TRANSITIONS OF CARE: COLLABORATIVE CARE TO REDUCE HOSPITAL READMISSION RATES
|
|
|
- Egbert Waters
- 6 years ago
- Views:
Transcription
1 TRANSITIONS OF CARE: COLLABORATIVE CARE TO REDUCE HOSPITAL READMISSION RATES Speakers Stacey Frede, PharmD, BCACP, CDE Manager of Clinical Program Development, The Kroger Co. Eric Wright, PharmD, MPH, Co-Director and Professor, Geisinger Center for Pharmacy Innovation and Outcomes 1
2 Objectives 1. Recognize the challenges and systemic barriers that hinder effective transitions of care in patients with chronic illnesses. 2. Understand how patient health outcomes can be improved and affected by transitions of care from the hospital to community pharmacy settings. 3. Identify strategies to improve transitions across health care settings to reduce hospital readmission rates. 2
3 Self-Assessment Question #1 Barriers that hinder effective Transitions of Care include: a) HIE Interoperability b) Effective HC provider communication c) Data Agreements d) Costs of care e) All of the Above 3
4 Self-Assessment Question #2 Which of the following communication methods/modes were used by Kroger and/or Geisinger to transmit hospital information to community pharmacists? a) Secure b) Phone c) Fax d) B and C e) All of the above 4
5 Self-Assessment Question #3 Strategies to improve transitions of care involving pharmacists include: a) Inpatient to outpatient pharmacist communication b) Telephone follow-up within 7 days post discharge c) In-home visits d) Face-to face medication consultation e) All of the Above 5
6 Outline Introduction Kroger Experience Geisinger Experience Recent Results and Future Directions Self-Assessment Questions Discussion 6
7 Hospital Readmissions Historically, 20% of Medicare patients are readmitted to the hospital within 30 days of discharge Readmissions cost $25 billion each year In October of 2012, The Hospital Readmission Reduction Program (HRRP) began penalizing hospitals for excess 30 day readmissions in specific high risk groups Excess readmissions = # readmissions # predicted 1 Jencks SF, Williams MV, Coleman EA. Hospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360: ; 2 7
8 HRRP Summary Year Penalties Applied FY 2013 FY 2014 FY 2015 FY 2016 FY 2017 Dx of initial hospitalization MI, CHF, Pneumonia MI, CHF, Pneumonia MI, CHF, Pneumonia COPD Hip or knee replacement MI, CHF, Pneumonia COPD Hip or knee replacement MI, CHF, Pneumonia* COPD Hip or knee replacement, CABG Penalties: Percentage reduction in base payments on all Medicare inpatient admissions Maximum rate of penalty Percent of hospitals penalized 1% 2% 3% 3% 3% 64% 66% 78% 78% 79% Estimate of total penalties $290 million $227 million $428 million $420 million $528 million Boccuti C, Cisllias, G. Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program. KFF. Medicare/issue-brief/aiming-for-fewer-hospital-u-turns-the-medicare-hospital-readmission-reduction-program/. Last accessed August 9, 2017.
9 Pharmacist Role in Addressing Readmissions Major reasons for readmission Medication errors Adverse drug reactions Medication nonadherence Pharmacists are needed in transitions of care process Community pharmacists are already touching patients postdischarge Community pharmacists have established relationships with patients Community pharmacists have understanding of pre-admission medications 3 Ann Intern Med. 2003;138(3): ; 4 Ann Pharmacother. 2002;36(9):
10 Barriers to Pharmacists Addressing Readmissions Variable inpatient pharmacist role in discharge process Community pharmacist lack of knowledge of recent hospitalization Community pharmacist role as provider in healthcare team not established No incentive to provide direct counseling/mtm Technology interoperability Expense 10
11 We Still Have to Prove It Multiple projects have demonstrated effectiveness in reducing hospital readmissions Project RED (AHRQ/Boston University) Medication REACH (Einstein Healthcare Network) STAAR (Massachuetts/IHI) Variable use of pharmacists Collaboration for inpatient/outpatient pharmacists opportunity Outcomes of pharmacist involvement need to be evaluated Cassano, A. ASHP-APhA Medication Management in Care Transitions Best Practices. Feb ASHP_APhA_MedicationManagementinCareTransitionsBestPracticesReport2_2013.pdf; BMC Health Mitchell SE. BMC Health Serv Res. 2017; 17: 291. Implementation and adaptation of the Re-Engineered Discharge (RED) in five California hospitals: a qualitative research study. Published online 2017 Apr 19; BMJ Innov Jul; 1(3): ; Hosp Pharm Mar; 49(3):
 Foundation KROGER HEALTH The Kroger Co.")
12 KROGER EXPERIENCE CINCINNATI Stacey M. Frede, PharmD, BCACP, CDE Manager of Clinical Program Development The Kroger Co. *Supported by a grant from the National Association of Chain Drug Stores (NACDS) Foundation KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation

13 PHARMACY MAP HOLD for Rx Map KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation



14 KROGER PHARMACY SNAPSHOT Pharmacies Pharmacists Our Clinical Services Travel and adult vaccinations Wellness» Smoking Cessation» Fitness, Nutrition, Weight Management» Health Screenings/POCT Medication Synchronization Medication Therapy Management (MTM) Disease Management» Diabetes» Hypertension KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 14

15 TRANSITIONS OF CARE WORK Objective: Decrease 30 day readmission rates 2 hospitals, 9 pharmacies Patient identification and study consent at the hospital by discharge coordinators Faxed communication- discharge summary Face-to-face pharmacist visit Telephonic follow-up KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 15
16 TRANSITIONSRX Usual Care (n=60) Pharmacist (n=29) Adjusted OR 95%CI p-value 30-day Readmissions 12 (20%) 2 (6.9%) ( ) p=0.019 Pharmacists averaged 7 interventions per patient 41% required consultation with a prescriber 18 new therapies were initiated 10 unnecessary therapies were discontinued 9 medications were changed 8 doses of medication were altered 5 Luder HR, Frede SM, Kirby JA, Epplen K, Cavanaugh T, Martin-Boone JE, Conrad WR, Kuhlmann D, Heaton PC. TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate. J Am Pharm Assoc (2003) May 1;55(3): KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation

17 TRADITIONAL SYSTEM KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation

18 ULTIMATE GOAL KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation
19 TRANSITIONRX EXPANSION TEAM Health Council: Sheri Vogel, Lori McAleer, Richard Shonk, Kate Haralson, Tiffany Mattingly HealthBridge: David Burch, Tim Mattingly College of Pharmacy: Heidi Luder, Pam Heaton Kroger Pharmacy: Natalie Kunze, Jim Kirby, Suzi Francis This project was funded by the National Association of Chain Drugs Stores Foundation (NACDS) Foundation KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation
20 CINCINNATI EXPERIENCE Objectives Primary: to determine the impact of a community pharmacy-based transition of care program on 30 day-all-cause hospital readmission rate Secondary: to measure: 1) the number and type of pharmacists interventions, 2) patient satisfaction with discharge and the pharmacist s intervention, 3) primary and secondary medication non-adherence KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 20
21 CINCINNATI EXPERIENCE Sites expanded: KROGER HEALTH 3 Health Systems 60 Pharmacies, 200 Pharmacists Addressed Barriers from Pilot: Consenting Process The Kroger Co Confidential» Use of Research Center Paper Communication System» hbdirect transmission of Continuity of Care Document (CCD)» Health Information Exchange (HIE) transmission of data back to primary care provider» Readmission data from HIE. reconciliation/pages/default.aspx Associates Customers Food Core Partnerships Innovation 21
22 CINCINNATI EXPERIENCE Inclusion criteria: Greater than 18 years of age English-speaking Discharged to home Diagnosis of heart failure, pneumonia, MI, diabetes or COPD Exclusion criteria: Cognitive impairment Discharged to long term care facility KROGER HEALTH The Kroger Co Confidential. reconciliation/pages/default.aspx Associates Customers Food Core Partnerships Innovation 22
23 Hospital UCCP Call Center UCCP Call Center Patient is referred to study upon discharge Consents, randomizes, and enrolls patient in study Schedules appointment within 7 days of discharge Continuity of Care Document sent to Call Center via hbdirect; passed to Pharmacy for Intervention patients Kroger Pharmacy Kroger Pharmacy Kroger Pharmacy Pharmacist calls patient for follow-up 2 weeks after appointment Communicate with prescriber/pcp as needed; Document medication problems and interventions from appointment Patient presents for MTM appointment UCCP Call Center Calls Control Patient to complete survey within 30 days Kroger Pharmacy Alerted if patient is readmitted to hospital or the ER Alert transmitted for hospital visit to Call Center via hbdirect; passed to Pharmacy for Intervention patients
24 Hospital Eligible patient is identified, consented, randomized, and enrolled in study UCCP Call Center Schedules appointment within 7 days of discharge Continuity of Care Document sent to Call Center (all) and Pharmacy (intervention) via hbdirect Kroger Pharmacy Pharmacist calls patient for follow-up 2 weeks after appointment UCCP Call Center Calls Control Patient to complete survey within 30 days Kroger Pharmacy Communicate with prescriber/pcp as needed; Document medication problems and interventions from appointment Document medication Kroger problems Pharmacy and interventions from Alerted appointment if patient is readmitted to hospital or the ER Kroger Pharmacy Patient presents for MTM appointment Alert transmitted for hospital visit to Call Center and Pharmacy (intervention) via hbdirect

25 KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 25

26 KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 26
27 PHARMACY INTERVENTION Pharmacist provided a Comprehensive Medication Review (CMR) Focused education on: Acute issues as priority Red Flag warning signs Common medication errors with transitions Medication adherence Drug or dietary interactions Sent home with PMR, MAP, written education Follow-up Call- 2 weeks out KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 27

28 CLOSING THE GAPS Documented visit and interventions in Pharmacy system Recommendations and updated PMR sent to PCP hbdirect Phone/Fax PMR and inactive medication list shared with primary pharmacy Phone/Fax KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 28

29 READMISSION ALERTS KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 29
30 PRELIMINARY RESULTS Enrollment: July Jan 2017 Total: 403 enrolled Control: 189 Intervention: patients completed intervention KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 30
31 BASELINE CHARACTERISTICS Measure Kroger (n=214) Control (n=189) P-value Age, in yrs., Mean (± SD) 60.3 (12.9) 63.2 (12.2) 0.02 Gender Race/Ethnicity Plan Type Male Female White Black Other Medicaid Medicare Private Other Length of index hospitalization in days, Mean (± SD) 103 (48.1%) 111 (51.9%) 172 (80.4%) 39 (18.2%) 3 (1.4%) 31 (14.5%) 21 ( 9.8%) 25 (11.7%) 5 ( 2.3%) 108 (57.1%) 81 (42.9%) 147 (77.8%) 35 (18.5%) 6 (3.2%) 10 ( 5.3%) 24 (12.7%) 19 ( 10.1%) 6 ( 3.2%) 6.23 (3.9) 6.23 (4.9) < Prior Hospitalization, Yes 43 (20.1%) 41 (21.7%) 0.40 KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 31





32 PRELIMINARY RESULTS Patients Enrolled by Disease State 28% 12% 20% 23% Pneumonia COPD MI DM CHF Pharmacist Interventions 65 patients presented» 404 interventions» Avg. 6.2/patient 17% KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 32
33 LESSONS LEARNED It is feasible for community pharmacies to partner with area hospitals to assist with transitions in care. Pharmacists are ready, willing, and able to provide the much needed service; health systems are ready to partner CCD is an effective communication tool one-way! Building the relationships can be difficult Approvals needed at multiple levels -- need a champion Contracts took a long time Time to enroll patients Patients high no-show rate HIE implementation KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation
34 BARRIERS OF HIE IMPLEMENTATION IN THE COMMUNITY Data Governance Agreements Patient Consent Technical Difficulties Physician Communication Burden of Documentation Cost and Sustainability KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation
 Discrete clinical coding KROGER HEALTH The Kroger Co.")
35 THE NEW NORMAL Provider status Patient Impact Interoperable EHR Connectivity and alerting Standardized documentation HL7 Consolidated Clinical Document Architecture (C-CDA) Discrete clinical coding KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation
 systems supports interoperability by facilitating the sharing of patient information among information systems 6 Standardized Framework")
36 SYSTEMATIZED NOMENCLATURE OF MEDICINE CLINICAL TERMS (SNOMED CT) Becoming the gold standard for documenting and communicating patient care information Mapped to medication-related terms & definitions Integration of SNOMED CT into electronic medical record (EMR) systems supports interoperability by facilitating the sharing of patient information among information systems 6 Standardized Framework for Cross-Walking Medication Therapy Management (MTM) Services to SNOMED CT Codes, Joint Commission of Pharmacy Practitioners Workgroup, retrieved from accessed August 10, 2017; UMLS SNOMED CT Browser. National Library of Medicine, National Institute of Health KROGER HEALTH The Kroger Co Confidential Associates Customers Food Core Partnerships Innovation 36
37 Outline Introduction Kroger Experience Geisinger Experience Recent Results and Future Directions Self-Assessment Questions Discussion 37


38 Geisinger Experience Eric A. Wright, PharmD, MPH Co-Director, Professor Geisinger Center for Pharmacy Innovation and Outcomes *Supported by a grant from the National Association of Chain Drug Stores (NACDS) Foundation 38

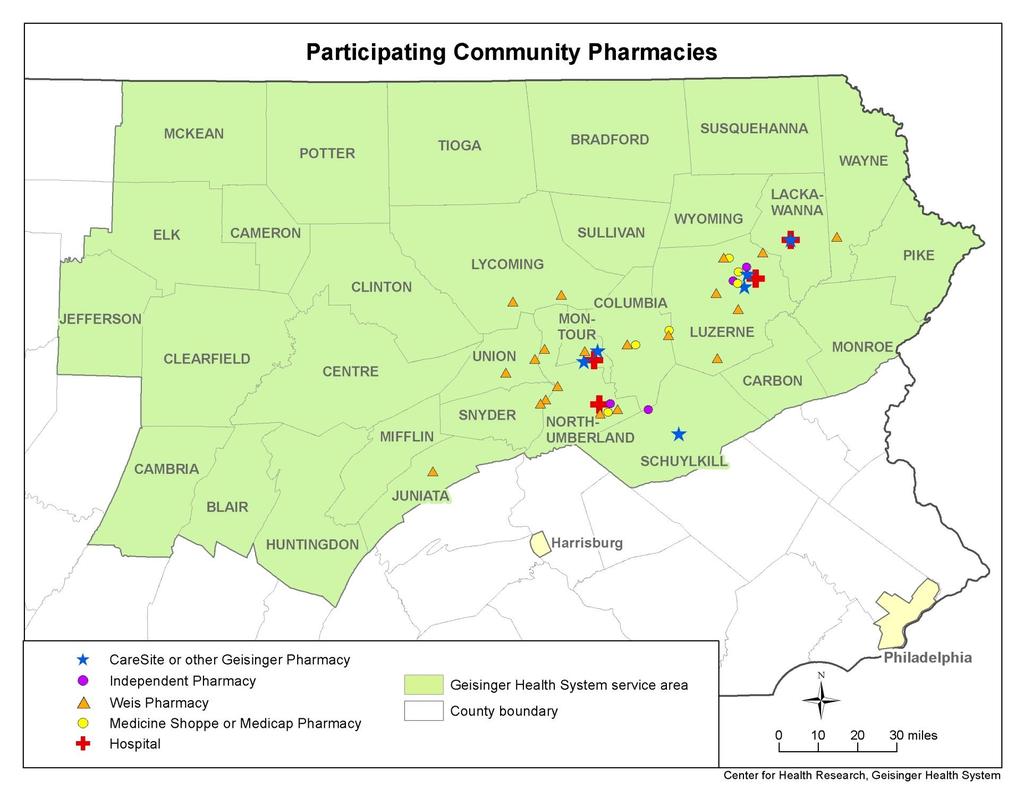
39 Thank you to this Amazing Collaborative Team! Geisinger - Lorraine Tusing, BA - Kelly Bolesta, PharmD - Kim Chaundy, BS - Jove Graham, PhD, MS - Christina Gregor, BS - Steve Gunderman, IT - Fred Leri, PharmD - Daniel Maeng, PhD - Richard Martin, MD - Charles Medico, PharmD, BCPS - Dean Parry, RPh - Rebecca Price, BS - Jim Younkin, BS - Lori Zaleski, RPh Collaborators -Rick Seipp, PharmD (Weis Markets) -Bruce Citsay, PharmD (Weis Markets) -John Fiacco, RPh (Medicine Shoppe) -Bette McDonald, RPh (Medicine Shoppe) -Karen Robinson, MSc, PhD (Johns Hopkins) 39

40 Geisinger Legacy Make my hospital right, make it the best. Abigail Geisinger

41 Geisinger - an Integrated Healthcare Delivery System 41


42 Geisinger - an Integrated Healthcare Delivery System 42
43 Geisinger Initiatives In Transitions Discharge Medication Program Case Nurse Management (Health Navigator) Transition bundle Pharmacist Medication Reconciliation Post-discharge Ambulatory Care Pharmacist Management Admission, Discharge, Transfer (ADT) alerts to PC providers through Health Exchange Bulger et al. Clin Med Res. 2010;8:

44 Current System Hospital Discharge? Community Pharmacy
45 Study Aims 1) Demonstrate the feasibility of connecting inpatient pharmacists to outpatient pharmacists using technology 2) To determine the impact of inpatient to outpatient pharmacist collaboration on clinical (E.g. readmissions, adherence) and economic outcomes among a group of high risk patients 45 45
46 Methods Design Prospective quasi-experimental study IRB-approved with waiver of informed consent Population >18 years Patients with high-risk conditions HF, MI, pneumonia, COPD, Diabetes Discharged to home from one of 4 hospitals EHR preferred pharmacy is participating in study 46
47 47
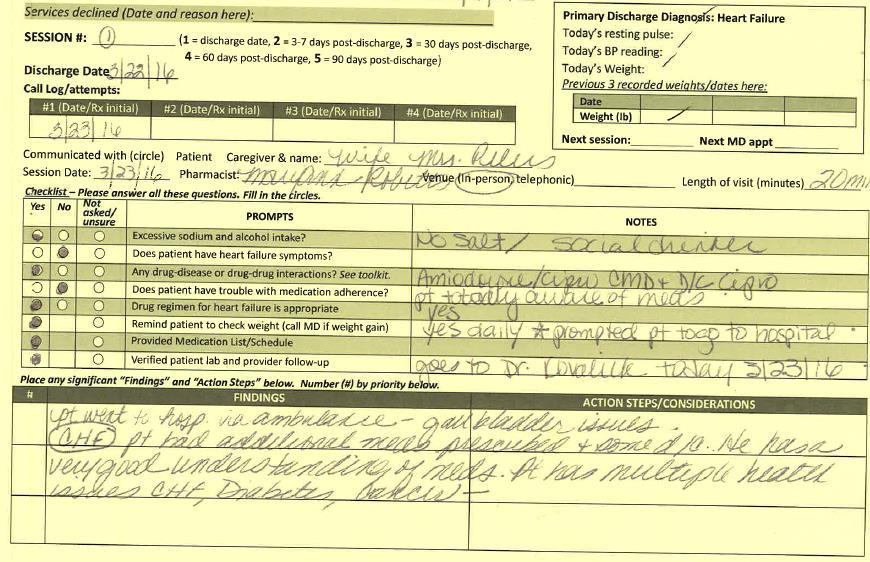
48 Methods Intervention Inpatient pharmacist medication reconciliation and counseling prior to discharge Send Direct Secure Messaging ( ) to community pharmacist Community pharmacist counseling/mtm 5 encounters - Day of discharge, call within 7 days, monthly x 3 Toolkit and education for providing services Control = Usual care Outcome 30-day all-cause readmissions Medication adherence Return on Investment Pharmacist perceptions 48
 Paste into Secure message (Orion) 6) Send to retail pharmacist Secure Message to Community Pharmacist Community")
 Follow-up at 3-7 days (call), 1, 2 and 3 months following")
49 Revised System Hospital Discharge 1) Perform Medication Reconciliation 2) Perform Discharge Counseling 3) Write EHR note 4) Copy note from EHR 5) Paste into Secure message (Orion) 6) Send to retail pharmacist Secure Message to Community Pharmacist Community Pharmacy 1) Message received in Orion inbox 2) Fax alert triggered 3) Secure Message read by pharmacist 4) Pharmacist assures medication pick-up, provides counseling and medication list 5) Follow-up at 3-7 days (call), 1, 2 and 3 months following discharge

50 Progress Note 50






51 Inclusion Population - Discharge to home from a Geisinger hospital - Age years at time of discharge - Diagnosis of heart failure, myocardial infarction, pneumonia, or chronic obstructive pulmonary disease, diabetes Intervention - 3,507 Screened touches D/C to home Intervention Participating pharmacy Verbal confirmation from patient Intervention Intention to treat: N = 615 Per protocol: n = 374 Control Non participating pharmacy Control (5:1) Intention to treat: N = 3075 Per protocol: n = 1870 Matched comparison Total available control cohort 42,184 Matched 5:1 51

52 Matching 52
53 Results Matching Intervention (ITT) (n=615) Comparison (ITT) (n=3075) Age, Mean (SD) 67 (13) 66 (14) Males 53% 53% White Race 99% 98% Charlson Comorbidity Index, mean (SD) 7.5 (4.3) 7.7 (4.6) Comorbidities Heart Failure ami COPD Diabetes Pneumonia 75% 31% 59% 76% 70% 76% 28% 58% 76% 70% Length of Stay in days, mean (SD) 5.1 (3.9) 5.0 (5.2) Number of medications at discharge, Mean per patient (SD) 19.1 (7.9) 18.6 (7.6) New prescriptions at discharge, Mean per patient (SD) 0.88 (1.2) 0.83 (1.1) 53
54 Number of Patients Inclusion Summary Enrollment from December 2014-September with available matches 61% with community note sent 60% with completed community pharmacy consultation 64% telephonic for first contact 34% 22% 17% 21% 6% Number of Community Pharmacy Visits 54
55 Initial Findings Connecting Inpatient and Outpatient pharmacists via Secure is feasible Despite feasibility, only 61% patients have a note sent to the community pharmacy Most patients received follow-up consultation by community pharmacists once discharged (most more than once), but some remain untouched 55
56 Pearls from Experience Interest exists Pharmacists/pharmacies can expand roles Health-systems are eager to collaborate Success requires Vision High-level support Collaboration across environments Consistent surveillance and evaluation 56
57 Pearls from Experience Keep patient-care focus Ideal initial contact within first 1-3 days Telephonic follow-up Talk with your technology providers about capabilities Keep in mind how new interventions merge with your current workflow Focus attention on patients in most need High risk conditions, medication-related problems, previous hospitalization Address legal, logistical and security concerns Learning curve exists Focus on Low-hanging fruit (e.g. adherence, medication reconciliation) Oversight of Follow-up improves capture 57
58 Outline Introduction Kroger Experience Geisinger Experience Recent Results and Future Directions Self-Assessment Questions Discussion 58
59 Readmission reduction since ACA N Engl J Med 2016; 374:

60 Evidence of Post-Discharge Pharmacist Impact on Rehospitalizations Oliveira et al J Patient Saf

61 Evidence of Post-Discharge Pharmacist Impact on Rehospitalizations Mekonnen AB, et al. BMJ Open 2016;6:e
62 Evidence of Post-Discharge Pharmacist Impact on Hospitalizations Pharm2Pharm: Inpatient to Outpatient pharmacist care Pellegrin et al. JAGS 65: ,
63 Evidence of Post-Discharge Pharmacist Impact on Rehospitalizations 63
64 Take Home Messages on Transitions Hospitals are seeing reduction in 30-day readmissions nationally Readmissions is a high-priority issue Many pharmacist-provided transitions of care interventions tested using inpatient, ambulatory and community pharmacists Outcomes using pharmacists look promising Wide-spread adoption depends on impact, scalability and sustainability 64
65 Outline Introduction Kroger Experience Geisinger Experience Recent Results and Future Directions Self-Assessment Questions Discussion 65
66 Self-Assessment Question #1 Barriers that hinder effective Transitions of Care include: a) HIE Interoperability b) Effective HC provider communication c) Data Agreements d) Costs of care e) All of the Above 66
67 Self-Assessment Question #2 Which of the following communication methods/modes were used by Kroger and/or Geisinger to transmit hospital information to community pharmacists? a) Secure b) Phone c) Fax d) B and C e) All of the above 67
68 Self-Assessment Question #3 Strategies to improve transitions of care involving pharmacists include: a) Inpatient to outpatient pharmacist communication b) Telephone follow-up within 7 days post discharge c) In-home visits d) Face-to face medication consultation e) All of the Above 68
69 Outline Introduction Kroger Experience Geisinger Experience Recent Results and Future Directions Self-Assessment Questions Discussion 69
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Medication Therapy Management
 Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge
 Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
New pharmacy practice opportunity: Enhancement of the transitions of care process
 New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
Deriving Value from a Health Information Exchange. HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017
 Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Brittany Turner, 2015 PharmD Candidate 1 Justin Campbell, PharmD 2 Katie McKinney, PharmD, MS, BCPS 2
 Discharge Medication Concierge Program: A pilot project in heart failure to reduce readmission rates, improve patient satisfaction, and increase pharmacy business metrics Brittany Turner, 2015 PharmD Candidate
Discharge Medication Concierge Program: A pilot project in heart failure to reduce readmission rates, improve patient satisfaction, and increase pharmacy business metrics Brittany Turner, 2015 PharmD Candidate
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Optimizing pharmaceutical care via Health Information Technology:
 Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future
 Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future Arnold Epstein MSU 2018 Health Care Policy Conference April 6, 2018 The Good Ole Days 2 Per Capita National Healthcare
Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future Arnold Epstein MSU 2018 Health Care Policy Conference April 6, 2018 The Good Ole Days 2 Per Capita National Healthcare
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Saint Agnes Hospital. Pharmacist utilization of the LACE tool to prevent hospital readmissions. Program/Project Description, including Goals:
 Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Benefits of National Provider Identifier
 Florida Pharmacy Association Professional Affairs Council Benefits of National Provider Identifier Written by: Kayla Mackanin, USF PharmD Candidate 2015, Professional Affairs Council Member Created on:
Florida Pharmacy Association Professional Affairs Council Benefits of National Provider Identifier Written by: Kayla Mackanin, USF PharmD Candidate 2015, Professional Affairs Council Member Created on:
IMPROVING MEDICATION RECONCILIATION WITH STANDARDS
 Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population
 Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Marshall Digital Scholar. Marshall University. Brittany Snodgrass. Charles K. Babcock Marshall University,
 Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service
 Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions
 1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
A Care Transitions Project
 Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
4/28/2017. Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC Presenter. Overview
 Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC 2017 Presenter Debra Demar, MS is the Community Liaison for White Cross Pharmacy, serving RI, MA and CT. She has
Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC 2017 Presenter Debra Demar, MS is the Community Liaison for White Cross Pharmacy, serving RI, MA and CT. She has
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care
 Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care Robert D. Rondinelli, MD, PhD Medical Director Rehabilitation Services Unity Point Health, Des Moines Paulette
Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care Robert D. Rondinelli, MD, PhD Medical Director Rehabilitation Services Unity Point Health, Des Moines Paulette
HCAHPS: Background and Significance Evidenced Based Recommendations
 HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Disclosures. Learning Objectives 4/26/2017. Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic
 Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
EHR Data Integration and Seamless Exchange of Clinical Information to Enable Next-Generation Pharmacy Services
 EHR Data Integration and Seamless Exchange of Clinical Information to Enable Next-Generation Pharmacy Services Presenter: Shelly Spiro RPh, FASCP Pharmacy HIT, Executive Director Objectives 1. Explain
EHR Data Integration and Seamless Exchange of Clinical Information to Enable Next-Generation Pharmacy Services Presenter: Shelly Spiro RPh, FASCP Pharmacy HIT, Executive Director Objectives 1. Explain
A Pharmacist Network for Integrated Medication Management in the Medical Home
 A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE
 PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE RAJEEV KUMAR MD FACP CHIEF MEDICAL OFFICER SYMBRIA OBJECTIVES Identify elements of key literature that describes post-hospital
PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE RAJEEV KUMAR MD FACP CHIEF MEDICAL OFFICER SYMBRIA OBJECTIVES Identify elements of key literature that describes post-hospital
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Practice Transformation Research Informing the Future Delivery of Healthcare: Insights from IHARP
 Practice Transformation Research Informing the Future Delivery of Healthcare: Insights from IHARP William T. Lee, BSPharm, MPA, FASCP Pharmacy System Director, Carilion Medical Center Gary R. Matzke, BS
Practice Transformation Research Informing the Future Delivery of Healthcare: Insights from IHARP William T. Lee, BSPharm, MPA, FASCP Pharmacy System Director, Carilion Medical Center Gary R. Matzke, BS
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Quality Data Model (QDM) Style Guide. QDM (version MAT) for Meaningful Use Stage 2
 Style Guide. QDM (version MAT) for Meaningful Use Stage 2") Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Monday, October 24, :15 a.m. to 10:45 a.m. Great Halls 1 & 2
 Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Transition from Hospital to Home: Importance of Medication Education and Reconciliation
 Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017
 Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Factors that Impact Readmission for Medicare and Medicaid HMO Inpatients
 The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
POST-ACUTE CARE Savings for Medicare Advantage Plans
 POST-ACUTE CARE Savings for Medicare Advantage Plans TABLE OF CONTENTS Homing In: The Roles of Care Management and Network Management...3 Care Management Opportunities...3 Identify the Most Efficient Care
POST-ACUTE CARE Savings for Medicare Advantage Plans TABLE OF CONTENTS Homing In: The Roles of Care Management and Network Management...3 Care Management Opportunities...3 Identify the Most Efficient Care
Page 2 of 29 Questions? Call
 Revised 7.29.2018 Contents Introduction. 3 OutcomesMTM Participation.. 3 User Access to Protected Health Information (PHI) 3 Participation from Various Settings..3 Retail 3 LTC/Assisted Living 3 Ambulatory
Revised 7.29.2018 Contents Introduction. 3 OutcomesMTM Participation.. 3 User Access to Protected Health Information (PHI) 3 Participation from Various Settings..3 Retail 3 LTC/Assisted Living 3 Ambulatory
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Synergy Through Integration:
 WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Medication Management Center
 Academic-Community Partnership to Implement Medication Therapy Management (MTM) Services in Rural Communities to Improve Adherence to Preventative Health Guidelines for Patients with Diabetes and/or Hypertension
Academic-Community Partnership to Implement Medication Therapy Management (MTM) Services in Rural Communities to Improve Adherence to Preventative Health Guidelines for Patients with Diabetes and/or Hypertension
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
IMPACT - Connecting Nursing Facilities and Home Care to the Healthcare System of the Future
 IMPACT - Connecting Nursing Facilities and Home Care to the Healthcare System of the Future MA Health Data Consortium CIO Forum January 17 th, 2013 Drs. Larry Garber and Terry O Malley Agenda IMPACT addressing
IMPACT - Connecting Nursing Facilities and Home Care to the Healthcare System of the Future MA Health Data Consortium CIO Forum January 17 th, 2013 Drs. Larry Garber and Terry O Malley Agenda IMPACT addressing
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project
 Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427