Mesosystems and pathways: Idealized design
|
|
|
- Gertrude Lynch
- 6 years ago
- Views:
Transcription
1 L14 These presenters have nothing to disclose Mesosystems and pathways: Idealized design Marjorie Godfrey PhD, MS, MSN Co-Director The Dartmouth Institute Microsystem Academy Tom Downes MB BS, MRCP, MBA, MPH (Harvard) Consultant Physician Clinical Lead for Quality Improvement Sheffield Teaching Hospitals NHS Foundation Trust, UK Institute for Healthcare Improvement Fellow 13:00 8 th December 2013 Activity P2 Please form a line in rank order of distance travelled to the Forum 1
2 Activity P3 Please form a line in rank order of distance travelled to the Forum Introduce yourself with: Name Place of work Role Expectation of the day Description Organizations are becoming more and more aware of the need to improve, coordinate, and design mesosystems of care that is, two or more microsystems and patient pathways. We will explore acquiring the essential skills of assessment, creating community, leveraging relationships across the organization, and developing leadership. 2
3 Objectives Identify and assess one mesosystem of care Practice designing and using the central data room to drive innovation and the monitoring of improvement Design an individual action-plan to assess, redesign, and monitor a mesosystem in your organization Agenda 1:00 Welcome, introductions & overview Margie 1:15 Charlotte story - What does Charlotte need? Table buzzing Tom 1:45 Define mesosystems and relationships - Improvement within the micro/meso/macro frame Margie - Participants identify a mesosystem 2:15 Key tools and processes to support redesign and continuous improvement Margie 2:30 Break 2:45 Oobeya Case Study Tom 3:15 Table teams work through case study using tools All in pairs 4:00 Report outs including how to apply in own setting All 4:20 Summary and lesson learned Tom + 4:30 Adjourn Margie 3
4 Healthcare inflation 4.3% per year over the last 30 years Driven by technology and expectation Only 0.4% attributable to ageing Need to deliver over 20% more care in 5 years time Need to deliver over 50% more care in 10 years time UNSUSTAINABLE Rises in healthcare spending: where will it end? Jon Appleby, BMJ 1 st November 2012 CHARLOTTE 4

5 High-Value Health Care Organizations SPECIFICATION AND PLANNING criteria-based decision making operationally and clinically INFRASTRUCTURE DESIGN match populations and pathways, involve staff and patient in outcomes reporting MEASUREMENT AND OVERSIGHT For process control and performance management CONFIDENTIAL - Internal Use Only SELF-STUDY Examine positive and negative deviance in care and outcomes Systems It is the nature of systems that smaller systems are embedded in bigger systems Selfcare system Systems Inside Systems Market / Geopolitical system Macrosystem Individual care-giver & patient system Microsystem Mesosystem
6 Systems Inside Systems Self-care system Market / Geopolitical system Macrosystem Individual care-giver & patient system Microsystem Mesosystem 11 Microsystems Every system is perfectly designed to get the results it gets Paul Batalden Smallest replicable unit in health care. Intersections between patients, families, health care professionals, technology, information Shared aim with process and business outcomes 6
7 Microsystems Are The Building Blocks That Come Together To Form Mesosystems & Macroorganizations The health system can be no better than the small systems 13 Transformation Equation Q HS = Q M1 + Q M2 + Q M3 + Q MN Note: Quality (Q) of the whole healthcare system (HS) is equal to the quality of care for individual patients within each microsystem (M 1 to M N ) that cares for the patient plus the handoffs -- of patients, information, and supporting services -- that occur between microsystems (+, +, +) that are involved in the care of each individual patient 7
8 It is easy to view the entire health care continuum as an elaborate network of microsystems that work together (more or less) to reduce the burden of illness for populations of people. Nelson, Splaine, Godfrey, et al, JQI, Dec When you put on your microsystem glasses Complexity of Care Delivery Pt & family voices Pt & family voices ED Cath Lab CCU Rehab 1-N 1-N T 1 T 2 Within, Between and Across Clinical Microsystems (Transitions and Handoffs) 8
9 Pt & family voices The Big Picture: Inverted Pyramid Q m1 + Q m2 + Q m3 + Q m4 = Q HS Pt & family voices ED Cath Lab CCU Patient & Family Voices Rehab 1-N 1-N T 1 T 2 A B C D E F Evidence Base Quality Metrics IOM - Chasm NQF - Metrics IHI 100K Local Competition Pay for Performance JCAHO, CMS, NCQA 2005, Trustees of Dartmouth College, Nelson, January IHI Whole System Metrics 9
10 Mesosystems Connect microsystems Surround microsystems Help or hinder microsystems in their work Mesosystems Mesosystem members are part of a community and have relationships and activities which frequently are not recognized, revealed, studied, discussed or improved but that might change with value based systems 10
11 Mesosystem Community The individual microsystems operate in ways that make or break the mesosystem as it attempts to provide high value care to individual patients and to clinical populations Share vision and mission? Good hand offs and transitions? Feed forward and feedback of information? Create a memory of patients and families? Regular communications and improvement? Schedule time to discuss and improve care across the mesosystem? Value stream design and patient & family centered co-design Mesosystems & Transitions Patient Pathways Phases of care Steps of care Hand Offs Feed Forward & Feedback Information Flow Memory 11


12 Cooperation, Collaboration Understanding the system Everything depends on each other Addressing technical issues is necessary but not sufficient We ve been doing process improvement for several years, and we think we re on the right track. But we ve tried a number of tools for process improvement, and they just don t address the relationship issues that are holding us back. -- CMO, Tenet Healthcare Systems 12
13 Group Health Cooperative People got better at performing their own tasks, but when they had to go beyond and connect with each other in response to an unexpected event or patient need, it didn t work as well. -Rob Reid, Medical Director, Primary Care Meso and Microsystems Microsystems w/in Mesosystem Tool: LEAN Efficient Mesosystem Owner/Leader (Authority Respected) Coach^ Pts with Needs Esther Outcomes Function Cost Satisfaction Clear Measurement Tracking * Each Microsystem Leader pair engaged activation must be enlightened MS Leadership Effective Reliable Role Optimization 13
14 Your Checklist 1. Get organized 1. Identify your population or pathway 2. Identify the mesosystem community 3. Consider the Big Room/Oobeyea Room 2. With the community, review data, map the patient journey 3. Value Stream Map 4. Identify key process and outcome measures 5. Through the eyes of the patients 6. Identify transitions & handoffs 7. Identify WASTE 8. Assess relationships through Mapping 9. Identify improvements to test, reflect, improve and repeat Just The Facts Subpopulation or Pathway Profile Demographics Remember the 5Ps..Focus on deep patient knowledge One page Just the Facts about your population Purpose Patients Professionals Processes Patterns (including relationships & communication) 14
15 Process Assessment Tools Just the Facts Mesosystem Assessment Workbook Clinical Value Compass Create Esther George or Charlotte Stopwatch & Pedometer Value Stream Mapping Tool/Cycle Time Spaghetti Diagram Tool 5 Whys Transitions and Handoffs Mesosystem Workbook Mesosystem Assessment Workbook The principal task of the mesosystem is to Enable the work of the microsystems for the population(s) of patients involved. ~ Paul Batalden Aim: 1.Assess and think about the mesosystem and the microsystems that form the mesosystem to gain insight of the between activities and processes where hand offs occur and identify processes and systems to improve the mesosystem to provide a smooth safe patient care journey. (one microsystem at a time) 2.Review what the mesosystem itself is doing to foster/develop the leadership and performance of the microsystem(s) to achieve a safe, effective, and smooth patient care experience. 3.Identify, recognize and enhance mesosystem community and relationships. 15
16 What is a Value Stream Map? A visual tool to show work flow and information flow/data, using: process time, wait time, lead time, and first time quality as system metrics. Why use a VSM? To open our eyes to existing problems, issues, and waste To identify shortfalls and process breakdowns, and to identify opportunities for improvement. PURPOSE: Visualize the work Build team consensus & perspective Point to problems Focus direction 16
17 Goals of VSM Focus on value for the patient/customer Simple & clear forms of communication Reduce waste Instill quality at each step Align resources to meet demands Improve flow of patients, information, etc. Empower staff to make continual improvements Caregivers have what they need when they need it Increase interdisciplinary understanding of the roles each team member plays Who s Involved? Need perspectives from people involved in the process from start to end Your Lead Improvement Team and any additional resources related to the selected process 17
18 Value Stream Map Process Adapted for Microsystems** 1. Clarify specific aim (from global aim & high-level flowchart) 2. Create Value Stream Map of CURRENT State** Include flow of information, documents, supplies, etc Identify customer at each step Include step data as possible 3. Perform observational walk Note customer/supplier & hand offs Measure time of each step and total cycle time of process 4. Design LEAN/improved process FUTURE State Determine delivery and quality requirements ** Review Value Stream Mapping Worksheet Quantifying the VSM Each step in the VSM will have specific information noted for it; cycle time, touch time, % value added, etc. This allows the team to assess the opportunities with each step: Increase % value added Decrease the difference between the cycle time and touch time Defining these measures. 18
19 Value Stream Map Data Sheets Name of Step INVENTORY WIP just before this step WIP on hand T-T TOUCH TIME # People Special Considerations C-T CYCLE TIME V-A VALUE ADDED C-O CHANGE OVER U-T UP TIME FPY FIRST PASS YIELD NOTES Orange used for Current state, Green for Future Value Stream Map Data Sheets Name of Step or Process Identify each step in the process you are analyzing Be sure to note concurrent processes or steps if they affect the flow of people or activities Process for handling inpatients vs. outpatients Don t overlook key documents or information that s required for each step 19


20 Value Stream Map Example 20
 Sent Location- Method-")

21 Transitions & Hand Offs Received Location- Method- Freq/24 hours (mesosystem) Sent Location- Method- Freq/24 hours MICROSYSTEM Most Frequent Received: Sent: Improvement Opportunities: Spaghetti Chart 42 21
22 Spaghetti Diagram movement path diagram a great waste observation tool even for people taking their very first steps pick up a pencil find a process to observe and you are ready to begin Spaghetti Diagram trace the movement of the person working within the process you are observing, just they way they are moving question the need for every strand solicit ideas from the people in the area do kaizen (improvement) and draw another spaghetti diagram ~ compare 22

23 Efficient Optimization of Roles Complete the Activity Tool 23
24 Create your Esther or Charlotte or George Review data and process Complete Through the Eyes Evidence Based What is the evidence? What is the best practice?? Benchmarking 24
25 Benchmarking Functional Status and Quality of Life Clinical Status Mortality: M = 0.7% D = 6.5% Satisfaction against Need Bowel Surgery Value Compass Costs Charges: M = $13,000 D = $35,000 LOS: M = 9 days D = 17 days Bowel Surgery: Functional Biological Mortality 0% vs 0% Costs 30 Day Re-admit 22% vs 4 % LOS 10.0 vs 6.6 Satisfaction Patient Satisfaction 83% vs 94% 25
26 c - 12/11/2013 The Clinical Value Compass Physical Mental Social/Role Risk Status Perceived Well-being Functional Health Status Biological Status Mortality Morbidity Costs Direct Medical Indirect Social Satisfaction Against Need Health Care Delivery Perceived Health Benefit 51 Your Checklist 1. Get organized 1. Identify your population or pathway 2. Identify the mesosystem community 3. Consider the Big Room/Oobeyea Room 2. With the community, review data, map the patient journey 3. Value Stream Map 4. Identify key process and outcome measures 5. Through the eyes of the patients 6. Identify transitions & handoffs 7. Identify WASTE 8. Assess relationships through Mapping 9. Identify improvements to test, reflect, improve and repeat 52 26
27 Relational Coordination. Findings Relationships shape the communication through which coordination occurs... Jody Hoffer-Gittell, PhD For better... Shared goals Shared knowledge Mutual respect Frequent communication Timely communication Problem-solving communication 27
28 Or worse Functional goals Specialized knowledge Lack of respect Infrequent communication Delayed communication Finger-pointing Institute of Medicine report The current system shows too little cooperation and teamwork. Instead, each discipline and type of organization tends to defend its authority at the expense of the total system s function. (2003) 28
29 Physicians and nurses recognize the problem The communication line just wasn t there. We thought it was, but it wasn t. We talk to nurses every day but we aren t really communicating. Miscommunication between the physician and the nurse is common because so many things are happening so quickly. But because patients are in and out so quickly, it s even more important to communicate well. Why does relational coordination matter? Relationships of shared goals, shared knowledge and mutual respect Help staff focus on the patient and provide an organizational culture that supports process improvement 29
30 Relational coordination: Connecting workers around the patient Nurses Case Managers Attending Physicians Nursing Assistants Patient and family Physical Therapists Social Workers Technicians Referring Physicians Administrators When does relational coordination matter most? Task interdependence What you do affects my ability to do my job, and vice versa Uncertainty, unpredictability We can t know everything we need to know Time constraints We can t waste time 30
31 Select for teamwork You can be the best social worker in the world, but if you can t work with the other disciplines, then you can t work here. Some are very good diagnostically. But it s the communication skills [we are looking for]. Measure team performance We have a Bone Team which includes the service line director, the case management supervisor, the head of rehab, the VP for nursing, the nurse manager, the clinical specialist, three social workers and three case managers. We generally look at system problems. 31
32 Resolve conflicts proactively We have a staff council that s largely responsible for information sharing among the departments. The staff council deals with medical policy and conflict resolution.... It s an informal body to air differences. It s more for problem solving. We have monthly meetings that are attended by all medical staff, including physicians, nursing, and social work. Make job boundaries flexible It s a question of what you d rather defend. That you did nothing, or that you tried to help, even if you may have gone beyond your licensing. I tell my nurses I d rather defend them doing too much than not enough. 32
33 Develop shared information systems Information systems are important for coordination, I think, but right now they are more a hope than a reality. Our chief information officer is building a clinical and administrative information system allowing patients to receive care anywhere across the continuum But for automation to work, it s important to get a format that s understood across all specialists. Measuring, mapping and improving relational coordination 33
34 Mapping relational coordination Work Group 1 Work Group 5 Client Work Group 2 Work Group 4 Work Group 3 Measuring relational coordination RC dimensions 1. Frequent communication 2. Timely communication 3. Accurate communication 4. Problem solving communication Survey questions How frequently do people in each of these groups communicate with you about [focal work process]? How timely is their communication with you about [focal work process]? How accurate is their communication with you about [focal work process]? When there is a problem in [focal work process], do people in these groups blame others or try to solve the problem? 5. Shared goals How much do people in these groups share your goals for [focal work process]? 6. Shared knowledge How much do people in these groups know about the work you do with [focal work process]? 7. Mutual respect How much do people in these groups respect the work you do with [focal work process]? 34
35 A Relational Model of Organizational Change Gittell, Edmondson & Schein, 2011 Structural Intervention Selection Training Conflict resolution Performance measures Rewards Meetings Boundary spanners Protocols Information systems Executive leadership Relational Intervention Psychological safety Relationship mapping Coaching/role modeling Relational Coordination Shared goals Shared knowledge Mutual respect Frequent communication Timely communication Accurate communication Problem-solving comm Mid-level leadership Work Process Intervention Process mapping Goal and role clarification Structured problem solving Performance Outcomes Quality Efficiency Worker well-being Front line leadership Summary High value organizations Specification and Planning Infrastructure Design Measurement & Oversight Self Study It s about the Patient And microsystems, mesosystems & macrosystems Relational Coordination Shared Goals Shared Knowledge Mutual Respect 35

36 A complex system problem 36


37 TOYOTA 37


38 2003 Toyota Corolla How do others design complex systems? Toyota Oobeya (Big Room) 38



39 First find a room A place to meet 39


40 The Big Room in Action Service Improvement GSM Matron General Manager For Medicine Discharge Liaison Physiotherapist Secretary Community Services manager Social Services Manager Senior registrar Physiotherapist gives an account of the test of change to get a patient home on the day they were discharged by the GSM consultant Improvement in health care is 20% technical and 80% human Marjorie Godfrey The Dartmouth Institute 40








41 PDSA tests of moving from post take to on take Let me introduce George 82 years old Lives independently and wants to continue doing so Widowed 5 years ago Has mild dementia Daughter lives locally Losing weight + poor mobility 41
42 Learning Your Way To Greatness No team can design a perfect system in advance, planning for every contingency and nuance. However,, people can discover great systems and keep discovering how to make them better. Idiosyncratic confluences and coincidences of people, processes, products, places and circumstances could create a hazardous situation where none had been known to exist. Dr. Steve Spear, The High Velocity Edge Implementation dates: April 2012 Consultant geriatricians on take 7 days per week May 2012 Frailty Unit process initially virtually Frailty Unit opens mid-may 42
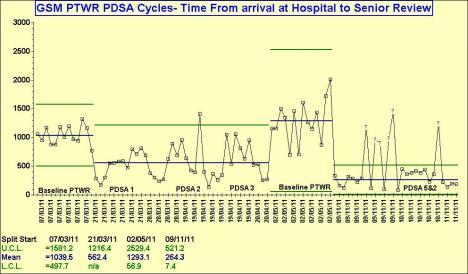
43 Outcome measure: 34% increase in discharge within 1 day Outcome measure: Bed occupancy reduced by over 60 beds 43
44 Was reduction in bed usage due to reduced admissions? No Balance measure: No increase in readmissions 44
45 Balance measure: Decreased mortality Discharge to Assess The future hospital will support a system of discharge to assess in physiotherapy and occupational therapy. Section 5.20 Future Hospital Report, Royal College of Physicians (September 2013) 45
46 Implementation dates: April 2012 Consultant geriatricians on take 7 days per week May 2012 Frailty Unit process initially virtually Frailty Unit opens mid-may September 2013 Testing of discharge to assess from base wards October 2013 Implementation of discharge to assess begins Weekly discharge count 46


47 Time waiting per pt 47
48 Thank you 48
IMPROVING QUALITY AND SAFETY WHERE PATIENTS, FAMILIES, AND CARE TEAMS MEET THE CLINICAL MICROSYSTEM
 IMPROVING QUALITY AND SAFETY WHERE PATIENTS, FAMILIES, AND CARE TEAMS MEET THE CLINICAL MICROSYSTEM Gautham Suresh, MD, MS Associate Professor of Pediatrics and Community & Family Medicine Medical Director,
IMPROVING QUALITY AND SAFETY WHERE PATIENTS, FAMILIES, AND CARE TEAMS MEET THE CLINICAL MICROSYSTEM Gautham Suresh, MD, MS Associate Professor of Pediatrics and Community & Family Medicine Medical Director,
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Continuous Value Improvement in Health Care
 webinar summary Continuous Value Improvement in Health Care Featuring Kedar Mate Chief Innovation and Education Officer Institute for Healthcare Improvement October 26, 2017 sponsored by webinar summary
webinar summary Continuous Value Improvement in Health Care Featuring Kedar Mate Chief Innovation and Education Officer Institute for Healthcare Improvement October 26, 2017 sponsored by webinar summary
Session 183, March 7, 2018 Sue Murphy, RN, BSN, MS, Chief Experience Officer, UChicago Medicine
 Chief Experience Officer: The New Leader Driving Innovation to Transform Healthcare for Patients, Families and Care Teams Session 183, March 7, 2018 Sue Murphy, RN, BSN, MS, Chief Experience Officer, UChicago
Chief Experience Officer: The New Leader Driving Innovation to Transform Healthcare for Patients, Families and Care Teams Session 183, March 7, 2018 Sue Murphy, RN, BSN, MS, Chief Experience Officer, UChicago
Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology
 Prepared for the Foundation of the American College of Healthcare Executives Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology Presented by: Sue Murphy Alison
Prepared for the Foundation of the American College of Healthcare Executives Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology Presented by: Sue Murphy Alison
Leadership for Transforming Health Care
 Presenters have nothing to disclose. Leadership for Transforming Health Care Partnerships with Patients and Families Barbara Balik, RN, EdD Kris White, RN, MBA November 4, 2014 This presenter has nothing
Presenters have nothing to disclose. Leadership for Transforming Health Care Partnerships with Patients and Families Barbara Balik, RN, EdD Kris White, RN, MBA November 4, 2014 This presenter has nothing
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Flow Coaching Academy programme
 Flow Coaching Academy programme Professor Tom Downes, MB BS, MRCP, MBA, MPH (Harvard) Clinical Lead for Quality Improvement Sheffield Teaching Hospitals Health Foundation / IHI QI Fellow 6 th July 2018
Flow Coaching Academy programme Professor Tom Downes, MB BS, MRCP, MBA, MPH (Harvard) Clinical Lead for Quality Improvement Sheffield Teaching Hospitals Health Foundation / IHI QI Fellow 6 th July 2018
Increased situational awareness to reduce undetected deterioration
 Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
Basic Knowledge of Clinical Microsystems. Success Characteristics of Great Clinical Microsystems Developing Microsystems
 Basic Knowledge of Clinical Microsystems Success Characteristics of Great Clinical Microsystems Developing Microsystems Marjorie M. Godfrey, PhD, MS, BSN Co-Director, The Dartmouth Institute Microsystem
Basic Knowledge of Clinical Microsystems Success Characteristics of Great Clinical Microsystems Developing Microsystems Marjorie M. Godfrey, PhD, MS, BSN Co-Director, The Dartmouth Institute Microsystem
Product and Network Innovation: Strategies to Achieve Triple Aim Success. Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013
 Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Creating a Lean Culture in Healthcare
 Creating a Lean Culture in Healthcare 0 Building Leaders Transforming Hospitals Improving Care 45 Years of Delivering Results 1 1 HealthTechS3 is a 45 year old, award-winning healthcare consulting and
Creating a Lean Culture in Healthcare 0 Building Leaders Transforming Hospitals Improving Care 45 Years of Delivering Results 1 1 HealthTechS3 is a 45 year old, award-winning healthcare consulting and
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Delivering Great Care with High Reliability The Orlando Health Journey
 FE5 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 11, 2017 Frank Federico, RPh Vice President Patricia McGaffigan, RN, MS, CPPS
FE5 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 11, 2017 Frank Federico, RPh Vice President Patricia McGaffigan, RN, MS, CPPS
Relational Coordination, Relational Leadership and the Transformation of Nursing. Tuesday, April 10 th, 2012
 Relational Coordination, Relational Leadership and the Transformation of Nursing Tuesday, April 10 th, 2012 1 Adobe Connect Reminders WELCOME! PLEASE MUTE YOUR COMPUTER Under System Preferences, click
Relational Coordination, Relational Leadership and the Transformation of Nursing Tuesday, April 10 th, 2012 1 Adobe Connect Reminders WELCOME! PLEASE MUTE YOUR COMPUTER Under System Preferences, click
Organization Review Process Guide Perinatal Care Certification
 Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management
 Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship
 Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care?
 Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
South Warwickshire s Whole System Approach Transforms Emergency Care. South Warwickshire NHS Foundation Trust
 South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
Are National Indicators Useful for Improvement Work? Exercises & Worksheets
 Session L5 These presenters have nothing to disclose These presenters have nothing to disclose Are National Indicators Useful for Improvement Work? Exercises & Worksheets Robert Lloyd, PhD Göran Henriks,
Session L5 These presenters have nothing to disclose These presenters have nothing to disclose Are National Indicators Useful for Improvement Work? Exercises & Worksheets Robert Lloyd, PhD Göran Henriks,
Operational Excellence at Lifespan. Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence
 Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
A Framework for Quality Improvement
 U019 - Integrating QI into the Derm Practice A Framework for Quality Improvement Margo Reeder, MD Assistant Professor Director of Quality Improvement UWSMPH July 30 2016 Quality is increasingly part of
U019 - Integrating QI into the Derm Practice A Framework for Quality Improvement Margo Reeder, MD Assistant Professor Director of Quality Improvement UWSMPH July 30 2016 Quality is increasingly part of
SFGH Strategic Plan
 SFGH Strategic Plan 2015-2018 Iman Nazeeri Simmons, Chief Operating Officer James Marks, Chief of Medical Staff 1 2 1 SFGH Strategy 2015-2018 3.5 Years of Lean Management Creating value for our patients
SFGH Strategic Plan 2015-2018 Iman Nazeeri Simmons, Chief Operating Officer James Marks, Chief of Medical Staff 1 2 1 SFGH Strategy 2015-2018 3.5 Years of Lean Management Creating value for our patients
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Leveraging Health Care IT Investment
 Leveraging Health Care IT Investment A Harvard Business Review Webinar featuring David M. Cutler and Robert S. Huckman Sponsored by OVERVIEW In recent years, health care organizations have made massive
Leveraging Health Care IT Investment A Harvard Business Review Webinar featuring David M. Cutler and Robert S. Huckman Sponsored by OVERVIEW In recent years, health care organizations have made massive
PERIOPERATIVE CONSULTING SERVICES
 SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
Delivering Great Care with High Reliability
 FE4 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 5, 2016 Joelle Baehrend, MA Director, Institute of Healthcare Improvement 1
FE4 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 5, 2016 Joelle Baehrend, MA Director, Institute of Healthcare Improvement 1
Leadership. David Dalton Chief Executive
 Leadership David Dalton Chief Executive Effective Modern Leadership Leaders at all levels are crucial in creating the culture of care and compassion in the NHS. Today s effective leaders in the NHS demonstrate
Leadership David Dalton Chief Executive Effective Modern Leadership Leaders at all levels are crucial in creating the culture of care and compassion in the NHS. Today s effective leaders in the NHS demonstrate
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Engaging Frontline Staff in Real-Time Improvement
 Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 Holland Bloorview Kids Rehabilitation Hospital 1 Overview Holland Bloorview continues to lead pediatric rehabilitation
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 Holland Bloorview Kids Rehabilitation Hospital 1 Overview Holland Bloorview continues to lead pediatric rehabilitation
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
What inspires your life can transform your career.
 OptumCare represents the thinking and innovation that the world has come to expect from our industry shaping team. It will provide you with the support services you need to thrive in a changing health
OptumCare represents the thinking and innovation that the world has come to expect from our industry shaping team. It will provide you with the support services you need to thrive in a changing health
HOW TO GET STARTED
 0.01 BUNDLING AND VALUE BASED CARE: Tony DiGioia, MD and Gigi Crowley HOW TO GET STARTED TONY@PFCUSA.ORG DEC 12 2017 40 Minutes 0.02 The existing deficiencies in health care cannot be corrected simply
0.01 BUNDLING AND VALUE BASED CARE: Tony DiGioia, MD and Gigi Crowley HOW TO GET STARTED TONY@PFCUSA.ORG DEC 12 2017 40 Minutes 0.02 The existing deficiencies in health care cannot be corrected simply
Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes
 Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes Sue Murphy, RN BSN MS Chief Experience Officer Becker's 3rd Annual Health IT + Revenue Cycle 2017 1
Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes Sue Murphy, RN BSN MS Chief Experience Officer Becker's 3rd Annual Health IT + Revenue Cycle 2017 1
Aclinical nurse leader (CNL) is an advanced generalist
 is an advanced generalist") Professional Issues Veronica Rankin Clinical Nurse Leader: A Role for the 21st Century Aclinical nurse leader (CNL) is an advanced generalist prepared at the master s degree level to oversee the lateral
Professional Issues Veronica Rankin Clinical Nurse Leader: A Role for the 21st Century Aclinical nurse leader (CNL) is an advanced generalist prepared at the master s degree level to oversee the lateral
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION
 UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
HealthPartners and the Triple Aim. IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners
 HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
Accountable Care: Clinical Integration is the Foundation
 Solutions for Value-Based Care Accountable Care: Clinical Integration is the Foundation CLINICAL INTEGRATION CARE COORDINATION ACO INFORMATION TECHNOLOGY FINANCIAL MANAGEMENT The Accountable Care Organization
Solutions for Value-Based Care Accountable Care: Clinical Integration is the Foundation CLINICAL INTEGRATION CARE COORDINATION ACO INFORMATION TECHNOLOGY FINANCIAL MANAGEMENT The Accountable Care Organization
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management
 The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
These Things (Don t Have to) Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013
 Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013") These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
Creating a Culture in Support of Patient Safety
 Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust Tel
 Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Leadership for Quality A Strategy for Marketplace Success. Requirements for Transformation. Typical State of Shared Vision. It All Starts With Urgency
 Virginia Mason Medical Center Leadership for Quality A Strategy for Marketplace Success Estes Park Institute January 2012 Gary S. Kaplan, MD, Chairman and CEO Virginia Mason Medical Center Seattle, Washington
Virginia Mason Medical Center Leadership for Quality A Strategy for Marketplace Success Estes Park Institute January 2012 Gary S. Kaplan, MD, Chairman and CEO Virginia Mason Medical Center Seattle, Washington
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
UPMC Passavant POLICY MANUAL
 UPMC Passavant POLICY MANUAL SUBJECT: Organizational Plan, Patient Care Services POLICY: 200.142 DATE: November 2015 INDEX TITLE: Nursing MISSION: Patient Care Services at UPMC Passavant is integral to
UPMC Passavant POLICY MANUAL SUBJECT: Organizational Plan, Patient Care Services POLICY: 200.142 DATE: November 2015 INDEX TITLE: Nursing MISSION: Patient Care Services at UPMC Passavant is integral to
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Quality Improvement in Health and Social Care
 Some Fundamentals on Quality Improvement in Health and Social Care Towards a Shared Understanding EPSO, Reykjavik, 2017-09-26 Johan Thor, MD, MPH, PhD Associate Professor E-mail: johan.thor@ju.se The death
Some Fundamentals on Quality Improvement in Health and Social Care Towards a Shared Understanding EPSO, Reykjavik, 2017-09-26 Johan Thor, MD, MPH, PhD Associate Professor E-mail: johan.thor@ju.se The death
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting
 Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project
 Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
Communication Challenges Overcoming the Barriers to Improve Quality. Presented by: Christy Brinkman LNHA Laura Seleen RN
 Communication Challenges Overcoming the Barriers to Improve Quality Presented by: Christy Brinkman LNHA Laura Seleen RN 6-16-16 Objectives The participant will be able to identify a process to follow to
Communication Challenges Overcoming the Barriers to Improve Quality Presented by: Christy Brinkman LNHA Laura Seleen RN 6-16-16 Objectives The participant will be able to identify a process to follow to
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Creating Exceptional Physician-Nurse Partnerships
 1 Creating Exceptional Physician-Nurse Partnerships Using Collaborative Partnerships to Raise the Standard of Care and Improve the Overall Patient Experience Your Speakers 2 Alan J. Conrad, MD, MMM,CPE,
1 Creating Exceptional Physician-Nurse Partnerships Using Collaborative Partnerships to Raise the Standard of Care and Improve the Overall Patient Experience Your Speakers 2 Alan J. Conrad, MD, MMM,CPE,
Nursing Home Walk of Fame Visiting What Really Works. Call in Number
 Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Pave Your Path: Improvement Science & Helpful Techniques
 Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
Pushing Case Management into the Future: Six Requirements to Drive Clinical and Financial Returns
 Pushing Case Management into the Future: Six Requirements to Drive Clinical and Financial Returns Authors: Loren Mann, Mark Werner, MD and Cynthia Bailey Hospital-based case management (CM) should be a
Pushing Case Management into the Future: Six Requirements to Drive Clinical and Financial Returns Authors: Loren Mann, Mark Werner, MD and Cynthia Bailey Hospital-based case management (CM) should be a
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments
 How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments Aravind Chandrasekaran PhD Peter Ward PhD Fisher College of Business Ohio State University
How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments Aravind Chandrasekaran PhD Peter Ward PhD Fisher College of Business Ohio State University
Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network
 Healthcare Quarterly ONLINE CASE STUDY Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network Jessica Meleskie and Katrina Wilson 1 Abstract The Grey Bruce Health
Healthcare Quarterly ONLINE CASE STUDY Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network Jessica Meleskie and Katrina Wilson 1 Abstract The Grey Bruce Health
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Objectives. Physician Leadership Engagement to Produce System Change
 Physician Leadership Engagement to Produce System Change David Swieskowski, MD, MBA Senior VP & Chief Accountable Care Officer Mercy Medical Center Des Moines, Iowa Objectives Discuss adoption of change
Physician Leadership Engagement to Produce System Change David Swieskowski, MD, MBA Senior VP & Chief Accountable Care Officer Mercy Medical Center Des Moines, Iowa Objectives Discuss adoption of change
Leading Quality Improvement
 June 9, 2015 These presenters have nothing to disclose Leading Quality Improvement Essentials for Managers Session 9: Empower Teams to Engage in Improvement Janet Porter, PhD Kathy Duncan, RN Today s Host
June 9, 2015 These presenters have nothing to disclose Leading Quality Improvement Essentials for Managers Session 9: Empower Teams to Engage in Improvement Janet Porter, PhD Kathy Duncan, RN Today s Host
8/10/2015. Module 1. A Fundamental Understanding of Quality. Management and its Application to Health Care
 Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
H ospital Voice. Oregon Community Hospitals. Lean Methods and Mindsets. The CEO Perspective. Taking Aim at Health Care Reform
 H ospital Voice A magazine for and about Oregon Community Hospitals A magazine for and about Oregon Community Hospitals Taking Aim at Health Care Reform Triple Aim to change health care for good The CEO
H ospital Voice A magazine for and about Oregon Community Hospitals A magazine for and about Oregon Community Hospitals Taking Aim at Health Care Reform Triple Aim to change health care for good The CEO
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Making system wide improvement in health care. Mats Bojestig MD Jönköping County Council, Sweden. When results get public
 Making system wide improvement in health care Mats Bojestig MD Jönköping County Council, Sweden When results get public 1 If people want take responibilty for their care are we with them? Improving clinical
Making system wide improvement in health care Mats Bojestig MD Jönköping County Council, Sweden When results get public 1 If people want take responibilty for their care are we with them? Improving clinical
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Root Cause Analysis LITE (RCA Lite)
") Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Patients and Professionals Partner to Redesign Inpatient Care
 Patients and Professionals Partner to Redesign Inpatient Care Mireille Brosseau Program Lead, Patient and Citizen Engagement Canadian Foundation for Healthcare Improvement (CFHI) Mario DiCarlo Patient
Patients and Professionals Partner to Redesign Inpatient Care Mireille Brosseau Program Lead, Patient and Citizen Engagement Canadian Foundation for Healthcare Improvement (CFHI) Mario DiCarlo Patient
Quality Improvement Plan (QIP): 2015/16 Progress Report
: 2015/16 Progress Report") Quality Improvement Plan (QIP): Progress Report Medication Reconciliation for Outpatient Clinics 1 % complete medication reconciliation on outpatient clinic visit assessments ( %; Pediatric Patients; Fiscal
Quality Improvement Plan (QIP): Progress Report Medication Reconciliation for Outpatient Clinics 1 % complete medication reconciliation on outpatient clinic visit assessments ( %; Pediatric Patients; Fiscal