Contents. Foreword. 1. Context
|
|
|
- Stella Gordon
- 6 years ago
- Views:
Transcription

1 Our Health, Our Future Hywel Dda Integrated Medium Term Plan 2016/17 to 2018/19 Work in Progress IMTP Draft for BP&PAC on 26 th January 2016 and Board Consideration on 28 th January
2 Contents Foreword 1. Context 2. Our Ambition 2016/17 to 2018/ The way we will do business our values 2.2 The difference we intend to make and why 2.3 Our top 10 strategic objectives and why we chose them 3. Integrated programmes for our 10 strategic objectives 3.1 The way we will bring all of plans together 3.2 Strategic objectives 1 to 8 Plans in support of their delivery including Prevention, General Practice Cluster Plans, Intermediate Care Funded Plans, Primary Care Delivery Agreements and Pathfinder Plans, Together for Health Delivery Plans, Mental Health Plans 3.3 Strategic objectives 9 and 10, the way we will bring all of our performance delivery patient access, waiting times for Outcome and Delivery Framework Targets plans for Diagnostics, Planned Care, Unscheduled Care, Women and Children s Services and our medium term financial plans (Quality Innovation Productivity Prevention (Prudency)) 3.4 Our strategic objectives with a particular emphasis on Quality and Safety 4. Supporting and enabling strategies 4.1 Our Organisational Strategy including Workforce Organisational Development, Staff Experience, Patient Experience, Public Engagement Quality Improvement and Communication 4.2 Our Governance 4.3 Our Equality Strategy and Welsh Language 4.4 Workforce and Organisational Development 4.5 Infrastructure, Estates & Capital Planning Assumptions 4.6 Information Management and Technology including Digital Health 4.7 Commissioning and Collaboratives, Innovation and Research and Development 4.8 Finance 5. Conclusion Annexes: 1. Health Need Assessment Summary 2. Draft mapping of plans to 10 Strategic Objectives 3. Public Health Plan 4. Primary Care Strategy 5a. Mental Health Integrated Medium Term Plan 5b. Mental Health Transformation 5c Mental Health Workstreams 6. Demand & Capacity Plans in Planned Care 7. Unscheduled care Delivery Unit Action Plan 8. Women & Children Royal College Action Plan 9. Governance 10a. Equality Strategy 10b. Welsh Language Skills Strategy 11. Workforce & Organisational Development 12a. Estates Strategy 12b. Capital Programme 13. Information Management & Technology 2
3 Foreword Expected from CEO Chapter 1: Context Hywel Dda University Health Board (University Health Board) covers the mainly rural counties of Carmarthenshire, Ceredigion and Pembrokeshire. Our responsibilities are to commission and provide healthcare for our resident population and this involves a full range of services from prevention, primary care, community, mental health and long-term care (continuing healthcare), hospital and very specialist care. To do this we are funded on a resident population basis which, whilst nationally equitable, does not deal with the fact that our geographical challenges means that we have four district general hospitals and primary and community services which cover over a quarter of the landmass of Wales, and as such is an expensive model of care. To provide services safely we rely on multiple staff rotas across all of our services which whilst trying to meet clinical standards have continued to prove challenging both in terms of recruitment and retention, and of course the exceptional costs to do this. This is especially the case in both the north and west of Hywel Dda, and whilst we are doing all we can to develop innovative staffing solutions, by their nature these have a lead-in time and require access to expertise that either through infrastructure or through Information Management and Technology we know we have to enable. Again, these solutions will incur a cost over and above the funded population share. In performance terms what this means is that our clinical teams which cover community and hospital services are smaller and more stretched than in an urban model, and as such do not have sufficient resilience to accommodate surges in demand or when there are staffing difficulties, namely sickness and vacancies. This means that we are moving towards improving productivity but we will only be able to do this if our services network more to flex and cover these factors as one hospital over four sites, and pursue hub and spoke models where clinically appropriate and to shift care more proactively from hospital care towards prevention, primary and community care. Obviously in terms of access and patient experience we will continue to provide services as close to home as possible, and where we are unable to do this we will optimise our Information Management and Technology /e-health solutions so that in their localities our patients can increasingly expect to receive more equitable access to specialist expertise. The NHS Finance (Wales) Act 2014 provides the legislative basis for the Integrated Medium Term Plan (IMTP). It requires the University Health Board to prepare a plan which sets out our strategy for complying with the financial duty while improving the health of people for whom we are responsible. Our Integrated Medium Term Plan sets the University Health Board s strategy to move towards compliance with our financial duty over the three year period of the plan, recognising that breakeven can only be delivered over a much longer planning cycle. Against the backdrop of a rural and ageing population and the service and workforce challenges already described, our baseline vacancies are manifesting themselves in premium variable pay of just over 34million per annum. The University Health Board has 9985 directly employed staff which equates to 43% of our budget. The current vacancies across the University Health Board in unit labour cost terms equate to approximately 700 whole time equivalents which means we are incurring high cost including agency, bank, medical locum and overtime payments to manage service demand. This is neither economically sustainable nor does it provide the highest quality of care. 3
4 As a consequence the University Health Board struggles to live within its funded resource allocation. It has been acknowledged that these structural challenges will mean that financial balance cannot be achieved over a three year planning period, and our clinical strategy will regear our resources to meet the University Health Board s strategic objectives through a patient experience and clinical lens, which evidences Quality, Innovation, Productivity, Prevention and Prudent healthcare (QIPP(P)). Our immediate 2016/17 year still results in a planned financial deficit of 25-30million. Over the next three year period of the Integrated Medium Term Plan this annual funding gap cannot be overcome and the cumulative deficit is around 75million. It is important that the University Health Board commitment remains to re-gear our services to come within our funding and to that end we are implementing a rigorous Programme Management approach which will cover up to 20 clinical, workforce and financial programmes/sub-programmes in-line with our strategic priorities. Hywel Dda s contextual position: Population of 383,900 (12% of Wales) across the three counties of Carmarthenshire, Ceredigion and Pembrokeshire, with pockets of both urban and rural deprivation and we are the second most sparsely populated Health Board Sustaining our primary, community and our four district general hospitals to ensure local access to care services wherever possible care closer to home and one hospital over four sites An ageing population, with a higher than average proportion of older people, in particular those aged 85 years and over, which leads to an increasing demand on services A recent history of difficult public and stakeholder relations, and controversial service change leading to the need to re-build trust and confidence with our population and stakeholders The increasing need to plan and deliver care in collaboration with external partners in health and social care, as well as planning to meet national priorities and legislation The Integrated Medium Term Plan produced for 2015/16 described plans to move from the stabilisation of services to optimising and transforming local health services. The key contextual challenges illustrate, that whilst progress has been made, the University Health Board continues to face significant challenges which we are seeking to stabilise as the cornerstone of our medium-term plan. In order to understand the context of our plan the 2016/17 to 2018/19, progress against 2015/16, prevention, care closer to home, General Practitioner cluster, mental health, primary and community monies and integrated health and social care funds and their deliverables shows where we have achieved some success, whilst they are still work-in-progress they remain the foundation of our plan. In particular the shift of services towards care closer to home, albeit we still have much to do is described more in chapter 3. Clinical Services Strategy Development We are reviewing and building our clinical services strategy with our clinicians, and by following a structured process through which we are highlighting the key opportunities and risks. We recognise that we have significant challenges to providing sustainable primary care, community and hospital services which are widely spread across both rural and more urban communities, and across four acute hospital sites. We also face significant challenges in recruiting to nursing, therapies and medical positions such as in General Practice, Emergency Medicine, Radiology, Radiography, Histopathology, Oncology, Respiratory, Acute Medicine, Surgery and Anaesthetics. For this reason we will be creative in our approach to finding solutions to our service and workforce challenges. We will embed the principles of Prudent Healthcare and the Hywel Dda University Health Board Population Health Approach, including involving our services users and public in participative 4
5 decision making as we create service solutions to allow us to communicate and discuss our challenges and proposals. We are conscious that there is inequalities and inequity of access in our population, and we will provide our services as close to home as possible, and only require people to travel when absolutely necessary. We will build our clinical strategy based on the needs of our population, and will drive improvements in prevention, health promotion, early intervention and reducing harm and variability, focussing significant effort on services which face the greatest challenge and risk. We will follow a systems approach and will challenge ourselves to make the best use of the resources across our system, and will ensure we drive the use of technology, information sharing and Information Technology capability to help our public and clinicians make the best decisions. We will collaborate closely with our partners through our Collaboratives (Mid- Wales Collaborative, All Wales Collaborative, A Regional Collaborative for Health, Health and Social Care Collaborative) and will maximise the involvement of the 3rd Sector. We are committed to supporting our clinicians to lead the Clinical Strategy development and implementation, and also develop the necessary clinical leadership capacity and capability to do this. Our General Practitioners leads have led the development of cluster plans for each of our 7 localities that are aimed at their local population need and we are developing our proactive care strategy. We held a listening event with clinical leads from all specialties on 14th and 15th January 2016 which provided an overview of the position of each specialty, the linkages with other specialties, and important information about each hospital site. We will be supporting our clinicians to guide how the cluster plans, site plans and speciality plans influence and inform each other to ensure that our services are best aligned to the needs of our population and are of high value. 5
6 Chapter 2: Our Ambition for 2016/17 to 2018/ The way we will do business and our values: Our draft organisational strategy seeks to develop a single organisational strategy to encompass the following: Organisational Development Staff Experience Patient Experience Public Engagement Quality Improvement Communications. Each of the above required some form of documented strategic direction in order to provide the organisation with clarity of purpose. It was therefore considered appropriate to attempt to link them (as they clearly overlap) and provide a strong visual and simple staff and public framework which links our values, plans, direction and objectives together. It was clear from talking to our staff that they would not see the value in a lengthy set of strategies which did not reflect the role they need to play and therefore the plan will be to have key work programmes underpinning this organisational strategy which sets out clarity of action required. As an example there will be no dedicated nursing strategy, a nursing work plan will be developed based on this organisational strategy and will set out practical steps to be taken to meet the key principles. Our overarching values will be: Integrity choosing to do the right thing every day Openness and honesty being transparent and accountable about what we are doing and planning to do Dignity treating people in a way that supports their self-respect Respect being polite and have due regard for the feelings, wishes and beliefs of others Fairness treating people in a way which is right and reasonable People focussed putting the population at the heart of what we do and how we do it Pride - having a sense of satisfaction and /or pleasure in our own and others success Excellence working as one to be the best that we can be. Our organisational strategy can be illustrated as follows: Our Organisational Strategy encompassing, Organisational Development, Staff Experience, Patient Experience, Public Engagement, Quality Improvement, Communications underpinned by our values 10 Strategic Objectives Our Priorities Patient and Communities Centred Quality Improvement Learning Organisation Leadership Improving Organisation 6
7 2.2 The difference we intend to make and why As a University Health Board, we have agreed that the difference we intend to make for the residents of Hywel Dda is encapsulated by the following: Prevention and early years intervention is the key to our long term mission to provide the best health care to our population We will be proactive in our support for our local population, particularly those living with health issues, and carers who support them If you think you have a health problem, rapid diagnosis will be in place so that you can get the treatment you need, if you need it We will be an efficient organization that does not expect you to travel unduly or wait unreasonably; is consistent, safe and of high quality, and, has a culture of transparency and learning when things go wrong All of these will run through our strategic objectives as common themes. In doing this, we also wanted the plan to be far more purposeful by reflecting: A sharper focus on actions we plan to take our plans will increasingly be framed in terms of what we intend to deliver, by when and with measurable targets to provide assurance on delivery and in governance terms who is charged with assuring delivery and through which Board Committee / Subcommittee Evidence that we have embraced the principles of Prudent Healthcare A strategic approach to workforce planning as whilst our workforce represents the greatest strength of the University Health Board, the challenges associated with recruitment and retention of staff with the right skills also represents the greatest risk to the sustainability of high quality clinical services. Addressing the challenge in these areas is central to, and underpins our planning. We recognise that the development of our clinical service strategy is at this stage a dynamic process, and our approach is to do the things we know must be done now, and acknowledge that not all of our challenges can be fixed at once. Needs assessment (Annex 1) is a key building block in enabling the understanding of the needs of our local residents. We continue to progress and develop our approach to needs assessment with our partners, and during 2015/16 this work has already supported the development of our delivery plans. Our needs assessment is helping us to prioritise activity, as we cannot take action on everything all at once and to support our work on developing the strategy for Hywel Dda, and to this end: We acknowledge the need for the approach to take account of the current and future needs of our communities and overall population from pre-birth to old age We are also looking beyond need alone, and ensuring that we are also examining local assets in our community/locality activity We are keen to highlight inequalities where we can within our needs assessment work given their impact on health and well being We are clear that the outcome of needs assessment activity is more than just a document the process is in itself valuable and informative for partners involved. Overall health in Hywel Dda, as measured by morbidity and mortality rates, is relatively good with life expectancy for both males and females being similar to the national average. However, there are some important issues around societal ageing, health inequalities and lifestyle choices that 7
8 need to be addressed if a sustainable health and social care service is to be achieved and maintained over the long term, in particular addressing the impact of frailty. Key Statistics Wales Hywel Dda Total population 3,092, ,900 Population aged 75 and over (%) Life expectancy at birth males (years) Life expectancy at birth females (years) Adults who are overweight or obese (%) Adults who smoke (%) Adults who drink above guidelines (%) MMR uptake (%) Live birth per 1,000 women aged Emergency hospital admissions (European age standardized rate per 1,000 population) Current population projections suggest that the total population of Hywel Dda will rise to 425,400 by 2033, with a rise in those aged over 65 years from 88,200 in 2013 to 127,700 by These estimates are based on assumptions about births, deaths and migration. The increase in the number of older people is likely to cause a rise in chronic conditions such as circulatory and respiratory diseases and cancers. Meeting the needs of these individuals will be a key challenge for the University Health Board. In the current economic climate, the relative (and absolute) increase in economically dependent and in some cases, care-dependent populations will pose particular challenges to communities. We will be working with Public Health Wales in 2016/17 to further develop our needs assessment approach given the new statutory requirements. To address the needs of the Social Services & Wellbeing Act and the Future Generations Act and to understand the level of deliverable ambition for Hywel Dda over a defined timeline, the need assessment work in 2016/17 will need to develop further in preparation for publicising our Well-being objectives under the Act. During the course of the development of the Integrated Medium Term Plan we intend to sign-post current and planned initiatives which are consistent with the aims of the Act. It is important to recognise that this is consistent with the existing direction of travel, which starts with the foundation of a robust needs assessment. 8
9 2.3 Our top 10 strategic objectives and why we chose them Our 10 Strategic Objectives: 1. To reduce overweight and obesity in our local population 2. To reduce the number of people who engage in risky behaviours and improve access to local support services 3. To improve the mental health and wellbeing of our local population through improved prevention and early intervention 4. To improve the prevention and management of cardiovascular disease in the local population 5. To increase survival rates for cancer through the earlier diagnosis, faster access to treatment, and improved survivorship programmes 6. To improve the management of patients with diabetes, reducing acute exacerbations and long term health and wellness increasing 7. To improve community based support for patients with respiratory illness and reducing the need for hospital based care 8. To improve the care and management of patients with frailty and/or dementia by being more proactive and consistent in our approach to care aimed at maintaining health and independence 9. To improve productivity and quality of our services using the principles of prudency and the opportunities to innovate 10. To deliver, as a minimum requirement, Outcome and Delivery Framework Targets and return the organisation to a sound financial footing over the lifetime of this plan. The rationale for each of our 10 strategic objectives, from a Public Health needs perspective for the first eight, is outlined below. Strategic Objective 1: Obesity and Overweight Obesity is regarded as the most challenging public health priority of the 21st century. Its increasing prevalence makes it one of the main risks for shortened life expectancy and greatly increases the risk of type 2 diabetes, cardiovascular disease and some cancers. At an annual cost of 73m to the health service in Wales, estimated at 8.4m for Hywel Dda, obesity places a significant burden on healthcare resources. Strategic Objective 2: Risky Behaviours Smoking - smoking places a significant burden of illness on the health of the Hywel Dda population, the effects of which place an unprecedented demand on Hywel Dda s Health and Social Care services across community, primary care and secondary care; and on the services provided by its partner organisations across statutory and voluntary sectors. The full impact of tobacco use on the health of individuals, communities and the population, and its impact on health services is wide-reaching. While overall death rates from smoking are falling, it still continues to be the largest single preventable cause of ill-health and premature death. Reducing smoking prevalence is a key action in the Tobacco Control Action Plan for Wales (Welsh Government, 2012) which sets out the aim to decrease adult smoking prevalence rates to 16% by Welsh Government indicates that reaching this target by 2020 will require a significant change in efforts to motivate and assist smokers to quit. Twenty percent of the adult population of Hywel Dda report smoking, that is approximately 62,000 people are smokers. Carmarthenshire exhibits a higher smoking prevalence rate of 20% compared with rates of 19% in Ceredigion and Pembrokeshire. Alcohol and Drug Misuse - those at risk of harm from alcohol misuse come from across the spectrum of society. They include chronic heavy drinkers, adults at home drinking at hazardous or harmful levels, and children and young adults who suffer from the consequences of parental alcohol misuse. The health impact of misuse of alcohol is considerable. More people die from 9
10 alcohol related causes than from breast cancer, cervical cancer, and methicillin-resistant Staphylococcus Aureus (MRSA) infection combined. Excessive alcohol consumption is a major cause of serious liver disease, which is often fatal. In addition, alcohol is a major contributing factor to the risk of cancer of the breast, mouth, gullet, stomach, liver, pancreas, colon and rectum. Foetal alcohol syndrome is also a risk to the babies of mothers who use alcohol. There is increasing recognition of the significant health harm that alcohol can cause. In Wales, 15 per cent of all hospital admissions are due to alcohol intoxication; with 30,000 hospital bed days related to alcohol each year and liver disease responsible for about 1600 admissions. The estimated health service cost in Wales of alcohol related chronic disease and alcohol related acute incidents are between 70 million and 85million each year. Most recent data on hospital admissions for the University Health Board show that over 5000 bed days were taken up by patients with alcohol related conditions at a cost to the University Health Board of over 5.2 million per year in inpatient treatment alone. Misuse of drugs, both legal and illegal, and other mind-altering substances such as solvents, can damage health in a variety of ways. These include fatal overdoses, addiction, mental health problems, infections caused by injecting, and the toxic effects of the many substances that dealers mix with the active substance. Although the greatest harms are associated with the use of illicit drugs, the misuse of prescription-only medicines and over the counter medicines continues to be a problem. There are estimated to be just under 20,000 problem drug users in Wales. The health service cost in Wales of problem drug use have been estimated at 17.6 million per year. Strategic Objective 3: Mental Health and Wellbeing The Together for Mental Health Strategy and Delivery Plan in conjunction with the local Mental Health and Wellbeing Strategy 2012/17 give a clear focus for the Hywel Dda community to work in partnership to improve the health and wellbeing gains for people who are experiencing, or have potential to experience, mental health problems. The overarching imperative and emphasis of the Strategy is the promotion of mental wellbeing, mental illness prevention, appropriate and easy access, early interventions and timely treatment. Effective and evidence based treatments and interventions will be accessed and delivered at the most appropriate stage and cohesively across services. The services we provide help people to develop, maintain, sustain and recover independence and better lives by helping them to achieve better mental health and well-being. Mental health problems range from common disorders of depression and anxiety, which affect between 8 12% of the population in any year, to two in 100 with the less common serious mental illnesses, such as schizophrenia. Estimates of the overall prevalence of mental distress suggest that one in four adults experience at least one diagnosable mental health problem in any one year. Between 1 in 10 and 1 in 15 new mothers experience post-natal depression. Mental health disorders in children and young people are equally as prevalent, with 1 in 10 children and young people aged five to sixteen suffering from a diagnosable mental health disorder. Between the ages of one to twelve 1 in 15 children young people deliberately self-harm. There were 341 suicides in those aged 15 years and over in Wales in 2011 (270 males and 71 females). In the last two years the rate in Wales has increased by 30% from a low of 10.7 deaths per 100,000 population in 2009 to 13.9 per 100,000 in This is the highest suicide rate seen in Wales since 2004, and the increase was seen in both males and females. Suicide rates within Hywel Dda are below the Welsh average in two of the three local authority areas, with the rate in Carmarthenshire significantly higher than the Welsh average and the fourth highest rate in Wales. Dementia is increasingly a major public health challenge with approximately 42,000 cases in Wales. By 2021 there is estimated to be a 31% increase in the number of people living with dementia. Some of the more rural areas, such as Pembrokeshire, will see the highest rises (44%). Over 10% of deaths in men 65 years of age and older and 15% of deaths in women in the same age group are attributable to dementia. 10
11 Strategic Objective 4: Cardiovascular Disease The Welsh Health Survey identifies that 20% of adults are being treated for high blood pressure and 9% for any heart condition, excluding high blood pressure. The most significant cause of heart related ill health and death is coronary heart disease (particularly angina and heart attack). Although death rates in Wales have been falling over the last three decades, they remain around 15% higher than in England. In addition, death rates vary significantly across Wales. The death rate in the most deprived fifth of wards is almost a third higher than in the least deprived fifth showing the pronounced impact of poverty and the socio-economic determinants of health. While coronary heart disease is a largely preventable cause of ill health and death, the latest figures show the major risk factors remain high as highlighted above.. Strategic Objective 5: Cancer It is estimated that around 1 in 3 people in Wales will be diagnosed with cancer before age 75. Around 4 in 10 will be diagnosed with cancer during their lifetime. The incidence rate is increasing. For the period , there was an average of around 16,100 new cases of cancer per year (cancer incidence increased by around 0.6% per year) and around 8,400 people died from cancer each year (an average decrease in death rates of 1% each year). The incidence of Cancer in the University Health Board is lower than the Welsh National average (Wales 630.9; Hywel Dda 619.0) (Cancer Incidence Rate (Per Cancer Site) 2009/13) and the Cancer Mortality rate in the University Health Board is significantly lower than the Welsh average (Wales 299.8; Hywel Dda 283.4) (Cancer Mortality Rate 2009/13) The most commonly diagnosed cancers are breast, lung, bowel and prostate cancer. Together these accounted for just over half of all new cases. There is wide variation in the rates of survival for different types of cancer. Among the commonest cancers the survival rate after 5 years varied from 7% for lung cancer to 78% for prostate cancer and 82% for breast cancer. Cancer has a greater impact in the more deprived areas of Wales. Strategic Objective 6: Diabetes In Hywel Dda there are in excess of 22,000 people registered with their General Practitioners with a diagnosis of diabetes (5.8%). It is widely accepted that Wales is facing a huge increase in the number of people with diabetes. Most of the increase is type 2 diabetes due to the ageing population and the increase in the number of overweight and obese people. People with diabetes have a substantially higher risk of serious illness, hospitalisation and premature death compared to the non-diabetic population. There is evidence to show that: The onset of type 2 diabetes can be delayed or even prevented Effective management of the condition increases life expectancy and reduces the risk of complications Support and self-management is the essential element of effective diabetic care Type 2 diabetes is more prevalent amongst less affluent populations. Those in the most deprived 1/5 th of the population are 1½ times more likely than average to have diabetes at any given age. 9% of those people living in the most deprived areas of Wales report being treated for diabetes compared to 6% of those living in the least deprived showing the pronounced impact of poverty and the socio-economic determinants of health. Strategic Objective 7: Respiratory Illness According to Health Statistics Wales (2013) one in seven adults (14%) in Wales reports being treated for a respiratory condition and respiratory diseases cause one in seven (15%) of all deaths in Wales. Both smoking and obesity are major contributory factors to the levels of respiratory disease. The European age-standardised mortality rate for all respiratory diseases in Hywel Dda residents in 2011 was 96 per 100,000 compared with 73 per 100,000 in Wales ( ; Public Health Wales Observatory, using ADDE/MYE (ONS). The rate for premature mortality (deaths under age 75) for respiratory disease in Hywel Dda residents decreased between 2002/07 however a gradual increase between 2008/10 can be seen. The gap in respiratory mortality (all 11
12 ages) between the least and most deprived between is evident. Mortality is much higher in the most deprived population, and for males the gap is widening. Improving the respiratory health of the population in Hywel Dda is a major challenge for health care providers and a key opportunity to improve the lives of patients and their families. Strategic Objective 8: Frailty and Dementia For older people living with frailty or complex needs, health and quality of life is vulnerable to sudden changes. A key feature of frailty is that it describes a person at a higher risk of a sudden deterioration in their physical and mental health. This will include people who could otherwise be very stable and low users of health services. Frail older adults have little or no reserve when faced with relatively minor illnesses, increasing the risk of hospital admission. The frail population group form a high proportion of people in the medical admissions units and a substantial proportion (60 70%) of overall hospital inpatients. Whilst 21% of the current Hywel Dda population is over 65, 55% of all emergency admissions are of people who are over 65, and due to their length of stay 78% of our emergency admission beds are taken up by people who are over 65 (this is 57% of all bed days in our hospitals): 55% of Hywel Dda residents who are over 65 report long-term health problems or disability that limits their ability to carry out day-today activities Dependence in 2 Activities of Daily Living predicts increased risk of complications in hospital A significant proportion of people who are over 65 will have lost 2 or more Activities of Daily Living from pre-morbid baseline (up to 60%) on admission to hospital. Frail older people usually have longer stays, higher mortality and rates of readmission, and they are more likely to be discharged to residential care. People with dementia stay far longer in hospital than other people who come in for the same procedure (at least 40 50% of bed days relating to emergency admission in Hywel Dda will relate to people who have dementia as part of their multi-morbidity) Most old people admitted to hospital will have multi-morbidity. The final two strategic objectives (9 and 10) have a corporate objective - Objectives 9 and 10: To improve productivity and quality of our services using the principles of prudency and opportunities to innovate & to deliver, as a minimum requirement, Outcome and Delivery Framework Targets and return the organisation to a sound financial footing over the lifetime of this plan. The need for these objectives stem from the NHS Wales Delivery Framework reflecting all of our service delivery over the 7 domains: Staying healthy Safe care Effective care Dignified care Timely care Individual care NHS staff and resources The reason why these objectives are important is that it is all about our residents and patients obtaining good access to timely, safe, high-quality services. In conjunction with our clinicians we will be approaching these through a quality, innovation, productivity, prevention and prudency (Quality, Innovation, Productivity, Prevention (Prudent)) lens (QIPP (P)). 12
13 Chapter 3: Integrated Programmes for our 10 Strategic Objectives 3.1 The way we will bring all of our plans together Delivery against all of the 10 strategic objectives will be managed through the Executive Programme Steering Group chaired by the Director of Finance, Planning and Performance onbehalf of the Chief Executive Officer and the governance is illustrated as follows: Executive Team Sub Committee Business Intelligence Unit identifies through benchmarking our future business opportunities Executive Programme Steering Group Programme Management Office holds the ring on all of the programmes 10 Strategic Objectives delivered through 10 Programmes QIPP(P) Sub-programmes of strategic objectives 9 and 10 Integrated Performance Management Team tracks in-year performance in its widest sense Enabling Work streams Organisational Strategy The Executive Programme Steering Group will oversee the delivery of 10 strategic objectives with the main success criteria being as follows: The Programmes supporting strategic objectives 1 to 8 will need to ensure delivery against health need, manage the growth in demand, and that the care quality and patient experience is consistent with our values set out earlier in the document and fundamentally they deliver on shifting services and resources to Primary and Community care and building on Primary Care cluster assessment. The Programmes supporting strategic objectives 9 and 10, comprise 10 subprogrammes/projects which deliver on the (Quality, Innovation, Productivity, Prevention (Prudent)) lens (QIPP (P)) principles and secure improved productivity and quality of our services using the principles of prudency and the opportunities to innovate and deliver, as a minimum requirement, Outcome and Delivery Framework Targets and return the organisation to a sound financial footing over the lifetime of this plan. The subprogrammes/projects are as follows: Sub-programme 1 - Referral management Sub-programme 2 - Acute care productivity and efficiency Sub-programme 3 - Medicines optimisation Sub-programme 4 - Learning disability shifts to community settings Sub-programme 5 - Unscheduled care improved flow Sub-programme 6 - Waiting lists management Sub-programme 7 - Patient care focus for clinicians Sub-programme 8 - Improved workforce planning to match forecasted demand Sub-programme 9 - Continuing healthcare Sub-programme 10 - Improved procurement. 13
14 The following diagram illustrates the fundamental principles that the strategic objectives are trying to achieve and in particular the shift of resources and care increasingly towards prevention, selfcare and proactive care closer to home. Shift of Care Focus on long-term conditions (heart failure/frailty/dementia/copd) More effective responses to urgent care needs Advance care planning/end-of-life care plans Targeted input into care homes Access to integrated services through robust patient pathways Clear operational performance framework integrated with GP processes Ready access to specialist advice when needed Improved integration with 1 and 2 responders via NHS pathways Front load senior decision process, including primary care, acute physicians and geriatricians General Practice and out of hours Community Support WAST Emergency Department Clinical Decision Unit Inpatient Ward Objective: a left shift Of activity across the system As a function of time; Yesterday s urgent cases are today s acute cases and tomorrow s chronic cases Optimise emergency cases: Evidence-based management Multidisciplinary input from Physiotherapists/occupational therapist and community nurses Access to intermediate/social care Cont: Front-line geriatricians/acute physicians input Effective information-sharing with primary care/secondary care/ Community Redesign to reduce LoS with social and multidisciplinary input using a pull system Effective discharge management Ambulatory care for falls/ long-term conditions How we will deliver this: successful Programme Management requires a number of key imperatives which includes having effective, coordinated and well executed leadership (Executive Programme Steering Group), clinical ownership and management which impacts positively on organisational culture (our Organisational Strategy), strong and consistent performance management (our internal performance meetings). To deliver successfully organisation will, for each of the strategic objectives, nominate an Executive Director as the Senior Responsible Officer on behalf of the Board. Each Programme will have a clinical lead and service leads as project directors. All of these Programmes will be supported by the Programme Management Office and the Business Intelligence Unit, with specific inputs as follows: Write-up of the programmes in language that increases clinical and front-line support and understanding reflecting the Organisational Strategy and its emphasis on quality improvement, being a learning organisation, leadership and an improving organisation (rather than cost saving) Promoting literature that promotes the interests of patients as well as performance and financial targets Through the Business Intelligence Unit developing business intelligence metrics, which will be used both to measure progress of the current programmes and to identify areas where future work programmes need to focus. The metrics will be developed and delivered as part of the role of the Business Intelligence Unit updating the Programme Management Office and the Executive Programme Steering Group. Intelligence from Wales Audit Office Reports, other external reviews e.g. Welsh Government Delivery Unit, reports commissioned by Hywel Dda, Locality Based Resourcing, Patient Level Costing & Other Costing Benchmarking data, Daily/Weekly/Monthly/Annual activity data reports and Prescribing data. From our Performance Management Team triangulating the business intelligence from inyear progress against key performance indicators that reflect quality, innovation, productivity and prevention activities and workforce measures as well as financial estimates and show a clear trajectory from the current state to the future planned. The Programme Management Office will monitor delivery of the plan to achieve this but will not be responsible for performance management of individual targets. 14
15 Staff based in the Programme Management Office will report to the Director of Finance, Planning & Performance. Other staff will be associated to the Programme Management Office as the work they are leading will be supported by the Programme Management Office and the reporting line for key pieces of work that deliver the plan will be through the Programme Management Office. A key task for the Programme Management Office early on will be the alignment of current plans, each of which contributes to the achievement of the 10 strategic objectives. The first draft of how the individual plans map to our 10 strategic objectives can be found in Annex 2. However, in summary the linkages can be illustrated as the table below Strategic Objective Welsh Government Delivery Agreements Welsh Government Cluster Plans Intermediate Care Fund Pathfinder Projects Together for Health Delivery Plans Population Health Approach 1. To reduce overweight and obesity in our local population 2. To reduce the number of people who engage in risky behaviours and improve access to local support services 3. To improve the mental health and wellbeing of our local population through improved prevention and early intervention 4. To improve the prevention and management of cardiovascular disease in the local population 5. To increase survival rates for cancer through earlier diagnosis, faster access to treatment, and improved survivorship programmes 6. To improve the management of patients with diabetes, reducing acute exacerbations and long term health and wellness increasing 7. To improve community based support for patients with respiratory illness and reducing the need for hospital based care 8. To improve the care and management for frail and/or dementia patients by being more proactive and consistent in our approach to care aimed at maintaining health and independence 9. To improve productivity and quality of our services using the principles of prudency and the opportunities to innovate 10. To deliver, as a minimum requirement, Outcome and Delivery Framework target delivery and return the organisation to a sound financial footing over the lifetime of this plan As an illustration below, the table details the alignment of current initiatives to three of our strategic objectives. Each objective has been allocated an Executive Lead and the detail below will need to be supplemented with additional core activities and metrics for delivery. 15
16 Delivery Agreements Cluster Plans Each Cluster to include: Lifestyle Advocate /GP Lead/Primary Care Locality Manager/Practi ce Manager Lead Intermediate Care Fund (ICF) Pathfinder Projects Together for Health Delivery Plans Population Health Programme / Groups Strategic Objective 2 - To reduce the number of people who engage in risky behaviours and improve access to local support services In Hospital Smoking Cessation Service - Extension to all sites Early Years Smoking Cessation Services Community Pharmacy Level 3 Smoking Cessation. Increase number of pharmacies involved. Smoking Cessation through MIND Smoke Free Site Signage County Led Prevention: Strengthening GP cluster prevention plans Lifestyle advocates in GP clusters Fully establish cluster teams Strategic Objective 6 - To improve the management of patients with diabetes, reducing acute exacerbations and long term health and wellness increasing Early years obesity prevention Fully establish cluster teams Pre-diabetes service (Ceredigion North and Ceredigion South) Psychological Support (South Ceredigion and Teifi) Pocket Medic Project (Pembs North) Extension of Rapid Response Service in Carms Enhanced Chronic Conditions Nurse Practitioners Service in Pembs Enhance patient education around specific conditions and appropriate services to meet their needs. Liver Diabetes Neurological Digestive and Urological (Cardiovascular and Metabolic) Strategic Objective 8 - To improve the care and management for frail and/or dementia patients by being more proactive and consistent in our approach to care aimed at maintaining health and independence Care Closer to Home: Carmarthenshire; Ceredigion and Pembrokeshire: strengthened capacity and capability in community resource teams Increase primary care nonmedical independent prescribing Health Care Staff - Enhanced flu vaccination programme Support for Primary Care to improve uptake of flu vaccination for 65+ Fully establish cluster teams Strengthen GP led frailty services (Towy/Taff) Establish GP led frailty service (Amman Gwendraeth) Dementia review service (Amman Gwendraeth) Advanced Care Planning Nurses Project (Pembrokeshire North) Medicines Management Pharmacist Pembs South) Extension of Rapid Response Service in Carms Health & Social Care Support Worker Pembrokeshire reablement Admission Prevention and Discharge Support PIVOT (Pembs), TOCALS (Carms) AAA (Ceredigion) Extension of Multi-disciplinary Assessment Support Team (MAST) to 7 day working Elderly and Neurological 16
17 Our current service plans which will help to deliver the 10 strategic objectives, but need to be realigned, are set out by patient pathway as follows: Prevention and Public Health Proactive Care, Primary & Community Care and Continuing Healthcare Mental Health and Learning Disabilities Rapid Access to Diagnostics Planned Care Unscheduled Care Women & Children End of Life These current service plans are not yet structured to directly align to the 10 strategic objectives and it is our intention that this is rectified for the March 2016 submission. 3.2 Strategic objectives 1 to 10 Plans in support of their delivery including Prevention, General Practitioners Cluster Plans, Intermediate Care Funded Plans, Primary Care Delivery Agreements and Pathfinder Plans, Together for Health Delivery Plans, Mental Health Plans Prevention and Public Health Our plans are embedded in our Public Health Strategy (Annex 3) and mainly focus on strategic objectives 1, 2 and 3 and set the necessary foundations for a more preventative focus in future years, and aim to reduce the risk associated with lifestyle choices whilst tackling inequalities. Based on the needs of our population, the following three general approaches will be fully utilised in 2016/17: Linking to Strategic Objectives 1 and 2 we will continue our work on lifestyle Advocacy in Primary Care. Since 2014 Public Health has worked with Primary Care and more latterly through the clusters. The success of the lifestyle advocate approach will enable further work with clusters on the prevention agenda, and acknowledges the pivotal role of primary care in supporting our communities to stay healthy Linking to Strategic Objectives 1 to 8 all Public Health elements to improve service quality. As we develop clinical leadership within the organisation the Public Health Directorate will ensure that all of the public health elements are included. Innovatively the Public Health Directorate became a direct manager and provider of health visiting, school nursing and substance misuse services in January 2016 which will embed prevention at the heart of our service delivery Linking to Strategic Objectives 1 to 8 ensuring an Early Years focus. In agreement with Public Health Wales we have agreed to ensure a focus on the early years, and in particular the first 1000 days of life. This also fits well with the introduction of the Healthy Child Programme from January 2016 now supported by the very innovative management arrangements. Our current (2015/16) three high level priority areas of work reflect strategic objectives 1 and 2, and are as follows: Tackling overweight and obesity (includes reducing sedentary behaviour) Tackling smoking cessation Tackling alcohol and substance misuse. In addition we have three lower level priority areas of work in our Public Health Plan as follows: 17
18 Immunisation and Vaccination During 2015/16 we have undertaken work to ensure plans are fit for purpose and refreshed Mental wellbeing (strategic objective 3) PANDAs (Dementia Prevention) (strategic objective 8) We will continue to ensure that community resilience work features strongly as an approach with our partners, and our needs assessment work and asset approach will further evolve in line with the various statutory requirements. This has always been a key approach for the team but 2016/17 will see further significant developments. Hywel Dda University Health Board and the Public Health Directorate are working closely with Public Health Wales to plan and implement prevention and wellbeing programme for 2016/ /19. During quarter 3 and quarter /16 a series of national workshops have taken place between Public Health Wales, local Public Health teams and Local Health Boards on priority prevention topics. An additional meeting took place in January 2016 between Public Health Wales and local Public Health Teams Integrated Medium Term Plan leads to discuss and co-ordinate the approach to public health planning. The Director of Public Health for the seven Local Health Boards meet regularly as a group to discuss strategic public health issues. In addition work is underway to develop a Memorandum of Understanding between Hywel Dda University Health Board and Public Health Wales to describe the multiple and complex arrangements between the organisations. The University Health Board continues to acknowledge that health inequalities are unacceptable. We will continue to work with partners to tackle this agenda and our focus on the first 1000 days of life (early years) will enable a refreshed focus to this work across the three counties and in our cluster planning work. Working closely with County Directors to ensure that there is a consistent approach to addressing inequalities across all the University Health Board activity. Our 2015/16 Welsh Government funding has underwritten the following action plans which are mainly the subject of Delivery Agreements. Further information on our key approaches is set out in the tables below, these represent live monitoring returns (December 2015) which are a key delivery mechanism for the University Health Board. What we said we would do (Welsh Government Delivery Agreement) Smoking cessation Community Pharmacy Level 3 Smoking Cessation Service In Hospital Smoking Cessation Service Early Years Smoking Cessation Service Smoking Cessation Services through MIND Smoke Free Signage What we have done Job descriptions and person specifications for agreed posts complete and recruitment under way. Project Initiation Document and service specification for the Early Years smoking cessation service is complete. Welsh Government Section 64 funding ( 160,000) has been received to extend this smoking cessation support service (developed in Hywel Dda) across Wales. Programme commenced April 1st 2015, funding will support a three year programme. (MIND) PHW agreed funding to implement smoke free sites policy including signage. (Signage) Training and promotional materials being developed for each primary care cluster through protected time for learning sessions and the Lifestyle Advocates Project. What will success deliver: Key metrics 5% of smokers make a quit attempt using smoking cessation services 40% of treated smokers are CO validated as quit at 4 weeks. Uptake of smoking cessation in pregnancy increased to 25%. Increase the number of smokers receiving cessation support services prior to elective surgery to a minimum of 20% Action focus how we will do it and by when The aim for 2015/16 will be continued roll-out of the maternity pilot with additional activity to develop a Health Visitor intervention, specifically to target the early years (0-5 years). Outcome and Delivery Framework Targets. 18
19 What we said we would do (Welsh Government Delivery Agreement) What we have done What will success deliver: Key metrics Extending this service to Pembrokeshire and Ceredigion is a key action in the Respiratory Disease Delivery Plan and will not only ensure equitable provision across the University Health Board area but will also target those smokers with chronic conditions and those waiting for elective surgery. This will improve patient outcomes and reduce health and social care costs. The business case includes financial details for 2015/16 and 2016/17 which will include further pharmacy recruitment to ensure an equitable service is provided across the University Health Board. Welsh Government Section 64 funding ( 160,000) has been received to extend this smoking cessation support service (developed in Hywel Dda) across Wales. This programme will commence on April 1st 2015 and the funding will support a three year programme of activity. Public Health Wales have agreed funding ( 20,000) to ensure smoke free sites policy is implemented and reinforced. What we said we would do Immunisations and vaccinations Achieving service sustainability Improving access What we have done Development of internal and external communications campaigns for seasonal flu including: Purchase of additional cool bags undertaken and bags disseminated to community staff Clinical advocates to support community and healthcare staff flu campaigns identified in primary and secondary care settings Discussions with primary care on additional call/recall initiative taken place. Launch mid January Additional template resources developed for primary care to support actions to canvass eligible patients who have not presented for seasonal flu vaccination What will success deliver: Key metrics Increase childhood immunisation rates to 95% at 4years by March 2016 Increase healthcare staff flu vaccination (focus includes community) uptake rates to a minimum of 50% by March 2016 (currently 37.1%). Increase primary care vaccination rates for over 65 s i.e. influenza to 75% Increase the uptake of shingles vaccination amongst the eligible population from 44.1% to at least the Welsh average of 51.6% Increase the uptake of pneumococcal vaccination Increase the uptake of flu vaccination with pregnant women to 75% Increase the uptake of pertussis vaccination with pregnant women Increase the uptake of flu vaccination with at risk groups aged 6 months 64 years old from 46.3% to 75% Action focus how we will do it and by when A mop up initiative between January and March 2016 of children aged 3-5 years old, identified from the Health Visitor caseload with outstanding immunisations. A nurse to organise the vaccinations in conjunction with the Health Visitors and Flying Start Health Visitors. Overall aim is to increase the Outcome and Delivery Framework Targets target above 95% in all areas of Hywel Dda, in line with the Welsh Government Healthy Child Wales Programme. Support the Occupational Health Service with added extra staff during the flu season. Ensuring staff are vaccinated against flu, allows services to maintain staff numbers which has an effect on patient care. Purchasing of leaflets, posters, investing in patient stories, resources and further training for flu vaccinators wherever their setting. Occupational health use different methods and settings to improve the access for staff to have their flu vaccine in order to achieve service sustainability. Support Primary Care by employing staff to assist surgeries that have low uptake rates of flu vaccination. Marketing and advertising of flu clinics. What we said we would do Ensure further integration between the various elements of the University Health Board Directorates to ensure a population health focus What we have done Discussions with Public Health Consultant lead for primary care to ensure fit with University Health Board work-plan. Focus required on analysis of primary care data to ensure needs assessment has increased data (and interpretation) from a primary care perspective to drive the required transformational change. What will success deliver: Key metrics A positive prevention story from each cluster in local press/social media by end Quarter /16. Each of the refreshed cluster plans demonstrating a strengthened needs profile which demonstrates a quantifiable link between the needs 19
20 improved access (e.g. to Public Health related services) move towards community settings (this would occur at all points of the pathway given links to partners in social care). Draft job description prepared. Secondment opportunity being explored to ensure that key work can commence asap in 2016, whilst awaiting the job matching. Public Health Directorate now includes School Nurse and Health Visitors. This is pivotal to work with primary care with a preventative, self care and early intervention focus. profile/assessment and the development plans. Smarter intelligence by the refreshed needs profile showing understanding of the complexity and modelling around ageing population. A new partnership approach evident in the new refreshed cluster plans. Action focus how we will do it and by when Appoint a senior staff member to act as a University Health Board staff member for Director Public Health thus facilitating planning and communication process. The overall work objectives are now clear given the ten strategic priorities have been agreed through this Plan. What we said we would do Promoting health and wellbeing and invest in prevention Countyled prevention To develop primary and community care prevention services for each of the 7 Hywel Dda GP clusters What we have done Annual Report of Director of Public Health focused on self care/community resilience and community/primary care and was published at end of November DirectorofPublicHealthAnnualReport %28Cymraeg%29.pdf DirectorofPublicHealthAnnualReport %28English%29.pdf This report used is as a basis for discussions with patients, groups and communities and as a tool for our County Directors. Report shared with the A Regional Collaboration for Health RCH wellbeing team, and the Mid Wales Healthcare collaborative (MWHC). Meeting/Mini workshop held with county Directors to agree our approach to Community Resilience and Self Care activity based on the DPH report. Theoretical models discussed and the potential for synergistic aims with current local activity including Clusters. Reports finalised. Expenditure for 2015/16 confirmed. Briefing now being finalised by Head of emergency planning re Local Resilience Forum What will success deliver: Key metrics A workshop to be held to raise awareness amongst the wider primary care workforce of cluster prevention work and activity required. By next Cluster plan refresh all cluster plans to demonstrate quantifiable links between needs and development work. A patient engagement event to be arranged in each county to understand and progress our thinking on self care /prevention/ resilience agenda. Action focus how we will do it and by when To ensure that prevention is a focus for each County Director/Commissioner with an increased focus on cluster leadership and through the primary care workforce. What we said we would do What we have done What will success deliver: Key metrics Promoting health and wellbeing and invest in prevention early years obesity prevention Implementing actions at levels 1 and 2 of the All Wales Obesity Pathway prioritising Maternal Women and Early Years will contribute to Local public health team members facilitating discussions between primary care clusters, Local Authority and Third Sector partners to raise awareness of community based obesity prevention initiatives, alcohol brief advice, and promotion of the 5 ways to wellbeing, Let s Walk groups etc. Meeting held with Health Visitor leads regarding the promotion of 10 steps to 10 midwives in each county to have undertaken the training Eating for 1 Healthy for 2 Based on our original healthy preschool data base of settings, 50 settings will have had specific contact in relation to the obesity/healthy eating agenda. A physical activity scheme for 20
21 preventing obesity in children and subsequent associated morbidity and service demand. healthy weight (in conjunction with Public Health Wales). The first of five training days for midwives was delivered on the 10th December and was attended by 17 Midwives. The remaining four dates (January March) advised to midwives Contract awarded to undertake research with professionals in Hywel Dda working in maternal and early years to gain insight into their perceptions about overweight and obesity to inform future interventions in primary care. A marketing brief has been issued to tender to develop a resource that promotes healthy eating in pregnancy, particularly to those with low literacy levels. Local public health and National Exercise Referral Co-ordinators developing a service specification and model in order to start delivery in the Pregnancy service April Action focus how we will do it and by when pregnant women will be developed in partnership with the three local authorities for roll out in Quarter /17. Year 1 Level 1 Strengthen Early Years obesity prevention programmes/ services across primary care and community settings. Work in partnership to identify and develop ways of promoting and implementing the 10 steps to a healthy weight Eating for 1, Healthy for 2 training package is delivered to midwives and given support to promote with pregnant women Work in partnership with leisure services to develop physical activity programme for pregnant women Year 2 Level 2 Actions as year one (following review) continued plus roll out training materials and information for professionals on recognising and acting on childhood obesity Year 3 Level 2 Actions from years 1 and 2 (following review) plus implement evidenced based interventions for children aged 2 who are overweight or obese What we said we would do What we have done What will success deliver: Key metrics Early Years, First 1000 Days The monies are currently To be developed if monies are The proposal is to work innovatively with our midwifery, health visiting and school nursing colleagues to further reach our population on public health type issues. awaiting approval from Welsh Government approved. Action focus how we will do it and by when We will work with our partners to deliver a range of prevention and early intervention services to support improved outcomes for children, young people and their families. In particular the focus on the first 1,000 days of life and addressing the shortage of School Health Nurses and Health Visitors required to fully implement the Healthy Child Wales programme will be a key to ensuring effective contributions to Early Years health outcomes. In addition, the University Health Board will continue to work in partnership with Local Authorities to develop services that enable the University Health Board to make a proactive contribution to the Welsh Government tackling poverty programmes, Flying Start, Families First, Communities First and Supporting People all have the potential to make a positive impact on reducing inequalities in health as well as addressing the wider determinants of health and wellbeing. Securing Welsh Government grant funding (via Local Authorities) is critical to maintaining the development of proactive early intervention and prevention services. Team around the Family arrangements in each county provide a framework for front line children s services staff e.g. Health Visitors and School Nurses to identify the holistic needs of families and work collaboratively with other agencies to ensure these are addressed. Encouraging that professionals in primary and secondary care to consider more holistic needs will also be a key challenge for demonstrating that the University Health Board is meeting its statutory obligations under the Social Services & Wellbeing Act. 21
22 And in governance terms, these actions will be performance managed as follows: Planning Directive, Welsh Government Objective/ Target / Guidance: NHS Wales Outcomes Framework Outcome and Delivery Framework Targets Executive Lead (Senior Responsible Officer): Director of Public Health Profiles / Trajectories Yr 1 Yr 2 Yr 3 Executive Performance Management Forum Performance Monitoring and Assurance Meeting Chaired by CEO Board Governance: Committee or Sub-Committee Responsibility: Business Planning and Performance Assurance Committee Understanding our population needs provides the foundation for our planning. Prevention is most effectively delivered on a local basis where a detailed understanding of need allows for more focused and targeted delivery. Primary Care clusters will increasingly be the focal point for locality planning and the delivery of Proactive Care Closer to Home and this is discussed in the next section Proactive Care, Primary & Community Care and Continuing Healthcare Linking to all our strategic objectives, our emerging proactive care strategy will provide a guiding framework to meet the more holistic needs of our whole population. Proactive care is a commitment between provider and patient co-production, where both parties take an active role in managing the patient s needs to enable the patient to sustain and increase their health and functional ability. It will specifically support the further development of the Primary Care Strategy (Annex 4), Cluster and Community plans for population health improvement and progressing the delivery of more Care Closer to Home including a focus on frailty and dementia. The following table sets out the wide range of co-production initiatives currently underway. Patient and public strategic & operational co-production We will engage, in a number of different ways, with our population to formulate our proactive care strategy in a way that has meaning, can be directly applied and shifts power to people for their own choices and decisions Currently well person Aligns to prevention, health promotion & self care Consistent messaging through Choose Well Provision of clear information & signposting Wellness & mindfulness Timely and responsive access to the right place first time Clear Health Literacy action plan Make every contact count Optimising local assets Enabling healthy lifestyle choices Living with a diagnosis Positive early diagnosis & education/support to enable self management & shared decision making Promotion of telehealth Clear escalation and access pathway for specialist advice & treatment Migration of treatments closer to home Rapid discharge from acute care Holistic management of multiple conditions Seamless integrated working and information sharing Frail & complex person Collaborative holistic & integrated multi-disciplinary assessment involving patient and carers Clear understanding of what matters most to the patient to define outcomes Proactive advice, information & signposting to impact on the maintenance of health and wellbeing Clear escalation and access pathway for acute care including sharing of information Seamless integrated working and information sharing Alignment with the Social Services & Well-being (Wales) Act 22
23 Our Proactive Care Strategy allows us to build on the positive start already made through evaluation, discussion and engagement with our population. This co-produced plan will be implemented throughout 2016/17. During this time the Locality and Primary care initiated projects will be making a difference. Co-production Evolving the current Primary Care Patient Participation Network and CHC Liaison meetings Developing the pilot with NW Inspirations to consider alternative approaches to engagement & co-production Learning lessons from Ophelia project & the LD Team Total Communication approach Building on the Let's Talk Health discussions Currently well person Whole Health Board implementation of the Lifestyle Advocates programme Enhance the Choose Well campaign and align the developmental primary and community services Further development of Commnunity Pharmacy first port of call services such as Triage & Treat, Common AIlement and Emergency Dispensing schemes Review Primary Care Access across all independent contractors further considering out of core hours provision Develop Health Board wide Primary and Community phlebotomy service Living with a diagnosis Review the Locality-led pre-diabetic service pilot and consider lessons for wider implementation aligned to the All Wales Diabetes Enhanced service review Review the self-help condition specific Pocket Medic videos and outcomes for patients within the pilot Localities Review QOF achievement and integration with community based chronic condition nurses Review the pathways to specialist advice, diagnositic and services to proactively manage care outside of hospital Enhance INR based service provision in Primary & Community services Review the implementation of the chronic condition dashboards and their impact in supporting service redesign Evaluate the benefit to the Primary Care multi-disciplinary team of the addition of Practice-based pharmacists, advanced practitioner paramedic and therapist roles. Frail & complex person Adopt a small experimental approach to a range of locality led frailty projects to refine and share/roll out what works well. Continue & review the impact of the Community Resource Teams in managing complex patients at home, mitigating admissions and long lengths of stay and supporting timely and effective discharge Continue & review the advanced care planning Locality-led pilot utilising the third sector with a view to embedding good practice across the Health Board Develop case finding strategies to identify people who will remain in their homes for longer if they have early support to develop anticipatory / advanced care plans including the evaluation of MSDi & Audit+ Further develop the integrated Primary Care integrated team around the General Practitioners list including the development of new roles Evaluate the Locality-led community Dementia clinics and consider HB-wide implementation Support service development that facilitates a planned approach to support vulnerable people to retain function and life skills 23
24 Foundation of a resilient primary care service Primary Care in its broadest context delivers over 90% of the interventions our population experience, therefore resilient primary care services provides the foundation on which the care for our population is built. During 2015/16 the investment of additional Primary Care funding has enabled the development of key interventions that promotes a strengthening of this foundation. These are best described against our 7 Pillars for Primary Care which complements the Proactive Care Strategy as follows. Perception & Access Accessible high quality comprehensive healthcare services for all communities which offers timely and appropriate access which can be trusted REVIEW & ENHANCE: principles of good access, extended hours enhanced service, telephone consultation & triage, Choose Well campaign, Investors in Carers and Engagement framework in line with our population and contractor feedback Delivery agreement funding : Improving access & Moving services through triage & treat Dental funding : enhancing general dental access, walk in services, urgent access and domicillary care Integration Generalist led integrated services to deliver personalised costeffective care which works seemlessly across providers Workforce Promote a greater understanding of the value that the generalist brings to the whole system, expand the capacity and diversity of the workforce REVIEW & ENHANCE : Locality based Multi-Disciplinary Team working with CRT including frailty and end of life pilots to develop Business Case fo further investment from 2017 Delivery agreement funding : Enhance Locality integration through supporting Primary Care Contractor backfill time REVIEW & ENHANCE : Locality based workforce plans to enable development of holistic integrated development of the PCST to test new roles and ways of working. Pacesetter & workforce funding : enhance the role variation and functionality of the Primary Care Support Team Estates & Equipment Investment in suitable community based premises for delivering care, teaching & research REVIEW & ENHANCE : Primary and community estate portfoli review to be refreshed and aligned with proactive care strategy and potential for new streams of funding Delivery agreement funding : Sustainability through developing primary care estate - improvement grants and to manage contract transistions Pacesetter funding : creating a primary care hub capable of delivering whole system services Dental funding : developing a special care dental hub and a Design to Smile dental hub IM&T Greater use of information & technology to improve health & care and to ensure seemless communication across organisational boundaries to benefit the patient journey REVIEW & ENHANCE : use of chronic condition dashboards, risk stratification tools and the enhanced development of primary care IT to include solutions for mobile working, online booking and timely transfer of patient informationn Funding Align incentives and priorities to enable strategy and more holistic community based outcomes Variation Monitor, review and consider variation across the Localities to consider ways of ensuring the best use of resources and the most equitable outcome for the population REVIEW & ENHANCE : Root and branch review of funding into primary care and whether it supports the broader Proactive Care Strategy, including an assessment of QOF and establishment of alternative funding mechanisms based on activity management Delivery agreement funding : Moving services - INR & phlebotomy Pacesetter funding : development of proactive care federations or merged practices around a capitated budget REVIEW & ENHANCE : Review of dashboard and activity information to support peer review discussions in cluster to drive service improvement and improved equity to servicess Dental funding : enhanced Dental Practice Adviser time 24
25 Primary Care Plans What we said we would do What we have done so far What are we going to do next 2016/17- Sustainability General Medical Services (GMS) in particular are facing increasing strain due to workload demand and recruitment challenges. Funding will therefore be used to support the diversification of the workforce, enhance recruitment, develop federated and cluster approaches to collaboration and ensure premises are fit for future models of working. Increase in the number of primary care professionally trained, receiving training or pending the commencement of a course of Non Medical Independent Prescribing Commencement date of course by March 2016 course has commenced. Increase in the self reported engagement in cluster working Baseline measure August 2015 British Medical Association survey to be used as a baseline. Improvement to the infrastructure to enable services to be delivered locally Improvement grant scheme to be developed August 2015 completed. Agree with Local Medical Committee and share with Practices September 2015 completed. Submissions received via clusters and University Health Board panel let Nov 2015 completed. 2018/19 Additional training programme to be commissioned by October 2015 Review measure March 2016 pending development and distribution in March. Finalised improvement projects March 2016 projects currently underway. Moving Services For year 1 the focus will be embedding the Triage and Treat services within community pharmacies and shifting more anti-coagulation services and phlebotomy services out of the hospital and into primary care. Increase in Community Pharmacies offering Triage & Treat & increase in number of contacts. In 2014/15 2 pharmacies offered this service, by the end of 2015/16 the target is to increase this to at least 10. Increase in phlebotomy services offered within General Medical Services On there were 2 pharmacies offering Triage and Treat, by the end of December 2015 this number had increased to 12. (This exceeded our original target of 10 by the end of 2015/16) A significant number of pharmacies across the Hywel Dda area have expressed an interest in joining the programme and our pharmacy team will be working to establish further training opportunities to build capacity in the pharmacy triage and treat service Patient Information Leaflets have been produced for each of the localities that have participating pharmacies. The University Health Board are particularly mindful of the negotiations ongoing at an All Wales level regarding General Medical Services phlebotomy and has withheld undertaking any actions until this is resolved. Funding is available through this delivery agreement to support the outcome of these negotiations once known. All Practices have been offered the opportunity of increasing to a point of care model with an appropriate machine and training provided. Deadlines for expressions of interest were 31 st 25
26 Improving Access Citizen perception, as well as, actual service delivery contributes significantly to the trust our communities have accessing primary care services. Funding will be used to engage with our population through the Choose Well campaign and through local conversations as well as enhancing workload management during core hours. Increase in opening hours over 47.5hours per week in General Medical Services. At the end of 2014/15, 81% of practices achieved this threshold and by the end of 2015/16 the aspiration is to exceed 85%. Increase in number of people reached with the Choose Well message. Between January and April 2015, direct contact was made with 567 people as well as broader social networking. Aim to increase this in 2016/17 to over 2000 direct contacts in addition to an enhanced social media campaign. Increase in number of Patient Participation Groups. In 2014/15 December. Early discussions have been held with acute services to align future funding to ensure any shift and utilisation of funding is sustainable. A number of cluster plans have identified phlebotomy as a priority and are taking local plans forward; the future model will need to align with these. Examples developed so far include the appointment of community phlebotomy staff embedded within communities, through to full service phlebotomy clinics serving a community. Each cluster has developed plans to further develop community phlebotomy provision. In some clusters this has seen practices employ community phlebotomy nurses, in another cluster we have seen the creation of a community drop in phlebotomy service in order to increase the amount of patients seen within a primary setting As at the end of September this had increased from 81% to 83%. Plan to further increase this and achieve 85% by the end of 2015/16. Access is part of the prioritisation criteria for the infrastructure/improvement grant scheme. 13 practices have undertaken training on 2 differing methods of managing their workload. An evaluation of the training and the subsequent outcomes is currently being undertaken. 10 practices have indicated that they have or will be making changes as a result of the training. Choose well promotion on the Hywel Dda Facebook page and twitter page. This also includes videos and leaflets. Choose Well attended the Pembrokeshire Show as well as Aberystwyth fresher s fair and had over 400 contacts and conversations. The Choose well leads from the Primary Care team have ensured that that every opportunity to engage with members of the public is seized. This includes Hywel Dda s regular Lets Talk Health events, Patient Participation Group groups and all staff inductions. To date we have reached 1400 direct interactions. The team continue to have Choose Well discussions at all corporate inductions to facilitate a cascade of awareness and information throughout the organisation, each month this reaches approximately 75 new employees. We have also developed an enhanced social media campaign in order to increase our message reach. 26
27 there were 3 representing a population of 44,000; in 2015/16 it is hoped that the number will increase to 6-8 with an increase of another 19 30,000 patients. In preparation for the onset of winter the team have increased social media activity in order to provide the public with greater awareness of the full range of services available to them. Work continues with eight General Practitioners practices currently seeking to develop a Patient Participation Group in 2015/16 or 2016/17. A number of the practices are facing challenges such as merging with a neighbour, taking on a second General Medical Services contract and sickness absence. Discussions are ongoing to support each practice to utilise these challenges to promote a strong start to the groups. In December a new Patient Participation Group formed in Ceredigion with members attending their first Patient Participation Group Network meeting. A patient engagement framework has been developed to support practices to progress towards improved engagement with their populations. This has been discussed broadly with patient groups and stakeholder, it will be launched January Connection has been made with the Coproduction Network in Wales to commence discussions to support patient advocates. Cluster Plans What we said we were going to do What we have done so far What are we going to do next 2016/17 (up to 2018/19) Establish 7 clusters / locality areas. Appoint 7 General Practitioners leads. Create 7 Primary care locality development managers. Recruit 7 practice manager leads. Clusters to include Public Health, Medicines Management, Community Resource Teams as well as colleagues from local authorities 7 clusters now fully established. 7 General Practitioners leads active. 7 Primary care locality development managers active. 2 practice manager leads in post. All clusters include representatives from Community Pharmacy, Dental, Optometrists and wider community services. Investigate new model of working / federations Build strong cluster relationships Initiate leadership training and strong management Appoint 5 further practice manager leads Ensure full active representation in every cluster meeting and in the planning process 27
28 What are we going to do next 2016/17 (up to 2018/19) by cluster Carmarthenshire Towy/Taf Locality Lifestyle Advocates - embedding healthy lifestyle and prevention by identifying enthusiastic individuals to become skilled advocates of lifestyle behaviour change: Year 1 - delivery of the Lifestyle Behaviour Change Interventions training; Year 2 - further training as identified by the advocates e.g. Mental Health First Aid; Foodwise; Alcohol Brief Intervention; Smoking Cessation; and to develop (in partnership with Public Health) performance indicators; and Year 3 - receive train the trainer training. Frailty - practices to nominate a clinical frailty lead to identify frail patients utilising a practice based information technology system. Patients to have a written Stay Well plan, which includes details of carer, health and social care summary, optimisation and maintenance plan, escalation and urgent care plan. General Practitioners to be offered training in frailty recognition. Support and extension of Multi-Disciplinary Team working in line with Multi-Disciplinary Team Best Practice Guidance. Training Budget - address training and workforce development. Evaluation of outcomes will include : Does the Lifestyle Advocate Programme lead to skilled and confident advocates actively promoting healthy lifestyle ethos and practice? (Advocates) Does an advocacy approach lead to an increase in activity to promote healthy lifestyles within Primary Care? (Clusters and practices) Number of stay well plans completed during year - Target of 20 plans per 1700 patients in the first year Number of low level assessments performed by Generic Technician Outcome of Generic Technician assessment Reduction in Occupational Therapy waiting list currently 12 weeks in 3Ts Improved recording and review of Multi-Disciplinary Team actions and follow-up Carmarthenshire Amman Gwendraeth Locality Lifestyle Advocates Programme As Towy Taf Locality Frailty Service The cluster has recognised frailty as a priority and developed a model which also incorporates the other cluster priority of resilient general practice. Integrated Frailty Service Pilot the cluster was unable to recruit a dedicated General Practitioner to lead on frailty across the area. It has now been agreed to have three separate pilots that come together to create an integrated frailty service. This is made up of 3 elements:- Care Home Pilot General Practitioners will visit all care homes within the cluster to offer services and reviews of their populations with regards to their frailty needs Cluster pharmacist A pharmacist will visit all care homes across the cluster to conduct medication reviews to support the General Practitioners. Cluster Advanced Nurse Practitioner (frailty) We will be appointing an advanced nurse practitioner to lead on frailty programmes across the cluster Primary Care Phlebotomy Service to continue with the provision of this service for non-housebound patients, delivered by phlebotomists across the locality; held in the General Practitioners practice. General Practitioner Dementia Review Clinic the Community Memory Clinic continues with a revised geographical spread to best meet local needs. January 2016 due to the success of the initial dementia clinics and continued support of the General Practitioners a second clinic was established in the South of the cluster area. This will allow us to offer a whole population service. Vision 360 All practices will be adopting this software. This will allow cross practice working, information sharing and the creation of continuous care for our population. Evaluation of outcomes will include : Increase in the number of medication and care reviews for frail patients Reduced case time spent undertaking phlebotomy by trained community nurses enabling more time for complex patients Increased support for dementia patients and higher diagnostic rate Carmarthenshire Llanelli Locality Lifestyle Advocates Programme as Towy Taf Locality Community Phlebotomy develop community based phlebotomy clinics in Llanelli with additional phlebotomists and re-locating hospital staff. One centre will run an appointment system for the initial 12 months, whilst the appointment centre is established. Further accommodation to be identified in Burry Port and the Llwynhendy/Llangennech areas. Training Education and Equipment Budget to support cluster development through training, education and provision of equipment, if need identified. 28
29 Multi Disciplinary Teams to support backfill of General Practitioners attendance at Multi-Disciplinary Team meetings. Chronic Obstructive Pulmonary Disease Plus Exercise Programme to expand this programme to improve access to community based combined education and exercise classes for people with Chronic Obstructive Pulmonary Disease. Evaluation of outcomes will include : Reduction in phlebotomy waiting times at Prince Philip Hospital; Improved coordination of care; Reduced emergency admissions North Ceredigion Locality Pre-Diabetes Care: to develop an integrated project to reduce the risk of developing diabetes. This project has General Practitioners surgeries working collaboratively with the dietetic department, Public Health Wales, Third Sector, Aberystwyth University, Education for patient volunteers, National Exercise Referral Scheme and lifestyle advocates, following NICE guidelines to proactively screen and identify those at risk. Once their risk score is known they will be signposted and encouraged to attend support services. As part of this, the Cluster is supporting the Lifestyle Advocates Programme (as Towy Taf Locality) and increase the capacity of the food wise programme delivery. 6 Practices have lifestyle advocates trained in delivering the Foodwise Programme. Practices have been screening and conducting 30 minute consultations with their at high risk patients. The researcher appointed to support the evaluation of the project Classes commenced delivering a bespoke exercise class for diabetic/obese National Exercise Referral Scheme are Planning to run Foodwise programmes EPP are supporting cluster with Foodwise delivery dates being set to begin 1 st programme Flu advert placed in local newspaper and Practices being proactive to encourage patients to have their flu vaccinations. Evaluation of outcomes will include : Number of people diagnosed as high risk of developing diabetes Number of those taking up the Foodwise and activity programmes Numbers continuing with a healthier lifestyle 12months later and number of people reducing their risk in a 12month follow up. Increase in numbers having the flu vaccination within the cluster from last year. South Ceredigion and Teifi Valley Locality Frailty and Chronic Conditions Nurse and Pharmacist - work collaboratively and assist General Practitioners Practices to avoid unplanned admission with proactive case findings and patient review of vulnerable patients who are not easy to reach. The Frailty and Chronic Disease Cluster Nurse will case manage people with long term conditions/complex needs, at a high risk of unplanned hospital admission with the aim of reducing unplanned admissions and improving health outcomes for that group. The Frailty and Chronic Conditions Cluster Pharmacist will lead and develop the role of the pharmacist working as part of a Multi-Disciplinary Team across a cluster of General Practitioners practices; provide expert pharmaceutical advice, in line with Prudent Prescribing principles and the promotion of evidence based clinically and cost effective medicines. Training New Staff/District Nurses - to assist finding appropriate patients it is planned to use the risk stratification software MSDI tool. The evaluation metrics will be looking at historic data sets of Accident and Emergency, attendances, unscheduled admissions and Out of Hours contacts and compare data to current to evaluate what changes and improvements have been made. Access Plans and Capacity/Demand to ensure practices are treating patients with the greatest illness first. This should impact on secondary care contacts - the same data sets will be examined. Multi-Disciplinary Team Pilot (end of March 2016) to create an environment of co-operation between agencies to resolve difficulties for patients with complex needs. Improvement to the quality of patient s lives and health and reduction in admissions - the same data sets will be examined to check the quantitative element. Additional Medicine Management Hours - to undertake specific audits. Commission Psychological Interventions - to improve the psychological management of patients with chronic diseases and empowerment of patients to take responsibility for their health and wellbeing. Evaluation of outcomes will include : Reductions in secondary care unplanned attendances and Out of Hours contacts for frail population Practices to undertake patient satisfaction surveys where systems have changed to Dr First or any other access changes. Review patient records of patients aged on 10 or more medications to see whether prescribing should be reviewed. 29
30 North Pembrokeshire Locality Community Phlebotomists to provide a phlebotomy service to primary care and community. Paul Sartori Advance Care Planning Nurses - appointment of 1.2 WTE (3 part-time posts linked to specific practices) Advanced Care Planning (ACP) Nurse Facilitators to the Paul Sartori Foundation. To assist practices in identifying people for whom Advanced Care Planning might be most urgent and relevant, and working with those patients to complete Plans; patients on the Palliative Care Register, and patients with chronic conditions. Includes funding for additional ad hoc counselling time for people in whom the process of Advanced Care Planning identifies a need. Advanced Care Planning can reduce avoidable hospital admissions form home and care homes, reduce healthcare costs, improve patient involvement in decision making, improve patient satisfaction with care services and reduce stress, depression and anxiety in the bereaved family members. Pembrokeshire Counselling Services - Improved access and further training and development of counsellors. Chronic Obstructive Pulmonary Disease+: EPP Chronic Obstructive Pulmonary Disease Self-Management and exercise programme with the aim of enabling Chronic Obstructive Pulmonary Disease patients to maintain their day to day activities for longer thus slowing the progression of the disease reducing the need to become dependent on others. Two programmes will run in early Pocket Medic A pilot project which allows clinicians to prescribe information to their patients to support the diagnosis provided in the surgery. It aims to help people revisit the information provided by General Practitioners and Practice Nurses and share it with their family if they wish. The information is in the form of a series of short films: about Type 2 Diabetes, Chronic Obstructive Pulmonary Disease, Wellbeing (depression and anxiety), Heart Failure and Post Cancer Survivorship. Pembrokeshire Young Person s Counselling Service - providing access to counselling service providing one day s counselling a week and linking in with the Crisis Counselling Service. The service will support young people presenting with low self-esteem, depression, sexual expressions, drug use, peer pressure, bereavement and anger issues. This links in with the funding of Pembrokeshire Counselling Service which has been put in place via cluster funding for the adult population. Evaluation of outcomes will include : Percentage of patients with an Advanced Care Plan in place Percentage of patients on Palliative Care Register with an Advance Care Plan in place Number of clients signposted out to alternative service provision from counselling service Pembrokeshire South Locality Community Phlebotomy Service to introduce a Community Phlebotomy Service attached to the District Nursing Service. 3 members of staff appointed Community Heart Failure Nurse - 0.5WTE for the south of the County to improve community cardiac services within South Pembrokeshire. Whilst the cluster mirrors the All Wales prevalence figure for Heart Failure (0.9%), access to a local cardiologist is limited. A community based nurse will support approximately 430 patients, improve medication management, and improve communication with General Practitioners, with a cluster based Health Promotion advisor appointed on an interim basis due to recruitment challenges Cluster Pharmacist work with General Practitioners practices within nursing and residential homes to undertake medication reviews; Prudent Prescribing Principles. Work with individual practices to improve systems and processes ensuring that discharge medications are correct and reviewed through appointment of a Community Pharmacist Evaluation of outcomes will include : Numbers of patients seen and medication reviews undertaken including the numbers of medications increased/reviewed and any cost savings identified. Numbers of people who have Advanced Care Plans in place and numbers of people who have been made aware of the need to have one in place Numbers of people accessing Community Obesity Programmes Increase in flu immunisations And in governance terms, these actions will be performance managed as follows: Planning Directive, Welsh Government Objective/ Target / Guidance: NHS Wales Outcomes Framework Outcome and Delivery Framework Targets Executive Lead (Senior Responsible Officer): Director of Commissioning/Therap ies and Health Science Profiles / Trajectories Yr Yr Yr Executive Performance Management Forum Performance Monitoring and Assurance Meeting Chaired by CEO Board Governance: Committee or Sub-Committee Responsibility: Business Planning and Performance Assurance Committee 30
31 Pro-active Community Care The University Health Board has established through successive Integrated Medium Term Plans the clear case for change in how we deliver services, particularly the need for increased integration of health and social care. This to respond to the requirements of the Social Services and Well-being (Wales) Act 2014, to place the individual at the centre with care services becoming increasingly accessible in local areas. To this end, our core aims for proactive care are: To deliver an end-to-end system of care with all our care partners in an integrated way to deliver prudent healthcare. To ensure patients and their families receive community services that are safe and of the highest quality and provide the best experience and outcomes as cost effectively and as locally as possible. As part of prudent healthcare, we want to develop community services which encourage a culture of self-management whilst helping and supporting people to optimise and maintain their own health, well-being and independence. To work with our population, our partners and our staff to deliver care that is responsive to local needs and addresses inequalities. Our intention remains to deliver service transformation which results in a significant shift in the way services are provided across hospitals and the community, with elements of care moving from hospitals to the community where safe and effective to do so. Delivering care in this way will support Care Closer to Home for our frail and elderly population. The delivery of community services are increasingly focused through Community Resource Teams. These provide a multidisciplinary approach to the management of patients in the community, preventing unnecessary admission to hospital. Complementary to the Community Resource Teams will be the development of enhanced facilitated discharge services, which will similarly provide a team approach to discharge facilitation. The Community Resource Teams and discharge liaison will improve patient flow through the health and social care system. Working with our local Government partners, in the Mid and West Wales Health and Social Care Collaborative, service investment has come through the Intermediate Care Fund, to fund key developments (known by different names, across the three counties) to ensure that patients are enabled to leave hospital, and receive more appropriate community based care. These are the Transfer of Care Advice Liaison Service (TOCALS), Multi Agency Support Team (MAST) and Admission Avoidance Assessment (AAA). These services work in an integrated system with Secondary Care services, and also dovetail with modernised practice such as Hot Clinics; the Frailty pathway including Rapid access multi-disciplinary frailty clinics; and improved patient management over seven days of the week. Our 2015/16 Welsh Government funding has underwritten the following action plans which are the main subject of Delivery Agreements. Further information on our key approaches is set out in the tables below, these represent live monitoring returns (December 2015) which are a key delivery mechanism for the University Health Board. Ceredigion What we said we would do What we have done so far What are we going to do next 2016/ /19 Develop senior posts to strengthen leadership and governance across the nursing services. The development of multidisciplinary working will support Primary Care and deliver care management and care plans for patients, focussing on those with Pilot Multi-Disciplinary Teams undertaken fortnightly in Newcastle Emlyn Surgery. A schedule of the roll out of Multi-Disciplinary Teams planned. Emphasised uptake of flu immunisations. Metrics to include the following. Increase in the number of people who have an Advance Care Plan - To increase by 10% across the Community Nursing Service Improvement in the number of those who choose preferred place of death To increase by 10% Increase in the number of patients 31
32 chronic conditions to improve selfmanagement and avoid unnecessary hospital admissions. Introduce the Community Resource Teams. Integration of the Health and Social Care Core Services Integrated Care Fund third sector integration facilitators Accessing alternatives to admission. Based on the frailty model to avoid unnecessary admissions and facilitate timely discharge. To support the reconfiguration of community nursing services: Increasing core community nursing capacity Introduce Community Resource Teams Provide additional specialist support Provide care co-ordination Provide a psychological service within general healthcare in order to meet the standards and guidelines for a range of conditions for psychological care. Provide a service that supports staff in the management of individuals with chronic conditions. This is an evidence based approach with the intention of improving selfmanagement and reducing the number of appointments with General Practitioners and reducing admissions to hospitals Improved management of the medically fit within Bronglais. Progress made in South Ceredigion with the implementation of the Core Community Nursing Service. Interim beds commissioned in nursing homes in and around Cardigan have been a successful and flexible option to those requiring a short term period of care. Developed a service model. Joint funded locality managers in post. Target intervention teams (short term / core social care and therapy services). Third sector integration facilitators embedded into weekly meetings in Bronglais. Strengthening of local 3 rd sector developments. Introduced a weekly meeting, involving multi-disciplinary team, drawn from the Community Resource Team. Posts have enabled the core nursing teams have been reconfigured to provide additional services, allowing the new recruits to backfill duties within the community, including: Specialist nurse in the minor injuries care. Introduction of leg clinics in Cardigan, and subsequent extension to the North Locality. A diabetic specialist nurse. A palliative care nurse in the North Locality to provide leadership across Ceredigion Lead psychologist appointed to provide leadership and management of services across the University Health Board Psychologists appointed to the pain service and musculoskeletal service 2 psychologist appointed to focus on the training of staff in primary care and community services to improve the management of individuals with chronic conditions accessing reablement To increase by 10% Reduction in number of care packages following reablement To decrease to 55% from the current level of 40% Reduction in admissions and readmission, Chronic Conditions Basket of Eight 10% reduction in chronic conditions admissions 15% reduction in chronic conditions readmissions 5% reduction in chronic conditions admissions Reduction in Delayed Transfers of Care Increase in carers assessment To increase by 5% Increase number of Multi-Disciplinary Teams taking place in General Practitioners practices To increase by 10% Each Continence nurse to reduce admissions by 1 per week based on prevalence of presenting conditions ( 3 nurses proposed) Multi-disciplinary meetings across all Primary Care services in Ceredigion. Community Resource Teams will be operational in the North Ceredigion Locality, following the transfer of resources from Tregaron Hospital, as the Clych Caron Capital project develops. Further development of interim leads across Ceredigion in response to need. A commissioning strategy to improve the resilience of the independent sector. Consolidation of service model, integrated governance and performance framework. Linked into the Community Resource Teams and multi-disciplinary discussions across Ceredigion. Improve the 3 rd Sector co-operation in line with the Health, Social Care and Wellbeing Act Further appointment of a psychologist for chronic condition management 32
33 Carmarthenshire What we said we would do What we have done so far What are we going to do next 2016/ /19 The new posts identified in Carmarthenshire will strengthen the model of service by providing a more proactive approach to care provision, more timely response and through using risk stratification, reducing demand for Unscheduled Care. Recruitment of the staff will provide Improved capacity in order to deliver the Community Resource Team model. Provide designated support to the discrete populations served by General Practitioners practices. Flexible and responsive workforce dependent on the level of activity within the communities and a reduction in duplication. Provide training, support, leadership and Governance to the Community Resource Team s. Including the wider commissioned services ie. Domiciliary care workers, Nursing Homes. The nurses will be based within the Community Resource Team (Community Resource Team) which are co-terminus with the Localities. Community Resource team expanded through appointment of 3 specialist Tissue Viability Nurses, 3 Continence Nurses and 3 Community Nursing Support Nurses split equally across the three localities. In advance of recruitment into these posts, current staffing has been enhanced through the use of Bank and additional hours. This has provided additional capacity for the Specialist and Community Nursing to work together to plan for the introduction of the new community service including a limited number of Leg Ulcer and Continence Clinics. In addition to the basic service development actions there has been a focus on the establishment of the governance framework, service baselining, delivery of a training and supervision programme. In advance of recruitment to the Community Nursing Support additional Health Care Support hours have been secured to strengthen core community nursing and release qualified nursing capacity to provide the more complex care and support care co-ordination. Outcome and Delivery Framework Targets Reduction in admissions and readmission, Chronic Conditions Basket of Eight 15% reduction in chronic conditions readmissions 5% reduction in chronic conditions admissions Baseline position: rolling 12 months ending Jan 15 (253 readmissions and 1245 admissions) Reduction in Delayed Transfers of Care (per 10,000 University Health Board population non mental health.) Baseline position: rolling 12 months ending June 15 ( 58.2) End of Life Care Increase in the number of people who have an Advance Care Plan - To increase by 10% across the Community Nursing Service % of patients who fulfilled their wish to die at preferred place of death (100% target) Re-ablement Number of people who have completed re-ablement: Number of people not needing ongoing support following reablement. Target 55%, current level of 40% Number of people needing reduced levels of care following re-ablement Carers Increase in carers assessment To increase by 5% Primary Care Roll out Primary Care based Multi-Disciplinary Teams in all practices. Establish baseline and agree Locality based targets to include frequency Specialist Nurses Establish leg ulcer clinics in each Locality Urinary Tract Infection related admissions to reduce by 3 per week. Consolidate posts and evaluate impact. Transfer of Care Advice & Liaison Service (TOCALS) 33
34 What we said we would do What we have done so far What are we going to do next 2016/ /19 To establish dedicated Multidisciplinary team at both acute hospital sites who will support the rapid assessment, care & discharge planning for people who are at increased risk of long term reduced level of function as a result of a hospital admission. This project will also incorporate the establishment of two Frailty Champion posts on Ward 1 in Prince Philip Hospital. Recruitment has been completed. Teams have been established in both Prince Philip Hospital and Glangwili. Impact has already been seen in improving patient flow in both acute hospitals. Review and integrate nursing roles within the teams including Discharge Liaison Nurses. Rapid Response Domiciliary Care Service This service will support the provision of increased care closer to home as part of the integrated community locality model by meeting the needs of local communities. Cartref Cynnes (Convalescence Beds) Enabling the lease of 2 apartments within the Cartref Cynnes Extra Care Facility to add to the range of intermediate accommodation available to people in Carmarthenshire for the purpose of enabling older people to improve their independence by providing a range of integrated services. Locality Community Resilience Co-ordinators This will mainstream the roles (previously known as Third Sector Health & Social Care Brokers) within the Integrated Services structure for Older Adults. 1 per locality. Health & Social Care Support Worker The purpose is to work across the health and social care interface. Specifically, up-skilling social care staff in order to improve the quality of their work as well as reducing pressures on community nursing. Team established Review of access underway and review of staffing structure to maximise care underway Teams available from December 2015 Recruitment complete Transfer current staff from Carmarthen Association of Voluntary Services to University Health Board. Pilot in Llys Y Bryn An implementation plan is currently being drawn up to roll out to two further Local Authority Care Homes in the County) move to what we have done to date) Integrate teams with other domiciliary care teams Evaluate impact and explore potential for additional beds Evaluate impact Evaluate outcomes Pembrokeshire What we said we would do What we have done so far What are we going to do next 2016/ /19 The vision for Care Closer to Home in Pembrokeshire is to have multidisciplinary teams aligned to General Practitioners clusters. Each General Practitioners practice to have a Multidisciplinary Team Meeting (Multi-Disciplinary Team) with General Practitioners, Community Resource Teams and including the Third Sector Broker. The Community & Primary Care management structure has been developed, consulted on and is now being taken forward. The Head of Adult Care has been appointed within the Local Authority and is appointing key leadership roles. Two Locality Managers have been appointed to provide leadership and Increase in the number of people who have an Advance Care Plan - to increase by 10% across the Community Nursing Service Additional funding for Paul Sartori for Advanced Care Planning in North. Improvement in the number of those who choose preferred place of death To increase by 10% - Increased Acute Response Team capacity. Increase in the number of patients accessing reablement To increase 34
35 What we said we would do What we have done so far What are we going to do next 2016/ /19 The aim is to identify individuals at risk of hospitalisation and manage their care in the Community. The focus is on integrated services, care and support for older people, particularly the frail elderly or those with complex needs including dementia. direction to the development of localities. Workshops are planned with these newly established Managerial teams of Community, Primary Care, Local Authority and 3 rd Sector to reestablish and realign the localities to the General Practitioner Clusters. Refocus the Community Resource Teams to support the General Practitioners cluster developments aligning with specific General Practitioners practices. Greater focus on the preventative agenda in early identification of those individuals at risk, frail and multiple co morbidities. Specifically: Establish and reinforce care coordination Improve capacity of the services provided Provide additional specialist support Provide increased therapy input Provide analysis of the local population needs and a Multi- Disciplinary Team response within the catchment area of each General Practitioners. Provide a joined up approach between the Local Authority, Health and Third Sector to ensure timely coordinated interventions within the Multi-Disciplinary Team process. Further enhance models of care to ensure robustness and support the broader cluster developments. Encouraging new ways of delivery resulting in increased resilience and self-care. Provide a skilled workforce and generic training for staff across Health and Social Care. Provide training, support, leadership and governance to the Community Resource Teams. Improve capacity in order to deliver Advanced Nurse Practitioner Frailty appointed due to commenced in post November Consultant Care of Elderly appointed to lead and support the development of the Frailty model within Pembrokeshire. Identifying pilot practices to introduce Audit + / Risk prediction tool to support the introduction of the Frailty model within Pembrokeshire. Pilot to formulate the preventative agenda in early identification of those individuals at risk, frail and multiple co morbidities. Additional Chronic Condition Nurse Practitioner is being recruited to give each Community Resource Team a dedicated Chronic Condition Nurse Practitioner to support and develop the Chronic condition service model. The South East Pembrokeshire model of integrated care has been developing a fully integrated provision of services; primary, community, Local authority and third sector acting as a way finder for the rest of the county. Ensure 100% completion of appraisal for community staff, Training needs analysis, Specialist training modules to develop community nursing staff. Development of 4 Leg Ulcer clinics. Community Phlebotomy service by 10% Reduction in number of care packages following reablement To decrease to 55% from the current level of 40% Reduction in admissions and readmission, Chronic Conditions Basket of Eight 10% reduction in chronic conditions admissions - Chronic Condition Nurse Practitioner 15% reduction in chronic conditions readmissions Heart Failure Nurse 5% reduction in chronic conditions admissions Acute Response Team Capacity, Multi Agency Support Team Reduction in Delayed Transfers of Care To meet Discharge Liaison Increase number of Multi-Disciplinary Teams taking place in General Practitioners practices To increase by 10% - Frailty Chronic Condition Nurse Practitioner Develop joint priorities with Local authority in driving forward integration in line with Welsh Government strategic direction and joint commissioning opportunities. Develop Localities developmental plans in line with General Practitioners clusters, further developing the Community Resource Team model within the County. Review and refine frailty model, realigning resources to further progress developments. Progress outcome of service review in South Pembrokeshire Health and Social Care Resource Centre, realigning resources to develop Community Resource Teams. Develop the commissioning strategy to improve the resilience and readiness of the independent sector. Consolidation of service model, integrated governance and performance framework. Introduce a programme of Multi- Disciplinary Team working across the 15 General Practitioner practices. Ensure engagement of General Practitioners, Primary Care, Local authority staff within the Community 35
36 What we said we would do What we have done so far What are we going to do next 2016/ /19 the Community Resource Team model and provide designated support to the discrete populations served by General Practitioners practices. established to support the General Practitioners practices. Resource Teams. Develop a frailty model supporting the delivery of care through the Community Resource Teams. Development of the Acute Response Team to ensure 24 hours community nursing service is strengthened. Heart Failure Clinical Nurse Specialist appointed. Improve the direct clinical support to General Practitioners through Multi- Disciplinary Team working, introducing care planning and regular reviews in order to increase the time available for General Practitioners to provide skilled medical support to patients. Introduce new roles to support the acuity of the population served. Develop a model of care for domiciliary home care. Provide greater choice to patients and their carers in receiving care at home, including end of life care. The development of the Multi-agency Assessment Support Team based in the Emergency Department at Withybush General Hospital, to provide 7 day service. Further development of hospice at home as identified in the palliative care strategy for Hywel Dda. Increase in nursing element of the team. The Intermediate Care Fund has supported the Occupational Therapist and Physiotherapist positions required to cover the 7 day working rota and provision of a community in reach service supporting Multi Agency Support Team. Consolidation of service model, integrated governance and performance framework, monitoring trends, quality outcomes. Proactive Care Long-term Healthcare (Continuing Healthcare) The long term vision for continuing healthcare focuses on delivery of prudent healthcare through the implementation of the integration agenda with Local Authorities and agreement on joint assessments, pooled budgets and a joint focus of commissioning from the Independent Sector for Long Term Care. In the interim, and for the 2015/ /18 financial years, the plan will be around embedding long-term Healthcare/Continuing Health Care within the core community services provision increasing the delivery of hands on care provision through the Community Resource Teams within each County. Central to delivering this will be the need for a change in culture within the University Health Board towards long-term care and the way patients with complex needs are assessed and managed. A key focus of the 2015/16 and 2016/17 plan is the development of in house domiciliary care provision that will deliver care to complex clients within their own homes, negating the need for the purchasing of care from the independent sector, resulting in the re-investment of resource with the Community Resource Teams. Supervised through the Community Resource Teams this work will significantly strengthen both the governance and financial arrangements around long-term care; enable increased economies of scale in Community Teams; reduce duplication and waste and move to a flexible model of care based on managed care approach in the delivery of care hours to patients. By April 2017, the University Health Board aims to be delivering 80% of Domiciliary Care through its core community provision. To increase the capacity and efficiencies of this shift of investment from the independent sector to the NHS for the delivery of domiciliary services, the University Health Board will deliver a number of additional schemes. Delivery of these schemes will ensure the best expectations and outcomes for our complex patients and their families. 36
37 Processes will be refined to ensure that assessment for long-term care is always undertaken in an appropriate setting and not on an acute ward. We plan to invest in strengthening reablement services to ensure that access to services is avoidable. It is forecasted that by enabling a culture and ethos where complex care cases are able to access re-ablement services routinely will enable the optimisation of outcomes and reduce the overall ongoing cost and care requirements to the organisation. It will also optimise care to patients who have long term needs. The integration of the service into the wider community service will provide for a re-balancing of equitable care with patients who have needs that make them eligible for long-term care offered the same suite of services including re-ablement as those with other conditions within the community setting. The broad vision will be for patients who have long term needs to access re-ablement for a period, post discharge and pre long-term care assessment. It is proposed that the assessment for longterm care would take place at the end of a 6 week re-ablement period. This model allows the opportunity for the patient to gain confidence and further convalescence time through the provision of integrated services in the community, before a determination is made regarding the longer term care requirements. Where a patient is not able to be discharged for re-ablement, we will invest in assessment beds within the Nursing Home Sector. The ethos of the assessment beds will be similar to the home based model, and will enable patients to reach their full potential and optimisation in their recovery prior to an assessment for Long Term Care provision and long term funding commitment. Where on-going long term funding is required following re-ablement/ assessment, we will revise and strengthen our Sustainability Policy to ensure that packages of care commissioned are fair, equitable and demonstrate value for money. We will support our care homes through the delivery of increased training programme predominately delivered through the Care Home Support Team. We will also review the options around increased focus from Primary Care in care homes through development of an enhanced service scheme. These additional services will focus on wellness and prevention of ill health and will aim to ensure that our care homes are able to manage more complex conditions within the homes, reducing the risk of hospital admission. In doing so, we will strengthen the delivery of the highest quality of care for our patients within Care Homes. And in governance terms, these actions will be performance managed as follows: Planning Directive, Welsh Government Objective/ Target / Guidance: NHS Wales Outcomes Framework As a Contributor to Outcome and Delivery Framework Targets Executive Lead (Senior Responsible Officer): Director of Therapies, Commissioning and Health Sciences Profiles / Trajectories Yr 1 Yr 2 Yr 3 Executive Performance Management Forum Performance Monitoring and Assurance Meeting Board Governance: Committee or Sub-Committee Responsibility: Business Planning and Performance Assurance Committee 37
38 Proactive care - Mental Health & Learning Disability Services (Strategic Objective 3) The mental health, learning disability and substance misuse needs of our society have changed significantly over the last decade. Treatment advances have seen many people who previously required hospital care being able to remain in their communities, supported by their families and friends and, when required, by services delivered by health, social care and third sector providers. The development of services has moved to more community focused care and treatment wherever it is appropriate and safe to do so. Recent Welsh Government guidance clearly promotes the need for a change in the way we provide mental health, learning disability and substance misuse services in our communities in Wales. The range of community services has extended significantly in recent years, but we now need to make sure that we are providing our services alongside other services in our communities to help build resilience in a joined up way, helping people to access the services that best meet their needs. The national strategic direction is to move services to more community focused delivery, and recent Welsh Government policy clearly indicates the changes needed in the way we deliver community based care in Wales. The focus on delivering community based models within mental health, learning disability and substance misuse services has been the strategic direction for many years following the closure of the historical large institutions, and the core values and drivers remain focussed on delivering services within and alongside local community infrastructures. The Together for Mental Health Strategy and Delivery Plan in conjunction with the local Mental Health and Wellbeing Strategy 2012/17 have given a clear focus for the Hywel Dda community to work in partnership to improve the health and wellbeing gains for people who are, or have potential to experience mental health problems. The overarching imperative and emphasis of the Strategy is the promotion of mental wellbeing, mental illness prevention, appropriate and easy access, early interventions and timely treatment. Effective and evidence based treatments and interventions will be accessed and delivered at the most appropriate stage and cohesively across services. The Substance Misuse Strategy for Wales 2008/18 Working Together to Reduce Harm is the Welsh Assembly Government s 10 year strategy for tackling the harms associated with the misuse of alcohol, drugs and other substances in Wales. The strategy defines the need to design services which aim to reduce the harm to individuals (particularly children and young people), their families and wider communities from the misuse of drugs and alcohol, whilst not stigmatising substance misuse. There also needs to be a focus on Improving the availability and quality of education, prevention and treatment services and related support, with a greater priority given than under the previous strategy to those related to alcohol. In 2007, the Welsh Government issued a new 'Statement on Policy and Practice for Adults with a Learning Disability'. This replaces previous strategy guidance and confirms a vision for the future based on the principle that all people with a learning disability are full citizens, equal in status and value to other citizens of the same age. Our services will be developed on the core values that people with a learning disability have the same rights to live healthy, productive and independent lives with appropriate and responsive treatment and support to develop their maximum potential. Our future services will have a greater focus on the promotion of mental wellbeing, preventing the development of mental illness, reducing the stigma and discrimination associated with mental ill health, offering appropriate and easy access to care and treatment, early intervention and timely treatment when needed. Mental health is equally as important as physical health, but this has not always been reflected in the way that services are provided and improved. We will deliver services that help people with mental health problems, learning disability and substance misuse difficulties 38
39 at an early enough stage, to prevent unnecessary admission to hospital, providing earlier support in their community to help them to get better more quickly. The Mental Health (Wales) Measure 2010 has provided a great opportunity for services to be delivered differently, and has enabled a more flexible and targeted use of resources ensuring that people receive the most appropriate support at the right time by the most appropriate service. Within Hywel Dda a major programme of service redesign is underway to enable the delivery of enhanced community mental health provision, with a resulting reduced reliance on in-patient services. The Transforming Mental Health programme is based on the Recovery Model which defines the philosophy of our future service. This means that the individual is supported to recover their life so that it feels worthwhile; so that they are working towards aspirations and goals that give value and meaning to their lives. Although they may not recover fully from their illness, they find themselves living in and contributing to the community. The delivery of our future service model is reliant on engagement with the wider system that supports people with a mental health problem or learning disability and therefore our services are dependent of a partnership approach to delivery. We are committed to co-design of our future models of care with our service users, carers and partners who are key members of our Transforming Mental Health programme group and associated engagement programme. Our service model is underpinned by evidence based psychological interventions, delivered in a timely manner by appropriately trained, competent practitioners. In order to impact on the mental health of future generations, the Hywel Dda community is committed to focussing its health and well-being services on young adults, through transition and into adult services. The promotion of personal strength, resilience, and recovery is key to our service model. Our Mental Health & Learning Disability service development is focussed on a progression model aimed at improving community resilience and enablement through choice, self-direction and control over our own lives, with an opportunity to move away from traditional services such as hospital and residential care. The full Mental Health & Learning Disabilities integrated medium term plan is contained in Annex 5a which provides the detailed delivery plan against the key priorities for service development: Transforming Mental Health Services Re-design of acute and community mental health service models (see Annex 5b). Enhanced Child and Adolescent Mental Health Services Development of Early Intervention in Psychosis, Perinatal Mental Health, Primary Care Mental Health, Crisis Assessment and Treatment service, Psychological Therapies service and neurodevelopmental services jointly with Children s services. Psychological Therapies Delivery of an integrated Psychological Service providing access to a range of Psychological interventions across primary and secondary care. Liaison Psychiatry service Delivery of site based liaison psychiatry pathway to improve patient flow, access, training and awareness alongside existing scheduled and unscheduled mental health services. Substance Misuse service the successful re-commissioning of all Tier 0-2 substance misuse services across the University Health Board area requires the realignment of the core Tier 3 service provision. Revised pathways and integrated working with the commissioned service will enhance the access to a range of support and intervention. Learning Disability model Re-design of in-patient, residential and community learning disability services to fit with the progression model and integrated community service support. Dementia diagnosis and support Commissioning of post-diagnostic community support workers linked closely to Primary Care and Memory Assessment services, developing a 39
40 revised pathway for diagnosis and support. The provision of enhanced Occupational Therapy provision on our older adult in-patient units is a key priority to optimise functioning. The additional Welsh Government funding confirmed in 2015/16 for Child and Adolescent Mental Health Services, Psychological Services, Liaison Psychiatry, Perinatal Mental Health and Dementia Support following approved bids will see significant growth in key service areas from 2016/17. This funding on a recurring basis is ring fenced in line with Welsh Government Mental Health budget ring-fencing review completed in The Directorate has been successful in bidding against identified service specific funding allocations in the current financial year. The following additional money is gained on a recurring basis and ring fenced in line with Welsh Government directive in relation Mental Health budgets. More detail on these is contained in Annex 5c. New Funding Allocations Current Status Actions Being Taken Development of Psychological Services - 236k Psychiatric Liaison Service - 654k These bids are at various stages of All new funded services are being planned in Development of Specialist Child and Adolescent approval, recruitment order to enhance current Mental Health Services - 873k and development from service provision. These Trusted to Care Occupational Therapy an operational services are not Interventions for Older Adult Inpatient units - perspective. The full duplicated and wherever 72k year effect will be possible will be provided Development of Peri-natal Services - Service realised within the next on an ageless basis. configuration is yet to be established 137k financial year, 2016/17 The following table provides an overview of key work streams for mental health and learning disabilities. More details can be found in Annex 5a & b. What we said we would do What we have done so far What are we going to do next 2016/ /19 Neuro-developmental service. Establish an integrated Neurodevelopmental service (Autistic Spectrum Disorder which will provide both a diagnostic and post diagnostic service which provides signposting and evidence based interventions for all children,young people and their families across Hywel Dda. Proposal submitted to Welsh Government and additional funding confirmed. Complete recruitment 2 posts outstanding. Ensure standardised referral criteria in line with defined diagnostic criteria, across the University Health Board to reduce variation. Address the current waiting list within Children s' Services (<550+), provide an equitable service across the University Health Board footprint with clear referral criteria which meets national standards, develop a range of evidence based support and interventions, and ensure strong links with the Local Authority, Third sector and service user/ carer groups. Designed a clinical pathway ensuring integration with existing Mental Health, Learning Disability and General Health services. Established Clinical Lead for Autistic Spectrum Disorder to develop clinical group to address standardisation of all assessments etc. Focused on the creation of a sustainable multidisciplinary team to ensure that those children who have been waiting the longest have been reviewed and provided with the relevant assessment/ diagnosis and sign posting, where appropriate, to the key agency who can offer ongoing support. Develop a communication strategy and establish link with Communications team to manage the growing interest in ASD locally and Nationally. Develop a Directory of Services. Engage with stakeholders and service users. 40
41 Perinatal Mental Health Service Establish collaborative working across Mental Health, Women s & Children s service and Primary care to deliver evidence based interventions to mothers experiencing mental health problems, working across health & social care to support families. Specialist Child and Adolescent mental Health (Child and Adolescent Mental Health Services) - Psychological Therapies Service Improve access to and promote equality in the provision of evidence-based Psychological Therapies across primary and secondary Child and Adolescent Mental Health Services. Child and Adolescent Mental Health Services Primary Mental Health Service Deliver a comprehensive primary care Child and Adolescent Mental Health Services service, supporting General Practitioners and Primary Care practitioners to access a primary care mental health assessment and signposting / escalation to other services as indicated, in line with Part 1 of the Mental Health (Wales) Measure Proposal submitted to Welsh Government and additional funding confirmed. Perinatal Mental Health Strategic and Medical lead recruited. Proposal submitted to Welsh Government and additional funding confirmed. Recruited staff for new service to deliver Cognitive Behavioural Therapy. Proposal submitted to Welsh Government and additional funding confirmed. Extended provision of primary team via recruitment of additional staff. Established a database to monitor all referrals to service and the number of referrals which are accepted, signposted or advice and consultation provided. Complete recruitment of team and embed within locality areas to establish local links with Women & Children s services, Primary Care and Social care services. Develop clinical pathway and integrated referral system, exploring opportunities for integrated records across services. Implement new Service model for Perinatal mental health services across all University Health Board sites. Fully implement an integrated psychological model for service delivery in line with evidence based practice. Continue process of increasing staff competencies in Psychological Therapies and consolidate competencies gained through training and experience. Extend opportunities to develop competencies in an expanded range of psychological therapies in collaboration with the wider Psychological Therapy services in the University Health Board. Establish base for co-located age inclusive Primary care mental health team. Continue to identify staff to undertake psychological training and or team to deliver low/ high intensity interventions as per the agreed training plan. Inform stakeholders of single point of referral and continue to provide training to Primary Care practitioners. Primary Mental Health workers to continue to work with schools and local child agencies to promote early intervention and prevention. 41
42 Child and Adolescent Mental Health Services Crisis Assessment and Treatment Services Develop an extended hours Crisis Intervention service to provide direct access to crisis assessment and intervention. Work alongside the Adult Mental Health Crisis and Home Treatment teams to provide specialist advice, and with the Emergency Department Teams, Street Triage and Children s Service to ensure a timely response to young people presenting in distress. Early Intervention Psychosis Expand existing service to provide a service from years, delivering evidence based Psychological and Family interventions aimed to improve the long term outcomes for individuals diagnosed with a Psychosis. Working with General Practitioners, Primary Care practitioners and the Primary Care mental health services. Proposal submitted to Welsh Government and additional funding confirmed. The new Crisis service has enabled provision of enhanced services for young people in crisis. The additional service and staff has enabled the Child and Adolescent Mental Health Services to initiate new systems to meet the new National Child and Adolescent Mental Health Services performance targets of emergency referrals (48 hours) and routine referrals (4 weeks). This is a change from 4 weeks and 16 weeks respectively. Proposal submitted to Welsh Government and additional funding confirmed. Completed review of current service provision and workforce / recruitment / skill gap analysis. Completed remodelling and develop new service specification with extension in age range to14-25 years. Implemented training programme for all staff in meeting the needs of young people. Establish database to monitor performance and measure compliance with national standards and enable Welsh Government reporting requirements. Implement Phase 3 of the proposed model which will ensure the provision of an integrated crisis model alongside the transformational change programme which will ensure any young person who presents in a crisis outside the current working hours will receive a timely responsive service to meet their needs. Audit effectiveness in preventing admissions / reducing number of days spent in hospital including admissions to age appropriate beds within the University Health Board. Strengthen the relationship between various teams and children s services. Implement revised service model. Strengthen relationship between Child and Adolescent Mental Health Services and adult mental health teams to improve transition and joint case work. Develop training plan for all staff to deliver evidence based Psychological Therapy Develop joint training programme and strengthen the clinical supervisory structures between services. 42
43 Dementia Support Workers Deliver post diagnostic support for individuals with Dementia and their families. Deliver dementia support services in partnership with the third sector, social care and community groups. Transforming Mental Health Programme Review and redesign of existing University Health Board Mental Health services. Complete a comprehensive formal engagement process to inform the coproduction of the future model and determine the process for ongoing engagement and / or consultation. (Full engagement document provided in appendices) Liaison Psychiatry Implement a Psychiatric Liaison service across the acute hospital sites. Funding of 114, 610 has been allocated for the development of Dementia Support workers. 3 Dementia Support Workers and a Dementia Support Manager have been recruited. Plans in place to start linking in with General Practitioners clusters/practices from January Complex service monitoring tool has been developed by the Alzheimer s Society to ensure that service outcomes can be measured. Funding of 71,697 has been allocated by Welsh Government to support the provision of meaningful activity and occupational therapy support on Older Adult Mental Health Inpatient units within the University Health Board. Multi-partner programme group established with 7 defined work streams (Finance, Estates & Information Technology, Clinical Pathways, Data & Evaluation, Communication & Engagement, Business Continuity, Workforce. Service User led engagement materials developed and widely circulated. A comprehensive Stakeholder engagement process has been established. International action learning sets established with Trieste Mental Health services, Italy, a World Health Organisation recognised provider, to assist with testing outputs from the programme group. Proposal submitted to Welsh Government and additional funding confirmed. Review of current numbers of Accident and Emergency Breaches undertaken, with ongoing monitoring To develop the interface between the memory Assessment services and primary care with the view that the Dementia Support Workers in the localities will be based within Primary Care. Memory assessment services will continue to develop increasing links into primary care with clinics provided in local communities and General Practitioners practices. Dementia support workers will support patients who receive a diagnosis and be engaged in the development of primary care delivery of Memory Assessment Services. Recruitment of additional Occupational Therapy support workers, as an integral part of the inpatient multidisciplinary team supporting the development of dementia supportive and friendly environments. External evaluation of engagement programme in February Presentation to University Health Board in March 2016 on the outcome of the engagement programme. Community Health Council decision on the next stage of continuous engagement or public consultation. Continuous engagement ongoing via Programme Group and Local Mental Health Partnership Board to ensure transparency and openness. Agree model and clinical pathways. Develop operational policy and outcome measures to enable Welsh Government reporting requirements. 43
44 Neuro-Psychology Develop a Consultant Neuro- Psychologist post, within MHLD. Integrated Psychological Therapies and Intervention Service Prepare a Mental Health costed plan for Psychological Therapies. Training Plan to follow the principle of Once for Wales basis and provide training places to practitioners from other Health Boards. in place. Improved relationships between Acute and mental health services via links established with Acute Site Managers and Mental health Locality Managers. Appointment to commence in February Psychology, psychotherapy and therapeutic day services have now been brought together as a group under one management and operational structure. The group also share the same professional leadership. Recruitment of 3 (band 5) Low Intensity Psychological Therapy Practitioner posts in both Primary Care Mental Health Services and Therapeutic Day Services. Training plan submitted in January 2016 and approved. Complete recruitment. Develop joint training plan. Implement agreed model. Establish a supervision and consultation network for other staff in order to improve the quality of assessment and skill up the staff. Explore innovative ways of recruiting to the Psychology post in order to assist with reducing waiting times. Finalise training arrangements and provide ongoing support and supervision network for staff that attend the training to ensure that skills are consolidated within practice. And in governance terms, these actions will be performance managed as follows: Planning Directive, Welsh Government Objective/ Target / Guidance: NHS Outcomes Framework Outcome and Delivery Framework Targets Delivery Plan Targets Executive Lead (Senior Responsible Officer): Deputy Chief Officer/Director of Operations Profiles / Trajectories Yr 1 Yr 2 Yr 3 Executive Performance Management Forum Mental Health Partnership Forum Board Governance: Committee or Sub-Committee Responsibility: Business Planning and Performance Assurance Committee Quality, Safety, Experience Assurance Committee Frailty and Dementia (Strategic Objective 8) Proactive specialist in-reach older persons assessment and liaison teams will be used to offer expert advice, follow-up and care co-ordination for older people throughout the hospital. In addition work has been initiated to look at the pathway for frail older people in each of the acute hospital sites. In moving forward we will be seeking to address the following priorities: Development of a frailty (including dementia) pathway for people accessing acute hospital Alternative places of safety to hospital admission Front door assessment Comprehensive geriatric assessment Designated acute frailty beds Rapid discharge through community in-reach 44
45 Effective care coordination Good dementia care to be everybody s business. Development of dementia pathways including those people with dementia as part of multimorbidity Standardised specialist memory services Primary care led approach Reliable approach to awareness of modifiable risk factors Community support systems for people with dementia and their carers Delivery of integrated care Interface with the acute hospital frailty pathway. 3.3 Strategic objectives 9 and 10, the way we will bring all of our performance delivery, Outcome and Delivery Framework Targets plans together and medium term financial plans (QUALITY, INNOVATION, PRODUCTIVITY, PREVENTION (PRUDENT)) Diagnostics, Planned Care, Unscheduled Care, Women and Children s Services Rapid Access Diagnostics A critical factor in our ability to deliver Proactive Care Closer to Home and strong secondary care services is appropriate and timely access to diagnostic services and reporting such as radiography, pathology and pharmacy. It is important to note the role of these services in safe admission avoidance and in facilitating timely discharge. The tables below evidence in summary form progress to date against plans and what we plan to do in 2016/17 up to 2018/19. Radiology What we said we were going to do Introduce additional reporting radiographers including chest & abdominal (backfill required) Recruitment of trainee sonographers based upon analysis of baseline demand Introduce rapid reporting for skeletal radiography for all Accident and Emergency/Minor Injury Introduce a single Radis system. What we have done so far 2 radiographers have qualified. Backfill recruited except Bronglais. Recruited radiographers in post by the end of January. Recruitment not yet progressed. In place, but inconsistent as this requires the presence of backfill staff (see above) and a single radis system (see below) Merger of Radis systems is in development nationally What are we going to do next 2016/17 (up to 2018/19) Continue training of reporting radiographers coupled with proposed recruitment of trainee assistant practitioners. Recruit trainee sonographers. Continue recruitment process at Bronglais, introduce cross-site reporting within the limitation imposed by separate radis systems. Await outcome of merger process Introduce extended working hours (evenings/ weekends) based upon baseline demand Extended working hours in place as staffing permits for scanning. Business case for 7/7 working submitted Continue to provide extending working whenever possible. Seek approval for funding to enable 7/7 working Recruitment of trainee assistant practitioners for future backfill for Not progressed. Recruit trainee assistant practitioners 45
46 What we said we were going to do reporting radiographers Continue drive to recruit consultant radiologists Decrease percentage of studies externally reported Commence planning of radiology services re-provision in Glangwili Replacement of Magnetic Resonance Imaging scanner at Bronglais What we have done so far Advertising in journals and amendment of contract offering an opportunity to opt out of oncall cover. Baseline work to be progressed Radiology and pathology to be considered in redevelopment of front-of-house at Glangwilli. Project group established, preferred site identified, costs being collated. What are we going to do next 2016/17 (up to 2018/19) Seek approval for overseas recruitment drive Continue to increase reporting by radiographers and use of locum agency radiologists Progress with planning/business case Subject to Welsh Government funding approval, replace scanner at Bronglais. Pathology What we said we were going to do Reconfigure existing laboratory space at Withybush to provide Blood Sciences laboratory Reconfigure existing laboratory space at Prince Philip to provide Blood Sciences laboratory Re-provision of Pathology facilities at Bronglais Hospital via the Front of House Scheme Support the rollout of the All Wales Laboratory Information Management System Cellular Pathology module Consolidate current Consultant Cellular Pathologist office accommodation to Teilo to release additional space for Cellular pathology laboratory use. What we have done so far Reconfiguration work completed. Unable to go live on 1 st September as planned due to issues with legacy data and voice recognition software all considered mandatory. Unable to progress office relocation. What are we going to do next 2016/17 (up to 2018/19) Implementation of new Clinical Chemistry equipment as part of the pathology wide managed service contract. Complete University Health Board wide Blood Transfusion Managed Service Contract tender exercise Complete Health Board wide Haematology /Coagulation Managed Service contract tender exercise. Implement All Wales Laboratory Information Management System Blood transfusion module Implement the All Wales Andrology model. Complete the rollout of Cellular Pathology Laboratory Information Management System module subject to availability of dependencies. Rollout digital dictation within Cellular pathology. Complete the consolidation of Cellular Pathology services to a single site. Pathology accommodation at Glangwili is not fit for purpose. Backlog of estates maintenance and health and safety issues. Segregation of tissue processors from cut up room Options to reduce exposure to formalin and xylene- closed system. Formaldehyde (reclassified to Cat 1 carcinogen) Office space for Consultants Identify career stage 4 tasks and functions to produce a new support worker role within Cellular Pathology 46
47 What we said we were going to do Achieve compliance with ISO 15189:2012 Compliance with Medicines and Healthcare Regulatory Products Authority standards Complete Human Tissue Authority compliance report Appointed an Advanced Biomedical Scientist (Research) in October Part of this new role is to liaise between Research and Development and Pathology for seeking approval from relevant pathology Leads to support clinical trials. What we have done so far Gap analysis completed Audit schedules in place Application for United Kingdom Accreditation Service inspection submitted for Blood Sciences and Microbiology Withybush Hospital Annual compliance reports completed and returned Completion of audits Tracking and trending incidents Governance meetings in place Standardisation of documentation. Submitted bid to Cancer innovation Fund new role to provide dedicated link between Cellular Pathology and Cancer Services Blood Sciences Band 3 staff to achieve Pathology Diploma, to release qualified staff time. Additional resource identified for ward based Band 2 phlebotomy staff to reduce pressure on junior doctors and ensure the correct level of skill is applied. Collaboration with Llanelli General Practitioners Cluster to identify funding for 2 posts to support Community phlebotomy in 3 locations. The TAT to seek approval from Pathology for trials has greatly improved due to the existence of this role. Currently Pathology have approved and are working on a range of trials Supporting pilot into the Use of calprotectin in Intensive Care Prince Philip Hospital as a marker of infection cost of test identified as a cost pressure within pathology but note potential benefits in other expenditure in other areas What are we going to do next 2016/17 (up to 2018/19) Application for UKAS inspection to be submitted for Blood Sciences Glangwili, Prince Philip and Bronglais Hospitals/Mortuary Continual quality improvement processes to be embedded Implement audit schedule Track and trend quality incidents Gap analysis against ISO15189:2012 standards If successful appoint to the new role. Develop a process to capture benefits, challenges etc. Training commenced for First cohort of staff these will progress to the technical modules. R&D are in the process of applying for a research licence for develop a Biobanking Centre to enable tissue banking activities covering a wide range of disease areas across University Health Board. This will require commitment from the Pathology Department to support tissue sampling activities on site, to be undertaken by the Advanced Biomedical Scientist (Research). Provide data from Laboratory Information Management System for use in prospective audit. 47
48 What we said we were going to do What we have done so far What are we going to do next 2016/17 (up to 2018/19) Action focus how we will do it and by when Review Pathology accommodation at Glangwili. Estates issues identified and proposals identified for improved flow. Complete the rollout of All Wales Laboratory Information Management System Mortuary module. Capital bids required to cover additional Mortuary Body Store capacity either as a permanent facility or mobile unit. All Wales proposal is for Public Health Wales to provide an All Wales Microbiology Service Support the governance framework as an enabler to increase use of Point of Care Testing where appropriate e.g. General Practitioners surgeries, to provide care closer to home. Improve connectivity Pharmacy What we said we were going to do Improve medicines management and clinical pharmacy services to patients with mental health and learning disabilities. Improve microbial stewardship across the sectors Develop pharmacy services within primary care supporting General Practitioners practices and Care Homes Increase the number of nonmedical prescribers pharmacist to support the development of patient centred services and improve access. Install ward automation units at ward level to improve access to medicines & reduce waste. Implementation of Medicine transfer by electronic discharge (MTed)) across the University Health Board What we have done so far Review of service provision has led to transfer of dispensing of dementia medication over to primary care clinicians supported by community dementia teams and services. Antibiotic pharmacists are in place (0.5WTE) in each hospital site leading on appropriate use of antimicrobials. A work plan has been agreed to ensure that regular audit and review is undertaken An app has been developed Updated guidelines across sectors. Links for ease of access for clinicians as point of care. Education sessions to junior and undergraduate staff. Funding for cluster pharmacist role has led to development of 2 posts in 2 clusters (South Pembrokeshire & South Ceredigion To target: Polypharmacy reviews Care home patients High risk patients (frequent flyers) 9 qualified pharmacists qualified,4 to commence January x Ward automation units in place in Glangwili site. These impact and benefits of these units will be assessed by March 2016 to determine future implementation. Funding from Welsh Government (Pharmacy Innovation) to put in place in 4 wards across the University Health Board. Project Board in place to oversee the implementation What are we going to do next 2016/17 (up to 2018/19) Complete the transfer for prescribing to primary care. This will allow for some development of the clinical services currently provided by the specialist mental health pharmacy team. Potential to develop the role of the non medical prescriber in services Continue to build on the activity of the Antimicrobial pharmacist in the acute sector. However the capacity to extend into primary care is very limited. A business case to support further capacity in primary care (where 80% of prescribing occurs) has been developed for consideration. Embed the posts into cluster working. Monitor and review the impact on patient care and General Practitioners capacity. Continue to develop services utilising the skills and further increase numbers of pharmacists trained On internal review, further implementation will be undertaken when capital finance is available. 4 wards ( 1 on each site) identified. Baseline data being collected. Trolleys & equipment ordered. Ready for first ward in January Remainder by March
49 What we said we were going to do Remedial work on the aseptic units across the University Health Board to bring in line with national standards. Longer term view to work collaboratively with Abertawe Bro Morgannwg University Health Board in the development of the service provision. What we have done so far Remedial work approved and set in motion to be completed by March What are we going to do next 2016/17 (up to 2018/19) Project Board set up in collaboration with Abertawe Bro Morgannwg University Health Board to determine the preferred option for service provision across West Wales. Business Case Justification has been approved by Welsh Government to progress the project Planned Care This section is specifically concerned with our planned care system, particularly elective outpatient and inpatient flows. The key performance indicator of the planned care system is waiting time. Our 2015/16 Integrated Medium Term Plan committed to stabilising our waiting times position and specifically avoiding further escalation of the numbers of people waiting more than 36 weeks from Referral to Treatment. The University Health Board is currently on track to meet with this objective by the end of March The University Health Board s ambition for 2016/17 is to eliminate waits in excess of 36 weeks by March During the year the University Health Board has strengthened its organisational capacity, including external support, to work with service delivery teams to establish robust demand and capacity analysis to underpin service plans and performance trajectories for 2016/17. Given the University Health Board s performance, unsurprisingly this work has highlighted recurrent capacity gaps and significant backlog pressures for the forthcoming year. Modelling and quantifying these pressures is enabling the University Health Board to focus its attention on the priority areas within the organisation where capacity and demand are out of balance. The final version of this Plan, in March 2016, will evidence detailed plans and the level of ambition for 2016/17, and will be the subject of detailed pro-formas as part of the full Integrated Medium Term Plan submission. Progress to date is included in Annex 6. The capacity and demand modelling analysis utilises the outputs of the specialty level Operational Delivery Plans (ODPs) that were introduced in April 2015 to determine recurrent capacity gaps, predict the March 2016 outturn and the additional activity required in 2016/17 to deliver the no 36 week breaches aspiration by March All the specialty specific Operational Delivery Plans contain planned and actual activity volumes for outpatient and where necessary inpatient / daycase treatment services from April 2015 through to March This information has been derived and input by the individual operational specialty teams and validated by the individual Service Delivery Management teams and the outputs have been correlated to enable the holistic analysis described. The results of the analysis are based on the University Health Board s Patient Tracking List position as at the 11 th January 2016 and take account of the following assumptions: the activity split by Core and Waiting List Initiative contained within the specialty level Operational Delivery Plans is correct planned activity to year end activity contained in the Operational Delivery Plans is deliverable. General Medicine has been included as a specialty and covers all sub-specialities. 49


50 Capacity Gap totals exclude any negative values as these are non-transferable between specialties. Neurology 36 week outpatient breaches will be resolved through outsourcing by March The impact of externally commissioned validation is likely to reduce the recurrent and backlog volumes required, but the impact cannot yet be quantified. The total capacity gap for inpatient / daycase treatments is inclusive of the recurrent and backlog gaps in outpatients. If the additional activity volumes can be delivered internally or through outsourcing, the University Health Board would have no patients breaching the 36 week target - however this cannot be assured with Surgical Outpatients still at a 26 week maximum wait. The following table contains the breakdown by specialty of the weekly recurrent capacity gaps for outpatients services across the University Health Board. The weekly capacity shortfall across the University Health Board for outpatient s services in 2015/16 year to date is per week, with Dermatology, General Surgery, General Medicine and Urology contributing the most significant shortfalls. In 2015/16 this gap has been partially filled through undertaking additional Waiting List Initiatives at a premium rate, however the shortfall has still resulted in the overall number of patients waiting for a New Outpatient appointment to increase by 1,660. The following table contains the breakdown by specialty of the weekly recurrent capacity gaps for inpatient / daycase services across the University Health Board. 50
51 The overall verall weekly capacity shortfall across Hywel Dda for inpatient/daycase for 2015/16 is 18.6 per week comprising Urology (8.1), (8.1) Orthopaedics (5.6) and Pain Management (4.9). These volumes are likely to be understated when the recurrent activity gaps in outpatients utpatients are taken into account, as seeing eeing an extra outpatients per week recurrently willl increase the recurrent demand for treatment. During 2015/16 this gap has been negated by undertaking additional waiting list initiatives (23.5 per week) this work is delivered at premium rate and is not sustainable, the additional activity and the shortfall in new outpatient activity has resulted in the overall number of patients waiting for treatment to decrease by 691. The following table,, given the caveat of o further validation, details the volumes of additional activity that would be required over and above the core levels achieved year to date 2015/16 to ensure that surgical new outpatients wait a maximum of 26 weeks, medical upto 36 weeks and all inpatient / daycase treatments upto 36 weeks. In order to generate the values, the projected hospital site year end position and the current backlogs waitings between 26 and 35 weeks were used. This modelling remains work in progress. It may not be operationally operationally or financially viable to achieve the activity volumes outlined above, especially if the schemes to modernise pathways, develop and implement referral criteria and optimise existing capacity levels only achieve at best a part year effect in 2016/17. Operational ational teams are working to develop comprehensive service plans for 2016/17 to respond to the individual specialty challenges outlined. Only provision of a full change programme of work across scheduled care services can assure that the referral to treatment treatment (and cancer) target position can be sufficiently improved, delivered and sustained. The programme may need to extend beyond March 2017 and will require the input of the integrated University Health Board teams to ensure its success. In order to alleviate iate this problem in 2016/17 plans will be prepared for each specialty that links to the University Health Boards Quality, uality, Innovation, Productivity, Prevention revention (Prudent) ( approach supported by the programme management office. The outpatient validation exercise currently underway underpins this approach and on-going on going plans will need to be prepared that consider the following approaches Referral management and the role of primary care in referral protocols and demand management in line with prudent healthcare health Optimising the capacity of specialities across sites to match demand 51
52 Engage with, and where necessary challenge, clinical practice, skill mix and efficiency of patient pathways to optimise capacity levels to meet, or reduce the capacity shortfall Consider outsourcing as a short term viable option for 2016/17 delivery, once all other options have been considered. The following tables summarise the current status and actions being undertaken which will be the subject of more detailed work to identify robust action plans particularly for 2016/17. Key Messages from Transform Your Health Your Future Stabilise Optimise Gynaecology Too much variation in Provision, Waiting Times & Access, Poor productivity Compliance with Standards Not maximizing sub specialisation potential in line with modern practice Privacy & Dignity No emergency / elective separation Patient experience challenges e.g. High Cancellation rates Orthopaedics Developing dedicated facilities so that more people will have their operation on a day or short stay basis and not need to stay so long in hospital Separating planned from unplanned care and will allow investment in pre-operative assessment services, delivered by General Practitioners or community team, and minimising cancellations and reducing significantly the risk of cross infection Consolidation of 2014/15 service transfers for Women s & Children s Improved Gynaecology pathways between Glangwili General Hospital and Withybush General Hospital. Community led Musculoskeletal triage service including Pain Services Hywel Dda Orthopaedic network to maximize sub specialization potential in line with modern practice Phase 2 development on Glangwili General Hospital site for Special Care Baby Unit and Obstetric unit will create capacity which will allow us to optimise Gynaecology services To maximize all efficiencies in outpatients, theatres and bed utilisation to All-Wales best in class specifically addressing Getting It Right First Time and Wales Audit Office recommendations. Scope the development of an elective inpatient centre of excellence in Gynaecology to: Split planned and unplanned Create critical mass to support sub-specialisation Improve Efficiency through theatres Improve Infection control Hospital Out-patients, diagnostics and day-case surgery to remain local as current. We will strengthen inpatient capacity and facilities on all 4 sites and scope the creation of an elective centre of excellence to accommodate increasing elective inpatient demand and workload. Otherwise inpatient Orthopaedics and Daycase surgery to remain local as current. Action to strengthen day surgery facilities and working across the University Health Board with follow up trauma fracture clinics in each county Ophthalmology Delivering in dedicated facilities to improve efficiency and reduce waiting times Cancer / Oncology & End of Life Care Inability to meet Standards Do not consistently meet the Outcome and Delivery Framework Targets targets Not all our Cancer Step improvement to deliver Referral To Treatment Implement oncology action plan Oncology Re-establish the Together for Health Cancer Board, and To maximize all efficiencies in outpatients, theatres to All-Wales best in class Achieve clarity on variation Fully functioning Multidisciplinary Teams Improved unbundling of parts Strengthen capacity on two sites Cancer services a major piece of work which needs to be scoped is transformation of surgical Cancer Services, and this will need to be undertaken in the next few months. In 52
53 Multidisciplinary Teams are linked Diagnostic Services are often a rate limiting step Not all of the commissioned activity occurs in contracted timescales Unsustainable Oncology Workforce model Clearer strategic direction reframe the plan to those actions critically needed over the next 5 years And progress targets for specific Multidisciplinary Teams in line with National Priorities of the pathways as part of the Cancer Network Significantly improved diagnostics Joined up working with our partners e.g. Macmillan, Marie Curie the meantime, this plan will concentrate on strengthening Oncology Services and End of Life Care. Planned Medicine Not maximizing sub-specialization potential in line with modern practice Too much variation Not meeting some Outcome and Delivery Framework Targets for example for Cardiology Diagnostics still a rate limiting factor Single handed practitioners Full evaluation of our delivery against the Together for Health Delivery Plans: Respiratory Diabetes Neurology Heart Disease Liver Optimise efficiency and productivity Action focus how we will do it and by when Improve Referral and Diagnostic Pathway Develop primary care based referral management system at practice level Develop the capacity of community based minor surgery by 5 % Sustain the management of musculoskeletal referrals Treat Day Surgery as the norm Increase overall day-case rate by 5 % from 85% to 90% Actively Manage Admission to Hospital Increase pre-assessment activity by 25% Increase day of admissions for surgery by 20% Reduce number of patients being admitted with no procedure performed by 25% Actively Manage Discharge and Length of Stay Reduce variation in length of stay Introduce estimated discharge date for 100% of elective patients Actively Manage Outpatient Capacity and Follow Up Achieve 1:1.5 new to follow up ratios for chosen specialties. Patient Focus Booking Evaluate patient focus booking Queuing theory and performance framework Improvement on the 26 week out-patient and in-patient target Unscheduled Care The University Health Board has been working with the Delivery Unit to strengthen unscheduled care. The illustration below summarises key recommended actions from their action plan (Annex 7) from which our action plan will be developed 53
54 Essentially unscheduled care is about patient flow across the whole system as indicated in the Delivery Unit schematic and the University Health Board acknowledges that we have to complete marginal gain in every part of the pathway in order to improve flow. To this end and for ease of understanding, we present initiatives that will improve the pathway and the actions plans currently in train. 54
55 Unscheduled Care Service Improvement to ensure Outcome and Delivery Framework Targets target Delivery Unscheduled Care: Emergency Departments Key Messages from Your Health Your Future Long waiting times at busy times Delayed access to senior clinical opinion and decision making Clinical governance challenge e.g. key specialty backup not available on all sites, with inconsistent assessment processes Lack of clarity of service provision Chronic recruitment and retention challenges Too many patients waiting too long in ambulances Stabilise Ensure safe staffing levels in Emergency Departments Optimise Prince Philip Unscheduled Care model Action focus how we will do it and by when Transform In addition to current Accident and Emergency services, we will have fully scoped the applicability of the Prince Philip Medical Model to Withybush and Bronglais this means that we can Sustain high quality acute medicine on all 4 sites with direct access to the Clinical Decisions Unit Deliver a frailty model integrated with community, primary and social care Keep all of our front doors open 24/7 Delays in patient discharge from wards and movement from Clinical Decisions Unit; Agreement of an Expected Day of Discharge within 24 hours of admission is not consistent -, 100% compliance required Clear, communicated discharge plan to be in place before Expected Day of Discharge Dec 2015 working with Acute Site Nurses Working with site teams to develop a weekly performance meeting focusing on previous week, understanding RCA and implementing actions focus on discharge planning. Nurse recruitment continues on all 4 sites but remains slow Poor Accident and Emergency flow: Education session for all junior Doctors in relation to Outcome and Delivery Framework Targets performance targets, accurate recording of care plans, efficient decision making and referral times, commenced Oct 2015 Paper to be submitted to board re development of Unscheduled Care Specialist roles 2pm to midnight, paper commenced Oct 2015 Review of medical staffing and nursing rotas versus attendee numbers, November 2015 The above actions will support both the 4 hour performance and a reduction in the 12 hour breaches. Improvement of ambulance handover; Clear identification of Accident and Emergency team leader with arm band Re-enforcement of team Leader having a joint responsibility with Welsh Ambulance Service Trust colleagues to update the HAS screens. Audit to be undertaken on all 4 sites in November 2015 to compare actual data with data provided by Welsh Ambulance Services Trust Issue of non utilisation of HAS screens and use of control raised with Welsh Ambulance Services Trust colleagues, monitoring ongoing The actions to support the 4 and 12 hour performance will also directly impact the ability to off load ambulances. The action tables below are a summary of our current plans and are subject to review and update to ensure alignment with the Delivery Unit and other reports. 55
56 Key Messages from Your Health Your Future Acute Medicine Inability to meet Royal College Guidance & Standards Single handed practitioners Recruitment & retention challenges Over-reliance on in-hospital and bedded models of care Too many patients staying too long in hospital Current model cannot meet future demand Sub-specialties require network solutions Stabilise Withybush General Integrated Medicine Model Prince Philip Front of House For Bronglais, this will be part of the emerging Mid Wales Study Collaborative Board For Glangwili, service as is now Optimise As part of this consolidation, Withybush Consultants will also extend part of their roles into supporting Proactive Care Closer to Home and strengthened Community & Primary Care & embracing the Frailty Model as part of the Accident and Emergency Front Door Transform Networked emergency medicine rosters, providing emergency subspecialisation expertise which could effectively allow us to operate as One Hospital over 4 Sites. Action focus how we will do it and by when General Integrated Medical (GIM) Service Model A new general medicine model is proposed for Withybush General Hospital to stabilise the position for Winter 2015/16. The model proposes the move to a 12 consultant GIM on-call model matched with 1:12 middle grade and 2 times 1:11 junior grade rotas. The original proposal included 2 consultants with interest in Respiratory medicine, however, given recruitment issues this alternative model does not include respiratory consultants but has specialist respiratory services reorganised according to a hub and spoke model operating out of Carmarthenshire. Respiratory Service Model A clinically led model has been approved that seeks to re-design the respiratory care model across the University Health Board. The options are based on our current service sustainability with particular to reference to consultant recruitment and retention. Capital enablement Prince Philip Hospital Front of House The redesign of Unscheduled Care in Prince Phillip will deliver a sustainable model for minor injuries and acute medicine. The focus will be around a Minor Injury Unit staffed with Enhanced Role General Practitioners working alongside Emergency Nurse Practitioner and a Consultant led Acute Medical Admissions Unit (16 beds) plus resuscitation and stroke beds and an Ambulatory Care area. It is anticipate that the medical model will go live in February 2016 with completion and co-location of community teams within the MIU by May A Business Justification Case has been submitted to Welsh Government Investment Infrastructure Board. A successful outcome to the submission has resulted in reimbursement of the full capital tender costs of the work and equipment at Prince Philip Hospital of 1.4m. 111 Pathfinder with Abertawe Bro Morgannwg University Health Board National implementation group established and decision taken that Abertawe Bro Morgannwg University Health Board will go live with a pilot 111 service in April 2016, this date has been postponed from October Following a trial period within Abertawe Bro Morgannwg University Health Board the 111 service will be subject to assessment. The second area to go live will be Carmarthenshire; the location decision is based upon the existing external contractual arrangements for delivery of call handling and triage for the General Practitioners Out of Hours Service. As part of the 111 model we are exploring alternative working practices that cut across current assumptions for unscheduled and emergency care, and as such standards may need to be explored to develop a robust and flexible workforce. The integrated 111 and General Practitioners Out of Hours pathfinder project within Abertawe Bro Morgannwg University Health Board will provide an opportunity to test employing a range of multidisciplinary professionals providing clinical advice and triage to patients the workforce profile is still be determined and it proposed that Health Boards need to consider what future requirements the local population needs to improve clinical pathways for musculoskeletal conditions and as a guide we believe that each Health Board should consider planning to train up an additional 1-1.5wte (Whole Time Equivalents) physiotherapists per Health Board. General Practitioners Out of Hours review 56
57 A review of General Practitioners Out of Hours Service is underway. Winter Planning A winter plan has been prepared which builds on the Seasonal/Pandemic Flu Plan, Major Incident Plan, Infections Outbreak Plans and Business Continuity Plans. The Plan has been completed covering both the winter pressures period and specifically for the two week festive break. A Red/Amber/Green RAG status report has been developed to inform the risk profiling of winter preparedness, the key area of risk focuses on workforce with implications both for safe management of core capacity and additional surge. A range of workforce actions are in place to mitigate where possible. The second area of concern highlighted is transport and consequently a Transport Strategy has been developed. Welsh Ambulance Services Trust action Plan As part of our joint working with Welsh Ambulance Services Trust the following actions have been agreed. Dedicated Ambulance Vehicle based within Withybush to support Women and Children s services Advanced Practitioners and Trainees supporting the Out of Hours General Practitioners service and the practice based General Practitioner services through the General Medical Services team Pathways of alternative care for patients with epilepsy, diabetes, falls Paramedic Pathfinder designed to support the above, and in addition to signpost appropriate treatments regimes for patients requiring care, but for whom Emergency Department would be inappropriate Hywel Dda and Welsh Ambulance Services Trust jointly established a dual-funded Project Manager role to support collaborative working whilst the reconfiguration of services progresses Welsh Ambulance Services Trust operational managers will maintain daily contact through teleconferences and joint meetings to ensure there is clear understanding of the bed-availability in all four sites Daily ambulance handover delay data will be regularly reviewed escalated as appropriate. In the event of the ED being unable to offload there is a jointly shared protocol to be followed Ambulance handover breaches will be monitored and are included as part of the escalation plan to ensure achievement of the 8 Minute Emergency Ambulance response target Welsh Ambulance Services Trust will ensure that planning assumptions and seasonal plans will be shared with other emergency services and 3 rd Sector partners through the Dyfed Powys Local Resilience Forum Emergency Surgery including Trauma and Anaesthetics Inability to meet Royal College Guidance & Standards Single handed practitioners Recruitment & retention challenges Sub-specialties require network solutions Too many patients staying too long in hospital Challenge to Core Trainees positions at Withybush Hospital For all emergency surgery services, these will continue as is now Scoping as per All Wales Health Collaborative planning work Action focus how we will do it and by when Networked emergency surgery rosters, providing emergency sub-specialisation expertise which could effectively allow us to operate as One Hospital over 4 Sites Women and Children s Following the report by the Royal College of Paediatrics and Child Health (RCPCH), work has commenced on implementing the recommendations from this report (Annex 8), including: Development of the Phase 2 Business Case with the project structure in place; Business Case writers having commenced work; and staff engaged on developing schedules of accommodation; Work continues to improve transport services for patients, with good use being made of the Voluntary Transport Services; Further strengthening of the Organisational Development Plan is being undertaken; The Dedicated Ambulance Vehicle remains an integral part of the service model and an extension to the contract will be formalised going forward. 57
58 The high principle recommendations that the Royal College of Paediatrics and Child Health presented in their summary report are reiterated in the final report. These are regarding: Patient Safety: The provision of maternity and children's services must continue to build on the current momentum with the major emphasis on provision of services that provide maximum safety for patients, but are sustainable in the long term, being cognisant of the geographical challenges of the area. We found no evidence that clinical outcomes had worsened since the changes and there is better compliance with professional standards. There is no clinical sense in reversing the major decisions of reconfiguration made one year ago. Clinical Accommodation: The further development of clinical excellence can only occur if the accommodation to deliver such care is appropriate and adequate for patient safety. Further delay with Phase Two is unacceptable and a potential risk to patient safety. Community Needs and Access to Services: Inevitably some decisions around reconfiguration will make access to safe services more difficult for some people. Alongside such changes, there therefore must be improvements in access to more routine care and the review recommends improved out patient services at Withybush to demonstrate commitment to patients and the public. The continued provision of a dedicated staffed ambulance for women and children must be supported, but the current consultant on-call arrangements for paediatric and obstetric/gynaecology out of hours are an inefficient use of resources which are hampering development of unified medical teams and these should be phased out. Recognition of Staff Commitment: The planning of care must involve all members of the clinical community and build on their professionalism, enthusiasm and commitment to patient welfare. Organisational Leadership: There needs to be more active and visible clinical leadership of women and children s services from the Board, and also at divisional and specialty level. Communication; The University Health Board needs to prioritise an active and evidencebased dialogue with patients, advisory groups and clinical staff to mitigate the misunderstandings and anxieties that have arisen in the past. An action plan will now be developed to provide a clear improvement plan for Women and Children s Services and specifically address the recommendations of the Royal College recommendations Key Messages from Your Health Your Future Optimise Transform Women and Children s Services Ensure standards are achieved across the University Health Board Sustainability of medical rosters Staffing efficiencies Stabilise Consolidation of 2014/15 service transfers for Women s & Children s Phase 2 development on Glangwilli site for Special Care Baby Unity Obstetric unit & Paediatrics Action focus how we will do it and by when Develop sustainable service model for Bronglais that meets standards Full report from Royal College received by Board in November 2015 and a University Health Board Action Plan has been developed to address the recommendations) Planning for Phase 2 development underway with joint Outline Business Case/Full Business Case targeted for Spring 2016 Additional review work being progressed with Neonatal Network with focus on training and expertise, clinical guidelines, staff rotation with tertiary units and achievement of LNU status 58
59 Organisation development programme to be commenced with clinical staff to support further integration of staff and services affected by service changes Further public communication and engagement initiatives to be prioritised to support service changes and build local public confidence RCPCH Evaluation Current Status Future Actions Formal evaluation of the extent to which the reconfiguration of Obstetric & Maternity, Paediatric and Neonatal services in 2014 has achieved the benefits criteria outlined below: Improved compliance with Royal College and Neonatal standards Stabilisation of medical rotas Improvements to medical training Provision of more care for children closer to home A reduction in the number of pregnant women over 30 weeks gestation who are transferred outside the University Health Board Swifter repatriation of babies transferred for neonatal care back to Hywel Dda Royal College of Paediatrics & Child Health invited to lead external review of service changes review undertaken July Interim report received by Board in September 2015: Services in general found to be safe with improving outcomes and better compliance with professional standards Urgent priority to progress Phase 2 development to address inadequacy of current facilities and to support further development of clinical excellence Utilisation of local midwifery led care is steadily increasing with very positive feedback from women who have used the service Glangwilli based obstetric service is meeting Royal College of Obstetricians standards re consultant cover and minimum deliveries to sustain training Neonatal nursing staffing levels are compliant with All Wales Standards for Neonatal Care. Numbers of infants sent outside University Health Board area for care has reduced Neonatal outreach service has improved care facilitating earlier discharge and care at home Further review of Neonatal services is required in partnership with Neonatal Network and Tertiary Unit to assess progress towards LNU status Paediatric service is compliant with the majority of Royal College Facing the Future standards with improved medical cover and compliant training rotas Paediatric nursing recruitment challenges remain Significant local public anxieties remain Opportunities exist for further provision of routine and outpatient based services more locally across University Health Board area Full report received by Board in November 2015 along with supporting University Health Board Action Plan to address recommendations Planning for Phase 2 development underway with business case targeted for Spring 2016 Additional review work being progressed with Neonatal Network with focus on training and expertise, clinical guidelines, staff rotation with tertiary units and achievement of LNU status Organisation development programme to be commenced with clinical staff to support further integration of staff and services affected by service changes Further public communication and engagement initiatives to be prioritised to support service changes and build local public confidence End of Life Care The Board published its Together for Health End of Life Care Delivery Plan in September 2013 and in December 2014 an update on the progress made against each of our priorities: Supporting living and dying well Detecting and identifying patients early Delivering fast, effective care Reducing the distress of terminal illness for the patient and their family During 2014/2015 examples of progress against these priorities including: The Official Opening of the Ty Cymorth Hospice on the Glangwili General Hospital site Delivery of the Core Curriculum Training Programme Recruitment of a Consultant in Palliative Care and a General Practitioners with a Special Interest 59
60 Positive evaluation of the initiative with Marie Curie to improve access for patients with Dementia to Palliative Care. Introduction of Anticipatory Grief Service in Carmarthenshire Continued support for the Third Sector in the provision of Palliative and End of Life Care services Integrated working with Third Sector and Independent Sector to deliver Hospice at Home Services across the three counties Roll out of MacMillan Information and Support Service Closer working, training and education within Care Homes in the Statutory and Independent Sector on Palliative and End of Life Care Use of Practice Development Plans and Cluster Plans to inform service developments Improved information sharing across all sectors Improved transition information between paediatric and adult services Steady improvement has been made against all outcome indicators: The percentage of General Practitioners patients who are on the Palliative Care Register is slightly higher than the Wales average (0.32% compared with 0.26% in 2013/14) The percentage of deaths in patient s own home is significantly higher than the Wales average (26.4% compared with 22.6% in 2014/15) The percentage of deaths in hospital is much lower than the Wales average (51.1% compared with 56.2% Although the number of Nursing Homes and Care Homes is lower than the Wales average, the percentage of deaths in Nursing Homes and Care Homes was higher (19.4% compared with 16.6%) The population in Hywel Dda is less deprived than in some other parts of Wales, but there are pockets of deprivation within its catchment area The percentage of Palliative Care patients who claim disability allowance is lower than in other parts of Wales The key actions ahead are Ensuring the same baseline of service is available in all three counties and in all seven localities Ensuring that Advance Care Planning is promoted effectively to enable people to express their wishes and care preferences Maintaining and developing partnership working across public, private and third sector organisations Ensuring adequate resources to support the provision of multidisciplinary training and education for the NHS and its partners. 3.4 Our strategic objectives with a particular emphasis on Quality and Safety The Quality, Safety and Experience Assurance Committee have prioritised five key areas of quality improvement during 2015/16 and are yet to be in a position to detail the 2016/17 action plan, but these will undoubtedly still continue as they constitute eight significant Quality and Safety improvement objectives as follows: Outpatient follow-up Harm and Mortality Measures Hospital & Community Acquired Infections Delays in Diagnosis Missed fractures Inpatient Falls Hospital Acquired Thrombosis Medication incidents Failure to Monitor. 60
61 A key quality initiative for the University Health Board to drive improvement in planned care services is reducing patients awaiting outpatient follow-up and those for whom capacity has not been identified to allow them to be seen by the target date. The following table summarises current status and action being taken: Outpatient Follow-up Current Status Task & Finish Group established to ensure that Follow Up care is prioritised and specifically to ensure that patients at risk of harm within the follow up backlog are prioritised and that risk is minimised. The programme of work has focussed on four key stages - Admin validation, Clinical Validation, treatment and modernisation of pathways. Alongside this programme of work a review of follow ups has been undertaken by the Auditor General for Wales and this report has identified a number of areas where the University Health Board needs to improve that have been incorporated into our forward plans. The key issue that is compromising our ability to take forward this programme has been one of resource as the same staff required to work on validation, treatment and modernisation of follow up care have been prioritising achievement of 2015/16 Referral to Treatment pathways. This has meant that as quickly as we have been able to validate and clear pathways an equivalent or greater number of follow up treatment episodes are being added to the backlog. Actions Being Taken to Progress Quality and Safety Improvement Objectives A revised programme structure and change programme is being established to address this issue. The programme of work under way within the University Health Board is focussing on a number of key stages: - Creation of a contact centre, ultimately Hywel Dda wide to ensure a consistent approach to closing pathways. Admin validation cleaning up the waiting lists and removing obvious duplicate entries or patients that have been seen and the pathway not closed. Establishing a new programme of training for waiting list and contact centre staff to ensure that there is a standardised approach to closing pathways. Clinical validation establishing consultant capacity through waiting list sessions to validate clinical notes and take a decision on the need for treatment. Reporting ensuring that any patient identified as being harmed by a delayed follow up is reported and lessons learned as part of this process of work. Agreement with General Practitioners colleagues on the process for discharge in the event that no follow up is needed. Review of Myrddin to ensure that the system is able to identify sub specialties and clinical conditions within the waiting list. Engaging clinical leads for each specialty in the prioritisation of their patients and the identification of those most at risk of harm. Establishment of a transformation programme for each specialty to map and redesign processes for follow up care, establish capacity needed and start the longer term modernisation of outpatient care across the University Health Board. Harm and Mortality Measures Our established quality and safety framework provides the Board and our patients and public with the assurance that our services are safe. We are committed to the transparent publication of a wide range of quality markers, safety indicators and mortality data and we constantly review our performance against best practice. The measurement of mortality statistics to help learn about the care we provide is well recognised. In June 2014 Professor Stephen Palmer published his report and independent review of the risk adjusted mortality data RAMI for Welsh Hospitals considering to what extent these measures provide valid information. Actions Being Taken that will continue in order to progress the Quality and Safety Improvement Objectives The University Health Board has taken forward the recommendations from Professor Palmer s report in which highlighted the importance of the key areas highlighted below. National Clinical Audits: The Clinical Audit Department for the University Health Board monitors participation of all National and Local Clinical Audits carried out across Hywel Dda, including community, Primary Care and mental health and learning disability Audit. This also includes the monitoring of all NCEPOD studies. The Department works with auditors, managers and clinicians to ensure that all national audits are supported, monitored and reported, and include a robust action plan for implementing recommendations. The Clinical Audit department is currently reviewing its function in relation to National Clinical Audits. Mortality Measures Within Clinical And Diagnostic Groups: We are in the process of reviewing mortality in disease specific groups working with the clinical specialist leads, and seeking to learn lessons from review. This includes acute and elective general surgery, and medical specialties such as cardiology, respiratory, stroke and sepsis. Our End Of Life group has undertaken a review of patients requiring palliative care in Glangwilli and is undertaking service improvement, and recruiting to additional palliative care posts. 61
62 Harm and Mortality Measures Professor Palmer made a number of recommendations as to how Health Boards should use clinical data effectively for quality improvement. National peer reviewed audits of clinical specialties are an important driver for clinical quality improvement. The use of condition specific mortality statistics at a University Health Board level is important to track changes in outcomes. There is a critical role in the review of hospital records and case note reviews. The accuracy and depth of coding (how we report our patient episode in hospital) is important and fundamental to developing any useful measurement of the quality of care. This requires the full participation of clinicians Actions Being Taken that will continue in order to progress the Quality and Safety Improvement Objectives Mortality Case Note review: In February 2010 the University Health Board commenced a continuous review of case notes of people who have died with the learning from these reviews is highlighted to clinical teams as well as a monthly report to the Executive Team. This process is evolving in line with the national mortality review process. For operational reasons, routine case note review in Carmarthenshire was temporarily discontinued in October However during the interval a more in-depth review of notes of selected surgical and medical cases has been undertaken. The mortality case note reviews recommenced in January 2016 in both Prince Philip and Glangwili Hospitals. Clinical Coding: Hywel Dda has had in depth analysis and investment into coding services and is % compliant within three months of leaving the hospital. Quality Metrics Reported to the Board: The Quality and Safety Sub- Committee on behalf of the Board has a suite of indicators to provide assurance to the Board on the safety of services. These indicators are published in a prominent place on the University Health Board internet site. In addition to this we publish our information in line with the Welsh Government publication scheme. Harm 2 Study: This 3 year research project led by Dr Sharon Mayor from Cardiff University involves a longitudinal measure of harm across NHS Wales. We have reviewed data for Bronglais General Hospital and Withybush General Hospital (Glangwili and Prince Philip data has yet to be received). We are starting to triangulate the study findings with the information we have on DATIX and what was found at the mortality reviews. The harm research provides an unbiased external scrutiny which has been useful to validate where we are and what we thought we knew from our existing systems and processes. Inpatient and Community C difficile & MRSA Actions Being Taken to progress this essential Quality and Safety Improvement Objective Our action and focus for the next 18 month period is on: Community acquired infection Antibiotic prescribing Devise management (e.g. lines) The introduction of the electronic system ICNET to strengthen the timeliness of information and monitoring. Some Success which we want to set as our baseline to improve upon: Now a Bevan Innovator in partnership with PHW based on our community work. 68% reduction in number of hospital in-patients (over age 65) acquiring Clostridium difficile infection C.difficile Rate 2008 = per 1000 admissions (over age 65). C diff rate = 3.77 per 1000 admissions April-Sept 2015 (all ages). MRSA Bacteraemia Rate per 100,000 population 2008/9 = 6. Current rate per 100,000 population Apr-Oct 15 = 2.67 What we know: High number of infections coming into hospital Urosepsis is Major Driver Blood Culture Positivity Rate 14% similar to All Wales, however, we take twice as many blood cultures. E. coli Bacteraemia have increased from 55 per 100,000 population in 2009 to 99.7 per 100,000 population in 2014 Top 5 Bacteraemia: 75% over 65 years of age (= 19% over age of 65, 28% over 70 and 28% over 80) Top 5 Bacteraemia: 62% Taken in Accident and Emergency or OPD. E. coli Bacteraemia: 70% taken in Accident and Emergency/ACDU. 62
63 Harm and Mortality Measures Actions Being Taken that will continue in order to progress the Quality and Safety Improvement Objectives Actions we are taking: Engaging, energising and empowering all staff and application of complexity science. Sepsis and associated use of invasive medical devices: o Implementation of Peripheral Venous Catheter Insertion & Blood Culture Sampling packs based on compliance audit data and Human Factors Studies. o Introduction of Chloraprepp for skin disinfection (incorporated into packs) in line with EPIC 3 guidance o Compliance Audit of ANTT Focus on IV therapy, Venepuncture, Peripheral cannulation, Catheterisation, Blood Cultures Antimicrobial Stewardship: o Audit of Antimicrobial Prescribing Compliance in line with guidance (web based tool developed) o IV to Oral Switch Focus o Antimicrobial Point Prevalence Survey o European Antimicrobial Awareness Day 18 th November Laboratory Sampling Practices & Influence: o Liaison with Urology, Care of Elderly & General Practice in relation to Urine Sampling o Procalcitonin testing (pilot Critical care Glangwili). Hand Hygiene (Overall percentage compliance, Breakdown by professional group, Breakdown by moment of hand hygiene) What are results of these actions evidencing? 10 less MRSA Bacteraemia April September 2015 compared to same period less E. Coli Bacteraemia April September 2015 compared to same period 2014 Blood culture contamination rate 2015 = % lower than 2014 data (consistent data across the University Health Board) less urine samples submitted (Carmarthenshire Lab data analysed) Quarter compared to same period Urine positivity rate remaining constant. Inpatient Falls Actions Being Taken to progress this essential Quality and Safety Improvement Objective Whilst the number of falls is consistent with other similar sized organisations, we are determined to do all we can to drive down both the number and severity of falls in our hospitals. This has been brought in to increased focus by the issuing of an improvement notice by the HSE related to the used of bed rails as a falls management tool. Our Action and focus will be Continue to get all wards to 100% compliance. Continued training and development especially of the nursing workforce. Improve understanding of SI reporting to ensure all appropriate incidents are escalated. The baseline we want these actions to improve upon: Inpatient Falls numerically high reporting (22-23%) of all incidents but similar to other providers (NRLS), and we are a lower reporter of severity compared to other Health Boards in Training & audit showing improving bedrails compliance (some wards now 100%), better assessment & use of equipment. Increased reporting from 2014 (same period 925) and for April to September 2015 (1251) have been reported. Although assumptions at this stage cannot be made we believe the focus on assessment and bed rails requirements have heightened awareness. Delays in Diagnosis and Missed Fractures Actions Being Taken to progress this essential Quality and Safety 63
64 Improvement Objective There are often delays in the pathway due to excessive waits for a radiological image to be taken, delays in radiology reporting following radiological investigation or interventional procedure, misinterpretation on image by junior nonradiology medical staff thus delaying diagnosis and treatment of patients. This affects both consultants and General Practitioners and has led to an increase in Grade 4/5 serious incidents and litigation. This relates to Emergency Departments in addition to radiology as issues occur if junior medical staff do not correctly specify or diagnose radiographs. Radiological Waiting Times improvement through investment The departments work to a standard on Inpatient imaging requests being managed within 24hours of the request being received. This is generally delivered. For non inpatient imaging the waiting times have fallen. At the end Oct 2014 we had 130 patients waiting more than the 8 week target with a maximum waiting time of 16 weeks. At the end Oct this year we have 28 patients waiting more than 8 weeks. Reporting and Missed Fractures improvement actions: An Action Plan and improved training for junior staff by Emergency Department Consultants is in place. Extended role Radiographer reporting is in place. New High Definition Monitors are Installed in appropriate locations. An Audit of Hips and C spines for 2014 (January to December) showed 0.3% missed fractures at initial presentation. To date no significant incidents reported related to missed Hip fractures/c Spine (Apr to date). Other improvement actions we intend to take: Hip and C Spine audit to be repeated for current calendar year. Continue to train and carry out Root Cause Analysis to learn from events when incidents occur Hospital Acquired Thrombosis Actions Being Taken to progress this essential Quality and Safety Improvement Objective The need to assess risk and monitor outcomes will be embedded, all sites are now reporting. How we intend to progress our actions comprise: The new Site Clinical Lead now has responsibility for implementation from October 2015 Now fully compliant with Welsh Government reporting requirements as of October Implementation of action plan monitor through Clinical Audit by Quality, Safety and Experience Assurance Committee (QSEAC) We will continue to audit to ensure compliance of reporting. Use Root Cause Analysis data assurance to review clinical practice and learn lessons. Link avoidable harm to redress. Medication incidents Actions Being Taken to progress this essential Quality and Safety Improvement Objective Patients receiving wrong medication as a result of transcription /prescription errors and the frequent omission of doses for inpatients leading to compromised patient care and an increase in patient morbidity and medication related admissions. Also cases relating allergy information not being considered and poor management around anti coagulation. How we intend to progress our actions comprise: Focussing on Missed doses. reviewing thematic issues by specialist Group Seeing Red Initiative. Monitor and Review by Quality, Safety and Experience Assurance Committee. Training and development Audit and learning from events. Safeguarding Adults and Children The risks for the University Health Board within Parts 2, 7 and 9 of the Social Services and Wellbeing Act (Wales) 2014 are clear in terms of the University Health Board s capacity and preparedness to discharge our statutory duties under this new legislation. The risks for the Health Board relate to the training implications for the Social Services and Wellbeing (Wales) Act
65 These are significant for the University Health Board and will need to be considered in partnership with the workforce and OD (Organisational Development) who will need to support delivery of the wider implications of the act, identify training plan, train the trainer etc. Specific risks associated with adult safeguarding include: The new definition of adult at risk, the duty to report and the duty to make enquiries. Each of these areas of the act, will require significant staff training; Additional professional and administrative capacity within the safeguarding adult team will be needed, to respond any enquiries/ allegations that are made against the Health Board. There will be a further requirement to ensure standardisation of processes across the University Health Board and the wider multi agency team are put in place eg A Regional Adult Safeguarding Board will need to considered, to support delivery of the act and agreement to look at standardising processes The new Adult Protection and Support Order This will again impact on training requirements of staff, There will be a need for specialised training to all clinical staff and consideration given to supervision of staff this can not be delivered within the current safeguarding resource. The Adult Practice Review process Statutory adult reviews will be required, there is no capacity to undertake these within current resource. The attendance in Adult Practice Review Panels; to learn from the reviews and identify feedback mechanisms across the University Health Board to ensure wider learning is also required under new act, again no capacity to deliver this within current resource. The need for Multi-agency engagement of Regional Safeguarding Adult Boards As above this will require additional adult safeguarding capacity to ensure an adequate University Health Board contribution and participation The need to provide funding support to Regional Safeguarding Adult Boards This resource will be required in order to ensure organisational reputation and partnership working are maintained as well as discharge of statutory duties And in governance terms, these actions will be performance managed as follows: Planning Directive, Welsh Government Objective/ Target / Guidance: NHS Outcomes Framework Outcome and Delivery Framework Targets Targets Executive Lead (Senior Responsible Officer): Director of Nursing, Quality and Patient Experience Profiles / Trajectories Yr 1 Yr 2 Yr 3 Executive Performance Management Forum Performance Monitoring and Assurance Meeting Chaired by CEO Board Governance: Committee or Sub-Committee Responsibility: Quality, Safety, Experience Assurance Committee 65
66 Chapter 4: Supporting and Enabling Strategies This chapter outlines our key supporting and enabling strategies which are drawn in the main from annexes to this Integrated Medium Term Plan. They summarise the positions and plans without which the University Health Board would be unable to effectively deliver the developments and improvements in clinical services and patient experience in the remainder of this document. 4.1 Organisational Strategy In order to deliver our 10 strategic objectives and the programmes of work that arise from them there is a need for a range of supporting and enabling strategies to be in place. Everything that we do needs to be underpinned by these and our actions and behaviours will demonstrate that we are in fact putting our values and prudent approach into action and living out in a very real way what legislation, standards and policies require us to do. It is easy to have rhetoric that aligns to these but what really builds public confidence and makes a difference is turning that into a culture and way of doing things on a day by day, project by project, patient by patient basis. It is that challenge we have set ourselves and that we want to rise to. The test of whether we are really embedding these values and principles will be our public, patient, carer, family and staff experience. Ultimately it will be what we do and how we do it that speaks so loudly that it overshadows anything we say. There has been significant new legislation from Welsh Government in the past year, The Wellbeing of Future Generations (Wales) Act, which has set an inspiring future vision for the Wales we want. In addition we are awaiting from the Welsh Language Commissioner our Welsh Language Standards. We want to respond to this legislation and the existing equality legislation by embracing the development of the wellbeing goals with our public sector partners and to implement both the spirit of the law and the clear duties and expectations of the University Health Board as a key public sector leader. We want to go beyond mere compliance with the Acts and really embed the aims in our strategies, actions, governance, approach to service delivery and the way we deliver our services on a day to day basis. One key way we will do this is to develop an Integrated Impact Assessment tool which allows us to be sure that each plan we put in place has taken account of the impact of the following: quality, equality, health inequality, finance, prudency, legal, information governance, the wellbeing goals, the Welsh language, those with sensory impairment or disability and more. This will be more than a checklist but become part of a culture of looking long term and really thinking through the impact of everything we plan so that we can avoid unintended consequences and put the right values at the heart of our decision making. We will also put governance at the heart of our organisation and engagement at the heart of all that we do. In 2015/16 we undertook a rigorous External Governance Review that gave us a clear route-map of what to put in place to make sure we had a governance structure and approach that was best practice and that would support the Board to make its decisions and assure itself that the services were delivering high quality, safe, sustainable services within the financial envelope it had. Those recommendations have largely been put in place and alongside a restructuring of the committee structures, risk management approach, change of accountabilities and revised scheme of delegation there has been vastly improved openness and transparency. However, structures are one thing and a culture of good governance is a longer journey and that is what we will focus over the next three years embedding a culture of sound decision making, risk management, assurance based on triangulated evidence and performance management and holding to people to account. 66
67 The way that we communicate and engage with our public, patients and staff demonstrates that we really do intend to be open and honest and to have a two way conversation where we really involve people in our decisions and our service planning and particularly when we are looking at making any changes to services. We have built back over the past year or so from a place where the public had little trust in the University Health Board. Through a series of more than 28 engagement events (including new virtual events online) and a lot of proactive communications have met with, listened and responded to our public. We fully intend to continue that dialogue and to be open and honest about what we are planning, how we are doing, what is going well and where we have fallen short. We want to work together in a new way and to find ways where our public, patients and staff can participate in decision making a both an individual level where shared decision making can happen between a patient and a clinician and at an organisational level where the public, patients, families, carers and staff can participate in decisions about service change and help us tackle some of the big challenges we face, together. We want this to become the hallmark of the way the University Health Board works and for it to bring better decisions and more meaningful change that really does improve things for everyone. We want to capture the passion that the people of West Wales have and join forces to improve the services of our National Health Service here in Hywel Dda. We will only do that by being very honest and open and inclusive and reaching out to hear those voices which are seldom heard as well as those who feel confident to articulate their views. This will mean we will engage differently and alongside the traditional methods people like to use to communicate through, to use the opportunities new technology and social media provide to reach new and wider audiences. Over the past 5 years we have invested heavily in partnership working, starting from a low base and building trust, relationships and networks with a range of public and third sector partners. We had a Director of Strategic Partnerships and team to undertake this work and to make sure that it became a hallmark of the way we worked. We now have long established, mature relationships with all our partners whether Local Authorities, Police, Fire and Rescue, Universities, the Third sector, Armed Forces and other patient groups. This is both at a strategic level through Local Service Boards and at a more local level through health and social care partnerships and third sector compacts. We have led the way on third sector partnership working and commissioning and now it feels that partnership working is just the way we do things in Hywel Dda. Throughout the whole of our organisation this approach is now a reality and so the need for a partnerships directorate is no longer needed. In the next three years we will be active leaders in our Public Service Boards as they become statutory partnerships and also throughout our many collaboratives. We will also develop a partnership governance framework to ensure that we are clear what our significant partnerships are and what framework they have in which to work. This will be developed with each of our partners to ensure that the same rigorous approach to performance management, risk management and registers, governance and decision making and probity and processes are followed and can provide assurance to both partners governing bodies, in our case the Board. Our draft organisational strategy seeks to develop a single organisational strategy to encompass themes to reflect: Organisational Development Staff Experience Patient Experience Public Engagement Quality Improvement Communications 67
 and provide a strong visual and simple staff and public framework which links our values, plans,")

68 Each of the above components required some form of documented strategic direction in order to provide the organisation with clarity of purpose within these key areas. It was therefore considered appropriate to attempt to link the themes (as they clearly overlap) and provide a strong visual and simple staff and public framework which links our values, plans, direction and objectives together. It was clear from talking to our staff that they would not see the value in a lengthy set of strategies which did not reflect the role they need to play and therefore the plan will be to have key work programmes underpinning this organisational strategy which sets out clarity of action required. As an example there will be no dedicated nursing strategy, a nursing work plan will be developed based on this organisational strategy and will set out practical steps to be taken to meet the key principles. Our overarching values will be: Integrity choosing to do the right thing every day Openness and honesty being transparent and accountable about what we are doing and planning to do Dignity treating people in a way that supports their self respect Respect being polite and have due regard for the feelings, wishes and beliefs of others Fairness treating people in a way which is right and reasonable People focussed putting the population at the heart of what we do and how we do it Pride - having a sense of satisfaction and /or pleasure in our own and others success Excellence working as one to be the best that we can be Our organisational strategy can be illustrated as follows: Our Organisational Strategy 10 Strategic Objectives Our Priorities Patient and Communities Centred Quality Improvement Learning Organisation Leadership Improving Organisation These four underpinning domains are illustrated further below 68
69 Centred on Communities Aim: The NHS is owned by every one of us. Hywel Dda University Health Board believes the only way to build the NHS of the future is to involve our staff, patients, carers and families, partners and communities to design and deliver good quality health services. Living health lives we believe each of us as an individual has a responsibility to make healthy lifestyle choices to improve and maintain our health. We will support you to live health lifestyles as well as provide services when needed. Building and sustaining healthy communities we fully embrace the spirit and the wellbeing long term goals of the Wellbeing and Future Generations (Wales) Act to help the organisation make sustainable decisions. We will develop a plan to make this a reality for the population we care for today and in the future. Working together to develop services and make better decisions we will only improve health and wellbeing by working with the public, patients and professionals as equal partners. We will care for those with the greatest need first, make the best use of skills, do only what is needed no more, no less and no harm and use evidence based practice consistently. Confidence and trust in the NHS we know that people highly value the NHS in west Wales. Our role as an organisation is to build and maintain that trust in the community. We will be open and honest with everyone when we communicate. We will listen to all views and seek out the seldom heard and quiet voices. Growing our own talent we believe our staff is our greatest strength. We will support our current and future staff to reach their potential and continue to learn, grow and develop. We will work with our communities, universities, local colleges and schools to raise the understanding of the organisation and consider working in health as a future career option. Centred on People Aim: Placing patients and their families at the centre of their care, all interventions and care will be personalised, coordinated and enabling; and all people that interact with us will be treated with respect, dignity and compassion. We will listen to, learn and act on feedback from our patients and their families; and our services will be designed and co-produced with the involvement of the population we serve and we will be a healthcare provider employer of choice in Wales, with staff that are respected and valued by colleagues, patients and the public. Understanding the patient s experience in accessible ways for all patients and carers so they can provide feedback to us and ensure that realistic and achievable actions are taken on the basis of this feedback; be it to share good practice or to make improvements and ensure that you know we have acted on that feedback. Patients as Partners in Care We want you to know that we will include you as full partners in your care. To do this, we will use a range of approaches and schemes such as Shared Decision Making and ensure that our patients understand what is happening with their care and provide good quality, accessible and clinically approved information to support discussions; as well a range of health literacy schemes. Co-designed Future Services We want to work in collaboration and with honesty with our patients and population, in order to co-design future services, ensuring that services are planned and designed around our patients. Patient Centred Workforce We want to support our staff to do their best at all times. We will create good first and lasting impressions, implementing schemes such as hellomynameis. To support this, we will provide a co-designed training programme for all staff, making explicit the expected standard of partnership working with all patients and their families, based on openness and transparency. Valued Workforce We want to improve on the work we do in ensuing appropriate support is offered and provided, either from within the organisation or from a third party, for staff who are involved in stressful or traumatic incidents or whose conduct or practice in work, is being investigated or scrutinised. Protecting Confidential Information We must clearly explain how we use all information about patients and staff and we will protect the confidentiality of all personal information. We will obtain consent prior to sharing any personal information with a third party. Where we need to make decisions about the use of information, on behalf of patients or staff we will ensure we act in their best interests. Quality improvement A learning organisation An improving organisation Leadership 69
70 A Learning Organisation Aim: Emphasise learning and promoting best practice across the University Health Board, Wales and healthcare across the UK the system is focused on learning, locally and nationally and makes extensive use of improvement methodology to test and implement the necessary changes. Near misses listen to our staff and patients to ensure we achieve improvements. System approach We will: Celebrate our successes and use these to embed best practice throughout the organisation. Use adverse events act as a window to allow improvement. Review monitor performance against other Organisations to ensure development Positive safety culture We will: Avoid, prevent and mitigate risks at all levels of the organisation. Ensure decisions relating to the management of adverse events are risk based, informed and transparent. Teamwork We will: Ensure everyone who works for our care system is valued as an essential and equal member of the team, Ensure everyone is empowered to work to the best of their ability. Encourage and foster team working to ensure effective patient care. Encourage and foster a culture if trust, mutual respect and open communication. Open about failures We will: Ensure errors are identified, reported and managed in a timely manner Ensure patients, service users and their families are told what went wrong and why. Review events quickly following their occurrence. Personal, professional and organisational accountability We will: Ensure everyone is responsible for taking action to provide good care to patients, services users, their families and carers. Ensure our workforce have the confidence and support to speak up when they see practice that endangers safety. Ensure all staff understand their roles and responsibilities Ensure our staff are supported and developed to fulfil their current roles and to develop into roles for the future. Just culture Assuring Quality We will: Individuals are treated fairly. Strengthen an Organisational culture is based upon the values of trust, openness, equality and diversity. Encourage and supports staff to recognise, report, learn from adverse events and implement service improvement. 70
71 Assuring Quality Aim: To provide Assurances that we are delivering on Quality there will be strong and effective leadership, the right infrastructure and commitment from all staff. Information will be reliable, measurable and used to make improvements to patient outcomes. Actions from key objectives will be monitored through appropriate Scrutiny processes. There will be clarity on what, how and why we are measuring to achieve the best possible outcome for our patients. Local ownership We will: Develop leaders who are clear about their professional accountability and who focus on delivering high standards of care. Develop an ethos where leaders benchmark and use accurate data to inform their local operational delivery plans.. Clear roles and responsibilities We will: Ensure that every staff member has clarity about accountability, roles and responsibilities. Be clear about the managerial structures within the organisation and clarify who are the identifiable owners of services, wards, pathways Be clear about reporting and monitoring lines of accountability. Smart quality objectives which are patient outcome focused Reliable Reporting Process Optimisation and Standardisation We will: Support the development of quality and safety objectives at Board and Operational Service level. Ensure objectives are person centred which support improved outcomes for care Ensure that objectives identified clearly demonstrate the impact of overall patient outcomes. We will: Ensure information is reported on agreed HB sources, such as the Risk Management System eg. DATIX, Health, and Care Metrics, and validated Dash Boards. Develop Patient Related Experience Measures and Patient Related Outcome Measures to support service development and continuous improvement. Invest in and develop the use of technology systems to support reliable data capture and reporting We will: Encourage the use of standardised operating procedures, which will form the basis of continuous improvement Encourage front line staff to assist in the formation of automated pathways, which will replace guidelines and provide feedback mechanisms to the developer of the pathways to ensure continuous improvement Outcome Measurement and monitoring We will: Involve staff at Leadership all levels to develop scrutiny processes and checks, to oversee the monitoring of agreed objectives and outcome measures. Ensure we benchmark services with the best to establish key outcome measures to support quality. 71
72 Leadership Aim: To have leaders who live our values and communicate our vision, and re-iterate at every level, the message that high-quality compassionate care is our core purpose. Our leaders work together to inspire confidence and innovation in individuals and teams by nurturing a positive culture, emphasising quality, safety, compassion, engagement and transparency. Person centred Leadership We will: Ensure our leaders role model our values and behaviours, Focus on delivering excellence in staff health and well-being. Attract and retain staff through being an employer of choice Visible Leadership We will: Ensure our leaders are visible Have regular contact with teams and individuals Underpin all that we do with our Values and Behaviours Framework. Maximise the benefits of Values Based Recruitment We will continually improve our staff and patient experience through excellent leadership Collective Leadership We will: Ensure we have high levels of team working and co-operation Increase the development and delivery of Team Based Working. Develop our staff through methods such as the Consultant Mentoring Programme, Provide access to coaching development and networking work with our managers to lead by example. Engaging Leadership Quality Leadership Values based Leadership We will: Strengthen our engagement with our Patients and wider community Listen to our public and patients using experiences to shape our planning. Develop our future workforce through work experience, careers, schools & colleges liaison Co-produce our services with our population. We will: Deliver supportive people management and leadership, Provide leadership and management development programmes. Expect our leaders to regularly feedback to teams and individuals Expect our leaders to set clear goals and give feedback on performance Use the PADR/Appraisal system to support individual development. We will: Revise and deliver our internal leadership development suite Ensure access to external programmes Deliver increased Improvement Capability through the Improving Quality Together programme. 72
73 An Improving Organisation Aim: Our whole system is focused on learning and delivering a high reliability service; built on meeting and exceeding standards and continually improving in all that we do. We listen to our staff, patients and our community and learn from our mistakes as well as our successes. We make extensive use of improvement methodology to test and implement changes. What we will improve We will improve services to patients by: Listening to what staff and patients tell us we will better understand our systems and services and will identify areas for improvement Develop a structured improvement plan. Using and analysing a wide variety of information we will create a culture which supports and sustains creativity and innovation and stimulate continuous learning and improvement. Our Approach One Team We will build a culture where: Staff feel positive about the organisations approach to quality and safety, teamwork and leadership. Staff and service users feel comfortable discussing errors and standards of care. The development of continuous learning and improvement is encouraged, facilitated and embedded into everyday practice and complements professional values and knowledge We will create a team approach to improvement where: Everyone who works for our care system is recognised as an essential and equal member of the team All staff and service users views, contribution and experience are valued, Everyone is treated well and empowered to work to the best of their ability. Innovation and creativity that comes from the diversity of each team member is maximised by adopting a multidisciplinary approach to all aspects of our work by explicitly fostering a culture of trust, mutual respect and open communication. Communication and Engagement We will provide systems that: Make it easy for staff and patients to raise concerns before they affect patient care. The safety and quality of patient care and the actions taken to prevent them happening again are measured monitored and reported Engage staff and patients in the development and implementation of improvement interventions, Use a systematic approach which is, evidence-based and context appropriate. Tell patients, service users and their families what went wrong and why. Review events frequently and quickly following their occurrence. All of our responsibility We will provide reliable services to patients, services users, their families and carers by: All staff will be responsible for creating a continuous improvement culture, Taking action to prevent adverse events Speaking up when they see practice that endangers safety, in line with the organisation s Raising concerns policy. Being explicit and clear about roles and responsibilities in relation to improvement. Ensuring that all individuals understand when they may be held accountable to their actions. 73
74 4.2 Governance The University Health Board has in place governance and assurance arrangements which are continually being developed and strengthened. During the year, Welsh Audit Office undertook the Structured Assessment 2015 (Year 6) review of the University Health Board which examined the arrangements to support good governance, (effective quality assurance) and the efficient, effective and economical use of resources. In governing the business, the assessment concluded that the organisation has continued to strengthen governance arrangements and has built a more open and engaging culture, although it is recognised that progress on some issues has been slow and fundamental issues still need to be addressed (including agreeing a clear strategic plan and strategic objectives, establishing a Board assurance framework and improving performance). In early 2015, the University Health Board commissioned an external review of its governance arrangements whose purpose was to identify how the University Health Board could strengthen its governance arrangements. The external review report identified a total of 58 recommendations covering structure and remit of the governance team, effectiveness of the Board and its Committees, complaints and incidents management and reporting, assurance process robustness, managing risk and partnership / inter-organisational governance arrangements. Good progress has been made in implementing these recommendations although deadlines have been extended for meeting some of these. Further details of our governance processes and structures can be found in Annex 9. 74
75 Board Audit & Risk Board BPPAC?Performance Assurance Board BPPAC BPPAC Sub Committees Maturity Assessment G and A Module Measures and Integrated Performance Reports Board Audit&Risk Board Local Partnerships Forum P.A. Group Board Audit & Risk Assurance Committee?Finance Sub Committee Values, Culture and Leadership Performance Database Integrated Plans Financial Management Internal Audit Domains - I.A. Cap / PFI Clinical Audit Safe Care, Compassionate Care 8 Quality Trigger Questions Are we providing safe care? Are we meeting required standards of effective care? Are we improving user experience? Are we providing efficient services within resources? Are we engaging the workforce? Are we providing accessible and equitable services? Are we improving population health? Are we working effectively with partners and stakeholders in planning for the future to Governance Structures Health and Care Standards Wider Public Sector - HSCWB Partnerships Volunteering Public Information and Transparency Board QSEAC Alignment to underpinning Committees Board BPPAC?CEAC (ECPSC) Audit Board Health Inspectorate Wales Reviews Wales Audit Office Structured Assessment Information Delivery Plan Group BPPAC Board Alignment to underpinning committees; QSEAC BPPAC MHLAC, Board BPPAC Audit Board 75
76 4.3 Our Equality Strategy & Welsh Language Equality Strategy - The Equality Act 2010 requires Health Boards and Trusts to pay due regard to the need to eliminate discrimination, harassment and victimisation, promote equality of opportunity and promote good relations (the General Duty) 1 The Public Sector Equality Duty for Wales (PSED) 2 requires Health Boards and Trusts to undertake a specific set of actions to demonstrate improved performance against the General Duty. The University Health Board has developed a set of equality objectives and published these equality objectives in its Strategic Equality Plan (Annex 10a). In line with the Duty, the University Health Board is currently reviewing it s stated objectives for 2012/16 and has undertaken a multi-agency joint public engagement exercise across the Dyfed Powys area. Draft objectives drawn up following this exercise for the period 2016/20 will be open for consultation prior to publication of approved objectives by 31 March The Duty places a requirement to undertake Equality Impact Assessments when developing, reviewing and revising policies and services. The Integrated Medium Term Plans should describe how these assessments inform planning and decision-making this is the Integrated Impact Assessment process described in the Organisational Strategy section. Welsh Language The University Health Board recognises the official status given to the Welsh language under the Welsh Language Act 1993 and the Welsh Language (Wales) Measure It aims to meet the statutory requirements through compliance with its own Welsh Language Scheme and the organisation is preparing for the introduction of the new Welsh Language Standards. Our aim is to provide services that satisfy the needs of Welsh speakers so that they are able to receive care that meets their needs in their own language as a core component of care. Communication in language of choice is a fundamental aspect of care that leads to better care, greater patient satisfaction and improved outcomes. As a principle the University Health Board promotes and facilitates the use of the language with the aim of treating the Welsh language no less favourably than the English language and actively works to enable Welsh speakers to use the language when dealing with the University Health Board. We aim to improve this further over the life of this plan by ensuring the delivery of the active offer concept, so public is automatically delivered of services in Welsh without the need to ask. We demonstrate further commitment to the integration of ownership in relation to the actions in the More Than Just Words framework in order to ensure that Welsh Language Officers are not solely responsible for the delivery of the strategy and that Welsh Language services are considered at the planning stage. The University Health Board s Welsh Language team is working with Primary Care to develop a planned approach to implementing the recommendations set out in the Welsh Language Commissioner s report into Primary Care. The University Health Board is also taking important steps by developing a Welsh Language Skills Strategy (Annex 10b) that focuses on: Bilingual Skills & Workforce Planning A Learning & Development Strategy and 1 The General Duty cover the protected characteristics of age, gender reassignment, disability, pregnancy and maternity, sex, sexual orientation, race, religion or belief, marriage and civil partnership. 2 Equality Act ( Statutory Duties) (Wales) Regulation
77 Strategic Recruitment including a Welsh Language Skills Matrix. As a healthcare provider, one of Hywel Dda University Health Board s objectives is to accurately assess people to be able to meet their needs, and the language needs and cultural identity of our service users must be considered as central to this assessment. Under the requirements for needs assessment under the Social Services and Well-being (Wales) Act 2014, the University Health Board will work with the three Local Authorities to collect data at a local level, and the outcomes of these assessments will in turn be used to inform service development. 4.4 Workforce and Organisational Development The aim of this refresh is to present current information on our University Health Board workforce, and update on progress in delivering the planned work described within the Integrated Medium Term Plan, the current and anticipated challenges over the next 12 months and the actions planned to mitigate the associated risks. The overarching strategic aims and detailed narrative associated with the themes is retained within the body of the core Integrated Medium Term Plan. Our current workforce profile The principles of Prudent Healthcare underpin all plans as does the investment in the development of our staff to maximise their full potential to deliver the prioritised service outcomes. The University Health Board will achieve this via number of workforce initiatives and techniques which are detailed within this refresh. Hywel Dda has 9,985 directly employed staff; which equates to 43% of our budget and does not include our Primary Care contractor workforce or the significant number of social care staff across our three Local Authorities. The current breakdown of the University Health Board by staff group as at 30 September 2015 is reflected in the table below. Staff Group WTE Headcount Add Prof Scientific and Technical Additional Clinical Services 1, Administrative and Clerical 1, Allied Health Professionals Estates and Ancillary Healthcare Scientists Medical and Dental Nursing and Midwifery Registered 2, Total 7, The current vacancies across the University Health Board as at 30 th September 2015 is 574 WTE, and the total variable pay spend is 15.5m (agency, bank, medical locum and overtime) during the year to manage service demand, plus cover for posts where we have gaps due to the recruitment challenges we face in some sub specialties. This is neither economically sustainable nor does it provide the highest quality of care. The current turnover rate by staff group based upon average turnover over the last 3 years provides additional recruitment vacancy figures for inclusion in our recruitment plan in year is reflected in the table below: 77
78 STAFF GROUP TURNOVER % FULL TIME EQUIVALENTS (FTE) Registered Nurses 6.54% Unregistered Nurses 4.81% Registered Physiotherapists 8.78% Registered Occupational Therapists 7.36% Registered Podiatry 3.04% Registered Speech and Language Therapists 4.53% Medical and Dental 15.16% Our key workforce characteristics are: Gender: our workforce is predominantly female with the majority of staff working full time. Welsh Language: based on the 60% return from staff used to collate the data on welsh language skills we currently have 18% of our staff who are proficient in using basic Welsh Language skills in the workplace and have achieved level 3 (intermediate), 4(higher) or 5 (proficient).the University Health Board takes our responsibility to provide bilingual services to our patients very seriously and have developed and begun to implement a bilingual skills strategy. Age profile: 34% of our total staff are between the ages of 46 & 55. There are very few employees below the age of 20. However when looking at the different staff groups the ranges and associated risk changes considerably. The tables below reflect the registered nursing and medical and dental profiles: Nursing and Midwifery Medical and Dental Key workforce challenges we currently face In summary the key workforce challenges are: the age profile and potential retirements National shortages for some professional groups recruitment and retention of staff the impact of the Safe Nurse Staffing Levels (Wales) Bill and nurse revalidation operational capacity to support the increase student numbers and new recruits particularly those from overseas. control of the variable pay expenditure modernising workforce models and practice, new roles and use of technology, rurality and the resultant impact upon recruitment and flexibility to use our workforce across services/localities in year unplanned service changes and developments with workforce impacts 78
79 Progress in delivering our 2015/16 Action Plan To date the Workforce and OD teams have: Reviewed the recruitment strategy and enhanced working practices by Use of social media via sites such as LinkedIn and Facebook to both recruit and to raise the profile of the University Health Board. Innovative advertising campaigns which include videos of service leads walking the patch and showing the units more actively. Overseas recruitment campaigns. Introduction of value and behavioural based recruitment selection criteria aligned with University Health Board values. Establishment of monitoring systems. Attendance at Careers fairs across the Country. Increased focus on work experience and links with local colleges and school as well as the LIFT initiative (13 applications received, 10 offered placements and 7 accepted). proactively linking with students in training nearing completion and arranging informative recruitment days with presentations from the Board, (of the 2 days run to date, the March 2015 day-54 attended and 50 recruited, and the day run in September attended and all were recruited.). Planning the development of staff pools with fixed but flexible hours. More imaginative initiatives support utilisation of volunteers to be the Employer of Choice. Improved PADR rates, current focussed work has increased the compliance rate to 43% in November. health and wellbeing services and staff benefits in place, and wellbeing days have been held on two main hospital sites with very good attendance. Management passport programme supporting management competence. Involve staff in improvement programmes. Begun work refining medical job planning. Hywel Dda is the first Health Board in Wales to appoint two Bevan Commission Fellows, and has a new appointment of a respiratory chair with Swansea University these are both important means which will help to attract and retain leading clinicians into Wales, creating a dynamic learning and innovative climate in which to live and work. Restructure of the resourcing (recruitment) teams to include medical recruitment to align working practices and efficiency. Results: New recruits to the University Health Board since 1 st April 2015 Starters Staff Group April December 2015 Additional Professional Scientific and Technical Additional Clinical Services Administration and Clerical Allied Health Professionals Estates and Ancillary Healthcare Scientists 3.40 Nursing & Midwifery Registered Total New recruits Thirty-eight European nurses have been offered posts since the summer of 2015 (20 will have commenced by 25 th January 2016), and 42 qualified nurses have been offered a post with the University Health Board from the first two SKYPE interviews in the Philippines. 79
80 There are aspects of the Workforce and OD work plan which still present a challenge and which the University Health Board recognise needs further work: Electronic Staff reported appraisal compliance rates as detailed above but detailed work plans now in place to support continued improvement. Sickness absence rates, the University Health Boards performance to date is less than satisfactory and a reduction in sickness absence has not been evident. To support this moving into next year a post has been created specifically to focus on supporting service to manage sickness absence and a staff physiotherapy access service established. The University Health Board recognises that the plan can only be delivered through strong and honest partnerships with staff and their representatives as well as through our engagement infrastructure. Partnership working is imperative if we wish to ensure a locality perspective to healthcare delivery. Next Steps for 2016/17 (detail within the workforce plan can be found in Annex 11) Stabilise the workforce to reduce variable pay as far as possible by continuing the current work streams as described. Increase capacity on the internal nurse bank to eradicate Healthcare Support Workers (HCSW) agency usage, and reduce reliance on nurse agencies particularly off contract agencies. Plan for 30 Physicians Associates by 2019 Further expand overseas recruitment to include Europe and Asia. Strengthen and deliver a speedier recruitment process by creating central control for the process. Increased attention to the retention agenda and the development of our current workforce to ensure turnover is reduced and a skilled workforce maintained. Become the best at delivering LIFT programme Refining and strengthening further the Bi Lingual Skills Strategy and the associated KPI to align with our modernised recruitment processes and the potential for further requirements within the new Act. Increased focus on how we can improve workforce retention rates through a range of work streams including: assessment of opportunities to retire and return for key experienced staff with specific role to mentor and develop skills of less experienced teams, focussed succession planning, leadership development and develop plans for our current workforce and structured exit interviews. Further development of primary care workforce plan to ensure community services are adequately resourced for the needs of the future. Modelling of the medical workforce to ensure services are provided in line with service plans contained within the Integrated Medium Term Plan eg respiratory medical model. The recruitment delivery plan for 2016/17 is based upon the vacancies within our current funded establishment and the known planned/funded developments and the projected turnover by profession. And in governance terms, these actions will be performance managed as follows: Planning Directive, Welsh Government Objective/ Target / Guidance: NHS Outcomes Framework Outcome and Delivery Executive Lead (Senior Responsible Officer): Director of Workforce and Organisational Development Profiles / Trajectories Yr 1 Yr 2 Yr 3 To follow Executive Performance Management Forum Workforce and OD Sub-Committee Board Governance: Committee or Sub-Committee Responsibility: Quality, Safety, Experience Assurance Committee 80
81 Framework Targets 4.5 Infrastructure, Estates & Capital Planning Assumptions Effective management of land and buildings is fundamental for the University Health Board achieving value for money, service delivery objectives, compliance standards and reduced operating costs. The University Health Board has in 2015/16 completed significant capital schemes to support the efficient delivery of unscheduled care services in Prince Philip and Bronglais Hospitals. Completion of these major schemes enables the University Health Board to move forward with an estates programme that is focussed on: Assurance of risk management and targeted investment to reduce risk; A framework for improving the condition, functionality, suitability and performance of the Estate with a focus on the patient environment; Assurance that clinical services will be supported by a safe, secure and appropriate environment; Strategic Capital investments that reflect service priorities A plan for change that enables progress to be measured and benchmarked Assurance that asset management costs are comparable with best in class A clear commitment to complying with national guidance in key areas including catering, cleanliness, maintenance and environmental management; A commitment that all unsuitable assets are appropriately managed through maintenance, adaptation or disposal; The key challenge for Hywel Dda is that 52% of the estate is between 30 and 65 years old, affecting both operational performance, and estates performance. Typically an aging estate can suffer from minimal insulation, single glazing and poor heating control. Sixty per-cent of our estate is over 30 years old and the impact on energy efficiency is demonstrated in that our consumption per m² is the highest in Wales. Our pioneering Energy Performance Contract (EPC) has been a strategic approach to improving our energy efficiency and mitigating cost and will be a continued focus. The assessment of backlog maintenance currently sits at 53M of which 23.8M is high or significant risk and the University Health Board manages this through a risk management and prioritisation process, to reduce corporate risk. An essential element of developing the University Health Board s Estates Strategy, currently in draft (Annex 12a) is the development of a forward plan for estate development in primary care that integrates both maintains and improves the core functionality of primary care, and supports the increasing demands on the community estate by the Care Closer to Home model. The University Health Board has established this process, and will complete prioritisation plans during early 2016/17 to ensure inclusion of assumptions for innovative funding pipeline projects. In service terms the University Health Board operates four significant hospitals each of which has a medium to long term future, and need to be configured both to support emerging changes in clinical service delivery and technological improvements, and to continually strive to provide a modern patient environment. In the community there is the requirement to support the delivery of care closer to home both through radical modernisation of the community hospital estate and improving the functionality and capacity of primary care premises. The objectives of our emerging Estates Strategy are therefore to address these key issues. Improve patient experience Focus on high risk High quality assets Focus on refurbishment of existing buildings rather than new build 81
82 Achieve best in class occupancy costs for our estate The Strategic Estates Programme is supported by a combination of effective prioritisation of the University Health Board s Discretionary Capital Allocation which is set at 4,947,000 and the submission of business cases to Welsh Government. Capital Planning Assumptions Our overall approach is that the Integrated Medium Term Plan must prioritise both capital developments in line with our strategic service direction and backlog maintenance, which is also informed by the current risks we hold as an organisation. The level of the discretionary capital allocation over the last few years has made it extremely difficult for the University Health Board to resolve risks around: infrastructure and statutory backlog replacement of medical equipment standardisation of medical equipment to enable cross site working rolling ward refurbishment programme to deal with statutory and infrastructure backlog replacement of major radiology equipment general rooms, CT & MRI significant upgrades of IT infrastructure The University Health Board has reviewed our future capital planning priorities on the assumption that the Discretionary Capital Allocation for the next few years does not increase from the 2015/16 allocation. Discretionary Capital at this level does mean that the University Health Board will have to approach Welsh Government with programme and project business cases which are for lower value schemes, as there is insufficient funding to support such developments from within the Discretionary Allocation. From April 2016 the only currently approved large scheme which the University Health Board will have on site is the remainder of the work on the Front of House Scheme in Bronglais. Consequently, there are some real opportunities to start to address our backlog maintenance and equipment replacement programmes, which is significant. Estates & Infrastructure Backlog: Services are currently provided from 4 acute sites, 5 Community Hospitals 2 Mental Health Inpatient Units and over 30 other sites. The building and infrastructure backlog maintenance cost associated with these properties currently stands at 52m ( 2.7m High, 20.6m Significant, 17.96m Moderate and 11.04m Low risk) To help tackle this, we have undertaken a programme of estates rationalisation since 2012 which has reduced floor area occupied by 8,256m 2, and we have further plans to reduce floor area by 3,388m 2 in the next months and possibly a further 7,484m 2 over the next 3 years as the development of locality plans progress. There are some new build schemes within our Integrated Medium Term Plan which are currently at Full Business Case stage which are also enablers to the delivery of Proactive Care Closer to Home, such as Cylch Caron and the re-provision of services in Cardigan. In these instances the new builds will reduce backlog on the sites that will be disposed and enable 21 st century healthcare in 21 st century buildings. Information Management & Technology (IM&T): The University Health Board has currently prioritised Information Management and Technology risks from an annual allocation of between 0.3m and 0.8m from the Discretionary Capital Programme. The Capital Development Plan & Risk Register holds a complete schedule of the Information Management and Technology investment required to deal with our current risks and future developments. Investment in the appropriate Information Management and Technology infrastructure will improve quality, safety 82
83 and improve outcomes and also eliminate duplication of effort by ensuring that the right person has access to the right information at the right time. We have prioritised these investments in our capital planning as we believe a shift- change in the Information Management & Technology infrastructure of the University Health Board could bring benefits to patients, service users, by investing in Tele-health, clinicians and other care professionals, by enabling them to provide Care Closer to Home by investing in the ability of staff to access information whilst mobile; and health service commissioners and providers, giving them the information they need to improve health outcomes and obtain the best value for the public money spent. One example of this will be the procurement of the Community Care Information and Communication Technology solution. To deal with all the current backlog issues and progress with this development work, the University Health Board will require around 12m over the next 5 years and will be the subject of a Programme Business Case. Replacement Equipment: In addition to the backlog issues around Information, Management & Technology and Estates the University Health Board currently has an additional 32m of equipment which is fully depreciated. Of this around 4m is out of support and at risk of being un-repairable in the event of breakdown. The equipment backlog figure includes the following equipment; Medical equipment, especially theatre, Critical Care, Accident & Emergency, Ward and Outpatients; Diagnostic pathology, radiology and endoscopy equipment, plus non-medical equipment such as decontamination equipment and Catering equipment such as dishwashers and industrial freezer units The University Health Board is therefore carrying a significant backlog risk and the current level of the discretionary capital allocation makes it impossible to replace all items as they come to the end of their expected asset lives. Discretionary capital is prioritised on a consistent risk score methodology. Current funding only allows a proportion of those items predominantly with a risk score of 20 or above to be purchased annually. This is the context in which the capital planning scenarios for Hywel Dda need to be considered for the Integrated Medium Term Plan from 2016/17. Capital Planning prioritisation: The University Health Board Capital Programme has been developed taking into consideration the Welsh Government prioritisation criteria of health gain, affordability, clinical and skills sustainability, equity and value for money. Consideration has also been given to the same key principles which also align with our strategic direction of Care Closer to Home. These developments must help tackle statutory and physical backlogs within the existing estate, help generate savings or invest to save, enable faster disposal of older non functionally suitable sites, and be enablers to the deliverability of changes to clinical services With these principles in mind, we have a schedule of 26 schemes (Annex 12b) which will help deal with current risks and key developments, details of which are in the table below, of which 4 are on site, 4 are being currently being actively progressed via business cases, 8 have feasibility or scoping work ongoing and 10 need to be prioritised by the University Health Board. A programme of this scale will require further prioritisation to ensure limited resources to drive the schemes forward are directed to the most appropriate areas. This will be developed further for the final March 2016 plan. The capital available will be based on the University Health Board s success in developing business cases that meet Welsh Governments investment criteria. The University Health Board also acknowledges that All Wales Capital is a scarce resource over the next few years. A key next step for the University Health Board will be to develop a work plan to progress the business cases for All Wales capital. This will require initial discussion with Welsh Government around the business case submission requirement. To enable this process the University Health Board is 83
84 proposing to invest discretionary capital in 2015/16 and 2016/17 to pump prime the development of business cases for the following: Scheme Current Status Year 1: 2016/17 Aseptic Unit Scoping work commenced BJC to Welsh Government Bronglais Front of House On Site Scheme conclusion Bronglais Fire Lift BJC Development Started on Site Cardiac Catheterisation Laboratory Scoping work commenced SOC/OBC to Welsh Government Chemotherapy Day Unit Withybush Ward 10 Scoping work commenced Mental Health: Acute Services PID Complete, Women & Children s Phase 2 Combined OBC/FBC commenced OBC/FBC to Welsh Government Prince Phillip Unscheduled Care On site Scheme conclusion Programme Business Information Management and Technology Business case writers appointed Case to Welsh Strategy Business Cases Government Catering SOC being developed Unscheduled Care Beds Glangwili On site Complete Unscheduled Care Beds, Bronglais To be complete early 2016 Complete Pathology Blood Sciences Phase 1 & 2 Phase 1 complete, Cardigan Integrated Care Cylch Caron Diagnostic Imaging Ward Refurbishments Energy Phase 2 Primary Care, Cross Hands Endoscopy Prince Phillip Medical Equipment Glangwili Hospital Site Review Bronglais Site Review incl Chemo Day Unit Withybush Site Review Day Surgery Deanery Training Post Graduate Phase 2 not yet commenced FBC to Welsh Government in February 2016 Work on FBC ongoing Not yet commenced Scoping work commenced Funding for progressing identified Not yet commenced Not yet commenced Initial scoping work commenced Not yet commenced Not yet commenced Not yet commenced Not yet commenced Not yet commenced On site FBC to Welsh Government June 2016 BJC to Welsh Government 4.6 Information Management & Technology including Digital Health Hywel Dda's Information Management and Technology system is currently delivered in support of four Acute Hospitals, seven Community Hospitals and numerous locations and settings in community settings. By far the majority of patient contacts are in these community settings and in patient s own homes, with links to critical clinical and diagnostic services in the main hospital sites requiring a dynamic and agile digital capability to meet the needs of a rapidly changing health service. A number of systems have been implemented over the last ten years including unique electronic patient identifiers, electronic recognition of staff, and system portals that enable both communication between data systems, and a summary of all electronic patient records to be available in a single view. The Wales Audit Office recently recognised that Hywel Dda was the 84
85 most advanced Health Board in Wales in implementation of these systems. Critically the digital capability of primary care, that currently holds the closest approximation to a single patient record, has been incrementally implemented. However there remains much to be done to achieve a system that can remove reliance on paper based systems, increase resilience, and broaden access for clinicians and patients alike. A core challenge for Hywel Dda is the infrastructure requirements to support the scale and pace of implementation of a digital NHS. The service has been grown from systems implemented in three previous organisations that have merged. Considerable progress has been made to deliver single, consistent systems across the University Health Board since merger The service is reliant on a potentially fragile server and end user hardware system, with challenging prospects for both capital and revenue investment. Each investment will therefore need to demonstrate benefits across the domains of improved outcomes for patients, patient safety, efficiency and cost effectiveness. Welsh Government recently set out its refreshed vision for a Digital NHS that includes: Information for you: People will be able to look after their own well-being and connect with health and social care more efficiently and effectively, with online access to information and their own records; undertaking a variety of health transactions directly, using technology, and using digital tools and apps to support self care, health monitoring and maintain independent living. Supporting professionals: Health and social care professionals will use digital tools and have improved access to information to do their jobs more effectively with improvements in quality, safety and efficiency. A once for Wales approach will create a solid platform for common standards and interoperability between systems and access to structured, electronic records in all care settings to join up and co-ordinate care for service users, patients and carers. Improvement and innovation: The health and social care system in Wales will make better use of available data and information to improve decision making, plan service change and drive improvement in quality and performance. Collaboration across the whole system, and with partners in industry and academia, will ensure digital advances and innovation is harnessed and by opening up the once for Wales technical platform allow greater flexibility and agility in the development of new services and applications. A planned future: Digital health and social care will be a key enabler of transformed service in Wales. Joint planning, partnership working and stakeholder engagement at local, regional and national level will ensure that the opportunities and ambitions are prioritised. In late 2015 the Welsh Audit Office published a Diagnostic Review of Information and Communication Technologies (ICT) Capacity and Resources in the University Health Board that indicated attention needs to focus on the following areas of improvement: Commitment to clinical Information and Communication Technologies Central management The University Health Board needs to improve the corporate commitment to clinical Information and Communication Technologies, by ensuring that: the strategy for Information and Communication Technologies is upto-date and supported by staff; the profile of Information and Communication Technologies is raised at the Executive Management Team; a clinical Information and Communication Technologies user group is established to improve engagement with clinicians; a clear Information and Communication Technologies benefits management programme is set out. To ensure that the totality of Information and Communication 85
86 of Information and Communication Technologies staff Training of staff Negative perceptions of medical staff Reliability of Information and Communication Technologies equipment Technologies resources within the University Health Board are used effectively, the University Health Board needs to understand the roles and responsibility of Information and Communication Technologies staff managed outside of the Information and Communication Technologies department to ensure that these roles are aligned with those within the central managed team and that they are used to their full potential. To ensure that staff are proficient in the use of the clinical systems, the University Health Board needs to ensure that appropriate and timely training is in place. This is particularly important in relation to new starters in order to prevent them from accessing the systems without having the appropriate training. The University Health Board needs to understand and address the negative perceptions from medical staff in relation to access, reliability and inability to use the clinical information systems that currently exist within the University Health Board to ensure that the systems potential is maximised. To minimise the extent to which there is lost time due to system failures, the University Health Board needs to ensure that the extent to which Information and Communication Technologies equipment is classed as out-of-life reduces During 2016 the University Health Board will approve a strategy, currently in draft (Annex 13) that responds both to Welsh Government and the Welsh Audit Office review recommendations. The strategy will focus on supporting the business strategy of the University Health Board and deliver in three key areas: Implementation and Adoption of Digital Solutions The University Health Board is committed to further implementation of the national health information infrastructure programmes lead by NHS Wales Informatics Service (NWIS) to build a system that further allows information to be seamlessly accessed and shared. Encouraging health sector participants to adopt and use digital systems and tools as they become available is key with an emphasis on: What informatics brings to delivering Integration & Modernisation - the service transformation agenda; What informatics contributes to improvements in Flow and Productivity very much in line with Prudent HealthCare principles; What informatics brings to improvement in Patient Experience & Communication; Stimulating Investment in Information Technology Infrastructure Stimulating investment in high priority computer systems and tools that can deliver tangible benefits to Hywel Dda consumers, care providers and health care managers will require consideration of the balance between revenue and capital approaches to infrastructure development, re-investment of associated efficiency and the procurement of strategic partners. Information Governance Strengthening the digital and information governance to include clinical leadership, assurance on governance, and delivery assurance. The mechanisms for joint planning of systems to meet Welsh Government requirements of shared planning of informatics in line with the Well being of Future Generations Act will need to be explored. 86
87 4.7 Commissioning and Collaboratives, Innovation and Research & Development The nature of Health and Social Care is that people move across artificial organisational and geographical borders and boundaries. Our collaborative and partnership arrangements are the mechanisms through which we plan and deliver services that take these movements of people into account. A Regional Collaboration for Health (ARCH) is the forum through which we will plan services in respect of our strategic relationship with Abertawe Bro Morgannwg University Health Board, where we have a significant patient flow. The Mid-Wales Collaborative seeks to consider the specific needs of our rural populations with partner NHS organisations with similar challenges and populations in Wales. The NHS Wales Collaborative is concerned with planning and implementing service change of national significance or impact to Wales. The Mid and West Wales Health and Social Care Collaborative provides a mechanism for tackling service issues at regional level in health and social care, where economies of scale at this level can be achieved, and where we address the requirements of the Social Care and Well-Being Act. Our Local Service Board arrangements are the mechanism for partnership working at County level and the means for delivering the requirements of the Well-being of Future Generations Act. A Regional Collaborative for Health (ARCH) ARCH is health and science working together to improve the health and wealth and wellbeing of the people of South West Wales. It will generate a future for the people of South West Wales which delivers better skills and economic outcomes. This world-class, visionary project is a collaborative between two University Health Boards, Abertawe Bro Morgannwg and Hywel Dda, and Swansea University. It spans the six local authorities covered by the Health Boards, the higher education sector and includes almost a million people. ARCH aims to break free from an outdated healthcare system designed over 50 years ago to replace it with an accessible one specifically planned for today s needs in purpose built or refurbished accommodation. It focuses on keeping people healthy or better managing disease when they are ill. ARCH also promotes research, training and skills, to help deliver a vibrant economy through investment, innovation and sustainable employment. The concept of ARCH is based around the development of Morriston Hospital as a Regional Centre of Excellence including academic, research and innovation links. As this Hospital is provides significant levels of specialist services to the Hywel Dda population, the University Health Board is engaged in the ARCH approach to ensure the impact of this long term planning arrangement is taken into account and links to other collaborative arrangements in our area. Mid Wales Health Care Collaborative In January 2014, the Welsh Government commissioned the Welsh Institute for Health and Social Care (WIHSC) to explore the options for the provision of high quality and sustainable healthcare services in Mid Wales. The Mid Wales Healthcare Study, published in October 2014, highlighted a number of issues and made twelve recommendations to ensure healthcare services in Mid Wales are effective for the population. The first recommendation was that a joint governance mechanism, The Mid Wales Healthcare Collaborative, should be established comprising the four healthcare organisations that cover mid-wales. The objectives of the Mid Wales Healthcare Collaborative are to implement the recommendations of the Mid Wales Healthcare Study in order to: Deliver a single integrated change programme, with full public and professional participation, which addresses the delivery of social care, primary care and specialist care as an integrated continuum, provided as close to home as possible; Address prevention as well as treatment, and promote prudent healthcare. Deliver a regional plan for Mid Wales. 87
88 The key achievement in its first year has been to establish the Collaborative as a structured planning process with a highly visible public and professional engagement programme. The planning & Co-ordination Group co-ordinates the development of service change plans across Mid Wales and considers the potential impact of implementation on other service areas across Wales. A Centre for Excellence in Rural Healthcare sub-committee has been established to develop plans in response to this recommendation from the Study. Innovation sub-groups have been established, led by the various partners as follows: Telehealth and Innovation (led by Betsi Cadwaladr University Health Board) Palliative Care / End of Life (led by Betsi Cadwaladr University Health Board) Mental Health and Learning Disabilities (led by Powys Teaching Health Board) Primary Care and Community Services (led by Powys Teaching Health Board) Bronglais General Hospital (led by Hywel Dda University Health Board) Health and Wellbeing (led by Hywel Dda University Health Board) Access and Transport (led by Welsh Ambulance Services NHS Trust) Mid and West Wales Health and Social Care Collaborative The Regional Collaborative was established in 2013 and includes partners within the Health and Social Care footprint of Hywel Dda and Powys Health Boards. The collaborative has a number of drivers including the Social Services and Well-being Act 2014 and the Framework for Delivering Integrated Health and Social Care for Older People with Complex Needs which required partners to accelerate the development of integrated services including the production of a shared statement of intent. At the start of the 2015/16 the Collaborative strengthened its governance arrangements reflecting the need to accommodate integration work across the region, and within the distinct footprints of both Health Boards. The Mid and West Wales Regional Implementation Plan (RIP) outlines the work required to meet the Social Services and Well-being Act. New governance arrangements were adopted by the Collaborative in April 2015 that provide the mechanism for developing detailed programmes of activity which address identified priorities within the context of the Social Care and Well-being Act and ensure statutory compliance from April Priorities identified by the regional Integrated Services Programme Board and Children s Services Programme Board include specific duties such as those relating to Information, Advice and Assistance, Advocacy, Integrated Assessment and Eligibility as well as the further remodelling and integration of key services. The regional Workforce Programme Board has focused initially on achieving strategic alignment between the Social Care Workforce Development Programme (SCWDP), Mid and West Wales Regional Implementation Plan and the Social Care in Partnership, alongside regional preparations for delivery of training on the Act. The regional Commissioning Programme Board has sought to identify and address opportunities for collaborative, cross-sector commissioning building within the Region. The Mid and West Wales Regional Implementation Plan also addresses 5 priorities identified at national level by ADSS Cymru in relation to the Act, namely: Workforce development and training needs Information, Advice and Assistance Supporting the development of new national and eligibility tools Performance management Planning and promoting preventative services The Delivering Transformation Grant (DTG) has been used to fund these activities, as well as discrete programme activities that fall within its parameters including regional enablers in the areas of children s services and learning disabilities. Additional funding for the Mid and West Wales Regional Implementation Plan is sourced from the Intermediate Care Fund (ICF), the Regional Collaboration Fund (RCF) and local agency budgets. The specific Intermediate Care 88
89 Fund programme is a substantial grant that has been used to develop and strengthen community health, social care and third sector responses to the needs of older people in three areas: Prevention in the Community; Reablement at the Core; and Reducing Admissions and Accelerating Discharge. The statutory requirements of the Act that come into force in April 2016 include two Regional Partnership Boards for mid and West Wales based on Health Board footprints: West Wales and Powys. Work is planned in the final quarter of 2015/16 to prepare for the new footprint requirements and ensure compliance for 2016/17 onwards. The level of grant funding from April 2016 has yet to be announced, and will be a key element of discussions on priorities and forward action planning, prior to submission of the final version of this Plan. NHS Wales Health Collaborative In October 2014, NHS Wales Chief Executives confirmed their intention to establish a new NHS Wales Health Collaborative to support them in delivering on areas of work that require an all- Wales focus. The core functions originally proposed for the Collaborative were: Joint planning of services where appropriate and agreed. Programme management of discrete pieces of work Research and evaluation of evidence to develop papers to support policy and strategy development The functions of the collaborative have been developed and specified during an establishment phase. During the past year Public Health Wales has agreed to host the Collaborative and its Director which has been established from the resources and functions of the: Chief Executives Support Office (CESO), the Programme Management Unit (PMU), and South Wales Health Collaborative (SWHC). A consistent programme approach to the work plan of the collaborative has been established the main components of which are: Strategic Programme Unit National Pathology Programme National Imaging Programme Lymphoedema Services Development Strategy Financial Information Strategy Programme Add to your life Health and Well-being Check for the over 50s Programme Business Unit NHS Wales/Novartis Outcomes Focused Joint Working project Implementation of Clinical Networks Review Unscheduled Care Improvement Programme Primary Care Network Measuring the Benefits of Technological Change Benefits of PHW delivered All Wales Microbiology Service Planning Unit Major Trauma Network Acute Medicine Model (South Wales) Surgical Specialties Model (South Wales) South East Wales Vascular Network Level 3 Neonatal Intensive Care Balancing Demand and Capacity Sexual Assault Services Specialist Services Specialised and tertiary services are those provided by a relatively small number of specialist centres, to populations greater than 1 million people. These services are typically high cost and low volume. The Welsh Health Specialised Services Committee (The Committee) is a Joint Committee of the seven Health Boards in Wales, and is responsible for the planning of specialised and tertiary services on their behalf. 89
90 The Commissioning Plan for Specialised Services for Wales 2016/19 sets out an integrated commissioning plan for specialised and tertiary services for the population of Wales for this financial year which The Committee will expect to commission on behalf of Local Health Boards, Health Boards including Hywel Dda The aim of The Committee is to ensure that these Services are planned and secured from providers that have the appropriate experience and expertise; are able to provide a robust and sustainable service; are safe for patients and are cost effective for NHS Wales. The seven Health Boards in Wales have agreed a three year commissioning strategy in order to Ensure equitable access to safe, effective, and sustainable specialised services for the people of Wales. The strategy also aims to raise awareness and understanding of specialised services and to ensure that specialised services help meet the Institute for Healthcare Improvement Triple Aim to: Improve the health of the population; Enhance the patient experience of care (including quality, access, and reliability); and Reduce, or at least control, the per capita cost of care. The key priorities for the six programme areas are set out in the following work programmes: Mental Health Cancer and Blood Cardiothoracic Neurosciences and Complex Conditions Renal Women and Children For 2016/17 the Committee have developed a set of commissioning intentions. During 2016/17, the University Health Board will continue to work with the Committee to deliver the priorities for the Welsh Health Specialised Services Committee Agenda and to look at further opportunities to improve the management of pathways between secondary care and tertiary services. In addition, as the University Health Board seeks increasing assurance regarding the patient experience and outcomes through commissioned activity, it is anticipated that the development of the Welsh Health Specialised Services Committee Quality Framework over the course of the next months will enable a greater focus on this important aspect of care. 2016/17 will provide a challenge for the Committee commissioning agenda, with the anticipated availability of a number of new high cost drugs. Hywel Dda will work with the Committee to identify these and develop options for their potential implementation. 4.8 Finance This section provides an update on work-in-progress in developing the financial plan for 2016/17, in the context of our current financial performance in 2015/16, which is a projected end of year deficit of 32.5m ( 41m before Welsh Government non- recurring support for Withybush General Hospital and Referral to Treatment Performance). Once adjusted for non-recurrent management actions and the full year effect of 2015/16 developments to support acute emergency medicine,, our rollover into 2016/17 is 49.34m deficit as follows: 90

91 New cost inflation and volume pressures are estimated at 25.63m, and it is likely that we will have some developments to manage gaps in service capacity. At present these are curtailed to 5m, although budget-holders have identified developments in excess of this, which at the time of the January 2016 submission, we are still in the course of reviewing. 91
92 Revenue Planning Assumptions for 2016/17 At this point in the year, there are many unconfirmed financial planning assumptions around the 2016/17 financial year. There are areas where we can make realistic assumptions but there are other areas where further discussion and decisions are required by the Executive Team and the Board before we can build them into the Integrated Medium Term Plan for 2016/17 and this is the work that will be undertaken from this point to the end of March In addition, there will be other areas where Welsh Government will need to advise, so provisionally at this time, our key assumptions are: Our recurrent allocation from Welsh Government in 2016/17 to commission and provide services for our residents will be 709.4m. This includes 38.7m structural deficit funding made available non-recurrently in 2015/16. In addition, it is assumed that the Welsh Government support of 5.690m for exceptional pressures in Withybush Hospital and 3.5m for performance will not be made recurrent in 2016/17. The 6m slippage on Delivery Plans and Dental in 2015/16 will not be available recurrently in 2016/17. Full year effect of the following developments in 2015/16 will be 5.5m (subject to verification as budget setting progresses) as follows: o Respiratory plan - 0.6m o Oncology Plan - 0.4m o Dental (re-provision of an element of 2015/16 slippage) - 0.3m o Emergency Medicine Ward Capacity - Afallon and Cadog - 2.2m o Medical Staffing for Withybush Hospital only - 2m These costs will in part be offset by the 3.16m Demographic/ Demand on Acute Services from the 2016/17 National Finance Agreement (NFA). NFA cost pressures are assumed to apply to Hywel Dda University Health Board at All Wales averages as discussed in the following sections, and for 2015/16 is 25.63m. Welsh Risk Pool cost pressures in 2016/17 are yet to be confirmed so no saving/cost pressure is assumed. Budget Setting has identified significantly more local cost pressures which are in the process of being reviewed by the Executive Team to inform Board discussion in February. Growth Funding of 24.2m is assumed as the Hywel Dda University Health Board consequential Welsh Government Barnett share of the UK Government uplift to the NHS (subject to decisions of Welsh Ministers) and will mostly offset 2016/17 inflation and volume cost pressures and the full year effect of 2015/16 developments. Further discussions are required regarding the use to which the potential 60m Integrated Care Fund monies can be put. At present this is assumed to be cost neutral. Contained within reserves from 2015/16 is 6.88m earmarked for the delivery of Tier 1 delivery, namely waiting times and A&E performance. We are in the process of reviewing the sufficiency of this in light of our demand and capacity plans and budget-holder business cases on the same. Draft Budget 2016/17 Comprehensive work has been undertaken over the last 4 months to further consolidate the zero based budgeting approach taken in 2015/16, particularly in the area of medical staffing which remained an un-clarified issue in the previous process, but with progress in job planning this year is now informing 2016/17. The 2016/17 budget-setting has identified recurrent issues in the cost base, activity cost pressures and unapproved service developments. In respect of the unapproved developments the vast majority have not started but are being signalled. There are supporting Business Cases which the Executive Team is in the process of reviewing for recommendation to Committees, and then to Board approval if considered necessary. 92

93 Many of these issues have not commenced, as they include significant policy changes such as 7 day working and more protected management time for ward sisters, which are decisions which only the Board can consider. Submissions from service leads indicate a potential gross budgetary activity related cost pressures particularly in drugs / development uplifts / workforce risk and workforce developments in excess of 53m before 2016/17 Continuing Health Care, pay and pensions costs. At the time of the January 2016 submission, the Executive Team are scrutinising these budget uplift requests in great detail with directorates and budget holders in order to present a budgetary plan to the Board that agrees, or otherwise, the root-causes of the position as follows: Unavoidable budgetary issues within 2015/16 base run rate (at NHS pay rates) Excess cost of variable pay which may need to be recognised to reflect the lead-in time for recruitment but is within 2015/16 forecast out-turn 2016/17 Inflationary cost and volume pressures (NFA) Full Year Effect of 2015/16 developments Signalled developments for 2016/17 through Business Cases which need detailed scrutiny as to their efficacy. At present it is assumed those cost pressures that fall outside of the underlying 2015/16 run rate or 2016/17 cost inflation and volume growth will be contained within the 5m 2016/17 developments detailed in the summary table, in addition to the full year effect of 2015/16 developments. Inflation / Growth Cost Pressures - The 2016/17 National Finance Agreement (NFA) which we will be testing budget-holder requests against, is detailed in the following table. However, there remain some unresolved aspects including; 93

94 The impact of Community Pharmacy Inflation/Cost Pressures has yet to be confirmed Continuing Health Care Phase 3 and 4 cost pressures are uncertain as is the timing of these being accrued. The impact on nursing homes of the Living Wage provisions has yet to be fully understood. Part of the cost pressure validation and challenge with budget holders will be to align, where possible their cost pressures issues with NFA provisions. Again, it should also be noted that the budget setting to date does not include assumptions for pay awards and pension increases with planning figures within the National Finance Agreement Savings What we said we d deliver in 2015/16: The year-end financial position for 2015/16 was forecast at m deficit. To do this required m of savings to be delivered. What we achieved: We identified schemes of 15.2m with 9.2m still unidentified. Against the challenging service position this year particularly regarding recruitment, delivery of savings has been difficult with a number of schemes slipping or being impossible to deliver against the extraordinary service and workforce circumstances in 2015/16, which have been partly acknowledged by Welsh Government with additional funding. This has led to the current forecast savings delivery of 9.419m summed up in the following table: What we plan to do in 2016/17: Even before the worsened position seen in 2015/16, the 2015/16 Integrated Medium term Plan indicated the requirement for a step up in savings delivery for 2016/17. This is now estimated at 28.4m. To try and identify how this level of saving can be achieved we are undertaking three main streams of work namely: Reviewing the savings schemes in 2015/16 which have not delivered as anticipated inyear to see if we can get a better full year effect impact in 2016/17 including realising secondary care savings through investment in community services and primary care, and now that some of the extraordinary workforce challenges in 2015/16 are improving against progress being made in recruitment; Working through the All-Wales sharing of savings schemes to examine whether opportunities identified by others can be implemented locally and sharing learning to see if they have managed to go further and quicker than us; Undertake a re-evaluation of potential savings opportunities (from a purely financial / benchmarking perspective) based on previous reviews and work undertaken locally. It will be for the Board with advice from service delivery leads to assess which of these options can be implemented in Hywel Dda. These will be accompanied by looking at areas for 94

95 potential cost avoidance and/or increased productivity and efficiency gains particularly from pathway re-design. Our savings delivery will be based on strong project management arrangements facilitated through a Programme Management Office as discussed in chapter 3, which fully align to the principles set out by the Audit Commission and Monitor as follows; Set out clearly an overall vision, improvement strategy and philosophy our 10 strategic objectives Ensure that the organisation culture facilitates transformation of services and improves patient experience our Organisational Strategy Develop long-term forecasts that support the longer-term transformation programmes supported by our Business Intelligence Unit. Involve all stakeholders at an early stage Organisational Strategy Identify suitable, tailored savings projects for each division/department that reflects their relative efficiency, using benchmarking data our Quality Innovation Productivity Prevention (Prudent) sub-programmes Set up a Executive Programme Steering Group to oversee Programme Delivery with clear governance and accountability Source: Delivering sustainable cost improvement programmes - Audit Commission and Monitor January 2012 Our QIPP (P) Programme (which stands for Quality, Innovation, Productivity, Prevention and Prudent Healthcare) Under the governance of the Executive Programme Steering Group, and support of the Programme Management Office and Business Intelligence Unit, the following table sets out the proposed sub-programme work streams and their targeted benefits in financial terms that form a key part of our savings planning for the next 3 years. All of these sub-programmes are contained within Strategic Objectives 9 and 10. Executives and Service leads are already being engaged in these areas to maximise the financial benefit delivery in 2016/17. 95
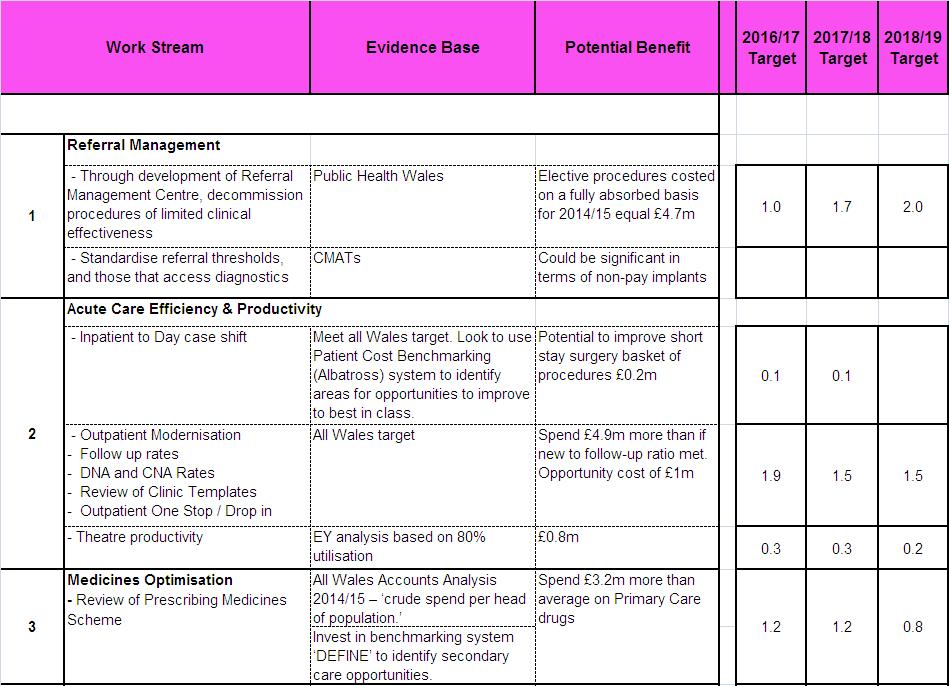
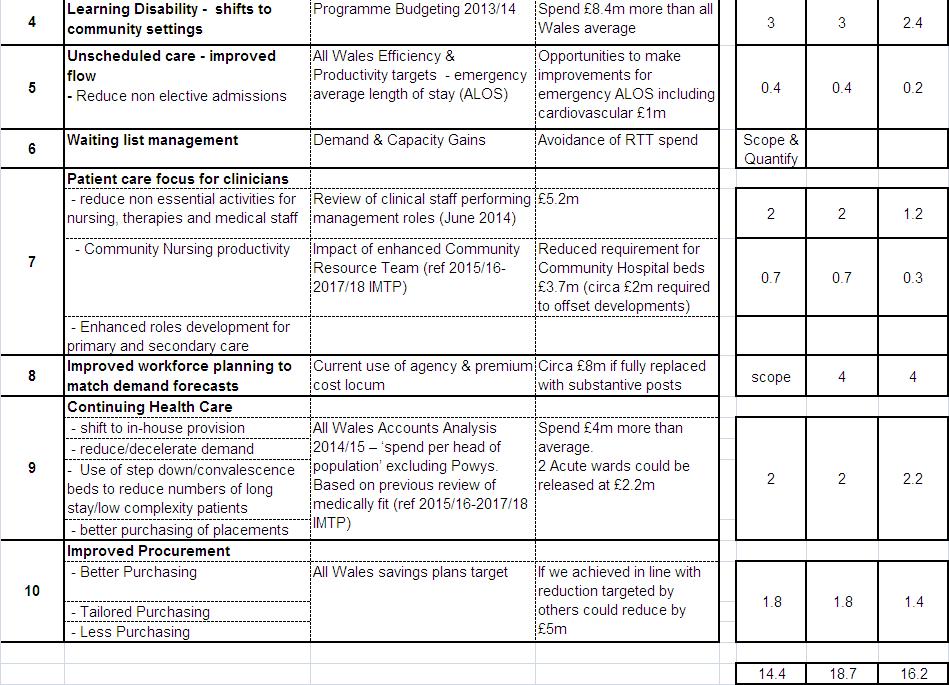
96 96
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Hywel Dda University Health Board Draft Operational Plan 2016/17 Version: 2 nd June 2016 Status: Work in Progress
 Hywel Dda University Health Board Draft Operational Plan 20/17 Version: 2 nd June 20 Status: Work in Progress Table of Contents Context... 2 Governance of the Plan... 4 Summary... 5 Strategic Objectives...
Hywel Dda University Health Board Draft Operational Plan 20/17 Version: 2 nd June 20 Status: Work in Progress Table of Contents Context... 2 Governance of the Plan... 4 Summary... 5 Strategic Objectives...
Powys Teaching Health Board. Respiratory Delivery Plan
 Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
RESPIRATORY HEALTH DELIVERY PLAN
 RESPIRATORY HEALTH DELIVERY PLAN 1. BACKGROUND AND CONTEXT Together for Health a Respiratory Health Delivery Plan was published in April 2014 and provides a framework for action by Health Boards and NHS
RESPIRATORY HEALTH DELIVERY PLAN 1. BACKGROUND AND CONTEXT Together for Health a Respiratory Health Delivery Plan was published in April 2014 and provides a framework for action by Health Boards and NHS
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Annex 3 Cluster Network Action Plan South Ceredigion and Teifi Valley Cluster Plan
 Annex 3 Network Action Plan 06-7 South Ceredigion and Teifi Valley Plan The Network Development Domain supports GP Practices to work to collaborate to: Understand local needs and priorities. Develop an
Annex 3 Network Action Plan 06-7 South Ceredigion and Teifi Valley Plan The Network Development Domain supports GP Practices to work to collaborate to: Understand local needs and priorities. Develop an
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Performance Evaluation Report Pembrokeshire County Council Social Services
 Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Worcestershire Public Health Directorate. Business plan 2011/12
 Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Medical and Clinical Services Directorate Clinical Strategy
 www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Living With Long Term Conditions A Policy Framework
 April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Our vision. Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey
 Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
Clinical Strategy. Transforming Healthcare in Fife
 Clinical Strategy Transforming Healthcare in Fife 2016-2021 Foreword This Clinical Strategy will shape the delivery of healthcare in Fife over the next five years and beyond and is our response to the
Clinical Strategy Transforming Healthcare in Fife 2016-2021 Foreword This Clinical Strategy will shape the delivery of healthcare in Fife over the next five years and beyond and is our response to the
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Agenda for the next Government
 Agenda for the next Government General election 2017 The Richmond Group of Charities We are the Richmond Group of Charities and we help people of all ages who have serious long term physical and mental
Agenda for the next Government General election 2017 The Richmond Group of Charities We are the Richmond Group of Charities and we help people of all ages who have serious long term physical and mental
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Transforming Clinical Services Help us improve our NHS for Mid and West Wales
 Transforming Clinical Services Help us improve our NHS for Mid and West Wales Safe, Sustainable, Accessible and Kind Contents About us What we are asking you to do Why things need to change Our challenges
Transforming Clinical Services Help us improve our NHS for Mid and West Wales Safe, Sustainable, Accessible and Kind Contents About us What we are asking you to do Why things need to change Our challenges
The prevention and self care workshop 16 th September Dr. Jenny Harries Regional Director PHE South Regional Office
 The prevention and self care workshop 16 th September 2016 Dr. Jenny Harries Regional Director PHE South Regional Office Jenny.harries@phe.gov.uk The health and wellbeing gap If the nation fails to get
The prevention and self care workshop 16 th September 2016 Dr. Jenny Harries Regional Director PHE South Regional Office Jenny.harries@phe.gov.uk The health and wellbeing gap If the nation fails to get
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Child Health 2020 A Strategic Framework for Children and Young People s Health
 Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
The future of mental health: the Taskforce 5 year forward view and beyond
 The future of mental health: the Taskforce 5 year forward view and beyond May 2016 Content Mental Health Taskforce Overview Achieving Better Access Safe, Effective and Compassionate Care Integrating Physical
The future of mental health: the Taskforce 5 year forward view and beyond May 2016 Content Mental Health Taskforce Overview Achieving Better Access Safe, Effective and Compassionate Care Integrating Physical
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health
 Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Cluster Network Action Plan Neath Cluster. Abertawe Bro Morgannwg University Health Board Neath Cluster Action Plan
 Cluster Network Action Plan 2016-17 Neath Cluster 1 Introduction The Neath Cluster Network includes a cluster of 8 GP practices, seven of the practices are engaged in GP training. The cluster network estate
Cluster Network Action Plan 2016-17 Neath Cluster 1 Introduction The Neath Cluster Network includes a cluster of 8 GP practices, seven of the practices are engaged in GP training. The cluster network estate
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS. September 2014
 OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
NHS Ayrshire and Arran. 1. Which of the following performance frameworks has the most influence on your budget decisions:
 A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
Lincolnshire JSNA: Chronic Obstructive Pulmonary Disease (COPD)
") Disease (COPD) What do we know? Summary is a long-term condition, which is affecting increasing numbers of people. There is a wide range of interventions to address COPD, from prevention to the ongoing
Disease (COPD) What do we know? Summary is a long-term condition, which is affecting increasing numbers of people. There is a wide range of interventions to address COPD, from prevention to the ongoing
Staff Health, Safety and Wellbeing Strategy
 Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Capital & Coast DHB System Level Measures Improvement Plan 2016/17
 Capital & Coast DHB System Level Measures Improvement Plan 2016/17 Written by: Astuti Balram, ICC Programme Manager, on behalf of the CCDHB Integrated Care Collaborative (ICC) Alliance Version 4 Released
Capital & Coast DHB System Level Measures Improvement Plan 2016/17 Written by: Astuti Balram, ICC Programme Manager, on behalf of the CCDHB Integrated Care Collaborative (ICC) Alliance Version 4 Released
A guide to NHS Bexley Clinical Commissioning Group
 A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
POPULATION HEALTH. Outcome Strategy. Outcome 1. Outcome I 01
 Section 2 Department Outcomes 1 Population Health Outcome 1 POPULATION HEALTH A reduction in the incidence of preventable mortality and morbidity, including through national public health initiatives,
Section 2 Department Outcomes 1 Population Health Outcome 1 POPULATION HEALTH A reduction in the incidence of preventable mortality and morbidity, including through national public health initiatives,
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
grampian clinical strategy
 healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
West Cheshire Clinical Commissioning Group
 West Cheshire Clinical Commissioning Group Strategic Commissioning Plan 2012 2017 01 Contents. 02 Foreword 04 Executive Summary 05 Section 1: Who We Are and Our Vision For Health Care in West Cheshire
West Cheshire Clinical Commissioning Group Strategic Commissioning Plan 2012 2017 01 Contents. 02 Foreword 04 Executive Summary 05 Section 1: Who We Are and Our Vision For Health Care in West Cheshire
Health and Wellbeing and You
 Health and Wellbeing and You The Big Picture There is a clear link between healthy and happy staff and improved patient outcomes. As an organisation we wish to be world class. Therefore we are aiming
Health and Wellbeing and You The Big Picture There is a clear link between healthy and happy staff and improved patient outcomes. As an organisation we wish to be world class. Therefore we are aiming
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Increasing Access to Medicines to Enhance Self Care
 Increasing Access to Medicines to Enhance Self Care Position Paper October 2009 Australian Self Medication Industry Inc Executive summary The Australian healthcare system is currently at a crossroads,
Increasing Access to Medicines to Enhance Self Care Position Paper October 2009 Australian Self Medication Industry Inc Executive summary The Australian healthcare system is currently at a crossroads,
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay. Statement of Intent
 Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay Statement of Intent March 2014 1 1. Introduction This document sets out our commitment to deliver integrated
Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay Statement of Intent March 2014 1 1. Introduction This document sets out our commitment to deliver integrated
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
ME-CFS and Fibromyalgia Delivery Plan
 ME-CFS and Fibromyalgia Delivery Plan 2015-2018 1 CONTENTS 1. BACKGROUND AND CONTEXT 3 1.1 The Vision 3 1.2 The Drivers 3 1.3 What do we want to achieve? 3 1.4 Prudent Healthcare 4 2. ORGANISATIONAL PROFILE
ME-CFS and Fibromyalgia Delivery Plan 2015-2018 1 CONTENTS 1. BACKGROUND AND CONTEXT 3 1.1 The Vision 3 1.2 The Drivers 3 1.3 What do we want to achieve? 3 1.4 Prudent Healthcare 4 2. ORGANISATIONAL PROFILE
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting. Meeting Date: 25 October Executive Lead: Rajesh Nadkarni
 Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
The North West London health and care partnership
 The North West London health and care partnership Sept 2017 The North West London health and care partnership Introduction In 2016, over 30 NHS organisations and local authorities came together to develop
The North West London health and care partnership Sept 2017 The North West London health and care partnership Introduction In 2016, over 30 NHS organisations and local authorities came together to develop
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Commissioning for Value insight pack
 Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Strategic Plan
 Strategic Plan 2013-2025 Toi Te Ora Public Health Service (Toi Te Ora) is one of 12 public health units funded by the Ministry of Health and is the public health unit for the Bay of Plenty and Lakes District
Strategic Plan 2013-2025 Toi Te Ora Public Health Service (Toi Te Ora) is one of 12 public health units funded by the Ministry of Health and is the public health unit for the Bay of Plenty and Lakes District
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Prospectus for the Procurement and. Commissioning of a Multi-Specialty. Community Provider (MCP) 1 P age
 1 P age") Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
Local Delivery Plan Guidance 2016/17
 The Scottish Government Directorate for Health Performance & Delivery Dear Colleague Local Delivery Plan Guidance 2016/17 Summary The LDP Guidance 2016-17 sets out the performance contract between the
The Scottish Government Directorate for Health Performance & Delivery Dear Colleague Local Delivery Plan Guidance 2016/17 Summary The LDP Guidance 2016-17 sets out the performance contract between the
The incentives framework for ACOs
 New care models The incentives framework for ACOs Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement, local ownership, national
New care models The incentives framework for ACOs Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement, local ownership, national