Telehealth/mHealth: Innovations in Improving Access to Care. Mark Carroll, MD Mose Herne, MPH, MS Mark Horton, OD, MD Lyle Ignace, MD, MPH
|
|
|
- Annice Mitchell
- 6 years ago
- Views:
Transcription

1 Telehealth/mHealth: Innovations in Improving Access to Care Mark Carroll, MD Mose Herne, MPH, MS Mark Horton, OD, MD Lyle Ignace, MD, MPH
2 Overview of Breakout Session Brief status of telehealth and mhealth in IHS Regulatory topics Credentialing and privileging Strategic opportunities Discussion

3 Facing the challenge of delivering health care where it s needed.











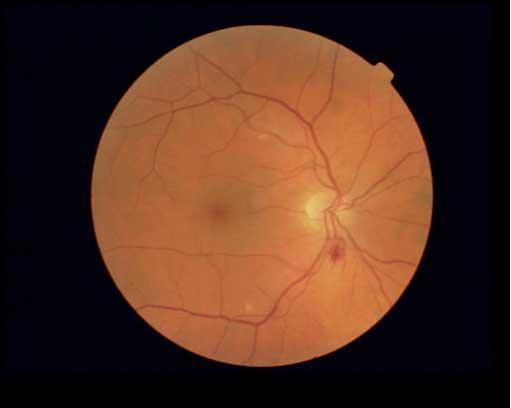
4 A Wide Range of Services AIDS-HIV care Behavioral Health Cardiology Dentistry Dermatology Diabetes care ENT Intensive care Rheumatology Neurology Nephrology Nutrition Ophthalmology - JVN Oncology/Palliative Care Pharmacy Radiology Rehab services Rheumatology Remote Monitoring Trauma Wound care

5 Patient-Centered Care Right care Right place Right time









6 Right Tool

7 Right Emphasis Relationships New tools and technologies must enhance relationships, especially if they are to be embraced and be effective in chronic care



8 The Mobile Revolution Audie A. Atienza, PhD
9 Audie A. Atienza, PhD

10 Audie A. Atienza, PhD

11 Audie A. Atienza, PhD





12 Remember : 1.5 Trillion Text Messages Sent in US 4.1 billion SMS messages sent daily Audie A. Atienza, PhD

13 50+ Case Studies Described Audie A. Atienza, PhD

14

 direct health care services, Tribally-operated health care services, and urban Indian health care services and resource centers.")


15 mhealth and Patient-Centered Care: Perspective from U.S. Indian Health Care M Carroll, MD 1 ; T Cullen, MD 1 ; M Horton, MD,OD 1 ; C Lamer, RPh 1 ; S Ferguson, PhD 2 ; M Veazie, DrPH 1 I Indian Health Service; 2 Alaska Native Tribal Health Consortium THE INDIAN HEALTH SYSTEM A comprehensive health delivery system for ~1.9 million American Indians and Alaska Natives. Serving members of 564 federally-recognized Tribes in 35 U.S. states. Comprised of Indian Health Service (IHS) direct health care services, Tribally-operated health care services, and urban Indian health care services and resource centers. USING mhealth IN AN EMERGING MODEL OF PATIENT-CENTERED CARE: THE 5 RIGHTS 1. RIGHT TOOL 2. RIGHT PLACE 3. RIGHT TIME 4. RIGHT SYSTEM OF CARE 5. RIGHT EMPHASIS: Relationships A RELATIONSHIP-CENTERED APPROACH Connected Care & Remote Monitoring Critical Triggers for Quality Improvement Effective Relationships Improved Self-care and Treatment Improved Outcomes & Value mhealth IN INDIAN HEALTH: CARE WHERE AND WHEN IT IS NEEDED The IHS and its Tribal partners are committed to the appropriate use of innovative tools and technologies to improve access to quality health care for American Indians and Alaskan Natives. mhealth: the integration of mobile technology, computing devices, and emerging delivery system capabilities into a patient-centered model of care. Innovative uses of mhealth tools in Indian health care include: Mobile deployment of services The IHS Joslin Vision Network Tele-Ophthalmology program to 14 facilities in AK and NC Mobile mammography, for communities in the Dakotas Remote monitoring programs in diverse geographies, for congestive heart failure and diabetes care CONSIDERATIONS FOR EXPANDED USE OF mhealth TOOLS New tools must be integrated into initiatives to improve models of care. A key example is the IHS Improving Patient Care initiative. Use of handheld mobile technologies and wireless monitoring devices must occur in strict compliance with emerging security and privacy standards. Patient health information must be part of the IHS and Tribal Electronic Health Records, for coordinated care at the health care facility and community level. mhealth services should complement developing work for personal health records and other key activities that expand access to health information for patients and communities. Cultural acceptance of new tools and technologies is vital to program development and must be a key component to mhealth project design.
16 Smartphone Adoption and Usage 83% of U.S. adults have a cell phone 35% of U.S. adults have a smartphone 87% use it to access internet or 25% use it as main access to internet 9% have apps to help track or manage health 17% have used phones to look up health info Pew Internet Project
17 Text Messaging 72% of adult cell phone users send or receive text messages Pew Internet Project, Sept 14, % of consumers prefer to receive a healthrelated task reminder through text messaging Consumer Health Information Corporation








18 HHS Text4Health Task Force (est. Nov 2010) Audie A. Atienza, PhD


19 text4baby Audie A. Atienza, PhD
20 mhealth: Access and Quality of Care Expanded models of care Remote patient monitoring Real-time support for dx and rx Innovative access to information, training, and education For care teams For patients communities Improved efforts at disease outbreak tracking and epidemiology


21

22

23 Last Mile Microwave Coverage
24
25






26
27 Social Media Standard Operating Procedures (SOPs) in final approval stage Facebook (updated version) social networking YouTube -video sharing Twitter - micro-blogging Flickr - photo sharing

28

29 FDA Proposed Rules: July 2011
30 Best Practices What are new privacy and security standards? IHS planning to establish guidelines for using mhealth communications for a variety of scenarios Health promotion and education Reminders Other communications
31 Care Coordination for Hypertension Care: Improving BP Control for Patients with Diabetes Lyle Ignace, MD, MPH July 27, 2011

32 GOAL: Care Coordination for Improved BP Management Improve BP Control for diabetic patients with poor BP control

33 TOOLS: Care Coordination for Improved BP Management Home BP monitoring cuffs and data transfer device/service Improved care coordination processes
34 Care Coordination for Improved BP Management DOES HOME BP MONITORING WORK? Many studies show significant reduction in patients BP, reducing risk for stroke, heart, disease, and other health problems Example: University of Toronto, Logan et al, implemented automated mobile phone-based telementoring Home BP monitoring data sent via mobile phone to care teams for DM patients with uncontrolled BP Systolic BP decreased by 9.1 mm Hg over one year, compared with 1.6 mm Hg decrease in control


35 In-home remote monitoring Courtesy of Bonnie Britton, RN
36 Hospital Bed Days and ER Visits Hospital Bed Days 6 mos. prior to Telehealth = 199 During 6 mos. Telehealth = 99 n=64 50% decrease prior to during 6-30 mos. post Telehealth = 70 65% decrease prior to 30 mos. post ER Visits 6 mos. prior to Telehealth = 27 During 6 mos. Telehealth = 5 81% decrease prior to during 6-30 mos. post Telehealth = 23 15% decrease prior to 30 mos. post Analyzed Charges are related to diseases being monitored Courtesy of Bonnie Britton, RN RCCHC/PPTN Patient Charge Data Ending June 2009
37 Total Charges Statistically significant difference between pre-, during, and posttelehealth charges p value = mos. prior to Telehealth = $1.34 M During 6 mos. Telehealth = $ 382 k 72% decrease 6-30 mos. post Telehealth = $483 k 64% decrease Analyzed Charges are related to diseases being monitored RCCHC/PPCTN Patient Charge Data Ending June 2009 Courtesy of Bonnie Britton, RN
38 Care Coordination for Improved TIMELINE: BP Management Pilot activity with 12 Improving Patient Care initiative sites To begin late summer/fall
39 Care Coordination for Improved EMPHASIS: BP Management The key part of this pilot is the care coordination team processes, not the facilitated access to home BP data
40 IHS/JVN Program Summer 2011 Update IHS NCC Meeting 27 July 2011 Mark B. Horton, OD, MD Phoenix Indian Medical Center Director, IHS/JVN Teleophthalmology Program

41 D M P r e v e l a n c e D R E x a m R a t e DM and DR In Indian Country Parallel Epidemics 180, , , , ,000 80,000 60,000 40,000 20,000 Doubling of DM prevalence during past decade Sustained 50% DR exam rate 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% '00 '02 '04 '06 '08 '10 0% Diabetic Retinopathy is the leading cause of new blindness Blindness due to DM/DR can be eliminated by timely Dx and Tx Conventional eye exams not a likely solution for timely DX
42 DR Exam Rate DR Surveillance in IHS: FY10 IHS (2010)- 53% (43% - 63%) DR eye exam rate 80% 70% 60% 50% 40% 30% 20% 10% 0% 51% 44% ABD ALA ALB BEM 63% 46% BIL CAL 59% 47% 43% NAS NAV OKL PHX 59% 55% 57% 43% POR TUC 53% DR Surveillance std of care failed in ~half of population with DM Urban and rural All socioeconomic groups AI/AN vs general US pop
43 DR Surveillance Reporting GPRA Performance Measure Performance Measure 2009 Target 2010 Target 2011 Target Headquarters Lead TREATMENT MEASURES Diabetes Group 6. Diabetic Retinopathy: Address the proportion of patients with diagnosed diabetes who receive an annual diabetic retinal examination. [outcome] During FY 2009, maintain the proportion of patients with diagnosed diabetes at all sites who receive an annual retinal examination at the FY 2008 level rate of 47% at all sites. During FY 2010, maintain the proportion of patients with diagnosed diabetes at all sites who receive an annual retinal examination of 55% at all sites. During FY 2010, maintain the proportion of patients with diagnosed diabetes at all sites who receive an annual retinal examination of 50.1% at all sites. Mark Horton

44 Cumulativee Annua Diabetic Retinopathy Surveillance IHS-JVN Teleophthalmology Program 78 physical/81 logical + 14 Portable Sites in 21 States IHS-JVN Exams , Program Year P R O J E C T E D
45 New IHS-JVN Developments Technical Software- RPMS/EHR interoperability Hardware- camera development Clinical- improved imaging protocols Operational- consortium deployments Business- Tribal collaborations
46 IHS-JVN CONOPS Summary Healthcare Facility JVN Server (PAO) National Reading Center (PIMC) JVN-RPMS/EHR Interoperability RPMS GIS 1 HL7 CDMP IE (Mirth) Automated Workflow JVN Image Acquisition Worstation Pt Demo 4 Image & Pt Info 3 2 Oracle DB Modality Worklist Provider DICOM PACS Image WebService JVN Application Server 8 Health Summary 5 7 JVN Diagnostic Display 6 Pull of clinical data into JVN Reader Push of JVN report and business information into RPMS/EHR RPMS GIS 9 CDMP IE (Mirth) 9 GIS RPMS EHR Consults Scheduling and Notification EHR Charge Posting EHR Charge Posting

47 Camera Development Current Technology Adapted from existing commercial device Wrong features Fragile Expensive Orphaned 40 lb - $20K - Manual - Discontinued - No Parts - In Development Designed for Tmed Light Small foot print Simi-automated Hardened $5-$10K DoD/University of Hi, others




48 New Clinical Protocols Extreme Remote Imaging protocol Mini-dilation Protocol Improve image gradeability and over-referrals Remote sites with extreme logistics Small sites with low volume imaging

49 New IHS-JVN Developments Consortium based deployments PORTLAND AREA DM PTS FY10 EXAM RATE FY10 CHEHALIS % NISQUALLY % SHOALWATER BAY 12 25% SKOKOMISH 40 5% SQUAXIN ISLAND % COWLITZ % TOTAL % Partnership for improved outcomes Operations Business Clinical
50 Tribal Collaboration Budget flat since 2002 Operational costs vs deployments and development Interest from related non-bens Urban Clinics, Hawai'i, Pacific Islanders IHCIA Reading Center franchise




51 IHS/JVN Program Summer 2011 Update IHS NCC Meeting 27 July 2011 Mark B. Horton, OD, MD Phoenix Indian Medical Center Director, IHS/JVN Teleophthalmology Program
52 REGULATORY UPDATE: Credentialing and Privileging
53 Credentialing and Privileging Requirements for Telemedicine Physicians and Practitioners Revisions to the Hospital and CAH Conditions of Participation (CMS-3227-F) June
54 Locating the Final Rule Published May 5, 2011, in the Federal Register: Medicare and Medicaid Programs: Changes Affecting Hospital and Critical Access Hospital (CAH) Conditions of Participation (CoPs): Telemedicine Credentialing and Privileging (CMS-3227-F) 76 FR 25550: 05/pdf/ pdf June 9,
55 Changes to the Hospital CoPs The hospital requirements for credentialing and privileging of medical staff are contained under the Governing Body ( ) and Medical Staff ( ) CoPs June 9,
56 Governing Body CoP Requires the governing body of the hospital ensure that an agreement exists with a distant-site hospital to provide telemedicine services and that the agreement specifies that the governing body of the distant-site hospital ensures that all current Governing Body CoP requirements ( (a)(1-7)) are met with regard to its physicians and practitioners providing telemedicine services. June 9,
57 Governing Body CoP (cont) The governing body of the hospital has the option of granting privileges based on the recommendations of its medical staff, which has relied upon information furnished by the distant-site hospital regarding privileges for individual physicians and practitioners providing telemedicine services. June 9,
58 Medical Staff CoP The hospital can rely on this information for its privileging decisions only if certain provisions (at (a)(3)) regarding the distant-site hospital, and the individual physicians and practitioners, were met regarding: Medicare-participation status of distant-site hospital Privileges of individual physicians and practitioners, including list of current privileges for each provided by distant-site hospital State License (does not apply to Indian health) Internal review for purposes of periodic appraisal of individuals providing telemedicine services, including adverse events/complaints June 9,

59 Changes to the CAH CoPs Critical Access Hospitals (CAHs) have CoP requirements under the Medicare regulations that are separate and distinct from the hospital CoPs. The term credentialing is used almost exclusively throughout the CAH CoPs. June 9,
60 Changes to the CAH CoPs (cont) The new CAH requirements for credentialing and privileging are under the Agreements ( ) and Periodic Evaluation and Performance Review ( ) CoPs. June 9,
61 Changes to CAH CoPs The requirements for CAHs are similar to those for hospitals, and/or designed to make the CAH credentialing and privileging requirements consistent with current hospital requirements (abbreviated slide) June 9,
62 Changes to CAH CoPs (cont) We also amended the Periodic Evaluation and Quality Assurance Review CoP (at (b)(4)) by adding a new paragraph that allows a distant-site hospital to evaluate the quality and appropriateness of the diagnosis and treatment furnished by the distant-site physicians and practitioners providing telemedicine services to the CAH s patients under an agreement between the CAH and a distant-site hospital June 9,
63 How does the final rule differ from the proposed rule we published in May 2010? First, we finalized the requirements proposed in the May 2010 NPRM with only minor clarifying revisions (e.g, specify in the provisions that the telemedicine agreement must be written). Based on public comment, we added new provisions to the final rule that will apply to the credentialing and privileging process and the agreements between hospitals and CAHs and nonhospital, distant-site telemedicine entities that provide telemedicine services (a)(9) and (a)(4) for hospitals; (c)(3) and (c)(4) for CAHs June 9,
64 How does the final rule differ from the proposed rule we published in May 2010? (cont) The new provisions will allow for the governing body of the hospital (or the CAH s governing body or responsible individual) to rely upon the credentialing and privileging decisions made by the distant-site telemedicine entity. The telemedicine entity s medical staff credentialing and privileging processes and standards must at least meet the CoPs related to credentialing and privileging. June 9,
65 What Are the Differences Between the Proposed Requirements and the New Provisions? These new provisions will require the governing body of the hospital (or the CAH s governing body or responsible individual): Through its written agreement with the distant-site telemedicine entity Ensure that the distant-site telemedicine entity as a contractor of services Furnishes its services in a manner that enables the hospital (or CAH) to comply with all applicable CoPs and standards for the contracted services Including the credentialing and privileging requirements regarding its physicians and practitioners providing telemedicine services June 9,
66 What effect will the final rule have on the CoPs? Will allow hospitals and CAHs to make full use of the telemedicine services offered by nonhospital telemedicine entities without the duplicative and burdensome task required by the traditional credentialing and privileging process. June 9,
67 Benefits for Hospitals and CAHs Will now allow hospitals and CAHs to take advantage of these streamlined credentialing and privileging options when using the telemedicine services of: Other Medicare-participating hospitals, Non-Medicare-participating telemedicine entities, or A combination of both types of service providers June 9,
68 What is a telemedicine entity? There is no statutory definition for a telemedicine entity contained in the Social Security Act. Therefore, for the purposes of this rule, we needed to define a distant-site telemedicine entity as one that (1) Provides telemedicine services; (2) Is not a Medicare-participating hospital; and (3) Provides contracted services in a manner that enables a hospital or CAH using its services to meet all applicable CoPs, particularly those requirements related to the credentialing and privileging of practitioners providing telemedicine services to the patients of a hospital or CAH. June 9,
69 The Importance of the Written Agreement Similar to our regulations proposed for hospitals and CAHs using the telemedicine services of distant-site Medicare participating hospitals, the written agreement between the hospital or CAH and the distant-site telemedicine entity will be the foundation for ensuring accountability on both sides. June 9,
70 Summary Proposed rule published May 26, 2010 CMS received over 100 comments from various stakeholders. Final rule published May 5, 2011 Effective date: July 5, 2011 The result of outreach efforts by CMS to the telemedicine stakeholder community Allows for a streamlined process for credentialing and privileging of telemedicine physicians and practitioners under written agreements between hospitals/cahs and distant-site non- Medicare-participating telemedicine entities and distant-site Medicare-participating hospitals June 9,
71 Summary (cont) Intent is to reduce burden and eliminate duplicative credentialing & privileging efforts by hospitals and CAHs that have telemedicine services agreements with distant-site telemedicine entities and Medicareparticipating hospitals CMS believes that the final rule will reduce the burden of the traditional credentialing and privileging process while still assuring accountability. June 9,
72 Note As per both CMS and Joint Commission, hospitals/cahs may accept credentialing and privileges for telemedicine practitioners from distant hospitals/dste without appointment of telemedicine practitioners to the local hospital/cah medical staff.
73 Next Steps for C & P Still awaiting new Joint Commission standards and interpretations New language has been drafted for the Indian Health Manual Facilities should review their med staff bylaws for compliance with new ruling Agreement templates are being drafted with OGC
74 STRATEGIC OPPORTUNITIES: Behavioral Health Business Planning

75
76 FORM FOLLOWS FUNCTION
77 What will be our new models of care? What will it take to implement those models of care? What will it take to support and sustain them?

78 April 2011 Telehealth Services Network This proposal was developed as a collaboration of many people. At the request of Dr. Susan Karol, IHS Chief Medical Officer, and Dr. Theresa Cullen, IHS Chief Information Officer, a Telehealth Planning Workgroup was formed. This workgroup led the planning and development of this proposal. Participants and contributors to the proposal development included: Tammy Brown, MPH, RD, BC-ADM, CDE Mark Carroll, MD Mandi Constantine, MEd Stewart Ferguson, PhD Chris Fore, PhD Jonathan Doggette Patrick Gormley Mark Horton, OD, MD Kathleen Keats, MBA, MSIT John Kokesh, MD Chris Lamer, RPh Jill Moses, MD, MPH Chris Patricoski, MD Diane Phillips, RD, LD, CDE Jay Shore, MD Peter Stuart, MD Mark Thomas, PE, MPH Mark Veazie, DrPH Chris Watson, RPh, MPH
79 Key Concepts Telehealth is a clinical mandate, not a technical initiative. We should: Provide a predictable level of service. Support local planning and decision making. Establish national coordination, planning and accountability. Improve efficiencies through regional and centralized services. Leverage existing expertise. 79
80 Telehealth Service Expansion Four key components: Clinical Telehealth Services (for primary and specialty care) Modernized Infrastructure Regional Telehealth Resource Centers for technical/coordination/training capacity National Program Support
81 Improving the Medical Home Clinical Service Telehealth Clinical Care Centers Discipline Behavioral Health Nutrition and dietetics Telehealth Modality Model of Care o Videoconferencing o Tiered model of service o Store-and-forward o Direct psychiatric care o Surge service for communities in crisis o 24/7 consultation and clinical evaluation o Education and training o Videoconferencing o Individual and group nutrition counseling services via videoconferencing Pharmacy o Videoconferencing o Store-and-forward o Remote monitoring o o o o o o Availability of advanced practice nutrition counseling On-site assistance in region with program development Regional telepharmacy service Centralized Mail Outpatient Pharmacy (CMOP) support After-hours pharmacy review Disease management assistance o o o o o Additional Description After-hours call will be shared among 5 regions for night/weekend service to emergency departments Intra-network consultation for advance practice needs (e.g. renal, geriatric care) Anticoagulation clinics Cardiovascular risk reduction monitoring Smoking cessation line April 2011
82 Improving the Medical Home (cont.) Clinical Service Specialist Consultation Population Health Consultation Discipline IHS JVN Teleophthalmology Dermatology, Cardiology, ENT, and ID Pop Health Support Network Telehealth Modality Model of Care o Store-and-forward o Expanded JVN I/T/U sites o o Portable service model for sites too small for fixed deployment Hybrid model possible for regional service delivery o Store-and-forward o As needed specialist consultation, assisting with initial consultation and ongoing treatment needs o o Videoconferencing o Store-and-forward o Network of coaches & consultants Knowledge management system o o o Additional Description Model will be based on DM prevalence and geographic specifics Services available via partial FTE or contract National coordination April 2011
83 Alternatives Analysis Behavioral Health Specialty Service Models On-site On-site + telehealth telehealth Scalability Poor Good Good Provider Challenging, expensive and Recruitment/Retention erratic Better Best 24/7 Coverage Dependent on clinic size Available Available Access to range of specialties Limited Available Available Educational Access Local/internet National/regional/ local National/regional Surge Response Poor Best Better Collegial Support Dependent on clinic size Opportunities Best Best depending on affiliation Care needed at other than Can adjust in less than full Can adjust in less than full Cost full FTE increments costly FTE increments FTE increments Limited by provider schedule Potentially available on Potentially available on Access and housing demand demand Cross-Coverage Dependent on clinic size Patient/Provider Safety Exposed to road/air travel hazards (sig in rural areas) National/regional coverage available Better National/regional coverage available Best April 2011
84 Alternatives Analysis Behavioral Health Specialty Service Models On-site On-site + telehealth telehealth Scalability Poor Good Good Provider Challenging, expensive and Recruitment/Retention erratic Better Best 24/7 Coverage Dependent on clinic size Available Available Access to range of specialties Limited Available Available Educational Access Local/internet National/regional/ local National/regional Surge Response Poor Best Better Collegial Support Dependent on clinic size Opportunities Best Best depending on affiliation Care needed at other than Can adjust in less than full Can adjust in less than full Cost full FTE increments costly FTE increments FTE increments Limited by provider schedule Potentially available on Potentially available on Access and housing demand demand Cross-Coverage Dependent on clinic size Patient/Provider Safety Exposed to road/air travel hazards (sig in rural areas) National/regional coverage available Better National/regional coverage available Best April 2011
85 Expanding Access to Quality Behavioral Health Services Mose Herne, MPH, MS July 27, 2011
86 Inpatient Mental Health Needs Significant challenges for IHS in meeting the inpatient mental health needs of its users Recommendations from 2011 assessment include: Expand behavioral health services in partnership with Tribes, local, State, and regional providers Capitalize on emerging technologies, i.e., telebehavioral health, to increase access to and quality of services for evaluation and treatment, enhance provider education through case consultation, and strive to prevent inpatient hospitalizations
87 Current Use of Tele-behavioral Health Improving access to behavioral health services: The National Tele-behavioral Health Center of Excellence (TBHCOE) was established to provide innovative and culturally competent technical assistance to increase: access to behavioral health services training in suicide prevention for behavioral health staff practicing in Indian Country Use of tele-behavioral health technology is on the rise Over 50 IHS and Tribal facilities in 8 IHS Areas are augmenting on-site behavioral health services with telebehavioral health services
88 TBHCE Support Activities TeleBehavioral Health Policies and Procedures Credentialing and Privileging guidelines Standardized Network Assessment TelePsychiatry formulary (in progress) Secure document sharing & messaging via AFHCAN (in progress) TeleBehavioral Health EHR template (pending) TeleBehavioral Health lab package (pending)
89 Goals of Tele-behavioral Health Improve quality and access to BH care Improve customer service Reform the IHS Transparency Tribal consultation NTAC and BH Workgroup
90 TBHCE Direct Services to I/T/U Psychiatry Adult Addictions Child/Adolescent Psychology Adult Child/Adolescent Individual Group Family
91 TBHCE Activities Coordinate 24/7 Coverage Credentialing National Standards Practice EHR Formulary AFHCAN Network Assessment Billing TA TeleVideo Support OIT Coordination mhealth Initiatives Program Evaluation New Technology Eval. Intensive case mgt Training TeleBH mhealth BH/Primary Care (CME) PHN/CHR training Cultural competence
92 TBHCE Indirect Services to I/T/U Education No-Cost CME to I/T/U Primary Care providers via televideo. Clinical Support Weekly Case Staffing to I/T/U Mental Health and Substance Abuse providers. Assessing and Treating Behavioral Health Issues in a Primary Care setting (piloting) Emphasis on dual diagnosis, suicide prevention, and chronically mentally ill (in progress)
93 Targeted Outcomes Increase access to BH services Increase quality of care through service coordination 24/7 support for mental health emergencies Use of innovative and multidisciplinary care models Prevent hospitalization/reduce length of stay Improve quality of life Leveraging existing programs, i.e. VA, SAMHSA, HRSA Collaboration across the system Customer service, i.e. directly addresses BH needs as outlined in numerous venues
94 BUSINESS UPDATE: Reimbursement Policy

95 Is telehealth cost-effective?
96 Better Question: Under what circumstances are new care models using telehealth tools costeffective?
 $0 2001 2002 2003 2004 2005 2006 2007 2008 2009 Primary Care Specialty Care SFerguson PhD,")
97 DATA FROM ALASKA $3,000,000 $2,500,000 $2,000,000 $1,500,000 $1,000,000 $500,000 Annual Travel Savings (by Case Role) $ Primary Care Specialty Care SFerguson PhD, ANTHC

98 Capistrant s Medicaid Grades G Capistrant, ATA, 2011 Red = A White = B Blue = C Grey = D Black = F
99 Expanding Reimbursement Incremental expansion in coverage by both Medicare and Medicaid programs CMS considering new approach to reviewing annual requests for additions to covered telehealth services Consideration within IHS for proposal to CMS re: national coverage determination for Indian health 99

100 Service to the point of need
101 Improved access for many types of care cannot occur without telehealth

102 Thank You
19 th Annual Western Regional Conference Women in Government May 21, 2016 Seattle, WA
 TELE TODAY 19 th Annual Western Regional Conference Women in Government May 21, 2016 Seattle, WA 877 707 7172 cchpca.org Mei Wa Kwong, JD Senior Policy Associate & Project Director DISCLAIMERS Any information
TELE TODAY 19 th Annual Western Regional Conference Women in Government May 21, 2016 Seattle, WA 877 707 7172 cchpca.org Mei Wa Kwong, JD Senior Policy Associate & Project Director DISCLAIMERS Any information
Telemedicine and Fair Market Value What You Need to Know
 Telemedicine and Fair Market Value What You Need to Know By Chris W. David, CPA/ABV, ASA August, 2017 Telemedicine (also known as telehealth) is a rapidly-evolving trend in the healthcare delivery space
Telemedicine and Fair Market Value What You Need to Know By Chris W. David, CPA/ABV, ASA August, 2017 Telemedicine (also known as telehealth) is a rapidly-evolving trend in the healthcare delivery space
Telehealth in Alaska. Cindy Roleff, MS, BSN, RN-BC Telehealth Program Development Manager AFHCAN / ANTHC
 Telehealth in Alaska Cindy Roleff, MS, BSN, RN-BC Telehealth Program Development Manager AFHCAN / ANTHC Why Telehealth? Patient Empowers them with additional choices Satisfaction Decreases disparities
Telehealth in Alaska Cindy Roleff, MS, BSN, RN-BC Telehealth Program Development Manager AFHCAN / ANTHC Why Telehealth? Patient Empowers them with additional choices Satisfaction Decreases disparities
Telehealth: Frequently Asked Questions
 Telehealth: Frequently Asked Questions WHAT IS TELEHEALTH? Telehealth is the use of electronic information and telecommunications technology to support: THE DELIVERY OF HEALTH CARE PATIENT AND PROFESSIONAL
Telehealth: Frequently Asked Questions WHAT IS TELEHEALTH? Telehealth is the use of electronic information and telecommunications technology to support: THE DELIVERY OF HEALTH CARE PATIENT AND PROFESSIONAL
Telehealth. Clinical Applications 6/28/2011 TELEHEALTH UPDATE: MONTANA AND BEYOND
 TELEHEALTH UPDATE: MONTANA AND BEYOND Telehealth Telehealth is the delivery of healthrelated services via telecommunications technologies Clinical Applications Allergy Cardiology * Dermatology Oncology
TELEHEALTH UPDATE: MONTANA AND BEYOND Telehealth Telehealth is the delivery of healthrelated services via telecommunications technologies Clinical Applications Allergy Cardiology * Dermatology Oncology
Opportunities to Leverage Telehealth Within Your ACO Strategy
 Opportunities to Leverage Telehealth Within Your ACO Strategy Shawn Valenta RRT, MHA Administrator of Telehealth Center for Telehealth Phillip Warr, MD Interim Chief Medical Officer Case Management and
Opportunities to Leverage Telehealth Within Your ACO Strategy Shawn Valenta RRT, MHA Administrator of Telehealth Center for Telehealth Phillip Warr, MD Interim Chief Medical Officer Case Management and
Telehealth Policy Barriers Fact Sheet
 FACT SHEET Telehealth Policy Barriers Fact Sheet Introduction August 2016 Telehealth has existed for decades in some form or another, but it is only in the last few years it has received increasing attention
FACT SHEET Telehealth Policy Barriers Fact Sheet Introduction August 2016 Telehealth has existed for decades in some form or another, but it is only in the last few years it has received increasing attention
Telehealth. Telehealth? 6/1/2016. A tool for enhancing health care, communication and information.
 Telehealth June 2016 Telehealth? A tool for enhancing health care, public Providing/receiving health, and health education health delivery care services and support, at using a distance. electronic communication
Telehealth June 2016 Telehealth? A tool for enhancing health care, public Providing/receiving health, and health education health delivery care services and support, at using a distance. electronic communication
Keeping Your Compliance Program in Pace with Rapidly Expanding TeleHealth Services
 Keeping Your Compliance Program in Pace with Rapidly Expanding TeleHealth Services In April 1924, an imaginative cover for the magazine Radio News foreshadowed telemedicine in its depiction of a "radio
Keeping Your Compliance Program in Pace with Rapidly Expanding TeleHealth Services In April 1924, an imaginative cover for the magazine Radio News foreshadowed telemedicine in its depiction of a "radio
Telemedicine Credentialing and Privileging
 Presenting a live 90-minute webinar with interactive Q&A Telemedicine Credentialing and Privileging Protecting Patient Privacy, Avoiding Fraud and Abuse Liability, Ensuring Quality of Care THURSDAY, AUGUST
Presenting a live 90-minute webinar with interactive Q&A Telemedicine Credentialing and Privileging Protecting Patient Privacy, Avoiding Fraud and Abuse Liability, Ensuring Quality of Care THURSDAY, AUGUST
Conflict of Interest Disclosure. Telemedicine: Credentialing And Best Practices. Learning Objectives. Learning Objectives. Telehealth.
 Conflict of Interest Disclosure Telemedicine: Credentialing And s Catherine M. Ballard Partner Bricker & Eckler LLP 614-227-8806/cballard@bricker.com Use the following statement or disclose any relationships
Conflict of Interest Disclosure Telemedicine: Credentialing And s Catherine M. Ballard Partner Bricker & Eckler LLP 614-227-8806/cballard@bricker.com Use the following statement or disclose any relationships
HIMSS Davies Award. Case Study #2. Joe Humphry MD, FACP, CPEHR Cori Takesue PsyD. December 13, 2017
 HIMSS Davies Award Case Study #2 LCHC Telehealth Joe Humphry MD, FACP, CPEHR Cori Takesue PsyD December 13, 2017 501(c)3 Non profit Organization Federally Qualified Health Center (FQHC) Provides services
HIMSS Davies Award Case Study #2 LCHC Telehealth Joe Humphry MD, FACP, CPEHR Cori Takesue PsyD December 13, 2017 501(c)3 Non profit Organization Federally Qualified Health Center (FQHC) Provides services
Legal Issues You Should Know April 25, 2018 In-House Counsel Conference
 1 TELEMEDICINE Legal Issues You Should Know April 25, 2018 In-House Counsel Conference Disclaimer: These materials and presentation are intended to be a general and brief summary of the law. This is not
1 TELEMEDICINE Legal Issues You Should Know April 25, 2018 In-House Counsel Conference Disclaimer: These materials and presentation are intended to be a general and brief summary of the law. This is not
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH
 WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
Telestroke Alaska Evidence Based Care Across the Great Frontier
 Telestroke Alaska Evidence Based Care Across the Great Frontier Presented by Dr. Christie Artuso Director, Neuroscience Services Providence Alaska Medical Center 1 2 Financial Disclosures I am a speaker
Telestroke Alaska Evidence Based Care Across the Great Frontier Presented by Dr. Christie Artuso Director, Neuroscience Services Providence Alaska Medical Center 1 2 Financial Disclosures I am a speaker
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
Telehealth 101. Telehealth Summit May 24, 2018
 Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Telehealth Reimbursement Policy in
 Telehealth Reimbursement Policy in New York State Greater New York Hospital Association Telehealth Webinar Series July 11, 2016 July 2016 2 Agenda Telehealth NY State Telehealth Parity Statutory Changes
Telehealth Reimbursement Policy in New York State Greater New York Hospital Association Telehealth Webinar Series July 11, 2016 July 2016 2 Agenda Telehealth NY State Telehealth Parity Statutory Changes
Center for Health and Technology Telehealth Education Program. Executive Overview
 Executive Overview 1. Technology-Enabled Health Understand the rationale for the use of advanced IT in healthcare Identify elements of a technology-enabled health care system Learn of the legal, regulatory
Executive Overview 1. Technology-Enabled Health Understand the rationale for the use of advanced IT in healthcare Identify elements of a technology-enabled health care system Learn of the legal, regulatory
TELEHEALTH & BEHAVIORAL HEALTH
 TELE & BEHAVIORAL NATIONAL COUNCIL FOR BEHAVIORAL INSTITUTE October 2, 2017 877-707-7172 cchpca.org Mei Wa Kwong, JD Policy Advisor & Project Director DISCLAIMERS Any information provided in today s talk
TELE & BEHAVIORAL NATIONAL COUNCIL FOR BEHAVIORAL INSTITUTE October 2, 2017 877-707-7172 cchpca.org Mei Wa Kwong, JD Policy Advisor & Project Director DISCLAIMERS Any information provided in today s talk
I. LIVE INTERACTIVE TELEDERMATOLOGY
 Position Statement on Teledermatology (Approved by the Board of Directors: February 22, 2002; Amended by the Board of Directors: May 22, 2004; November 9, 2013; August 9, 2014; May 16, 2015; March 7, 2016)
Position Statement on Teledermatology (Approved by the Board of Directors: February 22, 2002; Amended by the Board of Directors: May 22, 2004; November 9, 2013; August 9, 2014; May 16, 2015; March 7, 2016)
Telehealth and Children With Special Health Care Needs. Improving Access to Care and Care Coordination
 Telehealth and Children With Special Health Care Needs Improving Access to Care and Care Coordination Jacob Vigil, MSW Program Associate The Children s Partnership Mei Wa Kwong, JD Senior Policy Associate
Telehealth and Children With Special Health Care Needs Improving Access to Care and Care Coordination Jacob Vigil, MSW Program Associate The Children s Partnership Mei Wa Kwong, JD Senior Policy Associate
NATIONAL CONSORTIUM OF TELEHEALTH RESOURCE CENTERS
 NATIONAL CONSORTIUM OF TELE RESOURCE S For the California Telehealth Resource Center Conference May 17, 2018 877-707-7172 cchpca.org Mario Mei Guttierez Wa Kwong, JD DISCLAIMERS Any information provided
NATIONAL CONSORTIUM OF TELE RESOURCE S For the California Telehealth Resource Center Conference May 17, 2018 877-707-7172 cchpca.org Mario Mei Guttierez Wa Kwong, JD DISCLAIMERS Any information provided
APNP Hospitalist Program
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital. Ministry Health Care. Program Objectives. Catholic Health Assembly June 23, 2014
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
Past, Current, and Future State of Telehealth. Eric Wallace, MD, FASN Medical Director of Telehealth
 Past, Current, and Future State of Telehealth Eric Wallace, MD, FASN Medical Director of Telehealth The View from 2018 The view in 2017 2015 Medicare and Medicaid with reimbursement for telehealth BCBS-December
Past, Current, and Future State of Telehealth Eric Wallace, MD, FASN Medical Director of Telehealth The View from 2018 The view in 2017 2015 Medicare and Medicaid with reimbursement for telehealth BCBS-December
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Presenting a live 90-minute webinar with interactive Q&A. Today s faculty features:
 Presenting a live 90-minute webinar with interactive Q&A Telemedicine Credentialing and Privileging: Complying With the New CMS Rule Protecting Patient Privacy, Avoiding Fraud and Abuse Liability, Ensuring
Presenting a live 90-minute webinar with interactive Q&A Telemedicine Credentialing and Privileging: Complying With the New CMS Rule Protecting Patient Privacy, Avoiding Fraud and Abuse Liability, Ensuring
Disclosures. Objectives. Telemedicine to Improve Care for the Underserved. I have nothing to disclose
 Disclosures Telemedicine to Improve Care for the Underserved March 11, 2016 I have nothing to disclose George Su, MD Medical Director of Telehealth, San Francisco Department of Public Health Associate
Disclosures Telemedicine to Improve Care for the Underserved March 11, 2016 I have nothing to disclose George Su, MD Medical Director of Telehealth, San Francisco Department of Public Health Associate
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telehealth 101: Key Concepts for Starting and Sustaining
 Telehealth 101: Key Concepts for Starting and Sustaining Telehealth 101 Danielle Louder Program Director NETRC, MCD Public Health Andrew Solomon, MPH Project Manager NETRC Nina Antoniotti, PhD, MBA, RN
Telehealth 101: Key Concepts for Starting and Sustaining Telehealth 101 Danielle Louder Program Director NETRC, MCD Public Health Andrew Solomon, MPH Project Manager NETRC Nina Antoniotti, PhD, MBA, RN
MEDICARE ENROLLMENT, HEALTH STATUS, SERVICE USE AND PAYMENT DATA FOR AMERICAN INDIANS & ALASKA NATIVES
 American Indian & Alaska Native Data Project of the Centers for Medicare and Medicaid Services Tribal Technical Advisory Group MEDICARE ENROLLMENT, HEALTH STATUS, SERVICE USE AND PAYMENT DATA FOR AMERICAN
American Indian & Alaska Native Data Project of the Centers for Medicare and Medicaid Services Tribal Technical Advisory Group MEDICARE ENROLLMENT, HEALTH STATUS, SERVICE USE AND PAYMENT DATA FOR AMERICAN
Creative Solutions to Challenging Access Issues. The State of Telehealth in Our Region
 Creative Solutions to Challenging Access Issues The State of Telehealth in Our Region Nebraska Hospital Association - October 25, 2017 Telehealth: Telemedicine Remote Monitoring Store-and-Forward Direct-to-Consumer/Primary
Creative Solutions to Challenging Access Issues The State of Telehealth in Our Region Nebraska Hospital Association - October 25, 2017 Telehealth: Telemedicine Remote Monitoring Store-and-Forward Direct-to-Consumer/Primary
RECOVERY AUDIT CONTRACTORS
 RECOVERY AUDIT CONTRACTORS RAC SUBSCRIPTION SERVICE Being Proactive Telemedicine Rule and CMS Updates May 10, 2011 2011 Aegis Compliance & Ethics Center, LLP 1 Faculty Brian Annulis, JD Partner, Meade
RECOVERY AUDIT CONTRACTORS RAC SUBSCRIPTION SERVICE Being Proactive Telemedicine Rule and CMS Updates May 10, 2011 2011 Aegis Compliance & Ethics Center, LLP 1 Faculty Brian Annulis, JD Partner, Meade
JUL Dear Tribal Leader:
 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service JUL 26 2012 Indian Health Service Rockville MD 20852 Dear Tribal Leader: I am writing today to provide an update on progress on our agency priorities
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service JUL 26 2012 Indian Health Service Rockville MD 20852 Dear Tribal Leader: I am writing today to provide an update on progress on our agency priorities
Corporate Reimbursement Policy Telehealth
 Corporate Reimbursement Policy Telehealth File Name: Origination: Last Review Next Review: telehealth 11/1997 12/2017 12/2018 Description Telehealth is a potentially useful tool that, if employed appropriately,
Corporate Reimbursement Policy Telehealth File Name: Origination: Last Review Next Review: telehealth 11/1997 12/2017 12/2018 Description Telehealth is a potentially useful tool that, if employed appropriately,
Kern County s Health Care Coverage Initiative Network Structure: Interim Findings
 Kern County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The Health Care Coverage Initiative (HCCI) program in Kern County is known as the Kern Medical Center Health
Kern County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The Health Care Coverage Initiative (HCCI) program in Kern County is known as the Kern Medical Center Health
Building a Successful Telemedicine Program
 Building a Successful Telemedicine Program Part 1 Ronald S. Weinstein, MD Founding Director, Arizona Telemedicine Program First Telemedicine Case Massachusetts General Hospital April, 1968 Warren Street
Building a Successful Telemedicine Program Part 1 Ronald S. Weinstein, MD Founding Director, Arizona Telemedicine Program First Telemedicine Case Massachusetts General Hospital April, 1968 Warren Street
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Diving Into Telemedicine: Adventist Health s Virtual Care Network. Tuesday, July 25, 2017
 Diving Into Telemedicine: Adventist Health s Virtual Care Network Tuesday, July 25, 2017 Diving Into Telemedicine with Adventist Health Featured Presenters Dan McCafferty V.P. of Global Sales & Corporate
Diving Into Telemedicine: Adventist Health s Virtual Care Network Tuesday, July 25, 2017 Diving Into Telemedicine with Adventist Health Featured Presenters Dan McCafferty V.P. of Global Sales & Corporate
National Indian Health Board National REC. Presented By: Tom Kauley NIHB REC Consultant National Indian Health Board
 National Indian Health Board National REC Presented By: Tom Kauley NIHB REC Consultant National Indian Health Board National Indian Health Board Founded by Tribes in 1972 Advocates to Advance Health Care
National Indian Health Board National REC Presented By: Tom Kauley NIHB REC Consultant National Indian Health Board National Indian Health Board Founded by Tribes in 1972 Advocates to Advance Health Care
Telemedicine & Telehealth
 2014 NRTRC Telemedicine Conference Reaching Patients Far and Away: Telemedicine & Telehealth March 24, 2014 Jovanna McKinney Katherine Flynn, RN Yolanda Evans, MD MPH Disclosures Practice Gap: Lack of
2014 NRTRC Telemedicine Conference Reaching Patients Far and Away: Telemedicine & Telehealth March 24, 2014 Jovanna McKinney Katherine Flynn, RN Yolanda Evans, MD MPH Disclosures Practice Gap: Lack of
TELEHEALTH: THE FUTURE IS HERE!
 TELEHEALTH: THE FUTURE IS HERE! OPPORTUNITIES FOR CAPTIVES, TRADITIONAL INSURERS AND RISK MANAGEMENT PROFESSIONALS Paul Greve, J.D., RPLU Executive Vice President Willlis Healthcare Practice Gary Leonard
TELEHEALTH: THE FUTURE IS HERE! OPPORTUNITIES FOR CAPTIVES, TRADITIONAL INSURERS AND RISK MANAGEMENT PROFESSIONALS Paul Greve, J.D., RPLU Executive Vice President Willlis Healthcare Practice Gary Leonard
9/21/2017. Telemedicine vs. Telehealth. Telemedicine vs. Telehealth. Telemedicine vs. Telehealth. Time is Money. Disruptive Technology
 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients health status. Telemedicine The Virtual Experience
Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients health status. Telemedicine The Virtual Experience
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
MISSOURI TELEHEALTH NETWORK TRAINING CONFERENCE January 31, 2018 CENTER FOR CONNECTED HEALTH POLICY POLICY DISCLAIMERS
 LEGAL & REGULATORY ISSUES TO CONSIDER IN A TELE PROGRAM MISSOURI TELE NETWORK TRAINING CONFERENCE January 31, 2018 877-707-7172 cchpca.org Mei Wa Kwong, JD DISCLAIMERS Any information provided in today
LEGAL & REGULATORY ISSUES TO CONSIDER IN A TELE PROGRAM MISSOURI TELE NETWORK TRAINING CONFERENCE January 31, 2018 877-707-7172 cchpca.org Mei Wa Kwong, JD DISCLAIMERS Any information provided in today
MEANINGFUL USE STAGE FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
Certified Community Behavioral Health Clinics (CCBHCs): Overview of the National Demonstration Program to Improve Community Behavioral Health Services
: Overview of the National Demonstration Program to Improve Community Behavioral Health Services") Certified Community Behavioral Health Clinics (CCBHCs): Overview of the National Demonstration Program to Improve Community Behavioral Health Services Cynthia Kemp (SAMHSA) Mary Cieslicki (Center for Medicaid
Certified Community Behavioral Health Clinics (CCBHCs): Overview of the National Demonstration Program to Improve Community Behavioral Health Services Cynthia Kemp (SAMHSA) Mary Cieslicki (Center for Medicaid
HIMSS Davies Award. Case Study #1 Self Measured Blood Pressure Program. Joe Humphry MD, FACP, CPEHR, Jared Medieros, APRN Geneva Castro, RN
 HIMSS Davies Award Case Study #1 Self Measured Blood Pressure Program Joe Humphry MD, FACP, CPEHR, Jared Medieros, APRN Geneva Castro, RN December, 2017 501(c)3 Non profit Organization Federally Qualified
HIMSS Davies Award Case Study #1 Self Measured Blood Pressure Program Joe Humphry MD, FACP, CPEHR, Jared Medieros, APRN Geneva Castro, RN December, 2017 501(c)3 Non profit Organization Federally Qualified
u Telemedicine The Virtual Experience
 Telemedicine The Virtual Experience April 2017 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients
Telemedicine The Virtual Experience April 2017 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients
AI/AN Long Term Care Conference. Chronic Disease Management Through. Home Telehealth Monitoring. May 2, 2010 IHS. VA US Air Force US Army US Navy
 AI/AN Long Term Care Conference Chronic Disease Management Through Home Telehealth Monitoring May 2, 2010 Briefers: David T. Peters ANMC ANTHC IHS USCG VA US Air Force US Army US Navy Legal Authority --
AI/AN Long Term Care Conference Chronic Disease Management Through Home Telehealth Monitoring May 2, 2010 Briefers: David T. Peters ANMC ANTHC IHS USCG VA US Air Force US Army US Navy Legal Authority --
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Cheryl A Skiffington, CCO & Interim CFO Columbia County Health System
 Cheryl A Skiffington, CCO & Interim CFO Columbia County Health System Telemedicine is A mode of delivery The service provided is basically the same as if the patient and provider were face-to-face. A modifier
Cheryl A Skiffington, CCO & Interim CFO Columbia County Health System Telemedicine is A mode of delivery The service provided is basically the same as if the patient and provider were face-to-face. A modifier
Health Center Program Update
 Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Data Worksheet: Tele Behavioral Health Utilization / Veterans Services
 Department of Health and Social Services DIVISION OF BEHAVIORAL HEALTH Director s Office 3601 C Street, Suite 878 Anchorage, Alaska 99503-5924 Main: 907.269.3600 Toll Free: 800.770.3930 Fax: 907.269.3623
Department of Health and Social Services DIVISION OF BEHAVIORAL HEALTH Director s Office 3601 C Street, Suite 878 Anchorage, Alaska 99503-5924 Main: 907.269.3600 Toll Free: 800.770.3930 Fax: 907.269.3623
The Psychiatric Shortage:
 ational Council Medical Director Institute The Psychiatric Shortage: National Council Medical Causes and Solutions Director Institute Update National Council Medical Director Institute Medical directors
ational Council Medical Director Institute The Psychiatric Shortage: National Council Medical Causes and Solutions Director Institute Update National Council Medical Director Institute Medical directors
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
5/1/2017. Medicare Coverage Guidelines for DSMT and MNT Telehealth. Telehealth Defined
 Medicare Coverage Guidelines for DSMT and MNT Telehealth Mary Ann Hodorowicz, RDN, MBA, CDE Certified Endocrinology Coder Mary Ann Hodorowicz Consulting, LLC 4-30-17 MEDICARE DSMT - MNT TELEHEALH KEY TOPICS
Medicare Coverage Guidelines for DSMT and MNT Telehealth Mary Ann Hodorowicz, RDN, MBA, CDE Certified Endocrinology Coder Mary Ann Hodorowicz Consulting, LLC 4-30-17 MEDICARE DSMT - MNT TELEHEALH KEY TOPICS
Exploring Public Health Barriers and Opportunities in Eye Care: Role of Community Health Clinics
 Exploring Public Health Barriers and Opportunities in Eye Care: Role of Community Health Clinics Susan A. Primo, O.D., M.P.H., F.A.A.O. Director, Vision and Optical Services Emory Eye Center Professor
Exploring Public Health Barriers and Opportunities in Eye Care: Role of Community Health Clinics Susan A. Primo, O.D., M.P.H., F.A.A.O. Director, Vision and Optical Services Emory Eye Center Professor
3/27/2017. Historical Perspective. Innovative Model of Healthcare Delivery Using Telemedicine
 Innovative Model of Healthcare Delivery Using Telemedicine Vinita Kamath MS RDN MHA Clinical Director, Nutrition Therapy Cincinnati Children s Hospital Medical Center CNM Conference March 20, 2017 Outline
Innovative Model of Healthcare Delivery Using Telemedicine Vinita Kamath MS RDN MHA Clinical Director, Nutrition Therapy Cincinnati Children s Hospital Medical Center CNM Conference March 20, 2017 Outline
Jason C. Goldwater, MA, MPA Senior Director
 The History of Health Information Technology in 45 Minutes Jason C. Goldwater, MA, MPA Senior Director April 5, 2017 Agenda Where We are With Health Information Technology and Where We are Going The Alphabet
The History of Health Information Technology in 45 Minutes Jason C. Goldwater, MA, MPA Senior Director April 5, 2017 Agenda Where We are With Health Information Technology and Where We are Going The Alphabet
19/09/2017. Telehealth Legal and Regulatory Issues in Colorado and Beyond. Nathaniel Lacktman, October 2017
 Telehealth Legal and Regulatory Issues in Colorado and Beyond Nathaniel Lacktman, Esq. @Lacktman October 2017 1 2 1 Licensing 3 Licensing Physician offering care via telemedicine is subject to licensure
Telehealth Legal and Regulatory Issues in Colorado and Beyond Nathaniel Lacktman, Esq. @Lacktman October 2017 1 2 1 Licensing 3 Licensing Physician offering care via telemedicine is subject to licensure
Telehealth Legal and Compliance Issues. Nathaniel Lacktman, Anna Whites, Esq.
 Telehealth Legal and Compliance Issues Nathaniel Lacktman, Esq. @Lacktman Anna Whites, Esq. Anna Whites Law Office Attorney Advertising Prior results do not guarantee a similar outcome Models used are
Telehealth Legal and Compliance Issues Nathaniel Lacktman, Esq. @Lacktman Anna Whites, Esq. Anna Whites Law Office Attorney Advertising Prior results do not guarantee a similar outcome Models used are
Overview of Select Health Provisions FY 2015 Administration Budget Proposal
 Overview of Select Health Provisions FY 2015 Administration Budget Proposal On March 4, 2014, President Obama released his Administration s FY 2015 budget proposal to Congress. The budget contains a number
Overview of Select Health Provisions FY 2015 Administration Budget Proposal On March 4, 2014, President Obama released his Administration s FY 2015 budget proposal to Congress. The budget contains a number
THE TELEMEDICINE MARKET LANDSCAPE
 How Telehealth is Changing the Care Provided to Patients Anne Cadwell, The Permanente Medical Group THE TELEMEDICINE MARKET LANDSCAPE Approximately 1 million virtual doctor visits in the U.S. in 2015 1
How Telehealth is Changing the Care Provided to Patients Anne Cadwell, The Permanente Medical Group THE TELEMEDICINE MARKET LANDSCAPE Approximately 1 million virtual doctor visits in the U.S. in 2015 1
1. What are the requirements for Stage 1 of the HITECH Act for CPOE to qualify for incentive payments?
 CPPM Chapter 8 Review Questions 1. What are the requirements for Stage 1 of the HITECH Act for CPOE to qualify for incentive payments? a. At least 30% of the medications in the practice must be ordered
CPPM Chapter 8 Review Questions 1. What are the requirements for Stage 1 of the HITECH Act for CPOE to qualify for incentive payments? a. At least 30% of the medications in the practice must be ordered
TELEHEALTH REIMBURSEMENT
 FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 TELEHEALTH REIMBURSEMENT Telehealth is a well-established
FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 TELEHEALTH REIMBURSEMENT Telehealth is a well-established
Alpert Medical School of Brown University Clinical Psychology Internship Training Program Rotation Description
 Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Telemedicine Privacy and Security: Safeguarding Protected Health Information and Minimizing Risks of Disclosure
 Presenting a live 90-minute webinar with interactive Q&A Telemedicine Privacy and Security: Safeguarding Protected Health Information and Minimizing Risks of Disclosure THURSDAY, AUGUST 13, 2015 1pm Eastern
Presenting a live 90-minute webinar with interactive Q&A Telemedicine Privacy and Security: Safeguarding Protected Health Information and Minimizing Risks of Disclosure THURSDAY, AUGUST 13, 2015 1pm Eastern
HR Telehealth Enhancement Act of 2015
 HR 2066 - Telehealth Enhancement Act of 2015 Rep. Harper (R-MS), Rep. Thompson (D-CA), Rep. Black (R-TN) & Rep. Welch (D-VT) Author Intent: To promote and expand telehealth application under Medicare and
HR 2066 - Telehealth Enhancement Act of 2015 Rep. Harper (R-MS), Rep. Thompson (D-CA), Rep. Black (R-TN) & Rep. Welch (D-VT) Author Intent: To promote and expand telehealth application under Medicare and
Department of Health Care Services Integrating Telehealth Efforts. Joanne Peschko, MBA Health Program Specialist
 Department of Health Care Services Integrating Telehealth Efforts Joanne Peschko, MBA Health Program Specialist 1 Telehealth Programs Public Hospital Redesign and Incentives in Medi-Cal (PRIME) Managed
Department of Health Care Services Integrating Telehealth Efforts Joanne Peschko, MBA Health Program Specialist 1 Telehealth Programs Public Hospital Redesign and Incentives in Medi-Cal (PRIME) Managed
Oklahoma Health Care Authority. Telemedicine
 Oklahoma Health Care Authority Telemedicine Telemedicine Policy: OAC 317:30-3-27 Billing Technology 2 Telemedicine Applicability & Scope The purpose of the SoonerCare telemedicine is to improve access
Oklahoma Health Care Authority Telemedicine Telemedicine Policy: OAC 317:30-3-27 Billing Technology 2 Telemedicine Applicability & Scope The purpose of the SoonerCare telemedicine is to improve access
Telemedicine. Important Information. Telemedicine 5/6/2016. Lauren Prew
 Telemedicine Lauren Prew Important Information This presentation is similar to any other seminar designed to provide general information on pertinent legal topics. The statements made and any materials
Telemedicine Lauren Prew Important Information This presentation is similar to any other seminar designed to provide general information on pertinent legal topics. The statements made and any materials
Why Telehealth, Why Now?
 Promoting Access to Quality Care Through Technology and Innovation Why Telehealth, Why Now? Industry Webinar November 9, 2016 Panelists Bill Boling Owner/Principal Boling & Company bill@bolingandcompany.com
Promoting Access to Quality Care Through Technology and Innovation Why Telehealth, Why Now? Industry Webinar November 9, 2016 Panelists Bill Boling Owner/Principal Boling & Company bill@bolingandcompany.com
Telemedicine and Health Reform. Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center
 Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Chapter 7 Section 22.1
 TRICARE Policy Manual 6010.57-M, February 1, 2008 Medicine Chapter 7 Section 22.1 Issue Date: April 17, 2003 Authority: 32 CFR 199.4 and 32 CFR 199.14 1.0 DESCRIPTION 1.1 refers to the use of information
TRICARE Policy Manual 6010.57-M, February 1, 2008 Medicine Chapter 7 Section 22.1 Issue Date: April 17, 2003 Authority: 32 CFR 199.4 and 32 CFR 199.14 1.0 DESCRIPTION 1.1 refers to the use of information
TRANSFORMING HEALTH CARE WITH CONNECTED HEALTH TECHNOLOGY
 TRANSFORMING CARE WITH CONNECTED TECHNOLOGY TELE STATE TRENDS Florida Telehealth Advisory Council April 21, 2017 877-707-7172 cchpca.org Mario Gutierrez We are part of the Public Health Institute, an independent,
TRANSFORMING CARE WITH CONNECTED TECHNOLOGY TELE STATE TRENDS Florida Telehealth Advisory Council April 21, 2017 877-707-7172 cchpca.org Mario Gutierrez We are part of the Public Health Institute, an independent,
Telemedicine and Reimbursement
 Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
The Telemedicine Opportunity. Presented By: Marybeth McCall, MD
 The Telemedicine Opportunity Presented By: Marybeth McCall, MD 1962 Episode of the The Jetsons Presentation Objectives Identify telemedicine utilization projections Describe New York s Telemedicine Mandate
The Telemedicine Opportunity Presented By: Marybeth McCall, MD 1962 Episode of the The Jetsons Presentation Objectives Identify telemedicine utilization projections Describe New York s Telemedicine Mandate
Telehealth Landscape and Experience in Maine and Beyond
 Telehealth Landscape and Experience in Maine and Beyond September 22, 2017 Danielle Louder Program Director Northeast Telehealth Resource Center Co-Director - MCD Public Health About Us www.mcdph.org
Telehealth Landscape and Experience in Maine and Beyond September 22, 2017 Danielle Louder Program Director Northeast Telehealth Resource Center Co-Director - MCD Public Health About Us www.mcdph.org
Regents University of California Telehealth Network Ware County Telehealth Network
 TMC72 Response to Telemedicine Inquiry (Attachment and Appendix): The Health Resources and Services Administration (HRSA) oversees the Telehealth Network Grant Program (TNGP) which aims at: helping communities
TMC72 Response to Telemedicine Inquiry (Attachment and Appendix): The Health Resources and Services Administration (HRSA) oversees the Telehealth Network Grant Program (TNGP) which aims at: helping communities
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
Transforming Health Care with Telehealth: Today s Barriers and Tomorrow s Solutions
 Transforming Health Care with Telehealth: Today s Barriers and Tomorrow s Solutions Mario Gutierrez, Executive Director August 28, 2014 Webinar for the Northwest Telehealth Resource Center Center for Connected
Transforming Health Care with Telehealth: Today s Barriers and Tomorrow s Solutions Mario Gutierrez, Executive Director August 28, 2014 Webinar for the Northwest Telehealth Resource Center Center for Connected
H.R MEDICARE TELEHEALTH PARITY ACT OF 2017
 FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 H.R. 2550 MEDICARE TELEHEALTH PARITY ACT OF 2017 SPONSORS:
FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 H.R. 2550 MEDICARE TELEHEALTH PARITY ACT OF 2017 SPONSORS:
Comparison of the Health Provisions in HR 1 American Recovery and Reinvestment Act
 APPROPRIATIONS Comparative Effectiveness Research $1.1B for comparative effectiveness programs, including $300 M for AHRQ, $400 M for NIH, and $400 M for HHS. Establishes a Federal Coordinating Council.
APPROPRIATIONS Comparative Effectiveness Research $1.1B for comparative effectiveness programs, including $300 M for AHRQ, $400 M for NIH, and $400 M for HHS. Establishes a Federal Coordinating Council.
Albany Medical Center. AMCH PPS Clinical & Quality Affairs Committee
 Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Tara Foster, MS, RN Mingie Kang, MPH Mark Quail, MEd Brendon Smith, PhD Susan Kopp MBA, BSN, RN January
Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Tara Foster, MS, RN Mingie Kang, MPH Mark Quail, MEd Brendon Smith, PhD Susan Kopp MBA, BSN, RN January
Statewide Tribal Health Care Delivery Issues Log MH Medicaid Working Copy as of March 17, 2016
 Statewide Tribal Health Care Delivery Issues Log MH Medicaid Working Copy as of March 17, 2016 # Category Agency Issue Description/Analysis Next Steps Timeframe/Target Date 1 BH-BHO BHA Require BHOs to
Statewide Tribal Health Care Delivery Issues Log MH Medicaid Working Copy as of March 17, 2016 # Category Agency Issue Description/Analysis Next Steps Timeframe/Target Date 1 BH-BHO BHA Require BHOs to
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
RPM: Is It All It Is Cracked Up to Be?
 RPM: Is It All It Is Cracked Up to Be? Session 192, February 22, 2017 Hank Fanberg, Director of Innovation, Christus Health System Gregg Malkary, Managing Director, Spyglass Consulting Group 1 Speaker
RPM: Is It All It Is Cracked Up to Be? Session 192, February 22, 2017 Hank Fanberg, Director of Innovation, Christus Health System Gregg Malkary, Managing Director, Spyglass Consulting Group 1 Speaker
EXTENDED STAY PRIMARY CARE
 EXTENDED STAY PRIMARY CARE Working with Frontier Communities to Design Facilities that Work June 2000 Supported in part by the Federal Office of Rural Health Policy HRSA, DHHS Frontier Education Center
EXTENDED STAY PRIMARY CARE Working with Frontier Communities to Design Facilities that Work June 2000 Supported in part by the Federal Office of Rural Health Policy HRSA, DHHS Frontier Education Center
Telehealth: An Introduction to Implementation and Policy Considerations. Angela Evatt, M.A., M.P.P
 Telehealth: An Introduction to Implementation and Policy Considerations Angela Evatt, M.A., M.P.P Overview What is telehealth, how can it be used in care delivery, and what does it aim to accomplish? Value
Telehealth: An Introduction to Implementation and Policy Considerations Angela Evatt, M.A., M.P.P Overview What is telehealth, how can it be used in care delivery, and what does it aim to accomplish? Value
Cruising Through Key Legal Compliance Issues in Telemedicine
 April 12, 2018 Cruising Through Key Legal Compliance Issues in Telemedicine Presented by Cal Marshall 2018 Chambliss, Bahner & Stophel, P.C. All Rights Reserved. Chambliss, Bahner & Stophel, P.C. Liberty
April 12, 2018 Cruising Through Key Legal Compliance Issues in Telemedicine Presented by Cal Marshall 2018 Chambliss, Bahner & Stophel, P.C. All Rights Reserved. Chambliss, Bahner & Stophel, P.C. Liberty
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
The CCBHC: An Innovative Model of Care for Behavioral Health
 The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
Telemedicine Reimbursement. An Overview for Oregon
 Telemedicine Reimbursement An Overview for Oregon A Brief History - Medicare In 1997 the Balanced Budget Act first authorized Medicare to reimburse for telemedicine services Since 2000 there have been
Telemedicine Reimbursement An Overview for Oregon A Brief History - Medicare In 1997 the Balanced Budget Act first authorized Medicare to reimburse for telemedicine services Since 2000 there have been
Overview of the EHR Incentive Program Stage 2 Final Rule
 HIMSS applauds the Department of Health and Human Services for its diligence in writing this rule, particularly in light of the comments and recommendations made by our organization and other stakeholders.
HIMSS applauds the Department of Health and Human Services for its diligence in writing this rule, particularly in light of the comments and recommendations made by our organization and other stakeholders.
Expanding Urologic Practice Through Telehealth
 Expanding Urologic Practice Through Telehealth Great Lakes SUNA Chapter Spring Conference Chad Ellimoottil, MD, MS Assistant Professor of Urology Director of Telemedicine, Department of Urology ehealth
Expanding Urologic Practice Through Telehealth Great Lakes SUNA Chapter Spring Conference Chad Ellimoottil, MD, MS Assistant Professor of Urology Director of Telemedicine, Department of Urology ehealth
Chapter 2. Telehealth Regulatory Requirements
 Chapter 2 Telehealth Regulatory Requirements 2.1 Introduction Sometimes referred to as telehealth practice standards, the rules governing where and how telehealth may be used to deliver care are largely
Chapter 2 Telehealth Regulatory Requirements 2.1 Introduction Sometimes referred to as telehealth practice standards, the rules governing where and how telehealth may be used to deliver care are largely
Wired to Save Lives: A Virtual Hospital Experience
 Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has