Improving Patient Safety Through Accurate Medication Reconciliation
|
|
|
- Frederick Dixon
- 6 years ago
- Views:
Transcription

1 The University of San Francisco USF Scholarship: a digital Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall Improving Patient Safety Through Accurate Medication Reconciliation Dominique Watt University of San Francisco, dwatt116@gmail.com Follow this and additional works at: Part of the Nursing Commons Recommended Citation Watt, Dominique, "Improving Patient Safety Through Accurate Medication Reconciliation" (2015). Master's Projects and Capstones This Project/Capstone is brought to you for free and open access by the Theses, Dissertations, Capstones and Projects at USF Scholarship: a digital Gleeson Library Geschke Center. It has been accepted for inclusion in Master's Projects and Capstones by an authorized administrator of USF Scholarship: a digital Gleeson Library Geschke Center. For more information, please contact repository@usfca.edu.
2 Running Header: PROSPECTUS ELEMENTS 1 Prospectus Elements Dominique Watt University of San Francisco
3 PROSPECTUS ELEMENTS 2 Clinical Leadership Theme A medication error can occur anywhere in a patient s journey, especially since many different types of health professionals are involved in the process of medication administration. The National Patient Safety Agency (NPSA) reported that 1 in 10 patients experienced medication-related errors (NPSA, 2007). I have decided to focus on standardizing medication reconciliation as part of the national patient safety goal of using medications safely (Joint Commission, 2014). The clinical leadership theme my project is associated with is the Clinical Outcomes Management, educator role. We will be using teaching and learning techniques and incorporating best practices into our electronic health records and technology, in order to facilitate learning from the staff nurses. As a Clinical Nurse Leader (CNL), I will be managing the education and learning process for the new standardized process as well as evaluating the outcomes. Statement of the Problem 71 % of medication errors that result in fatality or serious harm are due to unclear prescriptions, wrong doses and frequency, drugs being omitted, and medication being delayed (NPSA, 2007). When these inconsistencies line up, as in the Swiss cheese model, the holes allow problems to pass through each layer and cause potential harm to the patient. Project overview The goal of the project, by standardizing medication reconciliation for registered nurses, is to have 80% of all medication reconciliations to be accurate and a decrease in medication error related safety incident reports to no more than 21 per fiscal year. This would represent a 50%
4 PROSPECTUS ELEMENTS 3 improvement from last fiscal year. With these improvements, we will be aligned with one of the 2015 Joint Commission National Patient Safety Goals (2014) of using medications safely. Rationale When I started analyzing the problem of medication errors on our unit, using a fishbone diagram (Figure 1), I found that we had many causes and this problem was complex and multi-layered. On the positive, we had staff who voiced that they were interested in improving our overall medication safety on the unit and volunteered to be a part of our medication administration task force. We performed a unit-based audit, which included patient identifiers, purpose of medications explained, and bar code scanning. We discovered that we were only compliant 40 % of the time. I then examined each patient s medication reconciliations for each day and found that no two patient s medication reconciliations were done the same way. We had variance in deleting medications if a patient was no longer taking them versus documenting the last dose as unknown. We also had discrepancies in adding free text notes to the medication if the dosage was different than what was listed, versus deleting the medication and entering it as a new medication with the correct dose. We had two safety events in one day related to incorrect medication reconciliation that took over an hour to resolve, delaying care and decreasing patient safety and satisfaction, as well as decreased nurse satisfaction. While performing a SWOT analysis, I found our strengths include clinically experienced nurses, both in outpatient and inpatient settings, which provides a diverse set of skills on our unit. Our nurses also give exceptionally compassionate care and have been recognized with hospital and national awards. This is displayed in many of our Press Ganey patient satisfaction survey results. Our weaknesses include the resistance or hesitance to change the current workflow in order to meet new needs of
5 PROSPECTUS ELEMENTS 4 the unit. The opportunities for this project are to meet one of the Joint Commission National Patient Safety Goals for 2015: use medications safely (Joint Commission 2014). The threats to this project are that the new standardized workflow and expectations may increase time required to complete tasks such as medication administration. We will be able to analyze our data with auditing the documentation in the electronic health record system by using reports as well as monitoring our safety incident reporting system frequency. By performing a value stream map of the process, we were able to identify the different layers of the issue (Figure 2) and noted that the RN is the first line of defense as well as the last line of defense with medication safety. When providing a cost benefit analysis, I found costs included the time involved with consultation of pharmacy, EPIC (electronic health record system), medication administration task force meetings with staff committee, and researching at other large Magnet institutions for best practices. This was approximately 120 hours of work for me and approximately $9240. Costs also included the education to staff from staff, separate cost of out of count time for super users to teach the workflow to staff, approximately 100 hours, divided by 4 super users, average hourly rate is $73/hour= $7300 total for super user time The benefits include improved patient safety with improving accuracy of medication reconciliation during the pre-operative admission process; improved effectiveness of nursing care with standardization of medication reconciliation done by creating a standard work flow which will guarantee the same results, every time; improve patient satisfaction by including patient in medication reconciliation and medication administration, as part of the Joint Commission National Patient Safety Goals of 2015: Use Medications Safely (Joint Commission, 2014). E-prescribing systems have been found to reduce medication errors by 85% and a net
6 PROSPECTUS ELEMENTS 5 cost savings of $400K in ambulatory settings, which my microsystem falls under (Burton et al, 2007). Bar Code Electronic Medication Administration System saved a large academic hospital $2.2M each year (Maviglia et. al, 2007). Stanford Health Care is considered a large academic hospital, which is my organization. The net benefit is using the $400 K savings listed above (Burton et al, 2007) and the costs of research and education, equaling $16,540 as a one-time cost, which means the net benefit of implementing this practice would be approximately $380, 000. Qualitative benefits are just as important as quantitative and include autonomy of nurses to be able to perform their nursing role with the education and best practices behind their practice, improved patient outcomes over long term, decreased costs associated to incorrect medication prescription and administration, improved patient satisfaction and increased patient involvement, and finally, decreased time of management involvement with investigation of medication errors due to decrease in medication errors Methodology The microsystem we are studying is an outpatient unit for cath angio pre and post procedure patients that sees approximately 40 to 50 patients daily and has an overnight observation unit. We have been examining the complex problem of medication administration errors and found there are inconsistencies with administration of medications and explaining the purpose of medications, using the bar coding and asking for 2 identifiers, as well as documenting medication reconciliation. We do the medication reconciliation for each patient upon admission. Since it is documented in our electronic health record system, it is easy to trackversus nurses explaining medications verbally and using 2 identifiers. It has a great impact because it affects the entire patient s stay and it is difficult to ascertain patients medications
7 PROSPECTUS ELEMENTS 6 after the procedure when they are post sedation. I have collaborated with staff nurses, pharmacy and now IT. It seems that medication reconciliation is something the organization is looking at standardizing. We will be developing a standard work process or guidelines for all RNs who complete medication reconciliation upon admission to follow. We will be able run reports in EPIC and see if our standard work has been followed. To track improvement, we are working with the pharmacy to identify if we have had less errors and incorrect reconciliations with our safety event reporting system. We will know if we are effective if we can reach and sustain 80% of all medications being reconciled correctly, in adjunct with a 50% decrease in safety event reports for the fiscal year As far as introducing this change, I will be utilizing John Kotter s theory. When I first went into management, I read the book Our Iceberg is Melting: Changing and Succeeding Under Any Conditions (Kotter, 2005), whose change theory includes eight steps. I try to use this theory whenever implementing a large-scale change. For my project, I established a sense of urgency when we had a near miss medication event by a well-respected and thorough nurse on our unit. She wanted to share her experience and mistake with the staff in hopes to improve our practice. Her presentation brought up many opportunities of improvement for our unit. Staff expressed awareness of the issue and I was able to create a powerful coalition of staff nurses interested in improving this issue. We have been meeting regularly and developed a vision of what issues are occurring and what our future state should be. These members are my informal leaders and are responsible in assisting me with communicating this vision. As staff nurses and informal leaders, they are respected and trusted by their peers and I have full confidence in their ability to empower others in our shared vision. With this project, as well as other responsibilities
8 PROSPECTUS ELEMENTS 7 of a manager, I try to be aligned with transformational leadership and give power to our staff in order to empower them and engage them. Our project task force has been working with pharmacy and our electronic health record (EPIC) team in order to create short term wins for our larger issue. It is a slow process as the problem has many layers, and if we continue to celebrate the small wins then we will continue to keep our staff engaged. This is part of the Clinical Nurse Leader (CNL) American Association of Colleges of Nursing (AACN) s competency to demonstrate effective communication, collaboration, and interpersonal relationships with members of the care delivery team across the continuum of care (AACN, 2013). With the project fully implemented, we will continue to review our progress in our daily huddles as part of the Plan-Do-Check-Act (PDCA) cycle and readjust as needed after the checking portion of the cycle. Once we have a revised, staff approved and tested standard work, we can use it seamlessly and it should not add time or tasks to the nurses work. Data Source/Literature Review The focus of my study has been unit assessment information and unit based, staff driven audits as well as a patient satisfaction story related to a medication error. It is appropriate for us to look into because we have a high frequency of medication reconciliations daily since we are a high volume outpatient unit. Also, as part of an organization overseen by the Joint Commission, it is important that we address their National Patient Safety Goals, which include medication safety. In order to find research on this topic, I used a PICO search. The term PICO stands for: P: Patient/Population : Who or What disease?
9 PROSPECTUS ELEMENTS 8 o Outpatients in a Cath Angio Department I: Intervention : Treatment of interest o Accurate Medication Reconciliation with patient including purpose/indication of each medication C: Comparison : Alternative/standard treatment o Current state- frequent (5-10 per week) discrepancies regarding medication reconciliation O: Outcome : What are you trying to accomplish, measure, improve, effect? o Improving patient safety by minimizing medication reconciliation discrepancies at admission, in order for patient to receive accurate medications through stay and post discharge I used Lane Library with Stanford University to perform a PICO search. Using the terms heart disease for patient populations (as most Cath Angio patients are here with heart disease) and medication reconciliation in intervention and safety in outcomes, I didn t find any relevant articles right away. Using the term Medication Reconciliation and Safety, I was able to find an article on medication reconciliation at admission and discharge, which is more specific to what I am looking for. I tried fewer categories (I and O of PICO) to see what resulted. Since our unit is
10 PROSPECTUS ELEMENTS 9 very unique, as we care for 5 different interventional services, it is hard to find like units. I will continue to test out the different categories in PICO to see what the best outcome is. In the article Medication reconciliation at admission and discharge: an analysis of prevalence and associated risk factors, authors Belda-Rustarazo, Cantero-Hinojosa, Salmeron- Garcia, Gonzalez-Garcia, Cabeza- Barrera and Galvez (2015), recognize medication errors as a major cause of morbidity and medication reconciliation as a strategy to prevent errors at points of care transition. The two-year study encompassed 814 patients and the most occurring error was drug omission. Risk factors were evaluated for each reconciliation. In the article Clinical and Financial Impact of Pharmacist Involvement in Discharge Medication Reconciliation at an Academic Medical Center: A Prospective Pilot Study, Sebaaly et. al, 2015, the authors who are all pharmacists, also stress that medication reconciliation is challenging. The study focused on the role of pharmacists in medication reconciliation, specifically discharges. It found the impact of pharmacy involvement and evaluation of medications upon discharge was significant in decreasing errors in a total of 77 patients in a large academic facility. Our microsystem has increased our usage of pharmacists during discharge education for anticoagulation medications. The qualitative results included staff stating they learned a lot about the new anticoagulation medications and the pharmacists have been very helpful to both patients and nurses. In the article Discharge Time Out: An Innovative Nurse Driven Protocol for Medication Reconciliation by Ruggiero et. al, 2014, researchers stated that a retrospective 2012 study showed that 71.2% of hospital discharges had at least one medication reconciliation error. The nurses at the University of Pennsylvania Hospital developed a time out process at discharge,
11 PROSPECTUS ELEMENTS 10 based on evidence-based practice. Pre implementation showed 77% of discrepancies upon discharge. Post implementation showed 21% of discrepancies upon discharge. This discharge time out can be easily integrated into nursing practice. We used this time out idea in our standard work and will train our staff to consider the discharge teaching to be considered an important aspect of our nursing care and treat it as important as time outs for procedures. In the article Impact of medication reconciliation and review on clinical outcomes by Lehnbom et. al, 2014, the authors examined the effect of medication reconciliation on clinical outcomes in acute care settings, community settings and long-term facilities. The authors performed a systematic review of 83 research articles. While medication reconciliation can identify discrepancies and decrease harm to patients, there was little evidence on how they impacted clinical outcomes. In the article A Quantitative Evaluation of Medication Histories and Reconciliation by Discipline, authors Kramer et. al, 2014, examined the different disciplines involved in medication reconciliation. Registered nurses, pharmacy technicians and pharmacists were all involved in the admission medication reconciliation and the patients had their admission reconciliation taken 3 different types, one by each discipline. The study showed that having a pharmacist review the medication reconciliation would save the hospital $397 per patient. In the article Make Time for Medication Reconciliation by Sarah Muegge, 2014, highlighted several medication discrepancies and the importance of care coordination amongst health care providers, also mentioning resources offered by the American Academy of Ambulatory Care Nursing. In her organization, it is encouraged that patients use the same pharmacy for all medication prescriptions in order to increase compliance and drug compatibility
12 PROSPECTUS ELEMENTS 11 safety. With this information and our electronic health record (EHR) system, we have been able to identify what pharmacies have prescribed medications and can contact the pharmacy if needed, by using the provided information. Timeline This project stemmed from safety issues occurring over the course of In August, I performed an assessment of my microsystem as part of the initial planning stage in the PDCA cycle. The problem was multilayered and extremely complex. It has also evolved since August. During the planning stage, I formed a group of staff nurses who volunteered to be a part of the committee. We created a sense of urgency, according to John Kotter s change theory (Kotter, 2005) and assessed our current state with observations and a baseline audit (see appendix 3). We originally tried to meet weekly, for an hour, but encountered challenges with staffing as most of the nurses were scheduled to work. September started and five incident reports were filed, over the course of two weeks, in regards to inaccurate medication reconciliation and patients receiving the incorrect dosage or not receiving their medications. In September, we reached out to the pharmacy quality manager for assistance in medication reconciliation. During this meeting, we learned that there is no true standard for medication reconciliation in the organization and the organization s quality department is hoping to give this responsibility to physicians as the primary recorder of the medication reconciliation process. This has yet to be done and will prove difficult in the outpatient areas as we have many patients arriving at the same time and a limited time to perform all the necessary preoperative documentation before procedure. The quality manager then recommended us to the ITS Program Manager for EHR Business Continuity and Regulatory Compliance in order to obtain the standard documentation for
13 PROSPECTUS ELEMENTS 12 medication reconciliation. This person also delivers the medication barcode scanning reports. In October, we were able to have our microsystem added. In October, we continued to audit our incident reports for frequency of medication reconciliation errors. There have been none so far. In November, we have developed a tool, under the guidance of the quality department and ITS program manager, for nurses to use when reconciling medications. This will be used for preparation for our new hospital as well. We had our committee and five other staff members use the tool to test its effectiveness. In December, we had hoped to implement the tool as part of the do step in the PDCA cycle. However, we are currently experiencing staffing shortages due to medical leaves and resignations so we have to postpone this step until January Early next year, we will check our progress and reevaluate the tool and process. While we are focusing on medication reconciliation, we are starting to make progress in other areas of our multi-layered problem of medication administration. The staff is celebrating the small successes, which is another step in Kotter s change theory. This timeline is illustrated in Figure 4. Expected Results As far as expected results, we have started to note some immeasurable ones thus far. Bringing visibility to this issue has begun the conversation of medication safety, including specifically medication reconciliation and examining our process rather than blaming others. There has been a shift in our culture to examine gaps or deviations in our standard process in order to create a streamlined workflow. As far as measurable expected results, I hope to see a 50% improvement in medication error related incident reports to 21 per fiscal year as well as be
14 PROSPECTUS ELEMENTS 13 compliant with 80% of our medication reconciliations according to the tool. We have not had any reports in the month of October or in November, so far. From the tool evaluation responses, all staff that tried the guide found it to be helpful. They wish to have more than one week to review it and see if there may be any more revisions needed. We are very pleased with the progress so far. Nursing Relevance Nursing has evolved from assisting physicians to becoming autonomous, independent healthcare providers, advocating for patient safety. I have seen our nurses in our microsystem grow as transformational leaders and role based practitioners by identifying a gap in our microsystem, and analyzing in order to improve patient safety and nursing care. We have also discovered a problem that seems to be relevant in the rest of the organization, as we have yet to find clear examples of standard practice for medication reconciliation. With empowerment to make changes in our microsystem, nursing satisfaction will improve. As nursing satisfaction improves, patient outcomes improve (McHugh et. al, 2015), which is our overall goal. Summary Report The goal of my CNL project was to improve medication reconciliation accuracy by standardizing our medication reconciliation process. With improving accuracy in 80% of our medication reconciliations, I aim to decrease the safety report incidences by 50% to 21 reports per fiscal year. My microsystem is an outpatient pre operative and postoperative cath angio unit. We see an average of patients daily.
15 PROSPECTUS ELEMENTS 14 Inspired by John Kotter s Change Theory(Kotter, 2005), I created a committee of staff members who wanted to improve medication errors on our unit. We used a fishbone diagram to first identify the causes of our inaccuracy with medication administration, including medication reconciliation. We then audited our staff during medication administration and reconciliation to identify the most common incorrect practices. With the help of the data from our safety event incident reporting system, we were able to conclude that most errors arise from inconsistent medication reconciliation due to lack of education. I contacted our information technology trainer for more resources. She was able to provide current articles on medication administration for outpatient settings, located in our Internet site portal. After interviewing the staff during huddles, I learned that our staff do not utilize this portal as they find the site confusing, I drafted a guide using screenshots from our EHR system and asked our committee to review it and try it during a medication reconciliation process (Figure 6). With their feedback and application trials, we revised it using the organization s standard work template (Figure 7). Our innovators and early majority members were identified through either membership of the committee or daily huddle participation. Our committee asked these members to trial the standard work last week during the preoperative phase. All of the five participants, in addition to the four-committee members, stated they learned something new regarding the correct way to perform medication reconciliation (Figure 5). This confirmed our theory that most incorrect practices were due to lack of education. In order to resolve this issue, we are going to formally train our staff in early 2016 on the new standardized process of medication reconciliation, using our standard work, and the EHR playground in which staff members can test out how to document medication reconciliations on created patient profiles.
16 PROSPECTUS ELEMENTS 15 In order to be sustainable, this new standard work will also be implemented in our orientation information packet for new hires and preceptors will be expected to teach to this process, once the staff is educated. Our medication administration safety committee plans to meet monthly and then quarterly. Our committee represents the champions of this project for the frontline staff and will be serving as resources to other staff members. We are optimistic in the success of this standard work tool and its effectiveness to minimize errors with medication reconciliation.

17 PROSPECTUS ELEMENTS 16 Appendices Figure 1. Fishbone diagram of the multiple causes of medication errors and specifically those related to medication reconciliation. Figure 2. Process Value Stream Mapping of Medication Reconciliation in our microsystem, starting and ending with the registered nurse.
18 PROSPECTUS ELEMENTS 17 Audit Survey (please complete 5 and to Dominique by 8/26/15) Name of RN being observed: Date: 1. Were the 5 rights performed before medication administration? a. Yes b. No 2. Was the patient scanned? a. Yes b. No 3. Was the medication scanned? a. Yes b. No 4. Was the RN interrupted or distracted during medication pass (from pyxis to patient)? a. Yes b. No 5. If a pain medication was administered, was the baseline and post intervention pain level documented? a. Yes b. No Figure 3: baseline medication administration audit for microsystem
19 PROSPECTUS ELEMENTS 18 August September October 2015 November December January assessment stage -audit, committee 1. incident reports filed regarding medication administration, focus changed to medication reconciliation as there was no consistent practice found during daily huddles with
20 PROSPECTUS ELEMENTS 19 staff 2. Met with pharmacy quality manager contacted ITS Program Manager for EHR Business Continuity and Regulatory Compliance and Director of Patient Safety Operations & Transformation for guidance on standardization of medication reconciliation, continued to audit the incident reports
21 PROSPECTUS ELEMENTS 20 related to medication errors Develop a tool for medication administration reconciliation Implement tool with committee educating staff- start with early majority and innovators Educate and Evaluate effectiveness of tool with survey for
22 PROSPECTUS ELEMENTS 21 staff RNs, review during daily huddles Figure 4 : Timeline for project Evaluation tool for Medication Reconciliation Standard Work 1. Please rate the effectiveness of the tool from 1 (least helpful) to 5 (extremely helpful) : 2. What did you find most helpful in standard work tool? 3. What did you find least helpful in standard work tool? 4. What would you like added to standard work tool? 5. What do you usually do if you have a question regarding medication reconciliation (resources, etc. )? Figure 5: Evaluation tool for Medication Reconciliation Standard Work


23 PROSPECTUS ELEMENTS 22 Medication Reconciliation How To Guide


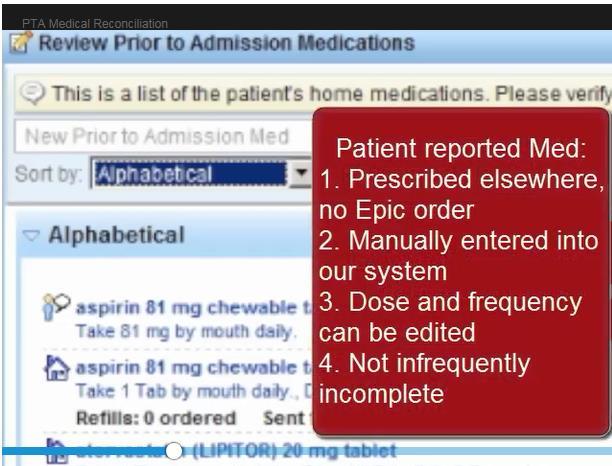
24 PROSPECTUS ELEMENTS 23 If there is a medication with no dosage, frequency, etc., delete it and enter complete medication with full dose, route, and frequency If the medication was prescribed, we cannot change dosage, etc. If it is a patient reported medication, we are able to change dosage, etc. If patient reports he has never taken medication, delete it with erroneous entry as reason When you are finished, you can MARK AS COMPLETE or incomplete if still missing medications, click add a note to specify if something is missing Then Mark as Reviewed If patient states they took the medication a week ago or a month ago, etc., please enter approximate date, otherwise it will show as unknown. Figure 6: First Draft of Medication Reconciliation Guide
25 PROSPECTUS ELEMENTS 24 Process Description: This standard work outlines the expectation and workflow for CAPR staff performing medication reconciliation during transfer of care phases: preop, post op and discharge Who Must Use this Process? : This standard work should be used at all times by Registered Nurses Process and Detailed Steps Outpatient arrives to CAPR 1. As part of pre op assessment, RN is to review medication reconciliation in the CAPR navigator a. Current medications listed- verify with patient to see if they are still taking i. Patient reported medication: visually represented by human icon by medication, can be edited ii. Prescribed medication: visually represented by house icon, ordered in EPIC, automatically added, cannot be edited only deleted when applicable b. If not taking a medication, use the X to remove. Medication can be viewed in historical tab c. Ask patient if they are taking any new medications not listed. i. Use the New Home Med search window to find medication and enter as much information as possible (name, dosage, frequency, last dose-enter specific date) ii. Review Rx dispenses tab in navigator. If a medication appears on list that is not correlated with order, add to medication list 2. Select status of this list : complete or incomplete. Add note if incomplete and as needed. This is important information for providers placing orders. 3. Mark as reviewed Postoperative phase in CAPR Figure 7: Medication Reconciliation Standard Work 1. If patient is staying overnight, review medication reconciliation tab. Verify medications with patient and dose times. a. Ask treatment team to order medications if necessary. Escalate any pending issues regarding medications. 2. Upon discharge, review medications with patient from the After Visit Summary (AVS). If any new medications are ordered, print Micromedex information for patient and include in AVS. a. For new anticoagulation medications, the OR pharmacy can be contacted to provide education b. Perform time out before discharging patient to confirm all medications are correct and ordered for pick up
26 PROSPECTUS ELEMENTS 25 References American Association Of Colleges Of Nursing (2013). Competencies and curricular expectations for clinical nurse leaders. Burton, M.M., Hope, C., Murray, M.D., et al. (2007). The cost of adverse drug events in ambulatory care. AMIA Annu Symp Proc, Edwards, S., & Axe, S. (2015). The 10 'R's of safe multidisciplinary drug administration. Nurse Prescribing, 13(8), p. Joint Commission. (2014, November 14). Hospital: 2015 National Patient Safety Goals. Retrieved September 11, 2015, from (Links to an external site.) Kotter, J., & Rathgeber, H. (2005). Our Iceberg is Melting: Changing and Succeeding Under Any Conditions. New York, NY: Audio Renaissance. Kramer, J. S., Stewart, M. R., Fogg, S. M., Schminke, B. C., Zackula, R. E., Nester, T. M., &... Goertzen, K. W. (2014). A Quantitative Evaluation of Medication Histories and Reconciliation by Discipline. Hospital Pharmacy, 49(9), p. doi: /hpj Lehnbom, E. C., Stewart, M. J., Manias, E., & Westbrook, J. I. (2014). Impact of medication reconciliation and review on clinical outcomes. The Annals Of Pharmacotherapy, 48(10), doi: / Maviglia, S.M., Yoo, J.Y., Franz, C., et al. (2007). Cost- benefit analysis of a hospital pharmacy bar code solution. Arch Intern Med, 167(8), Mchugh, M. D., Aiken, L. H., Eckenhoff, M. E., & Burns, L. R. (2015). Achieving Kaiser Permanente quality. Health Care Management Review, 1. doi: /hmr Muegge, S. (2014). Safety Corner: Make Time for Medication Reconciliation. AAACN Viewpoint, 36(3), p. National Patients Safety Agency. (2007). Safety in Doses: Medication Safety Incidents in the NHS. Retrieved October 8, 2015, from Nelson, E. C., Batalden, P. B., & Godfrey, M. M. (2007). 13. In Quality by design: A clinical microsystems approach(kindle ed.). Lebanon, NH: Center for the Evaluative Clinical Sciences at Dartmouth.
27 PROSPECTUS ELEMENTS 26 Ruggiero, J., Smith, J., Copeland, J., & Boxer, B. (2015). Discharge Time Out: An Innovative Nurse-Driven Protocol for Medication Reconciliation. MEDSURG Nursing, 24(3), p. Sebaaly, J., Parsons, L. B., Pilch, N. (., Bullington, W., Hayes, G. L., & Easterling, H. (2015). Clinical and Financial Impact of Pharmacist Involvement in Discharge Medication Reconciliation at an Academic Medical Center: A Prospective Pilot Study. Hospital Pharmacy, 50(6), p. doi: /hpj
Optimizing Electronic Healthcare Records and Improving Process in the Healthcare Clinic
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Optimizing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Optimizing
Improving Nurse-patient Communication about New Medicines
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
Improving Patient Safety: Reducing Medication Errors in the Microsystem
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-21-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-21-2015 Improving
Improving Pain Reassessment within One Hour Following the Administration of Pain Medication
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
Improving Patient Medication Reconciliation Participation and Compliance Through Education
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Improving
Obstetric Triage Improvement
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Obstetric
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Obstetric
IMPROVING COMMUNICATION AND SATISFACTION THROUGH HOURLY ROUNDS
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 IMPROVING
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 IMPROVING
Disclosure. SwedishAmerican Hospital A Division of UW Health. Learning Objectives. Medication History. Medication History 2/2/2017
 Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Educating medication aides about safe medication administration
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Educating
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Educating
Implementing Change to Decrease the Readmission Rate for Clients of a Care Transition Program
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Implementing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Implementing
Pharmacy Medication Reconciliation Workflow Emergency Department
 Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
University of Michigan Health System Program and Operations Analysis. Analysis of Problem Summary List and Medication Reconciliation Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
Improving Nurse Education on Research Informed Consent
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Infection Control: Reducing Hospital Acquired Central Line Bloodstream Infections
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Infection
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Infection
VAP Prevention in the CTICU
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 VAP
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 VAP
Reduce the Rooming Time
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Reduce
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Reduce
Prospectus Summary Brief: NICU Communication Improvement
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 Prospectus
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22-2015 Prospectus
Nurse Shift Handoff Report at the Patient's Bedside: Improving Nurse-to-Nurse Communication
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Nurse
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Nurse
USF Scholarship: a digital Gleeson Library Geschke Center
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-18-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-18-2015 Improving
Reducing Clostridium Difficile
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Reducing
Standardized Blood Transfusion Documentation
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-15-2016 Standardized
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-15-2016 Standardized
Reducing Avoidable Interruptions During the Medication Administration Process
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Reducing
Improving Hand Hygiene Compliance to Reduce CLABSI Rate in Oncology ICU
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22- Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22- Improving
REDUCTION OF PSYCHIATRIC PATIENT BOARDING IN THE ED
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
A Multi-Prong Fall Awareness Program to Reduce the Occurrence of Falls in a Skilled Nursing Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Multi-Prong
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Multi-Prong
Discharge by 11:00 AM and the Effects on Throughput
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 Discharge
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 Discharge
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Patient Satisfaction Related to Noise in the Coronary Care Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Patient
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Patient
Go! Guide: Medication Administration
 Go! Guide: Medication Administration Introduction Medication administration is one of the most important aspects of safe patient care. The EHR assists health care professionals with safety by providing
Go! Guide: Medication Administration Introduction Medication administration is one of the most important aspects of safe patient care. The EHR assists health care professionals with safety by providing
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Admission Handoff Between Emergency Department and Inpatient Units
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Admission
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Admission
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02
 Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Implementation of a Debrief Takeaway board
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Implementation
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Implementation
The Clinical Nurse Leader as Risk Anticipator: Optimizing the Completion and Accuracy of the Code Blue Recorder Sheet
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-9-2017 The
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-9-2017 The
Fall Reduction with Nursing Interventions
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Fall
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Fall
Learner Manual. Document Best Possible Medication History (BPMH)
") Learner Manual Document Best Possible Medication History (BPMH) Table of Contents Medication safety... 1 Medication errors impact everyone... 1 Who should obtain the BPMH?... 1 When is the BPMH obtained?...
Learner Manual Document Best Possible Medication History (BPMH) Table of Contents Medication safety... 1 Medication errors impact everyone... 1 Who should obtain the BPMH?... 1 When is the BPMH obtained?...
Impacting Patient Care Experiences: Hourly Rounding
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 5-22-2015 Impacting
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 5-22-2015 Impacting
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital. Final Report. Submitted To:
 Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
The Significance of Timing of Patient Daily Weights and the Barriers
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 The
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 The
Improving Patient Satisfaction through Reducing Nurse Overtime and Redesigning Nurse Staffing and Scheduling
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-18-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-18-2015 Improving
Barriers Encountered by Nurses and Nursing Assistants that Prevent Purposeful Rounding
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Barriers
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Barriers
Increasing CLABSI Bundle Compliance in the NICU
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-14-2017 Increasing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-14-2017 Increasing
Preventing HAPUs in High-Risk Cardiac Cath Patients Using Foam Dressing Protocol
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-16-2016 Preventing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-16-2016 Preventing
eprescribe Training for Nurses and Pharmacy Techs Net Access Home Medication Pathway Clinical Informatics - Oct 2015
 eprescribe Training for Nurses and Pharmacy Techs Net Access Home Medication Pathway Clinical Informatics - Oct 2015 Click Home Medications on the Navigator Home Medications Pathway Click on Select Default
eprescribe Training for Nurses and Pharmacy Techs Net Access Home Medication Pathway Clinical Informatics - Oct 2015 Click Home Medications on the Navigator Home Medications Pathway Click on Select Default
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Pharmacy Technicians and Interns: Charting New Territory
 Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Achieving safety in medication management through barcoding technology
 Achieving safety in medication management through barcoding technology Kara Marx, RN, FACHE, FHIMSS Vice President of Information Services Sharp Healthcare. SESSION OBJECTIVES Describe the primary activities
Achieving safety in medication management through barcoding technology Kara Marx, RN, FACHE, FHIMSS Vice President of Information Services Sharp Healthcare. SESSION OBJECTIVES Describe the primary activities
Improving Pain Reassessment and Documentation Through Nurse Education
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
A Multi-Phased Approach to Using Clinical Data to Drive Evidence-Based EMR Redesign. Kulik, Carole Marie; Foad, Wendy; Brown, Gretchen
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
A Roadmap for the Journey Home - A Supplemental Tool Guiding Patients from Hospital to Home
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Roadmap
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Roadmap
Reconciliation of Medicines on Admission to Hospital
 Reconciliation of Medicines on Admission to Hospital Policy Title State previous title where relevant. State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For
Reconciliation of Medicines on Admission to Hospital Policy Title State previous title where relevant. State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For
EMAR Pending Review. The purpose of Pending Review is to verify the orders received from the pharmacy.
 EMAR Pending Review This manual includes Pending Review, which is the confirmation that the information received from the pharmacy is correct. This is done by verification of the five (5) rights of medication
EMAR Pending Review This manual includes Pending Review, which is the confirmation that the information received from the pharmacy is correct. This is done by verification of the five (5) rights of medication
Fall Prevention in the Inpatient Setting
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-14-2017 Fall
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-14-2017 Fall
Reducing IV Infiltrates in the Neonatal Population
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Reducing
Medication Reconciliation: Preventing Errors and Improving Patient Outcomes
 Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
Preoperative Education: A Patient-Centered Care Approach
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Preoperative
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Preoperative
Decreasing Delayed Patient Transfers Prior to Shift Change
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Decreasing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Decreasing
STANDARDIZATION OF BODY IMAGING HUDDLE IN RADIOLOGY
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 STANDARDIZATION
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 STANDARDIZATION
SELF - ADMINISTRATION OF MEDICINES AND ADMINISTRATION OF MEDICINES SUPPORTED BY FAMILY/INFORMAL CARERS OF PATIENTS IN COMMUNITY NURSING
 CLINICAL PROTOCOL SELF - ADMINISTRATION OF MEDICINES AND ADMINISTRATION OF MEDICINES SUPPORTED BY FAMILY/INFORMAL CARERS OF PATIENTS IN COMMUNITY NURSING RATIONALE Medication errors can cause unnecessary
CLINICAL PROTOCOL SELF - ADMINISTRATION OF MEDICINES AND ADMINISTRATION OF MEDICINES SUPPORTED BY FAMILY/INFORMAL CARERS OF PATIENTS IN COMMUNITY NURSING RATIONALE Medication errors can cause unnecessary
University of Cincinnati Patient Centered Medical Home Leadership Decisions
 University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
Go! Guide: Adding Medication Administration History
 Go! Guide: Adding Medication Administration History Introduction Past medication administrations are often an integral part of a patient scenario. It may be important for students to review the patient
Go! Guide: Adding Medication Administration History Introduction Past medication administrations are often an integral part of a patient scenario. It may be important for students to review the patient
Improving Staff Responsiveness to Patient-Initiated Call Lights
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Reducing Patient Supply Waste Through Nurse Education to Improve Quality of Patient Care in the Clinical Microsystem
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Reducing
Hypertension Management Through Patient Education
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Hypertension
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Hypertension
Increasing Self Care Compliance with Follow-up Appointments
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-18-2015 Increasing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-18-2015 Increasing
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety
: Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety") Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Standardizing Telephone Triage Protocol
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Standardizing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Standardizing
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting
 patients from the Acute Care Setting to the Ambulatory Setting") Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting American College of Medical Practice Executives Case Study Submitted by Chantay Lucas,
Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting American College of Medical Practice Executives Case Study Submitted by Chantay Lucas,
Reducing Turnover Time to Improve Efficiency in the Operating Room
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 Reducing
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Reducing Wait Time of Chemotherapy and Biotherapy Administration to Inpatients by Increasing the Numbers of Chemotherapy Providers
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Reducing
BUSINESS CASE. Implementation of Bar code Medication Administration System at the Sault Area Hospital (SAH)
") BUSINESS CASE Implementation of Bar code Medication Administration System at the Sault Area Hospital (SAH) With the permission of the SAH, CSHP removed Date: August 25, 2009 content that would have identified
BUSINESS CASE Implementation of Bar code Medication Administration System at the Sault Area Hospital (SAH) With the permission of the SAH, CSHP removed Date: August 25, 2009 content that would have identified
Patient Safety It All Starts with Positive Patient Identity APRIL 14, 2016
 Patient Safety It All Starts with Positive Patient Identity APRIL 14, 2016 Maximizing patient safety and improving the quality of care is the ultimate goal for healthcare providers. Doing so requires staying
Patient Safety It All Starts with Positive Patient Identity APRIL 14, 2016 Maximizing patient safety and improving the quality of care is the ultimate goal for healthcare providers. Doing so requires staying
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
Chronic Pain Management in the Inpatient Care Setting
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Chronic
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Chronic
Making Differences Matter Redesign Ambulatory Medication Reconciliation
 Making Differences Matter Redesign Ambulatory Medication Reconciliation AMGA Annual Meeting April 5 2014 Presenters Thomas N. Atkins, MD MMM,FAAFP, FACPE, CPE Steven A. Mitnick MD MBA Katherine T. Manuel,
Making Differences Matter Redesign Ambulatory Medication Reconciliation AMGA Annual Meeting April 5 2014 Presenters Thomas N. Atkins, MD MMM,FAAFP, FACPE, CPE Steven A. Mitnick MD MBA Katherine T. Manuel,
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Introduction to the Parking Lot
 Introduction to the Parking Lot In ARK Epic training sessions, The Parking Lot" is used to capture all questions for which your trainer may not have an immediate answer during session. Your ARK Epic Training
Introduction to the Parking Lot In ARK Epic training sessions, The Parking Lot" is used to capture all questions for which your trainer may not have an immediate answer during session. Your ARK Epic Training
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Electronic Medical Records and Nursing Efficiency. Fatuma Abdullahi, Phuong Doan, Cheryl Edwards, June Kim, and Lori Thompson.
 Running Head: EMR S AND NURSING EFFICIENCY Electronic Medical Records 1 Electronic Medical Records and Nursing Efficiency Fatuma Abdullahi, Phuong Doan, Cheryl Edwards, June Kim, and Lori Thompson July
Running Head: EMR S AND NURSING EFFICIENCY Electronic Medical Records 1 Electronic Medical Records and Nursing Efficiency Fatuma Abdullahi, Phuong Doan, Cheryl Edwards, June Kim, and Lori Thompson July
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Improving Early Sepsis Identification on Inpatient Units
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 Improving
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
Medication Reconciliation with Pharmacy Technicians
 Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
UNIVERSITY OF CALIFORNIA, SAN FRANCISCO AUDIT SERVICES. UCSF Medical Center Hospital Charge Capture - Emergency Services Project #
 , SAN FRANCISCO AUDIT SERVICES UCSF Medical Center Hospital Charge Capture - Emergency Services Project #13-024 June 2013 Performed by: Sugako Amasaki, Principal Auditor Julia Travous, Manager (Protiviti)
, SAN FRANCISCO AUDIT SERVICES UCSF Medical Center Hospital Charge Capture - Emergency Services Project #13-024 June 2013 Performed by: Sugako Amasaki, Principal Auditor Julia Travous, Manager (Protiviti)
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Clearing the Pathway to Chemotherapy Certification for Inpatient Nurses
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-14-2017 Clearing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-14-2017 Clearing
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
eprescribing Information to Improve Medication Adherence
 eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when