Order Source Misattribution: The Impact on CPOE Metrics
|
|
|
- Amelia Miles
- 6 years ago
- Views:
Transcription


1 Order Source Misattribution: The Impact on CPOE Metrics Linda Catzoela, RN, BSN, Clinical Informaticist George Gellert, MD, MPH, MPA, Associate System CMIO CHRISTUS Health March 3, 2016
2 Co-authors and Conflict of Interest Linda Catzoela, RN, BSN George Gellert, MD, MPH, MPA Have no real or apparent conflicts of interest to report.
3 Agenda Benefits realized for the value of Health IT What is Order Source Misattribution? Common misuse of order source Impact to CPOE metrics and adoption Awareness to misattributions Root cause analysis Misattributions identified by groups Data analysis of written orders Order source analysis Impact of Misattribution on Physician Contract Management and Fulfillment Actionable steps to prevent/reduce misattribution Conclusion Questions
4 Learning Objectives 1. Identify the negative impact and magnitude of misattribution of order source on physician Computerized Provider Order Entry (CPOE) performance metrics, including its negative potential impact on physicians' confidence in use rate reporting and how it complicates physician contract fulfillment. 2. Evaluate and correct order source misattribution for a defined, limited period (e.g., 1 month) among key physician CPOE adopters (e.g., hospitalists), in order to accurately report individual physician and overall facility CPOE use rates. 3. Identify solutions, including preventive education across departments, to help mitigate the cause and effects of order source misattribution on physician CPOE use rate and compliance reporting.
5 Benefits Realized for the Value of Health IT S = Physicians endeavoring to adopt CPOE are deeply troubled by misattribution of orders to them. Reducing misattribution increases their confidence and satisfaction with individual CPOE use rate reporting. T = CPOE increases the safety of care delivery to patients, and so strong adoption by physicians is essential. Physicians who are dubious of their reported CPOE use due to order misattribution will be less willing to adopt CPOE. E = Order source attribution validation should eventually be automated within the EHR or enterprise data warehouse. This presentation will increase EHR and Business Intelligence vendors awareness of the significant negative impact of misattribution. P = CPOE facilitates provider engagement in care and population health. CPOE via evidence based clinical decision support improves clinical outcomes/quality and reduces error. S = Insofar as CPOE adoption reduces unnecessary diagnostic procedures, drug and other therapeutic use, it can yield savings in total care delivery.

6 What is Order Source Misattribution? Written Verbal Telephone Protocol Order Management Order Source Misattribution is the misuse of order source selection/attribution by nursing and ancillary departments which deflates physician CPOE use rates
7 Polling Question State your organization s assessment of CPOE misattribution 1. Unaware 2. Aware but not assessed 3. Assessed, not yet mitigated 4. Implementing solutions
8 CPOE Metric Calculation CCCC MMMMMM = N PPPPPPPP CCCC OOOOOO N TTTTT OOOOOO (CCCC, WWWWWWW, VVVVVV & TTTTTTTTT)
9 Order Source Selection for CPOE Computerized Provider Order Entry (CPOE) Meaningful Use was defined as direct order entry of laboratory, radiology, and pharmacy orders by physicians, nurse practitioners, physician assistants and residents Prior to CPOE, the most commonly used order source was written Implementation of CPOE required the creation of additional order source options in Electronic Health Record (EHR) systems
10 Order Source Selection for CPOE Additional order source options created unprecedented opportunities for misattribution of CPOE issued patient orders Each misattribution required analysis in order to determine its negative impact on CPOE metrics and individual physician use rate assessment
11 Neutral Order Sources Neutral order sources* are operational order sources not counted in either the numerator or denominator for determining CPOE use rates: Medication Therapy Management: used by Pharmacist when entering medication or laboratory orders as a result of a physician consult to dose and monitor therapy not outlined in a protocol Order Management: used when revising or entering new orders needed to complete or process an existing order * Caveat: Recommend policy documentation be in place for CPOE order sources
12 Neutral Order Sources Neutral order sources* are operational order sources not counted in either the numerator or denominator for determining CPOE use rates: Protocol: used when entering orders authorized as part of a physician order treatment or hospital protocol Standing Delegated Orders: used for orders/order sets approved by the medical staff for direct entry and implementation by nursing * Caveat: Recommend policy documentation be in place for CPOE order sources
13 Overview of Neutral Order Source Medication Therapy Management (Utilized by Pharmacy) Allow pharmacists to manage medications and related laboratory orders Order Management (Utilized by nurse/ancillary acting off existing orders) Allows nurses to manage and refine orders Protocol (Nurses acting on authorized order treatment) Standing Delegated Orders (Nurses acting on approved orders for direct entry) Allows nurses to enter orders based on hospital protocol Permits nurses to enter initial orders based on assessment according to policy

14 Example of Neutral Order Source Workflow PROVIDER enters orders for Electrolyte Protocol Order Source is PROVIDER Order calculated towards provider s CPOE use rate Patient care requires several orders from the Protocol Nurse enters 1 lab and 1 medication order in CPOE Correct Order Source Selected Yes No 2 orders negatively impact provider s CPOE use rate Order source of Protocol Orders have no impact on CPOE Metrics
15 Common Misuse of Order Source Order is part of a hospital practice or specialty protocol Subsequent orders generated by the protocol were entered as written by nursing or ancillary groups Example: Protocol to give Potassium if < 3.5 Nurse enters medication order for Potassium and does not select protocol as the order source
16 Common Misuse of Order Source Order is part of a conditional order Example: Order is part of a conditional order to draw blood cultures if temperature > 101 F Several days later, patient gets a temperature > 101 F Nurse selects written as the order source when entering order for blood cultures Nurse should have selected order management as the order source
17 Negative Impact on CPOE Metrics Identified early in CPOE use rate reports (distributed monthly to drive adoption) Identified number of orders, number orders by Provider, and CPOE % # of # Orders by Ordering Physician % CPOE Orders Provider TEST, MD % Caused clinicians to challenge the accuracy/credibility of use rates Required a detail breakdown of order source totals Contributed to physician dissatisfaction/distrust of reported use rates Affected contracted physician performance metrics
18 Informatics Involvement High volume order entry physicians ( e.g., hospitalists) are required to achieve established CPOE use rates Hospitalist group was willing to work with Informatics to determine the accuracy of use rate reporting CPOE use rate reports had to be broken down by order source: Telephone Verbal Written Provider
19 Informatics Involvement Ordering Physician Orders by Telephone Orders by Verbal Orders by Written Orders By Provider Total Orders % CPOE Opportunity Opportunity % of Total TEST, MD % %
20 Informatics Involvement CPOE usage report distributed monthly to include Order Source Hospitalist group questioned the overall number of written orders listed Charts randomly audited to determine usage of written orders by Hospitalist group Audit findings were that written orders generated by the hospitalist group were minimal to non-existent
21 Informatics Involvement Hospitalist group concerned with artificial deflation or negative bias on CPOE use rate metrics Requested that a systematic root cause analysis be conducted on order sources Analyses into the cause of order source misattribution determined that misuse of order source by nursing and ancillary were leading contributors to misattribution
22 Method to Complete Root Cause Analysis Focus on written orders exclusively attributed to Hospitalist group Written orders undetected by clinicians Hospitalists are unable to reject written orders misattributed to them Assessed for incorrect order source for a 1 month period
23 Method to Complete Root Cause Analysis Samples of selected month s orders were processed using analytical software and CPOE system data warehouse tool Each order was assessed and the order source attribution validated Orders validated by reviewing medical records or by the use of electronic audit trail Responsible parties for misattributed written orders were identified
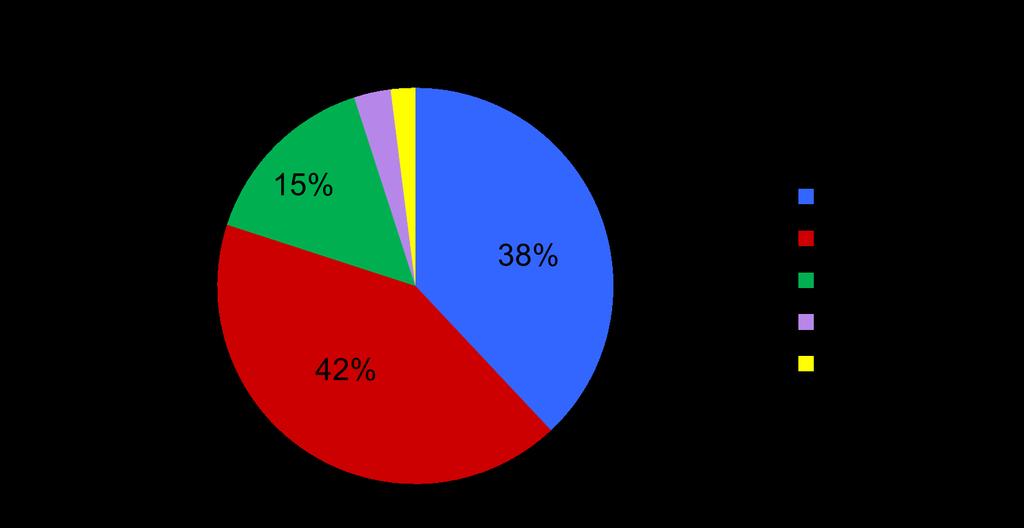
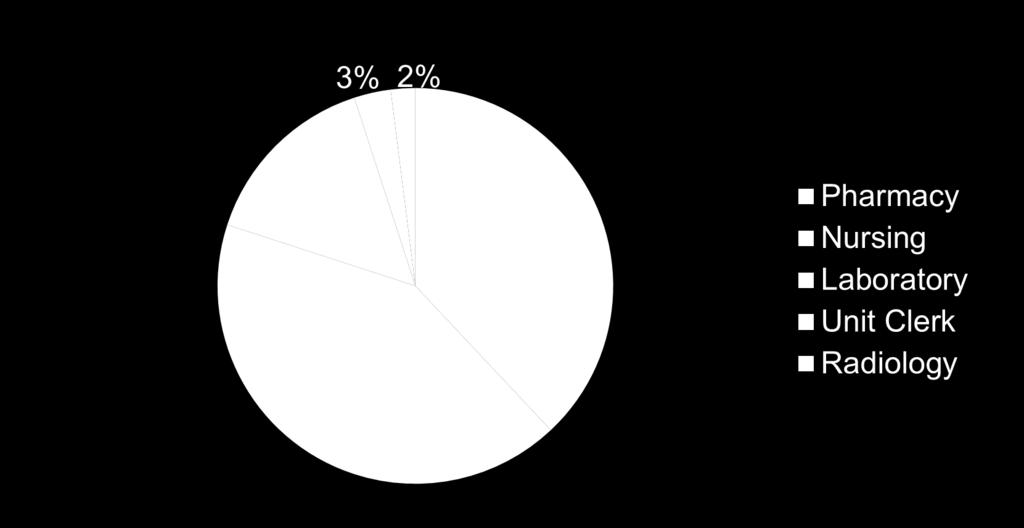
24 Misattribution Sources Identified by Group

25 Data Analysis Initial analysis identified 525 possible written orders that were attributed inaccurately to the sample providers group during the 1 month analysis period:
26 Reasons for CPOE Misattribution Illegible Signature: Pharmacy unable to determine signature on written order and used attending provider s name to process order Incorrect Provider: wrong provider entered at time of order Order Edited: original order placed by provider, then end user edited the order Telephone Order: end-user took telephone order and wrote the order on paper (orders written and scanned to Pharmacy are considered written)
27 Reasons for CPOE Misattribution Stat Order Edit: provider ordered procedure STAT, end-user edited and changed order Entry Error: error caused by duplicates entered by end-user No Electronic Order: select orders remain on paper, such as TPN No Order: no electronic or written order shown UTD: unable to determine source or cause of misattribution


28 Analysis for Incorrect Order Source Data analysis revealed 49% of misattributions were caused by incorrect order source selection Each was investigated to determine the correct order source

29 Use Rate Reporting Impact for Sample Group Sampled provider group s adjusted CPOE percentage -- By removing inaccurate written orders, group s CPOE monthly use rate increased by 4.1% A significant improvement in rate performance accuracy:
30 Impact of Misattribution on Physician Contract Management and Fulfillment Case Illustration: Hospitalist group had minimum acceptable CPOE use rates defined in group contract (e.g., 85% minimum) Incentive payments were to be paid for stretch performance objectives, for e.g., > 90% use rates for entire facility hospitalist group Group achieved 87% monthly reported use rates, but suspected misattribution, primarily from paper orders (unit clerks/nurses will attribute to a hospitalist when physician signature illegible due to their high order volume)
31 Impact of Misattribution on Physician Contract Management and Fulfillment Significant risk of hospitalists becoming demoralized due to inability to achieve payment incentives for actual 90+% CPOE performance A major political and operational liability given group s critical care role Once actual misattribution level was quantified (4% month over month), we were able to adjust performance expectations accordingly
32 Impact of Misattribution on Physician Contract Management and Fulfillment When hospitalists achieved 86% group CPOE use rate for a month, a 4% misattribution margin was added so their net performance was 90%+ Hospitalists could earn the group payment incentives they actually deserved
33 Actions to Prevent Misattribution End-users instructed to file and exit CPOE system when entering orders Daily monitoring of order entry by nursing and ancillary leadership Order Source Job Aid revamp to highlight examples of correct source and consequences when using the incorrect order source

34 Job Aid to Prevent Misattribution

35 Job Aid to Prevent Misattribution
36 Actions to Prevent Misattribution Order Source Job Aid used for recurrent periodic education of nursing and ancillary staff, focusing on the importance of preventing misattribution Correct use of Electronic Health Record data filters in the business intelligence software that generates CPOE use rates
37 Actions to Prevent Misattribution Review of additional workflows and processes with each department to identify source and magnitude of order misattributions Establishment of additional neutral order sources for operational orders, as well as conditional orders that could result in new orders
38 Conclusions Significant CPOE order misattribution may occur in a typical community general hospital Magnitude of order misattribution can be substantial, and important when performance metrics and payment incentives include CPOE performance Initial analysis identified 525 possible written orders were attributed inaccurately during a 1 month analysis period We uncovered a 4.1% misattribution rate among a sample group of important, high volume providers (e.g., hospitalists)
39 Conclusions Multiple departments may be the source of misattributions including nursing, pharmacy, ancillary and other non-providers Misattribution complicates the measurement of physician compliance with CPOE, particularly where minimum performance targets or objectives have been established in physician contracts Can also cause troubling frustrations among key physician groups incented to achieve stretch performance objectives but unable to due to misattribution
40 Conclusions Order source misattribution needs to be evaluated periodically in order to confirm validity and ensure physician end user trust of reported CPOE use rates Useful for facilities to conduct misattribution assessments periodically especially among high volume/high frequency CPOE using physicians Continuous ongoing efforts to prevent misattribution through education of source department personnel are imperative and needs to be supported by facility administrative and clinical leadership

41 Benefits Realized for the Value of Health IT S = Physicians endeavoring to adopt CPOE are deeply troubled by misattribution of orders to them. Reducing misattribution increases their confidence and satisfaction with individual CPOE use rate reporting. T = CPOE increases the safety of care delivery to patients, and so strong adoption by physicians is essential. Physicians who are dubious of their reported CPOE use due to order misattribution will be less willing to adopt CPOE. E = Order source attribution validation should eventually be automated within the EHR or enterprise data warehouse. This presentation will increase EHR and Business Intelligence vendors awareness of the significant negative impact of misattribution. P = CPOE facilitates provider engagement in care and population health. CPOE via evidence based clinical decision support improves clinical outcomes/quality and reduces error. S = Insofar as CPOE adoption reduces unnecessary diagnostic procedures, drug and other therapeutic use, it can yield savings in total care delivery.

42 Questions Linda Catzoela : linda.catzoela@christushealth.org George Gellert: ggellert33@gmail.com
Clinical Impact and Value of Workstation Single Sign-On. George A. Gellert, MD, MPH, MPA Associate CMIO, CHRISTUS Health San Antonio, Texas
 Clinical Impact and Value of Workstation Single Sign-On George A. Gellert, MD, MPH, MPA Associate CMIO, CHRISTUS Health San Antonio, Texas The Challenge: Providers using EHRs must maintain the security
Clinical Impact and Value of Workstation Single Sign-On George A. Gellert, MD, MPH, MPA Associate CMIO, CHRISTUS Health San Antonio, Texas The Challenge: Providers using EHRs must maintain the security
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Definition of Meaningful Use of Certified EHR Technology for Hospitals Approved by the HIMSS Board of Directors April 24, 2009
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 Definition of Meaningful Use of Certified EHR Technology for Hospitals Approved by
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 Definition of Meaningful Use of Certified EHR Technology for Hospitals Approved by
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Successful Clinical Process Redesign in a Connected Healthcare Community. Linus Diedling Allison Foley, MD Elliot Sternberg, MD Michelle Woodley, RN
 Successful Clinical Process Redesign in a Connected Healthcare Community Linus Diedling Allison Foley, MD Elliot Sternberg, MD Michelle Woodley, RN AGENDA Care Redesign from 3 Perspectives Chief Medical
Successful Clinical Process Redesign in a Connected Healthcare Community Linus Diedling Allison Foley, MD Elliot Sternberg, MD Michelle Woodley, RN AGENDA Care Redesign from 3 Perspectives Chief Medical
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Modified Stage 2 Meaningful Use: Objective #3 Computerized Provider Order Entry (CPOE) Massachusetts Medicaid EHR Incentive Payment Program
 Massachusetts Medicaid EHR Incentive Payment Program") Modified Stage 2 Meaningful Use: Objective #3 Computerized Provider Order Entry (CPOE) Massachusetts Medicaid EHR Incentive Payment Program July 7, 2016 Today s presenter: Al Wroblewski, PCMH CCE, Client
Modified Stage 2 Meaningful Use: Objective #3 Computerized Provider Order Entry (CPOE) Massachusetts Medicaid EHR Incentive Payment Program July 7, 2016 Today s presenter: Al Wroblewski, PCMH CCE, Client
Meaningful Use Is a Stepping Stone to Meaningful Care
 Meaningful Use Is a Stepping Stone to Meaningful Care Liz Johnson, RN-BC, MS, FCHIME, FHIMSS, CPHIMS Chief Clinical Informaticist and Vice President of Applied Clinical Informatics Tenet Healthcare Corporation
Meaningful Use Is a Stepping Stone to Meaningful Care Liz Johnson, RN-BC, MS, FCHIME, FHIMSS, CPHIMS Chief Clinical Informaticist and Vice President of Applied Clinical Informatics Tenet Healthcare Corporation
Automation and Information Technology
 4 Automation and Information Technology Positions Automation and Information Technology Ensuring Patient Safety and Data Integrity During Cyber-attacks (1701) To advocate that healthcare organizations
4 Automation and Information Technology Positions Automation and Information Technology Ensuring Patient Safety and Data Integrity During Cyber-attacks (1701) To advocate that healthcare organizations
INTEGRATED DATA ANALYTICS AND CARE WORKFLOW OPTIMIZATION
 INTEGRATED DATA ANALYTICS AND CARE WORKFLOW OPTIMIZATION CASE STUDY October 2016 1 AGENDA 1 2 3 INTRODUCTIONS Speaker and System 4 Q+A VALUE OF INTEGRATED DATA Why effective ACOs require EHR, Claims, and
INTEGRATED DATA ANALYTICS AND CARE WORKFLOW OPTIMIZATION CASE STUDY October 2016 1 AGENDA 1 2 3 INTRODUCTIONS Speaker and System 4 Q+A VALUE OF INTEGRATED DATA Why effective ACOs require EHR, Claims, and
Response to a Medication Error Tragedy and the Development of a Patient Safety Program. Dana-Farber Cancer Institute
 Response to a Medication Error Tragedy and the Development of a Patient Safety Program Dana-Farber Cancer Institute Institute of Medicine December 2010 Lawrence N Shulman, MD Chief Medical Officer and
Response to a Medication Error Tragedy and the Development of a Patient Safety Program Dana-Farber Cancer Institute Institute of Medicine December 2010 Lawrence N Shulman, MD Chief Medical Officer and
8/28/2014. Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Objectives of the Presentation
 Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Jerry Williamson MD. MJ. CHC. LHRM Objectives of the Presentation Definition of a Scribe Duties of a Scribe Regulatory
Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Jerry Williamson MD. MJ. CHC. LHRM Objectives of the Presentation Definition of a Scribe Duties of a Scribe Regulatory
End-to-end infusion safety. Safely manage infusions from order to administration
 End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
HIMSS 2011 Implementation of Standardized Terminologies Survey Results
 HIMSS 2011 Implementation of Standardized Terminologies Survey Results The current healthcare climate, with rising costs and decreased reimbursement, necessitates fiscal responsibility. Elements of the
HIMSS 2011 Implementation of Standardized Terminologies Survey Results The current healthcare climate, with rising costs and decreased reimbursement, necessitates fiscal responsibility. Elements of the
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Development and Implementation of a New Process for Handling Add-On Lab Orders at Duluth Clinic Ashland
 Development and Implementation of a New Process for Handling Add-On Lab Orders at Duluth Clinic Ashland Submitted by Pam Helgeson-Britton Director of Process Excellence & Organizational Productivity SMDC
Development and Implementation of a New Process for Handling Add-On Lab Orders at Duluth Clinic Ashland Submitted by Pam Helgeson-Britton Director of Process Excellence & Organizational Productivity SMDC
Value of HIT. Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017
 Value of HIT Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017 Value of HIT Value Score Pat Wise RN, MA, MS, FHIMSS COL (USA ret'd) Vice President, Health Information Systems Objectives
Value of HIT Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017 Value of HIT Value Score Pat Wise RN, MA, MS, FHIMSS COL (USA ret'd) Vice President, Health Information Systems Objectives
Tying It All Together: Informatics In Action
 Tying It All Together: Informatics In Action Sherri Hess, MS-IS, BSN, RN, Director of Nursing Informatics, Denver Health System Andrew Steele, MD, MPH, CMIO, Denver Health System Denver Health Integrated
Tying It All Together: Informatics In Action Sherri Hess, MS-IS, BSN, RN, Director of Nursing Informatics, Denver Health System Andrew Steele, MD, MPH, CMIO, Denver Health System Denver Health Integrated
Health Management Information Systems
 Health Management Information Systems Computerized Provider Order Entry (CPOE) Computerized Provider Order Entry (CPOE) Learning Objectives 1. Describe the purpose, attributes and functions of CPOE 2.
Health Management Information Systems Computerized Provider Order Entry (CPOE) Computerized Provider Order Entry (CPOE) Learning Objectives 1. Describe the purpose, attributes and functions of CPOE 2.
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance
 Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012
 A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
2. What is the main similarity between quality assurance and quality improvement?
 Chapter 6 Review Questions 1. Quality improvement focuses on: a. Individual clinicians or system users b. Routine measurement of performance c. Information technology issues d. Constant training 2. What
Chapter 6 Review Questions 1. Quality improvement focuses on: a. Individual clinicians or system users b. Routine measurement of performance c. Information technology issues d. Constant training 2. What
Evidence to Support Application of a Usability Assessment Tool for Nursing Documentation
 Janette Coble, MS, BSN, RN Staff Nurse, Neuroscience St. Louis Children s Hospital jcc6154@bjc.org Evidence to Support Application of a Usability Assessment Tool For Nursing Documentation Janette Coble,
Janette Coble, MS, BSN, RN Staff Nurse, Neuroscience St. Louis Children s Hospital jcc6154@bjc.org Evidence to Support Application of a Usability Assessment Tool For Nursing Documentation Janette Coble,
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Nursing Glue is the Magic to Make Things Work
 Nursing Glue is the Magic to Make Things Work Daniela Mahoney, RN danielamahoney@hisorg.com Improving workflow and patient outcomes through customized EHR consulting. CSOHIMSS 2008 Slide 1 Objectives Status
Nursing Glue is the Magic to Make Things Work Daniela Mahoney, RN danielamahoney@hisorg.com Improving workflow and patient outcomes through customized EHR consulting. CSOHIMSS 2008 Slide 1 Objectives Status
2011 Summer Institute in Nursing Informatics The Tenet Story
 2011 Summer Institute in Nursing Informatics The Tenet Story Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC VP of Applied Clinical Informatics HHS Health Information Technology Standards Committee Member Modern
2011 Summer Institute in Nursing Informatics The Tenet Story Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC VP of Applied Clinical Informatics HHS Health Information Technology Standards Committee Member Modern
Achieving HIMSS Level 7 Implications for HIM. Children s Health System of Texas
 Achieving HIMSS Level 7 Implications for HIM Children s Health System of Texas Katherine Lusk, MHSM, RHIA Chief Health Information Management & Exchange Officer Children s Health SM Four Campuses, 562
Achieving HIMSS Level 7 Implications for HIM Children s Health System of Texas Katherine Lusk, MHSM, RHIA Chief Health Information Management & Exchange Officer Children s Health SM Four Campuses, 562
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Electronic Physician Documentation: Increased Satisfaction
 Electronic Physician Documentation: Increased Satisfaction Session 222, February 23, 2017 Robert (Bob) Diamond, Sr. Vice President / CIO, Health Quest Kshitij (Tij) Saxena, MD, CMIO, Health Quest 1 Speaker
Electronic Physician Documentation: Increased Satisfaction Session 222, February 23, 2017 Robert (Bob) Diamond, Sr. Vice President / CIO, Health Quest Kshitij (Tij) Saxena, MD, CMIO, Health Quest 1 Speaker
Eligible Professional Core Measure Frequently Asked Questions
 Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
Eligible Professional Core Measure Frequently Asked Questions CPOE for Medication Orders 1. How should an EP who orders medications infrequently calculate the measure for the CPOE objective if the EP sees
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
MACRA Frequently Asked Questions
 Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
Qualifying for Medicare Incentive Payments with Crystal Practice Management. Version 1.0
 Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Disclosures. Relevant Financial Relationship(s): Nothing to Disclose. Off Label Usage: Nothing to Disclose 6/1/2017. Quality Indicators
: Nothing to Disclose. Off Label Usage: Nothing to Disclose 6/1/2017. Quality Indicators") Laurie Griesmann, Quality Specialist May 17, 2017 Disclosures Relevant Financial Relationship(s): Nothing to Disclose Off Label Usage: Nothing to Disclose 1 Objectives Define a quality indicator. Recognize
Laurie Griesmann, Quality Specialist May 17, 2017 Disclosures Relevant Financial Relationship(s): Nothing to Disclose Off Label Usage: Nothing to Disclose 1 Objectives Define a quality indicator. Recognize
Best Practices and Performance Measures for Systemic Treatment Computerized Prescriber Order Entry Systems (ST CPOE) in Chemotherapy Delivery
 in Chemotherapy Delivery") Best Practices and Performance Measures for Systemic Treatment Computerized Prescriber Order Entry Systems (ST CPOE) in Chemotherapy Delivery Dr. Vishal Kukreti, MD, FRCPC, MSc Clinical Lead, Systemic
Best Practices and Performance Measures for Systemic Treatment Computerized Prescriber Order Entry Systems (ST CPOE) in Chemotherapy Delivery Dr. Vishal Kukreti, MD, FRCPC, MSc Clinical Lead, Systemic
Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016
 Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016 Norris, Susan, Ph.D., Chief Clinical Officer, InfoMC Daniels, Allen S., Ed.D., Clinical Director,
Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016 Norris, Susan, Ph.D., Chief Clinical Officer, InfoMC Daniels, Allen S., Ed.D., Clinical Director,
Hardwiring Technology into Care Delivery to Increase HCAHPS
 Hardwiring Technology into Care Delivery to Increase HCAHPS March 1, 2016 Peggy Grant, Ph.D. Director of Innovation and Performance Improvement Community Regional Medical Center Conflict of Interest Peggy
Hardwiring Technology into Care Delivery to Increase HCAHPS March 1, 2016 Peggy Grant, Ph.D. Director of Innovation and Performance Improvement Community Regional Medical Center Conflict of Interest Peggy
A Better Prescription for Reducing Medication Errors and Maximizing the Value of Clinical Decision Support
 Clinical Drug Information A Better Prescription for Reducing Medication Errors and Maximizing the Value of Clinical Decision Support Medication errors are defined as preventable events that occur during
Clinical Drug Information A Better Prescription for Reducing Medication Errors and Maximizing the Value of Clinical Decision Support Medication errors are defined as preventable events that occur during
Minnesota Adverse Health Events Measurement Guide
 Minnesota Adverse Health Events Measurement Guide Prepared for the Minnesota Department of Health Revised December 2, 2015 is a nonprofit organization that leads collaboration and innovation in health
Minnesota Adverse Health Events Measurement Guide Prepared for the Minnesota Department of Health Revised December 2, 2015 is a nonprofit organization that leads collaboration and innovation in health
MEDICATION USE EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014
 TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
Text-based Document. Advancing Nursing Informatics to Improve Healthcare Quality and Outcomes. Authors Sensmeier, Joyce E.
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013
 GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
2011 Electronic Prescribing Incentive Program
 2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
2011 Electronic Prescribing Incentive Program Hardship Codes In 2012, the physician fee schedule amount for covered professional services furnished by an eligible professional who is not a successful electronic
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence
 PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
Bad Data s Effect on Population Health Performance
 Session #180: Bad Data s Effect on Population Health Performance Wednesday April 15, 2015 1-2pm Bill Gillis Chief Information Officer DISCLAIMER: The views and opinions expressed in this presentation are
Session #180: Bad Data s Effect on Population Health Performance Wednesday April 15, 2015 1-2pm Bill Gillis Chief Information Officer DISCLAIMER: The views and opinions expressed in this presentation are
Core Item: Clinical Outcomes/Value
 Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Patient Safety It All Starts with Positive Patient Identity APRIL 14, 2016
 Patient Safety It All Starts with Positive Patient Identity APRIL 14, 2016 Maximizing patient safety and improving the quality of care is the ultimate goal for healthcare providers. Doing so requires staying
Patient Safety It All Starts with Positive Patient Identity APRIL 14, 2016 Maximizing patient safety and improving the quality of care is the ultimate goal for healthcare providers. Doing so requires staying
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Belgian Meaningful Use Criteria for Mental Healthcare Hospitals and other non-general Hospitals
 Belgian Meaningful Use Criteria for Mental Healthcare Hospitals and other non-general Hospitals Introduction This document is the result the conclusion of the WG Belgian Meaningful Use Criteria for Mental
Belgian Meaningful Use Criteria for Mental Healthcare Hospitals and other non-general Hospitals Introduction This document is the result the conclusion of the WG Belgian Meaningful Use Criteria for Mental
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers
 Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers HIMSS Stage 7: What it Means Heart of America HIMSS and the Missouri Health Information Management Association
Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers HIMSS Stage 7: What it Means Heart of America HIMSS and the Missouri Health Information Management Association
Cloning and Other Compliance Risks in Electronic Medical Records
 Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy The MERU, HSE (2013)
 and in Radiotherapy The MERU, HSE (2013)") Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy 2010-2012 The MERU, HSE (2013) CONTENT Executive summary.. 2 Introduction 3 Incidents reported in
Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy 2010-2012 The MERU, HSE (2013) CONTENT Executive summary.. 2 Introduction 3 Incidents reported in
Meaningful Use and PCC EHR. Tim Proctor Users Conference 2017
 Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Informatics, PCMHs and ACOs: A Brave New World
 Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs. September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto
 2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
Paragon Clinician Hub for Physicians (PCH) Reference
 Reference") Paragon Clinician Hub for Physicians (PCH) Reference Logging in to the Clinician Hub Paragon Clinician Hub (PCH) is available on any Carroll Hospital Network. VMWare View must be utilized to open the application.
Paragon Clinician Hub for Physicians (PCH) Reference Logging in to the Clinician Hub Paragon Clinician Hub (PCH) is available on any Carroll Hospital Network. VMWare View must be utilized to open the application.
1. What are the requirements for Stage 1 of the HITECH Act for CPOE to qualify for incentive payments?
 CPPM Chapter 8 Review Questions 1. What are the requirements for Stage 1 of the HITECH Act for CPOE to qualify for incentive payments? a. At least 30% of the medications in the practice must be ordered
CPPM Chapter 8 Review Questions 1. What are the requirements for Stage 1 of the HITECH Act for CPOE to qualify for incentive payments? a. At least 30% of the medications in the practice must be ordered
eprescribe Training for Nurses and Pharmacy Techs Net Access Home Medication Pathway Clinical Informatics - Oct 2015
 eprescribe Training for Nurses and Pharmacy Techs Net Access Home Medication Pathway Clinical Informatics - Oct 2015 Click Home Medications on the Navigator Home Medications Pathway Click on Select Default
eprescribe Training for Nurses and Pharmacy Techs Net Access Home Medication Pathway Clinical Informatics - Oct 2015 Click Home Medications on the Navigator Home Medications Pathway Click on Select Default
Maintaining Excellence in Physician Nurse Communication with CPOE: A Nursing Informatics Team Approach
 Maintaining Excellence in Physician Nurse Communication with CPOE: A Nursing Informatics Team Approach Mary J. Wright, RN, MN, BC; Keith Frey, MD, MBA; Jeffery Scherer, MBA; and Debra Hilton, RN A B S
Maintaining Excellence in Physician Nurse Communication with CPOE: A Nursing Informatics Team Approach Mary J. Wright, RN, MN, BC; Keith Frey, MD, MBA; Jeffery Scherer, MBA; and Debra Hilton, RN A B S
The Value of Nursing Informatics. Julie D Luengas, RN-BC, BSN, MBA, FHIMSS
 The Value of Nursing Informatics Julie D Luengas, RN-BC, BSN, MBA, FHIMSS Objectives Define integration strategies to improve Quality Identify opportunities to improve workflow optimization with automated
The Value of Nursing Informatics Julie D Luengas, RN-BC, BSN, MBA, FHIMSS Objectives Define integration strategies to improve Quality Identify opportunities to improve workflow optimization with automated
2012 National Patient Safety Goals and National Priorities Partnership Goals addressed in this case study
 (ROI) University of California Davis Health System 2315 Stockton Blvd., Sacramento, CA 95817 Noel Sousa Finance Director noel.sousa@ucdmc.ucdavis.edu Michael Smith Financial Analyst michael.smith@ucdmc.ucdavis.edu
(ROI) University of California Davis Health System 2315 Stockton Blvd., Sacramento, CA 95817 Noel Sousa Finance Director noel.sousa@ucdmc.ucdavis.edu Michael Smith Financial Analyst michael.smith@ucdmc.ucdavis.edu
OHTAC Recommendation. Implementation and Use of Smart Medication Delivery Systems
 OHTAC Recommendation Implementation and Use of Smart Medication Delivery Systems July 2009 Background The Ontario Health Technology Advisory Committee (OHTAC) engaged the University Health Network s (UHN)
OHTAC Recommendation Implementation and Use of Smart Medication Delivery Systems July 2009 Background The Ontario Health Technology Advisory Committee (OHTAC) engaged the University Health Network s (UHN)
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Insights as a Service. Balaji R. Krishnapuram Distinguished Engineer, Director of Analytics, IBM Watson Health
 Insights as a Service Balaji R. Krishnapuram Distinguished Engineer, Director of Analytics, IBM Watson Health Data & Knowledge Explosion: New data about individuals, used in new ways helps determines health
Insights as a Service Balaji R. Krishnapuram Distinguished Engineer, Director of Analytics, IBM Watson Health Data & Knowledge Explosion: New data about individuals, used in new ways helps determines health
HIMSS Submission Leveraging HIT, Improving Quality & Safety
 HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
The Colorado ALTO Project
 Using Alternatives to Opioids (ALTOs) in Hospital Emergency Departments PRE-LAUNCH CHECKLIST Based on the 2017 Opioid Prescribing & Treatment Guidelines Colorado ALTO Project Champion Sets the direction
Using Alternatives to Opioids (ALTOs) in Hospital Emergency Departments PRE-LAUNCH CHECKLIST Based on the 2017 Opioid Prescribing & Treatment Guidelines Colorado ALTO Project Champion Sets the direction
Medical Assistant Credentialing Requirements for Your Client Practices. Eric Christensen Director of Client Services Healthcare Compliance Pros, Inc.
 Requirements for Your Client Practices Eric Christensen Director of Client Services Healthcare Compliance Pros, Inc. Requirements for Your Client Practices As of January 2013, under CMS guidelines, only
Requirements for Your Client Practices Eric Christensen Director of Client Services Healthcare Compliance Pros, Inc. Requirements for Your Client Practices As of January 2013, under CMS guidelines, only
Achieving Organizational Excellence Through Health
 Achieving Organizational Excellence Through Health IT @JohnHDaniels Objectives Identify the various HIMSS Awards and their focus Determine the challenges and the opportunities of affecting organizational
Achieving Organizational Excellence Through Health IT @JohnHDaniels Objectives Identify the various HIMSS Awards and their focus Determine the challenges and the opportunities of affecting organizational
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
Using Electronic Health Records for Antibiotic Stewardship
 Using Electronic Health Records for Antibiotic Stewardship STRENGTHEN YOUR LONG-TERM CARE STEWARDSHIP PROGRAM BY TRACKING AND REPORTING ELECTRONIC DATA Introduction Why Use Electronic Systems for Stewardship?
Using Electronic Health Records for Antibiotic Stewardship STRENGTHEN YOUR LONG-TERM CARE STEWARDSHIP PROGRAM BY TRACKING AND REPORTING ELECTRONIC DATA Introduction Why Use Electronic Systems for Stewardship?
Quick Guide to A3 Problem Solving
 Quick Guide to A3 Problem Solving What is it? Toyota Motor Corporation is famed for its ability to relentlessly improve operational performance. Central to this ability is the training of engineers, supervisors
Quick Guide to A3 Problem Solving What is it? Toyota Motor Corporation is famed for its ability to relentlessly improve operational performance. Central to this ability is the training of engineers, supervisors
Building a healthy legacy together. Presentation by Shelley Lipon, Executive Regional Director, Canada Health Infoway to ICTAM October 28, 2009
 Building a healthy legacy together Presentation by Shelley Lipon, Executive Regional Director, Canada Health Infoway to ICTAM October 28, 2009 Expectations What Canadians expect from their health care
Building a healthy legacy together Presentation by Shelley Lipon, Executive Regional Director, Canada Health Infoway to ICTAM October 28, 2009 Expectations What Canadians expect from their health care
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
Toward the Electronic Patient Record:
 June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
Is there an impact of Health Information Technology on Delivery and Quality of Patient Care?
 Is there an impact of Health Information Technology on Delivery and Quality of Patient Care? Amanda Hessels, PhD, MPH, RN, CIC, CPHQ Nurse Scientist Meridian Health, Ann May Center for Nursing 11.13.2014
Is there an impact of Health Information Technology on Delivery and Quality of Patient Care? Amanda Hessels, PhD, MPH, RN, CIC, CPHQ Nurse Scientist Meridian Health, Ann May Center for Nursing 11.13.2014
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Overview. Overview 01:55 PM 09/06/2017
 01:55 PM Inactive No Effective Date Date of Last Change 07/16/2017 08:34:13.108 AM Job Profile Name Director of Clinical Quality Informatics for Regulatory Performance- Enterprise Job Profile Summary Job
01:55 PM Inactive No Effective Date Date of Last Change 07/16/2017 08:34:13.108 AM Job Profile Name Director of Clinical Quality Informatics for Regulatory Performance- Enterprise Job Profile Summary Job
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using A Data Warehouse and Analytics to Drive Population Health Management
 Success Story Using A Data Warehouse and Analytics to Drive Population Health Management HEALTHCARE ORGANIZATION Large Medical Center TOP RESULTS Enabled pay-for-performance (P4P) incentive payment reporting
Success Story Using A Data Warehouse and Analytics to Drive Population Health Management HEALTHCARE ORGANIZATION Large Medical Center TOP RESULTS Enabled pay-for-performance (P4P) incentive payment reporting
How can oncology practices deliver better care? It starts with staying connected.
 How can oncology practices deliver better care? It starts with staying connected. A system rooted in oncology Compared to other EHRs that I ve used, iknowmed is the best EHR for medical oncology. Physician
How can oncology practices deliver better care? It starts with staying connected. A system rooted in oncology Compared to other EHRs that I ve used, iknowmed is the best EHR for medical oncology. Physician
Ontario Shores Journey to EMRAM Stage 7. October 21, 2015
 Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Reducing Infections and Improving Engagement St. Luke's Nephrology Associates. Contact Information: Robert Gayner, M.D., FASN
 BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
Licensed Pharmacy Technicians Scope of Practice
 Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Rules Based Orders. Good For Your Practice Today. And Tomorrow
 Rules Based Orders Good For Your Practice Today And Tomorrow Pat Wolfram Liaison Healthcare Director EMR-to-Lab Integration 971-255-9282 pwolfram@liaison.com What We ll Cover Today Adding Order Intelligence
Rules Based Orders Good For Your Practice Today And Tomorrow Pat Wolfram Liaison Healthcare Director EMR-to-Lab Integration 971-255-9282 pwolfram@liaison.com What We ll Cover Today Adding Order Intelligence
Successful disease management requires technology that can measure progress, show gaps
 Successful disease management requires technology that can measure progress, show gaps The days of health insurance payers relying on fee-for-service models to pay for healthcare services are rapidly fading.
Successful disease management requires technology that can measure progress, show gaps The days of health insurance payers relying on fee-for-service models to pay for healthcare services are rapidly fading.
GE Healthcare. Meaningful Use 2014 Prep: Core Part 1. Ramsey Antoun, Training Operations Coordinator December 12, 2013
 GE Healthcare Meaningful Use 2014 Prep: Core Part 1 Ramsey Antoun, Training Operations Coordinator December 12, 2013 2013 General Electric Company All rights reserved. This does not constitute a representation
GE Healthcare Meaningful Use 2014 Prep: Core Part 1 Ramsey Antoun, Training Operations Coordinator December 12, 2013 2013 General Electric Company All rights reserved. This does not constitute a representation