2/13/2018. Enhanced Recovery after Surgery (ERAS) in Gynecology
|
|
|
- Osborne Wheeler
- 6 years ago
- Views:
Transcription
1 Enhanced Recovery after Surgery (ERAS) in Gynecology J. Michael Straughn, Jr., MD Professor, Gynecologic Oncology University of Alabama at Birmingham Outline What is Enhanced Recovery after Surgery (ERAS)? Implementing an ERAS program for your patients Preoperative education Perioperative management Postoperative optimization Outcomes Others and UAB experience Page 2 Enhanced Recovery After Surgery (ERAS) Collection of best anesthesia and surgical practices bundled into a coordinated care pathway that benefits the patient and hospital by reducing length of stay, complications, readmissions, and cost Pathways have been successful in several surgical specialties Basse et al, patients undergoing colorectal surgery LOS 2 days Benefits are achieved by decreasing stress, maintaining normal physiologic function, and enhancing early mobilization Patients benefit from a multi-disciplinary approach to surgical care Page 3 1


2 Page 4 The ERAS Society was created in The mission of the ERAS Society To develop perioperative care To improve recovery through research, education, audit and implementation of evidence-based practice In 2005, the ERAS Study Group developed and published an evidencebased consensus protocol for patients undergoing colorectal surgery Page 5 Page 6 2
3 Page 7 Kalogera E, et al. Enhanced recovery in gynecologic surgery. Obstet Gynecol 2013;122: Retrospective cohort study at the Mayo Clinic Included cytoreductive surgery, staging, and prolapse surgery Historical control (241) vs. ERAS pathway (235) Cytoreductive cohort (81 vs. 78 patients) Less narcotic use in 48 hrs (80% reduction) with similar pain scores More nausea but no increase in ileus Decreased LOS (10 vs. 6 days), similar readmission rates (25.9% vs. 17.9%), and similar complication rates (63% vs. 72%) Page 8 Nelson G, et al. Enhanced recovery pathways in gynecologic oncology. Gynecol Oncol 2014;135: Systematic literature search on PubMed ERAS Society was contacted to identify any unpublished protocols 7 studies that examined the role of ERAS in gynecologic oncology patients No randomized control trials Page 9 3
4 Nelson G, et al. Enhanced recovery pathways in gynecologic oncology. Gynecol Oncol 2014;135: Common interventions included: Oral intake of fluids up to 2 hours before anesthesia Solids up to 6 hours before anesthesia Carbohydrate supplementation Intra- and postoperative euvolemia Aggressive nausea/vomiting prophylaxis Oral nutrition and ambulation the day of surgery Page 10 Nelson G, et al. Enhanced recovery pathways in gynecologic oncology. Gynecol Oncol 2014;135: Bowel preparations, NPO after midnight rule, nasogastric tubes, and intravenous opioids were discontinued Significant improvements in patient satisfaction, length of stay, and cost were observed in ERAS cohorts compared to historical controls Morbidity, mortality, and readmission rates were similar between groups Page 11 Nelson G, et al. Enhanced recovery pathways in gynecologic oncology. Gynecol Oncol 2014;135: ERAS is a safe perioperative management strategy for patients undergoing surgery for gynecologic malignancies ERAS reduces length of stay and cost, and is considered standard of care at a growing number of institutions There is a need for formalized evidence-based guidelines for patients with gynecologic cancer undergoing surgery Page 12 4
5 2 part evidence-based guidelines for Gynecologic Oncology published in 2016 Nelson G, et al. Guidelines for pre- and intra-operative care in gynecologic oncology surgery: ERAS Society recommendations Part I. Gynecol Oncol 2016;140: Nelson G, et al., Guidelines for postoperative care in gynecologic oncology surgery: ERAS Society recommendations - Part II. Gynecol Oncol 2016;140: Page 13 Implementing an ERAS program for your patients What is UAB care? Hospital wide-initiative focused on optimizing care for specific conditions and ensuring that redefined standards are applied Goals Improve quality of care Reduce variation Control cost Initiated ERAS programs for colorectal and urology Page 14 Implementing an ERAS program for your patients Implementation team and ERAS champion MDs (surgeons and anesthesia), nursing, administration, informatics Project goals Protocol development Leading Practice Guidelines (LPGs) Team STAFF, CLINIC, OR, PACT, PREOP, POSTOP Audit database to evaluate compliance and outcomes Page 15 5
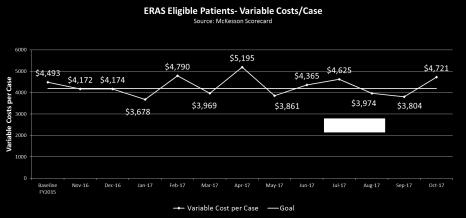
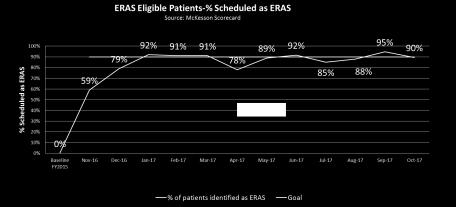
 Goal (FY 17 Q1) Average O/E LOS Index 1.07 0.95 Readmission % 6.71% 6.0% % of patients identified as ERAS 0% 90% SSI % 2.2% 1.")
6 18 Weeks 2/13/2018 Project Goals The ERAS pathway will address areas where there is room for improvement such as length of stay, variable cost per case, readmissions, and infections Current Performance (FY 15) Goal (FY 17 Q1) Average O/E LOS Index Readmission % 6.71% 6.0% % of patients identified as ERAS 0% 90% SSI % 2.2% 1.0% Variable cost per case $4,493 $4,200 Page 16 Dashboard Page 17 Protocol Development Discovery Assessment Process observation, staff interviews, data analysis, stakeholder feedback Work with administrative, physician, and nurse leaders to finalize project charter, develop LPGs, and ensure consensus Rapid Redesign Session 7/2016 Create Leading Practice Guidelines (LPGs) Develop Key Initiatives (KIs) First Implementation Meeting 9/2016 Assign key initiative teams Implementation Meetings Meet every two weeks to provide KI team updates Key Initiative (KI) Team Meetings Meet independently to implement solutions to achieve KI goals Educate Staff and Stakeholders Celebration and Project Closure 11/2016 Page 18 6

7 Protocol Development Page 19 Preoperative Education All patients with a planned laparotomy or hysterectomy are eligible for ERAS Transferred patients or those admitted from the ED can be enrolled as inpatients The surgeon introduces the ERAS concept followed by the clinic nurse reviewing the education booklet Teach Back method Surgery scheduled using the Anesthesia Type ERAS + General Intrathecal morphine Page 20 Preoperative Education Patients are enrolled into Emmi to view educational videos before surgery Patients with suspected malnutrition are started on Ensure TID until surgery The PACT appointment is scheduled at least 7 days prior to surgery No solid food after midnight Continue oral hydration with clear liquids up to 2 hours before surgery (arrival to hospital) Carbohydrate load with 400 ml Powerade or Gatorade 2 hours before surgery Page 21 7


8 Preoperative Education Page 22 Preoperative Education Page 23 Perioperative Management Patient is identified as ERAS at PACT Routine patient processing is done Medication reconciliation, medical interview, labs Patient education booklet/information is provided CHG bath instructions Regular diet until midnight Clear liquids until 2 hours before surgery Gatorade/Powerade AM of surgery (carbohydrate loading) Page 24 8
9 Perioperative Management Consent is obtained for intrathecal anesthesia and patient education questions are answered by a physician Patient role in recovery is reinforced Decreased narcotic use Early feeding Early ambulation Page 25 Perioperative Management Multimodal analgesic regimen is given prior to surgery Tylenol, Celebrex, Gabapentin Intrathecal injection recommended TAP (transverse abdominis plane) block PCA pump if not a candidate for intrathecal Intraoperative - Lidocaine infusion, Dexamethasone, Propofol Multimodal postoperative nausea/vomiting prophylaxis Page 26 Perioperative Management Intraoperative fluids Goal directed fluid management to maintain cardiac output while avoiding postoperative volume overload 800 cc/hour Limit crystalloid albumin for bolus if MAP < 60 mmhg Avoidance of normal saline LR or Plasmalyte Wound closure trays and change of gloves required Alexus wound protector for all planned bowel cases OR debriefing required Page 27 9
10 Complications 2/13/2018 Perioperative Management Hypoperfusion Organ dysfunction Adverse outcome Edema Organ dysfunction Adverse outcome OPTIMAL Hypovolemic Overloaded Volume Load Page 28 Perioperative Management ERAS Gyn Oncology PowerPlan Includes PACU and Post-op components Limited usage of narcotics in PACU Ice chips in PACU Initiate LR at 40 cc/hr If hypotensive, can give 250 cc bolus of LR or 5% albumin Page 29 Postoperative Optimization Day of Surgery Clears and advance as tolerated Out of bed 2 hours LR at 40 cc/hr POD 1 Regular diet with Ensure DC foley and IVFs by 0800 Out of bed 8 hrs staff to document activity Hemoglobin in AM with other labs as indicated Chewing gum recommended Page 30 10
11 Postoperative Optimization Multimodal Pain Control Acetaminophen 975 mg, Oral, Every 6 hours (scheduled) Oxycodone regular release (*24 hours after intrathecal) 2.5 mg, Oral, Every 4 hours, PRN Pain, Mild 5 mg, Oral, Every 4 hours, PRN Pain, Moderate 10 mg, Oral, Every 4 hours, PRN Pain, Severe Hydromorphone 0.4 mg, IV, Every 1 hour, PRN breakthrough pain Only if pain score >7 more than 1 hour after receiving oxycodone Notify MD if 2 doses required Page 31 Postoperative Optimization Based on age and weight of patient Ketorolac: mg, IV, Every 6 hours x 4 doses. Start 12 hours after preoperative Celebrex dose. Ibuprofen: mg, Oral, Every 6 hours. Start 6 hours after last dose of ketorolac If GFR <60 or patient unable to take NSAIDs for other reasons Tramadol: 100 mg, Oral, Every 6 hours. Begin on morning of POD1. For patients <65. Tramadol: 100 mg, Oral, Every 12 hours. Begin on morning of POD1. For patients >65 or with Cr clearance <30 ml/min Page 32 Postoperative Optimization Discharge planning starts on POD1 Documentation of daily weights, shower, and ambulation Discharge when tolerating diet, voiding, and adequate pain control Assess the need for narcotic prescription Lovenox for 21 days if cancer diagnosis or high risk Automated phone call with 72 hours of discharge Postop visit within 28 days Page 33 11
12 Outcomes Modesitt SS et al. Enhanced Recovery Implementation in Major Gynecologic Surgeries: Effect of Care Standardization. Obstet Gynecol 2016;128(3): Two ERAS protocols were developed Full pathway using regional anesthesia for open procedures Light pathway without regional anesthesia for vaginal and MIS Usual ERAS pathways A before-and-after study design compared clinical outcomes, costs, and patient satisfaction Page 34 Outcomes Modesitt SS et al. Enhanced Recovery Implementation in Major Gynecologic Surgeries: Effect of Care Standardization. Obstet Gynecol 2016;128(3): ERAS full protocol 136 patients compared with 211 historical controls Median LOS was reduced (2.0 vs. 3.0 days; P=.007) Reductions were seen in median intraoperative morphine equivalents (0.3 vs mg; P<.001) Immediate postoperative pain scores (3.7 vs. 5.0; P<.001) Total complications (21.3% vs. 40.2%; P=.004) Page 35 Outcomes Modesitt SS et al. Enhanced Recovery Implementation in Major Gynecologic Surgeries: Effect of Care Standardization. Obstet Gynecol 2016;128(3): ERAS light protocol 249 patients compared with 324 historical controls Decreased intraoperative morphine equivalents (0.0 vs mg; P<.001) and postoperative (15.0 vs mg; P<.001) 30-day hospital costs were significantly decreased in both ERAS groups $11,172 vs. $9,899; P<.001 $8,277 vs. $7,606; P<.001 Page 36 12
13 Outcomes Modesitt SS et al. Enhanced Recovery Implementation in Major Gynecologic Surgeries: Effect of Care Standardization. Obstet Gynecol 2016;128(3): Implementation of ERAS protocols in gynecologic surgery was associated with a substantial decrease in morphine administration, reduction in length of stay for open procedures, improved patient satisfaction and decreased hospital costs Page 37 Outcomes Dickson EL et al. Enhanced Recovery Program and Length of Stay After Laparotomy on a Gynecologic Oncology Service: A Randomized Controlled Trial. Obstet Gynecol 2017;129(2): Prospective, randomized, controlled trial comparing ERAS protocol with routine postoperative care among women undergoing laparotomy on the gynecologic oncology service A sample size of 50 per group was planned to achieve 80% power to detect a two-day difference in LOS 103 eligible patients were enrolled between 2013 and in the control group and 51 in the ERAS group Page 38 Outcomes Dickson EL et al. Enhanced Recovery Program and Length of Stay After Laparotomy on a Gynecologic Oncology Service: A Randomized Controlled Trial. Obstet Gynecol 2017;129(2): There was no difference in LOS between the two groups Median 3.0 days in both groups; P=.36 ERAS patients used less narcotics on day 0 (10.0 vs. 5.5 morphine equivalents; P=.09) and day 2 (10.0 vs 7.5 morphine equivalents; P=.05) No difference in ambulation, GI issues, complications, or readmissions Page 39 13


14 Outcomes Dickson EL et al. Enhanced Recovery Program and Length of Stay After Laparotomy on a Gynecologic Oncology Service: A Randomized Controlled Trial. Obstet Gynecol 2017;129(2): When compared with usual care, introducing a formal ERAS protocol did not significantly reduce LOS Of note, the historical LOS was 5 days Issues Few ERAS elements implemented, compliance not measured, use of ERAS tenets in the control arm Was this a poorly developed RCT? Page 40 UAB Outcomes Audit database to evaluate compliance and outcomes McKesson and Tableau Allison Todd, RN Quarterly ERAS meetings UAB Gynecologic Oncology Service Enrollment started November patients enrolled thru December 2017 UAB Gynecology Service Enrollment started December 2017 Page 41 UAB Outcomes Page 42 14



15 UAB Outcomes Page 43 UAB Outcomes Page 44 UAB Outcomes Page 45 15
16 UAB Outcomes Page 46 UAB Outcomes Page 47 UAB Outcomes Page 48 16
17 UAB Study Retrospective cohort study at UAB Gynecologic oncology patients undergoing elective laparotomy from 10/2016 6/2017 Managed on an ERAS protocol and a control group from the year prior to ERAS implementation Patients taking daily opioids prior to surgery were classified as chronic narcotic users and compared to non-narcotic users 376 patients were identified 197 in the control cohort and 179 in the ERAS cohort Smith HJ et al. SGO Annual Meeting, March 2018 Page 49 UAB Study Rates of chronic narcotic use were similar between cohorts 20.3% vs. 19.0%; p=0.75 In the ERAS cohort, chronic narcotic users required significantly more opioids at discharge (1,940 vs. 533 mg OME; p=0.002) They were also more likely to require additional narcotic prescriptions within 30 days of discharge 29.4% vs. 7.6%; p<0.001 Page 50 UAB Study LOS and readmission rates were similar in chronic narcotic users versus non-narcotic users There was no difference in postoperative pain score in chronic narcotic users in the ERAS cohort compared to control cohort (2.8 vs. 3.1; p=0.52), and no reduction in the amount of opioids prescribed at discharge (3,909 vs. 3,276 mg OME; p=0.61) In non-narcotic users, both postoperative pain scores (1.8 vs. 2.5; p<0.001) and the amount of opioids prescribed at discharge (1,940 vs. 2,610 mg OME; p<0.001) were significantly reduced with ERAS Page 51 17
18 UAB Study Implementation of ERAS improves pain control and decreases the amount of opioids prescribed at discharge in narcotic naïve gynecologic oncology patients. ERAS does not significantly improve postoperative pain control or decrease opioid use in chronic narcotic users. ERAS does decrease LOS. Page 52 Conclusions Nelson G et al. Enhanced recovery after surgery (ERAS ) in gynecologic oncology - Practical considerations for program development. Gynecol Oncol. 2017;147(3): Develop a multidisciplinary team and have a champion for the project Develop your ERAS protocol using the published guidelines Audit the program using a database to measure compliance and outcomes LOS, readmissions, complications Page 53 Acknowledgements UAB Care Anisa Xhaja, MHA, MSHQS Meredith Palmer, MSN, RN, CNL Jadwiga Wartak, MSHA Ben Taylor, MD ERAS Champions Dan Chu, MD Jeff Simmons, MD PACU Prentiss Lawson, MD Amanda Chambers, RN GYN Oncology Warner Huh, MD Charles A. Leath, MD Haller Smith, MD Danny Mounir, MD Bethany Fees, CRNP Clinic Terrell Halcomb, RN Carissa Purvis, RN Jennifer Kelley, RN OR Marquilla Brooks, RN Page 54 18
19 References Nelson G et al. Enhanced recovery after surgery (ERAS ) in gynecologic oncology - Practical considerations for program development. Gynecol Oncol. 2017;147(3): Nelson G et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: Enhanced Recovery After Surgery (ERAS ) Society recommendations Part I. Gynecol Oncol. 2016;140(2): Nelson G et al. Guidelines for postoperative care in gynecologic/oncology surgery: Enhanced Recovery After Surgery (ERAS ) Society recommendations - Part II. Gynecol Oncol. 2016;140(2): Miralpeix E et al. A call for new standard of care in perioperative gynecologic oncology practice: Impact of enhanced recovery after surgery (ERAS) programs. Gynecol Oncol. 2016;141(2): Nelson G et al. Enhanced recovery pathways in gynecologic oncology. Gynecol Oncol. 2014;135(3): Page 55 19
Enhanced Recovery After Surgery in OB/GYN
 Enhanced Recovery After Surgery in OB/GYN Audra Williams, MD Ashley Wright, MD University of Alabama at Birmingham Department of OB/GYN Women s Reproductive Healthcare Division Outline Brief background
Enhanced Recovery After Surgery in OB/GYN Audra Williams, MD Ashley Wright, MD University of Alabama at Birmingham Department of OB/GYN Women s Reproductive Healthcare Division Outline Brief background
9/29/2017. Enhanced Recovery After Surgery at the University of Virginia Medical Center. Disclosures. Objectives. None
 Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Creating Clinical Pathways
 Creating Clinical Pathways Michael Stifelman, MD Professor and Chairman of Urology Director, Urologic Oncology & Courtney DiBona, MSN, RN-BC Nurse Manager: Urology Why create clinical pathways? Institute
Creating Clinical Pathways Michael Stifelman, MD Professor and Chairman of Urology Director, Urologic Oncology & Courtney DiBona, MSN, RN-BC Nurse Manager: Urology Why create clinical pathways? Institute
Enhanced Recovery Implementing Meaningful Change
 Enhanced Recovery Implementing Meaningful Change Jeff Simmons MD Associate Professor UAB Department of Anesthesiology and Perioperative Medicine I have no relevant financial relationships to disclose.
Enhanced Recovery Implementing Meaningful Change Jeff Simmons MD Associate Professor UAB Department of Anesthesiology and Perioperative Medicine I have no relevant financial relationships to disclose.
Quality Improvement Initiative (QII): 2018 Options
: 2018 Options") Quality Improvement Implementation, Option A: Increase Surgeon Engagement Outcome Measure: SSI Summary: Surgeon Engagement is essential for the success of quality improvement programs within hospitals.
Quality Improvement Implementation, Option A: Increase Surgeon Engagement Outcome Measure: SSI Summary: Surgeon Engagement is essential for the success of quality improvement programs within hospitals.
Post-operative "Fast-Track" pathways for lung resection. Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic
 Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
Enhanced Recovery in NSQIP (ERIN): an update on the collaborative. Julie Thacker, LianeFeldman, and Julia Berian ACS NSQIP National Conference 2015
: an update on the collaborative. Julie Thacker, LianeFeldman, and Julia Berian ACS NSQIP National Conference 2015") Enhanced Recovery in NSQIP (ERIN): an update on the collaborative Julie Thacker, LianeFeldman, and Julia Berian ACS NSQIP National Conference 2015 No disclosures ERIN, ERAS, and ERP ERIN-Enhanced Recovery
Enhanced Recovery in NSQIP (ERIN): an update on the collaborative Julie Thacker, LianeFeldman, and Julia Berian ACS NSQIP National Conference 2015 No disclosures ERIN, ERAS, and ERP ERIN-Enhanced Recovery
Open Hysterectomy Enhanced Recovery (HER) (For elective benign hysterectomy, myomectomy and ovarian/adnexal surgery)
 (For elective benign hysterectomy, myomectomy and ovarian/adnexal surgery)") CLINICAL PATHWAY Open Hysterectomy Enhanced Recovery (HER) (For elective benign hysterectomy, myomectomy and ovarian/adnexal surgery) Pre-Admission Unit (PAU) Day of Surgery Pre-op Same Day Admission (SDA)
CLINICAL PATHWAY Open Hysterectomy Enhanced Recovery (HER) (For elective benign hysterectomy, myomectomy and ovarian/adnexal surgery) Pre-Admission Unit (PAU) Day of Surgery Pre-op Same Day Admission (SDA)
PSI 12 - Perioperative Pulmonary Embolism or Deep Vein Thrombosis Rate Opportunity
 MAY 2018 A MESSAGE FROM THE SAINT LUKE S CARE CMO Table of Contents PSI 12 - Perioperative Pulmonary Embolism or Deep Vein Thrombosis Rate Opportunity 1,2 NEW Order Sets & Documents 3 Saint Luke s Care
MAY 2018 A MESSAGE FROM THE SAINT LUKE S CARE CMO Table of Contents PSI 12 - Perioperative Pulmonary Embolism or Deep Vein Thrombosis Rate Opportunity 1,2 NEW Order Sets & Documents 3 Saint Luke s Care
Effect of Colon Bundle Implementation in a Community Hospital. Michael Barringer, MD, FACS CHS Cleveland
 Effect of Colon Bundle Implementation in a Community Hospital Michael Barringer, MD, FACS CHS Cleveland Doug Hobson, MD, Surgeon Champion Mike Barringer, MD, Surgeon Champion No Disclosures Except for
Effect of Colon Bundle Implementation in a Community Hospital Michael Barringer, MD, FACS CHS Cleveland Doug Hobson, MD, Surgeon Champion Mike Barringer, MD, Surgeon Champion No Disclosures Except for
Implementing an Enhanced Recovery Program for Surgery. Michael F. McGee, MD, FACS, FASCRS September 21, 2017
 Implementing an Enhanced Recovery Program for Surgery Michael F. McGee, MD, FACS, FASCRS September 21, 2017 Continuing Education Disclosures Commercial Support or Sponsorship None Speaker or planner relationships
Implementing an Enhanced Recovery Program for Surgery Michael F. McGee, MD, FACS, FASCRS September 21, 2017 Continuing Education Disclosures Commercial Support or Sponsorship None Speaker or planner relationships
Perioperative Surgical Home
 None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
? Prehab, immunonutrition. Safe surgical principles. Optimizing Preoperative Evaluation
 Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Combined SSI Bundles and ERAS in Colorectal Surgeries
 Combined SSI Bundles and ERAS in Colorectal Surgeries Joy Lanfranchi BSN, RN, CNOR, CMLSO Richard Bollin Jr. M.D. Kevin Kinzinger M.D. MBA, FACS, FASCRS Joanne Bonnot MSN, RN, BBA, NE-BC Claudia Skinner
Combined SSI Bundles and ERAS in Colorectal Surgeries Joy Lanfranchi BSN, RN, CNOR, CMLSO Richard Bollin Jr. M.D. Kevin Kinzinger M.D. MBA, FACS, FASCRS Joanne Bonnot MSN, RN, BBA, NE-BC Claudia Skinner
AHRQ Safety Program for Improving Surgical Care and Recovery. ACS Quality and Safety Conference New York City July 21, 2017
 AHRQ Safety Program for Improving Surgical Care and Recovery ACS Quality and Safety Conference New York City July 21, 2017 1 Project goals To measurably improve patient outcomes in five surgical areas
AHRQ Safety Program for Improving Surgical Care and Recovery ACS Quality and Safety Conference New York City July 21, 2017 1 Project goals To measurably improve patient outcomes in five surgical areas
TOTAL HIP REPLACEMENT FLOW SHEET
 TOTAL HIP REPLACEMENT FLOW SHEET Before Surgery: Nothing to eat or drink after midnight the night before surgery. Make sure you have a bowel movement the day before surgery. Be sure to attend your pre-op
TOTAL HIP REPLACEMENT FLOW SHEET Before Surgery: Nothing to eat or drink after midnight the night before surgery. Make sure you have a bowel movement the day before surgery. Be sure to attend your pre-op
Physician Executive Council. Using the Perioperative Surgical Home to Improve Joint Replacement
 Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Advisor Live Enhanced surgical recovery with perioperative goal-direcred therapy. October 16, #AdvisorLive
 Advisor Live Enhanced surgical recovery with perioperative goal-direcred therapy October 16, 2015 @PremierHA #AdvisorLive Download today s slides at www.premierinc.com/events Logistics Audio Use your computer
Advisor Live Enhanced surgical recovery with perioperative goal-direcred therapy October 16, 2015 @PremierHA #AdvisorLive Download today s slides at www.premierinc.com/events Logistics Audio Use your computer
Quality improvement for caesarean section - a multifactorial approach. Ian Wrench Consultant Anaesthetist Jessop Wing Obstetric Unit
 Quality improvement for caesarean section - a multifactorial approach. Ian Wrench Consultant Anaesthetist Jessop Wing Obstetric Unit Structure of talk: Rationale for introduction of enhanced recovery for
Quality improvement for caesarean section - a multifactorial approach. Ian Wrench Consultant Anaesthetist Jessop Wing Obstetric Unit Structure of talk: Rationale for introduction of enhanced recovery for
Enhanced recovery after surgery: the role of the PACU & Pre-op
 Enhanced recovery after surgery: the role of the PACU & Pre-op Magnus K. Teig BSc (Hons.) MBChB MRCP FRCA EDIC FFICM Assistant Professor Anesthesia & Neurosurgery Director UH PACU University of Michigan
Enhanced recovery after surgery: the role of the PACU & Pre-op Magnus K. Teig BSc (Hons.) MBChB MRCP FRCA EDIC FFICM Assistant Professor Anesthesia & Neurosurgery Director UH PACU University of Michigan
Surgical Oncology Manual: Patient Protocols: Daily Rounds:
 Surgical Oncology Manual: Patient Protocols: Daily Rounds: All inpatients must be seen by the chief resident or fellow prior to that day s OR cases. Multidisciplinary notes are to be completed for every
Surgical Oncology Manual: Patient Protocols: Daily Rounds: All inpatients must be seen by the chief resident or fellow prior to that day s OR cases. Multidisciplinary notes are to be completed for every
Enhanced Recovery after Surgery Considerations for Pathway Development and Implementation
 Enhanced Recovery after Surgery Considerations for Pathway Development and Implementation Table of Contents Purpose 2 Introduction 2 The Patient s Interdisciplinary Team 2 Culture and Leadership 3 Enhanced
Enhanced Recovery after Surgery Considerations for Pathway Development and Implementation Table of Contents Purpose 2 Introduction 2 The Patient s Interdisciplinary Team 2 Culture and Leadership 3 Enhanced
Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair
 or Atrial Septal Defect (ASD) Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay
 Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay Dear Prospective Patient: I have recently been informed that you are considering weight loss surgery at EMMC. As you know
Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay Dear Prospective Patient: I have recently been informed that you are considering weight loss surgery at EMMC. As you know
Euclid Hospital CMS BPCI Episode
 Euclid Hospital CMS BPCI Episode Two Paradigms in Health Care Reform Managing population 1 health, 2 PCMH Managing episodes of care, Bundled payments Health Status Baseline Episode Total Spend: Commercial
Euclid Hospital CMS BPCI Episode Two Paradigms in Health Care Reform Managing population 1 health, 2 PCMH Managing episodes of care, Bundled payments Health Status Baseline Episode Total Spend: Commercial
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
General OR-Stanford-CA-1 revised: Tuesday, February 02, 2016
 Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
C19: Patients at Home Hours After Total Joint Surgery
 C19: Patients at Home Hours After Total Joint Surgery Kaiser Permanente Santa Clara Chris Boyd, Area Manager, Senior Vice President Ashima Garg, MD, PhD, Orthopedic Surgeon Session Objectives Implement
C19: Patients at Home Hours After Total Joint Surgery Kaiser Permanente Santa Clara Chris Boyd, Area Manager, Senior Vice President Ashima Garg, MD, PhD, Orthopedic Surgeon Session Objectives Implement
Standardizing for Efficiency: Enhanced Recovery. Lillian S. Kao, MD, MS, CMQ July 23, 2018
 Standardizing for Efficiency: Enhanced Recovery Lillian S. Kao, MD, MS, CMQ July 23, 2018 Disclosures Small intestine section editor for UpToDate. ERAS Preoperative Intraoperative Postoperative Enhanced
Standardizing for Efficiency: Enhanced Recovery Lillian S. Kao, MD, MS, CMQ July 23, 2018 Disclosures Small intestine section editor for UpToDate. ERAS Preoperative Intraoperative Postoperative Enhanced
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty
 Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
Clinical Standardization
 Clinical Standardization Joe Sharma, MD, FACS, FACE Associate Professor of Surgery Director, of Endocrine Surgery Chief Quality Officer Emory University School of Medicine Disclosures Engineer US Navy
Clinical Standardization Joe Sharma, MD, FACS, FACE Associate Professor of Surgery Director, of Endocrine Surgery Chief Quality Officer Emory University School of Medicine Disclosures Engineer US Navy
Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital. What is Possible?
 for Elective Colon Resection Surgery at Vancouver General Hospital. What is Possible?") Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital What is Possible? BC Provincial Collaborative November 25, 2014 Disclosure Statement I do not have
Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital What is Possible? BC Provincial Collaborative November 25, 2014 Disclosure Statement I do not have
Strategy/Driver Prevention Strategies Action Strategies
 I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
Peri-operative Pain Management - a multi-disciplinary team-based approach
 Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative
 Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Colorectal Pathway: A Template for the Georgia Surgical Quality Collaborative
 Colorectal Pathway: A Template for the Georgia Surgical Quality Collaborative Disclosure Bryant Wilson, MD Relevant Financial Relationships: I have no actual or potential conflict of interest in relation
Colorectal Pathway: A Template for the Georgia Surgical Quality Collaborative Disclosure Bryant Wilson, MD Relevant Financial Relationships: I have no actual or potential conflict of interest in relation
EC OR ADULT OUTPATIENT SURGERY PLAN - Phase: PACU Orders
 - Phase: PACU Orders DETAILS Admit/Discharge/Transfer This plan should only be placed on a patient that is being discharged from outpatient surgery. If patient is being admitted, this plan should not be
- Phase: PACU Orders DETAILS Admit/Discharge/Transfer This plan should only be placed on a patient that is being discharged from outpatient surgery. If patient is being admitted, this plan should not be
Reducing Surgical Site Infections in Colon Surgery Patients
 Reducing Surgical Site Infections in Colon Surgery Patients Mercy Health St. Elizabeth Boardman Hospital A Catholic healthcare ministry serving Ohio and Kentucky Mercy Health St. Elizabeth Boardman Hospital
Reducing Surgical Site Infections in Colon Surgery Patients Mercy Health St. Elizabeth Boardman Hospital A Catholic healthcare ministry serving Ohio and Kentucky Mercy Health St. Elizabeth Boardman Hospital
Enhanced Recovery Programme
 Cancer Action Team Enhanced Recovery Programme Andy McMeeking National Cancer Action Team Andy.McMeeking@gstt.nhs.uk 18 th November 2009 Upper GI Lead Clinicians 1 Enhanced recovery Is a novel approach
Cancer Action Team Enhanced Recovery Programme Andy McMeeking National Cancer Action Team Andy.McMeeking@gstt.nhs.uk 18 th November 2009 Upper GI Lead Clinicians 1 Enhanced recovery Is a novel approach
Pre-Procedure/Surgical Instructions for Adults
 Pre-Procedure/Surgical Instructions for Adults Thank you for choosing Edward Hospital for your health care needs. Our goal is to be your partner to ensure that you will have a very good experience. Preparing
Pre-Procedure/Surgical Instructions for Adults Thank you for choosing Edward Hospital for your health care needs. Our goal is to be your partner to ensure that you will have a very good experience. Preparing
Dave Reeder, Quality Committee Chair. Dave Reeder, Quality Committee Chair. Dave Reeder, Quality Committee Chair. Dave Reeder, Dave Reeder,
 AGENDA Quality, Patient Care and Patient Experience Committee Meeting of the El Camino Hospital Board Monday, October 2 nd, 2017, 5:30 p.m. El Camino Hospital Conference Room A & B 2500 Grant Road, Mountain
AGENDA Quality, Patient Care and Patient Experience Committee Meeting of the El Camino Hospital Board Monday, October 2 nd, 2017, 5:30 p.m. El Camino Hospital Conference Room A & B 2500 Grant Road, Mountain
Clinical Fellowship Acute Pain Service
 Anesthesia and Perioperative Medicine Western University Acute Pain Service Program Directors Dr. Kevin Armstrong Dr. Qutaiba Tawfic Please visit the Acute Pain Service Fellowship site for most up-to-date
Anesthesia and Perioperative Medicine Western University Acute Pain Service Program Directors Dr. Kevin Armstrong Dr. Qutaiba Tawfic Please visit the Acute Pain Service Fellowship site for most up-to-date
Hip Replacement Modern Total Hip Replacement in an Ambulatory Surgery Center. A Brief History of Total Hip Replacement
 Modern Total Hip Replacement in an Ambulatory Surgery Center James T. Caillouette, M.D. Chairman Newport Orthopedic Institute 1 A Brief History of Total Hip Replacement Hip replacement 1990: LOS 7 Days
Modern Total Hip Replacement in an Ambulatory Surgery Center James T. Caillouette, M.D. Chairman Newport Orthopedic Institute 1 A Brief History of Total Hip Replacement Hip replacement 1990: LOS 7 Days
September 6, RE: CY 2017 Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems Proposed Rule
 September 6, 2016 VIA E-MAIL FILING Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1656-P P.O. Box 8013 Baltimore, MD 21244-1850 RE: CY 2017 Hospital Outpatient
September 6, 2016 VIA E-MAIL FILING Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1656-P P.O. Box 8013 Baltimore, MD 21244-1850 RE: CY 2017 Hospital Outpatient
Today medical providers are charged with delivering care
 The Joint Commission Journal on Quality and Patient Safety 2017; 43:524 533 CARE PROCESSES Optimizing an Enhanced Recovery Pathway Program: Development of a Postimplementation Audit Strategy Michael C.
The Joint Commission Journal on Quality and Patient Safety 2017; 43:524 533 CARE PROCESSES Optimizing an Enhanced Recovery Pathway Program: Development of a Postimplementation Audit Strategy Michael C.
CLINICAL PATHWAY. Surgical Services. Recurring Ventral Hernia
 CLINICAL PATHWAY Surgical Services Recurring Ventral Hernia Recurring Ventral Hernia Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts 1 CLINICAL PATHWAY 3
CLINICAL PATHWAY Surgical Services Recurring Ventral Hernia Recurring Ventral Hernia Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts 1 CLINICAL PATHWAY 3
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: OP49 Version: 4.0 Name of Policy: Patient Controlled Analgesia in Adult Patients Effective From: 28/11/2017 Date Ratified 21/09/2017 Ratified Medicines Group Review Date 01/09/2019 Sponsor Director
Policy No: OP49 Version: 4.0 Name of Policy: Patient Controlled Analgesia in Adult Patients Effective From: 28/11/2017 Date Ratified 21/09/2017 Ratified Medicines Group Review Date 01/09/2019 Sponsor Director
Neighborhood Hospital
 Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PRE OPERATIVE MANAGEMENT FOR PEDIATRIC HOSPITALISTS
 Before the Operating Room: PRE OPERATIVE MANAGEMENT FOR PEDIATRIC HOSPITALISTS Presenters: Anjna Melwani, MD Sonaly McClymont, MD David Rappaport, MD Sarah Denniston, MD David Pressel, MD Amy Vinson, MD
Before the Operating Room: PRE OPERATIVE MANAGEMENT FOR PEDIATRIC HOSPITALISTS Presenters: Anjna Melwani, MD Sonaly McClymont, MD David Rappaport, MD Sarah Denniston, MD David Pressel, MD Amy Vinson, MD
Why Focus on Perioperative Services?
 1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
Organizational Culture Change Results in Improvement in Outcomes, Value and Experience. Elizabeth C. Wick, M.D.
 Organizational Culture Change Results in Improvement in Outcomes, Value and Experience Elizabeth C. Wick, M.D. Objectives To describe the burden and complexity of surgical site infections To outline the
Organizational Culture Change Results in Improvement in Outcomes, Value and Experience Elizabeth C. Wick, M.D. Objectives To describe the burden and complexity of surgical site infections To outline the
IHI Expedition. Expedition: Preparing Care Teams for Bundled Payments Session 5: Care Team Redesign
 May 19, 2015 Begins at 1:00 PM IHI Expedition Expedition: Preparing Care Teams for Bundled Payments Session 5: Care Team Redesign Trisha Frick, MS, RN Nick Bassett, MBA Lucy Savitz, PhD, MBA Molly Bogan,
May 19, 2015 Begins at 1:00 PM IHI Expedition Expedition: Preparing Care Teams for Bundled Payments Session 5: Care Team Redesign Trisha Frick, MS, RN Nick Bassett, MBA Lucy Savitz, PhD, MBA Molly Bogan,
Whipple Procedure (Pancreaticoduodenectomy)
") Enhanced Recovery After Whipple Procedure (Pancreaticoduodenectomy) Your Path to Healing Your Pancreatic Surgical Oncology Team This expert team is an important part of the Pancreatic Surgery Program at
Enhanced Recovery After Whipple Procedure (Pancreaticoduodenectomy) Your Path to Healing Your Pancreatic Surgical Oncology Team This expert team is an important part of the Pancreatic Surgery Program at
Care of Patients Receiving Analgesia by Catheter Techniques Position Statement and Policy Considerations
 Care of Patients Receiving Analgesia by Catheter Techniques Position Statement and Policy Considerations Position Statement Registered nurses (RNs) are valuable members of the patient care team who are
Care of Patients Receiving Analgesia by Catheter Techniques Position Statement and Policy Considerations Position Statement Registered nurses (RNs) are valuable members of the patient care team who are
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Preparing for Surgery
 Preparing for Surgery Patient Education Guide This book is for You should arrive on (date) at (time) 6801 Airport Blvd. Mobile, AL (251) 633-1000 www.providencehospital.org providence hospital It is a
Preparing for Surgery Patient Education Guide This book is for You should arrive on (date) at (time) 6801 Airport Blvd. Mobile, AL (251) 633-1000 www.providencehospital.org providence hospital It is a
G: Surgical. College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 67
 G: Surgical College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 67 Major Competency Area: G Surgical Competency: G-1 Surgical Nursing Date: June 1, 2015 G-1-1 G-1-2 G-1-3
G: Surgical College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 67 Major Competency Area: G Surgical Competency: G-1 Surgical Nursing Date: June 1, 2015 G-1-1 G-1-2 G-1-3
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
Providing a Full Continuum of Care: The Cleveland Clinic Model
 Providing a Full Continuum of Care: The Cleveland Clinic Model Derrick Cetin, DO Obesity Medicine Clinical Assistant Professor Dept of Medicine Cleveland Clinic Lerner College of Medicine of Case Western
Providing a Full Continuum of Care: The Cleveland Clinic Model Derrick Cetin, DO Obesity Medicine Clinical Assistant Professor Dept of Medicine Cleveland Clinic Lerner College of Medicine of Case Western
Your facility is having a baby boom. The number of cesarean births is
 Clinical management Ensuring a comparable standard of care for cesarean deliveries Your facility is having a baby boom. The number of cesarean births is exceeding the obstetrical unit s capacity. Administrators
Clinical management Ensuring a comparable standard of care for cesarean deliveries Your facility is having a baby boom. The number of cesarean births is exceeding the obstetrical unit s capacity. Administrators
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
2018 DOM HealthCare Quality Symposium Poster Session
 Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Department of Anesthesiology and Pediatrics, Duke University School of Medicine, Durham, NC, USA
 JEPM Vol XVII, Issue III, July-December 2015 1 Original Article 1 Assistant Professor, Department of Anesthesiology and Pediatrics, Duke University School of Medicine, Durham, NC, USA 2 Resident Physician,
JEPM Vol XVII, Issue III, July-December 2015 1 Original Article 1 Assistant Professor, Department of Anesthesiology and Pediatrics, Duke University School of Medicine, Durham, NC, USA 2 Resident Physician,
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR.
 Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Enhanced Recovery: Measurement for Improvement Monthly Data Submission Guidance. Version 1.0
 Enhanced Recovery: Measurement for Improvement Monthly Data Submission Guidance Version 1.0 Document Control Version Version 1.0 Date Issued January 2014 Document To provide guidance for the monthly collection
Enhanced Recovery: Measurement for Improvement Monthly Data Submission Guidance Version 1.0 Document Control Version Version 1.0 Date Issued January 2014 Document To provide guidance for the monthly collection
4/10/2013. Learning Objective. Quality-Based Payment Models
 Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
CRNAs Value for Your Team and Bottom Line
 CRNAs Value for Your Team and Bottom Line Sarah Chacko, JD Assistant Director of State Government Affairs and Legal Lynn Reede, CRNA, DNP, MBA Senior Director, Professional Practice Becker s 13th Annual
CRNAs Value for Your Team and Bottom Line Sarah Chacko, JD Assistant Director of State Government Affairs and Legal Lynn Reede, CRNA, DNP, MBA Senior Director, Professional Practice Becker s 13th Annual
Beth Israel Deaconess Medical Center Perioperative Services Manual. Guidelines for Perioperative Handoffs from OR to receiving units.
 Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Clinical Pathway: Tetralogy of Fallot (TOF) Repair
 Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Tetralogy of Fallot (TOF) Repair Notes: (1) This pathway is a general guideline and variations can occur based on professional
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Tetralogy of Fallot (TOF) Repair Notes: (1) This pathway is a general guideline and variations can occur based on professional
Improving Compliance
 Improving Compliance * The following planners, speakers, moderators, and/or panelists of this CME activity have no relevant financial relationships with commercial interests to disclose: Mary B. Johnson
Improving Compliance * The following planners, speakers, moderators, and/or panelists of this CME activity have no relevant financial relationships with commercial interests to disclose: Mary B. Johnson
SCIP-Inf-2, SCIP-Inf-3, SCIP-Inf-4, SCIP-Inf- 9, SCIP-Inf-10, SCIP-VTE-1, SCIP-VTE-2 Anesthesia End Time 5
 Release Notes: Alphabetical Data Dictionary Version 3.3 Surgical Care Improvement Project (SCIP) - Data Dictionary The General Abstraction Guidelines explain the different sections of the data element
Release Notes: Alphabetical Data Dictionary Version 3.3 Surgical Care Improvement Project (SCIP) - Data Dictionary The General Abstraction Guidelines explain the different sections of the data element
Enhanced Recovery After. Colorectal Surgery. Your Path to Healing
 Enhanced Recovery After Colorectal Surgery Your Path to Healing Your Colorectal Surgical Oncology Team This expert team works together to give you the best care available. Based on your situation, you
Enhanced Recovery After Colorectal Surgery Your Path to Healing Your Colorectal Surgical Oncology Team This expert team works together to give you the best care available. Based on your situation, you
1. Introduction. 1 CMS section
 1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
Surgery guide. Prior to surgery. What to expect before, during and after your procedure.
 Surgery guide What to expect before, during and after your procedure. Prior to surgery Please complete the following one to two weeks before your scheduled surgery: Register with Texas Children s Pavilion
Surgery guide What to expect before, during and after your procedure. Prior to surgery Please complete the following one to two weeks before your scheduled surgery: Register with Texas Children s Pavilion
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath
 Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Quality Incentive Programs. By: Amy Yearwood RN, BSN Physicians Network Quality Manager Huntsville Hospital
 Quality Incentive Programs By: Amy Yearwood RN, BSN Physicians Network Quality Manager Huntsville Hospital Housekeeping 1. Using the control panel - Use the control panel on the right side of your screen
Quality Incentive Programs By: Amy Yearwood RN, BSN Physicians Network Quality Manager Huntsville Hospital Housekeeping 1. Using the control panel - Use the control panel on the right side of your screen
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
TEXAS CHILDREN S HOSPITAL EVIDENCE-BASED OUTCOMES CENTER Postoperative Gastrostomy Tube Management Evidence-Based Practice Course Evidence Summary
 TEXAS CHILDREN S HOSPITAL EVIDENCE-BASED OUTCOMES CENTER Postoperative Gastrostomy Tube Management Evidence-Based Practice Course Evidence Summary Inclusion Criteria Age 0-17 years Gastrostomy tube insertions
TEXAS CHILDREN S HOSPITAL EVIDENCE-BASED OUTCOMES CENTER Postoperative Gastrostomy Tube Management Evidence-Based Practice Course Evidence Summary Inclusion Criteria Age 0-17 years Gastrostomy tube insertions
Preparing for Surgery
 Preparing for Surgery Patient Education Guide This book is for You should arrive on (date) at (time) 3801 East Highway 98 Port St. Joe, FL (850) 229-5600 www.sacredheartonthegulf.org Sacred Heart Hospital
Preparing for Surgery Patient Education Guide This book is for You should arrive on (date) at (time) 3801 East Highway 98 Port St. Joe, FL (850) 229-5600 www.sacredheartonthegulf.org Sacred Heart Hospital
Hip Today Home Tomorrow:
 Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment
 Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
A Patient s Guide to Surgery
 A Patient s Guide to Surgery Welcome Welcome to Carolinas Medical Center-NorthEast. Our staff of skilled professionals look forward to providing the care you need. We want your stay to be pleasant and
A Patient s Guide to Surgery Welcome Welcome to Carolinas Medical Center-NorthEast. Our staff of skilled professionals look forward to providing the care you need. We want your stay to be pleasant and
Perioperative Fluid Utilization Variability and Association With Outcomes
 ORIGINAL ARTICLE Perioperative Fluid Utilization Variability and Association With Outcomes Considerations for Enhanced Recovery Efforts in Sample US Surgical Populations Julie K. M. Thacker, MD, William
ORIGINAL ARTICLE Perioperative Fluid Utilization Variability and Association With Outcomes Considerations for Enhanced Recovery Efforts in Sample US Surgical Populations Julie K. M. Thacker, MD, William
MQii Malnutrition Knowledge and Awareness Test
 MQii Malnutrition Knowledge and Awareness Test This test intends to assess hospital staff members knowledge of the impact of malnutrition and importance of optimal malnutrition care practices, specifically
MQii Malnutrition Knowledge and Awareness Test This test intends to assess hospital staff members knowledge of the impact of malnutrition and importance of optimal malnutrition care practices, specifically
Adult Patient Controlled Analgesia (PCA)
") Contents... 1 Policy... 1 Scope/Audience... 1 Associated Documents... 1 Statement... 2 Criteria... 2 Patient and Whanau Education... 2 Procedural Considerations... 3 Pre Administration... 3 Patient Monitoring...
Contents... 1 Policy... 1 Scope/Audience... 1 Associated Documents... 1 Statement... 2 Criteria... 2 Patient and Whanau Education... 2 Procedural Considerations... 3 Pre Administration... 3 Patient Monitoring...
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY. Dr. Paul Vercruysse M.D. Belgium
 ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
Empire BlueCross BlueShield Professional Reimbursement Policy
 Subject: Global Surgery NY Policy: 0012 Effective: 02/01/2014 05/31/2014 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
Subject: Global Surgery NY Policy: 0012 Effective: 02/01/2014 05/31/2014 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
Incident Reporting: Why it Matters
 Table of Contents Incident Reporting 1 IV Fluids Shortage 2 Asymptomatic Hypertension Treatment Recommendations 3 NEW Order Sets & Documents 4 SLC Shout Outs 4 National Shortage of IV Opioids 5 Saint Luke
Table of Contents Incident Reporting 1 IV Fluids Shortage 2 Asymptomatic Hypertension Treatment Recommendations 3 NEW Order Sets & Documents 4 SLC Shout Outs 4 National Shortage of IV Opioids 5 Saint Luke
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES
 UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
Understanding Diversion in the Pharmacy Kimberly S. New JD BSN RN
 Understanding Diversion in the Pharmacy Kimberly S. New JD BSN RN All Rights Reserved Scope of the Problem Diversion can t be prevented entirely Substantial safety, quality, regulatory and legal risk Mitigate
Understanding Diversion in the Pharmacy Kimberly S. New JD BSN RN All Rights Reserved Scope of the Problem Diversion can t be prevented entirely Substantial safety, quality, regulatory and legal risk Mitigate
Radical Prostatectomy Care Guide: A checklist of what to expect
 Radical Prostatectomy Care Guide: A checklist of what to expect Form: D-5473 How to prepare for your operation as an outpatient 1. Pre- Admission Visit Where to find us: Toronto General Hospital (TGH),
Radical Prostatectomy Care Guide: A checklist of what to expect Form: D-5473 How to prepare for your operation as an outpatient 1. Pre- Admission Visit Where to find us: Toronto General Hospital (TGH),
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
Laparoscopic Radical Nephrectomy
 Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you