Managing Clinical Risk Practice Guidance
|
|
|
- Eleanor Alexander
- 6 years ago
- Views:
Transcription

1 SH CP 28 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: These guidance notes are intended to help staff from Southern Health NHS Foundation Trust (SHFT) implement the policy, Risk Assessment and Management of Patients/Service Users. They should be read in conjunction with that policy. Risk assessment, risk, clinical risk, assessment. All clinical staff within the Mental Health Division Next Review Date: March 2019 Approved & Ratified by: AMH Performance & Assurance Board Date of meeting: 17 Date issued: Author: Sponsor: Brendan O Reilly, Lead Nurse - MH Division Liz Durrant, Area Manager AMH Tim Coupland, Head of Nursing, AHP and Quality- MH, LD & Social Care 1
2 Version Control Change Record Date Author Version Page Reason for Change Sept 14 Brendan O Reilly 2 All Revised to include principles of strengths-based recovery and positive risk-taking practice Amended to layout for ease of reading Aug Review date extended from Aug to Nov Oct Review date extended to 2015 Dec 2015 Liz Durrant 3 All Review undertaken Reviewers/contributors Name Position Version Reviewed & Date Mental Health, Learning Disabilities staff Various V1 July
3 Contents 1. Introduction 4 2. Risk Assessment Practice Principles 4 3. Risk Management Practice Principles 7 4. Staff Values - It is important as Clinicians we use strategies for 11 promoting Hope: 5. Other principles of working 12 Appendices A1 Actuarial Factors 16 A2 MAPPA arrangements 18 Page 3
4 1. Introduction These guidance notes are intended to help staff from Southern Health NHS Foundation Trust (SHFT) implement the policy, Risk Assessment and Management of Patients/Service Users. They should be read in conjunction with that policy. This document will also complement the SHFT training on managing risk. They have been adapted from the DH document Best Practice in Managing Risk (June 2007). In the foreword to that document, Professor Louis Appleby noted that good quality risk assessment helps to improve the safety of mental health services. He went onto say A good therapeutic relationship must include both sympathetic support and objective assessment of risk. The importance of embedding risk management in CPA was also emphasised. Critical Incident Reviews that have been carried out within SHFT over recent years have consistently identified risk assessment and risk management as areas for improvement in practice. This is also consistent with the findings of other independent reviews of serious incidents. 2. Risk Assessment Practice Principles (Adapted from Justifying Risk Decisions by Dr David Carson (2007) & Rethinking risk to others in mental health services (Royal College of Psychiatrists 2008) By definition, it is inevitable that harm will sometimes occur from risk taking, even with the highest quality decisions. When judging a risk decision both the assessment of the risk and the management of its implementation should be considered. The quality of risk decisions made by professional staff in SHFT will not be measured by whether harm does or does not result. Risk assessment is an assessment of a current situation, not itself a predictor of a particular event. Although accurate prediction is never possible in individual patients, some negative outcomes can be reduced in frequency by sensible contingency planning. Mental health professionals in SHFT must ensure that they have the necessary competencies to make risk decisions, including using approved relevant structured tools. Organisational contributions to poor quality risk decisions will always be considered along with the contribution of individual decision makers. Southern Health NHS Foundation Trust policy on Risk Assessment and Management of Patients/Service users describes the various risks which are covered by the policy. These risks can be grouped into one of four over-arching categories: Risk of harm to the patient including deliberate self harm, self neglect or the potential for abuse by others, to include the potential for actively or passively leaving the unit/department without the knowledge and agreement of staff 4
5 Risk of harm to others including physical violence or harm, verbal or psychological abuse, harassment, potential harm to others through passive or active unsafe actions including fire setting or other dangerous acts - to include the potential for actively or passively leaving the unit/department without the knowledge and agreement of staff Risk of damage to property including damage to fabric or structure of buildings or objects, including as a result of passive or active fire setting - to include the potential for actively or passively leaving the unit/department without the knowledge and agreement of staff. Risk to the Trust reputation and/or business profile if the Trust is shown to have failed to have robust systems and processes in place to identify and manage these risks. 2.1 Providing care proportionate to risk A fundamental principle of mental healthcare is that the level of security to which a patient is subjected should be as non-restrictive as possible and should be proportionate to the degree of risk that they actually present at the time. Risk assessment can be integral to deciding on the right level of intervention and support for a patient. When it is done properly using the principles of involvement, working together and individualised support risk management is empowering rather than disempowering for the patient and can be a vital part of recovery. 2.2 Risk Assessment- methodology and formulation Approaches to risk assessment have been broadly categorised into three groups: clinical, actuarial, and structured clinical judgement Actuarial approaches are based on addressing risk at a group level, but they cannot move from group to individual risk evaluations easily. Their accuracy is lowest in detecting rare events. They are able to predict at all only when the patient being assessed comes from the population for which the tool was developed. For actuarial factors please see appendix Clinical approaches provide individualised and contextualised assessments, but are vulnerable to individual bias and poor inter rater reliability. They have been reported, however, to achieve better than chance levels of accuracy. These approaches can be either structured or unstructured, or a combination of the two. Actuarial approaches are mainly structured and clinical approaches predominantly unstructured, although the latter may also have aspects of structured assessment. Unstructured assessment involves the selection and measurement of risk factors based on a mental health professional s clinical experience and theoretical orientation. Risk factors are combined in a holistic manner to develop a professional opinion about a person s level of risk in relation to violence Structured clinical (or professional) judgement is the approach that offers the most potential where violence risk management is the objective. This approach involves the practitioner making a judgement about risk on the basis of combining: an assessment of clearly defined factors derived from research; clinical experience and knowledge of the patient; and the patient s own view of their experience. 5
6 Tools using Structured Clinical Judgement such as the HCR 20 have been developed based on practice-based evidence; such tools are the most effective approach to violence risk management. Although, like the actuarial tools, these instruments are derived from research evidence, the clinician s discretion is seen as a vital element especially in relation to formulating the assessment of risk and preparing risk management plans based on the risk factors identified. The effectiveness of these tools can be hard to test, given their range of applications and the difficulty of measuring the prevented harm. Given their research focus, they may also exclude issues that the individual patient considers important although most structured clinical judgement tools offer practitioners the opportunity to add extra risk factors and considerations as required. Structured assessment is important in assessing suicide risk, but there are no instruments with a satisfactory evidence base. In this case, structured assessment means a systematic assessment of key risk factors and mental state leading to an informed clinical judgement Risk Factors and formulation A risk factor is a personal characteristic or circumstance that is linked to a negative event and that either causes or facilitates the event to occur. Risk factors can be categorised in a number of ways. Static risk factors are unchangeable, e.g. a history of child abuse or suicide attempts. Dynamic risk factors are those that change over time, e.g. misuse of alcohol. Dynamic factors can be aspects of the individual or aspects of their environment and social context, such as the attitudes of their carers or social deprivation. Because they are changeable, these factors are more amenable to management. Dynamic risk factors that are quite stable and change only slowly are called stable or chronic risk factors. Those factors that tend to change rapidly are known as acute risk factors or triggers and, as they do change rapidly, their influence on the level of risk may be short-lived. Particular sensitivity should be exercised when discussing historical factors from earlier in the life of the patient. The relevance and accuracy of these may need to be explained to the patient, and it is possible that carers may be unaware of these historical events or of their significance so many years on. Risk formulation is a process in which the practitioner decides how the risk might become acute or triggered. It identifies and describes predisposing, precipitating, perpetuating and protective factors, and also how these interact to produce risk. This formulation should be agreed with the patient and others involved in their care in advance, and should lead to an individualised risk management plan. Every risk formulation should have attached to it a plan for what to do when the warning signs become apparent. The plan should also include more general aspects of management, such as monitoring arrangements, therapeutic interventions, appropriate placements and employment needs. Further guidance on how to undertake a risk assessment can be found in appendix Fluidity of risk Risk can change sometimes over very short timescales. By definition, dynamic factors fluctuate in their contribution to the overall risk. Given the fluidity of risk, only the tools based on structured professional judgement are useful in monitoring change and engagement with the patient and carer. So there should be an established procedure to formally review the assessment of risk at regular intervals. However these reviews should not be rigidly limited to these time points. It is important that the 6
7 procedure has some flexibility so that, in particular circumstances, an earlier or more timely formal review can be undertaken. This also guards against a tick box mentality in completing risk assessment forms. All practitioners working with the patient need to be familiar with previous risk assessments so that they can be alert to changes in the level of risk. Particular attention should be paid to the relationship between substance misuse and changes in the risk of harm to self or others. It is crucial that patients and carers have access to someone whom they can contact in a crisis if the need arises, and that they are taken seriously if this occurs Finally, The Royal College of Psychiatrists (2008) has recommended a Tiered Approach to risk assessment. Rather than just using a standardised toolkit, they recommended that the structured clinical risk assessment should be constituted as a tiered approach to risk, within a framework of principles to guide its use. The use of clinical judgement should be an essential adjunct to this. A tiered approach should include: an examination of the patient s history a full mental state assessment, which should incorporate a short set of standard questions for use in all clinical situations, aimed at eliciting factors which increase the risk of violence (as described above). If risk is identified as significant in these assessments of the patient, this should trigger a more structured risk assessment process, with the use of an assessment tool that is appropriate for the group, and avoiding the notion that one size fits all. Full records should be kept and concerns raised by families should be responded to. In principle, their concerns should automatically trigger a more structured risk assessment. This type of risk assessment has several clear advantages. It does not require training in the use of a specific risk tool. It allows clinicians to use their clinical skills. It can be easily carried out and recorded as part of any clinical assessment of the patient. It can easily be incorporated into the CPA process. 3. Risk Management Practice Principles This guidance has been adapted from Best Practice in Managing Risk published by the Department of Health in 2007 (Department of Health 2007) which identifies 16 best practice points for effective risk management; Best practice involves making decisions based on knowledge of the research evidence, knowledge of the individual patient and their social context, knowledge of the patient s own experience, and clinical judgement. Positive risk management as part of a carefully constructed plan is a required competence for all mental health practitioners. Risk management should be conducted in a spirit of collaboration and based on a relationship between the patient and their carers that is as trusting as possible. Risk management must be built on recognition of the patient s strengths and should emphasise recovery. Risk management requires an organisational strategy as well as efforts by the individual practitioner. 7
8 Risk management involves developing flexible strategies aimed at preventing any negative event from occurring or, if this is not possible, minimising the harm caused. Risk management should take into account that risk can be both general and specific, and that good management can reduce and prevent harm. Knowledge and understanding of mental health legislation is an important component of risk management. The risk management plan should include a summary of all risks identified, formulations of the situations in which identified risks may occur, and actions to be taken by practitioners and the patient in response to crisis. Where suitable tools are available, risk management should be based on assessment using the structured clinical judgement approach. Risk assessment is integral to deciding on the most appropriate level of risk management and the right kind of intervention for a patient. All staff involved in risk management must be capable of demonstrating sensitivity and competence in relation to diversity in race, faith, age, gender, disability and sexual orientation. Risk management must always be based on awareness of the capacity for the patient s risk level to change over time, and recognition that each patient requires a consistent and individualised approach. Risk management plans should be developed by multidisciplinary and multiagency teams operating in an open, democratic and transparent culture that embraces reflective practice. All staff involved in risk management should receive relevant training, which should be updated at least every three years. A risk management plan is only as good as the time and effort put into communicating its findings to others. 3.1 Positive risk management Decisions about risk management involve improving the patient s quality of life and plans for recovery, while remaining aware of the safety needs of the patient, their carer and the public. Positive risk management as part of a carefully constructed plan is a desirable competence for all mental health practitioners, and will make risk management more effective. Positive risk management can be developed by using a collaborative approach and should work within the following principles: All individuals including vulnerable individuals have the right to take risks. An individual s right to take risks does not give them the right to put others at risk. Risk Management should involve working in partnership with adults who use services, family carers and advocates and recognise their different perspectives and views 8
9 It is essential for clinicians to listen to what the service user is saying about the gains from taking a risk and what they stand to lose if they are prevented from doing so. It is important when completing a risk assessment and safety plan to have a transparent discussion to assist the individual to understand the consequence of different actions/decisions. It is necessary for the service and clinicians to assist the service user to take positive risks once they have weighted up the consequence of such actions using accurate information that is collaborated. It will be vital for the clinician to understand what has worked or not in the past for the individual and why It is essential to build on the strengths of the individual and assist creativity including involving the family or carer in supporting the individual to make correct decisions relating to their own safety. It is by the clinician considering all the information available short terms goals are set to take appropriate positive risks as this will further enhance the therapeutic relationship between the service user and the clinician and may result in more long-term positive outcomes for the individual. It is important that services promote recovery and work with individuals to return to their normal routines as soon as possible following a relapse in their health and wellbeing. All individuals and agencies involved with the person working together to ensure the safety of the individual in collaboration with the individual and his/ her family/ carer. Over defensive practice is bad practice. Avoiding all possible risks is not good for the patient or society in the long term, and can be counterproductive, creating more problems than it solves. Any risk-related decision is likely to be acceptable if: it conforms with relevant guidelines; it is based on the best information available; it is documented; and the relevant people are informed. As long as a decision is based on the best evidence, information and clinical judgement available, it will be the best decision that can be made at the time. Positive risk management means being aware that risk can never be completely eliminated, and aware that management plans inevitably have to include decisions that carry some risk. This should be explicit in the decision-making process and should be discussed openly with the patient. 3.2 Positive risk management should take the following approach: working with the patient to identify what is likely to work; paying attention to the views of carers and others around the patient when deciding a plan of action; weighing up the potential benefits and harms of choosing one action over another; 9
10 being willing to take a decision that involves an element of risk because the potential positive benefits outweigh the risk; being clear to all involved about the potential benefits and the potential risks; developing plans and actions that support the positive potentials and priorities stated by the patient, and minimise the risks to the patient or others; ensuring that the patient, carer and others who might be affected are fully informed of the decision, the reasons for it and the associated plans; and using available resources and support to achieve a balance between a focus on achieving the desired outcomes and minimising the potential harmful outcome moving towards person centred safety planning Risk management in mental healthcare should be structured and consistent. It should be explicit to the patient and should involve the patient s own priorities. It should also include the structured clinical judgement outlined below. Decisions about care and security should not be based simply on the largely unstructured clinical approach, which could be subject to personal biases about the patient and may miss important factors such as the patient s strengths and resources or the views of the carer. These biases could lead to poor judgements where the risk is either overestimated or underestimated if key factors are missed. This is especially true if the judgements are made by an individual practitioner alone rather than by a clinical team working together. If it is not clear to the patient that their risk is being assessed, the principle of engagement is broken. Risk is dynamic and constantly changing in response to changing circumstances. Its assessment and management needs to be ongoing with contingency and safety plans agreed with the individual. These plans should be reviewed and updated by the MDT on a regular basis. Decisions will be based on clear reasoning using principles of multi-disciplinary and interagency working in proportion to the risk and impact to self and others. Risk management will involve everybody working in an integrated way to ensure positive outcomes for the individual and family/carer involved. 10
11 3.3 Monitoring & Regular reviews When monitoring a patient s risk to others, the supervising clinician should address the following questions: What events, occurrences, or circumstances might increase this person s violence risk? What factors might lead this person to consider or choose to act violently? What is the best way to monitor warning signs that this person s violence risk may be increasing? What events, occurrences, or circumstances should trigger a re-assessment of violence risk? While remaining flexible, risk management plans should include scheduled dates for reassessment, so that they are not simply amended as a reaction to a crisis or other events. These review requirements should be part of the risk management plan and not separate from it, and the patient and all those involved in their care should be involved in this review. Risk management plans should also include a clear statement of responsibility for carrying out specified tasks in the plan, as well as for reviewing them. From discussion with the patient, it is essential to anticipate what circumstances would trigger a review outside the normal timetable, as well as which times of year are particularly difficult. There should be scope for the patient or carer to request a review. In addition, the risk management plan should be revisited before and during time periods that are recognised to be associated with increased risk, for instance prior to leave, on return from leave and around the time of discharge. 4. Staff Values - It is important as Clinicians we use strategies for promoting Hope: Value the person as a unique human being; acknowledge positives and negotiate in a way that is helpful to the person who is showing signs of distress. Trust in the authenticity of what the person says, actively listen and empathise with the individuals position; believe in the person s potential and strength, sometimes this means looking beyond the signs of illness and disturbance presented. Accepting the person for who they are, reflect positives and be honest in your communications; assist the person to reflect on what is happening to them possibly due to a number of diverse factors. View set back and relapse as part of the individual s recovery journey. Tolerate the uncertainty about the person s future; be available to listen and explore alternative coping behaviours. Express and demonstrate genuine concern for the person s well-being, support access to a full range of treatments and information when the person is able to consider these. 11
12 Use person centred care planning; support the use of user developed work books such as the Wellness Recovery Action Planning. (WRAP) ( Adapted from 100 ways to support recovery- A guide for mental health professionals by Mike Slade 5. Other principles of working 5.1 Mental Health Act Given the nature of severe mental illness, there will always be circumstances in which decisions about the care plan are going to be dominated by immediate concerns about the safety of the patient and others. Lack of insight and non-adherence to treatment plans that have been put in place to reduce symptoms are particularly challenging aspects of the relationship between the patient and the practitioner. Psychopathological symptoms can seriously impact on a patient s ability to critically assess the implications of some of their actions, and this can result in unpredictable and potentially dangerous behaviour. In these situations, practitioners have to take decisions on behalf of a patient with their best interests in mind. The use of the Mental Health Act may well be part of the most appropriate risk management strategy here. A collaborative approach based on the principles of positive risk management is still the aim, but clearly this will require special efforts in these situations. 5.2 Risk management and the Care Programme Approach Risk management is part of the Care Programme Approach (CPA) and should be aligned closely with it. The CPA involves identifying specific interventions based on an individual s support needs, taking into account safety and risk issues. Care plans should be drawn up to meet all of the patient s needs, including those needs relating to risk. This creates a recorded management plan for the elements of risk to both self and others. The outcome of the risk assessment should also feed back into overall clinical management, since CPA should be applied in cases where there is an increased risk related to mental health problems of harming oneself or others. These steps help to support the continuity of care, which is essential for effective risk management. With risk management is a core part of the CPA process it therefore follows that CPA reviews must include a review of the risk assessment and the risk management plans. These will then inform the content of Crisis and Contingency Plans. 5.3 Supervision & Training Training within Divisions will be agreed on a bespoke basis e.g. the implementation of the Team-Based Risk Assessment and Management Practice Development Initiative in Mental Health Teams. This involves shifting from centralised to team based training. 5.4 Guidance on Recording of risk assessments All significant risk-related decisions should be recorded, signed within the EPR and using the specific tools agreed for the area of practice. Also, whenever it is not possible to follow an important principle of best practice, the reason for this should be documented, signed and dated. The patient and all those involved in their care should have the opportunity to contribute to this documentation and should be provided with copies. This information can be used collaboratively to plan future care. Negative and judgemental labels must be avoided, as they are a barrier to collaboration. A written record of the risk management plan allows practitioners to track changes in the level of risk and to note factors that have previously been considered important. This is particularly important when people have complex needs and are in contact with several agencies. Documentation also helps to protect practitioners in the event of a review. 12
13 5.5 Guidance on Recording risk incidents Whenever staff become aware that harm has occurred to the patient or to others, then the details must be recorded as precisely as possible in the patients clinical record. As a minimum this should include: What happened? What were the circumstances? What were the consequences? How does what happened relate to mental illness? 5.6 Disclosure and communication- general principles If particular individual or groups of victims have been identified in the risk assessment or incident, the supervising clinician should consider whether any steps could be taken to enhance the security of likely victims. Also whether there is any physical security or self-protective skills which could be employed to protect victims. It is likely that such work would be undertaken in conjunction with the Police as part of MAPPA or the Potentially Dangerous Offender protocol (see Appendix 2). Once a risk management plan has been developed or reviewed, it must become a live document and be communicated to the patient and all of those involved in providing their care. The risk management plan will only have a real purpose if it is shared between the relevant parties and used as a basis for joint action. The patient s consent for sharing information in this way should be sought, although the duty of confidentiality can be overridden if there is a clear risk of harm to others. The SHFT policy on information-sharing gives staff clear advice on this. Communication between mental health and learning disability teams, the community and patients families is essential for effective risk assessment. The importance of communicating and sharing information between members of mental health and learning disability teams has become even more crucial with the development of different teams such as AOT, CRHT in addition to CMHT s. Communication can often break down between mental health teams when patients move from one to another and that this can then hinder gaining a full picture of a person s history and, therefore, the assessment of risk. Staff should be aware of the SHFT policy on information-sharing, which gives advice on the need to know. If someone other than the patient is at risk, advice must be sought from the police public protection team or multi-agency public protection arrangements (MAPPA) so that an appropriate public protection plan can be activated. The rationale for any disclosure without consent, e.g. to prevent harm, must be clearly documented. 5.7 Team Working The practitioner may sometimes be working alone, but in most situations the best risk assessments and the most effective decisions are made by a team of experienced practitioners in consultation with the patient and carer. Decisions and assessments should also be based on collaboration between health and social care agencies in hospitals and in the community. In some cases they should be based on collaboration between general and specialist services. The judgements made in a risk assessment should be made in collaboration with others in the multidisciplinary team and with the patient and carer. In instances where the risk seems high, the involvement of senior colleagues to advise and support may be helpful. Multidisciplinary teams should think about the way that they operate and communicate: effective decision-making is more likely in an atmosphere of openness and transparency, where all views are welcomed and responsibility is shared. Teams 13
14 should consider the best way for them to resolve disagreements about a decision, to ensure that the best decisions are made and that team cohesion is preserved. Teams should also be alert to group processes such as the pressure to conform and the potential for groups to recommend more risky courses of action than an individual would. When working across agencies, a common understanding and language should be established for the issues that will be addressed. 5.8 Substance Misuse (Adapted from RCPsych report Rethinking risk to others in mental health services (Royal College of Psychiatrists 2008)). It has long been recognised that substance misuse is a significant factor in increasing the risk of violence to others in patients with mental disorder. Substance misuse is an important cause of all violence, both within and outside the home. The causal mechanisms are complex: drugs and alcohol have direct disinhibitory effects; the social or criminal milieu of substance misusers may encourage or sanction violence; some users fund their substance use through violent crimes, such as robbery; and the personal and social disintegration that accompanies dependence may lead to violence as a way of settling disputes and may contribute directly to domestic violence. Also, and crucially for mental health services, substance misuse makes the symptoms of mental illness worse. It may even cause serious mental illness and it greatly increases the risk of violence in schizophrenia or other serious mental illnesses. However complex the causal links, it is fair to conclude that the removal of substance misuse from the picture would result in a decrease in levels of violence. However substance misuse presents enormous problems and challenges for mental health services. Patients who misuse substances have an increased risk of relapse. Continuing substance misuse during relapse will in turn directly facilitate the expression of violence. In some patients the substance misuse causes the violence. There is a risk that serious mental illness may go unrecognised or untreated when there is coexisting substance misuse, as sometimes psychotic symptoms and challenging behaviour will be attributed solely to the substance use. There are simple measures that can be taken to reduce the risk of violence. Simply advising patients to avoid substances rarely works, but motivational interviewing, as well as more active attempts to encourage treatment for substance misuse or dependence, should form a component of routine clinical practice with patients who misuse or who are dependent on substances. The assessment of any patient with a substance misuse problem should include an enquiry about violence and particularly about domestic violence. In some cases clinicians will need to consider whether they have a duty to warn family members or partners who may be assessed as at risk. However, it is important to treat any mental illness effectively. Some acts of violence perpetrated by people with mental illness can arise directly from the symptoms of their condition. Here, effective treatment of the mental illness can reduce the future risk of violence. Other acts of violence have little or no direct link to mental illness. They can result from social or economic factors, and from misuse of alcohol or drugs. Monitoring and management of substance misuse should be an essential part of the care planning for patients whose risk assessment has identified this as a risk factor. However (as noted above) in practice, substance use is hard to monitor. If there is a history of violence, any sign of drug and alcohol misuse becoming out of control should trigger a reassessment of their risk. Finally, it must be accepted that any mental health service dealing with patients who misuse substances will have an increased rate of violent incidents; these do not indicate deficiencies in the service but are inherent in the challenge that faces all agencies. 14
15 5.9 Learning from Adverse Incidents and Good Practice Practitioners should be aware of the Incident Reporting, Recording and Reviewing Policy and Procedures which advises on the review of all incidents in SHFT. It is recognised that things can go wrong even when best practice has been used. However if this does happen then it is important to learn why, including identifying any mistakes that were made. Learning from near misses is vital to improving services, although not all lessons learned will require changes in practice they may not necessarily lead to better outcomes. SHFT promotes a culture of openness and honesty so that staff feel able to be honest about the decisions that they have taken, the basis on which they made their decisions, and how things might have been done differently and better: lessons can be learned and, where necessary, practices can be changed for the better. Training could also be improved as a result. It is important to remember that any decision is likely to be acceptable if it conformed to relevant guidelines, it was based on the best information available, it was documented and the relevant people were informed. The Trust places a very high emphasis on learning from adverse incidents. Incidents are carefully investigated in accordance with SIRI reporting procedures and the most serious incidents, those resulting in death or serious injury are reviewed for learning and sharing. 15

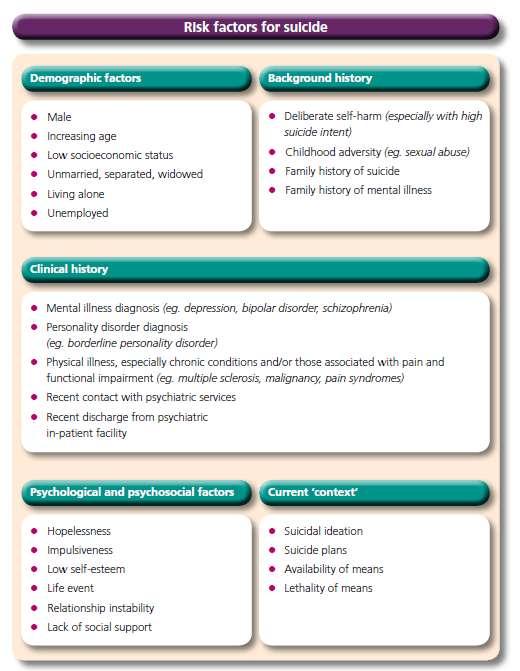
16 Appendix 1- Actuarial Factors The following risk factors for violence and suicide have been derived from the available research (Department of Health 2007): 16
17 17

18 Appendix 2- MAPPA arrangements Multi-Agency Public Protection Arrangements (MAPPA) Multi-Agency Public Protection Arrangements (MAPPA) began in the late 1990s with improved working relationships between Criminal Justice System agencies. The Police, Probation and Prison Services are the key bodies involved in managing risk within MAPPA. In addition a number of other agencies have a Duty to Cooperate with MAPPA. These include Health Service Organisations, i.e. NHS Trusts and PCTs. Offenders who commit sexual or violent offences and who receive a Hospital Order (or Guardianship) will be subject to MAPPA. MAPPA applies to patients who have been convicted of relevant violent or sexual offences. Offences are grouped into 3 categories: The MAPPA legislation imposes a duty on public bodies, including NHS Trust and PCTs to cooperate with the responsible authority for MAPPA. This includes the following obligations: A duty to cooperate in the provision of information to other MAPPA agencies in order to allow risk assessment and risk management. Duty for health professionals to consider as part of ongoing care planning whether there is a need to share information about persons who meet the criteria for MAPPA registration. 18
19 A duty on professionals to consider as an ongoing part of care planning whether there is a need to refer to the responsible authority for consideration for registration for MAPPA. Staff should refer to the policy, Confidentiality and Information Sharing: The Management of Service User Information - Interagency Policy for advice before sharing confidential information with other agencies including MAPPA. Practitioners should always discuss the disclosure of any clinical information to MAPPA with a Consultant Psychiatrist. References Carson D. (2007) Justifying Risk Decisions - Department of Health (2007) Best practice in managing risk - Royal College of Psychiatrists (2008) Rethinking risk to others in mental health services - Further Reading Bouch, J and Marshall, JJ (2005) Suicide risk: structured professional judgement Advan. Psychiatr. Treat., Mar 2005; 11: Clarke, I (2008) Learning from critical incidents Advan. Psychiatr. Treat., Nov 2008; 14: Fagin, L (2006) Repeated self-injury: perspectives from general psychiatry Advan. Psychiatr. Treat., May 2006; 12: Maden A. (2007) Treating violence. Oxford, Oxford University Press. Mullen, P. E. & Ogloff, J. R. P. (2008) Assessing and managing the risks of violence towards others. In New Oxford Textbook of Psychiatry (2nd edn). Oxford University Press. National Institute for Health and Clinical Excellence, Self-harm: The short term physical and psychological management and secondary prevention of self-harm in primary and secondary care, Clinical Guideline 16, NICE, London, July 2004 National Patient Safety Agency (2008) 7 Steps to patient safety in mental health. - Undrill, G (2007) The risks of risk assessment Advan. Psychiatr. Treat., Jul 2007; 13: University of Manchester, Avoidable Death: Five Year Report of the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness, University of Manchester,
Policy for the use of Leave under Section 17 of the Mental Health Act 1983 (as amended) Version: 9
 Version: 9") SH CP 52 Policy for the use of Leave under Section 17 of the Mental Health Act 1983 (as amended) Version: 9 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: Policy for
SH CP 52 Policy for the use of Leave under Section 17 of the Mental Health Act 1983 (as amended) Version: 9 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: Policy for
Care Programme Approach Policies and Procedures. Choice, Responsiveness, Integration & Shared Care
 Care Programme Approach Policies and Procedures Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose:
Care Programme Approach Policies and Procedures Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose:
The Cornwall Framework for the Assessment of Children, Young People and their Families
 The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under Section 17 of the Children Act 1989, local authorities are required to provide services for children
The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under Section 17 of the Children Act 1989, local authorities are required to provide services for children
Preventing suicide. A toolkit for community mental health
 Preventing suicide A toolkit for community mental health Foreword Over a quarter of people who take their own life have been in contact with mental health services in the previous year. While much improvement
Preventing suicide A toolkit for community mental health Foreword Over a quarter of people who take their own life have been in contact with mental health services in the previous year. While much improvement
Safeguarding Adults Policy March 2015
 Safeguarding Adults Policy 2015-16 March 2015 Document Control: Description Comment Title Document Number 1 Author Lindsay Ratapana Date Created March 2015 Date Last Amended Version 1 Approved By Quality
Safeguarding Adults Policy 2015-16 March 2015 Document Control: Description Comment Title Document Number 1 Author Lindsay Ratapana Date Created March 2015 Date Last Amended Version 1 Approved By Quality
Managing deliberate self-harm in young people
 Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: MH27 Version: 2.0 Name of Policy: Care Programme Approach & Care Co-ordination Effective From: 25/08/2015 Date Ratified 24/07/2015 Ratified Mental Health Committee Review Date 01/07/2017 Sponsor
Policy No: MH27 Version: 2.0 Name of Policy: Care Programme Approach & Care Co-ordination Effective From: 25/08/2015 Date Ratified 24/07/2015 Ratified Mental Health Committee Review Date 01/07/2017 Sponsor
APPROVAL OF MENTAL HEALTH CLINICAL RISK ASSESSMENT & MANAGEMENT POLICY
 FOR DECISION AGENDA ITEM 7.2 June 19 th 2012 APPROVAL OF MENTAL HEALTH CLINICAL RISK ASSESSMENT & MANAGEMENT POLICY Report of Paper prepared by Executive Nurse Director Divisional Nurse Mental Heath Executive
FOR DECISION AGENDA ITEM 7.2 June 19 th 2012 APPROVAL OF MENTAL HEALTH CLINICAL RISK ASSESSMENT & MANAGEMENT POLICY Report of Paper prepared by Executive Nurse Director Divisional Nurse Mental Heath Executive
Reducing Risk: Mental health team discussion framework May Contents
 Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Section 117 Policy The Mental Health Act 1983
 Section 117 Policy The Mental Health Act 1983 [as amended by the Mental Health Act 2007] DOCUMENT CONTROL: Version: 1 Ratified by: Mental Health Legislation Committee Date ratified: 2 November 2016 Name
Section 117 Policy The Mental Health Act 1983 [as amended by the Mental Health Act 2007] DOCUMENT CONTROL: Version: 1 Ratified by: Mental Health Legislation Committee Date ratified: 2 November 2016 Name
Page 1 of 18. Summary of Oxfordshire Safeguarding Adults Procedures
 Page 1 of 18 Summary of Oxfordshire Safeguarding Adults Procedures Page 2 of 18 Introduction This part of the procedures sets out clear expectations regarding the standards roles and responsibilities of
Page 1 of 18 Summary of Oxfordshire Safeguarding Adults Procedures Page 2 of 18 Introduction This part of the procedures sets out clear expectations regarding the standards roles and responsibilities of
Safeguarding Adults Policy
 Safeguarding Adults Policy Ratified Status Quality and Patient Safety Committee V2 Issued November 2015 Approved By Consultation Equality Impact Assessment Quality and Patient Safety Committee Safeguarding
Safeguarding Adults Policy Ratified Status Quality and Patient Safety Committee V2 Issued November 2015 Approved By Consultation Equality Impact Assessment Quality and Patient Safety Committee Safeguarding
Refocusing CPA: a summary of the key changes. Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust
 Refocusing CPA: a summary of the key changes Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust Introduction In March 2008, the Department of Health
Refocusing CPA: a summary of the key changes Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust Introduction In March 2008, the Department of Health
Summary guide: Safeguarding Adults: Pan Lancashire and Cumbria Multi Agency Policy and Procedures. For partner agencies staff and volunteers
 Summary guide: Safeguarding Adults: Pan Lancashire and Cumbria Multi Agency Policy and Procedures For partner agencies staff and volunteers 1 1. Introduction This Summary Guide is designed to provide straightforward
Summary guide: Safeguarding Adults: Pan Lancashire and Cumbria Multi Agency Policy and Procedures For partner agencies staff and volunteers 1 1. Introduction This Summary Guide is designed to provide straightforward
Non Attendance (Did Not Attend-DNA ) Policy. Executive Director of Nursing and Chief Operating Officer
 Policy. Executive Director of Nursing and Chief Operating Officer") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Non Attendance (Did Not Attend-DNA) NTW(C)06 Executive Director of Nursing and Chief Operating Officer Ann Marshall
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Non Attendance (Did Not Attend-DNA) NTW(C)06 Executive Director of Nursing and Chief Operating Officer Ann Marshall
Worcestershire Early Intervention Service. Operational Policy
 Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
Continuing Healthcare Policy
 Continuing Healthcare Policy 1 SUMMARY This policy describes the way in which Haringey Clinical Commissioning Group (HCCG) will make provision for the care of people who have been assessed as eligible
Continuing Healthcare Policy 1 SUMMARY This policy describes the way in which Haringey Clinical Commissioning Group (HCCG) will make provision for the care of people who have been assessed as eligible
Clinical Risk Assessment and Management in Mental Health & Learning Disability Services Policy
 Clinical Risk Assessment and Management in Mental Health & Learning Disability Services Policy Document Author Written By: MH & LD Clinical Quality & Safety Leads Authorised Authorised By: Chief Executive
Clinical Risk Assessment and Management in Mental Health & Learning Disability Services Policy Document Author Written By: MH & LD Clinical Quality & Safety Leads Authorised Authorised By: Chief Executive
Informal Patients to take Leave from Adult Mental Health Inpatient Wards. Standard Operating Procedure
 Informal Patients to take Leave from Adult Mental Health Inpatient Wards Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Quality Committee Date ratified: 16 June 2016 Name of originator/author:
Informal Patients to take Leave from Adult Mental Health Inpatient Wards Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Quality Committee Date ratified: 16 June 2016 Name of originator/author:
THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES
 THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES Interim Policy Implementation Guidance and Standards [July 2010] - 1 - CONTENTS 1. Introduction... 3 2. The guiding
THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES Interim Policy Implementation Guidance and Standards [July 2010] - 1 - CONTENTS 1. Introduction... 3 2. The guiding
DELIVERING THE CARE PROGRAMME APPROACH IN WALES
 DELIVERING THE CARE PROGRAMME APPROACH IN WALES Interim Policy Implementation Guidance [July 2010] - 2 - CONTENTS PART 1 Introduction and background... 5 1. Introduction... 5 2. Mental Health (Wales) Measure,
DELIVERING THE CARE PROGRAMME APPROACH IN WALES Interim Policy Implementation Guidance [July 2010] - 2 - CONTENTS PART 1 Introduction and background... 5 1. Introduction... 5 2. Mental Health (Wales) Measure,
(NAME OF HOME) 2.1 This policy is based on the Six Principles of Safeguarding that underpin all our safeguarding work within our service.
 2.1 This policy is based on the Six Principles of Safeguarding that underpin all our safeguarding work within our service.") Title: SAFEGUARDING POLICY 1.0 INTRODUCTION 1.1 Safeguarding means protecting people's health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It's fundamental
Title: SAFEGUARDING POLICY 1.0 INTRODUCTION 1.1 Safeguarding means protecting people's health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It's fundamental
SAFEGUARDING CHILDREN POLICY
 SAFEGUARDING CHILDREN POLICY The child s needs are paramount, and the needs and wishes of each child, be they a baby or infant, or an older child, should be put first Working Together 2015 p 8 Keeping
SAFEGUARDING CHILDREN POLICY The child s needs are paramount, and the needs and wishes of each child, be they a baby or infant, or an older child, should be put first Working Together 2015 p 8 Keeping
The CARE CERTIFICATE. Duty of Care. What you need to know. Standard THE CARE CERTIFICATE WORKBOOK
 The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
SAFEGUARDING CHILDEN POLICY. Policy Reference: Version: 1 Status: Approved
 SAFEGUARDING CHILDEN POLICY Policy Reference: Version: 1 Status: Approved Type: Clinical Policy Policy applies to : All services within SCH Serco Policy applies to (staff groups): All SCH Serco staff Policy
SAFEGUARDING CHILDEN POLICY Policy Reference: Version: 1 Status: Approved Type: Clinical Policy Policy applies to : All services within SCH Serco Policy applies to (staff groups): All SCH Serco staff Policy
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Wandsworth CCG. Continuing Healthcare Commissioning Policy
 Wandsworth CCG Continuing Healthcare Commissioning Policy Document Control Title Originator/author: Approval Body Wandsworth CCG Continuing Healthcare Commissioning Policy Alison Kirby / Munya Nhamo Wandsworth
Wandsworth CCG Continuing Healthcare Commissioning Policy Document Control Title Originator/author: Approval Body Wandsworth CCG Continuing Healthcare Commissioning Policy Alison Kirby / Munya Nhamo Wandsworth
Safeguarding Adults Policy
 Safeguarding Adults Policy Ratified Status Approved Final Issued December 2016 Approved By Consultation Equality Impact Assessment Distribution All Staff Date Amended following initial ratification November
Safeguarding Adults Policy Ratified Status Approved Final Issued December 2016 Approved By Consultation Equality Impact Assessment Distribution All Staff Date Amended following initial ratification November
Care Programme Approach
 Care Programme Approach Who Should Read This Policy Target Audience All Clinical Staff Care Coordinator Version 1.1 May 2017 Ref. Contents Page 1.0 Introduction 5 2.0 Purpose 5 3.0 Objectives 6 4.0 Process
Care Programme Approach Who Should Read This Policy Target Audience All Clinical Staff Care Coordinator Version 1.1 May 2017 Ref. Contents Page 1.0 Introduction 5 2.0 Purpose 5 3.0 Objectives 6 4.0 Process
Policy: A4 Alcohol and Illicit Drugs Procedure (Broadmoor Hospital only)
") Policy: A4 Alcohol and Illicit Drugs Procedure (Broadmoor Hospital only) Policy relates to: D2 Dual Diagnosis policy Version: A4/08 Ratified by: Policy Review Group Date ratified: 24 th September 2015
Policy: A4 Alcohol and Illicit Drugs Procedure (Broadmoor Hospital only) Policy relates to: D2 Dual Diagnosis policy Version: A4/08 Ratified by: Policy Review Group Date ratified: 24 th September 2015
Guide to the Continuing NHS Healthcare Assessment Process
 Guide to the Continuing NHS Healthcare Assessment Process Continuing NHS Healthcare (CHC) is a package of care arranged and funded solely by the NHS, where it has been assessed that the person s primary
Guide to the Continuing NHS Healthcare Assessment Process Continuing NHS Healthcare (CHC) is a package of care arranged and funded solely by the NHS, where it has been assessed that the person s primary
Care Programme Approach (CPA) Policy
 Policy") Care Programme Approach (CPA) Policy DOCUMENT CONTROL: Version: 10 Ratified by: Quality and Safety Sub Committee Date ratified: 3 May 2017 Name of originator/author: Nurse Consultant, AMHS Name of responsible
Care Programme Approach (CPA) Policy DOCUMENT CONTROL: Version: 10 Ratified by: Quality and Safety Sub Committee Date ratified: 3 May 2017 Name of originator/author: Nurse Consultant, AMHS Name of responsible
Care Programme Approach (CPA)
") Care Programme Approach (CPA) The Care Programme Approach (CPA) is a package of care that may be used to plan your mental health care. This factsheet explains what CPA is, when you should get and when
Care Programme Approach (CPA) The Care Programme Approach (CPA) is a package of care that may be used to plan your mental health care. This factsheet explains what CPA is, when you should get and when
Document Title Clinical Risk Assessment and Management Policy. Electronic Systems Development & Training Consultant Risk and Assurance Facilitator
 Document Title Clinical Risk Assessment and Management Policy Document Description Document Type Policy Service Application Trust Wide Version 1.2 Policy Reference no. POL 025 Lead Author(s) Name Bob Yardley
Document Title Clinical Risk Assessment and Management Policy Document Description Document Type Policy Service Application Trust Wide Version 1.2 Policy Reference no. POL 025 Lead Author(s) Name Bob Yardley
Hospital Discharge and Transfer Guidance. Choice, Responsiveness, Integration & Shared Care
 Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Mencap - Dorset Support Service
 Royal Mencap Society Mencap - Dorset Support Service Inspection report Unit 5, Prospect House Peverell Avenue East, Poundbury Dorchester Dorset DT1 3WE Date of inspection visit: 08 December 2016 Date of
Royal Mencap Society Mencap - Dorset Support Service Inspection report Unit 5, Prospect House Peverell Avenue East, Poundbury Dorchester Dorset DT1 3WE Date of inspection visit: 08 December 2016 Date of
SAFEGUARDING CHILDREN POLICY 2016
 POL 022 SAFEGUARDING CHILDREN POLICY 2016 Version 3.0 Ratified By Date Ratified NHS Wirral Clinical Commissioning Group :Quality, Performance & Finance Committee Author(s) Responsible Committee / Officers
POL 022 SAFEGUARDING CHILDREN POLICY 2016 Version 3.0 Ratified By Date Ratified NHS Wirral Clinical Commissioning Group :Quality, Performance & Finance Committee Author(s) Responsible Committee / Officers
A thematic review of six independent investigations. A report for NHS England, North Region
 A thematic review of six independent investigations A report for NHS England, North Region November 2014 Authors: Chris Brougham Liz Howes Verita 2014 Verita is a management consultancy that works with
A thematic review of six independent investigations A report for NHS England, North Region November 2014 Authors: Chris Brougham Liz Howes Verita 2014 Verita is a management consultancy that works with
Medical Consultant Change Request Procedure
 SH CP 154 Medical Consultant Change Request Procedure Version 1 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: This document outlines the Trust s procedure for requesting
SH CP 154 Medical Consultant Change Request Procedure Version 1 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: This document outlines the Trust s procedure for requesting
Adult Mental Health Team AMHT Standard Operating Procedure
 SH CP 198 Adult Mental Health Team AMHT Standard Operating Procedure Summary: Keywords: Target Audience: This Standard Operating Procedure describes the roles and functions of The Acute Mental Health Teams
SH CP 198 Adult Mental Health Team AMHT Standard Operating Procedure Summary: Keywords: Target Audience: This Standard Operating Procedure describes the roles and functions of The Acute Mental Health Teams
Clinical Supportive Observation, Intervention and Engagement of Service Users Policy
 Clinical Supportive Observation, Intervention and Engagement of Service Users Policy Document Control Summary Status: Version: Author/Title: Owner/Title: Approved by: Ratified: Related Trust Strategy and/or
Clinical Supportive Observation, Intervention and Engagement of Service Users Policy Document Control Summary Status: Version: Author/Title: Owner/Title: Approved by: Ratified: Related Trust Strategy and/or
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
The Cornwall Framework for the Assessment of Children, Young People and their Families
 The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under the Children Act 1989, local authorities are required to provide services for children in need
The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under the Children Act 1989, local authorities are required to provide services for children in need
Safeguarding through Commissioning Policy
 Safeguarding through Commissioning Policy Date December 2015 Document control Authors Reagender Kang, Roger Cornish Version 1.3 Amendments to Version 1 Amendments made by: Reagender Kang Designated Nurse
Safeguarding through Commissioning Policy Date December 2015 Document control Authors Reagender Kang, Roger Cornish Version 1.3 Amendments to Version 1 Amendments made by: Reagender Kang Designated Nurse
Framework for Managing Care Care Coordinators Handbook
 Ymddiriedolaeth GIG Gogledd Cymru North Wales NHS Trust (Central Area) Division of Mental Health, Learning Disability and Psychology Including Ymddiriedolaeth GIG Siroedd Conwy a Dinbych Adult Mental Health
Ymddiriedolaeth GIG Gogledd Cymru North Wales NHS Trust (Central Area) Division of Mental Health, Learning Disability and Psychology Including Ymddiriedolaeth GIG Siroedd Conwy a Dinbych Adult Mental Health
Adult Psychotherapist Specialist Personality Disorder (Mentalization Based Treatment)
") Job Title: dult Psychotherapist Specialist Personality Disorder (Mentalization Based Treatment) Band: 7 Hours: Department: Location: Reports to: Responsible for: 37.5 hours per week Croydon Personality
Job Title: dult Psychotherapist Specialist Personality Disorder (Mentalization Based Treatment) Band: 7 Hours: Department: Location: Reports to: Responsible for: 37.5 hours per week Croydon Personality
Luton Psychiatric Liaison Service (PLS) Job Description & Person Specification
 Job Description & Person Specification") Luton Psychiatric Liaison Service (PLS) Job Description & Person Specification Job Title: Psychiatric Liaison Nurse Practitioner Grade: Band 6 Hours: Responsible To: Accountable To: Location 37.5 Hours
Luton Psychiatric Liaison Service (PLS) Job Description & Person Specification Job Title: Psychiatric Liaison Nurse Practitioner Grade: Band 6 Hours: Responsible To: Accountable To: Location 37.5 Hours
Statement on the core values and attributes needed to study medicine
 Ceri Nursaw - Accessing Work Experience in Health and Care HEPP CPD conference 24 March 2015 Statement on the core values and attributes needed to study medicine Introduction This statement sets out the
Ceri Nursaw - Accessing Work Experience in Health and Care HEPP CPD conference 24 March 2015 Statement on the core values and attributes needed to study medicine Introduction This statement sets out the
Clinical Risk Assessment and Management Policy
 Clinical Risk Assessment and Management Policy For Individual Service Users Version: 8 Executive Lead: Lead Author: Approved Date: Approved By: Ratified Date: Ratified By: Issue Date: Review Date: Executive
Clinical Risk Assessment and Management Policy For Individual Service Users Version: 8 Executive Lead: Lead Author: Approved Date: Approved By: Ratified Date: Ratified By: Issue Date: Review Date: Executive
Core Domain You will be able to: You will know and understand: Leadership, Management and Team Working
 DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
ANEURIN BEVAN HEALTH BOARD & CAERPHILLY COUNTY BOROUGH COUNCIL ACTION PLAN
 ANEURIN BEVAN HEALTH BOARD & CAERPHILLY COUNTY BOROUGH COUNCIL RESPONSE TO THE REPORT BY HEALTH INSPECTORATE WALES REVIEW IN RESPECT OF: MR H AND THE PROVISION OF MENTAL HEALTH SERVICES, FOLLOWING THE
ANEURIN BEVAN HEALTH BOARD & CAERPHILLY COUNTY BOROUGH COUNCIL RESPONSE TO THE REPORT BY HEALTH INSPECTORATE WALES REVIEW IN RESPECT OF: MR H AND THE PROVISION OF MENTAL HEALTH SERVICES, FOLLOWING THE
Consultant and Speciality and Associate Specialists (SAS) Doctor Job Planning Procedure
 Doctor Job Planning Procedure") SH HR 70 Consultant and Speciality and Associate Specialists (SAS) Doctor Job Planning Procedure Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: This document outlines
SH HR 70 Consultant and Speciality and Associate Specialists (SAS) Doctor Job Planning Procedure Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: This document outlines
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process
 Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Fitness to Practise Policy and Procedures for Veterinary Nurse Students
 Fitness to Practise Policy and Procedures for Veterinary Nurse Students SEPTEMBER 2017 Fitness to Practise Policy and Procedures for Veterinary Nurse Students 1.1 Introduction: What is Fitness to Practise?
Fitness to Practise Policy and Procedures for Veterinary Nurse Students SEPTEMBER 2017 Fitness to Practise Policy and Procedures for Veterinary Nurse Students 1.1 Introduction: What is Fitness to Practise?
The NHS Constitution
 2 The NHS Constitution The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot
2 The NHS Constitution The NHS belongs to the people. It is there to improve our health and wellbeing, supporting us to keep mentally and physically well, to get better when we are ill and, when we cannot
ADASS Safeguarding Adults Policy Network. Guidance. June 2016
 ADASS Safeguarding Adults Policy Network Guidance June 2016 Out-of-Area Safeguarding Adults Arrangements Guidance for Inter-Authority Safeguarding Adults Enquiry and Protection Arrangements Table of Contents
ADASS Safeguarding Adults Policy Network Guidance June 2016 Out-of-Area Safeguarding Adults Arrangements Guidance for Inter-Authority Safeguarding Adults Enquiry and Protection Arrangements Table of Contents
HoNOS Frequently Asked Questions
 HoNOS Frequently Asked Questions The answers in this document are based on the information found on the Royal College of Psychiatrists webpage and policy adopted by Southern health Foundation Trust. If
HoNOS Frequently Asked Questions The answers in this document are based on the information found on the Royal College of Psychiatrists webpage and policy adopted by Southern health Foundation Trust. If
CLINICAL ASSESSMENT AND MANAGEMENT OF RISK OF HARM TO SELF AND OTHERS POLICY
 CLINICAL ASSESSMENT AND MANAGEMENT OF RISK OF HARM TO SELF AND OTHERS POLICY Version: 5 Ratified by: Date ratified: August 2015 Title of originator/author: Title of responsible committee/group: Date issued:
CLINICAL ASSESSMENT AND MANAGEMENT OF RISK OF HARM TO SELF AND OTHERS POLICY Version: 5 Ratified by: Date ratified: August 2015 Title of originator/author: Title of responsible committee/group: Date issued:
Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adult Reviews (SAR) Protocol
 Protocol") Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adult Reviews (SAR) Protocol SAR Process July 2014 (revised August 2017) Page 1 Contents 1. Introduction 2. Criteria 3.
Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adult Reviews (SAR) Protocol SAR Process July 2014 (revised August 2017) Page 1 Contents 1. Introduction 2. Criteria 3.
Safeguarding & Wellbeing Policy
 Safeguarding & Wellbeing Policy 4.0 June 17 June 19 (unless an earlier review is required by legislative changes) All Midland Staff, Contractors and Volunteers Rebekah Newton, Director of Retirement Living
Safeguarding & Wellbeing Policy 4.0 June 17 June 19 (unless an earlier review is required by legislative changes) All Midland Staff, Contractors and Volunteers Rebekah Newton, Director of Retirement Living
NORTH AYRSHIRE COUNCIL EDUCATION AND YOUTH EMPLOYMENT THE USE OF PHYSICAL INTERVENTION IN EDUCATIONAL ESTABLISHMENTS
 Appendix 1 NORTH AYRSHIRE COUNCIL EDUCATION AND YOUTH EMPLOYMENT THE USE OF PHYSICAL INTERVENTION IN EDUCATIONAL ESTABLISHMENTS Contents 1 Introduction Page 3 1.1 Purpose of this Policy Page 3 1.2 Rationale
Appendix 1 NORTH AYRSHIRE COUNCIL EDUCATION AND YOUTH EMPLOYMENT THE USE OF PHYSICAL INTERVENTION IN EDUCATIONAL ESTABLISHMENTS Contents 1 Introduction Page 3 1.1 Purpose of this Policy Page 3 1.2 Rationale
Mental Health Act Policy. Board library reference Document author Assured by Review cycle. Introduction Purpose or aim Scope...
 Mental Health Act Policy Board library reference Document author Assured by Review cycle P041 Associate Director of Governance, Quality and Regulatory Compliance Quality and Standards Committee 1 Year
Mental Health Act Policy Board library reference Document author Assured by Review cycle P041 Associate Director of Governance, Quality and Regulatory Compliance Quality and Standards Committee 1 Year
JOB DESCRIPTION. Specialist Looked After Children s Nurse
 JOB DESCRIPTION Job Title: Division/Department: Responsible to: Accountable to: Looked After Children Nurse Womens & Children Division / ESCAN Specialist Looked After Children s Nurse Specialist Looked
JOB DESCRIPTION Job Title: Division/Department: Responsible to: Accountable to: Looked After Children Nurse Womens & Children Division / ESCAN Specialist Looked After Children s Nurse Specialist Looked
SCDHSC0434 Lead practice for managing and disseminating records and reports
 Lead practice for managing and disseminating records and reports Overview This standard identifies requirements when you lead practice for managing and disseminating records and reports. This includes
Lead practice for managing and disseminating records and reports Overview This standard identifies requirements when you lead practice for managing and disseminating records and reports. This includes
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
NOT PROTECTIVELY MARKED
 POLICY / PROCEDURE Security Classification Disclosable under Freedom of Information Act 2000 NOT PROTECTIVELY MARKED Yes POLICY TITLE Welfare Services REFERENCE NUMBER A114 Version 1.1 POLICY OWNERSHIP
POLICY / PROCEDURE Security Classification Disclosable under Freedom of Information Act 2000 NOT PROTECTIVELY MARKED Yes POLICY TITLE Welfare Services REFERENCE NUMBER A114 Version 1.1 POLICY OWNERSHIP
CARE PROGRAMME APPROACH POLICY. Care Programme Approach. Quality and Safety Committee. Disclaimer
 CARE PROGRAMME APPROACH POLICY Reference No: UHB 118 Version No: 1 Previous Trust / LHB Ref No: T/226 Documents to read alongside this Policy Care Programme Approach Procedures Classification of document:
CARE PROGRAMME APPROACH POLICY Reference No: UHB 118 Version No: 1 Previous Trust / LHB Ref No: T/226 Documents to read alongside this Policy Care Programme Approach Procedures Classification of document:
An independent thematic review of investigations into the care and treatment provided to service users who committed a homicide and to a victim of
 An independent thematic review of investigations into the care and treatment provided to service users who committed a homicide and to a victim of homicide by Sussex Partnership NHS Foundation Trust: Extended
An independent thematic review of investigations into the care and treatment provided to service users who committed a homicide and to a victim of homicide by Sussex Partnership NHS Foundation Trust: Extended
Code of Professional Conduct and Ethics. Bord Clárchúcháin na dteiripeoirí Urlabhartha agus Teanga. Speech and Language Therapists Registration Board
 Speech and Language Therapists Registration Board Code of Professional Conduct and Ethics Bord Clárchúcháin na dteiripeoirí Urlabhartha agus Teanga Speech and Language Therapists Registration Board Note:
Speech and Language Therapists Registration Board Code of Professional Conduct and Ethics Bord Clárchúcháin na dteiripeoirí Urlabhartha agus Teanga Speech and Language Therapists Registration Board Note:
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Care and Treatment Review: Policy and Guidance
 Care and Treatment Review: Policy and Guidance With policy and guidance on Care, Education and Treatment Reviews for children and young people Easy Read Version 2017 1 Contents Foreword from Gavin Harding...
Care and Treatment Review: Policy and Guidance With policy and guidance on Care, Education and Treatment Reviews for children and young people Easy Read Version 2017 1 Contents Foreword from Gavin Harding...
Quality Assurance Framework Adults Services. Framework. Version: 1.2 Effective from: August 2016 Review date: June 2017
 Quality Assurance Framework Adults Services Framework Version: 1.2 Effective from: August 2016 Review date: June 2017 Signed off by: Sharon Gogan Title: Head of Adult Social Care Date: 20 th May 2014 Quality
Quality Assurance Framework Adults Services Framework Version: 1.2 Effective from: August 2016 Review date: June 2017 Signed off by: Sharon Gogan Title: Head of Adult Social Care Date: 20 th May 2014 Quality
Warwickshire. Domestic Abuse Multi-Agency Risk Assessment Conference (MARAC) Operating Protocol
 Operating Protocol") Warwickshire Domestic Abuse Multi-Agency Risk Assessment Conference (MARAC) Operating Protocol Contents 1 Introduction... 4 1.1 Multi-Agency Risk Assessment Conferences... 4 1.2 Multi Agency Risk Assessment
Warwickshire Domestic Abuse Multi-Agency Risk Assessment Conference (MARAC) Operating Protocol Contents 1 Introduction... 4 1.1 Multi-Agency Risk Assessment Conferences... 4 1.2 Multi Agency Risk Assessment
Safeguarding Vulnerable Adults Policy and Procedures
 155-159 Freeman Street, Grimsby, North East Lincolnshire, DN32 7AR Tel: 01472 240440 Safeguarding Vulnerable Adults Policy and Procedures The CPO Media policy adheres to the multi-agency policy, procedures
155-159 Freeman Street, Grimsby, North East Lincolnshire, DN32 7AR Tel: 01472 240440 Safeguarding Vulnerable Adults Policy and Procedures The CPO Media policy adheres to the multi-agency policy, procedures
Executive Director of Nursing and Operations. Liz Bowman Care Coordination Development Lead
 Document Title Reference Number Lead Officer Author(s) Ratified by Care Coordination (Incorporating Care Programme Approach (CPA)) Policy NTW(C)20 Executive Director of Nursing and Operations Liz Bowman
Document Title Reference Number Lead Officer Author(s) Ratified by Care Coordination (Incorporating Care Programme Approach (CPA)) Policy NTW(C)20 Executive Director of Nursing and Operations Liz Bowman
SAFEGUARDING ADULTS COMMISSIONING POLICY
 SAFEGUARDING ADULTS COMMISSIONING POLICY Director Responsible: Responsible person Target Audience: Name of Responsible Committee Nursing Matt O Connor Safeguarding Adults Lead All NHSBA staff and contractors
SAFEGUARDING ADULTS COMMISSIONING POLICY Director Responsible: Responsible person Target Audience: Name of Responsible Committee Nursing Matt O Connor Safeguarding Adults Lead All NHSBA staff and contractors
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY
 SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
Policies, Procedures, Guidelines and Protocols
 Title Policies, Procedures, Guidelines and Protocols Document Details Trust Ref No 2078-28878 Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director)
Title Policies, Procedures, Guidelines and Protocols Document Details Trust Ref No 2078-28878 Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director)
SAFEGUARDING ADULTS POLICY
 SAFEGUARDING ADULTS POLICY This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: POVA Operational
SAFEGUARDING ADULTS POLICY This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: POVA Operational
Lone worker policy. Director of Nursing Therapies Patient Partnership Author and contact number Safety and Security Lead
 Document level: Trustwide (TW) Code: GR33 Issue number: 3 Lone worker policy Lead executive Director of Nursing Therapies Patient Partnership Author and contact number Safety and Security Lead 01244 397618
Document level: Trustwide (TW) Code: GR33 Issue number: 3 Lone worker policy Lead executive Director of Nursing Therapies Patient Partnership Author and contact number Safety and Security Lead 01244 397618
POLICY & PROCEDURE FOR INCIDENT REPORTING
 POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
Leave for restricted patients the Ministry of Justice s approach
 Mental Health Unit GUIDANCE FOR RESPONSIBLE MEDICAL OFFICERS LEAVE OF ABSENCE FOR PATIENTS SUBJECT TO RESTRICTIONS (Restrictions under Mental Health Act 1983 sections 41, 45a & 49 and under the Criminal
Mental Health Unit GUIDANCE FOR RESPONSIBLE MEDICAL OFFICERS LEAVE OF ABSENCE FOR PATIENTS SUBJECT TO RESTRICTIONS (Restrictions under Mental Health Act 1983 sections 41, 45a & 49 and under the Criminal
The Code Standards of conduct, performance and ethics for chiropractors. Effective from 30 June 2016
 The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016 2 The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016
The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016 2 The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016
SCDHSC0450 Develop risk management plans to promote independence in daily living
 Develop risk management plans to promote independence in daily living Overview This standard identifies the requirements when developing risk management plans to promote independence in daily living. This
Develop risk management plans to promote independence in daily living Overview This standard identifies the requirements when developing risk management plans to promote independence in daily living. This
Policies, Procedures, Guidelines and Protocols
 Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Safeguarding Vulnerable Adults Policy
 POLICY & PROCEDURES PROTECTION OF VULNERABLE ADULTS This policy was written in conjunction with the Multi-Agency Safeguarding of Vulnerable Adults in Lincolnshire Policy STATEMENT The welfare of all vulnerable
POLICY & PROCEDURES PROTECTION OF VULNERABLE ADULTS This policy was written in conjunction with the Multi-Agency Safeguarding of Vulnerable Adults in Lincolnshire Policy STATEMENT The welfare of all vulnerable
This is the consultation responses analysis put together by the Hearing Aid Council and considered at their Council meeting on 12 November 2008
 Analysis of responses - Hearing Aid Council and Health Professions Council consultation on standards of proficiency and the threshold level of qualification for entry to the Hearing Aid Audiologists/Dispensers
Analysis of responses - Hearing Aid Council and Health Professions Council consultation on standards of proficiency and the threshold level of qualification for entry to the Hearing Aid Audiologists/Dispensers
SUICIDE PREVENTION POLICY
 SUICIDE PREVENTION POLICY DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Assurance Sub Group Date ratified: 25 October 2011 Name of originator/author: Patient Safety Lead Name of responsible Clinical
SUICIDE PREVENTION POLICY DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Assurance Sub Group Date ratified: 25 October 2011 Name of originator/author: Patient Safety Lead Name of responsible Clinical
The need for a distinct, radically different, visibly-led, strategic, proportionate, holistic, woman-centred, integrated approach
 The need for a distinct, radically different, visibly-led, strategic, proportionate, holistic, woman-centred, integrated approach Women in Forensic Services Workshop presentation Barcelona 5 February 2009
The need for a distinct, radically different, visibly-led, strategic, proportionate, holistic, woman-centred, integrated approach Women in Forensic Services Workshop presentation Barcelona 5 February 2009
Safeguarding Strategy
 1 Safeguarding Strategy 2017-2020 2 Contents Section Page No. 1 1.1 1.2 2.0 2.1 Introduction Legal Framework for Safeguarding What does Safeguarding cover? Our Duties Statutory Compliance for Safeguarding
1 Safeguarding Strategy 2017-2020 2 Contents Section Page No. 1 1.1 1.2 2.0 2.1 Introduction Legal Framework for Safeguarding What does Safeguarding cover? Our Duties Statutory Compliance for Safeguarding
Care Programme Approach (CPA): Standard Operating Procedure
: Standard Operating Procedure") Clinical Care Programme Approach (CPA): Standard Operating Procedure Document Control Summary Status: New Version: v1.2 Date: 22/09/15 Author/Owner/Title: Kenny Laing Deputy Director of Nursing Approved
Clinical Care Programme Approach (CPA): Standard Operating Procedure Document Control Summary Status: New Version: v1.2 Date: 22/09/15 Author/Owner/Title: Kenny Laing Deputy Director of Nursing Approved
Choice on Discharge Policy
 Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
CHILD PROTECTION POLICY
 BISHOPBRIGGS VILLAGE NURSERY SCOTTISH CHARITY NO. SC006583 CHILD PROTECTION POLICY At Bishopbriggs Village Nursery we follow East Dunbartonshire Council's Child Protection guidelines and intend to create
BISHOPBRIGGS VILLAGE NURSERY SCOTTISH CHARITY NO. SC006583 CHILD PROTECTION POLICY At Bishopbriggs Village Nursery we follow East Dunbartonshire Council's Child Protection guidelines and intend to create
EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST
 EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST STRATEGIC HEALTH AUTHORITY 1 Contents Page The Panel 3 1
EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST STRATEGIC HEALTH AUTHORITY 1 Contents Page The Panel 3 1
Procedure for Discharge from Inpatient Units including 48 hour Follow Up. (Wotton Lawn only)
") Procedure for Discharge from Inpatient Units including 48 hour Follow Up (Wotton Lawn only) Version: Version 3 Consultation: Ratified by: Date ratified: Name of originator/author: Date issued: July 2012
Procedure for Discharge from Inpatient Units including 48 hour Follow Up (Wotton Lawn only) Version: Version 3 Consultation: Ratified by: Date ratified: Name of originator/author: Date issued: July 2012
The Code. Professional standards of practice and behaviour for nurses and midwives
 The Code Professional standards of practice and behaviour for nurses and midwives Introduction The Code contains the professional standards that registered nurses and midwives must uphold. UK nurses and
The Code Professional standards of practice and behaviour for nurses and midwives Introduction The Code contains the professional standards that registered nurses and midwives must uphold. UK nurses and
CONTINUING HEALTHCARE POLICY
 BEFORE USING THIS POLICY ALWAYS ENSURE YOU ARE USING THE MOST UP TO DATE VERSION CONTINUING HEALTHCARE POLICY 1 SUMMARY This policy describes the way in which the five Primary Care Trusts in NHS North
BEFORE USING THIS POLICY ALWAYS ENSURE YOU ARE USING THE MOST UP TO DATE VERSION CONTINUING HEALTHCARE POLICY 1 SUMMARY This policy describes the way in which the five Primary Care Trusts in NHS North
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
This policy should be read in conjunction with all related policies and procedures. See the separate list in the Policies and Procedures file.
 Safeguarding Adults Policy and Procedure Related policies and procedures This policy should be read in conjunction with all related policies and procedures. See the separate list in the Policies and Procedures
Safeguarding Adults Policy and Procedure Related policies and procedures This policy should be read in conjunction with all related policies and procedures. See the separate list in the Policies and Procedures
POLICY AND PROCEDURE. Managing Actual & Potential Aggression. SoLO Life Opportunities. Introduction. Position Statement
 POLICY AND PROCEDURE Managing Actual & Potential Aggression Category: staff and volunteers/members SoLO Life Opportunities 38 Walnut Close Chelmsley Wood Birmingham B37 7PU Charity No. 1102297 England
POLICY AND PROCEDURE Managing Actual & Potential Aggression Category: staff and volunteers/members SoLO Life Opportunities 38 Walnut Close Chelmsley Wood Birmingham B37 7PU Charity No. 1102297 England