TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
|
|
|
- Derick Craig
- 6 years ago
- Views:
Transcription
1 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April b Agenda Item Chief Executive s Report Title Karen James Sponsoring Executive Director Tom Neve Author (s) To discuss and note the various items covered by Purpose this report. Some items previously considered by the Executive Previously considered by Management Team Executive Summary: Government to extend protections for NHS Whistle-blowers Consultation Plans have been published that will prohibit discrimination against whistle-blowers when they apply for jobs with NHS employers. Sir Bruce Keogh to step down from NHS England role Professor Sir Bruce Keogh has announced he will stand down as NHS England medical director at the end of the year, after 10 years in the role. NHS England national director to step down next month New care models director Samantha Jones is to step down next month to spend more time with her children. Related Trust Objectives Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? This report relates to all of the trust s corporate objectives Relates to all aspects of Board Assurance Framework and Significant Risk Report. This report impacts on the regulatory requirements from NHSI and the CQC May have some financial implications N/A Some items in the report have a direct impact on the organisation s sustainability Action required by the Board To note and discuss the items contained within the report
2 Chief Executive s Report Government to extend protections for NHS Whistle-blowers Consultation Plans have been published that will prohibit discrimination against whistle-blowers when they apply for jobs with NHS employers. These changes were a recommendation from Sir Robert Francis Freedom to Speak Up review which found a number of people struggled to find employment in the NHS after making protracted disclosures about patient safety. The consultation, Protecting whistle-blowers seeking jobs in the NHS seeks views on the draft regulations that aim to: Give the applicant a right to an employment tribunal if they have been discriminated against because it appears they have previously blown the whistle Set out a timeframe in which a complaint to the tribunal must be lodged Set out the remedies that the tribunal may or must award if a complaint is upheld Make a provision as to the amount of compensation that can be awarded Give the applicant a right to bring a claim in the county court or the High Court for breach of statutory duty in order to, among other things, restrain or prevent discriminatory conduct Treat discrimination of an applicant by a worker or agent of the prospective employed (NHS body) as if it were discrimination by the NHS body itself. The consultation on the Department of Health website closes on 12 May Sir Bruce Keogh to step down from NHS England role Professor Sir Bruce Keogh has announced he will stand down as NHS England medical director at the end of the year, after 10 years in the role. He will then take up a new role as chair of Birmingham Women s and Children s NHS Foundation Trust. NHS England national director to step down next month New care models director Samantha Jones is to step down next month to spend more time with her children. Ms Jones was appointed by NHS England in January 2015 to lead the vanguard programme to set up and test five new models of care outlined in the Five Year Forward View. The vanguard programme is in its final year. In the vanguards and national new care models team will increasingly focus on supporting the rest of the country to implement new care models. Louise Watson, currently deputy director for new care models, will take over as director.
3 IR35 regulations The IR35 regulations, which took effect at the beginning of April 2017, force offpayroll workers to pay the same level of tax as substantive employees, by making employers responsible for paying their tax and national insurance. This has resulted in locum doctors and other contractors at some trusts demanding significant uplifts in their pay, or threats not to come to work. In relation to this trust, it has resulted in some difficulties in covering the emergency department.
4 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item 7a Title Integrated Performance Report : March 2017 Sponsoring Executive Trish Cavanagh, Director of Operations Directors Brendan Ryan, Medical Director Amanda Bromley, Director of HR Claire Yarwood, Director of Finance Tracey McErlain-Burns, Chief Nurse Author (s) Peter Nuttall, Director of Performance & Informatics Purpose To note/receive Previously considered by This report has not been considered by any other meeting Executive Summary This Board Report includes an appendix showing the metrics and triggers included in the SOF. Not all metrics are currently measured, but work is being undertaken to ensure that: a. performance data is generated; and b. this report is developed to reflect the new Framework. The Trust reported failure of one of the performance metrics included in the SOF: the fourhour- wait target. Related Trust Objectives Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? Objective 1 - All patients receive harm-free care through the delivery of the Trust s Patient Safety Programme. Objective 2 - To improve the quality of patient care through the implementation of the Trust s agreed Quality Strategy. Objective 3 - To improve the patient experience through a personalised, responsive, compassionate and caring approach to the delivery of patient care. Objective 7 - To deliver against the required local and national frameworks in order to meet all the requirements of the Trust s operating licence and the commissioners requirements. Relates to all aspects of Board Assurance Framework and Significant Risk Report. This report indirectly impacts on CQC fundamental Standards of Care and licence requirements. Tameside and Glossop CCG may apply financial penalties for failing to achieve specific performance targets as detailed in the Contract. This is the Medical Director and Chief Nurse view on the impact of any service change Reflects current risks to the Trust s business and strategic objectives Action required by the Board The Board is asked to review the quality and performance standards noted in the Integrated Performance Report.
5 This page is intentionally blank INTEGRATED PERFORMANCE REPORT: April 2017 Board (March 2017 performance) Page 2
6 Board of Director s Meeting 27 th April 2017 Integrated Performance Report 2016/17 Contents Introduction 4 List of Acronyms 5 Dashboard March 2016/17 6 Exception Reports Medical Director/ Director of Operations Cancer 62-day target 7 Director of Operations Four-hour wait/ ambulance handover 8 Inpatient discharge summaries) 9 Director of Human Resources Staff attendance 10 Mandatory Training 11 Thresholds for Single Oversight Framework (SOF) metrics and triggers (draft) 13 INTEGRATED PERFORMANCE REPORT: April 2017 Board (March 2017 performance) Page 3
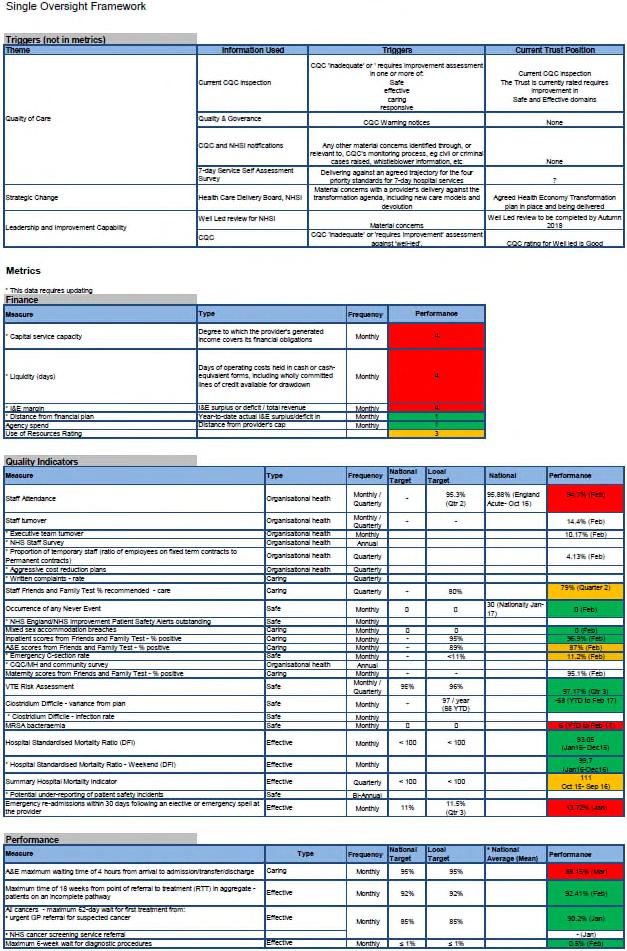
7 Integrated Performance Report March 2017 Performance Introduction This report provides the Trust Board with: an overview of the Trust s performance across a range of quality and operational indicators for the month of March 2017; and year-to-date performance, along with a RAG rating, to support the Board in evaluating performance against each indicator. Exception Reports Alongside the Quality and Performance Dashboard, the report includes exception reports, which respond to the performance data and allow the Executive Team and Trust Board to be assured of, and contribute to, plans to rectify performance and quality issues. All serious incidents are reported to Trust Board in Part 2 of the meeting for patient confidentiality reasons; therefore, no exception report is provided for this indicator. March Performance The Trust reported failure of one performance target included in the Single Oversight Framework (SOF): the four-hour- wait standard. This report includes exception reports for the following metrics: four-hour wait and ambulance handovers; Emergency Department and inpatient discharge summaries; staff attendance rate and mandatory training. Mortality In the latest Summary Hospital-level Mortality Indicator (SHMI) publication, THFT has a value of 111 for the period October September This value means that the SHMI is as expected. The hospital s Standardised Mortality Ratio (SMR) for the latest available twelve months (January 16 - December 16) is 93.05, which is better than expected but not statistically significantly so. Mixed-Sex Accommodation Breach The Trust reported its first mixed-sex accommodation breach of in March. The affected patient was delayed on ICU, over the weekend of the 18 th / 19 th March, as a result of the unavailability of suitable capacity on the medical wards. An assessment of the current escalation process and its application, particularly at weekends, is being undertaken. Referral-to-Treatment In March, the Trust met the national Referral-to-Treatment standard (incomplete pathways) with performance of 92.45% against the threshold of 92%. The Trust reported that no patients had a waiting time of more than 52 weeks at the end of March. Outpatient DNA Rate The outpatient DNA rate for March was 7.94%, which is significantly better than the 9.5% target. Stroke Targets The Trust Board is asked to note the Trust s banding of b for the SSNAP (Sentinel Stroke National Audit Programme) national stroke audit for the period August- November 2016, where the poorest performing trusts are classified as e and the best as a. The SSNAP audit includes 44 measures in 10 domains. The Trust s banding for the previous period was c. Emergency Readmissions within 30 days The 30-day readmission rate remains above the local target level of 10%, at 12.3% (year-to-date), although the rate has reduced steadily from around 14% in Appraisal It was not expected that the appraisal rate would reach the 90% target at the end of March, because the Appraisal Window opens on the 1 st April and managers were asked to wait until April and use the updated paperwork. Monitoring will recommence on the 1 st April. INTEGRATED PERFORMANCE REPORT: April 2017 Board (March 2017 performance) Page 4
8 List of Acronyms ADT C DIFF CIP CQC CT CWT DNA DPH DToC ED ENP ESDT ETD FFT GM GMCCN HSMR HAS IAU IR35 ICO MRSA MSA NWAS PTL RAID RCA REACT RIDDOR ROSIER RTT SAFER SALT SHMI SOP SSNAP STAR StEIS TIA TNA VTE WTE YTD Admission, Discharge, Transfer Clostridium difficile Cost Improvement Plan Care Quality Commission Computerised Tomography Cancer Waiting Times Did-not-Attend Director of Public Health Delayed Transfers of Care Emergency Department Emergency Nurse Practitioner Early Supported Discharge Team Education, Training and Development team Friends & Family Test Greater Manchester Greater Manchester & Cheshire Cancer Network Hospital Standardised Mortality Ratio Hospital Arrival Screen Integrated Assessment Unit Tax legislation relating to workers supplying services to clients via an intermediary Integrated Care Organisation Methicillin-resistant staphylococcus aureus Mixed-sex Accommodation North West Ambulance Service Patient Tracking List Rapid Assessment Interface and Discharge (psychiatry liaison service) Root Cause Analysis Rapid Assessment Emergency Care Team Reporting of Injuries, Diseases and Dangerous Occurrences Regulations Rule Out Stroke In the Emergency Room Referral-to-Treatment Patient Flow Bundle (Senior review; All patients with expected discharge date; Flow of patients at earliest time; Early discharge; Review of patients with extended lengths-of-stay) Speech and Language Therapy Summary Hospital-level Mortality Indicator Standard Operating Procedure Sentinel Stroke National Audit Programme Staff Accident Rate Strategic Executive Information System Transient Ischaemic Attack Training Needs Analysis Venous Thromboembolism Whole Time Equivalent Year-to-Date INTEGRATED PERFORMANCE REPORT: April 2017 Board (March 2017 performance) Page 5
9 THFT QUALITY ACCOUNT 2016/17 Quality Dashboard March 2017 Actual is upto March unless stated otherwise. * Governance indicators, which appear in Monitor's Risk Assessment Framework Target Actual 4-mth Actual Current 1-mth Staff Health & Safety Overall Clinical Quality Target Actual 4-mth Actual Current 1-mth Patient Access Target Actual 4-mth Actual Current 1-mth 16/17 16/17 Trend Month Period F'cast 16/17 16/17 Trend Month Period F'cast 16/17 16/17 Trend Month Period F'cast Mortality RIDDOR incidents reported Waiting times SMR (rolling 12 months- to Dec-16) NA Calendar days lost NA NA NA 18-week incomplete* 92% 92.81% 92.45% SHMI (rolling 12 months- to Sep 16) NA due to staff accidents RTT waits- incompletes (>52 weeks) Infection Prevention & Control Staff accident rate A&E < MRSA - actual cases YTD* (STAR) 4-hour wait* 95% 85.68% 88.24% C-difficile - actual cases YTD* N/A 63 6 N/A N/A Trolley waits in A&E (>12 hrs) C-difficile - avoidable cases YTD* (Feb- Target Actual 4-mth Actual Current 1-mth HAS compliance 95% 95.41% 96.43% 17) People NHS Safety Thermometer 16/17 16/17 Trend Month period F'cast Notify to Handover (30-60mins) Harm-free care (all harms) Harm-free care (new harms) Patient Safety VTE risk assessments (provisional) Medicines reconciled on admission (Feb-17) Nutrition risk assessment Emergency re-admissions within 30 days (Feb 17) Failure of safer-surgery process Serious Incidents reported (StEIS) NA 91.6% 92.2% NA NA Staff Attendance Q4: 96% 94.71% 94.9% Notify to Handover (>60mins) % 98.4% 97.9% Appraisals - rolling 12 mths 90% 71.60% 71.6% Cancer FFT- Staff Survey (quarterly) Cancer- Composite Indicator 8 NA 7 96% 96.83% 94.38% Recommend Treatment (Jul-Sep 16) 80% NA 79% Number achieved out of 8 (Feb-17) Recommend Work (Jul-Sep 16) 74% NA 74% 95% 83.13% 85.00% Mandatory Training Target Actual 4-mth Actual Current 1-mth Operational Efficiency 90% 96.5% 100% E-learming Info Gov 95% NA 73.3% 16/17 16/17 Trend Month Period F'cast Q4: 11% 12.28% 13.02% E-learming SG Children 95% NA 75.9% Outpatient slot utilisation 90% 87.42% 89.13% E-learming Infection Control 95% NA 85.0% Outpatient DNA rate 9.5% 9.31% 7.94% E-learming E-MH 95% NA 92.0% Theatre utilisation (capped) 90% 87.46% 86.94% E-learming E &D 95% NA 93.1% Cancelled operations- last-minute (provisional) 0.8% 1.20% 0.59% 'Duty of Candour' breaches E-learming SG Adults 95% NA 88.6% Urgent operations cancelled for a second time Never Events reported (StEIS) E-learming H&S 95% NA 88.2% Discharge Summaries Regulation 28 reports (inquests) Manual Handling 95% NA 86.9% A&E (within 48 hours) 95% 84.7% 89.8% Stroke Resus 95% NA 64.9% Inpatients (within 48 hours) 95% 80.8% 79.2% SSNAP DSC Stroke Indicators NA NA 7 NA NA Fire Safety 95% NA 83.6% Outpatients (within 5 days) 95% 82.0% 92.6% Number achieved out of 9 (Aug-Nov16) Mandatory training (Overall) 95% NA 81.2% Discharge Summary Quality Audit 100% NA 96.0% SSNAP Grading (Aug-Nov16) B NA B Delayed Transfers of Care- Days (Feb-17) NA 11, NA NA Safer Staffing Target Actual 4-mth Actual Current 1-mth Regulatory RN/RM hrs on shift (% of planned) TBC 93.4% 93.3% NA NA 16/17 16/17 Trend Month Period F'cast Target Actual 4-mth Actual Current Yr-end Finance HCA hrs on shift (% of planned) TBC 105.7% 104.4% NA NA Single Oversight Framework (Jan-Mar 17) NA 3-16/17 16/17 Trend Month Period F'cast CQC Rating* (Jan-Mar 17) - Good - Cum. Net surplus ( 'm) Patient Experience Target Actual 4-mth Actual Current 1-mth Cum. CIP (% of plan) 100% of plan 98.8% 72% 99% 16/17 16/17 Trend Month Period F'cast Cum. Capital ( k) FFTpositive responses (all) NA 89.7% 90.6% NA NA 1-month forecast 4-month trend Cum. CQUIN (% of plan) 70% of plan 97% 97% 97% FFTresponse rate (A&E/ Inpatients) 20% NA 21.38% The one-month forecast is an informed prediction of the next strong improvement Complaints received NA NA NA month's performance, which may be based on part-month data, operational intelligence and historical trends. improvement Complaints responded to within no change 90% 93.57% 92% agreed timescale deterioration Ombudsman cases upheld strong deterioration QUALITY ACCOUNT: April 2017 Board (March 2017 performance) Page 6
10 QUALITY ACCOUNT EXCEPTION REPORTS: Medical Director/ Director of Operations (1/1) Cancer Services Target Current Performance 62-day GP Referral to Treatment-Overall (reporting Period: February 2017) 85% 92.7% 4 Month Trend Previous Performance Forecast Acute trusts are required to support the NHS England/ Trust Development Authority/ Monitor commitment to Improving and Sustaining Cancer Performance. One action required of trusts is that they report tumour- sitespecific performance against the 62-day cancer target to their Board, irrespective of performance against the aggregate target. This report highlights the Trust s overall and tumour- site- specific performance against the 85% threshold. The period that it relates to is February 2017 and the position stated has been fully validated, in line with the Greater Manchester- wide Reallocation Policy. For the month of February 2017, the aggregate 62-day position was 92.7%, which means that the Trust met the national standard for the month. The reasons for the 4 breaches in February were as follows: 2 x complex / multi- tumour sites / patient comorbidities; 2 x internal diagnostic delays. Near Misses Acute trusts are also required to include, in the reports provided to their Board, data relating to patients treated within 48 hours of their breach date. Four patients were classified as near misses in the month of February. The near misses were the result of: 1 patient fitness review prior to surgery; 1 patient holiday; 2 external treatments (patients referred on/before day 42). Treated after day 104 A full breach analysis, and clinical assessment, must be conducted on patients with a total wait greater than 104 days. If harm has been caused by the treatment delay, a full Serious Incident investigation must be undertaken by the treating Trust. In February two of the Trust s patients were treated, post day- 104, at tertiary hospitals. These delays were the result of: an internal diagnostic delay; and delay at the tertiary provider. Both patients were referred to the tertiary provider on/ before day 42 of the pathway. Expected date to meet target NA Signed off by Janet Smart Signed off by Trish Cavanagh/ Brendan Ryan Page 7
11 QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (1/2) Patient Access- A&E 4-hour wait (Reporting period: March 2017) Target 95% Current Performance 88.24% 4 Month Trend Previous Performance Forecast Notify to Handover: mins (Reporting period: March 2017) 0 73 Notify to Handover: 60+ mins (Reporting period: March 2017) ISSUE The Trust did not meet the four-hour emergency care standard in March: Bed capacity across the organisation was problematic, causing delayed first assessments due to a lack of capacity in the Department; IAU remained escalated as a bedded area rather than functioning as originally planned; Reduced ambulatory-care service because of staffing shortages; National and local shortages of medical and nursing cover exacerbated by difficulties with IR35 regulation; Medical bed-pool occupancy was routinely at >96%; Delayed-transfers-of-care occupied 5.7% of the General and Acute bed pool, a reduction from 10% in January; Increased acuity, as measured using the Charlson Comorbidity Index (43% of patients with a Charlson comorbidity; 34% in ). ACTIONS NHSI s Head of Service Improvement significantly assured about the Trust s response to the challenges relating to emergency flow; Silver Command, including the deployment of Ward Liaison Officers, in place during February; Additional medical staffing resources deployed, especially on days of expected increased activity (Monday/Tuesday). PROPOSED ACTIONS NHSI to offer focused support concerning ED streaming; Pilot streaming for one month (Monday, Tuesday and Friday for four weeks) commencing 6th March; Visit to Derby Hospital to assess streaming model. Expected date to meet target Quarter 4 Signed off by Debbie Davies Signed off by Trish Cavanagh 0 16 Notify To Handover Time Aug- Sep- Oct mins 60+ Mins Nov- 16 Dec- 16 Jan- 17 Feb- 17 Mar- 17 YTD Page 8
12 QUALITY ACCOUNT EXCEPTION REPORTS: Director of Operations (2/2) Operational Efficiency Target Current Performance Discharge Summaries- A&E: (Reporting period: March 2017) 95% 89.8% 4 Month Trend Previous Performance Forecast Discharge Summaries- Inpatients: (Reporting period: March 2017) ISSUE Performance was below target for Emergency Department and inpatient discharge summaries. Performance against the outpatient- clinic letter standard improved again during February to 93% so that an exception report is not required. 80.5% of inpatient discharge summaries were completed within 48 hours in March, which is consistent with reporting from the most recent months. 89.8% of Emergency Department summaries were completed within 48 hours against the 95% standard. This performance represents a marginal deterioration from the performance in February but is a significant improvement upon performance in the months prior to that, as can be seen in the chart opposite. ACTIONS Review at the Patient Safety Board and feedback with proposed actions. Meeting with Director of Performance, Medical Director, Director of Quality and Governance and CCIO regarding strategy for discharge summaries. Significant improvements in performance may require increased digitisation: such options are being explored by the Health Records Group. PROPOSED ACTIONS Start development of ecas card, which will guarantee delivery of a summary within target; Develop reporting mechanism to directly target missing/ late summaries; Target areas of underperformance, such as General Medicine, Cardiology, General Surgery, Paediatrics and Trauma and Orthopaedics. ASSESSING IMPROVEMENT Using the bespoke performance reports. Expected date to meet target Quarter /18 Signed off by Geoff Lavelle 95% 79.2% Signed off by Trish Cavanagh Page 9
13 QUALITY ACCOUNT EXCEPTION REPORTS: Director of Human Resources (1/3) People Target Current Performance Staff Attendance: (Reporting period: March 2017) 96% 94.86% 4 Month Trend Previous Performance Forecast ISSUE The staff attendance rate was below the target for March, although there was a reduction in sickness (from 5.3% to 5.1%). PROPOSED ACTIONS The HR Business Partners are working closely with hotspot areas with high levels of absence and associated costs. Progress is being monitored via the monthly HR Divisional Management Team Meeting. Actions include: A review of all sickness cases, ensuring management plans are in place. Delivering 1:1, and small- group, training sessions to raise the profile of return- to- work interviews. A focus will be put on return- to- work compliance this month, given the recent increase in short- term sickness. Attendance Management Masterclass sessions were launched in February. The next session is scheduled for June and 22 managers are booked to attend. Discussions are underway with Staff Side with regards to the amendments to the Attendance Management Policy. The main change to the policy is the reduction of the Trust trigger levels. A full management toolkit will be released with the new policy. ASSESSING IMPROVEMENT Expect to see improved KPI performance, including an improvement in attendance and a decrease in costs associated with sickness absence including NHSP/Agency/Bank expenditure. Return-to-work interview compliance is also to be closely monitored. Expected date to meet target Quarter Signed off by Nicola Wilkinson Signed off by Amanda Bromley Page 10
 95% 83.")
14 QUALITY ACCOUNT EXCEPTION REPORTS: Director of Human Resources (2/2) QUALITY ACCOUNT EXCEPTION REPORTS: Director of Human Resources (2/2) People Target Current Performance Mandatory Training: (Reporting period: March 2017) 95% 83.3% 4 Month Trend Previous Performance Forecast ISSUE Mandatory Training performance did not meet the target of 95%: The Porters/ Domestics staff group was largely non-complaint for Mandatory Training upon transfer to the Trust (performance is 52.9%, up from 22%); this had a significant effect on the organisation s overall % performance. Community staff compliance (currently 77.6%, up from 67.8%) also reduced overall compliance upon transfer. Trust compliance, excluding these groups of staff, is 83.3% (see chart opposite). ACTIONS Close monitoring of, and the development of action plans for, individual subjects has had a positive impact on mandatory training elements. This includes reviewing what training should be provided on a face- to- face basis and which can be delivered via e-learning. Managers in areas with low compliance have been requested to provide action plans and trajectories for improvement. The gap analysis, relating to training in the Community services and for Porters and Domestics, continues Consideration is being given as to what sanctions can be applied to staff who are not compliant with mandatory training, and a review of approaches, taken by other trusts to this issue, is being undertaken. ASSESSING IMPROVEMENT Data is produced and assessed monthly, and sent to senior managers as soon as the data is produced. Expected date to meet target Quarter Signed off by L Harmer Signed off by Amanda Bromley Page 11
15 Indicator Quarter 1 Quarter 2 Quarter 3 Quarter 4 HSMR (amber if not statistically significant) SHMI (amber if not statistically significant) MRSA - actual cases C. difficile - actual cases Harm-free care (new harms) 98.5% 99% 99% 99% VTE risk assessments 96% 96% 96% 96% Medicines reconciled 95% 95% 95% 95% Nutrition risk assessment 90% 90% 90% 90% Re-admissions within 30 days 11.0% 11.0% 11.0% 11.0% Failure of the safer-surgery process Serious Incidents reported Duty of Candour breaches Never Events reported Regulation 28 reports Complaints response time 90% 90% 90% 90% Ombudsman cases upheld SSNAP Grading B B B B RIDDOR accidents reported Staff accident rate <10 <10 <10 <10 Staff attendance 95.0% 95.3% 95.7% 96.0% Appraisals 85% 90% 90% 90% Mandatory Training 95% 95% 95% 95% FFT Staff Survey- Recommend Treatment 80% 80% 80% 80% FFT Staff Survey- Recommned Working 74% 74% 74% 74% E-Learning Information Governance 95% 95% 95% 95% E-Learning Safe Guarding Children 95% 95% 95% 95% E-Learning Infection Control 95% 95% 95% 95% E-Learning E-MH 95% 95% 95% 95% E-Learning Equality and Diversity 95% 95% 95% 95% E-Learning Safe Guarding Adults 95% 95% 95% 95% E-Learning Health and Safety 95% 95% 95% 95% Manual Handling 95% 95% 95% 95% Resus 95% 95% 95% 95% Fire Safety 95% 95% 95% 95% 18-week incompleted 92% 92% 92% 92% RTT waits over 52 weeks (incompletes) hour wait 95% 95% 95% 95% Trolley waits in A&E HAS compliance 95% 95% 95% 95% Notify to Handover mins Notify to Handover ->60mins Outpatient Slot Utilisation 95% 95% 95% 95% Outpatient DNA rate 9.5% 9.5% 9.5% 9.5% Theatre utilisation (capped) 90% 90% 90% 90% Cancelled Operations (last minute) 0.8% 0.8% 0.8% 0.8% Urgent ops cancelled for 2nd time Discharge Summaries- A&E 95% 95% 95% 95% Discharge Summaries- Inpatients 95% 95% 95% 95% Clinical Letters- Outpatients 95% 95% 95% 95% Page 12
16 Page 13
17 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered by Safe Staffing Report Tracey McErlain-Burns, Interim Chief Nurse Tracey McErlain-Burns, Interim Chief Nurse To note/receive n/a Executive Summary In-line with the Hard Truths Commitments regarding the publishing of Staffing Data, the Trust Board are required to review staffing data on a monthly basis. This report has evolved over the past three months and this month it includes the results of the January 2017 Safer Nursing Care Tool analysis considered alongside professional judgement and NICE guidance on safe staffing levels for adult in-patients. The Board should note that some of the medical wards are underestablished and as such an urgent review of the models of care needs to be carried out. This review will be reported to the Board in June Finally in terms of summary the Board should note that the CQC requirement for having an Advanced Paediatric Life Support (APLS) trained nurse on each shift on the children s ward can now be achieved following completion of band 6 training. Related Trust Objectives Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? 1. All patients receive harm free care through the Trust s Patient Safety Programme. 2. To improve the quality of patient care through the implementation of the Trust s agreed Quality Strategy. 3. To improve the patient experience through a personalised, responsive, compassionate and caring approach to the delivery of patient care. CR734: Nurse vacancies, leadership and nurse staffing/ recruitment across medicine and the ability to provide safe care. AF3480: Failure to meet CQC registration requirements relating to staffing. AF3482: Failure to ensure adequate staffing levels to ensure patient safety and quality of services NHS England monthly requirement to publish and report Staffing Data The CQC report published 7 th February 2017 states that the Trust must ensure that there are appropriate numbers of nursing staff deployed to meet the needs of patients (medical services). The report also states that the Trust must ensure an advanced paediatric life support trained nurse is on each shift in Children s Services. There are no new immediate financial implications albeit the financial implications of international recruitment are being considered by the executive team. Yes where applicable in plans 1
18 How does this report affect Sustainability? The Trust is required to ensure staffing levels are adequate to meet patient safety and quality requirements. Action required by the Board The Trust Board is requested to receive this update and note the actions described and the assertive monitoring and management in place. 2
19 Background This is a monthly report to the Trust Board following National Quality Board (NQB) guidance issued in November 2013 to optimise nursing, midwifery and care staffing capacity and capability: How to ensure the right people, with the right skills, are in the right place at the right time: A guide to nursing, midwifery and care staffing capacity and capability. The guidance clearly sets out the expectations and requirements of the Trust to meet the Hard Truth s commitments (following the Mid Staffordshire report). In July 2016, the NQB published an updated set of expectations for nursing and midwifery staffing to assist NHS Provider Boards to take local decisions which will deliver high quality care for patients within the available staffing resource (Supporting NHS providers to deliver the right staff, with the right skills, in the right place, at the right time Safe sustainable and Productive Staffing, NQB, July 016). This updated guidance incorporates Lord Carter report findings, in setting out the key principles and tools that provider boards should use to measure and improve their use of staffing resources to ensure safe, sustainable and productive services. As advised in recent months the content of this report is evolving to ensure that the Board has a complete picture of matters relating to safe nurse staffing. Specifically this report includes a review of the Safer Nursing Care Tool data. Safe Staffing Update March 2017 Data Each month the data collection compares the number of nurse staff hours Planned against the number of nurse staff hours used Actual. This is collected by ward, by shift, and is reported by calendar month as a % fill rate by day and by night. Please refer to the Heat map (Appendix 1). This staffing information is published via NHS Choices. This data is currently available via our public website in a specific designated section Safe Staffing : ( Overall, Registered Nurse (RN) fill-rates remain constant (with minimal change) month on month, but unregistered (Healthcare Support Worker) fill rates fluctuate due to levels of enhanced care required (1:1 s) and additional support for RN shortfalls. The following graph highlights to the Board that unregistered fill rates for day and night shifts usually meet or exceed 100% 1 and registered fill rates for night shifts have recently improved to between %. Senior Nurse leaders review nurse staffing levels (actual against planned) several times a day and a conscious decision has been taken to increase the levels of fundamental care support by unregistered staff when registered nurses are not available to fill shifts. The registered nurse fill rate for day shifts is currently running at 89.9% which is marginally reduced in comparison to the rate of 91.1% for the month of February and the details in this report describe some of the actions being taken to address the shortfall. The reasons for the marginal reduction are firstly the inclusion of the 7 additional beds in the ward 31 establishment for a full month and increase in demand which was associated with the scheduling of annual leave. The latter is an issue that the Assistant Chief Nurses will address through tightened controls over roster sign off. 1 Fill rates dipped to 99% in the month of March due to annual leave. 3
20 % Fill Rate Average Fill Rates Registered Fill DAY Registered Fill NIGHT Unregistered Fill DAY Unregistered Fill NIGHT Exception Report March 2017 There were 5 inpatient areas with registered nurse/midwife fill rates <80% in March 2017 (Appendix 1 heatmap). Those areas were: 4 Ward 40 Ward 42 Ward 44 Ward 45 Ward 46 As reported to the Board last month ward 40 is trialling the inclusion of two registered chartered physiotherapists in the nursing establishment 6 days a week. Excluding those hours of registered practitioner input to care on the ward the fill rate is 79.9%. Inclusive of those hours the fill rate was 102%. The Board was advised last month that the Interim Chief Nurse was liaising with NHS England to seek clarity on whether the physiotherapy hours should be included in the unify return or not; making the case that they should because of the model being trialled. A response has now being received from NHS England and the advice is that these hours should not be included in the unify return however, NHS England noted the development of new models of care and will consider the inclusion again in the future when unify returns are reviewed. Wards 44, 45 and 46 have featured in this section of the Board report for several months due to fill rates being less than 80%. All three wards have 24 beds and their establishments are set at registered nurse to patient ratios of 1:8 during the daytime and 1:12 at night. A recent review of the Safer Nursing Care Tool data (expanded in a later section of this report) indicates that the establishment for wards 44 and 45 matches patient dependencies whereas on ward 46 the ward is under established to meet patient dependencies and as such new models of care will be explored. There are currently 4.89 whole time equivalent (wte) Registered Nurse vacancies on ward 44; 3.9wte vacancies on ward 45 and 5.29wte vacancies on ward 46. As such recruitment campaigns are being devised for these three areas. Ward 42 has not featured in the list of wards with less than 80% fill rate in recent months. The established RN to patient ratio is 1:8 on days and 1:10 on nights. There are currently vacancies on the ward and this ward has a considerable number of new members in the team (new recruits). Ahead of the Board meeting the Interim Chief Nurse and Assistant Chief Nurse will be meeting with the Ward Sisters of the medical wards to discuss models of care, retention, recruitment, capacity and demand. A verbal update will be provided at the Board meeting.
21 Since February 2017 this report has included details of the number and impact of escalation beds. In the month of March there was an average of 5 additional beds opened across ambulatory care, the day care unit, surgical unit and the heart care unit 2 which required 845 hours of nurse staffing (a combination of registered and unregistered) of which 411 hours were filled via NHS Professionals and the remaining hours were redeployed from other areas within the Trust. Requested Hours Filled / Worked Unfilled % Filled Ward 30 H C U % Ambulatory Integrated Assessment Unit % Day Surgery Unit % Surgical Unit % Total % Care Hours per Patient per Day (CHPPD) In recent months the heatmap attached at appendix 1 has included actual CHPPD; a measure used by NHS Improvement. This provides a consistent way of measuring the deployment of nurses and healthcare support workers and it needs to be used alongside acuity and skill mix. Planned CHPPD by ward and Trust has been added to the heatmap from February 2017 to show the hours required (based on nurse staffing establishments) versus that available. This draws attention to five wards with actual hours less than planned, which includes ward 41 which was not in the previous list of wards because it exceeded the 80% fill rate. It also draws attention to areas such as the surgical unit, critical care, the neonatal unit, children s unit, Stamford Unit and Shire Hill all of which exceeded their planned RN hours. This was largely due to reduced occupancy in those areas at times during the month of March, for example occupancy in the neonatal unit was 52%. The graph below shows the trend in actual CHPPD, as a total of days and nights, registered and unregistered, since the methodology was introduced. Benchmarking data is not yet available but it is anticipated that this may be available via NHS Improvement imminently CHPPD Trust Total CHPPD Total Planned 2 A reduction of 7 compared with the month of February
22 Safer Nursing care Tool (SNCT) In accordance with the NQB / Hard Truths guidance the Trust undertakes a review of nurse staffing establishments, using appropriate tools at least twice per annum. The latest Safer Nursing Care Tool (adult in-patient) review was conducted throughout January 2017 and the results were presented to a group of professionals comprising corporate nursing, divisional nursing, HR and finance colleagues on 28 March Each Ward Sister / Matron participated in the review of the staffing establishments in their own area. In summary a small number of areas would appear (based on the use of the SNCT) to be overestablished and some appear to be under-established. In a number of areas such as the heart care unit and acute care unit, together comprising the cardiology unit the SNCT does not adequately capture acuity and dependency and as such professional judgement is essential. Potentially efficiencies within the establishment could be achieved if the HCU and ACU were co-located. The planned orthopaedic unit and the emergency orthopaedic unit are both over established on SNCT analysis. The Board should note that the results of the January 2017 deployment have not been considered in isolation; averages over three deployments of SNCT in January 2016, June 2016 and January 2017 have been considered. The orthopaedic unit is part of the modern facilities and has a high percentage of single rooms cubicles which do demand higher staffing numbers for the purposes of observation made easier in more open wards. It is recommended that benchmarking information would be available from other Trusts and as such this will be requested by the Assistant Chief Nurse for the Surgical Division ahead of the next SNCT deployment. In the interim the Matron and Ward Sisters have been charged with having zero tolerance on the use of bank and agency staff based on establishment. The Surgical Unit would also appear to be over-established however it is noted that consultation is imminent with the Women s Health Unit part of which may be co-located with the surgical unit and therefore the outputs from the SNCT will be considered when finalising the establishment at the end of consultation. In relation to the medical wards and especially wards 40, 41, and 42 these are not established to meet a 1:8 ratio on days and some, together with wards 44 and 45 only achieve a 1:12 ratio on nights. Options for these wards need to be explored informed by the pilot on ward 40 and the fact that they are co-located. The simple solution of recommending an increase in RN establishment is not an adequate proposal given the level of vacancies and the temporary staffing fill rates. Solutions need to be identified and shared with the Board no later than June Finally in relation to the SNCT the review on 28 March identified that there has never been any validation built into the data collection and therefore this will be developed before the next deployment in June Validation would usually involve someone external to the ward reviewing the assessed dependencies of groups of patients. Going forward the Trust may chose to deploy other Health-roster modules including Safecare which would involve data collection every shift, every day benefiting not only twice per annum staffing establishment reviews but more importantly shift deployment and understanding of acuity and dependency. Safe Midwifery Staffing A detailed update on the midwifery staffing establishment was presented to Board in March 2017 along with a description of the framework being proposed as a replacement for the statutory supervision of midwives. On 07 April 2017 guidance of the A-EQUIP model of clinical midwifery supervision was published and this is now available of the NHS England website. The guidance describes transition from the statutory model of midwifery supervision to an employer led model of supervision. Until such time as 6
23 the Professional Midwifery Advocates (PMA) are prepared through a programme of education, the Trust as a provider of maternity services is required to deliver the non-statutory elements of the supervisor of midwives role through effective management and governance arrangements. Those arrangements are being led by the Head of Midwifery working with 11 of the previous (12) supervisors of midwives. Unlike statutory supervision which required providers to meet a 1:15 ratio of supervisors to midwives the PMA model can be flexible based on tasks, standards and the responsibilities of the PMA in organisations. The published guidance includes the competencies of the PMA and some role descriptors / profiles. Unlike the previous arrangements, the Head of Midwifery is now responsible for the selection of the PMAs. Now that the guidance has been published the Head of Midwifery, Deputy Chief Nurse, Divisional Director for Surgery and Women s Health, the Clinical Director for Women s Health and the Interim Chief Nurse will meet to recommend a model of clinical midwifery supervision with a view to that being presented to the Board by the Head of Midwifery in June Finally for this section of the report the Board is advised that following the dissolution of the Local Supervising Authority (LSA) NHS England has now appointed a new maternity leadership team. That team will be led by Mr Neil Tomlin and the Trust is in contact to arrange to meet him and his team. Community Nursing The Board has previously been advised of the concerns of the community nursing team regarding caseloads both in terms of the number of patients on caseloads and the complexity of those caseloads. Regular meetings with the community nursing team leaders are taking place and a community nursing (adults) action plan is now in place. An important component of that action plan is the case load review which has commenced together with a specialist review of the community nursing needs of all patients with a diagnosis of diabetes. Furthermore all patients requiring a continence assessment are now being assessed by the continence team rather than the community nursing team and the post of District Nurse Liaison is being appointed to. In March 2017 NHS Improvement released draft guidance on safe staffing management in community nursing settings. The guidance includes a literature review of the evidence to inform the setting of safe community nursing caseloads. Given the complexity and multifaceted nature of community nursing the literature review concludes that the notion of understanding safety in community nursing caseloads is still far from reach. As such a number of operational and strategic principles are proposed including the standardisation of data collection, avoidance of duplication, enriching learning and development environments, developing patient reported out-come measures and using canary markers to provide an early warning system, such as missed breaks. The guidance advocates the use of professional judgement in setting community nursing staffing levels. Currently all posts within the community nursing establishment are filled albeit there are staffing gaps due to sickness and other forms of absence. In recent weeks a small internal staffing bank has been established and it is planned for this to grow in the coming months. The new Assistant Chief Nurse Medicine has a community nursing background and therefore together with the Community Nursing Clinical Pathway Lead the current action plan will be reviewed to timetable a review of the staffing establishment informed by the published guidance. Updates will be included in future Board reports. Children and Young People 7
24 A must do action in the Care Quality Commission (CQC) report is to ensure that there is one nurse on duty on the children s ward trained and up to date in Advanced Paediatric Life Support (APLS) on each shift. Training of band 6 nurses was completed on 12 April enabling this action to be met. Having devised mechanisms to capture this on e-roster the Assistant Chief Nurse for Surgery and Women s and Children s Services will be accountable for ensuring that the requirement is met when signing off the rosters. Red Flags There were a total of 69 incidents with 163 Red Flags recorded via the incident reporting system with regards to Nurse Staffing for March 2017 this is due to the fact that multiple red flags can be reported on one incident 3. The number of red flags recorded can be broken down as follows:- Department Missed breaks Intentional rounding Total Ward Ward IAU Department 8 Missed breaks A shortfall of more than 8 hours or 25% of Registered Nurse time available compared with the actual requirement for the shift A shortfall of more than 8 hours or 3 A three fold increase on February 2017, as predicted. Intentional rounding Delay of 30 minutes in providing pain relief Delay of 30 minutes in Patient vital signs not assessed or recorded as outlined in the care plan Patient vital signs Unplanned omission in providing medication Unplanned omission Less than 2 registered nurses present on a ward during any shift Less than 2 Total
25 25% of Registered Nurse time available compared with the actual requirement for the shift providing pain relief not assessed or recorded as outlined in the care plan in providing medication registered nurses present on a ward during any shift A&E - Childrens 1 1 ACU Dewsnap Lane Clinic Hyde Clinic Mossley Clinic Surgical Unit Ward Ward Total The Board should note that there were no shifts with less than two registered nurses on duty during any shift. This is because the Interim Chief Nurse and the senior nursing team consider any such event to be an internal never event and as such must be prevented. There were a small number of occasions when the potential for only having one registered nurse on duty existed and in order to prevent this redeployment was managed. Strategies to Address Shortfalls in Nurse & Midwifery Staffing Levels The Trust has a range of strategies which include recruitment, workforce redesign through the creation of new roles, retention and flexible staffing solutions. This section of the report provides an update on some of those strategies. Recruitment & Retention During the month of March 6 Registered Nurses left the organisation; a total of 5.42 wte, and 11 Registered Nurses (10.29 wte) commenced employment with the Trust. However at any one time the Trust continues to experience a minimum of 100 RN vacancies. At the beginning of April the Executive Management Team (EMT) considered the proposal to invest in international recruitment and this has now progressed to the next stage of consideration. Meetings between colleagues in HR, Communications and the Interim Chief Nurse have taken place to look at redesigning our advertising and reach campaigns and the next recruitment open day will take place on a Saturday in June. Temporary Staffing The Trust works with NHS Professionals to provide a temporary staffing solution. In March 2017 the overall temporary staffing fill rate was 78.7%, up slightly on the fill rate in February 2017 and on regional comparative fill rates despite an 11.5% increase in demand. The top booking reasons remain vacancy, sickness, escalation and 1-1 specialling. 9

26 Of note whilst the new HMRC rules (IR35) have temporarily impacted on the shift uptake of some professional groups the Trust s Advanced Nurse Practitioners, Advanced Paediatric Nurse Practitioners and Emergency Nurse Practitioners have stepped up to strengthen rotas. Trainee Nurse Associates The Trust is part of the Nurse Associate pilot and had 20 Trainee Nurse Associates in post. The pilot is receiving very positive feedback to date however the number of trainees has now decreased to 18 due to the personal circumstances of 2 of the candidates. This will create a deficit in funds received from Health Education North West impacting on the financing of the Clinical Educator role. Nonrecurrently that will be avoided in year from underspends in the corporate nursing budget due to natural time-lags in recruitment of new personnel. In year a solution to the 1750 cost pressure for 2018/19 will be identified. Preceptorship The Trust continues to place importance of the preceptorship period of newly registered professionals. Twenty one preceptees joined the Trust on 03 April, 15 of whom are adult nurses. In March several members of the team led by the Preceptorship Lead attended the Ashton Sixth Form College to raise the profile of the Trust as an employer and to discuss career options. Discussions between the corporate nursing team and HR colleagues are taking place to understand if there are opportunities to work with other education establishments more frequently and what the return on that resource (time) investment might be. Summary Ensuring the correct numbers of suitably skilled Nurses, Midwives and Healthcare Support Workers are in post is essential for the delivery of safe and effective patient centred care. As described in this report there are a number of daily challenges not least due to vacancies and temporary staffing fill rates affecting the ability to have adequate numbers of suitably skilled nurses, midwives and HCSW on duty each day. The Safer Nursing Care data indicates that there are a number of wards under-established and some over-established and this data has been reviewed, for the first time jointly with nursing, HR and finance. It is clear that alternative models of safe staffing need to be quickly reviewed, informed by 10
27 the pilot on ward 40 for both the short and longer-term at the same time as exploring international recruitment to RN vacancies. Recommendations The Trust Board is asked to note the details of this report and the actions being taken. 11
28 Appendix 1 Inpatient Ward Compliments Complaints Moderate Harm + Incidents Falls with Harm MRSA C.Diff PU (+G2 only) FFT Positive (%) Registered Staff Fill Rate - Days % of Temp Staff Used Registered Staff Fill Rate - Nights % of Temp Staff Used Unregistered Staff Fill Rate - Days % of Temp Staff Used Unregistered Staff Fill Rate - Nights % of Temp Staff Used Planned Registered CHPPD Actual Registered CHPPD Planned Unregistered CHPPD Actual Unregistered CHPPD Planned Orthopaedic Unit % 95.4% 1.35% 98.6% 21.55% 106.1% 22.99% 154.6% 61.83% Surgical Unit % 94.3% 19.13% 99.2% 25.07% 89.3% 26.33% 109.0% 46.79% Emergency Orthopaedic Unit % 92.3% 3.50% 97.8% 40.75% 116.0% 20.68% 143.1% 37.41% Critical Care % 99.3% 11.28% 90.8% 34.41% 103.2% 13.15% N/A N/A AMU % 100.8% 16.40% 98.0% 44.81% 94.9% 14.11% 97.6% 22.83% Acute Cardiology Unit % Heart Care Unit % Heat map - Inpatient Ward Areas - March % 25.16% 110.5% 46.28% 121.8% 25.78% 102.4% 51.07% Ward % 84.3% 35.72% 90.7% 76.43% 101.1% 57.86% 100.1% 59.98% Ward % 79.9% 6.07% 99.6% 52.07% 81.3% 23.45% 118.5% 34.74% Ward % 84.4% 13.81% 97.8% 74.84% 98.4% 12.11% 100.6% 18.31% Ward % 72.8% 0.00% 99.3% 45.57% 110.0% 11.33% 114.8% 34.27% Ward % 73.7% 25.50% 100.0% 45.21% 146.1% 20.72% 132.2% 48.45% Ward % 76.7% 26.29% 98.3% 44.43% 103.1% 22.36% 100.8% 17.70% Ward % 73.4% 20.92% 82.4% 38.84% 109.5% 16.93% 182.4% 31.06% Ward 27 (Maternity) % 84.2% 25.41% 91.3% 7.17% 84.8% 9.94% 112.9% 11.79% NICU % 95.6% 12.38% 99.2% 14.87% 100.0% N/A N/A N/A Children's Unit % 95.0% 17.67% 95.7% 12.29% 69.8% 25.41% N/A 11.11% Stamford Unit % 10.94% 99.9% 63.28% 91.3% 21.54% 102.3% 62.18% % Stamford Unit % 5.42% 103.3% 45.22% 94.7% 30.24% 103.9% 40.84% Shire Hill % 100.2% 27.06% 99.7% 22.35% 90.5% 20.25% 91.8% 51.94% Inpatient Totals/Averages % 89.9% N/A 97.7% N/A 99.0% N/A 112.7% N/A Actual CHPPD TOTAL KEY Complaints Moderate Harm + Falls with Harm MRSA CDIFF PU(+G2) Staffing Fill Rates 0 - Green 0 - Green 0 - Green 0 - Green 0 - Green 0 - Green > 90% - Green >1- Amber >1 - Amber >1 - Amber >1 - Red >1- Amber >1 - Amber 80-90% - Amber >2 - Red >2 - Red > 2 - Red >2 - Red >2 - Red < 80% - Red NB: Please note that Inpt FFT Total shown does not include Community areas. 12
29 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item 7c Title Director of Finance Report - Month 12, March 2017) Sponsoring Executive Director Author (s) Purpose Previously considered by Claire Yarwood, Director of Finance Finance Team Discussion and Endorsement This paper has been reviewed by the Finance and Performance Committee Executive Summary: The financial position for the full year as at March 2017 is a 14.5m deficit which is 2.8m better than plan. Cash balances are slightly above plan. Related Trust Objectives 6 To deliver against the required local and national regulatory frameworks as part of the Greater Manchester Health and Social Care Devolution, securing the best economy efficiency and effectiveness in use of resources the Trust spends to deliver services both directly and through partner organisations. Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? 723 Failure to meet, deliver the Trust s financial plan In breach of licence None None Sustainability is subject to the outcome of the system wide review by the CPT Action required by the Board The Board are asked to discuss the contents of the report, recognise the risk and endorse the actions required.
30 Executive Summary Summary of Performance For the financial period to the 31 st March 2017, the Trust is reporting a normalised deficit of 13.3m which is 3.98m better than plan. The position is driven by the Trust receiving additional Sustainability and Transformation Funding from NHSI, and strong financial control measures implemented throughout the year. For the full year, the Trust has spent 12.7m on agency staffing, broadly in line with the NHS Improvement ceiling of 12.5m. The Trust has been reliant on agency usage to support winter pressures, and to cover medical vacancies in several areas where recruitment has been challenging. Plan ( '000) Actual ( '000) Variance ( '000) Plan ( '000) Actual ( '000) Variance ( '000) Plan ( '000) EBITDA (273) 2,107 2,384 (7,912) (4,811) 3,101 (7,922) Normalised Surplus/(Deficit) (1,056) 1,364 2,420 (17,300) (13,320) 3,980 (17,300) Net Deficit after Exceptional Costs (1,056) 844 1,900 (17,300) (13,993) 3,307 (17,300) Trust Efficiency Savings (43) 7,832 8, ,808 Use of Resources Metric Key I&E issues: Agency expenditure for the year end forecast is 12.7m so is broadly in line with the NHSI ceiling of 12.5m. A lot of hard work has been undertaken to strengthen control of agency usage within the Trust. The Trust Efficiency Savings target has been exceeded by 610k. This is an excellent achievement, although continued work is required in 2017/18 to increase the value of recurrent savings. Key Balance Sheet issues: Cash is c. 1.9m greater than planned. This is due to NHSI releasing STF earlier than planned. Better Payment Practice Code is currently below the target of 95% across all metrics, because the DH will only lend the Trust funding to meet the deficit plan, not improve the Trust creditor position. The annual capital plan of 3m has been delivered in full. Key Risks for 2017/18: The Trust has still not agreed as control total with NHSI. Failure to do so could result in additional financial implications not yet included in the 2017/18 financial plan. As the Trust is planning for a deficit, there is a requirement for a DH loan to fund it. The Trust will be subject to a higher interest rate for borrowing if a control total is not agreed. At the end of 2016/17, the Trust has loan liability of 54.8m. It is anticipated that this will increase to 78.1m in 2017/18. The Trust could be required to repay part of this liability in
31 Financial Overview - Dashboard Month 12 Full Year Plan ( '000) Actual ( '000) Variance ( '000) Plan ( '000) Actual ( '000) Variance ( '000) Income 17,227 22,384 5, , ,355 9,902 Expenditure - Pay 12,277 12, , ,501 (898) Expenditure- Non Pay 5,223 8,065 (2,841) 62,762 68,665 (5,903) EBITDA (273) 2,107 2,380 (7,912) (4,811) 3,101 Financing ,388 8, Normalised Surplus/(Deficit) (1,056) 1,364 2,420 (17,300) (13,320) 3,980 Exceptional Costs (520) (673) Net Surplus/(Deficit) (1,056) 844 1,900 (17,300) (13,993) 3,307 Deficit (% of Turnover) -6.1% 3.8% -8.5% -6.6% Trust Efficiency Savings (43) 7,832 8, Capital Expenditure ,016 2,937 (79) Cash and Equivalents 1,000 2,945 1,945 Use of Resources Metric Analysis of Income Elective 2,352 1,914 (438) 24,636 23,398 (1,238) Non Elective 4,207 4, ,037 52,816 1,779 Outpatients 2,447 2,310 (137) 27,788 27,398 (390) Other Clinical Income 7,273 10,465 3,192 87,525 91,369 3,844 Total Clinical Income 16,279 19,486 3, , ,981 3,995 Non Clinical Income 948 2,897 1,949 11,467 17,374 5,907 Total Income 17,226 22,384 5, , ,355 9,902 2
32 Breakdown of Deficit Improvement Planned 2016/17 Deficit (17.3) Balance Review (1) Sept m Notes Once indications suggested the Trust would not deliver the Q3 and Q4 A&E trajectory, mitigations were sought. Matched STF for Balance Sheet Review (1) 0.4 NHSI 'incentive' for improving the financial position. Balance Sheet Review (2) January Matched STF for Balance Sheet Review (2) 0.5 NHSI 'incentive' for improving the financial position. GM H&SC Partnership Transformation IM&T Review 0.5 Funding to offset previously incurred expenditure Matched STF for Transformation Funding 0.5 NHSI 'incentive' for improving the financial position. Bonus STF 1.0 NHSI additional payment for delivering a financial position better than planned. Revised Year End Deficit (13.4) 3

33 Valuing Care Productivity and Efficiency Programme 9,000 8,000 7,000 6,000 5,000 4,000 3,000 2,000 1,000 0 Year to Date Performance Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Plan Actual Recurrent Actions for 2017/18: Development and implementation of 2017/18 schemes. Working with the local health economy to develop system wide efficiency schemes. Month 12 Year to Date Annual Plan ( '000) Plan ( '000) Actual ( '000) Variance ( '000) Plan ( '000) Actual ( '000) Variance ( '000) Surgery and W&C 2, ,266 2,265 (1) Corporate 2, ,114 2, Medicine and CSS 2, (44) 2,951 3, Community Services (41) Grand Total 7, (43) 7,832 8, Key Messages The 2017/18 savings target has been exceeded by 653k. This attributable to the hard work from the operational and finance teams in identifying and delivering savings. Surgery and W&C: The division broadly delivered the target for the year. Corporate: The division overachieved the annual target due to non recurrent benefits. The division is working towards identifying recurrent savings for 2017/18. Medicine and CSS; The division exceeded the annual target by 188k. However, the majority of savings are non recurrent, and so work is ongoing to identify recurrent savings. Community Services: The savings target for 2016/17 has been achieved non recurrently. Invest to Save 70k was invested in a creating a new post for a medical staffing specialist within HR. This post has achieved the following; Supported an increase in Direct Engagement from 70% to over 90% resulting in a saving of over 150k. Supported the procurement of Brookson predicted annual saving of 200k although this could be offset by increased costs relating the implications of IR35 Is an integral part of the 2017/18 Medical Staffing TEP and is the lead for the majority of schemes. 4
.")
34 Financial Performance to Month Twelve (March 2017) Cumulative Financial Position 0-5,000-10,000 '000-15,000-20,000-25,000-30,000 Cumulative Plan Cumulative Actual Pay: is slightly worse than plan for the full year ( 898k, 0.6%). Underspends in the Community, Corporate and Surgery and Women and Children s divisions relating to vacancies are offset by overspends in Medicine and CSS staffing for escalation beds and the premium cost of temporary staff to cover vacancies. In addition, expenditure category changes in reserves are offset by corresponding underspends in non pay. Drugs: expenditure is overspent by 154k for the full year. Benefits relating to unrequired prior year anticipated expenditure is offset by activity related overspends across several areas. 347k of this is offset by income for PbR excluded drugs. Clinical Supplies: are overspent by 4.7m cumulatively to year end. This predominantly relates to expenditure plan category movements in reserves, which are offset by underspends on other types of expenditure, and overspends on medical and clinical equipment across all operational divisions. General Supplies: are overspent by 1.1m for the year to date. Expenditure plan category movements in reserves are offsetting overspends in the commercial sector (156 T&O cases, 30 General Surgery cases and 24 ENT cases- totalling 785k) and radiology private sector expenditure. Clinical Income: is cumulatively above plan by 3.9m, this includes an additional 2.4m of Sustainability and Transformation funding. Other Income: is better than plan by 6m, relating to recharges for staff and equipment funded by other organisations. This is predominantly offset by expenditure. 5
35 Pay Analysis Bank and Agency Key Messages Spend on bank and agency staff for the year to March 2017 is 19.5m which is c. 3.7m higher than in 2015/16. The Trust is now commissioned to provide Community Services for Tameside and Glossop, so bank and agency expenditure associated with this service in included in the 2016/17 figure. Bank usage has increased in comparison to the trend at the beginning of the year this is to support winter pressures. However, agency expenditure has been steadily decreasing since September '000 1,400 1,200 1, Tameside Rolling 12 Months Bank and Agency Expenditure Agency Bank Agency w/o credit Expenditure 1,000, , , , , , , , , ,000 0 Trust Agency Usage April 2014 to March 2017 Apr Jun Aug Oct Dec Feb Apr Jun Aug Oct Dec Feb Apr Jun Aug Oct Dec Feb Medical Nursing Other Trust Total Agency Spend The Trust has been assigned a year end ceiling of 12.5m total agency spend for 2016/17. Planned agency expenditure has been profiled based on the average of monthly expenditure over the last two years. The Trust spent 12.7m on agency for the full year, which is broadly on line with the NHSI ceiling. Overall, the pay budget is slightly above plan, however some of the overspend is offset by income to fund various staff posts. The Trust is also paying significantly for premium staffing costs due to the difficulties in recruiting certain staff groups. Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total Plan ( '000) ,043 1,065 1,106 1,033 1,038 1, ,053 1,054 1,102 12,499 Medical Actual ( '000) ,708 Nursing Actual ( '000) ,268 Other Actual ( '000) ,716 Total Actual ( '000) 1,115 1, ,148 1,306 1,205 1, ,109 12,692 Variance ( '000) (121) (165) (43) (273) (167) 48 (12) (7) (192) 6
36 NHS Improvement Agency Cap Key Messages On the 1 st April 2016, the NHS Improvement capped rates were reduced. The Trust has to report to NHSI on a weekly basis how many agency shifts are being used which exceed the capped rates. The latest return is shown below; Number of Shifts Exceeding the Staff Group Price Cap Week Ending 26/03/17 Nursing, Midwifery & Health Visitors 76 Scientific, Therapeutic and Technical 40.1 Medical & Dental 181 Administrative & Estates 0 Total 297 Actions A&E and General Medicine middle grade rotas have been redesigned to reduce the reliance on agency staffing. Substantive recruitment is now in progress, and some posts have been filled. Information by specific staff breaching the cap rate is being shared with the Executive Management Team on a weekly basis. A summary report is presented at the monthly Finance and Performance Committee for review. A review of medical staff recruitment and the impact on service delivery is ongoing. 7
37 Clinical Income - Contract Analysis Year to Date Commissioner Plan ( m) Actual ( m) Variance ( m) Annual Plan ( m) 15/16 Outturn ( m) Tameside and Glossop CCG (0.3) Oldham CCG Manchester CCG's (All) (0.1) Stockport CCG (0.0) NHS England Specialised Services Secondary Dental - NHS Area Team (0.1) Tameside MBC All Other Commissioners Grand Total Key Messages: Overall, clinical income is above plan by 3.9m. The Trust has a sophisticated block contract with Tameside and Glossop CCG has agreed a year end settlement. The value of over-performance blocked back to contract plan for Tameside and Glossop CCG year to date is 324k. Areas of overperformance in ambulatory care, non elective discharges and excess beddays are offset by underperformances in A&E, elective discharges and outpatients. Tameside MBC has provided funding to support costs incurred relating to delayed transfers of care. This funding offsets expenditure occurred by the use of spot beds. All Other Commissioners includes the Sustainability and Transformation funding (STF), of which the Trust is receiving 9.4m. 8
38 Income and Activity - Year to Date Activity '000 6,000 5,000 4,000 3,000 2,000 1, ,000-2,000 3,000 2,000 1, ,000-2,000-3,000-4,000-5,000-6,000-7,000 Clinical Income Variance by Point of Delivery Activity Variance by Point of Delivery A&E Critical Care Elective Daycase Non Elective Out-Patients Key Messages: Critical Care is under plan by 1m. Adult critical care is worse than plan by ( 613k, 321 bed days) and neonatal critical care is worse than plan by ( 396k, 639 bed days). Elective income is worse than plan by 841k, (494 procedures below plan). Under performances in Cardiology ( 176k), General Surgery ( 164k), Orthopaedics ( 197k) and Gynaecology ( 100k) are offset by small over performances in Breast Surgery, ENT and Paediatrics. Day-Case income is worse than plan by 397k (25 procedures below plan). Over performance in General Surgery ( 204k, 602 procedures above plan) is offset by underperformances in Colorectal Surgery ( 133k), General Medicine ( 166k), Pain Management ( 114k) and Plastic Surgery ( 90k). Non-Elective income is better than plan by 1.7m. Over performance in Obstetrics ( 334k), Paediatrics ( 377k) and Medicine ( 654k) is offset by under performance in General Surgery ( 396k) and Trauma and Orthopaedics ( 61k). Excess bed-days are above plan by 882k. Outpatient income is under performing by 389k, equating to 6,000 attendances. Over performances within Cardiology, Dermatology and Gynaecology are offset with underperformances in Anti Coagulant, Pain Management, Orthopaedics and Urology. Drugs and device income is cumulatively above plan by 347k. This is offset by corresponding overspends in expenditure. Other income additional STF funding of 9.3m and 1.5m additional funding from commissioners in relation to A&E and RTT pressures. 9
39 Pay Analysis Tameside Rolling 12 Months Pay Expenditure Key Messages: '000 14,000 9,000 4,000 '000 6,000 5,000 4,000 3,000 2,000 1,000 In Month Divisional Pay Analysis Bank Agency Payroll Budget Budget Bank Agency Payroll Pay expenditure is 898k worse than plan for the year to date. This is largely driven by expenditure category changes in reserves. * Community Services pay expenditure is underspent by 175k. This underspend has slowed down since the beginning of the year as teams have worked hard to recruit into vacancies. Corporate is underspent by 1.5m relating to vacancies across all Directorates The Corporate team have reviewed all budgets to ensure they accurately reflect service provision, and this will be reflected in the 2017/18 budgets. Surgery and W&C is underspent by 566k. This is due to vacancies relating to several specialties. Medicine and CSS is overspent by 914k. This largely relates to premium cost temporary staff to cover medical vacancies, as well as expenditure to staff unfunded escalation beds and additional staffing to support the CQC inspection. 0-1,000 Surgery and W&C Corporate Medicine and CSS Community Services * As per NHSI, once a budget is set by expenditure type for the financial plan, it cannot be changed. For example, when business cases are finalised in year it may be decided that a budget set for the commercial sector (non pay expenditure) at the beginning of the year would now be required for pay expenditure to perform the work in house. This category change would be transacted through reserves so the division has the appropriate budget in the correct expenditure category. 10
40 Divisional Performance (EBITDA) Month Twelve (March 2017) Month 12 Year to Date Division Plan ( '000) Actual ( '000) Variance ( '000) Plan ( '000) Actual ( '000) Variance ( '000) Surgery and W&C 1,529 1, ,588 15,236 (351) Corporate (3,083) (2,993) 90 (36,811) (36,076) 735 Medicine and CSS 874 (298) (1,172) 8,053 7,047 (1,006) Community Services (277) (360) (83) (1,767) (1,691) 76 Reserves 683 4,245 3,561 7,024 10,728 3,704 Trust EBITDA (274) 2,163 2,436 (7,913) (4,753) 3,154 Key Messages Surgery and W&C: Contribution is 351k worse than plan for the full year. This is driven by underperformance in clinical income, unfunded expenditure within the independent sector due to a shortfall in internal capacity and overspends on clinical prosthesis. Corporate: Full year contribution is 735k better than plan. This is largely driven by under-spends on pay expenditure relating to vacancies is offset by over-spends on non pay relating to efficiency savings targets. Medicine and CSS: Contribution is 1m worse than the full year. Minor over-performance on income is offset by overspends on pay relating to the premium costs covering vacancies, and activity related overspends on non pay. Community Services: Contribution is 76k better than plan for the full year which is due vacancies throughout the division. A significant number of these have no been recruited to, so the underspend has reduced in year. This is partially offset with the costs associated with running the Stamford Unit, an element of which are unfunded. EBITDA movement to Normalised Deficit position: The total Trust position is supported by a number of underperforming non operating expenditure budgets with an annual budget of 9.4m, which are not counted within the EBITDA. This is predominantly PDC payments ( 581k better than plan), depreciation ( 203k better than plan), exceptional costs ( 561k worse than plan) and interest payable ( 131k worse than plan). 11
41 Cash Flow, Capital Expenditure and Debtor and Creditor Analysis '000 25,000 20,000 15,000 10, Week Cash Flow from 13th March 2017 Forecast ( '000) Target Minimum Cash Reserve Category Balance ( '000) 0-30 Days ( '000) Days ( '000) Over 90Days ( '000) Total Sales Ledger Debtors 5,900 4, Total Aged Creditors 5,510 3, ,104 Top Five Debtors m Tameside MBC Other 1,563 1, NHS Tameside and Glossop CCG NHS NHS England North West (Manchester) NHS NHS England North West (Commissioning Hub) NHS Pennine Care NHS Foundation Trust NHS Top Five Creditors m NHS Professionals LTD Other Central Manchester University Hospitals NHS Found NHS NHS Tameside and Glossop CCG NHS Tameside MBC Other University Hospital of South Manchester NHS Fooun NHS '000 5, Capex Expenditure Capex Budget Capex Actual Key Messages: Cash: The March month end cash balance was 2.9m, above the 1m plan. This is due to the Trust receiving STF earlier than indicated by NHSI. The overall level of cash is forecast to remain at circa 1m across the next 13 weeks. Peaks in cash balances during this period reflect cash timing of receipt of monthly contract payments from NHS commissioners and payment to suppliers. Capital: Cumulatively, 2.9m of capital expenditure has been incurred as planned. Investments in 2016/17 included development of the Antenatal Clinic, upgrade of Critical Care and IT developments. Debtors: The majority of the debt relates to NHS debt. This has been reduced significantly in March. Loans: The cash support to the Trust is funded from an Interim Revenue Support Loan (IRSL) of 13.2m. For the remainder of the loan required to fund the deficit, the Trust agreed an uncommitted revenue support loan with DH, up to the value of 6.6m. The uncommitted loan can be withdrawn and full repayment requested at any time. The total distressed loan liability the Trust has at year end is 54.8m. Creditors: The creditor balances are predominantly current balances which will be settled in line with the Trust s payment terms. This is currently at 60 days due to the low levels of cash the organisation can maintain whilst operating in a deficit. Public Sector Payment Compliance (Target 95%): Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Total 30 Days Greater 30 Days NHS Value ( '000) 47,402 40, % 6, % NHS Number 2, % 1, % Non NHS Value ( '000) 116,632 77, % 34, % Non NHS Number 41,282 18, % 22, % 12
42 Statement of Financial Position (formerly Balance Sheet) as at 31 st March Dec Jan 2017 Actual '000 Actual ' Feb 2017 Actual ' Mar2017 Actual '000 Feb - Mar Movement '000 Total Non Current Assets 118, , , ,415 7,027 Current Assets Inventories - Stock - Finished Goods 1,619 1,426 1,743 1,430 (313) Trade & Other Receivables:- > NHS Trade Receivables 1,952 1,995 1,201 3,665 2,464 > Non NHS Trade Receivables ,235 1,489 Provision for doubtful debt (559) (559) (545) (594) (49) > PDC Dividend Receivable > Other Receivables 871 1, (368) > Accrued Income 4,348 4,128 5,573 5, > Prepayments - Non PFI Related 2,926 3,259 1,647 1,287 (360) Cash 1,247 1,028 1,235 2,945 1,710 Investments Total Current Assets 13,360 13,286 12,285 17,129 4,844 Current Liabilities Trade & Other Payables:- > NHS Trade Creditors (1,459) (1,599) (828) (1,899) (1,071) > Non NHS Trade Creditors (2,932) (2,836) (2,229) (3,612) (1,382) > Other Creditors (7,062) (7,199) (6,852) (6,992) (141) > Capital Creditors (61) (210) (123) (704) (581) Other Liabilities:- > Accruals (14,462) (13,157) (12,060) (10,862) 1,198 > Deferred Income (2,619) (3,874) (3,323) (2,342) 981 >PFI Leases (1,282) (1,282) (1,282) (1,336) (54) >PDC Dividend Creditor Provisions (179) (174) (337) (149) 188 Total Current Liabilities (30,057) (30,332) (27,035) (27,897) (862) Net Current Assets/Liabilities (16,697) (17,046) (14,750) (10,768) 3,983 Non Current Liabilities Other Financial Liabilities:- > Deferred Income 0 > PFI Leases (53,964) (53,855) (53,757) (53,594) 163 > Interim Revenue Support Loan - DOH (47,175) (48,150) (51,525) (54,801) (3,276) Provisions (767) (766) (681) (694) (13) Total Non Current Liabilities (101,906) (102,772) (105,963) (109,089) (3,126) TOTAL ASSETS EMPLOYED (369) (1,617) (2,325) 5,559 7,884 Financed By Taxpayers Equity PDC 53,285 53,285 53,285 53,285 0 Revaluation Reserve 29,298 29,298 29,298 35,287 5,989 I&E Reserve (33,588) (33,588) (33,588) (32,538) 1,050 I&E reserve 2014/15 (15,703) (15,703) (15,703) (15,703) 0 I&E reserve 2015/16 (20,779) (20,779) (20,779) (20,779) 0 TOTAL TAXPAYERS EQUITY (368) (1,616) (2,324) 5,559 7,883 13
43 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item 7d Title Significant Risk Report Sponsoring Executive Director Karen James Chief Executive Author (s) John Fletcher, Acting Director of Quality and Governance For discussion and agreement of future Purpose actions For approval To note/receive Previously considered by Risk Management Group, Service Quality and Operational Governance Group Executive Summary The Significant Risk Report provides details on all identified significant risk exposure through the Risk Register and Board Assurance Framework across services provided by the Trust. Related Trust Objectives Impacts on all Trust Objectives Risk Assurance risk impacted upon Impacts on all BAF and Risk Registers Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? Referred to if necessary in the paper Referred to if necessary in the paper Referred to if necessary in the paper How does this report affect Sustainability? Reflects current risks to the Trust s business and strategic objectives Action required by the Group Members are asked to discuss and consider the current position in relation to significant risks and the proposed changes to reporting and Trust Risk Strategy Page 1 of 29
44 April 2017 Significant Risk and BAF Report 1.0 Summary Narrative of April Significant Risk and BAF Paper This paper provides members with a report on the significant risk exposure through the Risk Register and Board Assurance Framework across services provided by the Trust. The recently revised format places more emphasis on the target risk score and timescales for achieving the target score and focusses attention on the gap between the current and target risk scores. A review of target risk scores is progressing to ensure achievement of the target is realistic and possible. Alongside the changes there will be focussed organisational development sessions to support the review of the risks in the context of the changes and the revision of the Risk Management Strategy Policy and Guidance. The risks included in this report have been subject to review by the Quality and Governance Unit following discussion with responsible Directors. The risks have been consistently and systematically reviewed in light of the regulatory requirements and mapped against the Trust s Strategic plans and responses to regulatory oversight which contain specific actions against identified risks. The Treatment Plans for these risks have been reviewed by responsible Directors and leads to ensure reflection of the assertive improvement work and current mitigations. Horizon scanning for future risks to ensure foresight and insight is continually taking place with systematic examination of information to identify potential threats, and vulnerabilities, and detect opportunities and options to reduce existing risks. Where applicable, necessary third party assurances are referred to. 1.1 The Trust has identified a range of significant risks to its strategic objectives, which are currently being mitigated, the impact of which could have a direct bearing on compliance with NHS Improvement Provider Licence, CQC registration or the achievement of corporate objectives, should the mitigation plans be ineffective. Currently, the significant risks relate to the following areas: Discharge processes and the management of the Urgent Care Pathway across the whole health economy Health economy capacity to manage patient flow and Urgent Care impacting on Emergency Department pressures Finance (Cost control, TEP delivery and liquidity) Information technology Medicines management Recruitment and Staffing Third party decisions /Transition to Integration Environmental monitoring Results Governance Page 2 of 29
45 The main controls and action plans for each significant risk have been reviewed and collated in the Trust s Risk Register. Our Risk management programme has incorporated the Corporate Risks (CR) and aligned them to the Board Assurance Framework (BAF). Updates against the BAF and Risk register significant risks are summarised in the analysis table in Appendix 1 and detailed risk information provided in Appendix Detailed updates against the BAF significant risks are included in this report. The Board have informed the principal risks described. The report reflects the revision of the BAF to include consideration of the potential impact of Greater Manchester Health and Social Care Devolution and external reconfiguration and the iterative development of Models of Care between acute, community, primary and social care providers. We continue to keep a line of sight on these and emergent risks through the Care Together Programme. The risks associated with Healthier Together implementation, Greater Manchester Health and Social Care Partnerships and the Care Together programmes are aligned through the Board as they emerge and are identified. The Director of Operations is currently overseeing the development of the risk assessments related to the five Neighbourhoods for inclusion in the risk register from April The BAF is being aligned to the 2017/18 Corporate Objectives and updated through a schedule of reviews by the Executive Directors, prior to next Trust Board. 1.3 New Significant Risks The following risks have been included within the report since the previous Trust Board meeting CR4302 Introduction of IR35 tax regulations on the 6th April 2017 may increase existing issues relating to medical and nursing staff. The risk has emerged following assessment of the impact of HMRC enforcement of Tax Law IR35 which relates to medical and nursing staff who are employed via an agency and being paid by a limited company which are now subject to normal PAYE and National Insurance. This has impacted specifically on medical staffing rotas and the ability to maintain medical staffing levels. The impact has the potential to impact on the consistency of supervision to trainee doctors. This is currently scoring 16 with a target score of 8. CR 4212 Delay/inability to obtain microbiology results This risk is concerned with the risk of inappropriately treating a significant infection due to delay/inability to obtain microbiology results. The risk has arisen out of delays in samples being transported to the Laboratories at Manchester, and delays in these being processed for cultures/microscopy. These are contributing to delays in results Page 3 of 29
46 being received from the Manchester Laboratory. The risk has been presented at Risk Management Group and is currently scoring 16 with a target score of 4 and a gap score of 12. Mitigations are in place to reduce the clinical risk, but there is impact on clinical time. 1.4 Reduction in Risk Scores None to report 1.5 Increased Risk Scores None to report 1.6 Other Notable Changes / Update Following the last Risk Management Group meeting divisions are focussing on revisiting the risk target scores and ensuring target scores are realistic and gap scores are aligned with the organisations risk appetite. Divisions will be supported by the Quality and Governance Unit in the new format and requirements. There will be a schedule of reviews by the Executive Directors supported by the Quality and Governance Unit to review the BAF in the context of the new corporate objectives for 2017/18. There will also be emphasis on reviewing the target score, gap score and risk appetite. 2.0 Recommendations Members are requested to note current significant risks, current controls and mitigations within the report. Page 4 of 29
47 Appendix 1 Summary of risks and analysis Risk Lead Key: BS: Board Secretary CEO: Chief Executive DoHR: Director of Human Resources MD: Medical Director DoE: Director of Estates CN: Chief Nurse DoP: Director of Performance & Informatics DoO: Director of Operations DoSP: Director of Strategy & Partnership DoF: Director of Finance DoQG: Director of Quality & Governance Risk Matrix Consequence Sub-Committee Key: AC: Audit Committee CoG: Council of Governors QGC: Quality & Governance Committee FPC: Finance & Performance Committee EMT: Executive Management Team SQOGG: Service Quality & Operational Governance Group IPCG: Infection Prevention & Control Group ISB: Internal Safeguarding Board IMTG: IM&T Group IG: Information Governance Group Likelihood Insignificant Minor Moderate Major Catastrophic Rare Low/Unlikely Possible High/Likely Almost ccertain Gap Score Matrix (Difference between Target Score and Current score) Gap score 0 Gap score 1-5 Gap score 6-9 Gap score 10 Gap score > 10 Risk target achieved Tolerable Close monitoring Concern Serious Direction of travel - Change since previous review Escalated De escalated Unchanged Target achieved Page 5 of 29
48 BAF Ref / Risk Ref Description Analysis of Risk Sub Committee Executive Lead Current Risk Score Risk Target Risk Target Gap Risk Appetite Guide Risk AF 1.24 (3483) If demands increase beyond predicted levels and outside current capacity, and the management of the urgent care pathway across the Health Economy is not undertaken in a cohesive and standardised way, this could result in delay, increased clinical risk and a reduced positive patient experience. The risk score remains in excess of the target score and continues to be closely monitored, The achievement of the target score is dependent on the transformation of services and pathways across the Health Economy. The Trust continues to engage with other service providers and to progress models of care to improve capacity and patient flow. QGC DoO DoSP Moderate AF 1.23 (3482) Medical Staffing - The ability to recruit to Consultant and Middle Grade posts due to national shortages in certain specialties i.e. Radiology, Medicine and A&E. This may impact on patient experience and the ability to provide safe care This risk remains at 20 and continues to be challenging. The risk is influenced by the national picture and availability of workforce. There still remains a significant operational risk profile against the BAF risk as the organisation continues to meet challenges in relation to medical staffing particularly speciality medical staff. International recruitment and alternative staffing models are being reviewed in difficult to recruit specialities. SQOGG DoHR MD Moderate AF 1.23 (734) Nursing Staff The ability to consistently sustain and maintain safe nurse staffing levels is compromised as a result of operational demand, use of escalation and additional capacity beds third party decisions and actions and continuous readmission challenges This risk remains at 20 and continues to be challenging. The risk is influenced by the national picture and availability of workforce. The Trust has been actively addressing staffing and has been utilizing a number of strategies to maintain consistent staffing levels, which include recruitment fast track events, skilling up of staff, and the recognition and certification of Health Care Workers. There still remains a significant operational risk profile against this BAF risk as the organisation continues to meet challenges around staffing particularly for registered nurses. SQOGG DoHR CN Moderate International recruitment and alternative staffing models are being reviewed in difficult to recruit specialities. AF2.2 (3485) Failure to deliver financial plans in line with National guidance from NHS Improvement This risk has remained static and links with other financial risks within the BAF. There are a number of monitoring processes in place and regular reporting to Trust Board. FPC DoF Moderate CR3618 linked If demands on the service outstrip capacity this may result in inability to Related closely to AF1.24 this risk score remains in excess of the target score and continues to be closely OG DoO Moderate Page 6 of 29
49 BAF Ref / Risk Ref Description Analysis of Risk Sub Committee Executive Lead Current Risk Score Risk Target Risk Target Gap Risk Appetite Guide with AF3489 deliver the 4 hour Emergency Access Standard. monitored, The achievement of the target score is dependent on the transformation of services across the health economy. The Trust continues to engage with other service providers and to progress models of care DoSP AF2.8 (3526) Failure to achieve VFM services and financial sustainability. This risk score has remained at 20 throughout the financial year and was reviewed at Audit Committee in February The risk continues to be closely monitored and assurance of the position provided through performance and financial reporting AC DoP Low AF2.9 (3527) AF5.1 (4059) Cash Management and Capital Investment Failure to achieve : a) cash/ liquidity targets, b) Capital Investment within planned resources c) Capital Absorption rate targets Failure to deliver Trust efficiency programme This risk was recently updated to reflect current terminology. The risk score reduced in Q1 2016/17 from 25 to 20 and has remained stable at 20 since this time. This BAF risk links closely with AF2.8 and AF2.9. There are a number of controls and assurance processes in place in relation to this risk which include internal audit. This risk emerged following the decision to separate a previous risk made following discussion at the Finance and Performance Committee in Q2 2016/17 the risk score remains at 20 AC FPC DoF DoF Low Low CR4201 Healthier Together Risk that the Trust will be in breach of its financial control limit due to the significant stranded costs caused by the reconfiguration of emergency and elective (cancer) general surgery as part of the Healthier Together Programme across Greater Manchester. This risk was identified in Quarter /17 and is being monitored closely. The risk score will be adjusted accordingly as mitigations and controls take effect. The Trust is continuing to engage with the Healthier Together clinical Advisory Group and the Trust Executives are being informed of any significant financial and/or clinical implications SQOGG DoO Low CR4183 There is a risk of delayed patient diagnosis and/or treatment as a result of lack of availability of radiologists/radiology staff in the service. This risk emerged in Quarter /17 and is being monitored closely. The risk score will be adjusted accordingly as mitigations and controls take effect. SQOGG DoO Low Page 7 of 29
50 BAF Ref / Risk Ref Description Analysis of Risk Sub Committee Executive Lead Current Risk Score Risk Target Risk Target Gap Risk Appetite Guide CR4012 Banking Trojans now using Locky ransomware resulting in potential data loss due to encryption This risk score saw an increase following the realisation of a ransomware occurrence. The risk is expected to be decreased following implementation of anti-ransomware software being procured IM&T Group DoP&I Moderate CR4147 Ability to consistently sustain and maintain a workforce with capability and capacity to deliver community nursing services This risk was identified following the transfer of the Community Services. The Division is reviewing options for alternative service delivery and staff skill requirements to further mitigate the risk. This risk was reviewed and reworded in March 2017 by the DoO and controls updated. OG DoO Moderate CR3472 The ability to consistently apply, sustain and maintain processes relating to the management of medicines This risk score has remained the same in Q1 and Q2 of 2016/17. Assertive work is being undertaken to understand and address the risks. Assurances are being scrutinised and challenged through the governance processes. This risk is currently being reworded and refocussed to more accurately reflect the specific areas of risk QGC, OG MD Moderate CR4219 Radiology requests on Lorenzo for in patients and out patients are being recorded as cancelled by the Radiology department without reference to the requesting clinician. This risk emerged in March 2017 and is undergoing further validation of information and evidence to support the score. SQOGG DoO Moderate CR4302 Introduction of IR35 Tax Regulations on the 6th April 2017 may increase existing issues relating to medical and nursing staff. This is a new risk and ongoing rota monitoring is in place to ensure mitigations are in place and to minimise the clinical risk. The risk is a National risk arising from a change in UK Tax Law this is impacting on the availability of Locum doctors. This also have a potential to impact on the nursing service and the supervision of doctors in training. RMG MD/DoO Moderate Page 8 of 29
51 BAF Ref / Risk Ref Description Analysis of Risk Sub Committee Executive Lead Current Risk Score Risk Target Risk Target Gap Risk Appetite Guide CR4212 Delay / inability to obtain microbiology results Risk of missing a significant infection due to delay/ antibiotics which may result in morbidity or inability to obtain microbiology results and therefore risk of mis-treating a patient with an inappropriate death. This is a new risk arising in Quarter /18 from the Division of Surgery Women and Children which has a specific area of focus within the Paediatric speciality. Mitigations are in place which is expected to reduce the risk these include active follow up of results. SQOGG MD High AF4.2 (3488) Failure to ensure on-going compliance with terms of NHS Improvement Provider Licence requirements This risk reduced from 25 to 15 in Quarter /17 as a result of positive assurances. There are no gaps in controls or assurances identified at this time. AC DoF Low AF4.8 (3491) Failure to have in place an IM&T infrastructure and service supporting the organisational objectives This risk score remains at 15 and has been static at 15 throughout this financial year to date. Although the risk score remains that same further assurances are being sought in relation to the integration of Community Services IMTG DoP Moderate CR3997 Inconsistent room temperatures in NICU This risk has remained static and following discussions at Risk Management Group in April 2017 assertive action has been requested by the Risk Management Group to resolve this issue via the Estates Department. SQOGG DoO Moderate CR4158 Transfer of microbiology laboratory to Manchester Royal Infirmary and relates to IT issues with Telepath and ICNet connectivity. This risk emerged with the transfer of microbiology services, manual systems for ensuring effective communication have been implemented to mitigate the risk and the risk is being closely monitored on an ongoing basis. SQOGG CN Moderate Direction of travel - Change since previous review Escalated Residual Risk Score (Current Risk) De escalated (Target Risk / Risk Appetite Threshold) Unchanged * New Risk Score Target achieved Page 9 of 29
52 Appendix 2 Detailed Risk Tables Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 3, Corporate Objective 4, Corporate Objective 5, Corporate Objective 6, Risk Description: If demands increase beyond predicted levels and outside current capacity, and the management of the urgent care pathway across the Health Economy is not undertaken in a cohesive and standardised way, this could result in delay, increased clinical risk and a reduced positive patient experience. Potentially this could lead to; Delays in treating 95% of patients within the 4 hour standard Increased levels of cancellations for elective surgery Increased financial cost of escalation areas Longer length of stay and associated complications. Graph of Risk over time Target score Risk score BAF Ref: AF1.24 Executive Director Lead Director of Operations Current Risk Score (L x C) 4 x 5 = 20 Target Risk Rating 2 x 5 = 10 Risk Appetite None low Moderate High Significant Risk Direction Unchanged Target Gap Score 10 Concern Risk ID number: AF 3483 Assurance Committee Quality & Governance Committee Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: The Trust is not willing to risk the ability of the organisation to delivery safe effective care or compliance with regulatory requirements Date When Target Risk score expected to be achieved Unable to quantify currently. Multiagency and Multi-organisational Agenda and transformation programme Controls: Working in partnership with external agencies to improve discharge process Care Together models of Care Work Patient flow list reviewed twice weekly to determine actions required for each patient A&E Delivery Group monitoring of recovery plan established across the health economy and monitored through the Finance and Performance, Operational Board and Executive Management Team meetings Internal escalation plans in place to maintain safe and effective care during periods of increased pressure Partnership working with other providers to ensure a long term strategy is in place regarding sustainability and service provision Community Care Model being extended to support existing structures Mitigating actions: (what more should we do?) Development of integration strategy and further models with key partners Implementation of Recovery Plan by all partners Risk source Third party review and internal monitoring, incidents, complaints and claims and Operational performance Rational for Risk appetite Current Reported performance information and impact on patient flow Assurance: (how do we know if the things we are doing are having an impact) Daily monitoring of bed capacity and ED Waiting times Waiting List Steering Group Activity Planning Monthly contract performance reporting to Executive Management Team & Board Monthly finance and activity reporting to Board MIAA audits Monthly submission of DTOC data Trust/Social Services Director level interface meetings A&E Delivery Group Gaps in assurance and actions not being actioned Third party action by other parties and stakeholders has impact upon organisation. Delays in delivery due to funding Anticipated effect of controls (Expected /risk score reduced) Reported at Board meeting aligned to performance trajectory and performance report Page 10 of 29
53 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 3, BAF Ref: AF1.23 Risk ID number: AF 3482 linked to CR1549 Risk Description: Medical Staffing - The ability to recruit to Consultant and Middle Grade posts due to national shortages in certain specialties i.e. Radiology, Medicine and A&E. This may impact on patient experience and the ability to provide safe care. Executive Director Lead Director of Human Resources Medical Director Current Risk Score (L x C) 4 x 5 = 20 Risk Direction Unchanged Assurance Committee Quality & Governance Committee Date of last review: April 2017 Target Risk Rating 2 x 5 = 10 Target Gap Score 10 Concern Date of next review: May 2017 Graph of Risk over time Target score Risk score Date When Target Risk score expected to be achieved Unable to quantify currently despite mitigations. Local and National agendas and changes influence the Trust s ability to achieve this target Controls: Workforce strategy Sickness Policy and monitoring Use of Agency and Locum staff to bridge the gap Temporary staff management monitoring Senior Managers receive daily staffing report summaries Capacity & Demand being reviewed through job planning process Robust job planning process Staffing monitoring via Quality Account dashboard and HR metrics. International recruitment Mitigating actions: (what more should we do?) Reports to Board and Executive Team Continuous recruitment in to the vacant posts is underway and to continue under monitoring Weekly monitoring of KPI s Stronger links to the annual Trust planning process Lack of workforce availability at an operational level leading to difficulty in recruitment Risk source Operational performance Risk Appetite None low Moderate High Significant Rationale for current score: There is a national shortage of Consultant and Middle Grade doctors in some specialties therefore there is additional reliance on Locum and Agency staffing to provide full staff compliment Rational for Risk appetite The Trust is not willing to risk the ability of the organisation to delivery safe effective care or compliance with regulatory requirements Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc.?): Improvement Plan HENW Review Action Plan monitored by Educational Governance and SQOGG Reports to Medical Staffing Group HR & OD Workforce Group Medical Staffing Expenditure Review Group (MSERG) Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps in assurance identified however implementation of real time operational management requires consistent application of agreed systems and processes by all staff at all levels across all divisions Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Reported at Board meeting aligned to performance trajectory/ performance report Page 11 of 29
54 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 2, Corporate Objective 3, BAF Ref: AF1.23 Risk ID number: CR734 Linked to CR 3909 and AF1.23 (3482) Risk Description : Nurse Staffing -The ability to consistently sustain and maintain safe nurse staffing levels is compromised as a result of operational demand, use of escalation and additional capacity beds, third party decisions and actions are continuous as admissions challenges Graph of Risk over time Target score Risk score Executive Director Lead Chief Nurse Current Risk Score (L x C) 4 x 5 = 20 Target Risk Rating 2 x 5 = 10 Risk Appetite None low Moderate High Significant Risk Direction Unchanged Target Gap Score 10 Concern Assurance Committee Quality & Governance Committee Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: Current operational processes and daily staffing reviews Date When Target Risk score expected to be achieved Unable to quantify as local and National agendas and changes influence the Trust s ability to achieve this. Controls: Workforce Strategy Recruitment open days Monitor safer staffing analysis/submission and oversight with Acuity and dependence reviews Nurse staffing are informed by National Guidance Continuous monitoring at each operational bed meeting. Monitoring of KPI s Ward level dashboards. Roster approval signed off by Ward Manager and Matron through e-rostering standards. Processes for authorisation to backfill in place Incident reporting systems analysis of variance Mitigating actions: (what more should we do?) Continuous recruitment in to the vacant posts is undertaken and continually monitored. Monitoring of KPIs. Utilisation of a partnership model and secondment opportunities from other trusts. Recruitment from abroad Return to Nursing and Pre nursing care Support Worker programme Weekly recruitment tracker to EMT Monthly Staffing Board Report to Trust Board informs this risk score. Risk source Operational performance, incidents and complaints Rational for Risk appetite; The Trust is not willing to risk the ability of the organisation to delivery safe effective care or compliance with regulatory requirements Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): NHSP monthly contract monitoring meetings E Rostering Reports to: Executive Management Team Quality & Governance Committee Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Decision of other parties Ability and availability of temporary staffing to meet demands Use of escalation areas and operational demand drawing from wider compliment of Trust resources. Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Reported at Board meeting aligned to performance trajectory and performance Page 12 of 29
55 Strategic Priority (Objective) Corporate Objective 6 BAF Ref: AF2.2 Risk ID number:af3485 Risk Description : Failure to deliver financial plans in line with FT (Provider Licence) compliance framework Graph of Risk over time Target score Risk score Executive Director Lead Director of Finance Current Risk Score (L x C) 4 x 5 = 20 Target Risk Rating 2 x 5 = 10 Risk Appetite None low Moderate High Significant Risk Direction Unchanged Target Gap Score 10 Concern Assurance Committee Finance & Performance Committee Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: Current financial performance. Service model for financial sustainability being implemented Date When Target Risk score expected to be achieved The delivery of the financial plan for 2017/18 should be achieved by April 2018 however this should be assessed in the context of the longer term financial plan Controls: Continued use of appropriate NHS Reference Costs information led by the Finance Department to ensure control and rigor of TEP delivery Finance Team work with budget holders to drive down costs and increase income and contribution margin and, with clinical teams, to exploit opportunities and repatriate activity and develop new markets Established Governance structure Ensure Divisional teams work with finance to review income, expenditure and TEP variances and to identify root cause analysis and where appropriate update systems and controls. Improvements to clinical coding team Standing Financial instructions Mitigating actions: (what more should we do?) Revised programme of financial management Certify that all material non-recurrent TEP's have also been subject to a rigorous QIA Fully develop schemes to deliver the TEP target on a recurrent basis. Develop and submit to regulators milestones and financial modelling Review of clinical coding and impact on income. Risk source Strategic Insight and Foresight Rational for Risk appetite The Trust not willing to risk the ability of the organisation to achieve NHS Improvement requirements and financial sustainability Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence Weekly EMT Performance and financial reports to Board Review of assurance and management structure/ meetings for TEP delivery Ensure PIDs and QIA are completed for each scheme Establish a recovery plan for all schemes not achieving targets Ensure Divisional infrastructure regularly review TEP Schemes, complete recovery plan and identify new schemes either in mitigation or for next financial year TEP programme alongside Improvement Plan to ensure they complement each other 2017/18 programme outline developed. Contractor meetings with the single Commissioner MIAA Audit Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Level of recording of non-recurrent TEP versus recurrent TEP. Timely planning of TEP programme to ensure future delivery Anticipated effect of controls Reported at Board meeting aligned to performance trajectory and performance report Page 13 of 29
56 Strategic Priority (Objective) Corporate Objective 2 Corporate Objective 6 Risk Description : If demands on the service outstrip capacity this may result in inability to deliver the 4 hour Emergency Access Standard BAF Ref: AF 1.1, 1.24 Executive Director Lead Director of Operations Risk ID number: CR3618 linked with AF3489 Assurance Committee Operational Group Current Risk Score (L x C) 4 x 5 = 20 Risk Direction Unchanged Date of last review: April 2017 Target Risk Rating 1 x 5 = 5 Target Gap Score 15 Serious Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Current Reported performance information and impact on patient flow Date When Target Risk score expected to be achieved Reduction of risk score is dependent on sustained proven performance and ability to influence external partners Controls: Additional ED Management Support and Infrastructure. Extended out of hours management presence. Bed meetings. Additional staffing (all services) Breach analysis and system resilience work. Mitigating actions: (what more should we do?) Daily management oversight on a patient by patient basis. On site management support overnight. In-reach from medical consultants to ED Trust wide focussed work regarding patient flow System resilience work Risk source Strategic Insight and Foresight Rational for Risk appetite The Trust is not willing to risk the ability of the organisation to delivery safe effective care Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): Emergency Department daily performance report Bed meeting reports Executive Team reports Board reports Divisional action plans and analysis of information Improvement Board Actions Detailed Improvement Plan and system resilience work. Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Impact of Third party action and third party decision e.g. impact of Primary care and Local Authority Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Reported at Board meeting aligned to performance trajectory and performance report Page 14 of 29
57 Strategic Priority (Objective) Corporate Objective 6, BAF Ref: AF2.8 Risk ID number: AF3526 Risk Description : Failure to achieve Value For Money (VFM) services and financial sustainability Executive Director Lead Director of Finance Executive Team Current Risk Score (L x C) 4 x 5 = 20 Risk Direction Unchanged Assurance Committee Finance & Performance Committee Date of last review: April 2017 Target Risk Rating 2 x 5 = 10 Target Gap Score 10 Concern Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: The Trust is currently working to a deficit plan, therefore is not currently financially sustainable Date When Target Risk score expected to be achieved Unable to quantify currently. The achievement of this for all services will only be realised with the achievement of a fully Integrated Care System Controls: Standing Financial Instructions (SFI s) in place Routine monthly service and financial meetings Regular monthly reporting to Executive Team and Board Monthly TEP reporting to Executive Team /Board Contract performance meetings Planned process Scheme of Delegation. Budgetary Systems and Procedures Appropriate insurance protection established Activity Planning income and activity Mitigating actions: (what more should we do?) Divisional action plans and recovery plans where required Implementation of CPT plan and formation of an integrated Care organisation Risk source Strategic Insight and Foresight Rational for Risk appetite The Trust is not willing to risk the ability of the organisation to achieve NHS Improvement requirements and financial sustainability Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): Strategic plan in place to work with other organisations to ensure sustainability going forward Audit Committee Finance and Performance Committee Trust Board Report. Internal and External Audit Reports to Audit Committee Annual (External) Audit. Annual Report to Trust Board on Financial Plans and Budgets for the new year Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps in assurance identified Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Reported at Board meeting aligned to performance trajectory and performance report Page 15 of 29
58 Strategic Priority (Objective) Corporate Objective 6 BAF Ref: AF2.9 Risk ID number: AF3527 Risk Description : Failure to achieve: a) Cash/ liquidity targets, b) Capital Investment within planned resources c) Capital Absorption rate targets Graph of Risk over time Target score Risk score Executive Director Lead Director of Finance Current Risk Score (L x C) 4 x 5 = 20 Target Risk Rating 2 x 5 = 10 Risk Appetite None low Moderate High Significant Risk Direction Unchanged Target Gap Score 10 Concern Assurance Committee Finance & Performance Committee Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: The Trust requires financial support to achieve liquidity targets and deliver the Trusts Efficiency Programme Date When Target Risk score expected to be achieved The delivery of the financial plan for 2016/17 should be achieved by April 2017 however this should be assessed in the context of the longer term financial plan Controls: SFIs and Scheme of Delegation. Budgetary Systems and Procedures Capital Budget Monitoring. Cash Flow monitoring and forecast against monthly profile over a two year forward look Treasury Management Policy Business case development controls. Monthly Board reports Rational for Risk appetite The Trust is not willing to risk the ability of the organisation to achieve NHS Improvement requirements and financial sustainability Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): Monthly finance reports to Finance and Performance Committee and Board Audit Committee reports (shadow investment committee) External Audit opinion on Accounts MIAA Audit Mitigating actions: (what more should we do?) Divisional action plans and recovery plans where required Implementation of CPT plan and formation of an Integrated Care Organisation Risk source Strategic Insight and Foresight Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps in assurance identified Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Reported at Board meeting aligned to performance trajectory and performance report Page 16 of 29
59 Strategic Priority (Objective) Corporate Objective 6, BAF Ref: AF5.1 Risk ID number: AF4059 Risk Description : Failure to deliver Trust Efficiency Programme Executive Director Lead Director of Finance Current Risk Score (L x C) 4 x 5 = 20 Risk Direction Unchanged Assurance Committee Finance & Performance Committee Date of last review: April 2017 Target Risk Rating 2 x 5 = 10 Target Gap Score 10 Concern Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: To be confirmed following Board development session Date When Target Risk score expected to be achieved Currently being reviewed to be reported at the next Board meeting aligned to performance trajectory Controls: Benchmarking with other organisations to ensure challenge and appropriateness of TEP Review of Lord Carter Report to ensure TEP reflects outputs of reports Ensuring valuing care efficiency programme is communicated effectively across the organisation Divisional structures performance manage delivery of TEP Mitigating actions: (what more should we do?) Revised programme of financial management Certify that all material non-recurrent TEP's have also been subject to a rigorous QIA Fully develop schemes to deliver the TEP target on a recurrent basis. Develop and submit to regulators milestones and financial modelling Review of clinical coding and impact on income. Risk source Strategic Insight and Foresight Rational for Risk appetite To be confirmed following Board development session Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): TEP Assurance Meeting Operations Board Finance and Performance Committee Trust Board Divisional Performance Groups Internal Audit VFM work covers arrangements in place to deliver TEP Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Level of recording of non-recurrent TEP versus recurrent TEP. Timely planning of TEP programme to ensure future delivery. Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Reported at Board meeting aligned to performance trajectory and performance report Page 17 of 29
60 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 4, Corporate Objective 5, Corporate Objective 6. BAF Ref: AF2.6, AF2.8 Risk ID number: CR 4201 Risk Description : Healthier Together Risk that the Trust will be in breach of its financial control limit due to the significant stranded costs caused by the reconfiguration of emergency and elective (cancer) general surgery as part of the Healthier Together Programme across Greater Manchester. Unless recurrent transformational funding is agreed the loss of income to the Trust would be far greater than the levels of costs which could be safely extracted. Currently GM is proposing to fund 2 years non recurrent stranded costs which would leave the organisation in serous financial deficit Executive Director Lead Director of Operations Current Risk Score (L x C) 4 x 5 = 20 Target Risk Rating 2 x 5 = 10 Risk Direction Unchanged Target Gap Score 10 Concern Assurance Committee SQOGG Date of last review: April 2017 Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Reconfiguration across Greater Manchester effecting services and financial income Date When Target Risk score expected to be achieved Unable to assess at this time Controls: (what are we currently doing about the risk?) Continue to engage with the Healthier Together Clinical Advisory Group and inform the Trust Executives of any significant financial and/or clinical implications. Ensure identified actions are worked through and completed Rational for Risk appetite The Trust is not willing to accept risk with the preference being for maintaining financial stability Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): Monitoring of data and financial position. Executive Management Team Board Reports Mitigating actions: (what more should we do?) Continue to attend HT clinical advisory group Input into key work streams, finance, human resources, cancer MDT. Contribute to and complete the outline business case and identification of stranded costs vs costs which can be influenced Completion of detailed bottom up analysis of stranded costs vs costs to be extracted. Risk source Operational performance and finance Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Ultimately the controls are third party reliant. Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Continued transformation and financial awareness. Page 18 of 29
61 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 3 BAF Ref: AF1.23 & CR3482 Risk ID number: CR 4183 Risk Description There is a risk of delayed patient diagnosis and/or treatment as a result of lack of availability of radiologists/radiology staff in the service. This is related to risk CR770, reduced sustainability of Radiology Services. This risk is multifaceted and impacts on activity and the ability of the department to undertake investigations within timescales, particularly to support the cancer pathways report investigations within timescales quality of service provided delivery of key objectives budgetary control reduction of backlogs (see risk no. 1880) Workload pressures - stress on the current workforce due to long working hours/complexity of work Executive Director Lead Director of Operations Current Risk Score (L x C) 5 x 4 = 20 Target Risk Rating 3 x 4 = 12 Risk Direction Unchanged Target Gap Score 8 Close monitoring Assurance Committee SQOGG Date of last review: April 2017 Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Current reported performance information Date When Target Risk score expected to be achieved July 2017 Controls: (what are we currently doing about the risk?) use of locum and agency radiologist reporting and direct clinical sessions EG ultrasound scanning and Breast interventions Radiographer reporting advanced practice Consultant Radiographer in post planned development of additional radiographer advanced practice outsourcing of CT and MR scanning and reporting use of WLI and ECP s Mitigating actions: (what more should we do?) submission of Radiology staffing paper to Executive Team in early 2017 Scoping exercise to identify possibility of support from local organisations across GM. Review of options to widen scope of practice/skill set of radiographer staff in the mid to longer term Risk source Risk register, and Operational performance Rational for Risk appetite The Trust is not willing to accept risk with the preference being for maintaining service stability Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): Reports to Divisional Governance meeting SQOGG Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Locum cover not sustainable in the long term due to high cost implication locum availability heavy reliance on very small substantive Consultant Team Anticipated effect of controls To be monitored closely to ensure impact is minimised Page 19 of 29
62 Strategic Priority (Objective) Corporate Objective 4, Corporate Objective 6 BAF Ref: AF4.8 Risk ID number: CR 4012 Risk Description : Banking Trojans now using Locky Ransomware and potential for data to be unavailable due to encryption of files Executive Director Lead Director of Performance & Informatics Assurance Committee IM&T Current Risk Score (L x C) 4 x 5 = 20 Risk Direction Unchanged Date of last review: April 2017 Graph of Risk over time Target score Risk score Target Risk Rating 2 x 5 = 10 Risk Appetite None low Moderate High Significant Target Gap Score 10 Concern Date of next review: May 2017 Rationale for current score: Current IM&T infrastructure and local intelligence Date When Target Risk score expected to be achieved Currently being reviewed to be reported at the next Board meeting aligned to performance trajectory Controls: (what are we currently doing about the risk?) ITIL (Information Technology Infrastructure Library) change Control process in place. IM&T Group structure. Risk Assessment in place with plans to mitigate. Strengthened structure to support service flow and ownership within IT. Mitigating actions: (what more should we do?) All user communication Propose to block macro s at point of entry into the Trust for all communications Review options to enforce disablement of Macros within Office or quarantine s with macros from none trusted sites User Training Information Security as part of mandatory training Review options to block the downloading of documents with macros enabled This would require significant investigation due to risk of impact. Purchase of software to reduce the risk further Risk source Operational performance Rational for Risk appetite The Trust is not willing to accept risk with the preference being for maintaining delivery systems Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): Monitoring of data/incidents. Executive Management Team Board Reports Exception Reports Audit Internal & External Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Ultimately the solution is operator reliant. Knowledge and Skills Gaps Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Continued stability and prevention of incidents. Embedding of best practice re user responsibility. Improved understanding, communication and visibility Page 20 of 29
63 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 2, Corporate Objective 3 BAF Ref: AF1.23 AF1.24 & AF4.6 Risk ID number: CR 4147 Risk Description : Ability to consistently sustain and maintain a workforce with capability and capacity to deliver community nursing services Executive Director Lead Divisional Directors and Head of Adult Services / Children, Young People & their Families Services Current Risk Score (L x C) Risk Direction 4 x 4 = 16 Unchanged Head of Assurance Committee Operational Group Date of last review: April 2017 Graph of Risk over time Target score Risk score Target Risk Rating 3 x 4 = 12 Risk Appetite None low Moderate High Significant Target Gap Score 4 Tolerable Date of next review: May 2017 Rationale for current score: Current IM&T infrastructure and local intelligence Date When Target Risk score expected to be achieved Unable to quantify at this time Controls: (what are we currently doing about the risk?) Continue to encourage self-management at all visits, particularly for administration of injections Review of existing workforce provision and exploration of options for transformation of services. Daily scoping of work across the whole service to try to minimise the mismatch between demand and capacity Mitigating actions: (what more should we do?) Engagement from finance and HR to support timely recruitment to current vacancies Review of resources and services to obtain a robust baseline and align existing skills and competencies with service requirements. Leadership model review Assess the need for further workforce development ensuring services are sufficiently resourced to meet service requirements Identify DN representation for each of the neighbourhoods and links with all GP practices. Continue to engage in and influence the development of integrated neighbourhoods and identify opportunities for new care models that transformation will enable Risk source Incidents, Complaints and Operational performance Rational for Risk appetite The Trust does not have any risk appetite for tolerating risk to quality of service Assurance: (how do we know if the things we are doing are having an impact and can we validate or evidence e.g.: Inspections; Committees; Working Groups; Reports; Monitoring Returns etc?): CRIG Service Quality and Operational Governance group and sub groups reporting to Quality and Governance Committee Regulatory compliance monitoring Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps identified Anticipated effect of controls (when is a reduction in risk trajectory expected /risk score reduced) Unable to quantify at the current time. Page 21 of 29
64 Strategic Priority (Objective) Corporate Objective 1, Risk Description : The ability to consistently apply, sustain and maintain processes relating to the management of medicines is compromised due to inappropriate prescribing of drugs/ineffective medicines management and/or theft/ loss of drugs Graph of Risk over time Target score Risk score BAF Ref: AF1.12 Executive Director Lead Medical Director, Director of Operations Current Risk Score (L x C) 4 x 4 = 16 Target Risk Rating 3 x 4 = 12 Risk Appetite None low Moderate High Significant Risk Direction Unchanged Target Gap Score 4 Tolerable Risk ID number: CR3472 linked with Risk CR656 Assurance Committee Quality and governance Committee, Operational Group Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: Current IM&T infrastructure and local intelligence Date When Target Risk score expected to be achieved It is expected that this risk score will reduce by Quarter 4 following assertive focus on medicines safety Controls: (what are we currently doing about the risk?) Medicines Management Committee Compliance with CAS Alerts for medicines Drugs and Therapeutic Group and Medicines Safety Work Stream Joint working arrangements with CCG re antibiotic prescribing Antimicrobial management Team Pharmacy stock control systems and procedures. Ward stock control systems and procedures. Review of Trust Medicines Policy Mitigating actions: (what more should we do?) Medicines management Patient Safety Work Stream and programme CQC assurance plan and agreed action Recommendations and actions following the MIAA Audit Report and the Review of Service to be completed. Risk source Incidents, Complaints and Operational performance Rational for Risk appetite The Trust does not have any risk appetite for tolerating medicines regulatory risks Assurance: Drug and Therapeutic Committee Service Quality and Operational Governance Group and sub groups reporting to Quality and Governance Committee which has the Chief Pharmacist as a member Safety Walk rounds Periodic progress reports to Safety Programme Board Audit Committee and Clinical Audit reports Internal Audit reviews regularly undertaken Pharmacy Dept. undertakes quarterly audits of compliance against Medicines Policy and Safety Thermometer monitoring against metrics. Regulatory compliance monitoring Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps identified Anticipated effect of controls Recommendations and actions following the MIAA Audit Report and the Review of Service will reduce the risk Page 22 of 29
65 Strategic Priority (Objective) Corporate Objective 1, Risk Description : Radiology requests on Lorenzo for in patients and out patients are being cancelled by the Radiology department without reference to the requesting clinician Graph of Risk over time Target score Risk score BAF Ref: AF1.12 Executive Director Lead Medical Director, Director of Operations, Current Risk Score (L x C) 4 x 4 = 16 Target Risk Rating 1 x 4 = 4 Risk Appetite None low Moderate High Significant Risk Direction Target Gap Score 12 Serious Risk ID number: CR4219 Assurance Committee Service Quality and Operational Governance Group Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: Current incident information and local intelligence Date When Target Risk score expected to be achieved Controls: (what are we currently doing about the risk?) Medicines Management Committee Patients that are cancelled are re-booked and letter sent to the Radiology department. Rational for Risk appetite The Trust does not have any risk appetite for tolerating clinical risks of this nature Assurance: Service Quality and Operational Governance Group and sub groups reporting to Quality and Governance Committee Periodic progress reports to local Quality and Safety Board Mitigating actions: (what more should we do?) Speak with and write to the management team in Radiology requesting immediate action. Radiology department are looking to invest in a system to solve the stated issue All Trust consultants to be ed informing them of the risk and potential compromise this may have to their practice Risk source Incidents, and Operational performance Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Radiology department are aware of the issue. Radiology state that they have a system in place to notify the relevant clinician. Clinicians are not aware of this system and have not received s. Anticipated effect of controls Recommendations and actions following and the review of system will reduce the risk Page 23 of 29
66 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 3 Risk Description: Introduction of IR35 tax regulations on the 6th April 2017 may increase existing issues relating to medical and nursing staff. BAF Ref: AF1.12 Executive Director Lead Medical Director, Director of Operations, Current Risk Score (L x C) 4 x 4 = 16 Risk Direction NEW* Risk ID number: CR4302 Assurance Committee Service Quality and Operational Governance Group Date of last review: April 2017 Target Risk Rating 2 x 4 = 8 Target Gap Score 8 Close monitoring Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Current staffing information and local intelligence Date When Target Risk score expected to be achieved This risk is still under assessment in relation to achievement of the target risk score Controls: (what are we currently doing about the risk?) Daily discussions with medical staffing team to optimise rotas. Substantive recruitment continues, including international recruitment Internal bank rates increased to try and mitigate financial impact on clinicians and encourage rota fill. Communication with clinicians to try and understand and mitigate their concerns/issues. Mitigating actions: (what more should we do?) Ongoing monitoring and oversight by Senior Managers and Clinicians Risk source Operational performance Rational for Risk appetite The Trust does not have any risk appetite for tolerating clinical risks of this nature Assurance: Service Quality and Operational Governance Group and sub groups reporting to Quality and Governance Committee and Trust Board Gaps in assurance and actions not being actioned (what additional assurances should we seek?) None identified Anticipated effect of controls Reduction in clinical risk and impact on services Page 24 of 29
67 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 6 Risk Description : Delays/inability to obtain microbiology results Risk of missing a significant infection due to delay/inability to obtain microbiology results and therefore risk of mis-treating a patient with an inappropriate antibiotics which may result in morbidity or death. Doctors time taken to chase results is a risk of less clinical time (more so at weekends/nights) to provide clinical care. Risk of delay in clinical decisions and prolonged hospital stay due to microbiology samples being delayed in being transported to Manchester, delay in being put for cultures and direct microscopy and delay in results being received from the Manchester Laboratory. BAF Ref: Risk ID number: 4212 Executive / Divisional Lead Medical Director Divisional Director Current Risk Score (L x C) 4 x 4 = 16 Target Risk Rating 1 x 4 = 4 Risk Direction NEW* Target Gap Score 12 Serious Assurance Committee Divisional Governance Meeting Date of last review: April 2017 Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Incidents Date When Target Risk score expected to be achieved Controls: (what are we currently doing about the risk?) Active chasing up of results. s to laboratory regarding risks of delay in samples being sent and viewed. Rationale for Risk appetite Inappropriate prescribing of Anti-biotics. Assurance: (how do we know if the things we are doing are having an impact) SQOGG Divisional Safety & Quality Group Mitigating actions: (what more should we do?) Directorate Manager for Diagnostic Services/Associate Divisional Director for Scheduled Care to liaise with CMFT regarding concerns. Risk source Clinical Risk Gaps in assurance and actions not being actioned Anticipated effect of controls (when reduction is risk trajectory expected /risk score reduced) To be agreed in line with Trust approach Page 25 of 29
68 Strategic Priority (Objective) Corporate Objective 5, Corporate Objective 7 Risk Description : Failure to ensure on-going compliance with NHS Improvement Provider Licence requirement BAF Ref: AF4.2 Executive Director Lead Company Secretary with Executive Team Risk ID number: AF3488 Assurance Committee Trust Board Current Risk Score (L x C) 4 x 5 = 15 Risk Direction Unchanged Date of last review: April 2017 Target Risk Rating 2 x 5 = 10 Target Gap Score 5 Tolerable Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Current IM&T infrastructure and local intelligence Date When Target Risk score expected to be achieved To be achieved and sustained on a continual basis Controls: (what are we currently doing about the risk?) Board reporting in line with FT provider licence requirements Board Financial reporting procedures fit for purpose FT metric performance framework Regular contact with Monitor and Board reporting re actions taken to maintain authorisation Mitigating actions: (what more should we do?) Continuous implementation of required actions by all staff at levels required Implementation of action plan re TEP identification and implementation of Trust Improvement Programme and Agreed Monitoring action Risk source NHS Improvement Provider licence requirements and Regulatory Monitoring Rational for Risk appetite The organisation is not prepared to accept risks to the ability of the Trust to maintain compliance with the Provider licence Assurance: Regular contact with NHS Improvement and Board reporting re actions taken to maintain authorisation Trust Board seminars Board Reports Financial governance infrastructure MIAA Audit review of Annual Report Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps in control identified Anticipated effect of controls It is anticipated that current controls and mitigations will align performance to ensure compliance Page 26 of 29
69 Strategic Priority (Objective) Corporate Objective 4, Corporate Objective 6 Risk Description: Failure to have in place an IM&T infrastructure and Service supporting the organisational objectives. (Linked to AF 4.8) Graph of Risk over time Target score Risk score BAF Ref: AF4.8 Executive Director Lead Director of Performance & Informatics Current Risk Score (L x C) Risk Direction 3 x 5 = 15 Unchanged Target Risk Rating 2 x 5 = 10 Risk Appetite None low Moderate High Significant Target Gap Score 5 Tolerable Risk ID number: AF3491 linked to CR3511 and 3604 Assurance Committee Quality & Governance Committee Date of last review: April 2017 Date of next review: May 2017 Rationale for current score: Current IM&T infrastructure and local intelligence Date When Target Risk score expected to be achieved Unable to quantify as assessment is still being undertaken in respect of additional IM&T risks transferred or arising out of the integration of services Controls: (what are we currently doing about the risk?) Director of Performance and Informatics Leadership. ITIL (Information Technology Infrastructure Library) change Control process in place. IM&T Group structure. Risk Register in place with plans to mitigate. Strengthened support service flow and ownership within IT Mitigating actions: (what more should we do?) Production of a detailed 1-3 year roadmap with 4-5 at a holistic level. Review of roadmap at key junctions, changes in business strategy or 6-monthly. Alignment of resource structure to meet the business model. Identification and mitigation plans reported via the risk board. IM&T Group in place to support developments across the Trust. Single points of failure to be identified and mitigated against. Departmental business plans in place in the event of an IT outage. Skills gaps to be addressed through training matrix. Funding for some elements of disaster recovery requirements Risk source Operational performance Rational for Risk appetite The Trust is not prepared to accept risks to the achievement of acceptable outcomes Assurance: Significant reduction in number of unscheduled outages impacting Trust services. Executive Management Team Board Reports Exception Reports Audit Internal & External (MIAA) Third party reviews and feedback Gaps in assurance and actions not being actioned (what additional assurances should we seek?) Lack in business understanding of the infrastructure supporting key services. Financial constraints. Technical refresh programme supporting the business strategy. Business strategy is not in place. Business leads not engaging with IT through Change Control and Service Desk. Skills Gaps. IM&T Group Anticipated effect of controls Continued stability as experienced over the last twelve months. Embedding of best practice utilising the ITIL model. Improved understanding, communication and visibility Page 27 of 29
70 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 2 BAF Ref: Risk ID number: CR3997 Risk Description : Inconsistent temperatures in NICU Clinical risk to babies dropping temperatures and nurses are giving, what could be considered as, conflicting advice to parents about wrapping babies. This is due to dropping temperatures in breastfeeding room and room 2 on NICU, due to fluctuating environmental temperature, especially at night and on cold days. This has the potential to lead to babies needing to be swaddled and/or put back into incubators. Executive Director Lead Director of Operations Current Risk Score (L x C) 5 x 3 = 15 Target Risk Rating 1 x 3 = 3 Risk Direction Target Gap Score 12 Serious Assurance Committee Service Quality and Operational Governance Group Date of last review: April 2017 Date of next review: May 2017 Graph of Risk over time Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Incident occurrence Date When Target Risk score expected to be achieved It is expected that this risk score will reduce by Quarter 4 following assertive focus on medicines safety Controls: (what are we currently doing about the risk?) Medicines Management Committee Breastfeeding room: doors are kept closed. Wall thermometers in situ; temperature monitoring is ongoing. Staff are advised to keep the door closed, when this is safe and feasible. Wall thermometers in situ; temperature monitoring is ongoing. Estates Manager continues to lead on the management of this risk; plan of action to fully rectify this issue remains outstanding. New vents installed to regulate temperature. Mitigating actions: (what more should we do?) Interim Head of Estates will review the building management system for anomalies. Director of Estates and Facilities has oversight of the NICU risk assessment to ensure awareness and for reflected risk assessment on estates to ensure cohesive team work to mitigate the risk. Risk source Incidents, Rational for Risk appetite The Trust does not have risk appetite for tolerating incidents of this nature Assurance: Service Quality and Operational Governance Group and sub groups reporting to Quality and Governance Committee Safety Walk rounds Periodic progress reports to local Quality and Safety Board Gaps in assurance and actions not being actioned (what additional assurances should we seek?) No gaps identified Anticipated effect of controls Monitoring is initially demonstrating controls may be stabilising the issue, it is expected the risk should be reducing once controls are demonstrating consistent compliance Page 28 of 29
71 Strategic Priority (Objective) Corporate Objective 1, Corporate Objective 6 BAF Ref: Risk ID number: CR4158 Risk Description: Transfer of the Microbiology laboratory Services to Manchester Royal Infirmary to begin earlier than anticipated, commencing October 2016, and relates to IT issues with Telepath and ICNet connectivity (IP Electronic Surveillance System). No ICNet connection for a period of 27 days whilst remedial works to solve the connectivity Issues takes place Executive Director Lead Chief Nurse Current Risk Score (L x C) 3 x 5 = 15 Risk Direction Unchanged Assurance Committee SQOGG Date of last review: April 2017 Target Risk Rating 3 x 3 = 9 Target Gap Score 6 Close monitoring Date of next review: May Target score Risk score Risk Appetite None low Moderate High Significant Rationale for current score: Current IM&T infrastructure and local intelligence Graph of Risk over time Date When Target Risk score expected to be achieved To be reviewed once the connectivity issues is resolved Controls: (what are we currently doing about the risk?) Notification by (NHS.net accounts) on a daily basis plus additional phone call with urgent results Manual opening of cases into ICNet and inputting of results. Rational for Risk appetite The Trust is not willing to accept risk of disruption brought about by business contingency and maintains an overall preference for safe delivery options Assurance: Provision of manual systems Daily monitoring of communication Mitigating actions: (what more should we do?) Business continuity plans in place Risk source Restructuring of service delivery of Microbiology to Manchester Royal Infirmary Gaps in assurance and actions not being actioned (what additional assurances should we seek?) External pressure and decisions influence the ability of the Trust to limit action Anticipated effect of controls With proposed actions implemented the Risk will reduce from a Major to a Moderate in Severity although will remain as a "red" risk Page 29 of 29
72 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 April 2017 Agenda Item 7e Title Sealed Documents Quarter /17 Sponsoring Executive Director Tom Neve Author (s) Tom Neve Purpose Previously considered by To notify the Board of the documents to which the Trust seal has been applied in Quarter 4 This report has not been considered by any other meeting Executive Summary The Trust s Seal has been applied on three occasions during Quarter 4 of the 2016/17 financial year Related Trust Objectives Objective 6 To deliver against the required local/national regulatory frameworks and standards, in addition to securing the most effective and efficient use of resources to deliver services that we provide directly or indirectly through out partner organisations Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? N/A Complies with the Trust s Standing Orders N/A N/A N/A Action required by the Board To note that the trust s seal has been used on three occasions during Q4 of the 2016/17 financial year
73 Sealed Documents Quarter 4 of 2016/17 The Trust s Standing Orders require a report to the Trust Board identifying all documents to which the Common Seal has been applied during the preceding quarter. These documents were secured and sealed under Tameside and Glossop Integrated Care NHS Foundation Trust. The Trust s seal was applied on the following occasions during quarter 4 of the 2016/17 financial year: 1. Lease for Stamford Unit from L and M 2. Deed of novation Consort Healthcare 3. Lease for Stamford Unit (replacement documents)
 John Fletcher, Director of Quality and Governance Purpose To note/receive Previously considered by Not applicable")
74 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item Title Sponsoring Non-Executive Director 8a Quality and Governance Committee Aggregated learning summary report attached Ms T Kalloo Author (s) John Fletcher, Director of Quality and Governance Purpose To note/receive Previously considered by Not applicable Executive Summary Summary aggregated learning report Related Trust Objectives Relates to all Corporate objectives Risk Assurance risk impacted upon Relates to all areas of risk Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? None identified None Not applicable Not applicable Action required by the Board The Board is asked to receive and note the Summary notes of the walkrounds undertaken and the Summary Aggregated Learning Report.
75 Quality and Governance Committee The Quality and Governance meeting took the form of assurance walk rounds. Walkround teams were convened with Non-executive Directors and Executive Directors supported by Quality and Governance Unit. The walkround process was unannounced to the areas visited. Real time assurances were sought and received on the implementation of work previously reported through the Governance processes to the Committee and Trust board. Members fed back that the process had provided assurance of implementation of the reported work programmes and the progress made to improve and ensure Quality and Safety of service provision. The reports from these walkrounds including any inconsistencies identified will be feedback to the Clinical and service leads to inform further improvement. The specific areas of focus in the walkrounds were to seek assurance that the actions identified from the CQC assurance plan had been implemented, to seek assurance on the pilot projects commenced and production of discharge letters in some medical areas were delivering the anticipated benefits and to speak to Porters and domestic staff following the transfer to an in house service. The areas visited were Maternity Ward 27, Neonatal Intensive Care unit (NICU), Medical Wards 31, 40, 41, 42, 46 the Whitehouse and a number of Domestics and Porters who were available. For each area the context of the review was identified and aligned to issues and previous assurance reports to the Committee with potential lines of enquiry being identified in relation to Observation, conversations with patients, relatives and staff as appropriate. The visit to the Maternity ward and the NICU are both located in the Charlesworth Building, the general fabric of the Charlesworth building was noted as a concern which would require further attention and assessment, and be considered in the estates strategy. However the contrast of this part of estate in the context of the newly upgraded Antenatal suite was noted. Despite this the feedback received from Patient and family members spoken to in both areas very positive about the care, treatment and services received. In the maternity ward the visitors were assured that the actions planned following the CQC inspection had been taken relating to replacement of furniture and fridge temperature monitoring appeared to be consistently monitored. The impact of the new ward manager was also noted. However, it was proposed that the ward environment could be further improved and decluttered with further actions agreed. Consideration was also discussed for what further work on the ward could take place to upgrade the facilities. Within the NICU unit it was noted that whilst most CQC actions were completed, some action were still being progressed, and improved ward communications were being refined and a communications book to be implemented. The issue of temperature control in one area was still a concern. Work to monitor this with Estates and Facilities had been progressed and changes made, however the issue had not been resolved, and was currently on the Risk register. It was agreed that the executives would escalate and review further with the Estates team to understand. In the medical wards the review team split to cover a greater number of areas. On ward 31 it was noted that there was a new ward manager on the ward and band 6 nurse being recruited to further strengthen the ward leadership. It was noted that the area was a specific focus of the Chief Nurse who was overseeing a weekly meeting and improvement work being undertaken which had commenced. This included staff recording feedback on what the shift had been like to work on a daily basis on the ward. Page 2 of 7
76 The ward felt calm and well organised, the CQC specific action re fridge temperature monitoring was taking place consistently, and positive feedback was again received from the patients spoken to. However, it was noted that recruitment of permanent staff continued to be an issues and the use of temporary and locum staff a cause for concern which was monitored several times daily and reported and escalated through the bed meetings to ensure safe staffing levels were maintained throughout the whole site. On Ward 40 the Respiratory ward a pilot project using Physiotherapists to support staffing resources appeared to be working very well and had been well received by the team members spoken to, and was providing addition support and training for ward staff to enhances their skills with the therapies offered on the ward. Whilst it was acknowledged that further nurse recruitment was required and being progressed, it was noted that pilot had developed good team working across disciplines. Assurance was noted on the other CQC actions and the feedback from patient was overwhelmingly positive. On ward 41 and 46 again the environment was reported to appear calm and well managed calm and well managed, assurance was noted that the CQC actions appeared to be consistently implemented and the new resuscitation trollies were noted to be in place and being monitored, again the patient feedback was positive. On ward 41 the area of the ward assigned to dementia care included a memories room used which the review team were impressed with. On Ward 42 Staff interaction with the patients was excellent, and the feedback again was positive, however there were some inconsistencies in the completion of some of the actions required noted, and the ward environment felt less well organised and cluttered. The issues identified were discussed with the Ward Manager and matron of the ward to identify support needed some delays in provision of discharge letter production had been identified and is being managed by the divisional management team. The improvement work achieved in the Whitehouse over 12 months ag was noted to have been maintained, and the staff spoken to were overwhelming ley positive about the continues achievement of the turnaround times for the discharge letters transcription undertaken. No delays were identified. It was noted that the Whitehouse building could do with some external maintenance which may benefit the internal state of the building. Of particular note was the staff notice board at the entrance which identified current information and the teams position with all mandatory training updates all staff talked positively about being up to date with all mandatory training and appraisals. The engagement with porters and domestics included two Porters who were new and had only been here four months and the other only two weeks. Both were very positive with no negative word to say. They had undertaken local induction and training. However the four domestics whilst happy with their working environment and the equipment available provided feedback that nothing had changed and was a lack of communication of what was taking place in the Trust. They identified that they met their supervisor regularly but had not had regular team meetings, however they had been notified that monthly team meetings were to commence, and hoped that this would improve communications. The issue was raised around the buffing of floors; Domestics informed the team that they are not allowed to buff as patients with dementia may think the shiny floor is water, however they did not believe they could remove all the marks on the floor without the buffers, and they were concerned that this may reflect on the perceived cleanliness of the Trust. This was agreed to be escalated with the management team. It was noted that the Domestic s and Porters spoken to were a credit to the service they all went and helped the patients, their attitude and demeanour was first class. Page 3 of 7
77 The committee noted the feedback and assurance provided. Specific feedback will be provided to the areas visited and issues identified escalated on the day of the visit or with the management teams Trish Kalloo April 2017 Page 4 of 7
78 Summary Aggregated Learning information Initial Data for March 2017 **still being validated Incidents reported March 2017 ** New incidents (reported in month- includes delayed reports) 938 Reported with Moderate harm 20 Reported with Major harm 2 Reported with Catastrophic harm 1 Never Event 0 RIDDOR reported incidents 1 Complaints and PALS issues New Complaints 40 New MP enquiry 0 New External complaint 0 New Enquiry 2 New PALS issues 154 Total issues received 199 Re opened Complaints 4 Issues /cases responded to 203 Complaints %age closed in agreed timescale 92% Average time to close issues/cases (working days) 12 Number issues time of monthly report 105 Ombudsman Cases upheld 0 Other Indicators Mortality reviews required 51 Initial Mortality reviews undertaken at time of report within 14 days 51 Inquests with TGH involvement closed /heard 7 Coroner-Prevention of Future Death report (Regulation 28) 0 Potential claims received in month 18 StEIS reports - Internal issue 7 StEIS reports - Never events 0 Safeguarding Adult cases - Allegation on hospital care 14 Safeguarding Adult cases - Allegation on other care 4 DOLS - Cases reported to Supervisory Body 10 PREVENT - Cases reported 0 Compliments 891 Page 5 of 7
79 Aggregated Dashboard December 2016 February 17 dashboard Incidents reported December 16 January 17 February 17 4 month avg trend New incidents (reported in month- includes delayed reports) Reported with Moderate harm Reported with Major harm Reported with Catastrophic harm Never Event RIDDOR reported incidents month avg trend Top Incident Causes reported with Moderate harm and above February 2017 Slips/Trips/Falls Pressure Ulcers Specimen Error Medication Failure To Follow Procedures Staffing Issues Complaints and Concerns December 16 January 17 February 17 4 month 12 month avg trend avg trend New Complaints New MP enquiry New External complaint New Enquiry New Concerns (PALS) issues Total issues received Re opened Complaints Issues /cases responded to Complaints %age closed in agreed timescale 96% 96% 97% Average time to close issues/cases (days) Ombudsman Cases upheld Complaints & Concerns by Month by Directorate Top issues reported in February 2017 related to Clinical Treatment Communications Prescribing Admissions & Discharges (Excl Delayed Discharge) Privacy, Dignity And Wellbeing Patient Care Page 6 of 7
80 Top issues reported in February 2017 related to Communications Appointments Clinical Treatment Values And Behaviours (Staff) Other Admissions & Discharges (Excl Delayed Discharge) Indicators December 16 January 17 February 17 4 month avg trend Mortality reviews required Mortality initial reviews undertaken (@time of reporting) Inquests with TGH involvement closed /heard Coroner-Prevention of Future Death report (Rule 43 ) Potential claims received in month Themes reported Morality themed feedback to Division for learning from reviews Consistent use of NEWS Record keeping standards DNAR Re-assessment and of patients Inquest and Coroner n/a Indicators December 16 January 17 February 17 4 month avg trend StEIS reports Internal issue StEIS reports Never events Safeguarding Adult cases Allegation on hospital care Safeguarding Adult cases Allegation on other care DOLS - Cases reported to Supervisory Body PREVENT Cases reported to Supervisory Body Compliments Themes reported 12 month avg trend 12 month avg trend StEIS Related to Infection control and patients admitted with Pressure ulcers Care related issues as above Adult Safeguarding allegations/issues relate to Pressure Ulcers General Care Physical Abuse Self-Neglect Page 7 of 7
81 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item 8b Title Minutes of the Audit Committee held on 21 ST February 2017 Sponsoring Executive Director Claire Yarwood - Director of Finance Author (s) Purpose Claire Yarwood - Director of Finance To inform the Board of the discussions held by the Audit Committee at its meeting in April Previously considered by Not previously considered. Executive Summary : The attached reflect the minutes of the Audit Committee which met in April Related Trust Objectives To deliver against the required local and national frameworks in order to meet all the requirements of the Trust s operating licence and the commissioners requirements Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? 723 Failure to ensure on-going compliance with the terms of FT Authorisation In breach of Licence None No Not Applicable Action required by the Board The Board is asked to note the minutes from the Audit Committee. 1
82 AUDIT COMMITTEE AGENDA ITEM 3 Date of Meeting: 21 st February 2017 Time: 9.00 am Location: Silver Springs Meeting Room Present Position Initial Mrs A Dray Non-Executive Director (Chairperson) AD Mr M Taylor Non-Executive Director MT In Attendance Ms C Yarwood Director of Finance CY Ms L Hulme Assistant Director of Finance, Financial Services LH Mr T Neve Trust Board Secretary TN Mr J Fletcher Head of Assurance & Governance JF Mrs D Chamberlain KPMG DC Mr M Holden Partner Governor MH Mrs J Bowles Porter Public Governor JBP Mr M Husaini Public Governor MH Mr N McQueen Mersey Internal Audit Agency Anti-Fraud Manager NM Mr Steve Connor Mersey Internal Audit Agency SC Ms S Dowbekin Mersey Internal Audit Agency SD Apologies Ms Karen James Chief Executive KJ Mr P Connellan Chairman PC Mrs T Kalloo Non-Executive Director TK Mr P Weller Director Quality and Governance PW Item No Description Action 01/2017 Apologies As above. 02/2017 Declaration of Interests None declared 03/2017 Minutes of the meeting held on 8 th December 2017 The minutes were approved subject to the following amendments: 57/2016 the sentence SD confirmed that the following Management requests have been finalised; Consultant Job Plans, Medical Locums and Well Led Self-Assessment Workshops is to be corrected to read SD confirmed that the Management request re Consultant Job Plans has been finalised. Those for Medical Locums and Well Led 2
83 Self-Assessment Workshops are outstanding 04/2017 Action Log The action log has been updated as per the discussion and is attached. 05/2017 Internal Audit Progress Report SD provided an update on the latest Internal Audit Progress Report and outlined the following key points. Work has been completed on follow ups and a management request for medical locums. As previous discussed at the Committee, management requests will be presented by management at a later date. The follow up report has two purposes, one to review the internal processes for managing internal audit recommendations and also to undertake an independent assessment of the position of the Internal Audit recommendations. It has been determined that the Trust has a robust process for monitoring recommendations and the independent assessment reconciles to what the Trust is stating. There are a number of pieces of work in progress and the overall plan is on schedule for completion by the end of the financial year. CY advised the Follow Up report has been presented to the Executive Team meeting. The outstanding items were discussed and it was stressed and acknowledged that any changes to the recommendations are documented to provide evidence for scrutiny Audit Committee Update The report was provided for information. awareness. SD highlighted the upcoming events for Assurance Framework Benchmarking Report The report was provided for information and consideration. SD highlighted the key points for information. The review focussed purely on Assurance Frameworks and no significant issues have been identified within the process. AD enquired if having a high number of risks is positive or negative, SD confirmed that it is not a negative sign as the risks are organisationally specific and reflects how the Board Assurance Framework is used. SC explained it is more about what works for the Trust and the average number is around fifteen and no judgement calls are being made in terms of what is right or wrong. CY advised that given where the organisation has come from in terms of being a Keogh Trust and the previous lack of 3
84 reporting around risks and issues the report is helpful to the Board around quality and safety as well as the financial position. JF added the report reflects the progress the organisation has made and confirmed high numbers are expected due to the integration and transformation work being undertaken. MT acknowledged the report endorses the fact that the Trust embraces risk culture and actions are undertaken to address the issues External Quality Assessment SC presented the report and explained there is a mandatory requirement for all Internal Audit Providers to have an independent assessment against the standards. As a result MIAA have been assessed as being fully compliant with the standards, with some areas for enhancements being identified. 06/2017 Anti-Fraud Progress Report NM presented the report and outlined the items of interest. The national fraud initiative has highlighted that the Trust had just under 500 duplicate matches in total and work is ongoing to resolve the issues. The Register of Interest is being reviewed and NM and SD have attended a Divisional Operational Board to provide information on conflicts of interests, register of interest and general fraud awareness training. NM has attended a Cardiology Business Group to provide a presentation of fraud awareness which included information on conflict and registers of interest and which interests need to be reported to the Trust. The local proactive protection exercise into Supplies and Stores is ongoing and the results are being written up and will be reported to the next meeting. MT asked if the exercise has highlighted any serious concerns. CY acknowledged there are some issues regarding protocols to work on but there are no serious issues from fraud perspective. It has been concluded that this exercise should have been conducted by Internal Audit rather than the Fraud Investigator. MT enquired if there is a material issue with regards to finance. CY advised she is not aware of any issues at this stage. There is one ongoing investigation from 2015/16 which has now been passed to the CPS to consider prosecution. The second investigation is in the initial enquiry stage Self Review Toolkit 4
85 NM presented the draft version and highlighted the changes to the report and asked for approval to submit to NHS Protect. AD highlighted the item which states that effectiveness is monitored by the fraud Survey and enquired whether a high number of responses have been received. NM replied that the responses have not been high. CY suggested exploring the options to introduce another method to collect the information. AD asked if conflict of interest has been rated as Green due the amount of work being undertaken to ensure the information is presented to groups of staff. NM confirmed his continued attendance at Divisional meetings (Medicine and Surgery) and advised that he is also presenting at meetings with Community staff. AD enquired how the national framework agreement related to the agency cap. CY advised that a national review of Agencies has been undertaken and a national agreement has been obtained to keep the prices under the cap. This is a way of nationally controlling the Agency prices. If Agencies meet the nationally set framework they can apply to be added to the Framework. If Agencies not on the Framework are used a report has to be submitted to NHSI. MT requested information regarding the internal challenge process which informed the outcome of the self-review. NH stated that NHS Protect challenge the submission should an inspection take place. CY acknowledged there are currently no internal forums to investigate issues around fraud and the options on how counter fraud will be utilised across the Acute and Community services are to be explored. CY outlined the benefits of the Anonymous telephone contact number. SC explained an internal Quality Assurance review across a number of clients has been undertaken which included calibration across the piece and advised this would provide some degree of assurance in terms of how the Trust stands against others and the consistency in terms of the way actions are undertaken Fraud Investigations Benchmarking Following the benchmarking exercise it has been determined that the Trust s policies and procedures provide the necessary information regarding reporting of any potential fraudulent issues. NM confirmed the Trust is comparable with other Trusts regarding the types of fraud reported. 07/2017 External Audit Audit Plan and Fees DC presented the report and outlined the key points. Materiality levels are 3.25m which has increased from last year and this is to recognise the increase in income following the transfer of the Community services. This means working towards a performance materiality of 2.4m and audit differences 5
86 over 160k will be reported. NHS income and NHS receivables is a new significant risk which recognises the uncertainty around Sustainability and Transformation funding and also the incentives for Commissioners and Providers to hit the control total and how this may impact on to agree of balance for the process at year end. Valuation of property plans and equipment was also considered a significant risk last year, due to the high value and potential for material misstatement. It has been recognised that the Trust has had a valuation in year and a paper is to be presented to a future meeting and will be reflected appropriately in the Accounts. Fraud risk from the management over ride controls and fraud risk from revenue recognition are the significant risks required by the Auditing Standards and all the audit processes are tailored to ensure they are covered throughout the audit. The next responsibility is reaching the value for money conclusion which is described in the report and the arrangements in place to achieve the outcomes are reviewed. The first initial risk assessment for the BFM value for money risks is the Management of the Trust s cash position and the second risk is the delivery of the Trust Efficiency Programme which is similar to the previous year and is around achieving the financial position and ensuring the correct arrangements are in place. The integration of Community services has been assessed as a risk which recognises there has been a significant transaction in-year as a new area of business has been taken on. The content of the Quality Account is reviewed to ensure it matches requirements and also to ensure this aligns to other information available. Two mandated and one local indicator (chosen by the Governors) are also reviewed to check the data quality to ensure this is reported appropriately. AD asked for clarity around the requirements for the Quality Account. JF replied that the work required for the Quality Account continues throughout the year, and the requirements for the Quality Account have not changed substantively. Therefore, the information received via the Quality and Governance Committee will support the vast majority of the metrics which are required to be reported through the Quality Accounts. Metrics which are not submitted to the Quality and Governance Committee are presented to Trust Board or Finance and Performance Committee as the information in the Quality Account also includes financial and performance information. AD enquired if any issues had been identified with outstanding debts with other NHS organisations. CY confirmed there are currently no issues to report. 6
87 7.2 - Technical Update DC highlighted two items for which actions should be considered, Publication of the national tariff and also the very Senior Manager Guidance. CY provided an update and advised that the new HRG 4 tariff has been implemented and the contract has been adjusted accordingly. As the contract has moved to a block contract there will be no impact in-year. The Senior Manager guidance has been adhered to in relation to the appointment of an Interim Chief Nurse. 08/2017 Charitable Funds Minutes 15th November The minutes were noted. 09/2017 Agreement of Final Accounts Timetable 2016/17 LH provided an overview of the timetable and advised the report highlights key submission dates for the Committee and includes the Audit Committee dates for April and May. A report is to be provided to Finance and Performance Committee prior to sign off and the new Non-Executive Directors are to be invited to attend. The Committee approved the timetable. 10/2017 Losses and Special Payments Quarter 3 LH advised that the total losses and special payments as at December is at 22k with thirteen new cases being reported. MT asked if the Pharmacy losses relate to medication which has gone over the expiry date. LH confirmed this is correct and advised that the high number stated for October was due to a manual input error which has since been corrected in the report. 11/2017 Update on work plan for Annual Governance Statement JF advised the work plan has been developed to provide context around how the Quality Governance Framework is routinely monitored and assessed throughout the year. The framework within the paper articulates the requirements and provides a commentary on how the requirements are being fulfilled. The point of note since the previous report is the provision of Community Services. CY reiterated this piece of work is not a requirement but is an example of really good practice which provides assurance that the work is being undertaken all year round and commended JF/PW and the Governance Team for the quality of the work produced. AD asked if issues are incremented each time. JF confirmed it is an incremental document and advised a lot of information will be iterative from year to year and the systems in place will identify assurance in-year that systems have been reproduced or recycled. 7
88 AD cited the statement that review work is taking place to support two or three areas and asked if there is an end point of the review to support the final version. JF advised a comprehensive Community Service review has been undertaken which involved over sixty staff and fifty visits. The review also included an MIAA audit and a report is to be published around the learning disability element and the results will inform the Community Services provision, provide assurance and highlight actions which may need to be taken around the requirements for CQC domains. JF advised no significant concerns were raised. The issues highlighted were around strengthening leadership structures within Community and these are currently being realigned within the organisation. It is anticipated that before the end of March a report will be available for distribution to Divisional Teams to provide an understanding of what actions are required. 12/2017 Review of the Risk register BAF recommendations JF highlighted the proposed changes to the Risk Management process and reporting arrangements and advised the proposal has been submitted to Risk Management Committee and is to be presented to Quality and Governance Committee and Trust Board. A review of the Risk Management processes and systems has been undertaken and advised that one of the concerns which has been identified is that focus is given to how the risks are graded and it is proposed to introduce the concept of a target risk gap score to refocus the organisation s view on which risks need to take priority. A change to the way the symbols are used to provide additional clarity has been suggested and the risk appetite has been rationalised. This will ensure the target risk rating will be vigorously assessed and the target scores set appropriately. This will also allow the opportunity for the Board and other elements of the organisation to apply a different rigour to the implementation and mitigation actions to achieve realist expectations of risk reduction. The other element to be included within future reports is the concept of heat mapping. The Committee were asked to adopt the revisions and recommendations to significantly strengthen the risk assessment process. AD enquired as to where the initiative came from. JF advised the motivation came from the need to reduce the risk exposure and highlight the opportunities for risk reduction. If the target risk is aligned correctly the appetite for managing the risks can be determined. DC advised that organisations are starting to look at risk appetite and is recognised as good practice. DC suggested a trajectory for the risk over time is included. JF confirmed that the anticipated target achievement date is to be added to the report. 8
89 MT commended the paper and observed the revisions provide more granularity and stated the gap scoring matrix is a good idea. MT also suggested working out the costs of managing this type of model. JF replied that if the focus is directed to the right place and people ask the right questions it should cost less overall. MT commented in relation to Trust Board risk target score metric that he felt it is unusual to see a gap score of 10 being the maximum score as all others have a range. JF explained the logic for the score given the maximum risk score is 25. However agreed that it should probably indicate greater than 10. A gap score of this magnitude scores would indicated that significant mitigation is possible but not yet achieved if the gap score is realistic. MT stated his approval of the addition of the graph of risk over time within the main papers. MT asked who sets the risk appetite and how is it agreed. JF explained Trust Board would set the this for the BAF risks and in terms of reviewing the Board Assurance Framework on an annual basis is one of the calibrations that if the report is accepted would be imposed by adopting the process. AD enquired how it will be determined that the changes are correct as there will not be a baseline of the movements of the risks. JF explained that the heat map analysis will be undertaken quarterly for the Board Assurance Framework risks. JF advised one of the solutions is to have a pre-mitigation risk and a post mitigation. CY suggested having a post project evaluation. The final document will be presented to a Trust Board development session for discussion and final approval. JF 13/2017 Outcome of Consultation of Managing Conflicts of Interest in the NHS TN provided a verbal update and advised NHSE have produced new guidance and the link will be distributed to all the Non-Executive Directors. The link is also to be added to the intranet and the policy is to be amended to include the revisions. TN Staff awareness sessions are to be arranged, along with including the information within payslips. 14/2017 Governance of the Care Together Programme AD explained a significant amount of work is being undertaken strategically around changes to the organisation going forward and expressed concerns around the understanding of how the Care Together governance arrangements mapped into the Trust s governance arrangements in order to be sighted on risks, opportunities and costs etc. CY highlighted an issue with the timing for approval of the Care Together Programme Board minutes. A meeting is to be arranged between AD and CY to discuss the issues in more detail. AD/CY 9
90 15/2017 Asset valuation and Impairment LH stated that the valuation of the assets has been identified as a significant risk and the paper details the actions undertaken to value land, buildings and equipment. The District Valuer has been on site and completed the valuation. Within the calculation a gross internal area has been used to calculate the valuation and this has changed from previous years and this is due to estates undertaking a more thorough calculation on the estates software system. Each change has been reviewed by Estates, finance and the District Valuer. The element of the building which is through the PFI has not previously been valued exclusive of VAT and as a result has reduced this element of the building value. The figures are indicative as they are calculated on the indices and when the valuation was performed it is showing that the valuation of the land and buildings have increased by around 6m. The valuation of Equipment has to ensure the assets are still in existence and in use and also that there are no indictors that the asset has impaired. A paper has been presented to the Executive Team meeting and Operational Board which outlines the responsibility for staff to manage the assets and communicate to Finance any indications of any potential impairing event. A list of the assets has been sent to each responsible Department Manager to determine whether the equipment is still in existence and in use. CY reiterated the issues around the gross internal area as this is a material change and advised that the organisation did not have any mapping software prior to the recent purchase of MICAD. A robust assessment has been undertaken and is now valued appropriately. AD asked how this cross references to the work which External Audit undertakes. DC advised it is recommended a paper to be brought to Audit Committee to provide the information and assurance and explained as part of the work the information will be taken and discussed with the District Valuer to separately gain assurance. The issue around the VAT on the PFI buildings will also be discussed. CY advised that Trusts are only required to complete a full valuation every five years and desk tops valuations can be undertaken in between. AD asked what impact will the 6m increase have on the Trust. CY confirmed this will increase the value on the balance sheet. LH explained it could also increase the depreciation charge which will have an impact on the I&E account. Once the indices have been completed the changes will be reflected within the accounts and the impact will be forecast. LH explained that the reduction in the PFI is classified as an impairment and this will 10
91 technically increase the deficit, but does not affect our control total as we are monitored against the deficit before technical adjustments. MT asked if this will create any issues with any of the External bodies. CY confirmed this is not the case. MT asked for assurance that the equipment audit has a robust process in place. LH explained the process and advised responses are being chased weekly and assistance has been offered to all departments. CY stated that this exercise will highlight any significant issues and actions can then be put in place to address these moving forward. The Committee approved the content of the report. 16/2017 Review of Audit Committee Work plan 2017 The workplan was amended as per discussion. 17/2017 Effectiveness of the Committee AD and LH to liaise to discuss and agree the process. AD/LH 18/2017 Internal Audit procurement MIAA representatives left the meeting for this agenda item. CY advised that the contract with MIAA is due to expire at the end of May and explained a procurement exercise for the internal audit function would normally be undertaken. However, on a Greater Manchester basis through the GM Health and Social Care Partnership a number of back office functions are being reviewed to establish if they can be provided more economically across Greater Manchester. Greater Manchester has been awarded Path Finder status which is a DoH and NHSI process which puts scrutiny, review and funding to evaluate whether systems should bring together back office functions. One of the assets in Greater Manchester is perceived to be Mersey Internal Audit Agency who work for a significant number of organisations across the North West. The proposal is for MIAA to become hosted by Greater Manchester and have an agreed plan over a three year period. The recommendation from the GMHSCP is for any Trust due to go out to the market for Internal Audit services over the next year to put this on hold until the process is put into place. The paper provided articulates the options available in terms of procurement methodology and provides a recommendation for option C to be undertaken. Option 11
92 C is to procure under the framework for one year with the possibility of extending for a further year if necessary. The paper has been presented to the Executive Team meeting and option C was recommended. The Audit Committee were asked to agree the recommendation. MT agreed to the recommendation in principle and asked if it is considered that MIAA provide value for money for the service they currently provide to the Trust and asked if they are challenging enough. CY stated in her opinion MIAA do provide value for money as the added element is the benchmarking across other organisations in the North West, development events are also available often at no charge to the Trust which also provide a network opportunity. TN agreed that the Trust gets value for money and added they can be challenging when necessary. DC confirmed that in her experience MIAA are providing good and challenging reports. The Committee endorsed undertaking Option C. 19/2017 Attendance Matrix The matrix was noted. 20/2017 Care Together Programme Board Minutes These were discussed under item 14/ /2017 Any other business There was no other business. 22/2017 Summary of points to escalate to Board Annual governance statement Review of the Risk Register and BAF Conflict of interest policy Asset valuation and impairment Internal audit procurement 23/2017 Date of Next Meeting: 25th April 9.00am Silver Springs Board Room 24/2017 Private Discussions with Internal and External Auditors 12
93 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item Title 8c Minutes of the Finance & Performance Committee held on 16 th February Sponsoring Executive Director Claire Yarwood - Director of Finance Author (s) Purpose Claire Yarwood - Director of Finance To inform the Board of the discussions held by the Finance & Performance Committee at its meeting in February Previously considered by Not previously considered Executive Summary : The attached reflect the minutes of the Finance and Performance Committee which met in February Related Trust Objectives Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? 5 Develop a strategic plan to secure clinical and financial sustainability for the Trust in conjunction with the Trust s strategic partners and key stakeholders 7 to deliver against local and national frameworks in order to meet all the requirements of the Trust s operating licence and the commissioners requirements. 723 Failure to meet, deliver Trust s financial plan In breach of Licence None No Review financial sustainability of organisation Action required by the Board The Board is asked to note the minutes from the Finance & Performance Committee. 1
 MT Mrs A Dray Non-Executive Director AD Mrs A Higgins Non-Executive Director AH Mrs C")
94 FINANCE AND PERFORMANCE COMMITTEE Agenda item 2 Date of Meeting: 16 th February 2017 Time: 2.00 pm Location: Board Room, Silver Springs Present Position Initial Mr M Taylor Non-Executive Director (Chair) MT Mrs A Dray Non-Executive Director AD Mrs A Higgins Non-Executive Director AH Mrs C Yarwood Director of Finance CY Mrs P Cavanagh Director of Operations TC Mr P Nuttall Director of Performance and Informatics PN In attendance Mr P Connellan Chairman PC Mrs K James Chief Executive KJ Ms A Bracegirdle Associate Director of Finance AB Ms J McShane Divisional Director of Operations (Surgery - W&C) JM Ms A Bromley Director of Human Resources (part meeting) ABr Additional attendees Ms W Brelsford Public Member Council of Governors WB Item No Description Action 15/2017 Apologies Ms S Derbyshire, Mrs G Parker 16/2017 Minutes of the previous meeting 19 th January /2017 Action log Minutes of the meeting were approved as an accurate record. Action log has been updated as per discussion and is attached. 18/2017 Trust Efficiency Programme 4.1 Month 10 report AB provided an update and advised 6.4m savings have been identified which is slightly better than plan. 1.9m of this are in year recurrent and it is forecast that the 7.8m will be delivered of which the fill year effect is for 4.3m recurrent savings. All the teams are still being encouraged to identify further recurrent savings and accelerate 2
95 2017/18 saving schemes where possible. AD asked if there is a formal process to deal with schemes which are not delivering. AB explained that all schemes are within the tracker and if it is forecast that the scheme will not deliver the Division will still have the same target to achieve so therefore a replacement scheme will have to be identified. CY advised if an investment had been agreed this would cease if it was decided the scheme would not deliver the savings /17 TEP Lessons Learned CY stated that as part of the Audit report on the Efficiency Programme there was a recommendation which suggested a formal lessons learned exercise was undertaken and the to-date lessons learned has been useful to help shape the programme for 2017/18. AH asked if the budget holders will use the savings monitoring tool, AB confirmed that it is planned for this to be available on the Trust intranet. AB advised there is also a section for the Local Health Economy (LHE) to add the data from their savings schemes in order to provide a LHE savings position. A discussion took place regarding providing the report via the intranet for NEDs to view. PN provided an update on the work being undertaken to enable external access to the intranet from non Trust devices. PC asked where the 25% of savings (Small change/big difference schemes) which have been returned to Departments has been spent on. CY explained a number of departments have offered the funds to be used towards their efficiency target. MT stated that the development of the TEP programme and presentation format has gone well in 2016/17 and was positive about the enhancements being put in place for next year and acknowledged that lessons have been learned. 4.3 Improvement in Theatre Utilisation JM provided an overview of the presentation and advised a target for saving of a full year effect of 140k TEP was agreed. A number of service improvements have been undertaken to improve start times and utilisation. Ensure all staff are aware of the schedule for the day. Working towards a 50 week elective programme. Early bed meeting arranged to ensure Theatres start on time. Theatre timetable has been realigned. Pre-op scheme Processes have been put in place for cancellations. Team Leaders have been assigned to each theatre corridor. A review of equipment was undertaken. The Golden Patient process was rolled out. Following a recommendation from an internal audit of theatres, a company called Four Eyes to support the improvement journey. A significant amount of work has taken place and theatre utilisation has increased. 3
96 JM advised that the Theatre Team have been shortlisted for an HSJ award and acknowledged the commitment of the team to continue to improve the service. Four Eyes have agreed to sponsor the table at the event in order for members of the team to attend. AD asked whether the early finishes have improved over the past few months. JM confirmed that there are still issues with cancellations due to bed pressures which have an impact on the early finishes /18 Medical Staffing Efficiency JM provided an update on medical staffing and advised the target of 620k has been increased by 60k as the Medical Staffing Business Partner was employed on a spend to save basis. The forecast of the current schemes has identified a gap of around 400k. Five core schemes have been identified to deliver the target going forward. A further 328k has been identified for cost avoidance. Overall 1m recurrent savings are anticipated at yearend. The schemes have been broken down into two categories, avoidance and efficiencies. There are two schemes in avoiding expenditure, increasing direct engagement and review and reduce payments above the cap and it is anticipated this will deliver around 328k. A tender exercise is being undertaken for a employing medical agency staff and the savings will come from the reduced commission fees. A 200k recurrent cost saving is anticipated. Discussions are being held with JLNC regarding part of the funding for Clinical Excellence Awards being put towards the TEP scheme and a decision as to whether or not to offer the awards is yet to be made. Job plans and on-call arrangements are being reviewed and 200k has been set as a target for this scheme. The scheme has been Red risk rated as some of the work is behind schedule. The challenge is to get the final job plans in place by the end of April at the latest. A test case has been completed within A&E and a system and process for oncall remuneration has been agreed with the BMA. CY explained the learning from the previous years experience is assisting with this year s process with a realistic and achievable target being agreed. KJ acknowledged that robust systems are now in place to facilitate the challenge with regards to job plans. 19/2017 Operational Performance 5.1 Performance Report PN highlighted the key points in the report. 2017/18 Activity Plans 2017/18 activity levels have been agreed at a high level and are now being split by specialty. 4
97 Outpatients AD asked if there have been any specific actions undertaken to reduce the DNA rates. TC explained that this work has been part of one of the service improvement projects and there has been a number of initiatives around text reminder system, more notice given to patients and moving to agreeing appointments over the telephone. A focused piece of work has been undertaken in Paediatrics which has reduced the rate significantly. Follow up rates have also been reviewed and telephone assessments have been introduced for some of the services. An advice and guidance service for patients who do not need a face-to-face appointment is also being introduced. Single Oversight Framework The framework is included within the report and around 90% of the metrics are now included. The remaining metrics will be included as soon as the information is available. The format of the report is to be reviewed to ensure the appropriate measures are included. Community Service KPIs The Information and Governance teams are undertaking a piece of work to agree the Community Service KPIs and develop a system in order to measure the KPIs. AH asked for a breakdown of the process undertaken to set the standards for next year in terms of performance targets. PN advised that most of the standards are set nationally and local target setting come through varies different areas for example the efficiency programme. AH enquired if there are any contractual issues from the Commissioners which are driving the standards. PN confirmed the contract KPIs are predominantly the same as the national standards. 5.2 Financial Performance Month 10 Summary Review AB provided a summary of the financial performance and advised that the Trust has a deficit of 14.1m at the end of January 2017 which is slightly better than plan. The Trust is now forecasting a year end deficit of 15.5m, which is better than the 17.3m deficit plan. As it was assumed that the STF funding would not be received due to the Q3 and Q4 A&E target not being achieved, mitigation was but in place though a balance sheet review which identified 400k which could be used to benefit the position. In January it was announced by NHSI that if the financial position was improved they would match the improvement by additional STF funding. As the position was improved by 400k an additional 400k was allocated. A balance sheet review is undertaken on a regular basis and an additional 500k has been identified which means further matched funding will be given from NHSI which results in the year-end deficit of 15.5m. In addition, the Trust is appealing the Q3 and Q4 STF funding related to delivery of A&E due to increased number of patients compared to the plan. Indications have suggested this appeal will be successful. Agency spend is 10.7m and it is forecast that the 12.5m NHSI target will be achieved. 5
98 A 17.3m loan has been agreed for this year due to the timing of the STF funding. The DH has advised the Trust will require two different types of loan a revenue support loan for 13.2m (interest of 1.5%). This is repayable in The remainder of the 17.3m is an uncommitted loan (value of 4.1m) for which the Trust can be asked to repay in full at any time. Capital expenditure is at 1.3m below the plan of 2.5m, but the forecast is to spend the full 3m as planned. CY advised a letter has been received from NHSI stating that the Trust is below the target spend and a return has been submitted to provide assurance that the funding will be spent by the end of the year. MT stated there is a risk around the independent sector expenditure. JM confirmed that no further expenditure is planned for the remainder of the year. PC emphasised that as the whole of Tameside and Glossop health economy will meet its targets for this year is good news in terms of the overall credibility. 5.3 NHS Improvement Agency Cap Report ABr provided an update and advised there is currently a reduction in agency expenditure above the capped rates, particularly within medical staffing and there is steady decline in nursing agency spend, although there has been a slight increase in early February due to sickness rates in some areas. There has been a marked reduction in medical agency usage above the capped rate since the HR Business Partner for Medical Staffing commenced in post and there is now a proactive stance around recruitment. The first of the three ED consultants have commenced in post and the other two consultants will be in post by the beginning of April. Work is continuing with Management Teams to review the vacancy gaps and ensure recruitment takes place in a timely way. There are still issues with recruiting to Band 5 nursing staff. A positive interview event took place at the end of January and twenty four posts were recruited to. Five of the staff can start immedicably and the rest will start later in the year. There has been an increase in short term sickness on some of the ward areas which has had an impact in early February and alternative options for recruitment are being considered. Discussions regarding international recruitment are taking place. There are currently seven WTE gaps within Theatres and the options to recruit to these posts are being explored. PC enquired if analysis is completed by day of the week and if there are any lessons to be learnt particularly in relation to sickness. ABr explained that there is a tendency for weekend shifts to experience more sickness and explained this is largely due to agency staff picking up weekend shifts due to the additional enhancement. AD asked what actions are being undertaken around retention. ABr advised there is a specific Recruitment and Retention plan which is discussed at the Executive Meeting each 6
99 week and an action plan has been put in place. A member of the HR team is contacting staff who have handed in their notice to ascertain what actions could have been taken for them to remain in post and the Exit Strategy is being reviewed to ensure exit interviews are undertaken effectively. A pilot is being undertaken to look at self-rostering and amending shift patterns to establish if this makes recruitment to nursing posts more attractive. A Preceptorship Nurse is o also working with newly qualified staff and the new starters to provide support and identify any issues. AH highlighted the high number of applications for the Clinic Fellow and Trust Grade Doctors. ABr confirmed that only the applicants who meet the person specification will be shortlisted. JM advised a rotation has been offered which has resulted in the high levels of applications. AB explained that the HR Medical Staffing team have been working with the Divisions and Operational Managers to look at different ways to attract applicants. A scoping exercise is being undertaken with the Clinical Skills Facilitators to undergo a training needs analysis to develop a training programme for nursing staff. AD asked if the cap level is likely to change on the 1 st April, AB advised there has been no notification received that the cap will change, but there will be an impact following the changes to the IR35 and meetings are being arranged to go through the implications to agency staff and agree actions. MT cited the section in the report which states it is projected there will be a cost of 13m against the cap of 12.5m, and in the Finance paper it is stated the target will be met. CY confirmed this anomaly is due to the timings of the report the agency report contains data which is a month behind the finance report. 5.4 Month 10 Contract Performance CY advised the paper outlines information on the performance against the various commissioner contracts. The Trust has over performed by 275k as at Month 10 which is predominantly from the other Commissioners other than Tameside and Glossop CCG. There is currently a block contract with T&G CCG which has been balanced back to zero variance. Concerns have been raised about the increased income relating to the Acute Cardiology Unit (ACU) as increased significantly from month 8. The coding of the activity on the ACU is being reviewed. MT requested an update report is provided to the next meeting. JM A year-end position has been agreed with Tameside and Glossop CCG which assumes there would not be an over performance on the contract. However, an additional 1.5m of income from Tameside Council in relation to delivery of performance targets has been agreed. CY provided an update following the contract meeting and advised the contract will be fully signed by the end of March
100 20/2017 Board Assurance Framework Risk Reporting CY advised the report details risks and the current scores. Each risk was reviewed and the scores amended accordingly. An explanation as to how the score is agreed is to be included within future reports. AB AF 2.1 = It was agreed to reduce the score to 8 AF 2.2 = It was agreed to reduce the score to 10 AF 2.8 = It was agreed the score remains at 20 AF 2.9 = It was agreed to reduce the score to 15 AF 5.1 = It was agreed to score remains at 12 TC enquired if achieving a deficit which is better than prediction is a risk to the Trust against agreeing the financial plan for next year. CY advised this would not be the case as the improvement is due to one off balance sheet items and funding allocations for the STF from NHSI. This issue has been raised with NHSI who have indicated this will not impact on the control total issued for 2017/18. 21/2017 Effectiveness of Finance and Performance Committee Review AB explained questionnaires are to be distributed for completion before the deadline and the results will be presented at the next Committee meeting. 22/2017 Transformation Savings Plan 23/ /2017 Workplan Item deferred to next meeting. Capital and Revenue Investment Group Minutes (January 2017) The minutes have been provided for information. The work plan was amended as per discussion. 25/2017 Summary of points to escalate to Board Agency Cap report TEP Improvement in Theatre Utilisation Medical Staffing Efficiency 26/2017 Any Other Business There was no other business 27/2017 Date of Next Meeting: 23 rd March 2017 at 2pm Silver Springs Board Room 8
101 TAMESIDE AND GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 27 th April 2017 Agenda Item 9a Title Corporate Objectives 2017/18 Sponsoring Executive Director Karen James Author (s) Purpose Executive Team To request endorsement of the Corporate Objectives for the 2017/18 financial year Previously considered by Discussed at Executive Management Team Executive Summary: The attached Corporate Objectives develop the key themes from the previous year whilst incorporating challenging success criteria to allow us to demonstrate the next phase of the trust s continuing improvement and integration journey Related Trust Objectives All Risk Assurance risk impacted upon Legal implications/regulatory requirements Financial Implications Has a quality impact assessment been undertaken? How does this report affect Sustainability? Relates to all aspects of Board Assurance Framework and Significant Risk Report. The successful achievement of the trust s corporate objectives will ensure the organisation complies with the legal and regulatory requirements of all its regulators The corporate objectives have a material impact on the financial sustainability of the trust. N/A The achievement of the Corporate Objectives directly impacts on the trust s future sustainability Action required by the Board To endorse the 2017/18 Corporate Objectives

102 Corporate Objectives 2017/18 Objective Draft 2017/18 Corporate Objectives Success Criteria We will maintain compliance with the CQC Fundamental To ensure our patients and users receive harm free care by Standards of Care improving the quality and safety of our services through the delivery of our Quality and Safety programme. We will maintain our overall CQC ratings at good and aspire to gain outstanding ratings in future service inspections We will maintain and or increase our incident reporting rate per 1000 bed days and aim to be in the top 25% of Trusts We will minimize levels of severe and catastrophic harm and be below the national average of 1% We will ensure our patient safety programme work streams uses metrics for anticipating and predicting 1. potential future harm in at least five of the work streams for 2017/18 We will achieve the identified CQUIN metric related to patient safety We will maintain or improve the completed eligible VTE risk assessment at an 98% or above We will continue to seek improvement of the Trust s mortality indices (HSMR and SHMI) and maintain them in the as expected or better than expected bandings We will continue to ensure learning from Deaths is part of the organisational learning and reported in line with the national requirements We will achieve the Single Oversight Framework metric 2. To improve our patient and service user experience through the delivery of a personalised, responsive, integrated, caring and compassionate approach to the delivery of care. related to emergency re-admissions within 30 days We will further reduce the number of KO41 complaints per 1000 patient contacts to below 1 complaint per 1,000 patient contacts 2
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 29 th June 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 29 th June 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
Tameside and Glossop Integrated Care NHS Foundation Trust. Board of Directors February Chair's Report
 Agenda Item 6 Tameside and Glossop Integrated Care NHS Foundation Trust Appointment of new Non-Executive Director Board of Directors February 2018 Chair's Report I am pleased to be able to confirm that
Agenda Item 6 Tameside and Glossop Integrated Care NHS Foundation Trust Appointment of new Non-Executive Director Board of Directors February 2018 Chair's Report I am pleased to be able to confirm that
Title Open and Honest Staffing Report April 2016
 Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Monthly Nurse Safer Staffing Report June and July 2018
 Monthly Nurse Safer Staffing Report June and July 2018 Trust Board September 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation
Monthly Nurse Safer Staffing Report June and July 2018 Trust Board September 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
The Royal Wolverhampton NHS Trust
 Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Monthly Nurse Safer Staffing Report October 2017
 Monthly Nurse Safer Staffing Report October 2017 Trust Board November 2017 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid
Monthly Nurse Safer Staffing Report October 2017 Trust Board November 2017 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST. Board Paper - Cover Sheet
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Date September 2017 Lead Director Report Title Nursing & Midwifery Staffing Three- Monthly Summary Nursing & Patient Services
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Date September 2017 Lead Director Report Title Nursing & Midwifery Staffing Three- Monthly Summary Nursing & Patient Services
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Status: Information Discussion Assurance Approval
 Report to: Trust Board Agenda item: Date of Meeting: July 2017 Report Title: Safe Nurse Staffing 6 Monthly Assurance Report Status: Information Discussion Assurance Approval X x Prepared by: Sarah Dodds,
Report to: Trust Board Agenda item: Date of Meeting: July 2017 Report Title: Safe Nurse Staffing 6 Monthly Assurance Report Status: Information Discussion Assurance Approval X x Prepared by: Sarah Dodds,
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
2017/18 Trust Balanced Scorecard
 ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
Safe Nurse Staffing Levels. June 2017
 Safe Nurse Staffing Levels Executive Summary June 2017 The purpose of this report is: 1. To provide an assurance with regard to the management of safe nursing and midwifery staffing for the month of June
Safe Nurse Staffing Levels Executive Summary June 2017 The purpose of this report is: 1. To provide an assurance with regard to the management of safe nursing and midwifery staffing for the month of June
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Monthly Nurse Safer Staffing Report May 2018
 Monthly Nurse Safer Staffing Report May 2018 Trust Board June 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid Staffordshire
Monthly Nurse Safer Staffing Report May 2018 Trust Board June 2018 Dr Shelley Dolan Chief Nurse /Chief Operating Officer 1 Monthly Nursing Report Introduction Following the investigation into Mid Staffordshire
INTEGRATED PERFORMANCE REPORT. BOARD OF DIRECTORS 20 September 2017
 INTEGRATED PERFORMANCE REPORT BOARD OF DIRECTORS 20 September 2017 1 S Section Page Executive Summary 4 Trust Performance Overview 7 Trust Performance Report by Exception 9 MSSA Bacteraemia - Actual numbers
INTEGRATED PERFORMANCE REPORT BOARD OF DIRECTORS 20 September 2017 1 S Section Page Executive Summary 4 Trust Performance Overview 7 Trust Performance Report by Exception 9 MSSA Bacteraemia - Actual numbers
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Section 1 - Key Performance Indicators
 Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014
 Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014 Presented for: Presented by: Author Previous Committees Information Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim
Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014 Presented for: Presented by: Author Previous Committees Information Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim
Link to Relevant CQC Domain: Safe Effective Caring Responsive Well Led
 Enclosure H Safe Staffing Trust Board Item: 12 Date 29 th November 2017 Enclosure: H Purpose of the Report: This report provides the Trust Board with an update on progress with meeting the safe staffing
Enclosure H Safe Staffing Trust Board Item: 12 Date 29 th November 2017 Enclosure: H Purpose of the Report: This report provides the Trust Board with an update on progress with meeting the safe staffing
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Governing Body. TITLE OF REPORT: Performance Report for period ending 31st December 2012
 - Governing Body DATE OF MEETING: TITLE OF REPORT: Performance Report for period ending 31st December 2012 KEY MESSAGES: We are responsible for securing improvements in the quality of care and health outcomes.
- Governing Body DATE OF MEETING: TITLE OF REPORT: Performance Report for period ending 31st December 2012 KEY MESSAGES: We are responsible for securing improvements in the quality of care and health outcomes.
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Quality & Safety Sub-Committee
 Quality & Safety Sub-Committee Agenda Item QS/029/16 Date: 17/03/2016 Report Title FOIA Exemption Prepared by Presented by Action required Supporting Executive Director Safer Staffing No Exemption Janet
Quality & Safety Sub-Committee Agenda Item QS/029/16 Date: 17/03/2016 Report Title FOIA Exemption Prepared by Presented by Action required Supporting Executive Director Safer Staffing No Exemption Janet
Quality Improvement Scorecard December 2016
 Mortality: HSMR Nat The improvement in performance has been maintained in year. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat The improvement in performance has been maintained in year. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Summarise the Impact of the Health Board Report Equality and diversity
 AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST. Board Paper - Cover Sheet
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Date 19 th December 2017 Lead Director Report Title Nursing & Midwifery Staffing Three- Monthly Summary Nursing & Patient
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Board Paper - Cover Sheet Date 19 th December 2017 Lead Director Report Title Nursing & Midwifery Staffing Three- Monthly Summary Nursing & Patient
SUMMARY REPORT. Board of Directors Date of meeting: 1 May P a g e
 SUMMARY REPORT Board of Directors Date of meeting: 1 May 2018 Subject Prepared by Approved by Presented by Safe Staffing Report Nursing and Midwifery Eileen Aylott Assistant Director of Nursing, Workforce
SUMMARY REPORT Board of Directors Date of meeting: 1 May 2018 Subject Prepared by Approved by Presented by Safe Staffing Report Nursing and Midwifery Eileen Aylott Assistant Director of Nursing, Workforce
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Policy Register No: Status: Public NURSING STAFFING SHORTFALL ESCALATION POLICY. NICE Guidelines July 2014 CQC Fundamental Standards: 17
 NURSING STAFFING SHORTFALL ESCALATION POLICY Policy Register No: 09114 Status: Public Developed in response to: National Quality Board Recommendations2013 NICE Guidelines July 2014 CQC Fundamental Standards:
NURSING STAFFING SHORTFALL ESCALATION POLICY Policy Register No: 09114 Status: Public Developed in response to: National Quality Board Recommendations2013 NICE Guidelines July 2014 CQC Fundamental Standards:
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing August 2017 (July 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Urgent Care Short Term Actions to Improve Performance
 To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
NQB safe sustainable and productive staffing
 NQB safe sustainable and productive staffing Jacqueline McKenna Deputy Director of Nursing NHS Improvement NHS Providers HR Network 21 July 2016 Patient Safety function from NHS England (including National
NQB safe sustainable and productive staffing Jacqueline McKenna Deputy Director of Nursing NHS Improvement NHS Providers HR Network 21 July 2016 Patient Safety function from NHS England (including National
NURSE STAFFING REPORT
 NURSE STAFFING REPORT INTRODUCTION This paper fulfills the nationally mandated, post Francis II requirement for monthly Board Reports detailing achievement against required nurse staffing levels. This
NURSE STAFFING REPORT INTRODUCTION This paper fulfills the nationally mandated, post Francis II requirement for monthly Board Reports detailing achievement against required nurse staffing levels. This
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
BOARD OF DIRECTORS MEETING 7th March 2018
 BOARD OF DIRECTORS MEETING 7th March 2018 Agenda Item TB058/18 Report Title Executive Lead Lead Officer Monthly Safer Staffing Report (January 2018) Sheila Lloyd Director of Nursing Midwifery Therapies
BOARD OF DIRECTORS MEETING 7th March 2018 Agenda Item TB058/18 Report Title Executive Lead Lead Officer Monthly Safer Staffing Report (January 2018) Sheila Lloyd Director of Nursing Midwifery Therapies
Trust Key Performance Indicators
 Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Agenda item A5(iii) PROVIDING CLINICAL ASSURANCE: CLINICAL ASSURANCE TOOLKIT (CAT), NURSE STAFFING, FRIENDS & FAMILY TEST (FFT) A SUMMARY REPORT EXECUTIVE
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST Agenda item A5(iii) PROVIDING CLINICAL ASSURANCE: CLINICAL ASSURANCE TOOLKIT (CAT), NURSE STAFFING, FRIENDS & FAMILY TEST (FFT) A SUMMARY REPORT EXECUTIVE
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10. Date of Meeting:.24 th March 2017.
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting:.24 th March 2017. TITLE OF REPORT: CCG Corporate Performance Report AUTHOR: Melissa Laskey Director of Service
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting:.24 th March 2017. TITLE OF REPORT: CCG Corporate Performance Report AUTHOR: Melissa Laskey Director of Service
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
Nursing and Midwifery Establishment review April 2017 Page 1
 Trust Board - July 217 Agenda Item: Nursing and Midwifery Establishment Review PURPOSE PREVIOUSLY CONSIDERED BY To provide the Board with the bi-annual review report for ward establishments for April 217
Trust Board - July 217 Agenda Item: Nursing and Midwifery Establishment Review PURPOSE PREVIOUSLY CONSIDERED BY To provide the Board with the bi-annual review report for ward establishments for April 217
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
July (Month 4) Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval
 Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval") BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Monthly Report on Nurse Levels for May 2016
 Meeting: Finance and Performance Committee Date: 27 th June 2016 Agenda Item: 7 Monthly Report on Nurse Levels for May 2016 Key Risks - Clinical: The delivery of safe, high quality care is a fundamental
Meeting: Finance and Performance Committee Date: 27 th June 2016 Agenda Item: 7 Monthly Report on Nurse Levels for May 2016 Key Risks - Clinical: The delivery of safe, high quality care is a fundamental
Report to: Trust Board 25 th April Enclosure 4. Title Integrated Performance Report March Sponsoring Executive Director
 Report to: Trust Board 25 th April 2013 Title Integrated Performance Report March 2013 Enclosure 4 Sponsoring Executive Director Author(s) Purpose Previously considered by Peter Herring Chief Executive
Report to: Trust Board 25 th April 2013 Title Integrated Performance Report March 2013 Enclosure 4 Sponsoring Executive Director Author(s) Purpose Previously considered by Peter Herring Chief Executive
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Agenda Item The report triangulates staffing levels against appropriate quality measures. The Report is provided to the Board for:
 To: Trust Board From: Michelle Rhodes, Director of Nursing Date: 2 nd May 2017 Essential Standards: Health and Social Care Act 2008 (Regulated Activities) Regulation 18: Staffing Title: Monthly Nursing/Midwifery
To: Trust Board From: Michelle Rhodes, Director of Nursing Date: 2 nd May 2017 Essential Standards: Health and Social Care Act 2008 (Regulated Activities) Regulation 18: Staffing Title: Monthly Nursing/Midwifery
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Safe staffing for nursing in A&E departments. NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015
 Safe staffing for nursing in A&E departments NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015 Safe staffing for nursing in A&E departments: NICE safe staffing guideline
Safe staffing for nursing in A&E departments NICE safe staffing guideline Draft for consultation, 16 January to 12 February 2015 Safe staffing for nursing in A&E departments: NICE safe staffing guideline
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
STAFFING ESCALATION TIMELINE
 STAFFING ESCALATION TIMELINE Date 2008 Staffing levels were first placed on the directorate risk register in 2008 and have been reviewed at subsequent directorate governance forums. 08.02.11 CQC visit
STAFFING ESCALATION TIMELINE Date 2008 Staffing levels were first placed on the directorate risk register in 2008 and have been reviewed at subsequent directorate governance forums. 08.02.11 CQC visit
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE HEALTHCARE GOVERNANCE COMMITTEE HELD ON 24 JULY 2017
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE HEALTHCARE GOVERNANCE COMMITTEE HELD ON 24 JULY 2017 Subject Monthly Staffing Report June 2017 Supporting TEG Member Professor
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE HEALTHCARE GOVERNANCE COMMITTEE HELD ON 24 JULY 2017 Subject Monthly Staffing Report June 2017 Supporting TEG Member Professor
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
Quality Governance and Risk Committee Safer Staffing Report January 2018
 Introduction Quality Governance and Risk Committee Safer Staffing Report January 2018 The Safe Staffing initiative is part of the NHS response to the Frances Report which called for greater openness and
Introduction Quality Governance and Risk Committee Safer Staffing Report January 2018 The Safe Staffing initiative is part of the NHS response to the Frances Report which called for greater openness and
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Appendix 1. Quality Update Report for Salford CCG Open Board. Salford Royal, Oaklands and other providers of clinical services November 2013
 Appendix 1 Quality Update Report for Salford CCG Open Board. Salford Royal, Oaklands and other providers of clinical services November 201 Contents Purpose of Paper... Ошибка! Закладка не определена. Greater
Appendix 1 Quality Update Report for Salford CCG Open Board. Salford Royal, Oaklands and other providers of clinical services November 201 Contents Purpose of Paper... Ошибка! Закладка не определена. Greater
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Physiotherapy outpatient services survey 2012
 14 Bedford Row, London WC1R 4ED Tel +44 (0)20 7306 6666 Web www.csp.org.uk Physiotherapy outpatient services survey 2012 reference PD103 issuing function Practice and Development date of issue March 2013
14 Bedford Row, London WC1R 4ED Tel +44 (0)20 7306 6666 Web www.csp.org.uk Physiotherapy outpatient services survey 2012 reference PD103 issuing function Practice and Development date of issue March 2013
UNIVERSITY HOSPITAL SOUTHAMPTON NHS FOUNDATION TRUST Trust Board meeting 27 th October 2016
 UNIVERSITY HOSPITAL SOUTHAMPTON NHS FOUNDATION TRUST Trust Board meeting 27 th October 2016 Title Sponsoring Executive Authors names & Job titles Ward Staffing nursing establishment 6 monthly review July
UNIVERSITY HOSPITAL SOUTHAMPTON NHS FOUNDATION TRUST Trust Board meeting 27 th October 2016 Title Sponsoring Executive Authors names & Job titles Ward Staffing nursing establishment 6 monthly review July
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Current policy context of safe staffing in A&E Departments
 Current policy context of safe staffing in A&E Departments Howard Catton, Head of Policy and International Affairs Hallam Conference Centre, London -18 th May 2015 Why is safe staffing so important? Right
Current policy context of safe staffing in A&E Departments Howard Catton, Head of Policy and International Affairs Hallam Conference Centre, London -18 th May 2015 Why is safe staffing so important? Right
Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September Executive Summary from CEO
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST PAGE 1 OF 2 Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September 2017 Executive Summary from CEO Paper
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST PAGE 1 OF 2 Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September 2017 Executive Summary from CEO Paper
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Waiting Times Report Strategic. Thematic Goals
 Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
CQC Quality Improvement Plan
 2018-19 CQC Quality Improvement Plan Date of Submission: 21/03/2018 Chief Executive: Lance McCarthy Chair Alan Burns Navigation Our Patients Our People Our Performance Our Places Key The table below identifies
2018-19 CQC Quality Improvement Plan Date of Submission: 21/03/2018 Chief Executive: Lance McCarthy Chair Alan Burns Navigation Our Patients Our People Our Performance Our Places Key The table below identifies
CQC IMPROVEMENT ACTION PLAN. Page 1 of 86 CQC Improvement Plan (Published 10/8/15)
") CQC IMPROVEMENT ACTION PLAN Page 1 of 86 CQC Improvement Plan (Published 10/8/15) Contents FOREWORD FROM THE CHIEF EXECUTIVE... 3 TRFT INSPECTION RATINGS... 4 AREAS FOR IMPROVEMENT... 5 ACTION PLAN MUST
CQC IMPROVEMENT ACTION PLAN Page 1 of 86 CQC Improvement Plan (Published 10/8/15) Contents FOREWORD FROM THE CHIEF EXECUTIVE... 3 TRFT INSPECTION RATINGS... 4 AREAS FOR IMPROVEMENT... 5 ACTION PLAN MUST