Technical Assistance Guide. Prescriber Report Cards
|
|
|
- Kellie Barber
- 6 years ago
- Views:
Transcription



1 Technical Assistance Guide Prescriber Report Cards Revised February 17, 2017 This project was supported by Grant No PM-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance is a component of the Office of Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice, the Office of Juvenile Justice and Delinquency Prevention, and the Office for Victims of Crime. Points of view or opinions in this document are those of the author and do not represent the official position or policies of the U.S. Department of Justice. March 15, 2016
2 Table of Contents Introduction... 3 Purpose... 3 Arizona... 4 Background... 4 Program Description... 4 Kentucky... 6 Background... 6 Program Description... 6 Ohio... 7 Background... 7 Program Description... 8 Prescribers Perspective... 9 Comments... 9 Recommendations... 9 Suggested Components of a Model Report Card Data File Generation Report Distribution and Retrieval Report Guidelines Acknowledgements Appendix A Specialty Groups Appendix B Arizona Report Card Sample Appendix C Kentucky Report Card Sample Appendix D Ohio Report Card Sample Appendix E Statistical Formula Examples
3 INTRODUCTION PDMPs play a vital role in reducing and preventing prescription drug abuse and drug overdose. When used intelligently and proactively, a PDMP will have a measurable effect on the efforts to stem the drug abuse epidemic. 1 As a central depository of information on the prescribing and dispensing of controlled substances a major role of the PDMP is making the data available to authorized users. States generally fulfill this role by disseminating PDMP information to authorized users through two kinds of reports commonly referred to as solicited and unsolicited. A solicited report is generated at the direct request of an authorized person in carrying out their professional responsibilities. The majority of solicited reports are initiated by health care providers (physician, dentist, pharmacist, etc.) who make queries to the PDMP in the course of prescribing or dispensing a controlled substance to a patient. In contrast, unsolicited reports are initiated solely by the PDMP and sent to authorized users. Unsolicited reports may be sent to inform a prescriber or dispenser about patients who may be engaged in doctor or pharmacy shopping or who may be at risk of adverse health events. PDMPs also send unsolicited reports to regulatory boards and law enforcement when a PDMP identifies questionable prescribing or dispensing activities. A new kind of report emerging among PDMPs is what we will refer to as a report card. This type of report provides a summary of a healthcare provider s own prescribing history, including their ranking compared to the average prescriber of the same specialty, and a summary or graphical representation of their prescribing history. The report card may also include a condensed description of patient prescription records, risk status, and other clinically relevant information. The use of report cards is a promising practice that not only provides an opportunity for selfexamination of a prescriber s practice as it pertains to their prescribing of controlled substances, but also provides a more efficient method for reviewing patient prescription histories and associated risk. Depending upon the PDMP, a report card may be a solicited report requested by the prescriber or sent as an unsolicited report to a prescriber. This technical assistance guide (TAG) will present examples of both. PURPOSE The Bureau of Justice Assistance (BJA) is interested in continuously advancing and maximizing PDMPs utility and effectiveness. Providing a prescriber with relevant and accurate information can positively influence his or her prescribing of controlled substances. Informing health care professionals of their standing among their peers and providing insightful, concise data summaries of patients meeting risk criteria may also assist them with their treatment decisions. BJA, through the PDMP Training and Technical Assistance Program (TTAP), seeks to support and assist PDMPs who may be interested in initiating a report card program. This guide will provide information about existing report card programs, examples of the reports and the data they include, and suggestions for a model report card. The information for this guide was compiled from interviews with the PDMP Administrators from three (3) states that have implemented a report card program; Arizona, Kentucky, and Ohio. Additionally, four (4) physicians were consulted to get a prescriber s perspective on the utility of the report and what elements should be considered for a model report card (see Acknowledgement section). 1 Office of National Drug Control Policy. Prescription Drug Monitoring Program Fact Sheet. April
4 ARIZONA Background In Arizona, the report card program was initiated by the Arizona Substance Abuse Partnership. The Partnership oversees substance abuse issues in the state and is comprised of representatives from the treatment community, regulatory boards, law enforcement, county coalitions, and local health departments. The Partnership encouraged the Arizona PDMP, which resides in the Board of Pharmacy, to develop the current report card program and suggested that it be piloted in several counties before expanding statewide. The goals of the pilot program were to reduce the number prescriptions issued for controlled substances by 10% and to reduce the overdose death rate by 2-4%. The pilot initially focused in four (4) counties (Yavapai, Pinal, Graham, and Greenlee) which were experiencing significantly high rates of deaths attributed to drug overdoses. One year into the pilot, a fifth county (Mohave) was added. The pilot was initially funded by the Arizona Criminal Justice Commission. Later, the Department of Health Services (DHS) provided additional funding to hire a program manager and a research analyst. The report card program was developed in-house by the Board of Pharmacy utilizing one (1) staff person who was devoted full-time in the development of the program. Although dispensed prescription data is collected and made available to authorized users through a data vendor, this particular report is designed to be generated by the PDMP. The data vendor provides a file containing the previous quarter s prescription data to the PDMP. The PDMP staff compiles, creates, and mails the report card reports to the prescribers. Since the major expense to operate this program is mailing the reports to the prescribers, to save on mailing costs, the program plans to distribute the reports via . Sending the reports via has been made possible by the recent legislation requiring prescribers to obtain a PDMP account and provide their address. If the address is not valid or has changed, the program will contact the prescriber to obtain a current account or the report will be mailed. The Arizona PDMP s staff includes a PDMP Director, Manager, Marketing Coordinator, analyst, and two (2) data entry positions which assist in the promotion of the report card program and increase use of the PDMP. Program Description The report is generated and distributed by the PDMP every quarter and is only sent to prescribers who have issued at least one (1) controlled substance prescription during the previous quarter. Each prescriber receives a report specific to their prescribing history. According to the Drug Enforcement Administration (DEA), Office of Diversion Control, there were approximately 31,000 registrants with authority to prescribe controlled substances in Arizona 2. Approximately 26,000 (84%) prescribers in Arizona receive the reports. Recently, prescribers were given authority to request their own reports. The report card categorizes each prescriber by specialty. The program is using the National Provider Identifier (NPI) file, maintained by the Centers for Medicare and Medicaid Services, to obtain taxonomy codes for each of the specialties. The NPI file has almost 1000 taxonomy codes; however, more than half of them are not related to the prescribing and even fewer related to controlled substance prescribing. To ensure that all specialties were covered, 2 Drug Enforcement Administration, Office of Diversion Control. Registrant Population by State and Business Activity. 4
5 the PDMP worked with the National Council for Prescription Drug Programs (NCPDP) to create a reference table. Their efforts identified 27 major specialties in which all prescribers were placed (see Appendix A). Prescribers who did not have an NPI number were contacted to obtain specialty information. The report card identifies five (5) major drugs: carisoprodol, benzodiazepines, hydrocodone, oxycodone, and other pain relievers. For each of these drug categories, the program counts the number of prescriptions and dosage units for solid, oral forms of these drugs. The report has several graphs showing the average number of prescriptions issued and doses prescribed in a given quarter for a specific prescriber with comparisons to others in the same specialty statewide (see Appendix B) As mentioned above, the report card was piloted within five (5) selected counties. About a year into the pilot project, the program began using standard deviation when comparing the prescription and dosage numbers in addition to the actual numbers of prescriptions and dosage units. The report card categorizes the prescriber s prescribing as follows: NORMAL- values are near the mean HIGH- values are one (1) standard deviation above the mean SEVERE values are two (2) standard deviations above the mean EXTREME- values are three (3) standard deviations above the mean The report also includes: Total number of the prescriber s patients receiving over 100 morphine milligram equivalents (MMEs) Total number of patients to whom the prescriber issued multiple controlled substance prescriptions Total number of patients receiving prescriptions from other prescribers for more than one (1) type of controlled substance Total number patients receiving controlled substances prescriptions from five (5) or more prescribers or visiting five (5) or more pharmacies A letter is sent with the report explaining the program and emphasizing that the purpose is to promote appropriate prescribing for the selected drugs (see Appendix B). A link to the Arizona Opioid Prescribing Guidelines is included as reference. The PDMP has seen evidence that more prescribers are querying the PDMP and have adjusted their prescribing habits. In Pinal County, the percentage of prescribers meeting the outlier criteria for total dosage units fell 26% and prescriber PDMP usage increased 14% in just one year. 3 3 PDMP Center of Excellence, Using PDMP Data to Guide Interventions with Possible At-Risk Prescribers, October
6 KENTUCKY Background Kentucky s interest in report cards began after attending a presentation describing the Arizona program at the 2014 National Data Driven and Multi-Disciplinary Grantees Meeting sponsored by BJA and hosted by TTAP 4. Kentucky originally patterned their program after Arizona s and had several discussions with the Arizona PDMP Administrator. Kentucky s PDMP, known as KASPER, originally intended to include a county-level report which compared a prescriber to other prescribers with similar specialties. However, during discussions with the KASPER Advisory Council and several prescribers in private practice, concerns were raised about the possibility that within counties that have few prescribers, the data could provide a misleading or skewed picture of the actual prescribing patterns. Thus, the report provides comparisons at the state-level and specialty-level. Kentucky s Prescriber Peer Review Report was implemented in December KASPER does all of its programming in-house. The development, testing, and production of the Prescriber Peer Review Report totaled approximately 200 hours and cost approximately $13,000. The entire project took approximately six (6) months to complete; four (4) months researching and obtaining approval for the project and two (2) months for development and testing. Information about accessing the report is provided under the What s New with KASPER section of their website and included as part of their KASPER training. They are also collaborating with the various medical regulatory boards to promote the report card program. The Kentucky Board of Medical Licensure featured the report card in its Winter 2016 newsletter. Program Description Kentucky requires all in-state DEA licensed prescribers to register with KASPER. At the time a prescriber registers, they are required to indicate their specialty from a drop-down list. The list includes 27 specialty areas (see Appendix A). Once registered, a prescriber logs into the KASPER system and has the option to generate the Prescriber Peer Review Report. Information for the report is based on the specialty noted by the prescriber at time of their enrollment with KASPER. It is important to note that prescribers may select any specialty area for comparison when generating this report. For example, a prescriber who designated their specialty as pediatrician can choose oncologist to see how their prescribing compares to that specialty. Authorization to request and receive the report is restricted to prescribers; delegates do not have that authority. On a weekly basis, the prescription data is configured to count the number of prescriptions and dosage units dispensed for the previous 90 days (i.e., during the first week in April, data is pulled from the start of January through the end of March; during the 2nd week of April, data is pulled from the 2nd week of January through the 1st week of April). The data are placed in a proxy table which becomes the source for generating the reports. The report is a single page which displays data for two (2) major categories: Prescription Counts and Dosage Counts (see Appendix C). Each category is displayed as actual numbers and within a bar chart. The drugs are divided into the therapeutic classes of benzodiazepines, opioids, sedatives and stimulants. These therapeutic classes are derived from the 4 BJA National Meeting on Data Driven Multi-Disciplinary Approaches to Reducing Rx Abuse National Meeting, February 25,
7 National Drug Code (NDC) Directory that KASPER uses. Prescription information is grouped and compiled based on the prescriber s DEA controlled substance registration number. The data for the two categories are shown as (a) the average for all Kentucky prescribers, (b) the average for prescribers within the selected specialty, and (c) the number for the requesting prescriber. Under consideration for enhancements to the report are the inclusion of the number of dosage units per prescription, morphine milligram equivalent (MME) calculations for a patient, and comparisons by a specific medication. The impact on KASPER system resources will be considered prior to implementing any enhancements. These reports became available in December 2015 and, as of this writing there has been limited, but positive feedback on this new feature. OHIO Background The Ohio PDMP, OARRS, does not allow prescribers to request a report of their prescribing history. However, in response to expressed needs of the prescriber community, the PDMP created a report called the Practice Insight Report. The purpose of the report is to provide a brief summary to each prescriber of their prescribing patterns. Discussions about developing this type of report first surfaced at a meeting, held in October 2013, sponsored by the Association of State and Territorial Health Officials (ASTHO) where several State of Ohio agencies (Board of Nursing, Board of Pharmacy, Bureau of Workers Compensation, Department of Aging, Department of Health, Department of Medicaid, Department of Mental Health and Addiction Services, Department of Public Safety, State Dental Board, State Medical Board, and Governor s Office), along with TTAP staff were present 5. Development of the Practice Insight Report required approximately one (1) month of work by the OARRS staff. The PDMP system did not need modifications; basic data queries were built to generate the report. The Board of Pharmacy publicized the Practice Insight Report in their monthly newsletter following its development. There are plans to create a video on the use of the report for prescribers. During the 18 months OARRS has been issuing reports to prescribers, there has been a new interest by the PDMP and prescribers to include a comparison of the individual prescribers to his/her peers or specialty in this report. The PDMP is currently working on this aspect of the report. As a condition of the Centers for Disease Control and Prevention (CDC) Prevention for States grant program, the PDMP provided the report, as an unsolicited report, to every prescriber. This report included a cover letter explaining how to interpret the report s contents and how the prescriber can generate the report from the PDMP website. The patient information is deidentified; however, the prescriber can obtain that information by requesting a patient-specific report or their personal Practice Insight Report. 5 PDMP Center of Excellence, Ohio Prescription Monitoring Workshop, October 30,
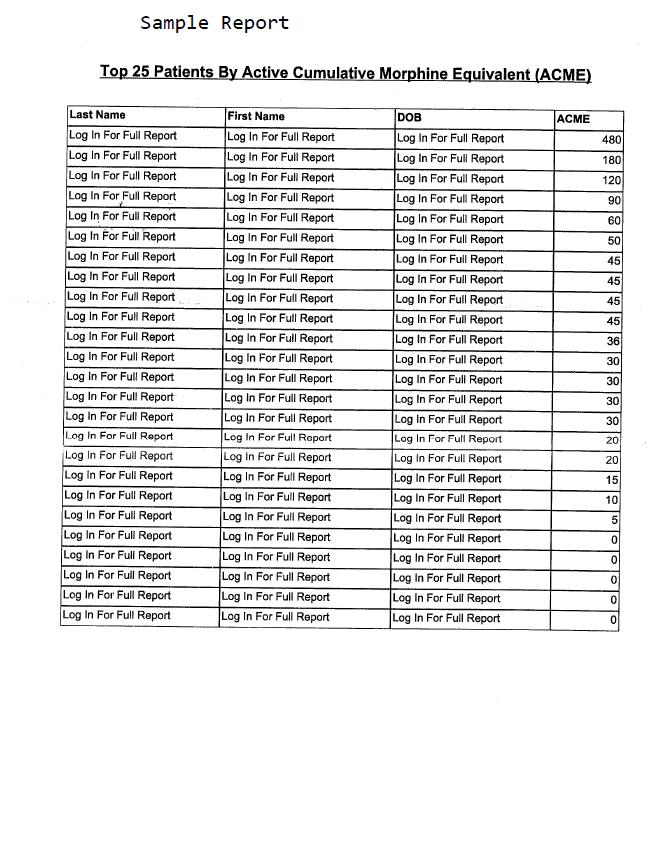
8 Program Description A prescriber can access the Practice Insight Report from the OARRS website in the same manner they would request a Patient Prescription History Report. The prescriber selects Practitioner instead of Patient for the type of report; no other information need be entered. The report is compiled based on the prescriber s DEA controlled substance registration number and the information is compiled into four (4) sections (see Appendix D): Top 25 patients by number of other prescribers visited in the previous 12 months o Patients are listed in descending order by the total count of other prescribers visited o Patient s last name, first name, date of birth, and prescriber count are displayed Top 25 patients by active cumulative morphine equivalent (ACME) (Ohio s acronym for MME) o Patients are listed in descending order by their ACME o Patient s last name, first name, date of birth, and ACME are displayed Top 10 medications prescribed in the previous 12 months for the prescriber s entire practice o Pie chart representation o Medication name and percentage of total prescriptions issued are displayed A listing of the prescriber s patients issued a controlled substances prescription in the previous 12 months o Alphabetical listing of all patients receiving prescriptions from prescriber o Patient s last name, first name, date of birth, and date that the last prescription was written are displayed The PDMP is considering several enhancements to the Practice Insight Report. These enhancements include: Adding peer comparisons by prescriber specialty Removing the pie chart of the top ten (10) medications prescribed as many prescribers have reported that it is confusing or little value to them Providing grouped reports containing information from all prescribers within a group practice or hospital setting Limiting prescription data in report to solid oral medications to increase accuracy of computations Creating metrics based on published prescribing guidelines Developing functionality in report that will allow a prescriber to view patient-specific information or drill down to specific prescriptions Since the report s inception, the feedback from the prescribers has been positive. To date, there has not been any formal evaluation of the report s effect on prescribing. In addition to the implementation of the report, Ohio has developed prescribing guidelines, so it may be difficult to determine which has had more of an impact on prescribing practices. 8
9 PRESCRIBERS PERSPECTIVE Along with examining the three (3) PDMP programs, TTAP reached out to the prescriber community to obtain their perspective on the usefulness of report cards. Four (4) nationally recognized experts were interviewed: Drs. Andrew Kolodny (Phoenix House), Greg Terman (University of Washington, Department of Anesthesiology and Pain Medicine), Bob Twillman (American Academy of Pain Management), and Scott Weiner (Brigham and Women s Hospital) (see Acknowledgement section). Before the interviews, the physicians were provided with a copy of the Arizona Report Card and accompanying letter (see Appendix B). Three (3) of the physicians shared the report with their colleagues, including emergency room physicians and several physicians who are reviewing the newly-released CDC draft opioid guidelines. Below is a summary of the comments and recommendations made by the physicians about the report card program. Comments The physicians and their colleagues unanimously liked the concept of providing information in this manner to a prescriber and felt that such a report would be beneficial to the prescriber in evaluating their prescribing practices. Each physician emphasized that the report card should be concise and not exceed two (2) pages in length to avoid information overload. They also felt that comparisons to other prescribers within the same specialty group were of great value to accurately assess prescribing habits. The physicians stressed the importance of an appropriately worded cover letter with the report card. To help ensure widespread acceptance and use, the wording should emphasize that the report card is simply a clinical tool for the prescriber s use and benefit. Recommendations The physicians offered recommendations of elements that would beneficial to include in a model report card program: The report cards should be sent by the PDMPs to every prescriber who has prescribed at least one (1) controlled substance, once or twice per year or, at most, quarterly. Prescribers should have the opportunity to request their own report online at their discretion. Allow the prescriber the option to select their specialty group when requesting their own report. Include information with helpful resources in the cover letter. For example, provide web links to information on prescribing guidelines, safe storage of medications, proper disposal of medications, etc. Provide detailed and complete explanations of the meaning of each element (e.g., chart, graph, table, number). Include a hyperlink with each report card element that allows the prescriber to obtain additional information about the patients associated with that element or, at a minimum, a hyperlink to retrieve a patient s complete PDMP report. Subject prescriber data that are determined to be outside the norm should be clearly denoted. To accommodate individuals that have difficulty differentiating colors, use patterns in conjunction with colors on charts/graphs. 9
10 Inform the prescribers of the number of patients they are treating who meet various risk factors and provide a method to easily retrieve PDMP information on those patients. Comparisons made to a prescriber s peers need only be at a statewide level; prescribing trends should not vary widely from one area of a state to another. Use a low threshold for patients with multiple provider episodes to alert prescribers of potential doctor shopping and/or drug interactions (i.e., total number of patients issued prescriptions from two (2) or more prescribers). Use daily morphine milligram equivalents (MMEs) instead of dosage units when comparing prescribing practices. This will avoid issues associated with compiling the dosage counts of medications that have varying strengths. The CDC has indicated that patients receiving 50 MMEs to 90 MMEs or more per day are at an increased risk of overdose. It would be beneficial to provide incremental information on the amounts patients receive (i.e., 40 MMEs, 60 MMEs, 80 MMEs). During the interviews with Drs. Twillman, Terman and Weiner, measuring effectiveness of the report cards was discussed. All agreed that it would be important to track the usage of the report cards and identify the impact on prescribing before and after a report card program was implemented. SUGGESTED COMPONENTS OF A MODEL REPORT CARD The following suggestions are the result of using the three (3) state report card examples and input from the four (4) doctors as a guide. PDMPs are urged to review the components and determine which are feasible with their system s capabilities, implementable with current resources, and applicable to the needs of prescribers in their state. Note: inclusion below is not intended to imply that all participants agree with every component listed. Peer Comparisons 1. Compare the prescriber s number of prescriptions issued per month by therapeutic class code or by specific substances to peer averages by specialty throughout the state. 2. Compare the prescriber s number of milligrams prescribed per month by therapeutic class code or by specific substances to peer averages by specialty throughout the state. Patient Risk Factors 3. Total number of patients receiving 90 MMEs or more per day. 4. Total number of patients receiving opioid medications for 30 days or more. 5. Total number of patients receiving opioids and benzodiazepines medications at the same time. 6. Total number of patients issued more than one (1) controlled substance prescription from the subject prescriber or other prescribers. 7. Total number of patients issued prescriptions from three (3) or more prescribers (multiple provider episodes). 8. Total number of patients filling prescriptions at three (3) or more pharmacies (multiple provider episodes). 9. Total number of patients with controlled substance prescriptions whose dispensing dates overlap. 10. Total number of patients obtaining refills on their prescriptions more than one (1) week early. 10
11 11. Total number of patients at various Risk levels. Risk levels can be determined by the number of risk indicators above (lines 3-10) that a patient meets. Risk levels range from 1 (patient meets the threshold for one risk indicator) to 8 (patient meets the threshold for all eight indicators). PDMPs should seek the guidance and expertise from the medical and treatment community or it s Advisory Council in establishing risk indicators and levels. Utilization 12. Total number of PDMP queries made by prescriber and a ratio of PDMP queries to the number of patients or prescriptions issued. Data File Generation In order to generate the data for these elements, some preparatory work should be completed to ensure accuracy, consistency, and processing efficiency: Patient information should be normalized and clustered. Information on the various methods to accomplish this are available: o Patient Linking Software Options Guide o Webinar on Linking Patients in PDMP Data Prescriber information should include their specialty. If this information is not part of the PDMP s prescriber file, there are other options: o Obtain the specialty from the appropriate regulatory/licensing board, if available o Include a specialty field as part of PDMP enrollment form o Use the specialty field from the NPI file and link to the existing prescriber file o Allow prescriber to select their specialty when report card is generated Categorize medications by class codes (i.e., benzodiazepines, opioids, sedatives, stimulants). The Food and Drug Administration (FDA) maintains a National Drug Code (NDC) Directory (note: NDCs can be obtained from other sources). Within the FDA NDC file, there is a Product File field (Pharm_Classes) which identifies the pharmacological class code for a medication. The above four (4) primary class codes are listed in many different ways; however, it is not difficult to identify and group them using a portion of the pharmacological class code definition string. Calculate the total milligrams prescribed or dispensed instead of quantity for comparisons to peers. Medications vary by strength and using the number of pills dispensed does not provide an accurate representation for evaluating the prescribing of a prescriber or the risk for a patient. For example, hydrocodone is available in 2.5mg, 5mg and 10mg tablets. A prescription for 100 tablets can result in a patient receiving 250mg, 500mg or 1000mg of hydrocodone. Within the FDA NDC file, there is a Product File which includes fields to identify the medication s strength: ACTIVE_NUMERATOR_STRENGTH and ACTIVE_INGRED_UNIT. To determine the total milligrams prescribed or dispensed, multiply the quantity by ACTIVE_NUMERATOR_STRENGTH (note: the ACTIVE_NUMERATOR_STRENGTH may need to be adjusted if the ACTIVE_INGRED_UNIT is not listed in milligrams). Base the comparisons of prescriptions issued and milligrams prescribed by calculating the prescriber s percentile ranking or variation (standard deviation) in relation to the average prescriber (see Appendix E for definitions and examples). o Standard deviation shows the amount of variation there is from the "average" (mean). o Percentile rank refers to the percentage of values that are equal to or less than a given value; commonly shown in deciles or quartiles. 11
12 Calculate the daily morphine milligram equivalents (MMEs) prescribed by the prescriber to each patient. Evidence suggests that a patient receiving more than 100mg MMEs is nine (9) times more likely to overdose, with 12% of those resulting in death 6. To calculate MMEs, multiply the medication s strength by the quantity dispensed and the MME conversion factor, then divide the answer by the number of days the medication is taken. The Centers for Disease Control and Prevention (CDC) developed and TTAP has made available a conversion table and Statistical Analysis System (SAS) program to assist in calculating MMEs: Calculating Daily Morphine Milligram Equivalents. Prescriptions are considered overlapping when at least two (2) controlled substance medications (usually opioids or opioids and benzodiazepines) are being taken at the same time by a patient. Typically, the time frame for the overlap is seven (7) days. For inclusion in the prescriber report card, it is the number of patients with overlapping prescriptions; not the number of prescriptions. The length of time a patient should take a medication is calculated using the dispensing date and the days supplied fields. If the prescriber does not indicate the number of days the prescribed medication should last, the dispensing pharmacist will determine the number of days based on the instructions for use indicated on the prescription or use an established formula within the pharmacy s software. In most instances this is accurate and reliable; however, when the prescriber indicates that the medication should be taken as needed, the accuracy and reliability are lessened. Refilling a prescription early implies that the patient may not be following the doctor s instructions for taking the medication. The quantity of medication prescribed will last a certain amount of time based on the instructions for use that a prescriber indicates. Patients are permitted to get the prescription refilled on or shortly before the medication runs out. For inclusion in the prescriber report card, it is the number of patients refilling at least one (1) prescription more than seven (7) days early; not the number of prescriptions that were refilled early. The method to determine which prescriptions were refilled early is the same as for overlapping prescriptions; based on the dispensing date and the days supplied fields. Report Distribution and Retrieval The value of the report cards will not be realized unless they are obtained and used by the prescriber. There are two (2) methods by which prescribers can obtain their report card; ideally, the PDMP should employ both methods. PDMP-Generated The reports should be generated at least once or twice a year and ed to all prescribers who have issued at least one (1) controlled substance prescription during the report s time frame. It is recommended that the reports be generated and sent no more than quarterly to avoid overwhelming the prescribers with too much information. It is recommended that these reports be generated in addition to other unsolicited reports or alerts that the PDMP may send. Self-Generated A prescriber should have the capacity to retrieve their own report card. This could be a separate report or included with their prescribing history report, if permitted under state law, administrative code, or policy. Self-generated reports would require the user query screen to be modified to include this type of report, but would be far less burdensome on the PDMP s resources than PDMP-generated report cards. If possible, it would be beneficial to allow the prescriber to set the parameters for some of the components, e.g. number of MMEs a patient is receiving, number of different prescribers issuing prescriptions to a patient, number of different pharmacies filling prescriptions for a patient). 6 Dunn et al, Opioid Prescriptions for Chronic Pain and Overdose. Ann Int Med 2010; 152:
13 To lessen the impact on PDMP functionality and reduce processing time, it is recommended that a separate data file be generated nightly or at least weekly which contains the previous three (3) to six (6) months data based on the date the medication was dispensed. Report Guidelines An aesthetically appealing and organized report card may improve the likelihood that the prescriber will readily review and quickly understand the report. Below are some suggestions for the layout and appearance: The report card should be brief to avoid overwhelming the prescriber with too much information; ideally one (1) to three (3) pages. The prescriber report card should include contextual information to ensure proper interpretation of the data. It is recommended to state that the report is a tool for the prescriber s use and benefit. Disclaimer language should be added stating the record source, statutory authority, dissemination of information, data limitations, etc. The elements included in the statistical analysis and compilation of the prescriber s data should be explained to avoid misinterpretation. The information on the report card should be arranged to allow for effortless review. The most important elements (i.e., patients at risk of adverse health events, multiple provider episodes) should be formatted to indicate various levels of concern (i.e., large or bold print, differing colors or patterns, asterisks). If the PDMP has the capability, pop-up text boxes or hyperlinks should be included so that the prescriber has the option to view more specific data associated with a report element; such as, patient information, prescription details, etc. ACKNOWLEDGEMENTS TTAP wishes to thank the below individuals for their expertise and assistance in preparing this guide: Dean Wright holds a Bachelor of Science degree in Pharmacy from the University of New Mexico, College of Pharmacy. Dean worked in retail and long-term care pharmacy settings until 1991 when he became a Compliance Officer for the Arizona State Board of Pharmacy. As a Compliance Officer, he conducted compliance visits at regulated facilities, investigated complaints and violations of state and federal drug laws. In 1994, in addition to his regular duties, Dean became the Board s rule writer. In August 2007, he left compliance and moved into the Board office to become the Director of the Board s Prescription Monitoring Program. Dave Hopkins is the Program Manager for the Kentucky All Schedule Prescription Electronic Reporting system also known as KASPER. KASPER is operated by the Office of Inspector General in the Kentucky Cabinet for Health and Family Services. In this position, he is responsible for KASPER training; managing federal Prescription Drug Monitoring Program Grants that provide funding support for the program; and for analysis and research using KASPER data. Mr. Hopkins graduated from The Ohio State University with a Bachelor of Science in Computer and Information Science, and has over 30 years experience in Information Technology consulting and project management. Mr. Hopkins is a member of the National Association of Drug Diversion Investigators, National Association of State Controlled Substances Authorities, and Vice-Chair of the RxCheck Governing Body. 13
14 Chad Garner is the current Director of OARRS, the Ohio prescription monitoring program. He has been employed by the Ohio State Board of Pharmacy since 2006, serving as the OARRS Database Administrator, the agency's Chief Technical Officer and now the Director of OARRS. Over the past 7 years, Chad has contributed to the efforts of the BJA/IJIS Prescription Monitoring Information Exchange (PMIX) subcommittee, the NABP Prescription Monitoring Program Interconnect (PMPi) steering committee and the Ohio Governor's Cabinet Opiate Action Team (GCOAT) Professional Education working group. Chad received his Bachelor of Science degree in Computer Science from Mount Vernon Nazarene University in Mount Vernon, Ohio. Andrew Kolodny, M.D., is the Chief Medical Officer of Phoenix House, a nonprofit addiction treatment organization and he is a senior scientist at the Heller School for Social Policy and Management at Brandeis University. Dr. Kolodny is also the Executive Director and co-founder of Physicians for Responsible Opioid Prescribing (PROP). Dr. Kolodny was previously the Chair of Psychiatry at Maimonides Medical Center in New York City. He has a long standing interest in Public Health. Prior to his position at Maimonides, he was the Medical Director for Special Projects in the Office of the Executive Deputy Commissioner for the New York City Department of Health and Mental Hygiene. For New York City, he helped develop and implement multiple programs to improve the health of New Yorkers and save lives, including city-wide buprenorphine programs, naloxone overdose prevention programs and emergency roombased screening, brief intervention and referral to treatment (SBIRT) programs for drug and alcohol misuse. Bob Twillman, Ph.D., is the Executive Director for the American Academy of Pain Management. In that capacity, Dr. Twillman is responsible for overseeing federal and state pain policy developments and advocating for those supporting an integrative approach to managing pain. He also serves as Chair of the Prescription Monitoring Program Advisory Committee for the Kansas Board of Pharmacy. Dr. Twillman received his Ph.D. in Clinical Psychology at the University of California in Los Angeles, and maintains a volunteer faculty appointment as Clinical Associate Professor of Psychiatry and Behavioral Sciences at the University of Kansas School Of Medicine in Kansas City, KS. Prior to taking his current position, Dr. Twillman was a full-time faculty member at the University of Kansas Medical Center, where he founded and directed the in-patient pain management program and was a co-founder of the hospital s Palliative Care Team. He has been actively involved in pain policy through his work with the Alliance of State Pain Initiatives and the American Pain Society for many years. Gregory Terman M.D., Ph.D., is professor of anesthesiology and pain medicine at the University of Washington based primarily at the University of Washington Medical Center (UWMC). He is currently director of the Acute Pain Service at UWMC. Dr. Terman earned his bachelor s degree at the College of William and Mary in Virginia. He completed his Ph.D. in behavioral neuroscience in the Department of Psychology at UCLA and his M.D. at the University of Miami. He completed his anesthesiology internship and residency, as well as pain medicine and pharmacology research fellowships at the University of Washington before joining the anesthesiology and pain medicine faculty. He is also a member of the University of Washington Graduate Program in Neuroscience and has run an NIH funded laboratory studying pain mechanisms since joining the Graduate Faculty. Nationally, Dr. Terman has served as president of the American Pain Society and is a special government employee for the FDA. 14
15 Scott Weiner M.D., MPH is an Assistant Professor of Emergency Medicine at Harvard Medical School and an Attending Emergency Physician in the Department of Emergency Medicine, Division of Health Policy Translation, at Brigham and Women s Hospital. Dr. Weiner completed medical school at the University of California, Irvine. He finished his residency training at the Harvard-Affiliated Emergency Medicine Program at Beth Israel Deaconess Medical Center in Boston and, subsequently, got his MPH degree at the Harvard School of Public Health. He serves as the Associated Fellowship Director for the Emergency Medicine Health Policy Research and Translation Fellowship at Brigham and Women s Hospital. Dr. Weiner s research focus in on identification of substance use disorder in the emergency department, particularly as it relates to prescription opioids. He has studied the effects of prescription drug monitoring programs (PDMPs) on prescribing behavior, in comparison to clinician gestalt and in relation to opioid risk-screening tools. His recent research evaluates opioid-prescribing behavior from the ED. He is also interested in implementation of prescribing guidelines and technological innovations that improve the care of ED patients presenting with pain. Dr. Weiner has authored more than 40 peer-reviewed papers over a decade of clinical and research experience. He has been funded by the NHLBI and was named as the 2015 Emergency Physician of the Year by the Massachusetts College of Emergency Physicians. 15

16 Appendix A Specialty Groups 16
17 Appendix B Arizona Report Card Sample 17
18 18
19 Appendix C Kentucky Report Card Sample 19
20 Appendix D Ohio Report Card Sample 20
21 21
22 22
23 Appendix E Statistical Formula Examples Standard Deviation To calculate the standard deviation, the mean and variance must be calculated. Variance is a measure of how the data are clustered around the mean. Standard deviation is found by taking the square root of the variance of the data sample. 1) The mean is determined by adding all the numbers in the data set, then dividing by the total number of values (n). 2) The variance is determined by subtracting the mean from each of the numbers in the data set, then computing the square for each, and adding the squared numbers together (called sum of squares ). 3) To determine the standard deviation, divide the sum of squares by the number of values in the data set (n) and calculate its square root. Standard deviations are determined by the number of square root values above or below the mean. Example: There are 5 prescribers who have issued 22, 37, 64, 81, and 138 prescriptions. Step 1: ( )=342 Mean: (342/5)=68.4 Step 2: ( )=-46.4; ( )=-31.4; ( )=-4.4; ( )=12.6; ( )=69.6 (-46.4*-46.4)= ; (-31.4*-31.4)=985.96; (-4.4*-4.4)=19.36; (12.6*12.6)=158.76; (69.6*69.6)= Sum of Squares: ( )= Step 3: ( /5)= ( )=42.98 One Standard Deviation: (42.98*1)+68.4= (>=68.5 and <=111.38) Two Standard Deviations: (42.98*2)+68.4= (>= and <=154.36) Three Standard Deviations: (42.98*3)+68.4= (>= and <=197.34) The prescribers who issued 64 and 81 prescriptions are within one (1) standard deviation above the mean; the prescriber who issued 138 prescriptions is within two (2) standard deviations above the mean. 23
24 Deciles Deciles are percentiles which divide a data set into ten (10) equal sections. There are nine (9) deciles in each distribution of values which correspond to the 10th, 20th, 30th,...90th percentiles. 1) Divide the total number of values by 10 to get the number of values within each decile. 2) Sort the values in the data set from smallest to largest. 3) Separate the values in the data set in groups of the number calculated in step 1. 4) The values within the highest 10 th are considered within the 9 th decile; the values within the lowest 10 th are considered within the 1 st decile. Example: There are 15 prescribers who have issued 7, 13, 22, 37, 48, 51, 64, 79, 81, 96, 103, 128, 138, 144, and 151 prescriptions. Step 1: (15)/10=1.5 Step 2: 7, 13, 22, 37, 48, 51, 64, 79, 81, 96, 103, 128, 138, 144, 151 Step 3: Each decile has 1.5 values within it. 1 st decile=1.5 2 nd decile=3.0 3 rd decile=4.5 4 th decile=6.0 5 th decile=7.5 6 th decile=9.0 7 th decile= th decile= th decile= th decile=15 The prescriber who issued 7 prescriptions is in the 1 st decile; which means that 90% of the prescribers issued more prescriptions. The prescribers who issued 13 and 22 prescriptions are in the 2 nd decile; which means that 80% of the prescribers issued more prescriptions. The prescribers who issued 144 and 151 prescriptions are in the 9 th decile; which means they issued more than 90% of the prescriptions. Quartiles Quartiles are percentiles which divide a data set into quarters; the first quartile (Q1) is the 25th percentile, the second quartile (Q2) is the 50th percentile or the median, and the 75th percentile is the third quartile (Q3). 1) Divide the total number of values by 4 to get the number of values within each quartile. 2) Sort the values in the data set from smallest to largest. 3) Separate the values in the data set in groups of the number calculated in step 1. 4) The values within the quarter are considered within the 3 rd quartile; the values within the lowest quarter are considered within the 1 st quartile. Example: There are 15 prescribers who have issued 7, 13, 22, 37, 48, 51, 64, 79, 81, 96, 103, 128, 138, 144, and 151 prescriptions. Step 1: (15)/4=3.75 Step 2: 7, 13, 22, 37, 48, 51, 64, 79, 81, 96, 103, 128, 138, 144, 151 Step 3: Each quartile has 3.75 values within it. 1 st quartile= nd quartile=7.5 3 rd quartile= th quartile=15.0 The prescribers who issued 7, 13 and 22 prescriptions are in the 1 st quartile; which means that 75% of the prescribers issued more prescriptions. The prescribers who issued 37, 48, 51 and 64 prescriptions are in the 2 nd quartile; which means that 50% of the prescribers issued more prescriptions. The prescribers who issued 128 or more prescriptions are in the 3 rd quartile; which means they issued more than 75% of the prescriptions. 24
Evidence-Based Practices to Optimize Prescriber Use of PDMPs
 Evidence-Based Practices to Optimize Prescriber Use of PDMPs Sheri Lawal, MPH, CHES Senior Associate, Substance Use Prevention and Treatment Initiative, The Pew Charitable Trusts Thomas Clark Research
Evidence-Based Practices to Optimize Prescriber Use of PDMPs Sheri Lawal, MPH, CHES Senior Associate, Substance Use Prevention and Treatment Initiative, The Pew Charitable Trusts Thomas Clark Research
Prescription Drug Monitoring Program (PDMP)
") Prescription Drug Monitoring Program (PDMP) West Virginia Information contained in this presentation is accurate as of October 2017 What is a Prescription Drug Monitoring Program? A PDMP/PMP is a statewide
Prescription Drug Monitoring Program (PDMP) West Virginia Information contained in this presentation is accurate as of October 2017 What is a Prescription Drug Monitoring Program? A PDMP/PMP is a statewide
Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels. Nick Snyder, Esq.
 Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels Nick Snyder, Esq. How Can We Impact Inappropriate Over-Prescribing of Opioids in Maine? What have other States or Organizations
Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels Nick Snyder, Esq. How Can We Impact Inappropriate Over-Prescribing of Opioids in Maine? What have other States or Organizations
(b) Is administered via a transdermal route; or
 Is administered via a transdermal route; or") ACTION: To Be Refiled DATE: 10/10/2018 2:31 PM 4723-9-10 Formulary; standards of prescribing for advanced practice registered nurses designated as clinical nurse specialists, certified nurse-midwives,
ACTION: To Be Refiled DATE: 10/10/2018 2:31 PM 4723-9-10 Formulary; standards of prescribing for advanced practice registered nurses designated as clinical nurse specialists, certified nurse-midwives,
Medication Assisted Treatment for Opioid Use Disorders Reporting Requirements
 This document is scheduled to be published in the Federal Register on 09/27/2016 and available online at https://federalregister.gov/d/2016-23277, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN SERVICES
This document is scheduled to be published in the Federal Register on 09/27/2016 and available online at https://federalregister.gov/d/2016-23277, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN SERVICES
Technical Assistance Guide. Enhancing PDMPs: A Comparison of Changes 2010 to 2016
 Technical Assistance Guide Enhancing PDMPs: A Comparison of Changes 2010 to 2016 December 2016 This project was supported by Grant No. 2014-PM-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau
Technical Assistance Guide Enhancing PDMPs: A Comparison of Changes 2010 to 2016 December 2016 This project was supported by Grant No. 2014-PM-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau
Ohio. Contact Information. State Registrant Totals and Population
 PDMP name: OARRS Agency responsible: State of Ohio Board of Pharmacy Agency type: Pharmacy Board PDMP email: info@pharmacy.ohio.gov PDMP website: www.ohiopmp.gov Enrollment website: https://ohio.pmpaware.net
PDMP name: OARRS Agency responsible: State of Ohio Board of Pharmacy Agency type: Pharmacy Board PDMP email: info@pharmacy.ohio.gov PDMP website: www.ohiopmp.gov Enrollment website: https://ohio.pmpaware.net
Kentucky. Kentucky Cabinet for Health and Family Services Office of Inspector General
 PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: Kentucky Kentucky Cabinet for Health and Family Services
PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: Kentucky Kentucky Cabinet for Health and Family Services
District of Columbia Prescription Drug Monitoring Program
 District of Columbia Prescription Drug Monitoring Program What Our Users Need to Know Health Regulation and Licensing Administration Pharmaceutical Control Division February 28, 2017 1 Mission Statement
District of Columbia Prescription Drug Monitoring Program What Our Users Need to Know Health Regulation and Licensing Administration Pharmaceutical Control Division February 28, 2017 1 Mission Statement
K-TRACS: Review of Program Data and a Qualitative Assessment Study
 K-TRACS: Review of Program Data and a Qualitative Assessment Study Amy Curry, MD Clinical Assistant Professor University of Kansas School of Medicine - Wichita Department of Family and Community Medicine
K-TRACS: Review of Program Data and a Qualitative Assessment Study Amy Curry, MD Clinical Assistant Professor University of Kansas School of Medicine - Wichita Department of Family and Community Medicine
Prescription Drug Monitoring Program (PDMP)
") Prescription Drug Monitoring Program (PDMP) New York State Information contained in this presentation is accurate as of September 2017 Meet the Speaker Anita Murray, R.Ph., Deputy Director Bureau of Narcotic
Prescription Drug Monitoring Program (PDMP) New York State Information contained in this presentation is accurate as of September 2017 Meet the Speaker Anita Murray, R.Ph., Deputy Director Bureau of Narcotic
Michigan. Contact Information. State Registrant Totals and Population. PDMP name: MAPS
 Michigan PDMP name: MAPS PDMP region: Agency responsible: Bureau of Professional Licensing, Drug Monitoring Section Agency type: Professional Licensing Agency PDMP email: BPL-MAPS@michigan.gov PDMP website:
Michigan PDMP name: MAPS PDMP region: Agency responsible: Bureau of Professional Licensing, Drug Monitoring Section Agency type: Professional Licensing Agency PDMP email: BPL-MAPS@michigan.gov PDMP website:
Nevada. Contact Information. State Registrant Totals and Population
 Statistics website: Long, Yenh - Program Administrator 431 W Plumb Ln Reno NV 89509 Office: (775) 687-5694 Fax: (775) 687-5161 Email: ylong@pharmacy.nv.gov Nevada PDMP name: Prescription Controlled Substance
Statistics website: Long, Yenh - Program Administrator 431 W Plumb Ln Reno NV 89509 Office: (775) 687-5694 Fax: (775) 687-5161 Email: ylong@pharmacy.nv.gov Nevada PDMP name: Prescription Controlled Substance
Massachusetts Prescription Monitoring Program
 Massachusetts Prescription Monitoring Program PDMP Training and Technical Assistance Center at Brandeis University in partnership with the Bureau of Justice Assistance August 8, 2012 Massachusetts Department
Massachusetts Prescription Monitoring Program PDMP Training and Technical Assistance Center at Brandeis University in partnership with the Bureau of Justice Assistance August 8, 2012 Massachusetts Department
Colorado. Contact Information
 Colorado PDMP name: Prescription Drug Monitoring Program PDMP region: Agency responsible: Colorado State Board of Pharmacy Agency type: Pharmacy Board PDMP email: pdmpinqr@state.co.us PDMP website: https://www.colorado.gov/pacific/dora/pdmp
Colorado PDMP name: Prescription Drug Monitoring Program PDMP region: Agency responsible: Colorado State Board of Pharmacy Agency type: Pharmacy Board PDMP email: pdmpinqr@state.co.us PDMP website: https://www.colorado.gov/pacific/dora/pdmp
New Mexico. Contact Information. State Registrant Totals and Population. PDMP name: NM PMP
 Statistics website: Ryba, Peter, PharmD - PMP Director 5500 San Antonio Drive NE, Suite C Albuquerque NM 87109 Office: (505) 222-9818 Fax: (505) 222-9845 Email: peter.ryba@state.nm.us New Mexico PDMP name:
Statistics website: Ryba, Peter, PharmD - PMP Director 5500 San Antonio Drive NE, Suite C Albuquerque NM 87109 Office: (505) 222-9818 Fax: (505) 222-9845 Email: peter.ryba@state.nm.us New Mexico PDMP name:
Massachusetts. Contact Information. State Registrant Totals and Population. PDMP name: MA Prescription Monitoring Program
 Massachusetts PDMP name: MA Prescription Monitoring Program PDMP region: Agency responsible: Department of Public Health Agency type: Department of Health PDMP email: mapmp.dph@massmail.state.ma.us PDMP
Massachusetts PDMP name: MA Prescription Monitoring Program PDMP region: Agency responsible: Department of Public Health Agency type: Department of Health PDMP email: mapmp.dph@massmail.state.ma.us PDMP
Maine Chronic Pain Collaborative 2 (ME CPC2) Chronic Pain Management Change Package for Primary Care Practices
 Chronic Pain Management Change Package for Primary Care Practices") Maine Chronic Pain Collaborative 2 (ME CPC2) Chronic Pain Management Change Package for Primary Care Practices These 10 change components are intended to support enhanced safety and improved patient care
Maine Chronic Pain Collaborative 2 (ME CPC2) Chronic Pain Management Change Package for Primary Care Practices These 10 change components are intended to support enhanced safety and improved patient care
North Carolina. Contact Information. State Registrant Totals and Population. PDMP region: PDMP name: Agency responsible:
 PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: North Carolina PDMP region: South North Carolina Department
PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: North Carolina PDMP region: South North Carolina Department
Alaska. Contact Information. State Registrant Totals and Population. PDMP name: AKPDMP
 Statistics website: Carrillo, Laura - PDMP Manager 550 W. 7th Ave, Ste 1500 Anchorage AK 99501 Office: (907) 269-8404 Fax: (907) 465-2974 Email: laura.carrillo@alaska.gov Alaska PDMP name: AKPDMP PDMP
Statistics website: Carrillo, Laura - PDMP Manager 550 W. 7th Ave, Ste 1500 Anchorage AK 99501 Office: (907) 269-8404 Fax: (907) 465-2974 Email: laura.carrillo@alaska.gov Alaska PDMP name: AKPDMP PDMP
Georgia DPH. Prescription Title Drug Heading Monitoring Program Program. Sheila Pierce April 2018
 Georgia DPH Prescription Title Drug Heading Monitoring Program Program Sheila Pierce April 2018 What is the PDMP? Legislative Mandates Registration Requirements How to use the PDMP Next Steps for Prescribers
Georgia DPH Prescription Title Drug Heading Monitoring Program Program Sheila Pierce April 2018 What is the PDMP? Legislative Mandates Registration Requirements How to use the PDMP Next Steps for Prescribers
STATE OF TEXAS TEXAS STATE BOARD OF PHARMACY
 STATE OF TEXAS TEXAS STATE BOARD OF PHARMACY REQUEST FOR INFORMATION NO. 515-15-0002 PRESCRIPTION DRUG MONITORING PROGRAM Reference: CLASS: 920 ITEM: 05 Posting Date: 12/08/2014 RESPONSE DEADLINE: 01/05/2015
STATE OF TEXAS TEXAS STATE BOARD OF PHARMACY REQUEST FOR INFORMATION NO. 515-15-0002 PRESCRIPTION DRUG MONITORING PROGRAM Reference: CLASS: 920 ITEM: 05 Posting Date: 12/08/2014 RESPONSE DEADLINE: 01/05/2015
Puerto Rico. Contact Information. State Registrant Totals and Population. PDMP name: PR PDMP
 Statistics website: Rodriguez, Cieni - Program Manager Carr. No. 2 Km 8.2, Bo. Juan Sanchez Bayamon, PR 00960 Office: (787) 763-7575 Fax: (787) 763-3152 Email: cieni.rodriguez@assmca.pr.gov Puerto Rico
Statistics website: Rodriguez, Cieni - Program Manager Carr. No. 2 Km 8.2, Bo. Juan Sanchez Bayamon, PR 00960 Office: (787) 763-7575 Fax: (787) 763-3152 Email: cieni.rodriguez@assmca.pr.gov Puerto Rico
Prescription Monitoring Program State Profiles - California
 Prescription Monitoring Program State Profiles - California Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control
Prescription Monitoring Program State Profiles - California Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control
PRESCRIBING IN NEVADA
 PRESCRIBING IN NEVADA An Inside Look at Changes to Nevada Laws Surrounding Prescribing Controlled Substances for the Treatment of Pain These changes to Nevada law do not impact the authority of practitioners
PRESCRIBING IN NEVADA An Inside Look at Changes to Nevada Laws Surrounding Prescribing Controlled Substances for the Treatment of Pain These changes to Nevada law do not impact the authority of practitioners
Annual Report to the Prescription Drug Monitoring Program Advisory Commission
 2015 Annual Report to the Prescription Drug Monitoring Program Advisory Commission PUBLIC HEALTH DIVISION Oregon Violent Death Reporting System Contents»» Acknowledgments... 1»» Executive summary... 2
2015 Annual Report to the Prescription Drug Monitoring Program Advisory Commission PUBLIC HEALTH DIVISION Oregon Violent Death Reporting System Contents»» Acknowledgments... 1»» Executive summary... 2
Prescription Monitoring Programs - Legislative Trends and Model Law Revision
 Prescription Drug Monitoring Programs Training and Technical Assistance Center Webinar Series National Alliance for Model State Drug Laws: Legislative Round-Up July 22, 2015 Prescription Monitoring Programs
Prescription Drug Monitoring Programs Training and Technical Assistance Center Webinar Series National Alliance for Model State Drug Laws: Legislative Round-Up July 22, 2015 Prescription Monitoring Programs
NATIONAL ASSOCIATION FOR STATE CONTROLLED SUBSTANCES AUTHORITIES (NASCSA) MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) COMMENT
 MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) COMMENT") 1 NATIONAL ASSOCIATION FOR STATE CONTROLLED SUBSTANCES AUTHORITIES (NASCSA) MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) SECTION 1. SHORT TITLE. This Act shall be known and may be cited as the
1 NATIONAL ASSOCIATION FOR STATE CONTROLLED SUBSTANCES AUTHORITIES (NASCSA) MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) SECTION 1. SHORT TITLE. This Act shall be known and may be cited as the
Tennessee. Contact Information. State Registrant Totals and Population. PDMP name: CSMD
 Statistics website: Bess, D. Todd - Director, CSMD Program 665 Mainstream Drive Nashville TN 37243 Office: (615) 253-1305 Fax: Email: david.bess@tn.gov Tennessee PDMP name: CSMD PDMP region: South Agency
Statistics website: Bess, D. Todd - Director, CSMD Program 665 Mainstream Drive Nashville TN 37243 Office: (615) 253-1305 Fax: Email: david.bess@tn.gov Tennessee PDMP name: CSMD PDMP region: South Agency
NCPDP s Recommendations for an Integrated, Interoperable Solution to Ensure Patient Safe Use of Controlled Substances
 National Council for Prescription Drug Programs White Paper NCPDP s Recommendations for an Integrated, Interoperable Solution to Ensure Patient Safe Use of This white paper details a plan to nationally
National Council for Prescription Drug Programs White Paper NCPDP s Recommendations for an Integrated, Interoperable Solution to Ensure Patient Safe Use of This white paper details a plan to nationally
RULES and REGULATIONS: PRESCRIBING CONTROLLED SUBSTANCES IN MS. Mississippi State Board of Medical Licensure June 24, 2016 Thomas Washington, CMBI
 RULES and REGULATIONS: PRESCRIBING CONTROLLED SUBSTANCES IN MS. Mississippi State Board of Medical Licensure June 24, 2016 Thomas Washington, CMBI This agency was created as an independent state agency
RULES and REGULATIONS: PRESCRIBING CONTROLLED SUBSTANCES IN MS. Mississippi State Board of Medical Licensure June 24, 2016 Thomas Washington, CMBI This agency was created as an independent state agency
Alabama. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Alabama Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Alabama Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
247 CMR: BOARD OF REGISTRATION IN PHARMACY
 247 CMR 9.00: CODE OF PROFESSIONAL CONDUCT; PROFESSIONAL STANDARDS FOR REGISTERED PHARMACISTS, PHARMACIES AND PHARMACY DEPART- MENTS Section 9.01: Code of Professional Conduct for Registered Pharmacists,
247 CMR 9.00: CODE OF PROFESSIONAL CONDUCT; PROFESSIONAL STANDARDS FOR REGISTERED PHARMACISTS, PHARMACIES AND PHARMACY DEPART- MENTS Section 9.01: Code of Professional Conduct for Registered Pharmacists,
Frequently Asked Questions
 1. What is dispensing? Frequently Asked Questions DO I NEED A PERMIT? Dispensing means the procedure which results in the receipt of a prescription drug by a patient. Dispensing includes: a. Interpretation
1. What is dispensing? Frequently Asked Questions DO I NEED A PERMIT? Dispensing means the procedure which results in the receipt of a prescription drug by a patient. Dispensing includes: a. Interpretation
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients
 Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
RULES OF THE TENNESSEE BOARD OF NURSING CHAPTER ADVANCED PRACTICE NURSES & CERTIFICATES OF FITNESS TO PRESCRIBE TABLE OF CONTENTS
 RULES OF THE TENNESSEE BOARD OF NURSING CHAPTER 1000-04 ADVANCED PRACTICE NURSES & CERTIFICATES TABLE OF CONTENTS 1000-04-.01 Purpose and Scope 1000-04-.07 Processing of Applications 1000-04-.02 Definitions
RULES OF THE TENNESSEE BOARD OF NURSING CHAPTER 1000-04 ADVANCED PRACTICE NURSES & CERTIFICATES TABLE OF CONTENTS 1000-04-.01 Purpose and Scope 1000-04-.07 Processing of Applications 1000-04-.02 Definitions
Prescription Drug Monitoring Program (PDMP)
") Prescription Drug Monitoring Program (PDMP) New Jersey Information contained in this presentation is accurate as of September 2017 Meet the Speaker Sindy Paul, MD, MPH, FACPM Medical Director - NJ Board
Prescription Drug Monitoring Program (PDMP) New Jersey Information contained in this presentation is accurate as of September 2017 Meet the Speaker Sindy Paul, MD, MPH, FACPM Medical Director - NJ Board
Mississippi. Contact Information. State Registrant Totals and Population
 Statistics website: Mueller, Stephanie - PMP Director 6360 I-55 North, Suite 400 Jackson, MS 39211 Office: (601) 899-0138 Fax: (601) 899-8904 Email: smueller@mbp.ms.gov Mississippi PDMP name: MS PMP Agency
Statistics website: Mueller, Stephanie - PMP Director 6360 I-55 North, Suite 400 Jackson, MS 39211 Office: (601) 899-0138 Fax: (601) 899-8904 Email: smueller@mbp.ms.gov Mississippi PDMP name: MS PMP Agency
MINNESOTA BOARD OF PHARMACY
 MINNESOTA BOARD OF PHARMACY Prescription Drug Waste Reduction Report. (In compliance with Minnesota Session Laws, 2010 First Special Session, Chapter 1, section 21) Cody Wiberg, Pharm.D., M.S., R.Ph. Executive
MINNESOTA BOARD OF PHARMACY Prescription Drug Waste Reduction Report. (In compliance with Minnesota Session Laws, 2010 First Special Session, Chapter 1, section 21) Cody Wiberg, Pharm.D., M.S., R.Ph. Executive
Prescription Monitoring Program State Profiles - Illinois
 Prescription Monitoring Program State Profiles - Illinois Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Monitoring Program State Profiles - Illinois Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Drug Monitoring Programs: Promising Practices to Maximize Their Effectiveness
 Prescription Drug Monitoring Programs: Promising Practices to Maximize Their Effectiveness Peter Kreiner, Ph.D. Prescription Monitoring Program Center of Excellence at Brandeis University NGA Meeting September
Prescription Drug Monitoring Programs: Promising Practices to Maximize Their Effectiveness Peter Kreiner, Ph.D. Prescription Monitoring Program Center of Excellence at Brandeis University NGA Meeting September
Oklahoma. Contact Information. Office: Fax: Statistics
 PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Vogt, Don - PMP Program Manager 419 NE 38th Terrace Oklahoma City OK 73105 Office: (405) 530-3140 Fax: (405) 524-7619 Email: dvogt@obn.state.ok.us
PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Vogt, Don - PMP Program Manager 419 NE 38th Terrace Oklahoma City OK 73105 Office: (405) 530-3140 Fax: (405) 524-7619 Email: dvogt@obn.state.ok.us
Policies Approved by the 2017 ASHP House of Delegates
 House of Delegates Policies Approved by the 2017 ASHP House of Delegates 1701 Ensuring Patient Safety and Data Integrity During Cyber-attacks Source: Council on Pharmacy Management To advocate that healthcare
House of Delegates Policies Approved by the 2017 ASHP House of Delegates 1701 Ensuring Patient Safety and Data Integrity During Cyber-attacks Source: Council on Pharmacy Management To advocate that healthcare
Medication Diversion and Prescription Drug Abuse in the Long Term Care Setting. Objectives
 Medication Diversion and Prescription Drug Abuse in the Long Term Care Setting Objectives Discuss: Learn about signs of potential diversion and recognize an impaired healthcare provider. Help to identify
Medication Diversion and Prescription Drug Abuse in the Long Term Care Setting Objectives Discuss: Learn about signs of potential diversion and recognize an impaired healthcare provider. Help to identify
NEW MEXICO PRACTITIONER S MANUAL
 NEW MEXICO PRACTITIONER S MANUAL An Informational Outline From the New Mexico Board of Pharmacy 5200 Oakland NE Suite A Albuquerque, New Mexico 87113 505-222-9830 800-565-9102 E-Mail: Debra.wilhite@state.nm.us
NEW MEXICO PRACTITIONER S MANUAL An Informational Outline From the New Mexico Board of Pharmacy 5200 Oakland NE Suite A Albuquerque, New Mexico 87113 505-222-9830 800-565-9102 E-Mail: Debra.wilhite@state.nm.us
Florida s New Law on Controlled Substance Prescribing
 FLORIDA MEDICAL ASSOCIATION Florida s New Law on Controlled Substance Prescribing HB 21, signed into law by Gov. Rick Scott on March 19, 2018, imposes a number of legal requirements on healthcare practitioners
FLORIDA MEDICAL ASSOCIATION Florida s New Law on Controlled Substance Prescribing HB 21, signed into law by Gov. Rick Scott on March 19, 2018, imposes a number of legal requirements on healthcare practitioners
SUBCHAPTER 32M - APPROVAL OF NURSE PRACTITIONERS
 SUBCHAPTER 32M - APPROVAL OF NURSE PRACTITIONERS 21 NCAC 32M.0101 DEFINITIONS The following definitions apply to this Subchapter: (1) "Approval to Practice" means authorization by the Medical Board and
SUBCHAPTER 32M - APPROVAL OF NURSE PRACTITIONERS 21 NCAC 32M.0101 DEFINITIONS The following definitions apply to this Subchapter: (1) "Approval to Practice" means authorization by the Medical Board and
Christopher W. Shanahan, MD, MPH, FACP
 Safe and Competent Opioid Prescribing: Optimizing Office Systems Christopher W. Shanahan, MD, MPH, FACP Assistant Professor of Medicine Boston University School of Medicine Boston Medical Center Certified:
Safe and Competent Opioid Prescribing: Optimizing Office Systems Christopher W. Shanahan, MD, MPH, FACP Assistant Professor of Medicine Boston University School of Medicine Boston Medical Center Certified:
Preventing Opioid Misuse and Potential Abuse: The Nurse's Role in Education. Authors Costello, Margaret; Thompson, Sarah B.
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
State of Kansas Department of Social and Rehabilitation Services Department on Aging Kansas Health Policy Authority
 State of Kansas Department of Social and Rehabilitation Services Department on Aging Kansas Health Policy Authority Notice of Proposed Nursing Facility Medicaid Rates for State Fiscal Year 2010; Methodology
State of Kansas Department of Social and Rehabilitation Services Department on Aging Kansas Health Policy Authority Notice of Proposed Nursing Facility Medicaid Rates for State Fiscal Year 2010; Methodology
Tennessee. Tennessee Department of Health, Tennessee Board of Pharmacy Pharmacy Board
 PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Tennessee Tennessee Department of Health, Tennessee Board of Pharmacy Pharmacy Board http://tn.gov/health/topic/csmd-board csmd.admin@tn.gov
PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Tennessee Tennessee Department of Health, Tennessee Board of Pharmacy Pharmacy Board http://tn.gov/health/topic/csmd-board csmd.admin@tn.gov
Prescriber Use of the PDMP: A Statewide Survey and Multistate Focus Groups
 Prescriber Use of the PDMP: A Statewide Survey and Multistate Focus Groups Richard Deyo, MD, MPH Depts. of Family Medicine & Internal Medicine, Oregon Health & Science University Jessica Irvine, MS Acumentra
Prescriber Use of the PDMP: A Statewide Survey and Multistate Focus Groups Richard Deyo, MD, MPH Depts. of Family Medicine & Internal Medicine, Oregon Health & Science University Jessica Irvine, MS Acumentra
How to Get the Most Out of Prescription Drug Monitoring Programs
 How to Get the Most Out of Prescription Drug Monitoring Programs Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-019-L03-P/T Activity Type: Knowledge-based Disclosures I own 40
How to Get the Most Out of Prescription Drug Monitoring Programs Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-019-L03-P/T Activity Type: Knowledge-based Disclosures I own 40
National Association of Boards of Pharmacy PMP Interconnect NABP
 National Association of Boards of Pharmacy PMP Interconnect NABP Problems with PMPs: Persons engaging in doctor shopping don t stay in one state, particularly areas that border other states Querying the
National Association of Boards of Pharmacy PMP Interconnect NABP Problems with PMPs: Persons engaging in doctor shopping don t stay in one state, particularly areas that border other states Querying the
TITLE 5 LEGISLATIVE RULE WEST VIRGINIA BOARD OF DENTISTRY SERIES 11 CONTINUING EDUCATION REQUIREMENTS
 TITLE 5 LEGISLATIVE RULE WEST VIRGINIA BOARD OF DENTISTRY SERIES 11 CONTINUING EDUCATION REQUIREMENTS 5-11-1. General. 1.1. Scope. This legislative rule establishes continuing education requirements for
TITLE 5 LEGISLATIVE RULE WEST VIRGINIA BOARD OF DENTISTRY SERIES 11 CONTINUING EDUCATION REQUIREMENTS 5-11-1. General. 1.1. Scope. This legislative rule establishes continuing education requirements for
eprescribing Information to Improve Medication Adherence
 eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
AN ACT. Be it enacted by the General Assembly of the State of Ohio:
 (131st General Assembly) (Substitute House Bill Number 124) AN ACT To amend section 4729.01 and to enact sections 4723.4810, 4729.282, 4730.432, and 4731.93 of the Revised Code regarding the authority
(131st General Assembly) (Substitute House Bill Number 124) AN ACT To amend section 4729.01 and to enact sections 4723.4810, 4729.282, 4730.432, and 4731.93 of the Revised Code regarding the authority
3. Practicing fraud, deceit, or misrepresentation in the practice of medicine.
 REGULATION MARKUP REGULATION NO. 2 The Arkansas Medical Practices Act authorizes the Arkansas State Medical Board to revoke or suspend the license issued by the Board to practice medicine if the holder
REGULATION MARKUP REGULATION NO. 2 The Arkansas Medical Practices Act authorizes the Arkansas State Medical Board to revoke or suspend the license issued by the Board to practice medicine if the holder
BJA COAP Category 5 Grantee Webinar Thursday, June 21, 2018
 BJA COAP Category 5 Grantee Webinar Thursday, June 21, 2018 BJA Update Tara Kunkel Senior Drug Policy Advisor IPA Bureau of Justice Assistance U.S. Department of Justice BJA Grant Project Update: Washington
BJA COAP Category 5 Grantee Webinar Thursday, June 21, 2018 BJA Update Tara Kunkel Senior Drug Policy Advisor IPA Bureau of Justice Assistance U.S. Department of Justice BJA Grant Project Update: Washington
10/4/12. Controlled Substances Dispensing Issues and Solutions. Objectives. Financial Disclosure
 Controlled Substances Dispensing Issues and Solutions Ronald W. Buzzeo, R.Ph. Chief Compliance Officer November 7, 2012 CE Code: Financial Disclosure I have no actual or potentially relevant financial
Controlled Substances Dispensing Issues and Solutions Ronald W. Buzzeo, R.Ph. Chief Compliance Officer November 7, 2012 CE Code: Financial Disclosure I have no actual or potentially relevant financial
SafetyFirst Alert. Improving Prescription/Order Writing. Illegible handwriting
 SafetyFirst Alert Massachusetts Coalition for the Prevention of Medical Errors January 2000 This issue of Safety First Alert is a publication of the Massachusetts Coalition for the Prevention of Medical
SafetyFirst Alert Massachusetts Coalition for the Prevention of Medical Errors January 2000 This issue of Safety First Alert is a publication of the Massachusetts Coalition for the Prevention of Medical
SCERC Needs Assessment Survey FY 2015/16 Oscar Arias Fernandez, MD, ScD and Dean Baker, MD, MPH
 INTRODUCTION SCERC Needs Assessment Survey FY 2015/16 Oscar Arias Fernandez, MD, ScD and Dean Baker, MD, MPH The continuous quality improvement process of our academic programs in the Southern California
INTRODUCTION SCERC Needs Assessment Survey FY 2015/16 Oscar Arias Fernandez, MD, ScD and Dean Baker, MD, MPH The continuous quality improvement process of our academic programs in the Southern California
REGULATION MARKUP REGULATION NO. 2
 REGULATION MARKUP REGULATION NO. 2 The Arkansas Medical Practices Act authorizes the Arkansas State Medical Board to revoke or suspend the license issued by the Board to practice medicine if the holder
REGULATION MARKUP REGULATION NO. 2 The Arkansas Medical Practices Act authorizes the Arkansas State Medical Board to revoke or suspend the license issued by the Board to practice medicine if the holder
Prescription Monitoring Program:
 Massachusetts Department of Public Health Prescription Monitoring Program: The Massachusetts Prescription Monitoring Tool (MassPAT) November 1, 2016 Goals of the Session Understand the mission and responsibilities
Massachusetts Department of Public Health Prescription Monitoring Program: The Massachusetts Prescription Monitoring Tool (MassPAT) November 1, 2016 Goals of the Session Understand the mission and responsibilities
NATIONAL PROGRESS REPORT
 2017 NATIONAL PROGRESS REPORT L ast year marked another chapter of growth and change in the story of the Surescripts Network Alliance. Together, we expanded the strength and number of our connections and
2017 NATIONAL PROGRESS REPORT L ast year marked another chapter of growth and change in the story of the Surescripts Network Alliance. Together, we expanded the strength and number of our connections and
2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH
 2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH Introduction to NCQA Credentialing Standards NAMSS Educational
2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH Introduction to NCQA Credentialing Standards NAMSS Educational
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM
 The Harvard Pilgrim Independence Plan SM") Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
UC Davis Pain Management Telehealth Academy
 UC Davis Pain Management Telehealth Academy Project ECHO Pain Management Telementoring Train the Trainers: Primary Care Pain Management Fellowship David J. Copenhaver, MD, MPH Associate Professor, Anesthesiology
UC Davis Pain Management Telehealth Academy Project ECHO Pain Management Telementoring Train the Trainers: Primary Care Pain Management Fellowship David J. Copenhaver, MD, MPH Associate Professor, Anesthesiology
InstyMeds Prescription Writer Tutorial
 InstyMeds Prescription Writer Tutorial July 2014 Log in to the InstyMeds Prescription Writer tool Important messages announcing the latest enhancements and notifications are located here. 1. Type in Username
InstyMeds Prescription Writer Tutorial July 2014 Log in to the InstyMeds Prescription Writer tool Important messages announcing the latest enhancements and notifications are located here. 1. Type in Username
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Issue Brief. E-Prescribing in California: Why Aren t We There Yet? Introduction. Current Status of E-Prescribing in California
 E-Prescribing in California: Why Aren t We There Yet? Introduction Electronic prescribing (e-prescribing) refers to the computer-based generation of a prescription, electronic transmission of the initial
E-Prescribing in California: Why Aren t We There Yet? Introduction Electronic prescribing (e-prescribing) refers to the computer-based generation of a prescription, electronic transmission of the initial
RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION
 RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION CHAPTER 0800-02-25 WORKERS COMPENSATION MEDICAL TREATMENT TABLE OF CONTENTS 0800-02-25-.01 Purpose and Scope
RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION CHAPTER 0800-02-25 WORKERS COMPENSATION MEDICAL TREATMENT TABLE OF CONTENTS 0800-02-25-.01 Purpose and Scope
Prescription Monitoring Program State Profiles - Texas
 Prescription Monitoring Program State Profiles - Texas Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Monitoring Program State Profiles - Texas Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Report of the Task Force on Prescription Monitoring Program Standards
 Report of the Task Force on Prescription Monitoring Program Standards Members Present: Gay Dodson (TX), chairperson; John Dorvee (ME); Danna Droz (OH); Allen F. Dulwick (OR); William Fitzpatrick (MO);
Report of the Task Force on Prescription Monitoring Program Standards Members Present: Gay Dodson (TX), chairperson; John Dorvee (ME); Danna Droz (OH); Allen F. Dulwick (OR); William Fitzpatrick (MO);
Osteopathic Advocacy: Partnering to Advance Sound Health Policy. Nicholas Schilligo, MS Associate Vice President, State Government Affairs
 Osteopathic Advocacy: Partnering to Advance Sound Health Policy Nicholas Schilligo, MS Associate Vice President, State Government Affairs Our Work Work with a variety of stakeholders to promote AOA policies
Osteopathic Advocacy: Partnering to Advance Sound Health Policy Nicholas Schilligo, MS Associate Vice President, State Government Affairs Our Work Work with a variety of stakeholders to promote AOA policies
H.B. 1, 1 st Extr. Sess. (Ky. 2012)
") State Statutes and Regulations Relative to Chronic Pain and Pain Management Emphasis on Pain Management Clinics Brief Summary of Federal Provisions June 2012 This project was supported by Cooperative Agreement
State Statutes and Regulations Relative to Chronic Pain and Pain Management Emphasis on Pain Management Clinics Brief Summary of Federal Provisions June 2012 This project was supported by Cooperative Agreement
Bold blue=new language Red strikethrough=deleted language Regular text=existing language Bold Green = new changes following public hearing
 Bold blue=new language Red strikethrough=deleted language Regular text=existing language Bold Green = new changes following public hearing 700.001: Definitions Delegate means an authorized support staff
Bold blue=new language Red strikethrough=deleted language Regular text=existing language Bold Green = new changes following public hearing 700.001: Definitions Delegate means an authorized support staff
KAREN D. McLIN 9929 NW State Road 45, High Springs, FL telephone: (813) (day); (386) (evening)
 (day); (386) (evening)") KAREN D. McLIN 9929 NW State Road 45, High Springs, FL 32643 telephone: (813) 758-6988 (day); (386) 454-7002 (evening) email: kdmclin@windstream.net EDUCATION: 2001-2003 Doctor of Pharmacy University of
KAREN D. McLIN 9929 NW State Road 45, High Springs, FL 32643 telephone: (813) 758-6988 (day); (386) 454-7002 (evening) email: kdmclin@windstream.net EDUCATION: 2001-2003 Doctor of Pharmacy University of
GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 2017 S 2 SENATE BILL 750* Health Care Committee Substitute Adopted 6/12/18
 GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 0 S SENATE BILL 0* Health Care Committee Substitute Adopted /1/ Short Title: Health-Local Confinement/Vet. Controlled Sub. (Public) Sponsors: Referred to: May,
GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 0 S SENATE BILL 0* Health Care Committee Substitute Adopted /1/ Short Title: Health-Local Confinement/Vet. Controlled Sub. (Public) Sponsors: Referred to: May,
Pharmacy Law Update for Pharmacists & Technicians October 1, 2017 Greg Baran, B.S., Pharm., M.A.
 Pharmacy Law Update for Pharmacists & Technicians October 1, 2017 Greg Baran, B.S., Pharm., M.A. Objectives: Pharmacist and Pharmacy Technician Learning Objectives: At the end of this activity, participants
Pharmacy Law Update for Pharmacists & Technicians October 1, 2017 Greg Baran, B.S., Pharm., M.A. Objectives: Pharmacist and Pharmacy Technician Learning Objectives: At the end of this activity, participants
Medication Module Tutorial
 Medication Module Tutorial An Introduction to the Medication module Whether completing a clinic patient evaluation, a hospital admission history and physical, a discharge summary, a hospital order set,
Medication Module Tutorial An Introduction to the Medication module Whether completing a clinic patient evaluation, a hospital admission history and physical, a discharge summary, a hospital order set,
South Carolina Reporting & Identification Prescription Tracking System (SCRIPTS)
") South Carolina Reporting & Identification Prescription Tracking System (SCRIPTS) Note! Contents are subject to change and are not a guarantee of payment. Webinar Reminders Webinar Reminders Agenda Welcome
South Carolina Reporting & Identification Prescription Tracking System (SCRIPTS) Note! Contents are subject to change and are not a guarantee of payment. Webinar Reminders Webinar Reminders Agenda Welcome
Centers for Medicare & Medicaid Services: Innovation Center New Direction
 Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
2017 ASAP MIDYEAR CONFERENCE THE FUTURE OF PRESCRIPTION DRUG MONITORING PROGRAMS (PMPS): HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L.
: HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L.") 2017 ASAP MIDYEAR CONFERENCE THE FUTURE OF PRESCRIPTION DRUG MONITORING PROGRAMS (PMPS): HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L. GREEN Disclosures Sherry Green is an employee of Na2onal
2017 ASAP MIDYEAR CONFERENCE THE FUTURE OF PRESCRIPTION DRUG MONITORING PROGRAMS (PMPS): HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L. GREEN Disclosures Sherry Green is an employee of Na2onal
POLICY FOR ANTICIPATORY PRESCRIBING FOR PATIENTS WITH A TERMINAL ILLNESS Just in Case
 POLICY FOR ANTICIPATORY PRESCRIBING FOR PATIENTS WITH A TERMINAL ILLNESS Just in Case DOCUMENT NO: DN116 Lead author/initiator(s): Sarah Woodley Community Health Services Pharmacist sarah.woodley@ccs.nhs.uk
POLICY FOR ANTICIPATORY PRESCRIBING FOR PATIENTS WITH A TERMINAL ILLNESS Just in Case DOCUMENT NO: DN116 Lead author/initiator(s): Sarah Woodley Community Health Services Pharmacist sarah.woodley@ccs.nhs.uk
Overview. Appriss Health Substance Use and Opioid Trends NarxCare Overview Live Demo
 Solution Overview Overview Appriss Health Substance Use and Opioid Trends NarxCare Overview Live Demo 2 Appriss Health Software provider for 42 of 52 PDMPs in U.S. Software provider for PMP Interconnect
Solution Overview Overview Appriss Health Substance Use and Opioid Trends NarxCare Overview Live Demo 2 Appriss Health Software provider for 42 of 52 PDMPs in U.S. Software provider for PMP Interconnect
NCPDP Work Group 11 Task Group: RxFill White Paper on Implementation Issues
 NCPDP Work Group 11 Task Group: RxFill White Paper on Implementation Issues Purpose: To highlight and provide a general overview of issues that arise in the implementation of RxFill transactions. The discussion
NCPDP Work Group 11 Task Group: RxFill White Paper on Implementation Issues Purpose: To highlight and provide a general overview of issues that arise in the implementation of RxFill transactions. The discussion
INSERT ORGANIZATION NAME
 INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
Pharmacy Pain Management Protocol Pharmacy Policy and Protocol
 Line of Business: Medicare and Medi-Cal Effective Date: November 18, 2015 Renewal Date: August 16, 2017 Pharmacy Pain Management Protocol Pharmacy Policy and Protocol This protocol has been developed through
Line of Business: Medicare and Medi-Cal Effective Date: November 18, 2015 Renewal Date: August 16, 2017 Pharmacy Pain Management Protocol Pharmacy Policy and Protocol This protocol has been developed through
Minnesota health care price transparency laws and rules
 Minnesota health care price transparency laws and rules Minnesota Statutes 2013 62J.81 DISCLOSURE OF PAYMENTS FOR HEALTH CARE SERVICES. Subdivision 1.Required disclosure of estimated payment. (a) A health
Minnesota health care price transparency laws and rules Minnesota Statutes 2013 62J.81 DISCLOSURE OF PAYMENTS FOR HEALTH CARE SERVICES. Subdivision 1.Required disclosure of estimated payment. (a) A health
Lethality Assessment Program Maryland Model (LAP)
") Lethality Assessment Program Maryland Model (LAP) Information Packet and Frequently Asked Questions (FAQ) Last revision: May 2015 This project was supported by Grant No. 2011-TA-AX-K111 awarded by the
Lethality Assessment Program Maryland Model (LAP) Information Packet and Frequently Asked Questions (FAQ) Last revision: May 2015 This project was supported by Grant No. 2011-TA-AX-K111 awarded by the
Forecasts of the Registered Nurse Workforce in California. June 7, 2005
 Forecasts of the Registered Nurse Workforce in California June 7, 2005 Conducted for the California Board of Registered Nursing Joanne Spetz, PhD Wendy Dyer, MS Center for California Health Workforce Studies
Forecasts of the Registered Nurse Workforce in California June 7, 2005 Conducted for the California Board of Registered Nursing Joanne Spetz, PhD Wendy Dyer, MS Center for California Health Workforce Studies
POLICIES, PENALTIES AND PROCEDURES
 POLICIES, PENALTIES AND PROCEDURES Policies exist to eliminate confusion and define for all people involved how things will be done in our practice. That way there is no misunderstanding and no perception
POLICIES, PENALTIES AND PROCEDURES Policies exist to eliminate confusion and define for all people involved how things will be done in our practice. That way there is no misunderstanding and no perception
Reporting Requirements and Exemptions to Reporting
 Reporting Requirements and Exemptions to Reporting Research current through May 2016. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Reporting Requirements and Exemptions to Reporting Research current through May 2016. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL
 PROVIDER MANUAL") THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL SUPPLEMENTAL INFORMATION This Supplement to the Optima Health Provider Manual is available for Providers who provide services
THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL SUPPLEMENTAL INFORMATION This Supplement to the Optima Health Provider Manual is available for Providers who provide services
Roadmaps to Health Community Grants
 40 YEARS OF IMPROVING HEALTH AND HEALTH CARE Roadmaps to Health Community Grants 2012 Call for Proposals Brief Proposal Deadline May 2, 2012 Program Overview (For complete details, refer to specific pages/sections
40 YEARS OF IMPROVING HEALTH AND HEALTH CARE Roadmaps to Health Community Grants 2012 Call for Proposals Brief Proposal Deadline May 2, 2012 Program Overview (For complete details, refer to specific pages/sections
Guidelines on the Keeping of Records in Respect of Medicinal Products when Conducting a Retail Pharmacy Business
 Guidelines on the Keeping of Records in Respect of Medicinal Products when Conducting a Retail Pharmacy Business to facilitate compliance with Regulation 12 of the Regulation of Retail Pharmacy Businesses
Guidelines on the Keeping of Records in Respect of Medicinal Products when Conducting a Retail Pharmacy Business to facilitate compliance with Regulation 12 of the Regulation of Retail Pharmacy Businesses
CHAPTER 29 PHARMACY TECHNICIANS
 CHAPTER 29 PHARMACY TECHNICIANS 29.1 HOSPITAL PHARMACY TECHNICIANS 1. Proper Identification as Pharmacy Technician 2. Policy and procedures regulating duties of technician and scope of responsibility 3.
CHAPTER 29 PHARMACY TECHNICIANS 29.1 HOSPITAL PHARMACY TECHNICIANS 1. Proper Identification as Pharmacy Technician 2. Policy and procedures regulating duties of technician and scope of responsibility 3.
DATA SOURCES AND METHODS
 DATA SOURCES AND METHODS In August 2006, the Department of Juvenile Justice s (DJJ) Quality Assurance, Technical Assistance and Research and Planning units were assigned to the Office of Program Accountability.
DATA SOURCES AND METHODS In August 2006, the Department of Juvenile Justice s (DJJ) Quality Assurance, Technical Assistance and Research and Planning units were assigned to the Office of Program Accountability.
ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-19 PAIN MANAGEMENT SEVICES TABLE OF CONTENTS
 Medical Examiners Chapter 540-X-19 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-19 PAIN MANAGEMENT SEVICES TABLE OF CONTENTS 540-X-19-.01 540-X-19-.02 540-X-19-.03 540-X-19-.04
Medical Examiners Chapter 540-X-19 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-19 PAIN MANAGEMENT SEVICES TABLE OF CONTENTS 540-X-19-.01 540-X-19-.02 540-X-19-.03 540-X-19-.04