WYOMING PREADMISSION SCREENING AND RESIDENT REVEW (PASRR) MANUAL
|
|
|
- Bernard Stuart Haynes
- 6 years ago
- Views:
Transcription

1 WYOMING PREADMISSION SCREENING AND RESIDENT REVEW (PASRR) MANUAL Version West 17 th Street, Suite 300A Cheyenne, WY Phone: Fax:
2 TABLE OF CONTENTS Section I: Introduction... 4 Definition... 4 History... 4 Authorization... 4 Purpose... 4 Policy... 4 Section II: PASRR Level I Definition and Process... 6 Section III: PASRR Level II Categorical Determinations... 8 Section IV: Individualized PASRR Level II Definition and Process Section V: Significant Change (Resident Review) Resident Review Significant Change in Condition Brief Interview for Mental Status (BIMS) Patient Health Questionnaire (PHQ-9) Resident Mood Interview Section VI: Inter-facility Transfer Policy Section VII: Roles and Responsibilities Nursing Facilities (NF) and Hospitals Public Health Nursing Concerning Referral Process for LT101 Referrals: Xerox Care and Quality Solutions Placement Support: Serious Mental Illness: Intellectual Disability and other Related Conditions Data Tracking: Reports: Quality Assurance: State Mental health Authority (SMHA) Responsibilities: State Mental Retardation Authority (SMRA) Responsibilities: Transferring Facility Responsibility (CFR (4)(II)) Office of Healthcare Licensing and Survey, PASRR and MDS PASRR, MDS and Significant Change Section VIII: Appeals Process
3 Purpose Initiating the Appeal and Fair Hearing Process Reconsideration Review Informal Conference Formal Hearing Section IX: Out of State Nursing Facility Placement Policy Enrollment: Section X: Swing Bed Facilities Section XI: Diversion/Transition Project OUT PACE PACE Program Services Home and Community Based Services: (HCBS) Long Term Care Home and Community Based Services Waiver Assisted Living Facility Home and Community Based Service Waiver Programs and Providers for Clients with Mental Illness Long Term Care Home and Community Based Services Waiver Section XII: Other Definitions Section XIII: References Section XIV: Appendix
4 Section I: Introduction Definition PASRR refers to Pre admission Screening and Resident Review, a federally mandated program that requires all states to develop a comprehensive process to pre screen all individuals applying for admission into Medicaid certified nursing facility care regardless of pay source. History The mandate was a U.S. Congress reaction to inappropriate institutionalization of persons with mental illness and/or intellectual disability (referred to as mental retardation in the mandate) and is included in The Omnibus Budget Reconciliation Act of 1987 (OBRA 87), also known as the Nursing Home Reform Act. The mandate requires a personalized assessment and personalized care recommendations for any person who may have mental health, intellectual disability or related conditions. The personalized assessment is used to identify individuals who may have mental health, developmental disabilities or related conditions, to create personalized care recommendations for those individuals, and provide a means to follow up to determine whether those needs are being met within the nursing facility. Authorization Pre admission Screening and Resident Reviews (PASRR s) are federally mandated screenings directed by the Medicaid Title XIX Program, Medicaid. Wyoming Medicaid or the Medicaid State Authority (MSA) is an office within the Division of healthcare financing (DHCF). The Department of Health, Mental Health and Substance Abuse Services Division and the Developmental Disabilities Division have final authority for mental illness (MI) and intellectual disability (MR/ID). The agent can delegate any function for which it has authority. Currently, Xerox Care and Quality Solutions (CQS), has been given delegation by the Division. Purpose Why do PASRR? The purpose of PASRR is to assess, through progressive screening, whether applicants for nursing facilities have a serious mental illness (MI) or intellectual disability (MR/ID), and if the nursing facility is an appropriate placement. For those who are currently in a nursing facility the PASRR is completed on those who have had a change in condition. Policy All persons needing admission to a Medicaid certified nursing facility must have a Preadmission Screening for possible mental illness (Level I). If mental illness appears to exist, the person must be referred for further evaluation (Level II). 4
5 All persons who reside in a nursing facility are subject to Resident Review if there is a substantial change in their mental or physical status which warrants a referral for an evaluation (Level II; See Section V for details). Persons may not be admitted to a nursing home until the Level I screening is completed and if necessary, until the Level II evaluation is completed. (Title XIX 1919(b)(3)(F) A nursing home must not admit any new resident who is mentally ill unless the State mental health authority has conducted a PASRR determination and was determined to need NF services. 42 CFR (m)--Prohibits admission without PASRR determination that NF services are needed.) Please note that our use of the terms mental illness and mental retardation is a strict reflection of the language used in the current Code of Federal Regulations (CFR) regarding PASRR. Valuable information PASRR is for all individuals applying for admission into Medicaid certified nursing facility care regardless of pay source All persons needing admission to a Medicaid certified nursing facility must have a Preadmission Screening for possible mental illness and/or intellectual disability (Level I) before admission A nursing home must not admit any new resident who is mentally ill unless the State mental health authority has conducted a PASRR determination and was determined to need NF services All persons who reside in a nursing facility are subject to Resident Review if there is a substantial change in their mental or physical status which warrants a referral for an evaluation (Level II). See Section V of this Manual for details. 5
6 Section II: PASRR Level I Definition and Process The first screening, PASRR Level I, assesses for potential mental illness and/or intellectual disability. All those who have a suspected or confirmed mental illness or intellectual disability must receive a more in-depth assessment, the Individualized PASRR Level II Evaluation. In order to complete the PASRR Level I: 1. Access the ACS/Xerox Provider Portal. If you do not have access contact ACS/Xerox at Option 3 to complete the Electronic Data Interchange (EDI) application and obtain a user name and password. 2. It is highly recommended to complete the ACS/Xerox tutorial for PASRR at: 3. Login in at the ACS/Xerox Provider Portal link located at: 4. Complete the PASRR Level I, filling in all areas and answering each question carefully. 5. When you get to the diagnosis sections they should be prioritized as you enter them. 6. If the PASRR Level I does not trigger MI and/or ID, print the PASRR Level I and place it in the client s chart. 7. If only a Level I is needed on a client, an LT101 is not required for the PASRR process. However, the Division of Healthcare Financing strongly recommends doing an LT101 on all admissions and is required for payment with Medicaid clients. 8. If the PASRR Level I triggers MI and/or ID there will be two possible next steps; be sure to read the summary and instructions: a) Individualized PASRR are required when, after screening, it is determined that the individual has indicators of serious mental illness (MI) or mental retardation/intellectual disabilities (MR/ID) therefore, review and evaluation of information regarding the individual s status and needs are required. If an individualized PASRR, send in the documents identified on the PASRR checklist, as detailed in Section IV of this Manual. b) Categorical decisions apply to people with MI or MR/ID conditions, as a way to expedite decisions regarding a person s needs when a full PASRR Level II assessment is not needed based on certain circumstances that are time limited or where need is clear (as defined by the State). If a Categorical Determination is triggered, you will need to fax to Xerox Care and Quality Solutions ( ) the following: PASRR Level I History and Physical within last 12 months Medication list (MAR) LT101 <90 days old Progress notes representing last seven (7) days of services and treatments Please see Section III for more information on Categorical Determinations. Xerox will file the Categorical Determination packet for possible future use and you will not receive any notifications. Valuable information 6
7 New PASRR fax number is Division of Healthcare Financing strongly recommends doing an LT101 on all admissions and it is required for payment with Medicaid clients. 7
8 Section III: PASRR Level II Categorical Determinations Categorical determinations permit states to omit the individualized Level II Evaluation in certain circumstances that are time limited or where need is clear. While categorical determinations do abbreviate the PASRR process, the function of the resulting determination is not different from an individualized determination and a determination document must be submitted to CQS prior to admission. Categorical determinations are not "exemptions" from the PASRR process. PASRR regulations permit the State Mental Health Authority (SMHA to develop categories based on certain diagnoses, levels of severity of illness, or need for a particular service such as a ventilator, that indicate that admission to a NF is normally needed. There also may be provisional admissions with time limits pending further assessment due to delirium, for emergency protective services not more than seven days, or for respite. (Longer stays would require a Level II Resident Review). These three provisional categories, at state option, may also carry a categorical determination that specialized services (SS) are not normally needed. A categorical determination that SS are needed is not allowed. This is to ensure, in states that provide SS for NF residents, that NF residents with SMI and/or MR/ID, receive individually planned SS. In states that do not provide SS to NF residents, this ensures that placement options will be addressed on an individualized basis. If sufficient, accurate, and current data are available following a Level I Identification for the evaluator to determine that an individual fits into a category established by the state authorities, then an individualized Level II Evaluation is not required, and the determination may be made categorically. Type of Categorical Question on Level I Categorical 4 1. A terminal illness, verified in writing by a physician? Categorical 5 2. Are comatose, ventilator dependent, functioning at brain stem level, have diagnosis of COPD, severe Parkinson's, Amyotrophic Lateral Sclerosis, CHF, Huntington's Disease, CVA, quadriplegia, advanced MS, muscular dystrophy, end stage renal disease, severe diabetic neuropathy or refractory anemia? 2a. If so, is the condition severe enough that he or she could not participate in evaluation or treatment? Categorical 6 3. If this individual has possible or (Exempted Hospital probable MI or MR/ID, does he or she Discharge) have a medical condition, subsequent to discharge from an acute care hospital, for which convalescent care is 8
9 Categorical 7 (Provisional Admission) Categorical 8 (Provisional Admission) likely to require LESS THAN 120 days of nursing facility services? 4. Require provisional placement for respite care or due to delirium not to exceed 14 days? 5. Require emergency placement for his/her safety not to exceed 7 days? Please note: If you answered yes to 1, 2 and 2a, 3, 4 or 5 of the previous questions then the PASRR Level I has triggered a Categorical Level II Determination. Fax to Xerox the following: PASRR Level I History and Physical within last 12 months Medication administration record (MAR) LT101 <90 days old Progress notes representing seven (7) days of services and treatments When submitting a Categorical Level II, you will not receive any documentation back from Xerox. Xerox stores the packet electronically and does not create a Determination Summary Report. If you answered yes to 2 and no to 2a it will trigger an individualized Level II Evaluation. Fax complete PASRR Level II packet to Xerox and wait for the determination. Xerox will send you a Determination Summary Report. If a client on the Home and Community Based Service (HCBS) waiver is moved to a NF for short term respite, it is considered an admission for purposes of PASRR and all policies and procedures must be followed for both the PASRR Level I and also Level II if MI or ID is identified. Valuable information Categorical determinations are not "exemptions" from the PASRR process Xerox does not send the facility a Determination Summary Report for Categorical Determinations The NF must keep track of the days allowed under the categorical exemption, complete the PASRR process and receive a completed determination before the end of the allowed exemption period, if the resident will remain in the facility beyond the expiration date of the categorical determination date. 9
10 Section IV: Individualized PASRR Level II Definition and Process PASRR Level II evaluations are in-depth reviews for nursing facility applicants and residents who are thought to have serious MI and/or MR/ID, to accurately assess whether an individual needs specialized services and/or nursing facility level of care. Level II evaluation packets are required to include: PASRR Level I Psychosocial evaluation (within the last 12 months from the date of the evaluation unless a change of condition has occurred, in which case a new psychosocial should occur at the time of changes - that includes: o the individual s past and present living arrangements describing successes and failures and medical and support systems and current family involvement in the evaluation and treatment) o cultural, language and ethnic origin and applicable adaptations required o evaluation of intellectual functioning, memory functioning and orientation, description of current attitudes and overt behaviors, affect, suicidal or homicidal ideation, paranoia, and degree of reality testing (presence and content of delusions) and hallucinations must be available. o a functional assessment of the individual s ability to engage in ADL s and IADL s that addresses monitoring of health status, self-administering and scheduling of medical treatment, self-monitoring of nutritional status, handling of money, dressing appropriately, and grooming. An accurate functional assessment is extremely important in determining an individual s appropriate placement) Current history and physical (within last 12 months or at change of condition, including: o medical history, o review of all body systems, o specific evaluation of the individual s neurological system in the areas of motor functioning, sensory functioning, gait, deep tendon reflexes, cranial nerves and abnormal reflexes) Psychiatric evaluation, if on file and less than two (2) years old LT101 less than 90 days old Current medications (medication administration record with name, dosage, administration frequency and route of administration) Progress notes representing last seven (7) days of services and treatments If MR/ID, a comprehensive medication history and IQ testing (within last 12 months) Informed Consent Form (If resident is unable to sign consent, a medical power of attorney (MPOA) must sign, or if resident is incompetent, legal representative must sign. Minimum Data Set (MDS) is strongly recommended for Significant Change reviews Fax the completed packet to Xerox Care and Quality Solutions at , for a Level II PASRR review to be completed. Determination of appropriateness for nursing facility placement is made by a qualified Clinician at Xerox with coordination between the Department of Health, 10
11 Mental Health and Substance Abuse Services Division and Medicaid as necessary. Qualified clinicians are defined per Wyoming State Statute, Wyoming Medicaid Program Manual, Community Mental Health Manual, Chapter 2, Section 01. Qualified clinicians include: o Licensed Professional Counselor o Licensed Addiction Therapist o Licensed Psychologist o Licensed Marriage and Family Therapist o License Physician o Licenses Psychiatric Nurse (Masters) o Licensed Advanced Practice Nurse (specialty area of psychiatric/mental health nursing) After review by the qualified clinician, the resulting document, known as the Determination Summary Report (DSR), is faxed within four (4) days of receipt of completed packet to: the individual in care of (C/O) the referring (discharging) or retaining facility and his/her legal representative, if applicable the admitting or retaining NF the admitting or retaining facility must place a copy of the DSR in the resident s chart for attending physician review the discharging hospital (if the individual is seeking NF admission from a hospital) A copy of the DSR is also sent to the Division of Healthcare Financing (DHCF) representative After review by the qualified clinician, the Notice of Determination (NOD) is faxed within four (4) days of receipt of completed packet to: the individual in C/O the referring or retaining facility and his/her legal representative, if applicable the Division of Healthcare Financing (DHCF) representative the Ombudsman for Long Term Care The fiscal agent will be notified by ed memo Sample communication documents are provided in the Appendix to this Manual. Clients who are screened for PASRR II are often in urgent need of structured care. Completion of PASRR screenings, evaluations, determinations and related paperwork, are TIME SENSITIVE; please submit all the required documentation listed above on the first submission to avoid delays in determinations. After the complete screening packet is received, experienced, qualified clinicians establish appropriate placement for the resident based on level of care needed. Valuable information Facilities should submit complete packets to facilitate the PASRR process LT101 must be less than 90 days old Completed packets must be legible and turned in an orderly manner, accompanied by the Checklist form identified in the Appendix to this Manual and available to download at WYHealth.net. 11
12 Section V: Significant Change (Resident Review) Resident Review Per CFR , a Resident Review, is to be completed on an annual basis for residents with either MI or MR to determine whether the resident s physical and mental condition requires the level of care and services which are being provided. Please note: CFR is not current concerning Resident Review. Revisions in 1996 resulted in changes within Sec [42 U.S.C. 1396r] (E) and replaced annual review with review upon a change in condition. The State of Wyoming has further defined the resident review as a significant change in condition. Significant Change in Condition An individual is considered to have a significant change in condition (improvement or decline and physical or mental) when the change results in the need to complete an update to the MDS or Plan of Care. Physical changes to a client s condition which result in a change of their level of functioning that would allow them into a less restrictive environment or requires a more restrictive environment would result in a significant change of condition. An updated Level I Screening should be completed and submitted within 14 days of the resident s status change to ensure appropriate services. Significant change does not apply to residents with a primary diagnosis of dementia including Alzheimer s disease or a related disorder, or a non primary diagnosis of dementia unless the primary diagnosis is a major mental disorder. Mental status changes that result in a new diagnosis or that trigger a significant change to the total score on the Brief Interview for Mental Status (BIMS) or the Patient Health Questionnaire (PHQ9) on the Minimum Data Set (MDS) would result in a significant change of condition. Brief Interview for Mental Status (BIMS) The BIMS is contained in Section C of the Minimum Data Set (MDS) 3.0 and is a structured test consisting of three components that are compiled into a total score. This score allows for comparison with future and past performance. The lowest possible score is 00 with the highest being 15. Total score reflects the client s cognitive status and can be interpreted as follows: Total Score Interpretation of Cognitive Status/Category Cognitively Intact Moderate Impairment Severe Impairment Any significant changes in the total score (e.g., change in Cognitive Status Category) could be interpreted as a significant change in the client s mental status. 12
13 Patient Health Questionnaire (PHQ-9) Resident Mood Interview The PHQ-9 is contained in Section D of the Minimum Data Set (MDS) 3.0 and is a validated interview that screens for symptoms of depression. It provides a standardized severity score that allows for comparison of symptoms multiple periods of time. PHQ 9 Provisional Diagnosis Treatment Recommendation Score 5-9 Minimal symptoms Support, educate to call if worse; return in 1 month Minor Depression Support, watchful waiting Dysthymia Antidepressant or psychotherapy Major Depression, Mild Antidepressant or psychotherapy Major Depression, Moderately Antidepressant or psychotherapy Severe > 20 Major Depression, Severe Antidepressant and psychotherapy (especially if not improved on monotherapy Any significant changes in the Provisional Diagnosis above could be interpreted as a significant change in the client s mood. Valuable information Revisions have replaced the annual review with a review upon a change in condition The Minimum Data Set (MDS) contains two assessment tools that can be used to objectively measure significant change If a significant change occurs, the facility has 14 days to submit an updated Level I Screen Significant change does not apply to residents with a primary diagnosis of dementia including Alzheimer s disease or a related disorder, or a non primary diagnosis of dementia unless the primary diagnosis is a major mental disorder. Submission of the Minimum Data Set (MDS) is highly recommended for Significant Change reviews. If deemed necessary, this document will be required for Significant Change reviews. 13
14 Section VI: Inter-facility Transfer Policy As previously indicated in this Manual, the purpose of PASRR Level II is multifunctional: 1) the assessment of the clients diagnoses; and 2) the verification of appropriate placement. When a transfer of a client occurs from one facility to another, a new PASRR Level I Screen, and if applicable, PASRR Level II Evaluation must be completed prior to admission. The admitting facility will not receive payment from Medicaid until the PASRR Level I is on file and a PASRR Level II Evaluation, if applicable, is completed in its entirety with the Division of Healthcare Financing (DHCF). A PASRR Level I will be considered valid for one (1) year unless a change of condition has occurred, in which case a new PASRR Level I Screen should occur at the time of change (within 14 days of the significant change). If the PASRR Level I triggers a PASRR Level II (potential for serious mental illness (MI) or intellectual disability (ID/MR) diagnosis), the PASRR II must also be completed within 3 weeks (if change of condition on an existing client) or prior to admission with a determination date from the State of Wyoming prior to admission, for payment moving forward. The contents of the PASRR Level II Evaluation packet for a patient transferring to another facility remain the same as identified in Section IV of this Manual: PASRR I Screen Psychosocial evaluation (within the last 12 months from the date of the evaluation unless a change of condition has occurred, in which case a new psychosocial should occur at the time of changes) Psychiatric evaluation (if on file and < 2 years old) LT101 <90 days old Current history and physical (within last 12 months of upon change of condition) Current medications Progress notes (reflecting last seven (7) days of services and treatments) Informed Consent Form (If resident is unable to sign consent, a medical power of attorney (MPOA) must sign, or if resident is incompetent, legal representative must sign) If ID, a comprehensive medication history and IQ Testing (within last 12 months) Minimum Data Set (MDS) is strongly recommended for Significant Change reviews Psychosocial Evaluations are valid for 12 months from the date of the evaluation unless a change of condition has occurred, in which case a new psychosocial should occur at the time of change. Valuable information A PASRR Level I will be considered valid for one (1) year unless a change of condition has occurred, in which case a new PASRR Level I Screen should occur at the time of change (within 14 days of the significant change) 14
15 A PASRR Level I Screen must be completed when a patient is transferred to another facility If applicable, a PASRR Level II Evaluation must be completed prior to the patient s admission to the receiving facility 15
16 Section VII: Roles and Responsibilities Referring Hospitals and Nursing Facilities (NF) 1. Log on to the ACS web portal, inc.com/index.html, and complete the PASRR Level I Screen. If a Level I PASRR indicates serious mental illness or intellectual disability/mental retardation, fax a completed packet to Xerox Care and Quality Solutions at for an individual Level II PASRR review to be completed. See Section III of this Manual for information on categorical determinations. If the Level I PASRR indicates no serious mental illness or intellectual disability, the client may be admitted. 2. Ensure that a complete individual Level II packet is sent. The requirement documents include: PASRR Fax coversheet PASRR Level I Screen Psychosocial within the last 12 months from the date of the evaluation unless a change of condition has occurred, in which case a new psychosocial should occur at the time of changes - that includes: o the individual s past and present living arrangements describing successes and failures and medical and support systems and current family involvement in the evaluation and treatment) o cultural, language and ethnic origin and applicable adaptations required o evaluation of intellectual functioning, memory functioning and orientation, description of current attitudes and overt behaviors, affect, suicidal or homicidal ideation, paranoia, and degree of reality testing (presence and content of delusions) and hallucinations must be available. o A functional assessment of the individual s ability to engage in ADL s and IADL s that addresses monitoring of health status, self-administering and scheduling of medical treatment, self-monitoring of nutritional status, handling of money, dressing appropriately, and grooming. An accurate functional assessment is extremely important in determining an individual s appropriate placement) Psychiatric evaluation (if on file and < 2 years old) LT101 <90 days old Current history and physical (within last 12 months or at change of conditions, including: o medical history, o review of all body systems, o specific evaluation of the individual s neurological system in the areas of motor functioning, sensory functioning, gait, deep tendon reflexes, cranial nerves and abnormal reflexes) Current medications(medication administration record with name, dosage, administration frequency and route of administration) Progress notes representing last seven (7) days of services and treatments Informed Consent Form If MR/ID, a comprehensive medication history and IQ Testing (within last 12 months) 16
17 Minimum Data Set (MDS) is strongly recommended for Significant Change reviews On the fax coversheet, you must include your name, phone number, fax number and address and purpose of request. A check list has been developed that must be completed and submitted with the packet. Templates for the fax cover sheet and checklist are found in the Appendix to this Manual and can be downloaded from WyHealth.net 3. Refer those persons who are in need of a current psychosocial evaluation to a local community mental health center. Prompt referrals are necessary as time is of the essence. 4. Refer those persons who are in need of a current LT101 evaluation to the Clinical Manager for Long Term Care, Wyoming Department of Health, Division of Healthcare Financing fax , via faxed LT101 request form. (See Public Health Nursing page 14 for complete referral process) 5. If there is a determination that NF placement is not appropriate, Xerox Care and Quality Solutions (CQS) will assist in the coordination of care in consultation with the resident and resident s family or legal representative and caregivers to: a. Arrange for safe orderly discharge of the resident. b. Prepare and orient the resident for such discharge. 6. File Level II Determination Summary and Notification in the patient s chart. The attending physician should be provided a copy of the Determination Summary Report. Public Health Nursing Concerning Referral Process for LT101 Referrals: There is a LT101 Request form available for use by facilities and hospitals to request LT101 assessments from the Clinical Manager for Long Term Care The form can be used effective from the date of this notice, and will be required through facsimile transmission for facilities and hospitals which began June 1, 2012, Fax # (307) The form can be accessed from the Wyoming Medicaid website for providers, on the forms page The form will need to be COMPLETE in order for the referral to be made to the Public Health Nursing Office LT101's must be requested on or before the day of admission to ensure Wyoming Medicaid payment Keep fax confirmations, and if there is a question as to whether or not the fax went through, call (307) to confirm receipt The date stamp on the form that is electronically received by the Division of Healthcare Financing via fax will be considered the provider referral date (should match the date on the request form) The Clinical Manager for Long Term Care will notify the facility if the LT101 is not referred to Public Health (i.e. the client has a current LT101) 17
18 LT101's are good for 90 days LT101's are required upon re-admission, after previous "discharge" "Discharge" does not include: temporary absence from the facility for treatment in a hospital, home visit, or community stay, provided such an absence is no longer than 30 consecutive days Wyoming Medicaid does not change the admit date, unless a discharge occurs The LT101 evaluation should be completed and received by the referral source within seven (7) calendar days upon actual referral. Leaving a copy of the LT101 in the patients chart is appreciated upon evaluation to expedite the PASRR process. Xerox Care and Quality Solutions A delegated authority at Xerox Care and Quality Solutions, Inc. (CQS) receives the referral and determines if all required documents are in the referral packet. If all documents are in the packet then the referral is assigned to a licensed reviewer. If the referral packet is incomplete then a Notice of Missing Documentation Letter is faxed or ed to the referral source. If the missing documentation is not received within 2 business days then an Administrative Closure Letter is faxed or ed to the referral source and mailed to client and/or guardian. When CQS, receives the missing documentation, the referral is then assigned to a licensed reviewer. The reviewer determines if the documents contain needed information and are representative of the client s current level of functioning. If not, additional information is requested within two (2) business days by fax or ing the referral source the Notice of Necessary Clinical Documentation Letter. After receiving additional information, if determination cannot be made, then outreach will be done via telephone to obtain additional information from the referring physician/provider. A copy of the Minimum Data Set (MDS) is strongly recommended for Significant Change reviews. If a determination can t be made without a copy of the MDS, this document will be required and the determination will be delayed until this document is received. PASRR Level II cases are reviewed in a multidisciplinary team conference. The multidisciplinary team includes a licensed professional counselor, licensed clinical social worker, registered nurse, masters prepared psychiatric nurse and utilization review assistant. The CQS Medical Director provides oversight and review of complex cases when needed. After receipt of all necessary documentation, the CQS licensed clinician completes a Determination Summary Report. If acute inpatient psychiatric care, known as Specialized Services (SS), is needed, Xerox CQS will assign a case manager to monitor and coordinate care After review by the CQS clinician, the resulting document, known as the Determination Summary Report (DSR), is faxed within four (4) days of receipt of completed packet to: the individual in care of (C/O) the referring (discharging) or retaining facility and his/her legal representative, if applicable the admitting or retaining NF 18
19 the admitting or retaining facility must place a copy of the DSR in the resident s chart for attending physician review the discharging hospital (if the individual is seeking NF admission from a hospital) A copy of the DSR is also sent to the Division of Healthcare Financing (DHCF) representative After review by the qualified clinician, the Notice of Determination (NOD) is faxed within four (4) days of receipt of completed packet to: the individual in C/O the referring or retaining facility and his/her legal representative, if applicable the Division of Healthcare Financing (DHCF) representative Ombudsman for Long Term Care The fiscal agent will be notified by ed memo Allow an average of 7 9 days for processing before billing. Sample communication documents are provided in the Appendix to this Manual. Placement Support: Xerox Care and Quality Solutions staff will provide placement support by phone: If the client is not appropriate for nursing facility placement, staff will begin Care Coordination within 1 business day to assist in finding an appropriate place for the client. If the client is not appropriate for nursing facility placement and the client requires SS, the staff will contact the referring facility within 1 business day to assist with SS placement. Serious Mental Illness: The determination of whether or not an individual has a serious mental illness involves reviewing the information available in the referral packet for any Diagnostic and Statistical Manual Fourth Edition Text Revision (DSM IV TR) diagnoses, use of psychotropic medications, and current and past outpatient or inpatient psychiatric care. The reviewer will review for any current disturbances in orientation, affect, mood, or behavior. Intellectual Disability and other Related Conditions: The determination of whether or not an individual has an intellectual disability or other related condition involves reviewing the information available in the referral packet for any Diagnostic and Statistical Manual Fourth Edition Text Revision (DSM IV TR) diagnoses or medical disorder, such as cerebral palsy or spina bifida. The evaluator will review documentation supporting the aforementioned conditions including medical records, psychological evaluation, functional assessment, and educational records. If SS are not recommended, the process is completed. Xerox Care and Quality Solutions will track completed Level II PASRR s and will report to the State monthly. Data Tracking: 19
20 The Xerox CQS data system will collect and store all information and documents that are submitted. This information will include the patient s mental health diagnosis and monitoring of SS recommended for patients deemed to meet criteria for a serious mental illness. This Structured Query Language (SQL)- based system tracks referrals; records outcomes including psychiatric diagnoses, the appropriateness of nursing facility placement, the need for SS; and plans of care while ensuring security and confidentiality. All data is in compliance with applicable federal and state laws (including HIPAA Privacy Rules, 45 C.F.R. Parts 160 and 164.) The monitoring of SS involves confirming the institutionalization of the client. Xerox CQS monitors and reports the status of SS recommendations on an annual basis. Reports: Xerox CQS provides data on the number of referrals for new admissions to nursing facilities, PASRR II screens, results of screening determinations, the number of residents requiring a Resident Review (RR) due to a significant change in their functioning, and referrals for which clinical record reviews and/or Level II evaluations are not completed due to situations such as the death of the patient, discharges/transfers from nursing facilities, those never admitted to nursing facilities, and those admitted for hospitalizations. Quality Assurance: Xerox CQS, maintains policies and procedures to assure excellence in the work process and end product. The Quality Assurance process involves evaluating completed referrals using specific protocols and guidelines to determine the accuracy of determinations and appropriateness of recommendations, if applicable, and the quality of work related to the PASRR Level II evaluations. This program provides for consistent and accurate review practices for determining the appropriateness for a nursing facility placement, need for SS, and the development of individualized plans of care when SS are deemed necessary. Inter rater reliability statistics are utilized to monitor the consistency and validity of the determinations. Results of the Quality Analyses are utilized to determine training needs and other quality improvement activities. State Mental health Authority (SMHA) Responsibilities: SMHA has delegated their function and responsibility as the mental health authority for the state of Wyoming to Xerox Care and Quality Solutions (CQS) for approval of the MI and ID determination review for Level II PASRR s. Below are some of the responsibilities CQS has been delegated by SMHA. State Mental Retardation Authority (SMRA) Responsibilities: SMRA has delegated their function and responsibility as the mental health authority for the state of Wyoming to Xerox Care and Quality Solutions (CQS) for approval of the MI and MR/ID determination review for Level II PASRR s. Below are some of the responsibilities CQS has been delegated by SMRA. Disposition Based on Results of Level II Evaluation 20
21 The Level II evaluation will result in determination of appropriate or inappropriate NF placement or need for Specialized Services. Placement refers either to admission or continued residence in a nursing facility. The meaning of Special Services, within the context of PASRR level II evaluations, refers to services specified by the State that: 1. Is developed and supervised by an interdisciplinary team, which includes a physician, qualified mental health professionals, and, as appropriate, other professionals. 2. Prescribes specified therapies and activities for the treatment of persons experiencing an acute episode of serious mental illness, which necessitates supervision by trained mental health personnel; and 3. Is directed toward diagnosing and reducing the resident s behavioral symptoms that necessitated institutionalization, improving his or her level of independent functioning, and achieving a functioning level (adaptive, functional, emotional etc.) that permits reduction in the intensity of mental health services to below the level of specialized services at the earliest possible time. In summary, specialized services are the level of services that would be provided in an institution or an inpatient psychiatric hospital. Types of determinations include the following: 1. Individual requires NF level of care but does not require specialized services. Placement is authorized. Mental health rehabilitation services may be recommended. 2. Individual does not require NF care and does not require specialized services. Placement is not authorized. Admission is denied. The nursing facility must arrange for orderly discharge and must prepare and orient the resident for discharge. 3. Individual does not require NF level of care but requires specialized services that cannot be provided in the NF. Placement is not authorized. Admission is denied. The nursing facility must arrange for orderly discharge and must prepare and orient the resident for discharge. The 30 month rule applies. 4. No evidence of a serious mental illness. Placement is authorized. No further screening is required. 5. No evidence of serious intellectual disability. Placement is authorized. No further screening is required. 6. Individual has a primary diagnosis of dementia or a secondary diagnosis of dementia when the primary diagnosis is not a serious mental illness. Placement is authorized. No further screening is required. 7. Individual is categorically appropriate due to terminal illness or severe medical condition. Placement is authorized. 8. The evaluation was incomplete due to death or discharge. These determinations carry the right of appeal as defined in 42 CFR Part and Chapter XIX of the State Medicaid Rules: Transferring Facility Responsibility (CFR (4)(II)) In cases of transfer of a resident with MI or MR/ID from a NF to a hospital or to another NF, the transferring NF is responsible for ensuring that copies of the resident s most recent PASRR and resident assessment reports accompany the transferring resident. 21
22 Office of Healthcare Licensing and Survey, PASRR and MDS 3.0 CMS and States will be monitoring PASRR activities partly through data entered into MDS 3.0 and onsite visits. The MDS 3.0 assessments will require providers to record PASRR data regarding an individual s pre screening, Level I screening and/or Level II resident review. PASRR requirements for MDS 3.0 can be found in Chapter 2 of the CMS Resident Assessment Instrument (RAI) Manual, Section S. PASRR, MDS and Significant Change If a significant change in status (SCSA) occurs for an individual known or suspected to have mental illness, intellectual disability, or condition related to mental retardation (as defined by 42CFR ), a referral to Xerox CQS for possible Level II PASRR evaluation must occur as required by Section 1919(e)(7)(B)(iii) of the Social Security Act. Resources for determining a SCSA as it relates to PASRR can be found in the MDS 3.0 RAI Manual Chapter 2. Inclusion of the Minimum Data Set (MDS) in the PASRR packet submitted to Xerox Care and Quality Services is strongly recommended for Significant Change reviews. The MDS has valuable information about the condition and functioning of the client that is useful for the reviewer in making a determination. MDS PASRR questions are a reminder to staff and a trigger to surveyors for PASRR tag. Failure to document pre screening evaluations, PASRR Level I, and if indicated all Level II requirements, (prior to admission or upon change in condition), subjects nursing facilities or swing beds to liability for: Survey deficiency (F285) Recouping federal financial participation monies (FFP) for all days prior to completion. Deficiencies in the areas of care planning and/or Quality of Life may occur if a provider does not follow recommendations or directives provided in a Level II determination letter. Department of Health reviews PASRR compliancy during their survey/certification of nursing homes and swing bed facilities. Valuable information Request LT101s and Psychosocial Evaluations early to avoid delays LT101 must be less than 90 days old Ensure that a complete individual Level II packet is sent. Incomplete packets will lead to delays in the process If a significant change in status (SCSA) occurs for an individual known or suspected to have mental illness, intellectual disability, or condition related to mental retardation (as defined by 42CFR ), a referral to Xerox Care and Quality Solutions for possible Level II PASRR evaluation must occur Inclusion of the Minimum Data Set (MDS) in the PASRR packet submitted to Xerox Care and Quality Services is strongly recommended for Significant Change reviews 22
23 Specialized services are the level of services that would be provided in an institution or an inpatient psychiatric hospital. 23
24 Section VIII: Appeals Process Purpose The purpose of this chapter is to ensure that individuals who were the subject of WY PASRR Level II evaluations have the right to appeal determinations in a fair and timely manner, consistent with state and federal law. Xerox Care and Quality Solutions has established a process policy (in accordance with the Division of Healthcare Financing [DHCF], Wyoming Department of Health Appeal Hearing policy) by which any applicant or their legal representative who is dissatisfied with the outcome of a Level II PASRR can appeal the decision. A copy of this procedure is available to referral sources, the applicant or legal representative upon request. Initiating the Appeal and Fair Hearing Process The patient is provided instructions for initiating the appeals process, per the Wyoming Medicaid Rules (Rules for Medicaid Administrative Hearings), in the Notice of Determination letter received via mail. The appeal must be requested in writing within 30 calendar days following the date of receipt of the determination letter. As explained in the letter, the request for an appeal should be faxed to or mailed to: Xerox Care and Quality Solutions. Inc. Attn: PASRR Coordinator P.O. Box 49 Cheyenne, WY (888) , ext Requests for a hearing are referred to the Xerox Care and Quality Solutions PASRR Coordinator and are date stamped upon receipt. From the date the appeal is received by Xerox Care and Quality Solutions, the DHCF has 20 days to review and respond to the appellant. A hearing must occur within 90 days of the PASRR Level II determination. Reconsideration Review When a hearing request is received, the Xerox Care and Quality Solutions PASRR Coordinator will conduct a Reconsideration Review in which the documentation available at the time of the initial determination is reviewed for accuracy. If any errors are noted, immediate action is taken to rectify the inaccuracy. The patient or their representative is immediately notified. If the appellant is satisfied with the correction, they may choose to withdraw their request in writing to the address above. 24
25 Informal Conference If no error is detected or in the event the appellant elects not to withdraw their request following an error correction, the Xerox Care and Quality Solutions PASRR Coordinator schedules a teleconference with the appellant or their representative. The patient or representative is advised the teleconference is optional and does not replace or delay the hearing process. If during the conference a satisfactory decision is made that satisfies the appellant, the request for a hearing may be withdrawn in writing to the address above. Formal Hearing All requests for a hearing are forwarded by the Xerox Care and Quality Solutions PASRR Coordinator to Renee Propps, Division of Healthcare Financing. The Facilities Manager will then forward all requests to the Office of Administrative Hearings (OAH) if reconsideration and/or informal teleconference do not result in resolution (within 7 business days). Only OAH can decide to reject an appeal. Xerox Care and Quality Solutions staff provides expert, telephone testimony in the event the case proceeds to a hearing. All actions to reduce or cancel benefits or services will be reviewed to determine whether or not the appeal was filed within the required 30 day time frame, thereby allowing any current benefits or services to continue until a decision can be rendered by the Hearing Officer. The potential decisions at any stage of the Appeal and Fair Hearing process include: Upheld: The determining authority concurs with the adverse determination or previous appeal decision. Partially Overturned: The determining authority modifies the adverse determination or previous appeal decision. Overturned: The determining authority does not concur with the adverse determination or previous appeal decision. The final decision is made by the DHCF following the Medicaid Rules (Rules for Medicaid Administrative Hearing) and no further administrative appeals are allowed. Valuable information An applicant or their legal representative who is dissatisfied with the outcome of a Level II PASRR can appeal the decision. DHCF has 20 days to review and respond to the appellant. A hearing must occur within 90 days of the PASRR Level II determination. The final decision is made by the DHCF following the Medicaid Rules (Rules for Medicaid Administrative Hearing) and no further administrative appeals are allowed. 25
26 Section IX: Out of State Nursing Facility Placement Policy Enrollment: If services are available in Wyoming within a reasonable distance from the recipient's home, the recipient must not utilize an out of state provider. Pursuant to Wyoming Medicaid Rule Ch 3, Section 6, Out of State Providers, documentation demonstrating one of the above circumstances and prior authorization through the Division of HealthCare Financing is required on all Nursing Home residents placed in out of state Nursing Facilities. If services are deemed appropriate for out of state nursing facility placement then: An LT101 (Functional Assessment) and Wyoming PASRR are required on all residents in order to receive payment on all nursing home services furnished outside the service area. Services furnished by a provider located outside the service area are not Medicaid reimbursable unless: The service is furnished in response to an emergency; The recipient is outside the service area and the recipient's health would be endangered if he/she were required to return to the service area; and LT101 and PASRR are required prior to admission. An LT101 can be obtained by faxing the LT101 request form for facilities and hospitals to the Clinical Manager for Long Term Care, Wyoming Department of Health, Division of Healthcare Financing at fax as soon as possible. The LT101 will be performed by phone in these situations, by a Wyoming Public Health Nurse. (See Public Health Nursing page 14 for complete referral process) A PASRR Level I should be completed on the ACS Provider Portal: 1. Access the ACS Provider Portal. If you do not have access contact ACS at Option 3 to complete the Electronic Data Interchange (EDI) application and obtain a user name and password. 2. It is highly recommended to complete the ACS tutorial for PASRR at 3. Login in at the ACS Provider Portal link located at to complete a PASRR Level I. If the resident will be out of state and placed for long term care the resident should become a Medicaid resident of that state. If obtaining another states residency is not applicable then a supporting document of medical necessity (according to the state of the facility) must be on file. If a resident is in WY and being transferred out of state then the LT101 should be performed face to face in the resident's county prior to leaving the state. 26
27 Valuable information If services are available in Wyoming within a reasonable distance from the recipient's home, the recipient must not utilize an out of state provider. An LT101 (Functional Assessment) and Wyoming PASRR are required on all residents in order to receive payment on all nursing home services furnished outside the service area. 27
28 Section X: Swing Bed Facilities Even though a swing bed facility is not technically a certified nursing facility (NF), it still has to comply with some of the NF requirements. Those requirements include PASRR, Section 1913 of the Social Security Act which defines swing beds and clearly requires that swing bed facilities comply with all requirements of section 1919(b) through 1919(d) with respect to the NF services offered. Section 1919(e)(7) of the Social Security Act and Chapter 42 of the Code of Federal Regulations, Sections through specify the requirements for pre admission screening resident reviews for individuals with mental illness, intellectual disabilities/mental retardation and developmental disabilities. Federal regulations require that PASRR screenings take place prior to admission to the swing bed. A client that receives swing bed services is not subject to the requirements of the PASRR II until the client remains in a swing bed for more than thirty (30) consecutive days. Then the client is subject to the requirements of Chapter 19, PASRR requirements. For clients meeting the criteria of CFR (b)(2) as an exempted hospital discharge, the requirements of Chapter 19 must be satisfied on or before the fortieth (40) calendar day after admission. The failure to timely complete the requirements of Chapter 19 shall result in nonpayment for services provided after the fortieth (40) consecutive day and until the date the PASRR requirements are satisfied. Valuable information Swing bed facilities comply with all requirements of section 1919(b) through 1919(d) with respect to the NF services offered. Federal regulations require that PASRR screenings take place prior to admission to the swing bed. A client that receives swing bed services is not subject to the requirements of the PASRR II until the client remains in a swing bed for more than thirty (30) consecutive days. For clients meeting the criteria of CFR (b)(2) as an exempted hospital discharge, the requirements of Chapter 19 must be satisfied on or before the fortieth (40) calendar day after admission. The failure to timely complete the requirements of Chapter 19 shall result in nonpayment for services provided after the fortieth (40) consecutive day and until the date the PASRR requirements are satisfied. 28
29 Section XI: Diversion/Transition When a client has been assessed through the PASRR process and deemed inappropriate for placement to a nursing facility, multiple options exist for the transition/diversion and assistance of care. Following is a list of a few of Wyoming s resources that work toward this goal. Project OUT Project OUT is a short term Medicaid and state funded intervention and assistance program that helps consumers overcome the barriers to living independently in the community. The program provides targeted case management and a limited financial resource to assist with some of the costs of transferring out of or diverting from a nursing home. Costs might include moving or storage expenses, rental or utility deposits, household items, furniture, personal alert systems, grab bars or other assistive devices, as well as limited transportation services following the transition or diversion process. Project OUT links the consumer to community services and long term care programs that may provide the on going support needed for consumers to live independently. To be eligible for Project OUT services, a consumer must be a Wyoming resident, at least 18 years of age, and Medicaid eligible. If during the transition or diversion process Medicaid eligibility must be determined, state dollars will fund the assistance. Wyoming defines a diversion as a person at risk of needing nursing facility care being able to remain in the community or a person who has been in a nursing facility for six months or less being able to return to the community to live. As predicted, the number of transitions compared to diversions continues to decrease. Identifying nursing home residents who want to return to the community through Minimum Data Set (MDS) collected by the nursing homes and increased education and outreach have resulted in consumers being educated earlier about their longterm care options. Remaining in the community or returning earlier to the community not only is the easiest and most desirable for the consumer, it is the least costly for the State. Each Project OUT client collaborates with a Project OUT transition specialist, his or her healthcare provider and/or discharge planner to create a transition or diversion plan which includes those services and supports that are necessary to facilitate independent living. Project OUT will continue to strive to increase awareness of the program within every Wyoming community. As more healthcare providers, discharge planners, and families become aware of the services available through Project OUT, the number of consumers helped by the program is expected to increase. Anita Fox, Program Manager, can be contacted at or Anita.Fox@wyo.gov. 29
30 PACE The Program of All inclusive Care for the Elderly (PACE) model is centered on the belief that it is better for the well being of seniors with chronic care needs and their families to be served in the community whenever possible. PACE serves individuals who are age 55 or older, certified by their state to need nursing home care, are able to live safely in the community at the time of enrollment, and live in a PACE service area. Although all PACE participants must be certified to need nursing home care to enroll in PACE, only about seven percent of PACE participants nationally reside in a nursing home. If a PACE enrollee does need nursing home care, the PACE program pays for it and continues to coordinate the enrollee's care. PACE Program Services Delivering all needed medical and supportive services, the program is able to provide the entire continuum of care and services to seniors with chronic care needs while maintaining their independence in their homes for as long as possible. Care and services include: Adult day care that offers nursing; physical, occupational and recreational therapies; meals; nutritional counseling; social work and personal care Medical care provided by a PACE physician familiar with the history, needs and preferences of each participant Home health care and personal care All necessary prescription drugs Social services Medical specialists such as audiology, dentistry, optometry, podiatry, and speech therapy Respite care Hospital and nursing home care when necessary PACE is a relatively new program in WY as of CMS approval of the State Plan on 09/06/11 to be effective 10/01/11. Currently Wyoming has one interested PACE provider who is looking to be in business by July 1, Anita Fox, Program Manager, can be contacted at or Anita.Fox@wyo.gov. Home and Community Based Services: (HCBS) There are two types of Home and Community Based Service waiver programs: Long Term Care Home and Community Based Services Waiver Services under this waiver include the following: Case Management: Assistance to identify an individual's needs, to locate, coordinate, and monitor social and medical services to meet the needs of the client. 30
31 Personal Care: A certified nurse aide assigned to care for the client in the home, providing help with activities of daily living such as bathing, dressing, meal preparation, and grocery shopping. Respite Care: Care that is provided for a short period of time to relieve a regular caregiver. If the care is provided in the home it is provided by a certified nurse aide. Home Delivered Meals: One or two meals delivered to a client's home or to a day care facility on a scheduled basis. Personal Emergency Response System: An electronic alarm system that a client wears which summons help in an emergency. Non Medical transportation: Transportation service provided to non medical activities that cannot be arranged by any other means. Adult Day Care: A structured program in a licensed setting that provides a variety of health, social, and related support services for part of the day, but less than 24 hour care. Skilled Nursing: Services which are within the scope of Wyoming's Nurse Practice Act that will prevent institutionalization and are not covered by home health. Consumer Directed Care Option: This option allows qualified waiver participants to obtain, hire and fire their own personal care attendant. With this option the client serves as the employer of their own personal care attendant. Services under this option are: o Care Coordination: Under this option, this service replaces Case Management. o Self Help Assistant: Under this option, this service replaces Personal Care. o Fiscal Management: Fiscal management services provide payroll and tax reporting activities for the Self Help Assistant. Assisted Living Facility Home and Community Based Service Waiver Services under this waiver include the following: Case Management: Assistance to identify an individual's needs; and to locate, coordinate, and monitor social and medical services to meet the needs. Daily Care: Assisted living facilities receive a daily rate at one of three levels of reimbursement which are based on a client's LT101 score. Further information on this program can be found at: 31
32 Programs and Providers for Clients with Mental Illness Clients who have been diagnosed with a mental illness and deemed inappropriate for nursing facility placement can still receive services through any of the aforementioned programs. In addition or simultaneous to those services Wyoming Medicaid covers rehabilitative services for mental health and substance abuse disorders via community mental health and substance abuse treatment centers, psychiatrists, psychologists, psychiatric APRN s, and licensed mental health professionals. Valuable information When a client has been assessed through the PASRR process and deemed inappropriate for placement to a nursing facility, multiple options exist for the transition/diversion and assistance of care. Project OUT is a short term Medicaid and state funded intervention and assistance program that helps consumers overcome the barriers to living independently in the community. PACE serves individuals who are age 55 or older, certified by their state to need nursing home care, are able to live safely in the community at the time of enrollment, and live in a PACE service area. There are two types of Home and Community Based Service waiver programs: Long Term Care Home and Community Based Services Waiver Assisted Living Facility Home and Community Based Service Waiver 32
33 Section XII: Other Definitions Mental Illness An individual is considered to have a serious mental illness (MI) if the individual meets the following requirements on diagnosis, level of impairment and duration of illness: The individual has a major mental disorder diagnosable under the Diagnostic and Statistical Manual of Disorder. This mental disorder is (A) A schizophrenic, mood, paranoid, panic or other severe anxiety disorder; somatoform disorder; personality disorder; other psychotic disorder; or another mental disorder that may lead to a chronic disability; but (B) Not a primary diagnosis of dementia, including Alzheimer's disease or a related disorder, or a non-primary diagnosis of dementia unless the primary diagnosis is a major mental disorder as defined in paragraph (b)(1)(i)(a) of this section. For all pertinent details of definition please refer to Per CFR Intellectual Disability - Mental Retardation An individual is considered to have an intellectual disability (ID) - mental retardation (MR) if he or she has A level of intellectual dysfunction (mild, moderate, severe or profound), referred to as retardation in the American Association on Mental Retardation's Manual on Classification in Mental Retardation (1983). For all pertinent details of definition please refer to Per CFR Resident Review Per CFR is to be completed on an annual basis for residents with either MI or MR to determine whether the resident s physical and mental condition requires the level of care and services which are being provided. Please note: CFR is not current concerning Resident Review. Revisions in 1996 resulted in changes within Sec [42 U.S.C. 1396r] (E) and replaced annual review with review upon a change in condition. The State of Wyoming has further defined the resident review as a significant change in condition. Significant Change in Condition An individual is considered to have a significant change in condition (improvement or decline and physical or mental) when the change results in an update to the MDS or Plan of Care. LT101 An evaluation of medical necessity including a review by a medical evaluator of an applicant s or recipient s physical and mental condition for the purpose of determining whether the individual requires nursing facility level of care. These determinations are only valid for 90 days after the date of review. 33
34 LT101 Referral A referral is made by contacting the Clinical Manager for Long Term Care, Wyoming Department of Health, Division of Healthcare Financing at fax via faxed LT101 request form for facilities and hospitals, as soon as possible. (See Public Health Nursing page 14 for complete referral process) LT101 Score A score is assigned to each component of the LT101 evaluation and an overall score results in a placement summary which is one of the following: 1. Has 13 or more points. Client may be served either in a Nursing Facility or Swing Bed OR on either the HCBS LTC or ALF waiver. 2. DOES NOT have 13 points, but placement remains medically necessary to maintain optimal functioning and maintain the continued safety and welfare of the client. 3. DOES NOT have 13 points, and DOES NOT meet the medical necessity criteria for long term care. PASRR Definition of Specialized Services for Mental Illness Specialized services for mental illness means the services specified by the State which, combined with services provided by the NF, results in continuous and aggressive implementation of an individualized plan of mental health care that: 1. Is developed and supervised by an interdisciplinary team, which includes a physician, qualified mental health professionals and, as appropriate, other professionals. 2. Prescribes specified therapies and activities for the treatment of persons experiencing an acute episode of serious mental illness, which necessitates supervision by trained mental health personnel; and 3. Is directed toward diagnosing and reducing the resident s behavioral symptoms that necessitated institutionalization, improving his or her level of independent functioning, and achieving a functioning level that permits reduction in the intensity of mental health services to below the level of specialized services at the earliest possible time. In summary, specialized services for mental illness are the level of services that would be provided in an institution for mental diseases or an inpatient psychiatric hospital. 34
35 Section XIII: References Xerox Fiscal Agent Web Portal inc.com/ Xerox Fiscal Agent Registration inc.com/wy/general/registrationhome.do Xerox Fiscal Agent Provider Home inc.com/provider_home.html DHCF, Division of Mental Health & Substance Abuse DHCF, Division of Developmental Disabilities DHCF, Division of Healthcare Financing, Medicaid DHCF, Medicaid Rules Chapter 19 PASRR Rules Chapter 22 LT101 Rules e CFR DHCF, PASRR State Plan Amendment Attachment 4.39 and 4.39A Diagnosis Codes Requiring a Level II inc.com/institutional.html 35
36 Section XIV: Appendix 36
37 P.O. Box 49 Cheyenne, WY Phone: Fax: PASRR Fax Coversheet PASRR REQUEST TO: Xerox Care and Quality Solutions, Inc. PASRR UR Assistant FROM: FACILITY: FAX: PHONE: Fax: TOTAL NUMBER OF PAGES: PHONE DATE: : RE: PASRR Level II Referral CC: Urgent Request from NF - Patient at NF Urgent Request from Referring Facility Ready for transfer Routine Request from Referring Facility Categorical Determination Review PASRR Review for Expiring Categorical Determination Period Change in Condition Review Other Comments: 37
38 P.O. Box 49 Cheyenne, WY Phone: Fax: Required Documents for Pre-Admissions Screenings Check Below all Documents Included Required Documents for Pre admission Screenings: PASRR Level I (from ACS provider portal) LT101 Functional Assessment, < 90 days old (from PHN) Current medications (medication administration record with drug, dosage, frequency and route of administration) Current history and physical within last 12 months including: Medical history Medication history Treatment/Hospitalization history Review of all body systems Neurological exam Differential diagnosis Psychosocial Evaluation (from CMHC) within last 12 months including: Past and current living arrangements Educational and work history Family & social history Psychiatric history Substance use/abuse history Mental Status Evaluation Estimated level of cognitive functioning Medical support needs Medication management Summary of strengths Cultural, language and ethnic origin and applicable adaptations required Diagnosis on all five Axis Functional assessment of the individual s ability to engage in ADL s Outcome/Disposition Psychiatric evaluation, if on file and less than two (2) years old Progress notes representing last seven (7) days of services and treatments If MR/ID, psychological evaluation within last 12 months to include: Comprehensive medication history Adaptive functioning, achievement, and intellectual testing with validated instruments Informed Consent Form Please submit this form after your fax cover page with the required documents in your packet. Please do not fax incomplete packets. Fax complete packet to Attention: PASRR UR Assistant 38
39 P.O. Box 49 Cheyenne, WY Phone: Fax: Required Documents for Categorical Determinations Check Below all Documents Included Required Documents for Pre admission Screenings: PASRR Level I (from ACS provider portal) LT101 Functional Assessment, <90 days old (from PHN) Current medications (medication administration record with drug, dosage, frequency and route of administration) Current history and physical within last 12 months including: Medical history Medication history Treatment/Hospitalization history Review of all body systems Neurological exam Differential diagnosis Progress notes representing last seven (7) days of services and treatments Informed Consent Form Please submit this form after your fax cover page with the required documents in your packet. Please do not fax incomplete packets. Fax complete packet to Attention: PASRR UR Assistant 39
40 P.O. Box 49 Cheyenne, WY Phone: Fax: Required Documents for PASRR Screening for Residents Needing NF Placement Beyond the End of Categorical Exemption Period Check Below all Documents Included Required Documents for Pre admission Screenings: PASRR Level I (from ACS provider portal) LT101 Functional Assessment, < 90 days old (from PHN) Current medications (medication administration record with drug, dosage, frequency and route of administration) Current history and physical within last 12 months including: Medical history Medication history Treatment/Hospitalization history Review of all body systems Neurological exam Differential diagnosis Psychosocial Evaluation (from CMHC) within last 12 months including: Past and current living arrangements Educational and work history Family & social history Psychiatric history Substance use/abuse history Mental Status Evaluation Estimated level of cognitive functioning Medical support needs Medication management Summary of strengths Cultural, language and ethnic origin and applicable adaptations required Diagnosis on all five Axis Functional assessment of the individual s ability to engage in ADL s Outcome/Disposition Psychiatric evaluation, if on file and less than two (2) years old Progress notes representing last seven (7) days of services and treatments If MR/ID, psychological evaluation within last 12 months to include: Comprehensive medication history Adaptive functioning, achievement, and intellectual testing with validated instruments Informed Consent Form Please submit this form after your fax cover page with the required documents in your packet. Please do not fax incomplete packets. Fax complete packet to Attention: PASRR UR Assistant 40
41 P.O. Box 49 Cheyenne, WY Phone: Fax: Required Documents for Resident Review (Significant Change) Screenings: Required Documents for Resident Review (Significant Change) Screenings: Check Below all Documents Included PASRR Level I (from ACS provider portal) LT101 Functional Assessment, <90 days old (from PHN) Previous Level II referral packet, if applicable Current medications (medication administration record with drug, dosage, frequency and route of administration) Current history and physical at change of conditions, including: Medical history Medication history Treatment/Hospitalization history Review of all body systems Neurological exam Differential diagnosis Psychosocial Evaluation (from CMHC) at change of condition including: Past and current living arrangements Educational and work history Family & social history Psychiatric history Substance use/abuse history Mental Status Evaluation Estimated level of cognitive functioning Medical support needs Medication management Summary of strengths Cultural, language and ethnic origin and applicable adaptations required Diagnosis on all five Axis Functional assessment of the individual s ability to engage in ADL s Outcome/Disposition Psychiatric evaluation, if on file and less than two (2) years old Progress notes representing last seven (7) days of services and treatments If MR/ID, psychological evaluation (within last 12 months) to include: Comprehensive medication history Adaptive functioning, achievement, and intellectual testing with validated instruments Informed Consent Form Minimum Data Set (MDS) is strongly recommended for Significant Change Please submit this form after your fax cover page with the required documents in your packet. Please do not fax incomplete packets. Fax complete packet to Attention: PASRR UR Assistant 41
42 P.O. Box 49 Cheyenne, WY Phone: Fax:
43 P.O. Box 49 Cheyenne, WY Phone: Fax: WYOMING DEPARTMENT OF HEALTH DIVISION OF HEALTHCARE FINANCING WYOMING MEDICAID PASRR LEVEL II INFORMED CONSENT FORM NAME: SOCIAL SECURITY #: The Level II PASRR determination notices are adapted to the race, ethnicity, language, and means of communication used by the individual being evaluated. Please fill in the following: RACE: ETHNICITY: PRIMARY LANGUAGE: PERFERRED METHOD OF COMMUNICATION (Written, oral, sign, etc.) An assessment is required for all persons applying for or receiving assistance for long term care. In order to evaluate my needs, I am giving my consent to the following: I agree to an assessment to identify my need for long term care, and to determine if my needs can be met in the community instead of a nursing facility. I authorize Wyoming Department of Health (WDH) and Xerox Care and Quality Solutions (CQS) staff to access my medical records. I understand and agree that WDH and CQS may need to talk to my doctor and other health professionals. I also understand that they may need to interview family members, close friends and social services professionals about my situation. Individual or Representative Signature (Indicate Relationship if signed by Representative) Please enter Contact Information above (address, phone, fax, ) Date 43
44 P.O. Box 49 Cheyenne, WY Phone: Fax: Wyoming PASRR Level II Evaluation Receipt of Referral Packet Notice of Missing Required Documentation Date: mm/dd/yyyy Name of Current Facility: Facility Contact Name: Fax Number: ### ###-#### RE: REQUEST FOR REQUIRED DOCUMENTS* The purpose of this letter is to request copies of medical records as allowed by the Health Insurance Portability and Accountability Act (HIPAA) and the Department of Health and Human Services regulations. Xerox Care and Quality Solutions, Inc. (CQS) was awarded a contract with the Office of Healthcare Financing to serve as the PASRR Level II Review vendor for Wyoming. We have received a request to complete a PASRR Level II Evaluation on: Patient Name: Date of Birth: mm/dd/yyyy Consumer Social Security Number: ###-##-#### In order to conduct the PASRR Level II Review, we are requesting that you fax copies of the following required documents: Please fax the above documents to If you are unable to obtain the required document(s) listed above, please send what you have obtained and call us at the number below to discuss any outstanding documents. This information should be faxed as quickly as possible, but no later than close of business on mm/dd/yyyy (2 days from when the letter was sent). If you have any questions about this request, contact the PASRR Coordinator toll free at *This letter has been faxed to the patient s current facility, if applicable, and a copy is on file with CQS for the Office of Healthcare Financing. 44
45 P.O. Box 49 Cheyenne, WY Phone: Fax: Wyoming PASRR Level II Evaluation Receipt of Referral Packet Notice of Request for Necessary Clinical Documentation Date: mm/dd/yyyy Name of Current Facility: Facility Contact Name: Fax Number: ### ###-#### RE: REQUEST FOR NECESSARY CLINICAL DOCUMENTATION* The purpose of this letter is to request copies of medical records as allowed by the Health Insurance Portability and Accountability Act (HIPAA) and the Department of Health and Human Services regulations. Xerox Care and Quality Solutions, Inc. was awarded a contract with the Office of Healthcare Financing to serve as the PASRR Level II Review vendor for Wyoming. We have received a request to complete a PASRR Level II Evaluation on: Patient Name: Date of Birth: mm/dd/yyyy Consumer Social Security Number: ###-##-#### In order to conduct the PASRR Level II Review, we are requesting that you fax copies of the following required information: Please fax the above documents to If you are unable to obtain the required document(s) listed above, please send what you have obtained and call us at the number below to discuss any outstanding documents. This information should be faxed as quickly as possible, but no later than close of business on mm/dd/yyyy (2 days from when the letter was sent). If you have any questions about this request, contact the PASRR Coordinator, toll free at *This letter has been faxed to the patient s current facility, if applicable, and a copy is on file with CQS for the Office of Healthcare Financing. 45
46 P.O. Box 49 Cheyenne, WY Phone: Fax: Wyoming PASRR Level II Evaluation Administrative Closure Letter Date: mm/dd/yyyy Name of Current Facility: Facility Contact Name: Fax Number: ### ###-#### RE: ADMINISTRATIVE CLOSURE DUE TO INCOMPLETE DOCUMENTATION* The purpose of this letter is to inform you that the PASRR Level II Evaluation you requested for: Patient Name: Date of Birth: mm/dd/yyyy Consumer Social Security Number: ###-##-#### could not be completed due to incomplete documentation. If a PASRR Level II Evaluation is still needed, please fax a complete referral packet to This information should be faxed as quickly as possible to ensure compliance with federal regulations and reimbursement for services. If you have any questions, please contact the PASRR Coordinator toll free at *Notification of this Administrative Closure has been sent to the patient or their legal representative, Ombudsman for LTC, and a copy to the Division of Healthcare Financing representative. [Name of Reviewer] [Reviewer s Title and Professional Credentials] CC: Legal Representative (if applicable) Ombudsman for Long Term Care, Analyn Reader Division of Healthcare Financing, Department of Health Representative, Renee Propps 46
47 504 West 17 th Street, Suite 300A Cheyenne, WY Phone: Fax: Wyoming PASRR Level II Determination Summary Report (DSR) Date of Level II Determination: [date] Date of Request for Additional Information: [date] Date of Receipt of Complete Documentation Package: [date] Date of notification by Fax: [date] Consumer Information Name: [Patient Name] Date of Birth: [DOB] Social Security Number: [###-##-####] Medicaid #: Medicare #: Secondary Insurance: Current Facility Name/Location: [Facility Name/Location] Summary of Medical and Social History: [Enter demographic information, past and current living arrangements, educational and work history, estimated level of cognitive functioning, family and social history] [Enter LASRR Level I and LT101 findings] [Enter LT101 results (results must be less than 60 days old). Indicate score and interpretation of results] Medical History [Enter medical history; medical diagnoses including date of onset; medication regimen; side effects; allergies; compliance with medications; history of hospitalizations/treatments; and medical support needs] Psychosocial Evaluation [Enter complete psychiatric history; psychiatric diagnoses with date of onset, substance use/abuse history including drug of choice, usage, treatments, and insight regarding use] [Enter ALL mental status evaluation results from Psychosocial Evaluation] (Externalizing and internalizing behaviors; past suicidal behaviors and history; homicidal and suicidal ideations and intentions; mood and affect; and reality testing. [Enter supplemental assessment results, if applicable. Includes Geriatric Depression Scale or other validated instrument][enter evaluator s diagnostic impressions. Full 5-Axis diagnosis is required (including GAF Score) along with indication if diagnosis is primary or secondary] 47
48 Page # PASRR Level II Determination Summary Report [Patient Name] [Enter evaluator s opinion regarding if the patient was: 1.) experiencing an acute episode of a serious mental disorder, 2.) if they required specialized services, and 3.) if the person was a danger to self or others] [Cultural, language and ethnic origin and applicable adaptations required] [Enter patient s social supports, strengths, positive traits, and areas of concern] [Enter other mental health or professional services needed] Functional Status [Enter information supporting statement regarding appropriateness of nursing facility placement. Add the patient s ability to perform ADLs and if needs can be met in a less restrictive environment. List what assistance is required and indicate what services are needed to maintain residence in a less restrictive environment] [Enter daily living supports available and needed; ability to access community resources, communicate, and attend to financial matters] [Enter recommendations regarding services that may be needed at the nursing facility, such as psychiatric medication management, physical therapy, wander guard, etc.)] [Enter narrative regarding appropriateness of nursing facility placement] Outcome / Disposition Meets the state definition of serious mental illness? [Yes or No] Meets the state definition of an intellectual disability (mental retardation)? [Yes or No] Note: If there is an indication of possible intellectual disability, the determination MUST be reviewed by Psychologist Nursing Facility Appropriate? [Yes or No] Are Specialized Services Recommended? [Yes or No] Date of Fax to: Resident in care/of the facility: [date faxed] Admitting Facility and Physician: [date faxed] (Facility to place copy of DSR in resident s chart for attending physician Referring (Discharging) Facility (if different from admitting facility): [date faxed] Division of Healthcare Financing Representative (Renee Propps): [date faxed] [place electronic signature here] Reviewers: [enter Reviewer name] [Enter title and professional credentials] 48
49 Page # PASRR Level II Determination Summary Report [Patient Name] For questions regarding this PASRR Level II Evaluation Determination Report please call the PASRR Coordinator at (888) You may also submit written inquires to Xerox Care and Quality Solutions, P.O. Box 49, Cheyenne, WY or fax toll free to
50 504 West 17 th Street, Suite 300A Cheyenne, WY Phone: Fax: Wyoming PASRR Level II Notice of Determination (NOD) [Date] [Patient Name] C/O [Facility Name] [Street Address] [City, State, Zip] Re: Wyoming PASRR Level II Review Dear [Patient Name]: This letter is to inform you that the PASRR/MI Review for you was completed on [date]. Our Level II review has determined: Nursing Facility Placement is appropriate. Specialized Services are not required. Nursing Facility Placement is appropriate. Specialized Services are required. Specialized services must be provided in accordance with the requirements outlined In Section 4250 of the Wyoming State Medicaid Manual. Nursing Facility Level of Care is inappropriate. Specialized Services are not required. Placement is not authorized; Medicaid payment will be denied. Nursing Facility Level of Care is inappropriate. This individual requires Specialized Services that cannot be provided in the NF. Placement is not authorized; Medicaid payment will be denied. This individual is categorically appropriate due to terminal illness or severe medical condition. This individual has no serious mental illness or mental retardation, or has a primary diagnosis of dementia. No further review or referral is required. Other: A copy of the results and any recommendations from this review, have been sent to the Medicaid Office at the Wyoming Department of Health, current facility if applicable, attending physician, consumer or legal representative, and the Wyoming Ombudsman for Long Term Care. If you disagree with this determination, you have the right to appeal this decision by contacting us in writing at Xerox Care and Quality Solutions, P.O. Box 49, Cheyenne, WY or fax toll free to , within 30 days from the date of this decision. For questions regarding this letter please call the PASRR Coordinator at (888) extension Sincerely, Robert Monger, M.D., CQS Medical Director Cc: Analyn Reader, Ombudsman for LTC Legal representative if applicable *Specialized Services, within the context of PASRR/MI level II evaluations, refers to acute inpatient psychiatric care
51 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II DATE: CLIENT NAME: SOCIAL SECURITY: DATE OF BIRTH: MEDICAID #: (IF NO MEDICAID #, LEAVE BLANK) REFERRING NURSING FACILITY OR AGENCY: PHONE: PSYCHOSOCIAL HISTORY AND MEDICAL NEEDS PAST AND CURRENT LIVING ARRANGEMENTS (Lived alone, required community supports, assisted living facility, etc.): EDUCATIONAL AND WORK HISTORY (Grades completed, special educational needs, work history): Estimated level of cognitive functioning: Extremely Low Borderline Low Average Average Above Average Superior FAMILY AND SOCIAL HISTORY (Marital status, significant life events, legal history, hobbies, history of mental illness in family): MEDICAL DIAGNOSES WITH DATE OF ONSET (List all current medical disorders and date of diagnosis): (Diagnosis) (Date of Onset/Diagnosis) MEDICAL SUPPORT NEEDS (Durable medical equipment needed, in home nursing services, hearing aids, glasses): 51
52 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II MEDICATIONS and MEDICATION MANAGEMENT (List all medications including psychotropics, the patient s compliance, and reported side effects) (Medication and dosage) (Compliance) (Reported side effects) DAILY LIVING SUPPORTS AVAILABLE AND NEEDED (Family assist, live in aid, in home nursing needed but not available): CULTURAL, LANGUAGE, AND ETHNIC ORIGIN (and applicable adaptations required): ACTIVITIES OF DAILY LIVING/ IADL (RESIDENT S ABILITY TO ACCESS COMMUNITY RESOURCES, COMMUNICATE, AND TO MANAGE PERSONAL FINANCES (Ability to schedule a medical appointment, manage finances, communicate with others, available of transportation to community resources, shopping, laundry, housekeeping, etc): PSYCHIATRIC/SUBSTANCE USE HISTORY COMPLETE PSYCHIATRIC HISTORY (Include all psychiatric hospitalizations and outpatient treatments. List all diagnoses, duration of inpatient stays and treatment, compliance with treatment, etc.). COPIES OF DISCHARGE SUMMARIES FOR THE PAST TWO (2) YEARS ARE REQUIRED. 52
53 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II PSYCHIATRIC DIAGNOSES WITH DATE OF ONSET (List all current psychiatric disorders and date of diagnosis): (Diagnosis) (Date of Onset/Diagnosis) SUBSTANCE USE/ABUSE HISTORY (Inpatient and outpatient treatment with diagnoses and date of onset. Include substance name, method and frequency of use, duration of use and/or abstinence, and patient s insight regarding use): MENTAL STATUS EVALUATION ORIENTATION: Ask for the date (day, month, year, and day of the week) and current location. Record response as well as whether or not client is correct or incorrect. REGISTRATION: Name three objects (enter below) and have person repeat them back. Give one point for each correct answer on the first trial Then repeat them (up to 6x) until all three are learned. [Number of trials ] ATTENTION AND CALCULATION: Ask the client to begin with 100 and count backwards by 7. Stop after five subtractions. Check correct answers Alternatively spell "world" backwards if client unable or unwilling to do math D L R O W RECALL: Ask for the names of the three objects learned above. Check each correct answer
54 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II DESCRIPTION OF CURRENT ATTITUDES AND OVERT BEHAVIORS (Describe behaviors that may be suggestive of a serious psychiatric illness. See optional Behavioral Observation Checklist for possible descriptions): MOOD AND AFFECT (If patient has s/s of depression you may use optional Geriatric Depression Scale): SUICIDAL/HOMICIDAL IDEATION (Past and current, passive versus active ideations, last attempt, plan and means available to hurt self): DEGREE OF REALITY TESTING (Presence and content of hallucinations and/or delusions, fixed or loose, command, etc.): SUMMARY OF CLIENT S STRENGTHS, WEAKNESSES, AND NEEDS: EVALUATOR S DIAGNOSTIC IMPRESSIONS Must include DSM Code and indicate if diagnosis is Primary or Secondary. Complete each of the five (5) Axis, including GAF score. AXIS I: Primary Secondary Primary Secondary Primary Secondary Primary Secondary AXIS II: Primary Secondary Primary Secondary Primary Secondary 54
55 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II AXIS III: AXIS IV: AXIS V (See page 10 for GAF criteria): CURRENT PAST YEAR PLEASE COMPLETE THE FOLLOWING: If the client DOES NOT have a primary diagnosis of dementia, but DOES have a primary or secondary diagnosis or a serious mental disorder 1, the client: is is not does does not is is not experiencing an acute episode of this serious mental disorder. require specialized services (the level of services provided in an institution for mental diseases or an inpatient psychiatric hospital). dangerous to self or others. If specialized services for mental health (the level of services provided in psychiatric inpatient setting) are needed, identify all of these services to meet client s needs, regardless of availability of those services. 1 Major Mental Illness: The definition for MI under these regulations is a psychiatric disorder of thought and/or mood which significantly impairs judgment, behavior, capacity to recognize reality, or ability to cope with the ordinary demands of life (Schizophrenia, Depression, Major Affective Disorders, Schizoaffective Disorders, Atypical Psychosis, including any other DSM IV Psychotic Disorder. Excludes: Dementia, Alzheimer s Disease, Alcoholism, Substance Abuse, Mood Disorders or delirium due to General Medical Condition, Epilepsy, Mental Retardation, and Developmental Disorders). 55
56 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II If specialized services for mental health are NOT needed, but client needs (or is receiving) other mental health services, please list these below: COMMENTS: Date of Evaluation Evaluator s signature Name of Mental Health Center PRINT NAME AND DEGREE 56
57 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II Appearance Attitude Facial Expression Eye Contact Motor Activity Gait Speech Mood Affect Perception Thought Processes Thought Content Attention/Concentration Orientation Abstract Reasoning Memory Insight Judgment Appetite Sleep Normal grooming/hygiene Disheveled Obese Underweight Bizarre Other (describe) Calm Cooperative Guarded Suspicious Hostile Withdrawn Attentive Other (describe) Sad Happy Vacant Other (describe) Good Fair Poor Intermittent Other (describe) Unremarkable Restless Uncoordinated Tics Purposeless movement Retardation Hyperactive Other (describe) Unremarkable Shuffles Stiff Leans Brisk Other Normal Rapid Slow Impaired Fluency Loud Aphasic Mute Dysphasic Neologisms Pressured Other (describe) Euthymic Anxious Irritable Depressed Elevated Angry Other (describe) Full Range Labile Flat Inappropriate Blunted Constricted Appropriate Other (describe) Hallucinations Delusions Illusions Depersonalization Derealization None of the Above Other (describe) Goal-directed Logical Disorganized Incoherent Loose Circumstantial Tangential Illogical Blocked Flight of Ideas Impoverished Other (describe) Suicidal Homicidal Delusional Obsessions Compulsions Phobias Suspiciousness Paranoia Ideas of Reference Somatic Preoccupation Other (describe) Unimpaired Mildly Impaired Moderately Impaired Severely Impaired Person Place Time Situation Normal Concrete Poor Other Intact Impaired Recent Impaired Remote Impaired Immediate Confabulation Adequate Poor/Minimal None/Denial Other (describe) Good Fair Poor Other (describe) Normal Decreased Increased Other No complaints Interrupted Early A.M. Waking Insomnia Medication Dependent Hypersomnia Other (describe) 57
58 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II GERIATRIC DEPRESSION SCALE (GDS) Number Question Response 1. Are you basically satisfied with your life? Yes No 2. Have you dropped many of your activities and interests? Yes No 3. Do you feel that your life is empty? Yes No 4. Do you often get bored? Yes No 5. Are you in good spirits most of the time? Yes No 6. Are you afraid that something bad is going to happen to you? Yes No 7. Do you feel happy most of the time? Yes No 8. Do you often feel helpless? Yes No 9. Do you prefer to stay at home, rather than going out and doing new things? Yes No 10. Do you feel you have more problems with memory than most? Yes No 11. Do you think it is wonderful to be alive now? Yes No 12. Do you feel pretty worthless the way you are now? Yes No 13. Do you feel full of energy? Yes No 14. Do you feel that your situation is hopeless? Yes No 15. Do you think that most people are better off than you are? Yes No Total: Score 1 point for each bolded answer. /15 58

59 PSYCHOSOCIAL EVALUATION FOR PASRR LEVEL II Global Assessment of Functioning (GAF) The Global Assessment of Functioning (GAF) is a numeric scale (0 through 100) used by mental health clinicians and doctors to rate the social, occupational and psychological functioning of adults. The scale is presented and described in the DSM-IV-TR on page 32. Children and adolescents under the age of 18 are evaluated on the Children s Global Assessment Scale, or C-GAS Superior functioning in a wide range of activities, life's problems never seem to get out of hand, is sought out by others because of his or her many qualities. No symptoms Absent or minimal symptoms, good functioning in all areas, interested and involved in a wide range of activities, socially effective, generally satisfied with life, no more than everyday problems or concerns If symptoms are present they are transient and expectable reactions to psychosocial stresses; no more than slight impairment in social, occupational, or school functioning Some mild symptoms OR some difficulty in social, occupational, or school functioning, but generally functioning pretty well, has some meaningful interpersonal relationships Moderate symptoms OR any moderate difficulty in social, occupational, or school functioning Serious symptoms OR any serious impairment in social, occupational, or school functioning Some impairment in reality testing or communication OR major impairment in several areas, such as work or school, family relations, judgment, thinking, or mood Behavior is considerably influenced by delusions or hallucinations OR serious impairment in communications or judgment OR inability to function in all areas Some danger of hurting self or others OR occasionally fails to maintain minimal personal hygiene OR gross impairment in communication Persistent danger of severely hurting self or others OR persistent inability to maintain Minimum personal hygiene OR serious suicidal act with clear expectation of death. 0 Not enough information available to provide GAF 59
60 Level I PASRR screening completed on the ACS/Xerox website and indicates serious MI/ID. Required Documents Contact info: fax, phone and name of referral source Consent Form PASRR Level 1 LT101<60 days old Current H&P/current med hx Progress notes Psych Evaluation If ID Comprehensive med hx needed and IQ Testing Yes Are all required documents included in the referral packet? Yes No Referral assigned to reviewer. Documents contain needed information and are representative of patients current levels of functioning. Referral routed to Xerox CQS (Routed by fax, contact info on Xerox/ACS) Fax number Attn: PASRR Coordinator: Fax number site) No No need for PASRR Level II okay to admit Notice of Missing Required Documentation letter faxed or ed to referral source. Missing documentation is to be received within 2 business days. Yes No No Additional information requested from referral source. Referral pended for 2 business days. Yes Can Determination be made? Referral administratively closed. Administrative Closure letter sent to referral source sent via or faxed and mailed to patient or guardian. Outreach will be done via telephone to get additional information from the referring physician/provider. No Yes Determination is made within 4 business days. Determination Summary Report is faxed to facility and Ombudsman. Notice of Determination letter is mailed to the patient/ legal guardian. If Specialized Services are needed a recommended plan of care is included as part of the Determination Summary. MEMO to Xerox: jennefer.rolf@xerox.com, tia.taylor@xerox.com, and angelica.espinoza@xerox.com. Are Specialized Services Recommended? Process is complete: Tracking of completed PASRRs will be reported to state monthly. No Yes If yes, Xerox will monitor compliance with Plan of Care recommendations and outcomes. A letter will be sent to the facility to request documentation. 60
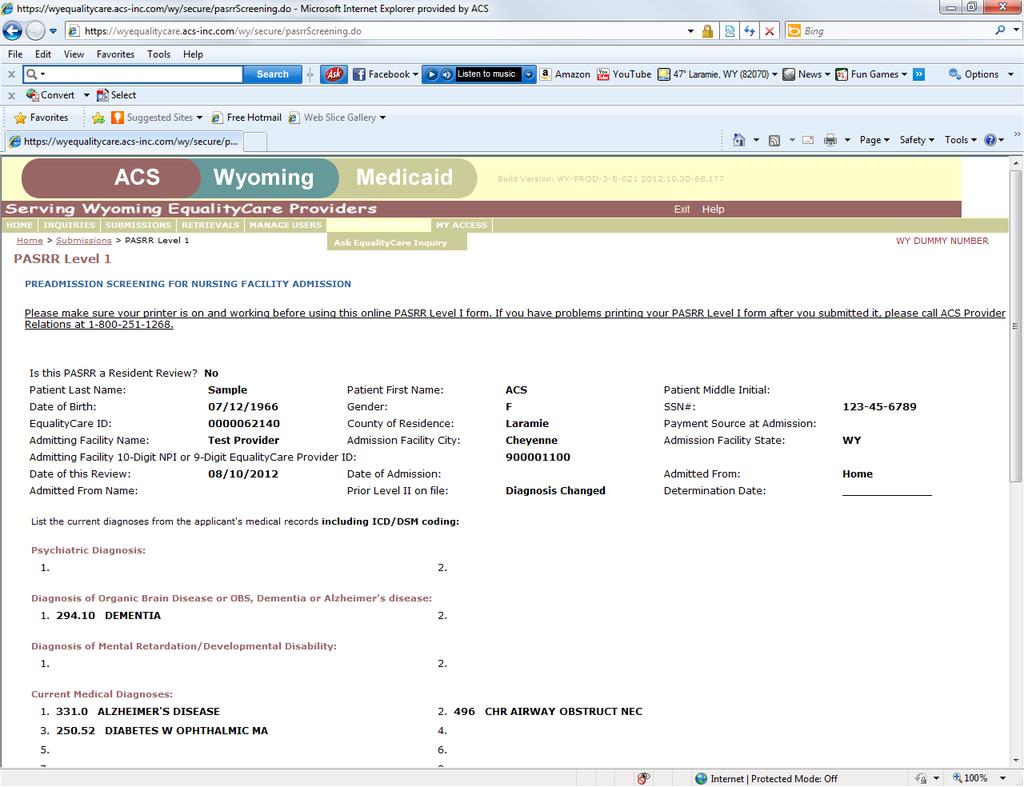
61 61
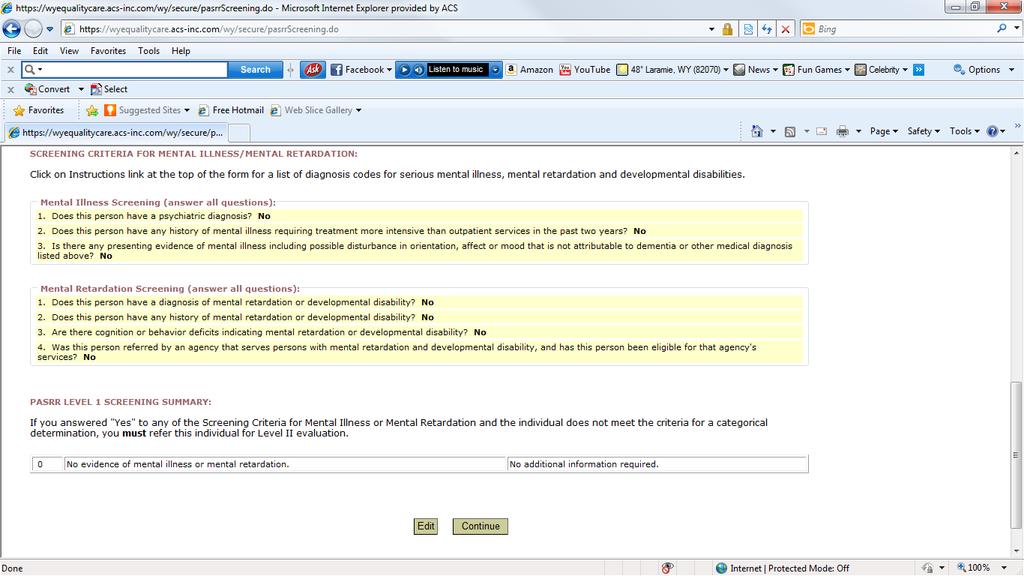
62 62
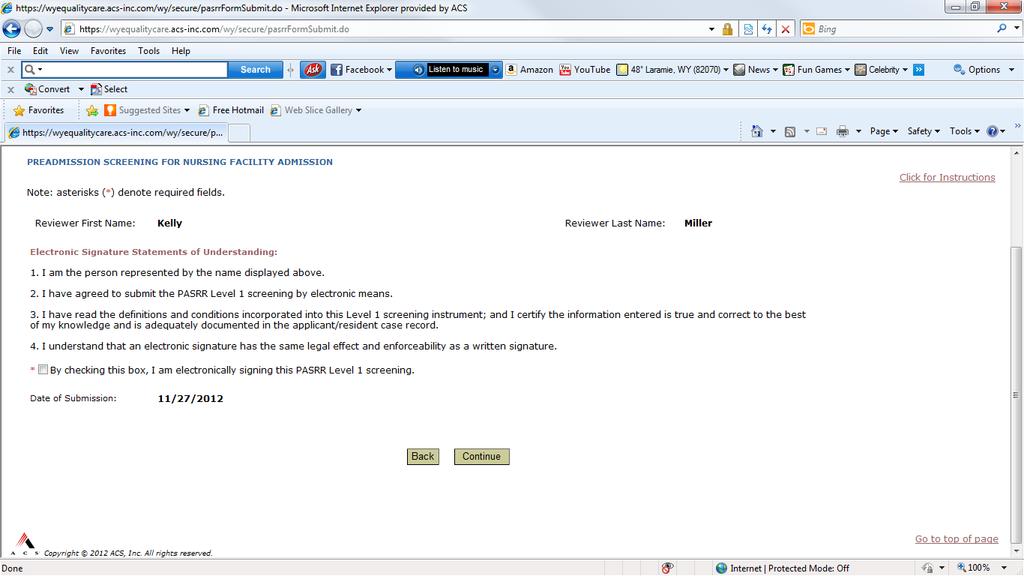
63 63
59G Preadmission Screening and Resident Review.
 59G-1.040 Preadmission Screening and Resident Review. (1) Purpose. This rule applies to all Florida Medicaid-certified nursing facilities (NF), regardless of payer source; all providers rendering NF services
59G-1.040 Preadmission Screening and Resident Review. (1) Purpose. This rule applies to all Florida Medicaid-certified nursing facilities (NF), regardless of payer source; all providers rendering NF services
# December 29, 2000
 #00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
#00-53-3 December 29, 2000 Minnesota Department of Human Services 444 Lafayette Rd. St. Paul, MN 55155 OF INTEREST TO! County Social Service Directors/Supervisors! County Designated LMHA for PASRR! County
The Power and Possibility of PASRR Webinar Series Webinar Assistance
 The Power and Possibility of PASRR Webinar Series Webinar Assistance http://www.pasrrassist.org/resources/webinar-assistance-and-faqs Call-in through one of two ways listed below: Telephone: 1. Locate
The Power and Possibility of PASRR Webinar Series Webinar Assistance http://www.pasrrassist.org/resources/webinar-assistance-and-faqs Call-in through one of two ways listed below: Telephone: 1. Locate
PASRR LEVEL I INSTRUCTIONS FOR OHCA FORM LTC-300A PURPOSE
 PLEASE READ THE FOLLOWING INSTRUCTIONS THOROUGHLY. IF YOU HAVE ANY QUESTIONS OR IF ANY PART IS NOT UNDERSTOOD, PLEASE CONTACT OHCA/LOCEU. PURPOSE The LTC-300A is used to meet Federal requirements for PASRR
PLEASE READ THE FOLLOWING INSTRUCTIONS THOROUGHLY. IF YOU HAVE ANY QUESTIONS OR IF ANY PART IS NOT UNDERSTOOD, PLEASE CONTACT OHCA/LOCEU. PURPOSE The LTC-300A is used to meet Federal requirements for PASRR
Chapter Two. Preadmission Screening and Annual Resident Review (PASARR)
") Preadmission Screening and Annual Resident Review (PASARR) Introduction The information in this chapter addresses Preadmission Screening and Annual Resident Review (PASARR) requirements for applicants
Preadmission Screening and Annual Resident Review (PASARR) Introduction The information in this chapter addresses Preadmission Screening and Annual Resident Review (PASARR) requirements for applicants
New Mexico Department of Health Developmental Disabilities Supports Division PASRR
 New Mexico Department of Health Developmental Disabilities Supports Division PASRR Presented by Sandyeva Martinez, LMSW PASRR Program Manager/Supervisor 1 What is PASRR? Pre Admission Screening and Resident
New Mexico Department of Health Developmental Disabilities Supports Division PASRR Presented by Sandyeva Martinez, LMSW PASRR Program Manager/Supervisor 1 What is PASRR? Pre Admission Screening and Resident
OBRA 87 & PASRR? Training Goals
 Alabama Department of Mental Health Alabama Medicaid Certified Nursing Homes Preadmission Screening & Resident Review (PASRR) for Mental Illness Intellectual Disability & Related Condition Angela Howard
Alabama Department of Mental Health Alabama Medicaid Certified Nursing Homes Preadmission Screening & Resident Review (PASRR) for Mental Illness Intellectual Disability & Related Condition Angela Howard
In Arkansas 02/20/2014 1
 In Arkansas 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures B. OLTC Procedures II. Pre-Admission Screening
In Arkansas 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures B. OLTC Procedures II. Pre-Admission Screening
Medicaid RAC Audit Results
 Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Understanding PASRR Categorical Decisions
 Understanding PASRR Categorical Decisions May, 2011 PTAC/NAPP PASRR web series Nancy Shanley Chairman of the Board of Directors, National Association of PASRR Professionals Consultant, PASRR Technical
Understanding PASRR Categorical Decisions May, 2011 PTAC/NAPP PASRR web series Nancy Shanley Chairman of the Board of Directors, National Association of PASRR Professionals Consultant, PASRR Technical
Sherri Proffer, RN, Program Manager. Dorothy Ukegbu, RN Coordinator, 02/20/2014 1
 Sherri Proffer, RN, Program Manager Dorothy Ukegbu, RN Coordinator, 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures
Sherri Proffer, RN, Program Manager Dorothy Ukegbu, RN Coordinator, 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures
Preadmission Screening (PASRR) Medicaid Certified Nursing Facilities DEPARTMENT OF HUMAN SERVICES MED-QUEST DIVISION 2018
 Medicaid Certified Nursing Facilities DEPARTMENT OF HUMAN SERVICES MED-QUEST DIVISION 2018") Preadmission Screening (PASRR) Medicaid Certified Nursing Facilities DEPARTMENT OF HUMAN SERVICES MED-QUEST DIVISION 2018 1 Agenda History Specialized Services in Hawaii CMS Review of Hawaii s PASRR Process
Preadmission Screening (PASRR) Medicaid Certified Nursing Facilities DEPARTMENT OF HUMAN SERVICES MED-QUEST DIVISION 2018 1 Agenda History Specialized Services in Hawaii CMS Review of Hawaii s PASRR Process
PASRR 101: Collaboration and A Successful PASRR Program
 PASRR 101: Collaboration and A Successful PASRR Program P A S R R 1 0 1 - T H E P A S R R T E C H N I C A L A S S I S T A N C E C E N T E R ( P T A C ) S T A T E T R A I N I N G S L I D E S & I N G R E
PASRR 101: Collaboration and A Successful PASRR Program P A S R R 1 0 1 - T H E P A S R R T E C H N I C A L A S S I S T A N C E C E N T E R ( P T A C ) S T A T E T R A I N I N G S L I D E S & I N G R E
FREQUENTLY ASKED QUESTIONS FOR PROVIDERS
 FREQUENTLY ASKED QUESTIONS FOR PROVIDERS TN PASRR REIMPLEMENTATION DEVELOPED: 10.5.16 REVISED: 10.17.16 Contents PASRR... 1 1. Does the person have to have be in TN to submit a PASRR?... 1 2. When does
FREQUENTLY ASKED QUESTIONS FOR PROVIDERS TN PASRR REIMPLEMENTATION DEVELOPED: 10.5.16 REVISED: 10.17.16 Contents PASRR... 1 1. Does the person have to have be in TN to submit a PASRR?... 1 2. When does
PASRR AND LEVEL OF CARE SCREENING PROCEDURES FOR LONG TERM CARE SERVICES
 PASRR AND LEVEL OF CARE SCREENING PROCEDURES FOR LONG TERM CARE SERVICES Developed: 08.18.11 Revised 6.23.2017 The policies and procedures in this document are approved and signed by Program Manager prior
PASRR AND LEVEL OF CARE SCREENING PROCEDURES FOR LONG TERM CARE SERVICES Developed: 08.18.11 Revised 6.23.2017 The policies and procedures in this document are approved and signed by Program Manager prior
What is a retrospective Level of Care and what is the process for submitting a retrospective Level of Care?
 Last updated 9/14/2011 The following are Frequently Asked Questions (FAQs) associated with Connecticut Level of Care and PASRR Level I/II processes. To read to the corresponding response to the questions
Last updated 9/14/2011 The following are Frequently Asked Questions (FAQs) associated with Connecticut Level of Care and PASRR Level I/II processes. To read to the corresponding response to the questions
PreAdmission Screening/Resident Review(PASRR) Level I Assessment (Form : DMA-613)
 Level I Assessment (Form : DMA-613)") PreAdmission Screening/Resident Review(PASRR) Level I Assessment (Form DMA-613) Please provide the required information for this PA request on this page. When you have completed entering the data for this
PreAdmission Screening/Resident Review(PASRR) Level I Assessment (Form DMA-613) Please provide the required information for this PA request on this page. When you have completed entering the data for this
WEBSTARS Instructions
 I. General Information On-line Submission of Screening and Tracking Information A. The Tracking Form Return to table of contents The Tracking Form is a way for Ascend (and the DDS) and NF providers to
I. General Information On-line Submission of Screening and Tracking Information A. The Tracking Form Return to table of contents The Tracking Form is a way for Ascend (and the DDS) and NF providers to
PENNSYLVANIA PREADMISSION SCREENING RESIDENT REVIEW (PASRR) IDENTIFICATION LEVEL I FORM (Revised 9/1/2018)
 IDENTIFICATION LEVEL I FORM (Revised 9/1/2018)") PENNSYLVANIA PREADMISSION SCREENING RESIDENT REVIEW (PASRR) IDENTIFICATION LEVEL I FORM (Revised 9/1/2018) This process applies to all nursing facility (NF) applicants, regardless of payer source. All
PENNSYLVANIA PREADMISSION SCREENING RESIDENT REVIEW (PASRR) IDENTIFICATION LEVEL I FORM (Revised 9/1/2018) This process applies to all nursing facility (NF) applicants, regardless of payer source. All
PASRR AND LEVEL OF CARE SCREENING PROCEDURES FOR LONG TERM CARE SERVICES
 PASRR AND LEVEL OF CARE SCREENING PROCEDURES FOR LONG TERM CARE SERVICES Developed: 11.10.09 Revised: 6.28.13 The policies and procedures in this document are approved and signed by Operations Director
PASRR AND LEVEL OF CARE SCREENING PROCEDURES FOR LONG TERM CARE SERVICES Developed: 11.10.09 Revised: 6.28.13 The policies and procedures in this document are approved and signed by Operations Director
Iowa PASRR for Providers. A brief introduction to
 Iowa PASRR for Providers A brief introduction to Iowa s PASRR process 1 Why are PASRR Level I screens and Level II evaluations important? Mental health services in nursing facilities make a difference
Iowa PASRR for Providers A brief introduction to Iowa s PASRR process 1 Why are PASRR Level I screens and Level II evaluations important? Mental health services in nursing facilities make a difference
Preadmission Screening for Medicaid Certified Nursing Facilities. Department of Human Services Med-QUEST Division 2016
 Preadmission Screening for Medicaid Certified Nursing Facilities Department of Human Services Med-QUEST Division 2016 1 Agenda History Specialized Services Hawaii s Revised Level I Screening Tool Level
Preadmission Screening for Medicaid Certified Nursing Facilities Department of Human Services Med-QUEST Division 2016 1 Agenda History Specialized Services Hawaii s Revised Level I Screening Tool Level
Applicant Name Last, First Social Security Number Date of Birth. Applicant s Address City State Zip Code
 MAP-409 COMMONWEALTH OF KENTUCKY DEPARTMENT FOR MEDICAID SERVICES PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) NURSING FACILITY IDENTIFICATION SCREEN (LEVEL I) Revised March 2007 Applicant Name
MAP-409 COMMONWEALTH OF KENTUCKY DEPARTMENT FOR MEDICAID SERVICES PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) NURSING FACILITY IDENTIFICATION SCREEN (LEVEL I) Revised March 2007 Applicant Name
PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) LEVEL I SCREEN
 LEVEL I SCREEN") NEW JERSEY DEPARTMENT OF HUMAN SERVICES PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) LEVEL I SCREEN Please print and complete all questions. This form must be completed for all applicants PRIOR
NEW JERSEY DEPARTMENT OF HUMAN SERVICES PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) LEVEL I SCREEN Please print and complete all questions. This form must be completed for all applicants PRIOR
Michelle Newberry Missouri Project Director Bock Associates
 Michelle Newberry Missouri Project Director Bock Associates bockmo@embarqmail.com Kathy Schafer Registered Nurse Clinical Operations Department of Mental Health Kathy.Schafer@dmh.mo.gov Ammanda Ott FAN
Michelle Newberry Missouri Project Director Bock Associates bockmo@embarqmail.com Kathy Schafer Registered Nurse Clinical Operations Department of Mental Health Kathy.Schafer@dmh.mo.gov Ammanda Ott FAN
ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-41 PSYCHIATRIC TREATMENT FACILITIES TABLE OF CONTENTS
 ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-41 PSYCHIATRIC TREATMENT FACILITIES TABLE OF CONTENTS 560-X-41-.01 560-X-41-.02 560-X-41-.03 560-X-41-.04 560-X-41-.05 560-X-41-.06 560-X-41-.07
ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-41 PSYCHIATRIC TREATMENT FACILITIES TABLE OF CONTENTS 560-X-41-.01 560-X-41-.02 560-X-41-.03 560-X-41-.04 560-X-41-.05 560-X-41-.06 560-X-41-.07
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE
 MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE SUBJECT BY NUMBER: ISSUE DATE: September 8, 1995 EFFECTIVE DATE: September 8, 1995 Mental Health Services Provided
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE SUBJECT BY NUMBER: ISSUE DATE: September 8, 1995 EFFECTIVE DATE: September 8, 1995 Mental Health Services Provided
Intermediate care facilities for the mentally retarded (ICF/MR)
") CodeofCol or adoregul at i ons Sec r et ar yofst at e St at eofcol or ado DEPARTMENT OF HEALTH CARE POLICY AND FINANCING Medical Services Board MEDICAL ASSISTANCE - SECTION 8.400 10 CCR 2505-10 8.400 [Editor
CodeofCol or adoregul at i ons Sec r et ar yofst at e St at eofcol or ado DEPARTMENT OF HEALTH CARE POLICY AND FINANCING Medical Services Board MEDICAL ASSISTANCE - SECTION 8.400 10 CCR 2505-10 8.400 [Editor
P A S R R L E V E L I SCREEN I T E M S
 D E M O G R A P H I C S Is this the individual s state of residence? Type of identification: Current Location: What is the individual s method of payment for nursing facility care? What has been his/her
D E M O G R A P H I C S Is this the individual s state of residence? Type of identification: Current Location: What is the individual s method of payment for nursing facility care? What has been his/her
MEDICAL ASSISTANCE BULLETIN
 MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER September 8, 1995 September 8, 1995 1153-95-01 SUBJECT Accessing Outpatient Wraparound
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER September 8, 1995 September 8, 1995 1153-95-01 SUBJECT Accessing Outpatient Wraparound
PASRR IN SKILLED NURSING Regulatory Overview
 PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
Comprehensive Community Services (CCS) File Review Checklist Comprehensive
 File Review Checklist Comprehensive") This is a sample form developed by the "CCS Statewide QA/QI Work Group", and is available to CCS sites as a sample for consideration of use, modification, and customization. There is no implicit or explicit
This is a sample form developed by the "CCS Statewide QA/QI Work Group", and is available to CCS sites as a sample for consideration of use, modification, and customization. There is no implicit or explicit
Provider Certification Standards Adult Day Care
 Provider Certification Standards Adult Day Care December 2015 1 Definitions: Activities of Daily Living (ADL s)- Includes but is not limited to the following personal care activities: bathing, dressing,
Provider Certification Standards Adult Day Care December 2015 1 Definitions: Activities of Daily Living (ADL s)- Includes but is not limited to the following personal care activities: bathing, dressing,
INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual
 INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual DEVELOPMENT DATE: 2.2.2016 MOST RECENT REVISION: 9.19.2016 2016 ASCEND MANAGEMENT INNOVATIONS LLC.
INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual DEVELOPMENT DATE: 2.2.2016 MOST RECENT REVISION: 9.19.2016 2016 ASCEND MANAGEMENT INNOVATIONS LLC.
Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria. Effective August 1, 2014
 Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria Effective August 1, 2014 1 Table of Contents Florida Medicaid Handbook... 3 Clinical Practice Guidelines... 3 Description
Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria Effective August 1, 2014 1 Table of Contents Florida Medicaid Handbook... 3 Clinical Practice Guidelines... 3 Description
Iowa Department of Human Services
 DATE: June 4, 2012 Iowa Department of Human Services Terry E. Branstad Kim Reynolds Charles M. Palmer Governor Lt. Governor Director TO: FROM: RE: General Hospital, Nursing Facility and Skilled Nursing
DATE: June 4, 2012 Iowa Department of Human Services Terry E. Branstad Kim Reynolds Charles M. Palmer Governor Lt. Governor Director TO: FROM: RE: General Hospital, Nursing Facility and Skilled Nursing
PASRR IN SKILLED NURSING Regulatory Overview
 PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
WYOMING MEDICAID PROGRAM
 WYOMING MEDICAID PROGRAM COMMUNITY MENTAL HEALTH & SUBSTANCE USE TREATMENT SERVICES MANUAL MENTAL HEALTH/SUBSTANCE USE REHABILITATION OPTION EPSDT CHILD & ADOLESCENT MENTAL HEALTH SERVICES TARGETED CASE
WYOMING MEDICAID PROGRAM COMMUNITY MENTAL HEALTH & SUBSTANCE USE TREATMENT SERVICES MANUAL MENTAL HEALTH/SUBSTANCE USE REHABILITATION OPTION EPSDT CHILD & ADOLESCENT MENTAL HEALTH SERVICES TARGETED CASE
INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual
 INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual DEVELOPMENT DATE: 2.2.2016 MOST RECENT REVISION: 8.3.2016 2016 ASCEND MANAGEMENT INNOVATIONS LLC.
INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual DEVELOPMENT DATE: 2.2.2016 MOST RECENT REVISION: 8.3.2016 2016 ASCEND MANAGEMENT INNOVATIONS LLC.
MDS 3.0 and PASRR. 10/12/2010 Webinar for NAPP members. Dan Timmel CMS PASRR Technical Assistance Center. Slides prepared by Breck Douglas (9/10)
") MDS 3.0 and PASRR 10/12/2010 Webinar for NAPP members Dan Timmel CMS PASRR Technical Assistance Center Slides prepared by Breck Douglas (9/10) Agenda What is MDS? How and why does it affect me? Review
MDS 3.0 and PASRR 10/12/2010 Webinar for NAPP members Dan Timmel CMS PASRR Technical Assistance Center Slides prepared by Breck Douglas (9/10) Agenda What is MDS? How and why does it affect me? Review
presentation will provide an overview of the history and purpose of PASRR
 Welcome to Ascend s PASRR training for Iowa PASRR Providers. The information in this presentation will provide an overview of the history and purpose of PASRR 1 Ascend, A MAXIMUS Company is an internationally
Welcome to Ascend s PASRR training for Iowa PASRR Providers. The information in this presentation will provide an overview of the history and purpose of PASRR 1 Ascend, A MAXIMUS Company is an internationally
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services.
 907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
Clinical Utilization Management Guideline
 Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Florida Medicaid. Community Behavioral Health Services Coverage and Limitations Handbook. Agency for Health Care Administration
 Florida Medicaid Community Behavioral Health Services Coverage and Limitations Handbook Agency for Health Care Administration UPDATE LOG COMMUNITY BEHAVIORAL HEALTH SERVICES COVERAGE AND LIMITATIONS HANDBOOK
Florida Medicaid Community Behavioral Health Services Coverage and Limitations Handbook Agency for Health Care Administration UPDATE LOG COMMUNITY BEHAVIORAL HEALTH SERVICES COVERAGE AND LIMITATIONS HANDBOOK
Behavioral Health Outpatient Authorization Request Self Service. User Guide
 Behavioral Health Self Behavioral Health Outpatient Authorization Request Self Service User Guide Introduction Tufts Health Plan Network Health has created this user guide to illustrate how to navigate
Behavioral Health Self Behavioral Health Outpatient Authorization Request Self Service User Guide Introduction Tufts Health Plan Network Health has created this user guide to illustrate how to navigate
Texas Medicaid. Provider Procedures Manual. Provider Handbooks. Telecommunication Services Handbook
 Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
STAR+PLUS through UnitedHealthcare Community Plan
 STAR+PLUS through UnitedHealthcare Community Plan Optum 06012014 Who We Are United Behavioral Health (UBH) was created February 2, 1997, through a merger of U.S. Behavioral Health, Inc. (USBH) and United
STAR+PLUS through UnitedHealthcare Community Plan Optum 06012014 Who We Are United Behavioral Health (UBH) was created February 2, 1997, through a merger of U.S. Behavioral Health, Inc. (USBH) and United
INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual
 INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual DEVELOPMENT DATE: 2.2.2016 MOST RECENT REVISION: 6.29.2016 2016 ASCEND MANAGEMENT INNOVATIONS LLC.
INDIANA PASRR Level I & Level of Care Screening Procedures for Long Term Care Services Provider Manual DEVELOPMENT DATE: 2.2.2016 MOST RECENT REVISION: 6.29.2016 2016 ASCEND MANAGEMENT INNOVATIONS LLC.
Self-Evaluation for States Preadmission Screening and Resident Review (PASRR)
") PASRR Self-Assessment DRAFT 3/12/2008 12:58:00 PM page 1 Self-Evaluation for States Preadmission Screening and Resident Review (PASRR) Purpose of this self-evaluation: 1. To clarify the Federal requirements
PASRR Self-Assessment DRAFT 3/12/2008 12:58:00 PM page 1 Self-Evaluation for States Preadmission Screening and Resident Review (PASRR) Purpose of this self-evaluation: 1. To clarify the Federal requirements
Strategies in Intellectual and Developmental Disabilities (IDD) and Mental Illness (MI) PASRR Program Collaboration
 and Mental Illness (MI) PASRR Program Collaboration") Strategies in Intellectual and Developmental Disabilities (IDD) and Mental Illness (MI) PASRR Program Collaboration NAPP Board Members Ellen Olsen LCSW, MBA Janet Spinelli PhD, PCNS Andrea Womack MA January
Strategies in Intellectual and Developmental Disabilities (IDD) and Mental Illness (MI) PASRR Program Collaboration NAPP Board Members Ellen Olsen LCSW, MBA Janet Spinelli PhD, PCNS Andrea Womack MA January
SECTION A: IDENTIFICATION INFORMATION. A0100: Facility Provider Numbers. Item Rationale. Coding Instructions
 SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
SECTION A: IDENTIFICATION INFORMATION Intent: The intent of this section is to obtain key information to uniquely identify each resident, the home in which he or she resides, and the reasons for assessment.
Provider Frequently Asked Questions
 Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Archived SECTION 13 - BENEFITS AND LIMITATIONS. Section 13 - Benefits and Limitations
 SECTION 13 - BENEFITS AND LIMITATIONS 13.1 GENERAL INFORMATION...5 13.1.A FUNDING SOURCES...5 13.1.B SUPPLEMENTAL SECURITY INCOME (SSI)...6 13.1.C LICENSED FACILITIES/CERTIFIED FACILITIES...6 13.1.D MEDICARE
SECTION 13 - BENEFITS AND LIMITATIONS 13.1 GENERAL INFORMATION...5 13.1.A FUNDING SOURCES...5 13.1.B SUPPLEMENTAL SECURITY INCOME (SSI)...6 13.1.C LICENSED FACILITIES/CERTIFIED FACILITIES...6 13.1.D MEDICARE
Prepublication Requirements
 Prepublication Requirements Standards Revisions for Swing Bed Final Rule in Critical Access Hospitals The Joint Commission has approved the following revisions for prepublication. While revised requirements
Prepublication Requirements Standards Revisions for Swing Bed Final Rule in Critical Access Hospitals The Joint Commission has approved the following revisions for prepublication. While revised requirements
DEFINITIONS (c)(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :
(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :") F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
Behavioral health provider overview
 Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
State of Alaska Department of Health and Social Services. Community-Based Youth Residential Behavioral Health Services Review Provider Manual
 State of Alaska Department of Health and Social Services Community-Based Youth Residential Behavioral Health Services Review Provider Manual February 2018 TABLE OF CONTENTS Section 1: Qualis Health Care
State of Alaska Department of Health and Social Services Community-Based Youth Residential Behavioral Health Services Review Provider Manual February 2018 TABLE OF CONTENTS Section 1: Qualis Health Care
State of Connecticut REGULATION of. Department of Social Services. Payment of Behavioral Health Clinic Services
 R-39 Rev. 03/2012 (Title page) Page 1 of 17 IMPORTANT: Read instructions on back of last page (Certification Page) before completing this form. Failure to comply with instructions may cause disapproval
R-39 Rev. 03/2012 (Title page) Page 1 of 17 IMPORTANT: Read instructions on back of last page (Certification Page) before completing this form. Failure to comply with instructions may cause disapproval
Macomb County Community Mental Health Level of Care Training Manual
 1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
1 Macomb County Community Mental Health Level of Care Training Manual Introduction Services to Medicaid recipients are based on medical necessity for the service and not specific diagnoses. Services may
Psychiatric Services Provider Manual 10/9/2007. Covered Services and Limitations CHAPTER IV COVERED SERVICES AND LIMITATIONS. Manual Title.
 Subject Revision Date CHAPTER COVERED SERVICES AND LIMITATIONS Subject Revision Date i CHAPTER TABLE OF CONTENTS Inpatient Psychiatric Services (Acute Hospital and Residential) 1 Acute Care Hospitals 1
Subject Revision Date CHAPTER COVERED SERVICES AND LIMITATIONS Subject Revision Date i CHAPTER TABLE OF CONTENTS Inpatient Psychiatric Services (Acute Hospital and Residential) 1 Acute Care Hospitals 1
Fourth, a 7000 Hospital Exemption cannot be issued for an individual who is in a hospital psychiatric unit.
 Information for Lesson 6 Hospital Exemption Information (Formerly Convalescent Stays and Various Scenarios Involving Hospital Exemptions-) For the HENS (Hospital Exemption Notification System) website
Information for Lesson 6 Hospital Exemption Information (Formerly Convalescent Stays and Various Scenarios Involving Hospital Exemptions-) For the HENS (Hospital Exemption Notification System) website
NEW YORK STATE DEPARTMENT OF HEALTH SCREEN/PASRR FREQUENTLY ASKED QUESTIONS (FAQ) OCTOBER 2009
 OCTOBER 2009") NEW YORK STATE DEPARTMENT OF HEALTH SCREEN/PASRR FREQUENTLY ASKED QUESTIONS (FAQ) OCTOBER 2009 SCREENER QUALIFICATIONS Q1. How do I know if I am qualified to complete SCREEN Form: DOH-695 (2/2009)? A1.
NEW YORK STATE DEPARTMENT OF HEALTH SCREEN/PASRR FREQUENTLY ASKED QUESTIONS (FAQ) OCTOBER 2009 SCREENER QUALIFICATIONS Q1. How do I know if I am qualified to complete SCREEN Form: DOH-695 (2/2009)? A1.
STATE OF CONNECTICUT. Department of Mental Health and Addiction Services. Concerning. DMHAS General Assistance Behavioral Health Program
 Page 1 of 81 pages Concerning Subject Matter of Regulation DMHAS General Assistance Behavioral Health Program a The Regulations of Connecticut State Agencies are amended by adding sections 17a-453a-1 to
Page 1 of 81 pages Concerning Subject Matter of Regulation DMHAS General Assistance Behavioral Health Program a The Regulations of Connecticut State Agencies are amended by adding sections 17a-453a-1 to
Pre-Admission Screening and Resident Review
 Pre-Admission Screening and Resident Review Mary Heim LICSW June 2017 PASARR Topics Covered Purpose Regulations MN PASARR Process Services Survey Process Resources Why does the PASARR program exist? PASARR
Pre-Admission Screening and Resident Review Mary Heim LICSW June 2017 PASARR Topics Covered Purpose Regulations MN PASARR Process Services Survey Process Resources Why does the PASARR program exist? PASARR
Interactive Voice Registration (IVR) System Manual WASHINGTON STREET, SUITE 310 BOSTON, MA (800)
 System Manual WASHINGTON STREET, SUITE 310 BOSTON, MA (800)") Interactive Voice Registration (IVR) System Manual 1000 WASHINGTON STREET, SUITE 310 BOSTON, MA 02118-5002 (800) 495-0086 www.masspartnership.com TABLE OF CONTENTS INTRODUCTION... 3 IVR INSTRUCTIONS...
Interactive Voice Registration (IVR) System Manual 1000 WASHINGTON STREET, SUITE 310 BOSTON, MA 02118-5002 (800) 495-0086 www.masspartnership.com TABLE OF CONTENTS INTRODUCTION... 3 IVR INSTRUCTIONS...
Leveraging PASRR to Support Community Placements
 1 Leveraging PASRR to Support Community Placements PASRR as a Vital Tool for Long- Term Care Rebalancing 26th National HCBS Conference, Atlanta, GA, September 28, 2010 Sponsored by the CMS PASRR Technical
1 Leveraging PASRR to Support Community Placements PASRR as a Vital Tool for Long- Term Care Rebalancing 26th National HCBS Conference, Atlanta, GA, September 28, 2010 Sponsored by the CMS PASRR Technical
Florida Medicaid. Early Intervention Services Coverage and Limitations Handbook. Agency for Health Care Administration
 Florida Medicaid Early Intervention Services Coverage and Limitations Handbook Agency for Health Care Administration CHARLIE CRIST GOVERNOR ANDREW C. AGWUNOBI, M.D. SECRETARY January 4, 2008 Dear Medicaid
Florida Medicaid Early Intervention Services Coverage and Limitations Handbook Agency for Health Care Administration CHARLIE CRIST GOVERNOR ANDREW C. AGWUNOBI, M.D. SECRETARY January 4, 2008 Dear Medicaid
907 KAR 1:044. Coverage provisions and requirements regarding community mental health center behavioral health services.
 907 KAR 1:044. Coverage provisions and requirements regarding community mental health center behavioral health services. RELATES TO: KRS 194A.060, 205.520(3), 205.8451(9), 422.317, 434.840-434.860, 42
907 KAR 1:044. Coverage provisions and requirements regarding community mental health center behavioral health services. RELATES TO: KRS 194A.060, 205.520(3), 205.8451(9), 422.317, 434.840-434.860, 42
Long Term Care (LTC) Facility Authorization Request
 Facility Authorization Request") State of Alaska Department of Health and Social Services Senior and Disabilities Services Long Term Care (LTC) Facility Authorization Request This form may be completed by hospital discharge staff or a
State of Alaska Department of Health and Social Services Senior and Disabilities Services Long Term Care (LTC) Facility Authorization Request This form may be completed by hospital discharge staff or a
Mental Health and Substance Abuse Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE
 Mental Health Substance Abuse Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE NUMBER: OMHSAS 01-01 ISSUE DATE: 2-01-01 EFFECTIVE DATE: Immediately SUBJECT BY Nursing Home Reform Implementation
Mental Health Substance Abuse Bulletin COMMONWEALTH OF PENNSYLVANIA * DEPARTMENT OF PUBLIC WELFARE NUMBER: OMHSAS 01-01 ISSUE DATE: 2-01-01 EFFECTIVE DATE: Immediately SUBJECT BY Nursing Home Reform Implementation
Chapter 14: Long Term Care
 I N D I A N A H E A L T H C O V E R A G E P R O G R A M S P R O V I D E R M A N U A L Chapter 14: Long Term Care Library Reference Number: PRPR10004 14-1 Chapter 14 Indiana Health Coverage Programs Provider
I N D I A N A H E A L T H C O V E R A G E P R O G R A M S P R O V I D E R M A N U A L Chapter 14: Long Term Care Library Reference Number: PRPR10004 14-1 Chapter 14 Indiana Health Coverage Programs Provider
Interactive Voice Registration (IVR) System Manual WASHINGTON STREET, SUITE 310 BOSTON, MA
 System Manual WASHINGTON STREET, SUITE 310 BOSTON, MA") Interactive Voice Registration (IVR) System Manual 1000 WASHINGTON STREET, SUITE 310 BOSTON, MA 02118-5002 1-800-495-0086 www.masspartnership.com TABLE OF CONTENTS INTRODUCTION... 3 IVR INSTRUCTIONS...
Interactive Voice Registration (IVR) System Manual 1000 WASHINGTON STREET, SUITE 310 BOSTON, MA 02118-5002 1-800-495-0086 www.masspartnership.com TABLE OF CONTENTS INTRODUCTION... 3 IVR INSTRUCTIONS...
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance. UM Retrospective Review Services.
 KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
Romney, WV May 9, 2011
 State of West Virginia DEPARTMENT OF HEALTH AND HUMAN RESOURCES Office of Inspector General Board of Review Earl Ray Tomblin P.O. Box 1736 Governor Romney, WV 26757 Michael J. Lewis, M.D., Ph.D Cabinet
State of West Virginia DEPARTMENT OF HEALTH AND HUMAN RESOURCES Office of Inspector General Board of Review Earl Ray Tomblin P.O. Box 1736 Governor Romney, WV 26757 Michael J. Lewis, M.D., Ph.D Cabinet
Georgia Department of Behavioral Health & Developmental Disabilities FOR. Effective Date: January 1, 2018 (Posted: December 1, 2017)
") Georgia Department of Behavioral Health & Developmental Disabilities PROVIDER MANUAL FOR COMMUNITY DEVELOPMENTAL DISABILITY PROVIDERS OF STATE-FUNDED DEVELOPMENTAL DISABILITY SERVICES FISCAL YEAR 2018
Georgia Department of Behavioral Health & Developmental Disabilities PROVIDER MANUAL FOR COMMUNITY DEVELOPMENTAL DISABILITY PROVIDERS OF STATE-FUNDED DEVELOPMENTAL DISABILITY SERVICES FISCAL YEAR 2018
Pre-admission Screening and Resident Review (PASRR) The Current Climate of PASRR
 The Current Climate of PASRR") Pre-admission Screening and Resident Review (PASRR) The Current Climate of PASRR Trends in Quality and Person-Centered Care 1 Topics of Discussion Understanding PASRR Trending shows states are increasing
Pre-admission Screening and Resident Review (PASRR) The Current Climate of PASRR Trends in Quality and Person-Centered Care 1 Topics of Discussion Understanding PASRR Trending shows states are increasing
Mississippi Medicaid Autism Spectrum Disorder Services for EPSDT Eligible Beneficiaries Provider Manual
 Mississippi Medicaid Services for EPSDT Eligible Beneficiaries Provider Manual Effective Date: July 1, 2017 Services for Introduction: eqhealth Solutions Services (ASD) Utilization Management Program includes
Mississippi Medicaid Services for EPSDT Eligible Beneficiaries Provider Manual Effective Date: July 1, 2017 Services for Introduction: eqhealth Solutions Services (ASD) Utilization Management Program includes
ABOUT AHCA AND FLORIDA MEDICAID
 Section I Introduction About AHCA and Florida Medicaid ABOUT AHCA AND FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency)
Section I Introduction About AHCA and Florida Medicaid ABOUT AHCA AND FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency)
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
Chapter 2 Provider Responsibilities Unit 6: Behavioral Health Care Specialists
 Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
LOUISIANA MEDICAID PROGRAM ISSUED: 06/09/17 REPLACED: CHAPTER 2: BEHAVIORAL HEALTH SERVICES SECTION 2.2: OUTPATIENT SERVICES PAGE(S) 8
 8") Licensed Practitioner Outpatient Therapy includes: Individual; Family; Group; Outpatient psychotherapy; Mental health assessment; Evaluation; Testing; Medication management; Psychiatric evaluation; Medication
Licensed Practitioner Outpatient Therapy includes: Individual; Family; Group; Outpatient psychotherapy; Mental health assessment; Evaluation; Testing; Medication management; Psychiatric evaluation; Medication
Basic Training in Medi-Cal Documentation
 Basic Training in Medi-Cal Documentation Sara Kashing, J.D. Staff Attorney The Therapist May/June 2012 Since 1998, Medi-Cal mental health services have been provided through county-based Mental Health
Basic Training in Medi-Cal Documentation Sara Kashing, J.D. Staff Attorney The Therapist May/June 2012 Since 1998, Medi-Cal mental health services have been provided through county-based Mental Health
Covered Behavioral Health Services
 Behavioral Health Services Covered Behavioral Health Services Cenpatico, Buckeye s behavioral health affiliate, has been delegated the provision of covered mental health and substance use disorder services
Behavioral Health Services Covered Behavioral Health Services Cenpatico, Buckeye s behavioral health affiliate, has been delegated the provision of covered mental health and substance use disorder services
PIONEER CENTER NORTH PIONEER CENTER EAST Substance Use Disorder (SUD) Residential Adult Long Term Care Statement of Work
 Residential Adult Long Term Care Statement of Work") PIONEER CENTER NORTH PIONEER CENTER EAST Substance Use Disorder (SUD) Residential Adult Long Term Care Statement of Work I. WORK STATEMENT The Contractor shall provide SUD residential treatment in the
PIONEER CENTER NORTH PIONEER CENTER EAST Substance Use Disorder (SUD) Residential Adult Long Term Care Statement of Work I. WORK STATEMENT The Contractor shall provide SUD residential treatment in the
Preadmission Screening Resident Review (PASRR) Instruction Manual
 Instruction Manual") Alabama Department of Mental Health and Mental Retardation Omnibus Budge Reconciliation Act (OBRA) Preadmission Screening Resident Review (PASRR) Instruction Manual May 2009 Table of Contents PASRR Process
Alabama Department of Mental Health and Mental Retardation Omnibus Budge Reconciliation Act (OBRA) Preadmission Screening Resident Review (PASRR) Instruction Manual May 2009 Table of Contents PASRR Process
CHILDREN'S MENTAL HEALTH ACT
 40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
IV. Clinical Policies and Procedures
 A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
General PASRR/LOC Questions
 General PASRR/LOC Questions 1. Q: What is the purpose of PASRR? A: The purpose of PASRR is to identify nursing facility applicants with serious mental illness and/or mental retardation or a related condition
General PASRR/LOC Questions 1. Q: What is the purpose of PASRR? A: The purpose of PASRR is to identify nursing facility applicants with serious mental illness and/or mental retardation or a related condition
Ryan White Part A. Quality Management
 Quality Management Mental Health Services Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part A grant
Quality Management Mental Health Services Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part A grant
Wilhide Consulting, Inc. (c) 1
 1") Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
CHAPTER 24 ACCREDITATION OF PROVIDERS OF SERVICES TO PERSONS WITH MENTAL ILLNESS, MENTAL RETARDATION, AND DEVELOPMENTAL DISABILITIES PREAMBLE
 Human Services[441] Ch 24, p.1 CHAPTER 24 ACCREDITATION OF PROVIDERS OF SERVICES TO PERSONS WITH MENTAL ILLNESS, MENTAL RETARDATION, AND DEVELOPMENTAL DISABILITIES PREAMBLE The mental health, mental retardation,
Human Services[441] Ch 24, p.1 CHAPTER 24 ACCREDITATION OF PROVIDERS OF SERVICES TO PERSONS WITH MENTAL ILLNESS, MENTAL RETARDATION, AND DEVELOPMENTAL DISABILITIES PREAMBLE The mental health, mental retardation,
FREQUENTLY ASKED QUESTIONS Iowa PASRR Onsite Provider Training 10/18/ /21/2016
 Below you will find the frequently asked questions for the multi location Onsite Provider Training conducted. Answers to these questions were based on knowledge and policy as of 10/18/2016. Due to policy
Below you will find the frequently asked questions for the multi location Onsite Provider Training conducted. Answers to these questions were based on knowledge and policy as of 10/18/2016. Due to policy
UTILIZATION MANAGEMENT Section 4. Overview The Plan s Utilization Management (UM)
") Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
PENNSYLVANIA DEPARTMENT OF HUMAN SERVICES OFFICE OF LONG-TERM LIVING OBRA. Preadmission Screening Resident Review Identification Form.
 PENNSYLVANIA DEPARTMENT OF HUMAN SERVICES OFFICE OF LONG-TERM LIVING OBRA Preadmission Screening Resident Review Identification Form (Level I Tool) April 2017 1 Objectives for this Webinar Overview of
PENNSYLVANIA DEPARTMENT OF HUMAN SERVICES OFFICE OF LONG-TERM LIVING OBRA Preadmission Screening Resident Review Identification Form (Level I Tool) April 2017 1 Objectives for this Webinar Overview of
OUTPATIENT BEHAVIORAL HEALTH CSHCN SERVICES PROGRAM PROVIDER MANUAL
 OUTPATIENT BEHAVIORAL HEALTH CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 OUTPATIENT BEHAVIORAL HEALTH Table of Contents 29.1 Enrollment......................................................................
OUTPATIENT BEHAVIORAL HEALTH CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 OUTPATIENT BEHAVIORAL HEALTH Table of Contents 29.1 Enrollment......................................................................
MDS 3.0: What Leadership Needs to Know
 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
Service Review Criteria
 Client Name: SAR#: Administrative Review Process notes: When documenting call outs to provider, please document the call in a patient note in Alpha the day the call is made. tes should be coded as Care
Client Name: SAR#: Administrative Review Process notes: When documenting call outs to provider, please document the call in a patient note in Alpha the day the call is made. tes should be coded as Care
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT October 1, 2012 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT October 1, 2012 Children s Mental Health
STATE OF CONNECTICUT DEPARTMENT OF DEVELOPMENTAL SERVICES
 STATE OF CONNECTICUT DEPARTMENT OF DEVELOPMENTAL SERVICES Procedure No. I.E.PR.003 Issue Date: October 28, 2003 Subject: Behavior Modifying Medications Effective Date: Upon Release Section: Health and
STATE OF CONNECTICUT DEPARTMENT OF DEVELOPMENTAL SERVICES Procedure No. I.E.PR.003 Issue Date: October 28, 2003 Subject: Behavior Modifying Medications Effective Date: Upon Release Section: Health and