Impact of performance-based financing on primary health care services in Haiti
|
|
|
- Mitchell Quinn
- 6 years ago
- Views:
Transcription
1 Impact of performance-based financing on primary health care services in Haiti Wu Zeng, MD, MS, PhD*, Marion Cros, MA, MS**, Katherine M. Dilley, MPH**, Donald S. Shepard, PhD* * Schneider Institutes for Health Policy, Heller School, Brandeis University ** Center for Health Services, Management Sciences for Health, 784 Memorial Dr., Cambridge, MA Corresponding author: Donald S. Shepard, Schneider Institutes for Health Policy, Heller School, MS035, Brandeis University, Waltham, MA USA, shepard@brandeis.edu; Tel: ; Fax: Length: Abstract: 299 words; text: 5,490 words (excluding tables, figures, and references) Keywords: performance-based financing, health financing, primary health care, maternal-child health services, Haiti Abbreviated running title: Performance-based financing in Haiti 1
2 Key messages: The addition of performance-based incentives to training and technical assistance for 27 nongovernmental health facilities in Haiti increased key services over a three-year period by 39% more than training and technical assistance alone. For children under age one and pregnant women, the increases in services were statistically significant and large (1.7 to 2.2 times the baseline rates). Incentives proved more effective and substantially less expensive than training and technical assistance alone. 2
3 Abstract To strengthen Haiti s primary health care (PHC) system, the country first piloted performance-based financing (PBF) in 1999 and subsequently expanded the approach to most internationally funded non-government organizations. PBF complements support (training and technical assistance). This study evaluates a) the separate impact of PBF and international support on PHC s service delivery; b) the combined impact of PBF and technical assistance on PHC s service delivery; and c) the costs of PBF implementation in Haiti. To minimize the risk of facilities neglecting potential non-incentivized services, the incentivized indicators were randomly chosen at the end of each year. We obtained quantities of key services from four departments for 217 health centers (15 with PBF and 202 without) from 2008 through 2010, computed quarterly growth rates, and analyzed the results using a difference-in-differences approach by comparing the growth of incentivized and non-incentivized services between PBF and non-pbf facilities. To interpret the statistical analyses, we also interviewed staff in four facilities. Whereas international support added 39% to base costs of PHC, incentive payments added only 6%. Support alone increased the quantities of PHC services over three years by 35% (2.7%/quarter). However, support plus incentives increased these amounts by 87% over three years (5.7%/quarter) compared to facilities with neither input. Incentive alone was associated with a net 39% increase over this period, and more than doubled the growth of services (p<0.05). Interview findings found no adverse impacts and, in fact, indicated beneficial impacts on quality. Incentives proved to be a relatively inexpensive, well accepted, and a very effective complement to support, suggesting that a small amount of money, strategically used, can substantially improve PHC. Haiti s experience, after more than a decade of use, indicates that incentives are an effective tool to strengthen PHC. 3
4 Introduction To help meet the Millennium Development Goals in developing countries and improve the quality and efficiency of health care in industrialized countries, policymakers have implemented pay-for-performance (P4P), performance-based financing (PBF) or performancebased incentives (PBI) in health systems. The Performance-Based Incentives Working Group at the Center for Global Development defines PBF/PBI as the transfer of money or material goods from a funder or other supporter to a recipient, conditional on the recipient taking a measurable action or achieving a predetermined performance target (Eichler et al. 2009). The goal of tying payment to performance is to promote hard work, innovation, and improvements along specified dimensions. In developing countries, performance of facilities operating under a PBF scheme is often measured by the quantities of essential services (e.g., vaccinations or prenatal care) provided to vulnerable populations, while sometimes also including indicators of quality of care. Major international donors, such as the World Health Organization, the World Bank, and the United States Agency for International Development (USAID) have supported projects with PBF elements (Soeters et al. 2011; The AIDSTAR-Two Project 2011). A rigorous randomized trial from Rwanda reported favorable results (Basinga et al. 2011). Other applications of this approach, in many cases with apparently favorable results, occurred in Afghanistan, Burundi, Cambodia, Democratic Republic of the Congo, Haiti, Kenya, Liberia, Sudan, and Uganda (Rusa et al. 2009; Sabri et al. 2007; Soeters et al. 2006). Concurrent increases in resources or poorly controlled evaluations, however, often confounded the interpretation of existing experience. Additionally, policy makers are advised to look for potential adverse effects, such as neglecting non-incentivized services, reducing quality of care, expensive monitoring structures, and short lived benefits, and to encourage more controlled evaluations in a variety of contexts (Ireland et al. 2011). This evaluation from Haiti seeks to address these concerns. Haiti is one of the least developed countries in the world, ranking 145th out of 169 countries in the United Nations Human Development Index (United Nations Development Programme 2010). While the performance of Haiti s health system is improving, the country still ranks worst in health indicators in the Western Hemisphere. In 2008, the infant mortality rate was 61 per 1,000 live births in comparison with global average of 43 and regional average of 20. The under-five years of age mortality rate was 87 per 1,000 births, which is higher than the global average (80) and regional average (18). The maternal mortality ratio was 300 deaths per 100,000 live births, while the regional and global average maternal mortality ratios are 66 and 260, respectively (World Health Organization 2008). The main causes of death in children under age five are acute respiratory infection, and pneumonia in particular, as well as diarrheal diseases (World Health Organization 2006). The three-year United Nations sanctioned embargo from 1991 to 1994 left Haiti with a weak health system and an underserved population. Primary health care (PHC) became a key priority and the strategic focus of Haiti s National Health Policy, published in 1996 and revised in 1999 (Ministère de la Sante Publique et de la Population 1999). 4
5 PBF was initiated in 1999 in three health facilities of nongovernmental organizations (NGOs) delivering PHC services through the Santé pour le Développement et la Stabilité d Haïti (SDSH) Project implemented by Management Sciences for Health (MSH) and funded by USAID. The preliminary evaluation showed great success from PBF, with a substantial increase in rates of completely vaccinated children and of prenatal care among pregnant women (Eichler et al. 2001). MSH then scaled up the PBF initiative, and, by 2005, all 29 NGOs supported by USAID were operating under a PBF scheme. An evaluation in 2009 found that NGO health facilities enrolled in the scheme performed better than those in the rest of Haiti in complete immunization coverage, prenatal care, assisted deliveries, and postnatal care (Eichler et al. 2001; Eichler and Levine 2009). The tenets of the MSH PBF scheme include regular, accurate, and timely monitoring and reporting; technical assistance to organizations to help them understand, set, and meet targets; suggestions for corrective actions if goals are not met; and an innovative mechanism of selecting incentivized indicators. MSH s support (technical assistance and training) includes procurement procedures, minor renovations to the facilities, and advice on community mobilization, communication, public relations, and promotion of family planning. This evaluation examines the PBF scheme in place through 2010, which applied to all NGOs served by SDSH. This scheme paid a varying percentage of budgeted spending (the expected cost of delivery of a full package of services based on historical costs of service delivery) to each contracted NGO each year based on its performance on the selected indicators. Each year, MSH worked with each NGO to set targets and incentives for candidate services based on the organization s historical performance and to agree on the budget. MSH disbursed 95% of budgeted funding to NGOs on a quarterly basis after receiving required information from them (e.g. data reporting and action plan), and kept 5% of budgeted funding as incentives. Thus the NGO received lowest percentage (95%) of its budgeted funding if it met none of its service targets and the highest percentage (105%) if it achieved all the targeted goals set by SDSH by the end of each year. The budgeting assumed that, on average, a facility would earn 50% of this possible 10 percentage points of bonus. For the study years, on average, facilities received 60% of their maximum bonus, corresponding to 6% of budgeted spending through incentives. The NGO had the discretion about how to use its bonus. While the amount of additional resources was modest, these incentives sought to focus the organization s attention on critical but underutilized PHC, such as vaccinations, prenatal and postnatal care, and institutional deliveries. To allow for timely assessment of NGOs performance, data were reported monthly by each facility to the MSH office in Port-au-Prince for monitoring and payment by MSH and, separately, by each facility to the department (provincial) office for incorporation into the country s health information system. The contract model, instituted before the start of the study period, randomly selects one indicator for payment in each category of services (such as HIV/AIDS or maternal health) just after the end of each year. Depending on services available in health facilities, there are often four to five indicators selected for actual payment. This approach prevents NGOs from knowing beforehand which services will be incentivized and neglecting non-incentivized services. It also reduces the likelihood that the NGOs will try to game the system by falsifying 5
6 data and minimizes administrative costs, as only data for the selected indicator need to be validated. Table 1 lists the potential indicators used in 2011 for incentives. <Insert Table 1 about here> While previous evaluations have described the design and initial functioning of PBF in Haiti (Eichler and Levine 2009; Eichler et al. 2001), facility-level data for a controlled evaluation were not previously available. This evaluation is the first to use data from Haiti s health information system, which became active in 2009, to evaluate PBF. As suggested by Ireland et al. (2011), several contextual factors in Haiti should be noted. First, PBF operates in a sophisticated, multi-layered environment within which the contracting NGOs often have multiple sites, with multiple health care providers at each site. Second, since training and technical assistance are prominent features of the SDSH project, we hypothesized that the incentives to facilities have had a synergistic effect, magnifying the interest of facility managers and providers in applying the lessons from the technical assistance and training. Finally, because incentives had been integrated into facility operations and financing for over 11 years by the end of the evaluation period, we hypothesized that incentives augmented the facilities ability to improve their output, resulting in a higher compound growth rate. Compounded over time, changes in growth rates, if found, would be very powerful effects. To reflect these factors, this evaluation covers the maximum period (three-years) available from Haiti s health information system and combines quantitative and qualitative methods. This evaluation addresses these issues through a controlled design comparing PBF and control facilities (which were conventionally funded via cost reimbursement or fixed budget). In all, this study aims to assess for the period from 2008 through 2010: (a) the separate impact of PBF and technical assistance on delivery of PHC services; (b) the combined impact of technical assistance and PBF on service delivery; and (c) the costs of PBF implementation. Methods Quantitative component. The earthquake on Jan. 12, 2010 destroyed the Ministry of Health building, other national computers, and much of Haiti s West department (which includes Port-au-Prince, where the earthquake was centered, and which accounted for 40% of total NGO facilities (31 out of 77) and 7% of total public facilities (5 out of 70) supported by SDSH in Haiti in Therefore, the quantitative component of this study relied on health information system at the department (provincial) level data in Haiti from 2008 through Our analysis included data from all the 217 health facilities in four departments (Northeast, North, South, and Central). Of these facilities, 15 were implementing PBF (all NGO facilities), while the remaining 202 facilities were not (a mix of public and NGO facilities with a majority of public ones). The public facilities were often different from NGO facilities in terms of less autonomy and flexibility in resource allocation and management, etc. This data set was independent of the one MSH used for determining incentive payments. It is important to note 6
7 that the loss of quantitative data from the West department may have resulted in our underestimating the impact of technical assistance as well as PBF because the West department probably received more rigorous monitoring and evaluation. To assess the quality of departmental data, at least for health facilities that implement PBF, we obtained a data set from the MSH Haiti office consisting of volumes of services for the same years for the same 15 SDSH-supported facilities. As MSH conducted data verification periodically to avoid over-reporting of service provision from health centers by interviewing a small sample of patients, we hypothesized that the data from MSH were reported accurately. Thus the consistency checking of the data from department and MSH would allow us to examine the quality of department data for implementing analyses. From the 48 indicators in the MSH data set, we identified the following four, which were also in the data from the health information system: number of DPT vaccinations, number of completely vaccinated children, number of women receiving their third prenatal visit, and number of women delivering in a health institution. We created a validation index defined as the ratio of difference (Source1 Source2) to the mean over all facilities of Source1, where Source1 is data from departments (government system) and Source2 represents data from MSH. Table 2 shows the means and standard deviations of indicators from the two sources, as well as the validation index. These findings show that the data are reasonably accurate. The median values are zero and the mean differences are small fractions, below 15% in magnitude. Furthermore, the signs of the differences do not reveal systematic bias. Whereas the MSH data were higher for three indicators (number of completely vaccinated children, number of DPT vaccinations, number of women receiving their third prenatal visit), they were lower for the fourth indicator (institutional delivery). The high standard deviation reflects the presence of a few outliers for each indicator, where the greatest upper outliers showed deviations of 11, 8, 7, and 5 times the mean. <Insert Table 2 about here> Our quantitative analysis examined the most robust available PHC service indicators: all types of consultations (i.e. generic) for children under 1 year of age, children aged 1 4, children aged 5 14, pregnant women, and adults excluding pregnant women. The PBF scheme pays providers primarily based on indicators related to maternal-child health, such as vaccinations, prenatal, and postnatal care. We did not include HIV/AIDS services in the analysis because many health centers did not provide those services. We created two summary indexes: one for potentially incentivized services (consultations for children under age 1, aged 1 4, and pregnant women) and one for non-incentivized services (consultations for children aged 4 15, and other adults). In both descriptive and regression analyses we used quarterly, rather than annual observations, to increase statistical power. To control for the individual health facility effects, 7
8 we used a random-effects model after controlling for seasonal (quarterly) variation and time trends, as follows: log( services) it = b0 + b1 PBFi + b2 timet + b3pbfi * timet + B4 quarter t + α + ε i it where i denotes the health facility and t is time (i.e., the number of quarters, where 1 is the first quarter of 2008). The dependent variables (log services) are the natural logarithms of the volumes of the categories of services provided by health facilities. PBF is a dummy variable indicating whether the health facility was implementing PBF or not (0 for no and 1 for yes), and time is coded from 1 to 12 to measure the time trend in quarters. The key variable is the interaction term between PBF and time, which shows the differential growth rate between PBF and non-pbf facilities. This variable indicates the net impact of PBF. The variable quarter is a vector of three dummy variables to adjust for seasonal variation, with the first quarter (January through March) as the reference group. The variableα is the individual health facility effect, and ε is random error. To separate the effect of incentives from technical assistance and it training offered to all sites, we compared the coefficients of interaction terms between incentivized and non-incentivized services, using a seemingly unrelated regression. This difference indicates the pure effect of the incentives. Using both the difference-in-difference approach as well as random-effects model would alleviate the concerns regarding the comparability between control and PBF facilities in evaluating the effect of PBF. Qualitative study. The qualitative study consisted of 12 interviews in four PBF NGOs based in the West Department in Haiti. The sample of NGOs was selected based on geography, varied levels of performance, security, and proximity to Port-au-Prince. Geography: All four interview sites were in the West Department, where 31% of health facilities in Haiti are located. MSH sponsors 27 NGOs in Haiti, which provide health services in 77 health delivery points. Of the 77 health delivery points, 31 are located in the West (Ministère de la Sante Publique et de la Population 2005). Varied levels of performance: Discussions with NGOs achieving different levels of performance allowed us to capture information about both the weaknesses and strengths of the PBF policy. We selected two low-performing NGOs (i.e., attaining less than 80% of the maternal and child health target indicators), and two high-performing sites (attaining at least 80% of these indicators) based on 2010 performance. Security: All the sites were in secure (relatively safe) regions to allow the research team to conduct interviews at the health delivery points run by the NGOs. Proximity to Port-au-Prince: All the sites visited were within a one- to two-hour drive from Port-au-Prince. A four-member research team with expertise in public health and health service research conducted interviews, with at least two members present for each interview. Each interview lasted one hour on average. Most interviews were performed in French. All subjects were told that their participation was voluntary and that individual responses would remain confidential. Six respondents were NGO managers or senior management staff, and six were managers of service delivery points or medical staff. As neither the qualitative nor quantitative i 8
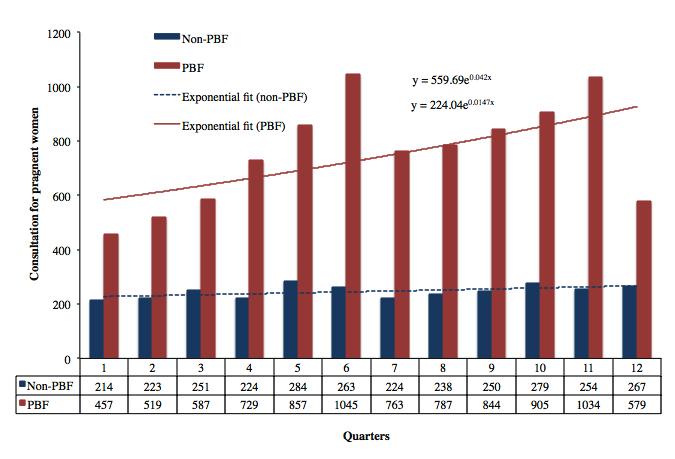
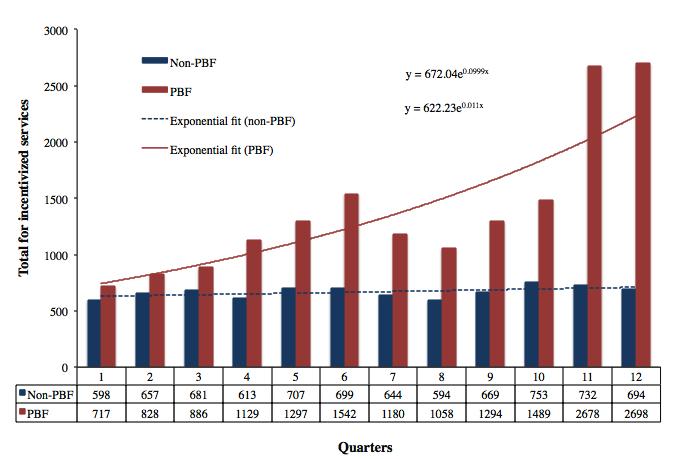
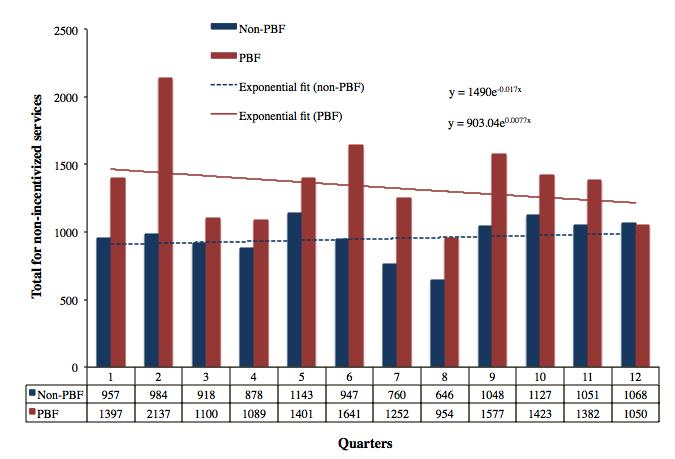
9 components entailed obtaining or accessing patient-level data, the study was not considered human studies research. Results Quantitative study. To illustrate the data for an individual service, Figure 1 shows the average number of consultations for pregnant women by quarter. The fitted (ordinary leastsquares) trend line indicates that the rate of growth of this service in PBF facilities (4.2%/quarter) exceeded that in non-pbf facilities (1.5%/quarter), but there is substantial variability from one quarter to the next. Other individual services (not shown here) exhibited similar tends and variability. <Figure 1 about here> These trends have to be interpreted with caution, however. First, we have data only for 12 quarters. Second, the service volumes are substantially higher during the last two quarters in PBF facilities; these observations may have raised the growth rate in the intervention group. Third, the sample size for the intervention group is small, with only 15 facilities. With a much smaller sample size than the control group of 202, the averages of PBF facilities are less stable. Figures 2 and 3 graph the summary indexes for incentivized services and nonincentivized services. As expected, the summary index for incentivized services shows a higher growth rate of 10.0%/quarter in PBF-implementing facilities, compared to 1.1%/quarter in non- PBF-implementing facilities. The corresponding summary for non-incentivized services show the opposite pattern from the incentivized services: a higher growth rate of 0.8%/quarter in the non-pbf-implementing facilities versus -1.7%/quarter in PBF-implementing facilities. <Figure 2 about here> <Figure 3 about here> Table 3 summarizes the regression results from the random effects models. PBF increased utilization of consultations for children under age 1 by 9.4%/quarter, 5.7%/quarter for children aged 1 4, and 4.0%/quarter for pregnant women. While the consultations for children 5 14 also increased, we did not find higher utilization for consultation for other adults. In sum, the incentivized services grew by 5.7%/quarter, while the non-incentivized services grew by 2.7%/quarter. When we compared the growth rates between incentivized and non- 9
10 incentivized services, the difference of 3.0%/quarter was statistically significant (p = 0.05, Chi square = 3.71). <Insert Table 3 about here> The cumulative effect of these growth rates over the three-year period of analysis is shown in Figure 4. Over the three years, the incentivized services grew by 87%, indicating the combined effect of incentives and the strengthened monitoring and technical assistance. The non-incentivized services grew by 35%, reflecting the strengthened monitoring and technical assistance. Thus, the estimated pure effect of the incentives (3.0%/quarter) led to a cumulative 39% improvement over the three-year period. <Figure 4 about here> As shown in the descriptive results, quarters 11 and 12 may contain some outliers. Table 4 shows the use of the data in the first 10 quarters to conduct the sensitivity analysis for the regression results. After excluding the last two quarters from the analysis, the positive growth rate for incentivized services, such as consultation for children under age one and pregnant women, remains statistically significant, while the growth rate for services that were not incentivized showed no statistical difference. <Insert Table 4 about here> The summary index shows a growth rate of 5.3%/quarter for incentivized services and no statistical significance for non-incentivized services (3.4%/quarter), in spite of a positive trend toward encouraging utilization of services. However, the difference in growth rates between the two types of facilities of 1.9%/quarter is not statistically significant (p = 0.24, Chi square = 1.38). Thus, non-incentivized services did not perform significantly lower than incentivized services. Qualitative study. Overall, the qualitative study identified several contributors to the improvement in incentivized services at PBF facilities, especially better management, higher accountability for results, and increased staff motivation. Management and technical staff interviewed at NGOs had a good understanding of the PBF system. The medical staff had excellent knowledge of the target indicators they were supposed to achieve, but they did not always link them with the bonus that NGOs would 10
11 receive from SDSH. Discussions with NGOs and health care providers indicated that a sound monitoring system was in place for reporting to SDSH in conjunction with the PBF mechanisms. The bonus (up to 10% of a contract s budgeted amount) was usually redistributed by NGOs at the facility level. In some cases, the bonus was used to upgrade health facilities and mobile health clinics. In other cases, the NGO provided individual incentives to medical staff based on their performance in order to motivate them. They rewarded community health workers (termed health agents) and medical staff by organizing parties, providing small gifts, and presenting certificates of performance. Interviews at the management and service delivery levels showed that PBF improved the coverage of services and revealed no instances of adverse quality impacts and several beneficial changes. For example, PBF reportedly encouraged NGO staff to be proactive in encouraging women and children to visit the clinic for recommended services and to internalize a sense of accountability for their work. Most NGOs have seen positive effects from PBF at the service delivery level because it has led to more effective management, through systematic planning and monitoring. In addition, the bonus policy and target indicators make medical staff more accountable for results. Resources. To interpret the magnitudes of incentive payments, it is useful to relate them to other budget categories. The SDSH project years that most closely match the time period of this evaluation are its basic period of August 3, 2007 through August 2, According to the SDSH summary budget for 2009, the budget for direct costs of services by MSH over those three years totaled US$47.65 million. The average annual budget of $15.88 million per year consists of $11.07 million (70%) for contracted health facilities (NGOs and public facilities in target zones), and $4.81 million (30%) consumed by MSH for support (monitoring and technical assistance). The payments to health facilities can be decomposed into basic amounts ($10.44 million) and the budget for potential award fees or incentives (estimated at 6% of the basic amount, or $0.63 million). Of the amounts spent by MSH on internal costs, project managers attribute approximately 85% ($4.09 million) to support, while the remaining 15% ($0.72 million) went to project administration. MSH provides technical support and training to maintain or improve quality of services and organizational development support for strengthening the health system elements required for effective health service delivery, including the areas of leadership and governance, health management information system, service organization, health care workforce, financial management, and drug management. In SDSH supported sites, technical assistance often consists of two fulltime technical and financial officers in each of the 10 districts. Technical and financial officers are respectively responsible for 3 to 5 SDSH supported sites and assist district health authorities in monitoring sites health outputs, implementing new health programs and managing their finances. On a monthly basis, SDSH headquarter monitoring unit assesses the health outputs of the Minimum Package of Services components (e.g. HIV/AIDS/TB, reproductive and sexual health, and nutrition and child Health) across all supported sites. In addition, SDSH headquarter technical units (e.g. HIV/AIDS/TB, reproductive health, child health, capacity building/training unit) provide support in upgrading protocols and standards of the 11
12 Minimum Package of Services and implementing them among supported sites through, among other activities, trainings. All these activities raise awareness of facility staff on resource management and target of health outputs, and contribute to better performance in SDSH supported sites. These breakdowns show that the budget for support was 39.2% of the basic costs. Current levels of incentives are small in relation to both basic and support costs, and support costs more than six times that for incentives. In terms of staffing, the project has about 60 technical staff based in Port-au-Prince or in departments. Together, they support 66 organizations (27 NGOs and 39 public facilities) across the country. By all measures, the resources for training and technical assistance are substantial. The synergistic value of incentives in reinforcing the application of this support is potentially very large. Discussion Consistent with PBF evaluations in other countries, such as Rwanda and the Democratic Republic of Congo (Basinga et al. 2011; Soeters et al. 2011), our results show that PBF has led to the improvement of health care delivery in Haiti. As noted, with both incentives and support, PHC services increased by 87% over three years, whereas with support alone, the change was only 35%. As the effects are multiplicative, PBF alone was associated with a net 39% increase (i.e., 1.87/1.35 1) over this period.. We found that improvements related to the use of PBF were particularly associated with the utilization of services for children under age one and for pregnant women. This was not surprising, since the major services utilized by these two population groups, such as vaccinations, prenatal and postnatal care, and attended delivery, are the key indicators tied to incentives. The interviews found that PBF was valued by all staff at health facilities. As indicated in the previous evaluation, facilities receiving PBF enjoy more flexibility in spending these payments compared to revenues from cost-based reimbursement, which requires carefully justified expenditures (Eichler and Levine 2009). Under PBF, NGOs were able to negotiate their budgets, provide services at known prices, and receive reimbursement quarterly. Thus, incentives offered health facilities greater autonomy to allocate their budgets. Incentives also encouraged staff at all levels of the NGOs, from service providers to senior managers, to pay attention to the facility s performance indicators, thereby strengthening facility management. The facility director generally assigned targets to community health workers, convened routine meetings, monitored and evaluated staff members performance, and formulated strategies to help staff to face challenges in meeting the targets. Those behavioral and management changes induced by PBF were critical drivers for improving the performance of health facilities. Rwanda has been widely cited for its effective PBF scheme (Ireland et al. 2011). An important difference between Rwanda s and Haiti s PBF schemes is the way in which payments are distributed. Unlike Rwanda, where the payments are linked to units of service (e.g., 12
13 payment of $0.09 for an initial prenatal visit), Haiti s payment scheme was attached to targeted coverage of maternal child services. The payment mechanism in Haiti may help mitigate concerns that health providers focus too much on services with high payment rates (e.g., attended delivery in Rwanda) and neglect those with lower rates (Basinga et al. 2011). Haiti s innovation of randomly selecting indicators for monitoring and evaluation appeared to further address this concern. Among the specific incentivized services, we did not find a statistically significant impact of PBF on services for children aged 1 4, for whom the key services are follow-up vaccinations, providing vitamin A, monitoring nutrition status, and treatment of pneumonia and diarrhea. One explanation is that compared to the services for children less than 1 year old and pregnant women, some of these services for children aged 1 4 may be regarded as less critical by service providers. As expected, we did not find a statistically significant impact of PBF on the two indicators for non-incentivized services: consultations for children aged 5 14 years, and consultations for other adults. But these results also point in a positive direction with higher growth rates in PBF-implementing facilities. The improvement is possibly due to three factors: First, the beneficial management innovations and technical assistance incorporated into PBF systems encourage provision of more services. Second, with the improvements in key services for children under five and pregnant women, health facilities are gaining greater trust by the communities they serve, and more people, in turn, are more willing to seek care in these health facilities. Third, incentivized services may spill over into non-incentivized services. For example, treatment of sexually transmitted infections, a potentially incentivized indicator, may encourage subsequent adult consultations, a non-incentivized indicator. As of 2012, PBF has been implemented in Haiti for 13 years since the pilot study in 1999 and for 7 years since the scale-up in Unless the use of PBF expands to more health facilities, the current growth rate does not indicate that there will be a continued positive trend in the future, since demand may become saturated. In 2011, MSH, with the support from the Government of Haiti, expanded the PBF scheme to more public health facilities, starting with those that needed the resources most. As of April 2012, there were 81 private and 79 public facilities under the PBF scheme, covering 42% of total population in Haiti. The Government of Haiti has decided to develop the capacity to pay incentives to public facilities directly, and will be working with USAID, the World Bank, and MSH to develop a system to integrate PBF programs (for public and private facilities) that are operational in all 10 departments. With more health facilities in the PBF scheme, several policy initiatives would be helpful to maintain the momentum of PBF in improving utilization and the quality of medical services. First, as some services may be saturated after many years of implementation of PBF, it would be beneficial to include more indicators on quality of services for the payment of incentives. Second, expansion of customized contracts with NGOs may serve the growing diversity of participating NGOs (e.g., in terms of stage of development and type of ownership). Some NGOs may not provide HIV/AIDS services, so the percentage of incentives for meeting each target must be adjusted compared to NGOs providing all potential incentivized medical services. Third, the inclusion of the demand side (e.g. community based health insurance) incentives is likely to enhance the effect of PBF in increasing the use of under- 13
14 utilized services to achieve MDGs, as has been found elsewhere (Shepard et al. 2012; Palmer et al. 2004). Limitations of the study. Several limitations must be acknowledged. First, our quantitative data could examine only the quantity, and not the quality of services. However, financial incentives were modest and generally indirect and the qualitative comments of those interviewed identified no adverse effects and suggested some potential improvements to quality. Therefore, we do not think this limitation was serious. Second, our control group (facilities with neither PBF nor support) consisted primarily of public facilities, and might have differed in some systematic way from the incentivized facilities. Two techniques use of longitudinal data for estimating the effect of PBF and use of difference-in-difference to isolate the effect of incentives helped us to adjust for both baseline and systematic differences between PBF and non-pbf facilities. As SDSH targeted poor-performing health facilities for implementing PBF since the scale up in 2005, our methodology may have underestimated the impact of PBF. Third, the data in the control group were not verified, and thus we were not able to assess the quality of the reporting in those health centers. If there were a systematic overreporting of service delivery in health centers in the control group, we may be underestimating the impact of the PBF. Fourth, although our sample of 15 PBF health faculties accounts for 37.5% of the total of 40 PBF health facilities supported by SDSH in the four departments, the sample size of 15 is small from a statistical perspective, which results in a higher probability of type II errors and the lack of statistical significance for some services that were hypothesized to be statistically significant, such as consultations for children aged 1-4. Conclusions Despite the absence of a standard policy on the distribution of incentives to direct care providers, this study found enthusiasm about incentives at all levels. Overall, the incentives seem to work synergistically with technical assistance under the PBF scheme. While modest incentives were associated with notable growth rates in incentivized services, slightly higher incentives and more frequent disbursement would likely strengthen the impact even more. Given the current low share of incentives in the total budget and their high impact, we recommend doubling incentives to an average of 10% of basic costs. We also recommend that incentives be paid quarterly rather than annually. This would make the incentives payment consistent with SDSH s current disbursement schedule for basic services and provide more frequent reinforcement. We recommend that facilities be sure to distribute a portion of the incentives to its staff, so they personally receive benefit from their extra work. This distribution should apply to health workers at all levels, especially the lower levels. The health agents (community health workers), the lowest paid workers, have a critical role in encouraging vulnerable populations to seek services and would likely respond very favorably to receiving a portion of the incentives directly. In conclusion, this study suggests that appropriately designed PBF incentive systems helped hold health facilities and staff accountable for the outputs that are directly related to beneficial outcomes. Hence, this mechanism is likely to accelerate progress toward the Millennium Development Goals (Montagu et al. 2011) to reduce child and maternal mortality. 14
15 References Basinga P, Gertler PJ, Binagwaho A, et al Effect on maternal and child health services in Rwanda of payment to primary health-care providers for performance: an impact evaluation. Lancet, 377: Eichler R, Auxila P, Pollock J Output-based health care: Paying for performance in Haiti. Public Policy in the Private Sector, Note 236: World Bank. Online at: Eichler R, Levine R Performance Incentives for Global Health: Potential and Pitfalls. Washington, DC: Center for Global Development. Online at: Ireland M, Paul E, Dujardin B Can performance-based financing be used to reform health systems in developing countries? Bulletin of the World Health Organization, 89: Ministère de la Sante Publique et de la Population Politique Nationale de la Sante d'haïti. Port-au-Prince, Haiti: Ministère de la Sante Publique et de la Population, République d'haïti. Ministère de la Sante Publique et de la Population Liste des Institutions Sanitaires. Portau-Prince, Haiti: Ministère de la Sante Publique et de la Population, République d'haïti. Montagu D, Yamey G Pay-for-performance and the Millennium Development Goals. Lancet, 377: Palmer N, Mueller DH, Gilson L, Mills A, Haines A Health financing to promote access in low income settings-how much do we know? Lancet, 364: Rusa L, Ngirabega Jde D, Janssen W, et al Performance-based financing for better quality of services in Rwandan health centres: 3-year experience. Tropical Medicine and International Health, 14: Sabri B, Siddiqi S, Ahmed AM, Kakar FK, Perrot J Towards sustainable delivery of health services in Afghanistan: options for the future. Bulletin of the World Health Organization, 85: Shepard DS, Zeng W, Amico P, Rwiyereka AK, Avila-Figueroa C A controlled study of funding for human immunodeficiency virus/acquired immunodeficiency syndrome as resource capacity building in the health system in Rwanda. The American journal of tropical medicine and hygiene, 86:
16 Soeters R, Habineza C, Peerenboom PB Performance-based financing and changing the district health system: experience from Rwanda. Bulletin of the World Health Organization, 84: Soeters R, Peerenboom BP, Mushagalusa P, Kimanuka C Performance-based financing experiment improved health care in the Democratic Republic of Congo. Health Affairs, 30: The AIDSTAR-Two Project The PBF Handbook: Designing and Implementing Effective Performance-Based Financing Programs, Version 1.0. Cambridge, MA: Management Sciences for Health. Online at: United Nations Development Programme Human Development Report. New York: United Nations Development Programme. Online at: World Health Organization Mortality Country Fact Sheet Online at: World Health Organization Haiti's Health Profile. Geneva: World Health Organziation. Online at: 16
17 Table 1. List of potential indicators for incentives by dimension Number Description I. Child health services Percentage of children under 5 years affected in nutrition programs (children 1 weighed) 2 Percentage of children 6-59 months who received at least one dose of Vitamin A 3 Percentage of children <1 year who received complete diphtheria, pertussis, tetanus (DTP3) vaccination II. Maternal health services 4 Percentage of pregnant women for whom the birth plan was prepared at the first prenatal visit 5 Percentage of pregnant women attending the first prenatal visit in the first trimester 6 Percentage of new mothers who received a postnatal home follow-up visit in the range of 0-3 days after delivery 7 Percentage of pregnant women who received three antenatal care visits 8 Percentage of new mothers who received a postnatal visit III. HIV/AIDS services 9 Number of people tested for HIV 10 Number of pregnant women tested for HIV IV. TB detection 11 Number of new TB cases detected by sputum 12 Number of TB cases tested for HIV V. Quality of services 13 Self-perceived quality of services at health centers 14 medical waste treatment meets the standards of MSPP 17
18 Table 2. Summary statistics for four indicators for validation Mean±SD Health-facility Indicators quarter-year (Department data) (MSH data) (validation index) periods (N) Complete vaccination 46.67± ± ± Key vaccination dose a 53.74± ± ± Three prenatal care visits 38.98± ± ± Institutional delivery 18.29± ± ± a Third dose of diphtheria-pertussis-tetanus vaccine (to children). SD denotes standard deviation Table 3. Differences in growth rates between PBF and non-pbf facilities (PBF Non-PBF facilities) from the random-effects regression models Service (consultation for) Difference in growth rates Z value P value Children < 1 9.4%*** Children %*** Pregnant women 4.0%* Children %* Other adults 2.8% All incentivized services 5.7%*** Non-incentivized services 2.7% Notes: * denotes p < 0.05, ***denotes p < 0.001; the number of observations is 1,
19 Table 4. Sensitivity analyses of differences in growth rates between PBF and non-pbf facilities (PBF Non-PBF facilities) Service (consultation for) Difference in growth rates Z value P value Children < 1 7.7%*** Children % Pregnant women 5.7%* Children % Other adults 4.5% Incentivized services 5.3%*** Non-incentivized services 3.4% Notes: * denotes p <0.05, *** denotes p <0.001; the number of observations is 1,466 19
20 Legend for figures: Figure 1. Average number of consultations for pregnant women (incentivized services) by non- PBF (n=202) and PBF facilities (n=15), Figure 2. Average number for total incentivized services by non-pbf (n=202) and PBF facilities (n=15), Figure 3. Average number for total non-incentivized services by non-pbf (n=202) and PBF facilities (n=15), Figure 4. Cumulative growth over three years (12 quarters) under alternative growth rates 20
21
22
23
24
25 APPENDIX Interview guide for NGO Management Level (CEO and Technical Director) Start Time of Interview: End Time: Recorder: YES NO Starting Year of PBF: Part I. General Questions Date of interview Position of interviewed person How long have you been in this position? Tell us about your background Name of the visited NGO Département Commune NGO s address Contact Information Phone number PART II. General Services What are the major diseases among the population served? What are the major services your facility is providing? HIV/AIDS (PMTCT, VCT) ARV ART TB Maternal Health (ANC, Delivery, PNC) Child health 21
26 (Immunization, Nutrition, Vitamin A, Diarrhea management, Pneumonia management) Reproductive Health and Family Planning (FP Counseling, LT FP, STI) How many service facilities/delivery points does your NGO support? Do they have a list of target indicators? Do you decide to breakdown the target indicators by facility? How do you monitor your staff s performance? How does your staff get paid? How do you split this list of target indicators by facility? How many facilities do you support? How do you monitor the quality of services? What proportion of your annual budget is provided through MSH? No Yes Part III. Performance-based Financing 1. How many facilities under this NGO are engaged in PBF? 2. On what date did this NGO first participate in PBF? Month Day Year 3. Did you receive a bonus for achieving targets or indicators? 4. What did you do to achieve this bonus payment? 5. If you received a bonus payment, how did you use it? What is the breakdown of the bonus? 6. What s percentage of bonus is kept by the NGO? 7. What s percentage of the bonus is allocated to facilities or delivery points 8. How do you decide to allocate the bonus across NGO and facility level? 9. Why have you decided to structure the bonus this way? 10. What do you get from structuring the bonus in this way? 22
27 Part III. Impact and Expectation 11. Since the introduction of PBF, can you list some of the ways in which improved operations of your facilities have led to improved health outcomes? 12. Could you please provide examples? (Please see the questions below to guide the interviewee) 12.1 Before the PBF, how did you monitor the performance of the providers? (Management) 12.2 Did you use the bonus to buy equipment? 12.3 Did you use the bonus to motivate your staff? Did it help them to provide more services? 12.4 How has PBF affected management, inputs, outputs, process, motivation of staff, leadership, coordination among staff, and quality of services? 13. What are some of the challenges that your NGO have faced? 14. What are some of the solutions your NGO use to address these challenges? 15. Did you use PBF as a response to address these challenges? 16. What are the main successes of your NGO? 17. Was PBF one contributor to this success? 18. How you categorize your experience with PBF? 19. Do you have any recommendations to improve the management of PBF? 23
28 Interview guide for the Financial Administrator / Manager at NGO level Part I. Personal information 1. Title 2. How long have you been in this position? 3. What is your background? 4. What is your contact information? Phone Part II. Financing of the health center 5. What percentage of the health center s funding comes from MSH? What are other sources of funding? Please list the sources and amount of the funding, starting from the year of PBF implementation to the date of the interview. Does this NGO maintain financial reports? 6. Are there any major in-kind donations? If so specify or give examples. 7. How has the funding been distributed? E.g. What percentage is used at the NGO and at the delivery level? What percentage is used for services provision? What percentage is used for salary of staff, and what percentage is for purchasing new facilities in the most recent time period? 8. How has the PBF been distributed? E.g. What percentage is used at the NGO and at the delivery level? What percentage is used for services provision? What percentage is used for salary of staff, and what percentage is for purchasing new facilities in the most recent time period. Part III. Payment 9. How do you get paid? 10. Are there any incentives associated with your performance or that of your colleagues in your department? 11. How does the NGO evaluate your performance? Part IV. Impact and Expectation 12. What is the impact of PBF on the financial health of the overall NGO management? 13. Could you please provide examples? 14. Since you have been a staff member, when was the most difficult time for the NGO financially? 15. How did your NGO manage that period? 16. Did PBF help address this financial difficulty? 17. What are the main successes of your NGO? 24
Performance-based financing (PBF) has been used
 has been used") January 2017 PERFORMANCE-BASED FINANCING IMPROVES QUANTITY AND QUALITY OF HEALTH SERVICES IN HAITI Photo by Colin Gilmartin Performance-based financing (PBF) has been used increasingly to improve the quantity
January 2017 PERFORMANCE-BASED FINANCING IMPROVES QUANTITY AND QUALITY OF HEALTH SERVICES IN HAITI Photo by Colin Gilmartin Performance-based financing (PBF) has been used increasingly to improve the quantity
Performance-based financing for better quality of services in Rwandan health centres: 3-year experience
 Tropical Medicine and International Health doi:10.1111/j.1365-3156.2009.02292.x volume 14 no 7 pp 830 837 july 2009 Performance-based financing for better quality of services in Rwandan health centres:
Tropical Medicine and International Health doi:10.1111/j.1365-3156.2009.02292.x volume 14 no 7 pp 830 837 july 2009 Performance-based financing for better quality of services in Rwandan health centres:
In recent years, the Democratic Republic of the Congo
 January 2017 PERFORMANCE-BASED FINANCING IMPROVES HEALTH FACILITY PERFORMANCE AND PATIENT CARE IN THE DEMOCRATIC REPUBLIC OF THE CONGO Photo by Rebecca Weaver/MSH In recent years, the Democratic Republic
January 2017 PERFORMANCE-BASED FINANCING IMPROVES HEALTH FACILITY PERFORMANCE AND PATIENT CARE IN THE DEMOCRATIC REPUBLIC OF THE CONGO Photo by Rebecca Weaver/MSH In recent years, the Democratic Republic
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
UHC. Moving toward. Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
QUALITY OF CARE IN PERFORMANCE-BASED INCENTIVES PROGRAMS
 QUALITY OF CARE IN PERFORMANCE-BASED INCENTIVES PROGRAMS MOZAMBIQUE CASE STUDY April 2016 This case study was funded by the United States Agency for International Development under Translating Research
QUALITY OF CARE IN PERFORMANCE-BASED INCENTIVES PROGRAMS MOZAMBIQUE CASE STUDY April 2016 This case study was funded by the United States Agency for International Development under Translating Research
Democratic Republic of Congo
 World Health Organization Project Proposal Democratic Republic of Congo OVERVIEW Target country: Democratic Republic of Congo Beneficiary population: 8 million (population affected by the humanitarian
World Health Organization Project Proposal Democratic Republic of Congo OVERVIEW Target country: Democratic Republic of Congo Beneficiary population: 8 million (population affected by the humanitarian
Microbicides Readiness Assessment Tool A tool for diagnosing and planning for the introduction of microbicides in public-sector health facilities
 Microbicides Readiness Assessment Tool A tool for diagnosing and planning for the introduction of microbicides in public-sector health facilities BACKGROUND This tool is intended to help evaluate the extent
Microbicides Readiness Assessment Tool A tool for diagnosing and planning for the introduction of microbicides in public-sector health facilities BACKGROUND This tool is intended to help evaluate the extent
Appendix. We used matched-pair cluster-randomization to assign the. twenty-eight towns to intervention and control. Each cluster,
 Yip W, Powell-Jackson T, Chen W, Hu M, Fe E, Hu M, et al. Capitation combined with payfor-performance improves antibiotic prescribing practices in rural China. Health Aff (Millwood). 2014;33(3). Published
Yip W, Powell-Jackson T, Chen W, Hu M, Fe E, Hu M, et al. Capitation combined with payfor-performance improves antibiotic prescribing practices in rural China. Health Aff (Millwood). 2014;33(3). Published
RBF in Zimbabwe Results & Lessons from Mid-term Review. Ronald Mutasa, Task Team Leader, World Bank May 7, 2013
 RBF in Zimbabwe Results & Lessons from Mid-term Review Ronald Mutasa, Task Team Leader, World Bank May 7, 2013 Outline Country Context Technical Design Implementation Timeline Midterm Review Results Evaluation
RBF in Zimbabwe Results & Lessons from Mid-term Review Ronald Mutasa, Task Team Leader, World Bank May 7, 2013 Outline Country Context Technical Design Implementation Timeline Midterm Review Results Evaluation
Pay-for-performance experiments in health care. Mattias Lundberg, World Bank SIEF Regional Impact Evaluation Workshop Sarajevo, Bosnia September 2009
 Pay-for-performance experiments in health care Mattias Lundberg, World Bank SIEF Regional Impact Evaluation Workshop Sarajevo, Bosnia September 2009 Outline Background What s the problem? Agency and information
Pay-for-performance experiments in health care Mattias Lundberg, World Bank SIEF Regional Impact Evaluation Workshop Sarajevo, Bosnia September 2009 Outline Background What s the problem? Agency and information
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Report on the Pilot Survey on Obtaining Occupational Exposure Data in Interventional Cardiology
 Report on the Pilot Survey on Obtaining Occupational Exposure Data in Interventional Cardiology Working Group on Interventional Cardiology (WGIC) Information System on Occupational Exposure in Medicine,
Report on the Pilot Survey on Obtaining Occupational Exposure Data in Interventional Cardiology Working Group on Interventional Cardiology (WGIC) Information System on Occupational Exposure in Medicine,
Toward Development of a Rural Retention Strategy in Lao People s Democratic Republic: Understanding Health Worker Preferences
 Toward Development of a Rural Retention Strategy in Lao People s Democratic Republic: Understanding Health Worker Preferences January 2012 Wanda Jaskiewicz, IntraHealth International Outavong Phathammavong,
Toward Development of a Rural Retention Strategy in Lao People s Democratic Republic: Understanding Health Worker Preferences January 2012 Wanda Jaskiewicz, IntraHealth International Outavong Phathammavong,
The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England
 Report by the Comptroller and Auditor General The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England Ordered by the House of Commons to be printed 14 February 2000 LONDON:
Report by the Comptroller and Auditor General The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England Ordered by the House of Commons to be printed 14 February 2000 LONDON:
Acronyms and Abbreviations
 Redacted Acronyms and Abbreviations CES CIP FP ISDP MCHIP MOH NGO OFDA PHC PHCC PITC PPH USAID WES Central Equatoria State County Implementing Partner Family Planning Integrated Service Delivery Project
Redacted Acronyms and Abbreviations CES CIP FP ISDP MCHIP MOH NGO OFDA PHC PHCC PITC PPH USAID WES Central Equatoria State County Implementing Partner Family Planning Integrated Service Delivery Project
Working Paper Series
 The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
The Financial Benefits of Critical Access Hospital Conversion for FY 1999 and FY 2000 Converters Working Paper Series Jeffrey Stensland, Ph.D. Project HOPE (and currently MedPAC) Gestur Davidson, Ph.D.
Contracts and Grants between Nonprofits and Government
 br I e f # 03 DeC. 2013 Government-Nonprofit Contracting Relationships www.urban.org INsIDe this IssUe In 2012, local, state, and federal governments worked with nearly 56,000 nonprofit organizations.
br I e f # 03 DeC. 2013 Government-Nonprofit Contracting Relationships www.urban.org INsIDe this IssUe In 2012, local, state, and federal governments worked with nearly 56,000 nonprofit organizations.
Association of Fundraising Professionals State of Fundraising 2005 Report
 Association of Fundraising Professionals State of Fundraising 2005 Report For more information, contact Walter Sczudlo (wsczudlo@afpnet.org) Or Michael Nilsen (mnilsen@afpnet.org) Association of Fundraising
Association of Fundraising Professionals State of Fundraising 2005 Report For more information, contact Walter Sczudlo (wsczudlo@afpnet.org) Or Michael Nilsen (mnilsen@afpnet.org) Association of Fundraising
Managing Programmes to Improve Child Health Overview. Department of Child and Adolescent Health and Development
 Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
U.S. Funding for International Maternal & Child Health
 April 2016 Issue Brief U.S. Funding for International Maternal & Child Health SUMMARY The U.S. government has a long history of supporting international maternal and child health (MCH) efforts, including
April 2016 Issue Brief U.S. Funding for International Maternal & Child Health SUMMARY The U.S. government has a long history of supporting international maternal and child health (MCH) efforts, including
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
#HealthForAll ichc2017.org
 #HealthForAll ichc2017.org Rwanda Community Performance Based Financing David Kamanda Planning, Health Financing & Information System Rwanda Ministry of Health Outline Overview of Rwandan Health System
#HealthForAll ichc2017.org Rwanda Community Performance Based Financing David Kamanda Planning, Health Financing & Information System Rwanda Ministry of Health Outline Overview of Rwandan Health System
The Contribution of the Contract and Verification Agencies in the Improvement of Health Facility Governance in Burkina Faso
 The Contribution of the Contract and Verification Agencies in the Improvement of Health Facility Governance in Burkina Faso Zénab K. KOUANDA 1, Moussa KABORE 2, Abdoulaye SOROMOYE 3 1 Coordinator, Contract
The Contribution of the Contract and Verification Agencies in the Improvement of Health Facility Governance in Burkina Faso Zénab K. KOUANDA 1, Moussa KABORE 2, Abdoulaye SOROMOYE 3 1 Coordinator, Contract
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health
 Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Performance-based Incentives to Improve Health Status of Mothers and Newborns: What Does the Evidence Show?
 J HEALTH POPUL NUTR 2013 Dec;31(4) Suppl 2:S36-S47 ISSN 1606-0997 $ 5.00+0.20 INTERNATIONAL CENTRE FOR DIARRHOEAL DISEASE RESEARCH, BANGLADESH Performance-based Incentives to Improve Health Status of Mothers
J HEALTH POPUL NUTR 2013 Dec;31(4) Suppl 2:S36-S47 ISSN 1606-0997 $ 5.00+0.20 INTERNATIONAL CENTRE FOR DIARRHOEAL DISEASE RESEARCH, BANGLADESH Performance-based Incentives to Improve Health Status of Mothers
Voucher schemes in the health sector.
 Voucher schemes in the health sector. The experience of German Financial Cooperation. KfW Entwicklungsbank is a competent and strategic advisor on current development issues. Reducing poverty, securing
Voucher schemes in the health sector. The experience of German Financial Cooperation. KfW Entwicklungsbank is a competent and strategic advisor on current development issues. Reducing poverty, securing
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Common Errors on the T3010 related to fundraising costs. Know how to avoid them
 Common Errors on the T3010 related to fundraising costs Know how to avoid them 1 Focus of presentation Many errors that charities make in the reporting of their fundraising expenses on the T3010 occur
Common Errors on the T3010 related to fundraising costs Know how to avoid them 1 Focus of presentation Many errors that charities make in the reporting of their fundraising expenses on the T3010 occur
A Comparison of Job Responsibility and Activities between Registered Dietitians with a Bachelor's Degree and Those with a Master's Degree
 Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 11-17-2010 A Comparison of Job Responsibility and Activities between Registered Dietitians
Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 11-17-2010 A Comparison of Job Responsibility and Activities between Registered Dietitians
Community CCT in Indonesia The Generasi Project
 Community CCT in Indonesia The Generasi Project November 12 th, 2008 Junko Onishi jonishi@jhsph.edu Two Pilot Projects In 2007 GoI started two pilot projects: Household CCT the traditional model Quarterly
Community CCT in Indonesia The Generasi Project November 12 th, 2008 Junko Onishi jonishi@jhsph.edu Two Pilot Projects In 2007 GoI started two pilot projects: Household CCT the traditional model Quarterly
Analysis of Nursing Workload in Primary Care
 Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Contents. Acronyms Why Performance-based Incentives? What is PBI? Types of PBI programs...5
 Performance-BASED INCENTIVES Primer FOR usaid missions July 2010 Contents Acronyms...2 1. Why Performance-based Incentives?...3 1.1 What is PBI?...4 1.2 Types of PBI programs...5 2. What Should USAID
Performance-BASED INCENTIVES Primer FOR usaid missions July 2010 Contents Acronyms...2 1. Why Performance-based Incentives?...3 1.1 What is PBI?...4 1.2 Types of PBI programs...5 2. What Should USAID
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
Nursing skill mix and staffing levels for safe patient care
 EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
Selected Strategies to Improve Access to and Quality of Urban Primary Health Care. Abdullah Baqui, DrPH, MPH, MBBS Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Health System Analysis for Better. Peter Berman The World Bank Jakarta, Indonesia February 8, 2011 Based on Berman and Bitran forthcoming 2011
 Health System Analysis for Better Health System Strengthening Peter Berman The World Bank Jakarta, Indonesia February 8, 2011 Based on Berman and Bitran forthcoming 2011 Health Systems Analysis: Can be
Health System Analysis for Better Health System Strengthening Peter Berman The World Bank Jakarta, Indonesia February 8, 2011 Based on Berman and Bitran forthcoming 2011 Health Systems Analysis: Can be
Aboriginal Community Controlled Health Service Funding. Report to the Sector. Uning Marlina Judith Dwyer Kim O Donnell Josée Lavoie Patrick Sullivan
 Aboriginal Community Controlled Health Service Funding Report to the Sector Uning Marlina Judith Dwyer Kim O Donnell Josée Lavoie Patrick Sullivan Aboriginal Community Controlled Health Service (ACCHS)
Aboriginal Community Controlled Health Service Funding Report to the Sector Uning Marlina Judith Dwyer Kim O Donnell Josée Lavoie Patrick Sullivan Aboriginal Community Controlled Health Service (ACCHS)
MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW
 06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
In 2012, the Regional Committee passed a
 Strengthening health systems for universal health coverage In 2012, the Regional Committee passed a resolution endorsing a proposed roadmap on strengthening health systems as a strategic priority, as well
Strengthening health systems for universal health coverage In 2012, the Regional Committee passed a resolution endorsing a proposed roadmap on strengthening health systems as a strategic priority, as well
FMO External Monitoring Manual
 FMO External Monitoring Manual The EEA Financial Mechanism & The Norwegian Financial Mechanism Page 1 of 28 Table of contents 1 Introduction...4 2 Objective...4 3 The monitoring plan...4 4 The monitoring
FMO External Monitoring Manual The EEA Financial Mechanism & The Norwegian Financial Mechanism Page 1 of 28 Table of contents 1 Introduction...4 2 Objective...4 3 The monitoring plan...4 4 The monitoring
Uzbekistan: Woman and Child Health Development Project
 Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
REGIONAL COMMITTEE FOR AFRICA AFR/RC54/12 Rev June Fifty-fourth session Brazzaville, Republic of Congo, 30 August 3 September 2004
 WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR AFRICA ORGANISATION MONDIALE DE LA SANTE BUREAU REGIONAL DE L AFRIQUE ORGANIZAÇÃO MUNDIAL DE SAÚDE ESCRITÓRIO REGIONAL AFRICANO REGIONAL COMMITTEE FOR AFRICA
WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR AFRICA ORGANISATION MONDIALE DE LA SANTE BUREAU REGIONAL DE L AFRIQUE ORGANIZAÇÃO MUNDIAL DE SAÚDE ESCRITÓRIO REGIONAL AFRICANO REGIONAL COMMITTEE FOR AFRICA
Executive Summary. Rouselle Flores Lavado (ID03P001)
") Executive Summary Rouselle Flores Lavado (ID03P001) The dissertation analyzes barriers to health care utilization in the Philippines. It starts with a review of the Philippine health sector and an analysis
Executive Summary Rouselle Flores Lavado (ID03P001) The dissertation analyzes barriers to health care utilization in the Philippines. It starts with a review of the Philippine health sector and an analysis
Clarifications III. Published on 8 February A) Eligible countries. B) Eligible sectors and technologies
 Eligible countries. B) Eligible sectors and technologies") 5 th Call of the NAMA Facility Clarifications III Published on 8 February 2018 Contents A) Eligible countries...1 B) Eligible sectors and technologies...1 C) Eligible applicants...2 D) Eligible support
5 th Call of the NAMA Facility Clarifications III Published on 8 February 2018 Contents A) Eligible countries...1 B) Eligible sectors and technologies...1 C) Eligible applicants...2 D) Eligible support
Population Council, Bangladesh INTRODUCTION
 Performance-based Incentive for Improving Quality Maternal Health Care Services in Bangladesh Mohammad Masudul Alam 1, Ubaidur Rob 1, Md. Noorunnabi Talukder 1, Farhana Akter 1 1 Population Council, Bangladesh
Performance-based Incentive for Improving Quality Maternal Health Care Services in Bangladesh Mohammad Masudul Alam 1, Ubaidur Rob 1, Md. Noorunnabi Talukder 1, Farhana Akter 1 1 Population Council, Bangladesh
COUNTRY PROFILE: LIBERIA LIBERIA COMMUNITY HEALTH PROGRAMS JANUARY 2014
 COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
Global Health Evidence Summit. Community and Formal Health System Support for Enhanced Community Health Worker Performance
 Global Health Evidence Summit Community and Formal Health System Support for Enhanced Community Health Worker Performance I. Global Health Evidence Summits President Obama s Global Health Initiative (GHI)
Global Health Evidence Summit Community and Formal Health System Support for Enhanced Community Health Worker Performance I. Global Health Evidence Summits President Obama s Global Health Initiative (GHI)
Study of Enhanced Quality of Care Assessment Instruments in Senegal s Performance-Based Financing Program
 Study of Enhanced Quality of Care Assessment Instruments in Senegal s Performance-Based Financing Program Presenter: April Williamson, Program Officer, R4D Global Maternal and Newborn Health Conference
Study of Enhanced Quality of Care Assessment Instruments in Senegal s Performance-Based Financing Program Presenter: April Williamson, Program Officer, R4D Global Maternal and Newborn Health Conference
Healthy Eating Research 2018 Call for Proposals
 Healthy Eating Research 2018 Call for Proposals Frequently Asked Questions 2018 Call for Proposals Frequently Asked Questions Table of Contents 1) Round 11 Grants... 2 2) Eligibility... 5 3) Proposal Content
Healthy Eating Research 2018 Call for Proposals Frequently Asked Questions 2018 Call for Proposals Frequently Asked Questions Table of Contents 1) Round 11 Grants... 2 2) Eligibility... 5 3) Proposal Content
TERMS OF REFERENCE WASH CONTEXT ANALYSIS IN LIBERIA, SIERRA LEONE AND TOGO
 USAID West Africa Water Supply, Sanitation, and Hygiene Program (USAID WA-WASH) TERMS OF REFERENCE WASH CONTEXT ANALYSIS IN LIBERIA, SIERRA LEONE AND TOGO Assessment of WASH Sector Strengths, Weaknesses,
USAID West Africa Water Supply, Sanitation, and Hygiene Program (USAID WA-WASH) TERMS OF REFERENCE WASH CONTEXT ANALYSIS IN LIBERIA, SIERRA LEONE AND TOGO Assessment of WASH Sector Strengths, Weaknesses,
Adapting a Health Systems Strengthening Model to Improve Access to Health Services in a Factory A Pilot Project in Haiti
 DECEMBER 2016 BRIEF Adapting a Health Systems Strengthening Model to Improve Access to Health Services in a Factory A Pilot Project in Haiti The pilot intervention described in this brief took place at
DECEMBER 2016 BRIEF Adapting a Health Systems Strengthening Model to Improve Access to Health Services in a Factory A Pilot Project in Haiti The pilot intervention described in this brief took place at
Essential Newborn Care Corps. Evaluation of program to rebrand traditional birth attendants as health promoters in Sierra Leone
 Essential Newborn Care Corps Evaluation of program to rebrand traditional birth attendants as health promoters in Sierra Leone Challenge Sierra Leone is estimated to have the world s highest maternal mortality
Essential Newborn Care Corps Evaluation of program to rebrand traditional birth attendants as health promoters in Sierra Leone Challenge Sierra Leone is estimated to have the world s highest maternal mortality
Impact of Financial and Operational Interventions Funded by the Flex Program
 Impact of Financial and Operational Interventions Funded by the Flex Program KEY FINDINGS Flex Monitoring Team Policy Brief #41 Rebecca Garr Whitaker, MSPH; George H. Pink, PhD; G. Mark Holmes, PhD University
Impact of Financial and Operational Interventions Funded by the Flex Program KEY FINDINGS Flex Monitoring Team Policy Brief #41 Rebecca Garr Whitaker, MSPH; George H. Pink, PhD; G. Mark Holmes, PhD University
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
2014 MASTER PROJECT LIST
 Promoting Integrated Care for Dual Eligibles (PRIDE) This project addressed a set of organizational challenges that high performing plans must resolve in order to scale up to serve larger numbers of dual
Promoting Integrated Care for Dual Eligibles (PRIDE) This project addressed a set of organizational challenges that high performing plans must resolve in order to scale up to serve larger numbers of dual
Assessing Health Needs and Capacity of Health Facilities
 In rural remote settings, the community health needs may seem so daunting that it is difficult to know how to proceed and prioritize. Prior to the actual on the ground assessment, the desktop evaluation
In rural remote settings, the community health needs may seem so daunting that it is difficult to know how to proceed and prioritize. Prior to the actual on the ground assessment, the desktop evaluation
Ethiopia Health MDG Support Program for Results
 Ethiopia Health MDG Support Program for Results Health outcome/output EDHS EDHS Change 2005 2011 Under 5 Mortality Rate 123 88 Decreased by 28% Infant Mortality Rate 77 59 Decreased by 23% Stunting in
Ethiopia Health MDG Support Program for Results Health outcome/output EDHS EDHS Change 2005 2011 Under 5 Mortality Rate 123 88 Decreased by 28% Infant Mortality Rate 77 59 Decreased by 23% Stunting in
Grant Aid Projects/Standard Indicator Reference (Health)
") Examples of Setting Indicators for Each Development Strategic Objective Grant Aid Projects/Standard Indicator Reference (Health) Sector Development strategic objectives (*) Mid-term objectives Sub-targets
Examples of Setting Indicators for Each Development Strategic Objective Grant Aid Projects/Standard Indicator Reference (Health) Sector Development strategic objectives (*) Mid-term objectives Sub-targets
Measuring the Cost of Patient Care in a Massachusetts Health Center Environment 2012 Financial Data
 Primary Care Provider Costs Measuring the Cost of Patient Care in a Massachusetts Health Center Environment 0 Financial Data Massachusetts Respondents Alexander, Aronson, Finning & Co., P.C. (AAF) was
Primary Care Provider Costs Measuring the Cost of Patient Care in a Massachusetts Health Center Environment 0 Financial Data Massachusetts Respondents Alexander, Aronson, Finning & Co., P.C. (AAF) was
How can the township health system be strengthened in Myanmar?
 How can the township health system be strengthened in Myanmar? Policy Note #3 Myanmar Health Systems in Transition No. 3 A WPR/2015/DHS/003 World Health Organization (on behalf of the Asia Pacific Observatory
How can the township health system be strengthened in Myanmar? Policy Note #3 Myanmar Health Systems in Transition No. 3 A WPR/2015/DHS/003 World Health Organization (on behalf of the Asia Pacific Observatory
Guidelines for Development and Reimbursement of Originating Site Fees for Maryland s Telepsychiatry Program
 Guidelines for Development and Reimbursement of Originating Site Fees for Maryland s Telepsychiatry Program Prepared For: Executive Committee Meeting 24 May 2010 Serving Caroline, Dorchester, Garrett,
Guidelines for Development and Reimbursement of Originating Site Fees for Maryland s Telepsychiatry Program Prepared For: Executive Committee Meeting 24 May 2010 Serving Caroline, Dorchester, Garrett,
Volunteers and Donors in Arts and Culture Organizations in Canada in 2013
 Volunteers and Donors in Arts and Culture Organizations in Canada in 2013 Vol. 13 No. 3 Prepared by Kelly Hill Hill Strategies Research Inc., February 2016 ISBN 978-1-926674-40-7; Statistical Insights
Volunteers and Donors in Arts and Culture Organizations in Canada in 2013 Vol. 13 No. 3 Prepared by Kelly Hill Hill Strategies Research Inc., February 2016 ISBN 978-1-926674-40-7; Statistical Insights
NBER WORKING PAPER SERIES USING PERFORMANCE INCENTIVES TO IMPROVE MEDICAL CARE PRODUCTIVITY AND HEALTH OUTCOMES. Paul Gertler Christel Vermeersch
 NBER WORKING PAPER SERIES USING PERFORMANCE INCENTIVES TO IMPROVE MEDICAL CARE PRODUCTIVITY AND HEALTH OUTCOMES Paul Gertler Christel Vermeersch Working Paper 19046 http://www.nber.org/papers/w19046 NATIONAL
NBER WORKING PAPER SERIES USING PERFORMANCE INCENTIVES TO IMPROVE MEDICAL CARE PRODUCTIVITY AND HEALTH OUTCOMES Paul Gertler Christel Vermeersch Working Paper 19046 http://www.nber.org/papers/w19046 NATIONAL
Rutgers School of Nursing-Camden
 Rutgers School of Nursing-Camden Rutgers University School of Nursing-Camden Doctor of Nursing Practice (DNP) Student Capstone Handbook 2014/2015 1 1. Introduction: The DNP capstone project should demonstrate
Rutgers School of Nursing-Camden Rutgers University School of Nursing-Camden Doctor of Nursing Practice (DNP) Student Capstone Handbook 2014/2015 1 1. Introduction: The DNP capstone project should demonstrate
The Effect of Performance-Based Financial Incentives on Improving Health Care Provision in Burundi: A Controlled Cohort Study
 Global Journal of Health Science; Vol. 7, No. 3; 2015 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education The Effect of Performance-Based Financial Incentives on Improving
Global Journal of Health Science; Vol. 7, No. 3; 2015 ISSN 1916-9736 E-ISSN 1916-9744 Published by Canadian Center of Science and Education The Effect of Performance-Based Financial Incentives on Improving
OUR UNDERWRITERS. We extend our appreciation to the underwriters for their invaluable support.
 OUR UNDERWRITERS We extend our appreciation to the underwriters for their invaluable support. 2 OUR ADVOCATES We extend our appreciation to the following organizations and businesses for their generous
OUR UNDERWRITERS We extend our appreciation to the underwriters for their invaluable support. 2 OUR ADVOCATES We extend our appreciation to the following organizations and businesses for their generous
Use of External Consultants
 Summary Introduction The Department of Transportation and Works (the Department) is responsible for the administration, supervision, control, regulation, management and direction of all matters relating
Summary Introduction The Department of Transportation and Works (the Department) is responsible for the administration, supervision, control, regulation, management and direction of all matters relating
$3,203m 73% Global investment in. neglected disease R&D. $420m Funding to PDPs
 94FINDINGS - FUNDING FLOWS FUNDING FLOWS Organisations can invest in neglected disease R&D in two main ways: by funding their own in-house research (internal investment, also referred to as intramural
94FINDINGS - FUNDING FLOWS FUNDING FLOWS Organisations can invest in neglected disease R&D in two main ways: by funding their own in-house research (internal investment, also referred to as intramural
Primary care P4P in Portugal
 Primary care P4P in Portugal Country Background Note: Portugal Alexandre Lourenço, Nova School of Business and Economics, Coimbra Hospital and University Centre February 2016 1 Primary care P4P in Portugal
Primary care P4P in Portugal Country Background Note: Portugal Alexandre Lourenço, Nova School of Business and Economics, Coimbra Hospital and University Centre February 2016 1 Primary care P4P in Portugal
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
ORGANIZATION OF SERVICES AND EFFICIENCY IN HEALTH SYSTEM PERFORMANCE
 ORGANIZATION OF SERVICES AND EFFICIENCY IN HEALTH SYSTEM PERFORMANCE Do we need to focus more attention on PHC? Daniel H. Kress Deputy Director, Global Primary Health Care and Health Financing December
ORGANIZATION OF SERVICES AND EFFICIENCY IN HEALTH SYSTEM PERFORMANCE Do we need to focus more attention on PHC? Daniel H. Kress Deputy Director, Global Primary Health Care and Health Financing December
USAID/Philippines Health Project
 USAID/Philippines Health Project 2017-2021 Redacted Concept Paper As of January 24, 2017 A. Introduction This Concept Paper is a key step in the process for designing a sector-wide USAID/Philippines Project
USAID/Philippines Health Project 2017-2021 Redacted Concept Paper As of January 24, 2017 A. Introduction This Concept Paper is a key step in the process for designing a sector-wide USAID/Philippines Project
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
Nursing and Personal Care: Funding Increase Survey
 Nursing and Personal Care: Funding Increase Survey Prepared for: Ministry of Health and Long-Term Care Long Term Care Facilities Branch 5 th Floor, Hepburn Block 80 Grosvenor Street Toronto, Ontario Prepared
Nursing and Personal Care: Funding Increase Survey Prepared for: Ministry of Health and Long-Term Care Long Term Care Facilities Branch 5 th Floor, Hepburn Block 80 Grosvenor Street Toronto, Ontario Prepared
Grant Performance and Payments at the Global Fund
 Grant Performance and Payments at the Global Fund Victoria Fan, Denizhan Duran, Rachel Silverman, and Amanda Glassman Abstract Center for Global Development 1800 Massachusetts Ave NW Third Floor Washington
Grant Performance and Payments at the Global Fund Victoria Fan, Denizhan Duran, Rachel Silverman, and Amanda Glassman Abstract Center for Global Development 1800 Massachusetts Ave NW Third Floor Washington
GAO. DEPOT MAINTENANCE The Navy s Decision to Stop F/A-18 Repairs at Ogden Air Logistics Center
 GAO United States General Accounting Office Report to the Honorable James V. Hansen, House of Representatives December 1995 DEPOT MAINTENANCE The Navy s Decision to Stop F/A-18 Repairs at Ogden Air Logistics
GAO United States General Accounting Office Report to the Honorable James V. Hansen, House of Representatives December 1995 DEPOT MAINTENANCE The Navy s Decision to Stop F/A-18 Repairs at Ogden Air Logistics
University of Michigan Health System. Current State Analysis of the Main Adult Emergency Department
 University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
Final Report No. 101 April Trends in Skilled Nursing Facility and Swing Bed Use in Rural Areas Following the Medicare Modernization Act of 2003
 Final Report No. 101 April 2011 Trends in Skilled Nursing Facility and Swing Bed Use in Rural Areas Following the Medicare Modernization Act of 2003 The North Carolina Rural Health Research & Policy Analysis
Final Report No. 101 April 2011 Trends in Skilled Nursing Facility and Swing Bed Use in Rural Areas Following the Medicare Modernization Act of 2003 The North Carolina Rural Health Research & Policy Analysis
FULTON COUNTY, GEORGIA OFFICE OF INTERNAL AUDIT FRESH and HUMAN SERVICES GRANT REVIEW
 FULTON COUNTY, GEORGIA OFFICE OF INTERNAL AUDIT FRESH and HUMAN SERVICES GRANT REVIEW June 5, 2015 TABLE OF CONTENTS PAGE Introduction... 1 Background... 1 Objective... 1 Scope... 2 Methodology... 2 Findings
FULTON COUNTY, GEORGIA OFFICE OF INTERNAL AUDIT FRESH and HUMAN SERVICES GRANT REVIEW June 5, 2015 TABLE OF CONTENTS PAGE Introduction... 1 Background... 1 Objective... 1 Scope... 2 Methodology... 2 Findings
GUIDELINES FOR HEALTH SYSTEM ASSESSMENT
 GUIDELINES FOR HEALTH SYSTEM ASSESSMENT Myanmar June 13 2009 Map: Planned Priority Townships for Health System Strengthening 2008-2011 1 TABLE OF CONTENTS BOOK 1 SURVEYOR GUIDELINES List of Figures...
GUIDELINES FOR HEALTH SYSTEM ASSESSMENT Myanmar June 13 2009 Map: Planned Priority Townships for Health System Strengthening 2008-2011 1 TABLE OF CONTENTS BOOK 1 SURVEYOR GUIDELINES List of Figures...
Period of June 2008 June 2011 Partner Country s Implementing Organization: Federal Cooperation
 Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
GLOBAL REACH OF CERF PARTNERSHIPS
 Page 1 The introduction of a new CERF narrative reporting framework in 2013 has improved the overall quality of reporting by Resident and Humanitarian Coordinators on the use of CERF funds (RC/HC reports)
Page 1 The introduction of a new CERF narrative reporting framework in 2013 has improved the overall quality of reporting by Resident and Humanitarian Coordinators on the use of CERF funds (RC/HC reports)
Table of Contents. Overview. Demographics Section One
 Table of Contents Overview Introduction Purpose... x Description... x What s New?... x Data Collection... x Response Rate... x How to Use This Report Report Organization... xi Appendices... xi Additional
Table of Contents Overview Introduction Purpose... x Description... x What s New?... x Data Collection... x Response Rate... x How to Use This Report Report Organization... xi Appendices... xi Additional
Making the Business Case
 Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients
 Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
HIV/AIDS Monitor: Guide to the Data Analyzed in The Numbers Behind The Stories
 HIV/AIDS Monitor: Guide to the Data Analyzed in The Numbers Behind The Stories 1. Data Limitations 2. Data errors 3. Using the data The data here are drawn from the Country Operational Plan and Reporting
HIV/AIDS Monitor: Guide to the Data Analyzed in The Numbers Behind The Stories 1. Data Limitations 2. Data errors 3. Using the data The data here are drawn from the Country Operational Plan and Reporting
TC911 SERVICE COORDINATION PROGRAM
 TC911 SERVICE COORDINATION PROGRAM ANALYSIS OF PROGRAM IMPACTS & SUSTAINABILITY CONDUCTED BY: Bill Wright, PhD Sarah Tran, MPH Jennifer Matson, MPH The Center for Outcomes Research & Education Providence
TC911 SERVICE COORDINATION PROGRAM ANALYSIS OF PROGRAM IMPACTS & SUSTAINABILITY CONDUCTED BY: Bill Wright, PhD Sarah Tran, MPH Jennifer Matson, MPH The Center for Outcomes Research & Education Providence
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative. May 4, :00-2:00pm ET
 Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative May 4, 2017 1:00-2:00pm ET Highlights and Key Takeaways MAC members participated in the virtual
Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative May 4, 2017 1:00-2:00pm ET Highlights and Key Takeaways MAC members participated in the virtual
Charlotte Banks Staff Involvement Lead. Stage 1 only (no negative impacts identified) Stage 2 recommended (negative impacts identified)
 Stage 2 recommended (negative impacts identified)") Paper Recommendation DECISION NOTE Reporting to: Trust Board are asked to note the contents of the Trusts NHS Staff Survey 2017/18 Results and support. Trust Board Date 29 March 2018 Paper Title NHS Staff
Paper Recommendation DECISION NOTE Reporting to: Trust Board are asked to note the contents of the Trusts NHS Staff Survey 2017/18 Results and support. Trust Board Date 29 March 2018 Paper Title NHS Staff
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
Contracting Out Health Service Delivery in Afghanistan
 Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
NATIONAL LOTTERY CHARITIES BOARD England. Mapping grants to deprived communities
 NATIONAL LOTTERY CHARITIES BOARD England Mapping grants to deprived communities JANUARY 2000 Mapping grants to deprived communities 2 Introduction This paper summarises the findings from a research project
NATIONAL LOTTERY CHARITIES BOARD England Mapping grants to deprived communities JANUARY 2000 Mapping grants to deprived communities 2 Introduction This paper summarises the findings from a research project
PERFORMANCE BASED FINANCING IN BURUNDI
 PERFORMANCE BASED FINANCING IN BURUNDI By Dr BASENYA Olivier President of the PBF Steering Committee in BURUNDI Director General of the National Institute of Public Health OUTLINE OF THE PRESENTATION INTRODUCTION
PERFORMANCE BASED FINANCING IN BURUNDI By Dr BASENYA Olivier President of the PBF Steering Committee in BURUNDI Director General of the National Institute of Public Health OUTLINE OF THE PRESENTATION INTRODUCTION
THE GLOBAL FUND to Fight AIDS, Tuberculosis and Malaria
 THE GLOBAL FUND to Fight AIDS, Tuberculosis and Malaria Guidelines for Performance-Based Funding Table of Contents 1. Introduction 2. Overview 3. The Grant Agreement: Intended Program Results and Budget
THE GLOBAL FUND to Fight AIDS, Tuberculosis and Malaria Guidelines for Performance-Based Funding Table of Contents 1. Introduction 2. Overview 3. The Grant Agreement: Intended Program Results and Budget
Nepal - Health Facility Survey 2015
 Microdata Library Nepal - Health Facility Survey 2015 Ministry of Health (MoH) - Government of Nepal, Health Development Partners (HDPs) - Government of Nepal Report generated on: February 24, 2017 Visit
Microdata Library Nepal - Health Facility Survey 2015 Ministry of Health (MoH) - Government of Nepal, Health Development Partners (HDPs) - Government of Nepal Report generated on: February 24, 2017 Visit
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
Making pregnancy safer: assessment tool for the quality of hospital care for mothers and newborn babies. Guideline appraisal
 Shahad Mahmoud Hussein - Soba University Hospital, Khartoum, Sudan - Training Course in Sexual and Reproductive Health Research 2010 Mohamed Awad Ahmed Adam - Faculty of Medicine, University of Khartoum,
Shahad Mahmoud Hussein - Soba University Hospital, Khartoum, Sudan - Training Course in Sexual and Reproductive Health Research 2010 Mohamed Awad Ahmed Adam - Faculty of Medicine, University of Khartoum,