NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING. 28 November 2017, am. Boardroom, Hilldale, Wigan Road, L39 2JW
|
|
|
- Collin Day
- 6 years ago
- Views:
Transcription
1 Item WLCCGB NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING 28 November 2017, am Boardroom, Hilldale, Wigan Road, L39 2JW Time Agenda item Action Presenter 11/17/ Welcome Chair 11/17/ Declaration of Interests All 11/17/ Minutes of previous meeting held on 26 September 2017 DR Chair 11/17/ Matters arising - Action sheet DR Chair Communication 11/17/ Chair s update I Chair 11/17/ Chief Officer s update I Mike Maguire Governance 11/17/ Risk management process I Paul Kingan Operational Management Section 11/17/ Integrated business report D Paul Kingan 11/17/ Children s and Adults policy DR Claire Heneghan 11/17/ Safeguarding Children and Adults annual report DR Claire Heneghan 11/17/ Declaration of Interests I Paul Kingan 11/17/ Social prescribing procurement DR Kathryn Kavanagh Consent items 11/17/ Minutes of sub-committees: - Primary Care Commissioning Committee September Finance and QIPP Committee 1 September and October Quality and Safety Committee 24 October Executive Committee 12 September 7 November 2017 Other minutes/action notes: - Lancashire Health and Wellbeing Board September West Lancashire Community Safety Partnership July Alliance Local Delivery September Joint Committee of CCGs September 2017 Other Business 11/17/ Any other business I Chair Date and Time of Next Meeting 23 January 2018, am, Boardroom, Hilldale 15 minutes to be allocated for questions from members of the public based on agenda items. I Chair
2 I Information D-Discussion DR Decision Required Members of the governing body will be available after the close of the meeting for informal discussion, time permitting
3 Meeting Title: West Lancashire Clinical Commissioning Governing Body Meeting Time: am Present: Dr John Caine, Chair Mike Maguire, Chief Officer Douglas Soper, Lay Member Greg Mitten, Vice-Chair / Lay Member Steve Gross, Lay Member Paul Kingan, Chief Officer/Deputy Chief Officer Dr Bapi Biswas, GP Executive Lead Dr Peter Gregory, GP Executive Lead Dr Rakesh Jaidka, GP Executive Lead Dr Vikul Mittal, GP Executive Lead Minutes D R A F T Date: 26 September 2017 Venue: Parbold Village Hall, Parbold In attendance: Cathy Ashcroft, Executive Assistant Gail Godson, Director, Healthwatch Lancashire Jackie Moran, Head of Quality, Performance and Contracting For item 09/17/11 and 09/17/12: Gary Raphael, Finance Director, Healthier Lancashire and South Cumbria For item 09/17/17: Nicola Baxter, Head of Medicines Optimisation Dawn Threlfall, Medicines Optimisation Technician Apologies: Mike Kirby, Director of Corporate Commissioning, Lancashire County Council (in attendance) Sakthi Karunanithi, Director of Public Health and Wellbeing (in attendance) Dr John (Jack) Kinsey, GP Executive Lead Claire Heneghan, Chief Nurse Dr Adam Robinson, Secondary Care Consultant Agenda Summary of Discussion Item WLCCGB/ 09/17/01 Welcome and apologies for absence The meeting of the West Lancashire Clinical Commissioning Group Governing Body was opened by Dr John Caine. There were four members of the public present and no questions had been received from the public in respect of the agenda. Those present were informed that the Annual General Meeting will take place immediately following the Governing Body meeting. The agenda was amended for items 11 and 12 to be addressed following item 6. Action 09/17/02 Declarations of interests Dr John Caine reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of West Lancashire CCG. Declarations declared by governing body members are listed in the CCG s Register of Interests. The register is available either via the secretary to the governing body or the CCG website at the following link: Declarations of interest from sub committees. None declared No declarations were declared. 09/17/03 Minutes of previous meeting held on 25 July 2017 The minutes of the meeting held on 25 July were approved as a correct record West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 1 of 8
4 with one minor amendment: Page 2, top of page; 05/17/02 Declarations of interest. Gail Godson declared an interest in item 12. Choice and Equity Policy, because she owns a home care company. The chair deemed this to be a significant interest 09/17/04 Matters arising The action sheet was updated. COMMUNICATION 09/17/05 Chair s update The report provided members with an update on both strategic and operational issues since the last meeting. John Caine highlighted key areas of interest: Right Care this is a national NHS England supported programme committed to delivering best care to patients whilst utilising NHS money efficiently. All three RightCare priority submissions have been made: musculoskeletal (MSK), chronic pain and respiratory. The CCG will report back quarterly to NHS England on the improvements in these areas. Urgent Care the falls car pilot has been extended to the end of the financial year to further assess the impact of the service. The current data shows that over 60% of patients were seen at home and did not require hospital admission, which reduces pressure on the ambulance service. Greg Mitten highlighted the positive feedback from patients in terms of agencies working together. The current mix of agencies is being looked at to develop the relationship with social prescribing. Changes to Prescribing following public consultation, the CCG announced the cessation to fund certain types of medicines or treatments with little evidence of real clinical benefit, that are readily available over the counter. This also included gluten-free products. Self-Care this is to encourage the community to self-care and avoid unnecessary visits to GP practices and A&E. Fact sheets and materials have been circulated and can be provided by the CCG. Annual General Meeting (AGM) the AGM, in association with the CVS health network, will follow the Governing Body meeting and all are welcome to attend. Duty to Involve Report the annual report highlights how the CCG have involved others in their work over the last year. It demonstrates the CCG s commitment to patient and public participation and involvement of wider stakeholders. The report is available from the CCG on request. Care for You this is a system-wide local programme to determine the future model of in-hospital care, including A&E services, based on the needs of residents in Southport, Formby and West Lancashire. It will build on previous local work around clinical and financial sustainability of Southport and Ormskirk Hospital NHS Trust (the Trust). It was reported that this programme differs from the previous in that the management team at the Trust is different and this process is more clinically led. The previous process focussed on the sustainability of Southport and Ormskirk Hospitals, whereas Care for You focusses on locality health needs and has a broader remit. In terms of the process feeding into Sustainability and Transformation Plans (STP), the CCG look to the Mersey STP for Acute services, where Andrew Gibson is looking at patch-based solutions and health economies in. In response to a question about the current risk presented by a number of fragile services at the Trust with a greater patient flow to other Trusts, this is being looked into by subgroups in terms of patient use of services. The options from this programme are required in 12 months. West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 2 of 8
5 Ophthalmology the CCG is in the process of procurement of a tier 2 ophthalmology and age related macular degeneration service. Patients are welcome to join a patient focus group in October. Primary Care since the CCG became a level 3 co-commissioner in primary care in April, much work has taken place through the Primary Care Commissioning Committee and GP Membership. Neighbourhood working continues and initiatives such as the access to GPs through extended hours pilot continues. New roles are being considered for Clinical Pharmacists and Care Navigators. The governing body: Noted the contents of the report 09/17/06 Chief Officer s update The report provided members with an update on both strategic and operational issues since the last meeting. Mike Maguire highlighted key areas of interest: Quality Southport and Ormskirk Hospital NHS Trust (the Trust) have achieved all their must do actions from their Care Quality Action plan, with the exception of refurbishment of a ward; dementia strategy and staffing issues. An improvement plan has been developed to improve North West Ambulance Services (NWAS) turnaround response times. In terms of quality improvement, the Quality and Safety Committee continue to monitor quality and the Collaborative Commissioning Forum will continue to scrutinise in detail the Trust s progress. Better Care Fund the Improved Better Care Fund aims to provide extra support to social and health care to further reduce delays in transfers of care. Lancashire County Council will receive 28 million in and the six CCGs are working with the council to develop improvement schemes. The CCG will receive approximately 330 thousand nonrecurrent funding to pump prime its local plan, as agreed with the council. The funding will contribute to the recruitment of occupational therapists, social workers and develop intermediate care in the community. Joint Health Since November 2016, GP orthopaedic referrals have been made directly to Joint Health (MSK) at the Trust. In total, 7,679 referrals have been seen which is an average of 850 patients per month. The process has moved beyond the pilot phase and is progressing. Community Health Services and Urgent Care Services the CCG will continue to work with Virgin Care, who took over the delivery of the services on 1 May. Focus is on transformation over the next five years particularly on the first two years. Local residents can join the Citizen s Panel to help shape future community and urgent care services. Mental Health the CCG has completed a huge scoping exercise to collect views on what modern mental health services should look like. The CCG will work closely with Lancashire Care NHS Foundation Trust to redesign services with local people s views at the forefront. A new safe area in the children s A&E department has been commissioned. The Improving Access to Psychological Therapies will begin working with patients with long-term conditions. The service at Birchwood Crisis Centre will be extended for another 18 months, with extremely positive feedback received from users. A clinician has been commissioned to work with the Children s and Adolescent Mental Health team, linking with schools and GPs. Chronic Pain - as the CCG has been an outlier in this area, a procurement process has commenced to identify a chronic pain specialist known as ihelp. The Innovation Partnership process is being used to develop a service-solution. The governing body: noted the content of the report West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 3 of 8
6 GOVERNANCE 09/17/07 Risk Management Process The current risk process and approach has been refreshed to produce an improved risk register and Board Assurance Framework (BAF). The Audit Committee had endorsed the changes to the report and the main changes were highlighted as follows: The risk reporting process has been strengthened with a step-by-step guide. Key risks have not changed, but have been consolidated into themes. There is one collective risk relating to recruitment and retention issues, scored at 16 for the Trust, which also reflects the risk on the Trust s risk register and its risk rating. Up and coming risks have been added by Paul Kingan and Smita Shetty. New risks include cyber attack An emerging risk is the new landscape of the NHS with changes from STPs, across boundary working and how the CCG needs to adapt. Doug Soper felt the changes were welcome and questioned the unchanged level of some risks following the refresh. Paul Kingan confirmed that the risks initial score would be checked. Smita Shetty was thanked for her contribution to the refresh. The governing body: noted the content and accepted the refreshed format. 09/17/08 Pan-Lancashire Clinical Commissioning Policies The pan-lancashire clinical commissioning policies have been updated centrally and will be presented to all Lancashire CCG Governing Bodies for approval, however in future approval will be sought from the Joint Committee of CCGs. The policies have been presented at the CCG Clinical Executive Committee, where their approval was recommended to the Governing Body. The policies are for the following areas: Surgical release of trigger finger Surgical release of carpal tunnel Male circumcision Tonsillectomy Endoscopic procedures on the knee joint cavity The governing body: approved the polices which will go live on 2 October /17/09 Human Resource Policies The human resource polices for Maternity Leave and Adoption Leave had been presented at the CCG Clinical Executive Committee who recommended their approval by the Governing Body. The governing body: approved the policies 09/17/10 Conflict of Interest Policy The Conflict of Interest policy had been presented at the Clinical Executive Committee and Audit Committee, where it was recommended for approval by the Governing Body. The minor amendments mainly relate to gifts and hospitality as follows: Gifts from suppliers should be refused (except low value promotional aids under the value of 6) Modest gifts from other sources eg patients, families, under the value of 50 may be accepted and do not need to be declared Meals and refreshments under the value of 25 may be accepted and not declared o A value between 25 and 75 may be accepted and must be declared West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 4 of 8
7 o Over the value of 75 should be refused (unless exceptional circumstances apply). National training in conflict of interest for CCGs is still awaited. Mersey Internal Audit Agency will provide a brief training session hopefully timed to consolidate the national training. The governing body: approved the policy. 09/17/11 Lancashire and South Cumbria Sustainability and Transformation Partnership Governance arrangements The governance arrangements have been discussed at the Clinical Executive Committee and other committees. Areas to note in the report include: The arrival of STP Boards, which are a national mandate, to spearhead the STPs. A memorandum of understanding between NHS England /Improvement and Blackpool and the Fylde coast, which is an Accountable Care System (ACS), details the requirements of the ACS. The roles of the groups within the STP were outlined and demonstrate the new relationship with CCGs, NHS England and NHS Improvement. West Lancashire CCG is known as a Local Delivery Partnership (LDP) and differs from other CCGs due to the crossboundary working, its council in West Lancashire and its main provider in Merseyside. When asked about decision-making and whether one CCG could stop a process because universal agreement was required, Gary Raphael confirmed that CCGs, Local Authorities and Trusts are not being asked for agreement, but for support to work together. The workstreams should reflect the priorities of each LDP area across Lancashire and South Cumbria, local health economies and neighbourhoods, which are essential going ahead. There may be a need to look at a specialist service provider going forward. Gary Raphael stated that although decisions are made centrally, it is essential that a proper process be followed to make decisions for local populations. The risk the CCG faces being part of two different STP areas was highlighted in terms of movement of specialist services. Better use of technology with Skype to participate in meetings was suggested and chat rooms are being considered. Have Your Say events are taking place in Lancashire and Gail Godson stated the need to articulate decisions being made to keep the public informed. It was agreed that work with other agencies to improve communications, reduce jargon and explain the complexities was important. Effective working with the community had been demonstrated following the recent mental health events where community recommendations had resulted in discussion between the CCG and Lancashire Care Foundation Trust to reshape services. VCFS will play a role in the self-care programme and there is a need to work together to achieve this. The CCG could demonstrate how the CCG and the council are already providing this work. Time is a priority to allow consultation and partnership working. The governing body: agreed to support the revised structure 09/17/12 Development of Shared Decision Making for the Joint Committee of CCGs The Joint Committee of CCGs, which meets in public, has been in place of approximately a year. Paul Kingan and Doug Soper represent the CCG on the joint meeting. Governance has been developed and the committee requires seven of the eight CCG members to agree for a decision to be passed. A legal framework does not allow the committee to make all the decisions that the STP Board would wish to make as the power to make decisions will need to be delegated to the joint committee by the individual CCGs. The paper outlines where decisions on specific areas are requested to be delegated. The paper lists the areas of decisions the committee anticipates wanting to West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 5 of 8
8 address at this point in time (Appendix 1) and another list of those to focus on next year (Appendix 2). The CCG is asked to delegate decision making in these areas. The proposed delegated decisions on mental health services was discussed. In respect of Appendix 1, the CCG had been working on the redesign of local mental health services for 18 months with engagement from local users and Lancashire Care Foundation Trust. Mike Maguire felt that most CCGs would wish to agree community mental health services locally and not assume a Pan- Lancashire model. It was assumed that funding in CCG baselines included IAPT, which would need to be continued on a recurring basis, with decisions made together. As mental health could be one of the top four national priorities, consistency is needed around decisions for requirements and working together. The language in appendix 2 was questioned in terms of the shift from LDP to STP decision-making and the importance of local conversation. The appendices are written to be informative and clear. In appendix 1, Adult mental health and dementia refer to operating at both a local and STP level. Rakesh Jaidka highlighted a need to agree on the outcomes and the LDP needs, to achieve this. This standard has to be achieved. The governing body: approved the delegation of joint decision-making through the Joint Committee of CCGs , of the decisions in appendix 1 with the following caveat regarding Mental Health Services: Recognising the difference in population needs will be considered in the delivery of the local solution. 09/17/13 Constitution The CCG Constitution document was presented. A few minor changes had been made to committee names, frequency of meetings and the reduction in the number of GP practices due to their amalgamation. Final approval is required from the GP Membership Council before the Constitution is submitted to NHS England for approval. The governing body: approved the Constitution, which requires ratification by the GP Membership Council. 09/17/14 EPRR Self-Assessment The CCG has full met the self-assessment criteria. The outstanding areas identified in the previous year s assessment has been completed with the CCG achieving full compliance. Improved measures of emergency preparedness which are now in place include: updated emergency plans, desk-top exercises, the positive management of the cyber-attack. The governing body: approved the EPRR self-assessment 09/17/15 Risk Management Strategy The Risk Management Strategy, formerly called the Integrated Risk Assurance Framework, sets out the roles and responsibilities of the organisation and those working within the organisation. The strategy has been strengthened with specific roles assigned to senior managers. The Clinical Executive Committee have recommended the strategies approval at the Governing Body. The governing body: approved the risk management strategy OPERATIONAL MANAGEMENT SECTION 09/17/16 Integrated Business Report (IBR) The report provided summary information on the financial position and activity West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 6 of 8
9 performance of the CCG to July and the financial position for August It also included quality and performance analysis for community based targets for Southport and Ormskirk Hospital NHS Trust. Paul Kingan highlighted some key areas within the report: The finance performance is rated as amber and is discussed at the CCG Finance and QIPP Committee. The CCG is unlikely to achieve its business rules this year due to current financial pressures. It is expected that a minimum of a break-even financial position and the risk reserve for the NHS England will be delivered. Further QIPP savings schemes need to be identified. Referral rates have reduced the reason is complex as referrals have reduced due to a redirection to joint healthcare (MSK) and the result of the cyber-attack on referral data. Scrutiny of hospital referrals is required. Planned care is currently underplan (eg MSK) Unplanned care it was recently established that the GP Assessment Unit is not following the normal service model and is focussing on follow-up activity and not initial admission to hospital wards. The CCG business analyst is working on this issue and sharing data with Sefton. Paul Kingan will report back at the next meeting. PK Jackie Moran reported on the quality and performance section of the IBR: Mixed-sex accommodation this is still an issue, but the Trust want to designate a full floor to assign patients to specific areas. MRSA and C. Difficile infection is rated at green. A&E waiting times this is still an issue and the government and NHS England are focussed on this. In future any related changes will need to be quantified in terms of the effect on A&E. Medical director at the Trust since the medical director s exclusion from the Trust, Dr Paul Mansour is covering this role. It is anticipated an advertisement for a substantive chief executive officer will be placed shortly. 2-week breast waiting this is below target and relates to a low number of patients at Aintree and Wrightington, Wigan and Leigh Hospitals. The delay relates to capacity issues and patient choice. The governing body: noted the content of the IBR. 09/17/17 Prescribing Hubs Nicola Baxter and Dawn Threlfall joined the meeting to present the paper, which provided an update on the work of the prescribing hub and for a decision on expanding the service. The prescribing hub in Skelmersdale Family Practice has been set up as proof of concept and work continues with Beacon Primary Care, who have an established hub. The prescribing hub has shown the following benefits: advice to patients about their prescribing has been well received; patient queries made to practice staff have reduced, from the baseline in March there has been a reduction in unnecessary prescribing; standardised systems have been put in place resulting in releasing some time for the GP; and an issue was identified in one community pharmacy which is now under investigation. The medicine co-ordinators within the practice are instrumental in supporting the hub. As drug prices increase this becomes high a financial pressure. The Governing Body are asked to: Fund three prescribing hubs across West Lancashire cost per hub is ,000 West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 7 of 8
10 Agree the roll in of other practices into the Skelmersdale and Northern parishes hub Agree that practices should pool back office staff, including medicines coordinators to support this new way of working The medicines optimisation team will support the role out and continued development of the hubs, they will work with the hub staff to ensure safe practice. This will include the already established hub in beacon primary care, this will support a learning culture Agree the proposed reporting structure Two practices are working towards the prescribing changes and hub working. It was agreed that discussion with the medicine co-ordinators will be arranged to clarify their roles going forward. The Clinical Executive Committee, GP Membership Council and the Finance and QIPP Committee support this proposal. Progress would be monitored through the Medicines Management and Quality and Safety Committee. Good news stories from open dialogue with patients had resulted in repeat prescriptions for two expensive drugs, which were no longer necessary, being cancelled. Going forward the team are considering working with taking blood and nurse practitioners. The governing body: approved the proposal and funding as set out above. CONSENT ITEMS 09/17/18 Minutes of sub-committees: - Primary Care Commissioning Committee July Finance and QIPP Committee 1 August Executive Committee 18 July 5 September 2017 Other minutes/action notes: - Lancashire Health and Wellbeing Board June and August Alliance Local Delivery July Joint Committee of CCGs July 2017 The governing body: noted the papers and comments above. Other business 09/17/19 Any other business None Meeting closed at am Date and time to next meeting: 28 November 2017, am, Boardroom, Hilldale, Wigan Road, Ormskirk West Lancashire Clinical Commissioning Group Governing Body meeting 26 September 2017 Page 8 of 8
11 Agenda item no: WLCCGB West Lancashire CCG Governing Body meeting Action sheet Action Lead Date required by Action completed 09/17/16 Integrated Business Report (IBR) GP Assessment Unit is focussing on follow-up activity and not initial admission to hospital wards. The CCG business analyst is working on this issue and sharing data with Sefton. Paul Kingan will report back at the next meeting. Paul Kingan 28 November /17/04 Chief officers update: Mental Health There was an expression of confidence in referrals being accepted in adult mental health, whereas referrals to the CAMHs are not always accepted, but signposted to other services. Mike Maguire will consider this issue. 05/17/09 Integrated Business Report (IBR) Paul Kingan will present a review of the coding of emergency cases at a future Executive Committee meeting. Mike Maguire 26 September 2017 Paul Kingan 26 September 2017 The GPs raised any issues at the CAMHs training session. The redesign of mental health will focus on the recruitment of a primary care worker. The paper has been presented. The statistics are in line with population trends. The increase at Southport Hospital is being looked into. Page 1 of 1
12 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT DATE OF BOARD MEETING: 28 November 2017 WLCCGB 11/17/05 TITLE OF REPORT: Chair s update BRIEFING POINTS: Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience) please outline impact YES 2. Commissioning of hospital and community services please outline YES impact 3. Commissioning and performance management of GP Prescribing YES please outline impact 4. Delivering Financial Balance please outline impact YES 5. Development of the commissioning group as a commissioning YES organisation please outline impact B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk NO number) have any legal implications promote effective governance practice 2. Additional resource implications YES (either financial or staffing resources) 3. Health Inequalities NO 4. Equality and Inclusion and Human Rights Requirements NO Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement YES 6. Patient and Public Engagement YES PAPER PREPARED BY: PAPER PRESENTED BY: Marco Giannini, communication and engagement manager Dr John Caine, chair Chair s update West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
13 WEST LANCASHIRE CLINICAL COMMISSIONING GOVERNING BODY CHAIR S UPDATE PURPOSE This report provides an update on both strategic and operational issues of interest to governing body members in the months since the last meeting. ISSUES ARISING URGENT CARE 1. As winter fast approaches, a number of initiatives are underway to help support A&E during this period. 2. GP streaming at Southport A&E has begun. The Trust are implementing the Golden Patient, which will mean each ward will identify a patient for discharge by 10am every day to encourage discharges before lunchtime. Streaming of patients into four lanes for discharge has also been implemented, however this is being monitored and is taking time to implement fully. 3. The discharge team are re-locating to the GP Out Of Hours (OOH) building on the Acute site, which will free up an office so that CORE 24 Mental Health liaison will be on-site at Southport, which is expected to have significant improved impact on the operation of the team. 4. West Lancashire s proposals for the ibcf (Extended Better Care Fund) are underway and this includes creating a community hub for intermediate care, development of trainee posts for Health Care Assistants and integrating local social work and community therapy teams to work jointly. The social care team will be recruited in November and the apprenticeship scheme is in development with Virgin Care. Further scoping work is required for the Community Hub before plans are progressed. SELF CARE 5. The CCG s Medicines Management Team have now implemented their new gluten free and self-care policies, which came into effect as of 4 September MEDICINES WASTE 6. A period of engagement will begin shortly around the new prescribing hub (POD), which is currently a pilot based out of Skelmersdale. 7. Work has commenced with Evergreen to trial a prescribing hub/practice/ccg website for patients to order medication, make appointments and access their medical records. 8. The medicines optimisation team currently run a care home service, proactively reviewing patients medication. They are reviewing the service to expand the team to have a wider skill mix and be part of the multi-disciplinary team Chair s update West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
14 ORCHA 9. Work has begun with ORCHA who are working with the CCG in developing a platform that will allow patients and clinical staff to select the best/most appropriate health related apps. This will help to promote self-care amongst our population and improve medicines adherence. NHS West Lancashire CCG is the first CCG in the country to adopt this platform. CLINICAL POLICIES 10. The CCG has been involved in a number of pan-lancashire policy consultations. 11. The policies out to consultation include: cosmetic procedures and treatments, three gynaecological policies and one hip related policy. 12. The CCG will be holding a public listening event at Hilldale on Wednesday 29 November from 5pm until 7pm on the topic of our plans for cosmetic procedures and treatments. Members of the public are encouraged to attend and are asked to let the CCG know that they would like to come by ing myview@westlancashireccg.nhs.uk. 13. Full details on the policy consultations are available from the news section of the CCG s website: PRIMARY CARE 14. The Skelmersdale walk-in centre is now open from 8am until 8pm. It was previously open until 5.30pm. This is adding an extra level of primary care to our residents. Recommendation 15. Members are asked to note the content of the report. Dr John Caine Chair November 2017 Chair s update West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
15 WLCCGB 11/17/06 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT DATE OF BOARD MEETING: 28 November 2017 TITLE OF REPORT: Chief officer s update BRIEFING POINTS: Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience) please outline impact YES 2. Commissioning of hospital and community services please outline YES impact 3. Commissioning and performance management of GP Prescribing NO please outline impact 4. Delivering Financial Balance please outline impact YES 5. Development of the commissioning group as a commissioning YES organisation please outline impact B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number) NO have any legal implications promote effective governance practice 2. Additional resource implications YES (either financial or staffing resources) 3. Health Inequalities NO 4. Equality and Inclusion and Human Rights Requirements NO Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement YES 6. Patient and Public Engagement YES PAPER PREPARED BY: Marco Giannini, communication and engagement manager PAPER PRESENTED BY: Mike Maguire, chief officer Chief Officer s update West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
16 WEST LANCASHIRE CLINICAL COMMISSIONING GOVERNING BODY CHIEF OFFICER S UPDATE PURPOSE This report provides an update on both strategic and operational issues of interest to governing body members in the months since the last meeting. ISSUES ARISING COMMUNITY HEALTH SERVICES AND URGENT CARE SERVICES 1. Virgin Care has been delivering community health services and urgent care services since 1 May We continue to work with Virgin Care and focus on the transformation needed over the next five years, focusing particularly on the first two years. This will relate to our primary care strategy (as a level 3 primary care co-commissioner). 3. Recruitment of additional community staff to support respiratory, IV Therapy and Tissue viability all of which will help to provide care closer to home for those involved. 4. A new IT system has also been introduced in the Walk in Centre in Skelmersdale, which is consistent with that utilised in the Ormskirk Health Centre. This will help with share information across sites, tells us the clinical detail of why patients are attending and help us to meet more specific service requirements in the future. 5. Mobile working for community staff; having hand held devices will mean that they will have patient notes to hand and be able to write their notes directly into those same notes; there will be less need for staff to continually travel to and from their base, they can travel from patient to patient - thereby making the most productive use of their time and increased patient contact. This is to be a phased approach, focussing in one neighbourhood to begin with. 6. Virgin Care have now appointed a new communications and engagement lead for West Lancashire, Rebecca Solari will now be focussing on developing the new patient engagement group, which will allow patients and members of the public to help shape community and urgent care services locally by offering views and experiences. The Citizen s Panel is open to anyone living in West Lancashire. Find out more and sign up here: 7. In addition to the governance framework already in place, the CCG and new provider have recently developed an additional forum which will allow even more regular, detailed discussions between both parties regarding the transformation of services. QUALITY 8. Southport and Ormskirk NHS Hospital Trust s temporary Medical Director has addressed issues relating to medical staffing shortages at the Contract and Clinical Quality Review meeting. This issue has particularly impacted maternity and AED services. Discussions are ongoing across the health economy to mitigate the associated risks. Chief Officer s update West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
17 9. Concerns have been raised with regards to the Trust s AQUA Mortality Report. To provide assurance to the CCG, the Trust will present their new governance arrangements at January s Contract and Clinical Quality Review meeting 10. A Section 65 issued by the Care Quality Commission requires Southport and Ormskirk NHS Trust to provide an explanation in relation to the outstanding 5000 patients requiring follow-up. 11. At the CCG s Quality and Safety Committee in October there was consensus that risks associated with quality of clinical services at Southport and Ormskirk NHS Trust were significant enough to be escalated to the Executive Committee. 12. There has been one reported case of MRSA Bacteraemia at Southport and Ormskirk NHS Trust. Following the post-infection review, the case of MRSA was attributed to the Trust. The action plan produced by the Trust has been shared with the CCG. 13. There are further changes to the senior leadership team within Southport and Ormskirk NHS Hospitals Trust. The director of nursing has been successful in obtaining an alternative post. MENTAL HEALTH 14. The CCG and Lancashire Care Foundation Trust met in November to review gateways and milestones which had previously been agreed as part of our mental health scoping exercise with local residents and stakeholders. CHRONIC PAIN 15. The CCG s new chronic pain procurement process is proceeding well. 16. To date, two bids have been received and phase 1 (the design phase) of the tendering process will soon begin. WELL SKELMERSDALE 17. The Well Skelmersdale programme has teamed up with the School of Social Entrepreneurs North West to launch a new 12-week social entrepreneurs programme called the Skelmersdale Social Innovators Start Up Programme. EXAMINE YOUR OPTIONS 18. As we approach the festive period, the CCG is now preparing its winter messages. This will include press releases and digital messages throughout December reminding residents of the many services available to them if they fall ill, the importance of self-care and how they can avoid any unnecessary GP and A&E visits, the importance of using A&E appropriately, pharmacy opening hours, the extended hours service and walk-in centres. Recommendation 19. Members are asked to note the content of the report. Mike Maguire Chief Officer November 2017 Chief Officer s update West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
18 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT DATE OF MEETING: 28 November 2017 Agenda item: WLCCGGB 11/17/07 TITLE OF REPORT: BRIEFING POINTS: WLCCG s Risk Management Process Amendments to our Corporate Risk Register and Risk Report: Reviewed and updated our current risks New risks added Closed a risk Does this report its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience) please outline impact No 2. Commissioning of hospital and community services please outline impact No 3. Commissioning and performance management of GP Prescribing please outline impact No 4. Delivering Financial Balance please outline impact No 5. Development of the commissioning group as a commissioning organisation please outline impact Part of governance arrangements No B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number) have any legal implications promote effective governance practice Provides overview and updates on all strategic and operational risks 2. Additional resource implications (either financial or staffing resources) We have amended the presentation style of the Risk Report for our Governing Body, which gives a brief summary of the new, updated, emerging and closed risks followed by a streamlined version of risks of scores 12 & above. Yes Yes 3. Health Inequalities No 4. Equality and Inclusion and Human Rights Requirements Has an Equality Impact and Risk Assessment been carried out? N/A 5. Clinical Engagement N/A 6. Patient and Public Engagement N/A REPORT PREPARED BY: REPORT PRESENT BY: Smita Shetty, Service Redesign Manager (Corporate) Paul Kingan, Chief Finance Officer Risk Management Process West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November 2017

 categorised as follows: 0 Low Risk Unlikely to cause problems 4 Moderate Risk Needs to be resolved or accepted")


19 Risk Register & Governing Board Assurance Framework Introduction The Board Assurance Framework (BAF) is a key part of the CCG s governance arrangements. It is the principal way by which the CCG holds itself to account; it helps to clarify and quantify risks that could compromise delivery of our strategic objectives. The CCG Risk Register has been reviewed to reflect the up to date position as at 17 November The CCG Risk Register has 23 risks (out of which 12 risks with a score of 12 and above) categorised as follows: 0 Low Risk Unlikely to cause problems 4 Moderate Risk Needs to be resolved or accepted at Departmental level 14 High Risk Needs to be resolved or accepted at Departmental level 5 Extreme Risk To be resolved or accepted at CCG Level NEW RISKS CCG59 - There is a risk of a gap in service for paediatric audiology due to the current provider serving notice on the service and the negotiated extension coming to an end. CCG60 - there is a risk of a gap in some paediatric services as a result of due diligence undertaken by the Trust during procurement of community services which did not raise issues with the delivery of some paediatric service provision, these are now coming to light as patients present. UPDATED RISKS CCG08 - CQPG has been reinvigorated but Trust Executive engagement from the Trust has been poor. Joint CQC action plan and risk summit and Executive Improvement Board has focussed the trust on more quality issues CCG25 - Consideration being given to how to achieve running costs target. Running costs being monitored monthly. Staffing requirements reviewed as and when vacancies arise CCG41 - The CCG is routinely checking whether any unwarranted specialist activity is inappropriately being charged as part of general activity. The CCG is also raising queries with the specialist commissioning team regarding budget allocation transfers. CCG44 - There is also a new governance structure for the health economy group working that facilitates better joint working for clinicians across sectors e.g. "Connecting the clinicians" events. EMERGING RISK O There are currently no emerging risks. CLOSED RISKS CCG23 Children being discharged from CAMHS too early at 16 when they should remain with service until 18. CAMHS transition will be increased to 18 years from April 2018 Current CAMHS patients are still transitioning at 16 years but no incidents have occurred because of this for at least the last 10 months. Irrespective of age the person is still receiving a specialist MH service as they have done for many years. A pan-lancs transformation work stream is ongoing and the age transition issue is not unique to West Lancs. CC61 there is a risk of unsafe obstetric services at Southport and Ormskirk Hospitals NHS Trust from November CCG56 - The Sophos Zero Date Protection system which is called exploit prevention has now been rolled to all PCs in the CCG and its GPs. This is the system that stopped the cyber-attack in other trusts. All other risks contain the same risk score as previously determined.
20 CCG Delivery 08/11/17 CCG Delivery 24/11/2017 Risk ID Date Added Current Risk Score Last Review Date Corporate Objective Description of Risk Controls to Mitigate Risk Gaps in Control Measures Gaps in Assurance Sources Actions Required Risk Lead Executive Lead Assurance Status Risk that Southport & Ormskirk Hospitals NHS Trust (S&OHT) will fail to provide a fully staffed, quality and safe obstetric, gynaecology and maternity services for patients from November 2017 due to a shortage in Middle Grade Doctors. Discussions across the Merseyside and Southport and Ormskirk Health System Senior Executives and Clinical Leads to find a solution. W Lancs CCG Executives are playing a prime role in the delivery of a solution The Mersey Women and Children s Vanguard is exploring wider network solutions across all providers 20 Uncertainty of allocation of Middle Grades from the Deanery Recruitment of middle grades and consultants underway; success of recruitment process unknown at present Alternative models of care have to be sustainable, appropriate and safe for the local population Lack of assurances of the delivery of safe services over the next 12 months to allow for the development of new models of care delivery. S&OHT are proactively exploring how to increase and adapt current staffing structures to support delivery of safe services and seeking additional resources wherever possible via mutual aid across the local system. Monthly meetings take place with all partners in the local health system to identify solutions in the short term and develop sustainable options for the medium to long term. Assurance being formally requested of the Board of S&OHT that the delivery of safe services can be maintained at least for the next 12 months. CH Chief Officer Risk of main acute provider failing to meet required levels of delivery and performance due to a number of issues including service quality, financial outlook and senior staff changes. Discussions at Quality Committee Discussions with hospital chair and Board to Board meetings and Executive Improvement Board meetings. There is also a new governance structure for the health economy group working that facilitates better joint working for clinicians across sectors e.g. "Connecting the clinicians" events. 16 Performance data often retrospective and time lag exists. Queries and letters not responded to on time.. Assurance around the impact of solutions on West Lancs population patient flows. In addition to the regular formal meetings in respect of quality and contract performance, the CCG will continue to maintain involvement in the Executive Improvement Board which oversees a number of improvement actions including recommendations from the latest CQC report. The CCG will also ensure it can influence any future STP-wide work programmes in relation to acute care and associated formal decision-making. JM Chief Finance Officer
21 CCG Delivery 08/11/17 CCG Delivery 08/11/17 CCG Delivery 31/08/17 There are no clear case management arrangements for those individuals who may be subject to a domestic DoL There is no oversight of individuals resulting in potential safeguarding risks and people being subject to an unauthorised DoL. The CSU have appointed a lead for quality and safety who will take a lead on the safeguarding arrangements for these individuals. CCG Safeguarding team are sited on identified cases and provide expert advice and signposting to legal team for Court of Protection referral. CSU have process in place to inform CCG as domestic DoL cases are identified. CHC documentation amended to reflect screening against the Acid Test Criteria. 16 No clear documented case management. Resource requirements need to be established. CSU to establish resource requirements and determine if additional resource is required to reflect workload. Case management arrangements not yet agreed. CH Chief Nurse Fragility of Hospital services relating to workforce recruitment and retention issues at the Trust. This includes Patient safety issues in relation to the Cardiology, Radiology & Dermatology services at Southport and Ormskirk Trust and issues in respect of backlog of follow up patients. IPA process - financial instability, increasing costs, and assurances on quality of assessments Through Suitability & Transformation Plans, working practices are being reviewed and are encouraged to work strategically within their local health economy. Resource management, planning eventualities shared organisational actions, etc. are being drawn through these plans. Reviews of high cost complex cases. Examining the information MLCSU sends to CCG. Undertaking further training for GPs on process. Participation at IPA Programme Board meetings 16 Timely recruitment and resource planning. 12 None identified at present Urgent cases have appointments scheduled. Alternative provider expanding services in Cardiology. Senior Service Redesign Manager will update monthly or sooner. Operational Services Manager has been contacted with regards to monthly updates. Undertake reviews and complete training for GPs on process. CCG scrutinising the accuracy of the financial forecast produced by the CSU Developing new commissioning processes in partnership with CSU. Continued scrutiny of CSU Broadcare data. The CCG has accepted the CSU's QIPP proposal - this will increase the capacity of the CSU IPA team and the frequency of case reviews. These additional reviews are currently progressing, with the CCG's investment anticipated to be more than offset by the savings made. The CCG is participating in a detailed review of the Detailed Service Offer (DSO) aimed at developing a new SLA to replace the 2013 DSO including prioritisation of what matters most to CCGs in delivering the programme within available budgets. JM PJ Chief Nurse Chief Nurse
22 CCG Contracts 31/08/17 CCG Contracts 08/11/17 CCG Delivery 25/08/17 Services users are potentially at risk of harm due to unlawful deprivation of liberty within hospital care home and supported living following the Cheshire West judgement in March Failure to Achieve Financial Balance 2017/18. LSAB MCA subgroup in place to ensure practice is consistent across Lancashire footprint. MCA/adult leads of CCGs providing expert advice and support around management of individual complex cases. Collaborative working with LCC around the use of the ADASS prioritisation tool. Collaborative working with CSU, CCG and LCC to develop COP prioritisation tool to identify potential domiciliary DoL's. Robust financial controls (ledger) and budget setting. Finance Recovery plan in operation to bolster initial financial and QIPP plan. 12 Timely notification and management of cases where application to Court of Protection may be required. CSU has no access to Broadcare to identify patients. CCG to determine which service is best placed to be commissioned to case manage CHC patients residing in their own homes and supported tenancy to ensure compliance with Cheshire West recommendations. 12 Planned Care Budgets need careful monitoring due to potential impact on CCG financial position. Close working relationships with CSU in the management Broadcare Reports. Seek assurance that the care and treatment plans for CHC commissioned packages of care have been reviewed and where a DoLS is identified least restrictive measures are in place. Work streams continue and the overall performance continues to be monitored. Continuous monitoring of financial position and take mitigating action when budgetary variances arise. Successful implementation of QIPP schemes. Seek clarity from NHS England on treatment of 0.5% nonrecurrent funds set aside by the CCG. The CCG did not deliver a 1% surplus in 2016/17 as per NHS England's Business Rules and will have to repay this shortfall from 2017/18 resources CH PJ Chief Nurse Chief Finance Officer There are no quality assurance arrangements or contracts in place for individuals in receipt of a CHC funded domiciliary health package of care. The risk is a commissioning gap resulting in a lack of governance arrangements impacting from a safeguarding perspective. There is an increased risk of harm to individuals due to a lack of quality assurance. Following the submission of a paper to the CCB July 2016 the work stream has been allocated to the Healthier Lancashire Group. Safeguarding team work closely with multi agency partners where there are identified safeguarding risks. CSU complex cases team sign off individual packages of care once a care plan has been presented and meets needs. CSU Safeguarding team work closely with multi agency partners. 12 Lack of governance arrangements when monitoring the ongoing packages of care or when an individual needs change. Limited resource available to provide the ongoing review of packages from the complex cases team. Safeguarding team are sited on complex cases. Safeguarding team become involved when safeguarding risks become apparent. CCG representative on the Healthier Lancashire Work stream. Quest 4 Care will enable significant improvement in assurance regarding the service delivery. A senior clinical CCG representative will be engaged in the development of Quest for care and its application. CH Chief Nurse
23 CCG57CCgCCG Delivery 08/11/17 CCG Delivery 31/08/17 Quest 4 Care proposal being trialled Pan Lancashire - joint health and social care contract management system that is being trialled with a domiciliary care provider in collaboration with our local provider. Local Delivery System (LDS) plans as part of the Merseyside Sustainability & Transformation Plan (STP) do not fully take account of the patient flows from West Lancashire to Mersey providers We are involved in the planning process and are able to influence the decisions taken. 12 MM Chief Officer Inability to deliver corporate objectives as a result of budget cuts in Local Authorities (including 4M reduction in Public Health funding). This has impacted on the CCG in terms of services provided by the Local Authorities; reduction in capacity and knowledge and relationships with key stakeholders; thereby increasing demand and strain on NHS services. Consolidation of two WLCCG risks (38 and 43) Chair of HWB Board has written to the Secretary of State on behalf on the Board. Regular meetings with Public Health. There is joint work across Lancashire as part of the Healthier Lancashire STP plan to work towards better health and social care integration by This currently includes work as part of the Better Care Fund and also Learning Disability. 12 None identified. None identified Ensure partnership arrangements are robust. CCG is in regular contact with LCC over the financial impact. A senior officer from LCC attends the governing body meetings to provide any updates. The CCG is also working collaboratively across Lancashire as part of the BCF and Healthier Lancashire work with LCC and the other CCG s. Any jointly identified risks are being identified and monitored, including the impact of budget cuts. Lancashire Health & Wellbeing Board to have discussion to determine what it will mean for the future of Public Health. Chair of H&W Being Board to write to the Secretary of State on behalf on the Board that any soft evidence on the impact of Local Authority cuts should be forwarded to Director of Public Health. PK Chief Officer
24 CCG Delivery CCG Delivery LCC Cabinet took a paper considering the impact of scaling back to statutory services. This is an area that we are monitoring in terms of LCC decisions and resulting impact. Continue to monitor any impact through comments received by the CCG. Liaison with LCC commissioning leads to ensure CCG Exec and Membership are briefed on updates regarding mobilisation of newly awarded contracts. The Council has reserves for 2 years which helps to mitigate against various service budget cuts in the near future. There is a risk of a gap in service for paediatric audiology due to the current provider serving notice on the service and the negotiated extension coming to an end. Managerial discussions to extend the contract with S&OHT AO discussion with new provider CEO about expediting the negotiation and mobilisation of the new service Managerial discussion with peers at new provider to make this shift happen 12 Dependent on capacity at the new provider who is currently mobilising another new service for another provider Managerial discussions to extend the contract with S&OHT AO discussion with new provider CEO about expediting the negotiation and mobilisation of the new service Managerial discussion with peers at new provider to make this shift happen JM Chief Finance Officer There is a risk of a gap in some paediatric services as a result of due diligence undertaken by the Trust during procurement of community services which did not raise issues with the delivery of some paediatric service provision, these are now coming to light as patients present. Urgent short term cover for these services are being put in place 12 Dependent on available skills and capacity of provider to respond to these gaps in service and cover these as quickly as required. We don t know currently in what services there might also be a problem until they arise so the mapping of services must be undertaken urgently Discussions with local providers to understand these gaps, how they have arisen and about how to cover these gaps in the short term Longer term mapping, modelling and reprocurement is urgently necessary to reduce this risk JM Chief Finance Officer
25 CCG Delivery CCG Delivery CCG Engagement 08/11/17 Lack of engagement of providers in the quality agenda leading to a lack of understanding and consistency between partners regarding outcomes of specific schemes. CQPG has been reinvigorated but Trust Executive engagement from the Trust has been poor. Joint CQC action plan and risk summit and Executive Improvement Board has focussed the trust on more quality issues 9 Significant issues are still regular arising from the trust which are causing Quality Committee concern Engagement of trust staff with GPs in our membership and in closer to you events as these tend to clash with our membership meetings Op forum is no longer functioning GPS and CCG concerns are represented through the quality and contracting process Updates still continue to be given at membership via the Chairman's update Engagement of the trust staff and GPs is via the LDS discussions now and Care for You events escalate quality committee concerns formally to lead CCG for their onward transmission to NHSE and NHSi JM Chief Nurse Failure to deliver service priorities to plan including QIPP targets Monitoring of progress and financial performance of QIPP schemes via new project management office (PMO). QIPP savings of 5.063m included in 2017/18 Financial Plan submitted to NHS England Recovery plan presented to Finance Committee on 7/11/17 9 Cross reference QIPP programme to redesign programme. Continuously refresh assumptions around QIPP programme outcomes and embed services. Adoption of Right Care methodology and associated benchmarking data to inform future direction of QIPP. PJ Chief Finance Officer Increasing financial risk in relation to the CCG taking on specialist services cocommissioning and the associated budget. The CCG is routinely checking whether any unwarranted specialist activity is inappropriately being charged as part of general activity. The CCG is also raising queries with the specialist commissioning team regarding budget allocation transfers. 9 Not always easy to identify inappropriate activity. Understanding Lancashire and Merseyside wide allocations in relation to key providers. The CCG has raised queries with the specialist commissioning team and is following these up on a regular basis. PK Chief Finance Officer
26 CCG Delivery 01/08/17 CCG Delivery 24/10/17 Business Continuity for example (the recent Cyber Attack) when the ransomware called WannaCry swept across the UK, locking computers and demanding payment for them to be unlocked. The NHS in the UK was particularly badly hit. Officials in Britain's National Cyber Security Centre (NCSC) began their own investigation and concluded their assessment in recent weeks. The ransomware did not target Britain or the NHS specifically, and may well have been a moneymaking scheme that got out of control, particularly since the hackers do not appear to have retrieved any of the ransom money as yet. Installed Microsoft Service Pack latest update and antivirus updates on all affected IT Devices. Ad-hoc spot checks of IT devices to ensure virus updates and Microsoft Service packs have been updated The Sophos Zero Date Protection system which is called exploit prevention has now been rolled to all PCs in the CCG and its GPs. This is the system that stopped the cyber-attack in other trusts. The CC are planning on moving all PCs to Windows 10 but we are currently waiting for the funding to be release by NHS England. 9 Conflicting and delayed comms from National leads. None identified Raising awareness amongst staff to be more vigilant and to refer to guidance published NHS Digital M&LCSU need to: monitor and implement new antivirus and Microsoft Security packs to IT devices. Carry out Ad-hoc spot checks of IT devices to ensure virus updates and Microsoft Service packs have been updated. Implementation of secondary (if possible) antivirus software to provide an additional defence. Explore a more secure virtual infrastructure SS Chief Finance Officer The cyber-attack affected some IT equipment within the CSU, Corporate CCG offices and GP Practice estates and has highlighted that some CSU and client s IT equipment is vulnerable to a malware/virus attack. These devices could become inoperable and require IT engineering resources to rebuild or reimage the IT equipment resulting in significant business impact for the CS, its CCG clients and frontline users such as those in GP Primary Care. Patients in receipt of NHS funded care potentially at risk of harm as their health and care needs may not be addressed due to gaps in the commissioning of the CHC service in respect of care planning and case management. Lack of capacity in CHC team resulting in routine reviews behind scheduled. CSU commissioned to manage CHC process. Monthly exception reporting care homes from CSU. Quarterly reporting on CHC from CSU. Additional reviews now being undertaken following the adoption of the CSU's QIPP proposal. 8 The CCG is participating in a detailed review of the Detailed Service Offer (DSO) aimed at developing a new SLA to replace the 2013 DSO including prioritisation of what matters most to CCGs in delivering the programme within available budgets. PJ Chief Nurse
27 CCG Contracts CCG Delivery CCG Delivery 25/08/17 CCG Delivery 25/08/17 Risks relating to MCA and DoLS quality assurance arrangements & compliance for patients diagnosed with learning disabilities, detained in secure settings where arrangements are being made for discharge in line with the Transforming Care agenda. There is a backlog of Court of Protection (COP) applications resulting in the potential for unauthorised DoLS Working arrangements for MASH require a redesign due to the current operating model not being fit for purpose. And there being a lack of strategic partnership. Insufficient health contribution will impact on timeliness of information sharing and decision making and may result in poorer outcomes for children and adults at risk. Lack of commissioning policies to drive individual patient funding decisions. Patients currently remain under section of the Mental Health Act whilst arrangements are being considered. Where appropriate COP applications will be submitted by social care. MASH multiagency steering group in place with CCG Designated Nurse representation to agree strategic direction for MASH including children and adults. Task and finish groups in place to review targeted work areas including a locality based approach, adult MASH to be incorporated into existing work streams Existing legacy policies being utilised. 8 A sustained operational process is in place to identify patients where a referral to the COP is required. CCG safeguarding involved in CSU monthly meetings to discuss complex cases and potential legal input. 6 Demand in workload and contribution required from a health perspective to cover both adults and children Task and finish work streams agreed to focus on clearer pathways for early help including response to Domestic Abuse, review IT systems and establish a single front door into MASH for referrals with 3 locality aligned teams based in MASH. Central Lancashire pilot of new way of working to commence following review of diagnostic in August/ September. Designated Nurses to monitor progress against agreed timescales. 6 Develop a new suite of policies. The CCG needs to establish clear governance arrangements for adopting polices CH CH SS Chief Nurse Chief Nurse Chief Finance Officer Continual review of commissioning policies is being undertaken. 5 newly written policies just adopted by the CCG Awaiting more updates from Pan Lancashire work Running costs outstrip available resource Consideration being given to how to achieve running costs target. Running costs being monitored monthly. Staffing requirements reviewed as and when vacancies arise 6 Finance monitor running costs on a monthly basis. Resources have been freed up by not replacing staff like for like. PJ Chief Finance Officer
28 CCG Delivery 25/08/17 CCG Delivery 25/08/17 There is no case management of adults and children who are allocated a personal health budget (PHB) with a package of care and there is no oversight of adults in receipt of PHB s where the LA have transferred care arrangements to the CCG for a CHC package resulting in potential safeguarding risks. CSU quality and safety lead in place to oversee this area of work. 6 CSU to provide update to CCG on progress. CCG safeguarding team to be sighted on any safeguarding issues. NHS England are participating in End of Life Care PHB programme which will enable the CCG to resolve some issues locally. CH Chief Nurse Health assessments for children looked after have not consistently been undertaken within statutory timescales and may result in the child not achieving their full potential as individual health needs not identified and addressed in a timely manner. Review health assessments have improved and sustained however no improvement with initial health assessments. Service specification in place with LCFT which requires them to coordinate the health assessment process and to quality assure assessments. S&O community paeds commissioned to undertake initial health assessments and adoption medicals for children 0-18 years. LAC multi agency recovery plan supported by tracking meetings and exception reporting. 4 Interdependencies with the LA and the IHA process IHA are not completed within times scales LAC multi agency recovery action plan supported by tracking meetings and exception reporting. Working with LCC/LCFT, Designated Drs for LAC. Scrutiny and regular reporting received from LCC/LCFT. LCFT are currently undertaking an audit to identify delays in the IHA process. Consideration being given to streamlining the IHA process but this will require changes to the current service specification and agreement by all partners CH Chief Nurse

29 Assurance and Governance A workshop was held on 26 th June with Senior Management and key risk owners to gain an overview of current and emerging risks. Since the workshop, new measures have been implemented to strengthen the Risk Reporting Process. The new Risk Reporting Process was discussed at the last Audit Committee meeting. We have amended the presentation style of the Risk Report for our Governing Body, which gives a brief summary of the new, updated, emerging and closed risks followed by a streamlined version of risks of scores 12 & above. We have also designed and developed a step by step How to...guide to log new risks and supports the Risk Management Process. We will be rolling this out to staff with the implementation of our Project Management Office function which will facilitate the Risk Management Process. How to...log a NEW Risk.pdf
30 Agenda item no: WLCCGB 11/17/08 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERING BODY REPORT DATE OF BOARD MEETING: 28 November 2017 TITLE OF REPORT: Integrated Business Report BRIEFING POINTS: This report provides summary information on the financial and activity performance of West Lancashire Clinical Commissioning Group for July 2017 and a financial position for August Quality and performance analysis is also provided for community based targets and for the Southport and Ormskirk Hospitals. Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient Yes experience) please outline impact The report outlines quality and performance issues relevant to the CCG and describes key actions to address these. 2. Commissioning of hospital and community services please outline impact The report includes financial and activity information in relation to commissioned services and highlights areas of risk and actions. 3. Commissioning and performance management of GP Prescribing please outline impact 4. Delivering Financial Balance please outline impact Yes The report summarises the financial position of the CCG and highlights areas of financial risk. 5. Development of the commissioning group as a commissioning organisation please outline impact This report will support the CCG in developing clear and credible plans. B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework have any legal implications promote effective governance practice Yes Links to financial risks. 2. Additional resource implications No (either financial or staffing resources) 3. Health Inequalities Yes Links to health outcomes framework (all five domains) 4. Equality and Inclusion and Human Rights Requirements No Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement No 6. Patient and Public Engagement No REPORT PREPARED BY: Paul Kingan, Chief finance officer Integrated Business Report West Lancashire Clinical Commissioning Group Governing Body 28 November 2017 Yes No Yes
31 West Lancashire Clinical Commissioning Group Integrated Business Report November 2017 (Reporting Period September 2017) 1 P a g e
32 TABLE OF CONTENTS 1 Executive Summary 3 2 Financial Position 4 3 QIPP 8 4 Individual Patient Activity 9 5 Right Care 11 6 Planned Care: Referrals 13 7 Planned Care: ereferrals Service 15 8 Planned Care: Acute Contract 16 9 Unplanned Care: Acute Contract Prescribing Mental Health Quality and Performance a West Lancashire CCG Performance Dashboard 26 b Southport and Ormskirk Hospitals NHS Trust Integrated Performance Dashboard 30 c Areas of Under-Performance 31 d Patients Waiting by Weeks 35 f Friends and Family Test 37 g Safety Thermometer Complaints GP Comments, Concerns and Issues with Healthcare Providers Serious and Untoward Incident Reporting 39 2 P a g e
33 1. Executive Summary This report provides summary information on the activity performance of West Lancashire Clinical Commissioning Group for September 2017 and a financial position as at October Quality and performance analysis is also provided for community based targets and for Southport and Ormskirk Hospitals NHS Trust. CCG Position Highlights FINANCIAL PERFORMANCE CCG Forecast Position (Surplus) Quantified Net Risks Risk Adjusted Forecast (Surplus) Value 2.997m 1.000m 1.997m Better Payments Practice Code >95% QIPP Forecast Savings (Plan 5.063m) DEMAND GP referrals Other referrals PLANNED CARE Total planned care PBR UNPLANNED CARE Total unplanned care PBR PRESCRIBING Prescribing Budget 4.137m Footprint CCG CCG CCG CCG CCG CCG Key Performance Indicators YTD Key information from this report NHS West Lancashire CCG For the 2017/18 financial year the CCG is forecasting a surplus of 2.997m, in line with that required by NHS England. However, there are significant risks to the delivery of this position. The CCG is currently quantifying the aggregate net value of these to be 1.000m, producing a risk-adjusted surplus of 1.997m. This figure is unchanged from the previous month. Indicative performance to the end of September 2017 against the planned care element of all contracts is under plan by 740k. The performance over the same period against the planned care element of the Southport and Ormskirk Hospitals NHS Trust contract only is under plan by 893k. Indicative performance to the end of September 2017 against the unplanned care element of all contracts is over plan by 639k. Unplanned care performance for the same period against the Southport and Ormskirk Hospitals NHS Trust contract is over plan by 185k. NHS Constitution indicators RTT 18 Weeks wait (admitted) Accident and Emergency 4 hours Cancer Waits 62 days Ambulance Category a Calls Footprint CCG CCG CCG CCG Performance issues The 4-hour Accident and Emergency target continues to be an issue with Southport and Ormskirk, Wrightington, Wigan and Leigh and Lancashire Teaching Hospitals NHS Trusts all failing the 95% target. Other key targets Friends and Family CCG MRSA attributable to CCG CCG C. difficile CCG The 12-hour Accident and Emergency Trolley Waits target has been exceeded at Southport and Ormskirk Hospitals NHS Trust these relate to Mental Health patients. Cancer 14-day urgent target breast CCG Southport and Ormskirk Hospitals NHS Trust have been identified as the second worst performing Acute Trust in England for Hospital Mortality (SHMI). 3 P a g e
34 2. Financial Position NHS West Lancashire CCG Financial Position as at Month 07 (October) 2017/18 Year to Date Full Year Budget Expenditure Variance Budget Forecast Forecast Variance Acute services Acute 43,025 43, ,778 75,243 1,465 Ambulance services 1,858 1, ,184 3,184 0 Sub-total Acute Services 44,883 45, ,962 78,427 1,465 Mental Health Services Mental Health 6,563 6, ,366 11, Learning Difficulties 1,052 1, ,804 1, Sub-total Mental Health Services 7,615 7, ,170 13, Community Health Services Community 9,892 9, ,957 17, Sub-total Community Services 9,892 9, ,957 17, Continuing Care Services Individual Packages 4,784 5, ,202 9,544 1,342 Funded Nursing Care (97) 1,332 1,166 (166) Sub-total Continuing Care Services 5,561 6, ,534 10,710 1,176 Primary Care Services Enhanced & Tier 2 Services ,274 1, GP IT Prescribing 11,152 10,460 (692) 19,118 17,932 (1,186) Primary Care Co-Commissioning 7,469 7,367 (102) 13,675 13,500 (175) Sub-total Primary Care Services 19,748 19,002 (746) 34,725 33,446 (1,279) Other Budgets/Reserves Running Costs 1,390 1, ,383 2,383 0 NHS Property Services (202) 1,360 1,014 (346) Urgent Care 2,247 2,244 (3) 3,851 3,846 (5) Other Corporate Costs (9) 1,042 1,027 (15) Other Programme Services (59) 1,493 1,392 (101) Seasonal Resilience Reserves (0.5% Non-recurrent) Reserves (0.5% Contingency) (438) (751) Reserves (Other) (386) 1, (662) Sub-total Other Programme Services 7,418 6,321 (1,097) 12,714 10,834 (1,880) Total - Commissioning services 95,117 95, , ,062 0 Planned Surplus 1,748 0 (1,748) 2,997 0 (2,997) Grand Total 96,865 95,117 (1,748) 167, ,062 (2,997) For the 2017/18 financial year the CCG is forecasting a surplus of 2.997m, in line with that required by NHS England. This figure comprises the CCG s cumulative surplus of 1.584m plus an additional 1.413m which relates to the CCG s under delivery against its surplus target in 2016/17 - this must be repaid in 2017/18. 4 P a g e
35 Key points to note are: Acute Services Month 6 activity monitoring information indicates significant forecast underperformance ( 772k) at Southport and Ormskirk Hospitals NHS Trust, although this figure is 110k lower than last month. The Trust is currently experiencing an underlying year on year reduction in GP referrals of 18% and this has translated into forecast underperformance of 840k for Daycases and 314k for Inpatient Elective surgery. Offsetting this is a marked increase in the Trust s activity in March, which was 450k higher than forecasted. As the position stated in the CCG s 2016/17 final accounts was based on the forecasted level, the resulting financial pressure therefore impacts on the 2017/18 financial position. Several of the CCG s other Acute contracts are however overperforming significantly most notably at Wrightington, Wigan and Leigh NHS Trust (forecast 905k above budget) and Aintree Hospitals NHS Trust ( 651k). It is probable that these variances represent a continuation of a shift in market share away from Southport and Ormskirk Hospitals NHS Trust. QIPP savings of 2.874m have been applied to this line. Under delivery on these schemes is highly likely to cause an associated financial pressure as the year progresses. Mental Health Services The CCG has been notified of a potential financial pressure relating to Out of Area Placements (OAPs). A risk share for such costs has been agreed between Lancashire Care Foundation Trust (LCFT) and the Lancashire CCGs, although given commissioner investment in schemes to avoid such placements the CCG expects that associated expenditure is considerably lower than the previous year. An initial estimate of the CCG s share of this issue is 90k. Additionally the CCG has offered to settle a longstanding dispute with LCFT regarding Psychology funding and this has been factored into the position. Individual Packages The CCG is now forecasting a pressure of 1.342m this represents a considerable increase of 825k in just one month. 683k relates to the forecast cost of new packages, two of which are each in excess of 100k pa. The CCG is undertaking further work to understand expenditure trends in this area and Midlands and Lancashire CSU are currently developing a proposal to improve the value for money of Individual Packages in West Lancashire. This will be presented at December s Finance and QIPP Committee. Funded Nursing Care Expenditure for April to September is approximately 12% lower than budgeted; if this trend is maintained this will deliver an underspend of 165k. Prescribing - The performance of the Prescribing budget, and the delivery of planned QIPP savings of 900k, will be critical to the CCG delivering its financial targets in 2017/18. Based on the encouraging data currently available for the 2017/18 financial year the CCG is reporting a forecast surplus of 1.186m. However, volatility in the prices of certain drugs mean this position is not settled will be subject to refinement in the coming months. More detailed analysis of Prescribing expenditure is provided in Section 10. Reserves 0.5% (Non-recurrent) Consistent with NHS England s planning guidance the CCG has set aside 0.5% of its allocation as a contribution towards a national risk reserve of 830m. Release of the risk reserve to each local system will be dependent on delivery of its control total, subject to a satisfactory national financial position. Reserves 0.5% (Contingency) - As was the case for 2016/17 and previous years, the CCGs has created a 0.5% contingency to manage in-year pressures and risks. Given the financial pressures that have already arisen, and the marked deterioration in the Individual Packages budgetary position, the entire contingency has now been deployed and the resultant underspend is factored into the CCG s Month 7 forecast. Reserves (Other) This surplus, helping to offset the various financial pressures above, predominantly relates to a market rent allocation the CCG has received. The CCG had already prudently budgeted for the associated costs. 5 P a g e
36 Financial Risk There are risks to the delivery of the reported financial position. These are quantified as below: Risk Risk Adjusted Value ( m) Commentary QIPP Under Delivery Failure to deliver forecast QIPP savings in 2017/18 Acute Services Possible pressure from additional overperformance Prescribing Possible pressure from new/increased package costs Sub Total Risks Mitigations Risk Adjusted Value ( m) Commentary Contingency Held Contingency already fully deployed Sub Total Mitigations Net Risk Value By far the largest risk to the CCG s financial position is under-delivery against its 5.063m QIPP savings programme. If the risks crystallised as above the CCG s surplus would fall to 1.997m. Allocated Resources The CCG s annual budget for 2017/18 is m. This is derived as follows: In addition to its duty on delivering a 2.997m surplus the CCG has other financial responsibilities: Better Payment Practice Code (BPPC) 000 Initial CCG Programme Allocation 150,017 Initial CCG Running Cost Allocation 2,355 Business Rules - Co Commissioning 160 Winter Resilience 117 IR Changes (341) HRG4+ changes (2,131) Primary Care Delegated budget 13, /17 Surplus/Deficit Carry Forward 1,584 Care Navigators and Medical Assistants Training 19 NHS WiFi 75 Market Rent Adjustment 907 Paramedic Rebanding Additional Funding HSCN - GP Funding 2 Transfer 17/18 for Minor Ailment Scheme (Pharmacy) 25 GP Access 2017/ /18 Working at scale 113 CYP Crisis Acceleration Funding - North 162 Total Resources (as at Month 07) 167,061 The Better Payment Practice Code requires the CCG to pay valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is later. The CCG s target is for 95% of invoices (both by value and volume) to be paid within this criteria. Below is the 2017/18 cumulative performance against these requirements: 6 P a g e
37 NHS Non-NHS Cash Management Target Cumulative Performance Year to Date Value 95% Volume 95% Value 95% Volume 95% On Target for Year End The CCG must not utilise more cash than it has available, both on a monthly and annual basis. It must manage its cash flow accordingly whilst ensuring there are sufficient funds available to pay suppliers and meet the BPPC targets listed above. NHS England issued the CCG with a Maximum Cash Drawdown (MCD) for 2017/18 of m. 000 Maximum Cash Drawdown 2017/18 163,796 YTD Cash Drawdown 85,060 YTD Oxygen and Prescribing 10,873 Cash Available for Remainder of Year 67,863 7 P a g e
38 3. QIPP Each year the CCG is required to balance the continually increasing demand for services with a finite amount of resources. Therefore the CCG seeks to negotiate the best value for money it can achieve from its contracts, whilst also seeking to achieve Quality, Innovation, Productivity and Performance (QIPP) gains. These savings may be either cash releasing or non-cash releasing but need to have a recurrent effect if the CCG is to derive a sustainable financial benefit. The CCG s Financial Plan identified 8 QIPP schemes for 2017/2018. These had an aggregate value of 4.684m, with a further 0.379m being classed as unidentified, giving a total savings target of 5.063m. Two additional schemes (Ophthalmology and Estates) have been subsequently added to the Programme, but it is probable that some schemes will not deliver all planned savings. The CCG must therefore continue to devise schemes that drive efficiencies to enable it to deliver services within its allocated resources. A description, scheme leads, financial performance (expected savings compared to planned levels) and project status for each are shown in the table below. ID Scheme Name Description 1 Community Procurement - Impact on emergency activity 2 Prescribing 3 Musculoskeletal Redesign Project 4 Right Care Redesigned community services will reduce emergency admissions and A&E attendances Savings from more efficient and effective prescribing of medicines Savings from avoided inpatient and outpatient activity Savings identified from the Right Care opportunities analysis (additional to schemes separately identified) Managerial Lead Year to Date Full Year Planned Forecast Planned Forecast Clinical Lead Savings Savings Savings Savings k k k k Update/Actions Pending New provider in period of 'safe transfer' prior to C Heneghan C Heneghan , transformation initiatives N Baxter P Gregory Medicines waste campaign operational in addition to 1,400 Prescribing for Clinical Need. Prescribing Ordering Direct (POD) initiative commenced in Skelmersdale. Joint Health service operational & producing marked P Kingan P Gregory reduction in elective activity. Oversight from Joint Health Programme Board Right Care data has been analysed. Potential J Moran C Heneghan opportunities are being considered MLCSU have recruited staff and 43 patient reviews have 5 Individual Patient Activity Reduction in CHC placement costs P Jones C Heneghan been completed. 6 Pain Management Redesign of service M Maguire V Mittal Procurement processes have commenced 7 Discharge to Assess A greater proportion of assessments to be undertaken in community based settings M Maguire C Heneghan Scheme will require additional capacity 8 Contract Review Review of grants made to non-nhs organisations to ensure alignment with CCG strategy J Moran J Rimmer Review completed 9 Ophthalmology The CCG will be commissioning a community Ophthalmology triage and treatment service alongside re-commissioning macular services M Greene J Rimmer V Mittal R Jaidka Prospective providers submitted bids September these are being evaluated 10 Estates 11 Unidentified Rationalisation of CCG Estate to reduce charges levied by NHS Property Services Schemes must be identified in year in order to bridge this financial gap in the QIPP plan P Kingan J Caine Total 2,322 1,649 5,063 4,137 % Delivery 71% 82% The figures shown in the table above will continue to be reviewed, refined and updated as the schemes develop and further analysis of supporting data is carried out. More sophisticated analysis will take place as the year progresses and more data on the performance of schemes becomes available to the CCG. 8 P a g e

39 4. Individual Patient Activity Current Activity Midlands and Lancashire CSU (MLCSU) provides commissioning support services on behalf of the CCG for Individual Patient Activity (IPA). The graph below itemises the spend for 2017/18 by categories of care and compares the spend to 2016/17. The largest spend by category is Continuing Healthcare, the graph/table below illustrates the number and type of packages the CCG has been responsible for over the 12 months to September As at September 2017, this amounted to 129 packages. Retrospective Cases On 15 March 2012, the Department of Health announced the introduction of deadlines for individuals to request an assessment of eligibility for NHS Continuing Healthcare (NHS CHC) funding, for previously unassessed cases during the period 1 April March Lancashire CCGs received almost 2,000 initial applications. In early 2015, NHSE instructed CCGs to provide an eligibility outcome on all cases received by March 2017, which was revised soon after to a shortened deadline of 30 September Because of this requirement the CCGs commissioned MLCSU to provide additional support to manage this caseload. MLCSU completed all 148 reviews relating to West Lancashire CCG by the 30 September deadline. However, work continues on disputes, complaints and Subject Access Requests received in relation to eligibility decisions. 9 P a g e

40 Court of Protection The following table provides a Lancashire-wide breakdown on active, inactive and pending Court of Protection cases: Court of Protection Cases CCG Active Inactive Pending Blackburn with Darwen CCG Chorley and south Ribble CCG East Lancashire CCG Fylde and Wyre CCG Greater Preston CCG Lancashire North CCG West Lancashire CCG All CCGs Location of Assessments The CCG has been set a target for the number of CHC assessments taking place in an acute setting. Fewer than 15% of assessments should take place in this environment. The graph below details recent performance. 10 P a g e
 to highlight areas where outcomes could be improved or spend reduced. Dr.")
41 5. Right Care West Lancashire CCG is in the second wave of the Right Care rollout to Clinical Commissioning Groups. Right Care is a benchmarking tool that compares West Lancashire CCG to 10 similar CCGs (as shown in the graphs below) to highlight areas where outcomes could be improved or spend reduced. Dr. Mark Johnston has been appointed West Lancashire CCG s Right Care Delivery Partner and will be working with the CCG throughout the Right Care Process. To begin with, West Lancashire CCG has chosen to focus on 3 areas identified by the Right Care Programme which are listed below. These areas link well with current areas of development at West Lancashire CCG. Musculo Skeletal System Elective Spend Neurological Problems Primary Care Prescribing Spend Problems of the Respiratory System Elective Spend and Primary Care Prescribing Spend Reporting to be included in the IBR focusing on the progress of NHS Right Care will be developed over the coming months as the Right Care Programme is better understood. Full detail of the NHS Right Care Programme can be found at: Extracts, included below, form the latest Where to Look Right Care pack for West Lancashire CCG which was published in January The full pack, which includes guidance on how to interpret the data, can be found at: 11 P a g e

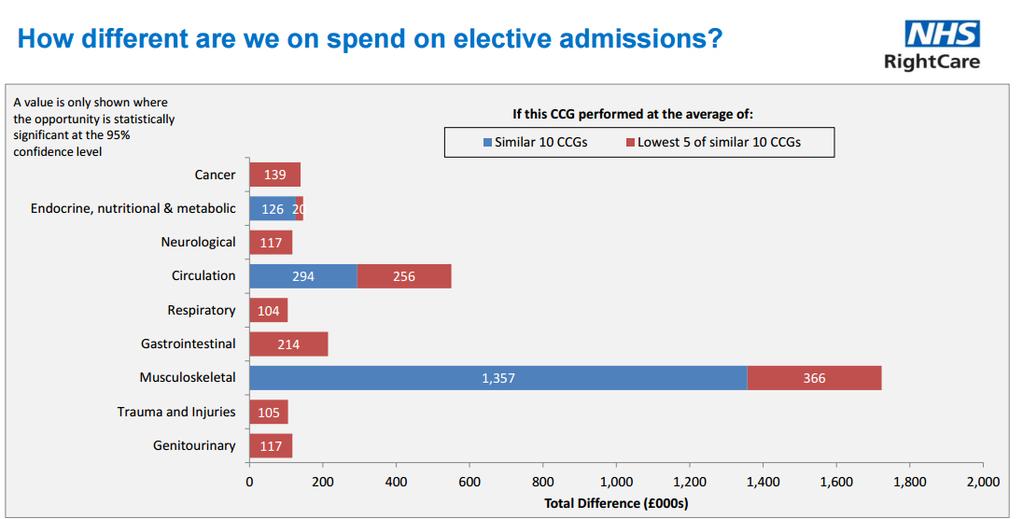
42 12 P a g e
43 6. Planned Care: Referrals The following section provides an overview of referrals to Secondary Care up to the end of September 2017 comparing referrals activity for financial years 2016/17 and 2017/18. This report differs from previous IBRs as steps have been taken to remove Physiotherapy GP referrals at Southport and Ormskirk Hospitals NHS Trust. The issue being that the Trust stopped recording Physiotherapy GP Referrals in March 2017 as this activity represented a direct referral to the Joint Health Service rather than Acute care. In 2016/17 there were 2492 GP referrals to Physiotherapy recorded at Southport and Ormskirk Hospitals NHS Trust, in 2017/18 there have been no referrals recorded. This approach is consistent with the referrals counting methodology used by NHS England to monitor CCG performance. Chart A (below) shows numbers of referrals for West Lancashire CCG across all Lancashire providers and Merseyside providers. Overall, there has been an increase of 1445 (5.27%) in all sources of referrals year to date compared to the same period last year. GP referrals have reduced by 3.59%, a decrease of 568 when comparing the same period 2016/17 to 2017/18. Significant in this reduction is the effects of Joint Health MCAS service and a requirement that all Orthopaedic Referrals to Secondary Care received after 30 October 2016 are triaged by this service. Across all providers GP referrals to Trauma and Orthopaedics have fallen by 47.79% (843 referrals) comparing April to September 2017/18 with the same period in 2016/17. If the effects of the Joint Health MCAS service are removed from GP referrals data, referrals have increased by 275 across all providers. Hospital referrals have increased by 29.62% (2147 referrals). This considerable increase can be ascribed to Southport and Ormskirk Hospitals. This increase is of concern and additional work is required to identify the source of these referrals, and any activity and cost pressures caused by this activity. Other referrals have decreased by 3.11% (134 referrals); this does not appear significant. It should be noted that NHS England monitors CCG Performance against GP written referrals made as recorded in the Monthly Activity Report (MAR) rather than using a local return (to MLCSU) for Lancashire and Merseyside providers. As of September 2017, the MAR Position for GP referrals for 2017/18 shows a 9.76% decrease compared to the same period 2016/17. The principal reason for this difference is that MAR only reports on referrals to consultant led services. 13 P a g e
44 An additional issue identified is that Ramsay Operations does not supply correct numbers of referrals to MAR and typically understates referrals by 30%. Ramsay have confirmed that their MAR return is incorrect and have explained the source of the error, but have not indicated how they intend to correct this. Work is ongoing to align the two data sources to ensure consistent reporting in future reports. The remainder of comments in this section relate to data supplied by the MLCSU local return. Comparison of Referrals Financial Year to Date 2016/17 to 2017/18 -September 2017 Referral Source Variance Variance % All % GP % Hospital % Other % West Lancashire CCGs main secondary care provider, Southport and Ormskirk Hospitals NHS Trust, has seen referrals increase by 0.02% in all sources (4 referrals); GP referrals have decreased by 1629 (-17.95%) compared to the same period last financial year. The overall market share in total referrals for Southport and Ormskirk Hospitals NHS Trust has decreased by 2.91% compared to the same period last year, while the market share for GP referrals has decreased by 8.54%. The specialties with the most significant decreases in GP referrals at Southport and Ormskirk Hospitals are Dermatology 60.1% decrease (922 referrals); Ophthalmology 12.2% decrease (144 referrals); Cardiology 28.4% decrease (111 referrals); Midwife Episodes 58.8% decrease (110 referrals); Rheumatology 38.1% decrease (96 referrals); Respiratory Medicine 27.6% decrease (88 referrals); Urology 17.9% decrease (82 referrals); Gastroenterology 25.4% decrease (74 referrals) and ENT 5.3% decrease (50 referrals). The decline in Dermatology referrals is related to restrictions being placed on the use of the ereferrals for this specialty. Significant increases in GP Referrals at Southport and Ormskirk Hospitals are Clinical Physiology 48.3% increase (171 referrals) and Gynaecology 6.5% increase (44 referrals). Our second main provider, Wrightington, Wigan and Leigh NHS Foundation Trust, has seen an 10.32% decrease in GP referrals (156) from 2016/17 to 2017/18. The most significant decreases in GP referrals have been in Trauma and Orthopaedics 46.1% decrease (250 referrals); Oral Surgery 93.3% decrease (56 referrals); Breast Surgery 13.5% decrease (31 referrals), General Surgery 30% decrease (15 referrals) and Pain Management 66.6% decrease (14 referrals). The most significant increases were; Rheumatology 175.9% increase (51 referrals); Dermatology 200.0% increase (40 referrals); Cardiology 59.6% increase (37 referrals) and General Medicine 65.3% increase (32 referrals). Overall market share for Wrightington, Wigan and Leigh NHS Foundation Trust total referrals decreased by 1.23% compared to same period 2016/17. University Hospitals Aintree Trust has seen an increase in GP Referrals of 145 (22.2%) when compared to same period 2016/17. This is mostly attributed to Breast Surgery an increase of 31.9% (66 referrals); Gastroenterology an increase of 88.5% (23 referrals); Cardiology an increase of 77.1% (27 referrals); Endocrinology with a decrease of 34.3% (12 referrals) and General Medicine with a decrease of 42.1% (8 referrals). Overall market share for University Hospitals Aintree total referrals increased by 0.61% compared to same period last year. St Helens and Knowsley has seen an increase of 1228 GP Referrals (304.0%) when compared to the same period last year. This is mainly attributed to Dermatology with 856 additional GP Referrals (1358.7%), Breast Surgery with 61 additional GP Referrals (145.2%), Plastic Surgery an increase of 58 GP Referrals (78.4%) and Gastroenterology an increase of 46 GP Referrals (766.7%). It is assumed that the increase in Dermatology referrals is related to the restrictions on GP referrals to the Dermatology service at Southport and Ormskirk Hospitals that became effective in February Overall market share for St Helens and Knowsley total referrals increased by 4.84% compared to same period 2016/17. Ramsay Healthcare (mainly Renacres Hospital) has seen a decrease of 691 GP referrals (-24.0%) for April-September 2017/18 compared to the same period in 2016/17. These decreases in referrals occurred mainly in Trauma and Orthopaedics with a reduction of 493 referrals (-65.0%); Gynaecology with a reduction of 107 referrals (-26.2%); General Surgery with a reduction of 107 referrals (-31.3%) and ENT with a reduction of 60 referrals (-28.3%). This is partially offset by an increase of 73 referrals in Pain Management (36.0%) and 34 referrals in Gastroenterology (7.5%). Overall market share of total referrals for Ramsey Healthcare decreased by 2.92% compared to same period in 2016/ P a g e
45 7. Planned Care: ereferrals Service (previously Choose and Book) Performance for September 2017 shows a marginal increase to 76.6% compared to the achievement of 75.2% in July Both these figures are considerably below the 80% target which West Lancashire CCG were supposed to achieve by March 2017 to be eligible for the ereferral Quality Premium. For 2017/18 there is no financial incentive for West Lancashire CCG to achieve 80% of all GP Referrals being made via the ereferrals service, However, achievement of the target is still expected. The September 2017 figure for ereferrals is based upon weekly bookings data up to 30 April 2017 and monthly data for the period 01 May 2017 to 30 September Because weekly data is subject to additional data cleansing it is possible that this May/September position will change most probably downwards. At present NHS Digital is indicating that a review of their processes by the NHS Small Numbers Panel is preventing the publication of weekly bookings data beyond 30 April The ereferral Quality Premium for 2016/17 was designed to increase the proportion of GP Referrals made by ereferrals. The referral Quality Premium (QP) was worth 1 per head of patient population approximately 112k, and to be eligible NHS West Lancashire CCG had to meet a level of 80% by March 2017 (March 2017 performance only). The failure of West Lancashire CCG to achieve a 1% financial surplus for 2016/17 meant that Quality Premium payments were not appropriate. Up until February 2017 there was a high degree of probability that the 80% target would be achieved in 2016/17 using the same measures as NHS Digital. However, in March 2017 Southport and Ormskirk Hospitals encountered service difficulties with Dermatology and refused to accept ereferrals into this service. This had a twofold effect, with Southport and Ormskirk Hospitals only taking paper referrals and additionally most referrals going to St Helens and Knowsley NHS Trust who do not accept Dermatology referrals via ereferrals. The 80% ereferrals target is to be measured by comparing all new ereferrals for outpatient attendances in a month (numerator) with the number of GP referrals (denominator) reported via the UNIFY Monthly Activity Report (MAR). To allow for dental activity the MAR GP Referrals in the denominator are reduced by 5.2%. ereferrals performance using these measures is shown as series 2015/16 and 2016/17 on the graph above. Work to meet the overall aims of improving the efficiency of referral processes for practices and local providers has continued. Input from the Health and Social Care Information Centre (HSCIC) has commenced and they are in the process of compiling reports to identify problem areas that can be addressed to improve ereferrals utilisation as reported using Monthly Activity Return (MAR). 15 P a g e
46 8. Planned Care: Acute Contract All Providers Performance up to the end of September 2017 against the planned care element of the contract is shown below in Table 2a. This shows the planned care element of the contracts is under plan by 740K. While the greatest variance is seen in Daycases (under plan by 432K), and Outpatient First Attendances (under plan by 249K). The greatest specialty level variance is Trauma and Orthopaedics with an underperformance of 479K across all providers. Table 2a: Planned Care to Month 6 (September) 2017/18 - All Providers Activity Cost Point of Delivery (POD) Plan Actual Variance Plan Actual Variance Daycase ,252,747 4,820, ,999 Elective ,481,788 3,329, ,770 Elective Excess Bed Days ,229 71,135-24,094 Outpatient First Attendance ,395,844 2,146, ,846 Outpatient Follow Up Attendance ,612,059 2,462, ,691 Outpatient Procedure ,958,620 2,194, ,883 Diagnostic Imaging , ,725 31,721 Grand Total ,421,292 15,681, ,796 Southport and Ormskirk Hospitals NHS Trust Performance up to the end of September 2017 against the Planned Care element of the contract is shown below in Table 2b. This shows that the Planned Care element of the contract is under plan by 893K. The most significant variance being in Daycases. The most significant variances within Daycases are Trauma and Orthopaedics with an underperformance of 130K; Pain Management with an underperformance of 110K and General Surgery with an underperformance of 105K. Table 2b: Planned Care to Month 6 (September) 2017/18 - Southport and Ormskirk Hospitals Activity Cost Point of Delivery (POD) Plan Actual Variance Plan Actual Variance Daycase ,393,136 1,939, ,512 Elective ,317,822 1,154, ,000 Elective Excess Bed Days ,833 29,435-7,398 Outpatient First Attendance ,071, , ,969 Outpatient Follow Up Attendance ,352,956 1,167, ,033 Outpatient Procedure ,330,733 1,427,241 96,508 Diagnostic Imaging , ,530 33,058 Grand Total ,778,798 6,885, ,347 All Other Providers Performance up to the end of September 2017 against the Planned Care element of the contract is shown below in Table 2c. This shows the Planned Care element of the contract is over plan by 154K. The largest performance differences within this are Outpatient Procedures (overperformance of 139K) and Outpatient First Attendances (underperformance of 35K). Table 2c: Planned Care to Month 6 (September) 2017/18 - All Other Providers Activity Cost Provider Plan Actual Variance Plan Actual Variance Wrightington, Wigan and Leigh NHSFT ,314,712 2,407,084 92,372 Ramsay Operations (UK) ,799,300 1,759,160-40,141 Aintree University Hospitals NHSFT ,099,422 1,140,629 41,207 Royal Liverpool and Broadgreen Hospitals NHSFT , ,989 12,486 St Helen's and Knowsley Hospitals NHSFT , ,563 46,560 Lancashire Teaching Hospitals NHSFT , ,839 89,333 Other ,659,047 1,570,780-88,267 Grand Total ,642,494 8,796, ,551 *Includes points-of-delivery as per Tables 2a and 2b 16 P a g e
47 Key Risks and Actions Although Planned Care is significantly below target at the end of September 2017 it should be noted that the May 2017 cyber-attack led to significant cancellations of Planned Care activity at Southport and Ormskirk Hospitals NHS Trust. The Trust has since made significant efforts to recover this position, and is targeting an increased in Planned Care activity in the remainder of the 2017/18 financial year to achieve a financial recovery plan submitted to NHS England. Concerns have been raised with Southport and Ormskirk Hospitals regarding the overperformance in Outpatient Procedures and Diagnostic Imaging combined with an underperformance in Outpatient First and Follow Up Attendances. Some issues have been identified with the planning process for 2017/18 which could have contributed towards this imbalance, while some changes to clinical practice have resulted in an increase in Outpatient Procedures. It should be noted that the structure of the 2017/18 tariff means that these movements between Outpatient Attendances and Outpatient Procedures are not financially significant. The change from an underperformance of 4K in June 2017 to an overperformance of 92K in September 2017 at Wrightington, Wigan and Leigh Hospitals NHSFT is a concern. The increase in costs occurs in Trauma and Orthopaedic Elective. Investigation is ongoing to establish if this is simply a blip in activity, or a consequence of patient choice for patients being referred on from the Joint Health MCAS service with more complex conditions. Both Wigan Borough CCG and Wrightington, Wigan and Leigh Hospitals NHSFT have been notified by letter of the requirement that all Orthopaedic referrals must be triaged and authorised by the Joint Health MCAS service. The continuing overperformance at Lancashire Teaching Hospitals NHSFT is a concern and currently unexplained, the only suggestion from the host CCG being that planned Care has been overperforming as the Trust attempts to improve its RTT performance. Overperformance at St Helens and Knowsley Hospitals NHSFT is in line with the increase in GP referrals over the previous 12 months and represents a market share shift from Southport and Ormskirk Hospitals NHST. Although Ramsay Operations (mainly Renacres Hospital) is currently indicating an underperformance, this is due to special circumstances and may be concealing other problem areas. The primary cause of the underperformance continuing falls in Orthopaedic activity believed to be caused by the Joint Health MCAS scheme. These factors are masking the continued significant overperformance in Pain Management at this provider. 17 P a g e
48 9. Unplanned Care: Acute Contract All Providers Performance up to the end of September 2017 against the Unplanned Care element of the contract is shown below in Table 3a. Overall, the unplanned care element of the contract is over plan by 639K. This is caused by significant overperformance from the GP Assessment Unit at 420K over plan and Accident and Emergency which is 126K above plan. See below for variances for Southport and Ormskirk Hospitals NHS Trust. Table 3a: Unplanned Care to Month 6 (September) 2017/18 - All Providers Activity Cost Point of Delivery (POD) Plan Actual Variance Plan Actual Variance Accident and Emergency ,124,685 2,250, ,920 GP Assessment Unit , , ,427 Non-Elective ,867,339 8,030, ,214 Non-Elective Short Stay , ,513-14,903 Non-Elective Same Day Emergency Care , ,414 19,225 Non-Elective Excess Bed Days , ,744-85,300 Non-Elective Non-Emergency ,569,285 1,579,260 9,974 Non-Elective Threshold Adjustment ,387-7,552 8,835 Grand Total ,953,276 13,591, ,556 Southport and Ormskirk Hospitals NHS Trust Performance up to the end of September 2017 against the Unplanned Care element of the contract is shown below in table 3b. Overall, the unplanned care element of the contract is over plan by 185K. The movement in Unplanned Care variance between July 2017 and September 2017 of 312K (from under plan by 127K to over plan by 185K) is significant and of concern. The principal movements within this change occurred in Points of Delivery GP Assessment Unit with an increase in variance of 190K and Non-Elective with an increase in variance of 116K. Table 3b: Unplanned Care to Month 6 (September) 2017/18 - Southport and Ormskirk Hospitals Activity Cost Point of Delivery (POD) Plan Actual Variance Plan Actual Variance Accident and Emergency ,661,866 1,752,138 90,272 GP Assessment Unit , , ,427 Non-Elective ,778,842 5,566, ,035 Non-Elective Short Stay , ,913-23,070 Non-Elective Same Day Emergency Care , ,500 8,849 Non-Elective Excess Bed Days , ,769-58,983 Non-Elective Non-Emergency ,319,417 1,290,521-28,895 Non-Elective Non-Emergency Excess Bed Days ,729 6,739-11,990 Grand Total ,852,556 10,037, ,574 The GP Assessment Unit began operating as part of the Accident and Emergency Department at Southport and Ormskirk Hospitals in April It is used by the Trust to assess patients and partly to manage the 4-hour waiting target in Accident and Emergency. Prior to implementation of this scheme, the Trust suggests that patients would have incurred both an Accident and Emergency attendance and a Non-Elective spell. Growth in GP Assessment Unit activity during 2016/17 was significant, caused partly by an extension to the opening hours of the service and partly by the Trust using the GPAU to manage 4-hour Accident and Emergency waits more efficiently. 18 P a g e
49 All Other Providers Performance up to the end of September 2017 against the Unplanned Care element of the contract is shown below in Table 3c. Overall, the Unplanned Care element of the contract is over plan by 453K. The most significant variance amongst the major providers is general overperformance at Wrightington, Wigan and Leigh NHSFT which is 251K over plan. Overperformance for Other (lower value contracts) is significant at 67K and is primarily at Liverpool Heart and Chest NHSFT ( 41K, 31.6%), University Hospitals of South Manchester NHSFT ( 31K) and Salford Royal NHSFT ( 23K, 155.2%). Table 3c: Unplanned Care to Month 6 (September) 2017/18 - All Other Providers Activity Cost Provider Plan Actual Variance Plan Actual Variance Wrightington, Wigan and Leigh NHSFT ,336,484 1,587, ,531 Aintree University Hospitals NHSFT , ,344 97,706 Lancashire Teaching Hospitals NHSFT , ,138-39,169 Royal Liverpool and Broadgreen Hospitals NHSFT , ,065-14,841 St Helen's and Knowsley Hospitals NHSFT , ,858 91,032 Other , ,843 67,492 Grand Total ,104,511 3,557, ,751 Key Risks and Actions The overperformance recorded by the GP Assessment Unit at Southport and Ormskirk Hospitals is of concern given the rapid growth in activity experienced there in 2016/17. Investigations have highlighted two significant changes to recording practice by the Trust since June The CCG position is that these coding and counting changes are contrary to Service Conditions 28.8 and of the NHS Standard Contract. Were West Lancashire CCG not to pay for this increase in activity a saving of 341K for the period April to September 2017 would be realised. West Lancashire CCG have written to Southport and Ormskirk Hospitals regarding the unauthorised increases in counting of GPAU activity. In March 2017 NHS England mandated that for all hospital episodes where sepsis occurred should be coded as the primary diagnosis rather than as a secondary diagnosis. This change to coding practice has been adopted by most acute providers, and appears to have been accompanied by an increase in the coding of sepsis. Coding sepsis as the primary diagnosis affects the HRG generated for the hospital spell and as a result increases cost. NHS England has also indicated that this change should be treated as a Code of Conduct change and as a result it should be cost neutral for 2017/18. Work has only been carried out for Southport and Ormskirk Hospitals to date this indicating that the Unplanned Care position for this provider should be adjusted downwards by approximately 7k per month. These adjustments will need agreeing with acute providers. The overperformance in Unplanned Care activity at Wrightington, Wigan and Leigh Hospitals is of concern and should be investigated in detail. The cost of emergency admissions at this Trust is overperforming by 18.8% while Accident and Emergency attendances at this Trust have only increased by 2.5%. Work should be undertaken to establish the cause of this financial overperformance which appears to be activity driven as the difference in unit cost between plan and actual is only 1% for admitted unplanned care. 19 P a g e
. The MMC s remit encompasses all systems, policies and procedures designed to ensure the safe, secure and cost-effective use of medicines.")
50 10. Prescribing To address the West Lancashire CCG Medicines Management duties as defined by the National Prescribing Centre s Medicines Management Competency Framework, West Lancashire CCG has set up a Medicines Management Committee (MMC). The MMC s remit encompasses all systems, policies and procedures designed to ensure the safe, secure and cost-effective use of medicines. For financial year 2017/18 West Lancashire CCG prescribing spend is 260K below budget (3.36%). This is based upon an annual budget of 18,661,414 which has been phased to correspond with dispensing days in each calendar month. This budget includes a 900k QIPP reduction. CCG Year to Date - August 2017/18 Budget Spend Variance Variance % Blackburn with Darwen 9,789,043 10,684, , % Blackpool 13,626,045 13,169, , % Chorley and South Ribble 11,097,046 11,505, , % East Lancashire 26,335,875 25,302,420-1,033, % Fylde and Wyre 11,557,461 11,376, , % Greater Preston 12,924,669 13,438, , % Morecambe Bay 22,899,598 West Lancashire 7,734,665 7,474, , % Grand Total 93,064, ,850, , % Morecambe Bay excluded from variance calculations owing to absence of a budget West Lancashire CCGs prescribing spend to the end of August 2017/18 is significantly lower, 352k (4.5%), than the corresponding period in 2016/17. This suggests West Lancashire CCG is reducing prescribing costs, most likely through the Waste Campaign which was launched late in the 2016/17 financial year. A national reduction in the costs of medicines covered by Category M has been announced from August However, the CCG has been informed that the benefit of these price reductions will be retained nationally by NHS England rather than reducing costs to CCGs to create a system risk reserve. In August, the CCG s prescribing costs have been adjusted by 21k to enable this benefit to be retained by NHS England. This adjustment is not included in the tables above and below. Further to this, the CCG is being adversely affected by shortages of multiple generic medications. The shortage of generic versions results in the CCG paying a higher price for these medicines. It is estimated that the financial pressure to the CCG in 2017/18 arising from generic shortages is 750k higher than the financial pressure in the previous year. 20 P a g e
51 The medicines waste campaign continues to progress, repeat prescription review services are being introduced (PODS) and the prescribing of self-care medicines is being limited. The CCG has also benefited from a significant price reduction in Pregabalin effective from August. The combination of the medicines management team s efforts and the windfall pregabalin saving mean that the CCG can more than offset the cost pressures discussed. The CCG is forecasting a prescribing underspend of 1.1 million in 2017/18. This position has been arrived at by extrapolating forward August costs for the remainder of the financial year. The table below shows the average prescribing cost year to date per APU (Astro Prescribing Unit a weighted population to take account of the differing prescribing costs with age and gender) for Lancashire CCGs. West Lancashire CCG has the third lowest cost per APU of the eight Lancashire CCGs, and has also demonstrated the second best reduction in spend per APU across the region. CCG Spend per APU Year to Date - August 2017/ Variance Blackburn with Darwen % Blackpool % Chorley and South Ribble % East Lancashire % Fylde and Wyre % Greater Preston % Morecambe Bay % West Lancashire % The table below details the spend and spend per APU for each GP Practice up to August 2017 along with comparative figures for the same period 2016/17. West Lancashire CCG Prescribing Performance 2017/18 to August / /18 Code Prescriber Name Spend Spend per APU Budget* Spend Variance Spend per APU P81201 Ashurst Primary Care 262, , ,573 9, P81695 Aughton Surgery 365, , ,268 2, P81112 Beacon Primary Care 940, , ,186-69, P81138 Burscough Family Practice 190, , ,627-1, P81727 County Road Surgery 170, , ,542 18, P81136 Dr A Bisarya 171, , ,110 5, P81084 Hall Green Surgery 543, , ,886-9, P81646 Lathom House Surgery 350, , ,208-11, P81039 Manor Primary Care 297, , ,903 7, P81758 Matthew Ryder Clinic 163, , ,693-7, P81772 North Meols Medical Centre 260, , ,298-44, P81014 Ormskirk Medical Practice 711, , ,710-24, P81096 Parbold Surgery 457, , ,359 7, P81041 Parkgate Surgery 441, , ,440-8, P81208 Skelmersdale Practice 968, , ,213-43, P81674 Stanley Court Surgery 364, , ,700-4, P81710 Tarleton Group Practice 527, , ,096-4, P81045 The Elms Practice 389, , ,540-60, P81177 Viran Medical Centre 159, , ,882-26, '*Budget to August 2017 is calculated as 41.45% of the 2017/18 annual budget for Prescriber - Based upon number of prescribing days. Table does not include all prescribing spend and budget - only active GP Practices are included. 21 P a g e
52 11. Mental Health Lancashire Care Foundation Trust The contract value for Lancashire Care Foundation Trust (LCFT) mental health services is 10.0m. The LCFT contract is for a range of mental health services such as rehabilitation, community mental health teams, hospital liaison, memory assessment, CAMHS child psychology and prison in-reach. Below is activity for 2017/18 by month up to the end of September Quarter 1 Quarter 2 Quarter 3 Quarter 4 Year to Metric Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Date ADHD Contacts Adult Ward Occupied Bed Days Adult/PICU Ward Admissions Adult/PICU Ward Discharges CCTT Teams - Accepted Referrals CCTT Teams - Contacts CMHT Contacts CMHT Referrals Community Restart Teams - Accepted Referrals 0 CRHT Face to Face Contacts - 18 to CRHT Face to Face Contacts - Below CRHT Face to Face Contacts - Over CRHT Teams - Referrals CRHT Telephone Contacts - 18 to CRHT Telephone Contacts - Below CRHT Telephone Contacts - Over Criminal Justice Liaison - Contacts Eating Disorder Service - Contacts Eating Disorder Service - Referrals Eating Disorder Service DNAs - Follow Up Contacts Eating Disorder Service DNAs - New Contacts Hospital Liaison Contacts Hospital Liaison Referrals MAS Teams - Contacts MAS Teams - Referrals Older Adult (Dementia) Inpatient Ward Discharges Older Adult (Dementia) Ward Occupied Bed Days Older Adult (Dementia) Inpatient 90 Day ReAdmissions Older Adult (Dementia) Inpatient Ward Admissions Older Adult (Functional) Inpatient Ward Discharges Older Adult (Functional) Ward Occupied Bed Days PICU Ward Occupied Bed Days PICU Wards - Transfers In RITT Contacts RITT Referrals Dementia For 2016/17 the Dementia Diagnostic Rate Target was monitored against a fixed estimate of the number of patients with dementia (Prevalence) this figure being based upon population profile. For 2016/17 this figure was estimated at 1483 patients. For 2017/18 a planning figure of 1426 patients was used. However, rather than monitoring against this figure, NHS Digital is monitoring against an estimate of prevalence based on the current CCG registered population. The CCG Diagnostic Rate Target is that at least 67% of patients with dementia have been diagnosed. Because the population with dementia suffers significant mortality it is necessary to maintain referrals to the Memory Assessment Service (MAS) to ensure that the CCG Diagnostic Rate Target is maintained. The table below shows performance against the CCG Dementia Diagnostic Rate Target. Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Diagnosed Patients Estimated Prevalence Demantia Diagnosis Rate 72.81% 73.50% 74.36% 75.77% 75.44% 74.63% 22 P a g e
53 West Lancashire CCG are holding a strong position against the target of 67% for Dementia Diagnosis Rate. It should be noted that these numbers are from the NHS Digital web site and are adjusted for any GP Practices where monthly diagnosis data is not available. To obtain a diagnosis of dementia for a patient it is necessary for GP practices to refer patients to the Memory Assessment Service (MAS) operated by Lancashire Care Foundation Trust. For West Lancashire CCG MAS waits have begun to reduce dramatically recently due to the older adult service stopping unnecessary annual reviews and, as of week commencing 8 May, anyone referred to the MAS will be offered an appointment within two weeks. This will be the best performance in Lancashire. The table below summarises MAS performance for West Lancashire CCG patients in 2017/18. Memory Assesment Service Metric Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Number of referrals to MAS Number of referrals accepted by MAS Number of referrals rejected by MAS Number of assesments by MAS Average (mean) wait to assesment (weeks) Waiting list at month end Average (mean) wait to diagnosis (Weeks) Number diagnosed Number diagnosed with dementia Practice level Information Practice level diagnosis rates are no longer produced by NHS Digital but provide a useful guide to progress against target. They indicate practices where the diagnostic rate is lower than anticipated which could indicate a lower than normal rate of referral to the MAS. To carry out this analysis the percentage of the CCG over-65 population registered with each practice is used to factor the CCG level of prevalence. Number of Registered over 65 Patients with a Dementia Diagnosis 2017/18 Performance as of September 2017 Patients % of CCG Share of CCG Diagnosis GP Practice Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Aged 65 Yr+ Patients 65+ Prevalence Rate % Beacon Primary Care % % Parkgate Surgery % % Ormskirk Medical Practice % % Aughton Surgery % % Lathom House Surgery % % Hall Green Surgery % % Burscough Family Practice % % The Elms Practice % % Ashurst Primary Care % % Skelmersdale Practice % % County Road Surgery % % Stanley Court Surgery % % Viran Medical Centre % % Parbold Surgery % % Matthew Ryder Clinic % % Manor Primary Care % % Tarleton Group Practice % % Dr A Bisarya % % GP List Size as of September P a g e
54 Care Programme Approach (CPA) follow-up within 7 days Research demonstrates that patients are more likely to commit suicide in the immediate days following discharge from a Mental Health Acute bed. Therefore, discharge is followed up with a meeting with a Mental Health Professional within 7 days of discharge to reduce this risk. (LCFT have a desirable 48-hour target). The national target is that 95% of all discharged patients are seen within 7 days. The table below summarises Lancashire Care Foundation Trust activity for West Lancashire CCG patients during 2017/18. West Lancashire CCG failed the 95% target in June and July 2017 due to a single person not receiving follow-up within 7 days. The low numbers being discharged will mean that even one fail will send us below the national target. Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Eligible Current Month Sucessful Current Month Sucessful Rate Current Month 100.0% 100.0% 90.0% 90.9% 100.0% 100.0% 95% Year to Date 100.0% 100.0% 96.9% 95.3% 96.3% 96.9% 95% Adult Psychological Therapy (Mindsmatter) For Adult Psychological Therapy, the number of patients with a need (Prevalence) is estimated at This is defined as the number of West Lancashire CCG patients who have depression and/or anxiety disorders. This is a local estimate based upon the Psychiatric Morbidity Survey. The table below summarises the year to date performance for West Lancashire CCG patients with the Lancashire Care Foundation Trust IAPT service. Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Referrals Current Month Year to Date Access Rate Current Month 13.5% 18.1% 16.1% 12.9% 17.8% 14.6% 15.0% Year to Date 13.5% 15.8% 15.9% 15.2% 15.7% 15.5% 15.0% Recovery Completed Treatment Moved to recovery Not at Caseness Current Month 54.0% 53.0% 67.1% 54.0% 65.6% 53.2% 50.0% Year to Date 54.0% 53.5% 58.3% 57.3% 58.9% 57.8% 50.0% Reliable Improvement Referral to receipt of 6 weeks or less welcome call from 7 to 18 weeks Service Greater than 18 weeks Current Month < 6 weeks 98.5% 98.6% 97.9% 97.3% 96.6% 97.0% 75.0% Year to Date < 6 weeks 98.5% 98.6% 98.3% 98.1% 97.7% 97.6% 75.0% Current Month < 18 weeks 98.5% 100.0% 100.0% 100.0% 100.0% 100.0% 95.0% Year to Date < 18 weeks 98.5% 99.6% 99.8% 99.8% 99.9% 99.9% 95.0% Referral to Discharge 6 weeks or less from Treatment 7 to 18 weeks Greater than 18 weeks Current Month < 6 weeks 98.5% 94.1% 97.3% 93.9% 98.6% 92.7% 75.0% Year to Date < 6 weeks 98.5% 96.3% 96.7% 96.0% 96.6% 95.8% 75.0% Current Month < 18 weeks 98.5% 100.0% 100.0% 100.0% 100.0% 100.0% 95.0% Year to Date < 18 weeks 98.5% 99.3% 99.5% 99.6% 99.7% 99.8% 95.0% The Access Rate national target is for 15% of patients with a need to have been referred to the Lancashire Care IAPT service during the financial year this equates to 174 patients per month. The Recovery target is that at least 50% of patients completing treatment with the APT service will be considered recovered. This is calculated as: (Number moved to Recovery)/ (Number Completed Treatment Number not at Caseness) Patients not at Caseness are defined as patients who on entry to the service were below the clinical cut off point for psychometric scoring measures for both depression and anxiety. Because recovery is measured against these criteria these patients are excluded from the recovery calculation. 24 P a g e
55 Reliable Improvement is defined as patients who demonstrate a statistically significant improvement in psychometric scoring measures for either depression or anxiety between the beginning of treatment and being discharged by the IAPT service. Referral to Treatment times in the preceding table relate to the wait between referral to the IAPT service and the welcome call made by the service to the client. These are the waits that patients often refer to when speaking to their GP. Following the welcome call, patients are allocated to one of three waiting lists; the time between allocation and the start of treatment Is shown in the table below. Psychological Wellbeing Practitioners Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Less than 6 Weeks to 17 weeks Weeks and Over Current Month < 6 Weeks 84.2% 87.7% 95.5% 95.7% 93.1% 81.6% 75.0% Year to Date < 6 Weeks 84.2% 85.9% 88.4% 90.2% 90.9% 89.2% 75.0% Current Month < 18 weeks 98.8% 100.0% 100.0% 100.0% 100.0% 100.0% 95.0% Year to Date < 18 Weeks 98.8% 99.4% 99.5% 99.6% 99.7% 99.8% 95.0% Waiting List Profile Cognitive Behavioral Therapists Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Less than 6 Weeks to 17 weeks Weeks and Over Current Month < 6 Weeks 60.3% 70.4% 63.9% 55.8% 56.0% 73.1% 75.0% Year to Date < 6 Weeks 60.3% 65.2% 64.7% 62.7% 61.5% 63.3% 75.0% Current Month < 18 weeks 96.6% 98.1% 95.1% 96.2% 98.0% 100.0% 95.0% Year to Date < 18 Weeks 96.6% 97.3% 96.5% 96.4% 96.7% 97.2% 95.0% Waiting List Profile Counsellors Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Less than 6 Weeks to 17 weeks Weeks and Over Current Month < 6 Weeks 41.4% 38.6% 30.6% 25.7% 30.6% 37.7% 75.0% Year to Date < 6 Weeks 41.4% 40.0% 36.7% 34.0% 33.3% 34.0% 75.0% Current Month < 18 weeks 86.9% 78.2% 80.6% 68.3% 69.4% 74.5% 95.0% Year to Date < 18 Weeks 86.9% 82.5% 81.8% 78.5% 76.6% 76.2% 95.0% Waiting List Profile All Services Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Target Less than 6 Weeks to 17 weeks Weeks and Over Current Month < 6 Weeks 66.8% 68.1% 63.4% 64.6% 67.2% 65.7% 75.0% Year to Date < 6 Weeks 66.8% 67.4% 66.2% 65.8% 66.1% 66.0% 75.0% Current Month < 18 weeks 94.7% 92.4% 91.4% 88.4% 89.8% 91.6% 95.0% Year to Date < 18 Weeks 94.7% 93.6% 92.9% 91.8% 91.4% 91.4% 95.0% Waiting List Profile 25 P a g e
56 12. Quality and Performance 12a West Lancashire CCG Performance Dashboard Preventing People from Dying Prematurely Metric Reporting Level 2017/18 Q1 Q2 Q3 Q4 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Cancer Waiting Times % Patients seen within two weeks for an urgent GP referral for suspected cancer. RAG G R G G G G G West Lancashire CCG Actual 96.23% 92.45% 96.21% 95.42% 96.26% 97.63% 95.79% % of patients seen within 2 weeks for an urgent referral for breast symptoms. Target 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% RAG R R R G G R R West Lancashire CCG Actual 91.84% 92.11% 89.74% 95.00% 96.30% 92.00% 92.96% % of patients receiving definitive treatment within 1 month of a cancer diagnosis. Target 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% RAG G G G G G G G West Lancashire CCG Actual % 98.11% % 98.21% 98.21% 97.56% 98.69% % of patients receiving subsequent treatment for cancer within 31 days (Surgery). Target 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% RAG G R G G G G G % of patients receiving subsequent treatment for cancer w ithin 31 days (Drug Treatments). % of patients receiving subsequent treatment for cancer w ithin 31 days (Radiotherapy Treatments). % of patients receiving 1st definitive treatment for cancer w ithin 2 months (62 days). % of patients receiving treatment for cancer w ithin 62 days from an NHS Cancer Screening Service. % of patients receiving treatment for cancer within 62 days upgrade their priority. West Lancashire CCG West Lancashire CCG West Lancashire CCG West Lancashire CCG West Lancashire CCG West Lancashire CCG Actual % 85.71% % % % % 97.37% Target 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% RAG R R G G G G G Actual 93.75% 96.00% % % % % 98.18% Target 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% RAG G G G G G R G Actual % % % % % 93.33% 99.04% Target 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% RAG G G R R G R R Actual 86.36% 86.96% 77.78% 72.00% 86.21% 79.17% 81.56% Target 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% 85.00% RAG G G G R R G G Actual % % % 75.00% 50.00% % 91.30% Target 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% RAG Actual 88.24% 77.78% 80.00% 90.00% % % 88.89% Target 26 P a g e
57 Metric Reporting Level 2017/18 Q1 Q2 Q3 Q4 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Ambulance Category A Calls Response Time (Red1). RAG R R R R R West Lancashire CCG Actual 53.13% 50.00% 32.60% 55.56% 46.98% Category A (Red 2) 8 Minute Response Time. Category A calls responded to within 19 minutes. North West Ambulance Service NHS Trust West Lancashire CCG North West Ambulance Service NHS Trust West Lancashire CCG North West Ambulance Service NHS Trust Target 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% RAG R R R R R Actual 70.08% 65.92% 62.53% 64.67% 65.77% Target 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% RAG R R R R R Actual 53.57% 54.18% 46.90% 44.32% 49.70% Target 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% RAG R R R R R Actual 68.94% 64.43% 64.68% 64.17% 65.51% Target 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% 75.00% RAG R R R R R Actual 85.05% 83.61% 73.30% 74.41% 79.00% Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% RAG R R R R R Actual 92.54% 90.08% 89.39% 89.80% 90.43% Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 27 P a g e
58 Ensuring that People Have a Positive Experience of Care Metric Reporting Level 2017/18 Q1 Q2 Q3 Q4 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD EMSA Mixed sex accommodation breaches - All Providers. RAG R R R R R R R West Lancashire CCG Actual Mixed Sex Accommodation - MSA Breach Rate. Target RAG R R R R R R R West Lancashire CCG Actual Target Referral to Treatment (RTT) & Diagnostics % of all Incomplete RTT pathways within 18 weeks. RAG G G G G G G G West Lancashire CCG Actual 95.75% 94.96% 95.15% 94.88% 94.96% 95.10% 95.14% Referral to Treatment RTT - No of Incomplete Pathways Waiting >52 weeks. Target 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% RAG G G G G G G G West Lancashire CCG Actual % of patients waiting 6 weeks or more for a diagnostic test. Target RAG R R R R R R R West Lancashire CCG Actual 3.13% 3.83% 1.56% 1.22% 2.39% 2.01% 2.34% Target 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 1.00% 28 P a g e
59 Treating and Caring for People in a Safe Environment and Protect them from Avoidable Harm Metric Reporting Level 2017/18 Q1 Q2 Q3 Q4 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD HCAI Number of MRSA Bacteraemias. RAG G G G G G R R West Lancashire CCG YTD Number of C.Difficile infections. Target RAG G G G G G G G West Lancashire CCG YTD Target Accident & Emergency 4-Hour A&E Waiting Time Target (Monthly Aggregate based on HES 15/16 ratio). West Lancashire CCG RAG R R R R R R R Actual 91.17% 89.48% 90.07% 88.32% 88.14% 85.69% 88.87% A&E Attendances: Type 1. A&E Attendances: All Types. 12 Hour Trolley w aits in A&E. Southport and Ormskirk Hospitals NHS Trust 29 P a g e Southport and Ormskirk Hospitals NHS Trust Wrightington Wigan and Leigh NHS Foundation Trust Lancashire Teaching Hospitals NHS Foundation Trust Southport and Ormskirk Hospitals NHS Trust Wrightington Wigan and Leigh NHS Foundation Trust Lancashire Teaching Hospitals NHS Foundation Trust Wrightington Wigan and Leigh NHS Foundation Trust Lancashire Teaching Hospitals NHS Foundation Trust Target 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% RAG Actual 6,177 6,720 6,368 6,714 6,018 6,195 38,192 Target RAG Actual 7,250 7,706 7,737 7,796 7,212 7,320 45,021 Target RAG Actual 5,639 5,895 5,352 5,758 5,495 5,501 33,640 Target RAG R G G G G G G Actual 11,007 20,532 30,231 40,313 49,538 59,014 59,014 Target 11,005 22,825 34,106 45,859 56,619 67,894 77,939 87,799 97, , , ,978 67,894 RAG G R R R R R R Actual 7,250 14,956 22,693 30,489 37,701 45,021 45,021 Target 7,300 14,700 22,100 29,800 37,200 44,600 52,200 59,800 67,300 74,800 81,700 89,300 89,300 RAG G R R R R R R Actual 11,981 24,827 36,982 49,842 61,609 73,641 73,641 Target 12,475 22,307 32,477 43,799 54,744 65,891 77,143 88,138 98, , , ,867 65,891 RAG R R G R G G R Actual Target RAG G G G G G G G Actual Target RAG G G G G G R R Actual Target
60 12b Southport and Ormskirk Hospitals NHS Trust Integrated Performance Dashboard 2016/ /18 Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Q2 Q3 Q4 Q1 Q2 YTD Target 18 Weeks - Ongoing - % <18 Weeks - Trust 92.8 % 92.7 % 92.7 % 92.0 % 92.6 % 92.9 % 94.1 % 94.1 % 93.4 % 94.0 % 94.0 % 93.7 % 94.2 % 92.8 % 92.0 % 94.1 % 94.0 % 94.2 % 94.2 % 92.0% A&E - Left Department Without Being Seen Rate (LWBS) - Trust 2.05 % 1.71 % 1.60 % 2.00 % 1.64 % 1.37 % 2.14 % 1.60 % 1.70 % 1.60 % 2.40 % 2.10 % 2.50 % N/A N/A N/A N/A N/A N/A 5.00% A&E - Time to Initial Assessment - 95th Percentile - Trust N/A N/A N/A N/A N/A N/A 15 A&E - Time to Treatment - Median - Trust N/A N/A N/A N/A N/A N/A 60 A&E - Total Time - 95th Percentile - Trust N/A N/A N/A N/A N/A N/A 240 A&E - Total Time in A&E - 4 Hour % - Trust Overall % % % % % % % % % % % % % % % % % % 100.0% A&E - Total Time in A&E - 4 Hour % - RVY % % % % % % % % % % % % % % % % % % 100.0% A&E - Unplanned Re-attendance Rate (within 7 days) - Trust 0.87 % 1.18 % 1.02 % 0.81 % 1.28 % 0.97 % 0.86 % 0.83 % 0.98 % 1.02 % 1.21 % 0.94 % 0.98 % N/A N/A N/A N/A N/A N/A 5.00% ALOS - Elective - Trust ALOS - Non-Elective - Trust ALOS - Overall - Trust Cancelled Operations - % of Total Electives in Month 0.53 % 0.92 % 0.62 % 0.49 % 0.80 % 0.23 % 0.50 % 0.68 % 0.50 % 0.60% Cancer 14 Day - Urgent GP Referral Suspected Cancer 96.1 % 94.3 % 94.9 % 95.8 % 93.5 % 94.7 % 94.2 % 94.9 % 91.9 % 95.8 % 95.0 % 96.3 % 95.0 % 95.0 % 94.2 % 94.4 % 95.6 % 93.0% Cancer 31 Day - Decision to Treatment 96.4 % 97.7 % 98.3 % % 96.0 % % % % 98.3 % 98.1 % % 96.0 % 98.1 % 98.7 % 98.8 % 98.9 % 98.3 % 96.0% Cancer 31 Day - Subsequent Treatment - Drug Therapy % NTR % NTR NTR % % NTR % % NTR % % % % % % 98.0% Cancer 31 Day - Subsequent Treatment - Surgery % % % % % % % 80.0 % % % % % % % % 87.5 % % 94.0% Cancer 62 Day - GP Referral to Treatment 80.7 % 83.6 % 76.7 % 80.6 % 85.7 % 76.5 % 78.6 % 86.7 % 84.3 % 76.1 % 77.9 % 77.4 % 85.6 % 79.9 % 81.0 % 82.1 % 77.7 % 85.0% Cancer 62 Day - Screening Referral to Treatment NTR % NTR % NTR % % % NTR NTR % NTR 90.9 % % % % % 90.0% Diagnostics waiting time: percentage >= 6 weeks - All Tests 0.16 % 0.43 % 0.58 % 1.86 % 3.06 % 1.51 % 1.26 % 4.55 % 5.88 % 1.89 % 1.50 % 2.35 % 2.23 % N/A N/A N/A N/A N/A N/A 0.01 DSSA Breaches - Trust HR - Agency Staff Costs 6.55 % 7.53 % 5.96 % 7.83 % 5.97 % 7.14 % 7.19 % 5.22 % 5.44 % 4.77 % 4.76 % 5.25 % 5.58 % N/A N/A N/A N/A N/A N/A 4.00% HR - Sickness Absence Rate - Trust 5.49 % 5.94 % 5.56 % 5.72 % 5.61 % 5.65 % 5.13 % 4.80 % 4.75 % 5.14 % 5.31 % 4.80 % 5.12 % 5.34 % 5.74 % 5.46 % 4.89 % 5.08 % 4.98 % 4.00% IC - Clostridium Difficile - Trust IC - Incidence of MRSA - Trust IC - MRSA Screening - Elective Admissions - Trust 97.0 % 99.4 % 98.0 % 99.0 % 99.0 % 99.0 % 99.5 % % 98.2 % 96.0 % 97.0 % 99.6 % N/A N/A N/A N/A N/A N/A 100.0% IC - MRSA Screening - Emergency Admissions - Trust 83.0 % 90.0 % 86.0 % 88.0 % 92.0 % 86.0 % 89.0 % 90.0 % 87.0 % 86.0 % 88.0 % 88.0 % N/A N/A N/A N/A N/A N/A 100.0% Mortality - HSMR 12 Month Rolling Total - Trust Mortality - HSMR Monthly - Trust N/A N/A N/A N/A N/A 90 RM - Never Events - Trust RM - Patient Falls - by 1,000 bed days RM - Steis Reportable Incidents - Trust Stroke/TIA - Stroke 90% Stay on ASU 64.5 % 56.7 % 56.7 % 58.1 % 60.7 % 52.0 % 53.9 % 43.6 % 54.3 % 42.9 % 48.7 % 52.8 % 48.3 % 57.3 % 57.3 % 55.4 % 47.1 % 50.0 % 48.5 % 80.0% Stroke/TIA - TIA - High Risk Treated within 24Hrs 25.0 % 0.0 % 62.5 % 22.2 % 8.3 % 8.3 % 26.7 % 33.3 % 0.0 % 0.0 % 0.0 % 25.0 % 0.0 % 40.0 % 31.8 % 15.4 % 6.3 % 5.0 % 5.6 % 60.0% TV - Hospital Acquired Grade 2 Pressure Sores TV - Hospital Acquired Grade 3 Pressure Sores TV - Hospital Acquired Grade 4 Pressure Sores TV - Hospital Acquired Pressure Sores - Grades VTE Prophylaxis Assessment - Trust 96.5 % 96.9 % 97.7 % 96.2 % 97.7 % 97.7 % 98.1 % 98.8 % 98.1 % 97.7 % 99.1 % 98.5 % 97.3 % N/A N/A N/A N/A N/A N/A 2016/ /18 30 P a g e


61 12 Months Activity 12 Months Activity 12c Areas of Under-Performance for West Lancashire CCG Several areas of underperformance are reported to end of August 2017 year to date. The detail below is presented by indicator for each of these areas with actions identified as required and ongoing, seeking to improve performance. For each indicator which is underperforming Year to Date in August 2017 there is a Sparkline graph which shows the monthly performance of the indicator over the previous 12 months. Months where the indicator achieved target are represented by a green line, underperformance by a red line and the target by a blue line. The vertical amber line represents the division between 2016/17 and 2017/18 financial years. West Lancashire CCG Business Intelligence is investigating local areas of underperformance and how this compares to the performance of our local peer CCGs. Cancer Waiting Times % of patients seen within 2 weeks for an urgent referral for breast symptoms. Target: 93% Current Performance YTD: 92.96% Current Issues: April and May performance was below target. In both cases the breach was caused by a single patient choosing to delay the start of treatment for personal reasons. Despite exceeding the target in June, July and August, year to date performance remains below target. Improvement Plans: This target is rarely breached, but low activity levels mean a single case is sufficient to cause a breach in month. No further action has been initiated. % of patients receiving 1 st definitive treatment for cancer within 2 months (62 days). Target: 85% Current Performance YTD: 81.56% Current Issues: August performance of 85.21% was within target; however, June performance of 77.78%, July performance of 72.00% and September performance of 79.17% means the Year to Date Target of 85% is not being met. In August there were seven breaches six of these being patients who were first seen at Southport and Ormskirk Hospitals. Four breaches in June, Seven breaches in July. Improvement Plans: Low activity levels mean a single case is sufficient to cause a breach of this target in month. No further action has been initiated. 31 P a g e



62 12 Months Activity 12 Months Activity 12 Months Activity Ambulance Indicator: Ambulance Response Times CCG Target: 95% (All Cat A) 75% (Red 1) 75% (Red 2) Current Performance YTD: 79.0% 47.0% 49.7% Current Issues: Issues with Ambulance Turnarounds have impacted on Ambulance response times. Turnaround target performance continues to be challenging due to bed pressures and lack of flow within Acute Trusts. During 2016/17, the North West Ambulance Service have experienced increases in call volumes. However, the main impact on response times continues to be delays with patient handover at Accident and Emergency. In February 2017 handover delays at Southport and Ormskirk Hospitals NHS Trust increased to 24.5% of ambulances waiting 30 minutes or more. These Indicators are no longer reported, the latest figures being for July New indicators are expected to be reported from November Until the revised indicators are available July performance will be reported. All Category A calls responded to within 19 minutes: performance has failed to meet the 95% target for West Lancashire CCG for the year to July NWAS performance is also under the 95% target at 90.4%. Category A Calls (Red 1) performance has failed to meet the 75% target for West Lancashire CCG for the year to July NWAS performance also failed to meet the 75% target at 66.8%. Category A Calls (Red 2) performance has failed to meet the 75% target for West Lancashire CCG for the year to July NWAS performance has also failed the 75% target at 65.5%. Improvement Plans: With Commissioner support, NWAS are undertaking analysis of the additional factors affecting performance, which may be added to the existing monitoring dashboard that is discussed at the weekly performance meetings, the NWAS Contracting Group and the Strategic Partnership Board. Some of the additional actions being considered include: Identification of how the red/green code set has changed following AMPDS v.13 being implemented Use of Auto Dispatch within the existing NWAS CAD system Recruitment of an additional 23 call handlers to specifically manage outbound calls Analysis of the effect on performance of delays in call pickups EMSA Mixed Sex Accommodation Breaches All Providers Target: 0 Current Performance YTD: 29 Current Issues: One Mixed Sex Accommodation Breach in April three in May four in June thirteen in July and four in August and September means the annual target of 0 breaches cannot be met. Improvement Plans: This activity relates to Critical Care and Stroke patients at Southport and Ormskirk Hospitals. The Trusts are in the process of reconfiguring the Stroke Care facilities to minimise these issues. Referral to Treatment (RTT) and Diagnostics % of patients waiting 6 weeks or more for a diagnostic test. Target: 1.0% Current Performance YTD: 2.34% Current Issues: This is an issue at Southport and Ormskirk Hospitals, primarily within Cardiology concerning echocardiography and ultrasound tests. Underperformance increased steadily since initially breaching the 1% target in December 2016, peaking at 5.88% of patients waiting over 6 weeks for a diagnostic test in May A major factor in the large number of breaches in May 2017 was the cyber-attack which resulted in the cancellation of a significant number of diagnostic tests. The deterioration in performance in August and September 2017 has been attributed to staffing issues within echocardiography with 50% of departmental staff being unavailable. Improvement Plans: Southport and Ormskirk Hospitals have improved performance significantly in June and July and are organising additional radiology sessions to bring this indicator back on track. No plans have been identified to deal with the echocardiography staff shortfall. 32 P a g e


63 12 Months Activity 12 Months Activity 12 Months Activity Treating and Caring for People in a Safe Environment and Protect them from Avoidable Harm Number of MRSA Bacteraemias. Target: 0 Current Performance YTD: 1 Current Issues: A case of MRSA Bacteraemia was detected in a West Lancashire patient while an inpatient at Southport and Ormskirk NHS Trust on 26th September Following the post-infection review, the case of MRSA was attributed to the Trust with poor cannula care identified as the root cause. The review also identified issues with documentation and observations as well as delays in reporting on the specimen and delays in receiving appropriate treatment. Improvement Plans: Southport and Ormskirk Hospitals carried out a full review of this case. The Action Plan produced has been shared with the CCG. Accident and Emergency 4-Hour Accident and Emergency Waiting Time Target Target: 95.0% Current Performance YTD: 88.87% Current Issues: Performance is consistently below the 95% target. Improvement Plans: A&E continues to experience pressures. The A&E Delivery Board; Southport Subgroup held a Winter planning workshop on 31st August Plans include: Development of a clinical design group to have an action learning set/solution focused approach Providers to identify procedures and processes of low priority which we don t need to do in January to release capacity in the system Development of winter flying squad team. Development of daily multi-agency discharge huddle which joins all flow critical providers Development of internal and external communications protocol to identify go to person at time of escalation. Work up schemes to test out as PDSAs during October. 12-Hour Trolley Waits in Accident and Emergency Target: 0 Current Performance YTD: 14 Current Issues: Three 12-hour trolley waits in April nine in May and two in July all at Southport and Ormskirk Hospitals and relating to the admission of mental health patients mean the annual target of 0 waits cannot be achieved. There were two 12-hour trolley waits at Lancashire Teaching Hospitals NHSFT in September 2017; however, neither related to a West Lancashire CCG patient. Improvement Plans: West Lancashire CCG met with Mersey Care and Southport and Ormskirk Hospitals Accident and Emergency representatives to discuss Mental Health 12-hour breaches. A Task and Finish Group will be established to improve escalation processes, interaction between Mersey Care and Lancashire Care FT Mental Health Services and to explore reciprocal arrangements for West Lancashire patients who attend Mersey Trust Accident and Emergency, but require Lancashire Care FT Mental Health Services. 33 P a g e
 Non-Elective Length of Stay.")

64 12 Months Activity 12 Months Activity Average Length of Stay Average Length of Stay (ALOS) Non-Elective Southport and Ormskirk Hospitals Target: 4.3 Current Performance YTD: 5.35 Current Issues: Southport and Ormskirk Hospitals NHS Trust currently exceed the national target of 4.3 days for average (mean) Non-Elective Length of Stay. This is mainly due to an ageing population and difficulties finding suitable post discharge accommodation. Improvement Plans: ECIP has highlighted to Southport and Ormskirk Hospitals NHS Trust that Non-Elective Length of Stay is significantly higher than other Trusts and needs to be improved. Urology moved to Ormskirk on 14 December to make way for the expanded 15a Ward which will become an integrated discharge hub; this will include a discharge lounge. Work on improving discharge processes is also part of the ECIP work as mentioned under Accident and Emergency performance. Hospital Mortality Hospital Mortality HSMR 12 Month Rolling Total - Southport and Ormskirk Hospitals Target: 100 Current Performance : Current Issues: Southport and Ormskirk Hospitals NHS Trust are significantly above the expected level of 100. This has also been confirmed by the publication of Standardised Hospital Mortality Index figures for the 12 months to December 2016 where Southport and Ormskirk Hospitals Trust had the second worst Mortality Index for an English Acute Trust (116). Up until late 2016 a combination of data processing issues with the Southport and Ormskirk Hospitals Patient Administration System and the data cleansing process used by NHS Digital for HES data resulted in the mortality at the Trust being significantly underestimated in these statistics. After several months of reporting with these errors corrected it is evident that mortality is a major concern and no longer a data issue. Improvement Plans: Southport and Ormskirk Hospitals have established a Mortality Review Group; however, this activity has been assumed by the Hospital Senior Management Team and as a result they feel that CCG participation in this review is inappropriate. To date no explanation for the high rates has been provided. 34 P a g e
65 12d West Lancashire CCG Patients Waiting To understand how many patients were still waiting for procedures or outpatient appointments, the numbers of patients waiting for all incomplete pathways for all Trusts have been included in the graph below. More detailed reports on RTT waiters are available via Aristotle spotlight reports. For West Lancashire CCG patients, in September 2017, there were 6331 patients in total with an Incomplete Pathway. Of these, 6021 (95.1%) are under 18 Weeks and 310 over 18 Weeks. The table below shows the providers with the highest number of incomplete patient pathways for West Lancashire CCG patients in September Of these providers five have achieved the 92% target. The best performer is Ramsay Operations (UK) (mainly Renacres Hospital) with 98.3%, followed by Wrightington, Wigan and Leigh NHS Foundation Trust with 98.0%. Southport and Ormskirk Hospitals NHS Trust, the most significant Secondary Care provider for West Lancashire CCG, achieved 95.7%. Trust Under 18 Weeks Over 18 Weeks Total % Under 18 Weeks RAG Southport and Ormskirk Hospitals NHS Trust % G Wrightington, Wigan and Leigh NHSFT % G Ramsay Operations (UK) % G St Helens and Knowsley Hospital Services NHS Trust % G Lancashire Teaching Hospitals NHSFT % R Aintree University Hospital NHS Foundation Trust % G Royal Liverpool and Broadgreen University Hospitals NHS Trust % R 35 P a g e
66 The table below shows the specialties at the main providers where the 92% target was not achieved for West Lancashire CCG patients in September Southport and Ormskirk Hospitals NHS Trust Rheumatology 85.1% Wrightington, Wigan and Leigh NHSFT Plastic Surgery 83.3% General Surgery 86.7% St Helens and Knowsley Hospital Services NHS Trust General Surgery 87.5% ENT 88.2% Gastroenterology 88.9% Lancashire Teaching Hospitals NHSFT General Medicine 63.6% Plastic Surgery 70.0% Urology 73.7% General Surgery 79.3% Gastroenterology 81.8% Neurology 87.5% Ophthalmology 88.9% Aintree University Hospital NHS Foundation Trust Urology 86.7% Respiratory Medicine 88.2% Ophthalmology 89.8% Gastroenterology 90.9% Royal Liverpool and Broadgreen University Hospitals NHS Trust Gastroenterology 64.3% Other 75.0% General Surgery 75.0% Trauma & Orthopaedics 78.0% Cardiology 84.6% Dermatology 90.4% Urology 91.7% Although West Lancashire CCG experienced a decline in 18-week Referrals to Treatment performance during 2016/17, this pattern is reflected both nationally and for other local CCGs. The table below shows West Lancashire CCG performance for 2017/18 compared to other local CCGs. CCG Name Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Chorley and South Ribble CCG 89.9% 90.6% 91.1% 89.4% 89.7% 89.7% % % % % % % 90.1% Greater Preston CCG 90.3% 90.5% 90.8% 89.1% 89.1% 88.8% % % % % % % 89.8% Liverpool CCG 91.4% 91.2% 90.5% 90.3% 89.9% 89.3% % % % % % % 90.4% South Sefton CCG 93.7% 94.2% 93.6% 92.6% 92.4% 92.3% % % % % % % 93.1% Southport and Formby CCG 94.3% 93.6% 93.9% 93.6% 93.4% 93.4% % % % % % % 93.7% West Lancashire CCG 95.8% 95.0% 95.1% 94.9% 95.0% 95.1% % % % % % % 95.1% The chart below indicates the number of patient pathways by which the major providers for West Lancashire CCG overperform or underperform the 92% Referral to Treatment target in September P a g e

67 12e Friends and Family Test This report has not been updated for September 2017 due to technical issues occurring this month. It should be noted that although the proportion of positive responses to the Friends and Family Test at Southport and Ormskirk Hospitals NHST are high the actual response rates are significantly below the National Average. For example, the National Response Rate for Inpatients is 26.4% whereas at Southport and Ormskirk Hospitals NHST only 13.3% of discharged patients responded. 37 P a g e
68 12g Safety Thermometer On one day each month, hospital Trusts are required to check to see how many of their patients suffered certain types of harm whilst in their care. This measure is known as the Safety Thermometer. The Safety Thermometer looks at four harms: pressure ulcers, falls, blood clots and urine infections for those patients who have a urinary catheter in place. This helps Trusts to understand where they need to make improvements. The graph and table below indicates the percentage of patients at each trust who did not suffer harm in any of the four categories. 38 P a g e
69 13. Complaints GP Comments, Concerns and Issues with Healthcare Providers August 2017 This report has not been updated for September 2017 owing to personnel issues in the NHS West Lancashire CCG Business Intelligence Team. In August 2017, there were eighteen issues raised by GPs, in contrast to July when there were four. This is the highest number of GP issues raised in the last 12 months Ten of the GP comments were regarding details of baby s hospital checks not being forwarded, five were regarding discharge letters being sent to an incorrect GP Practice, two regarding diagnostic testing reports being sent to the incorrect practice and one comment regarding general communication. Issues raised by GPs concern two providers, Southport and Ormskirk Hospitals NHS Trust and St Helens and Knowsley Hospitals NHS Trust. Virtually all issues are Information Governance with reports being sent to the wrong GP practice, this indicates that Southport and Ormskirk Hospitals NHS Trust are not verifying GP details correctly in particular checking patient details against the national spine. St Helens and Knowsley Hospitals NHS Trust are affected because Southport and Ormskirk Hospitals subcontract Direct Access Pathology activity to. 14. Serious Untoward Incidents During September, one new StEIS incident were reported involving West Lancashire CCG registered patients. This incident occurred at Southport and Ormskirk Hospitals NHS Trust and was reported within the 48-hour timescale. Four StEIS incidents were closed, one with Lancashire Care Foundation Trust and three with Southport and Ormskirk Hospitals NHS Trust. Five Root Cause Analysis Reports were due in September 2017, two from Lancashire Care NHS Foundation Trust and two from Southport and Ormskirk hospitals NHS Trust and one from Lancashire Teaching Hospitals NHS Foundation Trust. Lancashire Teaching Hospitals NHS Foundation Trust achieved the 60 working days timescale for submission while Lancashire Care NHS Foundation Trust achieved the 60-day target for one submission and delivered the second report within an agreed extension. Both the RCA Reports for Southport and Ormskirk Hospitals NHS Trust had agreed extension requests and of these one report has been received while the second is still within the agreed deadline extension. The RCA report received for Southport and Ormskirk Hospitals NHS Trust was originally due on 20/04/2017 and had been subject to four extension requests. As at 30 September 2017, 17 StEIS incidents remain open involving West Lancashire CCG patients. The majority of these are from Southport and Ormskirk Hospitals NHS Trust (10 in total). Of these 17 open incidents, the highest reported incidence is in the category apparent/actual/suspected self-inflicted harm with four incidents in total. 39 P a g e
70 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT DATE OF BOARD MEETING: 28 November 2017 WLCCGB 11/17/09 TITLE OF REPORT: CCG Safeguarding Children and Adult s Policy BRIEFING POINTS: The policy details the safeguarding arrangements which must be in place to ensure the CCG fulfils its statutory duties and responsibilities. It also provides clear service standards against which all healthcare providers will be monitored to ensure that safeguarding arrangements within commissioned services are appropriate. The updated version has been strengthened in line with current legislation and guidance in consultation with pan-lancashire CCG Designated Leads. The changes of note include: Guidance on appropriate behaviours for staff in and outside of work The Care Act and Prevent Categories of abuse have been amended to include Female Genital Mutilation and Child Sexual Exploitation Safeguarding standards have been updated for commissioned services LSCB revised Section 11 requirements have been added to the CCG Safeguarding and Accountability Framework self-assessment Reference is made to safeguarding and MCA standards being incorporated into commissioning processes and service specifications The amendments to the policy have been considered and approved by and the Quality and Safety Committee prior to being submitted to the Governing Body for ratification. Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience) please outline impact x 2. Commissioning of hospital and community services please outline impact x 3. Commissioning and performance management of GP Prescribing please x outline impact 4. Delivering Financial Balance please outline impact x 5. Development of the commissioning group as a commissioning organisation x please outline impact B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number) have any legal implications x CCG Safeguarding Children and Adult s policy West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
71 promote effective governance practice 2. Additional resource implications x (either financial or staffing resources) 3. Health Inequalities x 4. Equality and Inclusion and Human Rights Requirements X Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement x 6. Patient and Public Engagement x PAPER PREPARED BY: Lorraine Elliott, Designated Lead Nurse for Safeguarding Adults MCA Louise Burton, Designated Lead Nurse for Safeguarding Children PAPER PRESENTED BY: Claire Heneghan, Chief Nurse CCG Safeguarding Children and Adult s policy West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
72 NHS West Lancashire Clinical Commissioning Group Safeguarding Children and Adults Policy Incorporating standards for Safeguarding and Mental Capacity Act for the CCG and Commissioned Services Document Reference: Document Title: Version: 6.0 Supersedes: 5.0 Author: Authors Designation: Consultation Group: Date Ratified: West Lancashire CCG Safeguarding Children and Adults Policy, incorporating standards for Mental Capacity Act for the CCG and Commissioned Services Lorraine Elliott and Louise Burton Designated Leads Nurses Review Date: August 2019 Pan-Lancashire Safeguarding Designated Safeguarding / Mental Capacity Act Leads Safeguarding Children and Adults Policy V6 Page 1 of 68
73 Version Control Version Date Author Status Head of Safeguarding Final Head of Safeguarding Draft Head of Safeguarding Head of Safeguarding Draft Draft Head of Safeguarding Final Head of Safeguarding Final Head of Safeguarding Final Designated Lead Nurses Designated Lead Nurses Final Final Comment / Details of Amendments Waiting for feedback from patient group Waiting for ratification by Q&I committee before going to Governing Body for final ratification Endorsed by the Joint Quality and Improvement Committee Approved by the Chorley and South Ribble CCG Governing Body Amended to reflect changes to legislation and national guidance Approved by CCG Safeguarding Assurance Group / Joint Quality and Performance Committee Amended to reflect changes to legislation and statutory and national guidance including the Care Act 2014, the Counter-Terrorism and Security Act 2015 and the revised NHS Safeguarding and Assurance Framework Amended review date as this hadn t been amended following ratification of policy in January 2016 Revised in line with current legislation and guidance and to reflect NHSE Accountability and Assurance Framework Assessment Safeguarding Children and Adults Policy V6 Page 2 of 68
74 Circulation List Prior to approval, this Policy was circulated to the following for consultation: Contracting and Safeguarding Leads across pan-lancashire CCGs Members of the CCG Quality and Safety Committee Following approval this Policy document will be circulated to: All CCG staff To be incorporated within contract arrangements with all commissioned services Equality Impact Assessment This policy has been reviewed by the Equality and Diversity Lead and revision of the Equality Impact Assessment is not required Safeguarding Children and Adults Policy V6 Page 3 of 68
75 CONTENTS PAGE 1.0 INTRODUCTION Scope Principles Definitions ROLES AND RESPONSIBILITIES General Roles and Responsibilities of the CCG Chief Officer CCG Board Lead with responsibility for safeguarding CCG Safeguarding Team CCG Individual Staff Members including GP Member Practices GUIDANCE ON APPROPRIATE BEHAVIOURS GOVERNANCE ARRANGEMENTS Safeguarding Assurance Group Safeguarding Training Safe Recruitment Practices Managing Allegations CCG Safeguarding Team contact details IMPLEMENTATION Method of monitoring compliance BREACHES OF POLICY CATEGORIES OF ABUSE Children Adults PREVENT GUIDANCE FOR RAISING SAFEGUARDING CONCERNS REFERENCE DOCUMENTS AND GLOSSARY 18 APPENDICES Appendix 1: What to do if an adult is at risk of harm 21 Appendix 2: What to do if you have concerns a child is being abused 22 Appendix 3: Information Sharing Guidance 24 Appendix 4: Safeguarding Children and Adults Training for CCG staff 26 Appendix 5: Audit Tool for CCG commissioned services 35 Appendix 6: Audit Tool for CCG Commissioned Care Homes with Nursing 48 Appendix 7: Audit Tool for CCG compliance with Section 11 requirements 55 Appendix 8: CCG Safeguarding accountability flowchart Safeguarding Children and Adults Policy V6 Page 4 of 68
76 1.0 INTRODUCTION The Clinical Commissioning Group (CCG) as with all other NHS bodies has a statutory duty to ensure that it makes arrangements to safeguard and promote the welfare of children and young people, that reflect the needs of the children they deal with; and to protect adults from abuse or the risk of abuse. This policy details the safeguarding arrangements that must be in place to ensure the CCG fulfils its statutory duties and responsibilities In discharging these statutory duties/responsibilities account must be taken of: HM Government (2014) The Care Act The Children Act (1989 and 2004) DH (2017) Care and Support Statutory Guidance NHS England (July 2015) Safeguarding Vulnerable People in the NHS Accountability and Assurance Framework HM Government (March 2015) Working Together to Safeguard Children DH, DfE (March 2015) Statutory Guidance on Promoting the Health and Wellbeing of Looked After Children Department for Constitutional Affairs (2007) Mental Capacity Act 2005: Code of Practice DH 2011 Safeguarding Adults: The Role of Health Services The policies and procedures of Lancashire Safeguarding Children Board (LSCB) and Lancashire Safeguarding Adults Board (LSAB). HM Government (2011) Prevent Strategy Please see Section 11.0 for links to the above policies and procedures As a commissioning organisation the CCG is required to ensure that all health providers from whom it commissions services have comprehensive single and multi-agency policies and procedures in place. In addition, providers are linked into the Local Safeguarding Boards and contribute to multi-agency working This policy has two functions: it details the roles and responsibilities of the CCG as a commissioning organisation and that of its employees and GP member practices. The policy also provides clear service standards against which healthcare providers, including independent providers and voluntary, community and faith sectors will be monitored to ensure that all service users are protected from abuse and the risk of abuse Safeguarding is not a substitute for: Providers responsibilities to provide safe and high quality care and support Commissioners regularly assuring themselves of the safety and effectiveness of commissioned services The Care Quality Commission ensuring that regulated providers comply with the fundamental standards of care or by taking enforcement action Safeguarding Children and Adults Policy V6 Page 5 of 68
77 1.1 Scope This policy aims to ensure that no act or omission by the CCG as a commissioning organisation, or via the services it commissions, puts a service user at risk; and that robust systems are in place to safeguard and promote the welfare of children and to protect adults at risk of harm, including the implementation of the Mental Capacity Act (MCA) Where the CCG is identified as the lead commissioner it will notify associate commissioners of a provider s non-compliance with the standards contained in this policy, or of any serious incident that has compromised the safety and welfare of a child/adult resident within their population. 1.2 Principles In developing this policy the CCG recognises that safeguarding children and adults is a shared responsibility. There is a need for effective joint working between agencies and professionals that have different roles and expertise if vulnerable groups in society are to be protected from harm. In order to achieve effective joint working there must be constructive relationships at all levels, promoted and supported by: A commitment of senior managers and board members to seek continuous improvement with regards to safeguarding both within the work of the CCG and within commissioned services Clear lines of accountability within the CCG for safeguarding To work with the CCG to incorporate safeguarding and MCA standards into commissioning processes and service specifications Service developments that take account of the need to safeguard all service users and informed where appropriate, by the views of service users Staff training and continuing professional development to promote staff understanding of their roles and responsibilities Appropriate supervision and support for staff in relation to safeguarding practice Safe working practices including recruitment and vetting procedures. Effective interagency working, including effective information sharing The above principles reflect the expectations of the NHS Safeguarding Assurance and Accountability Framework and statutory guidance as referenced within this policy. The CCG will monitor themselves on an annual basis against a set of standards (appendix 7) reporting to the Safeguarding Assurance Group, which reports to the Quality and Performance Committee on the findings including any actions required to ensure full compliance The CCG is committed to a human rights based approach, which ensures that employees and the community that we serve are treated with fairness, respect, equality, dignity and autonomy (FREDA) and that individuals or groups are not discriminated against on the basis of their protected characteristics Safeguarding Children and Adults Policy V6 Page 6 of 68
78 1.2.3 In line with equality legislation, this policy aims to safeguard children, young people and adults who may be at risk of abuse irrespective of their protected characteristics as outlined in the Equality Act The nine protected characteristics being: age, gender, race, disability, marriage/civil partnership, maternity/pregnancy, religion/belief, sexual orientation and gender reassignment. 1.3 Definitions (categories of abuse are detailed in section 10) Children: in this policy, as in the Children Act 1989 and 2004, a child is anyone who has not yet reached their 18 th birthday. Children therefore means children and young people throughout Safeguarding and promoting the welfare of children is defined in Working Together to Safeguard Children (2015) as: Protecting children from maltreatment Preventing impairment of children's health or development Ensuring that children are growing up in circumstances consistent with the provision of safe and effective care Taking action to enable all children to have the best life chances Child protection: is part of safeguarding and promoting welfare. This refers to the activity that is undertaken to protect specific children who are suffering, or are likely to suffer, significant harm Young carers: these are children and young people who assume important caring responsibilities for parents, siblings or other family members; who maybe disabled, have physical or mental health problems, or misuse drugs or alcohol Looked After Children: The term looked after children and young people is generally used to mean those looked after by the state, according to relevant national legislation, which differs between England, Northern Ireland, Scotland and Wales. This includes those who are subject to an interim care order, care order in relation to the (Children Act 1989 section 31, 38) or temporarily classed as looked after on a planned basis for short breaks or respite care. The term is also used to describe accommodated (the Children Act 1989, section 20) children and young people who are looked after on a voluntary basis at the request of, or by agreement with their parents. These children are referred to as children in care The Care Act, 2014, Principles for Adult Safeguarding Empowerment - presumption of person led decisions and informed consent Protection - support and representation for those in greatest need Prevention - it is better to take action before harm occurs Proportionality proportionate and least intrusive response appropriate to the risk presented Partnership - local solutions through services working with their communities; communities have a part to play in preventing, detecting and reporting neglect and abuse Safeguarding Children and Adults Policy V6 Page 7 of 68
79 Accountability - accountability and transparency in delivering safeguarding Safeguarding Adults Safeguarding means protecting an adult s right to live in safety, free from abuse and neglect. It is about people and organisations working together to prevent and reduce both the risks and experience of abuse or neglect. At the same time making sure that the adult s wellbeing is promoted. This includes having regard to their views, wishes, feelings and beliefs in deciding on any action. This must recognise that adults sometimes have complex interpersonal relationships and maybe unclear or unrealistic about their personal circumstances. The Care Act requires agencies to work together to develop shared strategies for safeguarding adults. All health, social care professionals and care workers play a key role in safeguarding adults at risk, who are in receipt of health or care services. It is everybody s responsibility to protect adults at risk from abuse, harm and omissions of care Adult at risk (of abuse and neglect): Safeguarding duties apply to an adult aged 18 or over and who: Has needs for care and support (whether the local authority is meeting any of those needs) Is experiencing, or is at risk of abuse or neglect As a result of those care needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect The adult experiencing, or at risk of abuse or neglect will hereafter be referred to as the adult throughout this policy. 2.0 ROLES AND RESPONSIBILITIES FOR SAFEGUARDING 2.1 General Roles and Responsibilities of the CCG The ultimate accountability for safeguarding sits with the Chief Officer. Failure to have systems and processes in place to protect children and adults in the commissioning process, or by providers of health care that the CCG commission, would result in failure to meet statutory and non-statutory constitutional and governance requirements Fundamentally the role of the CCG is to work with others to ensure that critical services are in place to respond to children and adults and delivering improved outcomes and life chances for the most vulnerable The CCG must demonstrate appropriate systems are in place for discharging statutory duties in terms of safeguarding. These include: Safeguarding Children and Adults Policy V6 Page 8 of 68
80 The CCG must establish and maintain constitutional and governance arrangements with capacity and capability to deliver safeguarding duties and responsibilities A clear line of accountability for safeguarding, reflected in governance arrangements Clear policies setting out the commitment and approach to safeguarding including safe recruitment practices and arrangements for dealing with allegations against people who work with children and adults as appropriate Seeking assurance from all commissioned services, both NHS and independent healthcare providers, throughout the year to ensure continuous improvement Staff training in recognising and reporting safeguarding issues, appropriate supervision and ensuring staff are competent to carry out their roles and responsibilities Effective inter-agency working with the local authority, the police and third sector organisations, which includes arrangements to co-operate with the local authority in the operation of the Local Safeguarding Boards and Health and Wellbeing Board To employ or secure the expertise of a Designated Doctor and Nurse for Safeguarding Children; a Designated Doctor and Nurse and for Looked After Children (LAC); a Designated Paediatrician for Child Deaths To have an Adult Safeguarding Lead, which includes MCA and Deprivation of Liberty Safeguards (DoLS) supported by relevant policies and training Effective systems for responding to abuse and neglect Ensuring effective arrangements for information sharing Work with the local authority to enable access to community resources that can reduce social and physical isolation for adults Supporting the development of a positive learning culture across partners for safeguarding adults to ensure that organisations are not unduly risk adverse 2.2 Chief Officer Ensures that the health contribution to safeguarding and promoting the welfare of children and adults is discharged effectively across the whole local health economy through the organisation s commissioning arrangements Ensures that the organisation not only commissions specific clinical services but exercises a public health responsibility in ensuring that all service users are safeguarded from abuse or the risk of abuse Ensures that safeguarding children and adults is identified as a key priority area in all strategic planning processes Ensures that safeguarding children and adults is integral to clinical governance and audit arrangements Ensures that all providers from whom services are commissioned have comprehensive single and multi-agency policies and procedures for safeguarding, which are in line with the Local Safeguarding Boards policies and procedures, and are easily accessible for staff at all levels Ensures that all contracts for the delivery of health care include clear service standards for safeguarding children and adults; these service standards are Safeguarding Children and Adults Policy V6 Page 9 of 68
81 monitored thereby providing assurance that service users are effectively safeguarded Ensures that all staff in contact with children, adults who are parents/carers in the course of their normal duties are trained and competent to be alert to the potential indicators of abuse or neglect for children and adults and know how to act on those concerns in line with local guidance Ensures the CCG co-operates with the local authority in the operation of the Local Safeguarding Boards Ensures that all health organisations with whom the CCG has commissioning arrangements have links with their Local Safeguarding Boards; that there is appropriate representation at an appropriate level of seniority and that health workers contribute to multi-agency working Ensures that any system and processes that include decision making about an individual patient (e.g. funding panels) takes account of the requirements of the MCA; this includes ensuring that actions and decisions are documented in a way that demonstrates compliance with the Act. 2.3 CCG Board Lead with Responsibility for Safeguarding Ensures that the CCG has management and accountability structures that deliver safe and effective services in accordance with statutory, national and local guidance for safeguarding and LAC Ensures that service plans/specifications/contracts/invitations to tender etc. include reference to the standards expected for safeguarding children and adults Ensures that safe recruitment practices are adhered to in line with national and local guidance and that safeguarding responsibilities are reflected in all job descriptions Ensures that staff in contact with children and adults in the course of their duties are trained and competent to be alert to the potential indicators of abuse or neglect and know how to act on those concerns in line with local guidance 2.4 CCG Safeguarding Team (Designated and Professional Leads for Safeguarding and MCA) Designated leads will work across the local health system to support other professionals in their agencies on all aspects of safeguarding To ensure the CCGs meet the requirements of the MCA, including DoLS To ensure that safeguarding children and adults is an integral part of the CCG s clinical governance framework To promote, influence and develop safeguarding training on a single and inter-agency basis - to meet the training needs of staff To provide clinical advice on the development and monitoring of the safeguarding aspects of CCG contracts To undertake serious case reviews / case management reviews / domestic homicide reviews / safeguarding adult reviews on behalf of health commissioners and for quality assuring the health content Safeguarding Children and Adults Policy V6 Page 10 of 68
82 To fulfil the role of the Nominated Senior Officer where there is an allegation against a person who works with children / adults; including, ensuring the CCG operates within the Local Safeguarding Boards policies and procedures; to provide a coordinating role in these instances, resolving any interagency issues that may arise and liaising with the Safeguarding Boards as necessary To provide advanced expert knowledge and advice on safeguarding children and adults / MCA to a wide range of professional groups and organisations / agencies; where necessary taking responsibility for the oversight of complex cases To undertake statutory designated safeguarding functions as outlined in statutory guidance and as detailed in the Intercollegiate Documents (RCPCH 2012/14) The designated doctor and nurse functions to be incorporated into the job role / plan of those individuals designated to hold the role of designated nurse and designated doctor for safeguarding children and LAC To provide an annual report on safeguarding which will be considered by the governing body 2.5 Individual Staff Members including GP Member Practices To be alert to the potential indicators of abuse or neglect for children and adults and know how to act on those concerns in line with local guidance To undertake training in accordance with their roles and responsibilities as outlined by the training frameworks of the Intercollegiate Document so that they maintain their skills and are familiar with procedures aimed at safeguarding children and adults Understand the principles of confidentiality and information sharing in line with local and government guidance To contribute, when requested to do so, to multi-agency meetings established to ensure safeguarding arrangements Appendices at the back of this document provide guidance as to what action needs to be taken where there are concerns that a child or an adult at risk is being abused. 3.0 GUIDANCE ON APPROPRIATE BEHAVIOURS 3.1 The CCG is committed to valuing all employees and has a responsibility to establish requirements in standards of work to be achieved by its staff. All staff have a responsibility to maintain public confidence and must uphold high standards of personal conduct both within and outside of their work setting. Staff must not act in a way which could bring the CCG into disrepute and must act in accordance with their relevant professional bodies where appropriate. 3.2 The CCG expects that all staff are: Professional and honest Work in partnership with others to achieve our goals Listen and learn, and be willing to change based on what we hear Safeguarding Children and Adults Policy V6 Page 11 of 68
83 To respect and care for our staff, the people we work with and our local community To protect and invest the public funds that are given to us in a well-managed way 3.3 Staff are advised to take precautions with their use of social media in a personal capacity and are advised that expectations set out within the Information Governance Handbook apply whether using it for a work purpose or at home for personal use. 3.4 All staff must follow the guidance outlined within the safeguarding policy and it must be read in conjunction with the Information Governance Handbook, Complaints and Whistle Blowing policies. 4.0 GOVERNANCE ARRANGEMENTS 4.1 Safeguarding Assurance Group The Safeguarding Assurance Group will not replicate existing multi / single agency forums To ensure that safeguarding is integral to the governance arrangements of the CCG a Safeguarding Assurance Group has been established which reports directly into the Joint CCG Quality and Performance Committee. The purpose of the group is to provide assurance on the effectiveness of the safeguarding arrangements in place within commissioned services and the CCG; ensuring that safeguarding is integral to quality and audit arrangements within the CCG. The Safeguarding Assurance Group will also ensure that the CCG is kept informed of national and local initiatives for safeguarding and will oversee the implementation of learning from reviews and audits that are aimed at driving improvements to safeguard children and adults. 4.2 Safeguarding Training A safeguarding training matrix details the training expected of all CCG employees, including agency staff and CCG members. The matrix can be found at Appendix Safe Recruitment Practices Recruiting managers shall seek guidance from Human Resources, to determine the level of Disclosure and Barring Service (DBS) check required for the role. Where a DBS check is required, the manager shall ensure clearance is obtained before the applicant commences employment. 4.4 Managing allegations against persons who work with children, young people or adults at risk Where there are concerns that a member of staff, either directly or non-directly employed by the CCG, is behaving in a way that demonstrates unsuitability for Safeguarding Children and Adults Policy V6 Page 12 of 68
84 working with children, young people or adults at risk, in their present position, or in any capacity this must be reported to the CCG Designated Lead for Safeguarding The allegation or concern may arise either in the employees/professionals work or private life. Examples include: Commitment of a criminal offence against or related to children, young people or adults Failing to work collaboratively with social care agencies when issues about care of children, young people or adults for whom they have caring responsibilities are being investigated Behaving towards children, young people or adults, in a manner that indicates they are unsuitable to work with this client group Where an allegation or concern arises relates to the individuals private life such as perpetration of domestic abuse; behaviours to his / her own children; or behaviour to others which may impact upon the safety of children / adults to whom they owe a duty of care Where inadequate steps have been taken to protect vulnerable individuals from the impact of violence or abuse and neglect All concerns and allegations will be considered in line with the Local Safeguarding Boards policy relevant to managing allegations against persons who work with children, young people or adults. The designated safeguarding lead will inform the Local Authority Designated Officer (LADO) of all allegations that come to their attention In instances where the allegation suggests that a child/young person or adult is at risk of significant harm the case must be referred to the respective local authority in line with Lancashire Safeguarding Children Board and Lancashire Safeguarding Adult Board policies and procedures. 4.5 CCG Safeguarding Team contact details Designated Lead Nurse for Safeguarding Children and Looked After Children Deputy Designated Nurse for Safeguarding Children Designated Lead Nurse for Safeguarding Adults and Mental Capacity Act Deputy Designated Professional for Safeguarding Adults and Mental Capacity Act Safeguarding Administration Team csrccg.safeguarding@nhs.net IMPLEMENTATION 5.1 Method of Monitoring Compliance The standards expected of the CCG and all healthcare providers are detailed in the appendices. Compliance will be measured by annual audit an audit tool will Safeguarding Children and Adults Policy V6 Page 13 of 68
85 be made available to all providers to facilitate the recording of information. The audit tool should be completed using the RAG definitions outlined in the Procedure for Monitoring Safeguarding Children and Adults at Risk via Provider Contracts. 6.0 BREACHES OF POLICY 6.1 This policy is mandatory. Where it is not possible to comply with the policy or a decision is taken to depart from it, this must be notified to the CCG Safeguarding Team to enable the level of risk to be assessed and an action plan formulated. 6.2 Where the CCG is a lead commissioner it will notify associate commissioners of a provider s non-compliance with the standards contained in this policy, including action taken where there has been a significant breach. 7.0 CATEGORIES OF ABUSE 7.1 Children For children s safeguarding, the categories of abuse are taken from Working Together to Safeguard Children. Abuse is defined as a form of maltreatment of a child. Somebody may abuse or neglect a child by inflicting harm, or by failing to act to prevent harm. Children may be abused in a family, in an institutional or community setting, or via the internet by those known to them or, more rarely, by others. A child may be abused by an adult or adults, or another child or children Physical abuse: A form of abuse which may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning, female genital mutilation (FGM) suffocating or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child Emotional abuse: The persistent emotional maltreatment of a child such as to cause severe and persistent adverse effects on the child s emotional development. It may involve conveying to a child that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may include not giving the child opportunities to express their views, deliberately silencing them or making fun of what they say or how they communicate. It may feature age or developmentally inappropriate expectations being imposed on children. These may include interactions that are beyond a child s developmental capability, as well as overprotection and limitation of exploration and learning, or preventing the child participating in normal social interaction. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying (including cyber bullying), causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of emotional abuse is involved in all types of maltreatment of a child, though it may occur alone Safeguarding Children and Adults Policy V6 Page 14 of 68
86 7.1.4 Sexual abuse: Involves forcing or enticing a child or young person to take part in sexual activities, this may not necessarily always involve a high level of violence, the child may not always be aware they are being abused or know what is happening. The activities may involve physical contact, including assault by penetration (for example, rape or oral sex) or non-penetrative acts such as masturbation, kissing, rubbing and touching outside of clothing. They may also include non-contact activities, such as involving children in looking at, or in the production of, sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse (including via the internet). Sexual abuse is not solely perpetrated by adult males. Women can also commit acts of sexual abuse, as can other children. Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity Neglect: The persistent failure to meet a child s basic physical and/or psychological needs, likely to result in the serious impairment of the child s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to: provide adequate food, clothing and shelter (including exclusion from home or abandonment) protect a child from physical and emotional harm or danger ensure adequate supervision (including the use of inadequate care-givers) ensure access to appropriate medical care or treatment it may also include neglect of or unresponsiveness to a child s basic emotional needs 7.2 Adults The Care Act outlines the categories of abuse - Physical abuse: including assault, hitting, slapping, pushing and misuse of medication, restraint or inappropriate physical sanctions Domestic abuse: including psychological, physical, sexual, financial, emotional abuse; so called honour based violence, forced marriage and FGM Sexual abuse: including rape, indecent exposure, sexual harassment, inappropriate looking or touching, sexual teasing or innuendo, sexual photography, subjection to pornography or witnessing sexual acts, indecent exposure and sexual assault or sexual acts to which the adult has not consented or was pressured into consenting Psychological abuse: including emotional abuse, threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, cyber bullying, isolation or unreasonable and unjustified withdrawal of services or supportive networks Safeguarding Children and Adults Policy V6 Page 15 of 68
87 Financial or material abuse: including theft, fraud, internet scamming, coercion in relation to an adult s financial affairs or arrangements, including in connection with wills, property, inheritance or financial transactions, or the misuse or misappropriation of property, possessions or benefits Modern slavery: encompasses slavery, human trafficking and forced labour and domestic servitude. Traffickers and slave masters use whatever means they have at their disposal to coerce, deceive and force individuals into a life of abuse, servitude and inhumane treatment Discriminatory abuse: including forms of harassment, slurs or similar treatment; because of race, gender and gender identity, age, disability, sexual orientation or religion Organisational abuse: including neglect and poor care practice within an institution or specific care setting such as a hospital or care home, for example, or in relation to care provided in one s own home. This may range from one off incidents to on-going ill-treatment. It can be through neglect or poor professional practice as a result of the structure, policies, processes and practices within an organisation Neglect and acts of omission: including ignoring medical, emotional or physical care needs, failure to provide access to appropriate health, care and support or educational services, the withholding of the necessities of life, such as medication, adequate nutrition and heating Self-neglect: this covers a wide range of behaviour neglecting to care for one s personal hygiene, health or surroundings and includes behaviour such as hoarding 8.0 PREVENT 8.1 Prevent (radicalisation of vulnerable people): Prevent is one of the four key principles of the CONTEST strategy, which aims to stop people becoming terrorists or supporting terrorism. The Prevent Strategy addresses all forms of terrorism including extreme right wing but continues to prioritise according to the threat posed to our national security. The aim of Prevent is to stop people from becoming terrorists or supporting terrorism and operates in the pre-criminal space i.e. before any criminal activity has taken place. Radicalisation refers to the process by which people come to support, and in some cases to participate in terrorism Violent Extremism as defined by the Crown Prosecution Service (CPS) as the demonstration of unacceptable behaviour by using any means or medium to express views which: - foment, justify or glorify terrorist violence in furtherance of particular beliefs - seek to provoke others to terrorist acts Safeguarding Children and Adults Policy V6 Page 16 of 68
88 - foment other serious criminal activity or seek to provoke others to serious criminal acts - foster hatred which might lead to inter-community violence in the UK 8.2 Given the very high numbers of people who come into contact with health professionals, health services are a critical partner in Prevent. There are many opportunities for healthcare staff to help protect people from radicalisation. The key challenge is to ensure that healthcare workers can identify the signs that someone is vulnerable to radicalisation, interpret those signs correctly and access the relevant support. 8.3 Channel is a multi-agency process within Prevent, which aims to support those who may be vulnerable to being drawn into violent extremism. It works by Identifying individuals who may be at risk, assessing the nature and extent of the risk and where necessary referring cases to a multi-agency panel, which decides on the most appropriate support package to divert and support the individual at risk. 8.4 Channel aims to draw vulnerable individuals away from violent extremism before they become involved in criminal activity. Partnership working and effective information sharing is crucial in ensuring that multi-agency partners are able to build a comprehensive picture of an individual s vulnerability and therefore provide the appropriate type and level of support to safeguard the individual at risk. 8.5 Healthcare professionals may meet and treat people who are vulnerable to radicalisation. People with mental health needs or learning difficulties may be more easily drawn into terrorism. It is also known that some people without obvious vulnerabilities have been connected to terrorist acts. 9.0 GUIDANCE FOR RAISING SAFEGUARDING CONCERNS 9.1 It is important that all staff who work with adults, children, young people and their families are able to identify, assess and manage risks when dealing with safeguarding concerns. Furthermore staff should report and respond to these at the appropriate level. To assist with this, multi-agency guidance has been developed to aid decision making that ensures the most appropriate and proportionate response for the individuals involved. These should be used in conjunction with practitioners own multi-agency procedures. Lancashire Continuum of Need and Thresholds Guidance (Children) Lancashire Guidance for Safeguarding Concerns (Adults) 10.0 REFERENCE DOCUMENTS 10.1 In developing this policy account has been taken of the following statutory and non-statutory guidance, best practice guidance and the policies and procedures of the Local Safeguarding Boards Safeguarding Children and Adults Policy V6 Page 17 of 68
89 Statutory Guidance and Legislation Department for Constitutional Affairs (2007) Mental Capacity Act 2005: Code of Practice, TSO: London HM Government (2014) The Care Act The Children Act (1989 and 2004) The Human Rights Act (1998) Department of Health (2014) Care and Support Statutory Guidance Department of Health, London Department of Health et al (2015) Statutory guidance on Promoting the Health and well-being of Looked After Children, Nottingham, DCSF publications HM Government (2011) Safeguarding children who may have been trafficked, DCSF publications HM Government (2008) Safeguarding Children in whom illness is fabricated or induced, DCSF publications HM Government (2014) The Right to Choose: multi-agency statutory guidance for dealing with Forced marriage, Forced Marriage Unit: London HM Government (2015) Working Together to Safeguard Children Nottingham, DCSF publications HM Government (2016) Multi-agency statutory guidance on Female Genital Mutilation HM Government (2014) Multi-agency statutory guidance for dealing with cases of Forced Marriage, Forced Marriage Unit: London Ministry of Justice (2008) Deprivation of Liberty Safeguards Code of Practice to supplement Mental Capacity Act 2005, London TSO HM Government (2011) Prevent Strategy Counter Terrorism and Security Act (2015) Non-statutory guidance Children s Workforce Development Council (March 2010) Early identification, assessment of needs and intervention. The Common Assessment Framework for Children and Young People: A practitioner s guide, CWCD DH (2017) FGM Safeguarding Pathway DH (2016) FGM Risk and Safeguarding. Guidance for professionals. DH (June 2012) The Functions of Clinical Commissioning Groups (updated to reflect the final Health and Social Care Act 2012) DH (March, 2011) Adult Safeguarding: The Role of Health Services Lancashire Safeguarding Adults Board Guidance for Safeguarding Concerns 2017 DH (May, 2011) Statement of Government Policy on Adult Safeguarding Safeguarding Children and Adults Policy V6 Page 18 of 68
90 DH (Nov, 2011), Building Partnerships, Staying Safe. - The Health Sector Contribution to HM Governments Prevent Strategy. Guidance for Healthcare organisations. HM Government (2006) What to do if you re worried a child is being abused, DCSF publications HM Government (2009) Safeguarding children and young people from sexual exploitation: supplementary guidance to Working together to safeguard children DCSF publications HM Government (2015) Information Sharing: Advice for practitioners providing safeguarding services to children, young people, parents and carers, DCSF publications Ministry of Justice, Department of Health (2014) Mental Capacity Act: government response to the House of Lords Select Committee report NHS Commissioning Board July 2015 Safeguarding Vulnerable people in the NHS - accountability and assurance framework Royal College Paediatrics and Child Health et al (2014) Safeguarding Children and Young people: Roles and Competencies for Health Care Staff. Intercollegiate Document supported by the Department of Health. Royal College Paediatrics and Child Health et al (2015) Looked after children: Knowledge, skills and competences of healthcare staff. Intercollegiate Role Framework (RCPCH, 2015) NHS England (2017) Prevent Training and Competences Framework Best practice guidance Department of Health (2004) Core Standard 5 of the National Service Framework for Children Young People and Maternity Services plus those elements beyond standard 5 that deal with safeguarding and promoting the welfare of children Department of Health (2009) Responding to domestic abuse: a handbook for health professionals HM Government. (July 2011). The United Kingdom s Strategy for Countering International Terrorism, from Home Office. National Institute for Health and Clinical Excellence (2016) When to suspect child maltreatment, Nice clinical guideline 89 National Institute for Healthcare Excellence (2013) NICE support for commissioning for the health and well-being of looked after children and young people. National Institute for Healthcare Excellence (2014) Domestic abuse and violence Nice PH 50 RCPCH et al (2012) Standards for Children and young People in Emergency Care Settings; Intercollegiate standards Lancashire Safeguarding Children Board Policies, Procedures and Practice Guidance Lancashire Safeguarding Adult Board Policies, Procedures and Practice Guidance Safeguarding Children and Adults Policy V6 Page 19 of 68
91 Care Quality Commission - Care Quality Commission (2015) Guidance about compliance: Essential Standards of Quality and Safety Disclose and Barring Service - The primary role of the Disclosure and Barring Service (DBS) is to help employers make safer recruitment decisions and prevent unsuitable people from working with vulnerable groups including children. Glossary CAF CCG LAC DoLS MCA LSCB LSAB VCFS Common Assessment Framework Clinical Commissioning Group Looked After Children Deprivation of Liberty Safeguards Mental Capacity Act Local Safeguarding Children Board Local Safeguarding Adult Board Voluntary, Community and Faith Service Safeguarding Children and Adults Policy V6 Page 20 of 68


: 0300 123 6722 Who to contact in the Police Public Protection Unit: Tel: 101 and request to speak to the PPU for the area in")
92 Appendix 1 What to do if an adult is at risk of harm Abuse discovered or suspected Is the adult at risk of immediate danger or in need of emergency medical treatment? And/or has a crime been committed? And/or is there a need to protect forensic evidence? Is anyone at risk of harm e.g. another adult or child? Yes No Contact the Duty Social Worker In adult s social care or contact the CCG Safeguarding Adult Lead for advice Contact emergency service e.g. police ambulance or GP No Safeguarding adults issue confirmed? Yes Referral to Lancashire Safeguarding Adults Enquiry Team Document all discussions held, actions taken, decision made including who was informed and who was spoken to All information to be passed to designated professional for safeguarding on next working day Record incident on DATIX or incident reporting form Who to contact in Adult Social Care: Lancashire Safeguarding Adults Enquiry Team: Emergency Duty Team (every day out of hours): Who to contact in the Police Public Protection Unit: Tel: 101 and request to speak to the PPU for the area in which the person resides. In an emergency contact the police on 999 Who to contact for local NHS advice: Lead Nurse for Safeguarding Adults and Mental Capacity Act Implementation for the Clinical Commissioning Group Tel: Safeguarding Administrator: Tel: Staff should update their knowledge by accessing regular training and be familiar with local safeguarding policies, including those of the Local Safeguarding Adults Board Safeguarding Children and Adults Policy V6 Page 21 of 68
93 Appendix 2 What to do if you are worried a child is being abused Abuse may take the form of physical abuse, sexual abuse, emotional abuse or neglect Any member of staff who believes that a child may be suffering, or is likely to suffer significant harm should always refer their concerns to Children s Social Care. (There should always be an opportunity to discuss your concerns with a manager, named professional or qualified social worker, but never delay emergency action to protect a child). Are you concerned a child is suffering or likely to suffer harm, for example: You may observe an injury or signs of neglect You are given information or observe emotional abuse A child discloses abuse You are concerned for the safety of a child or unborn baby Step 1 Inform parents/carers that you will refer to Children s Social Care UNLESS The child may be put at increased risk of further harm (e.g. suspected sexual abuse, suspected fabricated or induced illness, female genital mutilation, increased risk to child, forced marriage) or there is a risk to your own personal safety. Step 2 Step 3 Make a telephone referral to Children s Social Care (Tel: ) Follow up referral in writing within 24 hours Document all discussions held, actions taken, decisions made including who was spoken to (for physical injuries document injuries observed). Where a CAF has been completed, forward this with the written referral. Children s Social Care acknowledge receipt of referral and decide on next course of action. If the referrer has not received an acknowledgement within 3 working days contact Children s Social Care again. You may be requested to provide further reports/information or attend multi-agency meetings Step 4 Who to contact in Children s Social Care Duty Social Worker (Mon to Fri 8:45 to 5:00pm) Tel: Emergency Duty Team (out of hours) Tel: Who to contact in the Police Public Protection Unit Tel: 101 Request to speak to the PPU for the area in which the child resides Who to contact for local NHS advice Designated Nurse Safeguarding Children Tel: Lead GP Safeguarding/Named Doctor Tel: Designated Doctor Safeguarding Children Tel: (Contact the switch board at Lancashire Teaching Hospitals NHS Foundation Trust who will put you through to the Designated Doctor) In an emergency contact the police on 999 Appendix 2 Staff should update their knowledge by accessing regular training and be familiar with local safeguarding policies, including those of Lancashire Safeguarding Children Board. Possible signs and indicators of abuse and neglect can be found overleaf Safeguarding Children and Adults Policy V6 Page 22 of 68 August 2015

94 Safeguarding Children and Adults Policy V6 Page 23 of 68
95 Appendix Safeguarding Children and Adults Policy V6 Page 24 of 68

96 Safeguarding Children and Adults Policy V6 Page 25 of 68
97 Appendix 4 Safeguarding Children and Adults Training for CCG staff All Healthcare staff have a duty to safeguard and protect the welfare of children and adults. Safeguarding children and adults training is therefore mandatory for all staff engaged in services for children and adults to ensure that you retain the competences appropriate to your role and follow the relevant professional guidance. This document aims to provide guidance on the requirements and resources available to CCG staff. Safeguarding Children Training Level 1 all CCG staff are required to undertake level 1 training (this is the minimum entry level for all staff working in healthcare settings) Level 2 - all staff who have any contact with children, young people and/or parents/carers are required to undertake level 2 training Levels 3, 4, 5 are applicable to Designated Professionals & Named Leads NB: The training requirements for the roles of Chair, CEOs, Executive Board leads and Board members will be described separately in this table Target Group Level and suggested content Training opportunities available Level 1 - All staff working in health care settings: CCG staff groups All non- clinical staff, administrative, domestics, Board level Executives & non executives, lay members Training must be accessed on induction or within 6 weeks of taking up the post Competencies should be reviewed annually as part of staff appraisal in conjunction with individual learning and development plans. Over a three-year period staff should receive refresher training equivalent to a minimum of 2 hours. What is abuse and neglect How to recognise abuse and neglect To be able to understand the impact a parent/carer s physical and mental health can have on the well-being of a child or young person, including the impact of domestic violence To be able to understand the risks associated with the internet and online social networking Appropriate action to take if an individual has concerns MLCSU Learning Management System (LMS) Level 1 accessed via: MLCSU Learning Lancs LSCB e-learning level 1 accessed via: Lancs E-Learning The e-learning programme can also be accessed as part of refresher training Safeguarding Children and Adults Policy V6 Page 26 of 68
98 Target Group Level and suggested content Training opportunities available Level 2 - All staff who have any contact with children, young people and/or parents/carers CCG staff groups Includes: administrators for safeguarding teams, quality performance specialists, equality and diversity lead, engagement and patient experience lead, engagement assistant & customer care & patient experience officers Training should be undertaken within six months of coming into post. Competencies should be reviewed annually as part of staff appraisal in conjunction with individual learning and development plans. Over a three-year period staff should receive refresher training equivalent to a minimum of 3-4 hours. Training should be tailored to the roles of individuals. Documentation and information sharing Professional roles and responsibilities Impact of parent/carers physical and mental health on the wellbeing of the child in order to be able to identify a child/young person at risk Using the common assessment framework Using professional and clinical knowledge and understanding of what constitutes child maltreatment and how to recognise signs of abuse and neglect To be aware of the risk of Female Genital Mutilation (FGM) and be able to refer appropriately for further care and support To be able to identify and refer a child suspected of being a victim of trafficking and/or sexual exploitation To be aware of the risk factors for radicalisation and know who to contact regarding preventative action and support Acting in accordance with statutory and non- statutory guidance and legislation All staff undertaking Level 2 training must also undertake a CSE (Child Sexual Exploitation) e-learning module. MLCSU Learning Management System (LMS) Level 2 accessed via: MLCSU Learning Lancs LSCB e-learning level 2 accessed via: Lancs E-Learning Lancashire Safeguarding Children Boards LSCB policies and procedures accessed at: Lancs Online Procedures
99 Target Group Level and suggested content Training opportunities available Level 3 - All clinical staff working predominately with children and or their families who contribute to assessing, planning, intervening and evaluating the needs of a child and parenting capacity where there are safeguarding /child protection concerns. CCG staff groups Designated Professionals and Named Leads to be competent at this level. To be able to identify possible signs of sexual, physical, or emotional abuse or neglect using child and family- focused approach To be able to know what constitutes child maltreatment including the effects of carer/parental behaviour on children and young people Identify, assess and meet the needs of children where there are safeguarding concerns The impact of parenting issues such as domestic abuse, substance misuse on parenting capacity and the interagency response Recognising the importance of family history and functioning Working with family members including the lack of co-operation and superficial compliance within the context of the role Awareness of interagency policy / national guidance, implications of legislation Information sharing, confidentiality and consent; Remit and role of Local Safeguarding Children Boards Interagency frameworks for safeguarding including the Common Assessment framework (CAF); Team around the Child and the role of the Lead Professional. Additional specialist competencies Interagency working Contributing to serious case reviews/critical incidents/child death overview processes Applying lessons learnt from audit and serious case reviews to improve practice Advising others on appropriate information sharing Lancashire Safeguarding Children s Board Multi-Agency Training (Level 3 and above) Lancashire Safeguarding Children Common Assessment Framework CAF /Continuum Of Need CON training CAF Training Information and guidance re working with children who are looked after Promoting the health and Well-being of Looked After Children (DH 2015) Promoting Health doc Information on domestic violence, forced marriage and honour based violence Information on working with sexually active young people accessed at Lancs Procedures
100 Target Group Level and suggested content Training opportunities available Level 4 - Specialist roles and Named Leads CCG staff groups Designated Professionals and Named Leads to be competent at this level. NB: Those undertaking level 4 training do not need to repeat level 1, 2 or 3 training as it is anticipated that an update will be encompassed in level 4 training Competence should be reviewed annually as part of staff appraisal in conjunction with individual learning and development plan Named professionals should attend a minimum of 24 hours of education, training and learning over a three-year period. This should include nonclinical knowledge acquisition such as management, appraisal and supervision training. To be able to contribute to the development of robust internal safeguarding/child protection policy, guidelines, and protocols as a member of the safeguarding team To be able to know how to provide specialist advice to practitioners, both actively and reactively including clarification about organisational policies, legal issues and the management of child protection cases To be able to work effectively with colleagues from other organisations, providing advice as appropriate e.g. concerning safeguarding/child protection policy and legal frameworks, the health management of child protection concerns. To be able to know how to undertake and contribute to serious case reviews/case management/significant case reviews, individual management views/individual agency reviews/internal management reviews, this will include the undertaking of chronologies, the development of action plans where appropriate, and leading internal management reviews as part of this To be able to be a trained provider of safeguarding/child protection supervision and/or support To be able to lead/oversee safeguarding quality assurance and improvement processes To be able to undertake risk assessments of organisational ability to safeguard/protect children and young people To be able to support colleagues in challenging views offered by other professionals, as appropriate To be able to support colleagues in challenging views offered by other professionals, as appropriate Please refer to all training opportunities available in level 3 Named professionals should participate regularly in support groups or peer support networks for specialist professionals at a local and national level, according to professional guidelines (attendance should be recorded) Named professionals should complete a management programme with a focus on leadership and change management within three years of taking up their post Named Professionals responsible for training of doctors are expected to have appropriate education
101 Target Group Level and suggested content Training opportunities available Level 5 - Specialists roles Designated professional staff groups CCG staff groups Designated professionals NB: Training at level 5 will include the training required at levels 1-4 and will negate the need to undertake refresher training at levels 1-4 in addition to level 5. Designated professionals should attend a minimum of 24 hours of education, training and learning over a three-year period. This should include non-clinical knowledge acquisition such as management, appraisal, supervision training and the context of other professionals work To be able to know how to conduct a training needs analysis, and how to commission, plan, design, deliver, and evaluate safeguarding/child protection single and inter-agency training and teaching for staff across the health community To be able to know how to take a lead role in: o Leading /overseeing safeguarding/child protection quality assurance and improvement across the health community. o The implementation of national guidelines and auditing the effectiveness and quality of services across the health community against quality standards. o Service development conducting the health component of serious case reviews/ case management reviews/significant case reviews drawing conclusions and developing an agreed action plan to address lessons learnt. o Strategic and professional leadership across the health community on all aspects of safeguarding/ child protection. o Multi-disciplinary team reviews. o Regional and national safeguarding/child protection clinical networks (where appropriate). To be able to know how to give appropriate advice to specialist safeguarding/child protection professionals working within organisations To be able to know how to provide expert advice on increasing quality, productivity, and improving health outcomes for vulnerable children and those where there are safeguarding concerns To be able to oversee safeguarding/child protection quality assurance processes across the whole health community. To be able to know how to provide expert advice to service planners Please refer to all training opportunities available in level 3 Designated professionals should participate regularly in support groups or peer support Networks for specialist professionals at a local, regional, and national level according to professional guidelines (and their attendance should be recorded) An executive level management programme with a focus on leadership and change Management should be completed within three years of taking up the post
102 Target Group Level and suggested content Training opportunities available and commissioners, to ensure all services commissioned meet the statutory requirement to safeguard of children. To be able to know how to influence improvements in safeguarding/child protection services across the health community. To be able to monitor services across the health community to ensure adherence to legislation, policy and key statutory and nonstatutory guidance. To be able to reconcile differences of opinion among colleagues from different organisations and agencies. To be able to proactively deal with strategic communications and the media on safeguarding/ child protection across the health community. To be able to know how to work with public health officers to undertake robust safeguarding/child protection population-based needs assessments that establish current and future health needs and service requirements across the health community. To be able to provide an evidence base for decisions around investment and disinvestment in services to improve the health of the local population and to safeguard/protect children and young people and articulate these decisions to executive officers. Board Level for Chief Executive Officers, Trust and Health Board Executive and non-executive directors/members, commissioning body Directors All board members must have knowledge equivalent to all staff working within the healthcare setting (level 1) as well as Board level specific competences as identified below: Demonstrates an awareness and understanding of child maltreatment Demonstrates an understanding of appropriate referral mechanisms and information sharing A bespoke package of training should be offered that incorporates Level one and additional Board level specific competencies for this staff group. All boards should have access to safeguarding advice and expertise through designated or named leads.
103 Target Group Level and suggested content Training opportunities available Demonstrates clear lines of accountability and governance within and across organisations for the commissioning and provision of services designed to safeguard and promote the welfare of children Demonstrates an awareness and understanding of effective board level leadership for the organisations safeguarding arrangements Demonstrates an awareness and understanding of arrangements to share relevant information Demonstrates an awareness and understanding of effective arrangements in place for the recruitment and appointment of staff, as well as safe whistle blowing Demonstrates an awareness and understanding of the need for appropriate safeguarding supervision and support for staff including undertaking safeguarding training Demonstrates collaborative working with lead and nominated professionals across agencies Safeguarding Adults Training Target Group Level and suggested content Training opportunities available All CCG staff Introduction to safeguarding adult training What is abuse and neglect How to recognise abuse and neglect Appropriate action to take if an individual has concerns. Refresher training at a minimum every three years. The e-learning programme can also be accessed as part of refresher training The Lancashire Safeguarding Adults Board (LSAB) E learning Level 1 Lancs LSAB MLCSU Learning Management System Level 1 accessed via: MLCSU Learning
104 Target Group Level and suggested content Training opportunities available All CCG staff who have contact with service users All CCG staff Safeguarding Adults What you need to know What is abuse and neglect Understanding the terms vulnerable and adults at risk How to recognise potential or actual abusive situations An overview of the background legislation and guidance Recognition of local pathways and safeguarding structures Understanding of CQC outcome 7 expectations Understanding the Mental Capacity Act (MCA) and the Deprivation of Liberty Safeguards (DoLS) Awareness of the legal framework underpinning the MCA 2005 and the DoLS safeguards Roles and responsibilities in respect of this legislation Guidance on completing capacity assessments and applying the best interests check list What protection the Act offers for people providing care or treatment PREVENT Learning Outcomes Increased awareness and understanding of risk relating to individuals being radicalised; an understanding of appropriate referral mechanisms and information sharing; an awareness of the Channel process; awareness that Prevent aims to tackle all forms of terrorism and that the health sector contribution operates in the pre-criminal space. Pan Lancashire and Cumbria multi agency safeguarding adult procedures manual RCGP Toolkit Safeguarding Adults MCA and DOLS E Learning programme SCIE website rning/index.asp CCG Safeguarding and Mental Capacity Act standards for commissioned services appendix 4 safeguarding standards for GP member practices can be accessed on the CCG websites. Mental Capacity Act code of practice ions/mental-capacity-act-code-ofpractice MLCSU Learning Management System Basic Prevent awareness accessed via: MLCSU Learning
105 Appendix 5 Part 1: Audit Tool to Monitor Safeguarding Arrangements for CCG Commissioned Services Organisation: Person completing the audit tool (include designation, contact details including ) Dated audit tool completed Useful links : Local Safeguarding Children Board policies/procedures Local Safeguarding Adult Board policies/ procedures Please do not send any personal identifiable information when providing evidence Rag rating key: Green Amber Red Fully compliant (remains subject to continuous quality improvement) Partially compliant - plans in place to ensure full compliance and progress is being made within agreed timescales Non-compliant (standards not met / actions have not been completed within agreed timescales) Standard Components of standard Evidence (embed or attach evidence including audits) 1. Governance / Accountability 1.1 (S11) It should be clear who has overall responsibility for the agency s contribution to safeguarding and what the lines of accountability are from each staff member up through the organisation through to the person with Board lead demonstrating specific safeguarding competence in line with National & Local Guidance Job descriptions clearly identify safeguarding responsibilities All staff know both how & who to report concerns about a child / adult at risk of harm SELF RAG CCG RAG Page 35 of 68
106 Standard Components of standard Evidence (embed or attach evidence including audits) ultimate responsibility 1.2 The organisation is linked into the Local Safeguarding Children Board (LSCB) and Local Safeguarding Adult Board (LSAB) 1.3 The organisation regularly reviews the arrangements in place for safeguarding and MCA The organisation is able to demonstrate engagement with the Board and subgroups The governing body should receive regular reports on their arrangements for safeguarding and MCA implementation SELF RAG CCG RAG 1.4 An adverse incident reporting system is in place which identifies circumstances and /or incidents which have compromised the safety and welfare of patients All STEIS and significant safeguarding incidents in relation to patient safety and welfare are to be reported to the Designated Lead for Safeguarding Services capture and have clear records of the key themes/learning from any significant safeguarding incidents and how learning is being implemented. Complaints are considered in the context of safeguarding 1.5 A programme of internal audit and review is in place that enables the organisation to continuously improve the protection of all service users from abuse or the risk of abuse Audits are to include: progress on action to implement recommendations from learning reviews: SCRs, SARs, DHRs, Internal Management Reviews and recommendations from inspections Page 36 of 68
107 Standard Components of standard Evidence (embed or attach evidence including audits) SELF RAG CCG RAG 2. Leadership 2.1 (S11) Senior managers will need to demonstrate leadership; be informed about and take responsibility for the actions of their staff who are providing services to the children and their families Designated senior officers for safeguarding are in place and visible across the organisation Senior managers can evidence effective monitoring of service delivery Ensure that your agency is compliant with SCR actions 2.2 There is a named lead for safeguarding children, CSE and a named lead for adults at risk. The focus for the named professionals is safeguarding within their own organisation Safeguarding leads will have sufficient time, support and flexibility to carry out their responsibilities this should be detailed in their job plans The Commissioner is kept informed at all times of the identity of the Safeguarding Leads 2.3 There is a named lead for MCA the focus for named professionals is MCA MCA Leads must have in-depth, applied knowledge of MCA/DoLS and must have protected study time Page 37 of 68
108 Standard Components of standard Evidence (embed or attach evidence including audits) implementation within their own organisation to ensure they keep their knowledge up to date to ensure: Awareness of relevant case law To provide support and advice to clinicians in individual cases and in supervision of staff where there are complex cases. SELF RAG CCG RAG 3. Service Development Review 3.1 (S11) In delivering, developing, reviewing and commissioning of services, the views and wishes of the child and adults at risk are clearly sought and respected. - In the delivery of services (including decisions made on behalf of service users), the voice of the child (and voice of the parent to promote family friendly services) is regularly sought through participation and joint enterprise/joint decision making activities. - In the development, review and commissioning of services, procedures, policies and strategies that impact on children s lives and that of their families are considered through active participation activities and through responsibilities under the Equalities Act (2010). - To assist your organisation to be child centred, policy and procedures exist that direct staff on taking account of children s views, involve Page 38 of 68
109 Standard Components of standard Evidence (embed or attach evidence including audits) children/service users in decision making and share power/responsibility with children/service users in decision making. SELF RAG CCG RAG 4. Safeguarding policies, procedures and guidance (see supporting sheet to identify those that are relevant to your organisation) 4.1 (S11) The agencies responsibilities towards children and adults at risk is clearly stated in policies and procedures that are available for all staff A statement of responsibilities (as per section 11 guidance) is visible in policies and procedures Policies and guidance refer to the LSCB / LSAB multi-agency procedures Prevent Duty/Counter Terrorism is reflected in policies and guidance These procedures are accessible and understood by all staff Policies and procedures are updated regularly to reflect any structural, departmental and legal changes All policies and procedures must be audited and reviewed at a minimum 2 yearly to evaluate their effectiveness and to ensure they are working in practice Services delivered by the agency or commissioned by the agency are designed to safeguard and promote the welfare of children and adults at Page 39 of 68
110 Standard Components of standard Evidence (embed or attach evidence including audits) risk SELF RAG CCG RAG 5. Domestic Abuse including Forced Marriage and Honour Based Violence, Female Genital Mutilation 5.1 The organisation takes account of national and local guidance to safeguard including recognition and response to those children and adults experiencing domestic abuse Policies and guidance refer to the LSCB / LSAB multi-agency procedures These procedures are accessible and understood by all staff Policies and procedures are updated regularly to reflect any structural, departmental and legal changes Policies and procedures must be audited and reviewed to evaluate their effectiveness and to ensure they are working in practice. 6. Information sharing 6.1 (S11) Effective information sharing by professionals is central to safeguarding and promoting the welfare of children and adults at risk of harm There are robust single / multi agency protocols and agreements for information sharing in line with national and local guidance Evidence that practitioners understand their responsibilities and know when to share information 7. Inter-agency working Page 40 of 68
111 Standard Components of standard Evidence (embed or attach evidence including audits) 7.1 (S11) Agencies and staff work together to safeguard and promote the welfare of children and vulnerable adults Evidence of leadership to enable joint working Evidence of practitioner s working together effectively and attending multi-agency meetings Evidence that Early Help/Support is being used appropriately and effectively Evidence of engagement in, and contribution to, safeguarding processes/enquiries e.g. attendance at child protection, CiN/adult safeguarding meetings, audit schedule to demonstrate commitment to multi-agency work & that staff contribute to agreed assessment processes (CAF and single assessments) SELF RAG CCG RAG 8. Safer recruitment practices 8.1 (S11) Robust recruitment and vetting procedures should be put in place to prevent unsuitable people from working with children and adults at risk All recruitment staff are appropriately trained in safe recruitment All appropriate staff receive a DBS check in line with national/local guidance Legal requirements are understood and in place Page 41 of 68
112 Standard Components of standard Evidence (embed or attach evidence including audits) Role of LADO understood and procedures in place Staff has access to policy detailing who the named senior officer is in relation to managing allegations SELF RAG CCG RAG 9. Supervision and support 9.1 (S11) Safeguarding supervision should be effective and available to all - Staff working with children and adults at risk receive appropriate regular supervision (including reviews of practice) - Supervision policy in and meets LSCB guidance standards - Evidence that staff feel able to raise concerns about organisational effectiveness/concerns (including whistleblowing) 10. Staff training and continuing professional development 10.1 (S11) Staff should have an understanding of both their roles and responsibilities for safeguarding children, children looked after and adults and those of other professionals and organisations. All training should be in line with the relevant intercollegiate document outlining staff roles and competencies and LSCB/AB procedures: Staff have received level 1 safeguarding children and know how to identify safeguarding needs at induction or within 6 weeks of Page 42 of 68
113 Standard Components of standard Evidence (embed or attach evidence including audits) taking up the post (include %) Staff have received safeguarding adults training at induction or within 6 weeks of taking up the post (include %) Appropriate staff have received safeguarding children level 2 and above single agency (include %) and multi-agency training MCA awareness should be included in staff induction programme and mandatory training Appropriate staff have received MCA training (include %) Staff who require Level 2 safeguarding children s training have undertaken level 1 CSE e- learning All necessary staff have completed the Contest/Counter Terrorism awareness training SELF RAG CCG RAG NB: The shaded sections highlight standards that are included in the LSCB section 11 audit Page 43 of 68
114 Part 2: Additional Requirements Organisations will need to ensure that they have appropriate governance arrangements, policies and procedures in place to reflect the services they provide. Section 1: details the policies that need to be in place for all providers of NHS care. Section 2: details the governance arrangements, policies, procedures and guidance that should be in place within the larger providers of acute care & community health services. Section 3: details the additional procedures that need to be in place within emergency care settings. Section 4: details the additional procedures that need to be in place in ambulance services, urgent care/walk in centres/minor injury units, acute services, emergency departments The list is not exhaustive and organisations need to always be mindful of changes to legislation and statutory/national/local guidance. Section 1: ALL PROVIDER ORGANISATIONS Safeguarding children policy Safeguarding adult policy Complaints and whistle blowing policies promoting staff being able to raise concerns about organisational effectiveness in respect to safeguarding Safe recruitment practices in line with LSCB/SAB and NHS Employers guidance and the recommendations of the Lampard report (post Savile) Arrangements for dealing with allegations against people who work with children and adults at risk as appropriate Information sharing & confidentiality policy MCA/DoLS policy this can be incorporated into the safeguarding policy for smaller providers To be registered with the Care Quality Commission (CQC) To undertake an annual audit of its conduct in relation to compliance with required safeguarding standards Section 2: LARGE PROVIDERS OF ACUTE AND COMMUNITY HEALTH SERVICES At a minimum an annual report should be presented at board level with the expectation that this will be made public, there is an expectation that there will be also regular reporting on safeguarding to governance/quality committees Named professionals have a key role in promoting good professional practice and in supporting the safeguarding system. They should work collaboratively with the organisations designated professionals and the LSCB/SAB Under the Health and Social care Act 2012 it is mandated to record FGM patient data under the FGM Enhanced Dataset Prevent as applicable to the service being provided and as agreed by the coordinating commissioner in consultation with the Regional Prevent Coordinator Include in its policies and procedures, and comply with, the principles contained in the Government Prevent Strategy and the Prevent Guidance and Toolkit SELF RAG SELF RAG CCG RAG CCG RAG Page 44 of 68
115 Include in its policies and procedures a programme to raise awareness of the Governments Prevent Strategy among staff and volunteers in line with the NHS England Prevent Training and Competencies Framework; a WRAP delivery plan that is sufficiently resourced with WRAP facilitators All NHS Trusts providing services for children must identify a named doctor and named nurse for safeguarding children; (where maternity services are provided, a named midwife for safeguarding children will be identified) Where organisations may have integrated specific services focused on children for example under Transforming Community Services children s community services may have integrated with Mental Health Trust in this instance there must be named professionals for children s community services and also named professionals for the mental health trust. REF: Intercollegiate document There is an operational framework/policy detailing the levels of supervision required for staff specific to their roles and responsibilities including a gap analysis. This framework meets LSCB/LSAB guidance for supervision Named Safeguarding/MCA leads, seek advice and access regular formal supervision from designated professionals for complex issues or where concerns may have to be escalated Where providers commission services evidence is required that they comply with S11 duty Section 2.1 additional guidance required of larger providers of acute and community health services Sudden unexpected deaths in childhood Child Sexual Exploitation Private fostering Fabricated Induced Illness (FII) Children missing education Missing from Home Domestic Abuse Forced Marriage and Honour Based Violence Female Genital Mutilation (including national reporting) Working with Children who self- harm or who have potential for suicide Historical Sexual Abuse Common Assessment Framework and local continuum of need Practitioners working with sexually active children under 18 years Self Neglect Covert Medication Deprivation of Liberty SELF RAG CCG RAG Page 45 of 68
116 E safety to incorporate the Lampard recommendations post Saville: To have a robust trust wide policy setting out how access by patients and visitors to the internet, social media networks and other social media activities such as blogs and Twitter is managed and where necessary restricted. The policy to be widely publicised to staff, patients and visitors and to be regularly reviewed and updated as necessary Clear way of identifying those children who are subject to a child protection plan and are looked after Conflict Resolution/Escalation Policies Managing allegations against staff working with children and adults in line with LSCB/AB guidance Policy for agreeing to and managing visits by celebrities, VIPs and other officials 2.2 This section is relevant to healthcare providers offering in-patient facilities to children under 18 years only Clear guidance as to the discharge of children for whom there are child protection concerns The CCG and the Local Authority shall be notified of any child (normally resident in CCG area) likely to be accommodated for a consecutive period of at least 3 months; or with the intention of accommodating him/her for such a period (ref s.85 & s.86 CA1989) 2.3 This section is relevant to providers of in-patient facilities and community services for adults Guidance on the use of restraint in line with Mental Capacity Act 2005 & DoLS All inpatient mental health services have policies and procedures relating to children visiting inpatients as set out in the Guidance on the Visiting of Psychiatric Patients by Children (HS 1999/222:LAC (99)32), to NHS Trusts 2.4 This section is relevant to community providers and acute trusts where they are commissioned to undertake statutory health assessments for children looked after Clear protocols and procedures in relation to completion of statutory health assessments Provision of services appropriate for children looked after in accordance with statutory guidance Section 3: THIS SECTION IS RELEVANT TO EMERGENCY CARE SETTINGS Local procedures for making enquiries to find out whether a child is subject to a child protection plan /child looked after; this will be CP-IS once implemented All attendances for children under 18 years to A&E, ambulatory care units, walk in centres and minor injury units should be notified to the child s GP Guidance on parents/carers who may seek medical care from a number of sources in order to conceal the repeated nature of a child s injuries Guidance on the use of restraint in line with Mental Capacity Act 2005 & DoLS SELF RAG SELF RAG SELF RAG SELF RAG CCG RAG CCG RAG CCG RAG CCG RAG Page 46 of 68
117 Section 4: THIS SECTION IS RELEVANT TO AMBULANCE SERVICES, URGENT CARE/WALK IN CENTRES/MINOR INJURY UNITS, ACUTE SERVICES, A&E The provider must co-operate fully and liaise appropriately with 3 rd party providers of social care services in relation to, and must take reasonable steps towards, the implementation of the Child Protection Information Sharing Project SELF RAG CCG RAG Page 47 of 68
118 Appendix 6 Organisation: Part 1 - Audit Tool to monitor Safeguarding Arrangements for CCG Commissioned Care Homes with Nursing Person completing the audit tool (include designation, contact details including ) Dated audit tool completed Useful links : Local Safeguarding Children Board policies/procedures Local Safeguarding Adult Board policies/ procedures Rag rating key: Green Amber Please do not send any personal identifiable information when providing evidence Fully compliant (remains subject to continuous quality improvement) Partially compliant - plans in place to ensure full compliance and progress is being made within agreed timescales Red Non-compliant (standards not met / actions have not been completed within agreed timescales) Standard Components of standard Evidence (embed or attach evidence including audits) 1. Governance / Accountability CH RAG CCG RAG 1.3 It should be clear who has overall responsibility for the agency s contribution to safeguarding and what the lines of accountability are from each staff member up through the organisation through to the person with ultimate responsibility 1.4 The organisation is linked into the Local Safeguarding Forums, including Provider Forums Organisation lead demonstrating specific safeguarding competence in line with National & Local Guidance Job descriptions clearly identify safeguarding responsibilities All staff know both how & who to report concerns about a child / adult at risk of harm The organisation is able to evidence membership of Community Provider Forums and knowledge of LSAB activity Page 48 of 68
119 Standard Components of standard Evidence (embed or attach evidence including audits) 1.6 The organisation regularly reviews the arrangements for safeguarding and MCA Organisation reviews and monitors safeguarding and MCA implementation CH RAG CCG RAG 1.7 An adverse incident reporting system is in place which identifies circumstances and /or incidents which have compromised the safety and welfare of patients 1.8 A programme of internal audit and review is in place that enables the organisation to continuously improve the protection of all service users from abuse or the risk of abuse All STEIS/SI reporting in relation to patient safety and welfare are to be reported to the Commissioning Support Unit Commissioners provided with a regular report (interval to be agreed between the provider and the commissioner but must be at least annually) of key themes/learning from STEIS/SI that involve safeguarding Complaints are considered in the context of safeguarding Audits are to include: Progress on any action plans that have been requested of the service which would impact on quality of care 2. Leadership 2.4 Senior managers will need to demonstrate leadership; be informed about and take responsibility for the actions of their staff who are providing services to vulnerable adults Safeguarding Leads are in place and visible across the organisation Senior managers can evidence effective monitoring of service delivery Safeguarding leads will have sufficient time, support and flexibility to carry out their responsibilities this should be detailed in their job plans Page 49 of 68
120 Standard Components of standard Evidence (embed or attach evidence including audits) evidence of safeguarding roles and responsibilities CH RAG CCG RAG 2.5 There is a named lead for MCA the focus for named professionals is MCA implementation within their own organisation. - There is evidence that patient care plans are regularly reviewed and that least restrictive practices are applied - There is evidence that deprivation of liberty applications are made for all patients who lack capacity to consent to their treatment plan or place of treatment & followed up proportionately 3. Safeguarding policies, procedures and guidance (see supporting sheet to identify those that are relevant to your organisation) 3.1 The organisation has a safeguarding policy and procedure in place which covers adults and children and are accessible and understood by all staff Staff are able to identify and respond to abuse and seek support and advice as necessary Policy and procedures are updated regularly to reflect any structural, departmental and legal changes All policies and guidance refer to LSAB multi-agency procedures Policies are compliant with the Care Act and cover all 10 forms of recognised abuse Guidance around what the PREVENT agenda is and what to do where there are concerns of radicalisation Policy and procedures include direct reference to good information sharing practice in relation to safeguarding The policy demonstrates that the organisation takes account of national Page 50 of 68
121 Standard Components of standard Evidence (embed or attach evidence including audits) 4. Inter-agency working and local guidance to safeguarding and protection of adults experiencing domestic abuse All policies and procedures must be audited and reviewed at a minimum 2 yearly to evaluate their effectiveness and to ensure they are working in practice Complaints and whistle blowing policies are in place which promote staff to raise concerns around organisation effectiveness in relation to safeguarding CH RAG CCG RAG 4.1 Contribution to safeguarding enquiries and engagement in the safeguarding process including safeguarding adult reviews Engagement in, and contribution to, safeguarding processes/enquiries, safeguarding meetings and learning reviews Engagement in an Quality Improvement Plans (QIP) Engagement in assessment processes 5. Safer recruitment practices 5.1 Robust recruitment and vetting procedures should be put in place to prevent unsuitable people from working with adults and children at risk All recruitment staff are appropriately trained in safe recruitment All appropriate staff receive a DBS check in line with national/local guidance Staff have access to policies detailing how to manage staff allegations and concerns Page 51 of 68
122 Standard Components of standard Evidence (embed or attach evidence including audits) 6. Supervision and support CH RAG CCG RAG 6.1 Supervision should be effective and available to all - Staff working with adults at risk receive appropriate regular supervision (including reviews of practice) which is appropriately recorded and evidence that themes are translated in to service improvement 7. Staff training and continuing professional development 7.1 Staff should have an understanding of both their roles and responsibilities for safeguarding children and adults There is a learning and development framework for safeguarding and MCA implementation that takes into account local and national guidance and roles & responsibilities All staff have received level 1 safeguarding children at induction or within 6 weeks of taking up the post (include % for both) Staff have received basic safeguarding training for adults MCA awareness should be included in staff induction programme & mandatory training All staff have received MCA training (include %) Staff members who are undertaking a lead role in safeguarding or MCA must have in depth applied knowledge and protected time to keep updated All necessary staff have completed Prevent / Counter Terrorism awareness Page 52 of 68
123 Standard Components of standard Evidence (embed or attach evidence including audits) training Training to be audited to ensure its quality and effectiveness CH RAG CCG RAG The list is not exhaustive and organisations need to always be mindful of changes to legislation and statutory/national/local guidance. Page 53 of 68
124 Part 2 Additional requirements Organisations will need to ensure that they have appropriate governance arrangements, policies and procedures in place to reflect the services they provide. Please see below a list of documents which must be submitted as a minimum with your return. The list is not exhaustive and organisations need to always be mindful of changes to legislation and statutory/national/local guidance. Safeguarding Policy (to include Adults and Children) Mental Capacity Act Policy this can be incorporated into the safeguarding policy for smaller providers. The MCA policy must be in line with the Mental Capacity Act Code of Practice 2007 Guidance on the use of restraint in line with Mental Capacity Act 2005 & DOLS Complaints and whistle blowing policies promoting staff being able to raise concerns about organisational effectiveness in respect to safeguarding Safe recruitment Policy Policy which covers arrangements for dealing with allegations against people who work with vulnerable people and children as appropriate Information sharing & confidentiality policy Prevent Policy (This may be included in the Safeguarding Policy) Supervision Policy (This may be included in the Safeguarding Policy) Policy for agreeing to and managing visits by celebrities, VIPs and other officials. Safeguarding Audit Programme CH RAG CCG RAG Page 54 of 68
125 Appendix 7 CCG: Audit Tool to measure CCG compliance with the NHS Assurance and Accountability Framework for Safeguarding (Safeguarding Vulnerable People in the NHS 2015) and Section 11 Children Act Dated audit tool completed Useful links : Local Safeguarding Children Board policies/procedures Local Safeguarding Adult Board policies/ procedures Rag rating key: Green Amber Red Fully compliant (remains subject to continuous quality improvement) Partially compliant - plans in place to ensure full compliance and progress is being made within agreed timescales Non-compliant (standards not met / actions have not been completed within agreed timescales) Standard Components of standard Evidence (embed or attach evidence including audits) RAG 1. Accountability 1.1 There is a clear line of accountability for safeguarding, reflected in CCG governance arrangements (SVP p.21) A named executive to take overall leadership responsibility for the organisations safeguarding arrangements (SVP p.21) 1.2 (s.11) It should be clear who has overall responsibility for the agency s contribution to safeguarding and what the lines of accountability are from each staff member up Board lead demonstrating specific safeguarding competence in line with National & Local Guidance Job descriptions clearly identify safeguarding responsibilities Page 55 of 68
126 Standard Components of standard Evidence (embed or attach evidence including audits) RAG through the organisation through to the person with ultimate responsibility All staff know both how & who to report concerns about a child / adult at risk of harm 1.3 There are effective systems for responding to abuse and neglect (SVP p.21). 1.4 NHS England in conjunction with CCGs to consider where there are risks and gaps in services to develop an action plan to mitigate against the risk (SVP p.30) 2.1 S11) Senior managers will need to demonstrate leadership; be informed about and take responsibility for the actions of their staff who are providing services to the children and their families Designated senior officers for safeguarding are in place and visible across the organisation Senior managers can evidence effective monitoring of service delivery Ensure that your agency is compliant with SCR Actions Page 56 of 68
127 Standard Components of standard Evidence (embed or attach evidence including audits) RAG 2.2 To employ or secure the expertise of Designated Doctors and Nurses for Safeguarding Children and for Looked After Children; and a Designated Paediatrician for unexpected deaths in childhood. The role of the designated professional to be explicitly defined in the job description for sufficient time, funding. (SVP p22) Designated clinical experts embedded into the clinical decision making of the organisation, with the authority to work within local health economies to influence local thinking and practice (SVP p.22). Clear accountability and performance management arrangements are essential; key elements include: o As single subject experts, peer-topeer supervision is vital to ensuring designated professionals continue to develop in practice in line with agreed best practice. o Designated leads must have direct access to the Executive Board lead for safeguarding to ensure that there is the right level of influence of safeguarding in commissioning process o The CCG Accountable Officer (or other executive level nominee) should meet regularly with the designated professional to review safeguarding o Where designated doctors are continuing to undertake clinical duties in addition to their clinical advice role in safeguarding, it is important that there is clarity about the two roles the CCG will need to input into the job planning, appraisal and revalidation process. (SVP p.23) Page 57 of 68
128 Standard Components of standard Where there is more than 1 CCG per LSAB/LSCB area, CCGs may want to consider developing lead or hosting arrangements for their designated professional team, or a clinical network arrangements. Where a designated professional (most likely designated doctor for safeguarding children or a designated professional for Looked after Children) is employed within a provider organisation, the CCG will need to have a service level agreement, with the organisation that sets out the practitioner s responsibilities and the support they should expect in fulfilling their designated role. To employ, or have arrangements in place to secure the expertise of a consultant paediatrician whose designated responsibilities are to provide advice on the commissioning of: paediatric services from paediatricians with expertise in undertaking enquiries into unexpected deaths in childhood; from medical investigative services; and the organisation of such services (WT p.90) Recommended minimum WTE/PAs as per the intercollegiate document o Designated nurse safeguarding children; 1 dedicated WTE Designated Nurse for a child population of 70,000, supported by Evidence (embed or attach evidence including audits) RAG Page 58 of 68
129 Standard o o o Components of standard 0.5WTE administrative support. Designated Doctor Safeguarding Children; PAs per week according to the size of the districts covered. (p97 intercollegiate) Designated Nurse Looked After Children; 1 dedicated WTE for a child population of 70,000 supported by 0.5 WTE administrative support Designated Doctor Looked After children; A minimum of 2 PAs per 400 Looked after children population (excludes operational activity) Evidence (embed or attach evidence including audits) RAG 2.3 To have a Designated Adult Safeguarding Manager (DASM) which should include an Adult Safeguarding lead role and to have a Designated Mental Capacity Act (MCA) Lead; supported by relevant policies and training. (SVP p. 21) N.B. The DASM can include both roles of Safeguarding Adult and MCA Leads Designated clinical experts embedded into the clinical decision making of the organisation, with the authority to work within local health economies to influence local thinking and practice (SVP p.22). Clear accountability and performance management arrangements are essential; key elements include: o As single subject experts, peer-topeer supervision is vital to ensuring designated professionals continue to develop in practice in line with agreed best practice. o Designated leads must have direct access to the Executive Board lead for safeguarding to ensure that there is the right level of influence of safeguarding in commissioning Page 59 of 68
130 Standard Components of standard Evidence (embed or attach evidence including audits) RAG process o The CCG Accountable Officer (or other executive level nominee) should meet regularly with the designated professional to review safeguarding NB: An intercollegiate document for safeguarding adults incorporating MCA is currently being devised nationally. Until this is published there is no guidance as to the WTE required. 2.4 Supporting the development of a positive learning culture across partners for safeguarding to ensure that organisations are not unduly risk adverse (SVP p.21) 3. Commitment/Safeguarding Policies, Procedures and Guidance 3.1 (S11) The agency s responsibilities towards children / adults at risk is clearly stated in policies and procedures that are available for all staff. Statement of responsibilities (as per section 11) is visible in policies & guidance Policies and guidance refer to the LSCB/LSAB multi-agency procedures Prevent Duty/Counter Terrorism is reflected in policies and guidance This is accessible and understood by all staff Policies and procedures are updated Page 60 of 68
131 Standard Components of standard Evidence (embed or attach evidence including audits) RAG regularly to reflect any structural, departmental and legal changes All policies and procedures must be audited and reviewed at a minimum 2 yearly to evaluate their effectiveness and to ensure they are working in practice Services delivered by the agency or commissioned by the agency are designed to safeguard and promote the welfare of children and adults at risk 4. Service Development Review 4.1 (S11) In delivering, developing, reviewing and commissioning of services, the views and wishes of the child and adults at risk are clearly sought and respected In the delivery of services (including decisions made on behalf of service users), the voice of the child (and voice of the parent to promote family friendly services) is regularly sought through participation and joint enterprise/joint decision making activities. In the development, review and commissioning of services, procedures, policies and strategies that impact on children s lives and that of their families are considered through active participation activities and through responsibilities under the Equalities Act (2010). To assist your organisation to be child centred, policy and procedures exist that direct staff on taking account of Page 61 of 68
132 4. Safeguardin Standard Components of standard children s views, involve children/service users in decision making and share power/responsibility with children/service users in decision making. Evidence (embed or attach evidence including audits) RAG 5.1 CCGs as commissioners of local health services are assured that the organisations from which they commission have effective safeguarding arrangements in place (SVP p.20). A statement of responsibilities (as per section 11 guidance) is visible in policies and procedures Policies and guidance refer to the LSCB / LSAB multi-agency procedures Prevent Duty/Counter Terrorism is reflected in policies and guidance These procedures are accessible and understood by all staff Policies and procedures are updated regularly to reflect any structural, departmental and legal changes All policies and procedures must be audited and reviewed at a minimum 2 yearly to evaluate their effectiveness and to ensure they are working in practice Services delivered by the agency or commissioned by the agency are designed to safeguard and promote the welfare of Page 62 of 68
133 Standard Components of standard children and adults at risk 6. Primary Care (co-commissioning) and safeguarding 6.1 Primary care commissioners are required to ensure there is named GP/named professional capacity to support primary care services in discharging their safeguarding duties (SVP append 1) The capacity is funded through the primary care budget but it is for local determination exactly how this is done and what employment arrangements are adopted (SVP p.28) Capacity commissioned locally needs to reflect local needs as set out in the JSNA - strongly recommended that two named GP sessions per 220,000 population is secured as a minimum. (SVP p.28) The named GP roles covers safeguarding of children it is recommended that NHS England /primary care commissioner and local CCG clinical leaders consider commissioning a cluster model of named safeguarding clinicians with a range of experience. This could include child safeguarding, safeguarding people of all ages with mental health issues, safeguarding CLA and care leavers, adult safeguarding including domestic abuse safeguarding in elderly care and dementia and safeguarding in institutions including care homes (SVP p.29) Arrangements are in place for training primary care professionals (SVP app 6)` Evidence (embed or attach evidence including audits) RAG 7. Information sharing 7.1 (S11) Effective information sharing by professionals is central to safeguarding and promoting the welfare of children and adults at risk of There are robust single / multi agency protocols and agreements for information sharing in line with national and local guidance Page 63 of 68
134 Standard Components of standard Evidence (embed or attach evidence including audits) RAG harm (SVP p.21) Evidence that practitioners understand their responsibilities and know when to share information 8. Inter-agency working 8.1 (S11) Agencies and staff work together to safeguard and promote the welfare of children and adults at risk Evidence of leadership to enable joint working Evidence of practitioner s working together effectively Early Help/Support is being used appropriately and effectively Evidence of engagement in, and contribution to, safeguarding processes/enquiries e.g. attendance at child protection, CiN/adult safeguarding meetings, audit schedule to demonstrate commitment to multi-agency work & that staff contribute to agreed assessment processes (CAF and single assessments) 8.2 Effective interagency working is in place with the local authority, police and 3 rd sector organisations (svp p.21) To co-operate with the local authority in the operation of the Local Safeguarding Children Board (LSCB), Local Safeguarding Adult Board (LSAB), and Health and Wellbeing Board (SVP p.21) CCG representatives at the LSCB must be accompanied by their designated professional to ensure their professional expertise is effectively linked into the local safeguarding arrangements (SVP p.23). When asked by the local authority for help Page 64 of 68
135 Standard Components of standard Evidence (embed or attach evidence including audits) RAG in enabling the LA to discharge its safeguarding duties, the CCG must help, as long as it is compatible with the CCGs own duties and does not hamper the discharge of the CCGs own functions. (SVP p13) To co-operate with the local authority in order to promote the wellbeing of children in general and to protect them from harm and neglect in particular (SVP p13) Work with the local authority to enable access to community resources that can reduce social and physical isolation for adults (SVP p To participate, when asked to do so, in a statutory review by providing a panel member. (SVP p.18) To provide a panel member, provide oversight of health involvement at panel meetings, ensure that recommendations and actions are achievable, and disseminate learning across the NHS local (SVP p.18) 9. Safer recruitment practices 9.1 (S11) Robust recruitment and vetting procedures should be put in place to prevent unsuitable people from working with children and vulnerable adults All recruitment staff are appropriately trained in safe recruitment All appropriate staff receive a DBS check in line with national/local guidance Legal requirements are understood and in place Role of LADO understood and procedures in place Page 65 of 68
136 Standard Components of standard Evidence (embed or attach evidence including audits) RAG Staff has access to policy detailing who the named senior officer is in relation to managing allegations 9.2 Clear policies setting out the commitment, and approach, to safeguarding including safe recruitment practices and arrangements for dealing with allegations against people who work with children and adults as appropriate (SVP p.21) 10.1 (S.11) Safeguarding supervision should be effective and available to all All staff working with children and adults at risk receive appropriate regular supervision (including reviews of practice) Evidence that staff feel able to raise concerns about organisational effectiveness/concerns (including whistleblowing) 11.1 (S11) Staff should have an understanding of both their roles and responsibilities for safeguarding children, children looked after and Staff have received level 1 safeguarding children and know how to identify safeguarding needs at induction or within 6 weeks of taking up the post (include %) staff have received safeguarding adults Page 66 of 68
137 Standard Components of standard Evidence (embed or attach evidence including audits) RAG those of other professionals and organisations. training at induction or within 6 weeks of taking up the post (include %) appropriate staff have received safeguarding children level 2 and above single agency (include %) and multiagency training MCA awareness should be included in staff induction programme & mandatory training appropriate staff have received MCA training (include %) staff who require Level 2 safeguarding children s training have undertaken level 1 CSE e-learning all necessary staff have completed the Contest/Counter Terrorism awareness training 11.2 Training of staff in recognising and reporting safeguarding issues, appropriate supervision and ensuring staff are competent to carry out their roles and responsibilities (SVP p.21). Training in line with the intercollegiate documents and local and national guidance NB: The shaded sections highlight standards that are included in the LSCB section 11 audit Page 67 of 68

138 Appendix 8 INDIVIDUAL ACCOUNTABILITY Accountable Officer SAFEGUARDING ACCOUNTABILITY FLOWCHART STRUCTURES/COMMITTEES Deputy Accountable Officer SAFEGUARDING SERVICE Designated Lead Nurses Deputy Designated Nurse / Professional Lead GP for Safeguarding Safeguarding Administration Governing Body Quality and Performance Committee LSCB LSAB Designated Doctor for Safeguarding Designated Doctor for LAC Safeguarding Assurance Group Page 68 of 68
139 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT WLCCGB 11/17/10 DATE OF BOARD MEETING: 28 November 2017 TITLE OF REPORT: Safeguarding Children and Adults Annual Report 2016/17 BRIEFING POINTS: This annual report reviews the work over 2016/17, providing assurance that the CCG has discharged its statutory responsibility to safeguard the welfare of children and adults across the health services it commissions. Information is included in respect to national changes and developments; it also highlights how the challenges relating to safeguarding are being managed. The report describes achievements and priorities for the year ahead. Some key achievements include the CCG s involvement in the development of the pan- Lancashire media resource and e-book and the collaborative work with external partners to raise awareness and provide local guidance on female genital mutilation. The CCG has been subject to considerable external scrutiny during 2016/17 including a Care Quality Commission review undertaken in respect to safeguarding children and looked after children across health services of Lancashire and an audit carried out by NHS England of the CCG s safeguarding arrangements. There continues to be a significant amount of development from both a national and local perspective. The report demonstrates that multi-agency working is integral to safeguarding and requires a partnership approach in the identification of developments and service gaps. Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience) please outline impact X 2. Commissioning of hospital and community services please outline X impact 3. Commissioning and performance management of GP Prescribing X please outline impact 4. Delivering Financial Balance please outline impact X 5. Development of the commissioning group as a commissioning X organisation please outline impact B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number) have any legal implications promote effective governance practice X Safeguarding Children and Adults Annual report 2016/17 West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
140 2. Additional resource implications X (either financial or staffing resources) 3. Health Inequalities X 4. Equality and Inclusion and Human Rights Requirements N/A Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement X 6. Patient and Public Engagement X PAPER PREPARED BY: Lorraine Elliott, Designated Lead Nurse for Safeguarding Adults and MCA Louise Burton, Designated Lead Nurse for Safeguarding Children PAPER PRESENTED BY: Claire Heneghan, Chief Nurse Safeguarding Children and Adults Annual report 2016/17 West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November

141 NHS West Lancashire Safeguarding Annual Report
142 Contents Executive Summary Page Introduction Safeguarding Governance and Accountability Arrangements Safeguarding Arrangements within the CCG Safeguarding Assurance in relation to Commissioned Services External Scrutiny of Safeguarding Arrangements CQC Section 11 of the Children Act 2004 Lancashire Children Services Improvement Journey Safeguarding and General Practice Training Policy and document development Multi-Agency Working Safeguarding Children The Wood Report Child Sexual Exploitation Female Genital Mutilation Child Protection Information Sharing project Safeguarding and Looked After Children Activity National Profile of Looked After Children Looked After Children Health Provision Unaccompanied Asylum Seeking Children Pan-Lancashire Sudden Unexpected Death in Childhood Services Improvements Lancashire Safeguarding Children Board Serious Case Reviews Mental Capacity Act and Deprivation of Liberty Safeguarding Safeguarding Adults Making Safeguarding Personal Care Homes Safeguarding Adult Activity Lancashire Safeguarding Adult Board Safeguarding Adults Reviews Domestic Homicide Review 23 Page 2 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
143 10.0 Prevent Multi-Agency Safeguarding Hub Conclusion Contributors to this Report 25 Appendix 1 Safeguarding team flowchart 26 Page 3 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
144 Executive summary The annual safeguarding report provides an update on developments nationally and locally and demonstrates that the Clinical Commissioning Group (CCG) is continuing to meet its statutory responsibilities to safeguard and promote the wellbeing of children, adults at risk including Mental Capacity Act (MCA) implementation. The report sets out achievements made during 2016/17 and describes the priorities for the year ahead. A particular highlight has been the CCG s involvement in the development of the pan- Lancashire media resource and e-book. This work has showcased Lancashire health and social care economy as a proactive partner in improving learning opportunities and awareness of the MCA. The resource was successfully featured in the annual report of Baroness Finlay, Chair of the National MCA Forum. An exciting development for the year ahead will be responding to the findings of a ground breaking pan-lancashire research study to determine how MCA is applied in everyday practice. The CCG lead for Female Genital Mutilation (FGM) has worked in collaboration with external partners to raise awareness and to provide local guidance. Although the number of suspected FGM cases is not high; Lancashire has seen an increase in reported cases to Children s Social Care. Learning and development is at the heart of the team s values; having a practice educator as part of the team has afforded provision of a specialist placement for a final year MSc student social worker. This learning experience has been a success both for the student who went on to secure employment but also for the team s continuing development. The CCG has been subject to considerable external scrutiny during 2016/17. A Care Quality Commission review has been undertaken in respect to safeguarding children and looked after children across health services of Lancashire and an audit carried out by NHS England of the CCG s safeguarding arrangements. Both reviews offered an opportunity to provide assurance and to serve as a prompt for any improvements. Although effective systems were found to be in place areas for improvement could be made. The action plans from both reviews have been progressed. The team are dedicated to improvement of practice and are enthusiastic partners in a series of themed multi-agency audits commenced under the remit of Lancashire Safeguarding Children and Adult Boards. The Boards have adopted the Welsh methodology for undertaking both Serious Case Reviews and Safeguarding Adult Reviews, although at different stages of implementation significant progress has been made. The challenge for the year ahead will be to continue to progress service developments through a period of national policy change, without losing sight of what matters the most; promoting the welfare of Lancashire s children and adults at risk. Page 4 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
145 1.0 Introduction 1.1 This is the fourth safeguarding annual report for the Clinical Commissioning Group (CCG). It outlines progress and developments from a national and local context from 1 April 2016 until 31 March The report will focus on key areas and provide an overview of the CCG responsibilities in respect to safeguarding children, adults and Mental Capacity Act (MCA) implementation. The report will demonstrate how the CCG is meeting its statutory requirements and responses to local challenges across the health economy. 2.0 Safeguarding Governance and Accountability Arrangements 2.1 Safeguarding Arrangements within the CCG Accountability for safeguarding rests with the Chief Officer of the CCG in meeting statutory and non-statutory constitutional and governance requirements. This includes having systems and processes in place to protect children and adults at risk within the commissioning process and by monitoring of health provider services commissioned by the CCG To ensure that the CCG is fulfilling its statutory responsibilities for safeguarding, a quarterly activity report is tabled at the CCG Quality and Safety Committee. The purpose of the group is to provide assurance on the effectiveness of the safeguarding arrangements ensuring that safeguarding is integral to quality and audit arrangements within the CCG The safeguarding team has developed considerably over recent years with seven members in 2016, see appendix 1. The new structure is working well: the team is jointly led by a Designated Lead Nurse for Safeguarding Adults / MCA and a Designated Lead Nurse for Safeguarding Children reporting to the Chief Nurse. An area that requires strengthening is around consistent administration support The joint leadership roles bring together a combination of subject matter, clinical expertise and a collaborative approach in ensuring that the CCG complies with its statutory duties. The Designated Leads are supported by two Deputies who are integral in meeting the demand of the ever increasing safeguarding agenda. The recruitment of the Deputy Designated Nurse for Safeguarding Children has contributed to the safeguarding team achieving priorities for 2016/ The CCG employ a GP lead for Safeguarding, two sessions equivalent to eight hours is commissioned on a monthly basis and this includes the role of safeguarding adults / MCA. This role is instrumental in the provision of advice and expertise to GP practices. The Named GP will continue to be supported by the wider safeguarding team to drive forward improvements and strengthen safeguarding arrangements within Primary Care. Page 5 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
146 2.1.5 A number of other statutory posts are commissioned from a provider organisation; including those of Designated Doctor for safeguarding children and Designated Doctor for Looked after Children (LAC) The team provide specialist expert advice to the CCG, partner agencies and health organisations across the health economy. Safeguarding assurance is a key aspect of all contractual arrangements As a member of Lancashire Children and Adult Safeguarding Boards, the CCG contributes to the work of the Boards both financially and through the work undertaken by the CCG Safeguarding team. This includes membership of the subgroups of the Boards; contributing to multi-agency audits and peer reviews; providing the health perspective on a range of topics and contributing to statutory learning reviews A key success for 2016 included the CCG being utilised as a specialist placement for a final year MSc Student Social Worker. The benefit of having a Practice Educator within the CCG safeguarding team has afforded a multifaceted learning experience to meet the requirements of the professional capabilities framework for social workers. The student secured full time employment at a Hospital Trust as the Safeguarding Adult Practitioner. 2.2 Safeguarding Assurance in relation to Commissioned Services The CCG monitor all commissioned services including the care home sector and voluntary, community and faith sector (VCFS), against safeguarding standards. These standards are reviewed in line with current guidance and legislation and form part of the annual contract as a system of audit Outcomes of the audit have resulted in the development of a sample policy for VCFS to support smaller providers in their identification and response to safeguarding. In addition, safeguarding workshops have been implemented to support care homes and VCFS with the completion of their audits. The first session was delivered in February 2017 for care homes with positive feedback Evidence indicators have also been developed to support the audit process in analysing the data The CCG continue to be a key partner in the development of the quality improvement process (QIP) to support care providers to maintain quality and safety in care homes. This has included leading QIP meetings and provision of additional services to support failing providers. This has been integral to keeping services safe and functioning during closure and alternatively supporting recovery preventing the need for closure; for further information see section A priority for 2017/18 will be to strengthen safeguarding and MCA involvement within quality visits for commissioned services. The aim is to support the assurance process by monitoring understanding of safeguarding Page 6 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
147 responsibilities, patient experience and to identify gaps and future service development opportunities. 2.3 External Scrutiny of Safeguarding Arrangements The CCG has participated in a series of NHS England assurance visits to demonstrate compliance with Safeguarding Vulnerable People in the NHS Accountability and Assurance Framework, April and wider objectives. This involved completion of a self-assessment and development of an action plan, which has been finalised during the reporting period. 2.4 CQC A CQC review of safeguarding children and looked after children (LAC) across health services of Lancashire has been undertaken. The CQC report published in August 2016 provided a narrative account of the quality of health services for LAC and the effectiveness of safeguarding arrangements within health for all children. The report acknowledged good practice and made recommendations for improvement. Organisational action plans informed a Lancashire wide action plan, which was submitted to CQC with positive feedback. 2.5 Section 11 of the Children Act Section 11 sets out agencies responsibilities in safeguarding children. The LSCB conducts an annual section 11 audit of all member organisations safeguarding arrangements and following submission is subject to scrutiny by the Quality Assurance and Performance Improvement sub group of the LSCB. The requirements have been revised by the LSCB and the CCG s submission demonstrated compliance in all areas except training. An action plan has been developed to strengthen compliance against Level 2 safeguarding children s training; this will to be a priority for 2017/ Lancashire Children Services Improvement Journey Progress has been made to implement the Lancashire Children s Service Improvement Plan following an Ofsted Inspection, which took place The aim is for progress to be sustained, moving beyond compliance and towards a consistent application of good practice that improves outcomes for children. The established Lancashire Children s Services Improvement Board continues to monitor and direct progress towards improved performance. More information can be found here. 2.7 Key priorities 2017/18 Achieve compliance with level 2 safeguarding children s training 1 Safeguarding Vulnerable People in the NHS Accountability and Assurance Framework, NHS England, 2015 Page 7 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
148 Strengthen safeguarding and MCA participation within commissioned services 3.0 Safeguarding and General Practice Primary Care has been supported in a variety of ways during 2016/17 to promote safeguarding knowledge and awareness. 3.1 Training Primary care have been provided opportunities to participate in an existing rolling programme of safeguarding training, to support with appraisal and CQC requirements. In addition, an expert speaker, high profile Barrister and Lecturer was commissioned to provide two sessions on MCA / DoLS, case law and Court of Protection (CoP). All sessions were well evaluated. A priority for 2017/18 is to hold a safeguarding workshop within the CCG locality. 3.2 Policy and Document Development A sample GP policy for domestic abuse has been developed to support Primary Care in the identification and response to domestic abuse. The policy has been shared across pan-lancashire CCGs to promote consistency and includes the referral process for the new Victim Support Services in Lancashire. This new service offers support for victims of domestic abuse, sexual violence, honour based abuse, forced marriage and female genital mutilation (FGM) Safeguarding sample policies for both adults and children clearly set out responsibilities for Primary Care. The sample adult policy has been reviewed to reflect local and national developments. The policy provides an evidence based resource and links into the local safeguarding board. The review of the sample children s policy is a priority for 2017/ Multi-Agency Working Multi-agency working is integral to safeguarding though can be challenging. Communication systems have been developed to strengthen information sharing between health and children social care (CSC) in respect to safeguarding and LAC The team hold bi-monthly meetings with Child and Family Health Service (CFHS) managers specifically to discuss communication between Primary Care and the health visiting/school nursing service. GPs are now informed when a Common Assessment Framework is opened or closed by the CFHS to enable the GP to contribute Regular Strengthening Links meetings are in place. The role of GPs is included in the social worker s induction booklet and a process for linking social worker team managers with GP practices is ongoing as part of this work stream. Changes have been put in place to improve communication Page 8 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
149 surrounding child protection conference invites and reports and this will be reaudited as a priority for 2017/ The safeguarding team are working towards implementing a Safeguarding Leads / Champion model across Primary Care. This will promote standardisation and consistency in line with other CCGs across Lancashire. A priority for 2017/18 will be to work with Primary Care to consider inclusion of the model within the GP quality contract and embed into practice The above developments meet the recommendations highlighted within the CQC Review, see section Key priorities 2017/18 Hold a safeguarding workshop within the CCG locality Continuation of strengthening systems between Primary Care and CSC Work with Primary Care commissioning to consider inclusion of the Safeguarding Lead / Champion model within the GP quality contract 4.0 Safeguarding Children 4.1 The Wood Report - review of the role and functions of Local Safeguarding Children Boards The Wood Review commissioned by the Government in 2016, has made directions and intentions relating to areas relevant to the CCG s safeguarding responsibilities and organisational arrangements A fundamental review of the role and functions of Local Safeguarding Children Boards found that they were not sufficiently operational in ensuring effective safeguarding in their specific areas. The review found widespread agreement that the current system needs to change to a new model that will ensure collective accountability across the system The proposal is to introduce a stronger but more flexible statutory framework which will give the three key agencies (Police, Health and Local Authorities) the freedom to determine how they organise themselves to work together to safeguard and promote the welfare of children in their local area. In addition, the review makes reference to a number of areas, including services for LAC, proposed changes to the arrangements for Serious Case Reviews (SCRs) and Child Death Reviews There will be implications for the CCG as it is not clear what resources may be necessary to meet the proposed arrangements. Consideration of independent scrutiny and governance is unknown. The message from the Wood review is that local partnership working is essential. Therefore 2017/2018 may see the 2 The Wood Report, review of the role and functions of Local Safeguarding Children Boards, March 2016 Page 9 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
150 need to determine future multi-agency safeguarding arrangements across Lancashire. 4.2 Child Sexual Exploitation Child Sexual Exploitation (CSE) can affect any child or young person and is one of the biggest risks to all our children and young people with devastating emotional and physical health consequences. February 2017 saw the review of the CSE definition and the introduction of a guide for practitioners, local leaders and decision makers working to protect children from CSE CSE definition was amended to state:- Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity (a) in exchange for something the victim needs or wants, and / or (b) for the financial advantage or increased status of the perpetrator or facilitator. The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact; it can also occur through the use of technology Locally, the specialist safeguarding practitioner role based within the multiagency CSE team, which was jointly commissioned with Public Health for a 12 month period, expired August Unfortunately, future joint commissioned arrangements with Public Health were not agreed. An additional, 12 months non-recurrent funding has since been agreed by both Chorley and South Ribble and Greater Preston CCGs to ensure continued CSE health provision across central Lancashire. To support sustainability a priority for 2017/18 will be to present a business case to seek funding from the CCG, due to the service being delivered across West Lancashire To influence future direction and address sustainability, the CSE task group of the LSCB is undertaking a time-limited piece of work that will scope services that are provided and funding streams. It is intended that the outcome of the work will be the development of a pan-lancashire integrated service offer which will link seamlessly with the pathway for vulnerable children CSE will continue to be a key priority area for 2017/ Female Genital Mutilation Female Genital Mutilation (FGM) refers to procedures that intentionally alter or cause injury to the female genital organs for non-medical reasons. FGM has been illegal in the United Kingdom (UK) since 1985, with the law being strengthened in 2003 to prevent girls travelling from the UK and undergoing FGM abroad There have been significant legislative changes during 2015/16, which introduced a number of responsibilities for professionals, employers and Page 10 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
151 organisations in respect to FGM. The reporting period has seen the introduction of the Multi-Agency Statutory Guidance on Female Genital Mutilation 3. The guidance is issued under the FGM Act It encourages agencies to co-operate and work together to protect and support those at risk of, or who have undergone, FGM and outlines three main functions: To provide information on FGM To provide strategic guidance on FGM To provide advice and support to front-line professionals The guidance underpins the terms of reference for the recently introduced pan-lancashire Multi-Agency FGM Task and Finish group chaired by the CCG FGM Lead. This work stream sits under the Forced Marriage / Honour Based Abuse / FGM Steering Group, which reports to the pan-lancashire Domestic Abuse Board. Work under development includes: reviewing pathways and scoping single agency training provision across pan-lancashire and the development of a multi-agency safeguarding pathway for FGM NHS England North Regional FGM subgroup work plan is now in place to ensure the FGM priorities are delivered. These work streams will contribute to a regional repository as a resource for health professionals. The CCG FGM lead attends the regional sub group and has been pivotal in providing advice and support within the CCG and to wider partners. A FGM Conference is planned for 2017/ Child Protection Information Sharing project Child Protection Information Sharing (CP-IS) is a national system (across England) that connects children s social care IT systems with those used by NHS in unscheduled care settings. CP-IS ensures that health and social care staff have a more complete picture of a child's interactions with health and social care services. This enables them to work more closely together and to provide earlier interventions for children who are considered vulnerable and at risk Lancashire is a good example of Local Authority (LA) and health working together as a number of hospital trusts have gone live with CP-IS. Implementation of CP-IS in a staged approach has commenced within Ormskirk Hospital. Within the reporting period, CP-IS has been rolled out within the paediatric accident and emergency department and will be implemented within maternity in the year ahead. 3 Multi-Agency Statutory Guidance on Female Genital Mutilation, April 2016 Page 11 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
152 4.5 Safeguarding and Looked After Children Activity Child Protection Table 1: Number of children, by social care district, subject to a child protection plan (CP) as of 30 March 2016 and March 2017, including rate per 10,000 population. March 16 Per 10,000 March 17 Per 10,000 % increase Chorley and SR % Preston % West Lancashire % Lancashire 1, , % The rates of children subject to CP plans have fallen from October 2016 following an increase in the previous year Looked after Children Table 2: Number of children in the care of Lancashire County Council (LCC), by social care district, as of March 2016 and March 2017, including rate per 10,000 population. March 16 Per 10,000 March 17 Per 10,000 % increase Chorley and SR % Preston % West Lancashire % Lancashire 1, , % There is a continued upward trend of LAC locally, which is consistent with the rising numbers nationally. Lancashire LAC rate remains above the National average but below the North West average despite the 10% increase. 4.6 National Profile of Looked After Children Demographical data regarding LAC has been taken from statistical first release which provides national and LA level information on the outcomes for children who have been looked after continuously for at least 12 months at 31 March 2016 by LAs in England At 31 March 2016, there were 70,440 LAC in England, an increase of 970 (1%) on 2015, and an increase of 3,370 (5%) on In 2012, 59 children per 10,000 of the population were looked after; in 2016 the rate was 60 children per 10,000 of the population The rise over time reflects the higher number of children starting to be looked after than ceasing. In particular, in the latest year, there has been a rise in the number of unaccompanied asylum seeking children (UASC) in care, with 3,440 UASC entering care and 1,980 leaving care. The removal of UASC from the count of LAC, shows a decrease in the LAC population of 500 (1%) since Page 12 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
153 4.6.4 Table 3: Indicates the number of LAC for central Lancashire as of March 2017 Number of LAC originating from Lancashire 596 Number of LAC originating from out of area but placed in Lancashire 283 Total number of LAC children Interestingly, the numbers of out of area children placed in Lancashire have reduced slightly over the reporting period. A large number of out of area LAC originate from neighbouring LAs. There is scope for improvement in understanding the exact numbers A challenge has been the increasing number of independent providers opening new residential units within the central Lancashire area. At the time of reporting there were 45 independent and four LA Children Referral Units. Many of the establishments offer provision for LAC with extremely complex needs and many of which originate from out of area. 4.7 Looked After Children Health Provision During 2016/17 LCC has notified CCGs and providers of their intention to cease current funding arrangements in relation to LAC health assessments across Lancashire, from April This included the withdrawal of 41,100 from central Lancashire and a total removal of 103,000 from the overall LAC health provision across Lancashire The CCGs across central Lancashire commission initial health assessments (IHA), which are undertaken by community paediatricians. Review health assessments (RHAs) are mostly carried out by health visitors and school nurses as part of the 0-19 service, commissioned by the Public Health Directorate of the LA. The funding provided by LCC contributed to the health assessments / provision for those children who are out of main stream school and those harder to reach The CCGs responsibilities are outlined in Promoting the Health and Wellbeing of Looked After Children ; in particular the CCGs duty to cooperate with requests from LAs, to undertake health assessments and quality assurance of the health plans. In addition, it was anticipated that the impact of LCC s disinvestment would result in a considerable reduction in the system s capacity to meet the health needs of LAC In response the CCGs across central Lancashire agreed to meet the financial deficit. The current service specification has been reviewed to include additionalities around LAC who are harder to reach; subsequently enabling the continued delivery of high quality service in respect to LAC originating from and placed in central Lancashire Table 4: refers to the number of requests for initial health assessments (IHA) and review health assessments (RHA) during 2016/17 for central Lancashire Page 13 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
154 Health assessments requested and completed within timescale Q1 Q2 Q3 Q4 No of IHA requested No of IHA completed within timescale No of RHA requested No of RHA completed within timescale RHAs continue to be completed within the statutory timeframes; however IHAs compliance rates remain low due to a series of co-dependant multi-agency challenges that are being addressed. There will be a continued drive through 2017/18 to improve the quality and performance of IHAs with a focus on partnership working arrangements. Performance is reported by exception as part of case tracking to support improvements Work streams have been established to streamline the notification and health assessment process. It is intended that this will include consideration of the SDQ pathway and care planning in a staged approach. This work streams sits under the Lancashire Multi-Agency LAC Action Plan group, which was initially established to support the joint recovery of the timeliness of health assessments. The group has since evolved to include other service improvement areas relating to LAC The introduction of a LAC pregnancy pathway to ensure robust and timely information is shared between relevant health organisations and LAC nurses is an area for improvement identified in the CQC review see section The pathway will enable additional support for the LAC during pregnancy where vulnerability may be increased A LAC professional network group has been re-established to support pan- Lancashire s contribution to the work of NHSE Regional network for LAC, which feeds into the National work plan 4.8 Unaccompanied Asylum Seeking Children Unaccompanied asylum seeking children (UASC) have been arriving in the UK under an ongoing Home Office programme as part of the resettlement scheme for vulnerable children. It is recognised that these children will have very different needs to other LAC. The complexities they may present with are not only physical but emotional; they may require intensive support and management of their emotional health and well-being due to the trauma they have experienced along their journey Health professionals and the wider health economy will play a vital role in the offer of support and provision of services related to meeting their health needs. Current numbers of UASC are increasing locally, a percentage are also the victim of human trafficking and have entered the country via harmful routes. It is difficult to determine a precise figure, as information known is limited. A priority for 2017/18 is to monitor the numbers of USAC placed within Page 14 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
155 central Lancashire and the emerging health impact to inform commissioning arrangements Unaccompanied Asylum Seeking Children - Health and Wellbeing Needs Assessment was published October This document aims to anticipate the health and wellbeing needs of UASC, to identify strengths and gaps within the local child care systems and inform the development of services. In addition, an UASC Health Website has been launched providing health resources and guidance which can be accessed through this link Pan-Lancashire Sudden Unexpected Death in Childhood Service Improvements The Sudden Unexpected Death in Childhood Service (SUDC) nurse-led service is commissioned jointly by the eight CCGs covering pan-lancashire. The service is provided by Lancashire Care Foundation Trust and is aimed at both ensuring any unexpected child death meets with a multi-agency response and providing a SUDC response from a health perspective. Since the inception of the service eight years ago, the number of unexpected deaths each year has remained consistent, however 2016/17 has seen an increase in the total number of deaths to 58, this represents an increase of nine. This is the highest number of deaths pan-lancashire has recorded to date. Out of these child deaths, 17 related to central Lancashire During the reporting period the service has been subject to a review commissioned by the Child Death Overview Panel (CDOP). The purpose of the review was to consider the SUDC service in line with the requirements and intended outcomes of the statutory guidance, Working Together to Safeguard Children, Chapter 5 (HM Government 2015) 4. The review detailed that the service was not consistently involved in the initial response for two thirds of unexpected deaths out of hours and the SUDC response deviated from the requirements of Working Together An option to extend the current SUDC service to become a seven day service model has been favoured by the CCG Accountable Officers across pan- Lancashire. This development will improve the equity of response and increase the SUDC nurse involvement from the outset for more cases. Moreover, it will ensure compliance with Working Together and improve practice in line with Baroness Kennedy SUDC guidelines published November 2016 accessed here A steering group has been established to support the service improvements. The group is accountable to CDOP who reports into pan-lancashire Children Boards. The group will make recommendations to inform CDOP's work programme. This will continue to be a priority into 2017/18. 4 Working Together to Safeguard Children. A guide to inter-agency working to safeguard and promote the welfare of children, March 2015 Page 15 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
156 5.0 Lancashire Safeguarding Children Board 5.1 The CCG supports the work of the LSCB and partner agencies, examples are outlined below: 5.2 The Lancashire Safeguarding Children s Board (LSCB) has led on an action identified as part of LCC s improvement process to refresh the thresholds guidance in relation to the continuum of need (CON). The refresh undertaken incorporated a risk assessment model and the changes were launched July 16. The LSCB has agreed the final version of the multi-agency risk sensible model toolkit, which has been developed to support professionals when considering risk/need, when undertaking a referral and work with families. The toolkit needs to be considered in conjunction with the CON to support with understanding thresholds of intervention. 5.3 Multi-agency audit activity is being undertaken in respect to the processes around safeguarding children and young people. Audits commenced in August 2016 as part of a themed rolling programme with child in need and early help. GP Practices have been involved and have engaged well with the process. This engagement has been mirrored in the second round of audits in respect to transitions. A third audit has been undertaken focussing on complex cases involving CSE in Lancashire. 5.4 Findings will be presented to the LSCB and shared with multi-agency partners to implement any identified learning. Early themes indicate consistent issues around information sharing. An emerging theme included a lack of professional curiosity around early CSE indicators. In response to the initial findings the sample GP policy for safeguarding children will be strengthened to include indicators of sexual abuse and exploitation and an on-line survey will be undertaken across Primary Care to identify barriers that may impact on information sharing. 5.5 Actions will be monitored by the LSCB quality assurance and performance improvement subgroup. Additional information on the work of the board, including board minutes, can be accessed here. 5.6 Serious Case Reviews A SCR is a local enquiry carried out where a child has died or been seriously harmed and abuse and neglect is suspected, and there is cause for concern about professionals working together. There have been a significant number of SCRs reviews and referrals pending during the reporting period, which has expedited the need to review current practice in respect to undertaking SCRs. In response Lancashire have adapted the Welsh model learning and review framework for undertaking SCRs and there are plans for this way of working to be evaluated. The LSCB have recently been contacted by the Scottish Parliament and have been asked to present on Lancashire s interpretation of using the Welsh Model in respect to both a children and adults perspective; a date is set in the next reporting year. Page 16 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
157 5.6.2 During the reporting period in respect to central Lancashire; Child LA s SCR report and learning brief has been published. The publication of Child G and Child LD s SCR report has been delayed due to parallel proceedings however learning briefs have been published for both Child G - 13 month old infant was found unresponsive in bed with their father in March The learning brief was published in October 2015; publication of the associated report has been delayed due to parallel proceedings. Learning has not been delayed pending publication, all agencies involved in the case have implemented action plans to address the identified learning. It is anticipated that Child G will be published June 2017 along with a number of other SCRs. The key learning points include: Thinking the unthinkable Importance of parental history to inform future risk assessment Rule of optimism The impact of adult behaviour on children considering what the child sees, feels, thinks and fears Child LA - aged 17 years, sadly died at home after being found collapsed September Primary concerns related to neglect, CSE and missing from home episodes. The child and family were known to services Child LD - aged 22 months, sustained a suspected skull fracture and other injuries following a fall from an upstairs window of the family home, August The child and family were known to services and the criminal investigation is on-going. 5.7 Key learning for the CCG includes - Reminding staff of their legal responsibilities for children up to the age of 18 years of age Strengthening supervision arrangements Highlighting the importance of historical information to inform risk, including information about historical sexual abuse Raising awareness of and the ability to act in identifying and protecting children who are at risk or experiencing sexual abuse, including familial risk indicators Further information is available on the LSCB website. 5.8 Key priorities for 2017/18 Develop a sustainable CSE model for health provision across central Lancashire Development of a multi-agency safeguarding pathway for FGM Review LAC service specification Improve the quality and performance of IHAs with a focus on partnership working arrangements Page 17 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
158 Conduct on-line survey across Primary Care relating to information sharing and barriers to escalating concerns Strengthen the sample GP policy for safeguarding children Support the developments for improving the SUDC Nurse-led service 6.0 Mental Capacity Act and Deprivation of Liberty Safeguards 6.1 The MCA is a ground breaking piece of legislation, which establishes a framework of protection of rights for people who may through disability, injury or illness have impaired mental capacity, or who are at risk of being wrongly thought to lack mental capacity because of a diagnostic label or some aspect of their appearance or behaviour. 6.2 The Act, implemented in 2007, applies to everyone involved in the care, treatment and support of people aged 16 and over who may be unable to make all or some decisions for themselves. The Act applies to approximately 2 million people and sets out how professionals should support and care for people who may lack capacity. It also outlines how people can prepare in advance for a time when they may lack capacity. 6.3 The Law Commission s consultation paper on DoLS 5 was published in July The safeguarding team submitted a response to the consultation, outlining recommendations for the reform of MCA and DoLS. The Law Commission have since published recommendations replacing DoLS with the Liberty Protection Safeguards, further information can be found here. 6.4 The safeguarding team are instrumental in developing initiatives to support MCA implementation. This involves addressing local challenges from a regional and national perspective including sharing and dissemination of best practice. NHS England North Regional MCA subgroup work plan is in place to ensure MCA objectives are delivered. The LSAB MCA implementation group feeds local challenges into the regional group. The CCG MCA Lead attends the regional sub group and provides advice and support across the health economy. 6.5 The provision of expert advice is provided in managing complex and Court of Protection (CoP) cases. Further work is required to strengthen COP processes for Continuing Health Care (CHC) packages of care. Collaborative working with the LA is essential to support health and social care services, including multi-agency training using local leads, case law/ legal updates. In order to strengthen learning and development a multiagency MCA training strategy has been proposed for 2017/ A pan-lancashire MCA research study commissioned by NHS England has been undertaken to determine how the Act is applied in everyday practice across LA and health commissioned services. This innovative research study will be reported in 2017/18. 5 Law Commission, Mental Capacity and Deprivation of Liberty A Consultation Paper 2015 Page 18 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
159 6.7 Priorities for 2017/18 Development and implementation of a CoP prioritisation tool for individuals in receipt of CHC packages of care Development of a process to strengthen and standardise CoP applications Consideration of the recommendations outlined in the Pan-Lancashire research study Development of a Lancashire wide MCA learning and development strategy 7.0 Safeguarding Adults 7.1 Protecting adults at risk of abuse or neglect is a key part of the CCG s role along with a focus on quality and patient experience being integral to working arrangements. 7.2 The following section outlines key developments throughout the reporting period in respect to safeguarding adults at both a national and local level. 7.3 The Care Act statutory guidance was updated in October 2016, which has seen a number of amendments. This includes the management of selfneglect around the identification and management of risk being incorporated into the assessment process. 7.4 Domestic abuse has been strengthened to reflect the new offence of controlling and coercive behaviour, which closes the gap between intimate partners who still live together, providing better protection and allowing for earlier intervention and prevention. 7.5 Safeguarding Adults Boards are required to establish a framework for how allegations against people working with adults with care and support needs are managed. Work is progressing locally to strengthen practice in relation to maintaining compliance with the Care Act. 7.6 Making Safeguarding Personal Making Safeguarding Personal (MSP) underpinned by the Care Act focuses on engaging with people about the outcomes they wish to achieve from a safeguarding intervention. The aim is to understand the range of interventions to utilise, depending on an individual's wishes and circumstances In the event of a safeguarding enquiry the individuals preferred safeguarding outcomes must be incorporated into recording systems and then monitored to see how effectively they have been met Challenges are evident in practice in supporting healthcare staff to develop skills and confidence around risk management in MSP and in changing 6 The Care Act 2014, HM Government, 2014 Page 19 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
160 practices from outputs to an outcome focus. Time and resources are required to embed MSP, along with skilling up the workforce in dealing with unrealistic views about specific outcomes. 7.7 Care Homes The CCGs are an active partner in the RADAR and Quality Improvement Process (QIP) offering safeguarding and MCA expertise, as well as access to community and primary care services for additional support. Over the reporting period there has been a reduction of care homes in the QIP process, which may be due to the implementation of additional early intervention; a joint targeted approach by the CCGs and LA Within the reporting period three care homes with nursing have been managed by the QIP process. Providers have demonstrated with additional support they are able to implement the required improvements, however there are continued challenges in ensuring providers embed and sustain the service improvements. Themes derived from QIP include: Poor leadership, Recruitment and retention pressures of registered nurses Lack of access to robust training and supervision Poor quality record keeping /care and support planning Inconsistency in MCA compliance The Safeguarding / MCA champion model continues to grow from strength to strength. The model has proved to be an effective mechanism to enhance safeguarding and MCA practice across the care home sector within Lancashire. The development of workshops has enabled a forum for champions to network, share best practice and lessons learnt; along with presentations from expert speakers. This successful model has influenced the development and replication of a similar model across Primary Care. 7.8 Safeguarding Adult Activity Safeguarding alerts received by LCC continue to increase year on year. The associated increase may be a result of a significant amount of service development and awareness raising in relation to roles and responsibilities of services, coupled with the LA message that no alert is a bad alert. Subsequently making a safeguarding alert can sometimes be seen as a method to escalate concerns but not necessarily where there are safeguarding concerns. The CCG team have seen an increase in referrals where there is a health component to the safeguarding enquiry and at the initial stages of the alert prior to the alert being stepped up to a safeguarding enquiry. Work is required to support agencies use a risk based approach when making safeguarding alerts by the development of a best practice guidance document. Page 20 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
161 Table 6: Total number of safeguarding adult alerts received by LCC April 15 March 16 April 16 March 17 Chorley and SR Preston West Lancashire Lancashire Challenges remain in ensuring alerts are triaged and prioritised accordingly along with manging the backlog of referrals referred into the Multi-Agency Safeguarding Hub (MASH). Work is in progress to develop a guidance document for providers when raising safeguarding alerts, to support a consistent approach. The purpose is to assist providers and practitioners to identify the level of support and response required when abuse is suspected or identified. Responses must be directed at reducing vulnerability and risk management to promote the wellbeing of adults at risk of abuse. Table 7: Total number of alerts received progressing to a safeguarding enquiry from the 1 April 2016 to 31 March 2017 Social care district/service Number of safeguarding alerts received by LCC per district Page 21 of 26 Alerts progressing to a safeguarding enquiry NHS West Lancashire CCG Safeguarding Annual Report 2016/17 % of alerts that substantiated Chorley and SR (38%) 1126 (47%) Preston (39%) 754 (46%) West Lancashire (37%) 459 (49%) Lancashire (40%) 5193 (46%) On average less than 40% of the alerts progressed to a safeguarding enquiry. This may be attributable to the alerts not meeting the threshold for enquiry. In these cases referrals are signposted or referred on to more appropriate services, such as complaints teams and /or disciplinary procedures. In addition, agencies may require further staff training to support appropriate referrals into the LA Learning from substantiated safeguarding enquiries continues to identify organisational themes, some are outlined below: Professional and individual accountability including leadership Limited MCA / DoLS implementation Lack of robust care and support planning Poor management of resident to resident type incidents 8.0 Lancashire Safeguarding Adult Board (LSAB) 8.1 The Board is responsible for providing the strategic direction for safeguarding across the county; ensuring that all agencies work together to minimise the risk of abuse to adults at risk and to protect those subject to abuse.
162 8.2 Within the reporting period the board has strengthened arrangements within its combined business function, which has successfully supported the adult agenda and its subgroups. The development of a LSAB website has been instrumental in enabling agencies and the public to access key information. 8.3 The introduction of a new sub group for quality, audit and performance has facilitated the development and implementation of a programme of multiagency audits. This has enabled a multi-agency forum where safeguarding quality assurance issues can be discussed. The first multi-agency audit completed, considered domestic abuse aged 16 and over and intimate partners. 8.4 Findings will be reported on during the next reporting period. Early themes indicate issues around information sharing and a lack of enquiry around domestic abuse in older adults where dementia may be a feature. 8.5 There continues to be gap in the multi agency management of self-neglect. A task and finish group has been established to progress the development of a self-neglect pathway. The purpose of the pathway is to support individuals where there is no perpetrator of abuse and the adult has mental capacity to make choices about their care and support needs. 8.6 Additional information on the work of the board, including board minutes, can be accessed here. 8.7 Safeguarding Adult Reviews Safeguarding Adult Reviews (SARs) are a statutory process as outlined within the Care Act The purpose of a SAR is to identify and apply lessons learnt from cases where there is reasonable cause for concern about how the Board, its members or other relevant organisations worked together in any particular case, so as to prevent risks of abuse or neglect arising in the future. Although determined locally according to the specific circumstance the criteria for undertaking a SAR is broad and a more streamlined criteria is required The role of the SAR panel has been promoted throughout multiagency partnerships. Within the reporting period a total of eleven referrals have been received by the SAR subgroup. Four met the threshold for a SAR and two are pending decisions There has been significant progress during the year based on the successful implementation of the Welsh methodology for undertaking SARs. The first SAR has been completed and is due to be published later in A further three SARs have been commissioned using a tendering process, along with the development of contracts for independent reviewers A resource pack has been developed which includes roles and responsibilities of panel members/ Independent Reviewer / Independent Chair and Business Coordinator, learning event briefing, certificate for learning event, and a seven Page 22 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
163 minute briefing on the Welsh methodology. A system has also been set up to enable prospective chairs to observe a full SAR prior to undertaking the chairing role; this provides an opportunity for new chairs to receive shadowing opportunities prior to undertaking a full SAR. 8.8 Key priorities for 2017/18 include Strengthening MSP by development and implementation of an audit framework to provide assurance that MSP principles are embedded in local practice Development of guidance to support providers in raising safeguarding alerts A focus on older adults and the management of domestic abuse Implementation of the recommendations from multi-agency audit findings Review of the Welsh model to ensure it is specific to safeguarding adult review process and strengthen arrangements for monitoring multi-agency actions plans and dissemination of learning 9.0 Domestic Homicide Review (DHR) 9.1 DHRs were established under a statutory basis under section 9 of the Domestic Violence, Crime and Victims Act (2004) 7. The DHR statutory guidance published December 2016 was amended to include NHS England and CCGs as statutory partners. The purpose is to contribute to a better understanding of the nature of domestic violence and abuse and to highlight good practice. 9.2 The Community Safety Partnership commissioned a DHR within the central Lancashire footprint following the homicide of a local male. The report has been submitted to the Home Office for approval and publication. Key findings include: A lack of awareness of male victims of domestic abuse, including female perpetrators of domestic abuse, which are under-represented in the field of research Strengthening risk assessment, information sharing and safeguarding procedures for adults, children and families and application to the whole family unit Domestic abuse screening and flagging records within the GP practice 10.0 Prevent 10.1 Section 26 of the Counter Terrorism and Security Act places a duty on health services to have due regard to the need to prevent individuals from being drawn into terrorism. The key challenge for services is to ensure that where there are signs that someone has been drawn into terrorism, health 7 Domestic Violence, Crime and Victims Act (2004), HM Government, Counter Terrorism and Security Act 2015, HM Government, 2015 Page 23 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
164 professionals are trained to recognise the signs and know how to access support Channel is a voluntary, confidential programme, which provides support to people who are vulnerable to being drawn into terrorism. It operates across the country through LA-chaired multi-agency panels and is not any form of criminal or civil sanction The CCG Prevent Lead works closely with the Regional Prevent Coordinator and acts as the single point of contact for referrals into the Channel panel Lancashire is participating in the Dovetail pilot, trialling a new method of delivery for the Channel programme, which sees LA taking the lead on the coordination of activities. Nine sites are testing a variety of models. The aim of the pilot is to assess the feasibility of transferring the Channel programme and its case management responsibilities to the LA, thus reducing the police s role in the Channel process Over the reporting period a rolling programme of Wrap 3 has been delivered, by the CCG safeguarding team to increase awareness of responsibilities within the Prevent agenda. The sessions have been well evaluated and themes have been highlighted during two of the sessions, which prompted two referrals. An increase in demand for Wrap 3 training has been seen due to the numbers of staff who require face to face training. In response, the CCG has approached the LA regarding the introduction of a joint training pool Referrals into the CCG to access Prevent advice remain low, further work is required to establish the cause Multi-Agency Safeguarding Hub 11.1 The LSCB led a multi-agency review of the functioning of the Multi-Agency Safeguarding Hub (MASH) diagnostic which concluded July 2016; with the outcome being that the MASH was in need of redesign. An independent consultant has been commissioned by the LSCB to scope the implications of the MASH diagnostic and to make proposals on how to progress a service redesign. The establishment of work streams reporting to the MASH strategic steering group has been agreed and work commenced with all stakeholders. All partners are working towards a fully integrated MASH providing a single point of access for all children s social care and safeguarding adult referrals. This is a first step in the move to a single front door and will include a removal of the distinction between MASH and Children s Assessment and Referral Team. In the longer term, a single point of contact will: Reduce the number of processes Allow the potential of the exercise of professional judgement at the earliest stage Improve demand management Improve timeliness of communication Optimise the potential for decisions to be made within 24 hours of contact Page 24 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
165 11.2 Although there is a common understanding around the issues with processes and what needs to change there have been a number of challenges, despite this the pace of development of the MASH has increased Priorities for 2017/18 include - Continued delivery of the Wrap 3 programme Strengthen Prevent awareness through the care home Safeguarding Champion / GP Leads / Champion models Continue to influence the strategic direction of MASH 12.0 Conclusion 12.1 The safeguarding agenda is complex and arrangements are frequently under review, often due to national drivers and local challenges. Safeguarding is multifaceted and continues to evolve in line with national policy, legislation and findings from learning reviews The CCG will continue to work collaboratively, as effective safeguarding depends on multi-agency working to ensure all children, young people and adults at risk of harm are protected; and are at the centre of care and service development Contributors to this Report Lorraine Elliott Louise Burton Linda Whitworth Kristy Atkinson Diane Kinsella Page 25 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
166 Appendix 1 Page 26 of NHS West Lancashire CCG Safeguarding Annual Report 2016/17
167 Agenda item no: WLCCGB 11/17/11 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP BOARD REPORT DATE OF BOARD MEETING: TITLE OF REPORT: 28 November 2017 Declaration of Members Interests - Update BRIEFING POINTS: To record the declared interests of the members of West Lancashire Clinical Commissioning Governing Body Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient No experience) please outline impact 2. Commissioning of hospital and community services please No outline impact 3. Commissioning and performance management of GP Prescribing No please outline impact 4. Delivering Financial Balance please outline impact No 5. Development of the commissioning group as a commissioning Yes organisation please outline impact Will provide the commissioning board and commissioning group with practical experience of implementing good governance practices B. Governance please outline impact Yes 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number) have any legal implications promote effective governance practice The report promotes good governance practices. It provides a summary of the declared interests of members. 2. Additional resource implications No (either financial or staffing resources) 3. Health Inequalities No 4. Equality and Inclusion and Human Rights Requirements No Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement No 6. Patient and Public Engagement No REPORT PRESENTED BY: Paul Kingan, Chief Finance Officer Declaration of members interests West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
168 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP BOARD DECLARATION OF MEMBERS INTERESTS - UPDATE BACKGROUND 1. The purpose of this report is to record the declared interests of the members of West Lancashire Commissioning Governing Body. 2. The register was updated in November 2017 to provide an up to date position of declarations of interest for the members of the Governing Body. 3. This register will be available to view on the West Lancashire CCG website on 30 November ACTIONS 4. The Governing Body is asked to: a. note the declared interests of its members. Declaration of members interests West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November
169 Financial Interest Non-Financial Professional Interest Non-Financial Personal Interest Register of declaration of interests for the Governing Body members November 2017 Name Current position (s) held in the CCG i.e. Governing Body member; Committee member; Member practice; CCG employee or other Declared Interest (Name of the organisation and nature of business) Type of Interest Is the interest direct or indirect? Nature of Interest Date of Interest Action taken to mitigate risk From To Adam Robinson Secondary care consultant on Board Salford Royal Foundation Trust X Direct Consultant and Chair of medicine 2013 Ongoing Declared on this form Pharmaceutical companies X Direct Continue to work with a number of pharmaceutical companies as advisor and speaker Ongoing Claire Heneghan Chief Nurse NIL All payments and contract in line with ABPI regulations Douglas Richard Soper Lay member audit and governance NIL
170 Dr Bapi Sujoy Biswas * GP executive lead Beacon Primary Care X Direct Partner Also, own buildings in which PDS use space (Railway Road) and pay rent. Deliver a variety of commissioned enhanced services as per website Ongoing Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy. North Meols Medical Centre X X Direct Partner Ongoing (removed October 2017) Family Surgery Birkdale X Direct Partner Sefton Tier 2 cardiology based here Present Viran Medical Centre X Direct Partner Present Barbonel Services Company provides services to Beacon Primary Care Beacon Primary Care X Direct Director and shareholder Indirect Wife works for practice Present Present
171 R&B Medical Indirect Shareholder Present R&B Medical X Direct Director and shareholder. Providing property management services to family surgery Present Beacon Primary Care X Direct Bidding for pain service Declared Chair to decide if fundamental or significant Noted as procurement DoI on Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in line with the conflict of interest policy. Dr John Caine * Chair Parbold practice X Direct Partner in GP practice (Ceased in July 2017) Southport and Ormskirk NHS Trust and Warrington and Halton General Hospital Indirect Spouse working as ANP (Paediatrics) April December 2017 ongoing Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy.
172 British Geriatric Society X Direct Member October 2016 Ongoing Beacon Primary Care X Direct Currently working as a sessional GP for Beacon Primary Care Ongoing Noted as procurement DoI on Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in line with the conflict of interest Dr John Paul Kinsey* GP executive lead Parbold surgery, 4 The Green, Parbold X Direct Partner (3 days per week) JPK medical Ltd X Direct Owner, director and 2015 Ongoing shareholder (70%). Out of hours work and other income is paid into this company Ongoing Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy. Manchester postgraduate deanery X Direct Primary care medical educator and programme director, as an educator at Preston Ongoing
173 Dr John Paul Kinsey* (Continued) OWLS CIC Ltd - work shifts X Direct Independent practitioners for GP services in West Lancashire 2008 Ongoing Aintree NHS Foundation Trust Indirect Wife works as Macmillan upper GI cancer nurse specialist 2015 Ongoing JPK medical Ltd Indirect Wife is a shareholder (30%) and co-owner Akea Life Indirect Brother-in-law setting up the private GP service company: to provide GP services and weight loss services Ongoing (removed ) 2015 Ongoing Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy Akea Life X Direct Working some shifts for private GP service. No managerial input or directorship Ongoing
174 GP Federation; PWLS CIC Ltd X Direct Practice member. Practice is a member of the developing federation organisation Ongoing Dr Rakesh Jaidka* CCG Executive OWLs West Lancashire Federation of primary care X Direct Director Ongoing Interest declared, included on the register and documented at meeting when relevant. Local Medical Council X Direct Representative for West Lancashire Ongoing JAIGURU Limited X Direct Work out of hours shifts for OWLS and Director of company Ongoing Skelmersdale Family Practice, Birleywood Health Centre WN8 9BW St Raphael s dental practice X Direct GP partner Ongoing X Indirect Wife works as dentist at practice in Upholland Ongoing Dr Peter Gregory* Clinical executive Parkgate Surgery X Direct Partner in practice. Surgery provides minor surgery and family planning services. Current Ongoing Declared
175 Dr Peter Gregory* (continued) OWLs CIC (GP Federation) OWLs has a subcontract with Virgincare to provide GP cover to OOH. X Direct Medical Director and member Current Ongoing Declare on COI register and when relevant during executive meetings. OWLs provides extended access. OWLS is in a joint bid with WLCVS in the social prescribing pilot. Dr Vikul Mittal* GP Executive Lead Tarleton Group Practice West Lancashire GP Federation OWLs CIC Ltd X Direct GP partner and trainer Since joining the CCG as GP executive X Direct Director. OWLs has a subcontract with Virgin Care to provide OOH GP services and run extended access pilot. Also involved in social prescribing bid. Mid 2017 Ongoing Ongoing Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy.
176 Dr Vikul Mittal* (continued) Practice X Direct Perform minor surgery/injections North Locality (Federation) X Direct Lead Late 2017 Ongoing Greg Mitten Lay member patient and public involvement, Chair of the CCG Quality and Safety Committee Southport and Ormskirk District General Hospital St Helens and Whiston Trust West Lancashire Community for Voluntary Services Indirect Wife, Dr Rashmi Gupta is a consultant microbiologist Employed by this Trust X Direct Chief Officer. WLCVS and VCFS member organisations could potentially be one of the supplier for this service. Since joining the CCG as GP executive Noted as procurement DoI on Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in line with the conflict of interest 2009 Ongoing Noted as procurement DoI on Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in line with the conflict of interest Lancashire Association of CVS (Charity) X Direct Director. Voluntary position. Organisation could potentially be one of the supplier organisations 2009 Ongoing Interest noted, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy.
177 Greg Mitten (continued) One West Lancashire X Direct Chair. Strategic partnership. Voluntary position Ongoing Lancashire West LAG (RDPE) Board X Direct Chair. Voluntary position Ongoing Mike Maguire Chief officer Range of companies One Lancashire X Direct Strategic VCFS Partnership for Lancashire Voluntary position. Indirect Spouse undertakes occasional market research assignments Ongoing August 2016 Ongoing Standing declaration. Interest notes, will be reviewed and discussed. Where a conflict emerges it will be dealt with in accordance with the conflict of interest policy. Paul Kingan Chief finance officer NIL Stephen Gross Lay member NIL *As agreed at the Governing Body meeting on 28 January 2014, please note that all principal GPs in West Lancashire are default members of the Out of Hours service.
178 WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY REPORT DATE OF BOARD MEETING: 28 November 2017 WLCCGB 11/17/12 TITLE OF REPORT: Contract Award Recommendation Report Social Prescribing BRIEFING POINTS: Recommended Provider for approval. Does this report / its recommendations have implications and impact with regard to the following: A. Commissioning Board s Aims and Objectives 1. Quality (including patient safety, clinical effectiveness and patient experience) please outline impact 2. Commissioning of hospital and community services please outline impact 3. Commissioning and performance management of GP Prescribing please outline impact 4. Delivering Financial Balance please outline impact 5. Development of the commissioning group as a commissioning organisation please outline impact X B. Governance please outline impact 1. Does this report: provide the Commissioning Board with assurance against any of the risks identified in the assurance framework (identify risk number) have any legal implications promote effective governance practice 2. Additional resource implications (either financial or staffing resources) 3. Health Inequalities X 4. Equality and Inclusion and Human Rights Requirements Yes Has an Equality Impact and Risk Assessment been carried out? 5. Clinical Engagement 6. Patient and Public Engagement PAPER PREPARED BY: PAPER PRESENTED BY: Kathryn Kavanagh Lead Health Inequalities Paula Williams Procurement Manager Kathryn Kavanagh Lead Health Inequalities Contract Award Recommendation Report Social Prescribing West Lancashire Clinical Commissioning Group Governing Body Meeting 28 November





179 MIDLANDS AND LANCASHIRE CSU CONTRACT AWARD RECOMMENDATION REPORT Social Prescribing Contract Award Recommendation Report NHS West Lancashire CCG Report Prepared By: Kathryn Kavanagh, Lead Manager Health Inequalities, WLCCG P.Williams, Procurement Manager, Midlands & Lancashire CSU
180 Contents 1. Participating Organisations 2. Background 3. Procurement Process 4. Recommendation

181 1. Participating Organisations The Commissioning Organisation for this procurement is: NHS West Lancashire CCG 2. Background Across West Lancashire there is a range in life expectancy, for males this difference spans from 83 years in Derby ward compared with 73.6 years in Tanhouse, a difference of 9.4 years. For females, life expectancy ranges from 87.6 years in Tarleton to 76.1 years in Birch Green, a difference of 11.5 years. These differences are patterned by deprivation, lifestyles and other social and economic influences. It is recognised that the health services can t do everything that is needed by itself to reverse the flow of costly avoidable illness required to narrow this gap in life expectancy; however it can become a more activist agent of health-related social change, leading a range of new approaches to improving health and wellbeing. Highlighted in the GP 5 Year Forward View (GP5YFV) Social Prescribing models can support wider integration across the health and social care system by enabling GP s to access practical, community-based support for their patients. Social Prescribing is a structured process through which the prescriber works with their patient to address the wider social and lifestyle issues that impact on their health. It is based upon an assetbased approach to health, understanding that health is a positive state of wellbeing rather than considering health as an absence of illness and disease. It is based upon the principles of coproduction, personalization, choice and control to achieve and maintain wellbeing. Importantly, it is something performed with people, not to them or for them. There can be different levels to Social Prescribing as shown in the diagram below.
182 Social Prescribing schemes can involve a variety of activities which are typically provided by voluntary and community sector organisations, but services for onwards referral may include those commissioned by the statutory sector. Examples include volunteering, arts activities, group learning, gardening, befriending, cookery, healthy eating advice and a range of sports. There are many different models for Social Prescribing, but most involve a Social Prescriber who works with people to address areas of behaviour change and access local sources of support. The Bromley by Bow Centre in London is one of the oldest and best-known Social Prescribing projects. Staff at the Centre work with patients, often over several session to help them get involved in more than 30 local services ranging from swimming lessons to legal advice. The aim of the service is to provide core, additional and enhanced services. Aims of the service The key aims of the service are to develop an approach that: Provision of a holistic approach to health & wellbeing based upon an asset-based approach to wellbeing. Based upon the principles of co-production, personalisation, choice and control Patient centred service which is simple to access. Integrated from a patient s perspective with other service providers, delivering seamless wrap around range of services that minimise the impact of social and lifestyle issues that impact on health. Facilitated access to prescribed services where needed Objectives and functions of the Skelmersdale Social Prescribing Hub: Provision of a holistic approach (as described above) to health and wellbeing that places greater emphasis on preventative measures that reduce the progression towards Long Term Conditions (LTC) or prevent the worsening health for individuals with existing LTC s. Coordination and aligning of existing Social Prescribing activity and related resources across the Skelmersdale neighbourhood. Harmonisation of the Social Prescribing offer across providers, ensuring that individuals in contact with SP services are met with the same quality interaction and support to onward services. This would be reflected in the harmonization of the case-management process used across SP services and the wellbeing assessment tools used. Coordination of the training programme for social prescribers and organisations who are the recipient of clients. Provide a focal point for the changing relationship between clinician and patient. Supporting this changing dynamic by engaging the service and wider team with Better Conversations, Solution Focused Shared Decision Making (SFSDM) and evidence-based behaviour change methodologies. Training will include but not be limited to Data Protection, Safeguarding, Motivational Interviewing techniques Health Promotion and Mental Health First Aid. In partnership with the local Primary Care Federation, working with GP practices on a neighbourhood basis to risk stratify the population, and develop intelligence driven population health profiles that drive proactive, anticipatory, joined up community-led support.
183 Development of strong relationships between VCFS, wider NHS structures and other providers who can support the approach. Provide the link between VCFS sector and emerging multidisciplinary teams in Skelmersdale. Provide robust evidence based on utilisation rates and outcomes, linking with Well Skelmersdale evaluation. Work with Well Skelmersdale associates and the VCFS sector and other providers to maintain a local Directory of Services, identifying gaps in local services where necessary (see digital section below). Work with Well Skelmersdale associates and the VCFS sector and other providers to enhance the mapping and identification of community assets and community activators that is already being undertaken under the banner of Well Skelmersdale. 3. Procurement Processes Evaluation Panel An Evaluation Panel was established, consisting of the members shown in Annex A. All evaluators were asked to complete a Confidentiality Agreement and a Declaration of Interest form at the start of the ITT stage when bidders were known. Expression of Interest The request for Information (RFI) was advertised on Contracts Finder on the 18 th July 2017 and closed on the 28 th July Contracts Finder (an eprocurement tool) requested expressions of interest to participate in an open procurement process in line with the Public Contracts Regulations All parties that responded to this RFI were invited to participate in the Invitation to Tender exercise. To express an interest in the providing the service, potential bidders prompted to register on the BRAVO e-tendering website where they gained access to the Tender Questionnaire which they were to complete online. Expressions of Interest were received from 24 suppliers. Invitation to Tender An Invitation to Tender (ITT) was published on 11 th September 2017 with a closing date of 11 th October 2017 using the Bravo e-procurement system. Four bids were received.
184 Evaluation Process The evaluation methodology for assessing the ITT responses was published in the ITT. The Quality Section of the ITT was broken down into a number of sub sections which were weighted according to their relative importance, as detailed in the table below. The table below sets out the scoring methodology for the questions: SECTION Evaluation Criteria Part 1 (A) - Potential Supplier Pass/Fail Details Part 2 (B) - Exclusion Criteria Pass/Fail Part 3 (C) Financial Pass / Fail Part 4 (D) Quality B - Service delivery Scoring/weighting 59% Pass / Fail C - Financial Scoring/weighting 7% Pass / Fail D - IM & T For Information only Pass / Fail E - Quality Scoring/weighting 14% Pass / Fail F - Contracts Management Scoring/weighting 5% Pass / Fail G Workforce Scoring/weighting 15% Pass / Fail H - Health and Safety Pass / Fail I Equalities Pass / Fail Part 5 Declarations Pass/Fail Total 100% Each of the questions within sections D-H falling within the non-financial Evaluation Criteria were scored using the scoring methodology set out in the below Table. Scores were awarded based on the score category the response to the question best aligns to. Score Criteria 0 Omitted - The response has been omitted. 1 Very poor - The response completely misses the point of the question. 2 Poor - Requires major revision to the proposal to make it acceptable. Only partially answers the requirement, with major deficiencies and little relevant detail
185 proposed. 3 Acceptable - Response is acceptable but remains basic and could have been expanded upon. Response is sufficient but does not inspire. Good probability of success, weaknesses can be readily corrected. 4 Good - Response exceeds minimum expectations including as level of detail, which adds value to the bid. Great probability of success, no significant weaknesses noted. 5 Excellent response comprehensive and useful. High probability of success, no weaknesses noted. The response is innovative and includes a full description of techniques or measurements to be employed. The Financial section was evaluated on the lowest price for a response which met the pass criteria being awarded a score of 5. Then all other bids shall be scored on a pro rata basis in relation to the lowest price. The score is then subject to a multiplier to reflect the percentage value of the price criterion. The panel made an initial evaluation individually, after which a moderation meeting was held on the 14 th November Consensus scores were finalised during the moderation meetings. Evaluation Summary The final evaluation of the Tenders has led to the following outcomes: SECTION Bidder 1 Bidder 2 Bidder 3 Bidder 4 Part 1 (A) - Potential Pass Pass Pass Pass Supplier Details Part 2 (B) - Exclusion Pass Pass Pass Pass Criteria Part 3 (C) - Financial Pass Pass Pass Pass Part 4 (D) Quality B - Service delivery C - Financial 7.00 Pass 6.69 Pass 6.69 Pass 6.76 Pass D - IM & T E - Quality 5.60 Pass Pass Pass 8.40 Pass F - Contracts Management 3.00 Pass 4.00 Pass 4.00 Pass 3.00 Pass
186 G - Workforce 6.00 Fail Pass Pass Pass H - Health and Safety Fail Pass Pass Fail I Equalities Pass Pass Pass Pass Part 5 Declarations Pass Pass Pass Pass PRICE 67, , , ,325. VALUE OF BID The highest overall scoring bid was achieved by Bidder 2 - Out of Hours CIC in partnership with WLCVS. 4. Recommendation The panel recommend that the contract for this service is awarded to Out of Hours CIC in partnership with WLCVS.
187 Annex A Tender Evaluation Panel Scoring: SECTION Evaluators Part 1 (A) - Paula Williams (Midlands and Lancashire CSU) Potential Supplier Kathryn Kavanagh(West Lancashire CCG) Details Part 2 (B) - Paula Williams (Midlands and Lancashire CSU) Exclusion Criteria Part 3 (C) - Paul Jones (West Lancashire CCG) Financial Part 4 - Quality B - Service Kathryn Kavanagh(West Lancashire CCG) delivery Phil Winnard (West Lancashire CCG) C - Financial D - IM & T E - Quality F - Contracts Management G - Workforce H - Health and Safety I Equalities Part 5 Declarations Ron Cooper Independent representative Paul Jones (West Lancashire CCG) Cath Thomson (West Lancashire CCG) Ron Cooper Independent representative Allison Lumley (West Lancashire CCG) Kathryn Kavanagh(West Lancashire CCG) Phil Winnard (West Lancashire CCG) Jackie Moran (West Lancashire CCG) Joanna Rimmer (West Lancashire CCG) Allison Lumley (West Lancashire CCG) Karen Tordoff (West Lancashire CCG) Mark Jump (Midlands and Lancashire CSU) Catherine Bentley (Midlands and Lancashire CSU) Paula Williams (Midlands and Lancashire CSU)
188 Minutes Primary Care Commissioning Committee Venue: Boardroom, Hilldale, Ormskirk Date & Time: Tuesday 12 September 2017 at pm Attendees: In attendance: Mr S Gross Chair Dr J Caine West Lancashire CCG Chair Mr P Kingan Chief Finance Officer J Kane Administrative Officer Mr M Maguire Chief Officer Mrs J Charnock Primary Care Development Manager Mrs S Wood, Clinical Leadership Manager, NHS England North (Lancashire) Mr M Green Finance manager Mrs N Baxter Head of Medicines Optimisation L Anton Graduate Management Trainee Apologies: Dr A Robinson Secondary Care Consultant Mrs C Heneghan Chief Nurse Mr D Soper Lay Member Mrs J Moran Head of Quality, Performance and Contracting Agenda Item Summary of Discussion Lead 1. Welcome and apologies for absence Steve Gross introduced himself and welcomed the members of the Primary Care Commissioning Committee (PCCC) to the meeting of the committee. The apologies above were relayed. No members of the public were present. 2. Declaration of interest Steve Gross reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of West Lancashire CCG. Declarations declared by governing body members are listed in the CCG s Register of Interests. The register is available either via the secretary to the governing body or the CCG website at the following link: As at the previous Primary Care Commissioning meeting John Caine again declared a general interest in all items as he is employed as a sessional GP. As John Caine is a non-voting member the chair considered the declaration of interest and deemed this to be significant and not fundamental for all items under consideration today. 3. Minutes from the previous meeting The minutes were approved as a correct record with no amendments required. 4. Update on actions from previous meeting The action sheet was updated. Primary Care Commissioning Committee 12 September 2017 Page 1 of 5
189 Agenda Item Summary of Discussion Lead STRATEGIC ISSUES 5. Primary Care Strategy / working in neighbourhoods Jan Charnock updated that the Primary Care Strategy is on track and just requires the agreement on the neighbourhood development plan levels to be embedded before completion. Once this is done the strategy will go to the Membership for agreement. Jan expects that the strategy will be ready to return to the PCCC in November before ratification at the WLCCG Governing Body. Discussion followed on how performance issues will be managed. Jan and Sheena confirmed the process to the PCCC, depending on the level of severity issues will be discussed either at the between Quality Sub Group, a Quality Surveillance Group. Sheena offered NHSE support to work with WLCCG to set out a process highlighting how and where monitoring issues are managed. A flow chart or template will be created that shows how and where issues will be monitored. 6. Finance update Matt Greene gave a brief update reporting that there is no significant change since the last meeting. A question was raised regarding reserves, Matt confirmed the CCGs current position, which depending upon the range of resources has some leeway. Primary care benchmarking by CCG Paul Kingan presented information regarding where WLCCG sits in terms of funding compared with other CCGs in Lancashire, Cheshire and Merseyside. Figures shown are 2015/16 and are measured per weighted patient. The Global Sum refers to the funding formula used to determine contract payments. Matt referred to the Global Sum, Premises and QOF as being indicators of interest. Discussion then turned to the benchmarks and what they illustrate. It was agreed more work is required on premises payments work, this depends upon the set-up of individual practices, the notional cost of buildings, historically there has been a lack of investment in premises and unfortunately levels of previous investment have not been considered by NHSE. It was noted that CCGs must fund any increase in market rent, as such WLCCGs potential liabilities for premises need to be understood. It was agreed that Matt Greene will break figures down and the return with further analysis. Nicola Baxter commented that WLCCG appears low on prescribing, however this is more about reimbursement of costs and reflects the work taking place in practices. WLCCG is like Chorley and South Ribble in this respect. Further discussion took place on understanding the QOF quality element of the benchmarking and why WLCCG was positioned where it was. 7. Medicines management update: Prescribing hubs Nicola Baxter updated the Primary Care Commissioning Committee on the prescribing hub element of the Medicines managements programme. The idea Primary Care Commissioning Committee 12 September 2017 Page 2 of 5
190 Agenda Item Summary of Discussion to create hubs came from the Waste Campaign, where variation in prescribing had been highlighted. The proof of concept pilot was rolled out in Skelmersdale and the model has already generated interested in other areas. The model consolidates several practices prescribing into one place which reduces variation, improves quality and frees up clinical time. One GP involved has reported that Prescription Ordering Direct (POD) has freed up one hour per day. Nicola reported that cost savings are also being realised. This programme helps both Quality and QIPP programmes. The Medicines Team have recruited staff and a paper will be produced for the Governing Body next week. Other areas where a hub model can be explored further are in coding and scanning. Federation involvement was briefly a focus. Care homes Nicola then updated on the ongoing work with Care homes and embedding with community services. The team is reviewing what they do as a team and working to align in community with Virgin Care, however there has been a hiatus recently due to leave. Nicola will update on the position of this work after discussion with Claire. Community pharmacy Nicola then focussed on community pharmacy and a pharmacy integration fund. Sheena suggested Linda Bracewell and Keith Kendall are contacted for the Pharmacy Integration Fund, this funding stream from NHSE encourages involvement in this work and could provide central funding for Community Pharmacy. Nicola will contact as suggested. Nicola also updated on the minor ailment scheme, this will be reviewed and an update will follow. There is work looking about Hesketh Bank Pharmacy to see if provision can offer more to patients in that area, scoping the possibility of a Walk in Centre. Sheena directed to Healthy Living Pharmacies, a paper is in the process of being written that could bring in extra quality payment, Nicola and Sheena will meet to discuss further. Prescribing for clinical needs and gluten-free policy Nicola reported that queries regarding the recent changes in prescribing for clinical need have reduced. The team continues to implement changes through training reception staff, there is tech on the practices systems to remind of the changes and promote the self-care approach where appropriate. Another topic of discussion was the NHS Urgent Medicine Supply Advanced Service Pilot (NUMSAS), this is a pilot where a caller to 111 may be directed to community pharmacy for urgent prescriptions. It was agreed that communications around this should be increased to make full use of the benefits. Lead OPERATIONAL ISSUES 8. NHS England update Sheena Wood advised that as her contract was nearing an end she would not be attending future meetings and Sarah Bloy will be representing NHSE in her place. Sheena then provided an update for NHS England, highlighting the following: Primary Care Commissioning Committee 12 September 2017 Page 3 of 5
191 Agenda Item Summary of Discussion Lead NHSE update on resilience funds, this is a case by case application. Jan reported that WLCCG are low on the scale this year, the Federation received funds last year. Jan has requested a breakdown of the information on resilience for CCGs to see what everyone received this year. For Seven-day access there are some non-recurrent monies to tap into, Stephen Gough is the contact. Patient population per head - Sheena asked what the preferred model of care is going forward for primary care. The focus for WLCCG is manageable steps for neighbourhoods. A Primary Care Home Hub model is currently being adopted. As for the MOU, Sheena reports that setting up a meeting has proved difficult however Jan will Jackie Forshaw to resume actioning this. 9. Primary Care Practice update The first meeting for Viran is on Friday, yet the vision for the future unclear but it was agreed that patients will be given time to settle before any further change.is implemented. Hilda Yarker from H2A is gathering feedback from patients on their experience, WLCCG are currently awaiting the report and this will be used to inform the vision. This will ensure that WLCCG has the view from patients before going to procurement. Sheena will follow up on report progress. Beacon and North Meols have now one practice code. Brief discussion took place on an issue regarding EMIS and data transfer, Sheena will flag this to NHSE. Zero tolerance is up and running in Lancashire and South Cumbria, again some issues with EMIS, the link code is now established but this took longer than expected. MLCSU have been tasked with data management. Further discussion took place on the process. A brief update was given on actions taken following an issue with behavioural issues from a patient presenting with complex mental health and substance misuse needs. A caution has been issued to try and mitigate the issue. Steve Gross thanked Sheena for her contribution to the PCCC and wished her well for the future. 10. Practice Visits update Jan Charnock gave an update on the recent practice visits. Following on from a visit with one practice data has highlighted the need for a further visit. As was discussed earlier in the meeting any issues arising from visits will be addressed via the correct route with NHSE and WLCCG. The POD has sparked further interest in increasing working together. George Hurst continues to work on building and space options, it was suggested that Jim Goulden may be helpful in making best use of space and obtaining funding in this aspect. Primary Care Commissioning Committee 12 September 2017 Page 4 of 5
192 Agenda Item Summary of Discussion Jan will collate common themes raised by the practice meeting and will bring these back to the PCCC. Jan suggested the next round of visits start in January, this was agreed along with visits will now require just one GP and one manager to simplify the process. Lead 11. Workforce Enhanced Training Practice (ETP) Alison Lumley attended to present a paper outlining a proposal for WLCCG practices to join a Wigan Enhanced Training Practice initiative. This scheme develops placements in primary care for health care staff. West Lancashire have been approached by Wigan to be included, Alison recommended that the PCCC support the proposal as no downsides are foreseen. The proposal complements the Grow Your Own GP scheme and would increase recruitment opportunities. The committee members agreed to support the proposal. FOR INFORMATION Education for Workforce Transformation (CPD) Allocation 2017 Alison also presented this paper for consideration, advising on the CPD allocation. This is a flexible cash allocation for education for workforce. Alison and Claire managed the previous allocation and now have brought this to the PCCC for approval. The paper proposes the money is used to support Advanced Nurse Practitioners to complete their training. The committee members agreed to support the proposal. A brief conversation took place on international GPs and the interest in the area in take up of this scheme. The PCCC will continue to be updated on this. 12. Notes from the Primary Care Operation Group Not available (meeting only took place day the agenda was circulated) 13. Any other business None presented. Date and time of the next meeting The next meeting of the committee will take place on Tuesday 14 November at 1.30 pm, Boardroom, Hilldale. Primary Care Commissioning Committee 12 September 2017 Page 5 of 5
193 West Lancashire Clinical Commissioning Group Finance & QIPP Notes and Actions 5 September 2017 ` Item Discussion and decisions Actions Responsible officer Attendees Chair Mike Maguire Chief Officer Due Date Paul Kingan Chief Finance Officer Peter Gregory GP Executive Lead Bapi Biswas GP Executive Lead Greg Mitten Lay Member Stephen Gross Lay Member Jack Kinsey GP Executive Lead John Caine Chair Rakesh Jaidka - GP Executive Lead Vikul Mittal GP Executive Lead Doug Soper Lay Member Pauline Webster Administration Officer In Attendance Apologies Nicky Baxter Head of Medicines Optimisation Jackie Moran Head of Contracting, Performance & Quality Paul Jones Head of Finance Matt Greene Finance Manager George Hurst Estates Lead Joanna Rimmer Contract Support Officer Adam Robinson Secondary Care Consultant Karen Tordoff Lead Manager Service Redesign Claire Heneghan Chief Nurse
194 Declaration of Interest Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: Declaration of Interest Declarations of interest from sub committees; None declared. Item 3 Notes from previous meeting 1 August / matters arising / summary of actions Declarations of interest from today s meeting; None declared The committee reviewed the draft notes for ratification. Paul referred to item 3 of the draft notes re ABPI referrals, Claire Heneghan was having discussions with VC to resolve this issue. The committee agreed that the paragraph under item 3 was an accurate record. The notes were agreed as an accurate record. Matter arising/summary of actions: Fairfield Hospital Contracts summary - 7 September Fairfield commenced a Direct access MRI pilot restricted to 4 Practices (Parkgate, Dr Littler, Stanley Court, Manor Primary) Originally contract term 12 months Body areas: Knee, Cervical, Thoracic and Lumbar Spine and Pelvis / Hip Contract extended for a further 12months under the same conditions. Following a discussion at a Membership meeting it was agreed that the service should be opened up to all West Lancs Practices Further contract offered from 1 August 2017 for 12 months. Notification has gone out regarding this in the GP newsletter NHS Right Care Karen Tordoff has invited Dr Mark Johnston NHSE Right Care Delivery partner and Lead Clinician to the next meeting on 3 October 2017 Acute Visiting Service (AVS) Paul Kingan reports that AVS is under performing and under-utilised. Averages have reduced to 97 from 166 cases per month since transferring to the new AVS data to be discussed at next Transformation Board Jackie Moran
195 Item 4 QIPP Plan Overview and early forecast Item 5 Estates QIPP Update provider. This under performance could be costing the CCG up to 20k per month. Jackie to further discuss the data at the next Transition & Transformation Board with the new provider on 28 September 2017 Recruitment to new post - Head of Integration of Health & Social Care is still in process and has not yet gone to advert. Claire to provide update at next meeting in October. Estates QIPP update see item 5 Pipeline Schemes Procedures of limited clinical value (PLCV) Paul informed the committee that he has received comparative data from Southport and Formby CCG and ran through some of the figures showing an opportunity of 3.3m. Paul will keep the committee updated as he is analysing the data. PLCV will also be covered in the agenda under item 7 Blueteq Service and System. Paul Kingan gave a verbal update: The CCG needs to be planning around a gap of between 1m to 1.5m in QIPP savings. IBR August 2017 Paul referred to forecast of 83% - shortfall of 800k with risk of a further 800k 6 months to deliver 1m need a plan to achieve it. Realistically there is a need to reduce costs 1m to 1.5m through the following schemes: Procedures of Low Clinical Value (PLCV) Prescribing Better Care Fund (BCF) Acute Visiting Service (AVS) Joint Health Musculo-Skeletal (MSK) possibly overachieve on this scheme George Hurst gave a presentation entitled Estates Opportunities. A copy of the slides to be circulated. The slides covered the following: 28 September and feedback to the committee at the next meeting Update on recruitment to new post Update on PLCV Slides to be circulated to the committee Claire Heneghan Paul Kingan Pauline Webster Which property does the CCG pay for Property costs ODGH QIPP Opportunities Estate Strategy Implementation
196 There was a discussion around buildings which are under-utilised / disused on the ODGH site. Both the S&O Trust and CCG incur costs for these buildings and both organisations support rationalisation once services can be relocated. George informed the committee that the NHS Property Services Disposal policy was published recently which clarifies the process for demolishing buildings which are no longer needed. Item 6 Prescribing QIPP Proposals George in his capacity of Estates lead was requested by the Committee to write a letter today to NHS Property Services on behalf of West Lancs CCG, indicating that the CCG support the demolition of these buildings. February 2018 is the cut-off date and if things go ahead as planned which would allow the CCG to recognise a cost saving in the 2017/18 financial year. Nicola Baxter gave a presentation entitled Prescribing QIPP - Prescribing Hub update. A copy of the slides will be circulated. The slides covered the following: Letter to go to NHS Property Services Slides to be circulated to the committee George Hurst Pauline Webster Prescribing Risk Impact of the waste campaign The Emerging Picture The Workplan Prescribing Hub Proof of Concept Nicola gave an update describing the reasons for the risk in terms of the prescribing growth for West Lancs CCG which post waste campaign November 2016 was 10% higher than national growth and 4% higher than the same period last year. The committee had a discussion around drugs that have increased significantly in price, one particular drug has recently came off patent and is now classed as Category M, however, any Category M windfall savings will go back to NHSE. The significant increases in other drugs will remain a risk for the CCG. Medicines optimisation have a workplan in place/ waste campaign which has had an impact in terms of a reduction in costs. However, there is currently an investigation into a community Paul Kingan
197 pharmacy due to an significant increase in dispensing from May to June 2017 which potentially looks like the pharmacy has had a duplicate payment in June. Costs and numbers dispensed are around double. This will be further discussed in the Audit Committee meeting today. Nicola gave an update on the Prescribing Hub pilot scheme in Skelmersdale Family Practice. The Prescription Ordering Direct (POD) concept is part of the waste campaign. Nicola discussed the potential savings with the committee and described the added benefits for the patients, GP Practices and the CCG. Nicola talked about issues with over ordering and what is being ordered and what should have been stopped. NHSE advise is that Medicines Optimisation should meet with the area manager. Community Pharmacy dispensing increase to be discussed at Audit Committee today Nicola asked the committee for their recommendation to extend the scheme to neighbouring practices; Burscough and Ormskirk. Nicola ran through the set up costs for the 3 prescribing Hubs. The scheme is being supported by the medicines optimisation project manager, within existing team costs. 2 Band 4 technicians are being recruited to support the role out and continue support. If the hubs are rolled out to Burscough and Ormskirk, the CCG will need to look at the rooms in the premises and will require investment into IT resources i.e. computer kits. The committee took a vote and gave their recommendation. This will be taken to the Governing Body on 26 September 2017 for final approval. Referral issues around Procedures of Limited Clinical Value (PLVC) has been discussed at previous meetings. The Federation were asked to draft a plan on how Primary Care can address this. One option was to explore the Blueteq system operating across Sefton. Final Approval at Governing Body Slides to be circulated to the committee Nicky Baxter Item 7 Blueteq Service and System Prior Approval process Prior Approval is a process and a system to identify and authorise PLVC. Currently the PLVC policies are currently under review and being updated. Pauline Webster
198 Jonathan Roberts Prior Approval Case Manager, Midlands and Lancashire Commissioning Support Unit gave a presentation on the Prior Approval Service. A copy of the slides will be circulated. The slides covered the following: What is Prior Approval The Steps involved An Eligibility criteria flowchart What BlueTeq system looks like Benefits to GPs The CSU have taken a hard line stance and will challenge procedures that should not be carried out if they do not meet the eligibility criteria. The Prior Approval system/blueteq system was trialled last year and has been installed and implemented in NHS South Sefton, Southport & Formby CCGs. Q & A s Q. Can this system be run alongside Choose and Book system? A. Yes Q. Does the system generate patient information leaflets? A. Yes Q. What savings have been made? A. Currently there is no data available as the CSU is still reviewing month 1 position As the committee require more information/data on cost savings they were unable to make a recommendation. Jonathan has been asked to return to Finance & QIPP meeting in December and possible present at a future Membership meeting. Peter Grebory to invite Helen Fogg to the next Finance & QIPP meeting in October to discuss what can Primary Care do about the system. Prior Approval / BlueTeq system to be on December meeting agenda Invite Helen Fogg to next meeting Paul Kingan Peter Gregory
199 Item 8 - AOB Care Homes reducing admissions/proactive care due to time constraints/meeting running over time- this will be discussed at the Clinical Executive meeting on 19 September OWLs issue with VC re IT maintenance. CCG to investigate To be discussed at Clinical Execs 19 September 2017 OWLs IT kit John Caine Jackie Moran Next Meeting The next meeting will take place on Tuesday 3 October 2017.

200 Finance & QIPP Notes and Actions 3 October 2017 `Item Discussion and decisions Actions Responsible officer Attendees Chair Mike Maguire Chief Officer Paul Kingan Chief Finance Officer Peter Gregory GP Executive Lead Bapi Biswas GP Executive Lead Stephen Gross Lay Member Rakesh Jaidka - GP Executive Lead Vikul Mittal GP Executive Lead Doug Soper Lay Member Pauline Webster Administration Officer Adam Robinson Secondary Care Consultant Karen Tordoff Lead Manager Service Redesign Due Date In Attendance Apologies Nicola Baxter Head of Medicines Optimisation Paul Jones Head of Finance Matt Greene Finance Manager Joanne Kane Administration Officer Helen Fogg Federation Manager Dr Mark Johnston NHS RightCare Delivery Partner Debbie Dobson Practice Manager Jo DeBacker Practice Manager Linda Riley Director of Clinical Services, MLCSU Debbie Jackson Head of IPA Commissioning, MLCSU Linda Dobbing - Head of IPA, Complex Services, MLCSU Claire Heneghan Chief Nurse Jack Kinsey GP Executive Lead Jackie Moran Head of Contracting, Performance & Quality Greg Mitten Lay Member John Caine Chair
201 Declaration of Interest Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: Declaration of Interest Declarations of interest from sub committees; None declared. Declarations of interest from today s meeting; Peter Gregory GP Exec is a Director West Lancashire GP Federation OWLS CIC and all GP Execs declared an interest in: Item 6 - Procedures of limited clinical value (PLCV) in Primary Care as they are either current or potential providers. The Chair deemed this as significant but not fundamental but as there was no decision to make Peter and all GP Execs were allowed to take part in the discussion. Item 3 Notes from previous meeting 1 August / matters arising / summary of actions The committee reviewed the draft notes for ratification. The note were agreed as an accurate record subject to removing a sentence under Item 4 QIPP Plan Overview and early forecast. Matter arising/summary of actions: Acute Visiting Service Paul Kingan gave a verbal update on behalf of Jackie Moran. Jackie raised the issue of the service data showing that the service is underperforming and underutilised at the Transition and Transformation on 28 September with Virgin Care (VC). VC are well aware of the issues and are putting measures in place to improve uptake and are liaising with North West Ambulance Service (NWAS). Karen Tordoff informed the meeting that the first subgroup of Transition and Transformation Board is meeting next week which has been set up to discuss issues in more detail. Karen will feed back to the committee at the next meeting in November. Transition and Transformation subgroup feedback Karen Tordoff
202 Recruit new post Head of Integration of Health and Social Care still pending Estates Buildings under-utilised/disused on the ODGH site Paul Kingan gave an verbal update on behalf of George Hurst. NHS Property Services have formally given written notice to services to vacate the buildings. They are currently working with VC regarding the plans to move the Child Development Centre to Hillside and Diabetes centre around the option appraisal with VC re model of care and longer term options. As George was not present to inform the committee of the time scales involved Paul Kingan will enquire on time scales and feedback to the committee at the next meeting. Prescribing Hub scheme extension Nicola Baxter informed the committee that the extension was given final approval at the Governing Body on 26 September 2017 to roll out Hubs to Burscough and then Ormskirk. Concerns were raised around moving the Hub model to Ormskirk due to existing similar models in Practices so there may be some resistance/challenges. Discussions around this was to establish the Hub in Burscough first and see how that goes before rolling out to Ormskirk. Nicola will keep the committee informed of progress. Pauline confirmed that she has circulated the presentation slides from the last meeting. Nicola Baxter tabled a report on Community Pharmacy Irregularities relating to the Community Pharmacy increase in June Nicola discussed possible reasons for the spike in dispensing costs in June and given the information available from the Pharmacy it is unlikely that they gain much further insight without an investigation by internal audit. The committee agreed the next steps as outlined in the report. Nicola to update the committee on any progress. The report will be circulated with the notes for information. Blueteq service and system Pauline has invited Jonathan Roberts to the meeting on 5 December 2017 and has circulated the presentation slides. Care Home reducing admissions/proactive care was discussed outside this meeting at the Clinical Execs on 19 September Recruit new post update next meeting Estates time scales Community Pharmacy Claim irregularities Nicola to update on progress Report to be circulated electronically to the committee with notes Claire Heneghan Paul Kingan Nicola Baxter Pauline Webster Ongoing
203 OWLs IT issues still not resolved. Helen Fogg and Rakesh Jaidka to details to Mike Maguire to raise with VC Chief Executive Officer (CEO). Mike Maguire Rakesh Jaidka / Helen Fogg Item 4 QIPP Plan Overview and early forecast Item 5 NHS Rightcare Paul Kingan gave a verbal update: 5 months to deliver 1m. Shortfall on non-electives day reflections delivered via the community contract. Realistically there is a need to reduce costs 1m to 1.5m through the following schemes: Procedures of Low Clinical Value (PLCV) Referrals/contract challenges Prescribing Prescribing Hubs going well Better Care Fund (BCF) - Acute Visiting Service (AVS) Joint Health Musculo-Skeletal (MSK) possibly overachieve on this scheme Pain policy has changed which will affect a cohort of patients. S&O NHS Trust reviewing patient lists and are liaising with Renecres Hospital. This issue is being discussed at the next Clinical Executive meeting on 10 October NHS RightCare is a national NHS England (NHSE) supported programme committed to delivering the best care to patients, making the NHS s money go as far as possible and improving patient outcomes. NHS RightCare has been rolled out across local health economies in England, with all clinical commissioning groups (CCGs) provided with a dedicated Delivery Partner to help support and implement the RightCare approach. This support is provided at no cost to CCGs, together with other tools and analytical support of NHS RightCare. For more information on NHS RightCare please click on this link
204 Every clinical commissioning group in England has an allocated Delivery Partner to help implement the NHS RightCare approach. Dr Mark Johnston, is NHS West Lancashire CCG dedicated NHS Right Care Delivery Partner to help support and implement the Right Care approach. For the last 6 months Dr Johnston has been working with Karen Tordoff, Jackie Moran and Matt Greene and Paul Kingan. The CCG has been focusing on 3 programmes, MSK, Pain and Respiratory and these have been submitted to NHS RightCare. Dr Johnston gave a verbal update on the submissions which have been formally signed off by him and NHSE. Dr Johnston commented of the high quality of the submissions and plans that are in place and is also supporting between 8-15 CCGs in the peer group and rated West Lancashire CCG in the top 5 of this peer group. Dr Johnston acknowledged that West Lancashire CCG had limited further opportunities than other CCGs as it was not a significant outlier for most areas. In addition to the Programmes the CCG has identified, Dr Johnston informed the committee of further opportunities that warrant further investigation from the indicative data: Cancer in relation to Haematological admissions and high cost drugs (highest spend in peer group) Cardiovascular Disease (CVD) in relation to coronary heart disease in terms of variation against peer group. Opportunities in primary care secondary prevention in atrial fibrillation (AF) Gastroenterology in relation to spend being more than peer group and paediatric admissions coding issues. Genito-urinary (GU) in relation to financial opportunities around excessive admissions and procedures of limited clinical value (PLCV). Dr Johnston will send the CCG the NHS RightCare, commissioning value data and intelligence focus packs for the above opportunities. Focus packs Dr Johnston Post meeting note: Focus packs received
205 Dr Johnston will continue to work with and meet with the CCG team regarding the additional opportunities identified. Post meeting note: meeting set up for 23 November 2017 Paul Kingan thanked Karen, Jackie and Matt for all their hardwork so far with the submissions. Meeting to be set up Karen Tordoff Item 6 Procedures of Limited Clinical Value (PLCV) in Primary Care Peter Gregory lead a discussion around how they can resolve issues around patient referrals for PLCV in Primary Care. Suggestions included: Training schemes and empowering staff including Locums or appoint a designated person in GP Practice to oversee/review referrals and not proceed with referrals that are deemed as PLCV but this will have implications with Choose and Book system in place and that some GP may oppose an anonymous person stopping referrals going through. Locality models were discussed and localities working together Limited time with patient computer systems are in place with pop up menu so that GP can look at a glance/emis templates which automatically print out patient self-care leaflets when criteria does not meet the need for referral at that stage. Peter Gregory, Helen Fogg to present a draft scheme proposal at the next meeting. Bapi volunteered Jill Foster Practice Manager to help with this. Matt Greene to look at finance aspect. Draft Scheme Proposal Peter Gregory / Helen Fogg / Jill Foster / Matt Greene Item 7 Individual Patient Activity Linda Riley Director of Clinical Services, Debbie Jackson, Head of IPA Commissioning and Linda Dobbing,Head of IPA, Complex Services from Midlands and Lancashire Commissioning Support Unit jointly presented slides IPA/CHC QIPP. Slides to be circulated with notes Pauline Webster Linda lead the presentation and gave the background to IPA QIPP covering the methodology. Linda referred to a slide to savings against
206 plan specifically for the CCG and explained that QIPP reviews are quality-led and not financially-led so there is no target as such. The majority of reviews have been found to be appropriate and no changes recommended. Further QIPP opportunities have been identified in relation to an area where the CCG is slightly worse than national average is number eligible for CHC per 50k population. Based on Deloitte/ NHSE STP report conversion rate to eligible is better than the national average. Average CHC package costs are lower than national average and other recent work has shown that Lancashire, average CHC care packages cost around 100 per week lower than the national average. Other QIPP opportunities identified include; Review of FNC, Market Management, Care Brokerage, Reviews, Case Management and Personal Health Budgets (PHB). Mike asked the IPA team to work with the CCG team (Claire Heneghan, Charlotte McAllister and Paul Jones) and put together a Business Case bespoke to the CCG and present the proposal to the meeting in December. Business Case Linda Riley Linda Dobbing Debbie Jackson Item 8 - AOB There was no any other business discussed Next Meeting The next meeting will take place on Tuesday 7 November 2017.
207 Minutes Quality and Safety Committee Venue: Boardroom, Hilldale, Ormskirk Date & Time: Tuesday 24 October 2017 at pm Attendees: In attendance: Mr G Mitten Chair Miss C Ashcroft Executive assistant Dr J Kinsey GP lead Mrs G Godson Director, Healthwatch Lancashire Mrs J DeBacker Practice manager Mrs L Burton Designated lead nurse for safeguarding Ms C Tomlinson - Infection prevention and children control specialist nurse Mrs A Lumley Nursing and clinical quality lead Mrs J Moran Head of quality, performance Mrs K Atkinson - Deputy designated professional for and contracting safeguarding adults and MCA Mrs Claire Heneghan, Chief nurse Mr M Giannini Communications manager Mrs C McCabrey Senior Service Redesign Manager - from item 5c Apologies: Mrs L Elliott Lead nurse for safeguarding adults and mental capacity act (in attendance) Mrs A Sathiyanathan Quality assurance manager (in attendance) Dr R Jaidka GP lead Dr P Gregory GP lead Agenda Summary of Discussion Item CCGQIC 10/17/1 Welcome and apologies for absence Greg Mitten chaired the meeting and welcomed the members of the Quality and Safety Committee to the meeting. The apologies above were relayed. Lead 10/17/2 Declaration of interest Greg Mitten reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of West Lancashire CCG. Declarations declared by governing body members are listed in the CCG s Register of Interests. The register is available either via the secretary to the governing body or the CCG website at the following link: No declarations of interests were declared at the meeting. 10/17/3 Minutes from the previous meeting on 27 June 2017 The notes from the previous meeting were approved as a correct record of the meeting, with one amendment as follows: Page 3, Infection Control, Ecoli bacteraemia Carley Thompson should read Carley Tomlinson. 10/17/4 Matters arising action sheet The action sheet was updated. Quality and Safety Committee 24 October 2017 Page 1 of 7
208 Agenda Summary of Discussion Item CCGQIC 10/17/5 Patient Improvement The committee agreed that a separate report by exception for mental health would be helpful for future meetings. Lead a. Acute care quality agenda / quality assurance including mental health The key points raised (by exception) included: issues with staffing levels at Southport and Ormskirk Hospital NHS Trust (the Trust) across all specialities and specifically the maternity unit. CCGs, NHSI and NHS England are working with the Trust. The mortality data (SHMI) has been established. The deep-dive shows significant actions have been completed eg moving a theatre to the Ormskirk site. One case of MRSA had occurred in September. A few instances of delayed mental health assessments at Southport A&E have taken place. The Executive Committee had discussed waiting times for ADHD services and required a turnaround. Eating disorder services have no medical cover in the paediatric ward at Ormskirk. Greg Mitten confirmed that the Executive Committee had discussed the quality issues that day and a report will be escalated to the Executive Committee for a further decision. b. Primary care quality agenda / quality assurance The report was felt to be useful as it is also shared with NHS England and the key issues were raised. Practice data has been shared during practice visits. One prescribing practice is an outlier and a meeting with medicines optimisation has been arranged. Work on incident reporting and root cause analysis is taking place with NHS England, to develop a best practice model, which will be rolled out. The re-procurement for Viran Medical has commenced to follow the 18-month caretaker contract. A quality impact assessment will be undertaken. The CCG has established a Primary Care Commissioning Committee (PCCC) and a new reporting flow chart. Any primary care item which is not quality-related will go to the PCCC. c. Transition of community and urgent care services / quality assurance The Transition and Transformation Board (TTB) is a contractual meeting, which focuses on quality and performance with a Transitional sub-group focusing just on transformation. Allison Sathiyanathan attends the quality and performance meeting with Virgin Care sub-group of the TTB. Statutory and mandatory training has been undertaken, although affected by the cyber-attack, has now achieved 42%. A legacy serious incident case transferred from the community is ready to close. Three new appointments have been made: tissue viability nurse, medicines optimisation lead and communications manager. The posts are not all full-time and more appointments will follow to include IV therapy staff. Virgin care have completed their safeguarding training. The report should be titled Community and Urgent Care Services. d. Patient and participation CCG assessment The paper outlined the new approach to the assessment of patient and public participation. Assessment will be different in terms of CCG engagement and adhering to guidelines with the CCG more open to scrutiny. Quality and Safety Committee 24 October 2017 Page 2 of 7
209 Agenda Summary of Discussion Item CCGQIC 10/17/6 Safety 1. Integrated business report (IBR) Jackie Moran reported on the highlights from the IBR as follows: Work is focussing around musculoskeletal, pain and respiratory services. The next Membership Council will focus on respiratory with Virgin Care attending. Improved Access to Psychological Therapies the targets must be met to avoid challenges. Cancer targets targets continue to be missed, due to diagnostic bottlenecks and ECGs waits. The Trust are assessing where the bottlenecks are and whether MRI and CT scans could be provided in the community. Falls car this is in place and benefits should be achieved. Virgin Care have made some changes to improve the Acute Visiting Service (AVS) and are taking on their own employed staff. This means that they will now be able to develop better relationships with the NWAS teams to facilitate divert away from A&E as confidence in the AVS service develops thus helping to reduce conveyance and thus reduce ambulance turnaround times. Mixed sex accommodation this is an issue with critical care and stroke units, however it is anticipated that the stroke service will move to a larger ward where it will be possible to flip wards and have a separate rehabilitation ward. This will be discussed further at a future meeting. From a homecare perspective, Gail Godson stated there has been positive patient feedback. Mortality rate Following the Trust s issue with mortality data being incorrectly counted, this has now been resolved with a new figure of 116, which is high. Greg Mitten acknowledged the mortality rate which had been raised three years previously by the Quality and Safety Committee. Lead It was highlighted that west Lancashire only receive 7 hours of support from the Stroke Association, who with more hours could support an early associated stroke discharge. A meeting is needed with Carol McCabrey and Jackie Moran regarding the current specification and going forward. 2. Serious untoward incident report (SUI) June to September 2017 There is still an issue with the timeframe for reporting SUIs and root cause analysis (RCA). The committee agreed that a summary of future multiple reports would be welcome. The poor information within the reports from the Trust had been raised at a recent Collaborative Commissioning Forum and it was agreed that this should be raised. Safeguarding are providing oversight and review of any related SUIs. AS 3. Safeguarding children, young people and adults at risk i. Children s and Adults policy The policy has been updated with current legislation and guidance in consultation with pan-lancashire CCG Designated Leads. The key changes were highlighted as follows: Guidance on appropriate behaviours have been added. Female Genital Mutilation (FGM) has been added to the physical abuse category and child sexual exploitation has been added to the sexual abuse category. Prevent and Care Act sections have been strengthened. Much work has been undertaken to revise and streamline the safeguarding standards for Quality and Safety Committee 24 October 2017 Page 3 of 7
210 Agenda Item CCGQIC Summary of Discussion small and large providers and care homes (see appendices). A discussion took place in respect to child protection information sharing system (CP-IS), which is a national system where health is linked with children social care for example when a child presents at an unscheduled care setting CP-IS will identify if the child is a looked after child and subject to a child protection plan. When a child presents at an unscheduled care setting there is a system which will identify if the child is a Looked after child and subject to a child protection plan. The policy will be presented at the governing body on 28 November 2017 for ratification before being embedded into the contracts. Positive feedback had been received from smaller providers on the support provided on safeguarding. There was a discussion around FGM reporting and how robustly it is embedded within West Lancs. Jackie requested more data around children subject to CP plans and categories including CSE. In September there were 76 children subject to child protection plans. This information will be reported in the safeguarding activity report in future. The Quality and Safety Committee - approved the annual report and recommended its ratification at the Governing Body. ii. Safeguarding annual report The report highlights national changes and local developments, achievements and priorities for the year ahead. The CCG target audience for safeguarding level 2 training has been reviewed in line with the Intercollegiate document There are no concerns in terms of delivering the priorities, although timescales may not always be met. The Quality and Safety Committee - approved the annual report and recommended its ratification at the Governing Body. iii. Safeguarding activity report The report provides an update on safeguarding developments taking place across the health economy of West Lancashire. The following amber rated issues were highlighted: a. One care home in West Lancashire is in quality improvement process(qip). Another home previously in QIP is still being monitored. b. An online survey to primary care is taking place in response to findings of the Lancashire Safeguarding Children s Board (LSCB). Unfortunately, there have been no responses received from West Lancashire. Further discussions highlighted that the link to the survey may not have been circulated in error, this has been rectified. Alison Lumley requested to be copied into future articles published in the GP newsletter. Lead A meeting had already taken place with Peter Gregory regarding the plans for introducing the GP champion / lead model and a launch date will be agreed after a meeting with Peter Gregory on 31 October. Quality and Safety Committee 24 October 2017 Page 4 of 7
211 Agenda Item CCGQIC Summary of Discussion c. It was highlighted that an issue remained with the quality and timeliness of initial health assessments, exception reporting is provided to the CCG. To fully review the process with all local agencies, a workshop is taking place in Chorley and Preston 17 November with a view to undertake a similar process in West Lancashire. Feedback will be provided. d. Sudden Unexpected Death Child Service a steering group has been established to support the existing provider in plans for extending the current service. This was following a SUDC evaluation commissioned by CDOP noting that out of hours compliance with Working Together needed strengthening. A timeframe for implementation will be developed by the provider service. e. FGM there is a recognised gap in local service provision to support girls who have undergone FGM. This has been raised regionally. Trust House a specialised counselling was mentioned, it is a service in Preston, however it is unknown what services they offer at this time iv. Children and Social Work Act 2017 The report provided an overview of the Act and implications for the CCG. There is limited supporting information on the timescales for introduction of the different elements of the Act and there is no supporting guidance at this time. The LSCBs are being abolished and local Safeguarding Partners (CCGs, Local Authorities, chief officer of police) will need to form local safeguarding partnership arrangements. Various changes were highlighted including: Serious Case Reviews being replaced by Child Practice Reviews and a National Panel being established and the Department of Health will now lead on child death reviews as opposed to the Department of Education. Working Together guidance is being revised and a consultation will be launched in the near future. v. Managing risk around identification and prioritisation of Court of Protection referrals The report requires a decision on how we manage the DoLs in a community setting, which need to be authorised by the Court of Protection (COP). Work with the local authority assessed the prioritisation of risk. With a COP prioritisation tool has been successfully piloted by the local authority. It was felt that the report should be presented at the Executive Committee prior to Governing Body approval. Jackie Moran will discuss with Kristy Atkinson and Claire Heneghan before a recommendation can be made. 4. Care home report Kristy Atkinson had mentioned the two care homes in terms of QIP. The report provided a summary of where homes are, in respect of CQC ratings and provides an update where contracting meetings are involved. Lead JM / CH / KA 5. Infection prevention and control i. Lancashire Infection Prevention Team report Q1 Carley Tomlinson offered to pass on any questions about the report to Anita Watson. Quality and Safety Committee 24 October 2017 Page 5 of 7
212 Agenda Item CCGQIC Summary of Discussion ii. HCAI report Q2 Carley Tomlinson highlighted the key points from the report: The data has been reported for the CCG, Southport and Ormskirk Hospital NHS Trust (S&O), Aintree University Hospitals and Wrightington, Wigan and Leigh NHS Foundation Trust (WWL). MRSA bacteraemia no cases reported for the CCG to date this year. The acute Trusts have each reported one case to date. C. Difficile infection there have been 14 cases to date for the CCG, against a trajectory of for S&O, 38 for Aintree and 18 for WWL. Under lapses in care, there is one case of a non-acute CDI outstanding, which will be discussed at the December Post Infection Review meeting. A running total of cases will be included in the next report. MSSA there is no trajectory, but numbers of cases to date are 10 for the CCG, 4 for S&O, 17 for Aintree and 6 for WWL. E. coli cases recorded to date are 41 for the CCG, 17 for S&O, 33 for Aintree, 10 for WWL. Outbreaks in care homes outbreaks of diarrhoea and vomiting have been reported in four homes in west Lancashire in quarter 2. Support and advice are provided. Horizon scanning - an antibiotic passport/report is being developed and will be piloted with a GP practice, pharmacy and care home. Jane Mastin is working on the sepsis strategy. A comment will be passed on to Jane regarding involvement of Southport and Formby CCG as west Lancashire patients flow to Sefton. A draft E. coli strategy has been developed. A Care Home Conference had been well attended. Care home infection prevention is still going ahead. At a practice manager meeting, PPE concerns were raised and two GP practice visits have been arranged to audit IPC within the practice. 6. Prescribing report The report demonstrates the activity of the medicines management team. A QIPP savings value of 900,000 had been set, with a current forecast outturn of - 109,946. The medicine co-ordinators visit and support care homes and GP practices to try to deliver the savings. There is focus on the prescribing hubs, which look at systems on the prescribing journey. Skelmersdale Family Practice has created a safe environment for patient queries and more practices will be brought on board. There are prescriptions on the spine, which are not being filled on a consistent basis. Optimize is a safety net tied back into medicines management formulary. There are only three practices in the Ormskirk neighbourhood not on Optimize. Three practices have been identified to bring into the hub to address this. In response to a question, Nic Baxter explained that NHS Pharmacy To You, is an internet pharmacy which is not endorsed by the NHS. The pharmacy cannot always fulfil the prescription as it is based remotely. Nic Baxter will look into this and other internet pharmacies. Lead 7. Chief nurse This item was deferred. 10/17/7 Patient Experience Marco Giannini reported on the key issues from Patient Engagement Group as Quality and Safety Committee 24 October 2017 Page 6 of 7
213 Agenda Item CCGQIC Summary of Discussion follows: In Quarter 1, significant engagement work took place around the Viran Medical Centre, with responses from 411 patients received via the Trust, West Lancashire CVS and Healthwatch Lancashire. Complaints received by the Trust had reduced by 23% overall in from the previous year. Lead 10/17/8 Other a. Quality risk register The risk register will be collated at a workshop in between committee meetings and return to the January meeting. A brainstorm to ensure all aspects are caught will be included. b. Quality impact assessment (QIA) The reason for the QIAs being presented at the committee was unclear. An alternative could be online decision making. A decision whether they should be presented at the meeting will be brought to the next committee. 10/17/9 Minutes of meetings: Southport and Ormskirk Collaborative Commissioning Forum June and July 2017 Southport and Ormskirk Contract and Clinical Quality Review meeting May and July 2017 Southport and Ormskirk Executive Improvement Board July 2017 JM AL / AS Reports for information: Exception report August and September 2017 Quality and Performance Report continuing healthcare and independent sector mental health The Quality and Safety Committee noted the meeting notes and reports. 10/17/10 Any other business Gail Godson confirmed that the Chair of Healthwatch Lancashire had resigned and will take up a new role as a non-executive for the Sustainability Transformation Partnership. Best wishes were relayed to Mike Wedgeworth. Date and time of the next meeting Quality Group - Tuesday 28 November 2017 at pm, Boardroom, Hilldale Quality and Safety Committee Tuesday 23 January 2018 at pm Quality and Safety Committee 24 October 2017 Page 7 of 7
214 West Lancashire CCG Clinical Executive Committee Action and Notes 12/09/2017 Key Attendance Record of Attendance Non-Attendance (sickness, holiday, unknown) Attended meeting on behalf of CCG Member Adam Robinson T H Bapi Biswas Claire Heneghan H Debbie Dobson H H Doug Soper Greg Mitten H H H Jack Kinsey CL H H Jackie Moran H H Jo Debacker John Caine H H Mike Maguire H H Paul Kingan H Peter Gregory H Rakesh Jaidka H Vikul Mittal H Steve Gross H H 1
215 Item Discussion and decisions Actions Responsible officer Attendees Chair Jack Kinsey GP Executive Lead Due Date Bapi Biswas GP Executive Lead Debbie Dobson Practice manager Greg Mitten Lay Member Jo Debacker Practice Manager Anne-Marie Bridge Administration Officer John Caine WLCCG Chair Mike Maguire Chief Officer Peter Gregory GP Executive Lead Paul Kingan Chief Finance Officer Rakesh Jaidka - GP Executive Lead Stephen Gross Lay Member Vikul Mittal GP Executive Lead Doug Soper Lay Member Jackie Moran Head of Quality Performance & Contracting In attendance Apologies Declaration of Interest Jan Charnock - Primary Care Development Manager Karen Tordoff Lead Manager Service Redesign Laura Anton Graduate Management Trainee Adam Robinson Secondary Care Consultant Claire Heneghan Chief Nurse Mike Maguire reminded committee members of their obligation to declare any interest they may have on any issues arising at Clinical Executive Committee meetings which might conflict with the business of NHS West Lancashire Clinical Commissioning Group. Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: Declaration of Interest Declarations of interest from sub committees; 2
216 None declared. Declarations of interest from today s meeting; All GPs declared an interest in Item 6 Care Homes reducing admissions/proactive - what we do for this winter? Mike decided that the interest was significant but not fundamental. At this stage, all GPs take part in the discussion. Item 3 Primary Care Development/ Conflict of Interest E-meeting NHS England (NHSE) have corresponded with all GPs and the CCG in relation to 1 per head for the development of locality/neighbourhood working. OWLS federation have corresponded with the GPs and offered to act their behalf with the use of the monies. This has led to some confusion between OWLS and the CCG with regards to how the two parties thought these funds should be handled. The CCG subsequently asked OWLS to pause this process so discussions and clarification could be sought. After early discussion, it came to light that the correspondence from NHSE can be interpreted in different ways. The CCG were under the impression that this money was to go towards the transition and development of locality working and would be distributed by them. OWLS had read the correspondence as the money would go directly to the GPs. It was agreed that the first non-recurrent allocation should be used to support infrastructure for Primary Care at scale in line with one of the NHSE documents. Moving forward the recurrent allocation should be used to support progress across levels of neighbourhoods. Further discussion took place of how both parties felt that there was a definite need to show a united front to enable the development of localities and the transformation of primary care. In order to help advance this it was agreed that the membership meeting to be held on 14 September 2017 would be presented by both the CCG and OWLS to encourage the membership to move forward with locality working. Item 4 - Feedback from JCCCG Deferred to next meeting. 3
217 Item 5 Technology in Dermatology Item 6 Care homes reducing admissions/ proactive care what do we do for this winter? Item 7 Tranche 1 Policies Item 8 - Adoption policy Item 9 Notes from previous meeting Deferred to next meeting. Deferred to next meeting. All approved. Approved Agreed as correct record Next Meeting The next meeting will take place on Tuesday 19 September
218 West Lancashire CCG Clinical Executive Committee Action and Notes 19/09/2017 Key Attendance Record of Attendance Non-Attendance (sickness, holiday, unknown) Attended meeting on behalf of CCG Member Adam Robinson T H Bapi Biswas Claire Heneghan H Debbie Dobson H H Doug Soper Greg Mitten H H H Jack Kinsey CL H H Jackie Moran H H Jo Debacker John Caine H H Mike Maguire H Paul Kingan H Peter Gregory H Rakesh Jaidka H Vikul Mittal H Steve Gross H H 1
219 Item Discussion and decisions Actions Responsible officer Attendees Chair Peter Gregory GP Executive Lead Due Date Adam Robinson Secondary Care Consultant Bapi Biswas GP Executive Lead Debbie Dobson Practice manager Jack Kinsey GP Executive Lead Jo Debacker Practice Manager Joanne Kane Administration Officer John Caine WLCCG Chair Mike Maguire Chief Officer Paul Kingan Chief Finance Officer Rakesh Jaidka - GP Executive Lead Stephen Gross Lay Member Vikul Mittal GP Executive Lead In attendance Item 5 - Dermatology Case for change Apologies Declaration of Interest Jan Charnock - Primary Care Development Manager Karen Tordoff Lead Manager Service Redesign South Sefton Clinical Commissioning Group Karl McCluskey Chief Strategy and Outcomes Officer Judith Neilson - Service Implementation Manager, Liverpool CCG Christine Randall - GP, Cumberland House Surgery, GPwSI in Dermatology Claire Heneghan Chief Nurse Doug Soper Lay Member Greg Mitten Lay Member Jackie Moran - Head of contracting, performance and quality Peter Gregory reminded committee members of their obligation to declare any interest they may have on any issues arising at Clinical Executive Committee meetings which might conflict with the business of NHS West Lancashire Clinical Commissioning Group. Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: 2
220 Declaration of Interest Declarations of interest from sub committees; None declared. Declarations of interest from today s meeting; The chair was passed from Peter Gregory to Mike Maguire for a decision on the declaration of interest. All GPs declared an interest in Item 4 Technology in Dermatology, as GPs have potential to be providers in the future. As no final decision is to be made today and clinical input into the discussion is necessary the interest was decided to be significant but not fundamental. All GPs will be allowed to take part in the discussion. For Item 6 Care Homes reducing admissions/proactive - what we do for this winter? All GP members declared an interest. Mike decided that the interest was significant but not fundamental. At this stage, all GPs can take part in the discussion as there is no decision to be taken today. However, the chair will pass to Mike for the duration of both items and back to Peter Gregory to chair for the remaining items. Item 3 Feedback from JCCCG held on 7 September 2017 Operational Paul Kingan presented a short film shot at the last Joint Committee of Clinical Commissioning Groups (JCCCG). The film focussed on Urgent Care and Mental health and getting agreement on strategy. Discussion followed on delegation and what is and is not delegated. There was no final agreement reached on the scope for mental health commissioning. Tier 3 IAPT is expected to be an area of difficulty. It was noted that no details are yet agreed. The JCCCG is just finding its feet, how this relates to the STP is also unclear. Progress will continue to be reported back to the Exec Committee. Item 4 Technology in Dermatology Strategic & Service Redesign The chair passed to Mike Maguire for this item. Mike presented this item which highlights the potential to use technology to mitigate problems in dermatology access. WLCCG has approached a university 3
221 Item 5 Dermatology Case for change about a published paper about the success rate of artificial intelligence for moles in Dermatology. The algorithm checks their database containing skin disease images that are used to visually diagnose skin lesions. Tests so far show the algorithm matched dermatologist performance in identifying lesions. The university is ready to build an app and have approached venture capitalist to fund its development. Mike invited discussion on whether WLCCG would like to be involved in a pilot. The Exec committee raised what safeguards and cautions are built into the system, the algorithm is biased towards caution. GPs asked if the app provides a sequential history of change or a detailed history. The AIs accuracy increases as more data is received and the algorithm learns. The Committee agreed in principle to be involved in using this technology providing further assurances on checks and balances are sought, especially regarding Information Governance and ethics. The chair passed back to Peter Gregory for the next item. Karl McClusky, Judith Neilson and Chris Randall attended to present on their Dermatology Case for Change which is a collaborative approach to capacity issues in dermatology. Karl began with the background of this scheme. This was instigated approximately 12 months ago when several dermatologists left the Sefton area at the same time, recruitment was a struggle and referrals were closed. A Dermatology Review group was established to map and understand current provision. The group found that across the board there was a similar struggle to provide a sustainable quality service. There was no consistency in the way dermatology was commissioned and providers offered differing services. The thinking behind the Case for change model is that the consultant led model is no longer feasible and as such a four-tier clinical model has been proposed; 1. Self-care, community advice pharmacy etc 2. Management in primary care 3. Community Triage 4. Secondary Care Mike Maguire - add to a single item Exec Committee Agenda This model was taken to stakeholders at engagement events, where over 40 providers both NHS and private discussed the future model, looked for gaps and tested the model. From these several areas were identified for further work, these 4
222 were training, education and workforce. It was noted that Tele Dermatology will be utilised. Levels of activity and finance were then discussed, Sefton has outlined their assumptions that have been applied to current levels of activity, so from the current spend of 20 million there are expected to be 4.6 million saving across the sites identified. The committee then asked questions regarding the model, these included waiting times, if they had projected for increased demand, what consultant support was in place for GPSIs and the use of IT and innovation solutions. Sefton are now in the process of consulting with CCGs partners to secure agreement, which is needed by October. The next step would be procurement, the go live date being April The Exec Committee thanked Karl and colleagues for attending and will consider the proposal. Karl and colleague then left the meeting. It was agreed that further time would be needed to fully explore WLCCGs options. Following consideration of the two dermatology items on the agenda. It was agreed that WLCCG needed to explore what a modern primary care led dermatology service should look like. WLCCG should consider what we commission in the context of this work. Discussion to be scheduled for an hour on the 3 rd October. Item 6 Care homes reducing admissions/ proactive care what do we do for this winter? Hot Topic The chair passed to Mike again for the duration of the item. John Caine opened the discussion on the Care homes item. As winter is coming there is an urgent need to promote the enhanced care home scheme which would proactively reduce admission. There have been early schemes in place that have evidenced their effectiveness, the schemes have a QIPP element too that should be a focus. Clarity was requested on the role of GPs and Community services in reducing admissions. John confirmed while Virgin Care have a role, their approach and way of working is different. The proactive scheme proposed to date involves a weekly ward in Care homes, reviews on medications, falls, hydration and nutrition. The rounds also build 5
223 relationships with care homes, providing assurance and increasing their confidence in caring for the most vulnerable to admission. It was noted that much earlier planning was required and that there may be a need to increase use of AVS as a temporary solution while working on a longer-term scheme. Following discussion, it was noted that it had not been possible to reach agreement about the implementation of a proactive care home scheme. It was also noted that the conflict of interest for GPs had led to the issue becoming divisive at Membership. It was therefore agreed that the WLCCG officers should work up a proactive scheme for consideration, that the CCG would commission at the Primary Care Sub Committee. Item 7 West Lancashire CCG Constitution Item 8 - IBR Item 9 WLCCG Risk Register and GBAF Item 10 Notes from previous meeting E-meeting The WLCCG constitution was presented for comment prior to the Governing Body on 26 September. It was noted that there were no concerns raised regarding the constitution, this will now go to the Governing Body for ratification. The IBR was briefly discussed, there is an emerging issue regarding GP AU, more investigation into this will take place before next Tuesday s Governing Body where the IBR will be presented for ratification. The Risk Register and Governing Board Assurance Framework was then considered. There was a query regarding risks related to DoLs and whether these should form one amalgamated risk. Paul reported that at present these have been advised to remain separate however Claire will be consulted to reassess this on her return. The notes from the previous meeting were approved subject to the following amendment; Under Item 2 Declaration of Interest the notes should have stated that all GPs and Practice managers declared an interest in Item 3 Primary Care Development. As Chair Mike Maguire considered the interest which relates to funds potentially being given to practices or administered on their behalf. Mike, decided that the interests were significant but not fundamental. As item was for debate only with 6
224 any recommendations to be considered by the Primary Care Committee and the Governing body as required. In addition, the notes for this item states an agreement to use first chunk of nonrecurrent money will be to support infrastructure, however this should state a recommendation will be made to the Primary Care Sub Committee to use the first chunk of non-recurrent money to support infrastructure. Next Meeting The next meeting will take place on Tuesday 19 September
225 West Lancashire CCG Clinical Executive Committee Action and Notes 10/10/2017 Key Attendance Record of Attendance Non-Attendance (sickness, holiday, unknown) Attended meeting/course on behalf of CCG Member Adam Robinson T H Bapi Biswas Claire Heneghan H Debbie Dobson H H Doug Soper Greg Mitten H H H Jack Kinsey CL H H Jackie Moran H H Jo Debacker John Caine H H Mike Maguire H Paul Kingan H Peter Gregory H Rakesh Jaidka H Vikul Mittal H Steve Gross H 1
226 Item Discussion and decisions Actions Responsible officer Attendees Chair Peter Gregory GP Executive Lead Due Date Adam Robinson Secondary Care Consultant Bapi Biswas GP Executive Lead Jack Kinsey GP Executive Lead Jo Debacker Practice Manager Anne-Marie Bridge Administration Officer John Caine WLCCG Chair Mike Maguire Chief Officer Paul Kingan Chief Finance Officer Rakesh Jaidka - GP Executive Lead Vikul Mittal GP Executive Lead Doug Soper Lay Member Greg Mitten Lay Member In attendance Karen Tordoff Lead Manager Service Redesign Item 3 IAPT LTC Apologies Declaration of Interest Phil Winnard Mental Health Transformation Lead Laura Anton Project Manager Claire Heneghan Chief Nurse Jackie Moran - Head of contracting, performance and quality Debbie Dobson Practice manager Stephen Gross Lay Member Peter Gregory reminded committee members of their obligation to declare any interest they may have on any issues arising at Clinical Executive Committee meetings which might conflict with the business of NHS West Lancashire Clinical Commissioning Group. Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: Declaration of Interest 2
227 Declarations of interest from sub committees; None declared. Declarations of interest from today s meeting; The chair was passed from Peter Gregory to Mike Maguire for a decision on the declaration of interest. All GPs declared an interest in Item 4 Designing a modern primary care led dermatology/skin conditions service, as GPs have potential to be providers in the future. As no final decision is to be made today and clinical input into the discussion is necessary, the interest was decided to be significant but not fundamental. All GPs will be allowed to take part in the discussion. Strategic & Service Redesign Phil Winnard regarding the implementation of integrated IAPT for long term conditions. Phil highlighted the main points of the document and how this would concentrate on the long-term conditions of diabetes and COPD in the West Lancs area. After discussion there were several questions raised with regards to how the service would be delivered and funded. It was requested that more information was needed to support a decision to move forward and this would be brought back to the committee on the 24 th October Item 3 IAPT LTC Further information requested to come back to exec on 24 October 2017 Phil Winnard/ Paul Kingan Item 4 Designing a modern primary care led dermatology/ skin conditions service This session was a workshop for exec members to investigate options to design a modern primary care led dermatology/skin conditions service. E-meeting Item 5 Draft policy for assisted conception The draft policy for assisted conception was presented for comment. The policy was approved. 3
228 Item 6 - Grievance policy Item 10 Notes from previous meeting The Grievance Policy was presented for comment. It was clarified that there were not changes to this policy as it was only for review. There were no concerns raised and the policy was approved. The notes from the previous meeting were approved. Next Meeting The next meeting will take place on Tuesday 17 October
229 West Lancashire CCG Clinical Executive Committee Action and Notes 31/10/2017 Key Attendance Record of Attendance Non-Attendance (sickness, holiday, unknown) Attended meeting/course on behalf of CCG Member Adam Robinson Bapi Biswas Claire Heneghan H Debbie Dobson H Resigned Resigned Doug Soper Greg Mitten H H Jack Kinsey CL H H H Jackie Moran H H Jo Debacker John Caine H H Mike Maguire Paul Kingan H H Peter Gregory H H Rakesh Jaidka H H H Vikul Mittal H H H Steve Gross H 1
230 Item Discussion and decisions Actions Responsib le officer Attendees Chair Peter Gregory GP Executive Lead Adam Robinson Secondary Care Consultant Jo Debacker Practice Manager Pauline Webster Administration Officer John Caine WLCCG Chair Mike Maguire Chief Officer Paul Kingan Chief Finance Officer Doug Soper Lay Member Greg Mitten Lay Member Stephen Gross Lay Member Claire Heneghan Chief Nurse Jackie Moran - Head of Contracting, Performance and Quality Due Date In Attendance Item 3 EMIS Protocols Item 4 Pain, procedures of low clinical value Item 5 LCFT Milestones & Gateways Item 6 MSK & Joint Health Apologies Smitty Shetty Service Re-design Manager Barry Johnson Data Quality team MLCSU Donna Wright Data Quality team MLCSU Barry Lloyd Medicines Optimisation Carol McCabrey Senior Service Re-design Manager Matt Greene Senior Finance Manager Phil Winnard Mental Health Transformation Lead Ros Bosnor GP and Mental Health Clinical Lead Joanna Rimmer Contracts Manager Karen Tordoff Lead Service Re-design Manager Jan Wilson - MSK Physiotherapy Consultant, Outpatient Therapies / Joint Health Lead, S&O Hospital Trust Katie Mann Physiotherapist, S&O Hospital Trust Steve Shanahan Director of Finance, S&O Hospital Trust Rakesh Jaidka - GP Executive Lead Vikul Mittal GP Executive Lead Jack Kinsey GP Executive Lead Bapi Biswas GP Executive Lead 2
231 Declaration of Interest The Chair reminded committee members of their obligation to declare any interest they may have on any issues arising at Clinical Executive Committee meetings which might conflict with the business of NHS West Lancashire Clinical Commissioning Group. Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: Declaration of Interest Declarations of interest from sub committees: None declared. Declarations of interest from today s meeting: Bapi Biswas was not in attendance, however, he declared an interest in item 4 Pain in comments received as Beacon Primary Care may potentially provide services in this area in the future. This interest was noted in his absence. Operational Item 3 EMIS Protocols procedures of low clinical value (PLVC) Smita Shetty has been liaising and working with the MLCSU Policy team and Data Quality team and GP Execs and Practice Managers with regards to looking for a solution around 5 revised policies implemented 1 November 2017 and the management of Procedures of Low Clinical Value (PLCV). A potential cost effective solution is that there is capabililty within EMIS Protocols which has been designed and built on the revised policy criteria so that GP and Locums have the required information for patients and a way of ensuring a consistent approach in all GP Practices. MLCSU has been working with GP Execs to develop this and has been tested by 2 GP Execs. Barry Johnson gave a demonstration how this capability works in EMIS and that patient information leaflets can be generated and printed at the time of consultation. Barry described the data process mapping around how the policy criteria and read codes built into EMIS to look at data on patients records. If criteria is met, the patient is referred and if the criteria is not met, the patient is given an information leaflet that can be printed off. 3
232 A discussion and questions took place. A decision could not be made as the meeting was not quorate but they supported in principle that the 5 policies are piloted with an associated roll out programme, protected time is given to develop, that the appropriate EMIS training is given, and that learning from the medicines Optimisation team in terms of the experience with Scriptswitch and Optimise is fully considered. However, this was on the understanding that there would need to be effective communications, awareness raising and involvement of Practices. Other suggestions included linking with ORCHA and the IT Strategy. Barry Johnston to meet Barry Lloyd outside of the meeting to discuss medicines optimisation input and involvement and attend Medicines Optimisation meeting. Pilot and roll out to all GP Practices MLCSU to work with medicine s Optimisation team Smita Shetty Barry Johnston On-going On-going Operational Item 4 Pain, Procedures of Low Clinical Value Carol McCabrey presented a paper on options for an Interim chronic pain service with the purpose of getting Exec direction with regard to an interim chronic pain management service, until the new I-HELP service has been procured and is operational expected by Autumn A summary of options and background to current provision, activity and issues outlined in the paper was discussed and commented upon by the Execs. Currently there is no specialist community pain service for patients with chronic pain across West Lancashire. NICE have published two guidance documents around low back pain and sciatica in over 16 s which outline a change in the pathway, drawing attention to the holistic approach of first line intervention and a change of the pathway in the do not offer injections, especially relating to spinal injections. The key issues are: There will be no interim provision for West Lancs patients when the PLCV policy is entered into the contracts until the provider for the I-HELP service goes live in Autumn 2018 The CCG has received one formal complaint regarding the PLCV policy Carol with support from GP Execs, Finance and BI has done an Options Appraisal and the Execs discussed the 3 options in the paper. Execs asked 4
233 questions around what the implications for existing and new patients would be following NICE guidance. The meeting was not quorate so a decision could not be made. A fourth option was discussed and recommended by Execs around the services of an existing local Consultant in Pain Management working within a West Lancashire based organisation as an interim measure. Carol will return to Execs for a decision on 21 November and make it clear that if anything was put in place it would be an interim solution for 12 months. It was agreed that an effective communications plan would be needed when a decision has been made. Bring back to next Execs 21 November for a decision Carol McCabrey Item 5 LCFT Milestones & Gateways West Lancashire CCG has undertaken a huge scoping exercise in the last 12 months around what we need Mental Health services locally to look like in the future. A Milestones and Gateways draft report which outlines the CCG commissioning intentions was submitted to Lancashire Care Foundation Trust (LCFT) for consideration and comment. The report highlights tables of areas that the CCG would like LCFT to focus on and transform which is around what the local population have requested over the next 12 months. The draft outlines that a West Lancashire CCG Review panel would meet quarterly to review all milestones. The CCG accepts that there can be issues that can arise on working on certain projects and the CCG Review panel will then decide whether to extend the timescale so that LCFT can achieve the milestone/objective. The CCG has received a disappointing response to the Gateways and Milestones draft report from the LCFT Chief Operating Officer and this was discussed with the Execs. Collaborative commissioning Mike Maguire The Execs recommended that the CCG initially formally respond to the and request a face to face meeting with LCFT to challenge/understand their stance and bring back to a future Execs meeting to agree next steps. Formally respond to LCFT/set up meeting Mike Maguire Item 6 MSK and Joint Health Jan Wilson with support from Katie Mann and Steve Shannahan gave a presentation on Joint Health Integrated Musculoskeletal Care service redesign update. 5
234 Jan talked through a series of slides covering: Aims and Objections of re-design Where are we now? Achievements Next Steps Joint Health self referral pilot Jan talked in more detail around the self-referral pilot and general referral issues and the challenges with e-referrals and capacity. The service is looking to roll out self-referrals in all GP practices. The Execs acknowledged the good work that has been achieved to date and asked for more clarity around orthotics referrals as Virgin Care has not currently commissioned to provide orthotics for a particular patient cohort that the CCG thought was staying with the Trust. Orthotics referrals Jan Wilson Item 7 - Concerns with S&O Hospital Trust Greg Mitten and Jackie Moran tabled a report following issues related to recent performance of and information received from S&O Hospital Trust which was raised at the Quality and Safety Committee 24 October The committee feel compelled to escalate the concerns to the CCG Executive Committee for their decision on future actions. The Quality and Safety committee have serious concerns around quality and safety issues and the stability of the Trust in its current form and feel that this needs to be urgently escalated to NHSE and the Lead Commissioner Item 8 Membership Agenda 9 November 2017 Item 9 Notes from previous meeting The Execs recommended that Mike Maguire to further discuss the report with South Sefton, Southport and Formby CCG Chief Officer and make a recommendation to the Clinical Execs in the next 2 weeks. The Execs agreed the draft agenda subject to adding names next to items. Jackie Moran has ed the names and details to Joanne Kane and has invited Chris Goddard, Consultant Anaesthetist to the meeting. GP Executive Elections to be added to agenda. The notes from the previous meeting were approved subject to amendments to: Declarations of Interest: Raise concerns with Chief Officer SS,S&F CCG Agenda to be amended and circulated Mike Maguire Joanne Kane
235 Item 6 - which should state that Bapi Biswas interest was that PDS Medical rent a room from Railway Road Practice. Item 5 which should state that all GP s interest was as potential future providers of shared care in ADHD. Agenda item 3 ORCHA last paragraph, remove the wording at least 5 voting members with the caveat. AOB Viran Procurement 6month extension and procurement process. A reciprocal arrangement has been agreed for Blackburn with Darwin CCG to evaluate this procurement if West Lancashire CCG can supply 2 GP s to evaluate a similar procurement in Blackburn with Darwin. West Lancashire GP involvement in this procurement to be discussed at the next meeting. to be sent to all GP s Jackie Moran Debbie Dobson, Practice Manager has formally tendered her resignation from the Clinical Executive Committee. The Execs wanted to formally acknowledge Debbie s hard work and support to the committee that she has given during her time as a committee member. GP Elections are due next year for 3 GP Executives. They are invited to discuss further with Doug Soper. This will be raised at Membership Council meeting on 9 November as timescales can take between 6-8 weeks if anyone wants to put their name forward. A vote and decision by the Membership will need to be made by Spring Next Meeting The next meeting will take place on Tuesday 7 November GP Executive Elections Jackie Moran/ Doug Soper Ongoing 7
236 West Lancashire CCG Clinical Executive Committee Action and Notes 07/11/2017 Key Attendance Record of Attendance Non-Attendance (sickness, holiday, unknown) Attended meeting/course on behalf of CCG Member Adam Robinson Bapi Biswas Claire Heneghan Debbie Dobson Resigned Resigned Resigned Resigned Doug Soper Greg Mitten H Jack Kinsey H H H Jackie Moran Jo Debacker John Caine H H Mike Maguire Paul Kingan H H Peter Gregory H H Rakesh Jaidka H H H Vikul Mittal H H H Steve Gross H 1
237 Item Discussion and decisions Actions Responsible officer Attendees Chair Peter Gregory GP Executive Lead Due Date Adam Robinson Secondary Care Consultant Bapi Biswas GP Executive Lead Claire Heneghan Chief Nurse Doug Soper Lay Member Jack Kinsey GP Executive Lead Jackie Moran - Head of Contracting, Performance and Quality Jo Debacker Practice Manager Joanne Kane Administration Officer John Caine WLCCG Chair Mike Maguire Chief Officer Paul Kingan Chief Finance Officer Rakesh Jaidka - GP Executive Lead Stephen Gross Lay Member Vikul Mittal GP Executive Lead In Attendance Item 4 Social Prescribing Item 5 EMIS Protocols Item 6 GMTS Orientation Programme Item 8 Enhanced Care Apologies Kathryn Kavanagh Lead Manager Health Inequalities Paul Jones Head of Finance Smita Shetty Service Re-design Manager Laura Anton Project Manager Jan Charnock - Primary Care Development Manager Greg Mitten Lay Member 2
238 Declaration of Interest The Chair reminded committee members of their obligation to declare any interest they may have on any issues arising at Clinical Executive Committee meetings which might conflict with the business of NHS West Lancashire Clinical Commissioning Group. Declarations declared by governing body members are listed in the CCG s Register of Interests. The Register is available either via the secretary to the governing body or the CCG website at the following link: Declaration of Interest Declarations of interest from sub committees: None declared. Declarations of interest from today s meeting: Greg Mitten had declared an interest in Item 4 Social Prescribing via . He excluded himself from the meeting and gave his apologies for today. Due to their position within OWLs Peter Gregory, Rakesh Jaidka and Vikul Mittel declared an interest in Item 4 Social Prescribing. As Jack Kinsey works for OWLs he also declared an interest in Item 4 Social Prescribing. The Chair was passed from Peter Gregory to Mike Maguire. The Chair deemed all the declarations to be fundamental, therefore Peter, Rakesh, Vikul and Jack will leave the room for the duration of this item and not take part in the discussion or any vote. All GPs and Practice Managers declared an interest in Item 8 Enhanced Care. Mike Maguire was still acting as Chair and considered the declaration to be fundamental, as such all GPs and Practice managers would not be allowed to take part in the discussion or any decision and would be excluded from the room during this item. Following these decisions on the declarations of interest the Chair passed from Mike Maguire back to Peter Gregory. 3
239 Item 3 Joint Committee of CCGs Meeting 2 November 2017 Item 4 Social Prescribing Operational Paul Kingan reported on the last meeting of the Joint Committee of CCGs (JCCCG). Paul stated that in terms of delivery this is still at an early stage. A brief update was then given on key topics. Some workstreams are moving faster than others for example CAMHs and LD, however A&E proves to be slower. There was an estates workshop last week, progress was made toward agreeing some estates schemes. The Exec Committee will continue to be updated on progress with the JCCCG meetings. For this Item Mike Maguire took the Chair, Peter Gregory, Rakesh Jaidka, Vikul Mittel and Jack Kinsey left the meeting. Kathryn Kavanagh and Paul Jones presented a paper to the Exec Committee for a decision. The Department of Health has a fund for CCGs to develop an approach to social prescribing. While a pilot is already underway in West Lancashire, a successful application could allow WLCCG to scale this up and roll out across the patch. OWLS and CVS are working together to submit a bid as part of the procurement process. The deadline is 21 November. Discussion took place on how this would work with or potentially complicate the current social prescribing procurement. The risk attached to this was considered, Kathryn assured that close working is a requirement in procurement. Another condition attached to the fund is that development work in social prescribing must contribute to building an evidence base. It was noted that while the proposed redistribution of funding may prove problematic, it was agreed to support in the bid in principle at this stage. Item 5 EMIS Protocols procedures of low clinical value (PLVC) Peter Gregory, Rakesh Jaidka, Vikul Mittel and Jack Kinsey returned to the meeting. Mike passed the chair back to Peter Gregory. Smita Shetty was in attendance for discussion on an item returning to the Exec Committee from the previous week. The meeting had not been quorate and so was now presented to agree the best way forward. The key issue in respect of EMIS Protocol is that as West Lancashire patients can be treated in Merseyside, Greater Manchester or 4
240 Lancashire. So even though West Lancashire is signed up to Lancashire policies patients may be affected by different areas protocols depending upon where they access their care. While the difference between policies can be negligible, there is potential for inconsistency for the West Lancashire population. Discussion took place on a pragmatic solution to the problem, it was agreed that a North West or Nationwide solution would be ideal. However, there is no resolution expected from this route presently. Discussion then followed on what Primary Care can do to, what the Federation can influence and how coding could be used to drive a standardised protocol. Following the discussion today Smita will hold on the roll out of EMIS Protocols on procedures of low clinical value to allow a wider solution to be explored. Strategic & Service Redesign Item 6 - GMTS Orientation Programme Item 7 Update on Mental Health Milestones & Gateways Laura Anton presented slides to feedback on the Graduate Management Training Scheme (GMTS). The slides set out what Laura had been involved with during her time so far at WLCCG. There was a focus on what Laura had learned and what could have improved her experience. The feedback was positive with the only aspect that Laura felt would have been beneficial was time with S&O NHS Trust, unfortunately this had proved difficult to arrange. Overall Laura would recommend the scheme itself and WLCCG as a placement host. Mike Maguire gave an update on Mental Health and progress towards service improvement. At present agreement on the programme of change has not been reached. However, after recent discussion Mike was hopeful that progress will be made. The Exec Committee will continue to be updated on discussion with LCFT regarding this. 5
241 Item 8 Enhanced Care For this Item the Chair passed from Peter Gregory to Mike Maguire. All GPs and Practice Managers left the room for the duration of this item. It was acknowledged that while this item is more appropriate for the Primary Care Commissioning Committee (PCCC) Jan Charnock was in attendance and would provide an update on extended access in WLCCG. Jan reports that the pilot continues to provide Extended Access, at present West Lancashire is the only CCG in Lancashire meeting the target for this. The pilot will end on 31 March and therefore a decision will be required on how to manage this in future, WLCCG must confirm their approach. Further discussion on this will take place in the PCCC. Item 9 Notes from previous meeting AOB The notes from the previous meeting were approved subject to amendments to: Item 9 This currently states that GP Elections are due next year for 3 GP Executives. They are invited to discuss further with Doug Soper. This should have stated rather that the Exec Committee need to consider the roles bearing in mind the current makeup of the committee to make sure quoracy is consistently attainable. Discussion then took place on a request for two GPs to volunteer to be involved in a procurement moderation for Blackburn with Darwen CCG. After a brief discussion Peter Gregory and John Caine agreed to do this. Next Meeting The next meeting will take place on Tuesday 14 November
242 Lancashire Health and Wellbeing Board Minutes of the Meeting held on Tuesday, 5th September, 2017 at am in Committee Room 'C' - The Duke of Lancaster Room, County Hall, Preston Present: Chair County Councillor Geoff Driver CBE, Lancashire County Council Committee Members County Councillor Graham Gooch, Lancashire County Council County Councillor Geoff Driver CBE, Lancashire County Council County Councillor Phillippa Williamson, Lancashire County Council County Councillor Shaun Turner, Lancashire County Council Dr Sakthi Karunanithi, Director of Public Health and Wellbeing, LCC Louise Taylor, Corporate Director Operations and Delivery (LCC) Tony Pounder, Director of Adult Services Councillor Bridget Hilton, East Lancashire Health and Wellbeing Partnership and Central District Councillor Karen Partington, Chief Executive of Lancashire Teaching Hospitals Foundation Trust Jane Booth, Independent Chair, Lancashire Safeguarding Children's Board and Adult Board Jacqui Thompson, North Lancashire HWB Partnership Cllr Viv Willder, Fylde Coast District Council Rep Amanda Hatton, Director of Children's Services, LCC Councillor Tony Harrison, East Lancashire District Council Rep Councillor Margaret France, Central HWBP Adrian Leather, Third Sector Simon Burnett, West Lancashire Health and Wellbeing Partnership Tim Almond, Morecambe Bay CCG Jackie Hanson, East Lancs CCG Supt Andrea Barrow, Lancashire Constabulary Clare Platt, Lancashire County Council Sam Gorton, Lancashire County Council Apologies Dr Gora Bangi Dr Sumantra Mukerji Michael Wedgeworth Graham Urwin Gary Hall Dee Roach Dr John Caine Chorley and South Ribble CCG Greater Preston CCG Healthwatch Lancashire Chair NHS England, Lancashire and Greater Manchester Chief Executive, Chorley Council representing CEOs of Lancashire District Councils Lancashire Care NHS Foundation Trust (on behalf of Heather Tierney-Moore) West Lancashire CCG 1
243 1. Welcome, introductions and apologies Due to the absence of County Councillor Vivien Taylor, CC Driver was appointed as Chair for the meeting. Apologies were noted as above. New member as follows: DCC Sunita Gamblin replaces ACC Mark Bates, Lancashire Constabulary Adrian Leather replaces Sarah Swindley, Third Sector Replacements were as follows: County Councillor Shaun Turner for County Councillor Vivien Taylor, Lancashire County Council County Councillor Philippa Williamson for County Councillor Susie Charles, Lancashire County Council Simon Burnett for David Tilleray, West Lancashire Health and Wellbeing Partnership Tim Almond for Dr Alex Gaw, Lancashire North CCG Jackie Hanson for Mark Youlton, East Lancs CCG Supt Andrea Barrow for DCC Sunita Gamblin, Lancashire Constabulary 2. Disclosure of Pecuniary and Non-Pecuniary Interests There were no disclosures of interest in relation to items appearing on the agenda. 3. Minutes of the Last Meetings held on 20 June 2017 and 7 August 2017 Resolved: That the Board agreed the minutes of the last meetings with the following amendment to 7 August 2017 Minute Item 3 i) removal of the word 'That'. 4. Forward Plan and Action Sheet The Forward Plan is a working document and items will move by necessity. Additional items that need adding are: Pharmaceutical Needs Assessment (PNA) Child and Adolescent Mental Health Service (CAMHS) Joint Strategic Needs Assessment (JSNA) Health and Wellbeing Strategy Lancashire Safeguarding Adult's Board (LSAB) - Annual Report - November 2017 meeting Lancashire Safeguarding Children's Board (LSCB) - Annual Report - November 2017 meeting Members of the Board were requested to send any future items for consideration at a Board meeting to Sam Gorton, sam.gorton@lancashire.gov.uk. 2
244 5. Lancashire Health and Wellbeing Strategy Progress on the refresh of the Lancashire Health and Wellbeing Strategy was considered by the Board. Resolved: That: i) The Health and Wellbeing Board (HWBB) members share the draft Strategy with health and wellbeing partnership colleagues for comment. ii) The HWBB agrees the draft strategy and associated appendices as the basis of a workshop to be held on 16 October 2017 where the focus for the final strategy will be agreed. 6. Sustainability and Transformation Plan (STP) Carl Ashworth, NHS Midlands and Lancashire Commissioning Support Unit on behalf of the Lancashire and South Cumbria STP presented an update to the Board on the proposed new STP Governance Arrangements details attached. Upper tier local authority representatives are represented on the STP Board, with County Councillor Vivien Taylor as the Lancashire County Council representative. The STP Board has a relationship with the Joint Committee of Clinical Commissioning Groups (JCCCG) in that the JCCCG is the means by which Lancashire and South Cumbria wide commissioning decisions will be made. The HWBB noted that there is need to ensure a strong link between the STP Board and the HWBB. Further to discussion, Carl confirmed that the Public Engagement Policy is a key workstream of the STP. The HWBB felt a better understanding of the STP Governance Structure would be beneficial if a worked through example was provided and showed how it was followed through the structure. Resolved: That the Health and Wellbeing Board agreed that a worked through example be provided to the HWBB at the Workshop on 16 October Better Care Fund (BCF) Paul Robinson, NHS Midlands and Lancashire Commissioning Support Unit, informed the HWBB of the development of the Lancashire Better Care Fund (BCF) Plan for 2017/18/19 and sought the Board s approval of the plan. It is a two year plan covering 2017/18 and 2018/19 with some ability to review late in the first year. It covers three elements of funding - the core BCF, the new ibcf and the Disabled Facilities Grants monies. 3
245 The Lancashire BCF Plan is built upon a high level of involvement of a wide range of partners, and in particular health and social care. The plan again sees the growing influence and engagement with the Voluntary Sector and District Councils. It has used approaches to support decision making that have required detailed analyses of 2016/17 BCF schemes and the potential of new areas of spend. Its spending plans reflect the decisions to retain the existing BCF schemes and to use the ibcf schemes to innovate, plug gaps and build upon existing success. A key requirement within the BCF plan is to demonstrate the action to be taken to address the priority of reducing Delayed Transfers of Care. The plan describes how the BCF will act as an enabler within a wider system approach that will be led by the A&E delivery boards and coordinated through the Lancashire and South Cumbria Urgent Care Network. The HWBB felt there was a need for better understanding and a flexible approach to what does and does not work. There is a requirement to track and monitor benefits and outcomes. Hospitals are signing off the LDP Winter Plans. There is a need for clear metrics on a Lancashire footprint. Karen Partington, Lancashire Teaching Hospitals Foundation Trust, agreed to share work around this with Paul. There is a need to align and learn quickly and be really clear on measured outcomes going forward. Guidance that will come through later in the year will encourage better alignment across boundaries. Resolved: That the Health and Wellbeing Board agreed to: i) Endorse the approach taken in developing the Lancashire Better Care Fund plan 2017/18/19. ii) Approve the Lancashire Better Care Fund Plan 2017/18/19 and its submission to NHS England. iii) Agree a BCF reporting schedule to the board based upon that required by NHS England. iv) Request the BCF Steering Group strengthens performance management and evaluation of the schemes, so that their effectiveness is more clearly understood; and opportunities to move resources within and between schemes are identified, prior to any changes being agreed by the Board. v) Request the BCF Steering Group strengthen the risk and benefit sharing arrangements between the County Council and the Clinical Commissioning Groups (CCGs) under the Section 75 pooled budget arrangements. 4
246 8. Supporting Patients Choice to Avoid Long Hospital Stays The Supporting Patients Choices to Avoid Long Hospital Stays Policy has been developed locally by NHS organisation and local authorities operating within the Lancashire and South Cumbria Sustainability and Transformation Partnership. It is based on a national framework issued by NHS England. The aim of the policy is to provide accurate and timely information to patients about their choices when leaving hospital, improve patient flow and increase capacity within hospital to meet growing demand. To minimise delays and uncertainty about which organisation has funding responsibility for meeting the support needs of particular individuals in the context of this policy, a funding framework has also been developed by NHS and Local Authority partners within the Lancashire and South Cumbria Partnership. Resolved: That the Health and Wellbeing Board agreed to endorse the collaborative policy framework, as detailed at Appendices 'A' and 'B' of the report; and supported its adoption across the footprint of the Lancashire and South Cumbria Sustainability and Transformation Partnership. 9. LCC Adult Social Care Winter Plan The Lancashire County Council (LCC) Adult Social Care Winter Plan has been updated for 2017/18 to reflect the services in place and the social care planning and response to winter pressures. The plan includes information about various enhanced responses over the winter period and the proposed service developments through the improved Better Care Fund (ibcf) funding that aim to improve the situation around delayed transfers of care, which typically increase through the winter period. Whilst some of the funding for enhanced services are being met through the ibcf, there is however no formal designated resilience funding identified within these monies, and therefore further resilience discussions may need to take place with NHS partners around whole system planning. The plan will be shared both internally in LCC and with each A&E Delivery Board across Lancashire for inclusion in the system wide winter planning and delivery reporting. Resolved: That the Health and Wellbeing Board received and noted the LCC Adult Social Care Winter Plan. 10. Urgent Business There were no matters of urgent business received. 5
247 11. Date of Next Meeting The next scheduled meeting of the Board will be held at 10.00am on Tuesday, 14 November 2017 in Committee Room 'C' - Duke of Lancaster Room, County Hall, Preston. The workshop will be held on Monday, 16 October 2017 at 1.00pm-4.30pm at County Hall, Preston. County Hall Preston I Young Director of Governance, Finance and Public Services 6
248 WEST LANCASHIRE COMMUNITY SAFETY PARTNERSHIP HELD: 5 th July 2017 Commenced: 6.00 pm Finished: 6.45 pm PRESENT: David Tilleray - WLBC (CSP Chairman) Andrew Hill - WLBC Cliff Owens - WLBC Steve Mahon - WLBC Inspector Adrian Jolly - Lancashire Constabulary Bill Hancox - Edge Hill University Mark Lamb - Lancashire Fire and Rescue Michele Dacre - Cumbria and Lancashire CRC Lisa Sloan - Discover Conrad Jones - EHSU Lisa Larsen - Liberty Centre Abdul Kheratka - LCC Kathryn Kavanagh - WLCCG 1. WELCOME AND INTRODUCTIONS The Chairman welcomed colleagues to the meeting and introductions were made. 2. APOLOGIES Apologies for absence were received from: Gareth Dykes, Councillor Furey, County Councillor Fillis, Eleanor Maddocks, Greg Mitten, Councillor Wright, Gwen Bleasdale, Steff Hull, Fay Sherrington, Matt Hamer and Jill Halliwell. 3. MINUTES OF LAST MEETING/MATTERS ARISING The minutes of the last meeting were agreed as a true and accurate record. 4. PERFORMANCE MONITORING The Chairman, David Tilleray, invited partner agencies to provide a verbal overview of current performance. Inspector Adrian Jolly provided the Partnership with an overview of police performance figures highlighting that the overall crime trend is slightly upward but within the control limits. Inspector Jolly stated that dwelling burglaries have reduced gradually but added that due to changes in Home Office counting the focus in future will be on all burglaries including both residential, business and community. Adrian continued by adding that the category 'robbery' is showing a slight increase but there is no significant trend. 1
249 Adrian advised the Partnership that although we have recorded reductions against ASB he was concerned with reports of ASB in Burscough West Ward. He provided an overview of tactics the neighbourhood policing team have put in place to address the ASB issues including engagement with local schools and clubs. Steve Mahon provided the Partnership with an overview of performance on behalf of the ASB Team. Steve provided a summary of the performance information contained in members meeting packs and highlighted the team's first use of the new 'Absolute Grounds' for possession tool which contributed to one of four evictions obtained in the quarter. Steve also highlighted the team's contribution to the successful Criminal Behaviour Order obtained by the Police to keep a prolific burglar out of Ormskirk and Aughton. Inspector Jolly added that this was an excellent team effort. Lisa Sloan, Discover Drug and Alcohol Services advised that she has taken over as the local Service Manager from Liz Hopkins and continued by providing a comprehensive overview of the performance data contained in members meeting packs. In response to Kathryn Kavanagh's question on the significant increase in the number of new treatment journeys for alcohol referrals, Lisa responded that she would look further into this increase and report back. Mark Lamb provided the Partnership with a brief overview of performance for LF&RS. Mark advised that overall incident activity is down by 5.7% in comparison to the previous year's performance. Mark continued by providing a summary of the report stating that in 2016/17, 8 Wards accounted for 51.97% of all activity; in 2017/18, 7 of the 8 Wards are consistent, with Ashurst replacing Digmoor in contribution levels. Considering these 8 Wards for 2017/18 these account for 55% of all activity. For quarter 1 there have been 8 recorded deliberate vehicle fires; 3 occurring in close succession in Up Holland Ward. Mark advised that West Lancashire has recorded 13 ADF incidents. Mark provided an overview of the type of incidents and highlighted that of the 13 incidents, 12 had working smoke detection with 1 having none. Mark added that the crews will continue to focus on looking at vulnerability issues in these areas. The Chairman thanked colleagues for providing an update against their performance indicators. 5. CSP FUNDING UPDATE Andrew Hill provided the Partnership with an update against the CSP s funding allocation for 2017/18. Andrew advised that to date the CSP has received a total allocation of 17,000. This includes 10,000 available from the Police and Crime Commissioner of which 5,183 has been allocated, 5,000 from the Borough Council towards Bright Sparx and Fresher's and 2,000 from Housing towards the Community Action and Engagement Days. Andrew advised the Partnership that the Community Safety Team welcomes bids from partners towards the remaining allocation from the OPCC which must meet CSP and PCC priorities. 6. DCLG FUNDING UPDATE & VAWG BID NEWS Lisa Larsen provided an update on behalf of the Liberty Centre with regards to the successful Pan Lancashire DCLG Funding bid which West Lancashire CSP 2
250 contributed to developing. The Liberty Centre is the commissioned provider of the West Lancashire element of the bid which will assist women needing support in the area to remain safely in their own homes. The outreach provision will also support those with disabilities as they can be supported where they are based as well as helping those in remote rural communities. Lisa advised that she has been employed as the Domestic Abuse Development Worker and will assist the victims to access training and support them into employment. Lisa advised that role has got off to a strong start and she has already developed a caseload that she is actively supporting. The funding will also support a Complex Needs Support worker who will support victims accessing the service, allowing them to receive the required intensive support. While a Family Support Worker will enable high-level therapeutic needs among the wider family to be addressed, as well as minimising the risk of these children becoming future victims. Cliff Owens advised the Partnership that following a recent Home Office VAWG bid, he was very pleased to inform colleagues that we have received confirmation earlier today from the HO that the proposal entitled the West Lancashire Safe Teens project is successful. We have been offered the full amount of grant requested; which was 160,000 over three years. The 'Safe Teens' project will be delivered by a 'Safe Teens Development Worker,' who will be managed through the Liberty Centre. This is a new approach to tackle Violence against Women and Girls and only possible with this funding. The project will include working with schools and colleges to develop a zero-tolerance approach to Violence against Women and Girls. It will also provide a bystander s network, including parents, teachers and health service workers. The key CSP Partners involved in the bid were the Council, WLCCG and the Liberty Centre. 7. REVIEW OF LANCASHIRE CONSTABULARY'S FRONT LINE COUNTER PROVISION Andrew Hill provided the Partnership with an overview of the review of Lancashire Constabulary's front line counter provision. Andrew advised that details of the review were provided in a letter sent by Clive Grunshaw, Lancashire Police and Crime Commissioner. A copy of the letter included in members meeting packs outlined that Lancashire Constabulary has recently undertaken a review of its front counters to ensure they remain fit for purpose and are providing value for money for Lancashire residents as the way the public engages with the police continues to change. Andrew confirmed that the review does not involve changes to the way local areas are policed nor will it result in police stations closing. The Constabulary is proposing to reduce the number of counters that are open to the public from 23 to 13 and Ormskirk Police Station's counter is proposed to be closed as part of this cost saving exercise. The Chairman advised the Partnership that the Council will likely respond to the consultation exercise and asked if the Partnership would like to consider also providing a response to the review. It was noted that the Partnership did not express an intention to respond to the review. Update: No response submitted by WLBC. 3
251 8. FRESHERS PLANNING 2017 Andrew Hill provided an overview of the Fresher's multi-agency planning process for September Andrew advised that the Fresher's Group planning meeting was held on the 23 rd June with excellent support from contributing stakeholders. Andrew stated that the meeting was very productive and colleagues indicated that we will be in a position to replicate the successful initiatives from the 2016 plan. Andrew advised that additional Policing resources, up to 50 hours, will be allocated at key times with funding provided through the CSP which will complement the Policing Plan. Bill Hancox advised the Partnership that the way we develop and deliver the multiagency Fresher's Plan is very effective and highlights the excellent local partnership arrangements we have in place in West Lancashire. Bill continued by adding that this is evidenced by the positive response we receive from residents groups and the community who acknowledge the proactive approach. Bill stated that EHU is focused on the big influx of students for Welcome Sunday adding that we continue to cope better each year. Andrew Hill advised that the Fresher's Plan will be completed by early August and shared with partners. 9. COMMUNITY ACTION AND ENGAGEMENT EVENT 2017/18 Cliff Owens advised that on behalf of this Partnership the community safety team plan to deliver a further 12 Community Action and Engagement Events this year. The events will continue to have a strong community focus and key overarching aims include providing opportunities for agencies to positively engage the local community and strengthening the relationship with service providers. Other objectives include the prevention of signal crime, including criminal damage and ASB fires. Consideration was given to these factors when choosing the locations in consultation with colleagues from Fire and Rescue and the Police. Six events will be delivered to support the aims of Bright Sparx in October and a further six events have been scheduled for this summer. The summer engagement events will be rolled out over two weeks commencing the 8 th August. To promote the events and showcase the excellent partnership working that we have in West Lancashire, we have also organised a 'Community Information Day' on Thursday, 3rd August at the Concourse Shopping Centre. The support offered from colleagues has been fantastic and we have commitment from 27 organisations to attend the event and offer a wide range of advice and support to the community. We aim to promote the planned events through social media, a press release and through the Concourse Communication's team. Cliff concluded by stating we also welcome support from all CSP partners to promote the information day and action days through your networks and social media platforms. 10. PRIMARY SCHOOLS TEACHER TRAINING PROGRAMME Cliff stated that colleagues will recall that the CSE and Healthy Relationship project commissioned by this Partnership received national recognition at the Unsung Heroes Award held in March 2017.The commissioned project enabled Freedom 4
252 Personal Safety (FPS) in partnership with the Police to deliver CSE and Healthy Relationship training to hundreds of school children throughout secondary schools in West Lancashire. To build on the excellent work undertaken by FPS and the Deter Team we submitted a further successful bid to the Office of the Police and Crime Commissioner. FPS will again utilise the 'Train the Trainer' approach but will now aim to equip staff from up to 60 West Lancashire primary schools to deliver the project. Each participant will be required to run at least 3 lessons with their class on topics covered in the training which will include; safe and unsafe adults/grooming, healthy relationships and resilience. FPS will aim to deliver the programme on 5 dates, with approximately 12 participants on each day. Each participant will receive a resource pack with the course content to use in school. The sustainable project has the potential to annually reach 1,800 year 6 primary school children. Key aims include, tackling and reducing child sexual exploitation, safeguarding and protecting young people from harm and early identification of risk and appropriate intervention FPS will soon begin the process of attempting to engage all 60 primary schools in West Lancashire. Whilst this is an ambitious project, the objectives it will achieve in building resilience to help safeguard local children is invaluable. Cliff advised that he will ensure this Partnership is kept updated on progress. 11. ANY OTHER BUSINESS Mark Lamb advised the Partnership that LF&RS are continuing to engage the owners of Appley Bridge Quarry with regards to the installation of signage around the quarry. LF&RS are also making enquiries with Northern Rail regarding advertising space at Wigan Station to advise people of the dangers of swimming in open water. Mark concluded that LF&RS are still pursing options and potential funding. 12. DATE OF NEXT MEETING The next meeting of the West Lancashire CSP will be held on Wednesday the 4 th October 2017 at 6.00pm in the Council Chamber, at the Main Council Office, 52 Derby Street, Ormskirk, L39 2DF 5
, Ann Marr (StHK), Michelle Creed (Halton CCG), Leigh Thompson (Halton CCG), Tracy Hill (NWBH), Sheila")
253 Cheshire and Merseyside Sustainability and Transformation Plan Alliance Local Delivery System Leadership Group Meeting Notes of the meeting held on 12 th September 2017, 10am-12pm, Boardroom, Whiston Hospital ITEM N o AGENDA ITEM 1a,b&c Welcome & Introductions In attendance: Ingrid Fife (Chair), Ann Marr (StHK), Michelle Creed (Halton CCG), Leigh Thompson (Halton CCG), Tracy Hill (NWBH), Sheila Lloyd (S&O), Mel Roche (Public Health), Charlotte Smith (Public Health), Eileen O Meara (Halton BC), Wayne Longshaw (StHK), Colin Scales (Bridgewater), Mike Palin (St Helens Council), Sarah O Brien (St Helens CCG), Glenn Coleman (NHSE), Iain Stoddart (St Helens/Knowsley CCGs), Andrea McGee (WHH), Rachel Mellor (Bridgewater), Nicola Bunce (StHK) Apologies: Andrew Davies, Anne-Marie Stretch, Christine Walters, Gareth Davies, Dave Sweeney, David Parr, Dianne Johnson, Mike Harden, Mike Maguire, Simon Constable, Steven Broomhead, Maria Austin, Jason DaCosta, Andrew Pryce ACTION - Consider the capacity of the meeting room for future meetings (min capacity needs to be 20) Minutes The minutes of the meeting on 8 th August 2017 were accepted as a true record. Review of action log The action log has been updated accordingly. Action 141 was highlighted, as it is now red develop a programme of level 2 savings proposals. IS said that a significant amount of work has been done, but the finance group needs more information before a detailed breakdown can be provided. ACTION - Programme SROs to meet with Finance Leads Group to develop granularity of the delivery plans (NB to arrange). ACTION - In future the finance leads group to review any papers with financial assumptions before presentation to the leadership group SOB confirmed that the message coming from the Expo conference stated that funding is only available to those who are performing well. We also need to be able to articulate what we need investment for. CS confirmed that work in GM is very similar to the Alliance, but has attracted investment to support transition. ACTION CS to share the GM transformation business cases that BW has been involved in 1 P a g e
254 ACTION IS to make contact with the Steve Wilson, the GM DoF, to see if he can obtain copies of all business cases 2a SRO feedback from C&M FYFV Working Group 2 nd and 16th August 2017 AM discussed the STP leadership changes, with the appointment of Mel Pickup and Andrew Gibson and the re-focus of the STP delivery programme. The programme director role, currently filled by Joe Gibson, has been advertised. The North Mersey LDS is currently without a lead and the STP workforce lead has not yet been named. Finance: 2b Capital bids update Month 4 finance update Capital bids update The capital bids that were re-submitted were: o o o Halton Healthy New Towns ( 40m) Southport and Ormskirk (submitted via Care4U programme) IT resubmitted more service focused IS also confirmed that Knowsley CCG has received 1.1m of ETTF funding for 2017/18. ACTION IS to confirm with STP (Sam Simpson) that all the capital bids are being put forward to NHSE/I by C&M for the wave 2 capital ACTION Identify a new Alliance Estates Lead to work on the Alliance Estates returns/strategy Month 4 finance update There is a 6m deficit variance for the Alliance. There is a risk in the full year s forecasts. Southport and Ormskirk are waiting for NHSI to approve their revised plan which is a deficit of 18.1m. The are several areas of risk in the plans many are back loaded and are expected to deliver later in the year (due to CIP profiles, income & activity profiles and STF payment schedules). There is a further risk regarding the cash position of many of the provider organisations. ACTION - From month 5 the finance report to include cash SOB said she felt NEL was a major issue driving the financial position and asked what could we do differently as a system? LT confirmed that she has met with Dianne Johnson to discuss NEL mapping. CS said that the Integrated Community Services model may address NELs and DToCs, based on the evidence from Wigan and GM. 2 P a g e
255 ACTION - Gap analysis of NEL schemes locally compared to best practice to be reported at the next meeting (DJ) 2c Project leads milestones progress reports: Out of Hospital and Demand Management High Quality Hospital Care Corporate Services Workforce Out of Hospital and Demand Management LT gave a presentation on NEL attendances and admissions. EOM asked what the quick wins were, suggesting flu jabs and alcohol as key areas that could have a big impact on NELs. It was acknowledged that a lot of the things that need to be done require primary care. This can t be done immediately as there is no appointments/capacity available. There was a discussion on how the system could work together to improve the flu vaccination rate. This could be done by reaching further into care homes, workforce etc. There was agreement that this could be coordinated at Alliance level. ACTION EOM will contact NHSE/PHE to create a plan, and will work with SOB to prepare a co-ordinated approach to flu. CS asked about the use of a risk stratification tool and referred to work that was currently ongoing in Warrington where community matrons were being used to man mark the highest risk patients. There was however as yet no standard approach to risk stratification adopted across all Boroughs. High Quality Hospital Care WL delivered his presentation, showing that 2/3 of all bed days are used by those over 70 years of age. A small % reduction in this would make a huge difference to flow. ACTION WL to link into Rob Cooper s frailty work. Corporate Services AMcG delivered her presentation. There are estimated savings of 15.3m. This does not include estates, as it is predominantly part of high quality hospital care. Savings for last year are to be calculated but are approximately 6m. Workstream leads have been sent a template to complete for their milestones. This work is to be prioritised for completion in October. ACTION milestones for all areas to be ready for October, except comms and estates 3 P a g e
256 Workforce A paper update was provided, which was read through by TH on Anne-Marie Stretch s behalf. 2d Prevention Deep Dive Mel Roche and Charlotte Smith deliver their presentations. It was agreed in principle that a medicines management lead could be identified from within existing resources/capacity. Members of the group were supportive of the approach and each making a small investment ( 8-10k per organisation) on the basis of a coordinated approach across the Alliance and review of existing medicines management priorities. ACTION PH leads to present the business case to the DoFs group to discuss the financial detail and clarify where in the system financial benefits would be delivered. 2e Agenda for OD workshop ACTION all members to review the draft agenda and feedback any comments to NB ASAP 2f Joint Committee Progress Report This item was deferred to the October meeting Information items: 2g i. CVD Clinical Summit 13 th October ii. Strategic System Leadership Programme for STP Footprints NEXT MEETING 10:00 12:00, Tuesday 10 th October this meeting was cancelled 4 P a g e
257 Joint Committee of the Clinical Commissioning Groups (JCCCGs) Ratified minutes of the Joint Committee of the Clinical Commissioning Groups held on Thursday 7 th September 2017, 1pm 3pm at Chorley Town Hall Lancastrian Suite Chair Phil Watson (PW) Independent Chair JCCCGs Attended Voting Members (One vote per CCG) In attendance Alex Gaw Chair Morecambe Bay CCG Apologies Andrew Bennett Chief Officer Morecambe Bay CCG Attended Chris Clayton Chief Clinical Officer Blackburn with Darwen CCG Attended Sumantra Mukerji Chair Greater Preston CCG Attended Doug Soper Lay Member West Lancashire CCG Attended Susan Fairhead GP Member Blackpool CCG Attended Geoffrey O Donoghue Lay Member Chorley South Ribble CCG Attended Gora Bangi Chair Chorley South Ribble CCG Attended Graham Burgess Chair Blackburn with Darwen CCG Attended Mark Youlton Chief Officer East Lancashire CCG Apologies Jackie Hanson Director of Quality and East Lancashire CCG Attended Performance Tony Naughton Chief Clinical Officer Fylde and Wyre CCG Attended Mary Dowling Chair Fylde and Wyre CCG Attended Paul Kingan Chief Finance Officer West Lancashire CCG Attended Phil Huxley Chair East Lancashire CCG Attended Debbie Corcoran Lay Member for Patient & Greater Preston CCG Attended Public Involvement David Bonson Chief Operating Officer Blackpool CCG Attended Amanda Doyle STP Lead Healthier Lancs & South Cumbria Attended Andrew Bibby Director for Specialised NHS England Attended Services Andy Curran Medical Director Healthier Lancs & South Cumbria Attended Carl Ashworth Service Director Healthier Lancs & South Cumbria Attended Gary Hall Chief Executive Officer Chorley Council Attended Gary Raphael Finance Director Healthier Lancs & South Cumbria Attended Jane Higgs Director of Operations NHS England Attended Lawrence Conway Chief Executive Officer South Lakeland District Council Attended Sir Bill Taylor Chair Healthwatch Attended Debbie Nixon SRO Mental Health Healthier Lancs & South Cumbria Attended Neil Jack Chief Executive Blackpool Council Attended Sakthi Karunanithi Deputy Lancashire County Council Attended Hannah Milton Business Support Healthier Lancs & South Cumbria Attended Joint Committee Clinical Commissioning Group Page 1 of 9
258 Joint Committee of the Clinical Commissioning Groups (JCCCGs) Welcome and Introductions ACTION Info The Chair welcomed the members of the Committee to the formal meeting. He explained the status of the meeting and that the Committee had, for the first time, invited members of the public to a drop-in session prior to the meeting, in order to give them the opportunity to ask questions in advance of the meeting. He added that there would still be an option to ask questions when the meeting had finished. The Chair acknowledged Chris Clayton s departure from the Committee and thanked him on behalf of the Committee and other colleagues for all his efforts and hard work, both in Pennine Lancashire and also the wider STP. The Committee wished him well in his future role Apologies and Quoracy Info Apologies were received from Alex Gaw, Roy Fisher, Marie Williams and Mark Youlton. These were acknowledged and the meeting was declared quorate. RESOLVED: The Chair noted the apologies and declared the meeting quorate Declarations of Interest Info The Chair requested that the members declare any interests relating to items on the agenda. The Chair reminded those present that if, during the course of the discussion, a conflict of interest subsequently became apparent, it should be declared at that point. RESOLVED: None declared Minutes from the previous meeting on 6 th July 2017 amendments were discussed as follows: Page 1 Organisation name incorrect for Dr Sumantra Mukerji - Amendment: change to Greater Preston CCG. Page 2 - Minute from the Joint Committee meeting in March regarding the Terms of Reference Amendment: It was noted that the version of the Terms of Reference circulated most recently was not the final version approved by the Joint Committee. It was therefore agreed that the most recent version of the Terms of Reference would be recirculated to Committee members again, noting that further comments and revisions will be incorporated in March 2018, when they will be reviewed. Page 3 Primary Care Transformation item Amendment: Outcome of the discussion was that the JCCCG noted the proposals and the next steps to move them forward. Page 5 second paragraph governance item Amendment: Mary Dowling suggested that the action on this item did not fully reflect the discussion that took place at the meeting and proposed that it should be as follows: ACTION: The paper was noted and following today s discussion, the governance structure will be refined and forwarded to all Chief Executives and Accountable Officers of Trusts, CCGs and Local Authorities, so that they are able to provide formal feedback on the plans. This amendment was agreed. Info and action Joint Committee Clinical Commissioning Group Page 2 of 9
259 Joint Committee of the Clinical Commissioning Groups (JCCCGs) It was noted that there are some outstanding changes to be made to the minutes from the Joint Committee meeting in March. Mary Dowling has provided comments outside of this meeting and these will be incorporated and the minutes will be brought back to the Joint Committee in November for formal ratification. RESOLVED: The minutes of the meetings were accepted subject to the relevant changes being made Action Matrix Review STP Admin Team Info The Action Matrix from the previous meeting was reviewed as follows: 1. Hurdle and Evaluation Criteria: This item has been deferred to the next meeting. 2. Integrated diagnostics update: This item has been deferred to the next meeting. 3. JCCCG Terms of Reference (ToR) - Mary Dowling commented on the ToR and suggested that the Committee should have the final agreed version available to it. The general view was that because of the changes that are taking place in the various other associated groups, such as the STP Board being established and the change in emphasis on the Programme Board and the wider governance of the programme, it makes sense to wait until the end of the financial year to review these, once the new bodies have been in operation for a few months. Amanda Doyle agreed that the most recent ToR which are being worked to could be recirculated, accepting that these would be reviewed in March ACTION: Recirculate the most recent version of the ToR, once Mary s comments have been incorporated Any Other Business Declared: STP Admin Team Info The Chair asked the members of the Committee if they had any other business they wished to declare for discussion at the end of the meeting. Gary Raphael stated that he would like to discuss the position on capital bids. The Chair added that there would also be an opportunity for the public to ask questions at the end of the formal meeting Programme Overview Info Carl Ashworth presented a paper on the STP Outline Work Programme for 2017/18. Amanda Doyle added that this is an STP level work programme and the purpose for the update was to provide the Committee with an understanding of the overarching programme activities and how the work in Local Delivery Partnerships (LDPs) fits with the wider STP strategy. Joint Committee Clinical Commissioning Group Page 3 of 9
260 Joint Committee of the Clinical Commissioning Groups (JCCCGs) STP s are expected to make progress across the following areas: 1. Establishing STP governance arrangements 2. Delivery and assurance of system performance against NHS Constitution and other targets 3. Achievement of system sustainability 4. Transformed services that manage future demand in a different way 5. Designing future commissioning/provider arrangements through ACS and strategic commissioning developments So far, Senior Responsible Officers have identified decisions for the JCCCGs in 2017/18, to sign off clinical policies, agree process and evaluation criteria and agree a strategic commissioning model. The role of the JCCCGs in 2018/19 will be to sign off clinical policies and the short list of options for consultation. An MOU (Memorandum of Understanding) has been agreed between NHS England and the STP, which aligns regulatory responsibilities to support the work of the STP. NHS Improvement had not yet agreed their input to the MOU. Amanda Doyle commented that this will be a fluid piece of work, in that as people agree delegations to the Joint Committee, the work around those decisions will be added to this work plan. Mary Dowling expressed a concern regarding the decision making role of the Joint Committee in the context of the proposed STP governance arrangements. Amanda Doyle commented that the Committee can only be responsible for things that the individual CCGs delegate to it. She added that the role of the Joint Committee is really important in relation to some of the major issues, but unless the individual CCGs delegate the decision making around those things to the Committee, the work required cannot be progressed effectively. Amanda Doyle also suggested that as the STP matures and develops, the responsibilities for the Joint Committee are likely to increase. Mary Dowling said that it was her understanding that delegation had already occurred through the terms of reference of the Joint Committee and the Committee now awaited the proposals/business cases on the major issues it needed to decide. Amanda Doyle and Mary Dowling agreed to discuss this further outside of this meeting. Amanda Doyle stated that the Committee should be taking some responsibility for performance management in relation to the priority areas including quality. At present, no CCG has led her to believe that they are willing to delegate their own responsibility for this to the Committee; however, she added that she would welcome CCG s that would like to pursue a conversation about this. Phil Huxley queried how we would enable clinicians to engage in conversations if we are dealing with things more centrally via the Committee. Amanda Doyle added that we need to widen our engagement to people at all levels and bring their comments and feedback to the process. Joint Committee Clinical Commissioning Group Page 4 of 9
261 Joint Committee of the Clinical Commissioning Groups (JCCCGs) Mary Dowling congratulated Carl Ashworth on the work which had gone into his paper and added that it was very helpful in taking things further forward. She remained concerned that the role of the Joint Committee was not adequately reflected, particularly in relation to delivery and assurance of system priorities. The paper was well received and members were appreciative of the clarification this provides. RESOLUTION: The paper was noted Urgent Care Presentation Info Andrew Bennett introduced the presentations, highlighting the impacts of the Five Year Forward View in relation to commissioning. Lancashire and South Cumbria have an opportunity to develop new approaches to commissioning as follows: Collective: STP-wide e.g. through the Joint Committee. Place-based: in local health and care accountable care systems. Integrated: aligning resources and priorities with NHS England, Local Government and commissioning support services. The next steps were outlined as follows: A proposal has now gone to CCG Governing Bodies requesting delegated decision making into the Joint Committee for specific areas. A Commissioning Development Strategy will now be developed encompassing the next 2-3 years. Two case studies to be presented today Urgent and Emergency Care and Mental Health. David Bonson thanked Andrew Bennett for setting the scene and commenced his presentation on Urgent and Emergency Care. Key messages were discussed as follows: Urgent Care is a whole system not just A&E services. Urgent and Emergency Care Plan There are seven key priorities which will deliver transformation of Urgent and Emergency Care. These are: 1. NHS 111 Online being tested and rolled out during NHS 111 Calls by the end of 2017/18 the percentage of calls receiving clinical advice will exceed 50%. 3. GP Access by March 2019, patients will have access to evening and weekend appointments with general practice. 4. Urgent Treatment Centres standardise approach nationally. These facilities will open 12 hours per day and will be staffed by clinicians, with access to simple diagnostics. 5. Ambulances are currently under extreme pressure. Ensure right vehicles are despatched as quickly as possible and move to a hear and treat/see and treat model. Joint Committee Clinical Commissioning Group Page 5 of 9
262 Joint Committee of the Clinical Commissioning Groups (JCCCGs) 6. Hospitals Emergency departments are very congested. Ensure that only patients that need to be there are there and others are screened and signposted to the most appropriate service. 7. Hospital to Home Move on to home/more appropriate care setting at the earliest opportunity. A lot of work is going on regarding delayed transfers of care (DTOC). Urgent Treatment Centres - national service specification was published in July The aim is to have 150 Urgent Treatment Centres in place by 2017, with full coverage by December Key components of the specification are: o GP led service as part of multidisciplinary workforce o Open at least 12hrs a day, 7/365 o Direct booking from NHS111, ambulance services, GPs and Walk in o Access to simple diagnostics and X-ray facilities Performance The national expectation is that we achieve the standard of 90% of people seen within the 4 hour period by September 2017 and 95% by March Amanda Doyle thanked David Bonson for the presentation and asked if he could be more specific about the action that needs to be taken immediately. David Bonson responded by suggesting that there is a need to do a stock take of contracts for CCG s and providers, in order to move this work forward, in terms of where we are now against the national specification. There is a deadline for the end of September This is a very specific ask. The Lancashire and South Cumbria Urgent Care Workstream is co-ordinating this piece of work. David Bonson added that there is a need to quickly think about what the commissioning arrangements would look like to deliver the requirements described in the service specification. Lead commissioner arrangements are linked with the delegated decisions work. There will also be a requirement to work collaboratively with providers around the function of the whole of urgent care, with an integrated approach to managing the workforce to deliver this effectively. There is also a plan to use business intelligence to track the patient journey, to help with understanding patterns, demand and risks. The Chair asked if there were any questions. A discussion took place around recent A&E performance, which is currently a risk across the whole system. We are in a very challenged position and there is a need to focus on what we are going to do about it. Lancashire and South Cumbria have an opportunity to work collectively to improve performance across the system. Geoffrey O Donoghue asked whether the presentations could be circulated with the papers for the Joint Committee. Amanda Doyle responded to state that the NHS England Joint Committee Clinical Commissioning Group Page 6 of 9
263 Joint Committee of the Clinical Commissioning Groups (JCCCGs) Urgent Care Specification has already been cascaded and that the presentations that are used, do not always tell the full story, as they are used as a tool to aid full explanation and therefore there could be a risk of confusion and misinterpretation if they were on the website. The Joint Committee is asked to agree the following:- To proceed with the stock take of existing contracts with CCG s and Providers to take this work forward. RESOLUTION: The Joint Committee agreed this Mental Health Presentation Info Debbie Nixon and Andrew Bibby presented a slide deck, which built on David Bonson s Urgent Care presentation. Debbie Nixon explained that the Mental Health Five Year Forward View is very explicit and sets a complex direction of travel in the following priority areas: Children and young people s mental health Perinatal mental health Adult mental health: common mental health problems Adult mental health: community, acute and crisis care Adult mental health: secure care pathway Health and justice Suicide prevention In addition to the Mental Health Five Year Forward View, there is a requirement to deliver a Mental Health Delivery Plan, which is aimed at monitoring performance and delivery through one function. This is very prescriptive, particularly around workforce and the delivery of outcomes. There are some really clear milestones that need to be delivered. There will be a consistent high quality offer for mental health services, regardless of where people live. There will be a tiered approach to services as follows: Tier 1 services neighbourhood level Tier 2 services Local Delivery Partnerships Tier 3 services STP level Tier 4 services STP or inter STP There is currently significant variation across Lancashire and South Cumbria which needs addressing. There will be a consistency around the what, but local flexibility about the how (taking account of incidence; population density; demography; geography). There are also a range of services that are in the main commissioned by NHS England including children, health and justice, secure services for adults, inpatient services and perinatal services. There will be equitable access for the whole population. Joint Committee Clinical Commissioning Group Page 7 of 9
264 Joint Committee of the Clinical Commissioning Groups (JCCCGs) The tier approach aims to deliver seamless transition for patients, irrespective of where they are from. There is also a huge opportunity around prevention and reducing demand, supporting people in communities to play an active role in their health and care. We have seen recent improvements in our performance in mental health and we have been rewarded for this, in that we have received capital resource to improve perinatal inpatient services, hospital liaison and transformation resource for improving access. We have an opportunity for greater collaboration across the whole patch, to help us to progress at pace, improve clinical outcomes, utilise workforce effectively, manage performance through a single system and increase our overall productivity and efficiency. Lancashire and South Cumbria are doing well against some of the performance indicators, but we are not achieving all. Step changes are required to achieve national priorities and mandates. We need to look at things to implement collectively or consistently. Debbie Nixon suggested a slight amendment to the ask of the Joint Committee as outlined below. The JCCCG is asked to agree the following: To receive a detailed proposal for a revised operating model for the commissioning of mental health services. This aims to implement the national mental health and wellbeing strategy. RESOLUTION: The Joint Committee agreed this Any other business 1. Capital Gary Raphael presented a slide deck on the Capital Bid. He explained that we had been successful previously, despite the tight timescales we had to refine and submit the bids. Wave 1 success: Mental Health Inpatient scheme affecting Burnley and Chorley hospitals ( 5m to 10m scheme) A&E development at Blackburn Hospital ( 5m to 10m scheme) Gary Raphael explained that as part of Wave 2 (September 2017), we will be submitting a Lancashire & South Cumbria pathology scheme, covering all four acute trusts with an estimated cost of 31m. In addition to the pathology scheme, we had decided to make NHS England and NHS Improvement aware of the priority schemes for Lancashire and South Cumbria, in relation to urgent and emergency care services, in effect, the pipeline of developments that were not yet ready for wave 2 submission, but would be next in line. Joint Committee Clinical Commissioning Group Page 8 of 9
 Improvements to cancer treatment Patient experience improved in A&E Costs circa 35m over next 2 years The Joint Committee is asked to support the following:-")
265 Joint Committee of the Clinical Commissioning Groups (JCCCGs) The relevant submission was still in development, but so far the benefits and costs of this could be outlined as follows: Improvements to A&E and RTT (Referral to Treatment Time) Improvements to cancer treatment Patient experience improved in A&E Costs circa 35m over next 2 years The Joint Committee is asked to support the following:- Submission of this bid. RESOLUTION: The Joint Committee supported this. 2. The next Joint Committee meeting incorrect date on the agenda The Chair stated that the date of the next Joint Committee meeting was outlined incorrectly on the agenda. He confirmed the correct date as 2 nd November pm 3.00pm Morecambe Bay CCG - The Lecture Theatre, Moor Lane Mills, Moor Lane, Lancaster, Lancashire, LA1 1QD. A message will be communicated to the public via the website and via Local Delivery Partnership communication channels. The next JCCCG Meeting will be held on: 2 nd November 2017, 1.00pm 3.00pm - Morecambe Bay CCG - The Lecture Theatre, Moor Lane Mills, Moor Lane, Lancaster, Lancashire, LA1 1QD The Chair thanked the Committee members and members of the public for their attendance and closed the meeting prior to taking questions from members of the public. Topics discussed through the Public Questions: 1. Access to papers prior to the meeting, difficulties accessing the website and publicising the Joint Committee meetings dates via different channels. 2. Our confidence in achieving success. Joint Committee Clinical Commissioning Group Page 9 of 9
Register of declaration of interests for the Governing Body members March 2018
 Register of declaration of interests for the Governing Body members March 2018 Name Current position (s) held in the CCG i.e. Governing Body member; Committee member; Member practice; CCG employee or other
Register of declaration of interests for the Governing Body members March 2018 Name Current position (s) held in the CCG i.e. Governing Body member; Committee member; Member practice; CCG employee or other
NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING. 25 November 2014, 9:30-11:30
 Item WLCCGB NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING 25 November 2014, 9:30-11:30 Boardroom in Hilldale, Wigan Road, Ormskirk, Lancashire 15 minutes to be allocated for questions
Item WLCCGB NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING 25 November 2014, 9:30-11:30 Boardroom in Hilldale, Wigan Road, Ormskirk, Lancashire 15 minutes to be allocated for questions
NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING. 22 March 2016, 9.30 am am
 NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING 22 March 2016, 9.30 am 11.30 am Lathom North, Lancashire Manor Hotel, Prescott Road Pimbo, Skelmersdale, WN8 9QD 15 minutes to be
NHS WEST LANCASHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING 22 March 2016, 9.30 am 11.30 am Lathom North, Lancashire Manor Hotel, Prescott Road Pimbo, Skelmersdale, WN8 9QD 15 minutes to be
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12. Date of Meeting: 23 rd March 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome:
 TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
Update on NHS Central London CCG QIPP schemes
 Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Wolverhampton Clinical Commissioning Group 1
 Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10. Date of Meeting: 31 st August 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 15 December 2016 Agenda No: 3.3 Attachment: 04 Title of Document: Surgery Readiness Option Report Author: Andrew Moore (Programme Director
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 15 December 2016 Agenda No: 3.3 Attachment: 04 Title of Document: Surgery Readiness Option Report Author: Andrew Moore (Programme Director
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MEMORANDUM OF UNDERSTANDING
 MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
The Symphony Programme an example from the UK of integrated working between primary and secondary care. Jeremy Martin, Symphony Programme Director
 The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
PRIMARY CARE COMMISSIONING COMMITTEE MEETING
 PRIMARY CARE COMMISSIONING COMMITTEE MEETING Date of meeting Title of report 20 th June 2017 Agenda item number Unscheduled Primary Care Services for the Fylde Coast 7 Paper Presented by: Alison Kerfoot,
PRIMARY CARE COMMISSIONING COMMITTEE MEETING Date of meeting Title of report 20 th June 2017 Agenda item number Unscheduled Primary Care Services for the Fylde Coast 7 Paper Presented by: Alison Kerfoot,
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015
 NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015 Title Locality Committee Reports Q2 2015/16 Agenda Item: 13 Purpose (tick one only) Responsible Director(s) and Job Title
NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015 Title Locality Committee Reports Q2 2015/16 Agenda Item: 13 Purpose (tick one only) Responsible Director(s) and Job Title
Memorandum of understanding for shadow Accountable Care Systems
 Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
QUALITY IMPROVEMENT COMMITTEE
 : 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
: 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
BIRMINGHAM CITY COUNCIL
 BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
AGENDA ITEM NO: 046/17
 AGENDA ITEM NO: 046/17 GOVERNING BODY MEETING: Governing Body Meeting DATE OF MEETING: 13 th September 2017 REPORT AUTHOR AND JOB TITLE: Rebecca Knight Head of Assurance & Risk REPORT TITLE: STRATEGIC
AGENDA ITEM NO: 046/17 GOVERNING BODY MEETING: Governing Body Meeting DATE OF MEETING: 13 th September 2017 REPORT AUTHOR AND JOB TITLE: Rebecca Knight Head of Assurance & Risk REPORT TITLE: STRATEGIC
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Any Qualified Provider: your questions answered
 Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
Healthier Wigan Partnership Board. Richard Mundon Director of Strategy and Planning. Approve x Adopt Receive for information. On the BAF.
 Trust Board Agenda Item 6. Date: 31.05.17 Title of Report Purpose of the report and the key issues for consideration/decision Prepared by: me & Title Presented by: Action Required (please X) Strategic/Corporate
Trust Board Agenda Item 6. Date: 31.05.17 Title of Report Purpose of the report and the key issues for consideration/decision Prepared by: me & Title Presented by: Action Required (please X) Strategic/Corporate
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July C Hickson, Head of Management Accounts
 NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July 2013 9.4 Date of the meeting 18/09/2013 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS Dorset Clinical Commissioning Group Governing Body Meeting Financial Position as at 31 st July 2013 9.4 Date of the meeting 18/09/2013 Author Sponsoring GB member Purpose of report Recommendation Resource
5. Does this paper provide evidence of assurance against the Governing Body Assurance Framework?
 Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016
 Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Papers for the. West Kent Primary Care Commissioning Committee (Improving Access) Tuesday 21 st August at 4 4:30 pm
 Tuesday 21 st August at 4 4:30 pm") Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Croydon Clinical Commissioning Group Clinical Leadership Meeting Minutes
 Attachment 16 Appendix 1 Date: 13 July 2012 Time: 13 30 15 30 Location: Room 11.4, Leon House Present: Dev Malhotra, GP Board Member Bobby Abbot, GP Dipti Gandhi, Clinical Leader Brian Okumu, GP Clinical
Attachment 16 Appendix 1 Date: 13 July 2012 Time: 13 30 15 30 Location: Room 11.4, Leon House Present: Dev Malhotra, GP Board Member Bobby Abbot, GP Dipti Gandhi, Clinical Leader Brian Okumu, GP Clinical
Transforming Clinical Services. Our developing clinical strategy
 Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 25th July 2016 Title: Executive Summary: Action Requested: Author: Contact Details: Resource Implications: Equality and Diversity Assessment
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 25th July 2016 Title: Executive Summary: Action Requested: Author: Contact Details: Resource Implications: Equality and Diversity Assessment
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting
 Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality and Safety
 Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Title: Replacement of the Commissioning Advisory Forum Agenda Item: 9
 Meeting of Bristol Clinical Commissioning Group To be held on Tuesday, 2 July 2013 commencing at 1.30 pm in the BAWA Centre Title: Replacement of the Commissioning Advisory Forum Agenda Item: 9 1 Purpose
Meeting of Bristol Clinical Commissioning Group To be held on Tuesday, 2 July 2013 commencing at 1.30 pm in the BAWA Centre Title: Replacement of the Commissioning Advisory Forum Agenda Item: 9 1 Purpose
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Responding to a risk or priority in an area 1. London Borough of Sutton
 Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Blackpool CCG Governing Body Part I
 2 August 2016 Prioritising the Use of Resources Background Governing Body members are aware of the huge growing pressures on NHS finances nationally and locally. This is primarily due to the slowing down
2 August 2016 Prioritising the Use of Resources Background Governing Body members are aware of the huge growing pressures on NHS finances nationally and locally. This is primarily due to the slowing down
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Status Internal Purpose: The attached paper provides an update of progess made in UHMB
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Status Internal Purpose: The attached paper provides an update of progess made in UHMB
Chief Accountable Officer Director Transformation and Quality. Director Transformation and Quality Chief Accountable Officer
 Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April The Broadway, Wimbledon, SW19 1RH
 MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
CCG authorisation: the role of medicines management
 May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
EMERGENCY PRESSURES ESCALATION PROCEDURES
 OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Westminster Health and Wellbeing Board
 Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release