Safety Code 442.5; Mich. Comp. L ; N.Y. Pub. Health L c; 18 Vt. Stat. Ann Hargett v. VITAS Healthcare Corp., No. RG (Alameda Cty. Sup. Ct., Cal., 6 July 2011) (First Amended Complaint). A similar case was settled in Florida. C.D. Kollas, Emerging Liability Issues and the Policy-Practice Gap in Endof-Life Care, poster at American College of Legal Medicine conference, In re Kamrava, No (Medical Board of California, 1 June 2011) (Decision after Nonadoption), Factual Finding In re Kamrava, Factual Finding In re Kamrava, Factual Finding In re Kamrava, Factual Finding 41, In re Kamrava, Legal Conclusion In re Kamrava, Legal Conclusion 63A American Bar Association, Commission on Law and Aging, Resolution 106B, 22 July 2011, files_flutter/ _31_1_1_9_resolution_ summary.doc , accessed 12 August 2011; _annual_house_mtg_docs.html, accessed 12 August The resolution was later withdrawn.
237 Widener Law School Legal Studies Research Paper Series no Involuntary Passive Euthanasia in U.S. Courts: Reassessing the Judicial Treatment of Medical Futility Cases Thaddeus Mason Pope Widener University School of Law This paper can be downloaded without charge from The Social Science Research Network Electronic copy available at:
238 Electronic copy available at:
239 INVOLUNTARY PASSIVE EUTHANASIA IN U.S. ~ COURTS: REASSESSING THE JUDICIAL TREATMENT OF MEDICAL FUTILITY CASES Thaddeus Mason Pope* INTRODUCTION End-of-life care issues are marked with significant conflict.! A particularly common type of conflict is the llledical futility dispute, in which a patient's surrogate decision-lllaker dem.ands life-sustaining medical treatm.ent ("LSMT") that the patient's health care provider ("provider") deellls m.edically inappropriate. A leading treatise predicts that llledical futility disputes are "likely to occupy as much, if not m.ore [time and] judicial effort in the com.ing years as conventional end-of-life * Thaddeus Mason Pope serves as Assistant Professor of Law at the University of Memphis Cecil C. Humphreys School of Law, and is serving as Visiting Assistant Professor at the Widener University School of Law ( ). This paper was developed from a presentation for NAELA's November 2006 Advanced Elder Law Institute and was supported by a summer research grant from the University of Memphis. Thanks to Sandra Johnson and Kathy Cerminara for thoughtful comments on an earlier draft. 1. See generally Catherine M. Breen et al., Conflict Associated with Decisions to Limit Life-Sustaining Treatment in Intensive Care Units, 16 J. GEN. INTERNAL MED. 283, 285 (2001) (finding that conflict occurred in 780/0 of cases concerning the limitation of life-sustaining medical treatment); John M. Luce & Douglas B. White, The Pressure to Withhold or Withdraw Life-sustaining Therapy from Critically III Patients in the United States, 175 AM. J. RESPIRATORY & CRITICAL CARE MED. 1104, 1108 (2007) (arguing that "disagreements between families and clinicians on end-of-life care are commonplace in the United States."); Hasan Shanawani et ai, Meeting Physicians' Responsibilities in Providing End-oJ-Life Care, 133 CHEST 755, 780 (2008); Keith M. Swetz et al., Report of255 Clinical Ethics Consultations and Review ofthe Literature, 82 MAYO CLINIC PROC. 686, (2007) (finding that futility disputes are one of the primary reasons for hospital ethics consultations). 229 Electronic copy available at:
240 230 MARQUETTE ELDER'S ADVISOR [Vol. 9 cases have in the last three decades."2 While most futility' disputes are -resolved informally, informal resolution is deeply informed and shaped by the "shadow of the law."3 The perception of legal liability has a considerable impact on physicians' life support decisions. 4 In one recent survey, providers were asked why they followed the instructions of surrogates instead of doing what they felt was appropriate. Almost all the responding providers cited a "lack of legal support."s But that "shadow of the law" is misperceived. In assessing the judicial treatm.ent of futility cases, it appears that most of the medical, legal, and bioethical literature concludes that courts have generally disfavored providers. Some treatises observe that "the courts have not given the elder law practitioner much guidance in the area of medical futility./ 6 However, these assessments are based on limited and outdated sets of cases. This article provides a comprehensive review of futility cases over the twenty-five year period from 1983 to Based on this review, I argue that courts have generally neither prohibited nor punished the unilateral refusal of LSMT. Providers have regularly obtained both ex ante permission and ex post forgiveness for stopping LSMT without consent ALAN MEISEL & KATHY CERMINARA, THE RIGHT TO DIE: THE LAW OF END OF-LIFE DECISIONMAKING 13.01[0] (3d ed & Supp. 2007) [hereinafter THE RIGHT TO DIE]. See Pam Belluck, Even as Doctors Say Enough, Families Fight to Prolong Life, N.Y. TIMES, Mar. 27, 2005, at 1.1 ('''The most common case that comes before the ethics committees... are families now insisting on treatment that the doctors believe is unwarranted."'(quoting Dr. John J. Paris». 3. Robert H. Mnookin & Lewis Kornhauser, Bargaining in the Shadow of the Law: The Case ofdivorce, 88 YALE L.J. 950, 968 (1979). 4. See Henry S. Perkins et al., Impact oflegal Liability, Family Wishes, and Other 'External Factors' on Physicians' Life-Support Decisions, 89 AM. J. MED. 185 (1990); S. Van McCrary et al., Treatment Decisions for Terminally III Patients: Physicians' Legal Defensiveness and Knowledge ofmedical Law, 20 L. MED. & HEALTH CARE 364 (1992). See also Thaddeus M. Pope & Ellen A. Waldman, Mediation at the End oflife: Getting Beyond the Limits ofthe Talking Cure, 22 OHIO ST. J. ON DISP. RESO~. 143, (2007). 5. Robert Sibbald et al., Perceptions of "Futile Care" among Caregivers in Intensive Care Units, 177 CANADIAN MED. ASS'N J. 1201, 1203 (2007). 6. EDWIN KASSER, ELDER LAW AND GUARDIANSHIP IN NEW YORK 4:97 (2008). 7. This article is not an analysis of the legal risks entailed in unilateral withdrawal of LSMT, given the unavoidable material jurisdictional and factual
241 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 231 In Section One, I describe a futility dispute and the informal manner in which such a dispute is usually resolved. -I also discuss the current popular: perception that the judicial treatment of such disputes generally disfavors health' care providers. While few cases are litigated, the perception of the judicial treatment of futility disputes has an enormous impact on the infor:rp.al resolution of tens of thousands of disputes in the hospital context. Furthermore, I exam.ine the complete available universe of litigated futility cases. 8 These cases can arise either before LSMT is withdrawn (ex ante cases) or after LSMT is withdrawn (ex post cases). In Section Two, I differentiate three types of ex ante cases. First, providers have had increasing success securing judicial permission to replace the authorized surrogate decision-maker with another who will agree with the provider's recommendation. Second, providers have had increasing success obtaining declaratory relief allowing the refusal itself. Third, surrogates have typically been able to only temporarily enjoin the withdrawal of LSMT. In Section Three, I examine cases brought by surrogates after LSMT is withdrawn. These ex post cases are typically adjudicated in favor of providers. Surrogates either cannot establish that the standard of care requires continued LSMT, or they cannot establish causation and damages. Surrogates' variations. Rather, it is a broad examination of those futility disputes that have been litigated. 8. The leading treatise focuses primarily on reported cases. THE RIGHT TO DIE, supra note 2, at to (Supp. 2007). Since the universe of reported cases is rather limited, this article includes a discussion of unreported cases. Of course, since there is no systematic way to locate unreported cases, these are limited to cases discussed in the secondary literature. Cf Edward K. Cheng & Albert H. Yoon, Does Frye or Daubert Matter? A Study of Scientific Admissibility Standards, 91 VA. L. REV. 471, 480 (2005) (observing that "[M]ost state court opinions, particularly at the trial court level, are unpublished or available on Westlaw or Lexis.") (citing David E. Bernstein, Frye, Frye Again: The Past, Present, and Future of the General Acceptance Test, 41 JURIMETRICS J. 385, 389 (2001». Moreover, even some of these cases have been excluded because they are still in litigation. See, e.g., Allen v. Stanford Dniv. Med. Ctr., No CV (Santa Clara Sup. Ct. Mar. '4, 2008) (defendant's motion for summary judgment taken under submission).
242 232 MARQUETTE ELDER'S ADVISOR [Vol. 9 actions for damages typically succeed only where the provider's conduct is outrageous, when LSMT is withdrawn in an egregiously insensitive manner.' ". J conclude by noting some practical im.plications of my reassessment of the judicial treatment of futility cases. Elder law treatises observe that "a doctor usually will accede to the wishes of a fam.ily that insists that. Care be continued, even if the doctor believes that no benefit is being conferred."9 But while this may have been true in the early 1990s, it m.ay be far less true today. Elder law attorneys should counsel their clients to have realistic expectations of what m.edicine can and will offer. THE MISPERCEPTION THAT FUTILITY CASES DISFAVOR PROVIDERS.. Before embarking. on.an analysis of the judicial treatment of futility cases, the distinctive feawres of a futility case l!lust be clarified, and the judicial treatm.ent of such cases m.ust be placed in the appropriate context. Specifically, while most futility disputes are resolved informally, resolution is deeply influenced by the shadow of the law created by the m.uch slllaller univ.erse of court cases. WHATIs A FUTILITY DISPUTE? A medical, futility dispute arises when a pr<?vider seeks to stop treatment that the patient or surrogate wants continued. The provider judg~s LSMT to be of no benefit and wants to "stop the train" when the patient or surrogate says "keep going." IO The provider wants to stop LSMT even without consent of the patient or surrogate.ii Accordingly, a, tnedical 9. JOAN M. KRAUSKOPF ET AL., ELDERLAW: ADVOCACY FOR THE AGING 13:26 (2d ed. 1993). See ALISON BARNES ET AL., COUNSELING OLDER CLIENTS 317 (2d ed. 2005). 10. K. Francis Lee, Postoperative Futile Care: Stopping the Train When the Family Says "Keep Going, "15 THORACIC SURGERY CLINICS 481, 481 (2005). 11. Some writers identify Lebreton v. Rabito, 650 So.2d 1245 (La. App. 1995), as a futility case. But while the daughter brought a malpractice action for the
243 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 233 futility dispute is sometimes referred to as a "reverse end-oflife," 12 a "right to life,i/13 a "duty to die," 14 or even an "involuntary 15 euthanasial/ situation. The provider and surrogate disagree about the need for LSMT because they each have different goals. 16 The surrogate's goals may include cure, amelioration of disability, palliation of sym.ptoms, reversal of disease process, or prolongation of life. The provider, -on the other hand, may, under the circumstances, judge these goals to be impossible, virtually impossible, or otherwise inappropriate. 17 It was just this sort of disagreement underlying the recent high-profile case of "Baby Emilio.1/ On November 3, 2005, Emilio Lee Gonzales was born generally healthy; however, within a few weeks, he started exhibiting neurological abnormalities.18 By November 2006, Baby Emilio showed "global developmental delay and decreased muscle tone and reflexes," and he was soon diagnosed with Leigh's disease, a progressive neuron-metabolic disorder affecting the nervous withdrawal of LSMT by her father, her mother was the authorized decision-maker who had consented to the withdrawal. Id. at This was an intra-family dispute, not a futility dispute between a patient or surrogate and a provider. See also Anthony Colarossi, Man at Center of Living Will Battle Dies, S. FLA. SUN SENTINEL, Dec. 11, 2004, at 6B. 12. See, e.g., Thomas Wm. Mayo, Living and Dying in a Post-Schiavo World, 38 J. HEALTH L. 587, 602 n.68 (2006); THE RIGHT TO DIE, supra note 2, 13.01[B] at See, e.g., Leigh Middleditch, Jr. & Joel Trotter, The Right to Live, 5 ELDER L.J. 395 (1997) [hereinafter The Right to Live]; Nancy Neveloff Dubler, Conflict and Consensus at the End of Life, HASTINGS CENTER. REP. S19, S19 (Nov.-Dec. 2005); Wesley J. Smith, Suingfor the Right to Live, DAILY STANDARD, Mar. 9, See, e.g., The Right to Live, supra note See Mary Ann Roser, Debate Heats Up on 10-day Medical Law, AUSTIN AM. STATESMAN, Aug. 10, 2006, at B See Thomas W. Mayo, Health Care Law, 53 SMU L. REV. 1101, 1110 n.78 (2000) ("[T]he core dispute is... over what constitutes a 'benefit' to the patient..."); Griffin Trotter, Editorial Introduction: Futility in the 21st Century, 19 HEC FORUM 1, 1 (2007). 17. See Thaddeus Mason Pope, Medical Futility Statutes: No Safe Harbor to Unilaterally Refuse Life-Sustaining Treatment, 75 TENN. L. REV. I, (2007) (reviewing physiological futility, quantitative futility, and four versions of qualitative futility). 18. Verified Complaint Ex. B to Ex. 1, Gonzales v. Seton Family of Hospitals, No. A07CA267 (W.D. Tex. Apr. 4, 2007).
244 234 MARQUETTE ELDER'S ADVISOR [Vol. 9 system.. 19 In Decem.ber 2006, Baby Emilio was adm.itted to the PICD at Children's Hospital of Austin, where his neurological status worsened as his brain atrophied.20 He depended on a m.echanical ventilator for breathing and a nasojejunal tube for eating.21 Baby EIllilio was sem.i-com.atose, unable to m.ove his arm.s or legs, rarely opened his eyes, and could not em.pty his bladder. 22 He also had frequent seizures, and the providers had "great difficulty keeping his lungs inflated."23 Baby Em.ilio's providers deterillined that his condition was irreversible, and they believed that to continue treatment would only "serve to prolong his suffering without the possibility of cure."24 His providers felt that "the burdens associated with his current care plan outweigh[ed] any benefit EIllilio [might have been] receiving"25 and that his "aggressive treatm.ent plan am.ount[ed] to a nearly constant assault on Emilio's fundamental hum.an dignity."26 However, Baby Em.ilio's m.other, Catarina, dem.anded that the providers continue the aggressive treatment plan.' She refused to consent to the withdrawal of Baby Em.ilio's lifesustaining treatment,27 insisting that the providers maintain him until "Jesus takes him.."28 Catarina would not agree to the providers' recom.m.endations because "every moment of life he has to spend with her is of inestim.able value."29 During the winter of 2007, Catarina had m.ultiple conferences with Baby Emilio's providers to discuss his condition and treatment plan,30 but they could not reach a consensus. In February and March of 19. Id. at <ji Id. at Ex. B to Ex Id. 22. Id. 23. Id. at Ex. 0 to Ex. I, at Id. at Ex. A to Ex Id. at Ex. 0 to Ex. I, at Id. 27. Id. at <ji Id. at Ex. B to Ex. I, at Id. at <ji Id. at Ex. B to Ex. I, at 2.
245 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY , Catarina met not only with the providers, but also with the hospital's entire Neonatal/Pediatric Ethics Committee. 31 Again, no consensus was reached. 32 Soon thereafter, Catarina filed two separate lawsuits against both the Children's Hospital and the individual providers.33 WHILE FUTILITY DISPUTES ARE RARELYRESOLVED IN COURT, JUDICIAL TREATMENT CASTS A LONG, DARK SHADOW OVER THEIR INFORMAL RESOLUTION While the Gonzales case ended up in court, most futility disputes are resolved internally and informally by the medical team. Presumably after a medical team discusses a patient's treatment goals, the nature of a patient's condition, and the range of options, the team comes up with a treatment recommendation, with which most surrogates agree. For example, in a multi-center study by Prendergast and colleagues, fifty-seven percent of surrogates agreed immediately with a provider-recommended care-plan, and ninety percent moved toward agreement within five days. 34 In a more recent study, consensus was reached in fifty-one percent of cases after the first meeting, in sixty-nine percent of cases after a second meeting, and in ninety-seven percent of cases after a third meeting.35 Even if the provider and surrogate do not agree on a treatment, it is sometimes possible to transfer a patient to 31. Id. 32. Id. at Ex. D to Ex Gonzales v. Seton Family of Hospitals, No (Travis Cty. Probate Ct, Tex. filed Mar. 20, 2007); Gonzales v. Seton Family of Hospitals, No. A07CA267 (W.O. Tex. filed Apr. 4, 2007). 34. Thomas J. Prendergast, Resolving Conflicts Surrounding End-oj-Life Care, 5 NEW HORIZONS 62, 62 (1997). 35. Daniel Garros et al., Circumstances Surrounding End oj Life in a Pediatric Intensive Care Unit, 112 PEDIATRICS e371, e373 (2003). See Laurence J. Schneiderman et al., Effect oj Ethics Consultations on Nonbenejicial Life-Sustaining Treatments in the Intensive Care Setting: A Randomized Controlled Trial, 290 JAMA 1166, 1166 (2003) (concluding that ethics consults "were useful in resolving conflicts that may have inappropriately prolonged nonbeneficial... treatments.").
246 236 MARQUETTE ELDER'S ADVISOR [Vol. 9 another institution that is willing to coltiply with the surrogate~s treatment requests. 36 While this is rarely successful,37 it does som.etimes resolve additional disputes.38 When stopping LMST is against the-wishes of a patient or surrogate, providers should take unilateral action to stop LSMT only after diligently m.aking all the foregoing attempts to resolve the conflict. 39 While most cases will never reach this stage,40 a significant percentage will. 41 A recent five-year study of sixteen 36. The model futility policies of most institutional and professional associations provide for transfer. See, e.g., AMA COUNCIL ON ETHICAL AND JUDICIAL AFFAIRS, CODE OF MEDICAL ETHICS 2.035, 2.037, at ( ); AMA COUNCIL ON ETHICAL AND JUDICIAL AFFAIRS, MEDICAL FUTILITY IN END-OF LIFE CARE, 281 JAMA 937, 940 (1999). This is consistent with the law of tortuous abandonment, which requires physicians to assist their patients in finding a new provider before terminating a treatment relationship.,see Payton v. Weaver, 182 Cal. Rptr. 225, 229 (Cal. App. 1982); Stella L. Smetanka, Who Will Protect the 'Disruptive' Dialysis Patient?, 32 AM. J. L. & MED. 53, (2006). Exploring the possibility of transfer is also required by many state health care decision-making statutes. See generally Pope, Futility Statutes, supra note See Pope, Futility Statutes, supra note 17, at 60 n. 343 (collecting cites). 38. See, e.g., Todd Ackerman, Hospital to End Life Support: Houston Woman Faces Second Fight in 2 Months Over Husband's Care, HOUSTON CHRON., Apr. 28, 2005, at 5 (discussing how St. Luke's in Houston noted that "more than 30 facilities had rejected Nikolouzos before Avalon Place surprised them and agreed to take [him]."); Joan Beck, Use Medical Treatment to Save Every Damaged Baby?, ORLANDO SENTINEL, May 18, 1990, at A13 (The GAL for Baby L "found a pediatric neu~ologlst who was willing to do everything the mother wanted./i); Alexander M. Capron, Baby Ryan and Virtual Futility, HASTINGS CENTER REP. 20, 20 (Mar.-Apr. 1995) (noting that the parents of Ryan Nguyen found a facility willing to provide the requested treatment.); John J. Paris et ai., Physicians' Refusal ofrequested Treatment: The Case ofbaby L, 322 NEW ENG. J. MED. 1012, 1013 (1990) (parents transferred' Baby L's care to a consultant pediatric neurologist). 39. See MICHAEL D. CANTOR ET AL., Do-NoT-RESUSCITATE ORDERS AND MEDICAL FUTILITY: A REPORT BY THE NATIONAL ETHICS COMMITTEE OF THE VETERANS HEALTH ADMINISTRATION 1 (Dec. 2000) (arguing that unilateral decisions "should be rese-rved for exceptionally rare and extreme circumstanc~s after thorough attempts to resolve disagreements have failed"); THE RIGHT TO DIE, supra note 2, 13.04, at (noting that "sometimes only litigation can break the impasse between demanding families and resistant health care professionals."); Timothy Bowen & Andrew Saxton, New Developments in the Law - 'Withholding and Withdrawal ofmedical Treatment, 14(5) AUSTRALIAN HEALTH L. BULL. 57, 60 (2006). 40. See Troyen A. Brennan, Ethics Committees and Decisions to Limit Care, 260 JAMA 803, 807 (1988) ("In all cases [where unilateral DNR orders were entered], the families either_ ultimately accepted this reasoning or ceased insisting that invasive procedures be used."). 41. See Pope & Waldman, supra note 4, at See also Robert L. Fine, The Texas Advance Directives Act of1999: Politics and Reality, 13 HEC FORUM 59, 81 (2001) (five of 29 cases went through the whole process, though two died and three agreed
247 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 237 hospitals found that each hospital averaged one case per year in which it decided to unilaterally stop LSMT.42 Another study of nine hospitals found that the hospitals decided to unilaterally stop LSMT in two-percent of 2,842 cases. 43 Moreover, there are strong reasons to suspect that the rate of intractability will rise. 44 While few futility cases go to court, those that do exert a strong influence on the resolution of the other cases. 45 "[W]hile legal power is relevant only in the few disputes that enter the system.... [b]argaining endowm.ents are... relevant to many futility cases."46 Mediation occurs in the "shadow of the law," 47 in that both parties consider the likely range of results if the dispute were litigated. 48 After all, "if agreem.ent cannot be reached in the mediation session, a series of default rules... corn.es into play." 49 "[T]he outcorn.e that the law will impose if no agreement is reached gives each [party] certain bargaining chips - an before treatment was actually stopped); Pendergast, supra note 34 at 67 (finding 40/0 of disputes were intractable). 42. Emily Ramshaw, Children Fight to Save Mom, DALLAS MORNING NEWS, Aug. 18, About half these patients died or were transferred to other facilities before treatment was actually stopped. Id. 43. Testimony before the Tex. H. Comm. on Public Health (2005), in INTERIM REPORT 2006, at 36 (citing a written statement of Greg Hooser). 44. The reasons for surrogate insistence are becoming more prevalent. See Pope & Waldman, supra note 4, at At the same time, provider resistance may increase with changes in reimbursement and an increased focus on palliative care. Id. 45. Cf Roberts v. Stevens Clinic, 345 S.E.2d 791, 801 (W. Va. 1986) (I/[B]ecause less than six percent of all serious lawsuits are tried, the most important thing that courts do is to cast a shadow of legal rules within which litigants can craft their own custom-made settlements."); RANDALL R. BOVBJERG & BRIAN RAYMOND, PATIENT SAFETY, JUST COMPENSATION AND MEDICAL LIABILITY REFORM 11 (2003), available at (explaining how providers engage in "defensive medicine") (last visited Feb. 2, 2008). 46. Bethany Spielman, Bargaining about Futility, 23 J. L. MED. & ETHICS 136, 137 (1995). 47. Mnookin & Kornhauser, supra note 3, at Jeffrey W. Stempel, Forgetfulness, Fuzziness, Functionality, Fairness, and Freedom in Dispute Resolution: Serving Dispute Resolution Through Adjudication, 3 NEV. L.J. 305, 308 n.14 (2003). 49. NANCY NEVELOFF DUBLER & CAROL B. LIEBMAN, BIOETHICS MEDIATION: A GUIDE TO SHAPING SHARED SOLUTIONS 25 (2004).
248 238 MARQUETTE ELDER'S ADVISOR [Vol. 9 endowment of sorts." 50 Since a party typically will not agree to settle for an amount less than it would be awarded in litigation, such entitlements typically determine the m.inimum amount a party will accept in bargaining.51 Therefore, it appears that the party who can achieve a better litigation outcome will have a higher minimum settlement amount and greater bargaining power. PROVIDERS GENERALLY PERCEIVE THAT FUTILIlY CASES DISFAVOR THE UNILATERAL REFUSAL OF LSMT It is widely believed that surrogates, can achieve the better litigation outcome. "Numerous articles have warned physicians of the serious legal risk in unilaterally writing a DNR order..."52 Specifically, based on the outcomes of several well-publicized court cases, commentators consistently conclude that courts usually side with families and ag'ainst hospitals.53. Commentators conclude that IIcourts have not upheld the right of physicians to make unilateral judgments"54 and find that "courts are overriding ostensibly sound physician assessments... [and] dictating medical maintenance of... gravely debilitated patients." 55 This assessment is widely 50. Mnookin & Kornhauser, supra note 3, at See Jonathan M. Hyman & Lela P. Love, IfPortia Were a Mediator: An Inquiry into Justice in Mediation, 9 CLINICAL L. REV. 157, 162 (2003) (noting that "public law provides the norms that guide private dispute resolution. Parties often settle... by keeping in mind and balancing the entitlements the litigation system promises."); Stephen N. Subrin, A Traditionalist Looks at Mediation: It's Here to Stay and Much Better than I Thought, 3 NEV. L.J. 196, 227 (2003) ("[t]he results of mediation are frequently - I actually believe usually - dependent upon the range of potential results that would come from formal adjudication."). 52. Edward F. McArdle, New York's DNR Law: Groundbreaking Protection of Patient Autonomy or a Physician's Right to Make Medical Futility Determinations, 6 DEPAULJ. HEALTH CARE L. 55,71 (2002). 53. Jack K. Kilcullen et al., A Multilevel Examination ofa Critically III Patient, in THREE PATIENTS: INTERNATIONAL PERSPECTIVES ON INTENSIVE CARE AT THE END OF LIFE 123 (2002). 54. Paul R. Helft et al., The Rise and Fall ofthe Futility Movement, 343 NEW ENG. J. MED. 293, 295 (2000). ' 55. Norman L. Cantor, Can Healthcare Providers Obtain Judicial Intervention against Surrogates Who Demand 'Medically Inappropriate' Life Support for Incompetent Patients?, 24 CRITICAL CARE MED. 883, 884 (1996).
249 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 239 reprinted in medical journals,56 bioethics journals,57 and even in many law reviews. 58 While some authors have made more careful and qualified case assessments, they emphasize the uncertainty and risk See, e.g., Am. CoIl. of Obstetricians and Gynecologists, Committee Opinion No. 362: Medical Futility, 109 OBSTETRICS & GYNECOLOGY 791, 792 (2007) (noting that "litigation has generally resulted in courts supporting the views of patient or family //); Robert A. Burt, The Medical Futility Debate: Patient Choice, Physician Obligation, and End-of-Life Care, 5 J. PALLIATIVE MED. 249, 250 (2002) ("[C]ourts have rejected physician claims to use futility...//); Robert S. Chabon et al., The Case of Baby K, 331 NEW ENG. J. MED. 1383, 1383 (1994) ("In no reported case has a court ruled that a physician may... override a parent's wish to continue life support for his or her dying child."); Lewis L. Low & Larry J. Kaufman, Medical Futility and the Critically III Patient, 58 HAWAII MED. J. 58, 62 (1999) (lito date, the u.s. courts have refused to grant physicians and hospitals the power to override the opinions of family members on matters of futility.//); Stanley A. Nasraway, Unilateral Withdrawal of Life-Sustaining Treatment: Is It Time? Are We Ready?, 29 CRITICAL CARE MED. 215, 217 (2001); James E. Szalados, Discontinuation ofmechanical Ventilation at End-of-Life: The Ethical and Legal Boundaries ofphysician Conduct in Termination of Life Support, 23 CRITICAL CARE CLINICS 317, 325 (2007). 57. See, e.g., Peter A. Clark, Medical Futility in Pediatrics: Is It Time for a Public Policy?, 23 J. PUB. HEALTH POL'y 66, (2002); Robert A. Gatter, Jr. & John C. Moskop, From Futility to Triage, 20 J. MED. & PHIL. 191, 194 (1995). 58. See, e.g., Peter N. Cultice, Medical Futility: When Is Enough, Enough, 27 J. HEALTH & Hasp. L. 225 (1994); Judith Daar, Medical Futility and Implications for Physician Autonomy, 21 AM. J. L. & MED. 221, 223 (1995); Sandra H. Johnson et al., Legal and Institutional Policy Responses to Medical Futility, 30 HEALTH L.J. 21 (1997) ("[T]he courts have almost uniformly ordered continued treatment."); Patrick Moore, An End-of-Life Quandary in Need of a Statutory Response: When Patients Demand Life-Sustaining Treatment that Physicians Are Unwilling to Provide, 48 B.C. L. REV.43~439(2007). 59. See, e.g., NAT'L CTR. FOR STATE COURTS, GUIDELINES FOR STATE COURT DECISION MAKING IN LIFE SUSTAINING MEDICAL TREATMENT CASES 147 (2d ed. 1993) (finding that there is "as yet no consensus... on the legal ramifications associated with [futility]..."); Gordon B. Avery, Futility Considerations in the Neonatal leu, 22 SEMINARS PERINATOLOGY 216, (1998); Jesse A. Goldner et al., Responses to Medical Futility Claims, in HEALTH LAW HANDBOOK 401, 401 (1997) (noting that the current legal status of claims of medical futility is confusing); Sandra H. Johnson et al., Legal and Institutional Policy Responses to Medical Futility, 30 HEALTH L.J. 21 (1997); Alan Meisel, Ethics and Law: Physician-Assisted Dying, 8 J. PALLIATIVE MED. 609, 615 (2005); E. Haavi Morreim, Profoundly Diminished Life, 24 HASTINGS CENTER REP. 33, 36 Gan.-Feb. 1994) (noting that "[c]ourts have yet to offer guidance..."); John M. Luce & Douglas B. White, The Pressure to Withhold or Withdraw Life-sustaining Therapy from Critically III Patients in the United States, 175 AM. J. RESPIRATORY & CRITICAL CARE MED. 1104, 1106 (2007) (correctly noting that the Baby K and Wanglie cases did not "fac[e] the futility issue head on"); Nasraway, supra note 56, at 217 ("Unilateral withdrawal... is still uncharted territory."); Sibbald, supra note 5, at 1206 (noting there is little case law to guide decisionmaking in the face of patient or surrogate opposition); Karen Trotochaud, 'Medically Futile' Treatments Require More than Going to Court, CASE MANAGER, May-June 2006, at 60, 63 ("[L]egal cases have provided limited and confusing guidance...").
250 240 MARQUETTE ELDER'S ADVISOR [Vol. 9 Moreover, much of what providers have learned about litigated cases is distorted. "[A]s the information gets passed along, it gets simplified, and sometimes oversim.plified, and som.etim.es distorted, as in a children's gam.e of 'telephone.'" 60 After all, "[e]ven experts can succum.b to reductionist tendencies and lose sight of the subtleties.ii 61 In short, actual risks are likely overestimated by providers. 62 Both providers and surrogates seem to believe that substantive end-of-life medical decision-m.aking law favors surrogates. Both understand that surrogates have an effective "veto authority" over physician judgm.ent. 63 It appears that both expect the surrogates to likely win a litigated case if an agreem.ent is not reached in LSMT n~gotiations and mediation. It is this understanding that ultim.ately casts a shadow on negotiations, rather than actual law. 64 "The m.ost efficacious social facts in the actual hospital situation are [provider] perceptions them.selves, not the objective risks...."65 But this pejorative assessm.ent of providers' non-settlem.ent alternatives appears off-base. Not only have providers 60. Alan Meisel, The Role oflitigation in End oflife Care: A Reappraisal, HASTINGS CENTER REP. 547, S48 (Nov.-Dec. 2005). 61. Id. 62. Cf Regina Ohkyusen-Cawley et al., Institutional Policies on Determination of Medically Inappropriate Interventions: Use in Five Pediatric Patients, 8 PEDIATRIC CRITICAL CARE MED. 225, 225 (2007) ("[C]ourts have endorsed patient or surrogate insistence on continued intervention, possibly fostering the reluctance of medical professionals to limit nonbeneficial interventions."). Marshall Kapp argues that the legal risks in the early 1990s were not serious and concedes that physicians had "overblown anxiety." Marshall Kapp, Futile Medical Treatment: A Review of the Ethical Arguments and Legal Holdings, 9 J. GEN. INTERNAL MED. 170, 175 (1994). 63. Cf Jacquelyn Slomka, Clinical Ethics and the Culture of Conflict, HASTINGS CENTER REP. 45, 46 (Mar.-Apr. 2005) (noting that "[a]n increasingly litigious society as well as bioethical emphasis on patient and family autonomy... have led to physicians' disempowerment..."). 64. See Pope & Waldman, supra note 4. Cf Mark A. Hall, The Defensive Effect of Medical Practice Policies in Malpractice Litigation, 54 L. & CONTEMP. PROBLEMS 119, 119 (1991) ("[T]o the extent that a crisis is in fact widely perceived, it has the quality of a self-fulfilling prophecy..."); Spielman, ~upra note 46, at 137 ("[I]n the clinical setting... myths about the law often overshadow reality."). 65. Stephen Toulmin, Institutions and their Moral Constraints, in INTEGRITY IN HEALTH CARE INSTITUTIONS: HUMANE ENVIRONMENTS FOR TEACHING, INQUIRY, AND HEALING 21, 26 (Ruth E. Bulger & Stanley J. Reiser eds., 1990).
251 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 241 frequently p.revailed in futility cases, but they also have more legislative protection than ever before. 66 Some surrogates have successfully litigated cases against providers. But those cases are legally and factually unique, so they simply cannot support a sweeping statement that the surrogates are favored judicially in all futility cases. Ex ANTE ACTIONS: GOING TO COURT BEFORE LSMT IS WITHDRAWN There are seven basic ways to resolve a futility dispute: (1) the patient dies; (2) the surrogate accedes to the provider's recommendation; (3) the surrogate replaces the provider with another provider willing to provide the requested treatment; (4) the provider accedes to the surrogate's request; (5) the provider replaces the surrogate; (6) the provider overrides the surrogate; or (7) the surrogate overrides the provider. It appears that a dispute typically goes to court only when parties take one of the last three approaches. Court actions are brought forth by way of four basic procedural vehicles, which can be categorized as either ex ante or ex post cases. If the provider withdraws treatment without consent or judicial permission, the surrogate may sue for damages. These ex post cases are discussed in Section III. The other three procedural vehicles, which are categorized as ex ante cases, are discussed here in this section. The ex ante cases involve going to court before treatment is withdrawn. First, if the provider plans to replace the surrogate, he or she will do that before withdrawing LSMT. The goal of surrogate replacement is to secure the consent of a newlyauthorized decision-maker. Second, where a provider plans to override the surrogate and withdraw LSMT without consent, a provider can first seek declaratory relief or permission to stop 66. See Pope, Futility Statutes, supra note 17 (surveying state statutes that grant providers civil, criminal, and disciplinary immunity for refusing to comply with inappropriate treatment requests).
252 242 MARQUETTE ELDER'S ADVISOR [Vol. 9 treatment. Third, a surrogate can seek an injunction to continue the treatment. PROVIDER ACTIONS TO REPLACE THE SURROGATE OFTEN SUCCEED Sometimes providers ask courts to adjudicate the fitness of the current surrogate decision-maker rather than the underlying appropriateness of the LSMT. 67 Some have even suggested that this should be the preferred method of resolving futility disputes,68 given the body of jurisprudence concerning how to select surrogates for patients without capacity. 69 In early cases, courts were generally unwilling to negate a surrogate's right to make health care decisions on behalf.of a patient. 70 However, in more recent cases, providers have successfully replaced surrogates who demanded LSMT that providers deemed inappropriate. 67. Sometimes no surrogate is reasonably available. Such a case is not really a futility dispute because not only does no one challenge the provider, but also the provider is the authorized decision-maker in many jurisdictions. See, e.g., TENN. CODE. ANN (c)(5) (2006). Cf Sumeeta Varma & David Wendler, Medical Decision Making for Patients without Surrogates, 167 ARCHIVES INTERNAL MED. 1711, 1712 (2007); Douglas B. White et al., Life Support for Patients without a Surrogate Decision Maker: Who Decides?, 147 ANNALS INTERNAL MED. 34 (2007). 68. See Jeffrey P. Burns & Robert D. Truog, Futility: A Concept in Evolution, 132 CHEST 1987, (2007); Robert D. Truog, Tackling Futility in Texas, 357 NEW ENG. J. MED. 1558, 1559 (2007) (endorsing "existing pathways to challenge the legitimacy of the surrogate to make these decisions and to seek appointment of another decision maker"). See also Rasa Gustatis, Right to Refuse Life-Sustaining Treatment, 81 PEDIATRICS 317, 319 (1988) (suggesting the use of child abuse laws to override parental requests for inappropriate treatment). But cf Robert Schwartz, Autonomy, Futility, and the Limits ofmedicine, 1 CAMBRIDGE Q. HEALTHCARE ETHICS 159, 161 (1992) (arguing that the question whether Mr. Wanglie was his wife's best substitute decision-maker was the "wrong question," and "[t]he real question [should have been]... whether the continuation of ventilator support and gastrostomy feeding were among the reasonable medical alternatives that should have been available to Mrs. Wanglie or her surrogate decision-maker, whoever that might be."). 69. See generally THE RIGHT TO DIE, supra note 2, at (outlining the jurisprudence of selecting surrogate decision makers); CLAIRE C. OBADE, PATIENT CARE DECISION MAKING: A LEGAL GUIDE FOR PROVIDERS ch.11 (1991 & Supp. 2007) (explaining various methods for surrogate decision-making). 70. See Lee, supra note 10, at 487.
253 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 243 In re Wanglie is one of the earliest and most widelydiscussed ~ases.71 Helga Wanglie was an eighty-six year old woman who was in a persistent vegetative state and dependent on a ventilator as a result of cardiorespiratory arrest. 72 Her providers determined that she could never appreciate any benefit from continued LSMT, so they advised her husband Oliver to remove the ventilator. 73 However, Oliver would not consent to stopping LSMT. 74 The providers petitioned the local probate court to appoint a professional conservator to make health care decisions for Helga.75 The hospital-nominated conservator presumably would accede to the providers' recommendation to stop LSMT, unlike Oliver. Despite the provider's efforts, the probate court denied the petition and instead appointed Oliver as conservator. 76 The court noted that Oliver was Helga's husband of fifty-three years. 77 Moreover, his decision to continue LSMT did not constitute grounds to remove his decision-making authority. The court could not conclude that Oliver's decision to continue LSMT was inconsistent with Helga's preferences or best interests. 78 While Wanglie is certainly the most famous case from the early 1990s in which a court rejected a provider's attempt at "surrogate shopping," it is not the only case. 79 In Nguyen v. 71. In re Wanglie, No. PX (Minn. Probe Ct. Hennepin County June 28, 1991), reprinted in 7 ISSUES L. & MED. 369 (1991). 72. Id. at Id. at Id. 75. Id. at 371, Id. at 372, Id. at Id. 79. See, e.g., In re Baby K, 832 F. Supp. 1022, 1031 (E.D. Va. 1993) (ruling that the mother's decision to continue treatment was not lisa unreasonably harmful as to constitute child abuse or neglect"); Belcher v. Charleston Area Med. Center, 422 S.E.2d 827, 838 (W. Va. 1992) (while providers received consent to a DNR order from a 17-year-old's parents, the court held that consent was valid only if the boy lacked capacity to decide for himself); In re Doe, Civ. No. D (Ga. Super. Ct. Oct. 17, 1991) (mem.), aff'd, 418 S.E.2d 3, 7 (Ga. 1992) (holding that providers could not withdraw LSMT from a child with only the mother's consent where the child's
254 244 MARQUETTE ELDER'S ADVISOR [Vol. 9 Sacred Heart Medical Center, a Washington court rejected a provider's argument that a child's parents serving as surrogate decision-makers should be replaced because their decision to continue LSMT constituted child abuse. 80 Similarly, a District of Columbia court refused to replace a mother as surrogate decision-maker for her two-month-old baby simply because she requested continued LSMT. 81 Some commenters cite Wanglie and other cases from the early 1990s to conclude that the strategy of having an alternative decision maker appointed by the court is "rarely successful./ 82 But it appears that these early decisions have little relevance today. First, these decisions were narrow in focus, in that they foreclosed only one legal avenue for providers to override surrogate requests. While the answers to the legal questions asked in Wanglie and Nguyen disfavored providers, these are not the only questions relevant in medical futility cases. 83 Providers can also seek ex ante permission or ex post forgiveness for unilaterally refusing a surrogate's request. 84 Second, emboldened by empirical evidence attacking the accuracy of surrogate decisions,85 providers have been father was available). Professor Annas suggests Doe is not a futility case, but instead a dispute about who is the authoriz.ed decision-maker. George J. Annas, The Case ofbaby K, 331 NEW ENG. J. MED (1994). This is belied by the course of the litigation, which demonstrated that the hospital was hardly agnostic as to which parent had authority. It argued that "continued aggressive treatment... constituted medical abuse." In re Doe, 418 S.E.2d at Nguyen v. Sacred Heart Medical Center, 987 P.2d 636, 638 (Wash. Ct. App. 1999); John Altomare & Mark Bolde, Nguyen v. Sacred Heart Medical Center, 11 ISSUES L. & MED. 199, 200 (1995) (noting that while the hospital attempted to characterize continued treatment as "cruel and inhumane," the court held that the argument had no merit). 81. Benjamin Weiser, A Question ofletting Go: Child's Trauma Drives Doctors to Reexamine Ethical Role: The Case ofbaby Rena, WASH. POST, July 14, 1991, at AI. 82. Burns & Truog, supra note 68, at Cf. THE RIGHT TO DIE, supra note 2, 13.03[A], at Providers can also seek declaratory relief. See infra "Provider Actions For Declaratory Relief Often Succeed" notes and accompanying text. Or providers can proceed to withdraw LSMT and defend any subsequent damages case. See infra "Ex Post Actions: Going to Court After LSMT Is Withdrawn" notes and accompanying text. 85. Lauren G. Collins et al, The State ofadvance Care Planning: One Decade after SUPPORT, 23 AM. J. HOSPICE & PALLIATIVE MED. 378, (2006).
255 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 245 increasingly able to establish that surrogates refusing to follow recommendations to stop L5MT are not acting in patients' best interests.86 /IA patient's preservable existence might be so tortuous, painful, or filled with suffering that it would be deemed inhumane for a surrogate to dictate continued medical intervention."87 Even permanent unconsciousness is increasingly broadly recognized as a status in which a patient can derive zero benefit from continued L5MT.88 By the mid-1990s, judicial hostility to surrogate shopping began to wane.89 Courts began replacing surrogates in situations where the only ground for disqualification was the fact that the surrogate demanded L5MT for the patient contrary to provider recomm.endations. Courts are prepared to override 86. Courts seemed always prepared to allow surrogate shopping when a parent is decision-maker and a parent's own physical abuse caused a child's dependence on LSMT. For instance, one Pennsylvania case involved a mother who abused her two-year-old baby. Providers recommended stopping LSMT, but the baby's father refused because he was concerned about his wife's criminal liability. The hospital prepared to ask a court to appoint a guardian because the father was looking out for his wife's interests, not the interests of the child. Steve Twedt, Should Comatose Baby Live? Hospital, Dad Differ, PITT. POST-GAZETTE, June 3, 1990, at AI. The father then acceded to the hospital's recommendation to withdraw LSMT. Father Ends Life Support, PITT. POST-GAZETTE, June 24, 1990, at A3; Mary Pat Flaherty, Right to Die Decision Has Little Impact Here, PITT. POST-GAZETTE, June 27, 1990, at AI. Cf J.N. v. Sup. Ct., 67 Cal. App. 3d 384, 391 (Cal. Ct. App. 2007) (holding that guardian of minor has the burden of bringing expert testimony to prove that the LSMT is in the minor's best interest); D.K. v. Commonwealth, 221 S.W.3d 382, 384 (Ky. Ct. App. 2007) (permitting a guardian to remove LSMT once parental rights were permanently terminated); In re Matthew W., 903 A.2d 333, 335 (Me. 2006) (holding that a pre-termination protection order allowing DNR for minor without parental consent violated the parents' right to due process); In re Smith, 133 P.3d 924, (Or. Ct. App. 2006) (holding that a mother was not in a position to make decisions for her minor child where she chose not to be involved in the child's health care decisions on a regular basis); In re Stein, 821 N.E.2d 1008 (Ohio 2004) (finding that a limited guardian did not have the authority to withdraw LSMT when parental rights had not yet been permanately terminated); In re Tabatha R., 564 N.W.2d 598, 605 (Neb. 1997) (discussing due process rights of parents during termination of parental rights determination). 87. Cantor, supra note 55, at Id. at Cf Causey v. St. Francis Med. Ctr., 719 So. 2d 1072, 1076 (La. Ct. App. 1998) (noting that if a surrogate insists on inappropriate treatment, "the usual procedure... is to transfer the patient or go to court to replace the surrogate or override his decision." One argument is that the surrogate is not fulfilling his or her statutorilyprovided role. Another argument is "that the guardian or surrogate is guilty of abuse by insisting on care which is inhumane.").
256 246 MARQUETTE ELDER'S ADVISOR [Vol. 9 even well-intentioned surrogates whose demands for continued LSMT cause a patient unwarranted extr.eme suffering. 90 For example, in the case In re Mason, the Massachusetts General Hospital successfully moved the local probate court to "override" a health care agent's refusal to consent to a do not resuscitate ("DNR") order.91 In granting the hospital's petition, the court explained that since the agent was I'in denial" about his mother's deterioration and distrustful of her providers, he had not given "full consideration of acceptable medical alternatives."92 Silllilarly, in a case referred to as Baby Terry, the court replaced the parents of two-month-old Terry Achtabowski Jr. with a guardian.93 Baby Terry was born premature at twentythree weeks gestation, was dependent on a ventilator, and had a host of serious medical problems that m.ade his prognosis very bleak. 94 Since continued treatm.ent was painful and offered virtually no prospect for recovery, the Genesee County Department of Social Services alleged that Baby Terry's parents were neglectful in requesting continued treatment.95 The Michigan Probate Court did not find the parents neglectful, but it did determine that they were "incompetent" to decide what was best for their son. The court reasoned that the parents lacked the requisite capacity to m.ake medical decisions for their son because their demands for continued LSMT evidenced that they were emotionally unable to appreciate the circumstances.96 Most recently, in In re Howe, the Massachusetts Probate 90. Cf. In re Guardianship of Myers, 610 N.E.2d 663, 671 (Ohio Misc. 1993) (appointing guardian other than parents of permanently comatose minor where one parent refused to consent to stopping LSMT). 91. In re Mason, 669 N.E.2d 1081, 1085 (Mass. App. Ct. 1996). 92. Id. 93. James Bopp, Jr. & Richard E. Coleson, Child Abuse by Whom? Parental Rights and Judicial Competency Determinations: The Baby K and Baby Terry Cases, 20 OHIO N.D.L. REV. 821, (1994)-(citing In re Achtabowski, No. G GD (Mich. Prob~e Ct. July 3D, 1993)); Baby Dies, Was Focus of Battle, ORLANDO SENTINEL, Aug. 13, 19~, at AID. 94. Bopp & Coleson, supra note 93, at Id. at Id. at 826, 832.
257 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 247 Court initially seemed to return to the earlier hostile approach to surrogate shopping. The court ruled that where a surrogate decision-maker insisted on continued LSMT for her m.other, "the evidence is insufficient to warrant court usurpation of [a daughter's] role as her mother's health care agent.// 97 But as the patient's condition deteriorated, the daughter's decision to continue LSMT increasingly.diverged from the hospital's assessment of the patient's preferences and best interests. Several months later, the court suggested that the agent's own personal issues were "impacting her decisions// and urged the daughter to "refocus her assessment.//9~ A year later, the hospital again planned to remove LSMT, and the court denied the daughter's request for a temporary restraining order (TRO).99 The daughter soon agreed to withdraw LSMT "because she believed the court was prepared to rule against her.// IoD Surrogates are generally obligated to make health care decisions in accordance with the patient's preferences and best interests. IOI Particularly for a conscious or semi-conscious patient, continuing LSMT contrary to provider recommendations often contravenes patient preferences and best interests. 102 Consequently, surrogates who make such requests are often acting outside the scope of their authority and should be replaced with other decision makers. 97. In re Howe, No , 2004 WL , at *21 (Mass. Probe & Fam. Ct. Mar. 22, 2004). 98. Id. at * See Liz Kowalczyk, Plan to Take Woman off Life Support is Halted, BOSTON GLOBE, Feb. 23, 2005, at B Daughter Explains Agreement to End Care, BOSTON GLOBE, Mar. 23, 2005, at B See generally THE RIGHT TO DIE, supra note 2, at (discussing incompetent patients and surrogacy) Cf Nina A. Kohn & Jeremy A. Blumenthal, Designating Health Care Decision Makers for Patients Without Advance Directives: A Psychological Critique (forthcoming 2008); David I. Shalowitz et al., The Accuracy of Surrogate Decision Makers, 166 ARCHIVES INTERNAL MED. 493 (2006) (finding that surrogates incorrectly predicted patient preferences in one-third of cases).
258 248 MARQUETTE ELDER'S ADVISOR [Vol. 9 PROVIDER ACTIONS FOR DECLARATORYRELIEF OFTEN SUCCEED While the foregoing cases address the question-of who is the appropriate decision-m.aker for the patient, other cases m.ore directly address the appropriateness of the treatrn.ent itself. In these cases, providers ask the court to declare that the providers would not violate the law by refusing the requested LSMT. It appears that the generally accepted view is that it is easier for providers to ask for forgiveness than to ask for perrn.ission. Schneiderrn.an and -Capron warn' that "[p]hysicians should not expect the courts to give them. priorperrnission to forgo futile treatment."i03 Since judges do not want to rn.ake decisions that may lead to a patient's death, it is thought that courts typically deny provider requests for declaratory relief. lo4 In perhaps the most farn.ous futility case, In re Baby K, the court denied declaratory relief. los Baby K was born with anencephaly, a birth defect in which part of the skull and the higher brain are m.issing. lo6 While Baby K was later rn.oved to a nursing home, she was periodically transferred to Fairfax hospital due to breathing difficulties. lo7 "Because aggressive treatment would serve no therapeutic or palliative purpose [Baby K's providers] recommended that [she] only be provided 103. Lawrence J. Schneiderman & Alexander M. Capron, How Can Hospital Futility Policies Contribute to Establishing Standards oj Practice?, 9 CAMBRIDGE Q. HEALTHCARE ETHICS 524, 530 (2000) See, e.g., Goldner et al., supra note 59, at 407 ("[W]hen the issue has been presented in the context of a dispute... concerning prospective treatment... courts have almost consistently sided against the health care professionals..."); Diane E. Hoffman & Jack Schwartz, Who Decides Whether a Patient Lives or Dies?, TRIAL, Oct. 2006, at 30, 37; John M. Luce & Ann Alpers, End-oj-Life Care: What Do the American Courts Say, 29 CRITICAL CARE MED. N40, N41-41 (2001); William Meadow et al., Current Opinion in Pediatrics and Law 2001, 14 CURRENT OPINION IN PEDIATRICS 170, 171 (2002); John J. Paris et al., Howe v. MGH and Hudson v. Texas Children's Hospital: Two Approaches to Resolving Family-Physician Disputes in End-oj-Life Care, 26 J. PERINATOLOGY 726, 726 (2006); William Prip & Anna Moretti, Medical Futility: A Legal Perspective, in MEDICAL FUTILITY AND THE EVALUATION OF LIFE-SUSTAINING INTERVENTIONS 136, 152 (Marjorie B. Zucker & Howard D. Zucker eds., 1997) In re Baby K, 832 F. Supp (E.D. Va. 1993), aff'd, 16 F.3d 590 (4th eire 1994) In re Baby K, 16 F.3d at Id. at 593.
259 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 249 with supportive care."10b Baby K's mother would not consent, insisting that Baby K be provided with a ventilator. lo9 Baby K's providers asked the local federal district court if they were obligated to provide the requested LSMT.l10 However, the providers framed their claim under the Emergency Medical Treatment and Active Labor Act (EMTALA).111 While the court ruled that the providers were so obligated, that holding is limited to the peculiar facts of the case and the coincidental application of the federal statute. 112 Only because Baby K newly arrived at the hospital in an "emergency m.edical condition," was the hospital obligated to stabilize her condition.113 EMTALA's scope is limited and it "cannot be invoked to require treatment in the vast majority of futility cases." 114 Under current EMTALA law, Fairfax Hospital arguably would not have had any obligation to treat Baby K because both 108. Id. at Id. at Id. at V.S.C.A. 1395dd (Westlaw currentthrough Feb. 2,2008) The Fourth Circuit affirmed on only the EMTALA claim, but the district court also based its ruling both on Section 504 of the Rehabilitation Act of 1973, 29 U.S.C. 794(a), and on the Americans with Disabilities Act (ADA), 42 U.S.C (a). See In re Baby K, 832 F. Supp. at However, typically such claims cannot succeed in the futility context because the patient's need for LSMT is directly related to his or her disability. See generally Schiavo v. Schiavo, 403 F.3d 1289, 1294 (11th Cir. 2005) (noting that "[t]he Rehabilitation Act, like the ADA, was never intended to apply to decisions involving the termination of life support or medical treatment./i); Grzan v. Charter Hosp., 104 F.3d 116, (7th Cir. 1997) (reviewing cases and legislative history); Rideout v. Hershey Med. Ctr., 30 Pa. D. & C.4th at 1 95 (1995) (quoting Anderson v. Vniv. of Wis., 841 F.2d 737, 740 (7th Cir. 1988) that "the Rehabilitation Act forbids discrimination based upon stereotypes about a handicap, but it does not forbid decisions based on the actual attributes of the handicap./i); Johnson v. Thompson, 971 F.2d 1487, (10th Cir. 1992) (discussing discrimination based on the degree of a handicap and Section 504). On the other hand, while there is no positive constitutional right to medical care, later courts have agreed with the district court that decided the Baby K case and have held that unilateral refusals may conflict with the free exercise clause and constitutional parental rights. See Rideout, 30 Pa. D. & C.4th at 1 84; In re Baby K, 832 F. Supp. at In re Baby K, 16 F.3d at THE RIGHT TO DIE, supra note 2, at 13.06[C] (explaining that EMTALA does not apply to in-patients).
260 250 MARQUETTE ELDER'S ADVISOR [Vol. 9 she and her mother were inpatients. lis The In re Baby K court itself later clarified that EMTALA applies "only in the immediate aftermath of admitting [a patient] for emergency treatment," and that there can be no EMTALA violation for entry of an "anti-resuscitation order" after a good faith admission. 116 That interpretation has been confirmed in regulations and appellate opinions. 117 In most subsequent unilateral withdrawal cases courts have explicitly noted that since the patient was already admitted, EMTALA did not apply. lib In short, the Baby K holding is far lllore limited than generally understood. Furthermore, providers have frequently succeeded in obtaining declaratory relief to stop LSMT. Most of the reported cases involve providers securing judicial permission to stop LSMT for patients declared brain dead. 119 The notoriety of the Baby K decision effectively chilled providers from. seeking ex ante judicial permission to stop LSMT.120 But at least one court 115. See Thaddeus M. Pope, EMTALA: Its Application to Newborn Infants, 4 ABA HEALTH ESOUR~E No.7 (Mar. 2008) Bryan v. Rectors & Visitors of the Univ. of Va., 95 F.3d 349, (4th Cir. 1996) See Preston v. Meriter Hosp. Inc., 700 N.W.2d 158, (Wis. 2005) (Roggensack, J., dissenting); 42 C.F.R (a)(1)(ii) (2003) ("1 the hospital admits the individual as an inpatient... the hospital's obligation under [EMTALA] ends..."); 42 C.F.R (d)(2) (2007) (providing that "[i]f a hospital... admits that individual as an inpatient... the hospital has satisfied its special responsibilities under [EMTALA].") See, e.g., In re AMB, 640 N.W.2d 262, 289 (Mich. Ct. App. 2001) (holding that there was no EMTALA violation "when the staff made the decision to discontinue the medical interventions" after the baby had been admitted for more than one week); Causey, 719 So. 2d at 1075 (noting that "EMTALA provisions are not applicable to the present case [where the patient had already been admitted]."); Rideout, 30 Pa. D. & C. 4th at See also Gonzales, No (Travis Cty. Probate Ct, Tex. filed Mar. 20, 2007) (Guardian Ad Litem's Trial Brief on Legal Issues) See, e.g., In re Long Island Jewish Med. Ctr., 641 N.Y.S.2d 989 (Sup. Ct. 1996) (granting hospital authorization to withdraw LSMT from brain dead infant); In re Haymer, 450 N.E.2d 940, (Ill. App. Ct. 1983); Frank Bruni, Medical Certainty, Legal Limbo, N.Y. TIM:ES, Feb. 28, 1996, at B1 (reporting that a trial court granted relief to a hospital). Cf Dority v. Sup. Ct., 193 Cal. Rptr. 288 (1983) (noting that "[t]he medical profession need not go into court every time it declares brain death.... ") 120. Kathy L. Cerminara, Critical Essay: Musings on the Need to Convince. Some People with Disabilities that End-oj-Life.Decision-Making Advocates Are Not Out to Get Them, 37 Loy. U. CHI. L.J. 343, (2006).
261 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 251 has granted declaratory relief permitting providers to unilaterally withdraw LSMT from a living patient.121 SURROGATE ACTIONS FOR INJUNCTIVE RELIEF SUCCEED ONLY TEMPORARILY Just as providers may ask the court for a green light, surrogates may ask the court for a red light. In these cases surrogates ask the court to issue an injunction prohibiting the providers from stopping LSMT. For the same reason that providers are thought to be unlikely to obtain declaratory relief, surrogates are thought likely to be successful in obtaining injunctive relief. Two distinguished commentators recently observed that the "Courts may be more willing to order the provision of care consistent with.a patient's wishes when he or she is still alive..."122 Indeed, courts appear to regularly issue surrogate-sought injunctions, but the injunctions are only tem.porary in nature. Given the imminent irreparable injury viz. the patient's death, it is not surprising that courts grant immediate relief as an emergency procedure. 123 As the estimable Judge J. Skelly Wright explained, "the compelling reason for granting the writ was that a life hung in the balance. There was no time for research or reflection."124 A temporary injunction preserves the status quo, 121. See, e.g., Child & Family Servo of Cent. Manitoba v. R.L. and S.L.H., 154 D.L.R.4th 409, (1997) (noting that I/[t]here is no need for a consent from anyone for a doctor to refrain from... heroic measures to maintain the life of a patient in an irreversible vegetative state.") Hoffman & Schwartz, supra note 104, at 37. See Goldner et al., supra note 59, at 407 (I/[W]hen the issue has been presented in the context of a dispute... concerning prospective treatment... courts have almost consistently sided against the health care professionals..."); Schneiderman & Capron, supra note 103, at 530 (I/Physicians should not expect the courts to give them prior permission to forgo futile treatment....") Cf. Wright & Miller, 11A FED. PRACTICE & PROC (2d ed. 2007) In re President and Directors of Georgetown College, Inc., 331 F.2d 1000, 1009 (D.C. Cir. 1964). See also Cruzan v. Director, Missouri Dep't Health, 491 U.S (1990) ("An erroneous decision not to terminate results in a maintenance of the status quo.... An erroneous decision to withdraw life-sustaining treatment,
262 252 MARQUETTE ELDER'S ADVISOR [Vol. 9 pending a hearing. 125 For example, in cases where the patient is brain. dead, courts m.ay grant injunctions to either give the surrogate"accomm.odation" tim.e or permit a confirm.ation of the diagnosis. 126 The injunctions obtained by surrogates are only interim. m.easures. Courts seem. do not generally order indefinite -LSMT. For exalllpie, many surrogates have sought injunctions prohibiting providers from. rem.oving LSMT from. corpses. 127 While court~ m.ay grant temporary relief, they ultim.ately deny such Illotions. For exam.ple, in Fennell v. Emory Eastside Medical Center, the judge granted an injunction ordering the hospital to continue LSMT for Donald Fennell, a m.an who.had been declared brain dead. 128 Less th~n forty-eight hours later, the however, is not susceptible of correction.") See, e.g., Rotaru v. VancouverGen. Hosp. Intensive Care unit, 2008 BCSC (denying injunction ordering continued LSMT, but not dismissing the petition and allowing petitioner to gather more evidence); Golubchuk v. Salvation Army Grace Gen. Hosp., 2008 MBQB (granting interim injunction pending a trial of disputed issues of fact and law); Jin v. Calgary Health Region, 2007 ABQB ("I am mindful that the injunction is for a brief period and on balance I prefer to rescind the DNR order and preserve the status quo until there is either consensus or a legal determination on full evidence.") See, e.g., THE RIGHT TO DIE, supra note 2, 13.08[A], at 13-40; Dority v. Sup. Ct., 193 Cal. Rptr. at 288 (describing a hospital's policy of keeping brain dead children on life support "until the parents were emotionally able to realize what the medical opinion was" and suggesting that hospitals encourage parent consultation and participation) See, e.g., Cole v. Dniv. of Kansas Med. Center, No. 06-CV-830 (Wyandotte County Dist. Ct. Kan. 2006) (granting a TRO but dissolving it after the -diagnosis was independently confirmed); Alvarado v. N.Y. City Health & Hosp.. Corp., 547 N.Y.S.2d 190 (Sup. Ct. 1989)~ vacated and dismissed, 550 N".Y.S.2d 353 (App. Div. 1990) (where patient was later determined not brain dead); Dority v. Sup. Ct., 193 Cal. Rptr.. at 288 (denying par~nts' petition for writ of p~ohibition against removing LSMT from brain dead child). Cf. Megan Tench, End-oj-Life Lawsu"it Outliving Its Subject, BOSTON GLOBE, Dec. 6, 2006, at B3 (reporting denial of relief for Cho Fook Cheng). But cf. Shively v. Wesley Med. Center, No. 06-CV-640 (Sedgwick County Dist. Ct. Kan. Feb. 10, 2006) (granting TRO forbidding providers from performing the tests necessary to diagnose brain death); Brain Dead Girl Will Be Sent Home on Life Support, N.Y. TIMES, Feb. 19, 1994, at 9 (hospital agreed to cover expenses of home LSMT for Theresa Hamilton, who had been declared brain dead); Lois M. Collins & Linda Thomson, Jesse Loses His Battle with Brain Tumor, DESERET MORNING NEWS,. Nov. 20, 2004, at B.Ol (reporting that the Utah -Third District Court granted a TRO, which prevented a hospital from removing LSMT from brain dead Jesse Koochin) Andria Simmons, Death Not Just a Family Matter, ATLANTA }.-CONST., Dec. 14, 2007, at AI.
263 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 253 judge authorized the hospital to stop LSMT.129 It is well-settled that once a patient is determined brain dead, further treatment is not required. 130 Sim.ilarly, no court has ever granted a perm.anent injunction ordering continued LSMT for living patients. In Nguyen v. Sacred Heart Me.dical Center for example, the hospital refused. to place Baby ;Ryan on dialysis, despite his parents' request. 131 The court issued a TRO ordering the hospital to resume dialysis. 132 However, the fam.ily was soon able to transfer Baby Ryan to another facility, Inooting the,dispute. 133 The court never.ruled on the parents' petition for perm.anent injunction. 134 And in Baby L,.the probate judge appeared willing to approve the mother's p~tition for injunctive relief, but the issue was rendered m.oot when the m.other of the patient was able to transfer his care to another provider.135 Finally, a num.ber of surrogates in Texas have successfully enjoined the unilateral termination of LSMT.136 Such cases were widely reported in the press. 137 But again, these injunctions 129. Id See, e~g., Cavagnaro v. Hanover Ins. Co., 565 A.2d 728, 729 (N.J. Super. Ct. App. Div. 1989) (holding that treatment for a brain dead patient was not medically necessary, so insurer had no obligation to pay for it). Since provider obligations with respect to brain dead patients are comparatively more settled, they may not provide material guidance for other types of futility cases Altomare & Bolde, supra note 80, at Id. (citing Nguyen, No (TRO» Id. at Id. (holding that the TRO was dissolved and the petition for permanent injunction dismissed) See Paris et al., supra note 38, at See, e.g., Gonzales, No (Travis Cty. Probate Ct, Tex. filed Mar. 20, 2007); Hudson v. Texas Children's Hosp., 177 S.W.3d,232 (Tex. App. 2005); In re Nikolouzos, 179 S.W.3d 581 (Tex. App. 2005) (granting an injunctionuntil an appeal could be assigned); Ramshaw, supra note 42 (TRO granted for Ruthie Webster). In other cases, hospitals agreed to an extension just before a pending hearing. See, e.g., Todd Ackerman, Transfer Resolves Latest Futile Care Case, Hous. CHRON., July 31, See, e.g., Kristina Hermdobbler, Court Keeps Woman on Life Support, BEAUMONT ENTERPRISE, Aug. 11, 2006, at A.1 (reporting a TRO in the case of Daisy Conner); Bill Murphy, Comatose Surgeon Would Prefer Death, Hous. CHRON., Mar. 21, 2001, at 26 (reporting a TRO in the case of Joseph Ndiyob); Ramshaw, supra note 42 (reporting a TRO in the case of Ruthie Webster).
264 254 MARQUETTE ELDER'S ADVISOR [Vol. 9 were temporary in nature and granted pursuant to the unique Texas Advance Directives Act for a limited time and purpose. The Act allows a provider to unilaterally refuse LSMT after giving a surrogate ten days to find an alternate provider that will provide the requested LSMT.138 Texas courts have the power to extend the ten-day period if a surrogate shows that "there is a reasonable expectation that a physician or health care facility that will honor the patient's directive will be found if the time extension is granted." 139 Courts have no other authority or jurisdiction.140 While surrogates often- obtain injunctions prohibiting the removal of LSMT, these injunctions typically operate like TROs. They are short-terill stop-gap orders, pending a hearing several days later. 141 Courts norillally dissolve the temporary injunction and permit providers to stop LSMT. Providers are similarly successful when they initiate an ex ante action. Specifically, providers are increasingly successful in actions to replace a surrogate who demands non-recommended LSMT. Also, while seeking declaratory judgment remains an unpopular procedural vehicle, available precedent fails to indicate that such petitions would be unsuccessful TEX. HEALTH & SAFETY CODE ANN (e) (Vernon 2006). See, e.g., Lance Lightfoot, Incompetent Decisionmakers and Withdrawal of Life-Sustaining Treatment: A Case Study, 33 J. L. MED. & ETHICS 851, 854 (2005) (citing Final Order Denying Plaintiff's Request for an Extension of Time Under the Health & Safety Code Section (f), Hudson v. Texas Children's Hosp., No. 352,526 (Probate Ct., Harris County, Tex. Mar. 14, 2005». Nikolouzos v. St. Luke's Hosp., 162 S.W.3d 678, (Tex. App. 2005) (affirming the denial of TRO because petitioner did not show a probable transfer) TEX. HEALTH & SAFETY CODE ANN (g) (Vernon 2006) See Lightfoot, supra note 138, at 852. See also Nikolouzos, 162 S.W.3d at 683 (finding medical evidence "irrelevant" since the IJ'hospital's ethics committee has determined the care is inappropriate."); H. Comm. Pub. Health, Tex. H.R., Interim Report 2006, at 35 ("The court considers whether another provider who will honor the patient's directive is likely to be found; it does not address the issue of whether the decision to withdraw life support is valid.") Sometimes, the patient dies during the temporary injunction period, such that the injunction has a practically dispositive impact.
265 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 255 Ex POST ACTIONS: GOING TO COURT AFTER LSMT Is WITHDRAWN While providers are often successful in ex ante actions, they are almost uniformly successful in ex post actions. Providers usually prevail when a surrogate brings a lawsuit after the unilateral termination of LSMT.142 Indeed, usually a surrogate succeeds only if he or she shows that the provider's nonconsensual refusal of LSMT was so egregious as to constitute the tort of outrage. A surrogate bringing a dam.ages action on another legal theory rarely succeeds because the surrogate: (1) cannot establish that the standard of care required continued LSMT, (2) cannot establish causation and dam.ages, or (3) cannot rebut the provider's statutory right to refuse LSMT. SURROGATE ACTIONS FOR DAMAGES TYPICALLY SUCCEED ONLY WHEN PROVIDER CONDUCT IS OUTRAGEOUS Hoffm.an and Schwartz note that I/[p]laintiffs who seek dam.ages for the withholding or withdrawal of requested lifesaving treatm.ent m.ay fare better, especially when the facts indicate egregious conduct by hospital personnel." 143 In fact, a com.prehensive review of litigated futility cases appears to support an even stronger statetilent that surrogate actions for dam.ages typically succeed only when provider conduct is 142. See Ann Alpers, Respect for Patients Should Dominate Health Care Decisions, 170 W. J. MED. 291, 292 (1999) ("Physicians are likely to get better legal results when they refuse to provide non-beneficial treatment and then defend their decisions as consistent with professional standards than when they seek advance permission to withhold care."); Goldner, supra note 59, at 407 (finding that in cases "in which physicians have been sued... based upon their termination of life-sustaining treatment, the courts almost uniformly have displayed great deference to medical judgments"); Johnson et a1., supra note 59, at 23 (observing that in "malpractice and related litigation... the outcomes seem to be more deferential to professional standards of practice"); Lee, supra note 10, at 485 ("[W]hen legal action is brought by the surrogates following the death of the patient, some legal precedents seem to validate the physician's right to unilaterally withdraw life-sustaining treatments."); Luce & Alpers, supra note 104, at N Hoffman & Schwartz, supra note 104, at 37.
266 256 MARQUETTE ELDER'S ADVISOR [Vol. 9 outrageous. Furthermore, surrogates cannot establish outrageous conduct by pointing to the unilateral withdrawal of LSMT itself, but only by demonstrating that the manner in which it was withdrawn was outrageous. OUTRAGEOUS PROVIDER CONDUCT In Rideout v. Hershey Medical Center, the parents of threeyear-old Brianna Rideout favored aggressive treatment for her brain cancer. 144 As Brianna's condition deteriorated, her parents remained adamant, and providers planned to remove her ventilator without her parents' consent. 14S However, the providers did far more than withdraw LSMT. They assured Brianna's parents that they would remove her ventilator only when the parents were at Brianna's bedside. 146 Nevertheless, the providers removed the ventilator outside the parents' presence, as the parents were in the hospital patient advocate's office trying to obtain legal assistance. 147 Brianna's parents learned of the surprise disconnection when the hospital chaplain, who was in Brianna's room, announced it over the hospital's intercom system.148 The Pennsylvania Common Pleas Court held in favor of the parents' claims for negligent and intentional infliction of emotional distress,149 as the providers withdrew the ventilator in a secretive, insensitive, and disrespectful manner. Moreover, the providers specifically anticipated that the parents would have a strong emotional reaction because the providers had requested that city police officers be present.iso Similarly, in Manning v. Twin Falls Clinic & Hospital, the patient had chronic obstructive pulmonary disease (COPD) 144. Rideout, 30 Pa. D. & C. 4th at Id. at Id. at Id. at 63, Id. at Id. at Id. at 70.
267 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 257 resulting in decreased ability to transfer oxygen to his bloodstreatn. 1s1 The patient's condition was rapidly deteriorating, but contrary to his fatnily's objections, the providers moved him to another room without the aid of a portable oxygen unit. 152 This patient experienced respiratory distress and died. 1s3 The court affirtned a punitive damages verdict for infliction of etnotional distress. 154 Intentional infliction of emotional distress was also the cause of action in Estate ofbland v. Cigna Health Plan of Texas. ISS Bland, a tertninally ill AIDS patient, was dependent upon a ventilator. 156 Both Bland and his family insisted that he rem.ain on the ventilator. 1s7 However, the chair of the ethics committee ordered the ventilator removed, apparently at the direction of the Cigna medical director. This was done without consulting Bland, his family, or Bland's primary care physician. 1s8 The ventilator retnoval seemed both secretive and financially motivated. The intentional infliction of emotional distress is not a favored tort in the law. 159 It is particularly difficult to show that a provider's conduct was extreme and outrageous when the provider reasonably believed that her objective was not only legititnate but even professionally and ethically necessary and appropriate.160 Consequently, in the several futility cases in which recovery was allowed, it is no surprise that liability was pretnised not on the fact that providers unilaterally withdrew 151. Manning v. Twin Falls Clinic & Hosp., Inc., 830 P.2d 1185, 1187 (Idaho 1992) ld. at ld. at ld. at 1191, Bland v. Cigna Healthplan of Texas, Inc., No A (Harris County Tex. Dist. Ct., Apr. 25, 1995) (First Amended Petition III) ld. at I ld JOHN FLETCHER ET AL., INTRODUCTION TO CLINICAL ETHICS 272, 273 (2d ed. 2000); Mimi Swartz, Not What the Doctor Ordered, TEX. MONTHLY, Mar. 1995, at See J.D. LEE & BARRY LINDAHL, 3 MODERN TORT LAW: LIABILITY AND LITIGATION 32:3, 32-8 (Thomson/West 2006) See id. at
268 258 MARQUETTE ELDER'S ADVISOR [Vol. 9 LSMT, but rather, on how they did it. 161 THE UNILATERAL REFUSAL OF LSMT Is NOT PER SE OUTRAGEOUS In som.e cases, surrogates have alleged that the unilateral withdrawal of LSMT is itself outrageous conduct because it is done without consent and against patient or surrogate wishes. However, courts have consistently rejected this proposition. For exam.ple, in Gallups v. Cotter, Pamela Gallups, a minor, was rendered brain dead after a car accident. 162 Providers made at least eight confirm.ations of the brain death diagnosis. And they had six discussions with the family between June 28 and July 8, whereby they recom.m.ended rem.oving LSMT.163 While there was a dispute over whether consensus was reached, providers allegedly rem.oved Pam.ela from. life support against her parents' wishes. 164 Nevertheless, the court found no evidence of 1/recklessness."165 Courts have similarly denied claims for outrage or intentional infliction of einotional distress based solely on the fact that providers unilaterally withdrew LSMT froin a living Not only liability but even a lawsuit itself may be averted through considerate handling. See generally NANCY BERLINGER, AFTER HARM: MEDICAL ERROR AND THE ETIDCS OF FORGIVENESS (2005) (discussing "The 'I'm Sorry' Laws"); Pam Baggett, I'm Sorry: Apologizing for a Mistake Might Prevent a Lawsuit, TEX. MED., Jan. 2005, at 56; Jennifer K. Robbennolt, Apologies and Legal Settlement: An Empirical Examination, 102 MICH. L. REV. 460, 463 (2003) (arguing that apologies go a long way in reaching settlements); Charles Vincent et al., Why Do People Sue Doctors? A Study ofpatients and Relatives Taking Legal Action, 343 LANCET 1609, 1612 (1994) (explaining how patients' families often feel that there is a lack of information and apologies). For example, in Bryan v. UVA, the University of Virginia risk management department believed that the primary cause for the state and federal actions was a dispute over billing; when the hospital turned the account over to a collection agency, the family gave the demand letters to an attorney to review, who coincidentally noticed grounds for a lawsuit in a subsequent review of the medical records. FLETCHER ET AL., supra note 158, at Gallups v. Cotter, 534 So. 2d 585, 586 (Ala. 1988) Id. at Id. at Id. at 589 (holding that acting without consent is "insufficient... to show defendants acted intentionally or recklessly"). The court had already disposed of claims for wrongful death, breach of contract, and fraud. Id. at 587.
269 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 259 patient.166 For example, in Gilgunn v. Massachusetts General Hospital, the attending physician wrote a do not resuscitate order, despite the surrogate's demands for aggressive I treatment.167 The claim for negligent infliction of emotional distress proceeded to a jury.168 The jury returned a verdict for the providers. 169 OTHER SURROGATE ACTIONS FOR DAMAGES TYPICALLY Do NOT SUCCEED170 Hoffman and Schwartz observe that plaintiffs "face uncertainty when health care providers defend their action oil futility grounds."171 In fact, once we account for the outrage cases, plaintiffs face not uncertainty, but instead, probable failure. "[C]ourts are hesitant to penalize physicians who reasonably rely on what they perceive to be professional standards concerning effectiveness of treatment measures." See, e.g., Morgan v. Olds, 417 N.W.2d 232 (Iowa. App. 1987); Nguyen v. Sacred Heart Medical Center, 987 P.2d 634, 636 (Wash. App. 1999) (refusing to allow plaintiffs to pursue claim for outrage). Cf Hartsell v. Fort Sanders Reg'l Med. Center, 905 S.W.2d 944 (Tenn. Ct. App. 1995) (trial court dismissed the claim for outrage); Litz v. Robinson, 955 P.2d 113, (Idaho Ct. App. 1997) (involving a unilateral DNR); Strickland v. Deaconess Hosp., 735 P.2d 74 (Wash. Ct. App. 1987) (involving unilateral removal of a respirator) John J. Paris et al., Use ofa DNR Order Over Family Objections: The Case of Gilgunnn v. MGH, 14 J. INTENSIVE MED. 41,41-42 (1999) ld. at ld. at Actions fail for a variety of fact-specific reasons. For example, in Kranson V. Valley Crest Nursing Home, 755 F.2d 46 (3d Cir. 1985), the court found in favor of a nursing home that failed to provide CPR to a resident because the plaintiffs could not establish municipal liability. In Strickland, 735 P.2d at 78, plaintiffs lacked standing to bring claims for negligence and informed consent. See also Judge' Dismisses Suit over Death, ST. LOUIS POST DISPATCH, June 28, 1996, at 38 (a court dismissed a wrongful death case because patient Philip Taylor's agent lacked standing to challenge unilateral DNR). Criminal actions have also been unsuccessful. See, e.g., Grotti V. Texas, 209 S.W.3d 747 (Tex. App. 2006) (reversing physician's homicide conviction for occluding a patient's endotracheal tube because there was insufficient evidence that the patient was alive at the time); State V. Naramore, 965 P.2d 211, 216, 223 (Kan. Ct. App. 1998) (reversing physician's murder conviction for stopping LSMT he considered futile). In this section of this article, I discuss only the more common causes of action Hoffman & Schwartz, supra note 104, at Goldner et al., supra note 59, at 409; Prip & Moretti, supra note 104, at 152;
270 260 MARQUETTE ELDER'S ADVISOR [Vol. 9 Specifically, surrogates have difficulty establishing the prima facie elements of their tort-based theories. First, they can find it difficult to establish that the standard of care required continued LSMT. Second, given the patient's extreme fragility and illness, they cannot establish causation and damages. Third, they cannot rebut provider's statutory presumptive right to refuse LSMT. SURROGATES CANNOT ESTABLISH THAT THE STANDARD OF CARE REQUIRES CONTINUED LSMT In medical malpractice actions, plaintiffs must establish a breach of the applicable standard of care by the provider. 173 Therefore, unless plaintiffs have a federal or constitutional cause of action, a threshold requirement is showing that the unilateral refusal does not comply with the standard of care. 174 Plaintiffs have never been able to show that the standard of care requires continued LSMT for brain dead patients. 175 Similarly, in most of the reported cases, plaintiffs have been unable to establish that the standard of care requires continued LSMT for living patients. 176 As a consequence, courts ordinarily see Schneiderman & Capron, supra note 103, at BARRY R. FURROW ET AL., HEALTH LAW (2d ed. 2000); STEVEN E. PEGALIS, AMERICAN LAW OF MEDICAL MALPRACTICE (3d ed. 2007) In DeKalb Med. Center v. Hawkins, the plaintiff successfully resisted providers' attempt to characterize his claim for "tortuous termination of life support" as a medical malpractice action Ga. App. LEXIS 1269 (Nov. 29, 2007). Since the court allowed plaintiff to proceed on an intentional tort/wrongful death theory, he presu~ablywill not need to establish standard of care. In contrast, the court in Ussery v. Children's Healthcare of Atlanta, Inc. rejected plaintiff's intentional tort allegations, allowing them to pursue only their negligence claims. 656 S.E.2d 882 (Ga. App. 2008) See, e.g., Gallups v. Cotter, 534 So. 2d 585 (Ala. 1988) See, e.g., Berkeley v. Dowds, 61 Cal.Rptr.3d 304, 311 (Cal. Ct. App. 2007) (affirming demurrer where plaintiff's counsel conceded that defendant's conduct "was within the standard of care"); Gamble v. Perra, No (Tenn. Ct. App. Feb. 22, 2007) (affirming the dismissal of tort claims because the wife showed that neither the prescription of pain medication nor the failure to attempt CPR was outside the standard of care); Litz, 955 P.2d at 113 (affirming summary judgment in favor of providers who placed unilateral DNR order); Nguyen, 987 P.2d at 636 (affirming dismissal of malpractice action in case involving unilateral removal from dialysis); Preston, 700 N.W.2d at 163 (affirming the dismissal of causes of action for malpractice and informed consent); John J. Paris et al., Resuscitation of a
271 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 261 grant summary judgment in favor of providers because plaintiffs fail to introduce evidence showing that the standard of care required continued LSMT. For example, in Duensing v. Southwest Texas Methodist Hospital, providers stopped a patient's dialysis without the consent of the patient's surrogate. 177 The surrogate sued for tnedical malpractice, but presented no evidence showing that withdrawing dialysis was inconsistent with the standard of care. 17B The plaintiff 1/failed to establish expert testimony that terminating the dialysis of a terminally ill and mentally incapacitated patient even without the consent of the patient's fatnily was necessarily a breach of medical standards." 179 Moreover, the plaintiff's own experts conceded that the providers complied with the standard of care. 1BO Therefore, the court granted summary judgment in favor of the providers, and the u.s. Court of Appeals for the Fifth Circuit affirmed. 1B1 Similarly, in Kelly v. St. Peter's Hospice, a surrogate sued a New York hospice for medical malpractice involving his wife's treatment because, among other things, the hospice (1) did not provide sufficiently aggressive care, (2) used an excessive amount of morphine, and (3) failed to insert an IV line for nutrition and hydration. 1B2 The New York appellate court Micropreemie: The Case of MacDonald v. Milleville, 18 J. PERINATOLOGY 302 (1998) (holding physician had no obligation to seek authorization to cease resuscitation of 23-week gestation baby after ten minutes); Defendant-Respondent Brief in Baby K, 2003 WL , at *24-25 & *28 (plaintiff's expert did not establish the standard of care required resuscitation of anencephalic infant). Tellingly, attorney Mark Geragos never filed a promised lawsuit on behalf of Nataline Sarkisyan after Cigna determined that a liver transplant was not covered under Sarkisyan's medical plan. Alicia Chang, Cigna Faces Lawsuit in Death after Policy Fight, CHI. TRIB., Dec. 23, 2007, at Duensing v. Southwest Tex. Medical Hosp., No. SA-87-CA1119 (W.D. Tex. 1988), a!f'd sub nom. Duensing v. Ruff, No (5th Cir. Feb 3, 1990) Id Duensing v. Ruff, No at Id. at 4-5. Furthermore, the defendants' position was supported at least by a school of thought. See FURROW ET AL., supra note 173, at ; Jones v. Chidester, 610 A.2d 964, 966 (Pa. 1992) Duensing v. Southwest Tex. Medical Hasp., No. SA-87-CAll Kelly v. St. Peter's Hospice, 553 N.Y.S.2d 906, 907 (N.Y. App. Div. 1990) (noting that the husband was unaware that his wife had checked into hospice,
272 262 MARQUETTE ELDER'S ADVISOR [Vol. 9 affirm.ed sum.tnary judgm.ent in favor of the hospice because the plaintiff-surrogate failed to present evidence that the provider's treatm.ent departed from. acceptable tnedical practice. 183 In other cases, plaintiffs have introduced competent expert evidence regarding the standard of care, but juries have still largely held that the providers did not breach the standard. For exam.ple, in Gilgunn, the jury determined that the patient would have wanted LSMT, which her providers unilaterally withdrew.184 However, the jury concluded that none of the defendants were negligent because 1/the actions of the physicians and of the [hospital] were within the standard of care."18s Sitnilarly, in LaSalle Nat'l Trust v. Swedish Covenant Hospital, the court affirm.ed a verdict in favor of providers who adhered to a /Icompassionate care" policy and refused to provide aggressive treatrn.ent to an extretnely pretnature infant. 186 The jury concluded that unilaterally refusing LSMT did not breach the standard of care. 187 While the jury verdict lacks the force of law as a legal precedent, it is a powerful statetnent that the standard of care does not require all that the patient would have wanted. In other cases, plaintiffs have voluntarily distnissed their lawsuits upon realizing the weakness of their claitns. For exarn.ple, in Burks v. St. Joseph's Hospital, the plaintiffs voluntarily distnissed their. claillls for ntedical m.alpractice. l88 Soon after arriving at a Milwaukee em.ergency room., Shem.ika Burks gave birth to a severely prem.ature baby who weighed only seven ounces. l89 The hospital did not attem.pt to resuscitate the baby, which is typically for palliative treatment, not curative treatment) Id. at Paris et al., supra note 167, at Id LaSalle Nat'l Trust v. Swedish Covenant Hosp., 652 N.E.2d 1089, (Ill. App. C ) Id. at Burks v. S1. Joseph's Hasp., No. 95-CV , at 17:4-6 (Milwaukee County Cir. Ct., Wis. Apr. 29, 1996) (hearing on motion for summary judgment); Burks v. St. Joseph's Hasp., 596 N.W.2d 391, 393 (Wis. 1999) Burks, 596 N.W.2d at 392.
273 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 263 and the baby died three hours later. 19o The plaintiffs dismissed the malpractice suit, apparently upon realizing that they could not establish whether it was within the standard of care to resuscitate a 22-week-old fetus. 191 SURROGATES TYPICALLY CANNOT ESTABLISH CAUSATION AND DAMAGES Even when plaintiffs can establish a breach of the standard of care, they still can have difficulty establishing proof of causation or damages, particularly because the patients from whom LSMT is withdrawn are catastrophically ill. 192 In King v. Crowell Memorial Home, a son sued the nursing hom.e for treating his mother as DNR, even though his instructions were to use "any and all medical measures./ 193 While the case went to trial, the court granted the home a directed verdict because the son failed to present sufficient evidence that (1) his m.other was DNR at the time of her death, (2) his instructions were not followed, or (3) resuscitative measures would have been successful.194 In som.e jurisdictions the causation hurdle is lower, and plaintiffs need only show loss of a chance rather than "but-for causation.// 195 For example, in Wendland v. Sparks, a patient's physician unilaterally decided not to attempt CPR when the 190. Id Brief in Support of Defendant's Motion to Dismiss EMTALA Claim, at (Nov. 9, 1995); Reply Brief in Support of Defendant's Motion to Dismiss EMTALA Claim, at 4 (Apr. 22, 1996); from Mary Wolverton to Thad Pope (Aug. 6, 2007) (on file with author) See, e.g., Berkeley, 61 Cal Rptr. 3d at 308, 312 (finding no causal connection where the plaintiff alleged that the providers prematurely removed patient from ICU and denied him medically necessary services); Gray v. Woodville Health Center, 225 S.W.3d 613, 619 (Tex. App. 2006); Kranson, 755 F.2d at 46 (affirming the dismissal of a claim against municipal nursing home that failed to perform CPR on resident because of the lack of a causal nexus between th~ home's CPR policy and the resident's death) King v. Crowell Memorial Home, 622 N.W.2d 588,592 (Neb. 2001) Id. at See LEE & LINDAHL, supra note 159, at 25:88-91.
274 264 MARQUETTE ELDER'S ADVISOR [Vol. 9 patient suffered cardiorespiratory arrest. 196 While the patient had only a ten percent chance of leaving the hospital following CPR, the court held that "even a sm.all chance of survival is worth something,"197 and the court allowed the plaintiffs to pursue their malpractice action on a loss of chance theory.19b But the loss of chance theory alters not only the elem.ent of causation, but also the nature of the injury. Under this theory, the injury is not a patient's death, but the loss of chance itself. This may substantially lower available damages.199 Furthermore, plaintiffs are unlikely to bring low damages cases in the first place. 20D Even if the cases are brought, such cases are hard for surrogates to win. For example, in Velez v. Bethune, providers unilaterally withdrew LSMT from. a prem.ature infant, and a Georgia appellate court held that plaintiffs' claim for wrongful death was valid.201 "Dr. Velez had no right to decide, unilaterally, to discontinue medical treatment even if... the child was... in the process of dying."2d2 But, the court noted that the am.ount of dam.ages would be very low. 2D3 The case ultim.ately settled, and 196. Wendland v. Sparks, 574 N.W.2d 327, 328 (Iowa 1998) Id. at Id. at 333. The case later settled for an undisclosed amount. from Julie Davis to Thaddeus Pope (May 2, 2007) (on file with author) It must be noted that even low damages entails a report to the National Practitioner Data Bank, psychological distress, and other repercussions for the provider. BOVBJERG & RAYMOND, supra note 45, at 6; Subrin, supra note 51, at 206 (lithe entire litigation process is anxiety-provoking and privacy-invading."); Mitchell S. Cappell, A Baseless Malpractice Suit Still Cost Me, MED. ECON., Feb. 1, Low damages cases are unlikely to be brought. See LaRae Huycke & Mark M. Huycke, Characteristics ofpotential Plaintiffs in Malpractice Litigation, 120 ANNALS INTERNAL MED. 792, 785 (1994); Daniel Costello, Lacking Lawyers, Justice is Denied, L.A. TIMES, Dec. 29, 2007 (reporting the difficulty of obtaining a lawyer in cases with limited damages). But cf. Kathy L. Cerminara, Tracking the Storm: the Far Reaching Power ofthe Forces Propelling the Schiavo Cases, 35 STETSON L. REV. 147, (2005) (reviewing the involvement of special-interest groups); Jon B. Eisenberg, The Terri Schiavo Case: Following the Money, RECORDER, Mar. 4, 2005, at 4 (reporting how much of the Schiavo litigation was funded by conservative organizations like the Philanthropy Roundtable and Life Legal Defense Foundation) Velez v. Bethune, 466 S.E.2d 627 (Ga. Ct. App. 1995) (affirming the denial of provider's motion for summary judgment) Id. at Id.
275 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 265 the providers did not have to pay anything to the plaintiffs. 204 SURROGATES CANNOT REBUT PROVIDERS' STATUTORY RIGHT TO REFUSE LSMT Surrogates have encountered an additional hurdle, in addition to hurdles in establishing the prima facie elements of tort-based causes of action. In many states, health care decisions statutes grant providers the right to refuse LSMT if they deem. it m.edically or ethically inappropriate.205 For instance, the Virginia Health Care Decisions Act (HCDA) provides that "[n]othing in this article shall be construed to require a physician to prescribe or render m.edical treatment to a patient that the physician determ.ines to be medically or ethically inappropriate."206 A provider may unilaterally stop LSMT after giving a surrogate fourteen days to attem.pt transfer to another facility willing to provide the requested treatm.ent. 207 This Virginia statute had an apparently dispositive im.pact in at least one case. After the University of Virginia Hospital issued a unilateral DNR order- for Shirley Robertson, her surrogate brought an EMTALA action in federal court. 208 In Bryan v. Rectors & Visitors of UVA, the Fourth Circuit affirm.ed the dismissal of the EMTALA claim. and suggested that the plaintiff proceed in state court, noting that "[s]uch reprehensible disregard for one's patient" would constitute the "tort of abandonment."209 Subsequently, the plaintiff proceeded in state court,210 but later voluntarily dism.issed that action because of from Robin C. Correll to Thaddeus Pope (May II, 2007) (on file with author) See Pope, Futility Statutes, supra note 17 (arguing that only Texas' safe harbor is effective). But cf Maureen Kwiecinski, To Be Or Not to Be, Should Doctors Decide? Ethical and Legal Aspects ofmedical Futility Policies, 7 ELDER'S ADVISOR 313, (2006) (questioning the constitutionality of unilateral decision statutes) VA. CODE ANN (A) (West 2007) Id Bryan, 95 F.3d at Id. at Id.
276 266 MARQUETTE ELDER'S ADVISOR [Vol. 9 the Virginia HCDA.211 Similarly, the Louisiana Health Care Decisions Act provides that the act should not be 1/construed to require the application of medically inappropriate treatment... or to interfere with medical judgment with respect to the application of medical treatment or life-sustaining procedures."212 In Causey v. St. Francis Medical Center, providers unilaterally withdrew a ventilator and dialysis from a comatose patient with end-stage renal disease. 213 The appellate court affirm.ed the dismissal of the family's intentional battery tort action, observing that Louisiana providers are entitled to unilaterally withdraw LSMT so long as they comply with the standard of care. 214 Apart from unique outrage cases, actions against unilateral termination of LSMT have been unsuccessful. Surrogates have had enormous difficulty overcoming statutory authorization to refuse LSMT, establishing breach of the standard of care, and establishing causation and damages. The low success rate means not only that the risk of liability is lower than b,elieved, but also that fewer cases will even be brought against providers.215 CONCLUSION While the litigated futility cases do not articulate a clear and unequivocal right of providers to refuse LSMT that they deem mappropriate, these cases also do not support the supposed 211. Bryan v. Rectors & Visitors of the Univ. of Virginia, No. CL (Fauquier County, Va. Cir. Ct. Nov. 27, 1995) (Order of Nonsuit). It is also hard to establish tortuous abandonment because while providers may cease aggressive treatment, they continue comfort care. See Hartsell, 905 S.W.2d at LA. REV. STAT. ANN. 40: (A)(4) (2006) Causey, 719 So. 2d at Id. at 1075 (citing 40: (A)(4». The appellate court did remand the medical malpractice claim to a "medical review panel" to determine whether the providers met the standard of care. See Message from Jeffrey D. Gurrierro to Thad Pope (on file with author) See John A. Day, Should You Risk Taking the Case? TRIAL, Jan. 2008, at 20; Gary B. Pillersdorf, Criteria for Case Selection, in ATLA's LITIGATING TORT CASES (2007).
277 2008] ]UDICIA.L TREATMENT OF MEDICAL FUTILITY 267 right of surrogates to demand such care. Surrogates do not have nearly the amount of bargaining power that they are perceived to possess. Therefore, the fear of legal liability should not have the impact on provider decision-making that it has had. A reassessment of the judicial treatment of futility cases leads to an obvious implication for health care providers. Physicians make decisions regarding LSMT based largely on perceived constraints from the legal system. 216 The misperception of those constraints has led to the overtreatment of patients, causing unnecessary suffering and inappropriate use of scarce medical resources. 217 But firmer, more accurate shadows should produce better results. 218 With sufficient legal education, providers may be more willing to treat patients in a way they deem medically appropriate. 219 A reassessment of the judicial treatment of futility cases also leads to two practical implications for elder law attorneys. First, attorneys must educate their clients. It is a long-recognized role of the elder law attorney to advise her clients about advance directives. 220 As elders may have misconceptions about their future care,221 counseling should be directive. It should entail more than the passive documentation of a client's articulated treatment preferences.222 Attorneys should educate clients so 216. McCrary, supra note 4, at 373; Pope & Waldman, supra note 4, at Pope & Waldman, supra note 4, at Cf Alan Bavley & Julius A. Karash, As Life Ebbs, Bills Can Mount: Millions of Elderly Get Needless and Costly Medical Care as They Near Death, KANSAS CITY STAR, Jan. 1, 2007 (discussing the Dartmouth Atlas of Health Care) Ruth D. Raisfeld, Mediators Can Best Help Those Who Help The1nselves, N.Y.L.J., Dec. 1, 2003 (arguing that mediation is more successful with "objective criteria" such as an accurate understanding of "prevailing case law") McCrary, supra note 4, at 372. See also Perkins et al., supra note 4, at 192 (criticizing the impact of "external factors" on physician decision-making) Nat'l Acad. of Elder Law Attorneys, Preparing for End oflife, EYE ON ELDER ISSUES, Aug. 2004, available at Aug04.pdf (last visited Feb. 2, 2008) See, e.g., Catherine A. Marco & Roques M. Schears, ER Decisions to Withdrazv CPR, 9 AMAVIRTUAL MENTOR 174 (2007) See Ed de St. Aubin et al., Elders and End-of-Life Medical Decisions: Legal Context, Psychological Issues, and Recommendations to Attorneys Serving Seniors, 7 ELDER'S ADVISOR 259, (2006).
278 268 MARQUETTE ELDER'S ADVISOR [Vol. 9 that they have realistic expectations of what medicine can offer. 223 Second, attorneys should empower their clients. Elder law attorneys should be "articulate and forceful advocates so that their client's [treatment] preferences... are honored and understood."224 Sometimes after a careful, thorough discussion of treatment options, attorneys may discover that their client has a religious or cultural reason for wanting to continue LSMT, no matter how dire the circumstances. If so, they should advise their client that an advance directive can be used not only to decline treatm.ent but also to "request that all reasonable measures... be taken to sustain life."225 To be sure, even advance directives can be overridden in futility disputes. However, having clear written docum.entation of treatment preferences maximizes the chance that such preferences will be honored Id A. KIMBERLY DAYTON ET AL., ADVISING THE ELDERLY CLIENT 33.7 (2007); Barbara Weinschenk, End of Life Issues, ELDER LAW UPDATE 146, (Nat'l Bus. Inst. 2007) DAYTON ET AL., supra note 224, at Cf Eric R. Oalican, Older Clients and Long Term Care, DRAFTING ESTATE PLANS (Mass. CLE, Inc. 2007) (offering the following sample medical directive language: "I want my life to be prolonged to the greatest extent possible without regard to my condition, the chances I have for recover, or the cost of the procedures.").
279 Widener Law School Legal Studies Research Paper Series no Involuntary Passive Euthanasia in U.S. Courts: Reassessing the Judicial Treatment of Medical Futility Cases Thaddeus Mason Pope Widener University School of Law This paper can be downloaded without charge from The Social Science Research Network Electronic copy available at:

280 Electronic copy available at:

281 INVOLUNTARY PASSIVE EUTHANASIA IN U.S. ~ COURTS: REASSESSING THE JUDICIAL TREATMENT OF MEDICAL FUTILITY CASES Thaddeus Mason Pope* INTRODUCTION End-of-life care issues are marked with significant conflict.! A particularly common type of conflict is the llledical futility dispute, in which a patient's surrogate decision-lllaker dem.ands life-sustaining medical treatm.ent ("LSMT") that the patient's health care provider ("provider") deellls m.edically inappropriate. A leading treatise predicts that llledical futility disputes are "likely to occupy as much, if not m.ore [time and] judicial effort in the com.ing years as conventional end-of-life * Thaddeus Mason Pope serves as Assistant Professor of Law at the University of Memphis Cecil C. Humphreys School of Law, and is serving as Visiting Assistant Professor at the Widener University School of Law ( ). This paper was developed from a presentation for NAELA's November 2006 Advanced Elder Law Institute and was supported by a summer research grant from the University of Memphis. Thanks to Sandra Johnson and Kathy Cerminara for thoughtful comments on an earlier draft. 1. See generally Catherine M. Breen et al., Conflict Associated with Decisions to Limit Life-Sustaining Treatment in Intensive Care Units, 16 J. GEN. INTERNAL MED. 283, 285 (2001) (finding that conflict occurred in 780/0 of cases concerning the limitation of life-sustaining medical treatment); John M. Luce & Douglas B. White, The Pressure to Withhold or Withdraw Life-sustaining Therapy from Critically III Patients in the United States, 175 AM. J. RESPIRATORY & CRITICAL CARE MED. 1104, 1108 (2007) (arguing that "disagreements between families and clinicians on end-of-life care are commonplace in the United States."); Hasan Shanawani et ai, Meeting Physicians' Responsibilities in Providing End-oJ-Life Care, 133 CHEST 755, 780 (2008); Keith M. Swetz et al., Report of255 Clinical Ethics Consultations and Review ofthe Literature, 82 MAYO CLINIC PROC. 686, (2007) (finding that futility disputes are one of the primary reasons for hospital ethics consultations). 229 Electronic copy available at:

282 230 MARQUETTE ELDER'S ADVISOR [Vol. 9 cases have in the last three decades."2 While most futility' disputes are -resolved informally, informal resolution is deeply informed and shaped by the "shadow of the law."3 The perception of legal liability has a considerable impact on physicians' life support decisions. 4 In one recent survey, providers were asked why they followed the instructions of surrogates instead of doing what they felt was appropriate. Almost all the responding providers cited a "lack of legal support."s But that "shadow of the law" is misperceived. In assessing the judicial treatm.ent of futility cases, it appears that most of the medical, legal, and bioethical literature concludes that courts have generally disfavored providers. Some treatises observe that "the courts have not given the elder law practitioner much guidance in the area of medical futility./ 6 However, these assessments are based on limited and outdated sets of cases. This article provides a comprehensive review of futility cases over the twenty-five year period from 1983 to Based on this review, I argue that courts have generally neither prohibited nor punished the unilateral refusal of LSMT. Providers have regularly obtained both ex ante permission and ex post forgiveness for stopping LSMT without consent ALAN MEISEL & KATHY CERMINARA, THE RIGHT TO DIE: THE LAW OF END OF-LIFE DECISIONMAKING 13.01[0] (3d ed & Supp. 2007) [hereinafter THE RIGHT TO DIE]. See Pam Belluck, Even as Doctors Say Enough, Families Fight to Prolong Life, N.Y. TIMES, Mar. 27, 2005, at 1.1 ('''The most common case that comes before the ethics committees... are families now insisting on treatment that the doctors believe is unwarranted."'(quoting Dr. John J. Paris». 3. Robert H. Mnookin & Lewis Kornhauser, Bargaining in the Shadow of the Law: The Case ofdivorce, 88 YALE L.J. 950, 968 (1979). 4. See Henry S. Perkins et al., Impact oflegal Liability, Family Wishes, and Other 'External Factors' on Physicians' Life-Support Decisions, 89 AM. J. MED. 185 (1990); S. Van McCrary et al., Treatment Decisions for Terminally III Patients: Physicians' Legal Defensiveness and Knowledge ofmedical Law, 20 L. MED. & HEALTH CARE 364 (1992). See also Thaddeus M. Pope & Ellen A. Waldman, Mediation at the End oflife: Getting Beyond the Limits ofthe Talking Cure, 22 OHIO ST. J. ON DISP. RESO~. 143, (2007). 5. Robert Sibbald et al., Perceptions of "Futile Care" among Caregivers in Intensive Care Units, 177 CANADIAN MED. ASS'N J. 1201, 1203 (2007). 6. EDWIN KASSER, ELDER LAW AND GUARDIANSHIP IN NEW YORK 4:97 (2008). 7. This article is not an analysis of the legal risks entailed in unilateral withdrawal of LSMT, given the unavoidable material jurisdictional and factual
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 231 In Section One, I describe a futility dispute and the informal manner in which such a dispute is usually resolved.](/docs-images/79/79224697/images/283-0.jpg "-I also discuss the current popular: perception that the judicial treatment of such disputes generally disfavors health' care providers.")
283 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 231 In Section One, I describe a futility dispute and the informal manner in which such a dispute is usually resolved. -I also discuss the current popular: perception that the judicial treatment of such disputes generally disfavors health' care providers. While few cases are litigated, the perception of the judicial treatment of futility disputes has an enormous impact on the infor:rp.al resolution of tens of thousands of disputes in the hospital context. Furthermore, I exam.ine the complete available universe of litigated futility cases. 8 These cases can arise either before LSMT is withdrawn (ex ante cases) or after LSMT is withdrawn (ex post cases). In Section Two, I differentiate three types of ex ante cases. First, providers have had increasing success securing judicial permission to replace the authorized surrogate decision-maker with another who will agree with the provider's recommendation. Second, providers have had increasing success obtaining declaratory relief allowing the refusal itself. Third, surrogates have typically been able to only temporarily enjoin the withdrawal of LSMT. In Section Three, I examine cases brought by surrogates after LSMT is withdrawn. These ex post cases are typically adjudicated in favor of providers. Surrogates either cannot establish that the standard of care requires continued LSMT, or they cannot establish causation and damages. Surrogates' variations. Rather, it is a broad examination of those futility disputes that have been litigated. 8. The leading treatise focuses primarily on reported cases. THE RIGHT TO DIE, supra note 2, at to (Supp. 2007). Since the universe of reported cases is rather limited, this article includes a discussion of unreported cases. Of course, since there is no systematic way to locate unreported cases, these are limited to cases discussed in the secondary literature. Cf Edward K. Cheng & Albert H. Yoon, Does Frye or Daubert Matter? A Study of Scientific Admissibility Standards, 91 VA. L. REV. 471, 480 (2005) (observing that "[M]ost state court opinions, particularly at the trial court level, are unpublished or available on Westlaw or Lexis.") (citing David E. Bernstein, Frye, Frye Again: The Past, Present, and Future of the General Acceptance Test, 41 JURIMETRICS J. 385, 389 (2001». Moreover, even some of these cases have been excluded because they are still in litigation. See, e.g., Allen v. Stanford Dniv. Med. Ctr., No CV (Santa Clara Sup. Ct. Mar. '4, 2008) (defendant's motion for summary judgment taken under submission).

284 232 MARQUETTE ELDER'S ADVISOR [Vol. 9 actions for damages typically succeed only where the provider's conduct is outrageous, when LSMT is withdrawn in an egregiously insensitive manner.' ". J conclude by noting some practical im.plications of my reassessment of the judicial treatment of futility cases. Elder law treatises observe that "a doctor usually will accede to the wishes of a fam.ily that insists that. Care be continued, even if the doctor believes that no benefit is being conferred."9 But while this may have been true in the early 1990s, it m.ay be far less true today. Elder law attorneys should counsel their clients to have realistic expectations of what m.edicine can and will offer. THE MISPERCEPTION THAT FUTILITY CASES DISFAVOR PROVIDERS.. Before embarking. on.an analysis of the judicial treatment of futility cases, the distinctive feawres of a futility case l!lust be clarified, and the judicial treatm.ent of such cases m.ust be placed in the appropriate context. Specifically, while most futility disputes are resolved informally, resolution is deeply influenced by the shadow of the law created by the m.uch slllaller univ.erse of court cases. WHATIs A FUTILITY DISPUTE? A medical, futility dispute arises when a pr<?vider seeks to stop treatment that the patient or surrogate wants continued. The provider judg~s LSMT to be of no benefit and wants to "stop the train" when the patient or surrogate says "keep going." IO The provider wants to stop LSMT even without consent of the patient or surrogate.ii Accordingly, a, tnedical 9. JOAN M. KRAUSKOPF ET AL., ELDERLAW: ADVOCACY FOR THE AGING 13:26 (2d ed. 1993). See ALISON BARNES ET AL., COUNSELING OLDER CLIENTS 317 (2d ed. 2005). 10. K. Francis Lee, Postoperative Futile Care: Stopping the Train When the Family Says "Keep Going, "15 THORACIC SURGERY CLINICS 481, 481 (2005). 11. Some writers identify Lebreton v. Rabito, 650 So.2d 1245 (La. App. 1995), as a futility case. But while the daughter brought a malpractice action for the
285 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 233 futility dispute is sometimes referred to as a "reverse end-oflife," 12 a "right to life,i/13 a "duty to die," 14 or even an "involuntary 15 euthanasial/ situation. The provider and surrogate disagree about the need for LSMT because they each have different goals. 16 The surrogate's goals may include cure, amelioration of disability, palliation of sym.ptoms, reversal of disease process, or prolongation of life. The provider, -on the other hand, may, under the circumstances, judge these goals to be impossible, virtually impossible, or otherwise inappropriate. 17 It was just this sort of disagreement underlying the recent high-profile case of "Baby Emilio.1/ On November 3, 2005, Emilio Lee Gonzales was born generally healthy; however, within a few weeks, he started exhibiting neurological abnormalities.18 By November 2006, Baby Emilio showed "global developmental delay and decreased muscle tone and reflexes," and he was soon diagnosed with Leigh's disease, a progressive neuron-metabolic disorder affecting the nervous withdrawal of LSMT by her father, her mother was the authorized decision-maker who had consented to the withdrawal. Id. at This was an intra-family dispute, not a futility dispute between a patient or surrogate and a provider. See also Anthony Colarossi, Man at Center of Living Will Battle Dies, S. FLA. SUN SENTINEL, Dec. 11, 2004, at 6B. 12. See, e.g., Thomas Wm. Mayo, Living and Dying in a Post-Schiavo World, 38 J. HEALTH L. 587, 602 n.68 (2006); THE RIGHT TO DIE, supra note 2, 13.01[B] at See, e.g., Leigh Middleditch, Jr. & Joel Trotter, The Right to Live, 5 ELDER L.J. 395 (1997) [hereinafter The Right to Live]; Nancy Neveloff Dubler, Conflict and Consensus at the End of Life, HASTINGS CENTER. REP. S19, S19 (Nov.-Dec. 2005); Wesley J. Smith, Suingfor the Right to Live, DAILY STANDARD, Mar. 9, See, e.g., The Right to Live, supra note See Mary Ann Roser, Debate Heats Up on 10-day Medical Law, AUSTIN AM. STATESMAN, Aug. 10, 2006, at B See Thomas W. Mayo, Health Care Law, 53 SMU L. REV. 1101, 1110 n.78 (2000) ("[T]he core dispute is... over what constitutes a 'benefit' to the patient..."); Griffin Trotter, Editorial Introduction: Futility in the 21st Century, 19 HEC FORUM 1, 1 (2007). 17. See Thaddeus Mason Pope, Medical Futility Statutes: No Safe Harbor to Unilaterally Refuse Life-Sustaining Treatment, 75 TENN. L. REV. I, (2007) (reviewing physiological futility, quantitative futility, and four versions of qualitative futility). 18. Verified Complaint Ex. B to Ex. 1, Gonzales v. Seton Family of Hospitals, No. A07CA267 (W.D. Tex. Apr. 4, 2007).

286 234 MARQUETTE ELDER'S ADVISOR [Vol. 9 system.. 19 In Decem.ber 2006, Baby Emilio was adm.itted to the PICD at Children's Hospital of Austin, where his neurological status worsened as his brain atrophied.20 He depended on a m.echanical ventilator for breathing and a nasojejunal tube for eating.21 Baby EIllilio was sem.i-com.atose, unable to m.ove his arm.s or legs, rarely opened his eyes, and could not em.pty his bladder. 22 He also had frequent seizures, and the providers had "great difficulty keeping his lungs inflated."23 Baby Em.ilio's providers deterillined that his condition was irreversible, and they believed that to continue treatment would only "serve to prolong his suffering without the possibility of cure."24 His providers felt that "the burdens associated with his current care plan outweigh[ed] any benefit EIllilio [might have been] receiving"25 and that his "aggressive treatm.ent plan am.ount[ed] to a nearly constant assault on Emilio's fundamental hum.an dignity."26 However, Baby Em.ilio's m.other, Catarina, dem.anded that the providers continue the aggressive treatment plan.' She refused to consent to the withdrawal of Baby Em.ilio's lifesustaining treatment,27 insisting that the providers maintain him until "Jesus takes him.."28 Catarina would not agree to the providers' recom.m.endations because "every moment of life he has to spend with her is of inestim.able value."29 During the winter of 2007, Catarina had m.ultiple conferences with Baby Emilio's providers to discuss his condition and treatment plan,30 but they could not reach a consensus. In February and March of 19. Id. at <ji Id. at Ex. B to Ex Id. 22. Id. 23. Id. at Ex. 0 to Ex. I, at Id. at Ex. A to Ex Id. at Ex. 0 to Ex. I, at Id. 27. Id. at <ji Id. at Ex. B to Ex. I, at Id. at <ji Id. at Ex. B to Ex. I, at 2.
287 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY , Catarina met not only with the providers, but also with the hospital's entire Neonatal/Pediatric Ethics Committee. 31 Again, no consensus was reached. 32 Soon thereafter, Catarina filed two separate lawsuits against both the Children's Hospital and the individual providers.33 WHILE FUTILITY DISPUTES ARE RARELYRESOLVED IN COURT, JUDICIAL TREATMENT CASTS A LONG, DARK SHADOW OVER THEIR INFORMAL RESOLUTION While the Gonzales case ended up in court, most futility disputes are resolved internally and informally by the medical team. Presumably after a medical team discusses a patient's treatment goals, the nature of a patient's condition, and the range of options, the team comes up with a treatment recommendation, with which most surrogates agree. For example, in a multi-center study by Prendergast and colleagues, fifty-seven percent of surrogates agreed immediately with a provider-recommended care-plan, and ninety percent moved toward agreement within five days. 34 In a more recent study, consensus was reached in fifty-one percent of cases after the first meeting, in sixty-nine percent of cases after a second meeting, and in ninety-seven percent of cases after a third meeting.35 Even if the provider and surrogate do not agree on a treatment, it is sometimes possible to transfer a patient to 31. Id. 32. Id. at Ex. D to Ex Gonzales v. Seton Family of Hospitals, No (Travis Cty. Probate Ct, Tex. filed Mar. 20, 2007); Gonzales v. Seton Family of Hospitals, No. A07CA267 (W.O. Tex. filed Apr. 4, 2007). 34. Thomas J. Prendergast, Resolving Conflicts Surrounding End-oj-Life Care, 5 NEW HORIZONS 62, 62 (1997). 35. Daniel Garros et al., Circumstances Surrounding End oj Life in a Pediatric Intensive Care Unit, 112 PEDIATRICS e371, e373 (2003). See Laurence J. Schneiderman et al., Effect oj Ethics Consultations on Nonbenejicial Life-Sustaining Treatments in the Intensive Care Setting: A Randomized Controlled Trial, 290 JAMA 1166, 1166 (2003) (concluding that ethics consults "were useful in resolving conflicts that may have inappropriately prolonged nonbeneficial... treatments.").

288 236 MARQUETTE ELDER'S ADVISOR [Vol. 9 another institution that is willing to coltiply with the surrogate~s treatment requests. 36 While this is rarely successful,37 it does som.etimes resolve additional disputes.38 When stopping LMST is against the-wishes of a patient or surrogate, providers should take unilateral action to stop LSMT only after diligently m.aking all the foregoing attempts to resolve the conflict. 39 While most cases will never reach this stage,40 a significant percentage will. 41 A recent five-year study of sixteen 36. The model futility policies of most institutional and professional associations provide for transfer. See, e.g., AMA COUNCIL ON ETHICAL AND JUDICIAL AFFAIRS, CODE OF MEDICAL ETHICS 2.035, 2.037, at ( ); AMA COUNCIL ON ETHICAL AND JUDICIAL AFFAIRS, MEDICAL FUTILITY IN END-OF LIFE CARE, 281 JAMA 937, 940 (1999). This is consistent with the law of tortuous abandonment, which requires physicians to assist their patients in finding a new provider before terminating a treatment relationship.,see Payton v. Weaver, 182 Cal. Rptr. 225, 229 (Cal. App. 1982); Stella L. Smetanka, Who Will Protect the 'Disruptive' Dialysis Patient?, 32 AM. J. L. & MED. 53, (2006). Exploring the possibility of transfer is also required by many state health care decision-making statutes. See generally Pope, Futility Statutes, supra note See Pope, Futility Statutes, supra note 17, at 60 n. 343 (collecting cites). 38. See, e.g., Todd Ackerman, Hospital to End Life Support: Houston Woman Faces Second Fight in 2 Months Over Husband's Care, HOUSTON CHRON., Apr. 28, 2005, at 5 (discussing how St. Luke's in Houston noted that "more than 30 facilities had rejected Nikolouzos before Avalon Place surprised them and agreed to take [him]."); Joan Beck, Use Medical Treatment to Save Every Damaged Baby?, ORLANDO SENTINEL, May 18, 1990, at A13 (The GAL for Baby L "found a pediatric neu~ologlst who was willing to do everything the mother wanted./i); Alexander M. Capron, Baby Ryan and Virtual Futility, HASTINGS CENTER REP. 20, 20 (Mar.-Apr. 1995) (noting that the parents of Ryan Nguyen found a facility willing to provide the requested treatment.); John J. Paris et ai., Physicians' Refusal ofrequested Treatment: The Case ofbaby L, 322 NEW ENG. J. MED. 1012, 1013 (1990) (parents transferred' Baby L's care to a consultant pediatric neurologist). 39. See MICHAEL D. CANTOR ET AL., Do-NoT-RESUSCITATE ORDERS AND MEDICAL FUTILITY: A REPORT BY THE NATIONAL ETHICS COMMITTEE OF THE VETERANS HEALTH ADMINISTRATION 1 (Dec. 2000) (arguing that unilateral decisions "should be rese-rved for exceptionally rare and extreme circumstanc~s after thorough attempts to resolve disagreements have failed"); THE RIGHT TO DIE, supra note 2, 13.04, at (noting that "sometimes only litigation can break the impasse between demanding families and resistant health care professionals."); Timothy Bowen & Andrew Saxton, New Developments in the Law - 'Withholding and Withdrawal ofmedical Treatment, 14(5) AUSTRALIAN HEALTH L. BULL. 57, 60 (2006). 40. See Troyen A. Brennan, Ethics Committees and Decisions to Limit Care, 260 JAMA 803, 807 (1988) ("In all cases [where unilateral DNR orders were entered], the families either_ ultimately accepted this reasoning or ceased insisting that invasive procedures be used."). 41. See Pope & Waldman, supra note 4, at See also Robert L. Fine, The Texas Advance Directives Act of1999: Politics and Reality, 13 HEC FORUM 59, 81 (2001) (five of 29 cases went through the whole process, though two died and three agreed
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 237 hospitals found that each hospital averaged one case per year in which it decided to unilaterally stop LSMT.](/docs-images/79/79224697/images/289-0.jpg "42 Another study of nine hospitals found that the hospitals decided to unilaterally stop LSMT in two-percent of 2,842 cases.")
289 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 237 hospitals found that each hospital averaged one case per year in which it decided to unilaterally stop LSMT.42 Another study of nine hospitals found that the hospitals decided to unilaterally stop LSMT in two-percent of 2,842 cases. 43 Moreover, there are strong reasons to suspect that the rate of intractability will rise. 44 While few futility cases go to court, those that do exert a strong influence on the resolution of the other cases. 45 "[W]hile legal power is relevant only in the few disputes that enter the system.... [b]argaining endowm.ents are... relevant to many futility cases."46 Mediation occurs in the "shadow of the law," 47 in that both parties consider the likely range of results if the dispute were litigated. 48 After all, "if agreem.ent cannot be reached in the mediation session, a series of default rules... corn.es into play." 49 "[T]he outcorn.e that the law will impose if no agreement is reached gives each [party] certain bargaining chips - an before treatment was actually stopped); Pendergast, supra note 34 at 67 (finding 40/0 of disputes were intractable). 42. Emily Ramshaw, Children Fight to Save Mom, DALLAS MORNING NEWS, Aug. 18, About half these patients died or were transferred to other facilities before treatment was actually stopped. Id. 43. Testimony before the Tex. H. Comm. on Public Health (2005), in INTERIM REPORT 2006, at 36 (citing a written statement of Greg Hooser). 44. The reasons for surrogate insistence are becoming more prevalent. See Pope & Waldman, supra note 4, at At the same time, provider resistance may increase with changes in reimbursement and an increased focus on palliative care. Id. 45. Cf Roberts v. Stevens Clinic, 345 S.E.2d 791, 801 (W. Va. 1986) (I/[B]ecause less than six percent of all serious lawsuits are tried, the most important thing that courts do is to cast a shadow of legal rules within which litigants can craft their own custom-made settlements."); RANDALL R. BOVBJERG & BRIAN RAYMOND, PATIENT SAFETY, JUST COMPENSATION AND MEDICAL LIABILITY REFORM 11 (2003), available at (explaining how providers engage in "defensive medicine") (last visited Feb. 2, 2008). 46. Bethany Spielman, Bargaining about Futility, 23 J. L. MED. & ETHICS 136, 137 (1995). 47. Mnookin & Kornhauser, supra note 3, at Jeffrey W. Stempel, Forgetfulness, Fuzziness, Functionality, Fairness, and Freedom in Dispute Resolution: Serving Dispute Resolution Through Adjudication, 3 NEV. L.J. 305, 308 n.14 (2003). 49. NANCY NEVELOFF DUBLER & CAROL B. LIEBMAN, BIOETHICS MEDIATION: A GUIDE TO SHAPING SHARED SOLUTIONS 25 (2004).

290 238 MARQUETTE ELDER'S ADVISOR [Vol. 9 endowment of sorts." 50 Since a party typically will not agree to settle for an amount less than it would be awarded in litigation, such entitlements typically determine the m.inimum amount a party will accept in bargaining.51 Therefore, it appears that the party who can achieve a better litigation outcome will have a higher minimum settlement amount and greater bargaining power. PROVIDERS GENERALLY PERCEIVE THAT FUTILIlY CASES DISFAVOR THE UNILATERAL REFUSAL OF LSMT It is widely believed that surrogates, can achieve the better litigation outcome. "Numerous articles have warned physicians of the serious legal risk in unilaterally writing a DNR order..."52 Specifically, based on the outcomes of several well-publicized court cases, commentators consistently conclude that courts usually side with families and ag'ainst hospitals.53. Commentators conclude that IIcourts have not upheld the right of physicians to make unilateral judgments"54 and find that "courts are overriding ostensibly sound physician assessments... [and] dictating medical maintenance of... gravely debilitated patients." 55 This assessment is widely 50. Mnookin & Kornhauser, supra note 3, at See Jonathan M. Hyman & Lela P. Love, IfPortia Were a Mediator: An Inquiry into Justice in Mediation, 9 CLINICAL L. REV. 157, 162 (2003) (noting that "public law provides the norms that guide private dispute resolution. Parties often settle... by keeping in mind and balancing the entitlements the litigation system promises."); Stephen N. Subrin, A Traditionalist Looks at Mediation: It's Here to Stay and Much Better than I Thought, 3 NEV. L.J. 196, 227 (2003) ("[t]he results of mediation are frequently - I actually believe usually - dependent upon the range of potential results that would come from formal adjudication."). 52. Edward F. McArdle, New York's DNR Law: Groundbreaking Protection of Patient Autonomy or a Physician's Right to Make Medical Futility Determinations, 6 DEPAULJ. HEALTH CARE L. 55,71 (2002). 53. Jack K. Kilcullen et al., A Multilevel Examination ofa Critically III Patient, in THREE PATIENTS: INTERNATIONAL PERSPECTIVES ON INTENSIVE CARE AT THE END OF LIFE 123 (2002). 54. Paul R. Helft et al., The Rise and Fall ofthe Futility Movement, 343 NEW ENG. J. MED. 293, 295 (2000). ' 55. Norman L. Cantor, Can Healthcare Providers Obtain Judicial Intervention against Surrogates Who Demand 'Medically Inappropriate' Life Support for Incompetent Patients?, 24 CRITICAL CARE MED. 883, 884 (1996).
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 239 reprinted in medical journals,56 bioethics journals,57 and even in many law reviews.](/docs-images/79/79224697/images/291-0.jpg "58 While some authors have made more careful and qualified case assessments, they emphasize the uncertainty and risk. 59 56. See, e.g., Am. CoIl.")
291 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 239 reprinted in medical journals,56 bioethics journals,57 and even in many law reviews. 58 While some authors have made more careful and qualified case assessments, they emphasize the uncertainty and risk See, e.g., Am. CoIl. of Obstetricians and Gynecologists, Committee Opinion No. 362: Medical Futility, 109 OBSTETRICS & GYNECOLOGY 791, 792 (2007) (noting that "litigation has generally resulted in courts supporting the views of patient or family //); Robert A. Burt, The Medical Futility Debate: Patient Choice, Physician Obligation, and End-of-Life Care, 5 J. PALLIATIVE MED. 249, 250 (2002) ("[C]ourts have rejected physician claims to use futility...//); Robert S. Chabon et al., The Case of Baby K, 331 NEW ENG. J. MED. 1383, 1383 (1994) ("In no reported case has a court ruled that a physician may... override a parent's wish to continue life support for his or her dying child."); Lewis L. Low & Larry J. Kaufman, Medical Futility and the Critically III Patient, 58 HAWAII MED. J. 58, 62 (1999) (lito date, the u.s. courts have refused to grant physicians and hospitals the power to override the opinions of family members on matters of futility.//); Stanley A. Nasraway, Unilateral Withdrawal of Life-Sustaining Treatment: Is It Time? Are We Ready?, 29 CRITICAL CARE MED. 215, 217 (2001); James E. Szalados, Discontinuation ofmechanical Ventilation at End-of-Life: The Ethical and Legal Boundaries ofphysician Conduct in Termination of Life Support, 23 CRITICAL CARE CLINICS 317, 325 (2007). 57. See, e.g., Peter A. Clark, Medical Futility in Pediatrics: Is It Time for a Public Policy?, 23 J. PUB. HEALTH POL'y 66, (2002); Robert A. Gatter, Jr. & John C. Moskop, From Futility to Triage, 20 J. MED. & PHIL. 191, 194 (1995). 58. See, e.g., Peter N. Cultice, Medical Futility: When Is Enough, Enough, 27 J. HEALTH & Hasp. L. 225 (1994); Judith Daar, Medical Futility and Implications for Physician Autonomy, 21 AM. J. L. & MED. 221, 223 (1995); Sandra H. Johnson et al., Legal and Institutional Policy Responses to Medical Futility, 30 HEALTH L.J. 21 (1997) ("[T]he courts have almost uniformly ordered continued treatment."); Patrick Moore, An End-of-Life Quandary in Need of a Statutory Response: When Patients Demand Life-Sustaining Treatment that Physicians Are Unwilling to Provide, 48 B.C. L. REV.43~439(2007). 59. See, e.g., NAT'L CTR. FOR STATE COURTS, GUIDELINES FOR STATE COURT DECISION MAKING IN LIFE SUSTAINING MEDICAL TREATMENT CASES 147 (2d ed. 1993) (finding that there is "as yet no consensus... on the legal ramifications associated with [futility]..."); Gordon B. Avery, Futility Considerations in the Neonatal leu, 22 SEMINARS PERINATOLOGY 216, (1998); Jesse A. Goldner et al., Responses to Medical Futility Claims, in HEALTH LAW HANDBOOK 401, 401 (1997) (noting that the current legal status of claims of medical futility is confusing); Sandra H. Johnson et al., Legal and Institutional Policy Responses to Medical Futility, 30 HEALTH L.J. 21 (1997); Alan Meisel, Ethics and Law: Physician-Assisted Dying, 8 J. PALLIATIVE MED. 609, 615 (2005); E. Haavi Morreim, Profoundly Diminished Life, 24 HASTINGS CENTER REP. 33, 36 Gan.-Feb. 1994) (noting that "[c]ourts have yet to offer guidance..."); John M. Luce & Douglas B. White, The Pressure to Withhold or Withdraw Life-sustaining Therapy from Critically III Patients in the United States, 175 AM. J. RESPIRATORY & CRITICAL CARE MED. 1104, 1106 (2007) (correctly noting that the Baby K and Wanglie cases did not "fac[e] the futility issue head on"); Nasraway, supra note 56, at 217 ("Unilateral withdrawal... is still uncharted territory."); Sibbald, supra note 5, at 1206 (noting there is little case law to guide decisionmaking in the face of patient or surrogate opposition); Karen Trotochaud, 'Medically Futile' Treatments Require More than Going to Court, CASE MANAGER, May-June 2006, at 60, 63 ("[L]egal cases have provided limited and confusing guidance...").

292 240 MARQUETTE ELDER'S ADVISOR [Vol. 9 Moreover, much of what providers have learned about litigated cases is distorted. "[A]s the information gets passed along, it gets simplified, and sometimes oversim.plified, and som.etim.es distorted, as in a children's gam.e of 'telephone.'" 60 After all, "[e]ven experts can succum.b to reductionist tendencies and lose sight of the subtleties.ii 61 In short, actual risks are likely overestimated by providers. 62 Both providers and surrogates seem to believe that substantive end-of-life medical decision-m.aking law favors surrogates. Both understand that surrogates have an effective "veto authority" over physician judgm.ent. 63 It appears that both expect the surrogates to likely win a litigated case if an agreem.ent is not reached in LSMT n~gotiations and mediation. It is this understanding that ultim.ately casts a shadow on negotiations, rather than actual law. 64 "The m.ost efficacious social facts in the actual hospital situation are [provider] perceptions them.selves, not the objective risks...."65 But this pejorative assessm.ent of providers' non-settlem.ent alternatives appears off-base. Not only have providers 60. Alan Meisel, The Role oflitigation in End oflife Care: A Reappraisal, HASTINGS CENTER REP. 547, S48 (Nov.-Dec. 2005). 61. Id. 62. Cf Regina Ohkyusen-Cawley et al., Institutional Policies on Determination of Medically Inappropriate Interventions: Use in Five Pediatric Patients, 8 PEDIATRIC CRITICAL CARE MED. 225, 225 (2007) ("[C]ourts have endorsed patient or surrogate insistence on continued intervention, possibly fostering the reluctance of medical professionals to limit nonbeneficial interventions."). Marshall Kapp argues that the legal risks in the early 1990s were not serious and concedes that physicians had "overblown anxiety." Marshall Kapp, Futile Medical Treatment: A Review of the Ethical Arguments and Legal Holdings, 9 J. GEN. INTERNAL MED. 170, 175 (1994). 63. Cf Jacquelyn Slomka, Clinical Ethics and the Culture of Conflict, HASTINGS CENTER REP. 45, 46 (Mar.-Apr. 2005) (noting that "[a]n increasingly litigious society as well as bioethical emphasis on patient and family autonomy... have led to physicians' disempowerment..."). 64. See Pope & Waldman, supra note 4. Cf Mark A. Hall, The Defensive Effect of Medical Practice Policies in Malpractice Litigation, 54 L. & CONTEMP. PROBLEMS 119, 119 (1991) ("[T]o the extent that a crisis is in fact widely perceived, it has the quality of a self-fulfilling prophecy..."); Spielman, ~upra note 46, at 137 ("[I]n the clinical setting... myths about the law often overshadow reality."). 65. Stephen Toulmin, Institutions and their Moral Constraints, in INTEGRITY IN HEALTH CARE INSTITUTIONS: HUMANE ENVIRONMENTS FOR TEACHING, INQUIRY, AND HEALING 21, 26 (Ruth E. Bulger & Stanley J. Reiser eds., 1990).
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 241 frequently p.revailed in futility cases, but they also have more legislative protection than ever before.](/docs-images/79/79224697/images/293-0.jpg "66 Some surrogates have successfully litigated cases against providers.")
293 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 241 frequently p.revailed in futility cases, but they also have more legislative protection than ever before. 66 Some surrogates have successfully litigated cases against providers. But those cases are legally and factually unique, so they simply cannot support a sweeping statement that the surrogates are favored judicially in all futility cases. Ex ANTE ACTIONS: GOING TO COURT BEFORE LSMT IS WITHDRAWN There are seven basic ways to resolve a futility dispute: (1) the patient dies; (2) the surrogate accedes to the provider's recommendation; (3) the surrogate replaces the provider with another provider willing to provide the requested treatment; (4) the provider accedes to the surrogate's request; (5) the provider replaces the surrogate; (6) the provider overrides the surrogate; or (7) the surrogate overrides the provider. It appears that a dispute typically goes to court only when parties take one of the last three approaches. Court actions are brought forth by way of four basic procedural vehicles, which can be categorized as either ex ante or ex post cases. If the provider withdraws treatment without consent or judicial permission, the surrogate may sue for damages. These ex post cases are discussed in Section III. The other three procedural vehicles, which are categorized as ex ante cases, are discussed here in this section. The ex ante cases involve going to court before treatment is withdrawn. First, if the provider plans to replace the surrogate, he or she will do that before withdrawing LSMT. The goal of surrogate replacement is to secure the consent of a newlyauthorized decision-maker. Second, where a provider plans to override the surrogate and withdraw LSMT without consent, a provider can first seek declaratory relief or permission to stop 66. See Pope, Futility Statutes, supra note 17 (surveying state statutes that grant providers civil, criminal, and disciplinary immunity for refusing to comply with inappropriate treatment requests).
294 242 MARQUETTE ELDER'S ADVISOR [Vol. 9 treatment. Third, a surrogate can seek an injunction to continue the treatment. PROVIDER ACTIONS TO REPLACE THE SURROGATE OFTEN SUCCEED Sometimes providers ask courts to adjudicate the fitness of the current surrogate decision-maker rather than the underlying appropriateness of the LSMT. 67 Some have even suggested that this should be the preferred method of resolving futility disputes,68 given the body of jurisprudence concerning how to select surrogates for patients without capacity. 69 In early cases, courts were generally unwilling to negate a surrogate's right to make health care decisions on behalf.of a patient. 70 However, in more recent cases, providers have successfully replaced surrogates who demanded LSMT that providers deemed inappropriate. 67. Sometimes no surrogate is reasonably available. Such a case is not really a futility dispute because not only does no one challenge the provider, but also the provider is the authorized decision-maker in many jurisdictions. See, e.g., TENN. CODE. ANN (c)(5) (2006). Cf Sumeeta Varma & David Wendler, Medical Decision Making for Patients without Surrogates, 167 ARCHIVES INTERNAL MED. 1711, 1712 (2007); Douglas B. White et al., Life Support for Patients without a Surrogate Decision Maker: Who Decides?, 147 ANNALS INTERNAL MED. 34 (2007). 68. See Jeffrey P. Burns & Robert D. Truog, Futility: A Concept in Evolution, 132 CHEST 1987, (2007); Robert D. Truog, Tackling Futility in Texas, 357 NEW ENG. J. MED. 1558, 1559 (2007) (endorsing "existing pathways to challenge the legitimacy of the surrogate to make these decisions and to seek appointment of another decision maker"). See also Rasa Gustatis, Right to Refuse Life-Sustaining Treatment, 81 PEDIATRICS 317, 319 (1988) (suggesting the use of child abuse laws to override parental requests for inappropriate treatment). But cf Robert Schwartz, Autonomy, Futility, and the Limits ofmedicine, 1 CAMBRIDGE Q. HEALTHCARE ETHICS 159, 161 (1992) (arguing that the question whether Mr. Wanglie was his wife's best substitute decision-maker was the "wrong question," and "[t]he real question [should have been]... whether the continuation of ventilator support and gastrostomy feeding were among the reasonable medical alternatives that should have been available to Mrs. Wanglie or her surrogate decision-maker, whoever that might be."). 69. See generally THE RIGHT TO DIE, supra note 2, at (outlining the jurisprudence of selecting surrogate decision makers); CLAIRE C. OBADE, PATIENT CARE DECISION MAKING: A LEGAL GUIDE FOR PROVIDERS ch.11 (1991 & Supp. 2007) (explaining various methods for surrogate decision-making). 70. See Lee, supra note 10, at 487.
295 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 243 In re Wanglie is one of the earliest and most widelydiscussed ~ases.71 Helga Wanglie was an eighty-six year old woman who was in a persistent vegetative state and dependent on a ventilator as a result of cardiorespiratory arrest. 72 Her providers determined that she could never appreciate any benefit from continued LSMT, so they advised her husband Oliver to remove the ventilator. 73 However, Oliver would not consent to stopping LSMT. 74 The providers petitioned the local probate court to appoint a professional conservator to make health care decisions for Helga.75 The hospital-nominated conservator presumably would accede to the providers' recommendation to stop LSMT, unlike Oliver. Despite the provider's efforts, the probate court denied the petition and instead appointed Oliver as conservator. 76 The court noted that Oliver was Helga's husband of fifty-three years. 77 Moreover, his decision to continue LSMT did not constitute grounds to remove his decision-making authority. The court could not conclude that Oliver's decision to continue LSMT was inconsistent with Helga's preferences or best interests. 78 While Wanglie is certainly the most famous case from the early 1990s in which a court rejected a provider's attempt at "surrogate shopping," it is not the only case. 79 In Nguyen v. 71. In re Wanglie, No. PX (Minn. Probe Ct. Hennepin County June 28, 1991), reprinted in 7 ISSUES L. & MED. 369 (1991). 72. Id. at Id. at Id. 75. Id. at 371, Id. at 372, Id. at Id. 79. See, e.g., In re Baby K, 832 F. Supp. 1022, 1031 (E.D. Va. 1993) (ruling that the mother's decision to continue treatment was not lisa unreasonably harmful as to constitute child abuse or neglect"); Belcher v. Charleston Area Med. Center, 422 S.E.2d 827, 838 (W. Va. 1992) (while providers received consent to a DNR order from a 17-year-old's parents, the court held that consent was valid only if the boy lacked capacity to decide for himself); In re Doe, Civ. No. D (Ga. Super. Ct. Oct. 17, 1991) (mem.), aff'd, 418 S.E.2d 3, 7 (Ga. 1992) (holding that providers could not withdraw LSMT from a child with only the mother's consent where the child's

296 244 MARQUETTE ELDER'S ADVISOR [Vol. 9 Sacred Heart Medical Center, a Washington court rejected a provider's argument that a child's parents serving as surrogate decision-makers should be replaced because their decision to continue LSMT constituted child abuse. 80 Similarly, a District of Columbia court refused to replace a mother as surrogate decision-maker for her two-month-old baby simply because she requested continued LSMT. 81 Some commenters cite Wanglie and other cases from the early 1990s to conclude that the strategy of having an alternative decision maker appointed by the court is "rarely successful./ 82 But it appears that these early decisions have little relevance today. First, these decisions were narrow in focus, in that they foreclosed only one legal avenue for providers to override surrogate requests. While the answers to the legal questions asked in Wanglie and Nguyen disfavored providers, these are not the only questions relevant in medical futility cases. 83 Providers can also seek ex ante permission or ex post forgiveness for unilaterally refusing a surrogate's request. 84 Second, emboldened by empirical evidence attacking the accuracy of surrogate decisions,85 providers have been father was available). Professor Annas suggests Doe is not a futility case, but instead a dispute about who is the authoriz.ed decision-maker. George J. Annas, The Case ofbaby K, 331 NEW ENG. J. MED (1994). This is belied by the course of the litigation, which demonstrated that the hospital was hardly agnostic as to which parent had authority. It argued that "continued aggressive treatment... constituted medical abuse." In re Doe, 418 S.E.2d at Nguyen v. Sacred Heart Medical Center, 987 P.2d 636, 638 (Wash. Ct. App. 1999); John Altomare & Mark Bolde, Nguyen v. Sacred Heart Medical Center, 11 ISSUES L. & MED. 199, 200 (1995) (noting that while the hospital attempted to characterize continued treatment as "cruel and inhumane," the court held that the argument had no merit). 81. Benjamin Weiser, A Question ofletting Go: Child's Trauma Drives Doctors to Reexamine Ethical Role: The Case ofbaby Rena, WASH. POST, July 14, 1991, at AI. 82. Burns & Truog, supra note 68, at Cf. THE RIGHT TO DIE, supra note 2, 13.03[A], at Providers can also seek declaratory relief. See infra "Provider Actions For Declaratory Relief Often Succeed" notes and accompanying text. Or providers can proceed to withdraw LSMT and defend any subsequent damages case. See infra "Ex Post Actions: Going to Court After LSMT Is Withdrawn" notes and accompanying text. 85. Lauren G. Collins et al, The State ofadvance Care Planning: One Decade after SUPPORT, 23 AM. J. HOSPICE & PALLIATIVE MED. 378, (2006).
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 245 increasingly able to establish that surrogates refusing to follow recommendations to stop L5MT are not acting in patients' best interests.](/docs-images/79/79224697/images/297-0.jpg "86 /IA patient's preservable existence might be so tortuous, painful, or filled with suffering that it would be deemed inhumane for a surrogate to dictate continued medical intervention.")
297 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 245 increasingly able to establish that surrogates refusing to follow recommendations to stop L5MT are not acting in patients' best interests.86 /IA patient's preservable existence might be so tortuous, painful, or filled with suffering that it would be deemed inhumane for a surrogate to dictate continued medical intervention."87 Even permanent unconsciousness is increasingly broadly recognized as a status in which a patient can derive zero benefit from continued L5MT.88 By the mid-1990s, judicial hostility to surrogate shopping began to wane.89 Courts began replacing surrogates in situations where the only ground for disqualification was the fact that the surrogate demanded L5MT for the patient contrary to provider recomm.endations. Courts are prepared to override 86. Courts seemed always prepared to allow surrogate shopping when a parent is decision-maker and a parent's own physical abuse caused a child's dependence on LSMT. For instance, one Pennsylvania case involved a mother who abused her two-year-old baby. Providers recommended stopping LSMT, but the baby's father refused because he was concerned about his wife's criminal liability. The hospital prepared to ask a court to appoint a guardian because the father was looking out for his wife's interests, not the interests of the child. Steve Twedt, Should Comatose Baby Live? Hospital, Dad Differ, PITT. POST-GAZETTE, June 3, 1990, at AI. The father then acceded to the hospital's recommendation to withdraw LSMT. Father Ends Life Support, PITT. POST-GAZETTE, June 24, 1990, at A3; Mary Pat Flaherty, Right to Die Decision Has Little Impact Here, PITT. POST-GAZETTE, June 27, 1990, at AI. Cf J.N. v. Sup. Ct., 67 Cal. App. 3d 384, 391 (Cal. Ct. App. 2007) (holding that guardian of minor has the burden of bringing expert testimony to prove that the LSMT is in the minor's best interest); D.K. v. Commonwealth, 221 S.W.3d 382, 384 (Ky. Ct. App. 2007) (permitting a guardian to remove LSMT once parental rights were permanently terminated); In re Matthew W., 903 A.2d 333, 335 (Me. 2006) (holding that a pre-termination protection order allowing DNR for minor without parental consent violated the parents' right to due process); In re Smith, 133 P.3d 924, (Or. Ct. App. 2006) (holding that a mother was not in a position to make decisions for her minor child where she chose not to be involved in the child's health care decisions on a regular basis); In re Stein, 821 N.E.2d 1008 (Ohio 2004) (finding that a limited guardian did not have the authority to withdraw LSMT when parental rights had not yet been permanately terminated); In re Tabatha R., 564 N.W.2d 598, 605 (Neb. 1997) (discussing due process rights of parents during termination of parental rights determination). 87. Cantor, supra note 55, at Id. at Cf Causey v. St. Francis Med. Ctr., 719 So. 2d 1072, 1076 (La. Ct. App. 1998) (noting that if a surrogate insists on inappropriate treatment, "the usual procedure... is to transfer the patient or go to court to replace the surrogate or override his decision." One argument is that the surrogate is not fulfilling his or her statutorilyprovided role. Another argument is "that the guardian or surrogate is guilty of abuse by insisting on care which is inhumane.").

298 246 MARQUETTE ELDER'S ADVISOR [Vol. 9 even well-intentioned surrogates whose demands for continued LSMT cause a patient unwarranted extr.eme suffering. 90 For example, in the case In re Mason, the Massachusetts General Hospital successfully moved the local probate court to "override" a health care agent's refusal to consent to a do not resuscitate ("DNR") order.91 In granting the hospital's petition, the court explained that since the agent was I'in denial" about his mother's deterioration and distrustful of her providers, he had not given "full consideration of acceptable medical alternatives."92 Silllilarly, in a case referred to as Baby Terry, the court replaced the parents of two-month-old Terry Achtabowski Jr. with a guardian.93 Baby Terry was born premature at twentythree weeks gestation, was dependent on a ventilator, and had a host of serious medical problems that m.ade his prognosis very bleak. 94 Since continued treatm.ent was painful and offered virtually no prospect for recovery, the Genesee County Department of Social Services alleged that Baby Terry's parents were neglectful in requesting continued treatment.95 The Michigan Probate Court did not find the parents neglectful, but it did determine that they were "incompetent" to decide what was best for their son. The court reasoned that the parents lacked the requisite capacity to m.ake medical decisions for their son because their demands for continued LSMT evidenced that they were emotionally unable to appreciate the circumstances.96 Most recently, in In re Howe, the Massachusetts Probate 90. Cf. In re Guardianship of Myers, 610 N.E.2d 663, 671 (Ohio Misc. 1993) (appointing guardian other than parents of permanently comatose minor where one parent refused to consent to stopping LSMT). 91. In re Mason, 669 N.E.2d 1081, 1085 (Mass. App. Ct. 1996). 92. Id. 93. James Bopp, Jr. & Richard E. Coleson, Child Abuse by Whom? Parental Rights and Judicial Competency Determinations: The Baby K and Baby Terry Cases, 20 OHIO N.D.L. REV. 821, (1994)-(citing In re Achtabowski, No. G GD (Mich. Prob~e Ct. July 3D, 1993)); Baby Dies, Was Focus of Battle, ORLANDO SENTINEL, Aug. 13, 19~, at AID. 94. Bopp & Coleson, supra note 93, at Id. at Id. at 826, 832.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 247 Court initially seemed to return to the earlier hostile approach to surrogate shopping.](/docs-images/79/79224697/images/299-0.jpg "The court ruled that where a surrogate decision-maker insisted on continued LSMT for her m.")
299 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 247 Court initially seemed to return to the earlier hostile approach to surrogate shopping. The court ruled that where a surrogate decision-maker insisted on continued LSMT for her m.other, "the evidence is insufficient to warrant court usurpation of [a daughter's] role as her mother's health care agent.// 97 But as the patient's condition deteriorated, the daughter's decision to continue LSMT increasingly.diverged from the hospital's assessment of the patient's preferences and best interests. Several months later, the court suggested that the agent's own personal issues were "impacting her decisions// and urged the daughter to "refocus her assessment.//9~ A year later, the hospital again planned to remove LSMT, and the court denied the daughter's request for a temporary restraining order (TRO).99 The daughter soon agreed to withdraw LSMT "because she believed the court was prepared to rule against her.// IoD Surrogates are generally obligated to make health care decisions in accordance with the patient's preferences and best interests. IOI Particularly for a conscious or semi-conscious patient, continuing LSMT contrary to provider recommendations often contravenes patient preferences and best interests. 102 Consequently, surrogates who make such requests are often acting outside the scope of their authority and should be replaced with other decision makers. 97. In re Howe, No , 2004 WL , at *21 (Mass. Probe & Fam. Ct. Mar. 22, 2004). 98. Id. at * See Liz Kowalczyk, Plan to Take Woman off Life Support is Halted, BOSTON GLOBE, Feb. 23, 2005, at B Daughter Explains Agreement to End Care, BOSTON GLOBE, Mar. 23, 2005, at B See generally THE RIGHT TO DIE, supra note 2, at (discussing incompetent patients and surrogacy) Cf Nina A. Kohn & Jeremy A. Blumenthal, Designating Health Care Decision Makers for Patients Without Advance Directives: A Psychological Critique (forthcoming 2008); David I. Shalowitz et al., The Accuracy of Surrogate Decision Makers, 166 ARCHIVES INTERNAL MED. 493 (2006) (finding that surrogates incorrectly predicted patient preferences in one-third of cases).
300 248 MARQUETTE ELDER'S ADVISOR [Vol. 9 PROVIDER ACTIONS FOR DECLARATORYRELIEF OFTEN SUCCEED While the foregoing cases address the question-of who is the appropriate decision-m.aker for the patient, other cases m.ore directly address the appropriateness of the treatrn.ent itself. In these cases, providers ask the court to declare that the providers would not violate the law by refusing the requested LSMT. It appears that the generally accepted view is that it is easier for providers to ask for forgiveness than to ask for perrn.ission. Schneiderrn.an and -Capron warn' that "[p]hysicians should not expect the courts to give them. priorperrnission to forgo futile treatment."i03 Since judges do not want to rn.ake decisions that may lead to a patient's death, it is thought that courts typically deny provider requests for declaratory relief. lo4 In perhaps the most farn.ous futility case, In re Baby K, the court denied declaratory relief. los Baby K was born with anencephaly, a birth defect in which part of the skull and the higher brain are m.issing. lo6 While Baby K was later rn.oved to a nursing home, she was periodically transferred to Fairfax hospital due to breathing difficulties. lo7 "Because aggressive treatment would serve no therapeutic or palliative purpose [Baby K's providers] recommended that [she] only be provided 103. Lawrence J. Schneiderman & Alexander M. Capron, How Can Hospital Futility Policies Contribute to Establishing Standards oj Practice?, 9 CAMBRIDGE Q. HEALTHCARE ETHICS 524, 530 (2000) See, e.g., Goldner et al., supra note 59, at 407 ("[W]hen the issue has been presented in the context of a dispute... concerning prospective treatment... courts have almost consistently sided against the health care professionals..."); Diane E. Hoffman & Jack Schwartz, Who Decides Whether a Patient Lives or Dies?, TRIAL, Oct. 2006, at 30, 37; John M. Luce & Ann Alpers, End-oj-Life Care: What Do the American Courts Say, 29 CRITICAL CARE MED. N40, N41-41 (2001); William Meadow et al., Current Opinion in Pediatrics and Law 2001, 14 CURRENT OPINION IN PEDIATRICS 170, 171 (2002); John J. Paris et al., Howe v. MGH and Hudson v. Texas Children's Hospital: Two Approaches to Resolving Family-Physician Disputes in End-oj-Life Care, 26 J. PERINATOLOGY 726, 726 (2006); William Prip & Anna Moretti, Medical Futility: A Legal Perspective, in MEDICAL FUTILITY AND THE EVALUATION OF LIFE-SUSTAINING INTERVENTIONS 136, 152 (Marjorie B. Zucker & Howard D. Zucker eds., 1997) In re Baby K, 832 F. Supp (E.D. Va. 1993), aff'd, 16 F.3d 590 (4th eire 1994) In re Baby K, 16 F.3d at Id. at 593.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 249 with supportive care."10b Baby K's mother would not consent, insisting that Baby K be provided with a ventilator.](/docs-images/79/79224697/images/301-0.jpg "lo9 Baby K's providers asked the local federal district court if they were obligated to provide the requested LSMT.")
301 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 249 with supportive care."10b Baby K's mother would not consent, insisting that Baby K be provided with a ventilator. lo9 Baby K's providers asked the local federal district court if they were obligated to provide the requested LSMT.l10 However, the providers framed their claim under the Emergency Medical Treatment and Active Labor Act (EMTALA).111 While the court ruled that the providers were so obligated, that holding is limited to the peculiar facts of the case and the coincidental application of the federal statute. 112 Only because Baby K newly arrived at the hospital in an "emergency m.edical condition," was the hospital obligated to stabilize her condition.113 EMTALA's scope is limited and it "cannot be invoked to require treatment in the vast majority of futility cases." 114 Under current EMTALA law, Fairfax Hospital arguably would not have had any obligation to treat Baby K because both 108. Id. at Id. at Id. at V.S.C.A. 1395dd (Westlaw currentthrough Feb. 2,2008) The Fourth Circuit affirmed on only the EMTALA claim, but the district court also based its ruling both on Section 504 of the Rehabilitation Act of 1973, 29 U.S.C. 794(a), and on the Americans with Disabilities Act (ADA), 42 U.S.C (a). See In re Baby K, 832 F. Supp. at However, typically such claims cannot succeed in the futility context because the patient's need for LSMT is directly related to his or her disability. See generally Schiavo v. Schiavo, 403 F.3d 1289, 1294 (11th Cir. 2005) (noting that "[t]he Rehabilitation Act, like the ADA, was never intended to apply to decisions involving the termination of life support or medical treatment./i); Grzan v. Charter Hosp., 104 F.3d 116, (7th Cir. 1997) (reviewing cases and legislative history); Rideout v. Hershey Med. Ctr., 30 Pa. D. & C.4th at 1 95 (1995) (quoting Anderson v. Vniv. of Wis., 841 F.2d 737, 740 (7th Cir. 1988) that "the Rehabilitation Act forbids discrimination based upon stereotypes about a handicap, but it does not forbid decisions based on the actual attributes of the handicap./i); Johnson v. Thompson, 971 F.2d 1487, (10th Cir. 1992) (discussing discrimination based on the degree of a handicap and Section 504). On the other hand, while there is no positive constitutional right to medical care, later courts have agreed with the district court that decided the Baby K case and have held that unilateral refusals may conflict with the free exercise clause and constitutional parental rights. See Rideout, 30 Pa. D. & C.4th at 1 84; In re Baby K, 832 F. Supp. at In re Baby K, 16 F.3d at THE RIGHT TO DIE, supra note 2, at 13.06[C] (explaining that EMTALA does not apply to in-patients).

302 250 MARQUETTE ELDER'S ADVISOR [Vol. 9 she and her mother were inpatients. lis The In re Baby K court itself later clarified that EMTALA applies "only in the immediate aftermath of admitting [a patient] for emergency treatment," and that there can be no EMTALA violation for entry of an "anti-resuscitation order" after a good faith admission. 116 That interpretation has been confirmed in regulations and appellate opinions. 117 In most subsequent unilateral withdrawal cases courts have explicitly noted that since the patient was already admitted, EMTALA did not apply. lib In short, the Baby K holding is far lllore limited than generally understood. Furthermore, providers have frequently succeeded in obtaining declaratory relief to stop LSMT. Most of the reported cases involve providers securing judicial permission to stop LSMT for patients declared brain dead. 119 The notoriety of the Baby K decision effectively chilled providers from. seeking ex ante judicial permission to stop LSMT.120 But at least one court 115. See Thaddeus M. Pope, EMTALA: Its Application to Newborn Infants, 4 ABA HEALTH ESOUR~E No.7 (Mar. 2008) Bryan v. Rectors & Visitors of the Univ. of Va., 95 F.3d 349, (4th Cir. 1996) See Preston v. Meriter Hosp. Inc., 700 N.W.2d 158, (Wis. 2005) (Roggensack, J., dissenting); 42 C.F.R (a)(1)(ii) (2003) ("1 the hospital admits the individual as an inpatient... the hospital's obligation under [EMTALA] ends..."); 42 C.F.R (d)(2) (2007) (providing that "[i]f a hospital... admits that individual as an inpatient... the hospital has satisfied its special responsibilities under [EMTALA].") See, e.g., In re AMB, 640 N.W.2d 262, 289 (Mich. Ct. App. 2001) (holding that there was no EMTALA violation "when the staff made the decision to discontinue the medical interventions" after the baby had been admitted for more than one week); Causey, 719 So. 2d at 1075 (noting that "EMTALA provisions are not applicable to the present case [where the patient had already been admitted]."); Rideout, 30 Pa. D. & C. 4th at See also Gonzales, No (Travis Cty. Probate Ct, Tex. filed Mar. 20, 2007) (Guardian Ad Litem's Trial Brief on Legal Issues) See, e.g., In re Long Island Jewish Med. Ctr., 641 N.Y.S.2d 989 (Sup. Ct. 1996) (granting hospital authorization to withdraw LSMT from brain dead infant); In re Haymer, 450 N.E.2d 940, (Ill. App. Ct. 1983); Frank Bruni, Medical Certainty, Legal Limbo, N.Y. TIM:ES, Feb. 28, 1996, at B1 (reporting that a trial court granted relief to a hospital). Cf Dority v. Sup. Ct., 193 Cal. Rptr. 288 (1983) (noting that "[t]he medical profession need not go into court every time it declares brain death.... ") 120. Kathy L. Cerminara, Critical Essay: Musings on the Need to Convince. Some People with Disabilities that End-oj-Life.Decision-Making Advocates Are Not Out to Get Them, 37 Loy. U. CHI. L.J. 343, (2006).
303 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 251 has granted declaratory relief permitting providers to unilaterally withdraw LSMT from a living patient.121 SURROGATE ACTIONS FOR INJUNCTIVE RELIEF SUCCEED ONLY TEMPORARILY Just as providers may ask the court for a green light, surrogates may ask the court for a red light. In these cases surrogates ask the court to issue an injunction prohibiting the providers from stopping LSMT. For the same reason that providers are thought to be unlikely to obtain declaratory relief, surrogates are thought likely to be successful in obtaining injunctive relief. Two distinguished commentators recently observed that the "Courts may be more willing to order the provision of care consistent with.a patient's wishes when he or she is still alive..."122 Indeed, courts appear to regularly issue surrogate-sought injunctions, but the injunctions are only tem.porary in nature. Given the imminent irreparable injury viz. the patient's death, it is not surprising that courts grant immediate relief as an emergency procedure. 123 As the estimable Judge J. Skelly Wright explained, "the compelling reason for granting the writ was that a life hung in the balance. There was no time for research or reflection."124 A temporary injunction preserves the status quo, 121. See, e.g., Child & Family Servo of Cent. Manitoba v. R.L. and S.L.H., 154 D.L.R.4th 409, (1997) (noting that I/[t]here is no need for a consent from anyone for a doctor to refrain from... heroic measures to maintain the life of a patient in an irreversible vegetative state.") Hoffman & Schwartz, supra note 104, at 37. See Goldner et al., supra note 59, at 407 (I/[W]hen the issue has been presented in the context of a dispute... concerning prospective treatment... courts have almost consistently sided against the health care professionals..."); Schneiderman & Capron, supra note 103, at 530 (I/Physicians should not expect the courts to give them prior permission to forgo futile treatment....") Cf. Wright & Miller, 11A FED. PRACTICE & PROC (2d ed. 2007) In re President and Directors of Georgetown College, Inc., 331 F.2d 1000, 1009 (D.C. Cir. 1964). See also Cruzan v. Director, Missouri Dep't Health, 491 U.S (1990) ("An erroneous decision not to terminate results in a maintenance of the status quo.... An erroneous decision to withdraw life-sustaining treatment,

304 252 MARQUETTE ELDER'S ADVISOR [Vol. 9 pending a hearing. 125 For example, in cases where the patient is brain. dead, courts m.ay grant injunctions to either give the surrogate"accomm.odation" tim.e or permit a confirm.ation of the diagnosis. 126 The injunctions obtained by surrogates are only interim. m.easures. Courts seem. do not generally order indefinite -LSMT. For exalllpie, many surrogates have sought injunctions prohibiting providers from. rem.oving LSMT from. corpses. 127 While court~ m.ay grant temporary relief, they ultim.ately deny such Illotions. For exam.ple, in Fennell v. Emory Eastside Medical Center, the judge granted an injunction ordering the hospital to continue LSMT for Donald Fennell, a m.an who.had been declared brain dead. 128 Less th~n forty-eight hours later, the however, is not susceptible of correction.") See, e.g., Rotaru v. VancouverGen. Hosp. Intensive Care unit, 2008 BCSC (denying injunction ordering continued LSMT, but not dismissing the petition and allowing petitioner to gather more evidence); Golubchuk v. Salvation Army Grace Gen. Hosp., 2008 MBQB (granting interim injunction pending a trial of disputed issues of fact and law); Jin v. Calgary Health Region, 2007 ABQB ("I am mindful that the injunction is for a brief period and on balance I prefer to rescind the DNR order and preserve the status quo until there is either consensus or a legal determination on full evidence.") See, e.g., THE RIGHT TO DIE, supra note 2, 13.08[A], at 13-40; Dority v. Sup. Ct., 193 Cal. Rptr. at 288 (describing a hospital's policy of keeping brain dead children on life support "until the parents were emotionally able to realize what the medical opinion was" and suggesting that hospitals encourage parent consultation and participation) See, e.g., Cole v. Dniv. of Kansas Med. Center, No. 06-CV-830 (Wyandotte County Dist. Ct. Kan. 2006) (granting a TRO but dissolving it after the -diagnosis was independently confirmed); Alvarado v. N.Y. City Health & Hosp.. Corp., 547 N.Y.S.2d 190 (Sup. Ct. 1989)~ vacated and dismissed, 550 N".Y.S.2d 353 (App. Div. 1990) (where patient was later determined not brain dead); Dority v. Sup. Ct., 193 Cal. Rptr.. at 288 (denying par~nts' petition for writ of p~ohibition against removing LSMT from brain dead child). Cf. Megan Tench, End-oj-Life Lawsu"it Outliving Its Subject, BOSTON GLOBE, Dec. 6, 2006, at B3 (reporting denial of relief for Cho Fook Cheng). But cf. Shively v. Wesley Med. Center, No. 06-CV-640 (Sedgwick County Dist. Ct. Kan. Feb. 10, 2006) (granting TRO forbidding providers from performing the tests necessary to diagnose brain death); Brain Dead Girl Will Be Sent Home on Life Support, N.Y. TIMES, Feb. 19, 1994, at 9 (hospital agreed to cover expenses of home LSMT for Theresa Hamilton, who had been declared brain dead); Lois M. Collins & Linda Thomson, Jesse Loses His Battle with Brain Tumor, DESERET MORNING NEWS,. Nov. 20, 2004, at B.Ol (reporting that the Utah -Third District Court granted a TRO, which prevented a hospital from removing LSMT from brain dead Jesse Koochin) Andria Simmons, Death Not Just a Family Matter, ATLANTA }.-CONST., Dec. 14, 2007, at AI.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 253 judge authorized the hospital to stop LSMT.129 It is well-settled that once a patient is determined brain dead, further treatment is not required.](/docs-images/79/79224697/images/305-0.jpg "130 Sim.ilarly, no court has ever granted a perm.anent injunction ordering continued LSMT for living patients. In Nguyen v. Sacred Heart Me.dical Center for example, the hospital refused.")
305 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 253 judge authorized the hospital to stop LSMT.129 It is well-settled that once a patient is determined brain dead, further treatment is not required. 130 Sim.ilarly, no court has ever granted a perm.anent injunction ordering continued LSMT for living patients. In Nguyen v. Sacred Heart Me.dical Center for example, the hospital refused. to place Baby ;Ryan on dialysis, despite his parents' request. 131 The court issued a TRO ordering the hospital to resume dialysis. 132 However, the fam.ily was soon able to transfer Baby Ryan to another facility, Inooting the,dispute. 133 The court never.ruled on the parents' petition for perm.anent injunction. 134 And in Baby L,.the probate judge appeared willing to approve the mother's p~tition for injunctive relief, but the issue was rendered m.oot when the m.other of the patient was able to transfer his care to another provider.135 Finally, a num.ber of surrogates in Texas have successfully enjoined the unilateral termination of LSMT.136 Such cases were widely reported in the press. 137 But again, these injunctions 129. Id See, e~g., Cavagnaro v. Hanover Ins. Co., 565 A.2d 728, 729 (N.J. Super. Ct. App. Div. 1989) (holding that treatment for a brain dead patient was not medically necessary, so insurer had no obligation to pay for it). Since provider obligations with respect to brain dead patients are comparatively more settled, they may not provide material guidance for other types of futility cases Altomare & Bolde, supra note 80, at Id. (citing Nguyen, No (TRO» Id. at Id. (holding that the TRO was dissolved and the petition for permanent injunction dismissed) See Paris et al., supra note 38, at See, e.g., Gonzales, No (Travis Cty. Probate Ct, Tex. filed Mar. 20, 2007); Hudson v. Texas Children's Hosp., 177 S.W.3d,232 (Tex. App. 2005); In re Nikolouzos, 179 S.W.3d 581 (Tex. App. 2005) (granting an injunctionuntil an appeal could be assigned); Ramshaw, supra note 42 (TRO granted for Ruthie Webster). In other cases, hospitals agreed to an extension just before a pending hearing. See, e.g., Todd Ackerman, Transfer Resolves Latest Futile Care Case, Hous. CHRON., July 31, See, e.g., Kristina Hermdobbler, Court Keeps Woman on Life Support, BEAUMONT ENTERPRISE, Aug. 11, 2006, at A.1 (reporting a TRO in the case of Daisy Conner); Bill Murphy, Comatose Surgeon Would Prefer Death, Hous. CHRON., Mar. 21, 2001, at 26 (reporting a TRO in the case of Joseph Ndiyob); Ramshaw, supra note 42 (reporting a TRO in the case of Ruthie Webster).

306 254 MARQUETTE ELDER'S ADVISOR [Vol. 9 were temporary in nature and granted pursuant to the unique Texas Advance Directives Act for a limited time and purpose. The Act allows a provider to unilaterally refuse LSMT after giving a surrogate ten days to find an alternate provider that will provide the requested LSMT.138 Texas courts have the power to extend the ten-day period if a surrogate shows that "there is a reasonable expectation that a physician or health care facility that will honor the patient's directive will be found if the time extension is granted." 139 Courts have no other authority or jurisdiction.140 While surrogates often- obtain injunctions prohibiting the removal of LSMT, these injunctions typically operate like TROs. They are short-terill stop-gap orders, pending a hearing several days later. 141 Courts norillally dissolve the temporary injunction and permit providers to stop LSMT. Providers are similarly successful when they initiate an ex ante action. Specifically, providers are increasingly successful in actions to replace a surrogate who demands non-recommended LSMT. Also, while seeking declaratory judgment remains an unpopular procedural vehicle, available precedent fails to indicate that such petitions would be unsuccessful TEX. HEALTH & SAFETY CODE ANN (e) (Vernon 2006). See, e.g., Lance Lightfoot, Incompetent Decisionmakers and Withdrawal of Life-Sustaining Treatment: A Case Study, 33 J. L. MED. & ETHICS 851, 854 (2005) (citing Final Order Denying Plaintiff's Request for an Extension of Time Under the Health & Safety Code Section (f), Hudson v. Texas Children's Hosp., No. 352,526 (Probate Ct., Harris County, Tex. Mar. 14, 2005». Nikolouzos v. St. Luke's Hosp., 162 S.W.3d 678, (Tex. App. 2005) (affirming the denial of TRO because petitioner did not show a probable transfer) TEX. HEALTH & SAFETY CODE ANN (g) (Vernon 2006) See Lightfoot, supra note 138, at 852. See also Nikolouzos, 162 S.W.3d at 683 (finding medical evidence "irrelevant" since the IJ'hospital's ethics committee has determined the care is inappropriate."); H. Comm. Pub. Health, Tex. H.R., Interim Report 2006, at 35 ("The court considers whether another provider who will honor the patient's directive is likely to be found; it does not address the issue of whether the decision to withdraw life support is valid.") Sometimes, the patient dies during the temporary injunction period, such that the injunction has a practically dispositive impact.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 255 Ex POST ACTIONS: GOING TO COURT AFTER LSMT Is WITHDRAWN While providers are often successful in ex ante actions, they are almost uniformly successful](/docs-images/79/79224697/images/307-0.jpg "in ex post actions. Providers usually prevail when a surrogate brings a lawsuit after the unilateral termination of LSMT.")
307 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 255 Ex POST ACTIONS: GOING TO COURT AFTER LSMT Is WITHDRAWN While providers are often successful in ex ante actions, they are almost uniformly successful in ex post actions. Providers usually prevail when a surrogate brings a lawsuit after the unilateral termination of LSMT.142 Indeed, usually a surrogate succeeds only if he or she shows that the provider's nonconsensual refusal of LSMT was so egregious as to constitute the tort of outrage. A surrogate bringing a dam.ages action on another legal theory rarely succeeds because the surrogate: (1) cannot establish that the standard of care required continued LSMT, (2) cannot establish causation and dam.ages, or (3) cannot rebut the provider's statutory right to refuse LSMT. SURROGATE ACTIONS FOR DAMAGES TYPICALLY SUCCEED ONLY WHEN PROVIDER CONDUCT IS OUTRAGEOUS Hoffm.an and Schwartz note that I/[p]laintiffs who seek dam.ages for the withholding or withdrawal of requested lifesaving treatm.ent m.ay fare better, especially when the facts indicate egregious conduct by hospital personnel." 143 In fact, a com.prehensive review of litigated futility cases appears to support an even stronger statetilent that surrogate actions for dam.ages typically succeed only when provider conduct is 142. See Ann Alpers, Respect for Patients Should Dominate Health Care Decisions, 170 W. J. MED. 291, 292 (1999) ("Physicians are likely to get better legal results when they refuse to provide non-beneficial treatment and then defend their decisions as consistent with professional standards than when they seek advance permission to withhold care."); Goldner, supra note 59, at 407 (finding that in cases "in which physicians have been sued... based upon their termination of life-sustaining treatment, the courts almost uniformly have displayed great deference to medical judgments"); Johnson et a1., supra note 59, at 23 (observing that in "malpractice and related litigation... the outcomes seem to be more deferential to professional standards of practice"); Lee, supra note 10, at 485 ("[W]hen legal action is brought by the surrogates following the death of the patient, some legal precedents seem to validate the physician's right to unilaterally withdraw life-sustaining treatments."); Luce & Alpers, supra note 104, at N Hoffman & Schwartz, supra note 104, at 37.
308 256 MARQUETTE ELDER'S ADVISOR [Vol. 9 outrageous. Furthermore, surrogates cannot establish outrageous conduct by pointing to the unilateral withdrawal of LSMT itself, but only by demonstrating that the manner in which it was withdrawn was outrageous. OUTRAGEOUS PROVIDER CONDUCT In Rideout v. Hershey Medical Center, the parents of threeyear-old Brianna Rideout favored aggressive treatment for her brain cancer. 144 As Brianna's condition deteriorated, her parents remained adamant, and providers planned to remove her ventilator without her parents' consent. 14S However, the providers did far more than withdraw LSMT. They assured Brianna's parents that they would remove her ventilator only when the parents were at Brianna's bedside. 146 Nevertheless, the providers removed the ventilator outside the parents' presence, as the parents were in the hospital patient advocate's office trying to obtain legal assistance. 147 Brianna's parents learned of the surprise disconnection when the hospital chaplain, who was in Brianna's room, announced it over the hospital's intercom system.148 The Pennsylvania Common Pleas Court held in favor of the parents' claims for negligent and intentional infliction of emotional distress,149 as the providers withdrew the ventilator in a secretive, insensitive, and disrespectful manner. Moreover, the providers specifically anticipated that the parents would have a strong emotional reaction because the providers had requested that city police officers be present.iso Similarly, in Manning v. Twin Falls Clinic & Hospital, the patient had chronic obstructive pulmonary disease (COPD) 144. Rideout, 30 Pa. D. & C. 4th at Id. at Id. at Id. at 63, Id. at Id. at Id. at 70.
309 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 257 resulting in decreased ability to transfer oxygen to his bloodstreatn. 1s1 The patient's condition was rapidly deteriorating, but contrary to his fatnily's objections, the providers moved him to another room without the aid of a portable oxygen unit. 152 This patient experienced respiratory distress and died. 1s3 The court affirtned a punitive damages verdict for infliction of etnotional distress. 154 Intentional infliction of emotional distress was also the cause of action in Estate ofbland v. Cigna Health Plan of Texas. ISS Bland, a tertninally ill AIDS patient, was dependent upon a ventilator. 156 Both Bland and his family insisted that he rem.ain on the ventilator. 1s7 However, the chair of the ethics committee ordered the ventilator removed, apparently at the direction of the Cigna medical director. This was done without consulting Bland, his family, or Bland's primary care physician. 1s8 The ventilator retnoval seemed both secretive and financially motivated. The intentional infliction of emotional distress is not a favored tort in the law. 159 It is particularly difficult to show that a provider's conduct was extreme and outrageous when the provider reasonably believed that her objective was not only legititnate but even professionally and ethically necessary and appropriate.160 Consequently, in the several futility cases in which recovery was allowed, it is no surprise that liability was pretnised not on the fact that providers unilaterally withdrew 151. Manning v. Twin Falls Clinic & Hosp., Inc., 830 P.2d 1185, 1187 (Idaho 1992) ld. at ld. at ld. at 1191, Bland v. Cigna Healthplan of Texas, Inc., No A (Harris County Tex. Dist. Ct., Apr. 25, 1995) (First Amended Petition III) ld. at I ld JOHN FLETCHER ET AL., INTRODUCTION TO CLINICAL ETHICS 272, 273 (2d ed. 2000); Mimi Swartz, Not What the Doctor Ordered, TEX. MONTHLY, Mar. 1995, at See J.D. LEE & BARRY LINDAHL, 3 MODERN TORT LAW: LIABILITY AND LITIGATION 32:3, 32-8 (Thomson/West 2006) See id. at

310 258 MARQUETTE ELDER'S ADVISOR [Vol. 9 LSMT, but rather, on how they did it. 161 THE UNILATERAL REFUSAL OF LSMT Is NOT PER SE OUTRAGEOUS In som.e cases, surrogates have alleged that the unilateral withdrawal of LSMT is itself outrageous conduct because it is done without consent and against patient or surrogate wishes. However, courts have consistently rejected this proposition. For exam.ple, in Gallups v. Cotter, Pamela Gallups, a minor, was rendered brain dead after a car accident. 162 Providers made at least eight confirm.ations of the brain death diagnosis. And they had six discussions with the family between June 28 and July 8, whereby they recom.m.ended rem.oving LSMT.163 While there was a dispute over whether consensus was reached, providers allegedly rem.oved Pam.ela from. life support against her parents' wishes. 164 Nevertheless, the court found no evidence of 1/recklessness."165 Courts have similarly denied claims for outrage or intentional infliction of einotional distress based solely on the fact that providers unilaterally withdrew LSMT froin a living Not only liability but even a lawsuit itself may be averted through considerate handling. See generally NANCY BERLINGER, AFTER HARM: MEDICAL ERROR AND THE ETIDCS OF FORGIVENESS (2005) (discussing "The 'I'm Sorry' Laws"); Pam Baggett, I'm Sorry: Apologizing for a Mistake Might Prevent a Lawsuit, TEX. MED., Jan. 2005, at 56; Jennifer K. Robbennolt, Apologies and Legal Settlement: An Empirical Examination, 102 MICH. L. REV. 460, 463 (2003) (arguing that apologies go a long way in reaching settlements); Charles Vincent et al., Why Do People Sue Doctors? A Study ofpatients and Relatives Taking Legal Action, 343 LANCET 1609, 1612 (1994) (explaining how patients' families often feel that there is a lack of information and apologies). For example, in Bryan v. UVA, the University of Virginia risk management department believed that the primary cause for the state and federal actions was a dispute over billing; when the hospital turned the account over to a collection agency, the family gave the demand letters to an attorney to review, who coincidentally noticed grounds for a lawsuit in a subsequent review of the medical records. FLETCHER ET AL., supra note 158, at Gallups v. Cotter, 534 So. 2d 585, 586 (Ala. 1988) Id. at Id. at Id. at 589 (holding that acting without consent is "insufficient... to show defendants acted intentionally or recklessly"). The court had already disposed of claims for wrongful death, breach of contract, and fraud. Id. at 587.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 259 patient.166 For example, in Gilgunn v.](/docs-images/79/79224697/images/311-0.jpg "Massachusetts General Hospital, the attending physician wrote a do not resuscitate order, despite the surrogate's demands for aggressive I treatment.")
311 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 259 patient.166 For example, in Gilgunn v. Massachusetts General Hospital, the attending physician wrote a do not resuscitate order, despite the surrogate's demands for aggressive I treatment.167 The claim for negligent infliction of emotional distress proceeded to a jury.168 The jury returned a verdict for the providers. 169 OTHER SURROGATE ACTIONS FOR DAMAGES TYPICALLY Do NOT SUCCEED170 Hoffman and Schwartz observe that plaintiffs "face uncertainty when health care providers defend their action oil futility grounds."171 In fact, once we account for the outrage cases, plaintiffs face not uncertainty, but instead, probable failure. "[C]ourts are hesitant to penalize physicians who reasonably rely on what they perceive to be professional standards concerning effectiveness of treatment measures." See, e.g., Morgan v. Olds, 417 N.W.2d 232 (Iowa. App. 1987); Nguyen v. Sacred Heart Medical Center, 987 P.2d 634, 636 (Wash. App. 1999) (refusing to allow plaintiffs to pursue claim for outrage). Cf Hartsell v. Fort Sanders Reg'l Med. Center, 905 S.W.2d 944 (Tenn. Ct. App. 1995) (trial court dismissed the claim for outrage); Litz v. Robinson, 955 P.2d 113, (Idaho Ct. App. 1997) (involving a unilateral DNR); Strickland v. Deaconess Hosp., 735 P.2d 74 (Wash. Ct. App. 1987) (involving unilateral removal of a respirator) John J. Paris et al., Use ofa DNR Order Over Family Objections: The Case of Gilgunnn v. MGH, 14 J. INTENSIVE MED. 41,41-42 (1999) ld. at ld. at Actions fail for a variety of fact-specific reasons. For example, in Kranson V. Valley Crest Nursing Home, 755 F.2d 46 (3d Cir. 1985), the court found in favor of a nursing home that failed to provide CPR to a resident because the plaintiffs could not establish municipal liability. In Strickland, 735 P.2d at 78, plaintiffs lacked standing to bring claims for negligence and informed consent. See also Judge' Dismisses Suit over Death, ST. LOUIS POST DISPATCH, June 28, 1996, at 38 (a court dismissed a wrongful death case because patient Philip Taylor's agent lacked standing to challenge unilateral DNR). Criminal actions have also been unsuccessful. See, e.g., Grotti V. Texas, 209 S.W.3d 747 (Tex. App. 2006) (reversing physician's homicide conviction for occluding a patient's endotracheal tube because there was insufficient evidence that the patient was alive at the time); State V. Naramore, 965 P.2d 211, 216, 223 (Kan. Ct. App. 1998) (reversing physician's murder conviction for stopping LSMT he considered futile). In this section of this article, I discuss only the more common causes of action Hoffman & Schwartz, supra note 104, at Goldner et al., supra note 59, at 409; Prip & Moretti, supra note 104, at 152;

312 260 MARQUETTE ELDER'S ADVISOR [Vol. 9 Specifically, surrogates have difficulty establishing the prima facie elements of their tort-based theories. First, they can find it difficult to establish that the standard of care required continued LSMT. Second, given the patient's extreme fragility and illness, they cannot establish causation and damages. Third, they cannot rebut provider's statutory presumptive right to refuse LSMT. SURROGATES CANNOT ESTABLISH THAT THE STANDARD OF CARE REQUIRES CONTINUED LSMT In medical malpractice actions, plaintiffs must establish a breach of the applicable standard of care by the provider. 173 Therefore, unless plaintiffs have a federal or constitutional cause of action, a threshold requirement is showing that the unilateral refusal does not comply with the standard of care. 174 Plaintiffs have never been able to show that the standard of care requires continued LSMT for brain dead patients. 175 Similarly, in most of the reported cases, plaintiffs have been unable to establish that the standard of care requires continued LSMT for living patients. 176 As a consequence, courts ordinarily see Schneiderman & Capron, supra note 103, at BARRY R. FURROW ET AL., HEALTH LAW (2d ed. 2000); STEVEN E. PEGALIS, AMERICAN LAW OF MEDICAL MALPRACTICE (3d ed. 2007) In DeKalb Med. Center v. Hawkins, the plaintiff successfully resisted providers' attempt to characterize his claim for "tortuous termination of life support" as a medical malpractice action Ga. App. LEXIS 1269 (Nov. 29, 2007). Since the court allowed plaintiff to proceed on an intentional tort/wrongful death theory, he presu~ablywill not need to establish standard of care. In contrast, the court in Ussery v. Children's Healthcare of Atlanta, Inc. rejected plaintiff's intentional tort allegations, allowing them to pursue only their negligence claims. 656 S.E.2d 882 (Ga. App. 2008) See, e.g., Gallups v. Cotter, 534 So. 2d 585 (Ala. 1988) See, e.g., Berkeley v. Dowds, 61 Cal.Rptr.3d 304, 311 (Cal. Ct. App. 2007) (affirming demurrer where plaintiff's counsel conceded that defendant's conduct "was within the standard of care"); Gamble v. Perra, No (Tenn. Ct. App. Feb. 22, 2007) (affirming the dismissal of tort claims because the wife showed that neither the prescription of pain medication nor the failure to attempt CPR was outside the standard of care); Litz, 955 P.2d at 113 (affirming summary judgment in favor of providers who placed unilateral DNR order); Nguyen, 987 P.2d at 636 (affirming dismissal of malpractice action in case involving unilateral removal from dialysis); Preston, 700 N.W.2d at 163 (affirming the dismissal of causes of action for malpractice and informed consent); John J. Paris et al., Resuscitation of a
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 261 grant summary judgment in favor of providers because plaintiffs fail to introduce evidence showing that the standard of care required continued LSMT.](/docs-images/79/79224697/images/313-0.jpg "For example, in Duensing v. Southwest Texas Methodist Hospital, providers stopped a patient's dialysis without the consent of the patient's surrogate.")
313 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 261 grant summary judgment in favor of providers because plaintiffs fail to introduce evidence showing that the standard of care required continued LSMT. For example, in Duensing v. Southwest Texas Methodist Hospital, providers stopped a patient's dialysis without the consent of the patient's surrogate. 177 The surrogate sued for tnedical malpractice, but presented no evidence showing that withdrawing dialysis was inconsistent with the standard of care. 17B The plaintiff 1/failed to establish expert testimony that terminating the dialysis of a terminally ill and mentally incapacitated patient even without the consent of the patient's fatnily was necessarily a breach of medical standards." 179 Moreover, the plaintiff's own experts conceded that the providers complied with the standard of care. 1BO Therefore, the court granted summary judgment in favor of the providers, and the u.s. Court of Appeals for the Fifth Circuit affirmed. 1B1 Similarly, in Kelly v. St. Peter's Hospice, a surrogate sued a New York hospice for medical malpractice involving his wife's treatment because, among other things, the hospice (1) did not provide sufficiently aggressive care, (2) used an excessive amount of morphine, and (3) failed to insert an IV line for nutrition and hydration. 1B2 The New York appellate court Micropreemie: The Case of MacDonald v. Milleville, 18 J. PERINATOLOGY 302 (1998) (holding physician had no obligation to seek authorization to cease resuscitation of 23-week gestation baby after ten minutes); Defendant-Respondent Brief in Baby K, 2003 WL , at *24-25 & *28 (plaintiff's expert did not establish the standard of care required resuscitation of anencephalic infant). Tellingly, attorney Mark Geragos never filed a promised lawsuit on behalf of Nataline Sarkisyan after Cigna determined that a liver transplant was not covered under Sarkisyan's medical plan. Alicia Chang, Cigna Faces Lawsuit in Death after Policy Fight, CHI. TRIB., Dec. 23, 2007, at Duensing v. Southwest Tex. Medical Hosp., No. SA-87-CA1119 (W.D. Tex. 1988), a!f'd sub nom. Duensing v. Ruff, No (5th Cir. Feb 3, 1990) Id Duensing v. Ruff, No at Id. at 4-5. Furthermore, the defendants' position was supported at least by a school of thought. See FURROW ET AL., supra note 173, at ; Jones v. Chidester, 610 A.2d 964, 966 (Pa. 1992) Duensing v. Southwest Tex. Medical Hasp., No. SA-87-CAll Kelly v. St. Peter's Hospice, 553 N.Y.S.2d 906, 907 (N.Y. App. Div. 1990) (noting that the husband was unaware that his wife had checked into hospice,

314 262 MARQUETTE ELDER'S ADVISOR [Vol. 9 affirm.ed sum.tnary judgm.ent in favor of the hospice because the plaintiff-surrogate failed to present evidence that the provider's treatm.ent departed from. acceptable tnedical practice. 183 In other cases, plaintiffs have introduced competent expert evidence regarding the standard of care, but juries have still largely held that the providers did not breach the standard. For exam.ple, in Gilgunn, the jury determined that the patient would have wanted LSMT, which her providers unilaterally withdrew.184 However, the jury concluded that none of the defendants were negligent because 1/the actions of the physicians and of the [hospital] were within the standard of care."18s Sitnilarly, in LaSalle Nat'l Trust v. Swedish Covenant Hospital, the court affirm.ed a verdict in favor of providers who adhered to a /Icompassionate care" policy and refused to provide aggressive treatrn.ent to an extretnely pretnature infant. 186 The jury concluded that unilaterally refusing LSMT did not breach the standard of care. 187 While the jury verdict lacks the force of law as a legal precedent, it is a powerful statetnent that the standard of care does not require all that the patient would have wanted. In other cases, plaintiffs have voluntarily distnissed their lawsuits upon realizing the weakness of their claitns. For exarn.ple, in Burks v. St. Joseph's Hospital, the plaintiffs voluntarily distnissed their. claillls for ntedical m.alpractice. l88 Soon after arriving at a Milwaukee em.ergency room., Shem.ika Burks gave birth to a severely prem.ature baby who weighed only seven ounces. l89 The hospital did not attem.pt to resuscitate the baby, which is typically for palliative treatment, not curative treatment) Id. at Paris et al., supra note 167, at Id LaSalle Nat'l Trust v. Swedish Covenant Hosp., 652 N.E.2d 1089, (Ill. App. C ) Id. at Burks v. S1. Joseph's Hasp., No. 95-CV , at 17:4-6 (Milwaukee County Cir. Ct., Wis. Apr. 29, 1996) (hearing on motion for summary judgment); Burks v. St. Joseph's Hasp., 596 N.W.2d 391, 393 (Wis. 1999) Burks, 596 N.W.2d at 392.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 263 and the baby died three hours later.](/docs-images/79/79224697/images/315-0.jpg "19o The plaintiffs dismissed the malpractice suit, apparently upon realizing that they could not establish whether it was within the standard of care to resuscitate a 22-week-old fetus.")
315 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 263 and the baby died three hours later. 19o The plaintiffs dismissed the malpractice suit, apparently upon realizing that they could not establish whether it was within the standard of care to resuscitate a 22-week-old fetus. 191 SURROGATES TYPICALLY CANNOT ESTABLISH CAUSATION AND DAMAGES Even when plaintiffs can establish a breach of the standard of care, they still can have difficulty establishing proof of causation or damages, particularly because the patients from whom LSMT is withdrawn are catastrophically ill. 192 In King v. Crowell Memorial Home, a son sued the nursing hom.e for treating his mother as DNR, even though his instructions were to use "any and all medical measures./ 193 While the case went to trial, the court granted the home a directed verdict because the son failed to present sufficient evidence that (1) his m.other was DNR at the time of her death, (2) his instructions were not followed, or (3) resuscitative measures would have been successful.194 In som.e jurisdictions the causation hurdle is lower, and plaintiffs need only show loss of a chance rather than "but-for causation.// 195 For example, in Wendland v. Sparks, a patient's physician unilaterally decided not to attempt CPR when the 190. Id Brief in Support of Defendant's Motion to Dismiss EMTALA Claim, at (Nov. 9, 1995); Reply Brief in Support of Defendant's Motion to Dismiss EMTALA Claim, at 4 (Apr. 22, 1996); from Mary Wolverton to Thad Pope (Aug. 6, 2007) (on file with author) See, e.g., Berkeley, 61 Cal Rptr. 3d at 308, 312 (finding no causal connection where the plaintiff alleged that the providers prematurely removed patient from ICU and denied him medically necessary services); Gray v. Woodville Health Center, 225 S.W.3d 613, 619 (Tex. App. 2006); Kranson, 755 F.2d at 46 (affirming the dismissal of a claim against municipal nursing home that failed to perform CPR on resident because of the lack of a causal nexus between th~ home's CPR policy and the resident's death) King v. Crowell Memorial Home, 622 N.W.2d 588,592 (Neb. 2001) Id. at See LEE & LINDAHL, supra note 159, at 25:88-91.

316 264 MARQUETTE ELDER'S ADVISOR [Vol. 9 patient suffered cardiorespiratory arrest. 196 While the patient had only a ten percent chance of leaving the hospital following CPR, the court held that "even a sm.all chance of survival is worth something,"197 and the court allowed the plaintiffs to pursue their malpractice action on a loss of chance theory.19b But the loss of chance theory alters not only the elem.ent of causation, but also the nature of the injury. Under this theory, the injury is not a patient's death, but the loss of chance itself. This may substantially lower available damages.199 Furthermore, plaintiffs are unlikely to bring low damages cases in the first place. 20D Even if the cases are brought, such cases are hard for surrogates to win. For example, in Velez v. Bethune, providers unilaterally withdrew LSMT from. a prem.ature infant, and a Georgia appellate court held that plaintiffs' claim for wrongful death was valid.201 "Dr. Velez had no right to decide, unilaterally, to discontinue medical treatment even if... the child was... in the process of dying."2d2 But, the court noted that the am.ount of dam.ages would be very low. 2D3 The case ultim.ately settled, and 196. Wendland v. Sparks, 574 N.W.2d 327, 328 (Iowa 1998) Id. at Id. at 333. The case later settled for an undisclosed amount. from Julie Davis to Thaddeus Pope (May 2, 2007) (on file with author) It must be noted that even low damages entails a report to the National Practitioner Data Bank, psychological distress, and other repercussions for the provider. BOVBJERG & RAYMOND, supra note 45, at 6; Subrin, supra note 51, at 206 (lithe entire litigation process is anxiety-provoking and privacy-invading."); Mitchell S. Cappell, A Baseless Malpractice Suit Still Cost Me, MED. ECON., Feb. 1, Low damages cases are unlikely to be brought. See LaRae Huycke & Mark M. Huycke, Characteristics ofpotential Plaintiffs in Malpractice Litigation, 120 ANNALS INTERNAL MED. 792, 785 (1994); Daniel Costello, Lacking Lawyers, Justice is Denied, L.A. TIMES, Dec. 29, 2007 (reporting the difficulty of obtaining a lawyer in cases with limited damages). But cf. Kathy L. Cerminara, Tracking the Storm: the Far Reaching Power ofthe Forces Propelling the Schiavo Cases, 35 STETSON L. REV. 147, (2005) (reviewing the involvement of special-interest groups); Jon B. Eisenberg, The Terri Schiavo Case: Following the Money, RECORDER, Mar. 4, 2005, at 4 (reporting how much of the Schiavo litigation was funded by conservative organizations like the Philanthropy Roundtable and Life Legal Defense Foundation) Velez v. Bethune, 466 S.E.2d 627 (Ga. Ct. App. 1995) (affirming the denial of provider's motion for summary judgment) Id. at Id.
![2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 265 the providers did not have to pay anything to the plaintiffs.](/docs-images/79/79224697/images/317-0.jpg "204 SURROGATES CANNOT REBUT PROVIDERS' STATUTORY RIGHT TO REFUSE LSMT Surrogates have encountered an additional hurdle, in addition to hurdles in establishing the prima facie elements of tort-based")
317 2008] JUDICIAL TREATMENT OF MEDICAL FUTILITY 265 the providers did not have to pay anything to the plaintiffs. 204 SURROGATES CANNOT REBUT PROVIDERS' STATUTORY RIGHT TO REFUSE LSMT Surrogates have encountered an additional hurdle, in addition to hurdles in establishing the prima facie elements of tort-based causes of action. In many states, health care decisions statutes grant providers the right to refuse LSMT if they deem. it m.edically or ethically inappropriate.205 For instance, the Virginia Health Care Decisions Act (HCDA) provides that "[n]othing in this article shall be construed to require a physician to prescribe or render m.edical treatment to a patient that the physician determ.ines to be medically or ethically inappropriate."206 A provider may unilaterally stop LSMT after giving a surrogate fourteen days to attem.pt transfer to another facility willing to provide the requested treatm.ent. 207 This Virginia statute had an apparently dispositive im.pact in at least one case. After the University of Virginia Hospital issued a unilateral DNR order- for Shirley Robertson, her surrogate brought an EMTALA action in federal court. 208 In Bryan v. Rectors & Visitors of UVA, the Fourth Circuit affirm.ed the dismissal of the EMTALA claim. and suggested that the plaintiff proceed in state court, noting that "[s]uch reprehensible disregard for one's patient" would constitute the "tort of abandonment."209 Subsequently, the plaintiff proceeded in state court,210 but later voluntarily dism.issed that action because of from Robin C. Correll to Thaddeus Pope (May II, 2007) (on file with author) See Pope, Futility Statutes, supra note 17 (arguing that only Texas' safe harbor is effective). But cf Maureen Kwiecinski, To Be Or Not to Be, Should Doctors Decide? Ethical and Legal Aspects ofmedical Futility Policies, 7 ELDER'S ADVISOR 313, (2006) (questioning the constitutionality of unilateral decision statutes) VA. CODE ANN (A) (West 2007) Id Bryan, 95 F.3d at Id. at Id.

318 266 MARQUETTE ELDER'S ADVISOR [Vol. 9 the Virginia HCDA.211 Similarly, the Louisiana Health Care Decisions Act provides that the act should not be 1/construed to require the application of medically inappropriate treatment... or to interfere with medical judgment with respect to the application of medical treatment or life-sustaining procedures."212 In Causey v. St. Francis Medical Center, providers unilaterally withdrew a ventilator and dialysis from a comatose patient with end-stage renal disease. 213 The appellate court affirm.ed the dismissal of the family's intentional battery tort action, observing that Louisiana providers are entitled to unilaterally withdraw LSMT so long as they comply with the standard of care. 214 Apart from unique outrage cases, actions against unilateral termination of LSMT have been unsuccessful. Surrogates have had enormous difficulty overcoming statutory authorization to refuse LSMT, establishing breach of the standard of care, and establishing causation and damages. The low success rate means not only that the risk of liability is lower than b,elieved, but also that fewer cases will even be brought against providers.215 CONCLUSION While the litigated futility cases do not articulate a clear and unequivocal right of providers to refuse LSMT that they deem mappropriate, these cases also do not support the supposed 211. Bryan v. Rectors & Visitors of the Univ. of Virginia, No. CL (Fauquier County, Va. Cir. Ct. Nov. 27, 1995) (Order of Nonsuit). It is also hard to establish tortuous abandonment because while providers may cease aggressive treatment, they continue comfort care. See Hartsell, 905 S.W.2d at LA. REV. STAT. ANN. 40: (A)(4) (2006) Causey, 719 So. 2d at Id. at 1075 (citing 40: (A)(4». The appellate court did remand the medical malpractice claim to a "medical review panel" to determine whether the providers met the standard of care. See Message from Jeffrey D. Gurrierro to Thad Pope (on file with author) See John A. Day, Should You Risk Taking the Case? TRIAL, Jan. 2008, at 20; Gary B. Pillersdorf, Criteria for Case Selection, in ATLA's LITIGATING TORT CASES (2007).
319 2008] ]UDICIA.L TREATMENT OF MEDICAL FUTILITY 267 right of surrogates to demand such care. Surrogates do not have nearly the amount of bargaining power that they are perceived to possess. Therefore, the fear of legal liability should not have the impact on provider decision-making that it has had. A reassessment of the judicial treatment of futility cases leads to an obvious implication for health care providers. Physicians make decisions regarding LSMT based largely on perceived constraints from the legal system. 216 The misperception of those constraints has led to the overtreatment of patients, causing unnecessary suffering and inappropriate use of scarce medical resources. 217 But firmer, more accurate shadows should produce better results. 218 With sufficient legal education, providers may be more willing to treat patients in a way they deem medically appropriate. 219 A reassessment of the judicial treatment of futility cases also leads to two practical implications for elder law attorneys. First, attorneys must educate their clients. It is a long-recognized role of the elder law attorney to advise her clients about advance directives. 220 As elders may have misconceptions about their future care,221 counseling should be directive. It should entail more than the passive documentation of a client's articulated treatment preferences.222 Attorneys should educate clients so 216. McCrary, supra note 4, at 373; Pope & Waldman, supra note 4, at Pope & Waldman, supra note 4, at Cf Alan Bavley & Julius A. Karash, As Life Ebbs, Bills Can Mount: Millions of Elderly Get Needless and Costly Medical Care as They Near Death, KANSAS CITY STAR, Jan. 1, 2007 (discussing the Dartmouth Atlas of Health Care) Ruth D. Raisfeld, Mediators Can Best Help Those Who Help The1nselves, N.Y.L.J., Dec. 1, 2003 (arguing that mediation is more successful with "objective criteria" such as an accurate understanding of "prevailing case law") McCrary, supra note 4, at 372. See also Perkins et al., supra note 4, at 192 (criticizing the impact of "external factors" on physician decision-making) Nat'l Acad. of Elder Law Attorneys, Preparing for End oflife, EYE ON ELDER ISSUES, Aug. 2004, available at Aug04.pdf (last visited Feb. 2, 2008) See, e.g., Catherine A. Marco & Roques M. Schears, ER Decisions to Withdrazv CPR, 9 AMAVIRTUAL MENTOR 174 (2007) See Ed de St. Aubin et al., Elders and End-of-Life Medical Decisions: Legal Context, Psychological Issues, and Recommendations to Attorneys Serving Seniors, 7 ELDER'S ADVISOR 259, (2006).
320 268 MARQUETTE ELDER'S ADVISOR [Vol. 9 that they have realistic expectations of what medicine can offer. 223 Second, attorneys should empower their clients. Elder law attorneys should be "articulate and forceful advocates so that their client's [treatment] preferences... are honored and understood."224 Sometimes after a careful, thorough discussion of treatment options, attorneys may discover that their client has a religious or cultural reason for wanting to continue LSMT, no matter how dire the circumstances. If so, they should advise their client that an advance directive can be used not only to decline treatm.ent but also to "request that all reasonable measures... be taken to sustain life."225 To be sure, even advance directives can be overridden in futility disputes. However, having clear written docum.entation of treatment preferences maximizes the chance that such preferences will be honored Id A. KIMBERLY DAYTON ET AL., ADVISING THE ELDERLY CLIENT 33.7 (2007); Barbara Weinschenk, End of Life Issues, ELDER LAW UPDATE 146, (Nat'l Bus. Inst. 2007) DAYTON ET AL., supra note 224, at Cf Eric R. Oalican, Older Clients and Long Term Care, DRAFTING ESTATE PLANS (Mass. CLE, Inc. 2007) (offering the following sample medical directive language: "I want my life to be prolonged to the greatest extent possible without regard to my condition, the chances I have for recover, or the cost of the procedures.").
321 Widener Law School Legal Studies Research Paper Series no Surrogate Selection: An Increasingly Viable, But Limited, Solution to Intractable Futility Disputes Thaddeus Mason Pope Widener University School of Law This paper can be downloaded without charge from The Social Science Research Network Electronic copy available at:
322 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM SURROGATE SELECTION: AN INCREASINGLY VIABLE, BUT LIMITED, SOLUTION TO INTRACTABLE FUTILITY DISPUTES THADDEUS MASON POPE* INTRODUCTION I. THE NATURE AND PREVALENCE OF MEDICAL FUTILITY DISPUTES A. What Is a Medical Futility Dispute? Physician Reasons for Refusing Requested Treatment Surrogate Reasons for Requesting Non-recommended Treatment B. Prevalence of Futility Disputes C. Most Futility Disputes Are Resolved Collaboratively II. THE ROLE OF SURROGATES A. Types of Surrogates Patient-Designated Surrogates: Agents and Attorneys-in- Fact Physician-Designated Surrogates: Default Surrogates and Proxies Court-Designated Surrogates: Guardians and Conservators B. Duties of Surrogates Subjective Standard: Implement the Patient s Instructions * Associate Professor of Law, Widener University School of Law; Adjunct Professor of Medical Education, Albany Medical College. Thanks to Elaine Renoire, Robert Sibbald, and Robert Truog for feedback. Key arguments in this Article were presented during ethics rounds at the Medical College of Wisconsin in September 2009, at HCA in December 2009, and at Rady Children s Hospital in September Thanks to the participants at these events for valuable comments and suggestions. Thanks to Andrew Grous, Preet Bassi, and Mitchell Palazzo for their superb research assistance. This Article was supported by a generous summer research grant from Widener University. 183 Electronic copy available at:
323 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 184 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3: Substituted Judgment: Implement the Patient s Preferences Best Interests Standard: Promote the Patient s Welfare III. UNFAITHFUL SURROGATES SHOULD BE REPLACED A. Surrogate Performance Is Mediocre Surrogates Do Not Know Patient Preferences Surrogates Do Not Follow Patient Preferences Formalized Distrust of Surrogates Summary B. Rationale for Surrogate Replacement C. Method of Surrogate Replacement IV. JUDICIAL REPLACEMENT OF UNFAITHFUL SURROGATES A. Early U.S. Cases: B. Later U.S. Cases: Judicial Replacement of Surrogates Making Decisions Inconsistent with the Patient s Advance Directive Judicial Replacement of Surrogates Making Decisions Inconsistent with the Patient s Preferences or Best Interests Judicial Replacement of Surrogates Suffering a Material Conflict of Interest C. Ontario Capacity and Consent Board D. Queensland Guardianship and Administration Tribunal V. THE LIMITS OF SURROGATE SELECTION A. Surrogates Often Have Evidence to Demonstrate Congruity B. Providers Often Lack Sufficient Evidence to Demonstrate Surrogate Deviation Few Advance Directives are Available and Applicable Patient Preferences Are Rarely Clear and Strong Patients Want their Surrogates to Have Discretion C. Silver Lining: Best Interests Analysis CONCLUSION Electronic copy available at:
324 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 185 INTRODUCTION In 2009, the New England Journal of Medicine published a very popular interactive clinical case discussion: 1 A 56-year-old homeless man was found having a seizure and was transported to the hospital. 2 He was found to have a subarachnoid hemorrhage and acute hydrocephalus. He underwent intubation, and mechanical ventilation was started. A shunt was placed to relieve the hydrocephalus; cerebral angiography revealed a ruptured aneurysm of the anterior communicating cerebral artery and an un-ruptured aneurysm of the posterior cerebral artery.... The patient s condition did not improve over the next 3 days, and both the neurologist and the neurosurgeon opined that he had a chance of approximately 80 to 90% of being in a long-term persistent vegetative state and only a chance of 5 to 10% of any recovery. His prognosis, at best, was to have a severe disability that would leave him dependent on care by others. 3 The patient had not been in contact with his family for several years. He had a son who, under the law of the state, was the legal next of kin for making medical decisions if the patient was unable to do so himself. 4 The patient also had a brother and a mother; all three relatives lived 1500 miles away. They were contacted and told of the patient s situation. They were all in agreement that the patient would not want to live in a state in which he would be largely dependent on others for daily care and would have severely impaired cognition. However, the son described the patient as a fighter who would want aggressive care until the prognosis was much more certain. 5 Supportive care, including mechanical ventilation, was continued for the next 3 weeks, without any clinically significant change in the patient s neurologic state. During this time it was discovered that the patient had a very close relationship with a counselor at a homeless shelter with whom he had talked at least every couple of weeks. The counselor came to see the patient and related that the patient had told him that he wished to avoid 1. Arthur S. Slutsky & Leonard D. Hudson, Care of an Unresponsive Patient with a Poor Prognosis, 360 NEW ENG. J. MED. 527, 527 (2009). See also Patricia A. Kritek et al., Care of an Unresponsive Patient with a Poor Prognosis Polling Results, 360 NEW ENG. J. MED. e15, e15 (2009). 2. Slutsky & Hudson, supra note 1, at Id. 4. This article uses the term surrogate as a generic term for all substitute decision makers, whether they obtained their authority from patient appointment (e.g., agent, attorneyin-fact, healthcare representative), physician appointment (e.g., proxy), or court appointment (e.g., guardian, conservator). See ALAN MEISEL & KATHY L. CERMINARA, THE RIGHT TO DIE: THE LAW OF END-OF-LIFE DECISIONMAKING 3.04 (3d ed. Supp. 2010) [hereinafter RIGHT TO DIE]; see also supra notes 19 to 139 and accompanying text. 5. Id.
325 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 186 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 hospitals and that when his time came he wanted no aggressive medical care Given the lack of improvement in the patient s neurologic state, the extremely poor prognosis for any meaningful recovery of cognitive function, and the [subsequently-discovered] high probability of cancer, the care team strongly believed that all aggressive and supportive measures should be discontinued and the goals of care changed to those of providing comfort. The brother and mother, who had been quick to respond to queries from the beginning, agreed with the shift to comfort care. However, the son... disagreed. He had hardened his position, wanting full aggressive-care measures to be taken, including clipping of the aneurysm. 7 This is a futility dispute. 8 The patient s healthcare provider believed that the only appropriate treatment was comfort care. But the patient s surrogate refused to consent to this recommendation, and instead demanded treatments that, in the providers judgment, would cause more harm than benefit. This sort of conflict regularly occurs in hospitals and other healthcare facilities. 9 In the New England Journal of Medicine case, it is unclear whether the providers conflict with the surrogate was intractable. Consequently, many participants in the online poll rightly voted that an ethics consultation was appropriate. 10 After all, most such disputes are resolved through further communication and mediation. 11 The focus of this Article is on the avenues for resolution, if the futility dispute proves to be intractable. Many New England Journal of Medicine poll respondents wanted to simply override the son, but noted that they would not do so because of legal concerns. 12 Physicians are overwhelmingly reluctant to withhold or withdraw treatment without the 6. Id. 7. Id. 8. See generally K. Francis Lee, Postoperative Futile Care: Stopping the Train When the Family Says Keep Going, 15 THORACIC SURGERY CLINICS 481, 481 (2005) (discussing the definition of futile care). 9. See discussion infra Part I.B (discussing the prevalence of futility disputes). 10. See Kritek et al., supra note 1, at e See Thaddeus M. Pope & Ellen A. Waldman, Mediation at the End of Life: Getting Beyond the Limits of the Talking Cure, 23 OHIO ST. J. ON DISP. RESOL. 143, 149, (2007) (stating, Mediation looked like the magic Band-Aid to solve end-of-life conflicts. However, in a growing number of cases further communication results in the provider backing down and the surrogate getting the treatment that he wants.); Sandra H. Johnson et al., Legal and Institutional Policy Responses to Medical Futility, 30 J. HEALTH & HOSP. L. 21, 31 (1997) (explaining that the results of a Life Sustaining Treatment Survey showed that futility policies generally envision[] a primarily consultative, consensus-building approach, rather than an adjudicative or decision making approach ). 12. See Kritek et al., supra note 1, at e15-e16.
326 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 187 consent of the authorized decision maker. 13 Accordingly, without explicit permission to do otherwise, physicians generally comply with surrogate requests for treatment even when they think it is cruel and wrong. 14 Only under Texas law do physicians have clear permission to refuse to provide inappropriate treatment. 15 When providers and patients surrogates cannot agree on appropriate life-sustaining medical treatment ( LSMT ), the Texas Advance Directives Act ( TADA ) designates the hospital ethics committee as adjudicator of last resort. 16 If the hospital committee agrees that the requested treatment is inappropriate, the provider earns legal immunity for refusing to provide it. 17 The Idaho State Senate recently passed a bill to do the same thing. 18 And policymakers in other states have considered, or are now considering, similar legislation, albeit most are vaguer than TADA See Pope & Waldman, supra note 11, at See id. at (citing sources providing physicians reasons for continuing futile treatment). See also ALISON BARNES, A. FRANK JOHNS & NATHALIE MARTIN, COUNSELING OLDER CLIENTS 317 (2d ed. 2005); JOAN M. KRAUSKOPF ET AL., ELDER LAW: ADVOCACY FOR THE AGING 501 (2d ed. 1993) ( [A] doctor usually will accede to the wishes of a family that insists that care be continued, even if the doctor believes that no benefit is being conferred.... ); Robert Sibbald, James Downar & Laura Hawryluck, Perceptions of Futile Care Among Caregivers in Intensive Care Units, 177 CANADIAN MED. ASS N J. 1201, 1203 (2007) (finding that providers followed the instructions of surrogates instead of doing what they felt was appropriate because of a lack of legal support. ). 15. TEX. HEALTH & SAFETY CODE ANN (d), (a) (West 1999). 16. TEX. HEALTH & SAFETY CODE ANN (a) (West 1999). See generally Robert L. Fine, The Texas Advance Directives Act of 1999: Politics and Reality, 13 HEALTHCARE ETHICS COMMITTEE F. 59, 68 (2001) (discussing the purpose of the Texas Advance Directives Act of 1999); Thaddeus Mason Pope, Legal Briefing: Medical Futility and Assisted Suicide, 20 J. CLINICAL ETHICS 274, 275 (2009) [hereinafter Pope 2009] (discussing the multi-stage review process). 17. TEX. HEALTH & SAFETY CODE ANN (d) (West 1999). 18. S. 1114, 60th Leg., 1st Reg. Sess. 5(7) (Idaho 2009). 19. Thaddeus Mason Pope, Medical Futility Statutes: No Safe Harbor to Unilaterally Refuse Life-Sustaining Treatment, 75 TENN. L. REV. 1, 54, 58 (2007) [hereinafter Pope 2007] (As of 2007, New Mexico, Maine, Delaware, Alabama, Mississippi California, Hawaii, Tennessee, Alaska, and Wyoming have adopted the Uniform Health Care Decisions Act, which has provisions specifically designed to handle futility disputes. ) See also Fine, supra note 16, at 59 ( Every state has developed laws regulating end-of-life decisions, including various forms for advance directives. ); Pope 2007, supra note 19, at 53-54, (examining notable unilateral decision statutes); Monica Sethi, A Patient s Right to Direct Own Health Care vs. a Physician s Right to Decline to Provide Treatment, 29 BIFOCAL 21, 27 (2007) ( All but five states acknowledge a provider s right to refuse to comply with a patient s request for treatment. ). The medical societies in several states have been pushing for TADA-type legislation. See, e.g., California Medical Association House of Delegates, Resolutions & ; Washington State Medical Association House of Delegates, Resolution C-5 (A-09). See also Betancourt v. Trinitas Hospital, No. A T2 (N.J. Sup. Ct., App. Div. Aug.
327 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 188 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 But Harvard Medical School Professor Robert Truog argues that this tooprovider-friendly sort of internal dispute resolution legislation is both unnecessary and dangerous. 20 He argues that current healthcare decision laws in every state already give healthcare providers an adequate mechanism to avoid providing inappropriate medicine demanded by surrogates. Specifically, when a surrogate demands treatment that providers deem medically inappropriate, these surrogate selection laws often permit (or even encourage) providers to designate a different new surrogate from whom consent to withhold/withdraw can be obtained. 21 7, 2009) (Amicus brief of Medical Society of New Jersey and New Jersey Hospital Association asking an appellate court to adopt a TADA-type process). 20. See Jeffrey P. Burns & Robert D. Truog, Futility: A Concept in Evolution, 132 CHEST 1987, 1991 (2007) (expressing concern that TADA gives an unwarranted amount of power to the clinicians and hospitals over patients and families who hold unpopular beliefs or values ); Robert D. Truog, Counterpoint: The Texas Advance Directives Act Is Ethically Flawed: Medical Futility Disputes Must Be Resolved by a Fair Process, 136 CHEST 968, 969 (2009) [hereinafter Truog, Counterpoint] (suggesting that TADA s placement of the life-and-death decision in the hands of hospital ethics committees is too-provider friendly because [m]ost of these committee members are doctors, nurses, and other clinicians from the hospital community.... [thus] involvement of the hospital ethics committee fails to bring the diversity of the community into the deliberative process ); Robert D. Truog, Medical Futility, 25 GA. ST. U. L. REV. 985, 1000, 1002 (2009) [hereinafter Truog, Medical Futility] (criticizing TADA s due process approach as more illusory than real and suggesting that the internal dispute resolution is unnecessary); Robert D. Truog, Rebuttal from Dr. Truog, 136 CHEST 972, (2009) (suggesting that TADA is unnecessary and that ethics committees should not have unchecked decision-making power); Robert D. Truog, Tackling Medical Futility in Texas, 357 NEW ENG. J. MED. 1, 3 (2007) [hereinafter Truog 2007] (stating that internal dispute resolution in Texas is both unnecessary and runs the risk of becoming a rubber-stamp mechanism that does not respect diversity). This article focuses on Truog s argument that unilateral refusal legislation is unnecessary. Id. For a fuller explication on why such legislation might be dangerous, see Thaddeus Mason Pope, Multi-Institutional Healthcare Ethics Committees: The Procedurally Fair Internal Dispute Resolution Mechanism, 31 CAMPBELL L. REV. 257, 258 (2009) (expressing concern that healthcare ethics committees make treatment decisions that suffer from risks of corruption, bias, carelessness, and arbitrariness ). 21. This is my term, not Truog s; but the concept is the same. See Burns & Truog, supra note 20, at 1989, (discussing the procedure used by hospitals to have the court appoint an alternate decision maker and how that procedural approach has been translated into state law); Pope, supra note 19, at (stating that if the health care provider... doubt[s] that the surrogate s decision reflects the patient s actual preferences or best interests... providers may try to switch the legally authorized decision maker to one that will agree with their recommendation to cease LSMT ); Robert D. Truog, Correspondence, Tackling Medical Futility in Texas, 357 NEW ENG. J. MED. 1558, 1559 (2007) [hereinafter Truog, Correspondence] (responding to criticism in a letter to the journal editor by arguing for existing pathways to challenge the legitimacy of the surrogate to make these decisions and to seek appointment of another decision maker ). See also Rasa Gustaitis, Right to Refuse Life- Sustaining Treatment, 81 PEDIATRICS 317, 318, 321 (1988) (suggesting the use of child abuse laws to override parental requests for inappropriate treatment).
328 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 189 Truog argues that a mechanism like TADA is most useful, and most justified, when surrogates make decisions not in the best interests of patients. But in precisely such a situation, there is no need to resort to a TADA-type mechanism. Instead, Truog argues, the remedy should be to use existing pathways to challenge the legitimacy of the surrogate to make these decisions and to seek appointment of another decision maker. 22 The logic behind these surrogate selection laws is simple. A surrogate is the patient s agent and, as such, must act according to the patient s instructions, known preferences, and best interests. When a surrogate exceeds the scope of her authority, she can and should be replaced. 23 For example, providers took a surrogate selection approach in the famous Helga Wanglie case. 24 Instead of asking the court to directly determine that their recommended treatment was correct, providers instead asked the court only to make a procedural decision appointing a new surrogate. 25 This surrogate, in turn, would make the substantive decision (presumably in accordance with provider recommendations) Truog, Correspondence, supra note 21, at See also Truog, Counterpoint, supra note 20, at 969 (declaring I think a better approach would be for clinicians to be more proactive in legally challenging the decisional authority of the surrogates ); Truog, Medical Futility, supra note 20, at 995 ( When family members insist upon treatments that are causing pain or suffering, we need to be much more proactive in challenging their role as surrogate decision makers, and we need to seek to have them replaced.... ); Robert D. Truog, Futile Care Debate and Baby Doe: Resolving Difficult Cases When Further Treatment May Be Considered Futile, Georgia State University College of Law Baby Doe Symposium: The 25th Anniversary of the Baby Doe Rules: Perspectives from the Fields of Law, Health Care, Ethics, and Disability Policy (Feb. 13, 2009), /videos. Even one of TADA s authors admits that much of the motivation for unilateral refusal stems from distrust pf surrogates. Thomas Wm. Mayo, The Baby Doe Rules and Texas Futility Law in the ICU, 25 GA. ST. U. L. REV. 1003, 1013 (2009). But cf. Robert L. Schwartz, Autonomy, Futility, and the Limits of Medicine, 1 CAMBRIDGE Q. HEALTHCARE ETHICS 159, (1992) (arguing that the question of whether Mr. Wanglie was his wife s best substitute decision-maker was the wrong question, and [t]he real question [should have been] whether the continuation of ventilator support and gastrostomy feeding were among the reasonable medical alternatives that should have been available to Mrs. Wanglie or her surrogate decision maker, whoever that might be ). 23. See Peter B. Terry, Informed Consent in Clinical Medicine, 131 CHEST 563, 565 (2007) ( Occasionally, the legal surrogate does not act in the patient s best interest... In such instances, the physician must ensure... that someone who will act in the patient s best interest is named. ). 24. In re: The Conservatorship of Helga M. Wanglie, 7 ISSUES L. & MED. 369 (1991) [hereinafter In re Wanglie]. 25. Id. at 371, See id. at 371 (stating that the physician nominated a conservator to replace Helga Wanglie s husband as her surrogate).
329 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 190 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 In Section One, I describe the nature and prevalence of futility disputes. In Section Two, I describe the role of surrogates and the standards that they must apply when making medical treatment decisions on behalf of patients. Unfortunately, the available empirical evidence indicates that surrogates do a rather poor job of representing patient s preferences and interests. So, in Section Three, I argue that unfaithful surrogates should be replaced. In Section Four, I demonstrate that surrogate replacement is a proven and viable dispute resolution mechanism. While providers were ultimately unsuccessful in both Wanglie and similar cases during the early 1990s, surrogate selection has, more recently, proven to be a successful approach. Emblematic of this trend is a string of cases during 2008 and 2009 in which several courts replaced patients surrogates because they were demanding inappropriately aggressive end-of-life treatment. 27 Finally, in Section Five, I argue that while surrogate selection has become increasingly well grounded both in statutory standards and in judicial precedent, it remains only a partial solution to intractable futility disputes. To replace a surrogate requires evidence of a contradiction between the surrogate s decision and the patient s instructions, known preferences, or best interests. But, for two main reasons, providers will frequently be unable to demonstrate any such contradiction. First, providers will often lack enough evidence of patient instructions or preferences to demonstrate surrogate deviation. Second, in many cases, surrogate decisions will actually be in harmony with patient wishes. In sum, Professor Truog is right to endorse surrogate selection as a solution to intractable futility disputes. It is a mechanism that can work, and one that, where possible, should be preferred over power-shifting laws. Yet, since surrogate selection cannot resolve significant categories of conflict, we must still develop dispute resolution mechanisms to handle those remaining disputes in which providers conflict with irreplaceable surrogates. I. THE NATURE AND PREVALENCE OF MEDICAL FUTILITY DISPUTES Before turning to the role of the surrogate in Section II, it is useful to first establish some basic features of a medical futility dispute. In this Section, I shall briefly consider: (a) the nature and causes of medical futility disputes, (b) the prevalence of such disputes, and (c) the high rate of informal collaborative resolution. 27. See infra notes and accompanying text.
330 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 191 A. What Is a Medical Futility Dispute? A medical futility dispute arises when a provider seeks to stop treatment that the patient or surrogate wants continued. 28 The provider judges lifesustaining medical treatment to be of no benefit and wants to stop the train when the patient or surrogate says, Keep going! 29 The provider wants to stop LSMT even without consent of the patient or surrogate. Accordingly, a medical futility dispute is sometimes referred to as a reverse end-of-life, 30 a right to live or right to life, 31 a right to die or duty to die, 32 or even an involuntary euthanasia 33 situation. One recent futility case was presented to the Court of Queen s Bench of Alberta. 34 In October 2009, Isaiah May was born in Rocky Mountain House, Alberta after a long and difficult forty-hour delivery. 35 At some point, his umbilical chord got wrapped around his neck several times, cutting off the oxygen supply to his brain. 36 Isaiah was airlifted to Stollery Children s Hospital in Edmonton, where he was diagnosed with severe neonatal encephalopathy. 37 He was then dependent on mechanical ventilation See generally Lee, supra note 8 (discussing medical futility disputes between providers and surrogates in the context of postoperative care). 29. Id. 30. See, e.g., RIGHT TO DIE, supra note 4, at 13.01[B]. See also Thomas Wm. Mayo, Living and Dying in a Post-Schiavo World, 38 J. HEALTH L. 587, 602 n.68 (2005) (using the term reverse right-to-die ). 31. See, e.g., Nancy Neveloff Dubler, Conflict and Consensus at the End of Life, HASTINGS CENTER REP., Nov.-Dec. 2005, at S19, S19; Leigh B. Middleditch, Jr. & Joel H. Trotter, The Right to Live, 5 ELDER L.J. 395, 395, 402, 404 (1997); Wesley J. Smith, Suing for the Right to Live, WEEKLYSTANDARD.COM, Mar. 10, 2004, Content/Public/Articles/000/000/003/836zeecs.asp. 32. See, e.g., Smith, supra note See, e.g., Mary Ann Roser, Existing Medical Futility Law Works, Hospitals Say; Others at Hearing Disagree, AUSTIN AM.-STATESMAN, Aug. 10, 2006, at B Canadian Press, Court Adjourns Case of Rocky Couple Fighting to Keep Infant on Life Support, REDDEERADVOCATE.COM, Jan. 19, 2010, advocate/news/court_adjourns_case_of_couple_fighting_to_keep_infant_on_life_support_ html?mobile=true; Melissa Dominelli, Parents to Battle AHS, Hospital to Keep their Infant Son on Life Support, CTVEDMONTON.CA, Jan. 19, 2010, let/an/local/ctvnews/ /edm_lifesupport_100118/ /. 35. Dominelli, supra note Canadian Press, supra note Andrew Hanon, Court Allows Baby Isaiah s Life Support to Continue, CALGARYSUN.COM, Jan. 28, 2010 [hereinafter Life Support to Continue], sun.com/news/alberta/2010/01/28/ html. 38. See Canadian Press, supra note 34; Dominelli, supra note 34; Andrew Hanon, More Time to Line Up Specialists for Brain-Damaged Baby, TORONTOSUN.COM, Jan. 28, 2010
331 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 192 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 On January 13, 2010, Alberta Health Services sent Isaiah s parents a letter explaining his prognosis and their planned course of action. 39 The physicians informed the parents that Isaiah would not recover from the severe lack of oxygen during his birth and that as a result, he suffered anoxic brain injury and irreversible brain damage. 40 They went on to tell Isaiah s parents that he would not recover from his injuries. 41 Isaiah s doctors believed that all medical procedures had been exhausted. They wrote: Your treating physicians regretfully have come to the conclusion that withdrawal of active treatment is medically reasonable, ethically responsible and appropriate. We must put the interests of your son foremost and it is in his best interests to discontinue mechanical ventilation support. 42 The letter went on to say: Accordingly, it is with sadness that we are advising you that your treatment team will discontinue mechanical ventilation support to Isaiah after 2 p.m. Wednesday, January 20, Isaiah s parents disagreed with this prognosis and recommendation. They secured a temporary injunction against the removal of life support, so that they could obtain a second opinion. 44 Isaiah s parents argued that continued treatment was appropriate because Isaiah had already defied medical experts by living as long as he had and by growing and developing. 45 Isaiah s parents ultimately agreed to remove his ventilator after obtaining a second opinion, so subsequent court hearings were cancelled. 46 [hereinafter Brain-Damaged Baby], html. 39. Canadian Press, supra note Dominelli, supra note Id. 42. Andrew Hanon, Parents Get One-Week Reprieve for Baby on Life-Support, CALGARYSUN.COM, Jan. 20, 2010 [hereinafter Baby on Life Support], sun.com/news/alberta/2010/01/19/ html. 43. Canadian Press, supra note EdmontonJournal.com, Parents of Baby Isaiah Hope to Avoid Court Clash, VANCOUVERSUN.COM, Feb.20, 2010, Isaiah+parents+await+results+assessment/ /story.html; Brain-Damaged Baby, supra note 38; Lisa Priest, Baby Isaiah to Remain on Life Support - for Now, GLOBE & MAIL, Jan. 28, 2010, at A Brain-Damaged Baby, supra note 38; CBCNews, Parents Find Expert to Assess Baby on Life-Support, CBCNEWS, Jan. 27, 2010, edmonton-alberta-baby-isaiah-stays-on-ventilator.html#ixzz0e3ygoqlr (quoting Isaiah s father as saying that, [e]very time I hold him, he s non-stop moving, and he moves his head... He opens his eyes, his eyelids, a little bit and I mean, every little thing is an improvement, right? ). 46. CBC News, Baby Isaiah Dies in Edmonton Hospital, CBCNEWS, Mar. 11, 2010, (discussing the Mays decision to take Isaiah off of the ventilator).
332 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 193 Obviously, baby Isaiah lacked the capacity to make healthcare decisions for himself. 47 But even in futility disputes involving adult patients, the patient almost always lacks capacity. 48 Either because of encephalopathy related to the disorder or because she is sedated, the patient is almost never able to communicate with providers at the time a decision must be made. 49 Therefore, these decisions are almost always made by surrogates. Unfortunately, there is a significant rate of conflict between healthcare providers and surrogates. In most cases, the surrogate and the health care provider disagree over whether LSMT provides benefit because of a communication failure. 50 The surrogate and the provider perceive the situation differently. 51 In other cases, the disagreement is normative. 52 But, whether for factual or normative reasons, the provider and surrogate 47. Capacity is typically defined as an individual s ability to understand the significant benefits, risks and alternatives to proposed health care and to make and communicate a health-care decision. DEL. CODE ANN. tit. 16, 2501(d) (2003). See also ALA. CODE 22-8A-11(a)(1)a. (LexisNexis 2006) (allowing a surrogate in consultation with the attending physician to make LSMT decisions if the patient is no longer able to understand, appreciate, and direct his or her medical treatment ). 48. See e.g., Alexandre Lautrette et al., Surrogate Decision Makers for Incompetent ICU Patients: a European Perspective, 14 CURRENT OPINION CRITICAL CARE 714, 716 (2008) (discussing the capacity of patients and the use of surrogates in the ICU). 49. Id. at 715. See MANAGING DEATH IN THE ICU: THE TRANSITION FROM CURE TO COMFORT 236 (J. Randall Curtis & Gordon D. Rubenfeld eds., 2001); Thomas J. Prendergast et al., A National Survey of End-of-Life Care for Critically Ill Patients, 158 AM. J. RESPIRATORY CARE MED. 1163, 1166 (1998); Susan M. Parks & Laraine Winter, End-of-Life Decision Making for Cancer Patients, 36 PRIMARY CARE CLINICAL OFFICE PRACTICE 811, 813 (2009) ( Most Americans are decisionally incapacitated at the time of death, usually because of dementia, delirium, coma, or PVS. ); Maria J. Silveira et al., Advance Directives and Outcomes of Surrogate Decision Making before Death, 362 NEW ENG. J. MED. 1211, 1214 (2010); Elizabeth K. Vig et al., Beyond Substituted Judgment: How Surrogates Navigate Endof-Life Decision Making, 54 J. AM. GERIATRICS SOC Y 1688 (2006). But cf. Burke v. Gen. Med. Council [2005] EWCA Civ 1003, [2]-[5] (appeal taken from Eng.) (patient with capacity litigating a futility dispute concerning his own future treatment). 50. See Pope & Waldman, supra note 11, at 153 (suggesting that most surrogates eventually agree with the health care team s recommendation after the patient s condition and options are fully explained). See also ANTHONY BACK ET AL., MASTERING COMMUNICATION WITH SERIOUSLY ILL PATIENTS: BALANCING HONESTY WITH EMPATHY AND HOPE 1-6 (2009) (discussing the importance of physician communication skills in the context of seriously ill patients). 51. See David E. Weissman et al., The Family Meeting: Causes of Conflict, FAST FACTS AND CONCEPTS (2010), pdf. 52. See JOSEPH J. FINS, A PALLIATIVE ETHIC OF CARE: CLINICAL WISDOM AT LIFE S END 82, 84 (2006) (explaining how futility disputes result from clinicians and families operating upon different assumptions because of miscommunication concerning basic information about diagnosis, prognosis, and remaining [treatment] options ).
333 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 194 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 disagree because they have different goals. 53 The patient s goals might include cure, amelioration of disability, palliation of symptoms, reversal of disease processes, or prolongation of life. The provider, on the other hand, might judge these goals to be impossible, virtually impossible, or otherwise inappropriate under the circumstances. 54 There is, in short, a demonstrable gap between the goals of physicians and the goals of surrogates. In one recent study, seventy-two percent of the public thought that patients have a right to demand treatment that their physician s believe will not help. 55 Only forty-four percent of physicians agreed. 56 Similarly, twenty-one percent surrogates thought that even when doctors believe there is no hope of recovery, all efforts should continue indefinitely. 57 Only 2.5% physicians agreed Physician Reasons for Refusing Requested Treatment Healthcare providers have several reasons for wanting to refuse surrogate-requested LSMT. 59 First, they want to prevent patient suffering since aggressive treatment can cause just that. 60 It is unacceptable if there is no countervailing benefit to be achieved by the treatment. 61 Continued interventions can be inhumane, invasive, pointless, intrusive, cruel, burdensome, abusive, degrading, obscene, violent, or grotesque. 62 CPR, 53. Cf. Thomas Wm. Mayo, Health Care Law, 53 SMU L. REV. 1101, 1110 n.78 (2000) (describing the dispute as being what constitutes a benefit to the patient ). 54. Pope, supra note 19, at Lenworth M. Jacobs et al., Trauma Death: Views of the Public and Trauma Professionals on Death and Dying from Injuries, 143 ARCHIVES SURGERY 730, (2008). 56. Id. at Id. at 732 tbl Id. 59. However, some providers actually provide as much as or even more treatment than surrogates desire. 60. See LAWRENCE J. SCHNEIDERMAN & NANCY S. JECKER, WRONG MEDICINE: DOCTORS, PATIENTS, AND FUTILE TREATMENT 101 (1995). 61. Plaintiffs Verified Complaint at 8, Gonzales v. Seton Family of Hospitals, No. A07CA267 (W.D. Tex. Apr. 4, 2007) ( [T]he burden of his treatment outweighs the benefit to E.G. [Emilio] or his mother. ). 62. See, e.g., In re Doe, 418 S.E.2d 3, 4 (Ga. 1992) (Hospital alleged continued treatment would constitute medical abuse. ); Wendland v. Sparks, 574 N.W.2d 327, (Iowa 1998) (Doctor unilaterally decided not to attempt CPR as an act of mercy because he could not do it to her. ); In re Dinnerstein, 380 N.E.2d 134,137 (Mass. App. Ct. 1978) (characterizing LSMT as pointless, even cruel, prolongation of the act of dying ); Brief for Appellants at 3, In re Baby K, 16 F.3d 590 (4th Cir. 1994) (No ), 1993 WL ( This tragic case involves a parent s attempt to require physicians to provide to a dying infant treatment that is medically unreasonable, invasive, burdensome, inhumane, and inappropriate. ); John Altomare & Mark Bolde, Nguyen v. Sacred Heart Medical Center, 11 ISSUES L. & MED. 199, 200 (1995) (Hospital alleged continued treatment was inhumane. );
334 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 195 for example, can be painful, causing rib or sternal fractures in over fifty percent of cases. 63 Health care providers want to relieve and shorten patient suffering, not cause or prolong it. 64 Second, physicians want to protect patient autonomy. In many cases, the aggressive treatment demanded by a surrogate is treatment that the patient does not want. 65 And even when patient preferences are unknown, continued treatment is not always in the patient s best interests. 66 Furthermore, providing unwanted treatment not only violates the patient s bodily integrity, but also the patient s decisional autonomy by undermining the patient s wishes regarding the location of her death (e.g. at home) and utilizing estate resources to pay medical bills that the patient may have wanted to go to other uses (e.g. grandchildren s education). Third, physicians want to prevent family distress. If they act as though a medically inappropriate option were available, then that would create a psychological burden on surrogates to select that option. 67 Naturally, Martha Kessler, Court Orders Hospital to Comply with Decisions Made Under Health Proxy, 13 HEALTH L. REP. (BNA) 527, 527 (2004) (Massachusetts General Hospital successfully argued to a Boston court that CPR for Barbara Howe would be severe, invasive and harmful. ); Liz Kowalczyk, Hospital, Family Spar over End-of-Life Care, BOS. GLOBE, Mar. 11, 2005, at A1 ( [T]his inhumane travesty has gone far enough... This is the Massachusetts General Hospital, not Auschwitz. (quoting Dr. Edwin Cassem)). 63. SCHNEIDERMAN & JECKER, supra note 60, at 94 ( [A]ttempted cardiopulmonary resuscitation could involve forceful, even violent, efforts at compressing the chest cage to the point of fracturing ribs.... ); Yoshiaki Hashimoto et al., Forensic Aspects of Complications Resulting from Cardiopulmonary Resuscitation, 9 LEGAL MED. 94, 97 (2007) ( [W]e observed rib fractures in 52% of the cases [and] [s]ternal fractures were recognized in 39%. ). See generally Paul C. Sorum, Limiting Cardiopulmonary Resuscitation, 57 ALB. L. REV. 617, 617 (1994) ( The patient will usually receive the following interventions: manual compressions of the chest... one or more jolts of electricity to the chest... and intravenous medications and fluids. ). 64. See Alexander Morgan Capron, Abandoning a Waning Life, HASTINGS CENTER REP., July-Aug. 1995, at 24, 24 (Unilateral termination can avoid mistreating the patient. ); SCHNEIDERMAN & JECKER, supra note 60, at (The Hippocratic Oath supports physicians refraining from providing futile care.). Cf. John C. Fletcher, The Baby K Case: Ethical and Legal Considerations of Disputes About Futility, II BIOLAW S:219, S:224 (describing a situation where the physicians initially provided LSMT with the hope that the surrogate would decide to have it removed). 65. In re Livadas, No. 08/ (N.Y. Apr. 28, 2008). 66. See generally Bernstein v. Superior Court, No. B212067, 2009 WL (Cal. Ct. App. Feb. 2, 2009). 67. See, e.g., George J. Annas, Asking the Courts to Set the Standard of Emergency Care The Case of Baby K, 330 NEW ENG. J. MED. 1542, 1543 (1994) (calling the provision of mechanical ventilation to Baby K after birth a medical misjudgment that gave the mother a false impression); Allan S. Brett, Futility Revisited: Reflections on the Perspectives of Families, Physicians, and Institutions, 17 HEATHCARE ETHICS COMMITTEE F. 276, 281, 282 (2005) (arguing that when a physician believes that additional treatment is inappropriate he should
335 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 196 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 families want to take at least all reasonable measures. Furthermore, it is unfair and deceptive to offer an option where there really is none. 68 Often the surrogate wants the burden of decision lifted from her. 69 And even if not the surrogate, other family members are often relieved to see the patient s preferences or best interests protected. 70 Fourth, physicians want to preserve the integrity of the medical profession. Those in the health profession surely must have some role in defining the ends and goals of medicine because the medical profession is a self-governing one with its own standards of professional practice. 71 The integrity of the medical profession is an important societal interest that must be balanced against patient autonomy. 72 Many health care providers express that view and justify it to the family). But cf. Fletcher, supra note 64, at S:224 (suggesting that the court documents in Baby K showed the physicians had good reasons to intubate). 68. See Howard Brody, The Physician s Role in Determining Futility, 42 J. AM. GERIATRICS SOC Y 875, (1994) (suggesting that it is unethical to mislead patients by falsely raising hopes); Terese Hudson, Are Futile-Care Policies the Answer?: Providers Struggle with Decisions for Patients Near the End of Life, HOSPS. & HEALTH NETWORKS, Feb. 20, 1994, at 26, (quoting John Popovich as saying that physicians who offer futile, meaningless care are charlatans ); John J. Paris et al., Has the Emphasis on Autonomy Gone Too Far? Insights from Dostoevsky on Parental Decisionmaking in the NICU, 15 CAMBRIDGE Q. HEALTHCARE ETHICS 147, 150 (2006) (arguing that when faced with futile LSMT for an infant, a physician should explain to the parent(s) that additional aggressive interventions or escalation of treatment will be unavailing and then emphasize that comfort care will be continued in order to prevent giving parents false hopes and unrealistic expectations ); Tom Tomlinson & Diane Czlonka, Futility and Hospital Policy, HASTINGS CENTER REP., May-June 1995, at 28, 28, (Offering futile care is a bogus choice and a deception, and instead providers should seek acceptance of plan rather than consent. ). 69. See Ursula K. Braun et al., Reconceptualizing the Experience of Surrogate Decision Making: Reports vs. Genuine Decisions, 7 ANNALS FAM. MED. 249, 253(2009) ( Requests to do everything should therefore initially be understood as a request for help with managing the [surrogate] decision-making burden. ). 70. See generally Fine, supra note 16, at See Eric Gampel, Does Professional Autonomy Protect Medical Futility Judgments?, 20 BIOETHICS 92, 97 (2006) ( [A]n HCP may refuse treatments which the medical profession gauges to be inappropriate, i.e. as being inconsistent with the basic goals and values of medicine. This would mean that each HCP inherits a right of refusal from the right of the medical profession to be a self-governing body, one which defines its own standards of professional practice. ). 72. See Washington v. Glucksberg, 521 U.S. 702, 731 (1997) ( The State also has an interest in protecting the integrity and ethics of the medical profession. ); Superintendent of Belchertown State Sch. v. Saikewicz, 370 N.E.2d 417, 426 (Mass. 1977) ( Prevailing medical ethical practice does not... demand that all efforts toward life prolongation be made.... [T]he prevailing ethical practice seems to be to recognize that the dying are more often in need of comfort than treatment. ); In re Quinlan, 355 A.2d 647, 663 (N.J. 1976) ( The claimed interests of the State in this case are essentially the preservation and sanctity of human life and defense of the right of the physician to administer medical treatment according to his
336 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 197 do not consider the practice of medicine to include measures aimed solely at maintaining corporeal existence and perpetuating biological function. 73 Under these circumstances, providers feel that it is just wrong to provide treatment. 74 It is bad medicine, medicine being used for the wrong ends. 75 Moreover, they find it gruesome, distressing, and demoralizing to provide treatment that harms patients. 76 best judgment. ); Matthew S. Ferguson, Ethical Postures of Futility and California s Uniform Health Care Decisions Act, 75 S. CAL. L. REV. 1217, 1239 (2002) (noting that the UHCDA attempts to protect the ethical integrity of the medical profession). The legal profession is similar in this respect. While generally the client is in charge, lawyers can withdraw if the client insists upon taking action that the lawyer considers repugnant.... AMERICAN BAR ASSOCIATION, MODEL RULES OF PROFESSIONAL CONDUCT R. 1.16(b)(4) (2008). Lawyers also have obligations under Rule 11 they cannot file frivolous lawsuits even if the client demands it. See Jerold S. Solovy & Laura A. Kaster, Signing Pleadings, Motions, and Other Papers; Representations to the Court; Sanctions, in 2 MOORE S FEDERAL PRACTICE 11.11[5] (3d ed. 2009). 73. COLL. OF PHYSICIANS & SURGEONS OF MANITOBA, STATEMENT NO. 1602: WITHHOLDING AND WITHDRAWING LIFE-SUSTAINING TREATMENT 15-S4 (2008), statements/1602.pdf (listing guiding principles for withholding and withdrawing life-sustaining treatment). 74. See Benjamin Weiser, The Case of Baby Rena: Who Decides When Care Is Futile? A Question of Letting Go: A Child s Trauma Drives Doctors to Reexamine Ethical Role, WASH. POST, July 14, 1991, at Al ( It was medicine being used for the wrong ends, and not only was it being used for the wrong ends, but it had a bad effect. It was making the child suffer. ). 75. Id. 76. See ROBERT ZUSSMAN, INTENSIVE CARE: MEDICAL ETHICS AND THE MEDICAL PROFESSION 109 (1992) (noting that doctors are inclined toward activism ); Robert A. Burt, The Medical Futility Debate: Patient Choice, Physician Obligation, and End-of-Life Care, 5 J. PALLIATIVE MED. 249, 252 (2002) (recognizing that providing treatment can be distressing for physicians); Stacey Burling, Penn Hospital to Limit Its Care in Futile Cases: Severely Brain-Damaged Patients Won t Get Certain Treatments, as a Rule, PHILA. INQUIRER, Nov. 4, 2002, at A1 (describing a situation where providing treatment was gruesome); Jan Hoffman, The Last Word on the Last Breath, N.Y. TIMES, Oct. 10, 2006, at F1 ( [D]oing CPR [to PVS and end-stage patients], felt not only pointless, but like I was administering final blows to someone who had already had a hard enough life. (quoting Dr. Daniel Sulmasy)); Hudson, supra note 68, at 26 (stating that physicians find some LSMT demoralizing); Liz Kowalczyk, Mortal Differences Divide Hospital and Patient s Family, BOST. GLOBE, Sept. 28, 2003, at A1 (nurse refused to participate in continued aggressive treatment of Barbara Howe); Kowalczyk, supra note 62, at A26 ( Howe s longtime doctors and nurses believe... that keeping her alive is tantamount to torture. ); Elisabeth Rosenthal, Rules on Reviving the Dying Bring Undue Suffering, Doctors Contend, N.Y TIMES, Oct. 4, 1990, at A1 ( Doctors and nurses... describe anger and anguish at being forced by a patient or family to inflict pain on the dying, knowing that it is to no avail. ); Weiser, supra note 74 (Physicians and nurses viewed every day that Baby Rena spent in the ICU as a day of torture and viewed themselves as the torturers. ); Gregory Scott Loeben, Medical Futility and the Goals of Medicine (1999) (unpublished Ph.D. dissertation, University of Arizona) (on file with Journal of Health Law and Policy, Saint Louis University) ( If such judgments are meant to benefit anyone, it makes more sense to say that it is the physician... uncomfortable with the role [he is] being asked to play.... ). Cf. TOM L.
337 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 198 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 Fifth, physicians want to reduce moral distress. 77 Numerous measures show high levels of moral distress among healthcare providers, especially nurses, in situations where they are obligated to provide inappropriate treatment. 78 This moral distress can drive people from the profession and thus reduce access. 79 It can also reduce staffing levels and make people operate less well, adversely impacting other patients quality of care. 80 Sixth, physicians want to responsibly steward scarce resources. This includes hard resources like intensive care unit ( ICU ) beds. 81 In under- BEAUCHAMP & JAMES F. CHILDRESS, PRINCIPLES OF BIOMEDICAL ETHICS 38 (5th ed. 2001) (defending the physician s right of conscientious objection where the patient request is for something medically unconscionable ). 77. See generally Karen M. Gutierrez, Critical Care Nurses Perceptions of and Responses to Moral Distress, 24 DIMENSIONS CRITICAL CARE NURSING 229, 229 (2005) (defining moral distress as the feelings and experiences which result from a moral conflict where one knows the correct action to take but constraints lead to either inability to implement this action or an attempt to carry out moral action which fails to resolve the conflict ); Ann B. Hamric et al., Moral Distress in Health Care Professionals: What Is It and What Can We Do About It?, PHAROS, Winter, 2006, at 17, 18 (discussing physician moral distress); Connie M. Ulrich et al., Moral Distress: A Growing Problem in the Health Professions?, HASTINGS CENTER REP. Jan.- Feb. 2010, at 20, 21 (recognizing the negative effects of moral distress on healthcare providers). 78. See, e.g., Anita Catlin et al., A Potential Neonatal Nurse Response to Care Orders that Cause Suffering at the End of Life? A Study of a Concept, 27 NEONATAL NETWORK 101, 102 (2008) (collecting quotations and authority); Edouard Ferrand et al., Discrepancies Between Perceptions by Physicians and Nursing Staff of Intensive Care Unit End-of-Life Decisions, 167 AM. J. RESPIRATORY & CRITICAL CARE MED. 1310, 1313 (2003) (reporting the results of a study designed to evaluate the perceptions of physicians and nursing staff concerning ICU end-of-life decisions); Ann B. Hamric, Moral Distress and Nurse-Physician Relationships, 12 VIRTUAL MENTOR 6, 7-8 (2010) (discussing evidence that supports that both physicians and nurses experience moral distress); Lilia Susana Meltzer & Loucine Missak Huckabay, Critical Care Nurses Perceptions of Futile Care and Its Effect on Burnout, 13 AM. J. CRITICAL CARE 202, 202 (2004). 79. See Ann B. Hamric & Leslie J. Blackhall, Nurse-Physician Perspectives on the Care of Dying Patients in Intensive Care Units: Collaboration, Moral Distress, and Ethical Climate, 35 CRITICAL CARE MED. 422, 426 (2007) ( Almost half (45%) of the RNs had left (17%) or considered leaving (28%) a position because of moral distress. ). 80. See Ellen H. Elpern et al., Moral Distress of Staff Nurses in a Medical Intensive Care Unit, 14 AM. J. CRITICAL CARE 523, 529 (2005); Judith M. Wilkinson, Moral Distress in Nursing Practice: Experience and Effect, 23 NURSING F. 16, 23 (1987) ( One of the most common, but unsuccessful, coping behaviors was avoidance of patients or of job situations. ); Meltzer & Huckabay, supra note 78, at 206 ( The frequency with which critical care nurses encountered moral distress situations involving futile care was directly and significantly related... to the experience of emotional exhaustion... [which] occurs when a person s appraisal of occupational stressors exceeds his or her coping capabilities.... ). 81. See George A. Skowronski, Bed Rationing and Allocation in the Intensive Care Unit, 7 CURRENT OPINION CRITICAL CARE 480, (2001)(describing ICU beds as scarce resources).
338 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 199 bedded regions, an ICU bed used by a patient in a persistent vegetative state with multi-organ failure is the very same bed that could be used to achieve recovery for an accident victim. 82 Physicians are also concerned with stewarding soft resources (e.g. dollars). 83 The billions spent treating persistent vegetative state ( PVS ) patients could be used to cover more people who now have no coverage. As costs rise, premiums rise, and access drops Surrogate Reasons for Requesting Non-recommended Treatment While most surrogates accede to provider recommendations to move to comfort care, significant subsets of surrogates are often inclined to request that everything [be] done. 85 There are many reasons that surrogates insist on continuing treatment their health care providers consider medically inappropriate. First, surrogates might think that the healthcare providers prognosis is wrong because of skepticism about their prognostic abilities. 86 Or the distrust might go deeper. Surrogates might distrust that they are receiving proper care either because of their race, 87 socioeconomic status, See generally Robert K. Oye & Paul E. Bellamy, Patterns of Resource Consumption in Medical Intensive Care, 99 CHEST 685, 685 (1991) (explaining study on ICU resources used on futile medical treatment). 83. See Daniel P. Sulmasy et al., Physicians Ethical Beliefs About Cost-Control Arrangements, 160 ARCHIVES INTERNAL MED. 649, (2000) (discussing the financial incentives for physicians to control costs). But see Lawrence J. Schneiderman et al., Medical Futility: Response to Critiques, 125 ANNALS INTERNAL MED. 669, 673 (1996) (arguing that medical futility should have nothing to do with saving money or rationing resources). There are other justice-based concerns. See Michael Niederman & Jeffrey Berger, The Delivery of Futile Care Is Harmful to Other Patients, 38 CRITICAL CARE MED. S518 (2010). 84. Ezekiel J. Emanuel, The Cost-Coverage Trade-off: It s Health Care Costs, Stupid, 299 JAMA 947, (2008). 85. See, e.g., John Ellement, Woman Suing MGH Tells Court of Distress, BOS. GLOBE, Apr. 8, 1995, at 18. See also SCHNEIDERMAN & JECKER, supra note 60, at (Parents demanded vigorous measures to keep their daughter alive.); Donalee Moulton, Death, Denial and the Law, 40 MED. POST, May 4, 2004, at 29 ( [T]here is a greater sense of entitlement among patients, who are more likely to challenge doctors and question medical decisions. ). 86. Lucas S. Zier et al., Doubt and Belief in Physicians Ability to Prognosticate During Critical Illness: The Perspective of Surrogate Decision Makers, 36 CRITICAL CARE MED. 2341, 2342, 2345 (2008) (Eighty-eight percent of study participants expressed doubt in physicians ability to prognosticate. ). See also Pam Belluck, Even as Doctors Say Enough, Families Fight to Prolong Life, N.Y. TIMES, Mar. 27, 2005, at A1 (reporting that some patients and families... are skeptical of doctors interpretations or intentions ). 87. See FINS, supra note 52, at ( An especially difficult dynamic can arise when the family believes that the patient s dire condition was precipitated by a medical error or if they are suspicious that substandard care is being provided because the patient is from a traditionally marginalized population. ); Lee, supra note 8, at 483 (recognizing concerns among African Americans regarding healthcare discrimination); Kathryn L. Moseley et al.,
339 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 200 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 or their provider s financial incentives. 89 A significant volume of scientific literature demonstrates that patients from racial and ethnic minorities more frequently and more adamantly demand LSMT. 90 Second, even if not distrustful, surrogates might be in denial or under a therapeutic illusion that the patient could recover or that a new therapy will come along. 91 Easy access to medical information online makes Futility in Evolution, 21 CLINICS GERIATRIC MED. 211, (2005) (discussing contributing factors to minorities, publicly insured patients, and uninsured patients suspicion of physician motives); Mary Ellen Wojtasiewicz, Damage Compounded: Disparities, Distrust, and Disparate Impact in End-of-Life Conflict Resolution Policies, AM. J. BIOETHICS, Sept.-Oct. 2006, at 8, 9 (discussing race-specific vulnerability in LSMT decisions). 88. Kevin Fiscella, Socioeconomic Status Disparities in Healthcare Outcomes: Selection Bias or Biased Treatment?, 42 MED. CARE 939, (2004) (stating that the relationship between socioeconomic status and health care quality includes patients attitudes and beliefs ). 89. See Pope & Waldman, supra note 11, at (discussing patients concerns regarding physician financial incentives). 90. See generally William Bayer et al., Attitudes Toward Life-Sustaining Interventions Among Ambulatory Black and White Patients, 16 ETHNICITY & DISEASE 914, 914, 917 (2006) (confirming previous studies that show Black patients are more likely to use life-sustaining treatment than White patients); Ursula K. Braun et al., Decreasing Use of Percutaneous Endoscopic Gastronomy Tube Feeding for Veterans with Dementia Racial Differences Remain, 53 J. AM. GERIATRICS SOC Y 242, 242, (2005) (finding that African Americans are more likely to receive a PEG tube than Caucasians ); Marion Danis, Improving End-of-Life Care in the Intensive Care Unit: What s to Be Learned from Outcomes Research?, 6 NEW HORIZONS 110, 113 (1998) (finding that nonwhite patients receive more DNR orders); Michael N. Diringer et al., Factors Associated with Withdrawal of Mechanical Ventilation in a Neurology/Neurosurgery Intensive Care Unit, 29 CRITICAL CARE MED. 1792, 1796 (2001) (discussing studies which found that African American patients want more life-sustaining treatments and are less likely to withdraw such treatment); Joanne Mills Garrett et al., Life- Sustaining Treatments During Terminal Illness: Who Wants What?, 8 J. GEN. INTERNAL MED. 361, 364 (1993) ( Black patients were almost three times as likely as white patients... to want more [life-sustaining] treatment. ); Faith P. Hopp & Sonia A. Duffy, Racial Variations in End-of-Life Care, 48 J. AM. GERIATRICS SOC Y 658, 661 (2000) (describing a study which found that blacks were less likely than whites to engage in advance care planning and to limit care at the time of death ); Hilary Waldman, End-of-Life Care, Viewed in Stark Black and White, L.A. TIMES, Feb. 6, 2006, at F5 (reporting that many African Americans have reservations about end-of-life palliative care and are less likely than whites to sign living wills or DNR orders). But see Amber E. Barnato et al., Racial Variation in End-of-Life Intensive Care Use: A Race or Hospital Effect?, 41 HEALTH SERVICES RES. 2219, 2228 (2006) (arguing that differences were attributable to the use of hospitals with higher ICU use rather than to racial differences). 91. See Stacey A. Tovino & William J. Winslade, A Primer on the Law and Ethics of Treatment, Research, and Public Policy in the Context of Severe Traumatic Brain Injury, 14 ANNALS HEALTH L. 1, 2-3 n.5, 26, 26 n.153 (2005) (discussing therapeutic illusion where patients have false hopes despite the lack of future benefit ); Middleditch, Jr. & Trotter, supra note 31, at (discussing Society s Increasing Denial of Death ).
340 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 201 surrogates more confident in opposing providers recommendations. 92 Even in the face of clear and dire medical facts, family members often hold out hope that the patient will beat the odds. 93 In one study, thirty-two percent of surrogates elected to continue treatment for patients with less than one percent survival estimate. 94 Even more shocking is that eighteen percent wanted to continue treatment even when there was zero chance of survival. 95 Third, even when they truly appreciate that the odds are exceedingly slim, surrogates might believe that those odds are still worth pursuing. They might believe that God will perform a miracle. 96 Or they might otherwise be 92. Julie Sneider, End-of-Life Decisions: Medical Ethics Experts See Shift in Care Disputes, MILWAUKEE BUS. J., Apr. 22, 2005, at A See Todd Ackerman, Hospital Rules to Unplug Baby Girl/Leukemia Patient s Parents Scramble to Find New Care Facility, HOUS. CHRON., Apr. 30, 2005, at B1, available at (reporting that the mother of Knya Dismuke-Howard, a 6-month old with leukemia in her brain, multiple organ failure, and a life-threatening antibiotic-resistant infection believed her daughter could beat the odds... She s a fighter. ); Belluck, supra note 86, at A1 ( Extraordinary medical advances have stoked the hopes of families. ); Clare Dyer, Doctors Need Not Ventilate Baby to Prolong His Life, 329 BRIT. MED. J. 995, 995 (2004) (reporting that the mother of a terminally ill infant rejected medical advice because her baby was a fighter and had lived longer than doctors had predicted ); Bill Murphy, Life-and-Death Matter Goes to Court, HOUS. CHRON., Mar. 18, 2001, at 37A (reporting that relatives opposed to removing life support don t share the conclusion that his condition is hopeless ). Cf. In re Guardianship of Schiavo, 851 So.2d 182, 186 (Fla. Dist. Ct. App. 2003) ( [W]e understand why a parent... would hold out hope.... If Mrs. Schiavo were our own daughter, we could not but hold to such a faith. ). 94. Lucas S. Zier et al., Surrogate Decision Makers Responses to Physicians Predictions of Medical Futility, 136 CHEST 110, 114 (2009). 95. Id. 96. Jacobs et al., supra note 55, at 734 (finding that more than sixty percent of the public believe that a person in a PVS state can be saved by a miracle). See, e.g., In re Baby K, 832 F. Supp. 1022, 1026 (E.D. Va. 1993) ( The mother opposes the discontinuation... because she believes that all human life has value... that God will work a miracle.... ); Lee, supra note 8, at 483 (stating religious views that [God] will pull [the patient] through ); Lois M. Collins & Linda Thomson, Boy Focus of Life-Death Battle: Parents Hope for Miracle; Doctors Say He Is Dead, DESERET MORNING NEWS, Oct. 14, 2004, available at news.com/article/ /boy-focus-of-life-death-battle.html (The parents sought an injunction to stop physicians from disconnecting their son from life support even though he was declared dead because they believed he was a small miracle away from recovering. ); Parents Fear Home Delay May Keep Miracle Baby Charlotte in Hospital, BIRMINGHAM POST [UK], Jan. 7, 2006, /is_2006_Jan_7/parents-fear-home-delay-miracle/ai_n /?tag=content;col1 (reporting that the parents of Charlotte Wyatt are committed Christians who believe that miracles do happen ).
341 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 202 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 compelled by religious or cultural traditions. 97 Disputes involving these somotivated surrogates tend to be the most intractable. 98 Fourth, surrogates may feel a sense of responsibility or guilt with respect to their relationship to the patient. 99 They might be too grief stricken to stop treatment. 100 Or they might consistent with the technological imperative in American medicine 101 simply have a sense that the patient is entitled to 97. See, e.g., Rideout v. Hershey Med. Ctr., 30 Pa. D. & C.4th 57, 85 (C.P. Dauphin County 1995) (parents opposed to removing ventilator from daughter because of religious belief that all human life... has value and should be protected ); James Bopp, Jr. & Richard E. Coleson, Child Abuse by Whom? Parental Rights and Judicial Competency Determinations: The Baby K and Baby Terry Cases, 20 OHIO N.U. L. REV. 821, 841 (1994) ( I cannot make that decision to terminate life. God did not give me that power. (quoting Brief of Appellant, In re Achtabowski, No AV (Mich. Cir. Ct. Aug. 12, 1993) (No ), at 39)); Bill Murphy, Comatose Man Dies After Battle over Life Support: Family Cited Spiritual Beliefs, HOUS. CHRON., Mar. 23, 2001, at 29A, available at CDA/archives/archive.mpl?id=2001_ (reporting that family was spiritually and culturally opposed to removing life support ); John Carvel, Muslim Family Lose Right-to-Life Appeal, GUARDIAN, Sept. 2, 2005, uknews (noting the family s religious conviction ); Lee, supra note 8, at 483 (suggesting that some surrogates respond that nobody should be making decisions for God ); Emily Ramshaw, Children Try to Keep Their Mother Alive, DALLAS MORNING NEWS, Aug. 18, 2006, at 1B ( Ruthie Webster[] is deeply religious and believes only God should give and take life. ); Benjamin Weiser, supra note 74 (discussing the religious views of Baby Rena s father). 98. Zier et al., supra note 94, at Hoffman, supra note 76, at F1 ( Families often believe that consenting to a DNR order implies they are giving up on their loved one, signing a death warrant. ); Lee, supra note 8, at 483 (citing a possible response to a physician s call for an end to futile care as, I m not sure I can live with myself for the rest of my life if I let you pull the tube on him ); Paris et al., supra note 68, at ; Arthur U. Rivin, Futile Care Policy: Lessons Learned from Three Years Experience in a Community Hospital, 166 W. J. MED. 389, 392 tbl.1 (1997) (identifying [s]ense of heavy responsibility or guilt as reason why family surrogates want continued futile care); Ann Wlazelek, Pendulum Swings in Life-Saving Efforts: Hospitals Policies on Doing All They Can to Keep Patients Alive Have Changed, MORNING CALL, June 13, 2004, ( It s dangerous to give the family the last word since guilt and a desire to do everything for mom or pop makes it emotionally impossible to stop any treatment. (quoting Arthur Caplan)) Rivin, supra note 99, at 392 tbl.1. See, e.g., Capron, supra note 64, at (reporting that Massachusetts General wrote a unilateral DNR because the family s unpreparedness for their mother s death did not justify mistreating the patient ); Ezekiel J. Emanuel & Linda L. Emanuel, Proxy Decision Making for Incompetent Patients: An Ethical and Empirical Analysis, 267 JAMA 2067, (1992) (discussing how surrogates face psychological stress when deciding to terminate life-sustaining treatments for loved ones) The mindset is that because we can use a given technology, we should use that technology. See generally VICTOR R. FUCHS, WHO SHALL LIVE? HEALTH, ECONOMICS, AND SOCIAL CHOICE (1974) (discussing how the technological imperative might be a contributing factor to rising health care costs); Kathy L. Cerminara, Dealing with Dying: How Insurers Can Help Patients Seeking Last-Chance Therapies (Even When the Answer Is No ), 15 HEALTH MATRIX 285, 296 (2005) (commenting on the technological imperative in American
342 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 203 everything. 102 Whatever the reason, more and more surrogates want their health care providers to do everything. 103 B. Prevalence of Futility Disputes A leading health law treatise predicts that medical futility disputes are likely to occupy as much, if not more [time and] judicial effort in the coming years as conventional end-of-life cases have in the last three decades. 104 And the numbers are beginning to bear this out. 105 Nearly medicine); Robert L. Fine, The History of Institutional Ethics at Baylor University Medical Center, 17 BAYLOR U. MED. CTR. PROC. 73, (2004) (stating the position taken by those who believe in the technological imperative) See, e.g., Arthur E. Kopelman, Understanding, Avoiding, and Resolving End-of-Life Conflicts in the NICU, 73 MOUNT SINAI J. MED. 580, 582, 584 (2006) (discussing the patient perspective that every life has great value and should be saved ); Alan Meisel, The Role of Litigation in End of Life Care: A Reappraisal, HASTINGS CENTER REP., Nov.-Dec. 2005, at S47, S49 ( A vocal proportion of the population... believes that life per se is a pearl beyond price and must be preserved at all costs... This set of beliefs [is] known as vitalism.... ); Rivin, supra note 99, at 392 tbl.2 (explaining that some doctors view themselves as clinical warriors fighting death); James J. Walter, Medical Futility An Ethical Issue for Clinicians and Patients, PRACTICAL BIOETHICS, Summer 2005, at 1, 1 ( The distraught family is at the bedside, demanding that everything be done to save their mother s life. ). Particularly where LSMT is covered by insurance, it is easy for surrogates to insist on continued treatment. All the costs (economic, emotional, etc.) are externalities. The insurer (through other policyholders) pays. Health care providers, particularly nurses, bear the emotional burden of treating the patient. Cf. Robert M. Taylor & John D. Lantos, The Politics of Medical Futility, 11 ISSUES L. & MED. 3, 9 (1995) (discussing the burden to medical professionals and to the other members of the insurance pool ). See also Todd Ackerman, St. Luke s Postpones Removal of Life Support, HOUS. CHRON., Mar. 12, 2005, at B1 ( [T]he family understands there is no hope... [but] the decision when life support is removed should be ours, not a corporation s. ) See News Release, Pew Res. Ctr. People & Press, More Americans Discussing and Planning End-of-Life Treatment: Strong Public Support for Right to Die (January 5, 2006) (reporting that between 1990 and 2005, the percent of Americans who wanted a doctor to do everything increased from fifteen percent to twenty-two percent). See also Sneider, supra note 92 ( [M]ore families are challenging doctors who believe additional medical treatment of a critically ill patient is unwarranted. ) RIGHT TO DIE, supra note 4, at 13.01[D] See, e.g., Belluck, supra note 86, at Al ( The most common case that comes before the ethics committees... are families now insisting on treatment that the doctors believe is unwarranted. (quoting Dr. John J. Paris)); Ron Hamel, A Critical Juncture: Surveys of Ethicists and Mission Leaders Indicate Concerns About the Future of Ethics in the Catholic Health Ministry, HEALTH PROGRESS, Mar.-Apr. 2009, at 12, 17 ( The most frequently mentioned issues... were end-of-life care and futile treatment. ); John M. Luce & Douglas B. White, The Pressure to Withhold or Withdraw Life-Sustaining Therapy from Critically Ill Patients in the United States, 175 AM. J. RESPIRATORY & CRITICAL CARE MED. 1104, 1107 (2007) ( [D]isagreements between families and clinicians on end-of-life care are commonplace in the United States. ); Renie Schapiro, Power of Attorney Won t Solve All Issues at End of Life, MILWAUKEE J.-SENTINEL, May 19, 2008, at 2G ( This scenario is a composite of cases... that
343 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 204 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 one-third of ICU patients had conflicts associated with their care. 106 One recent study identified 974 futility disputes in sixteen hospitals over an average four-year period. 107 Futility disputes are regularly identified as the single biggest ethical dilemma facing North American hospitals. 108 They now constitute the number one ethical challenge among the public in health care. 109 The debate over who decides when continued LSMT is inappropriate is one of the most important and contentious in medical ethics. 110 It has become a pressing issue of our times, whether we like it or not! 111 C. Most Futility Disputes Are Resolved Collaboratively While Alberta s Isaiah May case ended up in court, most futility disputes are resolved internally and informally by the health care team. Allowing surrogates enough time is critically important to help them understand the situation and to let them assimilate with what is happening. 112 After the team discusses the patient s goals for treatment, the nature of the patient s condition, and the range of options, most surrogates eventually come to agree with the team s recommendation. For example, in a multi-center study by Prendergast and colleagues, fifty-seven percent of surrogates agreed immediately with a providerrecommended care-plan, and ninety percent moved toward agreement within five days. 113 In a more recent study, Garros and colleagues found that consensus was reached in fifty-one percent of cases at the first meeting, in sixty-nine percent of cases after a second meeting, and ninety-seven regularly occur in hospitals and other health care facilities. ); Keith M. Swetz et al., Report of 255 Clinical Ethics Consultations and Review of the Literature, 82 MAYO CLINIC PROC. 686, 688 (2007) (finding that futility disputes are one of the primary reasons for hospital ethics consultations) Nathalie Danjoux Meth et al., Conflicts in the ICU: Perspectives of Administrators and Clinicians, 35 INTENSIVE CARE MED. 2068, 2069 (2009) Emily Ramshaw, Bills Challenge Limits for Terminal Patients: Some Say 10 Days to Transfer Isn t Enough Before Treatment Ends, DALLAS MORNING NEWS, Feb. 15, 2007, at 1A See Reuters, Death and Dying: When Is It Time to Let Go?, CNN.COM, July 31, 2007, Jonathan M. Breslin et al., Top 10 Health Care Ethics Challenges Facing the Public: Views of Toronto Bioethicists, 6 BMC MED. ETHICS tbl.1 (2005) Steven H. Miles, Medical Futility, 20 L. MED. & HEALTH CARE 310, 310 (1992) AYUL M. ZAMIR, INTERN BETH 157 (2006) A. A. Eduard Verhagen et al., Conflicts About End-of-Life Decisions in NICUs in the Netherlands, 124 PEDIATRICS e112, e117 (2009) Thomas J. Prendergast, Resolving Conflicts Surrounding End-of-Life Care, 5 NEW HORIZONS 62, 67 (1997).
344 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 205 percent of cases after a third meeting. 114 In an even broader study of nearly 3,000 disputes, consensus was reached in all but sixty-five. 115 In short, futility disputes are usually resolved collaboratively by the treatment team and the family. 116 Even when not settled there, multidisciplinary ethics consultation helps families accept treatment limitation in nearly ninety percent of cases. 117 The focus of this article is on the remaining intractable disputes: How to proceed when impasse persists remains an unsettled controversy. 118 But first, we must more closely examine a key party to such disputes, the patient s surrogate decision maker. II. THE ROLE OF SURROGATES Patient autonomy is valued so highly in the United States that the patient does not lose the right of self-determination when she loses the capacity to make healthcare decisions for herself. Our individualistic consensus places such a strong emphasis on the value of the patient that medical decisions should continue to be guided by that voice as much as possible, even when the patient has lost decision-making capacity. 119 A key method by which the patient can preserve her autonomy is by designating another person to direct the course of her medical treatment upon her incapacity. 120 For the sake of clarity and economy, I refer to this substitute decision maker as a surrogate. 121 In fact, there are three different types of surrogates. In this Section, I first describe these three basic types. I then explain the decision-making standards and criteria that these surrogates must employ when making healthcare decisions on behalf of incapacitated patients See Daniel Garros et al., Circumstances Surrounding End of Life in a Pediatric Intensive Care Unit, 112 PEDIATRICS e371, e373 (2003) Robert L. Fine, Point: The Texas Advance Directives Act Effectively and Ethically Resolves Disputes About Medical Futility, 136 CHEST 963, 963, 967 (2009) ( [B]asic clinical ethics consultation alone... brought closure to... 86% of explicit futility cases. ) Robert L. Fine, Correspondence, Tackling Medical Futility in Texas, 357 NEW ENG. J. MED. 1558, 1558 (2007) (responding to an article of the same name authored by Prof. Truog) Fine, supra note 115, at Mark D. Siegel, End-of-Life Decision Making in the ICU, 30 CLINICS CHEST MED. 181, 189 (2009) Bruce Jennings, Ethical Dilemmas in Surrogate Decision Making, in LIVING WITH GRIEF: ETHICAL DILEMMAS AT THE END OF LIFE 157, 158 (Kenneth J. Doka et al. eds., 2005) See generally William M. Lamers, Jr., Autonomy, Consent, and Advance Directives, in LIVING WITH GRIEF: ETHICAL DILEMMAS AT THE END OF LIFE 106, , 117 (Kenneth J. Doka et al. eds., 2005) (explaining the concept of autonomy and the use of advance directives) See RIGHT TO DIE, supra note 4, at 3.02[B].
345 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 206 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 A. Types of Surrogates There are three basic types of surrogates, corresponding to the three basic ways through which surrogates get their decision-making authority. 122 First, the patient herself can designate her surrogate in an advance directive. This type of agent is normally referred to as an agent or attorney-infact. 123 Second, the court can appoint a surrogate. This type of surrogate is normally referred to as a guardian or conservator. 124 Third, if neither of these is available, the healthcare provider can designate a surrogate pursuant to rules for default decision makers. This type of surrogate is normally referred to as a surrogate or proxy Patient-Designated Surrogates: Agents and Attorneys-in-Fact Every state legislature has established a decision-making process that allows competent patients to appoint an agent to decide about healthcare in the event that they become unable to decide for themselves. 126 This appointment can be made through a simple form typically referred to as an advance directive or durable power of attorney for healthcare. 127 Furthermore, even if a patient has not undertaken the execution formalities to appoint an agent, they can often designate a surrogate, even orally. 128 Such a designation is made directly by the patient to healthcare providers, letting them know whom the patient wants to speak on her behalf See generally id. at (outlining the jurisprudence of selecting surrogate decision makers) Id. at 7.01[B][5] Id. at 3.04[C], 7.01[B][6] Id., at 7.01[B][6]. Sometimes no surrogate is reasonably available. Such a case is not really a futility dispute because not only does no one challenge the provider, but also the provider is the authorized decision-maker in many jurisdictions. See, e.g., TENN. CODE ANN (c)(5) (2006) (providing the authority for a physician to become the decisionmaker for a patient if no eligible surrogate is available). Cf. Sumeeta Varma & David Wendler, Medical Decision Making for Patients Without Surrogates, 167 ARCHIVES INTERNAL MED. 1711, (2007) (discussing the challenges presented by patients without surrogates); Douglas B. White et al., Life Support for Patients Without a Surrogate Decision Maker: Who Decides?, 147 ANNALS INTERNAL MED. 34, (2007) (documenting the difficulty and frequency of life support decisions made for patients without surrogates). See also BLACK S LAW DICTIONARY 1346 (9th ed. 2009) (defining proxy ) See generally RIGHT TO DIE, supra note 4, at 7.01[A], 7.13 tbl Id. at 7.01 [A]-[B] Id. at 7.03[B][2]. See, e.g., TENN. CODE ANN (a) (2006) See, e.g., ALASKA STAT (2008); CAL. PROB. CODE 4711, 4714 (West 2009); DEL. CODE ANN. Health & Safety 16, 2507 (2003); HAW. REV. STAT. ANN. 327E-5 (LexisNexis 2008); MISS. CODE ANN (2005). See generally CHARLES P. SABATINO, U.S. DEP T HEALTH & HUMAN SERVS., ADVANCE DIRECTIVES AND ADVANCE CARE PLANNING: LEGAL AND POLICY ISSUES 22 (2007),
346 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 207 Upon a determination that the patient has lost capacity, the agent typically has the right to make all healthcare decisions that the patient could have made for herself, unless the patient has explicitly limited the agent s authority. 130 And providers must comply with the healthcare decisions made in good faith by an agent to the same extent that they must comply with decisions made by the patient herself Physician-Designated Surrogates: Default Surrogates and Proxies If the patient has neither appointed an agent nor designated a surrogate, or if none is reasonably available at the time a decision must be made, then the healthcare provider can designate a surrogate. 132 The provider makes the designation on the patient s behalf pursuant to default surrogate statutes in almost every state. 133 These statutes specify a priority list of individuals whom the physician should or must designate. 134 Typically, at the top of this hierarchy are the patient s spouse, adult child, parent, and adult sibling. 135 These relatives are likely not only to know the convictions and beliefs of the patient but also to be concerned for the reports/2007/adacplpi.pdf (discussing oral instructional directives and oral designation of surrogates) See RIGHT TO DIE, supra note 4, at 7.01[B][4] AM. MED. ASS N, COUNCIL ON ETHICAL AND JUDICIAL AFF., CODE OF MEDICAL ETHICS OF THE AMERICAN MEDICAL ASSOCIATION 252 (2008) [hereinafter AMA CODE OF ETHICS] ( Physicians should recognize the proxy or surrogate as an extension of the patient, entitled to the same respect as the competent patient. ) This type of surrogate is sometimes referred to as a proxy. See, e.g., FLA. STAT. ANN (West 2005) New York (until June 2010) and Missouri currently lack effective mechanisms for physician-designation of surrogates. Thaddeus Mason Pope, Legal Briefing: Advance Care Planning, 20 J. CLINICAL ETHICS 362, (2009); Susan E. Hickman et al., The POLST (Physician Orders for Life-Sustaining Treatment) Paradigm to Improve End-of-Life Care: Potential State Legal Barriers to Implementation, 36 J.L. MED. & ETHICS 119, 126 (2008) Sometimes the list is not prioritized, in which case the surrogate can be selected from anyone anywhere on the list. See, e.g., COLO. REV. STAT (2009); MICH. COMP. LAWS ANN (West 2009); TENN. CODE ANN (c) (2008); N.D. CENT. CODE (2002) Hickman et al., supra note 133, at 122. Sometimes the surrogates of a certain class are evenly divided, such that a court-appointed guardian may need to make the decision. This happened in the case of Jason Childress, whose parents could not agree whether to consent to the University of Virginia s removal of life support. See Va. Law. Wkly., A Family Divided Leaves Life-or-Death Decision to Man s Guardian, VA. LAW. WKLY., Sept. 8, 2003, available at death-decision-to-mans-guardian/. Such situations are outside the scope of this article.
347 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 208 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 patient. Since most patients do not engage in adequate advance care planning, default surrogates are the most numerous type of surrogate Court-Designated Surrogates: Guardians and Conservators The final way in which a person can become a substitute decision maker for a patient is to get appointed by a court. For patients without capacity, it is sometimes necessary to petition a court to appoint a guardian or conservator. The petition is usually filed by a relative or by the administrator of a long-term care facility where the patient resides. 137 After the appointment, the court supervises the guardian s choices on behalf of the patient, to ensure that the patient is getting appropriate medical care. 138 Because this process can be cumbersome and expensive, comparatively few surrogates are guardians. 139 B. Duties of Surrogates Whether patient-, physician-, or court-designated, a surrogate is an extension of the patient. 140 The surrogate stands in the shoes of the patient. Accordingly, the surrogate must make the medical choice that the patient, if competent, would have made and not one that the surrogate might make for himself or herself The surrogate is obligated to suppress his or her own judgment in favor of channeling what the [patient] would have done. 142 A well-respected how-to guide for surrogates advises 136. Alan Meisel & Bruce Jennings, Ethics, End-of-Life Care, and the Law: Overview, in LIVING WITH GRIEF: ETHICAL DILEMMAS AT THE END OF LIFE 72 (Kenneth J. Doka et al. eds., 2005) Kris Bulcroft et al., Elderly Wards and Their Legal Guardians: Analysis of County Probate Records in Ohio and Washington, 31 GERONTOLOGIST 156, 157 (1991). See generally PETER J. BUTTARO, LEGAL GUIDE FOR LONG-TERM CARE ADMINISTRATORS (Emily L.H. Buttaro ed., 1999) See Naomi Karp & Erica F. Wood, Guardianship Monitoring: A National Survey of Court Practices, 37 STETSON L. REV. 143, 146 (2007) (noting that court monitoring of guardians is required to ensure the welfare of incapacitated persons.... ) See Meisel & Jennings, supra note 136, at AMA CODE OF ETHICS, supra note 131, at In re Guardianship of Browning, 568 So. 2d 4, 13 (Fla. 1990). See also Lawrence A. Frolik, Is a Guardian the Alter Ego of the Ward?, 37 STETSON L. REV. 53, 63 ( [T]he law favors... doing what the ward would have done. ); id. at 65 ( [I]f the guardian is expected to act as the ward would have acted but for the incapacity, then the guardian is essentially the agent of the ward.... ); id. at 67 ( [T]he substituted-judgment doctrine is the overwhelming choice.... ) Frolik, supra note 141, at 65. See also RESTATEMENT (THIRD) OF AGENCY 8.01 cmt. b (2005) ( [T]he general fiduciary principle requires that the agent subordinate the agent s interests to those of the principal and place the principal s interests first.... ); In re Martin,
348 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 209 them to decide as the patient would, even if the decision goes against the way you would decide for yourself. 143 The standards for surrogate decision-making are basically the same for all three types of surrogates. 144 These standards are usually specified in state statutes, and there is substantial uniformity across the country. 145 There is generally a three-step hierarchy. 146 Surrogates should apply these standards sequentially in the order given: [1] expressed wishes, [2] substituted judgment, and then [3] best interest Subjective Standard: Implement the Patient s Instructions Sometimes, before losing capacity, the patient might have spoken directly to the issue of life-sustaining treatment, expressing a very clear preference for or against it in certain circumstances. Such instructions are normally memorialized in an advance directive or a living will. 148 In such cases, the advance directive becomes a self-initiating consent 538 N.W.2d 399, 408 (Mich. 1995) ( [T]he right the surrogate is seeking to effectuate is the incompetent patient s right to control his own life.... ) AM. BAR. ASS N COMM N ON LAW & AGING, MAKING MEDICAL DECISIONS FOR SOMEONE ELSE: A HOW-TO GUIDE 4 (2009), available at guide2009.pdf (emphasis added). See also Jennings, supra note 119, at 163 ( The surrogate is expressly forbidden to make the decision based on what the surrogate would want done. Surrogates must not project their own hopes, fears, emotions, expectations or beliefs onto the patient. ) See Frolik, supra note 141, at 85 ( [T]here is no defensible reason to apply different requirements to proxies whose authority arises from judicial appointment, statutory designation, or having been named by the principal. ); CLAIRE C. OBADE, PATIENT CARE DECISION-MAKING: A LEGAL GUIDE FOR PROVIDERS 11:9 (Thomson/West 2008) (explaining various methods for surrogate decision-making) See, e.g., WIS. STAT (5) ( ) ( The health care agent shall act in good faith consistently with the desires of the principal... In the absence of a specific directive by the principal or if the principal s desires are unknown, the health care agent shall, in good faith, act in the best interests of the principal in exercising his or her authority. ) RIGHT TO DIE, supra note 4, at 4.01[B] James L. Bernat, Ethical Issues in the Treatment of Severe Brain Injury: The Impact of New Technologies, ANNALS N.Y. ACAD. SCI., Mar. 2009, at 117, 123. Admittedly, the de facto standard is agreement. See RIGHT TO DIE, supra note 4, at There may indeed be a chasm between the statutorily specified standards and those that are applied at the bedside. See, e.g., Berger et al., Surrogate Decision Making: Reconciling Ethical Theory and Clinical Practice, 149 ANNALS INTERNAL MED. 48, 48 (2008). But it is outside the scope of this article to evaluate or analyze the merits of the decision-making standards. The mission of this article is to examine how and to what extent those standards can be used to resolve futility disputes Usually these are written and witnessed documents that follow the IF... THEN... format, where the IF refers to a hypothetical mental or physical condition and the THEN indicates the person s wishes regarding treatment and care. See Meisel & Jennings, supra note 136, at 76.
349 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 210 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 document. 149 Where such formal documentation is available, the surrogate s role is no longer that of decision maker, so much as that of reporter or enforcer of the patient s preferences. 150 The surrogate is charged merely with implementing what the patient has already actually decided. 151 In such situations, the surrogate s discretion is normally constrained by the patient s written instructions. 152 Massachusetts law, for example, provides: An agent shall have the authority to make any and all health care decisions on the principal s behalf that the principal could make, including decisions about life-sustaining treatment, subject, however, to any express limitations in the health care proxy. 153 The agent, after all, is only a second-best means to protecting patient autonomy. Almost always preferable is subjective first-hand evidence, evidence of the patient s very own decisions about her healthcare treatment Substituted Judgment: Implement the Patient s Preferences While theoretically the most straightforward standard, the circumstances rarely provide for application of the subjective standard. First, few patients have left specific treatment instructions. 155 Second, even when patients have 149. Casey Frank, Surrogate Decision-Making for Friendless Patients, COLO. LAW., Apr. 2005, at 71, Braun et al., supra note 69, at See generally RIGHT TO DIE, supra note 4, at 4.05 [A] (noting that under the subjective standard, the surrogate makes any decisions regarding forgoing life-sustaining treatment based on instructions the patient actually gave before losing decisionmaking ability); ALA. CODE 22-8A-6 (2006) ( An individual designated to make decisions regarding the providing, withholding, or withdrawing of life-sustaining treatment... for another... shall make those decisions according to the specific instructions or directions given to him or her in the designation or other document or by the individual making the designation. ) This is true unless the patient specifically granted otherwise. See infra notes 432 to 433 and accompanying text. See also RIGHT TO DIE, supra note 4, at 4.05 [B] (noting that the subjective standard gives no credence to speculation on the surrogate s behalf, but rather requires actual knowledge of the patient s wishes) MASS. ANN. LAWS ch. 201D 5 (LexisNexis 2009) (emphasis added) See, e.g., In re Estate of Longeway, 549 N.E.2d 292, 299 (Ill. 1989) ( [T]he surrogate first tries to determine if the patient had expressed explicit intent regarding this type of medical treatment.... ) SABATINO, supra note 129, at See News Release, Am. Bar Ass n, ABA- Commissioned Poll Finds More than Twice as Many Americans Talk About Planning For Healthcare Emergencies than Take Action (May 14, 2008), available at net.org/abanet/media/release/news_release.cfm?releaseid=345 (stating that less than thirty percent of Americans have advance directives); Honoring Final Wishes: How to Respect [Americans ] Choices at the End of Life: Hearing Before the S. Comm. on Aging, 110th Cong. 3 (2008) (statement of Sen. Sheldon Whitehouse) ( Even among terminally ill patients fewer than 50 percent have an advanced directive in their medical record. ).
350 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 211 memorialized written instructions, they are often unavailable at the time a decision must be made. 156 Third, even when instructions are available, they often fail to address the situation at hand. 157 Consequently, surrogates usually must instead apply the substituted judgment standard. Without express, specific instructions to guide them, surrogates must engage in some speculation and infer the patient s wishes from her prior statements and conduct. 158 In short, [w]hen there is evidence of the patient s preferences and values, [then] decisions concerning the patient s care should be made by substituted judgment. 159 In describing the substituted judgment standard, the AMA Code of Medical Ethics states: 156. Not only has a minority of the population completed advance directives, but also most advance directives in that subset are ineffective because either their existence or location is unknown. See statement of Sen. Whitehouse, supra note 155 ( [R]oughly 70 percent of physicians whose patients have advance directives do not know about them. ) As discussed below, this is demanding because it requires that the instructions (1) be directed at the treatment in question, (2) be clear and unequivocal, (3) concern the patient s own situation, (4) be solemn circumstances. RIGHT TO DIE, supra note 4, at 4.06[A]. Furthermore, even if the advance directive were available and clearly addressed the situation at hand, it might not reflect the patient s preferences. See, e.g., Henry S. Perkins, Controlling Death: The False Promise of Advance Directives, 147 ANNALS INTERNAL MED. 51, 53 (2007) (discussing that patient preferences often are compromised by poor proxy interpretation or from non-compliance with the advance directive by physicians). It is difficult for patients to anticipate their future preferences under new and different medical conditions. Therefore, instructional advance directives often fail to capture important preferences and priorities of patients. Consequently, clinical care may not be consistent with patient preferences. See, e.g., Angela Fagerlin & Carl E. Schneider, Enough: The Failure of the Living Will, HASTINGS CENTER REP., Mar.-Apr. 2004, at 30, 38-39; Daniel P. Hickey, The Disutility of Advance Directives: We Know the Problems, but Are There Solutions?, 36 J. HEALTH L. 455, (2003) (discussing the difficulties involved with completing advance directives); NICHOLAS A. CHRISTAKIS, DEATH FORETOLD: PROPHECY AND PROGNOSIS IN MEDICAL CARE 55 (1999) (explaining that advance directives involve a sort of hypothetical prognosis ). On the other hand, better informed consent tools appear able to address some of these problems. See also Angelo E. Volandes et al., Using Video Images to Improve the Accuracy of Surrogate Decision- Making: A Randomized Controlled Trial, 10 J. AM. MED. DIRECTORS ASS N 575, 578 (2009) (Surrogates receiving video decision support tool after verbal narrative made significantly better predications of what their loved ones would have wanted in an advanced dementia situation than those receiving only a verbal narrative.); Angelo E. Volandes et al., Overcoming Educational Barriers for Advance Care Planning in Latinos with Video Images, 11 J. PALLIATIVE MED. 700, 701 (2008) (studying the use of video images for improving advance care planning among Latinos) See RIGHT TO DIE, supra note 4, at 4.02[A]; In re Estate of Longeway, 549 N.E.2d at 299 ( Where no clear intent exists, the patient s personal value system must guide the surrogate.... ) AMA CODE OF ETHICS, supra note 131, at 252.
351 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 212 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 This entails considering the patient s advance directive (if any), the patient s views about life and how it should be lived, how the patient has constructed his or her identity or life story, and the patient s attitudes towards sickness, suffering, and certain medical procedures. 160 Alabama law similarly provides: The surrogate shall consult with the attending physician and make decisions permitted herein that conform as closely as possible to what the patient would have done or intended under the circumstances, taking into account any evidence of the patient s religious, spiritual, personal, philosophical, and moral beliefs and ethics, to the extent these are known to the surrogate. Where possible, the surrogate shall consider how the patient would have weighed the burdens and benefits of initiating or continuing life-sustaining treatment... against the burdens and benefits to the patient of that treatment The law in other states is substantially similar. 162 Massachusetts, for example, provides: [T]he agent shall make health care decisions...in accordance with the agent s assessment of the principal s wishes, including the principal s religious and moral beliefs Best Interests Standard: Promote the Patient s Welfare Sometimes, there is no reliable evidence of either the patient s expressed wishes or her values and preferences. In such cases, neither the subjective nor the substituted judgment standard can be applied. Therefore, the surrogate must shift her focus from the autonomy of the patient to the welfare of the patient. 164 In the absence of patient-centric evidence, the surrogate must rely on more objective grounds. 165 This decision-making 160. Id. If the advance directive specifically addresses the treatment at issue, then the surrogate would apply the subjective standard. But since advance directives are often not that clearly applicable, they often provide broad guidance rather than specific answers. Id. See also id. at 83 ( In making a substituted judgment, decision makers may consider the patient s advance directive (if any); the patient s values about life and the way it should be lived; and the patient s attitudes towards sickness, suffering, medical procedures, and death. ) ALA. CODE 22-8A-11(c) (2006); see also id. 22-8A See, e.g., MD. CODE ANN., Health-Gen (c)(1) (LexisNexis 2009); In re Westchester Cnty. Med. Ctr., 531 N.E.2d 607, 619 (N.Y. 1988) ( [W]hen implementing substituted judgment... a surrogate... effectuates as nearly as possible the decision the incompetent would make if he or she were able to state it. ) (internal citations omitted) MASS. ANN. LAWS ch. 201D 5 (LexisNexis 2009) See, e.g., FLA. STAT (1)(b) (2009) ( If there is no indication of what the principal would have chosen, the surrogate may consider the patient s best interest.... ); MD. CODE ANN., Health-Gen (c)(1) (LexisNexis 2009) ( [I]f the wishes of the patient are unknown or unclear, [base decisions] on the patient s best interest. ) RIGHT TO DIE, supra note 4, at 4.07[B].
352 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 213 criterion is referred to as the best interest standard. 166 The Code of Medical Ethics provides: If there is no reasonable basis on which to interpret how a patient would have decided, the decision should be based on the best interests of the patient, or the outcome that would best promote the patient s well-being. 167 The law across the United States is substantially similar. Massachusetts, for example, provides: [I]f the principal s wishes are unknown... the agent shall make health care decisions... in accordance with the agent s assessment of the principal s best interests. 168 For example, even if we know little or nothing about what life-sustaining treatment a particular patient might have desired, we can still determine what the hypothetical reasonable person would want. Few individuals would want to be kept alive only to suffer from their underlying illness, especially where the treatment caused pain, side effects, indignity, embarrassment, frustration, and/or emotional suffering. 169 The Code of Medical Ethics more fully articulates the best interest standard: Factors that should be considered when weighing the harms and benefits of various treatment options include the pain and suffering associated with treatment, the degree of and potential for benefit, and any impairments that may result from treatment. 170 Other factors a surrogate might consider include: (1) [the patient s] physical, sensory, emotional, and cognitive functioning; (2) the quality of life, life expectancy and prognosis for recovery with and without treatment; (3) the various treatment options... (9) the degree of humiliation, dependence, and loss of dignity resulting from the condition and treatment In the futility context, [a] patient s preservable existence 166. Id AMA CODE OF ETHICS, supra note 131, at 252 (emphasis added). See also id. at 83 ( If there is not adequate evidence of the incompetent patient s preferences and values, the decision should be based on the best interests of the patient (what outcome would most likely promote the patient s well-being). ) MASS. ANN. LAWS ch. 201D 5 (LexisNexis 2009) (also requiring full consideration of acceptable medical alternatives ) See Woods v. Commonwealth of Ky., 142 S.W.3d 24, 35 (Ky. 2004) (discussing the factors that a court should consider when determining whether to withdraw life-sustaining treatment for an incapacitated person) AMA CODE OF ETHICS, supra note 131, at 252; see also Frolik, supra note 141, at 71 ( The best-interests standard is in effect a signal of best practices. ) See Woods, 142 S.W.3d at 35 (Ky. 2004). In a surprising application of the best interest test, the Kentucky Court of Appeals upheld the lower court s ruling that it was in a patient s best interest to donate a kidney to his brother because the patient was emotionally and psychologically dependent on him. Strunk v. Strunk, 445 S.W.2d 145, 146, 149 (Ky. Ct. App. 1969).
353 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 214 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 might be so tortuous, painful, or filled with suffering that it would be deemed inhumane for a surrogate to dictate continued medical intervention. 172 Even permanent unconsciousness is increasingly broadly recognized as a status in which a patient can derive zero benefit from continued LSMT. 173 Notably, the Code specifically anticipates that surrogates might be guided by irrelevant concerns. It cautions: One way to ensure that a decision using the best interest standard is not inappropriately influenced by the surrogate s own values is to determine the course of treatment that most reasonable persons would choose for themselves in similar circumstances. 174 III. UNFAITHFUL SURROGATES SHOULD BE REPLACED While the use of surrogates is a key vehicle for promoting and protecting patients prospective autonomy, surrogates are not always diligent and faithful agents. 175 Surrogates are frequently inaccurate in implementing patient preferences. Sometimes, they misinterpret or misapply the patient s instructions or wishes. Other times, they deliberately ignore patient instructions and preferences. Whether culpable or not, these unfaithful surrogates are violating the required decision-making standards. And they should be replaced Norman L. Cantor, Can Healthcare Providers Obtain Judicial Intervention Against Surrogates Who Demand Medically Inappropriate Life Support for Incompetent Patients?, 24 CRITICAL CARE MED. 883, 884 (1996) Id. at AMA CODE OF ETHICS, supra note 131, at 252 (emphasis added). See also JAMES L. BERNAT, ETHICAL ISSUES IN NEUROLOGY 89 (Lippincott Williams & Wilkins 2008) ( The best interest standard... attempts to be objective, [but] remains inherently subjective. ); Frolik, supra note 141, at 61 ( How should the guardian choose... doing what the guardian might think is best based upon the values of the guardian... These can be eliminated as lacking any foundation in law. ); id. at 70 ( [W]e can hardly expect them to ignore their own values, morality, and ethics in favor of what some mythical reasonable person would do. ) See generally Robert S. Olick & Paul W. Armstrong, Health Care Directives, in 15B NEW JERSEY PRACTICE SERIES, LEGAL FORMS 37:29 (4th ed. 2009) ( In practice the health care proxy will not always adequately represent the patient s interests. ) While this Article focuses on defending surrogate selection as an option for resolving some intractable futility disputes, there are other good reasons for surrogate selection. For example, complying with a maverick agent can expose the provider to liability. See, e.g., Scheible v. Joseph L. Morse Geriatric Ctr., 988 So. (2d) 1130, (Fla. Dist. Ct. App. 2008); Kathleen E. Wherthey, Cause of Action to Recover Damages for Health Care Provider s Failure to Comply with Advance Directive, in 16 CAUSES OF ACTION 2d 83, 89 (2008); Holly Fernandez Lynch et al., Compliance with Advance Directives: Wrongful Living and Tort Law Incentives, 29 J. LEGAL MED. 133, 145 (2008) (discussing the case of Edward Winter).
354 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 215 A. Surrogate Performance Is Mediocre Unfortunately, surrogates often perform rather poorly. 177 Either (1) they do not know patient preferences or (2) they do not follow them. 1. Surrogates Do Not Know Patient Preferences Both the subjective standard and substituted judgment standard require that the surrogate make treatment decisions that reflect the patient s preferences and values. But surrogates, unfortunately, are often uninformed or misinformed about what the patient s treatment preferences and values actually are. A number of empirical studies over the past few years confirm that the choices surrogates make for patients are often not the same choices that patients would make for themselves. 178 A recent meta-review of sixteen 177. K.A. Bramstedt, Questioning the Decision-Making Capacity of Surrogates, 33 INTERNAL MED. J. 257, 258 (2003) See id.; Lauren G. Collins et al., The State of Advance Care Planning: One Decade After SUPPORT, 23 AM. J. HOSPICE & PALLIATIVE MED. 378, (2006); Terri R. Fried et al., Valuing the Outcomes of Treatment: Do Patients and Their Caregivers Agree?, 163 ARCHIVES INTERNAL MED. 2073, 2077 (2003); Daniel S. Gardner & Betty J. Kramer, End-of-Life Concerns and Care Preferences: Congruence among Terminally Ill Elders and their Family Caregivers, 60 OMEGA 273 (2010); Sara M. Moorman & Deborah Carr, Spouses Effectiveness as End-of-Life Health Care Surrogates: Accuracy, Uncertainty, and Errors of Overtreatment or Undertreatment, 48 GERONTOLOGIST 811, 818 ( Despite widespread reliance on spouses, our results show that surrogates are accurate in just 62% and 77% of cases, in pain and cognitive impairment scenarios, respectively. ); Rachel A. Pruchno et al., Predictors of Patient Treatment Preferences and Spouse Substituted Judgments: The Case of Dialysis Continuation, 26 MED. DECISION MAKING 112, 119 (2006) (finding inaccurate substituted judgment because patients and surrogates used different criteria in formulating judgments about continuation of life-sustaining treatment and had different perceptions about the patients conditions); William.D. Smucker et al., Modal Preferences Predict Elderly Patients Life-Sustaining Treatment Choices as well as Patients Chosen Surrogates Do, 20 MED. DECISION MAKING 271, 276 (2000). See also RIGHT TO DIE, supra note 4, at 3.16[C][2]; Magali Ciroldi et al., Ability of Family Members to Predict Patient s Consent to Critical Care Research, 33 INTENSIVE CARE MED. 807, 809 (2007); Michael Coppolino & Lynn Ackerson, Do Surrogate Decision Makers Provide Accurate Consent for Intensive Care Research?, 119 CHEST 603, (2001); Nina A. Kohn & Jeremy A. Blumenthal, Designating Health Care Decisionmakers for Patients Without Advance Directives: A Psychological Critique, 42 GA. L. REV. 979, (2008); Anand V. Mantravadi et al., Accuracy of Surrogate Decision Making in Elective Surgery, 33 J. CATARACT & REFRACTIVE SURGERY 2091, 2092 (2007). But see Linus Broström & Mats Johansson, Surrogates Have Not Been Shown to Make Inaccurate Substituted Judgments, 20 J. CLINICAL ETHICS 266, 266 (2009); Mats Johansson & Linus Broström, Counterfactual Reasoning in Surrogate Decision Making Another Look, BIOETHICS (forthcoming 2010); Mats Johansson & Linus Broström, Turning Failures into Successes: A Methodological Shortcoming in Empirical Research on Surrogate Accuracy, 29 THEORETICAL MED. & BIOETHICS 17, 18 (2008) (addressing a methodological shortcoming evident in a significant number of studies on substitute decision-making).
355 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 216 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 studies indicated that, overall, surrogates predict patient s treatment preferences with just sixty-eight percent accuracy. 179 A more recent study found even lower accuracy. 180 Indeed, these are hardly new findings. This same dubious surrogate performance has been repeatedly measured and documented for over two decades. 181 One aspect of these prediction studies is particularly notable for futility disputes. Not only do surrogates make inaccurate substituted judgments, but also that inaccuracy leans predominantly in one direction. Surrogate inaccuracy is strongly biased toward overestimating patient desires for treatment. 182 In other words, a surrogate is more likely to request aggressive 179. David I. Shalowitz et al., The Accuracy of Surrogate Decision Makers: A Systematic Review, 166 ARCHIVES INTERNAL MED. 493, 495 (2006) (Surrogate accuracy in dementia scenarios was only 58%.) Inés Maria Barrio-Cantalejo et al., Advance Directives and Proxies Predictions About Patients Treatment Preferences, 16 NURSING ETHICS 93, 105 (2009) ( The overall ability of the proxies in this study to predict the patients preferences was %.... ) See Ezekiel J. Emanuel & Linda E. Emanuel, Proxy Decision Making for Incompetent Patients: An Ethical and Empirical Analysis, 267 JAMA 2067, 2069 (1992); Muriel Gillick et al., A Patient-Centered Approach to Advance Medical Planning in the Nursing Home, 47 J. AM. GERIATRICS SOC Y 227, 228 (1999); Jan Hare et al., Agreement Between Patients and Their Self-Selected Surrogates on Difficult Medical Decisions, 152 ARCHIVES INTERNAL MED. 1049, 1049, 1052 (1992); Peter M. Layde et al., Surrogates Predictions of Seriously Ill Patients Resuscitation Preferences, 4 ARCHIVES FAM. MED. 518, (1995); Joseph G. Ouslander et al., Health Care Decisions Among Elderly Long-Term Care Residents and Their Potential Proxies, 149 ARCHIVES INTERNAL MED. 1367, (1989); Robert A. Pearlman et al., Spousal Understanding of Patient Quality of Life: Implications for Surrogate Decisions, 3 J. CLINICAL ETHICS 114, 114, 117 (1992); Allison B. Seckler et al., Substituted Judgment: How Accurate Are Proxy Predictions?, 115 ANNALS INTERNAL MED. 92, (1991) (discussing discrepancies between patients end-of-life preferences and proxies substituted judgment decision for patients); Jeremiah Suhl et al., Myth of Substituted Judgment: Surrogate Decision Making Regarding Life Support Is Unreliable, 154 ARCHIVES INTERNAL MED. 90, 93 (1994) (finding patient-surrogate agreement just 59.6% of the time); Daniel P. Sulmasy et al., The Accuracy of Substituted Judgments in Patients with Terminal Diagnoses, 128 ANNALS INTERNAL MED. 621, 623 (1998); Nancy R. Zweibel & Christine K. Cassel, Treatment Choices at the End of Life: A Comparison of Decisions by Older Patients and Their Physician-Selected Proxies, 29 GERONTOLOGIST 615, 616, 618 (1989) See Peter H. Ditto et al., Advance Directives as Acts of Communication: A Randomized Controlled Trial, 161 ARCHIVES INTERNAL MED. 421, 424 (2001); Hare et al., supra note 181, at 1051, 1052 (finding patient-surrogate agreement only seventy percent of the time); Pearlman et al., supra note 181, at 117, 119 tbls. 3 & 4; Shalowitz et al., supra note 179, at 495; Suhl et al., supra note 181, at 93-94; Richard F. Uhlmann et al., Physicians and Spouses Predictions of Elderly Patients Resuscitation Preferences, 43 J. GERONTOLOGY M115, M117 (1988) (finding that spouses overestimated patients preferences for resuscitation decisions, significantly so in some situations). See also SHARON KAUFMAN, AND A TIME TO DIE: HOW HOSPITALS SHAPE THE END OF LIFE (2005); Laraine Winter & Susan M. Parks, Family Discord and Proxy Decision Makers End-of-Life Treatment Decisions, 11 J. PALLIATIVE MED (2008).
356 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 217 life-sustaining treatment for a patient than the patient would for herself. 183 Therefore, in many futility disputes, the treatment that surrogates request, and that providers want to refuse, is treatment that the patient probably does not even want. None of this evidence is surprising given the widely observed failure of patients to discuss end-of-life planning with their prospective surrogates. 184 Patients themselves do not reflect on their end-of-life care, so it is unclear if they have even formed preferences to communicate to surrogates. 185 This is only exacerbated by the fact that patient preferences change over time. 186 In short, surrogates are presumed to be the best substitute decision makers for patients. But the available evidence seems to cast serious doubt on the basis for this presumption. 2. Surrogates Do Not Follow Patient Preferences While surrogate knowledge of patient preferences is a necessary condition, it is hardly a sufficient condition for application of the subjective and substituted judgment standards. Surrogates must also be willing and able to make decisions on the basis of that knowledge. And, on the best interest standard, surrogates must be willing and able to make a decision on the basis of what will best promote the patient s well being. Unfortunately, surrogates are often not up to the challenge. 187 We cannot ignore the 183. Laura Zettel-Watson et al., Actual and Perceived Gender Differences in the Accuracy of Surrogate Decisions About Life-Sustaining Medical Treatment Among Older Spouses, 32 DEATH STUDIES 273, (2008) (Husbands commited significantly more overtreatment errors than did wives acting as surrogates ) See Betty S. Black et al., Surrogate Decision Makers Understanding of Dementia Patients Prior Wishes for End-of-Life Care, 21 J. AGING & HEALTH 627, 629 (2009) (discussing studies finding that patients were reluctant to think about, discuss, or plan for serious future illness ). See also Terri R. Fried et al., Understanding Advance Care Planning as a Process of Health Behavior Change, 57 J. AM. GERIATRICS SOC Y 1547, 1547, 1552 (2009). On the other hand, some evidence suggests that this would not improve the rate of agreement. See Shalowitz, supra note 179, at See generally Louise Harmon, Falling Off the Vine: Legal Fictions and the Doctrine of Substituted Judgment, 100 YALE L.J. 1 (1990) (discussing cases in which patients had not reflected upon or communicated their choices for end-of-life care) See Marion Danis, Stability of Choices about Life-Sustaining Treatments, 120 ANNALS INTERNALS MED. 567 (1994) (showing that 40% of patients who said they wanted life-sustaining treatments, said no to those treatments two years later); Marsha N. Wittink et al., Stability of Preferences for End-of-Life Treatment After 3 Years of Follow-up, 168 ARCHIVES INTERNAL MED. 2125, (2008) (discussing a study where preferences for life-sustaining treatment showed changes over time) David Orentlicher, The Limitations of Legislation, 53 MD. L. REV. 1255, (1994); see also Kohn & Blumenthal, supra note 178, at Physicians exacerbate this by asking surrogates what they want to do. Physicians should instead ask surrogates what the patient would have chosen. Id. at
357 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 218 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 possibility that a surrogate might act contrary to the wishes of the patient. 188 First, surrogates frequently do not understand the clinical status of the patients whom they represent. 189 Less than half, regardless of educational level, had adequate knowledge of what was going on and what would happen [to the patient]. 190 Both for this reason and due to a belief in miracles, nearly ninety percent of surrogates doubt the physician s prognosis. 191 But to accurately apply the patient s wishes or determine best interests, the surrogate must comprehend the clinical information and the consequences of the options presented. Second, many surrogates have clinically diagnosable conditions such as stress, depression, and anxiety. 192 These psychological problems may 188. In re Browning, 568 So. 2d 4, 15 (Fla. 1990) Elizabeth A. Boyd et al., It s Not Just What the Doctor Tells Me Factors that Influence Surrogate Decision Makers Perceptions of Prognosis, 38 Critical Care Med (2010); Susan J. Lee Char et al., A Randomized Trial of Two Methods to Disclosing Prognosis to Surrogate Decision Makers in Intensive Care Units, 182 AM. J. RESPIRATORY & CRITICAL CARE MED. 905, 909 (2010) ( [S]urrogates prognostic estimates were on average more than twice as optimistic as the physician s prognostic estimate. ); Robert M. Rodriguez et al., A Prospective Study of Primary Surrogate Decision Makers Knowledge of Intensive Care, 36 CRITICAL CARE MED. 1633, 1633, 1635 (2008) (finding only fifty percent of surrogates had a good understanding of the patient s care); Margaret L. Rothman et al., The Validity of Proxy Generated Scores as Measures of Patient Health Status, 29 MED. CARE 115 (1991) James W. Jones & Lawrence B. McCullough, Dominions of Surrogate Opinions: Who Is in Charge?, 49 J. VASCULAR SURGERY 249, 249 (2009) Lucas S. Zier et al., Doubt and Belief in Physicians Ability to Prognosticate During Critical Illness: The Perspective of Surrogate Decision Makers, 36 CRITICAL CARE MED. 2341, (2008) See generally Elie Azoulay et al., Risk of Post-Traumatic Stress Symptoms in Family Members of Intensive Care Unit Patients, 171 AM. J. RESPIRATORY & CRITICAL CARE MED. 987, (2005) (finding many family members of critically ill patients experience posttraumatic stress reactions and/or symptoms of anxiety and depression); Lauris C. Kaldijan et al., Dementia Goals of Care and Personhood: A Study of Surrogate Decision Makers Beliefs and Values, AM. J. HOSPICE & PALLIATIVE MED. (forthcoming 2010); Virginia Lemiale et al., Health Related Quality of Life in Family Members of ICU Patients, 13 J. PALLIATIVE MED (2010); Jennifer McAdam et al., Symptom Experiences of Family Members of ICU Patients at High Risk of Dying, 38 CRITICAL CARE MED (2010); Jennifer L. McAdam & Kathleen Puntillo, Symptoms Experienced by Family Members of Patients in Intensive Care Units, 18 AM. J. CRITICAL CARE 200, (2009) (discussing prevalence rates of traumatic stress levels, depression, and anxiety in family members of patients in intensive care); Marie Cécile Poncet et al., Burnout Syndrome in Critical Care Nursing Staff, 175 AM. J. RESPIRATORY & CRITICAL CARE MED. 698, 698, (2007) (discussing how stress can cause burnout syndrome for nurses involved with making end-of-life decisions); Frédéric Pochard et al., Symptoms of Anxiety and Depression in Family Members of Intensive Care Unit Patients Before Discharge or Death: A Prospective Multicenter Study, 20 J. CRITICAL CARE 90, (2005) (discussing prevalence of symptoms of anxiety and depression in family members and spouses of ICU patients); Frédéric Pochard et al., Symptoms of Anxiety and Depression in Family Members of
358 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 219 impair the surrogate s own decision-making capacity. 193 The surrogate may fail to exercise sound and informed judgment, or will find it too difficult to accept personal responsibility for carrying out the patient s wishes. 194 In short, a serious question arises about the surrogate s fitness to serve. 195 Third, surrogates often cannot distinguish their own preferences from those of the patient. 196 There are two leading psychological explanations for this tendency. Surrogates may act on assumed similarity by assuming that she and the patient hold similar preferences and thus allowing her own preferences to guide the decision. 197 Surrogates may also be affected by projection bias, because they have difficulty disregarding their current preferences formed under current circumstances even though they are irrelevant both to the patient and to the patient s condition. 198 Intensive Care Unit Patients: Ethical Hypothesis Regarding Decision-Making Capacity, 29 CRITICAL CARE MED. 1893, 1894, 1896 (2001) (discussing prevalence of symptoms of anxiety and depression, and risk of posttraumatic stress disorder in family members of ICU patients); Mark D. Siegel et al., Psychiatric Illness in the Next of Kin of Patients Who Die in the Intensive Care Unit, 36 CRITICAL CARE MED. 1722, (2008) (discussing how many next of kin of patients in ICU have major depression or other psychiatric illnesses); Erika K. Tross et al., Care Associated with Symptoms of Depression and PTSD among Family Members of those Who Die in the ICU, CHEST (forthcoming 2010); Virginia P. Tilden et al., Family Decision-Making to Withdraw Life-Sustaining Treatments from Hospitalized Patients, 50 NURSING RES. 105, (2001) (discussing stress levels of family members making decisions to withdraw treatments) See RIGHT TO DIE, supra note 4, at See also Prendergast, supra note 113, at (discussing why fiduciaries should intercede in situations where surrogates insist on continued care even when it conflicts with the patient s interests and does not improve the patient s health) Olick & Armstrong, supra note 175, at 37: RIGHT TO DIE, supra note 4, at 3.24[C][2] Moorman & Carr, supra note 178, at 812. See also Yoram Bar-Tal et al., Whose Informational Needs Are Considered? A Comparison Between Cancer Patients and Their Spouses Perceptions of Their Own and Their Partners Knowledge and Informational Needs, 60 SOC. SCI. & MED. 1459, (2005); Collins et al., supra note 178, at 379; Angela Fagerlin et al., Projection in Surrogate Decisions About Life-Sustaining Medical Treatments, 20 HEALTH PSYCH. 166, , 171, 173 (2001); Melissa A. Z. Marks & Hal R. Arkes, Patient and Surrogate Disagreement in End-of-Life Decisions: Can Surrogates Accurately Predict Patients Preferences?, 28 MED. DECISION MAKING 524, 529 (2008) ( [W]hen surrogates must make difficult, end-of-life decisions for a loved one... their wishes for the patient tend to enter into surrogates predictions of patients preferences.... [S]urrogates often are unable to discriminate between what they want for the patient and what the patient would want for himself or herself. ); Rachel A. Pruchno et al., Spouse as Health Care Proxy for Dialysis Patients: Whose Preferences Matter?, 45 GERONTOLOGIST 812, (2005); Rebecca Sudore & Terri R. Fried, Redefining the Planning in Advance Care Planning: Preparing for End-of-Life Decision Making, 153 ANNALS INTERNAL MED. 256, 256 (2010) ( Surrogates may use their own hopes, desires, and needs to inform their decisions. ) (collecting cites) Sara M. Moorman et al., Do Older Adults Know Their Spouses End-of-Life Treatment Preferences?, 31 RES. ON AGING 463, 466 (2009) Id. at , 482.
359 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 220 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 Fourth, surrogates may base their decisions on factors external to the patient. 199 They may have dubious motives in that they are looking out for their own interests rather than the patient s interests. 200 Some surrogates make decisions to avoid the guilt from making a death-hastening decision or to avoid criticism from other family members as having made the decision. 201 Other surrogates make deliberately and intentionally selfish decisions This non-patient focus obtains outside the futility context, for example, where surrogates make decisions: (i) to involve the patient in experimental treatment that holds no benefit to the patient, (ii) to donate the patient s organs, or (iii) to harvest the patient s gamete material where there is no evidence that the patient planned to procreate. While sometimes permissible, such decisions are presumptively disallowed. See Cornelia Beck & Valorie Shue, Surrogate Decision-Making and Related Issues, 17 ALZHEIMER DISEASE & ASSOCIATED DISORDERS S12, S13, S15 (2003) (discussing (i) experimental treatment that holds no benefit to the patient); Marcia Sue DeWolf Bosek, Organ Donation and Surrogate Decision-Making: An Ethical Analysis, 8 J. NURSING ADMIN. HEALTHCARE L., ETHICS, & REG. 38, 38 (2006) (discussing (ii) surrogate decisions regarding organ donation); Frances R. Batzer et al., Postmortem Parenthood and the Need for a Protocol with Posthumous Sperm Procurement, 79 FERTILITY & STERILITY 1263, 1265 (2003) (discussing (iii) surrogate decisions regarding postmortem gamete procurement). Cf. Fine, supra note 115, at 1558 ( [N]ever use a patient as a means to the family s end. ) Fine, supra note 115, at See, e.g., BERNAT, supra note 174, at 93 ( Conflicts of interest can occur when the surrogate s decision is made more in her own interest than in the patient s interest. Equally disturbing are the reports of cases in which the surrogate has chosen a course of treatment or non-treatment that is diametrically opposite the one which the physician understood the patient to want when the patient was competent. ); Ann Alpers & Bernard Lo, Avoiding Family Feuds: Responding to Surrogate Demands for Life-Sustaining Interventions, 27 J.L. MED. & ETHICS 74, 74, (1999); Muriel R. Gillick & Terri Fried, The Limits of Proxy Decision Making: Undertreatment, 4 CAMBRIDGE Q. HEALTHCARE ETHICS 172, (1995); John Hardwig, The Problem of Proxies with Interests of Their Own: Toward a Better Theory of Proxy Decisions, 4 J. CLINICAL ETHICS 20, (1993); John Arthur McClung, Time and Language in Bioethics: When Patient and Proxy Appear to Disagree, 6 J. CLINICAL ETHICS 39, 39, (1995); Olick & Armstrong, supra note 175, at 37:29 ( Some may find following the patient s wishes contrary to the dictates of personal morality or conscience. ); Jeffrey Spike & Jane Greenlaw, Ethics Consultation: Refusal of Beneficial Treatment by a Surrogate Decision Maker, 23 J.L. MED. & ETHICS 202, (1995); Peter B. Terry et al., End-of-Life Decision Making: When Patients and Surrogates Disagree, 10 J. CLINICAL ETHICS 286, 290, 292 (1999) See A Tale of Two Patients, (Nov. 10, 2007, 11:25 AM) ( [N]obody wants to be accused [of] killing off grandma or grandpa. ) See Olick & Armstrong, supra note 175, at 37:29 ( In rare cases the proxy will act on the basis of improper or selfish motivations, financial or otherwise the classic example is the family member driven by the prospect of inheriting substantial wealth. ); LORI A. STIEGEL & ELLEN VANCLEAVE KLEM, AARP PUB. POLICY INST., POWER OF ATTORNEY ABUSE: WHAT STATES CAN DO ABOUT IT: A COMPARISON OF CURRENT STATE LAWS WITH THE NEW UNIFORM POWER OF ATTORNEY ACT 4 (2008); see infra notes 331 to 362.
360 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION Formalized Distrust of Surrogates There has long been a tension between the quick and easy identification of surrogates, on the one hand, and the inclusion of cumbersome procedural safeguards, on the other hand. 203 Today, the balance has been struck in favor of quick and easy identification. 204 There are no rigorous procedures for patient- and physician-designated surrogates precisely because they were enacted primarily to avoid the expense of full guardianship or conservatorship proceedings. 205 Still, recognizing the deficiencies of surrogate decision-making, most states have various special limitations on consent by surrogates. 206 There is perhaps no better example of the formalized distrust of surrogates than the U.S. Supreme Court s Cruzan decision. 207 The court held that the U.S. Constitution permitted Missouri to impose a procedural safeguard requiring the surrogate to have clear and convincing evidence of the patient s wishes. 208 The court was concerned that the views of a surrogate would not necessarily be the same as that patient s would have been had she been confronted with...her situation while competent. 209 Because the patient herself specifically chooses them, agents are accorded greater trust. They are often given more discretion than physicianor court-designated surrogates. 210 For example, often only patient-selected 203. See generally Karna Halverson, Voluntary Admission and Treatment of Incompetent Persons with a Mental Illness, 32 WM. MITCHELL L. REV. 161, (2005) (discussing different approaches for identifying surrogates, and the statutes used to simplify the process or create safeguards) Cf. id.at 187 (discussing the inflexibility of consent laws and suggesting revisions that would permit family or friends to consent to treatment of an incompetent patient ) PRESIDENT S COMM N FOR THE STUDY OF ETHICAL PROBLEMS IN MED. & BIOEMED. & BEHAVIORAL RES., DECIDING TO FOREGO LIFE-SUSTAINING TREATMENT 147 (1983), quoted in SABATINO, supra note 129, at 9, 28 ( The judiciary has had neither the resources nor the expertise for taking on responsibility in all such cases. ) See SABATINO, supra note 129, at ( Only eight states follow the Uniform Health-Care Decisions Act model that places no limitations on default surrogates. ); Abigail Petersen, Survey of States Health Care Decision-Making Standards, 28 BIFOCAL 53, (2007) (listing types of limitations); A.M. v. Benes, [1999] CanLII 3807 [11] (ON C.A.) (Rejecting a good faith test for surrogates, the Ontario Court of Justice explained such a test would fail to screen out the results of rank stupidity, or carelessness, or well-meant fanaticism or palpable illusion. ) Cruzan v. Dir., Mo. Dept. of Health, 497 U.S. 261 (Mo. 1990) Id. at Id. at See, e.g., S.I. v. R.S., 877 N.Y.S.2d 860, 866 (Supp. 2009) ( Petitioners have failed to establish any ground upon which the agent should be removed, they have not established that the agent is acting in bad faith; nor have they proffered any proof that would warrant overriding the agent s decision on the grounds that the decision was made in bad faith or that it was not in accordance with PHL 2982(1) or (2). Mere speculation or hope, regardless of
361 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 222 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 surrogates can (a) refuse life-sustaining treatment even when the patient is in a terminal condition or permanently unconscious, 211 (b) refuse artificial nutrition and hydration, 212 or (c) in New York (before June 2010), refuse life-sustaining interventions other than CPR. 213 But most surrogates are not patient-designated. And Cruzan is hardly the only example of the limitations of such surrogates. For example, in Wendland, the California Supreme Court held that the patient s wife and court-appointed conservator did not have the authority to consent to the removal of his life-sustaining medical treatment. 214 Had the patient been in a persistent vegetative state instead of a minimally conscious state, the wife would have had that authority. 215 This illustrates a general inverse correlation rule: The better off the patient, the narrower the scope of surrogate authority. 216 Unfortunately, these safeguards are usually designed to work in only one direction, like installing a railing on only one side of a pedestrian bridge. Specifically, the safeguards ensure that surrogates only consent to the withholding and withdrawing of treatment in accordance with patient wishes or best interests. They focus far less on assuring that surrogate consent to continuing treatment is in accordance with patient wishes or best interests. 4. Summary The vehicles for promoting and protecting patients prospective autonomy are imperfect. Still, the benefits of surrogate decision-making outweigh its risks. While substituted judgment has its problems, other how heartfelt, can not override the agent s decisions, which have priority over other surrogates. ). Still, not even agents can consent to some interventions. See, e.g., CAL. PROB. CODE 4711 (West 2009) See, e.g., ALASKA STAT (2008); DEL. CODE ANN. tit. 16, 2507 (2003); 755 ILL. COMP. STAT. 40/1-65 (2008); LA. REV. STAT. ANN. 40: (2008); ME. REV. STAT. ANN. tit. 18-A, (1998); N.C. GEN. STAT (2009); OHIO REV. CODE ANN (West 2005) See, e.g., KY. REV. STAT. ANN (LexisNexis 2007); OHIO REV. CODE ANN (West 2005) See Pope, supra note 133, at (2009) (discussing how a New York law will allow surrogates to make additional life-sustaining treatment decisions) Wendland v. Wendland, 28 P.3d 151, 154, (Cal. 2001) See id. at 175 (The holding does not affect permanently unconscious patients, including those who are comatose or in a persistent vegetative state. ) See generally In re Conroy, 486 A.2d 1209 (N.J. 1985) (discussing limitations on surrogate authority when the patient is not brain dead, comatose, or in a chronic vegetative state ).
362 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 223 standards have problems of their own. 217 Surrogates, after all, are still more accurate than physicians. 218 And even if no decision were made on the patient s behalf, we would still have to determine a status quo. That would itself constitute a decision made for the patient, indeed, one that may not reflect the patient s own preferences and values. Consequently, I have reviewed this empirical evidence on surrogate decision-making not to suggest that we should not have surrogates. Rather, I provide this background for context. Knowing surrogate deficiencies should make us less reluctant to replace surrogates in those situations, at the margins, where a presumption can be rebutted that the surrogate is acting pursuant to the required decision-making standards See Linus Broström & Mats Johansson, A Virtue-Ethical Approach to Substituted Judgment, 25 ETHICS & MED. 107, (2009), citing ALLEN E. BUCHANAN & DAN W. BROCK, DECIDING FOR OTHERS: THE ETHICS OF SURROGATE DECISION MAKING (1989) See, e.g., Kristen M. Coppola et al., Accuracy of Primary Care and Hospital-Based Physicians Predictions of Elderly Outpatients Treatment Preferences With and Without Advance Directives, 161 ARCHIVES INTERNAL MED. 431, 435 (2001); G.S. Fischer et al., Patient Knowledge and Physician Predictions of Treatment Preferences after Discussion of Advance Directives, 13 J. GEN. INTERNAL MED. 447 (1998); Seckler et al., supra note 181, at 94, 95; Uhlmann et al., supra note 182, at M117. Physicians tend to base their decision on a subjective assessment of the patient s quality of life that is less favorable than the patient s own assessment. See Robert A. Pearlman & Richard F. Uhlmann, Quality of Life in Chronic Diseases: Perceptions of Elderly Patients, 43 J. GERONTOLOGY M25, M27-28 (1988) Making it too easy for a physician to challenge a surrogate would open the door to unjustified paternalism, where someone who does not agree with a physicians [sic] recommendation might be thought to have questionable motives. Letter from John Doherty, Directing Attorney, AIDS Legal Servs., to Stan Ulrich, Assistant Executive Sec y, Cal. Law Revision Comm n (Nov. 29, 1999) (on file with the Cal. Law Revision Comm n as Study L- 4003: Second Supplement to Memorandum 99-82). In one study, thirteen percent of physicians reported that they and the surrogate disagreed about the right thing to do. Torke et al., Physicians Experience with Surrogate Decision Making for Hospitalized Adults, 24 J. GEN. INTERNAL MED. 1023, 1026 (2009). Just as judges cannot and should not disregard all jury findings with which they disagree, hardly all of these surrogates can or should be replaced. Physicians must generally comply with the surrogate s reasonable interpretation of the patient s advance directive. See, e.g., DEL. CODE ANN. tit. 16, 2508(d)(1) (2003). This limits the scope of the physician to simply select a surrogate who agrees with the physician s recommendation. Cal. Law Revision Comm n Staff Memorandum 98-63: Health Care Decisions: Comments on Tentative Recommendation 4 (Sept. 18, 1998) (on file with the Cal. Law Revision Comm n). Reliance on surrogate decisions seems inescapable. Daniel P. Sulmasy et al., The Accuracy of Substituted Judgment in Patients with Terminal Diagnoses, 128 ANNALS INTERNAL MED. 621, 629 (1998).
363 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 224 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 B. Rationale for Surrogate Replacement Surrogates are generally obligated to make health care decisions in accordance with the patient s preferences and best interests. 220 Particularly for a conscious or semi-conscious patient, continuing LSMT contrary to provider recommendations often contravenes patient preferences and/or best interests. Consequently, surrogates who make such requests are often acting outside the scope of their authority and should be replaced with other decision makers. 221 The Code of Medical Ethics advises: Though the surrogate s decision for the incompetent patient should almost always be accepted by the physician, there are four situations that may require either institutional or judicial review and/or intervention in the decision-making process:... (3) a health care provider believes that the family s decision is clearly not what the patient would have decided if competent; and (4) a health care provider believes that the decision is not a decision that could reasonably be judged to be in the patient s best interests See generally RIGHT TO DIE, supra note 4, at (discussing incompetent patients and surrogacy); DEP T OF VETERANS AFFAIRS, VETERANS HEALTH ADMINISTRATION HANDBOOK : INFORMED CONSENT FOR CLINICAL TREATMENTS AND PROCEDURES 14b.(1)(c) (2009) ( The surrogate s decision must be based on substituted judgment or, if the patient s values and wishes are unknown, on the patient s best interests... If the practitioner considers the surrogate to be clearly acting contrary to the patient s values and wishes or the patient s best interests, the practitioner must notify the Chief of Staff, or designee, and consult with the local IntegratedEthics program officer or Regional Counsel.... ). Cf. In re Orshansky, 804 A.2d 1077, 1081, 1103 (D.C. 2002) (discussing a situation where a health care proxy is trying to make health care decisions in the best interest of the patient) See BERNAT, supra note 174 at 189 (arguing for judicial recourse when there is evidence that a surrogate is deciding for reasons that are not altruistic ); Cantor, supra note 172, at 885 ( Courts should be willing to curb surrogates unexplained deviations from a course widely understood to be consistent with a patient s best interests and likely wishes. ); Gerald Kierzek et al., Advance Directives and Surrogate Decision Making before Death, 363 NEW ENG. J. MED. 295, 295 (2010) (rightly being surprised by the [de facto] authority of a surrogate to override all decisions even when surrogate decisions are inconsistent with the patient s written preferences ); Bernard Lo et al., The Wendland Case Withdrawing Life Support from Incompetent Patients Who Are Not Terminally Ill, 346 NEW ENG. J. MED. 1489, (2002) ( The assumption that the spouse should be the surrogate decision maker can be overturned for example, if the couple has separated or if there has been domestic violence. Also, physicians should not follow a spouse s decision if it contradicts previously expressed wishes of the patient that are so specific and to the point that they would meet the legal standard of clear and convincing evidence. ); Mark R. Tonelli, Withdraw Life Support on the Basis of Substituted Judgment, 360 NEW ENG J. MED. 530, 530 (2009) ( The choices of legal surrogates do not necessarily represent substituted judgments, nor should substituted judgments be taken at face value. Due diligence is required to ascertain whether a substituted judgment seems to be a valid expression of a patient s previously held goals and values. ) AMA CODE OF ETHICS, supra note 131, 2.20.
364 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 225 An appellate court similarly observed that when a surrogate insists on inappropriate treatment the usual procedure... is to... go to court to replace the surrogate or override his decision. 223 For example, surrogate selection was a major issue in the Schiavo case. Michael Schiavo was the surrogate for his wife Terri. 224 He instructed providers to remove her feeding tube because Terri would not have wanted to remain in a persistent vegetative state. 225 Terri s parents challenged Michael and argued that he was an unfit surrogate. 226 However, they also indicated that they would insist Terri be given treatment even if she had provided clear directives otherwise. 227 They thereby disqualified themselves from ever being appointed proxies.... because they had declared that they would ignore the fundamental ethical and legal requirements of a proper surrogate. 228 Many state statutes specifically provide for surrogate replacement. 229 Massachusetts, for example, provides that a health care provider... may 223. Causey v. St. Francis Med. Ctr., 719 So. 2d 1072, 1076 n.3 (La. Ct. App. 1998). In addition to the argument that the surrogate is not fulfilling his or her statutorily-provided role, the court observed that surrogate selection would be appropriate where the guardian or surrogate is guilty of abuse by insisting on care which is inhumane. Id In re Schiavo, 780 So. 2d 176, 177 (Fla. Dist. Ct. App. 2001). See also C. Christopher Hook & Paul S. Mueller, The Terri Schiavo Saga: The Making of a Tragedy and Lessons Learned, 80 MAYO CLINIC PROC. 1449, 1450 (2005) In re Schiavo, 780 So. 2d at 178, 180 ( Her statements to her friends and family about the dying process were few and they were oral. Nevertheless, those statements... gave the trial court sufficient basis to made the decision for her. ); Hook & Mueller, supra note 224, at In re Schiavo, 780 So. 2d at See also Hook & Mueller, supra note 224, at (discussing how the Schindlers disagreed with Michael s decision to remove Terri s feeding tube, and how the court appointed a second guardian ad litem to better serve Terri s interests) Hook & Mueller, supra note 224, at 1451, Id. at See, e.g., ALASKA STAT (2008) (discussing circumstances when the primary health provider may decline to comply with a surrogate decision and notify the appropriate health care institution); DEL. CODE ANN. tit. 16, 2511 (2003) (discussing circumstances when the Court of Chancery can be petitioned for appointment of a guardian); MASS. ANN. LAWS ch. 201D, 17 (LexisNexis 1994) (discussing circumstances when a special court proceeding can be commenced to override an agent s decision); N.Y. PUB. HEALTH LAW 2992 (McKinney 2007) (discussing circumstances when a special court proceeding can be commenced to remove an agent or override an agent s decision); OHIO REV. CODE ANN (West 2005) (discussing circumstances when a court hearing can be held to determine whether a surrogate decision should be confirmed or reversed); TEX. HEALTH & SAFETY CODE (g) (providing that any person in a class of default surrogates can apply for temporary guardianship to challenge the decision of the designated surrogate). Cf. Thomas J. Balch, Are There Checks and Balances on Terminating the Lives of Children with Disabilities, 25 GA. ST. U. L. REV. 959, 967 n.32 (2009). In a related context, the Revised
365 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 226 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 commence a special proceeding... [to] override the agent s decision about health care treatment on the grounds that: the decision was made in bad faith or the decision is not in accordance with [the decision-making] standards. 230 Florida similarly permits a provider to seek an expedited judicial intervention if the provider believes the surrogate s decision is not in accord with the patient s known desires or best interests. 231 While other states provide no special judicial mechanism with which to replace surrogates, they do clearly and firmly state that surrogates acting inconsistently with specified decision-making standards do not have authority to speak for the patient. The Delaware Healthcare Decisions Act, for example, provides that healthcare providers should comply with healthcare decisions for the patient made by a person then authorized to make health-care decisions for the patient to the extent the agent or surrogate is permitted. 232 C. Method of Surrogate Replacement When the surrogate seems to be making choices not in accordance with the patient s best interest, it is up to the treating physician to confirm that the surrogate is deciding in accordance with the patient s stated preferences or known values. 233 But because the informal resolution of futility disputes is so often successful, providers should exhaust such mechanisms before taking formal action to replace the surrogate. 234 After Uniform Anatomical Gift Act, now adopted in most states, precludes family members from overriding donor consent to organ donation. See Thaddeus Mason Pope, Legal Briefing: Organ Donation and Allocation, 21 J. CLINICAL ETHICS 243 (2010) MASS. ANN. LAWS ch. 201D, 17 (LexisNexis 1994). See also N.Y. PUB. HEALTH LAW 2992 (McKinney 2007) (discussing similar circumstances when a special court proceeding can be commenced to remove an agent or override an agent s decision) FLA. STAT. ANN (1), (1)(b) (West 2005) DEL. CODE ANN. tit. 16, 2508(d)(2) (2003) (emphasis added) Kathryn J. Rowland et al., Surgical Futility: Aggressive Surgery on the Severely Demented, 145 SURGERY 351, 353 (2009) See Franz-Josef Illhardt, Conflict Between a Patient s Family and the Medical Team, 19 HEATHCARE ETHICS COMMITTEE FORUM 381, 383 (2007) ( An initial subject raised... was the feasibility of having the power-of-attorney withdrawn from the daughter, since it had become obvious that she was acting more in her own than in her mother s interest. But was that really so? ); id. at 386 (concluding that consensus can often be reached by: (i) allowing the surrogate to adapt to her role, (ii) educating the surrogate about her role, and (iii) and making sure that the surrogate understands the clinical information); Meisel & Jennings, supra note 136, at 76 (explaining that most surrogates initially opposed to stopping LSMT ultimately agree to its termination ). See generally Pope & Waldman, supra note 11. In one recent case, the court rejected an attempt at surrogate selection before consensus building efforts had been attempted. In re DP, 2010 CanLII (Ont. C.C.B.) (dismissing Form G Application).
366 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 227 all, being a surrogate is not an easy job. 235 Illogical thinking might not reflect a careless, reckless, or malicious surrogate, but rather an uninformed or emotionally burdened surrogate. In one recently published account, a nursing home called a resident s surrogate. Your aunt has lower gastrointestinal bleeding. Do you want us to send her to the hospital? 236 The surrogate said she that would discuss it with her husband and call back. 237 The surrogate soon decided to send her aunt to the hospital. 238 But then, just as she was walking to the kitchen to return the call, the surrogate heard her aunt s familiar refrain from recent months: Pray for me to die. 239 The surrogate explained, I knew if the decision were hers to make she would refuse to go to the hospital. I called the nursing home and told staff not to send her. 240 In another recent account, the physician explained to the surrogate that her father s heart [was] weak, his kidneys [were] failing, and his lungs [were] filling with fluid. 241 The physician then asked, Does your father want us to employ extreme measures...? 242 The surrogate was conflicted. 243 She wanted to stop the insane cycle of hospitalizations and heroic life-saving treatments that were not helping her father: He is dying. And I am exhausted.... I want my life back. 244 The surrogate was acutely tempted to answer [no]. 245 But she instead gave the physician the answer that she knew to be true, even though both she and the physician thought it unreasonable. 246 While these two surrogates were faithful, their decisions were hard. Surrogates are performing a new role, for the first time, under difficult circumstances. Therefore, healthcare providers should make every effort to 235. See, e.g., Hannah I. Lipman, Surrogate Decision Making, 17 AM. J. GERIATRIC CARDIOLOGY 120 (2008); His Last Wish: Carrying Out End-of-Life Requests Not a Simple Matter, FOSTERS.COM, Feb. 1, 2009, /GJCOMMUNITY_01/ (detailing a surrogate s difficult decision not to pursue bypass surgery for a 75-year-old with lymphoma and dementia) Louise Szabo, My Aunt s Life Was in My Hands, GLOBE & MAIL, Jan. 21, 2010, article Id Id Id Id Alicia von Stamwitz, An Ill Father, a Life-or-Death Decision, N.Y. TIMES, Jan. 26, 2010, at D5, available at Id Id Id Id See id.
367 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 228 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 clarify the situation. 247 Specifically, they should do two things. First, they should advise the surrogate of the duties of a good surrogate decision maker. 248 Second, they should make sure that the surrogate understands the prognostic information about the patient. 249 If good communication about prognosis and the role of surrogates does not work, mediation often works. The Code of Medical Ethics advises that [w]hen a physician believes that a decision is clearly not what the patient would have decided, could not be reasonably judged to be within the patient s best interests, or primarily serves the interest of a surrogate or a third party, an ethics committee should be consulted before requesting court intervention. 250 Usually, conflict will dissipate when communication improves, misunderstandings are corrected, and emotional and spiritual needs are met. 251 While surrogate replacement may be an option for some intractable disputes, most futility disputes will not become intractable See, e.g., See David E. Weissman et al., Helping Surrogates Make Decisions, FAST FACTS AND CONCEPTS (2010), See Braun et al., supra note 69, at 252 ( To reduce this burden [of decision], the physician should point out that the decision has already been made by the patient. The task at hand is to respect and implement the patient s decision. ); AMA CODE OF ETHICS, supra note 131, 2.20 ( Physicians should... explain to surrogate decision makers that decisions regarding withholding or withdrawing life-sustaining treatment should be based on substituted judgment (what the patient would have decided).... ); Viki Kind, Helping the Family Make the Difficult Decisions, KindEthics.com (Jan. 30, 2009), ( First, stop asking, What do you want us to do? And instead ask, What would (the patient s name) want us to [do]?... Secondly, you need to educate the family about their role as the decision maker.... ); Meth, supra note 106, at 2076 (recommending [e]ducation of SDMs legal obligations ); Rowland, supra note 233, at 352 (recommending that providers remind family members or appointed guardians that it is important to choose a course of therapy as the patient would choose for herself ). Cf. GENERAL MED. COUNCIL, TREATMENT AND CARE TOWARDS THE END OF LIFE: GOOD PRACTICE IN DECISION MAKING 21 (2010), available at pdf_ pdf (making clear their role is just to advise on patient wishes, views, beliefs) See Latifat Apatira et al., Hope, Truth, and Preparing for Death: Perspectives of Surrogate Decision Makers, 149 ANNALS INTERNAL MED. 861, 867 (2008) AMA CODE OF ETHICS, supra note 131, Many cases will go undetected. [M]edical professionals cannot guard against improper motives... because they are neither suited by training nor situation to discover such impropriety. In re Hamlin, 689 P.2d 1372, 1381 (Wash. 1984) (Rosellini, J., dissenting). I analyze surrogate selection as a dispute resolution option for those cases in which providers do know or suspect the surrogate is unfaithful Mark D. Siegel, End-of-Life Decision Making in the ICU, 30 CLINICS CHEST MED. 181, 186 (2009).
368 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 229 Therefore, it will often be best to delay treatment decisions while the surrogate comes to terms with the patient s illness. 252 IV. JUDICIAL REPLACEMENT OF UNFAITHFUL SURROGATES For the small but significant subset of cases in which intramural and informal dispute resolution mechanisms fail, surrogate replacement may be an option. Indeed, it may be a legal obligation. So, why is it so underutilized? 253 The main obstacle to wider acceptance of surrogate selection has not been doubt of its appropriateness, but rather of its efficacy. 254 The standard operating procedure in most institutions seems to be accede to the surrogate s demands for treatment if the surrogate cannot be convinced to accept the physician s recommendation to forgo it. 255 In one recent study, seventeen percent of physicians responded that [i]f a family member or health care surrogate is making health care decisions that clearly go against the wishes stated in the patient s living will, they 252. Alexia M. Torke, The Physician-Surrogate Relationship, 167 ARCHIVES INTERNAL MED. 1117, 1120 (2007). Of course, delaying too long will undermine the patient s autonomy and/or best interests Some providers recognize it as an option. See, e.g., Posting of Tayyab Ali to New Eng. J. Med., commentbox (Feb. 02, 2009) (last visited Aug. 11, 2010) ( I wish we had a committee... who can make binding judgments in these situations to override unrealistic choices by surrogate decision makers. ); postings of Anthony Gagliardi, Ramón Trevino-Frutos, Stephen Workman, Donald Winston, Anne-Marie Hill, Luciano Corrêa da Silva Müller, George Schroeder, Giovanni Codacci-Pisanelli, Tom Mayo to New England J. Med., (2009) (last visited Aug. 11, 2010); Jennifer Frank, Refusal: Deciding to Pull the Plug, 23 J. AM. BOARD FAM. MED. 671, 673 (2010) ( I disregard what the familes request if they go against what the patient would want.... ) See Meth, supra note 106, at 2075 ( [L]egal recourse is avoided as health-care providers perceive that the legal forum fails to provide informed and timely resolution.... [P]hysicians may err on the side of caution by continuing life-sustaining interventions, even if treatment is believed to be against the patients wishes. ); Thaddeus Mason Pope, Involuntary Passive Euthanasia in U.S. Courts: Reassessing the Judicial Treatment of Medical Futility Cases, 9 MARQ. ELDER S ADVISOR 229, 267 (2008) ( [F]ear of legal liability should not have the impact on provider decision-making that it has had. ) Meisel & Jennings, supra note 136, at 76. In the New England Journal of Medicine poll, many respondents admitted that they would cave in to the unfaithful son s demands because of legal concerns. See postings of Adolfo Anchondo, Aarti Jerath, John Lace, James Holmlund, Marc Hirsch, B Douglas, Alvin Fuse, Moises Malowany, Albert Fuchs, Casey Hager, David Mehr, George Schroeder, Russell Buhr, Audrey Peterson to New England J. Med., box (2009). See also Kritek 2009, supra note 1, at e16 (reporting that many respondents believed they were limited, by legal concerns. ).
369 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 230 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 would follow the family s wishes and not the living will. 256 It is, in short, often easier to accede and provide treatment. In such cases, patients are often quite near death anyway, and they die in a relatively short time while treatment continues to be administered. 257 But the available legal precedent suggests that this reluctance to seek judicial surrogate replacement is unwarranted. 258 Admittedly, in early futility cases, courts were generally unwilling to negate a surrogate s right to make health care decisions on behalf of a patient. 259 But in more recent cases, providers have repeatedly successfully replaced surrogates who demanded LSMT that providers deemed inappropriate Dan M. Westphal & Stefanie Andrea McKee, End-of-Life Decision Making in the Intensive Care Unit: Physician and Nurse Perspectives, 24 AM. J. MED. QUALITY 222, 225 tbl. 3 (2009) (reporting that seventy-two percent of physicians but ninety-one percent of nurses would follow the living will). See also id. at 226 (reporting that the main reason physicians would follow family wishes that clearly go against the... patient s living will was fear of litigation ); BERNAT, supra note 174, at 84 ( A patient or family s verbal or veiled threat to pursue legal action often is sufficient to win whatever demand either makes on the physician. ); Berger et al., supra note 147, at 49 ( Despite substantial evidence of surrogate inaccuracy... many physicians do not require surrogates to adhere to patients known wishes, and physicians often treat incapacitated patients contrary to expressed preferences. ); Charlie Corke & Jill Mann, Effect of a Supplement Clarifying Patients Intentions on Doctors Willingness to Follow the Wishes of an Agent with Medical Enduring Power of Attorney, 11 CRITICAL CARE & RESUSCITATION 215, 217 (2009) (finding only forty percent of surveyed physicians believed that they had a duty to overrule a surrogate s wrong decision); Jennifer Murphy et al., Withdrawal of Care in a Potentially Curable Patient, 147 SURGERY 441, 443 (2010) ( [T]here might be legal consequences of failing to comply with the requests of the DPA. ) Meisel & Jennings, supra note 136, at BERNAT, supra note 174, at 83 ( If physicians, in their usual practice of following the law, find that doing so in a particular instance clearly produces more harm than good to a patient or others, if possible, they should contact a hospital attorney and seek a court order legally authorizing them to make an exception to the law. ); id. at 84 (arguing that rather than capitulating to the demand, physicians should courageously stand by their medical judgments ); Lo et al., supra note 221, at 1492 (arguing that physicians should accept a degree of legal uncertainty in order to do what is ethically and clinically appropriate ) See Cantor, supra note 172, at 886 ( [P]roviders can seek a judicial declaration that the surrogate is acting improperly; but the judicial route is currently likely to fail.... ); Lee, supra note 8, at 487; RIGHT TO DIE, supra note 4, 3.16[b][3] (observing that few cases have addressed the issue of the appropriate person to serve as judicially appointed guardian) It is rarely necessary for the replacement of surrogates to be made by a court. Physicians normally themselves have the authority to determine whom they will recognize as a valid surrogate. Still, most physicians want the legal comfort of a judicial declaration. In any case, it is important to review the appellate precedent because this cases a shadow on how surrogate selection will occur in the wards. Cf. Pope & Waldman, supra note 11, at 149 (discussing the application of mediation in end-of-life care).
370 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 231 A. Early U.S. Cases: In re Wanglie is one of the earliest and most widely discussed medical futility cases. 261 Helga Wanglie was an eighty-six year old woman who was in a persistent vegetative state and dependent on a ventilator as a result of cardio-respiratory arrest. 262 Her providers determined that she could never appreciate any benefit from continued LSMT, so they advised her husband, Oliver, to remove the ventilator. 263 However, Oliver would not consent to stopping LSMT. 264 The providers petitioned the local probate court to appoint a professional conservator to make health care decisions for Helga. 265 The hospital-nominated conservator presumably would accede to the providers recommendation to stop LSMT, although at the time of the appointment he was not familiar with the facts of the case. 266 Despite the provider s efforts, the probate court denied the petition and instead appointed Oliver as conservator. 267 The court noted that Oliver was Helga s husband of fiftythree years. 268 Moreover, his decision to continue LSMT did not constitute grounds to remove his decision-making authority. 269 The court could not conclude that Oliver s decision to continue LSMT was inconsistent with Helga s preferences or best interests. 270 While Wanglie is certainly the most famous case from the early 1990s in which a court rejected a provider s attempt at surrogate selection, it is not the only case. 271 In Nguyen v. Sacred Heart Medical Center, a Washington court rejected a provider s argument that a child s parents serving as surrogate decision-makers should be replaced because their decision to continue LSMT constituted child abuse. 272 Similarly, a District of Columbia 261. In re Wanglie, supra note 24, at Id. at Id. at Id Id. at 371, In Re Wanglie, supra note 24, at Id. at 372, Id. at Id. at Id. at See In re Doe, 418 S.E.2d 3, 7 (Ga. 1992) (holding that providers could not withdraw LSMT from a child with only the mother s consent where the child s father was available). Professor Annas suggests Doe is not a futility case, but instead a dispute about who is the authorized decision-maker. George J. Annas, The Case of Baby K, 331 NEW ENG. J. MED. 1383, 1385 (1994). This is belied by the course of the litigation, which demonstrated that the hospital was hardly agnostic as to which parent had authority. It argued that continued aggressive treatment... constituted medical abuse. In re Doe, 418 S.E.2d at See Nguyen v. Sacred Heart Medical Center, 987 P.2d 634, 638 (Wash. Ct. App. 1999); John Altomare & Mark Bolde, Nguyen v. Sacred Heart Medical Center, 11 ISSUES L. &
371 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 232 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 court refused to replace a mother as surrogate decision-maker for her critically ill two-month-old baby simply because she requested continued LSMT. 273 Some commentators cite Wanglie and other cases from the early 1990s to conclude that the strategy of having an alternative decision maker appointed by the court is rarely successful. 274 But it appears that these early decisions have little relevance today. 275 Emboldened by empirical evidence attacking the accuracy of surrogate decisions, 276 providers have been increasingly able to establish that surrogates refusing to follow recommendations to stop LSMT are not acting in patients preferences or best interests. 277 B. Later U.S. Cases: By the mid-1990s, judicial hostility to surrogate shopping began to wane. Courts began regularly replacing surrogates in three types of cases. First, they replaced surrogates who made decisions inconsistent with instructions in the patient s advance directive. Second, courts replaced surrogates who requested treatment inconsistent with the patient s preferences or best interests. Third, courts replaced surrogates who suffered from a material conflict of interest. 1. Judicial Replacement of Surrogates Making Decisions Inconsistent with the Patient s Advance Directive Advance directives are not always clear, and providers should comply with surrogate decisions so long as the surrogate interprets the advance MED. 199, 200 (1995) (noting that while the hospital attempted to characterize continued treatment as cruel and inhumane, the court held that the argument had no merit). This abuse argument had also failed in earlier cases. See, e.g., In re Baby K, 832 F.Supp. 1022, 1031 (E.D.Va. 1993) (ruling that the mother s decision to continue treatment was not so unreasonably harmful as to constitute child abuse or neglect ) Benjamin Weiser, A Question of Letting Go: Child s Trauma Drives Doctors to Reexamine Ethical Role, WASH. POST, July 14, 1991, at A18 (detailing the case of baby Rena) Burns & Truog, supra note 20, at While the answers to the legal questions asked in Wanglie and Nguyen disfavored providers, these are not the only questions relevant in medical futility cases. Cf. RIGHT TO DIE, supra note 4, 13.03[A]. Providers can also seek ex ante permission or ex post forgiveness for unilaterally refusing a surrogate s request, declaratory relief, or providers can proceed to withdraw LSMT and defend any subsequent damages case. See generally Pope 2007, supra note 19, at 42-78; Pope 2009, supra note 16, at See supra notes 178 to 181 and accompanying text See infra Part B.
372 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 233 directive in good faith in light of available information and circumstances. 278 But when the surrogate s interpretation becomes seriously strained or obviously wrong, the surrogate has exceeded the scope of her authority. In these situations, courts have not hesitated to replace such surrogates. Perhaps the most significant of these decisions is In re Livadas year-old Dorothy Livadas was in a persistent vegetative state and dependent on a PEG tube and a ventilator. 280 Her daughter and healthcare agent, Ianthe, wanted health care providers to continue this treatment because her mother was not done. 281 But health care providers did not think that was the right decision for Livadas. 282 In April 2008, a New York trial court appointed Catholic Family Center as Livadas guardian, a decision later affirmed by the appellate division. 283 The court replaced Ianthe as surrogate decision maker both because her demands for aggressive treatment contradicted instructions in her mother s advance directive and because she fail[ed] to appreciate her mother s true medical condition and lack[ed] the objectivity and insight to make necessary decisions. 284 The California Court of Appeal similarly endorsed surrogate selection in Cardoza v. USC University Hospital. 285 While the court did not replace a surrogate, it strongly indicated that there are clear limits to the scope of a surrogate s authority. 286 Healthcare providers complied with decisions of an 278. See In re Drabick, 200 Cal.App.3d 185, 200 (Cal. Ct. App. 1988) (holding the court should confine its involvement to ensuring that surrogate has made a good faith decision relying on medical advice) In re Livadas, No. 08/ (N.Y. Apr. 28, 2008) Id. at 2. See also Justina Wang & Gary Craig, In the Gray Area Between Life, Death, DEMOCRAT & CHRON., Aug. 11, 2008, at 1A In re Livadas, No. 08/037030, at 2. See also Wang & Craig, supra note 280, at 1A In re Livadas, No. 08/037030, at 4-6. See also Wang & Craig, supra note 280, at 8A; Gary Craig & Justina Wang, Removal of Life Support Allowed, DEMOCRAT & CHRON., Aug. 21, 2008, at1a In re Livadas, No. 08/037030, at 14, See also Wang & Craig, supra note 280, at 8A; Craig & Wang, supra note 282, at 6A In re Livadas, No. 08/037030, at A few weeks after its appointment, CFC, the new guardian, authorized the removal of Livadas life support based on the numerous legal documents, including a 2005 living will, Livadas had signed. Id. at 3. Observe that while Livadas living will clearly applied to her then-present circumstances, the result was still premised on the assumption that Livadas living will accurately represented her preferences. Id. Ianthe argued that since Livadas signed many legal papers the same day she signed her living will, it is unlikely that she put much thought into it. Id. at 8-9. Indeed, it is likely that many living wills (instructional advance directives) accurately reflect the preferences of declarants. Still, the presumption is that they do, and Ianthe could not bear the heavy burden of rebutting this presumption Cardoza v. USC Univ. Hosp., No. B195092, 2008 WL (Cal. Ct. App. 2008) Id. at *5.
373 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 234 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 appointed health care agent, a son of the patient, to continue aggressive interventions for his mother. 287 But the agent s sister (and patient s daughter) brought a lawsuit alleging that providers failed to comply with her mother s advance directive. 288 Since the surrogate had no authority to contravene instructions and preferences memorialized in the advance directive, the hospital could not have complied with the surrogate s decisions in good faith. 289 Therefore, the court held that the hospital was not entitled to immunity. 290 The hospital, the court implied, should have replaced the surrogate Judicial Replacement of Surrogates Making Decisions Inconsistent with the Patient s Preferences or Best Interests Replacing a surrogate who is making decisions contrary to a patient s advance directive may be an easy case. 292 But the courts have not stopped there. They have been replacing surrogates in situations where the only ground for disqualification was the fact that the surrogate demanded LSMT for the patient contrary to provider recommendations. 293 Courts are prepared to override even well-intentioned surrogates whose demands for continued LSMT cause a patient unwarranted or extreme suffering. 294 For example, in In re Mason, the Massachusetts General Hospital successfully moved the local probate court to override a health care agent s refusal to consent to a do not resuscitate ( DNR ) order. 295 In granting the hospital s petition, the court explained that since the agent was 287. Id. at * Id Id. at * Id Cardoza,WL at * Cf. Cantor, supra note 172, at 887 n.16 (observing that the easier case is where the patient had, while previously competent, issued instructions rejecting life support in the circumstances now at hand ) See John Zick, Man s Life in Court s Hands, CORNING LEADER, June 22, 2009, see also Kisner v. W.V. Univ. Hosp., No. 10-C-190 (Monogalia Cty., WV Cir. Ct., Mar. 25, 2010) (Complaint) (alleging that the hospital intends to remove the Plaintiff as surrogate because of evidence that the patient would refuse the level of medical intervention and treatment decided by the Plaintiff ) Cf. In re Guardianship of Myers, 610 N.E.2d 663, 664 (Ohio Misc. 1993) (appointing guardian other than parents of permanently comatose minor where one parent refused to consent to stopping LSMT) In re Guardianship of Mason, 669 N.E.2d 1081, 1082 (Mass. App. Ct. 1996).
374 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 235 in denial about his mother s deterioration and distrustful of her providers, he had not given full consideration of acceptable medical alternatives. 296 Similarly, in the case of Gary Harvey, the court replaced the patient s wife as surrogate because she failed to follow medical advice. 297 In January 2006, Gary Harvey fell down his basement stairs, leaving him in a persistent vegetative state. 298 Providers soon determined that Harvey was suffering and had little to no chance of recovery. 299 While his wife, Sara, was initially appointed guardian, she showed a pattern of dangerous behavior. 300 So, in February 2007, a court replaced Sara because she failed to use good judgment and follow medical advice. 301 The new guardian, Chemung County, New York Department of Social Services, following the recommendation of the hospital ethics committee, asked the trial court to authorize both the issuance of a DNR order and the removal of the Harvey s artificial nutrition and hydration. 302 In a case referred to as Baby Terry, the court replaced the parents of two-month-old Terry Achtabowski Jr. with a guardian. 303 Baby Terry was born premature at twenty-three weeks gestation, was dependent on a ventilator, and had a host of serious medical problems that made his prognosis very bleak. 304 Since continued treatment was painful and offered virtually no prospect for recovery, the Genesee County, Michigan Department of Social Services alleged that Baby Terry s parents were neglectful in requesting continued treatment. 305 The Michigan Probate Court did not find the parents neglectful, but it did determine that they were 296. Id. at One might say that the surrogate lacks capacity, just as the patient herself lacked capacity, to understand and make the healthcare decisions at hand See Zick, supra note Id Id Scott Cook & Ted Fioraliso, Gary Harvey s Daughter Speaks Out, WENY.COM (Dec. 16, 2009), Zick, supra note 293 ( Sara Harvey says her husband is a fighter who would not want to give up. They think that I m in denial. ). See also Ray Finger, Wife Accused of Abuse Wants Guardianship of Husband, STAR GAZETTE, Sept. 18, 2009, at 6A ( In his February 2007 decision that denied Sara Harvey guardianship, state Supreme Court Judge Robert Mulvey said she had abused Gary Harvey and failed to follow medical advice. ) See Zick, supra note 293. The county guardian later withdrew its request to remove Harvey s feeding tube. John Zick, Comatose Man s Feeding Tube Won t be Removed, CORNING LEADER, July 28, 2009, Bopp, Jr. & Coleson, supra note 97, at (discussing the case of Baby Terry, In re Achtabowski, No. G GD (Mich. Probate Ct. July 30, 1993)); Baby Dies, Was Focus of Battle, ORLANDO SENTINEL, Aug. 13, 1993, at A10 (Parents could not block courtappointed guardian.) Bopp, Jr. & Coleson, supra note 97, at Id.
375 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 236 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 incompetent to decide what was best for their son. 306 The court reasoned that the parents lacked the requisite capacity to make medical decisions for their son because their demands for continued LSMT evidenced that they were emotionally unable to appreciate the circumstances. 307 In In re Howe, 308 the Massachusetts Probate Court initially seemed to return to the early 1990s hostile approach to surrogate selection. The court ruled that when a surrogate decision-maker insisted on continued LSMT for her mother, the evidence is insufficient to warrant court usurpation of [a daughter s] role as her mother s health care agent. 309 But as the patient s condition deteriorated further, the daughter s decision to continue LSMT increasingly diverged from the hospital s assessment of the patient s preferences and best interests. 310 Several months later, the court suggested that the surrogate s own personal issues were impacting her decisions and urged the daughter to refocus her assessment. 311 A year later, the hospital again planned to remove LSMT, and the court denied the daughter s request for a temporary restraining order (TRO). 312 The daughter soon agreed to withdraw LSMT because she thought the court would rule against her. 313 Finally, in Bernstein v. Superior Court, 314 the dispute was between two sons of a 79-year-old Alzheimer s patient. 315 One brother, Scott, had been the conservator. 316 But Scott had been demanding very aggressive care that offered the father no benefit, only significant suffering. 317 While healthcare providers were not a party to the dispute, they all thought that the treatments were inappropriate and futile. 318 On the basis of the providers 306. Id. at Id. at 826, 832. Cf. Linda C. Fentiman, Health Care Access for Children with Disabilities, 19 PACE L. REV. 245, (1999) (describing case as a troubling example of judicial and physician usurpation of parental authority to make decisions about the medical treatment of their children ) In re Howe, No. 03 P 1255, 2004 WL (Mass. Prob. & Fam. Ct. Mar. 22, 2004) Id. at * Id. at * Id. at *20, * See Liz Kowalczyk, Plan to Take Woman Off Life Support Is Halted, BOS. GLOBE, Feb. 23, 2005, at B Daughter Explains Agreement to End Care, BOS. GLOBE, Mar. 23, 2005, at B Bernstein v. Sup. Ct. Ventura Cty., No. B212067, 2009 WL (Cal. Ct. App. Feb. 2, 2009) Id. at * Id Id. at * Id. at *4-5.
376 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 237 testimony, the other brother, Ilya, successfully replaced Scott as conservator Judicial Replacement of Surrogates Suffering a Material Conflict of Interest While courts replace surrogates requesting treatment contrary to patient instructions, preferences, and best interests, perhaps the easiest surrogate for courts to replace is one with a material conflict of interest. In the prescient 1997 film Critical Care, the daughter of a terminally ill man demanded that healthcare providers sustain her father. 320 She claimed that this is what her father would have wanted. 321 In fact, if the father lived for three more weeks, the daughter would inherit $10 million. 322 If the father died sooner, another daughter from another marriage would inherit the money. 323 Clearly, surrogates basing their treatment decisions on such selfish, non-patient-oriented reasons should be replaced. 324 And they are Id. at *10-11, CRITICAL CARE (Live Entertainment 1997). Such a motive obtained more generally in 2009, because the inheritance tax was lifted for deaths in Laura Saunders, Rich Cling to Life to Beat Tax Man, WALL ST. J., Dec. 30, 2009, at A1, available at article/sb html. One New York lawyer explained, in late December 2009, I have two clients on life support, and the families are struggling with whether to continue heroic measures for a few more days. Id. Of course, surrogates making such decisions on such a basis is not problematic if that is what the patient wanted. [S]ome clients are putting provisions into their health-care proxies allowing whoever makes end-of-life medical decisions to consider changes in estate-tax law. Id CRITICAL CARE, supra note Id Id. See also Maura Possley, Family Members Upset with Care of Elderly Aunt, SOUTHTOWN STAR, Mar. 26, 2010 (describing a case eerily similar to that depicted in CRITICAL CARE) See, e.g., Files v. State, 826 So. 2d 906 (Ala. Crim. App. 2001) (affirming conviction for criminally negligent homicide of conservator, sole heir of her aunt s estate, who diluted and discontinued her aunt s feeding tube); Lois Shepherd, Terri Schiavo: Unsettling the Settled, 37 LOY. U. CHI. L. REV. 297, 304 (2006) (observing that the Schindlers claimed that Michael Schiavo was motivated by money to remove Terri s feeding tube, but that the trial court found no basis for those charges); Jenette Sturges, Public Guardian Often Can Help the Helpless, NAPERVILLE SUN, July 26, 2010 (reporting the case of Mary Rauschenberger, in which the county guardian obtained a DNR order on the physician s recommendation, despite the objections of family members who were living off the patient s trust). Not only do such conflicted decisions violate general fiduciary obligations but they may also violate specific prohibitions. See, e.g., ALA. CODE 22-8A-11(c) (LexisNexis 2006) ( The decision to provide, withdraw, or withhold life-sustaining treatment... by the surrogate shall be made... without consideration of the financial benefit or burden which will accrue to the surrogate or the health care provider as a result of the decision. ).
377 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 238 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 In In re Rochester General Hospital, 325 Mr. Levin was admitted to the hospital for certain medical problems experienced while a patient in a nursing home. 326 Mr. Levin s adult son had been granted a health care proxy and appointed surrogate decision maker under a power of attorney. 327 But the son refused to cooperate in obtaining Medicaid reimbursement to cover the hospital expenses, apparently because he had wrongfully withheld his father s property. 328 The hospital commenced a special proceeding for the appointment of guardian. 329 The court granted the petition, explaining that it entertain[ed] serious doubts as to [the son s] ability to make future decisions pursuant to the health care proxy. 330 Not all conflicts are financial in nature. 331 For example, in In re Martin, 332 the mother of a patient challenged the appropriateness of the patient s wife as surrogate. 333 The Michigan Court of Appeals held that it was error for the trial court to have not considered evidence of the possible bias, prejudice, conflict of interest, or improper motive. 334 Such evidence would indicate that the wife was not a suitable surrogate In re Rochester Gen. Hosp., 601 N.Y.S.2d 375 (N.Y. 1993) Id. at Id Id. at 377, Id. at Id. at 379. Financial conflicts of interest often lead to breaches of fiduciary duty not only in the healthcare context but also in the context of the ward s estate. See, e.g., Grahl v. Davis, 971 S.W.2d 373, 380 (Tenn. 1998) (holding that the conservator breached her fiduciary duties for allowing redemption of certificates without court approval and for dealing with the property to attain personal benefit); Bryan v. Holzer, 589 So. 2d 648, 660 (Miss. 1991) (holding that the conservator using ward s funds for his own use violated fiduciary duties); In re Guardianship of Lawrence, 563 So. 2d 195, 197 (Fla. Dist. Ct. App. 1990) (holding that the guardian violated fiduciary duties by taking compensation and mismanaging funds). In October 2009, a Manhattan jury convicted the son of philanthropist Brooke Astor, on charges that he defrauded his mother and stole tens of millions of dollars from her as she suffered from Alzheimer s. John Eligon, Mrs. Astor s Son Guilty of Taking Tens of Millions, N.Y. TIMES, Oct. 9, 2009, at A1, available at region/09astor.html; Joseph A. Rosenberg, Regrettably Unfair: Brook Astor and the Other Elderly in New York, 30 PACE L. REV (2010) See, e.g., RIGHT TO DIE, supra note 4, at 3.24[C] (Conflicts can be emotional in nature as well.); STANLEY A. TERMAN, PEACEFUL TRANSITIONS: AN IRONCLAD STRATEGY TO DIE HOW AND WHEN YOU WANT (2009) In re Martin, 517 N.W.2d 749 (Mich. Ct. App. 1994), rev d on other grounds, 538 N.W.2d 399 (Mich. 1995) Id. at Id. at Id. at 754.
378 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 239 More starkly, in June 2009, Pedro Rosabal killed his two children, then turned the gun on himself and ended up on life support. 336 Legal and ethical experts agreed that it would be inappropriate for decisions regarding Rosabal s treatment to end up in the hands of his wife (the dead children s mother). 337 In a recent Arizona case, the patient s wife was removed as surrogate because of demonstrated animosity and enmity. 338 In 2007, Jesse Ramirez and his then-wife, Rebecca were involved in a terrible rollover car crash. 339 Jesse suffered a broken neck, fractured skull, punctured lung, broken ribs, and fractured face. 340 He was comatose in a minimally conscious state. 341 Just nine days later, even before Jesse s prognosis was certain, Rebecca directed the removal of his feeding tube. 342 But Jesse s siblings and parents objected. 343 They alleged that Rebecca had exceeded the scope of her authority. 344 Not only was there was marital discord but the couple had also been in a heated argument right at the time of the accident. 345 Based on this evidence, the Maricopa County Superior Court appointed an independent guardian. 346 Jesse s nutrition and hydration was resumed, and he was later discharged. 347 Sadly, one type of conflicted surrogate whom courts regularly replace is the parent whose very own physical abuse caused a child s dependence on LSMT. 348 For example, in the case of Michael Arzuaga-Guevara, life 336. Cindy George & Paige Hewitt, Kids Deaths Put Hospital in Ethical Quandary, HOUS. CHRON., June 18, 2009, Id Gary Grado, Judge Orders Life Support for Hospice Patient, E. VALLEY TRIB., June 15, 2007, at A Id Id Id Id Grado, supra note Id. Gary Grado, Crash Survivor s Case Spurs New State Law for Incapacitated People, E. VALLEY TRIB., July 19, 2009, at A Grado supra note 338; Grado supra note Grado, supra note Grado, supra note 344. See also Dennis Wagner, Man Wakes After Order to End Life Support, USA TODAY, June 27, 2007, at 3A, available at nation/ comatose_n.htm (stating Ramirez awoke from his coma eighteen days after his wife instructed his physicians to remove life support and was able to sit up and communicate with visitors). A similar issue arose when Different Strokes actor Gary Coleman s ex-wife Shannon Price directed the removal of his life support. Nancy Dillon, Gary Coleman s Wife on Why She Yanked His Life Support: He Wouldn t Have Made It Anyway, N.Y. DAILY NEWS, June 3, See, e.g., Hernandez v. Abel. No. 2:06-CV MBS (D.S.C. Feb. 4, 2008) (granting summary judgment to defendants and rejecting arguments of father convicted of
379 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 240 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 support was withdrawn from a critically injured infant, over the objections of his father who was in jail on assault and related charges in connection with Michael s injuries. 349 Another case involved a mother who abused her twoyear-old baby. 350 Providers recommended stopping LSMT, but the baby s father refused because he was concerned about his wife s criminal liability. 351 The hospital prepared to ask a court to appoint a guardian because the father was looking out for his wife s interests, not the interests of the child patient. 352 child abuse that he was wrongly excluded from the removal decision); J. M. Appel, Mixed Motives, Mixed Outcomes When Accused Parents Won t Agree to Withdraw Care, 35 J. MED. ETHICS 635, 635 (2009) (reviewing cases in which accused parents... argued against disconnecting but in each instance, the courts ruled against the accused parent ); Julie Akiko Gladsjo et al., Termination of Life Support After Severe Child Abuse: The Role of a Guardian ad Litem, 113 PEDIATRICS e141, e (2004) (explaining the American Academy for Pediatrics recommendation that in severe child abuse cases the accused parents may have a conflict of interest due to legal liability and it may be necessary for a court to appoint a guardian ad litem for medical decision-making); Vanessa Miller, Boulder County Officials Discuss Injured Infant s Future, COLORADODAILY.COM, July 29, 2009, daily.com/ci_ ?iadid=search- xzz0ga8ad0xo ( In cases where parents are suspected of being responsible for their child s injuries... they can t participate in the decision of whether to remove a child from life support. ). Surrogates are also replaced in the opposite situation, where they refuse to consent to treatment with life-saving benefits and minimal risks. See, e.g., Thaddeus Mason Pope, Legal Update, 20 J. CLINICAL ETHICS 287, 288 (2009) (reviewing recent cases) In re Michael Arzuaga-Guevara, 794 A.2d 579, 581 (Del. 2001). See also In re Truselo, 846 A.2d 256, 264, 274 (Del. Fam. Ct. 2000) (determining that for child severely shaken and dropped that his best interests [was] to forego the use of heroic medical efforts to resuscitate him, that the ventilator should be removed, and that he should receive comfort measures only) Steve Twedt, Should Comatose Baby Live? Hospital, Dad Differ, PITTSBURGH PRESS, June 3, 1990, at A Id Id. The father then acceded to the hospital s recommendation to withdraw LSMT. J. Kenneth Evans, Boy s Death Is Homicide, Mother May Be Charged, PITTSBURGH POST-GAZETTE, June 25, 1990, at 1; Mary Pat Flaherty, Right-to-Die Decision Has Little Impact Here, PITTSBURGH PRESS, June 27, 1990, at A1. Cf. J.N. v. Sup. Ct., 67 Cal. Rptr. 3d 384, 391 (Cal. Ct. App. 2007) (holding that guardian of minor has the burden of bringing expert testimony to prove that the LSMT is in the minor s best interest); D.K. v. Commonwealth, 221 S.W.3d 382, 384 (Ky. Ct. App. 2007) (permitting a guardian to remove LSMT once parental rights were permanently terminated); In re Matthew W., 903 A.2d 333, 335 (Me. 2006) (holding that a pre-termination protection order allowing DNR for minor without parental consent violated the parents right to due process); In re Tabatha R., 564 N.W.2d 598, 605 (Neb. 1997) (discussing due process rights of parents during termination of parental rights determination); In re Stein, 821 N.E.2d 1008, 1013 (Ohio 2004) (finding that a limited guardian did not have the authority to withdraw LSMT when parental rights had not yet been permanently terminated); In re Smith, 133 P.3d 924, (Or. Ct. App. 2006) (holding
380 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 241 It is important to emphasize that since surrogates are usually family members, they will be personally impacted by the patient s death, for example, in terms of inheritance, pensions, and government benefits. There is usually a conflict of interest. But this alone is insufficient to disqualify the surrogate. Instead, the moving party must establish a material conflict of interest. Otherwise, the very concept of surrogate decision-making would be swallowed by this exception. [T]he issue is not the existence of a conflict of interest, but its pervasiveness and its effect. 353 C. Ontario Capacity and Consent Board In Ontario, the Consent and Capacity Board ( CCB ) is a body created by the Ontario government under its Health Care Consent Act. 354 When in-house conflict resolution fails, CCB can mediate. If this mediation fails, CCB adjudicates The CCB is, in short, an independent, quasijudicial tribunal; a neutral, expert board which, in intractable treatment disputes, can make a legal, binding decision that can only be reversed on appeal through the courts. 356 Notably, the CCB is specially designed to ensure that substitute decision makers comply with the principles of substitute decision-making. 357 The CCB makes its own determination. If the CCB finds that the surrogate has not complied, then it directs the surrogate to consent to treatment as the CCB finds appropriate. 358 If the surrogate fails to do so, then the CCB passes the right to act as surrogate to the next eligible person. 359 The process is uncomplicated and expeditious. In a case where the healthcare provider judges that the surrogate is being unfaithful to the patient, the provider files a Form G application. 360 This is basically a petition for the CCB to determine whether the surrogate decision maker that a mother was not in a position to make decisions for her minor child where she chose not to be involved in the child s health care decisions on a regular basis) RIGHT TO DIE, supra note 4, at 3.24[C] Health Care Consent Act, 1996 S.O., ch. 2, 70(1) (Can.), available at (last visited Sept. 6, 2010) Mark Handelman & Bob Parke, The Beneficial Role of a Judicial Process When Everything Is Too Much?, HEALTHCARE Q., Sept. 2008, at 46, Id. at 50. See also Joaquin Zuckerberg, End-of-Life Decisions: A View from Ontario and Beyond, 16 EUR. J. HEALTH L. 139, (2009) (explaining how an administrative tribunal like the CCB may be better suited than courts to determine whether a surrogate has complied with the decision-making obligations) Health Care Consent Act 21 (outlining the principles for substitute decision-makers in refusing consent) Id. 36(4), 36(5) Id. 36(6), 36(6.1) Handelman & Parke, supra note 355, at 48.
381 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 242 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 complied with the principles for substitute decision-making. 361 The CCB sits in expert panels comprised of a lawyer, a psychiatrist, and a public member. 362 Due both to an interest in expeditious decision-making and to the expertise of the CCB, the Ontario Court of Justice reviews CCB decisions under a deferential reasonableness standard of review. 363 Regularly, when providers recommend treatment that includes the withholding or withdrawal of life-sustaining medical treatment, the CCB directs reluctant surrogates to consent. 364 For example, in the 2009 case of In re N, an 85-year-old patient was in septic shock, had numerous infections, kidney failure, and widespread skin breakdown. 365 She was experiencing pain, was dependent on a mechanical ventilator, and had almost no ability to come off it. 366 For these reasons, N s treating physician proposed withdrawing life support and beginning palliative care. 367 But N s surrogate, Mr. NP, would not consent to this plan of treatment. 368 Therefore, the physician brought a Form G application to the CCB to determine if that refusal was in accordance with the principles for... refusing consent to treatment. 369 The CCB held that the patient had expressed no prior capable wish that pertained to the circumstances. 370 Furthermore, because Mr. NP did not accept the medical opinion of the intensivists that N was in a state where there was no hope of recovery, the Board held that he could not possibly consider what N would have wanted if she was aware of those expert medical opinions[.] 371 Therefore, the Board had to determine not 361. Health Care Consent Act See In re E, 2009 CanLII (Ont. C.C.B.) at 5 ( The onus is always on the health practitioner.... ) CONSENT & CAPACITY BD., ANNUAL REPORT 2007/ (2008), available at Barbulov v. Cirone, 2009 CanLII (Ont. S.C.) at 7-8 (collecting authority). In recent cases, the Ontario Superior Court of Justice has repeatedly affirmed the CCB. See, e.g., Grover v. Butler, 2009 CanLII (Ont. S.C.) at 13 (holding that the Board s decision that patient s prior capable wish was inapplicable was reasonable both in fact and in law ) See, e.g., In re E, 2009 CanLII 28625, at 37 (directing that son comply with no-cpr, no-ventilator treatment plan of his father s physician); Barbulov, 2009 CanLII 15889, at 31. (affirming CCB direction that son consent to the no-cpr, no-dialysis treatment plan proposed by his father s physician) In re N, 2009 CanLII (Ont. C.C.B.) at 1, Id. at 1, Id. at 1, Id Id. at In re N, 2009 CanLII 42576, at Id. at 13.
382 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 243 whether the surrogate was acting in accord with the patient s wishes, but whether the surrogate was acting in her best interests. 372 The CCB held that the surrogate was not acting in the patient s best interests. 373 N had less than 1% chance of being off life support... She had no quality of life. She suffered from pain. Her physical condition was going to continue to deteriorate. There was no prospect that there would be any improvement in her condition. 374 The Board recognized that the family held out hope, but found that the family s hope was not at all realistic. 375 The Board found that the surrogate was blinded by [his] obvious love for N and could not view her situation objectively. 376 Accordingly, the CCB directed Mr. NP to consent to the proposed treatment plan. 377 Remarkably, the CCB has reached similar results, even in cases where the surrogate s decision had some warrant in the patient s own prior directions. While such evidence would appear to be a material obstacle to surrogate selection, the CCB is able to overcome it. The Board often finds that the patient s prior expressed preferences are inapplicable either because they are insufficiently clear or because they did not sufficiently anticipate the patient s current, very different circumstances. 378 D. Queensland Guardianship and Administration Tribunal Similar to the CCB is the Queensland Guardianship and Administration Tribunal ( QGAAT ). 379 The Tribunal has a multidisciplinary composition 372. Id Id. at In re N, 2009 CanLII 42576, at Id Id Id. The CCB gave Mr. NP approximately 48 hours to consent to treatment in accordance with its decision See, e.g., Conway v. Jacques 2002 CanLII (ON C.A.) at 70, 80 (The court affirmed the CCB where the surrogate refused to consent to anti-psychotic medication for the patient because the patient had refused when he had capacity years earlier. The CCB found that the patient s wish was not applicable since currently available medication was more effective and had fewer side effects than medication available when patient articulated preferences.); In re E, 2009 CanLII (Ont. C.C.B.) at 28 (finding that prior comments of patient were not precise and lacked particularly, refusing any mechanical or literal application of prior wishes, and thus employing best interest analysis); Id. at 36 ( [I]t is not open to the family to propose a treatment plan. Treatment plans are proposed by physicians and must be consented to by the substitute decision maker... the consent... must be correct. ); Barbulov v. Cirone, 2009 CanLII (Ont. S.C.) at 20 (finding power of attorney instrument had no weight since patient had given no prior instructions about a POA; did not read the POA [and] had limited command of written English ) Victoria has a similar mechanism under its Guardianship and Administration Act See Guardianship and Administration Act 1986, 42L-42M (2008) (Austl.). If a surrogate withholds consent to treatment and the provider thinks the surrogate is not making
383 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 244 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 comprised of at least a lawyer and a professional with extensive knowledge or experience of persons with impaired decision-making. 380 If there is a dispute about who should act as guardian 381 or concern about the suitability of a proposed guardian or someone believes inappropriate decisions are being made... by substituted decision makers, then the Tribunal may appoint the Adult Guardian, an independent statutory officer, to look after the interests of an adult with impaired decision-making ability. 382 For example, in In re AAC, providers determined that continuing lifesustaining measures for AAC was inappropriate because AAC s brain function had ceased due to cardiac arrest. 383 But AAC s children, who were the default surrogates ( statutory health attorneys ), refused to allow the withdrawal of life sustaining measures. 384 So, providers requested that an Adult Guardian consent to withdrawal, on the basis that the children s refusal to withdraw was inconsistent with good medical practice. 385 The Adult Guardian consented. 386 The Tribunal rejected the children s challenge to that decision. 387 V. THE LIMITS OF SURROGATE SELECTION Surrogate selection is a statutorily- and judicially-recognized option for resolving intractable futility disputes. But practical problems in application the right decision, the provider can provide the surrogate with a notice (Section 42M Notice) within three days of the refusal. Id. The notice advises the surrogate that they can apply to the Victorian Civil and Administrative Tribunal (VCAT) if they want to prevent the provider from proceeding. Id. If the surrogate does nothing, the practitioner can proceed. Id. If the surrogate makes an application, VCAT will decide whether the treatment can proceed. Id Id. at GUARDIANSHIP & ADMIN. TRIBUNAL, GUARDIANSHIP AND ADMINISTRATION TRIBUNAL: ANNUAL REPORT (2008). This entity was later amalgamated into the Queensland Civil and Administrative Tribunal Id. at In re AAC [2009] QGAAT 27 at [4]. The proceeding was brought by her child to challenge the Adult Guardian s decision. Id. at [7]-[8]. The Public Guardian can withdraw LSMT where continuation is inconsistent with good medical practice. Id. at [60]. See also In re SAJ [2007] QGAAT 62 at [1], [52] (holding that the continuation of artificial hydration to an eighty-six year old man who was a victim of multiple strokes did not constitute good medical practice); In re HG [2006] QGAAT 26 at [107] (holding that the continuation of artificial hydration and artificial nutrition was inconsistent with good medical practice) In re AAC, QGAAT at [5] Id. at [6], [60]. Good medical practice is defined in the controlling statute as (a) the recognized [sic] medical standards, practices and procedures of the medical profession in Australia; and (b) the recognized [sic] ethical standards of the medical profession in Australia. Guardianship and Administration Act 2000, Schedule 2, 5B In re AAC, QGAAT at [7] Id. at [60]-[62].
384 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 245 limit its use. 388 Surrogate selection cannot be successfully applied in several significant subsets of medical futility disputes. For three reasons, it will often be difficult to demonstrate a surrogate s deviation from required decision-making standards. First, surrogates often have sufficient evidence to demonstrate congruity between their decision and the patient s preferences. For example, surrogates might establish both that the patient belongs to a certain religion and that the tenets of that religion requires continued LSMT. Second, there will often be no available advance directive and little or no evidence of patient preferences. Therefore, it will be extremely difficult or impossible to demonstrate any contradiction between a patient s autonomy and a surrogate s decision. Third, even on the best interest standard, the benefit-burden balance is often not so obviously and severely imbalanced to justify usurping the surrogate s discretion and decision-making power. A. Surrogates Often Have Evidence to Demonstrate Congruity Perhaps the most obvious and the most significant limit to surrogate selection as a means for resolving futility disputes is that not all surrogates demanding medically inappropriate treatment are unfaithful. Sometimes, surrogates have solid evidence that they are making the very decisions that the patient would have wanted made on her behalf. After all, one cannot replace a good surrogate. 389 Take, for example, a recently reported case of a sixty-four year-old man found to have an incurable cancer of the esophagus. 390 Because of the patient s unawareness and his very poor prognosis, his providers believed that continued ICU care was inappropriate. 391 But the patient s surrogate insisted that he remain in the ICU, on ventilator support and on a full code 388. In addition to the problems described below concerning the merits for surrogate replacement, the time and cost of the judicial process may exceed the potential benefits. On the other hand, providers can replace surrogates without court involvement. See, e.g., 20 PA. CONS. STAT. ANN. 5431(a)(3) (providing immunity for refusing to comply with a surrogate based on a good faith belief that the surrogate was not complying with the standards for substitute decision making) For example, in only one case was the CCB s replacement of a surrogate reversed by the Ontario Superior Court of Justice. Scardoni v. Hawryluck, 2004 CanLII (ON S.C.) at 31. In that case, the Court found that the evidence indicated that the patient really did desire the treatment requested by her surrogate. Id. at 24. See also In re Univ. Hosp. SUNY Upstate Med. Univ., 754 N.Y.S.2d 153 (2002) (rejecting hospital s attempt to override surrogates through reliance on the patient advance directive because surrogates established that patient had revoked the advance directive) Robert D. Orr, Continuing Futile ICU Support at Relative s Insistence, 25 ETHICS & MED. 145, 145 (2009) Id.
385 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 246 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 status. 392 The surrogate explained that his deep religious faith (Methodist) required him to do everything possible to preserve life, and he was counting on God to perform a miracle. 393 Importantly, the surrogate further explained that that the patient was also a man of deep faith who would likewise insist on this approach. 394 It is unlikely that providers can replace this surrogate. Indeed, religion is at the bottom of most intractable futility disputes. 395 For example, in the widely-discussed Golubchuk case, physicians determined that eighty-four year-old Samuel Golubchuk had minimal brain function and that his chances for recovery [were] slim. 396 But Golubchuk s adult children argued that taking their father off life support would be a sin under their Orthodox Jewish faith. 397 Here, as in many cases, it was the patient s religion, and not just the surrogate s religion, that compelled continued treatment. Under such circumstances, it is difficult to replace such faithful surrogates. Surrogate selection seems inappropriate and inadequate to address this most common type of intractable futility dispute. 398 Furthermore, a practical reality seriously exacerbates this problem. Surrogates are a primary source of information about the patient s preferences and values. 399 So no matter what the applicable evidentiary standard, surrogates could manufacture or at least polish evidence to meet that standard. 400 And the limitations do not stop there Id Id Id See Pope & Waldman, supra note 11, at Carla Tonelli, Canada Life-Support Case Pits Religion vs. Science, REUTERS UK, Dec. 14, 2007, (discussing Golubchuk v. Salvation Army Grace Gen. Hosp., 2008 MBQB 49 (CanLII)) See id. at See Nat l Right to Life, Why the Need for a Will to Live?, euthanasia/willtolive/whyneedwtl.html (last visited Sept. 6, 2010). See also Texas Right to Life, Will to Live, (last visited Sept. 6, 2010) ( If you... do not want to be starved, dehydrated, or allowed to die simply because you have a disability, the medical community will be far more likely to respect your wishes if you sign a properly prepared Will to Live.... ) See A.M. v. Benes, [1999] CanLII 3807 (ON C.A.) at 10 ( The Board, though it may substitute its opinion for that of the S.D.M., must nonetheless take into account the S.D.M. s submissions on the incapable person s values, beliefs and non-binding wishes.... ) See Sandra H. Johnson, Quinlan and Cruzan: Beyond the Symbols, in HEALTH LAW AND BIOETHICS: CASES IN CONTEXT 53, (2009) (stating that after the U.S. Supreme Court upheld that constitutionality of Missouri s clear and convincing evidentiary standard, Judge Teel found that standard satisfied on remand and denied that he assisted in manufacturing evidence).
386 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 247 B. Providers Often Lack Sufficient Evidence to Demonstrate Surrogate Deviation In many futility disputes it will be difficult for providers to demonstrate that because surrogates demand continued treatment, they are being unfaithful to patient instructions or preferences. First, since applicable instructions are rarely available, cases like Livadas will be rare. 401 It is impossible to demonstrate surrogate deviation from patient instructions, if there are no such instructions in the first place. Second, there is a dearth of not only advance directives but also of any other evidence regarding patient preferences. Without such evidence, providers cannot demonstrate surrogate deviation. Third, even when patient instructions or evidence of patient wishes is available, patients often trust their surrogates discretion and want the surrogates to not be strictly bound by those instructions and wishes. 1. Few Advance Directives are Available and Applicable Notwithstanding many government and private initiatives, a majority of Americans do not complete advance directives. 402 Furthermore, even the minority that do complete advance directives often do so in an ineffective manner. 403 First, either the very existence or at least the location of the form is unknown at the time of treatment. 404 Second, even if the form is available, it is often not very informative anyway. 405 After all, most patients cannot possibly have anticipated and discussed their preferences in the numerous specific clinical states that later may occur. 406 One notable example of failed surrogate selection is In re University Hospital of the State University of New York Upstate Medical University. 407 Providers determined that patient Yvette Casimiro s condition satisfied her 401. See supra notes 280 to 284 and accompanying text. See also Kevin B. O Reilly, Defective Directives?, AM. MED. NEWS, Jan. 12, 2009, /01/05/prsa0105.htm See Charles P. Sabatino, The Evolution of Health Care Advance Planning Law and Policy, 88 MILBANK Q. 211, (2010); see also O Reilly, supra note Id Id Id; Muriel R. Gillick, The Challenge of Applying Advance Directives in Hospital Practice, 38 HOSP. PRACTICE 45 (2010) BERNAT, supra note 174, at 88. See also id. at 92 ( [I]t is ethically justifiable to overrule them... because an unexpected deterioration in the patient s health has rendered it no longer applicable. ); James L. Bernat & Lynn M. Peterson, Patient-Centered Informed Consent in Surgical Practice, 141 ARCHIVES SURGERY 86, 89 (2006); Ashwini Sehgal et al., How Strictly Do Dialysis Patients Want Their Advance Directives Followed?, 267 JAMA. 59, 62 (1992) In re Univ. Hosp. of State Univ., 754 N.Y.S.2d 153, 154 (N.Y. 2002).
387 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 248 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 advance directive such that it could invoke her expressed wishes that the life sustaining treatment be terminated. 408 When the surrogates refused to consent, providers went to court. 409 They argued that by their refusal and unwillingness to cooperate with the removal of these life sustaining systems, [the surrogates] are acting in contravention of the patient s directions and intent, and, therefore, they should be removed as health care agents But the court refused to replace the surrogate. 411 While the language of the advance directive clearly applied, the court found that it was unclear whether the patient realized the implications of her own advance directive. 412 Furthermore, the court credited the surrogates testimony concerning the patient s strongly expressed religious beliefs concerning who can take a life. 413 In short, while advance directives are presumed to be clear and convincing evidence of patient autonomy, that presumption can often be rebutted. 2. Patient Preferences Are Rarely Clear and Strong Just as it may be difficult to establish a contradiction between a surrogate s decision and a patient s advance directive, so too it will often be difficult to establish a contradiction between a surrogate s decision and evidence of patient treatment preferences. The reason, simply, is that there often is no such evidence. Indeed, recognition that surrogates would not have evidence was the point of the laws that gave them rights by status. 414 The absence of evidence regarding patient wishes is a significant obstacle to surrogate selection. For example, in 2006, Michigan internist Brian Drozdowski asked a Van Buren County probate court to allow [ninety-seven] year-old Hazel Wagner to be taken off a ventilator and have her feeding tube removed. Wagner, who already had kidney failure and dementia, had recently had a heart attack. In his request, Dr. Drozdowski said that Wagner had no chance of a meaningful recovery and that it was 408. Id. at Id. at Id. at Id. at In re Univ. Hosp. of State Univ. 754 N.Y.S.2d at Id. at See Jack Freer & Stephen Wear, Culture Wars in New York State: Ongoing Political Resistance by Religious Groups to the Family Health Care Decisions Act, 8 CHRISTIAN BIOETHICS 9, 9-10 (2002) (stating that in New York, surrogates not appointed by a court or advance directive have no status and can consent to stop aggressive treatment only with clear and convincing evidence of the patient s preferences).
388 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 249 unethical to keep her alive in her current condition. 415 Wagner had left no instructions and, by most accounts, had given no solid verbal indication of whether she would want to be kept alive using a feeding tube or ventilator. 416 For this reason, the judge denied Dr. Drozdowski s request and deferred to the surrogate s decision to continue treatment Patients Want their Surrogates to Have Discretion As demonstrated in the last two subsections, one serious obstacle to surrogate selection is that the requisite evidence to demonstrate surrogate unfaithfulness is often unavailable. 418 Providers often have no substantial evidence of patient instructions or wishes with which to establish surrogate deviation. 419 But even if there were such evidence, it still might not be sufficient to demonstrate that the surrogate was a maverick. 420 Surrogates often have permission to deviate from patient instructions and wishes. Many patients value trust over accuracy and prefer that their surrogates exercise judgment in response to actual clinical situations even if the surrogate s decisions depart from their expressed wishes. 421 A majority of terminally ill patients would prefer the decision of their surrogate even if it flatly contradicted explicit instructions in their living will See Bonnie Booth, Doctor s Request to End Patient s Care Denied, AM. MED. NEWS, June 12, 2006, at 22, 22, available at prca0612.htm Id Id See O Reilly, supra note See id Jeffrey T. Berger et al., supra note 147, at 49; O Reilly, supra note Jeffrey T. Berger, When Surrogates Responsibilities and Religious Concerns Intersect, 18 J. CLINICAL ETHICS 391, 392 (2007) (emphasis added); Berger et al., supra note 147, at 48. ( [M]any patients do not necessarily want their surrogates to adhere to their specific treatment preferences... but instead wish them to respond dynamically.... ); id. at 50 (suggesting that advance directives should indicate what role the content was intended to serve: binding, weighty but not binding, or merely informative ); J. McCarthy et al., Irish Views on Death and Dying: A National Survey, 36 J. MED. ETHICS 454, 455 (2010). See also Nikki Ayers Hawkins et al., Micromanaging Death: Process Preferences, Values, and Goals in Endof-Life Medical Decision Making, 45 GERONTOLOGIST 107, 108 (2005); Perkins, supra note 157, at 53; Christina M. Puchalski et al., Patients Who Want Their Family and Physician to Make Resuscitation Decisions for Them: Observations from SUPPORT and HELP, 48 J. AM. GERIATRICS SOC Y S84, S85 (2000); Sehgal et al., supra note 405, at Ashwini Seghal et al., How Strictly Do Dialysis Patients Want their Advance Directives Followed? 267 JAMA 59 (1992); Peter B. Terry et al., End-of-Life Decision Making: When Patients and Surrogates Disagree, 10 J. CLINICAL ETHICS 286, (1999). Cf. Rebecca L. Sudore, Can We Agree to Disagree, 302 JAMA 1629, 1630 (2009) ( [M]y grandfather s wishes were to have my grandmother make the decision she could live with. ).
389 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 250 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 While such flexibility does leave more room for error, it is a recognized advantage of surrogates over advance directives. 423 It is difficult for patients to anticipate all the permutations of clinical circumstances in which they might later find themselves. Surrogates, on the other hand, can respond dynamically to each situation and development. Nevertheless, while it will be difficult to replace a surrogate to whose discretion the patient has deferred, given the low use and availability of advance directives, such surrogates will be rare. Most surrogates are not designated by the patient (with or without discretion), but are clinically designated default surrogates. 424 Therefore, surrogates will often lack sufficient evidence to establish that the patient wanted them to have this discretion. C. Silver Lining: Best Interests Analysis It is important to observe that this lack of evidence limitation to surrogate selection may be substantially mitigated by the operation of the hierarchical decision-making standards. Specifically, if there is really no evidence of patient instructions or preferences, then neither the subjective standard nor the substituted judgment standard can be applied. In such cases, the appropriate decision-making standard is best interests. In short, the absence of relevant information means reversion to a best interest standard. As a purely objective standard, healthcare providers are in as good (or perhaps better) position as surrogates to determine the patient s best interests. 425 They are, after all, more experienced than surrogates at 423. See O Reilly, supra note 401. Some argue that patient-appointed surrogates have a greater moral authority than is now recognized at law. See Joseph J. Fins et al., Contracts, Covenants, and Advance Care Planning: An Empirical Study of the Moral Obligations of Patient and Proxy, 29 J. PAIN & SYMPTOM MANAGEMENT 55 (2005) See supra notes 132 to 136 and accompanying text. See also Charles P. Sabatino, The Legal and Functional Status of the Medical Proxy: Suggestions for Statutory Reform, 27 J.L. MED. & ETHICS 52, 55 (1999) Surrogates are regularly overruled on an application of the best interest standard. Cf. In re Storar, 420 N.E.2d 64, 79 (N.Y. 1981) (supporting a mother s surrogate decision to cease treatment for her mentally incompetent son); Braun et al., supra note 69, at 250, 252 (Since surrogates are only reporters under the subjective and substituted judgment standards, only under the best interest standard do surrogates engage in genuine surrogate decision making. ); Robert W. Sibbald & Paula Chidwick, Best Interests at the End of Life: A Review of Decisions Made by the Capacity and Consent Board of Ontario, 25 J. CRITICAL CARE 171 (2009). Still, we must keep in mind that, in the vast majority of situations, the best interests analysis is conducted by a combination of family members and healthcare professionals, and not formally by the courts. Marshall B, Kapp, Medical Decision-Making for Incapacitated Elders: A Therapeutic Interest Standard, INT L J. L. & PSYCH. n.21 (forthcoming 2010).
390 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 2010] SURROGATE SELECTION 251 assessing physical pain and suffering. Take, for example, the case of Mary Grover. 426 Mary suffered a brainstem stroke leaving her quadriplegic, dependent on a ventilator, and with diminished mental function. 427 Her healthcare providers proposed that the focus of Mary s care be comfort only. 428 But Marjorie Grover, Mary s surrogate and the oldest of her ten children, would not consent. 429 Marjorie correctly noted that at the patient s recent nursing home review, G s wish was to receive full resuscitative measures. 430 But the CCB still replaced Marjorie as surrogate. 431 The Board noted, Prior capable wishes are not to be applied mechanically or literally. 432 There was no evidence that Mary had her current circumstances in mind or that her wishes were applicable to those circumstances. 433 Moreover, Marjorie s evidence of Mary s values was quite vague. 434 Since there were no applicable instructions or evidence of Mary s preferences, the treatment decision had to be determined upon Mary s best interests. In applying this test, the surrogate s decision was accorded no deference. The Board was most influenced by the facts: (1) that Mary s other nine children all agreed with the proposed treatment plan; 435 and (2) that life-sustaining treatments would cause infections and hospitalizations but neither improve the overall quality of Mary s life nor lessen the disability. 436 Ultimately, the Board deferred to the recommendations of healthcare providers. The Board disregarded Marjorie s decision, finding that she was basing it on hope rather than on experienced medical opinions In re G, 2009 CanLII (ON C.C.B.); aff d, In re Grover, 2009 CanLII (ON S.C.) In re Grover, 2009 CanLII 16577, at Id. at Id. at 3-4; In re G, 2009 CanLII 25289, at 6, In re Grover, 2009 CanLII 16577, at In re G, 2009 CanLII 25289, at Id. at Id. at Id. at Id. at In re G, 2009 CanLII 25289, at Id. (The Board also noted that one of MG s siblings described MG as working her life plans around their mother. ). See also Barbulov v. Huston, 2010 Ont. Sup. Ct (2010) (affirming the CCB on a best interests standard because family members were misguided by their hope of recovery ).
391 POPE MACROED.DOCX (DO NOT DELETE) 11/2/ :07 AM 252 SAINT LOUIS UNIVERSITY JOURNAL OF HEALTH LAW & POLICY [Vol. 3:183 CONCLUSION Professor Truog is right to endorse surrogate selection as a solution to intractable futility disputes. 438 It is a mechanism that often works, and one that, when applicable, should be preferred over power-shifting laws. Yet, since surrogate selection cannot resolve significant categories of conflict, we must still develop dispute resolution mechanisms to handle those remaining disputes in which providers conflict with irreplaceable surrogates. In short, Truog is right to oppose the empowerment of intramural healthcare ethics committees to adjudicate futility disputes. 439 But he too quickly dismisses proposals for more legitimate, more independent ethics committees See Truog Medical Futility, supra note 20, at See Truog 2007, supra note 20, at See id. at 1-2; Truog, Correspondence, supra note 21, at I have outlined a dispute resolution mechanism for intractable futility disputes irresolvable through surrogate selection. See Pope, supra note 20.

392 Electronic copy available at:
393 Electronic copy available at:

394

395

396
397
VJ Periyakoil Productions presents
 VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
Advance Care Planning: the Clients Perspectives
 Dr. Yvonne Yi-wood Mak; Bradbury Hospice / Pamela Youde Nethersole Eastern Hospital Correspondence: fangmyw@yahoo.co.uk Definition Advance care planning [ACP] is a process of discussion among the patient,
Dr. Yvonne Yi-wood Mak; Bradbury Hospice / Pamela Youde Nethersole Eastern Hospital Correspondence: fangmyw@yahoo.co.uk Definition Advance care planning [ACP] is a process of discussion among the patient,
Educational Goals & Objectives
 Educational Goals & Objectives Primary care physicians are involved with patients over the course of their lives. Many of these patients will develop serious and/or life-threatening illnesses that affect
Educational Goals & Objectives Primary care physicians are involved with patients over the course of their lives. Many of these patients will develop serious and/or life-threatening illnesses that affect
Palliative and Hospice Care In the United States Jean Root, DO
 Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Overview of Presentation
 End-of-Life Issues: The Role of Hospice in The Nursing Home Susan C. Miller, Ph.D. Center for Gerontology & Health Care Research BROWN MEDICAL SCHOOL Overview of Presentation The rationale for the Medicare
End-of-Life Issues: The Role of Hospice in The Nursing Home Susan C. Miller, Ph.D. Center for Gerontology & Health Care Research BROWN MEDICAL SCHOOL Overview of Presentation The rationale for the Medicare
Hospice Care for anyone considering hospice
 A decision aid for Care for anyone considering hospice You or a loved one have been diagnosed with a serious illness that might not be curable. Many people find this scary or confusing. Some people feel
A decision aid for Care for anyone considering hospice You or a loved one have been diagnosed with a serious illness that might not be curable. Many people find this scary or confusing. Some people feel
Multidisciplinary care of a patient with heart failure. patient with heart failure. Dr Claire Hookey
 Multidisciplinary care of a patient with heart failure patient with heart failure Dr Claire Hookey Mr E.S 61 year old gentleman Referred to the hospice by the heart failure specialist nurse May 2010 Heart
Multidisciplinary care of a patient with heart failure patient with heart failure Dr Claire Hookey Mr E.S 61 year old gentleman Referred to the hospice by the heart failure specialist nurse May 2010 Heart
Communication & Shared Decision-Making
 Chapter 7: Communication & Shared Decision-Making STEP I CONDUCT AN AUDIT Key Item- the questions the TOOLKIT After-death Bereaved Family Member Interview asks communication and decision-making 1. Did
Chapter 7: Communication & Shared Decision-Making STEP I CONDUCT AN AUDIT Key Item- the questions the TOOLKIT After-death Bereaved Family Member Interview asks communication and decision-making 1. Did
End of Life Care in the ICU
 End of Life Care in the ICU C.M. Stafford, MD, FCCP Medical Director, Intensive Care Unit Chairman, Healthcare Ethics Committee Naval Medical Center San Diego The views expressed in this presentation are
End of Life Care in the ICU C.M. Stafford, MD, FCCP Medical Director, Intensive Care Unit Chairman, Healthcare Ethics Committee Naval Medical Center San Diego The views expressed in this presentation are
Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards
 Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards Dr Stephanie Chu Associate Consultant Department of Medicine Queen Elizabeth Hospital Hospital Authority Convention
Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards Dr Stephanie Chu Associate Consultant Department of Medicine Queen Elizabeth Hospital Hospital Authority Convention
Caregiving: Health Effects, Treatments, and Future Directions
 Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Your Results for: "NCLEX Review"
 Your Results for: "NCLEX Review" Site Title: Medical-Surgical Nursing Book Title: Medical-Surgical Nursing Location on Site: PART 1: MEDICAL-SURGICAL NURSING PRACTICE > Chapter 5: Nursing Care of Clients
Your Results for: "NCLEX Review" Site Title: Medical-Surgical Nursing Book Title: Medical-Surgical Nursing Location on Site: PART 1: MEDICAL-SURGICAL NURSING PRACTICE > Chapter 5: Nursing Care of Clients
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
Common Questions Asked by Patients Seeking Hospice Care
 Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
Advance Care Planning Communication Guide: Overview
 Advance Care Planning Communication Guide: Overview The INTERACT Advance Care Planning Communication Guide is designed to assist health professionals who work in Nursing Facilities to initiate and carry
Advance Care Planning Communication Guide: Overview The INTERACT Advance Care Planning Communication Guide is designed to assist health professionals who work in Nursing Facilities to initiate and carry
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Hospice Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 5 References... 6 Effective Date... 3/15/2014 Next Review
Cigna Medical Coverage Policy Subject Hospice Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 5 References... 6 Effective Date... 3/15/2014 Next Review
Children with Medical Complexity: A Unique Population with Unique Needs
 Children with Medical Complexity: A Unique Population with Unique Needs Nancy Murphy MD, Professor and Chief, Division of Pediatric PM&R, University of Utah School of Medicine Rishi Agrawal MD, MPH, Lurie
Children with Medical Complexity: A Unique Population with Unique Needs Nancy Murphy MD, Professor and Chief, Division of Pediatric PM&R, University of Utah School of Medicine Rishi Agrawal MD, MPH, Lurie
2 Palliative Care Communication
 2 Palliative Care Communication Issues Joshua Hauser Abstract Difficult conversations for patients and families can be challenging for physicians and other healthcare providers as well. Optimal preparation
2 Palliative Care Communication Issues Joshua Hauser Abstract Difficult conversations for patients and families can be challenging for physicians and other healthcare providers as well. Optimal preparation
Unit 301 Understand how to provide support when working in end of life care Supporting information
 Unit 301 Understand how to provide support when working in end of life care Supporting information Guidance This unit must be assessed in accordance with Skills for Care and Development s QCF Assessment
Unit 301 Understand how to provide support when working in end of life care Supporting information Guidance This unit must be assessed in accordance with Skills for Care and Development s QCF Assessment
What is palliative care?
 What is palliative care? Hamilton Health Sciences and surrounding communities Palliative care is a way of providing health care that focuses on improving the quality of life for you and your family when
What is palliative care? Hamilton Health Sciences and surrounding communities Palliative care is a way of providing health care that focuses on improving the quality of life for you and your family when
What do we promise people who are dying and those around them when we tell them about hospice care?
 Care Planning The Road to Meeting Patients and Families Where They Are Charlene Ross, MBA, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 602-740-0783 charlene@rchealthcaresolutions.com
Care Planning The Road to Meeting Patients and Families Where They Are Charlene Ross, MBA, MSN, RN Consultant/Educator R&C Healthcare Solutions & Hospice Fundamentals 602-740-0783 charlene@rchealthcaresolutions.com
While receiving hospice care services, non-hospice services may still be covered under other portions of the benefit plan.
 Medical Coverage Policy Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 0462 Hospice Care Table of Contents Coverage Policy... 1 Overview... 2 General Background...
Medical Coverage Policy Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 0462 Hospice Care Table of Contents Coverage Policy... 1 Overview... 2 General Background...
Path to Transformation Concept Paper Comments and Recommendations. Palliative Care Community Partners (PCCP)
") Path to Transformation Concept Paper Comments and Recommendations Palliative Care Community Partners (PCCP) c/o Hospice Care of America, Inc., 3815 N Mulford Rd, Rockford, IL / (815)316-2697 As part of
Path to Transformation Concept Paper Comments and Recommendations Palliative Care Community Partners (PCCP) c/o Hospice Care of America, Inc., 3815 N Mulford Rd, Rockford, IL / (815)316-2697 As part of
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee
 Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Hospital Transitions: A Guide for Professionals.
 Hospital Transitions: A Guide for Professionals 2017 www.medicarerights.org Medicare Rights Center The Medicare Rights Center is a national, nonprofit consumer service organization that works to ensure
Hospital Transitions: A Guide for Professionals 2017 www.medicarerights.org Medicare Rights Center The Medicare Rights Center is a national, nonprofit consumer service organization that works to ensure
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth
 Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
Individualised End of Life Care Plan for the Last Days or Hours of Life Patient name Hospital number Date of birth NHS number Informed by Five Priorities for Care: Recognise, Communicate, Involve, Support,
(f) Department means the New Hampshire department of health and human services.
 Department means the New Hampshire department of health and human services.") Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Adopted Rule 6/16/10. Effective: 7/1/10 1 Adopt He-W 544.01 544.16, cited and to read as follows: CHAPTER He-W 500 MEDICAL ASSISTANCE PART He-W 544 HOSPICE SERVICES He-W 544.01 Definitions. (a) Agent means
Leadership in Palliative Care: Strategies for APNs
 Leadership in Palliative Care: Strategies for APNs April 20, 2018 Lyn Ceronsky DNP, GNP, CHPCA, FPCN lcerons1@fairview.org System Director, Palliative Care Director, Fairview Palliative Care Leadership
Leadership in Palliative Care: Strategies for APNs April 20, 2018 Lyn Ceronsky DNP, GNP, CHPCA, FPCN lcerons1@fairview.org System Director, Palliative Care Director, Fairview Palliative Care Leadership
2015 National Training Program. History of Modern Hospice. Hospice Legislative History. Medicare s Coverage of Hospice Services
 2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
A Fresh Look at the Professional Consensus on the Ethics of End of Life Care What Good Can Ethics Guidelines Do?
 A Fresh Look at the Professional Consensus on the Ethics of End of Life Care What Good Can Ethics Guidelines Do? Bruce Jennings Center for Humans and Nature The Hastings Center Yale School of Public Health
A Fresh Look at the Professional Consensus on the Ethics of End of Life Care What Good Can Ethics Guidelines Do? Bruce Jennings Center for Humans and Nature The Hastings Center Yale School of Public Health
Palliative Care. Care for Adults With a Progressive, Life-Limiting Illness
 Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Palliative Care Care for Adults With a Progressive, Life-Limiting Illness Summary This quality standard addresses palliative care for people who are living with a serious, life-limiting illness, and for
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
Deciding Tomorrow... TODAY. Provider s Guide
 Deciding Tomorrow... TODAY. Provider s Guide No one should end the journey of life alone, afraid or in pain. Deciding Tomorrow Today is a program and toolkit developed by Nathan Adelson Hospice. The purpose
Deciding Tomorrow... TODAY. Provider s Guide No one should end the journey of life alone, afraid or in pain. Deciding Tomorrow Today is a program and toolkit developed by Nathan Adelson Hospice. The purpose
10/3/2016 PALLIATIVE CARE WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION. What, Who, Where and When
 PALLIATIVE CARE What, Who, Where and When Mary Grant, RN, MS ANP Connections Nurse Practitioner Palliative Care Program Oregon Region WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION The Center for
PALLIATIVE CARE What, Who, Where and When Mary Grant, RN, MS ANP Connections Nurse Practitioner Palliative Care Program Oregon Region WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION The Center for
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Talking to Your Doctor About Hospice Care
 Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
The Medicare Hospice Benefit. What Does It Mean to You and Your Patients?
 The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
Advance Care Planning: Goals of Care - Calgary Zone
 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning (and more)
") Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
National Standards Assessment Program. Quality Report
 National Standards Assessment Program Quality Report - March 2016 1 His Excellency General the Honourable Sir Peter Cosgrove AK MC (Retd), Governor-General of the Commonwealth of Australia, Patron Palliative
National Standards Assessment Program Quality Report - March 2016 1 His Excellency General the Honourable Sir Peter Cosgrove AK MC (Retd), Governor-General of the Commonwealth of Australia, Patron Palliative
Hospice Care For Dementia and Alzheimers Patients
 Hospice Care For Dementia and Alzheimers Patients Facing the end of life (as it has been known), is a very individual experience. The physical ailments are also experienced uniquely, even though the conditions
Hospice Care For Dementia and Alzheimers Patients Facing the end of life (as it has been known), is a very individual experience. The physical ailments are also experienced uniquely, even though the conditions
Providing Hospice Care in a SNF/NF or ICF/IID facility
 Providing Hospice Care in a SNF/NF or ICF/IID facility Education program Insert name of your hospice program Insert your logo Objectives Review the philosophy of hospice care and discuss what hospice care
Providing Hospice Care in a SNF/NF or ICF/IID facility Education program Insert name of your hospice program Insert your logo Objectives Review the philosophy of hospice care and discuss what hospice care
Appendix: Assessments from Coping with Cancer
 Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
Building the capacity for palliative care in residential homes for the elderly in Hong Kong
 Building the capacity for palliative care in residential homes for the elderly in Hong Kong Samantha Mei-che PANG RN, PhD, Professor School of Nursing, The Hong Kong Polytechnic University Why palliative
Building the capacity for palliative care in residential homes for the elderly in Hong Kong Samantha Mei-che PANG RN, PhD, Professor School of Nursing, The Hong Kong Polytechnic University Why palliative
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home. Your thoughts
 Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA. Introduction
 ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA Introduction There are two purposes to completing an Advance Directive for Receiving Oral Food and Fluids In Dementia. The first
ABOUT THE ADVANCE DIRECTIVE FOR RECEIVING ORAL FOOD AND FLUIDS IN DEMENTIA Introduction There are two purposes to completing an Advance Directive for Receiving Oral Food and Fluids In Dementia. The first
Advance Care Planning: Backgrounder. OMA s End-of-Life Care Strategy April 2014
 Advance Care Planning: Backgrounder OMA s End-of-Life Care Strategy April 2014 Definition/Legal Foundation Advance care planning (ACP) is a process of considering, discussing and planning for future health
Advance Care Planning: Backgrounder OMA s End-of-Life Care Strategy April 2014 Definition/Legal Foundation Advance care planning (ACP) is a process of considering, discussing and planning for future health
Be comfortable with comfort Meds
 DIAMOND PHARMACY SERVICES Be comfortable with comfort Meds Understanding Hospice medications Presented By: Daniel Barnes, RN Infusion RN Annual Educational Conference Thursday, April 16, 2015 1 Diamond
DIAMOND PHARMACY SERVICES Be comfortable with comfort Meds Understanding Hospice medications Presented By: Daniel Barnes, RN Infusion RN Annual Educational Conference Thursday, April 16, 2015 1 Diamond
Discussing Goals of Care
 Discussing Goals of Care Sarah Beth Harrington, MD UAMS Assistant Professor of Medicine Central Arkansas Veterans Healthcare System Chief of Palliative Care Objectives Understand the importance of discussing
Discussing Goals of Care Sarah Beth Harrington, MD UAMS Assistant Professor of Medicine Central Arkansas Veterans Healthcare System Chief of Palliative Care Objectives Understand the importance of discussing
DNACPR. Maire O Riordan 14 th January 2015
 DNACPR Maire O Riordan 14 th January 2015 Objectives NHS Scotland DNACPR policy Decision making framework and the forms DNACPR within ACP context Communicationwith patients, relatives and colleagues Background
DNACPR Maire O Riordan 14 th January 2015 Objectives NHS Scotland DNACPR policy Decision making framework and the forms DNACPR within ACP context Communicationwith patients, relatives and colleagues Background
Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference
 March 16, 2017 Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference Jeff Myers MD, MSEd, CCFP(PC) Nadia Incardona MD, MHSc, CCFP(EM) WHY this is timely JAMA,
March 16, 2017 Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference Jeff Myers MD, MSEd, CCFP(PC) Nadia Incardona MD, MHSc, CCFP(EM) WHY this is timely JAMA,
Better Ending. A Guide. for a A SSURE Y OUR F INAL W ISHES. Conversations Before the Crisis
 A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
A Guide for a Better Ending A SSURE Y OUR F INAL W ISHES Conversations Before the Crisis Information on Advance Care Planning and Documentation from Better Ending, a Program of the Central Massachusetts
Hospice Care for the Person with Cancer
 Hospice Care for the Person with Cancer Hospice is a special type of care designed to provide comfort, support and dignity to patients with a lifelimiting or terminal illness. For hospice purposes, a life-limiting
Hospice Care for the Person with Cancer Hospice is a special type of care designed to provide comfort, support and dignity to patients with a lifelimiting or terminal illness. For hospice purposes, a life-limiting
Caring for me Advanced Care Planning
 Caring for me Advanced Care Planning Supporting guidance for Healthcare Professionals and Administrative Staff This care plan is aimed as a guide to treatment and intended to aid the documentation of patient
Caring for me Advanced Care Planning Supporting guidance for Healthcare Professionals and Administrative Staff This care plan is aimed as a guide to treatment and intended to aid the documentation of patient
The Development of the Oncology Symptom Management Clinic
 The Development of the Oncology Symptom Management Clinic Submitted by: Catherine Brady-Copertino BSN, MS, OCN Executive Director Anne Arundel Medical Center s Geaton and JoAnn DeCesaris Cancer Institute
The Development of the Oncology Symptom Management Clinic Submitted by: Catherine Brady-Copertino BSN, MS, OCN Executive Director Anne Arundel Medical Center s Geaton and JoAnn DeCesaris Cancer Institute
VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES
 VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES Care Initiation: Critical Interventions VNAA Best Practice for Hospice and Palliative Care The first few days following a patient s admission to
VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES Care Initiation: Critical Interventions VNAA Best Practice for Hospice and Palliative Care The first few days following a patient s admission to
TEAMBUILDING CREATING A POSITIVE CULTURE IN HOSPICE CARE
 ...from the Middle Ages to the 21st Century TEAMBUILDING CREATING A POSITIVE CULTURE IN HOSPICE CARE Emily Bradford RN CHPN Director of Hospice Services VNA Middle Ages: 16th-18th Centuries: Religious
...from the Middle Ages to the 21st Century TEAMBUILDING CREATING A POSITIVE CULTURE IN HOSPICE CARE Emily Bradford RN CHPN Director of Hospice Services VNA Middle Ages: 16th-18th Centuries: Religious
COPD Management in the community
 COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
Challenging The 2015 PH Guidelines - comments from the Nurses. Wendy Gin-Sing RN MSc Pulmonary Hypertension CNS Imperial College Healthcare NHS Trust
 Challenging The 2015 PH Guidelines - comments from the Nurses Wendy Gin-Sing RN MSc Pulmonary Hypertension CNS Imperial College Healthcare NHS Trust Recommendations for pulmonary hypertension expert referral
Challenging The 2015 PH Guidelines - comments from the Nurses Wendy Gin-Sing RN MSc Pulmonary Hypertension CNS Imperial College Healthcare NHS Trust Recommendations for pulmonary hypertension expert referral
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Evaluation of of Resident Physician s. Do Not Resuscitate Orders Orders
 Evaluation of of Resident Physician s Understanding of Living of Living Wills and Wills Do and Not Do Not Resuscitate Orders Orders Colleen McQuown, MD Donald Kennedy,DO Danh Nguyen, DO Jennifer Frey,
Evaluation of of Resident Physician s Understanding of Living of Living Wills and Wills Do and Not Do Not Resuscitate Orders Orders Colleen McQuown, MD Donald Kennedy,DO Danh Nguyen, DO Jennifer Frey,
Honoring Patient Wishes
 Honoring Patient Wishes Nurses communication skills key to helping patients achieve end-of-life goals by Anna Mariani Reseigh Hearing the voice of the customer (VOC) is a goal for many industries. For
Honoring Patient Wishes Nurses communication skills key to helping patients achieve end-of-life goals by Anna Mariani Reseigh Hearing the voice of the customer (VOC) is a goal for many industries. For
Course Materials & Disclosure
 E L N E C End-of-Life Nursing Education Consortium Module 7 Loss, Grief, & Bereavement Course Materials & Disclosure Course materials including handout(s) and conflict of interest disclosure statement
E L N E C End-of-Life Nursing Education Consortium Module 7 Loss, Grief, & Bereavement Course Materials & Disclosure Course materials including handout(s) and conflict of interest disclosure statement
Policy for Admission to Adult Critical Care Services
 Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Partnering With Hospice to Improve Pain Management in the Nursing Home Setting
 People are living longer but are dying with more disabilities, often in nursing homes. Identification of those who are dying needs to be quicker to allow discussion of goals of care and to meet their individual
People are living longer but are dying with more disabilities, often in nursing homes. Identification of those who are dying needs to be quicker to allow discussion of goals of care and to meet their individual
HOSPICE IN MINNESOTA: A RURAL PROFILE
 JUNE 2003 HOSPICE IN MINNESOTA: A RURAL PROFILE Background Numerous national polls have found that when asked, most people would prefer to die in their own homes. 1 Contrary to these wishes, 75 percent
JUNE 2003 HOSPICE IN MINNESOTA: A RURAL PROFILE Background Numerous national polls have found that when asked, most people would prefer to die in their own homes. 1 Contrary to these wishes, 75 percent
I WOULD RECOMMEND INCORPORATING RECOMMENDATIONS INTO SHARED DECISION MAKING
 I WOULD RECOMMEND INCORPORATING RECOMMENDATIONS INTO SHARED DECISION MAKING JENNY WEI DO UNIVERSITY OF UTAH SCHOOL OF MEDICINE DEPARTMENT OF INTERNAL MEDICINE NOTHING TO DISCLOSE DISCLOSURES OBJECTIVES
I WOULD RECOMMEND INCORPORATING RECOMMENDATIONS INTO SHARED DECISION MAKING JENNY WEI DO UNIVERSITY OF UTAH SCHOOL OF MEDICINE DEPARTMENT OF INTERNAL MEDICINE NOTHING TO DISCLOSE DISCLOSURES OBJECTIVES
Hospice Continuous Home Care LEGACY HOSPICE
 Hospice Continuous Home Care LEGACY HOSPICE The Basics CONTINUOUS HOME CARE OF THE HOSPICE PATIENT What is Continuous Home Care? A day on which an individual who has elected to receive hospice care is
Hospice Continuous Home Care LEGACY HOSPICE The Basics CONTINUOUS HOME CARE OF THE HOSPICE PATIENT What is Continuous Home Care? A day on which an individual who has elected to receive hospice care is
Safety reporting in multi-site clinical trials in Palliative Care
 Safety reporting in multi-site clinical trials in Palliative Care Belinda Fazekas Linda Devilee Zac Vandersman David Currow Flinders University receives funding for PaCCSC from the Australian Government
Safety reporting in multi-site clinical trials in Palliative Care Belinda Fazekas Linda Devilee Zac Vandersman David Currow Flinders University receives funding for PaCCSC from the Australian Government
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces.
 End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Evolution of Hospice. Hospes: 1) Host 2) Guest, visitor 3) foreigner. Wholistic Care. hospice, hospitality, hostel
 Host 2) Guest, visitor 3) foreigner. Wholistic Care. hospice, hospitality, hostel") Evolution of Hospice Roman Empire 27 BC to 467 CE 500 L Hotel Dieu 1500 Our Lady s Hospice Dublin: Sister May Aikenhead 1879 St Christopher s Hospice London: Cicely Saunders 1967 Connecticut Hospice: Florence
Evolution of Hospice Roman Empire 27 BC to 467 CE 500 L Hotel Dieu 1500 Our Lady s Hospice Dublin: Sister May Aikenhead 1879 St Christopher s Hospice London: Cicely Saunders 1967 Connecticut Hospice: Florence
1/8/2018. Chapter 55. End-of-Life Care
 Chapter 55 End-of-Life Care Some deaths are sudden; others are expected. Health team members see death often. Death and dying mean helplessness and failure to cure. Your feelings about death affect the
Chapter 55 End-of-Life Care Some deaths are sudden; others are expected. Health team members see death often. Death and dying mean helplessness and failure to cure. Your feelings about death affect the
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit
 Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Palliative Care in Long-term Care: INNOVATIVE MODELS
 Palliative Care in Long-term Care: INNOVATIVE MODELS Betty Lim, MD Eileen R Chichin, PhD, RN & Laurie Posner, MD Care Settings for the Elderly Home Hospital Private House Assisted Living Facilities Residential
Palliative Care in Long-term Care: INNOVATIVE MODELS Betty Lim, MD Eileen R Chichin, PhD, RN & Laurie Posner, MD Care Settings for the Elderly Home Hospital Private House Assisted Living Facilities Residential
Chapter 4 Health and Illness
 Chapter 4 Health and Illness Definition of Health According to WHO, health is a state of complete physical, mental, and social wellbeing, not merely the absence of disease or infirmity Americans believe
Chapter 4 Health and Illness Definition of Health According to WHO, health is a state of complete physical, mental, and social wellbeing, not merely the absence of disease or infirmity Americans believe
START THE CONVERSATION
 START THE CONVERSATION SM conversation guide A public education initiative by vermont s non-profit vna s, home health and hospice agencies in partnership with vermont ethics network www.starttheconversationvt.org
START THE CONVERSATION SM conversation guide A public education initiative by vermont s non-profit vna s, home health and hospice agencies in partnership with vermont ethics network www.starttheconversationvt.org
Rock, Paper, Scissors
 Rock, Paper, Scissors Ideologies, Older People and End-of-Life Care Laura Green Doctoral Student University of Bradford, United Kingdom Aims Background & brief intro to study Present findings Contextualise
Rock, Paper, Scissors Ideologies, Older People and End-of-Life Care Laura Green Doctoral Student University of Bradford, United Kingdom Aims Background & brief intro to study Present findings Contextualise
Advance Care. Clinical. connections. ADVANCE CARE PLANNING: Uniting to Help Our Community
 Clinical connections A PUBLICATION FROM SUMMER 2018 IN THIS ISSUE 2 Conversations & Compassion at the End of Life 3 Palliative Care Partnership 4 ALS Educational Collaboration 5 Hospice Lightens Family
Clinical connections A PUBLICATION FROM SUMMER 2018 IN THIS ISSUE 2 Conversations & Compassion at the End of Life 3 Palliative Care Partnership 4 ALS Educational Collaboration 5 Hospice Lightens Family
Medications Changes from Hospital to Hospice
 Medications Changes from Hospital to Hospice March 15, 2013 Maxine DeLaCruz, MD Assistant Professor MD Anderson Cancer Center T. Hanh Trinh, MD Associate Medical Director Houston Hospice 1 Objectives To
Medications Changes from Hospital to Hospice March 15, 2013 Maxine DeLaCruz, MD Assistant Professor MD Anderson Cancer Center T. Hanh Trinh, MD Associate Medical Director Houston Hospice 1 Objectives To
RIGHTS OF PASSAGE A NEW APPROACH TO PALLIATIVE CARE. INSIDE Expert advice on HIV disclosure. The end of an era in Afghanistan
 Publications Mail Agreement Number 40062599 NOVEMBER 2013 VOLUME 109 NUMBER 9 RIGHTS OF PASSAGE A NEW APPROACH TO PALLIATIVE CARE INSIDE Expert advice on HIV disclosure The end of an era in Afghanistan
Publications Mail Agreement Number 40062599 NOVEMBER 2013 VOLUME 109 NUMBER 9 RIGHTS OF PASSAGE A NEW APPROACH TO PALLIATIVE CARE INSIDE Expert advice on HIV disclosure The end of an era in Afghanistan
Advance Care Planning
 Advance Care Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil, MD Course Director & Producer At the end of this session You
Advance Care Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil, MD Course Director & Producer At the end of this session You
Transfer Trauma: A Trip to the ER Can Put an Older Adult at Risk
 Transfer Trauma: A Trip to the ER Can Put an Older Adult at Risk Mukaila Raji, MD, MSC Professor and Director, Internal Medicine-Geriatrics Program Director, UTMB Geriatric Fellowship Department of Internal
Transfer Trauma: A Trip to the ER Can Put an Older Adult at Risk Mukaila Raji, MD, MSC Professor and Director, Internal Medicine-Geriatrics Program Director, UTMB Geriatric Fellowship Department of Internal
European Recommendations for End-of-Life Care for Adults in Departments of Emergency Medicine
 European Recommendations for End-of-Life Care for Adults in Departments of Emergency Medicine September 2017 European Recommendations for End-of-Life Care in Departments of Emergency Medicine * Summary
European Recommendations for End-of-Life Care for Adults in Departments of Emergency Medicine September 2017 European Recommendations for End-of-Life Care in Departments of Emergency Medicine * Summary
Communication with Surrogate Decision Makers. Shannon S. Carson, MD Associate Professor University of North Carolina
 Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
Communication with Surrogate Decision Makers Shannon S. Carson, MD Associate Professor University of North Carolina Role of Communication with Families in the ICU Sharing information about illness and
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Presentation Outline
 Enhancing Palliative and End of Life Care Services in Hospital Authority Dr Su Vui LO Director of Strategy and Planning Presentation Outline Background Recent initiatives Way forward 2 Background Hospital
Enhancing Palliative and End of Life Care Services in Hospital Authority Dr Su Vui LO Director of Strategy and Planning Presentation Outline Background Recent initiatives Way forward 2 Background Hospital
An individual may have one type of advance directive or may have both. They may also be combined in a single document.
 Advance Directives History In 1991, the Patient Self-Determination Act became a federal law. The act was signed into law to help ensure that patients preferences about medical treatment would be followed
Advance Directives History In 1991, the Patient Self-Determination Act became a federal law. The act was signed into law to help ensure that patients preferences about medical treatment would be followed
Dementia and End-of-Life Care
 Dementia and End-of-Life Care Part IV: What practical information should I know? About this resource The needs of people with dementia at the end of life* are unique and require special considerations.
Dementia and End-of-Life Care Part IV: What practical information should I know? About this resource The needs of people with dementia at the end of life* are unique and require special considerations.
Psychotropic Drug Use To Medicate or Not to Medicate?
 Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada.
 CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
MAKING YOUR WISHES KNOWN: Advance Care Planning Guide
 MAKING YOUR WISHES KNOWN: Advance Care Planning Guide ADVANCE CARE PLANNING The process of learning about the type of medical decisions that may need to be made, considering those decisions ahead of time
MAKING YOUR WISHES KNOWN: Advance Care Planning Guide ADVANCE CARE PLANNING The process of learning about the type of medical decisions that may need to be made, considering those decisions ahead of time
Hospice Clinical Record Review
 Purpose: Surveyors may use this worksheet when conducting clinical record reviews during a hospice survey. Directions: Fill in appropriate data. Table 1. Patient Information Patient Information Residence
Purpose: Surveyors may use this worksheet when conducting clinical record reviews during a hospice survey. Directions: Fill in appropriate data. Table 1. Patient Information Patient Information Residence
PROVIDER POLICIES & PROCEDURES
 PROVIDER POLICIES & PROCEDURES EXTENDED NURSING SERVICES The purpose of this document is to provide guidance to providers enrolled in the Connecticut Medical Assistance Program (CMAP) on the requirements
PROVIDER POLICIES & PROCEDURES EXTENDED NURSING SERVICES The purpose of this document is to provide guidance to providers enrolled in the Connecticut Medical Assistance Program (CMAP) on the requirements
Chapter 2: Patient Care Settings
 Chapter 2: Patient Care Settings MULTIPLE CHOICE 1. While the home health nurse is doing the entry to service assessment on a home-bound patient, the wife of the patient asks whether Medicare will cover
Chapter 2: Patient Care Settings MULTIPLE CHOICE 1. While the home health nurse is doing the entry to service assessment on a home-bound patient, the wife of the patient asks whether Medicare will cover