AIDS Foundation of Chicago. Ryan White Treatment Modernization ACT Standard Operating Procedures Effective: February 2017
|
|
|
- Barrie Boone
- 6 years ago
- Views:
Transcription
1 AIDS Foundation of Chicago Ryan White Treatment Modernization ACT Standard Operating Procedures Effective: February 2017
2 Appendix Order Appendix 1. Affidavit of Understanding for Uninsured Individuals Appendix 2. Invoice Template Appendix 3. Sample Inter-Agency Memorandums of Agreement Appendix 4. Authorization to Release Information Script Appendix 5. Authorization to Release Information (AFC) Appendix 6. Ryan White Authorization to Release Information (IDPH) Appendix 7. Foreign Language Translation Request Form Appendix 8. Sign Language Interpretation Request Form Appendix 9. IDPH Linguistics Procedure Appendix 10. Incident Report Appendix 11. Sample Agency Grievance Rights and Responsibilities Appendix 12. Grievance Tracking Form Appendix 13. Service Complaint Inquiry Form AFC Appendix 14. Grievance Form AFC Use Only Appendix 15: Confidentiality Violation Report Form (can be completed electronically in Provide) Appendix 16. Client Satisfaction Survey Template Appendix 17 Health Literacy Tool Appendix 18. Risk Assessment Tool Appendix 19. Client Screening and Placement (for AFC staff only) Appendix 20. Affordable Care Act Passport Form Appendix 21. Notice of Privacy Practices Appendix 22. Household Income Statement Appendix 23. Ryan White Initial Assessment Reassessment Checklist (Not Required) Appendix 24. Ryan White Client Intake & Reassessment Tool (Not Required) Appendix 25. Client Screening & Feedback Form (Not Required) Appendix 26. Medical Update Form (Recommended. Not Required) Appendix 27. Case Management Discharge Summary Appendix 28. Care Plan Template Appendix 29. Karnofsky Acuity Assessment Scale Tool Appendix 30. Sample Referral Letter & Verification Form Appendix 31. Case Conferencing Agenda Appendix 32. Case Conferencing Staffing Form Appendix 33. DRS Electronic Billing Verification Form Appendix 34. DRS Retroactive Billing Electronic Verification Form Appendix 35. Food Services Tracking Form Appendix 36. Housing & Utility Assistance Application
3 Appendix 37. IDPH Housing & Financial Assistance Procedure Appendix 38. Transportation Tracking Form Appendix 39. Fare Card Authorization & Reimbursement Request Form Appendix 40. MEDICARE Complaint Form Appendix 41. Notification of Change in Personnel and Training Request Form Appendix 42. New Case Manager and Supervisor Hire Form Appendix 43. Sample Medical Case Manager Job Description Appendix 43. Sample Medical Case Manager Job Description Appendix 44. Sample Non-Medical Case Manager Job Description Appendix 45. Request for Training Credit Application Appendix 46. Request for Conference Credit Application Appendix 47. Case Management Record Review Tool Appendix 48. Quarterly Report Appendix 49. Action Plan Appendix 50. Fiscal Supporting Documentation Appendix 51. Medical Case Management Chart Review Instrument Appendix 52. Medical Case Management Chart Review Tool Appendix 53. Non-Medical Chart Review Tool Appendix 54. Subcontractor Site Visit Review Form
4 ILLINOIS Department of Public Health Ryan White Part B Program AFFIDAVIT OF UNDERSTANDING FOR UNINSURED INDIVIDUALS Client First Name Middle Initial Client Last Name Social Security Number (Leave blank if no valid SS number for client) Date of Birth (mm/dd/yyyy) The Ryan White Part B Program is required to ensure that the program is the Payer of Last Resort for all services it provides. With the implementation of the Affordable Care Act, all persons have increased access to some form of insurance coverage. To ensure compliance with the Federal Payer of Last Resort requirements, all clients that do not have a form of insurance coverage that is able to coordinate with the Program are required to submit this completed for at every eligibility determination. There are a variety of options that clients may qualify for. These options include Traditional Medicaid, Expanded Medicaid/Managed Care Plans, Medicare, and Private Insurance including employer based plans, Illinois Marketplace Plans, and private insurance plans outside the Illinois Marketplace. If you have any questions, please contact your case manager or local Lead Agent to find the Medical Benefits Coordinator in your area (see back of document for contact listing). By signing this affidavit, I acknowledge and understand the statements below and agree to comply with any requirement identified herein. I understand that I am expected to enroll in health coverage through one of the ways listed above, to satisfy the Payer of Last Resort criteria. I understand that failure to meet this requirement could potentially affect future enrollments via waitlists, jeopardized eligibility, or negatively impact my enrollment due to cost saving requirements. I understand that the Ryan White Part B Program can assist with premium costs up to $750 per month for any health plan that qualifies for the program (please see criteria listed on back of document). I understand that if I enroll in health coverage, that my insurance plan(s) must meet the requirements listed on page 2 of this affidavit if I want to receive medication assistance or premium assistance services. If my plan does not meet these requirements, I will be unable to receive these services from the program. I understand that regardless of my citizenship or documentation status, I still have insurance coverage options available to me and that these options are outlined above. I understand that even if I am exempt under the Affordable Care Act legal enrollment requirements (Veterans Benefits or American Indian heritage), I still have Insurance coverage options available to me and that these options are outlined above. I understand that if I am not enrolled in the appropriate insurance coverage, I may incur fines and/or fees that will require payment. Medicare if you qualify for Medicare and do not enroll you will incur an additional LIFETIME fee for EACH YEAR you do not enroll. Marketplace/Private Insurance if you qualify for private insurance through the marketplace or outside the marketplace and do not enroll, you will incur a fine that will require payment when you file taxes. I understand that I will be required to submit this completed affidavit at every eligibility determination. Client Signature (age 12 and older) / / Date (Revised: 09/01/2016) Page 1 of 2
5 ILLINOIS Department of Public Health Ryan White Part B Program AFFIDAVIT OF UNDERSTANDING FOR UNINSURED INDIVIDUALS Plan requirements to qualify for Premium Assistance (not to exceed a combined total of $750/month): 1. The Illinois Department of Public Health must be able to pay the insurance company directly. a. Your premiums cannot be auto deducted from pay checks, Social Security checks, bank account, credit cards, etc. b. You will not be reimbursed for any premium payments you make. c. The insurance company must accept 3 rd party payments. 2. Your insurance plan must have prescription coverage included. a. Plan can also have Dental and/or Vision coverage. b. We cannot pay for Life Insurance portions of plans 3. Your insurance plan must allow CVS Specialty Pharmacy s Mail Order program to fill your prescriptions. 4. Your insurance plan s medication formulary must be representative of the IL Ryan White Part B Program formulary. 5. Cannot be a Medicare Part A or Part B plan. 6. When selecting an insurance plan through from the Illinois Marketplace you must: a. Elect the Advance Premium Tax Credit Option i. Documentation will be required b. Elect only silver plans from one of the approved providers. The list of approved providers can be found at XXXXXXXXXXXXXXXXXXXX. i. If you are age 50 or over and there are no silver plans available with a monthly premium of $750 or less, you can choose a bronze plan from the approved providers. For assistance from your local Medical Benefit Coordinator, contact your case manager or your regional Lead Agent: SIU School of Medicine - Springfield: Champaign Urbana Public Health District: UIC College of Medicine Peoria: AFC - Chicago: Winnebago County Health Department Rockford: Jackson County Health Department - Murphysboro: St. Clair County Health Department Belleville: Please feel free to give us a call if you have any questions. Contact us at if you have questions or concerns about this process. The Department wide TTY number is (for hearing impaired only). (Revised: 09/01/2016) Page 2 of 2
6 Appendix 2. Invoice Template AFC INVOICE TEMPLATE BILL TO: AIDS Foundation of Chicago INVOICE NUMBER AFC 200 W. Jackson Blvd. Suite 2200 INVOICE DATE Date Chicago, IL BILLING AGENT Name INVOICED TO RWID# # OF UNITS SERVICE PROVIDED UNIT COST AMOUNT SUBTOTAL Pay This Amount
7 Appendix 3. Sample Linkage Agreement Memorandum of Agreement Partner Organization AND Partner Organization Mission: The mission of (Agency Name) is to identify individuals newly diagnosed with HIV or HIV positive individuals who are not currently engaged in primary medical care for HIV treatment and link them into appropriate HIV care. Partner Organization Mission: Scope The goal of this relationship is to coordinate activities and collaborate to link HIV+ patients to medical care, and support them to remain in care. All parties are bound by the Illinois AIDS Confidentiality Act requirements regarding the release of an individual s HIV information, and HIPAA requirements regarding the release of personal identifying health information. The purpose of this project is to increase patient understanding of the benefits of being in treatment for HIV, while supporting individual choices about providers and treatment decisions.
8 Appendix 3. Sample Linkage Agreement (cont.) Staff Governed by this MOA: Responsibilities Agency : Name: Title: Address: Telephone: Address: Contact Information for Partner Organization Staff Governed by this MOA: Name: Title: Address: Telephone: Address: The organizations agree to the following tasks for this MOA (edit as necessary): (Agency ) agrees to: 1. Provide outreach and referrals for medical care at Partner Organization to HIV positive patients when appropriate. 2. Work with patients to continue to orient them to the care system and how their care will be delivered, clarifying various provider roles. 3. Ensure that patients have signed the Release of Information form for Partner Organization staff and services. (Partner Organization) agrees to: 1. Assist clients in accessing and engaging in HIV medical care. 2. When appropriate (immediate need for housing, transportation, etc), help patient connect with the case management system and other support services such as Behavioral Health, support groups and education groups. Timeline and Duration of this MOA This memorandum of agreement shall remain in effect for the period of one year from the date of its signatures below, unless modified in writing prior to this date.
9 Appendix 3. Sample Linkage Agreement (cont.) Confidentiality All parties are bound by the Illinois AIDS Confidentiality Act requirements regarding the release of an individual s HIV information, and HIPAA requirements regarding the release of personal identifying health information. The purpose of this project is to increase client understanding of the benefits of being in treatment for HIV, while supporting individual choices about providers and treatment decisions. Both entities agree to: 1. Ensure that clients referred between organizations have signed a HIPAA compliant Release of Information form (ROI) to permit the sharing of information between the two organizations. 2. Help eligible clients connect with the Ryan White case management system when appropriate (immediate need for housing, transportation, etc.). 3. Complete all state and local health department case reporting requirements and information to initiate partner services for all newly confirmed HIV+ individuals. Communication Use face-to-face contact, telephone and/or to clearly communicate expectations of any referrals, including how much feedback is desired of both organizations to meet the requirements of both organizations funders; if/how each organization will stay actively involved in the client s care. Termination Either party may terminate this MOA without cause by delivering written notice to terminate to all entities who signed the agreement below. If not renewed, the MOA will terminate in one year from the dates of the signatures below. Signatures On behalf of my organization, I wish to enter into this agreement and contribute to the shared goals of this memorandum. Signature Date Title Organization Signature Date Title Organization Signature Date Title Organization Signature Date Title Organization
10 Appendix 4. Authorization to Release Information Script Talking Points for Authorization to Release Information (AFC/IDPH) This form became effective on September, 2006, and was revised October 31, 2011 This form should be signed by all new clients, as well as continuing clients as soon as possible and no later than at their next scheduled reassessment. By signing these forms I understand that: My service information (including name) will be reported to the Illinois Department of Public Health s Direct Services Unit and Chicago Department of Public Health for the SOLE purposes of reporting service utilization; My information will be regarded with the highest privacy possible to ensure federal reporting standards. AFC users will remain the same and only two entities at IDPH (the Consortia Coordinator and the Data Coordinator) will have access to the reported information; My information will not be given out for surveillance or contact tracing purposes, but will only be reported for the purposes of service utilization tracking; My information is used to obtain health care and social services; I can terminate services at any time with a written request; I have the right to refuse to sign this Authorization form; and I have the right to request a copy of this Authorization form By signing these forms I give my permission to: Disclose my health information and case management records to the AIDS Foundation of Chicago and the other cooperative agencies; Have my information entered into the central database for the purpose of: o Statistical Reports o Ensure there is no duplication of services o Tracking service linkages and health status over time; Have my file reviewed by the AIDS Foundation of Chicago for quality assurance purposes; Have my name (IDPH only) or unique coded identifier (all other funding sources), service utilization information and limited demographic information sent to federal grant programs that support the AIDS Foundation of Chicago. The Consent to Release Information form is utilized to protect your confidentiality and ensure that your HIV status, risk factors, or use of services are not released without your written/documented consent. Your identifying information will only be released to parties outside of the Cooperative if required by law or federal funding requirements or to prevent harm to yourself or others. Your identifying information (name, date of birth, and HIV status) cannot be collected without your handwritten consent on the Consent for Release of Information form or the consent of a legal guardian. You may choose not to sign the Consent for Release of Information. However, if you decline to sign the form, you may jeopardize access to services.
11 Appendix 5: AFC Authorization to Release Information (English) CONSENT TO RELEASE INFORMATION Subject to the limitations and conditions set forth below, I, hereby consent to ( Provider/Case Manager ), acting through its employees or agents, to use and/or disclose my health information and medical records to the AIDS Foundation of Chicago, the Northeastern Illinois HIV/AIDS Case Management Cooperative (the Cooperative ) and/or any agencies that provide services through the Cooperative (collectively the Recipients ), as follows: (i) in connection with my participation in the centralized client database established by the AIDS Foundation of Chicago (the Database ) and the operation of the client database; (ii) to enable the AIDS Foundation of Chicago and the Cooperative to conduct quality assurance programs for individuals receiving case management services through the Cooperative; (iii) to avoid duplication of services by case management agencies; and (iv) in connection with the submission of reports and other data to funding sources. In connection with my enrollment in the Database, I hereby give my consent for the following information to be furnished to the AIDS Foundation of Chicago for entry into the Database: my name (when applicable), date of birth, mother s maiden name, and other demographic data. In addition, verification of HIV-positive status (if applicable) and dates of medical and case management service will be released to the AIDS Foundation. I understand that this information will be grouped together with that of other clients for the purpose of generating statistical reports, avoiding duplication of services and coordinating a system for service delivery to persons with HIV, their family members, and/or significant others and specifically authorize the use of such information for that purpose. I further allow the program staff of the AIDS Foundation of Chicago and its designated Oversight Committees of the Cooperative to review my individual service records as part of the Cooperative s quality assurance program. For the purposes of this consent, I acknowledge and agree that my service records include any and all records generated by any of the Provider agencies that participate in the Cooperative. Any information I provide for the purposes of receiving services will not be disclosed to any government agency or health department for purposes of surveillance, contact tracing, or any other purpose other than obtaining health care or social services, except (1) with my consent, (2) as required by law, or (3) if necessary, to prevent a serious attempt to inflict harm on myself or others. Security precautions will be maintained to prevent unauthorized access to the Database by anyone other than the program staff of the AIDS Foundation of Chicago. I give further consent to allow the AIDS Foundation of Chicago to report information that I provide in connection with my enrollment in the Database and in connection with my receipt of services to the federal grant programs that support the AIDS Foundation of Chicago. I understand that such information may be provided either in the aggregate or on an individualized basis. I understand that, in order to protect my privacy, any information that is provided on an individualized basis, with the exception of Part B funded service utilization, will be furnished using unique client codes, without names or other information that identifies me. I further understand that should I receive service funded under Part B of the Ryan White
12 CARE Act, certain information will be reported to the Direct Services Unit of the Illinois Department of Public Health, including: - demographic information, including but not limited to name, gender, race, ethnicity, and birth date; service utilization information; HIV/AIDS diagnosis and treatment information, if any; and mental health and/or substance use diagnosis, treatment, and service information, if any. I understand that this information will be shared for the purposes of evaluating Part B service utilization patterns, on-site service reviews, and when necessary to coordinate services. I further agree that the Direct Services Unit of the Illinois Department of Public Health may disclose this same type of information to my provider/case manager, and/or the Cooperative. I can terminate this consent by submitting a written request to any of the Recipients (agencies in the Cooperative) indicating that I no longer desire to receive services through the Cooperative, or my written revocation of this authorization, whichever occurs first. I understand that I may refuse to sign this consent and that may result in being denied services, if eligibility for services is based on the verification of my diagnosis and the release of that information. I understand that I have the right to receive a copy of this consent. I further understand that I may revoke this consent at any time by providing written notice of my intent to revoke this consent to Provider. This consent cannot be revoked to the extent that action has already been taken based on this consent. This consent is valid for a period of one year from the date of the actual client signature below. Provider will not use or disclose personal health information beyond the scope of this authorization without your written consent or authorization. Please note that, subject to applicable law, disclosed information may be subject to redisclosure by the recipient, and may no longer be considered to be protected health information pursuant to the Health Insurance Portability and Accountability Act of 1996 and the regulations promulgated thereunder. Signature of Client or Client s Legal Representative Print Name Date Relationship (if signed by person other than client) FORM REVISED 8/2006; EFFECTIVE DATE 9/12/2006
13 Appendix 5: AFC Authorization to Release Information (Spanish) CONSENTIMIENTO PARA TRANSFERIR INFORMACION Sujeto a las limitaciones y condiciones abajo expuestas, yo, por medio de la presente, doy mi consentimiento a ( Proveedor/Administrador de Casos ), actuando a través de sus empleados o agentes, a usar y/o revelar información sobre mi salud y mis archivos médicos a la Fundación de SIDA de Chicago, la Cooperativa de Manejo de Casos de VIH/SIDA del Noroeste de Illinois (la cooperativa ) y/o cualquier agencia que provee servicios a través de la cooperativa (colectivamente, los destinatarios ), para lo siguiente: (i) en conexión con mi participación en el banco central de datos establecido por la Fundación de SIDA de Chicago (el banco de datos ) y el manejo del mismo (ii) para permitir a la Fundación de SIDA de Chicago y a la Cooperativa conducir programas que garanticen la calidad de los servicios para los individuos que reciben manejo de casos a través de la cooperativa; (iii) para evitar duplicación de servicios en las agencias de manejo de casos; y (iv) en conexión con el suministro de reportes y otros datos a las entidades gubernamentales que proveen los fondos. En conexión con mi inscripción en el banco de datos, a través de este medio, doy mi consentimiento para que la siguiente información sea proporcionada a la Fundación de SIDA de Chicago para ser ingresada al banco de datos: mi nombre, fecha de nacimiento, mi número de seguro social, el apellido de mi madre, y otros datos demográficos. También entiendo que es mi responsabilidad verificar mi condición con respeto al VIH, (si, aplica) y fechas de tratamiento médico y servicio de manejo de casos que serán sometidos a la Fundación de SIDA de Chicago. Entiendo que esta información va a ser agrupada con la de otros clientes con el propósito de generar reportes estadísticos, evitar la duplicación de servicios y coordinar el sistema de entrega de servicios a personas con VIH, sus familiares y/o sus parejas y específicamente autorizo el uso de esta información para ese propósito. Además yo permito a los empleados de la Fundación de SIDA de Chicago y a los comités designados de la Cooperativa revisar mis archivos de servicios como parte del programa que garantiza la calidad de servicios de la Cooperativa. Como propósito de este consentimiento, yo reconozco y estoy de acuerdo en que mis archivos incluyen cualquier o todos los archivos generados por cualquier agencia proveedora de servicios que forma parte de la Cooperativa. Ninguna información que yo provea con el propósito de recibir servicios será revelada a ninguna agencia gubernamental ni al departamento de salud con propósitos de vigilancia, ubicación, o cualquier otro propósito que no sea obtener servicios médicos o sociales, exceptuando (1) con mi consentimiento, (2) si es requerido por la ley, o (3) de ser necesario, para prevenir una seria intención de ocasionar daño a otros o a mí mismo. Precauciones de seguridad se mantendrán para prevenir el acceso no autorizado al banco de datos por cualquier persona que no sea empleado de la Fundación de SIDA de Chicago. Yo doy consentimiento adicional para reportar información que yo provea en conexión con el banco de datos y en conexión con los servicios recibidos a través de fondos federales que apoyan a la Fundación SIDA de Chicago. Entiendo que esta información puede ser sometida en grupo o individualmente. Yo entiendo que, con el propósito de proteger mi privacidad, toda información sometida en forma individual con excepción de los servicios patrocinados por Parte B, serán proveídos con códigos individuales sin nombre ni ninguna información que me identifique.
14 Además, yo entiendo que si llego a recibir servicios bajo el Proyecto de ley Parte B de Ryan White, alguna información será reportada a la Unidad de Servicios Directos del Departamento de Salud Pública de Illinois, incluyendo: - información demográfica que incluye pero no está limitada a mi nombre, sexo, raza, número de seguro social, y fecha de nacimiento; información sobre servicios que he utilizado, diagnóstico de VIH/SIDA e información sobre mi tratamiento; información sobre servicios de salud mental o uso de drogas será compartido con el propósito de evaluar servicios proveídos, revisar archivos, o en casos donde el compartir información sea necesario para coordinar servicios. Yo puedo poner fin a este consentimiento presentando una solicitud por escrito a cualquiera de los Destinatarios (Agencias en las cooperativas) indicando que ya no deseo recibir servicios de la cooperativa o indicando mi revocación escrita a esta autorización. Yo entiendo que puedo rehusarme a firmar este consentimiento. Yo además entiendo que puedo suspender este consentimiento en cualquier momento presentando una nota por escrito al proveedor de servicios con mi intención de suspender este consentimiento. Este consentimiento no puede ser suspendido en la medida en que alguna acción ha sido tomada basada en este consentimiento. Este consentimiento es válido por el periodo de un año a partir de la fecha en que es firmado por el cliente El proveedor no usará o revelará información personal de salud más allá del propósito de esta autorización sin su autorización o consentimiento escrito. Por favor tenga en cuenta que, sujeto a la ley que aplica, la información revelada está sujeta a ser revelada a su vez por el que la recibe, y puede entonces no ser considerada información de salud protegida, en conformidad con al acta de transferibilidad y responsabilidad de seguro de salud de 1996 (HIPAA-Health Insurance Portability and Accountability Act of 1996) y las regulaciones promulgadas a partir de entonces. Firma del cliente o su representante legal Nombre Fecha Parentesco (Si es firmada por otra persona que no es el cliente)


15 Appendix 6: IDPH Authorization for Release of Health Information

16
17 Appendix 7. Foreign Language Translation Request Form Foreign Language Translation Request Form Case Management Agency Name: Case Manager Name: Date Completed: Requested date and time of service: Foreign Language Needed: Client Name: Visit Type: Intake Reassessment On-going case management contact Issues to be addressed in case management encounter: (Please include a brief narrative regarding the areas of service detailed in the encounter) Will the case manager be requesting this service again for this client? Yes No Anticipated frequency of translation service request for this client: AFC Staff Signature: Date: Vendor: Complete this form for every individual translation request and fax to Intake Manager at the AIDS Foundation (312) for approval. Service may not be rendered without prior approval.
18 Appendix 8. Sign Language Interpretation Request Form Sign Language Interpretation Request Form Case Management Agency Name: Case Manager Name: Date Completed: Requested date and time of service: Client Name: Visit Type: Intake Reassessment On-going case management contact Issues to be addressed in case management encounter: (Please include a brief narrative regarding the areas of service detailed in the encounter) Will the case manager be requesting this service again for this client? Yes No Anticipated frequency of translation service request for this client: AFC Staff Signature: Date: Vendor: Complete this form for every individual translation request and fax to Intake Manager at the AIDS Foundation (312) for approval. Service may not be rendered without prior approval.
19 ILLINOIS DEPARTMENT OF PUBLIC HEALTH (IDPH) RYAN WHITE PART B STANDARD OPERATING PROCEDURE Linguistic Services Effective Date: Page 1 of 2 Revised Date: V. PURPOSE The purpose is to define and provide guidance as to what is allowable for the Home and Community Based Health Services category of service, in accordance with HRSA standards. VI. DEFINITION Support for Linguistic Services including interpretation (oral) and translation (written) services, provided by qualified individuals as a component of HIV service delivery between the provider and the client, when such services are necessary to facilitate communication between the provider and client and/or support delivery of Ryan White-eligible services. VII. PROCEDURE PERFORMANCE MEASURE Documentation that: o o Linguistic services are being provided as a component of HIV service delivery between the provider and the client, to facilitate communication between the client and provider and the delivery of Ryan White-eligible services in both group and individual settings Services are provided by appropriately trained and qualified individuals holding appropriate State GRANTEE RESPONSIBILITY Develop the Request for Proposal (RFP), contract, Memorandum of Understanding (MOU)/Letter of Agreement (LOA) and/or statements of work language that: o o The range and types of linguistic services to be provided, including oral interpretation and written translation as needed to facilitate communications and service delivery Requirements for training and qualifications based on available State and local certification Monitor providers to assure that: o o Linguistic services are provided based on documented provider need in order for Ryan White clients to communicate with the provider and/or receive appropriate services Interpreters and translators have appropriate training and State or local certification Illinois Ryan White Part B Program Standard Operating Procedures Page 181 of 228
20 ILLINOIS DEPARTMENT OF PUBLIC HEALTH (IDPH) RYAN WHITE PART B STANDARD OPERATING PROCEDURE Linguistic Services Effective Date: Page 2 of 2 Revised Date: PROVIDER/SUBGRANTEE RESPONSIBILITY Document the provision of linguistic services, including: o o o o Number and types of providers requesting and receiving services Number of assignments Languages involved Types of services provided oral interpretation or written translation, and whether interpretation is for an individual client or a group Maintain documentation showing that interpreters and translators employed with Ryan White funds have appropriate training and hold relevant State and/or local certification VIII. EXCEPTIONS AND EXCLUSIONS Translation and Linguistic services (including oral, written, and sign language) must be given by a trained professional for any contact regarding Ryan White Part B as a whole. Family members or friends of the client are not to be utilized for these services, as this could unknowingly be a barrier to proper care and treatment of underlying issues that the client does not want to tell the family member or friend. Illinois Ryan White Part B Program Standard Operating Procedures Page 182 of 228
21 Appendix 10. Incident Reporting Form Incident Reporting Form Use this form to report any workplace accident, injury, incident, close call or illness. Return completed form to the Operations Supervisor, or Management. This is documenting: physical injury to or by the individual that requires a physician s treatment or admission to a hospital, or the death of any person, or emergency mental health treatment for the individual, or the intervention of law enforcement, or report of child abuse pursuant to Illinois Statutes 325 ILCS 5 Abused and Neglected Child Reporting Act or a report of dependent adult abuse pursuant to (320 ILCS 20/) Elder Abuse and Neglect Act., or Constitutes a prescription medication error or a pattern of medication errors a member s location being unknown by provider staff who are assigned protective oversight. Details of person injured or involved (to be filled in by person injured / involved if possible) Person Completing Report: Person(s) Involved: Equipment or Truck ID: Date: Event Details: Name of Individual served: Date of Event: Location of Event: Time of Event: Witnesses: Description of Events (Describe tasks being performed and sequence of events): *If more space is required please use the back of this sheet Was event / injury caused by an unsafe act (activity or movement) or an unsafe condition (machinery or weather)? Please explain:
22 Appendix 10. Incident Reporting Form TO BE COMPLETED ONLY IF LOST TIME/INJURY OR FIRST AID WAS REQUIRED Type of injury sustained: Cause of lost time/ injury or first aid: Was medical treatment necessary? Yes No If yes, name of hospital or physician: Action taken by organization to handle the situation: Resolution or follow up: Signature of Employee: Date: Signature of Supervisor: Date:
23 Appendix 11. Sample Agency Grievance Procedure Rights & Responsibilities SAMPLE AGENCY Client Grievance Procedure Rights & Responsibilities AGENCY believes in the dignity and worth of all individuals and holds that all persons have certain rights and responsibilities. Our goal as an agency is to ensure that all staff treats each individual we serve with the respect, dignity, and honor that benefits them. We also hold that each person seeking services from Erie should fully understand their rights, the rules and the regulations of the agency. AGENCY has been contracted to provide comprehensive case management services to individuals diagnosed with HIV/AIDS. Comprehensive case management is defined to mean a standardized process of client centered assessment case planning, service coordination, referral, advocacy, and follow up through which the multiple service needs of persons affected by HIV disease are met. AGENCY recognizes that clients have the following protection: 1. To remain anonymous, even though this may disqualify you from certain services. 2. To decline services at anytime. 3. To know at all times how and where to register complaints. 4. To know that all personal information is confidential and cannot be released without your consent. 5. To have freedom from mental and physical abuse and to have their civil rights respected. 6. To obtain the services of another organization without the consent of this organization and continue to receive non-duplicated care at that organization with or without help from AGENCY staff. 7. To not be excluded from services on the basis of race, ethnicity, sex, sexual orientation, physical disability, social and/or economic status/group member affiliation. 8. To appeal any fees assessed by the agency or to make an appeal for the reduction or waiver of fees assessed based on documented circumstances affecting the ability to pay. Client s Responsibilities: 1. Provide all information about his/her health as completely and accurately as possible. 2. Respect the privacy of other clients and families. 3. Keep all information learned about other clients and families in the strictest confidence. 4. Keep appointments, and when unable to do so for any reason, notify the appropriate staff. 5. You should maintain the level of contact agreed upon with your provider. 6. Be honest and open about your situation, and inform the case manager and/or medical provider if any changes in your situation. By participating fully in the case management/primary care relationship, you can obtain the best possible service we can provide. Grievance Procedure: In the event a client expresses a grievance with clinical or direct service case managers, the client has the right to speak to the following AGENCY staff. INSERT NAMES/TITLE OF STAFF HERE Staff Name Title Contact Information
24 Appendix 11. Sample Agency Grievance Procedure Rights & Responsibilities (Page 2) The following procedure for a complaint or concerns should be followed: 1. The complaint should be addressed in writing. The issue will be attempted to be resolved and addressed. 2. The final step at AGENCY will be to discuss the concerns with AGENCY Program Director. 3. If the client does not reach a satisfactory resolution by following the above procedure, or if they are not comfortable filing a grievance directly with AGENCY, the client may file a grievance with the Center for Conflict Resolution, , at any step during the procedure outlined above. I have read these rights and responsibilities listed above, or have had them read and explained to me and I fully understand them. I certify by my signature that I have received a copy of them for my future reference. Case Manager / Staff Witness Signature Date Client Signature Date
25 Appendix 12. Grievance Tracking Form AIDS FOUNDATION OF CHICAGO Northeastern Illinois HIV/AIDS Case Management Cooperative Grievance Tracking Form Client: Client Tract ID: Case Manager Name: Case Management Agency: Client receives case management services? Client received a copy of or signed the grievance procedure? Date: Client followed the agency grievance procedure? Agency has been contacted by AFC staff? Further action required by AFC staff: Complaint/Inquiry: Describe the nature of the complaint, include dates and time that the incident occurred and all agency staff that were involved. Final Outcome: What did the agency do to resolve the complaint/inquiry? Additional Comments: Case Manager Signature Date Client Signature Date
26 Appendix 13: AFC Service Complaint Inquiry Form SERVICE COMPLAINT/INQUIRY (For AFC STAFF USE ONLY) Date of Complaint AFC Staff Taking Complaint Client Name Client Address City Zip Code Phone # ( ) Name of caller (if other than client) Relationship to Client Phone # ( ) Does client receive case management services? - Yes No Case manager Agency Did client receive a copy of or sign the agency grievance procedure? Yes No Has the client followed the agency grievance procedure? Yes No Service Complaint/Inquiry-Describe the nature of the complaint, including dates that the incident occurred and all agency staff that were involved. Include any action steps client has already taken to resolve grievance.
27 Appendix 13: AFC Service Complaint Inquiry Form ACTION TAKEN BY AFC STAFF Date Agency was contacted by AFC Staff Name of Agency Staff Contacted Title Date Agency will provide written response to AFC Date Agency responded to complaint/inquiry Final Outcome What did the agency do to resolve the complaint/inquiry? Is any further action required by AFC staff? Yes No Comments: AFC Staff Signature
28 Appendix 14. Grievance Form AFC Use Only AIDS FOUNDATION OF CHICAGO NORTHEASTERN ILLINOIS HIV/AIDS CASE MANAGEMENT COOPERATIVE SERVICE COMPLAINT/INQUIRY (For AFC STAFF USE ONLY) Date of Complaint AFC Staff Taking Complaint Client Name Client Address City Zip Code Phone # ( ) Name of caller (if other than client) Relationship to Client Phone # ( ) Does client receive case management services? - Yes No Case manager Agency Did client receive a copy of or sign the agency grievance procedure? Yes No Has the client followed the agency grievance procedure? Yes No Service Complaint/Inquiry-Describe the nature of the complaint, including dates that the incident occurred and all agency staff that were involved. Include any action steps client has already taken to resolve grievance.
29 Appendix 14. Grievance Form AFC Use Only Page 2 ACTION TAKEN BY AFC STAFF Date Agency was contacted by AFC Staff Name of Agency Staff Contacted Title Date Agency will provide written response to AFC Date Agency responded to complaint/inquiry Final Outcome What did the agency do to resolve the complaint/inquiry? Is any further action required by AFC staff? Yes No Comments: AFC Staff Signature
30 Appendix 15. Confidentiality Violation Report Form Ryan White Case Management Program Electronic Health Record Confidentiality and Compliance Report Provide Enterprise functions as an Electronic Health Record (EHR) that contains Federal and Stated covered documentation and information required in our Program s daily operations. Violation of this confidentiality is an extreme matter, and if continued could result in termination and/or civil liability. This documentation must be completed, and returned to the AFC Ryan White Program. These will be kept as part of the Internal Compliance file, and may be used for reference in performance standards. Compliance Violation Information Provide User in violation: Date violation occurred: Date Violation reported: Please provide a summary of the violation: Corrective Action Plan Summary User Signature: Date: Supervisor Signature: Date:
31 Appendix 16. Client Satisfaction Survey Template Client Satisfaction Survey Template Please note that the Client Satisfaction Survey is not included because it changes year-to-year
32 Appendix 17. Health Literacy Assessment HEALTH LITERACY Question Scoring Response READ TO SUBJECT: This information is on the back of a container of a point of ice cream. 1. If you eat the entire container, how many calories will you eat? Answer: 1,000 is the only correct answer 2. If you are allowed to eat 60 grams of carbohydrates as a snack, how much ice cream could you have? Answer: Any of the following is correct: 1 cup (or any amount up to 1 cup), half the container. Note: If patient answers two servings, ask How much ice cream would that be if you were to measure it into a bowl? 3. Your doctor advises you to reduce the Answer: 33 is the only correct answer amount of saturated fat in your diet. You usually have 42 g of saturated fat each day, which includes one serving of ice cream. If you stop eating ice cream, how many grams of saturated fat would you be consuming each day? 4. If you usually eat 2,500 calories in a Answer: 10% is the only correct answer day, what percentage of your daily value of calories will you be eating if you eat one serving? READ TO SUBJECT: Pretend that you are allergic to the following substances: penicillin, peanuts, latex gloves, and bee stings. 5. Is it safe for you to eat this ice cream? Answer: No 6. (Ask only if the patient responds no to question 5): Why not? Answer: Because it has peanut oil. Interpretation: Score of 0-1 suggests high likelihood (50% or more) of limited literacy. Score of 2-3 indicates the possibility of limited literacy. Score of 4-6 almost always indicates adequate literacy. Total Score:

33
34 Appendix 18. Risk Assessment Tool Risk Assessment 1. How often would you say you have condomless (unprotected) vaginal, anal or oral sex? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused g. Not Applicable 2. How often do you use lubrication during sexual intercourse? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused g. Not Applicable 3. Which of the following sexually transmitted infections are curable? (check all that apply) a. Chlamydia d. Hepatitis C g. Herpes b. Hepatitis B e. Syphilis h. Don t Know c. Gonorrhea f. Human Papilloma Virus i. Refused 4. Which of the following sexually transmitted infections are not curable? (check all that apply) a. Chlamydia d. Hepatitis C g. Herpes b. Hepatitis B e. Syphilis h. Don t Know c. Gonorrhea f. Human Papilloma Virus i. Refused 5. Have you ever exchanged sex for money, drugs, alcohol, a place to stay, or material goods? a. Yes c. Don t Know b. No d. Refused 6. How often have you used drugs or alcohol before or during sex? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused 7. Have you used a needle to inject drugs into your veins or under your skin, including steroids? a. Yes c. Don t Know b. No d. Refused 8. Have any of your current or past sex partners ever inject drugs into their veins or under their skin, including steroids? c. Yes c. Don t Know d. No d. Refused 9. Have you shared needles for drugs or any other use with your sexual partners? a. Yes c. Don t Know b. No d. Refused 10. How often do you discuss your HIV status with your sexual partners? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused 11. How likely are you to have condomless (unprotected) sex if your viral load is undetectable? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused 12. How likely are you to have condomless (unprotected) sex with another HIV+ partner? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused 13. How likely are you to have condomless (unprotected) sex with a negative-partner? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused 14. How likely are you to have condomless (unprotected) sex with a negative-partner, if they were on PrEP)? a. Never c. Often e. Don t Know b. Some of the time d. All of the time f. Refused
35 Appendix 18. EVALUACIÓN DE RIESGO EVALUACIÓN DE RIESGO 1. Con que frecuencia dirías que tienes sex sexo vaginal, anal u oral sin protección? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó 2. Con qué frecuencia utilizas lubricación durante relaciones sexuales? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó 3. Cuáles de las siguientes infecciones de transmisión sexual son curables? a. Chlamydia d. Hepatitis C g. Herpes b. Hepatitis B e. sífilis h. No sé c. Gonorrea f. Virus de papiloma humano i. Se negó 4. Cuál de las siguientes infecciones de transmisión sexual no son curables? a. Chlamydia d. Hepatitis C g. Herpes b. Hepatitis B e. sífilis h. No sé c. Gonorrea f. Virus de papiloma humano i. Se negó 5. Ha intercambiado sexo por dinero, drogas, alcohol, un lugar para quedarse o bienes materiales? a. Sí c. No sé b. No d. Se negó 6. Con qué frecuencia usted ha utilizado drogas o alcohol antes o durante el sexo? a. Nunca c. Muchas veces e. No sabe b. De vez en cuando d. Todo el tiempo f. Se negó 7. Ha usado una aguja para inyectarse en las venas o debajo de la piel drogas, incluyendo esteroides? a. Sí c. No sé b. No d. Se negó 8. Ha tenido parejas sexuales actuales o antiguas, donde ellos se inyectaron drogas en las venas o debajo de la piel, incluyendo esteroides? a. Sí c. No sé b. No d. Se negó 9. Ha compartido agujas para el uso de drogas o cualquier otro uso con sus parejas sexuales? a. Sí c. No sé b. No d. Se negó
36 10. Con qué frecuencia discute su estatus de VIH con su pareja? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó 11. Qué probabilidades hay de tener relaciones sexuales (sin protección) si su carga viral es indetectable? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó 12. Qué probabilidades hay de tener relaciones sexuales (sin protección) si su pareja es VIH-positivo? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó 13. Qué probabilidades hay de que tener relaciones sexuales (sin protección) si su pareja es VIH-negativa? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó 14. Qué probabilidades hay de que tener relaciones sexuales (sin protección) si su pareja es VIH negativa, y estuviera tomando profilaxis pre-exposición (PrEP)? a. Nunca c. Muchas veces e. No saben b. De vez en cuando d. Todo el tiempo f. Se negó
37 Appendix 19. Client Screening & Placement Screening Form Client Screening & Placement Form Client ID: Agency: First Name: CODE DOB 1. What is your date of birth? Contact Date: Staff Name: Last Name: DEMOGRAPHICS month day year Gender Rlshp Address 2. What is your gender? 1 - Male 5 - Other (Describe: _ ) 2 - Female 6 - Doesn't know 3 - Transgender (Male to Female) 7 - Refused to answer 4 - Transgender (Female to Male) 3. What is your current relationship status? 1 - Single, Never Married 6 - Partnered 2 - Divorced 7 - Separated 3 - Widowed 8- Refused to Answer 4 - Married 5 - Engaged 4. What is your address? Street City State Illinois Zip Code Phone # 5. What is your phone number? Home Cellular Other Hispanic Race Country Language 6. Are you Hispanic or Latino? 1 - Yes, Hispanic /Latino 7 - Doesn t Know 2 - No, Non-Hispanic / Latino 8- Refused to Answer 7. What is your race? 1 - American Indian/Alsakan Native 5 - White 2 - Asian 7 - Doesn t Know 3 - Black / African American 8- Refused to Answer 4 - Native Hawaiian / Pacific Islander 8. What country were you born in? 9. What is your primary language? Note: If primary language is English, skip to next section. If primary language is other than English, go to question 10.
38 Appendix 19. Client Screening & Placement Screening Form Eng. Prof 10. Do you consider yourself to have limited English proficiency? 1 - Yes 7 - Doesn t Know 2 - No 8- Refused to Answer CODE GH1 GH2 1. When did you first test HIV-positive? 2. When did you last see a medical provider for HIV-related medical reasons? This could include a check-up with an HIV medical provider or another primary care provider whom you may have seen for HIV-related reasons. GENERAL HEALTH Month Day Year Month Day Year GH3 GH4 CODE??? 3. Are you currently taking HIV medications, also known as antiretroviral therapy? 1 - Yes 7 - Doesn t Know 2 - No 8- Refused to Answer 4. In general, would you say your health is: 1 - Excellent 5 - Poor 2 - Very Good 7 - Doesn t Know 3 - Good 8- Refused to Answer 4 - Fair 5. Compared to one year ago, how would you rate your health in general now? 1 - Much better now than one year ago 7 - Doesn t Know 2 - Somewhat better now than one year 8 - Refused to Answer ago 3 - About the same as one year ago 4 - Somewhat worse now than one year ago 5 - Much worse now than one year ago CODE DSS6 DISCLOSURE & SOCIAL SUPPORT 6. Among your close FRIENDS, how many know that you are HIV positive? 1 - None 5 - All 2 - A few 7 - Doesn t Know 3 - About half 8 - Refused to Answer 4 - Most 9 - Not applicable, no close friends
39 Appendix 19. Client Screening & Placement Screening Form DSS7 DSS8 DSS9 DSS9a 7. Among your close FAMILY, how many know that you are HIV positive? 1 - None 5 - All 2 - A few 7 - Doesn t Know 3 - About half 8 - Refused to Answer 4 - Most 9 - Not applicable, no close friends 8. Are there people who are close to you (family, friends, etc.) whom you want to tell that you are HIV+ but have not? 1 - Yes 7 - Doesn t Know 2 - No 8- Refused to Answer 9. Do you agree with the following statement? There are other people in my life that I am close to who are also HIV positive: 1 - Yes (Skip to Question 9a) 7 - Doesn t Know 2 - No 8- Refused to Answer 9a. Of these people, are some taking HIV medications that you know of? 1 - Yes (Skip to Question 9a) 7 - Doesn t Know 2 - No 8- Refused to Answer DSS Do you agree or disagree with the following statement? There are people I can depend on to help me if I really need it. 1 - Strongly Agree 7 - Doesn t Know 2 - Agree 8 - Refused to Answer 3 - Neither agree nor disagree 4 - Disagree 5 - Strongly disagree Note: If client says "Agree", ask "Would you say that you Strongly Agree or just Agree? Note: If client says "Disagree", ask "Would you say that you Disagree Agree or just Disagree? CODE STIGMA Instructions: The following questions are about your experiences living with HIV and how other people have reacted or how they might react if they knew you are HIV-positive. I am going to read some statements, and for each I want you to tell me whether it is true for you. The choices I would like you to use are not at all, rarely, sometimes, or often. Here is the first one S11 S I ve felt people avoid me because I have HIV. Would you say that for you this is true not at all, rarely, sometimes, or often? 1 - Not At All 2 - Rarely 3 - Sometimes 4 - Often 7 - Don t Know 8- Refused 12. I ve feared I would lose my friends if they learned about my HIV. 1 - Not At All 2 - Rarely 3 - Sometimes 4 - Often 7 - Don t Know 8- Refused S I ve thought other people were uncomfortable being with me because of my HIV. 1 - Not At All 2 - Rarely 3 - Sometimes 4 - Often 7 - Don t Know 8- Refused
40 Appendix 19. Client Screening & Placement Screening Form CODE S14 STIGMA 14. I ve avoided getting treatment because someone might find out about my HIV. 1 - Not At 2 - Rarely Often 7 - Don t 8- Refused All Sometimes Know CODE BELIEFS ABOUT MEDICATIONS Part 1 For All Clients: We are interested in your thoughts about taking medications. Please say whether you agree or disagree with each of the following statements about the general use of medications for any medical reasons. BAM Doctors prescribe too many medications. 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused BAM Medications do more harm than good. 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused BAM Doctors place too much trust in medications. 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused Note: If client says "Agree", ask "Would you say that you Strongly Agree or just Agree? Note: If client says "Disagree", ask "Would you say that you Disagree Agree or just Disagree? Part 2 for clients on ARVs only BAM18vA 18. Now I am going to ask you some questions about your HIV treatment and HIV medications. Thinking back over the past 30 days, please rate your ability to take all your HIV medications as prescribed. Would you say Very poor, poor, fair, good, very good, or excellent? 1 - Very Poor 6 - Excellent 2 - Poor 7 - Doesn t Know 3 - Fair 8- Refused to Answer 4 - Good 5 - Very good Part 3 for clients NOT ARVs: Now I would like to ask you about your thoughts about taking HIV medications. Even though you are not taking HIV medications, please say whether you agree or disagree with the following statements about what it would be like for you to take HIV medications. BAM18vB 18. Taking HIV medications on a schedule would be easy for me. 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused BAM19vB 19. I never want to take HIV medications 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused
41 Appendix 19. Client Screening & Placement Screening Form BAM20vB 20. I would not want people to know that I am taking HIV medications. 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused CODE SUBSTANCE ABUSE INSTRUCTIONS: I am going to change topics and ask you about alcohol and drug use. Remember that your responses are confidential. SAMISS1 1. How often do you have a drink containing alcohol? (Alcoholic drinks include one beer, one glass of wine, a mixed drink of hard liquor, or one wine cooler. Each of these counts as one drink, unless they have double shots, which would equal two drinks.) (If client does not drink, go to question #4.) 0 - Never 4-4 or more times per week 1 - Monthly or less 7 - Doesn t Know times per month 8- Refused to Answer times per week SAMISS2 2. How many drinks do you have on a typical day when you are drinking? drinks per day 4-10 or moer drinks per day drinks per day 7 - Doesn t Know drinks per day 8- Refused to Answer drinks per day CODE SAMISS3 SUBSTANCE ABUSE (Cont.) 3. How often do you have four or more drinks on one occasion? 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused SAMISS4 4. During the past 12 months, how often did you use non-prescription drugs to get high or to change the way you feel? 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused SAMISS5 5. During the past 12 months, how often did you use drugs prescribed to you or to someone else to get high or change the way you feel? 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused
42 Appendix 19. Client Screening & Placement Screening Form CODE SAMISS6 SUBSTANCE ABUSE (Cont.) 6. During the past 12 months, how often did you drink or use drugs more than you meant to? 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused SAMISS7 7. How often did you feel you wanted or needed to cut down on your drinking or drug use inthe past 12 months, and not been able to? 1 - Strongly Agree 2 - Agree 3 - Neither Agree / Disagree 4 - Disagree 5 - Strongly Disagree 7 - Don t Know 8- Refused DATA ENTRY Client considered positive for substance use symptoms if ANY of the following criteria are met: The sum of responses for Questions 1-3 is 5 The sum of responses for Questions 4-5 is 3 The sum of responses for Questions 6-7 is 1 Q1-3= Q4-5= Q6-7= SU Did client screen positive for substance abuse symptoms? 1 - Yes 2 - No CODE MENTAL HEALTH Now I am going to ask you some questions about your well-being or psychological health. SAMISS8 8. During the past 12 months, were you ever on medication/antidepressants for depression or nerve problems? 1 - Yes 2 - No 7 - Don t Know 8- Refused SAMISS9 9. During the past 12 months, was there ever a time when you felt sad, blue, or depressed for 2 weeks or more in a row? 1 - Yes 2 - No 7 - Don t Know 8- Refused SAMISS During the past 12 months, was there ever a time lasting 2 weeks or more when you lost interest in most things like hobbies, work, or activities that usually give you pleasure? 1 - Yes 2 - No 7 - Don t Know 8- Refused CODE SAMISS11 MENTAL HEALTH (Cont.) 11. During the past 12 months, did you ever have a period lasting 1 month or longer when most of the time you felt worried and anxious? 1 - Yes 2 - No 7 - Don t Know 8- Refused
43 Appendix 19. Client Screening & Placement Screening Form CODE SAMISS12 SAMISS13 MENTAL HEALTH (Cont.) 12. During the past 12 months, did you have a spell or an attack when all of a sudden you felt frightened, anxious, or very uneasy when most people would not be afraid or anxious? 1 - Yes 2 - No 7 - Don t Know 8- Refused 13. During the past 12 months, did you ever have a spell or an attack when for no reason your heart suddenly started to race, you feltfaint, or you couldn t catch your breath? (IF respondent volunteers only when having a heart attack or due to physical causes, mark NO.) 1 - Yes 2 - No 7 - Don t Know 8- Refused DATA ENTRY Patient considered positive for symptoms of mental illness if he/she responded yes to any mental health question. MH Yes MH Yes Did client screen positive for mental illness symptoms? 1 - Yes 2 - No Did client screen positive for co-occurring mental health substance use disorders? 1 - Yes 2 - No CODE SERVICES NEEDED I am going to read to you a list of services and resources. Please tell me which ones are ones that you currently need. (Screener check Yes or No for each) Code I need. 1 - Yes 2 - No 7 - Don t Know 8- Refused SVC22 SVC23 SVC24 SVC25 SVC26 SVC27 SVC28 SVC29 SVC30 SVC31 SVC Case management services, such as assistance in obtaining medical, legal, financial, and other needed services 23. Housing or shelter 24. Food or other basic needs 25. Dental services 26. HIV-Related Medical services 27. Non HIV-related medical services 28. Pharmacy or medication services (for HIV or non HIV reasons) 29. Mental Health services 30. Vocational/Job Training 31. Assistance with Benefits and Entitlements, such as Medicaid, SSI 32. Drug or alcohol abuse treatment
44 Appendix 19. Client Screening & Placement Screening Form SVC33 NOTE: If caller identifies more than one need, ask: Of those services, which one is the most urgent for you now? Document Here: CODE FUI1 FUI2 FUI3 FUI3a FOLLOW-UP INTERVIEW Follow Up Questions 1 - Yes 2 - No 7 - Don t Know 8- Refused 1. The AIDS Foundation of Chicago may want to call you back in the coming year or so to conduct a follow-up interview. Would it be alright if we called you back at that time? 2. Just to confirm, you can be reached at this telephone number: (READ BACK TELEPHONE NUMBER). Is this correct? 3. Are there any other alternative phone numbers where you can be reached? If Yes, answer 3a. What is the number, area code first.
45 Appendix 20: Affordable Health Care Act Passport Affordable Health Care Act Passport I currently get my medications from pharmacy or clinic. My medications are: Medical Provider Chart Please fill in the names of your care providers along with the hospital/clinic they are affiliated with Primary Care Physician Name Hospital /Clinic Affiliation Specialty Care Physician Name Hospital /Clinic Affiliation Other Specialists Hospital/Clinic Affiliation Mental Health Provider Name Hospital /Clinic Affiliation Psychiatrist Name Hospital /Clinic Affiliation Psychologist/Therapists Name Hospital /Clinic Affiliation Hospital Provider (last major hospitalization) Documents you need to provide: State ID or other form of identification with my picture Tax forms W2 form Pay stubs or checks from my job Social security card Piece of mail such as government mail, phone or utility bill, rent or lease receipt with my current address Under health care reform I think I qualify for health coverage. (Use the question tree in the following link to find out where you fit into health care reform).
46 ILLINOIS Department of Public Health Ryan White Part B Program Notice of Privacy Practices THE EFFECTIVE DATE OF THIS NOTICE IS April 1, THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. THIS NOTICE GIVES YOU INFORMATION REQUIRED BY LAW about the duties and privacy practices of the Illinois Department of Public Health s (IDPH) Ryan White Part B Program to protect the privacy of your personal health information. When IDPH provides you with pharmaceutical and/or premium assistance, medical case management, mental or physical health, dental, or social services, IDPH receives and maintains personal health information about you. IDPH may also receive and maintain financial and billing information about you. To help IDPH provide these comprehensive core and supportive care services to you, IDPH may contract with companies, social service agencies, or individuals. These contractors may also receive and maintain your personal information. IDPH will use and share only the minimum necessary health information that our staff and contractors need to do their jobs. IDPH and its contractors are required by law to (1) maintain the privacy of protected health information; (2) to provide you with notice of IDPH's legal duties and privacy practices with respect to your protected health information; and (3) to notify affected individuals of a breach of unsecured protected health information. This Notice describes how IDPH may use and disclose your information. It also describes your rights and IDPH's legal obligations with respect to your information. IDPH is required to follow the terms of this Notice until the Notice is replaced. IDPH reserves the right to change the terms of this Notice at any time. If IDPH makes changes to this Notice, the new Notice will be available in IDPH offices, upon request, and on our website: Any changes to our practices will apply to all of your personal health information maintained by IDPH. How IDPH May Use and Disclose Your Health Information IDPH may share your information without your authorization in the following ways: Treatment: IDPH can use your health information and share it with other professionals who are treating you in order to enhance coordination of comprehensive care services. For example: IDPH may disclose your personal health information to your doctor, at the doctor's request, for treatment by your doctor. Payment: IDPH can use and share your information for payment purposes. For example: IDPH may use or disclose your personal health information to provide eligibility information to your doctor when you receive treatment; to pay for claims for covered health care services; to pay for insurance premiums if eligible; to assist with payment of approved medical/pharmaceutical out-of-pocket costs; or to recover costs from other medical insurance or probate estates. Health Care Operations: IDPH can use and share your health information for IDPH operations, to improve your care, and to contact you when necessary. For example: IDPH or its contractors may use or disclose your personal health information (1) to conduct quality assessment and improvement activities; (2) to review applications for services; (3) to engage in care coordination or case management; (4) to manage, plan or develop IDPH's services and budget; (5) to coordinate services with another public benefit program; (6) to create or provide individualized service or treatment plans; or (7) to cooperate with State and federal auditors. Health Services: IDPH or its contractors may contact you to remind you of appointments or to give you information about treatment alternatives or other health-related benefits and services that may be helpful to you or your family. IDPH is allowed, and in some instances required, to share your information in other ways such as for public health and research. IDPH must meet conditions in the law before it can share your information for these purposes. Public Health and Safety Issues: IDPH can share health information about you with public health authorities for public health activities such as: preventing or controlling disease, injury, or disability; keeping vital records; avoiding a serious threat to the health or safety of a person or the public; and reporting suspected abuse, neglect, or domestic violence to governmental or social services agencies. IDPH also can share your health information with a governmental agency authorized to oversee government health care programs. Research: IDPH can use or share your information for health research in limited circumstances where the information will be protected by the researchers. As Required by Law: IDPH will share information about you if State or federal laws require it, including with the federal Health Insurance Portability and Accountability Act of 1996 (HIPAA) for a compliance review or complaint investigation or with a personal representative appointed by you or designated by law. Lawsuits and Legal Actions: IDPH can share health information about you in response to a court or administrative order, or in response to a subpoena. Public Health Activities and Public Health Reporting: IDPH is permitted to disclose protected health information for public health activities (such as surveillance and investigation), interventions and activities related to public health oversight; and to coordinate care and treatment with other IDPH Health Protection Entity s (e.g., Sexually Transmitted Disease Office) activities. Other Agencies: IDPH can share your information with another agency administering a government program providing public benefits, with respect to eligibility or enrollment information, and to better coordinate, administer and manage government programs and for treatment and care coordination of the Department s program. (Revised: 09/01/2016) Page 1 of 3
47 ILLINOIS Department of Public Health Ryan White Part B Program Notice of Privacy Practices IDPH follows the HIPAA guidelines. IDPH also follows any federal or State law that gives greater privacy protections than HIPAA. For example, IDPH follows the Illinois Mental Health and Developmental Disabilities Confidentiality Act concerning mental health records, 740 ILCS 110; the Illinois Personal Information Protection Act which protects personal information that is not otherwise lawfully made available to the general public from federal, State, or local government records, 815 ILCS 530; the federal Confidentiality of Alcohol and Drug Abuse Patient Records Act concerning the disclosure of drug or alcohol information, 42 U.S.C 290dd-2; 42 CFR Part 2; and the federal Family Educational Rights and Privacy Act concerning the privacy of education records, 20 U.S.C. 1232g; 34 CFR Part 99; 34 CFR Part 99 Our Responsibilities: IDPH is required by law to maintain the privacy and security of your protected health information. IDPH will notify you as required by law when there is a breach of your unsecured protected health information. In some circumstances IDPH's business associate may provide the notification to you. IDPH must follow the duties and privacy practices described in this Notice and give you a copy of it. IDPH will not use or share your information for any purposes not described in this Notice without your written permission. If you do authorize IDPH to use or disclose your health information, in most cases, you may revoke your written authorization at any time. Your revocation will be effective from the date IDPH receives the revocation. (Authorization and Revocation forms are available on IDPH's Ryan White Part B website.) IDPH is required to obtain your authorization prior to using or disclosing psychotherapy notes, except under the limited treatment, payment, and health care exceptions of 45 CFR (a)(2). IDPH does not market or sell your protected health information. However, IDPH would be required to obtain your authorization prior to selling any of your protected health information or disclosing any of your protected health information for marketing purposes. Your Rights: Communicate Confidentially: You can ask in writing that IDPH communicate with you by a reasonable alternative means or at a reasonable alternative location. For example, you may request that IDPH communicate with you by rather than by telephone, through a translator, or at home instead of your place of work. IDPH will agree to all reasonable requests. Request a Copy of this Privacy Notice: You are entitled to a paper copy of this Notice at any time, even if you have agreed to receive the Notice electronically. An electronic version of this Notice of Privacy Practices is also available on the IDPH website: Inspect and Amend Protected Health Info: You are entitled to inspect and copy your protected health information at any time. At the time of inspection you may request an amendment to your information. IDPH reserves the right to deny your request for amendment. Choose Someone to Act on Your Behalf: You may give someone a medical power of attorney, or a legal guardian may be appointed for you to exercise your rights and make choices about your health. Before IDPH takes any action, IDPH will confirm the person has this authority and can act on your behalf. Right to Accounting of Disclosures: You are entitled to receive an accounting of disclosures of protected health information as provided by 45 C.F.R File a Complaint: If you believe your privacy rights have been violated by IDPH, you have the right to complain to IDPH or to the Secretary of the U.S. Department of Health and Human Services. You may file a complaint with the IDPH Chief Privacy Officer, within 180 days of the suspected violation, at the address where you receive services listed below or you may file a complaint with the United States Department of Health and Human Services, Office for Civil Rights by sending a letter to 200 Independence Avenue, S.W., Washington, D.C ; or calling , or visiting IDPH will not retaliate against you for filing a complaint with either IDPH or with the U.S. Department of Health and Human Services. Your Choices: You have the right to request that IDPH restrict the uses or disclosures of your protected health information to carry out treatment, payment, for health care operations. Your requests must be clearly expressed. IDPH is not required to agree to your requests. IDPH does not engage in fundraising. However, you may opt out of receiving any fundraising communication from IDPH. Privacy Officer To request additional copies of this notice or to receive more information about IDPH's privacy practices or your rights, please contact the Chief Privacy Officer at the following address: Chief Privacy Officer Illinois Department of Public Health 535 West Jefferson Street, Fifth Floor Springfield, IL Telephone PrivacyOffice@idph.state.il.us (Revised: 09/01/2016) Page 2 of 3
48 ILLINOIS Department of Public Health Ryan White Part B Program Notice of Privacy Practices ACKNOWLEDGMENT OF RECEIPT Client First Name Middle Initial Client Last Name Social Security Number (Leave blank if no valid SS number for client) Date of Birth (mm/dd/yyyy) Please have the client/patient complete this acknowledgment of receipt of the Notice of Privacy Practices. Give customer a copy of this Notice and put the original in the medical or clinical record. I hereby acknowledge that I have received a copy of the IDPH Notice of Privacy Practices. I also recognize that I will be required to submit a completed Privacy Practice signature page at each 6 month eligibility determination. Client (age 12 and older) Date or Parent of Minor (clients age 11 and younger) Date or Legal Guardian Date ACUSE DE RECIBO El nombre del cliente La inicia media El apellido del cliente Número de Seguridad social (Permiso en blanco si no aplicable) Fecha de Nacimiento (mm/dd/yyyy) Por favor haga que el cliente / paciente complete este acuse de recibo del aviso de privacidad. Dar al cliente una copia de este aviso y poner el original en el expediente médico o clínico. Por la presente reconozco que he recibido una copia del Aviso de prácticas de privacidad IDPH. También reconozco que se me exigirá que presente una hoja de firma prácticas de privacidad completado en cada determinación de elegibilidad de 6 meses. Firma del cliente (12 años o más) Fecha o Firma de padre/madre del menor (11 años de edad o menos) Fecha o Firma del tutor legal Fecha (Revised: 09/01/2016) Page 3 of 3
49 ILLINOIS Department of Public Health Ryan White Part B Program HOUSEHOLD INCOME STATEMENT Client First Name Middle Initial Client Last Name Social Security Number (Leave blank if no valid SS number for client) Date of Birth (mm/dd/yyyy) Separate section must be filled out for each legal household member age 18 and over even if they do not earn income **All sources shaded that have an amount or are answered with a YES require additional supporting documentation** Wages, salaries, cash, tips Client CURRENT MONTHLY INCOME (cannot leave blank) Do you receive pay stubs (yes/no)? Alimony or spousal support received Self-employed, business income or loss IRA Distributions Pensions and annuities (veteran or employer based pensions, retirement or disabilities) Rental, real estate, partnerships, S Corporations, trusts Farm income or loss Unemployment Income Retirement from Social Security (SSA) Disability from Social Security (SSDI) Supplemental Income from Social Security (SSI) Other income (jury duty, gambling, etc.) Child Support, workers compensation Did you file a tax return (yes/no)? Comments (Additional room for comments on back) Name: Additional Legal Household Member over age 18 Wages, salaries, cash, tips, etc. CURRENT MONTHLY INCOME (cannot leave blank) Do you receive pay stubs (yes/no)? Alimony or spousal support received Self-employed, business income or loss IRA Distributions Pensions and annuities (veteran or employer based pensions, retirement or disabilities) Rental, real estate, partnerships, S Corporations, trusts Farm income or loss Unemployment Income Retirement from Social Security (SSA) Disability from Social Security (SSDI) Supplemental Income from Social Security (SSI) Other income (jury duty, gambling, etc.) Child Support, workers compensation Did this person file a tax return separately (yes/no)? (Revised: 9/1/2016) Page 1 of 2 You may use additional sheets as needed but signature page must accompany each set
50 ILLINOIS Department of Public Health Ryan White Part B Program HOUSEHOLD INCOME STATEMENT Name: Additional Legal Household Member over age 18 Additional Legal Household Member over age 18 CURRENT MONTHLY INCOME (cannot leave blank) Name: CURRENT MONTHLY INCOME (cannot leave blank) Wages, salaries, cash, tips Do you receive pay stubs (yes/no)? Alimony or spousal support received Self-employed, business income or loss IRA Distributions Pensions and annuities (veteran or employer based pensions, retirement or disabilities) Rental, real estate, partnerships, S Corporations, trusts Farm income or loss Unemployment Income Retirement from Social Security (SSA) Disability from Social Security (SSDI) Supplemental Income from Social Security (SSI) Other income (jury duty, gambling, etc.) Child Support, workers compensation Comments Did you file a tax return (yes/no)? Wages, salaries, cash, tips, etc. Do you receive pay stubs (yes/no)? Alimony or spousal support received Self-employed, business income or loss IRA Distributions Pensions and annuities (veteran or employer based pensions, retirement or disabilities) Rental, real estate, partnerships, S Corporations, trusts Farm income or loss Unemployment Income Retirement from Social Security (SSA) Disability from Social Security (SSDI) Supplemental Income from Social Security (SSI) Other income (jury duty, gambling, etc.) Child Support, workers compensation Did this person file a tax return separately (yes/no)? Client Signature Date (Revised: 9/1/2016) Page 2 of 2 You may use additional sheets as needed but signature page must accompany each set
51 Appendix 23. Ryan White Initial Assessment/Reassessment Checklist Ryan White Initial Assessment/Reassessment Checklist (To be completed at intake for all Ryan White clients) Forms/Documentation Client Screening Form/Placement Screening Form (from AFC) AFC Consent to Release Information (AFC form) RW Authorization to Release Form Eligibility Assessment Care Plan Medical Update Form to Physician (AFC form) Date Completed/Received Date Sent: Date Received: Client Photo ID (Driver s License/State ID) Client Proof of Residency (Any 2 of the following) Utility bill with client name and current address Driver s license or state ID with current address Documents issued by the state or federal government (i.e., a motor vehicle registration form, a current Illinois voter registration card, or a current Medicaid card) Current rental or lease agreement with client name Client Proof of Income Current pay stubs 1 months worth Most recent W2 forms Unemployment Benefits Statements Most recent SSI benefits statement Most recent Tax returns. If the client did not file taxes a copy of the Mock MAGI (Modified Adjusted Gross Income) Form For clients with no income, a mock MAGI form, signed and dated by client and CM Client copy of CD4 and Viral Load within the past 6months Client Proof of HIV Status (Part A Clients) Client s name must be on any of the following: Medical Assessment with diagnosis identified Official lab result with any detectable viral load Positive ELISA & Western Blot Positive Serology assay Positive DNA PCR assay Client Rights and Responsibilities (Agency Form) Client Grievance Policy (Agency Form) HIPAA Policy (when applicable) (Agency Form)
52 Appendix 24. Client Intake & Reassessment Form Date: CLIENT PROFILE: Client Intake & Reassessment Form Client First Name: Also Known As: Social Security Number: Client Last Name: Suffix: DEMOGRAPHIC INFORMATION Date of Birth: Current Age: Gender: Male Female Transgender Female to Male Transgender Male to Female Birth Gender: Male Female Married Single Divorced Widowed Legally Separated Civil Union Veteran s Status Yes No RACE (Check all that apply) Alaskan Native Asian Black / African-American Native American Native Hawaiian ETHNICITY Hispanic LANGUAGE & EDUCATION Primary Language: Pacific Islander White Other Unknown / Unreported Non-Hispanic Country of Origin: Married Single Divorced Widowed Legally Separated Civil Union RESIDENTIAL & CONTACT INFORMATION Current Address: City, State, Zip Code: Mailing Address: City, State, Zip Code: ADAP Medication Shipping Address: City, State, Zip Code: Okay to send mail: Yes No Okay to send mail: Yes No Okay to send meds: Yes No Primary Phone Number: Home Mobile If Mobile, okay to text Secondary Phone Number: Home Mobile If Mobile, okay to text Address: Yes, No, Don t
53 Appendix 24. Client Intake & Reassessment Form Initial Client Intake & Reassessment Form (continued) RESIDENCE INFORMATION (Current Residence Type) Apartment or home that you rent Permanent housing for formerly homeless persons Condo you own or house that you own Place not meant for habitation Domestic violence shelter Psychiatric hospital or other psychiatric facilities short term Emergency shelter Psychiatric hospital or other psychiatric facilities long term Foster Care home or foster care group home Psychiatric hospital or other psychiatric facilities long term Homeless from emergency shelters Place not meant for habitation Homeless from the streets Staying or living in FAMILY member s room apartment of house or house Hospital (Non Psychiatric) Staying or living in FRIEND S member s room apartment of house or house Hotel or motel paid for without emergency Substance Abuse facility or detox center voucher Jail prison or Juvenile detention facility Transitional housing for homeless person Other Describe Here: HOUSEHOLD Who do you live with? Person #1 First Name: Last Name: Relationship to you: Phone Number: Okay to contact Do you claim this person as a dependent or spouse on your tax returns? Yes No Date of Birth: Gender: Male Female Ethnicity: Proof of Income: Person #2 First Name: Last Name: Relationship to you: Phone Number: Okay to contact Do you claim this person as a dependent or spouse on your tax returns? Yes No Date of Birth: Gender: Male Female Ethnicity: Proof of Income: EMPLOYMENT STATUS Full-time Part-Time Unemployed/Lay-Off Self-Employed Retired Temporary / Contract Temporary Medical Disability INCOME Alimony / Spousal Support: $ Exempt Interest Dividend (1099-INT box 8): $ Business or self-employed income/loss Taxable Refund State/Local Income Taxes: $ (Schedule C or C-EZ): $ Capital Gain/Loss (Schedule D): $ Taxable Interest (1099-INT Form): $ Ordinary Dividends (1099-INT 1a):$ Tax-Exempt Interest (1099 INT box 8):$ Other Gains/Loss (Form 4797): $ Wages, Salaries, Tips (W-2):$
54 Appendix 24. Client Intake & Reassessment Form Initial Client Intake & Reassessment Form (continued) INCOME (continued) IRA Distribution taxable amount: $ Supplemental Social Security Income: $ Pension and Annuities: $ Other Child Support $ Rental Real Estate Trusts (Schedule E): $ Other Workman s Compensation $ Farm Income/Loss (Schedule F): $ Other Describe: Retirement Income from Social Security: $ Unemployment Income: $ Social Security Disability (SSDI): $ CURRENT HOUSEHOLD INCOME Alimony paid: $ IRA deduction: $ Business Expenses (2106 or 2106-EZ): $ Penalty on early withdrawer of savings $ Educator expenses: $ Self-employed health insurance deduction: $ Deductible from self-employment tax (Schedule Self-employed SEP, SIMPLE Plans: $ SE): $ Domestic production Activities (form 8903): Self-employed health insurance deduction: $ $ Health Saving Account (8889): $ Student loan Interest deduction $ Moving Expenses (3903): $ Tuition and Fees (form 1817): $ DISEASE STATUS Current Disease Status: CDC Defined AIDS HIV Positive / Not AIDS Date HIV Diagnosed: Date AIDS Diagnosed: IDENTIFIED RISK FACTORS Blood Transfusion Hemophilia Heterosexual Contact Intravenous Drug Use Men Who Have Sex with Other Men Mother-at-Risk (Perinatal) Others Undetermined ANTIRETROVIRAL THERAPY (ART) Therapy: Dual HAART None Salvage Single Unknown PHYSICIAN INFORMATION Primary Care Physician Name: Primary Care Facility: HIV Physician Name: HIV Facility Name:
55 Appendix 24. Client Intake & Reassessment Form Initial Client Intake & Reassessment Form (continued) BENEFITS Medicare Status: Active Applied No Benefit If Medicare Active, Medicare Coverage: Part A Part B Part C Part A & B Medicare Part D: Active Applied No Benefit Plan Name: Member ID# Bin # Benefit Phone # Medical Supplement Status: Active Applied No Benefit Plan Type: A B C D F G K L M N Plan Name: Member ID# Bin # Benefit Phone # Medicaid: Yes No INSURANCE Primary Private Insurance: Active Applied COBRA No Benefit If Active, Plan Name: Member ID# Group #: Benefit Phone # Is the Policy issued through an employer? Yes No Pharmacy coverage included? Yes No If COBRA, Start Date: End Date: Plan Name: Member ID# Group #: Benefit Phone # Is the Policy issued through an employer? Yes No Pharmacy coverage included? Yes No PRESCRIPTION ONLY BENEFIT PLAN STATUS Prescription Only: Active Applied No Benefit
56 Appendix 24. Client Intake & Reassessment Form Initial Client Intake & Reassessment Form (continued) If Prescription Only Active, Rx Plan Name: Rx Member ID# Rx Group #: Rx Benefit # Rx BIN # Benefit Phone # Premium Assistance requested? Yes No Are your premiums auto-deducted? Yes No Premium Amount: $ Are you overdue on a premium payment Yes No Premium Payment Frequency: Premium Payee information: DENTAL CARE ONLY BENEFIT STATUS Dental Care Only Status: Active Applied COBRA No Benefit Plan Name: Member ID# Group #: Benefit Phone # If Dental is COBRA, Start Date: End Date: Plan Name: Member ID# Group #: Benefit Phone # VISION ONLY BENEFIT STATUS Vision Care Only Status: Active Applied COBRA No Benefit Plan Name: Member ID# Group #: Benefit Phone # If Vision is COBRA Start Date: End Date: Plan Name: Member ID# Group #: Benefit Phone #
57 Appendix 25. Client Screening & Feedback Form AIDS FOUNDATION OF CHICAGO NORTHEASTERN ILLINOIS HIV/AIDS CASE MANAGEMENT COOPERATIVE DATE: / / CLIENT ID #: Client Eligibility Determination for Medical Case Management or Supportive Services Case Management: LAST NAME: FIRST NAME: MIDDLE INIT: DOB: / / SS#: - - Don t know/have SS# Refused SS# Geographic Eligibility: STREET ADDRESS: CITY: COUNTY: ZIP: CRITERIA: CM SCORE DATE OF HIV DIAGNOSIS (MM/DD/YYYY / / (18 months or less add 20 points) IF LESS THAN 18 MONTHS, ARE YOU EXPERIENCING DIFFICULTY DEALING WITH YOUR HIV DIAGNOSIS? Yes No (If yes add 5 points) DO YOU CURRENTLY HAVE A REGULAR PLACE TO GO FOR YOUR HIV MEDICAL CARE? Yes No (If no add 10 points) IF NO, WHY ARE YOU NOT SEEING A MEDICAL CARE PROVIDER FOR YOUR HIV? (TIME 1) DATE OF LAST HIV-RELATED MEDICAL APPOINTMENT? / / NUMBER OF MONTHS BETWEEN TIME 1 AND TIME 2: (TIME 2) DATE OF NEXT TO LAST HIV- RELATED MEDICAL APPOINTMENT, IF APPLICABLE? / / MONTHS (IF THE NUMBER OF MONTHS IS GREATER THAN 3, ADD 10 POINTS) ARE YOU CURRENTLY PRESCRIBED MEDICATIONS FOR HIV? Yes No IF YES, Thinking back over the past 30 days, rate your ability to take all your HIV medications as prescribed. Would you say very poor, poor, fair, good, very good, or excellent? Circle one. 1 Excellent 2 Very Good 3 Good 4 Fair 5 Poor 6 Very Poor 0 Don t Know 0 - Refused Please describe some of the reasons you have missed doses of your HIV medications:
58 Appendix 25. Client Screening & Feedback Form IF NO, REASON NOT ON HAART: Client Refused HAART payment assistance unavailable Intolerance due to side effects Not medically indicated Not ready (as determined by clinician) Other reason Unknown HOW WOULD YOU ASSESS YOUR KNOWLEDGE OF HOW HIV IMPACTS YOUR BODY? IN GENERAL, WOULD YOU SAY YOUR HEALTH IS: MEDICAL CONDITIONS THAT A DOCTOR, NURSE, OR OTHER MEDICAL PROVIDER HAS TOLD YOU THAT YOU HAVE: No understanding of HIV disease (5 pts) Basic understanding of HIV disease (3 pts) Comprehensive understanding of HIV disease (0 pts) Excellent (0 pts) Good (3 pts) Poor (5 pts) Very good (0 pts) Fair (4 pts) No Health History Hepatitis Hepatitis C Arthritis Epilepsy STI Hypertension Paralysis Asthma Liver Disease Tuberculosis Diabetes Heart Disease Obesity Stroke Cancer Obesity Endocarditis/Infection Of Heart Valve Other permanent numbness 1 point for every co-morbid condition ARE YOU OR YOUR PARTNER CURRENTLY PREGNANT? Yes (5 PTS) Refused No ( 0 PTS) IF, PREGNANT ARE YOU RECEIVING OR HAVE YOU RECEIVED PRENATAL CARE: Yes (5 PTS) No ( 0 PTS) Refused (0 points if not pregnant) HAVE YOU BEEN INCARCERATED IN THE LAST 12 MONTHS? Yes (5 PTS) Refused No ( 0 PTS) SUBSTANCE USE SCORE MENTAL HEALTH SCORE CO-OCCURING SU/MI Did client screen positive for substance abuse symptoms? 1- Yes (5 points) 2- No (0 points) Did client screen positive for mental illness symptoms? 1- Yes (5 points) 2- No (0 points) Did client screen positive for co-occurring mental health/substance use disorders? 1- Yes (5 points) 2- No (0 points) TOTAL CM SCORE
59 Appendix 25. Client Screening & Feedback Form Scoring for the Case Management Eligibility Scale: The following criteria make someone automatically eligible for Medical Case Management: Being HIV diagnosed within the last 6 months Not having an HIV primary care provider Co-occurring substance use issue and mental health issue Clients must score a minimum of a 70 (at a non-afc organization, or a 60 at AFC)to be eligible for Medical Case Management services. Clients who score below a 70 (or 60 at AFC) and do not meet the criteria listed above are Supportive Service clients. SUBSTANCE ABUSE I am going to change topics and ask you some sensitive questions about alcohol and drug use. Remember that your responses are confidential and you have the right to refuse to answer. Yes No 1. Have you felt the need to Cut down on your drinking or drug use? Do you feel Annoyed by people complaining about your drinking or dug use? Do you ever feel Guilty about your drinking or drug use? Do you ever drink an Eye-opener in the morning to relieve shakes? 1 0 Two or more affirmative responses suggest that the client has a substance problem and the client receives 5 points in the table above. Client refused to answer. ( Add 0 points) MENTAL HEALTH Total Now I am going to ask you some questions about your well-being or psychological health. 1. During the past 12 months, were you ever on medication/antidepressants for depression or nerve problems? 2. During the past 12 months, did you ever have a period lasting 1 month or longer when most of the time you felt worried and anxious? Yes No Any affirmative responses suggest that the client has symptoms for mental health issues and the client receives 5 points in the table above. Income Sources: SUPPORTIVE SERVICES NEEDS ASESSMENT (non-scored assessment) Total INCOME STABILITY: Has steady source of income Minimal unstable income No current income Insurance Sources: No Insurance
60 Appendix 26. Medical Update Form Medical Update Form Case Manager Data Entry Date: Month Day Year First Name: MI: Last Name: Date of Birth: CM Name: Phone Number: Month Day Year Agency Name: Fax Number: PROVIDER SECTION Provider Name: Provider Hospital/Clinic Affiliation: Provider Data Entry Provider Hospital/Clinic Address: Address City State Zip Diagnosis Information & Date of Diagnosis HIV Positive /Not AIDS HIV Positive /AIDS Status Unknown Mo/DD/Year CDC-Defined AIDS Mo/DD/Year Date of HIV Diagnosis Date of AIDs Diagnosis, if applicable Is this form being utilized to document proof of HIV status? Provider Medical Update Form Certification Provider Signature: Yes. If Yes, Provider must sign below. No Date:
61 Appendix 26. Medical Update Form Medical Update Form (continued) Antiretroviral Therapy (ART) History Is the patient currently prescribed antiretroviral Yes therapy? No. Explain below. No. The patient is not being prescribed antiretroviral therapy because (Describe below) INSERT REASON HERE Provider Data Entry Is the patient currently adherent to antiretroviral therapy? Yes No/don t know. Explain below. No. The patient is currently adherent to antiretroviral therapy because (Describe below) INSERT REASON HERE Last CD 4 Count: Last Viral Load Count: CD4 _Viral Load Count Date of Last CD4 Count: Date of Last Viral Load Count: Provider Data Entry Candidiasis (besides Oral Thrush) Pneumocystic Carinii Pneumonia (PCP) Retinitis Toxoplasmosis Recurrent Genital Herpes Human Papilloma Virus (HPV) Cytomegalovirus (CMV) Wasting Opportunistic Infection History Myobacterium Avium Complex (MAC) Cryptococcal Disease Lymphoma Syphilis Kaposi Sarcoma Histoplasmosis Tuberculosis Mycobacterium Tuberculosis Unknown/None Provider Data Entry Other Histories Yes No Other Mark X 1. Is the patient currently taking any PCP No, Not indicated prophylaxis? 2. Vaccinated against hepatitis A? (Complete Series) 3. Vaccinated against hepatitis B? (Complete Series) Documented Immunity Documented Immunity 4. Screened for Hepatitis C If Yes, What year? 5. Vaccinated against Pneumoccoccal Pneumonia? If Yes, What year?
62 Appendix 26. Medical Update Form Medical Update Form (continued) Was the client seen by a clinical care provider in the last 6 months? Yes No Provider Data Entry List the top 3 Clinical Goals: Goal #1: Goal #2: Total #of kept appointments in the last 12 months? Total # of kept appointments in the last 12 months? Goal #3: List the top 3 Case Management Goals: Goal #1: CASE MANAGER SECTION Goal #2: Case Manager Data Entry Goal #3: Primary Care & Clinical Needs to be Address through Case Management Domestic/Relationship/Family Concerns Substance Use General Care Coordination None Health Literacy Unknown Health/Medication Insurance (ADAP, Medicaid, County Cares, Manage Care Lost to Care Mental Health Medication Management Resource Identification/Referral Risk Reduction Counseling
63 Appendix 26. Medical Update Form Medical Update Form (continued) Clinical Counseling Provided by Clinical Care Team What counseling has been provided to the client by the clinical staff during this 6 month reporting period? Adherence Counseling Family planning/contraception HIV Risk Counseling Mental Health Evaluation Nutritional Counseling Smoking Cessation Substance Abuse Evaluation Treatment/Medication Adherence Case Manager Data Entry Are you requesting a case conference? Case Conferencing Request Yes No What will be the topics/agenda of the case conference? List reasons here: Case Manager Signature: Clinical Provider Signature: Case Manager & Provider Signatures Date Date
64 Appendix 27. Case Management Discharge Summary Date: Originating Agency Name: Case Manager Name: Client Name: Client ID: Client Notification Date: Case Management Discharge Summary CASE MANAGEMENT EXIT REASONS X Select one or more of the following reasons. Client disengaged after service began Client withdrew before service began Whereabouts unknown with no contacts in more than six months. Moved out of EMA service area Moved to assisted living / nursing facility. Incarceration Deceased Transferred to SSCM Transferred to MCM Transferred to DRS Transferred to PACPI DCFS Placement Not HIV Positive Duplicate Enrollment Violence/Threat/Theft/Violation of confidentiality of other clients or Violation of any other aspects of the agency policies. Client request / refused services / services are not needed VIOLATION OF RULES Client received the Rights & Responsibilities Client received the Grievance Procedures LOST TO CARE Yes/No Lost to Care Did the case manager send a certified letter to the client PRIOR to closing the case? DISCHARGE SUMMARY QUESTIONS: 1. Where the goals and objectives in the service plan achieved? Yes No Don t Know N/A If goals and objectives were not achieved, explain why: 2. Does the participant need further support or other services to assist him/her in maintaining well-being? Yes No Don t Know N/A If yes, list recommendations/referrals made for support and other services:
65 Appendix 27. Discharge Summary 3. At discharge/transfer/closure/termination from case management, was the client receiving medical care? Yes No Don t Know N/A If yes, describe how participant will continue to access medical care: Medical Provider Name: Hospital Affiliate Phone Number: 4. At discharge/transfer/closure/termination from case management, was the client taking medication? Yes No Don t Know N/A If yes, describe how the client will continue to access medications: TRANSFER INFORMATION (This is not entered into the client level database. Please notify the AFC to make the case assignment) New Agency Name: Date of Contact: Case Manager Name: Effective Transfer Date: Document Checklist Fax/ Date: Program Type: Additional Program Type: The following documents must be provided to the new agency: Letter notifying the client; detailed reason/scenario of incident Client full contact information HIV diagnosis documentation Most current enrollment form Most recent assessment/re-assessment Updated eligibility documentation Most recent benefits information Authorization to Release Information (AFC & IDPH), Care Plan with an overview of current case notes/open issues, etc. SIGNATURES: Case Manager Signature Date Supervisor Signature Date
66 Appendix 28: Care Plan Format Medical Case Management Care Plan Format The below elements must be used in all care plans created A problem Statement A long term Goal/ Goal Item A Short term goal/ Objective Tasks including Time Frames and Responsible Parties Description This is a statement that describes the underlying concerns a client may have This is a broad overarching goal that can be achieved in a 6 month/1 year time frame These are smaller goals that can be achieved within a period of 6 months The responsible parties can be either the client or the case manager Problem Statement Long Term Goal A Short Term Goals/Objectives Goal a Task 1 with person responsible and time frame Task 2 with person responsible and time frame Task 3 with person responsible and time frame
67 Appendix 29. Karnofsky Acuity Assessment Scale Tool The following scoring rubric measures functional impairment of HIV Continuity of Care dimensions. Medical / clinical Basic necessities/life skills Mental health Substance use Housing / living situation Support situation Insurance benefits Transportation HIV-related legal Cultural / linguistic needs Self-sufficiency in daily functioning HIV education and risk reduction Employment / income Medication adherence Karnofsky Score Dimensions & Frequency of Contact Ranked Score Description Need 1 - Low Normal activity. No complaints/signs of disease. Requires no assistance. Compliant with medical/treatment. MCM only needed to maintain eligibility. 2 Normal activity. Slight symptoms/signs of disease. Client executes services on their own. May need occasional assistance. Requires only MCM services. Client will initiate request for additional services. 3 Normal activity with effort. Some symptoms/signs of disease. Client mostly compliant medical/treatment. Has other service needs. May utilize MCM services. 4 Can take care of self but not engaged in normal work/personal activities. Mostly compliant with appointments but needs reminders and follow-up. Client receives MCM services with at least one other service. 5 Requires occasional assistance. Can take care of most needs. Needs appointment reminders or will miss appointments; follow up on how to obtain services. Client receives CM services with at least one other service. 6 Requires frequent help and medical care. Client needs reminders and misses appointments. Is not aware of services and/or is not able to seek out assistance on their own. Client receives MCM services with at least one other service. 7 Disabled, needing special care/assistance. Client s health has deteriorated. Misses appointments. Often noncompliant with services. Or is not able to see out assistance on their own. Utilizes multiple services. 8 Severely disabled. Hospital admission indicated but no risk of death. Has a Personal Assistant (PA) or needs constant coordination to receive services. Utilizes multiple services. 9 Very ill requiring hospitalization and supportive measures/treatment urgently. Client s health is very poor. Cannot care for daily needs. Has a Personal Assistant (PA) or needs constant coordination to receive services. Utilizes multiple RW services. 10 High Approaching death with rapidly progressive fatal disease processes. Client is near death and should receive focus as the client s physician recommends. Date: Case Management Agency Name: Case Manager Name: Client Name: OFFICE USE ONLY ++++ Karnofsky Score: Notes/Comments:
68 Appendix 30: Sample Referral Letter & Verification Form SAMPLE A Referral Introduction Letter Template Date Dear (name) I am writing to refer (client s name, include any other necessary information to verify identity such as date of birth or social security number) to (Agency Name) to receive (clarify the service you are referring them for). Enclosed is a completed referral form for your service. I am currently acting as a case manager for (enter client name) through the Northeastern Illinois HIV/AIDS Case Management Cooperative at (Case Management Agency Name). My role of case manager involves completing an assessment and then, in discussion with the client, drawing together a comprehensive care plan that addresses the clients needs in the categories of medical and support services. This care plan will be monitored and reviewed periodically to ensure that barriers to progression are being addressed and that interagency communication is supporting client efforts and the achievement of care plan goals. As part of the care planning and assessment process the need for (clients need) has been identified and your service has been identified as most appropriate service to address this need. (It may be appropriate to provide a rationale for the appropriateness of the referral i.e., motivation, attendance, family needs etc.). If you have any questions in relation to any aspect of the care plan, service delivery, or my role as case manager, please do not hesitate to contact me. I look forward to hearing from you. Sincerely, (name) (role/position) (service/project) (contact details: phone, and address)
69 Appendix 30: Sample Referral Letter & Verification Form AIDS FOUNDATION OF CHICAGO NORTHEASTERN ILLINOIS HIV/AIDS CASE MANAGEMENT COOPERATIVE Referral Plan Form Referral Verification Format: (this is a suggested format only. This document is not required to be in client charts, however this information must be captured in the client chart AND entered into the electronic client database) Client Information: FIRST NAME: MIDDLE INITIAL: LAST NAME: DOB: / / SS#: - - Don t know/have SS# Refused SS# Referral Date: / / Referral Recipient: (Agency receiving the referral) Referral Source: Refer From Provider: Refer from User (Case Manager): Location: Referral Status: Referral Made Turned Away Date referral was acknowledged by client: / / Referral Result Date: / / Pending Referral Status Comments:
70 Appendix 31: Case Conferencing Agenda Date: Client: Staff Present: Medical Case Management Case Conferencing Agenda Agenda Topics: 1. Client Case Staffing: a. Medical i. New infections (HIV and non-hiv related) ii. Hospitalizations iii. CD4/Viral Load iv. Appointment adherence v. Medication maintenance b. Oral Health c. Substance Use d. Psychological/Mental Health Issues e. Housing Concerns f. Food and Nutrition g. Income and Benefits h. Family and Support Networks i. Risk Reduction j. Other Challenges k. Discharges 2. Services/Resources Needed 3. Referrals 4. Old/New Issues 5. Additional Information/Announcements Notes:
71 Appendix 32: Case Conferencing Staffing Form Program: Medical Case Management Case Manager: Case Conferencing Staffing Form Name of Client: Date Issue/Status Goals/Intervention Person Responsible Medical: New Infections: Hospitalizations: CD4/Viral Load: Appointment Adherence: Medication Maintenance: Oral Health: Substance Abuse: Psychological/Mental Health: Housing Concerns: Food and Nutrition: Income and Benefits: Family and Support Networks: Risk Reduction: Other Challenges: Discharges:
72 Appendix 33. DRS Electronic Billing Verification Form DRS Electronic Billing Verification Form I verify that I have completed electronic entry of my agency s DRS billing submission via Client Track for the month of. I have run a copy of the DRS billing form to verify that my DRS billing is being accurately reflected in the report. Date: Name: Agency Name: Staff Signature Date Send only by fax to: AFC Fax
73 Appendix 34. DRS Retroactive Billing Electronic Verification Form DRS Retroactive Billing Electronic Verification Form I verify that I have completed electronic entry of my agency s DRS retroactive billing for the month of via Client Track. I have verified that my agency has not previously been reimbursed for these clients. I have requested and reviewed a copy of the DRS back billing form pulled from Client Track to verify that my DRS back billings is being accurately reflected in the report. Date: Name: Agency Name: Staff Signature Date Send only by fax to: AFC Fax
74 Appendix 35. Food Services Tracking Form Food Services Tracking Form Client Name: Case Manager Name: Client ID: Agency Name: Date Amount/Rides Type of Service (food voucher, basket, etc.) Emergency Reason Case Manager Signature Date Client Signature Date
75 Appendix 36. Housing & Utility Assistance Application Housing & Utility Assistance Application Housing Assistance Policy Subject: AFC Housing and Utility Assistance Application Date: November 25, 2014 PURPOSE: To set minimum eligibility criteria and standardize the process for distribution of multiple funding streams consistent with the guidelines established by those funding streams, which include the Illinois Department of Human Services (IDHS) State Homeless Prevention Funds, Emergency Food and Shelter Program (EFSP), Housing Opportunities for People With AIDS / Short Term Rental Mortgage Utility Assistance (HOPWA STRMU), and Ryan White Part A and Ryan White Part B, to clients participating in the Northeastern Illinois HIV/AIDS Case Management Cooperative with the AIDS Foundation of Chicago. It is at the discretion of AFC staff along with the guidelines established by the funding streams to determine which funding source, as previously mentioned, will be used in providing financial assistance to the client. POLICY: The AIDS Foundation of Chicago receives funding from a variety of sources to assist low income residents who reside in the following counties: Cook, DeKalb, DuPage, Grundy, Kane, Kendall, Lake, McHenry and Will. The principal purpose of this assistance is to stabilize individuals and families in their current home, to decrease the amount of time spent in shelters, and to help individuals and families secure and maintain affordable housing. Additionally, these funds are not intended to provide continuous or long-term assistance. These funds are defined as being a needs-based assistance program not an entitlement. Assistance from these funding streams is considered short-term help that is intended to promote long-term housing stability. AFC Housing and Utility Assistance (based on funding availability) can only be used for up to 4 payments in a 24-month period with only one payment allowed from each funding source and subject to the rules of that funding source. PROCEDURE: Eligibility criteria: 1. Households in imminent danger of eviction and/or, 2. Households in imminent danger of homelessness and/or, 3. Households in imminent danger of foreclosure (Note: they can t already be in the foreclosure process) and/or, 4. Households that are currently homeless. (Note: they need to be able to document the ability to afford rent and utilities in the future without this assistance) 5. For those households receiving funds from either HOPWA STRMU or Ryan White Part A, they must provide documentation showing that they are HIV+
76 Appendix 36. Housing & Utility Assistance Application All households must be able to document a temporary economic crisis beyond their control which includes: Loss of employment Medical Disability or emergency Loss or delay of a public benefit Natural Disaster Substantial change in household composition Victimization by criminal activity (including Domestic Violence) Illegal action by a landlord Displacement by government or private action Client is moving from Homelessness into permanent housing Client is moving into more affordable housing that promotes long term stability Types and Amounts of Assistance: o Any payment made cannot exceed $1, This is a cap. Actual payment amounts will always be determined by the documentation submitted on the applicant s lease, eviction notice, utility bill or mortgage statement as provided in the application. o Payments for security deposits must match the amount written on the client s lease. Any payment made, regardless of how much it may be below the cap amount, will be counted as one out of the four allowable payments in a 24-month period. It is allowable for a client to obtain both a rent payment and a utility payment in the same month with one application if the sum of both payments is still below the cap of $1, and there is adequate supporting documentation. This type of scenario, when properly documented, can be considered use of one out of the four allowable payments in a 24-month period. If a client requires assistance in an amount greater than the cap of $1, in the same application in order to prevent homelessness, it will be considered use of two payments in their four allowable payments in a 24-month period. The second payment MUST resolve the balance and MUST come from a different funding stream. AFC staff will determine, based on the application provided by the Case Manager, which funding source will be used to assist the client. AFC will first determine if the client s application meets the requirements of IDHS in order to receive funds. If IDHS funds are determined to be an ineligible source or if IDHS funds have been exhausted for the given period, AFC staff will then review EFSP as an alternate funding option. If EFSP funds are determined to be an ineligible source or if EFSP funds have been exhausted for the given period, AFC staff will then review HOPWA STRMU as an alternate funding option. If the client s application does not meet the necessary requirements of HOPWA STRMU or if HOPWA STRMU funds have been exhausted for that period, AFC staff will then review Ryan White Part A funding requirements in order to assist the client s application. Process to Obtain Assistance: Clients must complete the Step by Step application process with their assigned Case Manager and submit to the AIDS Foundation of Chicago for assistance.
77 Appendix 36. Housing & Utility Assistance Application Step One: Prior to completing any application forms the Case Manager must review the client for eligibility. At this time, the case manager and client should agree upon which of the eligible temporary economic crisis they are striving to document. Use the attached guide Documenting the Crisis to help determine eligibility. If it appears that the client is experiencing one of the eligible temporary economic crisis and will be able to document it, they should move on to step two. Step Two: The client must provide the case manager with all of the documentation that supports the temporary economic crisis that is being experienced. The attached guide Documenting the Crisis will help the case manager inform the client what must be submitted. Step Three: All of the application forms should be completed along with the case manager writing a narrative that describes the temporary economic crisis that is supported by the documentation. Step Four: The completed application with all of the supporting documentation can be submitted to AFC. Incomplete applications can be submitted to AFC and efforts will be made to help the case manager take steps to complete the application and potentially move it forward for approval. Submitting an application is not a guarantee of approval. If the client is not able to provide supporting documentation of an eligible temporary economic crisis, the case manager can move forward with submitting an incomplete application and AFC will provide an official denial letter. The denial letter from AFC will state all of the reasons for the application denial. The Case Manager should share the denial letter with the client and explain it if necessary. AFC s decisions will always be based on the narrative that is provided in the application and the documentation that is submitted to support it. The dissatisfied client can meet with the case manager supervisor who can further explain how the denial decision was made based on the ineligibility of the application of the lack of supporting documentation. Responsibilities of Client/Applicant: All applicants for AFC Housing and Utility Assistance must be enrolled in the central client registry at AFC and currently working with an AFC-funded program. Applicants must provide adequate documentation that they are experiencing a temporary economic crisis beyond their control. Applicants are not to engage in physically and/or verbally threatening behavior toward their case manager or AFC staff at any time. Physical or verbal threats will be cause for application denial. Discriminatory remarks and harassment in regards to but not limited to matters of race, color, national origin, creed, gender, sexual orientation or religion will be considered verbal threats and will be cause for application denial.
78 Appendix 36. Housing & Utility Assistance Application Responsibilities of Case Manager: 1. The Case Manager will work with the clients to submit all required forms and documentation. 2. If the client is deemed eligible for Ryan White Part A funds, the case manager will obtain approval and an Authorization Number on a Request for Reimbursement form from an AFC Housing Associate. This approval will allow the Case Manager s agency to cut a check to assist the client. 3. The Case Management agency must make the approved payment within 5 business days. The Case Manager must then return the Request for Reimbursement form along with a copy of the check within 5 business days of the expenditure of funds. 4. The AFC Housing and Utility Assistance Program requires that, if services are provided during AFC s fiscal year (July 1 st through June 30 th ), the Case Manager must attempt to contact the household to determine if they are still housed. This contact MUST be made during the month of September or October in the following fiscal year. In the event no one in the household can be contacted, the Case Manager must attempt to contact the landlord. For example: Client X received assistance anytime between July 2013 and June The Case Manager will attempt to make contact in either September or October of Responsibilities of AFC: 1. No payments will be made directly to the client; all payments will be made directly to a third party/vendor (property management company, utility company, building owner or mortgagor). 2. AFC will inform the case manager where the payment will be made from. Depending on the eligible funding stream, the payment may be cut out of the case manager s agency. In this case the case manager will receive a reimbursement form from AFC with an Authorization Number. The payment may also get cut from The Emergency Fund or from AFC. In all cases, copies of the checks will be kept in the client s file at AFC and sent to the client s case manager. 3. Clients who are dissatisfied with the process or results of their application for the AFC Housing and Utility Assistance Program will be provided the name and number of the AFC Housing Stabilization Manager, Alma Arroyo, Required Form: Housing & Utility Assistance Application
79 Appendix 36. Housing & Utility Assistance Application Documenting the Crisis The following documentation must be provided in order to support the eligible temporary economic crisis: Loss of employment: A termination letter from the previous employer that includes the final date of employment. Letters from the unemployment office with last date of employment. Medical Disability or emergency: Documentation from the medical provider that states the client was not able to work and earn their income as a result of a medical leave. The dates of when the medical leave occurred. A medical bill from a onetime essential procedure with paid receipt. If the client s only source of income is SSI or SSDI, a stay in the hospital has no impact on the client s income and therefore will not be an eligible reason for assistance. Loss or delay of a public benefit: Documentation from the public benefits office that states the change in benefits and the dates when it is occurring. Natural Disaster: Documentation that the client sought assistance from the American Red Cross or FEMA after the natural disaster impacted the client s home. Report from exterminator or documentation of mold indicating the client must move for safety reasons. Substantial change in household composition: If a person who was contributing financially to the household moves out, the client must be able to provide a lease or some other documentation that shows that the person was actually living there. Letter from the landlord stating the date the tenant moved out and the last month they contributed to the rent. Victimization by criminal activity (including Domestic Violence): A police report must be provided. If money was stolen there must be documentation that verifies how much money was stolen. Illegal action by a landlord: This is most commonly a result of the building going into foreclosure. If this is the case, all of the tenants should be provided with documentation ordering them to vacate the premises. Displacement by government or private action: Documentation from a third party that states that the client is required to move. Client is moving from Homelessness into permanent housing: A letter from a shelter or other social service agency that verifies that the client was homeless or a letter from the friend or family member that states the client must move out because they are not allowed to stay with them any longer as it is in violation of their lease. Client is moving into more affordable housing that promotes long term stability: a copy of the client s previous lease that shows they are now moving into a less expensive unit.
80 Appendix 36. Housing & Utility Assistance Application Required Documentation Overview The AFC Housing and Utility Assistance application requires up to (13) forms and documentation to be included. This document will provide a brief overview of each form, assisting the Case Manager in helping their clients gather and complete all needed forms when submitting an AFC Housing and Utility Assistance application. These forms include: Application Checklist Client Service Form (Including Budget & Signed Narrative) Temporary Economic Crisis Checklist Temporary Economic Crisis Supporting Documentation (i.e. letter from unemployment, police report, letter of homelessness etc.) IDHS Supportive Services Form IDHS Documentation Checklist Current Lease or Current Rental Agreement Form/Mortgage Payment Statement Notice of Eviction or Landlord Statement Form (if applicable) Copies of Past Due Utility Bills/Shut-off Notices (if applicable) Documentation of Current Income Copy of the client s ID Follow-Up Requirement Form Signed Release of Information Form Signed Rights/Responsibilities and Grievance Form Client Database Consent to Enroll Proof of HIV Status Ryan White Authorization to Release Form Proof of Ownership from Landlord (i.e. property tax statement or mortgage statement) Federal W9 and EIN Verification Letter (if not a management company landlord must submit a legible copy of social security card) Application Checklist This form is to be used as a cover sheet to the entire application indicating the client who is requesting assistance and the case manager who is submitting the application. It also serves as a checklist to confirm that all of the necessary application forms have been gathered. Please leave the bottom portion of the form blank where it states: DO NOT WRITE BELOW THIS LINE: AFC OFFICE USE ONLY. This is where AFC staff will internally keep track of the funding stream that the client is eligible for and how many payments the client may have received so far in a 24 month period. Client Service Form This form provides AFC needed demographic information on the client, including current address, race, household income as well as reason for assistance. It is important that clients along with their Case Managers review other funding streams as options in providing them assistance as warranted. This will include funding from CEDA / LIHEAP. It is up to the case manager to verify that the client has tried every resource possible before submitting this application. Below is an explanation of the race codes on the Client Service Form: AI/AN=American Indian/Native Alaskan A=Asian B/AA=Black/African American NH/OPI=Native Hawaiian/Other Pacific Islander W=White
81 Appendix 36. Housing & Utility Assistance Application AI/NA&W=American Indian/Native Alaskan White A&W=Asian and White B/AA&W=Black/African American and White AI/NA&B/AA=American Indian/Native Alaskan and Black/African American Other Multi Racial=also includes Hispanic and anyone who doesn t classify themselves Page 2 of Client Service Form (Budget and Narrative) The Case Manager must write a detailed description of the client s situation and what impact the assistance will have on the client s long term stability. It should include a Housing Plan that describes how the client will take steps to increase their income and reduce their expenses. The narrative should answer the questions of where did the client s money go instead of paying rent/utility and how will the client pay their expenses for next month on their own. Everything in the narrative must match the temporary economic crisis and must have supporting documentation. The purpose of the budget section is to show the client s total income versus their total expenses. The client must show that they DO NOT have a deficit. Additionally, the client must be able to show they can afford their bills in the future. The Case Manager should complete this form with their client to verify accuracy. This form MUST be signed and dated by the client ONLY. Temporary Economic Crisis Checklist The Temporary Economic Crisis checklist requires the Case Manager to identify the eligible emergency and/or crisis that the client is currently facing. Both the client and Case Manager MUST sign this document in certification that the information is accurate. Temporary Economic Crisis Supporting Documentation Supporting Documentation might include verifiable evidence of loss of job or other source of income, verifiable evidence from a healthcare professional of a hospitalization or inability to work. IDHS Supportive Services Form Case Managers must complete this form as part of the AFC Housing and Utility Assistance Application to indicate the kind of services and referrals the client is receiving through case management. The first five categories are mandatory in completing this document. Use the column that best describes the household and check the appropriate boxes, then total the number of checks at the bottom of the page. Regardless of whether or not the client receives funding from IDHS, this form must be completed and provided to AFC when applying for assistance to demonstrate the supportive services that are being provided. IDHS Documentation Checklist Like the previous IDHS document, this one goes into greater depth on the current status facing the client. Each category should be checked so that it corresponds to the information provided in the narrative. Like the IDHS Supportive Services Form, this document MUST also accompany each AFC Housing and Utility Assistance Application.
82 Appendix 36. Housing & Utility Assistance Application Current Lease or Rental Agreement Form/Mortgage Payment Statement Each client is responsible for providing a copy of their current written lease agreement or rental agreement form/mortgage payment statement when applying for assistance. A sample rental agreement form is provided if necessary. It is required that the written lease agreement include the length of lease, the amount of monthly rent, and both the client and the landlord signatures. The lease should have a start date on the 1 st day of month and an end date on the last date of a month. A lease that has an end date of Oct. 5, 2013 is only valid for the first five days of October. On Oct. 6 th it is considered to be expired. Even if the client is only applying for utility assistance, the client must still submit a copy of their written lease agreement or mortgage to show they are paying the utility for where they live. Notice of Eviction or Landlord Statement Form A sample Landlord Statement is provided if necessary. If the Landlord has already provided a notice with the same information, the sample Landlord Statement does not need to be used. Copies of Past Due Utility Bills/Shut-off Notices Each client is responsible in providing their Case Manager copies of the past due or shut-off notices from their utility companies in which funds are being requested. Payments for utilities (gas, electric, water) will be made directly to the utility company. Please make sure the client s account number is clearly visible. These documents are only required if the client is applying for utility assistance. A Utility Statement is included to serve as Documentation of Need. If the client is requesting utility assistance, this form must accompany the copy of the utility bill. Note that you must fill out the top and the bottom of the form and AFC staff will complete the rest if the application is moving forward. Documentation of Current Household Income Case Managers must obtain documentation of the client s entire household income. Clients with no income will not be eligible. The client must show that they DO NOT have a budget deficit. Additionally, the client must be able to show they have enough income to afford their bills in the future. Income documentation may include the current year s SSI or SSDI award letter, the current year s DHS award letter, copies of recent pay stubs, letter from employer (letter should be on company letter head and should include: rate of pay, number or hours worked, contact info of person who wrote letter), financial support from family (a letter should be submitted and include: amount given each month, length of time support will continue) the letter will have to be notarized and backing documentation to show that family member has income will have to be submitted (documentation can include: pay stubs, SSI/SSDI award letters etc.). Household members can be considered a dependent up to age 24 as long as they are a student. Household members over 18 who are NOT students must contribute to the household income. A copy of the client s ID The case manager should make a copy of the client s valid government issued photo ID. This can be the client s driver s license; State issued identification card or Veteran s Administration card. Follow-Up Requirement Form Whenever assistance is given to a client, the Case Manager MUST perform follow-up with the client in the following September or October to determine if the client has remained housed. In instances
83 Appendix 36. Housing & Utility Assistance Application when the Case Manager cannot contact the client, they must then attempt to make contact with the emergency contact or the landlord. This form must be included at the time of application to confirm that this requirement will be done in the future. Both the client and Case Manager MUST sign this form and submit with the application. Only the top and the bottom portions of the form must be completed at the time of application. The middle will be completed during the follow up period. Signed Release of Information Form All client applicants must complete and sign the Release of Information form that indicates where their information will be sent. This includes the case management agency and the AFC administrative office. Depending on the funding stream the client is approved for, it may also include The Emergency Fund administrative office. Signed Rights/Responsibilities and Grievance Form The client must sign this form as it is acknowledgement that both the eligibility criteria for assistance and the step by step application process have been explained to the client. This is also acknowledgement that the client has been informed how an application denial will be documented. Client Database Consent to Enroll The client must sign this form as it is acknowledgement that their information will be added to the centralized ClientTrack database. In addition, this consent allows for the Housing Advocates and Case Managers to see the client s enrollments in ClientTrack to facilitate referrals and service coordination. Proof of HIV Status Proof of HIV: CD4 and Viral load labs are required. If the client does not have a detectable viral load, in addition to the CD4 and viral load lab, at least one of the following is required. Doctor s signed, dated and certified note with diagnosis identified Positive ELISA screening with a confirmatory positive Western blot Positive Serology assay Positive HIV RNA PCR Positive DNA PCR assay Ryan White Authorization to Release Form If the applicant is HIV positive, this form MUST be completed and signed by client. This form must be signed AND dated by the client at least every 6 months. Proof of Ownership Payments for housing assistance will only be made to the owner of the building where the client lives, the Property Management Company or the mortgagor. If the payment check is to be made out to an individual person, proof of ownership in the form of a current property tax statement or a mortgage statement must be obtained. If the payment check is to be made out to a property management company or a mortgagor, proof of ownership is not needed. Federal W9 and Landlord Tax ID Number In order to be in compliance with IRS regulations, AFC requires that the landlord s Tax ID number be obtained on a federal W9 Form. If the landlord is an individual, this would be a Social Security number. If the landlord is a property management company they will have a Tax ID number for the business.
84 Appendix 36. Housing & Utility Assistance Application Landlord address on W9 should match current lease; checks will only be mailed to address on current W9 form. Please ensure that the form is filled in clearly and legibly. Landlords must also provide a copy of the Federal EIN form or Social Security card that matches the information they have filled in on the W9. This information is required by the IRS for payments to be made. Without it, assistance cannot be given.
85 Appendix 36. Housing & Utility Assistance Application AFC HOUSING AND UTILITY ASSISTANCE APPLICATION CHECKLIST (Please use this as a cover sheet) Client Last Name SS# - - First Name Date of Birth / / DOCUMENTATION CHECKLIST Client Service Form (Including Budget & Signed Narrative) Temporary Economic Crisis Checklist Temporary Economic Crisis Supporting Documentation (i.e. letter from unemployment, police report, letter of homelessness etc.) IDHS Supportive Services Form IDHS Documentation Checklist Current Lease or Current Rental Agreement Form/Mortgage Payment Statement Notice of Eviction or Landlord Statement Form (if applicable) Copies of Past Due Utility Bills/Shut-off Notices (if applicable) Documentation of Current Income Copy of the client s ID Follow-Up Requirement Form Signed Release of Information Form Signed Rights/Responsibilities and Grievance Form Client Database Consent to Enroll Proof of HIV Status Ryan White Authorization to Release Form Proof of Ownership from Landlord (i.e. property tax statement or mortgage statement) Federal W9 and EIN Verification Letter (if not a management company landlord must submit a legible copy of social security card) Case Manager Signature DO NOT WRITE BELOW THIS LINE: AFC OFFICE USE ONLY Client application meets the eligibility for: Date Reason for Eligibility: Including this application how many assistance payments has the client received in the past 24 month(s): ONE TWO THREE FOUR
86 Appendix 36. Housing & Utility Assistance Application Emergency Fund Client Service Form-State Homeless Prevention Fund Date: / / Partner Agency: AFC CC HHCS LCN 1. Client Information Does the person have a First Name Last Name DOB Hispanic Race Sex disability? Y N AI/AN A BL/AA NH/OP W AI/AN & M F Yes W A&W B/AA&W AI/AN & B/AA T Other/Multi-racial No Street Address Zip Code Phone # 1 Phone # 2 Monthly Referral Source Household Income 2. Household Information (include everyone else besides the client who lives in the household) $ HPCC External Internal First Name Last Name Age Hispanic Race Sex Y N AI/AN A BL/AA NH/OP W AI/AN & W A&W M F B/AA&W AI/AN & B/AA Other/Multi-racial Y N AI/AN A BL/AA NH/OP W AI/AN & W A&W M F B/AA&W AI/AN & B/AA Other/Multi-racial AI/AN A BL/AA NH/OP W AI/AN & W A&W Y N B/AA&W AI/AN & B/AA Other/Multi-racial M F AI/AN A BL/AA NH/OP W AI/AN & W A&W Y N B/AA&W AI/AN & B/AA Other/Multi-racial M F AI/AN A BL/AA NH/OP W AI/AN & W A&W Y N B/AA&W AI/AN & B/AA Other/Multi-racial M F 3. Program Eligibility 4. Coordination of Additional Services a. Have you received these funds in the last 24 months? Y N a. LIHEAP Coordination Already receiving LIHEAP b. Reason for assistance (check all that apply): Not receiving LIHEAP and helped to apply Natural disaster Not eligible for LIHEAP Homelessness Medical disability or emergency b. Food Stamp Coordination Illegal landlord action Already receiving food stamps Loss of delay of public benefit Not receiving food stamps and helped to apply Substantial change in household composition Not eligible to receive food stamps Displacement by private or government action Victimization by criminal activity c. Did this household require assistance with enrolling in or Loss of employment maintaining public benefits? Maintain/obtain subsidized housing Yes Other: No
87 Appendix 36. Housing & Utility Assistance Application 4. Prevention Services Reason for assistance Security Deposit Rent Mortgage Utility 1. To maintain current $ $ $ $ residence. 2. To move from $ $ $ $ residence to other permanent housing. 3. To move from a shelter $ $ $ $ to permanent housing. 5. Budget Monthly Household Income Employment SSI/SSDI VA Benefits TANF Unemployment Comp. Child Support Family Support Monthly Household Expenses Rent/Mortgage Gas Electricity Water Phone Food Transportation SNAP : $ Do not include in total Child Care Other: Other: Total $ Total $ Please write a brief narrative detailing the crisis that caused the client s situation and the impact of the assistance. Be sure to include any case management or referrals you provided to the client.(note: This information will be shared with staff of the Emergency Fund. I have received the services described in that document. I understand that I will be contacted in 9/14 and 10/14 and (Name Here) asked about the impact of this assistance. Client Signature Date
88 Appendix 36. Housing & Utility Assistance Application Temporary Economic Crisis Checklist Client Last Name First Name All Households Must Be Able to Document a Temporary Economic Crisis. These funds are not intended to provide continuous or long-term assistance. These funds are defined as being needs-based assistance, not an entitlement. Assistance from these funding streams is considered short-term help that is intended to promote long-term housing stability. If the client s temporary economic crisis does not appear below, please use this form to describe the situation and provide supporting documentation. Description of Emergency/Crisis: (check all that apply) Loss of Employment (termination letter from employer, unemployment application/documentation that shows date of final day of employment) Loss or delay of Public Benefit (with documentation PA, VA or SS letters) Medical disability or emergency (hospital bills, doctor s bills, or a doctor s note) Domestic violence situation (with police report) Natural Disaster (fire or flood report, etc) Substantial change in household composition (for example, proof of death of a household member) Victimization by criminal activity (with police report) Illegal action by a landlord Displacement by government or private action (letter from landlord informing the individual/household that they need to move) Client is moving from Homelessness into permanent housing Client is moving into more affordable housing that promotes long term stability Narrative/Explanation Here: I verify that the above information is accurate to the best of my knowledge Case Manager Signature Date Client Signature Date
89 Appendix 36. Housing & Utility Assistance Application IDHS Supportive Services Form Supportive Single Single Couple-no Couple w/ Male w/ Female Services Male Female child child child w/ child Case Management* Counseling-Financial* Food Stamp Screening* LIHEAP Screening* Six month follow-up* Advocacy Alcohol Abuse Services Child Care Children s Services Counseling-Life Skills Counseling-All Others Education Employment Services ESL Health/Dental Services HIV/AIDS Related Services Housing Placement/Inspection Legal Services/Referrals Mental Health Services Substance Abuse Services Transportation Children s Services Housing location/inspection Other: Total: *These 5 categories are mandatory for all clients receiving state prevention funds!
90 Appendix 36. Housing & Utility Assistance Application IDHS Homeless Prevention Program Documentation Checklist Initial Client Assessment The household must fall into one of these categories in order to be eligible: Imminent danger of eviction Imminent danger of foreclosure Imminent danger of homelessness Currently homeless The household must document a temporary economic crisis beyond its control, evidenced by at least one of the following conditions: loss of employment medical disability or emergency loss or delay of some form of public benefit natural disaster substantial change in household composition victimization by criminal activity illegal action by a landlord displacement by a government or private action some other condition which constitutes a hardship comparable to the one listed above: 2-year Eligibility Requirement The household is eligible to access assistance once every 2 years. All exceptions must be submitted to and approved by IDHS Homeless Prevention Program staff. Does the household meet the 2 year eligibility requirement? Yes No, but exception approved by IDHS program staff Income Verification The household must be able to demonstrate an ability to meet its future rental/utility obligations after assistance has been granted based on current or anticipated income: Employer verification/copy of Pay Stubs SSI/disability verification Unemployment Benefits Other: Rental (or Mortgage) Assistance/Arrearage Landlord agreement/lease Eviction/Five-Day/Past-Due Notice Mortgage Documentation/Repayment plan Records of payment Copy of check issued by agency Security Deposit Assistance Lease or rental agreement Receipt of payment or partial payment towards security deposit Copy of check issued by agency Utility Assistance/Arrearage Utility statement showing arrearage Shut-off notice or past due bills Copy of check issued by agency Follow-up Requirement Six months after the end of the fiscal year, the household must be followed-up with to determine their housing status. At the time of intake did you: Thoroughly explain your follow-up process to the household Collect adequate contact information, including a secondary number, to ensure a successful follow-up
91 Appendix 36. Housing & Utility Assistance Application Wrapping Up the Client File Am I collecting the necessary client data to ensure accurate reporting to the Department of Human Services? (ie household composition, gross monthly income, type of prevention assistance granted, food stamp status, LIHEAP status, supportive services).
92 Appendix 36. Housing & Utility Assistance Application DATE: HOUSING STABILITY LANDLORD STATEMENT (to be filled out by the landlord) TENANT INFORMATION: Client First Name: Address: Last Name: City, State, Zip: Amount of PAST DUE Rent: (amount requested) $ DO NOT WRITE IN THIS BOX AFC OFFICE USE ONLY Month(s) Past Due: Payment amount approved: $ Approved by (Staff initials): LANDLORD INFORMATION: Owner s Name or Management Company Name: Contact Person (Owner or legal representative of property): Mailing Address: City: State: Zip: Phone Number: I agree to accept a Housing Stability payment for this past due rent which will guarantee an additional 30 days of residence. By signing below I certify that I am the owner or legal representative of the owner, of the property listed under Tenant s Address above and that the information provided is true and accurate to the best of my knowledge. Property Owner or Legal Representative of Property
93 Appendix 36. Housing & Utility Assistance Application RENTAL AGREEMENT FORM This is a formal rental agreement between the Tenant and Landlord. The tenant shall be responsible for rent in the sum of $ per month, on a month-to-month, for the apartment listed below. Security deposit - $ Tenant is responsible for making direct payments to utility company for the cost following utilities: (check all that apply) Electric Cooking - Please specify (circle one) gas or electric stove Heating - Please specify (circle one) gas or electric Tenant does not pay for any utilities. All utilities are included in the cost of the rent. Address of apartment: Printed Name of Tenant Printed Name of Landlord Signature of Tenant Date Signature of Landlord Date Tenant Unit # Landlord Address Start Date of Agreement (Must begin on the 1 st of the month) Landlord City, State, Zip Code DO NOT WRITE BELOW THIS LINE AFC OFFICE USE ONLY Rental Agreement Valid for 12 Months from Date of Agreement Lease Start Date: Lease End Date:
94 Appendix 36. Housing & Utility Assistance Application Date: Utility Statement Client First Name: Address: Last Name: City, State, Zip: DO NOT FILL OUT THE INFORMATION IN BOX: AFC OFFICE USE ONLY Utility Information Company Name: Mailing Address: City, State, Zip Code: Amount Approved: Payment Date: Account Number: Client Signature Date Case Manager Signature Date Agency Name
95 Appendix 36. Housing & Utility Assistance Application Responsibilities of Client/Applicant: Client Rights/Responsibilities and Grievance Form 1. All applicants for AFC Housing and Utility Assistance must be enrolled in the central client registry at AFC and currently working with an AFC-funded program. 2. Applicants must provide adequate documentation that they are experiencing a temporary economic crisis beyond their control. 3. Applicants are not to engage in physically and/or verbally threatening behavior toward their case manager or AFC staff at any time. Physical or verbal threats will be cause for application denial. 4. Discriminatory remarks and harassment in regards to but not limited to matters of race, color, national origin, creed, gender, sexual orientation or religion will be considered verbal threats and will be cause for application denial. The following Step by Step application process with my assigned Case Manager has been explained to me: Step One: Prior to completing any application forms the Case Manager must review the client for eligibility. At this time, the case manager and client should agree upon which of the eligible temporary economic crisis they are striving to document. If it appears that the client is experiencing one of the eligible temporary economic crisis and will be able to document it, they should move on to step two. Step Two: The client must provide the case manager with all of the documentation that supports the temporary economic crisis that is being experienced. Step Three: All of the application forms should be completed along with the case manager writing a narrative that describes the temporary economic crisis that is supported by the documentation. Step Four: The completed application with all of the supporting documentation can be submitted to AFC. Incomplete applications can be submitted to AFC and efforts will be made to help the case manager take steps to complete the application and potentially move it forward for approval. Submitting an application is not a guarantee of approval. If the client is not able to provide supporting documentation of an eligible temporary economic crisis, the case manager can move forward with submitting an incomplete application and AFC will provide an official denial letter. The denial letter from AFC will state all of the reasons for the application denial. The Case Manager should share the denial letter with the client and explain it if necessary. AFC s decisions will always be based on the narrative in the application that is provided by the case manager and the documentation that is submitted to support it.
96 Appendix 36. Housing & Utility Assistance Application The dissatisfied client can meet with the case manager supervisor who can further explain how the denial decision was made based on the ineligibility of the application and the lack of supporting documentation.
97 Appendix 36. Housing & Utility Assistance Application I understand my rights and responsibilities and the grievance procedure. I also understand that this policy is specifically related to the AFC Housing and Utility Assistance application and it is not intended the replace the Grievance Procedure at my Case Management agency. Client Signature Date Case Manager Signature Date Agency Name
98 Appendix 36. Housing & Utility Assistance Application CONSENT TO ENROLL IN CENTRAL DATABASE AND APPLY FOR AFC HOUSING AND UTILITY ASSISTANCE I. CONSENT TO ENROLL IN CENTRAL DATABASE I, (enter client s name), consent to enroll in the centralized client database established by the AIDS Foundation of Chicago (the Database ) to assist and monitor the enrollment of persons receiving financial assistance through the AFC Housing and Utility Assistance application. In connection with my enrollment in the Database, I hereby allow the following information to be furnished to the AIDS Foundation of Chicago for entry into the Database: my name (where applicable), date of birth, any positive or negative HIV status and other demographic data. In addition depending on funding source; services or financial assistance received may be reported. I understand that this information will be grouped together with that of other clients for the purpose of generating statistical reports, avoiding duplication of services and coordinating a system for service delivery to persons with or at risk of HIV, their family members, and/or significant others and specifically authorize the use of such information for that purpose. Signature of Client or Client s Legal Representative Print Name Date Relationship (if signed by person other than Client)
99 Appendix 36. Housing & Utility Assistance Application CONSENT TO RELEASE INFORMATION Subject to the limitations and conditions set forth below, I, hereby consent to ( Provider/Housing Advocate ), acting through its employees or agents, to use and/or disclose my health information and medical records to the AIDS Foundation of Chicago, the Emergency Fund and/or any sub-contracted agencies that provide services through them, as follows: (i) in connection with my participation in the centralized client database established by the AIDS Foundation of Chicago (the Database ) and the operation of the client database; (ii) to allow sharing of my case management agency with my housing advocate. (iii) to allow sharing of my rent mortgage or utility assistance enrollments with my case management agency. (iv) to enable the AIDS Foundation of Chicago and the Cooperative to conduct quality assurance programs for individuals receiving case management services through the Cooperative; (iiv) to avoid duplication of services by case management agencies; and (vi) in connection with the submission of reports and other data to funding sources. In connection with my enrollment in the Database, I hereby give my consent for the following information to be furnished to the AIDS Foundation of Chicago for entry into the Database: my name (when applicable), date of birth, and other demographic data. In addition, verification of HIV positive status (if applicable) and dates of medical and case management service will be released to the AIDS Foundation. I understand that this information will be grouped together with that of other clients for the purpose of generating statistical reports, avoiding duplication of services and coordinating a system for service delivery to persons with HIV, their family members, and/or significant others and specifically authorize the use of such information for that purpose. I further allow the program staff of the AIDS Foundation of Chicago and its designated Oversight Committee to review my individual service records as part of the funders quality assurance program. For the purposes of this consent, I acknowledge and agree that my service records include any and all records generated by any of the Provider agencies that participate in the Ryan White Northeastern Illinois Cooperative, AFC Supportive Housing Programs or Financial Assistance Programs. Any information I provide for the purposes of receiving services will not be disclosed to any government agency or health department for purposes of surveillance, contact tracing, or any other purpose other than obtaining health care, housing, financial assistance or social services, except (1) with my consent, (2) as required by law, or (3) if necessary, to prevent a serious attempt to inflict harm on myself or others. Security precautions will be maintained to prevent unauthorized access to the Database by anyone other than the program staff of the AIDS Foundation of Chicago. I give further consent to allow the AIDS Foundation of Chicago to report information that I provide in connection with my enrollment in the Database and in connection with my receipt of services to the federal grant programs that support the AIDS Foundation of Chicago. I understand that such information may be provided either in the aggregate or on an individualized basis. I understand that, in order to protect my privacy, any information that is provided on an individualized basis, with the exception of Title II funded service utilization, will be furnished using unique client codes, without names or other information that identifies me. I further understand that should I receive service funded under Part A and B of the Ryan White CARE Act or IDPH HOPWA, certain information will be reported to the Direct Services Unit of the Illinois Department of Public Health and the Chicago Department of Public Health, including:
100 Appendix 36. Housing & Utility Assistance Application - demographic information, including but not limited to name, gender, race, ethnicity, and birth date; service utilization information; HIV/AIDS diagnosis and treatment information, if any; and mental health and/or substance use diagnosis, treatment, and service information, if any. I understand that this information will be shared for the purposes of evaluating Part A and B and IDPH HOPWA service utilization patterns, on-site service reviews, and when necessary to coordinate services. I can terminate this consent by submitting a written request to any of the Recipients (agencies in the Cooperative) indicating that I no longer desire to receive services through the Cooperative, or my written revocation of this authorization, whichever occurs first. I understand that I have the right to receive a copy of this consent. I further understand that I may revoke this consent at any time by providing written notice of my intent to revoke this consent to Provider. This consent cannot be revoked to the extent that action has already been taken based on this consent. This consent is valid for a period of two years from the date of the actual client signature below. Provider will not use or disclose personal health information beyond the scope of this authorization without your written consent or authorization. Please note that, subject to applicable law, disclosed information may be subject to redisclosure by the recipient, and may no longer be considered to be protected health information pursuant to the Health Insurance Portability and Accountability Act of 1996 and the regulations promulgated thereunder. Signature of Client or Client s Legal Representative Print Name Date Relationship (if signed by person other than client) Client must keep a copy of this for your records.
101 Appendix 36. Housing & Utility Assistance Application CLIENT INFORMATION: AFC HOUSING AND UTILITY ASSISTANCE FOLLOW UP REQUIREMENT Last Name First Name SS# - - Date of Birth / / Circle One: Single Male Single Female Couple: No Child Couple w/child Male w/child Female w/child Client received AFC Housing and Utility Assistance on: / / The program requires that if services are provided during the fiscal year (July 1, 2013 June 30, 2014) the case manager must attempt to contact the household to determine if they are still housed. This contact MUST be made during September or October of If rental assistance was provided and nobody in the household can be contacted, the case manager must attempt to contact the landlord. Please describe the results of the contact with the landlord Please describe the results of the contact with the client or the attempts at contact: Still housed in the same location Housed in a different location Homeless Deceased Unable to locate I authorize and understand that if my application for assistance is approved, my case manager will contact me, my emergency contact (below) or my landlord to determine if I am still housed. EmergencyContactName: Phone: Client Signature Date Case Manager Signature Date Agency Name
102 Appendix 36. Housing & Utility Assistance Application Dear Landlord or Property Manager, You are receiving this letter because a current or potential tenant has requested assistance from the AFC Housing Program which provides rental subsidies. The AFC Housing Program is a housing stability program designed to meet the financial needs of a participant by providing a direct rental payment to the landlord thus allowing the participant to access or maintain safe and affordable housing. In order to be in compliance with our state and federal funders as well as IRS requirements, the Finance Department at the AFC Housing Program requires that you provide a Tax ID number on the W9 Form that is attached. This is a Federal and State requirement that must be adhered to in order for us to make payments. If the landlord is an individual, the tax ID number will be either a Social Security number or an Individual Tax Identification Number (ITIN). If the landlord is a property management company the Tax ID number will be the Employer Identification Number (EIN) for the business. In order to ensure that you receive your payment in a timely manner, we request that you please complete the W9 form, writing as clearly and legibly as possible. Also, it is very important that the information matches the information on the Tax ID form exactly. Additionally, please provide us with a copy of your social security card, ITIN letter or federal Tax ID form, so we can ensure that the W9 form has been filled out correctly and to avoid delays in your payments. This information is gathered exclusively for the purpose of making payments to you so that the tenant can remain stably housed and will never be used for any other purpose We will always safeguard this information and respect your privacy. We use state of the art computer software to ensure that the information is protected. Thank you very much for your cooperation and for your commitment to providing safe and affordable housing for your tenants! AFC Housing Program PO Box 1022 Chicago, IL


103 Appendix 36. Housing & Utility Assistance Application
104 ILLINOIS DEPARTMENT OF PUBLIC HEALTH (IDPH) RYAN WHITE PART B STANDARD OPERATING PROCEDURE Housing and Emergency Financial Assistance Effective Date: Page 1 of 13 Revised Date: I. PURPOSE The purpose of this SOP is to provide coordinated and standardized guidance regarding Housing Services and Emergency Financial Assistance funded through multiple state and federal funding sources. II. DEFINITIONS HOPWA Housing Opportunities for Persons with HIV/AIDS is a source of funds provided by the United States Department of Housing and Urban Development (HUD). Ryan White Part B Ryan White Part B is a source of funds provided by the United States Department of Health Resources and Services Administration (HRSA). Housing Services Housing Services is the provision of assistance to support emergency, temporary or transitional housing to enable an individual or family to engage and maintain their HIV medical care. Housing related referral services include assessment, search for available affordable housing, and placement. Emergency Financial Assistance Emergency financial assistance is the provision of short-term payments to agencies or establishment of voucher programs to assist with emergency expenses related to essential utilities. III. PROCEDURE Eligibility To receive Housing Services or Emergency Financial Assistance clients must be eligible, enrolled in the Ryan White Part B program (see Eligibility Determinations SOP), and have a client specific Care Plan that addresses the housing needs and goals of the client. In addition, clients must have a household income at or below 80% of the area median income for the county in which the client resides. For those requesting Rent/Mortgage Assistance, the individual must provide proof of legal ability to occupy the residence and provide documentation of their responsibility to pay. For those requesting Emergency Financial Assistance, the individual must provide proof of their responsibility to pay said utilities. For further clarification please see category entitled Procedure-Allowable Costs. Illinois Ryan White Part B Program Standard Operating Procedures Page 115 of 228
105 ILLINOIS DEPARTMENT OF PUBLIC HEALTH (IDPH) RYAN WHITE PART B STANDARD OPERATING PROCEDURE Housing and Emergency Financial Assistance Effective Date: Page 2 of 13 Revised Date: Because the Program is a payer of last resort, clients must accept any assistance offered from Public Housing or other Housing Assistance Programs such as Section 8. Refusal to apply for or accept alternative housing will result in the client being ineligible for assistance. Case Managers must verify the availability of Public Housing or other assistance programs at each eligibility determination. o Screenshot of the public housing website indicating there is no current public housing is preferred, however if not available then An attestation from the case manager will be sufficient to meet this requirement. For more information on determining household income, see the Income Eligibility SOP. U.S. Department of Housing and Urban Development (HUD) policy notice PIH states that clients who are subject to a lifetime sex offender registration requirement under Public Law , section 578 are not eligible for assistance regardless of funding source. In addition, providers must verify that there are no individuals residing at the client s residence that are subject to a lifetime sex offender registration requirement. 1. Clients must be asked at each eligibility determination whether they or any individuals residing in the client s household are subject to a lifetime registration requirement under a state sex offender registration program. Clients must provide the legal name (first and last) of all individuals residing in the residence to the Program. Clients who are found to have intentionally falsified or failed to disclose this information when asked will have their assistance terminated. 2. Providers may utilize the Dru Sjodin National Sex Offender Website at to confirm that clients, household members, or other individuals residing in the residence are not lifetime registered sex offenders. 3. If it is determined that an individual residing in the residence is subject to lifetime sex offender registration, the provider must offer the family the opportunity to remove the individual from the household. If the family is unwilling to remove that individual from the household, the provider must not provide assistance with any funding source. 4. During site visits and chart reviews, the housing coordinator will verify that the results of the sex offender status verification is documented for clients receiving housing assistance. Illinois Ryan White Part B Program Standard Operating Procedures Page 116 of 228
106 ILLINOIS DEPARTMENT OF PUBLIC HEALTH (IDPH) RYAN WHITE PART B STANDARD OPERATING PROCEDURE Housing and Emergency Financial Assistance Effective Date: Page 3 of 13 Revised Date: IMPORTANT Clarifications Regarding HOPWA ONLY: Additional eligibility requirements related to HOPWA funded assistance only are that a client receiving assistance: o Must be currently housed o HOPWA funded services cannot be provided to homeless individuals or used for the purposes of move-in assistance. Move in assistance includes but is not limited to moving supplies, vehicle rentals, or moving services. Service Caps Both Housing Services and Emergency Financial Assistance have an annual service cap per client. The annual caps on the amount of assistance that can be provided are based on a calendar year and are shown in the table below. Service Name Annual Cap Housing Services $6,500 Emergency Financial Assistance $4,000 At no time can a service provided place the client over the annual cap. Clients cannot receive more than 5 months of assistance during any calendar year with HOPWA funds. Each rent/mortgage assistance service counts as 1 month of assistance. Clients can receive both rent or mortgage assistance and utility assistance in the same month which only counts as one month of assistance. Allowable Costs Housing Services To determine the amount of assistance that can be provided at any given time: 1. Providers must refer to the current Fair Market Rent or Rent Standard limits established for the area in which the client resides. To obtain the current limits, refer to the website below. The amount of assistance provided cannot exceed the lesser of: Fair Market Rent or Rent Standard limits established for the area in which the client resides, or Total monthly rent as defined by the rental/lease or mortgage agreement Illinois Ryan White Part B Program Standard Operating Procedures Page 117 of 228
107 ILLINOIS DEPARTMENT OF PUBLIC HEALTH (IDPH) RYAN WHITE PART B STANDARD OPERATING PROCEDURE Housing and Emergency Financial Assistance Effective Date: Page 4 of 13 Revised Date: PLUS Any allowable back owed amount (see Allowable Costs regarding requirements for past due amounts). The Program can provide assistance with the full rent/mortgage amount when the amount of assistance would exceed the Fair Market Rent or Rent Standard Limits if documentation of eviction notice is provided. 2. To assist with this calculation for how much is allowable in housing assistance the program has developed a Housing Assistance Worksheet. This worksheet must be completed and uploaded into the Payment Request record when documenting the assistance that was provided. a. A copy of the Housing Assistance Worksheet and accompanying instructions are provided at the end of this SOP. (see Appendix H: Housing Assistance Worksheet) b. Any requirement or standard outlined in the Housing Assistance Worksheet that is not meet must be addressed and documented in the Housing Plan and Progress Logs. i. Case Managers must make every effort to discuss these standards with clients and assist in developing a plan to promote compliance with the outlined standards. 3. If more than one client lives at the same residence; and each are listed on the lease/rental agreement; and are requesting assistance; then the total amount of allowable assistance must be divided among all clients according to the responsibilities outlined in the lease/rental agreement. Emergency Financial Assistance The amount of assistance that can be provided at any time cannot exceed the total amount currently due plus any allowable past due amount and/or any late fees or penalties (see below). Utility services being assisted must be in the client s name OR the client must provide documentation of their responsibility to pay the amount. This can be done by documenting a pattern of payment covering 2 consecutive months within the last 6 months. o Acceptable documentation includes but is not limited to bank statements or cash receipts. Household Supplies Housing supplies are only allowed for Housing Facilities. Housing supplies must be used for the facility, and cannot be provided to clients. Illinois Ryan White Part B Program Standard Operating Procedures Page 118 of 228
108 Appendix 38. Transportation Tracking Form Transportation Tracking Form Client Name: Case Manager Name: Client ID: Agency Name: Date Amount/Rides Type of Service (taxi, fare card, gas card, van, etc.) Reason for Ride Case Manager Signature Date Client Signature Date
109 Appendix 39. Fare Card Authorization & Reimbursement Request Form Fare Card Authorization & Reimbursement Request Form All requests for client fare cards MUST BE pre-approved by AFC in order to be reimbursed. Agencies must scan and a copy of this signed authorization form, a copy of the agency check used to purchase the client fare cards, a copy of the shipping form, a copy of the fare card receipt for purchase and the sales order form provided by Ventra or Pace to Alex Rhodes, AFC s Linkage to Care and Retention Associate at Arhodes@aidschicago.org within 15 business days of purchase. This Authorization Form is valid for only 20 business days from date of AFC authorization below and will be considered VOID after that time. Date of Request: Agency Name: Name of Person Making Request: Requestor s Phone Number: Agency Authorized Signature: Client Fare Cards: $ Client Metra Cards: $ Client Gas Cards: (Agencies are not $ allowed to purchase gas cards, please request them from AFC as part of your quarterly allocation). Total Authorization Amount: $ Case Manager Signature Date Client Signature Date
110 Appendix 40. Medicare Complaint Form Date: Agency Name: Staff Member: Date of Incident: Date/Time of Car Order: Car Company: Car Number: Pick-Up Address: Destination: Medicare Complaint Form Other No Show Round Trip One Way Comments/Explanation:
111 Appendix 41. New Case Manager and Supervisor Hire Form NOTIFICATION OF CHANGE IN AGENCY PERSONNEL AND TRAINING REQUEST AGENCY NAME AGENCY ADDRESS (service site) POSITION SUPERVISOR: Funding Source: Part A: (% FTE) Medical (% FTE) Intermediate Supportive Services Part B: (% FTE) Medical Corrections: (% FTE) PACPI: (%FTE) MAI (%FTE) DRS: (estimated % FTE) SHP: (%FTE) Will this staff person be a Provide user? YES NO New Hire: Start Date: Name: Phone #: Fax #: Does this position/staff member replace staff: YES NO Name: Last degree earned: Other training/certificates: Previous employment experience in social services: Skills and experience that qualify individual for case management: Change in Employment: Effective date: Reason: This form should be completed for any personnel changes for AFC-funded positions, and attached to staff resumes for all new hires. Personnel include case managers, and supervisors. Fax to AFC, Anthony Galloway Fax: T:Care/Program/Quality Assurance/Forms/New Case Manager and Supervisor Hire Form 2013
112 Appendix 42. Notification of Change in Personnel & Training Request Notification of Change in Personnel & Training Request AGENCY NAME AGENCY ADDRESS (service site) POSITION SUPERVISOR: Funding Source: Part A: (% FTE) Medical (% FTE) Intermediate Supportive Services Part B: (% FTE) Medical Corrections: (% FTE) PACPI: (%FTE) MAI: (%FTE) DRS: (estimated % FTE) SHP: (%FTE) Training Requested: Ryan White Orientation/Competencies Training DRS Home Services Training SHP Orientation Provide Training Will this staff person be a Provide user? YES NO New Hire: Start Date: Name: Phone #: Fax #: Does this position/staff member replace staff: YES NO Name: Last degree earned: Other training/certificates: Previous employment experience in social services: Skills and experience that qualify individual for case management: This form should be completed for any personnel changes for AFC-funded positions, and attached to staff resumes for all new hires. Personnel include case managers, and supervisors. Fax to AFC, Program Department
113 Appendix 43. Sample Medical Case Manager Job Description JOB SUMMARY This position is responsible for performing duties associated with conducting intakes and referrals for people living with HIV/AIDS who are seeking case management services. The Medical Case Manager will determine client eligibility for services, conduct an initial assessment of client needs, record basic demographic information in AFC s client-level database, and coordinate care with HIV primary care providers. Medical Case Management is the provision of a range of client-centered activities focused on improving health outcomes in support of the HIV care continuum. Medical Case Management includes all types of case management encounters (e.g., face-to-face, phone contact, and any other forms of communication). DUTIES: Initial assessment of service needs Development of a comprehensive, individualized care plan jointly with the client that includes short and long term goals focused on attaining, maintaining and achieving positive health outcomes Timely and coordinated access to medically appropriate levels of health and support services and continuity of care Continuous client monitoring to assess the efficacy of the care plan Re-evaluation of the care plan at least every 6 months with adaptations as necessary Ongoing assessment of the client s and other key family members needs and personal support systems Treatment adherence counseling to ensure readiness for and adherence to complex HIV treatments Client-specific advocacy and/or review of utilization of services Coordination of the care plan with client s primary care provider Work in conjunction with medical care providers (e.g. case conferencing, attending rounds); ensuring all clients are case conference at least twice per year Implement the medical treatment plan by providing counseling on medication, appointment and other treatment adherence issues Verify enrollment in medical care, and support enrollment of the uninsured in health care services Refer and link clients to appropriate services within the system of care that promote positive health outcomes, treatment adherence, and greater self-sufficiency. Monitor the client s follow-through with these services Provide access to Emergency Financial Assistance (EFA), (e.g. food vouchers, utility payment assistance, and transportation vouchers) as needed to promote and maintain positive health outcomes Evaluate effectiveness of services based upon client outcomes in the scope of work Enter and utilize the client level database for the tracking and reporting of all services provided Follow the Standard Operating Procedures of the AIDS Foundation of Chicago s Northeastern Illinois HIV/AIDS Case Management Collaborative In addition to providing the medically oriented services above, Medical Case Management may also provide benefits counseling by assisting eligible clients in obtaining access to other public and private programs for which they may be eligible (e.g., Medicaid, Medicare Part D, State Pharmacy Assistance Programs, Pharmaceutical Manufacturer s Patient Assistance Programs, other state or local health care and supportive services, and insurance plans through the health insurance Marketplaces/Exchanges).
114 Appendix 44. Sample Non-Medical Case Manager Job Description JOB SUMMARY This position is responsible for performing duties associated with conducting intakes and referrals for people living with HIV/AIDS who are seeking case management services. The Non-Medical Case Manager will determine client eligibility for services, conduct an initial assessment of client needs, record basic demographic information in AFC s client-level database, and work with client to ensure retention in HIV primary care. Non-Medical Case Management Services (NMCM) provide guidance and assistance in accessing medical, social, community, legal, financial, and other needed services. Non-Medical Case management services may also include assisting eligible clients to obtain access to other public and private programs for which they may be eligible, such as Medicaid, Medicare Part D, State Pharmacy Assistance Programs, Pharmaceutical Manufacturer s Patient Assistance Programs, other state or local health care and supportive services, or health insurance Marketplace plans. This service category includes several methods of communication including face-to-face, phone contact, and any other forms of communication. Non-Medical Case Management Services have as their objective providing guidance and assistance in improving access to needed services whereas Medical Case Management services have as their objective improving health care outcomes. Key activities include: Initial assessment of service needs Development of a comprehensive, individualized care plan jointly with the client that includes short and long term goals focused on attaining, maintaining and achieving positive health outcomes. Timely and coordinated access to appropriate levels of health and support services and continuity of care Continuous client monitoring to assess the efficacy of the care plan Re-evaluation of the care plan at least every 6 months with adaptations as necessary Ongoing assessment of the client s and other key family members needs and personal support systems Client-specific advocacy and/or review of utilization of services Coordination of the care plan with client s various service providers Implement the treatment plan by providing counseling, support and referrals on medication, appointment and other treatment adherence issues Verify enrollment in medical care, and support enrollment of the uninsured in health care services Refer and link clients to appropriate services within the system of care that promote positive health outcomes, treatment adherence, and greater self-sufficiency. Monitor the client s follow-through with these services Provide access to Emergency Financial Assistance (EFA), (e.g. food vouchers, utility payment assistance, and transportation vouchers) as needed to promote and maintain positive health outcomes Evaluate effectiveness of services based upon client outcomes in the scope of work Enter and utilize the client level database for the tracking and reporting of all services provided Follow the Standard Operating Procedures of the AIDS Foundation of Chicago s Northeastern Illinois HIV/AIDS Case Management Collaborative
115 Appendix 45: Request for Training Credit Application Form Request for Training Credit Form Please complete this form for each non-afc sponsored training that you have attended. You must complete all questions to receive credit. Agency: Case Manager: Name of Training: Date and Location of Training: Supervisor s signature Subject/Content of Training Place an X beside Number of Number of the appropriate sessions Hours topic area. Chemical Dependency Co-Morbid Disease (hypertension, diabetes, etc.) HIV Disease HIV Medications/Resistance Housing Intimate Partner Violence Mental Health Sexually Transmitted Disease/Infection Other: please list 1. Please explain whether and how the training met your expectations. 2. Please list the training objectives for the training. 3. Please explain how you will apply the knowledge gained. 4. Describe where you will share the knowledge gained.
116 Appendix 46: Request for Conference Credit Application Form Request for Conference Credit Application Form Please complete this form with information of sessions you attended during a non- AFC sponsored conference. You must complete all questions to receive credit. Agency: Case Manager: Conference Title: Date and Location of Conference: Supervisor s signature Workshop title Date and time Number of Number of sessions Hours 1. Please explain whether and how the conference met your expectations. 2. Please explain how you will apply the knowledge gained. 3. Describe where you will share the knowledge gained.
117
118 Appendix 47: Case Management Record Review Form CASE MANAGEMENT RECORD REVIEW FORM Use the following codes in documenting components in the case management service record: CRITERIA Yes No N/A Note Supervisor initials Record ID# Client Placement Screening form Intake date reasonable from screening date Completed intake/assessment/eligibility form Proof of HIV status CD4/Viral Load Completed care plan is up to date Care plan is signed by client and case manager AFC Release of information form RW Authorization to Release Information form Agency Release of Information form Rights and responsibilities form Grievance policy HIPAA Policy when applicable Photo ID Proof of residency Proof of Medical Insurance Proof of income Linkage to Primary Care is documented Medical Assessment form completed by physician. (Documentation otherwise) Treatment adherence counseling is documented Communication with medical provider is documented Medication list every six months Linkages/referrals made to other services are documented MAP information is included in chart with all required documentation Monitoring and intervention activities are included in progress notes Progress notes are dated Reassessment every six months (documentation otherwise) Discharge summary Case Conferencing notes Transportation and food services tracking form Supervisory notes in client record SERVICE RECORD INCLUDES Case Manager Name: Date: Supervisor Name: Supervisor Signature:
119 Definition of Terms for Chart Review Client placement screening form: presence of form will be assessed Intake date reasonable from screening date: date of initial intake will be compared to the date of referral to ensure timeliness of contact or contact attempts on the part of the case manager as per the Case Management Standard Operating Policies dated September 2014 Completed intake/assessment forms: presence and completeness of form will be assessed. Documentation of HIV Status: acceptable documentation of HIV status includes HOPWA Health Screening Form indicating HIV infection, positive viral load lab results with the patient s name, SSA disability certification naming HIV, DRS certification (residual capacity), written statement from a primary care physician, HIV antibody test results that include client s name. CD4/Viral Load: all charts must have documentation of CD4 and Viral load at least every 6 months. Acceptable documentation includes a print out from electronic medical record; a medical update form with documented CD4 and Viral load signed by a physician, Physician Assistant or Nurse; an affidavit from medical personnel documenting client CD4 and Viral Load Care plan in file and up to date: all charts must have a care plan that is no older than six months with appropriate documentation detailing the reason why a care plan has not been updated in the last six months. Service plan is signed by client and case manager: presence and completeness of form will be assessed as per the Case Management Operating Policies dated September AFC Release of information-signed & witnessed: AFC release of information must be present in all charts and must be updated every year. Agency- Release of information: releases of information must be present in all charts and documented for any collateral contact made on behalf of the client. All referrals and collateral contacts will be reviewed for the inclusion of a release of authorization allowing contact and information sharing to occur. RW Authorization to Release Information form: all clients must have this form fully completed and signed by the client every 6 months and scanned into the client database. Rights and responsibilities document- signed & witnessed: all client charts must include a client rights and responsibilities document that includes a clear grievance procedure and is signed by the client and witnessed by anyone 18 years of age or older (this may include but is not limited to the case manager). Grievance policy: presence and completeness of form will be assessed. HIPAA policy: Presence and completeness of form will be assessed if applicable.
120 Photo ID: Presence and completeness will be assessed Proof of residency: Presence and completeness will be assessed. The following will be accepted as proof of residency: Utility bill with client name and current address, driver s license or state ID with current address, documents issued by the state or federal government (i.e., a motor vehicle registration form, a current Illinois voter registration card, or a current Medicaid card), current rental or lease agreement with client name. Proof of Medical Insurance: Presence and completeness will be assessed. Acceptable documentation includes medical card and explanation of benefits document. Proof of Income: Presence and completeness of form will be assessed. The following will be accepted as proof of residency: Current pay stubs 1 months worth, most recent W2 forms, unemployment benefits statements, or most recent SSI benefits statement. For clients with no income, a verification letter must be completed, signed and dated by client and CM. Documentation of client enrollment in primary care: acceptable documentation of current client enrollment in primary care includes a note no greater than six months old documenting case manager knowledge of the client s primary care provider and status of kept appointments, lab values for client that are no greater than six months old, copies of prescriptions that are no greater than six months old, notes reflecting accompaniment to medical appointments or coordination of transportation to medical appointments (specified in note as based on medical need). Medical Assessment form: Presence and completeness of form every six months will be assessed or documentation detailing the reason why the form has not been updated in the last six months. Treatment adherence counseling: Presence of documentation and completeness of treatment adherence counseling at least 90 days apart, during the year. Communication with medical provider: Presence of documentation and completeness of communication with the medical provider at least 60 days apart, during the year. Medication list: Presence of documentation and completeness of treatment adherence counseling at least 90 days apart, during the year. Linkages/referrals made are documented: All referrals made will be reviewed to ensure appropriate documentation is kept for all referrals. MAP information: Presence and completeness of MAP (former ADAP) application will be assessed. Monitoring and intervention activities are included in progress notes: Client charts will be reviewed to ensure that client referrals, linkages made, and case notes are consistent with addressing client needs. When there are discrepancies, documentation is mandated for any exceptions to the above.
121 Progress notes are dated: Presence and completeness will be reviewed to ensure all notes are dated Re-assessment every six months (documentation otherwise): Charts will be reviewed to ensure that reassessments are done at minimum every six months. If greater than six months, documentation must justify that exception. Discharge plan: Presence and completeness of discharge plan will be assessed. Transportation and food services: Presence and completeness will be assessed Supervisory notes in client record: All client charts will be reviewed for evidence of some administrative review. Case notes of supervisory meetings or client file reviews are acceptable examples of documentation that will be allowed.
122 Appendix 48. Quarterly Progress Report Narrative Quarterly Progress Report Narrative Time Frame: Agency Name: Address: Phone: Project Administrator: Author of Report: Author s phone # and Part A funded agencies will electronically submit reports by 4:00 pm on the 10 th of June, September, December and March to MGrego@aidschicago.org. Part B funded agencies will electronically submit reports on the 10 th of July, October, January and April by 4:00 pm to BOsunmakinde@aidschicago.org. I. Scope of Services List the scope of services that your agency is funded to provide in each applicable category (Medical case management, Supportive case management, Outpatient Ambulatory Services, Early intervention Services, Mental Health, Substance Abuse (outpatient), Oral Health, Legal Services, Food Bank/Home delivered meals, Transitional Housing, Emergency Financial Assistance, Transportation) and describe your progress. Indicate the payer of the aforementioned services, Part A or Part B. If your agency receives both Part A & Part B funding through AFC, you will submit reports to the Part A and Part B Program Coordinators. II. Program Progress a. Describe activities to provide clients with harm reduction and risk reduction information for the prevention of secondary transmission. b) Describe how clients are screened for insurance coverage and third party funding sources at minimum every six months to ensure the program only serves eligible clients and that the Ryan White HIV/AIDS Program is the payer of last resort. c) Provide a description of activities conducted during the reporting period to pursue third-party payments for services subject to this agreement, including Medicaid, Medicare, and private insurance. If third-party payment was retroactively received, describe how the recovered funds were redirected for use in the Ryan White program.
123 d) Provide any additional narrative to describe successes not already discussed in Section II. Above, and their potential impact in HIV/AIDS direct services. III. Barriers or Trends a. Describe program and/or administrative including fiscal challenges that have occurred during this reporting period and their potential impact on your ability to provide HIV/AIDS direct services. Also, detail your plan to address those challenges including TA requests by AFC. Action Item: Expected Outcome: Target Completion Date: Completion Date: Key Steps Timeframe Responsible Party Status TA Needed/Requested b. Describe trends that have emerged within your program and their potential impact on your ability to provide HIV/AIDS direct services. IV. Staffing Changes a. Describe any personnel changes in this section and an action plan as to how your agency will resolve the issue, including trainings and certification process for new employees(s) using the template below. Action Item: Expected Outcome: Target Completion Date: Completion Date: Key Steps Timeframe Responsible Party Status TA Needed/Requested V. Quality Management a. Describe quality assurance/improvement activities related to your funded Part A/B direct services that occurred during this reporting period. Quality assurance/improvement activities should be linked to your organization s QM plan. QM indicators can measure accessibility, appropriateness, continuity, demographic characteristics, effectiveness, efficacy, patientsatisfaction, safety of the environment and timeliness of care.
124 V. Quality Management (continued) b. Describe the methods your agency employs to actively solicit consumer feedback and indicate how consumer feedback is incorporated within your agency. List specific areas of concern expressed by consumers and how the agency plans to address them. c. Describe case management supervisory activities conducted this quarter. (case management providers only) d. Please attach below progress reports related to quality management activities VI. Program Income and Client Charge a. In the following table, please report any program income that was generated by the Ryan White grant or earned as a result of the grant, including funds collected or recouped due to client s insurance or Medicaid eligibility identified after initial payment with Ryan White funds. Billing & Cost Sharing Retroactive Medicaid billing for any core services rendered through Ryan White. $ Cost Sharing from Ryan White and the client $ Amount b. Describe below how the recouped funds have been utilized.
125 Appendix 49. Action Plan Action Plan Grantee Name: Grantee Mailing Address: Principal Grantee Contact: Date: Action Item: Expected Outcome: Target Completion Date: Completion Date: Key Steps Timeframe Responsible Party Status TA Needed/Requested
126 Appendix 50. Fiscal Supporting Audit Document Fiscal Supporting Audit Document Required Supporting Audit Documentation PERSONNEL: Copy of the agency s personnel policies and procedures with required sections being Confidentiality Policy, Disclosure of Information, Background Check Policy, and Nondiscrimination section that includes language regarding Discrimination, Civil Rights and Human Rights. Personnel files for each employee funded through this grant. Files should have the following sections: Date of Hire, Job Description, Current Salary, Application/Resume, Staff evaluations, Background Checks, Current Contact/Emergency information and Annual Review of Personnel Policies and Procedures. (Will only need to review files to check off required sections) ORGANIZATION AND ADMINISTRATION: Copy of agency written accounting policies and procedures on file and internal controls have been established. Agency has following documents on file: Current Agreement and Budget, current Scopes of Services, copies of submitted vouchers or financial reports. Any subcontractor/consultant agreements funded thru this grant (i.e., physicians, therapists, etc.) Copy of agency s most recent bank reconciliation to tie out with accounting system in place. Staff allocation and payroll records of employees that are paid under this grant. Copy of Board of Directors meetings and by-laws and Code of Ethics. AUDIT INFORMATION: Copy of the most recent audited financial statements and OMB Circular A-133 single audit, if applicable. GOVERNMENT FILING REQUIREMENTS: Copy of agency s Annual Report to Illinois Secretary of State and proof of payment. Copy of federal payroll (941) reports and proof of payment. Copy of state payroll tax (IL 941) reports and proof of payment. Copy of IL unemployment UI-3/40 forms and proof of payment. Copy of form 1096, Annual Summary and Transmittal of U.S. Information Returns if paying any consultants requiring forms 1099-Misc. Copy of agency s IRS 501 (c)(3) determination letter. Copy of agency s annual federal IRS Form 990. Certificate of Liability malpractice insurance. REIMBURSEMENT REQUIREMENTS: Copy of the submitted monthly reimbursement voucher with supporting documentation to confirm 100% of the amount requested. For all shared costs, documented expense and cost allocation methodology. Please see Universal tool for additional requirements/documentation that will be reviewed at site visit.
127 Appendix 51. Medical Case Management Chart Review Instrument Points of Review Last Date (s) Prior to Review Period Medical Case Management Chart Review Instrument Date (s) Within the Review Period Met Not Met Weighted Total Documented Faceto-Face 4 Visit with Client Completed 2 Eligibility Assessment Present Completed Care 4 Plan Present Documented 1 Medical Visit Assessed 2 Medication List Documented Viral 1 Load Test Results Progress Note (s) 5 Discuss Care Coordination with the Client s Care Team (Physician, Mental Health Therapist, Housing Navigator, etc.) Progress Note (s) 3 Discuss Adherence Counseling with Client Client Chart 2 Includes Staffing Notes Agency Grievance 1 Form Agency Rights and 1 Responsibilities Form AFC Consent to 1 Release Form Total Score X X X X X

128 Appendix 52. Medical Case Management Chart Review Form Medical Case Management Chart Review Form
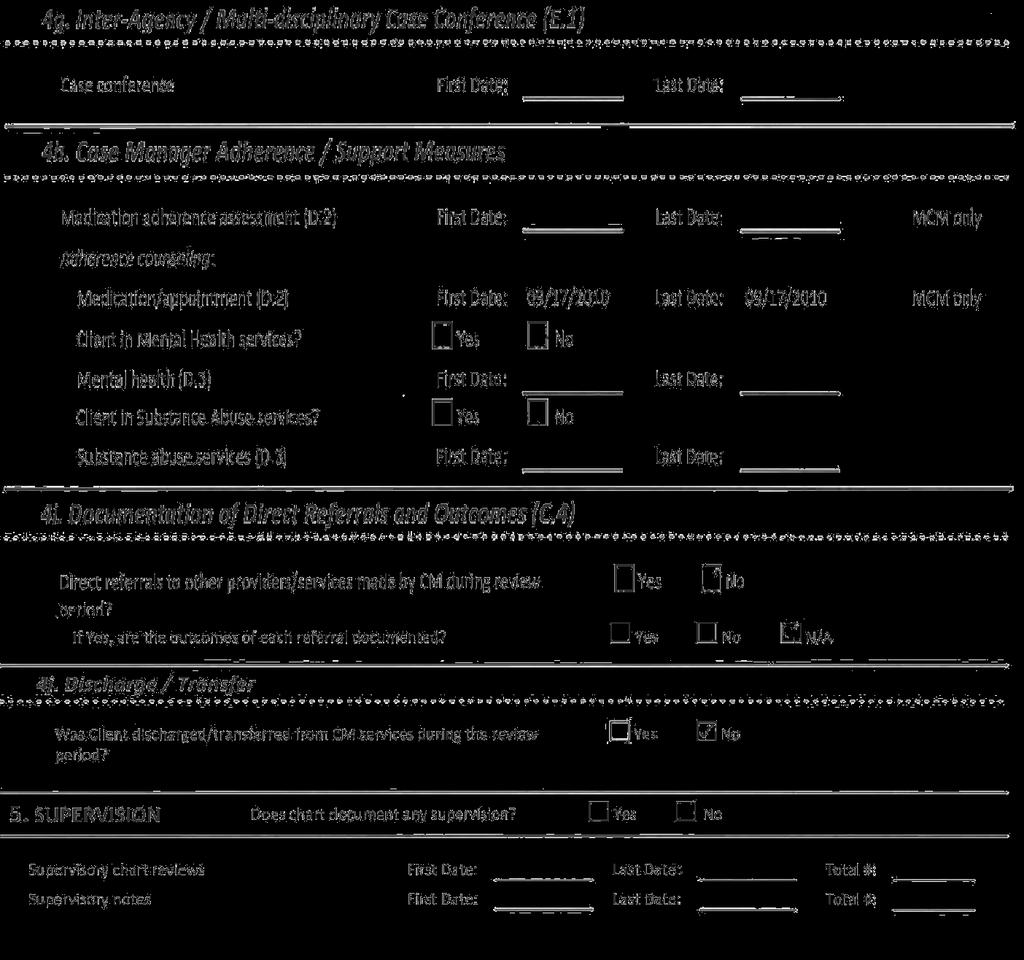

129
Policy and Procedures for Program Evaluation
 Chapter 6 Policy and Procedures for Program Evaluation Overview Evaluation of the Colorado Colorectal Screening Program will provide information about patient demographics and clinical outcomes necessary
Chapter 6 Policy and Procedures for Program Evaluation Overview Evaluation of the Colorado Colorectal Screening Program will provide information about patient demographics and clinical outcomes necessary
Santa Barbara County Public Health Department MEDIA GUIDE
 Santa Barbara County Public Health Department MEDIA GUIDE INTRODUCTION This guide is intended to assist the media in obtaining timely information from the Santa Barbara County Public Health Department
Santa Barbara County Public Health Department MEDIA GUIDE INTRODUCTION This guide is intended to assist the media in obtaining timely information from the Santa Barbara County Public Health Department
REFUSAL OF CARE AND/OR TRANSPORTATION
 Operations 21 Page 1 REFUSAL OF CARE AND/OR TRANSPORTATION APPROVED: 1 Purpose: 1.1 To determine when a person is identified as a patient in the EMS system. 1.2 To establish a standard process for the
Operations 21 Page 1 REFUSAL OF CARE AND/OR TRANSPORTATION APPROVED: 1 Purpose: 1.1 To determine when a person is identified as a patient in the EMS system. 1.2 To establish a standard process for the
PATIENT INFORMATION RESPONSIBLE PARTY INFORMATION NAME: DOB: SEX: M / F SOCIAL SECURITY # RELATIONSHIP TO PATIENT: PHONE #: CELL#: EMPLOYER:
 PATIENT INFORMATION NAME: DOB: SEX: MALE / FEMALE SOCIAL SECURITY #: MARITAL STATUS: ADDRESS: CITY: STATE: ZIP CODE: PHONE #: CELL#: E-MAIL: PATIENT'S EMPLOYER: OCCUPATION: WORK PHONE: WHERE IS THE BEST
PATIENT INFORMATION NAME: DOB: SEX: MALE / FEMALE SOCIAL SECURITY #: MARITAL STATUS: ADDRESS: CITY: STATE: ZIP CODE: PHONE #: CELL#: E-MAIL: PATIENT'S EMPLOYER: OCCUPATION: WORK PHONE: WHERE IS THE BEST
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Provider Quick Reference
 Provider Quick Reference Georgia Planning for Healthy Babies Program 1-800-454-3730 providers.amerigroup.com GAPEC-1771-17 Amerigroup Community Care has contracted with the Georgia Department of Community
Provider Quick Reference Georgia Planning for Healthy Babies Program 1-800-454-3730 providers.amerigroup.com GAPEC-1771-17 Amerigroup Community Care has contracted with the Georgia Department of Community
Initials of State and Out of State DL # Complete as Applicable
 Bridgeway Center Inc. Community & Court Education Services Enrollment Form Have you ever attended any classes at Bridgeway Center, Inc.? Yes No Today s Date First Name Middle Name Last Name / / Address
Bridgeway Center Inc. Community & Court Education Services Enrollment Form Have you ever attended any classes at Bridgeway Center, Inc.? Yes No Today s Date First Name Middle Name Last Name / / Address
NEW PATIENT PACKET. Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone. Address: Driver s License #:
 Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Patient s Name: NEW PATIENT PACKET Last Middle First Address: City: State: Zip: Home Phone: Cell Phone: Primary Contact: Home Phone Cell Phone Email Address: Driver s License #: DOB: Gender: Male Female
Family Care Health Centers
 Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
Family Care Health Centers New/Established Patient Information (Please Print) Account # Date: Circle One: New Patient or Established Patient Last: First: M.I. Date of Birth: Address: City: State: Zip:
INFORMED CONSENT FOR TREATMENT
 INFORMED CONSENT FOR TREATMENT I (name of client) agree and consent to participate in behavioral healthcare services offered and provided by Methodist Services - Community Counseling Services (CCS). I
INFORMED CONSENT FOR TREATMENT I (name of client) agree and consent to participate in behavioral healthcare services offered and provided by Methodist Services - Community Counseling Services (CCS). I
- Cardiac Catherization - Cardiac Angioplasty - Cardiac Bypass - MUGA - CT Scan
 Thank you for making an appointment with our office. We look forward to meeting you. Please help us to prepare for your appointment by gathering the information we will need to make the most of your time
Thank you for making an appointment with our office. We look forward to meeting you. Please help us to prepare for your appointment by gathering the information we will need to make the most of your time
PATIENT NOTICE. If you are already taking any of the above medications, your provider may want to talk to you about alternative treatments.
 PATIENT NOTICE Our goal at is to provide quality medical care. Because of our concern for your health and well-being, there are certain types of medications we may not be able to prescribe to you. Examples
PATIENT NOTICE Our goal at is to provide quality medical care. Because of our concern for your health and well-being, there are certain types of medications we may not be able to prescribe to you. Examples
PATIENT NOTICE. If you are already taking any of the above medications, your provider may want to talk to you about alternative treatments.
 PATIENT NOTICE Our goal at HOPES is to provide quality medical care. Because of our concern for your health and well-being, there are certain types of medications we may not be able to prescribe to you.
PATIENT NOTICE Our goal at HOPES is to provide quality medical care. Because of our concern for your health and well-being, there are certain types of medications we may not be able to prescribe to you.
Client Registration Form
 Client Registration Form Today s Date / / CLIENT INFORMATION (PLEASE PRESENT YOUR PHOTO IDENTIFICATION AND INSURANCE CARD WITH THIS PAPERWORK) Mr. Ms. Mrs. Legal Name: First Middle Last Suffix (Jr, Sr,
Client Registration Form Today s Date / / CLIENT INFORMATION (PLEASE PRESENT YOUR PHOTO IDENTIFICATION AND INSURANCE CARD WITH THIS PAPERWORK) Mr. Ms. Mrs. Legal Name: First Middle Last Suffix (Jr, Sr,
TRUCK DRIVER APPLICATION
 27154 County Road 13 / Johnstown, CO 80534 office 970.669.1463 / fax 970.669.1964 TRUCK DRIVER APPLICATION TO THE APPLICANT: GERRARD EXCAVATING, INC. DOES NOT DISCRIMINATE IN HIRING OR EMPLOY ON THE BASIS
27154 County Road 13 / Johnstown, CO 80534 office 970.669.1463 / fax 970.669.1964 TRUCK DRIVER APPLICATION TO THE APPLICANT: GERRARD EXCAVATING, INC. DOES NOT DISCRIMINATE IN HIRING OR EMPLOY ON THE BASIS
Adult Health History
 Adult Health History Name: DOB: Please list medications, including: vitamins, herbs, homeopathic remedies, and nonprescription medicines on the attached medication sheet. Medical History: High blood pressure
Adult Health History Name: DOB: Please list medications, including: vitamins, herbs, homeopathic remedies, and nonprescription medicines on the attached medication sheet. Medical History: High blood pressure
MAIN STREET RADIOLOGY
 MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
Re-Vita -Life. Sub-dermal Bio-identical Pellets
 Re-Vita -Life Sub-dermal Bio-identical Pellets Welcome and thank you for inquiring about Re-Vita-Life Bio-identical hormone replacement therapy. We have included a new patient information packet which
Re-Vita -Life Sub-dermal Bio-identical Pellets Welcome and thank you for inquiring about Re-Vita-Life Bio-identical hormone replacement therapy. We have included a new patient information packet which
ADMISSION CONSENTS. 1. Yes No Automobile Medical or No Fault insurance due to an accident?
 Patient Name: I.D. Number: Section A: Identifying Proper Payor ADMISSION CONSENTS Are services provided to you by Hospice reimbursements through health insurance other than Medicare due to one of the following
Patient Name: I.D. Number: Section A: Identifying Proper Payor ADMISSION CONSENTS Are services provided to you by Hospice reimbursements through health insurance other than Medicare due to one of the following
Medicaid Prepaid Mental Health Plan Information Handbook
 Medicaid Prepaid Mental Health Plan Information Handbook Prepaid Mental Health Services provided by Wasatch Mental Health Prepaid Substance Use Disorder Services provided by Utah County Department of Drug
Medicaid Prepaid Mental Health Plan Information Handbook Prepaid Mental Health Services provided by Wasatch Mental Health Prepaid Substance Use Disorder Services provided by Utah County Department of Drug
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Behavioral Health Services Handbook
 Behavioral Health Services Handbook Your Guide to the Medicaid Prepaid Mental Health Plan Mental Health and Substance Abuse Services In Carbon, Emery and Grand Counties Administrative Offices 105 West
Behavioral Health Services Handbook Your Guide to the Medicaid Prepaid Mental Health Plan Mental Health and Substance Abuse Services In Carbon, Emery and Grand Counties Administrative Offices 105 West
CATHOLIC CAMPAIGN FOR HUMAN DEVELOPMENT APPLICATION FOR LOCAL GRANTS ARCHDIOCESE OF OKLAHOMA CITY
 APPLICATION FOR LOCAL GRANTS ARCHDIOCESE OF OKLAHOMA CITY CAREFULLY READ CRITERIA FOR APPLYING COMPLETELY FILL OUT APPLICATION AND MAIL/FAX TO CCHD Local Committee Becky VanPool 1501 N. Classen Boulevard
APPLICATION FOR LOCAL GRANTS ARCHDIOCESE OF OKLAHOMA CITY CAREFULLY READ CRITERIA FOR APPLYING COMPLETELY FILL OUT APPLICATION AND MAIL/FAX TO CCHD Local Committee Becky VanPool 1501 N. Classen Boulevard
Dear Kaniksu Patient,
 Dear Kaniksu Patient, Welcome to Kaniksu Health Services (KHS), a Community Health Center that provides quality and affordable medical, pediatric, dental, behavioral health and veteran care, regardless
Dear Kaniksu Patient, Welcome to Kaniksu Health Services (KHS), a Community Health Center that provides quality and affordable medical, pediatric, dental, behavioral health and veteran care, regardless
Medicaid Prepaid Mental Health Plan
 Medicaid Prepaid Mental Health Plan Prepaid Mental Health Services provided by Wasatch Mental Health Prepaid Substance Use Disorder Services provided by Utah County Department of Drug and Alcohol Prevention
Medicaid Prepaid Mental Health Plan Prepaid Mental Health Services provided by Wasatch Mental Health Prepaid Substance Use Disorder Services provided by Utah County Department of Drug and Alcohol Prevention
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 HIV/AIDS SPECIALTY PLAN
 ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 HIV/AIDS SPECIALTY PLAN The provisions in Attachment II and the MMA Exhibit apply to this Specialty Plan, unless otherwise specified in this
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 HIV/AIDS SPECIALTY PLAN The provisions in Attachment II and the MMA Exhibit apply to this Specialty Plan, unless otherwise specified in this
EMPLOYMENT APPLICATION
 EMPLOYMENT APPLICATION Page 1 of 3 This Employment Application will remain active for one year from the date of completion APPLICANT INFORMATION Last Name First M.I. Date Street Apartment/Unit # City State
EMPLOYMENT APPLICATION Page 1 of 3 This Employment Application will remain active for one year from the date of completion APPLICANT INFORMATION Last Name First M.I. Date Street Apartment/Unit # City State
9.5 REFUSAL OF TREATMENT/TRANSPORT POLICY
 9.5 REFUSAL OF TREATMENT/TRANSPORT POLICY PURPOSE This policy outlines the evaluation of a patient refusing treatment or transport and the documentation expected when obtaining such a refusal. POLICY I.
9.5 REFUSAL OF TREATMENT/TRANSPORT POLICY PURPOSE This policy outlines the evaluation of a patient refusing treatment or transport and the documentation expected when obtaining such a refusal. POLICY I.
Alzheimer s Arkansas is pleased to provide you with information about the Family
 PLEASE READ ALL INFORMATION INCLUDED IN THIS GRANT APPLICATION Dear Caregiver: Alzheimer s Arkansas is pleased to provide you with information about the 2016-2017 Family Caregiver Support Program. Funding
PLEASE READ ALL INFORMATION INCLUDED IN THIS GRANT APPLICATION Dear Caregiver: Alzheimer s Arkansas is pleased to provide you with information about the 2016-2017 Family Caregiver Support Program. Funding
ENROLLMENT REQUIREMENTS FOR SLIDING FEE PATIENTS
 8515 Greenville Avenue, Suite N-210 Dallas, TX 75234 (214) 221-0855 ENROLLMENT REQUIREMENTS FOR SLIDING FEE PATIENTS 1. Proof of Household Income from everyone in the household who works Most recent pay
8515 Greenville Avenue, Suite N-210 Dallas, TX 75234 (214) 221-0855 ENROLLMENT REQUIREMENTS FOR SLIDING FEE PATIENTS 1. Proof of Household Income from everyone in the household who works Most recent pay
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES Effective Date: May 31, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
NOTICE OF PRIVACY PRACTICES Effective Date: May 31, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Chapter 6 Citizen Participation Plan
 Chapter 6 Citizen Participation Plan Every applicant and recipient of state of Oregon Community Development Block Grant (CDBG) funds must comply with the citizen participation requirements provided in
Chapter 6 Citizen Participation Plan Every applicant and recipient of state of Oregon Community Development Block Grant (CDBG) funds must comply with the citizen participation requirements provided in
We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal.
 Appointment Date: Appointment Time: Dear Orion Member, We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal. Enclosed
Appointment Date: Appointment Time: Dear Orion Member, We want to thank you for your interest in the Orion Weight Loss Program. We are looking forward to helping you reach your weight loss goal. Enclosed
Volunteer Application Package
 Volunteer Application Package April, 2016 This program is supported by the Georgia Department of Human Services/Division of Aging Services/GeorgiaCares Program with financial assistance, in whole or in
Volunteer Application Package April, 2016 This program is supported by the Georgia Department of Human Services/Division of Aging Services/GeorgiaCares Program with financial assistance, in whole or in
Clarke County School District Research Proposal Submission Guidance
 Clarke County School District Research Proposal Submission Guidance DISCLAIMER: Clarke County School District (CCSD) reserves the right to modify the research guidelines as needed. Therefore, CCSD reserves
Clarke County School District Research Proposal Submission Guidance DISCLAIMER: Clarke County School District (CCSD) reserves the right to modify the research guidelines as needed. Therefore, CCSD reserves
Pinellas County MPO Limited English Proficiency Plan
 Pinellas County MPO Prepared by the: Pinellas County Metropolitan Planning Organization 310 Court Street Clearwater, FL 33756 February 14, 2007 Revised March 18, 2013 LEP Plan Table of Contents Introduction...Page
Pinellas County MPO Prepared by the: Pinellas County Metropolitan Planning Organization 310 Court Street Clearwater, FL 33756 February 14, 2007 Revised March 18, 2013 LEP Plan Table of Contents Introduction...Page
PATIENT INFORMATION Please Print
 PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
PATIENT INFORMATION Please Print DATE Patient s Last Name First Name Middle Name Suffix Gender: q Male q Female Social Security Number of Birth Race Ethnic Group: q Hispanic q Non-Hispanic q Unknown Preferred
Avmed medicare. Keeping You Informed
 Avmed medicare Keeping You Informed Summer/July 2016 inside Your Primary Care Physician... 2 Preventive Healthcare... 2 Transferring Your Medical Records... 3 Mental Health Benefits... 3 Medical Technology...
Avmed medicare Keeping You Informed Summer/July 2016 inside Your Primary Care Physician... 2 Preventive Healthcare... 2 Transferring Your Medical Records... 3 Mental Health Benefits... 3 Medical Technology...
Girls RESIDENT Camp 2018 Camp Auxilium Registration Form (Please PRINT CLEARLY)
") Girls RESIDENT Camp 2018 Camp Auxilium Registration Form (Please PRINT CLEARLY) Week 1 Sunday June 24 Saturday June 30 Week 2 Sunday July 1 Saturday July 7 Week 3 Sunday July 8 Saturday July 14 Week 4
Girls RESIDENT Camp 2018 Camp Auxilium Registration Form (Please PRINT CLEARLY) Week 1 Sunday June 24 Saturday June 30 Week 2 Sunday July 1 Saturday July 7 Week 3 Sunday July 8 Saturday July 14 Week 4
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. WHY ARE YOU GETTING
NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. WHY ARE YOU GETTING
PATIENT REGISTRATION
 PATIENT REGISTRATION Patient Home Phone ( ) - Address Work Phone ( ) - City State Zip Cell Phone ( ) Birthdate Social Security # - - DL# E-Mail Address How did you hear about us? Billboard, Phone Book,
PATIENT REGISTRATION Patient Home Phone ( ) - Address Work Phone ( ) - City State Zip Cell Phone ( ) Birthdate Social Security # - - DL# E-Mail Address How did you hear about us? Billboard, Phone Book,
Midwestern University Clinic Patient Registration Form Please Print
 Midwestern University Clinic Patient Registration Form Please Print FOR OFFICE USE ONLY Pt Acct # Bill to Acct # Please check one: NEW PATIENT PATIENT UPDATE PATIENT INFORMATION Patient Name: (Last) (First)
Midwestern University Clinic Patient Registration Form Please Print FOR OFFICE USE ONLY Pt Acct # Bill to Acct # Please check one: NEW PATIENT PATIENT UPDATE PATIENT INFORMATION Patient Name: (Last) (First)
107 Commercial Street Mashpee, MA (fax)
") 107 Commercial Street Mashpee, MA 02649 508-477-7090 508-477-7028 (fax) www.chcofcapecod.org Welcome to your new medical home! We are excited to offer you high quality, integrated health care services
107 Commercial Street Mashpee, MA 02649 508-477-7090 508-477-7028 (fax) www.chcofcapecod.org Welcome to your new medical home! We are excited to offer you high quality, integrated health care services
FALLON TOTAL CARE. Enrollee Information
 Enrollee Information FALLON TOTAL CARE- Current Edition 12/2012 2 The following section provides an overview on FTC enrollee rights and responsibilities, appeals and grievances and resources available
Enrollee Information FALLON TOTAL CARE- Current Edition 12/2012 2 The following section provides an overview on FTC enrollee rights and responsibilities, appeals and grievances and resources available
PATIENT REGISTRATION FORM (ecw)
") PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
PATIENT INFORMATION PATIENT REGISTRATION FORM (ecw) (Please print) Patient s Name: (Last) (First) (MI) Address: City, State, Zip: Home: Cell: Work: E-Mail Address: DOB: Sex: Female Male Transgender Race:
HEALTH HISTORY QUESTIONNAIRE
 Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
RYAN WHITE TITLE I SERVICE STANDARDS
 RYAN WHITE TITLE I SERVICE STANDARDS 2 0 0 5 Chicago Area HIV Services Planning Council Chicago Department of Public Health Division of STD/HIV/AIDS Public Policy and Programs In collaboration with Midwest
RYAN WHITE TITLE I SERVICE STANDARDS 2 0 0 5 Chicago Area HIV Services Planning Council Chicago Department of Public Health Division of STD/HIV/AIDS Public Policy and Programs In collaboration with Midwest
PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD
 PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD General Consent for Treatment I have the legal right to consent to medical and surgical treatment because (a) I am the patient
PATIENT REGISTRATION FORM PARENTAL MEDICAL CONSENT FORM FOR A MINOR CHILD General Consent for Treatment I have the legal right to consent to medical and surgical treatment because (a) I am the patient
WELCOME. Payment will be expected at the time of service. Please remember our 24 hour cancellation notice.
 WELCOME Those of us at Crossroads Counseling want to thank you for choosing to work with us and we want to make your time with us as productive as possible. In order to expedite the intake process, please
WELCOME Those of us at Crossroads Counseling want to thank you for choosing to work with us and we want to make your time with us as productive as possible. In order to expedite the intake process, please
AMERICAN AMBULANCE SERVICE, INC.
 AMERICAN AMBULANCE SERVICE, INC. Proud to be a tobacco and smoke-free environment ONE AMERICAN WAY, NORWICH, CT 06360 VOLUNTEER APPLICATION GENERAL INFORMATION Date Name Last First MI Address Street City
AMERICAN AMBULANCE SERVICE, INC. Proud to be a tobacco and smoke-free environment ONE AMERICAN WAY, NORWICH, CT 06360 VOLUNTEER APPLICATION GENERAL INFORMATION Date Name Last First MI Address Street City
Welcome to The Brevard Health Alliance
 Welcome to The Brevard Health Alliance The Brevard Health Alliance, Inc. (BHA) is a Community Health Center serving Brevard County residents providing comprehensive medical services to all residents. It
Welcome to The Brevard Health Alliance The Brevard Health Alliance, Inc. (BHA) is a Community Health Center serving Brevard County residents providing comprehensive medical services to all residents. It
Paragon Infusion Centers Patient Information
 Paragon Infusion Centers Patient Information Please complete the following form as accurately as you are able. Inaccurate and/or incomplete information can delay our ability to authorize your treatments,
Paragon Infusion Centers Patient Information Please complete the following form as accurately as you are able. Inaccurate and/or incomplete information can delay our ability to authorize your treatments,
Santa Barbara County Public Health Department MEDIA GUIDE
 Santa Barbara County Public Health Department MEDIA GUIDE INTRODUCTION This guide is intended to assist the media in obtaining timely information from the Santa Barbara County Public Health Department
Santa Barbara County Public Health Department MEDIA GUIDE INTRODUCTION This guide is intended to assist the media in obtaining timely information from the Santa Barbara County Public Health Department
Welcome to LifeWorks NW.
 Welcome to LifeWorks NW. Everyone needs help at times, and we are glad to be here to provide support for you. We would like your time with us to be the best possible. Asking for help with an addiction
Welcome to LifeWorks NW. Everyone needs help at times, and we are glad to be here to provide support for you. We would like your time with us to be the best possible. Asking for help with an addiction
SPRING BRANCH COMMUNITY HEALTH CENTER
 Hillendahl Clinic 1615 Hillendahl Blvd., Suite 100 Houston, TX 77055 (713) 462-6565 Pitner Clinic 8575 Pitner Road Houston, TX 77080 (713) 462-6545 Mon, Wed, Fri: 8am-5pm Tues & Thurs: 8am-8pm 1 st & 3
Hillendahl Clinic 1615 Hillendahl Blvd., Suite 100 Houston, TX 77055 (713) 462-6565 Pitner Clinic 8575 Pitner Road Houston, TX 77080 (713) 462-6545 Mon, Wed, Fri: 8am-5pm Tues & Thurs: 8am-8pm 1 st & 3
CATHERINE FUND FINANCIAL AID APPLICATION March 2016
 GUIDELINES/ QUALIFICATIONS FOR Please read all Guidelines, Policies and Procedures, and Instructions before completing application. You must meet all guidelines for your application to be considered. 1.
GUIDELINES/ QUALIFICATIONS FOR Please read all Guidelines, Policies and Procedures, and Instructions before completing application. You must meet all guidelines for your application to be considered. 1.
Affordable Concierge New Patient Registration
 Affordable Concierge New Patient Registration Patient Information Last name: First name: MI: DOB: [ ] Male [ ] Female Home address: City: State: Zip: Billing address: [ ] Same as home City: State: Zip:
Affordable Concierge New Patient Registration Patient Information Last name: First name: MI: DOB: [ ] Male [ ] Female Home address: City: State: Zip: Billing address: [ ] Same as home City: State: Zip:
*3ADV* Patient Rights & Responsibilities Advanced Directive Page 1 of 2. Patient Rights & Responsibilities. Patient Label
 PATIENT RIGHTS Portneuf Medical Center encourages respect for the personal preferences and values of each individual and supports the Rights of each patient and resident of the Center, or their representative
PATIENT RIGHTS Portneuf Medical Center encourages respect for the personal preferences and values of each individual and supports the Rights of each patient and resident of the Center, or their representative
Member Handbook. HealthChoices Allegheny County
 Member Handbook HealthChoices Allegheny County Contents Welcome to Community Care! 3 About Community Care 6 Behavioral Health Services for HealthChoices Members 9 Getting Help 11 Your Rights and Responsibilities
Member Handbook HealthChoices Allegheny County Contents Welcome to Community Care! 3 About Community Care 6 Behavioral Health Services for HealthChoices Members 9 Getting Help 11 Your Rights and Responsibilities
REGISTRATION FORM (Minors)
") LEGAL NAME REGISTRATION FORM (Minors) Social Security#: Date of Birth: Sex: M or F Nickname: Religion: Church: Race (circle one): White Black-Asian AM Indian Alaska Native Native Hawaiian Pacific Islander-Unknown
LEGAL NAME REGISTRATION FORM (Minors) Social Security#: Date of Birth: Sex: M or F Nickname: Religion: Church: Race (circle one): White Black-Asian AM Indian Alaska Native Native Hawaiian Pacific Islander-Unknown
HOMELESS VETERAN REGISTRY NORTHWEST MINNESOTA
 STATE OF MINNESOTA MINNESOTA DEPARTMENT OF VETERANS AFFAIRS HOMELESS VETERAN REGISTRY NORTHWEST MINNESOTA TENNESSEN WARNING YOUR PRIVACY RIGHTS The State of Minnesota and its partners have committed to
STATE OF MINNESOTA MINNESOTA DEPARTMENT OF VETERANS AFFAIRS HOMELESS VETERAN REGISTRY NORTHWEST MINNESOTA TENNESSEN WARNING YOUR PRIVACY RIGHTS The State of Minnesota and its partners have committed to
Patient Registration Form Pediatrics
 Patient Registration Form Pediatrics For Office Use Only: Visit Date: Initials: PATIENT INFORMATION Preferred Language: English Spanish Other: Patient s Last Name First Middle Initial Date of Birth Sex
Patient Registration Form Pediatrics For Office Use Only: Visit Date: Initials: PATIENT INFORMATION Preferred Language: English Spanish Other: Patient s Last Name First Middle Initial Date of Birth Sex
Dear Patient, Welcome to Annadel Medical Group Urology.
 Dear Patient, Welcome to Annadel Medical Group Urology. Our priority is your health and we will strive for excellence in all aspects of medical care. Achieving this goal requires a partnership between
Dear Patient, Welcome to Annadel Medical Group Urology. Our priority is your health and we will strive for excellence in all aspects of medical care. Achieving this goal requires a partnership between
Lives (circle one): in assisted living with a relative alone
: in assisted living with a relative alone") Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Patient name: How did you hear about us? Lives (circle one): in assisted living with a relative alone Current address (include name of assisted living or independent living facility if applicable): Current
Patient Registration Form
 Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Date: Patient Registration Form First Name Middle Last Name... Sex: M F Preferred
Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Date: Patient Registration Form First Name Middle Last Name... Sex: M F Preferred
Ryan White Part A. Quality Management
 Quality Management Central Intake and Eligibility Determination (CIED) 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal
Quality Management Central Intake and Eligibility Determination (CIED) 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal
EMPLOYEE REPORT OF INJURY INCIDENT
 EMPLOYEE REPORT OF INJURY INCIDENT This checklist is to be completed by the INJURED EMPLOYEE with assistance from his/her immediate supervisor as necessary. The completed form should be signed by the injured
EMPLOYEE REPORT OF INJURY INCIDENT This checklist is to be completed by the INJURED EMPLOYEE with assistance from his/her immediate supervisor as necessary. The completed form should be signed by the injured
Information for Dual-Eligible Members with Secondary Coverage through California Regular Medi-Cal (Fee-for-Service)
") Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2011 December 31, 2011 Los Angeles County This publication is a supplement to the 2011 Positive (HMO SNP) Evidence
Information for Dual-Eligible Members with Secondary Coverage through California January 1, 2011 December 31, 2011 Los Angeles County This publication is a supplement to the 2011 Positive (HMO SNP) Evidence
Patient Privacy Requirements Beyond HIPAA
 Patient Privacy Requirements Beyond HIPAA Jane Hyatt Thorpe, J.D. School of Public Health and Health Services George Washington University Carrie Bill, J.D. Feldesman Tucker Leifer Fidell LLP The George
Patient Privacy Requirements Beyond HIPAA Jane Hyatt Thorpe, J.D. School of Public Health and Health Services George Washington University Carrie Bill, J.D. Feldesman Tucker Leifer Fidell LLP The George
EMPLOYMENT APPLICATION
 Travis County Human Resources Management Department 1010 Lavaca Street, 2 nd Floor (corner of West 11th & Lavaca) www.co.travis.tx.us P.O. Box 1748 Austin, TX 78767 (512) 854-9165 Voice EMPLOYMENT APPLICATION
Travis County Human Resources Management Department 1010 Lavaca Street, 2 nd Floor (corner of West 11th & Lavaca) www.co.travis.tx.us P.O. Box 1748 Austin, TX 78767 (512) 854-9165 Voice EMPLOYMENT APPLICATION
New Patient Information
 New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
APPLICATION FOR EMPLOYMENT EASTERN SHORE RURAL HEALTH SYSTEM, INC, Market Street, Onancock, VA 23417
 INSTRUCTIONS: Fill out this form as accurately as possible. If you are having trouble editing this file, please make sure Microsoft Word is in Normal or Print Layout by clicking View then Normal or Print
INSTRUCTIONS: Fill out this form as accurately as possible. If you are having trouble editing this file, please make sure Microsoft Word is in Normal or Print Layout by clicking View then Normal or Print
RESIDENT PHYSICIAN AGREEMENT THIS RESIDENT PHYSICIAN AGREEMENT (the Agreement ) is made by and between Wheaton Franciscan Inc., a Wisconsin nonprofit
 is made by and between Wheaton Franciscan Inc., a Wisconsin nonprofit") RESIDENT PHYSICIAN AGREEMENT THIS RESIDENT PHYSICIAN AGREEMENT (the Agreement ) is made by and between Wheaton Franciscan Inc., a Wisconsin nonprofit corporation ( Hospital ) and ( Resident ). In consideration
RESIDENT PHYSICIAN AGREEMENT THIS RESIDENT PHYSICIAN AGREEMENT (the Agreement ) is made by and between Wheaton Franciscan Inc., a Wisconsin nonprofit corporation ( Hospital ) and ( Resident ). In consideration
THE COUNSELING PLACE ADULT INTAKE FORM Yearly Family Income:
 Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
City of Florence, South Carolina Frozen Turkeys & Gift Cards Invitation to Bid No
 City of Florence, South Carolina Frozen Turkeys & Gift Cards Invitation to Bid No. 2015-40 Sealed bids will be received in the Office of Purchasing and Contracting, in the City Center, 324 W. Evans Street
City of Florence, South Carolina Frozen Turkeys & Gift Cards Invitation to Bid No. 2015-40 Sealed bids will be received in the Office of Purchasing and Contracting, in the City Center, 324 W. Evans Street
YMC Board Application DUE: Friday, May 18, 2018
 120 East Jones Street, Suite 110, Santa Maria, CA 93454 26 West Anapamu Street, Santa Barbara, CA 93101 Phone: 805-962-9164 ymc@fundforsantabarbara.org www.fundforsantabarbara.org YMC Board Application
120 East Jones Street, Suite 110, Santa Maria, CA 93454 26 West Anapamu Street, Santa Barbara, CA 93101 Phone: 805-962-9164 ymc@fundforsantabarbara.org www.fundforsantabarbara.org YMC Board Application
Thank you, in advance, for being a partner in your care.
 477 Cooper Road, Suite 220 Westerville, OH 43081 614-818-0215 Your appointment with: Dr. David H. Brown Dr. Jed W. Henry Dr. Adam J. Clemens is scheduled for. Welcome to our practice. It is our desire
477 Cooper Road, Suite 220 Westerville, OH 43081 614-818-0215 Your appointment with: Dr. David H. Brown Dr. Jed W. Henry Dr. Adam J. Clemens is scheduled for. Welcome to our practice. It is our desire
Volunteer Application
 Volunteer Application I. CONTACT INFORMATION Mr. Mrs. Name (first): (middle): (last): Ms. Home Address: City: State: Zip: Phone (home): E-mail Address: (business): (cell): Birth Date: Employer/School:
Volunteer Application I. CONTACT INFORMATION Mr. Mrs. Name (first): (middle): (last): Ms. Home Address: City: State: Zip: Phone (home): E-mail Address: (business): (cell): Birth Date: Employer/School:
HIPAA PRIVACY TRAINING
 HIPAA PRIVACY TRAINING HIPAA Privacy Training Objective Present a general overview of HIPAA and define important terms Understand the purpose of HIPAA and the Privacy Rule Understand the term Protected
HIPAA PRIVACY TRAINING HIPAA Privacy Training Objective Present a general overview of HIPAA and define important terms Understand the purpose of HIPAA and the Privacy Rule Understand the term Protected
Compliance Program Code of Conduct
 City and County of San Francisco Department of Public Health Compliance Program Code of Conduct Purpose of our Code of Conduct The Department of Public Health of the City and County of San Francisco is
City and County of San Francisco Department of Public Health Compliance Program Code of Conduct Purpose of our Code of Conduct The Department of Public Health of the City and County of San Francisco is
Columbia Medical Practice- Pediatrics Ken Klebanow M.D. and Associates
 HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
GENERAL INFORMATION. English Spanish Arabic Chinese French German Hmong Hindi Laotian Philippine Vietnamese Other
 **INCOMPLETE APPLICATIONS WILL DELAY THE CREDENTIALING PROCESS** 1. Please print or type ALL responses. 2. If you need additional space to complete a section, please attach additional sheets. 3. If you
**INCOMPLETE APPLICATIONS WILL DELAY THE CREDENTIALING PROCESS** 1. Please print or type ALL responses. 2. If you need additional space to complete a section, please attach additional sheets. 3. If you
CODAC BEHAVIORAL HEALTH SERVICES, INC.
 CODAC BEHAVIORAL HEALTH SERVICES, INC. Human Resources 1650 East Ft. Lowell Rd. Suite 202 Tucson, Arizona 85719 Administration: 520 327 4505 Human Resources: 520 202 1890 Fax: 520 202 1718 Website: www.codac.org
CODAC BEHAVIORAL HEALTH SERVICES, INC. Human Resources 1650 East Ft. Lowell Rd. Suite 202 Tucson, Arizona 85719 Administration: 520 327 4505 Human Resources: 520 202 1890 Fax: 520 202 1718 Website: www.codac.org
LifeBridge Health HIPAA Policy 4. Uses of Protected Health Information for Research
 LifeBridge Health HIPAA Policy 4 Uses of Protected Health Information for Research This Policy contains the following Sections: I. Policy II. III. IV. Definitions Applicability Procedures A. Individual
LifeBridge Health HIPAA Policy 4 Uses of Protected Health Information for Research This Policy contains the following Sections: I. Policy II. III. IV. Definitions Applicability Procedures A. Individual
CASE MANAGEMENT POLICY
 CASE MANAGEMENT POLICY Subject: Acuity Scale Determination Effective Date: March 21, 1996 Revised: October 25, 2007 Page 1 of 1 PURPOSE: To set a minimum standard across Cooperative agencies regarding
CASE MANAGEMENT POLICY Subject: Acuity Scale Determination Effective Date: March 21, 1996 Revised: October 25, 2007 Page 1 of 1 PURPOSE: To set a minimum standard across Cooperative agencies regarding
PATIENT INFORMATION. In Case of Emergency Notification
 PATIENT INFORMATION Patient Name Date Nickname DOB Age Sex Race/Ethnicity Language(s) spoken at home Person completing form Relation to Patient Patient Address City State Zip Phone # Other Phone Medical
PATIENT INFORMATION Patient Name Date Nickname DOB Age Sex Race/Ethnicity Language(s) spoken at home Person completing form Relation to Patient Patient Address City State Zip Phone # Other Phone Medical
Cadenza Center for Psychotherapy & the Arts, Inc. ADULT INTAKE
 Cadenza Center for Psychotherapy & the Arts, Inc. ADULT INTAKE Date: / / Name: Date of Birth: / / Age: Sex: M F ETHNIC ORIGIN: White Hispanic Haitian African American Other: PRIMARY LANGUAGE: English Spanish
Cadenza Center for Psychotherapy & the Arts, Inc. ADULT INTAKE Date: / / Name: Date of Birth: / / Age: Sex: M F ETHNIC ORIGIN: White Hispanic Haitian African American Other: PRIMARY LANGUAGE: English Spanish
NOTICE OF PRIVACY PRACTICES
 535 East 70th Street New York, NY 10021 (212) 606-1000 Specialists in Mobility NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE
535 East 70th Street New York, NY 10021 (212) 606-1000 Specialists in Mobility NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE
EVIDENCE OF COVERAGE Molina Medicare Options Plus HMO SNP
 Molina Medicare Options Plus HMO SNP Member Services CALL (800) 665-0898 Calls to this number are free. 7 days a week, 8 a.m. to 8 p.m., local time. Member Services also has free language interpreter services
Molina Medicare Options Plus HMO SNP Member Services CALL (800) 665-0898 Calls to this number are free. 7 days a week, 8 a.m. to 8 p.m., local time. Member Services also has free language interpreter services
Lalita Matta, MD Estrela Chaves, NP, CDE
 PERSONAL INFORMATION Name of Patient: Maiden Name: Social Security No.: Date of Birth: Home Address: City: State: Zip: Home Phone: Mobile Phone: Work Phone: Email Address: Race/ Ethnicity: Marital Status:
PERSONAL INFORMATION Name of Patient: Maiden Name: Social Security No.: Date of Birth: Home Address: City: State: Zip: Home Phone: Mobile Phone: Work Phone: Email Address: Race/ Ethnicity: Marital Status:
APPLICATION FOR EMPLOYMENT
 APPLICATION FOR EMPLOYMENT 895 Mary Dunn Road, Hyannis, MA 02601 (508) 778.5040 Fax: (508) 778.9642 www.capeabilities.org Accredited by The Commission on Accreditation of Rehabilitation Facilities Thank
APPLICATION FOR EMPLOYMENT 895 Mary Dunn Road, Hyannis, MA 02601 (508) 778.5040 Fax: (508) 778.9642 www.capeabilities.org Accredited by The Commission on Accreditation of Rehabilitation Facilities Thank
Indiana. Your Medical Record Rights in. (A Guide to Consumer Rights under HIPAA)
") Your Medical Record Rights in Indiana (A Guide to Consumer Rights under HIPAA) JOY PRITTS, JD NINA L. KUDSZUS HEALTH POLICY INSTITUTE GEORGETOWN UNIVERSITY Your Medical Record Rights in Indiana (A Guide
Your Medical Record Rights in Indiana (A Guide to Consumer Rights under HIPAA) JOY PRITTS, JD NINA L. KUDSZUS HEALTH POLICY INSTITUTE GEORGETOWN UNIVERSITY Your Medical Record Rights in Indiana (A Guide
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
YAI Family Reimbursement Program Guidelines PLEASE READ BEFORE COMPLETING APPLICATION
 YAI Family Reimbursement Program Guidelines PLEASE READ BEFORE COMPLETING APPLICATION YAI s Family Reimbursement Fund provides financial assistance to people with developmental disabilities who reside
YAI Family Reimbursement Program Guidelines PLEASE READ BEFORE COMPLETING APPLICATION YAI s Family Reimbursement Fund provides financial assistance to people with developmental disabilities who reside
1.2 ADULT CLIENT INTAKE FORM: Client Information
 1.2 ADULT CLIENT INTAKE FORM: Client Information FOR OFFICIAL USE ONLY: Client Number Effective Insurance No OH No CLIENT INFORMATION Client name of significant other CHILDREN INFORMATION of birth of birth
1.2 ADULT CLIENT INTAKE FORM: Client Information FOR OFFICIAL USE ONLY: Client Number Effective Insurance No OH No CLIENT INFORMATION Client name of significant other CHILDREN INFORMATION of birth of birth
Emergency Contact Name: Relationship: Home #: ( ) Cell #: ( ) Alternate #: ( ) Pharmacy Information Pharmacy Name: Phone #: ( ) Location:
 Cell #: ( ) Alternate #: ( ) Pharmacy Information Pharmacy Name: Phone #: ( ) Location:") New Patient Office Information Last Name: First Name: Initial Date of Birth: SSN # Marital Status: Single Married Divorced Widowed Address: City: State: Zip: Gender: M Parent/ Legal Guardian if Patient
New Patient Office Information Last Name: First Name: Initial Date of Birth: SSN # Marital Status: Single Married Divorced Widowed Address: City: State: Zip: Gender: M Parent/ Legal Guardian if Patient
STANDARDS OF CARE HIV AMBULATORY OUTPATIENT MEDICAL CARE STANDARDS I. DEFINITION OF SERVICES
 S OF CARE Oakland Transitional Grant Area Care and Treatment Services J ANUARY 2007 Office of AIDS Administration 1000 Broadway, Suite 310 Oakland, CA 94612 Tel: 510. 268.7630 Fax: 510.268-7631 AREAS OF
S OF CARE Oakland Transitional Grant Area Care and Treatment Services J ANUARY 2007 Office of AIDS Administration 1000 Broadway, Suite 310 Oakland, CA 94612 Tel: 510. 268.7630 Fax: 510.268-7631 AREAS OF
How did you hear about us? Patient s Last Name First Name Middle Initial. Patient s Social Security Number. Address Apt # City State Zip Code
 Who is responsible for this patient? Self Parent Employer Other How did you hear about us? Patient s Last Name First Name Middle Initial Patient s Social Security Number of Birth Address Apt # City State
Who is responsible for this patient? Self Parent Employer Other How did you hear about us? Patient s Last Name First Name Middle Initial Patient s Social Security Number of Birth Address Apt # City State
o Recipients must coordinate these testing services with other HIV prevention and testing programs to avoid duplication of efforts.
 E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology
 Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you
Houston Rheumatology Center Sabeen Najam, MD, PA Board Certified in Rheumatology Patient Health Questionnaire Patient s Name: Date of Birth: Drug / Food Allergies: Please list any and all allergies you