Technical Implementation Guide For
|
|
|
- Gladys Taylor
- 6 years ago
- Views:
Transcription

1 Technical Implementation Guide For NFPA Standard 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments Date Published: 15 Aug 2005
2 Preface This Technical Implementation Guide (TIG) provides standard determinations, interpretations, equivalencies, and deviations to implement the 2003 edition of National Fire Protection Association (NFPA) Standard 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments, in the Air Force. This TIG remains in effect until rescinded or one year following publication of a revised NFPA Standard All MAJCOM Civil Engineers, the USAF Academy Civil Engineer and the Air National Guard Civil Engineer have coordinated on this TIG. Correspondence in this regard is on file at HQ AFCESA/CEXF, Tyndall AFB FL. This TIG includes three attachments: 1. NFPA Standard 1582 Correlation Document 2. NFPA Standard 1582 Medical Questionnaire 3. Fire Fighter Physical Examination Schedule //SIGNED// 3 Mar 05 //SIGNED// 13 June 05, DONALD W. WARNER DAVID J. LOUIS Chief, Air Force Fire Protection COLONEL, USAF, MC, SFS HQ Air Force Civil Engineer Support Agency Chief, Occupational Medicine Air Force Medical Support Agency I have approved the deviations from NFPA Standard 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments, 2003 Edition, contained in this TIG. //SIGNED// 15 Aug 05 L. DEAN FOX, Major General, USAF The Civil Engineer DCS/Installations & Logistics
3 NFPA 1582 TECHNICAL INFORMATION GUIDE (TIG) NOTE: The NFPA text is not included in Column one to avoid copyright infringement, the Fire Department Physician will need access to the NFPA 1582 standard. This TIG and its attachments have been developed by the Air Force Medical Support Agency for use by the Fire department Physician. NFPA 1582 PROGRAM AF GUIDANCE CHAPTER 1 ADMINISTRATION 1.1 Scope. Implement as written 1.1.1* This standard shall apply to individuals involved in emergency response operations Implement as written N/A 1.2 Purpose. Implement as written Implement as written 1.2.2* Implement as written Implement as written 1.3 Implementation Implement as written, AHJ for deviations = HQ USAF/ILE AHJ for equivalency & interpretations = HQ AFCESA/CEXF 1.3.2* Implement as written 1.3.3* Implement as written CHAPTER 2 REFERENCED PUBLICATIONS All referenced publications can be found in the basic NFPA 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments, 2003 Edition CHAPTER 3 DEFINITIONS All referenced definitions can be found in the basic NFPA 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments, 2003 Edition Authority Having Jurisdiction In accordance with policy letter issued by HQ USAF/ILE, the AHJ for waivers is HQ USAF/ILE. The AHJ for determinations, equivalencies, and interpretations is HQ AFCESA/CEXF. The authority for medical determination at base level installations is the Fire Chief in coordination with Fire Department Physician
4 Candidate: A person who has made application to commence performance as a member of a fire department CHAPTER 4 ROLES AND RESPONSIBILITIES 4.1 Fire Department Responsibilities 4.1.1* Military firefighters will receive the candidate physical examination at their first physical after completing the Apprentice Fire Protection Course Implement as written Implement as written * Implement as written Implement as written 4.1.4* Exception: Air Force physicians who have completed Air Force specific courses in occupational medicine meet the intent of this section. The Occupational Health Installation Consultant will approve candidates before appointment as FD physician Implement as written Implement as written 4.1.7* Implement as written Implement as written Implement as written Implement as written Implement as written Implement as written * Implement as written. Also see Atch Implement as written 4.2 Fire Department Physician Responsibilities Implement as written Implement as written To include evaluations from other epidemiologic centers and other sources for indicators of a need for additional medical monitoring Implement as written Implement as written 4.2.6* Clarification: Base Level Fire Chief shall oversee development of a local Standard Operating Procedure with the coordination of Fire Department Physician Implement as written 4.3 Implement as written
5 CHAPTER 5 ESSENTIAL JOB TASKS 5.1 Essential Job Tasks and Descriptions Implement as written Implement as written. Fire chief using the core PD to develop essential job tasks Implement as written Physician Guidance: Implement as written Implement as written CHAPTER 6 MEDICAL EVALUATION OF CANDIDATES 6.1* Medical Evaluation. Implement as written 6.1.1* A Delete breast, pap smear and prostate exam as these has nothing to do with qualification for work. Urinalysis for leukocyte esterase has nothing to do with qualification for work. Polio, varicella and MMR should be done by the candidates own provider (US Prev Serv Task Force) Delete 8000 Hz frequency on audiograms (not part of OSHA std). CDC not recommending Hepatitis C to be monitored by employers. FF not considered high risk for TB; therefore no IPPD recommended routinely Implement as written 6.2 Medical Conditions Affecting Ability to Safely Perform Essential Job Tasks Implement as written FD Physician shall determine the ability of a member returning from a illness or injury Head and Neck Head. Implement as written Category B medical conditions shall include the Implement as written following: Neck Implement as written Implement as written 6.4 Eyes and Vision Implement as written Implement as written 6.5* Ears and Hearing. Implement as written
6 6.5.1 Implement as written Implement as written 6.6 Dental Implement as written Implement as written 6.7 Nose, Oropharynx, Trachea, Esophagus, and Larynx Implement as written Implement as written 6.8 Lungs and Chest Wall Implement as written Implement as written 6.9 Heart and Vascular System Heart Implement as written Implement as written Vascular System Implement as written Implement as written 6.10 Abdominal Organs and Gastrointestinal System Implement as written Implement as written Implement as written Implement as written 6.12 Urinary System Implement as written Implement as written Implement as written 6.13 Spine and Axial Skeleton Implement as written Implement as written 6.14 Extremities Implement as written Implement as written 6.15 Neurological Disorders Implement as written Implement as written Implement as written 6.17 Blood and Blood-Forming Organs Implement as written Implement as written 6.18 Endocrine and Metabolic Disorders Implement as written Implement as written 6.19 Systemic Diseases and Miscellaneous Conditions.
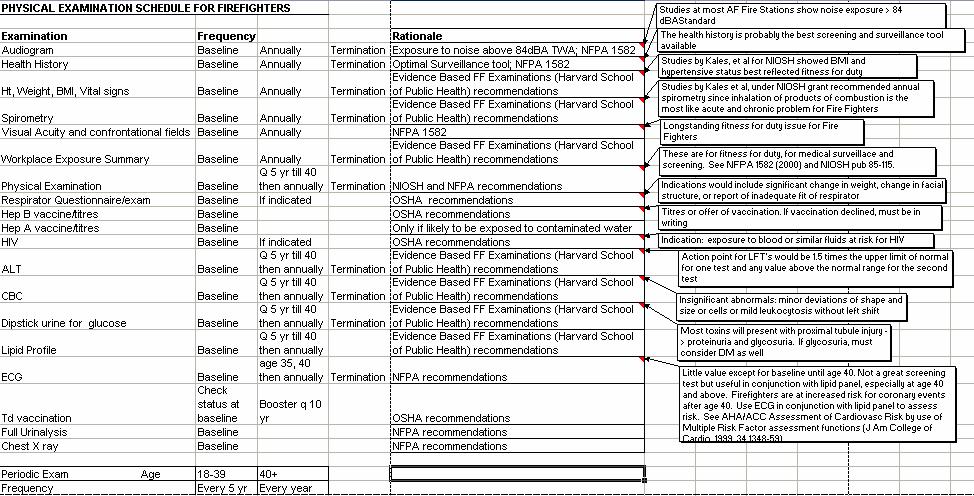
7 Implement as written Implement as written 6.20 Tumors and Malignant Diseases Implement as written Implement as written 6.21 Psychiatric Conditions Implement as written Implement as written 6.22 Chemicals, Drugs, and Medications Implement as written Exception: Smoking tobacco is not in itself a medical condition and should not be considered a disqualifier for otherwise healthy candidates. A firefighter who smokes will be offered enrollment in a smoker cessation program Implement as written Implement as written * Implement as written Chapter 7 Occupational Medical Evaluation of Members 7.1 General Medical records are managed by MTF s under their privacy protection policies As indicated by Fire Department Physician 7.1.3* Implement as written Implement as written 7.2 Member Education Regarding Medical Evaluation Program. Implement as written Implement as written Implement as written 7.3 Timing of the Annual Occupational Medical Evaluation of Members. Implement as written Implement as written The candidate s initial evaluation is the baseline examination and the firefighter should be re-examined annually afterward An ANNUAL exam includes: Ht Wt Blood pressure, audiogram PFT Interval Medical History. Then detailed supplemental exams are done every 3-5 years until age 40 when the supplemental exams are
8 done annually Implement as written Implement as written 7.4 Implement as written Exception: An ANNUAL exam includes: Ht Wt Blood pressure, audiogram PFT Interval Medical History. Then detailed supplemental exams are done every 3 years for and every 2 years for AND ANNUALLY STARTING AT AGE 40 (with blood work, ECG as indicated, etc) If clinically indicated in judgment of the physician An ANNUAL exam includes: Ht Wt Blood pressure, audiogram PFT Interval Medical History. Then detailed supplemental exams are done every 3-5 years until age 40 when the supplemental exams are done annually Plus ancillary tests as indicated including physical examination, blood test etc. The initial baseline exam will include all the above except the cancer screening and genitourinary exam 7.5 Medical History Implement as written Include off duty risk factors The fire department physician will review the TIG medical questionnaire given to the firefighters. 7.6 Physical Examination An annual exam includes: Ht Wt Blood pressure, audiogram PFT, Interval Medical History, with an extended examination as needed. A detailed supplemental exam is done every 3-5 years until age 40 when the supplemental exams are done annually. In addition to the items in the annual exam, the clinical portion of the detailed supplemental exam includes examination of the
9 Head, eyes, nose, throat, neck, cardiovascular and respiratory tract, the liver, lymph nodes, neurological system, musculoskeletal system, vision system, skin, and for hernias. The prostate, breast and genitourinary exams are not included * The laboratory and ancillary testing portion of the detailed supplemental examination will include complete blood count with differential, ALT, cholesterol/lipid profile, urinalysis for glucose Blood Tests. The laboratory and ancillary testing portion of the detailed supplemental examination will include complete blood count with differential, ALT, cholesterol/lipid profile, urinalysis for glucose Urinalysis for glucose during detailed examinations and in all firefighters aged 40 and over Audiology Hz may be omitted if technically difficult. Justification: OSHA currently requires testing to 6000 Hz Implement as written Implement as written 7.7 Spirometry. Implement as written 7.7.1* Implement as written 7.7.3* Results shall be corrected according to American Thoracic Society Implement as written (ATS) guidelines and normative equations found in Knudson et al. (1983) and the American College of Occupational and Environmental Medicine (2000). A See D Chest Radiographs Exception: Shall be repeated every 5 years if clinically indicated. Justification: not recommended by American Cancer Society or American Thoracic Society Implement as written 7.9 Electrocardiograms (EKG) * Exception: Perform a resting EKG as a part of the baseline medical
10 evaluation, again at age 35 and 40, the annually thereafter. Justification: The force of morbidity for cardiac events after age Implement as modified in * Implement as written 7.10 Mammography Mammography is not indicated as an occupational surveillance test May be accomplished by personal physician 7.11 CDC does not currently judge FF to be in a high risk group and is not recommending PPD s for them. CDC currently not recommending employers monitor Hepatitis C. MMR, Varicella, and polio vaccinations should be a part of the individual s personal medical care per the US Preventive Services Task force. Firefighters are not a high risk group for influenza. HIV screening should be event specific, related to specific occupational events that have put the firefighter at risk Heavy Metal Evaluation Implement as written Implement as written 7.13 Not recommended by the DoD Occupational Medical Working Group because of lack of causal factors Chapter 8 Annual Occupational Fitness Evaluation of Members 8.1 Weight and Body Composition. Implement as written Implement as written. 8.2 Annual Fitness Evaluation * Implement as written * * 9.1 Essential Job Tasks. Implement as written Implement as written 9.2 Medical Conditions. Implement as written
11 9.2.1 Implement as written The relevant task(s) shall be identified by number. Implement as written 9.3 Implement as written Implement as written 9.3.2* Implement as written 9.4* Cardiovascular Disorders. Implement as written Implement as written Implement as written 9.5 Vascular Disorders Implement as written Implement as written 9.6* Implement as written 9.7* Lung, Chest Wall, and Respiratory Disorders Implement as written 9.8 Infectious Diseases Implement as written Implement as written 9.9* Spine Disorders. Implement as written Implement as written Implement as written 9.10* Orthopedic Disorders. Implement as written Implement as written Implement as written 9.11 Disorders Involving Gastrointestinal Tract and Abdominal Viscera. Implement as written Implement as written Implement as written 9.12 Medical Conditions Involving Head, Eyes, Ears, Nose, Neck, or Implement as written Throat * Implement as written 9.13* Neurologic Disorders. Implement as written 9.14* Psychiatric and Psychologic Disorders. Implement as written Implement as written Implement as written 9.15* Substance Abuse. Implement as written Implement as written 9.16 Medications. Implement as written Physician Guidance: Implement as written Implement as written 9.17 Tumors Malignant or Benign Implement as written Implement as written
12 Fire Department Personnel Medical Questionnaire MEDICAL QUESTIONNAIRE NFPA 1582 MEDICAL QUESTIONNAIRE Job Position: Name: D.O.B: Age: Sex: M F Date of Exam: Physician: Head and Neck 1. Any skull deformities that may prevent the following: Proper wear of a helmet leaving head unprotected yes no Leading to improper respiratory mask seal yes no 2. Any neck condition(s) that may result in the inability to perform essential job tasks. yes no 3. Chronic neck pain yes no 4. Minimal range of motion yes no Eyes and Vision 5. Any vision problems that may result in the inability to perform essential job tasks. yes no 6. Do you wear contact lenses and/or spectacles yes no 7. Eye diseases: Retinal detachment yes no Progressive retinopathy yes no Optic neuritis yes no 8. Ophthalmological procedures: Radial keratotomy yes no Lasik procedure yes no Repair of retinal detachment yes no 9. Affected peripheral vision yes no Ears and Hearing 10. Chronic vertigo or impaired balance yes no 11. Hearing loss or damage yes no 12. Chronic ear ringing yes no 13. Do you wear protective hearing devices in noisy environments? yes no Dental 14. Do you wear any orthodontic appliances yes no 15. Any mandible or maxilla deformities that may prevent proper wear of protective equipment yes no Page 1
13 Fire Department Personnel Medical Questionnaire Nose, Oropharynx, Trachea, Esophagus, and Larynx 16. Recurrent nose bleeds yes no 17. Recurrent sinusitis yes no 18. Any nasal, oropharyngeal, tracheal, esophageal or laryngeal condition that may result in not being able to safely perform essential job tasks yes no 19. Difficulty smelling yes no 20. Difficulty speaking yes no Lungs and Chest Wall 21. Recurring Vomiting of Blood yes no 22. Pulmonary Hypertension yes no 23. Exposure to or Active tuberculosis yes no 24. Any illnesses or diseases of the respiratory system such as but not limited to: COPD, Hypoxemia, Asthma, Cystic Fibrosis, Pneumonia or Embolisms yes no 25. Any other pulmonary condition that may prevent you from being able to safely perform as a firefighter yes no Cardiovascular System 26. Recurrent syncope (fainting) yes no 27. Any conditions requiring the use of an implantable cardiac defibrillator or pacemaker yes no 28. Any cardiac dysrythmias such as but not limited to: SVT, PVC, Flutters, Fibrillations, AV Blocks, and Tachycardias yes no 29. Congestive Heart Failure yes no 30. Congenital abnormalities yes no 31. Hypertension yes no 32. Recurrent Chest Pain yes no 33. Myocardial Infarctions (Heart Attacks) yes no 34. Thoracic or abdominal aortic aneurysm yes no 35. Any other cardiovascular conditions that would result in the inability to perform essential job tasks yes no Abdominal Organs and Gastrointestinal System 36. Any gastrointestinal condition that may result in you not being able to safely perform essential job tasks such as but not limited to: Cholecystitis, Gastritis, GI bleeding Acute hepatitis, Hernia(s), Irritable bowel syndrome, Pancreatitis Diverticulitis, GI surgery, Ulcer(s), Asplenia, Cirrhosis, and/or Chronic active hepatitis yes no Page 2
14 Reproductive System Fire Department Personnel Medical Questionnaire 37. Any genital condition the may result in you not being able to perform essential job tasks yes no 38. Pregnancy, for its duration yes no Female 39. Difficult and painful menstruation yes no Female 40. Endometriosis, ovarian cysts, or other gynecologic conditions yes no Female 41. Testicular or epididymal mass yes no Male Urinary System 42. Any kidney diseases, renal failure, or insufficiency requiring continuous peritoneal dialysis or hemodialysis yes no 43. Any diseases of the ureter, bladder, prostate, or other conditions that may result in the inability to safely perform essential job tasks yes no Spine and Axial Skeleton 44. History of spinal surgeries or spinal surgery involving fusion of more than 2 vertebrae yes no 45. Any spinal or skeletal condition producing sensory or motor deficit(s), pain and or nerve compression yes no 46. Any spinal or skeletal condition that may result in the inability to safely perform essential job tasks yes no Extremities 47. Any type of hardware utilized metal plates or rods supporting bone during healing yes no 48. Amputation or congenital absence of any part of the upper or lower extremities yes no 49. History of joint surgery or total replacement yes no 50. Any history of extremity problems that may result in the inability to safely perform essential job tasks yes no Neurological Disorders 51. Any partial or full paralysis of a limb(s) yes no 52. History of Cerebrovascular Accidents or Transient Ischaemic Attacks yes no 53. History of seizures due to epilepsy to include: Simple partial, complex partial, generalized, and psychomotor seizure disorders yes no 54. Any neurological condition that may result in the inability to safely perform essential job tasks yes no Page 3
15 Skin Fire Department Personnel Medical Questionnaire 55. Any type of skin conditions of a chronic or recurrent nature that cause skin openings or inflammation or irritation of the skin surface yes no 56. Any dermatologic condition that may result in the inability to safely perform essential job tasks yes no Blood and Blood-Forming Organs 57. Sickle cell disease yes no 58. Clotting disorders yes no 59. Any other hematological condition that may result in the inability to safely perform essential job tasks yes no Tumors and Malignant Diseases 60. Any tumor or similar conditions that may result in the inability to safely perform essential job tasks yes no 61. Benign Tumors yes no Psychiatric Conditions 62. History of psychiatric condition or substance abuse yes no 63. Requirement for medications for a psychiatric condition that may result in the inability to safely perform essential job tasks yes no Chemicals, Drugs, and Medications Do you take: 64. Narcotics, including Methadone yes no 65. Sedatives-Hypnotics yes no 66. Beta-adrenergic blocking agents yes no 67. Heart medication(s) to include (HTN) high blood pressure yes no 68. Stimulants, Psychoactive agents, corticosteroids, Antihistamines, and Muscle relaxants yes no Endocrine and Metabolic Disorders Do you have a history of or currently being treated for: 69. Diabetes mellitus, which is treated with insulin yes no 70. Diabetes mellitus that is controlled on diet, exercise, and/or oral hypoglycemic agents yes no 71. Diseases of the adrenal gland, pituitary gland, or thyroid gland of clinical significance yes no 72. Any endocrine or metabolic condition that may result in the inability to perform essential job tasks yes no Page 4
16 Fire Department Personnel Medical Questionnaire Please list all medications that you are currently taking: OTHER 73. List any other jobs you have: 74. List any chemicals you use in those jobs: 75. Is there loud noise involved in those jobs? yes no 76. List your hobbies: 77. List any chemicals you use in those hobbies: 78. Has your health changed since your last examination? yes no 79. Did you have any unusual or unexpected exposures at work, yes no at another job or with your hobbies since your last examination? If you responded to any questions with YES please explain in more detail on the subject in the additional space provided. If you have any additional concerns, questions, or comments please annotate in the additional space provided. Page 5
17
S T A N D A R D O P E R A T I N G G U I D E L I N E
 S T A N D A R D O P E R A T I N G G U I D E L I N E Subject: Line of Duty Benefits Reference Number: SAP-DEP-048 Effective Date: July 1, 2013 Last Revision Date: N/A Signature of Approval: J. Dan Eggleston,
S T A N D A R D O P E R A T I N G G U I D E L I N E Subject: Line of Duty Benefits Reference Number: SAP-DEP-048 Effective Date: July 1, 2013 Last Revision Date: N/A Signature of Approval: J. Dan Eggleston,
Jacksonville State University Lurleen B. Wallace College of Nursing and Health Sciences Health Appraisal Form
 Jacksonville State University Lurleen B. Wallace College of Nursing and Health Sciences Health Appraisal Form Welcome to the Lurleen B. Wallace College of Nursing and Health Sciences at Jacksonville State
Jacksonville State University Lurleen B. Wallace College of Nursing and Health Sciences Health Appraisal Form Welcome to the Lurleen B. Wallace College of Nursing and Health Sciences at Jacksonville State
New Patient Registration Form NJR_NP_F100
 New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
New Patient Registration Form NJR_NP_F100 Patient Last Name First Name Middle Name Maiden Name Address (Street or Box) City State Zip Code Home Phone Number Cell Phone Number Work Phone Number E-Mail Patient
Medical Evaluation Program
 Medical Evaluation Program PURPOSE: To detail the procedures, controls and documentation necessary for administration of the Department s Medical Evaluation Program. To insure compliance with all applicable
Medical Evaluation Program PURPOSE: To detail the procedures, controls and documentation necessary for administration of the Department s Medical Evaluation Program. To insure compliance with all applicable
Descriptions: Provider Type and Specialty
 Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Patient Registration. City, State & Zip Code Date of Birth Age. Occupation: Family Physician: Married Single Other Spouse's Name
 *SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
*SHAREDID-42* Date of Birth: Page 1 of 2 Patient Registration Account # Patient Name Home Telephone # Work Telephone # Social Security Number Cell Telephone # Address Patient Sex City, State & Zip Code
Patient Name:,, Address: Phones:,, Home Work Cell. Primary Physician: Emergency Contact: Phone#:
 Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
NURSING COMPUTER SOFTWARE. Level 2- Semester 4. Advanced Medical Surgical Nursing/ Clinical Lab
 NURSING COMPUTER SOFTWARE Level 2- Semester 4 Nur 1210/ 1210L Advanced Medical Surgical Nursing/ Clinical Lab RECOMMENDED FOR ALL COURSES: Successful Test- taking Tips for Windows: (Copyright 1998) Test-Taking
NURSING COMPUTER SOFTWARE Level 2- Semester 4 Nur 1210/ 1210L Advanced Medical Surgical Nursing/ Clinical Lab RECOMMENDED FOR ALL COURSES: Successful Test- taking Tips for Windows: (Copyright 1998) Test-Taking
SPECIALTY SPECIFIC OBJECTIVES
 Family Medicine Residency Internal Medicine In-house II Rotation Rotation Goal Admission, evaluation, treatment and appropriate specialty consultation of adult hospitalized patients from either the ER,
Family Medicine Residency Internal Medicine In-house II Rotation Rotation Goal Admission, evaluation, treatment and appropriate specialty consultation of adult hospitalized patients from either the ER,
TESTING Computer Adaptive Testing (CAT)...1 Test Taking Strategies... 2
...1 Test Taking Strategies... 2") Table OF CONTENTS TESTING Computer Adaptive Testing (CAT)...1 Test Taking Strategies... 2 CONCEPTS OF NURSING PRACTICE Maslow s Hierarchy of Basic Human Needs...3 Steps in the Nursing Process... 4 The
Table OF CONTENTS TESTING Computer Adaptive Testing (CAT)...1 Test Taking Strategies... 2 CONCEPTS OF NURSING PRACTICE Maslow s Hierarchy of Basic Human Needs...3 Steps in the Nursing Process... 4 The
NURSING COMPUTER SOFTWARE. Level 1- Semester 2. Medical Surgical Nursing/ Clinical Lab
 NURSING COMPUTER SOFTWARE Level 1- Semester 2 Nur 1210/ 1210L Medical Surgical Nursing/ Clinical Lab RECOMMENDED FOR ALL COURSES: Successful Test- taking Tips for Windows: (Copyright 1998) Test-Taking
NURSING COMPUTER SOFTWARE Level 1- Semester 2 Nur 1210/ 1210L Medical Surgical Nursing/ Clinical Lab RECOMMENDED FOR ALL COURSES: Successful Test- taking Tips for Windows: (Copyright 1998) Test-Taking
Worker s Compensation Forms
 Patient Name: DOB: Employer Name: Address: Claim Number: Date of Injury/DOI: Description of Accident: Adjuster s Information Adjuster s Name: Adjuster s Phone Number: Fax Number: Workers Compensation Insurance
Patient Name: DOB: Employer Name: Address: Claim Number: Date of Injury/DOI: Description of Accident: Adjuster s Information Adjuster s Name: Adjuster s Phone Number: Fax Number: Workers Compensation Insurance
Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION. Cell Phone ( ) Employer s Name
 Employer s Name") Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION Name Last First M.I. Social Security. Home Address Street City State Zip Mailing Address
Please bring your ID and Medical/Dental Insurance cards to all appointments PATIENT REGISTRATION PATIENT INFORMATION Name Last First M.I. Social Security. Home Address Street City State Zip Mailing Address
Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM
 Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM TO THE PHYSICIAN: Southwestern College requires a physical examination for students enrolling in the Nursing and Health
Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM TO THE PHYSICIAN: Southwestern College requires a physical examination for students enrolling in the Nursing and Health
PATIENT INFORMATION INSURANCE INFORMATION
 PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
PATIENT INFORMATION Patient Name: Date of Birth: SSN: Cell Number: Cell Phone Provider: Home Number: Work Number: Home Address: City/State: Zip: Employer: Occupation: E-Mail: Relationship Status: S M W
Report of the Incidence and Prevalence of Diseases and other Health Related Issues in Saudi Arabia
 Report of the Incidence and Prevalence of Diseases and other Health Related Issues in Saudi Arabia A study for the SMLE Blueprint Project Heba AlManea Assessment Executive Specialist, SCFHS Dr Abdulmohsen
Report of the Incidence and Prevalence of Diseases and other Health Related Issues in Saudi Arabia A study for the SMLE Blueprint Project Heba AlManea Assessment Executive Specialist, SCFHS Dr Abdulmohsen
Department of State Academic Exchanges Participant Medical History and Examination Form
 Department of State Academic Exchanges Participant Medical History and Examination Form Having been selected to participate in a U.S. Department of State educational exchange program, you are required
Department of State Academic Exchanges Participant Medical History and Examination Form Having been selected to participate in a U.S. Department of State educational exchange program, you are required
FirstName: MiddleInitial: LastName: Student ID# LEHMAN COLLEGE DEPARTMENT OF NURSING READ ME FIRST
 FirstName: MiddleInitial: LastName: Student ID# Program: Generic/Accelerated (B.S.) RN-B.S Master s/post-master s Certificate Cohort/Online/Offsite: RN-BS MD-RN Master s ANNUAL HEALTH CLEARANCE REQUIREMENTS
FirstName: MiddleInitial: LastName: Student ID# Program: Generic/Accelerated (B.S.) RN-B.S Master s/post-master s Certificate Cohort/Online/Offsite: RN-BS MD-RN Master s ANNUAL HEALTH CLEARANCE REQUIREMENTS
Essentials for Clinical Documentation Integrity 2017
 Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
Essentials for Clinical Documentation Integrity 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101
Al al-bayt University. Nursing Faculty. Adult Health Nursing-1 ( ) Course Syllabus
 Course Syllabus") Al al-bayt University Nursing Faculty Adult Health Nursing-1 (1001221) Course Syllabus 2009/2010 1 Course Title: Adult Health Nursing-1 (1001221) Credit Hours: 3 Hours. Pre-requisite: (1001171) Date: first
Al al-bayt University Nursing Faculty Adult Health Nursing-1 (1001221) Course Syllabus 2009/2010 1 Course Title: Adult Health Nursing-1 (1001221) Credit Hours: 3 Hours. Pre-requisite: (1001171) Date: first
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS
 NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
Nursing Complex Health Alterations 1
 Western Technical College 10543109 Nursing Complex Health Alterations 1 Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 Complex Health Alterations
Western Technical College 10543109 Nursing Complex Health Alterations 1 Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 Complex Health Alterations
Allergies Drug Food Environmental. Previous Surgeries & Hospitalizations (Please list date, reason, and hospital)
") Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Allergies Drug Food Environmental Previous Surgeries & Hospitalizations (Please list date, reason, and hospital) Habits Do you ever use the following? If yes, how often? Tobacco Alcohol Recreational Drugs
Disclosure and Release of Health History and Immunization Requirements
 TO BE COMPLETED BY THE STUDENT: NURSING AND HEALTH OCCUPATIONAL PROGRAMS Disclosure and Release of Health History and Immunization Requirements Student s Name: Birth date: Last First Middle Month/Day/Year
TO BE COMPLETED BY THE STUDENT: NURSING AND HEALTH OCCUPATIONAL PROGRAMS Disclosure and Release of Health History and Immunization Requirements Student s Name: Birth date: Last First Middle Month/Day/Year
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
PATIENT INFORMATION. Address: Sex: City: State: address: Cell Phone: Home Phone: Work Phone: address: Cell Phone:
 PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
PATIENT INFORMATION Name: _ DOB: _ Age: Address: _Sex: City: _ State: _ Zip: _ Email address: Cell Phone: _ Home Phone: Work Phone: _ Responsible Party (if different from above) Name: DOB: Address: E-mail:
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
Health & Safety Packet for Incoming Students
 Health Occupations Division 707-256-7600 Health & Safety Packet for Incoming Students This packet has been designed to help Health Occupations students comply with CPR and health/physical documentation
Health Occupations Division 707-256-7600 Health & Safety Packet for Incoming Students This packet has been designed to help Health Occupations students comply with CPR and health/physical documentation
DRUG / MEDICATION ALLERGIES: (include: Type/Reaction)
") NASSAU CHEST PHYSICIANS PC MEDICAL QUESTIONNAIRE 1 DATE: PATIENT NAME: DOB: DRUG / MEDICATION ALLERGIES: (include: Type/Reaction) 9/1/2014 PHARMACY NAME PHARMACY PHONE PHARMACY Street Address City State
NASSAU CHEST PHYSICIANS PC MEDICAL QUESTIONNAIRE 1 DATE: PATIENT NAME: DOB: DRUG / MEDICATION ALLERGIES: (include: Type/Reaction) 9/1/2014 PHARMACY NAME PHARMACY PHONE PHARMACY Street Address City State
Sage Medical Center New Patient Forms
 Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Virginia Heartburn & Hernia Institute
 Virginia Heartburn & Hernia Institute PATIENT INFORMATION FORM (Please make sure to print clearly and sign at the bottom of this page) Patient s Last Name: First: Middle Initial: Marital Status: Married
Virginia Heartburn & Hernia Institute PATIENT INFORMATION FORM (Please make sure to print clearly and sign at the bottom of this page) Patient s Last Name: First: Middle Initial: Marital Status: Married
UWSMPH Clerkship Experience Requirements
 2016-2017 UWSMPH Clerkship Experience Requirements Students will use OASIS to check off each Clerkship Experience Requirement. The following conditions, procedures and learning activities must all be completed
2016-2017 UWSMPH Clerkship Experience Requirements Students will use OASIS to check off each Clerkship Experience Requirement. The following conditions, procedures and learning activities must all be completed
May Family Chiropractic Health Information and Health History Patient Name: Gender: Male Female
 1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
1 Health Information and Health History Patient Name: Gender: Male Female Marital Status: (Circle one) M S D W Other: Date of Birth / / Spouse Name: How many children: Patient Social Security Number: -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Allens Training Phone or
 Student Information Course Name Course code Contact details In Partial completion of Description of this unit against the qualification Descriptor What is covered in the course Employability Skills Pre-requisites
Student Information Course Name Course code Contact details In Partial completion of Description of this unit against the qualification Descriptor What is covered in the course Employability Skills Pre-requisites
FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty
 FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty Consent for Purposes of Treatment, Payment and Health Care Operations I consent to the use or disclosure of my protected health information by Florida
FLORIDA MEDICAL CLINIC, P.A. Your Life, Our Specialty Consent for Purposes of Treatment, Payment and Health Care Operations I consent to the use or disclosure of my protected health information by Florida
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Would you like to follow us on: Twitter Facebook Physician's Signature
 PATIENT REGISTRATION INFORMATION TODAY S DATE: / / Last Name First Name MI Soc. Sec. # Date of Birth Sex Male Female Patient Address Apt. City, State, Zip Single Married Divorced Widow Home Phone Work
PATIENT REGISTRATION INFORMATION TODAY S DATE: / / Last Name First Name MI Soc. Sec. # Date of Birth Sex Male Female Patient Address Apt. City, State, Zip Single Married Divorced Widow Home Phone Work
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
PATIENT INFORMATION (Please Print)
") PATIENT INFORMATION (Please Print) Patient Name: Home Phone: Patient Date of Birth: Cell Phone: Patient Social Security #: Sex: Consent to call? Yes No Consent to text? Yes No Address: Work Phone: City:
PATIENT INFORMATION (Please Print) Patient Name: Home Phone: Patient Date of Birth: Cell Phone: Patient Social Security #: Sex: Consent to call? Yes No Consent to text? Yes No Address: Work Phone: City:
Middle Initial: Street Address: City: Date of Birth: Age: Marital Status: Occupation: Employer: Name of Spouse: Emergency Contact:
 SALT LAKE EYE ASSOCIATES, LLC (801) 281-2020 1025 E 3300 S, SLC, Utah * Patient Information Sheet First Name: Last Name: Middle Initial: Referred By Family Doctor EMAIL Street Address: City: State: Zip:
SALT LAKE EYE ASSOCIATES, LLC (801) 281-2020 1025 E 3300 S, SLC, Utah * Patient Information Sheet First Name: Last Name: Middle Initial: Referred By Family Doctor EMAIL Street Address: City: State: Zip:
Library of Congress Cataloging-in-Publication Data
 Library of Congress Cataloging-in-Publication Data Names: Reinisch, Courtney, editor. Nursing Knowledge Center, publisher. Title: Family nurse practitioner review and resource manual / edited by Courtney
Library of Congress Cataloging-in-Publication Data Names: Reinisch, Courtney, editor. Nursing Knowledge Center, publisher. Title: Family nurse practitioner review and resource manual / edited by Courtney
Fullerton Physical Therapy and Sports Care, Inc.
 Fullerton Physical Therapy and Sports Care, Inc. Patient Information: Title Address Patient Name (Last, First, Middle initial) City/State/Zip Home Phone Work Phone Cell Phone Social Security DOB Gender
Fullerton Physical Therapy and Sports Care, Inc. Patient Information: Title Address Patient Name (Last, First, Middle initial) City/State/Zip Home Phone Work Phone Cell Phone Social Security DOB Gender
MRI Patient Screening and History
 Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
ADULT PATIENT INFORMATION. Patient Name: Last Name First Name Address: City: State: Zip Code: Phone #: Cell Phone #: Social Security:
 716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
PATIENT REGISTRATION. Street City State Zip WORK INJURY/ ACCIDENT
 PATIENT REGISTRATION, Last First M.I. SEX: Male Female DOB: / _/ AGE: MARITAL STATUS: SS#: - - PHYSICIAN: ADDRESS: Street City State Zip (HOME) (WORK) TEL: - - TEL: - _- CELL: - _- EMAIL: PRIMARY INSURANCE:
PATIENT REGISTRATION, Last First M.I. SEX: Male Female DOB: / _/ AGE: MARITAL STATUS: SS#: - - PHYSICIAN: ADDRESS: Street City State Zip (HOME) (WORK) TEL: - - TEL: - _- CELL: - _- EMAIL: PRIMARY INSURANCE:
Print Guardian Name (If not patient) DOB: Patients Name: (Last, First, MI): Circle One: - - / / Mailing Address: Apt. #: City: State: Zip Code:
 DOB: Patients Name: (Last, First, MI): Circle One: - - / / Mailing Address: Apt. #: City: State: Zip Code:") Patients Name: (Last, First, MI): SSN: DOB: Circle One: Male Mailing Address: Apt. #: City: State: Zip Code: Female Race: Ethnicity Primary Language: Home Phone: Preferred? Cell Phone: Preferred? Employer:
Patients Name: (Last, First, MI): SSN: DOB: Circle One: Male Mailing Address: Apt. #: City: State: Zip Code: Female Race: Ethnicity Primary Language: Home Phone: Preferred? Cell Phone: Preferred? Employer:
Piedmont Access to Health Services. Standing Orders for Patient Work-ups
 Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
GUIDELINE FOR CONDUCTING PRE-EMPLOYMENT MEDICAL EXAMINATION
 GUIDELINE FOR CONDUCTING PRE-EMPLOYMENT MEDICAL EXAMINATION 1.0 Introduction. Most employers require job applicants fulfil their requirements in term of qualification, experience and personal attributes
GUIDELINE FOR CONDUCTING PRE-EMPLOYMENT MEDICAL EXAMINATION 1.0 Introduction. Most employers require job applicants fulfil their requirements in term of qualification, experience and personal attributes
Change 135 Manual of the Medical Department U.S. Navy NAVMED P Oct 2009
 Change 135 Manual of the Medical Department U.S. Navy NAVMED P-117 30 Oct 2009 To: Holders of the Manual of the Medical Department 1. This Change Completely revises Chapter 15, Section IV, Article 15-107,
Change 135 Manual of the Medical Department U.S. Navy NAVMED P-117 30 Oct 2009 To: Holders of the Manual of the Medical Department 1. This Change Completely revises Chapter 15, Section IV, Article 15-107,
The Impact of Healthcare-associated Infections in Pennsylvania 2010
 The Impact Healthcare-associated Infections in Pennsylvania 2010 Pennsylvania Health Care Cost Containment Council February 2012 About PHC4 The Pennsylvania Health Care Cost Containment Council (PHC4)
The Impact Healthcare-associated Infections in Pennsylvania 2010 Pennsylvania Health Care Cost Containment Council February 2012 About PHC4 The Pennsylvania Health Care Cost Containment Council (PHC4)
SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely)
") SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely) Name: Former/ Maiden Name: Date of Birth: Age: Today s Date: *Language: Race: Ethnicity: *Do
SMG OB/GYN Lake Lansing St. Johns Returning Patient Questionnaire (Please print clearly and Fill out Entirely) Name: Former/ Maiden Name: Date of Birth: Age: Today s Date: *Language: Race: Ethnicity: *Do
Seasons Women s Care Patient Registration Form
 Seasons Women s Care Patient Registration Form Name: of Birth: Address: City: St: Zip Home Phone: Cell: Best Number: Email: Race or Ethnicity: Marital Status: SS# Drivers Lic#: Employer: Work# Occupation:
Seasons Women s Care Patient Registration Form Name: of Birth: Address: City: St: Zip Home Phone: Cell: Best Number: Email: Race or Ethnicity: Marital Status: SS# Drivers Lic#: Employer: Work# Occupation:
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group
 DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
DOUGLAS JAY SPRUNG MD, FACG, FACP The Gastroenterology Group Date: NAME: AGE: DOB: Why are you here to see the doctor today? REFERRED BY: INSURANCE HEALTH GRADES INTERNET FRIENDS/RELATIVES PCP OTHER: Medications
SoutheastHEALTH Occupation Medicine Clinic Patient Information Sheet
 SoutheastHEALTH Occupation Medicine Clinic Patient Information Sheet DATE Name (First, Middle, Last): Date of Birth: SSN: Mailing Address: City, State and Zip: Phone: Home Cell Other Alt Phone: Home Cell
SoutheastHEALTH Occupation Medicine Clinic Patient Information Sheet DATE Name (First, Middle, Last): Date of Birth: SSN: Mailing Address: City, State and Zip: Phone: Home Cell Other Alt Phone: Home Cell
Medicaid Benefits at a Glance
 Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
Burton M. Sundin, M.D. / Reps B. Sundin, M.D. Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: address:
: Address: Zip, City, State: Home#: Work#: Cell#: address:") Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
Date: Name (Last, First, MI): Address: Zip, City, State: Home#: Work#: Cell#: Email address: Patient Status: 1-Married 2 Single 3-Separated 4-Divorced 5-Widowed 6-Other Birthdate: Sex: Social Security#:
MOUNTAIN VIEW COLLEGE Health Record
 MOUNTAIN VIEW COLLEGE Health Record Date Name: DOB: Last First Middle Month Day Year Address: Street City & State Zip Telephone: Home Work Cell or VM I certify that I have: Health Questionnaire: To be
MOUNTAIN VIEW COLLEGE Health Record Date Name: DOB: Last First Middle Month Day Year Address: Street City & State Zip Telephone: Home Work Cell or VM I certify that I have: Health Questionnaire: To be
The Home Doctor. Registration Checklist
 The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
HISTORY AND PHYSICAL EXAM
 TO: PHYSICIAN COMPLETING THIS MEDICAL INFORMATION You are being presented papers for completion in reference to application for admission to The Virginia Home by a patient of yours. As you probably know,
TO: PHYSICIAN COMPLETING THIS MEDICAL INFORMATION You are being presented papers for completion in reference to application for admission to The Virginia Home by a patient of yours. As you probably know,
FIRE ACADEMY APPLICATION
 FIRE ACADEMY APPLICATION Dear Prospective Student: Thank you for your interest in the Fire Training Academy at Sandhills Community College. We have a team of highly qualified, experienced and dedicated
FIRE ACADEMY APPLICATION Dear Prospective Student: Thank you for your interest in the Fire Training Academy at Sandhills Community College. We have a team of highly qualified, experienced and dedicated
Welcome to the Southeastern Urology Associates meridianemr Patient Portal
 New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Harlem Hospital Center Department of Radiology. Residency Training Program ROTATION OBJECTIVE -- LEARN BASIC BODY CT, LEARN BASIC EMERGENCY CT.
 Harlem Hospital Center Department of Radiology Residency Training Program BODY CT: Goals and Objectives ROTATION 1 (Radiology Year 1) ROTATION OBJECTIVE -- LEARN BASIC BODY CT, LEARN BASIC EMERGENCY CT.
Harlem Hospital Center Department of Radiology Residency Training Program BODY CT: Goals and Objectives ROTATION 1 (Radiology Year 1) ROTATION OBJECTIVE -- LEARN BASIC BODY CT, LEARN BASIC EMERGENCY CT.
Benefits are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
PATIENT INFORMATION: CONTACT INFORMATION: EMERGENCY CONTACT: EMERGENCY PHONE: RESPONSIBLE PARTY (IF OTHER THAN PATIENT)
") PATIENT REGISTRATION PATIENT INFORMATION: NAME:,, (M.I.) ADDRESS:,, (Street) (City) (State) (Zip) SEX: MALE FEMALE DOB: / / AGE: MARITAL STATUS: SS #: / / REFERRING PHYSICIAN: CONTACT INFORMATION: (CELL):
PATIENT REGISTRATION PATIENT INFORMATION: NAME:,, (M.I.) ADDRESS:,, (Street) (City) (State) (Zip) SEX: MALE FEMALE DOB: / / AGE: MARITAL STATUS: SS #: / / REFERRING PHYSICIAN: CONTACT INFORMATION: (CELL):
LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W
 CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W") PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
NASCAR Medical Liaison Department Office: (386) Fax: (386)
 Fax: (386)") NASCAR Medical Liaison Department Office: (386) 310-6400 Fax: (386) 310-6405 Dear Driver, Please find enclosed the 2016 Driver History & Physical Examination, 2016 HIPAA Authorization for the Use and Disclosure
NASCAR Medical Liaison Department Office: (386) 310-6400 Fax: (386) 310-6405 Dear Driver, Please find enclosed the 2016 Driver History & Physical Examination, 2016 HIPAA Authorization for the Use and Disclosure
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA HEALTH PLANS INC.
 Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network Providers Annual Maximum Out-of-Pocket Amount $2,500 The maximum out-of-pocket limit applies to all
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network Providers Annual Maximum Out-of-Pocket Amount $2,500 The maximum out-of-pocket limit applies to all
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Nurse Aide. We reserve the right to cancel any class due to insufficient enrollment.
 Nurse Aide We reserve the right to cancel any class due to insufficient enrollment. **All clinical dates may vary according to site and instructor availability ABOUT THE NURSE AIDE PROGRAM The Nurse Aide
Nurse Aide We reserve the right to cancel any class due to insufficient enrollment. **All clinical dates may vary according to site and instructor availability ABOUT THE NURSE AIDE PROGRAM The Nurse Aide
Name DOB / / SS# / / Street Address City/State/Zip. Home ( ) - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -
 - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -") Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
If you have health insurance, please bring your insurance card(s) so that we may verify eligibility and bill correctly.
 so that we may verify eligibility and bill correctly.") Vimali Paul, MD David Alonso, MD Laura Loudermilk, FNP Joy Culp, FNP 85 Declaration Dr., Ste. 110 Chico, CA 95973 (530) 894-6600 phone (530) 894-1321 fax Dear Patient: Welcome to the practice! The forms
Vimali Paul, MD David Alonso, MD Laura Loudermilk, FNP Joy Culp, FNP 85 Declaration Dr., Ste. 110 Chico, CA 95973 (530) 894-6600 phone (530) 894-1321 fax Dear Patient: Welcome to the practice! The forms
Do not enclose these forms with any documents sent to other IMSA departments or representatives.
 IMSA Medical Liaison Department Toni Wright Senior Medical Liaison Coordinator Office: (386) 310-6434 Fax: (386) 310-6435 Ashlee Rice IMSA Medical Administrative Assistant Office: (386) 310-6438 Fax: (386)
IMSA Medical Liaison Department Toni Wright Senior Medical Liaison Coordinator Office: (386) 310-6434 Fax: (386) 310-6435 Ashlee Rice IMSA Medical Administrative Assistant Office: (386) 310-6438 Fax: (386)
Office Hours Our office hours are Monday through Friday 7:30 am to 5:30pm. Our office is closed on all major Holidays.
 Dear New Patient: We would like to welcome you to our practice. Our goal is to make your experience with us as pleasant as possible. In order to help us meet this goal we have listed some helpful hints
Dear New Patient: We would like to welcome you to our practice. Our goal is to make your experience with us as pleasant as possible. In order to help us meet this goal we have listed some helpful hints
NASHP s 30 th Annual State Health Policy Conference. Timeline of Tennessee Health Care Innovation Initiative
 STATE OF TENNESSEE NASHP s 30 th Annual State Health Policy Conference 10/25/2017 Timeline of Tennessee Health Care Innovation Initiative 2012 2013 2014 2015 2016 2017 1210 Stakeholder Meetings 16 Partnerships
STATE OF TENNESSEE NASHP s 30 th Annual State Health Policy Conference 10/25/2017 Timeline of Tennessee Health Care Innovation Initiative 2012 2013 2014 2015 2016 2017 1210 Stakeholder Meetings 16 Partnerships
MINNESOTA OCCUPATIONAL HEALTH 1661 St Anthony Avenue St Paul, MN Telephone (651) Fax (651)
 Fax (651)") MINNESOTA OCCUPATIONAL HEALTH 1661 St Anthony Avenue St Paul, MN 55104 Telephone (651) 968-5300 Fax (651) 730-3990 PERIODIC HAZMAT/ASBESTOS MEDICAL QUESTIONNAIRE Date: / / NAME: SS#: - - COMPANY: 1. OCCUPATIONAL
MINNESOTA OCCUPATIONAL HEALTH 1661 St Anthony Avenue St Paul, MN 55104 Telephone (651) 968-5300 Fax (651) 730-3990 PERIODIC HAZMAT/ASBESTOS MEDICAL QUESTIONNAIRE Date: / / NAME: SS#: - - COMPANY: 1. OCCUPATIONAL
(Please Print) PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )
 PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )") (Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
(Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
Patient Name DOB Sex M F
 Patient Name DOB Sex M F Social Security Ethnicity Marital Status Address City/State/Zip Email Race Preferred Language Employer Please check one box to indicate preferred number Home Phone Cell Phone Emergency
Patient Name DOB Sex M F Social Security Ethnicity Marital Status Address City/State/Zip Email Race Preferred Language Employer Please check one box to indicate preferred number Home Phone Cell Phone Emergency
Patient: Gender: Male Female. Mailing Address: Ethnicity: Not Hispanic or Latin Hispanic/Latin Home Phone #:
 5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
Benefits are effective January 01, 2017 through December 31, 2017
 Benefits are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of- Annual Deductible $0 This is the amount
Benefits are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of- Annual Deductible $0 This is the amount
Dodge. County. Schools
 Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
Dear New Patient: Sincerely, The Scheduling Staff
 Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
Dear New Patient: Welcome to Garden State Urology. The physicians in our group are board-certified, fellowship trained urologists who provide stateof-the-art care that rivals the finest academic institutions
SoutheastHEALTH Occupation Medicine Clinic Patient Information Sheet
 SoutheastHEALTH Occupation Medicine Clinic Patient Information Sheet DATE Name (First, Middle, Last): Date of Birth: SSN: Mailing Address: City, State and Zip: Phone: Home Cell Other Alt Phone: Home Cell
SoutheastHEALTH Occupation Medicine Clinic Patient Information Sheet DATE Name (First, Middle, Last): Date of Birth: SSN: Mailing Address: City, State and Zip: Phone: Home Cell Other Alt Phone: Home Cell
Patient Information: Last Name First Name MI. Address Apt/Room # City Zip. Community name (if not at home) Martial Status: S M W D
 Martial Status: S M W D") HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
Medical Examination Report Form (for Commercial Driver Medical Certification)
") Public Burden Statement A Federal agency may not conduct or sponsor, and a person is not required to respond to, nor shall a person be subject to a penalty for failure to comply with a collection of information
Public Burden Statement A Federal agency may not conduct or sponsor, and a person is not required to respond to, nor shall a person be subject to a penalty for failure to comply with a collection of information
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
PATIENT REGISTRATION FORM PATIENT INFORMATION Name: Date of Birth: Age: Address : Social Security #: City: Sex: Marital Status: State: Zip: Language: Pt Declines Home Phone#: Race: Pt Declines Work Phone#:
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network & Out-of- Annual Deductible This is the amount you have to pay out of pocket before the plan will pay
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network & Out-of- Annual Deductible This is the amount you have to pay out of pocket before the plan will pay
Welcome to our office! Please fill out this form as completely as possible and return it to the desk.
 Welcome to our office! Please fill out this form as completely as possible and return it to the desk. Name of Doctor you wish to see: Today's Date Name Email Address Address Home Male Female Cell City
Welcome to our office! Please fill out this form as completely as possible and return it to the desk. Name of Doctor you wish to see: Today's Date Name Email Address Address Home Male Female Cell City
Thank you for contacting the Saint Francis Center for Surgical Weight Loss.
 Saint Francis Center for Surgical Weight Loss 6005 Park Avenue Ste. 1011B, Memphis Tn. 38119 ***PLEASE NOTE This is our office, not our seminar address. Please see directions to our seminar location at
Saint Francis Center for Surgical Weight Loss 6005 Park Avenue Ste. 1011B, Memphis Tn. 38119 ***PLEASE NOTE This is our office, not our seminar address. Please see directions to our seminar location at
Family Medicine Division. Nyree Bryant DO George R. Davis DO
 Family Medicine Division Nyree Bryant DO George R. Davis DO 11/12/17 Dear New Patient, Welcome to Florida Medical Clinic! We are happy that you have made our office your choice for your medical care needs.
Family Medicine Division Nyree Bryant DO George R. Davis DO 11/12/17 Dear New Patient, Welcome to Florida Medical Clinic! We are happy that you have made our office your choice for your medical care needs.
Welcome to Hawaii Women s Healthcare
 Cheryl Lynn T. Rudy, M.D. Cheryl L. Leialoha, M.D. Erin C. Gertz, M.D. Laura A. Spector, D.O. Andrea Wieland, APRN Welcome to Hawaii Women s Healthcare Hawaii Women s Healthcare strives to provide you
Cheryl Lynn T. Rudy, M.D. Cheryl L. Leialoha, M.D. Erin C. Gertz, M.D. Laura A. Spector, D.O. Andrea Wieland, APRN Welcome to Hawaii Women s Healthcare Hawaii Women s Healthcare strives to provide you
COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF HEALTH CHAPTER 709, SUBCHAPTER F. STANDARDS FOR INPATIENT NONHOSPITAL ACTIVITIES SHORT-TERM DETOXIFICATION
 COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF HEALTH CHAPTER 709, SUBCHAPTER F. STANDARDS FOR INPATIENT NONHOSPITAL ACTIVITIES SHORT-TERM DETOXIFICATION 709.61. Exceptions to the general standards for free-standing
COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF HEALTH CHAPTER 709, SUBCHAPTER F. STANDARDS FOR INPATIENT NONHOSPITAL ACTIVITIES SHORT-TERM DETOXIFICATION 709.61. Exceptions to the general standards for free-standing
Crescent Community Clinic Application for Healthcare Services
 Crescent Community Clinic Application for Healthcare Services If you have been diagnosed with a dental concern, a chronic health or mental health condition, you may be eligible for free healthcare at the
Crescent Community Clinic Application for Healthcare Services If you have been diagnosed with a dental concern, a chronic health or mental health condition, you may be eligible for free healthcare at the
ESSENTIAL JOB FUNCTIONS:
 ESSENTIAL JOB FUNCTIONS: Perform fire-fighting tasks (e.g., hoseline operations, extensive crawling, lifting and carrying heavy objects, ventilating roofs or walls using power or hand tools, forcible entry),
ESSENTIAL JOB FUNCTIONS: Perform fire-fighting tasks (e.g., hoseline operations, extensive crawling, lifting and carrying heavy objects, ventilating roofs or walls using power or hand tools, forcible entry),
WITHOUT YOUR WRITTEN CONSENT, WE CAN NOT SPEAK TO ANYONE REGARDING YOUR MEDICAL CARE due to privacy laws. You have the right to list anyone you
 PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
PATIENT REGISTRATION FORM PLEASE PRINT : Referring Physician: Primary Care: Patient s Name: Last First: M.I. Address: City: State: Zip: Home Phone: Cell: Work: Email: Preferred Contact Method Race: Ethnicity:
Fax: Do not mail the forms!
 Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric
Associates in Pediatric and Adult Urology The Morristown Medical Center Health Pavilion 333 Mount Hope Avenue Suite 250 Rockaway, NJ 07866 973-895-6636 Dear New Patient: Welcome to Associates in Pediatric