Background Document for Consultation: Proposed Fraser Health Medical Governance Model
|
|
|
- Edmund McCarthy
- 6 years ago
- Views:
Transcription
1 Background Document for Consultation: Proposed Fraser Health Medical Governance Model Working Draft 6/19/2009 1
2 Table of Contents Introduction and Context Purpose of this Document 1 Clinical Integration 1 Program Management Overview 2 Proposed Medical Governance Structures Principles 6 Physician Leadership Positions 7 Roles and Accountabilities 8 Physician Compensation 8 Medical Staff Structure 9 Physician Leadership Development 10 Next Steps 11 Working Draft 6/19/2009 2
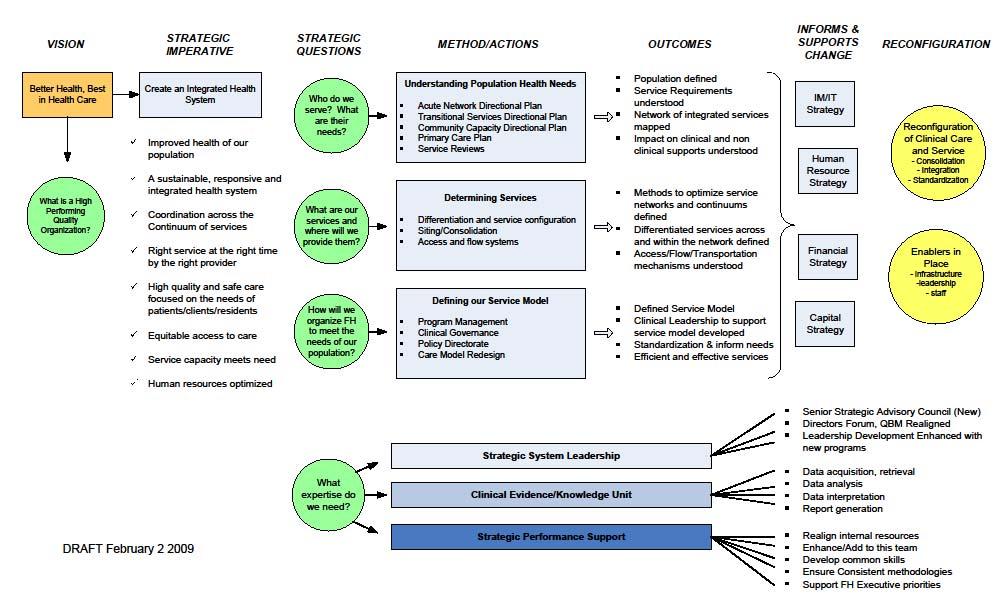
3 Introduction & Context The Purpose of this Document This document outlines a draft framework for the evolution of medical governance within Fraser Health, one which aligns with our proposed program management model and supports our broader strategy to develop an integrated health system. This document is intended to provide a starting point for discussions with medical leaders across Fraser Health. It describes key concepts including guiding principles, assumptions, governance structures, leadership roles and accountabilities. This has been developed based on experience and lessons learned from other jurisdictions and will be refined and elaborated on once consultation on this draft is concluded. The Context: Clinical Integration Developing an Integrated Health System is one of Fraser Health s six strategic imperatives aimed at ensuring we have a sustainable and responsive health system that meets the needs of Fraser Health residents. In addition to the work on Program Management, there are a number of other related initiatives underway that support clinical integration (Appendix 1) 5 Goals of Clinical Integration Increase understanding of system integration to reflect the needs of our population Align primary, acute and community networks to deliver the right care, in the right place Create integrated service, clinical governance and leadership models Use clinical information and technology to advance integration and quality of care and service Redesign the care delivery system to support leading practice and enhance efficiency Briefly, the Clinical Integration work falls into three broad grouping: Understanding Service Needs: these projects build on the work done over the last number of years to forecast our population s service needs in acute care, community care, transition support and primary care and how that fits with our current capacity. Determining How Services Will Be Delivered: This set of activities will help us determine how we will deliver services in the future to meet these demands. These are projects related to siting Working Draft 6/19/2009 3
4 and consolidation of services taking into account access, flow and transportation issues. Defining our Service Model: This final set of interrelated initiatives will help us define how Fraser Health will organize itself to deliver care and service. This initiative on program management and related ones on medical governance, care models, and professional practice are part of that process. Together, these initiatives will guide our planning and resource allocation as we move forward to achieve our vision of Better Health, Best in Health Care. Physician leaders have been and will continue to be engaged in all of these initiatives. Going forward, it is important that our Medical Staff Governance structure aligns with our proposed program management structure and that it supports our overall integration strategy. Program Management Model.Program Management is an organizational model where a defined leadership team is given the clinical and fiscal accountability for delivering, and/or arranging to deliver a set of services for a defined population or group. Program Types Fraser Health s programs will be organized around: Clinical Services Programs: These are programs that are organized along a service stream i.e. Services such as critical care, diagnostics, home care, or surgical care. A key focus of the Clinical Services programs will be to reduce variation in practice, streamline services, implement best practice and improve access to services. Clinical Population Programs: These programs are designed to meet the needs of a clinical population such as those with mental health and addictions issues, or renal disease. These programs function across the acute to community continuum and focus on coordinating functions / services and fostering multidisciplinary coordinated care. A key goal is to ensure that the patient/client s journey is seamless and that the care pathway is based on best / leading practice. Population Health Programs: The third type of program is that focused on a broader population such as the older adult, aboriginal population, or child and youth. These programs will deliver some services but clearly not all services. Their primary goal will be to influence health practice and policy for their defined populations across Fraser Health. Working Draft 6/19/2009 4
5 Most Health Authorities across the country that have implemented program management have a mix of these types due to the complexity and scope of the functions and relationships associated with operating a regional system for health. In addition to Fraser Health owned services, many programs will have contracts or agreements with non FH owned organizations / groups who provide care and service to this population. An integrated system will have strong partnerships across a range of stakeholders. Program Characteristics Program management supports stronger clinical governance or clinical accountability for continuous improvement of the quality of care and service. Every program will have a defined scope and the accountability to ensure that the services provided to the target population are effective and responsive, and consistent with evidence-based standards and performance metrics. The programs will ensure that all undertakings align with FH s strategic directions and themes and any specific MoH commitment or performance expectation. The programs will also have fiscal accountability for ensuring that the assigned resources are used to achieve optimal outcomes, with this reflected in a three year service plan. Program Characteristics Clinical and fiscal accountability Clearly defined leadership team with clinical governance responsibility Serves a defined population with a common set of needs Has a Fraser Health wide responsibility as defined by program scope. (Draft) Program Structure The proposed program structure for Fraser Health was determined using the following criteria as a lens to assess which services should be managed in a program and how quickly. These include criteria related to: Legitimacy (there is a clear rationale to have these services run as a program ) Feasibility (based on a number of factors related to HR, size, etc.) Process Used To Determine Programs Assessment criteria o Legitimacy o Feasibility o Support Lessons learned from other jurisdictions Support (there is strong enough support within the organization to move this forward or that support can be developed) These criteria are phased. The legitimacy lens was used as the first test as there was clearly no need to move to the others if that test failed. As indicated earlier, these criteria are a lens through which the SC and core team worked through and defined a draft structure. Working Draft 6/19/2009 5
6 The assessment was also guided by the lessons learned from other jurisdictions and the literature lessons related to size and number of programs for instance e.g. that a smaller number of larger programs was easier to manage than a proliferation of small programs. Program Roles and Accountabilities Exhibit 3 begins to outline the potential role and functions of the program in four broad areas. Exhibit 3. Proposed Roles and Accountabilities of the Programs Planning / Policy / Standardization / Service Delivery Models Develops a service plan which sets the strategic direction for the population or service for FH. Develops clinical service models, identifies opportunities that promote integration, standardization and consolidation across Fraser Health based on community, population and service needs and understanding of evidence based and leading practice models. Influences and/or sets policy and practice related to their population and / or service Represents FH externally on provincial committees or groups Operational Management / Partnerships / Workforce Planning Promotes great workplaces Establishes and manages the program budget in line with service plan. Seeks progressive partnerships with internal and external groups / bodies with key interfaces with the program. Conducts workforce planning (with HR and with the Division / Department Heads) Acts as the clinical, care and service expert for FH Monitors and reports on performance Quality Management Leads program-related improvement and quality initiatives, including overseeing quality and patient safety for the program/service; Develops a yearly quality performance work plan, which includes performance monitoring Oversees development, approval, and implementation policy and standards; Ensure implementation of standardized practice Leads accreditation and other auditing processes; follows up on recommendations and Required Organizational Practices; Addresses recommendations from audits, reports, surveys, and legislative requirements (e.g., Patient Quality Review Board, Patient Safety Reviews, Patient Satisfaction (Experience) Surveys, Office of the Auditor General Reports, Coroner Reports, etc.) Receives and actions direction from Fraser Health Quality Performance Committee and its four Sub-Committees (Safety & Risk Management; Medication and Therapeutics; Infection Prevention & Control; Medical Devices, Technology & Reprocessing) Academic Mandate Collaborates with partners to support the teaching / training mandate and goals of Fraser Health Identifies and supports the advancement of FH s research priorities Working Draft 6/19/2009 6
7 The above list of roles and accountabilities would be fine tuned during the implementation process and program specific indicators and monitoring mechanisms established. One of the goals of program management and the clinical integration imperative is to strengthen Fraser Health s clinical governance and bring more clinical / physician leadership to system wide planning and quality improvement. The restructuring of the medical governance with clear differentiation of the practice and program roles is key to achieving this goal. In the next section of this document key concepts of our proposed medical governance model are presented as a basis for discussion with physician leaders in Fraser Health. Working Draft 6/19/2009 7
8 Proposed Medical Governance Model: Key Concepts This model represents a significant shift in how physician leaders are engaged in Fraser Health. It is based on the premise that FH values physician expertise and ability to contribute to the health authority operations and quality and safety initiatives, and that more not less physician engagement and voice is important if we are to achieve our goals of clinical and operational excellence. There are two aspects to discussions around medical governance. The first is how is a medical staff is organized to self-govern. Under the current legislative framework, health authorities are expected to provide bylaws that define the structure of its medical staff. The organized medical staff is then accountable to the Board for the credentialing and privileging of its members. As well the organized medical staff is accountable for the quality of care provided by its members and for providing medical advice to the Board. The second aspect of medical governance relates to defining how the medical staff will be engaged by the health authority to assist in directing the planning and operations of the health authority. There is no doubt that the medical staff organization and the process of engagement has not kept pace with as Fraser Health has evolved from individual hospitals to the second largest, integrated health authority in Canada. A new model of medical governance is needed to reflect the current realities in Fraser health. Key assumptions underlying this model are: Fraser Health will move to full program management model over the next two fiscal years. The Medical Staff Bylaws and Rules & Regulations will be reviewed and revised as necessary to reflect the revised governance model and defined legislated responsibilities of the medical staff. Fraser Health is committed to a more integrated Lower Mainland clinical and operational service model. The physician leadership model will evolve over time as the program management model evolves. Physician leaders will be involved in the further development of Fraser Health s research and academic mandate. Working Draft 6/19/2009 8
9 Principles 1 The proposed governance has a number of guiding principles. 1. In accepting an appointment to FH Medical Staff, all physicians agree to contribute to the administrative responsibilities of the Department or Division to which they are assigned by attending meetings, participating in quality assurance activities, and assuming other leadership roles as determined collaboratively with the Department/Division Head. 2. Physician leadership positions at FH are appointed by FH senior administration and are accountable to the President & CEO and Board through one of the following mechanisms: MAC Committee structure; Clinical Department / Division Structure; Program Management Structure. 3. The physician leadership structure does not exist in isolation, but internally works in collaboration with the corresponding administrative and professional practice leaders and externally with relevant leadership structures within the medical education programs. 4. All physician leadership positions are term positions based on a written agreement or contract. Reappointment processes are agreed upon in advance and generally conform to policies outlined in the Medical Staff Rules. 5. Written leadership agreements are agreed to prior to all appointments. These are prepared and approved by the Medical Affairs Office and signed by both the incumbent and the appropriate FH Senior Leader. These include role and expectations of the position, reporting and accountability; compensation and non monetary perquisites, process for regular review and conditions required for renewal. Physician Leadership Positions Physician leadership positions in Fraser Health will fall into two broad categories. Roles and Responsibilities of Physician Leaders Position Role Department Heads, Division Heads, As mandated by the Medical Staff Bylaws and Associate Department Heads Rules and Regulations are responsible for Medical Staff professional practice and academic affairs Physician Program Leaders (PPL), Assistant Physician Program Leaders, Physician Leaders. i.e. they focus on the practitioner, Provide management support for the programs in conjunction with operational leaders; i.e. they focus on the program patients, residents and the care and service processes and outcomes. 1 Adapted from PHC Physician Leadership Guidelines (Third Draft) March 16, 2009 Working Draft 6/19/2009 9
10 The roles may not be independently exclusive of one another and there will be situations when one physician leader holds more than one role. Policy Statements Regarding Position Titles Each position title clearly identifies whether the position is part of the Departmental Structure or Program Management Structure. These titles are consistent with role and mandate of the position and should identify or suggest to whom that position reports. The terms Department Head, Division Head, Associate Head, and Assistant Head are used exclusively for Department and Division leaders. The terms Physician Program Director, Assistant Physician Program Director, and Physician Lead are exclusively used within the Program Management Structure. All physician program leadership positions, regardless of the title, report directly to the Physician Program Director who, as part of the program management team reports directly to the applicable Clinical Vice President. Wherever practical, physicians with Department/Division positions will also hold corresponding Program Management Positions. Roles and Accountabilities Department / Division Leadership Positions Medical Management Responsible for organization of the medical staff for the Department/Division including: Ensuring professional standards are established and maintained. Developing performance plans for each member and regularly evaluating members. Privileging and credentialing and advising HAMAC on reappointments, Resolving performance / behavioral issues as required. Physician resource planning (in conjunction with the program leaders), recruitment, retention, and mentorship. Program Management Leadership Positions Responsible with other members of the Program Team for the service delivery planning, budget development, operations and performance management of the program. (See Exhibit 3 ) Identifies physician resource requirements in collaboration with the Division / Department Head. Identifies quality of care concerns and refers to Division/Department Heads. Provides relevant program information to the Department/Division Heads as required Working Draft 6/19/
11 Responsible for developing, with members of the Department, standards of clinical practice for the Department and ensuring that the Department embers work within established standards. Establishing a quality assurance/quality improvement structure and program for the Department, which carriers out the functions of review, evaluation, and analysis of the quality of medical care and utilization of FHA resources. Monitoring and evaluating the utilization of FHA resources by members of the Department in order to ensure effective and efficient use of these resources. Responsible for leading Department / Division planning, setting annual objectives and participating in Fraser Health strategic planning. Responsible for providing leadership on all aspects of teaching and research within and related to Dept/Division including working with the Universities to ensure that education programs and research activities are being sufficiently promoted and supported. Responsible for all budgets under Department/Div control Participates on internal and external regional/provincial senior committees or task forces Meets regularly with VP Medicine to review professional practice, strategic directions, recruitment and retention and academic affairs. Quality of Care / Utilization Supports the Program s quality improvement and quality monitoring activities (Exhibit 3) Participates with the program team to implement evidence based clinical pathways and practice guidelines Planning Responsible with other Program Leaders for program clinical service planning including identifying opportunities for consolidation, integration, and more standardization of practice. Participates in capital planning as it impacts the program Academic Promotes the academic mandate including research within the program s multidisciplinary team Administration Responsible with program team for dayto-day management of program area and collaborates on budget planning. Participates on program committees and internal/external committees as needed. Meets regularly with the Operational Program Leader & VP to establish program priorities. Working Draft 6/19/
12 Physician Leadership Compensation The leadership within Fraser Health recognizes that in order to attract and retain quality physician leaders to these positions, it must provide compensation that reflects the time and responsibility of the position. This compensation model will need to be guided by a set of principles and be competitive with competitive with similar physician leadership positions in the provincial health authorities. More detailed work by a task group is recommended to work up a draft compensation grid. This work could be guided by The VCHA Medical Leadership Compensation Framework, the Physician Master Agreement negotiated between government and the BCMA. As part of this work, policies related to perquisites should be established. Medical Staff Structure The following recommendations are made in terms of structure. Health Authority Medical Advisory Committee (HAMAC) HAMAC will play a key role in supporting quality and patient safety in Fraser Health. It is the senior committee of the organized medical staff and interacts directly with the Board of Directors of Fraser Health. Given the proposed implementation of Program Management it is recommended that: Representatives from Physician Program Directors be invited to sit on HAMAC. The subcommittee structure be evaluated and consideration be given to establishing regional subcommittees in areas such as: Appointment and Reappointment, Privileging, and Quality. 2 Local Medical Advisory Committees (LMAC) It is proposed that local medical advisory groups continue and that their role evolves to one that represents the medical community from their respective geographical area including the general practitioner and community based physicians. The role of the LMACs would need to be explored in consultation with the medical community but could include addressing CME and advising on local / emerging needs. 2 Quality committees of HAMAC to align with the proposed FH Quality Management Framework. Working Draft 6/19/
13 Clinical Transformational Steering Committee (CTSC) One of the structures that is proposed to help FH strategically manage across programs, sites, and services is a FH Clinical Leadership Council. The Council would have representation from the administrative and physician program leads, operational Vice Presidents, and appropriated Physician Department / Division Heads. Their role would be to proactively manage cross program issues and ensure that the vision of moving to a clinically integrated system that is focused on delivering high quality standardized care in a sustainable manner is achieved. Site Leaders Group The new model does not envision site based medical directors although it is recognized that there will be a need for site based medical leaders. These site leaders will work along side a site based operational leader to ensure smooth operation of the hospital across the programs. These positions would be part time and one site leader could manage more than one site e.g. ARH and Mission Memorial Hospital. Medical Staff Associations It is expected that local medical staff associations will continue to meet. To further enhance communication with physicians it is suggested the Vice President of Medicine, other Vice Presidents and Senior Medical Directors, meet twice a year with the Medical Staff Associations Presidents in order to enhance the opportunity for improved input and dialogue. Working Draft 6/19/
14 Proposed Pathways of Physician Engagement BOARD CEO EXECUTIVE HAMAC VP MEDICAL LMACS CLINICAL TRANSITION STEERING COMMITTEE MEDICAL DIRECTORS GROUP LOCAL MEDICAL STAFF ASSOCIATIONS SUBCOMMITTEES SUBCOMMITTEES Leadership Competencies and Development The suggestions for re-designing the Medical Staff Governance structures that are outlined in this document will strengthen the organization s ability to integrate and standardize care throughout the health authority. These issues, however, will be challenging to implement and will more likely succeed if the physician leaders are provided with leadership education and supports. The physician leaders will be consulted regarding their needs in leadership development and the recommendations will most likely include: Systems processes and thinking Performance management Resource management Root cause analysis Conflict resolution Strategic planning Programs for leadership education as well as the development of a new infrastructure to support Department Heads are currently under development. Working Draft 6/19/
15 Next Steps It is proposed that: A Clinical Transformation Steering Committee, consisting of physician leaders and FHA executive be established to guide the further development and refinement of this governance structure including the compensation structure. This model be presented to HAMAC and the LMAC groups for review and comment, then circulated to physicians in FHA Representatives from FH Medical Executive host a series of conversations with FHA physician leaders to review the proposed model and seek feedback. Presentation of proposed model at QBM Further implementation planning with the CTAG group then initiate implementation of the model starting with the Physician Program leadership group. One of Fraser Health s strategic imperatives is Progressive Partnerships. This includes progressive partnerships with our physician leaders. The further evolution of Fraser Health s medical governance model is critical to our success in achieving a sustainable and responsive health system. **** Working Draft 6/19/

16 Appendix One: Clinical Integration Strategic Imperative Working Draft 6/19/2009 1
17 Working Draft 6/19/2009 2
The LHIN s role in creating integrated health service delivery systems
 PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
Interior Health Authority Board Manual 4.5 TERMS OF REFERENCE FOR THE QUALITY COMMITTEE
 Board Manual 4.5 1. PURPOSE (1) The Quality Committee (the Committee ) will assist the Board of Directors (the Board ) to ensure that the quality of patient, client and resident care meets an acceptable
Board Manual 4.5 1. PURPOSE (1) The Quality Committee (the Committee ) will assist the Board of Directors (the Board ) to ensure that the quality of patient, client and resident care meets an acceptable
Family and Community Support Services (FCSS) Program Review
 Program Review") Family and Community Support Services (FCSS) Program Review Judy Smith, Director Community Investment Community Services Department City of Edmonton 1100, CN Tower, 10004 104 Avenue Edmonton, Alberta,
Family and Community Support Services (FCSS) Program Review Judy Smith, Director Community Investment Community Services Department City of Edmonton 1100, CN Tower, 10004 104 Avenue Edmonton, Alberta,
J A N U A R Y 2,
 MEDICAL STAFF BYLAWS FRASER HEALTH AUTHOR ITY J A N U A R Y 2, 2 0 1 3 Page 2 of 39 TABLE OF CONTENTS TABLE OF CONTENTS... 2 INTRODUCTION... 4 PREAMBLE... 5 ARTICLE 1. DEFINITIONS... 7 ARTICLE 2. PURPOSE
MEDICAL STAFF BYLAWS FRASER HEALTH AUTHOR ITY J A N U A R Y 2, 2 0 1 3 Page 2 of 39 TABLE OF CONTENTS TABLE OF CONTENTS... 2 INTRODUCTION... 4 PREAMBLE... 5 ARTICLE 1. DEFINITIONS... 7 ARTICLE 2. PURPOSE
NWT Primary Community Care Framework
 NWT Primary Community Care Framework August 2002 Table of Contents Introduction... 1 National Perspective... 2 NWT Vision for Primary Community Care... 2 Principles... 3 The NWT Approach to Primary Community
NWT Primary Community Care Framework August 2002 Table of Contents Introduction... 1 National Perspective... 2 NWT Vision for Primary Community Care... 2 Principles... 3 The NWT Approach to Primary Community
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
QUINTE HEALTH CARE PRINCIPLES OF GOVERNANCE AND BOARD ACCOUNTABILITY
 QUINTE HEALTH CARE PRINCIPLES OF GOVERNANCE AND BOARD ACCOUNTABILITY 1. Quinte Health Care (QHC) is one hospital corporation with four interdependent sites. 2. The Board of Directors (Board) governs Quinte
QUINTE HEALTH CARE PRINCIPLES OF GOVERNANCE AND BOARD ACCOUNTABILITY 1. Quinte Health Care (QHC) is one hospital corporation with four interdependent sites. 2. The Board of Directors (Board) governs Quinte
EXECUTIVE COMPENSATION PROGRAM
 EXECUTIVE COMPENSATION PROGRAM 2 Background In 2010, the Province legislated a two-year compensation freeze for all non-unionized employees in the Broader Public Sector (BPS) which prohibited increases
EXECUTIVE COMPENSATION PROGRAM 2 Background In 2010, the Province legislated a two-year compensation freeze for all non-unionized employees in the Broader Public Sector (BPS) which prohibited increases
The Patients First Act Backgrounder
 December 7, 2016 The Patients First Act, 2016 is part of the government s Patients First: Action Plan for Health Care to create a more patient-centered health care system in Ontario. Ontario s 14 Local
December 7, 2016 The Patients First Act, 2016 is part of the government s Patients First: Action Plan for Health Care to create a more patient-centered health care system in Ontario. Ontario s 14 Local
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Grey Bruce Health Services. Executive Compensation Framework. January 2018
 Grey Bruce Health Services Executive Compensation Framework January 2018 2 Grey Bruce Health Service (GBHS) is in the process of establishing an Executive Compensation Framework, a new requirement of the
Grey Bruce Health Services Executive Compensation Framework January 2018 2 Grey Bruce Health Service (GBHS) is in the process of establishing an Executive Compensation Framework, a new requirement of the
Interprofessional Strategic Plan. Advancing Interprofessional Excellence through Collaboration
 Interprofessional Strategic Plan Advancing Interprofessional Excellence through Collaboration MESSAGE FROM EXECUTIVE VICE-PRESIDENT, PROGRAMS, CHIEF NURSING EXECUTIVE AND CHIEF HEALTH DISCIPLINES EXECUTIVE
Interprofessional Strategic Plan Advancing Interprofessional Excellence through Collaboration MESSAGE FROM EXECUTIVE VICE-PRESIDENT, PROGRAMS, CHIEF NURSING EXECUTIVE AND CHIEF HEALTH DISCIPLINES EXECUTIVE
Grey Bruce Health Services (GBHS) Executive Compensation Framework. February Final Copy
 Executive Compensation Framework. February Final Copy") Grey Bruce Health Services (GBHS) Executive Compensation Framework February 2018 Final Copy Grey Bruce Health Service has established an Executive Compensation Framework, a new requirement of the provincial
Grey Bruce Health Services (GBHS) Executive Compensation Framework February 2018 Final Copy Grey Bruce Health Service has established an Executive Compensation Framework, a new requirement of the provincial
Agenda Item 8.4 BRIEFING NOTE: Toronto Central Local Health Integration Network (LHIN)
") Agenda Item 8.4 BRIEFING NOTE: Toronto Central Local Health Integration Network (LHIN) SUBJECT: Voluntary Integration of the Assisted Living and Attendant Outreach Services from the Canadian Red Cross
Agenda Item 8.4 BRIEFING NOTE: Toronto Central Local Health Integration Network (LHIN) SUBJECT: Voluntary Integration of the Assisted Living and Attendant Outreach Services from the Canadian Red Cross
Report of the Auditor General to the Nova Scotia House of Assembly
 November 22, 2017 Report of the Auditor General to the Nova Scotia House of Assembly Performance Independence Integrity Impact November 22, 2017 Honourable Kevin Murphy Speaker House of Assembly Province
November 22, 2017 Report of the Auditor General to the Nova Scotia House of Assembly Performance Independence Integrity Impact November 22, 2017 Honourable Kevin Murphy Speaker House of Assembly Province
North East Behavioural Supports Ontario Sustainability Plan
 North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
RNAO s Framework for Nurse Executive Leadership
 1. Framework Overview The Framework for Nurse Executive Leadership is a unique model that is designed to delineate, shape and strengthen the evolving role of the nurse executive leader in Ontario and beyond.
1. Framework Overview The Framework for Nurse Executive Leadership is a unique model that is designed to delineate, shape and strengthen the evolving role of the nurse executive leader in Ontario and beyond.
Chapter 1 Health and Wellness and Nova Scotia Health Authority: Family Doctor Resourcing
 Chapter 1 Health and Wellness and Nova Scotia Health Authority: Family Doctor Resourcing Overall Conclusion: The department and the health authority are doing a poor job of publicly communicating their
Chapter 1 Health and Wellness and Nova Scotia Health Authority: Family Doctor Resourcing Overall Conclusion: The department and the health authority are doing a poor job of publicly communicating their
STANDING COMMITTEE ON PUBLIC ACCOUNTS
 STANDING COMMITTEE ON PUBLIC ACCOUNTS PHYSICIAN BILLING (SECTION 3.11, 2016 ANNUAL REPORT OF THE OFFICE OF THE AUDITOR GENERAL OF ONTARIO) 2 nd Session, 41 st Parliament 67 Elizabeth II ISBN 978-1-4868-1079-6
STANDING COMMITTEE ON PUBLIC ACCOUNTS PHYSICIAN BILLING (SECTION 3.11, 2016 ANNUAL REPORT OF THE OFFICE OF THE AUDITOR GENERAL OF ONTARIO) 2 nd Session, 41 st Parliament 67 Elizabeth II ISBN 978-1-4868-1079-6
Health Quality Ontario Business Plan
 Health Quality Ontario Business Plan 2017-20 October 2016 Table of Contents 1 Executive Summary...1 2 Mandate and Strategy...2 3 Environmental Scan...4 4 Programs and Activities...5 5 Risks... 18 6 Resources...
Health Quality Ontario Business Plan 2017-20 October 2016 Table of Contents 1 Executive Summary...1 2 Mandate and Strategy...2 3 Environmental Scan...4 4 Programs and Activities...5 5 Risks... 18 6 Resources...
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
ARH Strategic Plan:
 ARH Strategic Plan: 2017 2020 Table of Contents Section 1. Introduction 1.1 Why a Strategic Plan 1.2 Building on Previous Accomplishments 1.3 Where We Are Today 2. How We Developed Our New Plan: 2.1 Plan
ARH Strategic Plan: 2017 2020 Table of Contents Section 1. Introduction 1.1 Why a Strategic Plan 1.2 Building on Previous Accomplishments 1.3 Where We Are Today 2. How We Developed Our New Plan: 2.1 Plan
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Community Health Centre Program
 MINISTRY OF HEALTH AND LONG-TERM CARE Community Health Centre Program BACKGROUND The Ministry of Health and Long-Term Care s Community and Health Promotion Branch is responsible for administering and funding
MINISTRY OF HEALTH AND LONG-TERM CARE Community Health Centre Program BACKGROUND The Ministry of Health and Long-Term Care s Community and Health Promotion Branch is responsible for administering and funding
September Sub-Region Collaborative Meeting: Bramalea. September 13, 2018
 September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
Northern College Business Plan
 2018-2019 Northern College Business Plan Approved By The Board Of Governors May 8th, 2018 Table of Contents Executive Summary 3 Introduction 4 Vision, Mission And Guiding Principles 4 Business Plan Outline
2018-2019 Northern College Business Plan Approved By The Board Of Governors May 8th, 2018 Table of Contents Executive Summary 3 Introduction 4 Vision, Mission And Guiding Principles 4 Business Plan Outline
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP): 2015/16 Progress Report
: 2015/16 Progress Report") Quality Improvement Plan (QIP): Progress Report Medication Reconciliation for Outpatient Clinics 1 % complete medication reconciliation on outpatient clinic visit assessments ( %; Pediatric Patients; Fiscal
Quality Improvement Plan (QIP): Progress Report Medication Reconciliation for Outpatient Clinics 1 % complete medication reconciliation on outpatient clinic visit assessments ( %; Pediatric Patients; Fiscal
A S S E S S M E N T S
 A S S E S S M E N T S Community Design Assessment This process was developed to aid healthcare organizations in taking the pulse of their community prior to the start of capital improvement projects. A
A S S E S S M E N T S Community Design Assessment This process was developed to aid healthcare organizations in taking the pulse of their community prior to the start of capital improvement projects. A
Canadian Federation of Medical Students (CFMS) Wellness Committee: TERMS OF REFERENCE
 Wellness Committee: TERMS OF REFERENCE") Canadian Federation of Medical Students (CFMS) Wellness Committee: TERMS OF REFERENCE Drafted on April 14, 2014, by: Kayla Berst, CFMS Wellness Officer (2013-2014) Brandon Maser, CFMS VP Services (2013-2014)
Canadian Federation of Medical Students (CFMS) Wellness Committee: TERMS OF REFERENCE Drafted on April 14, 2014, by: Kayla Berst, CFMS Wellness Officer (2013-2014) Brandon Maser, CFMS VP Services (2013-2014)
Canada s National Nursing Assessment Service Launches New Strategic Plan
 Canada s National Nursing Assessment Service Launches New Strategic Plan Innovative Nursing Organization Poised for Growth Toronto, ON April 4, 2016 The National Nursing Assessment Service (NNAS) is pleased
Canada s National Nursing Assessment Service Launches New Strategic Plan Innovative Nursing Organization Poised for Growth Toronto, ON April 4, 2016 The National Nursing Assessment Service (NNAS) is pleased
Consultant Radiographers Education and CPD 2013
 Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
York Region Community Investment Strategy Report
 York Region Community Investment Strategy Report Page 1 Contents 1. INTRODUCTION:... 4 1.1 Principles... 4 Accountability... 4 Transparency... 4 Responsiveness... 4 1.2 Goals... 4 2. SCOPE:... 4 3. PURPOSE:...
York Region Community Investment Strategy Report Page 1 Contents 1. INTRODUCTION:... 4 1.1 Principles... 4 Accountability... 4 Transparency... 4 Responsiveness... 4 1.2 Goals... 4 2. SCOPE:... 4 3. PURPOSE:...
Higher Education Funding Reforms. Clinical Placements
 Higher Education Funding Reforms Clinical Placements Background The reforms announced in the Comprehensive Spending Review (CSR) in 2015 will lead to significant changes in the way health education funding
Higher Education Funding Reforms Clinical Placements Background The reforms announced in the Comprehensive Spending Review (CSR) in 2015 will lead to significant changes in the way health education funding
Pathology & Laboratory Medicine Lower Mainland Consolidation Project V3.10
 Pathology & Laboratory Medicine Lower Mainland Consolidation Project V3.10 Pathology and Laboratory Medicine and The Patient Care Pathway Laboratory testing is a critical component of the overall patient
Pathology & Laboratory Medicine Lower Mainland Consolidation Project V3.10 Pathology and Laboratory Medicine and The Patient Care Pathway Laboratory testing is a critical component of the overall patient
Health Sciences North Horizon Santé-Nord (QIP) Quality Improvement Plan
 Quality Improvement Plan") Health Sciences North Horizon Santé-Nord 2015 2016 (QIP) Quality Improvement Plan March 31, 2015 Overview HSN 2015-2016 Quality Improvement Plan Introduction Health Sciences North/Horizon Santé-Nord (HSN)
Health Sciences North Horizon Santé-Nord 2015 2016 (QIP) Quality Improvement Plan March 31, 2015 Overview HSN 2015-2016 Quality Improvement Plan Introduction Health Sciences North/Horizon Santé-Nord (HSN)
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 North Wellington Health Care 1 Overview North Wellington Health Care (NWHC) is a dynamic rural community hospital
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 North Wellington Health Care 1 Overview North Wellington Health Care (NWHC) is a dynamic rural community hospital
Board of Health and Local Health Integration Network Engagement Guideline, 2018
 Ministry of Health and Long-Term Care Board of Health and Local Health Integration Network Engagement Guideline, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective:
Ministry of Health and Long-Term Care Board of Health and Local Health Integration Network Engagement Guideline, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective:
Quality and Safety Committees
 Quality and Safety Committees Guidance and Resources This document replaces the previously published Quality and Safety Committee(s) Guidance and Sample Terms of Reference Document (May 2013). It forms
Quality and Safety Committees Guidance and Resources This document replaces the previously published Quality and Safety Committee(s) Guidance and Sample Terms of Reference Document (May 2013). It forms
Recommendation 1: All patients brought into St.
 Recommendation Accountability Response and Action Leads: Regional Emergency Department Head (Dr. Eric Grafstein) and Mental Health Physician Program Director/Department Head Psychiatry, Providence Health
Recommendation Accountability Response and Action Leads: Regional Emergency Department Head (Dr. Eric Grafstein) and Mental Health Physician Program Director/Department Head Psychiatry, Providence Health
FRENCH LANGUAGE HEALTH SERVICES STRATEGY
 FRENCH LANGUAGE HEALTH SERVICES STRATEGY 2016-2019 Table of Contents I. Introduction... 4 Partners... 4 A. Champlain LHIN IHSP... 4 B. South East LHIN IHSP... 5 C. Réseau Strategic Planning... 5 II. Goal
FRENCH LANGUAGE HEALTH SERVICES STRATEGY 2016-2019 Table of Contents I. Introduction... 4 Partners... 4 A. Champlain LHIN IHSP... 4 B. South East LHIN IHSP... 5 C. Réseau Strategic Planning... 5 II. Goal
RECOMMENDATION STATUS OVERVIEW
 Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Nova Scotia Health Authority Business Plan TABLE OF CONTENTS
 BUSINESS PLAN TABLE OF CONTENTS 1 Message from the President and CEO... 1 2 Our Strategic Plan... 2 3 Mandate... 3 4 Planning for the Future... 4 5 2018-19 Business Plan Priorities... 5 6 Research and
BUSINESS PLAN TABLE OF CONTENTS 1 Message from the President and CEO... 1 2 Our Strategic Plan... 2 3 Mandate... 3 4 Planning for the Future... 4 5 2018-19 Business Plan Priorities... 5 6 Research and
STRATEGIC PLAN Prepared by: Approved by the Board of Directors: June 25, June 2014 Page 1 of 12
 STRATEGIC PLAN 2014-2019 Prepared by: Approved by the Board of Directors: June 25, 2014 June 2014 Page 1 of 12 Section 1 Introduction Espanola General Hospital (EGH) was incorporated as a hospital in 1948.
STRATEGIC PLAN 2014-2019 Prepared by: Approved by the Board of Directors: June 25, 2014 June 2014 Page 1 of 12 Section 1 Introduction Espanola General Hospital (EGH) was incorporated as a hospital in 1948.
2014/15 Quality Improvement Plan (QIP) Narrative
 Narrative") 2014/15 Quality Improvement Plan (QIP) Narrative 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop a quality improvement plan.
2014/15 Quality Improvement Plan (QIP) Narrative 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop a quality improvement plan.
Quality Framework. for a High Performing Health and Wellness System in Nova Scotia
 Quality Framework for a High Performing Health and Wellness System in Nova Scotia Quality Framework for a High Performing Health and Wellness System in Nova Scotia Crown copyright, Province of Nova Scotia,
Quality Framework for a High Performing Health and Wellness System in Nova Scotia Quality Framework for a High Performing Health and Wellness System in Nova Scotia Crown copyright, Province of Nova Scotia,
Canadian Forces Liaison Council The Five - Year Strategic Plan
 http://www.cflc.forces.gc.ca Canadian Forces Liaison Council The Five - Year Strategic Plan 2009-2013 Table of Contents Message from the National Chair... 1 Foreword from the Chief Reserves and Cadets...
http://www.cflc.forces.gc.ca Canadian Forces Liaison Council The Five - Year Strategic Plan 2009-2013 Table of Contents Message from the National Chair... 1 Foreword from the Chief Reserves and Cadets...
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
A Span of Control Tool for Clinical Managers
 NURSING RESEARCH 83 A Span of Control Tool for Clinical Managers Robin Morash, RN, BNSc, MHS Clinical Manager, Geriatric Assessment Unit and Day Hospital Past Co-chair, Nursing Management Work Group The
NURSING RESEARCH 83 A Span of Control Tool for Clinical Managers Robin Morash, RN, BNSc, MHS Clinical Manager, Geriatric Assessment Unit and Day Hospital Past Co-chair, Nursing Management Work Group The
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
Integrated Leadership for Hospitals and Health Systems: Principles for Success
 Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Ontario Quality Standards Committee Draft Terms of Reference
 Ontario Quality Standards Committee Draft Terms of Reference 1. Introduction The Ontario Health Quality Council (Health Quality Ontario) officially commenced operation on April 1st, 2010. Created under
Ontario Quality Standards Committee Draft Terms of Reference 1. Introduction The Ontario Health Quality Council (Health Quality Ontario) officially commenced operation on April 1st, 2010. Created under
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Guelph Sustainable Neighbourhood Engagement Framework
 Guelph Sustainable Neighbourhood Engagement Framework Purpose Operational review initiated by Community Services Department City s role supporting neighbourhood groups Potential elimination of Community
Guelph Sustainable Neighbourhood Engagement Framework Purpose Operational review initiated by Community Services Department City s role supporting neighbourhood groups Potential elimination of Community
INVERCLYDE COMMUNITY HEALTH AND CARE PARTNERSHIP - DRAFT SCHEME OF ESTABLISHMENT
 EMBARGOED UNTIL DATE OF MEETING Greater Glasgow and Clyde NHS Board Board Meeting Tuesday 17 th August 2010 Board Paper No. 2010/34 Director of Corporate Planning and Policy/Lead NHS Director Glasgow City
EMBARGOED UNTIL DATE OF MEETING Greater Glasgow and Clyde NHS Board Board Meeting Tuesday 17 th August 2010 Board Paper No. 2010/34 Director of Corporate Planning and Policy/Lead NHS Director Glasgow City
Advisory Panel for Health Care Advancing the Academic Health System for the Future: Profiles in Academic Health System Leadership.
 Advisory Panel for Health Care Advancing the Academic Health System for the Future: Profiles in Academic Health System Leadership November, 2013 Project Focus and Methodology Project Focus This project
Advisory Panel for Health Care Advancing the Academic Health System for the Future: Profiles in Academic Health System Leadership November, 2013 Project Focus and Methodology Project Focus This project
Ministère de la Santé et des Soins de longue durée Bureau du ministre
 Ministry of Health and Long-Term Care Office of the Minister 10 th Floor, Hepburn Block 80 Grosvenor Street Toronto ON M7A 2C4 Tel 416-327-4300 Fax 416-326-1571 www.ontario.ca/health May 1, 2017 Ministère
Ministry of Health and Long-Term Care Office of the Minister 10 th Floor, Hepburn Block 80 Grosvenor Street Toronto ON M7A 2C4 Tel 416-327-4300 Fax 416-326-1571 www.ontario.ca/health May 1, 2017 Ministère
MINISTRY OF HEALTH PATIENT, P F A A TI MIL EN Y, TS C AR AS EGIVER PART AND NER SPU BLIC ENGAGEMENT FRAMEWORK
 MINISTRY OF HEALTH PATIENT, FAMILY, CAREGIVER AND PUBLIC ENGAGEMENT FRAMEWORK 2018 MINISTRY OF HEALTH PATIENT, FAMILY, CAREGIVER AND PUBLIC ENGAGEMENT FRAMEWORK 2018 Executive Summary The Ministry of Health
MINISTRY OF HEALTH PATIENT, FAMILY, CAREGIVER AND PUBLIC ENGAGEMENT FRAMEWORK 2018 MINISTRY OF HEALTH PATIENT, FAMILY, CAREGIVER AND PUBLIC ENGAGEMENT FRAMEWORK 2018 Executive Summary The Ministry of Health
Health and Wellness. Business Plan to restated. Accountability Statement
 Health and Wellness Business Plan 1999-2000 to 2001-02 - restated Accountability Statement As a result of government re-organization announced on May 25, 1999, the Ministry Business Plans included in Budget
Health and Wellness Business Plan 1999-2000 to 2001-02 - restated Accountability Statement As a result of government re-organization announced on May 25, 1999, the Ministry Business Plans included in Budget
March 15, Contact:
 Recommendations on how to strengthen the Local Health System Integration Act, 2006 to enable a People and Communities First approach to Health System Transformation March 15, 2016 Contact: Adrianna Tetley,
Recommendations on how to strengthen the Local Health System Integration Act, 2006 to enable a People and Communities First approach to Health System Transformation March 15, 2016 Contact: Adrianna Tetley,
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM
 Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/30/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Executive Job Codes and Descriptions
 Executive Job Codes and Descriptions Please note: The Executive Compensation Survey is designed to collect information on the highest level jobs reporting directly to the CEO, and/or jobs considered part
Executive Job Codes and Descriptions Please note: The Executive Compensation Survey is designed to collect information on the highest level jobs reporting directly to the CEO, and/or jobs considered part
Executive Summary. Leadership Toolkit for Redefining the H: Engaging Trustees and Communities
 Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
HQCA STRATEGIC FRAMEWORK AND BUSINESS PLAN
 HQCA STRATEGIC FRAMEWORK AND BUSINESS PLAN 2016 17 Message from the Board Chair and CEO We are pleased to share the HQCA s Strategic Framework and 2016-17 Business Plan. Now in our second year with
HQCA STRATEGIC FRAMEWORK AND BUSINESS PLAN 2016 17 Message from the Board Chair and CEO We are pleased to share the HQCA s Strategic Framework and 2016-17 Business Plan. Now in our second year with
Bon Secours Is Changing Its Approach TO ANNUAL MANDATORY TR AINING FOR NURSES
 Bon Secours Is Changing Its Approach TO ANNUAL MANDATORY TR AINING FOR NURSES From Bon Secours Health System: Sharon Confessore, Ph.D., Chief Learning Officer Pamela Hash DNP, RN, Associate System Chief
Bon Secours Is Changing Its Approach TO ANNUAL MANDATORY TR AINING FOR NURSES From Bon Secours Health System: Sharon Confessore, Ph.D., Chief Learning Officer Pamela Hash DNP, RN, Associate System Chief
Accountability Framework and Organizational Requirements
 Ministry of Health and Long-Term Care Accountability Framework and Organizational Requirements Consultation Document Population and Public Health Division May 2017 Ministry of Health and Long-Term Care
Ministry of Health and Long-Term Care Accountability Framework and Organizational Requirements Consultation Document Population and Public Health Division May 2017 Ministry of Health and Long-Term Care
Renville County, Minnesota Strategic Plan
 2015 2020 Strategic Plan In Renville County, our long heritage of farming has made us not only world class farmers, but also top-notch small business owners. We know that in today s competitive world,
2015 2020 Strategic Plan In Renville County, our long heritage of farming has made us not only world class farmers, but also top-notch small business owners. We know that in today s competitive world,
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing
 TO Hospital Advisory Committee FROM Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing DATE 26 August 2014 SUBJECT Mental Health Review MEMORANDUM
TO Hospital Advisory Committee FROM Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing DATE 26 August 2014 SUBJECT Mental Health Review MEMORANDUM
The Enduring Value of the Medical Staff Organization
 The Enduring Value of the Medical Staff Organization Session Code: MN07 Date: Monday, October 23 Time: 12:45 p.m. - 2:15 p.m. Total CE Credits: 1.5 Presenter(s): Arthur Snow, MD The Enduring Value of the
The Enduring Value of the Medical Staff Organization Session Code: MN07 Date: Monday, October 23 Time: 12:45 p.m. - 2:15 p.m. Total CE Credits: 1.5 Presenter(s): Arthur Snow, MD The Enduring Value of the
Response to Recommendations in Report: System Review of Tertiary Obstetric Services at the Victoria General Hospital
 Response to Recommendations in Report: System Review of Tertiary Obstetric Services at the Victoria General Hospital A report commissioned by the Vancouver Island Health Authority The System Review of
Response to Recommendations in Report: System Review of Tertiary Obstetric Services at the Victoria General Hospital A report commissioned by the Vancouver Island Health Authority The System Review of
MANITOBA PSYCHIATRIC NURSING PLANNING GROUP FINAL REPORT
 MANITOBA PSYCHIATRIC NURSING PLANNING GROUP FINAL REPORT November 2010 TABLE OF CONTENTS Acknowledgements...2 Executive Summary...3 Introduction...4 Psychiatric Nursing: Scope Of Practice...5 Background:
MANITOBA PSYCHIATRIC NURSING PLANNING GROUP FINAL REPORT November 2010 TABLE OF CONTENTS Acknowledgements...2 Executive Summary...3 Introduction...4 Psychiatric Nursing: Scope Of Practice...5 Background:
Central Zone Healthcare Plan. For Placement Only. Strategy Overview
 Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Indigenous Supportive Housing Program (ISHP)
") 2017 Expression of Interest Supportive Housing Investment Indigenous Supportive Housing Program (ISHP) Ontario Aboriginal Housing Services 1 Table of Contents Purpose... 3 Program Guidelines... 3 Eligibility
2017 Expression of Interest Supportive Housing Investment Indigenous Supportive Housing Program (ISHP) Ontario Aboriginal Housing Services 1 Table of Contents Purpose... 3 Program Guidelines... 3 Eligibility
PRIMARY HEALTH CARE TRANSFORMATION FAMILY CARE CLINIC APPLICATION KIT WAVE 1
 PRIMARY HEALTH CARE TRANSFORMATION FAMILY CARE CLINIC APPLICATION KIT WAVE 1 DRAFT FOR STAKEHOLDER ENGAGEMENT DECEMBER 20, 2012 FOREWORD Primary Health Care in Alberta Our Changing Society Alberta is changing
PRIMARY HEALTH CARE TRANSFORMATION FAMILY CARE CLINIC APPLICATION KIT WAVE 1 DRAFT FOR STAKEHOLDER ENGAGEMENT DECEMBER 20, 2012 FOREWORD Primary Health Care in Alberta Our Changing Society Alberta is changing
Nova Scotia s New Collaborative Care Model
 Nova Scotia s New Collaborative Care Model 1 Province of Nova Scotia Health Transformation: A partnership of the Department of Health, District Health Authorities, and the IWK Health Centre. 1 Why Nova
Nova Scotia s New Collaborative Care Model 1 Province of Nova Scotia Health Transformation: A partnership of the Department of Health, District Health Authorities, and the IWK Health Centre. 1 Why Nova
Approved Executive Compensation Policy and Framework Feb. 28, 2018 Executive Compensation Policy and Framework WOODSTOCK HOSPITAL
 Approved Executive Compensation Policy and Framework Feb. 28, 2018 Executive Compensation Policy and Framework WOODSTOCK HOSPITAL Organization (Full Name): Woodstock Hospital General Trust Last Name: Ziegler
Approved Executive Compensation Policy and Framework Feb. 28, 2018 Executive Compensation Policy and Framework WOODSTOCK HOSPITAL Organization (Full Name): Woodstock Hospital General Trust Last Name: Ziegler
STUDENT POPULATION BY ETHNIC GROUPS
 Application Narrative Section B 1. What is your school district s philosophy about the urgent need to retain the number of educators who are culturally and/or linguistically diverse in Oregon s PK-12 classrooms?
Application Narrative Section B 1. What is your school district s philosophy about the urgent need to retain the number of educators who are culturally and/or linguistically diverse in Oregon s PK-12 classrooms?
Position Number(s) Community Division/Region(s) 07-NEW Yellowknife Health Services/HQ
 Community Division/Region(s) 07-NEW Yellowknife Health Services/HQ") IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Territorial Manager, Laboratory & Diagnostic Imaging Position Number(s) Community Division/Region(s)
IDENTIFICATION Department Northwest Territories Health and Social Services Authority Position Title Territorial Manager, Laboratory & Diagnostic Imaging Position Number(s) Community Division/Region(s)
Integrated System of Care - Table of Contents
 Integrated System of Care - Table of Contents 1 Integrated System of Care Strategic Context 2 Ministry of Health Policy Framework Introduction Requirements for an Integrated Primary and Community Health
Integrated System of Care - Table of Contents 1 Integrated System of Care Strategic Context 2 Ministry of Health Policy Framework Introduction Requirements for an Integrated Primary and Community Health
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Mr. Tim Manning Board Chair Provincial Health Services Authority Burrard St. Vancouver BC V6Z 2H3. Dear Mr. Manning:
 1113936 Mr. Tim Manning Board Chair Provincial Health Services Authority 700-1380 Burrard St. Vancouver BC V6Z 2H3 Dear Mr. Manning: On behalf of Premier Horgan, thank you for your service to the people
1113936 Mr. Tim Manning Board Chair Provincial Health Services Authority 700-1380 Burrard St. Vancouver BC V6Z 2H3 Dear Mr. Manning: On behalf of Premier Horgan, thank you for your service to the people
for success Strategic Plan 1 Doctors Nova Scotia Strategic Plan Highlights
 A vision for success Doctors Nova Scotia 1 Doctors Nova Scotia 2012-2016 Strategic Plan Highlights Our Vision of Success A vision is a picture of the future desired end state. The vision of success for
A vision for success Doctors Nova Scotia 1 Doctors Nova Scotia 2012-2016 Strategic Plan Highlights Our Vision of Success A vision is a picture of the future desired end state. The vision of success for
Transplant Resource Guide
 Transplant Resource Guide The Transplant Resource Guide (TRG) and the supporting tools provide strategies, concepts and resources to enhance transplant program quality and value in our dynamic environment.
Transplant Resource Guide The Transplant Resource Guide (TRG) and the supporting tools provide strategies, concepts and resources to enhance transplant program quality and value in our dynamic environment.
Registered Nurse / Clinical Nurse Mental Health Community (Clozapine Clinic) Job Number Applications Closing Date 13 April 2018.
 Job Number Applications Closing Date 13 April 2018.") SA Health Job Pack Job Title Registered Nurse / Clinical Nurse Mental Health Community (Clozapine Clinic) Job Number 653546 Applications Closing Date 13 April 2018 Region / Division Health Service Location
SA Health Job Pack Job Title Registered Nurse / Clinical Nurse Mental Health Community (Clozapine Clinic) Job Number 653546 Applications Closing Date 13 April 2018 Region / Division Health Service Location
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Health System Outcomes and Measurement Framework
 Health System Outcomes and Measurement Framework December 2013 (Amended August 2014) Table of Contents Introduction... 2 Purpose of the Framework... 2 Overview of the Framework... 3 Logic Model Approach...
Health System Outcomes and Measurement Framework December 2013 (Amended August 2014) Table of Contents Introduction... 2 Purpose of the Framework... 2 Overview of the Framework... 3 Logic Model Approach...
Enabling Effective, Quality Population and Patient-Centred Care: A Provincial Strategy for Health Human Resources.
 Enabling Effective, Quality Population and Patient-Centred Care: A Provincial Strategy for Health Human Resources Strategic Context Executive Summary A key proposition set out in Setting Priorities for
Enabling Effective, Quality Population and Patient-Centred Care: A Provincial Strategy for Health Human Resources Strategic Context Executive Summary A key proposition set out in Setting Priorities for
Strategic Direction. Organizational Commitment. The Race for Relevance Framework
 Strategic Direction Organizational Commitment NSPE is committed to an ongoing process of continuous, organizational improvement in order to: remain relevant to the licensed professional engineers whom
Strategic Direction Organizational Commitment NSPE is committed to an ongoing process of continuous, organizational improvement in order to: remain relevant to the licensed professional engineers whom
Ministry of Health Patients as Partners Provincial Dialogue Report
 Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The Way Forward. Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador
 The Way Forward Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador 2 Table of Contents Introduction... 2 Background... 3 Vision and Values... 5 Governance... 6
The Way Forward Towards Recovery: The Mental Health and Addictions Action Plan for Newfoundland and Labrador 2 Table of Contents Introduction... 2 Background... 3 Vision and Values... 5 Governance... 6
Community Health Partnerships (CHPs) Scheme of Establishment for Glasgow City Community Health and Social Care Partnerships
 Scheme of Establishment for Glasgow City Community Health and Social Care Partnerships") EMBARGOED UNTIL MEETING Greater Glasgow NHS Board Board Meeting Tuesday 19 th April 2005 Board Paper No. 2005/33 Director of Planning and Community Care Community Health Partnerships (CHPs) Scheme of Establishment
EMBARGOED UNTIL MEETING Greater Glasgow NHS Board Board Meeting Tuesday 19 th April 2005 Board Paper No. 2005/33 Director of Planning and Community Care Community Health Partnerships (CHPs) Scheme of Establishment
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/26/2018 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/26/2018 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
DATE APPROVED SEPTEMBER 2010
 REASON FOR POLICY To delineate the Most Responsible Physician (MRP) key accountabilities and responsibilities for the admission, ongoing care, transfer of care, consultation and discharge processes for
REASON FOR POLICY To delineate the Most Responsible Physician (MRP) key accountabilities and responsibilities for the admission, ongoing care, transfer of care, consultation and discharge processes for
Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All
 Health Quality Branch Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All Ontario Long-Term Care Association Quality Forum June 12, 2013 Miin Alikhan Director,
Health Quality Branch Health System Funding Reform: Aligning Levers and Incentives to Achieve Excellent Care for All Ontario Long-Term Care Association Quality Forum June 12, 2013 Miin Alikhan Director,
Public Health within an Integrated Health System. Report of the Minister s Expert Panel on Public Health
 Public Health within an Integrated Health System Report of the Minister s Expert Panel on Public Health June 9, 2017 2 Table of Contents I. About the Expert Panel..4 Mandate....4 Membership......4 Desired
Public Health within an Integrated Health System Report of the Minister s Expert Panel on Public Health June 9, 2017 2 Table of Contents I. About the Expert Panel..4 Mandate....4 Membership......4 Desired
The 2006 ACCME Updated Accreditation Criteria
 The webinar will begin shortly. Please take a moment to answer the poll questions below. How many people are participating in this webinar at your location today? 1 2 3 4 5 6 7 8 or more Are you accredited
The webinar will begin shortly. Please take a moment to answer the poll questions below. How many people are participating in this webinar at your location today? 1 2 3 4 5 6 7 8 or more Are you accredited
Primary Health Care System Level Indicators. Presentation March 2015
 Primary Health Care System Level Indicators Presentation March 2015 1 Presentation Outline Background Alberta's Primary Health Care Strategy Evaluation Framework and Logic Model Measurement and Evaluation
Primary Health Care System Level Indicators Presentation March 2015 1 Presentation Outline Background Alberta's Primary Health Care Strategy Evaluation Framework and Logic Model Measurement and Evaluation