The Health Integration Collaborative A Year in the Making
|
|
|
- Pierce Bailey
- 6 years ago
- Views:
Transcription

1 The Health Integration Collaborative A Year in the Making Mary Jo Whitfield, VP of Behavioral Health Cheri DeBree, Director of Integrated Health
2 Presentation Objectives An overall look at integrated health practice A clinical/operational look at JFCS s Integrated Health Program as a possible model for integrative care. A practical look at how our electronic health record, NextGen, assists us throughout our program from beginning to end of a client s services with us. How reports generated from our electronic health record has allowed us to manage our program and helped us capture outcomes data.
3 Why Integrate Physical and Behavioral Health Care? Behavioral and physical health care have historically operated in silos. Health care integration is designed to: Improve patient access to care in a setting where patients are most comfortable. Reduce health care disparities. Contain costs by promoting a whole health approach. Improve patient outcomes through coordination of care.
4 Key Drivers of Integrated Health Patient Protection and Affordable Care Act State Health Insurance Exchanges Mental Health Parity Medicaid Expansion Maricopa County Regional Behavioral Health Authority Contract
5 National Driver: Affordable Care Act Health Insurance Exchanges Mental Health Parity Medicaid Expansion
6 Concepts Common to All Integrated Care Models Medical or Health Home Health Care Team Stepped Care Four Quadrant Clinical Integration

7 Four Quadrant Clinical Integration
8 Models of Integrated Care Coordinated Care Co-Located Care Transformed/Full Integration Virtual Integration
9 Jewish Family and Children s Services Who are we? Outpatient Behavioral Health Provider - Maricopa County In operation since 1935 JFCS is Currently serving 5,025 adults and 4,838 children and has about 90% Medicaid client population Our enrollment reflects the cultural diversity of our county Magellan Behavioral Health of Arizona Community Re-investment Grant
10 Integrated Health Program Data Program began May 1, ,400 clients served 700 active clients in the program typically 2,400 Health Risk Assessments have been collected 60% opt in rate as new clients to JFCS
11 Integrated Health Program Data Collaborative relationship with MIHS since August, 2010 Partnered with MIHS, a federally qualified Health center look alike 4 clinics across Maricopa County 8 Health Navigators






12 Integrated Health Client Demographics Women 80% Men 20% Age Demographics 60 + = 5% = 18% = 24% = 24% = 29% Age Ages Ages Ages Ages 60 +

13

14 Axis I Diagnosis Analysis

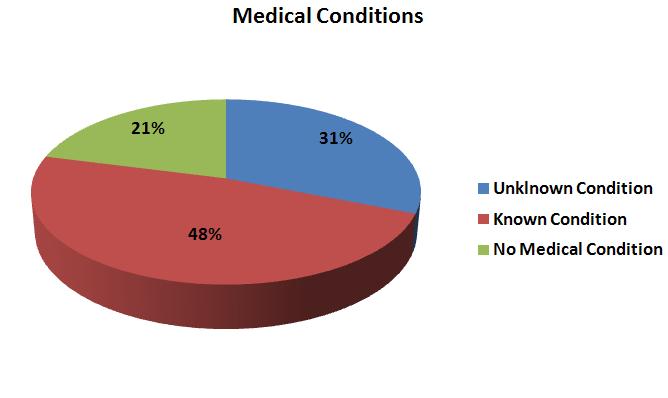
15 Axis III Medical Conditions Analysis

16 Chronic Disease Representation in the Integrated Health Client Population

17 With being overweight or obese being one of the lead health concerns with our clients, nutrition is discussed as part of our program.
18
19 Community Re-Investment Grant Objectives Objective 1: Assist behavioral health recipients in establishing/maintaining an ongoing, lasting relationship with a primary care provider. Objective 2: Facilitate improvements in the physical health of behavioral health recipients. Objective 3: Improve the mental health of behavioral health recipients. Objective 4: Enable behavioral health recipients to increase control over their health. Objective 5: Develop a health information infrastructure that includes an electronic medical record and shared health information for behavioral health recipients and their primary care and behavioral health providers.
20 Objective 1: PCP Relationship Investigate clients current relationship with Primary Care Physician (PCP) Is client is satisfied with current PCP Is client with Maricopa Integrated Health System already Assist client in changing PCP with AHCCCS PCP Notification auto faxed from EHR Assist client in scheduling first appointment with MIHS

21
22
23 Objective 2: Improved Physical Health Clients recent medical visits Client s satisfaction with current PCP Maricopa Integrated Health Systems Preventive screenings and testing Appointment planning Transportation to appointments if needed Compiling of medical records Medical decision making Advocate for the client Chronic Disease Self Management Stanford Best Practice Improved coordination and collaboration between medical and behavioral health through HIE and other efforts
24
 In Arizona, the average is even higher at 32")
25 Objective 3: Improved Mental Health People with mental health and substance use disorders die 25 years younger than the general population on average, according to a 2008 study done by the National Association of State Mental Health Program Directors (NASMHPD) In Arizona, the average is even higher at 32 years earlier

26
27 Client Quote on Integrated Care Services I have been a patient at JFCS for several years now and have received exceptional care. My life has improved since I first came here and I am grateful. However, since I was first introduced to Integrated Health by my peer navigator, the care I receive has become much more meaningful. Not just the behavioral health care, the physical health care I receive has improved as well. I say this because Adrienne has enlightened me to the fact that physical and emotional well being are inter-connected and cannot improve if either is neglected. - Anonymous satisfaction survey comment
28 Objective 4: Increased Control in Overall Health Teaching self management skills Decision making skills Health literacy skills equips clients to improved ability to manage health Empowerment skills Nutrition and exercise Information Resources Social Supports Chronic Disease Self Management WHAM
29 CDSMP Health Living Quotes from Clients After going to the CDSMP class, I learned a lot about how to take care of myself. I learned that I am not alone and that others suffer from similar health problems as me. I used to feel alone, but now I know I am not. - RS, CDSMP work shop participant I learned so much in the CDSMP class. People always stated that I was too young to be sick all the time and I felt ashamed about it. Now I realize that bad things happen to good people and I realize I can t compare myself to others. Just take care of myself so I can take care of my family. - BB, CDSMP work shop participant

30

31 Health Literacy is an important component of the IH Program



32 Relaxation and Stress Management Classes Quote from a enrolled client: The relaxation class helps me to cope with my problems better and helps me think in a more positive way. I really enjoy coming and being a part of this two days a week. I feel like it is empowering me, making me stronger as a person, more positive, and healthier in my lifestyle. This is a wonderful program. Nearly 60-90% of visits to healthcare professionals are either caused or exacerbated by stress. Dr. Herbert Benson: Institute of Mind-Body Medicine at Massachusetts General Hospital - SF, Integrated Health Client One of the most important components of human resiliency is social support. There is a lot of data supporting the importance of social supports in health outcomes.
33 The Relaxation Response Research shows the Relaxation Response is an essential resiliency self-management skill that is as predictable as medication in immediately reversing the stress-induced flight-or-fight response. -Benson, H. The Relaxation Response, William Morton and Company, 1975 Let s Do It!
34 EMPOWERING CLIENTS Helping clients gain the knowledge, skills, and attitudes for coping with changes in lifestyle and circumstances Learning to help themselves, management of their own care Greater confidence in themselves Increases clients understanding of the medical system Greater ability for the client to meet their own needs Gives clients knowledge that they can share with others
35 EMPOWERING CLIENTS Working our way out of a job from day one Encouraging ability to self care, cope and use active communication skills Enhancing ability to be assertive Providing access to information and resources Discussing various options and helping with decision-making process

36
37 Objective 5: Shared Health Information Continuity of Care Document: A patient summary containing a core data set of the most relevant administrative, demographic, and clinical information facts about a patient's healthcare, covering one or more healthcare encounters. It provides a means for one healthcare practitioner, system, or setting to aggregate all of the pertinent data about a patient and forward it to another practitioner, system, or setting to support the continuity of care. Six Mandated CCD Data Elements: 1. Header/Document Identifying Information 2. Patient Identifying Information. 3. Patient s Insurance and Financial Information. 4. Health Status of the Patient 5. Care Documentation includes some detail on the patient-clinician encounter history, such as the dates and times of recent and pertinent visits and the purposes of the visits and names of clinicians or providers 6. Care Plan Recommendation includes planned or scheduled tests, procedures or regimens of care.
38 Health Information Exchange JFCS and MIHS Sharing client data between JFCS and MIHS on two fronts utilizing the current CCD standard: JFCS can pull CCD from MIHS and bring in to EHR JFCS can pull CCD from our EHR and fax over to MIHS for inclusion in their client record

39 Scope of Integrated Health I feel empowered about my health because of the IHP (Integrated Health Program) - Anonymous satisfaction survey comment I was helped in finding a new and much better P.C.P, Thank you. Groups, workshops, PNP and counseling are all very helpful in dealing with my health. -Anonymous satisfaction survey comment

40 Health Risk Assessment Demo
41
42 Health Promotion Chronic Disease Self Management Healthy Living WHAM Whole Health Action Management Freedom from Smoking American Lung Association N.O.T. Not On Tobacco for youth American Lung Association Know Diabetes Greater Valley Area Health Education Center (GVAHEC) Know Heart Health Greater Valley Area Health Education Center (GVAHEC) Peer to Peer Smoking Cessation - Magellan Plan Well Eat Well Greater Valley Area Health Education Center Basic Tobacco Intervention Skills AZ Department of Health Services Tobacco Treatment Specialist Training AZ Department of Health Services COPD 101 Motivational Interviewing
43


44 CDSMP Evidence based best practice Created and tracked by Stanford Less expensive to get staff trained Trainings are easy to get in to Local support and meeting Great tools, exercises Weekly action plan very concrete Very well organized, easy to learn and teach Self management is core Great at fostering social supports within the group Gentle accountability Strong AZ presence Active list serve WHAM Evidence based best practice Specifically created by SAMHSA for behavioral health clients with chronic illnesses Low cost of participant materials Great tools Very well organized Very goal/action oriented Self Management is core Weekly action plan Big social component Relaxed, flexible Can be given to one person or in a group format Relaxation Response Catch it, Check it, Change it
45 CDSMP Not written for behavioral health population Participant materials higher $16 Not as flexible as WHAM Have to have a class of at least 6-8 to run (Stanford wants min. of 10) WHAM Expensive to train staff Difficult to bring WHAM training locally List serve not active enough Marketing materials not developed yet Little time for clients to expound, get support from the group Very concerned with sticking to the material, may not add anything from outside of CDSMP

46 Integrated Health Update Form
47 HRA Report Reporting HRA Comparison Report Integrated Health Update Report Client Caseload Tracker Report Daily staff productivity reports Billed services and unit reports Appointments kept, no billing has occurred
48 Outcomes PCP Relationship Outcomes and Baseline: We have assisted 66% of clients needing a better relationship with their PCP 75% of surveyed clients reported IH Program helped them develop better PCP relationship 86% of surveyed clients reported better coordination of care amongst health providers Improved Physical Health: We have delivered resources and information regarding health and wellness to 80% of our clients in the IH program 39% of clients needing screening or routine testing received it 55% Of clients walking in with untreated chronic medical disease, received medical appointment within 45 days of beginning the program 33% of clients that reported not managing their diabetes are now successfully managing it and have reduced their A1C levels to below 9% 77% of surveyed clients report they feel an improvement in overall physical health
49 Outcomes Improved Mental Health: Screen 100% of all IH clients for tobacco use, 112 have been given resources and information on tobacco cessation including formal classes and ASH Line referrals (29) To date, 5 IH clients have stopped the use of tobacco 42% of clients desiring to cut back or stop alcohol use did so 84% of surveyed clients reported be able to manage their symptoms better since joining the program Increased Control over Health: Almost 100 CDSMP participants 78% of surveyed clients reported they were functioning better overall since joining the program Overall Program Satisfaction: 93%
50 Client Quote on Integrated Care Services CLIENT VIDEO
51 Mary Jo Whitfield, MSW Vice President of Behavioral Health Cheri DeBree, MC Integrated Health Director 4747 N. 7 th Street, Suite 100 Phoenix, AZ Phoenix, Arizona
6/27/2014. THE NEW TECHNOLOGY LANDSCAPE Presentation Objectives. The Landscape Drives Metrics. Issues: Responding to Need. AZ Drivers/Priorities
 x == 6/27/2014 THE NEW TECHNOLOGY LANDSCAPE Presentation Objectives Using Business Analytics & Health Information Exchanges to Improve Practice & Sustain Organizations Business Metric Development Strategies
x == 6/27/2014 THE NEW TECHNOLOGY LANDSCAPE Presentation Objectives Using Business Analytics & Health Information Exchanges to Improve Practice & Sustain Organizations Business Metric Development Strategies
Arizona Living Well Institute
 HEALTH NET M A R C H 2 6, 2 0 1 5 J E N N A B U R K E, B S, C H E S I N T E R I M D I R E C T O R W W W. A Z L W I. O R G Agenda 1. 2. Learn of the background, structure and purpose of Healthy Living 3.
HEALTH NET M A R C H 2 6, 2 0 1 5 J E N N A B U R K E, B S, C H E S I N T E R I M D I R E C T O R W W W. A Z L W I. O R G Agenda 1. 2. Learn of the background, structure and purpose of Healthy Living 3.
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Using the Patient Activation Measure (PAM) to Promote Patient Engagement
 to Promote Patient Engagement") Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
MERCY HOSPITAL LEBANON COMMUNITY HEALTH IMPROVEMENT PLAN ( )
") MERCY HOSPITAL LEBANON COMMUNITY HEALTH IMPROVEMENT PLAN (2016-2019) An IRS-mandated Community Health Needs Assessment (CHNA) was recently completed for each hospital within the Central Community: * Hospital
MERCY HOSPITAL LEBANON COMMUNITY HEALTH IMPROVEMENT PLAN (2016-2019) An IRS-mandated Community Health Needs Assessment (CHNA) was recently completed for each hospital within the Central Community: * Hospital
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
How to Register and Setup Your Practice with HowsYourHealth. Go to the main start page of HowsYourHealth:
 How to Register and Setup Your Practice with HowsYourHealth Go to the main start page of HowsYourHealth: After you have registered you will receive a practice code and password. Save this information!
How to Register and Setup Your Practice with HowsYourHealth Go to the main start page of HowsYourHealth: After you have registered you will receive a practice code and password. Save this information!
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans
 Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Community Health Needs Assessment 2013 Oakwood Heritage Hospital Implementation Strategy
 Community Health Needs Assessment 2013 Oakwood Heritage Hospital Implementation Strategy Community Health Needs Assessment 2013 Oakwood Healthcare CHNA Implementation Strategy Community Health Needs Assessment
Community Health Needs Assessment 2013 Oakwood Heritage Hospital Implementation Strategy Community Health Needs Assessment 2013 Oakwood Healthcare CHNA Implementation Strategy Community Health Needs Assessment
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
 Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
Relationships: The Behavioral Health Consultant, Primary Care Physician, and Psychiatrist i t Healthcare Integration Webinar National Council for Community Behavioral Healthcare February 25, 2010 The Status
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Behavioral Health Services
 18 Behavioral Health Services Reviewed/Revised: 10/10/2017, 02/01/2017, 02/15/2016, 08/31/2015, 09/18/2014 INTRODUCTION The State of Arizona has contracted the administration of AHCCCS mental health and
18 Behavioral Health Services Reviewed/Revised: 10/10/2017, 02/01/2017, 02/15/2016, 08/31/2015, 09/18/2014 INTRODUCTION The State of Arizona has contracted the administration of AHCCCS mental health and
EVOLENT HEALTH, LLC. Asthma Program Description 2018
 EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Community Health Improvement Report
 SUBURBAN HOSPITAL 2016-2017 Health Improvement Report Behavioral Health: High Priority, Deliberate Approach The 2016 Health Needs Assessment (CHNA) process identified through primary and secondary data,
SUBURBAN HOSPITAL 2016-2017 Health Improvement Report Behavioral Health: High Priority, Deliberate Approach The 2016 Health Needs Assessment (CHNA) process identified through primary and secondary data,
COPD National Action Plan. COPD.nih.gov
 COPD National Action Plan COPD.nih.gov Kyle Mahan, MSM, RRT Vice President of KSRC DCE for Jefferson Community and Technical College RCP 14-ish Years AZ native. I am not from Kentucky, but I got here as
COPD National Action Plan COPD.nih.gov Kyle Mahan, MSM, RRT Vice President of KSRC DCE for Jefferson Community and Technical College RCP 14-ish Years AZ native. I am not from Kentucky, but I got here as
CASE MANAGEMENT TOOLS:
 CASE MANAGEMENT TOOLS: ENGAGING PATIENTS AS PARTNERS IN CARE September 19, 2017 Chinle Service Unit Diabetes Program Navajo Area Indian Health Service Miranda Williams Krista Haven CHINLE SERVICE UNIT
CASE MANAGEMENT TOOLS: ENGAGING PATIENTS AS PARTNERS IN CARE September 19, 2017 Chinle Service Unit Diabetes Program Navajo Area Indian Health Service Miranda Williams Krista Haven CHINLE SERVICE UNIT
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Profile: Integrating the Patient Activation Measure Into Health Coaching to Improve Patient Engagement
 MEASURING PATIENT ENGAGEMENT: HOW IS CAPACITY AND WILLINGNESS TO ENGAGE IN HEALTH CARE ASSESSED? 75 Profile: Integrating the Patient Activation Measure Into Health Coaching to Improve Patient Engagement
MEASURING PATIENT ENGAGEMENT: HOW IS CAPACITY AND WILLINGNESS TO ENGAGE IN HEALTH CARE ASSESSED? 75 Profile: Integrating the Patient Activation Measure Into Health Coaching to Improve Patient Engagement
EVOLENT HEALTH, LLC. Asthma Program Description 2017
 EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Central Zone Healthcare Plan. For Placement Only. Strategy Overview
 Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Building Connective Tissue for Integrated Care The Unfolding NH Medicaid Story. April 17, 2018
 Building Connective Tissue for Integrated Care The Unfolding NH Medicaid Story April 17, 2018 Who Are We Supporting In IDN-1? Source: MAeHC Analysis, NH Medicaid IDN Region 1 Data Book Release 1 Findings:
Building Connective Tissue for Integrated Care The Unfolding NH Medicaid Story April 17, 2018 Who Are We Supporting In IDN-1? Source: MAeHC Analysis, NH Medicaid IDN Region 1 Data Book Release 1 Findings:
The CCBHC: An Innovative Model of Care for Behavioral Health
 The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
Chapter 1: Responsibilities for Care in Community/Public Health Nursing Test Bank
 Chapter 1: Responsibilities for Care in Community/Public Health Nursing Test Bank MULTIPLE CHOICE 1. A community/public health nurse is best defined as a nurse who a. Applies concepts and knowledge from
Chapter 1: Responsibilities for Care in Community/Public Health Nursing Test Bank MULTIPLE CHOICE 1. A community/public health nurse is best defined as a nurse who a. Applies concepts and knowledge from
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare
: Billing, Codes and Need at Adelante Healthcare") Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Better health. Better bottom line.
 Better health. Better bottom line. Tailored well-being solutions to improve health and lower costs 847987 06/11 The Power of Well-Being To us, well-being is more than just promoting physical wellness.
Better health. Better bottom line. Tailored well-being solutions to improve health and lower costs 847987 06/11 The Power of Well-Being To us, well-being is more than just promoting physical wellness.
6/3/ National Wellness Conference. Developing Strategic Partnerships to improve the Health and Wellness of the Community. Session Objectives
 2015 National Wellness Conference Developing Strategic Partnerships to improve the Health and Wellness of the Community. Kimberly Sbardella, R.N. Manager, Community Health & Wellness Carolinas HealthCare
2015 National Wellness Conference Developing Strategic Partnerships to improve the Health and Wellness of the Community. Kimberly Sbardella, R.N. Manager, Community Health & Wellness Carolinas HealthCare
Health In Action Program
 WIN for Alaska and University of Alaska s Health In Action Program for Total Health And Wellness The Partnership Wellness Initiatives Network for Alaska, Inc. (WIN for Alaska) and University of Alaska
WIN for Alaska and University of Alaska s Health In Action Program for Total Health And Wellness The Partnership Wellness Initiatives Network for Alaska, Inc. (WIN for Alaska) and University of Alaska
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Brian Sheitman MD
 Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Patient and Family Engagement: Strategies to Improve Health
 Patient and Family Engagement: Strategies to Improve Health UHF & GNYHA 24 th Annual Symposium on Health Care Services in New York: Research and Practice David Cohen, MD, Maimonides Medical Center Overview
Patient and Family Engagement: Strategies to Improve Health UHF & GNYHA 24 th Annual Symposium on Health Care Services in New York: Research and Practice David Cohen, MD, Maimonides Medical Center Overview
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
VHA Preventive Care Program. Clinician/Educator Programs
 Behavioral Medicine Careers in the VA Health Care System: Clinician/Educator Positions Michael Goldstein, MD, Associate Chief Consultant for Preventive Medicine Margaret (Peg) Dundon, PhD, National Program
Behavioral Medicine Careers in the VA Health Care System: Clinician/Educator Positions Michael Goldstein, MD, Associate Chief Consultant for Preventive Medicine Margaret (Peg) Dundon, PhD, National Program
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Implementation Strategy Addressing Identified Community Health Needs
 2014-2017 Implementation Strategy Addressing Identified Community Health Needs Response to Schedule H Form 990 Table of Contents Page Overview of the Patient Protection and Affordable Care Act 3 Defined
2014-2017 Implementation Strategy Addressing Identified Community Health Needs Response to Schedule H Form 990 Table of Contents Page Overview of the Patient Protection and Affordable Care Act 3 Defined
Presenters: Gayle Alston MS. Gwenyth Johnson, MS. RD. LD. Cliff Burt, MPA
 Georgia Department of Human Services Implementing EBP for Family Caregivers Presenters: Gayle Alston MS. Gwenyth Johnson, MS. RD. LD. Cliff Burt, MPA Date: September 11, 2012 Vision, Mission and Core Values
Georgia Department of Human Services Implementing EBP for Family Caregivers Presenters: Gayle Alston MS. Gwenyth Johnson, MS. RD. LD. Cliff Burt, MPA Date: September 11, 2012 Vision, Mission and Core Values
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
MAA ACTIVITY CODES & EXAMPLES
 MAA ACTIVITY CODES & EXAMPLES CODE 1 OTHER PROGRAMS/ACTIVITIES Non Medi-Cal health and wellness activities Social services Educational services Teaching services Employment and job training Providing or
MAA ACTIVITY CODES & EXAMPLES CODE 1 OTHER PROGRAMS/ACTIVITIES Non Medi-Cal health and wellness activities Social services Educational services Teaching services Employment and job training Providing or
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
HW/ODH XDR CDS. Alliance of Chicago GE Centricity Qvera
 Use Case Title: Value Based Care Overview: Tim Jones a 54 year old male police officer has Diabetes and presents at his Primary Care Provider with an abnormal lab result. Follow his journey through Primary
Use Case Title: Value Based Care Overview: Tim Jones a 54 year old male police officer has Diabetes and presents at his Primary Care Provider with an abnormal lab result. Follow his journey through Primary
Behavioral Health Services
 18 Behavioral Health Services INTRODUCTION The State of Arizona has contracted the administration of AHCCCS mental health and substance abuse services program to Regional Behavioral Health Authorities
18 Behavioral Health Services INTRODUCTION The State of Arizona has contracted the administration of AHCCCS mental health and substance abuse services program to Regional Behavioral Health Authorities
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Number of individuals potentially accessing settings that have adopted policies to implement nutrition standards for health food
 Attachment 15 Wayne County Public Health Focus Area 1: Reduce Obesity in Children and Adults Do the suggested intervention(s) address a disparity? Yes No *Objective 1.3.2 targeting the low income population
Attachment 15 Wayne County Public Health Focus Area 1: Reduce Obesity in Children and Adults Do the suggested intervention(s) address a disparity? Yes No *Objective 1.3.2 targeting the low income population
Family and Youth Peer Support September 19, 2011, 2:00 4:00 p.m., ET
 Care Management Entity Quality Collaborative Technical Assistance Webinar Series Family and Youth Peer Support September 19, 2011, 2:00 4:00 p.m., ET For audio and to participate, dial: (866) 699-3239
Care Management Entity Quality Collaborative Technical Assistance Webinar Series Family and Youth Peer Support September 19, 2011, 2:00 4:00 p.m., ET For audio and to participate, dial: (866) 699-3239
Sheridan Community Hospital COMMUNITY HEALTH NEEDS ASSESSMENT (CHNA) IMPLEMENTATION PLAN
 IMPLEMENTATION PLAN") Sheridan Community Hospital COMMUNITY HEALTH NEEDS ASSESSMENT (CHNA) IMPLEMENTATION PLAN March 2016 March 2019 Health Needs Assessment Implementation Plan Sheridan Community Hospital Community Summary
Sheridan Community Hospital COMMUNITY HEALTH NEEDS ASSESSMENT (CHNA) IMPLEMENTATION PLAN March 2016 March 2019 Health Needs Assessment Implementation Plan Sheridan Community Hospital Community Summary
Listening to the Voices of Latinos in Omaha: Responses of Community-Based Health Care Providers
 Listening to the Voices of Latinos in Omaha: Responses of Community-Based Health Care Providers JUNE 2017 Listening to the Voices of Latinos in Omaha: Responses of Community-Based Health Care Providers
Listening to the Voices of Latinos in Omaha: Responses of Community-Based Health Care Providers JUNE 2017 Listening to the Voices of Latinos in Omaha: Responses of Community-Based Health Care Providers
What services does Open Door provide? Open Door provides prevention-focused services that extend beyond the exam room.
 What is Open Door? Open Door has been delivering top-notch health care services since 1973. We provide prevention-focused health care for low-income people in Westchester and Putnam, regardless of ability
What is Open Door? Open Door has been delivering top-notch health care services since 1973. We provide prevention-focused health care for low-income people in Westchester and Putnam, regardless of ability
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Women s Health: A Focus on Chronic Disease
 Women s Health: A Focus on Chronic Disease Sharon Moffatt, RN BSN MS Association of State and Territorial Health Official Chief of Health Promotion and Disease Prevention Overview Chronic Disease Prevention
Women s Health: A Focus on Chronic Disease Sharon Moffatt, RN BSN MS Association of State and Territorial Health Official Chief of Health Promotion and Disease Prevention Overview Chronic Disease Prevention
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement
 Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
St. Lawrence County Community Health Improvement Plan
 St. Lawrence County Community Health Improvement Plan November 1, 2013 Contents Executive Summary... 3 What are the health priorities facing St. Lawrence County?... 3 Prevent Chronic Disease... 3 Promote
St. Lawrence County Community Health Improvement Plan November 1, 2013 Contents Executive Summary... 3 What are the health priorities facing St. Lawrence County?... 3 Prevent Chronic Disease... 3 Promote
HEALTH LITERACY PROJECT
 HEALTH LITERACY PROJECT Joining Forces of Criminal Justice and Medicine September 2014 July 2015 1 2 If we want health equity, we need to make health literacy a priority...to give [the people] the tools
HEALTH LITERACY PROJECT Joining Forces of Criminal Justice and Medicine September 2014 July 2015 1 2 If we want health equity, we need to make health literacy a priority...to give [the people] the tools
2012 Community Health Needs Assessment
 Indiana University Health Goshen 2012 Community Health Needs Assessment A Report on Implementation Strategies to Address Community Health Needs Summary Report Our Commitment to You We are here for you,
Indiana University Health Goshen 2012 Community Health Needs Assessment A Report on Implementation Strategies to Address Community Health Needs Summary Report Our Commitment to You We are here for you,
Health Current: Roadmap Practice Transformation using Information & Data
 Health Current: Roadmap Practice Transformation using Information & Data Melissa A. Kotrys, MPH Chief Executive Officer July 2017 2 Arizona Health-e Connection is now Health Current. Powering the future
Health Current: Roadmap Practice Transformation using Information & Data Melissa A. Kotrys, MPH Chief Executive Officer July 2017 2 Arizona Health-e Connection is now Health Current. Powering the future
Employee Benefit Research Institute. Key Learnings for Employers from the Gallup Healthways Well-Being Index
 Employee Benefit Research Institute Key Learnings for Employers from the Gallup Healthways Well-Being Index John Harris Chief Wellness Officer VP Innovations Healthways john.harris@healthways.com December
Employee Benefit Research Institute Key Learnings for Employers from the Gallup Healthways Well-Being Index John Harris Chief Wellness Officer VP Innovations Healthways john.harris@healthways.com December
2016 BEHAVIORAL HEALTH GRANT OPPORTUNITY
 2016 BEHAVIORAL HEALTH GRANT OPPORTUNITY A. MICHIGAN HEALTH ENDOWMENT FUND OVERVIEW The Michigan Health Endowment Fund was established to improve the health of Michigan residents and reduce the cost of
2016 BEHAVIORAL HEALTH GRANT OPPORTUNITY A. MICHIGAN HEALTH ENDOWMENT FUND OVERVIEW The Michigan Health Endowment Fund was established to improve the health of Michigan residents and reduce the cost of
CareMore Special Needs Plans Model of Care. Annual Evaluation 2015 Performance
 CareMore Special Needs Plans Model of Care Annual Evaluation 2015 Performance The Special Needs Plans (SNPs) Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). Medicare SNPs limit
CareMore Special Needs Plans Model of Care Annual Evaluation 2015 Performance The Special Needs Plans (SNPs) Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). Medicare SNPs limit
Core Issues in Successful Integration of Behavioral Health and Primary Care: Part 1 and Part 2. Colorado Behavioral Health Association October 3, 2010
 Core Issues in Successful Integration of Behavioral Health and Primary Care: Part 1 and Part 2 Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that in order
Core Issues in Successful Integration of Behavioral Health and Primary Care: Part 1 and Part 2 Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that in order
Key Terms TBT = Technology Based Training (in Relias) F2F = Face to Face (In person training) TBD = To Be Determined
 F2F = Face to Face (In person training) TBD = To Be Determined") Instructions Key Terms TBT = Technology Based Training (in Relias) F2F = Face to Face (In person training) TBD = To Be Determined This document is called the Provider Course Equivalency Spreadsheet. The
Instructions Key Terms TBT = Technology Based Training (in Relias) F2F = Face to Face (In person training) TBD = To Be Determined This document is called the Provider Course Equivalency Spreadsheet. The
Community Health Plan. (Implementation Strategies)
") 2017-2019 Community Health Plan (Implementation Strategies) May 15, 2017 Community Health Needs Assessment Process Winter Park Memorial Hospital A Florida Hospital (the Hospital) conducted a Community
2017-2019 Community Health Plan (Implementation Strategies) May 15, 2017 Community Health Needs Assessment Process Winter Park Memorial Hospital A Florida Hospital (the Hospital) conducted a Community
Outline 11/17/2014. Overview of the Issue Program Overview Program Components Program Implementation
 Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
This study serves as an annual follow-up to the initial study conducted in 2016.
 Community Mental Health Association of Michigan: Center for Healthcare Research and Innovation Healthcare Integration and Coordination 2017/2018 Update Hundreds of innovative initiatives identified in
Community Mental Health Association of Michigan: Center for Healthcare Research and Innovation Healthcare Integration and Coordination 2017/2018 Update Hundreds of innovative initiatives identified in
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
Community Health Needs Assessment July 2015
 Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
OHIO PREGNANCY ASSOCIATED MORTALITY REVIEW (PAMR) TEAM ASSOCIATED FACTORS FORM
 TEAM ASSOCIATED FACTORS FORM") OHIO PREGNANCY ASSOCIATED MORTALITY REVIEW (PAMR) TEAM ASSOCIATED FACTORS FORM Please Circle: OFFICIAL WORKING COPY Case # DEATH REVIEW PROCESS 1. Estimate the degree of relevant information (records)
OHIO PREGNANCY ASSOCIATED MORTALITY REVIEW (PAMR) TEAM ASSOCIATED FACTORS FORM Please Circle: OFFICIAL WORKING COPY Case # DEATH REVIEW PROCESS 1. Estimate the degree of relevant information (records)
Motivational Interviewing and COPD Health Status Project 4 July-30 December 2016
 Project Overview Motivational Interviewing and COPD Health Status Project 4 July-30 December 2016 Applying the principles of motivational interviewing to everyday patient interactions has proven effective
Project Overview Motivational Interviewing and COPD Health Status Project 4 July-30 December 2016 Applying the principles of motivational interviewing to everyday patient interactions has proven effective
Good Samaritan Medical Center Community Benefits Plan 2014
 Good Samaritan Medical Center Community Benefits Plan 2014 This Addendum to the Community Benefits Plan 2014 is an addendum to the Community Benefits Plan approved by the Community Benefits Council on
Good Samaritan Medical Center Community Benefits Plan 2014 This Addendum to the Community Benefits Plan 2014 is an addendum to the Community Benefits Plan approved by the Community Benefits Council on
HEALTH AND BEHAVIOR ASSESSMENT & INTERVENTION
 Optum Coverage Determination Guideline HEALTH AND BEHAVIOR ASSESSMENT & INTERVENTION Policy Number: BH727HBAICDG_032017 Effective Date: May, 2017 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT
Optum Coverage Determination Guideline HEALTH AND BEHAVIOR ASSESSMENT & INTERVENTION Policy Number: BH727HBAICDG_032017 Effective Date: May, 2017 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT
Community Health Needs Assessment Implementation Plan
 Community Health Needs Assessment Implementation Plan 2016-2019 Introduction Sandoval Regional Medical Center (SRMC) serves patients in Sandoval County and the surrounding communities. As part of the Community
Community Health Needs Assessment Implementation Plan 2016-2019 Introduction Sandoval Regional Medical Center (SRMC) serves patients in Sandoval County and the surrounding communities. As part of the Community
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
Introduction to the Whole Person Integrated Care Model
 Introduction to the Whole Person Integrated Care Model North Carolina Council for Community Programs December 2016 Conference Pinehurst, North Carolina Excerpts from a note of encouragement and hope from
Introduction to the Whole Person Integrated Care Model North Carolina Council for Community Programs December 2016 Conference Pinehurst, North Carolina Excerpts from a note of encouragement and hope from
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
MERCY HOSPITAL BOONEVILLE COMMUNITY COMMUNITY HEALTH IMPROVEMENT PLAN ( )
") An IRS-mandated Community Health Needs Assessment (CHNA) was recently completed for the Booneville Community. For the purposes of this Community Health Improvement Plan the Booneville Community includes:
An IRS-mandated Community Health Needs Assessment (CHNA) was recently completed for the Booneville Community. For the purposes of this Community Health Improvement Plan the Booneville Community includes:
Community Counseling Centers, Inc. & North Country Health Care
 Community Counseling Centers, Inc. & North Country Health Care Holbrook & Show Low Navajo County Communities 9/28/11 The CCC multi-faceted approach to an integrated health program with North Country Health
Community Counseling Centers, Inc. & North Country Health Care Holbrook & Show Low Navajo County Communities 9/28/11 The CCC multi-faceted approach to an integrated health program with North Country Health
EDUCATION AND SUPPORT OF THE FAMILY THE ROLE OF THE PUBLIC HEALTH NURSE ANNE MCDONALD PHN PHIT PROJECT LEADER
 EDUCATION AND SUPPORT OF THE FAMILY THE ROLE OF THE PUBLIC HEALTH NURSE ANNE MCDONALD PHN PHIT PROJECT LEADER Public Health Nursing PHN is a generalist nurse with specialist education Postgraduate Diploma
EDUCATION AND SUPPORT OF THE FAMILY THE ROLE OF THE PUBLIC HEALTH NURSE ANNE MCDONALD PHN PHIT PROJECT LEADER Public Health Nursing PHN is a generalist nurse with specialist education Postgraduate Diploma
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Community Leadership Institute of Kentucky Request for Applications
 Community Leadership Institute of Kentucky Request for Applications Key Dates RFA Release Date: December 1, 2017 Applications due: January 10, 2018 Applicants Notified: February 9, 2018 Save the Required
Community Leadership Institute of Kentucky Request for Applications Key Dates RFA Release Date: December 1, 2017 Applications due: January 10, 2018 Applicants Notified: February 9, 2018 Save the Required
BHS Policies and Procedures
 BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
Tools for Better Health. Referral Toolkit. Health Care Providers
 Tools for Better Health Referral Toolkit Health Care Providers A guide to working with providers to establish a referral system for evidence-based self-management programs. Table of Contents How to Use
Tools for Better Health Referral Toolkit Health Care Providers A guide to working with providers to establish a referral system for evidence-based self-management programs. Table of Contents How to Use
Population Health Management Tools to Improve Care for Individuals and Populations of Patients
 June 1, 2015 Population Health Management Tools to Improve Care for Individuals and Populations of Patients Joel Diamond, MD, FAAP Building Population Health Information-powered clinical decision-making
June 1, 2015 Population Health Management Tools to Improve Care for Individuals and Populations of Patients Joel Diamond, MD, FAAP Building Population Health Information-powered clinical decision-making
A holistic approach to your wellbeing
 A holistic approach to your wellbeing Take control of your life with Ingenia Care Ingenia Care has been created to help you improve your level of independence and wellbeing by assisting you to access a
A holistic approach to your wellbeing Take control of your life with Ingenia Care Ingenia Care has been created to help you improve your level of independence and wellbeing by assisting you to access a
Regional Center for Border Health, Inc. San Luis Walk-In Clinic, Inc.
 Regional Center for Border Health, Inc. San Luis Walk-In Clinic, Inc. Community-Based Family Care Coordinator & Inter-Professional Patient Centered Care Model Initiative Amanda Aguirre, President & CEO
Regional Center for Border Health, Inc. San Luis Walk-In Clinic, Inc. Community-Based Family Care Coordinator & Inter-Professional Patient Centered Care Model Initiative Amanda Aguirre, President & CEO
Administrators. Medical Directors. 61% The negative impact on our hospital-based program s. 44% We will need to consider the most appropriate or most
 2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
Improving Mental Health Services in Schools
 House Select Committee on School Safety Student Health Working Group Improving Mental Health Services in Schools Mark T. Benton Department of Health and Human Services April 9, 2018 Unrecognized and untreated,
House Select Committee on School Safety Student Health Working Group Improving Mental Health Services in Schools Mark T. Benton Department of Health and Human Services April 9, 2018 Unrecognized and untreated,
Minnesota Accountable Health Model Accountable Communities for Health Grant Program
 Request for Proposals Minnesota Accountable Health Model Accountable Communities for Health Grant Program September 2, 2014 Page 1 of 79 Contents: 1. Overview... 3 2. Available Funding and Estimated Awards...
Request for Proposals Minnesota Accountable Health Model Accountable Communities for Health Grant Program September 2, 2014 Page 1 of 79 Contents: 1. Overview... 3 2. Available Funding and Estimated Awards...
2016 Community Health Needs Assessment Implementation Plan
 2016 Community Health Needs Assessment Following the 2016 Community Health Needs Assessment, Saint Mary s Hospital developed an Implementation Strategy to illustrate the hospital s specific programs and
2016 Community Health Needs Assessment Following the 2016 Community Health Needs Assessment, Saint Mary s Hospital developed an Implementation Strategy to illustrate the hospital s specific programs and
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs. September 20, 2017
 Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Healthy Communities Grant Application Form
 Healthy Communities Grant Application Form Crow Wing Energized along with the Statewide Health Improvement Program (SHIP) is working to help community members of Crow Wing County live longer, healthier
Healthy Communities Grant Application Form Crow Wing Energized along with the Statewide Health Improvement Program (SHIP) is working to help community members of Crow Wing County live longer, healthier
arizona health net a better decision sm Putting you at the center of everything we do.
 arizona health net a better decision sm Putting you at the center of everything we do. Nothing s more important than your health. When you re healthy, you want to stay healthy. When you re sick or have
arizona health net a better decision sm Putting you at the center of everything we do. Nothing s more important than your health. When you re healthy, you want to stay healthy. When you re sick or have