Fact-Finding on NRHM Facilities in Sikkim. Introduction
|
|
|
- Jonathan Hutchinson
- 6 years ago
- Views:
Transcription
1 Fact-Finding on NRHM Facilities in Sikkim 20 th 21 st May 2014 Introduction From May 20 th to 21 st 2014 two health activists from Delhi and Gangtok travelled to a District Hospital (DH), a Primary Health Centre (PHC), Pakyong PHC and Sir Thodup Namgyal Memorial (S.T.N.M.) Hospital Gangtok to investigate the standards of care of National Rural Health Mission (NRHM) facilities in Sikkim. At the various institutions the activists were able to speak to a wide range of people, including doctors, nurses, administrators and patients. While they were inspired to meet many dedicated medical professionals working hard for their communities, they found that every institution they visited failed to comply with basic NRHM service guarantees as set by the Indian Public Health Standards (IPHS). Allowing NRHM institutions to suffer from frequent electricity shortages, a lack of necessary equipment or severe understaffing that does not meet IPHS stipulations is a failure on the part of the state to protect the fundamental rights to life, health, and dignity enshrined in Article 21 of the Constitution. Below is a report of the outcomes of this two-day fact-finding, and the major issues of concern that the health activists would recommend to the NRHM as critical to be improved upon as soon as possible. Major Issues of Concern Based on visits to four facilities and interviews with medical professionals, patients, and families, the fact-finding team identified the following major issues of concern: 1. Roads and Transport. Almost every medical professional we spoke to said the biggest challenge they face is that of transportation given the dispersed population, difficult terrain and poor roads of the state. Although the Janani Shishu Suraksha Karyakram (JSSK) guarantees free transport from patients homes to the facilities, there are still no services in all of Sikkim to help patients reach the first level of care from their villages. A delay in reaching care, especially emergency obstetric care, is one of the primary causes of maternal mortality. According to the International Covenant on Economic, Social and Cultural Rights, which India is a state party to, the state has an obligation to create accessible health facilities. Sikkim should look to provide something similar to the 108 ambulances that exist in other states. In the meantime, it is vital that careful attention is made to ensure all those who are
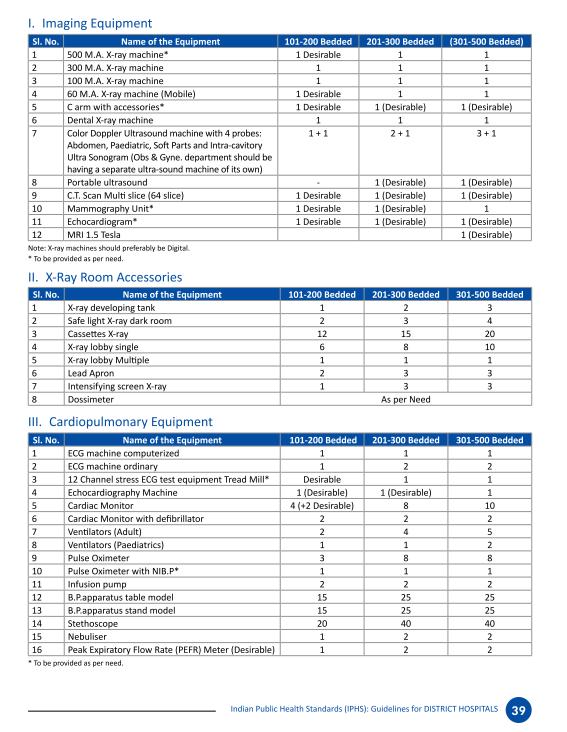
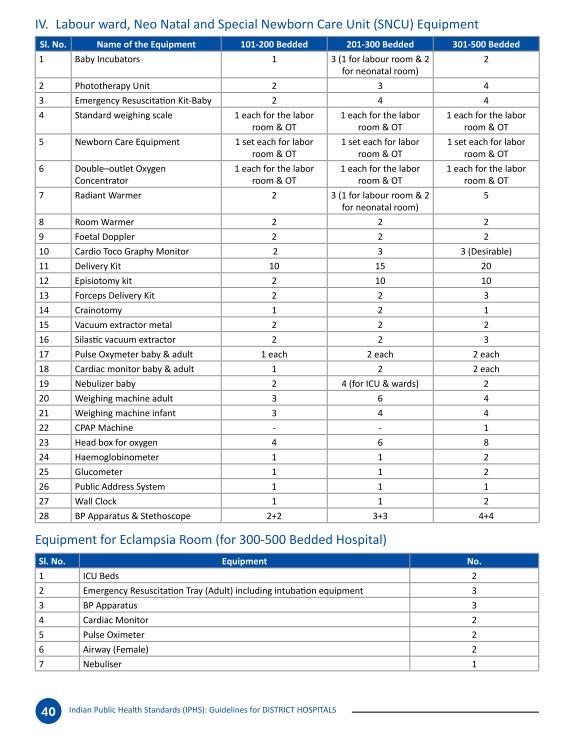
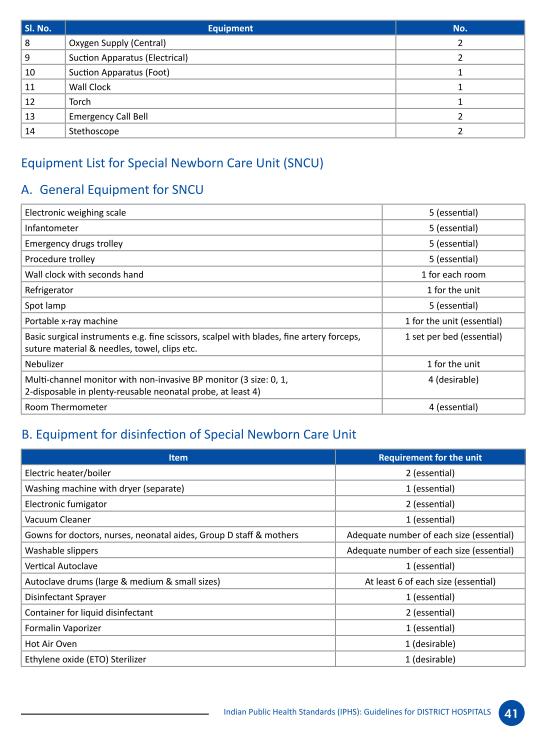
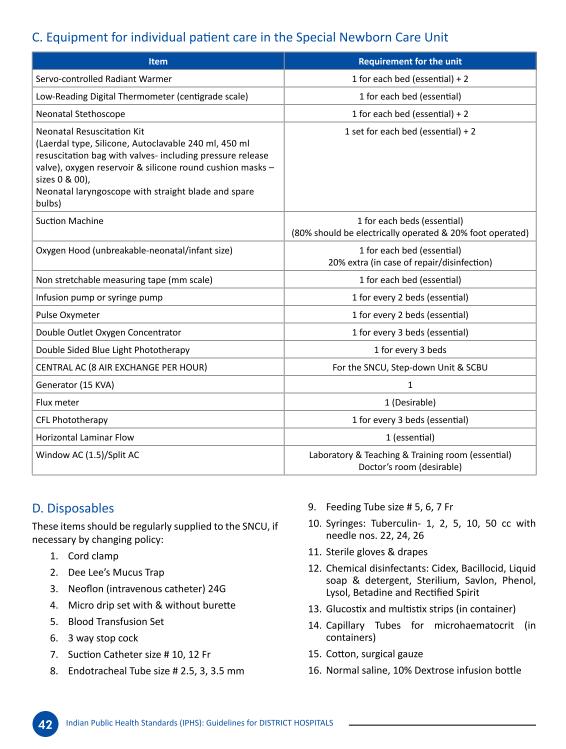
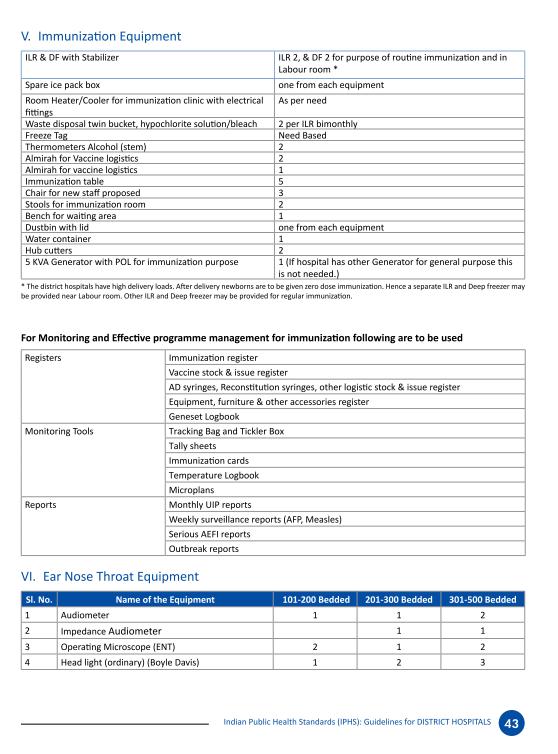
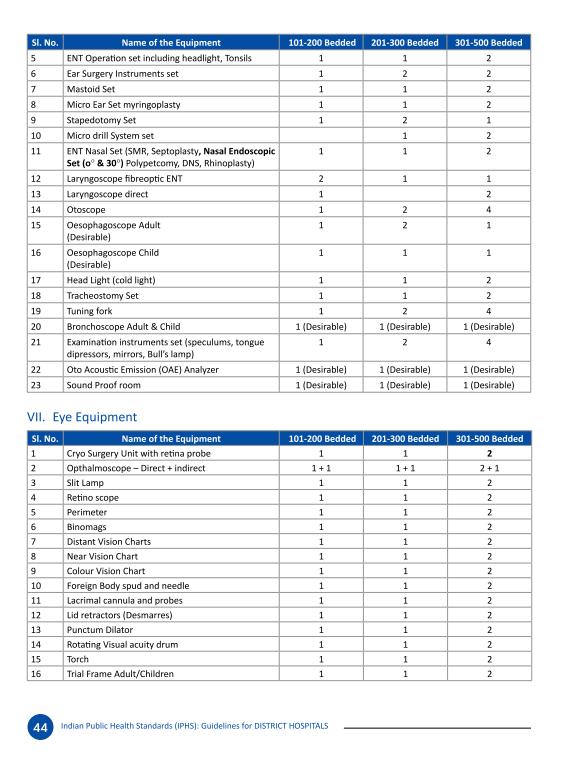
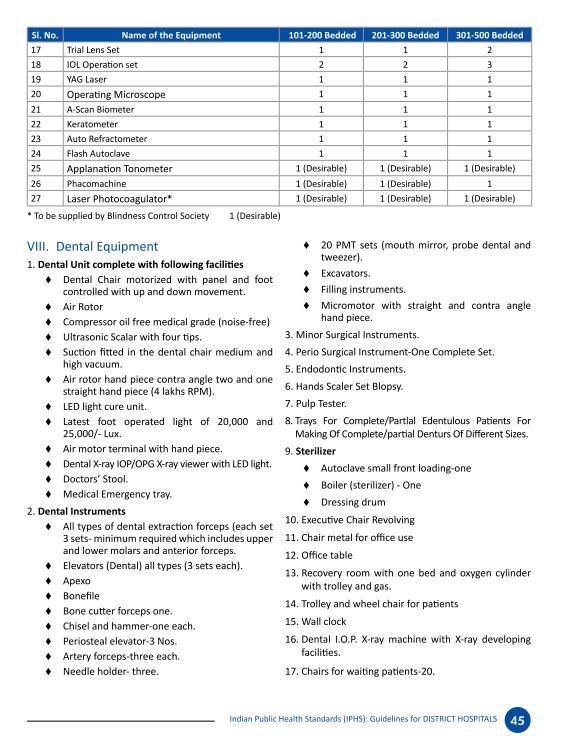
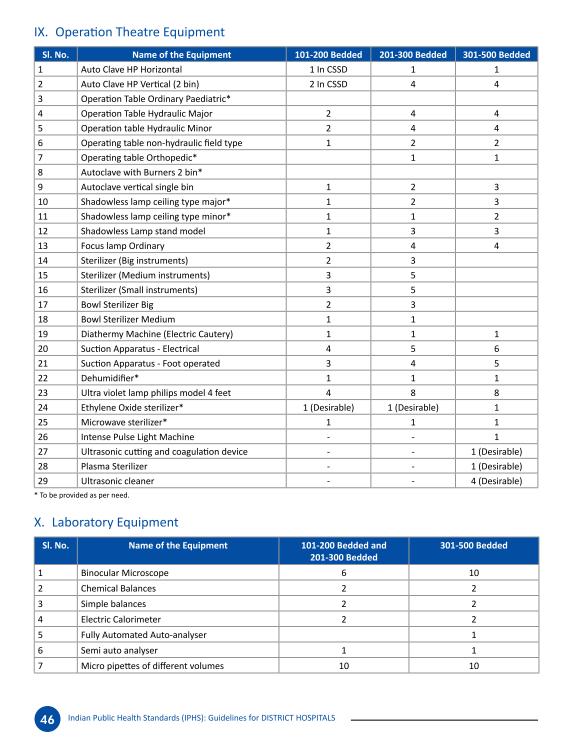
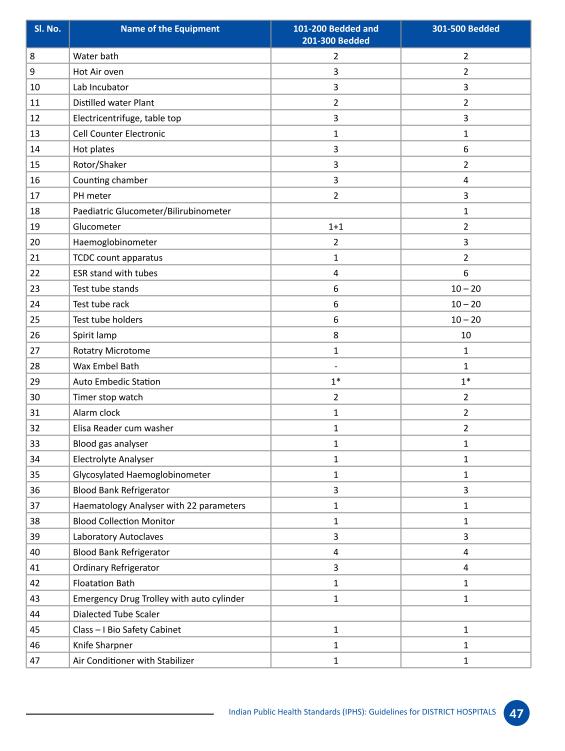
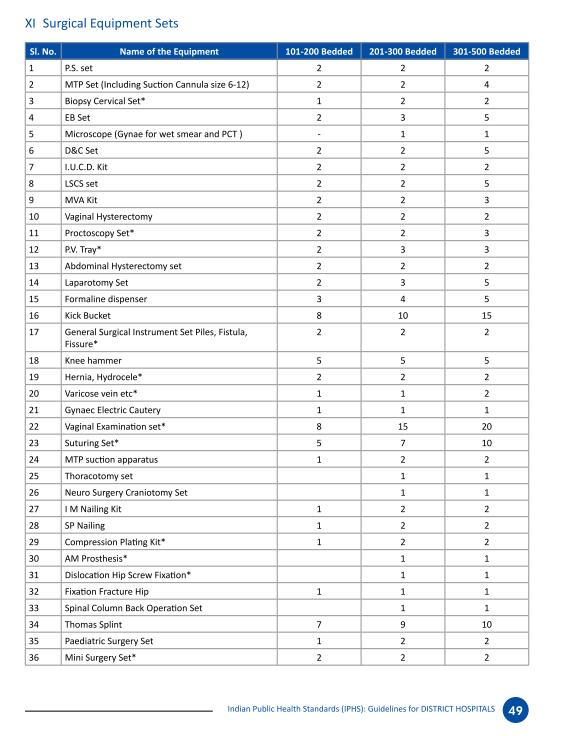
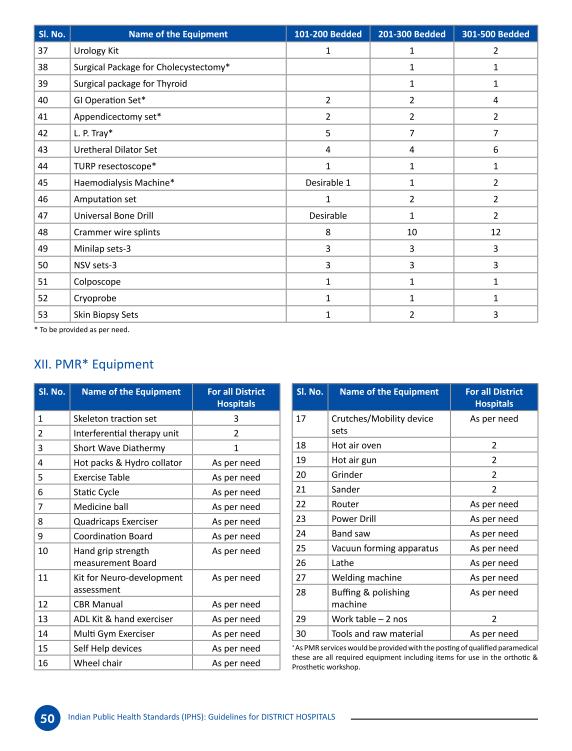
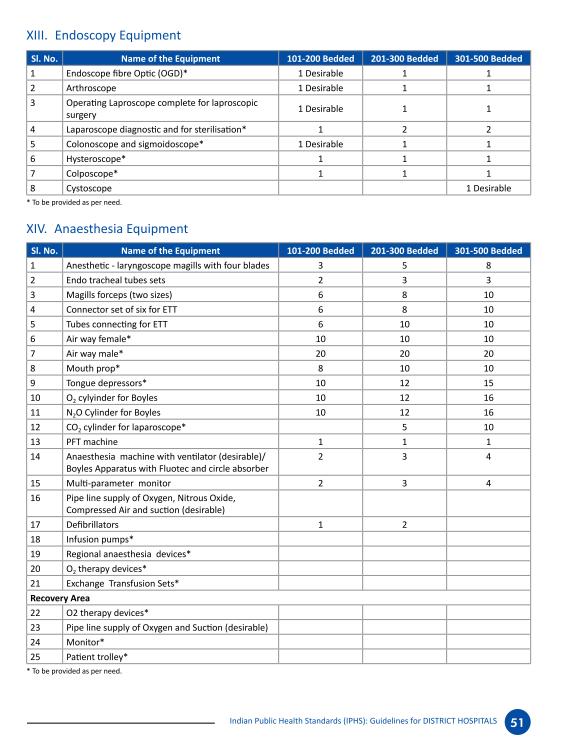
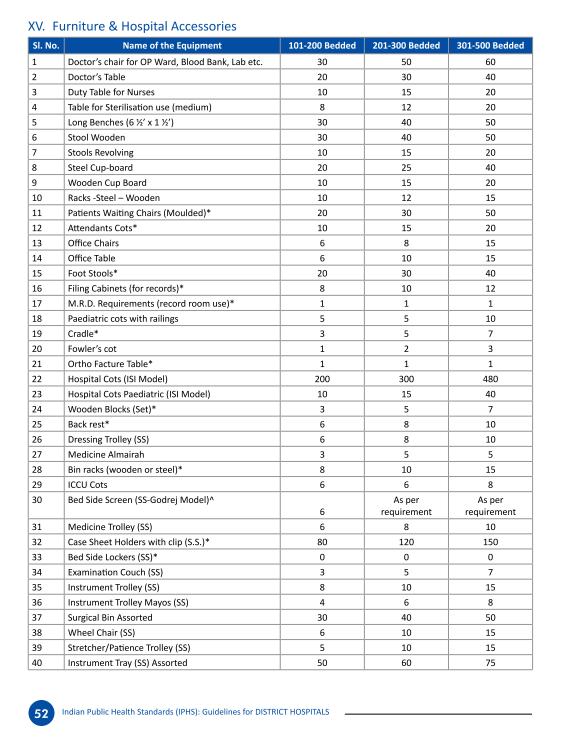
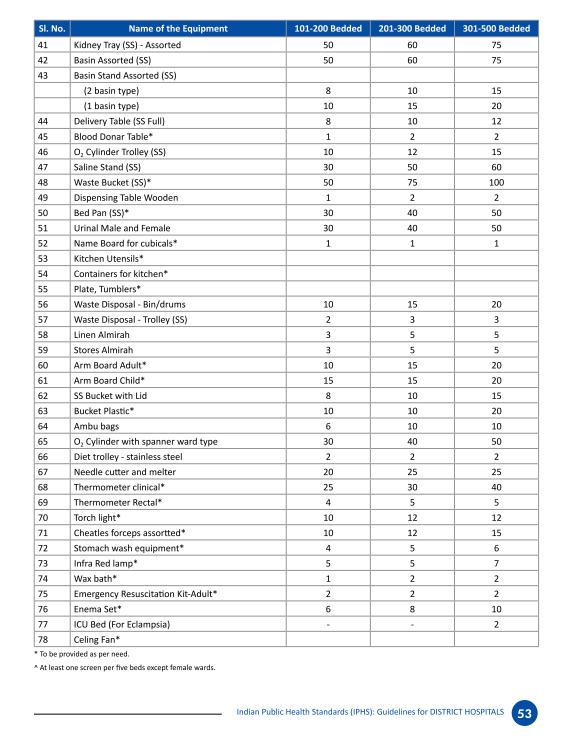
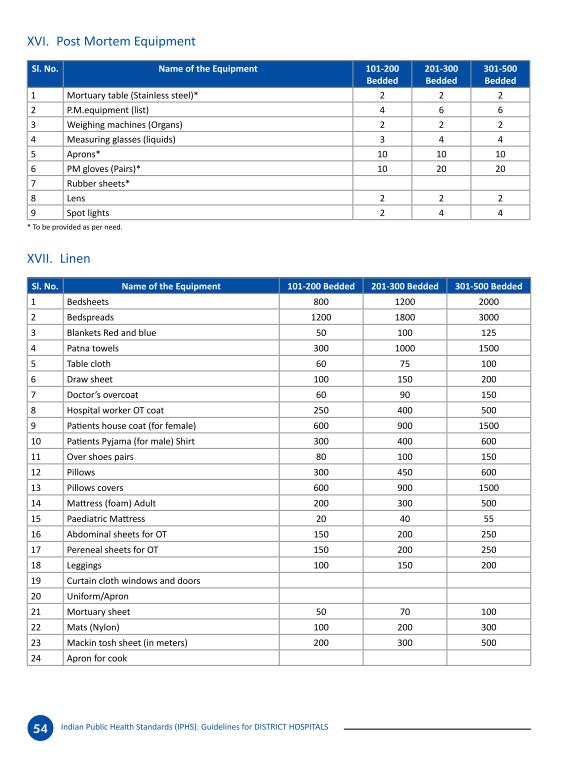
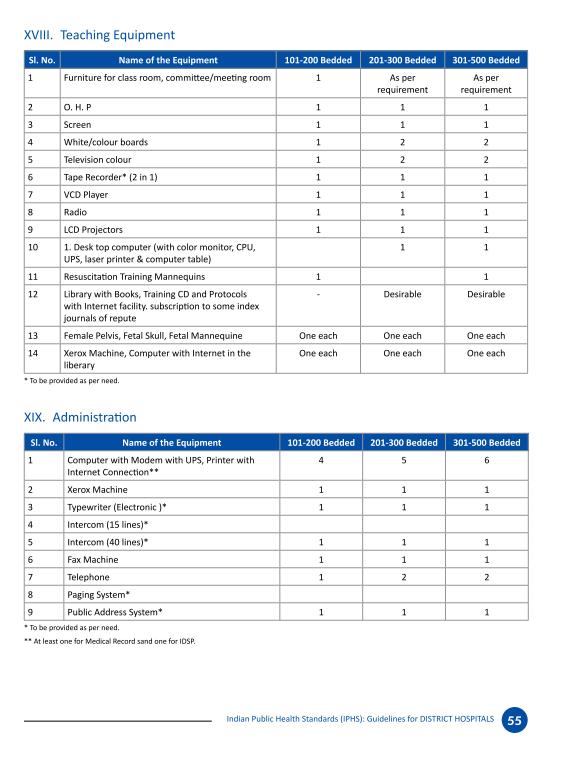
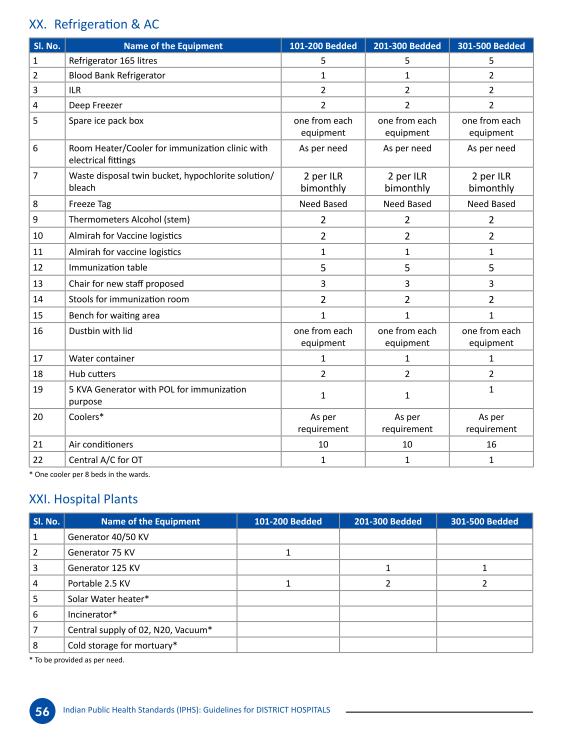
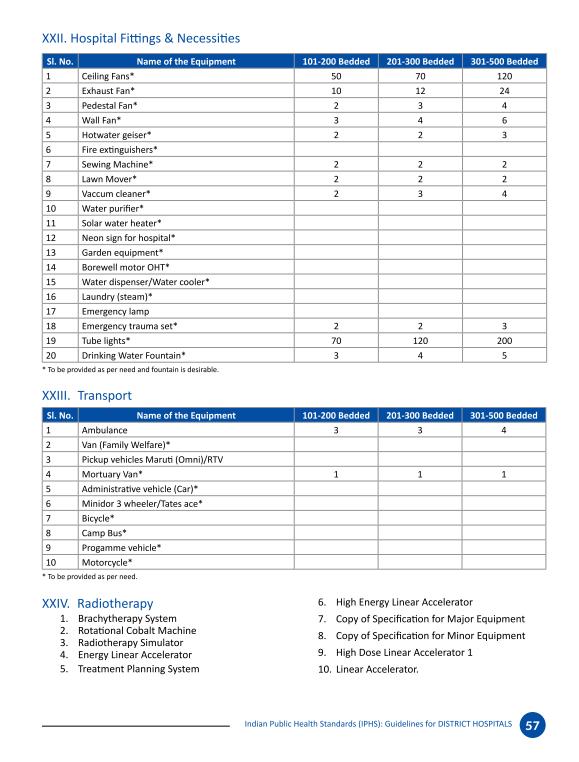
2 entitled to JSSK payments to help them cover the costs of private transportation receive them. The team also found that limited transportation results in substandard postnatal care and adequate discharge procedures as patients often rush to get back to their villages before the last shared taxi of the day, around 2pm. Doctors cannot keep patients for monitoring or provide adequate follow-up care. Under JSSK, the government has an obligation to provide adequate transport to pregnant and lactating women. Moreover, to ensure the right to health as enshrined in the Constitution, all patients should have easy access to health facilities. Therefore it is necessary that the District Hospitals provide transportation services to help patients get back to their villages. Another complaint we heard from doctors is that sometimes the hospital does not have money for petrol, so the ambulances are there, but cannot run. Some doctors are dedicated enough to pay for fuel out of their pocket but say they are still waiting for many years worth of reimbursements from the state. Any doctors currently awaiting reimbursement should receive it as soon as possible and care should be made to ensure sufficient funds are made available for fuel costs. 2. Staffing. Almost every institution we visited had complaints about insufficient staffing. The most necessary measure is to hire more nurses to ensure doctors have the support they need and avoid them spending time on simple procedures that nurses can handle. This will then free up doctors time for more urgent matters, as patients in critical condition wait several hours before seeing a doctor. It is also important to make sure all the DHs have all the necessary specialists under NRHM guarantees. Measures should also be taken to help remote outposts get sufficient staff by providing incentives. 3. Equipment. Every single institution we visited had some vital equipment that was either not available or broken. For example, DHs should have ECGs to prevent avoidable infant deaths, and basic lab facilities and a pathologist to prevent over-referring to STNM Gangtok. For these and other reasons, the state must ensure that all necessary equipment is made available at the appropriate institutional levels, with all the necessary parts and technicians for it to function. A list of necessary equipment according to the IPHS for Sub Centres, PHCs and DHs can be found below. When equipment is broken or parts are missing, doctors should not have to waste time making applications for over two years waiting for it to be fixed. In the meantime expensive equipment may rust or become unusable leading to a waste of resources. 4. Blood banks. Two District Hospitals in Sikkim are still not compliant with the Indian Public Health Standards (IPHS) in ensuring they are able to provide
3 this essential and life-saving facility. At the District Hospital we visited, funding has already been approved so we hope that the process is completed on time to prevent any further delay of this critical aspect of emergency care. 5. Operating theatres (OT). That the District Hospital visited below does not have an OT is shocking and a denial of life saving services for patients. PHCs should also have minor OTs as required under the IPHS, the one we visited did not have a minor OT, nor were any plans evident to construct one anytime soon. 6. Electricity. That the PHC visited below does not have electricity most days of the week is shocking and should not be the case. Electricity is vital to operate much life-saving equipment, and according to the IPHS must be available even at the Sub-Centre (SCs) and PHC level. We therefore demand that all PHCs in Sikkim get functioning generators as soon as possible, and SCs get invertors or solar equipment. 7. Referrals. STNM Hospital in Gangtok is still greatly overburdened. There are massive bed shortages and patients have to wait many hours before they are able to see a doctor. The state should implement a centralised and accountable referral system that sends patients to the most appropriate facility according to the patient s medical needs and provides patients with the following minimum information at the time of their referral: (1) the name of the referral facility, (2) the contact information of the referral facility, including the name, address, and phone number of the receiving staff member, (3) the reason for referral, (4) the diagnosis and treatment to be sought at the referral facility, (5) the contact information of the referring hospital in case of questions or concerns, (6) copies of all medical records and discharge slip(s), and (7) free transport for BPL patients. The state should also undertake a comprehensive investigation into referrals in the state. How many people come directly to STNM without being referred from their local NRHM institution? How many are referred from SCs, PHCs and DHs and for what reasons? How many die enroute? Where are most referrals coming from? These results should illuminate where interventions in the referral system are most urgent. 8. STNM Hospital Gangtok and Manipal Hospital. STNM itself makes many referrals to Manipal Hospital, a private institution, either because the cases are too complicated and STNM doesn t have the capacity to treat them, or it is too crowded. Because Manipal is a private hospital, patients have to pay for care, leaving many low-income patients unable to access emergency care due to prohibitive costs. As the highest level of government care in the state, STNM should ensure it has all the necessary equipment, staff and beds to deal with all cases. Patients should also not have to wait long hours to see a doctor
4 or get a bed. In the meantime, BPL and APL patients referred to Manipal from STNM should receive all care free of charge. 9. Trauma centre. Given the poor condition of roads in many parts of Sikkim, the risk of landslides and the high number of road accidents it is vital that DHs have trauma centres and resident orthopaedists to be able to deal with emergency cases. Such trauma patients cannot afford to make the long and difficult road journey to STNM Gangtok and often die enroute. 10. Medicines. We found several cases of drug shortages during our fact-finding, including iron folic acid and calcium pills necessary for women in pregnancy, hypertension medication and antacids. We met pregnant women who then had to buy the necessary pills from chemists at their own cost, when they should be available free of charge under the guarantees in the NRHM and the National List of Essential Medicines. Moreover, the High Court ordered the state to ensure adequate provisions of medicines in its order dated XXXXX. 11. Reproductive Services The DH we visited is no longer conducting medical termination of pregnancy (MTP), a guaranteed service under NRHM at that level of care. They also do not provide sterilizations. Women have to travel all the way to Gangtok s already overcrowded gynaecology ward to receive these basic reproductive services. Given that there is a high incidence of complications from illicit abortions it is clear that MTP is a highly needed service and the fact that women are not able to access it is greatly endangering their health. 12. JSY payments. ASHAs report difficulties with helping women receive their JSY checks (and therefore get their own payment) if the women do not have the necessary documentation to get a bank account, as all JSY payments are done through account transfers. This was particularly a problem in Pakyong PHC where there is a high population of migrant workers who often lack necessary documentation, like an ID card. Hospitals should be able to have the flexibility to give JSY payments by cash or check to such patients. 13. Sanitation. Much work needs to be done to ensure all toilets in all facilities are in good working condition, cleaned regularly and rules regarding men and women s toilets are upheld as per IPHS norms.
, the activists first spoke with an administrator: Blood Bank - The administrator told them that there is currently no blood bank at")

5 Findings 1. District Hospital The toilets on the ground floor were in complete disrepair and were very filthy. Hospital Administrator Upon arriving at the District Hospital (DH), the activists first spoke with an administrator: Blood Bank - The administrator told them that there is currently no blood bank at the hospital, but it will hopefully be completed by the end of May The hospital has written the proposal and apparently the funding has been approved. Referrals - The DH gets only about 2-3 referrals a month from the PHCs that come under it. This is because most patients choose to go straight from the PHC to STNM Hospital as they believe it offers better care than at the DH. They themselves do 7-8 referrals a month to STNM MMR and IMR - There were 2 maternal deaths in the last year, for which audits were completed. He did not have details on these audits or where we could get copies of them, but recommended we ask the gynaecologist. There were 13 infant mortalities in the last year, for which he recommended we speak to the paediatrician. Staffing - There are currently 9 doctors, of which 3 are specialists a gynaecologist, paediatrician and dental surgeon. They are still trying to fill some positions for more doctors. There are 10 nurses. There are 84 ASHAs under this hospital. Most of the
6 deliveries come through the ASHAs. JSY payments happen for all institutional deliveries and are made directly through the patient s bank account. Infrastructure - They have a generator so there are no problems with electricity. However internet is a big problem for them to complete their reporting and administration work. DOTS Programme Staff There are currently about 60 TB patients registered in this area. There are new strict rules about ensuring that all cases are registered, so they are quite sure these are all the cases. Often the ASHAs or anganwadi workers are helpful in referring TB patients to them. However, they have a small problem with alcoholic patients who often discontinue their drug regime because they do not want to give up alcohol, which cannot be taken with the medication. Senior Hospital Administrator This senior administrator was kind enough to speak with us and give us their honest perspective on the functioning of the hospital: Roads and Transportation This, compounded with the fact they are situated in an earthquake-prone area, is the biggest challenge they face. The hospital has 2 ambulances, which are only used for transporting patients to Gangtok. They normally make 3-4 journeys a day. The PHCs each have one ambulance that brings patients to the DH or Gangtok. It is quite rare that the PHCs send patients to the DH (1-2 times in a month). Mostly they are sent to Gangtok. Presently transport is working fine but sometimes they are not able to cope with demand. Many patients pay for private transportation. After the earthquake villagers had to walk to reach healthcare facilities. Even if it tried, the ambulance was unable to reach them. Currently there is still no vehicle available to transport patients or women in labour from their villages in an emergency to any health facility. Sometimes patients are even carried by hand. Referrals - Previously almost all patients would want to be transferred directly to Gangtok, however since November 2013 when they employed a gynaecologist and paediatrician many more stay. Before they were making over 200 referrals a month. Already this month they have done 32 referrals, and there are still 10 days of May left. ASHAs - To improve access to healthcare they have focused on training ASHAs. The hospital holds monthly trainings to improve ASHAs skills. They are trained to recognize complicated cases and make an effort to reach the most remote places. Often if an ASHA is going to a particularly far off place she will send messages a few
7 days before and call all patients to one particular place. Last month there was a training in a nearby PHC which the NRHM Director Sikkim attended he takes ASHAs very seriously. There are 27 ASHAs under this DH area alone, they are the backbone of the system. We are so grateful to our ASHAs go see for your own eyes how difficult it is to do the work they do. Even our doctors they are almost all ladies in Sikkim, and to be living in some of the remote PHCs is very difficult for them but they work hard. Mobile Medical Unit The MMU used to be sent out to a different place at least every day. However, since the earthquake many of the roads are very destroyed and this MMU bus can t pass them. It has a lot of equipment including a sonogram, x-ray equipment, etc., but is currently not being utilized. For now visits are made in a normal vehicle with 1-2 doctors, a nurse and pharmacist. Blood Bank / Operating Theatre - They have already started work on the blood bank, it should be completed in the next month. They are also starting construction of the operating theatre, which should be ready in the next 3 months. Once these two are complete they will need to make even fewer referrals. Staffing - They still need to hire one more specialists, though they didn t specify which posts. Right now every Friday the following specialists come from Gangtok for the day: A&T, ophthalmologist, psychologist, and others. This is one of the biggest challenges they face maintaining sufficient numbers of staff. Trauma Centre Speaking honestly with us, the administrator told us the thing the hospital actually needs most is a trauma centre. Road accidents is the biggest health problem they have to deal with, especially because of the bad road conditions described above; for six months of the year there are heavy rains and landslides. This is a health problem that also affects tourists greatly. Yet, they don t even have a trauma centre or a resident orthopaedic. Often casualties die on their way to STNM. Every year for the last few years they have sent a proposal for a trauma centre but they get no response. They generally get between 5-10 trauma cases a month. Paediatrician Importance of specialists in remote areas The paediatrician told us it feels good to be posted at the DH. This is especially because there are some patients that are too poor to be able to travel to Gangtok, so it is important that they are able to see a doctor locally. Roads and Transportation - The main challenge they have seen their patients face is the road conditions. Many of them live far away and it is difficult for them to reach the hospital in time. Also, when they do make it to the hospital, they have to leave by 2:30pm or they will not find a vehicle to take them back to their village so she cannot keep them for observation. Often because of the distance, parents do not bring their children back for follow-up appointments and instead show them to local
8 doctors or witchdoctors, which can be dangerous. They only make the long journey when it seems really serious, and by that time it is often too late. Lab facilities - They are also lacking good lab facilities. There is a basic lab here, but there is no pathologist, which creates problems. It takes too long to send samples to Gangtok and wait for results so they end up referring such cases. If it looks like the results will take time they usually recommend that the patients stay in Gangtok to wait for the results and see what follow-up care will be needed, but that is also expensive for patients. Infant Mortality - The main cause of infant mortality in this area is acute respiratory infections. Unfortunately they are also lacking ECG equipment, so many new-borns go undiagnosed. Staffing One of the biggest problems they face is that they are very understaffed, especially when it comes to nurses. Pharmacist Sometimes they face shortages with medicines, especially anti-hypertension drugs and antacids. Gynaecologist The AYUSH doctor was helping the gynaecologist with her consultations when we walked in. We, and a long line of patients, had been waiting several hours to meet her. It appears she is a busy woman and her services are highly in demand. The AYUSH doctor told us the biggest ailments she treats are hypertension, gastritis and diabetes. We were present while the gynaecologist was handling one consultation. She was discussing with the patient, and asked her who her ASHA is, supplying a few names of the ASHAs who work in the patient s area. She clearly knows the ASHAs well, and works closely with them. Maternal complications - The main causes of maternal complications are anaemia, which is quite common amongst women, and PI hypertension. Blood / OT - Most complications she refers to STNM because they do not have any blood facility or an OT. She knows that the OT and blood bank are in the process of being set up but doesn t know when they will be completed. They really need to be able to do blood transfusions to save lives. Staffing - The other main challenge is a big lack of nurses.
9 Maternal deaths - Of the two maternal deaths that took place in the last year, one was caused by atonic post-partum haemorrhage. The other was referred to STNM and she doesn t know the details. Contraception - Awareness of contraception is extremely high, although only about 60% of women use modern contraceptives. Most use injections. They don t do sterilizations at the DH. These are available at STNM, but the frequency is quite low. Medical termination of pregnancy Previously these used to happen more, about 7 a month, however now due to personal problems she is not performing them so there are fewer, despite the fact this is a guaranteed service under the NRHM. Patient in maternity ward This patient had just had a miscarriage. She was in her village and bleeding, so she came to the hospital. They did an ultrasound and the doctor told her she has lost the baby, so now she is waiting for it to be flushed out. She doesn t know the cause yet. Transport - It was very difficult for her to get here, transportation in this area is not easy. Challenges facing migrants - She does not know who the ASHA in her area is, and had not seen any, because she just moved here from West Sikkim.
10 2. Primary Health Centre Administrator The hospital is open from 10-2, or until the last patients of the day are finished. After that the doctor and two nurses live on site and all the locals know their numbers or how to find their homes so they are always on call. They usually have about patients a day. Currently there aren t any inpatients. Referrals and Transportation - They do several referrals to STNM a week. They have one ambulance, which makes these trips, which are almost always to Gangtok. Patients usually get to the PHC by taxi or walking. The SCs rarely refer patients to them but send the patients straight to the DH, or, more likely, Gangtok. Staffing - There are 2 doctors, but one is currently on maternity leave, altogether they have about 20 staff. This includes 3 nurses, 2 compounders, drivers, etc. Electricity The biggest problem they face is power cuts. They have a back up invertor, but whenever it rains which is very often there is no electricity. When the team visited, the facility did not have power. Medical Officer The doctor has been working here for 4-5 months. They usually have about 5-8 deliveries a month. Referrals - They do about 2 referrals a week. These referrals are almost always trauma cases or deliveries. They always send them to Gangtok since Mangan doesn t have the facilities to handle these cases. Equipment The facility requires, an x-ray, a minor OT, a generator, and an autoclave. They usually have oxygen cylinders. At this very moment they need to get them replaced, but they are always available on a monthly basis. Another problem they face is with maintenance of equipment. This is a very slow process and often they find nothing happens. All the equipment is there, and much of it is good, but unusable. This equipment is extremely important, especially for many trauma cases. For example, because there is no x-ray they have to send patients to the DH. Electricity - Electricity is a big problem. They used to have a generator but it broke a year ago. They made an application for it to be fixed and at some point someone came to look at it, but nothing has happened. They complained that these things always take a long time, if they happen at all.
11 Contraception - Most women use Mala or Mala-D for contraception. IUDs are less popular, although they are available at the PHC. No MTP is available, for that they have to go to the DH (the same one where we just heard that it is no longer available). However, people often take illegal medication to try and induce abortions, which causes problems. This happens because many people are hesitant to ask for an abortion and drugs are very easy to get. She gets at least 2 cases of complications from abortions a month, so it is quite common. They have wondered if it is due to a problem in their family planning programme. People often also appear to be quite shy about telling ASHAs they have conceived and don t feel comfortable to discuss these issues openly. Maternal and infant deaths - In January there was one maternal death at an SC under this PHC. It was a home delivery, and there was a uterine inversion. Luckily, home deliveries are much fewer these days. There was also one infant death in the last few months. He was born with a low birth weight, they referred the family to Gangtok, where he was treated, and then discharged but then unexpectedly died after being discharged. Staffing - NRHM has really strengthened the PHCs and SCs in the last few years. The main thing lacking now is staffing there is only one Assistant Nurse Midwife here and one Medical Officer (MO). The other MO is on maternity leave and there is no sub. So whenever the MO has to go somewhere the station is empty.
12 3. Pakyong Primary Health Centre Nurse There are three Medical Officers 1 dental surgeon, 1 chief medical officer, 1 general MO, 12 nurses (which amounts to more nurses than the DH above). They see patients a day, and have about 5-15 deliveries a month. They have one ambulance, which they use for referrals to Manipal or Gangtok, about 2-4 a day. In violation of NRHM service guarantees, they only do emergency MTPs if someone comes in with an incomplete abortion. Otherwise they refer the patients to STNM. ASHA The Reproductive and Child Health Centre at Pakyong is large, spacious and well equipped. The airport company recently donated it as part of its local CSR efforts. They don t actually do many deliveries here in Pakyong because many women prefer to go to STNM of their own accord since it is so close. In addition, all first deliveries are referred to STNM, as well as any complications. The few deliveries that take place in Pakyong are mostly with poor women from nearby villages who are unable to make it to Gangtok. The ASHA has been working in the area since Up until 2011 she was doing it as social work. Since then ASHAs have started to be paid by the state on a commission basis. She is also an ASHA facilitator for trainings and has 10 ASHAs working under her. She says support for ASHAs in Sikkim is very good there are lots of trainings, they have fully stocked kits that are easy to replenish. There are 37 ASHAs in the Pakyong area, all doing good work. Almost all births are institutional. There have been no maternal deaths in the last year. JSY Payments - With JSY they have a big problem with bank accounts. Many mothers are from outside Sikkim and don t have an ID card. Therefore it is not possible for them to get a bank account. So they don t receive JSY money, and neither do the ASHAs. In general ASHAs face problems with any patients who do not have sufficient documentation. Roads and Transportation - The biggest problem they face with maternal complications is that there are so many remote villages that are hard to reach. This is especially true during the monsoon season when many roads become unpassable. Sometimes ASHAs are forced to do emergency home deliveries, which they are trained to do. But they don t like doing that, it is difficult without support and equipment and it is often not clean. Thankfully so far, in the time that she has been an ASHA she has never had to deal with any complications.
13 Migrant patients - Another big problem that they face in the maternal and child health ward is inconsistency with patients attending the PHC. The reason they cited for this is the high number of migrant workers and their families who have moved to Pakyong in recent years to work on the airport. Many of them may come to the PHC for the first time in their last trimester, so all their check ups are late. Or, they may unexpectedly return back to their homes, not receiving all their check ups. The same is true for vaccinations for their children. Many families have gone back before their children have received their full immunization course. Doctor from DH Travelling from the Pakyong PHC, the activists met a doctor employed at a different DH who reported the following: Equipment - There is lots of expensive equipment at the hospital that is completely unused because one part might have been forgotten when the equipment was originally delivered, it might be lost now, or some part might be broken. Despite multiple inquiries for repair by doctors, they get little response and progress is very slow. Fuel and Transportation - While they do have an ambulance, often they do not have any money for fuel for the vehicle. As a doctor who cares deeply about the lives of her patients she believes the ambulance must continue its operations and for over a year paid for fuel for the ambulance out of her own pockets, and is still awaiting reimbursement. Often not all patients are able to get the ambulance services they need since there are only three. Therefore they have to decide who gets to use the ambulance by balancing economic ability to pay with urgency of the patient s condition. The remaining patients have to use private transportation.



14 4. STNM Hospital Gangtok Maternity Ward When we walked into the maternity ward at STNM Hospital it was 8:00pm. The corridor was filled with patients who had put down bedding ready to spend the night on the floor. We spoke to one woman who was lying on the floor who said she was bleeding and the doctor had asked her to stay, she didn t know what the problem was yet. She was waiting until she would be able to see the doctor the next day. She was in a lot of pain. Because it was so late we were unable to speak with any doctors, however we were able to speak to a room of nurses and nurse interns and several patients. The hospital has more than 10 deliveries a day, and up to 5 caesarean sections. Despite efforts to build new toilets outside for visitors, the toilets in the ward are still being used to male and female visitors, as well as to wash clothes and utensils in. There are signs that say, Women Only that are being completely disregarded. There needs to be someone there to enforce these rules to prevent the toilets from descending into the unhygienic state that we found them in.
15 Woman from North Sikkim The ASHA in her village was very good and she got all the necessary antenatal check-ups and 3 injections. Lack of trust in District Hospital - She didn t go to the District Hospital because she doesn t feel comfortable with the quality of care there. She feels safer to come to STNM. Paying for medicines - All of the medicines she has needed since she was pregnant including since she arrived at the hospital now she has had to pay for, except the calcium and iron pills. Couple from Tadong Shortage of pills - She came to STNM for all her ANCs, all medication was meant to be free. However, in the middle they ran out of iron and calcium pills and so she had to buy them herself from a chemist at her own cost. Woman from Pakyong She went to Pakyong PHC but her baby was facing the wrong direction, so they referred her here. The ASHAs were good and helped her to get to STNM and get medicines. Long waits for beds and to see doctor - She arrived her at 10am, and got a bed at 4pm. She saw a doctor finally at 7pm. She is still in labour. Woman from Laksam (West Sikkim) She first went to the small dispensary in Laksam where they gave her all the necessary injections during her pregnancy and the ASHA was very helpful. It is half an hour from where she lives to Geyzing DH, where she was referred for one of her antenatal check ups. They detected that there is water in her baby s brain so they referred her to Gangtok. Lack of beds - She and her husband arrived in Gangtok on May 2 nd, but there were no beds so they had to stay in a hotel for a night. They were admitted on May 3 rd and have been there since (May 21 st ). Her baby was born on the 16 th, and is currently in ICU. They are waiting for the baby to be discharged and then they will return to Laksem. Nurses Equipment - Biggest thing they need is a ventilator in the neonates ICU. There is also only one incubator. The ICU is overall not well equipped, so if the condition is serious or more than one baby needs an incubator then it is referred to Manipal. When we asked if they have enough equipment, they joked, Whatever was there when the Chogyal left, that s all we have, continuing to say that there are many shortages and a lot of equipment is quite old. For example, they don t have a baby suction, which is very important and right now they have to do it by hand.
16 Referrals - Even here referrals are made, any truly serious cases are referred to Manipal, but at the patient s own cost. Patients come from all districts, some come themselves and many are referred by the District Hospitals. Normally the staff at the district hospitals doesn t refer them straight away, but the patients request strongly to be referred directly upon arrival. Staffing - They are extremely understaffed with nurses. Especially for the evening and night shift when there are only two nurses for all the patients, and one doctor is on call. There are 6 doctors. Beds - Beds is also a big problem with a huge shortage. Sometimes there are patients lying on the floor stretching all the way out to the main gate. Patients are also discharged far too soon after delivery, even 2 hours afterwards in order to free up the beds. Maternal deaths - They have very few maternal deaths, though they were unable to give an exact number, but they said the major causes were lack of follow-up of ANCs, and eclampsia.
17 Sub Centres List of Necessary Equipment according to IPHS
18
19
20 Primary Health Centres
21
22
23
24
25

26 District Hospitals
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012
 Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh
 Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh 1 CHAPTER Deepak Kumar,* Manisha* and Archana Dwivedi** INTRODUCTION Himachal Pradesh (HP) is one
Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh 1 CHAPTER Deepak Kumar,* Manisha* and Archana Dwivedi** INTRODUCTION Himachal Pradesh (HP) is one
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur
 State Institute of Health & Family Welfare, Jaipur") Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Hospital Standards by Bureau of Indian. BIS Standards considered very resource. No such standards for primary health care
 Indian Public Health Standards State Institute of Health & Family Welfare, Jaipur Existing Standards Hospital Standards by Bureau of Indian Standards (BIS) BIS Standards considered very resource intensive
Indian Public Health Standards State Institute of Health & Family Welfare, Jaipur Existing Standards Hospital Standards by Bureau of Indian Standards (BIS) BIS Standards considered very resource intensive
Amendments for Auxiliary Nurses and Midwives syllabus and regulation
 Amendments for Auxiliary Nurses and Midwives syllabus and regulation Duration of the course : The total duration of the course is 2 year (18 months + 6 months internship) First Year : i. Total weeks -
Amendments for Auxiliary Nurses and Midwives syllabus and regulation Duration of the course : The total duration of the course is 2 year (18 months + 6 months internship) First Year : i. Total weeks -
HEALTH CARE FOR ASYLUM SEEKERS
 HEALTH CARE FOR ASYLUM SEEKERS 2 HEALTH CARE FOR ASYLUM SEEKERS DURING THE FIRST 15 MONTHS OF THEIR ASYLUM PROCEDURE / BEFORE THEY ARE ACCEPTED INTRODUCTION In Germany, medical care is organised in a way
HEALTH CARE FOR ASYLUM SEEKERS 2 HEALTH CARE FOR ASYLUM SEEKERS DURING THE FIRST 15 MONTHS OF THEIR ASYLUM PROCEDURE / BEFORE THEY ARE ACCEPTED INTRODUCTION In Germany, medical care is organised in a way
National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year
 National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year 2010-11 District :-Sriganganagar A RCH - TECHNICAL STRATEGIES & ACTIVITIES (RCH Flexible Pool) A.1 MATERNAL
National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year 2010-11 District :-Sriganganagar A RCH - TECHNICAL STRATEGIES & ACTIVITIES (RCH Flexible Pool) A.1 MATERNAL
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005
 Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Report to: Board of Directors Agenda item: 7 Date of Meeting: 28 February 2018
 Report to: Board of Directors Agenda item: 7 Date of Meeting: 28 February 2018 Title of Report: National Maternity Survey results 2017 Status: For information Board Sponsor: Helen Blanchard, Director of
Report to: Board of Directors Agenda item: 7 Date of Meeting: 28 February 2018 Title of Report: National Maternity Survey results 2017 Status: For information Board Sponsor: Helen Blanchard, Director of
Mama Rescue: An evoucher and Emergency Dispatch System for Ugandan Mothers
 Mama Rescue: An evoucher and Emergency Dispatch System for Ugandan Mothers Uganda suffers from a maternal mortality ratio of 336 deaths per 100,000 live births (2016),[1] and it is thought that 75% of
Mama Rescue: An evoucher and Emergency Dispatch System for Ugandan Mothers Uganda suffers from a maternal mortality ratio of 336 deaths per 100,000 live births (2016),[1] and it is thought that 75% of
National Patient Experience Survey UL Hospitals, Nenagh.
 National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
I. PROFORMA FOR PROGRESS REPORT
 PART 3. ANNEXURES I. PROFORMA FOR PROGRESS REPORT PROFORMAE FOR REPORT ON RURAL HEALTH STATISTICS (As on 31 st March, 2017) 141 GENERAL INSTRUCTION FOR FILLING THE PROFORMA 1. Please read all columns carefully
PART 3. ANNEXURES I. PROFORMA FOR PROGRESS REPORT PROFORMAE FOR REPORT ON RURAL HEALTH STATISTICS (As on 31 st March, 2017) 141 GENERAL INSTRUCTION FOR FILLING THE PROFORMA 1. Please read all columns carefully
YOU RE IN GOOD HANDS THANK YOU FOR CHOOSING ST VINCENT S PRIVATE HOSPITAL WERRIBEE
 YOU RE IN GOOD HANDS THANK YOU FOR CHOOSING ST VINCENT S PRIVATE HOSPITAL WERRIBEE Welcome to St Vincent s Private Hospital werribee From the moment you step through our doors we re looking out for you
YOU RE IN GOOD HANDS THANK YOU FOR CHOOSING ST VINCENT S PRIVATE HOSPITAL WERRIBEE Welcome to St Vincent s Private Hospital werribee From the moment you step through our doors we re looking out for you
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
Situation Analysis of MTP Facilities in Haryana
 Situation Analysis of MTP Facilities in Haryana Executive Summary Centre for Research in Development and Change (A Division Of Society for Operations Research and Training) Baroda 2004 The present study
Situation Analysis of MTP Facilities in Haryana Executive Summary Centre for Research in Development and Change (A Division Of Society for Operations Research and Training) Baroda 2004 The present study
DISTRICT BASED NORMATIVE COSTING MODEL
 DISTRICT BASED NORMATIVE COSTING MODEL Oxford Policy Management, University Gadjah Mada and GTZ Team 17 th April 2009 Contents Contents... 1 1 Introduction... 2 2 Part A: Need and Demand... 3 2.1 Epidemiology
DISTRICT BASED NORMATIVE COSTING MODEL Oxford Policy Management, University Gadjah Mada and GTZ Team 17 th April 2009 Contents Contents... 1 1 Introduction... 2 2 Part A: Need and Demand... 3 2.1 Epidemiology
CHAPTER 30 HEALTH AND FAMILY WELFARE
 CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
Eradicate Childhood Malnutrition, Madhya Pradesh, India
 Eradicate Childhood Malnutrition, Madhya Pradesh, India Date: May 6, 2017 I. Demographic Information 1. Districts and State: Barwani district in Madhya Pradesh, India 2. Organization: Real Medicine Foundation
Eradicate Childhood Malnutrition, Madhya Pradesh, India Date: May 6, 2017 I. Demographic Information 1. Districts and State: Barwani district in Madhya Pradesh, India 2. Organization: Real Medicine Foundation
Cover for pregnancy and childbirth
 Cover for pregnancy and childbirth 2017 How we cover pregnancy and childbirth in 2017 The Maternity Benefit covers day-to-day and in-hospital medical expenses for expectant mothers and newborns. Overview
Cover for pregnancy and childbirth 2017 How we cover pregnancy and childbirth in 2017 The Maternity Benefit covers day-to-day and in-hospital medical expenses for expectant mothers and newborns. Overview
 Miranda Ashton Destination: Zomba Central Hospital, Malawi Zomba is a town of 100 000 people in Southern Malawi. The hospital holds 600 beds and has 4 main departments: surgery, obs and gynae, general
Miranda Ashton Destination: Zomba Central Hospital, Malawi Zomba is a town of 100 000 people in Southern Malawi. The hospital holds 600 beds and has 4 main departments: surgery, obs and gynae, general
FINAL REPORT FOR DINING FOR WOMEN
 Organization Information a. Organization Name: One Heart World-Wide b. Program Title: Implementing a Network of Safety around mothers and newborns in Western Nepal c. Grant Amount: $50,000 USD d. Contact:
Organization Information a. Organization Name: One Heart World-Wide b. Program Title: Implementing a Network of Safety around mothers and newborns in Western Nepal c. Grant Amount: $50,000 USD d. Contact:
HOPE Final Report. 2. Program Outcomes: a. To establish an obstetric fistula team that will provide fistula repair surgeries on a yearround
 HOPE Final Report 1. a. Organization Name: HOPE Foundation for Women and Children of Bangladesh b. Program Title: Obstetric Fistula Team to Support Sustainable Fistula Program c. Grant Amount: $45,000
HOPE Final Report 1. a. Organization Name: HOPE Foundation for Women and Children of Bangladesh b. Program Title: Obstetric Fistula Team to Support Sustainable Fistula Program c. Grant Amount: $45,000
Visit to Rumbek Hospital, Lakes State, South Sudan: th September 2013
 Visit to Rumbek Hospital, Lakes State, South Sudan: 24-28 th September 2013 Introduction: South Sudan is the newest country in the world, having gained official independence from the North on 9 th July
Visit to Rumbek Hospital, Lakes State, South Sudan: 24-28 th September 2013 Introduction: South Sudan is the newest country in the world, having gained official independence from the North on 9 th July
Report Exchange Program At Faculty of Health Sciences Kobe University, Kobe City, Hyogo, Japan 9 May June 2015 Ms Supapitch Muanginn
 Report Exchange Program At Faculty of Health Sciences Kobe University, Kobe City, Hyogo, Japan 9 May 2015 6 June 2015 Ms Supapitch Muanginn Chiang Mai University, Chiang Mai, Thailand P a g e 2 Table of
Report Exchange Program At Faculty of Health Sciences Kobe University, Kobe City, Hyogo, Japan 9 May 2015 6 June 2015 Ms Supapitch Muanginn Chiang Mai University, Chiang Mai, Thailand P a g e 2 Table of
INDONESIA S COUNTRY REPORT
 The 4 th ASEAN & Japan High Level Officials Meeting on Caring Societies: Support to Vulnerable People in Welfare and Medical Services Collaboration of Social Welfare and Health Services, and Development
The 4 th ASEAN & Japan High Level Officials Meeting on Caring Societies: Support to Vulnerable People in Welfare and Medical Services Collaboration of Social Welfare and Health Services, and Development
Contracting Out Health Service Delivery in Afghanistan
 Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
The Right to Health in North Sinai Challenges and Community Solutions. (Executive Summary) The Right to Health in North Sinai - (Executive Summary)
 The Right to Health in North Sinai - (Executive Summary)") ! // November 2017 1 The Egyptian Initiative for Personal Rights The Right to Health in North Sinai Challenges and Community Solutions (Executive Summary) November 2017 ! 2 // November 2017 This document
! // November 2017 1 The Egyptian Initiative for Personal Rights The Right to Health in North Sinai Challenges and Community Solutions (Executive Summary) November 2017 ! 2 // November 2017 This document
National Patient Experience Survey South Tipperary General Hospital.
 National Patient Experience Survey 2017 South Tipperary General Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to
National Patient Experience Survey 2017 South Tipperary General Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to
HAPPY DAYS HEALTHY FUTURES
 HAPPY DAYS HEALTHY FUTURES PREGNANCY GUIDE 03 Thinking about having a baby? 05 Step 1 Choose the right product for you 09 Step 2 Choose an obstetrician 11 Step 3 Access Gap Cover scheme 13 Other information
HAPPY DAYS HEALTHY FUTURES PREGNANCY GUIDE 03 Thinking about having a baby? 05 Step 1 Choose the right product for you 09 Step 2 Choose an obstetrician 11 Step 3 Access Gap Cover scheme 13 Other information
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial
 Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial 24 April 2018 Katherine Semrau, PhD, MPH Health Systems Global Webinar Introductions Bejoy Nambiar Chair,
Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial 24 April 2018 Katherine Semrau, PhD, MPH Health Systems Global Webinar Introductions Bejoy Nambiar Chair,
CHC Inspection Protocol-Things to Look for
 CHC Inspection Protocol-Things to Look for Sr. No. Issues Comments 1. General Observations 1. There should be adequate signage in the city on main roads to inform where about of the CHC 2. Adequate signage
CHC Inspection Protocol-Things to Look for Sr. No. Issues Comments 1. General Observations 1. There should be adequate signage in the city on main roads to inform where about of the CHC 2. Adequate signage
Patient Experience Feedback Renal Medicine - Dialysis
 Patient Experience Feedback Renal Medicine - Dialysis Overall there was a very positive experience from all those surveyed Some very strong common themes ran throughout all respondents (see below), with
Patient Experience Feedback Renal Medicine - Dialysis Overall there was a very positive experience from all those surveyed Some very strong common themes ran throughout all respondents (see below), with
Addressing Delay 2: Transport and Communications To Improve Access to Obstetric Care
 Addressing Delay 2: Transport and Communications To Improve Access to Obstetric Care Daniel Murokora May 5, 2014 What Worked, What Did we Learn, How to Improve Regional Health Network Model SERVICES HCIV,
Addressing Delay 2: Transport and Communications To Improve Access to Obstetric Care Daniel Murokora May 5, 2014 What Worked, What Did we Learn, How to Improve Regional Health Network Model SERVICES HCIV,
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
Lactation. Patient Responsibility. AABC Birth Institute October 1-4, 2015 Scottsdale, AZ Lactation Billing & Patient Responsibility
 Lactation & Patient Responsibility The Affordable Care Act Provisions of the ACA have a big impact on how we are able to bill for lactation as well as other additional services. Some provisions increase
Lactation & Patient Responsibility The Affordable Care Act Provisions of the ACA have a big impact on how we are able to bill for lactation as well as other additional services. Some provisions increase
Review of Patient Experience of Elective Orthopaedic Services at Manchester Elective Orthopaedics Centre.
 Review of Patient Experience of Elective Orthopaedic Services at Manchester Elective Orthopaedics Centre. Report Summary The purpose of the report was to gather views from people using the elective orthopaedic
Review of Patient Experience of Elective Orthopaedic Services at Manchester Elective Orthopaedics Centre. Report Summary The purpose of the report was to gather views from people using the elective orthopaedic
Frontline Health Worker. Allied Health & Paramedics. Frontline Health Worker. Sector Health. Sub-Sector. Occupation
 Sector Health Sub-Sector Allied Health & Paramedics Occupation Frontline Health Worker Reference ID: HSS/ Q 8601, Version 1.0 NSQF level: 3 Frontline Health Worker Published by: All Rights Reserved, First
Sector Health Sub-Sector Allied Health & Paramedics Occupation Frontline Health Worker Reference ID: HSS/ Q 8601, Version 1.0 NSQF level: 3 Frontline Health Worker Published by: All Rights Reserved, First
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Orchard Home Care Services Limited
 Orchard Home Care Services Limited Orchard Home Care Inspection report 2 Ashfield Terrace Chester-le-street County Durham DH3 3PD Tel: 0191 389 0072 Website: www.cqc.org.uk Date of inspection visit: 12
Orchard Home Care Services Limited Orchard Home Care Inspection report 2 Ashfield Terrace Chester-le-street County Durham DH3 3PD Tel: 0191 389 0072 Website: www.cqc.org.uk Date of inspection visit: 12
Development of Educational Outreach Materials (Pregnancy Support Program)
") National Medical Foundation Primary Care Leadership Program GE/NMF PCLP Summer 2012 United neighborhood Health Services Service Project: Development of Educational Outreach Materials (Pregnancy Support
National Medical Foundation Primary Care Leadership Program GE/NMF PCLP Summer 2012 United neighborhood Health Services Service Project: Development of Educational Outreach Materials (Pregnancy Support
Operational Guidelines on. Maternal and Newborn Health
 Maternal and Newborn Health M E S S A G E The National Rural Health Mission has enabled several innovations to promote people s access to services. One of the most impressive of these is the Janani
Maternal and Newborn Health M E S S A G E The National Rural Health Mission has enabled several innovations to promote people s access to services. One of the most impressive of these is the Janani
Chapter 6 Planning for Comprehensive RH Services
 Chapter 6 Planning for Comprehensive RH Services This section outlines the steps to take to be ready to expand RH services when all the components of the MISP have been implemented. It is important to
Chapter 6 Planning for Comprehensive RH Services This section outlines the steps to take to be ready to expand RH services when all the components of the MISP have been implemented. It is important to
Worcestershire Acute Hospitals NHS Trust
 Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA.
 UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
Agency Headquarter Hospital Meshti Mela, Orakzai Agency
 Agency Headquarter Hospital Meshti Mela, Orakzai Agency Progress Report ober-ember, 217 Website: merf-pakistan.org Email: info@merf-pakistan.org I. Executive Summary Re-vitalization and strengthening health
Agency Headquarter Hospital Meshti Mela, Orakzai Agency Progress Report ober-ember, 217 Website: merf-pakistan.org Email: info@merf-pakistan.org I. Executive Summary Re-vitalization and strengthening health
Towards Quality Care for Patients. Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care
 Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Towards Quality Care for Patients Fast Track to Quality The Six Most Critical Areas for Patient-Centered Care National Department of Health 2011 National Core Standards for Health Establishments in South
Annie Hunter Head of Midwifery Isle of Wight NHS
 Annie Hunter Head of Midwifery Isle of Wight NHS The Isle of Wight has a population of 140,500, this doubles in the holiday season with the Island receiving approximately 2.8 million visitors each year.
Annie Hunter Head of Midwifery Isle of Wight NHS The Isle of Wight has a population of 140,500, this doubles in the holiday season with the Island receiving approximately 2.8 million visitors each year.
Final Technical Report Summary
 Final Technical Report Summary Development of Township Health Plans in Falam and Tedim Townships of Chin State, Myanmar Photo credit: Uzaib Saya Uzaib Saya, Than Naing Oo, David Collins, San San Min Management
Final Technical Report Summary Development of Township Health Plans in Falam and Tedim Townships of Chin State, Myanmar Photo credit: Uzaib Saya Uzaib Saya, Than Naing Oo, David Collins, San San Min Management
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA
 COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
PROJECT LIFE RAFT DESIGNING A LOWER COST INFANT INCUBATOR
 PROJECT LIFE RAFT DESIGNING A LOWER COST INFANT INCUBATOR Project Goal: The goal of this project is to develop a functioning prototype of a low-cost incubator and isolation unit for infant care in developing
PROJECT LIFE RAFT DESIGNING A LOWER COST INFANT INCUBATOR Project Goal: The goal of this project is to develop a functioning prototype of a low-cost incubator and isolation unit for infant care in developing
Improving Quality in Healthcare
 Improving Quality in Healthcare A practical guide for health care providers MARCH 2016 This guide report was prepared by University Research Co., LLC (URC) for review by the United States Agency for International
Improving Quality in Healthcare A practical guide for health care providers MARCH 2016 This guide report was prepared by University Research Co., LLC (URC) for review by the United States Agency for International
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
Developing an urgent care strategy for South Tees how you can have your say July/August 2015
 Developing an urgent care strategy for South Tees how you can have your say July/August 2015 Foreword Commissioning high quality, accessible urgent care services is a high priority for South Tees Clinical
Developing an urgent care strategy for South Tees how you can have your say July/August 2015 Foreword Commissioning high quality, accessible urgent care services is a high priority for South Tees Clinical
Your local NHS and you
 South Wales Programme Local Engagement Document Your local NHS and you Local NHS services in Cardiff and the Vale of Glamorgan are run by Cardiff and Vale University Health Board (UHB). The UHB is one
South Wales Programme Local Engagement Document Your local NHS and you Local NHS services in Cardiff and the Vale of Glamorgan are run by Cardiff and Vale University Health Board (UHB). The UHB is one
Catherine Hughson Kathryn Kearney Number of supervisors relinquishing role since last report:
 Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Maidstone Home Care Limited
 Maidstone Home Care Limited Maidstone Home Care Limited Inspection report Home Care House 61-63 Rochester Road Aylesford Kent ME20 7BS Date of inspection visit: 19 July 2016 Date of publication: 15 August
Maidstone Home Care Limited Maidstone Home Care Limited Inspection report Home Care House 61-63 Rochester Road Aylesford Kent ME20 7BS Date of inspection visit: 19 July 2016 Date of publication: 15 August
Enter and View Report FINAL
 Enter and View Report FINAL Name of Establishment: Birmingham Heartlands Hospital Maternity Services Postnatal Services Bordesley Green East Birmingham B9 5SS Date of Visit: Friday 27 th February 2015
Enter and View Report FINAL Name of Establishment: Birmingham Heartlands Hospital Maternity Services Postnatal Services Bordesley Green East Birmingham B9 5SS Date of Visit: Friday 27 th February 2015
Advance Health Care Planning: Making Your Wishes Known. MC rev0813
 Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Making a complaint about the NHS. The NHS and You. What you can expect from us What we expect from you NHS SCOTLAND
 Making a complaint about the NHS The NHS and You What you can expect from us What we expect from you NHS SCOTLAND Who is this leaflet for? This leaflet is for anyone who uses the NHS in any part of Scotland.
Making a complaint about the NHS The NHS and You What you can expect from us What we expect from you NHS SCOTLAND Who is this leaflet for? This leaflet is for anyone who uses the NHS in any part of Scotland.
Voucher Scheme for Equity in Health. Dr Nidhi Chaudhary Futures Group India
 Voucher Scheme for Equity in Health Dr Nidhi Chaudhary Futures Group India Challenges in Health System Low accessibility to health services High infant mortality rate Underutilization of services Low use
Voucher Scheme for Equity in Health Dr Nidhi Chaudhary Futures Group India Challenges in Health System Low accessibility to health services High infant mortality rate Underutilization of services Low use
Juba Teaching Hospital, South Sudan Health Systems Strengthening Project
 Juba Teaching Hospital, South Sudan Health Systems Strengthening Project Date: Prepared by: May 26, 2017 Dr. Taban Martin Vitale and Richard Anyama I. Demographic Information 1. City & State: Juba, Central
Juba Teaching Hospital, South Sudan Health Systems Strengthening Project Date: Prepared by: May 26, 2017 Dr. Taban Martin Vitale and Richard Anyama I. Demographic Information 1. City & State: Juba, Central
What will I do? Our HCSWs fall into three groups:
 As an HCSW, you will be a valued member of your team. Your focus will be on keeping patients at the centre of all we do, providing high quality care and living our Trust values: Together - Safe Kind Excellent.
As an HCSW, you will be a valued member of your team. Your focus will be on keeping patients at the centre of all we do, providing high quality care and living our Trust values: Together - Safe Kind Excellent.
You will be given five minutes at the end of the examination to complete the front of any answer books used. May/June 2016 LW3MED 2015/16 A 001
 On admission to the examination room, you should acquaint yourself with the instructions below. You must listen carefully to all instructions given by the invigilators. You may read the question paper,
On admission to the examination room, you should acquaint yourself with the instructions below. You must listen carefully to all instructions given by the invigilators. You may read the question paper,
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
St Mary s Birth Centre
 University Hospitals of Leicester NHS Trust St Mary s Birth Centre Quality report Thorpe Road Melton Mowbray Leicestershire LE13 1SJ Tel: 0300 303 1573 www.uhl-tr.nhs.uk Date of inspection visit: 13-16
University Hospitals of Leicester NHS Trust St Mary s Birth Centre Quality report Thorpe Road Melton Mowbray Leicestershire LE13 1SJ Tel: 0300 303 1573 www.uhl-tr.nhs.uk Date of inspection visit: 13-16
Trust Guideline for the Management of Postnatal Care: Planning, Information and Discharge Guideline
 Trust Guideline for the Management of Postnatal Care: Planning, A Clinical Guideline recommended for use In: Women s health - Obstetrics By: For: Key words: Written by: Obstetricians, Midwives, Paediatricians
Trust Guideline for the Management of Postnatal Care: Planning, A Clinical Guideline recommended for use In: Women s health - Obstetrics By: For: Key words: Written by: Obstetricians, Midwives, Paediatricians
REPORT: Healthcare services in Gulbarga District
 REPORT: Healthcare services in Gulbarga District Contents I. Introduction... 2 II. Healthcare in Aland Taluk... 2 Narona... 2 Kadaganchi... 4 Nehru Nagar Thanda... 6 Dangapur... 6 III. Healthcare in Afzalpur
REPORT: Healthcare services in Gulbarga District Contents I. Introduction... 2 II. Healthcare in Aland Taluk... 2 Narona... 2 Kadaganchi... 4 Nehru Nagar Thanda... 6 Dangapur... 6 III. Healthcare in Afzalpur
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW
 06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
Swindon Link Homecare
 Cleeve Hill Healthcare Limited Swindon Link Homecare Inspection report 41-51 Westlecott Road Old Town Swindon Wiltshire SN1 4EZ Date of inspection visit: 21 September 2016 Date of publication: 28 October
Cleeve Hill Healthcare Limited Swindon Link Homecare Inspection report 41-51 Westlecott Road Old Town Swindon Wiltshire SN1 4EZ Date of inspection visit: 21 September 2016 Date of publication: 28 October
PATIENT QUESTIONNAIRE Please help us make hospital care better.
 What is the survey about? PATIENT QUESTIONNAIRE Please help us make hospital care better. The National Patient Experience Survey is a new nationwide survey. It asks you for feedback about your most recent
What is the survey about? PATIENT QUESTIONNAIRE Please help us make hospital care better. The National Patient Experience Survey is a new nationwide survey. It asks you for feedback about your most recent
National findings from the 2013 Inpatients survey
 National findings from the 2013 Inpatients survey Introduction This report details the key findings from the 2013 survey of adult inpatient services. This is the eleventh survey and involved 156 acute
National findings from the 2013 Inpatients survey Introduction This report details the key findings from the 2013 survey of adult inpatient services. This is the eleventh survey and involved 156 acute
Leadership Forum: Promoting a Culture of Safety
 Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Speech to UNISON s Health Conference (25/04/2016)
") Speech to UNISON s Health Conference (25/04/2016) Thank you Wendy. It's a pleasure to be here today and to be addressing my first Unison Health Care Conference as Labour s Shadow Secretary of State for
Speech to UNISON s Health Conference (25/04/2016) Thank you Wendy. It's a pleasure to be here today and to be addressing my first Unison Health Care Conference as Labour s Shadow Secretary of State for
Addressing operational pressures across our maternity service. Our engagement document July 2018
 Addressing operational pressures across our maternity service Our engagement document July 218 Contents Introduction What is the problem How we currently staff our units What we need to do now The temporary
Addressing operational pressures across our maternity service Our engagement document July 218 Contents Introduction What is the problem How we currently staff our units What we need to do now The temporary
A Woman s Pathway to and Experience of Life-saving PPH and PE/E Care: Unmet Needs
 A Woman s Pathway to and Experience of Life-saving PPH and PE/E Care: Unmet Needs An Unfinished Agenda in Maternal Health: Meeting the Needs of Women with Preeclampsia/Eclampsia and Postpartum Hemorrhage
A Woman s Pathway to and Experience of Life-saving PPH and PE/E Care: Unmet Needs An Unfinished Agenda in Maternal Health: Meeting the Needs of Women with Preeclampsia/Eclampsia and Postpartum Hemorrhage
Healthwatch Knowsley Aintree University Hospitals Trust Service User Report Qtr. 1 ( )
") Healthwatch Knowsley Aintree University Hospitals Trust Service User Report Qtr. 1 (2016-17) 1 Contents About this report... 3 Snapshot... 3 Key... 4 Key Treatment & Care... 5 Key Facilities & Surroundings...
Healthwatch Knowsley Aintree University Hospitals Trust Service User Report Qtr. 1 (2016-17) 1 Contents About this report... 3 Snapshot... 3 Key... 4 Key Treatment & Care... 5 Key Facilities & Surroundings...
Betsi-Quthing Health Partnership. HCA Sharing Learning Sept 2018
 Betsi-Quthing Health Partnership HCA Sharing Learning Sept 2018 Outline 1. Betsi Quthing background 2. Brief overview on grant given by HCA 3. On how Betsi Quthing have assisted to build capacity of local
Betsi-Quthing Health Partnership HCA Sharing Learning Sept 2018 Outline 1. Betsi Quthing background 2. Brief overview on grant given by HCA 3. On how Betsi Quthing have assisted to build capacity of local
Alliance for Innovation on Maternal and Child Health Expanding Access to Care for Maternal and Child Health Populations Kentucky
 Alliance for Innovation on Maternal and Child Health Expanding Access to Care for Maternal and Child Health Populations Kentucky INTRODUCTION/BACKGROUND As part of the Alliance for Innovation on Maternal
Alliance for Innovation on Maternal and Child Health Expanding Access to Care for Maternal and Child Health Populations Kentucky INTRODUCTION/BACKGROUND As part of the Alliance for Innovation on Maternal
Benefits. Benefits Covered by UnitedHealthcare Community Plan
 Benefits Covered by UnitedHealthcare Community Plan As a member of UnitedHealthcare Community Plan, you are covered for the following MO HealthNet Managed Care services. (Remember to always show your current
Benefits Covered by UnitedHealthcare Community Plan As a member of UnitedHealthcare Community Plan, you are covered for the following MO HealthNet Managed Care services. (Remember to always show your current
MCH Programme in Vietnam Experiences for post Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam
 MCH Programme in Vietnam Experiences for post - 2015 Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam Current status: Under five mortality 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 58,0 45,8 26,8 24,4 24,1 22,5
MCH Programme in Vietnam Experiences for post - 2015 Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam Current status: Under five mortality 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 58,0 45,8 26,8 24,4 24,1 22,5
NEPAL EARTHQUAKE 2015 Country Update and Funding Request May 2015
 PEOPLE AFFECTED 4.2 million in urgent need of health services 2.8 million displaced 8,567 deaths 16 808 injured HEALTH SECTOR 1059 health facilities damaged (402 completely damaged) BENEFICIARIES WHO and
PEOPLE AFFECTED 4.2 million in urgent need of health services 2.8 million displaced 8,567 deaths 16 808 injured HEALTH SECTOR 1059 health facilities damaged (402 completely damaged) BENEFICIARIES WHO and
COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE D. Dr. Courtney Mazeroll
 COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE D Dr. Courtney Mazeroll OVERVIEW Dr. Courtney Mazeroll is a family physician, licensed to practise medicine
COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE D Dr. Courtney Mazeroll OVERVIEW Dr. Courtney Mazeroll is a family physician, licensed to practise medicine
Your guide to the National Standards for Safer Better Maternity Services
 Your guide to the National Standards for Safer Better Maternity Services Safer Better Care December 2016 Table of Contents About this guide...2 What is HIQA?...2 What are maternity services?...3 Why did
Your guide to the National Standards for Safer Better Maternity Services Safer Better Care December 2016 Table of Contents About this guide...2 What is HIQA?...2 What are maternity services?...3 Why did
Healthwatch Kent Enter & View Programme 2016 Winter Pressures Feb 2016
 Healthwatch Kent Enter & View Programme 2016 Winter Pressures Feb 2016 Healthwatch Kent undertook a series of visits to Accident & Emergency Departments in Kent to talk to staff and patients about their
Healthwatch Kent Enter & View Programme 2016 Winter Pressures Feb 2016 Healthwatch Kent undertook a series of visits to Accident & Emergency Departments in Kent to talk to staff and patients about their
Maternity benefit 2018
 Maternity benefit 2018 The Maternity benefit cover in-hospital and day-to-day medical expenses for expecting mothers and their newborns. Who we are The Malcor Medical Aid Scheme (referred to as the Scheme
Maternity benefit 2018 The Maternity benefit cover in-hospital and day-to-day medical expenses for expecting mothers and their newborns. Who we are The Malcor Medical Aid Scheme (referred to as the Scheme
Using Vouchers for Paying for Performance and Reaching the Poor: the Kenyan Safe Motherhood Initiative
 Using Vouchers for Paying for Performance and Reaching the Poor: the Kenyan Safe Motherhood Initiative Ben Bellows 1, Francis Kundu 2, Richard Muga 2, Julia Walsh 1, Malcolm Potts 1, Claus Janisch 3 1
Using Vouchers for Paying for Performance and Reaching the Poor: the Kenyan Safe Motherhood Initiative Ben Bellows 1, Francis Kundu 2, Richard Muga 2, Julia Walsh 1, Malcolm Potts 1, Claus Janisch 3 1
Milton Keynes University Hospital NHS Foundation Trust
 Milton Keynes University Hospital NHS Foundation Trust Enter and View Review of Staff/ Patient Communication Ward 17 and 18 September 2017 Contents Contents... 2 1 Introduction... 3 1.1 Details of the
Milton Keynes University Hospital NHS Foundation Trust Enter and View Review of Staff/ Patient Communication Ward 17 and 18 September 2017 Contents Contents... 2 1 Introduction... 3 1.1 Details of the
A Publication of the AIDS Law Unit, Legal Assistance Centre. Right to Health
 A Publication of the AIDS Law Unit, Legal Assistance Centre Right to Health Right to Health Table of Contents Chapter 1 What are human rights?... 1 Chapter 2 What is meant by the Right to Health?... 3
A Publication of the AIDS Law Unit, Legal Assistance Centre Right to Health Right to Health Table of Contents Chapter 1 What are human rights?... 1 Chapter 2 What is meant by the Right to Health?... 3
Semmelweis and the discovery of pathogens: Or why you need to wash your hands before touching patients.
 and the discovery of pathogens: Or why you need to wash your hands before touching patients. Cast Ignaz : Mary Bridget Nurse Agnes Nurse Barbara The Chief Doctor The nurse in charge of the maternity ward
and the discovery of pathogens: Or why you need to wash your hands before touching patients. Cast Ignaz : Mary Bridget Nurse Agnes Nurse Barbara The Chief Doctor The nurse in charge of the maternity ward
KANACHUR INSTITUTE OF MEDICAL SCIENCES UNIVERSITY ROAD, DERALAKATTE, MANGALORE INFRASTRUCTURE FACILITIES LAND DOCUMENTS
 KANACHUR INSTITUTE OF MEDICAL SCIENCES UNIVERSITY ROAD, DERALAKATTE, MANGALORE 575 018 INFRASTRUCTURE FACILITIES LAND DOCUMENTS. Reg. Doc. Date Survey Area (Acres) 1 (2604)2972/14-15 07.07.2014 333-1,
KANACHUR INSTITUTE OF MEDICAL SCIENCES UNIVERSITY ROAD, DERALAKATTE, MANGALORE 575 018 INFRASTRUCTURE FACILITIES LAND DOCUMENTS. Reg. Doc. Date Survey Area (Acres) 1 (2604)2972/14-15 07.07.2014 333-1,
Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn
 Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn Dr. M L Jain Director State Institute of Healthand and Family Welfare, Rajasthan Jaipur SIHFW: an ISO 9001: 2008 certified
Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn Dr. M L Jain Director State Institute of Healthand and Family Welfare, Rajasthan Jaipur SIHFW: an ISO 9001: 2008 certified
Having a baby at North Bristol NHS Trust
 Having a baby at North Bristol NHS Trust Exceptional healthcare, personally delivered Congratulations on your pregnancy! We hope that you will find this booklet helpful in providing you with useful information
Having a baby at North Bristol NHS Trust Exceptional healthcare, personally delivered Congratulations on your pregnancy! We hope that you will find this booklet helpful in providing you with useful information
Saint Mary s Birth Centre in Salford
 Saint Mary s Hospital Maternity Service Saint Mary s Hospital Saint Mary s Birth Centre in Salford Information For Patients From December 2011 Saint Mary s Hospital is offering women who live in Salford
Saint Mary s Hospital Maternity Service Saint Mary s Hospital Saint Mary s Birth Centre in Salford Information For Patients From December 2011 Saint Mary s Hospital is offering women who live in Salford
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Dent Blanche - Radcliffe-on-Trent 14A Main Road, Radcliffe-on-Trent,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Dent Blanche - Radcliffe-on-Trent 14A Main Road, Radcliffe-on-Trent,
Toolbox Talks. Access
 Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Case Study HEUTOWN DISTRICT: PLANNING AND RESOURCE ALLOCATION
 Case Study HEUTOWN DISTRICT: PLANNING AND RESOURCE ALLOCATION Di McIntyre Health Economics Unit, University of Cape Town, Cape Town, South Africa This case study may be copied and used in any formal academic
Case Study HEUTOWN DISTRICT: PLANNING AND RESOURCE ALLOCATION Di McIntyre Health Economics Unit, University of Cape Town, Cape Town, South Africa This case study may be copied and used in any formal academic
PRESENTATION ON UNIVERSAL HEALTH COVERAGE GOVERNMENT OF MEGHALAYA
 PRESENTATION ON UNIVERSAL HEALTH COVERAGE GOVERNMENT OF MEGHALAYA 1 1. Introduction General Background Indicator Meghalaya India Demographic Profile State Population Total (in lakhs) 29.64 12101. 02 State
PRESENTATION ON UNIVERSAL HEALTH COVERAGE GOVERNMENT OF MEGHALAYA 1 1. Introduction General Background Indicator Meghalaya India Demographic Profile State Population Total (in lakhs) 29.64 12101. 02 State