Royal Berkshire NHS Foundation Trust. Annual Report and Financial Statements for the period 1 April March 2015
|
|
|
- Lauren Pierce
- 6 years ago
- Views:
Transcription

1 Royal Berkshire NHS Foundation Trust Annual Report and Financial Statements for the period 1 April March
2 2
3 Royal Berkshire NHS Foundation Trust Annual Report and Financial Statements for the period 1 April March 2015 Presented to Parliament pursuant to Schedule 7, paragraph 25(4) (a) of the National Health Service Act
4 4
5 Annual Report 2014/15 Contents Page No Section 1 Chairman s and Chief Executive s Introduction 6 Section 2 Strategic Report Brief history of Trust Review of our business, including risks and uncertainties Strategy/business model Key performance indicators, including employee and environmental Staff breakdown by gender Refer to annual accounts Going Concern 8 Directors Report Directors About our care Our staff Stakeholder relations 15 Section 3 Governance arrangements Board of Directors Audit and Risk Committee Nominations and Remuneration Committee Council of Governors and membership 19 Section 4 Statutory information Financial performance Remuneration report Sustainability report Regulatory ratings Staff survey Disclosures in the public interest Compliance with the Monitor Code of Governance 37 Section 5 Statement of accounting officer s responsibilities 61 Section 6 Governance statement 62 Section 7 Quality Account Report 70 Section 8 Annual Accounts 153 5
6 1. Chairman s and Chief Executive Officer s introduction to the Annual Report There is no doubt that these continue to be challenging times for the NHS as a whole, including our Trust. Despite the increasing demand for services we recognise that we must manage within the finances available to us, we are constantly impressed by the positive feedback our teams receive and the support shown by their comments. We are proud of the ongoing improvements and developments across the Trust to deliver safe, high quality care. Early in the year the Care Quality Commission (CQC) released the results of its 2014 inspection. While there are lessons for us to learn the report does recognise the compassionate care provided here, and the respect and dignity with which patients are cared for. Over the year we have closely monitored our progress against an action plan to improve those areas identified where development was needed. The Trust was very pleased to welcome Jean O Callaghan as our new Chief Executive Officer in August We were grateful for Medical Director Alistair Flowerdew for providing interim leadership while we recruited to the role. In March 2015 Stephen Billingham stepped down from his role as Chairman and Non-executive Director Janet Rutherford was appointed Interim Chair while a permanent appointment is made. We would like to thank Stephen for the experience and expertise he has supported us with during his time with the Trust. We would also like to thank Jane May, Non-executive Director, who completed her term of office in September 2014 and to welcome Sue Hunt and Julian Dixon who join us as non-executive directors. Jean s appointment is reflective of the changes we are making to the way the Trust is run to ensure that we have effective leadership. We have made changes to our structure at Board and senior management level to make sure we are well placed in future to deliver the best possible care, against a sound financial performance. Demand on our Emergency Department (A&E) continues to test us we are seeing more elderly, frail patients and despite the measure we put in place to manage this higher level of complex demand, the challenge continues. We are pleased to have met the target for some months, and to only narrowly have missed it in others our focus now is on achieving consistency in delivering the access target month on month. We continue to work closely with our commissioners, local authorities, other trusts and stakeholders to improve the way services are delivered. During the year we also identified issues with recording around the 18-week referral to treatment pathway. Good progress was made on resolving these issues and delivering care to the patients involved. By year end the position was on target for admitted pathways, and better than scheduled for non-admitted pathways. The Trust group as a whole which includes the Trust s wholly owned subsidiary and the Royal Berkshire Charity, made a deficit of 9.0m in 2014/15 compared to a deficit of 6.6m in 2013/14. We have continued to see a growth in activity during the year with a corresponding increase in income, however costs have more than offset this increased income, in particular due to unfunded radiology costs, increased pay cost to validate and correct the Trust s waiting list and increased management costs. 6
7 In November 2014 Monitor announced an investigation into the Trust following concerns about our ability to meet national waiting times targets given the data issues we identified, and around our worse than expected financial position. A number of enforcement actions were agreed to rectify our position. The Trust continues to make progress against the agreed action plan and discussions with Monitor continue. We were extremely pleased with the opening of four refurbished dementia-friendly wards. The number of patients that we see with dementia is increasing and these wards provide a calmer environment that is easier to navigate, reducing stress for our patients. Staff have enthusiastically embraced the changes, introducing new activities to provide a more sociable and stimulating day for everyone. Our Cardiology team continue to deliver the fastest response times for heart attacks nationally. We were extremely proud of them for winning the Pride of Reading Healthcare Team of the Year award demonstrating how they are valued by local people. Prime Minister David Cameron took time to record a video message of congratulations to them too. The Cardiology team is just one group of staff who are working hard to make a difference to our patients. We continue to invest in our facilities we opened a new Acute Medical Unit which provides a ward environment for clinical staff to observe patients who need more time than a visit to A&E allows, but who don t need to be admitted to a ward. We have also opened two new operating theatres which will help us separate planned from emergency surgery, cutting waiting times and reducing cancellations. We would like to thank our Council of Governors for their ongoing work and support for the Trust. David Cooper, Public Governor for Reading, has stepped into the lead Governor role. We also appreciate the role played by our volunteers, and the charitable organisations that support us they all play a part in making life better for our patients and visitors. Most of all we want to thank our hard working and committed staff for their ongoing support and for ensuring we deliver the care our community requires. Janet Rutherford Chair Jean O Callaghan Chief Executive Officer 7
8 2. Strategic report About the Trust The Trust provides high quality acute medical and surgical services for our local communities of over 500,000 people. We also provide specialist services to a population of one million across Berkshire and its borders. With just over 4,500 staff we are one of the largest employers in the Reading area. The Trust provides services from the following bases: Royal Berkshire Hospital, Reading with just under 700 beds and capacity for over 200 day patients. The Prince Charles Eye Unit, Windsor, provides eye services to the patients of East Berkshire Dialysis services at a dedicated unit in Windsor West Berkshire Community Hospital - day surgery unit and the acute outpatients department. Royal Berkshire Bracknell Healthspace cancer, renal and outpatient services. Townland s Hospital, Henley outpatient services. We are a designated specialist centre in cancer, bariatric care, heart attack and stroke. We also provide specialist care as part of a care network through a local neonatal unit, an interventional radiology unit and a trauma unit. We are part of the critical care and vascular care networks. We have been an NHS foundation trust since June 2006 and we are pleased that the freedoms and responsibilities that this brings enables us to work with our members through our Council of Governors to shape our direction of travel, and that working with commissioners we can develop the services and facilities that are needed by our local communities. The directors are in agreement that there is no relevant audit data of which the auditors are unaware and each director has taken all necessary steps to make themselves aware of the relevant audit information. Our strategy Our Trust vision is to provide sustainable, and improving, high quality care for our local community. To achieve this we are committed to number of overarching strategic goals: High quality care: A commitment to high quality care that is safe, compassionate, effective and provides a positive experience. This will be underpinned by effective processes of clinical governance and risk management. Financial sustainability: Achieving financial stability, resilience and sustainability in the longer term that allows investment in front line services that are fit for the future. Transforming services: Ensuring our services meet the needs of the local population by responding to the changing needs of our patients, commissioners and the local health and social care environment in order to bring maximum benefit through integration. Organisational resilience and capability: Improving how we align all the components of our organisation that define us our estate, workforce (capacity and skills), technology, our culture of caring and learning and our leadership capability. 8
9 Central to our strategy is our view of the range of services we will be providing over the next three to five years. The Trust is clear that it will be: A major provider of A&E and medical and surgical emergency access services on the RBH site. Committed to development of more integrated care across both local hospital, communitybased and primary health services in order to deliver, with our partners, best care for patients throughout their healthcare journeys. Focussed on prevention, early intervention and keeping people healthy, as well as to provide excellent care for people who need treatment. Continue to develop as a centre of excellence for cancer, critical care, renal, heart attack management, stroke, trauma, spinal surgery, paediatric and neonatal services. Retain and develop a range of planned diagnostic and treatment services (which are clinically and financially viable, and support the wider provision of services in the Trust). The Trust will act in partnership with other organisations to provide and sustain high quality care, when this is the most appropriate solution. During 2015/16, the Trust will be developing a new Strategic Plan (supported by a Clinical Services Strategy). The development of this plan is part of a significant workstream reflective of our response, and that of the local health and social care economy, to the Five Year Forward View. This Strategic Plan will enable the Trust to refocus its longer-term goals and address the challenges faced by, not only the Trust, but also our partner providers, including primary care and our commissioner. The Board of Directors is responsible for adding value to, and promoting the success of, the organisation. Review of 2014/15 This year has been another challenging year for the Trust. The issues facing us are largely reflected across the NHS as the system continues to balance delivering high quality care against increasing demand and reducing financial resources. Following our Care Quality Inspection in early 2014, we received our inspection report in July The overall rating for the trust was requires improvement. The CQC rated us on five key areas as shown below: Are services at this trust safe? Requires improvement Are services at this trust effective? Good Are services at this trust caring? Good Are services at this trust responsive? Requires improvement Are services at this trust well led? Requires improvement CQC also rated services areas. Two areas receive a rating of outstanding - the highest mark given by the CQC. The critical care team is recognised for its caring interventions to support 9
10 patients, families, friends and staff, while end of life care received an outstanding rating for their responsiveness to patient needs. Services for children and young people were also highly praised, achieving a good rating against all five measures. The report sets out some clear challenges for us to address. Many of the challenges were already recognised and work was already underway to address areas such as the accessibility and security of medical records or staffing issues. Read the full report at Performance against national targets Despite the measures set in place last year, and additional work undertaken this year to expand our Emergency Department, the rising demand has continued to challenge us. Having achieved the target for the first four months of 2014/15 we were extremely disappointed to dip in performance and narrowly miss the target for the subsequent quarters. Referral to treatment times A&E Cancer access National standards 2014/15 RBFT 2014/15 RBFT 2013/14 % of admissions within 18 weeks from referral 90% 77.45% N/A % of non-admissions within 18 weeks from referral 95% 96.3% N/A % of incomplete pathways within 18 weeks 91.56% N/A % waiting less than 6 weeks from referral for a diagnostic test 99% 91.3% 96.9% % of A & E admission, transfer or discharge within 4 hours of arrival at A&E 95% 94.44% 92.1% % of service users referred urgently with suspected cancer by a GP waiting no more than 93% 90.7% 93.6% two weeks for first outpatient appointment % of service users referred urgently with breast symptoms (where cancer was not initially suspected) waiting no more than two weeks for first outpatient appointment % of service users waiting no more than one month (31 days) from diagnosis to first definitive treatment for all cancers % of service users waiting no more than two months (62 days) from urgent GP referral to first definitive treatment for cancer % of service users waiting no more than 62 days from referral from an NHS screening service to first definitive treatment for all cancers 93% 91.5% 93.9% 96% 97.2% 98.1% 85% 80.7% 86.2% 90% 88.6% 91.7% During 2014 an issue around data quality emerged which meant that we were not confident that the 18-week referral to treatment times reported were accurate. We agreed a reporting break with our regulator Monitor to enable us to investigate and address any issues. There were two clinical areas affected and the Trust took prompt action to ensure patients affected received a timely clinical review, and to make sure that the system issues were corrected. This issue was one, along with our financial position, that led Monitor to investigate the Trust and to initiate enforcement action. 10
11 The Trust was pleased to be ranked as one of the Top 40 Hospitals in by CHKS provider of healthcare intelligence and quality improvement services to the healthcare sector. These annual awards are based on the data submitted by Trusts across the country. The Trust was also invited to be one of the first trusts nationally to join the Sign up to Safety campaign. The programme is an NHS England initiative to deliver safer, harm free care across the NHS. It launched in June 2014 with the mission to strengthen patient safety in the NHS and make it the safest healthcare system in the world. PFI The Trust had no involvement in any Private Finance Initiative Contracts during the period 1 April 2014 to 31 March Building our presence In recent years the number of outpatient referrals made by GPs in Berkshire West has steadily increased as a result of growing population demand. We track our market share (the numbers of referrals that came to the Trust as a proportion of total referrals made) as a measure of how many patients chose to be treated at the Trust over other local providers. The graph below indicates the trend in our market share of new outpatients between 2011 and The trend in market share is different for elective (ie planned) surgical procedures. The following graph indicates that, whilst the Trust has increased the volume of elective surgery performed, our market share has decreased by around 7%. To an extent, some loss of market share in a growing market is to be expected initially, due to there being a range of providers for patients to choose from and the Trust having limited funds to rapidly invest in increasing capacity. However, there are some specific specialities, including orthopaedics, where market share has declined significantly and where in particular other providers are increasing their proportion of the more easier and profitable procedures. This has the potential to have an impact on the longerterm sustainability of some of our services. 11
12 To improve the quality of the patient experience, and in doing so, increase market share of elective surgery, the Trust has recently opened two new state of the art elective orthopaedic theatres. These are providing a greatly improved environment for patients as well as enabling the Trust to drive through a reduction in waiting times for elective surgery. It is this reduction in waiting times that we believe is the critical factor that will drive a greater proportion of patients to choose to have their surgery at the Trust. New developments Over the year the Trust has invested in facilities and service developments to improve the care we provide for our patients. We opened four dementia-friendly wards with financial support from the Department of Health. The wards have been designed to provide a calming environment which is easier to navigate. Feedback from patients and families has been very positive. We have also invested in two new operating theatres. The aim is to ensure that planned operations are not affected by peaks in demand for emergency surgery this can sometimes lead to cancellations which is frustrating for patients. This should also enable the Trust to better manage its waiting times for treatment in order to see patients more promptly. Meeting the waiting time targets for A&E has been an ongoing challenge and last year we described some of the steps we were taking to support staff in delivering timely care. This year we opened a new observation ward close to A&E which helps us monitor patients who do not need to be admitted to a ward but do need a period of time to stabilise before returning home. We also introduced two new campaigns to benefit patients. The Hello, my name is. is a national campaign started by a doctor following a spell of cancer treatment. She was struck by how few staff introduced themselves and we are encouraging all of our staff to start their conversations by giving their name. Forget me not is a campaign aimed at supporting patients with dementia. By placing the flower symbol above their beds, staff are instantly reminded that the patient has dementia and may therefore need more support. 12
13 As the year drew to a close we successfully won a tender to provide sexual health services. Research and development We have become a more diverse research active organisation with around 200 clinical trials running at the moment. Last year we were the fourth most active district general hospital in England with 5307 patients recruited into clinical trials. We also introduced National Institute for Health Research (NIHR) activity into more departments including Radiology, Trauma and Orthopaedics and Anaesthetics. Our staff As a Trust, we recognise that our staff are our most valuable asset. As such, our people are central to our success this past year, and integral to the delivery of our objectives and priorities into the future. The environment in which we operate is becoming ever more challenging but we are on a journey to make the Royal Berkshire NHS Foundation Trust the best place to work, learn and train and are committed to this as one of our aims. The Trust is a place our staff recommend as a place to work or receive treatment. The 2014 National Staff survey shows that we remain in the top 20% for staff engagement. We also performed better than last year with more staff having had health and safety training, and equality and diversity training in the last 12 months. We need to improve in some areas too: reporting errors, near misses or incidents witnessed in the last month reducing the number of staff reporting experiencing discrimination at work in last 12 months increasing the number of staff believing that the Trust provides equal opportunities for career progression. More information on the survey is presented on page 12. Our divide of male and female staff at the year end is: Female Male Directors (Executive and Non-executive) 7 5 Senior managers* All staff *Includes Agenda for Change bands 8 and 9, and senior manager spot salaries. The Trust sickness absence rate for end of March 2015 (12-month rolling absence) is 3.25%. Environmental, social, community and human rights issues A full report on our environmental impact is included on page 52. The Trust is keen to engage with the local community and does this in several ways. The main route is via the Trust membership which offers the local community the chance to get involved, and also to find out more about how we work with behind the scenes tours and health seminars. During the year we have also enhanced our approach to patient and public engagement and have appointed a number of patient leaders to work with us to encourage wider patient participation. Each of our policies has an equality impact assessment to assess its impact on service users and staff. The year end The Trust group as a whole which includes the Trust s wholly owned subsidiary and the Royal Berkshire Charity, made a deficit of 9.0m in 2014/15 compared to a deficit of 6.6m in 2013/14. 13
14 We have continued to see a growth in activity during the year with a corresponding increase in income, however costs have more than offset this increased income, in particular due to unfunded radiology costs, increased pay cost to validate and correct the Trust s waiting list and increased management costs. Preparation of these accounts These accounts have been prepared under a direction issued by Monitor under the National Health Service Act The Trust faces the following key risks over the coming year: Risk we fail to maintain financial stability Risk that our physical infrastructure is not of a sufficient standard Risk that our IM&T systems and process are not fit for purpose Risk that we will not achieve performance targets Going Concern As a foundation trust there is no presumption that the organisation is a going concern. After making enquiries the directors have a reasonable expectation that the Royal Berkshire NHS Foundation Trust has adequate resources to continue in operational existence for the foreseeable future. For this reason, they continue to adopt the going concern basis in preparing the accounts. Approval of this report Directors of the Trust have responsibility for preparing the annual report and accounts, and consider the annual report and accounts, taken as a whole, are fair, balanced and understandable and provide the information necessary for patients, regulators and other stakeholders to assess the NHS foundation trust s performance, business model and strategy. This report has been approved by the directors of the Trust. Signed Jean O Callaghan Chief Executive Officer Date: 27 May
15 Directors Report About our care The National Inpatient Survey results 2014 The results of the survey demonstrate that the Trust has improved significantly in five areas compared to the 2013 survey, while performance has deteriorated in two areas. Performance was maintained against 53 of the questions. The areas where we have improved significantly include the availability of nursing staff, hand hygiene and offering patients a choice of hospitals for admission. Our focus now will be on understanding where our performance has deteriorated and the measures we can take to address this. Working with the Care Quality Commission In March 2014 the Trust was inspected by the CQC under its new inspection regime. The team of 49 spent three days on site and visited a range of departments across the Trust with further follow up visits. The overall rating given to the Trust was requires improvement. Since the inspection we have been addressing any issues raised by the CQC team. Read the full report at Patient information Our patient information objectives are to promote inclusivity for all members of our community including producing individualised, easy read patient information for patients with a learning disability undergoing specific procedures, and working with the deaf community to help promote awareness resources. This year we have focussed on promoting our interpreting and translation services - all clinical areas have a poster explaining how to get an interpreter or translation in multi languages and there are statements to the same effect on our patient information leaflet web pages and included in most new patient leaflets Compliments and complaints The focus of the Trust is to improve the experience of the patient and ensure that we provide excellent care to them. We listen to and collect the views of our patients by various different methods, including surveys, complaints, Patient advice and Liaison Service (PALS) feedback and the Family and Friends Test. The information is used at ward, department and Trust-wide level to develop and improve our services. We received 431 formal complaints and 3226 PALS enquiries this year compared to 411 complaints and 2983 PALS enquiries in 2013/14. Four cases were referred to the Ombudsman. We received 415 compliments in addition to those sent directly to wards and departments. All compliments are passed to the Chief Executive Officer, who sends a letter back to the patient/family. They are also shared with the wards or departments as appropriate. The complaints policy was updated during the year and we are now closing more complaints within the Trust target of 25 days. In the year 2013/14 we closed 42% of complaints in 25 days, with an average overall handling time of 40 days. In the year 14/15 we closed 68% in 25 days with an average overall handling time of 26 days. Since November 2013, we have been asking complainants for feedback on how well their complaint was handled. The results are reviewed by the Patient and Staff Experience Committee in their meetings to shape future learning. The Patient Relations Managers attend nurse, healthcare assistant and Trust core inductions to raise awareness of PALS and complaints and the differences between them to ensure that patients receive a timely and appropriate response. 15
16 Quality of Service The Trust Board is committed to the delivery of high quality care and is accountable for the systems of assurance, internal control and risk management to ensure quality performance is monitored and managed. The Chief Executive is ultimately responsible for ensuring the Trust delivers a high quality service for all patients and for the delivery of and compliance with assurance, quality and performance targets. In 2014/15 the Board significantly reviewed the way in which we approach governing the quality of the services that we provide against Monitor s Quality Governance Framework. Further details of the approach to quality governance within the Trust and the processes adopted to achieve high quality safe patient care is set out more fully within the Quality Accounts on page 65 and in our Governance Statement on page 62. Stakeholder relations The Trust continues to work with our stakeholders in a range of ways. We have worked with both our commissioners and local authorities to create opportunities to move patients from our acute hospital into more suitable care as soon as appropriate. We have also worked with our commissioners to develop new services in response to emerging needs within the local population. Our local overview and scrutiny committees have been regularly attended and the Trust has worked to provide reports and updates on a number of topics including the appointments process and maternity services. More information on work with our patients, public and members can be found later in the report. Consultation and information The Trust has a formal recognition agreement with trade unions which outlines the main roles and responsibilities of all parties regarding the provision of information and consultation with employees. This process is supported by monthly meetings of the Joint Staff Consultative Committee and Joint Negotiating Committee together with fortnightly update meetings with staff side representatives and full time officers. Staff are routinely engaged in the Trust s business and performance through weekly cascade briefings, quarterly meetings with the CEO which are open to all staff and the staff newsletter which is published throughout the year. Information is routinely shared via the Trust intranet and views sought through online polls. Identifying potential financial risks The Trust has effective mechanisms in place to manage risk, in accordance with its risk management policy and strategy, supported by the Audit and Risk Committee, which has Board accountability. The Trust has low exposure to market risk being the risk that the fair value or cash flows of a financial instrument will fluctuate because of changes in market prices. In particular, the Trust is not exposed to price risk or credit risk and its exposure to interest risk is small because, with the exception of cash, its financial assets and liabilities are either at nil or fixed interest. The Trust s exposure to liquidity risk is only as a result of exposure to its challenging cost improvement programme. 16
17 Market risk This is the risk that the fair value or cash flows of a financial instrument will fluctuate because of changes in market prices. Interest Rate risk All the Trust's financial assets and liabilities, with the exception of cash held in UK banks, carry a nil or fixed rate of interest. The Trust is not, therefore, exposed to significant interest rate risks. Price risk The Trust does not deal with financial instruments other than loans with fixed interest rates and low value operating or finance leases. As a result the Trust is not exposed to a price risk. Credit risk The Trust is not exposed to credit risk. Liquidity / cash flow risk The Trust s exposure to liquidity / cashflow risk in relation to funding provided by the Commissioners is limited as it is government backed. In the event that the Trust does not deliver against the 2015/16 plan, and beyond, its cash will continue to deteriorate creating a heightened pressure on liquidity. Register of Board directors The register of Board directors at 31 March 2015 is as follows. For the latest register please see the Trust s website. Name Janet Rutherford Jean O Callaghan Bernadette Bluhm Caroline Ainslie Craig Anderson Lindsey Barker Paul Beal John Barrett Julian Dixon Brian Hendon Alison Hill Sue Hunt Designation Acting Chair Executive Director (Chief Executive) Executive Director (interim Chief Operating Officer) Executive Director (Director of Nursing) Executive Director (Director of Finance) Executive Director (Interim Medical Director) Executive Director (Director of HR and Organisational Development) Non-executive Director Non-executive Director Non-executive Director (Acting Senior Independent Director) Non-executive Director Non-executive Director (Acting Deputy Chair) 17
18 Directors statement In the case of each of the persons who are directors at the time the report is approved: a) so far as the director is aware, there is no relevant audit information of which the company s auditor is unaware, and b) they have taken all the steps that they ought to have taken as a director in order to make themselves aware of any relevant audit information and to establish that the company s auditor is aware of that information. 18
19 3. Governance arrangements Foundation trust The Trust became a foundation trust in Foundation trusts are public benefit corporations. They remain part of the NHS and the public sector. The Trust was required to demonstrate excellence in a number of areas to be granted foundation status. The benefits of foundation status include greater freedom to manage and control the Trust outside of national and regional NHS structures as well as operational benefits like being able to retain surpluses for future investment and borrow money for expansion of services. The staff and public members of the Trust elect governors to the Council. Other governors are appointed by key partners such as local authorities and our clinical commissioning group. The Council of Governors hold the Board of Directors to account and represent the views of the membership. The Board of Directors comprises both non-executive and executive directors and leads the organisation taking and managing the key financial and strategic issues. On behalf of the Board the chief executive and other senior staff manage the Trust on a day to day basis. The majority of governors on the council are publicly elected by public members of the Trust. The Council appoints the non-executive directors who have a voting majority on the Board. All Board members and governors meet the fit and proper person test as described in our provider licence. Further details on foundation trusts can be found on the Regulator s website: Board of Directors The Board of Directors of the Trust is a combined board meaning that it comprises both executive (paid staff) and non executive (appointed external) directors. Collectively, it has responsibility for: providing leadership to the organisation within a framework of prudent and effective controls sponsoring the appropriate culture, setting strategic direction, ensuring management capacity and capability, and monitoring and managing performance safeguarding values and ensuring the organisation s obligations to its key stakeholders are met facilitating the understanding on the part of governors of the role of the Board and the systems supporting its oversight of the Trust taking account of the NHS Constitution in all aspects of its work. The Board carries out the role envisaged within the Monitor Code of Governance, namely that its role is to provide active leadership of the Trust within a framework of prudent and effective controls which enables risk to be assessed and managed. As such, the Board: is responsible for ensuring compliance with the terms of authorisation, constitution, mandatory guidance issued by Monitor, relevant statutory requirements and contractual obligations. sets the strategic aims, taking into consideration the views of the Council of Governors, ensuring that the necessary financial and human resources are in place for the trust to meet its objectives and review management performance. 19
20 as a whole is responsible for ensuring the quality and safety of healthcare services, education, training and research delivered by the Trust and applying the principles and standards of clinical governance set out by the Department of Health, the Care Quality Commission, and other relevant NHS bodies. The Board ensures that the Trust exercises its functions effectively, efficiently and economically. sets the Trust s overall culture, its values and standards of conduct and ensures that its obligations to the public, its members, patients and other stakeholders are understood and met. The Trust has a code of conduct for Board directors based on the values of the NHS. It has been developed and will be reviewed by the Board once the new Chairman is in post. Deloitte has no other connection with the Trust. Board engagement with the Council and Members The Board takes active steps to ensure it interacts appropriately with the Council of Governors. The Board has agreed protocols in respect of communication with the Council and to help discharge its statutory duties. Board Directors attend Council s committees to provide support and information and to monitor progress on issues such as monitoring membership and membership engagement. The Council committee structure mirrors that of the Board. A lead executive, and a non executive director, also attends each of the Council's committees. There is also a quarterly joint meeting between the Board and the Council. Direct engagement with members takes place at the Trust s Annual Members Meeting where reviews of the year and forward plans are delivered and there is an open question and answer session. The register of Board directors at 31 March 2015 is as follows. For the latest register please see the Trust s website. Name Janet Rutherford Jean O Callaghan Bernadette Bluhm Caroline Ainslie Craig Anderson Lindsey Barker Paul Beal John Barrett Julian Dixon Brian Hendon Alison Hill Sue Hunt Designation Acting Chair Executive Director (Chief Executive) Executive Director (interim Chief Operating Officer) Executive Director (Director of Nursing) Executive Director (Director of Finance) Executive Director (Interim Medical Director) Executive Director (Director of HR and Organisational Development) Non-executive Director Non-executive Director Non-executive Director (Acting Senior Independent Director) Non-executive Director Non-executive Director (Acting Deputy Chair) During 2014/15 Janet Rutherford was deputy chair and senior independent director. However, when she assumed the role of Acting Chair from 27 February 2015, Sue Hunt was appointed acting deputy chair and Brian Hendon was appointed acting senior independent director. All nonexecutive directors are considered independent. 20
21 The Trust's Constitution specifies that non-executive directors are appointed for three year terms of office. Appointments can be terminated in accordance with Monitor's Code of Governance. Declarations of interest made by Board members are available on the Trust website. Changes to the Board during the year are set out on page 31. The Chairman must declare any significant interests to the Council of Governors prior to appointment. Janet Rutherford has declared no significant interests. Biographies Acting Chairman: Janet Rutherford, who joined in August 2012, was Director of Social Services for the former Berkshire County Council. She later became Director of Policy and Research at the Local Government Association. Chief Executive Officer: Jean O'Callaghan joined the Trust as Chief Executive in August Jean joined from Dorset County Hospital NHS Foundation Trust where she was Chief Executive for four years. Prior to Dorset, Jean was Chief Executive at Bedford Hospital NHS Trust for five years. Jean was CEO of the Canterbury District Health Board in New Zealand prior to joining the NHS, and is a nurse by background. Director of Nursing: Caroline Ainslie joined the Board in June She has held a number of senior roles, including divisional head of nursing and professions at Southampton, before moving to take on a strategic role as deputy chief nurse at South Central Strategic Health Authority. Director of Finance: Craig Anderson previously worked for Partnerships UK as Finance Director and has worked closely with a number of central government departments, such as the Department for Education, on the implementation of major infrastructure programs. Interim Medical Director: Lindsey Barker has worked at the Royal Berkshire Hospital since She is a Consultant Nephrologist and Physician and latterly Divisional Director of Medicine. Nationally, she has served the Royal College of Physicians in renal working parties and reports. Interim Chief Operating Officer: Bernie Bluhm joined as Interim Chief Operating Officer in September Bernie has a strong track record as a Chief Operating Officer within the acute sector with a permanent role at Surrey and Sussex Healthcare NHS Foundation Trust and as an interim at West Hertfordshire Hospitals NHS Foundation Trust. Director of Workforce and Organisational Development: Paul Beal joined as Director of Workforce and Organisational Development in October 2014 and has more than 20 years HR experience in the NHS in acute, community, mental health and commissioning organisations. Non-executive Director: John Barrett joined the Board of the Trust in 2007 and was reappointed in March He has substantial board level management experience in the information technology industry in the UK and internationally having been a Vice President at PictureTel Corporation, Digital Equipment Corporation and Deputy Chairman of Digital Equipment Company, UK. Non-executive Director: Julian Dixon joined as Non-Executive Director in December Julian has worked in leadership roles in the academic, healthcare and commercial sectors. 21
22 Julian is currently Managing Director at Strategic Health Connections, a consultancy which helps organisations to translate innovation into improved health and wealth outcomes. Non-executive Director: Brian Hendon joined in August With a background in finance, he has held a number of senior executive board positions with large private sector companies and also has extensive experience in non-executive roles including Thames Valley Housing Association. Non-executive Director: Alison Hill joined the Trust in December She worked as a GP in Oxfordshire, before pursuing a career in policy development and implementation in a series of health service and academic posts including Professional Policy Advisor to the Department of Health NHS Genetics Team and Director of Effective Practice Programme at the King s Fund. Non-executive Director: Sue Hunt joined the Trust in November She is a chartered accountant whose long career at KPMG spanned audit, mergers and acquisitions and healthcare consultancy. An experienced non-executive director Sue has current roles at Notting Hill Housing Group, CfBT Education Trust and The Satellite Applications Catapult Ltd. Review of Board performance Every three years the Board commissions an external evaluation in line with good practice. The most recent evaluation was carried out by Deloitte in November Executive Board members are also appraised on an individual basis. Board attendances April 2015 to March 2015 Board Clinical Governance Charity Remuneration & nominations Stephen Billingham 11/11 2/2 9/10 9/11 6/6 Janet Rutherford (NED/Acting 12/12 6/6 1/1 10/10 4/6 Chairman) Jean O Callaghan 7/7 3/4 6/6 5/6 3/3 Resources Audit & Risk Council of Governors Caroline Ainslie Craig Anderson (Director of Finance) Lindsey Barker * ** (Care Group Director/Acting Medical Director) 9/12 6/6 7/11 2/6 12/12 2/3 11/11 4/6 4/5 5/6 1/4 4/6 22
23 Paul Beal Sue Edees * Alistair Flowerdew **** Peter Malone * Brian Reid John Barrett Julian Dixon Brian Hendon Alison Hill Sue Hunt Jane May *** 3/3 3/9 2/4 2/5 5/12 1/6 2/4 5/6 3/6 5/9 4/4 5/8 1/5 3/5 2/2 9/12 6/6 9/10 6/6 2/6 4/4 2/2 1/1 10/12 10/10 8/11 6/6 3/6 10/12 8/10 5/6 3/6 5/5 2/3 4/4 2/2 7/8 7/8 6/7 7/8 3/5 *Care Group Directors were no longer Board members from December 2014 ** Acting Medical Director from November 2014 ***From 15 th September 2014 Jane May was Associate Non Executive Director **** For nominations business only The current formal committee structure of the Board is shown below. Trust Board Operational Performance & Finance Committee Exec lead Craig Anderson/Bernie Bluhm Audit & Risk Committee Exec lead Craig Anderson Clinical Governance Committee Exec leads Caroline Ainslie/ Lindsey Barker Resources Committee Exec lead Craig Anderson Charity Committee Execlead Craig Anderson Nominations & Remuneration Exec lead Paul Beal The main roles of each committee and group are as follows: Audit and Risk Committee The Committee reviews the effectiveness of financial systems for internal control and reporting and report to the Board of Directors on the levels of assurance. It also now co-ordinates and prioritises non-clinical governance and non clinical risk issues. It is responsible for ensuring and monitoring the regular review of risks identified against the board assurance framework and corporate risk register in order to embed risk management within the organisation. Charity Committee 23
24 The Royal Berkshire Charity (formally the Royal Berkshire NHS Foundation Trust Charity Fund Registration Number ) is governed by trustees acting through the Charity Committee. They are responsible for the overall management of charitable funds. Clinical Governance Committee The Committee provides assurance to the Board that appropriate clinical governance mechanisms are in place and effective throughout the organisation Nominations and Remuneration Committee The Committee oversees a formal, rigorous and transparent procedure for the appointment of the chief executive and the other Board executive directors. It advises and makes recommendations to the Board on executive and senior management remuneration and remuneration policy. See the Board remuneration report on page 39. Resources Committee The Committee gives detailed consideration to finance, estates, investment, IT and workforce issues. It advises the Executive and Board on issues to achieve the best value for money and use of resources. It seeks to ensure that agreed strategies for finance, estates and IT are developed, implemented, monitored and reviewed. Operational Performance and Finance The Committee scrutinises and makes recommendations to the Board on financial matters and operational performance. Audit and Risk Committee Composition The Audit and Risk Committee comprises non-executive directors. Discharging its responsibilities The Committee discharges the responsibilities delegated to it by the Board in the following ways: - the Committee has Board approved terms of reference - the Committee submits an annual programme of work to the Board for its approval - minutes of meetings are submitted to the Board - the chairman of the Committee gives regular verbal updates at the Board meetings. - The Committee prepares an annual report for the Board. The terms of reference of the Committee are reviewed annually by the Board to ensure their appropriateness and that they incorporate best practice as it develops. The work of the external auditors and the Committee has been carried out within a framework set by Monitor. The focus of this framework has been on the final accounts and the Statement of Internal Control. over the course of the year our external auditors have delivered a range of reports to the Committee. These include: the ISA260 report outlining the findings of the 2013/14 audit of the Trust s Group 2013/14 financial statements, and report following the audit for the Quality Accounts Management Letter for 2013/14 regular progress updates on the delivery of the audit and technical updates to members of the Audit Committee 24
25 the ISA260 report outlining the findings of the 2013/14 audit of the Royal Berkshire NHS Foundation Trust Charity the ISA260 report outlining the findings of the 2013/14 audit of Healthcare Facilities Management Services Limited Responsibility for appointment of external auditors rests with the Council of Governors. The contract with KPMG, our current auditors, expired on 31 March 2013 and the Committee recommended to the Council of Governors that the contract should be extended in order to ensure that the external and internal audit contracts are co-terminus. The Council of Governors agreed to extend the contract to 31 March The Committee s key focus was on follow up on internal audit recommendations and it has also extended into a broader role beyond its historic technical remit and has received updates on progress against the Quality Improvement Project Plans and IT at a number of its meetings. Ensuring external auditors independence The Trust has a policy in place for the engagement of the external auditors for non-audit work. This policy complies with all relevant auditing standards and follows industry practice in terms of defining prohibited work and setting out the approval and notification processes all non-audit work should be subject to. The policy is reviewed annually by the Audit and Risk Committee and they receive confirmation through KPMG progress reports presented to each of their meetings that it has been complied with. The Audit and Risk Committee believes that in this way the external auditors independence is ensured. It is the combined responsibility of the directors to prepare the annual financial statements and report. It is the auditors responsibility to report on whether the financial statements and Annual Report give a true and fair view. Auditors statement on reporting responsibilities It is the external auditor s responsibility on completion of their audit to issue: an opinion on financial statements: this confirms the accounts present a true and fair view of operations; and a conclusion on the Trust s use of resources: this confirms that no evidence has been identified to suggest resources are not being used effectively to deliver healthcare and other objectives. External auditors are also required to confirm aspects of the Quality Account Report, including a sample of indicators have been correctly prepared and presented. External auditors are required to report the findings of their audit to those charged with governance - for the Trust this is the Audit and Risk Committee. The FT Code of Governance states that this report must be sent to Monitor by the Trust. Nominations Committees There are two nominations committees one established by the Board of Directors for the appointment of executive directors and one established by the Council of Governors for the appointment of non-executive directors. 25
26 Board Nominations and Remuneration Committee This consists of all non-executive directors and the Chief Executive. No of meetings attended Nominations and Remuneration Committee /maximum no of meetings Stephen Billingham 9/10 John Barrett 9/10 Julian Dixon 2/2 Alistair Flowerdew* 2/4 Brian Hendon 10/10 Alison Hill 8/10 Sue Hunt 2/3 Jane May 7/8 Janet Rutherford 10/10 Jean O Callaghan * 6/6 * For nominations business only Council of Governors Nominations and Remuneration Committee The Committee consists of governors and for appointment duties is chaired by the chairman of the Trust. During 2014/15 this was Stephen Billingham. Responsibilities The Committee oversees the development, implementation and review of the policy for nonexecutive directors and the policy for governors. The Committee leads the process for the identification of non-executive directors. Duties: to establish and keep under annual review a policy for the composition of non-executive directors, which takes account of the membership strategy to receive from the Board recommendations on the skills and experience required in any nonexecutive director appointment to identify appropriate candidates for appointment as non-executive directors, seeking the advice of the chairman (or the deputy chairman in the case of appointing the chairman) and the Board throughout the process to establish and keep under annual review a policy for the composition of the Council of Governors, which takes account of the membership strategy to produce an annual work plan, for approval by the Council of Governors, setting out the priorities of the Committee for the coming year. The Committee reviews these terms of reference annually, making recommendations to the Council of Governors as appropriate. Board re-appointment process The process agreed by the Council of Governors, with the support of the Board of Directors, for the re-appointment of non-executive directors is as follows: 26
27 a) The reappointment of a non-executive director is considered by the Council s Nominations Committee, which will make a recommendation to the full Council b) The following information is submitted to the meeting at which the re-appointment is considered: A summary of the individual s last three years appraisals, submitted by the chairman of the Trust. In the case of the re-appointment of the chairman, this information will be submitted to the Committee by the senior independent director. A summary of the individual s attendance at Board and committee meetings since their appointment. An assessment, provided by the Chairman (or senior independent director in the case of the re-appointment of the chairman), of the balance of skills of the non-executive team on the Board and the individual s contribution to this. As background information to the discussion, the Committee will be provided with the Charter of Expectations, which sets out the skills required from, and the expectations of, Board members, and any employment advice from the Director of HR & Organisational Development. A statement by the individual seeking reappointment. c) The Nominations Committee will be entitled to request any further information that it deems necessary to be able to make a recommendation to the Board. Council of Governors The Council has several roles including: Constitutional: there are formal responsibilities set out in legislation and in our constitution, for example, appointing the chairman and non executive directors, approving the accounts and appointing external auditors. Providing assurance: governors assure themselves on behalf of the membership and community that the Trust s performance is as it should be. They examine performance and look at patient safety and quality issues. Representation: the Council is consulted on strategic and forward plans. It gives the views of membership, community and users to the Trust s Board. Become involved: governors are closely involved in the work of the Trust. They are briefed and informed but they also get involved in and lead on specific projects to improve the patient experience. The register of governors as at 31 March 2014 is set on the next page and also shows the constituency that each represents. For the latest register please see the Trust s website. 27
28 Register of Governors The following is the register of governors of the Royal Berkshire NHS Foundation Trust. It is maintained by the Trust Secretary. Name Constituency Term of office Attendance at Council meetings Ms. Deborah Sander Reading /6 Mr. Martyn Cooper Reading /6 Mr. Dave Dymond Reading /4 Mr. Jon Andrews Reading /1 Mr. David Cooper (Lead Governor) Reading /6 Mr. John McKenzie Wokingham /6 Mr. Tony Lloyd Wokingham /4 Mr. Tony Skuse Wokingham /6 Mr Jeremy Butler Mr. David Mihell Vacant East Berkshire & Borders East Berkshire & Borders East Berkshire & Borders / / Ms. Carol Bolderson Mr. Colin Lee Mr. David Rowark West Berkshire & Borders West Berkshire & Borders West Berkshire & Borders / / /1 Mr. Thomas Bune Southern Oxfordshire /6 Mr. Ian Clay Volunteer Governor /6 Staff Ms. Pamela Simmons Ms. Maria Walker- Reeves Staff: Health Care Assistant/Ancillary Staff: Admin/Management / Maternity leave 28
29 Mr. Charles McKenna Mr. Jonathan Mason Ms. Anne-Marie Probert Staff: Medical/Dental /4 Staff: Allied Health Professionals/Scientific Staff: Nursing/Midwifery / /6 Ms. Wendy Bower Ms. Jennie Ford Mr. Sanusi Koroma Mr. Peter Dooley Councillor Bet Tickner Councillor Bob Pitts Councillor Gordon Lundie Vacant Appointed by Berkshire West Federation of CCGs Appointed by Berkshire East Federation of CCGs Appointed by Reading Council for Racial Equality Appointed by Berkshire Carers Service Appointed by Reading Borough Council Appointed by Wokingham Borough Council Appointed by West Berkshire Council Youth rep appointed by Wokingham Borough Council / / / / / / / * Governors are elected by members of the relevant constituency unless stated otherwise. Declarations of interest made by governors are available on the Trust website. Changes to the Council during the year are set out on page 31. Governors work to influence the Trust and have an impact in several informal and formal ways. The formal committee structure of the Council is shown below. 29
30 Council of Governors Membership Committee Quorum = 4 Nominations and Remuneration Committee Quorum = 3 (2 public) Clinical Assurance Committee Quorum = 4 (1 public) Strategy Committee Quorum = 3 Business Assurance Committee Quorum = 3 public Exec Leads Director of HR & Exec Leads Director of Nursing/Medical Director Exec Lead Associate Director of Strategy Exec Lead Director of Finance The main roles of each group are as follows: Clinical Assurance Committee provides assurance to the Council on the performance of the Trust reviews the Trust s clinical performance briefs the Council on key assurance/scrutiny issues Business Assurance Committee provides assurance to the Council on the performance of the Trust reviews the Trust s financial and operational performance briefs the Council on key assurance/scrutiny issues Membership Committee develop, implement and review a membership strategy for the Trust develop a policy, implement agreed proposals and keep under review the Trust approach to engaging with the membership community recommend and review relationships and methods of communicating between governors and the membership review the membership of the Trust to ensure it is representative of those eligible to be members oversee preparations for the Annual Members Meeting Strategy Committee develops the Council s own objectives and monitors performance liaises with the Board and Executive on strategic planning issues, making sure the Council s views are heard develops the Council s approach to training and briefing governors. 30
31 The nominations and remuneration committees consider the salaries and appointments of the non- executive directors of the Board. Board attendance at Council of Governor meetings No. of meetings attended /Maximum no. of meetings Stephen Billingham 6/6 Caroline Ainslie 2/6 Craig Anderson 4/6 Lindsey Barker 4/6 John Barrett 2/6 Julian Dixon 1/1 Sue Edees 2/5 Alistair Flowerdew 3/6 Brian Hendon 3/6 Alison Hill 3/6 Sue Hunt 2/2 Peter Malone 1/5 Jane May 3/5 Jean O Callaghan 3/3 Janet Rutherford 4/6 Changes to the Board and Council of Governors The following were also Board directors during the year: Mr Stephen Billingham - Chairman Mrs Jane May Non-executive Director Dr Alistair Flowerdew Medical Director Dr Brian Reid - Acting Medical Director from November 2014 Dr Sue Edees* - Care Group Director Mr Peter Malone*- Care Group Director * Note: The Trust had three care group directors. Only one was a formally appointed and voting Board director at any given point with each rotating onto the Board for a six month period. Care group directors were no longer Board members from December 2014 The following were also governors during the year: Ms Margie Cutts Public Governor Dr Muhammed Abid Public Governor Mrs Vera Doe Public Governor (Lead Governor) Mrs Aileen Blackley Public Governor Mr Warren Fisher Staff Governor Councillor Alan Law Appointed Governor 31
32 Chair of the Audit and Risk Committee report The Trust Board have delegated authority to the Audit and Risk Committee, a non-executive committee of the Trust Board, to review the establishment and maintenance of an effective system of integrated governance, risk management and financial and non-financial non-clinical internal controls, which supports the achievement of the Trust s objectives. The Committee has no executive powers. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. In addition the Committee is required to satisfy itself that the Trust has adequate arrangements for countering fraud, for managing security of resources and has to review arrangements by which staff of the Trust may raise concerns via the Trust s Whistle Blowing policy. The Audit & Risk Committee consists of three Non-executive Directors members supported by professional advisors with Trust attendance provided by the Chief Executive Officer and the Director of Finance. The Committee meets privately on a regular basis with the Trust s Internal and External Auditors. During 2014/15 The Audit & Risk Committee has satisfied itself that the findings of assurance reports and other studies relating to the Trust, as drawn to its attention by the Board or by management, have been reviewed and the implications to the governance of the organisation considered. These reports include reports instigated by Monitor and Care Quality Commission and other professional bodies with responsibility for the performance of staff or functions (e.g. Royal Colleges, accreditation bodies, etc.). The Committee conducts an annual review of its effectiveness with its terms of reference and submits any findings and proposals for changes to the Board of Directors for consideration and once a year prepares an annual report. Both the review and the annual report are presented to the Board. No matters of concern were raised in the 2014/15 review. Financial reporting The Committee reviewed the Trust s accounts and Annual Governance Statement and how these are positioned within the wider Annual Report. To assist this review the Committee considered reports from management and from the internal and external auditors to assist the consideration of: the quality and acceptability of accounting policies, including their compliance with accounting standards; key judgements made in preparation of the financial statements; compliance with legal and regulatory requirements the clarity of disclosures and their compliance with relevant reporting requirements; whether the Annual Report as a whole is fair, balanced and understandable and provides the information necessary to assess the Trust s performance and strategy. The Committee reviewed the content of the annual report and accounts and advised the Board that, in its view, taken as a whole: it is fair, balanced and understandable and provides the information necessary for stakeholders to assess the Trust s performance, business model and strategy; 32
33 it is consistent with the draft Annual Governance Statement, Head of Internal Audit Opinion and feedback received from the external auditors. Significant financial judgements and reporting for 2014/15 The Committee considered a number of areas where significant financial judgements were taken which have influenced the financial statements: The Committee identified through discussion with both management and the external auditor the key risks of misstatement within the Trust s financial statements. The Committee discussed these risks with the external auditor at the time the external auditor s audit plan was reviewed and at the conclusion of the audit. The Committee also discussed these risks with management during the year and received a paper from management in advance of the year end. Set out below is a summary of how the Committee satisfied itself that these risks of misstatement had been appropriately addressed: Valuation of land, buildings and dwellings and intangible assets: We reviewed reports from management which explained the basis of valuation and the consideration of the need to recognise any impairments. We also considered the auditors views on the accounting treatment of these assets. We are satisfied that the valuation of these assets within the financial statements is consistent with management intention, and is in line with accepted accounting standards. Recognition of NHS Income: We received assurances from management in relation to the application of a consistent methodology for the recognition of income and provisioning of aged NHS debt. We also reviewed the outcomes from the Agreement of Balances exercise across the NHS as part of our consideration of the external auditor s report, to confirm that we had appropriately recognised income within the accounts. The adequacy of provisions; for example in relation to debtor balances and contractual disputes. External audit KPMG has provided External Audit services since the 1 April Audit and non-audit fees are set, monitored and reviewed throughout the year and are included in note 3.1 of the accounts. KPMG also provides some non-audit services to the Trust, during the year this included the provision of tax advisory and tax compliance services. The Committee receives a report of all non-audit services provided by KPMG at each meeting and have considered whether these services might result in any impairment of the auditor objectivity and independence. For all non-audit services delivered the Committee has concluded there is no risk of impairment of auditor objectivity and independence. During the Audit & Risk Committee meeting on t5 January 2014, the Committee reviewed and approved the external audit plan for the 2014/15 period. As part of the discussion at this meeting the Committee reviewed key risk areas highlighted by external audit in relation to the valuation of assets and recognition of NHS income. During the Audit & Risk Committee meeting on the 18 May 2015 the Committee reviewed the 2014/15 financial statements and KPMG s ISA260 Audit Highlights memorandum following the audit of the Group and Trust financial statements. Following this, the Committee recommended to the Board to approve the Annual Report and Financial Statements for the period ending 31 March
34 Internal audit and counter fraud services The Board uses external parties to deliver the internal audit and counter-fraud services. PwC has provided the Trust s internal audit service since March 2011.This service covers both financial and non-financial audits according to a risk-based plan agreed with the Audit Committee. During the year internal audit issued 12 reports which resulted in a total of 30 findings (12 high risk findings, 10 medium risk findings and 8 low risk findings). At each meeting the Committee receives a report from Management confirming the status of internal audit recommendations. Risk Following the re-organisation of Executive portfolios the responsibility for risk was transferred to the Director of Nursing. An external review of risk management processes was undertaken in November 2014 and a resultant action plan established. Regular updates will be provided to each meeting of the Committee to provide assurance of actions being addressed. Internal controls Through the internal audit plan the Committee review the financial and risk controls operating in the Trust, through and during the year also looked at the controls relating to data quality, estate and the patient environment, information governance and private patient activity. Action plans were put in place to address minor issues in operating processes. Fraud detection processes and whistle-blowing arrangements The Trust s counter fraud service is provided by Tiaa, who provide fraud awareness training, carry out reviews of areas at risk of fraud and investigate any reported frauds. The Committee reviewed the levels of fraud and theft reported and detected and the arrangements in place to prevent, minimise and detect fraud and bribery. No significant fraud was uncovered in the past year. Other areas reviewed In addition to the above areas of work the Committee has received reports on losses and special payment incurred by the Trust and considered the overall work of the risk management processes during the period. External Audit, Internal Audit and Counter Fraud Service Contracts The contracts for all three services are due to finish on 31 March A tender process will be taking place during 2015/16 to identify and appoint appropriate service contracts from 1 April Our membership This section sets out who is eligible to become a member of the Trust, our current membership numbers and our strategy and targets for recruiting new members. Our members can stand as governors, and are responsible for electing our governors. They get involved in the Trust through our membership newsletters, events, annual members meeting and as issues or topics arise that could be of interest such as consultation on services. 34
35 Eligibility Membership is open to two main groups: (a) Public, including patients and carers - people living within the five constituencies - people aged 16 and over (b) Staff employed by the Trust - all staff on a permanent contract or a contract of 12 months or more - all staff who are not already public members Categories of staff membership: - medical and dental staff - nursing and midwifery staff - allied health professions and scientific and technical staff - healthcare support workers (all disciplines) and ancillary staff - administrative, clerical and management staff. Boundaries of public membership Reading - All the electoral wards in Reading Borough Council (unitary authority) area. West Berkshire and borders All the electoral wards in West Berkshire Council (unitary authority) area. The following electoral wards from the Basingstoke and Deane Borough Council area of North Hampshire: Baughurst, Burghclere, Calleva, East Woodhay, Highclere and Bourne, Kingsclere, Pamber, Tadley North and Tadley South. The following electoral ward from the Test Valley Borough Council area of North Hampshire: Bourne Valley. East Berkshire and borders All the electoral wards in Bracknell Forest Borough Council (unitary authority) area. All the electoral wards in Slough Borough Council (unitary authority) area. All the electoral wards in the Royal Borough of Windsor and Maidenhead (unitary authority) area. The following electoral wards from South Bucks District Council area: Burnham, Beeches, Burnham Church, Burnham Lent Rise, Dorney and Burnham South, Farnham, Royal, Iver Heath, Iver Village and Rickings Park, Stoke Poges, Taplow, Wexham and Iver West. Southern Oxfordshire The following electoral wards from South Oxfordshire District Council area: Chiltern Woods, Cholsey and Wallingford South, Crowmarsh, Didcot All Saints, Didcot Ladygrove, Didcot Northbourne, Didcot Park, Goring, Hagbourne, Henley North, Henley South, Shiplake, Sonning Common, Wallingford North and Woodcote. Wokingham All electoral wards in Wokingham Borough Council (unitary authority) area. About our current membership At 31 March 2015 our public membership stood at 17,749 and our total membership at 23,458. The membership remains under represented in the younger age groups and the imbalance exists until we reach the 30+ age groups. The age category remain the highest 35
36 represented. However the Council of Governors agreed to maintain the membership at its current level for the year the Trust membership remains significantly higher than the average foundation trust membership. Public % of public membership East Berkshire and Borders 5,002 28% Reading 4,920 28% Southern Oxfordshire 1,004 5% West Berkshire and Borders 3,145 18% Wokingham 3,374 19% Other 304 2% Total 17, % Get in touch If you would like to contact our governors or directors, or to find out more about how you might get involved, please contact our membership office: Foundation Trust Membership Office Level 3 Main Reception Craven Rd Reading RG1 5AN Tel: or: foundation.trust@royalberkshire.nhs.uk or visit our website 36
37 4. Statutory information Finance performance The Trust group, which comprises the Trust, the Trust s wholly owned subsidiary and the Trust charity, made a deficit of 9.0m in 2014/15 compared to the deficit of 6.6m in 2013/14. In 2014/15 we continued to see growth in activity and in income, however costs more than offset income, in particular due to unfunded radiology costs, increased pay cost to validate and correct the Trust s waiting list and increased management costs. During the year the Trust failed to meet a number of performance standards with its contracts with Commissioners. The Commissioners sought to charge contract penalties which have been included within the deficit in the year The Trust has worked hard to reduce costs and delivered 15.2m of savings in 2014/15. However, this was only sufficient to offset the reduction in income due to reduced prices set by Monitor, the increase in cost due to pay and non pay inflation and loss of non recurrent income from 2013/14. The pay bill rose by 7.0m in 2014/15, with the largest increase, 2.8m, being in medical staff pay. Other areas where our pay cost increased significantly include IT and in validation work that we undertake on patient waiting list times. Ensuring our pay is controlled remains a key objective. The Trust plans to return to financial stability by the end of 2016/17. However the Trust does expect to report a deficit in 2015/16. This is contingent on us achieving extremely challenging levels of savings over the next year and to that end we have plans for both incremental and transformational programmes. Summary Financial Results comparison to prior year: 2014/ /14 Year on Year variance m Income Pay (209.7) (202.7) (7.0) Non-pay (130.5) (124.5) (6.0) Expenses (340.2) (327.2) (13.0) EBITDA (1.3) Depreciation / profit or loss on disposal (17.6) (17.1) (0.5) PDC Dividend (5.0) (4.8) (0.2) Net Interest payable (1.2) (1.3) 0.1 Other non-operating expenses (0.4) 0.1 (0.5) Reported (deficit) for the period (9.0) (6.6) (2.4) 37
38 Capital Expenditure The Trust spent 14.8m on capital expenditure in 2014/15, of which 2.3m was financed through leases. The focus of the Trust s capital expenditure plan was on medical equipment, including new MRI scanners, and investment in Engineering Compliance and Fire safety projects. Cashflow and Balance Sheet The Trust continued to hold a strong Statement of Financial Position mainly consisting of land and buildings owned by the Trust from which the Trust provides services to patients. The liquidity of the Trust declined in 2014/15, largely as a result of the lower trading results, and at the end of the year the Trust had cash or cash equivalent assets of 13.4m. The Trust has three loan facilities, totalling 36m, from the Foundation Trust Financing Facility, two to finance the development of the Royal Berkshire Bracknell Clinic and one to finance the Trust s Cerner EPR system. All of these loans have been fully drawn down and are being repaid. The Trust manages its cash position closely. Monitoring Trust Financial Performance The Trust s financial performance is reviewed through the weekly Executive meetings as well as at the monthly meeting of the full Trust Board, which takes a strategic view on the month s and annual financial results. Monitor assesses financial performance based on two criteria, debt cover and liquidity. Overall the Trust achieved a risk rating of 2 at the end of the year, within the range of one to four where four is the best performance. Policies for pensions and retirement benefits The Trust s policies for pensions and retirement benefits are set out on page 42 of this report. Details of senior employees remuneration can be found from page 39. Political or charitable donations The Trust did not make any political or charitable donations during the period 1 April 2014 to 31 March External auditor details The Trust s external auditors for 2014/15 were: KPMG LLP 15 Canada Square London E14 5GL Over the course of the year our external auditors have delivered a range of reports to the Committee. These include: Our audit plan for the period Progress update reports on the delivery of our audit work Technical update reports highlighting NHS FT and health sector issues of relevance for the Committee ISA 260 Audit Highlights Memorandum reports following our audit of the Group financial statements, and the financial statements of HFMS Limited and the Royal Berks Charity and Our Limited Assurance Opinion on the Trust s Quality Accounts. 38
39 KPMG s remuneration was 210k including VAT ( 196k including VAT in ) for the period 1 April 2014 to 31 March The liability limits have been agreed as: Audit Liability unlimited All other work up to 1m limit. Internal auditor details The Trust s internal auditors for 2014/15 were: Price Waterhouse Coopers LLP Docklands 161 Marsh Wall London E14 9SQ PwC s remuneration was 814,780 ( 182, /14) for the period 1 April 2014 to 31 March The above fees ( 512,982) include support provided by PwC to the Strategic Cost Reduction Programme. Charitable funds The Trust is supported by a number of charities. The Trust Charity is the Royal Berkshire NHS Foundation Trust Charity, which makes charitable grants to the Trust, often to contribute to capital projects. Under IAS 27 the Trust, as the Corporate Trust of the Charity, consolidates the financial statement of the Charity into these Financial Statements. The Royal Berkshire NHS Foundation Trust Charity does prepare its own financial statements, which are submitted to the Charity Commission. Remuneration report Annual Statement on Remuneration The Chief Executive started in post in August The appointment of the Chief Executive was recommended at the meeting of the Nominations and Remuneration Committee of the Trust Board held on 6 May At the meeting the salary level was also agreed. The Nominations and Remuneration Committee of the Trust Board met on 29 January 2015 in order to decide the remuneration of the Chief Executive and the other executive directors for the 2014/15 financial year. There were no changes to the remuneration of the Chief Executive, or the executive directors during the year, apart from the Director of Nursing. The Trust appointed a new Director of Workforce and Organisational Development and this was ratified by the Nominations and Remuneration Committee on 30 September
40 The appointment of a Chief Operating Officer was ratified by the Nominations and Remuneration Committee on 30 March The appointee will not take up post until June During the 2014/15 year one of the Care Group Directors acted into the Medical Director position. Senior Manager s Remuneration Policy Attracting and retaining talented directors and senior managers is essential for the successful delivery of the Trust s strategy and objectives within an increasingly competitive market place. The remuneration policy is designed with that in mind. The table on page 44 shows the remuneration package for senior managers (Executive Directors) including pension related benefits. The salary paid is inclusive of any overtime or allowances. The table also shows the salary/fees paid to Non-Executive Directors. No additional fees or other items, that could be considered to be remuneration in nature, are paid to the Non- Executive Directors. The definition of senior managers is those persons in senior positions having authority or responsibility for directing or controlling the major activities of the NHS Foundation Trust. For the purpose of reporting senior manager s remuneration in the table (below) and the pension benefits table this has taken to mean those executive directors holding voting rights on the board and also the Trust s non-executive directors. The senior manager s salary is payment for delivering the Executive Director role and for delivering the short and long-term strategic objectives of the Trust. Each Executive Director post is paid on a spot salary. The salaries are review on an annual basis when a decision is made whether to implement a pay award. There have been no new components added to the remuneration package or any changes to the existing components in this period therefore senior managers have not been consulted with regarding their remuneration policy. Annual Report on Remuneration Remuneration Committee The Remuneration Committee is responsible for agreeing, on behalf of the Board, the Trust s remuneration policy for directors and for determining the total individual remuneration package for these directors and senior staff earning over 75,000 per annum. Other staff employed in the Trust are on national terms and conditions of employment and are therefore determined at a national level. No of meetings attended Nominations and Remuneration Committee /maximum no of meetings Stephen Billingham (Chairman) (Chair of Committee) 9/10 John Barrett (Non Exec Director) 9/10 Julian Dixon (Non Exec Director) 2/2 Alistair Flowerdew* (Acting Chief Executive) 2/4 Brian Hendon (Non Exec Director) 10/10 Alison Hill (Non Exec Director) 8/10 Sue Hunt (Non Exec Director) 2/3 Jane May (Non Exec Director) 7/8 Janet Rutherford (Non Exec Director) 10/10 Jean O Callaghan * (Chief Executive) 6/6 40
41 * For nominations business only The Director of Workforce and Organisational Development provides advice or services to the Remuneration Committee. The nominations and remuneration committee uses the following survey guidance: - The Hay Survey, for public and not-for-profit sectors, which informs the Trust of salaries for equivalent roles across similar organisations - The Capita Salary surveys - The Income Data Services Report - Salary surveys conducted by the Foundation Trust Network The number of Remuneration Committee Meetings and individuals attendance at each meeting can be found in Section 3 above. Performance Related Pay The Trust does not currently operation a performance related pay scheme. Contractual Terms / Obligations All executive directors employed by the Trust are on standard contracts for senior managers which require a six month notice period. The executive director contract was subject to a full review during 2014/15. The Trust has not consulted with employees on the new contract as it is applicable to new appointments only. A number of the Executive Director roles were occupied by individual either on a fixed term contract or an interim basis during 2014/15. Payment for loss of office (redundancy) would be in line with Agenda for Change terms and conditions of employment. Service Contracts Obligations A contract for service is in place for any senior managers obtained via temporary, agency or contractor arrangements. The contract for service details the standard terms of business. The Trust will outline separately any specific obligations e.g. key deliverables. Service Contracts Name Designation Date Appointed End of Term of Office Mr Brian Hendon Non-Executive Director April 2012 July 2016 Ms Janet Rutherford Non-Executive Director April 2012 December 2015 Dr Alison Hill Non-Executive Director December 2013 December 2016 Mr Julian Dixon Non-Executive Director October 2014 October 2017 Ms Sue Hunt Non-Executive Director October 2014 October 2017 Mr Stephen Billingham Chairman July 2012 February 2015 Ms Jane May Non-Executive Director August 2013 September 2014* 41
42 * stayed on as an Associate NED until December 14 The notice period for Non-Executive Directors is one month. Salary and pension entitlements of senior managers The definition of senior managers is those persons in senior positions having authority or responsibility for directing or controlling the major activities of the NHS Foundation Trust. For the purpose of reporting senior manager's remuneration in the table (below) and the pension benefits table on page 47 this has been taken to mean those Executive Directors holding voting rights on the Board and also the Trusts'Non-Executive Directors. The Remuneration section of this report has been subject to audit. The pension related benefits for those Directors who have been in post for only part of the year have been calculated on a pro-rated basis to reflect that periodicity. Future Policy Table Salary / Fee Taxable Benefits Annual Performance Related Bonus Long Term Related Bonus Pension Related Benefits Support for the short and long-term strategic objectives of the FT Ensure the recruitment and retention of directors of sufficient calibre to deliver the Trust s objectives None disclosed None paid None paid Ensure the recruitment/ retention of directors of sufficient calibre to deliver the Trust s objectives How the component operates Paid in even twelfths None disclosed None paid None paid Contributions paid by both employee and employer Maximum payment None disclosed None paid None paid Lifetime allowance of 1m from April 2016 Framework used to assess performance Trust appraisal system None disclosed None paid None paid N/A Performance measures Tailored to the post concerned None disclosed None paid None paid N/A Performance period Concurrent with the financial year None disclosed None paid None paid N/A Amount paid for minimum level of performance and any further levels of Salaries / fees are agreed on appointment and set out in the contract of None disclosed None paid None paid N/A 42
43 performance employment Explanation of whether there are any provisions for recovery of sums paid to directors, or provisions for withholding payments Any overpayments may be recovered None disclosed None paid None paid N/A 43
44 Year to 31 March 2015 Name and Title Salary and fees Pension related benefits Total EXECUTIVE DIRECTORS Bands of 5,000 Bands of 2,500 Bands of 5, Jean O'Callaghan (From 01 Aug 14) Chief Executive Officer Alistair Flowerdew (From 18 Jan 14 to 31 Jul 14) Interim Chief Executive Officer Alistair Flowerdew (From 01 Aug 14 to 31 Mar 15) 5 Medical Director Brian Reid (To 31 Jul 14) Interim Medical Director Lindsey Barker (From 10 Nov 14 to 31 Mar 15) Interim Medical Director Craig Anderson Director of Finance Caroline Ainslie Director of Nursing Paul Beal (From 17 Dec 14) Director of Workforce and Organisational Development Bernie Bluhm (From 17 Dec 14) Interim Chief Operating Officer Peter Malone (To 30 Jun 14) Care Group Director 1 Sue Edees (From 01 Jul 14 to 17 Dec 14) Care Group Director NON-EXECUTIVE DIRECTORS Stephen Billingham - Chairman (To 27 Feb 15) Janet Rutherford (Acting Chair from 01 Mar 2015) John Barrett Brian Hendon Jane May (To 26 Nov 14) Alison Hill Susan Hunt ( From 29 Oct 14) Julian Dixon (From 26 Nov 14)
45 Notes 1 The appointment of care group directors to the Board was rotated every 6 months between the three care group leads, until 17 December 2014 when their Board role ceased Effective from 18th January 2014 Craig Anderson was appointed to the role of interim Deputy Chief Executive Officer in addition to his role as Finance Director. At the time of finalising the 2014/2015 pension disclosures the Trust was awaiting updated prior year information from the Pensions Agency relating to Jean O'Callaghan (Joined Trust August 2014). and Paul Beal (Joined Trust October 2014) The Trust has therefore not been able to make a meaningful calculation of in-year "Pension related benefits" for the year ending March 2015, for either of them. Interim Chief Operating Officer (Bernie Bluhm) is employed "off-payroll". The values shown above exclude VAT and an average agency mark-up charge, from that billed. Alistair Flowerdew remained contracted in post as Medical Director after standing down (from 10 Nov 2014 to 31 Mar 2015) even though Lindsey Barker was appointed to cover this role on an interim basis. Brian Reid ( Interim Medical Director) opted out of the NHS Pension scheme with effect from 1st April 2014 None of the directors received any Benefits in Kind in either years. Additionally no "taxable benefits", "annual performance-related bonuses" or "long-term performance-related bonuses" were paid. Posts occupied by more than one person during the year From To Chief Executive Officer Alistair Flowerdew (Interim) 01 April July 2014 Jean O'Callaghan 01 August March 2015 Medical Director Brian Reid (Interim) 01 April July 2014 Alistair Flowerdew 01 August March 2015 Lindsey Barker (Interim) 10 November March 2015 Chairman/Chair Stephen Billingham 01 April February 2015 Janet Rutherford (Interim) 01 March March
46 Name and Title Year to 31 March 2014 Salary and fees Payments-inlieu of notice and unpaid annual leave Pension related benefits Bands of Bands of Bands of Bands of 5,000 5,000 2,500 5, EXECUTIVE DIRECTORS Edward Donald (To 17 Jan 14) Chief Executive Officer Total Alistair Flowerdew (From 18 Jan 14 to 31 Mar 14) N/A Interim Chief Executive Officer Alistair Flowerdew (From 01 Apr 13 to 17 Jan 14 ) N/A Medical Director Brian Reid (From 18 Jan 14 to 31 Mar 14) N/A Interim Medical Director Craig Anderson N/A Director of Finance Caroline Ainslie N/A Director of Nursing Lindsey Barker (From 01 Feb 14 To 31 Mar 14) Care Group Director N/A Peter Malone (From 01 Aug 13 To 31 Jan 14) Care Group Director N/A Sue Edees (From 01 Apr 13 to 31 Jul 13) N/A Care Group Director 1 NON-EXECUTIVE DIRECTORS Stephen Billingham - Chairman N/A Janet Rutherford N/A Tim Caiger (To 03 Sep 13) 5-10 N/A John Barrett N/A Brian Hendon N/A Jane May N/A Alison Hill (From 1 Dec 13) 5-10 N/A Notes 1. The appointment of Care Group Directors to the Board was rotated every six months between the three Care Group leads. 2. At the time of finalising the 2013/2014 pension disclosures the Trust was awaiting updated prior year information from the Pensions Agency relating to Alistair Flowerdew (Joined Trust November 2012). The Trust was therefore not able to make a meaningful calculation of in-year "Pension related benefits" for Alistair Flowerdew for the year ending March Effective from 18th January 2014, Craig Anderson was appointed to the role of interim Deputy Chief Executive Officer in addition to his role as Finance Director. No annual performance-related bonuses or long-term performance-related bonuses were paid. 46
47 Pension Benefits! " # #! " # # $% # & ' ()! " # # * +,, -.! * %! * &'( / * + (', / -, 0$ -,!!!! " ""!!!! $" $## " #! # )" )" # # # "!!!! "! $!# $ "! 47
48 The "Pension Benefits" section of this report has been subject to audit. Notes 1. At the time of finalising the pension disclosures for the year ended March 2015 the Trust was awaiting updated information from the Pensions Agency relating to Jean O'Callaghan (joined Trust in August 2014) and Paul Beal (joined Trust in October 2014) for the year ending March The Trust was therefore unable to make a meaningful calculation of "Real increase in pension at age 60", "Real increase in pension lump sum at age 60" and "Real increase in cash equivalent transfer value" or show "Total accrued pension", associated "Lump sum" figures and "Cash equivalent transfer values"(cetv) for either Director for the year ending March Brian Reid (Interim Medical Director) opted out of the NHS Pension scheme with effect from 1st April It has therefore not been possible to show any figures for him for the year ended March 2015 or calculate the "Real increase in Pension at 60", "Real increase in Pension lump sum at 60" and "Real increase in CETV" between the two years in question. 3. The three Care Group Directors rotate onto the board in turn with a six-month tenure(until their Board role ceased effective from 17th December 2014) - see Remuneration table on page 46. The "Real increase in pension at age 60", "Real increase in pension lump sum at age 60" and "Real increase in CETV" have been calculated on a pro rata basis to reflect this. 4. Lindsey Barker's term as interim Medical Officer was from 10th November 2014 to 31st March The "Real increase in pension at age 60", "Real increase in pension lump sum at age 60" and "Real increase in CETV" figures shown for her have been calculated on a pro rata basis between these two dates. Bernadette Buhm (interim Chief Operating Officer) is employed "Off-payroll" and therefore has no NHS pension to be declared. Janet Rutherford has received an additional responsibility allowance for part of the year to cover her increased duties as interim Chair after Stephen Billingham stepped down. Fair pay disclosure Reporting bodies are required to disclose the relationship between the remuneration of the highest-paid director in their organisation and the median remuneration of the organisation s workforce. Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind as well as severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions. The "Fair Pay Disclosure" section of this report has been subject to audit. Year to 31 March 2015 Year to 31 March 2014 Band of Highest Paid Director s Total Remuneration Median Total Remuneration 28,791 30,130 Ratio
49 The banded annualised remuneration of the highest-paid director in the Trust in the financial year 2014/15 was 275, ,000 (2013/14, 195, ,000). This was 9.64 times (2013/ ) the median remuneration of the workforce including medical consultants remuneration, which was 28,791 (2013/14-30,130). The highest paid director on an annualised basis was the Chief Operating Officer. The Trust re-instigated this role during the year to address a number of operational issues that it had identified. The role during 2014/15 was undertaken by interim consultants with specific and extensive knowledge and experience in this area which resulted in a premia being paid. The Trust has appointed a permanent COO who starts on the 1 st June 2015 on an annual salary of 142,500. In 2014/15, one (2013/14, nil) individual received remuneration, on an annualised basis, in excess of the annualised remuneration of the highest-paid director. (Remuneration banding 295, ,000). Expenses paid to Directors and Governors The Expenses paid to Directors and Governors section of this Report has been subject to audit. The table below lists the total of reimbursed expenses paid to Directors and Governors Year to 31 March 2015 Year to 31 March 2014 Directors 14,441 9,803 Governors 1,212 1,619 Of the amount stated in respect of Directors expenses 3,210 was paid to Non-Executive Directors (2013/14 3,321). 8,000 was paid to the current Chief Executive and 2,000 was paid to the Interim Chief Executive in respect of re-location expenses. During the year there were, inclusive of non-executives, 18 directors in post (2013/14, 15). Of these 7 received expenses payments (2013/14, 4) Additionally there were 33 governors in post during the year (2013/14, 32) of which 4 were paid expenses (2013/14, 9). 49
50 Severance payments This section of the Annual Report has been subjected to audit. Exit package cost band Number of compulsory redundancies Number of other departures agreed < 10, ,000-25, ,001-50, , , , , , ,000 Total number of exit packages by type Total number of exit packages by cost band Total resource cost 125, , ,198 The payment for loss of office was a combination of redundancy pay and pay in lieu of notice. No other payments were made to the individual in connection with termination of services. Agreement Number Total Value of Agreements Voluntary redundancies including early retirement contractual costs 1 4,050 Mutually agreed resignations (MARS) contractual costs 2 63,362 Early retirements in the efficiency of the service contractual costs Contractual payments in lieu of notice ,813 Exit payments following employment tribunals or court orders Non contractual payments requiring HMT approval 1 114,298 Total: ,524 Of which: Non contractual payments made to individuals where the payment value was more than 12 months of their annual salary 0 0 Off payroll arrangements The Contracts for off payroll arrangements section of this report has been subject to audit. The Executive Directors have delegated authority to ensure that the Trust s procedures for the supply of temporary staff is applied to the provision of temporary staff ensuring that business continuity is maintained in accordance with appropriate legislative and regulatory standards. The Trust monitors, on a monthly basis, the reliance on off-payroll engagements by reviewing engagements costing more than 220 per day. 50
51 Off-payroll engagements as of 31 March 2015, for more than 220 per day and that last longer than six months No. of existing engagements as of 31 March Of which: No. that have existed for less than one year at a time of reporting 3 No. that have existed for between one and two years at time of reporting 4 No. that have existed for between two and three years at time of 4 reporting No. that have existed for between three and four years at time of 2 reporting No. that have existed for four or more years at time of reporting 0 The Trust can confirm that all existing off-payroll engagements, outlined above, have at some point been subject to a risk-based assessment as to whether assurance is required that the individual pays the right amount of tax and, where necessary, that assurance is being sought. All new off-payroll engagements or those that reached six months in duration, between 1 April 2014 and 31 March 2015, for more than 220 per day and that last longer than six months All new off-payroll engagements or those that reached six months in 4 duration, between 1 April 2014 and 31 March 2015, for more than 220 per day and that last longer than six months No. of the above which include contractual clauses giving the Trust the 4 right to request assurance in relation to income tax and National Insurance obligations No. for whom assurance has been requested 4 Of which: No. for whom assurance has been received 4 No. for whom assurance has been requested but not been received - No. that have been terminated as a result of assurance not being - received The Trust has not engaged any individual without including contractual clauses allowing the Trust to seek assurance as to their tax obligations. Any off-payroll engagements of board members and/or senior officials with significant financial responsibility, between 1 April 2014 and 31 March 2015 Any off-payroll engagements of board members and/or senior officials 3 with significant financial responsibility, between 1 April 2014 and 31 March 2015 No. of individuals that have been deemed board members and/or senior 18 officials with significant financial responsibility during the financial year. This figure should include both off-payroll and on-payroll engagements. The two senior officials with significant financial responsibility employed off-payroll between 1 April 2014 and 31 March 2015 were individuals who were engaged by the Trust to cover substantive roles whilst permanent employees were recruited. The first being the role of Director of Workforce and OD who was contracted between March and October 2014 and the second as interim Chief Operating Officer whose contract commenced in September 2014 and as at the end of the year was still employed. 51
52 Jean O Callaghan Chief Executive Officer Date: 27 May
53 Sustainability report During 2014/15, the Trust has continued to make progress with the challenge of reducing the size of its carbon footprint. Carbon Management Strategic Partnering: The Trust continues to work closely with the NHS Carbon Energy Fund (CEF) and Veolia plc who have responsibility for the operation of the boiler-house and the Combined Heat and Power (CHP) unit on the Royal Berkshire Hospital site. The CHP unit now generates a significant proportion of the electricity units used on the RBH site, and utilises the waste heat from this process to provide heating and hot water to the larger buildings on the site. Our Sustainability Performance: Greenhouse Gas Emissions Scope 1: Direct Emissions Information Greenhouse Gas Emissions Scope 1 Natural Gas: - Heating: 522 tco 2 - Electricity generation: 7,016 tco 2 Scope 2: Energy Indirect Emissions Scope 3: Official Travel Emissions - Total: 7,538 tco 2 Emissions Information Scope 2 Imported Electricity: 3,494 tco 2 These CO 2 emissions are based upon the latest DEFRA emissions factors for grid consumed electricity. Apart from a small number of electric cars, the Trust does not maintain a vehicle fleet and all patient transport services are contracted to the regional ambulance service and selected local service providers. Expenditure on purchase of energy: Natural Gas: 1,836k Expenditure on purchase of energy: Imported Electricity: 847k The Trust s annual spend on business travel was 289,319. However clinicians do provide clinical services across the community and staff incur travel costs during the course of their duties. Waste Minimisation and Management The data listed below relates to weights (in tonnes) of the various waste streams: Incinerated clinical waste weighing 303 tonnes 175k Non-burn clinical treatment weighing 572 tonnes 170k General waste to energy weighing 770 tonnes 125k Waste recovery & recycling weighing tonnes 13k Total waste weighing tonnes 482k Based on expenses mileage, this expenditure equates to approximately 518,000 miles for clinicians and staff. The data listed below is the financial costs for managing waste across the hospital Finite Resources Based on meter readings the hospital consumed a total of 202,000 cubic metres of water during 2014/15. The Trust spent 303k during 2014/15 on finite water resources Just over half of this water was extracted from a local borehole Achievements within the year The Trust is progressing its Good Corporate Citizenship reporting in support of a wider commitment to social and economic sustainability. 53
54 Our CHP scheme continues to deliver substantial annual carbon reductions over our baseline position. As one of the first projects to be successfully implemented through the Carbon and Energy Fund it provides a model for innovation across our peer group. The Trust has introduced electrically powered cars to reduce its Scope 3 travel emissions. Next steps Operational review of heating control systems on the RBH site Review use of motor speed controls and voltage optimisation Review of water saving opportunities Review of opportunities to use on-site generators in demand response mode Improved energy use metering to identify energy saving measure Summary The Trust continues to follow the long term strategic approach and is largely relying on technical solutions to bring incremental reductions in carbon footprint. The largest of these has been successfully implemented and is already delivering significant energy and carbon saving. By working with specialist contractors and our maintenance provider we are incrementally reducing energy consumption through good plant control and good housekeeping measures. We continue to work with our carbon champions on staff and patient engagement, which will be a focus area for Regulatory ratings As a foundation trust our activities are overseen by Monitor the independent regulator of Foundation Trusts. Monitor uses the Trust s Annual Plan and its in-year quarterly submissions to assign a risk rating for finance and governance for the Trust. Monitor uses these ratings to assess the risk of compliance with the Trust s Terms of Authorisation (to be a foundation trust), to guide the intensity of its monitoring and to signal its degree of concern with the specific issues identified and evaluated. With the change in regulatory regime in 2013/14 following the enactment of the NHS Act 2012 Foundation Trusts method of assessment was changed from the Financial Risk Rating under the Compliance Framework to the Continuity of Service Risk Rating under the Risk Assessment Framework. This change took place at the end of Q2 2013/14. The risk ratings achieved by the Trust for 2013/14 and 2014/15 are summarised in the tables below. Note that Financial Risk Rating was measured from 1 to 5, where 5 signifies the lowest risk and 1 the highest risk. The Continuity of Service Risk Rating is measured from 1 to 4, where 4 signifies the lowest risk. Under the Compliance Framework Annual Plan 2013/14 Q1 2013/14 Q2 2013/14 Q3 2013/14 Q4 2013/14 Financial risk rating N/A N/A Governance risk rating Amber/Green Red Red N/A N/A 54
55 Under the Risk Assessment Framework Annual Plan 2013/14 Q1 2013/14 Q2 2013/14 Q3 2013/14 Q4 2013/14 Continuity of service rating N/A N/A N/A 2 2 Governance rating N/A N/A N/A Issues identified Green Under the Risk Assessment Framework Annual Plan 2014/15 Q1 2014/15 Q2 2014/15 Q3 2014/15 Q4 2014/15 Continuity of service rating Governance rating Green Green Under review Red Red Continuity of service rating The Trust s Annual Plan for 2014/15 was Continuity of Service Risk Rating of 1 in the first quarter, rising to 3 by the end of the year, albeit that the excess over the minimum needed to support a rating of 3 was small. In practice the shortfall against the planned deficit resulted in reduced net cash receipts and with the Continuity of Risk Rating remaining at a 2. The Trust Board is committed to return the Trust to financial stability and expects to do so by the end of 2016/17. Staff survey results Commentary In 2014, the overall measure of staff engagement remained above the national average and in perhaps the key components of staff engagement - staff motivation at work - the Trust retained its position as a top 20% performer amongst all acute trusts. As a Trust we will continue to pursue our agenda to further enhance staff engagement focussing on the key enablers of staff engagement in areas including staff health and wellbeing, effective management and leadership and understanding and alignment to the Trusts vision and values - which we will refresh in Communication, feedback and harnessing the ideas and learning of our staff has remained a key feature of our work in 2014/15. We completed a second large scale staff listening programme where the views and opinions of hundreds of staff across the Trust were sought in areas such as our quality priorities and organisational development strategy. 55
56 Summary of performance Response rate Response Rate 2013/ /2015 Trust National Trust National Trust improvement/ average average deterioration 55% 49% 45% 42% Although our response rate has deteriorated, in 2014, the Trust moved to conduct an all staff survey compared to previous sample approaches. Over 2000 staff responded in 2014 compared to 450 in Areas of improvement/deterioration since 2013 survey Statistically significant improvement is reported on two key findings in 2014: 2013/ /2015 Statistically significant improvements KF10: % of staff receiving H&S training in last 12 months KF26: % of staff having E&D Training in last 12 months Trust National average Trust National average Trust improvement since 13/14 70% 76% 79% 77% 9% improvement (more staff receiving training) 63% 60% 76% 63% 13% improvement (more staff receiving training) Statistically significant deterioration is reported on two key findings in 2014 Statistically significant deteriorations KF3: Work Pressure felt by Staff KF19: % of staff experiencing harassment, bullying or abuse from staff in the last 12 months 2013/ /2015 Trust National Trust average National average Trust deterioration since 13/ = low work pressure; 5 = high work pressure 19% 24 23% 23% 4% increase (more staff experiencing harassment, bullying or abuse) 56
57 Top four ranked scores Top four ranking scores KF15: % of staff agreeing that they would feel secure raising concerns about unsafe clinical practice. KF2: % of staff agreeing that their role makes a difference to patients KF1: % of staff feeling satisfied with the quality of work and patient care they are able to deliver KF8: % of staff having well structures appraisals in the last 12 months 2013/ /2015 Trust National Trust National average average Trust improvement/deterioration since 12/ Question not directly comparable to 2013/ % improvement % deterioration % improvement Bottom four ranked scores Bottom four ranking scores KF13: % of staff reporting errors, near misses or incidents witnessed in the last month KF28: % of staff experiencing discrimination at work in the last 12 months 2013/ /2015 Trust National Trust average National average Trust improvement/deterioration since 13/ % improvement % deterioration KF5% % of staff working extra hours. KF21: % of staff reporting good communication between senior management and staff % deterioration % deterioration Action plans to address areas of concerns The 2014 survey does highlight some areas where we need to focus our efforts into the future and a detailed action plan for 2015/16, addressing key themes from the survey has been developed. The action plans focuses on improvements in the following domains: Staff health, safety and well being (including discrimination and bullying at work) Raising, reporting and responding to concerns Communication and staff engagement Work pressure felt by staff The quality of appraisals 57
58 Staff recommendation of the Trust as a place to work and receive treatment We have heard from staff that they are working longer. Many of our quality improvement projects are reducing inefficiencies and waste, supporting staff to work smarter not harder. We will continue to work hard to manage our significant capacity challenges and we continue to have large nursing recruitment drives to enhance our front line capacity and we have undertaken skill mix reviews utilising the safer nursing care tool to improve safety. We are committed to improving the staff experience here and we have undertaken large scale listening events to gather staff opinion, and local quarterly pulse surveys are in place to harness ideas. We ve also expanded our portfolio of flexible staff benefits offering staff the opportunity to access benefits such as bikes, computers, mobile phones and cars. Future priorities and targets A key focus for 2015/16 will be the development and delivery of the Trust s Health and Wellbeing strategy where we will look for a 10% improvement in survey findings of staff reporting that we take positive action on the health and wellbeing of staff. Improvements in the trusts performance relating to reported measures of bullying, harassment and discrimination at work - will also be a priority. We have a zero tolerance of bullying, harassment and discrimination and we will look to replicate the improvements we have made this year (fewer staff experiencing violence at work) through a range of interventions. Staff engagement and senior management communication will continue to be a focus. We will continue to deliver large-scale engagement events/forums for staff voice and feedback into Trustwide issues. During 2015 we will engage our staff in reviewing our organisational values and the behaviours framework that underpins them. Addressing the work pressure felt by staff will also be a priority through actions delivered through the Workforce Recruitment and Retention Board to improve the recruitment and retention of staff. Monitoring of the 15/16 action plan will be undertaken through the Board Resources committee and other forums such as the bi monthly Joint Staff Side Committee and the Staff and Patient Experience Committee. Disclosures in the public interest Equality and diversity Royal Berkshire NHS Foundation Trust is committed to embedding equality and diversity in all the services offered to patients, visitors and staff. We are committed to meeting our obligations under the Equality Act (2010). We remain a Stonewall Diversity Champion and Two Ticks employer. Health and safety At Royal Berkshire NHS Foundation Trust we have set the highest standards of health and safety for all our staff in the workplace, for members of the public, patients, and trust partners who come into our premises. We seek to continually improve safety in all locations and recognise that safety is something that everyone is responsible for. 58
59 Our policy therefore enables everyone who has an involvement at Royal Berkshire NHS Foundation Trust to have a role in improving safety and shows how this can be achieved. Occupational Health The department promotes both the physical and mental, health and well being of Trust staff recognising that the health and well being of our staff is key to enabling us to deliver consistently high quality care. During 2014/15 the Occupational Health department received just under 600 referrals from managers for advice on the health of their staff whilst a further 400 staff referred themselves to the department for advice. All new staff who have patient contact in their role continue to be checked for communicable disease status to help ensure we protect not only staff health but also that of our patients. A total of 46.9% of frontline staff took up the offer of a seasonal flu jab. The number of inoculation injuries increased to 200 during the year and the department has delivered further training and awareness around management and prevention of inoculation injuries with the OH nurses recently visiting all clinical areas. The department is engaging with various stakeholders within the Trust to continue the promotion of health and wellbeing for Trust staff to enable them to remain at work delivery high quality care to our patients. Sickness absence Work is continuing to reduce sickness absence in areas where rates are recorded above the Trust average. 2014/ /14 Number Number Total days lost 33,336 51,556 Total staff years 4,644 4,567 Average working days lost (per WTE) 7 11 Better Payment Practice Code measure of compliance Currently, the Trust is required to pay its all trade creditors in accordance with the Better Payment Practice Code. The target is to pay all trade creditors within 30 days of receipt of goods or a valid invoice (whichever is the later) unless other payment terms have been agreed with the supplier. Currently the percentage number of invoices the Trust pays within 30 days is 77% (87% were paid within 30 days in 2013/14). HM Treasury guidance The Trust has complied with the cost allocation and charging requirements set out in HM Treasury guidance. Data losses During 2014/15 there were seven data loss events recorded by the Trust as serious incidents. These were recorded at level 2 or above requiring the Trust to notify the Information Commissioner s Office. In 2013/14 there were nine incidents. The Trust has a commitment to encourage staff to report and investigate all relevant issues, even where the loss is considered minor. In each instance issues are investigated and actions taken where appropriate to mitigate against further occurrences. 59
60 Countering fraud and corruption The Trust is committed to promoting and maintaining an absolute standard of honesty and integrity in dealing with assets, expenditure and income. We are committed to the elimination of fraud and illegal acts within the Trust and ensure rigorous investigation and disciplinary or other action as appropriate. The Trust uses best practice as recommended by the NHS Counter Fraud and Security Management Service (CFSMS), and is also involved in the National Fraud Initiative, led by the Audit Commission. The Local Counter Fraud Specialist (LCFS) has during the past year continued with the work of raising staff awareness in relation to fraud. Income disclosure Section 43(2A) of the NHS Act 2006 (as amended by the Health & Social Care Act 2012) requires that the income from the provision of goods and services for the purposes of the health service in England must be greater than its income from the provision of goods and services for any other purposes. The Trust has met this requirement. Compliance with the Monitor Code of Governance The Board declares that, with the exception of the statement below, the Trust has met the requirements of the Monitor Code of Governance for the year 2014/15. Non-compliance is reported as follows: Code Provision C.2.2 Non-executive directors, including the chairman, should be appointed by the board of governors for specified terms subject to re-appointment thereafter at intervals of no more than three years and to the 2006 Act provisions relating to the removal of a director. The chairman should confirm to governors that, following formal performance evaluation, the performance of the individual proposed for re-election continues to be effective and to demonstrate commitment to the role. Any term beyond six years (e.g. two three-year terms) for a non-executive director should be subject to particularly rigorous review, and should take into account the need for progressive refreshing of the board. Non-executive directors may in exceptional circumstances serve longer than six years (e.g. two three-year terms following authorisation of the NHS foundation trust), but subject to annual re-appointment. Serving more than six years could be relevant to the determination of a non-executive director s independence (as set out in provision A.3.1). One Non Executive Director was appointed for a term of office of four years in The Authorised Constitution of the Trust was updated in 2013 and now stipulates that non-executive directors are appointed for a term of office of three years so any further appointments will be made for a period of three years. 60
61 6. Statement of accounting officer s responsibility 5. Statement of accounting officer s responsibilities Statement of the chief executive's responsibilities as the accounting officer of Royal Berkshire NHS Foundation Trust The NHS Act 2006 states that the chief executive is the accounting officer of the NHS foundation trust. The relevant responsibilities of the accounting officer, including their responsibility for the propriety and regularity of public finances for which they are answerable, and for the keeping of proper accounts, are set out in the NHS Foundation Trust Accounting Officer Memorandum issued by Monitor. Under the NHS Act 2006, Monitor has directed Royal Berkshire NHS Foundation Trust to prepare for each financial year a statement of accounts in the form and on the basis set out in the Accounts Direction. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of Royal Berkshire NHS Foundation Trust and of its income and expenditure, total recognised gains and losses and cash flows for the financial year. In preparing the accounts, the Accounting Officer is required to comply with the requirements of the NHS Foundation Trust Annual Reporting Manual and in particular to: observe the Accounts Direction issued by Monitor, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis make judgements and estimates on a reasonable basis state whether applicable accounting standards as set out in the NHS Foundation Trust Annual Reporting Manual have been followed, and disclose and explain any material departures in the financial statements ensure that the use of public funds complies with the relevant legislation, delegated authorities and guidance and prepare the financial statements on a going concern basis. The accounting officer is responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the NHS foundation trust and to enable him/her to ensure that the accounts comply with requirements outlined in the above mentioned Act. The Accounting Officer is also responsible for safeguarding the assets of the NHS Foundation Trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities. To the best of my knowledge and belief, I have properly discharged the responsibilities set out in Monitor's NHS Foundation Trust Accounting Officer Memorandum. Jean O Callaghan Chief Executive Officer Date: 27 May
62 6. Governance statement Scope of responsibility As Accounting Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the NHS Foundation Trust s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS Foundation Trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Foundation Trust Accounting Officer Memorandum. The purpose of the system of internal control The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of Royal Berkshire NHS Foundation Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in Royal Berkshire NHS Foundation Trust for the year ended 31 March 2015 and up to the date of approval of the annual report and accounts. Capacity to handle risk As Chief Executive, I am directly accountable to the Board of Directors in relation to the performance of the Trust. The authority for decision-making is, however, delegated to individual executive directors. Throughout 2014/15 we undertook a review of quality governance and risk management that resulted in changes to executive director s responsibilities to better align clinical and quality risk management leadership. Responsibility for the risk management process is delegated to executive directors who are supported in this by their own teams. Specific responsibility is as follows: Director of Finance financial and business development, health and safety Medical Director clinical governance Director of Nursing non financial risk management, assurance and legal services, safeguarding adults and children, patient safety and experience. In 2014/15 the leadership structures were reviewed and the role of Chief Operating Officer reintroduced to underpin the clinical leadership structure that was introduced in 2011/12. The care group director of operations role was strengthened to ensure greater accountability for operational and quality performance delivery. Throughout Quarters 2 and 3 of 2014/15 the preparation and review of the Corporate Risk Register and Board Assurance Framework by the Board slipped. Executive responsibility was transferred to the Director of Nursing in Quarter 4 and actions put in place to review the risk management and Board Assurance Framework. This work is progressing well and will be embedded throughout 2015/16. A new post of Deputy Director of Nursing and Governance has been appointed to provide additional capacity for the delivery of effective risk management. The Trust s risk manager has worked with the deputy director to review our risk management policy to reflect the changes in Executive roles and responsibilities and committee structures in the organisation. The risk manager is responsible for ensuring that staff are trained and equipped to manage risk in a way appropriate to their authority and duties. This is achieved through risk training programmes and 62
63 through supporting and facilitating departments and teams directly. All staff receive risk management information and training at mandatory corporate induction days. Organisational learning is communicated internally through a structure of committees that link through the organisation from ward to board and to local management teams. Hot topics and key learning is also cascaded through a number of internal communication mechanisms. Learning is supported by the consistent application of root cause analysis of incidents supported by a comprehensive suite of Trust policies regarding incident reporting. Risk and control framework The Trust recognises the need for a robust focus on the identification and management of risks. The overall aim of the Risk Management Strategy therefore is to ensure the safety of patients, staff and the public in supporting the delivery of affordable, quality, patient-centred services that achieve excellent results. In order to achieve this key objectives are outlined in the strategy: Compliance with relevant statutory, mandatory and professional requirements and maintenance of the Trust s registration with the Care Quality Commission (CQC) Consistent and effective risk management processes at all levels of the organisation The development of a learning culture to support improvements to the safety of services Integration of risk management into both Trust-wide and individual objective setting processes. A robust ward to Board risk process ensuring a clear understanding at Board level of the key risks facing the organisation. The Board considered the amount of risk it is prepared to accept in the pursuit of its strategic objectives and agreed its risk appetite statement in June The risk identification, assessment and risk register procedure is set out within the Trust s Risk Management Policy. Risks are identified as a result of incidents, complaints, claims or by proactive risk assessment and are scored using the Trust s scoring matrix. The policy clearly sets out how risks are scored, recorded, managed, escalated and de-escalated at all levels in the Trust through the committee structure from ward to board. Quality governance arrangements The Trust undertook a significant review of its Quality Governance arrangements in July The areas for improvement identified have driven the work programme for delivery of improvement to Quality Governance arrangements. Notable progress has been made in the following areas: Strategic Planning: Service and strategic planning frameworks are in place and are being implemented. Operational Plan, Clinical Services Strategy and Quality Strategy are all making progress and are on target for delivery. Risk management: With the appointment of a Head of Risk and revision of the Executive portfolio the Trust has completed its external review and good progress has been made improving risk management systems. Culture and workforce: Reviews and changes to senior roles, portfolios and governance structures have strengthened leadership, performance management and accountability. Foundation work has been completed in relation to improved reporting relating to workforce and in developing an organisational development strategy. Information management: Development of an integrated Board performance suite and Ward to Board reporting is in progress. This is supported by a programme focused on embedding robust data quality assurance. 63
64 During 2014/15 we have been subject to scrutiny from Monitor, the regulator of the NHS with respect to our 18-week referral to treatment times (RTT), A&E four-hour target and cancer waiting times. We have made significant improvements and these areas will continue to be a priority for us in the year to come. Governance structures Risk is managed on behalf of the Board through the Trust s governance structure. The committee structure was reviewed in 2014/15 and risk is managed through the following Board committees: Audit and Risk Committee Clinical Governance Committee Resources Committee Finance and Performance Committee. The Audit and Risk Committee oversees the delivery of effective risk management arrangements in the Trust. The key aims and objectives for risk management include: complying with legal and statutory requirements and meeting the requirements of external regulators and other relevant bodies providing guidance to assist with proactive risk management and risk reduction supporting the organisation in its approach to ensuring the safety of staff, patient and visitors. The Clinical Governance Committee enables the Board of Directors to obtain assurance that high standards of care are provided by the Trust and in particular that adequate and appropriate clinical governance structures, processes and controls are in place throughout the Trust. The key responsibilities of the CGC are: to ensure compliance with CQC essential standards and NICE guidance to be assured that risks to clinical quality are proactively identified, prioritised and managed to ensure effective learning is embedded from serious incidents, complaints and patient feedback to oversee the Trust s quality strategy, quality account and quality governance framework. The Quality Assurance and Learning Committee which reports to the CGC was introduced during 2014/15. Care Group Governance Committees now report to this committee, which has strengthened an integrated approach to the management of risk and shared learning across the organisation. Managing risk Incident reporting is encouraged across the Trust, which is reflected in the number of incidents reported each year. The Trust has seen an increase in incident reporting throughout the year. This has been encouraged through the Sign up to Safety campaign and monitored by the Patient Safety committee. The Board receives regular reports regarding numbers of incidents. Lessons learned from incidents are shared with the care groups and wider Trust through safety newsletters, hot topics and other mechanisms. Other risk management strategies include: the use of equality impact assessments as part of the development of business cases within the Trust. robust Quality Impact assessment process to assess the risk of cost improvement initiatives. 64
65 All the organisational risks (strategic and operational) identified have been classified and entered on to the Corporate Risk Register. The register is a live document that captures newly identified risks and allows risks that have been adequately treated to be removed from it. Each risk has a treatment plan and is allocated to an Executive ownership. An action plan has been drawn up for each risk, including proposed action, resource requirement, responsibilities, timescale reporting and monitoring requirements. Both the Register and action plans are presented to the Audit and Risk Committee, the Executive and the Board for assurance. The Trust was inspected by the Care Quality Commission during March On 24 June 2014 the CQC published the Quality Report of the Trust-wide inspection. The overall rating for the Trust was requires improvement and 7 compliance actions were identified. The Trust continues to implement its post inspection action plan and aims to be fully compliant by Quarter 3 of 2015/16. As an employer with staff entitled to membership of the NHS Pension Scheme, control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary, employer s contributions and payments into the Scheme are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations. Control measures are in place to ensure that all the organisation s obligations under equality, diversity and human rights legislation are complied with. The Trust has undertaken risk assessments and carbon reduction delivery plans are in place in accordance with emergency preparedness and civil contingency requirements, as based on UKCIP 2009 weather projects, to ensure that this organisation s obligations under the Climate Change Act and the Adaptation Reporting requirements are complied with. Current and future risks The principal risks, identified through this risk framework, to comply with the Trust licence are: Failure to sustainably achieve financial targets and cost improvement programmes Failure to maintain standards required to maintain licence to operate Failure to maintain and improve quality of care Failure to maintain and develop an estate fit for the future Scale of implementation of IT and Information systems impacts negatively on the functioning of the Trust and of clinical care Failure to ensure there are the right staff (numbers, skills and capability) in the right place Failure to develop the organisation to support the delivery of the Trust s vision Failure to maintain engagement with patients and other stakeholder groups Failure to respond appropriately to changes in the external environment impacts on viability. Annual Quality Report The Trust Quality Accounts for 2014/15 reflect a balanced assessment of our performance in respect of the last year and the priorities for 2015/16. Our assessment of the quality of our care reflects a balanced view of: 65
66 the action taken to deliver ever improving standards of quality in the care we provide (such as refurbishing and expanding our Critical Care unit, providing dementia friendly wards in elderly care and delivering more services seven days a week) the learning and experiences from major issues, initiatives and reports (such as the Francis, Berwick and Keogh reviews) the views and conclusions of our regulators such as the Care Quality Commission and Monitor feedback received from patients, partners and stakeholders in the community. The culmination of this is reflected in our quality strategy agreed during the course of the last year and our Quality Accounts achievements and priorities. The consultation undertaken with stakeholders and the public on our Quality Accounts priorities for 2014/15, and the feedback provided on our progress during 2013/14 provides the Board with confidence and assurance that the document, included within this Annual Report, presents a balanced review. The quality strategy, and our Quality Accounts, set out our plans for delivering care of the highest standards, which reflect the highest standards of patient safety, clinical effectiveness and provide an excellent patient experience. Both documents will be monitored over the course of the year to ensure that our ambitions are turned into reality. Underpinning this will be a comprehensive monitoring process to ensure that we know we are delivering quality care. This will encompass: the Executive and Care Groups meeting monthly to discuss and monitor progress against our quality indicators the monthly quality performance report to the Board periodic quality and safety reports regulatory assurance patient feedback. Data security Data Communications: The Trust has put in place appropriate measures to ensure the security of data and to ensure the risk of data loss is minimised. This is achieved in the following ways: Access to data: All applications are password controlled, the password policy issued by IT details the password requirements and the need to change passwords, and this is further enforced through forced password changes after 90 days on key applications. Remote connectivity to the Trusts applications is strictly controlled and only achieved by two factor authentication - user name / password plus RSA (Remote secure access) token with a 60 second refresh time. Third party access is only available under the terms laid out in the Information Governance Statement of Compliance issued by the NHS. This has been fully documented in the Access Control policy. Backup of data: The systems managed by IT have a daily, weekly, monthly backup cycle that is managed by the operations team in line with their operating procedures. Tape back-ups are stored in a fireproof safe, critical systems and monthly tapes are stored for a period of one year should the need arise to retrieve historical data. These back-up tapes would be used if there is a need to recover in the event of a disaster. 66
67 Threat intrusion: All PCs and servers have antivirus software installed and in addition a three-layer firewall is in place to reduce the risk of intrusion. The latest version of anti-virus software is distributed through an automated software deployment tool, and supplier notice boards are monitored regularly to ensure that newly identified threats are dealt with. Disposal of equipment: Disposal of equipment: any computer equipment or media that is replaced either through end of life refresh or due to a fault that cannot be repaired has the hard drive removed and granulated. Encryption / removable media In addition, the following policies are in the process of being implemented: Encryption Policy - all new laptops will be delivered with encryption software pre-loaded, this cannot be removed. All existing laptops are now encrypted. Removable Media Policy - this policy is in place and the Trust is planning to lock out any non-encrypted media devices such as memory sticks to ensure that if any patient data is copied it is secured. Data losses During 2014/15 there were seven data loss events recorded by the Trust as serious incidents. These were recorded at level 2 or above requiring the Trust to notify the Information Commissioner s Office. In 2013/14 there were nine incidents. The Trust has a commitment to encourage staff to report and investigate all relevant issues, even where the loss is considered minor. In each instance issues are investigated and actions taken where appropriate to mitigate against further occurrences. Review of economy, efficiency and effectiveness of the use of resources There are a number of processes used to deliver economy, efficiency and effectiveness of the use of resources. These include: use of Standing Financial Instructions. efficient use of electronic procurement with workflow. regular, systematic and risk based Internal Audit. detailed bottom-up process for budget setting and business cases. introduction of benchmarking techniques for services. financial and efficiency benchmarking at Trust level against other NHS foundation trusts. development of service level information, with an emphasis on service level reporting. and service level management. The Board of Directors sets the standards and has specified within the Standing Financial Instructions the appropriate delegated authority levels throughout the Trust. The Trust s efficiency programme has continued to focus on performance improvements and will continue to focus on operational, clinical, procurement, organisational and strategic opportunities. The emphasis in internal audit work is on risk management, governance and internal control processes. Individual assignments have also raised issues relating to economy, efficiency and effectiveness. Where scope for improvement, in terms of value for money was identified during an internal audit review, appropriate recommendations were made and action plans were agreed with management for implementation. 67
68 Public and patient involvement We wish to achieve a culture that consistently put patients need first. Patients are key and can be influential leaders who drive changes, provide constructive challenge and work with us to deliver high quality, safe care. The Trust currently works together with patient leaders and partners, who are volunteers from the public domain including patients, carers and representatives from a wide range of patient groups. This provides an opportunity for our leaders/partners to work together with the Trust in shaping the future of healthcare, establish priorities, improving the experience for both patients and carers and managing risks that impact on patients. The Trust recruited 15 patient leaders who completed an extensive training programme which enabled them to support our work. The first major project initiated by patient leaders, # hello my name is. campaign, launched in November The campaign has received enormous support from all staff and has helped us to improve communication with our patients. A further patient leadership recruitment drive is underway with an objective of recruiting another 20 patient leaders. Each year the Trust hosts two patient partnership standing conferences chaired by the Director of Nursing, where we engage with patients, staff, public and community groups. The conference enables us to share current and future initiatives and is a valuable networking opportunity for all concerned. Stakeholder engagement is referred to in more detail in the Directors Report on page 14 and in the Quality Account report on page 70. Review of effectiveness As Accounting Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, clinical audit and the executive managers and clinical leads within the NHS Trust who have responsibility for the development and maintenance of the internal control framework. I have drawn on the content of the Quality Account Report included in this Annual Report and other performance information available to me. My review is also informed by comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, the Audit and Risk Committee (and clinical governance/ quality committee, if appropriate) and a plan to address weaknesses and ensure continuous improvement of the system is in place. I have been specifically informed on the effectiveness of the system of internal control and the validity of the Corporate Governance Statement by the: Trust Board - through the regular review, adoption and approval of the Trust Corporate Risk Register, the Quality and Patient Safety reports and the Integrated Performance reports. Audit and Risk Committee through internal and external audit, reviewing the adequacy of internal control systems designed to minimise risk. Clinical Governance Committee - ensuring the effective working of clinical governance, both corporately and at care group level, including clinical audit and risk management. It also reviews reports on the quality assurance process and Quality Accounts data requirements demonstrating effectiveness and improvements in the quality and safety of our care for patients. 68
69 Audit and Risk Committee - ensuring overall co-ordination of risk management and monitoring of the action plans to address the risks identified in the Trust Corporate Risk Register. A number of factors have contributed to form the Head of Internal Audit opinion for the year. In March 2014 the Care Quality Commission inspected the Trust and their report, issued in June 2014, gave the Trust a requires improvement rating, then, in December, the Trust was subject to a number of enforcement actions from Monitor regarding the Trust s referral to treat target and its plan to eliminate the deficit. The Trust continues to make progress against the agreed action plan with each organisation. Also, in the Annual Report for both 2012/13 and 2013/14 the Trust highlighted delays in the programme of IT systems transformation. Whilst progress has been made in 2014/15 there are still shortcomings in the IT control environment that pose a risk to the Trust. Progress is being monitored by the Audit and Risk Committee. As a result, the Head of Internal Audit has reached an opinion of major improvement required on the Trust s overall system of controls, effectiveness and use of resources. Disclosure of public interest The Trust has complied with the cost allocation and charging guidance issues by HM Treasury. The directors consider the annual report and accounts, taken as a whole, is fair, balanced and understandable and provides the information necessary for patients, regulators and stakeholders to assess the Trust s performance, business model and strategy. Conclusion This report sets out an open and balanced reflection of the Trust s progress over the past year. The Board and Executive have a clear understanding of the issues facing the Trust and the work they must focus on during the 2015/16 financial year. Signed Jean O Callaghan Chief Executive Date: 27 May
70 7. Quality Account Report Part 1: Statement on quality from the Chief Executive Delivering high quality patient care is the guiding principle of the Royal Berkshire NHS Foundation Trust. Our purpose is to serve our patients and service users; we can only achieve this by ensuring that the patient comes first in everything that we do. We have prioritised patient safety and endeavour to support this through delivering effective outcomes and a positive patient experience. I want to thank our staff who constantly strive to deliver high quality care and provide a positive experience for patients and their carers/families. The Quality Account (also known as the Quality Report) provides us an opportunity to inform the public on what we have achieved in quality improvement over the last year and what the Trust intends to concentrate on during the coming year. We have made good progress in developing our Improvement Programme and driving forward priority improvements; we have redesigned our Quality Governance structure and embedded improvement in our structures and processes. We have made a number of significant achievements this year, including keeping patients safe from Clostridium Difficile infections, improving harm free care, reducing weekend mortality, improvements in medical records and improved processes in place for handling complaints received relating to staff behaviour and attitude. Despite a good start to the year in reducing cancelled operations we were not able to sustain this progress due to winter pressures. We continue with our nursing recruitment campaign and complete nursing skill mix reviews biannually to ensure we get our staffing levels right for the for the patients we look after. We have continued to work to revalidate our Doctors to ensure that they are up to date and fit to practice. Some highlights of our quality improvements achievements in 2014/2015 are: Being recognised as one of the best places to work by the Health Service Journal. Welcoming 15 patient leaders who are working in partnership with us to improve services across the organisation. The launch of the #hello my name is a campaign to enhance compassionate care. An award winning Cardiology Team Research and Development have made a significant contribution towards enhancing patient care including avoiding emergency admissions for older people, the management of pain in the Emergency Department, and evaluating a new blood test for earlier detection of acute kidney injury. We redesigned pathways to utilise the new Emergency Department (ED) Observation Ward that opened in October Prompt initial senior clinical assessment within ED and rapid referral if admission is required continues to aid flow within the department along with an ambulatory approach to medically expected patients within the Acute Medical Unit. These improvements are helping to support us to cope with the demand and pressure and deliver the 95% quality standard. During 2014/15 we have been subject to enforcement action from Monitor, the regulator of the NHS with respect to our 18-week referral to treatment times (RTT), ED 4 hour target and 70
71 cancer waiting times. We have made significant improvements and these areas will continue to be a priority for us in the year to come. On 24 June 2014, the CQC published the Quality Report of the Trust-wide inspection it undertook in March The overall rating for the Trust was requires improvement. A robust action plan has been implemented to focus on the risks identified. We have made significant strides in addressing the areas requiring improvement and will continue to do so in 2015/16. The Quality Account is by no means the only work we will be completing to improve our services. We are refreshing year 2 of our Quality Strategy to be implemented by 2018/19. This document is the foundation to support delivery of the highest quality healthcare services to our patients and sets our direction for making measurable enhancement to the quality of our services: Patient Safety: In 2015/16 we will continue to focus on improving our maternity services. Staffing and facilities have been improved and the unit obtained baby friendly status. In April we launched our Sign up to Safety Campaign designed to reduce avoidable harm to patients. We will also improve our ability to learn from incidents, further developing the right culture, systems and processes to enable us to learn from incidents and employ a zero tolerance to never events. To address these we know we need to further develop our learning structures. Clinical Effectiveness: Our immediate attention is on continuing to improve the quality and management of our patient medical records and waiting times for patients. These impact on patients and the efficient running of the hospital. We recognise that the current systems need to be improved. We therefore will be seeking to improve the quality of all the information that we use in relation to patients, supported by development of our clinical audit and governance process. We will undertake further work to reduce waiting times to ensure treatments are received at the right time. There will be particular focus on referral to treatment times and cancer waiting times. Patient Experience: We will be working to improve safe and timely discharge of our patients as well as developing administration systems to improve booking processes, reduce cancellations and improve access to the Trust. Culture: We recognise the most valuable tool we have for improving the quality of care is our workforce. We will continue to develop our organisation to ensure that we align all services on our culture of caring, learning and leadership. We accept that our focus on quality must be ongoing and relentless in order to deliver the services our patients and community deserve. I am very pleased to present this Quality Account to you and I believe that it is a fair and a balanced report on the quality of care at the Royal Berkshire NHS Foundation Trust. I also confirm that, to the best of my knowledge, the information contained within this report is accurate. Jean O Callaghan, Chief Executive 26 May
72 Introduction What is a Quality Account? Since 2009, all NHS hospitals must publish a Quality Account. The Quality Account is an annual report to the public by NHS providers of the quality of the services provided. Its purpose is to ensure NHS trusts demonstrate their commitment to delivering high quality care, openness and candour and to invite the stakeholders to contribute to determining the standards of care they desire and expect. This document is Royal Berkshire NHS Foundation Trust s ( the Trust ) Quality Account for 2014/15 and it is divided into three sections. Part 1: A statement from the Chief Executive on quality. We have also set out an introduction to the Trust and what quality means to us. Part 2: An outline of our quality improvement priorities for 2015/16. This includes how we have chosen those priorities through consultation. In this section we have included mandated statements of assurance from the Board on clinical audit, research, CQUIN payments and data quality. Part 3: We review 2014/15 and comment on our performance against our priorities for the year. We have also included highlights of other areas of quality improvement that have been important to us and to our patients. This includes information on national and mandated core indicators for 2014/15, including benchmarking. Annex: We have included statements from our local key stakeholders such as Healthwatch, Health and Wellbeing Boards and the Commissioners of the services we provide. 73
73 About Royal Berkshire NHS Foundation Trust Royal Berkshire NHS Foundation Trust provides high quality acute medical and surgical services for our local communities for over 500,000 people in Reading, Wokingham, West Berkshire and surrounding areas. We also provide specialist services to a population of one million across Berkshire and its borders. With just over 4,500 staff we are one of the largest employers in the Reading area. Our specialist centre is the Royal Berkshire Hospital in Reading, a large district general hospital with the expertise to treat patients requiring urgent or hyper-acute care. We provide services from the following bases: - Royal Berkshire Hospital, Reading with just under 700 beds and capacity for over 200 day patients. Additionally we have a number of community sites where we deliver ambulatory care and diagnostics. We continue to develop the range of services offered in the community to take a greater proportion and range of care nearer to, or at, patients homes (Figure 1). Figure 1: RBFT hospital sites 74
74 The Prince Charles Eye Unit, Windsor, provides eye services to the patients of East Berkshire. Dialysis services at a dedicated unit in Windsor. West Berkshire Community Hospital - day surgery unit and the acute outpatients department. Royal Berkshire Bracknell Healthspace cancer, renal and outpatient services. Townland s Hospital, Henley outpatient services. We have been an NHS foundation trust since June 2006 and we are pleased, with the freedom and responsibilities that this brings. It enables us to work with our members through our Council of Governors to shape our direction of travel. Working with Commissioners we can develop the services and facilities required by our local communities. We are a designated specialist centre in cancer, bariatric care, heart attack and stroke. We also provide specialist care as part of a care network through a local neonatal unit, an interventional radiology unit and a trauma unit. We are part of the critical care and vascular care networks. Our approach to quality Our commitment to quality is summarised in our vision to provide sustainable, and improving, high quality care for our local community. In support of this revised vision we are refreshing our Quality Strategy, containing our quality objectives and plans around strategic themes. These themes are: - High quality care: A commitment to deliver high quality care that is safe, compassionate and effective, which provides a positive experience. This will be underpinned by effective clinical governance and risk management processes. - Financial sustainability: Achieving financial stability, resilience and sustainability in the longer term that allows investment in front line services that are fit for the future. - Transforming services: Ensuring our services meet the needs of the local population by responding to the changing needs of our patients, Commissioners and the local health and social care environment in order to bring maximum benefit through integration. - Organisational resilience and capability: Improving how we align all the components of our organisation that define us our estate, workforce (capacity and skills), technology, our culture of caring and learning and our leadership capability. We know that one of the biggest risks to delivery of quality health care is affordability. We have set ambitious standards of care that we will seek to achieve by 2018/2019. However, we acknowledge that we have to deliver significant savings over this period. We have in place a robust Quality Impact Assessment 75
75 process which is used to measure and to monitor the potential impact that cost savings may have on the quality of care. Our mission is to always provide our patients with services that are safe, clinically effective and person centred: Patient Safety This is about treating and caring for people in a safe environment and how we ensure we protect them from any avoidable harm. Clinical effectiveness This is about whether or not a patient s care or treatment is successful. In other words did it have the impact it was supposed to have and did it achieve the best possible result for the patient? Patient experience Having patient-centred care is about ensuring that patients, relatives and carers have as positive experience as possible at every stage of the care or treatment provided. This is about their overall experience throughout the entire course of their treatment not just the result at the end. How do we know we are delivering quality care? The Trust Board is accountable for the systems of assurance, internal control and risk management and regularly monitors and reviews these at Trust Board level and via its committees. The Chief Executive is ultimately responsible for ensuring the Trust delivers a high quality service for all patients and for the delivery of and compliance with assurance, quality and performance targets. This responsibility is delegated to members of the Executive, such as the Medical Director, the Executive Director of Nursing, and to the Director of Finance for financial targets. The Executive Team and the Care Groups meet every month to discuss and monitor progress against our quality indicators. A scorecard is used to help the Trust monitor performance. This is supported by a dashboard which focuses attention on those areas that require further work. The quality scorecard and the actions are reviewed bi-monthly by the Clinical Governance Committee and are reported and discussed at the Trust Board every month. The Board is actively engaged in reviewing the quality of our services. The Chief Executive, Chairman and the Executive Director of Nursing take part in regular ward visits to meet staff and talk with patients. Throughout the year, we hold monthly Patient Safety and Patient Experience departmental visits. Teams consisting of executive directors, senior nurses, estates and facilities, corporate and operational managers visit all our sites to assess safety, the environment, patient experience, speaking with both staff and patients. The Trust Board gains assurance on quality through a number of reports including: The monthly Quality Performance Report (key performance indicator dashboard) Periodic quality and safety reports 76
76 Regulatory assurance including compliance with external regulators and Commissioners Patient experience/patient feedback Board visits to wards and departments Patient complaints Safeguarding The learning from incidents The Trust also monitor progress against CQUIN targets: Commissioning for Quality and Innovation (CQUIN) is a scheme designed to encourage NHS Trusts to improve quality and patient safety by setting targets and rewarding achievements of those targets through financial payments. These targets are set nationally, regionally and locally. Quality improvement journey We know our ability to learn from the past is critical to our ability to improve in the future. Therefore we have reflected on how we have achieved success in sustaining and growing improvement since 2011 (Figure 2). This helps us to reflect on those areas that are a greater challenge and that may warrant an increased profile and attention over a period longer than 12 months. Figure 2: 2011/ /16 Quality Improvement Priorities ) )" " ***to be added***./0 1 ( 2','3, 1 ( 45$' ','' 1 ( ','' 1 ( 2,'' ' 1 (,( ',(6 %7'$ 85$,'' '$45,((.'0 ',( '0 0 ' ' '',(,'3 '( 0 ' (,,, ' '0' 8 '( ( (3( '' ' (,(2090 '.,,( ' ( ',',(,,,( '0$ 2' 1 ( ',(' 0 ' (,',( ' '0' ',2+(, '''$ ' 77
77 Part 2: Priorities for Improvement in 2015/16 and Board Statements of Assurance 2.1 Priorities for improvement in 2015/16 Our high level Trust objectives are to ensure that patients are safe from harm, they receive clinically effective treatment and they have a positive experience whilst in our care. This year we have chosen six priorities for improvement that fall within these three high level groups. How did we choose our priorities for 2015/16? At any NHS organisation there are a large number of quality improvement initiatives being delivered at any one time, with a range of improvements happening across corporate departments and clinical care groups. It is necessary to focus our attention on a number of priority objectives that directly reflect what our partners, patients and staff are saying to us. Last year we developed our Quality Strategy which highlights our improvement priorities over the five years to 2018/9. We are currently refreshing the second year of this strategy. The Quality Account priorities form a key element of the Quality Strategy. It is our aim to align our priorities with those of our Commissioners and our patients and staff, to ensure that we have the supporting strategies that will underpin successful delivery. As a result, we are confident that these priorities will be meaningful and relevant to our key stakeholders, whilst ensuring that we continue to give appropriate purpose and focus to other priorities over a longer period. Patient Safety Reducing avoidable harm; providing safe care; and embedding sustainable mechanisms for patient safety improvement. Our chosen priorities are to: 1. Improve the reporting of patient safety incidents and the systems for learning from them 2. Improve the safety of our Maternity Service Clinical Effectiveness Treating patients effectively to improve their health and quality of life; continually monitoring clinical outcomes against agreed measures; and comparing our performance with other similar Trusts. Our chosen priorities are to: 3. Improve availability and quality of medical records 4. Reduce waiting times to ensure treatments are received at the right time Patient Experience Understanding what matters to our patients and improving their experience of care in hospital. Our chosen priorities are to: 5. Improve safe and timely discharge of patients 6. Improve administration systems to enhance booking processes, reducing cancellations and increasing access to hospital. Our approach this year has centred on three significant exercises: 78
78 Listening to our staff: for the second year running as part of our commitment to engage with our staff and capture feedback and suggestions for improvement, we held a large series of listening events across the Trust. In addition to the findings being reviewed by the Board, Executive and Care Groups the themes have been reflected in the list of quality priorities on which stakeholders were asked to prioritise for inclusion into the 2015/16 Quality Accounts. Strategic approach: We used the ideas and challenges presented by these discussions to refresh our longer-term Quality Strategy as our core driver for improvement. This sets out the steps we will take to make real and measurable improvements to the quality of services, underpinned by a robust programme of quality impact assessments. We have appointed a new Director of Organisational Development who plans to develop our Organisation Development strategy by June Stakeholder engagement: A long-list of quality objectives was identified as part of our five year strategy and we shared these with our stakeholders in February The various parties involved included our Commissioners, Healthwatch, Health and Wellbeing Boards, Governors, patients and our staff. Their feedback was used to identify the priorities we have included in our 2015/16 Quality Account (Figure 3). Figure 3: Quality Engagement process 79
79 Priority 1: Patient safety: To improve the safety of our Maternity Service Our Maternity Service Our maternity service is a core service within the Trust providing comprehensive obstetric and midwifery care for deliveries per annum. Over 90% of women living in Reading and Wokingham and around 50% of women living in Newbury choose to deliver their baby within the Royal Berkshire Foundation Trust (RBFT) service. We provide community and hospital care through pregnancy and delivery. Our service is designed to offer as much choice to women as possible both about their care and where they receive it. Our service ensures safety and quality of care is maintained within the decision making process. We participate in national initiatives for developing maternity care. In December 2014, we celebrated achieving Baby Friendly'status part of a global accreditation programme from UNICEF and the World Health Organisation designed to support breastfeeding and to strengthen mother-baby and family relationships Why have we chosen this priority? During 2014, our maternity service found itself at a crossroads where several external pressures (reaching capacity in birth numbers, a challenging recruiting environment, and an ageing building) resulted in a decline in the quality of service it aspired to. This was reflected in the 2014 CQC inspection which reported maternity services overall to be in need of improvement. The first step was to commission an external review of the service by the Royal College of Obstetricians and Gynaecologists. As a result an improvement programme was implemented in October The purpose of the improvement programme is to enable and support significant change in the way in which the maternity service carries out its functions, by meeting both the recommendations of the external review and the compliance criteria of the CQC. Of paramount importance is the service provides woman centred care to national standards in order to enhance the experience of women. The action plan is designed to deliver change in three phases; immediate (0-6 months), medium term (0-9 months), and long term (0 12 months+). It is based around the five evaluation criteria of the CQC and managed through three workstreams; safe and effective; caring and responsive; well led. The safe and effective work focuses on delivering change required to improve the current service model and includes management structures, governance; operational staffing; and improving the real estate to create a safer environment. The caring and responsive work focuses on listening to staff and feedback from women on our performance and the culture that underpins it. Inter professional teams will work together to identify and deliver improvement activities from the feedback in order to increase engagement, morale and improve women s satisfaction. The well-led workstream focuses on leadership and strategy to enable the future development of the service to meet the requirements of women and stakeholders. 80
80 What did we do in 2014/15? Reviewed our management structures to ensure there is greater accountability for service quality. Reviewed and improved the governance processes to provide robust assurance. Increased the consultant establishment by two to support the current birth rate. Commissioned a ventilation project on delivery suite to improve air exchange and temperature control. Reviewed feedback from both staff and women surveys to identify areas for improvement. Commenced a Strategic Leadership Programme supported by Thames Valley Leadership Academy. Completed benchmarking visits to other Trusts to identify new operating models and leading edge practices. How will we improve in 2015/16 In the next year we aim to: 1. Reinvigorate our vision, strategy for future development and planning so we can confidently meet our service needs. 2. Strengthen our service culture so it is characterised by strong professional relationships and team working with the ability to continuously improve embedded into the service. 3. Undertake a number of improvement projects including the implementation of the K2 maternal and foetal monitoring system. 4. Review the Kirkup report recommendations following events at Morecambe Bay. How will we monitor progress? Progress will be monitored through our Improvement Programme Board and overseen by the Trust Improvement Steering Group and also through our Quality Schedule which is monitored with our Commissioners. The programme has a number of key performance indicators which are measured monthly and demonstrate the impact the improvement work is having on the service. The key indicators we will monitor are the percentage of unexpected admission >37 weeks to NICU (Neonatal Intensive Care Unit and the midwife to birth ratio to support safer child birth. Priority 2: Patient Safety: Improve learning from patient safety incidents and our systems for learning from them Why have we chosen this priority? We aim at all times to provide a harm free environment but occasionally, despite our best efforts, patients encounter harm, for example if they slip or fall. We know that in order to be safe, we must promote an open culture for staff to report and learn from these events. The NLRS (national learning reporting system) highlighted the Trust as an outlier when benchmarked with other Trusts in the number of incidents reported per 100 admissions. We consider it very important that we learn when things go wrong, one way of learning is through reporting and managing incidents and we take this process very seriously. In 2014/15 we reported 10,129 patient safety incidents. 81
81 Incident reporting Incident reporting gives us an opportunity to learn from past events and to ensure that steps are taken to minimise recurrences. Research has shown the more incidents that are reported the more information is available about any issues and the more action can be taken to make healthcare safer for our patients, staff and visitors. What did we do in 2014/15? We have worked hard to increase our incident reporting over the year and have made steady progress and are no longer considered to be an outlier. How will we improve in 2015/16? We intend to implement the following: In April 2015 we will be launching our Sign up to Safety campaign. The campaign will be an opportunity to raise awareness of safety issues including the importance of an incident reporting culture and the importance of learning. As part of the campaign we will intend to recruit and develop 10 volunteers to become Safety Ambassadors and 20 staff to become Safety Makers. 1. We aim to improve the reporting of incidents. 2. We aim to improve our sharing of incidents outcomes and learning to relevant parties. 3. We will continue to drive a culture which encourages asking staff to speak up and speak out and zero tolerance to never events. How will we monitor progress? We have robust processes for the management of incidents and near misses where every incident is graded and analysed, and where required undergoes a root cause analysis report. Trends and themes are identified from the incidents and these are circulated across the organisation for action by care groups, directorates and departments and monitored through the clinical governance structure. The Patient Safety Committee will oversee implementation of this priority. Priority 3: Clinical effectiveness: Improving the availability and quality of medical records What did we do in 2014/15? Actions completed to date are as follows:- Changes to the way in which records are delivered to Outpatient Clinics to improve availability. Identification of 32 Champions from various staff groups across the Trust to help communicate and support the need for improvement with their peers. Development of KPIs (key performance indicators) to enable monitoring of progress going forwards. Feasibility study completed for implementation of electronic tagging to improve storage and availability of records. We undertook two main reviews that identified the extent of the problem with regard to records management. Security of Records Audit. Quality of Content Audit. 82
82 What is a medical record? Every patient has an individual medical record (sometimes called a health record) that contains personal information, age and address, treatments planned and received, any allergic reactions, prescribed medicines, and results of investigations carried out such as blood tests and x-rays. Why have we chosen this priority? (Continues to be a priority) The medical record is vitally important in supporting the clinical pathway and in the provision of safe patient care. We are increasingly aware the quality and availability of medical records needs to improve and a more robust approach to the management of health records is required. We have completed a consultation with external and internal stake holders (including staff, patients, Commissioners, Governors, Healthwatch and this was determined to be a priority), How will we improve in 2015/16? 1. An Improvement Plan for medical records has been agreed with key performance indicators which we will monitor. 2. Work stream Leads identified and regular meetings are held with working groups. 3. Progress and concerns are discussed at the monthly Steering Group Meetings and escalated to the Trust s Improvement Programme Steering Group. 4. Increase the availability of notes to clinical staff by the time of clinic appointments from 97.8% to 99%. 5. Increase the number of inpatient cases coded from notes to 80%. 6. Improve the content of medical records through regular audit and improvement activity. How will we improve in 2015/16? Medical Records management and processing will be reviewed and enhanced to provide a standardised way of working. Actions include: Standardised / improved storage facilities for wards and clinics. Provide alternative fit for purpose accommodation for the Health Records Department Off-site premises identified to bring in-house all medical records thus enhancing availability of records. Review of tracking locations across the Trust. Implement automatic requesting of notes for all wards to support weekend admissions. Training and education programme to be developed to include: o Level 1 Basic Information Governance Awareness o Level 2 Intermediate Consultant/Clinician level (Understanding the process, Quality of Content) o Level 3 High level users (day to day records management, Electronic Patient Records [EPR]) Complete monthly audits of the quality of content and the completeness of our medical records, and KPI reporting. Review current content of patient records with a view to standardise and streamline (reduce) the volume of paper. Load letters onto our Electronic Patient Record (EPR) Discharge Summaries, Results, GP Referrals, Outpatient Letters, and Operation/Theatre Notes. One view of co-modalities / allergies. 83
83 Agree our Information Technology (IT) Strategy leading to paper light processing. Enhance patient record availability by implementing latest volume and last volume unless full set of notes required by clinician. How will we monitor and report progress? KPIs are in place and will be monitored Trust-wide, at Care Group and local Clinical Governance meetings to ensure compliance and standards are maintained. Priority 4: Reducing waiting times to ensure treatments received at the right time National Standards The Referral to Treatment (RTT) operational standards is that 90 per cent of admitted and 95 percent of non-admitted patients should start consultant-led treatment within 18 weeks of referral. In order to sustain delivery of these standards, 92 per cent of patients who have not yet started treatment should have been waiting no more than 18 weeks. Why have we chosen this priority? Cancer Targets: Despite a marked improvement in Quarter 3, performance across all 5 reported Cancer standards the Trust failed to achieve the cancer 62 day (GP referral) target but remains on an improving trajectory. The Trust delivered sustained improvement across both 2 Week wait targets achieving national standards in quarter 4. The Cancer 2 week wait (2ww) Target failed in October due to a high number of capacity related breaches, primarily in endoscopy. These improved markedly in November and December. An additional endoscopy room is underway and the gastro team are looking at the provision for 6 day working. December 2014 performance dipped largely as a result of patient choice over the Christmas period. 18 week RTT Data reporting of 18 week RTT data was suspended for six months in 2014/15 due to ongoing validation processes in relation to its recording and reporting of RTT performance. A very challenging data cleansing plan was agreed with Monitor and commenced in November All milestones within this plan have been achieved, the main impact being the reduction in the size of the Trust Patient Tracking List from >80,000 patients to 26,000. Reporting resumed in January What did we do in 2014/15? We have been working with Planned Care and Informatics specialists to develop, implement and embed processes and disciplines, providing greater assurance to our Trust Board. 84
84 Figure 4: RBFT waiting times targets/indicators 2015/16 Q4 Targets or Indicators Not Met Target 2014/15 Quarter 4 (Actual) RTT 18 weeks - Admitted 90% 70.3% RTT 18 weeks - Non-admitted 95% 94.6% RTT 18 weeks incomplete pathways 92% 90.3% A&E Wait < 4 hours 95% 92.43% Cancer 62 Day Waits for first treatment (from urgent GP referral) 85% 80.4% How will we improve in 2015/16? We will be implementing our new patient flow programme of work which has six workstreams: Ambulatory Care Medicine; Ambulatory Care - Emergency Surgery; Effective Wards; Integrated Discharge; Elective Day Care Medicine and Elective Surgical Flow, including Theatres. The focus of the Patient Flow programme will enable a review of each element of pathways, use best practice and change processes to improve patient experience. This would combine aspects of the existing emergency care, length of stay and theatre programmes. 1. We aim to make our system efficient whilst improving the quality of care provided to our patients by designing a programme of work with the aim to promote boundaryless patient flow where we think about the patient journey beyond just the 4 walls of a hospital. 2. We aim to achieve the national targets for RTT, A&E access and Cancer waiting times. How will we monitor and report progress? Progress will be reviewed by the Patient Flow Steering Group which feeds into the Trust s Improvement Programme Board. Priority 5: Patient experience: Improving safety and timely discharge of patients Patient flow Improving patient flow is one way of improving services to our patients. Evidence suggests that improving patient flow also increases patient safety and is essential to ensuring that patients receive the right care, in the right place, at the right time, all of the time. It is essential that patient flow does not come at the expense of safety or reliability. Why have we chosen this priority? Right from admission it is important we are working to smooth and shorten the patient s pathway ensuring a safe and seamless transition from the hospital. In order to be able to meet our 4 hour access target we need to ensure that there are beds available in the hospital and the beds available enable our patients to be on the right ward. Patients on the right ward often have a better experience and a shorter length of stay. It is our intention to get the right patient to the right place at the right time. The longer we keep people in hospital the more risk they have of infections and 85
85 other safety concerns, such as pressure ulcers. If appropriate we aim to discharge patients back to their own environment as quickly and safely as possible as rehabilitation in the patient s home is more meaningful. What did we do in 2014/15? We are striving to make our system efficient whilst improve the quality of care provided to our patients by designing a programme of work with the aim to promote boundary-less patient flow where we think about the patient journey beyond just the 4 walls of a hospital. We are developing a Patient Flow Steering Group with 6 workstreams: Ambulatory Care Medicine; Ambulatory Care - Emergency Surgery; Effective Wards; Integrated Discharge; Elective Day Care Medicine and Elective Surgical Flow, including Theatres. The focus of the Patient Flow programme will enable a review of each element of pathways, use best practice and change processes to improve patient experience. This would combine aspects of the existing emergency care, length of stay and theatre programmes. How will we improve in 2015/16? We will consider and address the findings of the national Inpatient Survey undertaken by Picker. We review the comments made as part of the Friends and Family survey and address themes identified. We will be implementing our Patient Flow Steering Group, programme and workstreams: Continue our work striving for 24/7 working and increasing the number of discharges at weekends. We will work to improve the timely prescribing and dispending of medication. Two workstreams of the Patient Flow work programme are key to ensuring the safety and timely discharge of patients: Effective Wards Workstream Aim: to ensure the efficient flow of patients through the wards, ensuring each ward is ready to care for the next patient, and improving the patients' experience whilst on the ward as well as decreasing length of stay. This work will: - reduce the variation in discharge across the week - increase throughput per bed on each ward - enable a higher proportion of medication (TTOs) to be available prior to the day of discharge - deliver an effective process in place to unblock key bottlenecks e.g. timely therapy input We will continue to implement Integrated Discharge Workstream Aim: to reduce unnecessary delays in the transfer of patients out of the hospital once medically fit, to promote discharge to Hospital at Home pathways/ community services once medically stable and to safely decrease length of stay. This work will: - develop and implement hospital at home pathways for example implementing virtual ward rounds and other processes to enable patients to safely receive intravenous (IV) antibiotics, IV fluid or oxygen at home. - explore how to improve connectivity and enhance electronic communication between the hospital, GPs and out of hours services; - enable patients to be discharged to assess where patients need for care packages is assessed in their own home meaning patients spend less time in hospital, care needs are more accurate and patients are getting the right care package from the start. 86
86 enhanced recovery in our elderly care wards. - further integrate our Respiratory Team and reduce respiratory admissions. - reduce internal delays to patients reaching medically fit list e.g. delays in Section 2s. A Section 2 requires an NHS body to notify social services of a patient s likely need for community care services after discharge. 1. We will aim to increase the percentage of patients being discharged before noon 2. We will aim to reduce the number of patients being discharged after 9pm 3. Reduce delayed transfers of care How we will monitor and report progress Progress will be reviewed by the Patient Flow Steering Group which feeds into the Trust s Improvement Programme Board. Priority 6: Patient experience: Improving administration systems to improve booking processes, reducing cancellations and improve access to hospital Why have we chosen this priority? Concerns about clinical treatment, communication, administration, personal care and building, environment and equipment form the top themes regarding formal complaints. While actions are taken to address informal concerns raised via Patient Advice and Liaison Service (PALS) on an individual basis, learning from both PALS and formal complaints is shared across the care groups to address overarching themes. The number of complaints raised about administration was 58 during 2014/15, with the majority of complaints relating to behaviour and attitude (75). Improving our administration processes, better use of technology and roles will improve the patient journey and patient experience. What did we do in 2014/15? We have begun to review our administration processes, technology and administration roles that support a patient journey in order to align the clinical administration support to the clinical pathway of patients and provide a single point of access for patients and GPs. We have set up a Clinical Administration Programme Board to oversee the implementation of this work programme. There are four workstreams: Human Resources, Technology, Operations and Standards Operating Procedures and Estates and Facilities. These are to address the key areas which will be impacted in the programme. How will we improve in 2015/16? We intend to reconfigure the function of the patient services team and implement a new administration structure to support clinical pathways. This will involve development of a detailed structure, job descriptions, consultation and appointment of staff as well as detailed estates planning, technology planning, improving the IT and telephone infrastructure that support the teams. Communication and engagement will be key through all stages of this work programme. 87
87 We intend to implement a single point of contact for patients and GPs to their specialist care. 1. We intend to implement a new administration structure to support clinical administration to the clinical pathways. 2. We intend to implement a single point of contact for patients and GPs. 3. Reduce our DNA rate. 4. Reduce appointment cancellations. How we will monitor and report progress It is our aim to: - reduce appointment cancellations - increase the number of calls answered and reduce abandoned calls improve clinician experience and pathway delays by improving letter turnaround times reduce the number of patient complaints relating to administration improve the efficiency and consistency of clinics through improved management of consultant annual leave and robust cross cover at team level improve data quality and utilisation of EPR by standardising to best practice all workflows and standard operating procedures improve the administration staff job satisfaction by having clear career development in place improve the overall service experienced by our patients through customer service training and standardising practice provide greater control to the clinicians for managing their business We intend to measure the following: - Did not attend (DNA) rate The number of patient complaints relating to clinical administration Progress will be monitored through the Clinical Administration Steering Group and reported through the Improvement Programme Board Monitoring will be undertaken by the Care Groups and monthly reports on progress presented to the Board. 2.2 Statements of assurance from the Board As a provider of NHS services we are required to include statements of assurance from the Board on the quality of our data and governance arrangements within our Quality Accounts Review of our services During 2014/15 the Royal Berkshire NHS Foundation Trust provided and/or subcontracted 33 relevant health services. The Royal Berkshire NHS Foundation Trust has reviewed all the data available to them on the quality of care in 33 of these relevant health services. The income generated by the relevant health services reviewed in 2014/15 represents 100% of the total income generated from the provision of relevant health services by the Royal Berkshire NHS Foundation Trust for 2014/15. 88
88 2.2.2 Participation in national clinical audits and national confidential enquiries National clinical audit provides assurance that the care being delivered by our services is of the highest quality, in terms of clinical effectiveness, patient outcomes and patient experience, compared to both national best practice standards and other service providers nation-wide. Where the care being delivered does not meet these standards, it provides a stimulus for improvement in the quality of treatment and care. National clinical audits also provide a measure for organisations to be compared with other care providers across the country. National confidential enquiries are national reviews of high risk medical or surgical conditions which produce recommendations to be implemented to improve the quality of care being delivered to patients. During 2014/15 33 national clinical audits and three national confidential enquiries covered relevant health services that Royal Berkshire NHS Foundation Trust provides. During this period Royal Berkshire NHS Foundation Trust participated in 90.9% national clinical audits and 100% national confidential enquiries of the national clinical audits and national confidential enquiries which it was eligible to participate in. The national clinical audits and national confidential enquiries that Royal Berkshire NHS Foundation Trust was eligible to participate in during 2014/15 are as follows: 89
89 Figure 5 National clinical audits and national confidential enquiries participated in by the Royal Berkshire NHS Foundation Trust 2014/15 Title Participation Rate/Comment National Clinical Audits 1. Falls and Fragility Fractures Audit Programme 100% (FFFAP), National Hip Fracture Database (NHFD) 2. National Comparative Audit of Blood 100% Transfusion Audit of Transfusion in Adults and Children with Sickle Cell Disease 3. Renal Replacement Therapy (UK Renal 100% Registry) 4. Rheumatoid and early inflammatory arthritis 10 cases submitted denominator unknown 5. Emergency Laparotomy (NELA) 98% 6. Patient Reported Outcome Measures (PROMS) * Groin Hernia 43.4% Hip Replacement 53.5% Knee Replacement 65% Varicose Vein 43.5% * Figures based on the most recent data April 2014 to February Head and Neck Cancer (DAHNO) 100% 8. Bowel Cancer National Audit (NBOCAP) 100% 9. Oesophago-Gastric Cancer Audit (NOGCA) Data collection in progress deadline for submission May Lung Cancer Audit (NLCA) Data collection ongoing data entry deadline 1 st June Prostate Cancer Data collection ongoing data on 304 patients submitted (April- February 2015) 12. National Joint Registry 100% 13. Trauma Audit and Research Network (TARN) 100% 14. Acute Coronary Syndrome (MINAP) 100% 15. Cardiac Rhythm Management 100% 16. Coronary Angioplasty 100% 17. National Heart Failure Audit 85% (estimate) 18. Fitting Child (Care in Emergency 100% Departments) (CEM) 19. Mental Health (Care in Emergency Departments) (CEM) 23 cases submitted. Denominator unknown. 20. Older People (Care in Emergency Departments) (CEM) 30 cases submitted. Denominator unknown. 21. Adult Critical Care ICNARC 100% 22. National Pregnancy in Diabetes Audit (NPID) 100% 23. Epilepsy % 24. National Neonatal Audit Programme (NNAP) 100% 25. National Paediatric Diabetes Audit Data collection in progress data entry deadline 30/06/ Adult Community Acquired Pneumonia (BTS) Data collection in progress data entry deadline 31/05/ Pleural Procedures 45% 90
90 28. National Chronic Obstructive Pulmonary 50% Disease (RCP) 29. National Cardiac Arrest Audit 100% 30. Sentinel Stroke National Audit Programme 100% (SSNAP) National Confidential Enquiries 1. NCEPOD GI Haemorrhage 100% 2. NCEPOD Sepsis Study 100% 3. Maternal, infant and perinatal mortality 100% (confidential enquiry) Figure 6: National clinical audits and national confidential enquiries not participated in by the Royal Berkshire NHS Foundation Trust 2014/15 Title Reason for Non-Participation National Clinical Audits: 1. Congenital Heart Disease (Paediatric cardiac surgery) RBH not eligible to participate 2. National Adult Cardiac Surgery Audit RBH not eligible to participate 3. National Vascular Registry RBH not eligible to participate 4. Pulmonary Hypertension Audit RBH not eligible to participate 5. Chronic Kidney Disease in Primary Care 6. Prescribing Observatory for Mental Health (POMH) RBH not eligible to participate RBH not eligible to participate 7. Paediatric intensive care (PICANet) RBH not eligible to participate 8. National Diabetes Audit Adult Most adult out-patient diabetic care is provided by the Community; the Royal Berkshire Diabetes Centre only looks after children, adolescents, pump patients and pregnant women. It was therefore felt there were too few eligible patients to make it worthwhile for the RBH to participate in the adult element of the National Diabetes Audit programme. The Paediatric, Inpatient, and Pregnancy in Diabetes Audits are fully participated in by the RBH. 9. National Audit of Intermediate Care The aim of this audit is to review intermediate care a range of integrated services to promote faster recovery from illness, prevent unnecessary acute hospital admission and premature admission to long-term residential care, support timely discharge from hospital and maximise 91
91 independent living. It therefore covers a range of service providers, with just a small part relevant to acute care. Newbury and District CCG have not signed up to participate in this audit and so it was not felt worthwhile for the Trust to participate as the whole care pathway for these patients could not be assessed. This is not an NCAPOP audit therefore participation is optional. 10. Inflammatory Bowel Disease This round of the audit was concentrated on submitting patients Biologics data to a database. For this year the department did not have the manpower to support this data collection. For the forthcoming year this issue has been resolved. National Confidential Enquiries: 1. Mental health clinical outcome review programme: National Confidential Inquiry into Suicide and Homicide for people with Mental Illness (NCISH) RBH not eligible to participate Results of national clinical audits and national confidential enquiries The reports of 18 National Clinical Audits and three National Confidential Enquiries were reviewed by the provider in 2014/15. Some of the highlights from our national clinical audit results published in 2014/15 are given below: National Audit of Seizure Management Annual report (published January 2014) 73.3% of patients were reviewed by a Senior Registrar or Consultant (in comparison to 58% nationally); and 100% of patients were reviewed within 4 hours of arrival at ED (nationally 88.8%). At the Initial ED assessment all key diagnostic tests (temp/ pulse/ blood pressure/ Oxygen Sats/ Respiratory rate / GCS) were completed for 100% of patients. BTS Paediatric Asthma Audit (published March 2014) We have improved in three areas out of 5 identified as requiring improvement on the action plan for the previous round of the audit. We now have minimal use of Chest X-ray (3%) and have dramatically reduced usage since 2011 (61%). We now have less than average use of antibiotics (19%) and have reduced prescribing since 2011 (50%). We have improved checking and recording of inhaler technique before discharge 53% this year compared with only 14% in We are efficient at treating and promptly discharging our patients. The percentage of our patients staying 0-1 day (80%) is above the national average and increased since 2011 (53%). Hip Fracture Database (published September 2014) 92
92 For most of the indicators for this audit the Trust scored above or within the National average. 100% of patients had a falls risk assessment prior to discharge as well as a Bone Health Assessment completed. Inflammatory Bowel Disease Audit Annual Report (published June 2014) The Trust has Transitional care arrangements in place for adolescents (only 53% of hospitals audited had arrangements in place). Educational events are held for patients and families but less than half the hospitals audited offered this service. The Trust has low admission rates overall and a low non-elective surgery rate. There was also above average completion of the nutritional screening tool for patients. The Trust is committed to taking action where national clinical audits and confidential enquiries demonstrate that there are areas where our services could be improved. A selection of the quality improvement work which has taken place as a result of national clinical audits and confidential enquiries in 2014/15 is outlined below: National Paediatric Diabetes Audit (published October 2014) Business case for Paediatric Diabetes Specialist Nurse. Perform podiatry assessments in clinic for those patients not attending podiatry appointments. Targeted support for patients with high average blood sugar levels in order to prevent patients developing diabetes related complications. Hip Fracture Database (published September 2014) Trust bed reconfiguration allowed the formation of a hip fracture unit into which we are able to directly admit hip fracture patients. New ways of working at the front door may have helped but would be less effective than a hip fracture unit. Re-launch of A to Z for medical management of pre-operative fragility fracture patients. When new elective orthopaedic unit opens we will have daily Neck of Femur lists in theatre which will ease capacity. Results of local clinical audits Local-level clinical audit projects tend to be more specialised and smaller in scope than the national audit projects, but have the advantage of more rapid cycles of data collection and quality improvement work; this means patients can experience the benefits of the changes implemented more quickly. The reports of 21 local clinical audits were reviewed by the provider in 2014/15. Some examples of quality improvements that have been implemented as a result of local clinical audit activity in the Trust 2014/15 are given below: Empirical Antibiotic Treatment Audit Session on how to prescribe and review empirical antibiotic treatment as part of the compulsory teaching for foundation year (FY) doctors (FY1 and FY2). Smartphone application with the Adult Medicine Antibiotic Protocol. Inpatient Hypoglycaemia at RBH: Potential Causes, January 2015 Development of Hospital Hypoglycemia guidelines (to include section to identify and manage at risk patients). Admission sheet to include section to identify patients at risk. 93
93 Use of at risk bands for patients. Trustwide Audit of Healthcare Records Establish responsibilities from Record Keeping policy and disseminated this information to staff. Documented, processed, developed and disseminated via medical records champions and to all admin staff via ward and admin managers. Record keeping in Medical / Nursing induction. Patient safety hot topic developed. Healthcare Record Keeping Policy to be updated and policy launched with article in intranet emphasising standards, reasons for them and changes to policy. Comment to be included on audit feedback for specialty clinical governance meetings. Feedback to care pathways workstream on need for space to adequately document comments. Provide staff with information on where to purchase stamps if they wish to use them Participation in clinical research There were in excess of 5428 patients receiving NHS services provided or subcontracted by the Royal Berkshire NHS Foundation Trust as of 20 April 2015 that were recruited to participate in research approved by a research ethics committee. The Trust upholds its commitment to ensuring that National Institute for Health Research (NIHR) portfolio adopted studies are accessible for patients, relatives and staff to participate. An established infrastructure whereby clinical research runs effectively alongside usual clinical services and a workforce model that supports flexible working both within and across the Care Groups and Corporate areas whilst maintaining the high quality and standards of research conduct expected within the NHS. We are involved in conducting single and multi-centre research studies across the majority of clinical specialities. On the , there are 186 currently active studies and an additional 56 studies in the participant follow up phase. 138 (74.2%) of the active studies and 51 (91%) of the studies in follow up are NIHR adopted. Thirteen of the studies have been initiated by investigators at the Royal Berkshire NHS Foundation Trust. Over time, there has been a slow increase in the number and complexity of investigator initiated studies. This year the Trust is acting as the sole Research Sponsor for its very first multicentre, NIHR adopted, investigator initiated study called the POEM study. POEM (Prescription of Analgesia in Emergency Medicine), is a retrospective multicentre observational study that aims to assess the adequacy of pain management (according to the College of Emergency Medicine - CEM) in consecutive patients with confirmed long bone fracture or dislocations isolated to a single limb, presenting to Emergency Departments (EDs). In late 2014 the first collaborative National Institute of Health Research (NIHR) study that the Trust co-sponsored together with the University of Reading was published. 94
94 The study team developed a new test that could help more babies born underweight reach full mental development. ERIC (the Early Report by Infant Caregivers) is an easy to use assessment for parents to detect delayed learning in babies born prematurely or with low birth weight. And over a three year period, 300 pre-term or underweight babies were recruited and assessed as part of the study funded by the NIHR, Research for Patient Benefit programme. ERIC proved to be as effective at identifying cognitive problems as the Bayley Scales of Infant Development, the standard assessment currently used in clinics. ERIC has potential value as a quickly administered diagnostic instrument for the absence of early cognitive delay in 10- to 24-month-old preterm infants and as a screen for cognitive delay which has potentially huge impact on clinical practice. Development and validation of a parent-report measure for detection of cognitive delay in infancy; Developmental Medicine & Child Neurology. Volume 56, Issue 12, pages , December 2014 We have embraced the challenge of the government s commitment to working with the life sciences industry to deliver first class clinical research in the NHS. We exceeded our target for increasing the number of commercially funded studies by opening 8 more of these studies during this year. We have introduced research activity into departments with little or no previous track record of trials - radiology, anaesthetics (first pain study and first drug trial in the department for 22 years) and with the appointment of a research midwife who is an integral part of the paediatric research team. We now have the capability to offer opportunities to participate in research across the whole of Women and Children s services. Our research activity and infrastructure demonstrates our commitment to transparency and desire to improve patient outcomes and experience across the NHS. A number of our studies require additional monitoring and assessments and this contributes to keeping people well and out of hospital. Clinical research highlights our commitment to improving the quality, relevance, and focus of research, whilst adding value and offering the latest medical treatments and techniques to our local patient population CQUIN payment framework A proportion of Royal Berkshire NHS Foundation Trust income in was conditional on achieving quality improvement and innovation goals agreed between the Trust and its main Commissioners, NHS England and Berkshire West Clinical Commissioning Group (acting on behalf of all commissioning bodies in Berkshire East, Oxfordshire, Buckinghamshire, Hampshire and Surrey), through a quality incentive framework known as Commissioning for Quality Improvement and Innovation (CQUIN). Further details of the agreed goals for and the following 12 month period are available electronically at The figure below shows quarterly information about our compliance with the CQUIN framework. 95
95 Figure 7: RBFT CQUIN Performance Newbury District CCG Contract and Co-signatories Split of Total CQUIN value - % FFT - Staff - Implementation 3.00% 3.00% FFT - Outpatient Services & Day Surgery - Early Implementation 3.00% 3.00% FFT- A&E & Inpatient Services - Increased or maintained Response Rate 3.00% 3.00% FFT - Inpatient services - Increased Response Rate 3.00% 3.00% Dementia - Find, Assess, Investigate & Refer 3.00% 3.00% Dementia - Clinical Leadership 2.00% 2.00% Dementia - Supporting Carers of People with Dementia 3.00% 3.00% Split of Total CQUIN value - % 7 Day Working: Assessment by a consultant within 14 hours 30.00% 22.5%* Reduction in NEL Admissions (Hospital at Home) 15.00% 15.00% Reduction in NEL Admissions (Hospital at Home) 15.00% 15.00% End of Life 10.00% 10.00% G3/G4 Pressure Ulcers 10.00% 10.00% % of total CQUIN Value % 92.5% *CQUIN is still not finalised and is subject to audit with the Commissioners to determine final outturn. The percentage disclosed is the expected outturn. Split of NHS England Specialised Commissioning Contract Total CQUIN Achievement value - % FFT - Staff - Implementation 2.86% 2.86% FFT - Outpatient Services & Day Surgery - Early Implementation 2.86% 2.86% FFT- A&E & Inpatient Services - Increased or maintained Response Rate 2.86% 2.86% FFT - Inpatient services - Increased Response Rate 2.86% 2.86% Dementia - Find, Assess, Investigate & Refer 2.86% 2.86% Dementia - Clinical Leadership 2.86% 2.86% Dementia - Supporting Carers of People with Dementia 2.86% 2.86% G3/G4 Pressure Ulcers 13.33% 13.33% Shared Haemodialysis Care 13.33% 13.33% Specialised Service Quality Dashboard 13.33% 6.67% Neonatal Intensive Care Retinopathy of Prematurity Screening 13.33% 13.33% Improved Access to Breast Milk in Preterm Infants 13.33% 0.00% IVIG 13.33% 13.33% % of total CQUIN Value % 80.01% 96
96 In 2013/14 the Trust achieved 95% of its CQUIN targets and the resultant income from this source was 6,554,000. In 2014/15 the Trust it is estimated that the Trust will achieve 91% of its CQUIN targets and the resultant income from this source is estimated to be 6,240,000. The Trust is targeting broadly the same value of CQUIN income in 2015/16. A new CQUIN framework for has been agreed with our Commissioners, some of which are nationally mandated and all of which are intended to drive improvements in patient care. All topics will be subject to incentive payments the level of which depends on the extent of achievement. Topics for include: Dementia Sepsis Acute kidney injury Improving prescribing and dispensing of medication Increased involvement of Obstetric Consultant to ensure appropriateness of all emergency caesarean sections Hydration: safe intravenous (IV) fluid prescribing CQC Registration Compliance The Royal Berkshire NHS Foundation Trust is required to register with the Care Quality Commission (CQC) and its current registration status is Registered without conditions at its five registered locations. The Care Quality Commission has not taken enforcement action against the Royal Berkshire NHS Foundation Trust during 2014/15. CQC Inspections During 2014/15 Royal Berkshire NHS Foundation Trust has been subject to the following visits by the CQC. The CQC has not undertaken any inspections in which it has been the lead regulator in at the Trust. It will receive the Inspection Report from Ofsted following a 4-week inspection of West Berkshire Local Authority children s services, beginning on 4 March 2015, in which Ofsted is the lead regulator reviewing arrangements for children in need and safeguarding provision. On June , the CQC published the Quality Report of the Trust-wide inspection it undertook between March The overall rating for the Trust was requires improvement and the following ratings were given to the core services inspected, please see figure 8 below: 97

97 Figure 8: CQC Overall Ratings for RBFT Inspection June 2014 Accident and emergency Medical care (including older people s care) Surgery Intensive/critical care Maternity and family planning Services for children and young people End of life care Outpatients With the Quality Report the Trust was issued 7 Compliance Actions (areas in which the essential standards of quality and safety were not being met) in the following regulated activities: Figure 9: RBFT CQC Compliance Actions Regulation Description of regulation Regulated activity 9 Care & welfare of people who Treatment of disease, disorder or use services injury 16 Safety, availability and suitability of equipment 17 Respecting and involving people who use services 15 Safety and suitability of premises Surgical procedures Treatment of disease, disorder or injury Diagnostic and screening procedures Treatment of disease, disorder or injury Treatment of disease, disorder or injury Maternity & midwifery services 18 Consent to care and treatment Surgical procedures Maternity & midwifery services 22 Staffing Treatment of disease, disorder or injury Surgical procedures Maternity & midwifery services 20 Records Treatment of disease, disorder or injury 98
98 CQC Special Reviews The Royal Berkshire NHS Foundation Trust has not participated in any CQC special reviews or investigations by the CQC during the reporting period. In response to the CQC Report, the Trust has developed an action plan, which addresses how we will meet the requirements of the compliance actions and other actions specified by the CQC. Progress of the actions within the plan is regularly reviewed by the Trust Quality Assurance and Learning Committee and externally by the Clinical Commissioning Group and the Care Quality Commission. A number of initiatives have been implemented to provide assurance to the Board that the actions have been delivered, one of which is the Peer Review Scheme. This involves a regular programme of ward/departmental visits to test the evidence and assess assurance that improvements have been made. CQC Outliers There were no CQC Outlier Alerts in CQC Peer Review In January 2015, the Trust started a programme of internal peer review visits, the objective of which is to provide assurance that the issues identified by the Care Quality Commission (CQC) in its March 2015 Inspection of the Trust had been resolved and to celebrate areas of good practice. A team of 22 clinical and administrative staff visit wards and outpatient areas on an unannounced basis each month and make observations and speak to staff about their knowledge of specific areas of practice. By early May 2015, 41 visits will have been made to inpatient wards and outpatient areas with the following themes being the focus of each visit: Dementia, mental capacity act and deprivation of liberty awareness and training rates The maintenance request and response process Medical and nursing staffing levels The DNACPR process Sharps practice Ward based IT provision Medical equipment provision, servicing and training Patient information and access to translation services Patient documentation in medical notes The results from each visit are fed-back to ward staff and management teams and any Trust-wide action required as a result of the visits, identified at the monthly Peer Review Steering Group chaired by Caroline Ainslie, Director of Nursing. In June 2015, a team from the Trust will be visiting the Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust (RBCH) where it will spend a day undertaking peer review visits at the Bournemouth Hospital site. Also in June a team from RBCH will visit the Royal Berkshire Hospital site to carry out peer review visits in 10 wards and departments. The aim of these visits is to give staff at both Trusts an opportunity use the peer review skills they have already developed in making an 99
99 external assessment of practice at each hospital. The days will be a chance for staff at both Trusts to develop ongoing relationships with counterparts Data Quality The Royal Berkshire NHS Foundation Trust submitted records during 2014/15 to the Secondary Uses service for inclusion in the Hospital Episode Statistics which are included in the latest published data. Royal Berkshire NHS Foundation Trust will be taking the following actions to improve data quality: We will be implementing of a new data warehouse to serve as a centralised source of Trust information. This is turn will increase visibility of Trust data as well as support timely and efficient tracking of data quality issues across multiple datasets and sources. We monitor the accuracy of data in a number of ways including the Data Quality Outliers Review group. A number of workstreams dedicated to improving data quality (granularity, timeliness, completeness, validation and audit) are being planned for 2015/16 these include: Clinical Coding Closer clinical engagement with the coding team is necessary for increasing the quality of coded information. In 2014/15 significant progress was made in specialties such as respiratory medicine where the impact of improved clinical engagement can been seen in recent internal and external audits. In 2015/16 the Coding Department would be looking to work closely with more specialties is arranging regular reviews of coded finished consultant episode (FCE). In 2015/16 the Coding Department will be working closely with the Informatics Department to track key coding quality indicators in near real time. This approach to data quality is expected to increase the efficiency of the coding audit process and will allow us to review and correct before external submissions are made. Medical Records We will continue to work towards improving the content of its medical records. The Medical Records Improvement Programme has been implemented to coordinate and drive improvements to our medical records. Ward to Board The Trust has recently completed the Ward to Board project which centered on reviewing the data collection and assurance process for reporting of Key Performance Indicators (KPIs) from Ward to Board, this project has involved the development of a quality assurance framework which includes Information Quality Assurance Records (IQARs). In 2015/16 more work is planned to further implement and embed the use of the quality assurance framework in the organisation. 100
100 Data warehouse and Business Intelligence reporting We have begun the implementation of a new data warehouse that would serve as a centralised source of Trust information; this is turn would increase visibility of our data as well as support timely and efficient tracking of data quality issues across multiple datasets and sources. The implementation of a new business intelligence solution will also enable the reporting of Trust data in near real time, it is expected that this is turn would increase visibility and access of Trust data and further support a culture of resolving data quality issues in a timely fashion and at source. Improving the quality of external data submissions We will continue to engage in a joint programme of work with our local CCG (Clinical Commissioning Group) to triangulate and improve our data quality. A new joint programme is also being designed with NHS England to begin in 2015/16. This will involve reconciling Secondary Uses Services (SUS) submissions with billing (SLAM) to identify areas of missing or conflicting data. NHS number and General Medical Practice Code Validity The Trust provides submissions to the Secondary Uses System (SUS). This is a single source of comprehensive data which enables a range of reporting and analysis in the UK and is run by the NHS Information Centre. The Trust was rated green indicating that the percentages are equal to or greater than the national rate. The percentage of records in the published data that included the patient s valid NHS number was: Rating Accident & Emergency care Admitted Patient care Outpatient care % of valid NHS Numbers received % of valid Medical Practice Codes Green (97.77%) (99.6%) (99.8%) Green (100%) (100%) (100%) The Trust's Information Governance Assessment Report The Information Governance Toolkit (IGT) provides an overall measure of the quality of data systems, standards and processes. The score a trust achieves is therefore indicative of how well they have followed guidance and good practice. The Trust Information Governance Assessment Report overall score for 2014/15 was 80% (2013/14 was 77%) and the grading was red due to one assessment area scoring 1. In 2014/ % staff received mandatory training in Information Governance: 3883 staff received training; 1492 staff did not receive training. 101
101 Payment by Results Clinical Coding Audit Clinical coding is the process by which patient diagnosis and treatment is translated into standard, recognised codes that reflect the activity that happens to patients. The accuracy of this coding is a fundamental indicator of the accuracy of patient records. Royal Berkshire NHS Foundation Trust was subject to the Payment by Results clinical coding audit during the reporting period by the Audit Commission and the error rates reported in the latest published audit for that period for diagnoses and treatment coding (clinical coding) were 10%. Spells tested % of spells changing payment Clinical Coding % spells changing HRG % clinical codes incorre ct % diagnoses incorrect Primary Secondary % procedures incorrect Primary Secondary Other data items % spells with other data items incorrect % other data items incorrect Audit undertaken in February 2015 by external company final report not published at time of publication of this report. The results should not be extrapolated further than the actual sample audited. The following services were reviewed within the sample: respiratory and upper gastroenterology surgery. 102
102 Part 3: Review of quality performance Review against 2014/15 quality priorities In Part 3 of the Quality Account we review quality improvements that we have delivered throughout 2014/15. We have included actions we need to carry forward into 2015/16 to ensure our patients continue to receive the best possible care and experience. The following topics are covered in this section: Our 6 chosen 2014/15 Quality Account priorities: Target achieved Achieved Achieved Priority 1 Patient Safety: Keep patients safe from Clostridium Difficile infections. Priority 2 Patient Safety: Improve harm free care Achieved/Improvement Priority 3 Clinical Effectiveness: Improve weekend survival rates by reducing the weekend HSMR Improvement (nearly achieved) Achieved / Improvement Improvement Priority 4 Clinical Effectiveness: Improving the availability and quality of medical records Priority 5 Patient Experience: Improving our courtesy, communications and behaviours. Priority 6 Patient Experience: Improving patient experience by reducing cancellations 1. Other improvements in 2014/15 We prioritised six initiatives for improvement; below we have summarised our performance against these indicators. Progress has been monitored by the Trust Board throughout the year and where we have identified further improvement this has been carried forward to 2015/16 as we recognise that some of our priorities will take several years to fully implement. 103

103 Priority 1: Patient Safety: Keep patients safe from Clostridium Difficile infections. What did we do? We continue to reinforce to our staff the importance of effective hand hygiene, thorough environmental cleaning and prompt isolation of patients who are suspected of having infectious diarrhoea. This year we have focused on:- The multi-professional West Berkshire health economy group reviewing all reportable cases of Clostridium Difficile infections (CDI) across acute and community providers. This ensured relevant lessons were learnt promptly and provided a basis upon which individual organisations or GP practices can target further improvement activity to increase patient safety. We hosted a Clinical Commissioning Group infection control nurse to ensure effective cross organisational working. Staff awareness of patient s previous history of CDIs to minimise the risk of CDI reoccurring from antibiotic treatment or other patients being at risk of cross contamination. Re-emphasising the importance of hand washing around the Department of Health s standards five moments of hand hygiene. Ensuring initial empiric therapy is appropriately modified in response to microbiological results. The continued education of junior doctors and new nursing staff to minimise the number of patients acquiring CDI in the future. Did we achieve our target? Clostridium Difficile We aimed to have a maximum of 30 CDI cases in 2014/15, improving on our DH threshold of 40. We achieved 29 CDI cases (end March 2015). Figure 10: RBFT Trust Acquired Clostridium Difficile
104 Priority 2: Patient Safety: Improve harm free care What did we do? Pressure Ulcers Our Pressure Ulcer Steering Group oversees the pressure ulcer prevention and management work programme, in this included: We employed a senior staff nurse to join the Tissue Viability Team. Her role is to review all patients with a Trust acquired pressure ulcer and ensure that the ward staff have commenced the patient on the pressure ulcer prevention and management care pathway. This nurse undertakes spot audits on individual wards application of the care pathway, reports these results to the ward sister and matrons. Where necessary the post holder delivers ward based training to ensure that the staff have the knowledge and skills in pressure ulcer prevention and management. We reviewed our pressure relieving mattress provision to ensure that the Trust had enough equipment. To cope with higher demand in December and January this included hiring an additional 45 pressure relieving mattresses. Falls Our Falls Steering Group oversees the falls prevention and management work programme, in this included: Implementation of a Trust-wide action plan to address themes Ward specific action plans All falls where harm is sustained were assessed whether they are avoidable or unavoidable Revised our Root Cause Analysis (RCA) tool to ensure all contributing factors appropriately identified Fall champions have been appointed and have received falls training Education and falls awareness programmes have been linked to dementia training Venous thrombo embolism (VTE) Risk assessments are undertaken for all inpatients with appropriate prophylaxis prescribed We have implemented a validation process to review patients who have been identified in the Safety Thermometer as being treated for VTE prior or post admission Urinary tract infections following urinary catheters insertion (Cat UTI) The Catheter Associated Infection Quality Improvement project group have been reviewing and making improvements in the following areas: The need for catheterisation Selecting the appropriate catheter type Catheter insertion and aseptic technique Urinary catheter management Working with Berkshire Healthcare NHS Foundation Trust Education for patients and families Appropriate equipment selection Did we achieve our target? 105
105 Harm free care Our aim was to achieve 95% harm free care (as measured by incidence of all harms) and 98.5% (as measured by the Department of Health Safety Thermometer). The patient safety thermometer captures harms which have occurred prior to admission as well as new harms which have occurred since admission The four areas of harm measured by the patient safety thermometer: Pressure ulcers identifies pressure ulcers that were present when the patient was admitted or hospital acquired Falls identifies all falls the patient has experienced within 72 hours of the survey being performed Venous thrombo-embolism (VTE) identifies patients who are being treated for a VTE (deep vein thrombosis, pulmonary embolism) Urinary tract infections following urinary catheters insertion identifies patients who have a urinary catheter in place within 72 hours of the survey taking place and any patient being treated for a urinary tract infection (UTI) While for quarter 1, 2 and 3 we have not achieved the target of 95% harm free care we were above the national average in 10 of 12 months during 2014/15 and we achieved the 95% for every month in quarter 4. We have met the target of 98.5 % in new harms for 6 months of the year. Constant vigilance is required to maintain this level of performance as the operational challenges related to capacity and staffing levels continue to escalate. Figure 11: RBFT Safety Thermometer Performance against the harm free targets (All harm free and New harm free) 106
106 The table below summarises the national percentage of harm free care from the period of April March Figure 12: RBFT Performance in Department of Health Safety Thermometer Month Apr May Jun July Aug Sep Oct Nov Dec Jan Feb Mar % new harm free National Average % new harm free RBFT All harm free% Old PU% New PU% New VTE% Catheter & new UTI All harm free care target All harm free care actual New harm free target New harm free care actual 107

107 Severe Harm Falls: The Trust has continued to demonstrate improved performance with falls prevention. There were 20 high harm falls this year compared to 28 last year. Of the 20 falls root cause analysis has determined that 9 of these were unavoidable. Learning from avoidable falls has been incorporated into the falls action plan. Pressure Ulcers: There were no grade 3 or 4 hospital acquired pressure ulcers were reported in March. There were a total of 5 pressure ulcers reported over the financial year, however 1 was downgraded. The Trust has met the quality target for this year of reporting no more than 4 (grade 3 or 4) avoidable pressure ulcers. This compares to a total of 20 for the previous financial year. Figure 13: RBFT Pressure Ulcer performance April 2013 March 2015: reported grade 3 and 4 pressure ulcers +1 2/3 * 4 " ) )" " :, 0 ; ; :( /, & ; %2 Figure 14: RBFT Pressure Ulcer performance August 2014 to March 2015: reported grade 2 pressure ulcers 108
108 Priority 3: Clinical Effectiveness: Improve weekend survival rates by reducing the weekend HSMR harm free care What is HSMR? Hospital Standardised Mortality Ratio (HSMR) compares the number of deaths at each hospital in England and is a measure of quality. A score of 100 represents an expected level of deaths, a score lower than 100 represents less than expected deaths and a score of more than 100 more than expected deaths. An independent company Dr Foster Intelligence collates and reports HSMR. What did we do? We developed and continue to embed our quality improvement programmes for pneumonia, acute kidney injury (AKI), sepsis, theatre safety and delivering seven day working. We reviewed and continue to review patient deaths on a regular basis to identify to learn from potentially avoidable deaths. We are one of the leading trusts participating in the Sign up To Safety national campaign announced in June We have developed our strategic implementation plan to launch Trust wide in April 2015 with a focus in 6 key safety areas (never events, AKI, sepsis, right information, medication safety and addressing events that lead to clinical negligence claims). Sepsis prevention and management We have developed a sepsis identification tool. This tool advises staff to assume sepsis until otherwise demonstrated. The tool prompts staff to identify sepsis by using the Systemic Inflammatory Response Syndrome (SIRS) criteria, identifying a source of infection and signs of organ dysfunction. The sepsis identification tool informs staff to start the clock and complete intra venous Antibiotics, Fluid therapy, Oxygen, blood Cultures, Urine output, Serum lactate (AFOCUS management tool) within one hour. This is also highlighted to refer to critical care and outreach teams. We have worked with medical photography and clinical skills to develop a video to educate all nursing staff how to take a venous blood gas to enable faster lactate analysis and diagnosis. From September September 2014 a Sepsis Senior Staff Nurse was employed to provide sepsis education to staff in the Trust. We have provided all wards with a Sepsis Pink Pump which is an emergency piece of equipment to be used if a patient develops sepsis. This avoids delays in waiting for porters to bring a pump to the ward therefore allowing IV Antibiotics to be giving within the hour once prescribed. We worked closely with the sepsis champions throughout the Trust to give regular updates via s and bimonthly meetings assisting them as required. The Trust has developed a Sepsis action plan to improve both sepsis antibiotic administration and sepsis screening outcomes from our current baseline to improve performance during This is also part our commitment National Sign up to Safety campaign where we seek to reduce avoidable harm by 50% by The Quality Improvement team together with the Trust Sepsis Group and other multidisciplinary groups will implement the sepsis action plan with regards to: The recognition and assessment of sepsis Ongoing educational awareness for all hospital staff to raise awareness of sepsis care, through our sepsis master class training 109
109 Implementation and monitoring of the national CQUIN recommendations for sepsis Implement best Practice Benchmark in the treatment of inpatient sepsis through Dr Foster Global Comparators Score card Did we achieve our target? Our aim was to reduce our weekend Hospital Standardised Mortality Radio (HMSR) to the national benchmark of 100 or less by March 2015 and we have achieved a sustained and stable improvement over the year. Our weekend HSMR December 2013-November 2014 (the latest benchmarked data) is 89.4 and for weekends is 93.3 thus achieving our target. At the time of writing this report data from quarter 4 is not available as reports are received 3 months in arrears; we will continue to monitor this target. This Year Mortality Indicator Apr May Jun July Aug S e p t Oct Nov D e c J a n F e b M a r Q 4 Y T D Target/ Threshold 2014/15 Target Source Outturn 2013/14 HSMR 12 months rolling weekdays National Ave HSMR 12 months rolling weekend National Ave HSMR 12 months rolling all days N / A 100 National Ave HSMR weekdays National Ave HSMR weekend National Ave HSMR all days National Ave
110 Figure 15: RBFT Hospital Standardised Mortality Ration (HSMR) January 2014 to December weekends Figure 16: RBFT Hospital Standardised Mortality Ration (HSMR) January 2014 to December
111 Sepsis We build on improvements that our Surviving Sepsis Campaign achieved in 2014/15. It was our aim that 90% of all patients admitted to the Emergency Department with a suspicion of infection would receive antibiotics within one hour. Whilst we made improvements in this area our quarter 4 achievement was 52.4% and we have work to do in order to achieve our target. This target is one that has now been set as a national CQUIN for all acute trusts by NHS England for 2015/16 and this priority will continue, progress will be overseen internally as well as by our commissioners. Priority 4: Clinical Effectiveness: Improving the availability and quality of medical records What did we do? We have: Made changes to the way in which records are delivered to Outpatient Clinics to improve availability. Identified 32 Champions from various staff groups across the Trust to help communicate and support the need for improvement with their peers. We have developed of Key Performance Indicators (KPIs) to enable monitoring of progress going forwards. Completed a feasibility study completed for implementation of electronic tagging to improve storage and availability of records. We undertook two main reviews that helped us understand the extent of the problem with regard to records management (see review of priorities for full detail). Security of Records Audit 97 areas have been audited covering inpatients, outpatient clinics and admin offices. Activities reviewed included security and access, storage, processing and practice, IT governance, tracking and information governance awareness. Initial findings indicated that the majority of areas are low to medium risk and relating to behaviours/ways of working, records management training and information governance, storage and staff. There were three high risk areas that require immediate action. Quality of Content Audit Our 2014 Quality of Content Audit highlighted that although there has been an improvement in some areas, the quality of medical records was still below the standards we require. 112
112 Figure 17: RBFT Medical Records Quality of Content Audit 2014 Quality of Content Audit Preliminary Findings No. Question 2013 / / 15 1 Is the whole healthcare record in chronological order? 45% 79% 2 Is the outer covering of the healthcare record intact? 80% 92% 3 Does each page of the notes have an addressograph (or patient name/dob/nhs no) 13% 16% 4 Does each page of the notes have the location on the page? Not asked 8% 5 Was EDL printed off and filed in the notes? 68% 90% 6 Was there evidence of the discharge planning summary being started after admission? 28% 57% Q No Question 2013 / 14 Doctors Nurses Therapists 7 Total number of entries reviewed Number of entries in blue/ black ink? 96% 100% 99% 100% 9 Number of entries with date recorded 79% 97% 88% 99% 10 Number of entries with time recorded 79% 83% 78% 86% 11 Number of legible entries 82% 97% 98% 100% 12 Number of entries with bleep recorded Not asked 72% NA? NA? 13 Number of entries with a clear signature that identifies the author 61% 56% 37% 92% No Question 2013 / / VTE Prophylaxis administered 70% 63% 18 No of entries on drug chart reviewed Drug chart includes prescriber s signature and date 99% 99% 20 Drug chart includes date when treatment is started 100% 97% 21 Drug chart cancellations should be legibly crossed off, dated and signed by doctor Data to be 67% making the change reviewed 22 Drug chart IV antibiotics MUST be reviewed every 48 hours and documented 74% Data to be reviewed 23 Drug chart times of administration recorded 74% 96% 24 Allergy status recorded 86% 65% *Green= improvement from 2013/14 Red = results are worse than previous audit An action plan is in place to address these issues during 2015/16 see review of priorities on page 136 of this report. Did we achieve our target? In 2014/15 our target was to improve availability of medical records in outpatients before time of appointments from 96% to 98% by March An audit of 80 outpatient clinics in August demonstrated that 97.8% of records were present and available at the time of the patient s appointment. The next stage is to increase the availability of records to be available in clinic by 2pm prior to the day of appointment. We achieved our aim of having a detailed improvement plan was in place by June We also had the target of a step change in performance reducing unavailable notes by 50% on 2013/14 performance. 113
113 Priority 5: Patient Experience: Improving our courtesy, communications and behaviours We are committed to listening to the views of patients and members of the public in the form of complaints, concerns, comments and compliments and using this information as a means of addressing issues and improving and developing the quality of the services we provide. The Patient Relations Team deal with issues and concerns as soon as they arise, in order to try and remedy the situation as soon as possible, where this is not possible, they take a proactive role in managing the complaints received by the Trust. What did we do? Every written complaint received which related to negative staff behaviour was reviewed in line with the process and the relevant manager was asked to investigate. A new process for dealing with complaints received relating to staff behaviour and attitude has been implemented. Patient Relations Team Complaint received relating to staff behaviour/attitude First complaint for this staff member Second complaint for this staff member within six months Third complaint for this staff member within six months Logged with PRT and investigation completed Complaint well founded? Follow process for first complaint received Follow process for first complaint received Yes No - End Staff member to be supported to seek coaching** Formal performance management to be instigated Statement from staff member must provide assurance that reflection has been undertaken and discussed with line manager If relates to medical staff copy of complaint and final response shared with Medical Director Complaints training 51 people undertook complaints training in 2014/15 The objective of the training is to provide participants with the key skills to effectively improve their handling of patient complaints. During the one day programme, delegates; Gain a better understanding of their role within the complaints process and of the benefits of complaints Recognise the qualities needed to handle patient complaints Discover how to build rapport and engage with the patient 114

114 Demonstrate empathy whilst maintaining control of the conversation Establish the patient s needs through questions and listening Defuse difficult patient emotional responses Understand the use of positive and responsive language and adopting Plain English in both written and verbal communication Apply their learning to their own complaint situation We are currently evaluating feedback from the training and review the content of training. We intend to run further sessions in 2015/2016. Hello My Name is Campaign This year we launched the #hello my name is campaign to improve the communication between patients and staff. #hello my name was established by doctor and cancer sufferer Kate Granger. Kate was surprised at the number of staff she came into contact with during her treatment who did not introduce themselves. It is a simple change that can make a huge difference to our patients experience. The launch event was attended by members of our board, doctors, nurses, physiotherapists, and admin staff. The Hello My Name is Launch Did we achieve our target? We aimed to increase from 70 to 75 the net promoter score from patients. In December 2014 all NHS Trusts moved from completing the Net Promoter Score to completing the Friends and Family test: The NHS England review of the patient FFT, published in July 2014, recommended a move away from the Net Promoter Score (NPS) and the introduction of a simpler scoring system in order to increase the 115
115 relevance of the FFT data for NHS staff, patients and members of the public. Based on the findings of the review, NHS England is now calculating and presenting the FFT results as a percentage of respondents who would/would not recommend the service to their friends and family. This change was introduced in the first publication of Staff FFT results on 25 September 2014 and across all existing patient FFT settings on 2 October We consider we achieved this target: Figure 18: RBFT Friends and Family Recommendation Ratings Question 2012/13 score (Trust internal rolling monthly survey) 2013/14 ( Trust Internal Rolling monthly survey) March 2015 (Trust Internal Rolling Survey) Patients who would recommend this hospital to family and friends Rating Care as Good, Very Good or Excellent (subset rating care as Very Good or Excellent ) 96% 97% 98% 96% 96% 98% 84% 81% 89% 116
116 Complaints While we failed to reduce the percentage of complaints relating to attitude and behavior we have made improvements to our processes for handling complaints and to our response times. Figure February 2015 RBFT Complaints about behaviour Complaints Complaints about behaviour and attitude Number of Complaints Complaints average response time Number of PALS concerns Contract Contract days Contract Local 2982 N/A Figure 20: RBFT Complaints Performance Communication complaints breakdown by sub-subject 2012/ / /15 Behaviour and attitude Inadequate information Lack of information Patient not listened to/heard Conflicting information Incorrect information Breaking bad news Breach of confidentiality Referral between directorate Total
117 Figure 21: RBFT Complaints Performance Average number of day to close per month for each Care Group We have significantly improved the timeliness and quality of our complaint responses. Trust Networked Planned Urgent Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
118 Priority 6: Patient experience: Improving administration systems to improve booking processes, reducing cancellations and improve access to hospital Cancelled operations What did we do? The Trust theatre management team has continued with the project to improve the efficiency of our operating theatres, which includes reducing the number of operations cancelled on the day of surgery for non clinical reasons. Did we achieve our target? We aimed to continue to reduce the cancellation of operations on the day for both clinical and non clinical reasons to 0.5% which is an improvement of 0.2% on 2013/14 out turn. The national target is <0.8%. This has proved extremely challenging. The year to date performance stands at 0.7% with no significant difference from last year. Figure 22: RBFT Operations Cancelled for Non Clinical Reasons Inpatients Apr May Jun July Aug Sept Oct Nov Dec Jan Operations cancelled by the hospital on the day of surgery for nonclinical reasons Cancelled operations not rescheduled % 0.00 within 28 days 0.6% 0.7% 0.4% 0.9% 0.6% 0.7% 0.3% 0.8% 1.4% 0.9% 0.5% 0.00 % 0.00 % 6.06 % % 8.70 % 0.00 % 0.00 % % 5.41 % Feb Mar Q4 YTD % 0.9 % no 10.6 data % Target/ Outturn Threshold 2014/ /14 0.8% 0.7% 0.5% 0.55% 5.2% 5.0% 4.78% A number of issues have resulted in this performance. At the beginning of the year there were issues with medical staff sickness and estates. Following resolution performance improved through Quarter 2. The initiatives in place proved successful. However from October we have been challenged with the emergency access clinical standard impacting on patients cancelled due to there being no bed available. This had a significant impact on the reversal in performance through Quarter 3 as shown below in the graph which has excluded this category. 119
119 Figure 23: RBFT Cancelled Operations, breaches and rebooked within 28 days Cancelled Ops All Elective % Last min 28 day breaches % rebooked in 28 days for PCT Rebooked in 5 days Rebooked in 5 days % Apr , %99.41% % % % May , %99.29% % % % Jun , %99.56% % % % Q , %99.42% % % % Jul , %99.10% % 93.94% % Aug , %99.40% %89.47% % Sep , %99.34% % 91.30% % Q , %99.27% % 92.00% % Oct , %99.66% % % % Nov , %99.22% % % % Dec , %98.81% %86.11% % Q , %99.27% % 93.75% % Jan , %99.06% % 94.59% % Feb , %99.54% % 94.44% % Mar , %99.23% % 91.18% % Q , %99.27% % 93.26% % YTD , %99.31% % 94.43% % We are working with an external team to improve efficiency workstreams including pre-op, consent, list organisation, enhanced recovery and a bed booking system aligned to theatre lists. This work will continue through Rescheduled Outpatient Appointments What did we do? In addition to the Quality Account target our Trust s Improvement Board set a target to reduce the number of clinic appointments that were rescheduled to <9% of all appointments. A number of actions have been undertaken in identifying the reasons why appointments are rescheduled. In May cases these cancellations are legitimate, for example, on clinical review the referral is moved to another consultant or the patient is discharged. However we recognise the largest cause of the non-legitimate cancellations is due to late notice cancellations of clinics that have already been booked. 120
120 Did we achieve our target? Analysis of performance shows that during Quarter 2 and Quarter 3 had a performance of 10%. This is a marked improvement of the previous year. The first two months of Q4 show further improvement. Figure 24: RBFT Cancelled and Scheduled Appointments Date Range Appts Made Appts cancelled & rescheduled Appointments cancelled due to Admin No. % No. % 5 July - Sept ,345 14,776 7% 6,241 3% 5 Oct - Dec ,449 13,619 7% 7,016 3% 5 Jan-15 62,327 6,568 6% 1,896 3% 65 %2 6,233 3,983 < 2,108 )< 65 We aimed to have sustained reduction in the waiting times for first outpatient appointments to less than 6 weeks for all specialties. The current waiting times are listed below. The specialties are working with the NHS Intensive Support team to implement the IST capacity and demand model (a model that helps us to understand inpatient demand, variation by service/specialty and capacity levels to deliver a service). We aimed to improve the waiting times for an outpatient appointment in ophthalmology to a maximum of 6 weeks for a first appointment which is an improvement of 4 weeks when compared to performance in 2013/14. For Ophthalmology the waiting time for first outpatient appointment is 7.33 weeks, further improvement is needed. This will provide the teams with the information to put in place the correct capacity based on demand with a target waiting time. All specialties are expected to have waiting times less than 6 weeks within ; and will remain a target for The reduced waiting times are key to reducing rescheduling. By implementing a robust process of notification of cancelling clinics at 8 weeks or longer alongside the shorter waiting times there will be fewer requirements to reschedule. 121
121 Figure 25: RBFT Average Waiting Times as March 2015 Specialty CARDIOLOGY 5.46 COMMUNITY PAEDIATRICS 6.00 GASTROENTEROLOGY 6.69 OBSTETRICS 4.13 PAEDIATRICS 7.98 RESPIRATORY MEDICINE 8.34 RESPIRATORY PHYSIOLOGY 5.35 STROKE MEDICINE BREAST SURGERY 2.90 CLINICAL ONCOLOGY 3.96 COLORECTAL SURGERY 6.28 DENTAL MEDICINE SPECIALTIES 3.50 ENT 9.04 GENERAL SURGERY 6.28 GYNAECOLOGY 5.42 MAXILLO-FACIAL SURGERY OPHTHALMOLOGY 7.33 ORAL SURGERY 7.58 ORTHODONTICS PLASTIC SURGERY 4.70 TRAUMA & ORTHOPAEDICS 4.43 UPPER G I 5.94 UROLOGY 7.09 VASCULAR SURGERY 5.93 AUDIOLOGICAL MEDICINE 2.92 CLINICAL HAEMATOLOGY 6.06 GENITOURINARY MEDICINE 8.38 GERIATRIC MEDICINE 7.63 NEPHROLOGY 7.59 NEUROLOGY 9.71 PAIN MANAGEMENT 7.78 TRUST TOTAL 7.32 Average waits (weeks) 122

122 Other achievements and improvements we made in 2014/15 We undertook a range of work during to improve our services: Trust Improvement Programme We have developed our Quality Governance Structure and have a Trust Improvement Programme Steering Group, which oversees our key improvement projects. Figure 26: Royal Berkshire NHS Foundation Improvement Programme Board structure 123

123 Quality Committee Structure Figure 27: Royal Berkshire NHS Foundation Trust Quality Committee Structure Sign up to Safety We are one of the first 12 NHS organisations that have committed to Sign Up For Safety. Sign up to Safety s 3 year objective is to reduce avoidable harm by 50% and save 6,000 lives by June Our commitment statement June 2014 The key areas that our Trust sees as a priority of patient safety improvement are never events, sepsis, medication errors, medical records, clostridium difficile, acute kidney injury and pneumonia. Sign up to Safety will help provide a focus for our priorities but is also an exciting and valuable opportunity to share best practice and learn from, and be supported by, others. We want to stretch ourselves to improve and transform, embedding a culture of patient safety and continuous improvement. It will also be an impetus to aligning the work of the Patient Safety Federation (RBFT is host organisation) and the (future) Patient Safety Collaborative. There is the potential for innovative practice but at the same time Sign Up to Safety will really enable us to build on work we are already doing with a robust plan of improvement action. What is Sign Up to Safety? Sign up to Safety is an NHS England campaign designed to help realise the ambition of making the NHS the safest healthcare system in the world by creating a system devoted to continuous learning and improvement. This ambition is bigger than any individual or organisation and achieving it requires us all to unite behind this common purpose. 124

124 Sign up to Safety aims to deliver harm free care for every patient, every time, everywhere. It champions openness and honesty and supports everyone to improve the safety of patients. Figure 28: Sign Up To Safety Campaign Pledges Organisations and individuals who sign up to the campaign commit to setting out actions they will undertake in response to the five safety pledges: 1. Put safety first. Commit to reduce avoidable harm in the NHS by half and make public the goals and plans developed locally. 2. Continually learn. Make their organisations more resilient to risks, by acting on the feedback from patients and by constantly measuring and monitoring how safe their services are. 3. Honesty. Be transparent with people about their progress to tackle patient safety issues and support staff to be candid with patients and their families if something goes wrong. 4. Collaborate. Take a leading role in supporting local collaborative learning, so that improvements are made across all of the local services that patients use. 5. Support. Help people understand why things go wrong and how to put them right. Give staff the time and support to improve and celebrate the progress. CHKS Top 40 Hospitals We were named as one of the CHKS Top 40 Hospitals of These awards recognise top performing trusts and are based on the evaluation of 22 indicators of clinical effectiveness, health outcomes, efficiency, patient experience and quality of care. 125
125 Staff engagement / Staff survey NHS Staff Survey results 2014 For the 2014 national NHS Staff Survey we received 2,032 completed surveys. This gives us a valuable insight into how staff think we perform as a place to work and receive treatment. How do we compare to other trusts? We were proud that we are in the top 20% of trusts for: Staff motivation Feeling satisfied with the quality of work and patient care you are able to deliver Agreeing that your role makes a difference to patients Feeling secure to raise concerns about unsafe clinical practice Feeling that your role makes a difference to patients Having equality and diversity training in last 12 months Agreeing feedback from patients is used to make informed decisions by your department. We also performed better than the national average in a number of other areas including: Staff engagement o Staff felt they could contribute towards improvements at work o Staff recommend us as a place to work or receive treatment o Staff are motivated at work. Job satisfaction Well-structured appraisals Feeling able to contribute towards improvements Work-related stress Support from line managers Receiving health and safety training. What we have we improved on since last year s survey? This year more of staff reported having had health and safety training, and equality and diversity training in the last 12 months. Where are we doing worse than other trusts? While we are performing well in some important areas, we recognise we need to improve on areas we perform worse than average in: Reporting errors, near misses or incidents witnessed in the last month Experiencing discrimination at work in last 12 months Believing the Trust provides equal opportunities for career progression. Where are we performing worse than last year s survey? More staff reported that they: Feel work pressure Experience harassment, bullying or abuse from other staff. 126
126 What have we done with you feedback from the last survey? Staff feedback from the last survey placed us in the best 20% of acute trusts in a number of areas including your recommendation of the Trust as a place to work or receive treatment. But there were things that we needed to improve on. Staff said that on the front line they were working harder and for longer hours. What did we do about it? Quality improvement projects to reduce inefficiencies and waste, and supporting staff to work smarter not harder Worked hard to manage challenges around capacity and we continue to have nursing recruitment drives We supported initiatives such as the Schwartz Centre Rounds - a forum for hospital staff from all disciplines to discuss difficult emotional and social issues that arise in caring for patients Introduced more staff benefits so you can access initiatives such as loans for bikes, computers, mobile phones and cars. Staff said that they had not received health and safety training. What did we do about it? We made it a priority for all staff coming into the organisation and existing staff have the appropriate training from manual handling to fire safety. Now we are performing better than most other trusts in this area. What are we doing with this year s feedback? Our Executive Director of Workforce and Organisational Development will use this year s staff survey feedback and the feedback provided in the staff listening exercises to develop an Organisational Development Strategy for the Trust. The strategy will aim to improve our culture to make the Trust an even better place to work and receive care. Nursing recruitment and skill mix The National Quality Board advocates a twice yearly review of nurse staffing levels, with public Board level discussion to ratify and agree nurse staffing levels. Ward staffing levels were reviewed in July 2014 and January 2015 using a triangulated methodology; nationally recommended Safer Nursing Care Tool, triangulated with professional judgement, benchmarking and nurse sensitive indicators. A set of core principles were established to ensure consistency across all wards included in the review. Outcomes from the review are presented and agreed at the Trust Board Resources committee. On a monthly basis the Board receives a report outlining actual staff on duty on a shift by shift basis versus establishment levels for the previous month. This data is published on the Trust website and uploaded on NHS choices webpage. HSJ Best Places to Work (Sept 2014) We were recognised as one of the best places to work by the Health Service Journal (HSJ). We employ a total workforce of 4,642 highly motivated people, three quarters 127
127 of whom would recommend our Trust as a place to work and believe they can contribute towards improvements within the organisation. We will be hoping to maintain the low stress levels and work pressure felt by staff (2.88 out of 5). Implemented the Francis Report Action Plan We took a consultative Trust-wide approach to the Francis Report recommendations. A high level Francis Steering Group lead by the Medical Director and the Executive Director of Nursing reviewed the recommendations and considered that 100 recommendations were relevant under a number of themes, below. Progress against these is set out in the following pages. Quality information reporting and escalation Board leadership Complaints Mortality: certification and inquests relating to hospital death Patient and public involvement and engagement Culture and values: openness and candour Nursing, Medical training and education Care of the elderly. Since the Francis Report the Trust has progressed a number of significant improvement work streams including the Quality and Patient Engagement Strategies; the Quality Governance Framework, Board development; Board to Ward reporting; and the nursing skill mix review. Although improvement continues in all areas, there are three themes above that we know we need to make more progress and more effort. These have and continue to form the focus of our on-going improvement work: Information/data use and sharing Culture and values Handling and addressing complaints The Francis Report action plan was implemented, with key actions having been completed; some actions were devolved for Care Groups to implement. Structured listening exercise In February 2015 structured listening exercises took place across the organisation. Individual or small group discussions around a pre-set questionnaire were held with staff. Discussions were held with samples of staff from all clinical and non clinical (corporate) areas. In addition to this there were open forum events and staff could also complete a survey online. Feedback was received from over 800 staff. Staff appreciated being listened to; and the opportunity to express their views. Staff reporting feeling happy with their immediate managers and feeling engaged within their local teams. Staff reported feeling a need to improve the level of engagement with staff above their immediate level. Some staff reported feeling concerned about staffing levels. Leadership visibility and communication from leadership was felt to have improved since last year in some areas. Staff value the CEO briefing sessions and the weekly Round-Up (electronic Trust staff newsletter). A&E Performance There has been intense pressure on many Emergency Departments (ED) across the UK this winter and we have been no exception. We have worked hard to improve 128
128 patient access. We achieved a recovery in mid-january, a decline in performance in February and minimal variance in March. Whilst the Trust has not achieved the 95% compliance we have performed favourably compared with Trusts across the country through the winter period. Figure 29: Regional Accident and Emergency Weekly Performance 4 January 2015 to 5 April 2015 We have undertaken the following actions to achieve this: Setting and delivering operational standards within the key areas; ED/ Ambulatory / GP unit / AMU/ Short Stay to ensure right patient, right place right time. The Emergency Surgical Unit has been established within Hunter ward following a successful pilot The Trust have commenced a patient flow programme; o Surgical ambulatory o Improved same day o Discharge processes Review out of hours medical cover to respond to the evening flow from GPs Work with the ambulance teams to understand and predict for ambulance arrivals to the ED so that resources can be matched The Trust expects to be compliant with this standard for Q1 2015/16. Working with patients/partners to improve patient experience How we respond to patient and public feedback on their experiences of care in hospital is critical to ensuring the public can have trust and confidence in us as well as in maintaining staff morale. We learn from a wide range of sources including complaints and concerns, patient surveys and from key groups, such as our governors, our membership and more directly via the Patient Partnership Group. 129
129 The national inpatient survey (July 2013) reported responses to 85 questions and provides us with a snapshot of how we compare to national averages. The full report was published in February 2014 and can be viewed at In addition to the national and monthly Trust-wide surveys, we support approximately 30 different specialty level patient surveys, in diverse topics such as End of Life, Children s Services and the Discharge Lounge. The Friends and Family Test, introduced nationally in 2013, provides the opportunity for feedback from patients. A single question asks the person to indicate their likelihood of recommending the hospital to friends and family in need of care. We introduced the question in a staged approach to all areas last year and for 2014/15 intend to increase the uptake of responses in each area from our year end position of 29.12% in acute inpatients, 14.91% in ED and 15.07% in Maternity. Safeguarding vulnerable people and children Safeguarding vulnerable people has been a high priority throughout 2014/15 and will continue to be at all times. Key achievements of the Trust include: A written safeguarding training strategy including safeguarding adults, mental health, safeguarding children, mental capacity act, deprivation of liberty safeguards and The Prevent Strategy (Counter Terrorism Government policy). The Trust has achieved and in some cases exceeded compliance levels for staff being trained in safeguarding adults level 1 and in safeguarding children level 1, 2 and 3. The Trust has representatives at the Local Safeguarding Children Board and subgroups, Safeguarding Adult Board and subgroups and Learning Disability Partnership Boards. The safeguarding team has documented audit programmes for the year, which are reported via the Quality Assurance and Learning Committee. A Child Sexual Exploitation (CSE) group has been formed to ensure a robust Trust response to the National papers on CSE. The Trust has representation at local operational and strategic CSE groups and involvement in the Berkshire wide workshops to evaluate and improve the effectiveness of these groups. Adult safeguarding alerts are now recorded on the Datix incident reporting system. Cross cover for the safeguarding team has been assured. Mental capacity assessment forms have been piloted and rolled out Trust wide; they will be audited in April 2015 and there has been a significant amount of mental capacity assessment and deprivation of liberty awareness training provided to frontline staff. A Lead Nurse for Transition to adult services has been established in partnership with the Thames valley Strategic Clinical Network. Transition is the process of planning, preparing and moving from children s health care to adult health. This nurse is reviewing pathways for transition at RBFT and developing a new system of Ready, Steady, Go in select specialties to ensure transition is a controlled and planned process. This work is being led by the Trust, and the lead nurse will support colleagues across the network in the same project. 130

130 A Trust wide report of self harm and suicide and action plan was produced. Ligature audits Trust wide are being competed as part of ward risk assessment process. The Berkshire Rapid Response, following unexpected child death, protocol has been updated. Working with pre-hospital partners including Westcall and SCAS we have reviewed the Paediatric sepsis pathway in Berkshire West and supported education/training for primary care. NHS Trusts in England have been asked to draw up action plans in relation to the The report of the investigation into matters relating to Savile at Leeds Teaching Hospitals NHS Trust report within the next three months setting out how they will ensure patients are protected from potential sexual predators. A task and finish group will be established in April and chaired by Tricia Pease, Director of Nursing Urgent Care, and include representation across the Trust. Dementia care and training A quarter of patients in UK hospitals have a form of dementia, and the number is growing. Dementia will affect all of us in our work or our personal lives. In February 2009, the National Dementia Strategy was launched. It set requirements to ensure that all staff working in health and social care who might care for people with dementia should have the necessary skills. We are the only Trust in the Thames Valley to have met Health Education England s target to train 75% of staff on the issues faced by patients with dementia by December ,214 staff received training, which equates to 76% of our total staff. From April we will provide additional training for staff who work frequently with patients who have dementia. This will include training in the simulation centre and e- Learning. Figure 30: Health Education Thames Valley Number of Staff Trained in Dementia
131 Ensuring patients receive adequate food and fluid Ensuring our patients are adequately nourished is a highly important part of our caring intentions. We have a Trust Nutrition Steering Group that provides expert multidisciplinary leadership and guidance to our wards and addresses all elements of nutritional support. In , on average, 90% (compared to 91% in ) of patients were screened for signs of malnutrition within 48 hours of admission, using the nationally mandated Malnutrition Universal Screening Tool (MUST). The Trust has been inspected or undertaken specific audits relating to nutrition in with the following results: Environmental Health Office (EHO) Inspection 5 Star assessed as of Very good standard PLACE (Patient-led assessments of the care environment) 82.4% (previous 6 years 92-96%) CQC Picker report in Royal Berkshire Hospital was in the top 20% in the country. We are awaiting the 2014 results. Cardiology Our Cardiology Service was once again recognised as providing the fastest lifesaving treatment for heart attack patients / blood clots in the country. For the third year running our Cardiac Unit has been named the speediest 24/7 centre anywhere in England and Wales for providing patients with primary angioplasty treatment within 120 minutes of them calling the emergency services. The 120-minute target is regarded as the most important - and most challenging - one to meet. In the latest annual statistics released by the Myocardial Ischaemia National Audit Project (MINAP), the cardiac team are shown to be even more efficient in ensuring patients are treated as speedily as possible. Nationally the figures reveal that 58.9% of heart attack patients receive their treatment within the 120 minute timeline while at the Royal Berkshire Hospital the figure is 94.2%. The next best performing unit recorded 82.4%. Pride of Reading Awards Our Cardiology team has won the Health Team/Worker of the Year in this year s Pride of Reading Awards. This year, more Trust staff have been nominated for a Pride of Reading award than ever before. Teams and individuals throughout the Trust have been nominated by patients who believe our staff deserve to be recognised for going the extra mile. Mandated performance indicators 2014/15 Amended regulations from the Department of Health require trusts to include a core set of quality indicators in 2014/15 Quality Accounts. These mandated indicators are set out below. Where available, data has been drawn from the Health and Social Care Information Centre. 132
132 Summary Hospital-level Mortality Indicator Indicator Summary of Hospital level Mortality Indicator (SHMI) value and [OD banding] (2) (2) (2) (2) 1.79 Quarter /15* 1.3 (as at Jan 15) 1.7 (as at Jan 15) 1.1 (as at Jan 15) SHMI percentage of admitted patients whose deaths were included in the SHMI and whose treatment included palliative care 23.0% 23.3% 21.2% 23.4% 37.67% Quarter /15 * 24.6 (as at Jan 15) 24.2 (as at Jan 15) 26.9(as at Jan 15) Footnote: * The value and banding of the summary hospital-level mortality indicator ( SHMI ) for the Trust for the latest reporting period covers October 2013 to September 2014, at the time of writing this report there were no further data available. The Banding is for over-dispersion (OD Banding) and the Trust rated 2 of 7, with 1 being the best and 7 being the worst banding. The Summary Hospital-level Mortality Indicator (SHMI) reports on mortality at Trust level across the NHS in England. The SHMI is the ratio between the actual number of patients who die following a treatment at the Trust and the number that would be expected to die on the basis of average England figures, given the characteristics of the patients treated there. The SHMI covers all deaths reported of patients who were admitted to non-specialist, acute NHS trusts in England and either die while in hospital or within 30 days of discharge. The SHMI values are published along with bandings indicating whether a trust s SHMI value is as expected (band 2), higher than expected (band 1) or lower than expected (band 3). All trusts are encouraged to explore and understand the activity that underlies their SHMI using their own locally held information. The SHMI requires careful interpretation and should not be taken in isolation as a headline figure of trust performance. It is best treated as a smoke alarm'which warrants a follow-up. The SHMI is an indication of whether individual trusts are conforming to the national baseline of hospital-related mortality. Our overall SHMI for the past four years in the preceding table shows us to be in line with the national average with an as expected banding. 133
133 Patient reported outcome measures (PROMS) Indicator 2009 / / / / / /15 National Average NHS Best NHS Worst Patient reported outcome measure groin surgery adjusted average health gain (April to Sept 2014) * Patient reported outcome measure varicose vein adjusted average health gain Data not yet available * Patient reported outcome measure hip replacement adjusted average health gain (April to Sept 2014)* Patient reported outcome measure knee replacement adjusted average health gain (April to Sept 2014)* *Final year data not published until after the publication of this report Royal Berkshire NHS Foundation Trust considers that this data is as described for the following reasons: the data is collected for us by a contracted external organisation then provided to the national Health and Social Care Information Centre (HSCIC) which publishes them in their Quality Accounts section and from where we pull the information. The Trust undertakes very limited numbers of varicose vein surgery and the low numbers mean that for a six month period they cannot be reported without the risk of patient identification. There is therefore no adjusted average health gain to report at this time for varicose vein surgery. Royal Berkshire NHS Foundation Trust has taken the following actions to improve its score, and so the quality of its services, by reviewing the care of individual patients as case studies at general Surgical Clinical Governance meetings for groin hernia surgery and at monitoring the hip and knee PROMS within the Orthopaedic Clinical 134
134 Governance and Orthopaedic Business meetings for hip and knee replacement surgery. Percentage of patients aged 0-15 and 16 years or over readmitted to the Trust within 28 days of being discharged Indicator 2009/ / / / / / 15 National Average NHS Best NHS Worst Emergency readmissions to hospital of patients aged 0-15 within 28 days of discharge 8.93% 9.62% 8.93% 7.9% Trust data 7.2% Trust data 5.11% Trust data Emergency readmissions to hospital of patients aged 16 or over within 28 days of discharge 9.83% 9.45% % 6.8% Trust data 6.7% Trust data 4.29% Trust data Royal Berkshire NHS Foundation Trust considers that this data is as described for the following reasons: The Trust has completed readmission activity reconciliations with both the Clinical Commissioning Group (CCG) and the national SUS Readmission data extracts and has found its data to be in line with these external readmission sources Royal Berkshire NHS Foundation Trust has taken the following actions to improve its services, and so the quality of its services, by regularly reviewing the emergency admissions that appear to be related to the previous admission and ensuring that the care and treatment for these patients is reviewed by the relevant clinical team. 135
135 The percentage of staff employed by, or under contract to, the Trust during the reporting period who would recommend the Trust as a provider of care to their families or friends Indicator The percentage of staff employed by, or under contract to, the trust during the reporting period who would recommend the trust as a provider of care for their family and friends / / / / / /15 National Average NHS Best NHS Worst 65% 69% 71% 73% 74% 72% 66% 93% 36% The percentage of patients who would recommend the Trust to their family or friends The Trust's score from a single question survey which asks patients whether they would recommend the NHS service they have received to friends and family who need similar treatment or care. It is new non-statutory indicator for providers of NHS funded acute services for inpatients and patients discharged from our Emergency Department from April Figures in the following table are the combined score for inpatients and patients receiving treatment in our Emergency Department. The Response rate in 2014/15 was 29.6% Indicator 2013/14 The percentage of Patients who would recommend the trust to their family or friends 2014/15 xx% (restate) 92.06% National Average NHS Best 90.4% - - NHS Worst The Royal Berkshire NHS Foundation Trust considers these data are as described for the following reasons: the data is collected for us by a contracted external organisation then provided to the national Health and Social Care Information Centre (HSCIC) which publishes them in their Quality Accounts section and from where we pull the information. 136
136 Patients admitted to hospital who were risk assessed for venous thromboembolism Indicator 2009 / / / /1 3 Percentage of admitted patients risk assessed for venous thromboemb olism * Data published in February / /15 National Average NHS Best NHS Worst The Royal Berkshire NHS Foundation Trust has taken the following actions to improve its percentage, and so the quality of its services, by fostering an open reporting culture, involving key clinical staff to train others in the importance of risk assessment and collecting risk assessment data electronically. Clostridium Difficile (C difficile) Indicator 2009/ / / / / / 15 National Average NHS Best NHS Worst Rate of C difficile per 100,000 bed days for specimens taken from patients aged 2 years and over (Trust apportioned cases) Trust data Data not published The Royal Berkshire NHS Foundation Trust has taken the following actions to improve its rate, and so the quality of its services, by implementing actions focused on appropriate stool sampling; improved microbial prescribing; environmental cleaning; hand hygiene; and prompt isolation of affected patients. 137
137 Patient safety incidents Indicator 2009/ / / / / / 15 Natio nal Avera ge NHS Best NHS Worst Rate of patient safety incidents reported * per 100 admissions (%) per 1000 bed days (%) * Percentage of incidents resulting in severe harm or death Number of patient safety incidents Number of incidents resulting severe harm or death 0.5% 0.8% 0.8% 0.3% 0.3% 0.15%
138 Footnote * Patient safety incident data were extracted from the Trust s internal incident management system (DATIX) sourced for the time period, not the National Reporting Learning System as the NRLS publish data in arrears and therefore is not available for the full reporting period. * In 2014/15 the National Reporting and Learning System (NRLS) changed the way of measuring the rate of patient safety incidents from per 100 admissions to per 1000 bed days. There is no national comparative patient safety incident data available from the NRLS for 2014/15. At the Royal Berkshire NHS Foundation Trust there is a positive culture for reporting incidents. Between April 2014 and March ,129 incidents were reported. 139
139 Performance against other national indicators in 2014/15 The following table shows performance against mandated quality indicators relevant to Acute Trusts in the 2014/15 NHS Operating Framework. ***Data reported are end of year data and are reported to the Trust Board (unless otherwise advised) Safety Reduce the incidence of MRSA Venous thrombosis Risk Assessment Patient Experience National Patient Survey - Overall rating Data source: National PICKER Inpatient Survey Single sex accommodation - breaches Waiting Times Benchmark 2011/ / / % 94.7% 91.3% 95.6% 2014/ % 93% -data 93% 96% 98% What this means Low number is better Higher percent age is better Higher percent age is better Low number is better Admitted in 18 weeks percentage 90% 92.31% 91.8% 93.8% 77.45% Reporting holiday July 2014 to Dec 2014 Higher percent age is better Non admitted in 18 weeks percentage 95% 99.42% 99.2% 99.9% 96.34% Reporting holiday July 2014 to Dec 2015 Higher percent age is better 18 weeks Incomplete pathways 92% 89% 93.6% 94.4% 91.56% Reporting holiday July 2014 to Dec 2015 Higher percent age is better Diagnostics in 6 weeks % 99% 99.5% 99.4% 96.1% 91.3% Higher percent age is better 2 week wait for suspected cancer 93% 94.7% 93.0% 93.6% 90.70% Higher percent age is 140
140 Benchmark 2011/ / / /15 What this means better 31 day first treatment: all cancers 96% 96.5% 97.6% 98.1% 97.2% Higher percent age is better 62 day standard: all cancers 85% 85.0% 85.3% 86.2% 86.3% Higher percent age is better A&E attendance within 4 hours Types 1 & 2 Operations cancelled on the day for non clinical reasons Cancelled operations rebooked in 28 days 95% 95.66% 95.09% 92.1% 0.8% 2.70% 0.53% 0.55% 5.0% 2.64% 7.32% 4.78% 94.44% 0.69% 5.2% Higher percent age is better Lower percent age is better Lower percent age is better 141
141 Annex 1: Statements from commissioners, local Healthwatch organisations and Overview and Scrutiny Committees Berkshire West CCG and Berkshire East CCG Joint Response Executive Summary Berkshire West Clinical Commissioning Group (CCG) Federation has reviewed the Royal Berkshire NHS Foundation Trust Quality Account and is providing a joint response on behalf of Newbury and District CCG, South Reading CCG, North and West Reading CCG, Wokingham CCG, Slough CCG, Bracknell and Ascot CCG and Windsor Ascot and Maidenhead CCG, The Quality Account 2014/15 provides information across a wide range of quality measurers and gives a comprehensive view of quality of care provided by the Trust. There is evidence that the Trust has relied on both internal and external assurance mechanisms. The CCGs are satisfied as to the accuracy of the data contained in the Account and also that the Trusts 2014/15 Quality Account Priorities are those that were set out in the Trusts Vision and Strategic Objectives and five year plan. The CCGs agree that the 6 key priorities identified by the Trust are appropriate and in line with findings and discussions we have had with them throughout the year. History The Royal Berkshire NHS Foundation Trust is one of the largest general Hospital Foundation Trusts in the country. They provide acute medical and surgical services to Reading, Wokingham and West Berkshire and specialist services to a wider population across Berkshire and its borders. Underneath their Vision sits their strategic objectives and their five year plan which details how they aim to achieve their objectives. The Trust very much values the partnership working across the local health economy, and with their patients and the public. Berkshire West CCGs are pleased to continue working in partnership with them. Quality Account 2014/15 Their Quality Account for 2014/15 clearly identified their successes to date and also areas for further improvement. The CCG s support the Trust s openness and transparency and is committed to working with the Trust to achieve further improvements and successes in the areas identified within the Quality Account. This will be carried out through a number of both proactive and reactive mechanisms and collaborative and integral working. Priority 1: Patient safety: To improve the safety of our Maternity Service We are pleased that the Trust has reviewed and improved both its management structures, consultant establishment and governance processes ensuring greater accountability for service quality and robust assurance during 2014/15. We also welcome the Trust gathering and reviewing feedback from both the staff and women surveys to identify areas for improvement, which have assisted in the development of the Trusts maternity improvement plan going forwards. We are pleased that the Trust has chosen this as a priority area for 2015/16 and are encouraged by the Trusts plans to further improve the safety of their maternity service. Priority 2: Patient Safety: Improve learning from patient safety incidents and our systems for learning from them The Trust has worked hard in 2014/15 to increase their incident reporting and have made steady progress, which has resulted in the Trust no longer considered to be an outlier. Incident reporting is essential in providing an opportunity to learn from past events and to ensure that steps are taken to minimise recurrences. We welcome the Trust continuing to prioritise further improvement in this area, particularly their plan to 142
142 improve sharing of learning to relevant parties and their aim to drive a culture which encourages asking staff to speak up and speak out and zero tolerance of never events. Priority 3: Clinical effectiveness: Improving the availability and quality of medical records We welcome the extensive work that was undertaken in 2014/15 to improve the availability and quality of medical records. This included identifying champions from various staff groups to drive improvement, changes to the way in which records are delivered to outpatient clinics and the development of Key Performance Indicators (KPIs) to enable more robust monitoring of progress being made in this key area. We welcomed the Trust undertaking a security of records audit and quality of content audit to further inform required improvements going forward. We are again pleased that the Trust has chosen this as a quality priority for 2015/16. Good quality medical records are essential in supporting safe patient care and although a lot of progress has been made; there is still work to be done in this key area. Priority 4: Reducing waiting times to ensure treatments received at the right time During 2014/15 the Trust has worked extremely hard to improve waiting times. This has included working with Planned Care and Informatics specialists to develop, implement and embed processes and disciplines, providing greater assurance to the Trust Board and us as commissioners. Although there has been a significant improvement, the Trust has still failed to achieve the 62 day cancer target (GP referrals) and the 18 week referral to treatment target. We therefore welcome the Trust identifying reducing waiting times to ensure treatments received at the right time as a priority area to build on the work already undertaken this year. We support the plans outlined to make the Trusts system efficient whilst improving the quality of care provided to patients and the aim to achieve the national targets for RTT, A&E access and Cancer waiting times in 2015/16. Priority 5: Patient experience: Improving safety and timely discharge of patients We recognise the value of improving patient flow which can increase patient safety by ensuring they receive the right care, at the right time, all of the time. The Trust has worked hard on this area over 2014/15 and we welcome their plans to further develop this as a priority for 2015/16. We are encouraged by the Trust s vision to promote boundary-less patient flow where the patient s journey is thought about beyond just the 4 walls of the hospital. We fully support the Trusts plans and look forward to seeing the impact across 2015/16. Priority 6: Patient experience: Improving administration systems to improve booking processes, reducing cancellations and access to hospital We are aware that concerns about clinical treatment, communication, administration, personal care and building, environment and equipment form the top themes regarding formal complaints for the Trust and that the Trust has good systems and processes for sharing the learning across the organisation. We support that a focus on improving administration processes and better use of technology and roles will improve the patient journey and patient experience, so welcome this priority. We are particular pleased with the plan to provide a single point of access for patients and GPs, which we feel will greatly improve patient care and experience. Overall Following the publication of the Trust s CQC inspection on 24 th June 2014, where the Trust received an overall rating of requires improvement; we have seen the Trust 143
143 make significant progress in addressing the key areas of concern outlined in this report. We are pleased that the Trust has chosen to focus priorities on improving the safety of maternity services and improving the availability and quality of medical records, because these were key findings in the CQC report and although a vast amount of work has been undertaken over the past year, there is still work to be done. We acknowledge the work undertaken by the Trust to reduce the number of operations cancelled on the day of surgery for non-clinical reasons and share the Trusts disappointment at not achieving the improvement set out in last year s quality account, but accept that this was an ambitious target. We welcome the Trust continuing with the work they have started in this area to further improve. From the 2014/15 priorities patient safety: improve harm free care the Trust had a number of areas for improvement. One key area was falls and the Falls Steering Group has been overseeing the falls prevention and management work programme. Though falls are not identified as a 2015/16 priority the improvement momentum must be maintained so that progress can continue on a downward trajectory. This is because falls with harm as identified as a serious incident are still being reported by the Trust. The Trust has had a number of Never Events during 2014/15 which have resulted in learning for the Trust. The data for the Hospital Standardised Mortality Ratio (HMSR) was not available at the time of writing but from the available information deaths at weekends are still higher than during the week the CCG s will continue to review the data to ensure further improvement. We also acknowledge the hard work undertaken to improve performance in staff compliance with safeguarding children and adult training and are really pleased that the Trust has achieved full compliance with safeguarding children training levels 1, 2 and 3 and safeguarding adult training level 1 on 31 st March 2015, meeting national requirements. We support the Trust in its continuing focus on the positive results from 2014/15 priorities and their continuing work to further those improvement and strengthen priorities next year. Overall there have been many positive highlights for the Trust and assurance that they continue to offer high quality and safe care to our patients. The information in this Quality Account is provided from the Trust s data management systems and their quality improvement systems and to the best of our knowledge is accurate, and provides a true reflection of the organisation. Healthwatch West Berkshire Response Thank you for the opportunity to comment on this year s Quality Account. We have some general comments then a few specific ones related to particular sections. We are pleased to see improvements in a number of areas and achievements such as the positive staff survey, the Trust being rated by the Health Service Journal as one of the best places to work, and continued top performance for speedy cardiac treatment. Inevitably because of timescales, comments have to be on non-final drafts and we appreciate that there may be changes in the final version. Quality Accounts are an important way in which Trusts can formally report to local communities about quality and improvement. While we welcome the inclusion of a 144
144 glossary, we think more could be done in future, such as more consistent use of plain English, to make the report more accessible. Turning to the priorities for the coming year, we welcome these as areas requiring improvement (and are glad that Maternity Services are included, as we suggested last year). We were pleased to see the continued intention to take action on medical records, as this appears to be something which could have a wide-ranging impact on efficiency and effectiveness. However it is hard, from the information presented, to get a clear sense of a strategic way forward and particularly, as we mentioned last year, on how or when the move to electronic records will be achieved. In reviewing performance against last year s aims it would be helpful if there could be consistent reporting against all the aims set last year, which is not always the case (e.g., on weekend survival rates, there is no mention on success against the aim that 90% of patients admitted to ED with suspicion of infection receive antibiotics within one hour). In some cases there is no specific information on the targets. In others, information is presented but the narrative does not indicate whether the target has been achieved (e.g. there was a target last year under Priority 6, for ophthalmology waiting times and while the outturn figures are given, (in Fig 24, p.121 of the draft), whether the target was met is not specifically mentioned). Also it would be helpful to have some commentary on why targets have not been achieved (it may be for very good reasons) and what action is to be taken in future. On the Friends and Families test (FFT) (under Courtesy, Communications and Behaviours) the target was in terms of the net promoter score, which the text says was met, but the figure given (98%) is calculated on a different basis and this is not explained. It is not explained that the way the FFT is presented has been changed nationally, or to show calculations under the old and new methodology (although based on the figures given we calculate that the net promoter score for February 2015 would have been 78, which did meet the target). It is not clear why figures for complaints were only available for the first two quarters, up to the end of September rather than at least December (p.117 of the draft). Hopefully for the final version there will be figures for the whole year together with some commentary on whether the targets were met, if not why not and what remedial action is necessary. We were pleased to see that the staff survey has a number of responses in the top 20% of trusts and others that are better than average and that the Trust is rated as one of the best places to work by the HSJ. It is good to hear that the Francis Report action plan has been implemented, and the range of issues being addressed and recognition of continuing underlying issues where more progress is needed provides confidence in the seriousness with which this is being taken. The Trust is also to be to be congratulated on the Cardiac centre continuing to be the speediest in England and Wales for primary angioplasty treatment within 120 minutes. Healthwatch Reading Response Thank you for the opportunity to comment on your Quality Accounts. We welcome the priorities that have been set for this coming year, especially around patient safety 145
145 and patient experience: improving safety and timely discharge, which we have found to be a particular concern for patients and their families, as was demonstrated in the piece of work carried out by Healthwatch Reading last year supported by RBFT. It is a little disappointing that there is no reference to the Healthwatch report and how you have acted or committed to act on this to improve patient experience. There were key recommendations within the report around improving the way RBFT staff should improve the way they communicate discharge dates and times to people, as well as just getting people out quicker. We would look to see these are met, as they would improve the patient journey and experience. There is also little reference to integrated working and how you are working with others to improve this pathway. We welcome the complaints training that you have introduced for staff. In our advocacy role we have learnt how important showing genuine sympathy and talking to the patient openly as an equal is in the complaints process. Therefore even though we welcome the training element that includes 'demonstrating sympathy while maintaining control of the conversation'- we hope this would demonstrate equality in the conversation and not what sounds like talking 'to'the patient, rather than staff talking to patients as equals. We are keen to see that RBFT continues to meet its priority on improving communication by 'improving the quality of the response'to patient complaints. However we would be keen to see the evidence behind this, as we know that many clients we have dealt with have not been wholly satisfied with the response they have received. Therefore we feel that communication should remain a key priority for RBFT as this continues to be at the heart of most patient complaints. We welcome your pledge to the 'Sign up to Safety'campaign. However we would be keen to know how RBFT will go about changing staff attitudes and behaviours. What measures will you put in place? How will these be reported? In order to show that staff and concerned members of the public feel they can report openly. We also welcome the priority on Medical notes. In our recent Enter and View Visit to Ophthalmology at RBFT, we heard from a number of patients who were being delayed due to the unavailability of medical notes and would look to see improvements in this area. Finally we note that there is some final data missing within the report, which means we cannot provide complete comment over all the information. Thank you once again for the opportunity to comment and we hope to continue to work with RBFT to ensure that patient feedback and experience of services are best meeting local people's needs. Healthwatch Bracknell Forest Response Thank you for the opportunity to comment on your 2015 Quality Account. We note that there is an increasing focus on patient safety including reviewing serious incidents and learning from them to making maternity services safer. Healthwatch Bracknell Forest whist not having any specific evidence from the public in the previous year welcomes these priorities for 2015/16. We have received positive feedback about the services now offered from Brants Bridge within Bracknell however we have highlighted the need for Macmillan 146
146 volunteers to be stationed there as patients have expressed that service as invaluable. We note that you are making effective discharge a priority and we have received some feedback throughout the year from patients stating: discharge was at an inappropriate time (10PM) with no regard for transport and discharge paperwork bore no resemblance to my stay. The priority to make records better and enhance the discharge experience is very much welcomed. Other feedback throughout the year was on the quality of food that was described in several accounts as appalling and needing improvement. The cost to patients to watch TV and have some communication was highlighted as being expensive and patients have also stated they would like Wi-Fi throughout their stay to be free and available to all. Staff attitude in some areas has been criticised and we welcome the new initiatives to address poor staffing standards. Positive feedback was received on cancer and renal services at the main location as well as at Brants Bridge. We look forward to continuing to work with Royal Berkshire NHS Foundation Trust with the aim to improve patient engagement and experience. Wokingham Borough Council Health Overview and Scrutiny Committee response 'Members of the Wokingham Health Overview and Scrutiny Committee have reviewed the Trust's Draft Quality Account Report and have noted the priorities for 2015/16. The inclusion of 'Improving the safety of our maternity services'as a priority for next year is welcomed. Members were also pleased to note the success of the Cardiology Team, the level of staff who would recommend the Trust to Friends and Family and the number of readmissions within 28 days of discharge. Whilst it is disappointing that the Trust is likely to fail to achieve the Cancer 62 day target (GP referrals) and the Cancer two week wait targets (all cancers) it is encouraging to see that reducing waiting times to ensure treatments received at the right time is a priority for 2015/
147 Annex 2: Limited assurance by external auditors INDEPENDENT AUDITOR S REPORT TO THE COUNCIL OF GOVERNORS OF ROYAL BERKSHIRE NHS FOUNDATION TRUST ON THE QUALITY REPORT We have been engaged by the Council of Governors of Royal Berkshire NHS Foundation Trust to perform an independent assurance engagement in respect of Royal Berkshire NHS Foundation Trust s Quality Report for the year ended 31 March 2015 (the Quality Report ) and certain performance indicators contained therein. Scope and subject matter The indicators for the year ended 31 March 2015 subject to limited assurance consist of the following two national priority indicators: Percentage of incomplete pathways within 18 weeks for patients on incomplete pathways (Referral to Treatment incomplete pathways) Maximum waiting time of 62 days from urgent GP referral to first treatment for all cancers During 2014/15 the Trust agreed a reporting holiday in relation to its Referral to Treatment performance. As such management do not have reliable data to use in order to calculate the Trust s performance for this indicator for the 2014/15 period. We have been unable to perform testing in relation to this indicator and have excluded the provision of assurance in relation to the percentage of incomplete pathways within 18 weeks for patients on incomplete pathways from the scope of our work. In this opinion all references to the indicator refer to the national priority indicator: Maximum waiting time of 62 days from urgent GP referral to first treatment for all cancers. Respective responsibilities of the directors and auditors The directors are responsible for the content and the preparation of the Quality Report in accordance with the criteria set out in the NHS Foundation Trust Annual Reporting Manual issued by Monitor. Our responsibility is to form a conclusion, based on limited assurance procedures, on whether anything has come to our attention that causes us to believe that: the Quality Report is not prepared in all material respects in line with the criteria set out in the NHS Foundation Trust Annual Reporting Manual; the Quality Report is not consistent in all material respects with the sources specified in the Detailed Guidance for External Assurance on Quality Reports 2014/15 ( the Guidance ); and the indicator in the Quality Report identified as having been the subject of limited assurance in the Quality Report are not reasonably stated in all material respects in accordance with the NHS Foundation Trust Annual Reporting Manual and the six dimensions of data quality set out in the Guidance. We read the Quality Report and consider whether it addresses the content requirements of the NHS Foundation Trust Annual Reporting Manual and consider the implications for our report if we become aware of any material omissions. 148
148 We read the other information contained in the Quality Report and consider whether it is materially inconsistent with: board minutes for the period April 2014 to May 2015; papers relating to quality reported to the board over the period April 2014 to April 2015; feedback from Commissioners, dated 07/05/2015; feedback from governors, dated 05/05/2015; feedback from Healthwatch Bracknell Forest, dated 26/04/2015; feedback from Healthwatch West Berkshire, dated 05/05/2015; feedback from Healthwatch Reading, dated 25/04/2015; feedback from Wokingham Borough Council Health Overview and Scrutiny Committee, dated 24/04/2015; the trust s complaints report published under regulation 18 of the Local Authority Social Services and NHS Complaints Regulations 2009, dated 13/05/2014; the latest national patient survey, dated February 2015; the latest national staff survey, dated February 2015; Care Quality Commission Intelligent Monitoring Reports, dated July 2014 and December 2014; and the Head of Internal Audit s annual opinion over the trust s control environment, dated 18/05/2015. We consider the implications for our report if we become aware of any apparent misstatements or material inconsistencies with those documents (collectively, the documents ). Our responsibilities do not extend to any other information. We are in compliance with the applicable independence and competency requirements of the Institute of Chartered Accountants in England and Wales (ICAEW) Code of Ethics. Our team comprised assurance practitioners and relevant subject matter experts. This report, including the conclusion, has been prepared solely for the Council of Governors of Royal Berkshire NHS Foundation Trust as a body, to assist the Council of Governors in reporting the NHS Foundation Trust s quality agenda, performance and activities. We permit the disclosure of this report within the Annual Report for the year ended 31 March 2015, to enable the Council of Governors to demonstrate they have discharged their governance responsibilities by commissioning an independent assurance report in connection with the indicator. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Council of Governors as a body and Royal Berkshire NHS Foundation Trust for our work or this report, except where terms are expressly agreed and with our prior consent in writing. Assurance work performed We conducted this limited assurance engagement in accordance with International Standard on Assurance Engagements 3000 (Revised) Assurance Engagements other than Audits or Reviews of Historical Financial Information, issued by the International Auditing and Assurance Standards Board ( ISAE 3000 ). Our limited assurance procedures included: evaluating the design and implementation of the key processes and controls for managing and reporting the indicator making enquiries of management 149
149 testing key management controls limited testing, on a selective basis, of the data used to calculate the indicator back to supporting documentation comparing the content requirements of the NHS Foundation Trust Annual Reporting Manual to the categories reported in the Quality Report. reading the documents. A limited assurance engagement is smaller in scope than a reasonable assurance engagement. The nature, timing and extent of procedures for gathering sufficient appropriate evidence are deliberately limited relative to a reasonable assurance engagement Non-financial performance information is subject to more inherent limitations than financial information, given the characteristics of the subject matter and the methods used for determining such information. The absence of a significant body of established practice on which to draw allows for the selection of different, but acceptable measurement techniques which can result in materially different measurements and can affect comparability. The precision of different measurement techniques may also vary. Furthermore, the nature and methods used to determine such information, as well as the measurement criteria and the precision of these criteria, may change over time. It is important to read the quality report in the context of the criteria set out in the NHS Foundation Trust Annual Reporting Manual. The scope of our assurance work has not included governance over quality or the non-mandated indicator, which was determined locally by Royal Berkshire NHS Foundation Trust. Conclusion Based on the results of our procedures, nothing has come to our attention that causes us to believe that, for the year ended 31 March 2015: the Quality Report is not prepared in all material respects in line with the criteria set out in the NHS Foundation Trust Annual Reporting Manual; the Quality Report is not consistent in all material respects with the sources specified in the Guidance; and the indicator in the Quality Report subject to limited assurance has not been reasonably stated in all material respects in accordance with the NHS Foundation Trust Annual Reporting Manual and the six dimensions of data quality set out in the Guidance. KPMG LLP Chartered Accountants 15 Canada Square London E14 5GL 27 May
150 Annex 3: Statement of directors responsibilities for the quality report The directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each financial year. Monitor has issued guidance to NHS foundation trust boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that NHS foundation trust boards should put in place to support the data quality for the preparation of the quality report. In preparing the Quality Report, directors are required to take steps to satisfy themselves that: the content of the Quality Report meets the requirements set out in the NHS Foundation Trust Annual Reporting Manual 2014/15; the content of the Quality Report is not inconsistent with internal and external sources of information including: - Board minutes and papers for the period April 2014 to May Papers relating to Quality reported to the board over the period April 2014 to May Feedback from the commissioners dated 7 May Feedback from governors dated 5 May Feedback from Healthwatch Bracknell Forest dated 26 April Feedback from Healthwatch West Berkshire dated 05 May Feedback from Healthwatch Reading dated 25 April Feedback from Wokingham Borough Council Health Overview and Scrutiny Committee dated 24 April The Trust s complaints report published under regulation 18 of the Local Authority Social Services and NHS Complaints Regulations 2009, dated 13/05/2014; - The latest national patient survey February The latest national staff survey February The Head of Internal Audit s annual opinion over the trust s control environment dated 20 May CQC intelligent monitoring reports dates July 2014 and December The Quality Report presents a balanced picture of the NHS foundation trust s performance over the period covered; the performance information reported in the Quality Report is reliable and accurate; there are proper internal controls over the collection and reporting of the measures of performance included in the Quality Report, and these controls are subject to review to confirm that they are working effectively in practice; the data underpinning the measures of performance reported in the Quality Report is robust and reliable, conforms to specified data quality standards and prescribed definitions, is subject to appropriate scrutiny and review; and the Quality Report has been prepared in accordance with Monitor s annual reporting guidance (which incorporates the Quality Accounts regulations) (published at as well as the standards to support data quality for the preparation of the Quality Report (available at 151
151 The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the Quality Report. By order of the board Chairman Date : 27 May 2015 Chief Executive Officer Date : 27 May
152 7. Annual Accounts Index 153
153
154
155
156
157
158
159
160

161
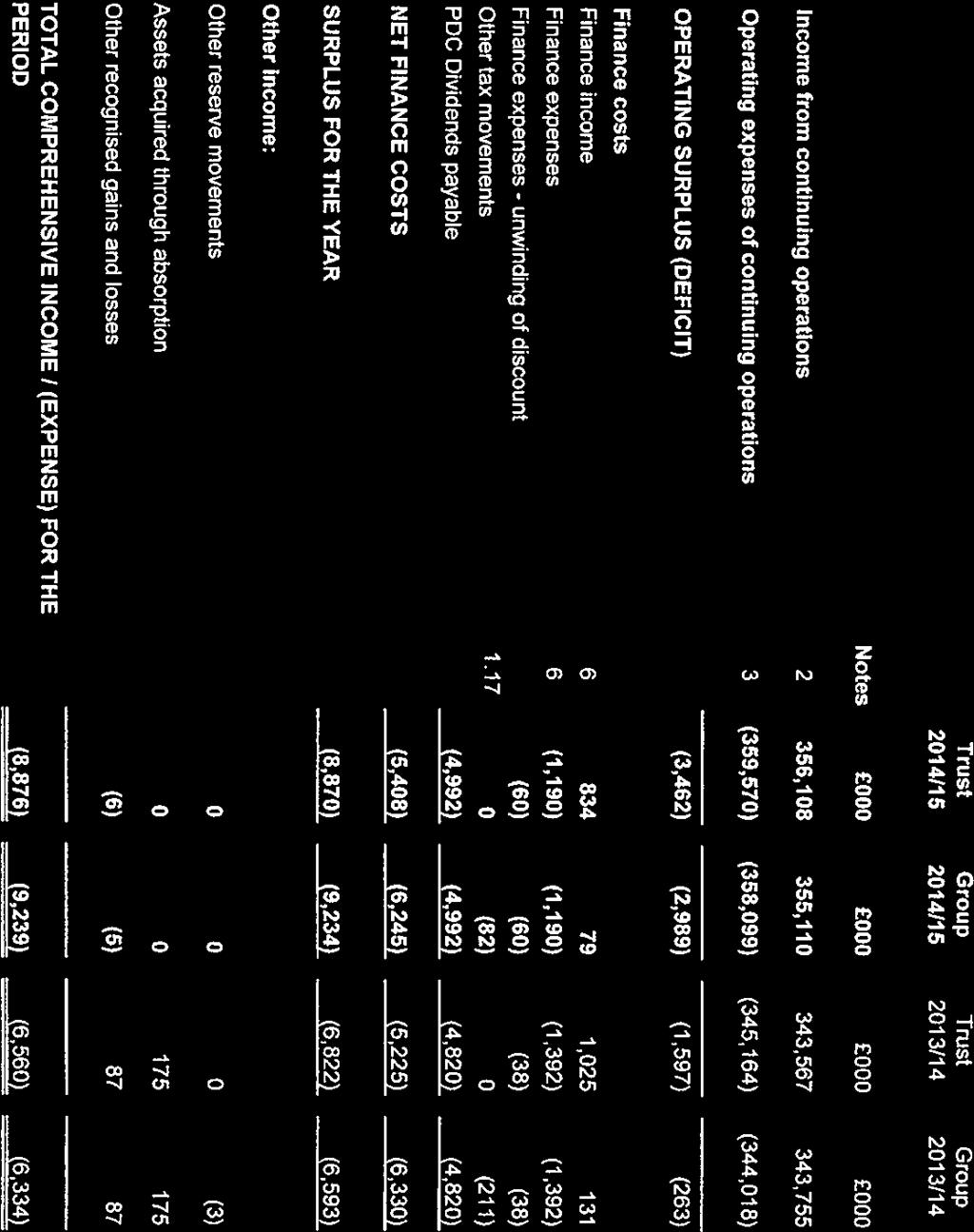
162
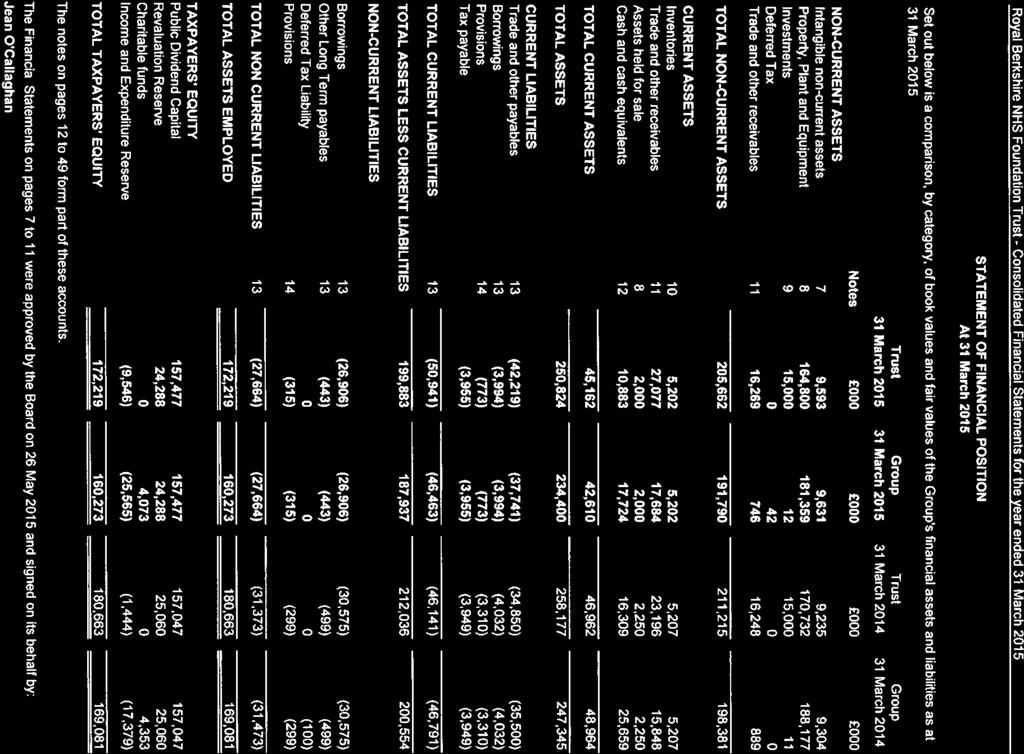
163
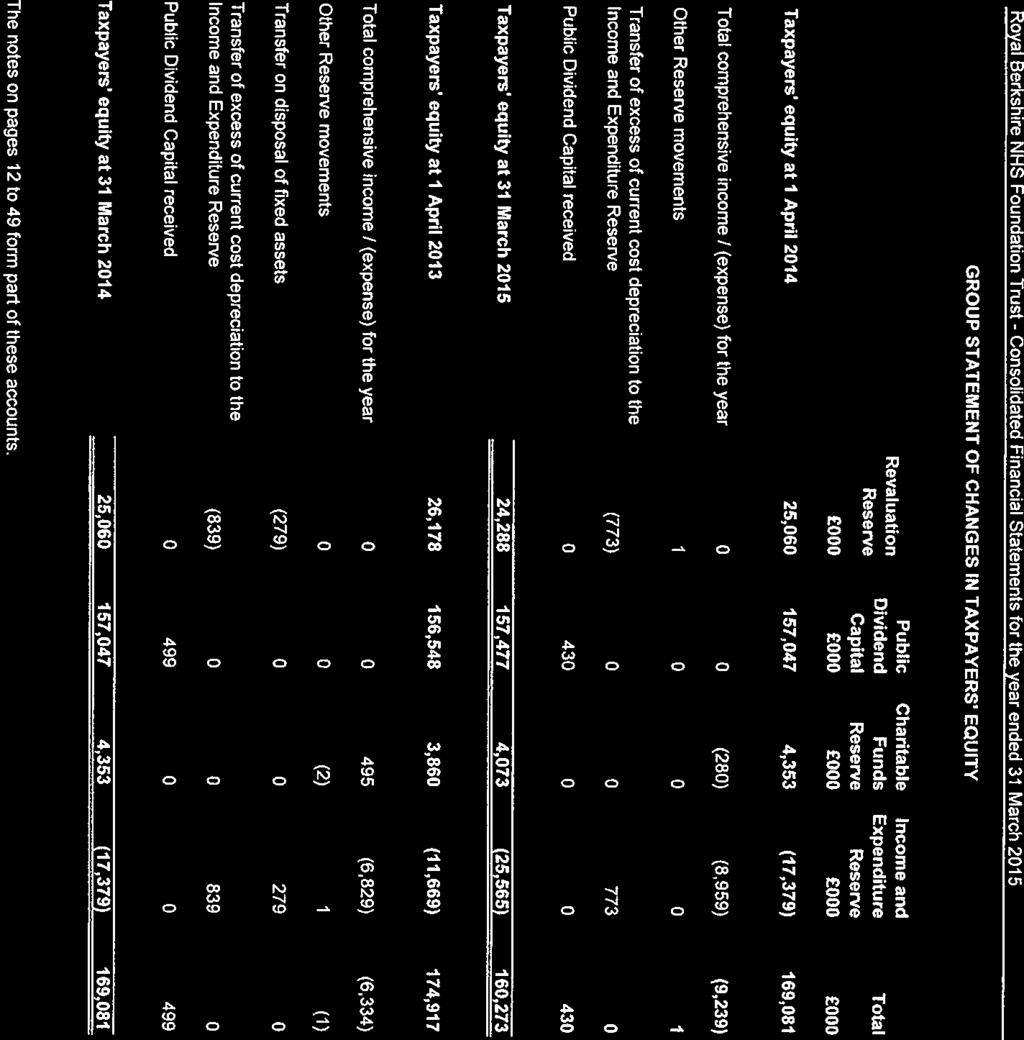
164
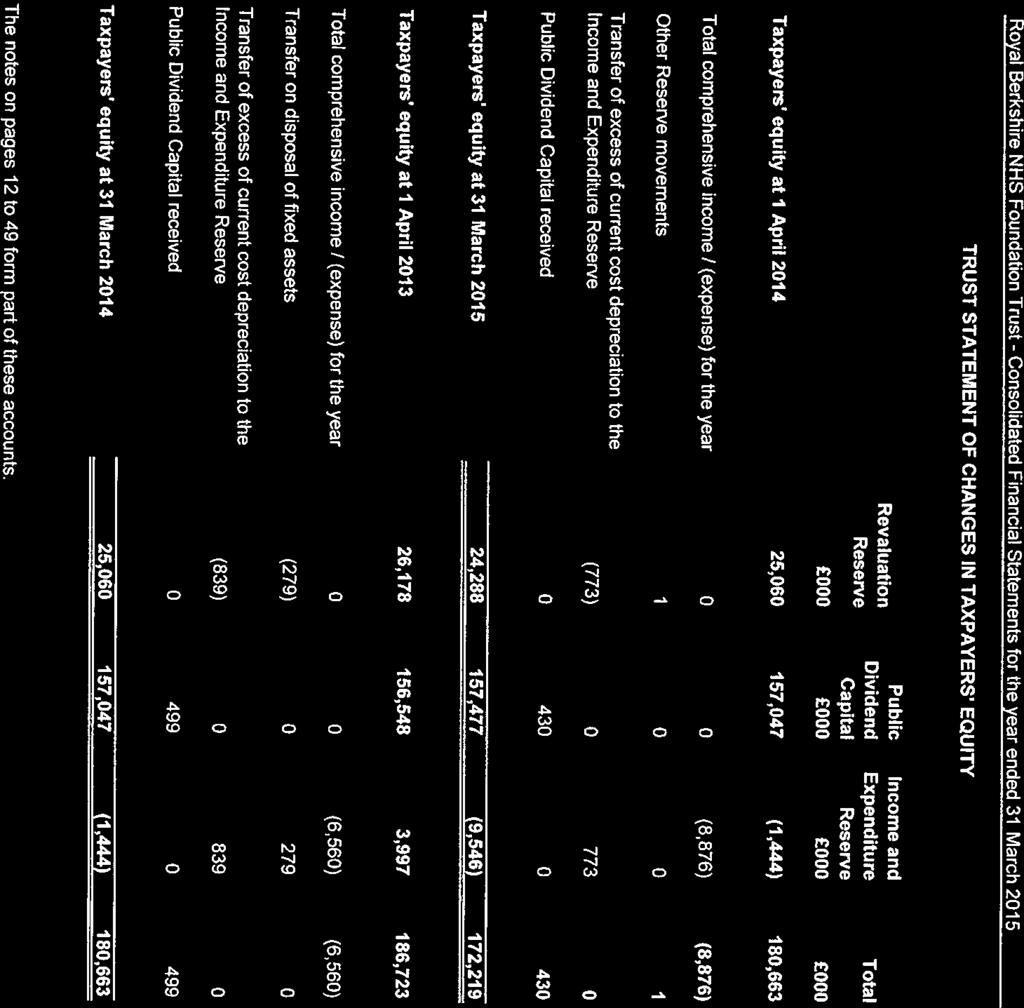
165
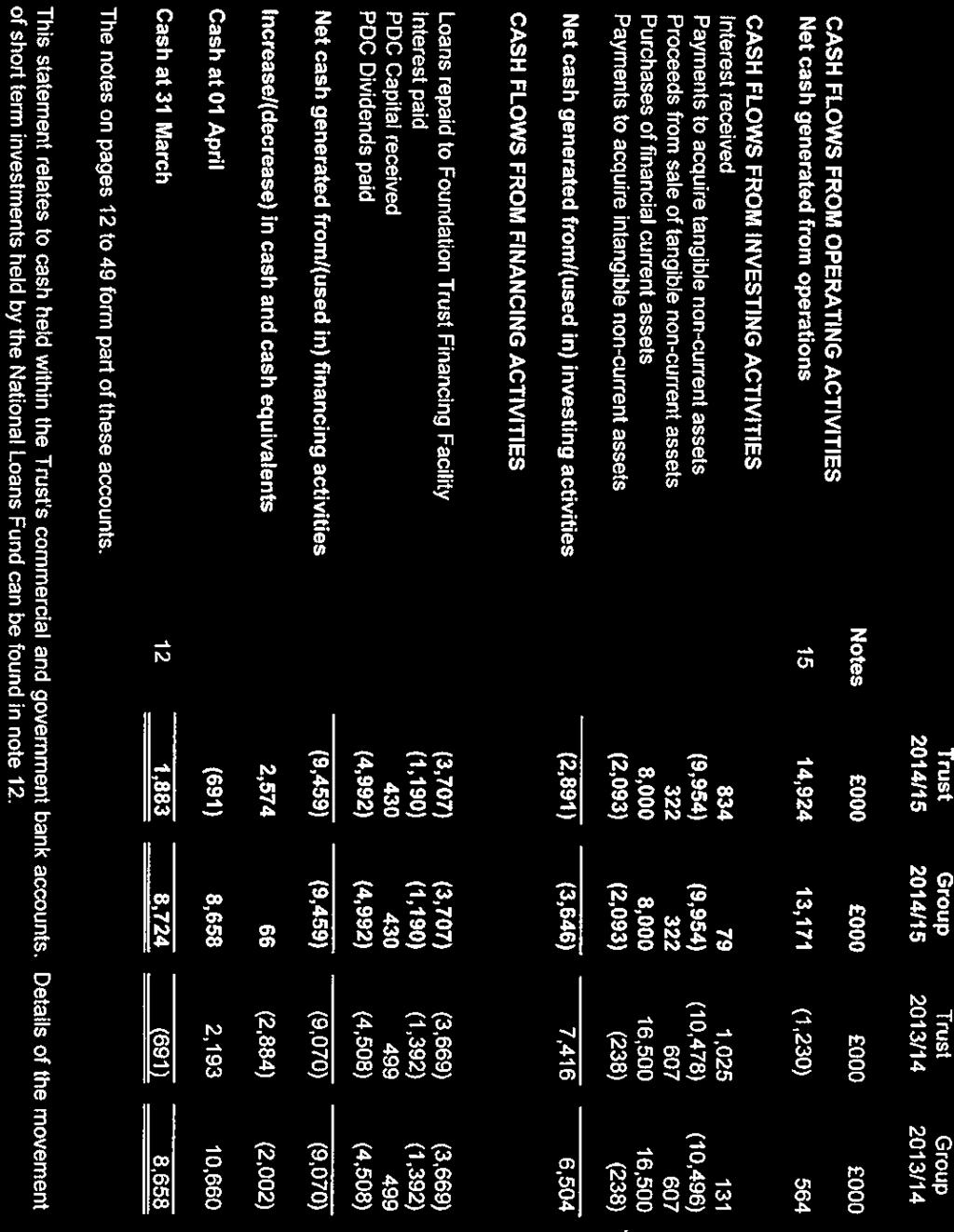
166
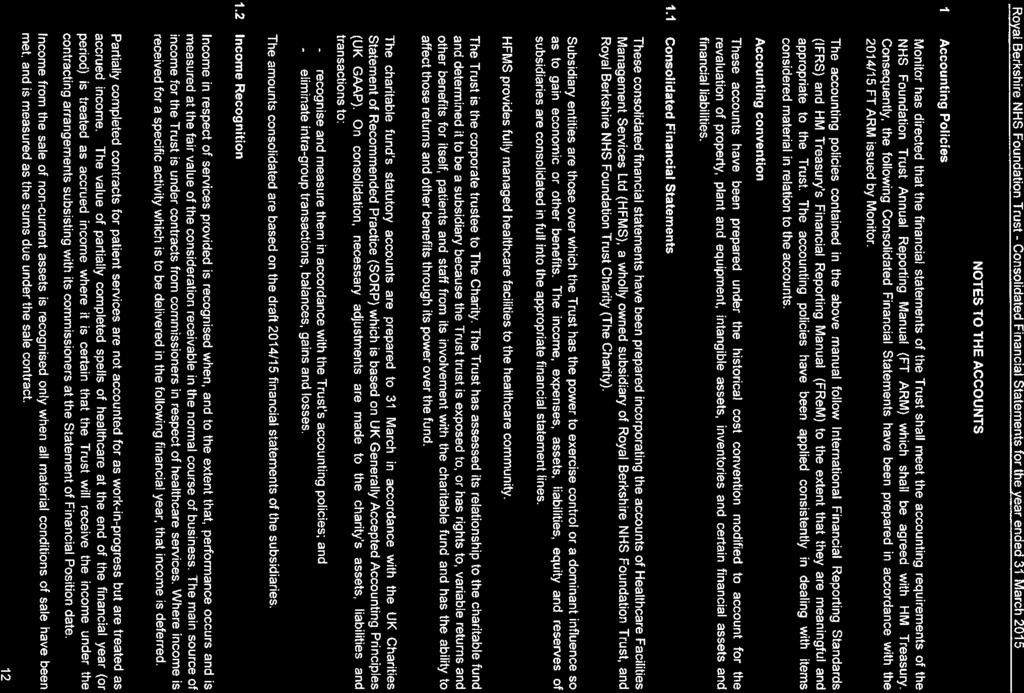
167
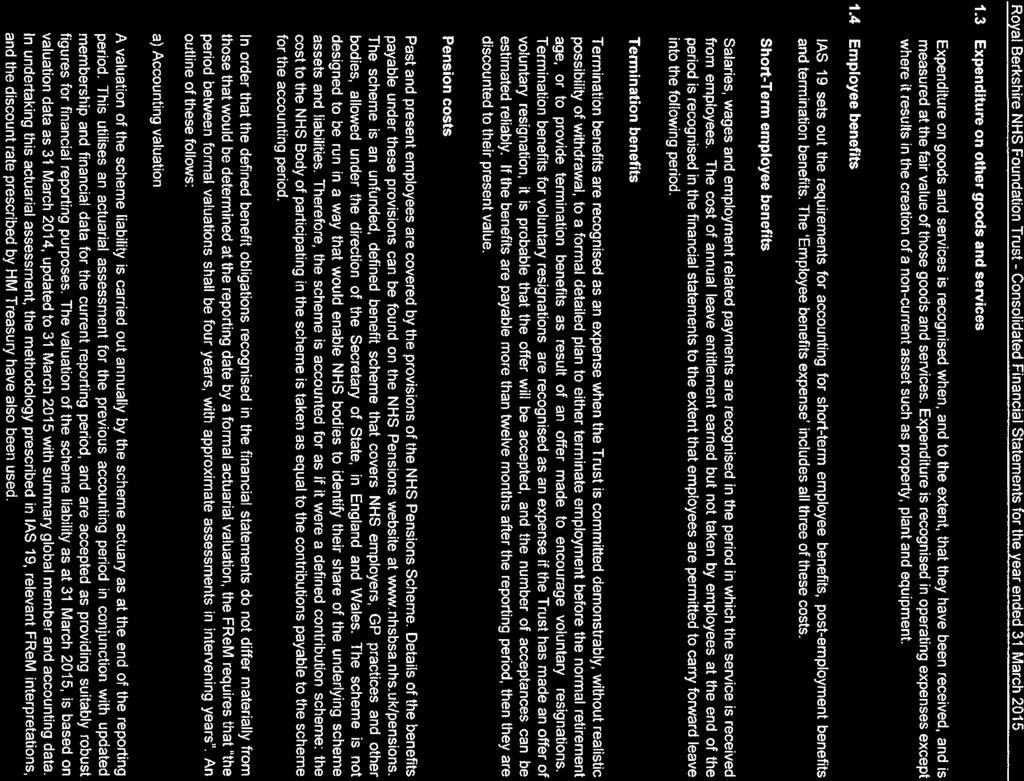
168
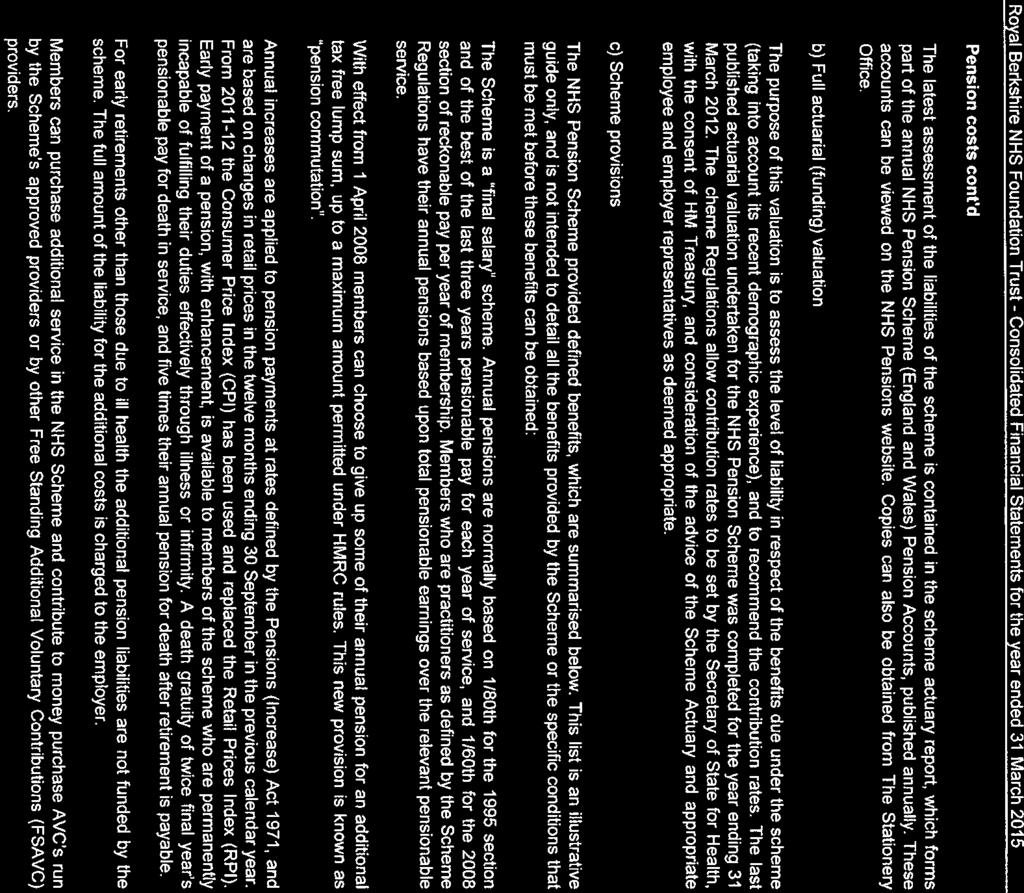
169
170
171
172
173
174
175
176
177
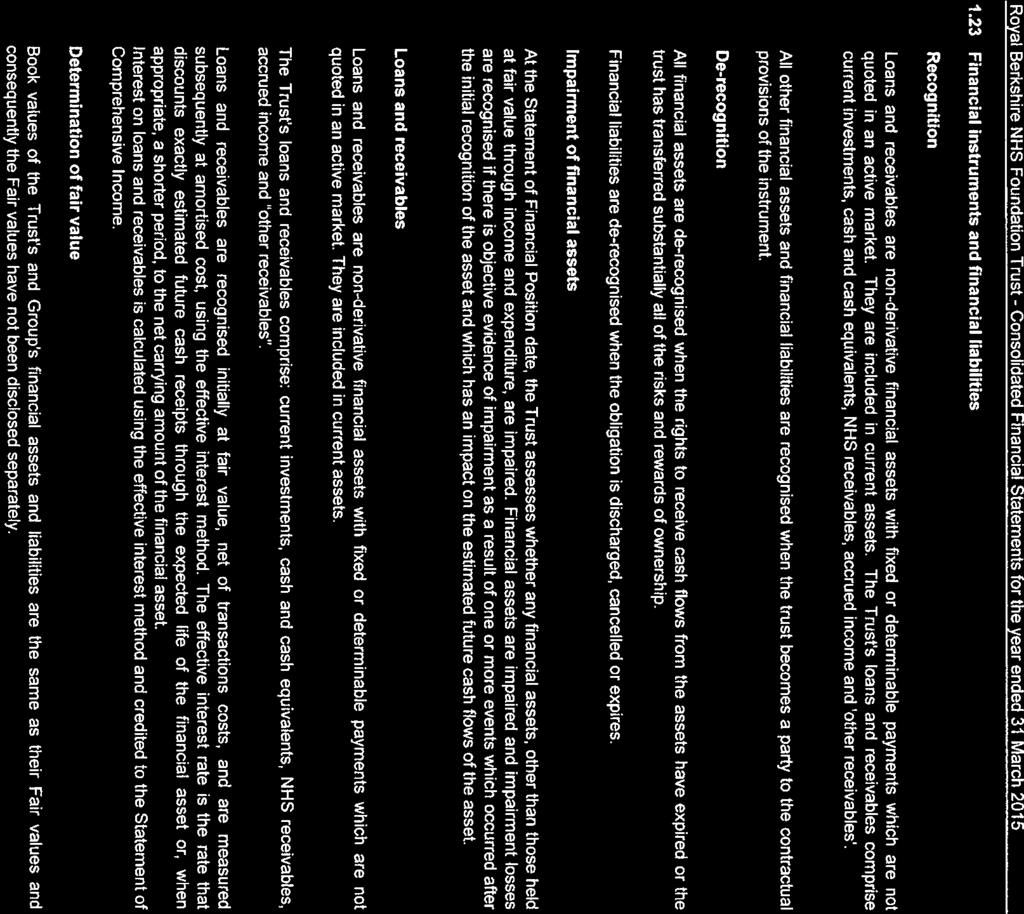
178
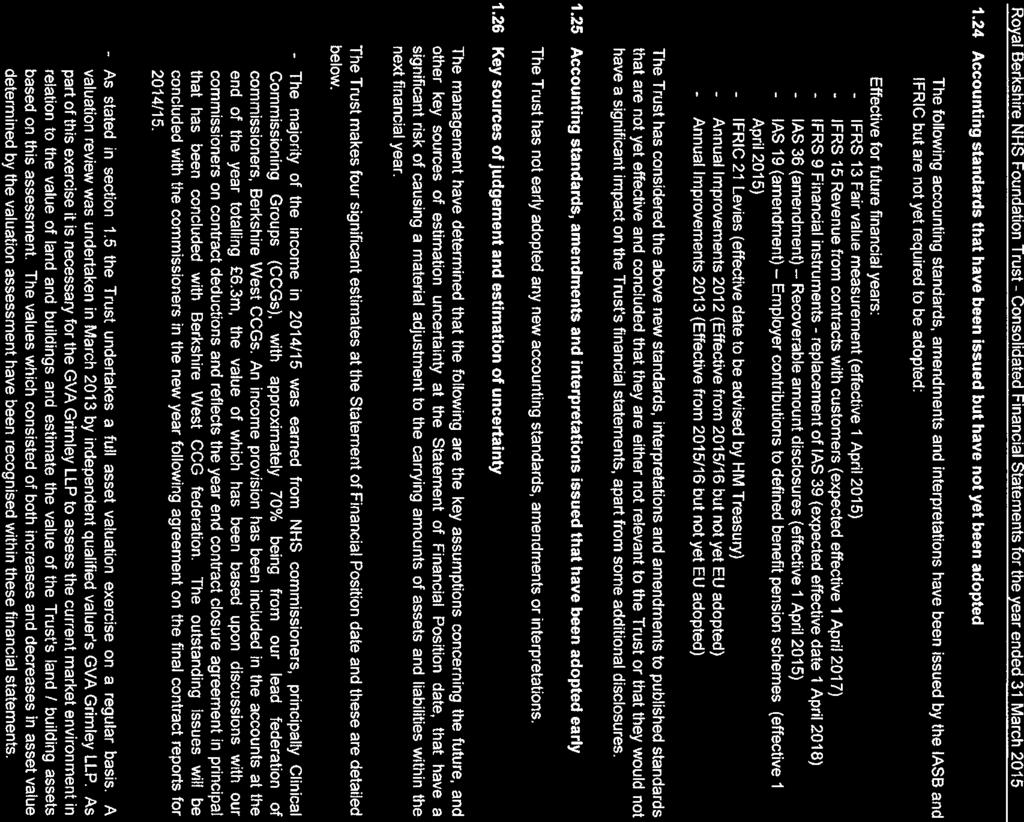
179
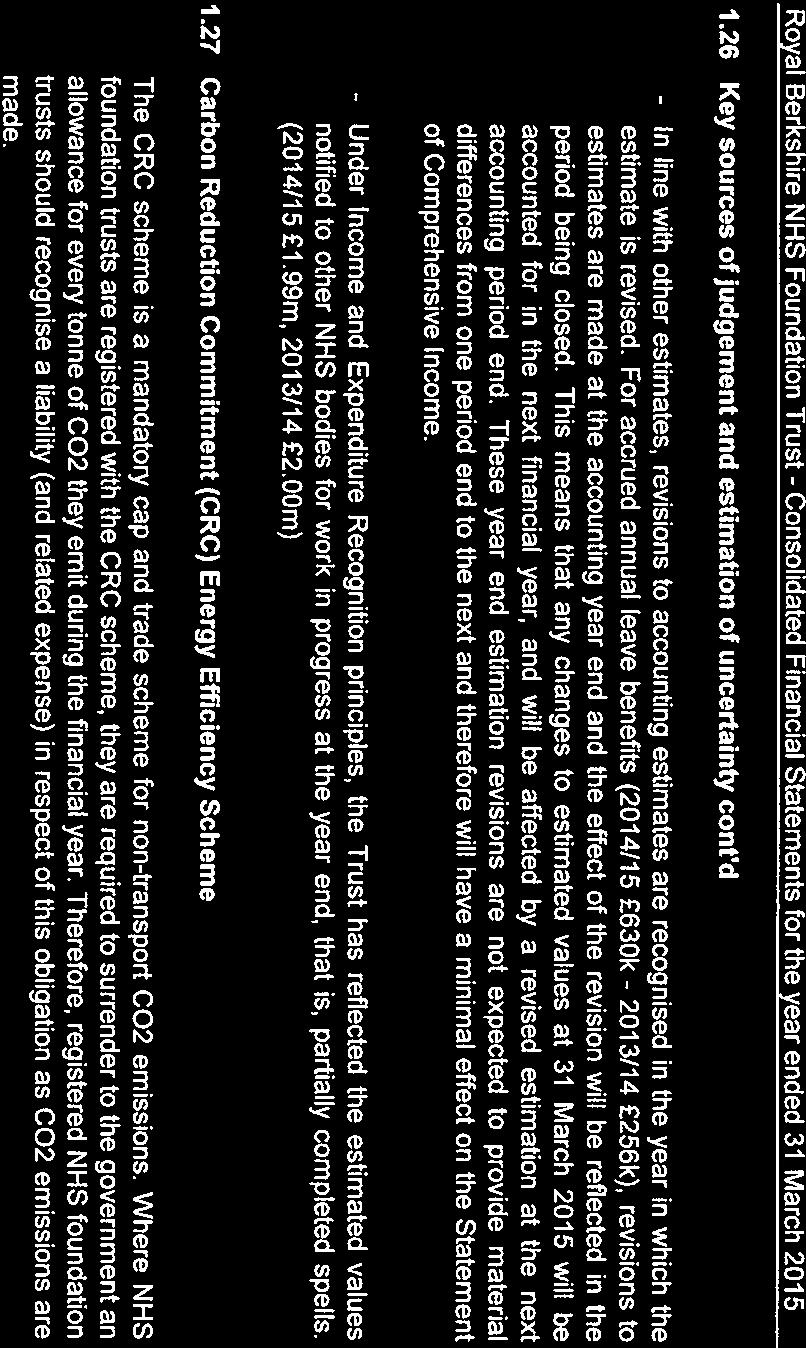
180
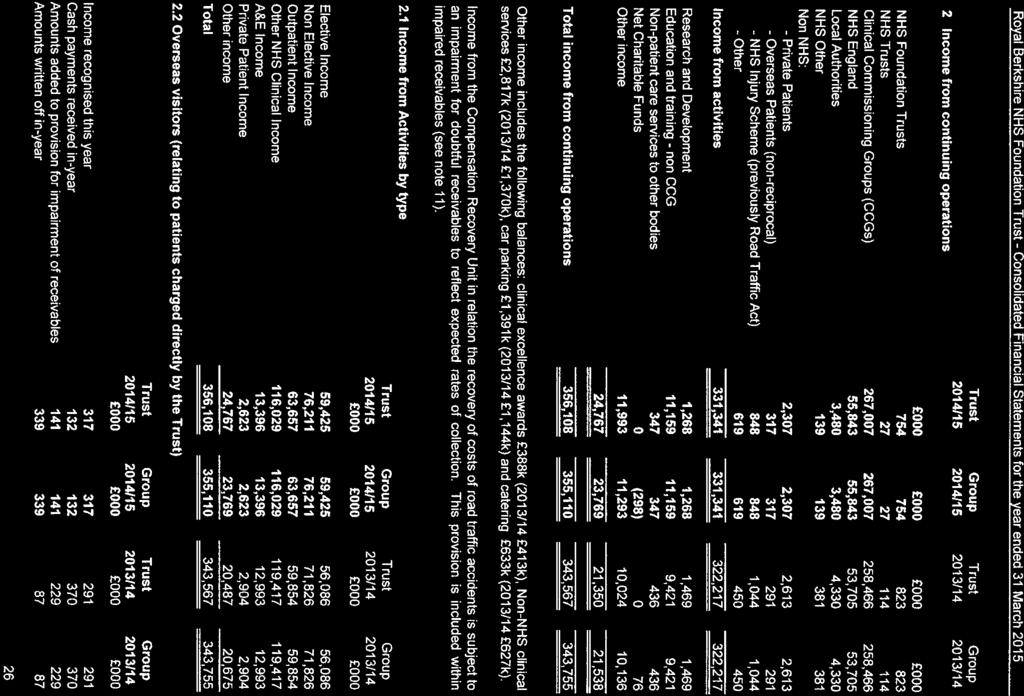
181
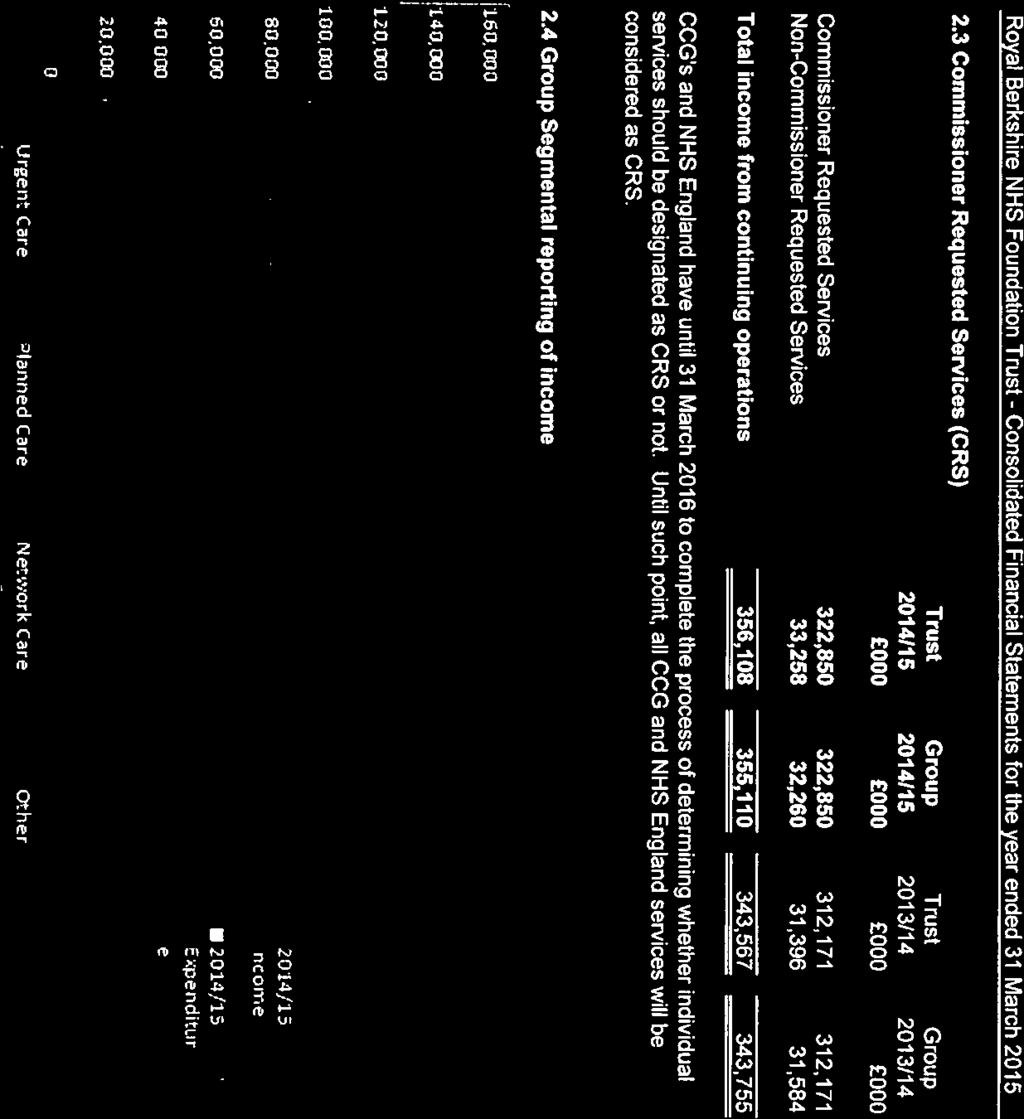
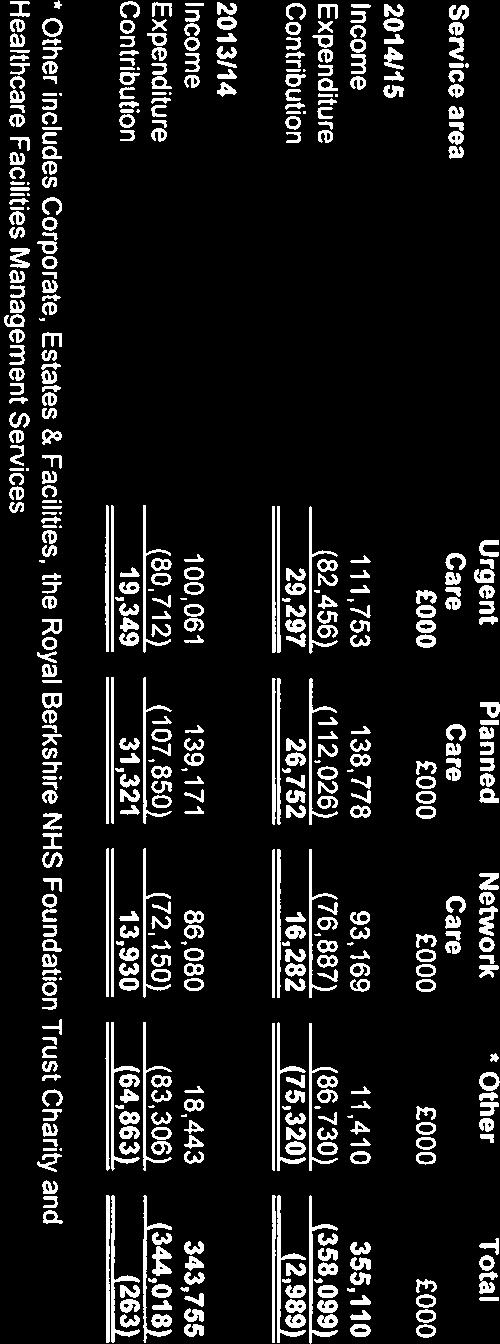
182
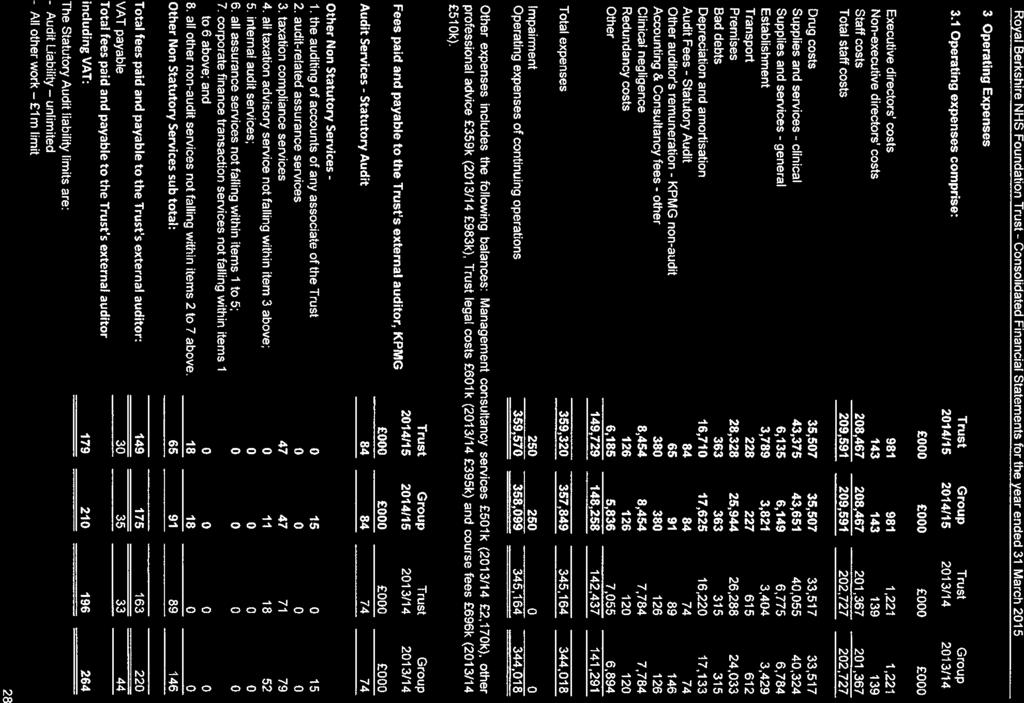
183
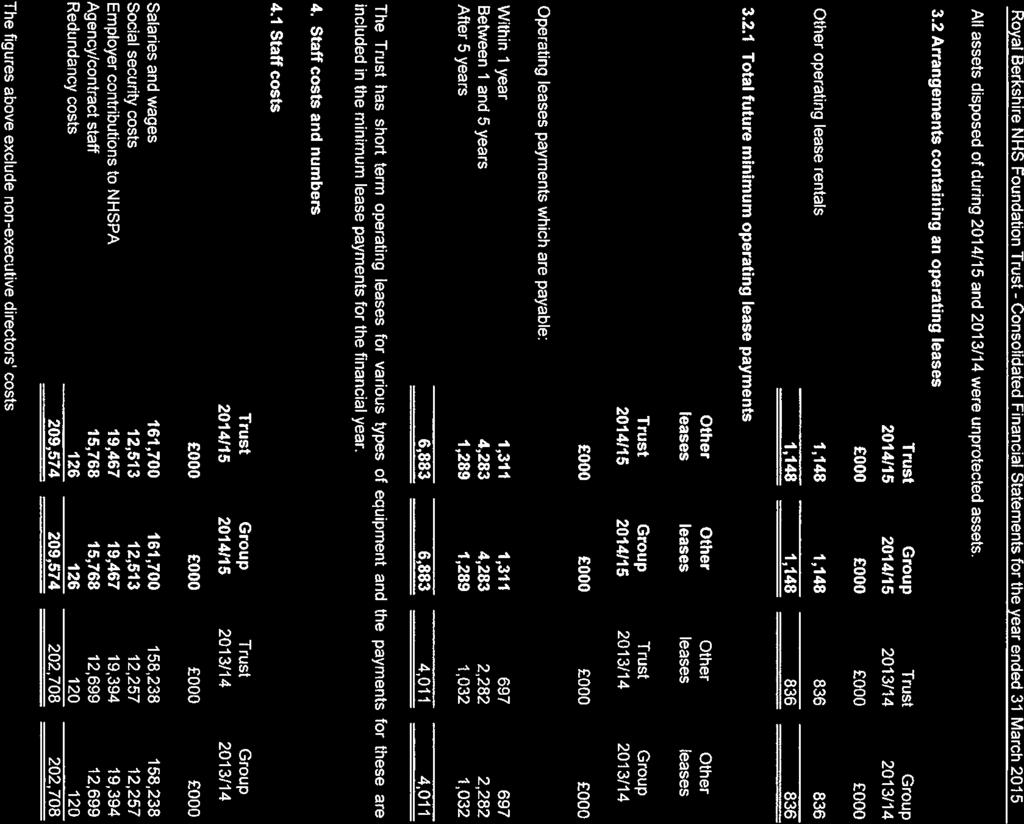
184
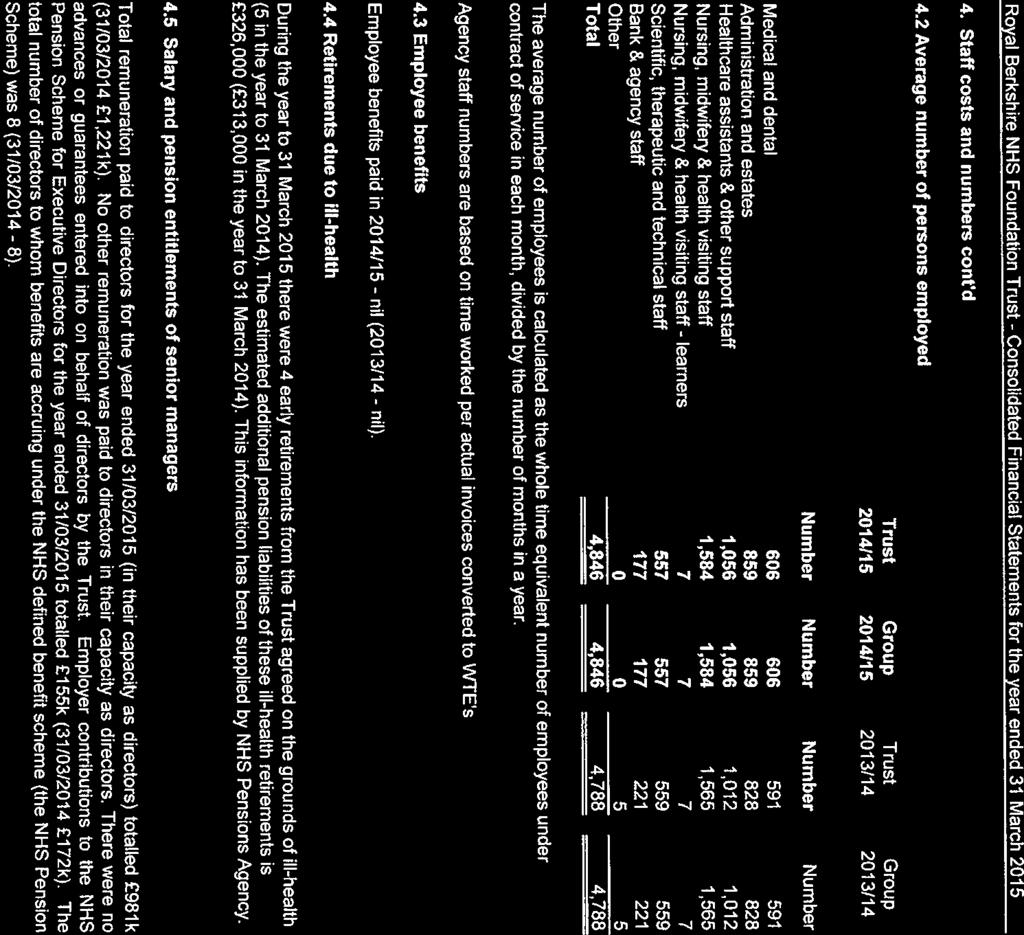
185
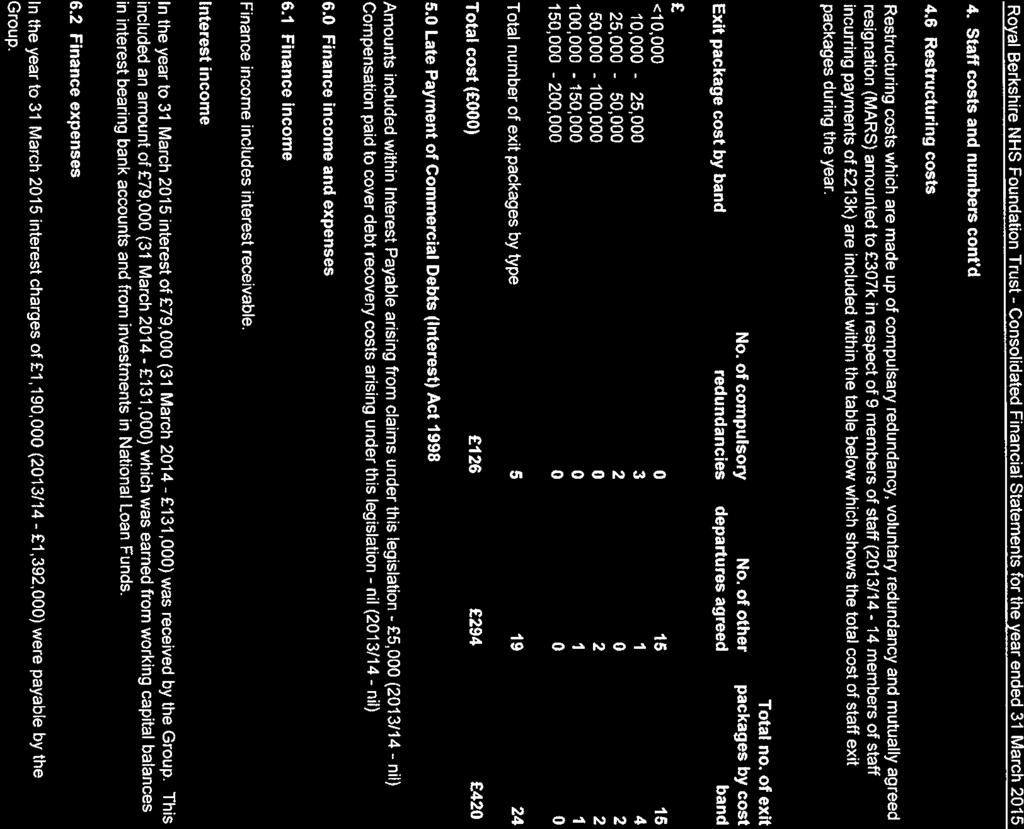
186
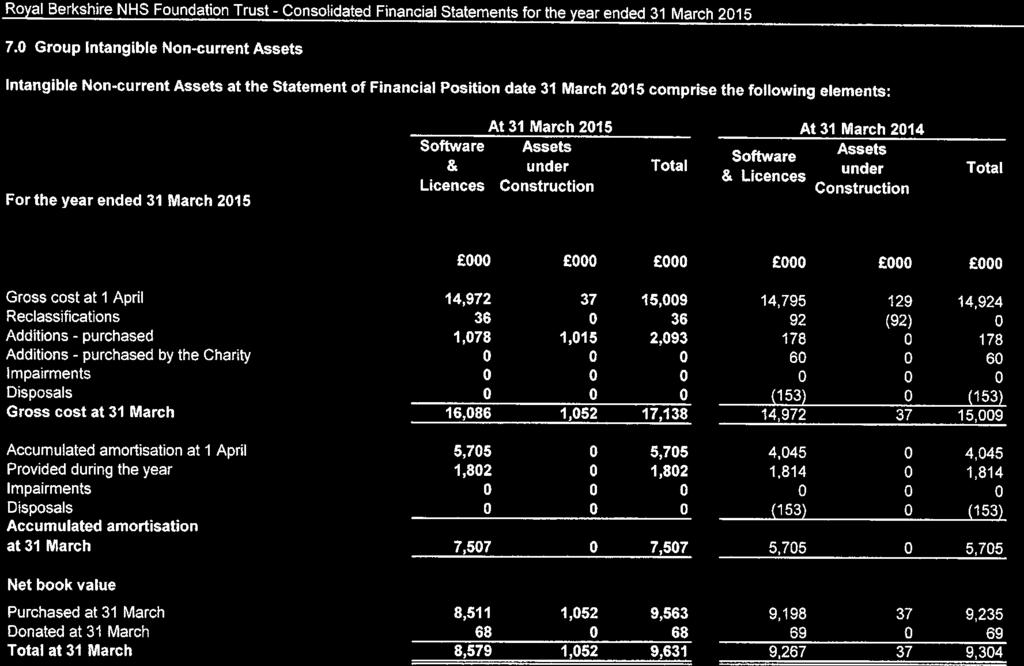
187
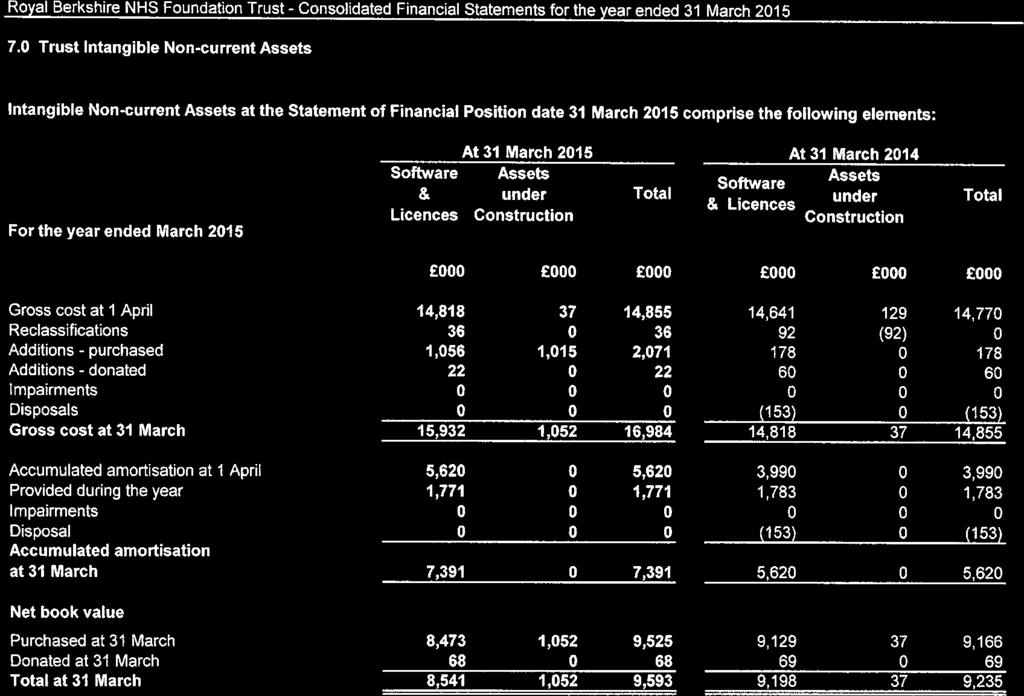
188
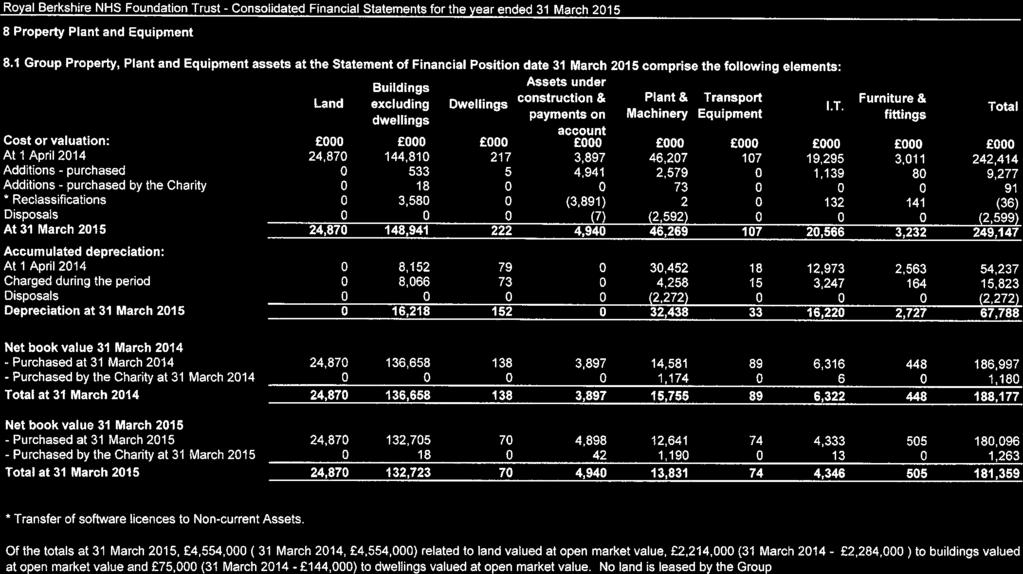
189
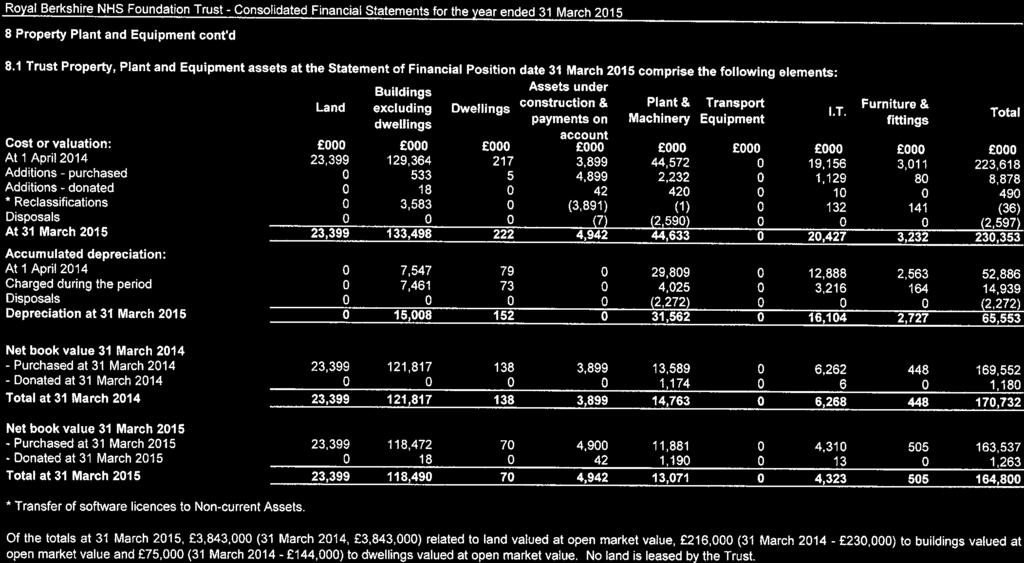
190
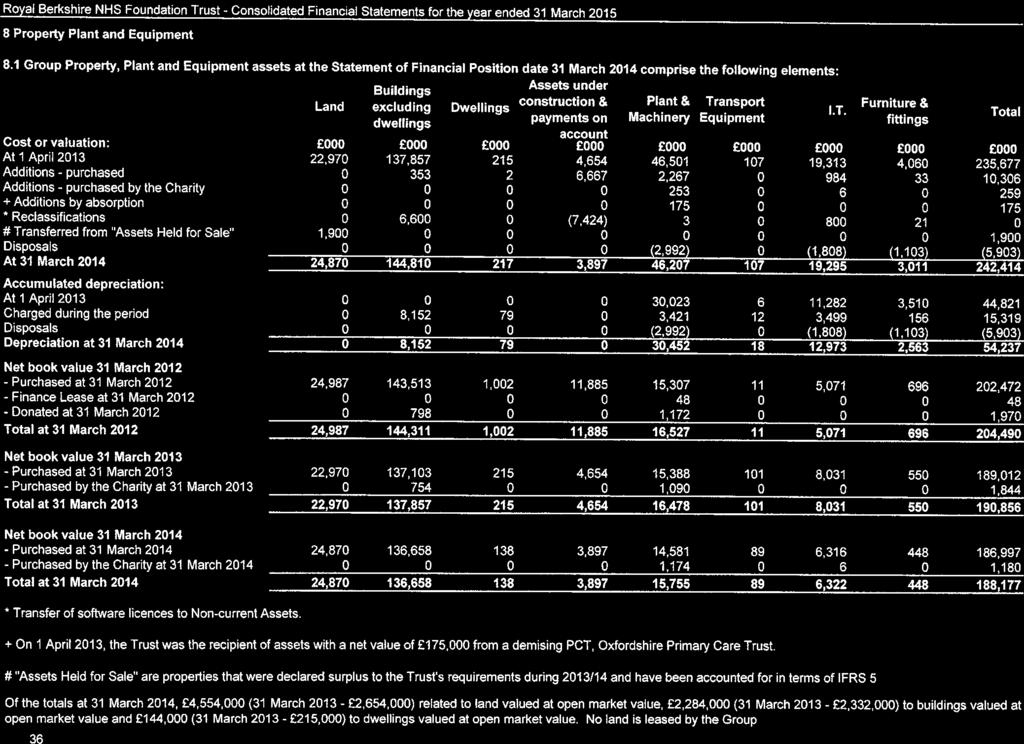
191
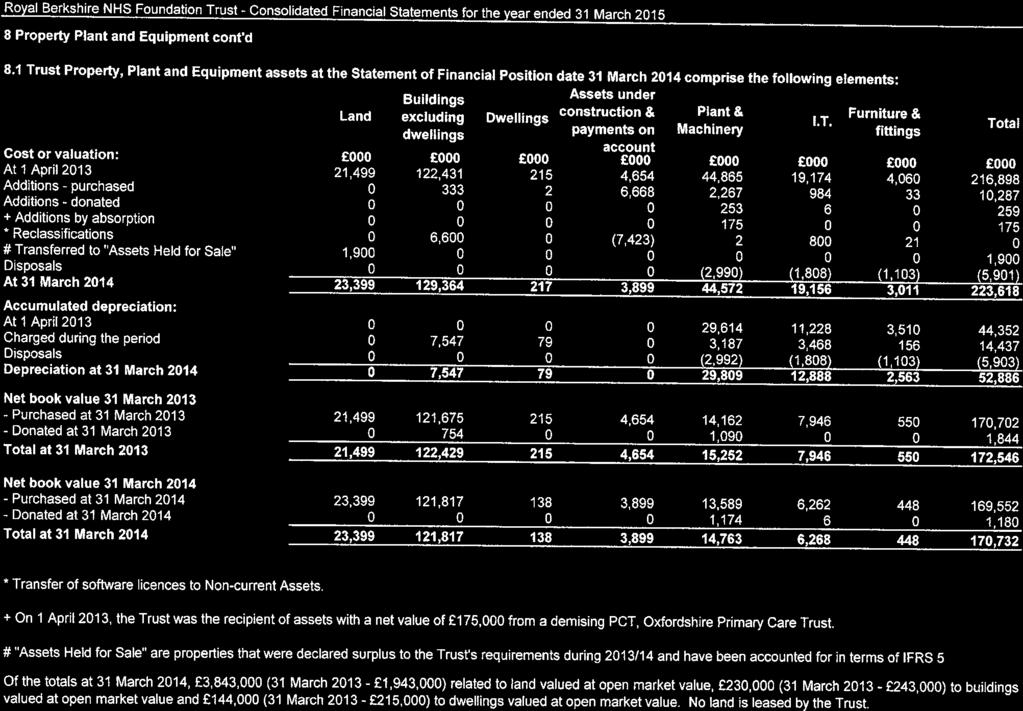
192
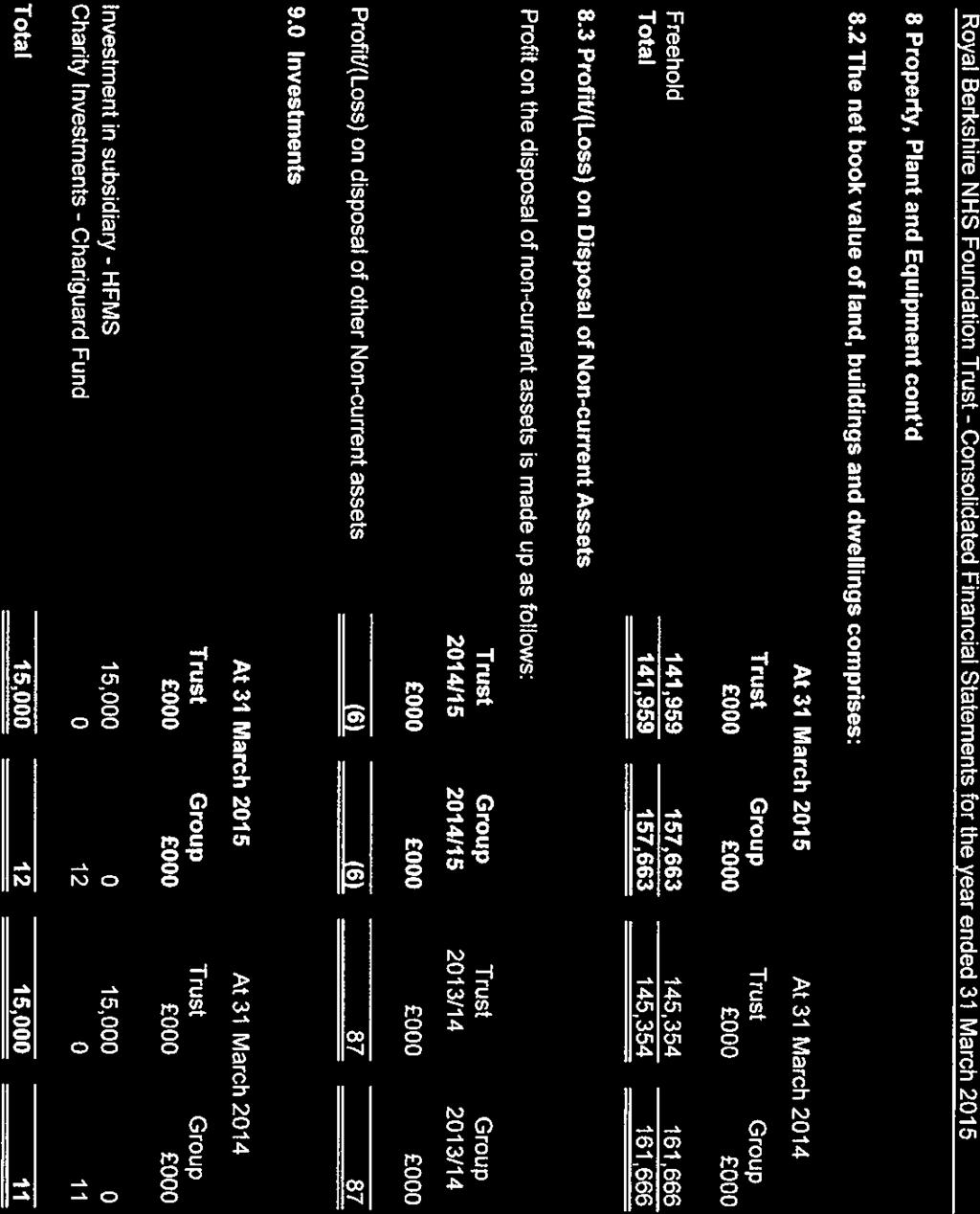
193
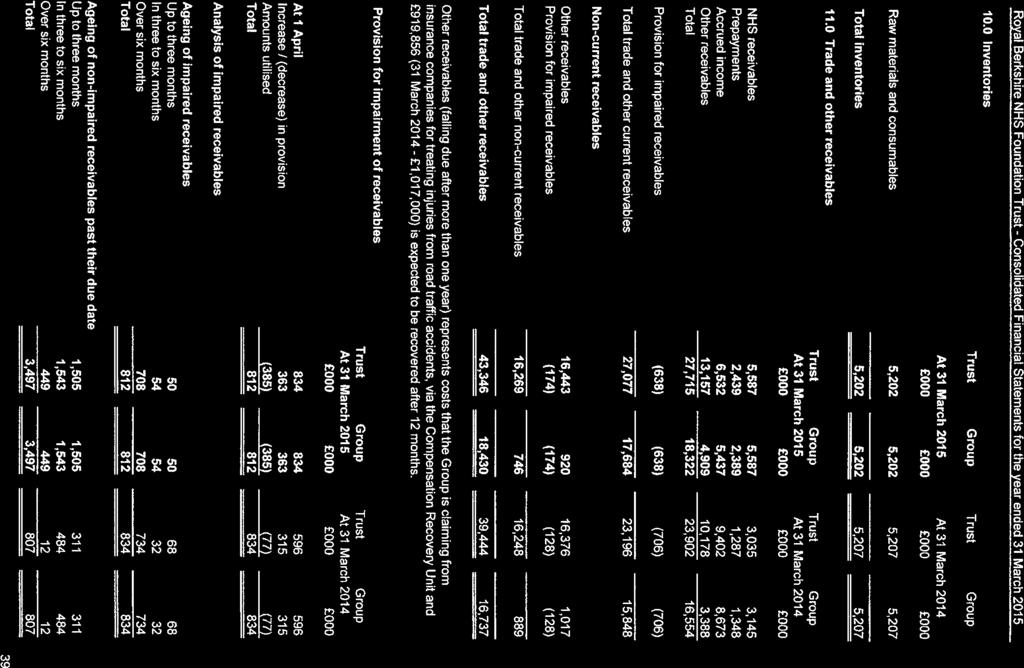
194
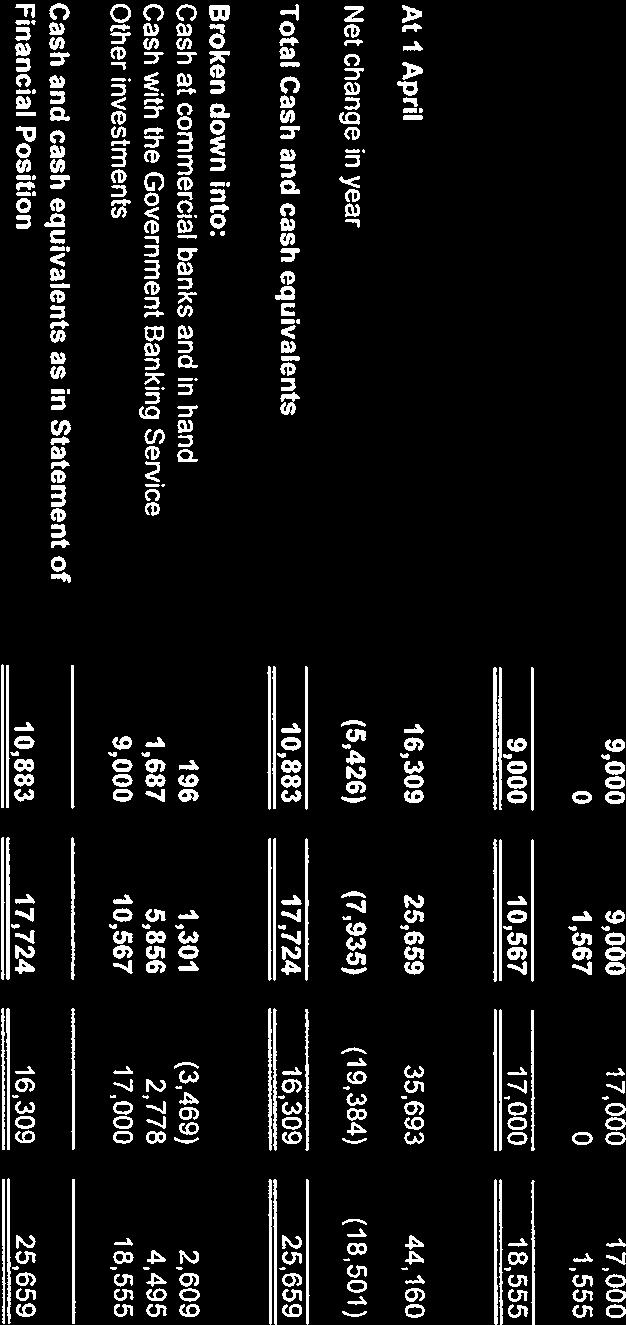
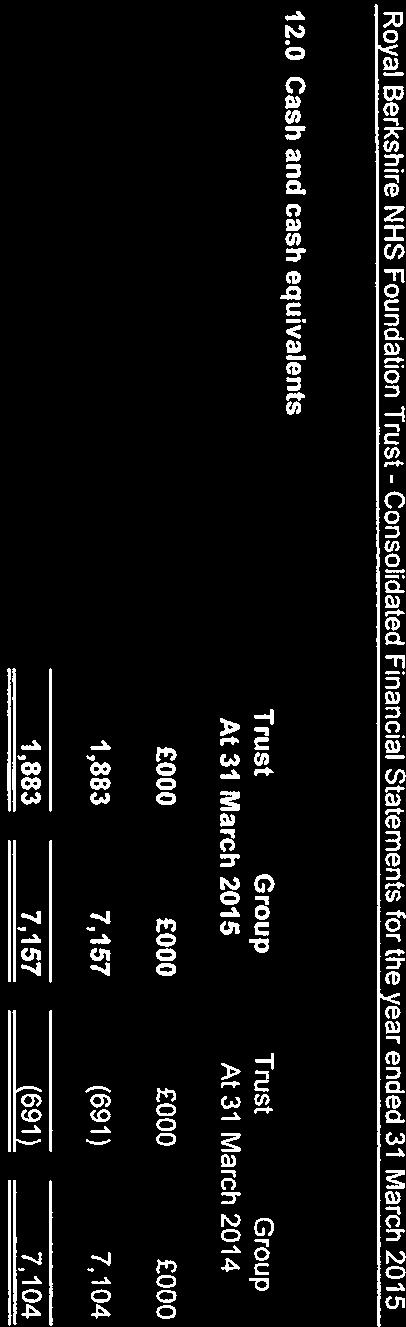
195
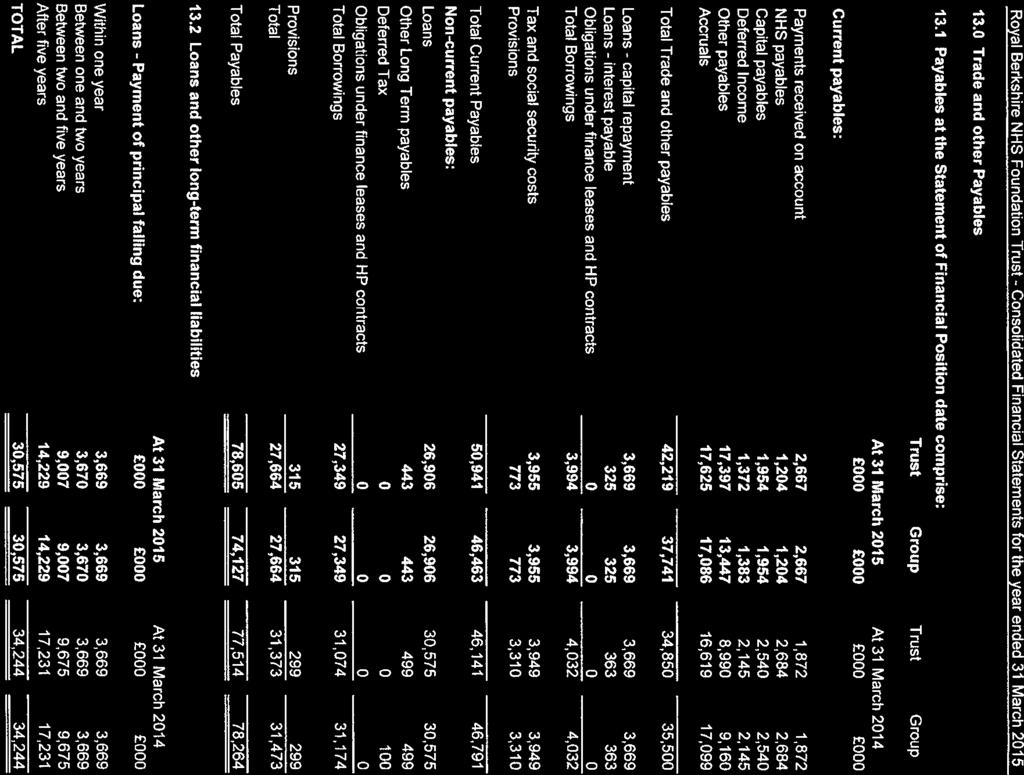
196
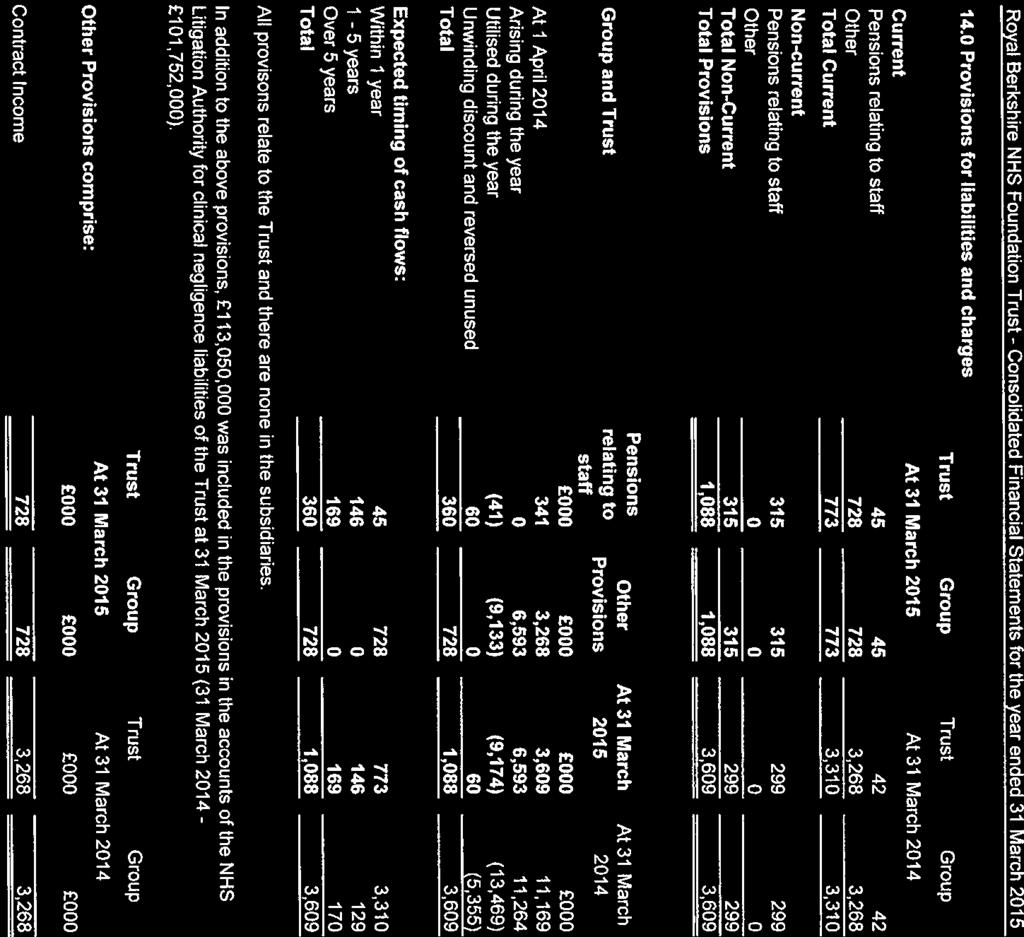
197
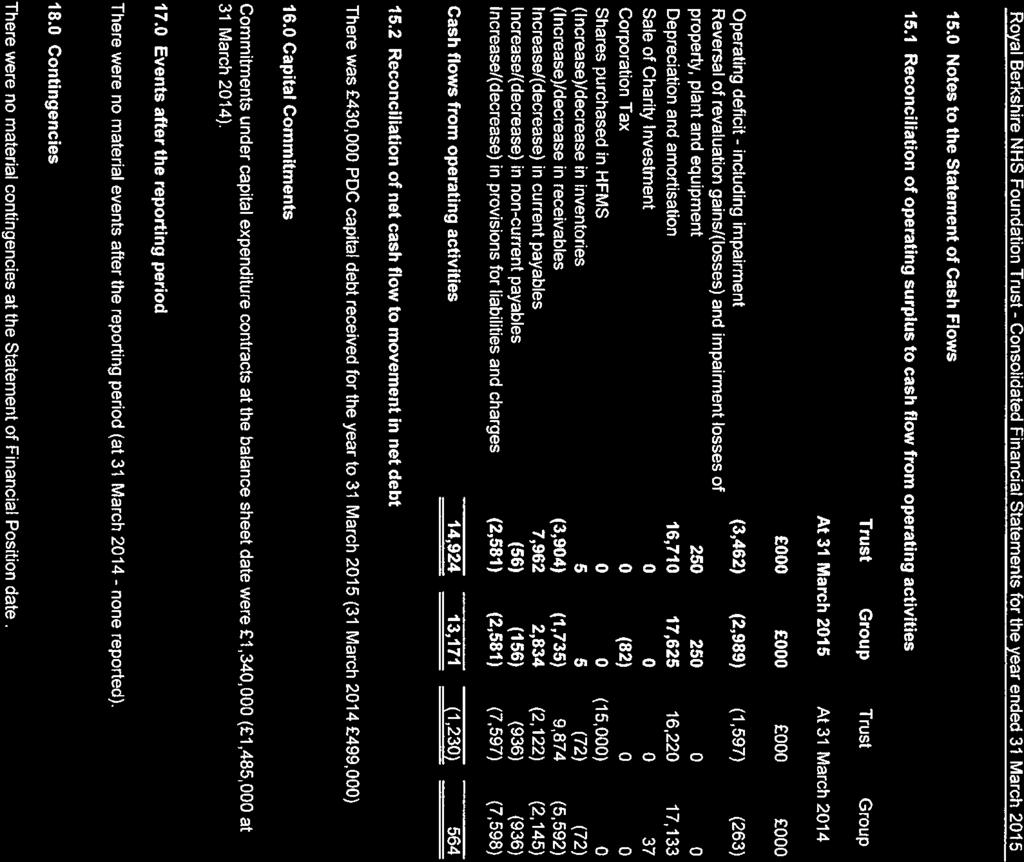
198
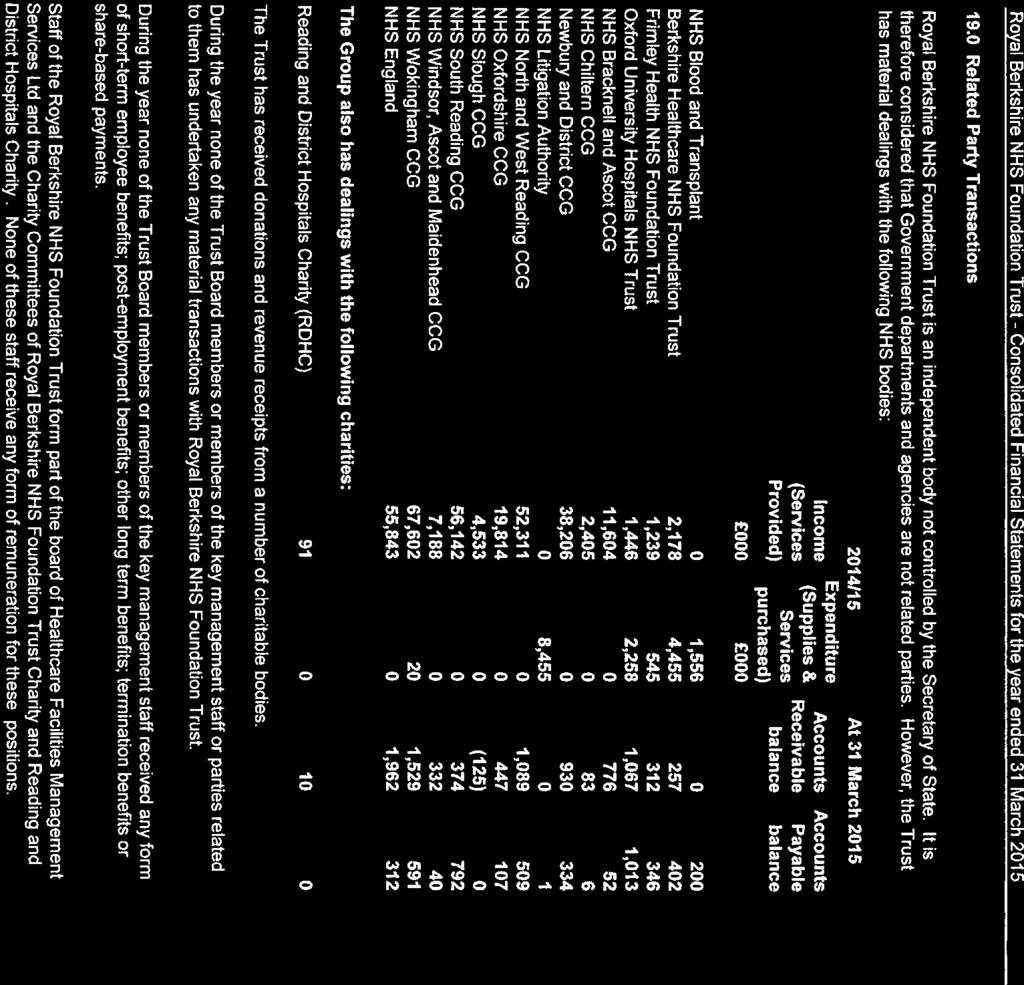
199
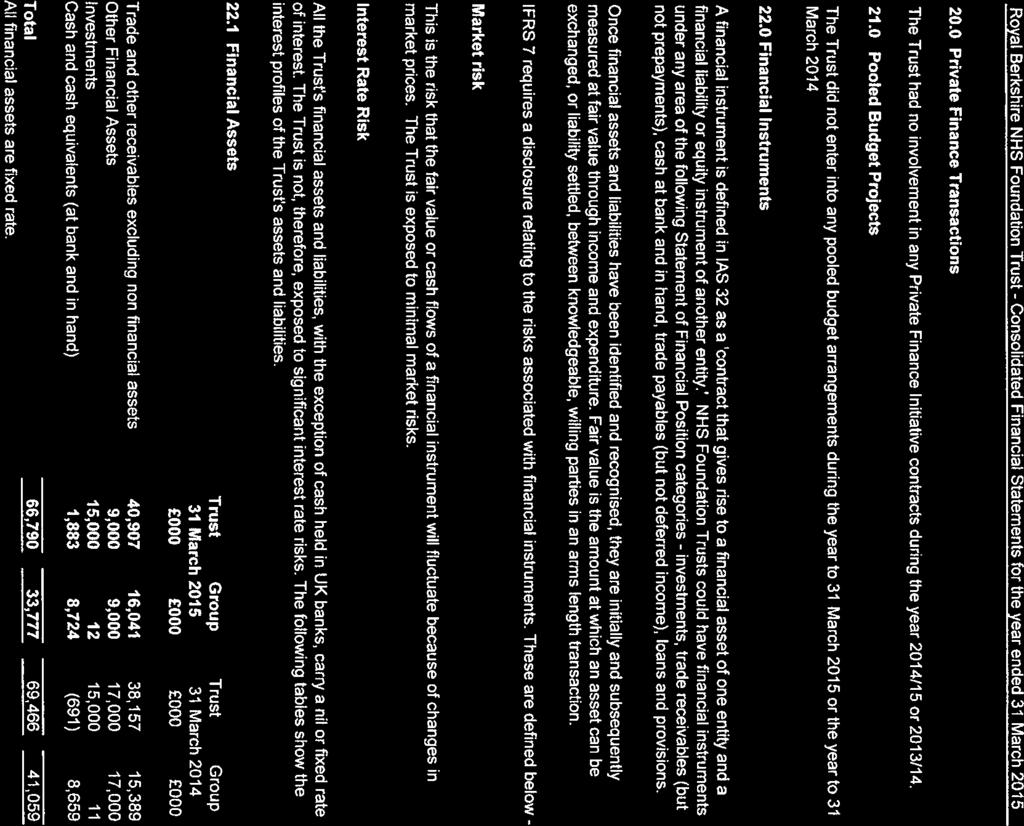
200
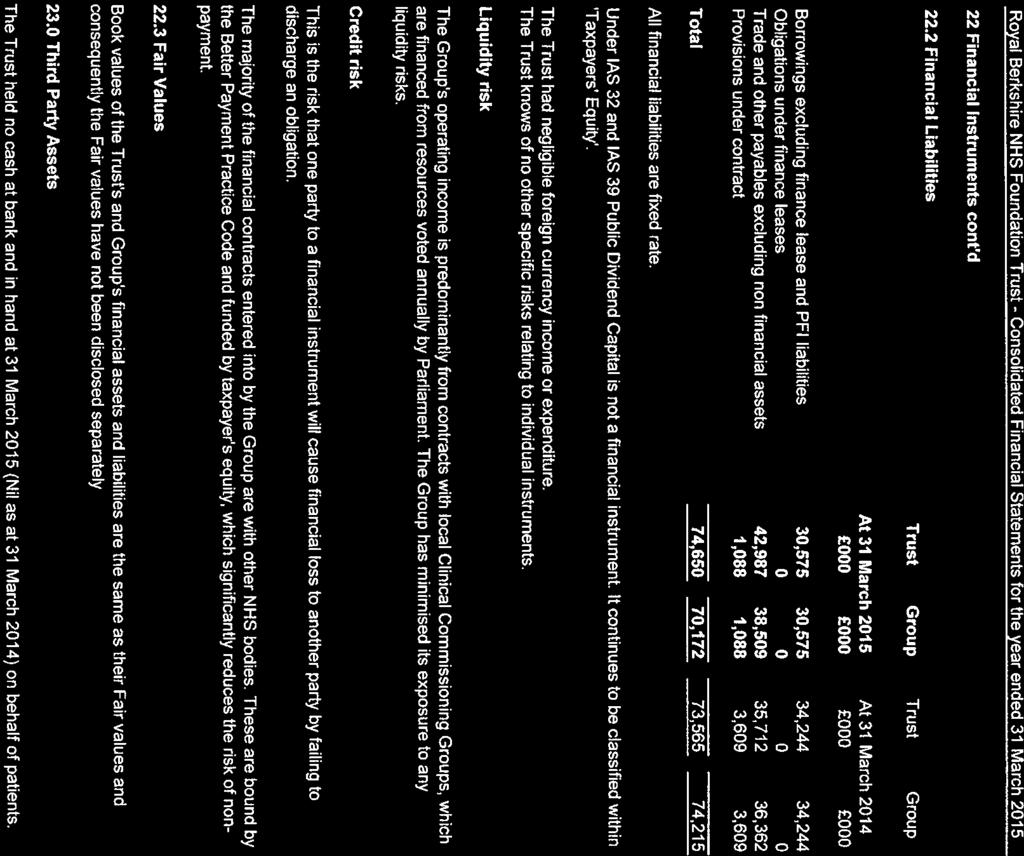
201
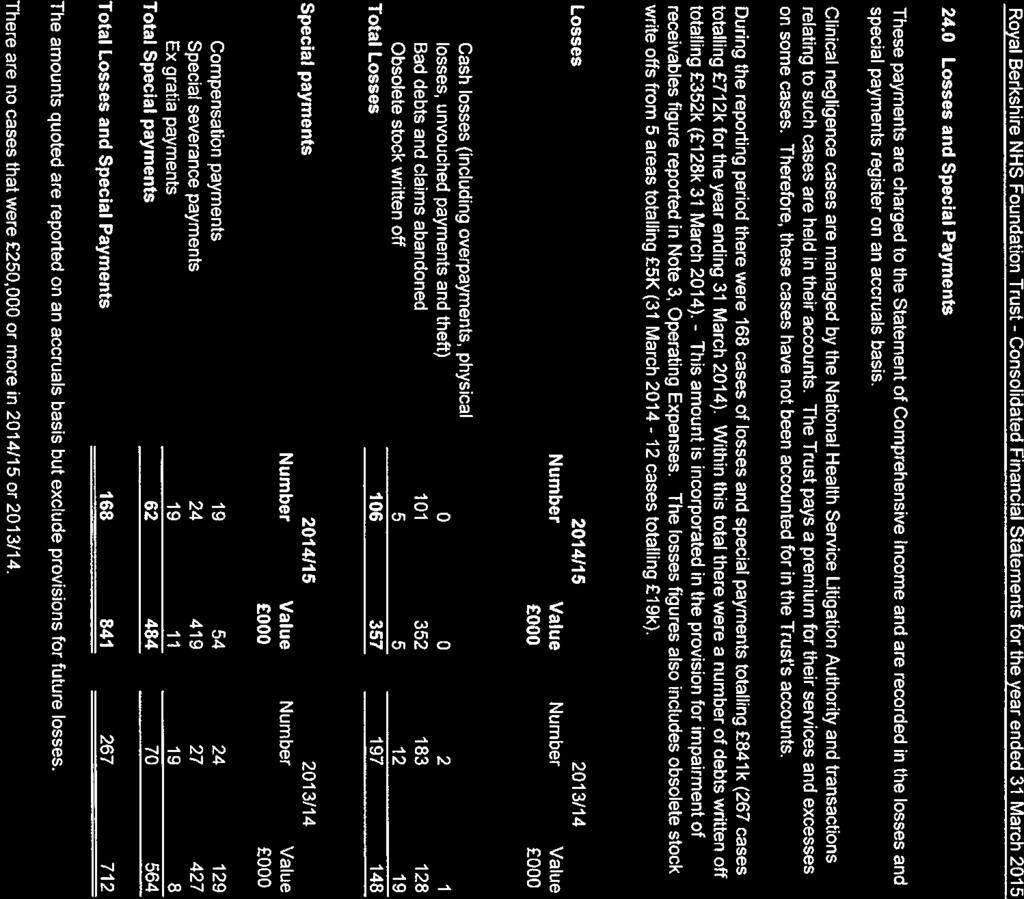
202
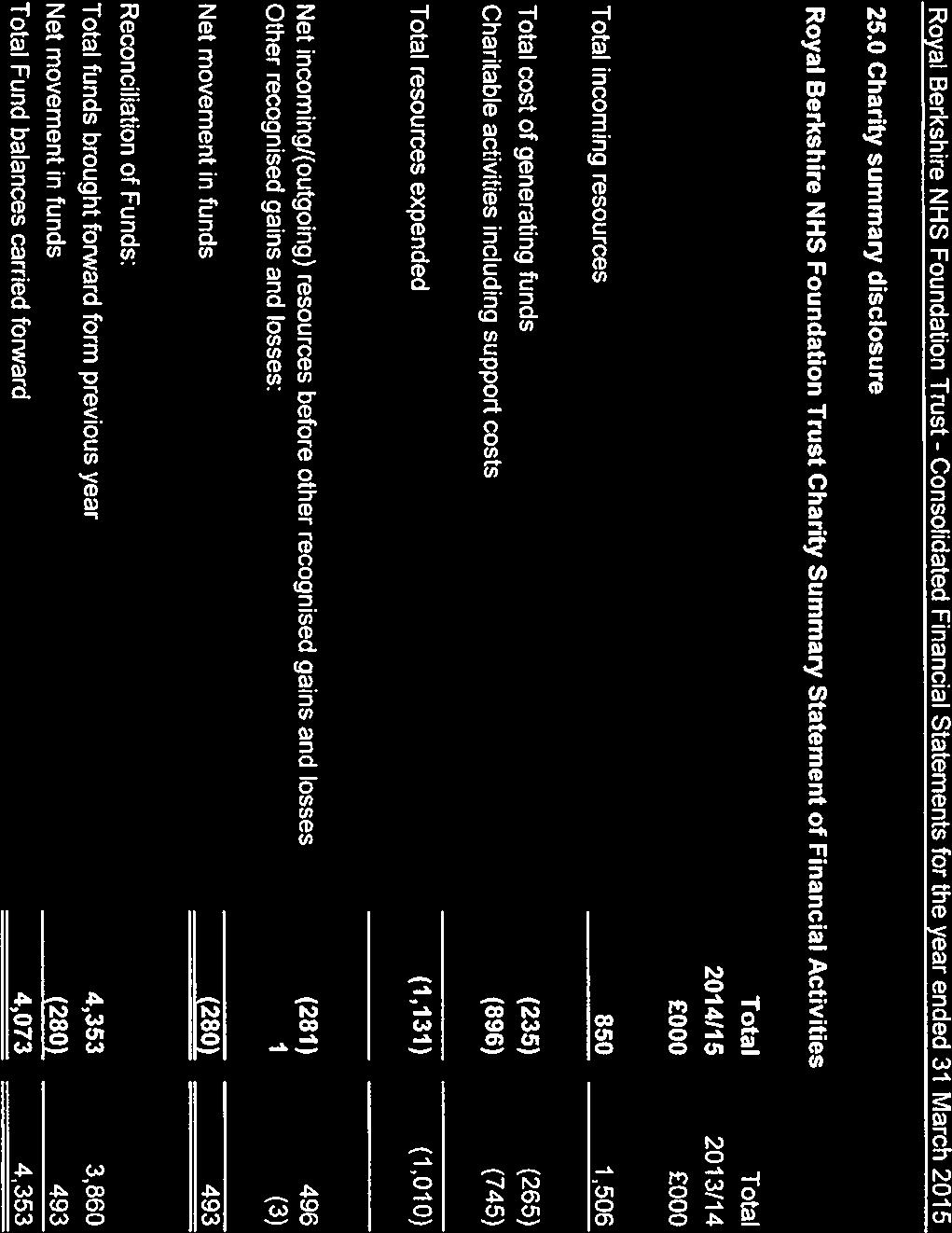
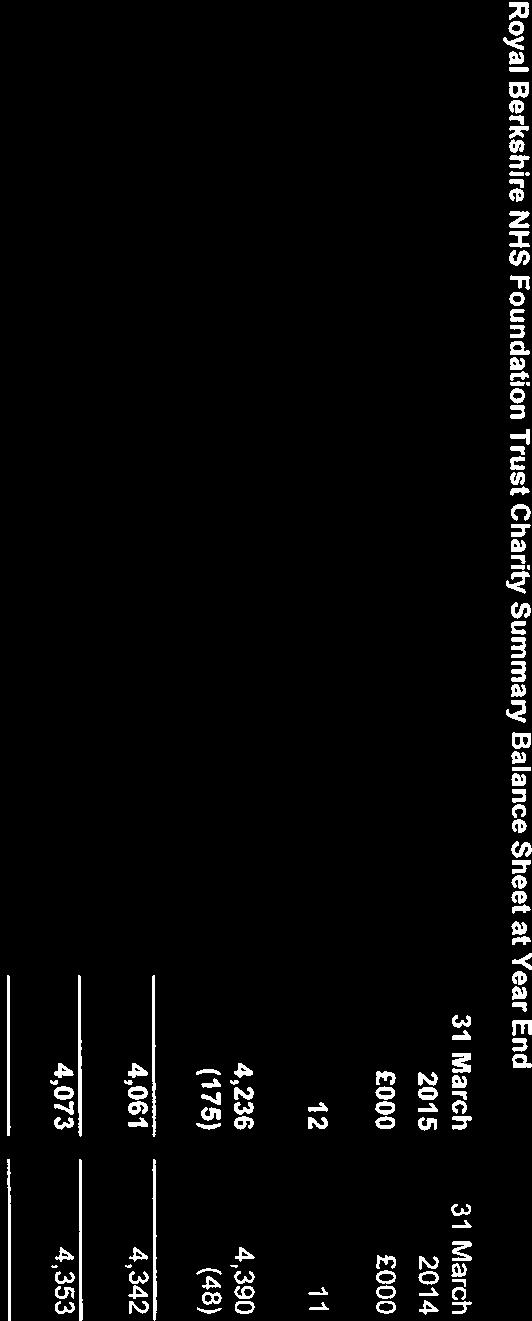
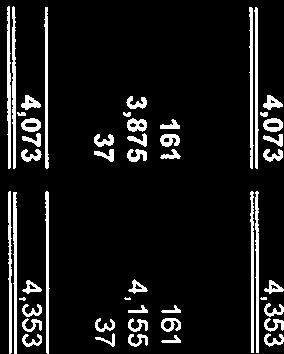
203
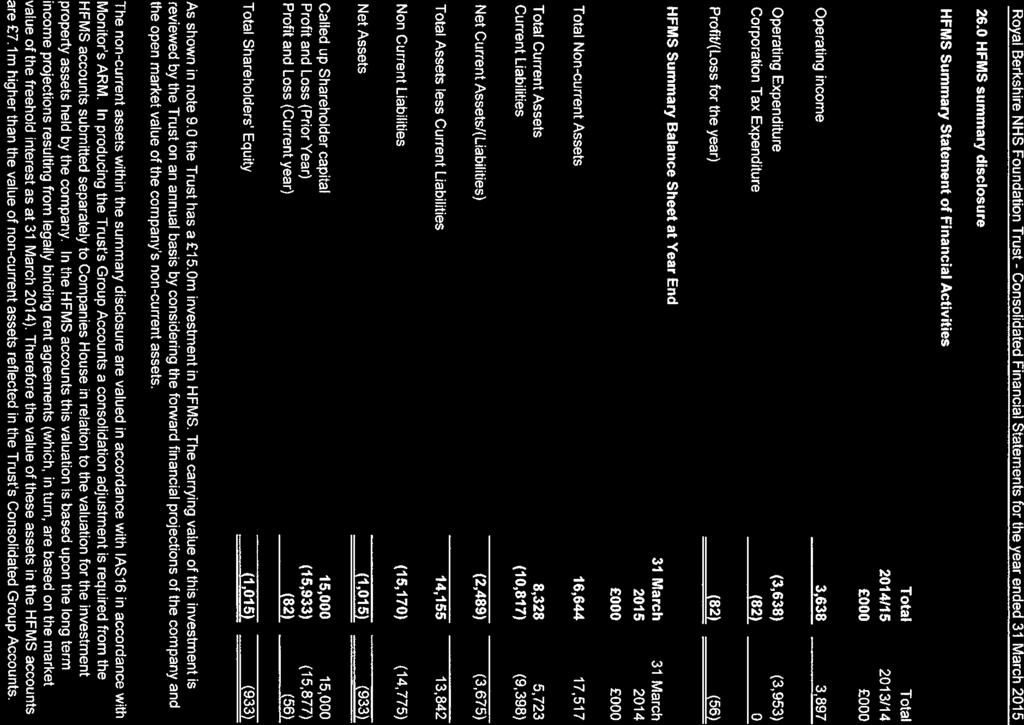
204
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Our Achievements. CQC Inspection 2016
 Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital
 The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital Introduction Supplementary Briefing Paper This paper provides more detailed
The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital Introduction Supplementary Briefing Paper This paper provides more detailed
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Annual Members Meeting 27 September Gillian Norton, Chairman
 Annual Members Meeting 27 September 2018 Gillian Norton, Chairman Council of Governors update Kathryn Harrison, Lead Governor Celebrating the NHS at 70 A short film Patient story Libby Keating I ve had
Annual Members Meeting 27 September 2018 Gillian Norton, Chairman Council of Governors update Kathryn Harrison, Lead Governor Celebrating the NHS at 70 A short film Patient story Libby Keating I ve had
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT
 KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
Non-Executive Director (two roles)
") Non-Executive Director (two roles) Candidate information We Care www.dbth.nhs.uk Providing Care Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust is one of Yorkshire s leading acute trusts,
Non-Executive Director (two roles) Candidate information We Care www.dbth.nhs.uk Providing Care Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust is one of Yorkshire s leading acute trusts,
CODE OF CONDUCT CODE OF ACCOUNTABILITY IN THE NHS
 CODE OF CONDUCT CODE OF ACCOUNTABILITY IN THE NHS CODE OF CONDUCT Public Service Values General Principles Openness and Public Responsibilities Public Service Values in Management Public Business and Private
CODE OF CONDUCT CODE OF ACCOUNTABILITY IN THE NHS CODE OF CONDUCT Public Service Values General Principles Openness and Public Responsibilities Public Service Values in Management Public Business and Private
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome:
 TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Standards conduct, accountability
 Standards of conduct, accountability and openness Standards of conduct, accountability and openness Throughout this document: members refers to all members of a board the Chair, the non-executives, the
Standards of conduct, accountability and openness Standards of conduct, accountability and openness Throughout this document: members refers to all members of a board the Chair, the non-executives, the
Quality Strategy (Refreshed March 2015)
") Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Shaping the future CQC s strategy for 2016 to 2021
 Shaping the future CQC s strategy for 2016 to 2021 CQC is the independent regulator of health and adult social care in England. We make sure health and social care services provide people with safe, effective,
Shaping the future CQC s strategy for 2016 to 2021 CQC is the independent regulator of health and adult social care in England. We make sure health and social care services provide people with safe, effective,
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EMBEDDING A PATIENT SAFETY CULTURE
 EMBEDDING A PATIENT SAFETY CULTURE October 2011 Robert J. Bell The NHS (2005) DEPARTMENT OF HEALTH STRATEGIC HEALTH AUTHORITIES PRIMARY CARE TRUSTS ACUTE CARE TRUSTS Manage and integrate primary care for
EMBEDDING A PATIENT SAFETY CULTURE October 2011 Robert J. Bell The NHS (2005) DEPARTMENT OF HEALTH STRATEGIC HEALTH AUTHORITIES PRIMARY CARE TRUSTS ACUTE CARE TRUSTS Manage and integrate primary care for
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
PATIENT ADVICE AND LIAISON SERVICE (PALS) ANNUAL REPORT
 ANNUAL REPORT") PATIENT ADVICE AND LIAISON SERVICE (PALS) ANNUAL REPORT 2007/08 CONTENTS Section Page 1. INTRODUCTION 3 2. ESTABLISHMENT OF PALS 3 2.1 Role of PALS 3 2.2 Providing advice and information 4 2.3 Resolving
PATIENT ADVICE AND LIAISON SERVICE (PALS) ANNUAL REPORT 2007/08 CONTENTS Section Page 1. INTRODUCTION 3 2. ESTABLISHMENT OF PALS 3 2.1 Role of PALS 3 2.2 Providing advice and information 4 2.3 Resolving
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Board pushes ahead with development plans
 Welcome to the latest edition of the bi-monthly newsletter produced by County Durham and Darlington NHS Foundation Trust for our partners across the health economy. To subscribe to this newsletter or to
Welcome to the latest edition of the bi-monthly newsletter produced by County Durham and Darlington NHS Foundation Trust for our partners across the health economy. To subscribe to this newsletter or to
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Thames Ambulance Service Ltd (TASL) Performance Report
 Performance Report") WEST LEICESTERSHIRE CLINICAL COMMISSIONING GROUP BOARD MEETING 8 th of May 2018 Title of the report: Section: Report by: Presented by: Thames Ambulance Service Ltd (TASL) Performance Report Public Joanna
WEST LEICESTERSHIRE CLINICAL COMMISSIONING GROUP BOARD MEETING 8 th of May 2018 Title of the report: Section: Report by: Presented by: Thames Ambulance Service Ltd (TASL) Performance Report Public Joanna
STATEMENT OF PURPOSE August Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008)
") 1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Welcome. Annual Members Meeting 7 September Excellence in specialist and community healthcare
 Welcome Annual Members Meeting 7 September 2017 Excellence in specialist and community healthcare Gillian Norton, Chairman Introduction Excellence in specialist and community healthcare Louise Peters,
Welcome Annual Members Meeting 7 September 2017 Excellence in specialist and community healthcare Gillian Norton, Chairman Introduction Excellence in specialist and community healthcare Louise Peters,
Airedale General Hospital
 Airedale NHS Foundation Trust Airedale General Hospital Quality report Skipton Road, Steeton Keighley BD20 6TD Telephone: 01535 652511 www.airedale-trust.nhs.uk Date of inspection visit: 19-20 and 27 September
Airedale NHS Foundation Trust Airedale General Hospital Quality report Skipton Road, Steeton Keighley BD20 6TD Telephone: 01535 652511 www.airedale-trust.nhs.uk Date of inspection visit: 19-20 and 27 September
NHS Equality Delivery System for Isle of Wight NHS Trust. Interim baseline assessment against the
 Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Sussex Health Care Audiology Ltd Dorking Hospital, Horsham Road,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Sussex Health Care Audiology Ltd Dorking Hospital, Horsham Road,
A fresh start for registration. Improving how we register providers of all health and adult social care services
 A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
IT ALL STARTS WITH YOU
 Email: jo.curtis@nhs.net IT ALL STARTS WITH YOU Tell us about your experience Help us improve NHS services This guide takes you through the different ways you can tell the NHS about your experiences, so
Email: jo.curtis@nhs.net IT ALL STARTS WITH YOU Tell us about your experience Help us improve NHS services This guide takes you through the different ways you can tell the NHS about your experiences, so
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Action required: To agree the process by which Governors will meet with the inspection team.
 Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Incorporating community services in Exeter, East and Mid Devon
 Incorporating community services in Exeter, East and Mid Devon NDDH Torridge North Devon Cornwall Plymouth Exeter Taunton H H NDDH H R R H H H H H H R R H H H H R H H H H H H H H H H H H NDDH H H H R
Incorporating community services in Exeter, East and Mid Devon NDDH Torridge North Devon Cornwall Plymouth Exeter Taunton H H NDDH H R R H H H H H H R R H H H H R H H H H H H H H H H H H NDDH H H H R
Library and Knowledge Services Annual Report
 Library and Knowledge Services Annual Report 2016-2017 West Hertfordshire Hospitals NHS Trust Katherine Teal Annual Report 2016-2017 Foreword This year has seen significant changes in the Library and Knowledge
Library and Knowledge Services Annual Report 2016-2017 West Hertfordshire Hospitals NHS Trust Katherine Teal Annual Report 2016-2017 Foreword This year has seen significant changes in the Library and Knowledge
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Quality Improvement Strategy 2017/ /21
 Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
The new CQC approach to hospital inspection. Ann Ford Head of Hospital Inspection (North West) June 2014
 June 2014") The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Rainbow Trust Childrens Charity 1
 Rainbow Trust Children's Charity Rainbow Trust Childrens Charity 1 Inspection report North Sands Business Centre Liberty Way Sunderland SR6 0QA Tel: 07825601369 Date of inspection visit: 19 June 2017 Date
Rainbow Trust Children's Charity Rainbow Trust Childrens Charity 1 Inspection report North Sands Business Centre Liberty Way Sunderland SR6 0QA Tel: 07825601369 Date of inspection visit: 19 June 2017 Date
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Agenda Item: REPORT TO PUBLIC BOARD MEETING 31 May 2012
 Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
corporate management plan
 corporate management plan 2012-2013 2 Contents 1. Introduction 2. Overview of the Trust 3. Our purpose, values and core objectives 4. Safety & Quality Corporate Objectives 5. Modernisation Corporate Objectives
corporate management plan 2012-2013 2 Contents 1. Introduction 2. Overview of the Trust 3. Our purpose, values and core objectives 4. Safety & Quality Corporate Objectives 5. Modernisation Corporate Objectives
JOB DESCRIPTION. The hospital has been consistently growing over the past few years, almost doubling since 2008.
 JOB DESCRIPTION JOB TITLE: Modern Matron CLINICAL UNIT: Paediatrics BASE: The Portland Hospital for Women and Children MANAGED BY: Children s Services Manager ACCOUNTABLE TO: Chief Nursing Officer HOSPITAL
JOB DESCRIPTION JOB TITLE: Modern Matron CLINICAL UNIT: Paediatrics BASE: The Portland Hospital for Women and Children MANAGED BY: Children s Services Manager ACCOUNTABLE TO: Chief Nursing Officer HOSPITAL
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Revalidation Annual Report
 Paper 31 14 Revalidation Annual Report 2013-14 Purpose of Document: To provide the Board with a report on the first year s experience with medical revalidation in Public Health Wales. Board/Committee to-
Paper 31 14 Revalidation Annual Report 2013-14 Purpose of Document: To provide the Board with a report on the first year s experience with medical revalidation in Public Health Wales. Board/Committee to-
National Inpatient Survey. Director of Nursing and Quality
 Reporting to: Title Sponsoring Director Trust Board National Inpatient Survey Director of Nursing and Quality Paper 6 Author(s) Sarah Bloomfield, Director of Nursing and Quality, Sally Allen, Clinical
Reporting to: Title Sponsoring Director Trust Board National Inpatient Survey Director of Nursing and Quality Paper 6 Author(s) Sarah Bloomfield, Director of Nursing and Quality, Sally Allen, Clinical
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
CQC say our staff give OUTSTANDING care!
 CQC SPECIAL Issue 513 14 February 2017 CQC say our staff give OUTSTANDING care! As you will hopefully know by now, the reports from the latest Care Quality Commission (CQC) inspection that took place in
CQC SPECIAL Issue 513 14 February 2017 CQC say our staff give OUTSTANDING care! As you will hopefully know by now, the reports from the latest Care Quality Commission (CQC) inspection that took place in
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Better Healthcare in Bucks Reconfiguring acute services
 service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
Safeguarding review to assist Walsall Healthcare NHS Trust
 [Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
[Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
Delivering a choice of four providers: A practical implementation guide for PCTs. October 2005
 Delivering a choice of four providers: A practical implementation guide for PCTs October 2005 DH information reader box Policy HR / Workforce Management Planning Clinical Estates Performance IM & T Finance
Delivering a choice of four providers: A practical implementation guide for PCTs October 2005 DH information reader box Policy HR / Workforce Management Planning Clinical Estates Performance IM & T Finance
Introduction by Lindsey Barker Medical Director
 Contents Introduction by Lindsey Barker... 1 Trust headlines... 2 Elective orthopaedic unit has wow factor!... 2 New trust chairman Graham Sims started on 24 August... 3 RBFT ranked in top 100 NHS places
Contents Introduction by Lindsey Barker... 1 Trust headlines... 2 Elective orthopaedic unit has wow factor!... 2 New trust chairman Graham Sims started on 24 August... 3 RBFT ranked in top 100 NHS places
JOB DESCRIPTION. Head Nurse for Inpatient Services
 JOB DESCRIPTION POST: GRADE: ACCOUNTABLE TO: RESPONSIBLE TO: BASE: DBS CHECK: Head Nurse for Inpatient Services Band 8a Chief Executive Officer Director of Clinical Services Helen and Douglas House Enhanced
JOB DESCRIPTION POST: GRADE: ACCOUNTABLE TO: RESPONSIBLE TO: BASE: DBS CHECK: Head Nurse for Inpatient Services Band 8a Chief Executive Officer Director of Clinical Services Helen and Douglas House Enhanced
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Nightingales Home Care
 Nightingale's Care (Gloucester) Limited Nightingales Home Care Inspection report Unit C1, Spinnaker House Spinnaker Road, Hempsted Gloucester Gloucestershire GL2 5FD Tel: 01452310314 Website: www.homecare.nightingales.co.uk
Nightingale's Care (Gloucester) Limited Nightingales Home Care Inspection report Unit C1, Spinnaker House Spinnaker Road, Hempsted Gloucester Gloucestershire GL2 5FD Tel: 01452310314 Website: www.homecare.nightingales.co.uk
Visiting Professional Programme: Paediatric ICU
 Visiting Professional Programme: Paediatric ICU 1 Introduction The Guy s and St Thomas NHS Foundation Trust Paediatric ICU Visiting Professional Programme (VPP) is designed to provide international visiting
Visiting Professional Programme: Paediatric ICU 1 Introduction The Guy s and St Thomas NHS Foundation Trust Paediatric ICU Visiting Professional Programme (VPP) is designed to provide international visiting
Stairways. Harpenden Mencap. Overall rating for this service. Inspection report. Ratings. Good
 Harpenden Mencap Stairways Inspection report 19 Douglas Road Harpenden Hertfordshire AL5 2EN Tel: 01582460055 Website: www.harpendenmencap.org.uk Date of inspection visit: 12 January 2016 Date of publication:
Harpenden Mencap Stairways Inspection report 19 Douglas Road Harpenden Hertfordshire AL5 2EN Tel: 01582460055 Website: www.harpendenmencap.org.uk Date of inspection visit: 12 January 2016 Date of publication:
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST BOARD OF DIRECTORS. Emergency Department Progress Report
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST Date of meeting: 27 June Title / Subject: Status Purpose: Report of: Prepared by: BOARD OF DIRECTORS Public To update the Board of actions being
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST Date of meeting: 27 June Title / Subject: Status Purpose: Report of: Prepared by: BOARD OF DIRECTORS Public To update the Board of actions being
NHS CONSTITUTION (MARCH 2013) RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC
 RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC") NHS CONSTITUTION (MARCH 2013) RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC APPENDIX A Access to Health Services o Receive NHS services free of charge, apart from certain limited exceptions sanctioned
NHS CONSTITUTION (MARCH 2013) RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC APPENDIX A Access to Health Services o Receive NHS services free of charge, apart from certain limited exceptions sanctioned
Quality Assurance Committee Annual Report April 2017 March 2018
 Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
West Hertfordshire Hospitals NHS Trust. Operational Plan 2016/17. Summary
 West Hertfordshire Hospitals NHS Trust Operational Plan 2016/17 Summary 22 August 2016 Contents 1. Introduction........................... 3 2. Your Care, Your Future and WHHT clinical and organisational
West Hertfordshire Hospitals NHS Trust Operational Plan 2016/17 Summary 22 August 2016 Contents 1. Introduction........................... 3 2. Your Care, Your Future and WHHT clinical and organisational
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT
 EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT Agenda Item No. 7 23 rd January 2008 1. Christmas Day Visit From Mayor of Stevenage and General Secretary, Royal College of Nursing Alison
EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT Agenda Item No. 7 23 rd January 2008 1. Christmas Day Visit From Mayor of Stevenage and General Secretary, Royal College of Nursing Alison
Radis Community Care (Nottingham)
") G P Homecare Limited Radis Community Care (Nottingham) Inspection report 12A Chilwell Road Beeston Nottingham Nottinghamshire NG9 1EJ Date of inspection visit: 08 August 2017 Date of publication: 14 September
G P Homecare Limited Radis Community Care (Nottingham) Inspection report 12A Chilwell Road Beeston Nottingham Nottinghamshire NG9 1EJ Date of inspection visit: 08 August 2017 Date of publication: 14 September
Maidstone and Tunbridge Wells NHS Trust
 Maidstone and Tunbridge Wells NHS Trust Quality report Tonbridge Road Pembury Tunbridge Wells Kent TN2 4QJ Tel: 01892 823535 www.mtw.nhs.uk Date of inspection visit: 14-16 October 2014 Date of publication:
Maidstone and Tunbridge Wells NHS Trust Quality report Tonbridge Road Pembury Tunbridge Wells Kent TN2 4QJ Tel: 01892 823535 www.mtw.nhs.uk Date of inspection visit: 14-16 October 2014 Date of publication:
How CQC monitors, inspects and regulates NHS trusts. June 2017
 How CQC monitors, inspects and regulates NHS trusts June 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor and inspect NHS trusts... 2 CQC Insight... 2 Provider information request...
How CQC monitors, inspects and regulates NHS trusts June 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor and inspect NHS trusts... 2 CQC Insight... 2 Provider information request...
Trust Board Meeting 05 May 2016
 Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Public Services Reform (Scotland) Bill. Scottish Independent Hospitals Association
 Bill. Scottish Independent Hospitals Association") Public Services Reform (Scotland) Bill Scottish Independent Hospitals Association The following submission is presented to the Health and Sport Committee of the Scottish Government as an outline of the
Public Services Reform (Scotland) Bill Scottish Independent Hospitals Association The following submission is presented to the Health and Sport Committee of the Scottish Government as an outline of the
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Barnet Health Overview and Scrutiny Committee 6 October 2016
 Barnet Health Overview and Scrutiny Committee 6 October 2016 Title Health Tourism Report of Wards Status Urgent Key Enclosures Officer Contact Details Barnet Clinical Commissioning Group All Public No
Barnet Health Overview and Scrutiny Committee 6 October 2016 Title Health Tourism Report of Wards Status Urgent Key Enclosures Officer Contact Details Barnet Clinical Commissioning Group All Public No
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Annual Complaints Report 2017/2018
 . Annual Complaints Report 2017/2018 CCG Information Reader Box Document Purpose CCG Website Link Title Author For information www.easterncheshireccg.nhs.uk NHS Eastern Cheshire Clinical Commissioning
. Annual Complaints Report 2017/2018 CCG Information Reader Box Document Purpose CCG Website Link Title Author For information www.easterncheshireccg.nhs.uk NHS Eastern Cheshire Clinical Commissioning
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST. PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control
 Documentation Control") NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
COMMON GROUND EAST REGION. DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing
 COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National