QUALITY & SAFETY COMMITTEE
|
|
|
- Hillary Parker
- 6 years ago
- Views:
Transcription
1 QUALITY & SAFETY COMMITTEE COMPLAINTS TO THE PUBLIC SERVICES OMBUDSMAN FOR WALES- INVESTIGATION FINDINGS Meeting Date: 9 th June 20 Author: Sponsoring Executive Director: Report Presented by: Committee/Group who have received or considered this paper: Jennifer Cooper, Concerns Manager Sue Morgan, Executive Director of Nursing/Service Improvement Sue Morgan, Executive Director of Nursing/Service Improvement Executive Management Board Trust Organisational Learning Committee Trust Resolution to: (please tick) Approve: Endorse: Discuss: Note: Recommendation: The Trust Quality & Safety Committee is asked to NOTE this report detailing two Ombudsman complaint investigations. This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well This report supports the following Health & Care Standards: Governance, Leadership and Accountability Safe Care Effective Care Dignified Care Timely Care Individual Care
2 2 Ombudsman Report COMPLAINTS TO THE PUBLIC SERIVCES OMBUDSMAN FOR WALES - INVESTIGATION FINDINGS 1. Introduction / Background: Individuals who remain dissatisfied with the management or outcome of the Trust s investigation of their concerns are advised they can take their concerns to the Public Services Ombudsman for Wales (PSOW). The PSOW has legal powers to look into complaints about public services in Wales from members of the public. If the PSOW decides to investigate and concludes from its investigation that the Trust is at fault and the individual has suffered as a result, it will make recommendations on what the Trust should do to put things right. 2. Timing During 20/ two complaints against the Trust were referred to the Ombudsman. One was referred out of time for investigation and was subsequently not taken forward by the Ombudsman. A second complaint was taken forward for investigation, the outcome of which is detailed within this report. The Trust s Annual Letter from the PSOW, which provides individual details in respect of the Trust as well as national statistics and trends, is expected in July Description In March 20 the Trust received the findings and recommendations from the PSOW s investigation of two separate complaints; Case Number & upheld complaint against Abertawe Bro Morgannwg University Health Board and Velindre NHS Trust; and Case Number partly upheld complaint against Aneurin Bevan University Health Board (details of which have been shared with the Trust by the PSOW given its involvement in AB HB s original investigation of the complaint and implications for the Trust arising from the PSOW s recommendations). 4. Financial Impact: There are no financial considerations in respect of this report. 5. Quality, Equality, Safety and Patient Experience Impact: The opportunities for learning that are identified from the investigation of concerns, both by the Trust and the PSOW, support the Trust in its commitment to continuously improve every aspect of the services it delivers. The PSOW s investigation findings and recommendations have identified learning points in respect of (i) the follow up care provided to patients after treatment; and (ii) processes for seeking informed consent. These learning points have been fully Page 2
3 3 Ombudsman Report considered both in respect of the individual cases investigated and their service wide implications. 6. Considerations for the Committee: For the purposes of updating the Committee, the PSOW s anonymised summary of each case (which can be used in information published by the PSOW) is presented below. Further details on each case are available, on request, from Jennifer Cooper, Concerns Manager. Summary of a Report issued under Section 21 of the Public Services Ombudsman (Wales) Act 2005 Case Number & Abertawe Bro Morgannwg University Health Board and Velindre NHS Trust Mrs A complained that the Health Board failed to diagnose her husband s secondary cancer despite him undergoing many investigations. She said there was also a delay in him being seen by the Urology Department. Mrs A said that despite her husband s deteriorating health, no measures were put in place for him to have palliative care. This led to poor pain control. In addition Mrs A complained that the Trust s Consultant Oncologist failed to recognise her husband s symptoms and examine him during a consultation. Mrs A said that she had described her husband s symptoms to the Consultant Oncologist and that these included loss of appetite, weight loss and a hoarse voice. The Ombudsman s investigation identified shortcomings in the care provided to Mrs A s husband by the Health Board and the Trust and upheld Mrs A s complaint. The Ombudsman recommended that both the Health Board and the Trust apologise to Mrs A for the shortcomings found. He also recommended that the Health Board pay Mrs A 350 for the difficulties her husband encountered around an endoscopy scan and for the distress caused by the failure to make a referral for nutritional support. March 20 Summary of a Report issued under Section 21 of the Public Services Ombudsman (Wales) Act 2005 Case Number Aneurin Bevan University Health Board Mr B complained about the standard of care provided to his late sister Ms C when she had surgery and underwent chemotherapy for breast cancer. She sadly died as a result of the chemotherapy treatment. He complained that Ms C had been discharged from hospital too soon following surgery, the district nursing care provided post operatively was variable and whether the risks of treatment had been fully explained to Ms C as part of the process for consenting to the treatment. The Ombudsman partly upheld the complaint. He found that: The standard of inpatient care and the decision to discharge Ms C were both reasonable. However, there were some shortcomings in care in that a Page 3
4 4 Ombudsman Report psychological assessment should have been completed and a nutritional assessment on admission. It was impossible to judge the standard of district nursing care as the Health Board could not locate the district nursing records; this in itself was an injustice to Ms C s family. Whilst there is some difference in the oncology community about the wording used on consent forms, in Ms C s case it would have been appropriate to use the term life-threatening infection. The Ombudsman recommended: (a) (b) (c) (d) (e) a written apology to Mrs C s family; a financial payment of 750 to MS C s family to reflect the loss of Ms C s district nursing notes; a review of the wording used in its consent forms for chemotherapy treatment to include, where appropriate, the possibility of life-threatening infection; satisfactory procedures for the Health Board to retrieve district nursing notes when patients stop receiving district nursing services; and verification via appropriate clinical records audit that MUST and psychological assessments are being completed for patients when indicated. March Next Steps The Committee is asked to NOTE the contents of this report. The Trust has complied with the recommendation identified in Case Number & Evidence of compliance has been provided to the PSOW. Though no formal recommendations have been identified for the Trust in respect of Case Number the Trust has provided a commitment to review the wording of both its consent forms and patient information leaflets to ensure the possibility of life threatening infection is explicitly stated whenever appropriate. The Trust will provide the PSOW with an informal update on progress against this improvement action by mid June 20. Progress against the PSOW s recommendations will be monitored through to completion by the Velindre Cancer Centre Concerns Forum. Page 4
5 Quality and Safety Committee The National Wound Audit 20: Report for NHS Wales Meeting Date: 9 th June 20 Author: Sponsoring Executive Director: Report Presented by: Committee/Group who have received or considered this paper: Jayne Elias Assistant Director of Nursing and Service Improvement Professor Susan Morgan, Executive Director of Nursing and Service Improvement Jayne Elias Assistant Director of Nursing and Service Improvement National Quality and Safety Forum Trust Resolution to: (please tick) Approve: Endorse: Discuss: Note: Recommendation: The Quality and Safety Committee is asked to note the findings of the National Wound Audit 20 This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well
6 2 [Report Title] 1. Introduction / Background: The National Wound Audit was commissioned by the Chief Nursing Officer for Wales and was undertaken in all Health Boards and Velindre NHS Trust between 28 th September 20 and 2 nd October Timing The National Wound Audit 20 report was received by the National Quality Forum meeting on 25 th April Description: The report sets out high level findings from the national audit. Although no recommendations were made the report sets out 10 key messages for NHS Wales. 4. Financial Impact: There are no specific financial considerations to bring to the notice of the Quality and safety Committee 5. Quality, Equality, Safety and Patient Experience Impact. The appropriate management of wounds/pressure ulcers is fundamental to patient experience. The Trust uses the skin care bundle to prevent avoidable pressure damage. The Pressure Ulcer group undertake a root cause analysis of all hospital acquired pressure ulcers to ascertain if there are lessons to inform practice development. This report is related to Standard 2.2 Preventing Pressure and Tissue Damage of the Health and Care Standards. 6. Considerations for Board / Committee The audit was undertaken across NHS Wales between 28 th September 20 and 2 nd October 20. The report was presented to the National Quality Safety Forum in April 20. The number of Velindre NHS Trust patients who were eligible for inclusion in the audit was very small (26), particularly in the context of the larger Health Boards (>1000). The Report does not make any recommendations for practice however identified 10 key messages for NHS Wales 7. Next Steps Pressure Ulcer Group have been asked to review the findings of the National Wound Audit 20, and to consider learning in the context of local services. Page 2

7 The National Wound Audit 20 Report for NHS Wales
8 Contents The National Wound Audit Contents... 1 Introduction... 1 Results... 3 Demographic data... 4 Pressure ulcers, moisture lesions and classification... 5 Patient support surfaces... 6 Other wounds encountered during the audit Key messages from the wound audit for NHS Wales References Introduction Pressure ulcers remain a significant challenge for NHS Wales given the large numbers of patients who present with, or develop these skin and soft tissue wounds. For individuals who have one or more pressure ulcers increased pain may be experienced, hospital stays may be longer and health related quality of life reduced (Welsh Wound Network 2010). While data upon pressure ulcer occurrence is routinely collected across much of NHS Wales the accuracy of this data is often questioned by clinicians and management. In 2014 a national audit of pressure ulceration across acute care in NHS Wales was proposed by the Chief Nurse with one goal of this audit being to identify how many moisture lesions are incorrectly classified as pressure ulcers (moisture lesions are skin wounds caused by urine and/or faeces and perspiration which is in continuous contact with intact skin of the perineum, buttocks, groins, inner thighs, natal cleft, skin folds and where skin is in contact with skin, All Wales Tissue Viability Nurse Forum and All Wales Continence Forum, 2014). Correct management of moisture lesions and pressure ulcers differs and incorrect classification may result in patients receiving inappropriate treatment for their moisture lesions. Preparation for the audit consumed almost 12 months with the project led by the Welsh Wound Innovation Centre (WWIC) working with the Lead for Patient Safety and Patient Experience (Chief Nurse s Office). A proposal describing the audit methodology was circulated from the Chief Nurse to all Health Board Directors of Nursing and Tissue Viability 1
9 Nurses. Detailed discussions occurred between each Health Board and WWIC to determine the scope of the audit within each Health Board with a number of issues arising such as consent, capacity to undertake the audit and the inclusion of wound aetiologies other than pressure ulcers and moisture lesions. It was agreed that WWIC would help provide staff to assist the audit where required and that while only pressure ulcers and moisture lesions would be visually inspected other wound aetiologies would be reported but not seen by the audit team. While this audit primarily aimed at collecting data in Acute and District General Hospitals a number of community hospitals were also included while Powys Teaching Health Board audited all patients within its community hospitals. To collect pressure ulcer occurrence data accurately the audit broadly utilised the methodology developed and reported by the European Pressure Ulcer Advisory Panel (EPUAP, Vanderwee et al 2007) where the skin of each patient who consents is visually examined from head to toe and all pressure ulcers reported. In each clinical area a date and time for the audit visit was agreed with clinical staff with the ward staff completing a form reporting pressure ulcers present from all in patients at midnight of the night before the audit visit. A clinician and a data collector visited each clinical area, the clinician sought consent from each in patient with their skin examined if consent was provided. No skin inspections were undertaken among mental health patients. If the skin inspection identified a pressure ulcer or moisture lesion that was not recorded on the form completed by the ward staff, then these wounds were also recorded. All data was captured on paper (completed by ward staff) and electronically using ipads with hardware and Information Technology support provided by Medstrom, a supplier of pressure redistributing equipment. The audit was conducted collaboratively across Wales bringing together the tissue viability nurses within each Health Board, WWIC clinical staff and a wide range of clinical and nonclinical staff from the wound care industry in Wales. Medstrom, using a series of Excel files, undertook initial data cleaning to remove duplicated data and identify missing data. Excel files containing data from single Health Boards were then circulated to each Health Board s Tissue Viability Nurses to check the accuracy of the data gathered within their Health Board. WWIC then created an SPSS (Version 23.0, SPSS Inc.) data file bringing together all the data for analysis. An initial report upon the audit data including recommendations for practice was prepared for the Chief Nursing Officer and Directors of Nursing with subsequent issue of individual Health Board reports. This document expands upon the initial report given that WWIC has further cleaned the complex data set to reveal more information upon aspects of the audit such as pressure redistributing support surface use, the other wounds encountered during the audit and errors in the classification of pressure ulcers and moisture lesions. A summary of the key findings between the original and final report are as follows: * One additional patient with a pressure ulcer was identified on cleaning the data file making 748 patients with pressure ulcers, the overall prevalence rate of patients 2
10 with pressure ulcers remains unchanged at 8.9% of which 50.4% (n=337) were hospital acquired with the origin of a further 80 (10.7%) patients pressure ulcers unknown. * 95% confidence intervals have been presented for the overall pressure ulcer prevalence and for each Health Board s pressure ulcer prevalence. These provide greater understanding of the likely variability in the prevalence were similar surveys to be conducted in future. * 51.7% (n=4282) of patients where an assessment of risk was recorded were considered to be at medium to high risk of developing pressure ulcers. * 5178 (64.2%) patients had their skin inspected with no change from the total shown in Figure 5 of the original report. * One hundred and sixty five (18.2%) of the 907 pressure ulcers encountered during the audit had not been reported by clinical staff prior to the audit. In the original report 8 of 906 (18.5%) pressure ulcers were reported to have been reported by the audit team rather than clinical staff. * One hundred and sixty five pressure ulcers were reported to be incorrectly classified when seen by the audit team (18.2%), in the original report 4/906 (18.1%) pressure ulcers were incorrectly classified. These minor changes reflect the additional patient found to have a pressure ulcer and a small number of errors in the data file observed on cleaning the data. * The data upon pressure redistributing mattresses has been condensed from 20 categories in the original report to six allowing clearer interpretation of the inappropriate allocation of mattress resources to patients. The number of patients allocated foam mattresses when at high risk of pressure ulcer developed increased from 646 in the original report to 663 due to the data cleaning identifying further mattresses allocated to patients. The number of low risk patients allocated dynamic mattress replacements also changed from 29 to 36 upon data cleaning. * New information has been added in the final report to illustrate mattress allocation by severity of pressure ulcers. This data was not included in the original report. * The original report noted that the majority of wounds other than pressure ulcers, moisture lesions and surgical wounds were unknown (n=474). Cleaning of the datafile has allowed identification of all bar 1 wounds. Results The audit was undertaken during the period 28 th September 20 to October 2 nd 20 and across Wales collected data upon 8365 patients, of whom 748 (8.9%) were reported or observed to have pressure ulcers. The 95% confidence interval around the proportion with 3
11 pressure ulcers was 8.29% to 9.51% suggesting that if the survey was repeated 95% of prevalence calculations would fall between these two limits. The scale of the audit is perhaps best represented by the person days required to gather the data and represents a significant undertaking by all staff involved. Within the tables presented in this report the denominator may be lower than 8365 patients given varying quantities of missing data in each analysis. Demographic data Table 1. Distribution of patients included in the 20 wound audit across Wales. Health Board/NHS Trust Abertawe Bro Morgannwg UHB Aneurin Bevan UHB Betsi Cadwaladr UHB Cardiff & Vale UHB Patients Gender (M:F; %M) :891 (44.7%) :926 (42.0%) :731 (46.4%) :898 (45.6%) Cwm Taf UHB 982 4:566 (42.4%) Hywel Dda UHB :519 (46.4%) Powys Teaching Health Board Velindre Trust NHS 7 53:114 (31.7%) 26 12:14 (46.2%) TOTAL :4659 (44.3%) Age (mode age band) Pressure ulcer risk (mode risk group) Number of Medium and High risk patients (n, % of all patients) Low 687 (42.6%) Low 726 (45.7%) Low 709 (52.1%) High 992 (60.5%) High 666 (67.9%) Not at risk 372 (38.0%) High 118 (70.7%) Low 12 (46.2%) Low 4282 (51.7%) 4
12 From Table 1; The majority of patients were elderly and female. Across Wales 51.7% (4282/8279) of patients where an assessment of risk was recorded were considered to be at medium to high risk of developing pressure ulcers. Pressure ulcers, moisture lesions and classification Table 2. The pressure ulcers and moisture lesions encountered across Wales. Number patients with pressure ulcers Number of patients with skin inspected Reason for no skin inspection Mental Health Patient Declined Off ward Too ill Unable to consent Number of patients with new pressure ulcers found during the audit Number of patients with incorrect classification of pressure ulcers Category III reported as II Category II reported as I Cat. II reported as moisture lesion Reported classification missing Number of pressure ulcers encountered Highest number of pressure ulcers per patient 748/8365 (8.9%) 5178/ Pressure ulcer maximum severity I II III IV Unstageable Deep Tissue Injury Body site where most severe pressure ulcer occurred Sacrum Heel Buttock Other 5 Origin of most severe PU Inherited: Incident Unknown Number of medical device related pressure ulcers 907 Number of moisture lesions reported 6 Number of moisture lesions reported as pressure ulcers Number of pressure ulcers reported as moisture lesions : From Table 2; 5178 (64.2%) of all patients had their skin inspected during the audit. 5
13 One hundred and sixty five (18.2%) pressure ulcers were found during the audit who had not been reported by clinical staff prior to the audit. One hundred and sixty five (18.2%) pressure ulcers were incorrectly classified. The most common errors were reporting category III pressure ulcers as partial thickness category II wounds; reporting category II wounds as category I skin damage and reporting category II pressure ulcers as moisture lesions. Two category IV pressure ulcers were reported to the audit teams as a moisture lesion and a category I pressure ulcer. Almost two thirds of the instances where pressure ulcers were stated to be incorrectly classified the original category of the wounds were not reported. One patient had a total of six pressure ulcers. Most pressure ulcers were of category I or II severity however 117 full thickness wounds (category III and IV) were reported with a further 51 wounds considered unstageable given extensive slough and necrotic tissue within the wound bed all of these were likely to be full thickness wounds. Three hundred and thirty seven (50.4%) patients developed their pressure ulcers while receiving care. Among the incident pressure ulcers were 27 category III, 10 category IV and 22 unstageable wounds. The origin of the pressure ulcers experienced by 80 patients (10.7%) was unknown. Moisture lesions were relatively common with 362 patients (4.3%) affected with no instances of moisture lesions being reported as pressure ulcers and only 6 cases of pressure ulcers being reported as moisture lesions. Very few pressure ulcers were directly related to the use and positioning of medical devices with only 33 medical device related pressure ulcers identified. Patient support surfaces A wide range of patient support surfaces were encountered during the audit for use while the patient rests in bed. These have been simplified for analysis into six categories foam mattress, other static mattresses and overlays, low air loss/specialty bed, mattress with static and dynamic capability (hybrid), dynamic mattress overlays and dynamic mattress replacement systems Table 3). Table 4 highlights how the six categories of mattress were allocated to patients at different degrees of vulnerability to developing pressure ulcers. 6
14 Table 3. Reducing the categories of pressure redistributing support surface. Foam mattress Other static mattress/overlay Mattress category Low Air Loss/Specialty bed Hybrid product Foam Repose Arise Invacare hybrid Dolphin Affinity Mercury Advance Dynamic overlay AlphaExcel B Wave Dynamic replacement Cairwave Nimbus Trinova Primo Duo 2 Autologic Alpha Relief Alpha Active P.R.O. Matt Table 3 illustrates the mattress descriptions from Figure 6 in the original report placed under the six broad categories used in this report. The 20 categories from the original report were completed by Other and Unknown. Table 4. Allocation of mattresses by level of vulnerability to pressure ulcer development. Risk of pressure ulcer development Product type None Low Medium High Foam mattress Other static mattress/overlay Low Air Loss/Specialty bed Hybrid product Dynamic overlay Dynamic replacement TOTAL From Table 4; Most foam mattresses were allocated to those at no risk of pressure ulcer development while dynamic mattress replacements were primarily used in the care of patients at high risk of pressure ulcer development. 7
15 663 (32.4%) patients at high risk of pressure ulcer development rested on foam mattresses while 36 patients considered not to be at risk were allocated dynamic mattress replacements. The mattress allocated to 1308 (.6%) patients was unreported. Table 5. The allocation of pressure redistributing mattresses by the severity of pressure ulcer. Pressure ulcer classification Product type I II III IV Deep Tissue Injury Unstageable Unknown Foam mattress Other static mattress/overlay Low Air Loss Hybrid product Dynamic overlay Dynamic replacement TOTAL From Table 5, Dynamic replacement mattresses were used in the treatment of all categories of pressure ulcer including Deep Tissue Injury and Unstageable ulcers. Foam and static mattresses were primarily allocated where patients had category I or II pressure ulcers. 8 people with unstageable (full thickness) pressure ulcers were allocated foam mattresses while 49 people with category I ulcers were nursed upon dynamic replacement mattresses. Other wounds encountered during the audit. While the survey was intended to capture the number of people with pressure ulcers and moisture lesions other wound aetiologies were recorded. Of the 8365 patients included in the audit 2546 (30.4%) either had a pressure ulcer, a moisture lesion or other wound, with 56 having both a pressure ulcer and a moisture lesion. Table 6 lists the most common other wound aetiologies recorded, there were a wide range of other wound aetiologies and anatomical locations reported to be wounded, however each of these affected fewer than 30 patients. 8
16 Table 6. Most common other wound aetiologies recorded in the 20 wound audit. Wound aetiology Number of patients Closed surgical wound 841 Other surgical wound 55 Infected surgical wound 43 Dehisced surgical wound 35 Skin tear 2 Leg Ulcer 196 Diabetic Foot Ulcer 56 Traumatic wound 40 Lymphoedema a 37 Wound diagnosis or location unknown 1 a Skin and soft tissue condition recorded given challenge of management. Key messages from the wound audit for NHS Wales. 1. Pressure ulcers affected 748 (8.9%) of all surveyed patients with 8 patients having full thickness pressure ulcers. This survey was the first national audit of pressure ulcers across the devolved nations of the United Kingdom. 2. One hundred and sixty five pressure ulcers were found during the audit although not reported by clinical staff. This represents 18.2% of all pressure ulcers encountered during the survey and illustrates the value of conducting detailed skin inspection to ascertain robust data upon wound occurrence. 3. One hundred and sixty five pressure ulcers classifications were incorrect although data upon these errors was only reported in one third of all cases. Further work on pressure ulcer classification may help improve the reporting of pressure ulcers within Wales. 4. Most pressure ulcers encountered were of category I or II severity however there were 8 full thickness category III, IV or unstageable pressure ulcers, of these more severe wounds 59 developed post admission. This cross sectional survey was not able to determine why patients had developed full thickness pressure ulcers whereas a Root Cause Analysis approach may cast light on why these severe pressure ulcers developed within NHS Wales care facilities. 5. In eighty (10.7%) patients with pressure ulcers it was unknown whether the wound had developed pre or post admission. Focus should perhaps be given to the importance of reporting pressure ulcer origins during assessment at A&E or on admission to the ward. 6. Moisture lesions were commonly encountered with 362 (4.3%) patients experiencing these wounds. No moisture lesion had been incorrectly defined as 9
17 a pressure ulcer and only 6 pressure ulcers incorrectly classified as moisture lesions suggesting appropriate education was available upon the differentiation between these two wound aetiologies. 7. Few medical device related pressure ulcers were encountered with only 33 patients affected % of all patients had their skin inspected during the audit. Where skin was not seen during the audit, over 1000 mental health patients had been excluded from skin inspection with 684 patients declining to give consent for their skin to be seen. Future detailed audit work may wish to consider the use of patient information to help explain the purpose of wound audits. 9. There were inconsistencies within the allocation of support surfaces based upon vulnerability to pressure ulcer development or in management of existing ulcers. It is possible that mattress allocation would not have been based solely upon a risk assessment score but the common use of foam mattresses among high risk patients and use of dynamic replacement mattresses in the treatment of category I pressure ulcers indicates that mattress allocation may be improved with the potential for cost reductions across NHS Wales. 10. Just over 30% (n=2546) of all patients surveyed had a pressure ulcer, a moisture lesion or another wound type (surgical wounds, skin tears and leg ulcers being the most common). The high prevalence of wounds within NHS Wales is likely to lead to increased staff time given to wound healing, increased demands upon the tissue viability services and additional cost for each Health Board. References All Wales Tissue Viability Nurse Forum and All Wales Continence Forum (2014). The All Wales Best Practice Statement on the Prevention and Management of Moisture Lesions. Wounds UK, accessed on 23 rd February 20 at Moisture_Lesions_final_final.pdf. Vanderwee K, Clark M, Dealey C, Gunningberg L, Defloor T (2007). Pressure ulcer prevalence in Europe: a pilot study. Journal of Evaluation in Clinical Practice. 13(2): Welsh Wound Network (2010). Pressure ulcers: Just the facts. Accessed 23 rd February 20 at content/uploads/2013/05/wwn_new_print.pdf. 10
18
19 QUALITY & SAFETY COMMITTEE Patient Experience Quarterly Report (Jan Feb Mar 20) Meeting Date: Author: Sponsoring Executive Director: Report Presented by: Committee/Group who have received or considered this paper: Kate Hammond, Patient Experience Manager VCC Prof Susan Morgan Lisa Miller, General Manager VCC Trust Organisational Learning Committee Trust Resolution to: (please tick) Approve: Endorse: Discuss: Note: Recommendation: The purpose of this report is for the group to discuss patient experience feedback collected during the period and the identified key themes and improvement actions. This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well This report supports the following Health & Care Standards: Individual Care Timely Care Dignified Care Safe Care
20 2 Effective Care 1. Introduction / Background 1.1. Feedback is hugely important to informing and understanding the patient experience at Velindre Cancer Centre. Patient surveys are completed during face-to-face conversations, online & picked up from feedback stands in key areas of the hospital. We also collect data from patient stories, comment cards and responses via social media The purpose of this report is for the group to discuss patient feedback during the period and the identified key themes and service improvement actions. 2. Timing: 2.1. This report is based on the activity during the period January to March Description: 3.1. Please see appendix 1 for the activity considered during this period. 4. Financial Impact: N/A 5. Quality, Equality, Safety and Patient Experience Impact: 5.1. Listening and learning from patient feedback is fundamental to improving the overall patient experience Velindre is working on increasing the amount of patient feedback we collect via a suite of methods in order to better inform service improvements and draw on key trends. 6. Considerations for Board / Committee: 6.1. The Committee is asked to consider the report The Learning Committee should consider if the themes identified in the report and the actions to improve demonstrate learning from listening to patients. 7. Next Steps: 7.1. The Committee are asked to DISCUSS the report. Appendix 1 Division/Service area: Organisational Learning Highlight Report Velindre Cancer Centre Kate Hammond Patient Experience Manager, Velindre Cancer Centre
21 3 Reporting period: January 20 March 20 Information analysed Patient Experience data Key Trends Identified Key Themes to Celebrate Gratitude and appreciation from our patients and their families Excellence and professionalism of staff Care and kindness Supportive & welcoming atmosphere Teamwork Key Themes for Improvement Waiting times Radiotherapy machine breakdowns Terminology used when communicating with patients Car Parking Number of disabled parking spaces available Radiotherapy machine breakdowns Kate Hammond Patient Experience Manager, Velindre Cancer Centre

22 4 Patient Experience Report Velindre Cancer Centre January February - March 20 If an encounter with a hospital in a time of unpleasant circumstances can be described as bittersweet, Velindre made my difficult experience oddly enough quite pleasant, maybe even enjoyable. Kate Hammond Patient Experience Manager, Velindre Cancer Centre
 Repondents 50% Female 83% 50% Male During January, February and March 20, we carried out 44 face-to-face interviews. online surveys were completed & 12 snapshot surveys.")

23 5 Patient Experience Surveys January, February and March 20 Jan, Feb, March 80 surveys completed 44% Face to Face 19% Snapshot Survey 24% Online Survey 14% Independent Overall Satisfaction Score (9/10 or above) Repondents 50% Female 83% 50% Male During January, February and March 20, we carried out 44 face-to-face interviews. online surveys were completed & 12 snapshot surveys. A further 8 surveys were submitted independently. The responses to each feedback method are combined to give an overall experience picture. We aim for 80% of the overall satisfaction scoring 9 or above. This quarter we achieved our target at 83% Kate Hammond Patient Experience Manager, Velindre Cancer Centre Overall Satisfaction Scores 58% (33) patients rated their experience as 10/10. 25% (14) patients rated their experience as 9/10. 14% (8) patients rated their experience as 8/10. 2% (1) patient rated their experience as 7/10. 2% (1) patient rated their experience as 5/10 I feel that everyone at Velindre does the utmost to make what is a very worrying & confusing time, as comfortable as possible
24 6 The Patient Experience refers to the quality and value of all of the interactions direct and indirect, clinical and non clinical spanning the entire duration of the patient/provider relationship. Deloitte LLP the sum of all interactions, shaped by an organisation s culture, that influence patient perceptions, across the continuum of care. The Beryl Institute. Kate Hammond Patient Experience Manager, Velindre Cancer Centre
25 7 The patient experience is not just one encounter, but spans over time and includes many touch points during our relationship with patients, carers, family members & the public. The patient experience is not just about a survey or a buzzword. This is about a shared commitment to listening & learning across the whole organisation. It is fundamental that everyone understands and values the importance of delivering an excellent patient experience which is embedded within our culture; Patients are at the heart of everything we do. Creating a good Patient Experience 1. Every role matters 2. Every interaction matters 3. Every perception matters 4. You matter Kate Hammond Patient Experience Manager, Velindre Cancer Centre
 o First")
26 8 How do we measure experience? The NHS in Wales has adopted a service user experience framework which identifies the three key determinants of a Good service user experience (based on national and local published evidence) o First and Lasting Impressions o Receiving care in a Safe, Supportive, Healing Environment o Understanding & Involvement in Care These three domains can be used to support the use & design of a range of feedback methods to help us understand the patient experience. It is recommended that a mixture of methods is used wherever possible in order to obtain a balanced understanding. The framework also includes a set of core questions which are used across all NHS organisations in Wales. At Velindre Cancer Centre, we have face-to-face conversations with our patients based around these core questions. These conversation opportunities enable us to capture the data in a meaningful way, where any issues identified can be discussed openly & often dealt with immediately. Kate Hammond Patient Experience Manager, Velindre Cancer Centre

27 9 The Framework in Action Why is it important to us? What s in it for our patients? Offering a means for patients to express their thoughts, wishes, ideas & personal experiences reinforces the patient-centred approach to our work and empowers patients to make their voice heard. What s in it for our staff? Patient feedback gives us as staff an opportunity to understand what care is like from the patient s perspective. Hearing patients talking about their experiences in their own words helps us to see care through their eyes and hear about the things that are most important to them. What s in it for Velindre? Patients are at the heart of everything we do. Feedback both good and bad - is fundamental to the way we shape our service for today & tomorrow. Kate Hammond Patient Experience Manager, Velindre Cancer Centre

28 10 How are we listening? We undertake the National Survey on a monthly basis during face-to-face conversations. A full version of this survey is now also available online as well as a shorter snapshot version for those who prefer fewer questions to complete. In addition to the National Survey, we also capture experience information via Patient Stories. These stories can be produced in various formats written, video, digital story, audio and graphic. Our Social Media channels offer a further means for patients and their families to comment on their experience at Velindre Cancer Centre as well as the placement of Comment Cards in key areas of the hospital. Professor Sue Morgan, Executive Director of Nursing & Service Improvement would like to thank everyone who took part in this month s survey. We are always striving to find better ways of delivering our services and we use the feedback from these surveys to learn and improve. Month by Month Our target is 80% of our patients rating their experience as 9 or above. Once again we have achieved our target this quarter, despite a dip during February where a greater number of surveys completed independently led to an overall lower score. Kate Hammond Patient Experience Manager, Velindre Cancer Centre

29 25% 56% 11 Patient Experience Surveys January February March 20 During this period Velindre Cancer Centre collected the views of 80 patients: 44 face-to-face interviews, 12 snapshot, online and 8 independent surveys. We are attempting to increase the number of completed surveys each month in order to represent the views of a greater number of patients. We hope that by introducing new methods to collect feedback in new formats we will be able to encourage an increase in responses. 10/10 56% (45) patients rated their experience as 10/10. 9/10 25% (20) patients rated their experience as 9/10. Kate Hammond Patient Experience Manager, Velindre Cancer Centre
30 Do you feel that people were polite to you? 12 94% Always 6% Usually Do you feel that you were: i) Listened to? 91% Always 9% Usually ii) Given all the information you needed? 86% Always 12% Usually 2% Sometimes Do you feel you were given enough privacy? 93% Always 5% Usually 2% Sometimes Were you: i) Given the support you needed to help with any communication needs? 27% Always 2% Usually 72% Not Applicable ii) Able to speak in Welsh to staff if you needed to? 100% Not Applicable From the time you realised you needed to use this service, do you feel you had to wait: 80% A short time % A little longer than needed 5% Longer than needed How clean was it? 95% Very clean 5% Fairly clean Kate Hammond Patient Experience Manager, Velindre Cancer Centre
31 13 Did you see staff clean their hands before they cared for you? 79% Always 10% Usually 11% Don t know Did you feel that everything you needed for your care was available? 89% Always 11% Usually If you asked for assistance: i) Did you get it? 95% Always 3% Usually 2% Sometimes ii) Get it when you needed it? 90% Always 10% Usually Were you involved as much as you wanted to be in decisions about your care? 95% Always 5% Usually Were things explained to you in a way that you could understand? 89% Always 10% Usually 2% Sometimes Did you feel you understood what was happening in your care? 77% Always 18% Usually 5% Sometimes Kate Hammond Patient Experience Manager, Velindre Cancer Centre

32 14 Yes! If an encounter with a hospital in a time of unpleasant circumstances can be described as bittersweet Velindre made my difficult experience oddly enough quite pleasant, maybe even enjoyable. All staff were extremely polite and courteous. Professionalism was at the forefront and communication levels were more then adequate. All the staff were fantastic. Polite. Friendly, knowledgable staff. Clean and pleasant surroundings. Positive atmosphere. The care, dedication and the work of all the nurses, doctors, cleaners, caterers is second to none. The Velindre is a shining example of excellence of which we should be proud in this age of shocking NHS cutbacks. I am very pleased with the speed that the staff were on my admission. Very pleased with staff at Velindre. Food was good also. Lovely staff, so kind to me It would be hard to find fault with any of the staff or the treatment I have so far received. They are always polite and efficient, make sure they are looked after well. Doctors, nurses, catering staff and care well above average. Food and general care excellent Everyone from the doctors and nurses to the catering and cleaning staff were very friendly & would help in any way possible to make my stay more pleasant. Just taking the time to chat makes a big impact to my day. Also if I ring the bell for assistance someone is always there within a few moments. Brilliant. Staff are very friendly. Way the nurses look after you. Really lovely experience! Staff go out of their way to help you - not just in this unit - but all over the hospital. Kate Hammond Patient Experience Manager, Velindre Cancer Centre
33 Pharmacist took time to sort things. Can't fault this place or the care as a cancer patient. I'm sure Velindre will come out at 100% and if not I want to know why! Compassionate staff. Everyone who works here very kind and polite, if I needed help I would get quickly seen to. If you need help there is nothing they won't do Make you feel at ease and everyone has a smile. It's like a family unit. Planning for blood transfusion was quick and good. Staff are brilliant and the atmosphere is great. Pager holder is fab always at the end of a phone. All staff were extremely kind and pleasant, receptionists and particularly the radiologists,who are a special type of person. The staff were very helpful and friendly I think I received the best of professional care from those brilliant nurses. The staff are amazing especially when you consider how draining this job must be. Everybody there so helpful and understanding in difficult situations very often. You cured me. Thank you. Such lovely staff, all of them My Mum was able to come with me for support, without her I wouldn't have made it this far. And staff were 100% there for me too. All staff could not do enough to ensure you were relaxed. I felt I was in the care of dedicated professional staff in whom I had every confidence I was very impressed by the care and dedication given to me by the staff at the Chemotherapy Day Unit. The staff are excellent. The whole experience was amazing. Amazing friendly supportive staff. I felt like the staff knew me personally and made it their business to put me at ease every time I come. I was petrified of Velindre before I went, first class staff in every department. Every member of staff (cleaners on ward, volunteers, Kate Hammond Patient Experience Manager, Velindre Cancer Centre
34 receptionist, nurses, doctors, radiotherapy etc. that I came in contact with that worked at Velindre Hospital were all lovely, understanding, reasurring, supportive and helpful and worked as a team. I have never experienced anything like it at other hospitals that I have attended. It made my radiotherapy and chemotherapy treatment so much easier. Also the transport arranged to get me to and from the hospital every day during my treatment was brilliant I don t know how I would have managed without it. Any problems during treatment were dealt with as and when they happened. Also the assistance given in dealing with my PIP claim was great. Manner of staff. The staff were brilliant, everyone from volunteers to consultants were so helpful and caring. Friendly staff. The staff are all exceptional. Nurses were kind, caring & compassionate staff. Inspire patients to feel confident about their treatment. Velindre should be used as a model for other hospitals in Wales. Staff are excellent, made me feel at ease and comfortable as possible. Everyone friendly, nice & caring. Staff are professional. I feel all my needs have been met. After first chemo was able to swallow. Hope it continues. I found that pharmacist Judy Banfield answered my questions & explained things more fully than anyone I had spoken with previously, concerning my illness. She took the time to explain what I could expect to experience from my treatment in a way that I was able to comprehend. Excellent staff The friendliness of the staff. Kate Hammond Patient Experience Manager, Velindre Cancer Centre


35 17 There are some things you can't! Issues of finance and availability of machines in Radiotherapy. Nothing comes to mind - a good experience. Waiting time for treatment - initial chemotherapy 11am, only had in the evening. Had to stay in longer. Not really. I'd like to thank everyone involved in my treatment at this difficult time. My response to question 13 probably says it all! (10/10) Many thanks to all concerned. Sometimes I found it difficult to understand terminology used by the Drs but my partner understood more than me and explained after the Dr left. If more disabled parking spaces could be made available, as searching for a space can be very stressful. There were a lot of delays on radiotherapy machines? Are more needed? More parking spaces maybe? Given the circumstances, I don't think it could be better than it was. Short of staff on occasions More plugs by the bed Nothing I can think of, all good. Bit of extra hanging space around bed. No- I feel that everyone at Velindre does the utmost to make what is a very worrying & confusing time, as comfortable as possible Everything was brilliant but when I was admitted to chemo inpatients, I requested a doctor early one Kate Hammond Patient Experience Manager, Velindre Cancer Centre
36 18 morning as my prescription needed changing in order to give me a headache tablet, but I waited approx 8 hours until one came, but she said she wasn't aware even though I'd chased it up during the day (this was on a Sunday last year) So I suffered with a very bad headache all day. Apart from that, everyone was excellent. On request technical language was explained in layman's terms, but I did have to ask the Dr to explain so I could understand. No I feel very well cared for. Parking Consultant was kind of confusing (From treatment in uclh I had the same nurse and same radiotherapy machine every time) sticking to the same machine would help. My team information with pictures would be nice. Planning was too far away from treatment 4 week wait. Continuity would be good...in London the light was always off for treatment at Velindre light is always on. I would like the choice. Time it takes for blood to be reported. Another trolley round for tea in the afternoon would be good. Buzzer on chairs to call nurses. Time sometimes can take longer and have to wait a long time. Maybe a small TV in LA7 and 8 waiting area. Couldn't think of anything else sorry. You're too good! It was a problem sometimes to keep my bladder full not knowing when I was going to be called. Upon entering the chemo unit a simple acknowledgement would be very welcome. Especially to first timers who were not given chemo ed and did not know what to expect. The staff are amazing once you are seated but it seems to be a common theme that new arrivals are ignored upon entering the unit. Kate Hammond Patient Experience Manager, Velindre Cancer Centre

37 19 The loudspeaker in the waiting room difficult to understand. The 'Velindre' spelling is wrong. It's a Welsh name and there's no 'v' in Welsh, therefore it should be Felindre (Milltown). Thank you Felindre for everything. My father spent 4 weeks on ASU ward and recently passed away. We would love to thank all the staff for looking after him so well through this terrible time and how great the staff were with his relatives. We asked for money in lieu of flowers and the donation would be to your hospital. A big thank you to all the excellent staff, especially the radiographers, at Velindre who have supported my Dad through his first stage of treatment (radiotherapy plus chemo tablets) which finished today. Thank you so much for all that you do.xx My mum has been suffering without knowledge of cancer until recently!! She has nothing but praise to the felindre staff thank you so much for making her so comfortable x I owe Velindre my life and will be eternally grateful. Kate Hammond Patient Experience Manager, Velindre Cancer Centre
38 20 Velindre stories My elderly mum underwent 2 weeks of palliative radiotherapy. She was often confused and scared. The team who treated her were just fantastic, always kind and patient, helping to put her at ease. They were also brilliant in taking care of me while I was bringing my mum to have her treatment daily. I cannot thank them enough for the kindness shown. The team were on was LA3. They were quite simply brilliant. The kindness and endless patience they showed towards my mum (and me) was exemplary and hugely appreciated. They helped make a very difficult time that little bit easier, I simply cannot praise or thank them enough. I was dreading my first visit to Velindre with my dear mum because I thought it would be a very depressing place. However, I have to say that it was the most uplifting and inspirational place I have ever visited. Everybody smiles, despite their own painful story. Thanks to Velindre, I got another Christmas with my mum. You are all truly remarkable - thank you. Kate Hammond Patient Experience Manager, Velindre Cancer Centre



39 21 Velindre Stories Kate Hammond Patient Experience Manager, Velindre Cancer Centre
40 22 Key Themes to Celebrate Gratitude and appreciation from our patients and their families Excellence and professionalism of staff Care and kindness Supportive & welcoming atmosphere Teamwork Key Themes for Improvement Waiting times Radiotherapy machine breakdowns Terminology used when communicating with patients Car Parking Number of disabled parking spaces available Radiotherapy machine breakdowns Kate Hammond Patient Experience Manager, Velindre Cancer Centre
41 23 Actions to improve.update From previous reports. Investigate the comments made about catering Response: The menu is under review and we are hopeful to launch the new menu by the end of January. Develop some ideas to make the main corridor more colourful and visually appealing Response: We are working on some artwork concepts that will not only make the corridor more visually appealing, but also highlight the amazing work of our fundraisers and help us celebrate our 60th Anniversary. Watch this space! Look at purchasing more pillows & continue to try to provide patients with as many pillows as they need Response: We ordered 30 additional pillows at the end of December. This month we are working with our Estates team & colleagues to identify the source of an unpleasant odour in our pharmacy department. This was brought to our attention via the new How Did We Do? comment cards. An update will follow. We are also collating an update on the work done to resolve parking issues at Velindre which we will be able to share with patients & visitors to the hospital. Kate Hammond Patient Experience Manager, Velindre Cancer Centre


42 24 You said we did You said we d like to have a better idea of how long waiting times might be. We did install display screens in our Outpatients department which show approximate waiting times for each clinic that day. The displays are updated by staff working in the clinics and so far the response has been overwhelmingly positive. Huge thanks to Mark Harvey, Alison Johnson & our colleagues in IT for their contribution to the successful implementation! We are now working with colleagues in Radiotherapy to introduce a similar display. Kate Hammond Patient Experience Manager, Velindre Cancer Centre




43 25 You said the chairs in Outpatients are too low & difficult to get up from. We did purchase new chairs for the department with arm-rests to make it easier for patients. Before After And the old chairs although not suitable for our needs - have been put to good use too... As part of the refurbishment of the outpatients area, 100 outpatient chairs were no longer required. Our aim was to reuse the chairs in order to give them a good home and reduce the environmental impact of disposal to landfill. After being unable to reuse the chairs at other divisions and hosted organisations within the Trust, we contacted other NHS Wales Health Boards through the Welsh Health Environmental Forum, achieving the following: 10 chairs have been donated to Powys Local Health Board 30 chairs have been donated to Welsh Ambulance Services NHS Trust The remaining 60 chairs have been re-used through an ISO 9001 quality and ISO14001 environmental accredited furniture recycling company. The chairs will be re-distributed throughout the third sector to local businesses and charities, with any surplus chairs being taken apart and every bit recycled. Kate Hammond Patient Experience Manager, Velindre Cancer Centre





44 26 You said it s difficult to find your way around Velindre. I need a map! We did update our signage with coloured coding to make it clearer and easier to find your way around. We also produced new maps which are on display around the hospital. Before After Kate Hammond Patient Experience Manager, Velindre Cancer Centre

45 PATIENT LIAISON GROUP (PLG) ANNUAL REPORT This has been another very busy and productive year for the PLG with all our members contributing. Thanks as usual to Helen Davies for all her support and to Roger Pratt and Eleri Girt for their meeting notes. We were very pleased to welcome two new members this year: Edward Tapper who has been a patient and James Thompson who was a carer for his wife. They join the existing members who are Lesley Radley (Chair), Sue Youngman, Janet Pope, Malcolm Pope, Malcolm Griffiths, Ray Price, Roger Pratt, Keith Cass, Derek Ford, Barbara Burbidge, Helen Jeffreys, Eleri Girt and Sally Anstey. Although Derek has not been well enough to attend the meetings this year he has contributed to the Head and Neck Clinical Effectiveness meeting where he was able to compare his treatment for this cancer with his previous treatment. He is also involved in developing a patient story. PLG members have contributed to professional training for student nurses both at Cardiff University and the University of South Wales. Our members spoke to the students about their experiences both as patients and as carers. Feedback from the sessions has been excellent and they were able to question our members about all aspects of their illnesses and their care. We have also contributed to the Foundations of Care course at Velindre and more recently Lesley Radley has spoken to the SHO s at Velindre from her perspective as a nurse, patient, carer and chair of the PLG. Our monthly PLG meetings have been very well attended with regular updates and discussions with consultants, management, senior nurses, therapists and radiotherapy staff. We are also very pleased when members of the Board are able to attend and not only to hear the work we are involved in but also contribute to the discussions. Ray Singh and Steve Ham have attended on a regular basis. Our members have been involved this year in helping with the production of DVDs on Metastatic Cord Compression and DNACPR. The DNACPR DVDs were produced in two versions, one for patients and one for junior doctors. We have also commented on the new patient alert cards for chemotherapy. The other areas where we continue to have an input and my thanks go to all involved: Malcolm Pope organises the packing of the information bags on a regular basis as these are still very popular. Malcolm Griffiths and now Edward Tapper assist with the monthly radiotherapy evenings. Sue Youngman produces the newsletter. Edward Tapper and James Thompson have assisted with this year s annual audit.
46 This year we have contributed to many other groups at Velindre. The patient/carer voice is now heard and well accepted. Many of our members are involved with the Transforming Cancer Services programme which we all feel is vital for continuing excellent care for patients and their carers not just at Velindre but in the whole catchment area. We have noticed that we are being contacted more and more by colleagues at Velindre, and that we are able to contribute the patient s voice to their work. Conclusion Once again thanks to all for their input to the PLG this year. Next year we plan to meet with Lisa and Andrea to discuss various issues about how the group functions. We want to be sure that the work we do is effective and is the best use of our skills and resources. Signed: L.M. Radley Dated: December 2nd 20
47 Quality and Safety Committee Welsh Blood Service Donor Experience Report Meeting Date: Author: Sponsoring Executive Director: Report Presented by: Committee/Group who have received or considered this paper: 24 th May 20 Joanne Allan Cath O Brien Joanne Allan N/A Trust Resolution to: (please tick those which apply) Approve: Endorse: Discuss: Note: Recommendation: This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick those which apply) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well This report supports the following Health & Care Standards: Individual Care Timely Care Dignified Care Safe Care Effective Care
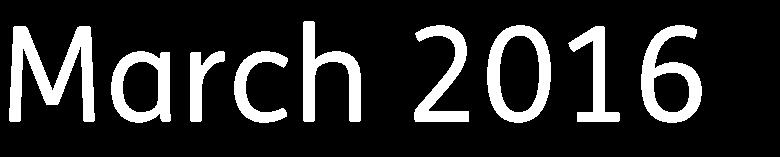
48 1. Introduction / Background In order to obtain donor feedback regarding the services we provide, surveys are sent via to donors who have attended clinics. The esurvey asks specific questions about our service such as appointments, waiting times, insertion of the needle etc and provides donors with the opportunity to leave general comments and score key service deliverables. The feedback received from donors enables us to identify lessons that can be learned and support the Welsh Blood Service to continuously improve the donor experience. 2. Timing: 2.1. This report covers the period January 20 to March Description: ,628 donors attended Welsh Blood Service donation clinics in quarter 4, Electronic surveys were sent to 10,194 donors during Q4 with 2,847 responses being received. The response rate to the esurvey for this quarter was 29%, this is an increase of 2.5% when compared to the response rates in quarter Financial Impact: 4.1. None 5. Key Trends and Learning 5.1 See appendix 1 for Key Trends and Learning 6. Considerations for Board / Committee: 6.1. The committee are asked to discuss this report 7. Next Steps: 7.1 See appendix 1 for next steps Appendix 1 Donor Experience Report Q4 January March 20 Page 2




49 Page 3
50 Page 4
51 Page 5

52 Page 6



53 Page 7


54 Page 8

55 Page 9
56 Page 10

























57 Page 11
58 Page 12
59 Page 13


60 The lady who was training to put needles in on the th in Port Talbot did a cracking job, no bruise. Well done. The staff at Parc and Dare today were amazing A big thank you to all the Welsh Blood Service team for looking after us My 53 rd donation today, in Rhiwbina. Good Service, Great Staff. Thank you!! #feelgoodfriday I had an amazing first experience giving blood yesterday in Abergavenny. #willbeback #lovelystaff #dontbenervous Big thanks to staff in Ammonford for making my first donation so fast and easy! Page 14
61 1 Quality & Safety Committee Quality & Safety Committee Care Decisions for Last Days of Life Meeting Date: 9 th June 20 Author: Sponsoring Executive Director: Report Presented by: Committee/Group who have received or considered this paper: Viv Cooper, Head of Nursing, VCC Dr Mark Taubert, Clinical Director Palliative Medicine, VCC Andrea Hague, Director of VCC Viv Cooper, Head of Nursing Executive Management Board Senior Management Team, VCC Trust Resolution to: (please tick) Approve: Endorse: Discuss: Note: Recommendation: The EMB are asked to note the contents of the Welsh Health Circular (WHC/20/004) Care Decisions for Last Days of Life This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well This report supports the following Health & Care Standards: Page 1
62 2 Quality & Safety Committee 1. Introduction / Background 1.1 This document summarises the all Wales approach and recommendations as set out in the Welsh Health Circular about Care Decisions to Chief Executives of Health Boards and Trusts for Last Days of life (WHC/20/004). The quality of care provided to a dying patient has a direct effect on that person s last moments, but it also has a lasting effect on families, friends, proxy and carers. Good quality end of life care and good communication between professionals and families supports individuals at the end of life and helps families to cope with bereavement. 1.2 It is important for all health care professionals, regardless of specialty, to consider the end of life care wishes of their patients as part of the basic care they provide to patients. The existing All Wales Integrated Care Priorities (ICP) for use in the last days of life was replaced on 1 April 20 with an update document and has been renamed the Care Decisions for the Last Days of Life, and has been developed by the Palliative Care Implementation Group with support from end-of-life care leads from each Health Board and Trust, and also the Royal Colleges. The document has been informed by a trial and has also been devised with End-of life care reports from England and Wales from recent years, in particular the Neuberger review on the Liverpool Care Pathway in England, which called for a move away from tick-box approaches in end of life care. 1.3 In 20 a sub group of the Palliative Clinical Implementation Group was established to develop an educational package to support the introduction of the document which was approved by the Welsh End of Life Care Implementation Board, chaired by Velindre NHS Chief Executive, Steve Ham, in September Timing: 2.1 The aim of the Chief Medical Officer s Welsh Health Circular is to inform all Health Boards and Trusts in Wales of the replacement of the ICP by the Care Decisions for the Last Days of Life in 20. The Chief Medical Officer has requested that staff be made aware and conversant with its requirements and fully equipped to provide the level of consistent care appropriate to patients and those important to them in the last few days of life, and for local Health Boards and Trusts to work effectively with their partners. 2.2 The Care Decisions for the Last Days of Life should be considered and put into practice alongside, and in conjunction with, key health publications such as Together for Health: Delivering End of Life Care - A delivery plan for NHS Wales and its Partners up to 20 and the 20 NICE guidance Care of the Dying Adult to ensure the wishes of the patient and those important to them are accounted for. 2.3 This work will support the priorities set out in the End of Life Care delivery plan by assisting implementation by April 20 and to take forward the End of Life Care delivery plan. A training package has been developed by palliative care leads within Health Boards. Educational departments in Health Boards and Trusts should aid the delivery of training packages and the intranet can be used as a repository to the training packages and videos that have been created and are available here: 3. Description: 3.1 Velindre Cancer Centre has a Specialist Palliative Care Unit and pride themselves in the provision of excellent and compassionate end of life care, with 24/7 availability of staff. While the overall aim is to support patients to die in the community and not in hospital, some patients who are admitted deteriorate quickly while they are inpatients and request to stay here, and Velindre prides itself as a provider of some of the best compassionate palliative care in the world. 3.2 Velindre is a European Society of Medical Oncology (ESMO) accredited centre for integrated oncology and palliative care. This care is not just delivered by the specialist team, but by all staff including oncologists, domestics, radiotherapists, physios, AHPs, supportive care staff, healthcare assistants, nurses and administrative support staff, to name just a few. Page 2
63 3 Quality & Safety Committee 3.3 Velindre currently use the Integrated Care Priorities for the Last days of life and the use of this document is audited at national level and at local level via the mortality meetings. The content, underpinnings and philosophy of the Care Decisions document has been presented at the annual Velindre Site Specific Team (SST) meeting for palliative care in March this year by Helen Way, Senior Palliative Care Nurse at Velindre Cancer Centre. 3.4 Operationally the implementation will require the new Care Decisions document has a section requiring staff to ensure the patients bedside care plans are updated and reflect the care they now need in terms of physical and psychological symptom management. In a previous Fundamentals of Care audit it was noted there was a lack of bedside documentation in the patients bedside care plan regarding symptom management (although plans were in the patients notes). Thus the new document should help address this as care will work with the wards during its implementation to embed the palliative care plan into the bedside care plans. The new document should also support Velindre in achieving palliative symptom management outcomes for Fundamentals of Care. 3.5 VCC piloted the new document on all 3 inpatient wards last year and it has also been piloted in all the Health Boards throughout Wales. The changes and new content for the document have come from the More Care Less Pathway Dying without Dignity and recommendations from similar reports. 4. Financial Impact: 4.1 Funding from the additional 10m announced last year for the ten delivery plans, has been made available to Health Boards and Trusts who will be working with the voluntary sector to provide training for the roll out of the Care Decisions for the Last Days of Life. Directors of Finance have received a letter with details of the funding received for this purpose from the Major Health Conditions Policy Division Vivienne.collins@wales.gsi.gov.uk 4.2 The main resource implications are in respect of the time for education and implementation. 5. Quality, Equality, Safety and Patient Experience Impact: 5.1 As outlined above the quality of care provided to a dying patient has a direct effect on that person s last moments, but also a lasting effect on families, friends, proxy and carers. Quality end of life supports individuals and end of life helps families to cope with bereavement. 6. Considerations for Board / Committee: 6.1 The Quality & Safety Committee are asked to note the contents of the Welsh Health Circular (WHC/20/004) Care Decisions for Last Days of Life, as set out by Welsh Government Health Circular from Chief Medical Officer, Ruth Hussey and the progress within VCC. Page 3
 : Vivienne Collins, Healthcare")
64 WHC/20/004 WELSH HEALTH CIRCULAR Issue Date: 1 March 20 Title: Care Decisions for the Last Days of Life STATUS: INFORMATION CATEGORY: HEALTH PROFESSIONAL LETTER Date of Expiry / Review: Annually For Action by: Health boards and trusts Action required by: 1 April 20 Sender: Dr Ruth Hussey, Chief Medical Officer / Medical Director DHSS Welsh Government Contact(s) : Vivienne Collins, Healthcare Policy, Welsh Government, Cathays Park 2, CF10 3NQ; Enclosure(s): None (see hyper links)
65 Dr Ruth Hussey CB OBE Prif Swyddog Meddygol/Cyfarwyddwr Meddygol, GIG Cymru Chief Medical Officer/Medical Director NHS Wales To: Chief Executives, NHS Wales Cc: Health board and trust end of life care leads March 20 Dear Chief Executives CARE DECISIONS FOR THE LAST DAYS OF LIFE A key element of patient need, and those of their families, is good end of life care. The purpose of this Welsh Health Circular is to highlight the importance of the continuation of patient care through to the very end of life, irrespective of physical or mental health conditions. The updated policy is set out in the document Care Decisions for the Last Days of Life. This document, which will replace the current All Wales Integrated Care Priorities (ICP) for use in the last days of life with effect from 1 April 20, is available on health board and trust websites. DoL%20Care%20Decisions%20V5.3.pdf Health board palliative care teams will lead on implementing the training package for the implementation of the Care Decisions for the Last Days of Life. This can be accessed using the following link &Itemid=244 Background The quality of care provided to a dying patient has a lasting effect on families and carers. Good quality end of life care and good communication between professionals and families supports individuals at the end of life and helps families to cope with bereavement. It is important all health care professionals, regardless of specialty, consider the end of life care wishes of their patients as part of the basic care they provide to patients. The existing All Wales Integrated Care Priorities for use in the last days of life is being phased out and should not be used after 31 March 20. The refreshed document, Care Decisions for the Last Days of Life, has been developed by the Palliative Clinical Implementation Group with the support of
66 the end of life care clinical lead from each health board. The document has been informed by a trial and responses to a consultation. Last year a sub group of the Palliative Clinical Implementation Group was established to develop an educational package to support the introduction of the document which was approved by the End of Life Care Implementation Board in September 20. Implementation The aim of this Welsh Health Circular is to inform all health boards and trusts in Wales of the replacement of the ICP by the Care Decisions for the Last Days of Life with effect from 1 April 20. We want to ensure that staff are conversant with its requirements and fully equipped to provide the level of consistent care appropriate to patients and those important to them in the last few days of life, and for local health boards and trusts to work effectively with their partners. The Care Decisions for the Last Days of Life should be considered and put into practice alongside, and in conjunction with, key health publications such as Together for Health: Delivering End of Life Care - A delivery plan for NHS Wales and its Partners up to 20 and the 20 NICE guidance Care of the Dying Adult to ensure the wishes of the patient and those important to them are accounted for. This work will support the priorities set out in the End of Life Care delivery plan by assisting implementation by April 20 and to take forward the End of Life Care delivery plan. A training package has been developed by palliative care leads within health boards. Palliative care clinical leads will assist with the dissemination of this information. Funding Funding from the additional 10m announced last year for the ten delivery plans, has been made available to health boards and trusts who will be working with the voluntary sector to provide training for the roll out of the Care Decisions for the Last Days of Life. Your Directors of Finance will have received a letter with details of the funding received for this purpose. If you have any general comments, please contact the Major Health Conditions Policy Division through Vivienne.collins@wales.gsi.gov.uk tel: Or for specific information please contact Veronica Snow, Programme Manager, End of Life Care Implementation Board on or Yours sincerely
67 DR RUTH HUSSEY CB OBE
68 Quality & Safety Committee WBS Regulatory & Accreditation Update Meeting Date: 9 th June 20 Author: Sponsoring Executive Director: Report Presented by: Committee/Group who have received or considered this paper: Joan Jones Cath O Brien Joan Jones/Cath O Brien N/A Trust Resolution to: (please tick) Approve: Endorse: Discuss: Note: Recommendation: This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well This report supports the following Health & Care Standards: Safe Care
69 2 [Report Title] 1. Introduction / Background 1.1 The WBS is heavily regulated and licensed by: Blood Safety & Quality Regulations SI 50/2005 (inspected by MHRA) this includes the Blood Establishment Authorisation and the Wholesale Dealers License Human Tissue Act 2004 (inspected by Human Tissue Authority) In addition the WBS is accredited by Clinical Pathology Accreditation (CPA) which is moving to UKAS accreditation (ISO 189 & 17043) and the European Federation of Immunogenetics (EFI). 1.2 The WBS works under a Quality Management System (QMS) that is maintained and continually improved in accordance with all relevant standards. 2. Timing: 2.1. This report covers the period January to March 20 (Quarter 4). 3. Description: 3.1. The MHRA conducted their biennial inspection for the retention of the Blood Establishment Authorisation (BEA) and the Wholesale Dealers Licence (WDL) with 2 inspectors during the first week of December 20. The actions identified by the WBS were accepted and to date there is one action outstanding with a closure date of the end of June UKAS undertook an inspection of the H&I External Quality Assurance scheme in December. The non-compliances have been actioned and accepted by UKAS In March 20 the MHRA conducted the first of 2 inspections to ascertain that the N Wales (Wrexham) base and the collection teams transferred from NHSBT to WBS met the requirements of the BSQR. The first inspection reviewed the data migration of NHSBT donors from PULSE to eprogesa and the equipment and facilities in the laboratory area of the stock holding unit in Wrexham. This was to allow the WBS to proceed with the implementation date of the 2 nd May 20. There were no critical or major deficiencies identified and just 4 others. The actions to address these were accepted by the MHRA and are currently being acted upon At the beginning of May the MHRA inspected both the Wrexham and Bangor collection teams and the N W Wales (Bangor) base. There were no critical or major deficiencies identified and again just 4 others. The actions to address these are being developed. This was an extremely positive result as both collections teams were in their first week of operation post a 2 week training period. 4. Financial Impact: 4.1. No financial impact has been identified other than resources within QA systems are still not at full capacity. 5. Quality, Equality, Safety and Patient Experience Impact: 5.1. One Serious Adverse Blood Reaction & Event (SABRE) was reported externally to the MHRA. Donor attended session and stated that he had stayed in a rural subsistence Page 2
70 3 [Report Title] farming area in S America for more than 4 weeks - staying in huts with mud walls and thatched roofs. Donor stated he has previously declared this but no Chagas test on record. There may have been confusion in that screener may not have realised Chagas test and T cruzi are the same. Donor permanently deferred and training material updated to use both terms in referring to the disease There were no serious adverse events of donation recorded this quarter 5.3. There were no component quality exceptions reported this quarter 6. Considerations for Board / Committee: 6.1. The committee are asked to note this report 7. Next Steps: 7.1. Continue completing the actions identified to address the non-conformances identified at the MHRA inspections and maintaining the Quality Management System. Page 3

71 Medicines management at Velindre Cancer Centre Velindre NHS Trust Audit year: Issued: November 20 Document reference: 496A20
72 Status of report This document has been prepared as part of work performed in accordance with statutory functions. In the event of receiving a request for information to which this document may be relevant, attention is drawn to the Code of Practice issued under section 45 of the Freedom of Information Act The section 45 Code sets out the practice in the handling of requests that is expected of public authorities, including consultation with relevant third parties. In relation to this document, the Auditor General for Wales and the Wales Audit Office are relevant third parties. Any enquiries regarding disclosure or re-use of this document should be sent to the Wales Audit Office at info.officer@audit.wales. The team who delivered the work comprised Stephen Lisle, Stephen Pittey and Nigel Blewitt. Page 2 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
73 Contents We found many good aspects of medicines management in the cancer centre. However, the pharmacy team is struggling to meet demand, facilities do not fully comply with requirements and there is not a clear strategy for driving improvement. Summary report Background 4 Key findings 6 Recommendations 8 Detailed report Part 1. Corporate arrangements 10 Pharmacy benefits from a high profile in the hospital but there is scope for more medical engagement in corporate medicines management issues and there is not yet a robust strategy to drive future developments Part 2. Workforce The involvement of pharmacists in clinics is positive but the pharmacy team is struggling to meet demand and pharmacy s input on the wards is too inconsistent Part 3. Facilities 26 Pharmacy facilities are cramped and do not fully comply with key requirements. There are ongoing issues associated with medicine storage in pharmacy and on the wards Part 4. Processes 30 The Trust has some good medicines management processes including use of electronic prescribing, timely reconciliations and the role of non-medical prescribers. There are issues with information exchange with primary care, controlled drug checks, and lack of selfadministration Part 5. Monitoring Medicines-related performance data is not used routinely enough to promote improvement and while there are good aspects of learning from incidents, more work is required to understand why pharmacists safety interventions are more frequent than average 41 Appendices Methodology 47 Page 3 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
 2. 2. Medicines management covers much more than the purchase of drugs.")
74 Summary report Background 1. The most common therapeutic intervention in the NHS is prescribing of medicines. 1 In , Welsh health bodies spent 258 million on purchasing drugs (eight per cent more than ) Medicines management covers much more than the purchase of drugs. The term covers all the processes and behaviours that influence the clinical and cost-effective use of medicines as well as positive outcomes for patients. 3. Patients medicines need to be managed well to ensure their treatment and recovery is optimised and to ensure value for money is secured from their medication. Exhibit 1 shows the main sources of harm to patients from poor medicines management. Exhibit 1: Key facts about the three main sources of harm from medicines Source: The footnotes contain the sources of data on adverse reactions 3, prescribing errors 4 and non-adherence 5, Lives Plus 2 Wales Audit Office analysis of NHS financial returns, including expenditure within primary care and secondary care. 3 Pirmohamed et al, Adverse drug reactions as cause of admission to hospital: prospective analysis of patients, British Medical Journal, 2004; 329(7456), Lewis et al, Prevalence, incidence and nature of prescribing errors in hospital inpatients: a systematic review, Drug Saf 2009; 32: Lives Plus, Achieving prudent healthcare in NHS Wales, June Royal Pharmaceutical Society of Great Britain, From Compliance to Concordance Achieving Partnership in Medicine-Taking, RPSGB, London, Shapps, Grant, A bitter pill to swallow: A report into the cost of wasted medicine in the NHS, June Page 4 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
75 4. In May 2014, an independent review 7 at Abertawe Bro Morgannwg University Health Board, called Trusted to Care (The Andrews Report), highlighted serious problems related to several aspects of patient care, but it also raised specific issues about administration and recording of medicines. After Trusted to Care, the Minister for Health and Social Services ordered unannounced spot checks on a sample of wards at 20 hospitals across Wales. The main findings from the spot checks were the need to improve standards in medicine administration and storage, as well as completing drug charts. 5. Trusted to Care also emphasised the importance of all types of healthcare professionals working together to manage patients medicines. Pharmacy staff are at the centre of medicines management but staff from all disciplines have a major role to play, as set out in guidance from representative bodies 8,9. Patients also need to be empowered to help them get the best out of their medication. 6. Prudent prescribing of medicines is a key focus within the Welsh Government s prudent healthcare agenda. The principles of prudent healthcare are to minimise avoidable harm, carry out the minimum appropriate intervention and promote equity between people who provide and use services. The key aspects of prudent prescribing are therefore about safe prescribing that minimises adverse drug reactions, conservative prescribing to avoid patients taking medicines unnecessarily, and fully involving patients in decisions about their own care. 7. Medicines management is a quickly changing agenda because of new technologies, new drugs, and the redesign of services. Given that medicines expenditure is one of the highest areas of NHS spending, austerity is also driving change in medicines management, with organisations revisiting treatment pathways to ensure clinically-appropriate and cost effective treatments are provided at the right time. For these reasons we consider it is now a good time to look at the issues across Wales. 8. Our study focuses on aspects of medicines management that directly impact on inpatients at acute hospitals. We cover medication information provided by GPs to support admissions, medication reviews that patients receive during their stay, the support patients are given to take their medicines and the arrangements to ensure good medicines management after discharge. We exclude procurement and largely exclude the supply of medicines. 9. In this report we refer to the position at Velindre Cancer Centre within Velindre NHS Trust (the Trust). We make comparisons with health boards across Wales and we present data from ward visits and patient reviews conducted across three wards in the cancer centre. When reviewing this information it is important to note that due to the differing nature of Velindre s services, comparisons with other health boards need to be treated with caution. Appendix 1 shows full details of our methodology. 10. At the Trust our review sought to answer the following question: Are there safe, efficient and effective arrangements for inpatient medicines management at Velindre Cancer Centre? 11. The key findings from our work are set out below and are considered further in the more detailed section of the report. 7 Professor June Andrews, Mark Butler, Trusted to care: An independent review of the Princess of Wales Hospital and Neath Port Talbot Hospital at Abertawe Bro Morgannwg University Health Board, May Nursing and Midwifery Council, Standards for Medicines Management. 9 General Medical Council, Good practice in prescribing and managing medicines and devices, 31 January Page 5 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
76 Key findings 12. Our overall conclusion is: We found many good aspects of medicines management in the cancer centre. However, the pharmacy team is struggling to meet demand, facilities do not fully comply with requirements and there is not a clear strategy for driving improvement. The table below sets out our key findings in more detail: Corporate arrangements: Pharmacy benefits from a high profile in the hospital but there is scope for more medical engagement in corporate medicines management issues and there is not yet a robust strategy to drive future developments Lines of accountability are clear in Pharmacy but there is minimal medical staff leadership of medicines management and scope for more medical engagement in the Medicines Management Committee. The Trust has a medicines management strategy but it is too high level and is not yet driving improvement and prioritisation of medicines management services. Pharmacy has a relatively high profile in the cancer centre and the ongoing internal Pharmacy Capacity Review should further raise awareness of pharmacy issues at all levels of the organisation. Medicines account for 70 per cent of non-pay expenditure in the cancer centre but the medicines savings plan focuses only on one initiative. The Trust s individual patient funding request committee considers more applications and requires more pharmacy staff time than in other Welsh health bodies. Workforce: The involvement of pharmacists in clinics is positive but the pharmacy team is struggling to meet demand and pharmacy s input on the wards is too inconsistent The medicines management workforce clearly feels under pressure and the Trust now needs to decide on an approach to manage capacity constraints and consider different ways of delivering services. While the Pharmacy Capacity Review suggests more staff are needed, the calculation may understate the actual resource required. This is because the review does not take into account the increasing demand for pharmacy services, and also because it focuses on the way that pharmacy resources are currently used, not the way that resources should be used in future. The amount of pharmacy resource allocated to training and development is less than the Welsh average but doctors and nurses had positive views about being able to keep their medicines skills up to date. Relationships are good between pharmacists and other ward staff but not as good as in other health boards, possibly due to inconsistency in pharmacy involvement on the wards. Doctors and nurses told us that pharmacy services are generally accessible despite pharmacy opening hours being slightly less than average. Facilities: Pharmacy facilities are cramped and do not fully comply with key requirements. There are ongoing issues associated with medicine storage in pharmacy and on the wards Pharmacy facilities are cramped and not all key requirements are met in relation to pharmacy s location, boundary security and storage of items above the floor. Patient feedback suggests the pharmacy is a long walk from outpatients and there have been instances of unauthorised personnel accessing the pharmacy corridor. Work is ongoing to address deficiencies in the aseptic unit and, in line with the rest of Wales, the preparation of injectable medicines on the wards is not regularly audited. There is more work to do to strike the right balance between ensuring medicines are stored securely on the wards whilst at the same time ensuring they are easily accessible without unnecessary delays. We saw two instances where medicines were stored within reach of treatment room windows that were kept ajar. Page 6 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
77 Processes: The Trust has some good processes including use of electronic prescribing, timely reconciliations and the role of non-medical prescribers. There are issues with information exchange with primary care, controlled drug checks, and lack of self-administration. Staff had generally negative views about the quality of information provided by GPs and technicians are spending valuable time chasing information about patients medications from primary care. The majority of patients had their medicines reconciled within one day of admission although compared with the rest of Wales, fewer patients in the Trust received a comprehensive medication review. The Trust uses the standard drug chart for all patients and we found good recording of patients allergy status but there is scope to improve the recording of the dates of medication history and medicines reconciliation. The Trust s medical staff were more positive than in the rest of Wales regarding the usefulness of the formulary although some scope remains to make the British National Formulary more readily available. Velindre has used an electronic prescribing system for many years and is in a good position to share its learning with the rest of Wales The Trust has developed the role of prescribing pharmacists more than the rest of Wales and while there are clear benefits of this approach, it is also taking pharmacists away from their core tasks. The Trust had comparatively few cases when it was unclear whether a drug had been administered or omitted. However, there is variation between wards in the way that controlled drugs are checked and there is no policy for patients to self-administer their medicines. The Trust has comparatively few patients with compliance issues and whilst the pharmacy team is spending little time educating patients on the wards, the technician-led oral chemotherapy education service is an example of good practice. Pharmacists, nurses and doctors agreed that the most common reasons for medicines-related delays to discharge were waiting for prescriptions to be written and delays in dispensary. There is also scope to better communicate with primary care upon discharge about patients medicines. The Trust is taking a number of good actions to improve the way it uses antimicrobial medicines. There is further scope to improve the recording of treatment durations on drug charts. Monitoring: Medicines-related performance data is not used routinely enough to promote improvement and while there are good aspects of learning from incidents, more work is required to understand why pharmacists safety interventions are more frequent than average. There is some scope to improve the use and sharing of performance data to promote further improvement in medicines management. The rate of safety interventions carried out by pharmacists was higher than the rest of Wales and there was conflicting data on the rate of medication-related admissions. There are some good aspects of the way that lessons are learnt from medication errors but the pharmacy team s views were less positive than in the rest of Wales and further work is required to understand the comparatively high proportion of incidents that are medicines related. Page 7 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
78 Recommendations R1 Corporate arrangements: In relation to Part 1 of the report, the Trust should: a. Increase medical engagement in corporate medicines management issues, possibly by rotating the chair of the Medicines Management Committee (MMC) around the hospital s consultant staff. b. Linked with the development of the Strategic Outline Plan for cancer services, engage with staff and patients about the strategic direction of medicines management, culminating in the development of a detailed strategy. c. Consider developing a broader financial plan for medicines management. The plan should avoid impacting on the quality of care but should assess whether there is scope for efficiencies through improved drug procurement or by delivering services in different ways. R2 Workforce: In relation to Part 2 of the report, the Trust should: a. Bolster the Pharmacy Capacity Review so that it considers the extent of increasing demand, the possible future model of services and compares staff numbers and skill mix with other cancer centres. b. Consider using the Trust s Service Improvement Team or other resources to explore the potential benefits of the alternative approaches to using nursing and pharmacy resources more efficiently that are discussed in this report. c. Improve continuity of pharmacy input by ensuring each ward has a specific, named pharmacist that is routinely available as the main point of contact. R3 Facilities: In relation to Part 3 of the report, the Trust should: a. Improve the boundary security of the pharmacy department by ensuring the double doors to the main stores are kept closed and by considering an alternative to the current pin code entry system. b. Implement regular ward audits of the preparation of injectable medicines and drug fridge temperatures. c. Develop a plan to improve the security of medicines storage on the wards that addresses the issues identified in this report regarding medicines within reach of open windows and unlocked medicines cupboards. d. Expedite the implementation of the recommendations of the All Wales Pharmaceutical Quality Assurance Specialist to improve the aseptic facilities and ensure progress is reported to the MMC. R4 Processes: In relation to Part 4 of the report, the Trust should: a. Ensure drug charts record dates of medication histories and reconciliations, particularly when being rewritten. b. Work in partnership with the NHS Wales Informatics Service to set out a clear timescale and funding plan for implementing the Individual Health Record (IHR) and the Medicines Transcribing Electronic Discharge (MTeD) system. c. Schedule a detailed discussion at the Medicines Management Committee with the aim of coming to a corporate decision on the potential to introduce a policy of patient self-administration. d. Taking into account the forthcoming guidance from the national Medicines Administration, Recording, Review and Storage (MARRS) Group, come to a formal decision on the appropriateness of single-nurse checking of controlled drugs administration. e. Learn from the national work on Prudent Prescribing to develop an action plan to increase pharmacy s focus on identifying patients compliance needs, educating/counselling patients, improving medicines information and supporting patients to take their medicines properly. f. Develop a funded and timebound plan for introducing discharge medication reviews (DMRs). Page 8 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
79 R5 Monitoring: In relation to Part 5 of the report, the Trust should: a. Review its portfolio of medicines management performance indicators to ensure performance is frequently monitored and shared with staff, and work with the health boards to regularly benchmark performance. b. Analyse the rate of safety interventions by pharmacists to identify root causes and decide whether more should be done to prevent errors and near misses, rather than correcting them once they have been made. c. Analyse the reasons why the proportion of incidents that were medication-related has decreased since 2008 and to understand the comparatively negative views of pharmacy staff about the reporting of incidents. d. Ensure the functions of the Medication Safety Officer role are routinely being carried out. Page 9 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
80 Part 1 Corporate arrangements for medicines management Pharmacy benefits from a high profile in the hospital but there is scope for more medical engagement in corporate medicines management issues and there is not yet a robust strategy to drive future developments Leadership and accountability structures Lines of accountability are clear in Pharmacy but there is minimal medical staff leadership of medicines management and scope for more medical engagement in the Medicines Management Committee 13. Effective leadership and clear lines of accountability are vital components of any healthcare service. Medicines management is slightly complicated in that it encompasses services and processes spanning pharmacy, nursing and medical staff. Nevertheless, it is still important that there are clear senior accountabilities and structures. 14. In the Trust, the Medical Director is the executive lead for medicines management and the Head of Nursing is the nursing lead for medicines management. There are no other leadership roles within the medical or nursing staffs that relate specifically to medicines management. The Medical Director recognises the potential benefits of introducing a specific role for one of his consultants to act as a leader for medicines management.. The Professional Standards for Hospital Pharmacy Services 10 (the Standards) state that there should be clear lines of professional and organisational responsibility within the pharmacy service. The Trust has a clear structure where, below the Chief Pharmacist, there is a management tier of four posts. The management tier includes two principal pharmacists, one responsible for aseptic services and the other responsible for clinical services, as well as the lead pharmacist for clinical trials and the pharmaceutical procurement and IT manager.. Exhibit 2 shows that in our survey across Wales, 69 per cent of pharmacy staff agreed or strongly agreed with the statement There are clear lines of accountability in the pharmacy team. The equivalent figure in the Trust was similar to the all-wales position at 70 per cent. 10 Royal Pharmaceutical Society, Professional Standards for Hospital Pharmacy Services, July Page 10 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
81 Exhibit 2: Pharmacy staff at the Trust generally agreed with the statement There are clear lines of accountability in the pharmacy team 60% 50% Velindre NHS Trust Wales Percentage of Respondents 40% 30% 20% 10% 0% Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Don't know Source: Wales Audit Office Survey of Pharmacy Staff 17. The Standards also state that health bodies should have a medicines management group as a focal point for the development of medicines policy, procedures and guidance. The Trust has a Medicines Management Committee (MMC) whose role it is to ensure that medicines are used safely and cost-effectively and to ensure that medicines are used in accordance with accepted current best practice. 18. The medicines group should be multidisciplinary to reflect the fact that medicines management is the responsibility of a number of clinical professional groupings. Nursing staff make up 20 per cent of the MMC s membership (compared with an average of nine per cent across Wales) and medical staff make up 50 per cent of the membership (compared with 46 per cent across Wales). 19. There is scope for greater medical staff engagement in the MMC. The terms of reference of the group state that the MMC should be chaired by a consultant but it is currently chaired by the Chief Pharmacist. The agenda is also largely driven by the Pharmacy Department. The Medical Director recognises the importance of the committee and acknowledges that it does not yet have a high enough profile amongst medical staff. Strategy for medicines management The Trust has a medicines management strategy but it is too high level and is not yet driving improvement and prioritisation of medicines management services 20. The Trust should have a clear strategic vision for medicines management. Velindre s Medicines Management Strategy is a two-page document that was developed by the Chief Pharmacist in 2014, with input from the Medical Director and was signed off by the MMC. It sets out general principles related to safety, efficiency, effectiveness, good clinical governance and risk management, and the Page 11 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
82 delivery of medicines through a proactive process adapted according to local and national needs and drivers. 21. The Trust recognises that the strategy is high level and we concluded that it is not specific enough about setting out the priority areas for the future direction of services. The strategy also appears to have been developed with little engagement with staff involved in medicines management services or patients who receive services. 22. We surveyed pharmacy staff for their views on the strategy. The results showed that 34 per cent of pharmacy staff agreed or strongly agreed that they had been consulted and were able to contribute to the strategy, compared to 30 per cent for Wales. The survey also showed that 40 per cent of pharmacy staff agreed or strongly agreed that the organisation has an effective strategy for medicines management, compared to 66 per cent for Wales. 23. As described in Part 2 of this report medicines management services are under pressure. With staff at many levels finding it difficult to deliver their core tasks within the available time, it could be argued that development of a strategy is a low priority. We consider that head room needs to be found to fully develop the strategic approach for medicines management to ensure long-term solutions are found to the current pressures and to better guide decisions about which services should be prioritised and which services should be withdrawn at times of particular pressure. Profile and influence of pharmacy within the wider organisation Pharmacy has a relatively high profile in the cancer centre and the ongoing internal Pharmacy Capacity Review should further raise awareness of pharmacy issues at all levels of the organisation 24. If the pharmacy team is to have sufficient profile and influence within the organisation, it should have adequate representation at the Trust s senior decision-making forums. Velindre s pharmacy team is better represented on senior committees than in the health boards. The pharmacy team is represented on the most senior committees responsible for quality and safety, clinical governance and risk management. Cwm Taf was the only health board where pharmacy was represented on the most senior committee responsible for quality and safety. None of the health boards pharmacy teams was represented on the committee responsible for clinical governance or risk management. 25. During our audit, staff told us about the relatively high profile of pharmacy within the cancer centre. The size of the hospital is one factor in this, as is the pharmacy team s detailed involvement in chemotherapy. Staff that had worked in other organisations reflected on the higher profile of pharmacy within the cancer centre. 26. The profile of pharmacy issues has been raised at the Trust s Quality and Safety Committee by the consideration of the Pharmacy and Medicines Management Annual Report. Further, the ongoing Pharmacy Capacity Review that has the potential to raise the profile of pharmacy even higher. The review was initiated by the Pharmacy Department, with agreement of the hospital s senior management team, to assess the appropriateness of current staffing levels. The involvement of the Head of Nursing as a critical friend for the review may help ensure independence and broader awareness raising of the issues being faced in pharmacy. It will be important that the findings from the Pharmacy Capacity Review are reported at a Trust level. Page 12 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
83 27. Pharmacy teams should be able to influence the design of services that involve medicines. This is because when new consultant posts, clinics and services are introduced, this inevitably impacts on pharmacy service delivery. The Trust s pharmacy team has slightly more input in such matters than compared with other teams across Wales. Whilst the Trust s pharmacy team has no involvement in decisions to introduce new consultants, it is fully involved in decisions regarding the introduction of new services. Where the Trust is considering introducing a new clinic or expanding an existing clinic, the pharmacy team s involvement would include providing information on drug costs and medicines service implications from change. Financial management of medicines management Medicines account for 70 per cent of non-pay expenditure in the cancer centre but the medicines savings plan focuses on only one initiative 28. Financial management and monitoring are particularly important in relation to medicines management due to the high expenditure on drugs within NHS Wales. Medicines accounts for 70 per cent (nearly 18 million) of the non-pay expenditure of Velindre Cancer Centre. 29. In 20-, the cancer centre has set a savings target of 275,000 related to medicines. The savings are intended to come from rolling out the use of a national framework contract to deliver medicines to patients homes and thereby secure efficiencies. These savings had been intended to be made in previous years but implementation of the project has slipped because of delays in finalising the national framework contract. Given the extent of medicines expenditure in the cancer centre we were surprised not to see a broader savings plan. 30. In response to our survey, 50 per cent of pharmacy staff disagreed or strongly disagreed with the statement Financial savings made in pharmacy services are not impacting on patient outcomes compared with 24 per cent across Wales. This is a slightly surprising result given the lack of a broad savings plan related to medicines. Individual patient funding requests The Trust s individual patient funding request committee considers more applications and requires more pharmacy staff time than in other Welsh health bodies 31. Individual patient funding requests (IPFRs) are usually requests from clinicians who want health body approval to use medicines that are not normally funded by the NHS. Health bodies need robust processes and effective IPFR panels to ensure appropriate decision-making regarding these requests. An all-wales report from April 2014 recommended that the panels that handle IPFR requests should have at least two lay members, and applications should be screened and signed by a clinical lead or head of department in advance of meetings At the Trust, the IPFR Advisory Committee is different to the IPFR panels in health boards. The committee screens requests from Trust consultants and if deemed appropriate, refers the request to the health board where the patient resides. 11 National IPFR Review Group, Review of the individual patient funding request process, April Page 13 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
84 33. The committee meets weekly and does not have any lay members. Preparatory work is undertaken by the pharmacy team s High Cost Drugs Administrator and clinical support outside of meetings is provided by the Chief Pharmacist. 34. During 2014-, the IPFR Advisory Committee at the Trust considered 96 applications regarding medicines, which was higher than the Wales average of This is likely to be due to the comparatively high number of oncology drugs that are developed. The total amount of time spent by the Trust s pharmacy team on supporting and attending these meetings was also higher than the average for Wales (353 hours compared with the Welsh average of 193 hours). 12 The Wales average is for Betsi Cadwaladr discounted from Wales average: the majority of applications at BCU are not managed through the IPFR panel. Page 14 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
85 Part 2 The medicines management workforce The involvement of pharmacists in clinics is positive but the pharmacy team is struggling to meet demand and pharmacy s input on the wards is too inconsistent Workload pressures The medicines management workforce clearly feels under pressure and the Trust now needs to decide on an approach to manage capacity constraints and consider different ways of delivering services 35. Our work across Wales highlighted general perceptions of high workload and too few staff. During our fieldwork at the Trust, staff from all disciplines talked about the pharmacy service being under pressure and struggling to meet demand. In the Trust, 87 per cent of pharmacy staff disagreed or strongly disagreed with the statement: There are enough pharmacy staff at this organisation for me to do my job properly. This compares with 60 per cent across Wales. 36. Exhibit 3 shows the extent to which staff agreed with the statement: I have time to carry out all of my work. Exhibit 3: Pharmacy staff generally disagreed or strongly disagreed with the statement I have time to carry out all of my work and to a similar extent to the rest of Wales 50% 40% Velindre NHS Trust Wales Percentage of Respondents 30% 20% 10% 0% Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Source: Wales Audit Office Survey of Pharmacy Staff 37. We were told about the senior members of the pharmacy team having limited time to attend meetings, manage their teams and focus on the development of services. Page of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
86 38. We were also told about the following workforce pressures in relation to the pharmacy team s clinical work on the wards: A general lack of time to complete tasks on the wards. The Chief Pharmacist recently recorded an incident on the Datix system related to a member of staff s increased workload. Rotas are tight under normal circumstances but when staff are absent from work for any reason, there can be more acute workforce pressures. Valuable time is used by technicians on the wards chasing information from primary care regarding patients existing medications. These issues are discussed further in paragraphs 83 to 84. The involvement of pharmacists as non-medical prescribers in outpatient clinics has potential benefits for patients and relieves pressures on these busy clinics. However, the clinics drain pharmacy resource from the wards. At times of pressure, important pharmacy services are withdrawn from the wards to maintain core pharmacy services. The withdrawn services include the discharge dispensing carried out on the wards and the medicines management role of technicians on the wards. This was a matter of particular frustration for some staff. 39. The Trust has implemented a number of changes in the dispensary in an attempt to reduce workload pressures. These changes include the rolling out of WP10 forms that are prescriptions that allow outpatients to have their medicines dispensed in community pharmacies instead of at the hospital dispensary. Other changes include the use of Lean 13 to streamline working practices, and the decision to take clinical trial dispensing out of the hands of the normal dispensary staff and instead allocate this task to the Clinical Trials Team. However, staff told us that workforce pressures remain in the dispensary including staff struggling to fulfil their management roles due to the frequent need to deliver front line services and difficulties in releasing staff for training and personal development. 40. Staff also told us about workforce pressures within the aseptic unit. We were told that increased demand meant that there is not sufficient time for planning and horizon scanning. We were also told that by having the aseptic unit split over two floors, valuable time is wasted by staff travelling up and down stairs. 41. The internal Pharmacy Capacity Review concluded that if pharmacy continues working in its current ways, the quality and safety of the current service will decrease and that Velindre Cancer Centre will be at risk of non-compliance with a number of regulatory and professional standards. 42. Exhibit 4 suggests some potential ways in which the pharmacy service could make better use of its resources. Many of these ideas were generated by the Pharmacy Department. These are not formal recommendations, and we recognise that some actions are more workable than others but the ideas are presented as food for thought to the Trust. 13 Lean thinking is an approach to improving the value secured from any process. It focuses on mapping the current process, then identifying and eliminating waste. It is an approach commonly used in manufacturing but is also used in public services. Page of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
87 Exhibit 4: The Trust may want to consider several options for making better use of pharmacy resources Possible actions Reduce the workload associated with labelling of medicines by purchasing overlabelled medicines from a pre-packing unit. Purchasing ready-made intravenous chemotherapy medicines to free up aseptic and dispensing staff capacity. Purchasing a pharmacy robot to dispense medicines. This reduces the requirement on dispensary staff and reduces picking errors. Patients typically require six cycles of oral chemotherapy. Each cycle requires a course of medicine to be dispensed. Resource could be saved if more than one cycle could be dispensed at once. Relocate services to ensure the aseptic unit is no longer split across two floors, thereby reducing the need to spread staff across two areas. Spread the pharmacy workload over longer hours to prevent peaks and troughs in activity and to ensure the resource is better matched to demand. Replacement of the current emergency medicine store with an automated vending machine. The Pharmacy Capacity Review estimates this will save 11 hours a month of pharmacy time. Analyse the nature of the phone calls to the pharmacy department with a view to providing better information to prevent the workload associated with phone call queries. Roll out of homecare services (as mentioned in paragraph 29). Ongoing work will focus on the provision of oral chemotherapy within patients homes but there is potential to extend to intravenous treatment. This may not reduce the overall workload but may have the benefit of moving some workload out of the cramped and busy pharmacy department. Barriers Cost and lack of space to store the purchased items. Cost and lack of space to store the purchased items. Lack of physical space in the current dispensary. Patients would have to follow complicated instructions. Medicines could be wasted if patients prescriptions change between cycles. Cost, lack of space, disruption to services. Risk of spreading the pharmacy service too thinly. None. This is being implemented. Time to carry out the analysis. May require additional staffing to manage and administer the contracts with homecare service providers. There are also governance risks associated with moving to this service model. Source: Wales Audit Office 43. Our review suggested there is scope to use the nursing resource in more efficient ways in relation to medicines management. We identified the following issues: As the newly-installed drug cupboards in the cancer centre are fitted with individual locks, we observed nursing staff spending valuable time trying to find relevant keys to access drugs. We were told about the increasing amount of nursing time that is being dedicated to drug administration rounds. It is essential that sufficient time and attention are given to the high-risk processes on drugs rounds. However, there may be scope to map the various tasks taken in drugs rounds with a view to saving time and securing efficiencies. Page 17 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
88 We were also told about valuable nurse time being used in carrying out routine checks of controlled drugs cupboards on the wards. In one instance, two senior nurses were engaged in this checking for 45 minutes. It is important that these drugs are regularly checked but there may be scope to review and rationalise the stock held in controlled drug cupboards on the wards to minimise the time taken on such tasks. Staff numbers and skill mix While the Pharmacy Capacity Review suggests more staff are needed, the calculation may understate the actual resource required 44. Pharmacy teams should have the right skill mix, capability and capacity to manage patients medicines effectively as well as develop and provide broader pharmacy services. Health bodies across Wales carried out a resource mapping exercise of their own pharmacy teams during late Exhibit 5 highlights some of the staffing indicators from that exercise and, unsurprisingly, it suggests that the make-up of the pharmacy team at the cancer centre differs considerably from the teams in acute hospitals in Wales. Velindre has a more senior grade mix of pharmacists, which causes the average cost per pharmacist to be higher than the rest of Wales. This is not unexpected given the highly specialised nature of services at Velindre, and hence the need for higher skilled pharmacists. Velindre also has a comparatively high number and cost of pharmacists and technicians per occupied bed day. It is difficult to make meaningful comparisons between Velindre and the health boards on these metrics because Velindre delivers much of its care through the Outpatients Department, and therefore the number of occupied bed days at Velindre is comparatively small. 14 Exhibit 5: The staffing profile for Velindre varies from that observed across Wales although it is difficult to make meaningful comparisons due to the different nature of services at the cancer centre Wales average Velindre NHS Trust Staff numbers and skill mix Total pharmacists and technicians in post (WTE) Ratio of pharmacists to technicians 51:49 40:60 Pharmacists and technicians (WTE) per 100,000 occupied bed days Staffing Average cost per WTE: Pharmacist 63,600 70,800 costs Average cost per WTE: Technician 35,900 36,700 Pharmacist and technician: cost per occupied bed day We used activity data on daily occupied beds from Stats Wales as an indicator of the pharmacy team s workload. Gross costs are based on the mid-point of each pay band and include rota, superannuation and national insurance allowances. Hourly cost is based on calculating the total WTE of pharmacists and technicians in each pay band, then multiplying these figures by the gross cost per hour (assuming 37.5 hours per week for 52 weeks of the year) at the mid-point of each band, then summing the totals across all bands. Page 18 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
89 Source: Resource Mapping Exercise carried out by pharmacy teams across Wales (2014), Stats Wales NHS beds by organisation and site ( ). These data include only acute-based staff and our analysis excludes the time/resource dedicated to primary care and community pharmacy activities. At the time of resource mapping Velindre had 10.5 WTE pharmacists,.4 WTE technicians and 3.7 WTE assistants. The figures for Velindre include staff from the Clinical Trials Team. 46. As at July 20, the Trust had a pharmacy team consisting of 8.2 whole time equivalent (WTE) pharmacists, 11.8 WTE pharmacy technicians and 3.7 WTE assistant technical officers. The Pharmacy Capacity Review has suggested that to deliver pharmacy services in a manner that is considered safe and effective, the following additional staff would be required: 2.8 WTE pharmacists, 1.4 WTE pharmacy technicians and 1.9 WTE assistant technical officers. 47. We have not tested the calculations contained in the Pharmacy Capacity Review, however, we believe there is a risk that the review might have understated the additional pharmacy resource required. The review provides details of the way in which pharmacy resources are currently used; it does not consider how the resource should be used. The review does not consider the future model of services that should be provided and the resource that will be required to deliver that model. Finally, the review also does not quantify the extent to which demand for pharmacy services is currently increasing. The next phase of the internal Pharmacy Capacity Review is due to consider these issues. Training and development The amount of pharmacy resource allocated to training and development is less than the Welsh average but doctors and nurses had positive views about being able to keep their medicines skills up to date 48. In our survey, 33 per cent of pharmacy staff in the Trust disagreed or strongly disagreed with the statement I am getting sufficient training, learning and development, which was very similar to the 34 per cent figure for the rest of Wales. Data from the resource mapping exercise shows that pharmacy staff in the Trust spent, on average, five per cent of their time on receiving and delivering training, education and personal development over the past year. This compares with nine per cent across Wales The Quality Delivery Plan 18 for the NHS in Wales said that health boards should train 25 per cent of their staff in quality improvement methodologies by the end of March Across the rest of Wales, the proportion of secondary care pharmacy staff trained to at least bronze level in the Improving Quality Together methodology led by 1000 Lives Plus was 27 per cent 19, ranging from 10 to 67 per cent. In the Trust, 77 per cent of secondary care pharmacy staff are trained to at least bronze level, well above the Welsh average. These data were sourced from the Pharmacy Capacity Review, July 20. These figures do not include staff from the Clinical Trials Team. 17 Resource Mapping activity data relating to pharmacist and technician staff groups across primary and secondary care. 18 Welsh Government, Achieving Excellence: the Quality Delivery Plan for the NHS in Wales , Calculation of the Wales average excludes an incomplete response from Hywel Dda. Page 19 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
90 50. Training for nursing and medical staff can be a key success factor in contributing to good, multidisciplinary engagement in medicines management. The Professional Standards for Hospital Pharmacy Services (the Standards) state that pharmacy should support induction and ongoing training of clinical staff. Across Wales, health boards fund an average of 0.7 WTE pharmacy staff to deliver training to medical staff. The Trust has no staff funded for this role. 51. Due to their relatively limited experience, junior medical staff are one staff group that is in particular need of training in medicines management. At the Trust, the pharmacy team is involved in junior doctor induction. These sessions cover the use of antibiotics, thromboprophylaxis and chemotherapy. Pharmacists are also providing continued support to junior doctors through their interactions on the wards. 52. Nurse training on medicines involves all new staff, regardless of how long they have been qualified, undertaking a medicines management study day. The day is provided by Cardiff and Vale University Health Board. Staff are also required to complete workbooks on oral and intravenous medicines administration. A competency assessment is required for staff using syringe drivers. 53. In our survey, 57 per cent of doctors and 56 per cent of nurses agreed or strongly agreed with the statement: It is easy for me to keep my medicines management skills up to date. This compared with 35 per cent of doctors and 47 per cent of nurses across Wales. 54. Doctors and pharmacy staff have differing views on the controls in place to monitor medical prescribers. In our survey, 17 per cent of pharmacy staff, 65 per cent of doctors and 37 per cent of nurses agreed or strongly agreed with the statement: The Trust has good controls in place to monitor the performance of medical prescribers. This compared with 23 per cent of pharmacy staff, 29 per cent of doctors and 32 per cent of nurses across Wales. Clinical pharmacy services Relationships are good between pharmacists and other ward staff but not as good as in other health boards, possibly due to inconsistency in pharmacy involvement on the wards 55. Clinical pharmacy describes the activity of pharmacy teams in ward and clinic settings. This activity involves direct involvement with patients, giving advice to other healthcare professionals and playing a full part of the multidisciplinary team approach to managing people s medicines. The Standards say that pharmacists should be integrated into clinical teams and provide safe and appropriate clinical care directly to patients. 56. The NHS Wales pharmacy resource mapping exercise carried out across Wales in late 2014 showed that the Trust s pharmacists and technicians typically spent nine per cent of their time directly supporting wards and clinics. Whilst this is lower than the average of 32 per cent across Wales 20 we recognise that this is an example where Velindre s different model of services makes it particularly difficult to compare with other organisations in Wales. 57. Exhibit 6 summarises some of the key data we collected in our clinical pharmacy review that covered three wards at Velindre Cancer Centre (details of these wards can be found at Appendix 1). The exhibit also shows data from our staff surveys and wider audit, relating to relationships and clinical pharmacy services on the wards. 20 Resource Mapping activity data relating to pharmacist and technician staff groups across primary and secondary care. Page 20 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
91 Exhibit 6: There is mixed performance in the Trust in relation to clinical pharmacy services Indicator Velindre Wales Observations % pharmacy staff saying there were good or excellent relationships with medical staff % pharmacy staff saying there were good or excellent relationships with nursing staff 64% 77% Good relationships between pharmacy, medical staff and nursing staff are essential for an effective multidisciplinary approach to medicines management. Ninety-six per cent of medical staff agreed that relationships with pharmacy were good or excellent. 76% 88% Ninety-six per cent of nursing staff shared this view. The positive relationships were mentioned to us several times during our hospital visits. Wards with a named pharmacist 1 of 3 wards Wards with a named technician All wards 50% 91% Allocating named pharmacists and technicians to specific wards can assist with working relationships. Only one ward at the Trust has a named pharmacist. All wards have a named technician. Across Wales the majority of wards have a named pharmacist assigned to them, and half have a named technician. Wards with no visiting service from pharmacy Wards with a seven-day visiting service % of pharmacy team recommendations that led to changes (from clinical pharmacy review) % pharmacy staff that agreed or strongly agreed that they are able to influence the prescribing behaviour of doctors and nurses (from staff survey) None None 11% 5% If there is no routine visiting service to the ward this may suggest that better links need to be forged between pharmacy and the ward teams. The Trust compares well against the rest of Wales. All wards receive a six-day visiting service with oncall support available on Sundays. 92% 40% 79% 68% We looked at recommendations made by pharmacy teams about the type and dosage of drug and we calculated the proportion of these recommendations that were followed. If pharmacy staff are unable to influence prescribers this suggests relationships should be strengthened. Source: Clinical Pharmacy Review, staff surveys, Core Medicines Management Tool. 58. Our audit suggests there is scope to improve the consistency of pharmacy input on the wards. We concluded this because: As shown in the exhibit above, only one of the wards has a named pharmacist, whereas across Wales, 91 per cent of wards have named pharmacists. We were told that during a single week, up to four different pharmacists may provide clinical services to a single ward. The Trust s self-assessment against the Standards recognises the inconsistency at ward level saying a mixture of different pharmacist/pharmacy technicians covering the same ward, sometimes on a daily basis. The self-assessment proposes that rotas should be reviewed to ascertain whether more consistent cover is achievable. Page 21 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
92 At interview, staff said that the lack of continuity in pharmacy input on the wards can cause inefficiencies and safety issues. Staff said that frequent changes in pharmacists can make it difficult for the pharmacist to get up to speed with the individual clinical needs and risks of each patient. We were also told that the lack of continuity from a named pharmacist means that ward staff may not know the best person to contact when they have medicines-related queries. Such queries from ward staff are frequently directed to the Principal Pharmacist as the first point of call. This escalation of issues to the Principal Pharmacist reduces the Principal Pharmacist s capacity and can mean that ward pharmacists are not aware of clinical issues on the wards. The lack of named pharmacists on the wards can mean there is inconsistent support available to technicians carrying out the medicines management work on the wards. 59. Exhibit 7 shows that during our clinical pharmacy review, the average time that pharmacy teams spent on the ward per visit was about the average seen across Wales. The number of patients reviewed per hour of visiting was also around the Wales average for all three wards Exhibit 7: Comparison across Wales of the time pharmacy teams spent on the wards per visit and the number of patients they reviewed per hour Average time on ward per visit (minutes) Average number of patients reviewed (per hour) Chemo IP 1st Floor ASU 0 Chemo IP 1st Floor ASU Source: Wales Audit Office Clinical Pharmacy Review 60. Exhibit 8 shows details of the pharmacist and technician workload, during our sampled ward visits, in relation to the supply of medicines. We recorded three types of supply: supply of medicines to inpatients, supply of to take out medicines when patients are due to be discharged, and supply of monitored dosage systems (MDS), which are multi-compartment boxes to help patients remember which medicines to take. Our clinical pharmacy review showed that supplying medicines to inpatients represented a greater proportion of the pharmacy team s workload than the Welsh average. Page 22 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
93 Exhibit 8: Supplying medicines to inpatients represents a greater proportion of the pharmacy team s workload at Velindre than across the rest of Wales Inpatient Supply To Take Out supply Monitored Dosage Systems Wales Velindre 0% 20% 40% 60% 80% 100% Source: Wales Audit Office Clinical Pharmacy Review (ward visit) 61. Exhibit 8 shows that in Velindre, no MDSs were supplied to patients. The dispensary does not prepare MDSs due to lack of facilities and resources. If a patient requires an MDS, the ward-based medic writes the prescription and the pharmacy team then contacts the patient s community pharmacist to arrange dispensing upon discharge. The Trust s self-assessment against the Standards recognises that the process for arranging MDS systems for patients needs to be streamlined. 62. Ward rounds are a route by which pharmacy staff can work closely with the rest of the multidisciplinary team to contribute to patient care. Our results from across Wales suggest there is scope for pharmacy teams to be more frequently involved in ward rounds, as just one per cent of the 673 visits recorded in our clinical pharmacy review were as part of ward rounds. In the Trust, none of the visits was recorded as a post-take ward round. Our survey highlighted differing views about the statement: Clinical pharmacy staff are regularly involved in multidisciplinary ward rounds. Ten per cent of pharmacy staff, 65 per cent of doctors and 23 per cent of nurses agreed or strongly agreed. 63. Exhibit 9 shows the pharmacy staff s views on how their team could be more effective and compares their opinions with those of doctors and nurses. Whilst pharmacy and nursing staff think the priority should be to improve continuity of pharmacy staff on the wards, medical staff said the top priority should be to improve discharge processes. Page 23 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
94 Exhibit 9: Staff views on the scope for making the pharmacy team more effective Priority Views of pharmacy staff Views of doctors Views of nurses 1 (Highest) Improve the continuity of pharmacy staff who support the ward/patients. Improve/put in place processes to support discharge. Improve the continuity of pharmacy staff who support the ward/patients. 2 Increase the amount of time spent on the wards. 3 Improve/put in place processes to support discharge. 4 Take part in post-take ward rounds. 5 Change the timing of the routine visits to wards. 6 Improve/put in place an on-call service. Take part in post-take ward rounds. Improve the continuity of pharmacy staff who support the ward/patients. Increase the amount of time spent on the wards. Change the timing of the routine visits to wards. Improve/put in place an on-call service. Improve/put in place processes to support discharge. Take part in post-take ward rounds. Increase the amount of time spent on the wards. Improve/put in place an on-call service. Change the timing of the routine visits to wards. Source: Wales Audit Office Surveys of Pharmacy Staff and Medical Staff Opening hours and access to the pharmacy workforce Doctors and nurses told us that pharmacy services are generally accessible despite the pharmacy opening hours being slightly less than average 64. Pharmacy services should be accessible to healthcare staff at the times when they are most needed. The Royal Pharmaceutical Society has highlighted problems with the availability of pharmacy services outside normal working hours. The Society reports that limited availability of hospital pharmacy services, particularly at weekends, can result in more missed doses and prescription errors, a lack of medicines reconciliation and prolonged waits for discharge medication Exhibit 10 shows the Trust s pharmacy service opening hours compared with the average across Wales. In addition to the hours shown in the table, the Trust s pharmacy team is available on-call at all times, which is also the case at all other health bodies in Wales. 21 Royal Pharmaceutical Society, Seven Day Services in Hospital Pharmacy: Giving patients the care they deserve, 2014 Page 24 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
95 Exhibit 10: Pharmacy service opening hours at Velindre are below the Welsh average Hospital Total number of hours open to A&E/ outpatients Total number of hours open to provide clinical services to the wards Mon-Fri Sat-Sun Mon-Fri Sat-Sun Velindre Wales average Source: Wales Audit Office Core Medicines Management Tool 66. Exhibit 11 shows the results of our survey of medical and nursing staff in relation to the accessibility and responsiveness of pharmacy services. Exhibit 11: Medical and nursing staff in Velindre were generally more positive than the rest of Wales about the access and responsiveness of the pharmacy team Velindre Wales It is easy to contact the pharmacy team in normal working hours % medical staff that agreed or strongly agreed 100% 85% % nursing staff that agreed or strongly agreed 96% 91% It is easy to contact the pharmacy team outside normal working hours % medical staff that agreed or strongly agreed 61% 30% % nursing staff that agreed or strongly agreed 66% 52% The pharmacy team responds in reasonable timescales to my requests in normal working hours % medical staff that agreed or strongly agreed 95% 81% % nursing staff that agreed or strongly agreed 80% 83% The pharmacy team responds in reasonable timescales to my requests outside normal working hours % medical staff that agreed or strongly agreed 67% 29% % nursing staff that agreed or strongly agreed 59% 51% Source: Wales Audit Office Surveys of Medical and Nursing staff. 67. During our fieldwork, nursing and medical staff told us about good access to pharmacy during normal working hours. We heard about pharmacy staff being easy to contact via the phone or bleep system and that they were always responsive and helpful. Nursing and medical staff also said that the out-of-hours arrangements for an on-call pharmacist and emergency medicine store worked well, although they were said to be rarely used. A number of staff said it would be helpful to have pharmacy staff carrying out routine discharge dispensing on Sundays and after 4.30 pm on weekdays. Page 25 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
96 Part 3 Medicines management facilities Pharmacy facilities are cramped and do not fully comply with key requirements. There are ongoing issues associated with medicine storage in pharmacy and on the wards Compliance with key requirements for pharmacy facilities Pharmacy facilities are cramped and not all key requirements are met. Patient feedback suggests the pharmacy is not ideally located and there is scope to improve boundary security 68. Our visit to the pharmacy department at Velindre Cancer Centre highlighted the cramped working conditions of pharmacy staff. The dispensary and pharmacy storage area are small and this issue has been recognised in the Trust s risk register. 69. A Welsh Health Building Note 22 describes key requirements for the design, layout and facilities of hospital pharmacies. The table below shows the requirements in italics and shows whether the facilities of the Velindre Cancer Centre pharmacy comply (), partially comply () or do not comply (). Findings Location Is the pharmacy on the ground floor and accessible from the main corridors/circulation routes? The pharmacy is on the ground floor but is quite a distance from outpatients. Feedback from patients has mentioned the long walk to pharmacy. The Trust is considering a satellite pharmacy in outpatients. Boundary security Is entry to pharmacy strictly controlled through the use of swipe cards or similar? Entry to pharmacy is via an electronic pin system at the door to the pharmacy corridor. We were told about one instance where a member of the public, waiting in the pharmacy waiting area, watched a member of staff input the pin code, then input the code themselves to gain entry to the pharmacy corridor. We were also told about instances of volunteers gaining access to the corridor inappropriately. We saw that the double doors from the general store to the outside of the hospital were kept open. This represents a security risk. 22 NHS Wales Shared Services Partnership, Pharmacy and radiopharmacy facilities, Welsh Health Building Note WHBN 14-01, 2014 Page 26 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
97 Findings Storage area and temperature Were all items stored above the floor? Boxes in the pharmacy storage area were seen on the floor, apparently due to the lack of space elsewhere. Are there good arrangements to regulate the temperature below 25 degrees, particularly in areas used to store bulk items? The pharmacy store room is air conditioned, although the main store area is not. Controlled drugs Is there a separate, lockable and alarmed controlled drugs store? The dispensary has a separated, locked controlled drugs cupboard. The keys are kept by the dispensary pharmacist. The cupboard is not alarmed although the pharmacy department is alarmed out of hours. Emergency medicine store Is there a specific store where medicines can be accessed when pharmacy is not staffed? The emergency store is a wooden cupboard in the pharmacy corridor although a new automatic vending machine is now in place and will soon replace the emergency store. Is there a clear system for recording which items have been taken from the emergency store? The current system relies on nursing staff completing a form. The patient details are not always fully completed, although the vending machine will ensure a more detailed audit trail. Dispensary Does the dispensary have benches and worktops of a colour that contrasts with white medicine labels? The worktops in the dispensary are speckled green. Does the dispensary have dedicated hand washing facilities? There is a sink but it is not used solely for hand washing, it is also used for drink preparation. Source: Wales Audit Office observations of hospital pharmacies Preparation of aseptics and injectable medicines Work is ongoing to address deficiencies in the aseptic unit and in line with the rest of Wales, the preparation of injectable medicines on the wards is not regularly audited 70. Aseptic facilities are sterile units used to prepare high-risk medicines such as chemotherapy injections, intravenous feeds for premature babies and certain antibiotics. The aseptic unit at Velindre Cancer Centre was last inspected by the All Wales Pharmaceutical Quality Assurance Specialist Pharmacist in February The report highlighted no critical deficiencies but it did highlight some major deficiencies that required action within three months. Some of the issues referred to within the report included: no independent quality assurance lead on site at Velindre; rust being evident on light panels in the isolator rooms; Page 27 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
98 the need to deep clean the vinyl floor in high-traffic areas in the isolator room; unsafe tray-stacking practices; a lack of space to allow separation of pre and post-checking processes; and part-used vials retained for use later in the day but were not stored in a sufficient environment. 71. The aseptic audit report has been considered by the Chief Pharmacist and presented to the cancer centre s Senior Management Team. The aseptic team monitors actions against the improvement plan every month although the team acknowledges that it would like to have seen more rapid progress in some areas. 72. Some injectable medicines are prepared on the wards rather than in an aseptic unit. These preparation processes should be subject to annual audits but across Wales we found that such audits are rarely carried out. 23 On our ward visits, staff were not aware of any audits or risk assessments of injectable medicines preparation. However, whilst the Trust told us that no wards had conducted an audit of aseptic practices in the past year, it also stated that all three wards had a risk assessment in place. Facilities for storing medicines on the wards There is more work to do to strike the right balance between ensuring medicines are stored securely on the wards whilst at the same time ensuring they are easily accessible without unnecessary delays. We saw two instances where medicines were stored within reach of treatment room windows that were kept ajar. 73. In February 2014, Healthcare Inspectorate Wales inspected the Active Support Unit at the cancer centre and highlighted some issues with the security and storage of medicines. 24 The report highlighted risks of potential access to medication by unauthorised persons due to the fridge and drug cupboards not being locked. 74. Following the Trusted to Care report, spot checks were undertaken across Wales regarding the safe and secure storage of medications on wards. At the Trust these spot checks were carried out in June 2014 and found the following: Active Support Unit Patients reported that they received medication at the right time. Staff were viewed giving out medicines in line with professional standards. First Floor Ward Medication was safely locked away in patient lockers but the treatment room and the drugs fridge were unlocked. Staff were viewed giving out medicines in line with professional standards. Chemotherapy Inpatient Unit All patients were aware of the medication they were taking and all patients were wearing identification bands with clear information. Patients own drugs cupboards were in use and worked effectively. 75. In October 2014, in response to Trusted to Care, the Trust set up a task and finish group, consisting of pharmacists and nursing staff to address the medicines-related aspects of the report. The group, chaired by the Director of Nursing and Service Improvement, established an assurance framework to map work planned or in progress within the Trust against the 14 recommendations specified in the report. The actions set out in the framework are numerous and include: revision of the medicines administration policy; 23 National Patient Safety Agency, Patient safety alert 20, 28 March Healthcare Inspectorate Wales, Unannounced Dignity and Essential Care Inspection, 6 February Page 28 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
99 introduction of audits of missed doses; revisions to the arrangements for nurse training on medicines; maintenance of a database on medicines-related incidents; refresher training to all pharmacy staff about professional standards and code of practice; and a spot check audit of drugs left on patients lockers and completion of prescription charts. 76. In June and July 20 we visited the inpatient wards at Velindre Cancer Centre. Our observations and conversations with staff during these visits revealed some ongoing storage issues. Our findings are summarised below: First Floor Ward A treatment room has recently been refurbished and provides generous space for storage. However, the pin code entry system bleeps loudly and is potentially disruptive to nearby patients. Nursing staff also told us about the frustration and inefficient use of time caused by having separate keys for separate drugs cupboards. We found that whilst the outside door to the room was locked, three drawers were unlocked. Chemotherapy Inpatients Unit The treatment room was locked but medicines cupboards were unlocked. The chemotherapy treatment room was locked using a new electronic pin code system. The fridge was unlocked and the window to this ground floor room was ajar. A cytotoxic extravasation kit was within reach of the window. Chemotherapy medication and intravenous fluids were stored on open shelves (although the Trust said this is necessary for the medication to reach room temperature before administration). Active Support Unit The treatment room was unlocked but the cupboards inside were locked. The window to this ground floor room was ajar and a box of Pabrinex (intravenous high potency injection) was reachable, as was the medical sharps box. 77. Our clinical pharmacy review found that all of the 32 patients (100 per cent) reviewed had a functioning, lockable cabinet. This compares with 94 per cent across Wales. 78. The introduction of automated vending machines to store and dispense medicines on the wards can improve security, audit trails and can release pharmacy and nursing staff time. None of the Trust s wards have automated vending machines in operation, compared with an eight per cent average across Wales. There is a vending machine in the Chemotherapy Inpatient Unit (which is not yet functional) and another is due to be used to replace the emergency medicines store near the Pharmacy Department. 79. The Trusted to Care spot checks across Wales revealed issues with the refrigeration of medicines on the wards. During our ward visits, we found that the fridge in CIU was kept unlocked and that staff on all wards were unsure about the roles and responsibilities for monitoring fridge temperatures. Page 29 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
100 Part 4 Medicines management processes The Trust has good medicines management processes including the use of electronic prescribing, timeliness of reconciliations and the role of non-medical prescribers. There are issues related to information exchange with primary care, controlled drug checks, and lack of self-administration Admission information from GPs Staff had generally negative views about the quality of information provided by GPs and technicians are spending valuable time chasing information about patients medications from primary care 80. When patients are admitted, good communication between the GP practice and the hospital can prevent errors and inaccuracies about people s medicines. If the interface between primary and secondary care is not managed properly it can be an area of high-risk in relation to medicines management. 81. In our survey, 24 per cent of hospital doctors, 27 per cent of pharmacy staff and 34 per cent of nurses in the Trust agreed or strongly agreed with the statement that admission information for elective patients was sufficient. Across Wales the results were 37 per cent of doctors, 26 per cent of pharmacy staff and 40 per cent of nurses agreeing or strongly agreeing. 82. For emergency patients, only 18 per cent of hospital doctors, seven per cent of pharmacy staff and 12 per cent of nurses agreed or strongly agreed with the statement that it is easy to access sufficient written/electronic information about patients' existing medication. The results for the rest of Wales were 11 per cent of doctors, 11 per cent of pharmacy staff and 13 per cent agreeing or strongly agreeing with the statement. 83. The Trust does not have guidance for GPs to stipulate what information to provide when their patients are admitted. Interviewees recognised that the transfer of medication information between primary and secondary care is a risk area for the Trust. We were told about pharmacy technicians spending considerable time telephoning GP practices and exchanging faxes to secure medicines information. For each patient, this process typically takes 10 to minutes but can take as long as 50 minutes. 84. The Individual Health Record (IHR) is an electronic system that contains a summary of the information held by GPs about their patients. The IHR system is being piloted for use in medicines reconciliation at Cardiff and Vale University Health Board. The IHR system allows pharmacists to directly access GP-held information about patients medicines. Evaluations at Cardiff and Vale suggest use of IHR saves an average of seven minutes of pharmacy time per patient reconciled. In , there were 1,231 emergency admissions to Velindre, which equates to an average of 3.4 per day. If IHR was used for each of these admissions, this would have saved approximately 24 minutes of pharmacy time per day. Given the safety improvements possible through IHR and potentially significant time savings possible, both for pharmacy staff and in general practices, it is important that the Trust works with partners to expedite the roll out of IHR. Page 30 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
101 Medicines reconciliation and review in hospital The majority of patients had their medicines reconciled within one day of admission although compared with the rest of Wales, fewer patients in the Trust received a comprehensive medication review 85. Medicines reconciliation is a checking process, often led by a pharmacist, to ensure that when a patient moves in or out of hospital, they are followed by accurate and complete medication information. The Professional Standards for Hospital Pharmacy Services (the Standards) state that within 24 hours of admission, patients medicines should be reconciled to avoid unintentional changes to their medication 25. Of the 32 patients seen as part of our clinical pharmacy review, 29 (91 per cent) had received their reconciliation within one day of their admission 26. This compares favourably against the average across Wales of 64 per cent. The Trust s own data on medicines reconciliation timeliness shows that in the first eight months of 2014, more than 85 per cent of patients had their medicines reconciled within 24 hours of admission During their hospital stay, patients should have their medicines reviewed regularly. In response to our survey, 64 per cent of pharmacy staff, 87 per cent of doctors and 68 per cent of nurses agreed or strongly agreed with the statement: Patients receive medication reviews (by any member of the multidisciplinary team) frequently during their hospital stay. For Wales as a whole, 66 per cent of pharmacy staff, 67 per cent of doctors and 66 per cent of nurses agreed or strongly agreed with the statement. 87. Our clinical pharmacy review showed that these medication reviews are almost exclusively carried out by pharmacists, with only six per cent across Wales being carried out by doctors. At Velindre, all of the patients recorded in our clinical pharmacy review had their medication reviews undertaken by a pharmacist. Only five ( per cent) of the patients from our sample at Velindre received a comprehensive medication review 28. The relevant figure for the rest of Wales was 44 per cent. The Trust believes it would not be appropriate for its staff to carry out comprehensive medication reviews on patients as a matter of routine. This is because the cancer centre s medical staff are specialist oncologists but are not experts in managing conditions and medicines other than those related to cancer. 25 National Prescribing Centre, Medicines reconciliation: A guide to implementation. 26 Figure represents patients whose medicines review date was either the same day as admission or the following day. 27 These data were taken from a Trust document entitled, Current Pharmacy Services Overview, September Pharmacy teams carrying out the clinical pharmacy review were asked to use evidence from the patient notes to identify the highest level of medication review that had occurred, ranging from None through to Full review which includes drug history taking, review of history and clinical notes and discussion with patients on concordance. Page 31 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
102 Medicines administration charts The Trust uses the standard drug chart for all patients and we found good recording of patients allergy status but there is scope to improve the recording of the dates of medication history and medicines reconciliation 88. The medicines management process in hospital relies heavily on safe and effective record keeping. Drug charts should be used by staff to record what medicines patients have been prescribed, the required dosage and to record clearly the times when doses were given. A standard drug chart has been developed in Wales, called the Inpatient Medication Administration Record and approved by the Royal College of Physicians. A separate chart called the Long Stay Medication Administration Record should be used for patients who remain in hospital for long periods. Our drug chart review in the Trust found that all patients had the standard inpatient form. In the rest of Wales as a whole, 93.3 per cent of patients had the standard form, 6.4 per cent had the Long Stay Inpatient Medication Administration Record and 0.3 per cent had a non-standard form of chart. 89. We found scope to improve the recording of dates when medicines reconciliations and medication histories were undertaken. Our drug chart review of 26 patients across the Trust found that only 12 patients had the date of their medication history recorded and had the dates of the medicines reconciliation recorded. 90. When a patient is prescribed many medicines, more than one drug chart may be necessary. We found that in these instances, important information about the patient was often not transferred to the front page of the new drugs charts. Such missing information included dates of admission as well as date of medication history, date of medicines reconciliation and details of the patient s compliance issues. 91. Whatever type of drug chart is in use, there should be a record of the patient s allergies and sensitivities to medications. Allergic reactions are a serious risk to patient safety and a common source of drug error. Our drug chart review of 26 patients across the Trust found that all patients (100 per cent) had their allergy status recorded on the drug chart. This compares with 98 per cent across Wales. Formulary processes The Trust s medical staff were more positive than in the rest of Wales regarding the usefulness of the formulary although some scope remains to make the British National Formulary more readily available 92. A formulary is a health body s preferred list of medicines that staff can use as a reference document to ensure safe and cost-effective prescribing. The Trust does not have a Velindre-specific formulary. Until January 2014, the Trust used the joint Bro-Taf (south) formulary but it now uses the formulary of Cardiff and Vale University Health Board. The Trust informs us that a local formulary is currently under development. 93. In response to the survey for this audit, 87 per cent of hospital doctors and 71 per cent of nurses said they agreed or strongly agreed that the formulary (and supporting documents/guidance) met their needs. The corresponding figures in the rest of Wales were 45 per cent and 74 per cent. Page 32 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
103 94. The British National Formulary (BNF) is published to provide prescribers, pharmacists, and other healthcare professionals with up-to-date, consistent information about medicines. It is important that staff on the wards can readily access the most up-to-date version of the BNF. Exhibit 12 shows the percentage of medical staff that agreed or strongly agreed with the statements about the BNF when on the wards. Exhibit 12: Medical staff in the Trust were more positive than those in the rest of Wales about computer access to the BNF but some scope remains to make the BNF more readily available Velindre Wales The most up-to-date version of the BNF is readily available in hard copy 61% 60% I can easily access the BNF using a computer 52% 40% I tend to access the BNF using a smartphone 8% 22% Source: Wales Audit Office survey of medical staff Electronic prescribing Velindre has used an electronic prescribing system for many years and is in a good position to share its learning with the rest of Wales 95. Electronic prescribing is the computer-based generation, transmission and filing of a prescription for medication. Electronic prescribing systems in secondary care can allow quicker, safer and cost-effective transfer of information 29. These systems provide a considerable opportunity to influence the prescribing behaviour of secondary care clinicians by reinforcing and reminding staff about the health body s prescribing priorities. 96. Health boards across Wales told us that none of their wards have electronic prescribing processes in place. However, Velindre has had an electronic prescribing system called Chemocare in place for many years. Chemocare is a system for prescribing chemotherapy and other medicines that patients may require when undergoing chemotherapy. It does not cover general prescribing. 97. Staff expressed generally positive views about the Chemocare system. We consider that the Trust is in a good position to share with the rest of Wales its experiences of implementing and using the system as part of any national work to develop general electronic prescribing systems. The Trust would also benefit from development of general electronic prescribing systems in Wales as Chemocare only covers chemotherapy and not other types of medication. 98. Our fieldwork did reveal three issues related to the use of Chemocare in Velindre: The first issue is that not all junior doctors have access to the system Lives Plus, Achieving prudent healthcare in NHS Wales, June 2014 Page 33 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
104 The second issue is a potential risk of double prescribing in relation to supportive medications. Supportive medications include antisickness drugs that counteract the side effects of chemotherapy. It is possible for patients to be prescribed supportive medications through Chemocare, as well as through hand-written drug charts on the wards. Staff told us that the use of two prescribing systems means that the checking of prescriptions has to be thorough to ensure there are no duplicates. Senior staff consider the risks to be minimal. The third issue is that the pharmacy team is currently responsible for keeping Chemocare up to date by carrying out such tasks as adding new drugs to the system. This is a drain on pharmacy team resources. Non-medical prescribing The Trust has developed the role of prescribing pharmacists more than the rest of Wales and while there are clear benefits of this approach, it is also taking pharmacists away from their core tasks 99. Training pharmacists, nurses and other non-medical staff as prescribers can improve patient access to medicines advice and expertise, contribute to more flexible team working and result in more streamlined care Health bodies across Wales struggled to provide us with comprehensive data on the number of non-medical prescribers within their staff, and they particularly struggled to provide the number of these staff that were regularly using their skills. Across the rest of Wales, health boards report having between 44 and 303 supplementary prescribers in place. Four health boards provided information about the proportion of nurses and pharmacists that were regularly prescribing, but only two recorded this information for other non-medical staff groups. This Trust was able to provide good information and told us that it has 17 nurses, six pharmacists and two other healthcare professionals that were registered as prescribers and were regularly practising In response to our survey, 63 per cent of pharmacy staff, 87 per cent of doctors and 50 per cent of nurses in the Trust agreed or strongly agreed with the statement: Staff trained in non-medical prescribing are regularly using these skills. These figures compare well with the rest of Wales which were 29 per cent for pharmacy staff, 28 per cent for doctors and 33 per cent for nurses Our clinical pharmacy review showed that pharmacy staff rarely prescribe on the wards, the average across Wales being 1.5 prescriptions per 100 patients reviewed. At the Trust, pharmacy staff wrote no prescriptions Exhibit 13 shows how the Trust compares to other bodies in Wales relating to non-medical prescribing policies. 30 Supplementary prescribers can only prescribe in partnership with a doctor or dentist. Independent prescribers can prescribe for any medical condition within their area of competence. Page 34 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
105 Exhibit 13: The Trust had three of the four key non-medical prescribing policies in place Does the Trust have these policies in place? Velindre Wales Criteria for selecting staff to train as non-medical prescribers Mechanism for recording non-medical prescribers and sharing this list with appropriate directorates Support mechanisms for ensuring non-medical prescribers maintain their knowledge Competency requirements to maintain validation as a non-medical prescriber No Yes Yes Yes In place at five health boards In place at all health boards In place at all health boards In place at three health boards Source: Wales Audit Office Core Medicines Management Tool 104. The Trust monitors the quality of non-medical prescribing (NMP) through quarterly NMP meetings and annual competency assessments. In response to our survey, Velindre staff were more positive than staff in the rest of Wales about the way in which NMP performance was monitored. In the Trust 34 per cent of pharmacy staff, 70 per cent of doctors and 43 per cent of nurses agreed or strongly agreed with the statement: The Health Board/Trust has good controls in place to monitor the performance of non-medical prescribers. In the rest of Wales the figures were 14 per cent for pharmacy staff, 14 per cent for doctors and 24 per cent for nurses Velindre uses nurses as prescribers in outpatient clinics and on the wards and pharmacists are used as prescribers in eight outpatient clinics. Staff from all disciplines told us about the wide-ranging benefits of pharmacy and nursing input as prescribers. Benefits include the opportunity for pharmacy, nursing and medical staff to work closer together and learn from one another. Pharmacy and nursing involvement also means that additional resource is available to meet demand at these busy clinics We were also told about some issues with this model of services. The pharmacy service is supporting eight outpatient clinics but is backfilled for only four clinics. The involvement in clinics is therefore draining pharmacy resource from core tasks. We were also told that when nursing staff are trained as prescribers, they are effectively taken away from other nursing roles and are therefore also depleting nursing resources. The Trust is now commencing a project to assess the effectiveness of non-medical prescribing. A project manager has been employed for two years to carry out a stocktake of non-medical prescribing, to assess whether it provides value for money and to develop recommendations for the future. Administration of medicines The Trust had comparatively few cases when it was unclear whether a drug had been administered or omitted. However, there is variation between wards in the way that controlled drugs are checked and there is no policy for patients to self-administer their medicines 107. Trusted to Care highlighted serious problems in the way that medicines are administered and recorded. All organisations have produced actions plans to respond to Trusted to Care and the Trust has carried out a range of other actions, including the introduction of a regular audit of omitted and delayed doses. The findings of these audits are reported to the Head of Nursing as well as the cancer centre s Senior Management Team. Page 35 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
106 108. In response to our survey, 67 per cent of pharmacy staff, 52 per cent of doctors and 77 per cent of nurses agreed or strongly agreed with the statement: The organisation has taken appropriate action in relation to Trusted to Care (the Andrews Report). This compares with 82 per cent of pharmacy staff, 34 per cent of doctors and 66 per cent of nurses across Wales Trusted to Care mentions delayed and omitted doses, and particular problems with confused and immobile patients being unable to take their pills without supervision and therefore not getting their medication on time, or at all. There can be justified reasons why a dose is missed, such as the patient refusing to take their medicines. However, sometimes doses are missed because the drug is not available on the ward or sometimes poor record keeping means it is not clear from the drugs chart whether a dose has been omitted or not. The latter is particularly dangerous because when the drugs chart has not been properly completed, as it risks the patient being given their medication twice The clinical pharmacy review carried out by pharmacy staff covered 32 patients over a 24-hour period across the Trust s three wards. It identified a total of 13 occasions where a dose was omitted. There were six occasions when the patient refused their medicine, two occasions when the drug was not given at the prescriber s request, two occasions when the patient was not on the ward, two occasions when the reason for non-administration was given as other and one occasion where the reason for the missed dose was because a drug was not available. There were no occasions where records were regarded as unclear about the omission of a dose We also looked at drugs charts when we visited the cancer centre. We reviewed the drug charts of 26 patients across three wards. In each ward we found one case where it was unclear whether a drug had been administered or omitted. This represented a rate of 1.2 instances per 10 patients reviewed. The corresponding figure in the rest of Wales was 2.5 instances per 10 patients The standards of the Nursing and Midwifery Council state that a policy must be in place and adhered to in assessing the competence of an individual to support a patient in taking medication. Those standards also set out the responsibility of nursing staff in assessing patients competence to self-administer their medicines. We found that none of the wards in the Trust have a procedure for self-administration (compared with 25 per cent of wards across Wales) and no patients were self-administering. Across Wales our clinical pharmacy review found that very few patients were administering their own medicines. Out of 1,026 patients audited, only 12 were self-administering and only three of these had been risk-assessed. A further 120 patients were self-administering in a limited way During our interviews, some staff at the Trust told us about the potential benefits for patients if a policy of self-administration was introduced at the cancer centre. Staff told us about the risk of current practices institutionalising patients and the Trust s self-assessment against the Professional Standards for Hospital Pharmacy Services (the Standards) also recognises a medium rated risk related to the lack of a self-administration policy The Trust s procedures for checking and administering controlled drugs vary within the cancer centre. Current procedures dictate that two nurses must be involved in the checking of controlled drugs at the Chemotherapy Inpatient Unit, whilst a process of single nurse checking is in place at the First Floor Ward. The Trust has set up a working party to look at this issue and is engaging with the ongoing work of the national Medicines Administration, Recording, Review and Storage (MARRS) Group. That group was due to issue its guidance at the time of drafting. Page 36 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
107 Supporting patients with compliance The Trust has comparatively few patients with compliance issues and whilst the pharmacy team is spending little time educating patients on the wards, the technician-led oral chemotherapy education service is an example of good practice 1. Studies 31 have shown that up to half of all patients do not take their medicines as intended. Not taking medicines appropriately has important implications for patient safety and can result in considerable waste. This may be because patients do not fully understand the instructions for taking their medicines or because they are physically unable to administer the medicines themselves. NHS bodies should make information readily available and proactively identify patients who need extra support in taking their medicines. 1. The results of our clinical pharmacy review found that none of the patients reviewed in the Trust were considered to have compliance issues or difficulties taking their medicines in line with advice. This was the only site in Wales where such compliance issues were not found. Across Wales, one in five reviewed patients was found to have compliance issues We scored organisations by considering the actions they take to support people to comply with their medicines 32. The Trust scored 13 out of a possible 32 points, compared with an average of 17 across Wales. This comparatively low score reflects a limitation placed on patients to self-administer their medicines: monitored dose systems are never applied at the Trust, and patients are not assessed on their ability to open medicine containers. Although the Trust explores patient difficulties in taking their medication while they are in hospital, this information is not routinely conveyed to their primary care providers on discharge home Across Wales we found that pharmacy teams are struggling to spend enough time educating patients on their medication. In the clinical pharmacy review across Wales we found that only six per cent of patients or carers were educated on an aspect of their medication. In the Trust, this figure was just one per cent Despite the apparent lack of time spent on educating patients on the wards, we found an example of potential good practice in the Trust in relation to more general education of patients. The Chemotherapy Education Service involves pharmacy technicians educating patients on their oral chemotherapy. Patients are educated on how and when to take their medicines and are made aware of side effects and complications. The service means that patients can be dispensed with day one and day eight of their medicine at the same time, thereby avoiding the need for patients to come back to hospital for their second dose. The education service has recently recorded a video in English and Welsh that will be given to patients as a DVD to take home. This joint project with the charity Tenovus aims to reinforce the messages provided by the education service and further improve patient understanding of their chemotherapy treatment and medication Lives Plus, Achieving prudent healthcare in NHS Wales, June We considered whether patients are assessed on their ability to open containers, whether patients are counselled for complex and high risk medication, whether reminder charts and monitored dosage systems are used, whether targeted written information is given, whether education groups are in existence and whether GPs are made aware of patients compliance issues. Page 37 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
108 120. Hospital pharmacies across Wales are not generally doing enough to provide medicines information to patient groups with particular information needs. The Trust s pharmacy provides no specific information for young children (the Trust does not provide chemotherapy to children and teenagers although it does provide radiotherapy to these patients) or patients with visual impairments but it does provide information for patients using non-english languages. Across the 18 hospitals we surveyed in the rest of Wales, five produce targeted information for young children, seven cater for the visually impaired, and eight provide medicines information in non-english languages The Standards state that patients should be able to call a helpline to discuss their medicines. This can be particularly important in supporting discharged patients who are unsure about their medication regime. Across Wales we concluded that some pharmacy helplines are under-utilised despite their importance in helping patients manage their medicines. The Trust does not routinely provide a contact phone number to patients in case of any medication problems following discharge although the hospital pharmacy is open and available to take calls from patients for 45 hours during the week and three hours at weekends. The Trust has not analysed the nature of calls from patients. Such analysis might allow the development of frequently asked questions to prevent commonlyoccurring patient queries. Exhibit 14 summarises key data about the Trust s pharmacy phone line. Exhibit 14: The helpline at Velindre is open for more hours than average during the week but its level of utilisation is about the same as that seen across Wales Total no. of hours open (Mon-Fri) Total no. of hours open (Sat-Sun) Average no. of contacts per 100 hours of opening Velindre Wales average Source: Wales Audit Office Core Medicines Management Tool Supporting discharge Pharmacists, nurses and doctors agree that the most common reasons for medicines-related delays to discharge were waiting for prescriptions to be written and delays in dispensary. There is also scope to better communicate with primary care upon discharge about patients medicines 122. It is good practice for hospital staff to begin planning a patient s discharge as soon as possible. 34 By estimating the date of their discharge this can ensure all staff are working towards the same timescale and can prevent unnecessary delays. Across Wales we found that 47 per cent of patients reviewed through the clinical pharmacy review had an estimated date of discharge. This Trust showed a similar profile, with 41 per cent of patients having an estimated date of discharge. 33 The Wales average is calculated across 12 hospital sites where a helpline service is provided. Six sites do not provide a dedicated helpline, but three of these do offer patients a contact number in case of medication problems following discharge. 34 College of Emergency Medicine, The Silver Book: Quality Care for Older People with Urgent and Emergency Care Needs, June Page 38 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
109 123. A patient s discharge from hospital can be delayed for various reasons. During our ward visits, some nursing and medical staff did express frustration at delays in pharmacy in relation to discharge medications. Pharmacy staff told us that there can be delays but some of this is caused by under resourcing and some of it is because of delays from medical staff in writing up the prescription. Exhibit summarises the views expressed in our survey from pharmacy staff, nurses and doctors about the most common causes of delays to discharge that are medicines-related. Exhibit : All staff groups agreed that the two most common reasons for medicines-related delays to discharge were waiting for prescriptions to be written and delays in dispensary Views of pharmacy staff Views of nurses Views of doctors 1 (most common) Waiting for prescription to be written Waiting for medicines to be dispensed in the dispensary Waiting for prescription to be written 2 Waiting for medicines to be dispensed in the dispensary 3 Waiting for medicines to be delivered to the ward 4 Waiting for the to take out (TTO) to be assembled on the ward 5 Waiting for prescription to be clinically checked Waiting for prescription to be written Waiting for medicines to be delivered to the ward Waiting for prescription to be clinically checked Waiting for the TTO to be assembled on the ward Waiting for medicines to be dispensed in the dispensary Waiting for medicines to be delivered to the ward Waiting for prescription to be clinically checked Waiting for the TTO to be assembled on the ward Source: Wales Audit Office surveys of pharmacists and medical staff 124. The process for preparing patients discharge medications varies by ward. At the First Floor Ward and the Active Support Unit, pharmacy technicians dispense the take-home medicines but at the Chemotherapy Inpatient Unit, nursing staff have to take the prescription to the dispensary for it to be dispensed. Staff we interviewed expressed some frustration at this variation and about the delays they can sometimes experience when taking prescriptions to the dispensary When patients are discharged from hospital, the interface between the hospital and the patient s GP is vital to ensure safe and effective medicines management. The Standards state that arrangements should ensure accurate information about the patient s medicines is transferred to the healthcare professional(s) taking over care of the patient at the time of the transfer. The Trust does have a standard template that sets out the information to be provided to GPs upon a patient s discharge, and the template applies to all specialties. Across the rest of Wales, 17 out of 18 hospitals that we reviewed have a similar template in place, but only 10 of these apply it across all specialties The Standards state that organisations should monitor the accuracy, legibility and timeliness of information transfer. The Trust has not monitored the quality and timeliness of its discharge information during the past two years In our survey, 56 per cent of pharmacy staff, 70 per cent of doctors and 60 per cent of nurses agreed or strongly agreed with the statement: The discharge information about patients medicines provided to GPs is of high quality. This compared with 41 per cent of pharmacy staff, 30 per cent of doctors and 43 per cent of nurses across the rest of Wales. Page 39 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
110 128. The Medical Director recognised that there is scope to improve the way in which discharge information is provided to primary care colleagues. He said that GPs have expressed some negative views about the quality and timeliness of discharge information and that there is some frustration that primary care cannot access the Trust s electronic CANISC system. The Trust hopes that future implementation of the Medicines Transcribing and Electronic Discharge (MTeD) system will improve the provision of discharge information to primary care staff When a patient is being discharged from hospital, staff may request that community pharmacists carry out a Discharge Medicines Review (DMR) soon after the patient s return home. These DMRs aim to ensure changes to patients medicines initiated in hospital are continued appropriately in the community. The reviews also ensure patients are supported in adhering to their medication regime. An independent review of the DMR service in Wales estimated that each DMR costs and that DMRs have an approximate 3:1 return on investment due to avoiding emergency department attendances, hospital admissions and medicines wastage. 35 The Trust does not use the DMR process but in its self-assessment against the Standards, it states an intention to develop a proposal on how best to provide the DMR service. Antimicrobial stewardship The Trust is taking a number of good actions to improve the way it uses antimicrobial medicines. There is further scope to improve the recording of treatment durations on drug charts 130. Resistance to antibiotics has increased in Wales. 36 The All-Wales Action Plan on antimicrobial stewardship talks about the importance of promoting good antimicrobial prescribing through audit. In the past year, the Trust has audited the following aspects of antimicrobial use across all service areas: point prevalence, the emergence of problem organisms and has carried out other studies 37. Costs, defined daily doses and comparisons between current practices and known local antibiotic resistance problems have yet to be audited. Only two health boards in Wales have audited all five of these topics. The scope of our audit did not cover the findings from these audits The Trust has an antimicrobial prescribing strategy in place, and guidelines covering prescribing for each clinical indication have been implemented across all specialties and directorates. All areas receive feedback on their antimicrobial prescribing, although this feedback is not extended to isolate the practice of individual clinicians. Guidelines relating to prescribing for surgical prophylaxis have not been disseminated The Trust has taken other actions to improve antimicrobial stewardship. These actions include an education programme for ward-based doctors, the introduction of consultant microbiologist ward rounds, antimicrobial treatment guidelines are on the Trust s intranet and the introduction of a dedicated antimicrobial pharmacist. Many health boards are now using stickers on drug charts to prompt prescribers to specify the required duration of antimicrobial treatment. Velindre was planning to introduce these stickers at the time of drafting. During our fieldwork, we were told that whilst prescribers in the Trust are getting better at specifying durations, there remains scope for improvement. 35 Cardiff University, Evaluation of the discharge medicines review service, March Public Health Wales, Antimicrobial resistance and usage in Wales ( ), November For example, studies of the implication of anti-microbial choices on particular patient groups. Page 40 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
111 Part 5 Monitoring pharmacy services Medicines-related performance data is not used routinely enough to promote improvement and while there are good aspects of learning from incidents, more work is required to understand why pharmacists safety interventions are more frequent than average Performance reporting There is some scope to improve the use and sharing of performance data to promote further improvement in medicines management 133. The Professional Standards for Hospital Pharmacy Services (the Standards) state that agreed key performance indicators should be in place to enable internal and external assessment of performance As part of our document request, we asked for examples of the Trust s main medicines management performance reports or performance scorecards from the past six months. We reviewed the Velindre NHS Trust Performance Review 2014-, which covers performance, quality and safety across the cancer centre, Welsh Blood Service and the Trust s Corporate division. The performance review only includes three indicators that are relevant to medicines management including: antibiotic prescribing compliance with documenting indication for use as at March 20, performance has reached 100 per cent compliance in all but two months in the past year; antibiotic prescribing compliance with documenting duration/review date as at March 20, monthly compliance had not reached higher than 80 per cent and was typically between 30 and 50 per cent; and NICE compliance this section of the performance review lists actions taken to implement NICE guidance We were also provided with a document from September 2014 entitled the Current Pharmacy Services Overview Report. This report gave data on average waiting times for systemic anti-cancer therapy (SACT) and non-sact prescriptions in the cancer centre. Performance on both of these measures was consistently better than the target Finally we reviewed the Pharmacy and Medicines Management Annual Report which covered data on the following indicators: medicines reconciliation within 24 hours, percentage of discharge prescriptions dispensed at ward level and completion of hospital acquired thrombosis (HAT) risk assessment Our survey found that 57 per cent of pharmacy staff agreed with the statement: I am regularly given an opportunity to see data relating to the pharmacy team s performance. This compares with 39 per cent across Wales. Page 41 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
112 138. During our visits to the cancer centre we concluded that there is scope for medicines-related performance data to be more consistently publicised to staff. We were told about some data being sent to staff by , or posted on the pharmacy noticeboard on an ad hoc basis but this was not routine. Some staff talked about data being collected but without any dissemination of the results It is good practice for performance to be benchmarked against other relevant organisations. The Trust is involved in a benchmarking relationship with Clatterbridge Cancer Centre but when we requested examples of benchmarking with Clatterbridge on medicines management related performance, the Trust was not able to provide us with any. The Trust has, however, been sharing medicines-related benchmarking information with other Welsh organisations since These data consider issues such as missed doses and the standard of record keeping on drug charts We asked organisations to provide examples of how they monitored patient experience in relation to medicines management. Velindre was able to provide several examples, such as a pharmacy-related survey of outpatients and a medicines-related survey of inpatient satisfaction of medicines information. The latter included comparisons between Velindre and other health bodies in Wales and the results for Velindre were amongst the most positive. Safety interventions and medication-related admissions The rate of safety interventions carried out by pharmacists was higher than the rest of Wales and there was conflicting data on the rate of medication-related admissions 141. Medicines management is a complicated set of processes and there is potential for things to go wrong at numerous stages. The absolute focus for health bodies should be in ensuring safe practices. Where errors or incidents are identified in relation to medicines, health bodies should act decisively and openly to learn lessons and prevent repeat incidents In our survey, 83 per cent of pharmacy staff, 100 per cent of doctors and 94 per cent of nurses agreed or strongly agreed that: I would feel safe having my medicines managed at this hospital. Across Wales, 74 per cent of pharmacy staff, 64 per cent of doctors and 78 per cent of nurses agreed or strongly agreed with the statement When something goes wrong with someone s medication it can directly cause an admission to hospital. Exhibit shows the results of a national audit on the rate at which patients were admitted to hospital as a result of problems with their medication. The rate of these admissions at the Trust is below the Welsh average. Data is taken from the NHS Wales Informatics Service but is complicated by the fact that coding teams take differing approaches to coding the causes of admissions. The scale of the problem with medication-related admissions is therefore potentially understated. Page 42 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
113 Exhibit : The proportion of admissions that are medication-related appears below the all-wales average Wales Velindre Cwm Taf Abertawe Bro Morgannwg Cardiff & Vale Hywel Dda Aneurin Bevan Betsi Cadwaladr Powys 0.0% 0.2% 0.4% 0.6% 0.8% Percentage of admissions that were medication-related Source: NHS Wales Informatics Service. Data by the health body providing care, cover 1 July 2012 to 31 June Our clinical pharmacy review also looked at medication-related admissions and found a considerably higher proportion of medication-related admissions than in the exhibit above. At the Trust, 22 per cent of patients seen by the pharmacy team were considered to be admitted due to a medication-related issue 38. This was the highest across Wales where the average was 10 per cent. The Trust believes its comparatively high rate of medication-related admissions is not unexpected. The Chemotherapy Inpatient Unit was included in these data and chemotherapy-related toxicity is a common and expected medication-related complication in these patients Part of the pharmacy team s role is to make important interventions when a patient s safety is at risk. Such patient safety interventions may be necessary, for example, to ensure that patients with a medication allergy are not prescribed those drugs and ensuring that insulin-dependent diabetic patients are correctly prescribed their insulin. Our clinical pharmacy review identified 12 occasions in the Trust where pharmacy teams intervened because a patient s medication regime could have significantly compromised their safety. This represents a rate of 5.8 occurrences for every 100 patients reviewed. Across the rest of Wales, the average was 4.1 occurrences for every 100 patients reviewed. The rate in Velindre is high enough to suggest that the pharmacy team is commonly acting as a backstop to find and correct errors in medicines management processes. The Trust should consider these data further and decide whether more pharmacy team resources should be diverted to addressing the root causes and stopping errors and near misses happening, rather than correcting them once they have been made. 38 Patients were deemed to have a medication-related admission if the documented, initial diagnosis included a possible problem with medication, including adverse drug reaction, non-compliance, non-evidence based prescribing, dispensing error, poor medication advice etc. Page 43 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
114 Learning when things go wrong There are some good aspects of the way that lessons are learnt from medication errors but the pharmacy team s views were less positive than in the rest of Wales and further work is required to understand the comparatively high proportion of incidents that are medicines related 146. Health bodies should report all patient safety incidents to the National Reporting and Learning System (NRLS) so that national analyses and comparisons can be made. Exhibit 17 shows the number of medication-related incidents reported as a percentage of all incidents reported to the NRLS. The exhibit shows that the proportion of incidents that were medicines related has been typically much higher than the average in the rest of Wales. This proportion has reduced in Velindre since The Trust should carry out further work to understand this pattern, as the recent reduction could represent a positive trend showing improved safety regarding medicines usage or it may be the result of a reduced willingness from staff to report such incidents. Exhibit 17: The proportion of incidents that were medication related in Velindre has been significantly higher than in the rest of Wales although this proportion has reduced since 2011 Medication incidents as % of all incidents 20% 18% % 14% 12% 10% 8% 6% 4% 2% 0% Wales Velindre Source: NRLS, NHS Commissioning Board Special Health Authority 147. Exhibit 18 shows the types of medication-related incidents that were reported by the Trust to the NRLS. The most common category of incident was Administration/supply of a medicine from a clinical area which covers all stages of the administration process from reviewing the prescription, selecting the correct medicine, identifying the correct patient and administering the dose. Page 44 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
115 Exhibit 18: Medication-related incidents in the Trust are most commonly associated with the administration and supply of medicines from clinical areas Administration / supply of a medicine from a clinical area Prescribing Preparation of medicines in all locations / dispensing in a pharmacy Other Monitoring / follow-up of medicine use 141 Advice Supply or use of over-the-counter (OTC) medicine Source: NRLS, NHS Commissioning Board Special Health Authority (1 April 2008 to 31 March 2014). Further detail on the categories can be found at the following link s/md01.htm 148. In our survey, only 50 per cent of pharmacy staff agreed or strongly agreed with the statement Medicines-related incidents/errors are reported and handled appropriately at this hospital, compared with 71 per cent across the rest of Wales. When asked whether they agree with the statement Information obtained through incident/error reports is used to make patient care safer, 60 per cent agreed or strongly agreed (compared with 70 per cent across the rest of Wales). During our visits to the cancer centre, some staff said that incidents may not be reported due to a lack of time Whilst the Trust has designated one of its principal pharmacists as the organisation s Medication Safety Officer, this role is not being regularly undertaken. The role should involve taking a lead on medication safety within the Trust and leading the Medication Safety Group. However, we were told that due to competing demands on this person s time, this role is not routinely being fulfilled. 0. The cancer centre does have two supernumerary patient safety champions amongst the nursing staff. These champions play a key role in learning from incidents, supporting staff involved in incidents and identifying patterns of errors and mistakes. When a medicine-related incident is reported, the champion will meet with the individual involved and look at trend data to see if there is a history of that individual being involved in incidents. The champion and the member of staff agree an action plan, which is then signed off by the Head of Nursing. The member of staff also completes a reflective document that aims to assist their individual learning. Page 45 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
116 1. Serious medication incidents are reported to the Serious Clinical Incident Forum (SCIF). If immediate learning is required, a speedy cascade is used to disseminate the key messages to staff. More routine sharing of messages is done through the production of a newsletter by the pharmacy team. Less serious incidents may be reported to the MMC. The Trust s self-assessment against the Standards acknowledges that there is no single committee that takes overall responsibility for medication errors and incidents. 2. Some patients can suffer negative impacts from taking their medication which are known as adverse drug reactions. Some reactions are unexpected but some are predictable. The Academy of Medical Royal Colleges 39 has calculated that 4 in 100 hospital bed days are caused by adverse drug reactions in the United Kingdom. Using this value, adverse reactions in the Trust represent an approximate cost of 230,000 per year in bed days alone When patients experience adverse reactions as a result of their medicines, staff should report these events to the MHRA via the Yellow Card Scheme. Our clinical pharmacy review identified just one occasion where pharmacy teams identified symptoms of potential adverse drug reactions or side-effects when reviewing patients. This represents a rate of five occurrences for every 1,000 patients reviewed and closely matches the average across Wales (six occurrences per 1,000 patients). 4. In our survey, 36 per cent of pharmacy staff, 74 per cent of doctors and 44 per cent of nurses agreed or strongly agreed with the statement: Use of the Yellow Card Scheme is promoted effectively in this Trust. This compared with 59 per cent of pharmacy staff, 31 per cent of doctors and 29 per cent of nurses across Wales. 39 The Academy of Medical Royal Colleges, Protecting resources, promoting value: A doctor s guide to cutting waste in clinical care, November Stats Wales data shows that the total number of occupied bed days in the Trust in was 14,0 and the cost of an inpatient bed day across Wales is 413 on average. Page 46 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
117 Appendix 1 Methodology Our audit consisted of the following methods: Method Core medicines management tool Document request Clinical pharmacy review Interviews Walkthroughs Surveys of medical and nursing staff Survey of pharmacy staff Use of existing data Detail The core tool was the main source of corporate-level data that we requested from the Trust. The tool was an Excel-based spread sheet. We requested and reviewed approximately 30 documents from the Trust. The clinical pharmacy review was completed by pharmacy teams on the following wards at Velindre Cancer Centre: First Floor Ward Active Support Unit Chemotherapy Inpatient Unit The tool aimed to record activity of pharmacy teams during ward visits. We interviewed a number of staff including: Medical Director, Chief Pharmacist, Principal Pharmacists, Head of Nursing, Pharmacists, Technicians, Ward managers, Patient Safety Champion, Nursing Staff and Medical Staff. We visited the pharmacy, dispensary and inpatient wards within Velindre Cancer Centre. We carried out observations, interviews and drug chart reviews. We carried out an online survey of a sample of medical and nursing staff to ask their views on the effectiveness of medicines management within the organisation. We received 23 responses from doctors, 19 of whom were consultants. Across the rest of Wales we received 413 responses from doctors. In the Trust we received 45 responses from nurses (and across the rest of Wales we received 377 responses from nurses). We carried out an online survey pharmacy staff to ask their views on the effectiveness of medicines management within the organisation. We received 30 responses in total. Across the rest of Wales we received 407 responses from pharmacy staff. We used existing sources of data wherever possible such as incident data from the NRLS, data from the Cardiff University review of the DMR Service and the NHS Wales pharmacy resource mapping exercise Page 47 of 48 - Medicines management at Velindre Cancer Centre - Velindre NHS Trust
118
119 Velindre NHS Trust Quality & Safety Committee Report Delivering Excellence Progress report Meeting Date: 9 th June 20 Author: Sponsoring Executive Director: Report Presented by: James Houston, Planning & Service Development Manager Professor Sue Morgan, Executive Director of Nursing & Service Improvement Andrea Hague, Divisional Director VCC Cath O Brien, Divisional Director WBS Trust Resolution to: (please tick) Approve: Endorse: Discuss: Note: Recommendation: The Committee is asked to DISCUSS the contents of this report. This report supports the following Trust objectives as set out in the Integrated Medium Term Plan: (please tick) Equitable and timely services Providing evidence based care and research which is clinically effective Supporting our staff to excel Safe and reliable services First class patient /donor experience Spending every pound well This report supports the following Health & Care Standards: Standard 2.2 Preventing Pressure and Tissue Damage Standard 2.8 Blood Management Standard 3.1 Safe and Clinically Effective Care Standard 6.1 Planning Care to Promote Independence

120 2 Delivering Excellence Progress report 1. Introduction / Background 1.1 This report provides an update to the Quality & Safety Committee with respect to progress against the Velindre NHS Trust s three year strategic plan - Delivering Excellence and against Trust wide key performance metrics. 2. Timing: 2.1 Reporting period to April Description: 3.1 The Progress Report has been developed and produced by the Trust Planning & Performance team and provides a summary of progress against the Level 1 & 2 objectives and performance metrics in the three year plan which fall under the remit of the Quality & Safety Committee. Definitions of the priority levels are shown below: 4. Financial Impact: 4.1 There are no direct financial implications contained within this report and delivery of the performance metrics presented in the report and work associated with delivering improved performance supports sound financial governance across the Trust. 5. Quality, Equality, Safety and Patient Experience Impact: 5.1 The current performance reporting and monitoring system is predicated upon identifying performance issues and supporting effective decision making at service and operational levels to drive forward continuous improvement in the quality, equality, safety and experience for our patients. 6. Considerations for Committee: 6.1 The report identifies the following objectives / performance measures that have fallen below the agreed target and reported as Red. These are highlighted to the committee as requiring further discussion. Safe & Reliable Services Level 1: (i) (ii) (iii) VCC 033: 0 Velindre hospital acquired pressure ulcers; 1 in April 20. VCC 139: 95% compliance with CAUTI maintenance care bundle; April 20: 83% VCC 142: 100% compliance with skin care bundle; April 20: 67% Page 2
121 3 Delivering Excellence Progress report (iv) VCC 034a: 90% patients to have a documented thromboprophylaxis risk assessment on admission; April 20: 69% First Class Patient Experience Level 2: (v) (vi) VCC 143: 95% hand hygiene compliance (average non inpatient areas); April 20: 87% VCC 144: 95% hand hygiene compliance (average inpatient areas); April 20: 78% Highlighted Measures Level 3: (vii) VCC 146: Antibiotic Prescribing- 100% compliance with documenting duration/review date; April 20: 60% Welsh Blood Service: (i) 60% red cells issued less than 14 days old April 20: 40% 7. Next Steps: 7.1 The Committee is asked to discuss the content of the report and paper, and where required, identify additional mitigating actions to support continuous improvement. Page 3

122 Quality & Safety Committee Delivering Excellence Reporting Period - April 20
123 April 20 Quality & Safety Committee Contents Keys... 2 Section 1 At a Glance Summary - Service Performance Status... 3 Velindre Cancer Centre... 3 Safe and Reliable Services... 3 First Class Patient Experience... 5 Level 3 Highlighted Measures... 6 At a Glance Summary Progress against 3 Year Plan Objectives... 7 Corporate Services... 9 At a Glance Summary Progress against 3 Year Plan Objectives... 9 Welsh Blood Service First Class Donor Experience At a Glance Summary Progress against 3 Year Plan Objective Section 2 Progress against Strategic Priorities Velindre Cancer Centre Safe and Reliable Services Our Key Performance Metrics First Class Patient Experience Our Key Performance Metrics Areas for improvement and areas to celebrate Corporate Services No level 1 Measures or level 2 Exceptions Welsh Blood Service First Class Donor Experience Our Key Performance Metrics

124 April 20 Quality & Safety Committee Keys Green Red Service Performance Target achieved this month Target not achieved this month Green Amber Red Closed Purple Grey Delivery again Plan Actively managed processes proceeding as planned - no major risks or issues identified Problems have surfaced, considered manageable in the normal course Serious problems have surfaced make Senior Management Team aware Major issues remain unsolved- on hold until resolved - senior executive engaged Deliverable activity at feasibility/initiation stage Risk Status Likelihood and impact of non - achievement. 2
125 April 20 Quality & Safety Committee Section 1 At a Glance Summary - Service Performance Status Velindre Cancer Centre Safe and Reliable Services Metric Level 1 VCC 025- Death within 30 days of chemotherapy VCC 032a- 0 C.diff cases VCC 032b- 0 MRSA cases VCC 032c- 0 MSSA cases VCC Velindre hospital acquired pressure ulcers VCC unexpected inpatient deaths VCC % Compliance with CAUTI insertion care bundles VCC % Compliance with CAUTI maintenance care bundle May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report Metric under development Q&S Q&S Q&S Q&S Q&S Q&S 18 83% 97% 100% 75% 75% 100% 92% 50% 59% 67% 83% 83% Q&S % 100% 100% 94% 100% 100% 100% 100% 94% 100% 93% 100% Q&S 21 Page No. 3
126 April 20 Quality & Safety Committee Metric VCC % compliance with CVC insertion care bundle VCC % compliance with skin care bundle VCC 034a 90% patients to have a documented thromboproxphylaxis risk assessment on admission VCC 034b 100% eligible patients prescribed thromboprophylaxis May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% Q&S 21 83% 100% 64% 100% 77% 100% 77% 100% 100% 100% 100% 67% Q&S 22 58% 48% 69% 56% 68% 85% 75% 93% 93% 62% 47% 69% Q&S % 96% 96% 100% 100% 100% 100% 100% 100% 100% 100% 100% Q&S 24 Page No. Metric Level 2 VCC % hand hygiene compliance (average- non inpatient areas) VCC % hand hygiene compliance (average- inpatient areas) VCC 036- Mortality Review of 100% of inpatient deaths May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report 82% 78% 82% 94% 98% 69% 93% 86% 100% 88% 90% 87% Q&S % 33% 75% 83% 91% 99% 91% 95% 100% 94% 74% 78% Q&S % 100% 100% No inpatient deaths 100% No inpatient deaths 100% 100% No inpatient deaths Page No. 100% 100% Q&S N/A 4
127 April 20 Quality & Safety Committee First Class Patient Experience Metric Level 1 VCC 044- >80% patient overall experience rated 9 and above May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report 100% 100% 75% 86% 80% 93% 85% 87% 100% 65% 97% 94% Q&S 28 Page No. Metric Level 2 May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report Page No. VCC 046- On the day waiting times in outpatients less than 20 minutes VCC % of palliative care patients have an POS-S or equivalent assessment within 24 hours of referral 44% 44% 57% 48% 47% 50% 54% 55% 52% 56% No data provided 45% Q&S N/A 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% Q&S N/A 5
128 April 20 Quality & Safety Committee Level 3 Highlighted Measures Metric Level 3 VCC 146- Antibiotic Prescribing- 100% compliance with documenting duration/review date May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report 44% 71% 67% 50% 88% 100% 84% 84% 90% 75% 88% 60% Q&S N/A Page No. 6
129 First Class Patient Experience Safe and Reliable Services Equitable and Timely Access to Services April 20 Quality & Safety Committee At a Glance Summary Progress against 3 Year Plan Objectives Strategic Theme Objective Level Status VCC 031- Review of Clinical nurse specialists and key workers to ensure appropriate service provision VCC104 Implement the agreed recommendations from the internal pharmacy review, the Welsh Audit Office report and the MHRA inspection report in order to improve the quality of the medicines management service. This is collectively termed the Medicines Management Action Plan 20 to 2017 Forecast Status Risk Assuring Committee Highlight Report Page No. 2 Q&S N/A 2 Q&S N/A VCC032 Reduce healthcare associated infections to zero 1 Progress reported in Section 2 Q&S 14 VCC033 Reduce Velindre acquired pressure ulcers to zero 1 Progress reported in Section 2 Q&S VCC034 Ensure that all inpatients received documented thrombosis risk assessments on admissions 1 Progress reported in Section 2 Q&S 23 VCC 039- Improve oversight of medication related errors to comply with NHS Wales standards 2 Q&S N/A VCC 028- Ensure that patients who take oral SACTs are able to make fully 2 Q&S informed decisions to facilitate medication adherence N/A VCC044 Increase positive patient experience levels through the collection of views and opinions from a wider sample of patients including outreach settings 1 Q&S 28 VCC 045- Ensure that people living with and beyond cancer have a personalised assessment, information and care plan and are empowered to manage their 2 Q&S N/A condition VCC050 Establish an assessment unit at VCC 2 Q&S N/A VCC 057- Increase the number of patients that die in their preferred place. Increase the number of patients who access their preferred place of care. 2 Q&S N/A VCC % of palliative care patients have an POS-S (palliative care outcome scale) or equivalent assessment within 24 hours of referral 2 Progress reported in Section 2 Q&S N/A VCC111 Improve feedback mechanisms for patients 2 Q&S N/A 7
130 Providing Evidence Based Care and Research April 20 Quality & Safety Committee Strategic Theme Objective Level Status Forecast Status Risk Assuring Committee Highlight Report Page No. VCC 029- Introduce and evaluate use of oncotype testing 2 Q&S N/A VCC118 Review structure and resources for Quality and Safety support provided by Cancer Services Management Offices 2 Q&S N/A 8
131 Organisational Learning Service Improvement April 20 Quality & Safety Committee Corporate Services At a Glance Summary Progress against 3 Year Plan Objectives Area Objective Level Status Forecast Status Risk Assuring Committee Highlight Report Page No. SI 01 Stimulate generation of the right ideas to take forward SI 02 Strengthening the arrangements for our international health links 2 Q&S N/A 2 Q&S N/A SI 03 Enable the spread of learning OL 01 - Provide opportunities for patients, donors and carers to provide feedback in order to help staff build effective care partnerships OL 02 - Have in place fully functional reporting systems to enable collection and analysis of patient, donor and carer feedback in order to facilitate learning OL 03 - Develop communication structures to enable the spread of learning across the organisation 2 Q&S N/A 2 Q&S N/A 2 Q&S N/A 2 Q&S N/A 9
132 March 20 Quality & Safety Committee Welsh Blood Service Level 2 Metric May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report Page No. 60% red cells issued less than 14 days old 33% 45% 75% 66% 66% 79% 79% 64% 52% 39% 32% 40% Q&S N/A First Class Donor Experience Level 1 Metric May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report Page No. 70% of blood donors scoring 9/10 for satisfaction with overall service 72% 67% 67% 71% 77% 77% 77% 76% 81% 82% 81% 89% Q&S 37 (new target of 71% 10
133 First Class Donor Experience Safe and Reliable Services April 20 Quality & Safety Committee Metric May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr Assuring Committee Highlight Report Page No. beginning April 20) 100 % of concerns answered within 30 days 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% Q&S 38 At a Glance Summary Progress against 3 Year Plan Objective Strategic Theme Objective Level Status Forecast Status Risk Assuring Committee Highlight Report Page No. WBS007 Maintain external regulatory compliance: (MHRA/HTA/EFI/WMDA) 1 Q&S 40 WBS Keep abreast of mandated changes to testing and emerging clinical priorities including: (I) PAS and NAT HEV, and (ii) Pathogen Inactivation 1 Q&S 41 WBS010 Retain wholesaling license 2 Q&S N/A WBS Continue to improve satisfaction ratings from our donors 1 Progress reported in Section 2 Q&S 37 11
134 April 20 Quality & Safety Committee Strategic Theme Objective Level Status Forecast Status Risk Assuring Committee Highlight Report Page No. WBS 0 - Respond to all concerns in a timely and effective way (links to donor satisfaction) 1 Q&S 41 WBS 0 Continue to improve donation experience 2 Q&S 42 12
135 April 20 Quality & Safety Committee Section 2 Progress against Strategic Priorities Velindre Cancer Centre Safe and Reliable Services Our Key Performance Metrics Level 1 VCC 025- Death within 30 days of Chemotherapy Primary Responsibility for Assurance: Quality & Safety Committee Progress against actions within the IMTP: Month Status Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept Story behind progress and performance : The NCEPOD agreed rate is 2% and VCC continuously report levels at under 2%. The SACT Board have agreed that death within 30 days of chemotherapy data will be reported as an overall quarterly % rate. Action(s) and dates for improvement: Risks and Issues: A measures specification will be written and signed off by the SACT Board in 20. Expression of interest for this measure to be reported via the Chemocare reporting package has been submitted to SACT board (to enable a systematic report- currently manual process) but was not prioritized Discussion to be had re: way forward in terms of systematic reporting of overall quarterly rate at June SACT Board Analyzing the data and producing a quarterly figure is time intensivetherefore a detailed report cannot be produced on a quarterly basis within the current resources. Current pressures within pharmacy and lack of clinical and technical support for Chemocare has led to a ceasing of provision of Crystal reports from the system such as SACT dataset, death within 30 days etc. Accountable manager: Associate Clinical Director SACT lead 13
136 April 20 Quality & Safety Committee VCC 032a- Number of Velindre Acquired C.diff Infections Primary Responsibility for Assurance: Quality & Safety Committee 10 Healthcare Associated Infections (HCAI) - C diff (All Ages) May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- No. of Velindre acquired infections No. of non-velindre acquired infections Target Progress against actions within the IMTP: Month Status Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept Story behind progress and performance : Action(s) and dates for improvement: Risks and Issues: Accountable manager: Performance still on target for year beginning April 20. Low rate of C. diff maintained with one case of Velindre acquired in April. Continued active surveillance for cases, symptomatic patient s e.g. C. diff. or GDH +ve. Weekly ICD/Team/Antimicrobial pharmacist ward round promoting prudent prescribing. Continued cleanliness and clinical practice audits Proactive isolation of diarrhoea cases Increased risk if: 1. Failure to comply with antimicrobial prescribing policy 2. Failure to adhere to standard precautions, isolate promptly and maintain environmental cleanliness. 3. Failure to promptly manage GDH +ve cases 4. Transfer of infected cases to Velindre hospital. Head of Nursing 14
137 April 20 Quality & Safety Committee VCC 032b/032c- Number of Velindre Acquired MRSA and MSSA infections Primary Responsibility for Assurance: Quality & Safety Committee 10 Healthcare Associated Infection (HCAI) - MRSA (Bacteraemia) May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- No. of Velindre acquired infections No. of non-velindre acquired infections Target 10 Healthcare Associated Infections (HCAI) - MSSA (Bacteraemia) May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- No. of Velindre acquired infections No. of non-velindre acquired infections Target Progress against actions within the IMTP: Month Status Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept Story behind progress and performance : Action(s) and dates for improvement: Low rate of MRSA and MSSA bacteraemia; 1 case of Velindre acquired MSSA related to a CVC. Continued active surveillance for cases. Investigation of source/root cause in each case identified. Continued work on clinical IV management Active screening and audit to identify MRSA colonised patients ANTT working group established and champions identified to aid
138 April 20 Quality & Safety Committee Risks and Issues: Accountable manager: rolling out across the Trust. Increased risk if: 1. Failure to comply with MRSA screening policy 2. Placement of CVC lines in MRSA positive patients 3. Failure to adhere to standard precautions and clinical practices for ANTT in IV care e.g. phlebotomy, CVC, PVC. Head of Nursing VCC 033- Velindre acquired pressure ulcers to zero Primary Responsibility for Assurance: Quality & Safety Committee 10 Velindre Acquired Pressure Ulcers May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- No. of Pressure Ulcers Target 10 Grading of Velindre Acquired Pressure Ulcers May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- Moisture Lesions Grade 1 Grade 2 Grade 3 Grade 4 Deep Tissue Injury/Unstage-able
139 April 20 Quality & Safety Committee Progress against actions within the IMTP: Month Status Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept Story behind progress and performance : There were 1 Velindre acquired pressure ulcers for the month of April 20 Grade 2 Grade 2 Patient admitted to ASU with a spinal cord compression, developed a grade 2 pressure area to bridge of nose due to the need for wearing of a CPAP mask which the patient required every night to aid breathing, due to a long term medical condition. The pressure area was treated with an appropriate cream and an adhesive dressing. All pressure ulcers were treated according to policy. Datix incident forms were completed and photos taken of the affected area. Action(s) and dates for improvement: Risks and Issues: Accountable manager: Active management, reporting and monitoring in place. All staff informed of pressure ulcers at ward meeting None Head of Nursing 17
 and dates for improvement: Risks and Issues:")
140 April 20 Quality & Safety Committee VCC 138- Number of unexpected deaths Primary Responsibility for Assurance: Quality & Safety Committee 10 Number of Unexpected Inpatient Deaths May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- Number of Unexpected Inpatient Deaths Target Story behind progress and performance : Action(s) and dates for improvement: Risks and Issues: Accountable manager: There were no unexpected inpatient deaths during this period. None Head of Nursing VCC 037- Number and severity of concerns Primary Responsibility for Assurance: Quality & Safety Committee VCC Concerns May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- Incidents Complaints Claims 18

141 April 20 Quality & Safety Committee 80 VCC Incident Types May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- Health and Safety Patients and Clients (Clinical) Information Governance Operational and Organisational Quality Assurance 80 Severity of VCC Incidents May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- No injury Low Minor Medium Major Catastrophic Death Severity of VCC Complaints May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- Grade 1 Grade 2 Grade 3 Grade 4 19
IQC/2013/48 Improvement and Quality Committee October 2013
 Item 9.4 IQC/2013/48 Improvement and Quality Committee October 2013 Pressure Ulcer Prevalence Improvement Plan 1. SITUATION AND BACKGROUND This paper is to update the Improvement and Quality Committee
Item 9.4 IQC/2013/48 Improvement and Quality Committee October 2013 Pressure Ulcer Prevalence Improvement Plan 1. SITUATION AND BACKGROUND This paper is to update the Improvement and Quality Committee
Maidstone Home Care Limited
 Maidstone Home Care Limited Maidstone Home Care Limited Inspection report Home Care House 61-63 Rochester Road Aylesford Kent ME20 7BS Date of inspection visit: 19 July 2016 Date of publication: 15 August
Maidstone Home Care Limited Maidstone Home Care Limited Inspection report Home Care House 61-63 Rochester Road Aylesford Kent ME20 7BS Date of inspection visit: 19 July 2016 Date of publication: 15 August
Healthwatch Knowsley Aintree University Hospitals Trust Service User Report Qtr. 1 ( )
") Healthwatch Knowsley Aintree University Hospitals Trust Service User Report Qtr. 1 (2016-17) 1 Contents About this report... 3 Snapshot... 3 Key... 4 Key Treatment & Care... 5 Key Facilities & Surroundings...
Healthwatch Knowsley Aintree University Hospitals Trust Service User Report Qtr. 1 (2016-17) 1 Contents About this report... 3 Snapshot... 3 Key... 4 Key Treatment & Care... 5 Key Facilities & Surroundings...
Non-emergency patient transport: the picture across Wales
 Non-emergency patient transport: the picture across Wales January 2018 0 P a g e Accessible formats If you would like this publication in an alternative format and/or language, please contact us. You can
Non-emergency patient transport: the picture across Wales January 2018 0 P a g e Accessible formats If you would like this publication in an alternative format and/or language, please contact us. You can
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET
 NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 17 th August 2017 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 17 th August 2017 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
PUBLIC SERVICES OMBUDSMAN WALES PROGRESS WITH CORRECTIVE ACTION PLANS. Assistant Director of Patient Safety & Quality
 PUBLIC SERVICES OMBUDSMAN WALES PROGRESS WITH CORRECTIVE ACTION PLANS AGENDA ITEM 2.2 21 June 2011 Report of Paper prepared by Nurse Director Assistant Director of Patient Safety & Quality Executive Summary
PUBLIC SERVICES OMBUDSMAN WALES PROGRESS WITH CORRECTIVE ACTION PLANS AGENDA ITEM 2.2 21 June 2011 Report of Paper prepared by Nurse Director Assistant Director of Patient Safety & Quality Executive Summary
Kestrel House. A S Care Limited. Overall rating for this service. Inspection report. Ratings. Good
 A S Care Limited Kestrel House Inspection report Kestrel House 14-16 Lower Brunswick Street Leeds West Yorkshire LS2 7PU Tel: 01132428822 Website: www.carewatch.co.uk Date of inspection visit: 31 May 2016
A S Care Limited Kestrel House Inspection report Kestrel House 14-16 Lower Brunswick Street Leeds West Yorkshire LS2 7PU Tel: 01132428822 Website: www.carewatch.co.uk Date of inspection visit: 31 May 2016
PRESSURE ULCER PREVENTION SIMPLIFIED
 10 PRESSURE ULCER PREVENTION SIMPLIFIED This simplified leaflet is intended to give you information about pressure ulcer and aid your clinical practice PRESSURE ULCER PREVENTION SIMPLIFIED Pressure ulcer
10 PRESSURE ULCER PREVENTION SIMPLIFIED This simplified leaflet is intended to give you information about pressure ulcer and aid your clinical practice PRESSURE ULCER PREVENTION SIMPLIFIED Pressure ulcer
What is this Guide for?
 Continuing NHS Healthcare (CHC) is a package of services that is arranged and funded solely by the NHS, for those people who have been assessed as having a primary health need. The issue is one of need.
Continuing NHS Healthcare (CHC) is a package of services that is arranged and funded solely by the NHS, for those people who have been assessed as having a primary health need. The issue is one of need.
Continuing NHS Health Care Quarterly Update April 2015
 SUMMARY REPORT ABM University Health Board Subject Prepared by Approved by Continuing NHS Health Care Quarterly Update April 2015 Date of Meeting: 30 th July 2015 Agenda item: 7 (ii) Christine Williams
SUMMARY REPORT ABM University Health Board Subject Prepared by Approved by Continuing NHS Health Care Quarterly Update April 2015 Date of Meeting: 30 th July 2015 Agenda item: 7 (ii) Christine Williams
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET
 NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 1 st September 2016 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
NHS WALES INFORMATICS SERVICE DATA QUALITY STATUS REPORT ADMITTED PATIENT CARE DATA SET Version: 1.0 Date: 1 st September 2016 Data Set Title Admitted Patient Care data set (APC ds) Sponsor Welsh Government
National Patient Experience Survey Mater Misericordiae University Hospital.
 National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
Healthwatch Knowsley St Helens & Knowsley NHS Trust Patient Experience Report Qtr
 Healthwatch Knowsley St Helens & Knowsley NHS Trust Patient Experience Report Qtr. 1 2017-18 1 Contents About this report... 3 Snapshot... 4 Sentiment Tracker... 5 Friends & Family Test... 5 Key Themes...
Healthwatch Knowsley St Helens & Knowsley NHS Trust Patient Experience Report Qtr. 1 2017-18 1 Contents About this report... 3 Snapshot... 4 Sentiment Tracker... 5 Friends & Family Test... 5 Key Themes...
National Patient Experience Survey UL Hospitals, Nenagh.
 National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
To Approve To Note To Assure. N/A Overall Income: N/A N/A N/A. Link to Business Plan:
 Patient Story Community Nursing/ Pressure Ulcers Agenda Item: 1 Reference: WCT14/15-096 Meeting Name: Trust Board Meeting Date: 4 August 2014 Lead Director: Sandra Christie Job Title: Director of Quality
Patient Story Community Nursing/ Pressure Ulcers Agenda Item: 1 Reference: WCT14/15-096 Meeting Name: Trust Board Meeting Date: 4 August 2014 Lead Director: Sandra Christie Job Title: Director of Quality
Somerset Care Community (Taunton Deane)
") Somerset Care Limited Somerset Care Community (Taunton Deane) Inspection report Huish House Huish Close Taunton Somerset TA1 2EP Tel: 01823447120 Date of inspection visit: 11 January 2016 12 January 2016
Somerset Care Limited Somerset Care Community (Taunton Deane) Inspection report Huish House Huish Close Taunton Somerset TA1 2EP Tel: 01823447120 Date of inspection visit: 11 January 2016 12 January 2016
Newsletter Spring 2017
 Newsletter Spring 2017 Primary Care's important role in cancer services I m a GP, with a practice in Ebbw Vale and for the last few years I ve been involved with initiatives that look at the role of primary
Newsletter Spring 2017 Primary Care's important role in cancer services I m a GP, with a practice in Ebbw Vale and for the last few years I ve been involved with initiatives that look at the role of primary
Fordingbridge. Hearts At Home Care Limited. Overall rating for this service. Inspection report. Ratings. Requires Improvement
 Hearts At Home Care Limited Fordingbridge Inspection report 54 Avon Meade Fordingbridge Hampshire SP6 1QR Tel: 01425657329 Website: www.heartsathomecare.co.uk Date of inspection visit: 25 July 2017 26
Hearts At Home Care Limited Fordingbridge Inspection report 54 Avon Meade Fordingbridge Hampshire SP6 1QR Tel: 01425657329 Website: www.heartsathomecare.co.uk Date of inspection visit: 25 July 2017 26
A1 Home Care. A1 Home Care Ltd. Overall rating for this service. Inspection report. Ratings. Good
 A1 Home Care Ltd A1 Home Care Inspection report Units 16-19 Robjohns House, Navigation Road Chelmsford Essex CM2 6ND Date of inspection visit: 06 April 2017 Date of publication: 08 June 2017 Tel: 01245354774
A1 Home Care Ltd A1 Home Care Inspection report Units 16-19 Robjohns House, Navigation Road Chelmsford Essex CM2 6ND Date of inspection visit: 06 April 2017 Date of publication: 08 June 2017 Tel: 01245354774
Adult Practice Review Report
 Adult Practice Review Report North Wales Safeguarding Adults Board (NWSAB) Concise Adult Practice Review Re: APR2/2016/Conwy 1. Brief outline of circumstances resulting in the Review 1.1 Patient A died
Adult Practice Review Report North Wales Safeguarding Adults Board (NWSAB) Concise Adult Practice Review Re: APR2/2016/Conwy 1. Brief outline of circumstances resulting in the Review 1.1 Patient A died
NHS Borders Feedback and Complaints Annual Report
 NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
A concern means any complaint, claim or reported patient safety incident.
 PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
All Wales Fundamentals of Care Audit
 All Wales Fundamentals of Care Audit A summary of the NHS organisations compliance with the standards based on 2011 audit Author: Nursing Directorate, Welsh Government February 2012 i Digital ISBN 978
All Wales Fundamentals of Care Audit A summary of the NHS organisations compliance with the standards based on 2011 audit Author: Nursing Directorate, Welsh Government February 2012 i Digital ISBN 978
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
September Workforce pressures in the NHS
 September 2017 Workforce pressures in the NHS 2 Contents Foreword 3 Introduction and methodology 5 What professionals told us 6 The biggest workforce issues 7 The impact on professionals and people with
September 2017 Workforce pressures in the NHS 2 Contents Foreword 3 Introduction and methodology 5 What professionals told us 6 The biggest workforce issues 7 The impact on professionals and people with
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 1 st December 2010
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 1 st December 2010 Agenda Item: 9 Paper No: E Title: Management of Pressure Ulcers Purpose: For Information Summary: This paper provides a report on the
Story Street Walk-in Service
 Story Street Walk-in Service Service User Engagement www.hullccg.nhs.uk NHSHullCCG @NHSHullCCG Page 2 Story Street Walk-in Service Service User Engagement Introduction The Walk-in Service is based in the
Story Street Walk-in Service Service User Engagement www.hullccg.nhs.uk NHSHullCCG @NHSHullCCG Page 2 Story Street Walk-in Service Service User Engagement Introduction The Walk-in Service is based in the
National Cancer Patient Experience Survey National Results Summary
 National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
National Cancer Patient Experience Survey 2016 National Results Summary Index 4 Executive Summary 8 Methodology 9 Response rates and confidence intervals 10 Comparisons with previous years 11 This report
N/A 98.6% July - 31 July. Radiology Day Case Unit. Your recommend scores. Scores for all services (with > 4 reviews)
") Queen Alexandra Hospital Radiology Day Case Unit Date 01 July - 31 July Your recommend scores Average score for all questions 1 2 3 4 4.91 Reviews this period 69 Response rate N/A Star Score4.91 % Likely
Queen Alexandra Hospital Radiology Day Case Unit Date 01 July - 31 July Your recommend scores Average score for all questions 1 2 3 4 4.91 Reviews this period 69 Response rate N/A Star Score4.91 % Likely
Angel Care Tamworth Limited
 Angel Care Tamworth Limited Angel Care Tamworth Limited Inspection report Unit 4, Anker Court Bonehill Road Tamworth Staffordshire B78 3HP Date of inspection visit: 14 August 2017 Date of publication:
Angel Care Tamworth Limited Angel Care Tamworth Limited Inspection report Unit 4, Anker Court Bonehill Road Tamworth Staffordshire B78 3HP Date of inspection visit: 14 August 2017 Date of publication:
The investigation of a complaint by Mr D against Cwm Taf University Health Board. A report by the Public Services Ombudsman for Wales Case:
 The investigation of a complaint by Mr D against Cwm Taf University Health Board A report by the Public Services Ombudsman for Wales Case: 201604327 Contents Page Introduction 1 Summary 2 The complaint
The investigation of a complaint by Mr D against Cwm Taf University Health Board A report by the Public Services Ombudsman for Wales Case: 201604327 Contents Page Introduction 1 Summary 2 The complaint
Sheffield. Juventa 4 Care Ltd. Overall rating for this service. Inspection report. Ratings. Good
 Juventa 4 Care Ltd Sheffield Inspection report 26 Halsall Drive Sheffield South Yorkshire S9 4JD Tel: 07908635025 Date of inspection visit: 15 September 2017 18 September 2017 Date of publication: 11 October
Juventa 4 Care Ltd Sheffield Inspection report 26 Halsall Drive Sheffield South Yorkshire S9 4JD Tel: 07908635025 Date of inspection visit: 15 September 2017 18 September 2017 Date of publication: 11 October
Swindon Link Homecare
 Cleeve Hill Healthcare Limited Swindon Link Homecare Inspection report 41-51 Westlecott Road Old Town Swindon Wiltshire SN1 4EZ Date of inspection visit: 21 September 2016 Date of publication: 28 October
Cleeve Hill Healthcare Limited Swindon Link Homecare Inspection report 41-51 Westlecott Road Old Town Swindon Wiltshire SN1 4EZ Date of inspection visit: 21 September 2016 Date of publication: 28 October
Moorleigh Residential Care Home Limited
 Moorleigh Residential Care Home Limited Moorleigh Residential Care Home Inspection report Lummaton Cross, Barton, Torquay. TQ2 8ET Tel: 01803 326978 Website: Date of inspection visit: 14 April 2015 Date
Moorleigh Residential Care Home Limited Moorleigh Residential Care Home Inspection report Lummaton Cross, Barton, Torquay. TQ2 8ET Tel: 01803 326978 Website: Date of inspection visit: 14 April 2015 Date
Implementation of Quality Framework Update
 Joint Committee Meeting 26 January 2016 Title of the Committee Paper Framework Update Executive Lead: Director of Nursing & Quality Assurance Author: Director of Nursing & Quality Assurance Contact Details
Joint Committee Meeting 26 January 2016 Title of the Committee Paper Framework Update Executive Lead: Director of Nursing & Quality Assurance Author: Director of Nursing & Quality Assurance Contact Details
Root Cause Analysis for Pressure Ulceration This tool MUST be completed electronically paper copies will not be accepted.
 Root Cause Analysis for Pressure Ulceration This tool MUST be completed electronically paper copies will not be accepted. What is this for? This root cause analysis (RCA) tool is used when a patient acquires
Root Cause Analysis for Pressure Ulceration This tool MUST be completed electronically paper copies will not be accepted. What is this for? This root cause analysis (RCA) tool is used when a patient acquires
REPORT TO IMPROVING PATIENT EXPERIENCE COMMITTEE
 REPORT TO IMPROVING PATIENT EXPERIENCE COMMITTEE Date: Agenda No: 10 Date Paper produced: 25 th July 2014 Sponsoring Director (responsible for signing off report): Author: Paper Title: National Cancer
REPORT TO IMPROVING PATIENT EXPERIENCE COMMITTEE Date: Agenda No: 10 Date Paper produced: 25 th July 2014 Sponsoring Director (responsible for signing off report): Author: Paper Title: National Cancer
Milton Keynes University Hospital NHS Foundation Trust
 Milton Keynes University Hospital NHS Foundation Trust Enter and View Review of Staff/ Patient Communication Ward 17 and 18 September 2017 Contents Contents... 2 1 Introduction... 3 1.1 Details of the
Milton Keynes University Hospital NHS Foundation Trust Enter and View Review of Staff/ Patient Communication Ward 17 and 18 September 2017 Contents Contents... 2 1 Introduction... 3 1.1 Details of the
The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales.
 Welsh Affairs Committee. Purpose: The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales. Contact: Nesta Lloyd Jones, Policy and Public Affairs
Welsh Affairs Committee. Purpose: The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales. Contact: Nesta Lloyd Jones, Policy and Public Affairs
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Listening and Learning from Feedback. Framework for Assuring Service User Experience 2015???
 Listening and Learning from Feedback Framework for Assuring Service User Experience 2015 Introduction The Framework for Assuring Service User Experience has been updated to include the need to gain feedback
Listening and Learning from Feedback Framework for Assuring Service User Experience 2015 Introduction The Framework for Assuring Service User Experience has been updated to include the need to gain feedback
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Aneurin Bevan University Health Board Clinical Record Keeping Policy
 N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Guide to the Continuing NHS Healthcare Assessment Process
 Guide to the Continuing NHS Healthcare Assessment Process Continuing NHS Healthcare (CHC) is a package of care arranged and funded solely by the NHS, where it has been assessed that the person s primary
Guide to the Continuing NHS Healthcare Assessment Process Continuing NHS Healthcare (CHC) is a package of care arranged and funded solely by the NHS, where it has been assessed that the person s primary
Analysis of Continence Service In Teesside
 Analysis of Continence Service In Teesside Feedback September 2017 Introduction Local Healthwatches have been set up across England to create a strong, independent consumer champion with the aim to: Strengthen
Analysis of Continence Service In Teesside Feedback September 2017 Introduction Local Healthwatches have been set up across England to create a strong, independent consumer champion with the aim to: Strengthen
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
NHS Nottingham West CCG Latest survey results
 NHS Nottingham West Latest survey results 2017 publication Version 1 Public 1 Contents This slide pack provides results for the following topic areas: Background, introduction and guidance.... Slide 3
NHS Nottingham West Latest survey results 2017 publication Version 1 Public 1 Contents This slide pack provides results for the following topic areas: Background, introduction and guidance.... Slide 3
St Quentin Senior Living, Residential & Nursing Homes
 St. Quentin Residential Home Limited St Quentin Senior Living, Residential & Nursing Homes Inspection report Sandy Lane Newcastle Under Lyme Staffordshire ST5 0LZ Tel: 01782617056 Website: www.stquentin.org.uk
St. Quentin Residential Home Limited St Quentin Senior Living, Residential & Nursing Homes Inspection report Sandy Lane Newcastle Under Lyme Staffordshire ST5 0LZ Tel: 01782617056 Website: www.stquentin.org.uk
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014
 Agenda item 7(v) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014 1. INTRODUCTION AND OVERVIEW The Cancer Patient Experience Survey
Agenda item 7(v) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014 1. INTRODUCTION AND OVERVIEW The Cancer Patient Experience Survey
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Heart Homecare Ltd. Heart Homecare Ltd. Overall rating for this service. Inspection report. Ratings. Good
 Heart Homecare Ltd Heart Homecare Ltd Inspection report Unit G2 Wises Oast Business Centre Wises Lane Sittingbourne Kent ME9 8LR Date of inspection visit: 07 March 2017 Date of publication: 30 March 2017
Heart Homecare Ltd Heart Homecare Ltd Inspection report Unit G2 Wises Oast Business Centre Wises Lane Sittingbourne Kent ME9 8LR Date of inspection visit: 07 March 2017 Date of publication: 30 March 2017
Open and Honest Care in your Local Hospitals
 Open and Honest Care in your Local Hospitals The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospitals The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
AGENDA ITEM: JANUARY 2018 MENTAL HEALTH SERVICE REPATRIATION: PROJECT CLOSURE. Subject :
 AGENDA ITEM: 2.5 BOARD MEETING Subject : Approved and Presented by: Prepared by: Other Committees and meetings considered at: Considered by Executive Committee on: DATE OF MEETING: 31 JANUARY 2018 MENTAL
AGENDA ITEM: 2.5 BOARD MEETING Subject : Approved and Presented by: Prepared by: Other Committees and meetings considered at: Considered by Executive Committee on: DATE OF MEETING: 31 JANUARY 2018 MENTAL
Parliamentary and Health Service Ombudsman. Complaints about the NHS in England: Quarter
 Parliamentary and Health Service Ombudsman Complaints about the NHS in England: Quarter 1 2018-19 Contents Our role 3 The purpose of this report 3 Our data 3 Our process 3 Step one: initial checks 4 Step
Parliamentary and Health Service Ombudsman Complaints about the NHS in England: Quarter 1 2018-19 Contents Our role 3 The purpose of this report 3 Our data 3 Our process 3 Step one: initial checks 4 Step
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
REPORT ON LOCAL PATIENTS PARTICIPATION FOR THE COURTLAND SURGERY ILFORD
 REPORT ON LOCAL PATIENTS PARTICIPATION FOR THE COURTLAND SURGERY ILFORD February 2012 Local Participation Report 1 Background Patients Reference Group Following the guidance by Primary Medical Services
REPORT ON LOCAL PATIENTS PARTICIPATION FOR THE COURTLAND SURGERY ILFORD February 2012 Local Participation Report 1 Background Patients Reference Group Following the guidance by Primary Medical Services
Sanctuary Home Care Ltd - Enfield
 Sanctuary Home Care Limited Sanctuary Home Care Ltd - Enfield Inspection report Skinners Court 1 Pellipar Close, Enfield London N13 4AE Tel: 02084478668 Date of inspection visit: 21 April 2017 Date of
Sanctuary Home Care Limited Sanctuary Home Care Ltd - Enfield Inspection report Skinners Court 1 Pellipar Close, Enfield London N13 4AE Tel: 02084478668 Date of inspection visit: 21 April 2017 Date of
BOARD OF DIRECTORS PAPER COVER SHEET. Meeting Date: 27 May 2009
 BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 27 May 2009 Agenda Item: 9 Paper No: F Title: PATIENT SURVEY 2008 BENCHMARK REPORT Purpose: To present the Care Quality Commission benchmarking report
BOARD OF DIRECTORS PAPER COVER SHEET Meeting Date: 27 May 2009 Agenda Item: 9 Paper No: F Title: PATIENT SURVEY 2008 BENCHMARK REPORT Purpose: To present the Care Quality Commission benchmarking report
Patient Experience Report Tissue Viability
 Patient Experience Report Tissue Viability August 2015 Making a difference. Demonstrating Effectiveness of care. Nine patient s experience:- staff fantastic could not have been treated any better, thank
Patient Experience Report Tissue Viability August 2015 Making a difference. Demonstrating Effectiveness of care. Nine patient s experience:- staff fantastic could not have been treated any better, thank
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
An investigation into Lower Leg Ulceration in Northern Ireland
 An investigation into Lower Leg Ulceration in Northern Ireland March 13 Contents Foreword List of Tables List of Figures Page number iii iv v-vi Introduction to Audit 1 Aim 2 Objectives 2 Audit Methodology
An investigation into Lower Leg Ulceration in Northern Ireland March 13 Contents Foreword List of Tables List of Figures Page number iii iv v-vi Introduction to Audit 1 Aim 2 Objectives 2 Audit Methodology
Patient survey report National children's inpatient and day case survey 2014 The Mid Yorkshire Hospitals NHS Trust
 Patient survey report 2014 National children's inpatient and day case survey 2014 National NHS patient survey programme National children's inpatient and day case survey 2014 The Care Quality Commission
Patient survey report 2014 National children's inpatient and day case survey 2014 National NHS patient survey programme National children's inpatient and day case survey 2014 The Care Quality Commission
THE PAPER IS ALIGNED TO THE DELIVERY OF THE FOLLOWING STRATEGIC OBJECTIVE(S) AND HEALTH AND CARE STANDARD(S):
 AND HEALTH AND CARE STANDARD(S):") AGENDA ITEM: 4.1 MENTAL HEALTH AND LEARNING DISABILITIES COMMITTEE DATE OF MEETING: 29 JANUARY 2018 Subject : REPATRIATION PROJECT Approved and Alan Lawrie, Director of Primary and Community Presented
AGENDA ITEM: 4.1 MENTAL HEALTH AND LEARNING DISABILITIES COMMITTEE DATE OF MEETING: 29 JANUARY 2018 Subject : REPATRIATION PROJECT Approved and Alan Lawrie, Director of Primary and Community Presented
Orchard Home Care Services Limited
 Orchard Home Care Services Limited Orchard Home Care Inspection report 2 Ashfield Terrace Chester-le-street County Durham DH3 3PD Tel: 0191 389 0072 Website: www.cqc.org.uk Date of inspection visit: 12
Orchard Home Care Services Limited Orchard Home Care Inspection report 2 Ashfield Terrace Chester-le-street County Durham DH3 3PD Tel: 0191 389 0072 Website: www.cqc.org.uk Date of inspection visit: 12
NHS Rushcliffe CCG Latest survey results
 R/GB/17/195 NHS Rushcliffe Latest survey results 2017 publication Version 1 Public 1 Contents This slide pack provides results for the following topic areas: Background, introduction and guidance.... Slide
R/GB/17/195 NHS Rushcliffe Latest survey results 2017 publication Version 1 Public 1 Contents This slide pack provides results for the following topic areas: Background, introduction and guidance.... Slide
cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL GOVERNANCE STATEMENT 2015/16
 EASC Agenda Item 4.5 Appendix 1 To: Mrs Allison Williams, Chief Executive, Cwm Taf University Health Board cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL
EASC Agenda Item 4.5 Appendix 1 To: Mrs Allison Williams, Chief Executive, Cwm Taf University Health Board cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Marie Curie Hospice Liverpool Speke Road, Woolton, Liverpool,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Marie Curie Hospice Liverpool Speke Road, Woolton, Liverpool,
VELINDRE NHS TRUST PUBLIC TRUST BOARD REPORT. Procurement Services. Andy Butler, Director of Finance, NWSSP
 VELINDRE NHS TRUST PUBLIC TRUST BOARD REPORT Meeting Date: 24 th September 2015 Agenda Item: 2.5 Report Author: Executive Sponsor: Presented by: Matthew Perrott, Senior Category Manager, NWSSP Procurement
VELINDRE NHS TRUST PUBLIC TRUST BOARD REPORT Meeting Date: 24 th September 2015 Agenda Item: 2.5 Report Author: Executive Sponsor: Presented by: Matthew Perrott, Senior Category Manager, NWSSP Procurement
Open and Honest Care in your Local NHS Trust
 Open and Honest Care in your Local NHS Trust The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local NHS Trust The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Essential Nursing and Care Services
 Essential Nursing & Care Services Ltd Essential Nursing and Care Services Inspection report Unit 7 Concept Park, Innovation Close Poole Dorset BH12 4QT Date of inspection visit: 09 February 2016 10 February
Essential Nursing & Care Services Ltd Essential Nursing and Care Services Inspection report Unit 7 Concept Park, Innovation Close Poole Dorset BH12 4QT Date of inspection visit: 09 February 2016 10 February
Contents. Contents. Executive Summary page 2. 1 Introduction page 3. 2 Background information page 4. 3 What we did page 7. 4 What we found out page 8
 Wexham Park Hospital Patient Discharge Report Consumer October 2014 Contents Contents Executive Summary page 2 1 Introduction page 3 2 Background information page 4 3 What we did page 7 4 What we found
Wexham Park Hospital Patient Discharge Report Consumer October 2014 Contents Contents Executive Summary page 2 1 Introduction page 3 2 Background information page 4 3 What we did page 7 4 What we found
NHS HIGHLAND. Significant Event Report
 ` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
The developing role of the nurse in wound management: Research. Prof Sue Bale OBE
 The developing role of the nurse in wound management: Research Prof Sue Bale OBE Background I qualified in 1978 (RGN, NDN Part1 Obs) Graduated from Newcastle upon Tyne Polytechnic the in last cohort of
The developing role of the nurse in wound management: Research Prof Sue Bale OBE Background I qualified in 1978 (RGN, NDN Part1 Obs) Graduated from Newcastle upon Tyne Polytechnic the in last cohort of
Supporting people who need Palliative and End of Life Care in the Community. Giving people a choice
 Supporting people who need Palliative and End of Life Care in the Community Giving people a choice Introduction People who are terminally ill or at the end of their life need excellent nursing and medical
Supporting people who need Palliative and End of Life Care in the Community Giving people a choice Introduction People who are terminally ill or at the end of their life need excellent nursing and medical
Monitoring the Mental Health Act 2015/16 SUMMARY
 Monitoring the Mental Health Act 2015/16 SUMMARY Foreword The work of monitoring the Mental Health Act 1983 (MHA) is a distinct but supportive role to CQC s wider regulatory task. It is distinct, in part,
Monitoring the Mental Health Act 2015/16 SUMMARY Foreword The work of monitoring the Mental Health Act 1983 (MHA) is a distinct but supportive role to CQC s wider regulatory task. It is distinct, in part,
106,717 people accessed mental health. 192,192 access A&E. 1,011,942 patient contacts with community staff. 2,245,439 patient contacts
 Employs 15,285 2,245,439 patient contacts 192,192 Assisted 91,360 Dispensed 13,598,605 prescription items** 38,107 1,011,942 patient contacts with Across 11 clusters, 540,850 people are registered with
Employs 15,285 2,245,439 patient contacts 192,192 Assisted 91,360 Dispensed 13,598,605 prescription items** 38,107 1,011,942 patient contacts with Across 11 clusters, 540,850 people are registered with
Appendix Five Decision Pathway Pressure Ulcers and safeguarding Adults (A3 format)
") Appendix Five Decision Pathway Pressure Ulcers and safeguarding Adults (A3 format) Pressure ulcer is observed. Concern is raised that a person has significant skin damage. Category / Grade 3 and 4 or Multiple
Appendix Five Decision Pathway Pressure Ulcers and safeguarding Adults (A3 format) Pressure ulcer is observed. Concern is raised that a person has significant skin damage. Category / Grade 3 and 4 or Multiple
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Independent investigation into the death of Mr David Adkins a prisoner at HMP Whatton on 14 September 2016
 Independent investigation into the death of Mr David Adkins a prisoner at HMP Whatton on 14 September 2016 Crown copyright 2015 This publication is licensed under the terms of the Open Government Licence
Independent investigation into the death of Mr David Adkins a prisoner at HMP Whatton on 14 September 2016 Crown copyright 2015 This publication is licensed under the terms of the Open Government Licence
Continuing NHS Healthcare for Adults in Wales. Preparing you for a CHC Eligibility Meeting
 Continuing NHS Healthcare for Adults in Wales Preparing you for a CHC Eligibility Meeting August 2016 Mae r ddogfen yma hefyd ar gael yn Gymraeg. This document is also available in Welsh. Crown copyright
Continuing NHS Healthcare for Adults in Wales Preparing you for a CHC Eligibility Meeting August 2016 Mae r ddogfen yma hefyd ar gael yn Gymraeg. This document is also available in Welsh. Crown copyright
Care Bundle Wound Care Guidance
 Care Bundle Wound Care Guidance A wound may be defined as a break in the structure of an organ or tissue caused by an external agent; for example, a bruise, cut, or burn (Oxford Living Dictionaries, 2017).
Care Bundle Wound Care Guidance A wound may be defined as a break in the structure of an organ or tissue caused by an external agent; for example, a bruise, cut, or burn (Oxford Living Dictionaries, 2017).
Julia Galliers and Stephanie Wilson, CHCID, City University London, UK
 DATA GATHERING FOR THE SAFER HANDOVER PROJECT Julia Galliers and Stephanie Wilson, CHCID, City University London, UK Introduction The terminology issue Introduction The Safer Handover project was initiated
DATA GATHERING FOR THE SAFER HANDOVER PROJECT Julia Galliers and Stephanie Wilson, CHCID, City University London, UK Introduction The terminology issue Introduction The Safer Handover project was initiated
Tissue Viability Referral Pathway. April 2017
 Tissue Viability Referral Pathway V4 April 2017 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities...
Tissue Viability Referral Pathway V4 April 2017 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities...
ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS. To approve. This paper supports the standards
 BOARD MEETING 25 FEBRUARY 2015 AGENDA ITEM 2.1 ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS Report of Paper prepared by Purpose of Paper Action/Decision required Link to Doing Well, Doing Better: Standards
BOARD MEETING 25 FEBRUARY 2015 AGENDA ITEM 2.1 ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS Report of Paper prepared by Purpose of Paper Action/Decision required Link to Doing Well, Doing Better: Standards
Mel McEvoy, Nurse Consultant in Palliative Care 12 th January 2013
 Family s Voice improving communication during end of life care. Trust Member Event Mel McEvoy, Nurse Consultant in Palliative Care 12 th January 2013 Overview Making a difference Results from the year
Family s Voice improving communication during end of life care. Trust Member Event Mel McEvoy, Nurse Consultant in Palliative Care 12 th January 2013 Overview Making a difference Results from the year
Marie Curie Nursing Service - Care at Home Support Service Care at Home Marie Curie Hospice - Glasgow 133 Balornock Road Stobhill Hospital Grounds
 Marie Curie Nursing Service - Care at Home Support Service Care at Home Marie Curie Hospice - Glasgow 133 Balornock Road Stobhill Hospital Grounds Springburn Glasgow G21 3US Telephone: 0141 531 1355 Inspected
Marie Curie Nursing Service - Care at Home Support Service Care at Home Marie Curie Hospice - Glasgow 133 Balornock Road Stobhill Hospital Grounds Springburn Glasgow G21 3US Telephone: 0141 531 1355 Inspected
Executive Summary 10 th September Dr. Richard Wagland. Dr. Mike Bracher. Dr. Ana Ibanez Esqueda. Professor Penny Schofield
 Experiences of Care of Patients with Cancer of Unknown Primary (CUP): Analysis of the 2010, 2011-12 & 2013 Cancer Patient Experience Survey (CPES) England. Executive Summary 10 th September 2015 Dr. Richard
Experiences of Care of Patients with Cancer of Unknown Primary (CUP): Analysis of the 2010, 2011-12 & 2013 Cancer Patient Experience Survey (CPES) England. Executive Summary 10 th September 2015 Dr. Richard
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Interserve Healthcare Liverpool
 Interserve Healthcare Limited Interserve Healthcare Liverpool Inspection report 2nd Floor, Cunard Building Water Street Liverpool Merseyside L3 1EL Date of inspection visit: 08 August 2017 Date of publication:
Interserve Healthcare Limited Interserve Healthcare Liverpool Inspection report 2nd Floor, Cunard Building Water Street Liverpool Merseyside L3 1EL Date of inspection visit: 08 August 2017 Date of publication:
National Cancer Patient Experience Survey National Results Summary
 National Cancer Patient Experience Survey 2015 National Results Summary Introduction As in previous years, we are hugely grateful to the tens of thousands of cancer patients who responded to this survey,
National Cancer Patient Experience Survey 2015 National Results Summary Introduction As in previous years, we are hugely grateful to the tens of thousands of cancer patients who responded to this survey,
NHS Kingston CCG Latest survey results
 NHS Kingston Latest survey results 2017 publication Version 1 Public 1 Contents This slide pack provides results for the following topic areas: Background, introduction and guidance.... Slide 3 Overall
NHS Kingston Latest survey results 2017 publication Version 1 Public 1 Contents This slide pack provides results for the following topic areas: Background, introduction and guidance.... Slide 3 Overall
Renacres Hall Hospital Patient Engagement Report
 Renacres Hall Hospital Patient Engagement Report Report summarising feedback from Patient Engagement activities between 5th November 2015 and 30th March 2016. V.2.3 V1.3 Introduction Healthwatch Lancashire
Renacres Hall Hospital Patient Engagement Report Report summarising feedback from Patient Engagement activities between 5th November 2015 and 30th March 2016. V.2.3 V1.3 Introduction Healthwatch Lancashire
Reducing Avoidable Heel Pressure Ulcers through education/active monitoring
 Reducing Avoidable Heel Pressure Ulcers through education/active monitoring United Lincolnshire Hospitals NHS Trust Mark Collier, Lead Nurse - Tissue Viability United Lincolnshire Hospitals NHS Trust mark.collier@ulh.nhs.uk
Reducing Avoidable Heel Pressure Ulcers through education/active monitoring United Lincolnshire Hospitals NHS Trust Mark Collier, Lead Nurse - Tissue Viability United Lincolnshire Hospitals NHS Trust mark.collier@ulh.nhs.uk
Appendix 5. Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures
 Appendix 5 Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to
Appendix 5 Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to
Pressure ulcers: revised definition and measurement. Summary and recommendations
 Pressure ulcers: revised definition and measurement Summary and recommendations June 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that are
Pressure ulcers: revised definition and measurement Summary and recommendations June 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that are
Radis Community Care (Nottingham)
") G P Homecare Limited Radis Community Care (Nottingham) Inspection report 12A Chilwell Road Beeston Nottingham Nottinghamshire NG9 1EJ Date of inspection visit: 08 August 2017 Date of publication: 14 September
G P Homecare Limited Radis Community Care (Nottingham) Inspection report 12A Chilwell Road Beeston Nottingham Nottinghamshire NG9 1EJ Date of inspection visit: 08 August 2017 Date of publication: 14 September
Toolbox Talks. Access
 Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that