The Hillingdon Hospitals NHS Foundation Trust. Meeting of the Board of Directors
|
|
|
- Florence Conley
- 6 years ago
- Views:
Transcription
1 The Hillingdon Hospitals NHS Foundation Trust Meeting of the Board of Directors Wednesday 30 th July 2014, 2pm Furze Conference Room, Hillingdon Hospital Paper Timings * a) Introductory business 5 mins 1. Welcome and apologies for absence - 2. Declaration of hospitality or amendments to the Register of Interests - 3. Minutes of the Board meeting held in Public on 25 th June Actions Log 5. Declaration of Any Other Business - 6. Patient Story and Putting People First Report (TM) 10 mins 7. Chief Executive s Report (SDG) 5 mins b) Strategy 8. Final Strategic Plan (KMO) 5 mins 9. Hillingdon Strategic Site Masterplan (PW) 15 mins 10. Delivering the Strategy (KMO) 10 mins 11. Emergency Care Reconfiguration Project Update (PW) 10 mins c) Quality, Operational & Financial Performance 12. Bullying, Harassment and Career Progression: Follow up from the 2013 National Staff Survey (CG) 10 mins 13. Safer Staffing Planned and Actual Staffing Levels (TM) 10 mins 14. Quality & Operational Performance Report (KMO/TM) 15 mins 15. Financial Report (PW) 10 mins /15 Quarter 1 Transformation and QIPP update (KMO) 10 mins 17. Annual Report on Medical Appraisal and Revalidation (RGM) 10 mins 18. Patient led Assessment of the Care Environment (PLACE) 2014 Results 10 mins
2 (PW) 19. Infection Control Annual Report 2013/14 (TM) 5mins d) Risk 20. The Integrated Risk Register (TM) 10 mins 21. Board Assurance Framework (TM) 10 mins 22. Health & Safety Report (PW) 10 mins e) Regulatory 23. Care Quality Commission Inspection (TM) 10 mins f) Other 24. Audit & Assurance Committee Annual Report 2013/14 (KA) 5 mins 25. Issues arising from the Board Committees 15 mins 26. Closure of a Dormant Trust Bank Account (PW) Use of Trust Seal Any Other Business Questions from the Public - - Date of next meeting: Wednesday 27 th August 2014, 2pm, Board Room, Mount Vernon Hospital * NB timings are indicative only: the Chair may decide to vary the timings and order.
3 ITEM 3 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST MINUTES OF THE MEETING OF THE BOARD OF DIRECTORS HELD ON WEDNESDAY 25 th JUNE 2014 IN THE FURZE CONFERENCE ROOM, HILLINGDON HOSPITAL Meeting held in public Present: Katey Adderley (KA) Carol Bode (CB) Shane DeGaris (SDG) Soraya Dhillon (SDh) Abbas Khakoo (AK) Karl Munslow Ong (KMO) Theresa Murphy (TM) Pradip Patel (PP) James Reid (JR) Craig Rowland (CR) David Searle (DS) Paul Wratten (PW) In Attendance: Claire Gore (CG) David Coombs (DC) Apologies: Lis Paice (LP) Also Present: Noreen Rice (NR)* Graham Bartram Don Dakin Jack Creagh Five members of public Non-Executive Director Non-Executive Director Chief Executive Non-Executive Director Medical Director Chief Operating Officer Executive Director of the Patient Experience & Nursing Deputy Chairman and Non-Executive Director Interim Chair Non-Executive Director Executive Director of Corporate Development Finance Director Director of People Trust Secretary (minutes) Non-Executive Director Emergency Care Service Manager Public Governor Public Governor Staff Governor * for item 05/06/2014 Declaration of Hospitality or Amendments to Register of Interests None declared. ACTION 1
4 01/06/2014 ACTION Minutes of the last Meeting The draft minutes of the Board meeting held in public on 28 th May 2014 were approved as an accurate record. 02/06/2014 Actions Log 03/06/2014 Declaration of Any Other Business The Board reviewed the actions arising from the Board meeting held in public on 28 th May 2014 and those outstanding from previous meetings. The Board agreed that those actions marked xx could be closed. It was agreed that the previously circulated paper on Governor development would be taken at the end of the meeting. 04/06/ /06/2014 Patient Story and Putting People First TM welcomed NR to the meeting who outlined the patient story of a 92 year old gentleman who was brought to the A&E department following a cardiac arrest at home and subsequent resuscitation by his daughter. NR stated that the gentleman was joined by a large number of close relatives. NR stated that it was apparent that the patient would not survive and it was important to find a suitable environment for the patient and his family. NR stated that the A&E resus unit was extremely busy with two other two acutely unwell patients. NR outlined the action taken by the A&E department to provide an alternative location to care for the patient and to support the family for the likely forthcoming bereavement. TM stated that this was a difficult case, but praised NR and the team. TM stated that the size of the resus unit was a key issue and this is being addressed with the current emergency care project. TM stated the option given to the family was not ideal, but highlighted the highly positive feedback from the family about the way the situation was handled and that they were involved in the decision about where to care for the patient. PP stated that dignity and respect are key in providing care. PP stated that this case demonstrates these values in action and highlight the importance of involving a patient s family in sensitive discussions. SDh welcomed how the Trust adopted a compassionate approach to managing a challenging situation. JR praised NR and the team for how the situation was handled. JR stated that having visited the A&E resus unit he agreed that this needs to be addressed. 2
5 TM presented the Putting People First report that included the Trust s performance in the Family and Friends Test (FFT) in May. TM stated that it was a very challenging month for the Trust which is shown in the FFT results and several other aspects of performance to be discussed later in the meeting. TM stated that the overall FFT score dropped compared to April, with 11 wards seeing a reduction in their score. ACTION TM highlighted the benchmarking information provided, including the very positive position of the Trust in terms of the low proportion of negative responses received. TM stated that the results are reviewed in detail at the ward level with the matrons and ward managers; the challenge now is to get greater traction on addressing the negative comments. AK suggested that the data is presented in the same format as for the rest of the quality report with information provided on the FFT score in the previous year, most recent month, and current year to date. CB asked whether staffing pressures could be a factor in the dip in FFT score. TM agreed that this could be a factor given the redeployment of staff between wards in response to the activity levels. JR highlighted that the extra capacity wards were the lowest performing on the FFT and stated that these issues will be part of the discussion later in the meeting on the activity pressures. The Board noted the report and agreed to the revised reporting proposed by AK. TM 06/06/2014 Chief Executive s Report SDG presented the report that updated the Board on a range of local, regional and national publications and developments. SDG stated that the Trust continues to maintain its green governance rating and achieve the performance indicators set out by Monitor. SDG stated that the financial position is however more challenging and will be picked up later in the meeting. SDG highlighted that the Board has commissioned KPMG to undertake a review of the Trust s governance, taking account of the Care Quality Commission and Monitor definitions of a well-led organisation. SDG stated that KPMG will be observing various meetings in July as part of this review. SDG highlighted the recent action being taken at the national level to prepare for winter and address backlogs for waiting 3
6 lists for treatment. SDG stated that once the implications of this for the Hillingdon health economy are clearer, KMO will brief a future Board meeting. ACTION SDG asked DS to update the Board on the emergency care project. DS stated that the overall project remains on track, but that there has been a small delay to the Clinical Decision Unit works since the report was produced. The Board noted the report. 07/06/2014 Shaping a Healthier Future Progress Update KMO presented the report that provided an update on the implementation of the Shaping a Healthier Future (SaHF) programme at the Trust. KMO stated that the Trust is closely involved in the discussions on the transition plans to deliver changes to maternity and A&E services at other hospitals proposed under SaHF. KMO stated that the outline business cases are being reviewed by the central SaHF team. KMO stated that a key aspect of this assurance process will be the affordability of the business cases, both in terms of each Trust s ability to service the investment and the overall affordability of the SaHF programme. KMO stated that the current aim is to bring the revised outline business case to the July Board for approval, but this is dependent on the Trust receiving feedback from this assurance process. TM highlighted that there has been a 24% increase in occupancy of the resus unit over the last two months. KMO stated that this has been due to a 12.5% increase in the number of patients, plus there has been an increase in the length of time that patients are staying in the unit. JR asked whether the transfer of Marina ward to Mount Vernon is on track given this appears to be central to the plans to provide an interim solution to create capacity for 500 births from Ealing hospital. KMO stated that there are several options for providing the capacity for patients currently seen on Marina ward which would enable the Trust to provide this short term maternity capacity. SDh asked how staff are being engaged in the transitional arrangements and the future plans. KMO stated that the senior clinical leads - the Head of Midwifery and the Associate Clinical Director for Obstetrics - together with the Assistant Director of Operations for the divisions, are leading this work and have numerous mechanisms for engaging staff in the 4
7 transition and wider plans. KMO stated that the challenge is that the timings for any changes are not within the Trust s control. SDG agreed that there has been significant engagement by the Executives and senior management; however the issue is about the level of uncertainty due to factors outside of the Trust s control. SDG stated that this engagement will need to remain an areas of focus given that the uncertainty is likely to continue before the proposals for Ealing hospital are finalised. SDG stated that it is important to ensure staff understand that the plans around the initial 500 births from Ealing hospital are distinct to the longer-term significant increase in maternity activity under SaHF. ACTION DS noted that the capital costs for the SaHF works are currently being refined and asked for confirmation that the business case will include the costs of reproviding any facilities that are temporarily or permanently displaced by the works, most notably car parking spaces. JR assured DS and the public present that the Board will not lose sight of the implications of the proposals on the car parking capacity. PP thanked KMO for his work in overseeing the significant changes affecting the Trust, whilst simultaneously addressing the significant day to day operational challenges. KMO thanked PP for this comments and stated that he, TM and AK are very mindful of the pressures on the operational teams, plus the support provided by PW, CG, DS and their teams. The Board noted the report. 08/06/2014 Safer Staffing: Nursing and Midwifery Establishment Review (Inpatient Areas) and Planned & Actual Staffing Levels May 2014 JR prefaced the discussion by stating that he could assure the public that the Trust is open and honest, and therefore the data presented represents the true situation. JR stated that as shown in the data, there are challenges with aspects of nursing staffing; hence this detailed paper and the following paper on recruitment and retention. TM presented the report that included the six monthly establishment review of the nursing and midwifery staff, and provided the planned and actual staffing levels for each inpatient ward in May. TM outlined the contents of the reports on a page by page basis, and highlighted the methodology by which the establishment review has been undertaken. TM highlighted how an additional 658k has been invested in nursing and midwifery staffing following the establishment review. 5
8 TM highlighted the temporary staffing usage and the shift fill rates. TM highlighted that the Trust has a rolling recruitment programme and 50 high quality staff were recruited at a recent recruitment event. TM stated that retention is a key factor that needs to be addressed. TM stated that one factor is how to balance stability for staff with the need to redeploy staff between wards based on acuity pressures. ACTION TM talked through the planned and actual staffing levels in May. TM highlighted the actions that have been taken in response to the staffing levels falling below those planned, which included herself and the matrons working clinically on wards. TM stated that for next month, information on pressure ulcers and infection control will be added to the report. CR stated that he found the reports extremely helpful. CR referred to the chart on the second page of the report on the funded whole time equivalent (WTE) against the recommended WTE. CR asked whether this establishment is based solely on the Safer Nursing Care Tool (SNCT) or whether it reflects the judgement of the ward manager on the level of staffing required. TM stated that it reflects the judgement of the ward managers as a result of the dependency of the patients on the ward. KA noted that the report references several different sets of recommendations about staffing levels from national organisations. KA asked whether the Trust has used these recommendations to produce a single agreed staffing level, and if so, whether this is the establishment figure shown in the chart referred to by CR. TM stated that the chart is based on the SNCT acuity tool. KMO highlighted that the funded WTE in the chart does not take account of increases in staffing that may be put in place based on the acuity at a particular time, i.e. to provide 1:1 care to a patient. SDh stated that in addition to the data it is important to look at softer issues such as how staff are feeling on the ground, and whether the matrons and ward manager feel they have sufficient staff. SDh suggested that the Board should discuss its aspirations for staffing levels at a future meeting. SDh asked about the processes for flexing staff across the organisation in response to activity pressures at a given time. TM stated that this is an important role of the matrons. TM stated that staffing levels are reviewed twice a day, with a view to balancing risk across the organisation. TM stated that temporary staff may also be sought, as shown by the level of expenditure on temporary staff in recent months. TM stated that out of hours, the site practitioners have a key role in managing the staffing levels across the hospital. TM stated that whilst the process is effective at managing risk, the movement of staff impacts on staff retention. 6
9 ACTION SDG stated that the clinical and operational teams are working hard each day to make decisions on staffing, and management will not override clinical requests for staff, as is reflected in the level of agency spend in the finance report. SDG stated that despite the investment that was made based on TM s professional judgement, the data shows that the Trust does have some issues around staffing levels. SDG stated that this is being addressed through the recruitment and retention strategy. CB stated that she has confidence in TM and the team managing the risk at a day to day basis, but stated that there is a need for the Board to take a step back and look at whether the Trust is transforming ways of working to address these issues; for example to enable early discharge. CB highlighted the importance of taking a more forward look at staffing requirements through forecasting, rather than solely looking back at past fill rates. CG agreed and stated that this is part of the work on workforce transformation. PP highlighted the importance of trusting the judgement of ward managers and matrons given their proximity to the patients. PP highlighted the work undertaken in his organisation to plan staffing requirements and offered to facilitate the sharing of this practice. SDG thanked PP for this offer and asked CG to take this up. JR stated that despite the investment in nursing staff, there remained two areas that had a shift rated red for the registered nurse to patient ratio on the establishment. JR asked TM whether she was comfortable with this situation. TM stated that she felt reconfiguring the shift patterns on Drayton ward would address the red rating on that ward; whilst the red rating for the night shift on Trinity ward reflects how the staff are deployed. TM stated that it is also important to factor in bed occupancy as Trinity ward is often not fully occupied at night. SDG asked that TM brings back a narrative to the Board on the red and amber rated shifts on establishment that outlines what is being to done to address these, or the mitigations in place to make the level of risk acceptable. JR stated that there has been an increase of approximately 50% in the use of temporary staff since the end of 2013 and asked whether this is due to the opening of the escalation wards or other factors. KMO suggested that this is picked up as part of the discussion on the financial and operational performance reports later in the meeting. AK echoed SDh s and KA s comments and stated that he is not clear on the Trust s aspiration for staffing levels. AK stated that it is important to be clear on whether the Trust is setting 7
10 levels at those defined by the Royal College of Nursing as providing basic safe care level or ideal good quality care. ACTION SDh stated that the expenditure on agency spend is bad spend and the Board should be challenging itself to spend this on substantive staff. The Board: 1. Noted the report. 2. Requested information to the July Board on the red and amber rated shifts on staff to patient ratios by establishment, which outlines the action being taken to address these, or the mitigations to enable this to be an acceptable risk. 3. Agreed that the next six monthly establishment review should outline how professional judgment has been factored into the recommended staffing, and which of the national recommendations have been met in setting the establishment. TM TM 09/06/2014 Recruitment and Retention Strategy CG presented the recruitment and retention strategy for the Board s review. CG stated that the strategy is focused on the nursing and midwifery workforce but is applicable to the whole workforce. CG outlined the aims of the strategy, which include decreased spend on agency and bank staff by reducing the level of turnover and the time taken to recruit to posts. CG highlighted the wide range of initiatives being explored, including linkages with universities and colleges, exploring the impact of improving the accommodation at Mount Vernon, and of increasing the rate paid to staff working through the bank. CG stated that the reasons why staff leave the organisation are also being explored, through strengthened exit interviews, and her and TM undertaking focus groups with staff. CB stated that the report includes all of the key aspects of a recruitment and retention strategy. CB asked whether the Trust is considering partnering with a recruitment supplier or specialist given this is not the Trust s core business. CB suggested that there could also be scope for entering into a partnership to improve the staff accommodation. CB referred to the linkages with education providers and stated that this issue has also been raised in discussions with Governors on member engagement. CB stated that there is scope for the Governors to engage with schools which could assist both with membership engagement and also future staff recruitment. CG stated that she is writing a business case for an experienced recruitment specialist to assist with the delivery of the strategy over the next six months. 8
11 ACTION PP agreed that there is scope to learn lessons from external organisations. In relation to staff choosing to work through an agency for a higher hourly rate, PP highlighted the importance of demonstrating to staff the total benefits package of working for the Trust compared to an agency, such as annual leave and pension entitlements. SDh encouraged linkages with the universities within commuting distance from the Trust who are often seeking to assist their graduates gain employment. The Board: 1. Supported the recruitment and retention strategy. 2. Requested short progress reports on recruitment in three months, and on retention in six months. CG 10/06/2014 Serious Incident Investigations TM presented the report that provided an overview of the management of Serious Incident (SI) investigations, as requested by the Board. TM stated that a significant number of the Trust s SI panel investigations fail to meet the deadline of 45 working days for providing the report to the Commissioning Support Unit (CSU). TM stated that the CSU have praised the quality of the Trust s investigation reports. TM stated that a factor in missing the deadline is that all panel reports are signed off by the Board, whereas in other Trusts these are usually signed off by an Executive Director. TM stated that the CSU have suggested that a report is provided to the CSU following review by an Executive Director and then amendments required by the Board are subsequently provided to the CSU. TM stated that the report also included information on the policy in place for investigating Incidents of Concern which are often near misses for SIs. TM highlighted the importance of following through on actions arising from investigations into IoCs. TM highlighted the benchmarking on reported SIs and Never Events and stated that the Trust is broadly in line with the other Trusts in North West London, with the exception of Chelsea & Westminster Hospital and West Middlesex Hospital. TM stated that this could reflect variations in patient safety, or that these Trusts have higher reporting levels. JR stated that whilst chair of the Quality & Risk Committee (QRC) he requested that IoCs are reported to the QRC in future. JR stated that he very strongly believes that the SI reports should come to the Board before submission to the 9
12 CSU given the Board often identify amendments that are required to strengthen reports, and also that the investigations often raise issues of concern that require the Board s attention. JR stated that he would support other changes to make the SI investigation process more efficient, such as a smaller skilled group of staff who investigate SIs. ACTION SDG referred to the benchmarking and stated that the Care Quality Commission risk banding and the conclusions of the quality governance review provide assurance that the Trust s reporting levels and Board scrutiny of SI reports are appropriate. AK and KA stated the approach of compressing the panel meeting into a single session was trialled, but the logistics were too challenging in terms of gaining the required witness statements. KA stated that it was not practical to hold a long single meeting and the panel need to review the report at a second meeting in order to consider whether the questions in the terms of reference have been addressed by the draft report. KA stated that what can be improved is the length of time between the panel meetings, which is affected by the availability of the clinical staff on the panel. DS highlighted the important role of the Investigating Officer (IO) bringing together the information and producing the investigation report that addresses the relevant questions. DS stated that he would support a dedicated resource for the IO role if this would improve the timeliness of producing the reports. DS stated that it is important not to compromise on the quality of the report and the report must be of sufficient high quality that the Chief Executive can personally present it to the family involved in the SI. SDG stated that the thoroughness and quality of the report is the key factor. SDG stated that he has not had a complaint from a family that the report has taken too long to produce and stated the feedback from families is positive that the Board is taking the incident seriously by reviewing the investigation report. The Board: 1. Noted the report. 2. Strongly supported the process of SI investigation reports being approved by the Board before submission to the CSU. 3. Agreed that in addition to this scrutiny of the full report, SIs and the lessons learnt should be summarised to the Board on a quarterly basis. 11/06/2014 Dementia Strategy: Implementation Update 10
13 TM presented the report that provided an update on progress with implementing the Trust s dementia strategy in 2013/14. TM highlighted the progress made in delivering the four themes of the strategy and highlighted the priorities for the year ahead. ACTION TM stated that the Trust is working closely with partners in the health, social care and voluntary sector to deliver the strategy. TM stated that future priorities will include greater use of technology and integrated care plans. JR referred to the formal opening of the refurbished Beaconsfield East ward the previous day and congratulated the nursing, estates and other staff involved in the delivery of this project. PP noted that the dementia awareness training is focused on the care of the elderly wards. PP stated that elderly patients are often in wards across the hospital and asked that this training is prioritised across the Trust given the benefits to patients. CG stated that the teams are very mindful of the importance of this training and it is being given appropriate focus. AK stated that he, Richard Grocott-Mason (fellow joint Medical Director) and TM are promoting the importance of dementia screening assessments to the medical staff. The Board noted the progress to date and endorsed the activities in 2014/15 to continue the work programme. 12/06/2014 Quality and Operational Performance Report KMO presented the quality and operational performance report for May. KMO stated a number of the key issues in the report have already been highlighted earlier in the meeting. KMO stated that whilst the Trust continues to be rated green on the Monitor indicators, there has been unprecedented levels of non-elective admissions. KMO stated that the A&E resuscitation unit is under great pressure, and there has been a large increase in the number of patients requiring treatment in the High Dependency Unit (HDU). KMO stated that the Trust is working with partners to understand the reason for these pressures, which are being seen across North West London and nationally. KMO stated that the London Ambulance Service has also been under huge pressure. KMO stated that there has been good partnership working with health and social care partners, and the Trust and Hillingdon CCG agreed to jointly fund 15 spot purchase beds to alleviate pressure in the hospital from patients waiting for continuing healthcare assessments. KMO stated that the 11
14 Trust and partners are also working to identify the reasons for the activity pressures. ACTION KMO highlighted the changes to the performance report to reflect the new contact with the commissioners. KMO stated that work is underway to revise the report to include greater trend analysis. TM highlighted that it has been 12 months since the Trust last had an MRSA bacteraemia, and there has been one c-diff infection in 2014/15 to date. TM stated that two unrelated patients at the Trust have tested positive for antibiotic resistant bacteria known as Carbapenemasme-producing Enterobacteriaceae (CPE). TM stated that the Trust has performed a risk assessment and has taken measures to ensure the organism does not spread to other patients. TM outlined the Trust s position on falls, pressure ulcers and complaints. AK highlighted that there is no updated mortality information available from Dr Foster. JR asked whether the process for making decisions to open escalation beds is sufficiently robust and takes account of the views of the Nursing and Medical Directors. KMO confirmed that the process is robust and is driven by patient safety. KMO stated that decisions are made on the basis of patient acuity in the A&E department. KMO stated that lessons have been learnt from recent years when decisions were on occasion made out of hours, and he feels that decisions are now taken appropriately. KMO stated that the key issue to work with partners to reduce the demand on the hospital. TM stated that any escalation ward will have nurse and medical leadership, and the process for opening these wards has been discussed with the Clinical Directors. TM highlighted that the demography of the Trust s patients has changed, with the average age of patients on a surgical ward recently being 80 years old. TM stated that increasingly whilst patients may be medically fit, they may still require assistance with care needs such as washing and dressing. AK stated that the process has changed in that the operational teams flag earlier when an escalation ward may be required, which enables the required staff to be arranged. AK stated that if escalation wards are not opened then pressures build up in A&E, which is not in patients interests. PP stated that the pressures will not go away, and therefore the Trust must look at how to solve this issue in the long-term. SDh asked whether enough has been done on issues such as rapid discharge, or looking to provide treatment to patients in alternative environments. KMO stated that these all form part 12
15 of the Trust s transformation workstreams, including ambulatory care and early supported discharge. ACTION AK stated that issues around the volume of work was raised at a recent junior doctor feedback session. AK stated that he and TM are meeting with a group of junior doctors from the session to seek further information on these concerns, and this will be included in a forthcoming Board report on junior doctor feedback. The Board noted the report. 13/06/2014 Financial Report 14/06/2014 QIPP Report PW presented the finance report for May and stated that the Trust ended the second month of the financial year behind plan by 512k, with a deficit of 696k. PW stated that this reflects the discussion earlier in the meeting about the staffing and activity pressures. PW stated that the Trust s Continuity of Services risk rating remains a 3, but has reduced to 2.5. PW stated that revenue is not a concern, and the QIPP plan is overachieving against the phased plan; the issue is the operating costs. PW stated that discretionary pay costs after two months of the financial year are 1m overspent. PW stated that this spend would have been 40% lower had it been through substantive staff, and it is the key factor in the variance to plan. PW stated that other Trusts are experiencing similar challenges and an unprecedented number of Trusts are reporting deficits in the first two months of the year, with staffing and activity pressures causing financial challenges. PW stated that by next month further information should be available on the extent of additional funds that may be made available nationally. SDG stated that the issue is clear; the activity levels and the escalation wards are causing financial challenges. SDG stated that the priority is to work with partners to reduce activity so that the escalation wards can be closed; and recruit substantive staff and improve staff retention to reduce spend on temporary staff. The Board noted the report and agreed that there would be a further more detailed discussion at the July Board based on the reforecast position after the first quarter of the financial year. 13
16 KMO presented the update on the 2014/15 QIPP programme and stated that in month two, 529k savings were achieved. KMO stated that the current risk adjusted forecast is 7.9m, which has increased by 400k compared to month one. ACTION KMO stated that the activity pressures are a risk to the improving inpatient care project savings and mitigating actions are being examined. KMO stated that similarly, the Trust is working closely with Hillingdon CCG around the risks to the CCG s QIPP programme from the activity pressures. KMO highlighted the information provided in the report on discharge and pharmacy as requested by the Board. The Board noted the report. 15/06/2014 Update on Clinical Records Department Relocation KMO presented the report that updated the Board on progress with the relocation of the clinical records library to an off-site facility. KMO stated that the health and safety risks for the staff have been addressed through the move, as have the risks to the records security. KMO stated that the operational teams are still working through some of the initial teething problems from the new service. KMO stated that the initial indications are that the move was managed within the budget; however a fuller financial analysis will be presented to the Board. JR asked whether the frequency of instances where notes are not available since the move has reduced. KMO stated that this has not been fully resolved, but has significantly improved since the initial teething problems. The Board noted the report. 16/06/2014 Care Quality Commission Inspection TM presented the report that outlined the process for how the Care Quality Commission (CQC) will undertake its forthcoming inspection of the Trust, and the preparations being made by the Trust for this. PP asked whether the project manager role is full-time and the individual has the appropriate skills. TM stated that this role is shared between two senior individuals; TM stated that she is also in discussions with the Programme Management Office (PMO) about the scope for additional support. SDG stated that the project managers have the appropriate seniority and skills, but he would follow-up outside of the meeting whether additional support is required. 14
17 ACTION The Board noted the report and agreed to receive regular progress updates. 17/06/2014 NHS Constitution TM and CG presented the report that outlined the assurance as to the Trust s compliance with the NHS Constitution. The Board noted the report and the assurance as to the Trust s compliance with the NHS Constitution. 18/06/2014 London Cancer Alliance Indemnity SDG presented the report that asked the Board to authorise the Trust signing an indemnity by members of the London Cancer Alliance (LCA) for any losses incurred by the Royal Marsden Foundation Trust (RMH) as a result of the RMH s hosting of the LCA. SDG stated that whilst in theory there is an unlimited liability, there are a number of mitigations to this, including the financial subscriptions from members that would be used to off-set any liabilities. SDG stated that importantly, the Trust is now a Board member of the LCA and therefore has an influence on the decisions that could incur a liability. PW stated that if the LCA staff are NHS employees undertaking NHS duties then they would be covered by the NHS Litigation Authority. PW stated that the liability for this indemnity is therefore in effect about issues the LCA may have with funding. The Board agreed to the Chief Executive signing the indemnity cover to The Royal Marsden Hospital NHS Foundation Trust for losses and liabilities suffered by the Royal Marsden arising out of the hosting of LCA activities. 19/06/2014 Issues Arising from the Board Committees CR provided a verbal update from the Transformation Committee meeting held on 9 th June. CR stated that one of the issues discussed, the QIPP programme, has already been covered earlier in this meeting. CR stated that the Committee received a paper on service developments and tenders for the first time. CR stated that the Committee was pleased to note the additional income being secured from new contracts and agreed to receive reports on forthcoming tenders bi-monthly, with a report on service developments every six months. 15
18 CR stated that the Trust s new ICT Director attended the meeting and provided an update on the delivery of the informatics strategy and his perspective on the Trust s position on ICT. CR stated that the Director will be bringing a further paper to the Committee s next meeting. ACTION 20/06/2014 Use of the Trust Seal The Board noted the use of the Trust Seal on the Deed of Trust relating to a bank account between Atlantic Data Ltd and the beneficiaries for the supply of electronic Disclosure and Barring Service applications. 21/06/2014 Any Other Business Governor Development CB presented the short report from herself and the Lead Governor on the key issues arising from the Governor development day held on 6 th June. CB stated that the issues included Governors getting to know each other and the NEDs better, and the information provided to the Governors. CB stated that the report is presented for the Board s information and initial comment. DS asked for clarification on the reference to briefing Governors on national matters of public interest. JR stated that he has reinforced to Governors that the Trust s position is that where the Trust is mentioned in the media or may feature in reports then the Governors will be briefed, such as on staffing. JR stated that he has advised Governors that it is not possible to provide a commentary on the numerous articles that feature in the media each day about the NHS. JR stated that several of the issues in the report have already been discussed; JR stated that these will be discussed further and fed back to the July Council of Governors meeting. The Board noted the report. 22/06/2014 Questions from the Public Mrs Thomas advised the Board that she had written to the London Ambulance Service (LAS) following two long waits for an ambulance. Mrs Thomas advised the Board that she had received a response from the Chief Executive of the LAS who advised that the LAS had been provided with additional resources in light of the pressures being faced. Mrs Thomas stated that when she last attended the Board she raised a number of issues with her husband s discharge summary. Mrs Thomas stated that on the Friday after the 16
19 Board meeting she received a letter in the post from AK with corrected discharge information. Mrs Thomas thanked AK for addressing these issues so promptly. ACTION Mrs Thomas referred to information provided to a recent Board meeting about the cancellation of operations and highlighted the importance of the role performed by the staff who prepare the documentation for theatres. Mrs Thomas welcomed that Consultants are receiving training on communication. Mrs Thomas suggested that the Trust speaks to the developers of St Andrews Park in Uxbridge about affordable housing for nurses. Mrs Thomas stated that she would like to visit the refurbished Beaconsfield East ward and would also like to attend the listening event being held by the CQC during its inspection of the Trust. Mrs Cook thanked the Trust for the opportunity to visit Beaconsfield East ward, which was very good. Mrs Cook asked whether the number of beds on the ward has reduced and also queried the staffing levels as she had not seen any nurses on the visit. TM stated that the bed numbers were reduced as part of the refurbishment in order to improve the care environment. TM stated that the ward is staffed for 20 beds, as outlined in the report earlier in the meeting. TM stated that some of the experienced staff from the ward have been temporarily redeployed to the escalation wards at times. Mrs Cook asked whether the red non-slip socks have made a difference to the number of patient falls. TM stated that the socks have helped reduce falls, but highlighted that there are range of factors that can lead to falls. TM stated that this is an area of close focus for the nursing staff. Mr Bartram referred to the proposed transfer of maternity activity from Hillingdon to Ealing and asked whether there have been discussions with Transport for London (TfL) about improving the transport links between Ealing and Hillingdon Hospital. KMO and SDG advised that there is a transport group for the central Shaping a Healthier Future (SaHF) programme that is reviewing bus routes. KMO highlighted that as part of SaHF, more services will also be provided in the community. Mr Bartram referred to the staffing levels shown for May and asked about the percentages. JR stated that these refer to the percentage of filled shifts from the funded establishment. Mr Bartram stated that this could be made clearer. Mr Bartram suggested that the Trust should speak to Hillingdon Council and the Greater London Authority about the scope for funding to bring the Mount Vernon accommodation into use for key workers. 17
20 ACTION Date of Next Meeting Mr Bartram highlighted the importance of ensuring that escalation wards have sufficient supplies such as bedding and drugs before they are opened. KMO stated that this is included in a detailed checklist that is completed prior to a ward being opened. Mr Bartram asked whether the reasons for the activity pressures have been analysed. KMO stated that initial analysis did not identify a common theme so this is being explored further. Mr Bishop stated that in his view the activity surge is due to the pressure on GP services. Mr Bishop stated that the Trust must prepare itself for the impact on A&E once the changes take place at other hospitals under SaHF. SDG stated that the Trust is closely involved in the extensive work to prepare for the closure of the A&E department at Central Middlesex Hospital. Mr Bishop referred to the contract won by the Trust to provide pathology services to Ealing GPs and asked why the Trust is not able to start providing this service on the required date. KMO stated that the contract is a positive development in that the Trust is bringing NHS work back to the NHS. KMO stated that the Trust is starting the service on the date required by the GPs, and there are robust arrangements in place to ensure this. Mr Bishop asked about the implications for the staff currently working for the private provider that delivers the service and whether they would be made redundant or transferred to the Trust. KMO stated that the Trust is currently awaiting the TUPE details from the current provider, and without this information he cannot comment further. However he expected that the Trust will most likely require additional staff given the increased workload. Mr Bishop asked why the Trust is engaging KPMG to review the Board and Council of Governors. JR stated that as part of good corporate governance the Trust is required to have an external assessment of its governance. Mr Bishop asked whether patient falls could be due to staffing levels. TM stated that this could be a factor. Mrs Davis supported Mr Bartram s comments about the Mount Vernon accommodation. Mrs Davis suggested that the Trust also asks the Foundation Trust members whether they could assist in providing temporary or long-term accommodation for nursing staff. 18
21 ACTION The next meeting is scheduled to take place on Wednesday 30 th July 2014, at 2.00pm in the Furze Conference Room, Hillingdon Hospital. James Reid Interim Chair Date. 19
22 ITEM 4 Actions arising from Board Meetings held in Public Note: actions marked xx are proposed for Board sign-off as completed. June 2014 Action ref: Action Action with 06/06/2014 Putting People First Report 08/06/2014 Safer Staffing 09/06/2014 Recruitment and Retention Strategy FFT data to be presented in the same format as for the rest of the quality report with information provided on the FFT score in the previous year, most recent month, and current year to date. (a) July Board to receive narrative on the red and amber rated shifts on staff to patient ratios by establishment, which outlines the action being taken to address these, or the mitigations to enable this to be an acceptable risk. (b) Next six monthly establishment review to outline how professional judgment has been factored into the recommended staffing, and which of the national recommendations have been met in setting the establishment. Board to receive short progress reports on recruitment in three months, and on retention in six months. Target date to complete Progress/evidence that completed TM July 2014 Done. FFT data amended in Putting People First Report. TM July 2014 Done. Included within the planned and actual staffing report. TM Dec 2014 To be covered in next establishment review in December CG Sept and Dec 2014 Reports scheduled for September and December respectively. Board confirmed completed XX XX May 2014 Action ref: Action Action with 14/05/2014 Finance Report July Board to include deep-dive of the forecast year-end position based on the first quarter s performance. Target date to complete Progress/evidence that completed PW July 2014 Done. Detailed reforecast provided to July Board. Board confirmed completed XX 1
23 April 2014 Action ref: Action Action with 10/04/2014 Equality, Diversity & Human Rights Report 14/04/2014 CQC Survey of Adult Inpatients March 2014 Follow-up report to be provided that outlines the action being taken in respect of bullying and harassment, and career progression. Top-line information on the Trust s internal patient experience survey to be added to the Putting People First report. Target date to complete Progress/evidence that completed CG July 2014 Done. Presented to July Board. XX TM July 2014 Done. Q1 results Provided to the July Board. Board confirmed completed XX Action ref: Action Action with 18/03/2014 Corporate Comms Report Future reports to include further information on the communication s team support for patient and public engagement events. Target date to complete Progress/evidence that completed DS Sept 2014 Requirement noted and will be included. Board confirmed completed December 2013 Action ref: Action Action with 10/12/2013 Meeting Nutritional Needs in Hospital Board to receive an annual report that includes information on the impact and effectiveness of the Trust s processes to support patients nutritional needs. TM Target date to complete June 2014 Progress/evidence that completed Scheduled for June Report deferred to August in light of operational pressures. Board confirmed completed September 2013 Action ref: Action Action with 13/09/2013 Research & Development Annual Report Trust s Research & Development Strategy to be reviewed and presented to the Board, with consideration given to increasing the role of non-medical staff on research and development. RGM / AK Target date to complete Sept 2014 Progress/evidence that completed Proposed to be presented as part of the next report in September Board confirmed completed 2
24 May 2013 Action ref: Action Action with 15/05/2013 Quality & Operational Performance Report (b) Rolling two year trend to be provided for the workforce indicators included in the workforce strategic trend analysis. Target date to complete Progress/evidence that completed CG TBC Interim Head of Workforce Planning appointed and initial meeting held to receive NED feedback. On work programme to be delivered in the 2 nd Quarter Board confirmed completed 3
25 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST ITEM 6 Board Meeting in Public 30 th July 2014 REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Bev Hall, Deputy Director of Nursing and Patient Experience Theresa Murphy, Executive Director of Nursing and the Patient Experience DATE: 30 th July 2014 SUBJECT: Putting People First Report Trust Strategic Priority To create a patient centred organisation, to deliver improvements in patient experience and the quality of care we provide. Summary This report provides the Board with patient experience survey results. The Trust is on target to achieve the end of year target of a 40% response rate for inpatients for the Friends and Family Test (FFT) and extremely likely is the most selected response across inpatients, maternity and A&E FFT. The FFT was rolled out to day care units and a number of high volume outpatient clinics in June, with a phased approach to bring the other clinics on board. The revised local inpatient survey is aligned with the CQC Intelligent Monitoring Framework. The highest scoring indicators in Quarter one are 95% for being treated with respect and dignity and 92% for confidence and trust in doctors and nurses. A strategic patient experience improvement plan has been developed; this includes a number of Trust wide initiatives linked to areas of care identified as important to patients. Board Action Required The Board is asked to review the report and: 1. Note the first quarter results from the revised local survey and the progress towards achieving response rate targets for the FFT. 2. Confirm support for the actions set out as part of the improving patient experience action plan. Equality Impact Assessment: There is no positive or negative impact from this report. 1

26 1. Friends and Family Test Putting People First Report The Friends and Family Test (FFT) was implemented across all inpatient wards and the A&E department in April 2013 and Maternity in September FFT scores are calculated by using the proportion of patients who would strongly recommend minus those who would not recommend or who are indifferent. The high level scores for June are shown below, alongside the 2013/14 year end and 2014/15 year to date result. Survey 2013/14 April May June YTD Overall Trust Inpatients A&E Maternity The Trust met the Quarter 1 response rate targets, set as part of a CQUIN scheme; meaning that the A&E response rate was no less than 15% and the inpatient response rate was no less than 20%. Further rewards are available linked to increasing response rates throughout the year, peaking at 40% for inpatients in March Each ward has an individual target to support achieving this target. More detailed information about each group is contained below. Friends and Family Test Score for A&E The Friends and Family Test score for A&E in May is 59, this is based on 416 responses giving a response rate of 22%. This is a significant increase from May. The distribution of responses across each possible answer is shown in the graph. The bars have been coloured to show promoters in green, passive in amber and detractors light to dark shades of red. A&E Response Distribution Don't Know Extremely unlikely Unlikely Neither likely or unlikely Likely Extremely likely

27 Friends and Family Test Score for Inpatients The Friends and Family Test score for inpatients in June is 67. This is based on 525 responses giving a response rate of 38.4%. The distribution of responses across each possible answer is shown in the graph. Inpatient Response Distribution Don't Know Extremely unlikely Unlikely Neither likely or unlikely Likely Extremely likely Results by ward The table below shows the June FFT scores by ward, alongside the 2013/14 year end score and 2014/15 year to date score. The table is organised in descending order, based on the last month s data. Ward 2013/14 YTD (01) Apr (02) May (03) Jun YTD Trinity FFT Score Response Rate 73.0% 89.7% 88.5% 105.5% 94.1% Pinewood FFT Score Response Rate 39.2% 56.5% 22.9% 38.5% 37.1% B east FFT Score Response Rate 45.7% 53.9% 33.3% 50.0% 45.0% CCU FFT Score Response Rate 34.6% 36.7% 11.5% 29.6% 26.5% Drayton FFT Score Response Rate 42.3% 41.2% 28.0% 46.5% 38.5% Kennedy FFT Score Response Rate 45.7% 61.2% 53.6% 55.4% 56.8% Grange FFT Score Response Rate 37.9% 27.5% 23.8% 11.5% 22.3% Bevan FFT Score Response Rate 40.8% 31.7% 24.6% 23.1% 27.3% Stroke Unit FFT Score Response Rate 50.7% 82.1% 62.2% 97.0% 78.3% 3
28 Marina FFT Score Response Rate 25.1% 27.5% 16.4% 32.3% 25.3% Hayes FFT Score Response Rate 61.8% 73.3% 47.4% 71.7% 65.4% EAU FFT Score Response Rate 35.9% 41.5% 43.0% 34.2% 39.6% Lister FFT Score Response Rate 22.5% 0.0% 0.0% 55.6% 22.0% Edmunds FFT Score Response Rate 24.1% 108.3% 35.7% 63.2% 66.7% Jersey FFT Score Response Rate 40.1% 34.5% 27.5% 26.6% 29.8% Churchill FFT Score Response Rate 38.7% 37.0% 12.7% 0.0% 15.6% Alderbourne FFT Score Response Rate 90.5% 100.0% 46.2% 8.3% 43.8% Summary: Ten wards increased their score Four wards had a lower score Two wards stayed the same as last month There were no responses from Churchill ward ( extra capacity) during June A selection of comments from the June survey are shown below using the Never and Always events framework. Never Events - attitudes and actions that patients should never experience 1 Care was good. Only complaint arrived at 07.30, told to undress and put on robe but didn t go down for operation until Care was excellent, but sadly had to wait for medications before discharge 3 Nurses really helpful but I was being discharged at 1pm and eventually got away at 6.30pm, I had to come back for my medication Always Events attitudes and actions that patients should always experience Everybody carries their tasks to a high degree. Always asking if you require anything just press the buzzer for anything. Excellent job by all Excellent care and attention from the sisters and nurses. They display a caring attitude which is essential when dealing with clients with dementia. The staff were very efficient and friendly. They treat everyone very well. I was particularly impressed by the care that they took with patients who found it difficult to eat. Gently persuading and cajoling without any sign of annoyance. Their patience with older and sometimes confused patients was only to be admired 4 Cold water served would be great 5 More physio needed at the weekend Today I had what you call a Health Care Assistant looking after me, Well what can I say, I would never have known as she was so good. I had the best care and attention that I could have had and I spend a great deal of time in hospital 6 Staff were friendly and informative. There were long (1 hour) periods of waiting with no contact. A quick ok every 15 minutes or so would be great Better communication, my doctor said discharge letter was with the nurse and the nurse said that she didn t have the letter. Comments two and three in the always events column appear to demonstrate that a judgement about likelihood to recommend may also be influenced by how staff behave towards other patients, especially those felt to be more vulnerable. It is very rewarding to 4
29 read these comments and number one, all of which highlight that nursing staff are putting the fundamentals of care first. Wards that do not already have them fitted have been encouraged to order chilled water systems, this is especially important during the hot weather and when trying to encourage patients to take regular fluids (Comment four). Comment six relates to A&E; nursing staff within the department are reviewing how the proactive care approach could be adapted to suit this setting. The proactive care approach involves regular checks on patients using a number of scheduled prompts related to comfort, safety and information. Friends and Family Test for Maternity The Friends and Family Test was implemented in Maternity in September. The question is asked at four key touch points: antenatal care, labour/birth, postnatal ward and community postnatal care. The May maternity FFT scores and response numbers and rates are shown in the table below. Please note labour/birth number of responses includes labour ward, home births and Katherine birthing unit. Touch points April May June Response rate Responses Antenatal (36 weeks) % 36 Labour/birth % 90 Postnatal ward % 84 Postnatal community service The highest score continues to be thee labour/birth touch point. No FFT surveys were returned from community postnatal services. Some of the comments associated with these negative scores are shown in the never events column below will be scrutinised to gain insight into what is important to mothers Comments indicating that improvement is Positive Comments required 1 Week day staff were great but some night and weekends staff were rude unhelpful and made you feel unsafe. Best treatment that I received was from a student nurse and her mentor 2 Too loud at night with doors and cabinets slamming Staff always available to assist and help 3 All staff have been very polite but I have been constantly confused and passed between people when trying to book appointments. No clear direction about who to go to for what and who will book what appointment Staff were really compassionate and understanding, really treating me with respect Each and every midwife and doctor was approachable and kind. My anxieties were dealt with over and over again with a very humanistic touch. I would recommend my case midwives and the care that they provide to all patients even high risk. 4 Waiting time Happy to see the same midwife as she knows me and the quality of care is consistent gives good advice and has made me feel comfortable throughout my pregnancy 5 Follow birth plan, do not try to suggest things that are against the parents wishes, be more caring not just robots Friendly staff, answered my questions clearly and kept me informed The Maternity FFT response remains a challenge due to the amount of touch points (4) required throughout the woman s journey. All commentary from FFT is fed back to staff via the Ward Manager. The vast majority of comments were positive with women happy to recommend our service, however where negative comments have been received they are reflected upon with the Team and 5
30 actions identified to minimise a reoccurrence. The wards use the you said- we did board to show the changes implemented. The Postnatal Community FFT response had a 0% return for June which was extremely disappointing. Following this the process for collecting information was reviewed and all community staff given individual letters reminding them of the need to promote the FFT survey as well as reminding women on their Day 5 visit that the response will be collected at their discharge on day 10. The Community Manager will continue to monitor the returns. We continue to see an increase in the antenatal responses month on month with ongoing promotion of completion. Response Distribution The distribution of responses for each touch point and across each possible answer is shown in the graph Maternity Response Distribution Antenatal Birth Postnatal ward Community postnatal Extremely likely Likely Neither likely or unlikely Unlikely Extremely unlikely Don't Know Friends and Family Test for Outpatients and Day Care Final guidance on implementation of the FFT to all other healthcare areas was due to be published on 16 th July 2014, however this has been delayed. The Trust has already begun a phased implementation into two other service areas; outpatients and day care. This has involved patients in six high volume outpatient departments and four day care facilities offering the FFT to their patients. In total 333 patients receiving day care services and 1830 attending outpatient clinics completed an FFT card. The June high level results are shown below. Area Score Response Oral Surgery Pre-assessment THH Pre-assessment MVH Trauma and Orthopaedics THH Trauma and Orthopaedics MVH Ophthalmology THH Ophthalmology MVH Cardiology THH Rheumatology THH Rheumatology MVH
31 Haematology THH Haematology MVH Elderly Day Hospital Surgical day care unit (female) Surgical day care unit (male) Trinity day care unit Staff in these areas have responded very positively to both implementing the FFT and the results. The results have been discussed at the divisional governance forums and displayed in the areas. Within Outpatients each sister has a folder with their own results to share with their team and identify where improvements are needed. The results do appear to show that with the exception of haematology, Mount Vernon equivalent clinics appear to be rated higher than those on the Hillingdon site. Outpatients at Mount Vernon are now directly line managed by the Nursing Services Manager and Matrons for Outpatients at Hillingdon, this will enable best practice to be shared across both divisions. The FFT will be implemented to further clinics over the next few months and Matron is planning to analyse the comments in more depth to identify always and never events for this cohort of patients. Regular updates will be provided to the Trust Board on implementation and performance. 2. Local Inpatient Survey Results The local inpatient survey was reviewed and revised early in The questions asked now are aligned with those used as part of the CQC Intelligent Monitoring Framework and also reflect the areas where the Trust is focused on improving. As importantly, these are areas where patients have highlighted the most problems in our national patient survey and also matter most to patients. The survey is now undertaken quarterly, results for Q1 are shown in the table below. Indicator/Question Q1 YTD Compassionate Care 88% 88% Did you find someone to talk to about worries and fears? 85% 85% Do you feel that you got enough emotional support from staff? 90% 90% Meeting Physical Needs 88% 88% Did you get enough help from staff to eat your meals? 87% 87% Were you involved as much as you wanted to be in decisions about your care and 86% 86% treatment? Did staff do all they could to help control your pain? 91% 91% Treated with respect and dignity 95% 95% Overall, did you feel that you were treated with dignity and respect? 95% 95% Building Trusting Relationships 92% 92% Did you have confidence and Trust in the doctors treating you? 91% 91% Did you have confidence and Trust in the nurses treating you? 93% 93% Overall 89% 89% Overall, I had a very poor very good experience ( 0= very poor & 10 = very good) 89% 89% Communication and Information 85% 85% When you had important questions to ask a nurse, did you get answers that you could 85% 85% understand? When you had important questions to ask a doctor, did you get answers that you could understand? 85% 85% The Trust uses the same methodology as the national survey for our local survey. Patients have the same range of responses; usually yes, always or definitely, yes, 7
32 sometimes or to some extent and no, with responses weighted to calculate the score. The percentage of patients who respond for each possible answer is available to Trust staff in more detailed reports if required. The blue rows show the indicators, with the cluster of questions that make up the composite score set out below. The Board has set an improvement target of 92% for the overall question; the Experience and Engagement Group (EEG) will discuss and agree targets for the remaining indicators. A strategic patient experience improvement plan has been developed, this includes a number of Trust-wide initiatives aligned to the areas covered in the survey. These include: Supporting the national Hello my name is initiative with the launch of a local campaign A number of approaches to raise awareness of who to speak to about worries or concerns, including: introducing daily matron rounds during visiting times, members of the PALS team proactively visiting wards, and posters with ward sister and matron photographs and contact details. Developing and implementing an admission standard to ensure there is a consistent approach to safely admitting both elective and emergency patients and settling them into the ward routine and environment. Divisional teams will support implementation of the strategic improvement plan and focus on specific areas of improvements within their wards and departments. Progress on the improvement plans will be monitored through the EEG. 8
33 ITEM 7 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: Trust Board Shane DeGaris, Chief Executive DATE: 30 th July 2014 SUBJECT: Chief Executive s Report Trust Strategic Priority: The report is relevant to all of the Strategic Priorities. Summary: The attached report updates the Board on a range of issues including local, regional and national strategic developments, recent publications, and developments at the Trust not otherwise covered in the Board papers. As such, it seeks to provide context to the Board s discussions. Board Action Required: The Board is asked to note and comment on the report. 1
34 1. Finance and performance Chief Executive s Report The Trust has achieved all of the Monitor compliance standards for the ninth quarter in a row. All the cancer standards were achieved with particularly strong performance of almost 100% against the 31 day targets. Referral to treatment times also remained strong and the Trust remains one of the top performing hospitals in the country for compliance against the 18 week standards. This performance was achieved in the face of ongoing activity pressures, with non-elective inpatient activity 25% above plan for the quarter. The Trust ended the quarter behind its financial plan with a 0.4m deficit. However, the Trust's QIPP programme was ahead of the plan. For the most part the deficit was due to the extremely high level of agency staff expenditure required to service the additional unplanned emergency surge pressure capacity noted above. Despite the deficit, the Trust retained a continuity of services risk rating of 3 but going forward has very little financial headroom before this reduces to a Executive Director and Corporate Department Restructure Following a consultation with the affected staff, a revised Executive Director and Corporate department structure was implemented on 1 st July. The changes seek to address the leadership challenges the organisation will face in the next five years as well as supporting the Trust to delivering our ambitious strategy. The key changes include: The Director of Corporate Development has become the Director of Strategy and Business Development, taking on responsibility for strategy and business development from the Chief Operating Officer portfolio. Corporate and Clinical Governance have been integrated under the Director of Nursing and Patient Experience, headed up a Deputy Director of Nursing and Integrated Governance. The post of Director of Estates and Development has been deleted and a new role of the Director of Strategic Estate Development and Asset Management has been established. The Trust Secretary role reports directly to the CEO with additional responsibilities. The Health and Safety portfolio now sits under the Finance Director. 3. Strategic update Shaping a Healthier Future (SaHF) The Trust programme team has continued to prepare the business case for capital development which will help future proof the Trust against the increasing demands upon its emergency and maternity services following implementation of the SaHF programme. High and significant backlog maintenance has also been included. 2
35 Whilst a draft outline business case (OBC) has been submitted into the SaHF assurance process, work continues to improve and refine the details of the various schemes and the supporting financial information. Communications activities have been initiated and changes to clinical models of care are being evaluated. The Trust entered the formal assurance process with a launch meeting on 26 th June with the consortium employed by NHS NW London. A significant information request has been received and the team are working to respond to this and revise sections of the OBC accordingly to meet NHS England and NHS Trust Development Authority (TDA) requirements. Engagement with the Foundation Trust Network The Foundation Trust Network (FTN) is the membership organisation and trade association of NHS acute hospitals and community, mental health and ambulance services. I was delighted to welcome the FTN s Chief Executive, Chris Hopson, to Hillingdon Hospital on 30 th June. This was an excellent opportunity to showcase our successes and also brief Chris on some of our challenges, particularly around the current non-elective demand and our estate. The following day, I shared a speaking platform with Mark Turner, Regional Director at Monitor, at the FTN s annual Governance conference which was attended by several hundred senior leaders from across the NHS. In my presentation I sought to provide an FT perspective on Monitor s new annual planning process that was introduced this year, and outline the approach we took as a Board to the strategic planning process. Kings Fund Quarterly Monitoring Report The Board may be interested to note the key headlines in the latest quarterly monitoring report of the NHS produced by the Kings Fund. The report examines the views of NHS Finance Directors as well as NHS performance data. The report highlights the challenges being faced and report that: 1 in 4 Trusts forecast ending the year in deficit 55% of Clinical Commissioning Groups are planning for emergency activity to decrease this year, compared to only 8% of Trusts The proportion of patients who waited more than four hours in A&E in the quarter was the highest for this quarter since 2004/5 The number of people on waiting lists for treatment in hospital is now at its highest level for six years at over 3 million. It also reports that the number of nurses, midwives and health visitors has increased by almost 9,000 in the last six months to nearly 315,000 the highest on record. 4. Regulatory update Monitor study on smaller hospitals 3
36 As the Board is aware, in 2013 Monitor commenced a review into the effect the size of a hospital has on performance. Monitor analysed a wide range of clinical and financial indicators in order to test whether there are any special factors that affect the performance of hospitals with less than 700 beds (which usually have an income of less than 300m). Monitor found some evidence that size affects financial performance, especially in the latest reviewed period (2013/14). However, Monitor concluded that the size of an organisation explained only a limited amount of the difference in financial performance between hospitals. Whilst some smaller providers were performing poorly, many were performing well. Monitor found that whilst size, or factors related to size, may be important, there are likely to be several other important factors. Monitor found that one factor affecting financial performance was the proportion of work undertaken under the NHS national tariff - with smaller providers tending to proportionally do more of this work. Monitor also found some evidence that when size is controlled for, having more than one acute site (measured by the presence of an A&E department) relates negatively on financial performance. Monitor also found some evidence that again when size is controlled for, providers with more service specialities tend to have worse financial outcomes. Monitor note this suggests there are unlikely to be financial benefits from widening the scope of services without the additional activity attracting revenue to cover the costs. The study refers to the various literature on the economies of scale of hospital providers. Monitor note that much of the hospital-level empirical research covering various countries suggests that economies of scale may exist up to 200 beds, but that hospitals with more than 600 beds show diseconomies of scale. Monitor note that even the smallest English acute providers (those with operating revenue below 200 million) have an average total bed base of 435. These conclusions support the Board s discussions which have noted the importance of the right type of scale. Monitor conclude that most of the variation in financial performance cannot be explained by factors that can be easily measured. Monitor suggest that this variability in performance is likely to be due to softer factors such as The quality of relationships among different players in a local health economy The financial health of other providers in the area The reputation of a provider Buyer power in procurement The leadership at a provider The quality of internal relationships between management and clinicians The longer-term historic circumstances of the provider. Monitor s analysis of a variety of clinical measures gave a mixed picture of the relationship between size and quality with no clear indication that smaller providers were performing worse. 4
37 However, Monitor identify that whilst providers of all sizes are experiencing financial pressures, there is a trend in smaller providers performing worse financially, which could be caused by increasingly intense staffing models. Monitor note that smaller providers are likely to find it increasingly hard to keep pace with these changing recommendations and expectations around workforce. Input-based standards, such as minimum consultant numbers, or other pressures to increase the levels of staff coverage, can increase the fixed costs associated with the provision of a service and increase the minimum efficient scale of that service. In light of this, the report concludes by highlighting the importance of smaller hospitals: working differently with community providers to deliver better out-of-hospital care, or exploring new ways to integrate primary, community and social care with lower risk urgent and elective care. Adopting innovative approaches to staffing such as appointing new nurse specialists or physician associates, or using new technologies such as telemedicine, or making staff appointments jointly with neighbouring hospitals. Building effective partnerships or networks between acute providers and major centres. Again, these actions are in line with the Trust s strategy of working closely with health and social care organisations in Hillingdon to integrate care, whilst exploring partnerships and networks with other providers on particular pathways. The full report can be accessed at eracuteproviders-report.pdf. Fundamental standards of care Following recent consultation, the Government has announced legislation which introduces fundamental standards for health and social care providers. The fundamental standards are part of the Government s response to the Francis Inquiry and, subject to parliamentary approval, will become law in April The standards define the basic standards of safety and quality that should always be met and will be used as part of the Care Quality Commission s (CQC) regulation and inspection of care providers. The CQC will be able to hold providers to account if they are not being met, including through the courts where appropriate. Registration with the CQC will also be dependent on compliance. The duty of candour will require NHS bodies to be open and transparent with service users about their care and treatment, including when it goes wrong. The fit and proper persons requirement means that all Directors of NHS bodies must meet the test of being fit and proper persons for their role. Under the legislation the CQC will be able to insist on the removal of directors that fail the test. 5
38 5. Recent Trust events The Trust was pleased to twice welcome The Mayor of Hillingdon to commemorative events in July. On 4 th July The Worshipful the Mayor of Hillingdon, Cllr Catherine Dann, helped celebrate the NHS' 66th anniversary with a Unison organised event at Hillingdon Hospital, which included a cake and speeches, before returning on 17 th July to officially open the new 1 million MRI scanner room which treats more than 500 patients a month. The scanner is one of the hospital's most in demand pieces of equipment and the updated version is key to maintaining patient flow and quick accurate diagnosis. These events followed last month s successful official opening of the refurbished Beaconsfield East ward with its dementia friendly facilities by Baroness Cumberlege. Shane DeGaris Chief Executive 21 st July
39 ITEM 8 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Liz Weller, Head of Business Planning Karl Munslow Ong, Chief Operating Officer DATE: 30 th July 2014 SUBJECT: Annual Planning: Final 14/15 Strategic Plan Trust Strategic Priority: The Trust s Annual Plan 2014/15 is focused on the achievement of all Trust objectives. Summary The second phase of the Monitor review focuses on the robustness of Foundation Trusts strategies to deliver high quality patient care on a sustainable basis. At the Board Seminar on 11 th June the Board reviewed the draft Strategic Plan, and issues arising at that meeting were addressed in the final version. This was submitted according to the deadline on 30 th June Attached is the version that will be published on Monitor s and the Trust s websites. Board Action Required: The Board is asked to note the attached summary Strategic Plan for 2014/15 that was submitted to Monitor on 30 th June and will be published on both Monitor s and the Trust s website. Equality Impact Assessment: N/A there is no positive or negative impact from this report.

40 Strategic Plan Document for
41 1. Trust Vision, Mission & Strategy The Trust vision is: To put compassionate care, safety and quality at the heart of everything we do. Beneath that vision sits the mission: To be the preferred, integrated provider of healthcare for Hillingdon and the surrounding population, with a major acute hospital as a hub. Our strategy sets out the Trust s ambition for the next 5 years through 4 key pillars, known as our strategic priorities, and supporting strategic objectives. Underneath sit actions and measures of success which are agreed each year by the Board. The actions and measures of success flow down into divisional business plans and from there into individual s personal development plans, to ensure a golden thread running down the organisation from the board to ward. The Trust strategy in the form of the priorities, objectives, actions and measures of success are captured each year within a single page document known as Strategy on a Page, which is widely distributed throughout the organisation. STRATEGIC PRIORITIES STRATEGIC OBJECTIVES To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide A clinically led service strategy that responds to the needs of patients and other health and social care partners To deliver high quality care in the most efficient way To develop sufficient sustainable scale to enable us to improve and grow healthcare services for our communities 1. Fully comply with licence to operate/ regulators 2. Improve the quality of care and clinical effectiveness 3. Improve patient and carer experience 4. Improve patient safety 5. Work with CCG collaboratively to improve services within available resources 6. Improve Patient & Public involvement 7. Engage clinicians to develop innovation and expansion of services 8. Deliver healthcare more efficiently 9. Improve and invest in IT to support service improvement 10.Modernise & reconfigure the Estate & Facilities to meet the needs of our clinical services 11.Maximise staff contribution to transforming the way we deliver our services 12.Develop a service plan in response to SaHF 13.Develop strategic alliances with appropriate partners 2. Market analysis and context 2.1 Context in North West London The population of NW London is growing and life expectancy is improving: population is forecast to increase by approximately 141,000 people from 2 million to 2.15 million over the period to Life expectancy has grown by an average of 3 years over the last 10 years, particularly due to early diagnosis and improved treatments resulting in fewer people dying prematurely from diseases such as cancer, heart disease and stroke. There is currently a difference of up to 17 years in life expectancy in different wards in NW London (NWL). This difference is heavily correlated with deprivation and is caused by a number of factors including: living conditions, diet, levels of smoking and drinking, access to sport and leisure activities, social and support networks, as well as barriers to healthcare such as language and literacy. Some 300,000 people in NWL have diabetes, asthma, coronary heart disease, chronic obstructive pulmonary disease or cystic fibrosis. More needs to be done to prevent ill health and to improve access to GP and community care. Much can be done through successful promotion of public health information and 2
42 campaigns that assist people to take personal responsibility for their own health. Also, more proactive primary care and better integrated working needs is required so that the health and social care system works seamlessly to support everyone to lead healthier lives. There have been vastly different levels of funding across the sector for different settings of care and on long term conditions, with Hillingdon significantly below the average for both. Patient experience across NWL is low compared to other regions. Mortality rates vary significantly between trusts, and weekday vs weekend, and readmission rates vary considerably from one hospital to another. There is considerable variation in the availability of senior experienced staff to care for patients between hospitals and from weekday to weekend, and particularly for specialist services. It is increasingly difficult to provide a broad range of services 24/7 across 9 acute hospital sites: 4 NWL hospitals have a smaller than average catchment population, and all but one are smaller than the Royal College of Surgeon s preferred catchment size. The Royal Colleges have recommended increased consultant presence, in particular to cover emergency and maternity services. Achieving such increased coverage is a huge challenge nationally as well as in NW London: Units need to serve a sufficiently large population so that they are busy enough out-of-hours for staff to maintain their skills in dealing with complications. This is a particular issue for senior staff who must also spend time fulfilling other responsibilities Only larger units can afford to employ an increased number of senior staff, with many smaller units already being on the margins of economic viability due to junior doctors now working fewer hours There are insufficient staff available to provide such increased cover across all units, even if it could be afforded and skills could be maintained. Three overarching principles form NHS NWL s vision for care: that health services need to be: localised where possible; centralised where necessary; and in all settings, integrated across health, social care and local authority providers to ensure seamless patient care. Local clinicians have developed visions for emergency and urgent care, maternity and paediatrics. These include quick access to high quality care, 24/7, and expectant mothers having the choice to deliver at home if appropriate, or with immediate access to supporting services if needed. The 8 NWL CCGs have agreed a vision to transform out-of-hospital care which will centre on the patient and ensure people receive the right care, in the right place, at the right time. The Shaping a Healthier Future (SaHF) programme was established in Nov 2011 and builds on significant work by clinicians to develop suitable models of care. In February 2013 the NW London Joint Committee of Primary Care Trusts agreed the following recommendations for service change: To adopt the NW London acute and out of hospital standards, service models and clinical specialty interdependencies for major, local, elective and specialist hospitals To adopt the model of care based on five major acute hospitals To coordinate implementation of out of hospital strategies in conjunction with the above changes 2.2 Hillingdon Healthcare Needs It is estimated that there are 273,900 people living in Hillingdon, 19.5% are under 15 years of age and 12.9% are over 65. This compares with 18.7% under 15's and 11.1% over 65's in London. From Sub National Population Projection figures the population of Hillingdon is expected to rise linearly by approximately 4,500 each year for the next 10 years. According to the 2011 Census in Hillingdon, 52% of the population were White British, 8% were White Other and 40% were from black and minority ethnic (BME) groups including 25% of the population that are Asian (figures sourced from 2013 Joint Strategic Needs Assessment, Hillingdon Clinical Commissioning Group (CCG)). There are around 4,200 births to Hillingdon residents each year. Over 80% of these babies are delivered at the Trust. This is a significantly higher birth rate than in England as a whole. The rate of women smoking during pregnancy in Hillingdon is significantly higher than the London average with 10% of pregnant women in the borough smoking at the time of delivery. There is a significantly higher rate of emergency caesarean sections in Hillingdon compared to England The proportion of babies born with low birth weight is significantly higher than the national average. 3
43 Current estimates suggest that there are currently 36,200 people aged over 65 living in Hillingdon. This figure is projected to increase by 13.3% by 2020 to 38,600. The numbers of people aged 85 and over is expected to increase by 10% to 5,400 within this period. There are estimated to be 4,778 frail elderly households living in the borough and nearly a quarter of these are thought to be living in unsuitable housing. Stroke is a condition that mainly affects older people and is one of the main causes of disability. In 2008/9 (the last year for which validated data is available) 3,209 people were reported by GPs as living with stroke. This is projected to increase to 4,351 by The number of adults aged 18 to 64 with a serious visual impairment is projected to increase by 3.5% by 2015 to 114. The majority of people with a moderate to severe sight impairment are in the over 75 age group and the number is projected to increase by 6.6% by 2015 to 2,244. The number in the 65 to 74 age group is expected to increase by 8.9% to 1,075. These figures are significant because of the linkages between sight loss and a loss of independence arising injuries sustained as a result of falls. There are also projected to be significant increases in the number of people with a moderate to severe hearing impairment. As expected, the largest concentration is amongst the 65+ age group, which is projected to increase by 8.2% to 16,164. There are currently an estimated 15,176 diabetics in Hillingdon. The rising prevalence of diabetes is due to an ageing population and unhealthy lifestyles leading to obesity. The number of people with diabetes is expected to increase in Hillingdon to 18,974 by A major challenge for health service is improvement in prevention and early detection of diabetes. Other lifestyle factors and risky behaviours contribute enormously to long-term (and short-term) health. The most significant of these in the Hillingdon area are: Obesity In Hillingdon, 23% of adult population is estimated to be obese, which is the same as London but slightly lower than England (24%). Physical activity rates of physical activity are worse than the England, London and Northwest London rates. Smoking the estimated 2011/12 prevalence of smoking in Hillingdon (17.6%) is lower than the estimated proportions for England (20.0%) and London (18.9%). Alcohol attributable hospital admissions and alcohol-related recorded crimes are worse (higher) than the England average. 2.3 Integrated Care North West London (NWL) has had Integrated Care pilots (ICPs) running for a number of years and a Whole Systems Integrated Care Programme is viewed as the next stage in the journey to provide a seamless model of health and social care. Much of the work to date has involved looking at condition specific issues such as diabetes and care of the elderly given the respective challenges they present. This has had significant involvement from our clinicians in each of these specialties but as the model evolves, there is a movement away from condition specific pathways to a more holistic whole patient approach, although still underpinned by the input of specialist expertise. The Whole Systems Vision is underpinned by 3 principles: i. People will be empowered to direct their care and support and to receive care they need in their homes or local community ii. GPs will be at the centre of organising and coordinating peoples care iii. Our systems will enable and not hinder the provision of integrated care. Hillingdon CCG submitted an expression of interest (EOI) supported in principle by CNWL, THHFT, GP s and third sector, initially planning to support the elderly and frail population in Hillingdon. The integrated model is expected to include: The GP as the professional, with overall responsibility for the patient including approval of MDT care plans Multi-Disciplinary Teams (MDTs), drawn from the Provider Network, to deliver care and the use of care coordinators to support delivery of desired outcomes. The GP as the lead MDT professional will 4
44 draw in whatever additional support (consultant, social care etc.) is needed from the Provider Network to ensure care plan outcomes are delivered A focus on supporting self-care and independence The use of capitated budgets and longer term contracts to increase incentives for primary and secondary prevention Through the Better Care Fund, pooling commissioning budgets relating to services commissioned for older people and exploring further pooling as part of this initiative Risk stratification Embedding ICP and its functions into the network The most important next step will be to co-create the new model of care in detail and to consider the related implications. Hillingdon s CCG Chair is currently arranging local meetings to clarify and to begin to develop a shared commissioner/provider vision on how Hillingdon healthcare might look in the future. Public Health will also join this group. The NWL ICP enters into a transition phase going into 14/15, dovetailing into the whole systems Integration programme within Hillingdon. Commissioners are currently putting a detailed service specification together which also sees some of the projects evolving into substantive models of care with a focus on outcomes monitoring. Some projects have been mainstreamed going forward; one example is the Falls Assisted Discharge Service and Falls Outpatient Clinic. Both services are set to continue, the assisted discharge is being incorporated into the Trust s early supported discharge model known as Home Safe (section 3.4.4) and the falls outpatient clinic is being commissioned separately by the CCG. 2.4 Capacity Analysis The SaHF programme used 7 criteria to establish the appropriate number of major hospitals in NW London, to ensure appropriate capacity, quality of care, patient access and safety: i. The correct care setting model to deliver high quality care: clinicians agreed that clinical standards could not be met if the 9 current acute sites became major hospitals, due to lack of staff with sufficient skills & experience, and the costs involved in providing staff on a 12-24/7 basis. ii. Consider the 9 existing major hospitals only rather than new sites, due to capital build costs and timescales iii. There should be enough major hospitals to support the population of NW London: clinicians considered evidence about the factors contributing to high quality care, including senior staff presence, patient volumes to ensure staff build and maintain skills, technology requirements, and interdependencies between acute services and the required clinical support. The resulting decision was that there should be no more than five major hospitals iv. The number of major hospitals must be viable in the medium term: it was agreed that having less than 5 major acutes would require a large number of service moves simultaneously across the region, increasing the likelihood of a long implementation timeframe and large capital investment requirements. No existing sites had the capacity to deliver the volumes of activity in an option with less than 5 major acutes. v. Ensure a good geographical spread of major hospitals across NW London: travel analysis showed the volumes of patients who would experience an increase in travel times, if residents there had to go to their next nearest hospital. vi. Use sites currently delivering high quality major hospital services to determine major hospital sites. vii. Geographic distribution of the remaining sites is proposed to minimise the impact of changes on local residents As part of this programme evaluation, an income and expenditure, activity and beds forecast was produced, taking into account planned service changes from hospitals changing from acute hospitals to local hospitals, most notably from the Trust s perspective, Ealing hospital. The table below shows the prediction of underlying changes required to deliver reconfigured service levels at Hillingdon. 5
45 13/14 activity 14/15 Activity 15/16 Activity 16/17 Activity 17/18 Activity Post Reconfigur ation Activity Movement - 13/14 to 17/18 A&E 54,112 55,137 56,222 57,353 58,510 61,887 7,775 Critical Care 4,028 4,184 4,347 4,516 4,691 5,165 1,137 Elective 16,456 16,670 16,891 17,118 17,346 21,032 4,576 Maternity (births) 4,033 4,193 4,359 4,532 4,711 6,020 1,987 Non Elective 23,724 22,720 21,702 20,637 19,498 22,039-1,685 Outpatient 295, , , , , ,724-83, , , , , , ,867-69,660 An Outline Business Case for Maternity, Theatres, Critical Care, A&E and backlog maintenance has been developed by the Trust to meet the strategic requirements of the SaHF programme. Delivery should ensure that Hillingdon Hospital is able to manage projected future patient demand of both its traditional population base and the expected patient flows from maternity and non-elective services at Ealing Hospital Workforce assumptions The proposed re-shaping of Ealing Hospital through the SaHF programme will have significant implications for the both the Maternity and Accident and Emergency departments in terms of numbers and skill mix with an increased need for paediatricians, midwives, maternity support workers, nurses and A&E consultants. This programme together with the development of more integrated pathways of care across acute and community settings will require significant changes to our workforce configuration. A detailed plan is currently being developed to ensure that the workforce is of the requisite size, meets quality standards and is equipped with the necessary skills to deliver the revised pathways of care. Two new A&E consultants have already been appointed to meet some of the new Emergency Care standards. Based on the activity assumptions contained within the Outline Business Case, modelling of the workforce has been undertaken for maternity staffing. Further work is currently being undertaken to determine the impact upon other specialties. Workforce Risks As with most other acute providers, the Trust faces recruitment and retention risks related to a number of staffing groups. This most obviously applies to qualified nurses as our biggest cohort of staff, particularly in light of the Francis and Keogh reviews which has seen demand for these posts rise significantly. Whilst we have been fortunate to date in attracting additional A&E consultant staff, we are clear that this presents a challenging area for future recruitment and retention. Other challenged medical specialties include paediatrics, anaesthetics, obstetrics, acute medicine and care of the elderly. The development of our workforce strategy looks to mitigate many of these risks through structured recruitment and retention plans, work with Health Education North West London (HENWL) regarding education and training and creating stronger links with education and health organisations. Out of Hospital Care The drive to provide care closer to home will undoubtedly impact on the delivery of services and the staff who deliver those services. The majority of changes in terms of enhanced skills are for those currently delivering care in the community setting; GPs, community and practice nurses and work is currently underway through HENWL to develop those skills. However, the envisaged changes to patient pathways and integrated care will undoubtedly mean that our clinical and medical workforce will need to be increasingly mobile, work in multi-disciplinary teams and be more IT literate to deliver care in an out of hospital setting. Care Co-ordinators have recently been appointed to support the drive towards patient centred care delivered in an OOH setting. The Trust has also recently introduced the Home Safe Early Supported Discharge programme which has already seen some changes to the shape and locality of patient care e.g. therapists visiting patients in a home setting. Increasingly clinics are being delivered in an OOH setting e.g. dermatology, ophthalmology, diabetes and antenatal clinics. These will undoubtedly continue to expand. 6
46 New Quality Standards and 7 Day Working The drive towards providing Seven Day Services including 16 hour/7 day a week consultant cover (24/7 in maternity) together with a requirement for a consultant assessment within 12 hours and the other emerging standards of care) present the Trust with significant challenges. Where possible job plans are being reviewed to meet the additional requirements and funding has already been provided from the quality fund to increase consultant presence in A&E and paediatrics. An analysis of how the trust meets the London Quality Standards and residual gaps has been undertaken and further work is currently being undertaken to prioritise how and where the gaps can be closed. Work is also starting to take place around how network solutions with other providers can help to meet quality standards in an efficient and sustainable way. Following the Cavendish review and the resultant Safer Staffing initiative, a review was undertaken of the nursing and midwifery staffing levels across the Trust. Several areas were identified as having insufficient levels of staffing and additional funding has been made available through the Quality Fund to provide additional staff. However, an overall reduction in the pay bill needs to be achieved. A number of QIPP programmes have been implemented which include a review of non-clinical support workers; benchmarking exercises have indicated that the Trust is an outlier in terms of the number of staff at bands 7 and above and work has commenced to streamline and rationalise these roles wherever possible. Workforce Plan Early in 2014 the Trust submitted an outline Workforce Development and Education Plan to HENWL to meet, where possible, the Health Education England and HENWL key priorities of: Emergency Care and Urgent Care Pathways The OOH/primary care and community workforce Developing community education provider networks Bands 1-4 staff End of Life and cancer pathways The key Organisational Development (OD) deliverables that will be encompassed within the Trust s workforce plan are as follows: Manage the development and implementation of relevant programmes to engage staff through a culture that promotes involvement, capability and quality in all areas of the Trust s work. Develop, implement and sustain the Trust Culture, values and behaviours through the integration of the CARES framework into all Trust processes and initiatives Contribute to the development of a learning organisation through appropriate OD interventions that encourage personal and organisational growth, reflection, innovation and team building Oversee the annual staff survey and use the results to inform and transform the level of engagement of staff, by developing corporate and local improvement plans Manage the human dimensions of organisational change, whether this is a small departmental change or a big divisional re-organisation so that it is seen as a positive experience. 2.5 Scenario Modelling The scenario modelling set out below illustrates our chosen strategic option (1a), which is aligned to the agreed sector wide reconfiguration (SaHF) and is principally supported by our local commissioner through the alignment of our shared long term financial model. The different scenarios describe variations to assumptions that impact our key service lines, and demonstrate a clear understanding of the key sensitivities that ultimately impact our declaration of sustainability. In light of the above analysis and specifically the planned Shaping Healthier Future initiative in NW London, the Trust have included the following possible scenarios in the financial model. Scenario 1: SaHF programme delivers in full, with 40m Public Dividend Capital (PDC) funded capital Scenario 1a: SaHF programme delivers in full, with 80m PDC funded capital Scenario 2: SaHF programme only delivers partially, with no associated capital funding available The Trust does not consider that a pure do nothing scenario is applicable in the context of SaHF and the changes at Ealing Hospital Trust. 7
47 2.5.1 Scenario 1: SaHF Programme delivers in full with 40m PDC The base strategy assumes SaHF will be implemented by 2017/18. Until this point the Trust will lose significant activity and associated revenue that is planned to be moved out-of-hospital by commissioners. In 2017/18 SaHF plans for the Trust to gain sufficient activity and revenue from Ealing Hospital to replace what is lost in the intervening years. During this SaHF implementation period the Trust will require 29.6m of fixed cost transitional support from top-sliced NWL commissioners funds to be able to remain financially viable. This builds on the process that commenced in 2013/14 when the Trust received 3m non-recurrent transitional financial support from the outer-cluster CCGs and continued in 2014/15 with a further agreed package of 5.5 m. Funding for quality investments is built into the financial strategy at 2.1m per annum until 2018/19 when it reduces to match the national tariff assumptions for the Trust of 0.5m. Capital Funding In addition to 45m of ongoing investment the strategy, also incorporates an additional 40m PDC capital required to deliver the SaHF programme. The SaHF investment in backlog maintenance (BLM) is estimated as 18m and includes the Trust s prioritised High and Significant BLM and Infrastructure works. This will make a material difference to the Trust s immediate needs to improve its estate over the next two to three years. It does not however create a sustainable maintainable position for the largest component of the Trust s retained estate in the longer term beyond five years. Although capital works undertaken within the Trust s capital programme has been able to mitigate the consequential impact of the deteriorating estate, the Trust are becoming increasingly concerned at its continuing ability to manage the estate on a sticking plaster approach. The Trust s long- term sustainability is affected by the lack of capital to address the Tower and Podium as an increasing proportion of its capital programme has to be used to reactively respond to infrastructure failures and other high risk works. Risk Rating Overall, the financial strategy as set out will only achieve modest financial surpluses of less than 1% in each financial year as a direct result of the Trust being in planned receipt of SaHF transition support funding. It will however, maintain a continuity of services risk rating of 3 (2.5) throughout the entire strategic planning period. 14/ / / / / Surplus/(Deficit) before ,823 Exceptionals Surplus/(Deficit) after Exceptionals (8,055) 324 (19,655) 208 1,823 14/15 15/16 16/17 17/18 18/19 Continuity of Service Risk Rating Scenario 1a: SaHF programme delivers in full, with 80m PDC funded capital The Trust is also continuing to explore under the scenario set out above, how it can access a further 40m of capital investment required to keep physical infrastructure fit for purpose. Assuming PDC can be accessed, this would be possible within the constraints of the financial strategy whilst still maintaining a continuity of services risk rating of 3 (2.5) in each year. 14/ / / / / Surplus/(Deficit) before (302) 663 Exceptionals Surplus/(Deficit) after Exceptionals (8,055) 324 (19,655) (302) /15 15/16 16/17 17/18 18/19 Continuity of Service Risk Rating
48 The most recent Estate condition survey was produced by Ove Arup & Partners Ltd (Arup) in February As a consequence of concerns raised in areas of the estate and infrastructure that were not readily visible to survey, a series of more detailed reports were additionally commissioned to produce a more rounded account of the works required on the Hillingdon site. The additional reports included: Electrical Distribution - Capacity and resilience. Medical Gases - Capacity and resilience. Upgrading theatre ventilation systems Tower & Podium structural, fenestration and facade works It was clear to the Trust that a large proportion of remedial works required were outside of what would be traditionally identified as backlog maintenance. Based on the indicative costs produced as a by-product of the Arup survey and the costs included in the above reports, the estimated investment required to raise the condition of the Hillingdon estate to an acceptable condition is circa 40m on top of the 17.69m identified under SAHF Scenario 2: SaHF programme only delivers partially, with no associated capital funding available The Trust has developed a separate financial strategy to address the likely downside scenario that would result should the SaHF programme not be fully realised. Due to the interlinked nature of the commissioners out-of-hospital strategy aligned to SaHF this scenario is based on only 75% of the related QIPP being delivered but also that the Trust will not receive any further fixed cost transitional funding beyond what has already been agreed for 2014/15. It also assumes even though the SaHF programme does not continue the planned changes in relation to Ealing Hospital s Maternity and A&E service reconfigurations will happen in full regardless given how advanced these are. For the other SaHF programme changes it has been assumed that only 30% of the planned activity from A&E and non-elective services will transfer to the Trust. In addition, the Trust has not included the 40m SaHF related additional capital investment and its associated revenue statement costs. Therefore, only the 45m ongoing capital investment will be planned. Risk Rating In order to mitigate the downside scenario the Trust would need to reduce our contingency in 2018/19 to 1%, a reduction of 1m, defer 1.0m of quality investment from 2017/18 to 2018/19, and further reduce quality investment planned for 2017/18 by 0.5m. During 2015/16 and 2016/17 our continuity of services risk rating will fall to a 1 before recovering to 2 in 2017/18. Without an injection of cash (PDC) however, it will not be able to restore the rating to a 3 in the foreseeable future. 2.6 Alignment of findings with LHE partners The 5-year financial strategy of the Trust has been based on the joint health economy financial planning work that was undertaken with external consultancy support. This aligned Trust and local Commissioner financial plans with the strategic commissioning North West London (NWL) Sector acute reconfiguration intentions of Shaping a Healthier Future (SaHF). This incorporates both revenue and capital assumptions and is consistent with the Outline Business Case submitted for review to the SaHF project team. Scenario 2 is set within a different context than the agreed alignment with health economy partners around SaHF. Therefore, not all the principles of the base case will apply. This will have financial implications on all local health economy partners, especially in relation to out of hospital strategies and the extent of commissioner QIPP that can be realistically achieved. More specifically, HCCG's relatively aggressive QIPP was a function of their underlying financial position. All other factors being equal achieving a lower level of QIPP delivery would therefore put a strain on the overall resources available for the commissioner unless replacement QIPP initiatives could be developed, agreed and implemented. However, since their out of hospital strategy was put in place HCCG's resource allocation has been significantly increased and as a consequence they will have additional financial headroom that can be utilised to mitigate the financial impact of lower QIPP and the resultant higher than planned provider spend. The CCG have also agreed a more formalised collaborative approach with the other 7 CCGs in the sector to pool financial risk across the North West London health economy. This in turn 9
49 should provide further assurance around HCCG s ability to support both its own and the Trust's financial requirements given the net surpluses that the 8 CCGs generate as region. 3. Risk to sustainability and strategic options 3.1 Estate Development and Rationalisation The Trust estate strategy is to continue to deliver services from its two existing hospital sites but also to develop its outreach community facilities in locations in Hillingdon and surrounding boroughs. The Hillingdon Hospital will continue to be the acute medical site and Mount Vernon will serve as the elective treatment centre with the addition of some medical rehabilitation wards and a skin centre. In recent years the hospital premises have suffered from serious infrastructure underinvestment arising from historic decision making about the failed PFI build. The Trust seeks to use the SAHF funding to rectify this to the greatest extent possible, however as noted in section 2.5, additional capital sums of 40m are being sought to create a sustainable hospital environment that is fit for patient care in the longer term Scenario 1: SaHF programme delivers in full The Hillingdon Hospital Site The Trust has developed a master plan for the Hillingdon site, consistent with SAHF plans, which will see patient accommodation progressively move out from the old annex corridor wards into the tower block. This will be achieved by the reduction in overall bed requirements arising from the out of hospital strategy plus the transfer of some acute medical patients from the tower to the new Acute Medical Unit. SAHF plans will also see the development of an extension to the maternity building, A&E and ICU. Mount Vernon Site The Trust serves as landlord on the Mount Vernon site to a number of tenants, most notably the Mount Vernon Cancer Centre run by East and North Hertfordshire NHS Trust. In a number of cases the tenancy is not formalised with lease arrangements. The strategy for the site is to rationalise the estate so that the Trust can focus on running its clinical services from two principal buildings, the modern 2011 Treatment Centre and the Medical Block. An associated objective is to provide East and North Hertfordshire with their own area of land on a proper leased basis so they can invest and develop their objectives for the Mount Vernon Cancer centre. The Mount Vernon site will not be affected to any material degree by SAHF. Community Locations The Trust already runs outpatient services for some specialties such as ophthalmology and dermatology from out of hospital locations using premises rented from GP practices. In addition, antenatal clinics are run from a number of different Children s Centres across the borough. The strategy, consistent with SAHF, is to increase the number of services provided from community locations. In this respect the Trust will plan to make appropriate use of the three proposed CCG community hubs but may also develop further community locations in Hillingdon. The Trust will also specifically seek to develop community premises in the west of Ealing Scenario 2: SaHF programme only delivers partially, no capital funding The Hillingdon Hospital Site In the scenario where SAHF is only partially implemented the Trust will accommodate the smaller amount of additional maternity activity by reconfiguration of existing estates footprint. If the out of hospital strategy fails or is only partially successful then it will only be possible to partially implement the site Master plan to exit the old annex corridor wards. The absence of capital funding under this scenario will mean that backlog maintenance will continue to be underfunded. The hospital estate will continue to deteriorate and although this will not affect sustainability over the 5 year time horizon it will create a very significant problem for the longer term. 10
50 Mount Vernon Site There will be no material difference to plans for the Mount Vernon site under this scenario however the lack of capital funding will again affect the ability to carry out appropriate back log maintenance. Community Locations If the out of hospital strategy fails and the Hillingdon CCG does not develop community hub premises then the Trust will seek to identify its own community healthcare locations in Hillingdon and Ealing in particular. 3.2 Transformation Programme This year the Trust has endeavoured to develop and drive a longer term transformation programme which has greater engagement and leadership of clinical teams. Tactical opportunities are now limited and in the coming years the focus needs to be very much on internal transformation programmes, with a growing emphasis on health economy opportunities specifically around integrated care. The 14/15 programme is a 7.5m programme made up of both single year schemes and larger transformational schemes which are planned to deliver over 2-3 years. Over the past 3 years QIPP achievement has increased from 4.5m in 11/12 to 6.3m in 12/13 and 8.2m in 13/14. The plan for future years is to continue to achieve 7.5m year on year. This will be very challenging and will need a different approach to that which has been used in previous years. The 3-5 year Transformation programme for Hillingdon starts to build on the longer term trustwide schemes already being taken forward and incorporates potential system wide improvements around SaHF and integrated care which will support the delivery of longer term savings across the system. In 13/14 the Trust invested in a Programme Management Office which has both supported the assurance of the QIPP programme and also provided significant delivery support such as identification, planning, driving and tracking of schemes and change programmes. The future, more complex, transformation programme will require this to continue alongside a new approach which begins to upskill local teams in their ability to plan and drive programmes of work. This skills transfer and cultural change has started but there will be a greater emphasis on this in 14/15 and future years. Engagement will also be key: all projects this year have a clinical lead but clinical champions will be identified to drive forward complex programmes of work. The transformation strategy which is in development begins to review the workforce requirements in terms of skills, capacity, capability and clinical leaders/champions that will be required in coming years to drive and deliver this challenging agenda. 3.3 Key service lines strategies underpinning Major Acute status Under the Shaping a Healthier Future model, the Trust is one of the five major acute hospitals in NW London and as such will continue to provide a full range of acute clinical services. Major Hospitals must have sufficient scale to support a range of clinically interdependent services and to provide high quality services for patients with urgent and/or complex needs. At their core they must be equipped and staffed to support a 24/7 A&E with 24/7 urgent surgery and medicine and a level 3 ICU. Major hospitals will also provide a psychiatric liaison service as well as maternity services with appropriate consultant cover alongside interventional radiology services. In NW London each major hospital will also provide local hospital services, with specialist staff and equipment to support the networks of GP practices where much care in the future will be delivered. For other service lines, the strategy differs somewhat between planned and unplanned care. For planned care (includes outpatients, direct access diagnostics, elective daycase and inpatient care, and rehabilitation) the strategy is for growth, both organic and inorganic where clinically appropriate and profitable. The Trust will aim to grow Hillingdon market share through repatriation of activity from other providers and expand in key co-located boroughs. We will ensure that we streamline pathways to make them value for money to commissioners (including movement of unplanned activities to planned activities). For unplanned care (A&E attendances, ambulatory care, hot clinics or rapid access services, non-elective admissions and critical care), THHFT will look to lead the appropriate prevention of unplanned attendances or admissions, and become a leading provider of ambulatory models of care. We will support the provision of high quality clinical care delivered in the most appropriate clinical setting, first time. Growth should only be inorganic through planned service reconfiguration. For all service lines, planned service developments will need to satisfy the following criteria: 11
51 1. Can we provide this service safely and to a high quality? 2. Will the service make a positive contribution or defend our market position (where the alternative is a greater loss to the organisation)? 3. Will the service development either support the expansion of us as a community or integrated service provider, or help our position as a major acute hospital under SaHF? 4. Can we deliver this for ourselves or do we need a partner to support this development? For both planned and unplanned care, THHFT will provide high quality, safe services with clear measurable outcomes, resulting in excellent staff and patient feedback. We will provide easy efficient access in the most appropriate clinical setting (including community or acute sites), and will work with partners to integrate health and social care and align commissioner and Trust strategies wherever possible. The Trust will seek to improve its brand development and increase market reach through planned networks and strategic collaborations. 3.4 Scenario modelling key service line evaluations Two scenarios (1 and 2) as described in para 2.5 above are considered in light of the key service lines below Scenario modelling for Maternity Services i) Scenario 1: SaHF programme delivers in full A business case is currently being developed to support the expansion of maternity services from 4,200 to 6,000 births, as a result of the reduction in the number of maternity units in NW London and demographic change, in line with the SaHF DMBC assumptions. 21 standards were identified in the DMBC. Those relating to quantifiable changes are as follows: hours (24/7) of obstetric consultant presence on the labour ward 2 Midwifery staffing ratios to achieve a minimum of one midwife to 30 births. 3 One consultant midwife for every 900 expected normal births. 4 1:1 care during established labour from a midwife. 10 Consultant obstetric anaesthetist present on the labour ward for a minimum of 40 hours a week. Units with > 5,000 deliveries a year, an epidural rate >35%, or a caesarean section rate >25%, to provide extra consultant anaesthetist cover during periods of heavy workload /7 access to a supervising consultant obstetric anaesthetist who undertakes regular obstetric sessions. 14 All labour wards to have onsite access to a monitored and nursed facility with appropriately trained staff. The intention is to create additional capacity throughout all maternity services which will include both consultant and midwifery led environments. Women will be risk assessed to identify those suitable for the delivery at the Midwifery Led Unit (MLU). The additional capacity both in estate and staffing will enable a flexible service enabling women and families to have greater choice of the maternity care and place of delivery. By creating a MLU, the model of care will change provision from a transitional ward concept to a Labour/Delivery/Recovery/Postnatal (LDRP) model where women will be admitted to rooms and remain there until discharge. Partners will be encouraged to stay throughout. LDRP rooms should be as nonclinical as possible with comfortable home-style ambience and should enable self-management in privacy wherever possible. The preferred option would create a new MLU and transitional care environment and would also include a significant refurbishment of the existing unit with the introduction of a HDU facility on Labour Ward and an increase in recovery space to meet modern health building standards. In addition this would include a new environment for Triage to improve privacy and dignity. Scenario 2: SaHF programme only delivers partially, no capital funding Under this scenario the services continue to operate from the existing facilities and would accommodate an increase of up to a maximum of 4,800 deliveries. Minor capital works to achieve this level of births have 12
52 been identified for the transitional period. The Trust would be unable to spend significantly on necessary backlog maintenance to remove a substantial proportion of the known historical backlog. There would be no strategic expansion of the facility in terms of added capacity to cope with future increased demand. The Trust would not be able to improve patient choice and would be the only Trust in NWL without a midwifery unit. Whereas it is feasible for the unit to continue to provide a good quality service at these levels of activity, the way in which the facility is set out will always be sub-optimal in terms of current best practice Scenario modelling for Specialist Rehabilitation Under both scenarios the plan is the same, as it is based on a gap analysis in the market that is applicable in both instances. The Hillingdon Alderbourne Rehabilitation Unit (ARU) has been designated as a level 2b unit providing care for category A and B patients to a population of approximately 350,000. A The ARU catchment area is predominantly Hillingdon borough, but as the reputation of the unit has grown over the past several years as a competent provider of specialist rehabilitation, referrals have been increasing from Harrow, Hounslow, Ealing and Berkshire. In addition, the unit has close links with Neurology and Neurosurgery at Charing Cross which has resulted in an increasing number of referrals from West London, not only for its inpatient rehabilitation beds but also for its specialist outpatient activity. The clinical teams provide multi-disciplinary, goal orientated rehabilitation for patients with predominantly, though not exclusively, complex neurological conditions. Areas for additional expansion include complex musculoskeletal rehabilitation including polytrauma and amputee rehabilitation. The ARU admits patients over the age of 18, with no upper age limit; however the patient must have needs or goals which can be met through specialist rehabilitation. There is clear evidence of under provision of specialist rehabilitation in London and adjoining areas with specialist rehabilitation beds in the region oversubscribed by a ratio of 5:1 to 3:1. The reported ratio of unmet need is commensurate with the steadily increasing number of referrals and is demonstrated by the current over subscription of referrals to ARU by 100%. The ARU currently has over 200 referrals per year for 20 beds and is able to admit in the region of 110 patients per year. In addition to the opportunities provided by under provision in the capital, the geographic location of Hillingdon and Mount Vernon Hospitals mean that THHFT is ideally located to draw in activity from the surrounding counties of Buckinghamshire, Hertfordshire and Berkshire. The next (westerly) significant specialist rehabilitation unit is situated at Stoke Mandeville Hospital, approximately 30 miles from THHFT. In winter 2013/14, in order to scope potential demand the ARU clinical team worked with other rehabilitation providers and trusts requiring rehabilitation services to improve local networks and pathways. This included: Increasing links with the Major Trauma unit at St Mary s hospital through the NWL Major Trauma rehabilitation group and through shadowing opportunities for therapy staff. Following discussions with St Mary s it is anticipated that transfers to Mount Vernon will require the use of 4 beds. Discussions with the RNOH to develop a hub and spoke service for non-complex SCI patients with an anticipated requirement for 1-2 beds. The development of close working relations with neurological services at Charing Cross Hospital which will generate inpatient activity requiring 2 further beds. Development of clinical relationships with external trusts to raise awareness and build confidence in the service anticipated requirement 3 beds. A new 16 bed rehabilitation ward is planned to open on the Mount Vernon site in summer 2014; estates works are under way at the time of writing, as is recruitment. The expectation is that the number of referrals from Hillingdon CCG residents will remain at the current level but the Trust will be able to offer specialist rehabilitation to patients out of borough who are in need. This will be predominantly through increased links with St Mary s Hospital (Major Trauma Unit) and RNOH Scenario modelling for Radiology Increases in demand and changes in standards are driving the need for the Trust to use network solutions to deliver Radiology out of hours reporting and Interventional Radiology. This will be the case in both scenario 1 (full SAHF) and scenario 2 (Partial SAHF). The only difference between the scenarios will be 13
53 that in scenario 2, the reduced amount of maternity activity will affect the requirements for the number of sonographers. A nominal sum has been included in the quality initiative fund to meet future requirements Radiology Reporting Radiology demand has been increasing continuously for the last 5 years and it is expected that the key drivers of demand (general population increase, over 60 s, long term conditions) will remain unchanged for the next 5 years. This has created a pressure on reporting capacity. In addition, the NHS operating framework (and the resulting London Health Programme service model) placed further pressure for faster turn-around times by specifying that all hospitals admitting medical and surgical emergencies should have access to all key diagnostic services in a timely manner 24 hours a day, seven days a week to support clinical decision making: Critical: Imaging and reporting within 1 hour. Urgent: Imaging and reporting within 12 hours. All non-urgent: Imaging and reporting within 24 hours. A business case is currently being considered to increase resource through a quality investment at the Trust which would address current reporting performance, particularly during the 5 day week. However, whilst extra capacity during 9am 5pm weekdays can be achieved by recruiting additional local resource, the solution for out of hours reporting is best achieved using a network or outsourced arrangement. A number of outsource providers have been considered however the most economical solution will be to create an out of hours reporting network for North West London. This will be a strategic objective for the next 5 years and work is already underway to explore options with other potential partners. Interventional Radiology Interventional Radiology services are required on an emergency basis for several specialties including gastroenterology, renal, obstetrics and gynaecology. The Trust has only 2 IR consultants and like many acute hospitals cannot maintain an emergency rota in isolation. The reconfiguration of vascular services in North West London reduced the amount of local non-emergency work for interventional radiology providing further incentive to find a network solution for this service. This work will be taken forward as part of the SaHF reconfiguration with a plan to consider regional network solutions across acute providers Scenario modelling: Acute Medicine The Trust is redesigning its emergency care facilities to support the delivery of a more integrated model of care, both within the acute setting, and more widely with other health and social care partners. A summary of some of the main principles that have been adopted for this programme are expressed below in the form of a measureable benefits: Patients should be seen by the right person in the right place, first time Reduced duplication of clinical input to patient pathways National clinical quality standards will be met The current Emergency Department targets would continue to be met Admission to hospital will be avoided wherever possible When admission is unavoidable, the aim will be for patient to be discharged in to a more appropriate care when clinically appropriate to do so The same standard of care will be available over an extended day 7 days a week The main components of the new care model that are either new or materially redesigned are described below: Acute Admissions Ward A new 48-bedded Acute Admissions ward will be built and linked by a new corridor to be adjacent to the existing A&E, whilst also improving patient access to diagnostics. This will provide beds for the majority of emergency admissions, and will be the ward that the majority of patients who have a length of stay less than 72 hours will be admitted to and discharged from. The ward will have two side rooms which provide a negative pressure environment for nursing tuberculosis infected patients, the first of their kind in the Trust, 14
54 as well as a further six single rooms. The ward will also have a suite of 3 consulting rooms to house the ambulatory emergency care service. As well as the general improvements set out above, further benefits will accrue as a consequence of this new facility such as: The co-location of patients will enable the acute physicians and surgeons to work more efficiently with the majority of acute admissions on one ward, stopping safari ward rounds. Reduction in the number of different medical staff who admit and review the same patient. Changes in the patient pathway to have direct admission of GP heralded patients to the new ward. Reduction in the number of times a patient moves on to different inpatient wards. Decommissioning of at least one inpatient ward and the relocation of two other wards on the annex corridor ward. Faster access to senior decision makers: there will also be a dedicated junior doctor ward team improving continuity of care for patients. The ambulatory emergency care service will allow GP s to have access to consultant opinion; will provide an environment in which patients can have a clinical review and receive treatment; keeping the patient in the community; and will also reduce readmission rates. There will be a multidisciplinary approach to the care of the patients which will include social services, physiotherapy and occupational therapy and mental health services with the focus on safe efficient discharge. The large majority of emergency admissions will be managed by acute physicians for the first 72 hours of their stay, with the clear philosophy of getting them fit for discharge as soon as possible. This has obvious quality and patient experience benefits such as to minimise the number of patient moves, increase continuity of care and reduce length of stay, which will translate to the potential closure of 18 beds. This will also be a lower cost model which will allow the Trust to reduce its operating revenue. Majors & Clinical Decisions Unit (CDU) Hillingdon CCG s Commissioning Intensions 2013/14 identified the need to redirect patients from A&E to the UCC and to improve case management in the community of regular attenders. A&E attendances have risen year on year which has created capacity issues for the department, and the reduction in available space in the A&E caused by the creation of the UCC has resulted in an inadequately sized A&E. This, together with the lack of space for ambulance deliveries, has contributed to the Trust being financially penalised regularly for inability to achieve a satisfactory flow through the department. A capacity model was prepared comparing activity to national norms, resulting in a requirement for 33 treatment spaces compared to the current 23 treatment spaces: a shortfall of 10 cubicles. The existing cubicles are also significantly below current space standards. The Trust has produced a case for additional A&E majors cubicles under the SaHF initiative. There will also be, as part of the new Acute Medical Unit, a new assessment area known as Rapid Assessment and Triage (RAT) which will facilitate a quicker clinical assessment, in which diagnostics can be ordered and the patient streamed to the appropriate area, with a target handover time of 15 minutes. In summary, the benefits that are projected to be delivered include: Earlier clinical assessment of patients. Reduced clinical risk and improved patient care and experience through the provision of an increased number of cubicles to provide assessment and treatment. Reduction in the number of patients waiting 3 hours for first assessment. The RAT service will allow diagnostics to be ordered and carried out earlier in the patient s pathway. Reduction in the length of stay in the department of major s patients. Supporting the overall objective of delivering patient care in the most appropriate care setting. There will be an improved patient experience for adults and paediatrics, as well as a better working environment for staff. The co-location of the admissions ward and A&E means that the length of time it takes to move patients is reduced, releasing nursing and portering time. The change in the patient pathway for GP heralded patients will mean that the A&E doctors will not clerk the patient as there will be a single clerking process on the new ward, reducing the amount of medical time involved in this patient pathway. 15
55 Paediatric Emergency Care The paediatric emergency care service will be reconfigured to centralise paediatric functions that include the paediatric cubicles, a Short Stay Paediatric Assessment Unit (SSPAU), a short stay paediatric unit for medically complex children which will be adjacent to Paediatric UCC cubicles. Expected benefits include: Creation of a community healthcare ambiance for the paediatric waiting and treatment areas which feels less clinical to patients. Improved patient experience and continuity of care. Reduction in length of time of first assessment and in length of stay. Reduction in the risk of transferring and treating patients on the paediatric ward. Increased number of patients redirected to appropriate alternative community care. The expansion of the number of beds in the SSPAU will produce a productivity benefit for the paediatricians, which will be reinvested in more patient contact. The scope of the service will also have an impact on the amount of paediatric inpatient beds which can be closed. Further work is required to fully model and outline the implications of the planned paediatric model of are although the estate proposals support a level of flexibility in the use and function of the clinical space. Home Safe The Home Safe model is an early supported discharge initiative as a result of an innovative 3 year CQUIN beginning in Its aim is to improve the interface between local primary and secondary care providers when reacting to the needs of the local frail older population. The project focuses on providing a seamless service for patients aged 65+ who have been admitted to the Emergency Assessment Unit and been identified as appropriate for a Comprehensive Geriatric Assessment (CGA) centred approach to their care. By commissioning specialist support from local community partners in health, social care and the voluntary sector, patients can be rapidly turned around in the initial days of admission, reducing their length of stay and enabling them to return home with additional support on a temporary or more long-term basis. This model of care will expand to offer eligible patients who have already been admitted onto the base wards opportunities to receive early supported discharge using the same comprehensive multi-disciplinary principles. Falls assessment and discharge services and THH respiratory nurse specialist outreach team also contribute and deliver the early supported discharge service. Scenario 2: The impact of reconfiguring the provider landscape in NWL has been modelled by commissioners to include additional A&E attendances per year for Hillingdon from the downsizing of Ealing s A&E; however Commissioners also propose that much of this increased activity will be offset by changes in out of hospital services. Under scenario 2, only 75% of the commissioner QIPP would be delivered including through the out of hospital strategy. In this event, and without SaHF investment in additional majors cubicles, the existing A&E facility would be unable to cope with the volumes of patients, causing major delays in ambulance handover and patient waits Scenario modelling Pathology Pathology services at THHFT are currently provided in-house by a very well established and respected team. The service provides the full range of tests for Hillingdon and Mount Vernon hospitals but also has a number of external contracts including the Mount Vernon Cancer Centre, GP direct access services in Hillingdon and GP direct access services in Hounslow and parts of Buckinghamshire. On the 14th May 2014 the Trust was successful in winning the tender to provide GP direct access services to Ealing. Subject to contract, this service will commence on 1st October With the addition of the Ealing work the total number of tests performed per annum will rise by 50% from the current level of circa 5m to 7.5m. The economies of scale arising from these contracts mean that the Trust net cost of pathology tests is favourably low. Looking forward the Trust is engaged in detailed planning for the NWL Modernising Pathology project with partners Imperial College Healthcare NHS Trust, Chelsea and Westminster NHS Foundation Trust and West Middlesex University Hospital. The objective is to create a joint venture that will run a centralised pathology lab for all cold pathology testing. The timescales for this venture are approximately 3 years. As 16
56 part of the negotiations for the creation of this venture the Trust has ensured that it will retain the current benefit of the low net cost of pathology tests. Any further efficiencies gains arising from the JV will be shared amongst the partners. It should be noted that neither the Ealing contract nor any potential benefits from the Modernising Pathology JV have been included in the long term financial model at this stage. i) Scenario 1: SaHF programme delivers in full Under the scenario where SAHF is implemented in full, we expect the Trust to experience a minor increase in demand for Pathology tests associated with the increase in maternity and A&E activity. The out of hospital strategy is not expected to affect pathology demand but rather to transfer the location of some of the sample collection to community locations. The small overall increase in demand will therefore be accommodated by the in house facilities until such time as the Modernising Pathology reconfiguration takes place. ii) Scenario 2: SaHF programme only delivers partially, no capital funding If SAHF is only partially implemented we still expect to see an increase in maternity activity however as described above this will have only a minor impact on overall Pathology test volumes Scenario Modelling for Dermatology In May 2014 the CCG commenced a competitive tender process for the provision of a consultant led community dermatology service in Hillingdon. When the full tender specification is available THHFT will decide whether it is commercially attractive to bid for this work. If the Trust does not bid, or if it loses the tender then a proportion of the current revenue, outpatient and daycase work will transfer to another provider. The exact proportion is not known until the tender spec is issued. In all scenarios the Trust plans to pursue its goal of developing a specialist skin centre for secondary/tertiary treatment, probably on the Mount Vernon site. This will bring additional revenue which will either grow the dermatology service or compensate for the loss of the community outpatient work if THHFT does not win the tender. The developments in dermatology described above apply under both the scenario 1 (full SAHF) and scenario 2 (partial SAHF) Scenario modelling Research & Development THHFT has a long history of participating in multi-centre research particularly in the areas of Cancer, Paediatrics, Cardiology, Haematology, Vascular and General Medicine that covers all the different types of studies; funded and unfunded both as chief investigator and as principal investigator. These have included commercial and non-commercial studies, the latter encompassing NIHR portfolio adopted studies and Student/Nursing /University research projects (MSc s, PhD s). The principal aim of the R&D department remains to protect the patients, the staff, the general public and the Trust from misadventure, whilst encouraging and permitting active research. Established Active Research Areas Haematology Cancer (Colorectal / Breast / Urology / Prostate) Ophthalmology (NIHR funded research) Stroke medicine Cardiology Active Areas for Targeted Development Diabetes Critical Care Ophthalmology (clinical trials) Urology Breast Surgery Rheumatology / musculoskeletal Paediatrics Reproductive health 17
57 Respiratory Orthopaedics Hepatology Ophthalmology is currently the most progressed of these initiatives. There is scope to monopolise on key reputational developments over the last year which includes being selected as the European training site for Novartis and the recruitment of a research and development consultant who is now the ophthalmic specialty lead for NW London Clinical Research Network (CRN). We have successfully bid for five clinical trials with a further seven planned. In the latest development THHFT have been selected for the Roche trials for new treatment of Dry AMD, one of 18 sites nationally and the only centre in NW London. Combined with a strong marketing strategy these are key building blocks that secures the Trust s position as a regional ophthalmology centre. High quality R&D is best undertaken in partnership with other institutions and the Trust recognises that strong collaborative partnerships with Brunel University and other local universities are crucial for the success of our research activity. Alongside this, THHFT needs a strong relationship with the CRN to attract both the projects and the subsequent funding of research management and activity costs Scenario Modelling for Community Care Growth through New Business A key part of the Trust s strategy over the next five years is to grow business by tendering for contracts to run community based services in surrounding geographies. This will be relevant in all SAHF scenarios assuming that CCGs continue to put services out for competitive tendering as required by the 2010 Health and Social Care Act. Running community health services will help to develop capabilities in integrated care and the Trust would expect to partner with other providers such as CNWL where appropriate. The Hillingdon community health service is currently run by CNWL under a contract awarded in 2011 which is understood to be for three years extendable to 5 years. The immediate focus for THHFT growth is therefore in neighbouring geographies although there are significant potential collaboration opportunities with CNWL in Hillingdon as part of the Whole System Integrated Care Pilot and Better Care Fund initiative. There has been quite a wide variation in the amount of tender activity taking place in different CCGs. This probably reflects differences in quality of existing provision, the finances of the health economy as well as management philosophy. In recent months Ealing CCG has been particularly active and it is expected that other neighbouring CCGs will start to catch up over the coming years. Services that lend themselves to delivery in the community include dermatology, MSK, diabetes, ophthalmology. Contract values vary substantially but are typically in the range of 2m- 3m per annum. A single contract therefore offers the potential for a material contribution to Trust sustainability assuming it can be won at a reasonable gross margin. To deliver on this strategy the Trust needs to develop its estates and IT infrastructure to deliver services in surrounding geographies. It also needs to develop systems of clinical and operational governance to ensure that remote services are safe and of high quality. Development of this capability will also help the Trust prepare to win defensive bids for the retention of any of its Hillingdon services that may be put out for tender by the CCG. 18
58 ITEM 9 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Steve Turner, Project Director Emergency Care Redevelopment and Strategic Estate Development Paul Wratten, Finance Director DATE: 30 th July 2014 SUBJECT: Hillingdon Strategic Site Masterplan Trust Strategic Priority: This paper supports all of the Trust s Strategic Priorities Summary: The purpose of this paper is to provide details of and request Board approval to submit the Hillingdon Hospital Strategic Site Masterplan to local authority planners. Board Action Required: The Board is requested to approve the submission to London Borough of Hillingdon of an application for Planning Permission for the Hillingdon Hospital Strategic Site Masterplan. Equality Impact Assessment: N/A there is no positive or negative impact from this report
59 Hillingdon Strategic Site Masterplan 1. Introduction The Hillingdon Hospitals NHS Foundation Trust is fully committed to preparing a strategic masterplan for the Hillingdon Hospital site. The scope for the production of a strategic masterplan is set out in broad terms within the clauses of a S106 Agreement that is related to the planning permission for the Acute Medical Unit (AMU) building granted on 14 th August The strategic masterplan will provide the framework for the determination of all future planning applications on the site and will obviate the requirement for future planning applications to be accompanied by an Environmental Impact Assessment. In summary, the purpose of the strategic masterplan is to: Provide a realistic long-term strategy for the redevelopment of the site. It will be based around retention and refurbishment of the tower block and podium. It will be implementable on an incremental basis according to the availability of funding. It demonstrates the Trust remains ambitious for the Hillingdon Hospital site and is committed to significantly enhancing the fabric of the hospital for the benefit of patients, staff and visitors. It will enable clinical and operational strategies to be based upon how the site will evolve in the future. The strategic masterplan will provide a sound basis for planning future growth. It will be based upon the following key principles: Centralise: Concentrate new development around the main core. Peripheral buildings are for non-operational and ancillary uses. Efficient and flexible: Simple forms, double banked wards, optimisation of land and buildings. Legibility: Creation of clear entrances and internal routes through the use of hospital streets. Segregated visitor and staff parking: Clear servicing strategy. Low energy solutions: In accordance with the Trust s sustainability plan. The strategic masterplan will not show a detailed design but it will set out broad principles for how the site can be developed in the future. It will not be building specific; the word strategic in the title is important. It will demonstrate to the Council the Trust has assessed the site against a wide range of development criteria. The Council will use it to ensure new buildings will not be undertaken on an ad-hoc or unplanned basis. It is not intended to be a strait jacket but it will demonstrate a longterm vision for the site. 2
60 2. Shaping a Healthier Future (SaHF) NHS North West London has indicated the Hillingdon Hospital site is a future major hospital in the emerging reconfigured health economy. The provision of a masterplan for the site will help to direct future investment in buildings and infrastructure in accordance with the objectives of Shaping a Healthier Future. 3. The Vision for the Site The vision for the Hospital follows a number of general aims that have been articulated by the Trust. These include adhering to the principles of good design and best clinical practice and to: Build a Major Hospital with a comprehensive range of modern services for the local population. Create a built environment that will be welcoming and comfortable with a sense of well-being for patients with well-designed clinical spaces. Provide services which, developed with the community, will provide the best care for local people. Use advanced information technology and medical equipment to support these services. Encourage easy access with good public transport and improved car parking. Create a legible and easily understood approach for vehicles and pedestrians in order to optimise efficient access and egress for users and visitors alike. Create a landscaped setting that will enhance the appearance of the new building(s) in addition to creating shaded amenity areas for patients, staff and visitors. The strategic masterplan provides a mechanism to achieve this vision. It is anticipated new buildings will be located adjacent to the existing tower block and podium. The existing points of access will be reinforced and linked to healthcare streets within this building. This will create a more legible internal layout for visitors, patients and staff. 4. The Strategic Masterplan Planning Application The application for planning permission and supporting masterplan will address the methodology and content as set out in Schedule 2 of the S106 Agreement to attain a realistic and achievable strategy for the redevelopment of the site. It will be an over-arching strategic masterplan demonstrating how the Hospital Site as a whole will be redeveloped in a phased, coherent, sustainable, strategic and comprehensive manner. It will also take account of the functional and financial restrictions under which the Trust has to operate. 3
61 5. Engagement Workshops were held with service, estates and Governor participation to enable the masterplan to be prepared. Presentations of the draft masterplan were given to the Trust Management Executive, Patients in Partnership and to the June Board Seminar as part of the consultation process. 6. Costs The costs of developing the masterplan to this stage have been funded by SaHF. The costs of completing the masterplan to the satisfaction of the London Borough of Hillingdon are included within the SaHF Outline Business Case. The capital cost to deliver the masterplan has not been calculated in any detail as there is currently no planned funding route for the Trust to be able to finance a redevelopment programme of this scale. 4
62
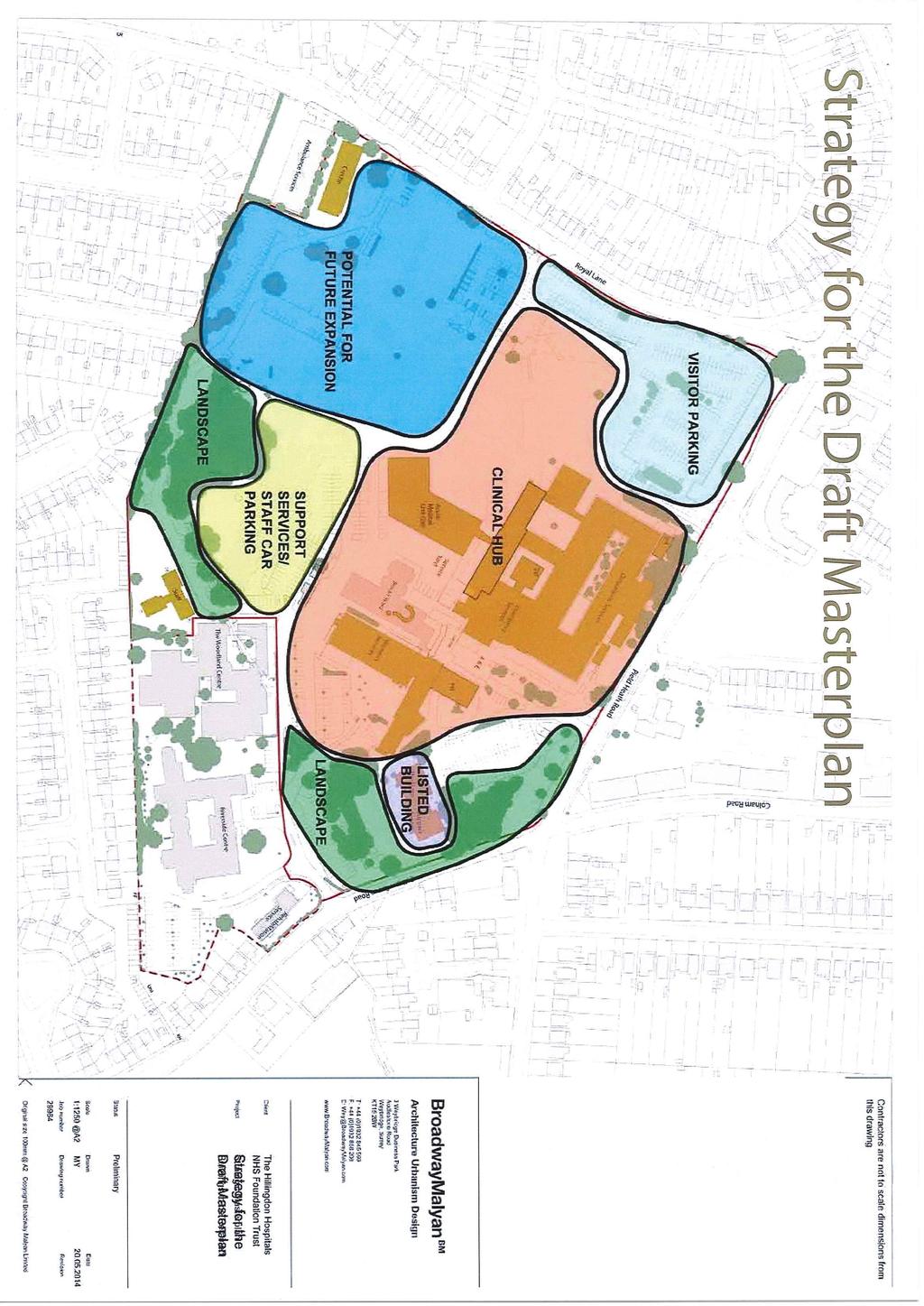
63
64
65 ITEM 10 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: SPONSOR: Trust Board Liz Weller, Head of Business Planning Karl MunslowOng, Chief Operating Officer DATE: 30 th July 2014 SUBJECT: Delivering the Strategy 2014/15 Trust Strategic Priority This paper supports all of the Trust s Strategic Priorities. Summary: The purpose of this paper is to provide the Board with an update on delivery of the Trust s Strategy 2014/15. The attached report summarises progress against the Board agreed objectives for the first quarter to June 2014, and highlights any material concerns for the Board s attention. Whilst there are some objectives where issues are registered, these will be brought to the Board for review as part of the normal planned Board cycle. There are no issues considered as needing escalation for urgent Board review. Board Action Required: The Board is asked to review and discuss the report summarising performance against the Trust s Business Plan for quarter 1 of 2014/15. Equality Impact Assessment: N/A there is no positive or negative impact from this report
66 Trust Objectives 1. Fully comply with licence to operate/ regulators 2. Improve the quality of care and clinical effectiveness Exec DPEN MD 1415 Actions/ measures of success Comply with requirements of Monitor licence and CQC and other regulators Maintain Monitor risk rating green or amber/green Maintain CQC registration and address concerns from unannounced inspection Achieve the main objectives of the annual financial plan Continuity of Service Risk Ratio of at least 3 and an EBITDA of 14.1m Deliver the new Clinical Quality Strategy Achieve indicators within Clinical Quality Strategy Refresh targets within Quality Dashboard New metrics defined and monitored Board focus to date Qtr 4 submission to Monitor (April) Monthly Performance Reports Monthly Finance reports Transformation Committee reports Clinical Quality Strategy Action plan to QRC Qtr 1 Monthly Quality Dashboard and exception report Key issues flagged for Board attention CQC inspection Sept 14 Very limited headroom for CoSRR to remain at 3 primarily due to current high temporary staff spend Divisions currently completing action plans Targets updated M1 Planned Board Focus Monthly Performance Reports Qtr 1 submission to Monitor (July) Monthly Finance reports Transformation Committee reports Strategy monitored quarterly at QRC Monthly Quality Dashboard and exception report 3. Improve patient and carer experience DPEN Fully implement Friends and Family test across the trust, and apply lessons learned into practice. FFT in place in all required areas and targets met Trustwide improvement in Net Promoter Score of 15% (adult inpatients) Putting People First reports (benchmark with London & national data) - Agreement of 13/14 average as baseline required - Better than average in London for negative responses - Plan to roll out to Outpatient & Daycase facilities Qtr2 - Included as an option in paediatrics Monthly Performance Reports Putting People First reports
67 Trust Objectives 4. Improve patient safety Exec MD 1415 Actions/ measures of success Utilise learning from complaints to improve patient and family experiences at THH Reduction in complaints related to key themes Embed patient and carers stories at the Trust Board. Improvement in national patient survey metrics Continue to implement and embed London Health Programmes Emergency Care Standards in conjunction with Commissioners Prioritised plans in place and agreed with Commissioners Reduce variability of weekend v weekday HSMR Reduce weekend HSMR to at least London Average. Demonstrate improvement in achieving patient safety thermometer standards Reduce all harms to 95% and falls without harm by 20% Eradicate grade 3 and Board focus to date Annual complaints report Putting People First reports Patient Stories at EEG & Board Monthly Performance Reports High level update on LHP standards May 14 LHP standards self assessment review to QRC Qtr 1 Summary of mortality review process May 14 Dr Foster Palliative Care benchmark May 14 Trustwide mortality action plan QRC Qtr 1 Monthly Performance Reports Key issues flagged for Board attention - Key themes by division distilled & reported to EEG - Agreement of metrics as improvement in 9 CQC Intelligent Monitoring Framework questions required - Sample period will be Aug 14, feedback Qtr 4 LHP standards prioritised from quality investment fund - Palliative care coding just below London Average. - HSMR just above (5-10 points) London average ytd to Feb 14 (w/e 98.2% w/d 84.1%) but gap narrowing Harmfree care (all harms including old) 95%ytd. Bed base and staffing complement must be better aligned to reduce risk to target Planned Board Focus Complaints reports Themes across complaints, incidents, FFT & junior frontline staff feedback Qtr 2 Putting People First reports Patient Stories at EEG & Board Picker survey report Qtr 4 (NPS Qtr ) Monthly Performance Reports Month on month comparison of weekend and weekday mortality separately and against London average in Quality Dashboard Mortality review process Quality Report Monthly Performance Reports BSS = Board Strategy Session
68 Trust Objectives 5. Work with CCG collaboratively to improve services within available resources 6. Improve Patient & Public involvement Exec COO DPEN 1415 Actions/ measures of success 4 pressure ulcers and reduce grade 1 and 2 pressure ulcers by 30% Deliver in conjunction with CCG the shared health economy transformation programme Agreed schemes delivered Achieve year 1 of the shared integration plan 7 day working model Actively contribute to development & delivery of Better Care Fund in Hillingdon Deliver yr 1 actions for Better Care Fund plan Deliver year 3 of the FT Membership & Engagement Action Plan Increase membership by 10% Set out an action plan to improve engagement with membership including underrepresented groups. Establish a programme of events that will capture wider sections of the community, and reflect the patient groups. Board focus to date PwC stage 2 report will inform planning round for 2014/15 and beyond. Feedback on 14/15 contract agreement Monthly QIPP updates FT Membership Development & Engagement Report Qtr 1 FT Membership Development & Engagement Report Qtr 1 Key issues flagged for Board attention Key risk is non-delivery of CCGs QIPP particularly nonelective performance Initial draft of Whole Systems Integrated Care proposal agreed Agreed at April Trust Board that the focus in the year ahead will be on ensuring a representative and engaged membership rather than increasing by 10% Membership numbers very stable Qtr 1 2 successful maternity community events Qtr 1 Membership Development Engagement Group establishing ways of further engagement Planned Board Focus Monthly QIPP updates Quarterly Health and Social Care Integration updates to Board. Board to review and approve Integration Strategy - Qtr2. Action plan to CoG Qtr 2 BSS = Board Strategy Session
69 Trust Objectives 7. Engage clinicians to develop innovation and expansion of services 8. Deliver healthcare more efficiently 9. Improve and invest in IT to support service improvement 10. Modernise & reconfigure the Estate & Facilities to Exec COO COO FD DSBD 1415 Actions/ measures of success Deliver the clinical strategy for MVH Board agree aligned clinical & estate strategy Move to a clinically led divisional structure Divisional Directors and clinical service leads from agreed structure in place Expansion of skin centre, pathology and specialist rehab services Business case decision made and implemented according to plan. Roll out key ambulatory and outreach service models across key inpatient specialties Models in place for Medicine, Surgery and Gynaecology Clinical model for Acute Medical Unit in place Deliver yr 1 of the Informatics strategy Successful implementation of wireless networking Mobile devices in use in 2 clinical areas Deliver a Strategic Outline Case for Mount Vernon Outline Case decision made Board focus to date Update on MVH clinical site strategy Qtr 2 Key issues flagged for Board attention No material issues Clinical leads appointments process under way No material issues Rolled out community models for gynae, ophthalmology, urology No material issues No material issues Planned Board Focus Business cases for Skin Centre & Pathology Qtr 2 Finance Reports QIPP reports Transformation Committee Reports (Transformation Committee will see detailed 14/15 plans) First yr review of Strategy & deliverable to Transformation Committee Qtr 2 Review of Governance arrangements to Transformation Committee Qtr 2 Outline Strategy BSS Update Qtr3 BSS = Board Strategy Session
70 Trust Objectives meet the needs of our clinical services 11. Maximise staff contribution to transforming the way we deliver our services BSS = Board Strategy Session Exec DPD 1415 Actions/ measures of success Complete the Emergency Care Redevelopment project and other major capital schemes Major capital programmes delivered to operational users on time and to budget (Beaconsfield East, Labour ward and AMU) Secure Board approval for backlog investment and capital improvement requirements Board approved capital investment plan Stakeholder support for future strategic investment Implement Board decision on Car Parking business case Deliver the in-year PLACE improvement plan Completed action plan Implement yr 2 of Experience & Engagement Action Plan Action plan delivered Deliver Leadership development programme Leadership 100 programme delivered across 5 cohorts Implement yr 2 of Workforce & OD Strategy Board focus to date BSS Updates Board Finance reports CEO Monthly summary update on EC Project and EC Quarterly project updates Agreed capital programme Mar 14 SaHF draft OBC BSS updates PLACE improvement plan update May 14 Equality & Diversity action plan Qtr 1 Leadership Strategy implementation update Qtr 4 Staff Survey Results Qtr 4 Workforce and OD strategy Key issues flagged for Board attention - Beaconsfield East formally opened - Labour Ward due for completion Qtr2 - MPs & Regulator briefed on long term strategic investment plans - Planning application July 14 No material issues No material issues No material issues Planned Board Focus BSS Updates Board Finance reports CEO Monthly summary update on EC Project Quarterly project updates Monthly Finance reports SaHF OBC Qtr 2 BSS Updates National Report on PLACE audit outcome when national comparative data available (Qtr2) PLACE update Qtr4 Putting People First reports Leadership and Talent Management Strategy Qtr 2 Putting People First reports Organisational workforce and
71 Trust Objectives Exec 1415 Actions/ measures of success action plan Organisational & divisional workforce plans Improved staff survey metrics to national average Talent Management Strategy in place Equality & Diversity action plan in place Board focus to date to Transformation Committee in QTR 1 People and OD Strategy Board update in Qtr 1 Key issues flagged for Board attention Planned Board Focus OD plan to Board in Qtr2 12. Develop a service plan in response to SaHF 13. Develop strategic alliances with appropriate partners COO COO Publish a SaHF consistent Estate Strategy and develop FBCs for capital builds Board approved FBCs Agree activity and workforce transition plans with commissioners Agreed transition plans Formalise strategic relationships with RBHT and CNWL Jointly bid for a new service with a partner. Monthly SaHF updates BSS updates Enhanced support agreement reached with RBHT. Potential impact from Hammersmith & Central Middlesex A&E closures from September No material issues Trust/CNWL joint bid for Brent MSK shortlisted Business Cases to come to Trust Board in accordance with revised external timetables. SaHf Board Updates BSS updates Mini Board to Board with CNWL BSS = Board Strategy Session
72 ITEM 11 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Steve Turner, Project Director Emergency Care Redevelopment and Strategic Estate Development Paul Wratten, Finance Director DATE: 30 th July 2014 SUBJECT: Emergency Care Project Progress update Trust Strategic Priority: This paper supports all of the Trust s Strategic Priorities. Summary: The purpose of this paper is to provide the Board with a progress update on the implementation of the Emergency Care Project. Key Points to note: The contract with Kier is being delivered in accordance with the contractual timetable, and the contractor s predicted cost out-turn aligns to that previously reported to the Board. Board Action Required: The Board is asked to note the update, specifically that the project remains on track in terms of timing and cost. Equality Impact Assessment: N/A there is no positive or negative impact from this report
73 Emergency Care Project Progress update 1. The new Acute Medical Unit (AMU)/Endoscopy building The contractor Kier started on site on Monday 6 th January Demolitions, groundworks and foundations were completed by the end of April The 75 prefabricated new modules were successfully delivered to site during the month of May 2014 and the internal fitting out of the building is in progress starting with service pipes in the ceiling void. The main roof plant has started to arrive on site. 2. Enabling and other related refurbishment works (Jarvis) The consequential improvements to the kitchen that arose from the demolition works were completed at the end of May 2014 enabling the area to become fully operational in July All of the works needed to enable the Kier main contract to function as per the approved programme are now complete including the newly configured Clinical Decision Unit (CDU) that was operational from 17 th July The CDU was redesigned to create a corridor and bridge link between the A&E and the AMU. 3. Connections to existing infrastructure services The installation of the new electrical cable is ongoing with final connections planned for the end of July 2014 in accordance with the works programme. Works connected to the medical gases infrastructure, the additional generator and the steam main have started and are programmed to be delivered as per Kier s requirements. 4. Overall programme There is no change to report to the current agreed work programme (version 19). Version 19 indicates key contractual dates for the Trust including possession of the new 49 bed AMU ward and the new Endoscopy department in mid-november The ward is expected to be operational before the end of December 2014 while the Endoscopy Unit is planned to be operational at the end of February The above programme is consistent with the post project evaluation paper presented to the Board on 29 th January Timetable and Key Milestones Kier works to create the link between the new bridge and A&E in the tower block will start in August The link and the new building are programmed to be handed over to the Trust in mid-november
74 6. Financial forecast for the new building works (Kier) The total cost of the Kier contractual element of the project is forecast to be m. This remains within the capital budget set for the completion of the project this financial year. 7. Communications Recent communications about the AMU build have included weekly photos of the development available on the staff intranet. Two press releases with photos have been sent to the Uxbridge Gazette and both appeared in printed copy and on the paper s website. These stories focussed on the first module being lifted into place and the final piece being positioned. The Trust has tweeted regular photo updates of the build and these have often been retweeted by local news organisation, including GetWestLondon.co.uk and HillingdonTimes.co.uk. 3
75 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST ITEM 12 Board Meeting in Public 30 th July 2014 REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Inderjit Bhambra, Interim Head of HR Business Partnering Claire Gore, Director of People DATE: 30 th July 2014 SUBJECT: Bullying, Harassment and Career Progression: follow up from the 2013 National Staff Survey Trust Strategic Priority: To create a patient centred organisation to deliver improvements in the quality of care we provide. Summary: As requested by the Board when it reviewed the 2013 National Staff Survey results, this paper provides details of actions that are being undertaken in relation to bullying and harassment and career progression. The report provides the Board with an overview of the current position in relation to harassment and bullying, and details the work being progressed within the Divisions and Departments, by the CARES Ambassadors and by People and Development. The report also highlights the issues surrounding career progression both at a local and national level and the actions being taken to enhance progression, especially amongst underrepresented groups. Trust Board Action Required: The Trust Board is asked to: 1. Note the current position in relation to harassment, bullying and career progression. 2. Consider and comment on the actions being taken in relation to the issues raised in relation to bullying and harassment and career progression from the 2013 National staff Survey 3. Agree any further actions the Board feels appropriate. 1
76 Bullying, Harassment and Career Progression: Follow up from the 2013 National Staff Survey 1.0 Introduction and Background 1.1 The 2013 National Staff Survey report highlighted areas of improvement in the percentage of staff experiencing bullying and harassment either from staff or from patients and the public, and specific areas of concern relating to the frequency of reporting it when it is experienced (44%), in comparison to the previous year (50%) and the national 2013 figure of 44%. 45% of staff completed the survey. 1.2 In % of staff reported that they had never experienced bullying and harassment from patients or the public, compared with 71% in 2012; a slight improvement. The national comparison for 2013 is 72%. 1.3 Those who had never experienced bullying and harassment from staff, decreased from 78% in 2012 to 76%, a 2% difference, which is a slight improvement, however, slightly lower than the national figure of 75%. 1.4 Overall, 1% fewer staff from The Hillingdon Hospitals had never experienced bullying and harassment from the public than nationally in Overall, 1% more staff in the Trust had never experienced bullying and harassment from staff than nationally in Actions being Undertaken / Current Initiatives Staff Survey 2.1 Whilst the numbers of staff reporting that they had never experienced bullying and harassment from staff or patients and the public has improved and is either just below or above the national average, Hillingdon Hospitals NHS FT aspires to be in the top quartile in all areas of the staff survey and this was highlighted by the Board as an area for focus and improvement. This is the first year that the Trust has distilled the survey results down to a divisional/departmental level which has enabled us to highlight particular areas of concern. Divisional/Departmental results are attached at Appendix A. Where areas in the staff survey highlighted bullying and harassment concerns (either from patients or staff), specific action plans are being developed to explore the issues further. 2.2 Given the variance in results the divisions/departments are adopting slightly different approaches as follows: The Women s & Children s Division s approach is both service area and Departmental; members of staff have received an invitation to contact Organisational Development (OD) to state whether they would prefer to discuss bullying in focus groups or in one-to-one sessions. They are also looking at other areas which may be related, such as work pressure, job satisfaction, and support from the immediate line manager and recognition 2
77 from the Trust for the work they do. Different service areas are focusing on various combinations of allied topics according to the responses locally. HR and OD will be attending briefing dates in August and September to facilitate exploration, and engagement in future focus and planning. An action plan has been agreed. Cancer & Clinical Support Services staff will shortly be attending focus groups to explore concerns in more depth. An action plan will be developed following these focus groups. Surgery Division, similarly to Women s and Children s, is also approaching concerns from both a service area and Departmental perspective. Service area meetings to discuss survey results have taken place, with more in-depth meetings booked for July and August. An action plan will be developed following these meetings. Medicine Division has considered the survey results at the Divisional Management Meeting together with HR and OD representatives from People and Development, and members of the divisional management team are considering the development of an action plan. 2.3 The OD team will facilitate these focus groups and individual 1:1 meetings with staff to better understand the issues raised in relation to bullying and harassment with a view of assisting the Divisions in pulling together an action plan, which will be owned and monitored by the respective Divisions as will reporting progress to the Experience and Engagement Group. 2.4 Divisions will be supporting the programme by ensuring that staff are released to attend the focus groups and 1:1 sessions. 2.5 This concerted effort by the Divisions will help demonstrate to staff that their Division is keen on addressing concerns raised by them and that there is value in completing the National Staff Survey Questionnaire. CARES Group 2.6 A newly created Dignity at Work group which is chaired by the CARES Ambassadors is also looking at ways of promoting what staff can do in the event that they perceive they are subject to bullying and harassment. 2.7 This group will help signpost staff to support that is available, such as Occupational Health and the Employee Assistance Programme, whilst also directing staff to the Dignity at Work Policy. 2.8 As part of this work stream, the P&D department are creating a flow chart, which will help the CARES Ambassadors in their dealings with staff, in relation to what options are available to address the issue. 2.9 This group is also in the process of finalising posters which will highlight to all staff what behaviours / actions could be deemed as bullying and harassment, 3
78 Mediation and highlight what employees should do in the event that they are concerned about the behaviours of others. Once agreed and finalised, these posters will be put up in staff areas across the Trust by the CARES Ambassadors The OD Team are currently exploring options regarding a mediation service which could assist in resolving dignity at work complaints at local level, without the need to escalate to a formal investigation The aforementioned CARES Group are very supportive of this approach, and are keen to be involved in the process where possible and where practicable. Exit Interviews 2.12 Results of Exit Interview Questionnaires (EIQs) will be evaluated to ascertain if any themes in relation to bullying and harassment are evident Whilst the P&D Directorate recognise that insufficient data is available within the existing EIQs that have been completed (low uptake), the department have written out to and provided an EIQ to 128 staff that left the Organisation between September 2013 and May 2014, who had not completed an EIQ at the point of leaving with a view of capturing greater levels of intelligence To encourage a respectable return rate, ex-employees are being provided with a stamped addressed envelope to return their EIQ, and being offered an opportunity to meet with a P&D representative. 3.0 Career Progression 3.1 Career progression was highlighted as an issue within the 2013 National staff Survey and is also highlighted nationally as an issue for staff, particularly within Black and Minority Ethnic (BME) Groups. 3.2 The Agenda for Change (AfC) full-time equivalent (FTE) workforce at the Trust is comprised of 78% women and 22% men. However, women only represent 55% of the FTE workforce at band 8a and above; whilst men represent 45% of the workforce at this level although they only make up 22% of the total AfC workforce. Black and Minority Ethnic (BME) staff account for 9.53% of the AfC workforce on an FTE basis, and 6.32% of the FTE AfC staff at band 8a and above. Action being taken: 3.3 The Talent Management Process was expanded over 500 staff and included nursing staff from Band 7 upwards (non-nursing staff were included from band 8a upwards) in recognition of the need to develop these staff to support them progress to more senior positions or taken on broader roles 4
79 3.4 The Leadership 100 programme provided a development programme for nearly 120 staff across all disciplines and included personal coaching for individuals to support their own personal development 3.5 All nurse leaders were offered the opportunity to attend the Advance managing self and managing others programme. 3.6 An apprenticeship programme has been introduced and there are plans to expand this in the future. 3.7 On an annual basis the Trust is invited to request salary support places into Nurse, Midwifery and AHP undergraduate programmes. The salary support is provided by Health Education North West London (HENWL). After consultation with clinical areas requests are made to HENWL. Depending on workforce demand and commissioned numbers, the Trust is allocated places. Individuals are then invited to apply for a secondment position and after successful interview their names are forwarded to the Higher Education Institution (HEI) to undergo the HEI's selection process. The successful applicants will then undergo undergraduate professional training either on a full or part time basis. The individual will receive a salary as provided by HENWL for the duration of the secondment. The individual will still remain a hospital employee and return to the Trust as a registered practitioner following the secondment. 3.8 HENWL also support Foundation degrees by paying the fees for the course and study days backfill cost. This year the Trust is interviewing 20 HCAs for four allocated places. The selection process is very rigorous. Candidates that are not successful but have shown potential for development will be offered the opportunity to undertake one of the five Foundation degrees available. This will give the additional knowledge and skills required to undertake the undergraduate nursing programme in the future. 3.9 The Trust is piloting the Fundamental Certificate of Care for Band 1-4 to improve the quality of care and patient experience. In addition this will also give individuals additional skills which will enable them to progress within the service Work is being undertaken in partnership with Staff Side to improve the language skills of staff that require support in this area The selection tests used in recruitment/selection are being reviewed to ensure that they do not indirectly discriminate against particular groups and to ensure an even playing field The Leadership programme is being expanded to include opportunities for leaders from Band 3 upwards to enhance their knowledge and skills and as such increase their career opportunities The Director of People is a member of a London wide group entitled Unconscious Bias, which following the recent research undertaken by the Royal College of Nursing (RCN) is developing a strategy to address the issues of under representation and is also utilising senior diversity and inclusion connections 5
80 within the Metropolitan Police Service s (MPS) Department to advise and support initiatives going forward Integrate diversity within P&D to ensure that sufficient resources are directed to supporting the identified actions 4.0 Next Steps 4.1 The HR Business Partner team will analyse the results of the EIQs and highlight areas for improvement with the Divisions/departments and develop actions as appropriate. 4.2 Action plans will be developed in conjunction with the Assistant Director of Operations to address any bullying and harassment concerns that came out of the National Staff Survey, following the focus groups and 1:1 sessions. 4.3 These action plans will be presented to the Experience and Engagement Group as a staff engagement progress update The OD team are designing interventions as appropriate, whether team based activities or one-to-one meetings or mediation events as required on the basis of the outcomes from discovery meetings. These are more advanced in some Divisions than others, and progress is being driven jointly by the Divisions/Departments and People and Development A paper will be presented to the Executive Team for a decision on the proposal to train mediators, and implement a mediation service, to support re-building sustainable working relationships where they have broken down, or where staff experience discord. 4.6 Expand the leadership programmes to encompass a wider group of staff. 4.7 Develop local action plans to deliver the Unconscious Bias strategy. 4.8 Expand the apprenticeship programme. 4.9 Review recruitment and selection process to reduce the occurrence of any indirect discrimination. 5.0 Summary There is a considerable amount of work being undertaken at a local level to identify the issues that are impacting on our staff s well-being at work in terms of harassment and bullying and also to support staff who perceive that they are victims of such action. More work is required to both identify the causes and to implement the actions identified following the current diagnostic work being undertaken. The divisions and departments will be supported by the P&D Department and the actions monitored through the Experience and Engagement group. The initiatives in relation to career progression will continue to be 6
81 implemented at a local level and participation at a London wide level will ensure that best practice can be identified and implemented locally. 6.0 Board Action Required 1. Note the current position in relation to harassment, bullying and career progression. 2. Consider and comment on the actions being taken in relation to the issues raised in relation to bullying and harassment and career progression from the 2013 National staff Survey 3. Agree any further actions the Board feels appropriate. 7
82 ITEM 13 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Bev Hall, Deputy Director of Nursing Theresa Murphy, Director of the Patient Experience and Nursing DATE: 30 th July 2014 SUBJECT: Safer Staffing Planned and actual staffing levels Trust Strategic Priority: To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide. Summary: The report in appendix 1 sets out the fill rates and vacancy levels along with a number of Nurse Sensitive Outcome Indicators (NSOI). This month the Q1 results from selected questions from the local inpatient survey are included. The average fill rates for Registered Nurses (RN) for day shifts in June were slightly lower than in May; and there continues to be a better average fill rate for RN and care staff on nights. Vacancy levels and extra capacity beds continue to be the biggest challenge. Thirty eight new nurses and care staff have been recruited during the recent recruitment days. A total of 25 new nursing staff started work in July, and the Director of Patient Experience & Nursing is undertaking daily safe staffing reviews on the escalation wards. Divisional Senior Nurses review staffing levels on each shift and take action to ensure that patient care remains safe and effective. Clear escalation plans in place. NICE guidelines for safe staffing for adult inpatient wards, were published on 14 th July; the recommendations from these will be implemented. Board Action Required: The Board is asked to: 1. Review and note the information contained in the report and the actions in place to achieve and maintain safe staffing levels. 2. Discuss the ongoing impact of the number of extra-capacity beds open currently. Equality Impact Assessment: There is no positive or negative impact from this report. 1
83 1. Introduction Planned and Actual staffing levels This report provides the Trust Board with an overview of registered nursing, midwifery and care staff levels across day and night shifts in inpatient areas as outlined in the guidance published by the National Quality Board in November A table (Appendix 1) sets out the nursing fill rates by ward, providing an at a glance overview that also includes vacancy rates and a selection of Nurse Sensitive Outcome Indicators (NSOI) that may be associated with the impact of gaps in staffing levels. The NICE guidelines for Safe staffing for nursing in adult inpatient wards in acute hospitals, published on 14 th July, highlight a range of NSOI that could be used. A number of these, including results from the Quarter 1 local inpatient survey, have been included in the table. 2. Key Points This report has used information generated by the e-rostering system; the reported fill-rate is based on number of nursing hours deployed as a percentage of number of nursing hours planned in the rota. Our validation processes identified that on occasions when early and late shifts are compressed into one long day shift the lost hours will be included in the unfilled hours. The commentary included by the Women and Children s Division highlight this with an example. The new NICE guidelines recommend measuring the average amount of nursing time required throughout a 24-hour period for each of the ward's patients. The measurement should take into account the patient factors and nursing care activities. It could be expressed as nursing hours per patient to ensure ward nursing staff establishments are derived from individual patients needs (a measurement of nursing hours per patient enables the nursing needs of individual patients and different shift durations of the nursing staff to be more easily taken into account than with a nurse-to-patient ratio). This methodology will be used as part of our next establishment review. Our previous establishment reviews have focused on the number of nursing staff on each shift and the registered nurse to patient ratios, it is clear that the approach recommended by NICE will help to articulate the actual direct nursing contact time required, shift durations should then be set in the roster templates to ensure that the planned nursing hours can be met (this will be dependent on a full establishment, i.e. no vacancies). The staffing fill rates shown in Appendix 1 were submitted to NHS England on 10 th July, within the timescales set out by NHS England. High level information is provided on the Trust page on the NHS Choices website, and this report containing additional information is published on the Trust website on a dedicated staffing page. This report can also be accessed via a link on NHS Choices. Staffing during June remained challenging, contributory factors include: The volume of extra capacity beds open, ranging between beds Vacancy levels Acuity and Dependency of patients. 2
84 The table below shows the average fill rates for June across both sites. Site Day Night Average fill rate RN/RM % Average fill rate Care staff % Average fill rate RN/RM % Average fill rate Care Staff % Hillingdon 83.6% 89.8% 98.7% 108.6% Mount Vernon 80.4% 88.9% 93.8% 108.7% There is a better fill rate at nights across both sites, the figures also appear to show that additional nursing hours (exceeding the planned hours) were used. The Senior Sister/Matron may identify the need for additional nursing hours for a number of reasons: a) There is higher acuity or dependency of patients generally on the ward, compared to what would be usual for a specific ward; 1:1 care may not be required, but additional RN or care staff hours may be needed to provide care that is safe, effective and dignified. b) A requirement to special a patient (provide 1:1 observation or care) this may be necessary because the patient has been assessed as at high risk of harm to themselves or others due to a mental health condition. In these circumstances, and following a psychiatric assessment it may be necessary to arrange for additional support from a Registered Mental Health Nurse (RMN), where it is safe to do so a Health Care Assistant may be used. c) A patient may also require 1:1 observation or care because the patient has been assessed as at high risk of harm to themselves due to dementia, confusion, risk of absconding or risk of falling. The table below highlights the number of additional duties that were allocated by the Nursing Bank Office for Special Duties Specific Duty Number of duties Comment 1:1 special 216 Please see c) above Escort special 18 Example: A patient may require a nurse to escort them to another hospital for an investigation, clinic appointment or transfer. RMN special 104 Please see b) above Any requirement for additional nurses is reviewed on a shift by shift basis and agreed with the Matron or Senior Divisional Nurse. During June acuity and dependency assessments were carried out on the adult inpatient wards as part of a planned quarterly cycle, an overview of the results will be provided in the August report. Information from the assessment will be considered as part of the next establishment review. 3. Actions to address gaps Planned and actual staffing levels are reviewed on a shift by shift basis by the ward sister and matron and discussed at the daily bed meetings. Plans to ensure safe staffing are formulated and agreed at the daily bed meetings in conjunction with the Director of Patient Experience & Nursing. Where a shift is running below the planned level, staff will be especially vigilant to any aspects of care that is at risk of being missed and escalate their concerns to Senior Nurses for further action. 3
85 Actions are taken with the aim of maintaining safe and effective nursing care for our patients. Examples of actions taken to address any gaps in planned staffing levels include: Reallocation of staff from within the division or other divisions in the Trust Support from non-ward based nursing/midwifery or care staff Matron working clinically providing hands on care Requests for bank or agency staff. A recruitment open day, supported by nursing, the recruitment team and occupational health was held on Saturday 12 th July. 45 applicants were invited and 34 attended, an interview was rescheduled for one individual. In total 32 staff were recruited. The table below shows a breakdown of roles. Registered Nurse Health Care Assistant Substantive Roles Nurse Bank 2 1 Total In addition five registered nurses and one healthcare assistant were appointed for the Mount Vernon site on 30 th June. The recruitment day and interview format is being reviewed and revised as part of the Nursing Recruitment work stream. A further recruitment day is planned 16 th August. The Trust will also have a stand at the Royal College of Nursing Job Fair held in London on 5 th and 6 th September. A total of 25 new nursing staff started work in July. The table below shows a breakdown of roles. Registered Nurses 7 Health Care Assistants 18 Total 25 Divisional Overview Medical Division Russell Wernham, Assistant Director of Nursing, Medical Division The Division has been working to fill current vacancies within its wards and departments with the latest event recruiting 25 RNs. The Division has made contact with Bucks New University to look at developing a preceptorship programme to simplify student recruitment. The Division has also had the added pressure of an additional 72 beds open for the month of June. This has had an impact on senior staffing levels with the nursing numbers being adjusted to provide safe and effective cover across all patient areas. The medical matrons have also worked clinically during the month to ensure that ward and department areas are safe and that patient care is maintained. 4
86 Stroke Unit - Fill rates were consistently above the planned levels in June. The ward is established for 20 beds, but has physical capacity for an additional six beds should operational demand increase; when these beds are in use the ward staffing is increased to ensure safe and effective care for the increased number of patients. These beds were open throughout June, hence the staffing levels being above those originally planned. The ward has also had extra pressures on staffing to provide 1:1 care for both confused and psychiatric patients. Beaconsfield East - Day shifts were below planned levels. This is due the ward team supporting an additional ward that was opened temporarily due to increased operational demand. The ward Matron worked clinically on Beaconsfield East when necessary to ensure adequate nursing cover during the day, and the ward based multidisciplinary team also supported the nursing team wherever possible. The Division has now filled the band 6 vacancy caused by retirement in June. Drayton - Staffing levels were increased on nights due to patients needing specialing. The ward has a lower vacancy rate then the Divisional trend. CCU The fill-rate was below planned levels however this was for part shifts only and during the day; the acuity of patients was assessed to ensure levels were appropriate for acuity and dependency levels. The unit is situated at the end of Drayton ward, enabling nursing staff to work flexibly across both areas when required. Bevan The staffing on Bevan was increased to provide cover for an extra capacity ward that opened. There was also long term sickness on the ward in June. Edmunds Staffing was adjusted to ensure minimal cover overnight with backfill from HCAs. Surgical Division Sinead Fagan, Assistant Director of Nursing Surgical Division Trinity Although there were low fill rates throughout, actual staffing levels were appropriate for the number of patients on the ward as activity fluctuates but the planned numbers are based on an assumption of full occupancy. On any occasions where staffing is lower than assessed need, support is given by day care unit staff. The vacancy rate on Trinity has been higher than desired due to a number of staff being moved to support Edmunds ward. These vacancies are now advertised with recruitment taking place in early July. Jersey appears significantly under filled across both staff groups due to a mixture of sickness and vacancies during our day shifts. Both these areas have been addressed with staff members on phased return to work and recruitment taken place. In the interim the Matron is carrying out clinical duties when support is needed. Currently we have seen a small rise in falls and pressure ulcers within our nurse sensitive indicators; this may be linked to increased use of temporary staffing. Recruitment has taken place to fill these vacancies. We hope to be at appropriate establishment levels in September for the ward. 5
87 The acuity and dependency review is now completed for this quarter. We are awaiting this analysis. Kennedy also has areas where shifts have not been filled to the 100% with day hour requirement, mostly due to vacancies and sickness. Each day the clinical need and staffing levels are reviewed by the Sister and Matron with provisions made to cover where possible by reallocating staff from other surgical areas or Matron assisting in clinical practice. Registered Nurse fill rates at night were prioritised to ensure safe care, with additional one to one specials in place when required for specific patient conditions. The ward currently has a patient who requires a 1:1 special for 24hrs a day. Vacancies have now been recruited to and sickness management has been undertaken for those staff requiring it. ITU Staffing in ITU fluctuates depending on the patient criteria. ITU patients require a ratio of 1:1 (RN:Patient) where as some HDU patients can be nursed on a ratio of 1:2 (RN:Patients).This is monitored on a daily basis by the ITU senior nurse manager, with staffing levels adjusted accordingly in line with acuity and actual patient present on the unit during the month. Women and Children s Division - Anita Hutchins, Head of Midwifery This is not an accurate reflection of the unfilled shift allocation for maternity. The unfilled rate is less than 7%. This discrepancy is due to the allocation of long days (LD) shifts. The vast majority of maternity staff work long day shifts (12 hours) as opposed to the traditional early/late shifts (7.5 hours each = 15 hours for two members of staff), which on the current staff modelling appears as though there is a 3 hour shortfall per shift. However, as our rota is set for the Long Day shift pattern this is not a factor as there is no time needed for handover and the hours are allocated for direct clinical care. To demonstrate how the calculation is impacting on the figures: Antenatal ward- qualified staff Figures show a deficit of 286 hours for the month of June. For June Antenatal Ward had a total of 9 shifts not fully covered totalling 71 hours. The 286 hours is based on the cumulative 3 hours of LD shifts that have been filled over the month. Actions: E rostering team to work with the division to reflect the true rate of unfilled hours. The maternity service continues to follow the escalation and divert policy on a daily basis to ensure that the maternity unit is safely and appropriately staffed to manage the patient workload. Where unfilled shifts are identified the priority will be to ensure nights and weekends are covered as there is the potential to flex staffing during the weekdays. Where there are identified unexpected shortfalls in shift cover, e.g. due to sickness, then a review of activity and acuity will be undertaken to determine the need for shift fill. 6
88 NNU Suet-Mei Yoon, Ward Manager Staffing levels are flexed, in terms of numbers and skill mix to match the clinical need in terms of acuity and dependency of the babies on a shift-to-shift basis. This can cause a deviance from planned levels but will always match what is actually required. Presently, the Nursery Nurse of 0.88 wte is included in the RN figures and the HCA band 1 who does not work clinically is reflected in the care staff figures. This will be adjusted in future figures. Peter Pan Melissa Mellett, Assistant Director of Operations, Women s & Children Division The night shifts are over quota due to periods of time when children have been admitted needing an RMN. The day shifts that were not filled to the 100% standard, is due to maternity leave and short term/long term sickness. We have successfully appointed a fixed term contract to cover Maternity leave and continue to proactively manage sickness. Where there are shortfalls in the day shifts the ward is supported by staff from the paediatric day unit, multi-disciplinary team and or/the Matron. 4. Action from the June Board The Board received the establishment review report in May, this included an at a glance table indicating RN:patient and Staff 1 :patient ratios by ward. This showed that some wards had shifts that were rated as amber or red when benchmarked against best practice guidance. This narrative explains the plans to address these or mitigate any risks. It is important to note that the ratios have been calculated based on an assumption of 100% occupancy. Trinity ward receives only elective surgical admissions. Currently the ward is rarely fully occupied, the June acuity and dependency assessment has shown that 86% of the patients assessed were level 0 - normal ward patients, with 12% having increased dependency and just 2% a higher level of acuity. Action: The Senior Sister and Matron will continue to assess their patient profile and staffing levels, and may request additional staff via the nurse bank should patient needs exceed the actual level of nursing staff available. The establishment will be reviewed again this year and take into account any changes to the service or the patient profile. Hayes ward Acute admissions older people. Currently the staff: patient ratio is 1:4.2 on a late shift, the RCN guidance for older people recommends 1: Hayes ward staff work predominantly short shifts, this means that the staffing levels will exceed the RCN guidance during the shift overlap time. Action: Sister and Matron assess patient acuity and dependency every shift and indeed throughout the shift, where it is felt that additional staff are required due to increased acuity, dependency or a specific patient requirement the division will seek additional staff appropriate to the specific need, this may be an RN, HCA or RMN. The establishment will be reviewed again this year and take into account how frequently additional nurses have been required, nurse sensitive outcome indicators and staff and patient reports of insufficient staffing (all monitored through the planned and actual staffing template). 1 Please note that staff includes RN and care staff 7
89 Edmunds ward Older people rehabilitation ward. Currently the staff: patient ratio is 1:4.1 on a late and night shift, the RCN guidance for older people recommends 1: The establishment for this fairly new ward was planned to achieve an RN: patient ratio across all shifts at of less than 1:8. In addition the Senior Sister on Edmunds also works in a supervisory capacity (not usually taking an allocated case load) this means that she is able to provide additional hands on support on the ward should the need arise. Action: please see Hayes ward actions. Bevan ward - Medical ward (Haematology and gastroenterology) currently the RN: patient ratio is 1:8 on a late shift only. Drayton ward -Medical ward (cardiology and general medicine) currently the RN: patient ratio is 1:9 on a late shift only. Drayton and Bevan ward staff work a mixture of long days and short days so there will be additional nursing staff on the ward for part of the late shift on most days. Action: please see Hayes ward actions. The newly issued NICE guidance for safe staffing in adult inpatient wards sets out the recommended approach for establishing safe staffing establishments; this involves calculating the direct care nursing hours required by each patient on a ward, along with assessment of a range of other ward and nursing staff factors. This approach will be used for the next establishment review later this year, however in light of the current RN:patient ratios on the late shift on these wards, we will be testing this approach first in these areas and recommending further investment if this is required to ensure that we can safely and effectively meet the patient s needs on these two wards. 5. Next Steps Continued focus on recruitment through the Recruitment and Retention group which meets bi-weekly and is chaired by the Director of People. The Trust is currently in discussions with TMP Worldwide with regard to establishing a clear brand for the Trust and take forward new initiatives on advertising. This will be in collaboration with our communications department. TMP are also looking into raising the profile of the Trust through advertising on various media such as banner adverts on Google and the feasibility of 'micro sites' which will hold details of the Trust and specific departments and posts. In addition the Trust is running a series of recruitment days for Nurses and HCW's. These are held on Saturdays and applicants are interviewed and given offers on the same day. Estates are looking at refurbishing the Mount Vernon accommodation blocks several of which are currently in poor condition to support the Trust's recruitment incentives. 8
90 Appendix 1 STAFFING LEVELS June Data - JULY REPORT Environment Fill Rates Vacancies Nurse Sensitive Outcome Indicators Division Ward Overall gross Hospital Falls with no Friends and Comments Suboptimal Confidence Staff did Answers Finding Enough New PU Falls Beds Days Nights vacancy rate** Acquired harm / Falls Family Test from FFT: staffing & trust in all they you can someone to emotional ST ST Average fill rate- RN /Midwives % Average fill rate- Care Staff % Average fill rate- RN /Midwives % Average fill rate- Care Staff % Pressure Ulcers*** resulting in harm*** ( FFT ) score insufficient staffing levels incident reports*** nursing* could to control understand from talk to about worries/fears* support from staff* pain* nurses* Medicine Surgery Women & Children Ald % 86.4% 99.9% 105.0% 7.03% 3/1 94% 90% 81% 93% 94% B'east % 76.5% 98.3% 96.7% 33.29% 1 5/ % 87% 79% 76% 84% Bevan % 87.5% 103.3% 150.2% 24.81% 1 2/ % 80% 90% 75% 75% CCU % 98.9% 23.12% % 100% 83% 88% 86% 1 Drayton % 87.4% 96.7% 116.7% 9.27% % 80% 90% 50% 93% 1 EAU % 97.6% 100.5% 100.9% 21.0% % 94% 92% 83% 93% 4 Grange % 81.3% 96.7% 96.7% 19.5% 3 5/ % 86% 78% 81% 79% 5 Hayes % 94.6% 97.8% 103.3% 12.5% 5 7/ % 86% 59% 75% 83% 2 Stroke % 129.5% 120.9% 200.7% 22.1% 1 4/ % 90% 79% 84% 88% Edmunds % 108.5% 90.8% 119.3% % 93% 91% 91% 96% Jersey % 75.1% 98.9% 96.6% 23.5% % 99% 96% 97% 98% 1 1 Kennedy % 85.6% 105.4% 125.0% 26.1% 3 2/ % 88% 72% 71% 83% 1 ITU/HDU % 88.2% -0.64% 2 100% 100% 83% 100% 100% 1 1 Trinity % 65.3% 100.0% 96.0% 18.6% % 98% 84% 92% 99% Marina % 94.2% 105.0% 111.8% 5.8% % 86% 90% 86% 91% 2 Peter Pan % 84.7% 104.8% 8.34% 1 3 NNU 78.8% 191.0% 95.3% 11.89% 3 Alex 80.1% 92.7% 90.1% 99.7% -5.8% Kath 79.4% 84.7% 98.9% 100.0% 22.0% 2 91% 83% 86% 92% 78% Labour 73.3% 83.1% 97.6% 94.9% 3.8% *Q1 local inpatient survey ** June Vacancy Tracker *** Reported via Datix Incident Reporting System Medication errors*** 9
91 ITEM 14 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Joe Smyth, Director of Operational Performance Jacqueline Walker, Deputy Director of Nursing and Integrated Governance Karl Munslow Ong, Chief Operating Officer Theresa Murphy, Director of Patient Experience and Nursing DATE: 30 th July 2014 SUBJECT: Quality and Operational Performance Report for June 2014 Trust Strategic Priority: The report covers all of the Trust s Strategic Priorities. Summary: This report provides the Board with an analysis of performance to the end of June The report covers performance against the Monitor Risk Assessment Framework as well as national and local key performance indicators. Board Action Required: The Board is asked to review the Quality and Operational Performance Report and the actions being taken. Equality Impact Assessment: N/A there is no positive or negative impact from this report. 1

92 1. Introduction Quality and Operational Performance Report for June 2014 The purpose of this report is to provide assurance to the Board on compliance against the Monitor Risk Assessment Framework, national and local key performance indicators. It acknowledges significant and notable achievements, and highlights and discusses areas of concern or where performance has a less than favourable forecast. 2. Items of Note 2.1 Bed Occupancy There has been a significant increase in the number of non-elective admissions in the first quarter when compared to previous years. While length of stay savings continue to be delivered the sheer volume of activity means that the Trust was unable to close any of its escalation capacity. This is impacting on anticipated savings from the Improving Inpatient Care programme although commissioners acknowledge that there are unavoidable cost pressures for the Trust as a result of higher than anticipated emergency demand. 2

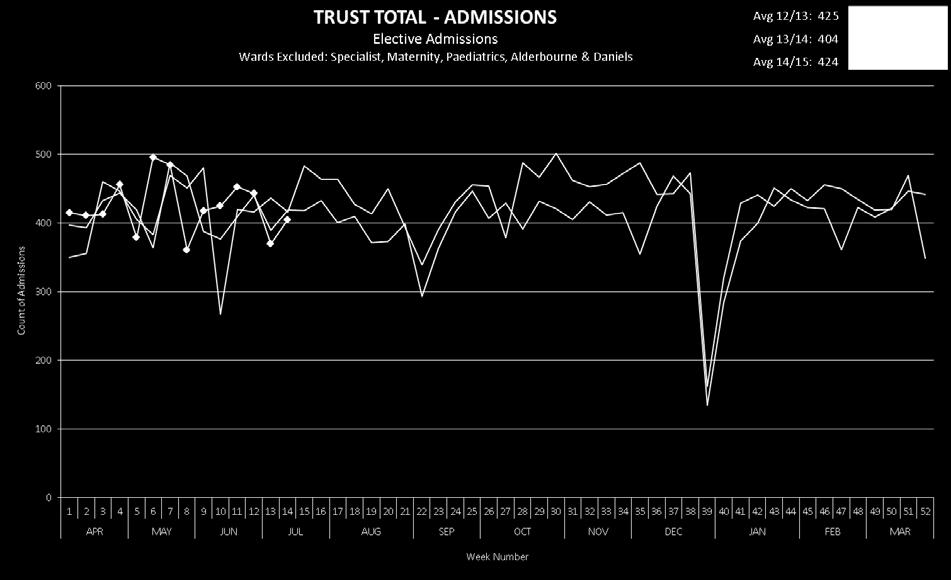
93 3
 were admitted requiring ongoing rehabilitation services with the remaining (41) admitted while awaiting complex placements to be arranged.")
94 2.2 Edmunds Ward To date 123 patients have been admitted to Edmunds ward. The majority (82) were admitted requiring ongoing rehabilitation services with the remaining (41) admitted while awaiting complex placements to be arranged. So far 73 patients have been discharged either home or to a nursing-home placement. In total 21 patients have been transferred back to Northwick Park for medical reasons. 2.3 Northwick Park Elective Work Number of Referrals received Number of New outpatient attendances Number of Follow up outpatient attendances Number of procedures undertaken To date June 14 14/15 Year to date The Trust is continuing to support North West London Hospitals Trust (NWLHT) to deliver its elective work programme. To date 254 patients have had their procedure at the Trust. The numbers of new referrals being received from NWLHT are decreasing. NWLHT have confirmed that going forwards they require capacity in different specialties and we are currently in discussions with both the Trust and local commissioners as to the level of ongoing support we can provide. 4
95 2.4 Resilience Planning RTT Following the pressure experienced during the winter of 2012/13, NHS England published the A&E Recovery Plan in May The plan brought together the national and regional A&E tripartite panels, comprised of representatives from NHS England, The NHS Trust Development Authority (NHS TDA), Monitor and the Association of Directors of Adult Social Services (ADASS). Recognising the good work undertaken by Urgent Care Working Groups, it was agreed that the roles of these groups should be expanded to include Elective Care. Bringing together both urgent and elective care within one planning process underlines the importance of whole system resilience. As part of the elective plan the Trust recently bid for monies to reduce the number of elective patients waiting more than 16 weeks for treatment, and was successful in securing 503k to improve the waiting times for at least 275 Hillingdon patients. Detailed implementation plans are currently being developed to increase capacity to facilitate a reduction in the waiting times which will include increasing diagnostic capacity in key modalities. All the additional elective work must be undertaken between July and the end of September. There may be the opportunity to support other Trusts with their additional elective activity during this period if there is sufficient capacity. 2.5 Neuro-Rehabilitation Expansion Mount Vernon There is a significant shortfall of Neuro-Rehabilitation capacity across the region. Patients often have to wait considerable amounts of time to access the Rehab services on the Alderbourne unit. In response to this need the Trust is expanding its Neuro-Rehab service by opening a new bespoke 16 bedded unit on Daniels Ward on the Mount Vernon site. Refurbishment work on the ward is progressing well with the service expected to commence towards the end of July. Both units will work together to provide an enhanced service for patients and their families. 2.6 Cancer Report Performance and Audit Cancer performance is being well maintained. It should be noted that out of the 16 organisations in the London Cancer Alliance (LCA) the Trust was one of five who achieved the 62 day standard consistently across the four quarters in 2013/14. The recent audit of the 62 day pathway by Deloitte noted no issues in the testing of data through to supporting recording. TIAA are currently undertaking a further audit of cancer services with a focus on governance, management arrangements and pathway escalation processes. 5
96 LCA Members Board The refreshed LCA Members Board met on 29 th May 2014 and received an update from the LCA Clinical Board about the proposed actions from baseline audits of existing services in gynaecology and urology. The audits were conducted against the original Model of Care for Cancer Services across London which aims to address areas of non-compliance, reduce variation across the LCA, improve patient experience and clinical outcomes. The significant issues to note for the Trust are detailed below: Gynaecology The pathway group recommended that the gynaecology unit hold a weekly multidisciplinary team (MDT) meeting and in July the team increased their meeting schedule to comply. Other recommendations from the audit concern the specialist site MDT (SSMDT) where patients requiring treatment at the tertiary centre (Hammersmith Hospital) are discussed. These recommendations are currently being considered by the Trust MDT Lead (Mr Nicholas). It is important to note that the Trust currently has a robust pathway with Hammersmith and strong communication links with members of the SSMTD. Urology The pathway group has agreed that transurethral resection of bladder tumour procedures should be undertaken by a designated urologist with an interest in bladder cancer. The Trust MDT Lead (Mr Pope) has written to the Chair of the Pathway group to ask for further clarification about the pathway for these patients as the Trust does not hold a specific MDT meeting for bladder cancers. CNS Mapping The LCA have undertaken an initial mapping exercise of Clinical Nurse Specialist functions and found notably that this role is vital in acting as a point of contact for patients. The work has clearly indicated that CNS roles must have clear job descriptions, a framework for development, and realistic caseloads to ensure the benefits of the post are maximised. The Trust level analysis is now being discussed and disseminated and will be presented at the Cancer Strategy Board. Recruitment to the Macmillan Lead Cancer Nurse is in progress with interviews scheduled for 10 th July Peer Review The peer review process for 2013/14 period is underway, an external assessment of the Breast Team in July 2014 found no immediate risks or serious concerns. Other teams are progressing through internal validation and self-assessment. 2.7 A&E planned Changes On 10 th September 2014 the A&E units at Central Middlesex and Hammersmith will be re-classified as minor injury units. Initial modelling indicates that patients will either attend their GP surgery or transfer to St Mary s or Northwick Park. 6
97 The impact on Northwick Park could be significant which would in turn increase the number of patients attending Hillingdon A&E. With this in mind the Trust requested that additional modelling be undertaken to assess the wider impact across the sector and help inform any further measures that may need to be taken to improve system resilience. Hillingdon A&E is being used as a pilot site to assess likely impacts of increases in self-referrals, Ambulance or GP Heralded arrivals. This will allow Trusts to plan for changes to existing flows and the resource required to manage the same. The modelling will incorporate changes to the available cubicles and the number and type of staff required to manage additional activity. 3. Quality Report Narrative Patient Safety Indicator (04) Hospital Acquired Infections Cdiff The Trust remains on two reported C diff cases to date with one in May and one in June, and is within the current threshold. Both patients had received antibiotics necessary for their treatment and root cause analysis investigation did not reveal any care or service delivery problems that may have contributed to their diagnosis. MRSA It is very disappointing that in July we have reported an MRSA bloodstream infection. This is currently under investigation by the infection control team and a root cause analysis with the clinical team is in progress. Patient Safety Indicator (05) - Patient Falls June saw the falls rate per 1000 bed-days increase to 4.7 against a target of 4; this was an increase of 0.7 compared with May. It has been noted that the falls rate also rose in June compared with May in the two previous years: in 2013 it rose from 4.2 to 6.7 and in 2012 it rose from 5.2 to 6.6. Although this year's increase is significantly lower than in previous years, data is being reviewed in an effort to identify any consistent underlying factors. June was the third consecutive month in which the rate of falls was above the Trust target for 2014/15. This target, which requires a 20% reduction from last year, is proving challenging on top of the reductions delivered in 2013/14. It is important to note that the quarterly average is lower than for the same quarter in both the two previous years (average 4.3 this year compared with 5.0 last year and 6.17 in 2012/13). To support further improvements in falls prevention TIAA will be auditing falls risk assessment processes and also outcomes of a selection of root cause analyses in falls resulting in fracture. The National Dementia Audit requires Executive Boards to receive information on falls in which patients with dementia can be identified. To support this Dementia has been added to Datix as a selectable contributory factor for falls. In June dementia was recorded as a contributory factor in 12 of the 168 reported falls, an increase of 7 7
98 compared with May. Work will continue over coming months to refine how this data is recorded and analysed to support improvements in care. Patient Safety Indicator (13) Serious Incidents The Trust is currently investigating two Serious Incidents one of which relates to a delayed diagnosis in a patient who needed urgent treatment and transfer to another hospital for a vascular emergency. It is expected that the report and action plan will be presented to the August Board meeting. The second case relates to a serious drug incident that affected three babies receiving intravenous antibiotics on the Neonatal Unit who developed a very severe reaction to the skin; this case has been escalated to the Medicines and Healthcare Products Regulatory Agency with regard to concern about potential problems with the product that was used. It is anticipated that this case will be presented to the September Board meeting. Two SI investigations have recently been completed; the investigation reports and action plans have been presented to and approved by the Trust Board and have been submitted to the Commissioning Support Unit for review. Actions are being progressed by the relevant divisions and progress will continue to be monitored by the Board until actions are complete. Learning to be shared and actions to drive improvement: The Enhanced Recovery Programme (ERP) document for colorectal surgery is to be reviewed The Colorectal Clinical Nurse Specialist will provide training sessions for staff re: ERP and signs and symptoms of complications Staff will receive further training on the standards of record keeping The use of fluid balance charts in the post-operative patient will be audited Staff to be instructed that bowel and urine output have to be strictly monitored post operatively for a minimum of 72 hours or until surgical review advises otherwise Staff to use the labour ward problem box (on the documentation) to highlight risk factors Review of the new handheld notes to add a column for weight on the antenatal clinic pages, as well as keeping it in the checklists Highlight the standards to all staff regarding the siting of an epidural within 1hr maximum of request by the patient Set up multidisciplinary training for all staff in the use of the ventouse machine Reflection by staff involved in how to improve communication processes in the context of stressful circumstances within labour ward and maternity theatre. Patient Safety Indicator (14) Never Events Unfortunately a Never Event was declared in June whereby the wrong gas (air instead of oxygen) was delivered to a patient in the A&E department. This case has been declared to the Commissioning Support Unit and is being investigated in line with the Trust s Serious Incident policy. 8
99 Patient Experience Indicator (17) - Friends and Family Test Net Promoter Score The Trust has set a stretching target for improving the inpatient and A&E Friends and Family Test Score by 15%. FFT results are calculated using a Net Promoter Score. The idea is simple: if you like using a certain product or doing business with a particular company you like to share this experience. From the answers given three groups of people can be distinguished. These are: Promoters - people who have had an experience which they would definitely recommend to others (extremely likely). Detractors - people who would probably not recommend you based on their experience, or couldn't say (neither likely or unlikely, unlikely and extremely unlikely). Passive - people who may recommend you but not strongly (likely). The score is calculated by subtracting the % of detractors from the % of promoters. The Trust has more promoters than any other group, with the passives being the next largest group. Actions taken to improve scores are based on the comments received each month, but because each patient will have their own unique set of factors that will influence their scores it is not possible to say with complete certainty that improving X will result in more patients moving from the passive group to the promoter group. Details about some of the improvement actions can be found in the monthly Putting People First Board report. Patient Experience Indicator (19a & 19b) Complaints Division % Numbers Commentary CCSS 100% Due - 5 Actions and learning from complaints monitored at Divisional Governance Meeting. Achieved - 5 Breach - 0 Surgery 100 % Due - 9 Achieved - 9 The common themes highlighted are lack of communication and cancellations or unavailable appointment. The division continues to stress the importance of the CARES values to all staff. Breach - 0 They are also trying to increase the numbers of staff attending the customer care courses and the Assistant Director of Nursing within the Division is ensuring that feedback is provided to areas that have received multiple complaints. W&C 100% Due - 5 The Division continues to work to ensure timely investigation and response to complaints. The Achieved - 5 recent trend of the complaints has seen a consistent theme on attitude. As part of the Division s response to the staff survey a group Breach - 0 including CARES ambassadors and staff from all areas has been created to review work pressure. Medicine 100% Due - 5 Several lessons learnt from complaints across the division which include: 9
100 Achieved - 5 Breach Providing clear information to patients on discharge - Communicating to patients when there are delays - The need to document all patient and family conversations in the medical record - Ensuring patients have enough information about their diagnosis The Trust acknowledged 100% of complaints within three days of receipt. 29 complaint responses were due in June and responses went out on all of these within the agreed timeframe, giving 100% performance. This was in spite of 3 weeks staff absence on annual leave within the Complaints Management Unit and is a reflection of the more effective working practices within the unit, the stronger working relationship with all Divisions and the focus by all on meeting or exceeding targets. Complaint Trends The graph below shows the Trust wide top ten subjects in June, compared with those logged in May. The most frequently mentioned subject areas continue to include attitude of medical and nursing staff as well as clinical care. Discharge is also an area which is appearing with more frequency and often concerns difficulties in discharge planning in conjunction with Social Services and the arrangement of packages of care. A meeting is currently being arranged between the Director of Nursing and the Integration Lead for Adult Social Services at Hillingdon Council in order to improve the discharge planning process. We were notified of one complaint being referred to the Ombudsman in June; this was referred back to the Trust for further local resolution and was the only reopened complaint this month. 10
101 We also received one final report from the Ombudsman on a case that has been under investigation since March 2014 and this was partially upheld on poor complaints handling because of excessive delays. We have issued our response in line with the Ombudsman s recommendations, providing details of the measures now in place to avoid such delays. The team performance in June demonstrates the effectiveness of these changes. 4. Monitor Performance Framework Compliance against the Monitor Performance Framework remains strong, and all indicators were achieved for the first quarter (April June 2014). 5. Contract KPIs Indicator 16 C section rate (emergency and elective) Amber Target 27% Elective Non Elective Total (15% & 12%) June 08.92% 13.54% 22.46% YTD 11.89% 15.98% 27.87% Following a high rate of caesarean sections for April an audit was undertaken at the beginning of May which included a review of all caesarean sections. As a consequence of the audit and its findings, a number of actions have been taken: processes for elective surgery reinforced; guideline for Vaginal Birth after Caesarean (VBAC) revised; daily multidisciplinary review of caesarean sections undertaken from the previous 24 hours; and general reinforcement of guidelines from the Consultant body around decision making. For the month of June there was significant reduction in the caesarean section rate. Whilst this is partially down to improved process there has also been a reduction of acuity. Acuity levels will fluctuate on a month by month basis and so this should act as a cautionary note to the good performance figures this month. Indicator 20 Patients not Readmitted within 28 days RED Target June Year to Date 0% 28.60% 05.10% In the month of June there were two Dermatology patients cancelled on the day of Mohs micrographic surgery due to the cryostat machine being out of order. The cryostat machine is integral to the Mohs surgery because it freezes the skin tissue which the surgeon removes during the procedure. The frozen tissue is then microscopically examined to establish if further tissue requires removal. These cancelled patients could not all be accommodated within 28 days due to the unavailability of the cryostat machine and also due to the unavailability of the Mohs surgeon. The Cancer and Clinic Support Services Division are developing plans to recruit a second Mohs surgeon to mitigate against these incidences. 11
102 Indicator 22 Type 1 A&E Performance RED Target June Year to Date 87.90% 87.90% No longer in contract but monitored by CCG In June the Trust achieved 95.6% for all type activity against the 4 hour performance standard, successfully ending the quarter above the expected standard of 95%. Achieving type 1 activity has continued to be a challenge in the face of increasing acuity and blue light conveyances. During June, 181 blue light ambulances attended the emergency department compared with 126 for the same time period last year, an increase of 43%. During quarter one the number of blue light arrivals increased by 137 when compared to the same period last year. This group of patients will often consume a significant amount of resources in terms of the requirement for immediacy of care delivered by senior personnel. This in turn will often impact on the throughput of the remaining patients in the department as resources are diverted to those in greatest need. In order to address the current level of demand, the Trust has recently made further investments in the senior medical team to increase capacity during peak periods to help improve patient flow. In addition, the number of emergency admissions to the Trust in month has increased by 350 when compared to June This suggests that patients coming to the emergency department have more complex needs, will take longer to assess and treat before admission to an inpatient bed. Comparison of inpatient admissions Year April May June The Trust is working with healthcare partners to address the issues of increasing acuity presenting through A&E and the resulting impact on bed capacity. Indicator 31 Emergency Readmissions 30 Days Target May Year to Date TBC 8.00% 8.30% The increased re-admission rate seen across the Trust during May dropped back to 8.0% in June, a level commensurate with April, although the year to date readmission rate at 8.3% remains higher than over the same period in 2013/14 when it was 7.7%. 12
103 Investigations have been carried out into the increase in General Surgery readmissions highlighted in last months report. The results of these investigations have since been shared with general surgeons and emerging trends relating to constipation, haematoma, and general abdominal pain have been discussed in detail at audit. The division is currently looking at enhancing the pathway for patients with 'stone' pain, through the development of the new surgical assessment short stay unit and patient pathways. Work is progressing on the development and implementation of our hospital wide system to promote timely, patient-focussed, clinical investigation at the point of readmission. Discussions have taken place with clinical directors and nursing service managers to ensure that they understand and support the system, and activities are now under way to develop the technical infrastructure that will underpin the readmissions investigation process. The trust is still working towards implementation at the end of July. The Trust also continues to work closely with colleagues in social care, primary, community and CCG to identify, review and support yearly investment schemes aimed at strengthening integration and reducing readmission rates and has submitted a bid to fund the recruitment of a full-time facilitator to support the point-ofreadmission review process. Indicator 32: Theatre Utilisation RED Target June YTD Utilisation 85% 78.1% 79.3% Productivity 95% 76% 77% Average cases per session Cancellations <0.8% 0.35% 0.63% Theatre utilisation and productivity performance remain below target. The Clinical Director for Surgery and the Associate Clinical Director for Anaesthetics have recently joined the monthly Theatre Steering Group. This increased clinician input has proved very beneficial and has allowed a refreshed list of practical issues impacting theatre utilisation and productivity to be devised. These issues have been grouped into work streams and each of these is now being led by a named Senior Manager who is responsible for reporting progress back to both the Operational and Steering Group. It is anticipated that the actions being taken and the different approach being adopted will deliver improved performance but there will be a time lag before this is reflected in performance data. This is in part due to the forward booking of lists. The late start audit performed in June is now complete and the results will be presented to the Theatre Steering Group Meeting on 24 th July An action plan will be devised to address issues identified. For the past month one of the Surgeons has been working closely with the Booking Team on his lists to see if giving Consultants more control over the booking of their lists results in improved productivity and utilisation. This performance data for this 13
104 clinician has improved illustrating that close working with Clinicians is vital to improving performance. Theatre cancellation performance has improved considerably and is currently within target for both June and year to date. Indicator 33 London Ambulance Service (LAS) 30 minute waits RED Target June Year to Date 100% 88.80% % 594 The recent increase in batching of ambulances during peak periods has impacted on the ability of the Emergency Department (ED) team to transfer patients to a cubicle within the 30 minute standard. In addition, essential building work has reduced space to treat patients within the ED which in turn has impacted on the ability to manage flow through the department. This essential work in the department is due to complete in July which will increase the cubicle capacity in the department and improve LAS handover times. Indicator 35 Appointment Slot Issue (ASI) RED Target May Year to Date < 10% 12.90% 16.30% The appointment slot issue (ASI) continues to be monitored at the Trust elective performance meeting and at divisional performance meetings. This month has seen continued pressure in the ENT CATS service, general eye service, one stop cataract service, rheumatology, hearing service, and coloproctology. The actions to address this are noted below: ENT- polling range extended Colorectal - paper referred patients booked to MVH clinics releasing capacity at THH Ophthalmology - Review outpatient clinics in line QIPP scheme, short term solution is being managed by increasing capacity through additional clinics Rheumatology - Exploring options for additional capacity at MVH Hearing service - Demand and capacity review underway. Indicator 36 FNOF patients in theatre within 36 Hrs RED Target June Year to Date 90% 71.4% 82.1% In the month of June there were 14 patients discharged following treatment for a Fractured Neck of Femur (FNOF). The average time to theatre for all 14 patients was 28 hours. Unfortunately four of these patients breached the standard for being taken to theatre within 36 hours. The Trust normally performs very well against this standard and there is a robust clinician led process for reviewing any patient that does not meet the standard. The regular Trauma Multi-Disciplinary Team (comprising of Orthopaedic Consultants, an Ortho Geriatrician, a Trauma Nurse, Orthopaedic ward nurses, an A&E Consultant and the T&O Service Manager) review each patient that has breached the standard and discuss individual cases. This process allows a review of 14
105 each patient pathway and ensures that where appropriate, lessons are learnt and breaches of this nature do not occur again. A summary of each breach analysis can be found below: 1 patient was delayed due to patient choice 2 patients were not medically fit or stable enough to be taken to theatre within 36 hours 1 patient was delayed to theatre as the fracture was not initially detected on arrival to A&E due to underlying complications and other medical complaints. As soon as the fracture was detected, the patient was referred to the Orthopaedic Team. This does occasionally happen and to minimise these occurrences Orthopaedic training is delivered regularly to A&E Doctors. Indicator 37 Re-admissions within 28 days AMBER Target June Year to Date < ( ) 103 ( ) These figures are derived from Dr. Foster information and cover the period April to December The benchmark is always 100, values grater then a 100 represent performance worse than expected. These ratios should always be interpreted in line with the accompanying confidence limits. The Trust consistently remains within the confidence limits. Indicator 41 Vacancy Rate RED Target June Year to Date < 8% 13.19% N/A A recruitment day was held on Saturday 7 th June 2014 which was successful in recruiting 25 nurses and 26 health care assistants. These nurses have not yet taken up post in the Trust and hence the vacancy rate remains unchanged from last month. Indicator 43 StaM% RED Target June Year to Date 80% 69.26% 69.26% 15
106 Quality Dashboard: Jun-2014 Clinical Effectiveness ID Indicator Source Performance in 2012/2013 Performance in 2013/2014 YTD Target 2013/2014 Apr-2013 May-2013 Jun-2013 Jul-2013 Aug-2013 Sep-2013 Oct-2013 Nov-2013 Dec-2013 Jan-2014 Feb-2014 Mar-2014 Clinical Effectiveness [01] Mortaility Indicators a HSMR* (aggregate) < b HSMR* (aggregate) Upper & Lower Limits ( ) ( ) n/a ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) c HSMR* (weekday) < Dr Foster d HSMR* (weekday) Upper & Lower Limits ( ) ( ) n/a ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) e HSMR* (weekend) < f HSMR* (weekend) Upper & Lower Limits ( ) ( ) n/a ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) ( ) [02] Palliative Care Coding* a THHFT Coding Rate 2.60% 2.90% TBC 3.36% 2.32% 3.36% 2.68% 4.42% 2.82% 3.52% 3.09% 2.52% 2.20% 2.36% 2.52% Dr Foster b National Coding rate 2.68% 2.94% TBC 2.77% 2.91% 2.90% 2.94% 3.00% 3.11% 3.06% 2.92% 2.77% 3.06% 3.01% 2.83% ID Indicator Source Performance in 2013/2014 Performance in 2014/2015 YTD Target 2014/2015 Apr-2014 May-2014 Jun-2014 Jul-2014 Aug-2014 Sep-2014 Oct-2014 Nov-2014 Dec-2014 Jan-2015 Feb-2015 Mar-2015 Clinical Effectiveness [01] Mortaility Indicators g SHMI n/a 0.89 h SHMI Banding As Expected As Expected [03] Crude Mortality (In-Hospital) HSCIC As Expected/ Lower Than Expected As Expected a Deaths (Absolute) n/a PAS b Mortality Rate 1.2% 1.1% n/a 1.1% 1.2% 1.2% * Dr Foster Basket of 56 Diagnosis groups
107 Quality Dashboard: Jun-2014 Patient Safety ID Indicator Source Performance in 2013/2014 Performance in 2014/2015 YTD Target 2014/2015 Apr-2014 May-2014 Jun-2014 Jul-2014 Aug-2014 Sep-2014 Oct-2014 Nov-2014 Dec-2014 Jan-2015 Feb-2015 Mar-2015 Patient Safety [04] Hospital Acquired Infections a MRSA 1 0 National: b MRSA cases per 100,000 beddays n/a c CDiff National: Infection (de minimis: 12) Control Team d Cdiff cases per 100,000 beddays n/a e E Coli 24 4 n/a f MSSA 4 2 n/a [05] Rate of Patient Falls per 1,000 beddays a All Falls b With Harm Clinical Governance [06] Patient Falls with Fracture (Datix / ir) <11 / Annual 8 3 <=1 / Month Medication Related Incidents per 100 [07] beddays n/a [08] VTE Compliance PAS 95.2% 92.3% 95% 95.0% 89.8% Ava. 28 Jul [09] VTE (Hospital Acquired) tbc [10] Attributable Pressure Ulcers a Volume (Grade 2,3,4) Clinical 170, 2, 1 41, 0, 0 120, 0, 0 10, 0, 0 18, 0, 0 13, 0, 0 Governance b Rate per 1,000 beddays (Datix / ir) [11] Safety Thermometer (Harm Free Care) a All Harms ST Tool 94.5% 95.4% 95% 95.0% 96.3% 95.0% b New Harms ST Tool 97.8% 98.5% 95% 98.7% 98.6% 98.0% [12] Patient Safety Incidents a Total Numbers n/a b Reporting Rate per 100 admissions > c Numbers Resulting in Harm Clinical n/a Governance d Percentage Resulkting in Harm (STEIS) 6.3% 6.4% <7% 6.2% 6.5% 6.6% [13] Serious Incidents (SI Panel) 10 1 n/a [14] Never Events
108 Quality Dashboard: Jun-2014 Patient Experience ID Indicator Source Performance in 2013/2014 Performance in 2014/2015 YTD Target 2014/2015 Apr-2014 May-2014 Jun-2014 Jul-2014 Aug-2014 Sep-2014 Oct-2014 Nov-2014 Dec-2014 Jan-2015 Feb-2015 Mar-2015 Patient Experience [15] Same Sex Breaches a Same Sex Breaches Operations Team b Rate per 1,000 FCEs Derived [16] FFT Response Rates a Accident & Emergency IWGC 18% 18.3% 20% 18.9% 14.2% 22.0% b Inpatients IWGC 40% 37.3% 30% 40.1% 33.7% 38.4% c Maternity IWGC 27% 18.0% n/a 22.0% 14.9% 17.5% [17] FFT - Net Promoter Score a Accident & Emergency IWGC b Inpatients IWGC c Maternity IWGC TBC [18] Overall Patient Experience a Inpatients Meridien 91% 89% >=88% 89% b Outpatients Meridien 87% 90% >=88% 90% c Maternity Meridien 86% 88% >=87% 88% [19] Complaints a Volume (Plan Agreed) Datix <40/month b Response Rate Datix 73.6% 86.2% >90% 79.4% 81.6% 100.0% [20] Number of Negative PALS Concerns PALS (Datix) n/a
109 The Hillingdon Hospital Trust Performance Report For the Month of Jun 2014 (Monitor KPIs) Traffic Light Key: [] - On target [] - Narrowly missing target [] - Significantly missing target Performance Movement Key: I - improvement S - static D - deterioration 2013/2014 Performance Jun Performance Year-to-date Performance 2014/2015 Target Year End Forecast 12 Month Trend Lead Exec Monitor governance risk weighting if in breach Current Month weighting Current Month Traffic Light Q1 Actual Q2 Forecast Q3 Forecast Q4 Forecast DQ Badge Monitor Risk Assessment Framework: Access and Outcomes metrics 1 Clostridium Difficile Infection National: 16 (de minimis : 12) 12 TM Cancer: Maintain two week cancer waits (all cancers) +^ 3 Cancer: Maintain two week cancer waits (breast symptoms except suspected cancer) +^ 4 All cancers: 31 days diagnosis to treatment for cancer (1st Treatment) +^ 5 All cancers: 31 days diagnosis to treatment for cancer (2nd or Subsequent Treatment - Surgery) +^ 6 All cancers: 31 days diagnosis to treatment for cancer (2nd or Subsequent Treatment - anti cancer drug treatments) +^ 97.9% 98.2% 98.4% 93% 98% KMO % 95.6% 95.5% 93% 95% KMO 99.3% 100.0% 99.2% 96% 99% KMO % 100.0% 100.0% 94% 100% KMO % 100.0% 100.0% 98% 100% KMO 0 7 All cancers: 62 days urgent GP referral to treatment for cancer +^ 90.3% 88.0% 90.9% 85% 90% KMO 0 8 All cancers: 62 days urgent referral to treatment for cancer (Screening) +^ Referral to treatment waiting times (admitted) Referral to treatment waiting times (non-admitted) Referral to treatment waiting times (incomplete) A&E: Total time in A&E less than 4 hours (A&E, MIU, UCC) Self certification against compliance with requirements regarding access to healthcare for people with a learning disability 97.8% 100.0% 100.0% 90% 98% KMO % 96.7% 96.7% 90% 97% KMO % 98.5% 98.5% 95% 99% KMO % 96.7% 97.0% 92% 97% KMO % 95.6% 95.6% 95% 96% KMO Fully Compliant Fully Compliant Fully Compliant Fully Compliant Fully Compliant 1.0 S TM N/A Notes: Monitor's Governance Rating under its RAF is now based on 5 categories (CQC Information, Access & Outcomes Metrics, Third Party Reports, Quality Governance Indicators and Financial Risk). The 13 indicators above reflect the Access & Outcomes Metrics only. The Second Page of the Glossary details the triggers for concern and the steps that lead to a specific Governance Rating. As there are numerous sources of information that will be used to derive the rating, it is not possible to give the full rating on this scorecard and so the rating that is reported here is based purely on the 13 indicators above. Key triggers in relation to those 13 indicators are: [a] 3 consecutive quarters' breaches of a single metric or a service performance score of 4 or greater. [b] Breaching pre-determined annual C. difficile threshold (either 3 quarters' breach of the year-to-date threshold or breaching the full year threshold at any time in the year) [c] Breaching the A&E waiting times target in two quarters over any 4 quarter period and in any additional quarter over the subsequent three quarters Monitor identifies potential material causes for concern in one or more No Governance categories (requiring further information Concern Evident or formal investigation), Monitor will replace the green rating with a description of the issue and steps taken to address it Regulatory Action + Indicator reported one month in arrears, ++ Indicator reported two months in arrears ^ Whilst Cancer Indicators are reported with a one month lag, the Current Month Traffic Light Column is based on the latest complete month available
110 The Hillingdon Hospital Trust Performance Report For the Month of Jun 2014 (Contract KPIs) 2013/2014 Performance Jun Performance Year-to-date Performance 2014/2015 Target 2014/2015 Year End Monthly Traffic Light Forecast Movement Lead Exec Comments Glossary Contract Indicators: Maternity 14 Obstetric 3rd/4th degree tears 1.98% 0.90% 2.05% <5 % 2% I AK/RGM RCOG target Obstetric 3rd/4th degree tears as a percentage of deliveries 15 Early access for women to maternity services by 12 weeks 6 days of their pregnancy [all] (excl late refs) [83.1%] (97.2%) [84.1%] (97.5%) [81.1%] (97.3%) 95.0% [83%] (97%) I KMO % of bookings having had a contact with service within 13 weeks of the booking. Exclusions apply to referrals after 10+6 weeks. 16 Caesarean section rate (Elective), [Non Elective] 26.8% (9.6%)[17.2%] 22.46% (8.92%)[13.54%] 27.87% (11.89%)[15.98%] 27% 27.0% I AK/RGM Elective and Non Elective caesarean sections as a percentage of all deliveries. Target is Royal College of Obs and Gynae recommendation 17 Infant health & inequalities: smoking during pregnancy 7.8% 7.4% 6.9% <10% 8% D KMO Actual percentage of smoking mothers 18 Infant health & inequalities: breastfeeding initiation 81.9% 85.5% 84.1% >=83% 83% I KMO Actual percentage of breast feeding mothers Contract Indicators: Cancelled Operations Cancelled operations: operations cancelled for non clinical reasons on day of admission or after admission. Patients not readmitted within 28 days of cancellation for non-clinical reasons on day of admission or after admission. 0.85% 0.35% 0.63% <0.8% 0.8% I KMO 0.0% 28.6% 5.1% 0% 5% D KMO Ratio of Cancelled Operations (meeting all SITREP - Situation Reports - criteria) to Elective Inpatient activity. % of Cancelled Operations (meeting all SITREP - Situation Reports - criteria) which do not get re-admitted within 28 days 21 Number of Urgent Operations Cancelled for a Second Time S KMO Contract Indicators: Waiting Times 22 A&E: Total time in A&E less than 4 hours: Type 1 A&E Only (ie excl MIU & UCC) 92.1% 87.9% 87.9% N/A (No longer in Contract but Monitored by CQC) 90% I KMO % of patients waiting less than 4 hours in A&E from arrival to discharge for a Type1 A&E Unit Only. Type 1 A&E Emergency departments are a CONSULTANT led 24 hour service with full resuscitation facilities and designated accommodation for the reception of accident and emergency PATIENTS 23 Trolley Waits: Patients Waiting over 12 hours S KMO Decision to Admit or A&E Treatment Complete to Patient Admission 24 First attendances at GUM service who were offered an appointment within 48 hours 100.0% 100.0% 100.0% 100% 100% S KMO % of first attendances in month who were offered an appt to be seen within 48 hours of contacting patient request (via telephone). 25 Maximum two-week wait for Rapid Access Chest Pain Clinics 100.0% 100.0% 100.0% >= 98% 100% S KMO % of patients with a GP Referral to a RACPC seen within 2 weeks. The standard only applies where the referral is received by the clinic within 24 hours of GP deciding to refer. 26 Percentage of patients waiting >6 weeks for a diagnostic test 0.003% 0.00% 0.04% <1% 0% S KMO Percentage of patients waiting over 6 wks for diagnostic tests at month end 27 All cancers: 62 days urgent referral to treatment for cancer (Consultant Upgrade) % 95.5% 95.8% TBC (was >=85% in 13/14) 97% D KMO 28 Referral to treatment waiting times (incomplete): patients waiting over 52 weeks S KMO Number of patients on incomplete RTT pathways, waiting 52+ weeks Contract Indicators: Other Performance Indicators 29 Stroke: Percentage of patients that have spent at least 90% of their time on the stroke unit 97.3% 100% 96.8% 80% 97% S KMO 30 Stroke: Percentage of high risk TIA patients who are treated within 24 hours 31 Emergency readmission within 30 days of discharge 8.0% 8.0% 8.3% 100% 100% 100.0% n/a 100% S KMO To be set following CCG Audit 8.0% I KMO Methodology taken from PBR Guidance - note that denominator also does not include PBR excluded activity for consistancy. Major Exclusions are patients aged <4 years old, patients with a cancer diagnosis & maternity patients 32 Theatre Utilisation (Newton Methodology) 82.8% 78.1% 79.3% 85% 83% D KMO 33 LAS Handover 30 min waits (actual / %) 1162 / 94.6% 197 / 88.8% 594 / 88.9% 100% 95% I KMO Sourced from LAS Portal 34 DNA Rates 9.1% 8.4% 8.5% 8.9% 8% D KMO Numerator = DNAs, Denominator = Attends + DNAs 35 Appointment Slot Issues (ASIs) 13.1% 12.9% 16.3% Q1:10% Q2:9% Q3:8% Q4:7% 10% D KMO ASIs as a % of DBS Bookings
111 The Hillingdon Hospital Trust Performance Report For the Month of Jun 2014 (Local KPIs) 2013/2014 Performance Jun Performance Year-to-date Performance 2014/2015 Target 2014/2015 Traffic Light Year End Forecast Monthly Movement Lead Exec Comments Glossary 36 Safety Fractured neck of femur patients in theatre within 36 hours % 71.4% 82.1% 90% 92% D AK/RGM May Data Fractured Neck of Femur (FNOF) patients operated on in theatre within 36 hours of admission as a % of total FNOF patients. Reported with a one month lag. 37 Readmissions within 28 days (benchmarked and casemix adjusted) ( ) ( ) ( ) < D KMO/ AK/RG M Monthly & YTD figure is still for Apr-13 to Dec- 13 Derived by Dr Foster. The benchmark is always 100, hence values greater than 100 represent performance worse than the benchmark, and values less than 100 represent performance better than the benchmark. This ratio should always be interpreted in the light of the accompanying confidence limits. It is standardised for diagnosis/procedure, subgroup, admission type, age, sex, deprivation, month of admission (for some respiratory diagnoses) and year. Important note: When analysing readmissions, admissions for the last 3 months (based on discharge date) are excluded. This is because it is impossible to calculate the outcome with any degree of certainty due to the time lag involved. We allow 1 month for the patient to be readmitted, 1 month for the patient to be discharged and 1-2 months for the data to be submitted to SUS (Secondary Uses Service - National database of hospital activity). 38 Trust Incidents Reported under RIDDOR TBC 33 D DS Trust incidents resulting in notification to the Health and Safety Executive under the Reporting of Injuries, Diseases and Dangersous Occurances Regulations (RIDDOR). 2012/2013 is based on a 7 day period Other 39 Personal Development Review (PDR) coverage 83.9% n/a n/a 90% n/a n/a CG New cycle not started 40 Trust sickness rate % 3.71% 3.40% 3% 3.1% D CG Jun Data 41 Trust vacancy rate 9.32% 13.19% N/A 8% 9.3% D CG Jun Data 42 Turnover rate 12.08% 0.90% 2.78% n/a 10.0% D CG Jun Data 43 STaM % 62.94% 69.26% 69.26% 80% 80% I CG Jun Data Feb 2014: The STaM figure is now populated from WIRED (excluding Local and Corporate Induction data) and based on the new Training Matrix. 44 ER Cases n/a 65 D CG Jun Data 45 Medical Staff Appraisals 30.40% 70.09% 70.09% 100% (by 31st May) n/a I RGM Jun Data Deadline Extended to end of May Response Time to FOI 75.0% 77.0% 74.0% n/a 75.0% D DC May Data FOI requests have a 20 working day turn around before they breach
112 Glossary - Jun Monitor Compliance Indicator Description Monitor Compliance Notes DQ Comments Healthcare Acquired Infections Clostridium Difficile Infection Inpatients with Specimens taken after 48 hours (attributable to Trust) Cancer Waiting Times (all indicators reported with a one month lag) Maintain two week cancer waits (all cancers) 2 % of patients with an 'Urgent GP referral' having been 'First Seen' within two weeks of referral. Maintain two week cancer waits (breast symptoms except suspected cancer) 3 % of patients first seen by a specialist within two weeks when urgently referred by GP with any breast symptom except suspected cancer. 31 days diagnosis to treatment for cancer (1st Treatment) 4 % of patients receiving first treatment within a maximum waiting time of 31-days from decision to treat, including patients with a recurrent cancer. 31 days diagnosis to treatment for cancer (2nd or Subsequent Treatment - Surgery) 5 % of patients receiving subsequent treatment (surgery) within a maximum waiting time of 31-days from decision to treat, including patients with a recurrent cancer 31 days diagnosis to treatment for cancer (2nd or Subsequent Treatment - anti cancer drug treatments) 6 % of patients receiving subsequent treatment (drug) within a maximum waiting time of 31-days from decision to treat, including patients with a recurrent cancer 62 days urgent GP referral to treatment for cancer 7 % of patients receiving first definitive treatment within 62-days of referral, following an urgent referral from a GP 62 days urgent referral to treatment for cancer (Screening) 8 % of patients receiving first definitive treatment within 62-days of referral, following a referral from an NHS Cancer Screening Service Referral to Treatment Waiting Times Admitted Pathways 9 % of patients that had treatment completed as an Inpatient within 18 weeks Non-Admitted Pathways 10 % of patients that had treatment completed in a setting other than Inpatients within 18 weeks Incomplete Pathways 11 % of patients waiting for treatment waiting less than 18 weeks Monitor s annual de minimis limit for cases of C. difficile is set at 12 Failure against either threshold represents a failure against the overall target. The target will not apply to trusts having five cases or fewer in a quarter. Monitor will not score trusts failing individual cancer thresholds but only reporting a single patient breach over the quarter. The target will not apply to trusts having five cases or fewer in a quarter. Monitor will not score trusts failing individual cancer thresholds but only reporting a single patient breach over the quarter. Failure against any threshold represents a failure against the overall target. The target will not apply to trusts having five cases or less in a quarter. Monitor will not score trusts failing individual cancer thresholds but only reporting a single patient breach over the quarter. Failure against either threshold represents a failure against the overall target. The target will not apply to trusts having five cases or less in a quarter. Monitor will not score trusts failing individual cancer thresholds but only reporting a single patient breach over the quarter Performance is measured on an aggregate (rather than specialty) basis and NHS foundation trusts are required to meet the threshold on a monthly basis. Consequently, any failure in one month is considered to be a quarterly failure for the purposes of the Compliance Framework. Failure in any month of a quarter following two quarters failure of the same measure represents a third successive quarter failure and should be reported via the exception reporting process. Will apply to consultant-led admitted, non-admitted and incomplete pathways provided. While failure against any threshold will score 1.0, the overall impact will be capped at 2.0. External Deloitte audit May '11 assessed data as 'Green'; meeting all key standards and aspects of data quality. Internal October 2013 data quality audit rated 'well above minimum requirements'. Rating remianed the same. Completeness - All records submitted. Timeliness - All patients were submitted in time for submission. Audit - External Parkhill audit has taken place on 01/03/2012 with a rating of 'Adequate Assurance'. Internal October 2013 data quality audit rated as 'Data quality is above minimum requirements'. Timeliness - Not all records are updated within 24 hours of activity. Audit - Internal October 2013 audit rated as 'Data quality is above minimum requirements'. Other Total time in A&E less than 4 hours (A&E, MIU, UCC) 12 % of patients waiting less than 4 hours in A&E from arrival to discharge Waiting time is assessed on a site basis: no activity from off-site partner organisations should be included. The 4-hour waiting time indicator will apply to minor injury units/walk in centres. This data is validated daily & weekly in time for the weekly SITREP return. In line with DH & Monitor requirements, the Trust is expected to incorporate and submit UCC data as part of Trust returns. Audit - Internal October 2013 audit rated as 'Urgent Action Required'. Four, 4 hour breaches found. Timeliness is within 24 hours of activity for all records but not real-time. Self certification against compliance with requirements regarding access to healthcare for people with a learning disability 13 Meeting the six criteria for meeting the needs of people with a learning disability, based on recommendations set out in Healthcare for All (DH, 2008) NHS foundation trust boards are required to certify that their trusts meet requirements a) to f) above at the annual plan stage and in each quarter. Failure to do so will result in the application of the service performance score for this indicator. n/a
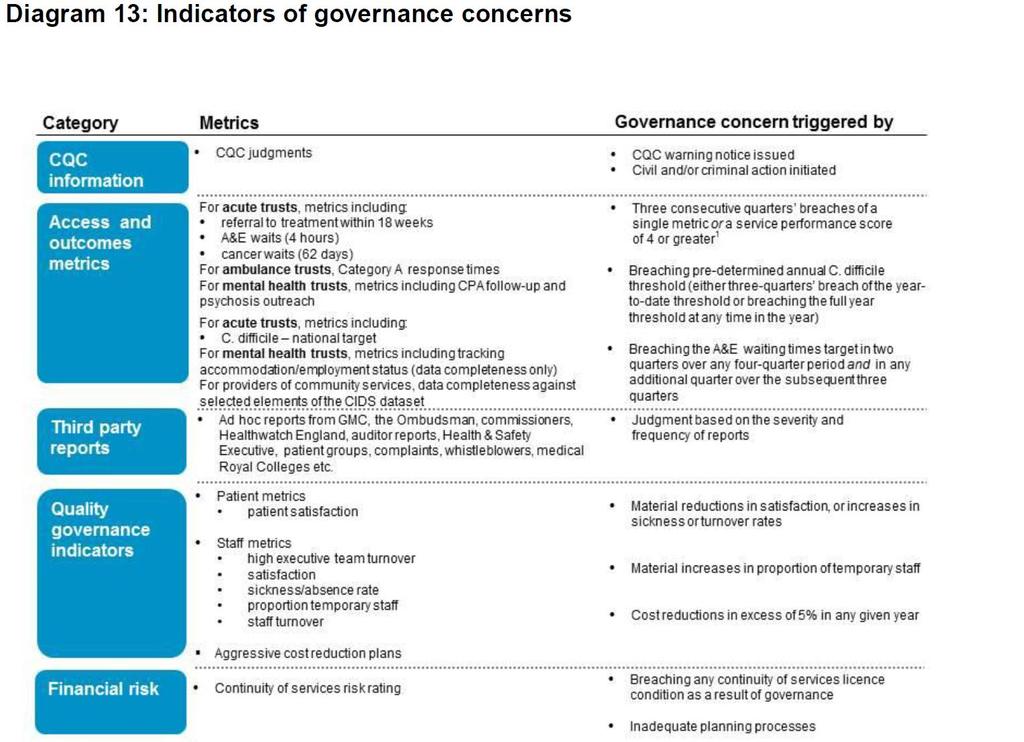
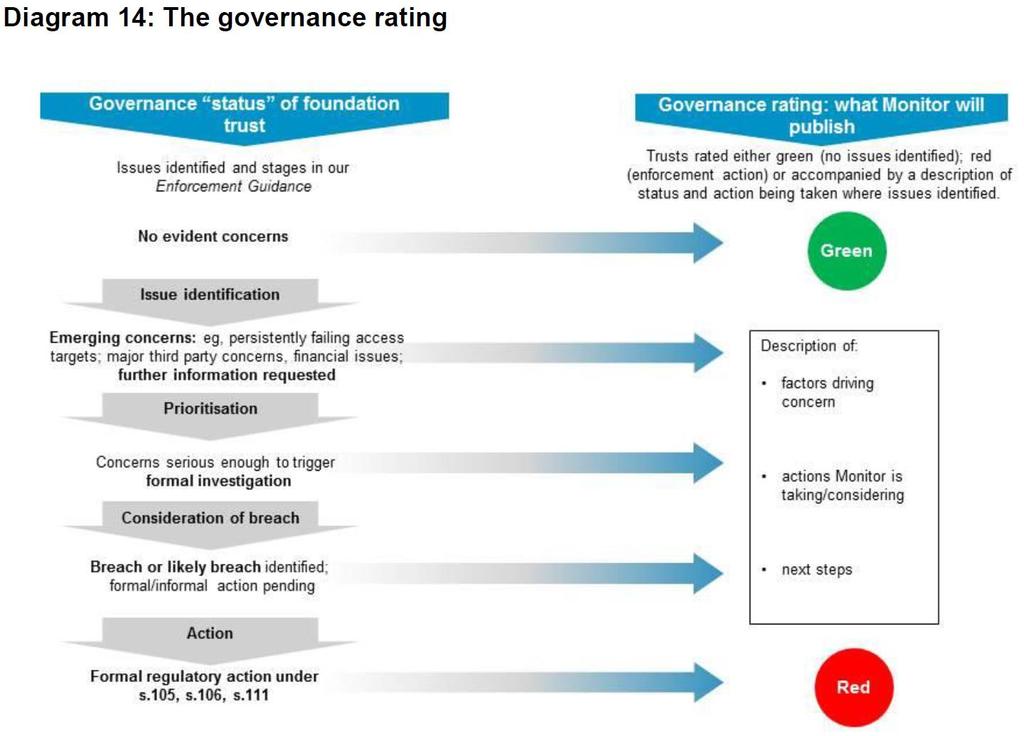
113
114 DQ Badge Data Quality Badge Granularity Completeness Timeliness Audit Not sufficient Sufficient Validation Source Assessment of Executive Director Exemplary Not yet assessed Exemplary (Dark Green) Sufficient (Light Green) Not sufficient (Red) Always available at HRG and/or patient level Granularity Available at speciality level Directorate level Timeliness Completeness Final validation Data entered realtime and available to access as of midnight previous day The lower of: 0% blanks or within national tolerance for data items used to calculate indicators Final sign off by Exec Director Data entered within 24hours of activity, data extract available daily Not applicable to this item Final sign off by Ops Manager Data not entered within 24 hours or extracts not available daily / unknown age The lower of: >0% blanks or exceeded national tolerance for data items used to calculate indicators No signoff or sign off by data entry staff Source Fully documented system with audit control Undocumented system or standardised and mapped manual process Undocumented manual process Audit Assessment of ED Consistent compliance for internal audit, tabled at a group listed in the DQ policy Exec Director would, on balance, vouch for data quality being exemplary Compliance for at least one local audit in the last 6 months, tabled at a group listed in the DQ Policy Exec Director would, on balance, vouch for data quality being sufficient No audit tabled at a group listed in the DQ Policy within last 12 months or compliance not acceptable Exec Director cannot vouch for data
115 April May June July August September October November December January February March Deaths Mortality Rate April May June July August September October November December January February March HSMR HSMR HSMR (to Mar-2014, Source: Dr Foster) & Crude Mortality Data (to Jun-2014, Source: PAS) 01 HSMR: 2010/2011 to 2013/2014 by Month 02 HSMR: 2010/2011 to 2013/2014 by Year 2011/ /2013 National Average 2010/ / Month / / / /2014 Year 03 Inpatient Deaths: 2010/2011 to 2014/2015* by Month 2010/ / / / /2015* 1.6% 04 Crude Mortality Rate: 2010/2011 to 2014/2015* by Year % 1.2% 1.0% 0.8% 0.6% 0.4% 0.2% 1.3% 1.3% 1.3% 1.2% 1.1% Month 0.0% 2010/ / / / /2015* Year
116 Mortality Rate HSMR (to Mar-2014, Source: Dr Foster) & Crude Mortality Data (to Jun-2014, Source: PAS) 07 Crude Mortality Rate: 2010/2011 to 2014/2015* by Admitting Day (Weekday vs Weekend) 2010/ / / / /2015* 9 HSMR: 2010/2011 to 2013/2014 THHFT vs London Providers (Weekdays only) 2010/ / / /2014 National Average 3.0% % 2.0% 1.5% 1.0% 0.5% 1.1% 1.1% 1.2% 1.0% 1.0% 2.0% 2.4% 2.1% 2.1% 1.6% NB THHFT HSMR for this category differs from all other categories due to application of Super Spell concept by Dr Foster. Specifically, if a Super Spell exists, the death is allocated to the first provider within the Super Spell 0.0% Weekday Admission Day Weekend 0 THHFT - Weekday Provider Group London SHA Providers - Weekday 10 HSMR: 2010/2011 to 2013/2014 THHFT vs London Providers (Weekends only) 2010/ / / /2014 National Average NB THHFT HSMR for this category differs from all other categories due to application of Super Spell concept by Dr Foster. Specifically, if a Super Spell exists, the death is allocated to the first provider within the Super Spell 0 THHFT - Weekend Provider Group London SHA Providers - Weekend
117 Measures of Infection Prevention and Control Mandatory Reporting June 2014 Performance in 2013/14 June Performance Year-to-Date Performance 1 MSSA blood stream infections (attributed to the Trust) NT 2 E Coli blood stream infections (attributed to the Trust) NT Local Reporting 2014/15 Target 3 Compliance with MRSA screening policy (elective) 98% 93% 92% 100% 4 Compliance with MRSA screening policy (non elective) 102% 82% 94% 100% 2014/15 traffic light Clinical Support Services 5 Number of needle stick injuries reported NT Local Monthly IP&C performance indicators 6 Uptake of mandatory IP&C training (clinical level 2) 86% 61% 59% >80% Medicine Surgery Women & Childrens Comments ICT point prevalance on audit Kennedy, Jersey, Trinity and Marina wards demonstrated 100% compliance to elective admission screening CT point prevalance on audit on surgical wards showed 92% compliance with non elective screening. ICT have developed a new pretest for clinical IP&C which is due to be launched at the end July so staff can attempt 10 random questions and if achieve 80% will be compliant for IP&C update for the year. 7 Uptake of mandatory IP&C training (clinical level 1) 85% 71% 66% >80% E-learning and face to face sessions available- performance being reviewed at ICC 8 Managerial Cleaning Audit - very high risk (VHR)* 94% 97% 96% >95% Managerial Cleaning Audit high risk (HR)* 95% 96% 97% >92% Compliance with restricted antibiotic policy 88% NM 88% >95% Data not available. 11 Compliance with hand hygiene policy 98% 98% 99% >95% Compliance with Bare Below Elbows 99% 100% 100% >95% Contamination of Blood Cultures 4% NM 3% NT Monthly High Impact Interventions (HIIs) 14 HII No. 1 - Central venous catheter care 100% 97% 98% >97% HII No. 2 - Peripheral line care (VIP) 98% 97% 98% >97% HII No. 5 - Ventilator care 98% 98% 97% >97% HII No. 6 - Urethral catheter care 93% 94% 97% >95% wards in medicine not compliant. Division to present their HCAI action plan to ICC in July which will include actions to address non compliance 18 HII No. 7 - Clostridium difficile care bundle 94% NA 94% >95% Data pending 19 New Quick Question Assessment - Environment 94% 96% 97% >90% HII No. 8 - New Quick Question Assessment - Clinical 20 Equipment 88% 97% 97% >90% Bi-annual / Annual IP&C local measures 21 Compliance with Isolation Policy 80% NM NM >90% Audit planned in August 22 Compliance to linen policy 89% NM NM >95% New linen contract in July, plan to audit after change embedded 23 HII No. 4 - Preventing surgical site infection 93% NA NA >85% Audit completed July, results pending NM = not measured NA = not available NT = No Target IP&C RAG rating for compliance of 95% IP&C RAG rating for compliance of 90% Compliance >95% Compliance>90% Partial Compliance 70%-94% Minimal Compliance 0%-69% Partial Compliance 70%- Minimal Compliance 0%-
118 PEOPLE DASHBOARD - Strategic Main summary: Executive Summary Month Ending May 2014 Sickness: Overall sickness across the Trust has increased, compared to the previous month (now 3.20%, was previously 3.03%) The overall sickness rate across the Trust for the month of May is more than the Trust target of 3% The Trust's YTD sickness rate is more than the target rate of 3% and is 3.16% The Following departments are currently exceeding the specified thresholds (3%): Surgical Wards = 7.08% Corporate, Estates & Facilities = 4.99% Medicine Division Admin = 6.68% Operational services = 4.04% CSS Admin = 5.63% Emergency Care = 3.41% Women's Services = 5.68% People % Development = 3.39% Medical Wards = 5.15% Theatres = 3.37% Surgery Division Admin = 3.29% Medicine, Corporate and Women's and Childrens have all exceeded the YTD sickness target of 3% with the Women's and Childrens Division having the highest YTD sickness rate at 4.23% Month 2 Sickness Comparison The estimated cost of sickness (YTD) is Action Plan Run additional training for managers in relation to managing sickness absence. Provide additional support for managers in relation to managing sickness absence. The P&D Department are now utilising a case management approach to resolving long term sickness cases. Spend Data: Bank spend in May 2014 increased by 4%, whilst agency spend also increased by 5% compared to the previous month At the end of Month 2, spend on Bank, Agency, Overtime, Waiting Lists and Additional Hours is already 1,870,202 At this point last year the spend was 2,658,780 which represents an 42.16% increase in spend for the same period year on year 3.20% 3.10% 3.00% 2.90% 2.80% 2.70% 2.60% 2.50% 2.76% 3.16% May 2013 May 2014 YTD Spend Comparison (Month 2) 1,400,000 1,200,000 1,000, , , , ,000 0 Bank Agency Overtime Waiting List Additional Work Hours/Sessions May 2013 May 2014 The Division of Medicine currently has the highest YTD spend at 1,256,594,79 PDR & STaM: PDR Doctors's Appraisals CSS N/A 72.73% Medicine N/A 66.15% Surgery N/A 70.73% W&C N/A 75.00% Corporate N/A Trust wide N/A 69.90% Trust Target N/A % Additional Comments: In order to try and reduce the vacancy rate further, substantive recruitment plans will be agreed with Directorates. Recruitment campaigns are ongoing for bank, with a view of increasing the pool of staff available. In order to get a better understanding of why staff are leaving, the P&D Department are analysing exit interview questionnaires.
119 Strategic Trend Analysis May-13 May-14 Establishment Bank Usage (wte) Agency Usage (wte) Permanent Staffing Levels Fixed term Staffing Levels Vacancy Rate (%) 7.65% 9.99% Turnover Rate (%) 1.21% 0.94% Sickness Rate (%) 2.76% 3.20%
120 PEOPLE DASHBOARD - Strategic Month Ending May 2014 Performance Negative Warning Positive Trust Target Highlights Movement on previous month Vacancies Bank ( ) Agency ( ) Sickness Turnover % Change on previous month 1% 4% 5% 4% 8% Comments Please note STaM figures will no longer be populated on the dashboard, STaM figures can be found on WIRED. Absence returns were not received from 18 departments. Total % FTE that did not submit an absence return = 9.89% - this figure represents that 282 staff have not had absences recorded against them Please note the PDR cylce has not yet commenced for this year, and doctors appraisals has been extended to the 31st May 2014 Please note that the Labour Turnover rate calculated on Permanent staff only WORKFORCE RESOURCES Area Funded establish. (wte) Permanent (wte) Fixed term (wte) Bank (wte) Agency (wte) Total Workforce (wte) % Temporary Workforce Vacancies (wte) Vacancies (%) Jobs advertised Time to recruit (from Advert to point of formal offer) Avarege Days CSS % % Medicine % % Surgery % % W&C % % Corporate % % Trust % % Trust Target n/a n/a 8.00% London Benchmark TBC n/a Bank & Agency spend over 24 Month Period ( ) Agency Bank % 10.00% Vacancy Trend over last 24 months (%) 8.00% 6.00% 4.00% 2.00% 0.00% CSS Medicine Surgery W&C Corporate Trust Area Bank ( ) Agency ( ) Overtime ( ) Waiting List ( ) Additional Work Hours/Session s ( ) Grand Sum 95,008 99,975 10,795 8,565 47, , , , , ,317 1,256, , ,319 4,008 10, , , ,612 98, , , , ,661 14, , , ,767 1,196,643 29,229 32, ,851 2,658,780.16
121 WORKFORCE PRODUCTIVITY Area % of working days lost through sickness (Current) % of working days lost through sickness (YTD) Average Days Sickness Year to date Previous Financial Year (2013/14) Estimated days (1/4/ /3/2015) Estimated Cost of sickness (Year to date) Short Term Sickness No. of staff with 3 episodes in last 6 months No. of cases with action taken Long Term Sickness No. of staff long term sick leave (current month) No. of cases with action taken Staff on maternity leave CSS 1.83% 1.92% , Medicine 3.66% 3.67% , Surgery 2.80% 2.97% , W&C 4.23% 4.09% , Corporate 3.84% 3.41% , Trust 3.20% 3.16% , Trust Target 3.00% n/a 4.50% 4.00% 3.50% 3.00% 2.50% 2.00% 1.50% 1.00% 0.50% 0.00% Sickness Trend over last 24 months (%) Turnover Trend over last 24 months (%) 20.00% 15.00% 10.00% 5.00% 0.00% Area New starters (Year to Date) Leavers (Year to Date) Current month Labour Turnover (%) Year to Date Previous Financial Year (2013/14) Estimated (1/4/ /3/2015) Nursing Turnover (%) Rolling 12 month Turnover (combined) Top 5 reasons for leaving (Year to Date) % of Leavers CSS % 1.90% 9.56% 11.37% 2.00% 11.00% End of Fixed Term 24.65% Medicine % 2.22% 17.04% 13.33% 2.46% 18.00% Relocation 17.80% Surgery % 1.62% 9.84% 9.74% 2.48% 11.00% Promotion 15.06% W&C % 2.70% 15.43% 16.22% 2.84% 17.00% Other\Not Known 4.10% Corporate % 1.13% 9.56% 11.37% 2.84% 11.00% Retirement Age 6.84% Trust wide % 1.84% 12.08% 11.03% 2.43% 14.00% London Average TBC STAFF EXPERIENCE AND DEVELOPMENT Area No. of Grievances raised (YTD) No. of Dignity at Work Complaints (YTD) No. of Disciplinary Cases (YTD) No. of Capability Cases (YTD) Area Dismissal - Capability (YTD) Dismissal - Conduct (YTD) Dismissal - Some Other Substantial Reason (YTD) Dismissal - Statutory reason (YTD) CSS CSS Medicine Medicine Surgery Surgery W&C W&C Corporate Corporate Trust wide Trust wide Area % of PDRs completed in current PDR cycle Doctors Appraisal % YTD No. of requests for funding (does not include contracted courses) CSS N/A 72.73% 28 Medicine N/A 66.15% 0 Surgery N/A 70.73% 2 W&C N/A 75.00% 5 Corporate N/A 7 Trust wide N/A 69.90% 42 Trust Target 90.00% % Notes/ Areas for Action 1. Unless otherwise indicated, figures are as at current month end 2. % Temporary Workforce includes bank & agency staff only 3. Vacancies are calculated using funded establishment provided by Finance and ESR staff in-post figures 4. RAG rating for sickness: 2.7% and below = Green; between 2.71% and 3% = Amber; Greater than 3% = Red 5. Cost of sickness is calculated using salary cost per day, adjusted OMP/ OSP cost (other costs such as agency are not included) 6. Turnover figures are calculated using leavers during a period and whole time equivalent in post; figures exclude fixed term/ temporary staff 7. Estimated figures are based on financial year to date performance 8. RAG rating for PDR and Doctors Appraisals: 100% = Green, between 51% and 99% = Amber, below 50% = Red 9. Disciplinary information includes those disciplined for PIN lapse
122 ITEM 15 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: Trust Board Paul Wratten, Finance Director DATE: 30 th July 2014 SUBJECT: June 2014 (Month 3) Financial Report Trust Strategic Priority: To deliver high quality care in the most efficient way. Summary: Attached is the full report and commentary covering the most recent financial performance (month 3) of the Trust to the end of the first quarter, June The Trust ended the period behind plan by 0.45m for the year-to-date with a deficit of 0.37m but with a continuity of services risk rating still at 3 (2.5). Earnings before Interest, Depreciation and Amortisation, EBITDA, was 3.22m, 0.37m behind plan and 6.2 % of turnover. Actual efficiency savings achieved were 1.47 m (3.0% of operating expenses) and 9.1% ahead of plan. Capital expenditure was 4.24m, 0.38m behind plan. Cash ended the month behind plan at 1.35m. The revised forecast position for this year demonstrates the high level of financial risk facing the Trust but also that the financial plan still remains achievable. This is a key performance report of the Trust s statutory financial compliance obligations as a licensed provider of NHS commissioned services. The attached report and commentary will form the basis of the Trust s first quarter financial submission to Monitor. Board Action Required: The Board is requested to review the report and discuss any further action required to maintain a continuity of services risk rating at 3 for the remaining quarters of this financial year. Equality Impact Assessment: N/A there is no positive or negative impact from this report.
123 FINANCIAL REPORT JUNE 2014 (MONTH 3) QUARTER 1, 2014/15 EXECUTIVE SUMMARY The June financial position was a surplus of 326k, 62k better than plan. EBITDA was 1,523k, 8.5%, of revenue, 88k better than plan. Year-to-date the actual position was a deficit of 370k, 450k worse than plan. EBITDA was 3,223k; 6.2% of revenue, 370k worse than plan. The Continuity of Services Risk Rating remained at 3 (2.5). The in-month surplus position improved the risk rating for capital service planning from 2 to 3. The rating for liquidity however, reduced from 3 to 2 due to in-month payments for the Emergency Care capital scheme of 2m. The Board should note the headroom before the overall rating reduces to 2 is now extremely limited. As highlighted to the Board in the last two months the main underlying pressure for the Trust remained the high level of pay expenditure; and agency staff in particular required to provide the capacity to meet very high non-elective activity levels that were planned to reduce after the winter months. The Board should note non-elective activity is currently 25% above the plan agreed with commissioners. YEAR-END FORECAST A full appraisal of the year-end forecast financial position was carried out based on actual first quarter revenues and costs. This is shown as appendix 1 to this report. The forecasting shows the straight-line position based on the actual first quarter results in a deficit of 1.5m. However, by incorporating margins from new revenue streams that are planned but not yet certain to be delivered a break-even position can still be achieved. This would mean delivering a 6.4% year-on-year increase in total revenue compared to the 5% growth achieved in the last financial year. However, this clearly comes with a significant level of risk demonstrated by the forecasting of a reasonable set of downside scenarios that would result in a deficit of 2.3m. The Board should note both the straight-line and downside forecasts would end in the Trust s Continuity of Services Risk Rating dropping below 3. KEY MESSAGES The Board should note the June position included 180k of over performance revenue in relation to the Trust s host commissioner contract for first quarter activity above the guaranteed minimum based on an agreed marginal rate of 45%. June results also reported a more positive revenue position in relation to a number of non-nhs lease agreements currently being renegotiated at Mount Vernon Hospital. Some of the gains relate to prior periods. NHS Clinical Revenue over-performed by 1,547k year-to-date mainly due to the non-recurrent receipt of funding to support winter pressures in April; 1 P age
124 contract over performance; increased provision of services in the community following commissioner initiation of new pathways and the opening of an offsite Ophthalmology service; increased income from excluded drugs and income above plan from Edmunds ward due to higher utilisation for North West London Hospitals NHS Trust patients. Re-provision of services in the community revenue was above plan reflecting the faster than anticipated transfer of hospital run services into a community based pathway. Non-NHS Clinical Revenue over-performed in month, due to increased income from overseas patients and is now 59k below plan year to-date. Other Operating Revenue over-recovered in month by 202k and returned to plan for the year to-date. The improvement in month reflected increased confidence from current commercial lease negotiations. Pay was above plan by 429k in June and agency expenditure in particular remained very high at 702k; 339k above plan and 470k higher than June last year. Although increased non-elective volume was a significant driver of increased agency costs other elements such as ward based staff levels and higher agency premiums were also important factors. Drugs costs were below plan for the month by 54k. This was despite excluded drugs income being 51k above plan. Clinical Supplies was 217k above plan for the most part directly linked to the higher than planned level of activity. Other operating expenses however, remained close to plan year to-date. Efficiency savings of 526k were delivered in June and this was 18k (3.4%) above plan. This was 180k lower than the level of savings delivered in June 2013 of 706k) though this largely reflected a different planned profile for savings. Year-to-date total savings of 1,465k were achieved. This was 122k, 9.1% ahead of plan and 3% of operating revenue. DIVISIONAL FINANCES Of the clinical divisions only Clinical Support Services ended the quarter achieving their overall financial plans. Medicine was overspent by 233k, 2.5%; an increase of 175k in-month. This was despite the financial benefits generated from Edmunds ward. Women & Children overspent by 58k, 1.2%; an in-month reduction of 25k. Surgery had the most significant overspend however of 343k, 3.3%; with an in-month increase of 96k. This was due to a combination of several factors including the largest under delivery of efficiency savings to-date. The Board should note a comparison of net expenditure by clinical division demonstrated these were all significantly higher year-to-date compared to 2013/14. 2 P age
125 Estates and Facilities overspent significantly by 453k, 10.5% to the end of June. Estates was 316k of this and facilities 137k. Of the total 122k was due to the division s QIPP shortfall. The Board should note the ever increasing pressure on estates costs linked to the age and condition of the Trust s physical infrastructure. CASH AND BALANCES The Trust ended the quarter with a 1.4m cash balance. This was a sharp 2.3m reduction from the end of May cash position. As planned the pressure on liquidity has increased as the Emergency Care capital scheme nears completion and the remaining contract payments made. The Board should note for this reason alone it is important the Trust achieves its planned cash flow from operating activities as current liquidity cannot withstand a significant deficit. In addition, there was a significant increase in accrued income indicating a delay in the issuing of invoices. This is being addressed together with improvements in general debtor management controls. The balance sheet reported a negative 1.7m net current liability position in line with the above. Capital expenditure of 4,242k to the end of June was 384k lower than plan. The shortfall was in relation to the timing of medical equipment and IT capital schemes. OTHER KEY STRATEGIC POINTS Births at 321 for the month were 10 higher than last June but only 2 higher than the comparable year-to-date position. New GP outpatient referrals were 753 (13.0%) higher than June last year from only one additional working day; year to-date activity increased by 1,044 (5.8%) again also from only one additional working day. A&E attendances in June averaged 226 per day compared to a post 1 st October 2013 UCC average of 210. This was an increase of 7.6%. Year-todate the increase was 4.9%. Emergency inpatient spells increased by 497 (23.7%) compared to June last year. Year-to-date emergency inpatient spells have increased by 826 (11.9%). Elective and day cases decreased by 185, 10.2% this month compared to last June from only one additional working day. Year-to-date spells increased by 204, 3.4%, indicating, even allowing for an additional working day, slowly increasing year-on-year demand. Equality Impact Assessment: N/A there is no positive or negative impact from this report. Paul Wratten Finance Director July P age
126 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Revenue Statement Revised Forecast As at Quarter /15 Appendix 1 Annual Straight Non Main Trust New Emergency RTT Quality Use of Year Yr on Yr Var to Plan Line Recurrent CCG QIPP Activity Resilience Pressures and Contingency End Forecast Annual From Q1 Items Revenue Delivery Initiatives Other Forecast Growth Plan 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s % 000s Operating Revenue NHS Clinical Revenue 177, , ,027 1,690 1, , % 13,121 Non-NHS Clinical Revenue 3,912 3, ,676 (2.1%) (236) Other Operating Revenue 23,648 23,712 (250) ,462 (0.1%) (186) Total Operating Revenue and Income 204, , ,027 1,690 1, , % 12,699 Operating Expenses Employee Benefits (130,832) (136,076) (650) (735) 647 (1,625) (750) (300) (712) 0 (140,201) 7.9% (9,369) Drugs (13,687) (14,028) 0 (1) 0 0 (100) (14,129) 6.9% (442) Clinical Supplies (20,730) (21,860) 0 (45) 0 (930) (150) (300) 0 0 (23,285) 11.1% (2,555) Other Operating Expenses (25,304) (24,724) (125) (100) 0 (300) 0 (25,249) (4.5%) 55 Total Operating Expenses (190,553) (196,688) (650) (781) 647 (2,680) (1,100) (600) (1,012) 0 (202,864) (6.5%) (12,311) EBITDA 14,123 12,892 (400) (653) 647 1, (1,012) , % 388 PFI & Lease Depreciation (1,339) (1,516) (1,516) 5.3% (177) Other Depreciation (6,959) (6,992) (100) 0 (7,092) 7.4% (133) Interest Receivable (15.8%) (1) Other Interest Payable (68) (84) (84) 23.5% (16) Interest Payable on Capital Investment Loans (268) (256) (256) (4.5%) 12 Interest Payable on LIFT Contract (1,352) (1,392) (1,392) 2.7% (40) Interest Payable on Other Finance Leases (184) (244) (244) 27.1% (60) PDC Dividend (3,904) (3,904) (3,904) 9.3% 0 Surplus(Deficit) before Exceptionals 66 (1,480) (400) (653) 647 1, (1,112) (27) Profit/(Loss) on the Disposal of Assets Impairments (8,121) (8,121) 0 (8,121) - (7,936) Surplus(Deficit) after Exceptionals (8,055) (1,480) (400) (653) 647 1, (9,233) 500 (8,082) - (7,963) Downside (1,480) (400) (653) (1,112) 500 (2,262) - ( ) variance indicates it is adverse
127 Appendix A THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Revenue Statement Period Ending 30th June 2014 (Month 3) Annual Yr on Yr Actual Actual Var Actual Var Year Yr on Yr Var Plan Growth to to-date Yr on Yr to-date This Yr on Yr This End Forecast to Outturn Growth Month Growth Month Forecast Growth Plan 000s % 000s % 000s 000s % 000s 000s % 000s Operating Revenue NHS Clinical Revenue 177, % 45, % 1,547 15, % , % 13,121 Non-NHS Clinical Revenue 3, % 919 (24.1%) (59) 396 (6.2%) 70 3,676 (2.1%) (236) Other Operating Revenue 23, % 5, % 15 2, % ,462 (0.1%) (186) Total Operating Revenue and Income 204, % 52, % 1,503 17, % , % 12,699 Operating Expenses Employee Benefits (130,832) 0.7% (34,019) 5.6% (1,213) (11,382) 7.6% (429) (140,201) 7.9% (9,369) Drugs (13,687) 3.5% (3,507) 14.2% (195) (1,059) 8.7% 54 (14,129) 6.9% (442) Clinical Supplies (20,730) (1.1%) (5,465) 3.3% (431) (1,895) 10.4% (217) (23,285) 11.1% (2,555) Other Operating Expenses (25,304) (4.3%) (6,181) 2.1% (34) (2,104) 8.2% (55) (25,249) (4.5%) 55 Total Operating Expenses (190,553) 0.0% (49,172) 5.4% (1,873) (16,440) 8.1% (647) (202,864) (6.5%) (12,311) EBITDA 14, % 3,223 (1.2%) (370) 1, % 88 14, % 388 PFI & Lease Depreciation (1,339) (7.0%) (379) 19.2% (46) (126) 18.9% (15) (1,516) 5.3% (177) Other Depreciation (6,959) 5.4% (1,748) 7.7% (8) (583) 8.0% (3) (7,092) 7.4% (133) Interest Receivable 17 (10.5%) 4 0.0% % 0 16 (15.8%) (1) Other Interest Payable (68) 0.0% (21) 31.3% (3) (7) 40.0% (1) (84) 23.5% (16) Interest Payable on Capital Investment Loans (268) 0.0% (64) (4.5%) 2 (22) 0.0% 0 (256) (4.5%) 12 Interest Payable on LIFT Contract (1,352) (0.2%) (348) 3.6% (9) (114) 1.8% (1) (1,392) 2.7% (40) Interest Payable on Other Finance Leases (184) (4.2%) (61) 56.4% (16) (21) 162.5% (6) (244) 27.1% (60) PDC Dividend (3,904) 9.3% (976) 3.8% (1) (325) 3.8% 0 (3,904) 9.3% 0 Surplus(Deficit) before Exceptionals 66 - (370) - (450) (27) Profit/(Loss) on the Disposal of Assets Impairments (8,121) (8,121) - (7,936) Surplus(Deficit) after Exceptionals (8,055) - (370) - (450) (8,082) - (7,963) EBITDA % 6.9% 6.2% (24.6%) 8.5% - 6.7% - Normalised Surplus (Deficit) % 0.0% (0.7%) (29.9%) 1.8% - 0.0% -
128 Appendix B Income and Expenditure Trend Analysis 000s Income Trend Analysis April 2012 to August ,000 18,750 18,500 18,250 18,000 17,750 17,500 17,250 17,000 16,750 16,500 16,250 16,000 15,750 15,500 15,250 15,000 AprMayJun Jul AugSep Oct NovDec Jan FebMar AprMayJun Jul Aug 000s Operating Expenses Trend Analysis April 2012 to August ,000 17,750 17,500 17,250 17,000 16,750 16,500 16,250 16,000 15,750 15,500 15,250 15,000 14,750 14,500 AprMayJun Jul AugSep OctNovDecJan FebMar AprMayJun Jul Aug Last Year This Year Trend Last Year This Year Trend 1,800 1,600 1,400 EBITDA Trend Analysis April 2012 to August Surplus/(Deficit) Against Plan April 2014 to March , s 1, s Apr MayJun Jul AugSep Oct NovDec Jan Feb Mar Apr MayJun Jul Aug Last Year This Year Trend -400 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Plan Actual
129 Appendix C THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Divisional Performance Summary Period Ending 30th June 2014 (Month 3) Annual Plan Actual Variance Variance Year-End Risk WTE's WTE's WTE's Change Plan Forecast to Substantiv Other Total from To-Date To-Date To-Date To-Date Variance Achieving Last 000's 000's 000's 000's % 000's 000's Target Month Clinical Support Services (25,554) (6,595) (6,607) (12) 0.2% 13 0 Medium (5) Medicine and Emergency Care (36,382) (9,350) (9,583) (233) 2.5% (58) (600) High Surgery (41,539) (10,542) (10,885) (343) 3.3% (236) (846) High Women & Children (19,930) (5,006) (5,064) (58) 1.2% (83) (350) High Estates and Facilities & Corporate Devt. (17,205) (4,313) (4,766) (453) 10.5% (357) (750) High Finance and Information (6,556) (1,639) (1,673) (34) 2.1% (41) 0 Low Corporate Nursing (1,689) (422) (420) 2 (0.5%) 19 0 Low Senior Management (1,741) (435) (444) (9) 2.1% 5 0 Low Human Resources (1,744) (436) (445) (9) 2.1% (44) 0 Low Education Centre (295) (74) (63) 11 (14.9%) (8) 0 Low Director of Operations (2,236) (559) (547) 12 (2.1%) (11) 0 Low Other Corporate and Reserves 154,937 39,451 40, (1.7%) 289 2,546 Low Total (370) (450) (562.5%) (512) 0 High 2, , Efficiency Savings Delivery by Division Period Ending 30th June 2014 (Month 3) Last Year Plan Plan Actual Variance Variance Year-End Worst Best Actual For Year To-Date To-Date To-Date To-Date Forecast Case Case 000's 000's 000's 000's 000's % 000's 000's 000's 000's Clinical Support Services 1,540 1, (35) (16.4%) (27) 1,566 1,436 1,601 Medicine and Emergency Care 1,405 1, % 22 1,505 1,152 1,856 Surgery 1,247 2, (156) (38.6%) (80) 1,348 1,168 1,595 Women & Children 722 1, (40) (25.0%) (34) Estates and Facilities & Corporate Devt. 1,126 1, (122) (39.0%) (96) ,192 Finance and Information (29) (29.0%) (19) Corporate Nursing % Human Resources % Director of Operations % Trustwide Savings 1, % Contingency - (1,500) (258) (100.0%) Total 8,185 7,500 1,343 1, % 104 7,558 6,347 8,657
130 Appendix D Efficiency Savings Delivery by Programme Period Ending 30th June 2014 (Month 3) Plan for the Year Plan To- Date Actual To- Date Variance To-Date Year-End Forecast Worst Case Best Case Efficiency Saving Project 000's 000's 000's 000's % 000's 000's 000's Seven Day Services & Improving Inpatient Care 1, % Accessible and Responsive Services (39) (27.7%) Building a Sustainable & Safer Nursing Workforce (13) (22.4%) Procurement 1, % 1, ,098 Reducing Reliance on temporary Staffing (21) (25.6%) Internal Referral Management Maximising utilisation of the MV Site 1, (8) (2.8%) 1,308 1,057 1,581 Other 3, (55) (6.7%) 3,548 3,230 3,908 Contingency (1,500) (258) % Total 7,500 1,343 1, % 7,558 6,347 8,657
131 Appendix E THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Analysis of Operating Expenses Period Ending 30th June 2014 (Month 3) Last Annual Budget Actual Var Actual Year Year Plan To-date To-date To-date Yr on Yr End Actual Growth Forecast 000s 000s 000s 000s 000s % 000s Pay Medical Staffing - Non-Training Grades (22,858) (23,020) (5,772) (6,143) (371) 7.2% (26,388) Medical Staffing - Training Grades (13,310) (13,404) (3,361) (3,333) % (13,954) Nurses & Midwives (38,107) (38,377) (9,623) (10,117) (494) 8.3% (40,970) Scientific, Therapeutic & Technical Staff (10,241) (10,313) (2,586) (2,750) (164) 9.7% (11,930) Other Clinical Staff (19,689) (19,828) (4,972) (5,182) (210) 4.8% (20,965) Non-Clinical Staff (25,708) (25,890) (6,492) (6,494) (2) 1.9% (25,994) Total Pay Costs (129,913) (130,832) (32,806) (34,019) (1,213) 5.6% (140,201) To note on Pay Agency Staff (4,707) (4,339) (1,088) (2,128) (1,040) 138.8% (8,500) Bank Staff (5,255) (5,255) (1,318) (1,577) (259) 39.9% (6,300) Discretionary Pay (2,728) (2,728) (684) (892) (208) 40.5% (3,900) Total (12,690) (12,322) (3,090) (4,597) (1,507) 73.3% (18,700) Non-Pay Clinical Supplies & Services (34,184) (34,417) (8,346) (8,972) (626) 7.3% (37,414) General Supplies & Sevices (3,361) (3,218) (782) (793) (11) 1.8% (3,291) Establishment (4,263) (4,081) (991) (1,108) (117) 10.4% (4,485) Premises and Fixed Plant (7,349) (7,035) (1,709) (1,965) (256) 9.7% (8,134) Ambulance Services (952) (911) (221) (214) 7 (6.1%) (924) Other Non-Pay (10,507) (10,059) (2,444) (2,101) 343 (6.6%) (8,415) Total Non-Pay Costs (60,616) (59,721) (14,493) (15,153) (660) 5.1% (62,663) Total Expenses (190,529) (190,553) (47,299) (49,172) (1,873) 5.4% (202,864)
132 Appendix F THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Thirteen Month Rolling Cashflow Report & Forecast Period Ending 30th June 2014 (Month 3) Monthly Analysis 2014/ / / / / / / / / / / / / / / /15 April May June July August September October November December January February March April May June Full Year Actual Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Actual 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s 000s Opening Cash 5,733 3,383 3,706 1,355 3,475 3, ,666 2,420 2,688 3,535 3,547 3,071 1,321 5,733 Receipts Healthcare Contracts 13,400 13,287 13,204 13,300 13,300 13,300 13,300 13,300 13,300 13,300 13,300 13,309 13,300 13,300 13, ,600 Other NHS 3,580 4,351 2,486 3,500 3,000 2,700 2,700 2,800 2,700 2,700 2,800 3,513 3,000 3,000 3,000 36,830 Commercial 1, ,000 1,000 1,000 1,000 1,037 1,100 1,100 1,100 1,398 1,000 1,000 1,000 12,000 PDC Dividend Receipt Payments Salaries & Wages (6,064) (6,183) (6,080) (6,100) (6,100) (6,100) (6,100) (6,100) (6,100) (6,100) (6,100) (6,037) (6,100) (6,100) (6,100) (73,164) Tax, N.I. & Pensions (4,521) (4,479) (4,600) (4,500) (4,500) (4,500) (4,500) (4,500) (4,500) (4,500) (4,500) (4,421) (4,500) (4,500) (4,500) (54,021) Other Expenses (8,414) (5,936) (5,583) (4,000) (5,500) (5,150) (4,889) (4,500) (4,666) (4,399) (4,673) (4,878) (6,173) (6,000) (6,000) (62,588) Dividend Payable (1,750) (1,750) (3,500) LIFT and Lease Payments (280) (280) (280) (280) (280) (280) (280) (280) (280) (280) (280) (280) (280) (280) (280) (3,360) Capital Payments (1,051) (1,000) (2,200) (800) (1,200) (1,100) (1,500) (812) (800) (1,553) (800) (523) (723) (1,000) (1,000) (13,339) Loans Repayments (325) (319) (644) Closing Cash 3,383 3,706 1,355 3,475 3, ,666 2,420 2,688 3,535 3,547 3,071 2, ,547 Weekly Analysis Week Week Week Week Week Week Week Week Week Week Week Comm Comm Comm Week Comm Week Comm Comm Comm Comm Comm Comm Comm Comm Comm 13 Week Rolling Forecast 1/6/14 8/6/14 15/6/14 22/6/14 29/6/14 6/7/14 13/7/14 20/7/14 27/7/14 3/8/14 10/8/14 17/8/14 24/8/14 Opening Cash 3,706 3,191 2,357 10,123 1,355 1, ,920 3,475 2,490 2,155 15,140 10,305 Receipts Healthcare Contracts , , , Other NHS , , , Commercial PDC Dividend Receipt Drawdown of Loans Payments Salaries & Wages (78) (84) (88) (5,830) (85) (85) (85) (5,845) (85) (85) (85) (85) (5,760) Tax, N.I. & Pensions 0 0 (4,600) (4,500) (4,500) 0 Other Expenses (1,000) (1,500) (1,500) (1,583) (1,000) (1,000) (1,000) (1,000) (1,000) (1,000) (1,000) (1,000) (1,500) Dividend Payable Lease Payments (280) 0 0 (280) (280) 0 0 Capital Expenditure (2,200) 0 0 (800) (1,200) 0 0 Loans Repayments Closing Cash 3,191 2,357 10,123 1,355 1, ,920 3,475 2,490 2,155 15,140 10,305 3,195 Creditor Stretch b/f (2,649) (2,860) (2,571) (2,282) (2,510) (2,721) (2,932) (3,143) (3,354) (4,165) (4,376) (4,587) (4,798) Expenditure (1,211) (1,211) (1,211) (1,811) (1,211) (1,211) (1,211) (1,211) (1,811) (1,211) (1,211) (1,211) (1,211) Payments 1,000 1,500 1,500 1,583 1,000 1,000 1,000 1,000 1,000 1,000 1,000 1,000 1,500 Creditor Stretch c/f (2,860) (2,571) (2,282) (2,510) (2,721) (2,932) (3,143) (3,354) (4,165) (4,376) (4,587) (4,798) (4,509)
133 Appendix G THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Statement of Financial Position Period Ending 30th June 2014 (Month 3) 31-Mar Jun-14 Movement 31-Mar-15 Actual Actual Actual Forecast 000's 000's 000's 000's Non-Current Assets Intangible Assets 2,141 2,023 (118) 2,141 Plant, Property and Equipment (Owned) 108, ,182 2, ,166 Plant, Property and Equipment (Leased) 15,658 15, ,638 Investment Property 14,816 14, ,816 Trade and other receivables 1,435 1,364 (71) 1,435 Total Non-Current Assets 143, ,073 2, ,196 Current Assets Inventories 2,943 3, ,943 NHS Trade Receivables 7,276 4,692 (2,584) 7,097 PDC Dividend Receivable Non-NHS Trade Receivables 1,288 1,018 (270) 1,134 Prepayments and Accrued Income 5,651 12,348 6,697 5,294 Cash and Cash Equivalents 5,733 1,355 (4,378) 3,547 Total Current Assets 23,038 22,741 (297) 20,015 Total Assets 166, ,814 1, ,211 Current Liabilities Trade Payables 4,327 6,055 1,728 5,943 Capital Payables and Accruals 1, (1,005) 1,023 Other Payables 6,063 5,514 (549) 6,785 Accruals and Deferred Income 5,204 8,802 3,598 5,465 PDC Dividend Payable Provisions (6) 168 Other Liabilities 3, (2,685) 3,245 Borrowing Capital Investment Loans LIFT Finance Leases 1,109 1, ,109 Net Current Assets/(Liabilities) 628 (1,726) (2,354) (4,294) Total Assets Less Current Liabilities 143, ,347 (310) 139,902 Non-Current Liabilities (amounts falling due after more than one year) Provisions 2,272 2, ,272 Borrowing Capital Investment Loans 6,685 6, ,295 LIFT 12,718 12,672 (46) 12,537 Finance Leases 3,956 4, ,297 Total Assets Employed 118, ,656 (370) 115,501 Taxpayers Equity Public Dividend Capital 71,456 71, ,456 Retained Earnings 24,207 23,837 (370) 16,827 Revaluation Reserve 22,363 22, ,218 Total Taxpayers' Equity 118, ,656 (370) 115,501
134 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Cash Flow Statement Period Ending 30th June 2014 (Month 3) 30-Jun Mar-15 Actual Forecast 000's 000's Cash flow generated from operating activities EBITDA 3,223 14,511 Excluding Non-Cash Items 0 0 Inventories (238) 0 NHS Trade Receivables 2, PDC Dividends Receivable Non-NHS Trade Receivables Other Receivables (6,697) 357 Movement in Long-Term Receivables 71 0 Trade Payables 1,728 1,616 Capital Payables and accruals (1,005) (700) Other Payables 4, Provisions (6) 0 Other Liabilities (2,685) 0 Total cash flow generated from operating activities 1,270 17,247 Appendix H Cash Flow fom investing activities : capital expenditure and receipts (4,242) (12,339) Cash Receipt from Asset Sales 0 0 Cash flow from financing activities Interest Interest Received on Cash Balance 4 16 Other Interest Payable (21) (84) Interest Paid on Capital Investment Loans (64) (256) Interest Paid on LIFT Contract (348) (1,392) Interest Paid on Finance Leases (61) (244) Capital Loans and Leases Repayment of Capital Investment Loans 0 (390) Repayment of LIFT Contract (46) (181) Additional funding by Finance Leases Repayment of Finance Lease Capital (304) (1,159) PDC Public Dividend Capital Received/Receivable 0 0 Proceeds on the Disposal of Assets 0 0 Dividends Paid (976) (3,904) Total cash Flow from financing activities (1,406) (7,094) Net cash (Outflow)/Inflow (4,378) (2,186) Opening Cash Balance 5,733 5,733 Closing Cash Balance 1,355 3,547
135 Appendix I THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Capital Expenditure Report Period Ending 30th June 2014 (Month 3) 2014/15 Actual Plan Variance Year-End Year-End Plan To-Date To-Date To-Date Forecast Variance 000s 000s 000s 000s 000s 000s Major Medical Equipment - Outright Purchase 1, (235) 1,300 0 Information Management Technology - Outright Purchase 1, (180) 1,500 0 Estates - Outright Purchase 3, (149) 3,900 0 Emergency Care Scheme 5,151 2,639 2, ,151 0 Replacement Lease Funded Equipment Contingency (166) Total 13,339 4,242 4,626 (384) 13,339 0
136 Appendix J THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Annual Forward Financial Plan Financial Risk Management - Base Plan Downside Scenarios Value Downside Impact Worst Case Impact Risk Events 000s Probability 000s Probability 000s Basis Risks to Financial Plan Non-delivery of efficiency savings 1, , ,500 75% achievement Non-achievement of CQUIN From planned 75% to achievement of 60% Contract penalties General risk from challenges and penalties Non-Hillingdon Activity Growth Non-HCCG activity only Expenditure reduction following HCCG QIPP 1, , ,533 HCCG QIPP schemes only Additional Winter cost and funding pressures 1, , In addition to planned amount General Quality & Compliance 1, Estimate Non-Pay inflation % higher than 2.5% built in the Annual Plan Value of Financial Risks 8,605 5,460 6,658 Mitigating Actions Use of annual plan QIPP contingency 1, , ,500 Incorporated into the Annual Plan Use of annual plan General contingency 1, , ,000 Incorporated into the Annual Plan Use of Contract penalty contingency Incorporated into the Annual Plan Delay new quality investment Remainder after all current commitments Increased Margins from Trading 1, , Pathology, Edmunds, Mount Vernon Balance sheet flexibilities Current assessed value Value of Mitigating Actions 6,000 5,113 4,375 Residual Risk 347 2,283 Normalised surplus (deficit) as a result of residual risk (281) (2,262) Headroom for CoSRR to remain a Resulting CoSRR 3 2
137 Appendix K THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST Continuity of Services Risk Rating and Other Financial Performance Metrics Period Ending 30th June 2014 (Month 3) 13/14 Continuity of Service Risk Rating 14/15 14/15 To-Date 14/15 15/16 Actual Rating Metric Plan Rating Actual Rating Forecast Rating Forecast Rating Capital Service Planning (0.4) 3 Liquidity (10.0) 2 (9.0) 2 (12.8) 2 (13.2) Weighted Average Overriding Rules Impact
138 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST CONTRACT INCOME Period Ending 30 June 2014 (Month 3) Appendix L Trust Position Hillingdon CCG Other North West London CCGs Specialised Commissioning Other Contracts Annual Financial Actual Var Actual Contract Actual Actual Contract Actual Actual Contract Actual Actual Contract Actual Actual Actual Actual YTD YTD Yr onyr YTD YTD Yr onyr YTD YTD Yr onyr YTD YTD Yr onyr YTD YTD Yr onyr Yr onyr Growth Growth Growth Growth Growth Growth 000's 000's % 000's 000's % 000's 000's % 000's 000's % 000's 000's % 000's % NCA's Inpatients Daycase (spells) % % % % % 44-13% Elective (Spells) % % % % % 41 51% Non-Elective (Spells) % % % % % % Total Inpatients % % % % % % Outpatients New (Attendance) % % % % % 32 2% Follow Up ( Attendance) % % % % % 36 16% Procedure (Attendance) % % % % % 39-3% Ward Attender % % % % % 0-13% Outpatient Unbundled % % % n/a 5 n/a Maternity Ante/Postnatal n/a % % 0 0 0% n/a 15 n/a Total Outpatients % % % % % 128-7% A&E (Attendance) % % % 0 0 n/a % 86-32% Total A&E % % % 0 0 n/a % 86-32% Critical Care % 0 0 n/a 0 0 n/a % 0 0 n/a 59 n/a Critical Care - Adults % % % 0 13 n/a % 71-18% Rehab - Specialist & Non specialist (bed days) % % % 0 9 n/a % 6 n/a Chemotherapy (spells) % 0 0 n/a 0 0 n/a % 0 0 n/a 0 n/a Direct Access (tests) % % % 0 0 n/a % 2-13% Excluded Drugs & Anti VEGF % % % % % % Block and other clinical income % % % % % % Transitional Funding n/a % 0 0 n/a 0 0 n/a 0 0 n/a 0 n/a Northwick Park SLA n/a 0 0 n/a 0 0 n/a 0 0 n/a 0 0 n/a 1700 n/a Winter pressures funding n/a 0 0 n/a 0 0 n/a 0 0 n/a 0 0 n/a 197 n/a Community n/a 0 0 n/a 0 0 n/a 0 0 n/a 0 0 n/a 502 n/a Overperformance n/a n/a 0 0 n/a 0 0 n/a 0 0 n/a 0 n/a CQUIN n/a n/a n/a n/a n/a 52 n/a Total Other Clinical Income % % % % % 4406 n/a Total Clinical Income % % % % % 5117 n/a Contract Variance
139 Appendix M THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST CONTRACT ACTIVITY Period Ending 30 June 2014 (Month 3) Trust Position Hillingdon CCG Other North West London CCGs Specialised Commissioning Other Contracts Activity Plan Activity Actual Var Var % Activity Plan Actual Var Activity Plan Actual Var Activity Actual Var Activity Actual Var Actual Plan YTD YTD YTD YTD YTD YTD YTD YTD YTD YTD YTD NCA's Inpatients Daycase (Spells) 20,634 5,035 5, % 3,702 3, (65) Elective (Spells) 3, (38) -4.3% (31) (13) 12 Non-Elective (Spells) 25,197 6,306 7,894 1, % 4,825 6,234 1, , Total Inpatients 49,414 12,215 14,116 1, % 9,202 10,854 1,652 1,621 1, (58) Outpatients New (Attendance) 95,808 23,737 22,996 (741) -3.1% 18,214 17,249 (965) 2,843 2,835 (8) ,341 2, Follow Up ( Attendance) 188,639 46,563 49,611 3, % 36,122 39,721 3,599 6,293 5,785 (508) (20) 3,390 3,328 (62) 459 Procedure (Attendance) 57,796 14,077 14, % 10,264 10, ,593 1,544 (49) ,963 2, Ward Attender 7,360 1, (932) -51.9% 1, (888) (51) 5 2 (3) Outpatient Unbundled 26,201 6,389 5,648 (741) -11.6% 5,371 4,452 (919) (173) 39 Maternity Ante/Postnatal 9,003 2,197 2,043 (154) -7.0% 1,755 1,658 (97) (57) Total Outpatients 384,807 94,758 95,899 1, % 73,306 74,574 1,268 11,749 11,234 (515) ,290 8, ,009 A&E (Attendance) 79,690 20,079 20,040 (39) -0.2% 13,035 13, ,530 2,893 (637) ,477 2, Total A&E 79,690 20,079 20,040 (39) -0.2% 13,035 13, ,530 2,893 (637) ,477 2, Critical Care - Neonatal 4, , % , Critical Care - Adults 3, (107) n/a (22) (87) (14) 48 Rehab - Specialist & Non specialist (bed days) 13,880 3,443 2,537 (906) -26.3% 2,529 1,559 (970) (315) Chemotherapy (spells) % Direct Access (tests) 1,126, , ,060 (3,207) -1.1% 273, ,007 (3,471) 11,385 11, ,280 1, Community 3,418 3,418 n/a 3,418 Total Other 1,148, , ,411 (424) n/a 276, ,205 (4,463) 12,345 12,099 (246) 1,228 1, ,406 1, ,609 Total 1,662, , ,466 2,579 n/a 372, ,140 (1,071) 29,245 27,956 (1,289) 2,053 2, ,960 13,997 1,037 5,792
140 Appendix N Activity Trend Analysis Spells/ Attendances A&E Activity July 2012 to November ,500 10,000 9,500 9,000 8,500 8,000 7,500 7,000 6,500 6,000 5,500 Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov This year Last Year Trend Spells/ Attendances All New Outpatient Referrals July 2012 to November ,000 6,800 6,600 6,400 6,200 6,000 5,800 5,600 5,400 5,200 5,000 Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov This year Last Year Trend Spells Inpatient Activity July 2012 to November ,800 2,700 2,600 2,500 2,400 2,300 2,200 2,100 2,000 1,900 1,800 1,700 Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Elective This year Emergency This year Elective Last Year Emergency Last Year Births Births July 2012 to November Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct This year Last Year Trend
141 ITEM 16 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Simal Patel, Associate Director of Programme Management Karl Munslow Ong, Chief Operating Officer DATE: 30 th July 2014 SUBJECT: 2014/15 Quarter 1 Transformation and QIPP update Trust Strategic Priority: To deliver high quality care in the most efficient way. Summary: At Q1 the YTD variance against the 9m plan is - 136k and + 122k against the 7.5m plan. The current risk adjusted forecast is at 7.7m which has reduced by 200k since M2 predominantly due to the forecasted slippage of the Marina scheme. The two areas of greatest risk are the Improving Inpatient Care programme and the aim to close beds as forecasted, and also the Nursing agency reduction scheme. All divisions have developed plans to mitigate against anticipated slippage or identify opportunities to reduce slippage that has already occurred. There are a number of risks against CCG QIPP schemes. The Trust is working closely with the CCG to support the collation and development of KPI data which can demonstrate the impact of their schemes. A 3 year transformation plan is currently being developed. The timeline proposed is a draft plan to be formulated by end of September with a view to have a final plan by the end of October; this will then inform the Trust s Transformation programme for 15/16. Board Action Required: The Board is asked to: 1. Review the risks around the Improving Inpatient Care programme and agree any further actions that need to be taken. 2. Review the mitigations that have been put in place and confirm any further actions that need to be taken. 3. Agree and confirm the timeline for the 3 year transformation plan
142 2014/15 Quarter 1 Transformation and QIPP update 1. Month 3 Performance Overview The table below outlines M3 (Q1) plan vs actuals. At M3 the plan to the 9m target was 587k, the actual delivered at M3 was 544k which has resulted in an in month negative variance of 44k. Against the 7.5m plan there is an in month over delivery of 18k. YTD variance against the 9m is equal to - 136k but the YTD variance against the 7.5m is + 122k. M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12 Total 14/15 Plan to 9m target ( ) 481, , , , , , , , , , , ,681 8,999,999 14/15 Plan to the 7.5m ( ) 383, , , , , , , , , , , ,516 7,500,000 14/15 Actuals ( ) 412, , ,493 1,464,970 Variance to the 9m ( ) -68,727-23,904-43, ,212 Variance to the 7.5m ( ) 28,721 75,512 17, ,128 This is illustrated graphically below and includes 13/14 actuals. *The phasing has been updated slightly to reflect the additional schemes which CCSS have now included into their plans phased from October. The table in section 3 outlines by division the reasons for slippage or non-delivery against the plan. 2. Risk adjusted forecast The table below outlines the risk adjusted programme value; the risk adjusted value is at 7.7m which has reduced by 200k since M2. The main reason for this is the projected slippage to the Marina ward scheme. The team are working up options to mitigate this slippage
143 ID Project Medicine Surgery CCSS W&C E&F Corporate Other Total 1 Improving Inpatient Care 500k 94k 0 295k k 2 Internal Referral Management 13k 13k 37k 1k k 3 Shaping the Nursing Workforce 57k 4k 0 13k 0 50k 0 125k 4 Maximising utilisation of the Mount 0 183k k 0 315k 5 Non-Nursing Temporary Staffing 85k 79k 17k 61k 17k k 6 Procurement Trust-wide project 50k 150k 25k 25k k 7 Accessible & Responsive Services 37k 34k 62k 18k k 14 Divisional Projects 1.3M 654k 1.6M 352k 853k 818k 0 5.6M Total Target Gap 2.0M 1.2M 1.8M 766k 871k 1.0M 0 7.7M 1.9M 2.1M 1.8M 1.0M 1.3M 987k - 9.0M - 161, k - 6, k 422k - 13, M - 3 -
144 3a. Divisional summary The table below outlines the main reasons for the gap against plan by division: Division YTD (Q1) plan ( ) YTD (Q1) actual ( ) YTD (Q1) variance ( ) (-ve underachieved) YTD (Q1) GAP ( ) (schemes yet to be identified)* Surgery 404, , ,373 84,440 Medicine 259, ,052 59,505 0 W&C 160, ,358-40,470 40,476 Main cause of the variance At M3 Surgery has underdelivered by 76k. This is predominantly due to a number of schemes which were due to start in M3 but have not started in line with plan. A large proportion of these are service developments which are anticipated to deliver the full amount through over-delivery in future months. The division have developed mitigation plans for schemes that have slipped and are working to pull these back in line with the plan. Q1 delivery for Medicine has been strong with the plan met or exceeded in all three months. Under delivery in Q1 against the plan is predominantly due to the Gap. The division are working to identify additional opportunities to close the gap; these include increased income from amenity room s review and additional radiology demand management schemes. The W&C QIPP programme holds significant risk as a large proportion of their QIPP programme is made up of a Cross-Div IIC scheme. Mitigation Plans Scheme level mitigations have been drafted. Service developments: greater availability of services at Mount Vernon has started to be implemented and there are plans in place to raise the awareness of these services. Education events have also been planned with GPs. Repatriation of activity has started although further work to influence flows is required and is being worked up. There are risks to future schemes, slippage avoidance plans have started to be developed. The division are doing a targeted review of nursing resignation reasons to improve the impact of rolling recruitment. A&E workforce redesign substantive posts have been advertised (mitigate agency spend), this is likely to slip due to actions being carried out later than planned. The division is looking into international recruitment to reduce the issues they have had with junior doctor recruitment. Additional opportunities are being scoped
145 CCSS 214, ,093-35,456 0 Estates 153,034 39, , ,805 Facilities 157, ,553-31,325 23,478 CORP 236, ,525-26,626 0 Trustwide 224, Delivering to plan. The gap remains closed in the division with additional values phased towards the end of the year. At the close of Q1 non-delivery totals 35k (17%). This is driven primarily by smaller schemes that have slipped. MRI productivity non-delivery due to settling in phase of new machine to realise improved throughput. Division is mitigating by identifying training needs and upskilling staff. Two other schemes which will slip as they require further planning and work-up, the PMO will be working with the division to support this. It is likely that these will slip for another couple of months. The variance at Q1 is predominantly due to the gap that Estates currently have. They have a total gap of 361k which has been phased over 12 months. The division have identified a potential opportunity to save through a workforce review but further work is required to review the proposal, assess risks and understand the impact of any proposed changes. Estates employed an energy manager on 9th June. (As yet no QIPPs identified) Facilities have under-delivered in month against the plan, this is predominantly due to a few schemes e.g. leases which have not yet delivered but when they do they will deliver in full and therefore offset the slippage. The team have identified opportunities to close the gap, these are currently being costed. The variance is driven by 1 scheme which is a contract charge which does hold some risk, if this delivers then the full amount will be realised, there is a risk that this will not be delivered in year. The consolidation of IT contracts scheme is currently being worked up, the team are confident that this can deliver the full value but it will take a few months for the work up to be completed. Radiology the team are looking at realising improved productivity benefits through undertaking additional work which has been requested from a private commissioner. Clear milestones for the next 2 months are being outlined to prevent further slippage for high risk schemes. A couple of quick win workforce review schemes (to reduce temporary spend) are being progressed with a confirmed timeline by M4. The full workforce review is being further reviewed and tested. Additional schemes have been identified; Energy efficiency opportunities and also a small maintenance contract opportunity. This area is likely to over recover, areas of slippage are planned to catch-up through the year. The consolidation of IT contracts scheme now has a working group set-up and work is underway. It is anticipated that this scheme will catch up on delivery through the year. *This column shows the Q3 unidentified schemes value. Most divisions still have a proportion of their target which does not yet have worked up schemes, this values has been phased over 12 months and is contributing to a ve monthly variance. In some cases e.g. Estates their Q1 variance is completely due to the proportion of their target which does not yet have any schemes identified - 5 -

146 3b. Mitigation plans Each of the divisions has outlined a mitigation plan which identifies options to reduce further slippage and/or identify ways in which to close gaps created due to the slippage. A summary of these plans has been included in the table above. 4. Trust-wide schemes a. Improving Inpatient Care The key to the success of this programme is the Ward Based Standards workstream. The group has now been re-established and specific workstreams around reviewing and improving the TTA processes are currently underway. There are key issues to resolve with regards to the Marina closure which are currently being worked through. Other factors impacting on the programme are the increased use of escalation beds driven by increased admissions and patient acuity. There is a risk to the original plan to reduce the numbers of beds due to the increased activity; emergency admissions to the Trust in month (June) have risen by 350 (20%) when compared with June 2013, which is impacting the Trust s ability to reduce the bed base down to the non-winter baseline. The additional activity is predominantly Hillingdon patients; the impact of this is being discussed with the CCG to look at what actions can be taken to manage demand more effectively. The AMU Future group is in the process of reviewing the clinical model and agreeing the revised pathways. Next steps include: Development of detailed project plan with monthly milestones for the Ward Based Standards workstream. Finalising medical cover arrangements plans for elective gynae to move to Mount Vernon. To work up the financial impact of the increased activity. b. Seven Day Services Seven Day services will have a separate governance structure and formally report to the IIC Steering Board as below. The Seven Day working group is being set up and will be chaired by a clinician and include representation from operations. This group will recommend the priorities for seven day working and agree the key milestones and deliverables. A multi-agency task and finish group has been set up and the group is undertaking a multi-agency gap analysis of services delivered across whole system
147 c. Shaping the Nursing Workforce This scheme has been flagged as high risk due to year to date delivery and increased nursing expenditure. This is driven by the number of vacant posts and to a significant extent by operational bed pressures and numbers of escalation beds open. To date, three recruitment days have been held which have had varied success. One of the biggest challenges is the retention rate as this is largely offsetting the recruitment efforts. Recruitment is further being ramped up and the group is working closely with the communications department and using social media to boost the recruitment drive. Facilities are currently working up options to increase the amount of staff accommodation available. Next steps for this programme include: Options for UK and overseas recruitment to be scoped in more details Nursing to work with P&D to implement retention strategies for areas with high staff turnover. Completion of non-ward based nursing review and diary carding exercise to be revisited for identified areas d. Responsive and Accessible Services (RAS) RAS has focused on consolidating the scope and purpose of this multi-year crossdivisional project and has started to pull together key milestones for year 1 delivery. Domain [1] is focused on improving the incoming contacts into the Trust. A baseline of issues and complaints is being assessed via PALS and Trust complaints. This will inform the work going forward. Domain [2] is reviewing booking processes and work is progressing to work-up what further booking activity can be moved to central Outpatient Appointment Centre team. Domain [3] is at a baseline stage to understand the quality of letters with a focus on surgery. Divisional teams are currently working this up. Domain [4] - innovation in outpatient care is progressing with divisional representatives who have identified potential clinics to be moved to a Telemedicine setting. This is being worked up with clinical colleagues in medicine, surgery and W&C. e. Maximising the utilisation of the Mount Vernon site The review of maximising theatre usage on the site continues alongside the ward moves that are being progressed within the IIC project. The group have started to also consider the potential commercial opportunities for the site. A marketing plan for the Mount Vernon site is being drafted and specialty specific plans have started to be put into action. f. Non-Nursing Temporary Staffing The initial phase of this programme of work has focused on a baseline assessment of the key challenge areas. Plans are in development for work streams including medical locum rate standardisation and reduction in the use of premium rate - 7 -
148 resources. g. Internal Referral Management This project is progressing in line with the actions set out in the original plan although the timelines have slipped slightly due to the time required to ensure the relevant clinical engagement occurs around pathway decisions. Implementation of Pathology decision support defining test intervals / frequency on ICE electronic ordercomms is underway. Diagnostic pathways and guidelines for new hip and knee referrals have been agreed. A review of externally sent tests is being undertaken with a view to understand what can be brought back into the Trust and options for best value SLAs to be set up around the others. Next steps include agreeing guidelines for the colorectal cancer pathway and beginning an audit of obstetric scanning. h. Procurement A diagnostic of the Trust s non pay spend has been undertaken by an external consultant; initial results show that there are minimal quick win opportunities around supplier pricing negotiations. The analysis shows that there are pockets of opportunity but these are spread across a large number of products which could make the effort to achieve outweigh the potential financial benefit. The second Clinical Supplies and Effectiveness Committee was held, with a focus on the development of current procurement processes and controls. Further work is still required to ensure sufficient clinical engagement. 5. CCG QIPP Programme The CCG QIPP programme has a Q1 negative variance of 940k which is predominantly driven by the schemes outlined below: Admission avoidance Gynaecology Ambulatory Emergency Care shared project. Their admission avoidance programme has been seeing fewer patients than expected. An end to end review of the pathways has been planned to rectify the deficit on this programme however, latest figures are indicating an upturn in activity. The Trust is working with the CCG to understand why rapid response activity has reduced. The CCG are planning to verify this in their M4 report. There have been a few challenges with the Gynae pathway; there have been significant problems with ensuring that the referral pathways are followed, THH are supporting both the CCG and GPs to improve compliance with the new referral pathway. It is expected that these actions will lead to an immediate step change. A deep dive into the Ambulatory care service by the Trust is due to be carried out to understand in more detail the KPIs and also the benefits which have been realised through the service
149 The CCG have identified a number of additional schemes to mitigate against slippage and support closure of their current gap, these schemes are in the process of being worked into plans. KPIs for the planned care schemes need to be tracked and monitored; The Trust has outlined an action plan to develop dashboards for these schemes. Divisions are starting to work through ways in which to reduce cost in line with the reduced income through the new elective care pathways. Now that more of these pathways are embedded, a detailed review is underway to ensure that they are streamlined and care is delivered by the most appropriate professional in the most cost effective way. 6. Transformation 3 year plan The longer term transformation plan is to be worked up over the coming months. This will start to review the long term financial plan which provides an underlying assumption of the year on year savings required and also the impact of CCG QIPP. With this in mind, the transformation plan will start to consider more innovative options for improving the efficiency of pathways and models of care whilst maintaining and improving quality. As discussed in previous papers, the approach taken in previous years to realise QIPP savings will need to evolve as there is minimal opportunity to realise savings through traditional tactical schemes. The plan will consider in more detail the potential opportunity of joint transformation schemes which can streamline pathways across the system and therefore reduce organisational bottlenecks which often prove costly. The paper will also begin to consider the reasons behind spend and how much can be avoided through proactive cross organisational planning initiatives rather than current spend spikes which are due to reactive responses to often predictable events. The timeline proposed is a draft plan to be developed by end of September with a view to have a final plan by the end of October; this will then inform the Trust s Transformation programme for 2015/
150 ITEM 17 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Siobhan Ferguson, Interim Employee Services Manager Dr Richard Grocott-Mason, Joint Medical Director and Responsible Officer DATE: 30 th July 2014 SUBJECT: Annual report on Medical Appraisal and Revalidation Trust Strategic Priority: To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide. Summary: The Trust Board has a statutory duty to ensure that the Trust discharges its responsibility as a Designated Body in the Revalidation of Medical Staff. This paper outlines the obligations and provides a breakdown of performance in the financial year The format is in compliance with the Framework of Quality Assurance required by NHS England. It includes data on the number of completed appraisals, reasons for gaps, and the number of doctors who have had recommendations made. There is also data on the numbers of doctors who have been subject to a GMC process in the year. Key successes are the establishment of a comprehensive electronic system for Medical Appraisal; training of sufficient Appraisers and case investigators; and work to improve the participation and quality of appraisals. Over the next year more work is required with quality assurance of the process. All of the statutory requirements have been met. Board Action Required: The Board is asked to approve the annual report, and mandate the Chief Executive or Chairman to sign the Annual Statement of Compliance (attachment 1). Equality Impact Assessment: N/A there is no positive or negative impact from this report 1
151 1. Executive summary Annual report on Medical Appraisal and Revalidation The purpose of this report is to provide assurance to the Board that The Hillingdon Hospitals NHS Foundation Trust has systems operating effectively to carry out it s responsibility as a Designated Body. This is the first annual report to the Board in this format and is reporting on the Trust s performance for the financial year 2013/2014. The Responsible Officer (RO) submitted the Annual Organisational Audit to NHS England in May This annual report to the Board contains all of that submitted information with further assurance to the Board. The Trust is required to return a statement of compliance after the approval of this report. All doctors with a prescribed connection to the Trust have been allocated a revalidation date by the General Medical Council (GMC). Richard Grocott-Mason, Joint Medical Director, is the Responsible Officer (RO) and undertakes the duty of ensuring that there are processes and procedures in place to ensure the revalidation of all medical staff. The Trust is the Designated Body for 239 doctors. In , 48 positive recommendations for revalidation were made and 5 requests for deferral were made and accepted by the GMC. 203 doctors had an appraisal in the Trust. This paper also outlines the numbers of doctors involved in remediation, concerns or GMC processes. 2. Purpose of the Paper 3. Background To provide Board with assurance that The Hillingdon Hospitals NHS FT and the Responsible Officer are executing their duties in respect of Revalidation. To allow the Board to approve the statement of compliance. Medical Revalidation was introduced in the UK on 3 rd December On this date the Trust assumed a formal role in the regulation of doctors by becoming a designated body with some specific legal requirements. Revalidation is the process by which the GMC confirms that a doctor s licence to practice will continue. Its purpose is to assure patients and the public, employers and other healthcare professionals that licensed doctors are up to date and fit to practice; to improve patient safety and increase public trust and confidence in the medical system. Board members are required To monitor the frequency and quality of medical appraisals in the Trust Check there are effective systems in place for monitoring the conduct and performance of their doctors Confirm that feedback from patients is sought periodically so that their views can inform the appraisal and revalidation process. 2
152 A previous paper was presented to the Board in September This annual report is in the format developed by NHS England as a Framework of Quality Assurance. Once approved the Trust is required to return a statement of compliance signed by the Chief Executive or Chairman by 31 st August The Trust has appointed a Medical Appraisal and Revalidation Administrator to support the Responsible Officer in managing the Medical Revalidation and appraisal processes and maintaining an important link with Equiniti who were appointed by the Trust to provide the revalidation management system to our doctors. The Trust monitors on a monthly basis the frequency of medical appraisals in the organisation. This is reported via the Board Dashboard and the divisional People Dashboards. All appraises will undergo during the five year revalidation cycle a 360 degree assessment whereby feedback from patients and colleagues will be sought. All doctors undergo a pre-employment background checks in accordance with the NHS Employment Checks Standards to ensure that medical practitioners have the qualifications and experience appropriate to the work performed. During 2013 we were awarded 5,000 from the Revalidation Support Team to facilitate training sessions to support revalidation in non-consultant grade doctors. Approximately 40 Associate Specialist Doctors attended this training to increase their understanding of the appraisal and revalidation process and its importance. 4. Governance Arrangements Our current governance arrangements are as follows: The Trust are responsible for all doctors including Consultants, Staff and Associate Grade Doctors, Locums (short and long term), Trust Grade Doctors. The revalidation process for trainee doctors is the responsibility of the London Deanery. The Medical Appraisal and Revalidation administrator has the responsibility of maintaining an accurate list of doctors who have a prescribed connection with the Trust. Appraisals are monitored on a monthly basis to ensure that doctors are undertaking appraisals via Dashboards and the Trust compiles quarterly requests which previously went to the Revalidation Support Team and this now is sent to NHS England. The Revalidation Officer and Interim Employee Services Manager meet regularly to ensure that doctors are regularly engaging with the process for Medical Appraisals and Revalidation. It is the individual responsibility of all doctors to ensure that they have an annual appraisal and that they collect the required supporting information. The Trust has a list of trained appraisers and has sufficient appraisers for the number of appraisals required. All doctors have an account with an electronic system for managing their appraisal (Equiniti). It is possible within this system to know when an appraisal is due, and therefore to start to alert when this has been missed. For all of the doctors requiring a recommendation from the RO, their appraisal data has been personally reviewed by the RO, including the 360 feedback. Doctors who have not had an appraisal within the appropriate time have been flagged to the Responsible Officer who is taking individual action with each of these doctors. The 3
153 Trust is currently being audited by TIAA Internal Audit around Medical Appraisals and it is expected some recommendations will be presented to assist the Medical Revalidation team. a. Policy and Guidance Medical Appraisal Policy for Revalidation Policy for Rehabilitation and Remediation Policy and Procedure (for Medical Staff) 5. Medical Appraisal a. Appraisal and Revalidation Performance Data There are 239 doctors for whom we are currently the designated body. This is broken down as 140 Consultants, 42 staff grade, associate specialist or specialty doctor, and 57 doctors who are either locums or non-training grade Trust doctors. Each doctor has been allocated a date for revalidation by the GMC over the next 5 years. At the time of the Annual Organisational Audit 203/239 (85%) doctors had been documented to have had an appraisal in this year. Some of these doctors have subsequently completed their 2013/14 appraisal late, within the first 2 months of the new financial year. This represents a considerable improvement on the previous year s return of 34%. There are a small number of doctors who have been very slow in engaging with the process. The majority of the gap is a result of doctors joining the Trust part way through the year, who have either had appraisals at previous Trusts, or just been awarded CCT and been appointed to their first Consultant post. A small number of doctors are on career breaks or maternity leave (Appendix A). There are 4 trained case investigators - three consultants and one SAS Doctor, who are able to lead investigations into concerns about doctors performance. b. Appraisers The Trust has 42 trained Appraisers. The annual appraisal process is now electronic. The Trust provides doctors with an electronic system for annual appraisal (Equiniti 360). This allows each doctor to collect their portfolio of supporting information, as recommended by the GMC Good Medical Practice Guide. It also administers and analyses 360 degree feedback from colleagues and patients. This has to be provided at least once in every five year revalidation cycle by each doctor. Initially this system was only available for Consultants and permanent staff but is will be extended to all those for whom the Trust is the designated body. The Trust is working hard to ensure that all staff are on the Equiniti Revalidation Management System. Regular Webinar sessions are run by our revalidation management (Equiniti RMS) provider to ensure all doctors understand how to use the system for the appraisal and revalidation processes. 4
154 c. Quality Assurance This is one of the key areas for the Trust to focus for this year to improve, but during the first year we have spent most time focussing on ensuring that all are on the electronic system, we have enough trained appraisers and all the doctors are having their appraisals. The RO has personally reviewed the appraisal data for 48 doctors who required a recommendation to the GMC. In 5 cases there was not sufficient supporting information available and so their date for revalidation was deferred. In many of these cases the delay was in the time taken to complete the 360 colleague and patient feedback. In the coming year we are planning to establish a more formal feedback audit on the quality of appraisals, the quality of supporting information and the personal development plans. In addition, we have held a couple of appraiser meetings but this needs to become a more regular event. d. Access, security and confidentiality There are no information governance issues to report during 2013/ Revalidation Recommendations Number of recommendations between April 2013 March 2014 = 48 All recommendations have been completed on time; with 43 positive recommendations, and 5 deferrals. The deferrals were all done to allow the doctors to gather more supporting information to meet all the GMC requirements for revalidation. There were no notifications of non-engagement. (Appendix B) 7. Recruitment and engagement background checks All doctors are subject to the NHS Employment Checks Standards which include those checks that are required by law. These include verification of: Identity Right to Work Professional Registrations and Qualifications Employment History and References Occupational Health Criminal Records The Trust has appointed a Medical Appraisal and Revalidation Administrator to support the Responsible Officer in managing the Medical Revalidation and appraisal processes and maintaining an important link with Equiniti who were appointed by the Trust to provide the revalidation management system to our doctors. 8. Monitoring Performance All doctors require annual appraisal to meet the requirements of revalidation. The Trust is committed to ensure that adequate resources are provided to facilitate this. A 360 assessment with colleague and patient feedback is provided once every five 5
155 year revalidation cycle which will be discussed with their appraiser during their appraisal. Performance is monitored through quarterly returns to NHS England, of the number of appraisals completed each quarter as a proportion of those that were due, and the Annual Organisational Audit (AOA). In this year, the accuracy of data was a problem, but now that all doctors are set up on the electronic system and the Revalidation administrator is in post it is anticipated that data accuracy will be greatly improved. 9. Responding to Concerns and Remediation There is a policy on remediation and responding to concerns and this was authorised and ratified by the Joint Local Negotiating Committee (JLNC) in June The data on the numbers of doctors involved in formal concerns processes is shown in Appendix C. There have been 3 doctors in which the Trust has led a formal process to investigate concerns about their practice. 1 doctor was restricted from any clinical practice for 2 weeks and then returned to work with supervision and restrictions until the end of their contract. A larger number of doctors have had varying levels of investigation from the GMC. This number includes some trainee doctors for whom the Trust is not the Designated Body. It also includes a number of doctors who are no longer employed at the Trust. Many of the investigations have arisen from the GMC making enquires in response to patient complaints to them. In 1 case a single patient complaint resulted in 6 doctors being investigated. The outcome of this was written advice to 1 junior doctor and no action or criticism for the other 5. The doctor erased from the Medical Register had been dismissed by the Trust in Risk and Issues 10.1 The 2013 Annual return identified two areas in which the Trust was not fully compliant with the standard, as updated from the previous ORSA guidelines. The actions were planned and are listed below: Risk/Issue Action Q4.10 Absence of remediation policy Remediation policy written. Approved by LNC July 2013 and JLNC in September 2013 Q3.3 Absence of missed or incomplete appraisal audit Reviewing our processes to ensure that doctors have been appraised, recorded on Equiniti and on ESR. Any appraisals not taken place referred to the Responsible Officer for further action to take place. 11. Corrective Actions, Improvement Plan and Next Steps Processes are in place to manage the appraisal and revalidation process, which has been effective in allowing the RO to make timely recommendations to the GMC in 6
156 2013/14. The main area of improvement is quality assurance of medical appraisals. A number of actions will be put in place to achieve this, including audit of feedback data, appraiser training and group meetings, audit of personal development plans and quality of supporting information provided. More work needs to be undertaken to understand the processes around doctors on temporary and short term contracts with the revalidation and medical processes. We will be focussing on reviewing the feedback from appraisees and appraisers comments where they have used the Equiniti system. We will be focusing and looking for best practice from other organisations to continue to improve the experience of appraisals and revalidation at the Trust. 12. Recommendations The Board is asked to accept this report. The Board is asked to approve the Statement of Compliance document confirming that the organisation, as a designated body, is in compliance with the regulations, to be signed by the Chief Executive for return to NHS England before 31 st August
157 Annual Report Appendix A Audit of all missed or incomplete appraisals audit Doctor factors (total) 24 Maternity leave during the majority of the appraisal due window 3 Sickness absence during the majority of the appraisal due window 0 Prolonged leave during the majority of the appraisal due window 2 Suspension during the majority of the appraisal due window 0 New starter within 3 month of appraisal due date 1 New starter more than 3 months from appraisal due date 9 Postponed due to incomplete portfolio/insufficient supporting information Appraisal outputs not signed off by doctor within 28 days Lack of time of doctor 0 Lack of engagement of doctor 9 Other doctor factors (describe) Appraiser factors Number Unplanned absence of appraiser 0 Appraisal outputs not signed off by appraiser within 28 days 0 Lack of time of appraiser 0 Other appraiser factors (describe) 0 (describe) Organisational factors Number Administration or management factors 0 Failure of electronic information systems 0 Insufficient numbers of trained appraisers 0 Other organisational factors (describe) 8
158 Annual Report Appendix B Audit of revalidation recommendations Revalidation recommendations between 1 April 2013 to 31 March 2014 Recommendations completed on time (within the GMC recommendation window) Late recommendations (completed, but after the GMC recommendation window closed) 48 0 Missed recommendations (not completed) 0 TOTAL 48 Primary reason for all late/missed recommendations For any late or missed recommendations only one primary reason must be identified No responsible officer in post 0 New starter/new prescribed connection established within 2 weeks of revalidation due date New starter/new prescribed connection established more than 2 weeks from revalidation due date 0 0 Unaware the doctor had a prescribed connection 0 Unaware of the doctor s revalidation due date 0 Administrative error 0 Responsible officer error 0 Inadequate resources or support for the responsible officer role 0 Other 0 Describe other TOTAL [sum of (late) + (missed)] 0 9
159 Audit of concerns about a doctor s practice Concerns about a doctor s practice High level Annual Report Appendix C Medium level Low level Number of doctors with concerns about their practice in the last 12 months Explanatory note: Enter the total number of doctors with concerns in the last 12 months. It is recognised that there may be several types of concern but please record the primary concern Capability concerns (as the primary category) 1 1 in the last 12 months Conduct concerns (as the primary category) in the last 12 months Health concerns (as the primary category) in 0 the last 12 months Remediation/Reskilling/Retraining/Rehabilitation Numbers of doctors with whom the designated body has a prescribed connection as at 31 March 2014 who have undergone formal remediation between 1 April 2013 and 31 March 2014 Formal remediation is a planned and managed programme of interventions or a single intervention e.g. coaching, retraining which is implemented as a 2 consequence of a concern about a doctor s practice A doctor should be included here if they were undergoing remediation at any point during the year Consultants (permanent employed staff including honorary contract holders, 1 NHS and other government /public body staff) Staff grade, associate specialist, specialty doctor (permanent employed staff 1 including hospital practitioners, clinical assistants who do not have a prescribed connection elsewhere, NHS and other government /public body staff) General practitioner (for NHS England area teams only; doctors on a medical 0 performers list, Armed Forces) Trainee: doctor on national postgraduate training scheme (for local education 0 and training boards only; doctors on national training programmes) Doctors with practising privileges (this is usually for independent healthcare 0 providers, however practising privileges may also rarely be awarded by NHS organisations. All doctors with practising privileges who have a prescribed connection should be included in this section, irrespective of their grade) Temporary or short-term contract holders (temporary employed staff including 0 locums who are directly employed, trust doctors, locums for service, clinical research fellows, trainees not on national training schemes, doctors with fixedterm employment contracts, etc) All DBs Other (including all responsible officers, and doctors registered with a locum 0 agency, members of faculties/professional bodies, some management/leadership roles, research, civil service, other employed or contracted doctors, doctors in wholly independent practice, etc) All DBs TOTALS 2 Other Actions/Interventions Total 10
160 Local Actions: Number of doctors who were suspended/excluded from practice between 1 April 1 and 31 March: Explanatory note: All suspensions which have been commenced or completed between 1 April and 31 March should be included Duration of suspension: 2 weeks Explanatory note: All suspensions which have been commenced or completed between 1 April and 31 March should be included Less than 1 week 1 week to 1 month 1 3 months 3-6 months 6-12 months Number of doctors who have had local restrictions placed on their practice in the 2 last 12 months? GMC Actions: Number Number of doctors who: Were referred to the GMC between 1 April and 31 March 18 Underwent or are currently undergoing GMC Fitness to Practice procedures between 1 April and 31 March Had conditions placed on their practice by the GMC or undertakings agreed with the GMC between 1 April and 31 March Had their registration/licence suspended by the GMC between 1 April and 31 March 4 (only 1 still employed at THH; 3 others trainees) 1 Were erased from the GMC register between 1 April and 31 March 1 National Clinical Assessment Service actions: Number Number of doctors about whom NCAS has been contacted between 1 April and 31 March: For advice 3 For investigation 0 For assessment 0 Number of NCAS investigations performed 0 Number of NCAS assessments performed
161 Attachment 1 Statement of Compliance Designated Body Statement of Compliance The board/executive management team [delete as applicable] of [Insert official name of designated body] has carried out and submitted an annual organisational audit (AOA) of its compliance with The Medical Profession (Responsible Officers) Regulations 2010 (as amended in 2013) and can confirm that: 1. A licensed medical practitioner with appropriate training and suitable capacity has been nominated or appointed as a responsible officer; Comments: 2. An accurate record of all licensed medical practitioners with a prescribed connection to the designated body is maintained; Comments: 3. There are sufficient numbers of trained appraisers to carry out annual medical appraisals for all licensed medical practitioners; Comments: 4. Medical appraisers participate in ongoing performance review and training / development activities, to include peer review and calibration of professional judgements (Quality Assurance of Medical Appraisers or equivalent); Comments: 5. All licensed medical practitioners 1 either have an annual appraisal in keeping with GMC requirements (MAG or equivalent) or, where this does not occur, there is full understanding of the reasons why and suitable action taken; Comments: 6. There are effective systems in place for monitoring the conduct and performance of all licensed medical practitioners 1, which includes [but is not limited to] monitoring: in-house training, clinical outcomes data, significant events, complaints, and feedback from patients and colleagues, ensuring that information about these is provided for doctors to include at their appraisal; Comments: 7. There is a process established for responding to concerns about any licensed medical practitioners 1 fitness to practise; Comments: 1 Doctors with a prescribed connection to the designated body on the date of reporting. 1
162 8. There is a process for obtaining and sharing information of note about any licensed medical practitioners fitness to practise between this organisation s responsible officer and other responsible officers (or persons with appropriate governance responsibility) in other places where licensed medical practitioners work; Comments: 9. The appropriate pre-employment background checks (including preengagement for Locums) are carried out to ensure that all licenced medical practitioners 2 have qualifications and experience appropriate to the work performed; and Comments: 10. A development plan is in place that addresses any identified weaknesses or gaps in compliance to the regulations. Comments: Signed on behalf of the designated body Name: _ Signed: [chief executive or chairman a board member (or executive if no board exists)] Date: 2 Doctors with a prescribed connection to the designated body on the date of reporting. 2
163 ITEM 18 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Steve Wedgwood, Head of Facilities Operations Paul Wratten, Finance Director DATE: 30 th July 2014 SUBJECT: Patient Led Assessment of the Care Environment (PLACE) 2014 Results Trust Strategic Priority: To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide. Summary: This paper updates the Board on the 2014 Patient Led Assessment of the Care Environment (PLACE). It gives high level detail of the Hillingdon and Mount Vernon PLACE domain results. The Board should be aware that the national averages for each domain and how the Trust compares will not be known until 27 th August Hillingdon Hospital domain results have all improved since Three of the four Mount Vernon Hospital results have worsened since 2013 but other than privacy, dignity and wellbeing, still score higher than Hillingdon. The food and hydration result at Mount Vernon, which was above the national average, has further improved since The PLACE Improvement Plan with actions for improvement is being currently drafted and will be discussed with the PLACE Improvement Group and then will be presented to the Board in September Board Action Required: The Board is asked to note the 2014 PLACE Improvement assessment scores and the process to develop the PLACE Improvement Plan. Equality Impact Assessment: Improving the estate and facilities services enables positive adjustment to specific user needs. 1
164 Patient Led Assessment of the Care Environment (PLACE) 2014 Results 1. The 2014 PLACE results The 2014 PLACE scores for the Trust have now been received and are summarised in the table below showing a comparison to the 2013 results and where scores have improved or worsened. The national average scores for each domain enabling the Trust to see how it compares to other Trusts is planned to be issued by the HSCIC (Health & Social Care Information Centre) on 27 th August The process in 2014 involved eighteen patient assessors and thirteen staff assessors undertaking four days of PLACE assessments. The range of scores on the PLACE assessment sheets for each area were Pass, Qualified Pass and Fail. Domain/Score 2013 Hillingdon % Score 2014 Hillingdon % Score +/- % 2013 Mount Vernon % Score 2014 Mount Vernon % Score +/- % Cleanliness Privacy, dignity & wellbeing Condition, appearance and maintenance Food & Hydration Key Points Hillingdon Hospital: The assessment took place over three days and covered 10 wards, 6 outpatient areas, A&E, all public areas and the grounds. all Hillingdon scores improved; in terms of privacy, dignity and wellbeing the outpatient team did a lot to improve these issues in the reception areas that has principally led to the large improvement this year; despite scores improving across all domains there are still issues to be addressed across cleaning (domestic, nursing and estates cleaning); and condition, maintenance and appearance (buildings and grounds). 2
165 Mount Vernon Hospital: The assessment took place in one day and covered the wards the Trust operates services from, all outpatient areas, Minor Injuries, all public areas and the grounds. three of the four domain results worsened only the food and hydration domain result improved; in 2014 more areas were assessed (i.e. nine areas in 2013 and fourteen areas in 2014) an increase of 55% more areas; the additional areas assessed at Mount Vernon were Edmunds Ward, Trinity Day Care, Pre-Assessment, Elderly Day and Blood Tests; the scores for grounds and buildings maintenance reduced; the score for signage improved to a pass; internal decoration in communal areas reduced; the Blood Tests area was assessed this year for the first time and it had fails across all condition, maintenance and appearance areas; X Ray and MIU were assessed in both years but their scores this year fell on all condition, maintenance and appearance areas; there were issues over privacy, dignity and wellbeing in Blood Tests (around reception privacy and seating) and Elderly Day (around cubicle curtain length) which as fails dropped the scores in those areas. 3. The PLACE Improvement Plan Following the PLACE assessment in 2013 an Improvement Plan was developed and has been monitored through the PLACE Improvement Group. It should be noted that that there has been a significant amount of improvement taking place since the 2013 assessment particularly at Hillingdon. These developments have included: significant investment in both patient chairs, reception and waiting room chairs and wheelchairs responding to both the PLACE assessment and patient feedback; improvements to the Hillingdon outpatient reception and waiting area arrangements creating a waiting zone barrier to improve privacy so that conversations between staff and patients are not overheard including better signage and some changes to layout; improvements to external and internal signage and way finding with the involvement of five members of Hillingdon Healthwatch and the provision of new roadside, car park and external signs; as well as new internal entrance, reception, junction and corridor signs; a matron prioritised redecoration programme at Hillingdon to ensure that patient environments are as bright and chip free as possible and an emphasis on dealing with lighting, flooring, carpentry works and maintenance issues; reinforcement by matrons and communication bulletins of the requirement for maintaining a tidy patient environment; 3
166 a review of waste segregation and waste bins to ensure that any that need to be replaced or to have soft closers fitted to reduce noise impacts are highlighted for replacement by the relevant ward or clinical area; significant investment in new technology cleaning equipment and work undertaken to review cleaning processes and structures to improve standards. The 2014 PLACE Improvement Plan is currently being drafted for discussion at the PLACE Improvement Group and will be presented to the Board following the announcement of the national results on 27 th August
167 ITEM 19 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Fiona Jarvis, Lead Nurse Infection Prevention and Control Theresa Murphy, Director of Infection Prevention and Control (DIPC) DATE : 30 th July 2014 SUBJECT: Infection Prevention & Control Annual Report Trust Strategic Priority: To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide. To deliver high quality care in the most efficient way. Summary This annual report fulfils the Trust s statutory requirement under section 1.3 of the Health and Social Care Act 2008 for the Director of Infection Prevention and Control (DIPC) to provide a report on infection control activity across the organisation. This report covers the period 1 st April st March This report includes performance for infection prevention and control for the previous year. The key items to note are as follows: Clostridium difficile infections were reduced by 48% reporting only 12 cases from a threshold of 14 No ward closures due to confirmed/suspected Norovirus through the winter period, an achievement never seen before A rise of other resistant bacteria in particular Carbapenemase-producing Enterobacteriaeae Achievement of compliance for Aseptic Non Touch Technique (ANTT) Delivery of the Trust s three year IP&C Strategy Orthopaedic Surgical Site Infection (SSI) rates for repair fractured neck of femur remain above the national average (the organisation was highlighted as an outlier); the actions that have been identified to reduce SSI. Ongoing work on antimicrobial stewardship
168 Care Quality Commission inspection report from November and actions taken by the Trust and Infection Control Team. Board Action Required: The Board is asked to review and discuss the report and note the recommendations for 2014/15 which are currently being addressed by the Infection Control Team. Equality Impact Assessment: N/A there is no positive or negative impact from this report.

169 Infection Prevention and Control Annual Report 1 st April st March 2014 Produced by: The Director of Infection Prevention and Control Written by: Lead Nurse Infection Prevention & Control Reviewing the period: April March 2014 Approved by Infection Control Committee: July 2014 Received by Trust Board: July 2014
170 Table of Contents Section: Page: 1 Introduction 4 2 Infection Control Roles and Governance Structures Within the Trust 2.1 Corporate Responsibility 2.2 Infection Prevention and Control team and Members 2.3 Infection Control Committee 2.4 Internal Reporting Arrangements 2.5 Reports to the Executive Team and Trust Board 2.6 Risk Register Infection Control Resources Within the Trust 6 4 Infection Control in 2014/15: The Local Picture 4.1 Aseptic Non Touch Technique 4.2 Infection Prevention and Control Strategy Mandatory Surveillance During 2014/ Mandatory reporting Meticillin Resistant Staphylococcus aureus (MRSA) Meticillin Sensitive Staphylococcus aureus (MSSA) Surveillance of Clostridium difficile toxins Escherichia coli bacteraemia Surveillance Glycopeptide Resistant Enterococcal (GRE) bacteraemia 5.2 Other Resistant Bacteria 5.3 Surgical Site Infection Orthopaedic Caesarean Section The Infection Control Team: Other Core Activity During 2014/ Education and Training 6.2 Supporting and Working with Infection Control Link Staff 6.3 Implementation of the European Directive on Safer Sharps 6.4 Audit and Monitoring 6.5 Working with the Patients and Public 6.6 Working to Ensure Optimum Hospital Hygiene Cleaning and Catering Services 6.7 Sterile Services 6.8 Redesigning Environments and New Builds Endoscopy Infection Control Policy and Procedures Within the Trust 19 8 Outbreaks and Incidents at the Trust in 2014/ Pandemic Influenza 8.2 Gastroenteritis / Norovirus 8.3 Needlestick incidents and Prevention of Needlestick injuries 8.4 Legionella and Water Quality Monitoring Management of Antibiotics Prescribing at the Trust in 2014/ Safety and Quality in Infection Control: Statutory Duties 10.1 Care Quality Commission Annual Report Infection Prevention and Control April 2013-March 2014
171 11 Measures of Infection Prevention and Control: Shaping Practice to Improve Performance Looking Forward to 2014/ Conclusion Acronyms Appendix A : IP&C Policies Appendix B: IP&C Strategy Metrics 28-3 Annual Report Infection Prevention and Control April 2013-March 2014
172 1 Introduction to the Report This is the annual report from the Director of Infection Prevention and Control (DIPC) providing information on infection prevention and control activity across the organisation. The purpose of this report is to provide detail to our patients, public, staff, Trust Board, Commissioners and Monitor on the infection control agenda for the previous year. This report covers the period from 1 st April st March 2014 and provides performance against national targets for: Meticillin Resistant Staphylococcus Aureus (MRSA) bacteraemia figures, Clostridium difficile Toxin (CDT) rates, Healthcare associated infections Other key activities and audit for the year. Infection prevention and control remains a key patient safety and quality focus for the organisation. This year was the first year NHS England set all MRSA bloodstream infections targets as nil, as they continue to pursue a zero tolerance approach to Health Care Associated Infections (HCAI). A zero target for MRSA, coupled with a significant reduction in the Clostridium difficile threshold, proved very challenging for the Trust at a time when there is greater scrutiny and challenge for reducing HCAI. Whilst the Trust did not achieve the MRSA bloodstream infection target, performance was sustained with only 1 case reported. Key achievements for 2013/14 include:. Clostridium difficile infections were reduced by 48% reporting only 12 cases from a threshold of 14 No ward closures due to confirmed/suspected Norovirus through the winter period, an achievement never seen before. 2 Infection Control Roles and Governance Structures Within the Trust 2.1 Corporate Responsibility The Hillingdon Hospitals NHS Foundation Trust maintains a full compliment of staff for infection prevention and control as required under the Health and Social Care Act. The Director Infection Prevention and Control (DIPC) is both an Executive member of the board and also the Director of Nursing and Patient Experience. The Trust has two Consultant Microbiologists, one of whom holds the position of infection control doctor and they continue to provide specialist advice and microbiology support on a 24hour basis. The specialist nursing team and antimicrobial pharmacist are available during office hours Monday to Friday. 2.2 Infection Prevention and Control (IPC) Team and Members In May 2013 the Trust appointed a new Director of Nursing and Patient Experience and as a result a new DIPC. Whilst this new appointment did not affect the specialist nursing team, it did bring to the organisation an experienced DIPC and returned the - 4 Annual Report Infection Prevention and Control April 2013-March 2014
 report an overview of the infection control agenda and progress throughout the year to the Quality and Risk Committee (QRC).")
173 team to full strength with the return of the Deputy DIPC and Deputy Director of Nursing. Infection control team members consist of: 2.3 The Infection Control Committee The Infection Control Committee (ICC) report an overview of the infection control agenda and progress throughout the year to the Quality and Risk Committee (QRC). ICC is a key forum for the development and performance management of the infection control agenda across the organisation. The Committee meets bi monthly and is chaired by the DIPC with key representation from across the organisation. Membership includes the ICT, a number of senior management and senior nurses, the Occupational Health Department, clinical governance staff, Pharmacy, Estates and Facilities staff and external bodies such as the local Public Health England (PHE) Health Protection Unit and Hillingdon Community Health (HCH). A change in the NHS and consequently the community with the establishment of Clinical Commissioning Groups (CCGs) has seen the Infection Control Committee for HCH no longer exist. Whilst the Infection Control Nurses from HCH attend the Trust s ICC it is challenging to collaboratively drive forward the IP&C agenda across the health economy when there is no current ICC in the CCG. 2.4 Internal Reporting Arrangements New to 2013/14 is a Patient Safety and Quality Report submitted quarterly. This report includes key information on the Trust s quality and safety priorities reflecting the new Clinical Quality Strategy. Infection control includes performance against National objectives as well as progress on local trust initiatives and has been well received across the organisation. Infection Prevention and Control (IP&C) is also discussed monthly via divisional dashboards at the Divisional Reviews with the Executive Team. These divisional dashboards include HCAI data, overall IP&C performance and compliance to antimicrobial prescribing. - 5 Annual Report Infection Prevention and Control April 2013-March 2014


174 2.5 Reports to the Executive Team and Trust Board The Infection Control Team provide a range of measures to the Board monthly which include cleaning scores, infection control audit results, compliance to restricted antimicrobial prescribing, MRSA screening and other initiatives. IP&C performance is also commented on in the monthly performance report so that direct feedback on post infection reviews or root cause analysis is provided to the Board and any necessary actions. 2.6 Risk Register The Trust includes the risk of HCAI on the corporate risk register. The risk is updated and reviewed every 2 months at ICC, in order to reflect current priorities and activities; and is presented to QRC for discussion and scrutiny. 3 Infection Control Resources Within the Trust The ICT continues to have a budget that is predominately staff pay. The team does however continue to work closely with the procurement department to ensure the Trust purchases quality products, that are fit for purpose and deliver value for money. In 2013 the ICT developed a business case to upgrade the current IT system ICNet to the newer version NG. As part of this process the ICT bid in round one of the Nursing Technology Fund (2013/14) to support this initiative. Whilst this was not successful the organisation is planning to bid in the second round in the Spring Infection Control in 2014/15: The Local Picture Some of the key activities over the past 12 months are outlined below: 4.1 Aseptic Non Touch Technique (ANTT) ANTT is now an established technique across the Trust and remains key in reducing intravenous (IV) related blood stream infections. Annual reassessments are undertaken in each division, supported by the ICT. Across the organisation ANTT was above 95% by the end of the year. The performance by division is demonstrated in the chart below: Divisional ANTT 2014 Competencies 100% 98% 99% 100% 95% 90% 85% 91% Medicine Surgery W&C CSS Medicine Surgery W&C CSS - 6 Annual Report Infection Prevention and Control April 2013-March 2014

175 4.2 Infection Prevention and Control Strategy In the third and final year of the IP&C strategy the Trust successfully achieved a number of measures (refer Appendix B) Those not achieved fully have been included in the annual HCAI action plan and will form the basis of the new trust IP&C 3 year strategy, these included: C section surveillance Further improvement in Antimicrobial prescribing and stewardship 5 The Infection Control Team: Mandatory Surveillance During 2013/ Mandatory Reporting The Trust reports the following mandatory HCAI statistics to both the Trust Board and Public Health England (PHE) on a monthly basis. Meticillin Resistant Staphylococcus aureus (MRSA) bacteraemia Clostridium difficile infection Meticillin Sensitive Staphylococcus aureus (MSSA) bacteraemia Escherichia coli (E coli) bacteraemia The Trust follows guidance for HCAI associated deaths. Where MRSA or C.diff is included as a part 1A, 1B or 1C on a death certificate it is entered onto the Strategic Executive Information System (STEIS). Inclusion criteria in this data set are any incidents of C diff on the same ward if two or more cases were reported in one week or three in a month. A Root Cause Analysis (RCA) is undertaken on such cases and they are presented to ICC for monitoring and scrutiny of any arising actions. In 2013/14 there were 3 cases reported under this guidance as detailed below: Reason for STEIS report Number of cases MRSA on death certificate 2 C diff on death certificate 1 Two cases C diff on 1 ward in a week 0 Included in the above data is an MRSA case which was attributed to the CCG and died shortly after admission and the MRSA case which was attributed to the organisation sadly died. All of the above cases had root cause analysis (RCAs). - 7 Annual Report Infection Prevention and Control April 2013-March 2014
176 5.1.1 Meticillin Resistant Staphylococcus aureus (MRSA) With the new NHS landscape and emergence of CCGs also came a change to the MRSA bloodstream infection objectives and methods of attributing cases to organisations. Any Trust reporting a positive MRSA blood stream infection will be expected to complete a Post Infection Review (PIR). The organisation for leading the case is responsible for completing a PIR within 1 week of the date of assignment (acute providers will be assigned the PIR for samples taken after the 1 st two days of admission and the CCG for those admitted septic.) The outcome of the PIR should establish the organisation to which the bacteraemia should be finally assigned. The final assignment will identify the organisation best placed to ensure that any lessons learned are acted upon. It was envisioned that with this new system there would be greater partnership working across the health economy. The variety of MRSA objectives was abolished for 2013/14 with a zero tolerance approach to MRSA bloodstream infections, therefore all organisations has a target of zero for the year. The following graph illustrates the MRSA bacteraemia reported by month for 2013/14; including those attributed to the CCG. The Trust reported one MRSA bacteraemia in May this was a complex case with the patient having multiple hospital admissions including treatment in a specialist unit at another acute Trust. The root cause analysis included both acute trusts and there was learning identified for both organisations, however under the current system cases could only be attributed to either the acute trust taking the specimen or the CCG. This case was therefore attributed to The Hillingdon Hospitals NHS Foundation Trust. Of the four cases attributed to the CCG three of these underwent an arbitration process. This involved the ICT from both the acute trust and CCG and Public Health England and this was facilitated by the Director of Public Health. The process looked at the PIR and evidence from both organisations to demonstrate that policies were followed and that patient safety was maintained and quality care delivered. After the review, cases were attributed to either the CCG or Trust by the Director of Public Health. In all three cases the Trust was able to demonstrate robust documentation and all were attributed to the CCG. - 8 Annual Report Infection Prevention and Control April 2013-March 2014
 and has reported six cases or fewer in the year to date, the MRSA")
177 MRSA bloodstream infections since 2003 Whilst the Trust was disappointed to not achieve the national target it did meet those set by Monitor and sustained performance. The Monitor framework states Where an NHS Foundation Trust has an annual MRSA objective of six cases or fewer (the de minimis limit) and has reported six cases or fewer in the year to date, the MRSA objective will not apply for the purposes of Monitor s Compliance Framework. MRSA screening remains an important part of the patient pathway and certainly provided evidence for the PIRs. Currently the Trust can only provide MRSA screening data based on the number of admissions, either emergency or elective against screening requests via our laboratory system Sunquest. In order to get an accurate picture of MRSA screening which is able to provide patient specific data the Trust would need to invest in the upgrade to the ICNet system as this would then be available at the touch of a button. MRSA screening for 2013/14 is detailed below: Group Activity Type YTD Pathology MRSA Screenings PAS Admissions Elective Screening Rate % 97.7% Pathology MRSA Screenings PAS Admissions Emergency Screening Rate % 92.8% Meticillin Sensitive Staphylococcus aureus (MSSA) The Department of Health have applied the same data definition previously attributing cases as per MRSA bacteraemia. There is currently no PIR process for these cases or national target so they are assigned by time from admission to specimen being taken. - 9 Annual Report Infection Prevention and Control April 2013-March 2014

178 5.1.3 Surveillance of Clostridium difficile toxins The annual objective for C. difficile was significantly reduced from the previous year s number to just 14. This was a significant challenge for the organisation having finished 3 years with between cases. A case attributed to the acute organisation is defined as a case where the sample was taken on the fourth day or later of an admission to that trust (where the day of admission is day one). Following the previous year s root cause analysis the Trust was aware that a proportion of the positive cases were associated with inappropriate sampling. In order to improve clinical practice and provide more accurate information for teams on bowel management the ICT developed a new Bristol stool chart with the multidisciplinary team. This was successfully passed through the clinical records committee and is now used in clinical practice. 2013/14 demonstrated a significant reduction on previous year s numbers reporting 12 cases which was a 48% reduction. This met both national and Monitor targets for the year. C diff cases for 2013/14 The chart below details the number of cases per month Escherichia coli (E coli) bacteraemia E. coli is a species of bacteria commonly found in the intestines of humans and animals. There are many different types of E. coli, and while some live in the intestine quite harmlessly, others may cause disease Annual Report Infection Prevention and Control April 2013-March 2014
179 There is no objective or target associated with this bacteramia and it is not included in London performance data. However E coli bacteraemia contribute to a high number of blood stream infections and the significant effect on both the patient and burden on the health economy should not be underestimanted. In total there were 149 E coli blood stream infections for 2013/14 with the siginifcant number of patients admitted with septicaemia. By using the same data definitions as MRSA and MSSA attributed cases, the Trust has reported the following cases as represented in the following graph Surveillance of Glycopeptide Resistant Enterococcal (GRE) Bacteraemia GRE are resistant to glycopeptides (antibiotics such as vancomycin) and have been nationally reported since During 2013/14 the Trust reported no cases, with the last reported case being in Although the incidence remains low the ICT will continue to monitor and report cases. 5.2 Other Resistant Bacteria Carbapenemase-producing Enterobacteriaeae The Trust has received both a letter from Public Health England and a Patient Safety Alert in relation to carbapenemase-producing Enterobacteriaceae and other carbapenem-resistant organisms. Enterobacteriaceae are a large family of bacteria that usually live harmlessly in the gut of all humans and animals, but, in the wrong place, can cause serious infections. Worldwide, a small but increasing number of strains of enterobacteriaceae have become resistant to carbapenem antibiotics, which have been defined by WHO as critically important antibiotics. Increasing trends in sporadic infections, clusters and outbreaks of carbapenemase-producing Enterobacteriaceae (CPE) have been observed in a number of NHS trusts in England. There is a high risk of this problem becoming more widespread unless early and decisive action is taken by Trusts as these bacteria represent a significant challenge in terms of prevention, treatment and control. In the UK, we have a window of opportunity to prevent widespread problems caused by these organisms. Whilst we are seeing increasing numbers of carbapenemaseproducing Enterobacteriaceae, we have not yet reached the escalated situation seen in other countries. New guidance on the management and detection of these resistant organisms has been produced and the Infection Prevention and Control Team are reviewing current - 11 Annual Report Infection Prevention and Control April 2013-March 2014
180 policies and practice to ensure we meet these new recommendations. Crucial to these new guidelines is the ability to isolate a higher number of patients within the organisation. This is clearly a challenge for all trusts as isolation facilities are at a premium, and often risk based. If we are to fully implement the new guidance then in 2014 the ICT with the Trust will have to review the isolation facilities across the organisation and provide recommendations on how isolation facilities can be both improved and increased in number. 5.3 Surgical Site Infection Orthopaedic Surveillance of orthopaedic surgical site infection (SSI) is undertaken for both total hip replacements and repair of fractured neck of femur only. Whilst this meets our mandatory requirements for SSI the Trust would ideally like to extend this surveillance over additional surgical techniques. In the July - September 2013 submission period for total hip replacements and neck of femur the Trust saw an unusual peak in the number of surgical site infections. For this quarter the combined rates were 2% for hip replacement and 4.4% for repair neck of femur, with National data for hip replacement at 1.2% and neck of femur 1.7%. This resulted in the Trust being identified as an outlier by PHE, as we are outside national rates. In actual cases this represented four infections for neck of femur in one data collection period which triggered the orthopaedic and infection control team to review the cases. The increased incidence of cases was discussed at the divisional audit day and ICC in both January and March. Whilst initial investigation did not identify any immediate themes such as the same surgeon a more detailed case review was undertaken by the orthopaedic team. The Trust held a meeting with the wider multidisciplinary team focusing on surgical site infection, the report on the cases and to identify any further actions. In order to monitor the effectiveness of any change in practice the meeting agreed to currently take forward work on: Culture and behaviour within the theatre environment (including wearing of scrubs outside theatre areas) Maintenance of Normothermia- including pre, intra and post operative rewarming Skin decolonisation / washes prior to surgery Dressing changes on non orthopaedic specialist wards. Since 2013 the Trust has been reviewing the operating theatre environment and has a planned programme of works which includes re-commissioning of the theatres. Work on one orthopaedic theatre has been completed and the second orthopaedic theatre has planned maintenance in May 2014, with the remaining theatres to follow. Water testing for Pseudomonas aeruginosa was commenced in October 2013, as this is national guidance for critical care areas where patients are either immunocompromised or whose defences may have been breached ie: surgery. This will be undertaken as per guidance every 6 months. The Trust did identify taps which were positive and remedial work with re-testing was undertaken Annual Report Infection Prevention and Control April 2013-March 2014
181 It should be noted that we did not report any SSIs in neck of femur for the following two periods of surveillance but the increase in cases for July-September has clearly affected the combined 4 month data. There is only a small number of total hip replacements carried out at the Hillingdon site. The majority of cases, as they are elective are undertaken at Mount Vernon however patients with a Body Mass Index (BMI) over 40, ASA* 3 or 4 or require ITU admission are done at the Hillingdon site. The one reported case for July-September was very complex with a number of co-morbidities and high risk factors. PHE have responded to a recent communication from the Trust that they would note that only high risk cases are done at the Hillingdon site. (*The ASA score is a subjective assessment of a patient's overall health that is based on five classes (I to 5). 1 is patient has severe systemic disease that is not incapacitating to 5 Patient has incapacitating disease that is a constant threat to life.) The Trust is taking seriously this increased incidence and in collaboration with the Infection Control Team, there is a current business case to upgrade ICNet to the NG version and include the SSI module. This upgrade would enable real time monitoring and greater ownership by the clinicians involved. Our strategy, risk register and HCAI action plan all identify the need to expand SSI surveillance and for surgeons to have the ability to analyse and own their own data in order to understand patient outcomes and drive safer, quality care. Work on reducing surgical site infection is a priority for 2014/15. Surgical site infections are estimated to account for 15 per cent of all hospitalacquired infections and affect around 5 per cent of all patients undergoing a surgical procedure. (PHE 2012) Monitoring of surgical site infections is complicated; while many occur during hospitalisation, the majority manifest only after discharge, a phenomenon that has increased as hospitals have sought to reduce the length of inpatient stays. In these instances, the infection is often managed in primary care and is only recognised by the host institution if the patient is readmitted and these cases are typically not captured in monitoring/surveillance studies due to the manual nature limiting scope of surveillance. SSI data for 2013/14 is reflected in the table below Trust Procedure Number of Number of % SSI National data Site cases cases with SSI MVH Total hip % 1.2% replacement THH Neck of femur % 1.7% fracture THH Total hip replacement % 1.2% Caesarean section Recent studies have shown that C-section infection could be as high as 9.6% nationally in recent studies. The ICT have been working closely with the women and children s division in order to establish a C-section surveillance system as currently - 13 Annual Report Infection Prevention and Control April 2013-March 2014
182 the Trust does not have robust knowledge of current infection rates. With birth rates increasing and patient choice we need to be able to monitor rates in order to drive reductions, therefore encouraging more patients to choose the organisation. A data collection sheet has been agreed with the division but there remain challenges around receipt of completed data. A recent change in something as simple as the colour of the data collection form has seen a significant increase in the number of returns to the ICT office. In quarter 1 of 2014 it is anticipated that the Trust will have some robust data to analyse. 6 The Infection Control Team: Other Core Activity during 2013/14 The ICT remains focussed on patient safety, reductions in HCAI and that no person is harmed by a preventable infection. The team appreciate the focus and commitment from the members of staff across the organisation, including the Trust Board in ensuring they deliver safe quality care in a clean and suitable environment. 6.1 Education and Training The ICT continue to deliver IP&C training to all members of staff across the organisation; this training varies from regular formal sessions to individual bespoke delivery at a ward or department level saw a completely new approach for statutory and mandatory training across the organisation. Instrumental to these changes was the move to ensure that the organisation followed the core skills training framework outcomes for subject matters and included in this were refresher periods. The ICT had undertaken a risk based approach in previous years, establishing 3 levels of training. This new system has clinical and non-clinical staff only with refresher periods moving from every 2-3 years for clinical staff to annual and for non-clinical staff from once to every 3 years. The ICT worked closely with the STaM training advisory group as subject matter experts (SME) in IP&C. Concern was raised by the ICT at the time that current training, which was over 80% across the organisation, would drop significantly and measures would need to be in place to deliver extra-ordinary sessions. The Trust announced in January the new move for STaM training with details of the new fresher periods. An amnesty period from February to March was announced with a significant amount of additional sessions provided by SMEs. Linked to this transition was the movement of the current reporting for STaM to a new system as well as linking training records to ESR. Up to January 2014 the Trust was over 80% compliant in all levels of IP&C training. Data for January and February was not reported due to the amnesty, additional staff trained during this period is detailed below: Training Number of Staff attended Non-clinical 76 Clinical Annual Report Infection Prevention and Control April 2013-March 2014
183 6.2 Supporting and Working with Infection Control Link Staff Link nurses from wards and departments have a pivotal role as the member of the team in order to drive forward the IP&C agenda. Each clinical area has a named link nurse and in some departments and wards there are two members of staff who support each other in this role. The ICT held one link nurse study day in 2013 with representation from a number of specialist staff. A key item on this agenda was work around waste management. The Trust had just introduced new waste streams and it was essential that staff were clear on the use of the new offensive and alternative waste streams including new hard burn bins. 6.3 Implementation of the European Directive on Safer Sharps July 2013 saw the introduction of new safety engineered devices and a week of raised awareness on sharps, reporting and reducing risk. Educational stands were held in both the main entrance and staff canteen, where representatives from the new companies demonstrated their new products and were supported by the ICT, Health and Safety Team and Occupational Health. The new products had a staged roll out supervised by the procurement team and supported with ward/departmental training by the company representatives. The introduction of the new devices went smoothly as these products had been trialled in key clinical areas prior to final approval. Further work continued throughout the rest of the year with attention on risk assessments for those devices where safety engineered products are not availanble or practical. 6.4 Audit & Monitoring The Trust and ICT currently use the Meridian (Optimum) system to support audit and monitoring across the organisation. This system which is principally used for patient experience data, is also used for some IP&C audits but cannot be used for all measures due to limitations in the system. Currently the system is used for hand hygiene, VIP, Bare Below Elbows by the ward staff and for linen and isolation by the ICT. The Meridian system is due for contract review at the end of the year and the ICT is working closely with the audit department to ensure that the system is suitable for all of its users and provides appropriate data and reports for the organisation. The current audits & monitoring for IP&C in 2013/14 are detailed below: Compliance with Hand Hygiene policy (monthly) Compliance with Bare Below Elbows policy (monthly) Compliance with Isolation policy (annually) Compliance with Restricted Antibiotic Prescribing policy (quarterly) Compliance with Linen policy (annually) High Impact Intervention 1 Central Venous Catheter care (monthly) High Impact intervention 2 Peripheral Line Care (monthly) High Impact Intervention 4 Preventing Surgical site infection (bi annually) - 15 Annual Report Infection Prevention and Control April 2013-March 2014
 6.")
184 High Impact Intervention 5 Ventilator Care (monthly) High Impact Intervention 6 Urinary catheter care (monthly) High Impact Intervention 7 Clostridium difficile care bundle (monthly) High Impact Intervention 8 Cleaning and decontamination of clinical equipment (bi-weekly) 6.5 Working with the Patients and Public The Fighting Infection Together (FIT) is a public group that was established a number of years ago. This longstanding group is one of a kind with people passionate about infection prevention and the Trust as a whole. They provide a valuable interface, with a critical eye between the public, staff and the ICT. In addition to the support on infection control stands, producing and reading IP&C leaflets and general awareness raising, they provided significant support in the Trusts new hand hygiene products. In November 2013 after trials of new products the ICT with the FIT group and procurement department approved the move from our previous supply to our new supply Deb-cutan. This new product provided both a foam sanitiser and soap that was gentle to hands as well as outstanding product support with posters and our new bus stop signs. The new hand hygiene signage is clear, concise and eye catching with sanitiser signs in red throughout the organisation. New sanitiser signs in the main entrance 2013: 6.6 Working to Ensure Optimum Hospital Hygiene The Trust has undertaken a significant investment in order to ensure that we provide a clean, safe, suitable environment for our patients, staff, visitors and the organisation Cleaning & Catering services PLACE The new PLACE process has replaced the long standing PEAT (Patient Environment Access Team) process in It has been introduced to both revitalise the assessment of the patient environment process but also, more importantly, to ensure that there is a greater focus on patient involvement in the process. PLACE covers broadly the same areas as PEAT namely privacy and dignity, wellbeing, food, cleanliness and general maintenance of buildings and facilities. It focuses entirely on the care environment and does not stray into clinical care - 16 Annual Report Infection Prevention and Control April 2013-March 2014
185 provision or staff behaviours. It extends only to areas accessible to patients and the public (for example, wards, departments and common areas) and does not include staff areas, operating theatres, main kitchens or laboratories. In the past, all NHS providers have undertaken PEAT inspections and in the same way, PLACE will continue to provide an invaluable resource in assessing the care environment. This will directly support the provision of a high quality service to patients. The key feature of PLACE is the central role of patients in carrying out the assessments. At least 50 per cent of the team must be patients, and local Healthwatch must be offered the opportunity to be involved. Recruiting and training patient assessors is carried out locally and there is criteria outlining who is eligible and who is not available to become a patient assessor. The PLACE assessments took place at Hillingdon and Mount Vernon in April 2013 and involved patient and staff assessors including representatives from Facilities, Infection Control, Nursing and Estates. The four days of assessments covered wards, Minor Injuries Unit, Accident and Emergency, outpatients, internal public areas and grounds and buildings and generated almost 400 pages of assessment score sheets. The assessment scores covered the key areas of hygiene and cleanliness; condition, maintenance and appearance; privacy, dignity and wellbeing; and food and hydration. The results were published nationally in September 2013 with the Trust disappointed to be below national average for cleanliness; privacy, dignity and wellbeing; and condition and appearance at the Hillingdon site. Mount Vernon was above the national average in all of the key domains. On the plus side the Trust s food and hydration scores were above the national average. In 2013 the results were used to develop an Improvement Plan, which focused on the recurrent themes across the organisation that led to possible failure to meet the required standard or a qualified pass. This has resulted in a considerable amount of work that led to reception changes, new signage, new patient and waiting area chairs, new patient wheelchairs, an increased focus on cleanliness and hygiene and maintenance improvements. Domain/Score Hillingdon % Score Mount Vernon % Score HH/MVH % Combined Score National Average % Score Cleanliness Privacy, dignity & wellbeing Condition, appearance and maintenance Food & Hydration Annual Report Infection Prevention and Control April 2013-March 2014
186 Cleaning & Catering In August 2013 all cleaning and housekeeping rosters were reviewed and changed to ensure that they better met the size and infection control risk of an area, the work taking place there and the throughput. This led to many clinical areas receiving increased cleaning inputs and achieved savings through better productivity and utilisation of staff. The team engaged an external cleaning consultant to work with the team on cleaning processes, equipment and training. Working with infection control and nursing, for example, the cleaning team changed the processes and structure for cleaning outpatient areas to improve the standards. There were considerable catering service developments for both patient dining and retail services during the year with a new patient and retail kitchen being installed and new patient menus being introduced as well as a new HACCP manual developed to underpin food handling and safety. An internal audit was undertaken by TIAA to determine whether management had implemented adequate and effective operational and management controls over the Catering and Cleaning function. The audit included focus on: Policy and procedures to ensure the Trust s catering and cleaning services meet all applicable regulations and standards for NHS catering and cleaning services (Trust has identified standards and regulations for compliance; policies and procedure are in place; training is provided; cleaning arrangements are in place). And that Trust s catering and cleaning service complies with the requirements of CQC related standards (arrangements/action plans in place to ensure compliance). Overall the audit provided substantial assurance against the objectives. Linen The London procurement program with facilities led the work to tender the linen and sterile theatre packs contract in The infection control team played a crucial role in the tender assessment process participating in the tender assessment group to review the quality of linen and cleaning processes. Unfortunately the process in late 2013 needed to be repeated, from a contractual point of view, and this will take place in April and May Sterile Services The sterile services contract with IHSS continues to provide a good service to the organisation and is closely monitored by the facilities team in partnership with clinical services. Performance remains high on equipment turnaround times, which is encouraging as 2013 saw a number of additional trusts utilising the company and it is essential that standards are maintained. 6.8 Redesigning Environments and New Builds The ICT continue to work closely with the project team to ensure that the new designs and builds are fit for purpose, meet the Health Technical Guidance and provide a safe, clean environment. The new plans for 2013 included: Redesign and upgrade of the delivery suites in maternity New kitchen and catering facilities - 18 Annual Report Infection Prevention and Control April 2013-March 2014
187 Beaconsfield East dementia ward refurbishment Redesign and commissioning of the urgent care centre Re commissioning of orthopaedic theatre 1, including duct cleaning, recommissioning of the specialist airflow system and purchase of specialist ventilation for the prep room Endoscopy The Trust successfully redesigned and opened a new endoscopy unit at Mount Vernon. This new unit provides a spacious dedicated endoscopy unit with associated decontamination facilities. This new unit is the culmination of a number of years work to ensure the organisation s decontamination facilities meet Department of Health guidelines and provide a suitable environment for both patients and staff. The Hillingdon Hospital Endoscopy Unit will be completed as part of the new emergency admission unit on the ground floor in 2014/15. 7 Infection Control Policy and Procedure Within the Trust Infection Prevention and Control Policies are reviewed every three years or in light of new best practice or guidance. There are 28 policies found under the Policy Management Information System (PMiS) for infection control, which can be found in Appendix A. All policies now follow the Trust permitted format and are approved at the Infection Control Committee then ratified at the Clinical Governance Committee. 8 Outbreaks and Incidents at the Trust in 2013/ Pandemic Influenza The Pandemic Influenza Operational Policy is reviewed annually in preparation for the winter season by the ICT and links with the Trust s winter preparations and planning. This operational policy remains a flexible document that not only enables the Trust to react to a potential new pandemic but is also to respond to an increase in demand due to seasonal influenza activity or other possible increases in capacity due to either a Severe Acute Respiratory Syndrome (SARS) or the newer Middle East Respiratory Syndrome (MERS-CoV). An increase in influenza activity was not evident over the winter period, with relatively few confirmed flu patients admitted to the organisation. The Trust did however have a few suspected MERS-CoV patients admitted to the organisation in November This new respiratory syndrome is associated with travellers and residents from the Middle East. This year it was evident that with the high numbers of travellers returning from Hajj, the Trust could see potential admissions with suspected influenza or MERS-CoV. 8.2 Gastroenteritis/Norovirus Norovirus is always a particular challenge for organisations especially over the busy winter period. This virus is spread easily from one person to another and is highly infectious in nature. Whilst Norovirus activity remained high in the community setting and other organisations had wards closed for the first time in years the Trust did not close one ward or bay over winter due to confirmed/suspected Norovirus Annual Report Infection Prevention and Control April 2013-March 2014
188 Seasonal activity was lower in comparison to previous years as can be seen in the following chart from PHE. However the Trust still admitted cases with diarrhoea and vomiting and successfully managed them in side rooms without impact on the organisation. Possible contributing factors to the success of this year s management were: Recent change of Hand Hygiene product and awareness leading to greater compliance New pull up banners in the main entrances highlighting Norovirus A&E undertook a risk assessment for inpatients to identify those patients currently not symptomatic but had been in household/ contact with relative with known diarrhoea and vomiting, these patients were isolated as a precaution. 8.3 Needlestick Incidents and Prevention of Needlestick Injuries Occupational Health received 76 reports of needle stick injury for 2013/14, which is three more than the previous year. It was noted that there was a significant rise in reported needlestick injuries in July with 16 cases, compared with the usual 4-8 per month. This rise coincided with the month where the Trust had sharps awareness week and is possibly due to the promotion of reporting. Certainly towards the end of the year injuries from intravenous cannulae has significantly dropped due to the introduction of the safety engineered device. 8.4 Legionella & Water Quality Monitoring Legionella bacteria, which cause legionellosis, is an uncommon form of pneumonia and the majority of cases are reported as single (isolated) cases but outbreaks can and have occurred. Our duties, as an organisation, are provided in the approved Code of Practice and guidance Legionnaires' disease: The control of legionella bacteria in water systems (L8). This contains practical guidance on how to manage and control the risks in your system. Control and prevention of the disease is through treatment of the source of the infection, i.e. by treating the contaminated water systems, and good design and maintenance to prevent growth in the first place. The Trust continues to take this responsibility very seriously and is aware of the risks inherent in a multi building site with a number of older facilities. The Trust has a Water Quality group which meets regularly throughout the year monitoring Trust performance for both Legionella and Pseudomonas. In February 2014 the Trust - 20 Annual Report Infection Prevention and Control April 2013-March 2014
189 tested a number of outlets as part of re-commissioning of units back into general use following work or upgrades. A number of these outlets had positive counts and as a result were chlorinated and a revised system put in place to ensure that outlets under construction are tested and flushed just prior to handover. Testing for Pseudomonas aeruginosa P. aeruginosa is a Gram-negative bacterium, commonly found in wet or moist environments. It is commonly associated with disease in humans with the potential to cause infections in almost any organ or tissue, especially in patients compromised by underlying disease, age or immune deficiency or whose defences have been breached (for example, via a surgical site, tracheostomy or indwelling medical device such as a vascular catheter). In most cases, colonisation will precede infection. Some colonised patients will remain well but can act as sources for colonisation and infection of other patients. Its significance as a pathogen is exacerbated by its resistance to antibiotics, virulence factors and its ability to adapt to a wide range of environments. Contaminated water in a hospital setting can transmit P. aeruginosa to patients through the following ways: direct contact with the water through: ingesting bathing contact with mucous membranes or surgical site, or through splashing from water outlets or basins (where the flow from the outlet causes splashback from the surface); inhalation of aerosols from respiratory equipment, devices that produce an aerosol or open suctioning of wound irrigations; medical devices/equipment rinsed with contaminated water; indirect contact via healthcare workers hands following washing hands in contaminated water, from surfaces contaminated with water or from contaminated equipment such as reusable wash-bowls. The Trust has identified areas across the organisation for testing of P. aeruginosa and include ITU, NNU, Bevan and Theatres. In September 2013 the theatre complex at Hillingdon was tested for P. aeruginosa and some water outlets came back positive. As per guidance these outlets are taken out of use, remedial work is undertaken and then retesting of the water supply is undertaken. Only after a number of tests can the outlet be placed back in use. Unfortunately during routine testing for theatres one of the positive outlets was incorrectly labelled. This led to an incident of concern being raised and investigated by the Trust to ensure that patients and staff were protected. All testing was undertaken as per guidance with retesting in order to ensure results of <1 cfu/100ml. No patients in the two weeks following the incident isolated Pseudomonas species. The direct cause of the incident was attributed to human error exacerbated by a number of additional factors detailed in the report. In order to prevent a similar incident occurring the report recommended a number of actions which were contained in a Pseudomonas action plan, a new Standard Operating Procedure and signage was put into effect immediately Annual Report Infection Prevention and Control April 2013-March 2014
190 9 Management of Antibiotic Prescribing at the Trust in 2013/14 The scale of the threat of Anti-Microbial Resistance (AMR) and the case for action was set out in the Annual Report of the Chief Medical Officer published in March The UK Five Year Antimicrobial Resistance Strategy set out actions to address the key challenges to AMR. The overarching goal of the strategy is to slow the development and spread of AMR. It focuses activities around three strategic aims; improve the knowledge and understanding of AMR, conserve and steward the effectiveness of existing treatments, stimulate the development of new antibiotics, diagnostics and novel therapies. Antimicrobial prescribing & stewardship (APS) competencies have been developed by The Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection (ARHAI) and PHE; the goal is to improve the quality of antimicrobial treatment and stewardship and so reduce the risk of inadequate, inappropriate and ill effect of treatment. The aim is to improve the safety and quality of patient care, as well as contributing significantly to the reduction in the emergence and spread of antimicrobial resistance This year the Trust Antimicrobial Stewardship Group (ASG) started looking at Datix incidents related to antimicrobials, it continues to monitor spending on antimicrobials as well as Defined Daily Dosing (DDD)/1000 bed day report on selected restricted antibiotics. Ward pharmacists continue to report restricted antibiotic use to the antibiotic pharmacist, these are all reviewed by both the antibiotic pharmacist and the consultant microbiologists with the average number of reported prescriptions as 184/month The annual surgical prophylaxis audit which was completed in February 2014, showed that 78% of patients were given antibiotics as recommended in Surgical Prophylaxis Guideline. When looking at the timing of administration, in 88% of cases the correct surgical prophylaxis antibiotic was given at the correct time, this is an improvement from the 2012 audit. The Start Smart then Focus guidance and its subsequent action plan continue to be developed. The audit programme for antibiotic compliance has recently changed from monthly to quarterly. The frequency has been changed in collaboration with the clinical audit department and ensures that with the new quarterly data an action plan from divisions will be required to address low compliance. A recent meeting with the ADOs, NSMs and CDs strengthened the focus on antimicrobial prescribing with a commitment from specialties to undertake their own audits using a Trust template. This will provide data specific to the specialty in order to drive performance. The Trust Continues to take part in the European Antimicrobial Awareness day on 18 th November of each year - 22 Annual Report Infection Prevention and Control April 2013-March 2014
191 10 Safety and Quality In Infection Control: Statutory Duties & External Visits The Trust has an established assurance framework for IP&C as the safety of patients and staff, and quality care is a key consideration for all organisations. The Health and Social Care Act 2008 clearly reflects our duties and provides a collection of systems, processes and procedures in order to define the risks to achieve high quality care Care Quality Commission The Trust was inspected by the CQC over a number of days from 4 th -7 th October For Cleanliness and Infection Control the regulated outcome stipulates that; People should be cared for in a clean environment and protected from the risk of infection. The outcome of the inspection was reported by the CQC as the following: Whilst the trust had many positive infection control indicators and audits showed a low level of infection, we found a number of instances where the risks of the spread of infection were increased. We have judged that this has a minor impact on people who use the service, and have told the provider to take action. The provider was not meeting this standard The Trust was disappointed with the decision by the CQC which was based on: Isolation doors not shut on all occasions The use of a cordless phone-on one of the wards Lack of knowledge amongst clinical staff on curtain changes Cleaning of equipment Damaged flooring/ condition of the building As a result the Infection Control Team revised the current audit programme within the organisation following the inspection. A new quick question assessment (QQA) tool was devised using elements from the inspection such as correct use of personal protective equipment, isolation standards and inspection of equipment in the clinical area. This was then assessed twice a month and findings reported at both divisional and Board level. The Trust will continue to audit mattresses annually as well as adhoc inspections by staff to ensure damaged items are replaced. The Estates and Facilities team have a robust programme of audit for cleaning of the Trust and the supervising staff have all been given details of areas in which to pay particular attention ie: high level dusting. There is an existing PLACE improvement group which includes any Estates issues that require rectification eg: damage to floors, and this has already been identified and a report produced. There are a number of financial implications for the organisation in particular the maintenance of the Estate and repairs to the existing floors. A full report with costing on such repairs has been produced since the inspection Annual Report Infection Prevention and Control April 2013-March 2014
192 The Trust recognises that whilst it is not following best practice for closing all doors when isolating patients, this has to be balanced against the risk to the patient. It was explained during the inspection that as the doors are solid in some parts of the building, when we have a confused, critically ill or patient at risk of falls then doors cannot be closed for patient safety reasons. The Trust have however taken the comments into account and are investigating the possibility of replacing the doors in order to enable staff to patients clearly. During the inspection the frequency of curtain changing was identified as a risk as staff did not know the frequency of changes. The Trust does however have a named person responsible for all curtains, where records are kept and these were not requested during the visit. Staff know that they can request change of curtains when these are damaged or stained and therefore this is not considered a risk to people who use this service. The Trust considers that these minor points raised in the inspection did not pose a risk to patients or visitors. Where the inspection identified torn or damaged items these were already condemned or replaced. Equipment and the general ward environment is regularly inspected to ensure it meets standards. 11 Measures of Infection Prevention and Control: Shaping Practice to Improve Performance The ICT regularly review and update audit and monitoring to reflect both current practice and to highlight any areas for improvement. The IP&C measures have been used to drive performance and sustain best practice. In order to gain maximum impact and to challenge the divisions around performance the league table presentation was again reviewed and updated for 2013/14. Whilst the ICT does utilise the Meridian system this does not fully integrate all of the current audits and is time consuming to complete at ward level. It is essential in 2014 that when the audit system is reviewed that it is able to adapt to the ever increasing demands of the organisation and supports staff in their work. 12 Looking forward to 2014/15 As we come to the end of the year new objectives for 2014/15 are established. As with this year NHS England remain focused on a zero tolerance of MRSA blood stream infections and have set the same objective of zero. This remains a substantially challenging target across the NHS as the MRSA bloodstream infections we see today are now complex, multi-factoral events. New from April 2014 is that NHS England regional teams will take on the role of arbitrating disputed MRSA bacteraemia cases which was previously held by Local Authority based Directors of Public Health. NHS England and Public Health England have noted that the rate of improvement for C diff has slowed over recent years. There are indications that for some organisations at least, C diff levels may be approaching their irreducible minimum - 24 Annual Report Infection Prevention and Control April 2013-March 2014
193 level at which these infections will occur regardless of the quality care provided. Experts have now advised that a more flexible approach is now needed to objectives. The new changes are primarily focused on further encouraging organisations to look at each case they identify in order to understand what lessons they are able to learn in order to improve patient safety. Trusts have been divided into three cohorts for the purpose of calculating median C diff rates; these are: Teaching acute trusts Non teaching acute trusts CCGs Recommendations for 2014/15 1. Upgrade of ICNet to NG version to enable : Extended surgery interface and surgical site surveillance module Dedicated Surgical outcome reports to support surgical directorates with accurate rate reports on infection, readmission and mortality Provide accurate real-time performance data on surgical infection rates Enable real time Device Management tool to ensure that infection prevention team is supported with accurate denominator data and microbiology reports on device associated infections such as Catheter Associated Urinary Tract Infections (CA-UTI) and Central Line Associated Bacteraemia (CLABSI). Provide accurate MRSA screening data at both patient and ward level in order to drive performance 2. Review of Isolation Facilities In line with current guidance on isolation for new emerging infections the current siderooms will not provide the required facilities for both staff and patients. A risk assessment of the isolation facilities should be undertaken in order to assess how the organisation will meet the ever increasing demands for sideroom facilities. 13 Conclusion The Hillingdon Hospitals NHS Foundation Trust has infection prevention and control at the heart of its agenda. There have been significant achievements over the past year for the organisation balanced against some disappointing performance in PLACE and the CQC inspections. It is important that in this ever changing face of the NHS where we are faced with new targets, emerging infections and financial challenges that we ensure patients still receive safe quality care across the organisation. As ever infection prevention and control is not just the remit of the infection control team but it is everybody s responsibility and we would like to take the opportunity to thank staff, patients, public, governors and all our stakeholders for their continued support with this important agenda Annual Report Infection Prevention and Control April 2013-March 2014
194 14 Acronyms ANTT CCG C diff CQC DH DIPC FIT GRE HCAI HII HPA ICC ICN ICT IPC or IP&C ITU MRSA MSSA NNU PCO PEAT PHE PIR SMART UTI Aseptic Non Touch Technique Clinical Commissioning Group Clostridium difficile Care Quality Commission Department of Health Director of Infection Prevention and Control Fighting Infection Together Glycopeptide Resistant Enterococci Healthcare Associated Infection High Impact Intervention Health Protection Agency Infection Control Committee Infection Control Nurse Infection Control Team Infection Prevention and Control Intensive Therapy Unit Metecillin Resistant Staphylococcus Aureus Metecillin Sensitive Staphylococcus Aureus Neo-natal Unit Primary Care Organisation Patient Environment Action Team Public Health England Post Infection Review Specific, Measurable, Achievable, Realistic, Timely Urinary Tract Infection - 26 Annual Report Infection Prevention and Control April 2013-March 2014
195 15 Appendix A Infection Control Policies Policy Number Policy 240 Animals & Pets In Hospital 188 Aseptic Technique Policy 178 Care & Management of Patients in Hospital with Diarrhoea Policy 183 Central Venous Catheter Insertion and Maintenance (CVC) 179 Clostridium Difficile (C diff) Associated Diarrhoea 169 Decontamination of Medical Devices 245 Employment Health Screening (including food handlers and drivers) 177 Hand Washing 244 Immunisation Policy (Occupational Health ) 170 Isolation 185 Laundry Sorting 175 Meningitis including Meningococcal Septicaemia 174 MRSA Control (Methicillin-Resistant Staphylococcus) 167 Outbreak (Food Poisoning or Communicable Disease) 186 Re-use of Single Use Items Supplied for Single Use Only 165 Risks Associated with Infection Prevention and Control 166 Safe Handling & Removal of Infected Bodies 181 Scabies 172 Standard (Universal) Precautions 171 Surveillance 176 TB Prevention & Control 187 Transmissible Spongiform Encephalopathies (TSE) Creutzfeldt Jacob Disease (CJD) 231 Urinary Catheter 189 Varicela Zoster Virus (Chickenpox/Shinges) 180 Viral Haemorrhagic Fever (VHF)- suspected cases of 173 Visual Infusion Phlebitis (VIP) Score - 27 Annual Report Infection Prevention and Control April 2013-March 2014
196 Strategy Priority Area and Strategy Ref: 6.1 Culture & leadership 6.2 Accountabilities, responsibilities and organisational framework 6.3 Performance reporting Action Priority Comments Plan Ref: Q1 Q2 Q3 Q4 Nos. 7&9 Receive and review Divisional HCAI action plans at ICC G G G G All divisions HCAI action plans presented bimonthly Executive ward visits to include observation and discussion on IP&C measures G G G G Observation of care launched February 2013 Nos. 4,5&9 Nos. 3, 4, 5&8 6.4 Accessible information No Improving patient safety No. 5, 13&14 Sisters/Charge Nurses to enforce stricter IP&C measures embed visitors charter, revised signage, enforce BBE/hand hygiene etc (recs from People in Partnership group work) to be monitored through observation and discussion Discuss and endorse all RCA actions at executive level (trust attributed MRSA and CDI cases) and present actions to ICC New Post Infection Review (PIR) process to be used across the organisation in line with Public Health England (PHE guidance. In case of arbitration cases DIPC and Lead ICN to attend which includes ward appearance A A A G Visitors charter implemented, new signage on for Hand Hygiene now Trust wide. G G G G RCAs reviewed at ICC itemised on agenda. G G G G PIR process in place. 3 arbitration meetings attended to date all awarded to CCG ToR refreshed 2012 for ICC and included more active medical representation A A A A Regular representative from Surgical division still pending Antimicrobial Group to include revised membership, ensure robust annual action plan and bi-monthly reporting to ICC A A G New member to ASG includes Lead Pharmacist. Reporting is an agenda item on Each division to table one IP&C item at divisional governance forum per annum (e.g. antimicrobial stewardship) Receive and review the HCAI assurance framework based on H&S Care Act at ICC every six months Report key IP&C performance and compliance to ICC with exception reporting to QRC Committee Establish a surveillance system to enable performance reporting for SSI Caesarean section wounds Public website and staff Intranet information resources are to be reviewed and refreshed Refresh posters in accordance with People in Partnership group work suggestions A ICC and papers now received Dates to be confirmed and taken forward for 2014/15 G G HCAI Assurance Framework to ICC March. G G G G Robust reporting in place to ICC A A G SSI monitoring process agreed with W&C and date collection started March 2014 G G G G FIT group reviewed current public information. LICN reviews staff Intranet monthly to ensure all aspects up to date. A A G New posters for Hand Hygiene throughout Trust for hand hygiene. New Norovirus full pull up banners designed by FIT group in use. Ensure that the review of IP&C policies is on track A A G Programme of review in place for all ICC policies and included in HCAI action plan. Outbreak management procedures to be reviewed & amended based on learning from 2012/13 winter period Consider further and improved technology in relation to cleaning clinical areas post CDI/Norovirus etc G G G G D&V protocol reviewed and approved September New banners in use and updated Norovirus leaflet reviewed and agreed by FIT group *G Further discussion with Estates and Facilities planned for Quarter after new in house cleaning contract embedded. New microfiber system purchased by Facilities to replace current system.
197 6.6 Surveillance & reporting 6.7 Risk assessment & audit 6.8 Training & education 6.9 Partnership working Comply with the new EU directive on sharp safety which includes introduction safety engineered devices A A A A Sharp safety week in June. New Medical devices introduced July Further devices to be launched after trials No.&10 Improve antimicrobial prescribing compliance to >95% A A A A Start Smart then Focus action plan in progress and clinical specialties undertaking own audits. Compliance still not consistently above 95% but discussion and engagement has significantly improved across the organisation. ICT to validate local monitoring and performance to be published G G G G VIPS currently validated by ICT and urinary catheter audits. New QQA tool launched in November, adhoc validation. No. 12 Undertaken business case for ICNet upgrade to NG which includes SSI module and real time MRSA screening. Gain assurance that the replacement programme for hand wash basins is on schedule *G Business case complete. Not funded in 1 st round nursing technology fund and expression of interest submitted for 2 nd round funding * No budget for 2013/14 allocated to replace CHWB- 150K available for 2014/15 and audit planned April/May as major refurbs undertaken across organisation. Any new build/ refurb includes new CHWB Risk assessments to be completed for sharp safety where new devices not A A A A In progress, work only started in 2013 and will available be ongoing process as new devices available. Risk register for IP&C to be reviewed at ICC bimonthly and updated. G G G G Risk register updated bi monthly Nos. 1&3 Sustain compliance for IP&C training at > 80% A A G G Currently Trust overall performance 80% in all levels. New system to be launched Q3 across the organisation. Deliver more robust ANTT programme and achieve compliance at >95% by March 2014 A A G New process resulted in annual assessment for 2013/14, staff required to have annual review to be completed by March No. 6 Deliver annual joint IP&C awareness event with partners Due to change in PCT and new CCG there is currently no community ICC. Joint IP&C awareness event agreed for FIT member engagement to agree IP&C patient information. To be included in new PLACE assessment process G G G G FIT group reviewed IP&C leaflets Q2 and approved trial new hand hygiene products. FIT members included in PLACE assessments - 29 Annual Report Infection Prevention and Control April 2013-March 2014
198 ITEM 20 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Helen Cobb, Assistant Director Governance & Quality Standards Theresa Murphy, Director of Patient Experience & Nursing DATE: 30 th July 2014 SUBJECT: The Integrated Risk Register Trust Strategic Priority: The Integrated Risk Register impacts across all the Trust s Strategic Priorities. Summary: The Quality and Risk Committee (QRC) met on 16 th July and reviewed the high and medium level risks on the risk register. New high level risks: Risk Financial Performance 2014/15 Upgraded risks: Risk 41 - The Management of Legionella in Trust Premises Down-graded risks: Risk Statutory and Mandatory Training (high to medium) Risk Electrical - Single point of failure (high to medium) Risk Medical Record Library Building Working Environment at Hillingdon Hospital (high to medium) Board Action Required: The Board is asked to review and approve the high level risks on the Risk Register following consideration by the Quality & Risk Committee. Equality Impact Assessment: N/A there is no positive or negative impact from this report.
199 Integrated Corporate Risk Register July 2014 (High) Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 41 Risk assessor: Trevor Pollard Date assessed: 27/10/2006 Review Date: 19/12/2014 Verified: Yes Status: Active Last Updated: 09/07/2014 Sue Manthorpe Subject: The Management of Legionella in Trust Premises Hazard: Legionella bacterium contamination in hot and cold water domestic services. Type: Health & Safety Management level: Corporate Source: Legacy Data Source Description: reactive risk assessment following water reports indicating high levels of legionella growth Trust/Site: The Hillingdon Hospitals NHS Foundation Trust Specialty: Estates, Estates (MVH) Risk Registers: Estates, Mount Vernon (THH FT), Mount Vernon Site Risk lead: Edmund Fosbrook Handler: Sue Manthorpe Executive lead: David Searle Inadequate water management systems in place resulting in the spread of Legionellosis. Monthly hot and cold water temperature checks. Monthly biological sampling of hot and cold water systems Chemical treatment of water supply. Showerhead replacement and hose cleaning and descaling programme. Water sampling to determine level of contamination. Flushing of infrequently used outlets Effective use of the sampling and surveys to identify and carry out remedial works has now been fully implemented Inability to soften water supply to prevent lime scale build up on calorifiers inconsistent temperature controls due to plant room mechanical issues increasing legionella growth due to tank cleaning difficulties High C=5 L=3 L8 risk assessment programme and action plan in place Calorifiers are removed regularly and cleaned to prevent severe build-up of lime scale Annual management audit by external contractor Regular reports to the Infection Control Committee and health and Safety Committee to monitor management of Legionella work plan Action Action Ref: 925 Action lead: Edmund Fosbrook Due date: 09/09/2014 Action: Clean and disinfected tower block tanks Last updated: Action Action Ref: 926 Action lead: Edmund Fosbrook Due date: 09/09/2014 Action: remove or isolate Annex ward and areas water tanks switching to mains water supply Last updated: Progress Company identified to carry out cleaning of the tanks - dates of work to be confirmed. Last updated: Progress Pagett ward tank isolated. A plan and programme of work for all other tanks is being agreed with health and safety Last updated: The Hillingdon Hospitals NHS Foundation Trust Page 1 of 15
200 Action Action Ref: 927 Action lead: Edmund Fosbrook Due date: 09/09/2014 Action: Working with health and safety and infection control plan and carry out full system disinfection and flushing from tower block tanks Last updated: Action Action Ref: 453 Action lead: Edmund Fosbrook Due date: 08/12/2014 Action: L8 risk assessments completed for THH and MVH. Action plans to close identified gaps are now in place and are being monitored to ensure completion by agreed timelines Last updated: 09/07/2014 Sue Manthorpe Progress weekly extraordinary water quality meetings taking place to plan and agree process for full system disinfection Last updated: Progress SM 09/07/14 L8 risk assessments completed in February and work plan being prioritised SM 13/12/13 The Water quality meeting continues to monitor the testing and management of Legionella across the Trust. L& risk assessment action plan completion continues at a slow pace. 12/09/13 legionella sampling continues to show control of current water supply levels Legionella sampling results presented to June Water Quality Committee. Results for both Hillingdon and Mount Vernon Hospitals were clear. THH and MVH action plans are presented at the monthly water quality meetings where progress against agreed action plan timelines are monitored. Progress on the risk assessments continues and is included in the estates work plan for the next financial year. Failure to meet agree action plan timelines are escalated to the Health and Safety Committee Last updated: 09/07/2014 Sue Manthorpe The Hillingdon Hospitals NHS Foundation Trust Page 2 of 15
201 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 152 Risk assessor: Jacqueline Walker Date assessed: 18/09/2009 Review Date: 30/12/2014 Verified: Yes Status: Active Last Updated: 12/09/2013 Sue Manthorpe Subject: Decontamination of Endoscopes. Hazard: Inability to meet decontamination compliance standard (2f) in accordance with the Health and Social Care Act Low risk of patient infected by contaminated equipment or staff infected by environmental conditions of endoscope cleaning areas. Type: Clinical Management level: Corporate Source: External recommendation(s), Regulatory requirements Source Description: Regulatory - HTM2030 Trust/Site: The Hillingdon Hospitals NHS Foundation Trust Directorate: Medicine, Rehab & Emergency Care, Mount Vernon, Surgery, Women & Children Specialty: Estates, Infection Control Risk Registers: Estates, Medicine, Mount Vernon (THH FT), Infection Control, Acute Surgery, Gynaecology BAF: 1.1 Risk lead: Sue Batty Handler: Sue Manthorpe Executive lead: David Searle Closure of service if patient safety is not maintained in accordance with CQC registration. Patient harm due to cross contamination. Staff harm due to infection. * Annual audits are carried out by Authorised Engineer Decontamination with Endoscopy Manager, H&S, IC and Sterile Services Client Services Manager * Trust policies in place. * ICC/CGC/IRMC monitor action plans. * Annual review/risk assessment of decontamination conducted by Trust's authorised person. * Annual maintenance agreements with manufacturers/suppliers are in place. * All relevant local procedures available within key departments (endoscopy/outpatients). * Staff training available in key departments. Detailed training provided by manufacturers on annual basis for staff in scoping areas * Endoscope tracking system in place on both sites. * Scope User Group meetings. * Environmental restraints within Endoscopy areas, such as inadequate space and design, resulting in non-compliance with clean/dirty flows and adequate ventilation systems * Deloitte review in December * Not meeting HTM2030 for endoscopy decontamination * Cumberledge decontamination environment is of inadequate size and design High C=4 L=3 Action Progress Action Ref: 295 Action lead: Karen Blackbond Due date: 06/03/ /04/14 Action: Strategic solution for the clinical requirements of decontamination of endoscopes across the Trust to be agreed to ensure compliance with HTM 2030 and requirements of Health & Social Care Act (2008). Last updated: 07/02/2014 Sue Manthorpe New build solution for Endoscopy at THH underway and remains on schedule to be completed February /02/14 New build solution for Endoscopy at THH underway and on schedule to be completed February 2015 The Hillingdon Hospitals NHS Foundation Trust Page 3 of 15 The new build solution for endoscopy commences in January A solution to the Endoscopy suite at Hillingdon Hospital is part of the new build project and it is anticipated that this will be completed by December 2014 Solution has been changed:- Hillingdon site - new build project progressing 27/01/14: Endoscopy at MVH has now moved to the New Endoscopy Unit purpose built unit in the Treatment Centre. Endoscopy at Hillingdon is still ongoing as part of the new build project anticipated to be completed December Last updated: 09/04/2014 Sue Manthorpe
202 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 209 Risk assessor: Graham Smith Date assessed: 17/07/2013 Review Date: 17/07/2014 Verified: Yes Status: Active Last Updated: 08/04/2014 Margaret Boonstra Action Subject: Malfunction of CT Scanner at Hillingdon Hospital Hazard: Unavailability of machine resulting in suspension of service Type: Clinical Management level: Corporate Source: Incident(s), Other Source Description: Failure of CT scan leading to cancelling and rescheduling appointments To support Business case for acquiring a clinical system that can also provide backup for main and only CT scanner CT Scanner has broken down 9 times between March 2012 and April 2013 with loss of service. 06/11/2013 It has broken down again in Oct 2013 for 4 days. There has been a formal complaint (ID 3278) and initial proceedings for a claim (ID 764). Datix: W35040 CT scanner not operational Action Ref: 687 Action lead: Graham Smith Due date: 30/09/2014 Trust/Site: Hillingdon Hospital Directorate: Cancer & Clinical Support Services Specialty: Radiology Ward/Department: Radiology Risk Registers: Radiology BAF: 1.1,1.3 Risk lead: Graham Smith Handler: Margaret Boonstra Executive lead: Karl MunslowOng Delayed assessment and diagnosis as patient needs to be transferred off site for scanning. Repairs can be in excess of one day. On occasion has taken as long as four days Action: Replace the current gamma scanner with a Spec /CT scanner which will provide a degree of cover for the main CT scanner when being serviced or repaired. Last updated: 25/03/2014 Margaret Boonstra Agreement with Wexham Park Hospital to cover emergency service in the event of a mechanical breakdown Written record for alerting all relevant teams of scanner malfunction has been put in place Protocol in place for referring patients for CT scans - all referrals are checked and approved by Radiologist Consultant Clinical assessment prior to transfer of the patient is undertaken by attending clinician Progress Only 1 CT Scanner in the Trust which has broken down 9 times between March 2012 and April 2013 with loss of service and again in Oct 13 Management of patient during transfer and while attending at Wexham Park Hospital is uncertain. There is no control with regard to the timeliness of the transfer and return of the patient High C=4 L=3 Latest update: 05/06/2014 An initial allocation of funds has been made as part of the equipment capital plan. Quotes for equipment have been received. Currently arranging specification for the room development in order to invite quotes for the building work. Once complete the business case can be finished and submitted. On 14/15 Capital bid. Results in Feb/Mar /03/2014 It is anticipated that it will be accepted. The dept. has already begun consultation with building and radiation protection advisors. There is an anticipated completion date for this project of sept This project has now been submitted to the capital bid for approval.15/04/2014 Last updated: 05/06/2014 Margaret Boonstra The Hillingdon Hospitals NHS Foundation Trust Page 4 of 15
203 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 240 Risk assessor: Graham Smith Date assessed: 24/07/2013 Review Date: 24/07/2014 Verified: Yes Status: Active Last Updated: 07/04/2014 Jacqueline Walker Subject: Lack of Interventional Radiology on call Hazard: Unavailability of trained staff out of hours impacting on treatment, which is potentially life threatening Type: Clinical Management level: Corporate Source: Complaint(s), External recommendation(s) Source Description: Action plan within the report after the Adult Emergency Care Standards visit to the Trust 5th Sept The Trust arrangements failed the Quality and Safety Standards for Interventional Radiology in a hospital providing Acute Medicine, Surgery and Obstetrics. Action point in the report: For the Trust to develop a service to deliver the Standards. The Commissioned Standards for 13/14 are unchanged for Interventional Radiology. Concerns have also been raised from Surgical Consultants regarding the very poor level of formal cover for non-vascular interventional radiology out of hours. Trust/Site: Hillingdon Hospital, Mount Vernon Hospital Directorate: Cancer & Clinical Support Services Specialty: Radiology, Radiology (MVH) Ward/Department: Radiology, Radiology (MVH) Risk Registers: Radiology BAF: 1.1 Risk lead: Monica Whittle Handler: Margaret Boonstra Executive lead: Abbas Khakoo There is only one full time Interventional radiologist who is trained to do on-call at Hillingdon. If this Radiologist is not available, it could lead to delay in diagnosis or treatment. Northwick Park only provides cover for Vascular cases. Rapid access to Interventional radiology is required by Obstetric, Renal and Gastroenterology patients. Around 20 cases have been referred to other hospitals in the absence of interventional cover in the last year resulting in financial losses to the Trust. Hillingdon Hospital, having an Acute site status, must provide a robust Interventional cover process either on site or in collaboration with other Trusts. Acute site status is at risk in the absence of a robust Interventional Radiology process. Trained staff can be called at home to assist if available There is an agreement with Northwick Park to provide interventional cover only for Vascular cases. Patients outcomes are potentially adversely affected by delaying diagnosis and treatment e.g. leading to hysterectomy in obstetric patients, nephrectomy as a result of kidney failure Not all Radiologist are interventionally trained Current collaboration is only with Northwick Park for Vascular cases High C=4 L=3 Action Action Ref: 512 Action lead: Monica Whittle Due date: 29/09/2014 Action: Negotiate with other local hospital to develop a Regional Network of Interventional Radiologists to provide out of hours cover Last updated: 03/04/2014 Margaret Boonstra Progress Latest update: June 2014 There has been no progress with this action Discussions are ongoing with Northwick Park regarding setting up a Network service to cover 24hr Interventional service. MW has had discussions with Clinical Director for Northwick Park, Michelle Marshall (Dec 2013). We have agreed to work up a formal proposal. Jan 2014: Hillingdon Hospital C&CSS Division has submitted a bid for 340, from the Quality Reserve to enable development of staffing and patient pathways to support high quality Interventional Radiology. March 2014: This has not been successful Last updated: 17/06/2014 Margaret Boonstra The Hillingdon Hospitals NHS Foundation Trust Page 5 of 15
204 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 323 Risk assessor: John Saberton Date assessed: 01/01/2013 Review Date: 02/09/2014 Verified: Yes Status: Active Last Updated: 05/06/2014 Margaret Boonstra Action Subject: Cardiac Arrest Service provided to CNWL Hazard: Staff may not know where the specific ward area is as it is a different Trust and staff may be unable to access building to attend cardiac arrest in a timely way Resuscitation team will be unfamiliar with ward/trolley set up currently in place at CNWL Not all clinical areas in CNWL have a battery suction unit THH staff may opt to use the monitored LifePak 9 defibrillator (monophasic) not realising that the ward have a biphasic AED CNWL may incorrectly assess the patient and place a 2222 cardiac arrest call for a medical emergency or false alarm Type: Clinical Management level: Corporate Source: Incident(s), Proactive risk assessment Source Description: Incidents/proactive risk assessment relating to lack of SLA between the Trust and CNWL with regards to resuscitation service and availability of appropriate equipment on arrival. Ward/Department: Resuscitation, Riverside Centre Risk Registers: Nursing BAF: 1.1,1.3 Action Ref: 726 Action lead: John Saberton Due date: 02/09/2014 Risk lead: John Saberton Handler: Margaret Boonstra Executive lead: Abbas Khakoo Cardiac Arrest team unable to easily access CNWL s clinical areas and there may be a delay in getting the arrest team to the patient Staff will have access to an unfamiliar resuscitation trolley with old defibrillators, no EZ-IO or the CNWL grab bag with basic equipment The team will be unable to successfully clear a patient s airway using the equipment that is currently in place The staff have a biphasic AED but staff may not use this as there is no monitor. If the patient requires a shock there is roughly a 30% less chance of survival on the old LifePak defibrillator There is no other way of monitoring a patient other than using the defibrillator monitor. The team will have to wait for the ambulance to arrive to do any further investigations Action: Agree formal and documented SLA for resuscitation services provided to CNWL in line with Trust standards and implementation/training of staff for use of the new equipment Last updated: 05/06/2014 Margaret Boonstra Staff are all told on induction that we still cover CNWL for cardiac arrest calls. They are told where the ward areas are on the site and advised to walk around the site to familiarise themselves CNWL Resuscitation Officers train staff to open all doors to allow access to THH Resuscitation team CNWL staff have been asked to check the trolley daily so when the arrest team ask for equipment CNWL staff should be able to identify the equipment rather than THH staff looking through various drawers All areas have a hand pump suction unit. This can be used while a member of staff goes and gets the portable battery suction machine from another clinical area Staff attending the arrest should realise that all automated external defibrillators (AED) are biphasic. So although the Hillingdon arrest team may use the LifePak 9 for monitoring through if the patient requires defibrillation then they should be using the AED Anytime a cardiac arrest call is placed at CNWL, an ambulance should also be called so we are able to transfer the patient to A&E resuscitation room. Progress SLA agreed and signed between the Trust and CNWL for the provision of resuscitation services; the Trust has purchased resus equipment for use at CNWL; however, the equipment service agreement has to be put in place before the equipment can be released. Latest update 05/06/14 SLA agreed and signed between the Trust and CNWL for the provision of resuscitation services; the Trust has purchase the agreed equipment so it is universal across Trusts; delivery time 4-6 weeks. The CNWL have to agree an equipment maintenance contract before the equipment can be put into clinical areas. Last updated: 05/06/2014 Margaret Boonstra High C=4 L=3 The Hillingdon Hospitals NHS Foundation Trust Page 6 of 15
205 Risk Basics Subject/Hazard Areas Affected Risk Ref: 350 Risk assessor: Vicky Cook Date assessed: 01/10/2013 Review Date: 30/09/2014 Verified: Yes Status: Active Last Updated: 08/07/2014 Sarah Locke Action Subject: Suboptimal maternity staffing levels within midwife, obstetrics and anaesthetics Hazard: Inability to provide safe, effective and timely care to women and their babies on the maternity unit due a lack of staff (Midwives, Obstetric and Anaesthetics). Type: Clinical Management level: Corporate Source: Claim(s), Complaint(s), Incident(s), Proactive risk assessment Source Description: Claims and complaints have been received where the cause has been shortage of maternity staff. There have also been a number of incidents pertaining to the shortage of maternity staff. Directorate: Women & Children Specialty: Obstetrics Risk Registers: Obstetrics BAF: 1.1,1.3,3.5 Action Ref: 924 Action lead: Anita Hutchins Due date: 31/03/2015 Risk Controls Gaps Rating Risk lead: Anita Hutchins Handler: Sarah Locke Executive lead: Theresa Murphy The lack of staffing will give rise to: Increased rate of caesarean sections Increased rate of serious incidents CQC have already identified maternity staffing as a moderate risk during the October 2013 unplanned visit Inability to manage induction of labour processes in line with current guidelines which may lead to an increased risk of caesarean section, sepsis, Sis and Incidents of Concern. As induction of labour is commenced on the antenatal ward, the potential shortage of staff frequently leads to significant delays in women reaching the labour ward (greater than 24 hours) which results in deliveries occurring on the ward; failed induction or uterine sepsis. failure to act promptly to early warning signs leading to an increase in stillbirths/intrauterine Deaths (IUDs)/maternal mortality and morbidity resulting in SIs Increasing complaints and low satisfaction figures in the patient experience surveys both locally and nationally. This is likely to lead to reduced bookings through choose and book which in turn is likely to have a financial impact on the Trust Increasing staff sickness absence rate due to low staff morale and exhaustion. Delay in emergency/elective caesarean section due to the unavailability of an anaesthetic consultant. Action: Business plan under review identifying shortfalls in minimum recommended staffing levels across all maternity specialities. Last updated: The Escalation and Divert procedure allows for short term emergency flexing of staff when workload is high as well as allowing for a divert of mothers to other units. During normal working hours (08:00 to 17:00 mon to fri) staff can be relocated from other roles to help in clinical areas. Out of hours community midwives can be asked to work a shift. During the hours of 20:00 to 08:00 the consultant at home can be called in to assist if required. Use of bank/agency staff to fill the gaps. Progress Budgeted staffing levels do not meet RCOG Safer Childbirth 2007 recommendations. Diversion of mother to other units is frequently turned down as other units are struggling with their own service pressures. Moving staff across the unit is not always possible due to staff competencies and experience; it delays other work and increases pressure further on the areas also left without staff. Using out of hours community midwives can lead to breaking the working time directive as well as having exhausted staff working in a high pressured environment. On call consultant being called in to assist can lead to breaking the working time directive as well as having exhausted staff working in a high pressured environment. LSCS audits have identified the need for an out of hours consultant presence on the labour ward with regard to training and decision making. the level of competency of bank and agency staff or the required is not always available the availability of bank and agency staff is very limited leading to unfilled shifts or often fail to attend. High C=4 L=3 There has been an increase in Labour Ward Consultant presence to 114 hours per week. There has also been an increase in postnatal midwifery staffing levels. Community and labour ward staffing as well as anaesthetic and obstetric hours shortfalls still under review. Last updated: The Hillingdon Hospitals NHS Foundation Trust Page 7 of 15
206 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 382 Risk assessor: Paul Wratten Date assessed: 16/06/2014 Review Date: 17/07/2014 Verified: Yes Status: Active Last Updated: 01/07/2014 Helen Cobb Action Subject: Financial Performance 2014/15 Hazard: Deterioration in financial performance against plan Type: Corporate Management level: Corporate Source: Proactive risk assessment Source Description: Proactive risk assessment Trust/Site: The Hillingdon Hospitals NHS Foundation Trust Risk Registers: Finance Action Ref: 919 Action lead: Paul Wratten Due date: 31/03/2015 Action: Mitigation plan to cover any in-year under-delivery to be worked up. Last updated: 21/07/2014 Risk lead: Paul Wratten Handler: Hannah Hutchinson Executive lead: Paul Wratten Failure to achieve the required level of efficiency savings results in the Trust's financial risk rating dropping to 2. This would result in the Regulator raising serious concerns about the Trust's governance and its ability to remain compliant with its terms of authorisation. A more rigorous approach to CIP programme management performance and governance. Revised monthly and quarterly performance management framework. Forward plan based on prudent financial assumptions and flat activity. This includes a realistic CIP target. Monthly QIPP Board Monthly Board reporting. Transformation Committee further challenge areas of weak performance. Progress Mitigation plan to cover any in-year under delivery has not yet been worked up. Monthly Board report on savings includes progress of the mitigation plans being put in place. Last updated: High C=4 L=3 The Hillingdon Hospitals NHS Foundation Trust Page 8 of 15
207 Appendix RR1 Risks Re-graded Risk Rating Audit Total Records: 4 Risk Ref Consequence (Old) Likelihood (Old) Risk Level (Old) Consequence (Now) Likelihood (Now) Risk Level (Now) Management Level Date Updated 41 Moderate Possible Medium Critical Possible High Corporate 09/07/2014 Sue Manthorpe 343 Significant Possible High Moderate Possible Medium Corporate 03/07/2014 Sue Manthorpe 190 Significant Possible High Moderate Possible Medium Corporate 02/07/2014 Sue Manthorpe 175 Significant Probable High Significant Unlikely Medium Corporate 03/06/2014 John King Risk 41 page 1 above Risk 343, Risk 190 and Risk 175 below The Hillingdon Hospitals NHS Foundation Trust Page 9 of 15
208 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 343 Risk assessor: Tally Kandola Date assessed: 31/10/2013 Review Date: 30/04/2015 Verified: Yes Status: Active Last Updated: 03/07/2014 Sue Manthorpe Action Subject: Statutory and Mandatory Training Hazard: Patients or staff suffer avoidable injury because of lack of staff knowledge and competency in key areas of patient and staff safety due to poor uptake of Statutory and Mandatory training (e.g. fire, health and safety, infection control, safeguarding children, Local induction) Type: Corporate Management level: Corporate Source: Statutory requirements Source Description: Trust Internal monitoring system indicates failure to meet Trust set compliance target of 80% (and 95% for Information Governance Training) for STaM training External regulator visits highlighting concerns NHSLA/CNST assessments indicating gaps in assurance Trust/Site: Hillingdon Hospital Directorate: Cancer & Clinical Support Services, Clinical Governance, Corporate Development, Finance, Procurement, IT & Telecomms, Medicine, Rehab & Emergency Care, Mount Vernon, Operations, Patient Services & Nursing, People & Development, Surgery, Women & Children Risk Registers: NHSLA BAF: 1.1,1.3 Action Ref: 326 Action lead: Claire Gore Due date: 28/05/2015 Risk lead: Claire Gore Handler: Sue Manthorpe Executive lead: Claire Gore 1) Potential for serious injury or harm to patients due to staff's inappropriate use of equipment resulting from lack of knowledge, skills and competency. 2) Potential for serious injury or harm to patients because staff do not take appropriate action when required to do so; for example, how to raise the fire alarm 3) Staff injury due to their lack of skills, knowledge and/or processes 4) Not meeting recommendations of key drivers - legislation - policy - standards - best practice guidance. 5) Staff who are not compliant could be asked to step down from practicing - CQC/HSE/LFB 6) Reputation compromised as Trust has low levels of compliance and cannot meet best practice standards 7) May affect revalidation and other professional registration requirements. Action: To meet regulatory AND best practice requirements e.g. CQC/HSE/LFB/NHSLA/CNST: Managers are being informed that they must monitor staff attendance and utilise the L&D reports and follow up staff DNA's to training in line with Trust policy 1. Training Needs Assessment Matrix 2. Adequate, robust training programmes 3. Choice of learning methodologies, including e learning 4. Directorate/divisional KPIs and Dashboards 5. KSF PDR process (Core Dimensions/PDP) the new performance appraisal will require staff to be compliant with STaM training before pay progression 6. L&D monitoring processes producing attendance level and compliance reports via WIRED for managers to utilise 7. Statutory & Mandatory Performance Reporting via intranet and regular compliance reporting through Divisional Boards Progress 1. Statutory and Mandatory Training Policy processes are not being followed 2. Managers not releasing staff to attend training 3. Managers/Staff not booking training sessions 4. Managers not monitoring staff attendance, not utilising L&D reports and not following up staff DNA's to training in line with Trust policy 5. Lack of performance management of staff at all levels where low compliance is clearly indicated within divisions/directorates. 6. Unable to meet regulatory AND best practice requirements e.g. CQC/HSE/LFB/NHSLA/CNST Medium C=3 L=3 Following a meeting with the ADO's and the People and Development Director a plan to improve training attendance has been agreed. An 'amnesty' period until March 31st will allow staff to attend additional training sessions, to improve compliance. Further sanctions will then need to be agreed and implemented e.g. requests for external training will be refused. Where non-compliance and DNA is persistent, the mangers are being reminded by People and Development Business Managers, of their responsibility to performance manage staff at all levels where low compliance is clearly The Hillingdon Hospitals NHS Foundation Trust Page 10 of 15
209 indicated within divisions/directorates. The Trust policy indicates that sanctions against staff e.g. not able to attend external conferences will be imposed Last updated: 03/07/2014 Sue Manthorpe A meeting with ADO's, Director of People and Development and NHSLA/CNST Lead to discuss the issues of releasing staff for training and following up those who do not attend is scheduled for 7th January Data on STaM training and compliance levels is now sent to all divisional governance boards for action; Managers can also check staff compliance via the intra net records. People and Development Business managers will be reminding and supporting managers in applying the STaM policy processes for DNA training Action Action Ref: 325 Action lead: Claire Gore Due date: 29/05/2015 Action: 03/07/14 Data on STaM training and compliance levels is now available via WIRED for all divisional governance boards for action Managers are being reminded that they must follow the Trust Statutory and Mandatory Training Policy processes and must release staff to attend training, following up those who do not attend Managers are to being reminded to monitoring staff attendance, not utilising L&D reports and not following up staff DNA's to training in line with Trust policy Last updated: 03/07/2014 Sue Manthorpe Last updated: 09/04/2014 Sue Manthorpe Progress Following a meeting with the ADO's and the People and Development Director a plan to improve training attendance has been agreed. An 'amnesty' period until March 31st will allow staff to attend additional training sessions, to improve compliance. Further sanctions will then need to be agreed and implemented e.g. requests for external training will be refused. A meeting with ADO's, Director of People and Development and NHSLA/CNST Lead to discuss the issues of releasing staff for training and following up those who do not attend is scheduled for 7th January Learning and Development training booking system has been simplified to assist with booking processes and contains ability for staff to 'self-book' on to training. All staff can view their training status records via the Trust intra net Data on STaM training and compliance levels is now sent to all divisional governance boards for action Last updated: 09/04/2014 Sue Manthorpe The Hillingdon Hospitals NHS Foundation Trust Page 11 of 15
210 Risk Basics Subject/Hazard Areas Affected Risk Ref: 190 Risk assessor: John King Date assessed: 20/08/2012 Review Date: 30/12/2014 Verified: Yes Status: Active Last Updated: 02/07/2014 Sue Manthorpe Subject: Electrical - Single point of failure Hazard: Loss of electrical failure of 1000kVA transformer that serves main intake switchboard situated in Plant room A. Failure of main switchboard situated in Plant room A. This switchboard provides electrical services for the majority of the Tower Block and Podium Building Type: Health & Safety Management level: Corporate Source: Incident(s), Proactive risk assessment Source Description: incident Trust/Site: Hillingdon Hospital Specialty: Estates Risk Registers: Estates BAF: 3.4 Risk Controls Gaps Rating Risk lead: Sue Batty Handler: Sue Manthorpe Executive lead: Paul Wratten In the event of a failure of the 1000kVa transformer the electrical supply for the majority of the Tower Block and Podium would be supported by a generator situated in the Entrance road to Maternity. This generator provides 100% support with no emphasis on separate essential or not essential services. This is unconventional and the current single step load would appear to be just inside the capability of the generator. Inadvertent tripping of the switchboard can be caused by an excessive rise in temperature and humidity. The switchboard is located in a switch room within Plant room A, which also contains pipework from the steam system. Due to the age and poor integrity of the steam system, this leaves the switchboard vulnerable to steam leaks in adjacent Boiler Plant Room. Excessive rises in temperature and humidity can cause the bus-coupler to trip. As a result power would be lost to sections of the Main Tower Block and Podium. Stand-by generator maintenance improved Annual maintenance of electrical systems carried out. Electrical survey of site now complete Steam leaks repaired but due to age and condition of system offers limited resilience. Some protection installed to prevent adverse effects of steam leaks to switchboard weekly plant room checks implemented Switchboard resilience improved through repair and maintenance. Age and condition of electrical and mechanical infrastructure. Transformer replacements required UPS systems is obsolete and needs replacing Medium C=3 L=3 The main intake switchboard is configured as three separate sections A - B - C. Each section is interconnected via a bus bar coupler breaker/and or switch - fuse. The generator will only start and take load on a loss of incoming supply from the transformer. Therefore, any loss of supply on any individual section e.g. B and C will not be supported by the generator. This is a significant single point of failure. Action Action Ref: 433 Action lead: Edmund Fosbrook Due date: 30/12/2014 Action: Serious consideration should be given to the preparation of a feasibility study for upgrading the existing switch room and its associated generator support, to eliminate the single point of failure. In addition, the feasibility study should complete the original design of the integration of the Tower Block and Blue Building electrical infrastructure Last updated: 02/07/2014 Sue Manthorpe The Hillingdon Hospitals NHS Foundation Trust Page 12 of 15 Progress Switchboard Transformer replacement has commenced. CS advised of various work streams on Capital Programme 14/15 for completion of critical areas of UPS system in NNU, ITU, CCU and main theatres. 02/01/14 the work has now been tendered. 12/09/13 feasibility study completed and business case is currently being written for the redesign and reconfiguration of the electrical distribution boards. 26/03/13 identified areas have been scheduled in to the Estates Capital Plan for 13/14 Detailed technical study now complete. The options have been reviewed and are now being integrated in to the Capital Programme. Last updated: 02/07/2014 Sue Manthorpe
211 Action Action Ref: 434 Action lead: Edmund Fosbrook Due date: 27/03/2015 Action: An outline plan for electrical priorities across the Hillingdon site up to the year 2020 is being prepared. The cost and timing of upgrade of this switchboard will be part of this plan. The feasibility study will be planned for a suitable date within this long term plan. Last updated: 09/04/2014 Sue Manthorpe Progress Options appraisal has been presented to the Board CS advised of various work streams on Capital Programme 14/15 for completion of critical areas of UPS system in NNU, ITU, CCU and main theatres. 19/09/ Capital project running, funding has been set aside for the next financial year. There is a capital scheme for Plant Room A switch panel replacement by the 31st March /03/13 A further review has been done to align work with the A&E build. A five year plan has been produced by ETA Projects Ltd. The options have been reviewed and are now being integrated in to the Capital Programme Last updated: 02/07/2014 Sue Manthorpe The Hillingdon Hospitals NHS Foundation Trust Page 13 of 15
212 Risk Basics Subject/Hazard Areas Affected Risk Controls Gaps Rating Risk Ref: 175 Risk assessor: John King Date assessed: 18/05/2011 Review Date: 30/09/2014 Verified: Yes Status: Active Last Updated: 03/06/2014 John King Subject: Medical Record Library Building Working Environment at Hillingdon Hospital Hazard: Poor Lighting Insufficient Ventilation and Heating Water Penetration. Overcrowding of records on shelves and boxes Manual handling injuries Fire Insufficient amount of electrical sockets Sewage Smell. Type: Health & Safety Management level: Corporate Source: Regulatory requirements, Statutory requirements Source Description: Management of Health and Safety Regulations 1999 Workplace (Health, Safety and Welfare) Regulations 1992 Trust/Site: Hillingdon Hospital Directorate: Cancer & Clinical Support Services Ward/Department: Clinical Records (HH) Risk Registers: Medical Records, Estates BAF: 3.4 Risk lead: Kay Sandhu Handler: Sue Manthorpe Executive lead: Karl MunslowOng Poor lighting and persistent water damage to Permanent and Emergency lighting has left the department with insufficient lighting. Temporary lighting is in place but this has increased the risk of tripping hazards, eye strain and inability to retrieve records. The temporary lighting does not have emergency lighting capabilities. Insufficient Ventilation and Heating There is insufficient ventilation. The ventilation ducting is also dangerously low in parts of the podium and leaks water. This is putting the integrity of the records stored in this part of the library and the health and well-being of staff at risk. Water Penetration. The presence of stagnant water in buckets, guttering, various containers on shelves and drains poses a health and safety risk to staff working in the area and a risk to patient notes from water damage. There is an increased risk to staff, slips, trips and falls. The internal temporary guttering needs regular maintenance to prevent the build-up of stagnant water and lime scale deposits. Overcrowding. Records are stored on the floor resulting risk of trips and falls. Results in poor filing and increases risks of failure to provide notes for clinic. Manual Handling Risk of staff injury from incorrect manual handling Fire from combustible records stored in close proximity to electrical fittings Narrowed and partially obstructed fire escape routes Insufficient emergency lighting Poor working environment associated with all of the above Insufficient amount of electrical sockets Increased risk of fire due to paper records being in close proximity to overloaded electrical sockets and extension leads. Transitional programme in place to move records out of the podium area Programme of records management in place to eliminate storage of records on the floor. Robust tracking system for all records in place Reporting all incidents of leaks to Estates Staff trained in manual handling techniques and processes. Staff dress appropriately for environmental temperature levels Not all records have moved out of this location 1) Poor lighting and lack of emergency lighting. 2) Poor ventilation and heating systems 3) Full Structural survey needs to be undertaken to inform action plan on the management of the water penetration issues. 4) Poor storage and fire compartmentalisation increases risks due to fire 5) There is limited compliance with health and safety and fire safety regulations. Medium C=4 L=2 Sewage Smell. Recurrent smell of sewage throughout the department, posing a risk to the health and well-being of the staff in the department and disruption to the service as parts of the podium are uncomfortable to work in whilst the smell is present. The Hillingdon Hospitals NHS Foundation Trust Page 14 of 15
213 Action Action Ref: 886 Action lead: Kay Sandhu Due date: 04/08/2014 Action: To move all medical records to a more suitable environment Last updated: 02/07/2014 Sue Manthorpe Progress 03/06/14 - Majority of records have now been moved to Square One, however thee are still some still occupying the podium area. Once the area has been vacated it will be inspected by H&S and Estates before final closure. 07/04/14 On the 24th Match 2014 the process of moving active medical records to one central library located offsite at Building 4 square one, Southall Lane commenced. Weeded records will be held at MVH library. Records for patients returning to the Trust within 6 months of their last episode of care will be kept on site at the relevant hospital. It is anticipated that this work will be completed in 6 weeks time. Last updated: 02/07/2014 Sue Manthorpe The Hillingdon Hospitals NHS Foundation Trust Page 15 of 15
214 ITEM 21 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Helen Cobb, Assistant Director Governance & Quality Standards Theresa Murphy, Director of Patient Experience & Nursing DATE: 30 th July 2014 SUBJECT: The Board Assurance Framework Version 0.2 Trust Strategic Priority: The Board Assurance Framework (BAF) impacts across all strategic priorities. Summary: The BAF provides a structure and process that enables the organisation to focus on those risks that might compromise achieving its strategic objectives and the strength of internal control to prevent these risks occurring. The BAF maps out both the key controls in place to manage the principal risks, and also how sufficient assurance has been gained about the effectiveness of these controls. The BAF was last reviewed by the Board in January Since then the BAF has been reviewed at the meetings of the Quality & Risk Committee and Audit and Assurance Committee (AAC) in April and July The Board undertook the annual review of the BAF in May 2014 where three new risks were added these and any other new changes are highlighted in yellow. BAF version 0.2 The recent performance reports have been reviewed for trends and there have been three new red issues identified: Statutory and mandatory training Staff appraisals London Ambulance Service 30 minute waits BAF entries under risk 3.3 have been strengthened regarding Informatics following the AAC s deep dive at its April 2014 meeting. The revised strategic priorities and objectives for 2014/15 have been taken from the Board approved Strategy on a Page; the risks relating to these have been updated 1
215 following the annual review of the BAF risks at the May 2014 Board Strategy Session and the changes are reflected in version 0.2. The additional risks are: Failure to provide adequate patient safety standards leads to patient harm. Failure to ensure engagement with the Governors, members and the wider public leads to the Trust losing the confidence of the wider community and diminishes the Trust s reputation. Failure of the Trust to fully participate with Integrated Care across the whole patient pathway, potentially leads to unnecessary admissions and prolonged hospital stays affecting both patient experience and Trust performance. The AAC reviewed version 0.2 at their July meeting and undertook a closer look at the risks held by the Director of Patient Experience & Nursing. Some further work was identified to strengthen the assurances and controls against these risks. This work will be reflected in the next version of the BAF. Board Action Required The Board is asked to comment on and approve version 0.2 of the BAF. Equality Impact Assessment: N/A there is no positive or negative impact from this report. 2
216 Board Assurance Framework 2014/15 (Version 0.2) Our vision for The Hillingdon Hospitals NHS Foundation Trust is: To put compassionate care, safety and quality at the heart of everything we do Mission Statement: To meet the needs of our patients with high quality services and the best care on every occasion, in every setting, in every place and; To serve our community as a healthcare provider, working with our partners, through a culture from Board to ward which enshrines our values of Communication, Attitude, Responsibility, Equity and Safety (CARES).
217 STRATEGIC PRIORITIES, OBJECTIVES AND OVERARCHING TRUST RISKS FOR 2014/15 STRATEGIC PRIORITIES 1. To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide. 2. A clinically led service strategy that responds to the needs of patients and other health and social care partners 3. To deliver high quality care in the most efficient way 4. To develop sufficient sustainable scale to enable us to improve and grow healthcare services for our communities OBJECTIVES 1. Fully comply with licence to operate/ regulators 2. Improve the quality of care and clinical effectiveness 3. Improve patient and carer experience 4. Improve patient safety 1. Work with CCG collaboratively to improve services within available resources 2. Improve Patient & Public involvement 3. Engage clinicians to develop innovation and expansion of services 5. Deliver healthcare more efficiently 6. Improve and invest in IT to support service improvement 7. Modernise & reconfigure the Estate & Facilities to meet the needs of our clinical services 8. Maximise staff contribution to transforming the way we deliver our services 6. Develop a service plan in response to Shaping a Healthier Future 7. Develop strategic alliances with appropriate partners OVERARCHING TRUST RISKS A culture of high quality and an effective system of performance monitoring is not deeply embedded across the whole organisation causing failure in performance. Liquidity pressures inhibit our ability to maintain and improve quality and financial sustainability Failure to identify people at risk of harm or abuse and failure to implement safety measures to protect them leads to/results in lack of appropriate action. Failure to provide adequate patient safety standards leads to patient harm. Failure to engage with our clinicians to develop the optimal strategy for each service. Failure to engage with CCG to develop new pathways results in lost opportunities to the trust and suboptimal pathways for our patients. Failure to ensure engagement with the Governors, members and the wider public leads to the Trust losing the confidence of the wider community and diminishes the Trust s reputation. Given the state of the local health economy financial position and the Trust's investment needs starting from a low cash reserves base there is a risk of a lack of cash whether from an unplanned cash outflow or insufficient inflow that would cause failure of the Financial Plan Under delivery of QIPP leads to failure of the financial plan. Changing IT systems against limited investments funds may result in failing or inefficient IT. Fragile estate infrastructure and scale of long and short term investment required exceeds the Trust s financial capacity and leads to a failure of the financial plan. Risk of insufficient skilled managerial capacity and capability during periods of substantial change leads to poor financial and operational performance. Staff morale and motivation drops due to increasing demands and competing priorities during significant change, leading to reduced productivity, increased levels of sickness and turnover and reduced satisfaction and engagement. Risk that the Trusts size is insufficient to give financial sustainability in the medium term. Growth in key services e.g. A&E and maternity is not consistent with what has been planned in SaHF creating unmanageable and costly capacity issues. Failure to identify and implement other growth opportunities from suitable strategic alliances could restrict Trust development. Through unsustainable demand, uncontrolled delays to the delivery timelines and an inability to deliver the required clinical workforce Shaping a healthier future delivers precipitate, poorly planned change, which adversely impacts quality and safety Through an inability to meet the clinical standards, deliver the requisite workforce, deliver behavioural change, sustain expected patient experience and an unsustainable demand on the system Shaping a healthier future does not deliver the planned benefits to improve quality and safety of health and care across NW London Failure of the Trust to fully participate with Integrated Care across the whole patient pathway, potentially leads to unnecessary admissions and prolonged hospital stays affecting both patient experience and Trust performance.
218 References Inherent Risk/Threat Control Internal monitoring Ref no and What could prevent this What controls/systems are What monitoring links to objective being in place to assist in arrangements residual risk achieved? securing the delivery of the are in place? register and objective? compliance areas How effectively these a = risk controls are working? accepted Control Rating Assurance Evidence that shows management of risks and objectives being delivered Assurance rating Gaps in Control or Assurance Control Do the assurances identify that any of the controls are not working or are not fully implemented? Are further controls required? Assurance are there controls where no assurance is available? Action to meet gaps Action plans (or reference to action plans) to meet gaps in control or assurance By when Responsible Executive Director Operational Lead Principle Working Group CQC Regulations / NHSLA Risk Management Standards Strategic Priority 1 To create a patient centred organisation to deliver improvement in patient experience and the quality of care we provide 1.1 Risk Ref: 11, 19a, 30, 56, 93, 116, 141a, 143, 144, 152, 172, 184, 188, 189, 197, , 209, 240, 323, 324, , 342, 343, CQC Outcome 1, 4, 5, 6, 8, 9, 10, 11, 12, 13, 14, 16, 17, 21 NHSLA 1, 2, 3, 4, 5 A culture of high quality and an effective system of performance monitoring is not deeply embedded across the whole organisation causing failure in performance. Performance and quality targets monitored by Trust Board Divisional Executive Board monitoring Regular performance meetings with Department and Directorates National Audit results benchmarked against national best practice Experience and Engagement strategy sets out the Trust direction for improving experience Clinical Audit Programme identifies and prioritises external and internal must do audits Participation in Healthcare Quality Improvement Partnership National Programme Recently introduced Mortality Review Audit Process Mortality data reviewed by weekday vs weekend within Quality Dashboard Trust Board Quality and Operational Performance Reports Experience and Engagement Group Quality and Risk Committee & Clinical Governance Divisional Governance Boards Monthly Performance Reports provide adequate assurance May 2014 Care Quality Commission Review of compliance at Mount Vernon Jan substantial assurance Care Quality Commission Review of compliance at Hillingdon Hospital Oct 2013 adequate assurance FFT Comments reviewed monthly, with vast majority being complimentary NHSLA Level 2 assessed March 2014 provides substantial assurance CNST Maternity Level 2 compliance assessed March 2014 provides substantial assurance Deloitte Review of Quality Report May 2013 Monthly Quality Reports to Trust Board June 2014 Gap in Control Performance Indicator 33: LAS Handover 30 min waits (actual / % May 87.8% - Target 100% Gap in Control Performance indicator 40: Trust sickness rate May 3.2% Target 3% Gap in Control Performance Indicator 41: Trust vacancy rate May 9.99% Target 8% Gap in Control Performance Indicator 43: STAM % May 68.09% - Target 80% Gap in Control Performance Indicator 45: Medical Staff Appraisals May 68.7% - Target 100% Gap in Control Trust Mortality Rate above London average (but below national average) Improvement expected after completion of link corridor to new AMU building works. Sickness Absence Policy No 231, Health and Wellbeing Strategy and action plan in place Monthly rolling recruitment programme including open days. Figures based on new WIRED system Deadline extended Clinical Divisions to monitor mortality rates by speciality and take action where appropriate Monthly Monthly Chief Operating Officer Director of Operational Performance Medical Director
219 References Inherent Risk/Threat Control Internal monitoring 1.1 Risk Ref: 11, 19a, 30, 56, 93, 116, 141a, 143, 144, 152, 172, 184, 188, 189, 197, , 209, 240, 323, 324, , 342, 343, 350, 342 CQC Outcome 1, 4, 5, 6, 8, 9, 10, 11, 12, 13, 14, 16, 17, 21 NHSLA 1, 2, 3, 4, 5 A culture of high quality and an effective system of performance monitoring is not deeply embedded across the whole organisation causing failure in performance. (cont) Quality Performance monitoring from Dr Foster Trusts Incident Reporting Policy and process Monthly SI Update report and open action plans reviewed by Trust Board. SI s reported quarterly to monitor AVIA (Agency Visits, Inspections and Accreditations) database controls follow up of actions Implementation and monitoring of Patient related outcome measures (PROMS) Implementation and monitoring of NPSA Alerts Monitoring of CAS (Central Alert System) Quality Dashboard Divisional Governance Monitoring Assurance Monitor Governance rating for 2013/14 Green Q3 Monitor performance measures met for eight consecutive quarters. Reporting of Patient Safety Incidents through NRLS (6 monthly) shows above average with high reporting of low/no harm. Reported to Trust Board May 2014 CQC Intelligent Monitoring Report March 2014 Rated Band 6 lowest risk rating Reported quarterly Quality Governance Assessment to Trust Board December 2013 Inpatient, Outpatient and Maternity Local overall satisfaction survey targets for 2012/13 achieved April 2013 Gaps in Control or Action to meet gaps By Assurance when No gaps identified N/A N/A Gap in Control CQC Intelligent Monitoring Report March 2014 shows 1 area of risk identified. PROMs EQ-5D score: Knee Replacement Gap in Assurance Gaps identified - NPSA Alerts requiring audit Gap in Assurance Incomplete/inadequate keeping non-compliance with Trust Record Keeping Policy Quality and Risk Committee to over-see CQC Intelligent Monitoring Report and CQC Inspection report with associated action plans Recent Inpatient Survey shows Improvement in response to Q34 and Q68 Clinical Audits to be identified against relevant NPSA Alerts to be included on Trust Audit Plan. Action plan to address gaps to be monitored by via clinical audit processes Results of Observations of Care visits fed back to Wards/departments and actions to improve quality of record keeping included within corporate risk register Risk Ref: 188. Reviewed quarterly at Quality and Risk Committee. See also Monitored Quarterly Bimonthly Monitored quarterly Responsible Medical Director Observations of Care visits Nursing Dashboard Trust wide audit underway involving Critical Outreach Leads to provide assurance and identify areas for improvement around the escalation of a deteriorating patient in line with NEWs, PEWs and MEWs procedures. Sept 2014
220 References Inherent Risk/Threat Control Internal monitoring Assurance Gaps in Control or Assurance Action to meet gaps By when Responsible 1.2 Risk Ref: 381 & 382 Liquidity pressures inhibit our ability to maintain and improve quality and financial sustainability Clinical Dashboards monitored in all directorates and linked to CQUINs Patient Safety and Quality Report Quality report to Trust Board and Quality and Risk Committee NHSLA Report March 2014 provides substantial assurance at level 2 Gap in control Risk of deterioration of quality during busy winter months eg: Increase in Falls reporting Inadequate sharing of best practice Quality and availability of equipment Risks and actions to be monitored via risk register at Clinical Governance Committee, Quality and Risk Committee. Monitored quarterly Medical Director Dr Foster Hospital Quality Indicators Quality Impact Assessments of all service changes / cost improvements Clinical Assurance Panel (Chaired by Medical Director) Dr Foster Hospital Quality Indicators provide assurance that the Trust is not an outlier March 2014 Gap in Control Dr Foster Intelligence highlights Trust as an outlier for Neoplasms July 2013 Gap closed CCSS continues to monitor via balanced scorecard monthly Neoplasm Mortality remains within normal limits. Audit of all patient deaths in July 2013 by ACD for Cancer No avoidable deaths identified. May 2014 Completed Emergency Care Standards 3-5 year implementation programme Transformation Committee Emergency Care Standards 3-5 year programme has been produced and actions have been prioritised based on risk level. Sept 2013 Analysis and monitoring of Incidents Complaints and Claims actions Divisional Governance Boards Annual Complaints Report - May 2013 details 29% increase in complaints from 2011/12 Gap in Control Recurrent themes from complaints: Communication, Staff attitude and clinical care To be addressed by Divisions/Core Service Leads within CQC KLOE Assurance Templates July 2014 Executive Director of Patient Experience and Nursing Acuity and Dependency Tool Safer staffing assurance process recently introduced with monthly reporting to Trust Board Trust Board CQC Intelligent Monitoring Report March 2014 Rated Band 6 lowest risk rating Gap in Control Gap identified during CQC inspection Oct Not currently meeting best practice guidelines in all areas Planned and actual staffing levels reported to Trust Board. To be featured on NHS Choices and Trust Website June 2014 Completed Safer staffing meetings monthly/weekly Safer Staffing QIPP workstream monitored at Transformation Committee Divisional Governance Boards Evidence based tool used to review the Trusts establishment and skill mix October 2013 Staffing and skill mix review report presented to Trust Board. June 2014 Completed
221 References Inherent Risk/Threat Control Internal monitoring Assurance Gaps in Control or Assurance Action to meet gaps By when Responsible 1.3 Risk Ref: 11, 93, 116, 143, 172, 184, 186, 197, 209, 323, 324, 332, 335, & 350 CQC Outcome 4, 5, 6, 8, 9, 14, 16, 17, 21 NHSLA 1, 2, 3, 4, 5 Failure to identify people at risk of harm or abuse and failure to implement safety measures to protect them leads to/results in lack of appropriate action. Specialist risk assessment tools within nursing documentation identify patients at risk of harm. Topics include: Falls, Waterlow (pressure ulcers), Nutritional screening tool, VIP score, VTE etc Implementation of NEWS, PEWS and MEWS Trust policies and procedures including procedure for shift handover, which describes flagging of patients at risk, Slips, Trips and Falls Prevention and Management Policy and Prevention and management of Pressure Ulcers Prevention Policy Falls Group established And Root Cause analysis process in place for falls and pressure ulcers Monthly Clinical Effectiveness Checker Monthly Quality Performance review meetings with Director of Patient Experience and Nursing and wards Safeguarding Children and Young People (0-18 years) and Pan London Multi Agency Safeguarding Adults Policies Safeguarding assurance frameworks detail within risk register ref: 186 Safeguarding training available at different levels for differing post requirements Local Safeguarding Children Board (LSCB) and Safeguarding Adults Partnership Board (SAPB) provide clear processes across Health and Social Care Economy Quarterly Report to Quality and Risk Committee / Annual report to Trust Board Safeguarding Committee Monitoring quarterly Report from Care Quality Commission - Compliance visit on the 13 th January 2011 provides substantial assurance. Care Quality Commission Review of compliance at Hillingdon Hospital Oct 2013 adequate assurance. Outcome 4 Compliant. Measures of Care results for Sept 2013: Medicines Management, Record Keeping, Falls, Pressure Ulcers adequate assurance Safety Thermometer Nov 2013 Shows improvement in Harm Free Care. Year end 94.5% Result for 2012/ % NHSLA Report March 2014 provides substantial assurance at level 2 Observations of Care Oct 2013 Section 11 Audit - Compliance with section 11 of the Childrens Act Validated by LSCB in December NHS London - London-wide Overview Report Safeguarding Adults Self-Assessment and Assurance Framework (SAAF) March 2012 & 2013 provides substantial assurance. The Hillingdon Hospital referenced numerous times as examples of good practice. SAAF Validation event with partners September 2012 ratified by NHS London and SAPB Gap in Assurance Record keeping audit results poor Gap in Assurance Increase in incidents of Falls identified within Quality dashboard. Gap in Assurance Risks identified by the Trust with regard to Safe Staffing levels in Maternity and A&E Paediatrics / Moderate Concern raised by Care Quality Commission during inspection in October 2013 Gap in Assurance Current training levels are not at the Trust Board compliance level target of 80% Safeguarding Adults Training: 75.47% (Previously 71.80%) Safeguarding Children Level 1 Training: 72.71% (Previously 69.63%) Safeguarding Children Level 2 Training: 66.52% (Previously 57.53%) Safeguarding Children Level 3 Training: 51.77% (Previously 48.86%) Actions to address gaps have been detailed within Clinical Audit improvement process and incorporated into risk 188 on the corporate risk register. Preparation for CQC Inspection, supporting drive for improvement in documentation and record keeping. Falls Safe Care Bundle to be implemented. Refresh of Falls Group and future actions to be incorporated into Trust wide improvement plan. Actions detailed under 3.5 Safe Staffing for Maternity reviewed at Maternity Board. Business case to increase staffing levels being considered. Subject matter experts providing bespoke sessions in addition to the Trust wide training programme to improve compliance. STAM training compliance to be monitored through PDR process. Quarterly Review Sept 2014 See 3.5 March 2015 Executive Director of Patient Experience and Nursing Deputy Director of Nursing
222 References Inherent Risk/Threat Control Internal monitoring 1.3 Failure to identify people PAS Alert for children with LSCB and SAPB at risk of harm or abuse Child Protection Plans, monitoring Risk Ref: and failure to implement Learning Disability patients safety measures to and adults with adult protect them leads protection plans to/resu lts in lack of appropriate action (cont) 11, 93, 116, 143, 172, 184, 186, 197, 209, 323, 324, 332, 335, Borough-wide process for ensuring Deprivation of Liberty Safeguards and the requirements of the Mental Capacity Act are followed. Information available on intranet. Learning Disability performance indicator included in Trust Board report / Assurance LDSAAF- Lead by commissioners in place. Health section has been ratified by NHS London October LDSAAF- Lead by commissioners in place. Health section has been ratified by NHS London October Gaps in Control or Assurance Action to meet gaps By when Responsible No additional gaps identified N/A N/A Executive Director of Patient Experience and Nursing Deputy Director of Nursing 1.4 Risk Ref: 11, 19a, 30, 56, 93, 116, 141a, 143, 144, 152, 172, 184, 188, 189, 197, , 209, 240, 323, 324, 332 & 335, 342, 343, CQC Outcome 1, 4, 5, 6, 8, 9, 10, 11, 12, 13, 14, 16, 17, 21 NHSLA 1, 2, 3, 4, 5 Failure to provide adequate patient safety standards leads to patient harm CQC Steering Group Self Assessment / including Observations of Care & Peer Review Mock Assessments Core Services KLOE Templates Action plan from CQC Inspection Emergency Care Standards 3-5 year implementation programme Monitoring of CAS (Central Alert System) Implementation and monitoring of NPSA Alerts Review of risk register at CGC, QRC and Trust Board Incident management processes/learning from investigations Divisional and corporate scrutiny Clinical Audit Programme identified and prioritises audits of clinical guidelines Clinical Audit programme takes into account local and national priorities. AVIA (Agency Visits, Inspections and Accreditations) database controls follow up of actions Regular review of compliance against NICE guidelines Review of compliance with NCEPOD/MBRRACE-UK CQC Steering Group Quality and Risk Committee Clinical Audit & Effectiveness Committee Care Quality Commission Review of compliance at Mount Vernon Jan 2012 substantial assurance Care Quality Commission Review of compliance at Hillingdon Hospital Oct 2013 adequate assurance CQC Intelligent Monitoring Report June 2014 Rated Band 6 Lowest Band of risk Quality Governance Reviews conducted by KPMG in line with selfassessment Feb 2014 provides substantial assurance NRLS incident reporting good level of reporting above average for sector. (8.3 vs median of 7) April 2014 NHSLA Level 2 Assessed March 2014 substantial assurance CNST Level 2 compliance assessed March 2014 substantial assurance Gaps in Assurance Gaps in compliance identified during assessment by CQC and NHSLA Gap in Assurance The organisation does not participate in all relevant National Audits 91% participation in NCAPOP Audits Overall participation for quality reporting current figure is 86% 100% participation of National Confidential Enquiries Action plans in place to be driven forward by CQC Steering Group. Gaps identified to be risk assessed including escalation to risk register as required. Monitored Fortnightly August 2014 Director of Patient Experience and Nursing Assistant Director of Nursing
223 Strategic Priority 2 A clinically led service strategy that responds to the needs of patients and other health and social care partners 2.1 Failure to engage with CCG to develop new Trust participates in the Borough Winter Planning CQG Meeting to discuss quality Single winter plan developed jointly with CCG Gap in Control pathways results in lost group. impacts June 2013 Understanding of the On-going control clinical opportunities to the trust developing market system is working groups, which Joint bids to Integrated Contract Joint response to NHS and suboptimal incomplete. involved Trust Clinicians pathways for our care board and meetings to England Action plan on and GP s from the CCG. patients. development of integrated monitor business A&E June 2013 strategies. 2.2 Failure to engage with our clinicians to develop the optimal strategy for each service. Executive and clinical representation at CCG board. Medical Director and other senior staff attend CQG Director of Integrated Care leads on all external relationship development, including Social Services and CCG clinical pathways. All major cross divisional /organisational QIPP schemes have an appointed clinical lead. Improving Inpatient Care Programme is led by the CD for Medicine and supported by several consultant colleagues Monitoring of tender applications and results Chief Executive has written to consultants inviting time to set up clinical business units to be clinically led. Multiple clinical working groups to jointly develop services Monitored through Transformation Committee Board to Board meetings Jan 2014 Monitoring of delayed discharge and other joint projects - monthly Uptake of rapid response Access to community beds Dec 2013 Nominated clinical leads for all transformation projects Improving Inpatient Care steering board (monthly) is chaired by the Clinical Director for Medicine. Each operational group is led by a clinical lead for the relevant service. Business case to the CCG on expansion of Ambulatory Emergency Care was written and presented by an acute physician. Gap in Assurance Further work is required to expand the number of clinical staff developing and leading projects Progress monitored by Transformation Committee Revised Structure for improved clinical leadership launched and under ongoing development and will be reviewed at newly established monthly meeting. Ongoing Bimonthly Complete Chief Operating Officer Director of Operational Performance Chief Operating Officer/ 2.3 Risk Ref: Failure to ensure engagement with the Governors, members and the wider public leads to the Trust losing the confidence of the wider community and diminishes the Trust s reputation. Membership Development and Engagement Group set up to identify ways of effective engagement with public members People in Partnership to Attend PIP Meetings led by Governors Regular Governor Member Communication via Quarterly Pulse Magazine Opportunities for members to be involved in Focus Groups FT Office Quarterly report to Council of Governors Annual Report to Board Review of Patient Experience and Engagement January 2013 provides adequate assurance Gaps in Control Governor member engagement consistent across all constituencies Action plan to be developed by Membership Development and Engagement Group Oct 2014 Director of Patient Experience and Nursing Head of PPE
224 References Inherent Risk/Threat Control Internal monitoring Strategic Priority 3 To deliver high quality care in the most efficient way 3.1 Risk Ref: 381 & Risk Ref: 381 & 382 Given the state of the local health economy financial position and the Trust's investment needs starting from low cash reserves, there is a risk of a lack of cash whether from an unplanned cash outflow or insufficient inflow that would cause failure of the Financial Plan Under delivery of QIPP leads to failure of the financial plan. Board approved Annual Capital Plan Capital Planning review and allocation of funding Reduce debtor levels Tight treasury management and cash forecasting. Use of working capital facility as required. Prudent planning assumptions include commissioner demand management measures and the impact of contract clauses with financial penalties Monthly meetings with NWL Sector Commissioners to identify issues early and on a consistent basis Agreed robust mitigation plans are in place to manage the financial consequences of a reasonable reduction in revenue as a consequence of services being decommissioned. QIPP Programme Management Office QIPP Working Group Tight controls in place around QIPP monitoring and reporting. New Access Data based developed to track progress Monthly / Quarterly Divisional Performance Management Meetings Trust Board monitoring Long-Term Financial Model Monthly precontract management meetings Monthly reporting to Trust Board Transformation Committee Divisional Reviews Assurance Business Cases for major works reviewed by Transformation Committee and approved by Trust Board. In accordance with SFIs. Bi-monthly APR stage two financial stability report. Sept 2012 Annual Forward Finance Plan 2014/15 March 2014 & 5 Year Strategic Plan June 2014 Liquidity ratio reported to Trust Board monthly Working capital facility in place for 2014/15 and 2015/16 April 2014 The guaranteed minimum payment contract agreement will mitigate the financial impact of services being reduced and or decommissioned in 14/15. However, unless a new similar agreement is made in 15/16 and subsequent years prior to full SaHF Implementation, the risk will return Monthly QIPP Board Report Report to Transformation Committee June 2014 All shortfalls identified and tracked by PMO. Overseen by Transformation committee Reports to monthly divisional meetings Weekly update to Execs Gaps in Control or Assurance No Gaps Identified The APR stage 2 review identified that ideally the Trust should have 5m to 10m cash headroom. Options for this were explored from September 2012 onwards but none were found that the Trust would be allowed to implement in its current regulatory context. The Trust Board has approved a 14.9M working Capital Facility be put in place for the next 2 financial years. In the meantime the Trust s annual forward finance plan aims to build up cash headroom of 3m in 14/15 with the planned balance not falling below 1m in any one month.. Gap in Control Insufficient schemes identified to meet financial gap. Action to meet gaps By when Responsible N/A N/A Finance Director Continuous review with Division and Corporate directorates to identify additional schemes. Monthly report to the Trust Board. Quarterly review Chief Operating Officer/ Finance Director
225 References Inherent Risk/Threat Control Internal monitoring Assurance Gaps in Control or Assurance Action to meet gaps By when Responsible , 141a, 183, 279, 306, Changing IT systems against limited investments funds may result in failing or inefficient IT Informatics Steering Group. Chaired by MD with appropriate Executive representation. Business Case Approval Process Reported to the Transformation committee Informatics Steering Group IT Strategy in place with funding identified July 2013 Gap in Control IT system risks : Trusts Bleep system Risk Ref: Completed Water leak ingress into switchboard Risk assessments to be carried out and included onto corporate risk register Oct 2014 Finance Director Assistant Director IM&T Quarterly review of Medium and High corporate risks Detailed local risk register held within ICT Department Quality and Risk Committee Head of IT TIAA Risk Assessment carried out to identify future audit requirements - June 2013 Disaster recovery lack of 24-7 supplier support Lack of real time data entry resulting in failing or inefficient IT 3.4 Risk Ref: 40a. 41a, 44a, 132, 148a 149, 150a, 151, 152, 163a, 164, 166, 168, 175, 176, 183, 190, 193a, 279, 304, 306, 337 CQC Outcome 8, 11 NHSLA 3, 4 & 5 Fragile estate infrastructure and scale of long and short term investment required exceeds the Trust s financial capacity and leads to a failure of the financial plan. Condition Survey of Trust Estate carried out every 5 years to establish condition and risk Risk based prioritisation of work Board approved Annual Capital Plan Capital Planning review and allocation of funding Contingency level identified in Trust financial plan Procurement and Financial Authorisation Processes for Estates works Regular reports to Trust Board Survey informs risk based Estate Capital Investment plan Capital Programme Delivery Group Monthly Chaired by Executive Director of Corporate Development Bi-monthly Capital Programme review at Site Strategy Development Group chaired by CEO Capital Planning Meeting quarterly Chaired by Finance Director Directorate performance budget review monthly monitoring of revenue ARUP conditions survey review of the Trust estate completed FY 2013/14 Analysis carried out by CAPITA updates high and significant backlog maintenance Business Cases for major works approval in accordance with SFIs. Business planning and Executive Performance Review by Directorate Quarterly Gap in Control Long term strategic site investment plans SaHF Backlog maintenance investment to be detailed within SaHF Business Cases are planned for submission to the Board. Development of Hillingdon Site Master Plan A draft Hillingdon Site Master Plan has been developed for endorsement by the Trust Board Hillingdon Master plan consultation in progress, proposed submission date to LBH July 2014 July 2014 Sept 2014 Executive Director of Corporate Development Director of Estates and Facilities
226 References Inherent Risk/Threat Control Internal monitoring 3.5 Risk of insufficient Leadership Development Trust Board skilled managerial across the Trust Reporting Risk ref: capacity and capability 332 & 335 during periods of Business Planning Cycle 350 substantial change leads to poor financial and Set operational performance. Divisional Reviews 3.6 Staff morale and motivation drops due to increasing demands and competing priorities during significant change, leading to reduced productivity, increased levels of sickness and turnover and reduced satisfaction and engagement. Monthly workforce dashboards issued to Divisions and Trust Board Establishment data is regularly updated by finance and divisions Management / Committee Structure PDR (Personal and Performance Development Review) process Learning and Development Programme s for Managers Phased in Talent management process (including succession planning) Advance Programme Pilot for supanumery sisters/ward managers CARES Principles Establishment and development of CARES Ambassadors Customer Services Training Stress Awareness training for managers CARES link to PDR and Talent management CARES built into Recruitment and Selection Process Staff Suggestions Scheme Capability Policy Whistle Blowing Policy Trust Board Monitoring Assurance Staff Survey Results for 2012 Jan 2013 provides adequate assurance Care Quality Commission Review of compliance at Hillingdon Hospital Oct 2013 adequate assurance Dashboard discussed at Trust Board monthly and in DTMs (or equivalent) Annual Divisional Service Planning provides limited assurance People & Development Team working closely with Divisions to support and develop workforce - Dec 2013 Staff Survey Results for 2012 January 2013 provides adequate assurance Leadership 100 Programme and includes coaching skills. NHSLA Report March 2014 provides substantial assurance at level 2 Gaps in Control or Assurance Gap in control Limited knowledge around managing change Gap in control Moderate Staffing concern raised by CQC Gap in control Limited knowledge of managers around financial management and planning Gap in Control CARES implementation not consistent across recruitment and selection processes Gap in Control Awareness of policies and skills to implement Action to meet gaps Additional Managerial and Leadership Programme being developed to enhance skills across the Trust which will incorporate managing change. Recruitment and Retention Strategy developed, with accompanying action plan will be reviewed by Trust Board. Review of areas of high turnover including exit interviews Rolling recruitment plan in place. Additional staff appointment to enable recruitment drive. Leadership 100 Programme includes a module on how to write business cases, which is open to the wider management population People and Development to introduce minimum standards and value based recruitment Coaching for Managers Training to be developed as part of new Managerial and Leadership Programme. Coaching available for Leadership 100 Programme and includes coaching skills. By when Sept 2014 June 2014 Sept 2014 Monthly Completed Oct 2014 Sept 2014 Complete Responsible Director of People Director of People Disciplinary Policy
227 References Inherent Risk/Threat Control Internal monitoring 3.6 Staff morale and Dignity at work Policy Trust Board motivation drops due to (formerly Bulling and Monitoring increasing demands and Harassment) competing priorities Grievance Policy during significant change, leading to reduced productivity, Sickness Absence Policy increased levels of sickness and turnover Monthly meeting with OH and reduced satisfaction and HR review and and engagement monthly Employee (continued) relations issues Employee Awards Assurance Care Quality Commission Review of compliance at Hillingdon Hospital Oct 2013 adequate assurance Gaps in Control or Assurance Gap in control Moderate Staffing concern raised by CQC Action to meet gaps Recruitment and Retention Strategy developed, with accompanying action plan will be reviewed by Trust Board. Rolling recruitment plan in place. Additional staff appointment to enable recruitment drive. By when June 2014 Monthly Responsible Director of People Health and Well-being Strategy Sickness Absence Project Review of areas of high turnover including exit interviews Sept 2014 Strategic Priority 4 To develop sufficient sustainable scale to enable us to improve and grow healthcare services for our communities 4.1 Risk that the Trusts size inhibits financial sustainability in the medium term. 2014/15 contract with NWL builds in 5.9M transitional funding to support the Trust in-line with SaHF Trust Board Signed contract - April 2014, however this is for one year only. Agreement will need to be reached for intervening SAHF years. No Gaps identified N/A N/A PWC Joint health economy financial review completed to confirm SaHF Impact Dec Risk Ref: 337 Growth in key services e.g. A&E and maternity is not consistent with what has been planned in SaHF creating unmanageable capacity issues. Trust is a major acute Hospital under SaHF Medium term is considered a fixed point Detail analysis being undertaken of current GP activity. Monitoring report of geographical locations enabling us to identify increase in referrals. Tracking labour ward capacity linking to recruitment plans Monitoring activity and trends Market share data A&E activity analysed Trust Board Reviewed at departmental meetings and at Trust level ADO s weekly. SaHF formerly approved by secretary of state- Nov 2013 Business planning process 5 Year Strategy including downsize scenario that assumes SaHF is not fully implemented Weekly Activity report produced by Information and reviewed weekly at ADO Monitoring of 4 hour 95% target. LAS 15/30 minute turn around - Weekly Gap in Control Trust to identify opportunities for expansion and bring more work to THH Gap in Control Inability to respond to surges in demand Monitoring of all activity reviewed monthly at Divisional Reviews with the Director of Finance and the Chief Operating Officer - Plans submitted to expand both Maternity and A&E Additional staffing employed to cover surges Additional resources deployed thought-out winter, LOS reductions maintained. A&E target achieved for 2013/14 Monitored Monthly Regular review Director of Finance COO Chief Operating Officer / Director of Operational Performance
228 References Inherent Risk/Threat Control Internal monitoring 4.3 Failure to identify and The Hillingdon Hospital is Trust Board and implement other growth publically named as a fixed Exec monitoring opportunities from point within the NWL suitable strategic Strategy alliances could restrict Trust development. CEO is a member of the Programme Board for NWL and Medical Director is one of NWL Acute MDs represented Tracked through Transformation Committee Assurance Trust has been identified as a fixed point in the outcome of the NWL consultation document. Feb 2013 Gaps in Control or Assurance Gap in Control Lack of understanding of opportunities available. Action to meet gaps Market analysis strategy as 2.4 Trust has appointed a Business Development manager to identify potential opportunities. Trust developed business by approx. 12M in 2013/14 By when Monitored Monthly Responsible Chief Operating Officer Director of Operational Performance Trust is represented at the Integrated Management Board and on all project groups Trust exploring business development opportunities with other health and social care providers Trust appointed business development manager to research potential opportunities
229 References Inherent Risk/Threat Control Internal monitoring Through unsustainable demand, uncontrolled delays to the delivery timelines and an inability to deliver the required clinical workforce Shaping a healthier future delivers precipitate, poorly planned change, which adversely impacts quality and safety Through an inability to meet the clinical standards, deliver the requisite workforce, deliver behavioural change, sustain expected patient experience and an unsustainable demand on the system Shaping a healthier future does not deliver the planned benefits to improve quality and safety of health and care across NW London A programme implementation governance structure has been established to ensure that there is involvement from all major stakeholders and will monitor programme progress: Clinical Board - brings together all of NW London s medical leaders to ensure transition is being safely planned and managed and will coordinate collective action to address any issues as required. This group will be responsible for leading clinical implementation planning, in particular advising on safe sequencing of change and readiness for change (incorporating the programme four step decision making process). Further scenario testing and readiness exercises are to be carried out. Uncontrolled delays - dedicated resources have been put in place across all organisations to support the delivery of the programme. These are centrally supported by the programme zones and cross cutting workstreams, which includes the involvement of all major external stakeholders. The Implementation Programme Board will continue to review the overarching programme progress. Internal monitoring: Shaping a Healthier Future Programme Board and Trust Board External monitoring: SaHF Programme Board SaHF Clinical Board P1PP Project delivery boards SaHF Finance and Activity Modelling Group SaHF Programme Delivery Group NWL Collaboration Board NHS England Assurance Management of risks and delivery of objectives is evidenced through the following routes: Programme level Minutes of SaHF Programme Board Minutes of SaHF Clinical Board Trust level Minutes of HH SaHF Programme Board Minutes of HH Trust Board 14/15 service transition Mobilisation of Phase 1 priority projects (P1PPs)including Hammersmith Hospital A&E transition, Central Middlesex Hospital A&E transition, Maternity contingency planning P1PP Project Delivery Board minutes Hospital business case development Minutes of SaHF Finance & Activity Modelling Group Meeting record of Programme Delivery Group SaHF assurance process for hospital business cases. Gaps in Control or Assurance Clearly defined process for agreeing the 14/15 SaHF service transitions Action to meet gaps Service transition process has been defined and is being agreed in conjunction with CCGs, Providers and NHS England. Additional funds being made available by DoH NHS England to reduce waiting times. By when June 2014 Sep 2014 Responsible CE/COO COO
230 References Inherent Risk/Threat Control Internal monitoring Assurance Gaps in Control or Assurance Action to meet gaps By when Responsible 4.6 Risk Ref: Failure of the Trust to fully participate with Integrated Care across the whole patient pathway, potentially leads to unnecessary admissions and prolonged hospital stays affecting both patient experience and Trust performance. Full participation in WSIC for NWL and Hillingdon Project Full participation in Better Care Fund Pathway Full participation in Integrated Care Programme Full participation in 7 Day Services Improvement Programme Trust Board receives regular reports Improving Inpatient Care (IIC) Early Supported Discharge (Home Safe) CQIUN Fully compliant with CQUIN milestone for Quarter 1 Gap in Control WSIC and Better Care Not fully implemented yet (scheduled April 2015) Continue to co-design and support models of care to ensure integrated care July 2014 COO Director of Integrated Care Readmission root cause analysis Intermediate Care committee Information / IT Sharing CQUIN Early Supported Discharge (Home Safe) CQIUN Information / IT Sharing CQUIN CCG Fully compliant with CQUIN milestone for Quarter 1 Multi agency inpatient Reviews Bi Annual
231 Control Ratings Green Evidence of regular monitoring available / results of monitoring satisfactory Amber Control recently introduced, not fully embedded / Control process is not delivering adequate assurance / Shared ownership of control means Trust not fully in control concerns about processes outside of the Trusts Control Red Not controlled / no controls in place / no evidence available Assurance Ratings From Internal Audit (Parkhill Audit Agency) Substantial Adequate (Light amber) Limited (Dark amber) None Generally sound system of internal control designed and operating in a way that gives a reasonable likelihood that the system s objectives will be met. In our opinion the controls within the system, as currently laid down and operated, provide adequate assurance that risks material to the achievement of the organisation s objectives for the system are managed and controlled. However, some weakness in the design or inconsistent application of controls put the achievement of particular objectives at risk. Weaknesses in the design or inconsistent application of controls put the achievement of the objectives at risk in the areas reviewed. Weaknesses in control, or consistent non-compliance with key controls, could result (have resulted) in failure to achieve the organisation s objectives in the areas covered.
232 Care Quality Commission Essential Standards of Quality and Safety The essential standards of safety and quality are made up of the following outcomes described in the Guidance about Compliance that define the relevant safety and quality regulations: Outcome Regulation Description 1 17 Respecting and involving people who use services 2 18 Consent to care and treatment 4 9 Care and welfare of people who use services 5 14 Meeting nutritional needs 6 24 Co-operating with other providers 7 11 Safeguarding vulnerable people who use services 8 12 Cleanliness and infection control 9 13 Management of medicines Safety and suitable premises Safety, availability and suitability of equipment Requirements relating to workers Staffing Supporting workers Assessing and monitoring the quality of service provision Complaints Records These are outcomes relevant to NHS providers.
233 NHSLA Risk Management Standards 1 Standard Criterion Governance Learning from Experience Competent & Capable Workforce Safe Environment 1 Risk Management Strategy Clinical Audit Corporate Induction Secure Environment Acute, Community and Non-NHS Providers Supervision of Medical Staff in Training 2 Policy on Procedural Documents Incident Reporting Local Induction of Permanent Staff Violence & Aggression Patient Information & Consent 3 High Level Risk Committee(s) Concerns & Complaints Local Induction of Temporary Staff Slips, Trips & Falls (Staff & Others) Consent Training 4 Risk Management Process Claims Management Risk Management Training Slips, Trips & Falls (Patients) Maintenance of Medical Devices & Equipment 5 Risk Register Investigations Training Needs Analysis Moving & Handling Medical Devices Training 6 Dealing with External Recommendations Analysis & Improvement Risk Awareness Training for Senior Management Hand Hygiene Training Screening Procedures 7 Health Records Management Learning Lessons from Claims Moving & Handling Training Inoculation Incidents Diagnostic Testing Procedures 8 Health Record-Keeping Standards Best Practice - NICE Harassment & Bullying The Deteriorating Patient Transfusion 9 Professional Clinical Registration Best Practice - National Confidential Enquiries & Inquiries Supporting Staff Involved in an Incident, Complaint or Claim Clinical Handover of Care Venous Thromboembolism 10 Employment Checks Being Open Stress Discharge Medicines Management 1 Unchanged from the published 2012/13 NHSLA Standards
234 Risk Register Key Risk Ref: Description of Risk Risk Level Strategic Objective Link 11 Healthcare Associated Infection - Patients may suffer harm and experience discomfort due to contracting avoidable HCAI Medium 1.1 & a IV Fluids bulk storage facility doesn t have the capacity to store the volume of fluids that may be required Alternative storage space allocated in SSD Low - Accepted a Management of Asbestos - Failure to prevent or minimise the risk of disturbing asbestos and exposing people to the risk of asbestos related ill health Accepted by IRMC Medium - Accepted a Management of Legionella in Trust Premises Risk of Legionella bacterium contamination in hot and cold water domestic services Medium - Accepted a Egress does not comply with the requirements of DDA resulting difficulty in evacuating patients Accepted by IRMC Medium - Accepted Duplicate patient records on Trust Patient Information Systems Low High dependency children being cared for on a general paediatric ward without a designated paediatric high dependency unit Medium 1.1 & Pressure Ulcer - Patients may develop a preventable pressure ulcer (PU) whilst an inpatient in the Trust Medium & IT Communications Room - Failure of air conditioning unit/high temperature sensor not functioning, could lead to malfunction/damage of equipment Medium a IT Business Continuity - Hillingdon Hospital and Mount Vernon - Based on controls in place, risk is now deemed to be at an acceptable level Medium - Accepted Psychiatric patients may come to harm or cause harm to others either inside or outside the hospital whilst waiting to be assessed by the Psychiatric team Medium 1.1 & Risks of violence against patients and staff in A&E - this risk is linked with 143 relating to psychiatric patients in A&E Medium a Fire Detection and Alarm Systems and is not compatible with new fire detection and alarm systems put in to refurbished/new areas as required by Fire legislation 149 Containment of Fire - Insufficient compartmentalisation in some areas. Risk of serious injury or death from inhalation of smoke, fumes and asphyxiation. Medium - Accepted 3.4 Medium a Inadequate access to Tower Block for fire service in event of a fire. Delay in accessing areas of Tower Block affected by fire. Medium - Accepted Insufficient provision of emergency lighting - Delay and confusion in the evacuation of areas affected by fire Medium Decontamination of Endoscopes - Inability to meet decontamination compliance standard (2f) in accordance with the Health and Social Care Act 2008 High a Asbestos Containing Materials (ACM's) Used for Insulation of Pipework in Maternity Plant Room Accepted by IRMC Medium - Accepted Duct cleaning Low Use of Lifts in Tower Block in Event of fire. Lifts do not respond and ground when fire alarm system is activated. Low Decontamination of surgical instruments by external contractor - Instruments not returned to Service Level Specification Low A shortage of Paediatric staff means that paediatric A&E may not always be sufficiently staffed to attend to paediatric patients in a responsive and timely manner Medium 1.1 & Medical Record Library Building Working Environment at Hillingdon Hospital Medium Terrace Balcony Main Block Mount Vernon Hospital - Deterioration of balcony structure Low Generators fail to start up in the event of an electrical supply failure at the grid /unable to hold the load it supplies - Loss of power to the Trust Medium Failure to meet the required number of criterion in the standards in order to retain NHSLA level 1 Low 1.1 & 1.3
235 Risk Ref: Description of Risk Risk Level Strategic Objective Link 186 Safeguarding - Failure to identify vulnerable people at risk of harm or abuse Medium Incomplete/Inaccurate documentation may result in harm to patients/leave the Trust open to litigation/failure to achieve compliance with national standards. Medium Regulatory Risk: The Trust does not achieve 95% target for Information Governance Training Medium Electrical - Single point of failure - Loss of electrical failure of 1000kVA transformer that serves main intake switchboard situated in Plant room A High a Maternity Stairwell Medium - Accepted Management and Governance of Clinical Guidelines - Unable to effectively monitor clinical guideline production, updates and date specific reviews. Medium 1.1 & Healthcare Contract Penalties Low Failure to meet the required number of criterion in the standards in order to attain NHSLA level 2 at assessment Low Malfunction of CT scanner at Hillingdon Hospital High 1.1 & Lack of Interventional Radiology on call High 1.1 & Delays/failure in alarm sounding/visual display in switchboard puts patients/staff at potential risk Medium IT Workshop - Environment and Critical Equipment Cabinet Medium 3.3 & Cardiac Arrest Service provided to CNWL Medium 1.1 & Unavailability of Clinical Records Medium 1.1 & Potential of harm to children if there is an inadequate number of paediatric trained staff and in addition those with higher level of paediatric experience Medium 1.1 & High dependency children being cared for on a general paediatric ward that is not commissioned to deliver this level of service. Medium 1.1 & Emergency Care Reconfiguration - Reconfiguration project deadlines missed Medium 3.4 & Out of date Trust Policies Medium Risk Suboptimal maternity staffing levels within midwife, obstetrics and anaesthetics High 1.1, 1.3 & Internal Bleep system across both Hillingdon and Mount Vernon sites Medium Financial Performance Liquidity 2014/15 Medium 1.2, 3.1 & Financial Performance 2014/15 - Deterioration in financial performance against plan High 1.2, 3.1 & 3.2
236 ITEM 22 Board Meeting in Public 30 th July 2014 THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST REPORT TO: REPORT FROM: REPORT SPONSORED BY: Trust Board Sue Manthorpe, Assistant Director Health and Safety Paul Wratten, Finance Director DATE : 30th July 2014 SUBJECT: Health and Safety Report Trust Strategic Priority: To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide. To deliver high quality care in the most efficient way. Summary The Board has requested a quarterly report on the Trust s management of health and safety. This report covers the period 1 April 2014 to 30 th June This report includes performance against key health and safety incidents and RIDDOR information. It also covers emerging topics that require Board focus. The main ones are as follows: The increase in the number of Legionella positive water test results and the action being taken to manage this. Amendments to the legislation of the management of Legionella as this will have an impact on relevant Trust risk assessment processes. The current drive to strengthen the Trust s safety culture and in particular to support the participation of mangers on the health and safety Managing Safely course that aims to better instil the necessary health and safety knowledge and understanding of responsibilities. The reduction in the number of fire service attendances following Trust fire alarm activations as a result of the introduction of the seek and search process used by staff. The Board should note this process also alleviates potential costs from the fire authority that would otherwise impose an additional burden to the Trust.
237 Board Action Required: The Board is asked to review and discuss the report and note the significant points highlighted for this quarter. Equality Impact Assessment: N/A there is no positive or negative impact from this report.
238 Health and Safety Report 1. Incident Reporting 30 Accidents to staff Accidents to Staff 25 Counts of Incidents Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 2012/ / / During this quarter the 2 highest sub categories of the 53 reported accidents to staff were: Needlestick or sharps injury (18) and Slips trips and falls (11). The overall the number of accidents to staff has not increased this quarter and remains consistent with the previous quarter s report. 1.2 Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) There were 5 incidents reportable under RIDDOR in this quarter. Type of report Fracture Dangerous Occurrence Involving Description of Incident Actions Taken Location Staff Staff Member of staff fell in corridor and fractured ankle. Staff member was removing Cannula from patient s hand when blood and fluid sprayed into their eye. Patient was known to be Hep C positive. H&S inspected the area no trip hazards or damaged flooring staff member twisted and fell. The member of Staff attended A&E Occupational Health informed, follow up protocols followed as per Trust policy. Ward reminded that risk assessments must be carried out to identify high risk tasks and the necessary control measures, i.e wearing Bevan Alexandra Ward
239 Dangerous Occurrence 7 Day Absence 7 Day Absence N/K Staff Staff Vehicle entering MVH from Gate 2 drove the wrong way around roundabout, mounted roundabout and crashed into lamp post. Lamp post was bent to an angle of 45 degrees Security officer tripped over cable laying on ground Domestic/Catering staff member suffered bruising to arm when opening Damaged fridge door personal protective equipment, must be implemented No witnesses to incident. Trust Estates staff made area safe. Roundabout returned to use. Estates & Facilities to implemented additional signage on the roundabout Car park inspected Hole in paving slab (to allow cable to be fed to new ticket machine) to be installed. Estates have made the area safe until installation has been completed. Fridge door was found to be broken. It has now been repaired. Mount Vernon Treatment Centre Boulevard Mount Vernon Car Park G Mount Vernon Ward Areas of focus Water Safety There has been a rise in the number of legionella positive test results requiring standard remedial action methods of disinfection and increasing water temperatures to 60 degrees, by the estates team. As part of the Trust s continuing commitment to a robust water system management process, the Water Quality Group is monitoring the test results and actions being taken on a weekly basis to ensure that patient, staff and visitor safety are maintained. In addition, the corporate Legionella risk has been moved from medium to high until confirmation that Legionella growth has been reduced. Contractors The health and safety team continue to provide independent scrutiny and monitoring of the entire refurbishment and building project contractors across the Trust. Where concerns are raised, these are discussed with the appropriate personnel immediately and escalated through the relevant management channels as required. Key concerns raised are site security and access; ensuring the appropriate fire safety measures are in place; and the failure to wear the appropriate personal protective clothing. Fire Safety The Fire Safety Adviser reviews the number of fire calls received across the Trust in order to identify the reason for false alarms and to provide a strategy to reduce them. During this quarter there were a total of 8 fire alarm activations, 5 at Hillingdon Hospital, and 3 at Mount Vernon Hospital. The number of actual fire brigade call outs as a result of these incidents was 3. Since the introduction of the Seek and Search process in December 2013, operated by staff with support from the Fire Response Team, there has been a significant reduction in the number of calls to the fire service. This also alleviates potential costs, which are now in force, of the fire authority imposing additional burdens to the Trust.
 HSG274 Part 2 (Hot and cold water systems) provides a clearer distinction between legal requirements and guidance.")

240 Legislation update The Health and Safety Executive (HSE) has issued part 2 of the revised suite of guidance to help businesses understand how to manage Legionella. The Approved Code of Practice (ACOP) HSG274 Part 2 (Hot and cold water systems) provides a clearer distinction between legal requirements and guidance. A key change is the time frame for the review of risk assessments from 2 yearly to a more frequent review based on the information on control measures e.g. the level of Legionella growth found during water sample tests. The Trust legionella policy is being updated to ensure that it complies with the revised HSE guidance. Training The Trust has been reviewing of all its Statutory and Mandatory training provision to assess whether training can be provided through an e-learning route. As a result of this review some aspects of basic first level health and safety training will now be available through the e-learning route. Increasing participation in the Managing Safely managers course is a key target during this quarter and will be the main driver for the Trust to instil the necessary health and safety knowledge and understanding of responsibilities. Safety is a core part of our culture and the Trust s CARES values, and the continued strengthening of this culture will require ongoing senior leadership and support. 3. Security There were 89 security incidents reported during this quarter with the highest category being other security issues (25), however, there continues to be a reduction in the number of physical assaults on staff. The Trust Security Management Specialist (LSMS) continues to work with the health and safety team on security related issues. This working partnership assists with the Trust s health and safety compliance relating to risk assessments on violence and aggression, lone workers as well as security risks.
Title Open and Honest Staffing Report April 2016
 Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Draft Minutes. Agenda Item: 16
 Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014
 Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014 Presented for: Presented by: Author Previous Committees Information Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim
Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014 Presented for: Presented by: Author Previous Committees Information Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim
Report sponsor: Theresa Murphy, Director of the Patient Experience & Nursing
 Meeting of the Board of Directors public session Safer Staffing Planned and actual staffing levels Wednesday 29 th April 2015 Agenda item 12 Reason for item: This is a standard monthly report on the planned
Meeting of the Board of Directors public session Safer Staffing Planned and actual staffing levels Wednesday 29 th April 2015 Agenda item 12 Reason for item: This is a standard monthly report on the planned
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Agenda item A5(iii) PROVIDING CLINICAL ASSURANCE: CLINICAL ASSURANCE TOOLKIT (CAT), NURSE STAFFING, FRIENDS & FAMILY TEST (FFT) A SUMMARY REPORT EXECUTIVE
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Agenda item A5(iii) PROVIDING CLINICAL ASSURANCE: CLINICAL ASSURANCE TOOLKIT (CAT), NURSE STAFFING, FRIENDS & FAMILY TEST (FFT) A SUMMARY REPORT EXECUTIVE
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
Safe staffing for nursing in A&E departments. NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015
 Safe staffing for nursing in A&E departments NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015 Safe staffing for nursing in A&E departments: NICE safe staffing guideline
Safe staffing for nursing in A&E departments NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015 Safe staffing for nursing in A&E departments: NICE safe staffing guideline
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Status: Information Discussion Assurance Approval
 Report to: Trust Board Agenda item: Date of Meeting: July 2017 Report Title: Safe Nurse Staffing 6 Monthly Assurance Report Status: Information Discussion Assurance Approval X x Prepared by: Sarah Dodds,
Report to: Trust Board Agenda item: Date of Meeting: July 2017 Report Title: Safe Nurse Staffing 6 Monthly Assurance Report Status: Information Discussion Assurance Approval X x Prepared by: Sarah Dodds,
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Trust Board Meeting : Wednesday 11 March 2015 TB
 Trust Board Meeting : Wednesday 11 March 2015 Title Business Case for the Refurbishment and Reconfiguration of the bed based areas of the Emergency Assessment Unit at the John Radcliffe Hospital, to deliver
Trust Board Meeting : Wednesday 11 March 2015 Title Business Case for the Refurbishment and Reconfiguration of the bed based areas of the Emergency Assessment Unit at the John Radcliffe Hospital, to deliver
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led
 Enclosure H Safe Staffing Trust Board Item: 12 Date 29 th November 2017 Enclosure: H Purpose of the Report: This report provides the Trust Board with an update on progress with meeting the safe staffing
Enclosure H Safe Staffing Trust Board Item: 12 Date 29 th November 2017 Enclosure: H Purpose of the Report: This report provides the Trust Board with an update on progress with meeting the safe staffing
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
FOR: Information Assurance Discussion and input Decision/approval
 Nursing & Midwifery (N&M) Establishments Trust Board Meeting - Part 1 Item: 7.4 27 th November 2013 Enclosure: F Purpose of the Report: This paper sets out the Trusts current approach to nurse establishment
Nursing & Midwifery (N&M) Establishments Trust Board Meeting - Part 1 Item: 7.4 27 th November 2013 Enclosure: F Purpose of the Report: This paper sets out the Trusts current approach to nurse establishment
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Monthly Nurse Safer Staffing Report June and July 2018
 Monthly Nurse Safer Staffing Report June and July 2018 Trust Board September 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation
Monthly Nurse Safer Staffing Report June and July 2018 Trust Board September 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation
Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality and Safety
 Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Key facts and trends in acute care
 Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
NHS North West London
 NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS 22 FEBRUARY 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Richard Wilson, Quality Insight and Intelligence Director
 To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
SuRNICC Full Business Case. Benefits Realisation Strategy and Framework
 SuRNICC Full Business Case Benefits Realisation Strategy and Framework Purpose The purpose of this document is to set out the arrangements for the identification of potential benefits, their planning,
SuRNICC Full Business Case Benefits Realisation Strategy and Framework Purpose The purpose of this document is to set out the arrangements for the identification of potential benefits, their planning,
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
All Wales Nursing Principles for Nursing Staff
 All Wales Nursing Principles for Nursing Staff 1 Introduction The purpose of the paper is to respond to the Welsh Governments Staffing Principles for Nurse Staffing within Wales. These principles set out
All Wales Nursing Principles for Nursing Staff 1 Introduction The purpose of the paper is to respond to the Welsh Governments Staffing Principles for Nurse Staffing within Wales. These principles set out
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Quality and Safety Improvement Strategy
 Quality and Safety Improvement Strategy 2016-2021 Page 1 of 20 1. Purpose of this Strategy Patient safety and quality of care are at the heart of the NHS agenda. Treating and caring for people in a safe
Quality and Safety Improvement Strategy 2016-2021 Page 1 of 20 1. Purpose of this Strategy Patient safety and quality of care are at the heart of the NHS agenda. Treating and caring for people in a safe
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 29 th June 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 29 th June 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
Agenda Item. 12 July NHS North Cumbria CCG Primary Care Committee. Approval of ICC Primary Care Investment Proposals. Purpose of the Report
 NHS North Cumbria CCG Primary Care Committee Agenda Item 12 July 2018 6 Approval of ICC Primary Care Investment Proposals Purpose of the Report The purpose of this report is: - To formally ratify the decision
NHS North Cumbria CCG Primary Care Committee Agenda Item 12 July 2018 6 Approval of ICC Primary Care Investment Proposals Purpose of the Report The purpose of this report is: - To formally ratify the decision
QUALITY IMPROVEMENT COMMITTEE
 : 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
: 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
is asked to NOTE the update provided on fragile services.
 Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
A concern means any complaint, claim or reported patient safety incident.
 PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
Norfolk and Waveney STP. Meeting with East Suffolk Partnership 27 September 2017
 Norfolk and Waveney STP Meeting with East Suffolk Partnership 27 September 2017 2 The Norfolk and Waveney STP Members Waveney District Council Focus of Norfolk and Waveney STP Our plan is in line with
Norfolk and Waveney STP Meeting with East Suffolk Partnership 27 September 2017 2 The Norfolk and Waveney STP Members Waveney District Council Focus of Norfolk and Waveney STP Our plan is in line with
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
The new CQC approach to hospital inspection. Ann Ford Head of Hospital Inspection (North West) June 2014
 June 2014") The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
Trust Board Meeting: Wednesday 12 March 2014 TB Peer Review Programme Implementation Update
 Trust Board Meeting: Wednesday 12 March 2014 Title Peer Review Programme Implementation Update Status History For discussion Papers providing updates on the process and outcomes of the Peer Review Programme
Trust Board Meeting: Wednesday 12 March 2014 Title Peer Review Programme Implementation Update Status History For discussion Papers providing updates on the process and outcomes of the Peer Review Programme
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
NHS East and North Hertfordshire Clinical Commissioning Group. Quality Committee. Terms of Reference Version 4.0
 NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Specialist mental health services
 How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse
 TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Quality & Safety Sub-Committee
 Quality & Safety Sub-Committee Agenda Item QS/029/16 Date: 17/03/2016 Report Title FOIA Exemption Prepared by Presented by Action required Supporting Executive Director Safer Staffing No Exemption Janet
Quality & Safety Sub-Committee Agenda Item QS/029/16 Date: 17/03/2016 Report Title FOIA Exemption Prepared by Presented by Action required Supporting Executive Director Safer Staffing No Exemption Janet
THE SOCIAL CARE WALES (SPECIFICATION OF SOCIAL CARE WORKERS) (REGISTRATION) (AMENDMENT) REGULATIONS 2018
 (REGISTRATION) (AMENDMENT) REGULATIONS 2018") THE SOCIAL CARE WALES (SPECIFICATION OF SOCIAL CARE WORKERS) (REGISTRATION) (AMENDMENT) REGULATIONS 2018 This Explanatory Memorandum has been prepared by the Health and Social Services Department and is
THE SOCIAL CARE WALES (SPECIFICATION OF SOCIAL CARE WORKERS) (REGISTRATION) (AMENDMENT) REGULATIONS 2018 This Explanatory Memorandum has been prepared by the Health and Social Services Department and is
A fresh start for registration. Improving how we register providers of all health and adult social care services
 A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
Present: Mr B Reid OBE Chair of the Board of Directors Mr N Summers CBE Vice Chair of the Board of Directors. Mr G McEvoy Non-executive Director
 ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for