Strengthening institutional capacity for nursing training on HIV/AIDS & Tuberculosis (GFATM R7) KNOWLEDGE, ATTITUDE & PRACTICES OF NURSES TOWARDS TB
|
|
|
- Sophie Gilbert
- 6 years ago
- Views:
Transcription

1 KNOWLEDGE, ATTITUDE & PRACTICES OF NURSES TOWARDS TB BASALINE SURVEY 2014
2 KNOWLEDGE, ATTITUDE & PRACTICES OF NURSES TOWARDS TB BASALINE SURVEY
3
4 Table of contents Content Page Abbreviations 3 List of Tables 4 List of Figures 4 Executive Summary 6 1. Introduction TB burden in India RNTCP: Revised National TB Control Programme INC: Training of Nurses on TB case management Rationale Methodology Sample Framework Sample size Data collection Data Analyses Quality Assurance Limitations and Challenges Results Demographics Knowledge on TB Attitude and Practices towards TB Attitude and Practices Leading to Delay in TB Treatment Discussion Conclusions Recommendations 41 Annexure I: TB questionnaire for Nurses 42 2
5 Abbreviations AIDS Acquired immune deficiency syndrome ANM Auxiliary Nurse Midwife B.Sc (N) Bachelor of Science degree in Nursing DNEA Diploma in Nursing Education and Administration EQA External Quality Assessment GNM General Nursing Midwifery HIV Human immunodeficiency virus IRL Intermediate Reference Laboratory KAP Knowledge, Attitude and Practices MDRTB Multi Drug Resistant TB M.Sc (N) Master of science degree in Nursing NGO Non Governmental Organization NRL National Reference Laboratory PLHIV People Living with HIV and AIDS RNTCP Revised National Tuberculosis Control Programme STDC State Tuberculosis Training & Demonstration Centre TB Tuberculosis WHO World Health Organization XDR-TB Extensively Drug Resistant TB List Of Tables Table 1. TB burden in India 10 Table 2. MDR and TB-HIV burden in India 11 Table 3. Socio-demographic profile of respondents 25 Table 4. Resources available for capacity building of the 26 nurses Table 5. Knowledge of nurses about TB 29 Table 6. Knowledge score of nurses on TB 30 Table 7. Socio demographic characteristics of Nurses 31 and their association with knowledge score Table 8. Availability of resources and association with knowledge score 32 Table 9. Attitude and practices of nurses about 34 Tuberculosis Page No. Table 10. Table 11. Socio demographic variables and attitude and practices towards TB Availability of resources and attitude and practices towards TB
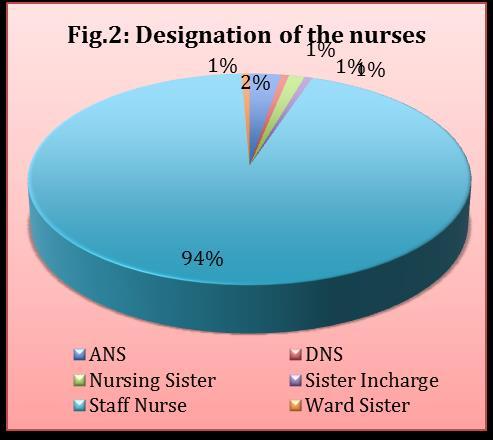
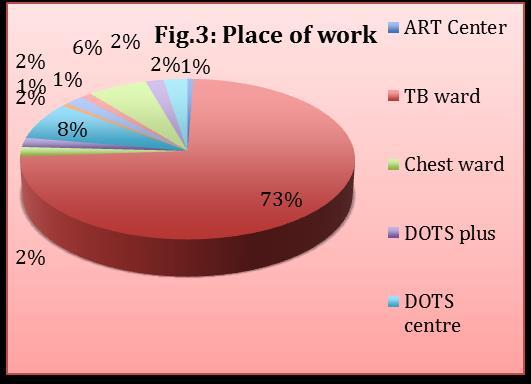
6 Table 12 Attitude and practices score of nurses and their association with knowledge about Tuberculosis 37 List Of Figures Page No. Fig. 1 District-wise coverage of PMDT services 13 Fig. 2 Designation of the nurse 22 Fig. 3 Place of posting 22 Fig. 4 Gender 23 Fig. 5 Age 23 Fig. 6 Qualification 23 Fig. 7 Yrs of service in current position 23 Fig. 8 Yrs of service 23 Fig. 9 Number of TB patients seen in a month 23 Fig. 10 Type of facility 24 Fig. 11 Resources available 24 Fig. 12 Criteria to identify TB suspect 27 Fig.13 Symptoms of TB 27 Fig.14 Investigations for diagnoses of TB 28 Fig. 15 TB cure strategy 29 Fig.16 Minimum duration of treatment of Pulmonary TB 29 Fig. 17 Can Reinfection Occur In Previously Treated 29 Case Fig. 18 What Is Recurrent TB? 29 Fig. 19 Attitude towards TB 33 Fig. 20 Prevention of TB 33 Fig. 21 Health education and counseling to TB patients 37 Fig. 22 Topics covered during health education 37 sessions Fig. 23 Resource material 37 Fig. 24 Source of educational material 37 Fig. 25 Causes of Delay in Seeking Treatment for TB 39 Fig. 26 Treatment Taken Prior To Accessing This 39 Facility Fig. 27 Delay In TB Diagnoses Longer Among 39 Fig. 28 Delay In MDR Treatment 39 4
7 Contributors Mr. T. Dileep Kumar, INC Dr. Asha Sharma, INC Mrs. K. Bharati, INC Dr. S. N. Misra, Futures Group Dr. Jayanti Singh, Futures Group Mrs. Shanta Misra, Futures Group Ms. Poornima Sharma, Futures Group Dr. Dilip Vaswani, Futures Group 5
8 Executive Summary Introduction: India is the second-most populous country in the world and has one fourth of the global incident TB cases occur in India annually. In 2012, out of the estimated global annual incidence of 8.6 million TB cases, 2.3 million were estimated to have occurred in India. Tuberculosis prevalence per lakh population has reduced from 465 in year 1990 to 230 in Incidence per lakh population has reduced from 216 in year 1990 to 176 in 2012.Tuberculosis mortality per lakh population has reduced from 38 in year 1990 to 22 in As per the WHO Global Report on Tuberculosis 2013, India accounts for 64,000 MDRTB cases out of 300,000 cases estimated globally to occur among the notified pulmonary TB cases annually. In 2013, TB suspects examination rate has further increased to 651 per 100,000 population. A total of smear positive TB patients were diagnosed and 14,10,880 patients were registered for treatment under RNTCP. Overall success rate of new and retreatment TB cases is 88% and 70% respectively. RNTCP has established a nationwide laboratory network of over 13,000 DMCs, which are supervised by the IRLs at the state level and NRLs and Central TB Division at the national level. INC supported by Futures Group International will be conducting training of nurses and ANMs on TB under GFATM project. Rationale: This KAP study investigates nurses regarding their knowledge, attitudes towards TB, and TB-care practices, and studies the related factors. The results of this study will be used to plan for better training provision in terms of strengthening nurses capabilities, hence improving patient care, and delivering higher quality services. The assessment survey is conceptualized to generate baseline data on nurses knowledge, attitude and practices for TB. Methodology: This is a cross sectional survey. This KAP survey was conducted through Nursing Colleges associated with GFATM project as SRs or SSRs. The Survey was offered to 10 nurses posted in DOTS centre, TB clinics and TB wards in tertiary hospitals or district hospitals in 20 districts across five zones throughout India during the months of June and July For the purpose of this survey, the districts and the DOTS centre/ TB clinic/ TB 6
9 wards in tertiary or district hospital within each zone were selected through judgmental sampling method and within the facility the nurses were selected randomly. A Semi structured questionnaire was used as a tool for this KAP study. Data were analyzed using SPSS version 17. The chi-square test was used in bivariate statistical analysis, to assess the relationship between the variables. Results: Majority of the respondent nurses were staff nurses and mostly posted at TB wards at the time of interview. 80.6% nurses responded having list of essential drugs. Guidelines on infection prevention and control were available to 88.5% respondents and 81.2% nurses had guidelines on management of drug resistant TB. More than half of the respondents did not receive any training on TB and 7 did not respond to this question. 75.2% of the respondents did not receive any TB update. 30.3% of the nurses do not know if there was TB focal person in their facility. Under criteria to identify TB suspect 91.5% of the nurses said contact of active TB cases, followed by people living with HIV/AIDS. Most know symptoms of TB were cough followed by fever and weight loss, with 98.8%, 91.5% and 90.3% response from the nurses. Night sweat and pallor was recognized, as may be symptom of TB in 64.2% and 48.5% of responses. Haemoptysis is recognized as a symptom of TB in 72.7% respondents and weakness in 76.4% responses. No response with antibiotics was responded positively by only 36.4%. Investigations conducted for identifying TB cases according to 98.8% nurses was sputum smear examination. 98.2% also mentioned chest X-ray. DOTS strategy for TB cure was responded by 98.8% of the nurses. Minimum duration of treatment for Pulmonary TB case as six months was responded by 88.5% of the nurses. 93.9% of the nurses said that reinfection could occur in previously treated case of TB. Recurrent TB was known to 72.7% of the nurses. The respondents score of knowledge of TB was excellent for 21.8%, good 35.8%, average 33.9% and 8.5 % had below average knowledge. 86.1% of the nurses recognized TB as a major public health treat. According to 97% of nurses nutritional support should be provided to the TB patients. 87.3% of the nurses said that vulnerable groups for TB are being identified, but 79.5% that vulnerable groups are being actively approached for TB screening. Covering of nose and mouth while coughing or 7
10 sneezing prevents infection spread according to 159 nurses followed by good nutrition. Misconceptions like practicing safe sex, avoiding sharing of dishes and hand shaking as per 25, 30 and 31 responses respectively can prevent TB infection. Education and counseling for TB is being offered to TB patients as per the responses in 92.6%, however 92.9% and 91.6% of nurses said HIV/TB co-infection counseling and MDR-TB education and counseling respectively is also offered is offered to patients. 150 nurses covered treatment adherence during health education session, followed by TB symptoms by 147 respondents. 27% and 25% of the nurses used booklets and pamphlets respectively. 29% did not respond regarding the type of resource material used by them. Source of educational material was mainly RNTCP (70%). Respondents with score of 2 or less had poorer knowledge about TB. Respondents with score 6 and more had 23.9% excellent knowledge, 35% good, 31.6% average and 9.4% poor knowledge of TB. 60% nurses said that delay is due to patients unawareness, followed by patients difficulty in accessing the health facility followed by TB patient s preference of informal health care providers. According to 12 responses the delay is due to time send in sending and receiving of test results and 2 responded as uncertainty regarding testing and treatment protocol is causing delay. Private sector providers treat 40% of the patients before they arriving to the health facility for TB, 24% are self treated, 25% by other government doctor and 4% by pharmacists and druggist. Time elapsed before diagnoses is about the same for both gender as per 32% of the responses, 31% felt it took longer among men, while 14% and 16% felt the delay longer among women and children respectively. 44% of the respondents said delay in treatment of MDR TB is mainly due to patient refusal, 24% said due to non-availability of second line of drugs, 11% due to shortage of MDR beds and 6% said that patient died before treatment initiation. Conclusions and recommendations: Slightly more than half (57.6%) of nurses have above average knowledge score. All nurses should, therefore, undergo TB training to increase or update their knowledge. Guidelines on PMDT and infection control should be provided to all nurses. Nodal person if possible should be available in all tertiary institutes. Comprehensive health education and counseling should be provided to all TB patients 8
11 focusing on MDR and TB-HIV co-infection cases. Health system factors leading to delay in treatment of TB including MDR as mentioned by nurses should be looked into, analyses and thereafter necessary actions should be taken by the TB control program authorities and locally at the facility by the concerned administrative person. Behaviour change communication strategy should be developed focusing to create awareness among patients to seek early treatment. MDR patients should be proactively counseled to overcome the hurdle of patients refusal in initiating treatment. 9
12 1. Introduction 1.1. TB burden in India India is the second-most populous country in the world and has one fourth of the global incident TB cases occur in India annually. In 2012, out of the estimated global annual incidence of 8.6 million TB cases, 2.3 million were estimated to have occurred in India. As per WHO estimations, Tuberculosis prevalence per lakh population has reduced from 465 in year 1990 to 230 in In absolute numbers, prevalence has reduced from 40 lakhs to 28 lakhs annually. Incidence per lakh population has reduced from 216 in year 1990 to 176 in 2012.Tuberculosis mortality per lakh population has reduced from 38 in year 1990 to 22 in In absolute numbers, morality due to TB has reduced from 3.3 lakhs to 2.7 lakhs annually. Table: 1 TB burden Number (Millions) (95% CI) Rate Per 100,000 Persons (95% CI) Incidence 2.2 ( ) 176 ( ) Prevalence 2.8 ( ) 230 ( ) Mortality 0.27 ( ) 22 (14 32) WHO estimated burden of tuberculosis in India, 2012 Table: 2 TB burden Number (Millions) Percent (95% (95% CI) CI) HIV among estimated incident TB patients 0.13 ( ) 5.6 ( ) MDR-TB among notified pulmonary TB patients ( ) MDR-TB among notified New pulmonary TB 2.2% ( ( ) patients 2.6%) MDR-TB among notified Re-treatment pulmonary ( ) TB patients 15% (11 19%) WHO estimated burden of tuberculosis in India,
13 India is one of the countries in the world with the highest burden of multidrug-resistant tuberculosis (MDR-TB). As per the WHO Global Report on Tuberculosis 2013, India accounts for 64,000 MDRTB cases out of 300,000 cases estimated globally to occur among the notified pulmonary TB cases annually. As per the Global Report on Tuberculosis 2013, there were an estimated 5,30,000 TB cases among children (under 15 years of age) and TB deaths (among HIV-negative children) in 2012 (6% and 8% of the global totals, respectively). It is one of the top 10 causes of childhood mortality. Though MDR-TB and XDR- TB is documented among paediatric age group, there are no estimates of overall burden, chiefly because of diagnostic difficulties and exclusion of children in most of the drug resistance surveys. India s TB control programme is on track as far as reduction in disease burden is concerned. There is 42% reduction in TB mortality rate by 2012 as compared to 1990 level. Similarly there is 51% reduction in TB prevalence rate by 2012 as compared to 1990 level. These estimations were based on RNTCP data, 7 Prevalence surveys in India conducted between , National ARTI surveys, mortality surveys conducted in RNTCP: Revised National TB Control Programme In 2013, TB suspects examination rate has further increased to 651 per 100,000 population. A total of smear positive TB patients were diagnosed and 14,10,880 patients were registered for treatment under RNTCP. Total case notification rate per 1,00,000 population was 113 which is decreasing since last 5 years. Incident TB case notification rate is also declining since last 5-6 years and in 2013 it was 91 per 1,00,000 population. Overall success rate of new and retreatment TB cases is 88% and 70% respectively. RNTCP has established a nationwide laboratory network of over 13,000 DMCs, which are supervised by the IRLs at the state level and NRLs and Central TB Division at the national level. One IRL has been designated in the STDC Public Health 11
.")
14 Laboratory/ Medical College of the respective state. Six NRLs have been established under RNTCP. The RNTCP aims to consolidate its laboratory network and organize a defined hierarchy for conducting sputum microscopy with external quality assessment (EQA). There are 51 RNTCP certified C&DST laboratories in the country, which include laboratories from the public sector (IRLs and medical colleges), private sector and operated by NGOs. After complete geographical coverage of the country for PMDT services, number of MDR TB suspects who were offered DST increased in 2013 with diagnosis of MDR TB cases, of which were put on treatment. With early diagnosis of MDR TB, the outcomes of treatment are expected to improve, however mortality and default are still around 20% each. Fig: 1 Source: TB INDIA 2014 Revised National TB Control Programme Annual Status Report The key activities undertaken for enhancements of programmatic management of drug resistant TB under RNTCP in India are summarized below: 12
15 India has introduced PMDT services in all 35 states on 24th March As on February 2014,PMDT services are available in all 35 states of the country across 704 districts covering the entire population (100%) of the country 110 DR TB wards established with airborne infection control measures by end of The country has shown an accelerated progress in scale up of PMDT diagnostic services as compared to the early implementation years from A total of 51 C-DST labs were established using various technologies- 37 Solid culture labs, 12 Liquid culture labs and 41 LPA labs MDR-TBsuspects were tested for MDR-TB and patients were initiated on MDR-TB treatment during Focused and periodic intensive PMDT review meetings at regional levels with key state officials were conducted in 2013 with the objective to closely monitor the progress made by every state in their PMDT scale up plans and to further accelerate the scale up of PMDT services by addressing challenges through timely intervention. Programme is in the process of developing guidelines and regulation of newer anti- TB drugs in India. To look into possibility of introduction of Bedaquiline in India a protocol for multi-centric study is being finalized for four selected sites in the country. Additional Human Resources: Each DRTB Centre is provided with a counselor. Counseling of DRTB patients and their families is important for compliance to treatment, identification and management of adverse reaction to drugs and to ensure social security. TB-HIV coordination is incrementally improving with 60% of the patients with known HIV status, and 90% of the HIV positive TB patients receiving Cotrimoxazole Preventive Therapy (CPT), and 84% receiving Anti-Retroviral Therapy (ART). However, outcomes of HIV positive TB patients continue to be poorer with less than 80% success rate amongst the new patients. Programme is considering to pilot daily anti-tb regimen to improve these outcomes. 13
16 Among new TB cases 5% of patients were in pediatric age-group (0-14 yrs). The National Technical Working Group (NTWG) on Paediatric TB has been constituted and its first meeting took place on July This committee has examined the current policy & practices and provides suggestions to CTD for improving situation of childhood TB INC Training of Nurses on TB case management Nurses working in primary health care are often the only health professionals available for TB prevention, detection, care, and treatment, and a competent nursing workforce is crucial for the success of TB programs. They are responsible for educating and supporting patients with TB, detecting medication side effects, educating and supporting patients at home through and follow-up clinics. Nurses are also responsible for screening those who have been in close contact with patients with infectious TB and perhaps running clinics for patients taking prophylactic TB treatment. Because of their frontline presence in all healthcare facilities and their diversity of skills, nurses are the natural allies in the fight against TB. Indian Nurses Council, nursing regulatory bodies, and schools of nursing are challenged to work closely with the national TB program to ensure continuous nursing competence and an expanded scope of practice in TB prevention and care. The objective of the training of nurses and ANMs on TB case management is to reach and sustain a situation where nurses at different levels of the health system have the knowledge and skills (in other words are competent) necessary to successfully implement and sustain TB control activities under RNTCP including the implementation of new and revised strategies PMDT and TB-HIV co infection. Additionally INC is also looking at longterm objective of this TB training to enhance nursing competence by integrating TB into the basic nursing curriculum and providing continuing education programs. 14
17 2. Rationale This KAP survey is a representative study of nurses to collect information on what is known, believed and done in relation to a TB. KAP survey data are essential to help plan, implement and evaluate TB trainings. This survey will gather information about what respondents know about TB, what they think about people with TB or about the health system response to TB, and causes of delay in TB treatment. KAP surveys can identify knowledge gaps, cultural beliefs, or behavioural patterns that may facilitate understanding and action, as well as pose problems or create barriers for TB control efforts. This study will help in identifying information about attitude and common practices with regards to TB. KAP surveys hope to identify training needs of the nurses and ANMs, problems and barriers in programme delivery, as well as solutions for improving quality and accessibility of services. The data collected will enable CTD and INC to set TB Training programme priorities. This KAP assessment covers: Understanding of TB infection and control including DOTS, PMDT and TB- HIV co-infection Knowledge about government program - RNTCP Knowledge regarding infection control Causes of delay in treatment Understanding the present practices of the nurses regarding TB patients Patient counseling Health education This study, therefore, investigates nurses regarding their knowledge, attitudes towards TB, and TB-care practices, and studies the related factors. The results of this study can be used to plan for better training provision in terms of strengthening nurses capabilities, hence improving patient care, and delivering higher quality services. The assessment 15
18 survey is conceptualized to generate baseline data on nurses knowledge, attitude and practices for TB. 3. Methodology 3.1. Sample Framework Knowledge, attitude and practices survey of nurses on TB was commissioned by Indian Nursing Council with the support from Futures Group International Pvt. Limited. This is a cross sectional survey. This KAP survey was conducted through Nursing Colleges associated with GFATM project as SRs or SSRs. The Survey was offered to nurses posted in DOTS centre, TB clinics and TB wards in tertiary hospitals or district hospitals. The survey was conducted in 20 districts under all 5 SRs across five zones throughout India during the months of June and July For the purpose of this survey, the districts and the DOTS centre/ TB clinic/ TB wards in tertiary or district hospital within each zone were selected through judgmental sampling method and within the facility the nurses were selected randomly. The distribution of districts according to the zones is as under: North Zone Delhi, Lucknow, Ludhiana, West Ahmedabad, Indore, Mumbai, Pune South Bangalore, Calicut, Hyderabad, Kozhikode, Kurnool, Madurai, Puduchery, Ramanathapuram East Raipur North East Chingmeirong Imphal, Guwahati, Kamrup, Kohima 16
19 3.2. Sample Size Each Nursing College conducting the survey interviewed 10 nurses posted at DOTS center, TB clinic or TB ward at tertiary hospital or District hospital or TB hospital. The nurses were chosen randomly at the health facility based on their availability. Inclusion criteria Nurses with some experience of working with the TB patients. They may be posted in TB ward, DOTS center or TB OPD at the tertiary level hospital. Willingness and availability of the nurse without interrupting the working of the facility. Exclusion criteria Nurses who have undergone GFATM TB training within 2 months 3.3. Data Collection The M.Sc or PhD nursing students from Nursing Colleges (preferably from non SR/SSRs to avoid bias), based in these districts were trained to conduct the KAP survey under the leadership of the principals of the respective colleges. The data collectors should not have undergone any GFATM training. Approximately 20 minutes were required for each interview. The nurses were approached and their recruitment in the survey was totally voluntary. Conscious efforts were put in to cause minimal disruption to the functioning of the healthcare facility. Variables Data collected included variables like age, sex, nursing qualification, years of service, place of present posting, training undergone for TB case management and infection control. 17
20 Assessment Tools A Semi structured questionnaire (Annexure I), consisting of five sections on general information about respondents and facility, knowledge and attitude towards TB and TB care practices, reasons for delay in TB treatment and patient education and counseling offered by respondents. Answers were categorized into either correct (if matching the medically correct answer from the RNTCP guidelines), or incorrect. One score was given for each of the correct answers. Futures group provided the overall survey structure, training and guidance. Ethical Consideration In Survey Administration Ethical clearence for this survey was obtained from CTD before the commencement of the survey. Permission to conduct this survey was requested and obtained from the concerned facility superintendent. The participation of nurses was completely voluntary. Informed consent of each participant was taken. It was explained to the participants that anonymity will be maintained and they have the option to decline the participation anytime. No personal identifiers was entered onto the survey form. Although the survey questionnaire was printed in English, the interview was conducted in vernacular language also for convenience and understanding of the respondents. All the forms have date, site and name of the interviewer Data Analysis Data were entered in Excel. The data were first checked for completeness and consistency by the coordinator appointed by the nursing college conducting the survey. Before final analysis, data were cleaned and questionnaires with missing variables, information or mistakes were left out of the analysis. Coding was also done at this stage. Data were 18
21 analyzed using SPSS version 17. The chi-square test was used in bivariate statistical analysis, to assess the relationship between each of the variables Quality Assurance Survey guidelines and tools were developed in consultation with Indian Nursing Council, CTD and Futures Group International. Nursing Colleges Principals and Training Coordinators were oriented for the survey, which was henceforth conducted under their guidance. PhD and MSC students from the respective colleges were identified for the purpose of conducting the interview. These identified students were trained to ensure that they thoroughly understood the survey methodology, the assessment questionnaire and the process of data collection from participants. A team supervisor supervised the interviews. At the end of each day, questionnaires were checked for errors and missing data in order to rectify this while still at the study site. Futures Group staff supervised a random 5% of the interviews. The nursing colleges were responsible for collecting the duly checked questionnaire and then sending them to Futures Group to be entered into the database Limitations and Challenges This is a KAP survey. There are few limitations to this assessment study. It is possible that there may be some element of bias since the data collectors and the local coordinators are from the nursing institutes and the respondents are also nurses. However students from the non-sr/ssr colleges were given preference. 19
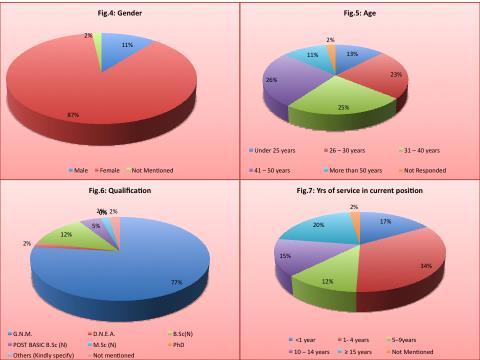
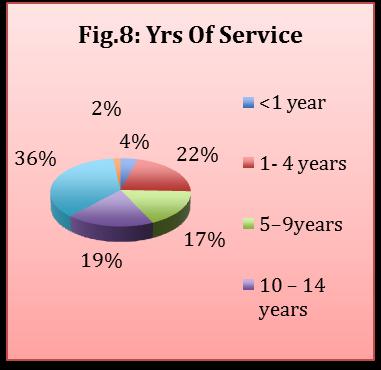
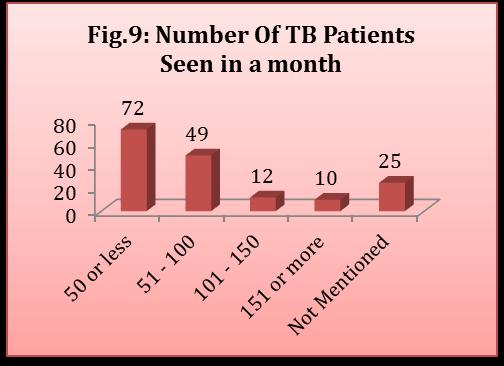
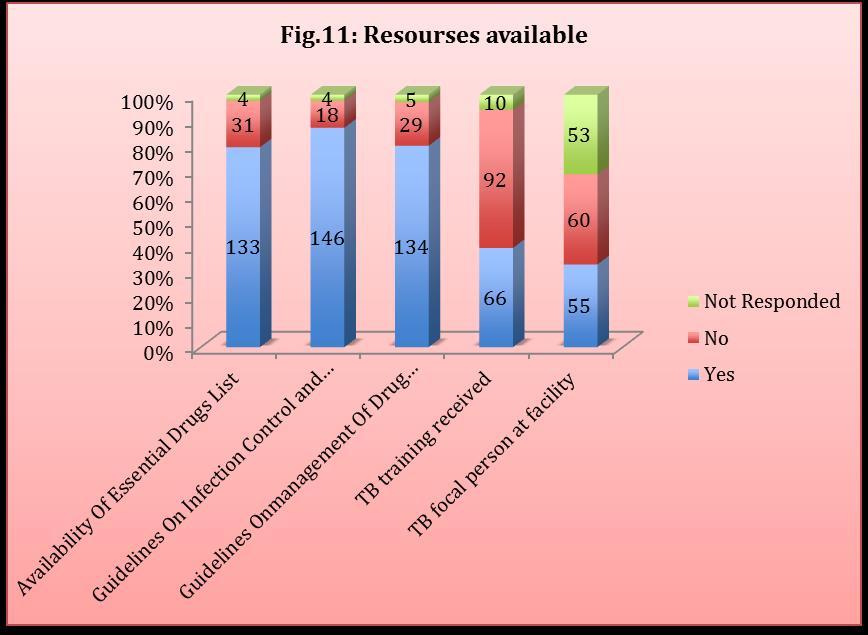
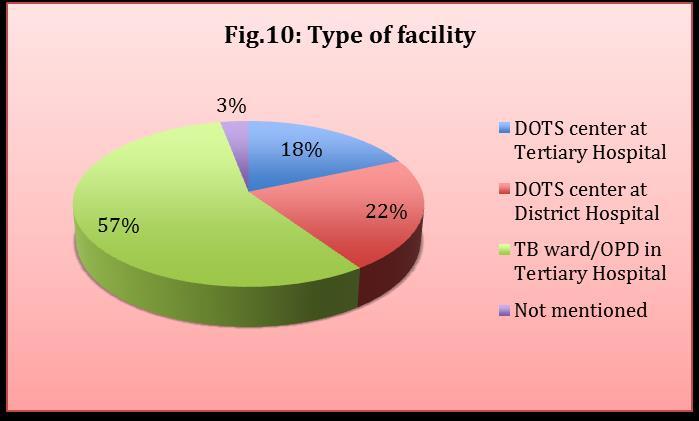
22 4. Results The results are based on 165 respondent nurses who completed the interview. Three forms had to be rejected, as they were incomplete Demographics Majority of the respondent nurses were staff nurses and mostly posted at TB wards at the time of interview. 89.1% of the respondents are female. Most of the respondents were between the age of 25 and 50. Only 12.7% and 11.5% of the respondents were under 25 years and more then fifty years respectively. 78.2% of the nurses taking the survey were G.N.M. while 12.7% were B.Sc (N). None of the respondent was PhD. Maximum number of nurses 34.5%, have been serving for 1 to 4 years at their current position, 20.6% more than 15 years, 17% less than one year. Among the respondents 37% had total services of more than 15 years, followed by 21.8%, 19.4%, 17.6 and 4.2% with total service bracket of 1 to 4 years, 10 to 14 years, 5 to 9 years and less than 1 year respectively. 43.6% attended less than 50 TB patients while 30.9% attended 50 to 100 TB patients per month. 20 nurses could not recall number of TB patients attended per month. Slightly more than of the nurses interviewed were from TB ward or OPD of a tertiary hospital, 22.4 % from the DOTS centre at the district hospital while 18.8% were from DOTS centre of a tertiary hospital. 133 nurses responded having list of essential drugs. Guidelines on infection prevention and control were available to 146 respondents and 134 nurses had guidelines on management of drug resistant TB. More than half of the respondents did not receive any training on TB and 7 did not respond to this question. 23 nurses received training on TB in 2014, 8 in 2013 and 25 received training before Of the nurses who received TB training 34.4% received one day training, 24.6% received 2 day training. 75.2% of the respondents did not receive any TB update. Those who do receive update the range is from one month to a year. 30.3% do not know if there was TB focal person in their facility. Table 3 and 4 and figures 2 to 14 shows the socio-demographic profile and resources available for capacity building of the respondents. 20
23 21
24 22
25 23
26 Table 3: Socio-demographic characteristics of the participants (N=165) Characteristics N % Gender Male Female Under 25 years years Age years years More than 50 years G.N.M Nursing Qualification D.N.E.A B.Sc (N) Post Basic B.Sc (N) M.Sc (N) <1 year years Years of Service in Current 5 9years Position years years <1 year years Total Years of Service 5 9years years years Number of TB cases/ suspects seen by the nurse per month Type of Health Facility Less than 50 cases More than Unknown DOTS center at Tertiary Hospital DOTS center at District Hospital TB ward/opd in Tertiary Hospital
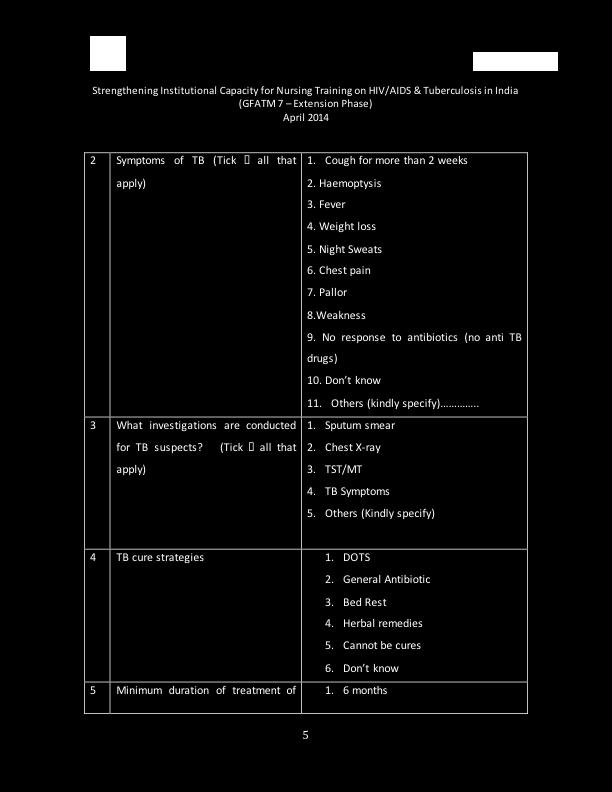
27 Table 4: Resources available for capacity building of the Nurses N % Yes Do you have an Essential Drugs List? No Do you have Guidelines on Infection Yes Prevention and Control? No Do you have Guidelines on the Yes management of Drug Resistant TB? No Yes Did you receive any training in TB? No No response Receive update on TB Yes No Do you have a TB focal person in the facility? Yes No No response Knowledge of TB Table 5 shows respondent nurses knowledge about TB. Under criteria to identify TB suspect 91.5% of the nurses said contact of active TB cases, followed by people living with HIV/AIDS. Most know symptoms of TB were cough followed by fever and weight loss, with 98.8%, 91.5% and 90.3% response from the nurses. Night sweat and pallor was recognized, as may be symptom of TB in 64.2% and 48.5% of responses. Haemoptysis is recognized as a symptom of TB in 72.7% respondents and weakness in 76.4% responses. No response with antibiotics was responded positively by only 36.4%. Investigations conducted for identifying TB cases according to 98.8% nurses was sputum smear examination. 98.2% also mentioned chest X-ray. DOTS strategy for TB cure was 25

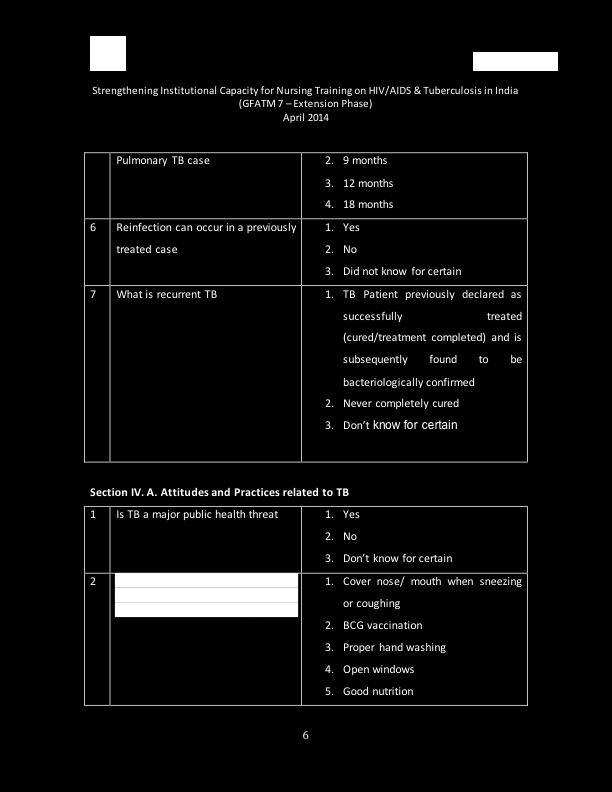
28 responded by 98.8% of the nurses. Minimum duration of treatment for Pulmonary TB case as six months was responded by 88.5% of the nurses. 93.9% of the nurses said that reinfection could occur in previously treated case of TB. Recurrent TB was known to 72.7% of the nurses. Seven respondents scored 100%, 6 of which are from Delhi and one from Mumbai. 26


29 Score was categorized in four categories, excellent, good, average and poor. The respondents score of knowledge of TB was excellent for 21.8%, good 35.8%, average 33.9% and 8.5 % had below average knowledge. (Table 6). 27
 What criteria are used to identify Homeless 52 (31.5) TB suspects? Health care worker 58 (35.2) Senior citizen 68 (41.2) Children under 5 yrs 61 (37.0) No response to antibiotics 58 (35.")
30 Table 5: Knowledge of nurses about TB Knowledge variable N (%) Contacts of active TB 151 (91.5) People living with HIV/ AIDS 113 (68.5) Prison inmates 37 (22.4) What criteria are used to identify Homeless 52 (31.5) TB suspects? Health care worker 58 (35.2) Senior citizen 68 (41.2) Children under 5 yrs 61 (37.0) No response to antibiotics 58 (35.2) Cough for more than 2 weeks 163 (98.8) Symptoms of TB Haemoptysis 120 (72.7) Fever 151 (91.5) Weight loss 149 (90.3) Night sweats 106 (64.2) 28
31 What investigations are conducted for TB suspects? Chest pain 116 (70.3) Pallor 80 (48.5) Weakness 126 (76.4) No response to antibiotics (no anti TB drugs) 60 (36.4) Sputum smear 163 (98.8) Chest X-ray 162 (98.2) TST/ MT 84 (50.9) TB symptoms 84 (50.9) TB cure: DOTS strategies 162 (98.2) Minimum duration of treatment of Pulmonary TB case: 6 months 146 (88.5) Re-infection can occur in a previously treated case 155 (93.9) What is recurrent TB 120 (72.7) Table 6: Knowledge score of nurses on TB Knowledge score N (%) Result (21.8) Excellent (35.8) Good (33.9) Average (8.5) Poor Socio demographic characteristics of Nurses and their association with knowledge score is shown in Table 7 and availability of resources and knowledge score is represented in Table 8. There is statistically significant association between socio-demographic variables of age (P= ), qualification (P= ), duration of service in the current position (P= ), total service (P= and type of facility (P= ) with knowledge. Gender is not significantly linked to knowledge score. Resources available to the nurses are statistically associated with the knowledge score, availability of guidelines on infection prevention and control (P= ), guidelines on PMDT (P= ), training on TB (P= ) and receiving updates on TB (P= ). Presence of focal person for TB is not linked to knowledge score. 50 respondents were not even aware of the presence of the focal person. 29
32 Table 7: Socio demographic characteristics of Nurses and their association with knowledge score. Characteristics Mean Excellent Good Average Poor SD Significance score N % N % N % N % Gender Age Nursing Qualification Years of Service in Current Position Total Years of Service Health Facility Male Female Under 25 years years years years More than 50 years X 2 = The P= The result is not significant at p < X 2 = P= The result is significant at p < G.N.M X 2 = P= D.N.E.A The result is B.Sc (N) significant at Post Basic p < B.Sc (N) M.Sc (N) <1 year X 2 = P= years The result is 5 9years significant at p < years 15 years <1 year X 2 = P= years The result is 5 9years significant at p < years 15 years DOTS center at Tertiary Hospital DOTS center at District Hospital TB ward/opd in Tertiary Hospital X 2 = P= The result is significant at p <
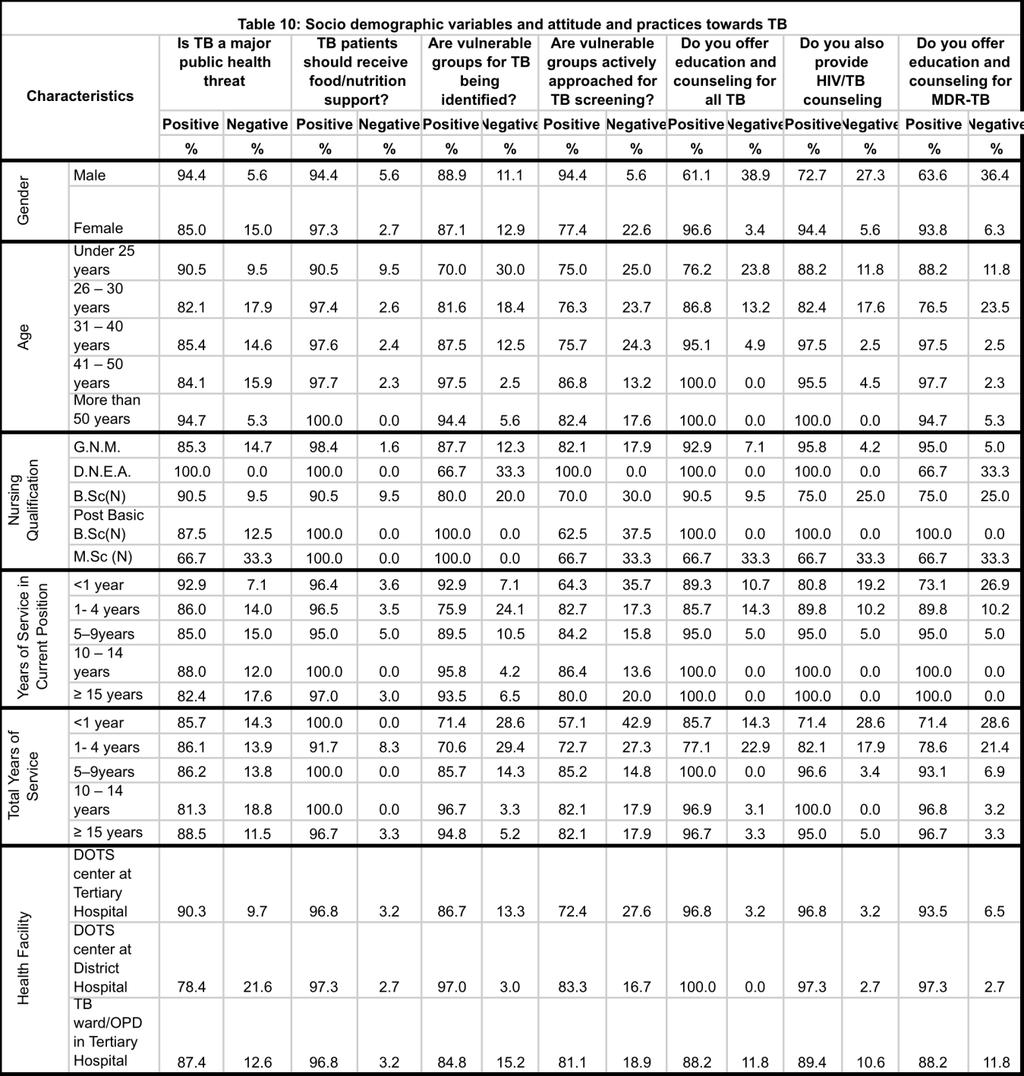
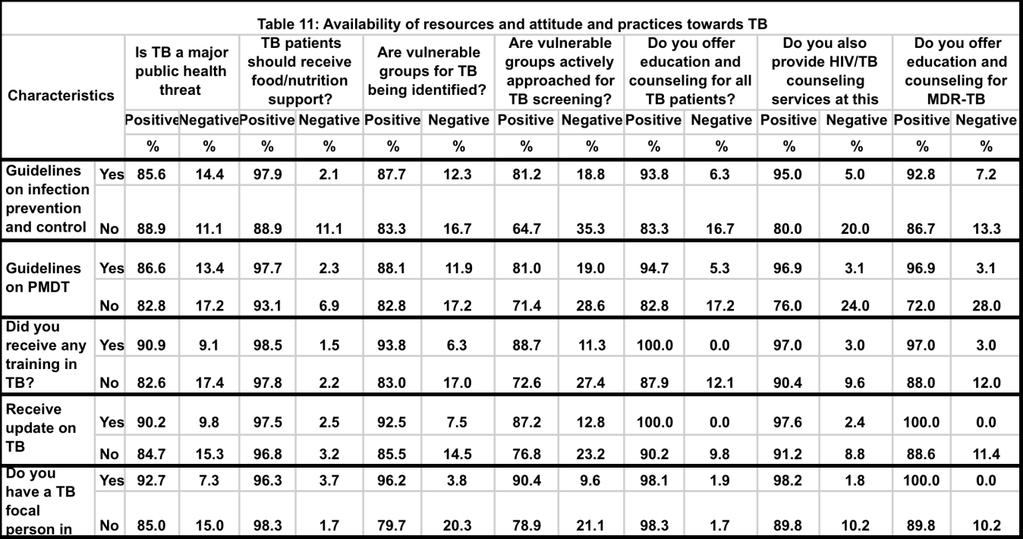
33 Table 8: Availability of resources and knowledge score Characteristics Guidelines on infection prevention and control Guidelines on PMDT Mean score SD Excellent Good Average Poor N (%) N (%) N (%) N (%) Significance Yes X 2 = The P-Value is The No result is significant at p < 0.05 X 2 = The P- Yes Value is The result is significant at p < 0.05 No Did you receive any training in TB? Receive update on TB Do you have a TB focal person in the facility Yes No Yes No Yes No X 2 = The P-Value is The result is significant at p < X 2 = The P-Value is The result is significant at p < X 2 = The P-Value is The result is not significant at p < Attitude and Practices towards TB Table 9 and figures 19 and 20 shows attitude and practice of respondent nurses about TB. 86.1% of the nurses recognized TB as a major public health treat. According to 97% of nurses nutritional support should be provided to the TB patients. 87.3% of the nurses said that vulnerable groups for TB are being identified, but 79.5% that vulnerable groups are being actively approached for TB screening. Covering of nose and mouth while coughing or 31


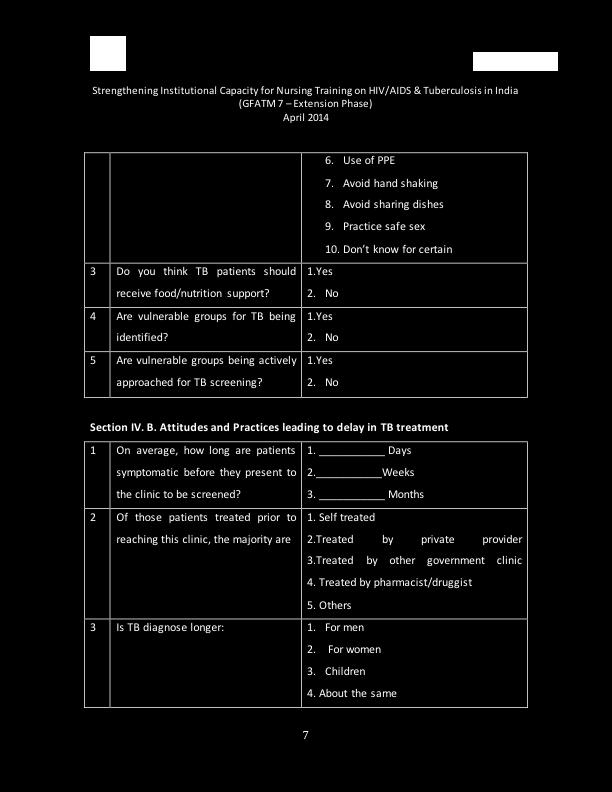
34 sneezing prevents infection spread according to 159 nurses followed by good nutrition. Practicing safe sex, avoiding sharing of dishes and hand shaking as per 25, 30 and 31 responses respectively can prevent TB infection. Table 10 and 11show attitude and practices of the nurses against Socio demographic variables and resources available to the nurses. 32
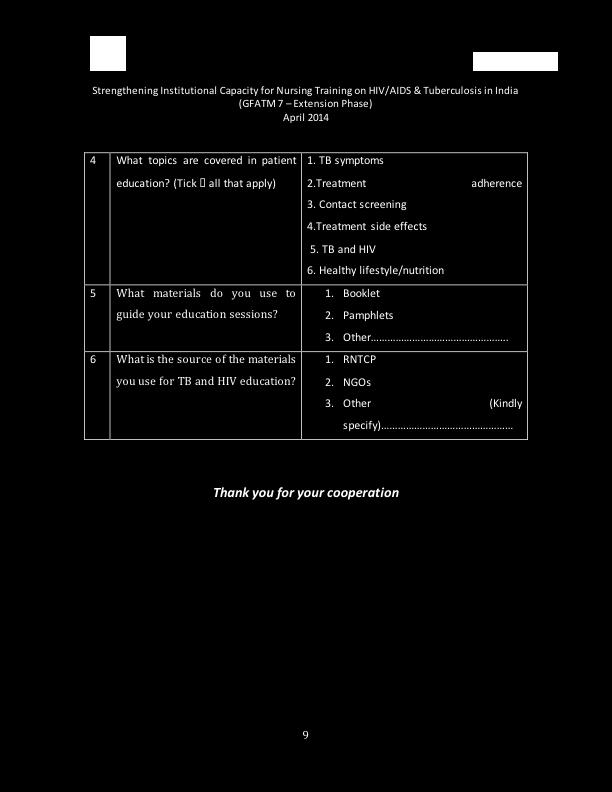
35 Table 9: Attitude and practices of nurses about Tuberculosis Positive % Negative % Is TB a major public health threat Do you think TB patients should receive food/nutrition support? Are vulnerable groups for TB being identified? Are vulnerable groups being actively approached for TB screening? Do you offer education and counseling for all TB patients? Do you also provide HIV/TB counseling services at this facility? Do you offer education and counseling for MDR-TB patients? Education and counseling for TB is being offered to TB patients as per the responses in 92.6%, however 92.9% and 91.6% of nurses said HIV/TB co-infection counseling and MDR-TB education and counseling respectively is also offered is offered to patients. 150 nurses covered treatment adherence during health education session, followed by TB symptoms by 147 respondents. 134 nurses dealt side effects during sessions, 130 nutrition and lifestyle, 128 counseled about contact screening and 125 about TB-HIV co-infection. 27% and 25% of the nurses used booklets and pamphlets respectively. 29% did not respond regarding the type of resource material used by them. Source of educational material was mainly RNTCP (70%). Figures 21, 22, 23 and 24 represent various aspects of education and counseling provided to the patients as well as type and source of the resource materials used by the nurses. 33
36 34
37 35

38 Table 12 show attitude and practices score of nurses and their association with about Tuberculosis. Respondents with score of 2 or less had poorer knowledge about TB. Respondents with score 6 and more had 23.9% excellent knowledge, 35% good, 31.6% average and 9.4% poor knowledge of TB. Table 12:Attitude and practices score of nurses and their association with knowledge about Tuberculosis Attitude and Knowledge about TB Practices score Excellent % Good % Average % Poor % to
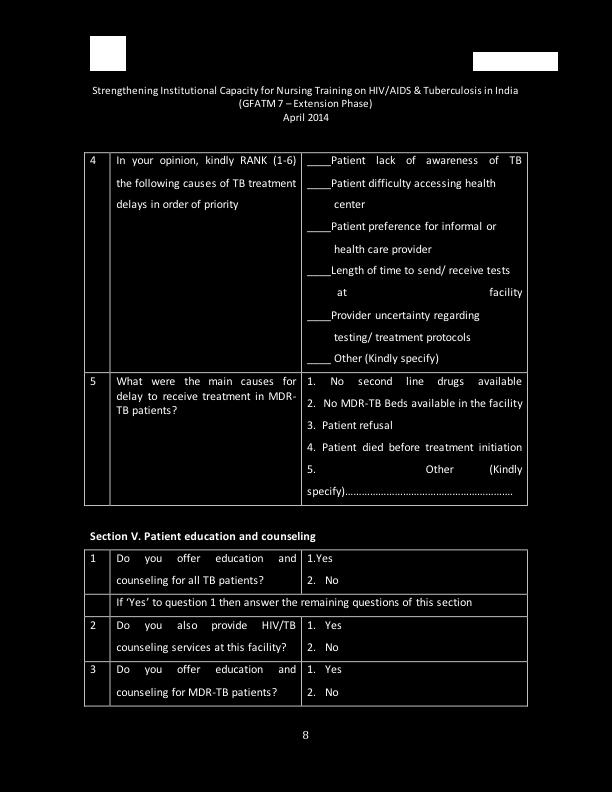
39 4.4. Attitude and Practices Leading to Delay in TB Treatment Approximately half of the respondents feel there is a delay of month plus between symptoms and the patient gets screened for TB. The range for this according to the responses is from few days to 6 to 12 months. 99 nurses said that delay is due to patients unawareness, followed by patients difficulty in accessing the health facility followed by TB patient s preference of informal health care providers. According to 12 responses the delay is due to time send in sending and receiving of test results and 2 responded as uncertainty regarding testing and treatment protocol is causing delay. Private sector providers treat 40% of the patients before they arriving to the health facility for TB, 24% are self treated, 25% by other government doctor and 4% by pharmacists and druggist. Time elapsed before diagnoses is about the same as per 32% of the responses, 31% felt it took longer among men, while 14% and 16% felt the delay longer among women and children respectively. 44% of the respondents said delay in treatment of MDR TB is mainly due to patient refusal, 24% said due to non-availability of second line of drugs, 11% due to shortage of MDR beds and 6% said that patient died before treatment initiation. Figures 25, 26, 27 and 28 show various causes of delay in treatment. 37

40 5.Discussion This KAP survey on TB shows that among respondent nurses, 21.8% had excellent knowledge on TB, 35.8% good, 33.9% average and 8.5% had poor knowledge. 91.5% 0f nurses identified contacts of active TB cases as suspect for TB followed by people living with HIV/AIDS in 68.5% of the responses. Other criteria like children, health workers and no improvement post antibiotic, homelessness for identifying a TB suspect were responded by less than 50% of the nurses. More than 90% of the nurses recognized cough for more than 2 weeks, fever and weight loss as symptoms of TB. Haemoptysis, chest pain and 38
41 weakness were responded by approximately 70% of the nurses. However knowledge of night sweat, pallor and no response to antibiotics as symptoms of TB was quite low. Majority of nurses considered sputum smear examination and X-ray as a diagnostic tool for tuberculosis. RNTCP guidelines do not encourage X ray as diagnostic tool due to high percentage of false positive. Almost all the nurses (162) had knowledge of DOTS strategy for TB treatment. Re-infection of TB can occur in cured TB cases was also know to 155 nurses. Regarding the awareness of correct definition of recurrent TB was 72.7%. Knowledge about minimum duration of treatment for pulmonary TB was among 88.5% on nurses. Gender and knowledge score are not significantly linked. Similarly presence of TB focal person is also not significantly linked to knowledge score of the nurses. Presence of guidelines for infection prevention and control and PMDT and updates on TB help in building capacity and knowledge on TB for nurses. TB training is significantly linked to knowledge on TB. This survey on nurses showed that age, qualification and service duration are associated with knowledge level on TB. More exposure and longer duration of work experience make nurse more knowledgeable and guide their attitude and practice in positive direction. Generally nurses had positive attitude towards TB patients. They recognize TB as major public health threat and most of them think that nutritional support should be provided to TB patients. Cough hygiene as means for preventing infection is answered by most of the nurses followed by BCG vaccination. There is a gap in identifying vulnerable groups for TB, which is further widened, as they are not being actively approached for screening of TB. Misconceptions like spread of TB infection through handshake, sharing if dishes and unsafe sex is prevalent. 32% of the nurses replied that delay in diagnoses for TB is about the same for both gender. About one third respondent it was more for men. Only14% said the delay in women is more while 16% said that delay is more among children. This is in contrast to most of the studies, which said that delay in diagnoses was more among female patients. Delay in treatment for TB as per the nurses is mostly due to patients unawareness and to a certain extent preference of private health care provider. Patient s refusal for MDR treatment is quite prevalent. However inaccessibility of TB centre, time lapse between sending and receiving of test result as well as uncertainty regarding testing and treatment protocol is also leading to delay in treatment. 39
42 Health system delay is further evident in case of treatment of MDR TB due to lack of lack line of drugs and non-availability of beds. Health education and counseling is provided by most of the nurses however there is a fall in percentage with regards to TB-HIV co-infection and MDR. Health education and counseling on TB symptoms and adherence to treatment is provided to most of the patients. Patients are less frequently counseled on topic like contact screening, side effects of drugs, importance of health lifestyle and diet and coinfection. Most of the educational material used by nurses is from RNTCP. Attitude and practices score was higher in respondents with excellent and good knowledge where as average and poor knowledge was associated with lower attitude and practice score. 6. Conclusions Slightly more than half (57.6%) of nurses have above average knowledge score. All nurses should, therefore, undergo TB training to increase or update their knowledge. Availability of guidelines on infection prevention and control and on PMDT has positive influence on the knowledge of the nurses. It was found that most of the nurses in this study had positive attitudes towards existing TB control strategy. In terms of their attitudes towards TB control systems, they believed in DOTS strategy. Delay in diagnoses of TB is same for both gender as per one third of nurses while another one-third said delay was more for men. However delay in diagnoses and treatment due to health system like time lag between the sending and receiving of test results, uncertainty regarding testing and treatment protocols, unavailability of second line of drug and shortage of hospital beds for MDR TB patients is also perceived occasionally by the nurses. Misconceptions regarding spread of TB infection by handshake, sharing of dishes or unsafe sex is prevalent among few nurses. Patients awareness is quite low which is leading cause of delay in treatment followed by preference of private providers by the patients in few cases. Patients are frequently refusing to start MDR treatment. 40
43 Studies have shown providers attitudes towards patients affects actual treatment success. It is believed that if patients perceived a stigma or felt negative attitude towards them, there was a greater tendency to drop out of treatment. Therefore, nurses attitude toward patients is key to achieving higher treatment success rate. Health education and counseling to TB patients is provided by most of the nurses but gap exists in the education and counseling provided to patients especially HIV-TB co-infection and MDR TB. Adherence counseling is provided to most of the patients but fewer receive counseling on contact screening, side effects of drugs, co-infections especially HIV and importance of lifestyle and nutrition. 7. Recommendations It is well established that providers knowledge levels impact directly upon the effectiveness of healthcare services. Based on the finding of KAP study TB training of nurses is critical for their knowledge gain and thereafter attitude and practices towards TB. Guidelines on PMDT and infection control should be provided to all nurses. Nodal person if possible should be available in all tertiary institutes. Comprehensive health education and counseling should be provided to all TB patients focusing on MDR and TB-HIV co-infection cases. Health system factors leading to delay in treatment of TB including MDR as mentioned by nurses should be looked into, analyses and thereafter necessary actions should be taken by the TB control program authorities and locally at the facility by the concerned administrative person. Behaviour change communication strategy should be developed focusing to create awareness among patients to seek early treatment. MDR patients should be proactively counseled to overcome the hurdle of patients refusal in initiating treatment. 41

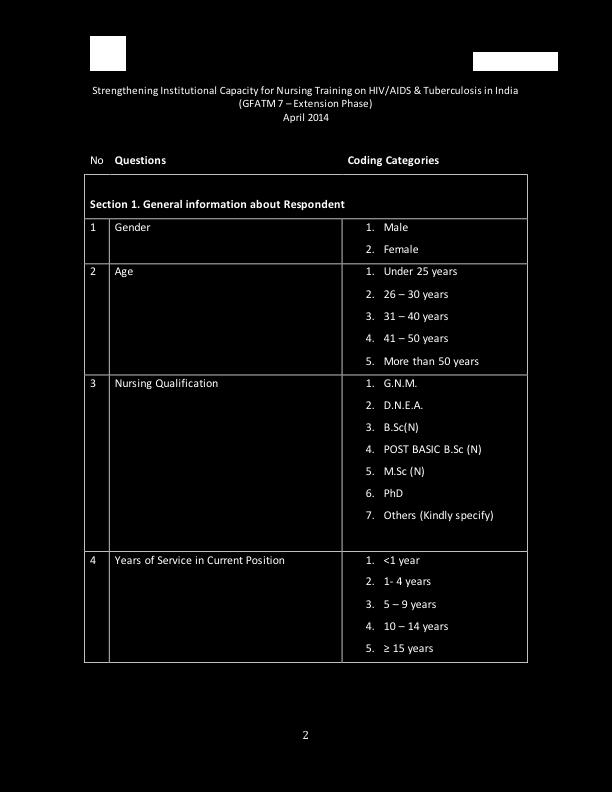
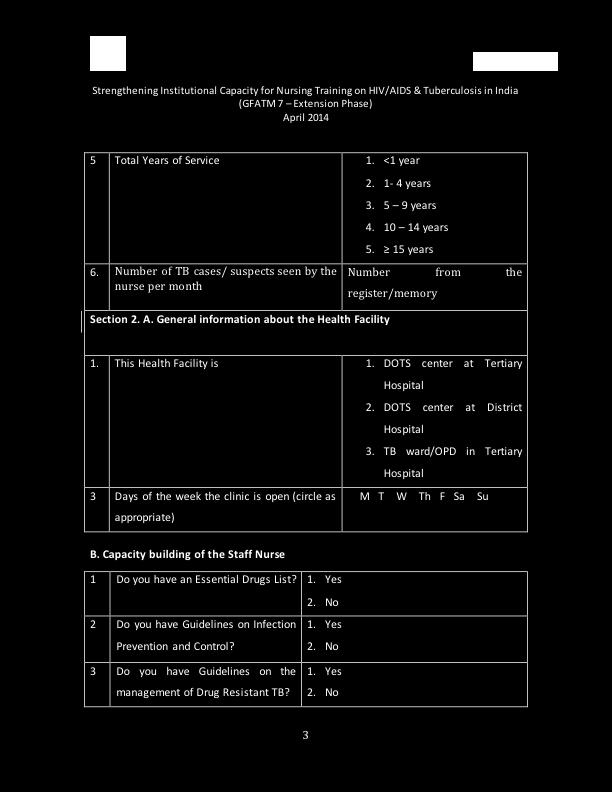
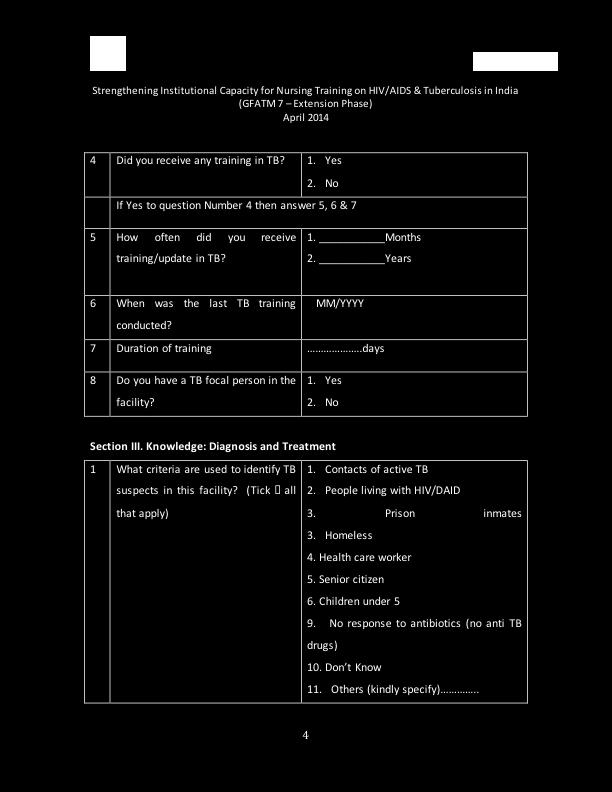
44 Annexure I: TB questionnaire for Nurses 42
45 43
46 44
47 45
48 46
49 47
50 48
51 49
52 50
KNOWLEDGE, ATTITUDE AND PRACTICE OF DOTS PROVIDERS UNDER RNTCP IN UJJAIN, MADHYA PRADESH
 Original Article KNOWLEDGE, ATTITUDE AND PRACTICE OF DOTS PROVIDERS UNDER RNTCP IN UJJAIN, MADHYA PRADESH Mayank Jain 1, Swarupa V Chakole 2, Amit S Pawaiya 1, Satish C Mehta 3 Financial Support: Non declared
Original Article KNOWLEDGE, ATTITUDE AND PRACTICE OF DOTS PROVIDERS UNDER RNTCP IN UJJAIN, MADHYA PRADESH Mayank Jain 1, Swarupa V Chakole 2, Amit S Pawaiya 1, Satish C Mehta 3 Financial Support: Non declared
Expanding Laboratory Capacity in India for the Diagnosis of Drug-Resistant TB
 Expanding Laboratory Capacity in India for the Diagnosis of Drug-Resistant TB Dr. Neeraj Raizada Medical Officer Project Leader, LPA and LC Projects Foundation for Innovative New diagnostics A non-profit
Expanding Laboratory Capacity in India for the Diagnosis of Drug-Resistant TB Dr. Neeraj Raizada Medical Officer Project Leader, LPA and LC Projects Foundation for Innovative New diagnostics A non-profit
Programmatic Management of MDR-TB in China: Progress, Plan and Challenge
 Programmatic Management of MDR-TB in China: Progress, Plan and Challenge Dr. Mingting Chen Researcher/Vice Director National Centre for Tuberculosis Control and Prevention of China CDC The People s Republic
Programmatic Management of MDR-TB in China: Progress, Plan and Challenge Dr. Mingting Chen Researcher/Vice Director National Centre for Tuberculosis Control and Prevention of China CDC The People s Republic
Terms of Reference Kazakhstan Health Review of TB Control Program
 1 Terms of Reference Kazakhstan Health Review of TB Control Program Objectives 1. In the context of the ongoing policy dialogue and collaboration between the World Bank and the Government of Kazakhstan
1 Terms of Reference Kazakhstan Health Review of TB Control Program Objectives 1. In the context of the ongoing policy dialogue and collaboration between the World Bank and the Government of Kazakhstan
MONITORING AND EVALUATION PLAN
 GHANA HEALTH SERVICE MONITORING AND EVALUATION PLAN National tb control programme Monitoring and evaluation plan for NTP INTRODUCTION The Health System Structure in Ghana The Health Service is organized
GHANA HEALTH SERVICE MONITORING AND EVALUATION PLAN National tb control programme Monitoring and evaluation plan for NTP INTRODUCTION The Health System Structure in Ghana The Health Service is organized
SOURCE OF LATEST ANTI-TB TREATMENT AMONGST RE-TREATMENT TB CASES REGISTERED UNDER RNTCP IN GUJARAT
 Original Article.. SOURCE OF LATEST ANTI-TB TREATMENT AMONGST RE-TREATMENT TB CASES REGISTERED UNDER RNTCP IN GUJARAT P Dave 1, K Rade 2, KR Pujara 3, R Solanki 4, B Modi 5, PG Patel 6, P Nimavat 7 1 Additional
Original Article.. SOURCE OF LATEST ANTI-TB TREATMENT AMONGST RE-TREATMENT TB CASES REGISTERED UNDER RNTCP IN GUJARAT P Dave 1, K Rade 2, KR Pujara 3, R Solanki 4, B Modi 5, PG Patel 6, P Nimavat 7 1 Additional
FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH. National Tuberculosis and Leprosy Control Programme. A Tuberculosis Infection Control Strategy
 FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH National Tuberculosis and Leprosy Control Programme FAST A Tuberculosis Infection Control Strategy 1 Acknowledgements This FAST Guide is developed
FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH National Tuberculosis and Leprosy Control Programme FAST A Tuberculosis Infection Control Strategy 1 Acknowledgements This FAST Guide is developed
Strengthening and Aligning Diagnosis and Treatment of Drug Resistant TB in India
 Strengthening and Aligning Diagnosis and Treatment of Drug Resistant TB in India Dr K S Sachdeva Additional Deputy Director General Central TB Division Ministry of Health & Family Welfare Government of
Strengthening and Aligning Diagnosis and Treatment of Drug Resistant TB in India Dr K S Sachdeva Additional Deputy Director General Central TB Division Ministry of Health & Family Welfare Government of
Strategy of TB laboratories for TB Control Program in Developing Countries
 Strategy of TB laboratories for TB Control Program in Developing Countries Borann SAR, MD, PhD, Institut Pasteur du Cambodge Phnom Penh, Cambodia TB Control Program Structure of TB Control Establish the
Strategy of TB laboratories for TB Control Program in Developing Countries Borann SAR, MD, PhD, Institut Pasteur du Cambodge Phnom Penh, Cambodia TB Control Program Structure of TB Control Establish the
FEDERAL MINISTRY OF HEALTH NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME TERMS OF REFERENCE FOR ZONAL CONSULTANTS MARCH, 2017
 FEDERAL MINISTRY OF HEALTH NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME EPIDEMIOLOGICAL ANALYSIS OF TUBERCULOSIS BURDEN AT NATIONAL AND SUB NATIONAL LEVEL (EPI ANALYSIS SURVEY) TERMS OF REFERENCE
FEDERAL MINISTRY OF HEALTH NATIONAL TUBERCULOSIS AND LEPROSY CONTROL PROGRAMME EPIDEMIOLOGICAL ANALYSIS OF TUBERCULOSIS BURDEN AT NATIONAL AND SUB NATIONAL LEVEL (EPI ANALYSIS SURVEY) TERMS OF REFERENCE
Annual Report. Strengthening Institutional Capacity for Nurses Training On HIV/AIDS in India (GFATM 7) (October September 10)
 (October September 10)") Annual Report Strengthening Institutional Capacity for Nurses Training On HIV/AIDS in India (GFATM 7) (October 2009- September 10) Annual Report 2009-10 1 Annual Report 2009-10 2 Contents Highlights 4
Annual Report Strengthening Institutional Capacity for Nurses Training On HIV/AIDS in India (GFATM 7) (October 2009- September 10) Annual Report 2009-10 1 Annual Report 2009-10 2 Contents Highlights 4
Performance of RNTCP NTI Bulletin 2003, 39 / 3&4, 19-23
 Performance of RNTCP NTI Bulletin 2003, 39 / 3&4, 19-23 PERFORMANCE OF RNTCP IN HIMACHAL PRADESH AND KERALA - A PERSPECTIVE COMPARISON SG Radhakrishna* & G Sumathi* SUMMARY Monitoring is a continuous assessment
Performance of RNTCP NTI Bulletin 2003, 39 / 3&4, 19-23 PERFORMANCE OF RNTCP IN HIMACHAL PRADESH AND KERALA - A PERSPECTIVE COMPARISON SG Radhakrishna* & G Sumathi* SUMMARY Monitoring is a continuous assessment
EXECUTIVE SUMMARY. 1. Introduction
 EXECUTIVE SUMMARY 1. Introduction As the staff nurses are the frontline workers at all areas in the hospital, a need was felt to see the effectiveness of American Heart Association (AHA) certified Basic
EXECUTIVE SUMMARY 1. Introduction As the staff nurses are the frontline workers at all areas in the hospital, a need was felt to see the effectiveness of American Heart Association (AHA) certified Basic
Tuberculosis Prevention and Control Protocol, 2018
 Ministry of Health and Long-Term Care Tuberculosis Prevention and Control Protocol, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective: January 1, 2018 or upon
Ministry of Health and Long-Term Care Tuberculosis Prevention and Control Protocol, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective: January 1, 2018 or upon
Country experience on engaging large hospitals - INDIA
 Ninth Meeting of the Sub- group on PPM for TB Care and Control and Global Workshop on Engaging Large Hospitals, 28-30 August 2013 Country experience on engaging large hospitals - INDIA Sreenivas A Nair
Ninth Meeting of the Sub- group on PPM for TB Care and Control and Global Workshop on Engaging Large Hospitals, 28-30 August 2013 Country experience on engaging large hospitals - INDIA Sreenivas A Nair
Practical Aspects of TB Infection Control
 Practical Aspects of TB Infection Control Sundari Mase, MD Division of TB Elimination, CDC TB Intensive Workshop October 1, 2014 National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention Division
Practical Aspects of TB Infection Control Sundari Mase, MD Division of TB Elimination, CDC TB Intensive Workshop October 1, 2014 National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention Division
International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 50-59
 Original article An Epidemiological Study of Tuberculosis Patient with Special Reference to Cost Incurred By Patient for the Treatment in an Urban Slum of Mumbai, Maharashtra Dnyaneshwar M. Gajbhare 1,
Original article An Epidemiological Study of Tuberculosis Patient with Special Reference to Cost Incurred By Patient for the Treatment in an Urban Slum of Mumbai, Maharashtra Dnyaneshwar M. Gajbhare 1,
Changing the paradigm of Programmatic Management of Drug-resistant TB
 Republic of Moldova Changing the paradigm of Programmatic Management of Drug-resistant TB Liliana Domente, Elena Romancenco GLI / GDI Partners Forum WHO Global TB Programme Geneva 27-30 April 2015 Republic
Republic of Moldova Changing the paradigm of Programmatic Management of Drug-resistant TB Liliana Domente, Elena Romancenco GLI / GDI Partners Forum WHO Global TB Programme Geneva 27-30 April 2015 Republic
Administrative Without, TB control fails. TB Infection Control What s New? Early disease prevention Modern cough etiquette
 Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual July, 2018 Page 1 TABLE OF CONTENTS APPENDIX B: INFECTION PREVENTION AND CONTROL... 2
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual July, 2018 Page 1 TABLE OF CONTENTS APPENDIX B: INFECTION PREVENTION AND CONTROL... 2
Management of patients with TB/HIV Gunta Kirvelaite
 Management of patients with TB/HIV Gunta Kirvelaite Riga East Clinical hospital, Centre for tuberculosis and lung diseases. Head of outpatient department. MDR TB physician. WHO Collaborating Centre for
Management of patients with TB/HIV Gunta Kirvelaite Riga East Clinical hospital, Centre for tuberculosis and lung diseases. Head of outpatient department. MDR TB physician. WHO Collaborating Centre for
Financial impact of TB illness
 Summary report Costs faced by (multidrug resistant) tuberculosis patients during diagnosis and treatment: report from a pilot study in Ethiopia, Indonesia and Kazakhstan Edine W. Tiemersma 1, David Collins
Summary report Costs faced by (multidrug resistant) tuberculosis patients during diagnosis and treatment: report from a pilot study in Ethiopia, Indonesia and Kazakhstan Edine W. Tiemersma 1, David Collins
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
FAST. A Tuberculosis Infection Control Strategy. cough
 FAST A Tuberculosis Infection Control Strategy FIRST EDITION: MARCH 2013 This handbook is made possible by the support of the American people through the United States Agency for International Development
FAST A Tuberculosis Infection Control Strategy FIRST EDITION: MARCH 2013 This handbook is made possible by the support of the American people through the United States Agency for International Development
Conclusion: Despite existing comprehensive feedback guidelines under RNTCP there was a lack of commitment in implementation of such guidelines.
 Status of Feedback on TB Cases Put on DOTS and Referred for Treatment: A Record Based Study from a Medical College in Dakshina Kannada District of Karnataka Abstract Dr J P, Majra, Dr Anjali Pal, Dr.ArpitaGur
Status of Feedback on TB Cases Put on DOTS and Referred for Treatment: A Record Based Study from a Medical College in Dakshina Kannada District of Karnataka Abstract Dr J P, Majra, Dr Anjali Pal, Dr.ArpitaGur
The State Health & Family Welfare Society (RNTCP), NHM invites applications for the following contractual posts for a period of one year.
, NHM invites applications for the following contractual posts for a period of one year.") The State Health & Family Welfare Society (RNTCP), NHM invites applications for the following contractual posts for a period of one year. Rc.No.RNTCP/180/AP/2017 TB-HIV Coordinator-State TB Cell, Vijayawada
The State Health & Family Welfare Society (RNTCP), NHM invites applications for the following contractual posts for a period of one year. Rc.No.RNTCP/180/AP/2017 TB-HIV Coordinator-State TB Cell, Vijayawada
TUBERCULOSIS CONTROL RESEARCH MATRIX
 TUBERCULOSIS CONTROL MATRIX 2014-2016 STRA- S1 S1 S1 S2 1.1. 80% of provinces and highly urbanized cities (HUC) include TB based on a set criteria within PIPH/ AIPH/ CIPH 1.3. Ninety percent (90%) of provinces
TUBERCULOSIS CONTROL MATRIX 2014-2016 STRA- S1 S1 S1 S2 1.1. 80% of provinces and highly urbanized cities (HUC) include TB based on a set criteria within PIPH/ AIPH/ CIPH 1.3. Ninety percent (90%) of provinces
Assessment of Knowledge on management of Pulmonary Tuberculosis under RNTCP among graduating Interns and Postgraduate students in RIMS Imphal.
 IOSR Journal of Nursing and Health Science (IOSR-JNHS e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 6, Issue 3 Ver. I (May. - June. 2017), PP 07-11 www.iosrjournals.org Assessment of Knowledge on management
IOSR Journal of Nursing and Health Science (IOSR-JNHS e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 6, Issue 3 Ver. I (May. - June. 2017), PP 07-11 www.iosrjournals.org Assessment of Knowledge on management
GUIDE: Reporting Template_Tuberculosis
 GUIDE: Reporting Template_Tuberculosis Narrative Report section Contract Number Project Title Contract Period Reporting Period Reporting Date (dd/mm/yyyy) explanation project start and end date in (DD/MM/YYYY)
GUIDE: Reporting Template_Tuberculosis Narrative Report section Contract Number Project Title Contract Period Reporting Period Reporting Date (dd/mm/yyyy) explanation project start and end date in (DD/MM/YYYY)
Momentum on Child TB: South East Asia (SEA)
") Momentum on Child TB: South East Asia (SEA) Dr. Shakil Ahmed MBBS, FCPS, MD Associate Professor of Pediatrics Shaheed Suhrawardy Medical College Bangladesh shakildr@gmail.com Child Mortality from TB: 2015
Momentum on Child TB: South East Asia (SEA) Dr. Shakil Ahmed MBBS, FCPS, MD Associate Professor of Pediatrics Shaheed Suhrawardy Medical College Bangladesh shakildr@gmail.com Child Mortality from TB: 2015
Effectiveness of Structured Teaching Programme on Bio-Medical Waste Management
 IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 3, Issue 3 Ver. II (May-Jun. 2014), PP 60-65 Effectiveness of Structured Teaching Programme on Bio-Medical
IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 3, Issue 3 Ver. II (May-Jun. 2014), PP 60-65 Effectiveness of Structured Teaching Programme on Bio-Medical
IHF Training Manual for TB and MDR-TB Control for Hospital/Clinic/Health Facility Managers Executive Summary 2
 EXECUTIVE SUMMARY International Hospital Federation Immeuble JB SAY, 13, Chemin du Levant, 01210 Ferney Voltaire, France Tel: +33 (0) 450 42 60 00 / Fax: +33 (0) 450 42 60 01 Email: info@ihf-fih.org /
EXECUTIVE SUMMARY International Hospital Federation Immeuble JB SAY, 13, Chemin du Levant, 01210 Ferney Voltaire, France Tel: +33 (0) 450 42 60 00 / Fax: +33 (0) 450 42 60 01 Email: info@ihf-fih.org /
AIRBORNE PATHOGENS. Airborne Pathogens: Microorganisms that may be present in the air and can cause diseases in exposed humans.
 MARICOPA COUNTY SHERIFF S OFFICE POLICY AND PROCEDURES Subject Related Information CRITICAL POLICY PURPOSE AIRBORNE PATHOGENS Supersedes CP-7 (8-14-15) Policy Number CP-7 Effective Date 01-04-17 The Office
MARICOPA COUNTY SHERIFF S OFFICE POLICY AND PROCEDURES Subject Related Information CRITICAL POLICY PURPOSE AIRBORNE PATHOGENS Supersedes CP-7 (8-14-15) Policy Number CP-7 Effective Date 01-04-17 The Office
Epidemiological review of TB disease in Sierra Leone
 Epidemiological review of TB disease in Sierra Leone October 2015 Laura Anderson WHO (Switzerland) Esther Hamblion WHO (Liberia) Contents 1. INTRODUCTION 4 2. PURPOSE 5 2.1 OBJECTIVES 5 2.2 PROPOSED OUTCOMES
Epidemiological review of TB disease in Sierra Leone October 2015 Laura Anderson WHO (Switzerland) Esther Hamblion WHO (Liberia) Contents 1. INTRODUCTION 4 2. PURPOSE 5 2.1 OBJECTIVES 5 2.2 PROPOSED OUTCOMES
Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
 and cure individuals with active TB disease") Tuberculosis (TB) Control and Prevention Program Program Purpose PHD/CHPB Evelyn Poppell, x5600 Rachel Kidanne, x5605 Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
Tuberculosis (TB) Control and Prevention Program Program Purpose PHD/CHPB Evelyn Poppell, x5600 Rachel Kidanne, x5605 Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
OPERATIONAL RESEARCH. What, Why and How? Dr. Rony Zachariah MD, PhD Operational Centre Brussels MSF- Luxembourg
 OPERATIONAL RESEARCH What, Why and How? Dr. Rony Zachariah MD, PhD Operational Centre Brussels MSF- Luxembourg rony.zachariah@brussels.msf.org What is operational research Search for knowledge on interventions,
OPERATIONAL RESEARCH What, Why and How? Dr. Rony Zachariah MD, PhD Operational Centre Brussels MSF- Luxembourg rony.zachariah@brussels.msf.org What is operational research Search for knowledge on interventions,
WHO policy on TB infection control in health care facilities, congregate settings and households.
 WHO policy on TB infection control in health care facilities, congregate settings and households. Rose Pray Stop TB, WHO Why should we develop a policy on TB infection control? To guide countries on what
WHO policy on TB infection control in health care facilities, congregate settings and households. Rose Pray Stop TB, WHO Why should we develop a policy on TB infection control? To guide countries on what
Philippine Strategic TB Elimination Plan: Phase 1 (PhilSTEP1)
") 2017 2022 Philippine Strategic TB Elimination Plan: Phase 1 (PhilSTEP1) 24 th PhilCAT Convention August 16, 2017 Dr. Anna Marie Celina Garfin NTP-DCPB, Department of Health Reasons for developing the NTP
2017 2022 Philippine Strategic TB Elimination Plan: Phase 1 (PhilSTEP1) 24 th PhilCAT Convention August 16, 2017 Dr. Anna Marie Celina Garfin NTP-DCPB, Department of Health Reasons for developing the NTP
CHAPTER 30 HEALTH AND FAMILY WELFARE
 CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
Overview: TB Case Management and Contact Investigation
 Overview: TB Case Management and Contact Investigation Karen A Martinek, RN, MPH Alaska DHSS, DPH, Section of Epidemiology Overview Define tuberculosis (TB) case management Describe the roles and responsibilities
Overview: TB Case Management and Contact Investigation Karen A Martinek, RN, MPH Alaska DHSS, DPH, Section of Epidemiology Overview Define tuberculosis (TB) case management Describe the roles and responsibilities
Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala. Sunil Kumar
 End TB Strategy Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala Sunil Kumar The END TB strategy challenges the world to envision the End of the Tuberculosis pandemic and
End TB Strategy Contextualising the End TB Strategy for a Push toward TB Elimination in Kerala Sunil Kumar The END TB strategy challenges the world to envision the End of the Tuberculosis pandemic and
"Discovery to Treatment" Window in Patients With Smear-Positive Pulmonary Tuberculosis
 ORIGINAL ARTICLE "Discovery to Treatment" Window in Patients With Smear-Positive Pulmonary Tuberculosis L C Loh, MRCP*, A Codati, MJamil*, Z Mohd Noor**, P Vijayasingham, FRCPI** IMU Lung Research, International
ORIGINAL ARTICLE "Discovery to Treatment" Window in Patients With Smear-Positive Pulmonary Tuberculosis L C Loh, MRCP*, A Codati, MJamil*, Z Mohd Noor**, P Vijayasingham, FRCPI** IMU Lung Research, International
Adherence with Evidence-based TB Standards and Guidelines in Selected Health Facilities in Kenya
 Quality Improvement of TB Services Adherence with Evidence-based TB Standards and Guidelines in Selected Health Facilities in Kenya April 2013 This study is made possible by the support of the American
Quality Improvement of TB Services Adherence with Evidence-based TB Standards and Guidelines in Selected Health Facilities in Kenya April 2013 This study is made possible by the support of the American
Author for Correspondence
 A STUDY ON KNOWLEDGE, ATTITUDE AND PRACTICES REGARDING BIOMEDICAL WASTE MANAGEMNT AMONG NURSING STAFF IN PRIVATE HOPITALS IN UDUPI CITY, KARNATAKA, INDIA * Md. Asadullah, Karthik G. K. and Dharmappa B.
A STUDY ON KNOWLEDGE, ATTITUDE AND PRACTICES REGARDING BIOMEDICAL WASTE MANAGEMNT AMONG NURSING STAFF IN PRIVATE HOPITALS IN UDUPI CITY, KARNATAKA, INDIA * Md. Asadullah, Karthik G. K. and Dharmappa B.
NORTHERN ZONE SAN MATEO COUNTY FIRE AGENCIES (Brisbane, Colma, Daly City, Pacifica and San Bruno) EMS - POLICY MANUAL
 EMS - POLICY MANUAL") POLICY STATEMENT Purpose: To provide a comprehensive exposure control plan which maximizes protection against occupational exposure to tuberculosis/respiratory conditions for all members of the Northern
POLICY STATEMENT Purpose: To provide a comprehensive exposure control plan which maximizes protection against occupational exposure to tuberculosis/respiratory conditions for all members of the Northern
Omobolanle Elizabeth Adekanye, RN 1 and Titilayo Dorothy Odetola, RN, BNSc, MSc 2
 IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 232 1959.p- ISSN: 232 194 Volume 3, Issue 5 Ver. III (Sep.-Oct. 214), PP 29-34 Awareness and Implementation of Integrated Management of Childhood
IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 232 1959.p- ISSN: 232 194 Volume 3, Issue 5 Ver. III (Sep.-Oct. 214), PP 29-34 Awareness and Implementation of Integrated Management of Childhood
Engagement of Workplace in TB Care and Control in Bangladesh. Dr. Md. Nazrul Islam Program Manager NTP Bangladesh
 Engagement of Workplace in TB Care and Control in Bangladesh 1 Dr. Md. Nazrul Islam Program Manager NTP Bangladesh Basic Facts about Bangladesh Area: 147570 sq. km Population: 145 million Administrative
Engagement of Workplace in TB Care and Control in Bangladesh 1 Dr. Md. Nazrul Islam Program Manager NTP Bangladesh Basic Facts about Bangladesh Area: 147570 sq. km Population: 145 million Administrative
Fundamentals of Nursing Case Management
 Fundamentals of Nursing Case Management Shea Rabley, RN, MN TB Nurse Educator Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures No relevant financial relationships No off-label investigational
Fundamentals of Nursing Case Management Shea Rabley, RN, MN TB Nurse Educator Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures No relevant financial relationships No off-label investigational
Directly Observed Therapy for Active TB Disease and Latent TB Infection
 Directly Observed Therapy for Active TB Disease and Latent TB Infection Policy Number TB-5001 Effective Date (original issue) September 6, 1995 Revision Date (most recent) June 26, 2008 Subject Matter
Directly Observed Therapy for Active TB Disease and Latent TB Infection Policy Number TB-5001 Effective Date (original issue) September 6, 1995 Revision Date (most recent) June 26, 2008 Subject Matter
Engaging the Private Retail Pharmaceutical Sector in TB Case Finding in Tanzania: Pilot Dissemination Meeting Report
 Engaging the Private Retail Pharmaceutical Sector in TB Case Finding in Tanzania: Pilot Dissemination Meeting Report February 2014 Engaging the Private Retail Pharmaceutical Sector in TB Case Finding
Engaging the Private Retail Pharmaceutical Sector in TB Case Finding in Tanzania: Pilot Dissemination Meeting Report February 2014 Engaging the Private Retail Pharmaceutical Sector in TB Case Finding
Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
 and cure individuals with active TB disease") Tuberculosis (TB) Control and Prevention Program Program Purpose Program Information PHD/CHPB Evelyn Poppell, x5600 Nga Nguyen, x5663 Prevent the transmission of tuberculosis (TB) and cure individuals
Tuberculosis (TB) Control and Prevention Program Program Purpose Program Information PHD/CHPB Evelyn Poppell, x5600 Nga Nguyen, x5663 Prevent the transmission of tuberculosis (TB) and cure individuals
Dyah Erti Mustikawati
 SCALING UP PPM IN INDONESIA Seventh Meeting of the Subgroup on Public-Private Mix for TB Care and Control 23-24 October 2011, Lille, France Dyah Erti Mustikawati NTP Manager MOH Indonesia Content Background
SCALING UP PPM IN INDONESIA Seventh Meeting of the Subgroup on Public-Private Mix for TB Care and Control 23-24 October 2011, Lille, France Dyah Erti Mustikawati NTP Manager MOH Indonesia Content Background
Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor
 Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor Overview- What gets measured, gets done Operation ASHA -serving more than 54 Lakh people in
Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor Overview- What gets measured, gets done Operation ASHA -serving more than 54 Lakh people in
Prevention and Care- Role of Pharmacists. Prafull Sheth, FIP Vice President
 Challenges in TB Prevention and Care- Role of Pharmacists Prafull Sheth, FIP Vice President Tuberculosis- Global Facts Disease of poverty, Contagious and Air borne Among the top ten causes of deaths 1.7
Challenges in TB Prevention and Care- Role of Pharmacists Prafull Sheth, FIP Vice President Tuberculosis- Global Facts Disease of poverty, Contagious and Air borne Among the top ten causes of deaths 1.7
Universal Access to MD TB Program in Cambodia. ITM, Antwerp 08 December Sam Sophan Cambodian Health Committee (CHC)
") Universal Access to MD TB Program in Cambodia ITM, Antwerp 08 December 2012 Sam Sophan Cambodian Health Committee (CHC) 1 Cambodia 2 Basic Info About Cambodia Location: South East Asia Border countries:
Universal Access to MD TB Program in Cambodia ITM, Antwerp 08 December 2012 Sam Sophan Cambodian Health Committee (CHC) 1 Cambodia 2 Basic Info About Cambodia Location: South East Asia Border countries:
How Do We Define Adherence? Improving Adherence to TB Treatment. Broad View of Adherence. What is adherence?
 How Do We Define Adherence? Improving Adherence to TB Treatment Lillian Pirog, RN, PNP Nurse Manager, Waymon C. Lattimore Practice NJMS Global Tuberculosis Institute What is adherence? A. Taking medication
How Do We Define Adherence? Improving Adherence to TB Treatment Lillian Pirog, RN, PNP Nurse Manager, Waymon C. Lattimore Practice NJMS Global Tuberculosis Institute What is adherence? A. Taking medication
Systematic Engagement of Hospitals Philippine Experience. Dr. Marl Mantala 8 th PPM Sub-group Meeting, 10 Nov. 2012, Kuala Lumpur
 Systematic Engagement of Hospitals Philippine Experience Dr. Marl Mantala 8 th PPM Sub-group Meeting, 10 Nov. 2012, Kuala Lumpur Flow of discussion Context Process Results Recommendations Philippines Population:
Systematic Engagement of Hospitals Philippine Experience Dr. Marl Mantala 8 th PPM Sub-group Meeting, 10 Nov. 2012, Kuala Lumpur Flow of discussion Context Process Results Recommendations Philippines Population:
Public Private Mix sub group meeting 23 October, 2011 Scale up PPM in Myanmar
 Public Private Mix sub group meeting 23 October, 2011 Scale up PPM in Myanmar Dr. Thandar Lwin Programme Manager National TB Programme, Myanmar Myanmar INDIA KACHIN BANGLA DESH CHIN RAKHINE SAGAING MAGWE
Public Private Mix sub group meeting 23 October, 2011 Scale up PPM in Myanmar Dr. Thandar Lwin Programme Manager National TB Programme, Myanmar Myanmar INDIA KACHIN BANGLA DESH CHIN RAKHINE SAGAING MAGWE
Tuberculosis surveillance in Suriname. Drs. B. Jubithana, MD M. Wongsokarijo, MSc
 Tuberculosis surveillance in Suriname Drs. B. Jubithana, MD M. Wongsokarijo, MSc Overview Background Current surveillance system in Suriname Prison outbreak Challenges Background Yearly around 120 cases,
Tuberculosis surveillance in Suriname Drs. B. Jubithana, MD M. Wongsokarijo, MSc Overview Background Current surveillance system in Suriname Prison outbreak Challenges Background Yearly around 120 cases,
Checklists for screening for active tuberculosis in high-risk groups
 Checklists for screening for active tuberculosis in high-risk groups General screening program considerations The following are aspects of design and implementation that should be considered before planning
Checklists for screening for active tuberculosis in high-risk groups General screening program considerations The following are aspects of design and implementation that should be considered before planning
Medical Student Research DELAY IN DIAGNOSIS OF TUBERCULOSIS IN PATIENTS PRESENTING TO A TERTIARY CARE HOSPITAL IN RURAL CENTRAL INDIA
 Medical Student Research DELAY IN DIAGNOSIS OF TUBERCULOSIS IN PATIENTS PRESENTING TO A TERTIARY CARE HOSPITAL IN RURAL CENTRAL INDIA PALLAVI DHANVIJ*, RAJNISH JOSHI**, SP KALANTRI** ABSTRACT Background
Medical Student Research DELAY IN DIAGNOSIS OF TUBERCULOSIS IN PATIENTS PRESENTING TO A TERTIARY CARE HOSPITAL IN RURAL CENTRAL INDIA PALLAVI DHANVIJ*, RAJNISH JOSHI**, SP KALANTRI** ABSTRACT Background
Tuberculosis: Surveillance and the Health Care Worker
 Tuberculosis: Surveillance and the Health Care Jo Fagan Director Public Health PHAC Delivering a Healthy WA Overview 1. Pre-employment assessment 2. Post-exposure follow-up 3. Routine follow up testing
Tuberculosis: Surveillance and the Health Care Jo Fagan Director Public Health PHAC Delivering a Healthy WA Overview 1. Pre-employment assessment 2. Post-exposure follow-up 3. Routine follow up testing
Social Action Plan (Including the Tribal Action Plan)
") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Revised National Tuberculosis Control Programme Social Action Plan (Including the Tribal
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Revised National Tuberculosis Control Programme Social Action Plan (Including the Tribal
WHO/HTM/TB/ Task analysis. The basis for development of training in management of tuberculosis
 WHO/HTM/TB/2005.354 Task analysis The basis for development of training in management of tuberculosis This document has been prepared in conjunction with the WHO training courses titled Management of tuberculosis:
WHO/HTM/TB/2005.354 Task analysis The basis for development of training in management of tuberculosis This document has been prepared in conjunction with the WHO training courses titled Management of tuberculosis:
Tuberculosis as an Occupational Disease. Molebogeng Malotle
 Tuberculosis as an Occupational Disease Molebogeng Malotle Introduction TB is a major global health problem Causes ill-health in millions of people each year Ranks the second leading cause of death from
Tuberculosis as an Occupational Disease Molebogeng Malotle Introduction TB is a major global health problem Causes ill-health in millions of people each year Ranks the second leading cause of death from
Republic of Indonesia
 Republic of Indonesia National Tuberculosis Program Remarks by the Honorable Ministry of Health on the Recommendation of the Tuberculosis Joint External Monitoring Mission 11-22 February 2013 First I would
Republic of Indonesia National Tuberculosis Program Remarks by the Honorable Ministry of Health on the Recommendation of the Tuberculosis Joint External Monitoring Mission 11-22 February 2013 First I would
Responsibilities of Public Health Departments to Control Tuberculosis
 Responsibilities of Public Health Departments to Control Tuberculosis Purpose: Tuberculosis (TB) is an airborne infectious disease that endangers communities. This document articulates the activities that
Responsibilities of Public Health Departments to Control Tuberculosis Purpose: Tuberculosis (TB) is an airborne infectious disease that endangers communities. This document articulates the activities that
Assessing Health Needs and Capacity of Health Facilities
 In rural remote settings, the community health needs may seem so daunting that it is difficult to know how to proceed and prioritize. Prior to the actual on the ground assessment, the desktop evaluation
In rural remote settings, the community health needs may seem so daunting that it is difficult to know how to proceed and prioritize. Prior to the actual on the ground assessment, the desktop evaluation
Ambulatory Care Day 1 for Multidrug Resistant Tuberculosis
 Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Tuberculosis in 2017: Searching for new solutions in the face of new challenges 6th TB Symposium Ministry of Health of the Republic of Belarus, Republican Scientific and Practical Center for Pulmonology
Effectiveness of Video Assisted Teaching Regarding Knowledge and Practice of Intra-Venous Cannulation for Under-five Children
 IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 5, Issue 5 Ver. VII (Sep. - Oct. 26), PP 10-15 www.iosrjournals.org Effectiveness of Video Assisted Teaching
IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 5, Issue 5 Ver. VII (Sep. - Oct. 26), PP 10-15 www.iosrjournals.org Effectiveness of Video Assisted Teaching
PhilHealth TB DOTS Out-patient Benefit Package
 PhilHealth TB DOTS Out-patient Benefit Package WHO Consultation Eliminating the Catastrophic Economic Burden of TB: Universal Health Coverage and Social Protection Opportunities April 29, 2013 Sao Paulo,
PhilHealth TB DOTS Out-patient Benefit Package WHO Consultation Eliminating the Catastrophic Economic Burden of TB: Universal Health Coverage and Social Protection Opportunities April 29, 2013 Sao Paulo,
BEST PRACTICE FOR THE CARE OF PATIENTS WITH TUBERCULOSIS
 BEST PRACTICE FOR THE CARE OF PATIENTS WITH TUBERCULOSIS A guide for low-income countries Second Edition 2017 This publication was made possible thanks to the support of the International Union Against
BEST PRACTICE FOR THE CARE OF PATIENTS WITH TUBERCULOSIS A guide for low-income countries Second Edition 2017 This publication was made possible thanks to the support of the International Union Against
Author's response to reviews
 Author's response to reviews Title: Quality the diagnostic process for tuberculosis in primary health centers (PHC) in Sidoarjo district, East Java, Indonesia Authors: Chatarina CU Wahyuni (chatrin03@yahoo.com)
Author's response to reviews Title: Quality the diagnostic process for tuberculosis in primary health centers (PHC) in Sidoarjo district, East Java, Indonesia Authors: Chatarina CU Wahyuni (chatrin03@yahoo.com)
Hello. Welcome to this webinar titled Preventing and Controlling Tuberculosis in Correctional Settings.
 Hello. Welcome to this webinar titled Preventing and Controlling Tuberculosis in Correctional Settings. This webinar was produced by the Minnesota Department of Health Tuberculosis Program. This is the
Hello. Welcome to this webinar titled Preventing and Controlling Tuberculosis in Correctional Settings. This webinar was produced by the Minnesota Department of Health Tuberculosis Program. This is the
Tuberculosis (TB) Procedure
 Procedure") Tuberculosis (TB) Procedure (IPC Manual) DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Policies Review and Approval Group Date ratified: 4 September 2018 Name of originator/author: RDaSH Community
Tuberculosis (TB) Procedure (IPC Manual) DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Policies Review and Approval Group Date ratified: 4 September 2018 Name of originator/author: RDaSH Community
NATIONAL SITUATION ASSESSMENT
 WHO/HTM/TB/2007.391 Public Private Mix for TB Care and Control A TOOL FOR NATIONAL SITUATION ASSESSMENT Acknowledgements This document was drafted by Kabir Sheikh with input from Mukund Uplekar and Knut
WHO/HTM/TB/2007.391 Public Private Mix for TB Care and Control A TOOL FOR NATIONAL SITUATION ASSESSMENT Acknowledgements This document was drafted by Kabir Sheikh with input from Mukund Uplekar and Knut
MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW
 06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
A Study to Assess Patient Safety Culture amongst a Category of Hospital Staff of a Teaching Hospital
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
TB Elimination. Respiratory Protection in Health-Care Settings
 TB Elimination Respiratory Protection in Health-Care Settings Introduction All health-care settings need an infection-control program designed to ensure prompt detection, airborne precautions, and treatment
TB Elimination Respiratory Protection in Health-Care Settings Introduction All health-care settings need an infection-control program designed to ensure prompt detection, airborne precautions, and treatment
Case-Finding for Pulmonary Tuberculosis in Penang
 ORIGINAL ARTICLE Case-Finding for Pulmonary Tuberculosis in Penang L N Hooi, MRCP Chest Clinic, Penang Hospital, Jalan Residensi, 70450 Penang ~p~mt;lry 1'h~ proce~s Qfcase-findip.g was studied in 100
ORIGINAL ARTICLE Case-Finding for Pulmonary Tuberculosis in Penang L N Hooi, MRCP Chest Clinic, Penang Hospital, Jalan Residensi, 70450 Penang ~p~mt;lry 1'h~ proce~s Qfcase-findip.g was studied in 100
Sathya Priya Kittusami. Gayathri Gurumurthy. Suma Prashant. Ashok Jhunjhunwala. CPR South 8/ CPR Africa September 5-7, 2013
 ICT- Enabled Treatment Adherence and Follow-up System Towards Successful Implementation of Revised National Tuberculosis Control Programme (RNTCP), India Sathya Priya Kittusami Gayathri Gurumurthy Suma
ICT- Enabled Treatment Adherence and Follow-up System Towards Successful Implementation of Revised National Tuberculosis Control Programme (RNTCP), India Sathya Priya Kittusami Gayathri Gurumurthy Suma
Florida Tuberculosis System of Care
 Table of Contents I. Introduction... 4 II. Florida s Charge... 5 III. Florida Tuberculosis System of Care... 5 IV. Florida Department of Health Tuberculosis Program... 7 V. Florida Department of Health
Table of Contents I. Introduction... 4 II. Florida s Charge... 5 III. Florida Tuberculosis System of Care... 5 IV. Florida Department of Health Tuberculosis Program... 7 V. Florida Department of Health
SURVEY ON THE KNOWLEDGE, ATTITUDES AND PRACTICES ON TUBERCULOSIS (TB) AMONG HEALTH CARE WORKERS IN KINGSTON & ST. ANDREW, JAMAICA
 AMONG HEALTH CARE WORKERS IN KINGSTON & ST. ANDREW, JAMAICA") UNIVERSITY OF LIVERPOOL SURVEY ON THE KNOWLEDGE, ATTITUDES AND PRACTICES ON TUBERCULOSIS (TB) AMONG HEALTH CARE WORKERS IN KINGSTON & ST. ANDREW, JAMAICA Zahra Nailah White Dissertation submitted in partial
UNIVERSITY OF LIVERPOOL SURVEY ON THE KNOWLEDGE, ATTITUDES AND PRACTICES ON TUBERCULOSIS (TB) AMONG HEALTH CARE WORKERS IN KINGSTON & ST. ANDREW, JAMAICA Zahra Nailah White Dissertation submitted in partial
MANAGING AND MONITORING THE TB PROGRAMME
 MANAGING AND MONITORING THE TB PROGRAMME Dr Lindiwe Mvusi 14 April 2016 Outline Burden of disease of TB globally Progress towards MDG targets Burden of disease of TB globally Monitoring and evaluation
MANAGING AND MONITORING THE TB PROGRAMME Dr Lindiwe Mvusi 14 April 2016 Outline Burden of disease of TB globally Progress towards MDG targets Burden of disease of TB globally Monitoring and evaluation
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Effectiveness of Self Instructional Module (SIM) on Current Trends of Vaccination in Terms
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Effectiveness of Self Instructional Module (SIM) on Current Trends of Vaccination in Terms
Regional Response Plan for Programmatic Management of Drug-resistant Tuberculosis
 Regional Response Plan for Programmatic Management of Drug-resistant Tuberculosis Report of meeting of WHO country offices focal points SEARO, New Delhi, 4 6 April 2011 Regional Office for South-East Asia
Regional Response Plan for Programmatic Management of Drug-resistant Tuberculosis Report of meeting of WHO country offices focal points SEARO, New Delhi, 4 6 April 2011 Regional Office for South-East Asia
Priority programmes and rural retention the example of TB. Karin Bergstrom Stop TB Department WHO, Geneva
 Priority programmes and rural retention the example of TB Karin Bergstrom Stop TB Department WHO, Geneva In this presentation I will briefly: review the TB situation in the world discuss "evidence" on
Priority programmes and rural retention the example of TB Karin Bergstrom Stop TB Department WHO, Geneva In this presentation I will briefly: review the TB situation in the world discuss "evidence" on
Statistical Analysis of the EPIRARE Survey on Registries Data Elements
 Deliverable D9.2 Statistical Analysis of the EPIRARE Survey on Registries Data Elements Michele Santoro, Michele Lipucci, Fabrizio Bianchi CONTENTS Overview of the documents produced by EPIRARE... 3 Disclaimer...
Deliverable D9.2 Statistical Analysis of the EPIRARE Survey on Registries Data Elements Michele Santoro, Michele Lipucci, Fabrizio Bianchi CONTENTS Overview of the documents produced by EPIRARE... 3 Disclaimer...
CHAPTER 3. Research methodology
 CHAPTER 3 Research methodology 3.1 INTRODUCTION This chapter describes the research methodology of the study, including sampling, data collection and ethical guidelines. Ethical considerations concern
CHAPTER 3 Research methodology 3.1 INTRODUCTION This chapter describes the research methodology of the study, including sampling, data collection and ethical guidelines. Ethical considerations concern
Student Health Form Howard Community College Health Science Division
 Name: HCC ID#: Student Health Form Howard Community College Health Science Division Student- Check program: Nursing: Fall: PN RN Day E/W Spring Accelerated Pathways (NURS-103) CVT: Dental Hygiene: MLT:
Name: HCC ID#: Student Health Form Howard Community College Health Science Division Student- Check program: Nursing: Fall: PN RN Day E/W Spring Accelerated Pathways (NURS-103) CVT: Dental Hygiene: MLT:
902 KAR 20:200. Tuberculosis (TB) testing for residents in long-term care settings.
 testing for residents in long-term care settings.") 0 KAR :0. Tuberculosis (TB) testing for residents in long-term care settings. The final version was copied on April, from the Kentucky Legislative Commission Website, http://www.lrc.ky.gov/kar/0/0/0.htm.
0 KAR :0. Tuberculosis (TB) testing for residents in long-term care settings. The final version was copied on April, from the Kentucky Legislative Commission Website, http://www.lrc.ky.gov/kar/0/0/0.htm.
TUBERCULOSIS TABLE OF CONTENTS TUBERCULOSIS CONTROL PLAN...2 ADMISSIONS...3 PROSPECTIVE EMPLOYEES...5
 TUBERCULOSIS TABLE OF CONTENTS TUBERCULOSIS CONTROL PLAN...2 ADMISSIONS...3 PROSPECTIVE EMPLOYEES...5 ANNUAL PERSONNEL SCREENING...5 EXPOSURE INCIDENTS...5 DOCUMENTATION OF OCCUPATIONAL EXPOSURE...5 PRE-PLACEMENT
TUBERCULOSIS TABLE OF CONTENTS TUBERCULOSIS CONTROL PLAN...2 ADMISSIONS...3 PROSPECTIVE EMPLOYEES...5 ANNUAL PERSONNEL SCREENING...5 EXPOSURE INCIDENTS...5 DOCUMENTATION OF OCCUPATIONAL EXPOSURE...5 PRE-PLACEMENT
2012 TB Laboratory Specimen Referral, Reporting & Transportation for diagnosis and management of MDR TB (January to June 2012)
") Questionnaire Serial No: 2012 TB Laboratory Specimen Referral, Reporting & Transportation for diagnosis and management of MDR TB (January to June 2012) Referring Facility Questionnaire Form 1 SECTION A:
Questionnaire Serial No: 2012 TB Laboratory Specimen Referral, Reporting & Transportation for diagnosis and management of MDR TB (January to June 2012) Referring Facility Questionnaire Form 1 SECTION A:
INTEGRATED SAFEGUARDS DATA SHEET APPRAISAL STAGE
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Copy Public Disclosure Copy Date ISDS Prepared/Updated: 02-Jan-2014
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Copy Public Disclosure Copy Date ISDS Prepared/Updated: 02-Jan-2014
TUBERCULOSIS INFECTION CONTROL
 OBJECTIVES TUBERCULOSIS INFECTION CONTROL At the end of this presentation, you will be able to: List infection control approaches to TB prevention and control Describe the type of protective equipment
OBJECTIVES TUBERCULOSIS INFECTION CONTROL At the end of this presentation, you will be able to: List infection control approaches to TB prevention and control Describe the type of protective equipment
BIOSTATISTICS CASE STUDY 2: Tests of Association for Categorical Data STUDENT VERSION
 STUDENT VERSION July 28, 2009 BIOSTAT Case Study 2: Time to Complete Exercise: 45 minutes LEARNING OBJECTIVES At the completion of this Case Study, participants should be able to: Compare two or more proportions
STUDENT VERSION July 28, 2009 BIOSTAT Case Study 2: Time to Complete Exercise: 45 minutes LEARNING OBJECTIVES At the completion of this Case Study, participants should be able to: Compare two or more proportions
TB PREVENTION AND CONTROL: WORKING WITH THE HOMELESS
 CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TB PREVENTION AND CONTROL: WORKING WITH THE HOMELESS OBJECTIVES Upon completion of this session, participants will be able to: 1. Explain the responsibilities
CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TB PREVENTION AND CONTROL: WORKING WITH THE HOMELESS OBJECTIVES Upon completion of this session, participants will be able to: 1. Explain the responsibilities
National Patient Safety Foundation at the AMA
 National Patient Safety Foundation at the AMA National Patient Safety Foundation at the AMA Public Opinion of Patient Safety Issues Research Findings Prepared for: National Patient Safety Foundation at
National Patient Safety Foundation at the AMA National Patient Safety Foundation at the AMA Public Opinion of Patient Safety Issues Research Findings Prepared for: National Patient Safety Foundation at
International Journal of Scientific and Research Publications, Volume 4, Issue 1, January ISSN
 International Journal of Scientific and Research Publications, Volume 4, Issue 1, January 2014 1 A study to assess the effectiveness of planned teaching programme on of staff nurses regarding prevention
International Journal of Scientific and Research Publications, Volume 4, Issue 1, January 2014 1 A study to assess the effectiveness of planned teaching programme on of staff nurses regarding prevention
FEDERAL MINISTRY OF HEALTH
 FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH NATIONAL TUBERCULOSIS, LEPROSY AND BURULI ULCER CONTROL PROGRAME. THE NEW ANTI-TB DRUG FORMULATIONS FOR CHILDREN: STRATEGIES FOR ROLL-OUT IN NIGERIA
FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH NATIONAL TUBERCULOSIS, LEPROSY AND BURULI ULCER CONTROL PROGRAME. THE NEW ANTI-TB DRUG FORMULATIONS FOR CHILDREN: STRATEGIES FOR ROLL-OUT IN NIGERIA