The Royal Marsden NHS Foundation Trust Quality Account for January and February 2016 presented to the March 2016 Board. Dr. Shelley Dolan, Chief Nurse
|
|
|
- Coleen Gilmore
- 6 years ago
- Views:
Transcription
1 The Royal Marsden NHS Foundation Trust Quality Account for January and February 2016 presented to the March 2016 Board. Dr. Shelley Dolan, Chief Nurse 1.0. Introduction The monthly Quality Account reports the current Trust performance against the targets for 2015/16 described in the Annual Quality Account (2014/15) under the following three nationally agreed categories: Safe care Effective care Improved Patient experience Data Quality Information and data at the Royal Marsden is produced by a centralised expert team separate from the clinical and operational teams. This separation and expertise is critical to ensure that the data is accurate and is not affected by the operational teams who are trying to comply with local and national improvement targets. All healthcare associated incidents, falls, medication incidents and pressure ulcers are reported locally onto the central Datix incident reporting system. The Datix analyst from the risk management team who is completely separate to the clinical care team compiles the reports for the quality account. All falls and medication incidents are also reviewed by subject matter experts to ensure accuracy and learning from themes. Every month a report is generated for each clinical area and if there is a reduction in reporting there is a central and local alert with action taken Safe Care 2.1. Reduction in Healthcare Associated Infections (MRSA bactereamia and C Difficile infections) Target: <31 C Difficile infections and <1 MRSA bactereamia 1
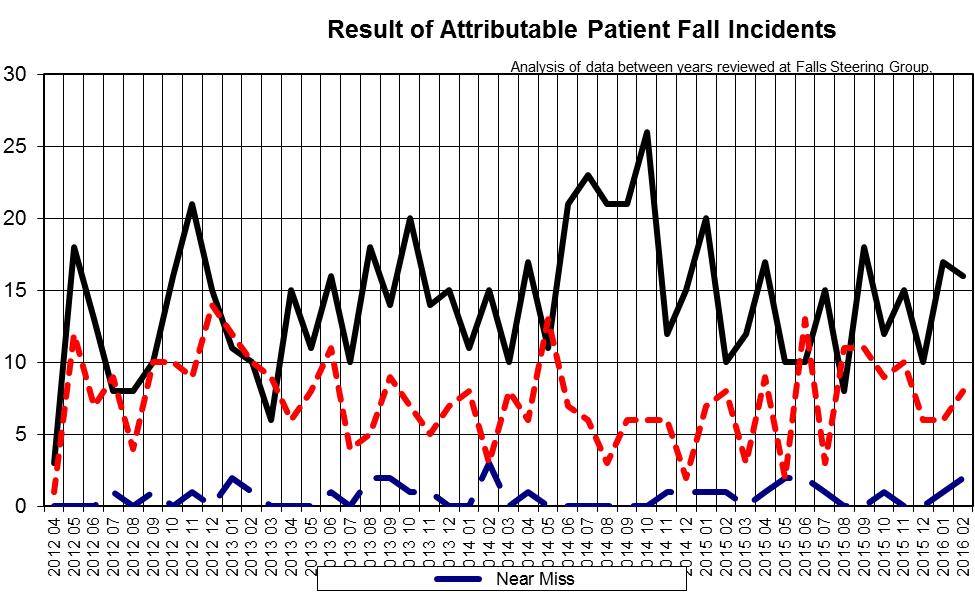
2 Table 2.1 No. Organism RM attributable January 16 RM attributable February 16 YTD Trajectory 1. MRSA * bactereamia 2. C.Difficile *MRSA has a target of zero but Monitor has a de minimus of six cases. Currently only three cases have been deemed attributable to cross infection throughout the year. This number will be finalised by the national team in April / June Rate of patient safety incidents and percentage resulting in severe harm or death To include: Reduction of severe/moderate risk medication errors Reduction of harm from falls Target: Reduction in the rate of patient safety incidents per 100 admissions and the proportion that have resulted in severe harm or death Performance: 2.3. (1) Reduction in Falls Target: < 0.7 moderate and above (resulting in harm) falls per 1000 bed days Year to date - to the end of February 2016 the Trust has met the target. 2
3 3
4 4
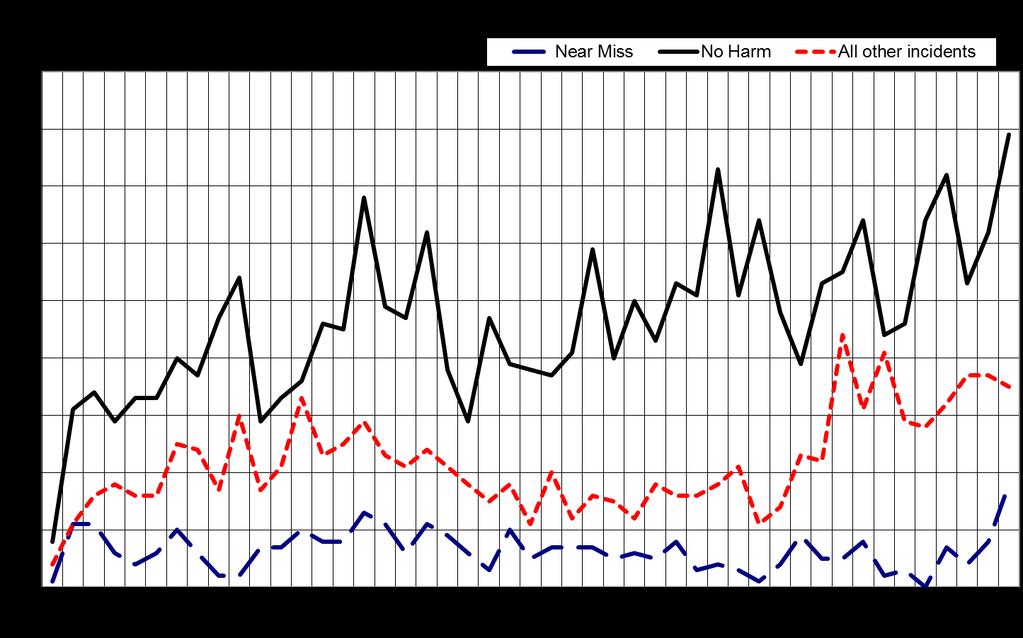
5 Severity of Patient Fall incidents: 3 - Severity - Current Period Total No Harm Low / Minor (Minimal harm) Moderate (Short term harm) Severe / Major (Permanent or long term harm) Death / Catastrophic (Caused by the incident) Totals: % Harm Patient Fall 20% 33% 14% 52% 16% 58% 38% 41% 40% 38% 25% 31% 35% 2.4. (2) Reduction in medication errors Target: To increase the reporting of near misses and decrease the incidents that cause actual harm (low<2 per 1000 bed days and moderate <0.17 per 1000 bed days). N.B. To place medication errors in perspective, annually 0.7% of all medicines administered result in a medication error. For February 2016, the figure is 0.08%. There has been a 20% increase in medication incidents categorised as near miss in comparison to the same period in 2014/2015. A streamlined near miss reporting method utilising the current IT system is now available for all Trust staff in order to encourage/facilitate an increase in the reporting of near miss incidents. In the current period, 1125 attributable medication incidents have been reported using the IT system Datix, of which 70% caused no harm. 331 incidents have been categorised as low severity and 6 incidents as moderate severity (resulting in harm), this represents 5.43 and 0.10 medication incidents per 1000 bed days respectively. As such, the Trust has missed the target relating to low severity medication incidents, however the target relating to moderate severity incidents has been met. 5
6 6
7 7
8 Severity of medication incidents: 3 - Severity - Current Period Total o Harm Low / Minor (Minimal harm) Moderate (Short term harm) Severe / Major (Permanent or long term harm) Death / Catastrophic (Caused by the incident) Totals: % Harm Medication Incidents 17% 30% 24% 40% 29% 40% 35% 25% 27% 37% 30% 24% 30% 2.5 Percentage of admitted patients risk assessed for Venous Thrombo-embolism (VTE) Target: 95% have completed VTE risk assessments Performance: The Trust consistently achieves >90% compliance with risk assessment (CQUIN target is 90%). All patients with confirmed VTE as reported by radiology undergo a Root Cause Analysis (RCAs). The VTE steering board monitor all confirmed VTE and scrutinise the RCAs. 8

9 3.0 Effective Care 3.2 Incidence of Trust acquired pressure ulcers The number and severity of healthcare acquired pressure ulcers are used internationally as a proxy for the effectiveness of care provision. Many people with cancer and or co-morbidity are more vulnerable to tissue damage for the following reasons; multiple hospital admissions, frailty, multiple drugs including high dose steroids (decreases skin elasticity), immobility, malnutrition or susceptibility to infection Data for this report was taken on 4 March (hospital) and on 2 March (SMCS) 2016 from DATIX. Data may have been updated since Total number of patients with the Trust (hospital/community services) attributable pressure ulcers for the month of January 2016: 52 [Hospital=20, Community services=32] February 2016: 47 [Hospital=14, Community services=33] For serious incident reporting to Steis [Strategic Executive Information System] as Hospital/Community Services. Number of patients with Trust attributable pressure ulcers at categories 3 and 4 for the month of January 2016: 10 [Hospital=0, Community services=10] February 2016: 5 [Hospital=0, Community services= 5] 9
10 3.2.5 Number of patients with Trust attributable category 3 and 4 pressure ulcers Number of patients with Trust attributable category 3 and 4 pressure ulcers, April February hospital community services 2 0 Apr Jun Aug Oct Dec Feb Apr Jun Aug Oct Dec Feb 10
11 Number of patients with Trust attributable pressure ulcers, all categories Patients with Trust attributable pressure ulcers, all categories, April February hospital community services 5 0 Apr Jun Aug Oct Dec Feb Apr Jun Aug Oct Dec Feb 11
12 Number of patients with Trust attributable pressure ulcer, monthly and cumulative totals April 2015 to February monthly hospital total hospital Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb monthly community services total community services 12
13 Description of European Pressure Ulcer Advisory Panel (EPUAP) pressure ulcer classification system. EPUAP Description of Stage 1 Non blanching redness of intact skin 2 Partial thickness skin loss or blister 3 Full thickness skin loss (fat visible) 4 Full thickness tissue loss (muscle/bone visible) 3.3. Emergency re-admissions to hospital within 28 days of discharge Target: Reduction in the number of avoidable re-admissions to hospital within 28 days of discharge Some emergency re-admissions following discharge from hospital are an unavoidable consequence of the original treatment, however some can be potentially avoided through ensuring the delivery of optimal treatment according to each patient s needs, careful planning and support for self care. It is important to note that some readmissions will inevitably include patients who are admitted with side effects of treatment therefore it may be difficult to explain any differences between RMH with other acute Trusts. Performance: Within 28 days of original admission there were the following emergency admissions: 13
14 14

15 4.0 Patient Experience 4.1 Reduction in chemotherapy waiting times and improvement in patient experience related to waiting times Target: Reduction in chemotherapy waiting times at Sutton/Chelsea and improvement in the patient experience related to waiting times Performance: Data in the following graphs are for all chemotherapy attendances, for NHS and Private Patients Table 1: Chelsea chemotherapy waiting times 15
16 Table 2: Sutton chemotherapy waiting times 16
17 Table 3: Chelsea and Sutton chemotherapy waiting times 17
18 Figure 1 Pre-prescribing >5days in advance: All Clinical units Figure 1 illustrates pre-prescribing performance >5days in advance. It demonstrates that there is a reduced performance at Chelsea (70-80%) when compared to the Sutton and Kingston units (~90%). The rates at Chelsea can be seen to have increased over the period and can in part be explained by a change in case mix. However, looking at the Breast unit as an example (Fig 2), it can be shown that across a group of patients where the chemotherapy regimens are essentially the same there is still significantly better adherence to pre-prescribing guidance at the Sutton and Kingston sites. It is unclear why there is such a difference in pre-prescribing rates and this now needs a greater focus. With this in mind, a new chemotherapy pharmacist has been employed on the Chelsea site to specifically work with clinical groups and clinicians to identify reasons for the reduced rate of pre-prescribing and improve this metric each month. This will start from March 2016 and will become part of the monthly metrics we share with clinical teams to drive improvement. 18
19 Figure 2 Pre-prescribing >5days in advance: Breast Unit Plans for improving turnaround of manufacturing of chemotherapy As 80% of the chemotherapy is manufactured from a third party partnership with an external company (Hospira ), the pharmacy department has been working with them to introduce a new way of manufacturing which will help speed up the supply of chemotherapy. The new method of manufacturing will also reduce the amount of chemotherapy that is wasted. The new systems will start in April 2016 and the impact of this will be monitored across RM. Improvements in waiting times for discharge and outpatient prescriptions: In quarter two 2015 there has been a significant change in the supply of discharge medication with commencement of a partnership with Boots the chemist. Boots dispense: Out-patient, day-case and discharge medication for patients at the Royal Marsden. We have also introduced prescription tracking technology at commencement of the partnership, this facilitates the monitoring of dispensing times for both outpatient and discharge prescriptions. 19

20 The Boots partnership has now been in place for six months and whilst a steady improvement has been seen in waiting times for patients across both sites, there are still some challenges, particularly on the Sutton site. The waiting times are longer in Sutton and some of this is due to the greater complexity of prescriptions especially from paediatrics and haematology, which need careful screening before being dispensed. Boots have to feedback performance against certain targets of which discharge is a key indicator and Q3 performance can be seen below. 20
21 We are working closely with Boots to ensure a high quality medicines management service is provided to patients. All targets are monitored monthly as part of performance review meetings, quarterly performance meetings will oversee the contract and provide strategic direction for service development. In addition a bi-weekly Quality Improvement group with both Boots and RMH staff has been set up to raise concerns and work jointly through to resolve them and improve the performance particularly on the Sutton site. 6.1 Ensure that we are responding to inpatient s personal needs The Friends and Family Test The NHS Friends and Family Test was announced by the Prime Minister on 25 May The national mandated question asked is: How likely are you to recommend our ward to friends and family if they need similar care or treatment? The patients then select their answer from the following Likert Scale: Extremely likely; Likely; Neither likely nor Unlikely; Unlikely; Extremely unlikely; Don t know. The Royal Marsden has then chosen to add a second question: What was good about your care and what could be improved? Patients answer this question with free text comments. January 887 responses overall: Inpatients 233, Day Care 352, Outpatient (OPD) 302 Inpatient: 26 patients made suggestions for improvement:- further to my last feedback today (over 4 hours ago) I am still waiting to be discharged. Your admin dept needs a serious overhaul. Medical may be your first priority but all areas contribute to the good running of a service! (still her 1 hour later) 21
22 I think there needs to be more evident senior level management of the work of more junior nurses and HCA s. As a patient it would be impossible to know who to call in case of a query. NICE guidelines, not followed for meds the only thing that could be improved was that at the weekend, the staff were over-stretched and perhaps not enough of them, and the night staff were not as particular with the ward or as friendly Due to an error with my drug chat I was waken at 11.30pm for a new canula to be put in and antibiotics given, but it couldn t be helped and everyone was very apologetic. the only thing instead of those flimsy curtains which, actually offer, very little privacy, could you not put frosted prospect curtains which you can push back when not in use and are easily cleaned We also asked all in-patients on discharge the following questions about their care. Score (out of 5) Were you treated with dignity and respect? 4.94 Did you feel involved enough in decisions made about you? 4.79 Did you receive timely information about your care and treatment? 4.76 Was the location clean? 4.88 Were you treated well by the staff looking after you? 4.94 Day care 20 patients made suggestions for improvement: Room for improvement unit was very busy today. There was a 3 hour delay and I was still there at 6.30 after 12:30 appointment. Also I had to spend all the time on the unit i.e. without my husband for company prior to the procedure. Often found the nurses were not rightly informed on what was going on with the patient s e.g unnecessary blood being taken which could have been done when cannulated more staff for the pharmacy 22
23 I did feel anxious on today s visit, as someone in the waiting area appeared to have a cold. As we all have an impaired immune system this is a worry. As a suggestion, maybe all patients and their companions could be asked at reception when looking in, if they have an active infection Score (out of 5) Were you treated with dignity and respect? 4.95 Did you feel involved enough in decisions made about you? 4.86 Did you receive timely information about your care and treatment? 4.84 Was the location clean? 4.91 Were you treated well by the staff looking after you? 4.97 OPD 11 patients made suggestions for improvement: I do have a minor suggestion and that is registration could be more private. Clerk asked questions re personal status in waiting room within hearing of other patients waiting 1 and a half hours for an appointment is not a good introduction to this hospital-seems to be a complete shambles. Signage from outside and within the grounds is none0existing I had no treatment today as my appointment had been cancelled but the letter telling me so had been headed confirmation of appointment like the previous letter which was a confirmation so I assumed it was just that and I didn t read it carefully enough. That was my fault but if only someone had bothered to head the letter change We also asked all out-patients on discharge the following questions about their care. Score (out of 5) Were you treated with dignity and respect? 4.85 Did you feel involved enough in decisions made about you? 4.77 Did you receive timely information about your care and treatment? 4.75 Was the location clean? 4.85 Were you treated well by the staff looking after you?
24 February overall 977 responses: Inpatients 242, Day Care 356, OPD 309 Inpatients 19 patients made suggestions for improvement: I felt hurriedly and prematurely discharged e.g. not shown how to get in/ out of bed. Not accompanied for my first walk after operation along the ward. Might have been help to have nil-by-mouth signs on bed to prevent catering staff offering food and very occasionally bringing meal to bed. There were four comments about the coldness of the ward bed areas and bathrooms. Faulty air con made the bay too cool/cold. Window seals in room 2 need attention-bad draught. We also asked all in-patients on discharge the following questions about their care. Score (out of 5) Were you treated with dignity and respect? 4.91 Did you feel involved enough in decisions made about you? 4.79 Did you receive timely information about your care and treatment? 4.78 Was the location clean? 4.87 Were you treated well by the staff looking after you?
25 Day care 44 patients made suggestions for improvement: Waiting times. one thing that could definitely be improved is the timing of appointments. My appointment was for 9am but as the anaesthetist have ward rounds, there is no chance of them getting to the ward before 1030/11am. So why the need to arrive at 9am? Sometime though, the wait is one hour and a half (drug trial). If it can be a bit less, it would be very helpful. 1) Decrease in waiting times between apt. time and arrival of drugs for the drip infusion. 2) Decrease in waiting time between apt time and seeing a consultant. 3) Conflict between consultant reports for future treatment. Sometimes quite big delays between appointment time and treatment starting. Could be improved: Waiting time. Waiting for chemo makes anxiety increase- 2hrs late is very hard to deal with. Sadly the open wards lack privacy and are loud and a little stressful to stay in an ideal world, rooms would be separate (and there would be more rooms). I realize that space and money is limited. We also asked all day case patients on discharge the following questions about their care. Score (out of 5) Were you treated with dignity and respect? 4.91 Did you feel involved enough in decisions made about you? 4.81 Did you receive timely information about your care and treatment? 4.77 Was the location clean? 4.88 Were you treated well by the staff looking after you?
26 OPD 10 patients made suggestions for improvement: There were three complaints about car parking. Waiting to get into the car park was lengthy, which does not help patient stress levels prior to appointments. Car park capacity does not seem to have increased over the last few decades, but patient numbers surely have. There were several comments about the reception staff. receptionists not always friendly- very stern especially the man. reception staff helpful and friendly. This is hit and miss depending on who you get, but majority of the time positive. There were several comments about waiting times. My husband had to wait an hour after his appointment and when he checked at the desk he was told that he seemed to have slipped through the net. Too long waiting to see doctor s waiting went for 45 mins then 1 hour then one and a half hours in a time of half hour, I get all uptight waiting this long, you expect a little wait. Why do you over book? We also asked all out-patients on discharge the following questions about their care. Score (out of 5) Were you treated with dignity and respect? 4.94 Did you feel involved enough in decisions made about you? 4.87 Did you receive timely information about your care and treatment? 4.82 Was the location clean? 4.93 Were you treated well by the staff looking after you?
27 National FFT inpatient results reporting: From November 2014 NHS England report a percentage of those who would recommend the Trust to friends and family. Inpatient data was collected for 170 Acute NHS trusts and independent sector providers. Nationally, the overall average inpatient percentage for those who would recommend the service to friends and family was 96% in December. The Trust is slightly below this with an average of 95% in December. Outpatient data was collected for 234 Acute NHS trusts and independent sector providers. Nationally the overall average outpatient percentage for those who would recommend outpatients to friends and family was 92% in December. The trust was above this with an average of 98% in December. The tables below shows the results for the Trust each quarter to date. At the time of reporting (9 th March 2016) national figures were available up to December Q2 Q3 Q4 Q1 Apr 2015 May 2015 June 2015 July 2015 Aug 2015 Sep 2015 Oct 2015 Nov 2015 Dec The Royal 94% 97% 99% 97% 96% 97% 97% 95% 97% 98% 95% 98% 95% Marsden percentage of inpatients who would recommend National average 94% 95% 95% 96% 95.5% 95.7% 95.8% 95.9% 96.0% 96% 96% 96% 96% Response number OUTPATIENTS The Royal Marsden percentage of outpatients who would recommend July 2015 Aug Sept 2015 Oct 2015 Nov 2015 Dec % 97% 96% 99% 97% 98% National average 92% 92% 92 % 92% 92% 92% Response number
28 7.1 Complaints by Directorate and Subject January Standard of Care Attitude Delay Diagnosis/Treatment Communication 1 0 Cancer Services Clinical Services Private Care Community Services There were nine complaints in January. There was no complaint for Clinical Services. Communication Communication prior and after surgery Communication around the handling of child protection procedures Communication around patient discharge Diagnosis/Treatment Review of symptoms and scans, and medical records accuracy Lack of referral and treatment offered 28
29 Concern about treatment at another Trust Delay Delay in physiotherapy appointment Attitude Concern with staff attitude at family planning clinic Standard of care Level of care provided by nursing team is below standard 4 Complaints by Directorate and Subject February Attitude Delay Diagnosis/Treatment Communication Environment 1 0 Cancer Services Clinical Services Private Care Community Services Estates 29
30 There were 11 complaints in February. There were no complaints for Private Care. Communication Lack of communication and clear information about test results Breach of confidentiality Poor verbal communication received as an inpatient Communication around health visiting service's decision to halt its intervention Diagnosis/Treatment Lack of care and concerned with risk of delay in treatment Delay in diagnosis of injury and concerns raised about surgical procedure Delay Delay in outpatients department Delay in appointment at clinic, unacceptably long waiting time Attitude Poor attitude of breast care nurse Attitude of physiotherapists and the treatment received at the health centre Environment Concerns with environment on Wilson Ward Safer staffing From June 2014 all Trusts are required by the Department of Health, Monitor and Care Quality Commission to be able to assure their Boards around the provision of nursing care on its wards and units. This new requirement follows the national failings in care at Mid Staffordshire NHS Foundation Trust and other Trusts since put on special measures. The final Francis report recommended that Boards regularly check that levels of nurse staffing are appropriate for good quality care. Therefore from June 2014 the RM Board has received a monthly summary of planned numbers of nurses and Health Care Assistants (HCA) during the day and at night, versus the actual numbers. It is also mandated that the Board receive a six monthly report from the Chief Nurse regarding all issues regarding Safe Nurse staffing across the Trust. Such a report has been presented to the June 2014 and January 2015, June Board and will be presented again in March
31 The following data is the planned and actual nurse staffing for January Overall the percentages are as follows: Average fill rate for night staff 97.7% Average fill rate for day staff 94.2% Average fill rate for Registered staff 94.9% Average fill rate for Care staff 99.0% Average Trust wide fill rate (All staff, night and day) 95.6% February 2016 Average fill rate for night staff 100.7% Average fill rate for day staff 96.6% Average fill rate for Registered staff 97.7% Average fill rate for Care staff 100.5% Average Trust wide fill rate (All staff, night and day) 98.2% 8.1 Nursing Leavers and Starters Report The tables below show the number of nurse starters and leavers over a two year period. In the financial year 2013/14 the number of nurse leavers equated to 12 nurses per month on average. For the current financial year more nurses have been recruited at this point than in the last financial year. In November 2014 the Chief Nurse began a monthly recruitment meeting to address the issues around recruitment and retention of nurses. For the first time in February the meeting was able to review the results of a small exit questionnaire, questionnaires were sent retrospectively to 35 nurses who had left and nine were returned. In all but one case the nurses left for personal or financial reasons. The questionnaires are now reviewed monthly. Board members will note below that the concerted work of nursing and HR, marketing and communications is finally showing positive results from June onwards more nurses were recruited than left the Trust. The Trust is holding national recruitment days on a Saturday which have thus far yielded 15 days and the next event is to be held on Saturday the 19 th March 2016 at Chelsea. The RM is keen to improve recruitment and retention of nurses particularly at bands 5 and 6 (junior and senior Staff Nurses). The new recruitment group is facilitating HR, senior nursing, marketing and communications to work together and look at innovative solutions. The Board will be kept updated on this important issue through regular reports at QAR. 31
32 Band 5-7 Nurses (2014/15) Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Total Starters (wte) Leavers (wte) Variance Band 5-7 Nurses (2015/16) Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Total Starters (wte) Leavers (wte) Variance
33 8.2 Leavers in January 2016 Area Job Title Nursing Leavers Bands 5-7 January 2016 Leaving LOS Band WTE Reason for leaving date Cancer Services Division Bud Flanagan East Staff Nurse 02/01/ y 3 m XR Voluntary Resignation - Health Bud Flanagan East Senior Staff Nurse 24/01/ y 2 m XR Voluntary Resignation - Promotion Bud Flanagan West Senior Staff Nurse 03/01/ y 2 m XR Voluntary Resignation - Promotion Ellis Ward Staff Nurse 24/01/ y 7 m XR Voluntary Resignation - Relocation Ellis Ward Sister/ Charge Nurse 01/01/ y 2 m XR Voluntary Resignation - Relocation Markus Ward Staff Nurse 10/01/ y 9 m XR Voluntary Resignation - Other Medical Day Unit (S) Staff Nurse 07/01/ y 3 m XR Voluntary Resignation - Other Clinical Services Division Horder Ward Staff Nurse 03/01/ y 8 m XR Voluntary Resignation - Promotion Outpatients (L) Senior Staff Nurse 05/01/ y 7 m XR Voluntary Resignation - Promotion Outpatients (L) Sister / Charge Nurse 10/01/ y 7 m XR Voluntary Resignation - Relocation Clinical Research Division Lerner Lung & Mesothelioma Research Research Nurse 30/01/ y 2 m XR Retirement - Age Oak Ward Senior Staff Nurse 24/01/ y 3 m XR Voluntary Resignation - Other Rehabilitation Research Research Nurse 14/01/ y 5 m XR Voluntary Resignation - Adult Dependants Community Services HV Merton Health Visitor 31/01/ y 3 m XR Voluntary Resignation Work Life Balance - Cost of Living (Travel, Accomodation) Respiratory Nursing Specialist Nurse Respiratory Medicine 04/01/ y 10 m XR Voluntary Resignation - Other Private Care GH Day Services Staff Nurse 31/01/ y 0 m XR Voluntary Resignation - Other GH Ward (1 & 2) Senior Staff Nurses 24/01/ y 3 m XR Voluntary Resignation - Relocation Total WTE Leavers
34 Leavers in February 2016 Nursing Leavers Bands 5-7 February 2016 Area Job Title Leaving date LOS Band WTE Reason for leaving Cancer Services Division Ellis Ward Staff Nurse 17/03/ y 5 m XR Voluntary Resig. - Relocation McElwain Ward Staff Nurse 06/03/ y 7 m XR Voluntary Resig. - Child Dependants Wilson Ward Staff Nurse 28/02/ y 10 m XR Voluntary Resig. - Relocation Burdett Coutts Ward Staff Nurse 18/03/ y 5 m XR Voluntary Resignation - Other Lung Unit (S) Clinical Nurse Specialist 29/03/ y 5 m XR Voluntary Resig. - Relocation Clinical Services Division Critical Care Unit (L) Staff Nurse 11/03/ y 2 m XR Voluntary Resig. - Relocation Critical Care Unit (L) Staff Nurse, Critical Care 10/03/ y 8 m XR Retirement - Age Endoscopy Staff Nurse 01/04/ y 6 m XR Voluntary Resign. - To undertake further Education or Training Theatres (L) Staff Nurse 07/02/ y 8 m XR Voluntary Resign. - To undertake further Education or Training Theatres (L) Staff Nurse 26/02/ y 6 m XR Voluntary Resig. - Better Reward Package Theatres (L) Theatre Sister 31/03/ y 8 m XR Volun. Early Retirement - with Actuarial Reduction Clinical Research Division New Cancer Research Networks Research Nurse - Kingston Hospital 01/02/ y 4 m XR Voluntary Resignation - Other Head and Neck Research Research Nurse 15/02/ y 3 m XR Voluntary Resignation - Other Community Services FP Medical Contraception & Sexual Health Nurse 07/02/ y 1 m XR Voluntary Resignation - Other East Merton Community Nurse 21/02/ y 11 m XR Voluntary Resig. - Relocation Rapid Response Rapid Response Nurse 31/03/ y 5 m XR Retirement - Age Raynes Park Community Nurse 14/02/ y 3 m XR Voluntary Resig. - Child Dependants Private Care GH Ward (1 & 2) Staff Nurse 25/05/ y 10 m XR Retirement - Age Total WTE Leavers Board Members are invited to note the performance of the Trust against the agreed national and local quality targets for January and February 2016 and the actions being taken. 34
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Open and Honest Care in your Local Hospitals
 Open and Honest Care in your Local Hospitals The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospitals The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Board of Directors Meeting Board Room, Chelsea
 Board of Directors Meeting Board Room, Chelsea Wednesday 29 March 2017, 10am 12pm Agenda 1. Welcome & Apologies for Absence No apologies to note. 2. Declarations of Interest (All) 3. Minutes of Public
Board of Directors Meeting Board Room, Chelsea Wednesday 29 March 2017, 10am 12pm Agenda 1. Welcome & Apologies for Absence No apologies to note. 2. Declarations of Interest (All) 3. Minutes of Public
NHS Borders Feedback and Complaints Annual Report
 NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S REPORT. BOARD OF DIRECTORS 21 st March 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS MEETING HELD MAY 2011
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST K EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS MEETING HELD MAY 2011 Subject Supporting TEG Member Author Status 1 Pharmacy and medicines management
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST K EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS MEETING HELD MAY 2011 Subject Supporting TEG Member Author Status 1 Pharmacy and medicines management
Monthly Nurse Safer Staffing Report October 2017
 Monthly Nurse Safer Staffing Report October 2017 Trust Board November 2017 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid
Monthly Nurse Safer Staffing Report October 2017 Trust Board November 2017 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid
Monthly Nurse Safer Staffing Report June and July 2018
 Monthly Nurse Safer Staffing Report June and July 2018 Trust Board September 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation
Monthly Nurse Safer Staffing Report June and July 2018 Trust Board September 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing August 2017 (July 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
Annual Report and Accounts 2013/14
 Annual Report and Accounts 2013/14 CQuality Account 2016/17 The Royal Marsden NHS Foundation Trust Front cover photo Filipe Carvalho, Advanced Nurse Practitioner in Colorectal cancer. D Quality Account
Annual Report and Accounts 2013/14 CQuality Account 2016/17 The Royal Marsden NHS Foundation Trust Front cover photo Filipe Carvalho, Advanced Nurse Practitioner in Colorectal cancer. D Quality Account
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Section 1 - Key Performance Indicators
 Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Integrated Quality Report
 Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Dartford and Gravesham NHS Trust. Susan Acott Chief Executive
 Dartford and Gravesham NHS Trust Susan Acott Chief Executive A First in Kent Retired policeman Richard Oliver aged 59 was the first patient to be fitted with the EMBLEM, Subcutaneous Implantable Cardiac
Dartford and Gravesham NHS Trust Susan Acott Chief Executive A First in Kent Retired policeman Richard Oliver aged 59 was the first patient to be fitted with the EMBLEM, Subcutaneous Implantable Cardiac
National Inpatient Survey. Director of Nursing and Quality
 Reporting to: Title Sponsoring Director Trust Board National Inpatient Survey Director of Nursing and Quality Paper 6 Author(s) Sarah Bloomfield, Director of Nursing and Quality, Sally Allen, Clinical
Reporting to: Title Sponsoring Director Trust Board National Inpatient Survey Director of Nursing and Quality Paper 6 Author(s) Sarah Bloomfield, Director of Nursing and Quality, Sally Allen, Clinical
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016)
 HR & OD Monthly Trust Report (September 2016)") Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
National findings from the 2013 Inpatients survey
 National findings from the 2013 Inpatients survey Introduction This report details the key findings from the 2013 survey of adult inpatient services. This is the eleventh survey and involved 156 acute
National findings from the 2013 Inpatients survey Introduction This report details the key findings from the 2013 survey of adult inpatient services. This is the eleventh survey and involved 156 acute
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Open and Honest Care in your local Trust
 Agenda Item: 3 Encl. 3.3 Open and Honest Care in your local Trust Open and Honest Report for Black Country Partnership NHS Foundation Trust February 2017 NHS England INFORMATION READER BOX Directorate
Agenda Item: 3 Encl. 3.3 Open and Honest Care in your local Trust Open and Honest Report for Black Country Partnership NHS Foundation Trust February 2017 NHS England INFORMATION READER BOX Directorate
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014
 Agenda item 7(v) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014 1. INTRODUCTION AND OVERVIEW The Cancer Patient Experience Survey
Agenda item 7(v) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014 1. INTRODUCTION AND OVERVIEW The Cancer Patient Experience Survey
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Northern Health - Acute Services. Evidence Based Practice Venous Thromboembolism Prevention
 Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
Northern Health - Acute Services Evidence Based Practice Venous Thromboembolism Prevention (VTE) Jeannette Kamar Christine Lamotte, Liam Carter Improving Patient Safety Preventing and Managing Venous Thromboembolism
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
PRIMARY CARE COMMISSIONING COMMITTEE
 PRIMARY CARE COMMISSIONING COMMITTEE 1. Date of Meeting: 2. Title of Report: Western Avenue Medical Centre Personal Medical Services (PMS) Reinvestment Report 3. Key Messages: The Personal Medical Services
PRIMARY CARE COMMISSIONING COMMITTEE 1. Date of Meeting: 2. Title of Report: Western Avenue Medical Centre Personal Medical Services (PMS) Reinvestment Report 3. Key Messages: The Personal Medical Services
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
BOARD MEETING. Document is for: (indicate with an x) Assurance x Information Decision. Executive Summary
 Assurance x Information Decision. Executive Summary") Document Title: Presenter: Author: Contact details for further information: BOARD MEETING Review of Pressure Ulcer Prevalence across DCHS services March June 2012 Kath Henderson, Chief Nurse Michelle O
Document Title: Presenter: Author: Contact details for further information: BOARD MEETING Review of Pressure Ulcer Prevalence across DCHS services March June 2012 Kath Henderson, Chief Nurse Michelle O
The Royal Wolverhampton NHS Trust
 Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Monthly Nurse Safer Staffing Report May 2018
 Monthly Nurse Safer Staffing Report May 2018 Trust Board June 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid Staffordshire
Monthly Nurse Safer Staffing Report May 2018 Trust Board June 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid Staffordshire
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Quality Improvement Scorecard December 2016
 Mortality: HSMR Nat The improvement in performance has been maintained in year. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat The improvement in performance has been maintained in year. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
National Patient Experience Survey Mater Misericordiae University Hospital.
 National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Governing Body. TITLE OF REPORT: Performance Report for period ending 31st December 2012
 - Governing Body DATE OF MEETING: TITLE OF REPORT: Performance Report for period ending 31st December 2012 KEY MESSAGES: We are responsible for securing improvements in the quality of care and health outcomes.
- Governing Body DATE OF MEETING: TITLE OF REPORT: Performance Report for period ending 31st December 2012 KEY MESSAGES: We are responsible for securing improvements in the quality of care and health outcomes.
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Pharmacy, Medicines and You. Principal Pharmacist Pharmaceutical Services Deputy Director of Pharmacy and Medicines Management
 Pharmacy, Medicines and You Wendy Robertson Liz Kemp Caroline Hind Principal Pharmacist Pharmaceutical Services Principal Pharmacist Pharmaceutical Services Deputy Director of Pharmacy and Medicines Management
Pharmacy, Medicines and You Wendy Robertson Liz Kemp Caroline Hind Principal Pharmacist Pharmaceutical Services Principal Pharmacist Pharmaceutical Services Deputy Director of Pharmacy and Medicines Management
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Sarah Bloomfield, Director of Nursing and Quality
 Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Complaints Report. Quarter 1, 2014/2015
 Complaints Report Quarter 1, 2014/2015 (1 st April 30 th June 2014) Authors: Tanya Tofts, Patient Support and Complaints Manager Chris Swonnell, Head of Quality (Patient Experience and Clinical Effectiveness)
Complaints Report Quarter 1, 2014/2015 (1 st April 30 th June 2014) Authors: Tanya Tofts, Patient Support and Complaints Manager Chris Swonnell, Head of Quality (Patient Experience and Clinical Effectiveness)
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Quarter /13 Quality Account (Quality and Safety)
") Airedale NHS Foundation Trust Board of Directors:23 rd January 213 Title: Quarter 2 212/13 Quality Account (Quality and Safety) Author: Alison Fuller, Assistant Director Healthcare Quarter 2 212/13 Quality
Airedale NHS Foundation Trust Board of Directors:23 rd January 213 Title: Quarter 2 212/13 Quality Account (Quality and Safety) Author: Alison Fuller, Assistant Director Healthcare Quarter 2 212/13 Quality
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
TRUST BOARD PART I SEPTEMBER 2011 Agenda Item Number: 145/11 Enclosure Number: (1)
") TRUST BOARD PART I SEPTEMBER 2011 Agenda Item Number: 145/11 Enclosure Number: (1) Subject: Prepared by: Sponsored by: Presented by: Purpose of paper Why is this paper going to the Trust Board? Key points
TRUST BOARD PART I SEPTEMBER 2011 Agenda Item Number: 145/11 Enclosure Number: (1) Subject: Prepared by: Sponsored by: Presented by: Purpose of paper Why is this paper going to the Trust Board? Key points
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST REDUCING HARM TISSUE VIABILITY PROGRESS REPORT
 Agenda item A5(iv) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST REDUCING HARM TISSUE VIABILITY PROGRESS REPORT EXECUTIVE SUMMARY The Tissue Viability Team assists wards and departments to reduce
Agenda item A5(iv) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST REDUCING HARM TISSUE VIABILITY PROGRESS REPORT EXECUTIVE SUMMARY The Tissue Viability Team assists wards and departments to reduce
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Patient Experience Annual Report
 Patient Experience Annual Report 1 April 2013 31 March 2014 Queen Victoria Hospital Patient Experience Annual Report 2 Overview This report includes an overview of activity for the financial year between
Patient Experience Annual Report 1 April 2013 31 March 2014 Queen Victoria Hospital Patient Experience Annual Report 2 Overview This report includes an overview of activity for the financial year between
Statement 2: Patients/carers are offered verbal and written information on VTE prevention as part of the admission process.
 THROMBOSIS GROUP Venous thromboembolism (VTE) is a collective term referring to deep vein thrombosis (DVT) and pulmonary embolism (PE). VTE is defined by the following ICD-10 codes: I80.0-I80.3, I80.8-I80.9,
THROMBOSIS GROUP Venous thromboembolism (VTE) is a collective term referring to deep vein thrombosis (DVT) and pulmonary embolism (PE). VTE is defined by the following ICD-10 codes: I80.0-I80.3, I80.8-I80.9,
PATIENT EXPERIENCE REPORT
 Improving Patient Experience PATIENT EXPERIENCE REPORT 1st July 2012 30th September 2012 Patient Experience Report - Page 2 Introduction The Patient Experience Report aims to present a rounded picture
Improving Patient Experience PATIENT EXPERIENCE REPORT 1st July 2012 30th September 2012 Patient Experience Report - Page 2 Introduction The Patient Experience Report aims to present a rounded picture
Andrea Croft RGN Lead Advanced Nurse Practitioner Anticoagulation. Welsh Nurse Director Thrombosis UK
 Andrea Croft RGN Lead Advanced Nurse Practitioner Anticoagulation Welsh Nurse Director Thrombosis UK Background Venous Thromboembolism (VTE), the collective term for deep vein thrombosis (DVT) and pulmonary
Andrea Croft RGN Lead Advanced Nurse Practitioner Anticoagulation Welsh Nurse Director Thrombosis UK Background Venous Thromboembolism (VTE), the collective term for deep vein thrombosis (DVT) and pulmonary
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Open and Honest Care in your local Trust. Open and Honest Report for. Black Country Partnership NHS Foundation Trust
 Open and Honest Care in your local Trust Open and Honest Report for Black Country Partnership NHS Foundation Trust May 2016 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations
Open and Honest Care in your local Trust Open and Honest Report for Black Country Partnership NHS Foundation Trust May 2016 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Patient survey report Survey of adult inpatients 2013 North Bristol NHS Trust
 Patient survey report 2013 Survey of adult inpatients 2013 National NHS patient survey programme Survey of adult inpatients 2013 The Care Quality Commission The Care Quality Commission (CQC) is the independent
Patient survey report 2013 Survey of adult inpatients 2013 National NHS patient survey programme Survey of adult inpatients 2013 The Care Quality Commission The Care Quality Commission (CQC) is the independent
National Cancer Patient Experience Survey National Results Summary
 National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
National Patient Experience Survey UL Hospitals, Nenagh.
 National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Review of Inpatient Nursing Establishment, Capacity and Capability Review
 Appendix 2 Review of Inpatient Nursing Establishment, Capacity and Capability Review Mental Health Group September 2015 Review March 2016 Author: Heidi Cater, Head of Nursing, Mental Health Page 1 of 15
Appendix 2 Review of Inpatient Nursing Establishment, Capacity and Capability Review Mental Health Group September 2015 Review March 2016 Author: Heidi Cater, Head of Nursing, Mental Health Page 1 of 15
Sheffield Teaching Hospitals NHS Foundation Trust
 Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
HCAHPS. Presented by: Bill Sexton. Proudly recognized as one of the Nation s Top 100 Critical Access Hospitals - ivantage Health Analytics
 HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.