Ohio Home Care Waiver Provider Application Process
|
|
|
- Belinda McKenzie
- 6 years ago
- Views:
Transcription








1 Ohio Home Care Waiver Provider Application Process

2 Provider Enrollment Website medicaid.ohio.gov



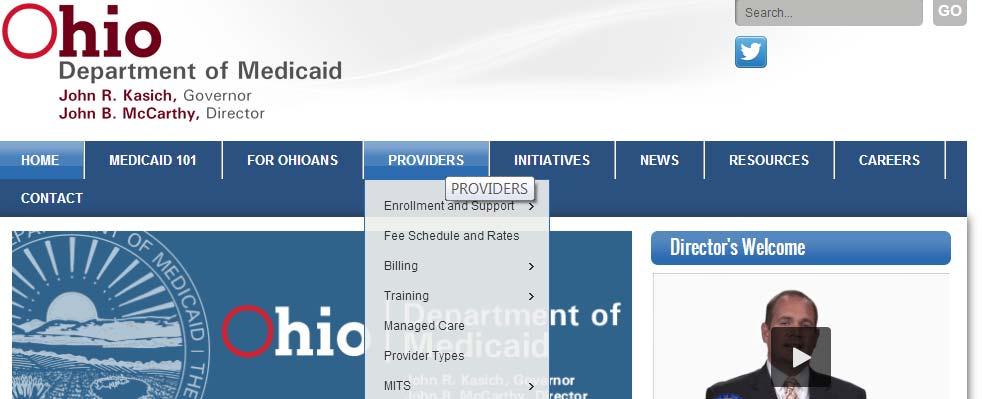
3 Hover over the Providers Tab


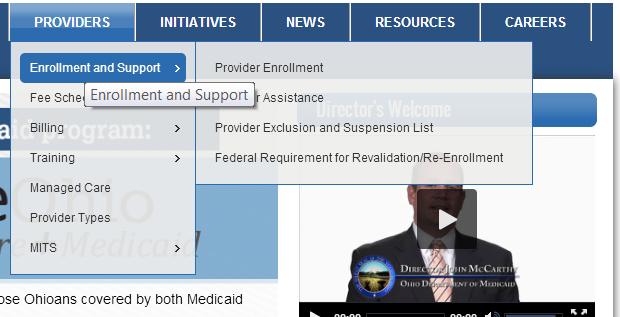
4 Hover over Enrollment and Support

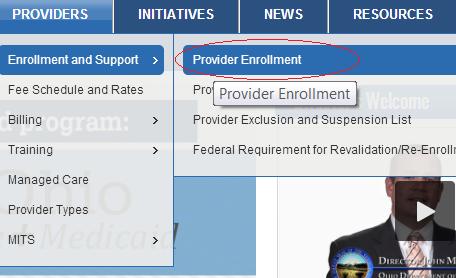
5 Click Provider Enrollment



6 On the next page, click Enroll as a New Provider




7 On this page, you will also find required application documents and a link to the MITS portal, located in the right margin as you scroll down the page.

8 After clicking Enroll as a New Provider, click I need to enroll as a provider to bill Ohio Medicaid Even if you are a previous provider and wish to re-enroll, a new application is needed.



9 This will expand the Instructions box. Click new application or continue application in the lower right corner. Continue application will resume an application in progress.

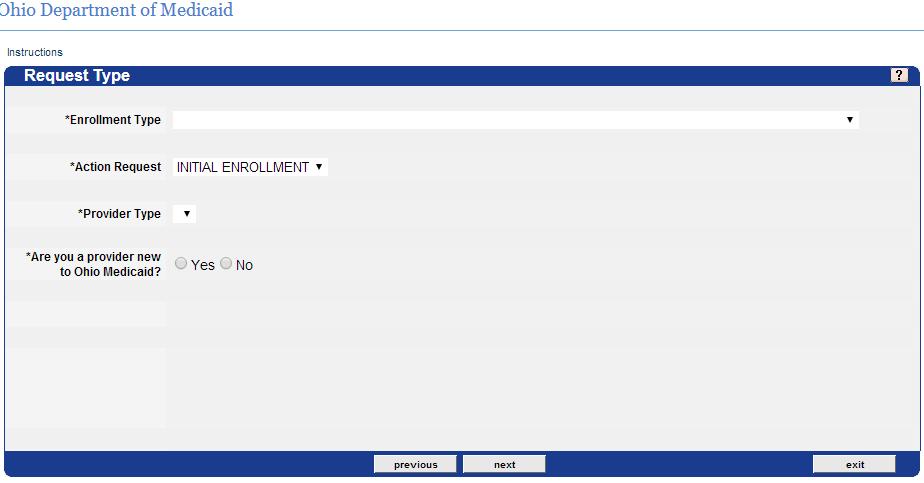
10 Application Page 2: Request Type


11 Application Page 2, Continued Select an enrollment type, either individual practitioner or organization. Please note that individuals should enroll as individual practitioners and not as organizations.



12 Application Page 2, Continued Choose the provider type for which you are applying.



13 Application Page 2, Continued If you are a re-enrolling provider, select No for the question Are you a provider new to Ohio Medicaid? and enter your 7- digit Medicaid number. If you are a new provider, select Yes.

14 Application Page 3: Identifying Information. Applicants will enter Identifying Information. Only fields marked with a * are required.
15 Application Fee for Agency Providers Agency providers will be prompted to pay an application fee. The fee is paid with the initial application and every 5 years at revalidation. Applicants will receive a confirmation number for the fee. This number must be entered in the Confirmation Number field at the bottom of the page. If the agency is a Medicare/Medicaid provider, and has paid the fee in the last 5years, answer YES to the Medicare or Medicaid application fee question and submit proof of payment with the application.


16 Application Fee for Agency Providers, Continued

17 Application Page 4: Tax Information On page 4, an ATN is assigned and tax information is needed. The IRS effective date should be today s date. The IRS end date auto-fills.

18 Application Page 4, Continued W-9 should be marked YES. Form 147 will be marked NO for individuals. Organizations that need Form 147 will check YES.



19 Application Page 5: DEA License This page requests DEA license information to administer drugs. Most applicants will not have a license to administer drugs and can click next.



20 Application Page 6: Address Information The Address Type needs to be practice location or the applicant will not be able to continue.


21 Application Page 7: Type and Specialty This page will auto fill for individuals. The primary specialty box needs to be checked. Organizations may pick other specialties using the drop down options.
22 Provider Type & Specialties TYPE SPECIALITY DESCRIPTION Other accredited Home Health Agency PCS - Personal Care Services Home Care Attendant RN LPN 45/ Home Meals 45/ Supplemental Transport Services 45/ Adult Day Health 45/ Supplemental Adaptive/Assistive Devices 45/ Home Delivered Meals 45/ Minor Home Modifications 45/ Out of Home Respite 45/ Emergency Response System Medicare Certified Home Health Agency


23 Application Page 8: Language Applicants may add any additional languages they speak.

24 Application Page 9: Group Affiliations Applicants affiliated with a group practice or practices would click add and fill in the information on this page. Most applicants will leave this page blank.

25 Application Page 10: Criminal Offense I Disclose convictions here.



26 Application Page 11: Criminal Offense II Disclose convictions here.


27 Application Page 12: Violations of State or Federal Law Disclose violations of State or Federal Law.


28 Application Page 13: Previously Participated For re-enrolling providers, that previously had a Medicaid provider number, click yes and enter the previous provider ID.


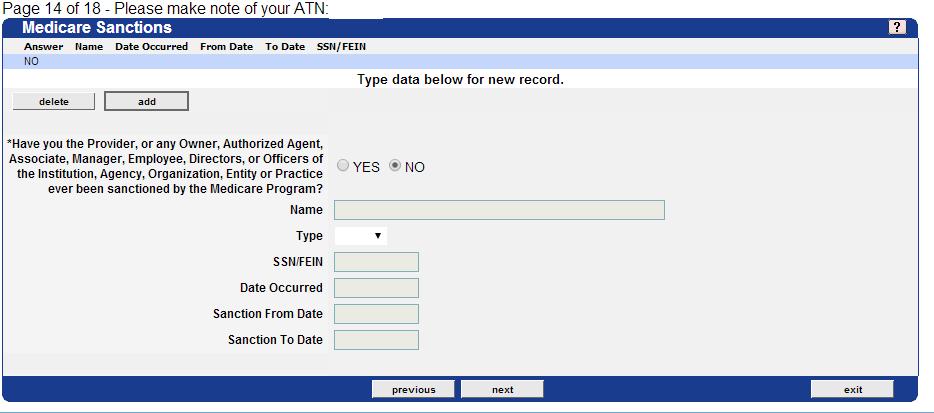
29 Application Page 14: Medicare Sanctions Any sanctions by the Medicare program must be entered.

30 Application Page 15: Addendum E To proceed all questions must be answered yes with the exception of the residency questions.


31 Application Page 15: Addendum E, Continued For LPNs, an RN supervisor s name and license number is needed.

32 Application Page 15: Addendum E, Continued Relationship to consumer: Check YES to indicate you meet the requirements to be the provider for the individual you will be providing services to. The provider cannot be the legally responsible family member. Legally responsible family members include Spouse Birth or adoptive parent (in the case of a minor) Foster caregiver

33 Application Page 15: Addendum E, Continued Check yes or no for each residency question. Applicants that have not been an Ohio resident for at least the last five years will need an FBI check in addition to a BCI background check to process the application.

34 Application Page 15: Addendum E, Continued The applicant must type an electronic signature at the bottom of the page.



35 Application Page 16: Certification Fill in Legal Entity Name and Individual Name. The primary practice address also needs to be completed. The Enrollment Checklist link provides a list of documents needed to complete the application.



36 Application Page 16: Certification, Continued All applicants must read and accept the terms. Use the scroll bar on the right of each section to read the terms and select I accept the terms and conditions.


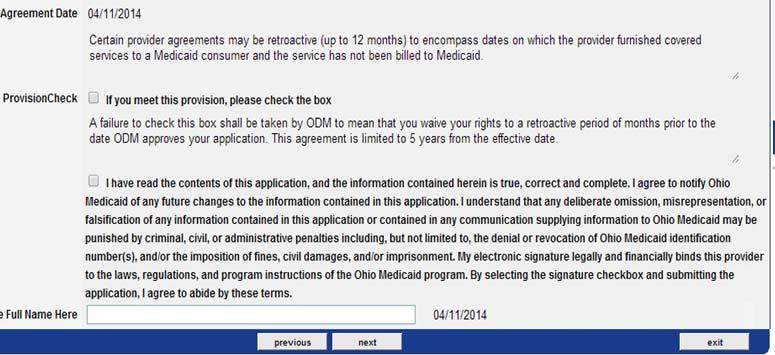
37 Application Page 16: Certification, Continued Check the provision check box and sign at the bottom.



38 Application Page 17: Documents Submission Type and Notes Applicants will choose mail or upload for application documents and add any comments they feel are helpful. Click submit at the bottom of the page to submit the application.




39 Application Page 18: Confirmation of Receipt A list of required documents will come up with address to send to. There are also links to upload documents and print the application.



40 Application Page 18: Confirmation of Receipt, Continued Note: the address on application is incorrect.
41 Please Mail Documents To: Public Consulting Group Home and Community-Based Provider Oversight Services 155 East Broad Street, 8 th Floor Columbus, Ohio Fax: OHProvidermaintenance@pcgus.com
42 Please Have Background Check Mailed to: Ohio Department of Medicaid Attn: BCI Coordinator PO Box Columbus, OH 43218
43 Uploading Documents after the Application Is Submitted


44 Go to the provider enrollment page and click Check Provider Enrollment Status



45 This will bring up a new page where applicants will enter the ATN assigned to the application and their last name. The last name must be in CAPS.


46 Applicants can check application and document status. At the bottom of the page, applicants can use the link to upload documents.



47 Click Upload required documents to upload new documents. Select the document type to upload and browse to select the document being uploaded.
Use the following to enter new patients into Horizon and to establish a patient for a pending admission. All referrals will be entered into Horizon.
 REFFERAL AND INTAKE SUMMARY Use the following to enter new patients into Horizon and to establish a patient for a pending admission. All referrals will be entered into Horizon. ROLES Supervisor/Nurse The
REFFERAL AND INTAKE SUMMARY Use the following to enter new patients into Horizon and to establish a patient for a pending admission. All referrals will be entered into Horizon. ROLES Supervisor/Nurse The
Reimbursements: Submit a Flat Rate Reimbursement
 Reimbursements: Submit a Flat Rate Reimbursement Overview Tax-Aide volunteers may elect to receive a one-time, flat-rate expense reimbursement for which volunteers receive $35 and volunteer leaders receive
Reimbursements: Submit a Flat Rate Reimbursement Overview Tax-Aide volunteers may elect to receive a one-time, flat-rate expense reimbursement for which volunteers receive $35 and volunteer leaders receive
Care Provider Background Screening Clearinghouse
 Agency for Health Care Administration Care Provider Background Screening Clearinghouse AHCA Clearinghouse Results Website Instruction Guide Updated May 2017 Page 1 of 47 Clearinghouse Results Website Overview...3
Agency for Health Care Administration Care Provider Background Screening Clearinghouse AHCA Clearinghouse Results Website Instruction Guide Updated May 2017 Page 1 of 47 Clearinghouse Results Website Overview...3
Intern Placement Tracking (IPT)
") Intern Placement Tracking (IPT) How-To Guide for Students Binghamton University College of Community and Public Affairs Department of Social Work Sophia Resciniti Director of Field Education PO Box 6000
Intern Placement Tracking (IPT) How-To Guide for Students Binghamton University College of Community and Public Affairs Department of Social Work Sophia Resciniti Director of Field Education PO Box 6000
Conflict of Interest Committee Submission Guide
 Conflict of Interest Committee Submission Guide Training materials for using IRBNet are available at: http://www.irbnetresources.org/ (userid: kettering, password: training) Guides and submission forms
Conflict of Interest Committee Submission Guide Training materials for using IRBNet are available at: http://www.irbnetresources.org/ (userid: kettering, password: training) Guides and submission forms
INDIVIDUAL FUNDING. Stella Yang SGA Treasurer August 2018
 INDIVIDUAL FUNDING Stella Yang SGA Treasurer August 2018 Accessing the Form 1. Read our funding guideline information on our SGA page on the WSU Website, or go to https://www.wichita.edu/student_life/sga/individual_funding_.php
INDIVIDUAL FUNDING Stella Yang SGA Treasurer August 2018 Accessing the Form 1. Read our funding guideline information on our SGA page on the WSU Website, or go to https://www.wichita.edu/student_life/sga/individual_funding_.php
Personal Emergency Response System
 LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Emergency Response System (Enrollment packet is subject
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Emergency Response System (Enrollment packet is subject
Supervised Independent Living (SIL)
") PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Supervised Independent Living (SIL) (Enrollment packet is subject to change without notice) PT89 07/10 GENERAL INFORMATION REGARDING
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Supervised Independent Living (SIL) (Enrollment packet is subject to change without notice) PT89 07/10 GENERAL INFORMATION REGARDING
RELATIVE/NEIGHBOR PROVIDER
 TABLE OF CONTENTS 301.1 GENERAL POLICY & REGULATION 301.2 DEFINITIONS & ACRONYMS 301.3 GOALS & OBJECTIVES 301.4 P/C RESPONSIBILITIES 301.5 CCIS RESPONSIBILITIES 301.6 PROVIDER RESPONSIBILITIES 301.7 IDENTIFYING
TABLE OF CONTENTS 301.1 GENERAL POLICY & REGULATION 301.2 DEFINITIONS & ACRONYMS 301.3 GOALS & OBJECTIVES 301.4 P/C RESPONSIBILITIES 301.5 CCIS RESPONSIBILITIES 301.6 PROVIDER RESPONSIBILITIES 301.7 IDENTIFYING
Guide to Provider Forms
 Guide to Provider Forms ACTION Add a Provider to the group YOU WILL NEED TO COMPLETE THE SECTIONS IDENTIFIED BELOW ON THE PROVIDER INFORMATION UPDATE FORM (PIF) AND ANY ADDITIONAL DOCUMENTS LISTED. ALL
Guide to Provider Forms ACTION Add a Provider to the group YOU WILL NEED TO COMPLETE THE SECTIONS IDENTIFIED BELOW ON THE PROVIDER INFORMATION UPDATE FORM (PIF) AND ANY ADDITIONAL DOCUMENTS LISTED. ALL
Ohio Home and Community-Based Service Waivers
 Ohio Home and Community-Based Service Waivers Ohio Home Care Waiver Provider Education and Technical Assistance www.pcghealth.com Training Overview Priorities for Ohio Home Care Waiver: Waiver Target Population
Ohio Home and Community-Based Service Waivers Ohio Home Care Waiver Provider Education and Technical Assistance www.pcghealth.com Training Overview Priorities for Ohio Home Care Waiver: Waiver Target Population
Novant Health Auxiliary Prince William Medical Center Haymarket Medical Center
 Novant Health Auxiliary Adult Volunteer Application Form (Application 18 Years of Age or Older and not currently enrolled in high school) Once you have completed this application please scan and email,
Novant Health Auxiliary Adult Volunteer Application Form (Application 18 Years of Age or Older and not currently enrolled in high school) Once you have completed this application please scan and email,
Application Process for Individual HCPs
 HCF Program Training Application Process for Individual HCPs HCF Program Training I Application Process I September 2015 1 This training is just a general overview and starting point for applicants Every
HCF Program Training Application Process for Individual HCPs HCF Program Training I Application Process I September 2015 1 This training is just a general overview and starting point for applicants Every
ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Rural Health Clinic
 Rural Health Clinic") LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Rural Health Clinic (Enrollment packet is subject to change without
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Rural Health Clinic (Enrollment packet is subject to change without
Carefully read the following information, application instructions, and the NCLEX Candidate Bulletin prior to completing the enclosed application.
 Executive Office of Health and Human Services Department of Public Health Bureau of Health Professions Licensure Board of Registration in Nursing www.mass.gov/dph/boards/rn The Commonwealth of Massachusetts
Executive Office of Health and Human Services Department of Public Health Bureau of Health Professions Licensure Board of Registration in Nursing www.mass.gov/dph/boards/rn The Commonwealth of Massachusetts
Requirements for Provider Type 21 Case Manager
 Requirements for Provider Type 21 Case Manager Specialty Code 076 Peer Support Services 211 Medical Assistance Case Management for HIV&AIDS 212 Medical Assistance Case Management for Under 21 213 Early
Requirements for Provider Type 21 Case Manager Specialty Code 076 Peer Support Services 211 Medical Assistance Case Management for HIV&AIDS 212 Medical Assistance Case Management for Under 21 213 Early
Medical Education and Research Cost (MERC) Grant Application Instructions for Sponsoring Institutions and Teaching Programs
 Grant Application Instructions for Sponsoring Institutions and Teaching Programs") for Sponsoring Institutions and Teaching Programs Data year: Fiscal Year 2016 Clinical Training Application deadline: October 31, 2017 Estimated distribution: April 30, 2018 For more information: http://www.health.state.mn.us/divs/hpsc/hep/merc/index.html
for Sponsoring Institutions and Teaching Programs Data year: Fiscal Year 2016 Clinical Training Application deadline: October 31, 2017 Estimated distribution: April 30, 2018 For more information: http://www.health.state.mn.us/divs/hpsc/hep/merc/index.html
What is your start date? (Date in which you plan to begin seeing patients in the hospital). Specialty SECTION I. IDENTIFICATION DATA
. Specialty SECTION I. IDENTIFICATION DATA") This Application is for Non-employed Clinical Assistants (RN, dental assistant, orthotist, etc) who wish to assist a supervising physician at one or more of our facilities. Advanced Practice Nurses (CRNA,
This Application is for Non-employed Clinical Assistants (RN, dental assistant, orthotist, etc) who wish to assist a supervising physician at one or more of our facilities. Advanced Practice Nurses (CRNA,
ECOLAB GIVING SITE FOR ALUMNI OF ALL ECOLAB SUBSIDIARIES
 ECOLAB GIVING SITE FOR ALUMNI OF ALL ECOLAB SUBSIDIARIES 1 Table of Contents Program Page 1. Giving Site Access 3-7 2. Matching Gifts: Education, Public Broadcasting 8-20 3. Dollars for Doers (FKA Volunteer
ECOLAB GIVING SITE FOR ALUMNI OF ALL ECOLAB SUBSIDIARIES 1 Table of Contents Program Page 1. Giving Site Access 3-7 2. Matching Gifts: Education, Public Broadcasting 8-20 3. Dollars for Doers (FKA Volunteer
PRACTICE INFORMATION AND LETTER AGREEMENT FORM. COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747
 PRACTICE INFORMATION AND LETTER AGREEMENT FORM COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747 PERSONAL DATA Last Name First Name License Number Tax I.D. Number for
PRACTICE INFORMATION AND LETTER AGREEMENT FORM COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747 PERSONAL DATA Last Name First Name License Number Tax I.D. Number for
LIBERTY DENTAL PLAN. Dental Hygienist - Credentialing Application. City: State: DEGREE: City: State: DEGREE:
 *Required Fields LIBERTY DENTAL PLAN Dental Hygienist - Credentialing Application Please complete one application per Dental Hygienist Demographic Information: Male Female *HYGIENIST NAME: RDH Other *DATE
*Required Fields LIBERTY DENTAL PLAN Dental Hygienist - Credentialing Application Please complete one application per Dental Hygienist Demographic Information: Male Female *HYGIENIST NAME: RDH Other *DATE
Personal Care Attendant
 LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Care Attendant (Enrollment packet is subject to change
LOUISIANA Department of HEALTH and HOSPITALS ENROLLMENT PACKET FOR THE LOUISIANA MEDICAL ASSISTANCE PROGRAM (Louisiana Medicaid Program) Personal Care Attendant (Enrollment packet is subject to change
NEW STUDENT HOUSING APPLICATION
 NEW STUDENT HOUSING APPLICATION Step-by-step guide to filling out the housing application for new students who wish to live on campus. Frequently Asked Questions about living on campus NEW REDHAWK NEXT
NEW STUDENT HOUSING APPLICATION Step-by-step guide to filling out the housing application for new students who wish to live on campus. Frequently Asked Questions about living on campus NEW REDHAWK NEXT
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST
 PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Children s Choice (Enrollment packet is subject to change without notice) Revised 01/15 GENERAL INFORMATION REGARDING WAIVER ENROLLMENTS
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Children s Choice (Enrollment packet is subject to change without notice) Revised 01/15 GENERAL INFORMATION REGARDING WAIVER ENROLLMENTS
Utah medical & controlled substance license instructions Division of Occupational and Physician Licensing (DOPL) rev: 8/9/16
 rev: 8/9/16") Utah medical & controlled substance license instructions Division of Occupational and Physician Licensing (DOPL) rev: 8/9/16 Programs Exempt from the Utah controlled substance license: ALL Pathology and
Utah medical & controlled substance license instructions Division of Occupational and Physician Licensing (DOPL) rev: 8/9/16 Programs Exempt from the Utah controlled substance license: ALL Pathology and
INSTRUCTIONS AND INFORMATION FOR APPLICATION FOR INITIAL NURSE LICENSURE BY EXAMINATION
 The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health Bureau of Health Professions Licensure www.mass.gov/dph/boards/rn INSTRUCTIONS AND INFORMATION
The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health Bureau of Health Professions Licensure www.mass.gov/dph/boards/rn INSTRUCTIONS AND INFORMATION
LIBERTY DENTAL PLAN. Provider Credentialing Application. (* Required Fields) *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )
 *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )") (Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
(Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
Home and Community Based Services (HCBS)/Long Term Services and Supports (LTSS) Provider Credentialing/Re-Credentialing Application
/Long Term Services and Supports (LTSS) Provider Credentialing/Re-Credentialing Application") Home and Community Based Services (HCBS)/Long Term Services and Supports (LTSS) Provider Credentialing/Re-Credentialing Application New Mexico General information Corporate name (as assigned on W-9): Doing
Home and Community Based Services (HCBS)/Long Term Services and Supports (LTSS) Provider Credentialing/Re-Credentialing Application New Mexico General information Corporate name (as assigned on W-9): Doing
PROVIDER INFORMATION UPDATE FORM CURRENT CONTRACT INFORMATION - ALL FIELDS IN THIS SECTION ARE REQUIRED
 PROVIDER INFORMATION UPDATE FORM CURRENT CONTRACT INFORMATION - ALL FIELDS IN THIS SECTION ARE REQUIRED 1. Type of Group: Ancillary Specialist PCP Hospital Urgent Care FQHC/RHC QFPP/ X Contracted Entity/Name:
PROVIDER INFORMATION UPDATE FORM CURRENT CONTRACT INFORMATION - ALL FIELDS IN THIS SECTION ARE REQUIRED 1. Type of Group: Ancillary Specialist PCP Hospital Urgent Care FQHC/RHC QFPP/ X Contracted Entity/Name:
Post-Production, Visual Effects and Digital Animation Grant GUIDE TO APPLICATION SUBMISSION
 Post-Production, Visual Effects and Digital Animation Grant GUIDE TO APPLICATION SUBMISSION Introduction This guide will assist Post-Production, Visual Effects and Digital Animation Grant (PPG) applicants
Post-Production, Visual Effects and Digital Animation Grant GUIDE TO APPLICATION SUBMISSION Introduction This guide will assist Post-Production, Visual Effects and Digital Animation Grant (PPG) applicants
BSN Application. Supporting Documents Checklist. Part A - To Be Submitted Online. Part B Slide Room Submission. Your Application Number is:
 BSN Application Supporting Documents Checklist Your Application Number is: 57789296 Print, complete and sign this page. This page must be submitted as the top sheet, along with all BSN Application materials
BSN Application Supporting Documents Checklist Your Application Number is: 57789296 Print, complete and sign this page. This page must be submitted as the top sheet, along with all BSN Application materials
Reimbursement for National Certification in a Clinical Specialty
 California Nurses Association Represented Registered Nurse / Nurse Practitioner Reimbursement for National Certification in a Clinical Specialty Kaiser Permanente Northern California Revised 2/2/17 National
California Nurses Association Represented Registered Nurse / Nurse Practitioner Reimbursement for National Certification in a Clinical Specialty Kaiser Permanente Northern California Revised 2/2/17 National
Application Checklist for Facilities
 Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for the facility to participate with
Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for the facility to participate with
Medical Education and Research Cost (MERC) Grant Application Instructions for Sponsoring Institutions and Teaching Programs
 Grant Application Instructions for Sponsoring Institutions and Teaching Programs") Grant Application Instructions for Sponsoring Institutions and Teaching Programs Data year: Fiscal Year 2017 Clinical Training Application deadline: October 31, 2018 Estimated distribution: April 30, 2019
Grant Application Instructions for Sponsoring Institutions and Teaching Programs Data year: Fiscal Year 2017 Clinical Training Application deadline: October 31, 2018 Estimated distribution: April 30, 2019
DEVELOPMENTAL DISABILITIES INDIVIDUAL LETTER OF INTENT
 DEVELOPMENTAL DISABILITIES INDIVIDUAL LETTER OF INTENT To ensure timely processing of your application, please return the following checklist completed Letter of Intent (LOI) and documents requested to:
DEVELOPMENTAL DISABILITIES INDIVIDUAL LETTER OF INTENT To ensure timely processing of your application, please return the following checklist completed Letter of Intent (LOI) and documents requested to:
Checklist for Nursing Program Students
 Checklist for Nursing Program Students It is recommended that students make copies of all documents for your personal record prior to submitting. Complete and upload the following forms to CastleBranch
Checklist for Nursing Program Students It is recommended that students make copies of all documents for your personal record prior to submitting. Complete and upload the following forms to CastleBranch
CAREERTECH INFORMATION MANAGEMENT SYSTEM (CTIMS) EDI PROCESS GUIDEBOOK IMD
 EDI PROCESS GUIDEBOOK IMD") CAREERTECH INFORMATION MANAGEMENT SYSTEM (CTIMS) EDI PROCESS GUIDEBOOK IMD June 27, 2017 Revised January 5, 2018 Table of Contents Logging in to CTIMS... 1 Help and Troubleshooting... 2 Roles... 4 Starting
CAREERTECH INFORMATION MANAGEMENT SYSTEM (CTIMS) EDI PROCESS GUIDEBOOK IMD June 27, 2017 Revised January 5, 2018 Table of Contents Logging in to CTIMS... 1 Help and Troubleshooting... 2 Roles... 4 Starting
Edith Cowan University Research Management System. Reviewing Research Proposals in ECURMS: A guide for Associate Deans (Research)
") Research Management System Reviewing Research Proposals in ECURMS: A guide for Associate Deans (Research) V5 - November 2016 Contents Introduction... 2 Processes... 2 Expression of Interest... 2 Pre-submission...
Research Management System Reviewing Research Proposals in ECURMS: A guide for Associate Deans (Research) V5 - November 2016 Contents Introduction... 2 Processes... 2 Expression of Interest... 2 Pre-submission...
Grant Program
 Preventive Controls Alliance Training Grant Program http://afdo.org/pcgrants REPORTING AND REIMBURSEMENT INSTRUCTIONS CALENDAR YEAR 2017 Providing funds for state, local, tribal, and territorial food safety
Preventive Controls Alliance Training Grant Program http://afdo.org/pcgrants REPORTING AND REIMBURSEMENT INSTRUCTIONS CALENDAR YEAR 2017 Providing funds for state, local, tribal, and territorial food safety
Henry County Community Foundation How to Access the Online Scholarship Application
 Henry County Community Foundation How to Access the Online Scholarship Application 1. Follow the link from the Foundation website to https://henrycountycfscholarships.communityforce.com/ You will be taken
Henry County Community Foundation How to Access the Online Scholarship Application 1. Follow the link from the Foundation website to https://henrycountycfscholarships.communityforce.com/ You will be taken
MS Medicaid Provider Enrollment
 MS Medicaid Provider Enrollment Agenda 1. Provider Enrollment Tips 2. Enrollment Package 3. General Application Information 4. Enroll Online Checking Application Status 7. Self Attestation 8. License Renewal
MS Medicaid Provider Enrollment Agenda 1. Provider Enrollment Tips 2. Enrollment Package 3. General Application Information 4. Enroll Online Checking Application Status 7. Self Attestation 8. License Renewal
INSTRUCTIONS AND INFORMATION APPLICATION FOR INITIAL NURSE LICENSURE BY EXAMINATION
 Revised April 4. 2016 The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health Division of Health Professions Licensure Board of Registration in Nursing
Revised April 4. 2016 The Commonwealth of Massachusetts Executive Office of Health and Human Services Department of Public Health Division of Health Professions Licensure Board of Registration in Nursing
Provider User Guide. Intensive Case Management Enhancements via NaviNet
 Provider User Guide Intensive Case Management Enhancements via NaviNet December 2017 Provider Guide: Intensive Case Management Program Table of Contents About the Intensive Case Management (ICM) Program...
Provider User Guide Intensive Case Management Enhancements via NaviNet December 2017 Provider Guide: Intensive Case Management Program Table of Contents About the Intensive Case Management (ICM) Program...
TX-UNPS CACFP Training Packet for Child & Adult Application Packet New or Renewal Applications
 TX-UNPS CACFP Training Packet for Child & Adult Application Packet New or Renewal Applications Child and Adult Care Food Program: Application Packet for Centers Have questions about CACFP forms, claims
TX-UNPS CACFP Training Packet for Child & Adult Application Packet New or Renewal Applications Child and Adult Care Food Program: Application Packet for Centers Have questions about CACFP forms, claims
Section. 13: Levels of Care: GI, Routine, Continuous Care, & Respite. Reviewed: June 13, Section Author(s): megging
: megging") Section 13: Levels of Care: GI, Routine, Continuous Care, & Respite Reviewed: June 13, 2012 Section Author(s): megging Section 13: Levels of Care 2 Section 13: Levels of Care Field Guide Section Contents
Section 13: Levels of Care: GI, Routine, Continuous Care, & Respite Reviewed: June 13, 2012 Section Author(s): megging Section 13: Levels of Care 2 Section 13: Levels of Care Field Guide Section Contents
Medical Assistance Provider Incentive Repository. User Guide. For Eligible Hospitals
 Medical Assistance Provider Incentive Repository User Guide For Eligible Hospitals February 25, 2013 Contents Introduction... 3 Before You Begin... 3 Complete your R&A registration.... 3 Identify one individual
Medical Assistance Provider Incentive Repository User Guide For Eligible Hospitals February 25, 2013 Contents Introduction... 3 Before You Begin... 3 Complete your R&A registration.... 3 Identify one individual
DEPARTMENT OF COUNSELOR EDUCATION AND FAMILY STUDIES. LiveText Field Experience Manual Practicum & Internship
 DEPARTMENT OF COUNSELOR EDUCATION AND FAMILY STUDIES LiveText Field Experience Manual Practicum & Internship 2018-2019 1 Table of Contents Introduction...3 How To Purchase LiveText...3 How To Register
DEPARTMENT OF COUNSELOR EDUCATION AND FAMILY STUDIES LiveText Field Experience Manual Practicum & Internship 2018-2019 1 Table of Contents Introduction...3 How To Purchase LiveText...3 How To Register
Fulbright Specialist Program: Host Institution Application Instructions
 Fulbright Specialist Program: Host Institution Application Instructions Thank you for your interest in submitting a project for the Fulbright Specialist Program. These instructions are intended to guide
Fulbright Specialist Program: Host Institution Application Instructions Thank you for your interest in submitting a project for the Fulbright Specialist Program. These instructions are intended to guide
Short Term Faculty Led Programs
 Substantive Edit In the first edit of a document, the substantive edit, the editor checks the organization and structure of information. During this phase, I moved two sections in the beginning of the
Substantive Edit In the first edit of a document, the substantive edit, the editor checks the organization and structure of information. During this phase, I moved two sections in the beginning of the
Overview What is effort? What is effort reporting? Why is Effort Reporting necessary?... 2
 Effort Certification Training Guide Contents Overview... 2 What is effort?... 2 What is effort reporting?... 2 Why is Effort Reporting necessary?... 2 Effort Certification Process: More than just Certification...
Effort Certification Training Guide Contents Overview... 2 What is effort?... 2 What is effort reporting?... 2 Why is Effort Reporting necessary?... 2 Effort Certification Process: More than just Certification...
Involved Portal: Donations & Matching Gifts
 Involved Portal: Donations & Matching Gifts Employee User Guide For Internal Use Only / Not for Distribution to the Public Table of Contents Credit Card Donations Page 2 Offline Donations & Matching Gifts
Involved Portal: Donations & Matching Gifts Employee User Guide For Internal Use Only / Not for Distribution to the Public Table of Contents Credit Card Donations Page 2 Offline Donations & Matching Gifts
To begin reporting with edwr reports, the responsible official of the water system or laboratory must request the edwr service.
 edwr Service Request To begin reporting with edwr reports, the responsible official of the water system or laboratory must request the edwr service. Note: will only be approving responsible officials (RO)
edwr Service Request To begin reporting with edwr reports, the responsible official of the water system or laboratory must request the edwr service. Note: will only be approving responsible officials (RO)
Name of Sex: M F Applicant: Last First Middle. Date of Birth: Social Security Number: Phone: ( ) City State Zip. Phone: ( ) City State Zip
 City State Zip. Phone: ( ) City State Zip") SCHNEIDER REGIONAL MEDICAL CENTER 9048 SUGAR ESTATE ST. THOMAS, U.S.V.I 00802 APPLICATION FOR TEMPORARY PRIVILEGES (USED FOR URGENT PATIENT NEED AND LOCUM TENENS) COMPLETE THE APPLICATION IN FULL. PRINT
SCHNEIDER REGIONAL MEDICAL CENTER 9048 SUGAR ESTATE ST. THOMAS, U.S.V.I 00802 APPLICATION FOR TEMPORARY PRIVILEGES (USED FOR URGENT PATIENT NEED AND LOCUM TENENS) COMPLETE THE APPLICATION IN FULL. PRINT
Presented by: Department of Health Care Services Provider Enrollment Division (PED) Wednesday, January 16, 2013
 Wednesday, January 16, 2013") Presented by: Department of Health Care Services Provider Enrollment Division (PED) Wednesday, January 16, 2013 2 1 3 4 2 5 6 3 7 Applications received by PED after 60 days will be reviewed as new applications.
Presented by: Department of Health Care Services Provider Enrollment Division (PED) Wednesday, January 16, 2013 2 1 3 4 2 5 6 3 7 Applications received by PED after 60 days will be reviewed as new applications.
How to request reliance by UNC on an external IRB or extend UNC IRB oversight to an external group or individual
 How to request reliance by UNC on an external IRB or extend UNC IRB oversight to an external group or individual A reliance agreement may be requested when you are collaborating with researchers external
How to request reliance by UNC on an external IRB or extend UNC IRB oversight to an external group or individual A reliance agreement may be requested when you are collaborating with researchers external
This letter is to let you know that you are due for re-credentialing as a participating provider for AmeriHealth Caritas Louisiana of Louisiana.
 ATTN: AmeriHealth Caritas Louisiana Providers RE: Provider Re-Credentialing CAQH ID: Dear Credentialing Contact: This letter is to let you know that you are due for re-credentialing as a participating
ATTN: AmeriHealth Caritas Louisiana Providers RE: Provider Re-Credentialing CAQH ID: Dear Credentialing Contact: This letter is to let you know that you are due for re-credentialing as a participating
CRNA INITIAL CREDENTIALING APPLICATION
 CRNA INITIAL CREDENTIALING APPLICATION Revised 01/12 GENERAL INSTRUCTIONS LocumTenens.com CVO must credential all providers prior to placement into any practice location. All information requested in this
CRNA INITIAL CREDENTIALING APPLICATION Revised 01/12 GENERAL INSTRUCTIONS LocumTenens.com CVO must credential all providers prior to placement into any practice location. All information requested in this
SOBA Employee Site Training Manual
 SOBA Employee Site Training Manual 1 What is EBenefits? EBenefits is CSEBA s benefits self-service website. EBenefits allows you to view, enroll in and make changes to your benefits information quickly,
SOBA Employee Site Training Manual 1 What is EBenefits? EBenefits is CSEBA s benefits self-service website. EBenefits allows you to view, enroll in and make changes to your benefits information quickly,
Ohio Long-Term Care Consumer Guide Residential Care Facility Entry Page
 Ohio Long-Term Care Consumer Guide Residential Care Facility Entry Page This form has been provided to you as part of the application process to become an ODA approved provider of Assisted Living Services.
Ohio Long-Term Care Consumer Guide Residential Care Facility Entry Page This form has been provided to you as part of the application process to become an ODA approved provider of Assisted Living Services.
Table of Contents INTRODUCTION NEW APPLICATION GETTING STARTED POST SUBMISSION. Return to Table of Contents
 External User Guide Table of Contents INTRODUCTION GETTING STARTED Mission Statement Commitment to Research G Vision Investigator/Sponsor Responsibilities Visiontracker Web Portal Registration New User
External User Guide Table of Contents INTRODUCTION GETTING STARTED Mission Statement Commitment to Research G Vision Investigator/Sponsor Responsibilities Visiontracker Web Portal Registration New User
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST
 PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) Assistive Devices (Enrollment packet is subject to change without notice) Revised 03/15 GENERAL INFORMATION FOR PROVIDER ENROLLMENT Provider
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid) Assistive Devices (Enrollment packet is subject to change without notice) Revised 03/15 GENERAL INFORMATION FOR PROVIDER ENROLLMENT Provider
Registered Dietician (Individual)
") PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Registered Dietician (Individual) (Enrollment packet is subject to change without notice) GENERAL INFORMATION FOR THE INDIVIDUAL REGISTERED
PROVIDER TYPE SPECIFIC PACKET/CHECKLIST (Louisiana Medicaid Program) Registered Dietician (Individual) (Enrollment packet is subject to change without notice) GENERAL INFORMATION FOR THE INDIVIDUAL REGISTERED
2015 SCHOLARSHIP PROGRAM
 LOS ANGELES POLICE RELIEF AND ASSISTANCE FOUNDATION 2015 SCHOLARSHIP PROGRAM The Los Angeles Police Relief and Assistance Foundation (LAPRAF) will be awarding four $10,000 scholarships to graduating seniors
LOS ANGELES POLICE RELIEF AND ASSISTANCE FOUNDATION 2015 SCHOLARSHIP PROGRAM The Los Angeles Police Relief and Assistance Foundation (LAPRAF) will be awarding four $10,000 scholarships to graduating seniors
Setup for Ohio Medicaid billing for DOS 7/1/2015 and later
 Setup for Ohio Medicaid billing for DOS 7/1/2015 and later OH Medicaid nursing and aide service rates and billing requirements changed effective July 1, 2015. Program changes have been made to accommodate
Setup for Ohio Medicaid billing for DOS 7/1/2015 and later OH Medicaid nursing and aide service rates and billing requirements changed effective July 1, 2015. Program changes have been made to accommodate
Kentucky National Background Check Program Webinar for BHDID
 Kentucky National Background Check Program Webinar for BHDID Office of the Inspector General KARES Helpdesk Team Regulation Status On March 15, 2016, the withdrew Kentucky s National Background Check Program
Kentucky National Background Check Program Webinar for BHDID Office of the Inspector General KARES Helpdesk Team Regulation Status On March 15, 2016, the withdrew Kentucky s National Background Check Program
Do not drop off applications at the fire division offices.
 Dear Firefighter/Paramedic Applicant: Thank you for your interest in employment with the City of Urbana. Please read this cover letter carefully prior to filling out the attached application packet for
Dear Firefighter/Paramedic Applicant: Thank you for your interest in employment with the City of Urbana. Please read this cover letter carefully prior to filling out the attached application packet for
Practitioners may be recredentialed at any time, but in no circumstance longer than a 36 month period.
 SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN RECREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-02 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed by contract
SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN RECREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-02 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed by contract
Atlas LabWorks User Guide Table of Contents
 http://lab.parkview.com Atlas LabWorks User Guide Table of Contents Technical Support 2 Online Directory of Services.......3 Log into Connect.Parkview.com Account... 4 Log into Atlas Account....6 Patient
http://lab.parkview.com Atlas LabWorks User Guide Table of Contents Technical Support 2 Online Directory of Services.......3 Log into Connect.Parkview.com Account... 4 Log into Atlas Account....6 Patient
CRIMINAL BACKGROUND CHECK by Division of Criminal Investigation (DCI)
") *All licenses expire December 31 of every EVEN year* This is a Legal Document. By completing and signing this document, you certify, under penalty of perjury and subject to the provisions of Wyo. Stat.
*All licenses expire December 31 of every EVEN year* This is a Legal Document. By completing and signing this document, you certify, under penalty of perjury and subject to the provisions of Wyo. Stat.
HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS
 HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS The following checklist can be used to verify that the regulatory requirements are addressed in hospice contracts
HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS The following checklist can be used to verify that the regulatory requirements are addressed in hospice contracts
Director James L Whalen. Reviewed/Revised by
 Approval Signature Title Body Worn Digital Recording Systems SOP Number PU50 Director James L Whalen Reviewed/Revised by 6/1/16 Lt. T. Barge 8/6/2015 RC 10/12/14 JRC 1/29/15 4/11/16 Last Revision Date
Approval Signature Title Body Worn Digital Recording Systems SOP Number PU50 Director James L Whalen Reviewed/Revised by 6/1/16 Lt. T. Barge 8/6/2015 RC 10/12/14 JRC 1/29/15 4/11/16 Last Revision Date
Summer Institute for the Gifted 2018 Online Application for Partner Organizations and Groups
 Summer Institute for the Gifted 2018 Online Application for Partner Organizations and Groups SIG utilizes an online application specifically designed for our partner organizations and groups to assist
Summer Institute for the Gifted 2018 Online Application for Partner Organizations and Groups SIG utilizes an online application specifically designed for our partner organizations and groups to assist
Avatar User Guide: Adult/Older Adult Treatment Plan of Care/ Reassessment City and County of San Francisco
 Avatar User Guide: Adult/Older Adult Treatment Plan of Care/ Reassessment City and County of San Francisco Page 1 of 19 Adult/Older Adult Treatment Plan of Care/Reassessment The purpose of this manual
Avatar User Guide: Adult/Older Adult Treatment Plan of Care/ Reassessment City and County of San Francisco Page 1 of 19 Adult/Older Adult Treatment Plan of Care/Reassessment The purpose of this manual
Professional Development Committee
 STEP 1: Go to the Grants & Sponsored Projects page, on the KU website. 1. The application guidelines are also available on this page for detailed information on categories, funding levels and allowable
STEP 1: Go to the Grants & Sponsored Projects page, on the KU website. 1. The application guidelines are also available on this page for detailed information on categories, funding levels and allowable
LEARNER USER GUIDE LEARNER USER GUIDE
 CAREER CONNECTION LEARNER USER GUIDE Capella University 5 South Sixth Street, Ninth Floor Minneapolis, MN 5540 TABLE OF CONTENTS Search... 3 Search Capella Network Jobs... 3 Create a Job Alert... 4 Designate
CAREER CONNECTION LEARNER USER GUIDE Capella University 5 South Sixth Street, Ninth Floor Minneapolis, MN 5540 TABLE OF CONTENTS Search... 3 Search Capella Network Jobs... 3 Create a Job Alert... 4 Designate
AbbVie Grant Management System (GMS) Requestor Training, Grant Request Training: General Program Support
 Requestor Training, Grant Request Training: General Program Support") AbbVie Grant Management System (GMS) Requestor Training, Grant Request Training: General Program Support After Reviewing this Module, You Will be Able to: Log Onto the GMS Setting up Your Security Password
AbbVie Grant Management System (GMS) Requestor Training, Grant Request Training: General Program Support After Reviewing this Module, You Will be Able to: Log Onto the GMS Setting up Your Security Password
FCC Form 460 for Consortia
 Healthcare Connect Fund Program FCC Form 460 for Consortia Rural Health Care Program I Healthcare Connect Fund Program 1 FCC Form 460 for Consortia Today s Speakers Paloma Costa RHC Program Outreach Camelia
Healthcare Connect Fund Program FCC Form 460 for Consortia Rural Health Care Program I Healthcare Connect Fund Program 1 FCC Form 460 for Consortia Today s Speakers Paloma Costa RHC Program Outreach Camelia
Home Health Orientation: Manager of Clinical Practice (MCP)/Clinical Manager (CM)/ Director of Clinical Management (DCM) Track
/Clinical Manager (CM)/ Director of Clinical Management (DCM) Track") Name Hire Date: Branch: A learner s progression will be based on their ability to demonstrate knowledge and competency to the satisfaction of their immediate Supervisor. Week 1 Attend Kindred at Home New
Name Hire Date: Branch: A learner s progression will be based on their ability to demonstrate knowledge and competency to the satisfaction of their immediate Supervisor. Week 1 Attend Kindred at Home New
CareTracker Patient Portal Tips
 CareTracker Patient Portal Tips by Phasis Group, LLC CONTENTS Purpose... 2 Patient Portal Manual and Help... 2 Requirements for Patient s Computer... 2 Operating System / Internet Browsers... 2 Internet
CareTracker Patient Portal Tips by Phasis Group, LLC CONTENTS Purpose... 2 Patient Portal Manual and Help... 2 Requirements for Patient s Computer... 2 Operating System / Internet Browsers... 2 Internet
NOTICE OF PRIVACY PRACTICES Full Length Version Effective Date: 4/19/2016
 Conrad l Pearson Clinic, P.C. NOTICE OF PRIVACY PRACTICES Full Length Version Effective Date: 4/19/2016 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
Conrad l Pearson Clinic, P.C. NOTICE OF PRIVACY PRACTICES Full Length Version Effective Date: 4/19/2016 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN
National Verifier Training: Eligibility. November 8, 2017
 National Verifier Training: Eligibility November 8, 2017 1 Housekeeping Audio is available through your computer s speakers The audience will remain on mute Enter questions at any time using the Questions
National Verifier Training: Eligibility November 8, 2017 1 Housekeeping Audio is available through your computer s speakers The audience will remain on mute Enter questions at any time using the Questions
Instructions for Navigating Your Awarded Grant
 Instructions for Navigating Your Awarded Grant proposalcentral s Post-Award allows grantees to submit progress reports, project documents, financial/budget information, communicate with the funding organization,
Instructions for Navigating Your Awarded Grant proposalcentral s Post-Award allows grantees to submit progress reports, project documents, financial/budget information, communicate with the funding organization,
Network Participant Credentialing Application
 Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
The Plan will not credential trainees who do not maintain a separate and distinct practice from their training practice.
 SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN INITIAL CREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-01 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed
SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN INITIAL CREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-01 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed
HIPAA Notice of Privacy Practices
 HIPAA Notice of Privacy Practices *HIPAA: Health Insurance Portability and Accountability Act Effective Date: April 14, 2003; rev. Dec. 1, 2003; Form # 030463 CAT: 15-Patient Data To reorder, log onto
HIPAA Notice of Privacy Practices *HIPAA: Health Insurance Portability and Accountability Act Effective Date: April 14, 2003; rev. Dec. 1, 2003; Form # 030463 CAT: 15-Patient Data To reorder, log onto
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
Educational Grant and Outcomes Database User Guide
 Educational Grant and Outcomes Database User Guide June 06 Table of Contents Getting Started System Tips and Useful Hints p.3 Where to Find Us p.4 Logging in as a Registered User p.5 Registering as a First-Time
Educational Grant and Outcomes Database User Guide June 06 Table of Contents Getting Started System Tips and Useful Hints p.3 Where to Find Us p.4 Logging in as a Registered User p.5 Registering as a First-Time
Credentialing Application
 Credentialing Application 1. NAME Last First MI Degree Gender 2. BIRTH, SOCIAL SECURITY & E-MAIL ADDRESS Date of Birth Social Security # E-Mail Address 3. PRACTICE, OFFICE & SPECIALTY INFORMATION 3.1 Please
Credentialing Application 1. NAME Last First MI Degree Gender 2. BIRTH, SOCIAL SECURITY & E-MAIL ADDRESS Date of Birth Social Security # E-Mail Address 3. PRACTICE, OFFICE & SPECIALTY INFORMATION 3.1 Please
Welcome to a tutorial on the abstract submission process for the 2014 AGU Fall Meeting.
 Welcome to a tutorial on the abstract submission process for the 2014 AGU Fall Meeting. NOTE: The abstract submission site is NEW this year. Please take a few moments to review this tutorial and become
Welcome to a tutorial on the abstract submission process for the 2014 AGU Fall Meeting. NOTE: The abstract submission site is NEW this year. Please take a few moments to review this tutorial and become
Creating A Patient Portal Link From More Patient Button
 Creating A Patient Portal Link From More Patient Button Go to More Patient and click on the Export PHI tab. From this tab, click on Create Patient Portal Link. Note: Allow Internet Based Delivery Of Reminders
Creating A Patient Portal Link From More Patient Button Go to More Patient and click on the Export PHI tab. From this tab, click on Create Patient Portal Link. Note: Allow Internet Based Delivery Of Reminders
Alphabet Soup of Provider Credentialing. Anne Hanzel Alta Partners, LLC
 Alphabet Soup of Provider Credentialing Anne Hanzel Alta Partners, LLC Why is Credentialing Important? Patient Safety Build practice base Allow for discounted amounts Direct link to managed care systems
Alphabet Soup of Provider Credentialing Anne Hanzel Alta Partners, LLC Why is Credentialing Important? Patient Safety Build practice base Allow for discounted amounts Direct link to managed care systems
Complete instructions are located online at and within the online application system.
 Information in this presentation is intended for the purpose of providing training for program directors and faculty that teach in Arkansas nursing programs. Content may be shared with nursing education
Information in this presentation is intended for the purpose of providing training for program directors and faculty that teach in Arkansas nursing programs. Content may be shared with nursing education
Cal State Apply Guide for MSN Applicants. 1. Go to https://www2.calstate.edu/apply, click on Graduate
 Cal State Apply Guide for MSN Applicants 1. Go to https://www2.calstate.edu/apply, click on Graduate 2. Click on Apply Now 3. If you have already created an account on the Cal State Apply website, enter
Cal State Apply Guide for MSN Applicants 1. Go to https://www2.calstate.edu/apply, click on Graduate 2. Click on Apply Now 3. If you have already created an account on the Cal State Apply website, enter
The Credentialing Process. Note! Contents are subject to change and are not a guarantee of payment.
 The Credentialing Process Note! Contents are subject to change and are not a guarantee of payment. Introduction to Credentialing BlueCross BlueShield of South Carolina, BlueChoice HealthPlan of South Carolina
The Credentialing Process Note! Contents are subject to change and are not a guarantee of payment. Introduction to Credentialing BlueCross BlueShield of South Carolina, BlueChoice HealthPlan of South Carolina
FY19 City of Virginia Beach Arts and Humanities Commission Project Grant
 Humanities Commission Project Grant Organization Information Thank you for applying to the Virginia Beach Arts and Humanities Commission. Provide all information requested below in the order listed. Submit
Humanities Commission Project Grant Organization Information Thank you for applying to the Virginia Beach Arts and Humanities Commission. Provide all information requested below in the order listed. Submit
SOUTH CAROLINA DEPARTMENT OF TRANSPORTATION Office of Public Transit. Grants Management System (GMS) User Guide
 User Guide") SOUTH CAROLINA DEPARTMENT OF TRANSPORTATION Office of Public Transit Grants Management System (GMS) User Guide Table of Contents User Accounts... 3 Create User Accounts... 3 Login Procedure... 3 Annual
SOUTH CAROLINA DEPARTMENT OF TRANSPORTATION Office of Public Transit Grants Management System (GMS) User Guide Table of Contents User Accounts... 3 Create User Accounts... 3 Login Procedure... 3 Annual
Type & Specialty pages Mark the specialty(s) you wish to enroll in. Attach required documents including license as specified.
 you wish to enroll in. Attach required documents including license as specified.") P O Box 3571 Below is a checklist for your convenience to help ensure that all forms are completed in their entirety. If any of the following items are not complete, do not contain original signatures,
P O Box 3571 Below is a checklist for your convenience to help ensure that all forms are completed in their entirety. If any of the following items are not complete, do not contain original signatures,
Certification of Employee Time and Effort
 Procedure: Policy: Number: Completing a Personnel Activity Report (PAR) Certification of Employee Time and Effort GP1200.3 ( ) Complete Revision Supersedes: Page: ( ) Partial Revision Page 1 of 21 ( X
Procedure: Policy: Number: Completing a Personnel Activity Report (PAR) Certification of Employee Time and Effort GP1200.3 ( ) Complete Revision Supersedes: Page: ( ) Partial Revision Page 1 of 21 ( X
eqsuite System Changes for Pediatric Behavioral Therapy PAR Submission Instructions
 eqsuite System Changes for Pediatric Behavioral Therapy PAR Submission Instructions This document is designed to help Behavior Therapy providers to submit initial prior authorization requests and modifications
eqsuite System Changes for Pediatric Behavioral Therapy PAR Submission Instructions This document is designed to help Behavior Therapy providers to submit initial prior authorization requests and modifications
Troubleshooting Audio
 Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines